CADTH Health Technology Review
Point-of-Care HIV and Syphilis Screening
Rapid Review
Authors: Kendra Brett, Nicole Askin
Abbreviations
CI
confidence interval
CrI
credible interval
DALY
disability-adjusted life-year
DTA
diagnostic test accuracy
FTA-ABS
fluorescent treponemal antibody absorption
ICER
incremental cost-effectiveness ratio
RCT
randomized controlled trial
RPR
rapid plasma reagin
STI
sexually transmitted infection
TPHA
Treponema pallidum hemagglutination assay
TPPA
Treponema pallidum particle agglutination
Key Messages
Dual point-of-care tests for HIV and syphilis and standalone point-of-care tests for syphilis may be useful in prenatal care for screening people for potential HIV and/or syphilis infections, based on findings from test accuracy studies.
In prenatal care, point-of-care tests for syphilis have the potential to be cost-effective and may increase the proportion of people screened and treated for syphilis.
Decision-makers should consider the potential for point-of-care HIV and syphilis screening to increase access to timely treatment for birthing parents and newborns, particularly in rural and remote communities and certain equity-deserving groups. However, the identified studies for this report provided few details about included populations, limiting an assessment of potential health inequities related to point-of-care screening.
None of the included studies used point-of-care tests for HIV or syphilis in people in labour.
We did not find any studies on the clinical utility or cost-effectiveness of dual point-of-care tests for HIV and syphilis that met our inclusion criteria.
We did not find any studies on the diagnostic test accuracy, clinical utility, or cost-effectiveness of standalone point-of-care tests for HIV that met our inclusion criteria.
Context and Policy Issues
What Are HIV and Syphilis?
HIV is a virus that attacks the body’s immune system, which during pregnancy can be transmitted to a child either in utero or at the time of delivery (i.e., vertical transmission). If antiretroviral therapy is initiated early in pregnancy, the risk of perinatal HIV transmission is minimized.1 In Canada, vertical transmission rates are less than 2%, but the rate can be as high as 25% if no interventions are taken during pregnancy, delivery, or the neonatal period.2 One cohort study found that 12.1% of all women living with HIV who gave birth in Ontario between 2006 and 2018 were diagnosed with HIV during pregnancy.1 Of those diagnosed with HIV during pregnancy, rates of diagnosis varied by trimester (23%, 54.9%, and 22.1%, in the first, second, and third trimesters, respectively).1
Syphilis is a curable sexually transmitted infection (STI) caused by the bacteria Treponema pallidum.3 Penicillin G benzathine is used to treat syphilis infection. A single dose is used for primary, secondary, or early latent stages of syphilis, and 3 doses are used for late latent or tertiary stages, or for syphilis infections with unknown duration.3 In Canada, the rate of syphilis infection has been increasing since 1997.4 There has been a rapid increase in syphilis infection among females, including those of reproductive age, as well as increases in congenital syphilis in babies.5 Congenital syphilis can occur through transplacental transmission of the bacteria during pregnancy or during delivery from contact with maternal secretions or blood, and it can cause adverse outcomes including perinatal death.3,4 In Canada, there were 53 cases of congenital syphilis in 2019 and 50 in 2020.5
What Is the Current Practice?
HIV testing is recommended early in pregnancy for all pregnancies,2,6 and rapid HIV testing is recommended at the time of labour or delivery in those with undocumented HIV status.2,7 In Canada, the standard practice for HIV screening during pregnancy is multistep serology testing. First, blood samples are screened for HIV antibodies with an enzyme immunoassay (e.g., a fourth generation HIV1 and HIV2 immunoassay). If the immunoassay is reactive, a more specific confirmatory test for HIV antibodies (e.g., a Western blot) is used to retest the blood sample.2,8 Point-of-care HIV testing may also be available in some settings (e.g., emergency departments) or situations (e.g., at the time of delivery when HIV status is undocumented); however, standard serological testing is required to confirm the diagnosis.7,8
Syphilis screening is recommended in Canada for all pregnant people during the first trimester or at the first prenatal visit, with repeat screening in pregnant people at high risk for infection at 28 to 32 weeks and again at delivery.9 Due to increasing rates of syphilis infection and 2 reported cases of congenital syphilis in 2019 in British Columbia, the provincial Health Authority issued interim guidance to screen for syphilis in all pregnant people at the time of delivery.10 Diagnostic screening of syphilis is done through serologic testing of a blood sample, using both treponemal and nontreponemal tests. Treponemal tests detect antibodies to T. pallidum and cannot distinguish between active or previously treated syphilis infection. These tests include treponemal-specific enzyme immunoassay, T. pallidum particle agglutination (TPPA), T. pallidum hemagglutination assay (TPHA), and fluorescent treponemal antibody absorption (FTA-ABS).3,9 Nontreponemal tests can indicate active or recent infection, and include rapid plasma reagin (RPR) and Venereal Disease Research Laboratory tests.3,9 In Canada, there are 2 serological screening algorithms. The traditional algorithm starts with a nontreponemal test to screen for infection, followed by 1 or 2 treponemal tests on positive samples to confirm syphilis. The reverse algorithm, favoured by most provinces in Canada, uses a treponemal test to screen for syphilis-specific antibodies, followed by a quantitative nontreponemal test to confirm positive test results and help determine the stage of infection.9
What Is Point-of-Care HIV and Syphilis Screening?
Point-of-care tests can be performed where care is provided, provide rapid turnaround for test results (e.g., within minutes), are visually interpreted, do not require sophisticated equipment or laboratory experience to perform, and use noninvasive specimens (e.g., finger prick blood sample).11 They can screen for HIV or syphilis alone, or may include dual testing for both syphilis and HIV antibodies.
Most commercially available point-of-care syphilis tests detect treponemal antibodies, and are not designed to distinguish between active and past syphilis infections.11 These tests are designed to screen for potential syphilis exposure (i.e., previous or current infection), but require additional nontreponemal testing to confirm an active syphilis diagnosis. Currently, there are no standalone point-of-care syphilis tests approved for use in Canada.
A standalone point-of-care test for HIV, the INSTI HIV Self Test (bioLytical Laboratories Inc., British Columbia), has been licensed for use as a Class 4 medical device by Health Canada since November 2020.12 In March 2023, a dual HIV and syphilis point-of-care antibody test, the INSTI Multiplex HIV-1/2 Syphilis Antibody Test (bioLytical Laboratories Inc., British Columbia, Canada), was licensed as a Class 4 medical device by Health Canada.12
Why Is It Important to Do This Review?
Laboratory tests take time to complete (e.g., 15 to 20 days for HIV) and often involve sending samples to external facilities with sophisticated laboratory equipment.8 As such, the test results are not available at the initial doctor-patient appointment and cannot have an immediate impact on treatment.11 Delays in obtaining results mean that people who test positive for HIV or syphilis only start treatment at the next health care visit and some may be lost to follow-up.
In Canada, certain groups are disproportionately affected by HIV, including people who use injection drugs; Indigenous people; members of the African, Caribbean, and Black community; and people who have immigrated to Canada from HIV endemic countries.13 There are structural barriers and health inequities that contribute to the inequitable occurrence of syphilis in specific groups, including lower income, insecure housing, rural or remote residence, lack of access to culturally appropriate health care, and experiences of stigma and discrimination within the health care system.14
Assuming adequate test performance, screening with point-of-care tests can provide a presumptive diagnosis during a clinic visit, which can help guide immediate treatment decisions in birthing parents or newborns. Rapid turnaround time for point-of-care tests may be especially useful for pregnant people who face barriers to accessing prenatal care or STI screening, people who may have difficulty returning for follow-up appointments (e.g., people in unstable housing, people without access to reliable transportation),3,11 people living in rural or remote areas, health care facilities with limited resources for laboratory testing, or people in labour with unknown HIV or syphilis status. In these settings, decision-makers need to determine effective screening practices to ensure timely treatment of HIV and/or syphilis for birthing parents and their newborns.
Objective
To support decision-making about point-of-care HIV and syphilis screening in people who are receiving prenatal care or people in labour, this Rapid Review summarizes and critically appraises available studies on the diagnostic test accuracy (DTA), clinical utility, and cost-effectiveness of point-of-care HIV and syphilis tests in these populations.
Research Questions
What is the diagnostic test accuracy of point-of-care HIV and syphilis screening for people who are receiving prenatal care and/or people in labour?
What is the clinical utility of point-of-care HIV and syphilis screening for people who are receiving prenatal care and/or in labour?
What is the cost-effectiveness of point-of-care HIV and syphilis for people who are receiving prenatal care and/or in labour?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, Cochrane Library, and the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were pregnancy/labour and point-of-care testing for HIV and/or syphilis. Comments, newspaper articles, editorials, and letters were excluded. Where possible, retrieval was limited to the human population. The search was completed on May 18, 2023, and limited to English-language documents published since January 1, 2018.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | People receiving prenatal care and/or individuals in labour |
Intervention | Point-of-care HIV and syphilis screening |
Reference standard | Q1: Standard serologic screening Q2, Q3: Not applicable |
Comparator | Q1: Not applicable Q2, Q3: Standard serologic screening |
Outcomes | Q1: Diagnostic test accuracy (e.g., sensitivity, specificity) Q2: Clinical utility (e.g., maternal fetal outcomes, time to treatment, morbidity, incidence of disease, mortality, quality of life) Q3: Cost-effectiveness (e.g., cost per QALY gained, ICER) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies, economic evaluations |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, if they were duplicate publications, or if they were published before 2018.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)15 for systematic reviews, the Drummond checklist16 for economic evaluations, and the Quality Assessment of Diagnostic Accuracy Studies 2 (QUADAS-2) checklist17 for DTA studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Equity Considerations
CADTH recognizes the need for and importance of equity considerations in health technology assessment. The Equity Checklist for Health Technology Assessment18 and PROGRESS-plus19 were used to guide considerations of equity in this Rapid Review. Relevant prompts were used to guide the assessment and reflection of the included studies, and in writing the Limitations and Conclusion sections of this report. We did not explicitly search for information related to sources of inequity or disadvantaged groups and access to prenatal HIV and syphilis screening.
Summary of Evidence
Quantity of Research Available
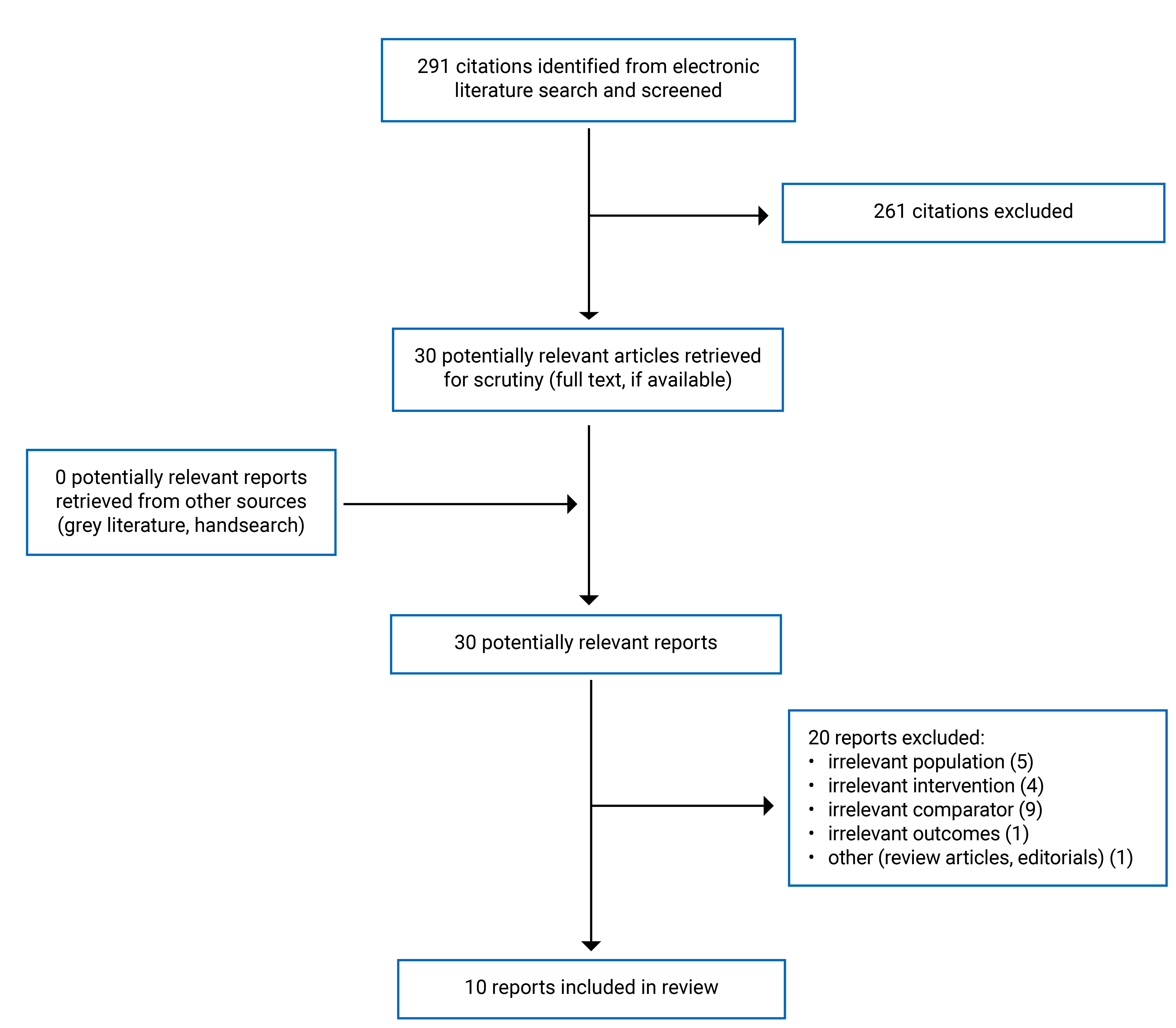
This report includes 3 systematic reviews,20-22 6 nonrandomized studies,23-28 and 1 economic evaluation.21 Study selection details are presented in Appendix 1. Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
Detailed characteristics of included publications are provided in Appendix 2. All of the included studies reported their population as “women,” and none distinguished sex from gender. While we have retained the original language used when reporting on these studies, we acknowledge that such language is not inclusive of trans and nonbinary persons.
Included Studies for Question 1: DTA
Dual Point-of-Care HIV and Syphilis Tests
Six cross-sectional studies were included that studied the DTA of dual point-of-care tests for HIV and syphilis in people receiving prenatal care.23-28 The studies were conducted in Brazil,23 Zambia,24 Uganda,25 Vietnam,26 South Sudan,27 and Nigeria.28 The studies included 180 to 4,550 pregnant women aged 15 years or older27 or 18 years or older23-26,28 attending routine antenatal care. Three studies specified that it was the first antenatal care visit.24,27,28 Blood samples for the index tests and reference standards were collected at the same visit.23-28
The index tests included the SD BIOLINE HIV/Syphilis Duo Test (6 studies)23-28 and the Chembio Dual Path Platform HIV-Syphilis Assay (1 study).24 The results of the dual rapid tests for HIV and syphilis were compared against separate reference tests by condition. For syphilis, all 6 studies used serological treponemal reference tests, including the FTA-ABS,23 TPPA,24,26 and TPHA.25,27,28 Three studies also used the nontreponemal RPR test to confirm active syphilis infection in the positive serology samples24,27,28 (i.e., similar to the reverse algorithm used in many Canadian provinces), but only 1 study24 specifically included RPR results in the DTA calculations to determine whether the point-of-care test could detect active syphilis infection; the other 2 studies27,28 considered the RPR test results as part of the discussion of their findings. For HIV, the serological reference tests were Genscreen Ultra HIV Ag-Ab23,28 and the Vironostika HIV1/2 Uniform II Ag/Ab.27 Three studies used rapid point-of-care tests for HIV as the reference standard (rather than standard serological testing) and were not relevant to this review.24-26
Outcomes included sensitivity and specificity (6 studies),23-28 positive predictive value and negative predictive value (2 studies),23,27 and accuracy performance (1 study).23
Point-of-Care Syphilis Tests
One systematic review was included on the DTA of rapid point-of-care syphilis tests to detect active syphilis in pregnant women attending antenatal care.22 The systematic review included studies that compared any rapid point-of-care syphilis test to a standard serological reference algorithm for syphilis where a nontreponemal (e.g., RPR) test was followed by a treponemal test. Studies with only 1 serology standard test were excluded. Five studies were included in the systematic review with a total of 14,985 pregnant women. The findings of the 5 studies were combined in a meta-analysis that reported sensitivity and specificity.
Included Studies for Question 2: Clinical Utility
One systematic review was included that examined the clinical utility of point-of-care syphilis tests in antenatal settings on pregnancy outcomes.20 This systematic review included 1 cluster randomized controlled trial (RCT) relevant to this report, which included 7,700 pregnant women attending antenatal care, and compared the SD Bioline Syphilis 3.0 rapid test to conventional serology testing for syphilis (RPR plus TPHA). Outcomes included the percentage of women receiving adequate syphilis treatment and the rate of congenital syphilis.
Included Studies for Question 3: Cost-Effectiveness
One systematic review of economic evaluations29 and 1 cost-effectiveness study21 on point-of-care syphilis testing in people receiving prenatal care were included.
The systematic review of economic evaluations examined point-of-care testing and treatment of STIs in pregnancy in low-income and middle-income countries (as defined by the World Bank).29 Relevant studies in the systematic review included 2 cost-effectiveness analyses and 1 cost-utility analysis comparing rapid syphilis tests with RPR laboratory testing in pregnant women. No information was provided on the type of point-of-care test or the population characteristics of the included studies. The authors reported whether or not the intervention was considered cost-effective based on the cost-effectiveness threshold established by each study.
The cost-effectiveness study21 assessed point-of-care syphilis testing and immediate treatment (of pregnant people who test positive) compared to standard laboratory tests (a nontreponemal test plus TPHA) with treatment at next follow-up visit in Brazil. The model was built with a lifetime horizon using the Brazilian public health system perspective. The focus of the model was on eliminating transmission of syphilis to the child and did not consider outcomes for the parent. The incremental cost-effectiveness ratio (ICER) was reported as cost per disability-adjusted life-year (DALY).
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
DTA Studies
The 6 DTA studies on dual point-of-care tests for HIV and syphilis23-28 used appropriate methods for patient selection and the patients match the population of interest in this report (i.e., people receiving prenatal care). However, 4 studies23,24,26,27 reported little to no information about the participants, which limits our understanding about the generalizability of the findings. The choice of index tests and the reference standard for syphilis matched those targeted by this review in all 6 studies, and the reference standard for HIV matched that targeted by this review in 3 studies.23,27,28 The other 3 studies used rapid point-of-care tests for HIV as the reference standard, which did not match this review.24-26 Three studies also used RPR testing to confirm whether the positive results from the treponemal reference standards were active syphilis infections, and considered these findings in their reports (as part of the DTA calculations or in the discussion of the findings).24,27,28 This reflects the screening algorithm used in Canada for active syphilis. The blood samples for all tests were collected at the same visit in each study, which reduced the likelihood that misclassification might occur due to the timing of the tests. Index tests were interpreted without knowledge of the reference standard in all studies, which reduced the potential for bias due to prior knowledge when interpreting the test results. In 5 studies,23-27 the reference standard was also interpreted without knowledge of the index test. In the other study,28 it was unclear whether the reference standard was interpreted without prior knowledge of the index test, or whether this may have introduced bias in the interpretation of the reference standard. In 1 study,24 only samples that tested positive with the reference standard were further tested with a confirmation test for active syphilis (i.e., RPR), which could bias the interpretation of the results of the RPR test. This study was also missing blood samples for the reference test from 34% of the recruited population, and it is unclear whether this could have introduced bias in the study due to potential population differences in those lost to follow-up.
The systematic review on the DTA of rapid point-of-care syphilis tests to detect active syphilis22 clearly stated its eligibility criteria and registered its protocol a priori, thus reducing the risk of reporting bias. A comprehensive search strategy was used and study selection was performed in duplicate, reducing the likelihood that relevant literature was missed. The inclusion criteria, sampling method, and index and reference tests of the included studies were well described, and appropriate statistical methods were used to conduct the meta-analysis. The population characteristics of the included studies only included the approximate age and the trimester of pregnancy, which may limit the generalizability of the findings. An appropriate tool was used to assess the risk of bias of the included studies, but the meta-analysis included all studies, regardless of risk of bias, which may have biased the results in favour of the point-of-care tests. This review assumed that different rapid tests by different manufacturers could be considered equivalent, and were combined in the meta-analysis to represent 1 index test.22 The heterogeneity in the index tests in this systematic review may limit the generalizability of the findings to the context of this report.
Clinical Utility Studies
The systematic review on the clinical utility of point-of-care syphilis tests20 clearly stated the population, intervention, and outcomes of interest. The comparator of interest was not clearly reported, the included studies were described with limited details, and it was not reported whether the review methods were established before the conduct of the review, thus increasing the risk of reporting bias. A comprehensive search strategy was used. Study selection was conducted by 1 reviewer, a list of excluded studies was not provided, and it was unclear whether data extraction was performed in duplicate, which increases the risk that relevant studies or details were missed or included in error. An appropriate tool was used to critically appraise the included studies, but the authors did not consider the risk of bias in the studies when interpreting the results.
Economic Evaluations
The systematic review of economic evaluations of point-of-care syphilis tests29 clearly stated the population, intervention, and outcomes of interest, however, the comparator of interest was not well defined. The authors registered their protocol a priori, thus reducing the risk of reporting bias. A comprehensive search strategy was used and study selection was conducted in duplicate, which reduces the risk that potential studies were missed. It was unclear whether data extraction was conducted in duplicate, a list of excluded studies was not provided, and limited information was provided on the included studies (e.g., sample size, population characteristics, and type of point-of-care tests were not reported). This limits our ability to assess whether the included studies were appropriately chosen and whether they are relevant to the current review. The comparator used in the 3 relevant studies was RPR alone (i.e., not in conjunction with a treponemal test), which does not align with the current practice in Canada for syphilis testing, which includes both treponemal and nontreponemal testing. This may limit the generalizability of findings, as these studies do not include the cost of treponemal testing. The authors acknowledged the degree of heterogeneity in the included studies and discussed the impacts of various limitations (e.g., time horizon or perspective not reported by multiple studies) on their findings.
The research question and objective of the economic evaluation set in Brazil21 were clearly stated. The intervention and comparators were appropriate; however, the specific types of point-of-care syphilis tests used were not reported, limiting their generalizability to this review. The lifetime time horizon was appropriate given the nature of congenital syphilis. The willingness-to-pay threshold was based on a published estimate for low-income to middle-income countries, and the authors selected the most conservative threshold suggested for Brazil (i.e., US$3,200). A probabilistic sensitivity analysis was conducted and credible intervals (CrIs) were reported, which strengthens the findings of the analysis. However, the full details of the sensitivity analysis were reported to be available in an online supplement that was not available at the time this review was written and could not be appraised. This economic evaluation did not include direct nonmedical costs or indirect costs, nor did it include the costs related to the training, consumables, and equipment required to perform the laboratory tests (due to nonavailability of the cost data). If the costs for the laboratory tests had been considered, the results of the cost-effectiveness analysis might differ in favour of the point-of-care tests. In addition, the treatment costs and follow-up costs were presumed to be the same for both testing strategies, with the difference in treatment compliance between strategies affecting total cost (i.e., probability of compliance with full treatment was lower for standard serological testing); however, it is unclear whether this method of estimating costs is appropriate. This model was focused on preventing the transmission of syphilis to the child, and did not include any maternal outcomes.
Summary of Findings
Appendix 4 presents the main study findings.
Diagnostic Accuracy of Dual Point-of-Care HIV and Syphilis Screening
Six cross-sectional studies23-28 were identified regarding the DTA of dual point-of-care HIV and syphilis tests in prenatal care. Three studies used a relevant reference standard for HIV23,27,28 and all 6 used a relevant reference standard for syphilis.23-28
For HIV Detection
SD BIOLINE HIV/Syphilis Duo Test Versus Genscreen Ultra HIV Ag-Ab
When compared to the Genscreen Ultra HIV Ag-Ab laboratory test for HIV,23,28 the SD BIOLINE HIV/Syphilis Duo Test had:
moderate to high sensitivity to detect HIV (85.8% [95% confidence interval [CI], 79.1% to 90.6%] to 100% [95% CI, 39.76% to 100%]; 2 studies)
high specificity to detect patients who do not have HIV (99.5% [95% CI, 99.3% to 99.7%] to 100% [95% CI, 99.06% to 100%]; 2 studies)
high proportion of people with correctly classified HIV status (100% accuracy [95% CI, 99.07% to 100%]; 1 study)
high positive predictive value (100%; 1 study)
high negative predictive value (100%; 1 study).
SD BIOLINE HIV/Syphilis Duo Test Versus Vironostika HIV1/2 Uniform II Ag/Ab
When compared to the Vironostika HIV1/2 Uniform II Ag/Ab laboratory test for HIV,27 the SD BIOLINE HIV/Syphilis Duo Test had:
high sensitivity to detect HIV (100% [95% CI, 63.1% to 100%])
high specificity to detect patients who do not have HIV (100% [95% CI, 99.2% to 100%])
high positive predictive value (100% [95% CI, 63.1% to 100%])
high negative predictive value (100% [95% CI, 99.2% to 100%]).
Overall Accuracy Results for HIV Detection
Dual point-of-care tests have moderate to high sensitivity to detect HIV infection. This means that, out of every 100 people with HIV, these tests will:
detect between 85 and 100 people with HIV
miss up to 15 people (i.e., false negatives).
The 95% CIs for these studies23,27,28 suggest that the ability of dual point-of-care tests to detect HIV could be as low as detecting 40 out of every 100 people with HIV (i.e., 60 false negatives) and could be as high as detecting 100 out of every 100 people with HIV (i.e., no false negatives).
Dual point-of-care tests have high specificity to detect those who do not have HIV. This means that, out of every 100 individuals who do not have HIV:
more than 99 people will test negative
less than 1 person will be wrongly diagnosed as having HIV (i.e., false positive) (3 studies).23,27,28
For Syphilis Detection
SD BIOLINE HIV/Syphilis Duo Test Versus FTA-ABS
When compared to the FTA-ABS laboratory test for syphilis,23 the SD BIOLINE HIV/Syphilis Duo Test had:
high sensitivity to detect current or previous syphilis infection (93.55% [95% CI, 78.58% to 99.21%])
high specificity to detect patients who do not have syphilis infection (100% [95% CI, 99% to 100%])
high proportion of people with correct syphilis status classification (99.50% accuracy [95% CI, 98.19% to 99.94%])
high positive predictive value (100%)
high negative predictive value (99.46% [95% CI, 97.95% to 99.86%]).
SD BIOLINE HIV/Syphilis Duo Test Versus TPPA
When compared to the TPPA laboratory test for syphilis,24,26 the SD BIOLINE HIV/Syphilis Duo Test had:
low sensitivity to detect current or previous syphilis infection (66.2% [95% CI, 59.4% to 72.4]; 1 study)
high specificity to detect patients who do not have syphilis infection (97.2% [95% CI, 96.4% to 97.9%] to 100% [95% CI, 98.0% to 100%]; 2 studies).
In 1 study,26 no women were diagnosed with syphilis, and the sensitivity of the point-of-care test could not be calculated.
SD BIOLINE HIV/Syphilis Duo Test Versus TPHA
When compared to the TPHA laboratory test for syphilis,25,27,28 the SD BIOLINE HIV/Syphilis Duo Test had:
moderate to high sensitivity to detect current or previous syphilis infection (86.4% [95% CI, 65.1% to 97.1%] to 100% [95% CI, 98.3% to 100%]; 2 studies)
high specificity to detect patients who do not have syphilis infection (99.9% [95% CI, 99.8% to 100%] to 100% [95% CI, 99.7% to 100%]; 3 studies)
high positive predictive value (100% [95% CI, 82.4% to 100%]; 1 study)
high negative predictive value (99.3% [95% CI, 97.9% to 99.9%]; 1 study).
In 1 study,28 sensitivity could not be calculated as there were no positive test results for both tests.
Chembio Dual Path Platform HIV-Syphilis Assay Versus TPPA
When compared to the TPPA laboratory test for syphilis,24 the Chembio Dual Path Platform HIV-Syphilis Assay had:
low sensitivity to detect current or previous syphilis infection (68.6% [95% CI, 61.9% to 74.6%])
high specificity to detect patients who do not have syphilis infection (98.5% [95% CI, 97.8% to 98.9%]).
Dual Point-of-Care Tests Versus TPPA and RPR
When compared to the combined results from TPPA and RPR titres to detect active syphilis infection, 1 study24 found:
moderate sensitivity for the SD BIOLINE HIV/Syphilis Duo Test to detect active syphilis infection (81.6% [95% CI, 72.7% to 88.1%])
moderate sensitivity for the Chembio Dual Path Platform HIV-Syphilis Assay to detect active syphilis infection (84.7% [95% CI, 76.1% to 90.6%]).
Overall Accuracy Results for Current or Previous Syphilis Infection
The sensitivity of dual point-of-care tests to detect syphilis infection varied by index test and reference standard (6 studies).23-28 This means that out of every 100 people with syphilis infection, these tests will:
detect between 66 and 100 people with current or previous syphilis infection
miss up to 34 people (i.e., false negatives).
The 95% CIs for these studies23-28 suggest that the ability of dual point-of-care tests to detect current or previous syphilis infection could be as low as detecting 59 out of every 100 people with current or previous syphilis infection (i.e., 41 false negatives) and could be as high as detecting 100 out of every 100 people with current or previous syphilis infection.
The dual point-of-care tests have high specificity to detect those who do not have syphilis infection. This means that out of every 100 individuals who do not have syphilis infection:
more than 97 people will test negative
up to 3 people may be wrongly diagnosed as having a current or previous syphilis infection (i.e., false positives).
Overall Accuracy Results for Active Syphilis Infection
Dual point-of-care tests have moderate sensitivity to detect active syphilis infections. This means that out of every 100 people with active syphilis, these tests will:
detect between 82 and 85 people with active syphilis
miss 15 to 18 people (i.e., false negatives).
The 95% CIs suggests that the ability of dual point-of-care tests to detect active syphilis could be as low as 73 out of every 100 people with active syphilis and as high as 91 out of every 100 people with active syphilis (1 study, testing 2 dual point-of-care tests).24
Diagnostic Accuracy of Point-of-Care HIV Screening
No relevant evidence was identified regarding the DTA of point-of-care HIV tests during prenatal care or for individuals in labour; therefore, no summary can be provided.
Diagnostic Accuracy of Point-of-Care Syphilis Screening
One systematic review and meta-analysis22 which included 5 relevant DTA studies evaluated the ability of point-of-care syphilis tests to detect active syphilis in prenatal care by comparing them to the traditional laboratory testing algorithm for active syphilis (i.e., a nontreponemal [e.g., RPR test] followed by a treponemal test).
For the point-of-care syphilis tests, this study22 reported:
moderate sensitivity to detect active syphilis infection (85% [95% CrI, 73% to 92%])
high specificity to detect patients who do not have active syphilis infection (98% [95% CrI, 95% to 98%]).
The prediction interval for sensitivity was wide (i.e., 57% to 96%) and the prediction interval for specificity was 88% to 100%.22 Wide prediction intervals reflect considerable between-study variability, likely due to the different index tests and reference standards that were used.
Overall Accuracy Results for Active Syphilis Infection
Standalone point-of-care syphilis tests have moderate sensitivity to detect active syphilis infections. This means that out of every 100 people with active syphilis, these tests will:
detect 85 people with active syphilis
miss 15 people with active syphilis (i.e., false negatives).
The 95% CIs suggest that point-of-care syphilis tests will detect between 73 and 92 out of every 100 people with active syphilis infection (i.e., between 8 and 27 cases will be missed; 1 systematic review with 5 DTA studies).22
These tests have very high specificity to detect patients who do not have active syphilis. This means that out of every 100 individuals who do not have active syphilis:
98 people will test negative
2 people will be wrongly diagnosed as having active syphilis (i.e., false positives; 1 systematic review with 5 DTA studies).22
Clinical Utility of Dual Point-of-Care HIV and Syphilis Screening
No relevant evidence was identified regarding the clinical utility of dual point-of-care HIV and syphilis tests during prenatal care or for people in labour; therefore, no summary can be provided.
Clinical Utility of Point-of-Care HIV Screening
No relevant evidence was identified regarding the clinical utility of point-of-care HIV tests during prenatal care or for people in labour; therefore, no summary can be provided.
Clinical Utility of Point-of-Care Syphilis Screening
One systematic review20 identified 1 relevant RCT. In prenatal care settings, when compared to the traditional algorithm for laboratory screening for syphilis (i.e., RPR and TPHA testing), point-of-care testing for syphilis resulted in:
more women receiving antenatal syphilis screening (99.9% versus 62.1% to 79.9%; statistically significant difference)
more women receiving adequate syphilis treatment (98.9% versus 89.6%; statistically significant difference)
93% reduction in congenital syphilis cases (0.13 cases versus 1.95 cases per 1,000 pregnancies; statistically significant difference).
Cost-Effectiveness of Dual Point-of-Care HIV and Syphilis Screening
No relevant evidence was identified regarding the cost-effectiveness of dual point-of-care HIV and syphilis tests during prenatal care or for people in labour; therefore, no summary can be provided.
Cost-Effectiveness of Point-of-Care HIV Screening
No relevant evidence was identified regarding the cost-effectiveness of point-of-care HIV tests during prenatal care or for people in labour; therefore, no summary can be provided.
Cost-Effectiveness of Point-of-Care Syphilis Screening
Point-of-care syphilis testing and treatment in pregnancy was reported to be cost-effective compared to RPR laboratory testing in low-income to middle-income countries; however, the willingness-to-pay thresholds for the relevant studies were not reported (1 systematic review of 3 studies).29
The Brazilian economic evaluation reported that point-of-care testing and treatment of syphilis in antenatal care resulted in an ICER of US$357.44 per DALY when compared to standard serology testing (i.e., nontreponemal test plus TPHA) with treatment at a follow-up visit. At a willingness-to-pay threshold of US$3,200 per DALY, the probability of the point-of-care testing and treatment strategy being cost-effective is 58%.21 Based on the cost-effectiveness acceptability curve, there is a similar probability of this intervention being cost-effective at higher willingness-to-pay thresholds.
Limitations
Overall Completeness of the Evidence
No evidence was found for the following; therefore, no conclusions can be formed on these research questions:
the DTA of point-of-care tests for HIV (standalone tests)
the clinical utility of dual point-of-care tests for HIV and syphilis
the clinical utility of point-of-care tests for HIV (standalone tests)
the cost-effectiveness of dual point-of-care tests for HIV and syphilis
the cost-effectiveness of point-of-care tests for HIV (standalone tests)
point-of-care HIV and/or syphilis screening for people in labour.
For the DTA studies, the small number of people who tested positive for HIV (3 studies23,27,28 with less than or equal to 3%) or syphilis (3 studies25-27 ranging from 0 to 2.1%) may have contributed to imprecision for sensitivity or specificity (i.e., wide CIs around the estimates) or made it not possible to calculate sensitivity.
Little to no population characteristic information was provided in 8 of the 10 studies in the review,20-24,26,27,29 and we were not able to consider the generalizability of these findings nor could we reflect on any potential areas of health inequity in these articles.
Generalizability of the Findings
None of the included studies were conducted in Canada, and none of the studies reported using the specific point-of-care tests for HIV and/or syphilis that are approved for use in Canada (i.e., the INSTI Multiplex HIV-1/2 Syphilis Antibody Test and the INSTI HIV Self Test [there are no standalone point-of-care syphilis tests approved for use in Canada]). The choice of index tests and the potentially different prevalence of HIV or syphilis in these countries compared to Canada may limit the generalizability of the findings of this Rapid Review to the Canadian health care context.
Applicability of the Index Test and Reference Standard
Our ability to assess the DTA of the dual point-of-care test to detect HIV was limited by the reference standards for HIV that were used in included studies. In Canada, the standard practice for HIV screening is serology testing, but some countries use rapid point-of-care tests for HIV as part of their testing algorithm. Three studies in this report used rapid point-of-care tests for HIV as the reference standard (rather than standard serological testing) and were not relevant to this review.24-26
The relevant studies in the systematic review of economic evaluations use RPR testing alone (i.e., not in conjunction with a treponemal test),29 which does not align with the Canadian approach for syphilis testing to include both treponemal and nontreponemal testing. This may limit the generalizability of findings as these studies do not include the cost of treponemal testing.
The systematic review of DTA studies was specifically looking at the performance of point-of-care syphilis tests to detect active syphilis in pregnancy. Current point-of-care syphilis tests are intended to detect the presence of syphilis antibodies, which may reflect a current or past syphilis infection (similar to a treponemal test) and are not designed to distinguish between active and past syphilis infections. Thus, the index tests and the reference standard used in this systematic review are measuring different target conditions (i.e., syphilis exposure versus active syphilis infection) which may affect the sensitivity and specificity results. However, screening pregnant people with the intent to identify those in need of treatment (i.e., screening for active syphilis infection) may be more valuable to health care providers than screening for syphilis exposure. As this systematic review was interested in detecting active syphilis infection, the authors excluded 9 studies because they only used 1 treponemal serology test (e.g., TPHA or TPPA) as the reference standard for syphilis testing.22 It is unknown whether these excluded studies would have met the inclusion criteria for this Rapid Review.
Equity Considerations
None of the included studies distinguished sex from gender, and all studies reported their population as “women.” While we have retained the original language used when reporting on these studies, we acknowledge that such language is not inclusive of trans and nonbinary persons. It is unknown whether any of the studies excluded trans or nonbinary people who were pregnant and receiving antenatal care.
One study25 reported the proportion of the population that had completed primary level education, and the proportion in a monogamous relationship, and 1 study28 reported the average time to reach the antenatal care clinic from home, but neither study considered these characteristics when summarizing or discussing the results. There was limited detail provided about the populations in the included studies, and none of the other studies reported characteristics that permitted an assessment of potential health inequities related to HIV and syphilis testing in a prenatal care setting.
This Rapid Review did not include a formal evaluation of the equity considerations, nor did it conduct a search explicitly for information related to inequity or groups that are underserved for point-of-care HIV or syphilis screening. Rather, the Equity Checklist for Health Technology Assessment18 and PROGRESS-plus19 were used to guide our discussion of equity considerations for this topic, primarily focusing on gaps in the included studies.
Conclusions and Implications for Decision- or Policy-Making
This report comprises 3 systematic reviews,20-22 6 cross-sectional studies,23-28 and 1 cost-effectiveness study21 regarding the DTA, clinical utility, and cost-effectiveness of point-of-care HIV and syphilis screening in prenatal care settings. No relevant evidence was identified regarding the use of these tests in people in labour.
HIV Point-of-Care Tests
Dual point-of care tests have moderate to high sensitivity for HIV, correctly detecting 85% to 100% of pregnant people with HIV. They also have high specificity for HIV, correctly classifying more than 99% of pregnant people who do not have HIV.23,27,28 The high specificity suggests that if a person receives a positive test result for HIV from a dual point-of-care test, we can be fairly certain that the person has an HIV infection. However, if a person receives a negative test result for HIV from a dual point-of-care test, there is a chance that it is a false-negative test result, and further testing would be required to confirm the diagnosis.
We did not identify any evidence about the cost-effectiveness or clinical utility of point-of-care tests for HIV that met inclusion criteria for this report.
Syphilis Point-of-Care Tests
Dual point-of care tests have low to high sensitivity to detect syphilis, correctly detecting 66% to 100% of pregnant people with current or previous syphilis infection. They also have high specificity for syphilis, correctly classifying more than 97% of pregnant people who do not have a current or previous syphilis infection.23-28 The high specificity suggests that if a person receives a positive syphilis test result from a dual point-of-care test, we can be fairly certain that the person has a current or previous syphilis infection. However, if a person receives a negative test result for syphilis from a dual point-of-care test, we cannot be certain they do not or have not had a syphilis infection (i.e., possible false-negative test result), and further testing would be required to confirm the diagnosis.
Both the dual point-of care tests and the standalone point-of-care syphilis tests have moderate sensitivity for active syphilis, correctly identifying 82% to 85% (dual tests)24 and 85% (standalone tests)22 of pregnant people with active syphilis infection. The specificity of the dual point-of-care tests to detect people who do not have active syphilis was not reported, which limits our understanding of the DTA of these tests for active syphilis infection. However, the standalone point-of-care syphilis tests have high specificity for active syphilis, correctly classifying 98% of pregnant people who do not have active syphilis.22 The high specificity of the standalone point-of-care syphilis tests suggests that if a person receives a positive result from a point-of-care syphilis test, we can be fairly certain that the patient has active syphilis. However, if a person receives a negative test from a point-of-care syphilis test, we cannot be certain they do not have an active syphilis infection (i.e., possible false-negative test result), and further testing would be required to confirm the diagnosis.
Limited evidence suggests that point-of-care syphilis screening in prenatal settings may increase the proportion of women screened and adequately treated for syphilis, and may reduce the number of cases of congenital syphilis, when compared to the traditional laboratory-based screening approach (1 systematic review of 1 study).20
In low-income to middle-income countries, point-of-care syphilis testing in pregnancy may be cost-effective compared to RPR (i.e., nontreponemal) laboratory testing alone (1 systematic review of 3 studies).29 However, RPR testing alone does not align with the standard approach for syphilis testing in Canada, which requires conducting both treponemal and nontreponemal testing, and these findings may not be generalizable to the Canadian health care context. In a cost-effectiveness analysis set in Brazil, a point-of-care test and treat strategy was likely to be cost-effective at a willingness-to-pay threshold of US$3,200 per DALY, when compared to a strategy of standard serology testing with treatment at subsequent follow-up (1 study).21
Considerations for Future Research
To help address health equity concerns in future studies, researchers should consider collecting equity-relevant population characteristics (e.g., gender, education, socioeconomic status, place of residence) to assess potential health inequities related to point-of-care HIV and syphilis screening in prenatal settings.
Researchers should also consider that certain equity-deserving groups may face barriers to accessing prenatal care (e.g., trans and nonbinary people,30 Indigenous people in Canada31) and should consider including pregnant people from diverse groups in future studies on point-of-care HIV and syphilis screening in prenatal settings. This may inform evaluations of the health system implications of using point-of-care screening tests beyond test accuracy, including whether they could be effective strategies to remove barriers to accessing timely and appropriate prenatal care in these populations.
While not included in their analysis, the authors of the systematic review of economic evaluations by Saweri et al.29 discussed the importance of incorporating equity considerations within economic evaluations of health interventions. The authors suggest that point-of-care testing and treatment strategies may have the potential to reduce inequalities in health care by diagnosing and treating sexually transmitted infections in a single visit to a health facility.29 To address health equity concerns in future economic evaluations, the systematic review authors recommend that future work should consider the distribution of costs and effects by equity-relevant variables such as socioeconomic status, location, ethnicity, or sex (i.e., a distributional cost-effectiveness analysis).29
Implications for Clinical Practice
Point-of-care syphilis tests have the potential to be cost-effective,21,29 and are likely to increase the proportion of people who are screened and treated for syphilis, which may reduce transmission of syphilis to the child.20
The findings of this report suggest that in prenatal care, dual point-of-care tests for HIV and syphilis and point-of-care syphilis tests would be a useful screening strategy for determining whether a person has a potential HIV or syphilis infection. If a person receives a positive result for HIV or syphilis with these tests, they are likely to have the infection and decisions around treatment and management could be expedited. These tests are less likely to misclassify those who are not infected with HIV or syphilis as having an HIV or syphilis infection. However, there is a risk that these tests may miss people who do have an HIV or syphilis infection (i.e., false negatives) and standard serological testing is needed to confirm the diagnosis.
Decision-makers should consider that point-of-care tests for HIV and syphilis are designed to screen people for potential HIV infections and syphilis exposure and that standard serological testing is needed to confirm the diagnosis of HIV and to distinguish between previous and active syphilis infections, for both positive and negative test results. However, given the risk of adverse pregnancy outcomes associated untreated syphilis, and that some populations may experience barriers in returning for follow-up visits to receive the results of a confirmatory diagnostic test, in some cases initiating syphilis treatment immediately following the results of the point-of-care test may outweigh the risk of overtreatment of birthing parents with a false-positive result.27 Similarly, antiretroviral treatment for HIV in newborns is recommended to start as early as possible after delivery, ideally within 6 hours of birth, and presumptive treatment may be initiated in the absence of confirmed test results for infants at highest risk of perinatal HIV acquisition.32
Decisions-makers should also consider that point-of-care tests have the potential to expand the availability of prenatal HIV and syphilis screening in rural and remote communities and in underserved facilities and/or communities. Point-of-care tests could expedite screening and treatment decisions in people who face barriers to accessing prenatal care or STI screening and who might be lost to follow-up using traditional testing strategies, including (but not limited to) people living in rural or remote areas, people who may have difficulty returning for follow-up appointments (e.g., due to a lack of paid time off for medical appointments, or lack of reliable transportation), or people who have experienced stigma or discrimination in health care. If used during labour or at the time of delivery, these screening tests can also provide the opportunity for timely treatment of the birthing parent and the newborn, rather than waiting days for results from standard laboratory tests before initiating treatment.
References
1.Shoemaker ES, Volpini K, Smith S, Loutfy M, Kendall C. Equitable timing of HIV diagnosis prior to pregnancy: a Canadian perspective. Cureus. 2021;13(7):e16691. PubMed
2.Canadian Paediatric Society. HIV in pregnancy: identification of intrapartum and perinatal HIV exposures 2019; https://cps.ca/en/documents/position/hiv-in-pregnancy. Accessed 2023 Jun 12.
3.Norwitz ER, Hicks CB. Syphilis in pregnancy In: Lockwood CJ, Marrazzo J, eds. UpToDate. Waltham (MA): UpToDate; 2022: http://www.uptodate.com. Accessed 2023 May 19.
4.Public Health Agency of Canada. Congenital syphilis fact sheet. 2007; https://www.canada.ca/en/public-health/services/infectious-diseases/sexual-health-sexually-transmitted-infections/congenital-syphilis-fact-sheet.html. Accessed 2023 Jun 12.
5.Public Health Agency of Canada. Syphilis guide: etiology and epidemiology. https://www.canada.ca/en/public-health/services/infectious-diseases/sexual-health-sexually-transmitted-infections/canadian-guidelines/syphilis/etiology-epidemiology.html. Accessed 2023 Jun 12.
6.Sax PE. Screening and diagnostic testing for HIV infection In: Hirsch MS, ed. UpToDate. Waltham (MA) UpToDate; 2021: http://www.uptodate.com. Accessed 2023 May 19.
7.Funai EF, Norwitz ER. Labor and delivery: management of the normal first stage In: Prabhu M, ed. UpToDate. Waltham (MA) UpToDate; 2023: http://www.uptodate.com. Accessed 2023 May 19.
8.Public Health Agency of Canada. Human immunodeficiency virus - HIV screening and testing guide. 2014; https://www.canada.ca/en/public-health/services/hiv-aids/hiv-screening-testing-guide.html#d. Accessed 2023 Jun 12.
9.Public Health Agency of Canada. Syphilis guide: screening and diagnostic testing. 2022; https://www.canada.ca/en/public-health/services/infectious-diseases/sexual-health-sexually-transmitted-infections/canadian-guidelines/syphilis/screening-diagnostic-testing.html. Accessed 2023 Jun 12.
10.Grennan T, van Schalkwyk J, Giesbrecht E. Interim guideline on syphilis screening in pregnancy. Vancouver (BC): Perinatal Services BC.; 2019: http://www.perinatalservicesbc.ca/Documents/Guidelines-Standards/Maternal/Guideline-syphilis-screening-in-pregnancy.pdf 023 Jun 12.
11.Naidu P, Tsang RS. Canadian Public Health Laboratory Network guidelines for the use of point-of-care tests for Treponema pallidum in Canada. J Assoc Med Microbiol Infect Dis Can. 2022;7(2):85-96. PubMed
12.Health Canada. Active licence listing by company: Biolytical Laboratories Inc. 2023; https://health-products.canada.ca/mdall-limh/information?companyId=116586&lang=eng. Accessed 2023 Jun 12.
13.Public Health Agency of Canada. Estimates of HIV incidence, prevalence and Canada’s progress on meeting the 90-90-90 HIV targets, 2020. 2022; https://www.canada.ca/en/public-health/services/publications/diseases-conditions/estimates-hiv-incidence-prevalence-canada-meeting-90-90-90-targets-2020.html. Accessed 2023 Jun 14.
14.Aho J, Lybeck C, Tetteh A, et al. Rising syphilis rates in Canada, 2011-2020. Can Commun Dis Rep. 2022;48(23):52-60. PubMed
15.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
16.Higgins JPT, Green S, editors. Figure 15.5.a: Drummond checklist (Drummond 1996). Cochrane handbook for systematic reviews of interventions. London (GB): The Cochrane Collaboration; 2011: http://handbook-5-1.cochrane.org/chapter_15/figure_15_5_a_drummond_checklist_drummond_1996.htm. Accessed 2023 Jun 12.
17.Whiting PF, Rutjes AW, Westwood ME, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155(8):529-536. PubMed
18.Benkhalti M, Espinoza M, Cookson R, Welch V, Tugwell P, Dagenais P. Development of a checklist to guide equity considerations in health technology assessment. Int J Technol Assess Health Care. 2021;37:e17. PubMed
19.O'Neill J, Tabish H, Welch V, et al. Applying an equity lens to interventions: using PROGRESS ensures consideration of socially stratifying factors to illuminate inequities in health. J Clin Epidemiol. 2014;67(1):56-64. PubMed
20.Brandenburger D, Ambrosino E. The impact of antenatal syphilis point of care testing on pregnancy outcomes: a systematic review. PLoS One. 2021;16(3):e0247649. PubMed
21.Romero CP, Marinho DS, Castro R, et al. Cost-effectiveness analysis of point-of-care rapid testing versus laboratory-based testing for antenatal screening of syphilis in Brazil. Value Health Reg Issues. 2020;23:61-69. PubMed
22.Phang Romero Casas C, Martyn-St James M, Hamilton J, Marinho DS, Castro R, Harnan S. Rapid diagnostic test for antenatal syphilis screening in low-income and middle-income countries: a systematic review and meta-analysis. BMJ Open. 2018;8(2):e018132. PubMed
23.Soares DC, Filho LCF, Souza Dos Reis H, et al. Assessment of the accuracy, usability and acceptability of a rapid test for the simultaneous diagnosis of syphilis and HIV infection in a real-life scenario in the Amazon region, Brazil. Diagnostics (Basel). 2023;13(4):20. PubMed
24.Kasaro MP, Bosomprah S, Taylor MM, et al. Field performance evaluation of dual rapid HIV and syphilis tests in three antenatal care clinics in Zambia. Int J STD AIDS. 2019;30(4):323-328. PubMed
25.Taremwa IM, Twelwanike A, Mwambi B, Atuhairwe C. Laboratory assessment of SD Bioline HIV/Syphilis Duo Kit among pregnant women attending antenatal clinic Mayuge Health Center III, East central Uganda. BMC Res Notes. 2019;12(1):238. PubMed
26.Withers K, Bristow C, Nguyen M, Stafylis C, Giang LM, Klausner JD. A field evaluation of a rapid dual immunoassay for human immunodeficiency virus and syphilis antibodies, Hanoi, Vietnam. Int J STD AIDS. 2019;30(2):173-180. PubMed
27.Lodiongo DK, B KB, G WD, et al. Field evaluation of SD BIOLINE HIV/Syphilis Duo assay among pregnant women attending routine antenatal care in Juba, South Sudan. PLoS One. 2018;13(10):e0205383. PubMed
28.Olugbenga I, Taiwo O, Laverty M, et al. Clinic-based evaluation study of the diagnostic accuracy of a dual rapid test for the screening of HIV and syphilis in pregnant women in Nigeria. PLoS One. 2018;13(7):e0198698. PubMed
29.Saweri OPM, Batura N, Al Adawiyah R, et al. Economic evaluation of point-of-care testing and treatment for sexually transmitted and genital infections in pregnancy in low- and middle-income countries: a systematic review. PLoS One. 2021;16(6):e0253135. PubMed
30.Kukura E. Reconceiving reproductive health systems: caring for trans, nonbinary, and gender-expansive people during pregnancy and childbirth. J Law Med Ethics. 2022;50(3):471-488. PubMed
31.Bacciaglia M, Neufeld HT, Neiterman E, Krishnan A, Johnston S, Wright K. Indigenous maternal health and health services within Canada: a scoping review. BMC Pregnancy Childbirth. 2023;23(1):327. PubMed
32.Clinicalinfo. Recommendations for the Use of antiretroviral drugs during pregnancy and interventions to reduce perinatal HIV Transmission in the united states. 2023; https://clinicalinfo.hiv.gov/en/guidelines/perinatal/management-infants-arv-hiv-exposure-infection. Accessed 2023 Jun 28.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study design, outcomes | Intervention and comparator(s) | Included studies | Population characteristics |
|---|---|---|---|---|
Brandenburger and Ambrosino 202120 Netherlands Funding: No specific funding received for this work | Systematic review of studies investigating the impact of antenatal syphilis point-of-care tests on pregnancy outcomes Literature searched until June 8, 2020 Adverse pregnancy outcomes related to syphilis | Intervention: Point-of-care syphilis test. Relevant study used SD Bioline Syphilis 3.0 Comparator: Conventional laboratory testing for syphilis. Relevant study used RPR and TPHA laboratory tests | Relevant to this report: 1 cluster RCT (published in 2009, conducted in Mongolia) | Pregnant women attending antenatal care N = 7,700 Age (years), mean (SD) Intervention: 26.9 (5.5) Control: 27 (7.5) Gestational age at first sampling, weeks (SD) Intervention: 14.1 (6.6) Control: 12 (4.8) |
Saweri et al. (2021)29 Australia Funding: UK Department for International Development, the UK Medical Research Council and the Wellcome Trust; the Australian National Health and Medical Research Council; the Swiss National Science Foundation | Systematic review of economic evaluations of point-of-care testing and treatment of sexually transmitted infections (including syphilis) in pregnancy in low- and middle-income countriesa Literature search completed April 2020 Cost-effectiveness (e.g., incremental cost per DALY averted) | Intervention: Point-of-care testing and treatment of syphilis Relevant interventions: Rapid syphilis tests Comparator: Alternative test or no screening Relevant comparator: RPR alone | 3 studies relevant to this report (1 cost-utility analysis and 2 cost-effectiveness analyses) published between 2006 and 2016 The studies were conducted in Tanzania, Haiti, and Peru One study conducted from the societal perspective and the provider perspective, and perspective not reported in 2 studies Time horizon not reported | Pregnant women in low-income and middle-income countriesa No additional details provided about the populations within each study |
Phang et al. (2018)22 Brazil Funding source: National Council for Scientific and Technological Development; Ministry of Science, Technology, Innovation and Communication Research Foundation of the State of Rio de Janeiro, and the Oswaldo Cruz Foundation | Systematic review and meta-analysis of DTA studies of point-of-care syphilis tests to detect active syphilis Literature searched until end of August 2017 QUADAS-2 tool used to assess risk of bias DTA studies only included if they reported test performance data (i.e., true positive, false positive, false negative, true negative) to calculate sensitivity and specificity | Index test: Rapid point-of-care immunochromatographic syphilis testsb Excluded: Studies using dual rapid tests Reference standard: Traditional algorithm for syphilis that used a nontreponemal test VDRL or RPR test followed by a treponemal test (e.g., TPHA, FTA-ABS, TPPA) Excluded: Studies with only 1 lab-based standard test (e.g., TPHA alone) | Five prospective DTA studies (published between 2006 and 2015), which only recruited patients with the suspected condition (i.e., single-gate design) from antenatal clinics or hospitals The studies were conducted in Brazil, South Africa, Mexico, India, Mozambique, and Bolivia, which the authors reported as “low-income and middle-income countries” based on the World Bank country classification | Pregnant women in antenatal care settings N, total = 14,985 N, range = 200 to 8,892 All women in third decade of life (reported in 3 studies) Stage of pregnancy: All women in second trimester (3 studies); 16%, 32%, and 52% in the first, second, and third trimesters, respectively (1 study); and not reported (1 study) |
DALY = disability-adjusted life-year; DTA = diagnostic test accuracy; FTA-ABS = Fluorescent Treponemal Antibody Absorption; QUADAS-2 = Quality Assessment of Diagnostic Accuracy Studies; RCT = randomized controlled trial; RPR = rapid plasma reagin; SD = standard deviation; TPHA = Treponema pallidum hemagglutination; TPPA = Treponema pallidum particle agglutination; VDRL = Venereal Diseases Research Laboratory test.
Note: All studies reported their population as “women.” We have retained the original language used by the studies and acknowledge that such language is not inclusive of trans and nonbinary persons.
aAs defined by the World Bank.
bTwo included studies used the SD Bioline V3.0 test (Standard Diagnostics, Korea), 2 studies used the Determine Syphilis TP test (Abbott Laboratories, US), and 1 study used the VisiTect Syphilis test (Omega Diagnostics, Scotland). Data synthesis assumed that different specific rapid tests (e.g., by different manufacturers) can be considered equivalent (i.e., only 1 index test).
Table 3: Characteristics of Included Diagnostic Test Accuracy Studies
Study citation, country, funding source | Study design, target condition(s) | Population characteristics | Index test(s) and reference standards | Outcomes |
|---|---|---|---|---|
Soares et al. (2023)23 Brazil Funding: Through the Pan American Health Organization and the Department of Chronic Diseases and Sexually Transmitted Infections | Cross-sectional study Participants recruited using convenience sample from 3 sites, from April to July 2021 Samples for index test and reference standard collected at same time Dual rapid test for HIV and syphilis compared against separate laboratory tests for each condition (reported by author as the “gold standard”) | 397 pregnant women aged 18 years or older attending routine antenatal care Age:
| Index test: SD BIOLINE HIV/Syphilis Duo Test for HIV and syphilis using fingerpick or whole blood sample Reference standard: For syphilis = FTA-ABS (Wama) treponemal laboratory test For HIV = 4th generation Genscreen Ultra HIV Ag-Ab (Bio-Rad) enzyme immunoassay | Sensitivity, specificity, positive predictive value, negative predictive value, accuracy performance (not further defined by the authors) |
Kasaro et al. (2019)24 Zambia Funding: WHO Department of Reproductive Health and Research, PATH, and the Bill and Melinda Gates foundation | Cross-sectional study Participants recruited from 3 antenatal clinics from September 2014 through June 30, 2015 Samples for index tests and reference standards collected at same time Testing 2 dual rapid diagnostic tests for HIV and syphilis compared against separate tests by condition. HIV results compared against alternative rapid tests (not relevant to this review). Syphilis results compared to serologic screening | Pregnant women 18 or older presenting to their first antenatal care visit Blood samples available for 2,121 women, but 3,213 were enrolled Age (years), median (IQR) = 25 (21 to 30) Gestational age (weeks), median (IQR) = 20 (16 to 24) | Index tests: SD BIOLINE HIV/Syphilis Duo Test (Standard Diagnostics, Korea) and Chembio Dual Path Platform HIV-Syphilis Assay (Medford, NY, US) Reference standard: For syphilis = TPPA treponemal test. Positive TPPA samples were tested with RPR to determine whether infection was active For HIV = 2 Rapid point-of-care tests, Determine (Alere Medical Company Limited, Japan) and Uni-Gold (Trinity Biotech, US) | Sensitivity and specificity |
Tarema et al. (2019)25 Uganda Funding: No funding received; HIV-Syphilis SD Bioline test kits were donated from MEDLINK LAB and SURGICALS LTD. | Cross-sectional study Participants recruited from 1 antenatal care unit from July 2018 to September 2018 Venous blood samples for index test and reference standards collected at same time and sent to a lab for all analyses Dual rapid test for HIV and syphilis compared against separate tests by condition. HIV results compared against alternative rapid tests (not relevant to this review). Syphilis results compared to serologic screening | 382 Pregnant women aged 18 to 49 years who did not know their HIV or syphilis status Age (years), mean (SD) = 25.8 (5.977) Completed primary level education, N (%) = 199 (52.1) Monogamous relationship, N (%) = 251 (65.7) | Index test: SD BIOLINE HIV/Syphilis Duo Test Reference standard: For syphilis = TPHA assay (BIOTEC Lab 21 Health care, Ltd., Dorset UK) For HIV = rapid point-of-care tests Determine HIV-1/2 (Abbott Laboratories, Ireland),HIV 1/2 Stat-Pak (Chembio Diagnostic, US) and (c) Uni-Gold recombinant HIV-1/2 (Trinity Biotech, Ireland) | Sensitivity, specificity |
Withers et al. (2019)26 Vietnam Funding: UCLA Center for AIDS research, UCLA Center for HIV Identification, Prevention and Treatment Services, and UCLA Center for World Health | Cross-sectional study Participants recruited by convenience sampling from and antenatal clinic between May 2017 and July 2017 Fingerpick sample for index test and venous blood sample for reference standards collected at same time Dual rapid test for HIV and syphilis compared against separate tests by condition. HIV results compared against an alternative rapid test (not relevant to this review). Syphilis results compared to serologic screening | 180 pregnant women 18 or older who were willing to be counselled, tested, and treated (if necessary) for HIV and syphilis | Index test: SD BIOLINE HIV/Syphilis Duo rapid test (Alere Inc., US) using whole blood collected using fingerpick Reference standard: For syphilis = TPPA (SERODIA-TPPA, Fujirebio Diagnostics, Japan) For HIV = Rapid point-of-care test BIOLINE HIV-1/2 3.0 (Standard Diagnostics Inc., Republic of Korea) | Sensitivity and specificity |
Londiongo et al. (2018)27 South Sudan Funding: Standard Diagnostics, Inc., Yongin, Gyeonggi, South Korea provided the SD Bioline Duo kits and financial support | Cross-sectional study Participants recruited from 4 facilities by convenience sampling between June 2016 and August 2016 One venous blood sample was collected and used for all tests Dual rapid test for HIV and syphilis compared against separate laboratory tests for each condition | 442 pregnant women aged 15 to 49 attending their first antenatal care visit | Index test: SD BIOLINE HIV/Syphilis Duo rapid test (Standard Diagnostics, Inc., Yongin, Gyeonggi, South Korea) Reference standard: For syphilis = TPHA (BIOTEC Lab21 Health care Ltd., UK) and RPR For HIV = Vironostika HIV1/2 Uniform II Ag/Ab ELISA test (BiomeÂrieux SA, France) | Sensitivity, specificity, positive predictive value, negative predictive value |
Olugbenga et al. (2018)28 Nigeria Funding: UNDP-UNFPA-UNICEF-WHO-World Bank Special Programme of Research, Development and Research Training in Human Reproduction | Cross-sectional study Patients recruited from 12 sites Fingerpick sample for index test and venous blood sample for reference standards collected at same visit | 4,550 pregnant women 18 or older attending their first antenatal care visit Age (years), median (IQR) = 30 (27 to 33) Gestational age (weeks), median (IQR) = 20 (16 to 28) Time taken to reach clinic from home, minutes (range) = 30 (30 to 50) | Index test: SD BIOLINE HIV/Syphilis Duo rapid test (Alere, US) Reference standard: For syphilis = TPHA. Positive samples were tested with RPR to determine whether infection was active For HIV = 4th generation Genscreen Ultra HIV Ag-Ab (Bio-Rad, Europe GMbH) enzyme immunoassay | Sensitivity, specificity |
CIA = chemiluminescence immunoassay; EIA = enzyme immunoassays; FTA-ABS = Fluorescent Treponemal Antibody Absorption; IQR = interquartile range; RPR = rapid plasma reagin; SD = standard deviation; TPHA = Treponema pallidum hemagglutination; TPPA = Treponema pallidum particle agglutination; UCLA = University of California Los Angeles.
Note: All studies reported their population as “women.” We have retained the original language used by the studies and acknowledge that such language is not inclusive of trans and nonbinary persons.
Table 4: Characteristics of the Included Economic Evaluation
Study citation, country, funding source | Type of analysis, time horizon, perspective | Population, intervention, and comparator | Modelling approach | Source of clinical, cost, and utility data used in analysis | Main assumptions |
|---|---|---|---|---|---|
Romero et al. (2020)21 Brazil Funding: Science without Borders (Brazil); Department of Science and Technology of Brazilian Ministry of Health; Brazilian Network for Health Technology Assessment | Analysis: Cost-effectiveness Time horizon: Lifetime Perspective: Brazilian public health system | Hypothetical cohort of all pregnant women (aged 10 to 49) who receive antenatal care and are at risk of syphilis. Singleton pregnancies only Intervention: Rapid point-of-care immunochromatographic syphilis test with same day treatment Comparator: Standard reference laboratory tests (VDRL plus TPHA) with treatment at follow-up visit | Decision analytic model Model incorporates 3 steps in antenatal care: syphilis testing, treatment prescription, and treatment adherence Effects and costs were discounted at 3% and 5% Focus is on eliminating mother-to-child syphilis transmission and model focuses on outcomes for the baby (does not include maternal outcomes) | Syphilis prevalence estimated from large hospital-based cohort study Sensitivity and specificity of the rapid test were from published literature (Phan et al.22) Micro-costing study was used to estimate costs for tests, personnel time, treatments, and inpatient care based on information from the Ministry of Health, the Unified Health System, national means, and expert opinion |
|
TPHA = Treponema pallidum hemagglutination; VDRL = Venereal Diseases Research Laboratory.
Note: This study reported their population as “women.” We have retained the original language used by the study and acknowledge that such language is not inclusive of trans and nonbinary persons.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 5: Strengths and Limitations of Systematic Reviews Using AMSTAR 215
Strengths | Limitations |
|---|---|
Brandenburger and Ambrosino (2021)20 | |
The population, intervention, and outcomes of interest were clearly stated. The authors explained their selections of study designs for inclusion in the review. The search was conducted in 3 databases, the full search strategy was provided, the authors searched reference lists of potentially relevant studies, and the search was conducted withing 24 months of publication. The Joanna Briggs Institute critical appraisal tool was used to assess the included studies. The authors declared no conflicts of interest, financial or otherwise. | The comparator was not clearly stated. It is unclear if the review methods were established before the conduct of the review. Authors did not provide justification for restricting to studies published in English. Study selection was conducted by a single reviewer. It was unclear whether data extraction or critical appraisal was performed by a single reviewer or in duplicate. Included studies were described with limited detail (e.g., population characteristics only included age, gestational age). A list of excluded studies with justifications for exclusion was not provided. The authors did not report the sources of funding for the included studies. The authors did not account for the risk of bias of the individual studies when interpreting the results. |
Saweri et al. (2021)29 | |
The population, intervention, and outcomes of interest were clearly stated. A protocol was registered in PROSPERO. Included full and partial economic evaluations. The search was conducted in 3 databases, search terms were provided, there were no language restrictions, the authors searched reference lists of relevant studies, and the search was conducted withing 24 months of publication. Two independent reviewers conducted study selection, and disagreements were resolved with a third reviewer. Two checklists were used to evaluate the comprehensiveness of the reporting and the methodology. Limitations of the studies were included in the discussion. The authors declared that they had no competing interests. The authors declare that the funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript. | The comparator of interest was not clearly stated. It was unclear whether data extraction or critical appraisal was performed by a single reviewer or in duplicate. A list of excluded studies with justifications for exclusion was not provided. Limited details were provided for the included studies. For instance, the populations were not described (e.g., number and characteristics) and the type of rapid tests were not reported. The comparator in the 3 relevant studies was RPR alone (i.e., not in conjunction with a treponemal test), which may limit the generalizability of the findings. The authors did not report the sources of funding for the included studies. |
Phang et al. (2018)22 | |
The population, index tests, reference standards, and outcomes of interest were clearly stated. An explicit statement was provided that the review methods were established before the conduct of the review (registered in PROSPERO). The authors explained their selections of study designs for inclusion in the review. The search was conducted in multiple databases, the full search strategy was provided, there were no language restrictions, the authors searched reference lists of relevant studies, and the search was conducted withing 24 months of publication. Full texts of potentially relevant studies were reviewed in duplicate. Data extraction was performed in duplicate. Description of included studies included inclusion criteria, definition of syphilis, sampling methods, index, and reference tests. A list of excluded studies and the reasons for exclusion was provided. Included studies were critically appraised using QUADAS-2 for diagnostic test accuracy studies. Appropriate statistical methods were used for the meta-analysis. The authors declared that they had no competing interests. The authors reported that the funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript. | Titles and abstracts were reviewed by a single reviewer. It was unclear whether critical appraisal was performed by a single reviewer or in duplicate. Population characteristics of included studies were described with limited detail (i.e., approximate age, trimester of pregnancy). The authors did not report the sources of funding for the included studies. The meta-analysis included all studies, regardless of risk of bias of the individual studies. The authors included studies using different index tests and reference standards but did not sufficiently explore or discuss the sources of heterogeneity observed in the results of the meta-analysis. |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; QUADAS-2 = Quality Assessment of Diagnostic Accuracy Studies 2.
Table 6: Strengths and Limitations of Diagnostic Test Accuracy Studies Using the QUADAS-2 Checklist17
Strengths | Limitations |
|---|---|
Soares et al. (2023)23 | |
Participants were recruited using a convenience sample. The study population, index test, and reference standard (for HIV and syphilis) match those targeted by the review question. The sample for the index test and the reference standard were collected at the same visit. Index test results were interpreted without knowledge of the results of the reference standard. Methods to conduct and interpret the index test were well described. Reference standard results were interpreted without knowledge of the index test. All patients received the same reference standard. The authors declared that they have no conflicts of interest. | Limited information provided about the participants (i.e., age only). Did not use RPR to confirm active syphilis infections. Small number of HIV (1.0%) infections, which may contribute to imprecision for sensitivity and specificity results. |
Kasaro et al. (2019)24 | |
Low risk that the selection of patients would have introduced bias. The study population, index test, and reference standard (for syphilis) match those targeted by the review question. The sample for the index test and the reference standard were collected at the same visit. Index test results were interpreted without knowledge of the results of the reference standard. RPR was used to confirm whether positive serology results were active syphilis infections. A subgroup analysis was conducted on all active syphilis cases (detected via TPPA and RPR testing). Methods to conduct and interpret the index test were well described. Reference standard results were interpreted without knowledge of the index test. All patients received the same primary reference standard. The authors declared that they have no conflicts of interest with respect to the research, authorship, and publication of the article. | Only samples that tested positive with the reference test were further tested with a confirmation test for active syphilis (rather than conducting an RPR test on all samples), which could bias the interpretation of those results. 34% of recruited patients were missing from the analysis due to missing blood samples for the reference test. It is unclear whether there are any differences in the population missing from the analysis. Limited information provided about the participants (i.e., age, gestational age). The reference standard for HIV did not match that targeted by this review. |
Tarema et al. (2019)25 | |
Low risk that the selection of patients would have introduced bias. The study population, index test, and reference standard (for syphilis) match those targeted by the review question. Population characteristics well described (e.g., age, education level, relationship status, religion, occupation) The sample for the index test and the reference standard were collected at the same visit. Index test results were interpreted without knowledge of the results of the reference standard. Methods to conduct and interpret the index test were well described. Reference standard results were interpreted without knowledge of the index test. All patients received the same primary reference standard. The authors declared that they have no competing interests. The authors declared that the donation of the test kits did not interfere with the study design, the result of the analysis, or their decision to publish. | Did not use RPR to confirm active syphilis infections. The reference standard for HIV did not match that targeted by this review. Small number of syphilis infections (2.1%), which may contribute to imprecision for sensitivity and specificity results. |
Withers et al. (2019)26 | |
Participants were recruited using a convenience sample. The study population, index test, and reference standard (for syphilis) match those targeted by the review question. The sample for the index test and the reference standard were collected at the same visit. Index test results were interpreted without knowledge of the results of the reference standard. Methods to conduct and interpret the index test were well described. Reference standard results were interpreted without knowledge of the index test. All patients received the same primary reference standard. | Population characteristics not provided separately for the subgroup of pregnant women. The reference standard for HIV did not match that targeted by this review. Did not use RPR to confirm active syphilis infections. None of the pregnant women tested positive for syphilis, thus it was not possible to calculate sensitivity and may contribute to imprecision for specificity results. It was not reported whether the authors had any competing interests. It was not reported whether the funding agency had any influence on the study design or manuscript preparation |
Londiongo et al. (2018)27 | |
Participants were recruited using a convenience sample. The study population, index test, and reference standard (for HIV and syphilis) match those targeted by the review question. RPR was used to confirm whether positive serology results were active syphilis infections, and these results were considered by the authors in the discussion section of the report. The sample for the index test and the reference standard were collected at the same visit. Reference standard results were interpreted without knowledge of the index test. All patients received the same primary reference standard. The authors declared that they have no competing interests. The authors declared that the funders had no role in the design or conduct of the study, data analysis, decision to publish, or preparation of the manuscript. | No population characteristics were reported. Small number of HIV (1.8%) and syphilis (0.09%) infections, which may contribute to imprecision for sensitivity and specificity results. |
Olugbenga et al. (2018)28 | |
Participants were recruited using a convenience sample. The study population, index test, and reference standard (for HIV and syphilis) match those targeted by the review question. Some population characteristics were reported (i.e., age, gestational age, time to reach clinic from home). RPR was used to confirm whether positive serology results were active syphilis infections, and these results were considered by the authors when discussing the results. The sample for the index test and the reference standard were collected at the same visit. All patients received the same primary reference standard. The authors declared that they have no competing interests. The authors declared that the funders had no role in the design or conduct of the study, data analysis, decision to publish, or preparation of the manuscript. | It is unclear whether the reference standard results were interpreted without the knowledge of the index test, and it is unclear whether this may have introduced bias in the interpretation of the reference standard. Small number of HIV (3.0%) infections, which may contribute to imprecision for sensitivity and specificity results. |
QUADAS-2 = Quality Assessment of Diagnostic Accuracy Studies 2; RPR = rapid plasma reagin; TPPA = Treponema pallidum particle agglutination.
Table 7: Strengths and Limitations of the Economic Evaluation Using the Drummond Checklist16
Strengths | Limitations |
|---|---|
Romero et al. (2020)21 | |
The research question and its economic importance were stated. The type of analysis, perspectives, and time horizon were clearly stated and appropriate. The interventions and comparators of interest were reported and were appropriate. The sensitivity and specificity of the rapid tests were from a published systematic review and meta-analysis. Source of cost data was reported. The analysis was done using a decision analytic model. The model parameters were described. Probabilistic sensitivity analysis was conducted and credible intervals were reported. The conclusions follow from the data reported and are accompanied by the appropriate caveats. The clinical assumptions are reasonable. The authors declared that the funders had no role in the design or conduct of the study, data analysis, decision to publish, or preparation of the manuscript. | The details of the patients from which the population were based and the measurement of effectiveness were estimated were not reported. The quantities of resource use were not reported separately from their unit costs. The treatment costs and follow-up costs were presumed to be the same for both strategies, with the total cost depending on the probabilities of treatment compliance (which differed between strategies). Unclear whether this method of estimating costs is appropriate. Did not include nonmedical costs or indirect costs (e.g., consumables, equipment to perform lab tests). Did not include maternal outcomes. Unclear how or why the 3% and 5% discount rates were selected. Authors reported that the full details of the sensitivity analysis were in an online supplement but it was not available, thus unclear whether sufficient details are provided. Major outcomes were not presented in a disaggregated form, limiting the interpretation of key drivers of cost. |
Appendix 4: Main Study Findings
Table 8: Summary of Findings by Outcome — DTA for Dual Point-of-Care Test HIV Detection
Study citation | Index test | Reference standard | Number of patients | Number with HIV (%) | Sensitivity, % (95% CI) | Specificity, % (95% CI) | PPV, % (95% CI) | NPV, % (95% CI) | Accuracy, % (95% CI) |
|---|---|---|---|---|---|---|---|---|---|
Soares et al. (2023)23 | SD BIOLINE HIV/Syphilis Duo Test | Genscreen Ultra HIV Ag-Ab | 397 | 4 (1.0) | 100 (39.76 to 100) | 100 (99.06 to 100) | 100 | 100 | 100 (99.07 to 100) |
Olugbenga et al. (2018)28 | SD BIOLINE HIV/Syphilis Duo test | Genscreen Ultra HIV Ag-Ab | 4,550 | 138 (3.0) | 85.8 (79.1 to 90.6) | 99.5 (99.3 to 99.7) | — | — | — |
Londiongo et al. (2018)27 | SD BIOLINE HIV/Syphilis Duo test | Vironostika HIV1/2 Uniform II Ag/Ab | 442 | 8 (1.8) | 100 (63.1 to 100) | 100 (99.2 to 100) | 100 (63.1 to 100) | 100 (99.2 to 100) | — |
CI = confidence interval; FTA-ABS = Fluorescent Treponemal Antibody Absorption; NPV = negative predictive value; PPV = positive predictive value.
Note: This table has not been copy-edited.
Table 9: Summary of Findings by Outcome — DTA of Dual Point-of-Care Test for Syphilis Detection
Study citation | Index test | Reference standard | Number of patients | Number with syphilis (%) | Sensitivity, % (95% CI) | Specificity, % (95% CI) | PPV, % (95% CI) | NPV, % (95% CI) | Accuracy, % (95% CI) |
|---|---|---|---|---|---|---|---|---|---|
Soares et al. (2023)23 | SD BIOLINE HIV/Syphilis Duo Test | FTA-ABS | 397 | 29 (7.3) | 93.55 (78.58 to 99.21) | 100 (99 to 100) | 100 | 99.46 (97.95 to 99.86) | 99.50 (98.19 to 99.94) |
Kasaro et al. (2019)24 | SD BIOLINE HIV/Syphilis Duo Test | TPPA | 2,119 | 205 (9.7) | 66.2 (59.4 to 72.4) | 97.2 (96.4 to 97.9) | — | — | — |
Withers et al. (2019)26 | SD BIOLINE HIV/Syphilis Duo test | TPPA | 108 | 0 | Not availablea | 100 (98.0 to 100) | — | — | — |
Tarema et al. (2019)25 | SD BIOLINE HIV/Syphilis Duo Test | TPHA | 382 | 8 (2.1) | 100 (98.3 to 100) | 100 (98.6 to 100) | — | — | — |
Londiongo et al. (2018)27 | SD BIOLINE HIV/Syphilis Duo test | TPHA | 442 | 22 (5) exposure | 86.4 (65.1 to 97.1) | 100 (99.1 to 100) | 100 (82.4 to 100) | 99.3 (97.9 to 99.9) | — |
Olugbenga et al. 2018)28 | SD BIOLINE HIV/Syphilis Duo test | TPHA | 4,550 | 4 (0.09) | Not availableb | 99.9 (99.8 to 100) | — | — | — |
Kasaro et al. (2019)24 | SD BIOLINE HIV/ Syphilis Duo Test | TPPA plus RPR titresc | 2,119 | 205 (9.7) | 81.6 (72.7 to 88.1) | — | — | — | — |
Chembio Dual Path Platform HIV-Syphilis Assay | TPPA | 68.6 (61.9 to 74.6) | 98.5 (97.8 to 98.9) | — | — | — | |||
Chembio Dual Path Platform HIV-Syphilis Assay | TPPA plus RPR titresc | 84.7 (76.1 to 90.6) | — | — | — | — |
CI = confidence interval; FTA-ABS = Fluorescent Treponemal Antibody Absorption; NPV = negative predictive value; PPV = positive predictive value; RPR = rapid plasma reagin; TPHA = Treponema pallidum hemagglutination; TPPA = Treponema pallidum particle agglutination.
aCould not be calculated because there were no positive results for syphilis antibodies.
bCould not be calculated because there were no positive results for the TPHA or the dual point-of-care test. Four specimens tested positive on TPHA but were not identified as positive with the dual test. RPR testing results for these 4 samples were indicative of nonactive syphilis.
cDetects active syphilis.
Note: This table has not been copy-edited.
Table 10: Summary of Findings by Outcome — DTA of Point-of-Care Syphilis Testing
Study citation | Study design | Index test and reference standard | Sensitivity | Specificity | ||
|---|---|---|---|---|---|---|
% (95% CrI) | 95% PrI, % | % (95% CrI) | 95% PrI, % | |||
Phang et al. (2018)22 | SR and meta-analysis of 5 DTA tests | Rapid POC syphilis test vs. traditional testing algorithma | 85 (73 to 92) | 57 to 96 | 98 (95 to 98) | 88 to 100 |
CrI = credible interval; FTA-ABS = Fluorescent Treponemal Antibody Absorption; POC = point-of-care; PrI = prediction interval; RPR = rapid plasma reagin; TPHA = Treponema pallidum hemagglutination; TPPA = Treponema pallidum particle agglutination; vs. = versus.
aStandard reference test algorithm includes a nontreponemal or RPR test followed by a treponemal test (e.g., TPHA, FTA-ABS, TPPA).
Note: This table has not been copy-edited.
Table 11: Summary of Findings by Outcome — Clinical Utility of Point-of-Care Syphilis Testing
Study citation | Study design | Intervention and control | Outcome | POCT | Lab testing | P value |
|---|---|---|---|---|---|---|
Brandenburger and Ambrosino 202120 | SR with 1 RCT | SD Bioline Syphilis 3.0 vs. RPR and TPHA | Receiving antenatal syphilis screening, % | 99.9 | First test: 79.9 Second test: 62.1 | < 0.001 |
Receiving adequate syphilis treatment,a % | 98.9 | 89.6 | 0.02 | |||
Congenital syphilis, per 1,000 pregnancies | 0.13b | 1.95 | < 0.002 |
CI = confidence interval; POCT = point-of-care test; RCT = randomized controlled trial; RPR = rapid plasma reagin; SR = systematic review; TPHA = Treponema pallidum hemagglutination; TPPA = Treponema pallidum particle agglutination; vs. = versus.
aThe definition of ‘adequate syphilis treatment’ was not reported in the systematic review.
bRepresents a 93% reduction in congenital syphilis cases compared to standard lab testing.
Note: This table has not been copy-edited.
Table 12: Summary of Findings — Economic Evaluations of Point-of-Care Syphilis Testing
Main study findings | Authors’ conclusion |
|---|---|
Saweri et al. (2021)29 | |
Point-of-care rapid syphilis testing and treatment was cost-effective compared to RPR in all 3 studies | “These studies also indicate that point-of-care testing and treatment for STIs is most cost-effective where access to alternative testing mechanisms is limited, including laboratory testing facilities.” (p. 15) “Our review indicates that point-of-care testing and treatment for syphilis in pregnancy is cost-effective in LMICs compared to laboratory-based testing.” (p. 18) |
Romero et al. (2020)21 | |
Total costs: POC strategy: US$2.63 per pregnant woman screened Lab testing strategy: US$2.48 per pregnant women screened POC vs. lab testing strategy: Incremental cost = US$0.15 (95% CrI, US$–1.56 to US$1.92) Probability POC is cost-saving vs. lab testing = 0.428 Incremental DALY = 0.00042 (95% CrI,–0.0036 to 0.0044) Probability POC is more beneficial than lab testing = 0.595 ICER (3% discount rate) = US$357.44 per DALY POC testing has a 58.42% chance of being the most cost-effective at a WTP threshold of US$3,200 per DALY ICER (5% discount rate) = US$342.29 per DALY POC testing has a 58.41% chance of being the most cost-effective at a WTP threshold of US$3,200 per DALY | “Antenatal syphilis screening with rapid point-of-care test incorporating treatment of positive women in the same day is a potentially cost-effective strategy.” (p. 18) |
CrI = credible interval; DALY = disability-adjusted life-years; ICER = incremental cost-effectiveness ratio; LMIC = low- to middle-income country; POC = point-of-care; RPR = rapid plasma reagin testing; STI = sexually transmitted infection; vs. = versus; WTP = willingness-to-pay.
Note: This table has not been copy-edited.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
CADTH Horizon scan: rapid point of care HIV testing [in progress]. Ottawa (ON); CADTH; 2023: https://www.cadth.ca/rapid-point-care-hiv-testing Accessed 2023 Jun 29.
Clark M, Grobelna A. CADTH Horizon scan: rapid syphilis testing. Can J Health Technol. 2022; 2(11). https://www.cadth.ca/rapid-syphilis-testing Accessed 2023 Jun 29.
Non-Randomized Studies
Woldesenbet SA, Kufa T, Barron P, et al. Assessment of readiness to transition from antenatal HIV surveillance surveys to PMTCT programme data-based HIV surveillance in South Africa: the 2017 Antenatal Sentinel HIV Survey. Int J Infect Dis. 2020;91:50-56. PubMed
Pereira LE, McCormick J, Dorji T, et al. Laboratory evaluation of a commercially available rapid syphilis test. J Clin Microbiol. 2018;56(10):10. PubMed
Pham MD, Wise A, Garcia ML, et al. Improving the coverage and accuracy of syphilis testing: the development of a novel rapid, point-of-care test for confirmatory testing of active syphilis infection and its early evaluation in China and South Africa. EClinicalMedicine. 2020;24:100440. PubMed
Economic Evaluations
Rodriguez PJ, Roberts DA, Meisner J, et al. Cost-effectiveness of dual maternal HIV and syphilis testing strategies in high and low HIV prevalence countries: a modelling study. Lancet Glob Health. 2021;9(1):e61-e71. PubMed
Note: Dual point-of-care HIV and syphilis test compared to standalone point-of-care HIV test, and results are not reported separately by HIV and syphilis.
Scott RK, Crochet S, Huang CC. Universal rapid human immunodeficiency virus screening at delivery: a cost-effectiveness analysis. Infect Dis Obstet Gynecol. 2018;2018():6024698.
Note: Point-of-care HIV screening compared to no screening.
Additional References
Pant Pai N, Daher J, Prashanth HR, et al. Will an innovative connected AideSmart! app-based multiplex, point-of-care screening strategy for HIV and related coinfections affect timely quality antenatal screening of rural Indian women? Results from a cross-sectional study in India. Sex Transm Infect. 2019;95(2):133-139. PubMed
Implementation
Zhang Y, Guy R, Camara H, et al. Barriers and facilitators to HIV and syphilis rapid diagnostic testing in antenatal care settings in low-income and middle-income countries: a systematic review. BMJ Glob Health. 2022;7(11):11. PubMed
Dassah ET, Adu-Sarkodie Y, Mayaud P. Rollout of rapid point of care tests for antenatal syphilis screening in Ghana: healthcare provider perspectives and experiences. BMC Health Serv Res. 2018;18(1):130. PubMed
Crochet S, Huang CC, Fries M, Scott RK. Implementation of universal rapid human immunodeficiency virus screening on labor and delivery. Ther Adv Infect Dis. 2018;5(2):47-54. PubMed
Wang Q, Chan PL, Newman LM, et al. Acceptability and feasibility of dual HIV and syphilis point-of-care testing for early detection of infection among pregnant women in China: a prospective study. BMJ Open. 2018;8(10):e020717. PubMed
Contributors: Elizabeth Carson
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca