CADTH Health Technology Review
Platelet-Rich Plasma Injections for Chronic Tendinopathies in the Upper Extremities
Rapid Review
Authors: Sara D. Khangura, Sharon Bailey
Abbreviations
AE
adverse event
ASES
American Shoulder and Elbow Surgeons
BCTQ
Boston Carpal Tunnel Syndrome Questionnaire
CMS
Constant-Murley score
CS
corticosteroid
DASH
Disabilities of the Arm, Shoulder and Hand
DN
dry needling
LP-PRPi
leukocyte-poor platelet-rich plasma injection
LR-PRPi
leukocyte-rich platelet-rich plasma injection
MA
meta-analysis
MCID
minimal clinically important difference
NMA
network meta-analysis
NR
not reported
PRPi
platelet-rich plasma injection
PRTEE
Patient-Rated Tennis Elbow Evaluation
PT
physiotherapy
RCT
randomized controlled trial
SPADI
Shoulder Pain and Disability Index
SR
systematic review
SST
Simple Shoulder Test score
UCLA
University of California Los Angeles
VAS
visual analog scale
VISA
Victorian Institute of Sports Assessment
WORC
Western Ontario Rotator Cuff Index
Research Question
What is the clinical effectiveness of platelet-rich plasma injections for the treatment of adults with chronic tendinopathies in the upper extremities?
Key Messages
Findings from evidence syntheses describing the comparative clinical effectiveness of platelet-rich plasma injection (PRPi) in the treatment of chronic tendinopathies of the upper extremities were variable.
Whereas findings describing function showed no clear demonstration of effect, some findings describing pain suggested there may be potential for a benefit of PRPi with higher concentrations of leukocytes or longer durations of follow-up.
Lack of a clear demonstration of the comparative clinical effectiveness of PRPi in chronic tendinopathies of the upper extremities does not currently support decision-making in favour of its use.
Context and Policy Issues
What Are Chronic Tendinopathies in the Upper Extremities?
Chronic, or persistent, tendinopathy is a common disorder that is characterized by pain and loss of function,1 and has been described as accounting for 30% of musculoskeletal conditions.2 Chronic tendinopathies represent a range of conditions, based on the location of the affected tendon, with chronic tendinopathies of the upper extremities occurring in the shoulder (e.g., rotator cuff), elbow (i.e., epicondylitis), or wrist and hand (e.g., carpal tunnel).3,4 Chronic tendinopathies of the upper extremities can cause pain, swelling, and can interfere with the daily activities (including performance in exercise and sport), as well as quality of life.2
Causes of chronic tendinopathies may vary, but they are often believed to be the result of overuse1 and/or impaired healing of injury.2,5 Risk factors for developing chronic tendinopathy include intrinsic factors (such as age and previous injury) and extrinsic factors (such as exposure to high-intensity exercise).1
What Is Platelet-Rich Plasma Injection?
Platelet-rich plasma (PRP) is a biologic treatment and blood product containing concentrated growth factors, which are thought to reduce inflammation and promote healing.2,6 PRP has been described as a general term for a therapy lacking standardization in its composition and administration.7 PRP has also been described as a costly intervention, incurring greater expense versus other nonsurgical therapies,8 and is not always reimbursed by payers or insurers.9
There are multiple treatments available for chronic tendinopathies — including those of the upper extremities — with conservative therapies including physiotherapy (PT) and/or systemic pharmacotherapy for pain.3,10 Other nonsurgical treatments include injection therapies to improve pain and function that may be used following more conservative therapies, such as corticosteroids (CSs), dry needling (DN), or platelet-rich plasma injection (PRPi).11 While PRPi is not thought to be curative, it has been hypothesized that pain and function may be improved in response to its administration.11
Why Is It Important to Do This Review?
The incidence of chronic tendinopathies, in general, has been on the rise and is thought to be associated with greater participation in recreational exercise and sport among middle-aged individuals.1 While no Canadian data specific to the incidence or prevalence of chronic tendinopathies in the upper extremities were identified, a survey of adults living in Canada indicated the shoulder, elbow, and wrist were among the top 20 most common sites of chronic pain.12 Notably, it has been suggested that tendinopathies of the upper extremities may respond differently to treatment than those of the lower extremities, based on factors associated with the central nervous system.3
Current recommendations for the nonsurgical management of chronic tendinopathies include physiotherapy and nonsteroidal anti-inflammatory drugs (NSAIDs); others, including PRPi, have been described as alternative treatments with limited evidence demonstrating clinical efficacy,3,7 which make decisions concerning the use of PRPi in chronic tendinopathies of the upper extremities challenging.
In 2019, Health Canada clarified its classification of PRP as a drug, confirming its distinction from cell therapies.13 Nonetheless, concern has been raised about this classification, which renders PRP broadly available in Canada despite the limited evidence demonstrating its effectiveness.14
Objective
To support decision-making about the use of PRPi in chronic tendinopathies of the upper extremities, we conducted this review to summarize recent, available evidence describing its clinical effectiveness.
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, and the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevance. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research question and selection criteria. The main search concepts were platelet-rich plasma injections and tendinopathies. Conference abstracts were excluded. Retrieval was limited to the human population. The search was completed on May 8, 2023, and limited to English-language documents published since January 1, 2018.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for eligibility. The final selection of full-text articles was based on the eligibility criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults with chronic tendinopathies in the upper extremities (e.g., lateral epicondylitis, rotator cuff tendinopathy) |
Intervention | Platelet-rich plasma injections |
Comparator | Usual care (e.g., no treatment with platelet-rich plasma injections, exercise or physiotherapy, cortisone injections, or nonsteroidal anti-inflammatory drugs) |
Outcomes | Clinical benefits (e.g., improvement in pain, function, mobility, quality of life, patient satisfaction) and harms (e.g., adverse events) |
Study designs | Health technology assessments and systematic reviews |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2018. Reports of acute tears and other injuries in which the tendon did not remain intact were interpreted as distinct from chronic tendinopathies, and were therefore excluded.1 Studies reporting PRPi comparisons with “alternative interventions” (i.e., not considered usual care), local anesthetic injections, whole blood injections, radiation, stem cell therapy, extracorporeal shockwave therapy, and hyaluronic acid injection, as well as studies reporting no comparator (i.e., single-arm studies), were excluded. Systematic reviews (SRs) in which all relevant studies were captured in other more recent or more comprehensive SRs were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically assessed by 1 reviewer using A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)15 for SRs, with additional considerations applied to overviews of reviews. The ISPOR checklist was used to critically assess network meta-analyses (NMAs).16 Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included review were summarized narratively.
Summary of Evidence
Quantity of Research Available
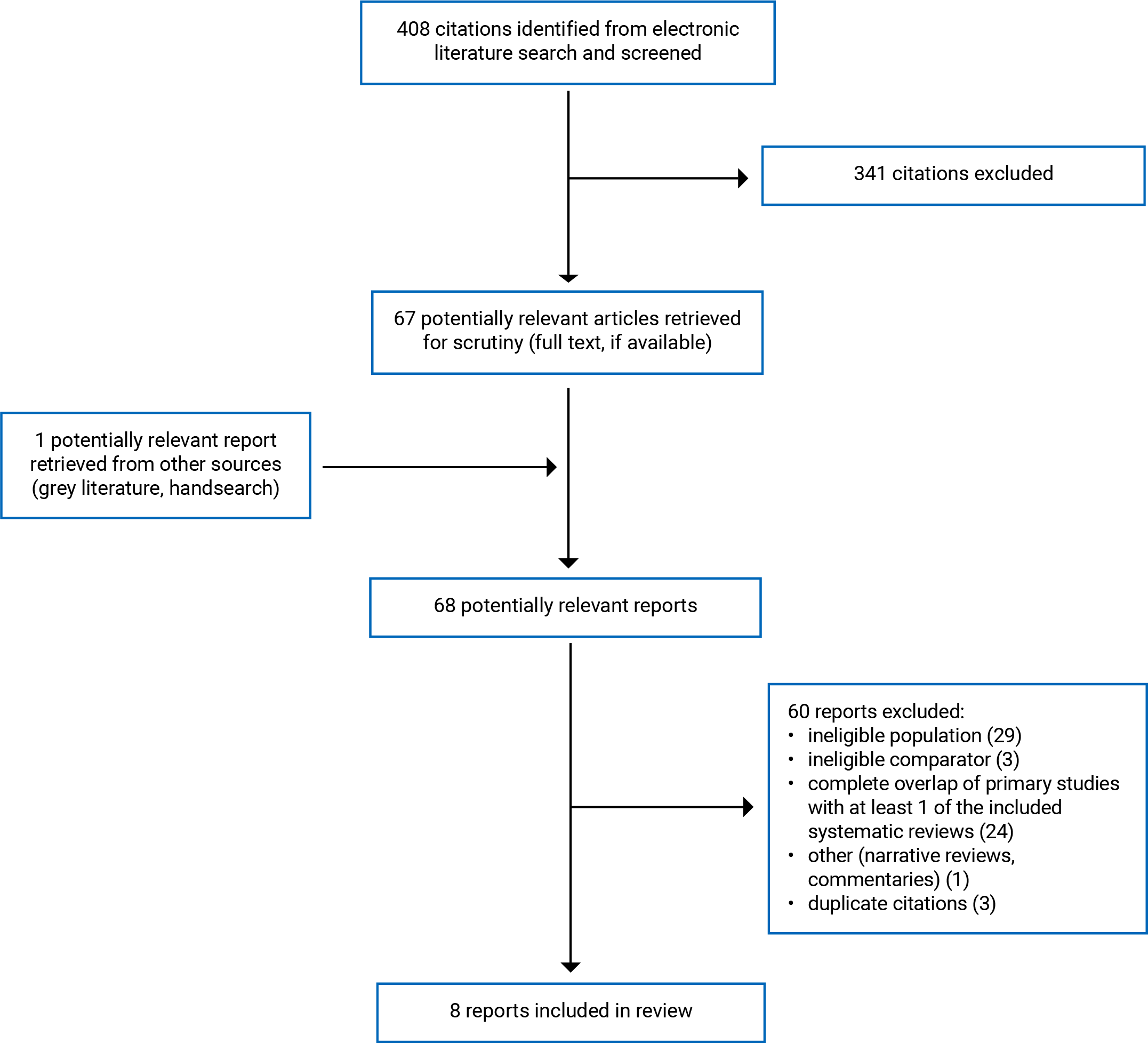
A total of 408 citations were identified in the literature search. Following screening of titles and abstracts, 341 citations were excluded and 67 potentially relevant reports from the electronic search were retrieved for full-text review. There was 1 potentially relevant publication retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 60 publications were excluded for various reasons, and 8 publications met the inclusion criteria and were included in this report. These comprised 2 overviews of SRs and meta-analyses (MAs),17,18 1 NMA,19 and 5 SRs.20-24 Appendix 1 presents the PRISMA25 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 6.
Summary of Study Characteristics
This review identified and summarized 2 overviews of SRs and MAs,17,18 1 NMA,19 and 5 SRs.20-24 Characteristics of included reviews are tabulated and detailed in Appendix 2.
Seven of the 8 reviews were broader in scope than the eligibility criteria for the current review, and included SRs, MAs, and primary studies that were not relevant to this report;17-21,23,24 thus, from the included reviews, only the subset of 42 unique studies that were relevant to this report were summarized. Of the relevant included primary studies in the NMA and SRs, there was considerable overlap, which is characterized in a matrix
The included overviews of SRs and MAs were conducted in the US17,18 and published in 201918 and 2020,17 with searches that spanned an unspecified start date to June 201718 and search database inception to February 2020.17 The NMA was conducted in India and published in 2022, with a search that spanned search database inception until June 2021.19 The 5 included SRs were conducted in Italy,20 China,21,24 Malaysia,22 and Australia,23 and were published between 2020 and 2023, with search time frames that ranged from 1946 (or search database inception) to March 2022.20-24 Authors of the NMA described use of a frequentist statistical framework to inform their methods.19
Patient populations included those with chronic tendinopathies of the shoulder (e.g., rotator cuff),17,21,22 elbow (i.e., lateral epicondylitis),17-19,23,24 or wrist and hand (e.g., carpal tunnel),20 with age either not reported17,24 or ranging between 18 years and 79 years.18-23 All of the reviews described investigations of PRPi, with 7 not distinguishing between types of PRPi based on leukocyte concentration,17,18,20-24 and 1 describing both leukocyte-poor PRPi (LP-PRPi) and leukocyte-rich PRPi (LR-PRPi).19 The included reviews compared PRPi with 1 or more multiple comparators, including saline (i.e., placebo) injections,17-20,22 steroids (either administered as CS injections, or with mode of administration not reported),17-21,23,24 DN,17,22,23 and/or PT.20,22 The included NMA19 reported network comparisons both of relevance and beyond the scope of the present review; specifically, between LP-PRPi, LR-PRPi, steroids, placebo (saline), laser therapy, local anesthetic, whole blood, and surgery. Only the relevant comparisons (i.e., PRPi with leukocyte concentrations not specified, LP-PRPi, or LR-PRPi versus placebo [saline] or steroids) were described in this report.
Outcomes included measures of function, including the American Shoulder and Elbow Surgeons (ASES) score, Boston Carpal Tunnel Syndrome Questionnaire (BCTQ), Constant-Murley score (CMS), Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire, Nirschl stage, Patient-Rated Tennis Elbow Evaluation (PRTEE), Shoulder Pain and Disability Index (SPADI), Simple Shoulder Test (SST) score, University of California Los Angeles (UCLA) shoulder rating scale score, and the Western Ontario Rotator Cuff (WORC) index score.17,19-23 Both of the overviews of SRs listed the measures described by included SRs, and described findings for pain and/or function across the included SRs narratively, without specifying which outcomes were measured by the scales and scores listed.17,18 This made it unclear as to which measures were used to render the findings described.17,18
Pain was reported in the 8 reviews, all of which described use of the visual analogue scale (VAS) for measurement.17-24 One of the overviews of reviews also reported use of the Pain Pressure Threshold (PPT) score.18
Other outcomes included symptom severity measured by the BCTQ (severity subscale),20 and adverse events (AEs).21-23 Of note, both of the overviews of SRs and MAs described the use of additional outcome measures that were not described by other reviews included in this report (i.e., Neer Test, Tegner Activity Scale, Lysholm Scale, Likert global assessment scale, EQ-5D, and Roles and Maudsley score); however, the outcomes that were measured by these scales or scores were not reported, nor was any other information.17,18
Follow-up of outcomes ranged from 1 week to 24 months in the 5 included SRs,20-24 but was not reported in the overviews of SRs and MAs,17,18 and was not clearly reported in the NMA (i.e., reported only as between 2 and 24, with the unit[s] of measurement not reported).19
Summary of Critical Appraisal
SRs and Overviews of SRs and MAs
Reporting
All of the 7 included SRs and overviews of SRs and MAs provided some description of their inclusion criteria;17-24 however, 3 reviews did not describe either the establishment of an a priori method or development of a review protocol.17,18,21 A pre-established method is important for informing the conduct of reviews and allows readers to assess any protocol deviations that could introduce a risk of bias to the findings of the review.15 The rationale for limiting inclusion of study designs was either not reported or not explicitly stated by the 5 included SRs and the NMA,19-24 whereas the overviews of SRs and MAs did provide some description of their rationale for limiting included studies to SRs.17,18
Included studies were described in sufficient detail by 3 SRs,21-23 whereas some information describing the intervention and/or comparator(s) (e.g., number of injections, dose, frequency) was missing in 4 reviews.17,18,20,24 The overviews of SRs and MAs had information missing on either the outcomes measured (i.e., including only the outcome measure without a description of what was being measured) or the measures used.17,18 Whereas 3 of the SRs were explicit in defining what constituted a minimal clinically important difference (MCID),21,23,24 both of the overviews of SRs and MAs and 2 SRs either did not define what constituted an MCID17,18,22 or did not explicitly define the MCID used.20
Four of the included reviews were explicit in reporting sources of funding,18,21,23,24 and 2 reported that no funding was received to support conduct of the review.17,22 One review did not report any information about source(s) of funding.20 This information is important for assessing any potential conflict of interest or risk of bias (RoB) introduced by funding source(s).
Finally, both of the overviews of SRs and MAs reported an analysis of overlap between primary studies in their included SRs and MAs.17,18
Search Strategy
While all of the included reviews performed searches in 2 or more relevant databases,17,18,20-24 and all but 117 reported the search keywords used, only 1 SR described consultation with an expert biomedical librarian in the development of the search strategy.23 A comprehensive search should draw from the expertise of an information specialist to ensure that the strategy uses adequate search terms and is sufficiently sensitive and specific.15 Further, whereas search time frames were clearly and explicitly reported by 4 of the included reviews,17,21,23,24 3 reviews did not clearly or completely report the dates of the search(es) conducted.18,20,22
Review Methods
Study selection was performed by 2 independent reviewers in 5 included reviews,17,18,21,23,24 whereas 2 reported no information on the number of reviewers that performed study selection.20,22 Four reviews reported that data abstraction was performed by 2 independent reviewers,17,20,21,23 and 3 either reported no information on the number of reviewers who completed data abstraction, or reported that it was performed by 1 reviewer.18,22,24 RoB assessments conducted by 2 independent reviewers were reported by all of the 7 included reviews summarized in this report.17,18,20-24 Duplicate study selection, data abstraction, and RoB assessment are important features of a robust method that reduce the risks of error and bias in the review.15
Neither of the overviews of SRs and MAs conducted any meta-analyses, summarizing their findings narratively.17,18 Of the 5 SRs, all reported findings from meta-analyses, with 1 describing appropriate statistical methods;23 however, it was unclear whether appropriate statistical methods were applied in the remaining 4 SRs, given the acknowledgement of heterogeneity across primary studies included in the MAs.20-22,24 Four of the 5 SRs described an assessment of the risk of publication bias,20-23 whereas 1 did not;24 however, only 1 provided a description of the potential impact of publication bias on the findings of the review,23 whereas 3 did not.20-22
Heterogeneity between the included studies and its potential impact on the findings of the review was reported in sufficient detail by 5 of the included reviews,18,21-24 while 2 either made a cursory mention of heterogeneity and/or did not describe its potential impact on the review findings.17,20
Network Meta-Analysis
The included NMA described populations, interventions, outcomes, and context that were relevant and applicable to the current review, and the included trials formed a network.19 The SR methods were appropriate, including a comprehensive search strategy, justification for the use of random effects models, and sensitivity analyses to explore heterogeneity; however, findings from individual studies were not provided, and it was unclear whether statistical methods were used to preserve within-study randomization.19 Further, while the results from direct and indirect comparisons were reported separately (as available), and an analysis of consistency was reported, there was some inconsistency observed between the direct and indirect estimates of effects.19 This inconsistency may be an indicator of insufficient transitivity (i.e., the requirement that indirect comparisons are drawn from studies that are sufficiently similar in their methods and any effect modifiers).16 Finally, the conclusions were fair and balanced and the authors reported no sources of funding or conflicts of interest.19
Additional details regarding the strengths and limitations of included reviews are provided in Appendix 3.
Summary of Findings
Clinical Effectiveness of PRPi
Function
Measures of function were reported in 7 of the 8 reviews included in this report,17-23 with 2 describing rotator cuff tendinopathy,17,21 4 describing lateral epicondylitis,18,19,22,23 and 1 describing tendinopathies of carpal tunnel syndrome.20 Across the conditions, comparisons, outcome measures, and follow-up time frames described, findings were mixed, with many indicating no difference between PRPi and comparators, and fewer indicating either a comparative benefit of PRPi or a comparative benefit of control interventions.17-23
Rotator Cuff Tendinopathy
One overview of SRs and MAs17 and 1 SR21 reported on various measures of function in patients with rotator cuff tendinopathies, describing findings from 1 SR (5 randomized controlled trials [RCTs]; number of patients not reported [NR])17 and 16 MAs (11 RCTs; number of patients ranging from 90 to 247),21 respectively (Table 8).
One overview of SRs reported findings from comparisons of PRPi with placebo or DN, noting that a “slight improvement” was observed in the PRPi group (data not provided; statistical or clinical significance not specified).17
Of the 16 MAs reported in 1 SR, all of the comparisons were between PRPi and CS, using 6 measures (ASES, CMS, DASH, SST, UCLA, WORC).21
At short-term follow-up (< 2 months):
no statistically significant difference between treatment groups was reported in 5 of the 6 measures (5 MAs; 3 RCTs to 6 RCTs; 90 patients to 217 patients)
a statistically significant benefit of PRPi was reported in DASH scores (although the threshold for clinical significance was not met) (1 MA; 5 RCTs; 169 patients).
At midterm follow-up (2 months to 6 months):
no statistically significant difference between treatment groups was observed in DASH scores (1 MA; 5 RCTs; 247 patients)
a statistically significant benefit of PRPi was reported in ASES, SST, and WORC scores (however, whereas the threshold for clinical significance was met for ASES and WORC scores, the threshold for clinical significance was not met for SST scores)(3 MAs; 3 RCTs to 5 RCTs; 90 patients to 189 patients)
a statistically significant benefit of CS was reported in CMS scores (although the threshold for clinical significance was not met) (1 MA; 5 RCTs; 129 patients).
At long-term follow-up (> 6 months):
no statistically significant difference between treatment groups was observed in ASES, SST, and UCLA scores (3 MAs; 2 RCTs to 4 RCTs; 90 patients to 189 patients)
a statistically significant benefit of PRPi was reported in CMS scores (although the threshold for clinical significance was not met) (1 MA; 6 RCTs; 217 patients)
a statistically significant benefit of CS was reported in DASH scores (although the threshold for clinical significance was not met) (1 MA; 3 RCTs; 127 patients).
Lateral Epicondylitis
Measures of function in lateral epicondylitis were reported in 1 overview of MAs,18 the NMA,19 and 2 SRs22,23 (Table 8).
PRPi was compared with placebo (saline) in the overview of MAs18 and the included NMA.19
PRPi was compared with CS in the overview of MAs,18 the NMA,19 and 1 SR.23
No statistically or clinically significant differences were demonstrated between treatment groups in 6 NMA comparisons (3 direct and 3 indirect comparisons) of DASH or PRTEE scores (number of patients and RCTs NR)19 as well as 1 SR describing various measures of function (2 RCTs; 30 patients to 60 patients; short-term follow-up).23
PRPi was described as effective in 1 overview of MAs (data not provided; statistical and clinical significance NR) (2 RCTs; number of patients NR)18 and was found to have demonstrated a statistically and clinically significant benefit in 1 SR describing various measures (1 RCT; 60 patients; midterm and longer-term follow-up).23
CS demonstrated a statistically and clinically significant improvement in 2 NMAs (1 direct and 1 indirect comparison) of DASH scores (number of patients and RCTs NR).19
Two SRs22,23 summarized evidence describing PRPi versus other comparators (i.e., DN, PT, and mixed comparisons).
No statistically significant difference was demonstrated between PRPi and control groups in 5 MAs (2 RCTs to 4 RCTs; 70 patients to 291 patients; DASH and SPADI scores)22 and 1 RCT (28 patients; measure NR).23
A statistically significant benefit of PRPi was demonstrated in 3 MAs (although clinical significance was NR) (2 RCTs; 70 patients to 228 patients; SPADI scores).22
Carpal Tunnel Syndrome
One SR reported findings from 3 RCTs describing a comparison of PRPi with several comparators (i.e., placebo, steroids, or PT) at 1 month to 12 months of follow-up using the BCTQ (functional score)20 (Table 8).
No statistically significant differences were observed between PRPi and placebo at 1 month to 12 months of follow-up in 1 RCT (48 patients), as well as at 1 month of follow-up in another RCT (98 patients).20
A statistically significant benefit of steroids was reported at 3 months of follow-up (1 RCT; 60 patients) as well as PT at 1 month to 6 months of follow-up (although clinical significance was NR) (1 RCT; 60 patients).20
Pain
Of the 7 included reviews that reported on pain,18-24 3 described chronic tendinopathies of the shoulder,21,22,24 3 of the elbow,18,19,23 and 1 of the wrist or hand.20 Across the conditions, comparisons, and follow-up time frames described, findings were again mixed, with some indicating no difference between PRPi and comparators, and others indicating a comparative benefit of PRPi18-24 (Table 9).
Rotator Cuff Tendinopathy
Two SRs described comparisons of PRPi with CS21,24 (Table 9).
One SR reported findings from 6 relevant RCTs.21
At short-term follow-up, 3 of 6 RCTs reported estimable data (with 3 not producing an estimable mean difference), 2 of which observed no statistically or clinically significant difference between treatment groups, while 1 reported a significant benefit of PRPi (range of 58 patients to 99 patients).
In an MA of 5 RCTs at midterm follow-up, a statistically and clinically significant benefit of PRPi was reported (157 patients).
At longer-term follow-up, findings from 3 RCTs were available, all of which reported a statistically significant benefit of PRPi (although only 1 RCT demonstrated a clinically significant benefit) (range of 60 patients to 99 patients).21
Another SR reporting findings from 1 RCT indicated no statistically significant difference between treatment groups at 1 month and 2 months of follow-up, but reported a statistically and clinically significant improvement in patients who received PRPi at 6 months of follow-up (83 patients).24
One SR described 5 MAs describing PRPi compared with saline (placebo), DN, or PT22 (Table 9).
At 1 month, 3 months, and 6 months of follow-up, no statistically significant difference between treatment groups was found (4 RCTs to 6 RCTs; 227 patients to 259 patients).
At 12 months of follow-up, a statistically significant benefit of PRPi was reported (although clinical significance was NR) (4 RCTs; 274 patients).
An MA combining the findings across follow-up durations found no statistically significant difference between treatment groups (8 RCTs; reported as 1,007 patients).22
Lateral Epicondylitis
One overview of MAs,18 1 NMA,19 and 1 SR23 reported information and/or data from comparisons of PRPi with CS (Table 9).
the overview of MAs narratively summarized information from 3 RCTs, with follow-up ranging from 12 weeks to 12 months across 2 RCTs (and NR in 1 RCT), reporting that PRPi was an effective treatment (data not provided and statistical and/or clinical significance NR).18
The SR reported data from 2 RCTs describing short-term (> 3 weeks to 6 weeks), midterm (> 6 weeks to 3 months) and longer-term (> 3 months to 6 months) follow-up.23
At short-term follow-up, both RCTs reported no statistically significant difference between PRPi and CS (90 patients).
At midterm and longer-term follow-up, 1 RCT reported a statistically and clinically significant benefit of PRPi (60 patients).
The NMA reported direct and indirect comparisons for both LP-PRPi and LR-PRPi.19
No statistically significant difference was found in either direct or indirect comparisons between LP-PRPi and CS, whereas a statistically and clinically significant benefit of LR-PRPi was reported for both comparisons.
One overview of MAs18 and 1 NMA19 reported information and/or data from comparisons of PRPi with placebo (saline) (Table 9).
The overview of MAs described information from 2 RCTs, with follow-up ranging from 8 weeks to more than 6 months (although follow-up was NR in 1 RCT); whereas 1 reported that PRPi demonstrated a significantly greater improvement, the other reported that PRPi demonstrated no comparative clinical benefit (data not provided and statistical and clinical significance NR).18
The NMA reported direct and indirect comparisons for both LP-PRPi and LR-PRPi.19
No statistically significant difference was found in either direct or indirect comparisons between LP-PRPi and CS, whereas a statistically and clinically significant benefit of LR-PRPi was reported for both comparisons.
One SR described data from 1 RCT comparing PRPi and DN at midterm and longer-term follow up23 (Table 9).
No statistically significant difference between treatment groups was found at either duration of follow-up (28 patients).
Carpal Tunnel Syndrome
One SR reported findings from 1 MA at 3 months of follow-up (2 RCTs; 158 patients) and 1 RCT at 6 months of follow-up (60 patients), with the comparator groups described only as “controls”20 (Table 9).
Both findings demonstrated a statistically significant benefit of PRPi (though, clinical significance was not defined or specified).
Symptom Severity
Carpal Tunnel Syndrome
One SR reported findings on symptom severity from 3 RCTs at 1 month, 3 months, 6 months, and 12 months of follow-up (range of 48 patients to 98 patients) comparing PRPi to placebo, steroids, or PT20 (Table 10).
At 1 month of follow-up, there was no statistically significant difference observed between treatment groups in any of the 3 RCTs.
At 3 months of follow-up, a statistically significant benefit of PRPi was demonstrated in all 3 RCTs (although clinical significance was not defined or specified).
At 6 months of follow-up, a statistically significant benefit of PRPi was demonstrated as compared to placebo (although clinical significance was not defined or specified) (1 RCT; 48 patients).
At 12 months of follow-up, there was no statistically significant difference between treatment groups as compared to placebo (1 RCT; 48 patients).
Adverse Events
Of the 3 SRs reporting on AEs,21-23 findings from 4 RCTs were summarized (Table 11).
Rotator Cuff Tendinopathy
Two SRs described AEs in tendinopathies of the rotator cuff21,22 (Table 11).
One SR described 2 RCTs comparing PRPi to CS (179 patients), indicating that lower rates of any AE and treatment failure were observed in the PRPi groups (data not provided, and statistical and clinical significance were NR).21
One SR described 1 RCT comparing PRPi to saline (84 patients), which described greater numbers of postinjection pain, frozen shoulder, and extension of lesion size in the PRPi groups (data not provided, and statistical and clinical significance were NR).22
Lateral Epicondylitis
One SR reported data from 1 RCT (28 patients), demonstrating no statistically significant difference between PRPi and DN in any AEs, or study withdrawals due to AEs23 (Table 11).
Unspecified Outcomes
Lateral Epicondylitis
Of the 2 overviews of SRs and MAs that reported on unspecified outcomes, providing only the names of measures used,17,18 both described findings from 1 SR17 and 1 MA,18 respectively, comparing PRPi to CS, and 1 described findings from 2 MAs comparing PRPi to placebo18 (Table 12).
Compared to CS, both overviews reported that PRPi was a more effective treatment option (data not provided, and statistical and clinical significance were NR).17,18
Compared to placebo, findings from 1 MA were described as indicating no clinical benefit of PRPi, whereas findings from the other MA were reported as demonstrating a significant benefit of PRPi (data not provided, and statistical and clinical significance were NR).18
Limitations
The literature describing PRPi in chronic tendinopathies of the upper extremities is ample, with a broad variety of conditions, treatment protocols, comparators, and outcomes described. Despite the large numbers of primary studies and reviews available on this topic, 1 of the key limitations observed in this review was primary studies with small sample sizes and variable findings described in the included reviews. A second key limitation was a lack of clarity and standardization in the reporting and descriptions of interventions, comparators, outcomes, and measures.
Of the 8 reviews identified and included in this report, 42 unique primary studies of relevance were described and summarized,17-24 with 7 of the reviews reporting primary studies with sample sizes ranging between 9 patients and 119 patients,17-24 whereas the overview of MAs reported a mean number of patients per primary study as 118.18 Small study sample sizes may not have sufficient power to render valid and/or consistent findings, making their interpretation in an evidence synthesis challenging. This expanding number of primary research studies with small sample sizes and effect sizes has been identified as a challenge to decision-making about optimal approaches to the use of PRPi elsewhere in the literature,8 corroborating the findings of this review.
A lack of clarity in the description of chronic tendinopathies in the literature was also observed, with broad references to tendinopathies, diseases, or disorders, often leaving it unclear as to whether the condition(s) being described were chronic or acute, for instance. This made the interpretation of some of the literature on this topic challenging and unclear, as it concerned the populations of interest. Variability in reporting was also a limitation identified in this review; for instance, authors of most of the included reviews acknowledged that PRPi is described inconsistently in the literature, making interpretation of the composition of the intervention (e.g., leukocyte concentrations) and treatment protocols challenging,18-22,24 and creating the potential to produce variable findings across primary studies. This inconsistency was consequently observed in the description of the use of PRPi in the reviews included in this report, with several reviews not reporting on key features of the intervention, such as number(s) of injections, dose(s), frequency of injections, and/or intervals between multiple injections.17-20,24 Similarly, comparator arms of relevant primary studies were not described in sufficient detail to understand their composition in 6 of the included reviews.17-20,24 These deficits in reporting leave uncertainty as to whether any possible differences in PRPi or comparison treatment protocols may have contributed to the variability in the findings of SRs included in this review. For instance, if 1 PRPi injection was used in some of the study treatment protocols while multiple injections were used in others, the findings of these studies may have been impacted; however, because insufficient information was provided, the potential for this variability to impact findings and interpretation cannot be ascertained.
Likewise, unclear reporting of the outcomes measured in the included overviews of SRs and MAs was a limitation observed in this review, i.e., with only the measures reported, it was unclear which outcomes were being described.17,18 This lack of clarity in the description of what was measured in the reviews summarized in this report limits the clarity and interpretation of its findings.
Further, most of the included reviews commented on methodological limitations and a low quality of included evidence as limitations to their findings,19-24 including small sample sizes, risks of bias, and heterogeneity.
Finally, none of the 8 reviews summarized in this report were conducted in in Canada.17-24 In addition, while 5 of the reviews did not describe the countries within which the included SRs, MAs, or primary studies were conducted,17-20,24 1 SR described relevant primary studies from non-Canadian countries only,23 and 2 SRs described 1 primary study each that was conducted in Canada.21,22 The apparent scarcity of Canadian data may limit the generalizability of the findings of this report to the Canadian context.
Conclusions and Implications for Decision- or Policy-Making
This report identified and summarized 2 overviews of SRs/MAs,17,18 1 NMA,19 and 5 SRs of primary studies20-24 describing the clinical effectiveness of PRPi for chronic tendinopathies of the upper extremities.
The populations, composition, and/or treatment protocols of PRPi, comparators, outcomes, and durations of follow-up were either unclear or variable across the included reviews, as were the findings. For instance, while some of the reported findings demonstrated no observed comparative effect(s) of PRPi in chronic tendinopathies of the upper extremities,18-23 others indicated a statistically significant benefit of PRPi,17-23 and some demonstrated a statistically significant benefit of control interventions.19,22 Nonetheless, the clinical significance of findings that favoured either PRPi or the comparator intervention was less often demonstrated (or not described). It may be notable that while there was no clear pattern of effect describing function, several findings favoured PRPi in terms of improvements in pain — particularly at longer durations of follow-up.18,20-22,24 Statistically and clinically significant improvements in pain were also reported by the included NMA when comparing LR-PRPi to saline or CS (although no significant differences were reported in the comparisons of LP-PRPi with saline or CS).19
The proliferation of studies investigating the use of PRPi for chronic tendinopathies in recent years has been analyzed and commented on repeatedly in the literature;8,26,27 similarly, the lack of consensus and certainty as to its clinical effectiveness has been highlighted.28 Factors contributing to this uncertainty have been outlined in the relevant literature, and are similar to those identified in this report (e.g., small RCTs of limited quality with no or small effect sizes,2 as well as considerable lack of clarity and/or variability in PRPi components and treatment protocols),6,27,29-31 which have been identified as challenges in drawing conclusions from the research investigating PRPi’s effectiveness. One of the included overviews summarized in this report made particular mention of the need for larger and more methodologically rigorous RCTs in the future, given the limited quality of existing primary research and the consequent lack of consensus across multiple evidence syntheses on the topic.18 Another pointed out that demonstrating the clinical effectiveness of PRPi as compared to placebo is a necessary precursor to investigation of its effectiveness against other interventions; that is, if PRPi is demonstrated to be effective against placebo, then its effectiveness against other interventions may be of interest, whereas if PRPi is demonstrated to have no comparative effect versus placebo, then further investigation of its effectiveness is not warranted.23,32
CADTH has conducted past reviews of the clinical evidence describing PRPi for other indications, including orthopedic conditions, trauma,33 and low back pain.34 While the conditions reviewed in those reports are not entirely relevant to the research question posed in this report, it is notable that both reports similarly identified a lack of conclusive evidence supporting the clinical effectiveness of PRPi, with both indicating some evidence to support its safety, but a lack of evidence to support efficacy.33,34
Despite the variability of the findings in the literature summarized in this review, there may yet be potential for the clinical effectiveness of PRPi, given that some of the findings summarized herein have demonstrated effectiveness; for instance, it may be that some formulations of PRPi are more effective than others, or that any effect of PRPi is observed at a longer (as opposed to shorter) duration of follow-up. It may also be that advances in the technology of platelet-rich therapies, such as platelet-rich fibrin35 and plasma gel,36 could hold promise for clearer or more consistent improvement in clinical outcomes among musculoskeletal conditions. Nonetheless, measurement of effectiveness that can support clinical and other decisions concerning the use of PRPi in chronic tendinopathies is necessarily supported by high-quality RCTs that use robust methods with sufficient sample sizes and standardized treatment protocols, and these remain a current limitation of the literature on this topic.6 The inconclusive state of the current evidence describing PRPi for chronic tendinopathies, combined with its high cost, has been highlighted as a point of caution, including assertions that the current use of PRPi is not supported by the available evidence.8,32,37
Given the inconsistency across the findings reported in the current literature summarized in this report that describes the comparative clinical effectiveness of PRPi in chronic tendinopathies of the upper extremities, the evidence is likely insufficient at this time to support decision-making in favour of its use.
References
1.Scott A, Rees J. Overview of overuse (persistent) tendinopathy. In: Fields KB, ed. UpToDate. Waltham (MA): UpToDate; 2023: http://www.uptodate.com. Accessed 2023 May 24
2.Dai W, Yan W, Leng X, et al. Efficacy of platelet-rich plasma versus placebo in the treatment of tendinopathy: a meta-analysis of randomized controlled trials. Clin J Sport Med. 2023;33(1):69-77. PubMed
3.Scott A, Purdam CR. Overview of the management of overuse (persistent) tendinopathy. In: Fields KB, ed. UpToDate. Waltham (MA): UpToDate; 2023: http://www.uptodate.com. Accessed 2023 May 25
4.Vivek K, Padma V. Efficacy of autologous platelet rich plasma injection in lateral epicondylitis and plantar fasciitis. Indian J Public Health Res Dev. 2019;10(11):4241-4245.
5.Abadin AA, Orr JP, Lloyd AR, Henning PT, Pourcho A. An evidence-based approach to orthobiologics for tendon disorders. Phys Med Rehabil Clin N Am. 2023;34(1):83-103. PubMed
6.Collins T, Alexander D, Barkatali B. Platelet-rich plasma: a narrative review. EFORT Open Rev. 2021;6(4):225-235. PubMed
7.Cook J, Young M. Biologic therapies for tendon and muscle injury. In: Fricker P, ed. UpToDate. Waltham (MA): UpToDate; 2023: http://www.uptodate.com. Accessed 2023 Jun 16.
8.LaBelle MW, Marcus RE. CORR synthesis: what is the role of platelet-rich plasma injection in the treatment of tendon disorders? Clin Orthop Relat Res. 2020;478(8):1817-1824. PubMed
9.Perry D, Ton J, Kolber MR. Platelet-rich plasma injections. Can Fam Physician. 2020;66(5):337. PubMed
10.Sheean AJ, Arner JW, Bradley JP. Proximal hamstring tendon injuries: diagnosis and management. Arthroscopy. 2021;37(2):435-437. PubMed
11.Marcolina A, Vu K, Chang Chien G. Peripheral joint injections. Phys Med Rehabil Clin N Am. 2022;33(2):267-306. Medline PubMed
12.Schopflocher D, Taenzer P, Jovey R. The prevalence of chronic pain in Canada. Pain Res Manag. 2011;16(6):445-450. PubMed
13.Health Canada. Information update: Health Canada clarifies position on platelet rich plasma treatments. 2019; https://recalls-rappels.canada.ca/en/alert-recall/health-canada-clarifies-position-platelet-rich-plasma-treatments. Accessed 2023 Jun 14.
14.CBC News. Platelet-rich plasma treatment classified as drug, Health Canada says. 2019; https://www.cbc.ca/news/health/platelet-rich-plasma-treatment-classification-1.5226906. Accessed 2023 Jun 15.
15.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
16.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. PubMed
17.Irby A, Gutierrez J, Chamberlin C, Thomas SJ, Rosen AB. Clinical management of tendinopathy: a systematic review of systematic reviews evaluating the effectiveness of tendinopathy treatments. Scand J Med Sci Sports. 2020;30(10):1810-1826. PubMed
18.Houck DA, Kraeutler MJ, Thornton LB, McCarty EC, Bravman JT. Treatment of lateral epicondylitis with autologous blood, platelet-rich plasma, or corticosteroid injections: a systematic review of overlapping meta-analyses. Orthop J Sports Med. 2019;7(3):2325967119831052. PubMed
19.Muthu S, Patel S, Gobbur A, et al. Platelet-rich plasma therapy ensures pain reduction in the management of lateral epicondylitis - a PRISMA-compliant network meta-analysis of randomized controlled trials. Expert Opin Biol Ther. 2022;22(4):535-546. PubMed
20.Masiello F, Pati I, Veropalumbo E, Pupella S, Cruciani M, De Angelis V. Ultrasound-guided injection of platelet-rich plasma for tendinopathies: a systematic review and meta-analysis. Blood Transfus. 2023;21(2):119-136. PubMed
21.Pang L, Xu Y, Li T, Li Y, Zhu J, Tang X. Platelet-rich plasma injection can be a viable alternative to corticosteroid injection for conservative treatment of rotator cuff disease: a meta-analysis of randomized controlled trials. Arthroscopy. 2023;39(2):402-421.e401. PubMed
22.A Hamid MS, Sazlina SG. Platelet-rich plasma for rotator cuff tendinopathy: a systematic review and meta-analysis. PLoS One. 2021;16(5):e0251111. PubMed
23.Karjalainen TV, Silagy M, O'Bryan E, Johnston RV, Cyril S, Buchbinder R. Autologous blood and platelet-rich plasma injection therapy for lateral elbow pain. Cochrane Database Syst Rev. 2021;9:CD010951. PubMed
24.Huang K, Giddins G, Wu LD. Platelet-rich plasma versus corticosteroid injections in the management of elbow epicondylitis and plantar fasciitis: an updated systematic review and meta-analysis. Am J Sports Med. 2020;48(10):2572-2585. PubMed
25.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
26.Cash C, Scott L, Walden RL, Kuhn A, Bowman E. Bibliometric analysis of the top 50 highly cited articles on platelet-rich plasma in osteoarthritis and tendinopathy. Regen Med. 2022;17(7):491-506. PubMed
27.Sheean AJ, Anz AW, Bradley JP. Platelet-rich plasma: fundamentals and clinical applications. Arthroscopy. 2021;37(9):2732-2734. PubMed
28.Filardo G, Di Matteo B, Kon E, Merli G, Marcacci M. Platelet-rich plasma in tendon-related disorders: results and indications. Knee Surg Sports Traumatol Arthrosc. 2018;26(7):1984-1999. PubMed
29.Adra M, El Ghazal N, Nakanishi H, et al. Platelet-rich plasma versus corticosteroid injections in the management of patients with rotator cuff disease: a systematic review and meta-analysis. J Orthop Res. 2023;41(1):7-20. PubMed
30.Feltri P, Gonalba GC, Boffa A, et al. Platelet-rich plasma does not improve clinical results in patients with rotator cuff disorders but reduces the retear rate. A systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2023;31(5):1940-1952. PubMed
31.Kemp JA, Olson MA, Tao MA, Burcal CJ. Platelet-rich plasma versus corticosteroid injection for the treatment of lateral epicondylitis: a systematic review of systematic reviews. Int J Sports Phys Ther. 2021;16(3):597-605. Medline PubMed
32.Karjalainen T, Richards B, Buchbinder R. Platelet-rich plasma injection for tennis elbow: did it ever work? BMJ Open Sport Exerc Med. 2022;8(1):e001258. PubMed
33.Platelet-rich plasma injections for wound healing and tissue rejuvenation: a review of clinical effectiveness, cost-effectiveness and guidelines. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2017: https://www.cadth.ca/platelet-rich-plasma-injections-wound-healing-and-tissue-rejuvenation-review-clinical-effectiveness. Accessed 2023 Jun 15.
34.Platelet rich plasma lumbar disc injections for lower back pain: clinical effectiveness, safety, and guidelines. (CADTH Rapid response report: summary of abstracts). Ottawa (ON): CADTH; 2014: https://www.cadth.ca/sites/default/files/pdf/htis/mar-2014/RB0649%20Platelet%20Rich%20Plasma%20Final.pdf. Accessed 2023 Jun 15.
35.Narayanaswamy R, Patro BP, Jeyaraman N, et al. Evolution and clinical advances of platelet-rich fibrin in musculoskeletal regeneration. Bioengineering (Basel). 2023;10(1):58. PubMed
36.Godoi TTF, Rodrigues BL, Huber SC, et al. Platelet-rich plasma gel matrix (PRP-GM): description of a new technique. Bioengineering (Basel). 2022;9(12):817. PubMed
37.Patricios J, Harmon KG, Drezner J. PRP use in sport and exercise medicine: be wary of science becoming the sham. Br J Sports Med. 2022;56(2):66-67. PubMed
38.Gummesson C, Atroshi I, Ekdahl C. The disabilities of the arm, shoulder and hand (DASH) outcome questionnaire: longitudinal construct validity and measuring self-rated health change after surgery. BMC Musculoskelet Disord. 2003;4:11. PubMed
39.Balestroni G, Bertolotti G. [EuroQol-5D (EQ-5D): an instrument for measuring quality of life]. Monaldi Arch Chest Dis. 2012;78(3):155-159. PubMed
40.Sun Z, Fan C. Validation of the Liverpool Elbow Score for evaluation of elbow stiffness. BMC Musculoskelet Disord. 2018;19(1):302. PubMed
41.Mustafa Ç, Kenan A, Murat B, Ilhan K, Havva Ç, Fikret T. Diagnostic values of clinical diagnostic tests in subacromial impingement syndrome. Ann Rheum Dis. 2000;59(1):44. PubMed
42.O’Conner FG, Howard TM, Fieseler CM, Nirschl RP. Managing overuse injuries: a systematic approach. Phys Sportsmed. 1997;25(5):88-113. PubMed
43.APTA. Pain Pressure Threshold (PPT). 2023; https://www.apta.org/patient-care/evidence-based-practice-resources/test-measures/pain-pressure-threshold-ppt#:~:text=The%20test%20determines%20the%20amount,direction%20relative%20to%20the%20muscle. Accessed 2023 Jun 29.
44.Braaksma C, Otte J, Wessel RN, Wolterbeek N. Investigation of the efficacy and safety of ultrasound standardized autologous blood injection as treatment for lateral epicondylitis. Clin Shoulder Elb. 2022;25(1):57-64. PubMed
45.NICE. Interventional procedure overview of extracorporeal shockwave therapy for refractory greater trochanteric pain syndrome 2010; https://www.nice.org.uk/guidance/ipg376/documents/extracorporeal-shockwave-therapy-for-refractory-greater-trochanteric-pain-syndrome-overview2#:~:text=The%20Roles%20and%20Maudsley%20score,worse%20than%20pre%2D%20treatment. Accessed 2023 Jun 29.
46.Tveitå EK, Ekeberg OM, Juel NG, Bautz-Holter E. Responsiveness of the Shoulder Pain and Disability Index in patients with adhesive capsulitis. BMC Musculoskelet Disord. 2008;9(1):161. PubMed
47.von der Heyde R, Droege K. 8 - Assessment of functional outcomes. In: Cooper C, ed. Fundamentals of Hand Therapy (Second Edition). St. Louis (US): Mosby; 2014:115-127.
48.Delgado DA, Lambert BS, Boutris N, et al. Validation of digital visual analog scale pain scoring with a traditional paper-based visual analog scale in adults. J Am Acad Orthop Surg Glob Res Rev. 2018;2(3):e088. PubMed
49.Richards RR, An KN, Bigliani LU, et al. A standardized method for the assessment of shoulder function. J Shoulder Elbow Surg. 1994;3(6):347-352. PubMed
50.Ozer K, Atan O. The addition of platelet-rich plasma to facial lipofilling: a double-blind, placebo-controlled, randomized trial. Plast Reconstr Surg. 2018;142(5):795e-796e. PubMed
51.Vrotsou K, Ávila M, Machón M, et al. Constant-Murley Score: systematic review and standardized evaluation in different shoulder pathologies. Qual Life Res. 2018;27(9):2217-2226. PubMed
52.Roy JS, Macdermid JC, Faber KJ, Drosdowech DS, Athwal GS. The simple shoulder test is responsive in assessing change following shoulder arthroplasty. J Orthop Sports Phys Ther. 2010;40(7):413-421. PubMed
53.Thamyongkit S, Wanitchanont T, Chulsomlee K, et al. The University of California-Los Angeles (UCLA) shoulder scale: translation, reliability and validation of a Thai version of UCLA shoulder scale in rotator cuff tear patients. BMC Musculoskelet Disord. 2022;23(1):65. PubMed
54.Jansen JP, Trikalinos T, Cappelleri JC, et al. Supplementary material to: Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of the Included Overviews of SRs and/or MAs
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Irby et al. (2020)17 US Funding source: Reported as none | SRs relevant to and summarized in this report: 2 of 25 included SRs Sources and dates searched: The sources searched were PubMed, Embase, CINAHL, Physiotherapy Evidence Database (PEDro), and the Cochrane Database from database inception to February 2020 | Included studies: 6 RCTs (1 SR), 5 RCTs (1 SR) Conditions: lateral epicondylitis; rotator cuff tendinopathy All eligible patients summarized in this report = range of 13 to 115 patients (1 SR); NR (1 SR) Intervention group, n = NR No other characteristics reported Comparator group, n = NR No other characteristics reported | Intervention: PRPi N injection(s), dose, frequency, interval(s) between injections = NR Comparators: CS injections (1 SR) N injection(s), dose, frequency, interval(s) between injections = NR Dry needling (1 SR) N injection(s), dose, frequency, interval(s) between injections = NR Placebo (1 SR) N injection(s), dose, frequency, interval(s) between injections = NR Others (1 SR) NSp | Outcome (measure): Pain (VASj), function (LES,c PREEg), NR (PRTEE,g Nirschl score,e SPADI,i WORC,k Neer Testd) Follow-up: NR |
Houck et al. (2019)18 US Funding Sources: Authors reported having received funds and/or royalties from Mitek, Smith and Nephew, Stryker, Zimmer Biomet, DePuy, Elsevier, DJ Orthopedics, Encore Medical, Shukla Medical, Open Payments Database (OPD) | MAs relevant to and summarized in this report: 5 of 9 included MAs Sources and dates searched: The sources searched were PubMed, Embase, and the Cochrane Library from an unspecified time point to June 2017 | Included studies: 84 RCTs (range of 8 RCTs to 27 RCTs per MA) Condition: lateral epicondylitis All eligible patients summarized in this report, n = NR Mean age: range, 43 years to 47 years Disease duration: range, 1 month to 18 months Intervention group, n = NR No other characteristics reported Comparator group, n = NR No other characteristics reported | Intervention: PRPi N injection(s), dose, frequency, interval(s) between injections = NR Comparators (relevant only): CS injections (4 MAs) N injection(s), dose, frequency, interval(s) between injections = NR Placebo (1 MA) N injection(s), dose, frequency, interval(s) between injections = NR | Outcome (measure): Pain (VAS,j PPTf), function (NR), NR (PRTEE,g DASHa score, EQ-5D,b Nirschl score,e Roles and Maudsleyh), adverse events (n) Follow-up: NR |
CINAHL = Cumulated Index to Nursing and Allied Health Literature; DASH = Disabilities of the Arm, Shoulder and Hand; LES = Liverpool Elbow Score; NR = not reported; NSp = not specified; PEDro = Physiotherapy Evidence Database; PPT = pressure pain threshold; PREE = Patient-Rated Elbow Evaluation; PRPi = platelet-rich plasma injection; PRTEE = Patient-Rated Tennis Elbow Evaluation; RCT = randomized controlled trial; SPADI = Shoulder Pain and Disability Index; SR = systematic review; TAS = Tegner Activity Scale; VAS = visual analogue scale; WORC = Western Ontario Rotator Cuff Index.
aDASH score: The DASH score ranges from 0 to 100, with 0 representing no disability or symptoms and higher scores representing increasing disability or symptoms.38
bEQ-5D: This measure is widely used in studies of health outcomes, with utility scores anchored at 0 for “death” and 1 for “perfect health.”39
cLES: The LES is scored from 0 to 10, with 0 representing the worst symptoms and function and increasing scores representing improved symptoms and function.40
dNeer Test: A clinical technique for determining shoulder pathology, with a dichotomous score of present or absent.41
eNirschl score: The Nirschl score ranges from 0 to 100, with 0 representing no disability or symptoms and higher scores representing increasing disability or symptoms.42
fPPT: The PPT is a clinical measure of pain in response to pressure applied by a clinician;43 no information on scoring was identified.
gPREE and PRTEE: The PREE and PRTEE are scored from 0 to 10, with 0 representing no pain or disability and higher scores representing increasing pain and/or disability.44
hRoles and Maudsley score: The Roles and Maudsley score ranges from 0 to 4, with 0 representing no pain or limits on activities and higher scores representing increasing pain and/or limits on activity.45
iSPADI: The SPADI is scored from 0 to 100, with 0 representing no pain or disability and higher scores representing increasing pain and/or disability.46
jVAS: The VAS is generally scored from 0 to 10, with 0 representing no pain and 10 representing the worst possible pain.48
kWORC: The WORC is scored from 0 to 100, with 0 representing the best possible quality of life and higher scores representing worsening quality of life.47
Table 3: Characteristics of the Included Network Meta-Analyses
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Muthu et al. (2022)19 India Funding sources: Reported as none | Primary studies relevant to and summarized in this report: 15 of 25 included RCTs Statistical approach to NMA: Frequentist Sources and dates searched: The sources searched were PubMed, Embase, Web of Science, and the Cochrane Library from database inception to June 2021 | Condition: lateral epicondylitis All eligible patients summarized in this report, n = 1,164 Mean age: range, 34 years to 52.6 years (15 RCTs) Male, n = 436 (12 RCTs); NR (3 RCTs) Female, n = 526 (12 RCTs); NR = 3 RCTs Intervention groups = 535 No other characteristics reported Comparator groups = 571 No other characteristics reported | Intervention: LR-PRPi, LP-PRPi N injections, dose, frequency, interval(s) between injections = NR Comparator: Saline (7 RCTs) N injections, dose, frequency, interval(s) between injections = NR CS (8 RCTs) N injections, dose, frequency, interval(s) between injections = NR | Outcomes (measures): Function (DASH,a PRTEEb), pain (VASc) Follow-up; range, 2 to 24 (unit of measurement of time NR) |
CS = corticosteroid; DASH = Disabilities of the Arm, Shoulder and Hand; LP-PRPi = leukocyte-poor platelet-rich plasma injection; LR-PRPi = leukocyte-rich platelet-rich plasma injection; NMA = network meta-analysis; NR = not reported; PRPi = platelet-rich plasma injection; PRTEE = Patient-Rated Tennis Elbow Evaluation; RCT = randomized controlled trial; VAS = visual analogue scale.
aDASH score: The DASH score ranges from 0 to 100, with 0 representing no disability or symptoms and higher scores representing increasing disability or symptoms.38
bPRTEE: The PRTEE is scored from 0 to 10, with 0 representing no pain or disability and higher scores representing increasing pain and/or disability.44
cVAS: The VAS is generally scored from 0 to 10, with 0 representing no pain and 10 representing the worst possible pain.48
Table 4: Characteristics of the Included SRs and Meta-Analyses
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Masiello et al. (2023)20 Italy Funding source: NR | Primary studies relevant to this review: 14 of 33 included RCTs, including MA Primary studies summarized in this report: 4 of the 14 eligible RCTs that were not included in the other SRs included in this report Sources and dates searched: The sources searched were MEDLINE, EMBASE, SCOPUS, OVID, and the Cochrane Library databases from an unspecified time point to November 2021 | Condition: carpal tunnel syndrome All eligible patients summarized in this report, n = 234 Age: range, 31 years to 77 years (3 SRs); NR (1 SR) Intervention group, n = 118 No other characteristics reported Comparator groups, n = 116 No other characteristics reported | Intervention: PRPi N injections, dose, frequency, interval(s) between injections = NR Comparator: Steroid (2 SRs) N injections, dose, frequency, interval(s) between injections = NR PT (1 SR) Type, frequency = NR Placebo (1 SR) N injections, dose, frequency, interval(s) between injections = NR | Outcomes (measures): Pain (VASi); function (BCTQb – functional score); severity (BCTQb – severity score) Follow-up: range, 3 months to 12 months |
Pang et al. (2023)21 China Funding Sources: National Natural Science Foundation of China (82072514), Science and Technology Department of Sichuan Province (2021YFS0238) | Primary studies relevant to and summarized in this report: 11 of 13 included RCTs Sources and dates searched: The sources searched were PubMed, EMBASE, the Cochrane Library, and Web of Science databases from 1990 to March 2022 | Condition: rotator cuff tendinopathies All eligible patients summarized in this report, n = 664 Mean age: range, 41.85 years to 57.33 years (10 RCTs); NR (1 RCT) Male sex, n = 207 (9 RCTs) Female sex, n = 331 (9 RCTs) Sex NR = 2 RCTs Intervention groups, n = 347 Symptom duration, months = 2.12 to 11.6 Comparator groups, n = 332 Symptom duration, months = 1.21 to 13.1 | Intervention: PRPi N injections = 1 (9 RCTs); 2 (1 RCT); 3 (1 RCT) Interval between > 1 injections = 7 days (1 RCT); 2 weeks (1 RCT) Dose: range, 2 mL to 6 mL (9 RCTs) Comparator: CS (11 RCTs) N injections: range, 1 (10 RCTs) to 2 (1 RCT) Corticosteroids used: methylprednisolone (2 RCTs), betamethasone (2 RCTs), triamcinolone acetonide (7 RCTs) Dose: range, 1 mL to 3 mL | Outcomes (measures): Pain (VASi); function (ASES,a CMS,c DASH,d SST,g UCLA,h WORCj); adverse events (n) Follow-up: range, 1 week to 24 months |
Hamid et al. (2021)22 Malaysia Funding sources: Reported as none | Primary studies relevant to and summarized in this report: 8 RCTs Sources and dates searched: The sources searched were CINAHL, MEDLINE, SCOPUS, SPORTSDiscus, and Web of Science databases from an unspecified time point to December 2020 | Condition: rotator cuff tendinopathy All eligible patients summarized in this report, n = 454 Age: range, 18 years to 79 years (6 RCTs); NR (2 RCTs) Intervention groups, n = 230 No other characteristics reported Comparator groups, n = 224 No other characteristics reported | Intervention: PRPi N injections = 1 (3 RCTs); 2 (2 RCTs); 3 (1 RCT) 4 (1 RCT); NR (1 RCT) Interval between > 1 injections = 1 week (1 RCT); 1 month (2 RCTs); NR (1 RCT) Dose: range, 2 mL to 6 mL (8 RCTs) Comparatorsa: Saline (4 RCTs) N injections: range, 1 (10 RCTs) to 2 (1 RCT) Dose: range, 1 to 3 mL PT (6 RCTs) Dry needling (1 RCT) N injections = 2 | Outcomes (measures): Function (DASH,d SPADIf); pain (VASi); adverse events (n) Follow-up: range, 12 weeks to 12 months |
Karjalainen et al. (2021)23 Australia Funding sources: Cabrini Institute, Cabrini Hospital, Australia; Monash University, Australia; National Health and Medical Research Council (NHMRC), Australia; NHMRC Senior Principal Research Fellowship | Primary studies relevant to this review: 15 of 32 included RCTs Primary studies summarized in this report: 3 of the 15 relevant RCTs that were not also included in the other reviews summarized in this report Sources and dates searched: The sources searched were CENTRAL, MEDLINE, Embase, Clinicaltrials.gov, WHO (WHO) International Clinical Trials Registry Platform (ICTRP) from 1946 to September 2020 | Condition: lateral epicondylitis All eligible patients summarized in this report, n = 115 Age: range, 18 years to 60 years (1 RCT); 18 years to NR (1 RCT); NR (1 RCT) Male sex, n = 24 (2 RCTs) Female sex, n = 34 (2 RCTs) Sex NR = 1 RCT Intervention groups, n = 58 Baseline VAS: range of mean scores, 8.0 to 8.07 (2 RCTs); NR (1 RCT) Baseline DASH scores, mean (SD) = 58.9 (10.5) (1 RCT) Baseline Nirschl stage, mean (SD) = 11.1 (14.3) (1 RCT) Comparator groups, n = 57 Baseline VAS: range of mean scores, 6.87 to 8.6 (2 RCTs); NR (1 RCT) Baseline DASH scores, mean (SD) = 57.3 (10.3) (1 RCT); NR (2 RCTs) Baseline Nirschl stage, mean (SD) = 22.9 (19.1) (1 RCT); NR (2 RCTs) | Intervention: PRPi N injections = 1 (2 RCTs); NR (1 RCT) Dose = 2 mL (1 RCT); NR (2 RCTs) Comparators: CS injection (2 RCTs) Type of CS: methylprednisolone (1 RCT); NR (1 RCT) N injections = 1 (1 RCT); NR (1 RCT) Dose = 40 mg (1 RCT); NR (1 RCT) Dry needling (1 RCT) N sessions = 1 | Outcomes (measures): Function (DASH,d Nirschl stagee); pain (VASi); adverse events (n) Follow-up: range, 6 weeks to 6 months |
Huang et al. (2020)24 China Funding sources: National Natural Science Foundation of China (grant 81871792); Scientific and Technological Plan of Traditional Chinese Medicine of Zhejiang Province (grant 2018ZB033); Medical and Health Science and Technology Project of Zhejiang Province (grants 2018KY324, 2020KY498) | Primary studies relevant to this review: 9 of 20 included RCTs Primary studies summarized in this report: 1 of the 9 eligible RCTs that was not also included in the other reviews summarized in this report Sources and dates searched: The sources searched were Cochrane Bone, Joint and Muscle Trauma Group Specialized Register, the Cochrane Central Register of Controlled Trials, MEDLINE, Embase, Web of Science, and the Cochrane Library from database inception to October 2018 | Condition: lateral epicondylitis All eligible patients summarized in this report, n = 83 Intervention group, n = 33 No other characteristics reported Comparator group, n = 50 No other characteristics reported | Intervention: PRPi N injections = NR Dose = 2 mL Comparator: CS injection N injections = NR Dose = 80 mg | Outcomes (measures): Pain (VASi) Follow-up: 1 month to 6 months |
ASES = American Shoulder and Elbow Surgeons; BCTQ = Boston Carpal Tunnel Syndrome Questionnaire; CMS = Constant-Murley score; DASH = Disabilities of the Arm, Shoulder and Hand; EQ-VAS = EuroQoL visual analogue scale; FSS = functional status scale; LP-PRPi = leukocyte-poor platelet-rich plasma injection; LR-PRPi = leukocyte-rich platelet-rich plasma injection; MA = meta-analysis; mg = milligram(s); NA = not applicable; NI = not interpretable; NR = not reported; NRS = nonrandomized study; PRPi = platelet-rich plasma injection; PT = physiotherapy; Q-DASH = Disabilities of the Arm, Shoulder and Hand Questionnaire; RCT = randomized controlled trial; SD = standard deviation; SPADI = Shoulder Pain and Disability Index; SR = systematic review; SSS = symptom severity scale; SST = Simple Shoulder Test score; UCLA = University of California Los Angeles; VAS = visual analogue scale; WORC = Western Ontario Rotator Cuff Index.
Note: Several studies were described as using combinations of control interventions.
aASES: The ASES is scored from 0 to 100, with 0 representing the worst pain and disability and higher scores representing less pain and/or disability.49
bBCTQ: The BCTQ is measured using a series of Likert scales with higher scores indicating worse function and symptom severity.50
cCMS: The CMS is scored from 0 to 100, with 0 representing the worst function and higher scores representing better function.51
dDASH score: The DASH score ranges from 0 to 100, with 0 representing no disability or symptoms and higher scores representing increasing disability or symptoms.38
eNirschl score: The Nirschl score ranges from 0 to 100, with 0 representing no disability or symptoms and higher scores representing increasing disability or symptoms.42
fSPADI: The SPADI is scored from 0 to 100, with 0 representing no pain or disability and higher scores representing increasing pain and/or disability.46
gSST: The SST is scored from 0 to 12, with 0 representing the worst function and higher scores representing better function.52
hUCLA shoulder rating scale: The UCLA shoulder rating scale is scored from 0 to 35, with 0 representing the worst function and higher scores representing better function.53
iVAS: The VAS is generally scored from 0 to 10, with 0 representing no pain and 10 representing the worst possible pain.48
jWORC: The WORC is scored from 0 to 100, with 0 representing the best possible quality of life and higher scores representing worsening quality of life.47
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 5: Strengths and Limitations of the Included Overviews of SRs Using AMSTAR 215 With Additional Items
Strengths | Limitations |
|---|---|
Irby (2020)17 | |
|
|
Houck (2019)18 | |
|
|
AMSTAR = A MeaSurement Tool to Assess systematic Reviews; MA = meta-analysis; MCID = minimal clinically important difference; NR = not reported; PICOS = population, intervention, comparator, outcome, study design; QUOROM = Quality of Reporting of Meta-analyses; RoB = risk of bias; SR = systematic review.
Table 6: Strengths and Limitations of the Included Network Meta-Analysis Using the ISPOR Questionnaire54
Strengths | Limitations |
|---|---|
Muthu (2022)19 | |
|
|
ISPOR = International Society for Pharmacoeconomics and Outcomes; MCID = minimal clinically important difference; SR = systematic review.
Table 7: Strengths and Limitations of the Included SRs and Meta-Analyses Using AMSTAR 215
Strengths | Limitations |
|---|---|
Masiello (2023)20 | |
|
|
Pang (2023)21 | |
|
|
Hamid (2021)22 | |
|
|
Karjalainen (2021)23 | |
|
|
Huang (2020)24 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; GRADE = Grading of Recommendations, Assessment, Development, and Evaluations; MA = meta-analysis; MCID = minimal clinically important difference; NR = not reported; PEDro = Physiotherapy Evidence Database; PICOS = population, intervention, comparator, outcome, study design; PROSPERO = International Prospective Register of Systematic Reviews; RCT = randomized controlled trial; RoB = risk of bias; SR = systematic review.
Appendix 4: Main Study Findings
Table 8: Summary of Findings by Outcome — Function
Review citation and data from included studies | Measure, summary statistic | N patients | Follow- up | Results | ||
|---|---|---|---|---|---|---|
PRPi | Comparator | Treatment group difference | ||||
Rotator cuff tendinopathy | ||||||
Pang et al. (2023)21 Findings from 3 MAs of 5 to 6 RCTs: Oudelaar (2021) Jo (2020) Barreto (2019) Say (2016) (no data for 2-month to 6-month follow-up) Shams (2016) Von Wehren (2016) | CMSa, mean (SD) | 201 | < 2 months | NR | CS NR | MD (95% CI), statistical significance = −0.02 (−2.12 to 2.08), NS |
123 | 2 months to 6 months | NR | CS NR | MD (95% CI), statistical significance = −3.56 (−6.47 to −0.65), SS favours CS | ||
217 | > 6 months | NR | CS NR | MD (95% CI), statistical significance = 9.29 (6.32 to 12.27), SS favours PRPi | ||
Pang et al. (2023)21 Findings from 3 MAs of 4 to 5 RCTs: Jo (2020) Kwong (2020) Sari (2020) (no data for > 6-month follow-up) Shams (2016) Von Wehren (2016) | ASESa, mean (SD) | 189 | < 2 months | NR | CS NR | MD (95% CI), statistical significance = −0.30 (−5.37 to 4.77), NS |
2 months to 6 months | NR | CS NR | MD (95% CI), statistical significance = 14.50 (9.19 to 19.82), SS favours PRPi | |||
117 | > 6 months | NR | CS NR | MD (95% CI), statistical significance = 5.22 (−0.64 to 11.07), NS | ||
Pang et al. (2023)21 Findings from 3 MAs of 3 RCTs: Jo (2020) Shams (2016) Von Wehren (2016) | SSTa, mean (SD) | 90 | < 2 months | NR | CS NR | MD (95% CI), statistical significance = −1.00 (−2.22 to 0.22), NS |
2 months to 6 months | NR | CS NR | MD (95% CI), statistical significance = 1.30 (0.16 to 2.44), SS favours PRPi | |||
> 6 months | NR | CS NR | MD (95% CI), statistical significance = 0.30 (−0.85 to 1.45), NS | |||
Pang et al. (2023)21 Findings from 3 MAs of 3 to 5 RCTs: Dadgostar (2021) (no data for > 6-month follow-up) Oudelaar (2021) Jo (2020) Barreto (2019) Pasin (2019) (no data for > 6-month follow-up) | DASHa, mean (SD) | 169 | < 2 months | NR | CS NR | MD (95% CI), statistical significance = 5.28 (2.07 to 8.48), SS favours PRPi |
247 | 2 months to 6 months | NR | CS NR | MD (95% CI), statistical significance = −2.26 (−5.02 to 0.51), NS | ||
127 | > 6 months | NR | CS NR | MD (95% CI), statistical significance = −7.00 (−8.47 to −5.53), SS favours CS | ||
Pang et al. (2023)21 Findings from 2 MAs of 2 to 3 RCTs: Jo (2020) Barreto (2019) Pasin (2019) (no data for > 6-month follow-up) | UCLAa, mean (SD) | 108 | < 2 months | NR | CS NR | MD (95% CI), statistical significance = 0.40 (−0.69 to 1.49), NS |
102 | > 6 months | NR | CS NR | MD (95% CI), statistical significance = 0.13 (−0.33 to 0.59), NS | ||
Pang et al. (2023)21 Findings from 2 MAs of 3 to 4 RCTs: Dadgostar (2021) Kwong (2020) Sabaah (2020) (no data for < 2-month follow-up) Sari (2020) | WORCa, mean (SD) | 217 | < 2 months | NR | CS NR | MD (95% CI), statistical significance = −3.07 (−6.68 to 0.54), NS |
157 | 2 months to 6 months | NR | CS NR | MD (95% CI), statistical significance = 8.19 (1.50 to 14.88), SS favours PRPi | ||
Irby et al. (2020)17 Findings from 1 SR (5 RCTs): Tsikopoulos (2016) | Tsikopoulos (2016) | |||||
NR; NRb | NR | NR | NR | DN, placebo NR | Reported as a slight clinical improvement in function with PRPi | |
Lateral epicondylitis | ||||||
Muthu et al. (2022)19 Findings from 7 NMAs (N RCTs NR) | DASHc, mean (SD) | NR | NR | LP-PRPi NR | Saline NR | Direct WMD (95% CI), statistical significance = −0.45 (−13.53 to 12.64), NS |
Pooled indirect WMD (95% CI), statistical significance = −0.45 (−13.53 to 12.64), NS | ||||||
NR | NR | LR-PRPi NR | Saline NR | Pooled indirect WMD (95% CI), statistical significance = −8.77 (−30.60 to 13.07), NS | ||
NR | NR | LP-PRPi NR | CS NR | Direct WMD (95% CI), statistical significance = −7.60 (−22.08 to 6.88), NS | ||
Pooled indirect WMD (95% CI), statistical significance = −7.60 (−22.08 to 6.88), NS | ||||||
NR | NR | LR-PRPi NR | CS NR | Direct WMD (95% CI), statistical significance = −15.92 (−25.71 to −6.13), SS favours CS | ||
Pooled indirect WMD (95% CI), statistical significance = −15.92 (−25.71 to −6.13), SS favours CS | ||||||
Muthu et al. (2022)19 Findings from 7 NMAs (N RCTs NR) | PRTEEc, mean (SD) | NR | NR | LP-PRPi NR | Saline NR | Pooled indirect effect of WMD, (95% CI), statistical significance = −5.97 (−16.64 to 4.71), NS |
NR | NR | LR-PRPi NR | Saline NR | Direct effect of WMD, 95% CI), statistical significance = −4.60 (−12.86 to 3.66), NS | ||
Pooled indirect effect of WMD, (95% CI), statistical significance = −3.96 (−11.87 to 3.94), NS | ||||||
NR | NR | LP-PRPi NR | CS NR | Direct effect of MD (95% CI), statistical significance = −2.50 (−10.76 to 5.76), NS | ||
Pooled indirect effect of WMD, (95% CI), statistical significance = −3.13 (−11.05 to 4.80), NS | ||||||
NR | NR | LR-PRPi NR | CS NR | Direct effect of WMD (95% CI), statistical significance = −2.40 (−10.66 to 5.86), NS | ||
Pooled indirect effect of WMD, (95% CI), statistical significance = −1.12 (−7.86 to 5.61), NS | ||||||
Hamid et al. (2021)22 Findings from 4 MAs of 2 to 4 RCTs: Centeno (2020) Nejati (2017) Wesner (2016) (Data for 6-month follow-up only) Ilhani (2015) (1 month data only) | DASHd, mean (SD) | 135 | 1 month | NR | PT NR | SMD (95% CI), statistical significance = 1.00 (−0.29 to 2.30), NS |
76 | 3 months | NR | PT NR | SMD (95% CI), statistical significance = 1.00 (−3.56 to 5.56), NS | ||
80 | 6 months | NR | Saline, PT NR | SMD (95% CI), statistical significance = −0.68 (−3.63 to 2.26), NS | ||
Reported as 291 | All time points | NR | Saline, PT NR | SMD (95% CI), statistical significance = 0.42 (−0.76 to 1.60), NS | ||
Hamid et al. (2021)22 Findings from 4 MAs of 2 RCTs: Rha (2012) Kesikburun (2013) | SPADId, mean (SD) | 70 | 1 month | NR | DN, PT, Saline NR | SMD (95% CI), statistical significance = −1.87 (−4.64 to 0.90), NS |
79 | 3 months | NR | DN, PT, Saline NR | SMD (95% CI), statistical significance = −0.57 (−1.03 to −0.12), SS favours PRPi | ||
79 | 6 months | NR | DN, PT, Saline NR | SMD (95% CI), statistical significance = −0.62 (−1.07 to −0.17), SS favours PRPi | ||
Reported as 228 | All time points | NR | DN, PT, Saline NR | SMD (95% CI), statistical significance = −0.91 (−1.49 to −0.32), SS favours PRPi | ||
Karjalainen et al. (2021)23 Findings from 3 RCTs: Martinez-Montiel (2015) Stenhouse (2013) Omar (2012) | Martinez-Montiel (2015) | |||||
NR (described as “various”)e, mean (SD) | 60 | > 3 weeks to 6 weeks | 60.3 (7.5) | CS 58.8 (7.1) | MD (95% CI), statistical significance = 1.50 (−2.20 to 5.20), NS | |
> 6 weeks to 3 months | 46.3 (5.1) | 64.3 (8.2) | MD (95% CI), statistical significance = –18.00 (−21.46 to −14.54), SS favours PRPi | |||
> 3 months to 6 months | 49.4 (6.14) | 67.7 (6.14) | MD (95% CI), statistical significance = −18.30 (−21.41 to −15.19), SS favours PRPi | |||
Stenhouse (2013) | ||||||
NR (described as “various”)e, mean (SD) | 28 | > 6 weeks to 3 months | 31.5 (18.2) | DN 28.7 (27.0) | MD (95% CI), statistical significance = 2.80 (−16.88 to 22.48), NS | |
> 3 months to 6 months | 51.1 (20.1) | 45.4 (31.8) | MD (95% CI), statistical significance = 5.70 (−14.36 to 25.76), NS | |||
Omar 2012 | ||||||
NR (described as “various”), mean (SD) | 30 | > 3 weeks to 6 weeks | 19.9 (12.9) | CS 20.2 (14.0) | MD (95% CI), statistical significance = −0.30 (−9.93 to 9.93), NS | |
Houck et al. (2019)18 Findings from 3 MAs (57 RCTs): Mi (2017) Dong (2015) Sayegh (2014) | Mi (2017) | |||||
NR; NRf | NR | 12 weeks to 12 months | NR | CS NR | PRPi is described as the most effective treatment (data not provided) | |
Dong (2015) | ||||||
NR; NRf | NR | 6 months | NR | CS NR | PRPi is described only as an effective treatment option (data not provided) | |
Sayegh (2014) | ||||||
NR; NRf | NR | NR | NR | Placebo NR | PRPi demonstrated no clinical benefit (data not provided) | |
Wrist and hand | ||||||
Masiello et al. (2023)20 Findings from 3 RCTs: Chen (2021) Senna (2019) Wu (2017) | BCTQg (functional score), mean (SD) | Chen (2021) | ||||
48 | 1 month | 1.9 (0.4) | Placebo 1.8 (0.4) | MD (95% CI), statistical significance = 0.10 (−0.13 to 0.33), NS | ||
3 months | 1.7 (0.4) | 1.7 (0.4) | MD (95% CI), statistical significance = 0.00 (−0.23 to 0.23), NS | |||
6 months | 1.5 (0.4) | 1.7 (0.4) | MD (95% CI), statistical significance = −0.20 (−0.43 to 0.03), NS | |||
12 months | 1.6 (0.4) | 1.7 (0.4) | MD (95% CI), statistical significance = –0.10 (−0.33 to 0.13), NS | |||
Senna (2019) | ||||||
98 | 1 month | 3.1 (0.4) | Steroid 3.0 (0.4) | MD (95% CI), statistical significance = 0.10 (−0.06 to 0.26), NS | ||
3 months | 2.1 (0.6) | 2.5 (0.6) | MD (95% CI), statistical significance = −0.40 (−0.64 to −0.16), SS favours control | |||
Wu (2017) | ||||||
60 | 1 month | 12.2 (3.0) | PT 14.4 (3.8) | MD (95% CI), statistical significance = −2.20 (−3.93 to −0.47), SS favours control | ||
3 months | 10.7 (2.1) | 13.6 (3.2) | MD (95% CI), statistical significance = −2.90 (−4.27 to −1.53), SS favours control | |||
6 months | 10.4 (2.6) | 12.9 (3.2) | MD (95% CI), statistical significance = −2.50 (−3.98 to −1.02), SS favours control | |||
ASES = American Shoulder and Elbow Surgeons; CI = confidence interval; CMS = Constant-Murley score; CS = corticosteroid; DASH = Disabilities of the Arm, Shoulder and Hand; DN = dry needling; LP-PRPi = leucocyte-poor platelet-rich plasma injection; LR-PRPi = leucocyte-rich platelet-rich plasma injection; MA = meta-analysis; MCID = minimal clinically important difference; MD = mean difference; NE = not estimable; NR = not reported; NS = not significant; PRPi = platelet-rich plasma injection; PRTEE = Patient-Rated Tennis Elbow Evaluation; PT = physiotherapy; RCT = randomized controlled trial; SD = standard deviation; SMD = standardized mean difference; SPADI = Shoulder Pain and Disability Index; SR = systematic review; SS = statistically significant; SST = Simple Shoulder Test score; UCLA = University of California Los Angeles; WMD = weighted mean difference; WORC = Western Ontario Rotator Cuff Index.
aThe MCIDs defined by Pang et al.21 were: CMS: a ≥ 10 point change; ASES: a ≥ 12 point change; SST: a ≥ 2 point change; DASH: a ≥ 10 point change; UCLA: a ≥ 3.5 point change; WORC: a ≥ 5 point change.
bThe MCIDs were NR by Irby et al.17
cThe MCIDs defined by Muthu et al.19 were: DASH: a ≥ 10 point change; PRTEE: NR.
dThe MCIDs were NR by Hamid et al.22
eThe MCIDs for measures of function and/or disability that used a 100-point scale were reported as ≥ 10 points.23
fThe MCIDs were NR by Houck et al.18
gThe MCID for the BCTQ was not defined by Masiello et al.20 but MCIDs were described collectively as follows: “Overall, most of the differences observed for the comparisons between groups at different time points were below the minimal clinically important difference, and at best indicate the possibility of a very marginal clinical benefit.” (p. 133)20
Note that this appendix has not been copy-edited.
Table 9: Summary of Findings by Outcome — Pain
Review citation and data from included studies | Measure(s); summary statistic | N patients | Follow-up | Results | ||
|---|---|---|---|---|---|---|
PRPi | Comparator | Treatment group difference | ||||
Rotator cuff tendinopathy | ||||||
Pang et al. (2023)21 Findings from 6 RCTs: Dadgostar (2021) Jo (2020) Kwong (2020) Sari (2020) Pasin (2019) Say (2016) | VASa; mean (SD) | Dadgostar (2021) | ||||
58 | < 2 months | −2.91 (2.21) | CS −1.69 (1.95) | MD (95% CI), statistical significance = −1.22 (−2.29 to −0.15), SS favours PRPi | ||
Jo (2020) | ||||||
57 | < 2 months | −0.8 (0.4) | CS −1.1 (0.3) | MD (95% CI) = NE | ||
> 6 months | −1.7 (0.3) | −0.8 (0.4) | MD (95% CI) = NE | |||
Kwong (2020) | ||||||
99 | < 2 months | −1.39 (2.5) | CS −1.2 (2.5) | MD (95% CI), statistical significance = −0.19 (−1.18 to 0.80), NS | ||
> 6 months | −2.16 (2.44) | −1.05 (2.62) | MD (95% CI), statistical significance = −1.11 (−2.11 to −0.11), SS favours PRPi | |||
Sari (2020) | ||||||
60 | < 2 months | −0.8 (1.0) | CS −3.2 (1.57) | MD (95% CI) = NE | ||
> 6 months | −3.06 (1.1) | −1.86 (1.24) | MD (95% CI), statistical significance = −1.20 (−1.79 to −0.61), SS favours PRPi | |||
Pasin (2019) | ||||||
60 | < 2 months | −3.50 (1.1) | CS −3.7 (1.2) | MD (95% CI), statistical significance = 0.20 (−0.38 to 0.78), NS | ||
Say (2016) | ||||||
60 | < 2 months | −2.4 (2.0) | CS −4.7 (1.4) | MD (95% CI) = NE | ||
69 | > 6 months | −2.2 (2.1) | −5.7 (1.3) | MD (95% CI), statistical significance = 3.50 (2.69 to 4.31), favours PRPi | ||
Pang et al. (2023)21 Findings from 1 MA of 5 RCTs: Dadgostar (2021) Jo (2020) Kwong (2020) Sabaah (2020) Sari (2020) | VASa; mean (SD) | 157 | 2 months to 6 months | NR | CS NR | MD (95% CI), statistical significance = −1.84 (−2.58 to −1.11), SS favours PRPi |
Hamid et al. (2021)22 Findings from 5 MAs of 4 to 8 RCTs: Centeno (2020) (no data for 12-month follow-up) Schwitzguebel (2019) (data for 12-month follow-up only) Ilhani (2015) (no data for 3-month or 6-month follow-up) Cai (2019) Nejati (2017) (no data for 12-month follow-up) Wesner (2016) (data for 6-month follow-up only) Kesikburun (2013) (no data for 1-month follow-up) Rha (2012) (data for 6-month follow-up only) | VASb; mean (SD) | 227 | 1 month | NR | Saline, PT NR | SMD (95% CI), statistical significance = 0.65 (−0.55 to 1.86), NS |
247 | 3 months | NR | Saline, PT NR | SMD (95% CI), statistical significance = 0.09 (−1.05 to 1.23), NS | ||
259 | 6 months | NR | Saline, DN, PT NR | SMD (95% CI), statistical significance = −0.46 (−1.06 to 0.14), NS | ||
274 | 12 months | NR | Saline, PT NR | SMD (95% CI), statistical significance = −0.46 (−0.70 to −0.21), SS favours PRPi | ||
Reported as 1,007 | All time points | NR | Saline, DN, PT NR | SMD (95% CI), statistical significance = −0.11 (−0.50 to 0.28), NS | ||
Huang et al. (2020)24 Findings from 1 RCT: Varshney (2017) | Varshney (2017) | |||||
VASc, mean (SD) | 83 | 1 month | 2.5 (0.9) | CS 2.3 (1.2) | SMD (95% CI), statistical significance = 0.18 (−0.26 to 0.62), NS | |
2 months | 1.6 (0.9) | 1.4 (0.8) | SMD (95% CI), statistical significance = 0.24 (−0.21 to 0.68), NS | |||
6 months | 0.7 (1.6) | 4.6 (1.5) | SMD (95% CI), statistical significance = −2.51 (−3.10 to −1.92), SS favours PRPi | |||
Lateral epicondylitis | ||||||
Muthu et al. (2022)19 Findings from 4 MAs (N RCTs, NR) | VASd; mean (SD) | NR | NR | LP-PRPi NR | Saline NR | Direct effect of WMD, (95% CI), statistical significance = −0.14 (−11.24 to 10.96), NS |
Pooled indirect effect of WMD, (95% CI), statistical significance = −5.65 (−14.71 to 3.41), NS | ||||||
NR | NR | LR-PRPi NR | Saline NR | Direct effect of WMD, (95% CI), statistical significance = −15.87 (−26.07 to −5.66), SS favours PRPi | ||
Pooled indirect effect of WMD, (95% CI), statistical significance = −14.87 (−23.18 to −6.39), SS favours PRPi | ||||||
NR | NR | LP-PRPi NR | CS NR | Direct effect of WMD, (95% CI), statistical significance = −13.00 (−33.22 to 7.22), NS | ||
Pooled indirect effect of WMD, (95% CI), statistical significance = −2.52 (−12.66 to 7.62), NS | ||||||
NR | NR | LR-PRPi NR | CS NR | Direct effect of WMD, (95% CI), statistical significance = −11.87 (−19.56 to −4.18), SS favours PRPi | ||
Pooled indirect effect of WMD, (95% CI), statistical significance = −11.66 (−18.85 to −4.46), SS favours PRPi | ||||||
Karjalainen et al. (2021)23 Findings from 3 RCTs: Martinez-Montiel (2015) Stenhouse (2013) Omar (2012) | Martinez-Montiel (2015) | |||||
VASe; mean (SD) | 60 | > 3 weeks to 6 weeks | 6.95 (1.7) | CS 6.35 (1.6) | MD (95% CI), statistical significance = 0.60 (−0.24 to 1.44), NS | |
> 6 weeks to 3 months | 4.1 (1.5) | 6.6 (1.6) | MD (95% CI), statistical significance = −2.50 (−3.28 to −1.72), SS favours PRPi | |||
> 3 months to 6 months | 5.05 (2.0) | 7.55 (1.7) | MD (95% CI), statistical significance = −2.50 (−3.44 to −1.56), SS favours PRPi | |||
Stenhouse (2013) | ||||||
VASe; mean (SD) | 28 | > 6 wk to 3 months | 5.88 (2.4) | DN 6.02 (2.9) | MD (95% CI), statistical significance = −0.14 (−2.13 to 1.85), NS | |
> 3 months to 6 months | 4.15 (3.3) | 4.5 (3.5) | MD (95% CI), statistical significance = −0.35 (−2.88 to 2.18), NS | |||
Omar (2012) | ||||||
VASe; mean (SD) | 30 | > 3 wk to 6 wk | 3.8 (1.9) | CS 4.3 (2.1) | MD (95% CI), statistical significance = −0.50 (−1.93 to 0.93), NS | |
Houck et al. (2019)18 Findings from 5 MAs (84 RCTs): Mi (2017) Arirachakaran (2015) Dong (2015) Sayegh (2014) Krogh (2012) | Mi (2017) | |||||
Pain intensity, VASf; NR | NR | 12 wk to 12 months | NR | CS NR | PRPi is described as the most effective treatment (data not provided) | |
Arirachakaran (2015) | ||||||
VAS, PPTf; NR | NR | NR | NR | CS NR | PRPi can improve pain (data not provided) | |
Dong (2015) | ||||||
Pain intensity, VASf; NR | NR | 6 months | NR | CS NR | PRPi is described only as an effective treatment option (data not provided) | |
Sayegh (2014) | ||||||
Pain intensity, VAS, PPTf; NR | NR | ≥ 6 months | NR | Placebo NR | PRPi demonstrated no clinical benefit (data not provided) | |
Krogh (2012) | ||||||
Pain intensity, VASf; NR | NR | Range of 8 and 52 wk | NR | Placebo NR | PRPi demonstrated a significantly greater improvement (data not provided) | |
Wrist and hand | ||||||
Masiello et al. (2023)20 Findings from 1 MA of 2 and 1 RCT: NRh | VASg; mean (SD) | 1 MA (2 RCTs) | ||||
158 | 3 months | NR | NR | MD (95% CI), statistical significance = −3.97 (−4.51 to −3.33), SS favours PRPi | ||
1 RCT | ||||||
60 | 6 months | NR | NR | MD (95% CI), statistical significance = −10.2 (−10.8 to −9.58), SS favours PRPi | ||
CI = confidence interval; CS = corticosteroid; DN = dry needling; LP-PRPi = leucocyte-poor platelet-rich plasma injection; LR-PRPi = leucocyte-rich platelet-rich plasma injection; MA = meta-analysis; MCID = minimal clinically important difference; MD = mean difference; NE = not estimable; NR = not reported; NS = not significant; PRPi = platelet-rich plasma injection; PPT = pressure pain threshold; PT = physiotherapy; RCT = randomized controlled trial; SD = standard deviation; SMD = standardized mean difference; SR = systematic review; SS = statistically significant; VAS = visual analogue scale; WMD = weighted mean difference.
aThe MCID defined by Pang et al.21 for the VAS was ≥ 1.4 cm change.
bThe MCID was NR by Hamid et al.22
cThe MCID defined by Huang et al.24 for the VAS was ≥ 1.0 point change.
dThe MCID defined by Muthu et al.19 for the VAS was ≥ 1.4 point change.
eThe MCID for measures of pain that used a 10-point scale were reported as ≥ 1.5 points.23
fThe MCIDs were NR by Houck et al.18
gThe MCID for the VAS was not defined by Masiello et al.,20 but MCIDs were described collectively as follows: “Overall, most of the differences observed for the comparisons between groups at different time points were below the minimal clinically important difference, and at best indicate the possibility of a very marginal clinical benefit.” (p. 133)20
hAuthors did not report or cite which RCTs reporting on pain data were summarized.
Note that this appendix has not been copy-edited.
Table 10: Summary of Findings by Outcome — Symptom Severity
Review citation and data from included studies | Measure, summary statistic | N patients | Follow- up | Results | ||
|---|---|---|---|---|---|---|
PRPi | Comparator | Treatment group difference | ||||
Wrist and hand | ||||||
Masiello et al. (2023)20 Findings from 3 RCTs: Chen (2021) Senna (2019) Wu (2017) | BCTQ (severity score)a, mean (SD) | Chen (2021) | ||||
48 | 1 month | 1.9 (0.4) | Placebo 2.1 (0.4) | MD (95% CI), statistical significance = −0.20 (−0.43 to 0.03), NS | ||
3 months | 1.7 (0.4) | 2.0 (0.4) | MD (95% CI), statistical significance = −0.30 (−0.68 to −0.12), SS favours PRPi | |||
6 months | 1.5 (0.4) | 1.9 (0.4) | MD (95% CI), statistical significance = −0.40 (−0.63 to −0.17), SS favours PRPi | |||
12 months | 1.5 (0.4) | 1.7 (0.4) | MD (95% CI), statistical significance = −0.20 (−0.43 to 0.03), NS | |||
Senna (2019) | ||||||
98 | 1 month | 2.4 (0.6) | Steroid 2.5 (0.5) | MD (95% CI), statistical significance = −0.10 (−0.32 to 0.12), NS | ||
3 months | 2.0 (0.7) | 2.4 (0.7) | MD (95% CI), statistical significance = −0.40 (−0.68 to −0.12), SS favours PRPi | |||
Wu (2017) | ||||||
60 | 1 month | 17.1 (3.2) | PT 18.4 (4.9) | MD (95% CI), statistical significance = −1.30 (−3.39 to 0.79), NS | ||
3 months | 15.7 (2.7) | 18.1 (5.4) | MD (95% CI), statistical significance = −2.40 (−4.56 to −0.24), SS favours PRPi | |||
6 months | 14.1 (2.4) | 16.2 (4.7) | MD (95% CI), statistical significance = −2.10 (−3.99 to −0.21), SS favours PRPi | |||
BCTQ = Boston Carpal Tunnel Syndrome Questionnaire; CI = confidence interval; MA = meta-analysis; MCID = minimal clinically important difference; MD = mean difference; NS = not significant; PRPi = platelet-rich plasma injection; PT = physiotherapy; RCT = randomized controlled trial; SD = standard deviation; SR = systematic review; SS = statistically significant.
aThe MCID for the BCTQ was not defined by Masiello et al.,20 but MCIDs were described collectively as follows: “Overall, most of the differences observed for the comparisons between groups at different time points were below the minimal clinically important difference, and at best indicate the possibility of a very marginal clinical benefit.” (p. 133)20
Note that this appendix has not been copy-edited.
Table 11: Summary of Findings by Outcome — Adverse Events
Review citation | Primary studies | Adverse event | Patients affected, n (%) | Treatment group difference | |
|---|---|---|---|---|---|
Intervention group | Comparator group | ||||
Rotator cuff tendinopathy | |||||
Pang et al. (2023)21 | Oudelaar (2021) | Any adverse event | 5 (NR) | CS 1 (NR) | NR |
Treatment failure | NR | NR | Significantly lower rates in the PRPi groups (data not provided) | ||
Kwong (2020) | Treatment failure | NR | CS NR | ||
Hamid et al. (2021)22 | Schwitzguebel (2019) | Postinjection pain, frozen shoulder, extension of lesion size | NR | Saline NR | While these AEs were observed in both groups, authors report that more AEs were observed in the PRPi (data not provided) |
Lateral epicondylitis | |||||
Karjalainen et al. (2021)23 | Stenhouse (2013) | Any adverse event | 2 (13) | DN 1 (8) | RR (95% CI), statistical significance = 1.73 (0.18 to 16.99), NS |
Study withdrawal due to adverse events | 2 (13) | 1 (8) | RR (95% CI), statistical significance = 1.73 (0.18 to 16.99), NS | ||
AE = adverse event; CI = confidence interval; MCID = minimal clinically important difference; NR = not reported; SR = systematic review.
Note: Information on MCIDs was NR for AEs.21-23
Note that this appendix has not been copy-edited.
Table 12: Summary of Findings by Outcome — Unspecified Outcomes
Review citation and data from included studies | Measure(s); summary statistic | N patients | Follow-up | Results | ||
|---|---|---|---|---|---|---|
PRPi | Comparator | Treatment group difference | ||||
Lateral epicondylitis | ||||||
Irby et al. (2020)17 Findings from 1 SR (1 RCT): de Vos (2014) | de Vos (2014) | |||||
NR | NR | NR | NR | CS NR | Reported as only 1 study showed positive comparative effect(s) of PRPi (data not provided) | |
Houck et al. (2019)18 Findings from 3 MAs (66 RCTs): Dong (2015) Sayegh (2014) Krogh (2012) | Dong (2015) | |||||
NR, NR | NR | 6 months | NR | CS NR | PRPi is described only as an effective treatment option (data not provided) | |
Sayegh (2014) | ||||||
PRTEE, DASH, Roles and Maudley, Likert scale, EQ-5D; NR | NR | ≥ 6 months | NR | Placebo NR | PRPi demonstrated no clinical benefit (data not provided) | |
Krogh (2012) | ||||||
PRTEE, Roles and Maudley, Nirschl scale; NR | NR | Range, 8 weeks to 52 weeks | NR | Placebo NR | PRPi demonstrated a significantly greater improvement (data not provided) | |
CS = corticosteroid; DASH = Disabilities of the Arm, Shoulder, and Hand; DN = dry needling; MA = meta-analysis; MCID = minimal clinically important difference; NR = not reported; PRPi = platelet-rich plasma injection; PRTEE = Patient-Rated Tennis Elbow Evaluation; RCT = randomized controlled trial; SR = systematic review; VISA = Victorian Institute of Sports Assessment.
Note: Information on MCIDs were NR for unspecified outcomes.17,18
Note that this appendix has not been copy-edited.
Appendix 5: Overlap Between Included SRs
Note that this appendix has not been copy-edited.
Table 13: Overlap in Relevant Primary Studies Between the Included SRs and Network Meta-Analysis
Primary study citation | Hamid (2021)22 | Huang (2020)24 | Karjalainen (2021)23 | Masiello (2023)20 | Muthu (2022)19 | Pang (2023)21 |
|---|---|---|---|---|---|---|
Shoulder | ||||||
Dadgostar (2021) | No | No | No | Yes | No | Yes |
Kwong (2021) | No | No | No | Yes | No | Yes |
Oudelaar (2021) | No | No | No | No | No | Yes |
Centeno (2020) | Yes | No | No | No | No | No |
Jo (2020) | No | No | No | No | No | Yes |
Sari (2020) | No | No | No | Yes | No | Yes |
Barreto (2019) | No | No | No | No | No | Yes |
Pasin (2019) | No | No | No | No | No | Yes |
Sabaah and Nasif (2019) | No | No | No | No | No | Yes |
Schwitzguebel (2019) | Yes | No | No | Yes | No | No |
Cai (2018) | Yes | No | No | No | No | No |
Nejati (2017) | Yes | No | No | Yes | No | No |
Say (2016) | No | No | No | No | No | Yes |
Shams (2016) | No | No | No | No | No | Yes |
Von Wehren (2016) | No | No | No | No | No | Yes |
Wesner (2016) | Yes | No | No | No | No | No |
Ilhani (2015) | Yes | No | No | No | No | No |
Kesikburun (2013) | Yes | No | No | Yes | No | No |
Rha (2013) | Yes | No | No | Yes | No | No |
Elbow | ||||||
Linnanmaki (2020) | No | No | Yes | No | Yes | No |
Lim (2018) | No | No | Yes | Yes | Yes | No |
Yerilkaya (2018) | No | No | Yes | No | Yes | No |
Schoffl (2017) | No | No | Yes | No | Yes | No |
Seetharamiaiah (2017) | No | Yes | No | No | Yes | No |
Varshney (2017) | No | Yes | No | No | No | No |
Montalvan (2016) | No | No | Yes | Yes | Yes | No |
Palacio (2016) | No | Yes | Yes | No | Yes | No |
Gautam (2015) | No | Yes | Yes | No | Yes | No |
Lebiedzinski (2015) | No | No | Yes | No | Yes | No |
Martinez-Montiel (2015) | No | No | Yes | No | No | No |
Yadav (2015) | No | Yes | Yes | No | Yes | No |
Khaliq (2014) | No | Yes | No | No | Yes | No |
Krogh (2013) | No | Yes | Yes | Yes | Yes | No |
Stenhouse (2013) | No | No | Yes | No | No | No |
Gosens (2011) | No | Yes | Yes | No | Yes | No |
Gupta (2011) | No | No | Yes | No | Yes | No |
Omar (2012) | No | Yes | Yes | No | No | No |
Peerbooms (2010) | No | No | No | No | Yes | No |
Wrist and/or hand | ||||||
Chen (2021) | No | No | No | Yes | No | No |
Senna (2019) | No | No | No | Yes | No | No |
Malahias (2017) | No | No | No | Yes | No | No |
Wu (2017) | No | No | No | Yes | No | No |
Appendix 6: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
PRPi for Indications Other Than Chronic Tendinopathies of the Lower Extremities
Platelet-rich plasma injections for wound healing and tissue rejuvenation: a review of clinical effectiveness, cost-effectiveness and guidelines. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2017: https://www.cadth.ca/platelet-rich-plasma-injections-wound-healing-and-tissue-rejuvenation-review-clinical-effectiveness. Accessed 2023 Jul 12.
Platelet rich plasma lumbar disc injections for lower back pain: clinical effectiveness, safety, and guidelines. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2014: https://www.cadth.ca/sites/default/files/pdf/htis/mar-2014/RB0649%20Platelet%20Rich%20Plasma%20Final.pdf . Accessed 2023 Jul 12.
Review Articles
Narrative Reviews (i.e., No Systematic Review Method)
Bhan K, Singh B. Efficacy of platelet-rich plasma injection in the management of rotator cuff tendinopathy: a review of the current literature. Cureus. 2022; 14(6): e26103. PubMed
Rosso C, Morrey ME, Schar MO, Grezda K. The role of platelet-rich plasma in shoulder pathologies: a critical review of the literature. EFORT Open Rev. 2023; 8(4): 213-222. PubMed
Vinod UDD, Chandra RM, Kranthi J, Chetamoni PC. The role of platelet-rich plasma in inducing musculoskeletal tissue healing in chronic tendinopathies. Eur J Mol Clin Med. 2022;9(3), 1618-1623.
Vukelic B, Abbey R, Knox J, Migdalski A. Which injections are effective for lateral epicondylitis? J Fam Pract. 2021;70(9): 461-463. PubMed
Wong JRY, Toth E, Rajesparan K, Rashid A. The use of platelet-rich plasma therapy in treating tennis elbow: a critical review of randomised control trials. J Clin Orthop Trauma. 2022 Sep;32:101965. PubMed
Additional References
Relevant Commentary
Hulsopple, C. Musculoskeletal therapies: musculoskeletal injection therapy. FP Essent. 2018 07;470:21-26. PubMed
Karjalainen T, Richards B, Buchbinder R. Platelet-rich plasma injection for tennis elbow: did it ever work? BMJ Open Sport Exerc Med. 2022;8(1):e001258. PubMed
Lai WC, Erickson BJ, Mlynarek RA, Wang D. Chronic lateral epicondylitis: challenges and solutions. Open Access J Sports Med. 2018;9:243-251. PubMed
Contributors: Chris Kamel
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca