CADTH Health Technology Review
Emergency Care Follow-Up for Children and Adolescents With Suicide Attempts or Ideation
Rapid Review
Authors: Candyce Hamel, Sinwan Basharat, Melissa Severn
Abbreviations
PICO
participants, interventions, comparators, outcomes
PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
RCT
randomized controlled trial
SR
systematic review
Key Messages
Death by suicide is the second-leading cause of death for young people in Canada. Because 10% to 15% of the people seen in hospital emergency departments for a suicide attempt will repeat the attempt within 12 months following their discharge, it is important to identify what interventions are effective for preventing further self-harm during this time.
Active follow-up care following an emergency department visit for a suicide attempt is common; however, it is unclear what type (e.g., text message, home visit) or timing (e.g., 24 hours, within 72 hours after emergency department discharge) of interventions is most effective for preventing further self-harm in people younger than 18 years. The objective of this review is to summarize the evidence regarding the clinical effectiveness of active contact and follow-up interventions, and the timing and duration of care, for children and adolescents (younger than 18 years) who present to emergency care for suicide attempts or suicide ideations.
For children and adolescents presenting to the emergency department for suicide attempts or ideation, telephone-based follow-up care initiated within 1 week of discharge may not affect the number of people who completed the full course of postdischarge treatment, the mean number of sessions attended, or the number of suicide deaths. This finding was based on evidence from 2 systematic reviews, each with 1 primary study relevant to this report. The small sample sizes of these studies (N = 64 and N = 97) and their limited or unclear quality should be considered when interpreting these results.
None of the relevant primary studies within the systematic reviews reported on mental health outcomes (e.g., depression, social functioning) or harms from the intervention.
No studies were found that evaluated the clinical effectiveness of other methods of active follow-up care or of different time durations of follow-up care for children and adolescents who present to emergency care for suicide attempts or suicide ideations that met our criteria for this review.
No evidence-based guidelines were identified that provided recommendations about timing, modality, and which health care professionals should be involved in follow-up care for children and adolescents who present to emergency care for suicide attempts or ideations that met our criteria for this review.
Guidance documents and guidelines for adults generally recommend that follow-up should occur within 48 hours, particularly for those with safety concerns of subsequent self-harm. These guidance documents also suggest different modalities for follow-up during that time, including telephone calls, visits, and electronic communication. Given the higher risk and potential vulnerability experienced by children and adolescents and the absence of formal clinical guidelines, person-centred follow-up care for all children and adolescents within 48 hours should be considered, similar to adults who present with high concerns.
Context and Policy Issues
In Canada, approximately 12 people die by suicide every day.1 For those aged between 10 and 19 years, death rates by suicide per 100,000 people are 4.9 in females and 7.4 in males;1 however, published data may underestimate true numbers due to stigma. In a 2019 Canadian survey of 6,800 adolescents (6,750 cisgender and 50 transgender), transgender adolescents were at increased risk of suicidal ideation (risk ratio = 4.95; 95% confidence interval [CI], 3.63 to 6.75) and having attempted suicide (risk ratio = 7.60; 95% CI, 4.76 to 12.10) compared with cisgender adolescents.2 Further, the COVID-19 pandemic has had an impact on the mental health of children and adolescents due to stress, unpredictability, and disruptions (e.g., school, social, family). A 2023 meta-analysis identified 42 studies in 18 countries and reported a 22% increase in emergency department visits for attempted suicide compared with prepandemic rates; the mean age of children presenting to the emergency department for an attempted suicide was 11.7 years.3
For every completed suicide in adolescents, there may be as many as 50 to 100 attempts.4 Several organizations, including the WHO, state that a previous suicide attempt is the single most important risk factor for suicide.5 Other risk factors include psychiatric disorders, family history of mood disorders, history of physical or sexual abuse, exposure to violence, and biologic factors.4 An evidence brief by the Mental Health Commission of Canada reported that 10% to 15% of people seen in a hospital emergency department for a suicide attempt will repeat the attempt within 12 months following discharge.6 Up to 70% of individuals who survive a suicide attempt do not attend their first outpatient appointment, so several follow-up and regular contact interventions can be implemented to help ensure the continuity of care for these individuals.6 These active follow-up interventions include telephone calls, text messages, emails, letters or postcards, and home visits. The National Institute for Health and Care Excellence (NICE) recommends the following: “If there are ongoing safety concerns for the person after an episode of self-harm, the mental health team, GP, team who carried out the psychosocial assessment or the team responsible for their care should provide initial aftercare within 48 hours of the psychosocial assessment.”7 Most recommendations regarding follow-up after an episode of self-harm or suicide attempt are developed using evidence generated from adults.
Several systematic reviews (SRs) have been published that evaluate the effectiveness of active follow-up care; however, they also include adult populations and/or other interventions.8-12 It is unclear what are the best interventions (e.g., text message, home visit) and the timing of these interventions (e.g., 24 hours, within 72 hours after emergency department discharge) specific to those younger than 18 years. The objective of this review is to summarize the evidence regarding the clinical effectiveness of early active contact and follow-up interventions, and the timing of initial follow-up care after discharge, for children and adolescents (younger than 18 years) who present to emergency care for suicide attempts or suicide ideations.
Research Questions
What is the clinical effectiveness of active contact and follow-up interventions for children and adolescents who present to emergency care for suicide attempts or suicide ideations?
What is the clinical effectiveness of different time durations for follow-up care for children and adolescents who present to emergency care for suicide attempts or suicide ideations?
What are the evidence-based guidelines about the timing, modality, and health care professionals involved in follow-up care for children and adolescents who present to emergency care for suicide attempts or ideations?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources, including MEDLINE, PsycINFO, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were suicide, emergency settings, and follow-up methods. The search was completed on June 16, 2023, and limited to English-language documents published since January 1, 2018.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1. Within the included SRs, when PICO (participants, interventions, comparators, outcomes) elements were not described in sufficient detail to be able to determine if a study was relevant to this report, an additional review of the abstracts was performed.
Criteria | Description |
|---|---|
Population | Children and adolescents (younger than 18 years) with attempted suicide or suicide ideation, presenting to emergency care (emergency departments) who are not subsequently admitted to the hospital |
Intervention | Q1: Active contact and follow-up care, with initial contact within 1 week of emergency department discharge Q2: Time durations from emergency department discharge for initial follow-up care (e.g., 24 hours, 48 hours, 72 hours) Q3: Follow-up care |
Comparator | Q1. Usual care (may include passive contact, general outpatient appointment, or no follow-up) Q2. Alternative time duration for follow-up care Q3. Not applicable |
Outcomes | Q1 and Q2. Clinical benefits (e.g., suicide behaviour or ideation, mental health outcomes, treatment engagement, or adherence or attendance) and harms Q3. Recommendations about follow-up care interventions or practices (e.g., best practices for timing of care, modality of care, health care professionals) |
Study designs |
|
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2018. SRs in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A Measurement Tool To Assess Systematic Reviews 2 (AMSTAR 2)13 for SRs. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
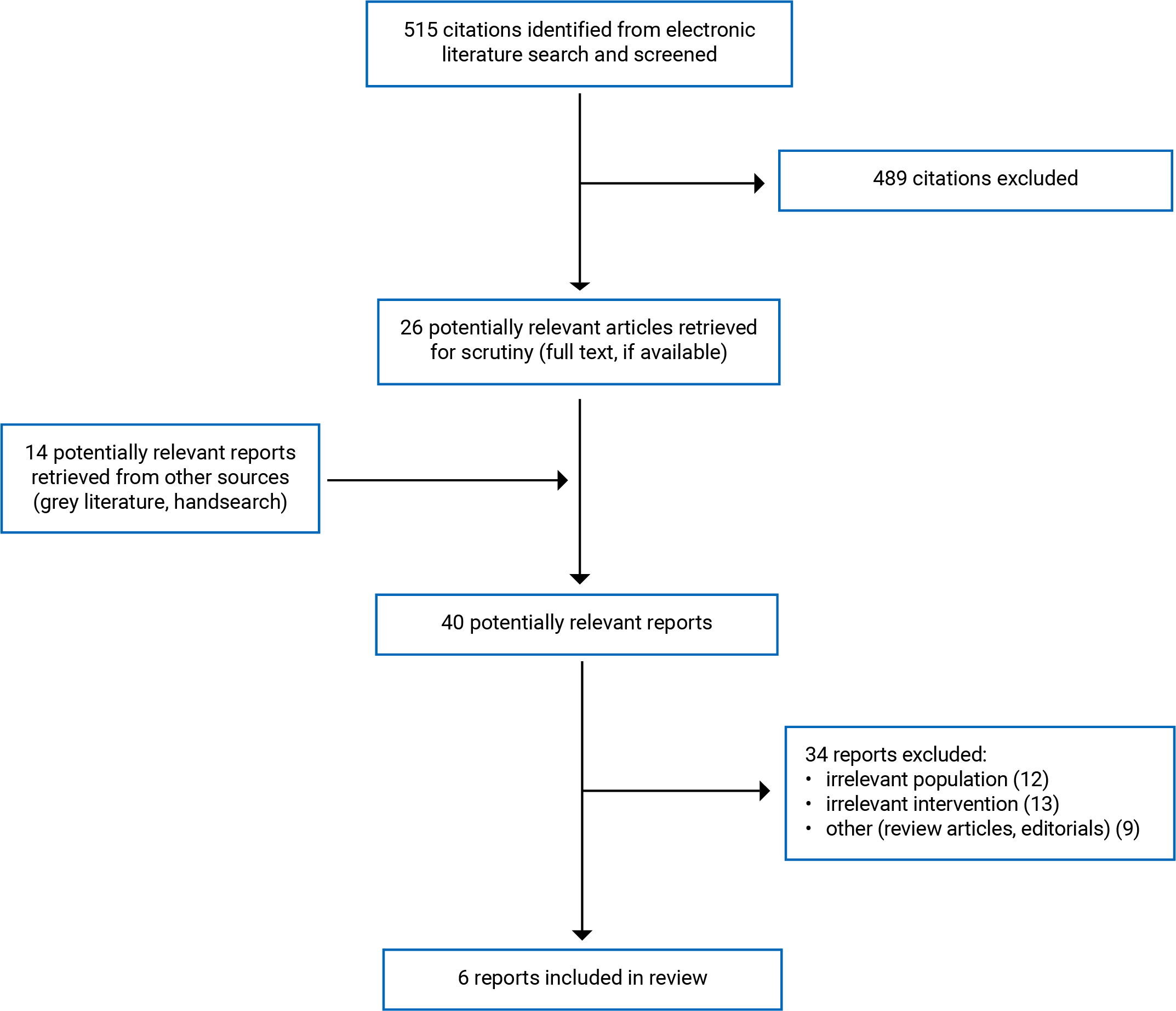
Quantity of Research Available
A total of 515 citations were identified in the literature search. Following screening of titles and abstracts, 489 citations were excluded and 26 potentially relevant reports from the electronic search were retrieved for full-text review. Fourteen potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 34 were excluded for various reasons; 6 SR publications met the inclusion criteria and are included in this report. Figure 1 presents the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)14 flow chart of the study selection. One included primary study overlapped in the SRs by Witt et al.15 and Doupnik et al.8 but the population was described as “adolescents hospitalized for suicide attempt” in the SR by Doupnik et al.8 (which would be excluded) and “patients presenting to hospital for suicide attempt necessitating medical care in either an emergency department or pediatrics ward of a general children’s hospital” in the SR by Witt et al.15 (which would be included). Because the SR by Witt et al.15 is well-reported and has no major limitations, we included the primary study as reported in this SR.
Additional references of potential interest are provided in Appendix 5. This includes primary studies in adults, reviews with participants who are adults, or participants for whom their age was not clearly defined, and a protocol for a randomized controlled trial (RCT). A brief summary of guidance documents describing follow-up protocols for adults visiting emergency care for suicide attempts or ideation is also presented in Appendix 5, Table 5.
Summary of Study Characteristics
All 6 SRs8,9,11,12,15,16 had broader inclusion criteria than the present review, and 4 SRs did not include any primary studies relevant to this review. For example, the SR by Skopp et al.11 included studies evaluating the Caring Contacts intervention, but there was no restriction on the population (e.g., adults, patients discharged from psychiatric care), and first contact may have been beyond 1 week after emergency department discharge. This was common among the other SRs, which included broader populations (e.g., adults, patients, hospitalized patients, adolescents presenting to emergency departments for nonpsychiatric reasons),8,9,12,15,16 irrelevant interventions (e.g., 1 session delivered in the hospital, first contact was beyond 1 week, school-based interventions, psychotherapy, pharmacotherapy),8,9,12,15,16 and noncomparative study designs (e.g., single group design, case report).12 In terms of the comprehensiveness of the literature search, most SRs did not have a restriction on publication date, with 1 including studies from January 1, 2000, to the date of the search.8 The end search dates ranged from January 20159 to May 31, 2021.12
The 2 SRs with relevant primary studies (Witt et al.15 and Chaudhary et al.16) each included 1 primary study relevant to this review. These 2 SRs will be described further in subsequent sections of this review, with the exception of the Summary of Critical Appraisal, which will discuss all 6 included SRs.
Additional details regarding the characteristics of included publications are provided in Table 2.
Study Design
The SRs were published in 202115 and 2020.16 Date ranges covered by their searches were up to July 4, 202015 and January 2019.16 The SR by Witt et al.15 included RCTs and the SR by Chaudhary et al.16 included RCTs and nonrandomized studies. There was no overlap in the relevant studies for these reviews because the SR by Witt et al.15 included an RCT and the SR by Chaudhary et al.16 included a nonrandomized clinical trial.
Country of Origin
The first authors for the 2 SRs were from Australia15 and Pakistan.16 Both primary studies were conducted in the US.
Patient Population
In the relevant primary studies in both SRs,15,16 the populations were adolescents who attempted suicide and were evaluated in the emergency department. The primary study in the SR by Witt et al.15 included participants who received medical attention in emergency departments and pediatric wards, although it is unclear what proportion were cared for in wards.
Interventions and Comparators
In the SR by Witt et al.,15 the relevant RCT evaluated an intervention described as a “compliance-enhanced intervention,” which included a single 1-hour session, delivered in the emergency department before discharge, to review expectations for outpatient treatment, address common treatment misconceptions, a verbal treatment contract, and a series of 4 telephone calls at 1, 2, 4, and 8 weeks after discharge (duration not reported). The intervention was delivered by 3 postdoctoral fellows in psychology (experience not reported). Treatment as usual (standard disposition planning) consisted of a “brief” (duration not reported) inpatient treatment and/or outpatient appointment, as appropriate.
In the SR by Chaudhary et al.,16 the relevant nonrandomized clinical trial evaluated an intervention that included 3 phone interviews over 8 weeks that were scheduled with patients and parents for 1, 2, and 6 weeks after discharge. These phone calls focused on treatment expectations, outpatient services, problems, concerns, and resistance of patients and their parents to attend predecided outpatient psychotherapy sessions. The intervention was delivered by a doctor-level clinician. The comparison group was described as treatment as usual, without further details.
Outcomes
Outcomes reported in the relevant primary studies within the SRs include:
psychotherapy session “no shows”16
completed the full course of treatment15
suicide deaths15
suicide reattempts16
repetition of self-harm at 6 months follow-up.15
In the SR by Witt et al.,15 repetition of self-harm was identified through self-report, collateral report, clinical records, or research monitoring systems, and suicide was identified through register-recorded deaths or reports from collateral informants, such as family members or neighbours. Depression, hopelessness, general functioning, social functioning, and suicidal ideation were also reported in the SR by Witt et al.,15 but with no data available.
Chaudhary et al.16 did not report on the outcomes of interest in the inclusion criteria, but outcomes related to suicide and self-harm were captured in the results tables (e.g., suicidal ideations, repetition of suicidal behaviour, rate of suicidal attempts after discharge from the hospital, completion of suicide, repetition of deliberate self-harm within 6 months of the initial incident, number of self-harm episodes after receiving treatment, readmission for self-poisoning), depression, hopelessness, social and psychological well-being, and outpatient services outcomes (e.g., engagement with outpatient services).
Summary of Critical Appraisal
Systematic Reviews
The SRs were assessed using AMSTAR 2.13 Among the 2 SRs with relevant primary studies, the SR by Witt et al.15 is a Cochrane review and was well conducted and reported, with no major limitations identified. Chaudhary et al.16 searched 2 electronic databases, did not restrict inclusion of studies based on language, provided a PRISMA flow diagram, and performed study selection and data extraction with 2 reviewers; however, there were several limitations in conduct and reporting. There was no mention of a registered protocol, it was unclear if supplemental searching was performed, elements of PICO were not well described in the eligibility criteria or for the included studies, a list of excluded studies was not provided, risk of bias was not formally done with a tool, there was no mention of assessment for publication bias, and the source of funding of the included primary studies and for the review itself was not reported.
There were strengths across the 4 SRs with no relevant primary studies. All searched 2 or more databases, provided a PRISMA flow diagram, reported declarations and conflicts of interest, and described the statistical analyses. However, there were differences in limitations in quality of conduct and reporting across the 4 SRs. Some quality criteria were not conducted or reported: publications were restricted to English publications,8,9,11,12 elements of PICO for the inclusion criteria were not well described,11,12 no details on the conduct for study selection and data extraction were provided,9 a list of excluded studies was not provided (with varying levels of details for exclusion in the PRISMA flow diagram),8,9,11,12 no details around how risk of bias was performed8,9,11 some PICO elements of the included studies were not well described,8,9,12 it was unclear if it was assessed,11 no details of funding for the included studies in the SR,8,9,11,12 and no details of funding source for the SR.11 It is possible that some studies included in the SRs met our inclusion criteria, but we were unable to determine this due to lack of details.
Additional details regarding the strengths and limitations of included publications are provided in Table 3.
Summary of Findings
Clinical Effectiveness of Active Contact and Follow-Up Interventions
Six SRs were identified that met the inclusion criteria for this research question, of which 2 contained relevant primary studies: 1 RCT from the SR by Witt et al.15 and 1 nonrandomized clinical trial from the SR by Chaudhary et al.16 There was no overlap of the relevant primary studies included in the SRs.
Adherence to Psychotherapy
Overall, there may be no difference in adherence to psychotherapy between those who received telephone follow-up care and those who received treatment as usual.
Evidence from 1 RCT in the SR by Witt et al.15 reported no significant difference in those patients who completed the full course of treatment for of the compliance-enhancement intervention compared with those who received treatment as usual (odds ratio [OR] = 1.59; 95% CI, 0.59 to 4.33). Evidence from 1 nonrandomized clinical trial identified in the SR by Chaudhary et al.16 reported psychotherapy “no shows” of 9% for those receiving telephone calls and 18% for those receiving treatment as usual (no statistical comparison reported).
Both primary studies in the SRs15,16 reported on the average number of sessions. The RCT in the SR by Witt et al.15 reported no difference in the average number of sessions attended between groups (mean difference = 1.30; 95% CI, −1.28 to 3.88), whereas the nonrandomized trial in the SR by Chaudhary et al.16 reported the mean number of sessions was 5.5 in the group receiving telephone calls compared with 3.9 in the treatment as usual group (no statistical comparison reported).
Number of Reattempts and Death by Suicide
Overall, there may be no difference in the number of reattempts or death by suicide between those who received telephone follow-up care and those who received treatment as usual.
The RCT in the SR by Witt et al.15 reported no deaths by suicide in either group by the final follow-up assessment. Additionally there was no significant difference between groups in patients repeating self-harm at 6 month follow-up (OR = 0.67; 95% CI, 0.15 to 3.08).15 Evidence from the nonrandomized trial in the SR by Chaudhary et al.16 reported that the group receiving telephone calls had 0% reattempted suicide, whereas the treatment as usual group had a 9% suicide reattempt rate.
Other Outcomes
Witt et al.15 sought evidence regarding depression, hopelessness, general functioning, social functioning, and suicidal ideation; no evidence was identified for these outcomes in the primary study relevant to this review.
Table 4 presents the main study findings.
Clinical Effectiveness of Time Durations for Follow-Up Care
No relevant evidence regarding the time durations for initiation of follow-up care for children and adolescents who presented to emergency care for suicide attempts or suicide ideations was identified; therefore, no summary can be provided.
Evidence-Based Guidelines About Timing, Modality, and Health Care Professional Involved in Follow-Up Care
No relevant evidence-based guidelines regarding the timing, modality, and health care professionals involved in follow-up care for children and adolescents who present to emergency care for suicide attempts or suicide ideations was identified; therefore, no summary can be provided.
Limitations
There were some limitations to the SRs that would prevent a definitive conclusion on clinical effectiveness of active contact and follow-up intervention for children and adolescents who present to emergency care for suicide attempts or suicide ideations.
Six SRs were included with inclusion criteria broader than the scope of this review, particularly around the populations and interventions included in the primary studies. In most reviews, there was poor reporting of the patient population and interventions, making it difficult to determine if primary studies were relevant to this review. Therefore, it is possible that some primary studies within the SRs were missed in this review (although a search of the abstract for the primary studies did not result in any studies that would meet the eligibility criteria of this review). Two SRs provided sufficient details to identify 2 relevant primary studies. The SR by Witt et al.15 was well conducted and reported; however, the relevant primary study was judged on 6 domains of risk of bias, with 3 judged as having “some concerns” and 3 judged as “high risk.” The quality of conduct and reporting for the SR by Chaudhary et al.16 was poor, and they did not perform a formal risk of bias assessment, with the limitation for the relevant primary study listed as “small sample size.”
Both relevant primary studies in the SRs were conducted in the US (1 in Northeast US, and the other did not provide any further details), with data from 1 emergency department (no further details about the setting reported), and sample sizes of 64 participants15 and 97 participants.16 These limit the generalizability because the capacity of emergency departments may differ across regions and countries and the participants in these studies may not be representative of all children and adolescents who present to emergency departments for suicidal ideation or attempts. The intervention in both primary studies evaluated telephone follow-up, which limits the generalizability of follow-up aftercare for other modalities (e.g., email, text message, home visit). Neither primary study in the SRs reported on mental health outcomes (e.g., depression, anxiety) or harms of the intervention.
No studies were identified that evaluated different time durations from emergency department discharge for follow-up care. Although the 2 relevant primary studies in the SRs reported on a different numbers of telephone calls, with the first call within 1 week of discharge, they were compared with treatment as usual, which was not reported or was missing details (i.e., duration), not with a different time duration.
No evidence-based guidelines that met our inclusion criteria were identified. One potential guideline by the National Institute for Health and Care Excellence (NICE) provided a recommendation on first point of contact within 48 hours after discharge,7 but was excluded because the recommendation was not specific to the child and adolescent population. This guideline has been listed in Appendix 5, Table 5.
Conclusions and Implications for Decision- or Policy-Making
The evidence is scarce about active contact and follow-up care in children and adolescents (younger than 18 years) who present to the emergency department with attempted suicide or suicide ideation but are not subsequently admitted. This review included 6 SRs,8,9,11,12,15,16 and the included primary studies were published from 1976 to 2021. Two SRs15,16 each identified 1 relevant primary study that evaluated telephone follow-up care; these primary studies were published in 1997 and 2002. Although other active follow-up care interventions were identified in the SRs, poor reporting of the PICO elements of the included studies limited the ability to identify other active follow-up interventions (e.g., email, text message, home visit) or relevant studies conducted in the past 20 years. When PICO elements were not clearly described within the SRs, an additional search for the abstracts was performed, which did not reveal any further relevant studies, although abstracts do not always sufficiently describe the PICO elements. There were no studies evaluating different time durations for follow-up care. An SR of primary studies using the same inclusion criteria as this Rapid Review may identify additional relevant studies because the population and intervention within the primary study would likely provide sufficient details to determine eligibility.
Although the 2 relevant primary studies within the SRs both evaluated telephone follow-up, there was a difference between the interventions. The compliance-enhancement approach included an additional 1-hour session before emergency department discharge and 1 additional telephone call. Evidence from the RCT evaluating the compliance-enhancement approach, included in the SR by Witt et al.,15 showed no significant differences between participants who received the single-session and follow-up telephone calls and participants who received treatment as usual in the number of deaths by suicide, those who completed the full course of treatment, or the average number of sessions attended. Chaudhary et al.16 reported means and rates but did not state whether there was a statistical difference between groups. The limitations of the included literature should be considered when interpreting the findings of this report. Although the SR by Witt et al.15 was well conducted and reported, the relevant primary study was at high risk of bias. Additionally, both relevant primary studies in the SRs15,16 had small sample sizes (N = 64 and N = 97), which affects the number of possible events, and the lack of observed significant differences could be due to sample size rather than lack of intervention effect.
Several reviews and primary studies have evaluated different modalities of follow-up care in adults, participants admitted to hospitals, or opportunistic screening of adolescents presenting to the emergency department for nonpsychiatric reasons, or with no comparison group.8,9,17-20 Although these sources generally indicated that active follow-up is associated with positive outcomes, such as reducing the risk of repeat suicide attempts and increasing connectedness to ongoing care for adults, it is unclear if these populations are generalizable to children and adolescents presenting to the emergency department due to suicidal ideations or attempts.
We did not identify any evidence-based guidelines regarding the timing, modality, or health care professionals involved in the follow-up care for people younger than 18 years who present to emergency care for suicide attempts or suicide ideations. However, guidance documents and guidelines for adults (refer to Appendix 5, Table 5) generally indicate that follow-up should occur within 48 hours, particularly for adults with safety concerns of subsequent self-harm. These guidance documents also suggest different modalities for follow-up during that time, including telephone calls, visits, and electronic communication. Given the higher risk and potential vulnerability experienced by children and adolescents, in the absence of formal clinical guidelines, ensuring person-centred follow-up care for all children and adolescents is provided within 48 hours may be considered, similar to adults presenting with high concerns. As the number of children and adolescents presenting to emergency departments for suicide attempts has increased since the COVID-19 pandemic,3 future research in this area should evaluate all modalities for active follow-up care, including text messages, telephone calls, email, and home visits specific to children and adolescents presenting to the emergency department due to suicidal ideation or attempt who are not admitted to hospital.
References
1.Public Health Agency of Canada. Suicide in Canada: Key statistics (infographic). 2023; https://www.canada.ca/en/public-health/services/publications/healthy-living/suicide-canada-key-statistics-infographic.html. Accessed 2023 July 2.
2.Kingsbury M, Hammond NG, Johnstone F, Colman I. Suicidality among sexual minority and transgender adolescents: a nationally representative population-based study of youth in Canada. CMAJ. 2022;194(22):E767-E774. PubMed
3.Madigan S, Korczak D, Vaillancourt T, et al. Comparison of paediatric emergency department visits for attempted suicide, self-harm, and suicidal ideation before and during the COVID-19 pandemic: a systematic review and meta-analysis. Lancet Psychiatry. 2023;10(5):342-351. PubMed
4.Kennebeck S, Bonin L. Suicidal behavior in children and adolescents: Epidemiology and risk factors. Waltham (MA): UpToDate; 2023.
5.World Health Organization. Suicide. 2021; https://www.who.int/news-room/fact-sheets/detail/suicide.
6.Mental Health Commission of Canada. Post-attempt follow-up and regular contact interventions. 2020. https://mentalhealthcommission.ca/wp-content/uploads/2021/09/Suicide_Care_Evidence_Brief_eng.pdf
7.Self-harm: assessment, management and preventing recurrence (NG225). London (GB): National Institute for Health and Care Excellence; 2022: https://www.nice.org.uk/guidance/ng225. Accessed 2023 Jul 2.
8.Doupnik SK, Rudd B, Schmutte T, et al. Association of Suicide Prevention Interventions With Subsequent Suicide Attempts, Linkage to Follow-up Care, and Depression Symptoms for Acute Care Settings: A Systematic Review and Meta-analysis. JAMA Psychiatry. 2020;77(10):1021-1030. PubMed
9.Inagaki M, Kawashima Y, Yonemoto N, Yamada M. Active contact and follow-up interventions to prevent repeat suicide attempts during high-risk periods among patients admitted to emergency departments for suicidal behavior: a systematic review and meta-analysis. BMC Psychiatry. 2019;19(1):44. PubMed
10.McIntyre H, Reeves V, Loughhead M, Hayes L, Procter N. Communication pathways from the emergency department to community mental health services: A systematic review. Int J Ment Health Nurs. 2022;31(6):1282-1299. PubMed
11.Skopp NA, Smolenski DJ, Bush NE, et al. Caring contacts for suicide prevention: A systematic review and meta-analysis. Psychol Serv. 2023;20(1):74-83. PubMed
12.Hou X, Wang J, Guo J, et al. Methods and efficacy of social support interventions in preventing suicide: a systematic review and meta-analysis. Evid Based Ment Health. 2022;25(1):29-35. PubMed
13.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
14.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
15.Witt K, Hetrick S, Rajaram G, et al. Interventions for self-harm in children and adolescents. Cochrane Database Syst Rev. 2021;(3):CD013667. PubMed
16.Chaudhary AMD, Memon RI, Dar SK, Bhullar DK, Dar KR, Naveed S. Suicide during Transition of Care: a Review of Targeted Interventions. Psychiatr Q. 2020;91(2):417-450. PubMed
17.King CA, Grupp-Phelan J, Brent D, et al. Predicting 3-month risk for adolescent suicide attempts among pediatric emergency department patients. J Child Psychol Psychiatry. 2019;60(10):1055-1064. PubMed
18.Martinez-Ales G, Jimenez-Sola E, Roman-Mazuecos E, et al. An Emergency Department-Initiated Intervention to Lower Relapse Risk after Attempted Suicide. Suicide Life Threat Behav. 2019;49(6):1587-1599. PubMed
19.Malakouti SK, Nojomi M, Ghanbari B, Rasouli N, Khaleghparast S, Farahani IG. Aftercare and suicide reattempt prevention in Tehran, Iran: Outcome of 12-month randomized controlled study. Crisis. 2022;43(1):18-27. PubMed
20.Fossi L, Debien C, Demarty A, Vaiva G, Messiah A. Suicide reattempt in a population-wide brief contact intervention to prevent suicide attempts: The VigilanS program, France. Eur Psychiatry. 2021;64(1). PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Skopp et al. (2023)11 US Funding source: NR | RCTs Studies published up to February 11, 2020 Included studies: 6 RCTs; 0 relevant to the present review | Broader review: Patients deemed by medical or behavioural health services to be at elevated risk for suicide. All included studies were in adults, with some studies including patients discharged from psychiatric care. | Eligible intervention: Caring Contacts (contacts were text-based, including email, letter, text message, or postcard). Most studies had follow-up care starting more than 1-week post emergency department discharge. Comparator: Not specified | Outcomes reported: All-cause mortality; suicide mortality; suicidal ideation; suicide attempts; emergency department readmissions; psychiatric inpatient and general admissions; representation for self-harm; medial evacuation; self-injury Follow-up: NR |
Hou et al. (2022)12 China Funding source: Authors have not declared specific grant from any funding agency in the public, commercial or not-for-profit sectors | Classification of social support interventions portion of review: all studies Meta-analysis: RCTs Studies published up to May 31, 2021 Included studies: 77 studies in classification review; 14 RCTs included in meta-analysis; 0 relevant to the present review | Broader review: Suicidal individuals Included studies were in adults, patients in psychiatric inpatient units, in hospital, or delivered to students in a school setting. | Eligible intervention: Studies aimed at preventing suicide through method(s) that directly provide social support. Many studies had follow-up care starting more than 1-week post emergency department discharge. Comparator: Treatment as usual or “the latter serving group” for comparative studies; No comparator for noncomparative studies | Outcomes reported: Suicide; suicide attempt; social support-related outcome Follow-up: NR |
Witt et al. (2021)15 Australia Funding source: National Institute for Health Research | RCTs Studies published up to July 4, 2020 Included studies: 17 RCTs; 1 RCT relevant to the present review | Broader review: Children and adolescents (up to 18 years of age) with a recent (within 6 months of trial entry) presentation to hospital or clinical service for self-harm (e.g., self-poisoning, self-injury) Some included studies had patients admitted to hospital. Relevant included study: Adolescents aged 12 to 18 years old presenting to hospital following a suicide attempt | Eligible interventions: Psychosocial or pharmacological treatments. Many studies evaluated cognitive-behavioural therapy, group therapy, dialectical behaviour therapy, mentalization based therapy, home-based family therapy, and pharmacological therapies. Comparator: Treatment as- usual, routine psychiatric care, enhanced usual care, active comparator, placebo, alternative pharmacological treatment, or a combination of these. Relevant intervention: Described as compliance-enhancement approach; a single 1-hour session, before emergency department discharge, to review expectations for outpatient treatment, address common treatment misconceptions, a verbal treatment contract, and a series of 4 telephone calls at 1, 2, 4 and 8 weeks' post-discharge (duration not reported). Intervention delivered by 3 postdoctoral fellows in psychology (experience not reported) Relevant comparator: Treatment as usual, a standard disposition planning consisting of a brief (duration not reported) inpatient treatment and/or an outpatient appointment, as appropriate | Outcomes reported in relevant primary study: adherence to psychotherapy; repeat self-harm and death by suicide Follow-up: Up to 2 years |
Chaudhary et al. (2020)16 Pakistan Funding source: NR | RCTs, nonrandomized clinical trials, cohort, descriptive analysis Studies published up to January 2019 Included studies: 30 RCTs, 8 nonrandomized clinical trials, 1 cohort study, 1 descriptive study; 1 nonrandomized clinical trial relevant to the present review | Broader review: No restriction on race, place, sex, age, and ethnicity were applied. Included studies were in adults, patients admitted to hospital, or patients in psychiatric inpatient units Relevant included study: Adolescents aged 12 to 18 years old seen at general hospital for a suicide attempt requiring medical care | Intervention: Interventions to target suicidal behaviours after discharge from a medical facility to the community Included studies had follow-up care starting more than 1-week post emergency department discharge, and sent letters to general practitioners, Comparator: NR Relevant intervention: Structured 3 telephone intervention with patients and parents at 1, 2, and 6 weeks following discharge; Intervention delivered by a doctor-level clinician Relevant comparator: Treatment as usual (not further described) | Outcomes reported in relevant primary study: School functioning; Suicidal behaviours, Psychotherapy visits Follow-up: NR |
Doupnik et al. (2020)8 US Funding source: National Institute of Mental Health of the National Institutes of Health | Studies with a comparison group Studies published January 1, 2000 to December 31, 2019 Included studies: 14 studies (design not reported); 0 relevant to the present review | Broader review: Patients with identified suicide risk Included studies were in adults, patients admitted to hospital, or adolescents seeking nonpsychiatric emergency department services | Intervention: Intervention (i.e., brief acute care suicide prevention) delivered in a single in-person encounter to patients with identified suicide risk. Interventions consisting solely of a brief follow-up contact were ineligible for inclusion Some studies had intervention delivered only during hospitalization Comparator: NR | Outcomes listed in PROSPERO: Suicide death; Suicide ideation; Suicide attempt; Suicide-related health care visit Outcomes included in meta-analysis: Subsequent suicide attempts; Linkage to follow-up care; Depression symptoms at follow-up Follow-up: NR |
Inagaki et al. (2019)9 Japan Funding source: Japan Agency for Medical Research and Development | RCTs Studies published up to January 2015 Included studies: 28 RCTs (14 RCTs for active follow-up); 0 relevant to the present review | Broader review: Participants had attempted suicidal behaviour within 1 month and had been admitted to an emergency department for their suicidal behaviour Most included studies were in adults. | Interventions: All interventions (e.g., psychosocial intervention, psychotherapy, pharmacotherapy). Included studies had follow-up care starting more than 1-week post emergency department discharge, continuous case management, and pharmacotherapy Comparator: Placebo, treatment as usual and other expected intervention Relevant interventions: Interventions in the trial was performed while the patients were in the emergency department or a subsequent ward; Active contact and follow-up interventions (intensive care plus outreach, brief interventions and contact, letter/postcard, telephone, and composite of letter/postcard and telephone) | Outcomes reported: Recurrence of attempted suicide or self-harm; Completed suicide; Any cause of death Follow-up: NR |
NR = not reported; RCT = randomized controlled trial.
Note this appendix has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Note this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Systematic Reviews Using AMSTAR 213
Strengths | Limitations |
|---|---|
Skopp et al. (2023)11 | |
|
|
Hou et al. (2022)12 | |
|
|
Witt et al. (2021)15 | |
|
|
Chaudhary et al. (2020)16 | |
|
|
Doupnik et al. (2020)8 | |
|
|
Inagaki et al. (2019)9 | |
|
|
AMSTAR 2 = A Measurement Tool to Assess Systematic Reviews 2; PICO = population, intervention, comparator, outcomes; PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Appendix 4: Main Study Findings
Note this appendix has not been copy-edited.
Table 4: Summary of Findings by Outcome
Variable | Witt et al. (2021)15 N = 64 | Chaudhary et al. (2020)16 N = 97 |
|---|---|---|
Adherence to psychotherapy | ||
Psychotherapy session “no shows” | NR | Intervention: 9% Comparison: 18% |
Completed the full course of treatment | Intervention: 17/29 Comparison: 16/34 OR 1.59, 95% CI 0.59 to 4.33 | NR |
Average number of sessions attended | Intervention: mean 7.70 sessions (SD 5.80, n = 29) Comparison: mean 6.40 sessions (SD 4.40, n = 34) MD 1.30 95% CI −1.28 to 3.88; N = 63 | Intervention: mean 5.5 sessions Comparison: mean 3.9 session |
Number of reattempts and death by suicide | ||
Suicide deaths | Intervention: 0 suicides Comparison: 0 suicides | NR |
Suicide reattempts | NR | Intervention: 0% reattempted Comparison: 9% reattempted |
Repetition of self-harm at 6 months follow-up | Intervention: 3/29 Comparison: 5/34 OR 0.67, 95% CI 0.15 to 3.08 Repeat self-harm episodes: Intervention vs comparison: mean 0.10 vs. 0.15 | NR |
Depression | ||
NA | No data available | NR |
Hopelessness | ||
NA | No data available | NR |
General functioning | ||
NA | No data available | NR |
Social functioning | ||
NA | No data available | NR |
Suicidal ideation | ||
NA | No data available | NR |
CI = confidence interval; MD = mean difference; N = number; NA = not applicable; NR = not reported; OR = odds ratio; SD = standard deviation.
Appendix 5: References and Guidance of Potential Interest
Note this appendix has not been copy-edited.
The subsequent list of potentially relevant articles includes studies that may be relevant but were not included in the main analysis as they did not fulfill the PICO criteria (primarily due to age of study population). However, note that interventions assessing follow-up care among adults was not within the scope of the literature search and therefore, there are likely other studies related to adult population not mentioned here.
Korczak et al. (2020) details an ongoing RCT in Canada about a youth specific suicide prevention intervention. Although the primary aim of the study is to assess the specific intervention within emergency care, monitoring the study results may be useful for developing follow-up protocols.
Informal Scan of Emergency Department Follow-Up Guidance or Protocols for Suicide Ideation or Attempts
Online scanning and grey literature searching identified the following publicly available guidance documents or resources related to follow-up care produced by jurisdictions in Canada or internationally). The scan was not systematic or comprehensive. In particular, Canadian jurisdictions and health care centres may have other resources that are not publicly or easily accessible. The scan was also limited to English-language resources.
Table 5 lists the identified guidance documents, protocols, or recommendations that mention follow-up care among other aspects of delivering care for self-harm or suicide prevention. The recommendations summarized in the table are specifically related to follow-up care for people who are not admitted into inpatient settings and have been discharged from emergency care or other acute settings. These resources generally indicate that active follow-up care is recognized as being an important part of the care pathway. The resources recommend different options for follow-up periods, modalities, and health care professionals, but the resources do not consistently provide specific details about modalities or health care professionals who should be involved. Some reports recommend multiple stages of follow-up (e.g., immediate follow-up and subsequent follow-up over a longer time period). Guidance specifically for children and adolescents (under 18 years) was not identified.
Table 5: Guidance Documents Describing Follow-Up Protocols for People Visiting Emergency Care for Suicide Attempts or Ideation
Jurisdiction | Organization or hospital | Recommendations or findings | Link |
|---|---|---|---|
Canada (pan-Canadian) | Mental Health Commission of Canada |
| Post-Attempt Followup and Regular Contact Interventions Evidence Brief on Suicide Care (publication date not clear) |
Canada (British Columbia) | BC Mental Health and Addiction Services |
| The Provincial Suicide Clinical Framework (January 2011) |
UK | The National Institute for Health and Care Excellence | Regarding initial after care following self-harm, guidelines recommend:
| Self-harm: assessment, management and preventing recurrence (September 2022) |
Australia | Black Dog Institute | A member of the suicide response team within emergency or acute care should ensure people:
| Guidelines for integrated suicide-related crisis and follow-up care in Emergency Departments and other acute settings (November 2017) |
US (California) | Mental Health Services Oversight and Accountability Commission | California has set an objective for all hospitals and emergency departments to:
| California’s Strategic Plan for Suicide Prevention 2020 – 2025 (December 2019) |
US (New York State) | NY Center for Practice Innovations |
| A Guide for Clinicians (2021) |
DCP = discharge care plan.
Potentially Relevant Articles With Adult or Unclear Population
Betz ME, Knoepke CE, Simpson S, et al. An interactive web-based lethal means safety decision aid for suicidal adults (Lock to Live): Pilot randomized controlled trial. J Med Internet Res. 2020;22(1):e16253. PubMed
Lopez-Goni JJ, et al. Effectiveness of a telephone prevention programme on the recurrence of suicidal behaviour. One-year follow-up. Psychiatry Res. 2021;302(114029). PubMed
Malakouti SK, et al. Aftercare and suicide reattempt prevention in Tehran, Iran: Outcome of 12-month randomized controlled study. Crisis. 2022;43(1):18-27. PubMed
Martinez-Ales G, et al. An Emergency Department-Initiated Intervention to Lower Relapse Risk after Attempted Suicide. Suicide Life Threat Behav. 2019;49(6):1587-1599. PubMed
Shand F, Woodward A, McGill K, et al. Suicide aftercare services: an Evidence Check rapid review brokered by the Sax Institute for the NSW Ministry of Health, 2019. https://www.saxinstitute.org.au/wp-content/uploads/2019_Suicide-Aftercare-Services-Report.pdf
Stanley B, Brown GK, Brenner LA, et al. Comparison of the Safety Planning Intervention With Follow-up vs Usual Care of Suicidal Patients Treated in the Emergency Department. JAMA Psychiatry. 2018;75(9):894-900. PubMed
Wilson MP, Moutier C, Wolf L, Nordstrom K, Schulz T, Betz ME. ED recommendations for suicide prevention in adults: The ICAR2E mnemonic and a systematic review of the literature. Am J Emerg Med. 2020;38(3):571-581. PubMed
Additional References
Wilson MP, Kaur J, Blake L, et al. Adherence to guideline creation recommendations for suicide prevention in the emergency department: A systematic review. Am J Emerg Med. 2021;50:553-560. PubMed
Korczak DJ, Finkelstein Y, Barwick M, et al. A suicide prevention strategy for youth presenting to the emergency department with suicide related behaviour: protocol for a randomized controlled trial. BMC Psychiatry. 2020;20(1):20. PubMed
Contributors: Kristen Moulton, Elizabeth Carson
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca