CADTH Health Technology Review
Somatropin for Short Stature
Rapid Review
Authors: Camille Santos, Jennifer Horton
Abbreviations
GH
growth hormone
IGF-I
insulin-like growth factor 1
ISS
idiopathic short stature
PES
Pediatric Endocrine Society
SDS
standard deviation score
SGA
small for gestational age
Key Messages
For children with short stature who were born small for gestational age, 1 guideline suggests increasing human growth hormone dose when treatment response is unsatisfactory, while aiming for normal insulin-like growth factor 1 levels.
For children with idiopathic short stature, 1 guideline recommends against the routine use of growth hormone. It suggests initiating growth hormone therapy on a case-by-case basis, with a starting dose ranging from 0.24 mg/kg/week to 0.47 mg/kg/week, as well as conducting an assessment 12 months after initiation to optimize dosage.
The development of recommendations from guidelines included in this report was challenged by limited relevant evidence, as well as heterogeneity of growth hormone dose and frequency and treatment response found in available literature. Future guidelines should also consider patient perspectives, resource implications, and the facilitators of and barriers to therapy within the context of health care systems in Canada.
Context and Policy Issues
What Is Short Stature?
An individual with short stature is at or below the third percentile for height within their respective age and sex category.1 Genetics (familial short stature) and constitutional growth delay are common and nonpathologic causes of short stature in children.2 However, short stature can be a manifestation of an underlying disease or condition, such as endocrine disorders (e.g., growth hormone deficiency), genetic disorders (e.g., Turner syndrome, Prader-Willi syndrome), and chronic illness (e.g., chronic kidney disease).2,3 It can also be a side effect of medication or an indication of malnutrition in children.2 The treatment of short stature is determined by its etiology,2 and associated psychosocial distress should be managed.1
Around 10% of babies born small for gestational age (SGA) are living with short stature well into adulthood.4 Babies born SGA are below the 10th percentile for weight for the number of weeks of pregnancy.5 Being born SGA can be caused by a variety of factors, such as inadequate supply of nutrients to the fetus or poor maternal health status.5 In addition to risk of short stature, babies born SGA are at risk of perinatal complications, such as premature delivery and hypoxic stress.5 In Canada, babies born SGA represented 8% of live births in 2016.6
In certain cases, short stature occurs without a known cause; this is referred to as idiopathic short stature (ISS).7 Children with ISS are born near or at average length and weight with no signs of an underlying disorder.7 To our knowledge, the number of children living with ISS in Canada is not readily available.
What Is Somatropin?
Growth hormone (GH) is a peptide hormone produced by the pituitary gland and is essential for human growth. It stimulates tissue, bone, and linear growth, as well as the metabolism of proteins, fats, and carbohydrates.8,9 Somatropin, a recombinant form of human GH, is used to treat a variety of conditions, such as growth hormone deficiency and short stature.4,10 In children, it aims to stimulate growth to ultimately achieve adult height in the normal range.1 Some potential side effects noted in the literature for GH therapy in children born SGA are impaired glucose tolerance, intracranial hypertension, pancreatitis, musculoskeletal complications, and aggravation of existing scoliosis.11-15 For children with ISS, some potential side effects of GH therapy are headaches, changes in mood, increased appetites, and gastrointestinal and musculoskeletal complications.11,12,14 There are also concerns regarding long-term use of GH therapy in children, specifically increased risk of mortality and cancer.3,10
Why Is It Important to Do This Review?
Currently, 6 somatropin products are approved for pediatric use in Canada,12-16 with the approval dependent on the underlying cause of short stature.17 The products approved for children born SGA are Genotropin,11 Humatrope,12 Norditropin,13 Omnitrope,14 and Saizen.15 For children with ISS, the approved somatropin products are Genotropin,11 Humatrope,12 and Omnitrope.14
The treatment of children with short stature born SGA and ISS is primarily privately funded in Canada,18 which can limit access to therapy. Evidence-based guidelines regarding somatropin use may be helpful to inform reimbursement criteria and clinical decision-making. This Rapid Review summarizes the recommendations related to the use of somatropin for children with short stature born SGA and children with ISS.
This report was informed by 2 published Reference Lists by CADTH: Somatropin for Short Stature Secondary to Small for Gestational Age19 and Somatropin for Idiopathic Short Stature.20 CADTH also published 2 Rapid Reviews on evidence-based guidelines related to the use of somatropin for other indications: 1 for children living with Turner syndrome21 and 1 for children living with GH deficiency.22
Objective
The purpose of this Rapid Review is to summarize and critically appraise evidence-based guidelines regarding the use of somatropin for the treatment of short stature, specifically for children born SGA and children with ISS.
Research Questions
What are the evidence-based guidelines regarding the use of growth hormone therapy for children with short stature secondary to being small for gestational age?
What are the evidence-based guidelines regarding the use of growth hormone therapy for children with idiopathic short stature?
Methods
Literature Search Methods
Limited literature searches were conducted for 2 previous CADTH reports19,20 by an information specialist on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, and the websites of Canadian and major international health technology agencies, as well as a focused internet search. Results of the searches for these reports were incorporated into the current reports and comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concept for the first search was human growth hormone.19 CADTH-developed search filters were applied to limit retrieval to guidelines. The search was completed on June 6, 2023, and limited to English-language documents published since January 1, 2013. The main search concepts for the second search were human growth hormone and idiopathic short stature.20 CADTH-developed search filters were applied to limit retrieval to guidelines. The search was completed on June 14, 2023, and limited to English-language documents published since January 1, 2013.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Q1: Children (< 18 years old) with short stature secondary to being small for gestational age Q2: Children (< 18 years old) with idiopathic short stature |
Intervention | All somatropin products |
Comparator | NA |
Outcomes | Recommendations regarding best practices (e.g., dose and timing of treatment, duration of treatment, laboratory cut-offs for eligibility, monitoring treatment response) |
Study designs | Evidence-based guidelines |
NA = not applicable.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or they were published before 2013. Guidelines with unclear or alternative methodology were not included in the text, but their characteristics and findings are presented in Appendix 5. Guidelines with alternative methodology were devoid of systematic methods to inform their development.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument23 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
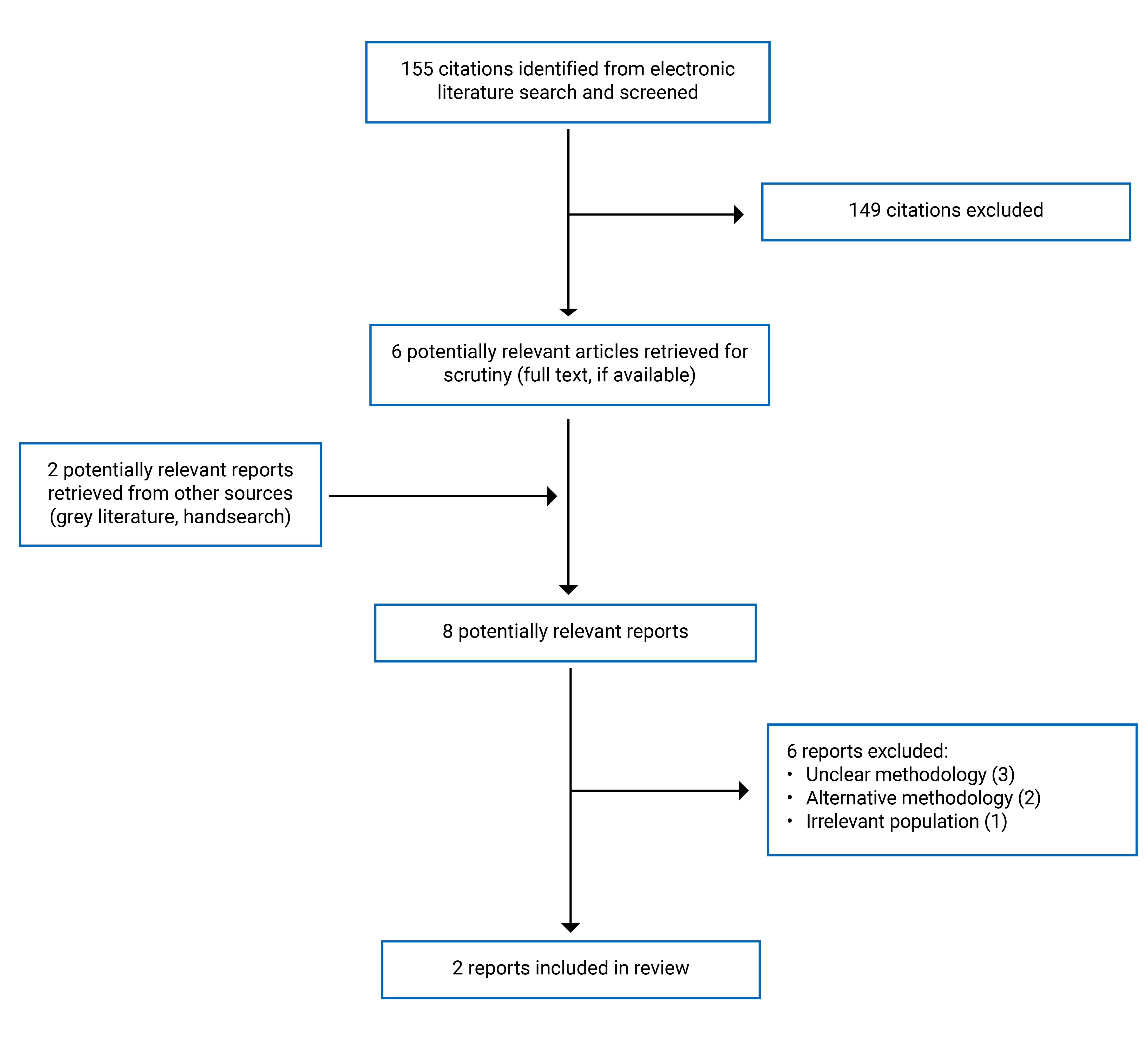
This report includes 2 evidence-based guidelines10,24 screened from 155 citations identified in the literature search. The study selection details are presented in Appendix 1. This report also includes 5 guidelines3,25-28 summarized in Appendix 5 with unclear or alternative methodology and therefore considered not to be evidence-based.
Summary of Guideline Characteristics
Detailed characteristics of included evidence-based guidelines are provided in Appendix 2.
Short Stature Secondary to SGA
We identified 1 position statement that provided recommendations regarding GH therapy in children with short stature secondary to SGA, published in 2016 by Allen et al.10 The European Society of Pediatric Endocrinology, GH Research Society, and the Pediatric Endocrine Society (PES) developed the position statement detailing the discussions regarding the safety of GH therapy for adults and children during an in-person workshop.10 They used 2 systematic reviews to inform their recommendations,29,30 and they sought a majority vote in cases where agreement was not reached.10 They did not assess the quality of evidence or strength of recommendations.10
Idiopathic Short Stature
We identified 1 guideline published in 2016 by the PES that provided recommendations regarding GH therapy in children and adolescents with ISS.24 Two reviewers conducted a systematic review for each research question and drafted recommendations. The reviewers appraised the quality of evidence using the Grading Recommendations, Assessment, Development, and Evaluation (GRADE) framework.24 A taskforce then sought consensus on the draft recommendations and assessed the strength of recommendations (strong or conditional).24
Summary of Critical Appraisal
Both guidelines provided a description of their overall objectives, key questions, and target populations to which they apply.10,24 The target users of the guidelines were inferred to be clinicians involved in the management of populations of interest treated with GH therapy.10,24
Both guidelines used systematic methods to search for evidence and detailed the voting process to finalize recommendations.10,24 A variety of relevant clinical and research professionals were involved in the development of both guidelines.10,24 However, it is unclear whether perspectives or preferences of their target populations were sought and if they influenced the development of recommendations for both guidelines. Although both guidelines were published in peer-reviewed journals, no explicit external review process was detailed.10,24 These factors may have implications on the feasibility and validity of the guidelines for clinical practice and decision-making.
The PES assessed the strength of its recommendations and quality of evidence, and spoke to the potential benefits, side effects, and risks of GH therapy from the literature.24 The same guideline detailed the link between the recommendation and supporting evidence.24 Conversely, the guideline by Allen and colleagues10 is a position statement intended to detail discussions regarding the safety of GH therapy. It excluded a formal quality assessment typically expected when developing evidence-based recommendations. Allen and colleagues10 acknowledged that data on the safety of GH therapy were primarily from postmarket surveillance data due to lack of relevant randomized controlled trials.10 This is reflected in the absence of cited evidence to support the relevant recommendation and the acknowledgement that the topic has not been thoroughly evaluated in the literature.10 Hence, the target users may feel uncertain about the quality of the recommendations outlined in the guideline by Allen and colleagues10 given the limited evidence to support the recommendation.
The relevant recommendations by the PES were specific and unambiguous,24 whereas the guideline by Allen and colleagues lacked specific information regarding dosage, as well as a definition for an appropriate treatment response.10 The guideline by the PES touched on the high cost of GH therapy, but the intent to consider and discuss the facilitators and barriers to implementation was not apparent in the publication. Similarly, the guideline by Allen and colleagues10 lacked discussion of the facilitators and barriers, and the potential resource implications of applying the relevant recommendations. These factors can have implications on the feasibility and appropriateness of providing GH therapy within the context of the individual receiving care. However, the recommendation from the guideline by Allen and colleagues10 provided guidance related to monitoring treatment response limited to insulin-like growth factor 1 (IGF-I) levels, which may help inform reimbursement criteria.
Each guideline disclosed the competing interests of its development group.10,24 The PES covered expenses related to an in-person meeting.24 None of the taskforce members received remuneration for other work from the PES or any commercial entity.24 However, it is unclear if and how reviewers who conducted the systematic review and drafted recommendations were compensated. The guideline by Allen and colleagues10 did not disclose how the competing interests were addressed and how the funding group may have influenced the development of recommendations.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Recommendations
Appendix 4 presents relevant recommendations from the evidence-based guidelines.
Short Stature Secondary to SGA
The position statement by Allen et al. (2016) focused on the safety of GH therapy and provided some guidance on monitoring treatment response.10 The guideline stated that GH dose can be increased within the recommended range in cases of unsatisfactory growth response, which can then result in IGF-I levels above normal (> + 2 standard deviation score [SDS]).10 While the guideline suggests that temporary increases in IGF-I levels do not likely present a safety concern, it recommends aiming for IGF-I levels within the normal range.10 This guideline did not specify the recommended GH dose or establish how unsatisfactory growth response is defined, nor did it provide the strength of the recommendation or assess the quality of underlying evidence.10
Idiopathic Short Stature
The PES recommends against the routine use of GH for every child with a height SDS less than or equal to −2.25 (conditional recommendation informed by moderate quality evidence), in consideration of the varied treatment response in the literature.24 They suggest shared decision-making and a case-by-case approach when initiating GH therapy, with an assessment of physical and psychological burdens and discussions of risks and benefits.24 They recommend a starting GH dose of 0.24 mg/kg/week, with some children requiring up to 0.47 mg/kg/week (conditional recommendation informed by low-quality evidence).24 After 12 months of GH therapy, the PES suggests a follow-up to optimize dosage by assessing height SDS and psychosocial impact (conditional recommendation informed by low-quality evidence).24
Limitations
Generalizability
The strategies used to search for evidence to inform both guidelines were inclusive and did not limit studies from certain populations.10,24 However, the guideline by the PES is limited to English-language studies, which may have excluded evidence from certain regions. It is unclear where studies used to inform both guidelines were conducted. Additionally, it is possible that relevant recommendations by the PES24 are applicable only to children living in the US, given that 1 recommendation is specific to FDA criteria approved for GH therapy in children with ISS.24 There is general alignment between the FDA and Health Canada regarding recommended doses for somatropin products available in Canada. However, Saizen is approved for children with ISS by the FDA but not by Health Canada.15,31 It is unclear how generalizable the guidelines and considered evidence are within the context of the health care systems and children living in Canada.
Heterogeneity, Quality, and Quantity of the Supporting Evidence
Both guidelines acknowledged the challenges in developing detailed and specific recommendations for GH therapy in children with short stature.10,24 The literature revealed a varied treatment response from children with short stature from GH therapy, and heterogeneity in frequency and dosage of GH in studies.10,24 Both guidelines acknowledged the limited number of studies available to inform recommendations related to GH therapy use.10,24 The guidelines by the PES24 rated available evidence used to inform recommendations for ISS from low to moderate. The guideline by Allen and colleagues24 was dependent on postmarket surveillance for data and identified a lack of randomized controlled trials assessing the safety of GH therapy. Additionally, the recommendation regarding IGF-I levels lacked supporting evidence regarding the risk of complications with levels above normal, and reflects discussions between experts.10
Quality of Guidelines for Children Born SGA
Target users may feel uncertain about implementing recommendations in the guideline by Allen and colleagues,10 given some methodological limitations in its development. Specifically, it lacked a formal assessment of the supporting evidence and did not assign strength to recommendations, which is characteristic of comprehensive and rigorous evidence-based guidelines. While the guideline is a position statement that provided insight on the discussions between experts related to the safety of GH therapy, the resulting recommendation had unclear links to the evidence.10
Patient Engagement and Implementation Considerations
Both guidelines did not explicitly consider the perspectives and preferences of children with short stature or their caretakers.10,24 The guidelines may have missed and disregarded relevant outcomes that are a priority to the target population. In terms of implementation considerations, the PES touched on the high cost of therapy,24 but both guidelines did not state any intent to consider facilitators of and barriers to GH therapy during development.
Conclusions and Implications for Decision- or Policy-Making
The height of children with short stature is below the average of their peers of the same age and sex. In Canada, a variety of somatropin products, or recombinant human GH, are approved for children with short stature born SGA and children with ISS.17 This Rapid Review summarized 2 evidence-based guidelines regarding the use and monitoring of GH therapy in children with short stature to inform clinical and policy decision-making. One guideline (a position statement) is relevant to children born SGA,10 whereas the other is relevant to children with ISS.24
Both guidelines recognized the potential benefit of GH therapy for children with short stature, but they also acknowledged the varied treatment frequency, dose, and response found in the literature.10,24 This led to ambiguity around appropriate dosing of GH and lack of specific and comprehensive monitoring criteria to initiate, modify, and discontinue therapy. For children born SGA, it is recommended to aim for normal IGF-I levels in children undergoing therapy, especially with GH doses at the higher end of recommended ranges. For children with ISS, the PES recommends a starting dose from 0.24 mg/kg/week to 0.47 mg/kg/week.24 However, the PES suggests a case-by-case approach versus routine use when considering GH therapy.24
There are some limitations to consider when using these guidelines to inform clinical and policy decision-making. The validity and feasibility of the relevant recommendations may be impacted by the absence of an external review and the perspectives of its target population.10,24 The recommendation regarding IGF-I levels for children born SGA undergoing GH therapy lacks supporting evidence and likely reflects expert opinion.10 This recommendation was derived from a position statement highlighting discussions between experts that lacked an assessment of evidence quality and recommendation strength.10 For children with ISS, the conditional recommendations were informed by low to moderate quality evidence.24 There was also minimal discussion about the feasibility of providing GH therapy and it is unclear to what extent these recommendations can be applied within the context of children with short stature living in Canada. Both guidelines acknowledged the challenges in developing specific recommendations given the heterogeneity in treatment response, frequency, and dosage in the literature, as well as the limited number of relevant studies and clinical data available.10,24 To supplement these findings, this Rapid Review provides a narrative summary, without critical appraisal, of related publications of potential interest that were not considered to be evidence-based guidelines in Appendix 5.
Considerations for Future Work
Future research and evidence-based guidelines regarding somatropin use for children with short stature should consider criteria to initiate, modify, and discontinue therapy, as well as when and how treatment response should be evaluated. Beyond safe IGF-I levels, the evidence-based guidelines lacked discussion around clinical parameters to monitor and a definition of a satisfactory growth response. These considerations would help further inform clinical and policy decision-making.
Implications for Clinical Practice and Decision-Making
The findings of this report suggest that somatropin may be appropriate for managing children with short stature secondary to SGA and children with ISS. However, treatment response, in terms of growth, can vary. This leads to uncertainty when initiating or modifying dosages, and when continuing somatropin to manage short stature for these indications. Health care professionals may need to exercise clinical judgment in assessing the appropriateness of somatropin for each child living with short stature receiving care. Decision-makers may require more specific and unambiguous guidance informed by high-quality evidence, perspectives of the target population, and formal review by external experts in the field to establish comprehensive reimbursement criteria for somatropin. The guideline should consider resource implications and the facilitators of and barriers to GH therapy in the context of Canada’s health care systems.
References
1.Rani D, Shrestha R, Kanchan T, Krishan K. Short Stature. Treasure Island (FL): StatPearls Publishing. 2023. https://www.ncbi.nlm.nih.gov/books/NBK556031/ Accessed 2023 Aug 4.
2.Richmond EJ, Rogol AD. Causes of Short Stature. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2023: www.uptodate.com Accessed 2023 Aug 4.
3.Collett-Solberg PF, Ambler G, Backeljauw PF, et al. Diagnosis, Genetics, and Therapy of Short Stature in Children: A Growth Hormone Research Society International Perspective. Horm Res Paediatr. 2019;92(1):1-14. PubMed
4.Deodati A, Cianfarani S. The Rationale for Growth Hormone Therapy in Children with Short Stature. J Clin Res Pediatr Endocrinol. 2017;9(Suppl 2):23-32. PubMed
5.Osuchukwu O, Reed J. Small for Gestational Age. Treasure Island (FL): StatPearls Publishing. 2022. https://www.ncbi.nlm.nih.gov/books/NBK563247/. Accessed 2023 Aug 2.
6.Why are babies in Canada getting Smaller? Ottawa (ON): Statistics Canada. 2022. https://www150.statcan.gc.ca/n1/pub/82-003-x/2022001/article/00001-eng.htm Accessed 2023 Aug 22.
7.Halas JG, Grimberg A. Dilemmas of growth hormone treatment for GH deficiency and idiopathic short stature: defining, distinguishing, and deciding. Minerva Pediatrica. 2020;72(3):206-225. PubMed
8.Health Link BC. Somatropin - Injection. https://www.healthlinkbc.ca/medications/somatropin-injection. 2021. Accessed 2023 Aug 4.
9.U.S. Food and Drug Administration. Somatropin information. Postmarket Drug Safety Information for Patients and Providers. 2015; https://www.fda.gov/drugs/postmarket-drug-safety-information-patients-and-providers/somatropin-information. Accessed 2023 Aug 4.
10.Allen DB, Backeljauw P, Bidlingmaier M, et al. GH safety workshop position paper: a critical appraisal of recombinant human GH therapy in children and adults. Eur J Endocrinol. 2016;174(2):P1-9. PubMed
11.Genotropin GoQuick (somatropin): 5mg, 5.3mg, 12mg pre-filled pen; and Genotropin MiniQuick (somatropin): 0.2mg, 0.4mg 0.6mg, 0.8mg, 1.0mg, 1.2mg, 1.4mg, 1.6mg, 1.8mg, and 2.0mg pre-filled syringe [product monograph]. Kirkland (QC): Pfizer Canada ULC. 2020 Jun 22. https://pdf.hres.ca/dpd_pm/00056686.PDF Accessed 2023 Aug 31.
12.Humatrope (somatropin for injection): 5mg vial; 6, 12, 24mg cartridges [product monograph]. Toronto (ON): Eli Lilly Canada Inc. 2020 Jun 19. https://pdf.hres.ca/dpd_pm/00056950.PDF Accessed 2023 Aug 31.
13.Norditropin FlexPro (somatropin): 5mg/1.5mL, 10mg/1.5mL, and 15mg/1.5mL solution for subcutaneous administration; and Norditropin NordiFlex (somatropin): 5mg/1.5mL, 10mg/1.5mL, and 15mg/1.5mL solution for subcutaneous administration [product monograph]. Mississauga (ON): Novo Nordisk Canada Inc. 2022 Jul 19. https://pdf.hres.ca/dpd_pm/00066739.PDF Accessed 2023 Aug 31.
14.Omnitrope (somatropin): 5.8mg/vial lyophilized powder for solution; and 5mg/1.5mL, 10mg/1.5mL, 15mg/1.5mL solution for injection [product monograph]. Boucherville (QC): Sandoz Canada Inc. 2022 Nov 1. https://pdf.hres.ca/dpd_pm/00068010.PDF Accessed 2023 Aug 31.
15.Saizen (somatropin): 5mg/vial lyophilized powder for injection; and 6mg, 12mg, 20mg solution for injection in a cartridge [product monograph]. Mississauga (ON): EMD Serono. 2020 Jun 8. https://pdf.hres.ca/dpd_pm/00056674.PDF Accessed 2023 Aug 31.
16.Nutropin AQ NuSpin (somatropin): 5mg/2mL, 10mg/2mL, 20mg/2mL injection device prefilled with cartridge [product monograph]. Mississauga (ON): Hoffmann-La Roche Limited. 2018 Jun 5. https://pdf.hres.ca/dpd_pm/00045938.PDF Accessed 2023 Aug 31.
17.Clinical Review Report: somatropin (Genotropin). Ottawa (ON): CADTH. 2014. https://www.cadth.ca/sites/default/files/cdr/clinical/SR0332_GenotropinGHD-A_CL_Report_e.pdf. Accessed 2023 Jul 20.
18.Deal C, Kirsch S, Chanoine JP, Lawrence S, Cummings E, Rosolowsky ET, Marks SD, Jia N, Child CJ; GeNeSIS National Board on behalf of the GeNeSIS Canada Investigators. Growth hormone treatment of Canadian children: results from the GeNeSIS phase IV prospective observational study. CMAJ Open. 2018;6(3):E372-E383. PubMed
19.Somatropin for Short Stature Secondary to Small for Gestational Age. Ottawa (ON): 2023. https://www.cadth.ca/somatropin-short-stature-secondary-small-gestational-age Accessed 2023 Jul 20.
20.Somatropin for Idiopathic Short Stature. Ottawa (ON): CADTH. 2023. https://www.cadth.ca/somatropin-idiopathic-short-stature Accessed 2023 Jul 20.
21.Somatropin for Turner Syndrome. Ottawa (ON): CADTH. 2023. https://www.cadth.ca/somatropin-turner-syndrome Accessed 2023 Aug 4.
22.Somatropin for Growth Hormone Deficiency. Ottawa (ON): CADTH. 2023. https://www.cadth.ca/somatropin-growth-hormone-deficiency Accessed 2023 Aug 4.
23.Agree Next Steps C. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2023 Aug 4.
24.Grimberg A, DiVall SA, Polychronakos C, et al. Guidelines for Growth Hormone and Insulin-Like Growth Factor-I Treatment in Children and Adolescents: Growth Hormone Deficiency, Idiopathic Short Stature, and Primary Insulin-Like Growth Factor-I Deficiency. Horm Res Paediatr. 2016;86(6):361-397. PubMed
25.Corripio-Collado R, Fernandez-Ramos C, Gonzalez-Casado I, Moreno-Macian F, Lopez-Siguero JP, Labarta-Aizpun JI. Delphi consensus on the diagnosis and treatment of patients with short stature in Spain: GROW-SENS study. J Endocrinol Invest. 2022;45(4):887-897. PubMed
26.Standard treatment guidelines 2022: Approach to short stature. Mumbai (India): Indian Academy of Pediatrics. 2022. https://iapindia.org/pdf/Ch-097-Approach-to-Short-Stature.pdf Accessed 2023 Jul 20.
27.Somatropin for the treatment of growth failure in children. Singapore (Singapore): Ministry of Health Singapore. 2017. https://www.ace-hta.gov.sg/healthcare-professionals/ace-technology-guidances/details/somatropin-for-the-treatment-of-growth-failure-in-children Accessed 2023 Jul 20.
28.Al Herbish AS, Almutair A, Bin Abbas B, et al. Diagnosis and management of growth disorders in Gulf Cooperation Council (GCC) countries: Current procedures and key recommendations for best practice. Int J Pediatr Adolesc Med. 2016;3(3):91-102. PubMed
29.Stochholm K, Johhannsson G. Reviewing the safety of GH replacement therapy in adults. Growth Horm IGF Res. 2015;25(4):149-157. PubMed
30.Deodati A, Ferroli BB, Cianfarani S. Association between growth hormone therapy and mortality, cancer and cardiovascular risk: Systematic review and meta-analysis. Growth Horm IGF Res. 2014;24(4):105-111. PubMed
31.Saizen (somatropin) for subcutaneous or intramuscular injection [label]. Rockland (MA): EMD Serono, Inc. 2007. https://www.accessdata.fda.gov/drugsatfda_docs/label/2007/019764s035lbl.pdf Accessed 2023 Aug 31.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Evidence-Based Guidelines
Intended users, target population | Relevant intervention and major outcomes considered | Evidence synthesis, collection, and assessment | Recommendation development and evaluation | Guideline validation |
|---|---|---|---|---|
Allen et al. (2016)10 | ||||
Intended users: Clinicians involved in the management of individuals treated with recombinant human GH therapy Target population: Adults and children treated with recombinant human GH therapy | Relevant intervention: Recombinant human GH therapy Outcomes considered: All-cause, cancer, and cardiovascular standard mortality ratio; SIR for cancer; RR for second neoplasms | Two published systematic reviews and available postmarket surveillance data were used as evidence. The quality of the evidence was not assessed because no RCTs on the safety of GH was identified. | The European Society of Pediatric Endocrinology, the GH Research Society, and the PES discussed the evidence and developed the final statements. When no agreement was reached on specific points, a majority vote was done. If a majority was not reached, statements were revised, and voting was done until consensus was reached. Representatives of pharmaceutical companies participated in discussions, but they were not involved in the writing and voting process. They reviewed the manuscript for factual errors about their data. | The position statement was published in a peer-reviewed journal. |
PES, Grimberg et al. (2016)24 | ||||
Intended Users: Clinicians involved in the management of children with GHD, ISS, or PIGFD Target Population: Children and adolescents with growth failure from GHD, ISS, or PIGFD | Relevant Intervention: GH treatment Outcomes considered: Adult height, mean height gain, growth response | A systematic review was conducted by 2 reviewers based on a series of key questions. The GRADE system was used to determine the quality of evidence (from very low to high). | The GRADE system was used to draft and evaluate recommendations (strong or conditional). A taskforce of 7 pediatric endocrinologists and 1 pediatric bioethicist discussed the draft recommendations and evidence to determine the strength of the recommendation (conditional or strong) at an in-person meeting. At least 6 of the 8 members of the taskforce must agree to achieve consensus. Any further deliberation regarding the recommendations were conducted via teleconference or email. | The guideline was published in a peer-reviewed journal. |
GH = growth hormone; GHD = growth hormone deficiency; GRADE = Grading of Recommendations, Assessment, Development, and Evaluations; ICER = incremental cost-effectiveness ratio; IGF-I = insulin-like growth factor 1; ISS = idiopathic short stature; PES = Pediatric Endocrine Society; PIGFD = primary insulin-like growth factor-I deficiency; RCT = randomized controlled trial; RR = relative risk; SIR = standardized incidence ratio; SMR = standard mortality ratio.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Guidelines Using AGREE II23
Item | Allen et al. (2016)10 | Pediatric Endocrine Society, Grimberg et al. (2016)24 |
|---|---|---|
Domain 1: Scope and purpose | ||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes |
Domain 2: Stakeholder involvement | ||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Unclear | Unclear |
6. The target users of the guideline are clearly defined. | Yes | Yes |
Domain 3: Rigour of development | ||
7. Systematic methods were used to search for evidence. | Yes | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Na | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes |
13. The guideline has been externally reviewed by experts before its publication. | No | No |
14. A procedure for updating the guideline is provided. | No | No |
Domain 4: Clarity of presentation | ||
15. The recommendations are specific and unambiguous. | No | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes |
17. Key recommendations are easily identifiable. | No | Yes |
Domain 5: Applicability | ||
18. The guideline describes facilitators and barriers to its application. | Unclear | Unclear |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Unclear | Unclear |
20. The potential resource implications of applying the recommendations have been considered. | Unclear | Unclear |
21. The guideline presents monitoring and/or auditing criteria. | Yes | No |
Domain 6: Editorial independence | ||
22. The views of the funding body have not influenced the content of the guideline. | Unclear | Unclear |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; NA = not applicable.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 4: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
Allen et al. (2016)10 | |
When the growth response is unsatisfactory in children with short stature born SGA, the GH dose can be increased within the recommended range. Aiming for IGF-I levels in the normal range is recommended. (p. 6) Supporting evidence: No evidence that raising IGF-I above the normal range (> + 2 SDS) increases risk of adverse events. However, guideline authors recognize that this has not been thoroughly evaluated in the literature. | Strength of recommendation: NR Quality of evidence: NR |
Pediatric Endocrine Society, Grimberg et al.(2016)24 | |
Recommendation 6.1. (p. 364 and 381) “In the USA, for the children who meet FDA criteria, we suggest a shared-decision making approach to pursuing GH treatment for a child with ISS. The decision can be made on a case-by-case basis after assessment of physical and psychological burdens, and discussions of risks and benefits. We recommend against the routine use of GH in every child with HtSDS ≤ −2.25. Technical Remark: While studies have shown GH treatment increases the main height of treated cohorts, there is marked interindividual variability in responses, including some individuals who do not respond to treatment.” Supporting evidence (p. 381):
| Strength of recommendation: Conditional Quality of evidence: Moderate |
Recommendation 6.2. (p. 365 and 381) “We suggest a follow-up assessment of benefit in HtSDS and psychosocial impact 12 months after GH initiation and dose optimization.” Supporting evidence (p. 381 to 382): First year change in growth in predictive models suggest that assessment in 12 months may be used to predict long-term response (2 studies using registry data). | Strength of recommendation: Conditional Quality of evidence: Low |
Recommendation 6.3. (p. 365 and 382) “Because there is overlap in response between dosing groups, we suggest initiating GH at a dose of 0.24 mg/kg/week, with some patients requiring up to 0.47 mg/kg/week.” Supporting evidence (p. 382 to 383):
| Strength of recommendation: Conditional Quality of evidence: Low |
GH = growth hormone; HtSDS = height standard deviation score; IGF-I = insulin-like growth factor 1; ISS = idiopathic short stature; NR = not reported; RCT = randomized controlled trial; SD = standard deviation; SDS = standard deviation score; SGA = small for gestational age.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
We summarized recommendations from guidelines considered not to be evidence-based identified in the literature search for this Rapid Review. The purpose of this narrative summary is to supplement the findings from evidence-based guidelines included in the main body of this report. The methods to develop the following guidelines were either unclear or used nonsystematic methods (alternative methodology); however, these publications were not critically appraised further. Refer to Table 5 (Characteristics of Guidelines With Alternative or Unclear Methodology) for characteristics of the guidelines included in this section.
The Ministry of Health Singapore recommends the use of somatropin for children with short stature secondary to SGA with poor catch-up. However, the ministry recommends against the use of somatropin for children with ISS.27 The Indian Academy of Pediatrics26 and the review by Al Herbish and colleagues28 provided a treatment approach for GH therapy for children with SGA and ISS. The guideline by Corripio-Collado and colleagues25 sought expert consensus on the initiation and exclusion criteria for GH therapy. The Growth Hormone Research Society International provides guidance related to GH dosing in older SGA patients, SDS targets for ISS, and the addition of gonadotropin hormone-releasing hormone (GnRH) for children SGA.3 Refer to Table 6 (Summary of Recommendations From Guidelines With Alternative or Unclear Methodology).
Table 5: Characteristics of Guidelines With Alternative or Unclear Methodology
Intended users, target population | Intervention and major outcomes considered | Evidence collection, synthesis, and assessment | Recommendation development | Guideline validation |
|---|---|---|---|---|
Corripio-Collado et al. (2022)25 | ||||
Intended users: Clinical practitioners Target population: Children with short stature in Spain | Relevant intervention: GH therapy Outcomes considered: NR | Qualitative survey to collect opinions of a group of experts | Delphi consensus | NR |
Indian Academy of Pediatrics (2022)26 | ||||
Intended users: Pediatricians in India Target population: Children with short stature | Relevant intervention: GH Outcomes considered: NR | NR | NR | NR |
Growth Hormone Research Society International (2019)3 | ||||
Intended users: Health care providers Target population: Children with short stature | Relevant intervention: rhGH Outcomes considered: NR | A nonsystematic review of GH therapy for children with short stature was published before discussions with subject matter experts.a Forty-six GH experts provided expert perspective on the diagnosis and therapy of short stature in children during an in-person workshop. | The document outlining discussions was revised by participants. In cases with lack of consensus, a majority vote was done. | The document was shared with academic attendees for final review after the meeting. |
Ministry of Health Singapore (2017)27 | ||||
Intended users: Policy and clinical decision-makers; health care professionals in Singapore Target population: Children with Growth Failure (i.e., ISS, SGA with poor catch-up growth) | Relevant intervention: Somatropin Outcomes considered: Height, HtSDS, growth velocity, ICER, cost impact | NR | A committee deliberates the findings of the review and makes recommendations. | The guidance is shared with public health care for revisions. |
Al Herbish et al. (2016)28 | ||||
Intended users: Pediatric health care professionals Target population: Individuals with growth disorders in Gulf Cooperation Council Countries | Relevant intervention: Human GH therapy for SGA and ISS Outcomes considered: NA | A nonsystematic review of published guidelines and studies. | NA | NA |
GH = growth hormone; HtSDS = height standard deviation score; ICER = incremental cost-effectiveness ratio; ISS = idiopathic short stature; NA = not applicable; NR = not reported.; SGA = small for gestational age.
aReview article by Collett-Solberg et al. (2019) as cited in the publication by the Growth Hormone Research Society International.3
Table 6: Summary of Recommendations From Guidelines With Alternative or Unclear Methodology
Recommendations and rationale |
|---|
Corripio-Collado et al. (2022)25 |
The criteria considered indispensable for starting GH treatment in children with short stature born SGA are:
|
Silver-Russell syndrome is not considered an exclusion criterion for initiating GH treatment in children with short stature born SGA (88% consensus). |
Indian Academy of Pediatrics(2022)26 |
Indications and criteria for growth hormone therapy for children with ISS:
|
Indications and criteria for growth hormone therapy for SGA infants:
|
Growth Hormone Research Society International (2019)3 |
“In certain conditions, such as with older SGA patients and in the late diagnosis of Turner syndrome, it is recommended that rhGH be started at a dose that is at the higher end of the approved range.” (p. 8) |
“In non-GHD conditions, such as ISS, IGF-I levels of approximately 1+ SDS or higher as usual, but the target should be adjusted on an individual bases based on auxological measurements.” (p. 8) |
“…adding a GnRH analogue to rhGH therapy may be considered for children with GHD or SGA and/or Silver-Russell syndrome patients if height SDS is low at pubertal onset” (p. 9) |
Ministry of Health Singapore (2017)27 |
“The Ministry of Health’s Drug Advisory Committee has recommended somatropin (recombinant growth hormone) for the treatment of children with short stature due to conditions associated with growth failure. Treatment with somatropin should always be initiated and monitored by paediatric endocrinologist with specialist expertise in managing growth disorders in children.” Specific conditions associated with growth failure include growth hormone deficiency, SGA with poor catch-up growth, Prader-Willi syndrome, and chronic renal failure. Rationale: The committee agreed that somatropin is clinically effective compared to placebo in increasing height, HtSDS, or growth velocity for conditions under evaluation. The committee expressed concerns that SGA with poor catch-up is determined subjectively leading to potential increase in use. |
“Somatropin is not recommended for the treatment of ISS.” Rationale:
|
Al Herbish et al. (2016)28 |
Recommended approach and human GH treatment for patients with SGA (birth weight/length < -SD):
Key comments:
|
Recommended approach and hGH treatment regimens for patients with ISS:
Key comments:
|
GH = growth hormone; GHD = growth hormone deficiency; GnRH = gonadotropin hormone-releasing hormone; HtSDS = height standard deviation score; ISS = idiopathic short stature; NA = not applicable; NR = not reported; SD = standard deviation; RCT = randomized controlled trial; rhGH = recombinant human growth hormone; SDS = standard deviation score; SGA = small for gestational age.
aBased on UK National Institute for Health and Care Excellence (NICE) / European Medicines Agency guidance as cited in the publication by Al Herbish and colleagues (2016).28
bBased on FDA guidance as cited in the publication by Al Herbish and colleagues (2016).28
Contributors: Elizabeth Carson, Kim Le
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca