CADTH Health Technology Review
Timing of Ventilator Circuit Tubing Replacement
Rapid Review
Authors: Zahra Jafari, Melissa Severn
Abbreviations
AGREE
Appraisal of Guidelines for REsearch and Evaluation
AMSTAR-2
A MeaSurement Tool to Assess systematic Reviews 2
MA
meta-analysis
OR
odds ratio
RCT
randomized controlled trial
RR
risk ratio
SCS
sequential comparison study
SR
systematic review
VAP
ventilator-associated pneumonia
VCTR
ventilator circuit tubing replacement
Key Messages
In adult patients with mechanical ventilation, more frequent ventilator circuit tubing replacement may increase the odds of ventilator-associated pneumonia, but the findings are imprecise.
In pediatric patients with mechanical ventilation, more frequent and less frequent intervals of ventilator circuit tubing replacement may result in similar a risk of ventilator-associated pneumonia, all-cause mortality, and ventilator-associated pneumonia mortality, and similar durations of mechanical ventilation and hospital stay.
For preterm neonates, children, and adult patients, it is recommended to replace the ventilator circuit tubing if it is visibly soiled, not functioning properly, or as recommended in the manufacturer's instructions.
We did not find any guidelines about fixed versus nonfixed ventilator circuit tubing replacement.
Context and Policy Issues
A mechanical ventilator — also known as a ventilator, respirator, or breathing machine — assumes respiratory function when an individual's natural breathing is insufficient.1 Various factors can necessitate ventilator use, with low oxygen levels or pronounced breath insufficiency due to conditions like pneumonia being the primary causes.1 The ventilator circuit encompasses tubing that transports gas from a positive pressure ventilator to the patient and includes any connected devices.2 This circuitry typically features 22 mm inner diameter tubing (adjustable for neonatal and pediatric cases) and links the ventilator to the patient. The ventilator circuit accommodates ancillary components such as heaters, humidifiers, filters, suction catheters, and therapeutic aerosol generators like nebulizers and inhalers. Collectively, these elements ensure effective ventilation and patient comfort during mechanical respiratory support.2
Ventilator-associated pneumonia (VAP) is a common infection acquired in the intensive care unit, with reported incidences ranging from 5% to 40%, depending on the setting and diagnostic criteria.3 Approximately 5% to 10% of patients with mechanical ventilation develop ventilator-associated events.4 The estimated mortality rate attributed to VAP is approximately 10%, with higher rates in surgical intensive care unit patients and those with average severity scores at admission.3 Prolonged mechanical ventilation, altered consciousness, burns, comorbidities, prior antibiotics, invasive procedures, and genetic polymorphisms are characterized as globally recognized VAP risk factors.5 Among vulnerable populations, neonates and children are more susceptible to VAP due to factors such as an immature immune system, incomplete mucosal barrier, lack of maternal immunoglobulins in preterm infants, and increased risk of aspiration.6 Common strategies used to prevent and control VAP are prevention bundles (including combined strategies, such as noninvasive positive pressure ventilation for respiratory failure, spontaneous breathing trials, elevated head of the bed to 30 to 45 degrees, and oral care) and drugs such as chlorhexidine, beta-lactam antibiotics, and probiotics.5
Careful evaluation of workflow, clinical outcomes, economic factors, and environmental impacts is crucial when adopting medical devices in health care management. This ensures that the medical devices not only meet the clinical needs of patients but also contribute to sustainable and cost-effective practices within health care settings.7 Nonetheless, recent studies comparing the environmental and cost-saving impacts of reusable and single-use devices highlight concerns about patient safety and increased labour and capital costs leading to the preference for single-use devices in many surgical settings.8 Despite this preference, in the pursuit of reducing negative environmental impacts and promoting sustainability, the concepts of the circular economy and life cycle assessments have gained attention in the medical device industry. The circular economy approach seeks to minimize waste and maximize the utilization of resources by designing devices that can be easily reused, recycled, or repurposed.9 However, barriers such as infection concerns, customer and manufacturer behaviours, and regulatory structures impact the full implementation of circularity in the medical device industry.8 To address these barriers, collaboration among health care professionals, manufacturers, policy-makers, and regulatory bodies will be needed to establish guidelines and standards that ensure patient safety while encouraging the adoption of more sustainable practices in medical device design, production, and disposal.8
In 2003, the US Centers for Disease Control and Prevention (CDC) recommended changing ventilator circuits only when visibly solid, rather than routinely at fixed intervals for all age groups.10,11 This recommendation was supported by randomized controlled trials (RCTs) conducted in adults, which demonstrated reduced health care costs and no increase in VAP rates when ventilator circuits were changed only when visibly solid.12-15 To update the current knowledge of ventilator circuit tubing replacement (VCTR), this report aims to summarize existing available evidence regarding the clinical effectiveness of different time intervals for VCTRs, as well as evidence-based guidelines for the replacement of ventilator circuits in patients with mechanical ventilation.
Research Questions
What is the clinical effectiveness of different fixed or nonfixed intervals for timing ventilator circuit tubing replacements for patients with mechanical ventilation?
What are the evidence-based guidelines regarding ventilator circuit replacement for patients with mechanical ventilation?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, CINAHL, the Cochrane Database of Systematic Reviews, the International HTA Database, and the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy included both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on research questions and selection criteria. The main search concepts were mechanical ventilation and timing of circuit replacement. The search was completed on July 6, 2023, and limited to English-language documents published since January 1, 2010.
Selection Criteria and Methods
One reviewer screened citations and selected studies. At the first level of screening, titles and abstracts were reviewed, and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Patients with mechanical ventilation in clinical settings |
Intervention | Timing of ventilator circuit tubing replacement or changes at different fixed or nonfixed intervals |
Comparator | Q1: Alternative fixed or nonfixed intervals for ventilator circuit tubing replacement or change Q2: NA |
Outcomes | Q1: Benefits and harms (e.g., ventilator-associated pneumonia, mortality, rates of infection, length of stay) Q2: Recommendations regarding ventilator tubing replacement (e.g., routine change vs. no routine change, fixed intervals, timing, and conditions for replacement) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies, evidence-based guidelines |
NA = not applicable; vs. = versus.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before January 1, 2010.
Critical Appraisal of Individual Studies
One reviewer critically appraised the included studies. The critical appraisal tools used were a MeaSurement Tool to Assess systematic Reviews (AMSTAR-2)16 for systematic reviews (SRs) and meta-analyses (MAs), and the Appraisal of Guidelines for REsearch and Evaluation (AGREE) II instrument17 for guidelines. Summary scores were not calculated for the studies; rather, the strengths and limitations observed among the included studies were summarized and described narratively in Appendix 3.
Summary of Evidence
Quantity of Research Available
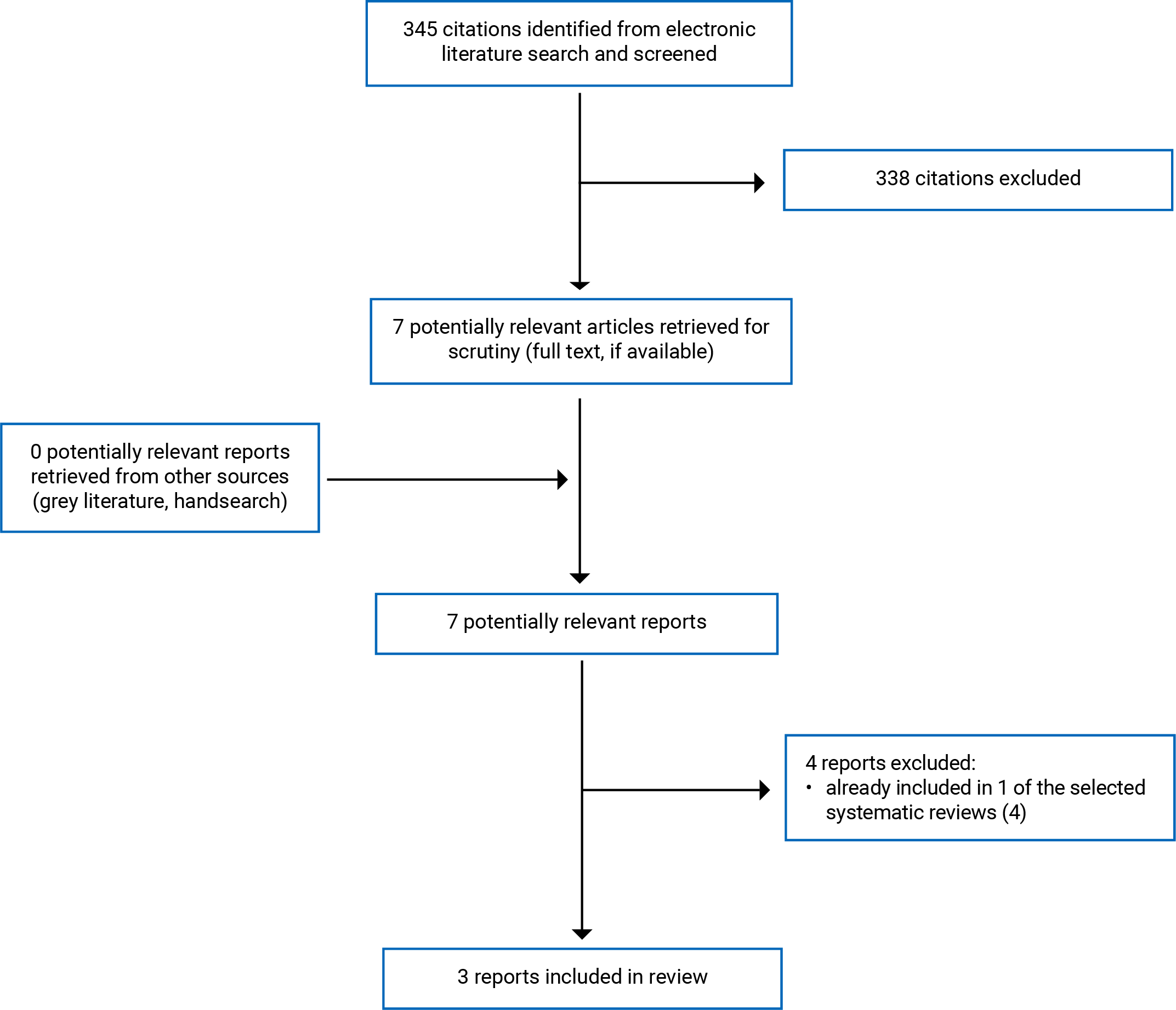
A total of 345 citations were identified in the literature search. Following the screening of titles and abstracts, 338 citations were excluded and 7 potentially relevant articles from the electronic search were retrieved for full-text review. No potentially relevant publications were identified from the grey literature search for full-text reviews. Of the 7 potentially relevant articles, 4 primary studies were excluded because they were already captured in 1 included SR.6 Three publications4,6,18 met the selection criteria and were included in this report.
Appendix 1 presents the PRISMA19 flow chart of the study selection. Additional references of potential interest are provided in Appendix 5.
Summary of the Study Characteristics
Three peer-reviewed publications consisting of 2 SRs with MAs6,18 and 1 guideline4 were included in this report.
Additional details regarding the characteristics of the included publications are provided in Appendix 2 (Table 2 and Table 3).
Study Design
Of the 3 publications that met the selection criteria for this report, 2 were SRs with MAs (including randomized and nonrandomized primary studies) on adult18 and pediatric6 patients. Of the 10 primary studies included in 1 SR on adults,18 8 studies (5 sequential comparison studies [SCSs] and 3 RCTs) were selected for MA. Of the 6 primary studies included in 1 SR on neonates and children,6 2 before-after studies were considered for MA.
The evidence-based guideline4 included in this report was a 2022 update of the Strategies to Prevent Ventilator-Associated Pneumonia in Acute Care Hospitals published in 2014,20 and was sponsored by the Society for Health care Epidemiology of America (SHEA) in collaboration with the Infectious Diseases Society of America (IDSA), the American Hospital Association (AHA), the Association for Professionals in Infection Control and Epidemiology (APICE), and the Joint Commission, with contributions from representatives of other organizations and societies with content expertise. The authors reported the use of tools to assess the quality of the evidence, but not the strengths of the recommendations (Table 3).
Country of Origin
The authors of 2 SRs with MAs6,18 and 1 guideline were based in India,6 China,18 and the US,4 respectively.
Patient Population
Of the 3 selected publications on patients requiring VCTR, 1 SR with MA6 was conducted on neonates and children, 1 SR with MA18 was performed on adults, and 1 guideline4 included preterm neonates, children, and adults.
Interventions and Comparators
In 1 SR with MA on neonates and children,6 VCTR at more frequent intervals (e.g., once in less than 7 days) was compared with less frequent (e.g., once weekly) intervals (Table 2).
In 1 SR with MA on adult patients,18 VCTR every 2 was compared with VCTR every 7 days, or once every 2 or 7 days was compared with no routine circuit change (Table 2).
In 1 included guideline,4 among described interventions, the timing of VCTR was the intervention relevant to this report (Table 3).
Outcomes
In adult patients, the outcome reported was the odds ratio (OR) of VAP.18
In pediatric patients, the outcomes reported were VAP,6 all-cause mortality rate before discharge,6 VAP-related mortality rate,6 duration of mechanical ventilation,6 duration of hospital stay,6 and incidence of bloodstream infections.6
Summary of the Critical Appraisal
Systematic Reviews
Of the 3 studies included in this report, 2 were SRs with MAs to examine the effect of VCTR intervals on VAP in children6 and adults18 on mechanical ventilation. We used the AMSTAR-2 checklist16 to evaluate the quality of the SRs and determine whether the most important elements of the SR methodology were reported (Table 4). The strengths of the SRs were in defining the research question and inclusion and exclusion criteria, describing the study design of the selected primary studies, using a comprehensive literature search strategy, conducting study selection and data extraction in duplicate, reporting potential sources of conflict of interest, and providing a list of excluded studies and justifying the exclusions. For the MAs, the authors reported risk ratios (RRs)6 or ORs18 of the VAP rate and the inconsistency index (I2). The I2 statistic describes the percentage of variation across studies due to heterogeneity rather than chance and is characterized as an intuitive and simple expression of the inconsistency of studies' results.21
The number of primary studies included in the 2 SRs was limited, consisting of 10 studies in the Han et al.18 SR on adults and 6 studies in the Abiramalatha et al.6 SR on neonates and children. Moreover, MAs were limited to 8 studies (5 SCSs and 3 RCTs) in the SR on adults18 and 2 before-after studies in the SR on neonates and children.6 In the SR on adult patients, the MA that combined the results of 5 SCSs did not yield a significant difference in the odds of VAP and had severe statistical heterogeneity. The authors then conducted a second MA of 4 SCSs that excluded a large-scale study from the analysis (based on the severity-of-illness scores of the patients), which yielded a significant difference in odds of VAP between the groups. However, it was unclear whether this was an ad hoc analysis or part of their planned statistical analysis, as the authors did not report sufficient details of their statistical analyses. The SR authors did not adequately examine publication bias, specifically small study bias, and its potential impact on outcomes. Small study effects refer to situations where smaller studies demonstrate varying, often larger, treatment effects compared to larger studies, posing a potential risk to the validity of SRs and MAs.22 Small study bias represents a specific type of publication bias in which smaller primary studies are more likely to be published when they exhibit positive results.23 Thus, the potential impact of small study bias (which could result in more extreme treatment effects)24 on the findings was unclear.
The risk of bias (RoB) in the primary studies included in the SR was assessed in 1 SR6 (using the Cochrane Effective Practice and Organization of Care [EPOC] Risk of Bias Tool), but the impact of RoB in individual studies was not accounted for in interpreting and discussing the review results in either study. In the other SR18 the authors did not assess the RoB of the primary studies. RoB in primary studies can distort the results and conclusions of an SR.25 If the RoB is not assessed or addressed, it can lead to misleading or inaccurate findings, potentially influencing subsequent decision-making or interventions.25 Further, RoB in primary studies may result in an overestimation of treatment effects. Biased studies tend to report more positive or exaggerated results, which can lead to an inflated perception of treatment effectiveness.26
Guidelines
The AGREE II Reporting Checklist17 (Table 5) was used for the critical appraisal of the guideline4 included in this report. The checklist is a tool to improve the completeness of reporting in guidelines and is intended to provide guidance to guideline developers, guideline users, guideline funders, peer reviewers, and journal editors about the essential components of a high-quality practice guideline.27 The checklist entails 6 quality domains (scope and purpose, stakeholder involvement, rigour and development, clarity of presentation, applicability, and editorial independence) and 23 key items.27
The areas clearly described or reported in the guideline were overall objectives; main questions; target patients; using a systematic search to identify, synthesize, and summarize evidence; the use of tools to assess the quality of evidence; the methods for formulating the recommendations; and the consideration of health benefits, side effects, and risks in formulating the recommendations. In the guideline, key recommendations were easily identifiable; recommendations were specific and unambiguous; and different options for the management of preterm neonates,4 children, and adults4 on mechanical ventilation were presented.
However, the included guideline4 did not specify a procedure for updating its recommendations, and it was uncertain if the strengths and limitations of the body of evidence were evaluated as it was not reported in the article. Assessing the limitations of the evidence can indicate whether the findings of an intervention (or treatment comparison) for a specific outcome are adequately protected against bias based on the study design (i.e., possess good internal validity).28
Summary of Findings
We identified 3 studies including 2 SRs with MAs and 1 guideline4 on patients requiring VCTR.
Appendix 4 presents the main outcomes of the included studies.
Findings Reported in Pediatric Patients With Mechanical Ventilation
Rate of VAP
The included SR6 found that the risk of VAP in pediatric patients with mechanical ventilation was similar when the following VCTR intervals were compared (Table 6):
once weekly versus less than 7 days (1 RCT and 1 MA of 2 before-after studies)
once in 3 days versus daily (1 RCT)
once in 1 week versus once in 2 weeks (1 retrospective study).
All-Cause Mortality Rate Before Discharge
The included SR6 found that the RR of all-cause mortality before discharge in pediatric patients was similar when the following VCTR intervals were compared (Table 6):
once weekly versus less than 7 days (1 RCT and 1 MA of 2 before-after studies)
once in 3 days versus daily (1 RCT).
The authors of the SR used the GRADE tool to assess the certainty of the evidence for the VAP rate and all-cause mortality rate before discharge, which was assessed as very low.
VAP-Related Mortality Rate
According to the included SR,6 the mortality rate in children with VAP was similar when the following VCRT intervals were compared (Table 6):
once weekly versus less than 7 days (1 RCT and 1 MA of 2 before-after studies)
once in 3 days versus daily (1 RCT).
Duration of Mechanical Ventilation
According to the included SR,6 the duration of mechanical ventilation (days) in pediatric patients was similar when the following VCTR intervals were compared (Table 6):
once weekly versus less than 7 days (1 RCT and 1 MA of 2 before-after studies)
once in 2 weeks versus once weekly (1 retrospective).
Duration of Hospital Stay
According to the included SR,6 the duration of hospital stay (days) in pediatric patients was similar when the following VCTR intervals were compared (Table 6):
once weekly versus less than 7 days (1 RCT and 1 before-after study)
once in 3 days versus daily (1 RCT).
Incidence of Bloodstream Infections
According to the included SR,6 the incidence of bloodstream infections in pediatric patients was similar for VCTR intervals of once weekly versus less than 7 days (1 RCT and 1 before-after study) (Table 6).
Findings Reported in Adult Patients With Mechanical Ventilation
Rate of VAP
In adults with mechanical ventilation, VCTR every 2 days compared with every 7 days may result in little to no increase in odds (OR = 1.501; 95% confidence interval [CI], 0.952 to 2.365) or in higher odds of VAP (OR = 1.93; 95% CI, 1.08 to 3.44) (Table 7);18 however, there is some uncertainty in the findings from this systematic review.
In adults with mechanical ventilation, VCTR every 2 days or every 7 days may result in little to no increase in the odds of VAP (OR = 1.126; 95% CI, 0.79 to 1.59) compared to no routine circuit changes (Table 7).
Recommendations for VCTR
According to a 2022 guideline for patients in all age groups (preterm neonates, children, and adults requiring mechanical ventilation),4 the ventilator circuit should only be replaced if it is visibly soiled, not functioning properly, or as recommended in the manufacturer’s instructions (Table 8). These recommendations were based on low-quality evidence for preterm neonates, and moderate-quality evidence for pediatric and adult patients.
Limitations
In the review of the clinical effectiveness of various fixed or nonfixed intervals for VCTR in patients with mechanical ventilation, we only identified 3 articles that met the selection criteria for this report. These articles consisted of 1 SR with MA (2010)18 in adults (including 10 primary studies published between 1992 and 2004), 1 SR with MA (2021)6 in neonates and children (including 6 primary studies published between 1995 and 2014), and 1 guideline (2022)4 in preterm neonates, children, and adults. The number of primary studies included in the 2 SRs was limited, and not all included studies were considered for MA. In addition, all of the primary studies captured in the SRs were published before 2014, and we did not find any primary studies that met the selection criteria and were published after 2014.
Regarding the potential harms associated with the VCRT intervals, negative aspects or disadvantages such as increased all-cause mortality rate before discharge, VAP-related mortality rate, duration of mechanical ventilation, and duration of hospital stay were only reported in 1 SR in pediatric patients.6
Regarding guidelines or recommendations, we only identified 1 guideline4 that met the section criteria for this report. We did not find any guidelines that specifically addressed routine versus no routine VCTR in patients with mechanical ventilation.
In addition, none of the 3 studies selected for this report, or the primary studies included in the 2 SRs6,18 were conducted in Canada. Therefore, the generalizability of the findings and the extent to which studies from other cultures and health system policies might contribute to the Canadian context remain uncertain and require further research.
Conclusions and Implications for Decision- or Policy-Making
This report comprises 2 SRs6,18 and 1 evidence-based guideline.4
In adult patients requiring mechanical ventilation,18 more frequent VCTR (i.e., every 2 days) may increase the odds of VAP compared to less frequent changes (i.e., every 7 days), but the findings are uncertain (1 SR with 2 MAs).18 In addition, occasionally changing the ventilator circuit tubing (i.e., every 2 days or every 7 days) may have similar odds of VAP compared to no routine circuit changes (1 SR with MA).18
In neonates and children requiring mechanical ventilation,6 the RR of VAP, all-cause mortality rate before discharge, bloodstream infections, and the mortality rate in patients with VAP, as well as the mean difference of the duration of mechanical ventilation and the duration of hospital stay, were similar for the 3 VCTR intervals that were compared (i.e., once per week versus less than 7 days, once in 3 days versus daily, and once per week versus once in 2 weeks) (1 SR with MA).
According to a 2022 guideline on preterm neonates, children, and adult patients requiring mechanical ventilation,4 the ventilator circuit should only be replaced if it appears soiled or is not functioning properly, or as per the manufacturer’s instructions.
We only found 3 publications meeting our inclusion criteria for this report. Overall, the relevant evidence was limited, and there were no recent primary studies identified (i.e., all of the relevant primary studies were captured by the included SRs and published in or before 2014). Additionally, the recommendations provided in 1 guideline might have been affected by the low to moderate quality of evidence used to develop the relevant recommendations. Furthermore, we identified no guidelines regarding routine versus no routine ventilator circuit changes. Given the low number and limitations of the included publications in this report, and as we identified no relevant study conducted in Canada, the generalizability of the findings and their contribution to the Canadian context are uncertain. Therefore, the findings reported should be interpreted with caution, and further research is suggested to inform decision-making.
When making decisions about ventilator circuit replacement, clinical decision-makers and policy-makers may also wish to consider the associated costs and environmental implications. This involves evaluating the financial implications of device usage, including expenses related to materials, sterilization, personnel time, and salaries,8 as well as the environmental impacts and sustainability of the medical devices. By taking into account these factors, health care decision-makers can strive for a sustainable choice of devices that are clinically effective and cost-effective, while minimizing environmental impact. Policy-makers may also wish to consider these factors when establishing guidelines and policies that promote sustainable device use.
References
1.Society AT. Mechanical Ventilation. Am J Respir Crit Care Med. Vol 1962020: https://www.thoracic.org/patients/patient-resources/resources/mechanical-ventilation.pdf. Accessed Aug 4, 2023.
2.D. H. The ventilator circuit. In: S. M, G. F, eds: UpToDate; 2022: https://cadthcanada.sharepoint.com/sites/projectdocs/Reference%20List%20%20Rapid%20Review/Forms/AllItems.aspx?id=%2Fsites%2Fprojectdocs%2FReference%20List%20%20Rapid%20Review%2FActive%20Projects%2FRC1498%20Ventilator%20Tubing%20Replacement%2F02%20Literature%20Search%2F02%20e%2DPublications%2FThe%20ventilator%20circuit%20%2D%20UpToDate%2Epdf&parent=%2Fsites%2Fprojectdocs%2FReference%20List%20%20Rapid%20Review%2FActive%20Projects%2FRC1498%20Ventilator%20Tubing%20Replacement%2F02%20Literature%20Search%2F02%20e%2DPublications. Accessed Aug 4, 2023.
3.Papazian L, Klompas M, Luyt CE. Ventilator-associated pneumonia in adults: a narrative review. Intensive Care Med. 2020;46(5):888-906. PubMed
4.Klompas M, Branson R, Cawcutt K, et al. Strategies to prevent ventilator-associated pneumonia, ventilator-associated events, and nonventilator hospital-acquired pneumonia in acute-care hospitals: 2022 Update. Infect Control Hosp Epidemiol. 2022;43(6):687-713. PubMed
5.Wu D, Wu C, Zhang S, Zhong Y. Risk Factors of Ventilator-Associated Pneumonia in Critically III Patients. Front Pharmacol. 2019;10:482. PubMed
6.Abiramalatha T, Ramaswamy VV, Thanigainathan S, Pullattayil AK, Kirubakaran R. Frequency of ventilator circuit changes to prevent ventilator-associated pneumonia in neonates and children-A systematic review and meta-analysis. Pediatr Pulmonol. 2021;56(6):1357-1365. PubMed
7.Nations. U. Sustainable Development Goals, 17 Goals to Transform our World. 2015: https://www.un.org/sustainabledevelopment/sustainable-development-goals/.
8.Sørensen BL, Larsen S, Andersen C. A review of environmental and economic aspects of medical devices, illustrated with a comparative study of double-lumen tubes used for one-lung ventilation. Environment, Development and Sustainability. 2022.
9.Circular Economy. Retrieved 2017: https://ellenmacarthurfoundation.org/topics/circular-economy-introduction/overview. Accessed July 15, 2023.
10.Tablan OC, Anderson LJ, Besser R BC, R. H. CDC; Healthcare Infection Control Practices Advisory Committee. Guidelines for preventing health‐care-associated pneumonia, 2003: recommendations of CDC and the Healthcare Infection Control Practices Advisory Committee. MMWR Recomm Rep. 2004;53(RR‐3):1‐36. PubMed
11.Klompas M, Branson R, Eichenwald EC, et al. Strategies to prevent ventilator-associated pneumonia in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35(8):915-936. PubMed
12.Lorente L, Lecuona M, Galván R, Ramos MJ, Mora ML, Sierra A. Periodically changing ventilator circuits is not necessary to prevent ventilator-associated pneumonia when a heat and moisture exchanger is used. Infect Control Hosp Epidemiol. 2004;25(12):1077-1082. PubMed
13.Dreyfuss D, Djedaini K, Weber P, et al. Prospective study of nosocomial pneumonia and of patient and circuit colonization during mechanical ventilation with circuit changes every 48 hours versus no change. Am Rev Respir Dis. 1991;143(4 Pt 1):738-743. PubMed
14.Kollef MH, Shapiro SD, Fraser VJ, et al. Mechanical ventilation with or without 7-day circuit changes. A randomized controlled trial. Ann Intern Med. 1995;123(3):168-174. PubMed
15.Long MN, Wickstrom G, Grimes A, Benton CF, Belcher B, Stamm AM. Prospective, randomized study of ventilator-associated pneumonia in patients with one versus three ventilator circuit changes per week. Infect Control Hosp Epidemiol. 1996;17(1):14-19. PubMed
16.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
17.Agree Next Steps C. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf.
18.Han J, Liu Y. Effect of ventilator circuit changes on ventilator-associated pneumonia: a systematic review and meta-analysis. Respir Care. 2010;55(4):467-474. PubMed
19.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
20.Klompas M, Branson R, Eichenwald EC, et al. Strategies to prevent ventilator-associated pneumonia in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35(8):915-936. PubMed
21.Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. Bmj. 2003;327(7414):557-560. PubMed
22.Hong C, Salanti G, Morton SC, et al. Testing small study effects in multivariate meta-analysis. Biometrics. 2020;76(4):1240-1250. PubMed
23.Schwarzer G, Carpenter JR, Rücker G. Meta-Analysis with R. Springer; Small-Study Effects in Meta-Analysis: https://link.springer.com/chapter/10.1007/978-3-319-21416-0_5. Accessed July 14, 2023.
24.Turner RM, Bird SM, Higgins JP. The impact of study size on meta-analyses: examination of underpowered studies in Cochrane reviews. PLoS One. 2013;8(3):e59202. PubMed
25.Pussegoda K, Turner L, Garritty C, et al. Systematic review adherence to methodological or reporting quality. Systematic reviews. 2017;6(1):131. PubMed
26.How Do You Know Which Health Care Effectiveness Research You Can Trust? A Guide to Study Design for the Perplexed. 2023: https://www.cdc.gov/pcd/issues/2015/15_0187.htm. Accessed July 14, 2023.
27.AGREE reporting checklist. 2023: https://www.agreetrust.org/resource-centre/agree-reporting-checklist/. Accessed 2023 May 16.
28.Berkman N, Lohr K, Ansari M, et al. Methods Guide for Effectiveness and Comparative Effectiveness Reviews. 2013.: https://www.ncbi.nlm.nih.gov/books/NBK174881/. Accessed August 10, 2023.
29.Lien TC, Lin MY, Chu CC, Kuo BI, Wang ED, Wang JH. Ventilator-associated pneumonia with circuit changes every 2 days versus every week. Zhonghua Yi Xue Za Zhi (Taipei). 2001;64(3):161-167. PubMed
30.Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. Bmj. 2008;336(7650):924-926. PubMed
31.Canadian Task Force on Preventive Health Care 2023: https://canadiantaskforce.ca/methods/grade/. Accessed July 15, 2023.
32.Lesson 3: Measures of Risk. CDC Web Archive; 2023: https://www.cdc.gov/csels/dsepd/ss1978/lesson3/section5.html#:~:text=A%20risk%20ratio%20greater%20than,actually%20protects%20against%20disease%20occurrence. Accessed July 12, 2023.
33.Interpreting the Results of Case-Control Studies. 2023: https://www.cdc.gov/training/SIC_CaseStudy/Interpreting_Odds_ptversion.pdf. Accessed July 12, 2023.
34.Higgins J, Thomas J, Chandler J, et al. Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022). Cochrane; 2022.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, objective, funding source | Study designs and characteristics of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Abiramalatha et al. (2021)6 India Funding source: NR | Design: SR and MA Total number of studies included: 6 (2 RCTs and 4 before-after studies) Total number of studies relevant to this report: 6 (2 before-after studies were included in the MA) Inclusion criteria:
Exclusion criteria:
| Population included: Neonates (term and preterm) and children (younger than 18 years) with mechanical ventilation Total N = 768 (range, 32 to 361) Number of patients included in the MA: 475 (range, 96 to 361) Age in all included studies: below 18 years Sex: NR | Interventions included: VCTR Comparison: Shorter VCTRs (e.g., once in less than 7 days) vs. longer VCTRs (e.g., once per week) | Outcome measure:
Follow-up: Between 1 year and 3 years |
Han et al. (2010)18 China Funding source: NR | Design: SR and MA Total number of studies included: 10, including 4 RCTs and 6 sequential comparison studies Total number of studies relevant to this report: 10 (5 sequential comparison studies and 3 RCTs were included in the MA) Inclusion criteria:
Exclusion criteria: Papers on mechanical ventilation in a subacute facility | Population included: Adult patients with mechanical ventilation Total N = 19,375
Number of patients included in the MA: 4,931
Age in all included studies: NR Sex: NR | Interventions included: VCTR Comparison: Circuit changes every 2 or 3 days vs. every 7 days | Outcome measure: VAP rate Follow-up: Between 5 months and 12 months |
MA = meta-analysis; NR = not reported; RCT = randomized controlled trial; SR = systematic review; VAP = ventilator-associated pneumonia; VCTR = ventilator circuit tubing replacement; vs. = versus.
Note that this appendix has not been copy-edited.
Table 3: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations for development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
Klompas et al. (2022)4 | ||||||
Intended users: Clinicians Target population: Preterm neonates, children, and adults requiring ventilator circuit tubing replacement (VCTRs) | To provide practical recommendations for acute care hospitals to prioritize and implement strategies for preventing VAP, and NV-HAP. |
| Through a comprehensive search strategy in 2 databases (PubMed and Embase) between January 2012 and July 2019; updated to August 2021. The articles’ abstracts were reviewed by panel members in a double-blind fashion. Exclusion criteria: NR. Synthesis: Using a standardized multiround rating process | Evidence quality was rated as high, moderate, or low based on the CDC’s HICPAC, GRADE,30 and the Canadian Task Force on Preventive Health Care.31 | The findings of the literature review were grouped based on evidence quality and the balance between beneficial and potentially unfavourable outcomes of interventions. Panel members discussed the summarized findings, recommendations, evidence quality, and categorization (essential practices, additional approaches, or unresolved matters) through virtual meetings. The panel then reviewed and approved the document and its recommendations. | Following the review and approval of the draft manuscript, the expert panel, 5 partnering organizations, stakeholder organizations, and CDC reviewed the document. Prior to dissemination, the guideline document was reviewed and approved by the SHEA Guidelines Committee, the IDSA Standards and Practice Guidelines Committee, the Boards of SHEA, IDSA, APICE, AHA, and the Joint Commission. |
AHA = American Hospital Association; APICE = Association for Professionals in Infection Control and Epidemiology; CDC = Centers for Disease Control and Prevention; GRADE = Grades of Recommendation, Assessment, Development, and Evaluation; HICPAC = Health Care Infection Control Practice Advisory Committee; IDSA = Infectious Diseases Society of America; NR = not reported; NV-HAP = nonventilator hospital-acquired pneumonia; SHEA = the Society for Health care Epidemiology of America; VAP = ventilator-associated pneumonia.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Included Systematic Reviews Using AMSTAR-216
Checklist items | Abiramalatha et al. (2021)6 | Han et al. (2010)18 |
|---|---|---|
1. Did the research questions and inclusion criteria for the review include the components of PICO? | Yes | Yes |
2. Did the report of the review contain an explicit statement that the review methods were established before the conduct of the review and did the report justify any significant deviations from the protocol? | Yes | No |
3. Did the review authors explain their selection of the study designs for inclusion in the review? | Yes | Yes |
4. Did the review authors use a comprehensive literature search strategy? | Yes | Yes |
5. Did the review authors perform study selection in duplicate? | Yes | Yes |
6. Did the review authors perform data extraction in duplicate? | Yes | Yes |
7. Did the review authors provide a list of excluded studies and justify the exclusions? | Yes | Yes |
8. Did the review authors describe the included studies in adequate detail? | No | Yes |
9. Did the review authors use a satisfactory technique for assessing the RoB in individual studies that were included in the review? | Yes | No |
10. Did the review authors report on the sources of funding for the studies included in the review? | No | No |
11. If meta-analysis was performed did the review authors use appropriate methods for the statistical combination of results? | Yes | Uncertain |
12. If meta-analysis was performed, did the review authors assess the potential impact of RoB in individual studies on the results of the meta-analysis or other evidence synthesis? | Yes | No |
13. Did the review authors account for RoB in individual studies when interpreting or discussing the results of the review? | No | No |
14. Did the review authors provide a satisfactory explanation for, and discussion of, any heterogeneity observed in the results of the review? | No | Yes |
15. If they performed quantitative synthesis did the review authors carry out an adequate investigation of publication bias (small study bias) and discuss its likely impact on the results of the review? | No | No |
16. Did the review authors report any potential sources of conflict of interest, including any funding they received for conducting the review? | Yes | Yes |
AMSTAR-2 = a MeaSurement Tool to Assess systematic Reviews – 2; PICO = population, intervention, comparator, outcome; RoB = risk of bias.
Table 5: Strengths and Limitations of Guidelines Using AGREE II Checklist17
Checklist items | Klompas et al. (2022)4 |
|---|---|
Domain 1: Scope and purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes |
Domain 2: Stakeholder involvement | |
4. The guideline development group includes individuals from all relevant professional groups. | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | No |
6. The target users of the guideline are clearly defined. | Yes |
Domain 3: Rigour of development | |
7. Systematic methods were used to search for evidence. | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Unclear |
10. The methods for formulating the recommendations are clearly described. | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes |
14. A procedure for updating the guideline is provided. | No |
Domain 4: Clarity of presentation | |
15. The recommendations are specific and unambiguous. | Yes |
16. The different options for the management of the condition or health issue are clearly presented. | Yes |
17. Key recommendations are easily identifiable. | Yes |
Domain 5: Applicability | |
18. The guideline describes the facilitators and barriers to its application. | Yes |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes |
20. The potential resource implications of applying the recommendations have been considered. | Yes |
21. The guideline presents monitoring and/or auditing criteria. | Yes |
Domain 6: Editorial independence | |
22. The views of the funding body have not influenced the content of the guideline. | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes |
AGREE II = Appraisal of Guidelines for REsearch and Evaluation II.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 6: Summary of Findings on VCTR Intervals in Neonates and Children in an SR by Abiramalatha et al. (2021)6
Outcomes | Number and study design | VCTR intervals | Total number of patients | RRa or MD (95% CI) | Finding (P value) | Certainty of evidence |
|---|---|---|---|---|---|---|
Rate of VAP | 1 RCT | Once weekly vs. less than 7 days | 176 | RR = 0.83 (0.38 to 1.81) | NSD (0.63) | VL |
MA of 2 before-after studies | Once weekly vs. less than 7 days | 457 | RR = 0.94 (0.49 to 1.81) | NSD (0.86) | VL | |
1 RCT | Once in 3 days vs. daily | NR | RR = 0.81 (0.43 to 1.36) | NSD (NR) | VL | |
1 retrospective | Once weekly vs. once in 2 weeks | NR | RR = 0.93 (0.36 to 2.36) | NSD (NR) | VL | |
All‐cause mortality rate before discharge | 1 RCT | Once weekly vs. less than 7 days | 176 | RR = 0.67 (0.34 to 1.30) | NSD (0.23) | VL |
MA of 2 before-after studies | Once weekly vs. less than 7 days | 457 | RR = 1.01 (0.63 to 1.64) | NSD (0.95) | VL | |
1 RCT | Once in 3 days vs. daily | NR | RR = 0.80 (0.29 to 2.21) | NSD (NR) | VL | |
Incidence of bloodstream Infections | 1 RCT | Once weekly vs. less than 7 days | 176 | RR = 0.11 (0.01 to 2.03) | NSD (NR) | NR |
1 before-after study | Once weekly vs. less than 7 days | 361 | RR = 0.87 (0.62 to 1.22) | NSD (NR) | NR | |
Mortality rate in children with VAP | 1 RCT | Once weekly vs. less than 7 days | 176 | RR = 0.66 (0.11 to 4.04) | NSD (NR) | NR |
MA of 2 before-after studies | Once weekly vs. less than 7 days | 457 | RR = 0.22 (0.86 to 5.71) | NSD (NR) | NR | |
1 RCT | Once in 3 days vs. daily | NR | RR = 1.76 (027 to 11.47) | NSD (NR) | NR | |
Duration of mechanical ventilation (days) | 1 RCT | Once weekly vs. less than 7 days | 176 | MD = 0.10 (−3.55 to 3.75) | NSD (NR) | NR |
MA of 2 before-after studies | Once weekly vs. less than 7 days | 457 | MD = 1.83 (−2.07 to 5.73) | NSD (NR) | NR | |
1 retrospective | Once weekly vs. once in 2 weeks | NR | MD = 3.00 (−18.10 to 24.10) | NSD (NR) | NR | |
Duration of hospital stay (days) | 1 RCT | Once weekly vs. less than 7 days | 176 | MD = −5.10 (−16.70 to 6.50) | NSD (NR) | NR |
1 before-after study | Once weekly vs. less than 7 days | 361 | MD = −4.00 (−13.69 to 5.69) | NSD (NR) | NR | |
1 RCT | Once in 3 days vs. daily | NR | MD = −1.39 (−22.63 to 19.85) | NSD (NR) | NR |
CI = confidence interval; MA = meta-analysis; MD = mean difference; NR = not reported; NSD = no significant difference; RCT = randomized controlled trial; RR = risk ratio; VAP = ventilator-associated pneumonia; VCTR = ventilator circuit tubing replacement; VL = very low.
aRR is the ratio of the risk of an event in 2 or more groups. A risk ratio greater than 1.0 indicates the increased risk of an event (here developing VAP) for the exposed group. A risk ratio less than 1.0 indicates a decreased risk for the exposed group, showing that perhaps exposure actually protects against disease occurrence.32
Table 7: Summary of Findings on VCTR Intervals in Adult Patients in an SR and MA by Han et al. (2010)18
Outcome | Number of studies included and study design | VCTR intervals | Total number of patients | ORa (95% CI) | Findings (P value) | Statistical heterogeneity of evidenceb |
|---|---|---|---|---|---|---|
Rate of VAP | 5 SCSsc | Every 2 days vs. every 7 days | 18,055 | 1.501 (0.952 to 2.365) | NR | Severe (P = 0.002; I2 = 0.764) |
4 SCSs | Every 2 days vs. every 7 days | 4,774 | 1.93 (1.08 to 3.44) | Significantly increased OR of VAP every 2 days vs. every 7 days (NR) | Moderate (P = 0.056; I2 = 0.604) | |
3 RCTs | Every 2 or 7 days vs. no routine circuit change | 667 | 1.126 (0.79 to 1.59) | Potentially increased OR of VAP every 2 or 3 days vs. every 7 days (NR) | No or mild (P = 0.85; I2 = 0.000) |
CI = confidence interval; I2 = inconsistency index; MA = meta-analysis; NR = not reported; OR = odds ratio; RCT = randomized controlled trial; SCS = sequential comparison study; VAP = ventilator-associated pneumonia; VCTR = ventilator circuit tubing replacement.
aThe OR indicates how much higher the odds of exposure are among patients than among controls. An OR of greater than 1.0 indicates that the odds of exposure (here developing VAP) among patients are higher than the odds of exposure among controls.33
bAccording to the Q-Cochrane test, I2 values between 0.0 and 39.9, 40.0 and 69.9, 70.0 and 89.9, and 90 and 100 correspond with no or mild, moderate, severe, and highly severe heterogeneity.34 I2 values for the first and second analyses suggest that the findings should be interpreted with caution.
CIn the MA including 5 SCSs, despite a tendency favouring less frequent circuit changes observed in 4 studies, a large study by Lien et al. (2001)29 enrolling 13,281 patients with and without a history of ICU admission, did not corroborate this pattern. The authors discussed that this finding was probably linked to low severity-of-illness scores and/or few risk factors for VAP, owing to the very low pneumonia rate in both ICU and non-ICU groups (around 3%). The second row of findings of the current table presents the findings of a subsequent MA excluding this study.
Table 8: Summary of Recommendations Regarding Timing of VCTR
Guidelines | Recommendations and supporting evidence | Evidence qualitya |
|---|---|---|
Klompas et al. (2022)4 | To lower VAP or VAE and minimize risks of harm in preterm neonates: “Change the ventilator circuit only if visibly soiled or malfunctioning (or per manufacturers’ instructions)” (p. 696) Supporting evidence: According to an SR of 6 studies in neonates and children (Abiramalatha et al. 2021),6 which reported no difference in VAP rates or mortality with 3-day vs. 7-day VCTR. | Low |
To lower VAP, VAE, and/or duration of mechanical ventilation in pediatric patients: “Change the ventilator circuit only if visibly soiled or malfunctioning (or per manufacturers’ instructions)” (p. 698) Supporting evidence: According to an SR of 6 studies in neonates and children (Abiramalatha et al. 2021),6 which reported no difference in VAP rates or mortality with 3-day vs. 7-day VCTR. | Moderate | |
To prevent VAP or VAE in adult patients: “Change the ventilator circuit only if visibly soiled or malfunctioning (or per manufacturers’ instructions)” (p. 691) Supporting evidence: According to the findings of 4 RCTs, already cited in the CDC recommendation (2003),10 which demonstrated no increase in VAP rates when ventilator circuits were changed only when visibly soiled.12-15 | Moderate |
CDC = US Centers for Disease Control and Prevention; RCTs = randomized controlled trials; VAE = ventilator-associated event; VAP = ventilator-associated pneumonia; VCTR = ventilator circuit tubing replacement.
aPanel members assessed the evidence supporting each recommendation as high (highly confident that the true effect lies close to that of the estimated size and direction of the effect), moderate (the true effect is likely to be close to the estimated size and direction of the effect, but there is a possibility that it is substantially different), or low (the true effect may be substantially different from the estimated size and direction of the effect).
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
The following publications were identified because they may provide additional information associated with this report.
Systematic Reviews
Flodgren G, Conterno LO, Mayhew A, Omar O, Pereira CR, Shepperd S. Interventions to improve professional adherence to guidelines for prevention of device-related infections. Cochrane Database Syst Rev. 2013(3):CD006559. PubMed
Pinto HJ, D'Silva F, Sanil TS. Knowledge and Practices of Endotracheal Suctioning amongst Nursing Professionals: A Systematic Review. Indian J Crit Care Med. 2020;24(1):23-32. PubMed
Reviews
Al-Tamimi M, Refaat F, Bani Issa W. Barriers to compliance with evidence-based guidelines for ventilator-associated pneumonia among critical care nurses: A scoping review. F1000Res. 2022;11:1551. PubMed
Karim HMR, Burns KEA, Ciobanu LD, et al. Noninvasive ventilation: education and training. A narrative analysis and an international consensus document. Adv Respir Med. 2019;87(1):36-45. PubMed
Craven DE, Hudcova J, Rashid J. Antibiotic therapy for ventilator-associated tracheobronchitis: a standard of care to reduce pneumonia, morbidity and costs? Curr Opin Pulm Med. 2015;21(3):250-259. PubMed
Umscheid CA, Mitchell MD, Doshi JA, Agarwal R, Williams K, Brennan PJ. Estimating the proportion of healthcare-associated infections that are reasonably preventable and the related mortality and costs. Infect Control Hosp Epidemiol. 2011;32(2):101-114. PubMed
Recommendations or Guidelines
File TM, Jr. Recommendations for treatment of hospital-acquired and ventilator-associated pneumonia: review of recent international guidelines. Clin Infect Dis. 2010;51 Suppl 1:S42-47. PubMed
Contributors: Kendra Brett
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as of the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, collecting, using, and disclosing by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca