CADTH Health Technology Review
Electrostimulation Devices for Wounds
Rapid Review
Authors: Qiukui Hao, Jennifer Horton, Angie Hamson
Acknowledgements
Many thanks to patient contributor, Stewart Midwinter, for his time and energy sharing his lived experiences and perspectives. His contribution was invaluable.
Abbreviations
CI
confidence interval
DC
direct current
ES
electrical stimulation
EST
electric stimulation therapy
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HVMPC
high-voltage monophasic pulsed current
IWGDF
International Working Group on the Diabetic Foot
LVBPC
low-voltage biphasic pulsed current
LVMPC
low-voltage monophasic pulsed current
NHS
National Health Service
NPWT
negative pressure wound therapy
PI
pressure injury
PROSPECT
procedure-specific postoperative pain management
QALY
quality-adjusted life-year
RCT
randomized controlled trial
RR
risk ratio
SMD
standardized mean difference
SWC
standard wound care
VLU
venous leg ulcer
WSA
wound surface area
Key Messages
We found that electrostimulation as an adjunct to usual wound care might be better than usual care alone for wound management without increasing the risk of adverse events.
Electrostimulation therapy may have greater effectiveness for patients with chronic wounds versus acute wounds or those with venous leg ulcers (VLUs) who do not have surgery compared with those who do have surgery.
Electrostimulation using pulsed current may have greater effectiveness on wound management than using direct current for patients with pressure ulcers.
Limited evidence from subgroup analyses suggests that the effectiveness of electrostimulation may be similar to negative pressure wound therapy (NPWT) in wound surface area (WSA) and time to complete wound healing.
One economic evaluation study used a within-trial time horizon (up to 24 weeks) and, based on the UK National Health Service perspective, suggests that electrostimulation is less costly and more effective than placebo at 24 weeks. We did not find any studies reporting on the cost-effectiveness between electrostimulation and NPWT that met the inclusion criteria for this report.
One guideline suggests using electrostimulation as an adjunct intervention for managing postoperative pain in patients who have undergone elective caesarean section; another guideline strongly recommends against physical therapies (including electrostimulation) for diabetic foot ulcer management.
A patient with lived experience of using an electrostimulation device for the treatment of a wound was involved in this report. He identified outcomes that are important to patients, primarily avoiding hospitalization and surgery, which were not outcomes reported in the identified literature. Considerations included the accessibility of the devices, training, and integration into homecare services.
Context and Policy Issues
Basic Principles of Wound Management
For optimal wound healing, it is important to follow basic principles such as wound bed preparation, wound dressing, and wound closure.1 Effective wound management usually involves a multidisciplinary team, consisting of primary care providers, specialists, physical therapists, and nursing staff whenever possible.2 Typically, wound management requires debridement and topical therapy to remove devitalized tissue, clear infection, and provide an appropriate moist environment. To enhance wound healing, clinicians may suggest other adjunctive therapies, such as hyperbaric oxygen therapy, ultrasound stimulation, electrostimulation, and electromagnetic energy stimulation.1,3
What Are Electrostimulation Devices?
Electrostimulation devices provide low-level currents via surface electrodes on the skin.4 There are multiple electrostimulation devices available with varying costs. For a particular device, the expenses could vary from a monthly fee of $125 to a 1-time purchase cost of $750.5 It is now feasible to develop a cost-effective electrostimulation device that costs less than US$70.6 The electrostimulation devices are generally safe, stable, and compact.4
How Might Electrostimulation Treatment Work?
There are several theories on how electrostimulation can aid wound healing, but a systematic review focusing on these theories to understand the mechanisms of electrostimulation on wound management has yet to be conducted so none of these theories have been fully established.7 According to prior research, electrostimulation has been found to affect all 4 phases of the healing process, including inflammatory, proliferative, epithelialization, and remodelling phases.7 The underlying effect of electrostimulation may involve the resolution of inflammation, increase of tissue blood flow, reduction in edema, increase of cell migration, angiogenesis, and collagen deposition in scars.4,8,9 Moreover, electrostimulation therapy has been found to be beneficial for individuals with spinal cord injuries who experience chronic wounds due to immobility and continuous pressure. The possible advantages of this treatment include that it promotes muscle hypertrophy and enhances muscle contraction.10
Why Is it Important to Do This Review?
Wounds have a major impact on one's quality of life, and their management has a significant economic impact on health care.11,12 In Canada’s health care facilities, the prevalence of pressure ulcers is estimated to be more than 25%, which is higher than the reported rates in the US (most studies have been conducted in the US) and the Netherlands (which has a higher prevalence rate than the international average).13
Increasing evidence suggests that electrostimulation is beneficial for wound management, and this therapy is becoming an important component of physical therapies for wound management.3 Health Quality Ontario and several guidelines suggest using electrostimulation as an adjunct therapy to standard wound care (SWC) for patients with pressure injuries.14,15 Despite the potential clinical effectiveness, electrostimulation has not gained much usage in clinical practice in Canada.15 In addition, medical insurance policies do not currently recognize electrostimulation as an essential treatment for managing wounds and do not cover its usage.16
Objectives
The purpose of this report is to provide a summary of the latest evidence on electrostimulation devices for wound management, including clinical effectiveness and safety, cost-effectiveness, and relevant clinical practice guidelines.
Research Questions
What is the clinical effectiveness of electrostimulation devices as an adjunct to usual care for the management of wounds?
What is the clinical effectiveness of electrostimulation devices versus negative pressure wound therapy for the management of wounds?
What is the cost-effectiveness of electrostimulation devices as an adjunct to usual care for the management of wounds?
What is the cost-effectiveness of electrostimulation devices versus negative pressure wound therapy for the management of wounds?
What are the evidence-based guidelines regarding the use of electrostimulation devices for the management of wounds?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources, including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were electrostimulation and wounds. No filters were applied to limit the retrieval by study type. A supplemental search was conducted with CADTH-developed search filters applied to limit retrieval to guidelines. Retrieval was limited to the human population. The search was completed on May 30, 2023, and limited to English-language documents published since January 1, 2018.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed, and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Individuals (of all ages) with acute or chronic wounds of any etiology |
Intervention | Electrostimulation devices as an adjunct to usual care |
Comparator | Q1 and Q3: Usual care alone (e.g., conventional dressings, compression bandages) or with sham electrostimulation Q2 and Q4: Negative pressure wound therapy as an adjunct to usual care Q5: Not applicable |
Outcomes | Q1 and Q2: Clinical benefits (e.g., pain, wound size, healing time, maceration, exudate, quality of life, treatment adherence, patient satisfaction) and harms (e.g., adverse events) Q3 and Q4: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained) Q5: Recommendations regarding best practices (e.g., appropriate patient populations or types of wounds, treatment protocols, contraindications, pediatric considerations, recommended devices) |
Study designs | Health technology assessments, systematic reviews for Q1 and Q2 with publication time restricted to 2022 onward, economic evaluations, evidence-based guidelines |
Exclusion Criteria
We excluded articles if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or if they were published before 2018 for the economic evaluation and evidence-based guidelines. For health technology assessment and systematic reviews that addressing the questions 1 and 2, articles published before 2022 were excluded due to substantial amount of literature identified during our search. We also excluded publications that are not published in the English language.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A Measurement Tool to Assess Systematic Reviews 2 (AMSTAR 2)17 for systematic reviews, the Drummond checklist18 for economic evaluations, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument19 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Patient Engagement
CADTH has adopted the CADTH Framework for Patient Engagement in Health Technology Assessment,20 which includes standards for patient involvement in individual health technology assessments and is used to support and guide CADTH activities involving patients. For this report, CADTH engaged a patient contributor with lived experience of an electrostimulation device for wound care.
Invitation to Participate and Consent
CADTH reached out through social media and by direct email to a patient advocacy group. The preliminary engagement request included an overview of this project, the purpose of engagement, and the nature of engagement activities. An interested individual was identified, and the CADTH Patient Engagement Officer obtained the person’s informed consent to share with CADTH staff their lived experience with a wound and their treatment with an electrostimulation device.
Engagement Activities
An individual contributor shared their personal experience by video call during the drafting of the report. Patient perspectives gained through engagement processes are used to understand relevance of outcomes of interest and to provide contexts or insights to inform the summary, limitation, and conclusion sections.
Patient involvement was reported using the Guidance for Reporting Involvement of Patients and the Public (version 2) (GRIPP2) short form reporting checklist,21 which is outlined in Appendix 6. Regarding outcomes, the patient contributor noted the importance of minimizing chances of being hospitalized or undergoing surgery.
Summary of Evidence
Quantity of Research Available
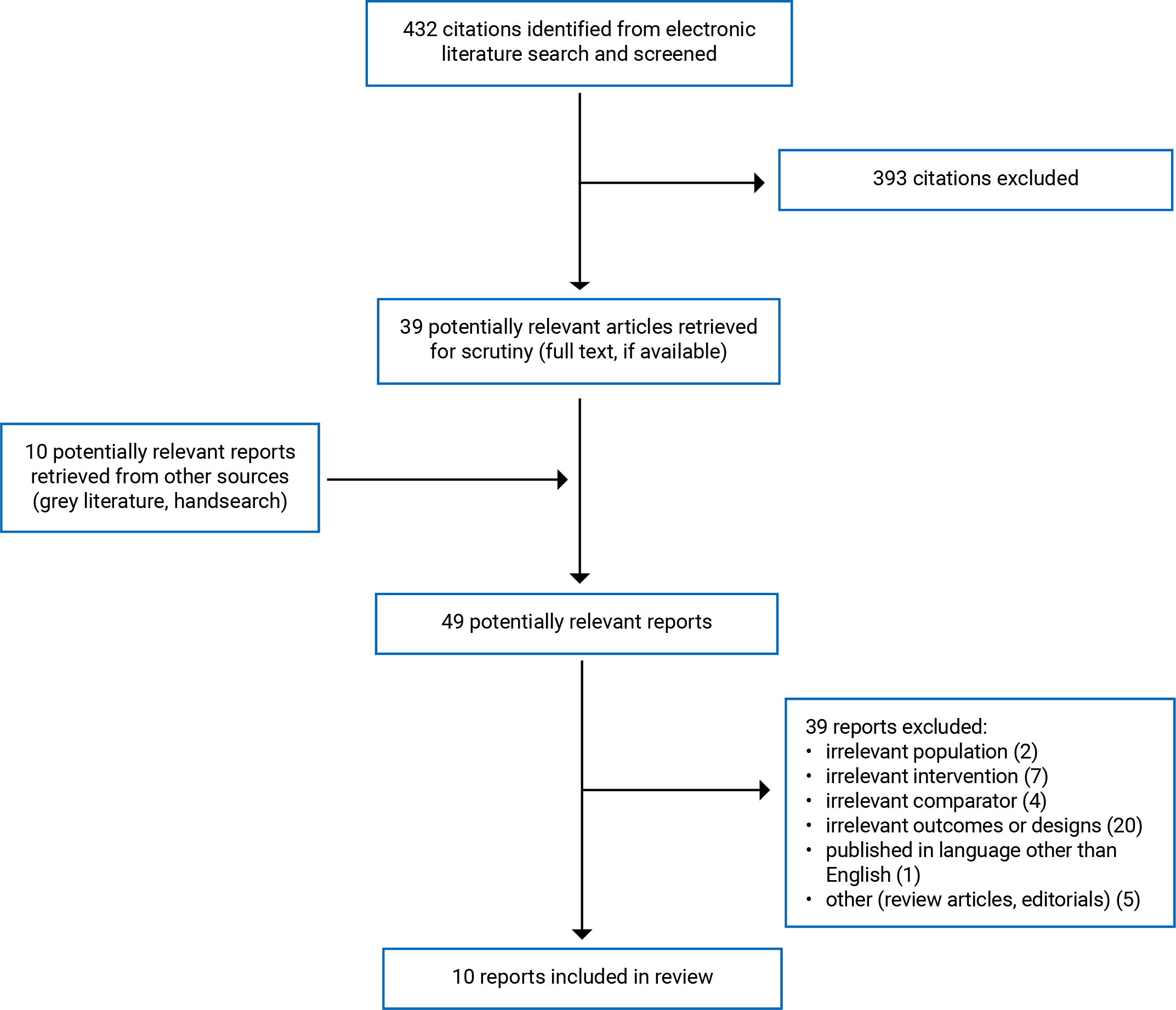
A total of 432 citations were identified in the literature search. Following screening of titles and abstracts, 393 citations were excluded and 39 potentially relevant reports from the electronic search were retrieved for full-text review. Ten potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 39 publications were excluded for various reasons and 10 publications met the inclusion criteria and were included in this report. These comprised 7 systematic reviews,1 economic evaluation, and 2 evidence-based guidelines. Appendix 1 presents the PRISMA22 flow chart of the study selection. Additional references of potential interest are provided in Appendix 7.
Summary of Study Characteristics
This report included 7 systematic reviews,23-29 1 economic evaluation,30 and 2 evidence-based guidelines.31,32 We did not identify any health technology assessments that met the inclusion criteria. Further, we did not come across any studies that reported surgery or hospitalization outcomes, which were identified as important during our patient engagement activities. Characteristics of included publications are provided in Appendix 2.
Included Studies for Question 1: Electrostimulation Versus Usual Care
We included 7 systematic reviews that examined the clinical effectiveness of electrostimulation devices as an additional treatment for wound management compared with usual care without electrostimulation. The included systematic reviews were conducted in Portugal,23,25 Poland,24 China,26,27 the UK,28 and Spain.29 Five systematic reviews23,26-29 included primary studies from various countries, such as Canada, Slovenia, Germany, Brazil, Italy, Poland, the UK, the US, Nigeria, Israel, Egypt, Spain, Iran, Colombia, Sweden, and Belgium. Three of the systematic reviews only considered eligible randomized controlled trials (RCTs),24,26,29 whereas the remaining reviews also incorporated observational studies23,25,28 or quasi-experimental studies27 in addition to RCTs. These systematic reviews included patients with venous leg ulcers (VLUs),23 pressure ulcers,24,26 diabetic ulcers,25,27,28 and both chronic and acute wounds.29
Electrostimulation varied in anatomical location, frequency, duration, and parameters in the included systematic reviews. One systematic review included 10 RCTs used high-voltage monophasic pulsed current (HVMPC), 2 RCTs used low-voltage monophasic pulsed current (LVMPC), 3 RCTs used low-voltage biphasic pulsed current (LVBPC), and 1 RCT low-intensity direct current. A systematic review was conducted on studies involving HVMPC.25 One systematic review included only studies with the current intensity of 1 mA or greater. Other systematic reviews included diverse electrostimulation methods23,26,28 or unclear details.27 The comparators were SWC with or without sham stimulation. Outcomes included healing rate, incidence of worsening of healing, wound surface area (WSA) measures, ulcer size, number of completely healed ulcers, time to healing, pain score, quality of life, adverse effects, and other outcomes, such as wound tissue granulation and capillary blood flow.
Included Studies for Question 2: Electrostimulation Versus Negative Pressure Wound Therapy
A systematic review29 included 1 RCT with 3 treatment groups for patients with burn wounds: electrostimulation plus SWC, negative pressure wound therapy (NPWT) plus SWC, and SWC. This systematic review conducted a subgroup analysis, using the data from the RCT, that compared electrostimulation with NPWT. Outcomes included WSA measures and time to healing; no adverse effects were reported for this comparison.
Included Cost-Effectiveness Study Regarding Electrostimulation Versus Placebo for Wound Management
We included 1 cost-utility analysis based on data from 1 RCT30 , which was included in 2 systematic reviews in this report.23,29 We have only provided details about the participants and the results pertaining to the economic assessment. The evaluation used a within-trial time horizon (8 weeks, 16 weeks, and 24 weeks) from the perspective of the UK National Health Service. The study enrolled 90 people with nonhealing leg ulcers. Patients in the intervention group were treated with an electrostimulation device for 12 days in addition to usual care, while patients in the control group were treated with usual care and a placebo device that looked the same as the electrostimulation device but did not deliver a microcurrent. The intervention group had a mean age of 71 years (SD = 15.0 years) and 60% were male, while the control group had a mean age of 68 years (SD = 15.1) and 50% were male. Data on effectiveness were gathered through the RCT, with the patients' utility values determined from participants’ responses to the EQ-5D-5L questionnaire. Quality-adjusted life-years (QALYs) were calculated at 8, 16, and 24 weeks following randomization. NHS tariffs from 2015 or 2016 were used to estimate national unit costs and were applied to health care resource usage to determine the cost per patient within each group. The authors compared the cost-effectiveness of 2 groups by calculating the incremental cost per QALY gained and the incremental cost for each additional healed patient.
Included Cost-Effectiveness Study Regarding Electrostimulation Versus Placebo for Wound Management
We did not find any studies that reported on the cost-effectiveness of electrostimulation compared with NPWT that met the inclusion criteria for this report.
Included Clinical Practice Guidelines Regarding Electrostimulation for Wound Management
We included 2 evidence-based clinical practice guidelines from International Working Group on the Diabetic Foot (IWGDF)31 and procedure-specific postoperative pain management (PROSPECT) working group.32 These guidelines are updated versions of 2 existing ones.
The IWGDF guideline development group comprised independent international experts in wound healing for diabetes-related foot ulcers that conducted an updated systematic review to identify relevant RCTs.31 The ratings of the quality of evidence and strength of recommendations were reported based on Grading of Recommendations Assessment, Development and Evaluation (GRADE) evidence to recommendation framework. A team of clinical experts, the IWGDF editorial board, and individuals with lived experience reviewed and assessed the guideline recommendations and rationales.
The PROSPECT guideline32 included recommendations for pain management in patients who undergo elective caesarean section under neuraxial anesthesia. The panel of experts (authors of the guideline were from Belgium, Sweden, and the US) followed their own methodology to obtain formal consensus and develop recommendations after conducting a systematic review. However, they did not specify how to interpret the strength of recommendations (Grades A to D). The PROSPECT working group used a modified Delphi approach to review recommendations and reach a consensus. The final document was approved by the working group and received support from the Obstetric Anesthetists’ Association’s executive committee.
Summary of Critical Appraisal
Systematic Reviews
In all 7 systematic reviews,23-29 the objective was clearly described, multiple databases were searched, and keywords or full search strategies and study selection flow charts were provided, the review authors declared no conflicts of interest, lists of included articles were presented, and the study characteristics were described. Two systematic reviews24,29 did not provided lists of excluded articles or the reasons for exclusion, and only 1 systematic review25 assessed the sources of funding in individual studies. Despite searching in multiple databases, 4 systematic reviews23,26,27,29 did not report performing a grey literature search and 4 systematic reviews23-25,29 did not report searching the Embase database specifically. These limitations may result in missing some studies (unpublished or studies conducted in Europe) or misidentification of potential publication bias.
At least 2 reviewers independently performed or verified the article selection and data extraction in 5 systematic reviews.23,26-29 Two reviewers independently conducted data extraction in 1 systematic review,24 but it was unclear how the article selection was performed. In the remaining systematic review,25 it was unclear how article selection and data extraction were conducted. The possibility of inappropriate inclusion or exclusion or errors in data extraction cannot be ruled out. Although all 7 systematic reviews assessed the risk of bias of the included individual studies and reported study quality, only 1 systematic review25 assessed the potential impact of study risk of bias on the interpretation of results. One systematic review27 judged that only 2 of 8 primary studies had a low risk of bias. Some subgroup analyses in this systematic review only included 2 primary studies; therefore, the results of these analyses may be driven by individual studies with high risk of bias.
Two systematic reviews9,13 assessed the quality of evidence using the GRADE framework. However, 1 of these reviews29 did not adhere completely to the GRADE principles because it rated up the certainty of evidence on pain and adverse events outcomes even when the risk difference was less than 0.20. Thus, the accuracy of the overall quality evidence on pain and adverse events was uncertain in this review.
Four systematic reviews25-27,29 conducted meta-analyses to compare effectiveness in several outcomes. Considering the significant clinical heterogeneities, such as diverse electrostimulation methods and wound types, it is uncertain whether pooling these data is suitable. The authors conducted subgroup analyses to examine some heterogeneities, including chronic or acute wounds and pulsed or direct currents of electrostimulation. However, none of the 4 systematic reviews assessed the credibility of their subgroup analyses.25-27,29 Two of the systematic reviews26,27 failed to mention the procedures used to manage trials with multiple arms (3 or more). When conducting a meta-analysis with a study that involves multiple or correlated comparisons, the Cochrane group suggests overcoming the unit-of-analysis error by combining groups to form a single pairwise comparison33 instead of dividing the shared group, which is a suboptimal approach. The authors of the 2 systematic reviews25,29 stated that they followed the Cochrane Group Guidelines to avoid double counting by splitting the shared control group. However, some forest plots presented in the 2 systematic reviews did not reflect this split.25,29 It is possible that the meta-analysis had unit-of-analysis error and double-counting issues, which could have influenced the outcome in favour of the intervention.
Economic Evaluation
The included economic evaluation study30 outlined its design and analysis perspective clearly, with thorough data collection and stated outcome measures. The authors of the study examined and interpreted the results and presented their conclusions with appropriate caveats. However, the primary objective of the study did not involve estimating the cost-effectiveness of electrostimulation, and the study lacks clarity in its research question and economic significance.30 Moreover, the study lacks details on currency price adjustments for inflation or conversion, and the intervention’s effectiveness measures were based on a single RCT rather than a synthesis or meta-analysis of estimates from multiple sources.30 The treatment effects from the single RCT align with the included meta-analysis in the healing outcomes, but the RCT indicates a higher treatment effect of WSA compared with the meta-analysis, with a 50% reduction30 versus a 30% reduction.25,26 It is worth noting that the time horizon for costs and benefits — which is up to 24 weeks — may be considered relatively short if taking into account the mean duration of nonhealing VLUs, which can last for more than 2 years. Additionally, more than 20% of patients still exhibited heavy exudate at the end of the study (after 24 weeks).30 This study was also conducted from the UK NHS perspective and may not necessarily apply to the health care system in Canada.
Evidence-Based Guidelines
In this report, we included 2 evidence-based guidelines,31,32 which had clear descriptions of objectives, scope, population, and target users. Their recommendation statements were stated and reviewed by members in related working groups, but they did not provide clear guidance on their applicability.
The IWGDF guidelines used the GRADE evidence to recommendation framework to formulate their recommendations and included individuals with lived experience and the IWGDF editorial board reviewed and assessed the guideline recommendations and rationales.31 However, the guideline panel did not provide a thorough explanation regarding why they made strong recommendations despite having low-quality evidence for electrostimulation and the evidence of electrostimulation was not clearly described.31,34 The authors of the IWGDF guidelines declared no conflicts of interest.
The PROSPECT guideline used their own methodology35 to develop recommendations but did not clarify the interpretation of recommendation strength, and the links between the evidence and the recommendations were unclear. The recommendation statement regarding electrostimulation was ambiguous. The PROSPECT working group reviewed and approved the final guideline, which also received support from the Obstetric Anesthetists’ Association. Although some authors of the guideline disclosed potential conflicts of interest and had received grants or consultation fees from industries, it remains unclear how these were addressed.
Additional details regarding the strengths and limitations of the included publications are provided in Appendix 3.
Summary of Findings
All 7 included systematic reviews23-29 compared the effectiveness of electrostimulation plus usual care with only usual care. One of the systematic reviews included data from 1 RCT comparing electrostimulation plus usual care with NPWT plus usual care.29 The review conducted a subgroup analysis for the comparison. Of the 7 systematic reviews included, 4 conducted a pooled meta-analysis25-27,29 while the remaining 3 systematic reviews23,24,28 provided narrative summaries of the individual studies' findings. We included 1 economic evaluation study30 about the cost-effectiveness of electrostimulation compared with placebo. There are 2 guidelines based on evidence that offer recommendations for electrostimulation in patients with diabetes-related foot ulcers31 and for postoperative pain management in patients undergoing an elective caesarean section with neuraxial anesthesia.32 We did not find any studies that reported outcomes that were considered important during our patient engagement activities, which included avoiding surgery and hospitalization.
Appendix 4 presents the main study findings. Due to some overlap in the studies included in the included systematic reviews, the pooled estimates or narrative summaries may be based on some of the same individual study data (Appendix 5).
Clinical Effectiveness of Electrostimulation Plus Usual Care Versus Usual Care
Wound Surface Area
Five systematic reviews24-27,29 have reported on the comparison of electrostimulation versus a control group (usual care with or without sham stimulation) in reducing WSA. The reports on WSA in these systematic reviews used various measures and statistical indicators, and there were inconsistencies in the results of the statistical tests among different populations:
Relative WSA reduction from baseline (3 systematic reviews: MD25,26 or SMD,27 the differences were statistically significant): 1 systematic review27 conducted a subgroup analysis and found no statistically significant subgroup effect between pulsed current and direct current or between leg ulcers and foot ulcers. One systematic review25 evaluated the overall evidence quality on this outcome as very low.
Raw WSA (2 systematic reviews26,29: cm2, the differences were statistically significant for patients with pressure ulcer,26 but not statistically significant for patients with all types of wounds with moderate certainty evidence29): Subgroup analysis in the 2 systematic reviews found statistically significant subgroup effects between pulsed current and direct current (larger effect was observed in the pulsed current subgroup in treating pressure ulcers),26 but no statistically significant subgroup effects between chronic and acute wounds.29
Qualitative summaries (1 systematic review24): WSA decreased more from baseline in the intervention group than that in the control group based on 9 RCTs.
Rate of Complete Healing
Three systematic reviews25,26,29 have reported on the comparison of electrostimulation versus a control (usual care with or without sham stimulation) in improving the rate of complete healing for diabetic ulcer and pressure ulcer. There were inconsistencies in the results of the statistical tests among different populations or subgroups:
Diabetic ulcers (1 systematic review25): There was no statistically significant difference between electrostimulation and control (usual care with or without sham stimulation).
Pressure ulcer (2 systematic reviews25,26): There was a statistically significant difference between electrostimulation and control (usual care with or without sham stimulation) (GRADE: moderate certainty from 1 systematic review25); subgroup analysis in 1 systematic review26 found statistically significant subgroup effects between pulsed current and direct current (larger effect was observed in the pulsed current subgroup; the effect in the direct current subgroup was not statistically significant).
All types of wounds (1 systematic review29): There was no statistically significant difference between electrostimulation and control (GRADE: very low certainty).
Rate of Nonhealing or Worsened Wounds
Two systematic reviews25,27 have reported that electrostimulation was statistically significantly more effective than a control group (usual care with or without sham stimulation) in reducing the rate of nonhealing or worsened (wound size increase) wounds for treating diabetic ulcers. One systematic review27 did not find statistically significant subgroup effects for electrostimulation between diabetic leg and foot ulcers.
Time to Complete Wound Healing
Two systematic reviews28,29 reported the time to complete wound healing. One systematic review29 has reported that electrostimulation was statistically significantly more effective than the control group (usual care with or without sham stimulation) in reducing the time to healing or the rate of worse healing wounds for treating different types of wounds. The systematic review found statistically significant subgroup effects between acute wounds and chronic wounds, with a larger effect observed in the chronic wounds subgroup; the effects in the acute wounds subgroup were not statistically significant.29 The other systematic review reported the difference between electrostimulation and control was not statistically significant.
Pain
Three systematic reviews23,25,29 have reported on the comparison of electrostimulation versus control in pain. According to 1 systematic review,29 the participants in the electrostimulation group experienced a statistically significant decrease in pain scores compared with those in the control group (GRADE: low certainty). However, 2 other systematic reviews23,25 offered qualitative summaries and noted inconsistent results in pain outcomes.
Exudate Levels
A systematic review provided qualitative summaries of the exudate level outcome, which showed inconsistent results. Electrostimulation reduced exudate levels in 1 study, but 2 other studies found no difference compared with the control group.
Adverse Events
According to 1 systematic review,29 the risk of adverse events among participants in the electrostimulation group was similar to that of the control group (GRADE: moderate certainty). In other systematic reviews reported on adverse events,23-26 it was found that most studies did not report these events. However, the few adverse events related to electrostimulation were minor and rare, and included uncomfortable sensations, infection, skin rash, itchiness, pain, or wound deterioration.
Other Outcomes
Several systematic reviews also report other outcomes such as percentage of wounds healed, composite healing outcomes, edema and function, quality of life, recurrence or development of new ulcers, and amputation. We have highlighted the following points in this report:
Percentage of wounds healed28: There was no statistically significant difference between electrostimulation and control at week 2 and week 4 (1 RCT); statistically significant differences were found between the 2 groups at week 8 (1 RCT) and week 12 (2 RCTs).
Composite healing outcomes: Electrostimulation appeared to be more effective than control treatment (usual care with or without sham stimulation) for patients who had not undergone surgical treatment for VLU. However, the benefit of electrostimulation compared to the control was not statistically significant for patients with VLUs who had undergone the surgery.23
Quality of life: According to 1 study in 1 systematic review,25 there were no statistically significant differences between electrostimulation and control.
Clinical Effectiveness of Electrostimulation Plus Usual Care Versus NPWT Plus Usual Care
A systematic review provided a subgroup analysis that compared the effectiveness of electrostimulation and NPWT in treating acute wounds. However, they did not observe any statistically significant differences in the following 2 outcomes:
raw WSA (1 subgroup analysis from 1 systematic review29)
time to complete wound healing (1 subgroup analysis from 1 systematic review29).
Cost-Effectiveness of Electrostimulation Versus Placebo
Evidence regarding the cost-effectiveness of electrostimulation versus placebo for patients with nonhealing VLUs was available from 1 economic evaluation.30
Measures of Cost-Effectiveness
Patients With Nonhealing VLUs
The results of the economic evaluation suggested that the incremental cost per QALY gained of the intervention (versus sham stimulation) was £4,480 at 8 weeks, £2,655 at 16 weeks, and –£2,388 at 24 weeks, and the incremental cost per each additional ulcer for the intervention (versus placebo) was £1,867 at 8 weeks, £1,850 at 16 weeks, and –£4,775 at 24 weeks. Electrostimulation was less costly and more effective at 24 weeks (dominant). The results were supported by sensitivity analyses conducted using bootstrapping sample methods. The estimated probability of the electrostimulation being cost-effective with a threshold of £20,000 per QALY was 88% at 8 weeks, 91% at 16 weeks, and 92% at 24 weeks.
Cost-Effectiveness of Electrostimulation Versus NPWT
We did not find any studies that reported on the cost-effectiveness of electrostimulation compared with NPWT that met the inclusion criteria for this report; therefore, no summary can be provided.
Guidelines Regarding the Use of Electrostimulation
Based on the low quality of evidence according to the GRADE evidence to recommendation framework, the IWGDF guideline strongly recommends against physical therapy interventions (which includes electrostimulation) for diabetic foot ulcer management and wound healing. Within the GRADE framework, a strong recommendation suggests that the majority of patients with diabetic foot ulcers should not undergo electrostimulation for wound healing. However, the guideline did not provide descriptions of evidence and the specific reasoning for the recommendation on electrostimulation. The guideline authors stated that limited (low-quality) evidence suggests physical therapies (including electrostimulation) may have a small positive impact on wound healing, with no substantial difference from usual care for patients with diabetic foot ulcers. Few negative effects were reported, and it is uncertain if physical therapies are more beneficial overall. In addition, these physical therapies are costly and resource-intensive and may not be suitable for all patients. Thus, the guideline did not recommend any physical therapies for managing diabetic foot ulcers.
The PROSPECT guideline provided the recommendation for managing postoperative pain in patients undergoing elective caesarean section with neuraxial anesthesia. The guideline suggests considering the use of electrostimulation as an analgesic adjunct for postoperative pain management (Grade A recommendation). The guideline did not cover the possible application of electrostimulation for wound healing. The quality of evidence supporting the recommendation was unclear. The guideline also lacked instructions on how to interpret the strength of recommendations, which is difficult for people who are trying to implement the recommendation. The clinical practice guidelines did not provide information on suggested electrostimulation parameters, frequency, and duration in the related recommendation, which might be another potential barrier for implementation.
Limitations
We found some methodological limitations in the body of evidence presented. In this report, we identified 7 systematic reviews to answer the research question on clinical effectiveness of electrostimulation plus usual care versus only usual care. Four23,25,27,28 of these reviews included observational studies or quasi-experimental studies with only a small number of RCTs with a low risk of bias (for example, 2 of 8 included RCTS were low risk of bias in 1 systematic review27). Therefore, the body of evidence may have selection bias, recall bias, or performance bias. None of the 4 systematic reviews with meta-analysis25-27,29 used the Cochrane-recommended approach to address the unit-of-analysis error that could potentially skew the pooled estimate in favour of electrostimulation.
The body of evidence also has substantial heterogeneity and inconsistency in some reported outcomes. Although 4 systematic reviews with meta-analysis25-27,29 carried out subgroup analysis to explore possible heterogeneity, they neglected to conduct a thorough assessment of the credibility of this analysis. Therefore, the observed subgroup effect may not be entirely reliable, and the interpretations of evidence regarding these subgroup analyses were limited.
In this report, we also found some evidence gaps. We could not identify a systematic review that specifically compared electrostimulation and NPWT. The only available evidence on this comparison comes from a subgroup analysis in 1 systematic review with small sample size (n = 15 for the NPWT arm).29 We also did not find any evidence on the cost-effectiveness of electrostimulation and NPWT. The only economic evaluation study conducted was in the UK from the perspective of the NHS, which compared electrostimulation to sham stimulation. We had to adjust our criteria for including studies for our research questions 1 and 2 due to the large volume of literature we found during our search, which may have caused some relevant studies to be missed. However, we provide the additional references of potential interest in Appendix 7. In addition, we did not find any evidence on patient satisfaction, hospitalization and surgery outcomes that were considered important during patient engagement activities (Appendix 6), but our patient contributor was satisfied with electrostimulation therapy and recommended it for wound healing, stating he did not experience noticeable side effects related to electrostimulation therapy.
Additionally, we did not find evidence-based guidelines or economic evaluations from Canada. In the 2 included guidelines, no panel member was from a Canadian institution. Thus, the generalizability of the findings to a Canadian setting was unclear.
Conclusions and Implications for Decision- or Policy-Making
In this report, we identified 7 systematic reviews23-29 that addressed the clinical effectiveness of electrostimulation as an adjunct to usual care for wound management. One economic evaluation study30 compared the cost-effectiveness of electrostimulation with placebo for treating patients with nonhealing VLUs. Two evidence-based practice guidelines regarding the use of electrostimulation as an adjunct treatment were included,31,32 1 for diabetic foot ulcers and another for postoperative pain management in patients who had undergone elective caesarean section with neuraxial anesthesia.
We identified 7 systematic reviews23-29 to address the clinical effectiveness of electrostimulation as an adjunct to usual care for various types of wound management, including chronic and acute wounds. Specifically, most eligible studies focused on pressure ulcers, diabetic ulcers, and VLUs. Based on both RCTs and observational studies, the evidence suggests that combining electrostimulation with usual wound care could be more effective than usual care alone in at least 1 measure of wound healing (WSA, rate of complete healing, rate of nonhealing or worsened wounds, time to complete wound healing) or pain outcomes. The evidence suggests that patients with chronic wounds or those who did not undergo surgery for VLUs experienced larger positive effects from electrostimulation compared with those with acute wounds or who received surgery for VLU. Similarly, electrostimulation using pulsed current had a greater effectiveness than direct current on would healing outcomes (WSA and rate of complete healing) for patients with pressure ulcers. No serious adverse effects related to electrostimulation were reported in all included systematic reviews.
We identified subgroup analyses in 1 systematic review,29 which suggested that the effectiveness of electrostimulation and NPWT may be similar in WSA reduction from baseline and time to complete wound healing. One economic evaluation study suggested that electrostimulation was less costly and more effective than placebo at 24 weeks (dominant). With a threshold of £20,000 per QALY, the estimated probabilities of electrostimulation being cost-effective were more than 88% at any follow-up time point.
The IWGDF guideline strongly recommends against physical therapies, including electrostimulation, for diabetic foot ulcer management based on low quality of evidence on effectiveness and the potential cost. However, the IWGDF guideline did not provide any recommendations specific to electrostimulation. Additionally, the evidence supporting these guidelines (which included only 6 citations related to electrostimulation) may not be as comprehensive as this report (7 systematic reviews) and the guidelines do not include any cost-effectiveness analysis comparing electrostimulation to a sham stimulation device. The PROSPECT guideline offered a grade A recommendation for using electrostimulation as an adjunct in managing postoperative pain in patients who have undergone elective caesarean section with neuraxial anesthesia.
The prognosis of an acute or minor wound is relatively good because most patients recover with usual care. One systematic review24 noted that electrostimulation should be used in patients with stage 2 to 4 pressure ulcers. Identifying individuals who would receive a significant benefit is crucial when considering electrostimulation referrals. Patients’ values and preferences, accessibility, and cost of using electrostimulation can also play a significant role in the decision-making process. During our patient engagement activities, another barrier was identified, which was the lack of proper training for using the electrostimulation device.
Considering the current limitations of the body of evidence, primary studies with robust designs and adequate sample sizes that address the relative effects of electrostimulation versus NPWT are needed. To obtain precise relative risk estimates, a thorough systematic review with robust methodology is required, particularly using a better approach to overcome the potential unit-of-analysis error when dealing with data from a single trial with multiple interested arms. Due to the potential bias and inconsistency across included primary studies in eligible systematic reviews, limitations of the body of evidence, and small sample size in the NPWT arm (n = 15), these findings need to be interpreted with caution.
References
1.Armstrong; DG, Meyr AJ. Basic principles of wound management In: Post TW, ed. UpToDate. UpToDate: Waltham (MA); 2022: www.uptodate.com. Accessed 2023 May 29.
2.Lindholm C, Searle R. Wound management for the 21st century: combining effectiveness and efficiency. Int Wound J. 2016;13 Suppl 2(Suppl 2):5-15.
3.Fernández-Guarino M, Bacci S, Pérez González LA, Bermejo-Martínez M, Cecilia-Matilla A, Hernández-Bule ML. The Role of Physical Therapies in Wound Healing and Assisted Scarring. Int J Mol Sci. 2023;24(8). PubMed
4.Luo R, Dai J, Zhang J, Li Z. Accelerated skin wound healing by electrical stimulation. Ad. 2021;10(16):2100557.
5.Mittmann N, Chan BC, Craven BC, Isogai PK, Houghton P. Evaluation of the cost-effectiveness of electrical stimulation therapy for pressure ulcers in spinal cord injury. Arch Phys Med Rehabil. 2011;92(6):866-872. PubMed
6.Stewart AM, Pretty CG, Chen X. Design and testing of a novel, low-cost, low-voltage, functional electrical stimulator. Paper presented at: 2016 12th IEEE/ASME International Conference on Mechatronic and Embedded Systems and Applications (MESA)2016.
7.Arora M, Harvey LA, Glinsky JV, et al. Electrical stimulation for treating pressure ulcers. Cochrane Database Syst Rev. 2020;1:CD012196. PubMed
8.Katoh K. Effects of Electrical Stimulation of the Cell: Wound Healing, Cell Proliferation, Apoptosis, and Signal Transduction. Med Sci (Basel). 2023;11(1). PubMed
9.Zhao M, Pu J, Forrester JV, McCaig CD. Membrane lipids, EGF receptors, and intracellular signals colocalize and are polarized in epithelial cells moving directionally in a physiological electric field. Faseb J. 2002;16(8):857-859. PubMed
10.Alberty M, Mayr W, Bersch I. Electrical Stimulation for Preventing Skin Injuries in Denervated Gluteal Muscles-Promising Perspectives from a Case Series and Narrative Review. Diagnostics (Basel). 2023;13(2). PubMed
11.Sen CK. Human wound and its burden: updated 2020 compendium of estimates. Adv Wound Care (New Rochelle). 2021;10(5):281-292. PubMed
12.Olsson M, Järbrink K, Divakar U, et al. The humanistic and economic burden of chronic wounds: A systematic review. Wound Repair Regen. 2019;27(1):114-125. PubMed
13.Woodbury MG, Houghton PE. Prevalence of pressure ulcers in Canadian healthcare settings. Ostomy Wound Manage. 2004;50:22-39. PubMed
14.Electrical Stimulation for Pressure Injuries. Toronto (ON): Health Quality Ontario; 2017: https://www.hqontario.ca/evidence-to-improve-care/health-technology-assessment/reviews-and-recommendations/electrical-stimulation-for-pressure-injuries. Accessed 2023 Jun 3.
15.Orr L, Houghton P, Holyoke P, Lala D. A Quasi-Experimental Evaluation of an Education Program for the Use of Electrical Stimulation Therapy to Heal Pressure Injuries. Wound Manag Prev. 2020;66(1):14-23. PubMed
16.Medical Coverage Policy: Electrical Stimulation and Electromagnetic Therapy for Wound Treatment. Providence (RI): Blue Cross Blue Shield of Rhode Island; 2013: https://www.bcbsri.com/sites/default/files/polices/Electrical_Stimulation_Electromagnetic_Therapy_for_Wound_Treatment.pdf. Accessed 2023 Jun 2.
17.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
18.Higgins JPT, Green S, editors. Figure 15.5.a: Drummond checklist (Drummond 1996). Cochrane handbook for systematic reviews of interventions. London (GB): The Cochrane Collaboration; 2011: http://handbook-5-1.cochrane.org/chapter_15/figure_15_5_a_drummond_checklist_drummond_1996.htm. Accessed 2023 Jun 5.
19.Agree Next Steps C. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2023 Jun 5.
20.CADTH framework for patient engagement in health technology assessment. Ottawa (ON): CADTH; 2022: https://www.cadth.ca/cadth-framework-patient-engagement-health-technology-assessment. Accessed 2023 Jun 19.
21.Staniszewska S, Brett J, Simera I, et al. GRIPP2 reporting checklists: tools to improve reporting of patient and public involvement in research. BMJ. 2017;358:j3453. PubMed
22.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
23.Borges D, Pires R, Ferreira J, Dias-Neto M. The effect of wound electrical stimulation in venous leg ulcer healing - a systematic review. J Vasc Surg Venous Lymphat Disord. 2023;15:15. PubMed
24.Szoltys-Brzezowska B, Bankowska A, Piejko L, et al. Electrical Stimulation in the Treatment of Pressure Injuries: A Systematic Review of Clinical Trials. Adv Skin Wound Care. 2023;36(6):292-302. PubMed
25.Girgis B, Carvalho D, Duarte JA. The effect of high-voltage monophasic pulsed current on diabetic ulcers and their potential pathophysiologic factors: A systematic review and meta-analysis. Wound Repair Regen. 2023;31(2):171-186. PubMed
26.Chen L, Ruan Y, Ma Y, Ge L, Han L. Effectiveness and safety of electrical stimulation for treating pressure ulcers: A systematic review and meta-analysis. Int J Nurs Pract. 2023;29(2):e13041. PubMed
27.Zheng Y, Du X, Yin L, Liu H. Effect of electrical stimulation on patients with diabetes-related ulcers: a systematic review and meta-analysis. BMC Endocr Disord. 2022;22(1):112. PubMed
28.Melotto G, Tunprasert T, Forss JR. The effects of electrical stimulation on diabetic ulcers of foot and lower limb: A systematic review. Int Wound J. 2022;19(7):1911-1933. PubMed
29.Avendano-Coy J, Lopez-Munoz P, Serrano-Munoz D, Comino-Suarez N, Avendano-Lopez C, Martin-Espinosa N. Electrical microcurrent stimulation therapy for wound healing: A meta-analysis of randomized clinical trials. J Tissue Viability. 2022;31(2):268-277. PubMed
30.Guest JF, Singh H, Rana K, Vowden P. Cost-effectiveness of an electroceutical device in treating non-healing venous leg ulcers: results of an RCT. J Wound Care. 2018;27(4):230-243. PubMed
31.Guidelines on interventions to enhance healing of foot ulcers in people with diabetes. International Working Group on the Diabetic Foot; 2023: https://iwgdfguidelines.org/wp-content/uploads/2023/05/IWGDF-2023-07-Wound-Healing-Guideline.pdf. Accessed 2023 Jun 2.
32.Roofthooft E, Joshi GP, Rawal N, Van de Velde M. PROSPECT guideline for elective caesarean section: updated systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia. 2021;76(5):665-680. PubMed
33.Higgins JPT ES, Li T. Chapter 23: Including variants on randomized trials. In: Higgins JPT TJ, Chandler J, Cumpston M, Li T, Page MJ, Welch VA., ed. Cochrane Handbook for Systematic Reviews of Interventions. Chichester (UK): John Wiley & Sons; 2022.
34.Schünemann HJ, Mustafa R, Brozek J, et al. GRADE Guidelines: 16. GRADE evidence to decision frameworks for tests in clinical practice and public health. J Clin Epidemiol. 2016;76:89-98. PubMed
35.Joshi GP, Van de Velde M, Kehlet H. Development of evidence-based recommendations for procedure-specific pain management: PROSPECT methodology. Anaesthesia. 2019;74(10):1298-1304. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Borges et al. (2023)23 Portugal Funding source: the authors declared no conflict of interest. | Study design: systematic review of RCTs and observational studies Number of included studies: 11 (8 RCTs and 3 case series) Countries: Canada, Slovenia, Germany, Brazil, Italy, Poland, UK, US | Patients with venous leg ulcers Number of participants: 716 (number in the individual studies ranged from 6 to 305) Mean age: 64.2 years Sex: male, 46.2% Disease duration: NR | Intervention: electrical stimulation with diverse methods: location, current forms, and electric stimulation parameters. Treatment duration: from 12 minutes to 12 consecutive days; the treatment was repeated 1 to 14 times weekly. Comparator: conventional therapy or placebo or baseline scores in the same group | Outcomes:
Follow-up: from 3 weeks to 60 weeks after treatment |
Szołtys-Brzezowska et al. (2023)24 Poland Funding source: the authors declared no financial conflict of interest. | Study design: systematic review of RCTs Number of included studies: 16 Country: NR | Patients with pressure injury Number of participants:793 with 890 pressure injuries Age: 10 to 95 years, predominantly adults Sex: NR Disease duration: NR Severity: from stage 2 to 4 when reported Etiologies for pressure injury: central nervous system injuries, advanced age-related conditions, immobilization after orthopedic interventions, diabetes, cardiovascular disease, or cerebrovascular accidents when reported. | Intervention: electrical stimulation with various electric currents: HVMPC, LVMPC, LVBPC, low-intensity direct current. Treatment duration: NR Comparator: SWC with or without sham electrical stimulation | Outcomes:
Follow-up: NR |
Girgis et al. (2023)25 Portugal Funding source: “Fundaçao para a Ciência e a Tecnologia (SFRH/BD/144090/2019)” | Study design: systematic review of RCTs and observational studies Number of included studies: 32: 17 RCTs, 2 cohort studies, 13 case series or reports Country: NR | Patients with diabetic ulcers Number of participants: 1,061 with 1,103 skin lesions Mean age: 56 to 73 years, when reported Sex: male: from 26% to 39%; female: 61% to 74%, when reported. Disease duration: NR Severity: NR | Intervention: electrical stimulation with HVMPC protocols. Mean treatment duration: 6 weeks to 14 weeks when reported Comparator: sham or no stimulation or baseline scores in the same group | Outcomes:
Follow-up: NR |
Chen et al. (2023)26 China Funding source: academic or government agencies in China and the authors declared no conflict of interest. | Study design: systematic review of RCTs Number of included studies: 17 Countries: US, Canada, Nigeria, Israel, Egypt, Poland, Spain | Patients with pressure ulcers Number of participants: 768 Mean age: 32 to 81 years, when reported Sex: male included in meta-analysis 39% in the intervention group and 34% in the control group Mean disease duration: from 5 days to 231 days Severity: from stage 1 to 5 when reported | Intervention: electrical stimulation with diverse methods Mean treatment duration: 4 weeks to 12 weeks when reported Comparator: SWC with or without sham stimulation | Outcomes:
Follow-up: NR |
Zheng et al. (2022)27 China Funding source: government agencies in Jilin province, China (JJKH20221068KJ) and the authors declared no conflict of interest. | Study design: systematic review of RCTs and quasi-experimental studies Number of included studies: 10 (8 included in the meta-analysis) Countries: US, Italy, Iran, Colombia | Patients with diabetes-related ulcers Number of participants: 352 Age: 48.4 to 65.1 years Sex: male from 58.3% to 91.4% Disease duration: NR Severity: NR | Intervention: electrical stimulation with unclear treatment detail Mean treatment duration: NR Comparator: SWC with or without placebo | Outcomes:
Median follow-up: 4 to 12 weeks |
Melotto et al. (2022)28 UK Funding source: University of Brighton and the authors declared no conflict of interest. | Study design: systematic review of RCTs and observational studies Number of included studies: 7 (5 RCTs and 2 cohort studies) Countries: US, Sweden, Iran | Patients with diabetic ulcers of foot and lower limb Number of participants: from 20 to 80 across included primary studies Age: 50 to 67.5 years Sex: male from 42% to 90% Mean disease duration: 1.8 to 14.7 months Severity: grades 1A, 2A in University of Texas Diabetic Wound Classification System or grade 2 in Wagner Ulcer Classification | Intervention: DC for 60 minutes, 3 times per week; monophasic high-voltage, asymmetric or symmetric biphasic PC (length from 20 minutes to 8 hours); frequency: from twice weekly to twice daily; length: from 4 weeks to 16 weeks. Comparator: SWC or personalized care with sham stimulation | Outcomes: Healing rates Follow-up: NR |
Avendano-Coy et al. (2022)29 Spain Funding source: no specific funding support and the authors declared no conflict of interest. | Study design: systematic review of RCTs Number of included studies: 7 Countries: Egypt, UK, Brazil, Italy, Belgium. | Adults with wounds (acute wounds, surgical wounds, chronic wounds, or pressure ulcers) Number of participants: 337 Age: 26 to 74 years Sex: male 68.5% | Intervention: electrical stimulation with diverse methods, but the current intensity ≥ 1 mA Comparator: SWC or NPWT | Outcomes:
Follow-up: NR |
DC = direct current; DW = degenerate wave current; HVPC = high-voltage pulsed current; HVMPC = high-voltage monophasic pulsed current; LVMPC = low-voltage monophasic pulsed current; LVBPC = low-voltage monophasic pulsed current; NA = not applicable; NPWT = negative pressure wound therapy; NR = not reported; PC = pulsed current; SWC = standard wound care; WSA = wound surface area.
Table 3: Characteristics of Included Economic Evaluation
Study citation country, funding source | Type of analysis, time horizon, perspective | Population characteristics | Intervention and comparator(s) | Approach | Source of clinical, cost, and utility data used in analysis | Main assumptions |
|---|---|---|---|---|---|---|
Guest et al. (2018)30 UK Funding source: manufacturer of the device; the authors declared no conflict of interest | Analysis: cost-utility analysis that was conducted based on an individual RCT Time horizon: within-trial horizon (up to 24 weeks) Perspective: the UK’s National Health Service | Adults with nonhealing venous leg ulcers from an RCT Number of participants:90 Mean age: 71 (SD: 15.0) in the intervention group; 68 (SD: 15.1) in the control group. Sex: 60% male in the intervention group; 50% in the control group. | Intervention: self-contained programmed electric microcurrent generator and 2 skin contact pads for 12 consecutive days Comparator: placebo device (identical in appearance but did not deliver an electric microcurrent) | To determine the cost-effectiveness between the 2 groups, the authors divided the estimated cost-difference by the estimated effect difference at the same time point. Outcome measures: incremental cost per QALY gained and incremental cost for each additional healed patient. Bootstrapping and deterministic sensitivity analyses were conducted. | National unit costs were obtained from NHS tariffs, at 2015 or 2016 prices, and applied to the amounts of health care resource use to estimate the cost per patient in each group. Effectiveness inputs were collected during the RCT. Patients’ utility values were calculated from the scores of the EQ-5D-5L questionnaires. QALYs at 8, 16 and 24 weeks after randomization were calculated. | The distribution of expected costs and QALYs were estimated using 10,000 subsets of the data from each group, based on random sampling. Deterministic sensitivity analyses were performed. |
EQ-5D-5L = EuroQol 5 Dimension 5 Level; NA = not applicable; NHS = National Health Service; NR = not reported; QALY = quality-adjusted life-year; RCT = randomized controlled trials; SD= standard deviation
Table 4: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
IWGDF (2023)31 | ||||||
Intended users: clinicians Target population: patients with diabetic foot ulcers Countries: Australia, Dominican Republic, UK, Germany, Ireland, Italy, US, India, UK | Wound management strategies: debridement, wound bed preparation and newer technologies to facilitate healing | Ten outcomes: complete would healing, time to healing, sustained healing, reduction in ulcer area, amputation, quality of life, maintenance of function and ability to perform activities of daily living, new infection, resource utilization, and mortality. | Systematic review of RCTs | GRADE methodology: “high,” “moderate,” “low” or “very low.” | Based on GRADE evidence to recommendation framework: the direction of the recommendation: “for” or “against;” the strength of recommendation: “strong” or “conditional.” | The guideline recommendations and rationales were reviewed by clinical experts and persons with lived experience who reviewed the clinical questions and the members of the IWGDF editorial board. Several external experts also reviewed the guideline manuscript. |
PROSPECT (2021)32 | ||||||
Intended users: clinicians Target population: patients with elective caesarean section under neuraxial anesthesia Countries: Belgium, Sweden, and US | Postoperative pain management strategies such as paracetamol, nonsteroidal anti-inflammatory drugs, opioids surgical techniques, TENS | Postoperative pain scores, analgesia use, patient satisfaction, adverse effects. | Systematic review of RCTs | PROSPECT methodology: grading of A-D according to the overall level of evidence by considering the quality of studies, consistency of evidence. | PROSPECT Working Group reviewed the proposed recommendations. A modified Delphi approach was used to achieve consensus. | PROSPECT working group approved the final document and the Obstetric Anesthetists’ Association Executive Committee offered their support for recommendations. |
GRADE = Grading of Recommendations, Assessment, Development and Evaluation; IWGDF = International Working Group on the Diabetic Foot; NA = not applicable; NR = not reported; PROSPECT = procedure-specific postoperative pain management; RCT = randomized controlled trials; TENS = transcutaneous electrical nerve stimulation.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 5: Strengths and Limitations of Systematic Reviews Using AMSTAR 217
Strengths | Limitations |
|---|---|
Borges et al. (2023)23 | |
The purpose of the study was clearly described. The protocol of this review was prospectively registered in the PROSPERO. Multiple databases were searched (PubMed, Scopus, and Web of Science). The search strategies were provided. The authors manually searched reference lists of pertinent reviews and studies. A flow chart of study selection was provided. The study selection process was clearly described and conducted by 2 reviewers. The list of excluded studies was provided. The data extractions were performed by one reviewer and verified by a second reviewer. The details of included studies were adequately described. The review authors assessed the RoB for eligible studies using the Cochrane risk of bias tool for RCTs and the Joanna Briggs Institute critical appraisal checklist for case series. The intervention and study designs of the individual study for inclusion were clearly described. The review authors reported no conflicts of interest. | The diagnostic criteria of venous leg ulcers, disease duration and background intervention were not clearly described. A grey literature search was not reported. The review authors did not report the funding sources for eligible studies. The review authors did not assess the potential impact of RoB in individual studies on result interpretations. |
Szołtys-Brzezowska et al. (2023)24 | |
The purpose of the study was clearly described. The study designs of the individual study for inclusion were clearly described. Multiple databases were searched (PubMed, EBSCO, MEDLINE, and Elsevier). The keywords in the search strategy were provided. A grey literature search (grey publications were conducted). A flow chart of study selection was provided. Two review authors independently assessed the RoB for eligible studies using the 10-item Physiotherapy Evidence Database scale. The data extractions were performed by 3 reviewers independently. The details of included studies in were adequately described. The review authors summarized the results according to different types of electrical stimulation devices. The review authors declared no conflicts of interest. | The diagnostic criteria of pressure injuries were not clearly described. It was unclear if the study selection was conducted by at least 2 authors independently. The list of excluded studies was not provided. The review authors did not report the funding sources for eligible studies. The review authors did not assess the potential impact of RoB in individual studies on results interpretation. The follow-up of outcome measures was unclear. |
Girgis et al. (2023)25 | |
The purpose of the study was clearly described. The study designs of the individual study for inclusion were clearly described. Multiple databases (PubMed, Scopus, Physiotherapy Evidence Database and Google Scholar) were searched. The search terms and full search strategies were described. The review authors assessed the RoB for RCTs and observational studies. Publication bias, sensitivity analyses and subgroup analyses were conducted. The list of excluded studies was provided. The review authors assess the overall quality of evidence using the GRADE framework. A flow chart of study selection was provided. The review authors reported the sources of funding for eligible studies. The review authors declared no conflicts of interest. | It was unclear if the study selection, data extraction and RoB were conducted by at least 2 authors independently. The diagnostic criteria of ulcers, disease duration, disease severity and background intervention were not clearly described. The follow-up of outcome measures was unclear. The authors stated that they followed the Cochrane Group Guidelines to avoid double counting by splitting the shared control group. However, some forest plots (figures 4 and 5) presented by them did not reflect this split. The authors did not assess the credibility of subgroup analyses. |
Chen et al. (2023)26 | |
The purpose of the study was clearly described. The protocol of this review was prospectively registered in the PROSPERO. The study designs of the individual study for inclusion were clearly described. Multiple databases were searched (PubMed, Embase, the Cochrane Library, Web of Science, g CNKI, SinoMed, VIP and WANFANG). The search terms and full search strategies were provided. The study selection process and data extraction were clearly described and conducted by 2 reviewers. The review authors assessed the RoB for RCTs using the Cochrane Collaboration RoB tool. A flow chart of study selection was provided. Publication bias assessments and subgroup analyses were conducted. The reasons for exclusion in the stage of full-text screening were provided. The details of included studies were adequately described. The review authors reported no conflicts of interest. | A grey literature search was not reported. The review authors did not report the sources of funding for eligible studies. The review authors did not assess the potential impact of RoB in individual studies on result interpretations. The follow-up of outcome measures was unclear. It was unclear how to handle trials with multiple arms (3 or more). The authors did not assess the credibility of subgroup analyses. |
Zheng (2022)27 | |
The purpose of the study was clearly described. The study designs of the individual study for inclusion were clearly described. Multiple databases were searched (Embase, MEDLINE, and Cochrane Library). The search terms and full search strategies were provided. The study selection process and data extraction were clearly described and conducted by 2 reviewers. The review authors assessed the RoB for RCTs using a revised Cochrane RoB tool. A flow chart of study selection was provided. Publication bias assessments and subgroup analyses were conducted. The reasons for exclusion in the stage of full-text screening were provided. The details of included studies were adequately described. The review authors reported no conflicts of interest. | A grey literature search was not reported. The review authors did not report the sources of funding for eligible studies. The review authors did not assess the potential impact of RoB in individual studies on result interpretations. The diagnostic criteria of diabetes-related ulcers, disease duration, disease severity and background intervention were not clearly described. The methods for outcome measures (ulcer area and healing rate) were unclear. It was unclear how to handle trials with multiple arms (3 or more). The authors did not assess the credibility of subgroup analyses. |
Melotto et al. (2022)28 | |
The purpose of the study, inclusion or exclusion criteria were clearly described. The protocol of this review was prospectively registered in the PROSPERO. The study designs of the individual study for inclusion were clearly described. Multiple databases were searched (Embase, MEDLINE, Cochrane Library, CINAHL Plus, AMED, Web of Science, PubMed). The grey literatures were searched through OpenGrey. The search terms and full search strategies were provided in the appendix. The study selection process and data extraction were clearly described and conducted by 2 reviewers. The reasons for exclusion were provided. The review authors assessed the RoB for included studies using CCAT. A flow chart of study selection was provided. The details of included studies were adequately described. The review authors reported no conflicts of interest. | The study selection process and data extraction were not clearly described. The review authors did not report the sources of funding for eligible studies. The review authors did not assess the potential impact of RoB in individual studies on result interpretations. The diagnostic criteria of ulcers and background intervention were not clearly described. The follow-up of outcome measures was unclear. |
Avendano-Coy et al. (2022)29 | |
The purpose of the study was clearly described. The protocol of this review was prospectively registered in the PROSPERO. The study designs of the individual study for inclusion were clearly described. Multiple databases were searched (PubMed, Google Scholar, Cochrane, CINAHL, Scopus, PEDro, and ProQuest). The detailed search terms were provided in appendix. The study selection process and data extraction were clearly described and conducted by at least 2 reviewers. The review authors assessed the RoB using Cochrane RoB tool. The review authors assess the overall quality of evidence using the GRADE framework. A flow chart of study selection was provided. The subgroup analyses were conducted. The details of included studies were adequately described. The review authors reported no conflicts of interest. | A grey literature search was not reported. The list of excluded studies was not provided. The review authors did not report the sources of funding for eligible studies. The review authors did not assess the potential impact of RoB in individual studies on result interpretations. The follow-up of outcome measures was unclear. When the number of included studies is less than 10, funnel plots are used to assess publication bias. The authors stated that they followed the Cochrane Group Guidelines to avoid double counting by splitting the shared control group. However, the forest plots presented by them did not reflect this split. The authors did not assess the credibility of subgroup analyses. |
AMSTAR 2 = A Measurement Tool to Assess Systematic Reviews 2; CCAT = Crowe Critical Appraisal Tool; GRADE = Grading of Recommendations, Assessment, Development and Evaluation; RCT = randomized controlled trial; RoB = risk of bias
Table 6: Strengths and Limitations of Economic Evaluation Using the Drummond Checklist18
Strengths | Limitations |
|---|---|
Guest et al. (2018)30 | |
Study design The population, intervention and the strategies being compared, and the outcome measures were clearly described. The perspective of the analysis was clearly stated. The form of economic evaluation was stated. Data collection The sources of effectiveness estimates and treatment costs were described. The design and results of the effectiveness were given. The primary outcome measures for the economic evaluation were clearly described. Methods to value health states and utility values were stated. Characteristics of the participants included in the cost-effectiveness analysis were described. Currency and price data are recorded. Analysis and interpretation of results Time horizon of costs and benefits were stated (i.e., 8, 16 and 24 weeks). Incremental analyses and probability of being cost-effective were reported. Details of statistical tests and confidence intervals were given. Major outcomes are presented in a disaggregated as well as aggregated form. The answer to the study question was given. Conclusions follow from the data reported and were accompanied by the appropriate caveats. | The research question, economic importance of the research question, and rationale for choosing alternative interventions compared were unclear. To estimate the cost-effectiveness of the intervention is not of the primary objectives of this study. The “cost-effectiveness” analysis probably was a “cost-utility” analysis. Quantities of resource were not reported separately from their unit costs. Methods for estimation of quantities and unit cost were not described. Details of currency of price adjustments for inflation or currency conversion were not given. Measures of intervention effectiveness were taken from a single RCT rather than a synthesis or meta-analysis of estimates from multiple sources. No discount rate was applied. Deterministic sensitivity analyses were performed but not clearly described. The time horizon of costs and benefits were short (up to 24 weeks) by considering the duration of the nonhealing venous leg ulcers. The findings of this UK-NHS based study may not be generalizable to the Canadian health system. |
NHS = National Health Service.
Table 7: Strengths and Limitations of Guidelines Using AGREE II19
Item | IWGDF (2023)31 | PROSPECT (2021)32 |
|---|---|---|
Domain 1: scope and purpose | ||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Not explicit but implied |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Not explicit but implied | Yes |
Domain 2: stakeholder involvement | ||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Not explicit but implied yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes | Unclear |
6. The target users of the guideline are clearly defined. | Yes | Yes |
Domain 3: rigour of development | ||
7. Systematic methods were used to search for evidence. | Yes | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes | Not explicit but implied |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | To some extent but lacked details. | To some extent but lacked details. |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Unclear |
13. The guideline has been externally reviewed by experts before its publication. | Yes | Yes |
14. A procedure for updating the guideline is provided. | Yes | No |
Domain 4: clarity of presentation | ||
15. The recommendations are specific and unambiguous. | Yes | No |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes |
Domain 5: applicability | ||
18. The guideline describes facilitators and barriers to its application. | No | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No | No |
20. The potential resource implications of applying the recommendations have been considered. | No | No |
21. The guideline presents monitoring and/or auditing criteria. | No | No |
Domain 6: editorial independence | ||
22. The views of the funding body have not influenced the content of the guideline. | Yes | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Conflicts of interest were declared but it was unclear how they were addressed. Several authors had received grants or consultation fees from industries.a |
AGREE II = Appraisal of Guidelines for Research and Evaluation II.
aPfizer, Baxter, Pacira, Sintetica, Grunenthal, Vifor Pharma, MSD, Nordic Pharma, Janssen Pharmaceuticals, Heron Therapeutics, Mundipharma, Grunenthal, Janssen-Cilag GmbH, Fresenius Kabi and AcelRx.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 8: Summary of Findings by Outcome — Wound Surface Area
Author (year) and study design | Number of studies | Statistics | Effect size/description | Population/subgroup | P | Notes |
|---|---|---|---|---|---|---|
Relative WSA reduction from baseline | ||||||
Girgis et al. (2023)25 Systematic review with 11 articles: 8 RCTs and 3 observational studies | 9 | Pooled MD (95% CI) | 32.97% (21.86% to 44.07%) | Pressure ulcer | < 0.001 | Intervention vs. control at 20 days to 12 weeks |
7 | Pooled MD (95% CI) | 33.76% (21.38% to 46.15%) | Pressure ulcer | < 0.001 | Intervention vs. control at 4 to 8 weeks (GRADE: very low) | |
Chen et al. (2023)26 Systematic review with 17 RCTs | 8 | Pooled MD (95% CI) | 29.7% (22.43% to 36.98%) | Pressure ulcer | < 0.001 | Intervention vs. control |
Zheng et al. (2022)27 Study design: systematic review of 8 RCTs and quasi-experimental studies | 7 | Pooled SMD (95% CI) | 2.56 (1.43 to 3.69) | Diabetes-related ulcers ulcer | < 0.001 | Intervention vs. control |
5 | Pooled SMD (95% CI) | 3.01 (1.62 to 4.39) | Pulsed current subgroup | NR | No statistical difference | |
2 | Pooled SMD (95% CI) | 1.45 (0.86 to 2.04) | Direct current subgroup | NR | ||
NR | Pooled SMD (95% CI) | 1.58 (1.03 to 2.13) | Leg ulcers subgroup | NR | No statistical difference | |
NR | Pooled SMD (95% CI) | 2.41 (0.88 to 3.94) | Foot ulcers subgroup | NR | ||
Raw WSA (cm2) | ||||||
Chen et al. (2023)26 Systematic review with 17 RCTs | 11 (overall) | Pooled MD (95% CI) | −1.76 (−3.24 to –0.28) | Pressure ulcer | < 0.001 | Intervention vs. control |
8 (pulsed current subgroup) | Pooled MD (95% CI) | −3.83 (−4.71 to –2.95) | Pressure ulcer | NR | Interaction P < 0.001 | |
2 (direct current subgroup) | Pooled MD (95% CI) | −2.67 (−4.40 to –0.95) | Pressure ulcer | NR | — | |
Avendano-Coy et al. (2022)29 Study design: systematic review of 7 RCTs | 3 | Pooled MD (95% CI) | −4.86 (−11.02 to 1.30) | All types of wounds | 0.12 | Intervention vs. control (GRADE: moderate) |
3 | Pooled MD (95% CI) | −8.26 (−10.52 to −6.01) | Control comparator subgroup | < 0.001 | Interaction P < 0.001 | |
1c | Pooled MD (95% CI) | −1.30 (−3.48 to 0.88) | NPWT comparator subgroup | 0.24 | ||
2 | Pooled MD (95% CI) | −5.64 (−24.84 to 13.56) | Chronic wounds subgroup | 0.56 | Interaction P = 0.94 | |
1 | Pooled MD (95% CI) | −4.79 (−11.65 to 2.07) | Acute wounds subgroup | 0.17 | ||
Qualitative summaries | ||||||
Szołtys-Brzezowska et al. (2023)24 Study design: systematic review of 16 RCTs | 9 | NR | “WSA decreased more in the EGS treated with HVMPC than in the CGs. (p. 294)” | Pressure Injuries | NR | Details of each RCT were available in the result section. |
CI = confidence interval; CGs = control groups; EGs = electrical stimulation groups; RR = risk ratio; NPWT = negative pressure wound therapy; NR = not reported; RCTs = Randomized controlled trials; MD = mean difference; SMD = standardized mean difference; WSA = wound surface area.
Table 9: Summary of Findings by Outcome — Rate of Complete Healing
Author (year) and study design | Number of studies | Statistics | Effect size | Population/subgroup | P | Notes |
|---|---|---|---|---|---|---|
Girgis et al. (2023)25 Systematic review with 11 articles: 8 RCTs and 3 observational studies | 2 | Pooled RR (95% CI) | 1.43 (0.92 to 2.24) | Diabetic ulcers | 0.30 | Intervention vs. control |
8 | Pooled RR (95% CI) | 2.08 (1.42 to 3.04) | Pressure ulcer | 0.0002 | Intervention vs. control (GRADE: moderate) | |
Chen et al. (2023)26 Systematic review with 17 RCTs | 9 | Pooled RR (95% CI) | 1.79 (1.09 to 2.92) | Pressure ulcers | 0.02 | Intervention vs. control |
8 | Pooled RR (95% CI) | 2.09 (1.22 to 3.58) | Pulsed current subgroup | 0.007a | Interaction P = 0.02 | |
1 | Pooled RR (95% CI) | 0.72 (0.34 to 1.53) | Direct current subgroup | 0.39a | ||
Avendano-Coy et al. (2022)29 Systematic review with 7 RCTs | 2 | Pooled RR (95% CI) | 2.04 (0.43 to 9.73) | All types of wounds | 0.37 | Intervention vs. control (GRADE: very low) |
CI = confidence interval; GRADE = Grading of Recommendations, Assessment, Development and Evaluation; NR = not reported; RCT = Randomized controlled trial; RR = risk ratio.
Table 10: Summary of Findings by Outcome — Rate of Nonhealing or Worsened Wounds
Author (year) and study design | Number of studies | Statistics | Effect size | Population/subgroup | P | Notes |
|---|---|---|---|---|---|---|
Rate of nonhealing wounds | ||||||
Zheng et al. (2022)27 Study design: systematic review of 8 RCTs and quasi-experimental studies | 4 | Pooled RR (95% CI) | 0.72 (0.54 to 0.96) | Diabetic ulcer | NR | Intervention vs. control |
NR | Pooled RR (95% CI) | 0.36 (0.13 to 0.99) | Leg ulcers subgroup | NR | No statistical difference | |
NR | Pooled RR (95% CI) | 0.71 (0.47 to 1.07) | Foot ulcers subgroup | NR | ||
Rate of worsened wounds | ||||||
Girgis et al. (2023)25 Systematic review with 32 articles: 17 RCTs and 15 observational studies | 5 | Pooled RR (95% CI) | 0.18 (0.06 to 0.60) | diabetic ulcer | 0.005 | Intervention vs. control (GRADE: moderate) |
CI = confidence interval; GRADE = Grading of Recommendations, Assessment, Development and Evaluation; NR = not reported; RCT = randomized controlled trial; RR = risk ratio.
Table 11: Summary of Findings by Outcome — Time to Complete Wound Healing
Author (year) and study design | Number of studies | Statistics | Effect size | Population/subgroup | P | Notes |
|---|---|---|---|---|---|---|
Time to complete wound healing (number of days) | ||||||
Avendano-Coy et al. (2022)29 Study design: systematic review of 7 RCTs | 4 | Pooled MD (95% CI) | −5.13 (−9.40 to −0.87) | All types of wounds | 0.02 | Intervention vs. control (GRADE: low) |
4 | Pooled MD (95% CI) | −7.04 (−11.93 to −2.14) | Control comparator subgroup | < 0.001 | Interaction P = 0.01 | |
1a | Pooled MD (95% CI) | 2.00 (−3.08 to 7.08) | NPWT comparator subgroup | 0.24 | ||
3 | Pooled MD (95% CI) | −2.93 (−6.50 to 0.65) | Acute wounds subgroup | 0.11 | Interaction P < 0.001 | |
1 | Pooled MD (95% CI) | −27.00 (−39.41 to −14.59) | Chronic wounds subgroup | 0.02 | ||
Melotto et al. (2022)28 Study design: systematic review of 5 RCTs and 2 observational studies | 1 RCT (Peters et al.) | Healing time (weeks) | Intervention: 6.8 ± 3.4 weeks Control: 6.9 ± 2.8 weeks MD: 0.1 weeks | Diabetic ulcers | No statistical significance | Burdge et al. found an average healing time for intervention was 14.2 ± 9.8 weeks. |
CI = confidence interval; GRADE = Grading of Recommendations, Assessment, Development and Evaluation; RCT = randomized controlled trial; MD = mean difference; NPWT = negative pressure wound therapy.
aThe study provided data for both control comparator and NPWT comparator.
Table 12: Summary of Findings by Outcome — Pain
Author (year) and study design | Number of studies | Statistics | Effect size/description | P | Notes |
|---|---|---|---|---|---|
Pain score | |||||
Avendano-Coy et al. (2022)29 Study design: systematic review of 7 RCTs | 4 | Pooled MD (95% CI) | −1.42 (−2.65 to −0.19) | 0.02 | Intervention vs. control (GRADE: low) |
Borges et al. (2023)23 Systematic review with 11 articles: 8 RCTs and 3 observational studies | 4 | NR | “Improvements in pain were reportedly much higher in the intervention groups than in the control groups. (p. 5)” | NR | NA |
1 (Guest et al.) | NR | “A significant reduction in pain at 12 months after starting EST. (p. 5)” | 0.001 | Before-after | |
1 (Ovens et al.) | NR | “Substantial pain reduction in 84% of patients within 2 weeks after beginning EST. (p. 5)” | NR | Before-after | |
Girgis et al. (2023)25 Systematic review with 32 articles: 17 RCTs and 15 observational studies | 5 | NR | “Similar pain improvement in both the treatment and control groups was found in two studies. Early reduction in postoperative wound pain was observed following HVMPC intervention. Another study also concluded that HVMPC intervention reduced pain in patients with chronic ulcers. Treatment was discontinued following a complaint of increased pain by a patient who had severe Raynaud's syndrome. (p. 177)” | NR | GRADE: very low |
Table 13: Summary of Findings by Outcome — Exudate Levels
Author (year) and study design | Number of studies | Statistics | Effect size/description | Population | P | Notes |
|---|---|---|---|---|---|---|
Borges et al. (2023)23 Systematic review with 11 articles: 8 RCTs and 3 observational studies | 1 | NR | “After EST, the patients’ exudate levels decreased compared with the controls. (p. 4)” | Patients with VLU who have been without surgery | NR | No |
2 | NR | “The exudate levels were similar between EST and control. (p. 4)” | Patients with VLU who had undergone surgery | NR | No | |
2 case series | NR | “Patients’ exudate levels were also reduced after EST. (p. 5)” | Patients with VLU with unclear surgical status | NR | Before-after |
EST = electric stimulation therapy; GRADE = Grading of Recommendations, Assessment, Development and Evaluation; NR = not reported; VLU = venous leg ulcer.
Table 14: Summary of Findings by Outcome — Adverse Events
Author (year) and study design | Number of studies | Statistics | Effect size/description | P | Notes |
|---|---|---|---|---|---|
Avendano-Coy et al. (2022)29 Study design: systematic review of 7 RCTs | 3 | Pooled RD (95% CI) | 0.05 (−0.06 to 0.17) | 0.34 | Intervention vs. control (GRADE: moderate) |
Chen et al. (2023)26 Systematic review with 17 RCTs | 3 | NR | Gary et al. (1991) “The only adverse events were the occurrence of uncomfortable sensation in both groups. (p. 9)” Adunsky et al. (2005) “Patients got excessive granulation of the treated PUs in young participants in generally good conditions. (p. 9)” Houghton et al. (2010) “Adverse effects were minor and rare. (p. 10)” | NR | Three of 13 RCTs reported adverse effects. |
Borges et al. (2023)23 Systematic review with 11 articles: 8 RCTs and 3 observational studies | 1 (Guest et al.) | NR | Adverse events include infection, skin rash, pain, wound deterioration. EST: 23% Placebo: 15% | NR | No |
Szołtys-Brzezowska et al. (2023)24 Study design: systematic review of 16 RCTs | 16 | NR | “In the 16 RCTs reviewed, ES had no adverse effects on the patients treated. (p. 300)” | NR | No |
Girgis et al. (2023)25 Systematic review with 32 articles: 17 RCTs and 15 observational studies | NR | NR | “Many of the identified studies did not report on adverse reactions. No adverse reactions were observed in a number of studies. Other studies, however, documented minor and rare reactions such as red, raised, itchy skin beneath the dispersive electrode that was attributed to contact dermatitis, and was resolved by using a non-adhesive carbon electrode, or applying hydrocortisone 2.5% ointment to the affected area for 1–2 weeks. (p. 178)” Other adverse reactions: complaints of stimulation intensity, increased pain (in a patient with severe Raynaud's syndrome). | NR | GRADE: low |
CI = confidence interval; EST = Electric stimulation therapy; GRADE = Grading of Recommendations, Assessment, Development and Evaluation; NR = not reported; RCT = randomized controlled trial; RR = risk ratio; RD = risk difference.
Table 15: Summary of Findings by Outcome — Other Healing Outcomes
Author (year) and study design | Number of studies | Statistics | Effect size/description | P | Notes |
|---|---|---|---|---|---|
Percentage of wounds healed | |||||
Melotto et al. (2022)28 Study design: systematic review of 5 RCTs and 2 observational studies | 1 RCT (Peters et al.) | Percentage | Intervention: 71% Control: 39% | < 0.05 | Week 12 |
1 RCT (Lundeberg et al.) | Percentage | Intervention: 42% Control: 15% | < 0.05 | Week 12 | |
1 RCT (Lundeberg et al.) | Percentage | Intervention: 25% Control: 11% | < 0.05 | Week 8 | |
1 RCT (Lundeberg et al.) | Percentage | Intervention: 12% Control: 7% | NR | Week 4 | |
1 RCT (Lundeberg et al.) | Percentage | Intervention: 0% Control: 4% | NR | Week 2 | |
Composite healing outcomes | |||||
Borges et al. (2023)23 Systematic review with 11 articles: 8 RCTs and 3 observational studies | 5 RCTs | NR | “Improvement in at least one VLU healing outcome after EST compared with the control groups. (p. 4)” | NR | statistically significant |
3 RCTs | NR | “Improvement in VLU healing outcomes observed in the patients who received EST. (p. 4)” | NR | No statistically significant | |
2 RCTs | NR | “EST appeared to be an efficient method of enhancing healing compared with the control groups. (p. 4)” | NR | Only for patients who had not undergone surgical treatment of VLU | |
3 case series | NR | “Improvement in the VLU healing outcomes after EST (p. 4)” | NR | Before-after comparison | |
4 | NR | “EST produced faster healing or led to accelerated wound closure compared with the control groups (p. 4)” | NR | NA | |
Szołtys-Brzezowska et al. (2023)24 Study design: systematic review of 16 RCTs | NR | NR | “Electrical stimulation also accelerated PI healing, stimulated granulation tissue growth, and improved periwound skin blood flow. (p. 294)” | NR | The electrical stimulation used HVMPC. |
1 (Gentzkow et al.) | NR | “Over 4 weeks of treatment, twice as many PIs in the ES group healed as in the CG. (p. 298)” Intervention group: 49.8% Control group: 23.4% | 0.042 | The electrical stimulation used LVMPC. | |
1 (Wood et al.) | NR | “Compared with 25 PIs (58%) that healed completely in the ES group, only 1 PI (3%) closed in the CG. Whereas 10 PIs in the CG increased in size, no PIs increased in size in the ES group. (p. 298)” | NR | The electrical stimulation used LVMPC. | |
1 (Jerčinović et al.) | NR | “the mean daily healing rate was not significantly different between the ES and the CG. (p. 299)” Intervention group: 5.7% Control group: 2.7% | > 0.05 | The electrical stimulation used LVBPC. | |
1 (Karba et al.) | NR | “the mean wound healing rate in the ES was statistically significantly greater than in the CG. (p. 298)” | < 0.05 | The electrical stimulation used LVBPC. | |
1 (Baker et al.) | NR | “The mean weekly rates of PI area reduction calculated for all wounds in ES1, ES2, ES3, and CG were 36.4%, 29.7%, 23.3%, and 32.7%. (p. 299)” ES1: rectangular asymmetrical pulses, 100 μs, 50 pps, 7 seconds on and 7 seconds off. ES2: rectangular symmetrical pulses, 300 μs, 50 pps, 7 seconds on and 7 seconds off. ES3: 4 mA, 10 μs, 1 pps, 7 seconds on and 7 seconds off. | > 0.05 | The electrical stimulation used LVBPC. | |
1 (Adunsky and Ohry et al.) | NR | “An absolute wound area reduction and a relative wound area reduction (percentage change in wound area from baseline) obtained after 6 weeks of treatment (45 days) favored the ES group: mean wound area decreased by 44% compared with 14% in the CG. Thereafter, the groups’ healing rates were similar. A logistic regression analysis determined that the probability of all wounds healing was greater for the ES than for the CG (odds ratio, 1.6; 95% CI, 0.4–4.73). (p. 299)” | NR | The electrical stimulation used Low-Intensity DC. | |
Melotto et al. (2022)28 Study design: systematic review of 5 RCTs and 2 observational studies | 1 RCT (Baker et al.) | Percentage | “a statistically significant weekly healing rate increase. (p. 1923)” Asymmetric biphasic intervention: 27.0% Symmetric biphasic intervention:16.4% Control group (sham intervention): 17.3% | < 0.05 | No |
5 RCTs | NA | “Although none of the RCTs presented a statistically significant healing rate improvement after 2 weeks from the beginning of the ES intervention compared with the CG, the healing rate reported after 2 weeks in all the selected studies is higher in the IG compared with the CG. (p. 1923)” | NA | No | |
Other patients report outcomes | |||||
Girgis et al. (2023)25 Systematic review with 32 articles: 17 RCTs and 15 observational studies | Edema and function | NA | “Reduced oedema and improved function were noted following HVMPC intervention in one study. (p. 177)” | NA | Omar et al. |
Quality of life | NA | “No significant differences in quality of life were observed in one study. (p. 177)” | NA | Ortiz et al. | |
Recurrence or development of new ulcers | NA | “One study documented recurrence or development of new ulcers, within 4 months of complete healing, in eight subjects in each group. (p. 177)” | NA | Houghton et al. | |
Amputation | NA | “Two patients, who had pre-existing contralateral major amputation and received HVMPC, underwent amputation in one study. (p. 177)_” “Two major amputations in the treatment group, compared with three in the control group, were reported in another study. (p. 177)” | NA | Goldman et al. (2002) and Goldman et al. (2003). | |
CG = control group; CI = confidence interval; ES = electric stimulation; EST = electric stimulation therapy; HVMPC = high-voltage monophasic pulsed current; IG = intervention group; NA = not applicable; NR = not reported; PI = Pressure Injuries; RCT = randomized controlled trial; VLU = venous leg ulcer.
Table 16: Summary of Findings by Outcome — Other Outcomes
Author (year) and study design | Outcomes | Effect size/description | Notes |
|---|---|---|---|
Girgis et al. (2023)25 Systematic review with 32 articles: 17 RCTs and 15 observational studies | Edema and function | “Reduced oedema and improved function were noted following HVMPC intervention in one study. (p. 177)” | Omar et al. |
Quality of life | “No significant differences in quality of life were observed in one study. (p. 177)” | Ortiz et al. | |
Recurrence or development of new ulcers | “One study documented recurrence or development of new ulcers, within 4 months of complete healing, in eight subjects in each group. (p. 177)” | Houghton et al. | |
Amputation | “Two patients, who had pre-existing contralateral major amputation and received HVMPC, underwent amputation in one study. (p. 177)_” “Two major amputations in the treatment group, compared with three in the control group, were reported in another study. (p. 177)” | Goldman et al. (2002) and Goldman et al. (2003). |
CI = confidence interval; NA = not applicable; NR = not reported; RR = risk ratio; RD = risk difference; DC = direct current; DW = degenerate wave current; HVPC = high-voltage pulsed current; HVMPC = high-voltage monophasic pulsed current; LVMPC = low-voltage monophasic pulsed current; LVBPC = low-voltage monophasic pulsed current; NA = not applicable; NPWT = negative pressure wound therapy; NR = not reported; PC = pulsed current; SWC = standard wound care; WSA = wound surface area.
Table 17: Summary of Findings of Included Economic Evaluation
Main study findings | Authors’ conclusion |
|---|---|
Guest et al. (2018)30 | |
Mean NHS cost per patient at 8 weeks
Mean NHS cost per patient at 16 weeks
Mean NHS cost per patient at 24 weeks
Mean number of QALYs per patient at 8 weeks
Mean number of QALYs per patient at 16 weeks
Mean number of QALYs per patient at 24 weeks
Probability of healing at 8 weeks
Probability of healing at 16 weeks
Probability of healing at 8 weeks
Incremental cost per QALY gained (vs. placebo)
Incremental cost for each additional healed ulcer (vs. placebo)
Sensitivity analyses
| “In conclusion, the study was confounded by unwarranted variation in the provision of wound care both within and between centres. Nevertheless, the use of the EAE resulted in some improved clinical outcomes and patient-reported outcomes for the same or less cost as standard care by 24 weeks (p. 242),” |
EAE = electroceutical device; NHS = National Health Service; QALY = quality-adjusted life-year.
Table 18: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
IWGDF (2023)31 | |
“Do not use any interventions reported in the field of physical therapies for wound healing in the management of diabetes-related foot ulcers. (p. 20)” (Recommendation 15) Physical therapies include electrical or electromagnetic stimulation and other therapies such as heat application, therapeutic ultrasound, compression, light and laser treatment, Extracorporeal Shock Wave Therapy ischemic preconditioning, therapeutic magnetic resonance, and connective tissue manipulation. Relevant supporting evidence: “We identified six studies investigating the use electrical or electromagnetic stimulation on some of our outcomes of importance. (p. 20)” | Strong recommendation (GRADE) based on low certainty of evidence. |
Roofthooft et al. (2021)32 | |
“Consider the use of transcutaneous electrical nerve stimulation as an analgesic adjunct. (p. 666)” in postoperative pain management for patients undergoing elective caesarean section performed under neuraxial anaesthesia. Relevant supporting evidence: “Several investigators reported on the beneficial effects of transcutaneous electrical nerve stimulation on pain scores, rescue analgesia use and patient satisfaction. (p. 671)” | Strength of recommendations: Grade A in PROSPECT methodology based on systematic reviews or RCTs.35 Quality of evidence: unclear |
GRADE = Grading of Recommendations, Assessment, Development and Evaluation; IWGDF = International Working Group on the Diabetic Foot; PROSPECT = procedure-specific postoperative pain management
Appendix 5: Overlap Between Included Systematic Reviews
Note that this appendix has not been copy-edited.
Table 19: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Borges et al. (2023)23 | Szołtys-Brzezowska et al. (2023)24 | Girgis et a. (2023)25 | Chen et al. (2023)26 | Zheng et al. (2022)27 | Melotto et al. (2022)28 | Avendano-Coy et al. (2022)29 |
|---|---|---|---|---|---|---|---|
Zulbaran-Rojas A, Park C, et al. J Diabetes Sci Technol. 2021; 19322968211035100 | — | — | — | — | Yes | — | — |
Elio C, Fontain V, et al. Acta Dermatovenerol Alp Pannonica Adriat. 2020; 29: 109-13. | Yes | — | — | — | — | — | — |
Ibrahim ZM, Waked IS, et al. J Wound Care. 2019; 28(4):214-9. | — | — | — | — | — | — | Yes |
Ovens L. Wounds UK. 2019; 15:78-84. | Yes | — | — | — | — | — | — |
Polak A, Kucio C, et al. Ostomy Wound Manage. 2018; 64(2):10-29. | — | Yes | Yes | Yes | — | — | — |
Guest JF, Singh H, et al. J Wound Care. 2018; 27: 230-43. | Yes | — | — | — | — | — | Yes |
García-Pérez, S., García-Ríos, M. C., et al. Advances in Skin & Wound Care. 2018; 31(10), 462-469. | — | — | — | Yes | — | — | — |
Gomes RC, Guirro EC, et al. Burns. 2018; 44(3):636-645. | — | — | Yes | — | — | — | — |
Sakabe FF, Sakabe DI, et al. Fisioterapia. 2018; 19(1):72-79. | — | — | Yes | — | — | — | — |
Polak A, Kloth LC, et al. Phys Ther. 2017; 97(8):777-89. | — | Yes | Yes | Yes | — | — | — |
Asadi MR, Torkaman G, et al. Res Clin Pract. 2017; 127:147-55. | — | — | — | — | Yes | Yes | — |
Karsli PB, Gurcay E, et al. Adv Skin Wound Care. 2017; 30(12):565-70. | — | Yes | Yes | Yes | — | — | — |
Santana de Souza AC, Lomasso Costa MM, et al. Fisioterapia. 2017; 18(6):676-685. | — | — | Yes | — | — | — | — |
Polak A, Taradaj J, et al. J Wound Care. 2016; 25(12):742-54. | — | Yes | Yes | Yes | — | — | — |
Polak A, Kloth LC, et al. Adv Skin Wound Care. 2016; 29(10):447-59. | — | Yes | Yes | Yes | — | — | — |
Zhou K, Schenk R, et al. Eur J Clin Invest. 2016; 46: 1017-23. | Yes | — | Yes | — | — | — | — |
Zhou K, Krug K, et al. Ostomy Wound Manage. 2016; 62(3):36-44. | — | — | Yes | — | — | — | — |
Asadi MR, Torkaman G, et al. J Babol Univ Med Sci. 2015; 17(7):7-14. | — | — | — | — | — | Yes | — |
Guest JF, Ayoub N, et al. J Wound Care. 2015; 24: 572, 574-580. | Yes | — | — | — | — | — | — |
Lessiani G, Galati V, et al. J Nov Physiother. 2014; 4:4 | — | — | — | — | — | — | Yes |
Mohajeri-Tehrani MR, Nasiripoor F, et al. J Rehabil Res Dev.2014; 51(5):815-24. | — | — | — | — | Yes | Yes | — |
Ortiz MCS, Villabona EH, et al. Rev Univ Ind Santander Salud. 2014; 46(2):107-117. | — | — | Yes | — | Yes | — | — |
Liani M, Trabassi E, et al. Primary Care Diabetes. 2014; 8(3):244-9. | — | — | — | — | Yes | — | — |
Malin EW, Galin CM, et al. Ann Plast Surg. 2013; 71(5):481-4. | — | — | — | — | — | — | Yes |
Gui MS, Guirro RRJ, et al. Fisioterapia e Pesquisa. 2013; 20:286-292. | — | — | Yes | — | — | — | — |
Santamato A, Panza F, et al. Rejuvenation Res. 2012; 15:281-7. | Yes | — | — | — | — | — | — |
Korelo RI, Valderramas S, et al. Rev Latino-Am Enferm. 2012; 20(4):753-60. | — | — | — | — | — | — | Yes |
Franek A, Kostur R, et al. Ostomy Wound Manag. 2012; 58(3):30-44. | — | Yes | Yes | Yes | — | — | — |
Taradaj J, Franek A, et al.Wounds. 2012; 24:215-26. | Yes | — | — | — | — | — | — |
Recio AC, Felter CE, et al. J Spinal Cord Med. 2012; 35(1):58-63. | — | — | Yes | — | — | — | — |
Franek A, Kostur R, et al. Wounds. 2011; 23(1):15-23. | — | — | Yes | — | — | — | — |
Petrofsky JS, Lawson D, et al. J Diab. 2010; 2(1):41-6. | — | — | — | — | Yes | — | — |
Houghton PE, Campbell KE, et al. Arch Phys Med Rehabil. 2010; 91(5):669-678. | — | Yes | Yes | Yes | — | — | — |
Lasko J, Kochik J, et al. Adv Skin Wound Care. 2010; 23(10): 446-449. | — | — | Yes | — | — | — | — |
Silva Ede F, Martins CC, et al. An Bras Dermatol. 2010; 85(4):567-569. | — | — | Yes | — | — | — | — |
Burdge JJ, Hartman JF, et al. Ostomy Wound Manage. 2009; 55(8): 30-38. | — | — | — | — | — | Yes | — |
Santos RP, Nascimento CA, et al. Fisioter Mov. 2009; 22: 615-23. | Yes | — | — | — | — | — | — |
Ahmad ET. Ann Burns Fire Disasters. 2008; 21(3):124-8. | — | Yes | Yes | Yes | — | — | — |
Jünger M, Arnold A, et al. Wound Repair regen. 2008; 16: 480-7. | Yes | — | — | — | — | — | — |
El-Husseini T, El-Kawy S, et al. Int Orthop. 2007; 31(2). | — | — | — | — | — | — | Yes |
Huckfeldt R, Flick AB, et al. J Burn Care Res. 2007; 28(5):703-7. | — | — | — | — | — | — | Yes |
Petrofsky JS, Lawson D, et al. Diabetes Technol Ther. 2007; 9(6):535-44. | — | — | — | — | Yes | — | — |
Franek A, Taradaj J, et al. Phlebologie. 2006; 35:127-33. | Yes | — | — | — | — | — | — |
Adunsky A and Ohry A.Arch Gerontol Geriatr. 2005; 41(3):261-9. | — | Yes | — | Yes | — | — | — |
Goldman R, Rosen M, et al. Adv Skin Wound Care.2004; 17(6): 284-294. | — | — | Yes | — | — | — | — |
Omar MT, El-Badawy AM, et al. Egypt J Plast Reconstr Surg. 2004; 28(2):141-146. | — | — | Yes | — | — | — | — |
Houghton PE, Kincaid CB, et al. Phys Ther. 2003; 83: 17-28. | Yes | — | Yes | — | — | — | — |
Goldman R, Brewley B, et al. Adv Skin Wound Care.2003; 16(2):79-89. | — | — | Yes | — | — | — | — |
Goldman RJ, Brewley BI, et al. Adv Skin Wound Care.2003; 16(7):363-366. | — | — | Yes | — | — | — | — |
Goldman RJ, Brewley BI, et al. Adv Skin Wound Care.2002; 15(3):112-120. | — | — | Yes | — | — | — | — |
Peters EJ, Lavery LA, et al. Arch Phys Med Rehabil. 2001; 82(6):721-725. | — | — | Yes | — | Yes | Yes | — |
Adegoke, B. O., and Badmos, K. A.African Journal of Medicine and Medical Sciences. 2001; 30(3), 195-197. | — | — | — | Yes | — | — | — |
Gilcreast DM, Stotts NA, et al. Wound Repair Regen.1998; 6(5):434-441. | — | — | Yes | — | — | — | — |
Elshazly F and Hassan A. Bull Fac Phys Ther Cairo Univ.1998; 3(1):61-68. | — | — | Yes | — | — | — | — |
Baker LL, Chambers R, et al. Diabetes Care. 1997; 20(3):405-12. | — | — | — | — | Yes | Yes | — |
Baker LL, Rubayi S, et al. Wound Repair Regen. 1996; 4(1):21-8. | — | Yes | — | Yes | — | — | — |
Karba R, Benko H, et al. Med Sci Res. 1995; 23(10):671-3. | — | Yes | — | — | — | — | — |
Jerčinović A, Karba R, et al. IEEE Trans Rehabil Eng. 1994; 2(4):225-33. | — | Yes | — | Yes | — | — | — |
Wood JM, Evans PE, et al. Arch Dermatol. 1993; 129:999-1009. | — | Yes | — | Yes | — | — | — |
Fitzgerald GK and Newsome D. Phys Ther.1993; 73(6):355-360. | — | — | Yes | — | — | — | — |
Lundeberg TCM, Eriksson SV, et al. Ann Plast Surg. 1992; 29(4):328-31. | — | — | — | — | Yes | Yes | — |
Griffin JW, Tooms RE, et al. Phys Ther. 1991; 71(6):433-442. | — | Yes | Yes | Yes | — | — | — |
Gentzkow G, Pollack S, et al. Wounds. 1991; 3(5):158-70. | — | Yes | — | Yes | — | — | — |
Kloth LC and Feedar JA. Phys Ther. 1988; 68(4):503-8. | — | Yes | Yes | Yes | — | — | — |
Akers TK and Gabrielson AL. Biomed Sci Instrum. 1984; 20:99-100. | — | — | Yes | — | — | — | — |
— = not included.
Appendix 6: Patient Involvement
Note that this appendix has not been copy-edited.
Table 20: Summary of Patient Involvement Using the Guidance for Reporting Involvement of Patients and the Public (Version 2) Short Form Reporting Checklist21
Section and topic | Item | Report section |
|---|---|---|
Aim | A patient living with quadriplegia who had used an electrostimulation device for the treatment of a pressure ulcer was engaged during the writing of this report. He shared his experience, thoughts, perspectives, and priorities to help contextualize the information gathered from the literature search. The purpose of the engagement was to offer a unique perspective of the treatment to allow for a more nuanced understanding of the literature and to add context to the findings reported in the literature. | Key Messages |
Methods | A request for engagement was disseminated through both social media and a relevant patient advocacy group, and an interested individual was identified. After giving informed consent, the patient participated in a semistructured dialogue with a Patient Engagement Officer and the Research Officer authoring this report via a 1-hour video call. A summary of the engagement discussion was prepared by the Patient Engagement Officer and shared with the patient, who confirmed that the contents reflected his experience and the discussion. This summary was subsequently shared with the Research Officer, who was able to refer to it while considering the evidence compiled during the literature search. | Methods |
Results of engagement | The researchers were made aware of the importance of 2 specific outcomes that mattered to the patient. In particular, the patient identified the need for avoiding surgery and hospitalization. He also raised issues for consideration, including the accessibility of devices, the need for training on the device for home therapy, and the need for adoption by home care providers. | Key Messages, summary of findings, limitation |
Discussion and conclusions | The patient contributor was highly engaged in the dialogue, openly sharing his personal experience living with a wound and his treatment experience with an electrostimulation device. He reported a high degree of satisfaction with the electrostimulation therapy, stating that he did not experience noticeable side effects. He recommended that other people with wounds could benefit from electrostimulation. He appreciates that electrostimulation therapy enabled him to avoid a flap surgery and its associated hospitalization for recovery. He prefers minimizing time spent in hospital whenever possible. The patient reported barriers to access, including the cost of purchasing the device, availability of the devices, access to training on how to use the device, and the need for home care nurses to be trained on how to administer treatment to those without family members who can apply the electrodes, etc. | Conclusion and implications |
Reflections/critical perspective | The success of patient engagement in the review is related to several factors. First, the patient was supported by a Patient Engagement Officer. Second, the Research Officer was receptive to patient involvement and consulted the summary of the engagement during their consideration of the clinical evidence. Finally, compensation was offered for patient contributor’s time and expertise. One limitation of our approach is that people need reliable internet access and access to a phone, computer, or tablet to contribute to CADTH’s work, which may exclude some voices. | NA |
NA = not applicable.
Appendix 7: References of Potential Interest
Systematic Reviews (Outside of Date Range)
Rajendran SB, Challen K, Wright KL, Hardy JG. Electrical Stimulation to Enhance Wound Healing. J Funct Biomater. 2021;12(2):19. PubMed
Milne J, Swift A, Smith J, Martin R. Electrical stimulation for pain reduction in hard-to-heal wound healing. J Wound Care. 2021;30(7):568-580. PubMed
Ofstead CL, Buro BL, Hopkins KM, Eiland JE. The impact of continuous electrical microcurrent on acute and hard-to-heal wounds: a systematic review. J Wound Care. 2020;29(Sup7):S6-S15.
Goodall RJ, Langridge B, Lane T, Davies AH, Shalhoub J. A Narrative Review of the Use of Neuromuscular Electrical Stimulation in Individuals With Diabetic Foot Ulceration. Int J Low Extrem Wounds. 2020;19(3):242-250. PubMed
Chen Z, Chen ZY, Liu WH, Li GS. Electric Stimulation as an Effective Adjunctive Therapy for Diabetic Foot Ulcer: A Meta-analysis of Randomized Controlled Trials. Adv Skin Wound Care. 2020;33(11):608-612. PubMed
Arora M, Harvey LA, Glinsky JV, et al. Electrical stimulation for treating pressure ulcers. Cochrane Database Syst Rev. 2020;1:CD012196. PubMed
Girgis B, Duarte JA. High Voltage Monophasic Pulsed Current (HVMPC) for stage II-IV pressure ulcer healing. A systematic review and meta-analysis. J Tissue Viability. 2018;27(4):274-284. PubMed
Randomized Controlled Trials
Zulbaran-Rojas A, Park C, El-Refaei N, Lepow B, Najafi B. Home-Based Electrical Stimulation to Accelerate Wound Healing-A Double-Blinded Randomized Control Trial. J Diabetes Sci Technol. 2023;17(1):15-24. PubMed
Bull RH, Clements D, Collarte AJ, Harding KG. The impact of a new intervention for venous leg ulcers: A within-patient controlled trial. Int Wound J. 2023 Feb 13. PubMed
Zhao Y, Zhang B, Wang Y, Liu J. Effectiveness of Neuromuscular Electrical Stimulation for Enhanced Recovery After Total Hip Replacement Surgery: A Randomized Controlled Trial. Geriatr Orthop Surg Rehabil. 2022;13:21514593221129528. PubMed
Yoshikawa Y, Hiramatsu T, Sugimoto M, Uemura M, Mori Y, Ichibori R. Efficacy of Low-frequency Monophasic Pulsed Microcurrent Stimulation Therapy in Undermining Pressure Injury: A Double-blind Crossover-controlled Study. Prog Rehabil Med. 2022;7:20220045. PubMed
Elfahl AM, Abd El Baky AM, Yousef MT, Elgohary HM. High Versus Low Frequency Transcutaneous Electric Nerve Stimulation On Chronic Venous Lower Limb Ulceration Randomized Controlled Trial. Int J Low Extrem Wounds. 2022:15347346221093860. PubMed
Avendano-Coy J, Martin-Espinosa NM, Ladrinan-Maestro A, Gomez-Soriano J, Suarez-Miranda MI, Lopez-Munoz P. Effectiveness of Microcurrent Therapy for Treating Pressure Ulcers in Older People: A Double-Blind, Controlled, Randomized Clinical Trial. Int J Environ Res Public Health. 2022;19(16):15. PubMed
Miguel MMV, Mathias-Santamaria IF, Rossato A, et al. Microcurrent electrotherapy improves palatal wound healing: Randomized clinical trial. J Periodontol. 2021;92(2):244-253. PubMed
Aquil S, Sharma H, Alharbi B, Pacoli K, Luke PP, Sener A. The impact of a muscle pump activator on incisional wound healing compared to standard stockings and compression devices in kidney and kidney-pancreas transplant recipients: A randomized controlled trial. Can Urol Assoc J. 2019;13(11):E341-E349. PubMed
Guidelines and Recommendations (Unclear Methods or No Specific Recommendation Regarding Electrostimulation)
Foundations of Best Practice for Skin and Wound Management. Wounds Canada. 2018. https://www.woundscanada.ca/health-care-professional/publications/dfc-2. Accessed 2023 Jun 2.
Additional References (Outside of Date Range)
Electrical Stimulation for Pressure Injuries. Toronto (ON): Health Quality Ontario. 2017. https://www.hqontario.ca/evidence-to-improve-care/health-technology-assessment/reviews-and-recommendations/electrical-stimulation-for-pressure-injuries. Assessed 2023 Jun 3.
Contributors: Chris Kamel, Calvin Young, Elizabeth Carson
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca