CADTH Health Technology Review
Direct-Acting Antivirals for Pediatric Chronic Hepatitis C Virus Infection
Rapid Review
Authors: Khai Tran, Kendra Brett, Melissa Walter
Abbreviations
AE
adverse event
CDEC
CADTH Canadian Drug Expert Committee
DAA
direct-acting antiviral
DORA
DAA fOr CuRe of HepAtitis
GLE
glecaprevir
GT
genotype
HCV
hepatitis C virus
PIB
pibrentasvir
RNA
ribonucleic acid
PedsQL
Pediatric Quality of Life Inventory
SOF
sofosbuvir
SVR
sustained virologic response
VEL
velpatasvir
Key Messages
Clinical evidence showed that treatment with glecaprevir-pibrentasvir for children and adolescents with chronic hepatitis C virus infection was efficacious with an overall sustained virologic response 12 weeks after treatment near 100%.
Glecaprevir-pibrentasvir treatment was well-tolerated as there were no serious adverse events or adverse events leading to treatment discontinuation. Most adverse events were mild.
We did not find any studies that evaluated the cost-effectiveness of glecaprevir-pibrentasvir for the treatment of chronic hepatitis C virus infection in pediatric patients.
We did not find any peer-reviewed studies that evaluated the clinical effectiveness of sofosbuvir-velpatasvir for the treatment of chronic hepatitis C virus infection in pediatric patients. Unpublished data in a conference abstract and clinical trial registry suggest effectiveness of sofosbuvir-velpatasvir, but the findings should be interpreted with cautions.
We did not find any studies that evaluated the cost-effectiveness of sofosbuvir-velpatasvir for the treatment of chronic hepatitis C virus infection in pediatric patients.
Context and Policy Issues
Hepatitis C virus (HCV) infection is a liver disease caused by single-stranded ribonucleic acid (RNA) virus of the family Flaviviridae.1 Acute infection occurs within the first 6 months.1 When the infection persists for more than 6 months, it is considered chronic.1 Adults and children differ in the mode of HCV infection (e.g., perinatal transmission in children, blood transfusion, sexual activities, or IV drug misuse in adults).1 Chronic HCV infection can lead to cirrhosis, a scarring of the liver, caused by long-term liver damage that increases the chance of developing liver failure or cancer.1 There are 7 HCV genotypes (GTs), with GT1 being the most prevalent worldwide.2 GT2 and GT3 are common in Latin America (5% to 30% of the HCV population), Europe (20% to 40% of the HCV population), and Asia (30% to 45% of the HCV population).3-5 GT4 is common in parts of Africa and the Middle East, GT5 is found in South Africa, GT6 is found primarily in South-east Asia, and GT7 is found in Central Africa.2
Data on the incidence rates of HCV infection (calculated as the number of cases per 100,000 population) in total, in male, and in female children and adolescents from 2013 to 2023 in Canada are present in Table 1, Table 2, and Table 3, respectively.6 For all children and adolescents, the incidence rates were highest in the age groups of those younger than 1 year and those aged 15 to 19 years (Table 1). The 5- to 9-year-old age group had the lowest incidence rates, followed by the 10- to 14-year-old age group and the 1- to 4-year-old age group (Table 1). These observations were true for both male (Table 2) and female (Table 3) children and adolescents. From 2013 to 2021, the incidence rates of both male and female children and adolescents aged 15 to 19 years decreased over time, from 6.56 in 2013 to 1.91 in 2021 in males (Table 2) and from 12.28 in 2013 to 5.85 in 2021 in females (Table 3). In this age group, the female to male incidence rate ratios ranged from 1.72 to 3.06, indicating that the incidence rates in females were 2 to 3 times higher than those in males. There were no apparent differences in the incidence rates among females and males in the other age groups.
Table 1: Incidence Rates of HCV Infection in All Children and Adolescents From 2013 to 2021
Age, years | Incidence rate, per 100,000 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | |
< 1 | 3.42 | 4.98 | 4.71 | 4.44 | 2.90 | 2.92 | 5.11 | 3.79 | 5.83 |
1 to 4 | 0.78 | 0.71 | 0.65 | 0.58 | 0.70 | 0.96 | 1.15 | 0.77 | 0.92 |
5 to 9 | 0.21 | 0.16 | 0.66 | 0.25 | 0.25 | 0.39 | 0.39 | 0.24 | 0.15 |
10 to 14 | 0.37 | 0.32 | 0.53 | 0.73 | 0.67 | 0.90 | 0.98 | 0.10 | 0.33 |
15 to 19 | 9.33 | 10.1 | 10.2 | 7.82 | 9.71 | 9.68 | 7.66 | 3.52 | 3.84 |
HCV = hepatitis C virus.
Table 2: Incidence Rates of HCV Infection in Male Children and Adolescents From 2013 to 2021
Age, years | Incidence rate, per 100,000 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | |
< 1 | 3.07 | 3.08 | 4.60 | 4.59 | 2.57 | 2.59 | 4.20 | 4.22 | 6.48 |
1 to 4 | 0.89 | 0.88 | 0.51 | 0.50 | 0.38 | 1.00 | 0.87 | 0.50 | 0.38 |
5 to 9 | 0.21 | 0 | 0.40 | 0.49 | 0.10 | 0.29 | 0.48 | 0.19 | 0.19 |
10 to 14 | 0.31 | 0.10 | 0.72 | 0.41 | 0.40 | 0.79 | 0.97 | 0 | 0.38 |
15 to 19 | 6.56 | 6.76 | 6.48 | 5.58 | 6.88 | 6.93 | 5.63 | 2.14 | 1.91 |
HCV = hepatitis C virus.
Table 3: Incidence Rates of HCV Infection in Female Children and Adolescents From 2013 to 2021
Age, years | Incidence rate, per 100,000 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | |
< 1 | 3.79 | 6.99 | 4.29 | 4.28 | 3.26 | 2.73 | 6.06 | 3.33 | 5.14 |
1 to 4 | 0.66 | 0.53 | 0.79 | 0.66 | 1.05 | 0.79 | 1.45 | 1.06 | 1.48 |
5 to 9 | 0.22 | 0.32 | 0.93 | 0 | 0.40 | 0.50 | 0.30 | 0.30 | 0.10 |
10 to 14 | 0.44 | 0.54 | 0.32 | 1.06 | 0.94 | 1.02 | 1.00 | 0.20 | 0.29 |
15 to 19 | 12.28 | 13.67 | 14.12 | 10.21 | 12.52 | 12.40 | 9.70 | 4.87 | 5.85 |
HCV = hepatitis C virus.
The estimated prevalence of HCV infection among Canadian youth aged 15 to 24 years was 0.2% according to statistical modelling estimates in 2007.7 However, the overall prevalence of HCV infection among Canadian youth (15 to 24 years) who injected drugs was 34.7%.7 Older youth (aged 20 to 24 years) who injected drugs were 5.2 times more likely to have HCV infection than younger youth (age 15 to 19 years) (41.5% versus 12.0%; odds ratio = 5.2; 95% confidence interval, 2.7 to 9.9).7 An epidemiological study found a higher prevalence of HCV infection in an Indigenous population in Manitoba than in the non-Indigenous population.8 In 2002, the estimated prevalence rates of HCV infection in Indigenous female and male children and adolescents (aged 0 to 17 years) were 103.1 per 100,000 and 35.3 per 100,000, respectively, compared to 25.0 per 100,000 and 21.4 per 100,000 non-Indigenous female and male counterparts.8 A population-based study of reported HCV diagnoses from 1998 to 2018 in Quebec reported that immigrants have been found to have a higher HCV prevalence (1.5 to 2 fold) compared with nonimmigrants.9 During this period, the prevalence rates of children who were immigrant and aged 0 to 9 years and adolescents aged 10 to 19 years were 4.8 per 100,000 and 4.9 per 100,000, respectively, compared with 1.4 per 100,000 and 3.4 per 100,000 in nonimmigrants.9
Before the introduction of direct-acting antivirals (DAAs), HCV infection was treated with pegylated interferon and ribavirin, which were associated with significant adverse reactions and yielded variable sustained virologic responses (SVRs).10 DAAs have been shown to be the most successful HCV cure when used in combination regimens, which typically include inhibitors targeting the NS3-4A, NS5A, and NS3B viral proteins.11 Health Canada has authorized 3 DAAs regimens, namely glecaprevir-pibrentasvir (GLE-PIB) (brand name Maviret) on August 16, 2017,12 sofosbuvir-velpatasvir (SOF-VEL) (brand name Epclusa) on July 11, 2016,13 and ledipasvir-sofosbuvir (brand name Harvoni) on October 15, 2014,14 for treatment of chronic HCV infection in pediatric populations.
The oral fixed-dose combination GLE-PIB is indicated for the treatment of chronic HCV GT1 to GT6 infections in adults and pediatric patients 3 years of age and older who are treatment-naive or treatment-experienced, with or without coinfection with HIV, and with or without compensated liver cirrhosis.12 The recommended dose for adolescents 12 years or older, weighing at least 45 kg, is 3 tablets of GLE-PIB 100 mg/40mg daily (total 300 mg/120mg). Children aged 3 or older, weighing 12 kg to 45 kg, receive GLE-PIB film-coated granules in sachets (50 mg/20 mg in each sachet); the number of sachets is based on body weight: 3 sachets (150 mg/60 mg) for children weighing 12 kg to less than 20 kg; 4 sachets (200 mg/80 mg) for children weighing 20 kg to less than 30 kg; and 5 sachets (250 mg/100 mg) for children weighing 30 kg to less than 45 kg. Treatment duration varies from 8 weeks to 16 weeks depending on cirrhosis status, HCV GT, and previous treatment.
The oral fixed-dose combination SOF-VEL is indicated for the treatment of chronic HCV GT1 to GT6 infections in adults and pediatric patients 12 years of age or older who weigh more than 30 kg and are without cirrhosis or with compensated cirrhosis.13 The recommended dose is 1 tablet of SOF-VEL (400 mg/100mg) once daily for 12 weeks.
In 2016, the CADTH Canadian Drug Expert Committee (CDEC) conducted a reimbursement review of SOF-VEL, and recommended that the drug be reimbursed for the treatment of chronic HCV infection in adults if the price was reduced.15 In 2017, CDEC also recommended that GLE-PIB be reimbursed for the treatment of adults with chronic HCV infection if the drug plan cost for GLE-PIB does not exceed the drug plan cost of treatment with the least costly DAA(s).16 None of these combination regimens have been reviewed by CDEC for the treatment of pediatric patients.
The American Association for the Study of Liver Diseases17 and the European Association for the Study of the Liver18 guidelines have updated their recommendations on the use of DAA regimens, including GLE-PIB and SOF-VEL for the treatment of pediatric patients. Despite the recent approval by Health Canada12,13 and recommendations from major guidelines17,18 on the use of GLE-PIB or SOF-VEL for the treatment of HCV infection in the pediatric population, clinical evidence was mainly derived from published and unpublished data from nonrandomized, open-label, single-arm studies,12,13,17,18 meaning the comparative clinical effectiveness and cost-effectiveness of these combination regimens with other alternative DAAs have yet to be addressed.
This report aims to summarize the clinical effectiveness and cost-effectiveness of GLE-PIB and/or SOF-VEL compared with each other, other DAA regimens, placebo, or no comparator for the treatment of HCV in pediatric patients. The evidence will help inform local reimbursement decisions.
Research Questions
What is the clinical effectiveness of GLE-PIB for the treatment of chronic HCV infection in pediatric patients?
What is the clinical effectiveness of SOF-VEL for the treatment of chronic HCV infection in pediatric patients?
What is the cost-effectiveness of GLE-PIB for the treatment of chronic HCV infection in pediatric patients?
What is the cost-effectiveness of SOF-VEL for the treatment of chronic HCV infection in pediatric patients?
Methods
Literature Search Methods
An information specialist conducted 2 literature searches on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, and the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approaches were customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategies comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The first search used the main search concepts glecaprevir-pibrentasvir (Maviret) and pediatrics. This search was completed on July 31, 2023, and limited to English-language documents published since January 1, 2013. The second search used the main search concepts sofosbuvir-velpatasvir (Epclusa) and pediatrics. This search was completed on August 11, 2023, and also limited to English-language documents published since January 1, 2013.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 4.
Criteria | Description |
|---|---|
Population | Q1 and Q3: Pediatric patients (aged 3 to < 18 years and weighing ≥ 12 kg) with chronic HCV infection Subgroup of interest: Patients aged 12 to < 18 years Q2 and Q4: Pediatric patients (aged 12 to < 18 years and weighing ≥ 30 kg) with chronic HCV infection without cirrhosis or with compensated cirrhosis |
Intervention | Q1 and Q3: Glecaprevir-pibrentasvir Q2 and Q4: Sofosbuvir-velpatasvir |
Comparator | Q1 and Q3: Alternative direct-acting antiviral regimens (i.e., ledipasvir-sofosbuvir, sofosbuvir-velpatasvir), placebo, no comparator Q2 and Q4: Alternative direct-acting antiviral regimens (e.g., ledipasvir-sofosbuvir, glecaprevir-pibrentasvir), placebo, no comparator |
Outcomes | Q1 and Q2: Clinical effectiveness (e.g., sustained virologic response, treatment failure, relapse, mortality [all-cause and liver-related], HRQoL) and safety (e.g., adverse events, severe adverse events) Q3 and Q4: Cost-effectiveness (i.e., incremental cost per health benefit or QALY gained) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies, economic evaluations |
HCV = hepatitis C virus; HRQoL = health-related quality of life; QALY = quality-adjusted life-year.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1 or were published before 2013. Primary studies published in a language other than English were also excluded.
Critical Appraisal of Individual Studies
One reviewer critically appraised the included publications using the Downs and Black checklist19 for nonrandomized studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
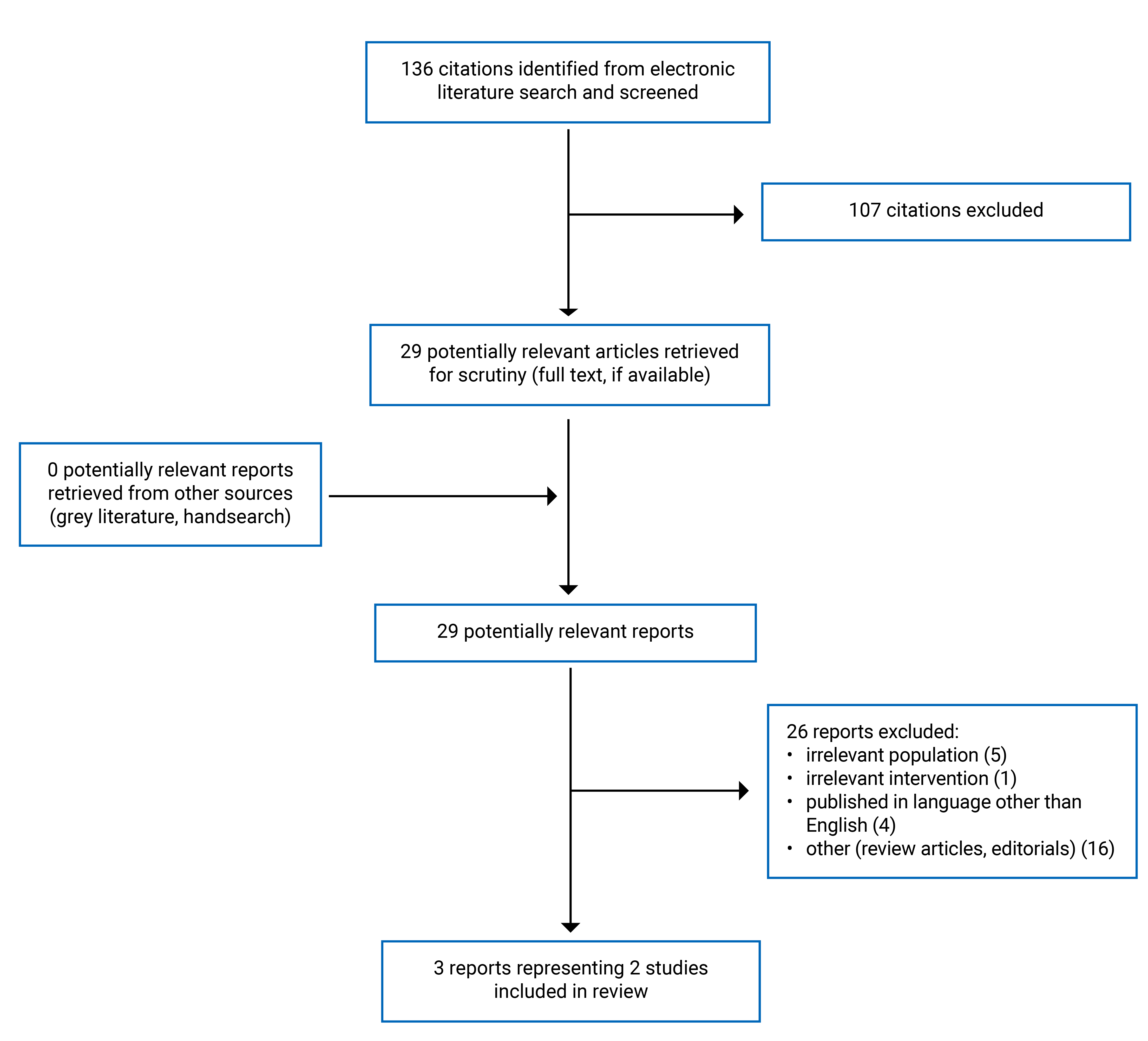
A total of 136 citations were identified in the literature search. Following screening of titles and abstracts, 107 citations were excluded and 29 potentially relevant reports from the electronic search were retrieved for full-text review. No potentially relevant publications were retrieved from the grey literature search for full-text review. Of 29 potentially relevant articles, 26 publications were excluded for various reasons, and 3 publications met the inclusion criteria and were included in this report. These were 2 nonrandomized studies of GLE-PIB (1 of which was published in 2 publications) presenting the results of different subpopulations. No relevant studies of SOF-VEL were identified. Appendix 1 presents the PRISMA20 flow chart of the study selection.
Summary of Study Characteristics
Additional details regarding the characteristics of the 2 included primary clinical studies of GLE-PIB21-23 are provided in Table 5, Appendix 2.
Study Design
Both included primary clinical studies21-23 were prospective, nonrandomized, open-label, single-arm, multicentre studies. The study by Mizuochi et al. (2023)21 was conducted in 13 Japanese pediatric centres and published in 2023, and the DORA (DAA fOr CuRe of HepAtitis) study was conducted in 38 sites in North America, Europe, and Japan, and was published as part 122 and part 223 in 2020 and 2021, respectively.
Country of Origin
The primary clinical studies were conducted by authors from Japan,21 and from countries22,23 including the US, Canada, the UK, Germany, Russia, Belgium, and Japan.
Patient Population
Eligible patients in the included studies21-23 were children and adolescents with chronic HCV GT 1 to 6 infections (defined as HCV RNA ≥ 1,000 IU/mL), who were treatment-naive or treatment-experienced, with or without compensated cirrhosis or coinfection with HIV.
The study by Mizuochi et al. (2023)21 enrolled 25 adolescents aged 12 to 17 years, 60% of whom were female and 40% of whom were male. The study only had patients with GT 1 to 2. Most patients (88%) were naive to HCV treatment, while 12% were experienced with prior HCV treatment with pegylated interferon and ribavirin. All patients were without cirrhosis or coinfected with human HIV or hepatitis B virus and had acquired HCV perinatally.
The multinational study by Jonas et al. (part 1, 2020, and part 2, 2021)22,23 was the DORA study:
DORA part 1 involved 47 adolescents aged 12 to 17 years, with 55% female and 45% male. Patients were of GT 1 to 4. The majority of patients were HCV treatment-naive (77%), while 23% were experienced with prior HCV treatment with pegylated interferon and ribavirin. All patients were without cirrhosis. Two patients (4%) coinfected with HIV were enrolled. The majority of patients had acquired HCV perinatally (85%).
DORA part 2 involved 80 children aged 3 to 11 years, which were divided into 3 subgroups based on age: 3 to 5 years (N = 24); 6 to 8 years (N = 27); 9 to 11 years (N = 29). In total, 55% of the patients were female and 45% were male. Patients were of GT 1 to 4. The majority of patients were treatment-naive (97.5%), while 2 patients who were treatment-experienced (2.5%) had been treated with pegylated interferon and ribavirin. None of the enrolled patients had cirrhosis. One patient (1%) coinfected with HIV was enrolled.
Interventions
In the study by Mizuochi et al. (2023)21 and part 1 of the DORA study,22 adolescents aged 12 to 17 years received 3 tablets of 100 mg GLE and 40 mg PIB (total = 300 mg/120 mg) orally with food once daily for 8, 12, or 16 weeks depending on HCV GT, cirrhosis status, and prior treatment experience.
In part 2 of the DORA study,23 children aged 3 to 11 years received GLE-PIB as small film-coated granules in sachets (50 mg/20 mg in each sachet) taken with a small amount of food once daily for 8, 12, or 16 weeks depending on HCV GT, cirrhosis status, and prior treatment experience. The final dose was given based on the child’s weight: 150 mg GLE and 60 mg PIB (3 sachets) for children weighing 12 kg to less than 20 kg; 200 mg GLE and 80 mg PIB (4 sachets) for children weighing 20 kg to less than 30 kg; and 250 mg GLE and 100 mg PIB (5 sachets) for children weighing 30 kg to less than 45 kg.
Outcomes
In the study by Mizuochi et al. (2023),21 the primary efficacy end point was SVR12, the percentage of patients attaining SVR 12 weeks after treatment, defined as an undetectable HCV RNA at 12 weeks after the last dose of study drug. HCV RNA was measured using a real-time reverse transcription-polymerase chain reaction assay. Safety and tolerability were evaluated by monitoring adverse events (AEs), laboratory values, physical examinations, and vital signs. Growth and development were also evaluated.
In both part 122 and part 223 of the DORA study, the primary efficacy end point was SVR12, defined as an HCV RNA of less than the lower limit of quantification (15 IU/mL) 12 weeks after the last actual dose of the study drug. Secondary outcomes were on-treatment virologic failure (i.e., breakthrough or failure to suppress at end of treatment), post-treatment relapse (i.e., HCV RNA was detectable following cessation of therapy), and HCV reinfection (i.e., reinfection at any time up to the last study visit). Safety and tolerability were evaluated by monitoring AEs and laboratory values. Part 1 of the DORA study22 also evaluated quality of life using the Pediatric Quality of Life Inventory (PedsQL), a patient-reported outcomes instrument validated in studies of the pediatric patients who have chronic health conditions.24 The 23 items in the PedsQL comprises 4 Generic Core Scales: Physical Functioning (8 items), Emotional Functioning (5 items), Social Functioning (5 items), and School Functioning (5 items). Two Summary Scores can be calculated as the Psychosocial Health Summary Score and the Physical Health Summary Score, as well as a Total Scale Score. Items on the PedsQL Generic Core Scales are reverse scored and transformed to a 0 to 100 scale. Higher scores indicate better HRQoL.
Summary of Critical Appraisal
The detailed quality assessments of the included studies are provided in Table 6, Appendix 3.
For reporting, both studies21-23 clearly described the objective of the study, the intervention of interest, the main outcomes, the main findings of the study, and the patient characteristics at baseline. Both studies evaluated the efficacy and safety outcomes of the intervention.
For external validity, it appears that patients in both studies21-23 enrolled from multiple centres were representative of the entire population from which they were recruited. The treatment settings (i.e., hospitals) in both studies21-23 appeared to be representative of the treatment received by most of the patients.
For internal validity, patients in both studies21-23 were treated for 8, 12, or 16 weeks according to GT, presence or absence of cirrhosis, and prior treatment status. The majority (96%) received an 8-week therapy in both studies.21-23 Statistical tests were used appropriately, and the main outcome measures were accurate and reliable. Both studies21-23 were prospective, nonrandomized, open-label, single-arm trial. Blinding is not feasible with an open-label study, and patients with knowledge of their assignment may drop out from the trial, leading to missing data. However, the intention-to-treat approach was used in the analysis, which included all patients who received at least 1 dose of the study drug. Backward imputation, where applicable, was used to impute missing data. Participants with missing data after backward imputation were counted as nonresponders. Sample size calculation was performed in the DORA study22,23 to adequately characterize the pharmacokinetics of the intervention. Overall, both studies had low risk of bias related to reporting and external and internal validity with respect to their primary purpose, which was the treatment of patients with chronic HCV.
Summary of Findings
Appendix 4 presents the main study findings, which were summarized by outcome, such as SVR12 (Table 7), safety and tolerability (Table 8), quality of life (Table 9), and growth and development (Table 10).
Clinical Effectiveness of GLE-PIB
Sustained Virologic Response
Patients Aged 12 to 17 Years
For adolescent aged 12 to 17 years, the overall SVR12 rates were 96% and 100% in the study by Mizuochi et al. (2023)21 and the part 1 of the DORA study,22 respectively.
Patients Aged 3 to 11 Years
For children aged 3 to 11 years evaluated in the part 2 of the DORA study,23 the overall SVR12 rates were 96%. When stratified by age groups, the SVR12 rates were 96%, 100%, and 93% in children aged 3 to 5 years, 6 to 8 years, and 9 to 11 years, respectively.
Safety and Tolerability
Patients Aged 12 to 17 Years
There were no AEs leading to discontinuation of the study drug in the study by Mizuochi et al. (2023)21 and part 1 of the DORA study.22 No patients had a serious AE or died during treatment.21,22 The most common AEs (occurring in ≥ 10% of patients) in the part 1 of the DORA study22 were nasopharyngitis, upper respiratory tract infection, vomiting, headache, pyrexia, fatigue, and oropharyngeal pain. No patients experienced clinically significant laboratory abnormalities, and there were no cases of liver-related toxicities or drug-induced liver injury.21,22 No patients experienced virologic failure, and no new HCV infections or reinfection were observed.21,22
Patients Aged 3 to 11 Years
In the part 2 of the DORA study,23 no patients had serious AEs or died during treatment. One 11-year-old patient discontinued treatment by day 4 due to a drug-related rash. The most common AEs were headache, vomiting, and diarrhea. No patients experienced clinically significant laboratory abnormalities, and there were no cases of liver-related toxicities or drug-induced liver injury. No patients experienced virologic failure, and there were no new HCV infections or reinfections. One 9-year-old patient relapsed after 4 weeks of treatment.
Quality of Life
Patients Aged 12 to 17 Years
In part 1 of the DORA study,22 available data from 44 patients aged 12 to 17 years showed improvements in total PedsQL score, Physical Health Summary Score, and Psychosocial Health Summary Score at the end of treatment compared with baseline.
Patients Aged 3 to 11 Years
This was not a reported outcome.
Growth and Development
Patients Aged 12 to 17 Years
Treatment of patients in the part 1 of the DORA study22 did not appear to have an impact on growth and development, as shown by a non–statistically significant mean change from baseline to post-treatment week 12 for body mass index and height z scores. In the study by Mizuochi et al. (2023),21 treatment appeared to affect body mass index z score, but not height z score.
Patients Aged 3 to 11 Years
This was not a reported outcome.
Clinical Effectiveness of SOF-VEL
We did not identify any published peer-reviewed studies assessing the clinical effectiveness of SOF-VEL for the treatment of chronic HCV infection in pediatric patients; therefore, no summary can be provided.
Cost-Effectiveness of GLE-PIB
We did not identify any studies assessing the cost-effectiveness of GLE-PIB for the treatment of chronic HCV infection in pediatric patients; therefore, no summary can be provided.
Cost-Effectiveness of SOF-VEL
We did not identify any studies assessing the cost-effectiveness of SOF-VEL for the treatment of chronic HCV infection in pediatric patients; therefore, no summary can be provided.
Limitations
The 2 clinical studies21-23 identified in this report had several limitations. Both studies were prospective, open-label, nonrandomized trials without a comparator. The clinical effectiveness and cost-effectiveness of GLE-PIB compared with other DAA regimens remains to be determined. As there is ample evidence from comparative and noncomparative studies in adult populations, few studies with limited study designs provided evidence for the efficacy and safety of GLE-PIB in pediatric patients with chronic HCV. Although the patients with all HCV GTs (1 to 6) were eligible in the studies, only HCV GTs 1 to 2 were enrolled in the study by Mizuochi et al. (2023)21 and HCV GTs 1 to 4, with the majority being HCV GT 1, were enrolled in the DORA study.22,23 Most patients were treatment-naive and none had cirrhosis (although cirrhosis was allowed by inclusion criteria). Likewise, no patients in the study by Mizuochi et al. (2023)21 had coinfection with HIV. Only 2 out of 47 patients in the part 1 of the DORA study,22 and 1 out 80 patients in the part 2 of the DORA study,23 were coinfected with HIV. Therefore, the clinical effectiveness and safety of those patients (i.e., HVC GTs 5 and 6, treatment-experienced, cirrhosis, and HIV coinfection) could not be directly evaluated.
Conclusions and Implications for Decision- or Policy-Making
We reviewed the evidence from 2 prospective, nonrandomized, open-label, single-arm, multicentre studies21-23 that evaluated the efficacy and safety of GLE-PIB in children (aged 3 to 11 years) and adolescents (aged 12 to 17 years) with chronic HCV. We did not identify any studies that evaluated the clinical effectiveness or cost-effectiveness of GLE-PIB compared with other DAA regimens or with placebo. We also did not identify any evidence about the clinical effectiveness or cost-effectiveness of SOF-VEL for the treatment of chronic HCV infection in pediatric patients that met the criteria for this report.
The product monograph for SOF-VEL13 indicates that the pharmacokinetics, safety, and efficacy of SOF-VEL in 102 pediatric patients aged 12 to 17 years has been established in an open-label trial. However, at the time of writing this report, the results of the study on SOF-VEL had only been published as a conference abstract25 and are not eligible for inclusion in this report. The study reported the safety and efficacy of SOF-VEL for the treatment of HCV in children and adolescents aged 3 to 17 years in a phase II, open-label trial, whose results were made available on the clinical trials registry (NCT03022981).26 The study enrolled 102 adolescents aged 12 to 17 years, 73 children aged 6 to 11 years, and 41 children aged 3 to 5 years. The groups’ SVR12 rates were 95%, 93%, and 83%, respectively. However, this study has not been published in a peer-reviewed journal and has not been critically appraised for methodological quality or risk of bias; thus, these findings should be interpreted with caution.
For GLE-PIB, clinical evidence from the included studies21,22 showed that adolescent patients (aged 12 to 17 years) with chronic HCV infection treated with an adult GLE-PIB regimen achieved overall SVR12 rates close to 100% for as short as 8 weeks of treatment. The dose of 300 mg GLE and 120 mg PIB appears to be safe in adolescents as there were no serious AEs or AEs leading to drug discontinuation. Treatment with GLE-PIB appears to improve quality of life, and does not appear to impact growth and development. A similar observation was found that treatment with weight-based oral granules in sachets of GLE-PIB was efficacious and well tolerated in children aged 3 to 5 years old, 6 to 8 years old, and 9 to 11 years old.23 There were no drug-related serious AEs, and most AEs were mild.
There were no patients with HCV GTs 5 or 6, or with cirrhosis, who were enrolled in the included studies (although they were allowed by inclusion criteria). Therefore, the efficacy and safety of GLE-PIB in those patient subgroups remain uncertain. Prospective multicentre controlled studies with larger study populations and more diverse HCV GTs will provide more information regarding GLE-PIB treatment in children and adolescents with chronic HCV infection. Whether or not GLE-PIB treatment in pediatric populations is cost-effective and affordable from the Canadian health care system perspective remains to be determined by an economic evaluation study. Evidence of the clinical effectiveness and cost-effectiveness of SOF-VEL for pediatric populations is also needed.
Treatment and management of chronic HCV with the intention to cure in pediatric populations will reduce the development of progressive liver injury and prevent further transmission of HCV when patients reach adulthood. In light of the current evidence, treatment with GLE-PIB would likely decrease the rates of HCV infection in children and adolescents.
References
1.Public Health Agency of Canada. Hepatitis C: Symptoms and treatment. 2023; https://www.canada.ca/en/public-health/services/diseases/hepatitis-c.html. Accessed 2023 Aug 14.
2.Smith DB, Bukh J, Kuiken C, et al. Expanded classification of hepatitis C virus into 7 genotypes and 67 subtypes: updated criteria and genotype assignment web resource. Hepatology. 2014;59(1):318-327. PubMed
3.Kershenobich D, Razavi HA, Sanchez-Avila JF, et al. Trends and projections of hepatitis C virus epidemiology in Latin America. Liver Int. 2011;31 Suppl 2:18-29. PubMed
4.Sievert W, Altraif I, Razavi HA, et al. A systematic review of hepatitis C virus epidemiology in Asia, Australia and Egypt. Liver Int. 2011;31 Suppl 2:61-80. PubMed
5.Manos MM, Shvachko VA, Murphy RC, Arduino JM, Shire NJ. Distribution of hepatitis C virus genotypes in a diverse US integrated health care population. J Med Virol. 2012;84(11):1744-1750. PubMed
6.Public Health Agency of Canada. Notifiable Diseases Online. 2023; https://diseases.canada.ca/notifiable/. Accessed 2023 Aug 3.
7.Epi-Update: Hepatitis C virus (HCV) in youth aged 15 to 24 years. Ottawa (ON): Public Health Agency of Canada; 2010: https://publications.gc.ca/collections/collection_2011/aspc-phac/HP40-53-2010-eng.pdf. Accessed 2023 Aug 3.
8.Uhanova J, Tate RB, Tataryn DJ, Minuk GY. The epidemiology of hepatitis C in a Canadian Indigenous population. Can J Gastroenterol. 2013;27(6):336-340. PubMed
9.Passos-Castilho AM, Murphy DG, Blouin K, et al. A population-based study of reported hepatitis C diagnoses from 1998 to 2018 in immigrants and nonimmigrants in Quebec, Canada. J Viral Hepat. 2023;30(8):656-666. PubMed
10.Motisi MA, Tamborino A, Parigi S, Galli L, de Martino M, Chiappini E. The use of antiviral drugs in children. J Chemother. 2022;34(2):73-86. PubMed
11.Ahmed A, Felmlee DJ. Mechanisms of Hepatitis C Viral Resistance to Direct Acting Antivirals. Viruses. 2015;7(12):6716-6729. PubMed
12.Maviret (glecaprevir/pibrentasvir): glecaprevir 100 mg / pibrentasvir 40 mg oral tablets; glecaprevir 50 mg / pibrentasvir 20 mg per sachet oral granules [product monograph]. St-Laurent (QC): AbbVie Corporation; 2022: https://pdf.hres.ca/dpd_pm/00065378.PDF. Accessed 2023 Aug 16.
13.Epclusa (sofosbuvir/velpatasvir): 400 mg/100 mg oral tablets [product monograph]. Mississauga (ON): Gilead Sciences Canada, Inc.; 2022: https://pdf.hres.ca/dpd_pm/00066982.PDF. Accessed 2023 Aug 16.
14.Harvoni (ledipasvir/sofosbuvir): 90 mg/400 mg oral tablets [product monograph]. Mississauga (ON): Gilead Sciences Canada, Inc.; 2021: https://www.gilead.ca/-/media/gilead-canada/pdfs/medicines/harvoni_english_pm_e170097-gs-012.pdf. Accessed 2023 Sep 6.
15.CADTH Drug Reimbursement Expert Review Committee final recommendation: sofosbuvir/velpatasvir (Epclusa — Gilead Sciences Canada, Inc.). Indication: Chronic Hepatitis C Virus Infection in Adults. Ottawa (ON): CADTH; 2016: https://www.cadth.ca/sites/default/files/cdr/complete/SR0486_complete_Epclusa-Oct-28-16.pdf. Accessed 2023 Aug 22.
16.CADTH Drug Reimbursement Expert Review Committee final recommendation: glecaprevir/pibrentasvir (Maviret — Abbvie Corporation). Indication: Chronic hepatitis C virus (HCV) infection. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/sites/default/files/cdr/complete/SR0523_Maviret_complete-Jan-25-18.pdf. Accessed 2023 Aug 22.
17.American Association for the Study of Liver Diseases, Infectious Diseases Society of America. HCV in Children. In: Recommendations for testing, managing, and treating hepatitis C. 2022; https://www.hcvguidelines.org/unique-populations/children. Accessed 2023 Aug 16.
18.European Association for the Study of the Liver. EASL recommendations on treatment of hepatitis C: Final update of the series. J Hepatol. 2020;73(5):1170-1218. PubMed
19.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
20.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
21.Mizuochi T, Iwama I, Inui A, et al. Real-world efficacy and safety of glecaprevir/pibrentasvir in Japanese adolescents with chronic hepatitis C: a prospective multicenter study. J Gastroenterol. 2023;58(4):405-412. PubMed
22.Jonas MM, Squires RH, Rhee SM, et al. Pharmacokinetics, Safety, and Efficacy of Glecaprevir/Pibrentasvir in Adolescents With Chronic Hepatitis C Virus: Part 1 of the DORA Study. Hepatology. 2020;71(2):456-462. PubMed
23.Jonas MM, Rhee S, Kelly DA, et al. Pharmacokinetics, Safety, and Efficacy of Glecaprevir/Pibrentasvir in Children With Chronic HCV: Part 2 of the DORA Study. Hepatology. 2021;74(1):19-27. PubMed
24.Varni JW, Seid M, Kurtin PS. PedsQL 4.0: reliability and validity of the Pediatric Quality of Life Inventory version 4.0 generic core scales in healthy and patient populations. Med Care. 2001;39(8):800-812. PubMed
25.Feld JJ, Foster GR, Bourliere M, et al. 907: Safety and efficacy of sofosbuvir/velpatasvir for the treatment of chronic hepatitis c infection in adolescents and children aged 3 to 17 years old through 24 weeks post-treatment. Hepatology. 2020;72(S1):554A. https://aasldpubs.onlinelibrary.wiley.com/doi/10.1002/hep.31579. Accessed 2023 Aug 22.
26.Gilead Sciences. NCT03022981: A Phase 2, Open-Label, Multicenter, Multi-cohort Study to Investigate the Safety and Efficacy of Sofosbuvir/Velpatasvir in Adolescents and Children With Chronic HCV Infection. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2020: https://clinicaltrials.gov/study/NCT03022981?tab=results. Accessed 2023 Aug 22.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 5: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of treatment |
|---|---|---|---|---|
Mizuochi et al. (2023)21 Japan Funding source: Research Program on Hepatitis from the Japanese Agency for Medical Research and Development | Nonrandomized, open-label, single arm, multicentre study (13 sites) Sample size calculation: NR ITT: Yes | Adolescents (N = 25) with chronic HIV genotype 1 to 2 infection, without cirrhosis or coinfection with HIV-1 or HBV. Median age (range), years: 13 (12 to 17) Sex, n (%):
HCV genotype, n (%):
Prior HCV treatment, n (%)
HIV-1 or HBV coinfection: 0 Perinatal transmission, n (%): 25 (100) | Intervention: Adult regimen of GLE and PIB (300 mg and 120 mg), orally with food once daily, for 8 to 12 weeks. Comparator: None | Outcomes:
Treatment, n (%):
|
Jonas et al. (2021)23 (Part 2 of DORA study) Multinational Funding source: AbbVie | Phase 2/3, nonrandomized, open-label, single arm, multicentre study (38 sites in North America, Europe and Japan). Sample size calculation: Yes ITT: Yes (all patients receiving at least 1 dose of study drug). | Children (N = 80) aged 3 to < 12 years with chronic HCV genotype 1 to 6 infection (HCV RNA ≥ 1,000 IU/mL), without cirrhosis. Median age (range), years: 7 (3 to 11) Sex, n (%):
Race, n (%):
HCV genotype, n (%):
Prior HCV treatment, n (%)
Stages of fibrosis, n (%):
HCV/HIV coinfection, n (%):
The population was divided into 3 subgroups:
| Intervention: Final dosages of GLE + PIB were based on weight at screening: • Subgroup 1 (12 kg to < 20 kg): GLE 150 mg + PIB 60 mg • Subgroup 2 (20 kg to < 30 kg): GLE 200 mg + PIB 80 mg • Subgroup 3 (30 kg to < 45 kg): GLE 250 mg + PIB 100 mg Pediatric formulations were prepared as small film-coated granules taken with a small amount of food once daily for 8, 12, or 16 weeks depending on HCV genotype, cirrhosis status, and prior treatment. Comparator: None | Outcomes:
Treatment, n (%):
|
Jonas et al. (2020)22 (Part 1 of DORA study) Multinational Funding source: AbbVie | Phase 2/3, nonrandomized, open-label, multicentre study (38 sites in North America, Europe and Japan). Sample size calculation: Yes ITT: Yes (all patients receiving at least 1 dose of study drug). | Adolescents (N = 47) aged 12 to 17 years with chronic HCV genotype 1 to 4 infection (HCV RNA ≥ 1,000 IU/mL), without cirrhosis. Median age (range), years: 14 (12 to 17) Sex, n (%):
Race, n (%):
HCV genotype, n (%):
Prior HCV treatment, n (%)
Stages of fibrosis, n (%):
HCV/HIV coinfection, n (%):
Perinatal transmission, n (%): 40 (85) | Intervention: Adult regimen of GLE and PIB (300 mg and 120 mg), orally with food once daily, for 8 to 16 weeks. Comparator: None | Outcomes:
Treatment, n (%):
|
AE = adverse event; DORA = DAA fOr CuRe of HepAtitis; GLE = Glecaprevir; HBV = hepatitis B virus; HCV = hepatitis C virus; HIV = HIV; INF = interferon; ITT = intention-to-treat; IU = international unit; PedsQL = Pediatric Quality of Life Inventory; PIB = Pibrentasvir; QoL = quality of life; RNA = ribonucleic acid; SVR 12 = sustained virologic response 12 weeks after treatment.
aSVR12 was defined as undetectable HCV-RNA (target not detected) at week 12 after the end of treatment.
bSVR12 was defined as HCV RNA less than the lower limit of quantification (15 IU/mL) 12 weeks after the last actual dose of the study drug.
cPedsQL scale is a patient-reported outcomes instrument validated in studies of the pediatric patients who have chronic health conditions. There are 23 items comprising 4 Generic Core Scales: Physical Functioning (8 items), Emotional Functioning (5 items), Social Functioning (5 items), and School Functioning (5 items). Two Summary Scores can be computed as the Psychosocial Health Summary Score and the Physical Health Summary Score, as well as a Total Scale Score. Higher scores indicate better health-related quality of life.
Note that this appendix has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 6: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist19
Strengths | Limitations |
|---|---|
Mizuochi et al. (2023)21 | |
Reporting:
External validity:
Internal validity – bias:
| Internal validity – confounding:
|
Jonas et al. (2020, 2021)22,23 (Part 1 and Part 2 of DORA Study) | |
Reporting:
External validity:
Internal validity – bias:
Internal validity – confounding: A sample size calculation was performed to adequately characterize the pharmacokinetics of the intervention. | Internal validity – confounding: This was a nonrandomized, open-label study, without a control group. Blinding was therefore not feasible as this is an open-label study. Patients with knowledge of the assignment may drop out from the trial, leading to missing data. |
ITT = intention-to-treat.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 7: Summary of Findings by Outcome — Sustained Virologic Response
Assessment | Mizuochi et al. (2023)21 | The DORA Study | ||||
|---|---|---|---|---|---|---|
Part 122 | Part 223 | |||||
12 to 17 years | 12 to 17 years | 3 to 5 years | 6 to 8 years | 9 to 11 years | 3 to 11 years | |
SVR12, % (n/N) | 96 (24/25) | 100 (47/47) | 96 (23/24) | 100 (27/27) | 93 (27/29) | 96.3 (77/80) |
95% CI, (%) | – | (92.4 to 100.0) | (80 to 99) | (88 to 100) | (78 to 98) | (90 to 99) |
CI = confidence interval; SVR12 = sustained virologic response 12 weeks after treatment.
Table 8: Summary of Findings by Outcome — Safety and Tolerability
Assessment | Mizuochi et al. (2023)21 | The DORA Study | |
|---|---|---|---|
Part 122 | Part 223 | ||
12 to 17 years | 12 to 17 years | 3 to 11 years | |
Adverse event, % (n/N) | |||
Any AE | 24 (6/25) | 87 (41/47) | 71 (57/80) |
Serious AE | 0 | 0 | 0 |
Discontinuation due to AE | 0 | 0 | 1 (1/80) |
All-cause mortality | – | 0 | 0 |
Details of AEs, % (n/N) | |||
Nasopharyngitis | – | 26 (12/47) | – |
Upper respiratory tract infection | – | 19 (9/47) | – |
Viral infection | 4 (1/25) | 0 | 5 (4/80) |
Abdominal pain | 4 (1/25) | 4 (2/47) | 4 (3/80) |
Nausea | 4 (1/25) | 9 (4/47) | 6 (5/80) |
Vomiting | – | 11 (5/47) | 14 (11/80) |
Diarrhea | – | 6 (3/47) | 14 (11/80) |
Headache | – | 17 (8/47) | 10 (8/80) |
Pyrexia | – | 11 (5/47) | 6 (5/80) |
Fatigue | – | 11 (5/47) | 9 (7/80) |
Oropharyngeal pain | – | 11 (5/47) | 1 (1/80) |
Pruritus | 4 (1/25) | 0 | 4 (3/80) |
Rash | 4 (1/25) | 2 (1/47) | 4 (3/80) |
Laboratory abnormalities, % (n/N) | |||
Virologic failure | 0 | 0 | 0 |
Post-treatment relapse | – | 0 | 1 (1/78) |
HCV reinfection | – | 0 | 0 |
Liver-related toxicities | 0 | 0 | 0 |
Drug-induced liver injury | 0 | 0 | 0 |
AE = adverse event.
Table 9: Summary of Findings by Outcome — Quality of Life
Assessment | The DORA Study, Part 122 | ||
|---|---|---|---|
Psychosocial score | Physical score | Total score | |
PedsQL, mean change from baseline (SD) | 2.4 (9.2) | 2.0 (9.2) | 2.3 (7.7) |
PedsQL = Pediatric Quality of Life Inventory; SD = standard deviation.
Table 10: Summary of Findings by Outcome — Growth and Development
Assessment | Mizuochi et al. (2023)21 | The DORA Study, Part 122 |
|---|---|---|
Height z score, mean change from baseline (SD) | + 0.02 (1.8); P = 0.93 | −0.1 (NR); NS |
BMI z score, mean change from baseline (SD) | + 0.11 (1.6); P = 0.03 | + 0.1 (NR); NS |
NR = not reported; NS = not statistically significant; SD = standard deviation.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca.