CADTH Health Technology Review
Riluzole for Amyotrophic Lateral Sclerosis Treatment
Rapid Review
Authors: Zahra Jafari, Quenby Mahood, Angie Hamson
Acknowledgement
Many thanks to patient contributor Scott Williams for his time and energy and for sharing his lived experiences and perspectives. His contribution was invaluable.
Abbreviations
AE
adverse event
ALS
amyotrophic lateral sclerosis
ALSFRS
Amyotrophic Lateral Sclerosis Functional Rating Scale
ALSFRS-R
Amyotrophic Lateral Sclerosis Functional Rating Scale-Revised
EC
expert consensus
EFNS
European Federation of Neurological Associations
FT9
Fine’til 9
HR
hazard ratio
MA
meta-analysis
QALY
quality-adjusted life-year
QoL
quality of life
RC
recurring cost
RCT
randomized controlled trial
RoB
risk of bias
SR
systematic review
TC
transition and/or “tollgate” cost
Key Messages
Treatment with riluzole may provide clinical benefits for patients with amyotrophic lateral sclerosis, including longer survival time, reduced risk of disease progression, and minor reversible adverse events, compared to no treatment with riluzole or a placebo.
We did not find any studies meeting our selection criteria on the clinical effectiveness of riluzole for patients with amyotrophic lateral sclerosis compared to alternative pharmacological therapies.
Riluzole may be cost-effective at generic drug costs for patients with amyotrophic lateral sclerosis. Evidence supporting this finding is limited, and further research is required to inform decision-making.
Riluzole is recommended for the treatment of amyotrophic lateral sclerosis, except for patients with progressive muscular atrophy, primary lateral sclerosis, or hereditary spastic paraplegia, and should be initiated promptly following disease diagnosis.
A patient with lived experience of riluzole treatment for amyotrophic lateral sclerosis was involved in this report. They identified outcomes that are important to patients, including slowing the progression of amyotrophic lateral sclerosis and minimal side effects from the medication.
Context and Policy Issues
Roughly 1,000 individuals in Canada receive a diagnosis of amyotrophic lateral sclerosis (ALS) annually.1 At any time, around 2,500 to 3,000 people live with this disease in Canada. ALS is a fatal neurodegenerative disease characterized by the progressive degeneration of upper and lower motor neurons.2,3 Clinical features of ALS include limb paralysis, muscle atrophy, difficulty speaking or swallowing, shortness of breath, respiratory failure, and weakness.3 The most common presentation involves limb onset, with about 70% of patients experiencing extremity weakness and mobility impairment.2 Bulbar onset with oropharyngeal muscle involvement affecting swallowing and speech is observed in 25% of patients.2 In addition to motor impairment, up to 50% of patients may experience cognitive or behavioural impairments due to degeneration in the frontal and temporal lobes.2,4 Over time, strength progressively declines, and patients typically die from respiratory failure within 5 years of diagnosis.2 Despite an increase in research publications in recent years, treatment options for ALS remain limited, and patient care is primarily focused on symptom management and improving function and quality of life (QoL).2,5 Ventilation via a tracheostomy may be suitable for patients with ALS. It is estimated that less than 10% of those with ALS receive life-prolonging ventilation via a tracheostomy, specifically those who desire life-prolonging treatment.6 According to a study published in 2014 on the economic burden of ALS in Canada, the expenses associated with symptom management and care encompass both direct and indirect costs. Direct costs consist of expenditures on equipment, home renovations, medication, aids, and medical services. Indirect costs, on the other hand, include income loss, early retirement, and caregiver absence. The average annual direct and indirect costs per patient reported in this study were $32,337 (with 61% being out-of-pocket expenses) and $56,821, respectively.7 However, the average expenses for caring for a single person with ALS have also been reported to range from $150,000 to $250,000.1
Riluzole, a glutamatergic antagonist, is a disease-modifying treatment shown to extend survival time in ALS,8 demonstrating reduced mortality9 and improved survival time10 in past studies. A Health Canada Notice of Compliance (dated April 27, 2022) exists for riluzole for patients with ALS.11 According to the product monograph, based on evidence from older clinical trials (last updated July 9, 2012),12 riluzole is not a cure for ALS, but represents an initial step toward prolonging survival time.13 The recommended dosage for achieving a survival benefit, as observed in clinical trials, is 50 mg every 12 hours. There was limited experience with riluzole overdose in humans, but neurologic and psychiatric symptoms have been reported as side effects in isolated cases.13
The purpose of this report is to summarize and critically appraise recent available evidence (including observational studies) on the clinical effectiveness and cost-effectiveness of riluzole for patients living with ALS, as well as to summarize evidence-based guidelines regarding the use of riluzole for the treatment of ALS. A current understanding of the clinical effectiveness and cost-effectiveness of riluzole and guidelines for its use may contribute to informed decision-making, particularly in light of the emerging adjunctive and alternative drugs for ALS currently under development.
Research Questions
What is the clinical effectiveness of riluzole for patients living with ALS compared to alternative pharmacological therapies?
What is the clinical effectiveness of riluzole for patients living with ALS compared to no treatment?
What is the cost-effectiveness of riluzole for patients living with ALS?
What are the evidence-based guidelines regarding the use of riluzole for the treatment of patients with ALS?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources, including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, and a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were riluzole (Rilutek) and amyotrophic lateral sclerosis. Comments, newspaper articles, editorials, letters, and conference abstracts were excluded. Retrieval was limited to the human population. The search was completed on May 5, 2023, and limited to English-language documents published since January 2011. This time frame was chosen as a Cochrane systematic review was published with a literature search completed in 2011.14
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Patients of any age living with ALS |
Intervention | Riluzole (any dose) |
Comparator | Q1 and Q3: Any alternative pharmacological therapy (e.g., AMX0035, oral or IV edaravone) Q2 and Q3: Placebo, no treatment (e.g., before and after comparison) Q4: Not applicable |
Outcomes | Q1 and Q2: Clinical benefits (e.g., disease progression, health-related quality of life measures, patient satisfaction, Amyotrophic Lateral Sclerosis Functional Rating Scale, survival) and harms (e.g., treatment-related adverse events) Q3: Cost-effectiveness (e.g., cost per QALY gained, ICER) Q4: Recommendations regarding the best use of riluzole for the treatment of patients living with ALS (e.g., recommended dose, treatment settings, treatment delivery, patient populations of interest) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies, economic evaluations, evidence-based guidelines |
ALS = amyotrophic lateral sclerosis; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before January 1, 2011.
Critical Appraisal of Individual Studies
One reviewer critically appraised the included studies. The critical appraisal tools used were a Measurement Tool to Assess Systematic Reviews (AMSTAR-2)15 for systematic review (SRs) and meta-analyses (MAs), the Downs and Black checklist16 for randomized controlled trials (RCTs), the Drummond checklist17 for economic evaluations, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument18 for guidelines. Summary scores were not calculated for the studies; rather, the strengths and limitations observed among the included studies were summarized and described narratively in Appendix 3.
Patient Engagement
CADTH has adopted the CADTH Framework for Patient Engagement in Health Technology Assessment,19 which includes standards for patient involvement in individual health technology assessments and is used to support and guide CADTH activities involving patients. For this report, CADTH engaged a patient contributor with lived experience with riluzole treatment for ALS.
Invitation to Participate and Consent
CADTH reached out to a patient advocacy group that supports people living with ALS. The preliminary engagement request included an overview of this project, the purpose of engagement, and the nature of engagement activities. An interested individual was identified, and the CADTH Patient Engagement Officer obtained the person’s informed consent to share with CADTH staff their lived experiences with ALS and the use of riluzole.
Engagement Activities
An individual contributor shared their personal experiences via video call during the drafting of the report. Patient perspectives gained through engagement processes were used to understand the relevance of reported outcomes in identified clinical effectiveness studies and to provide insights, background, and context to help inform the conclusion section.
Patient involvement was reported using the Guidance for Reporting Involvement of Patients and the Public (version 2) Short-Form reporting checklist20 (Table 22 in Appendix 6).
Summary of Evidence
Quantity of Research Available
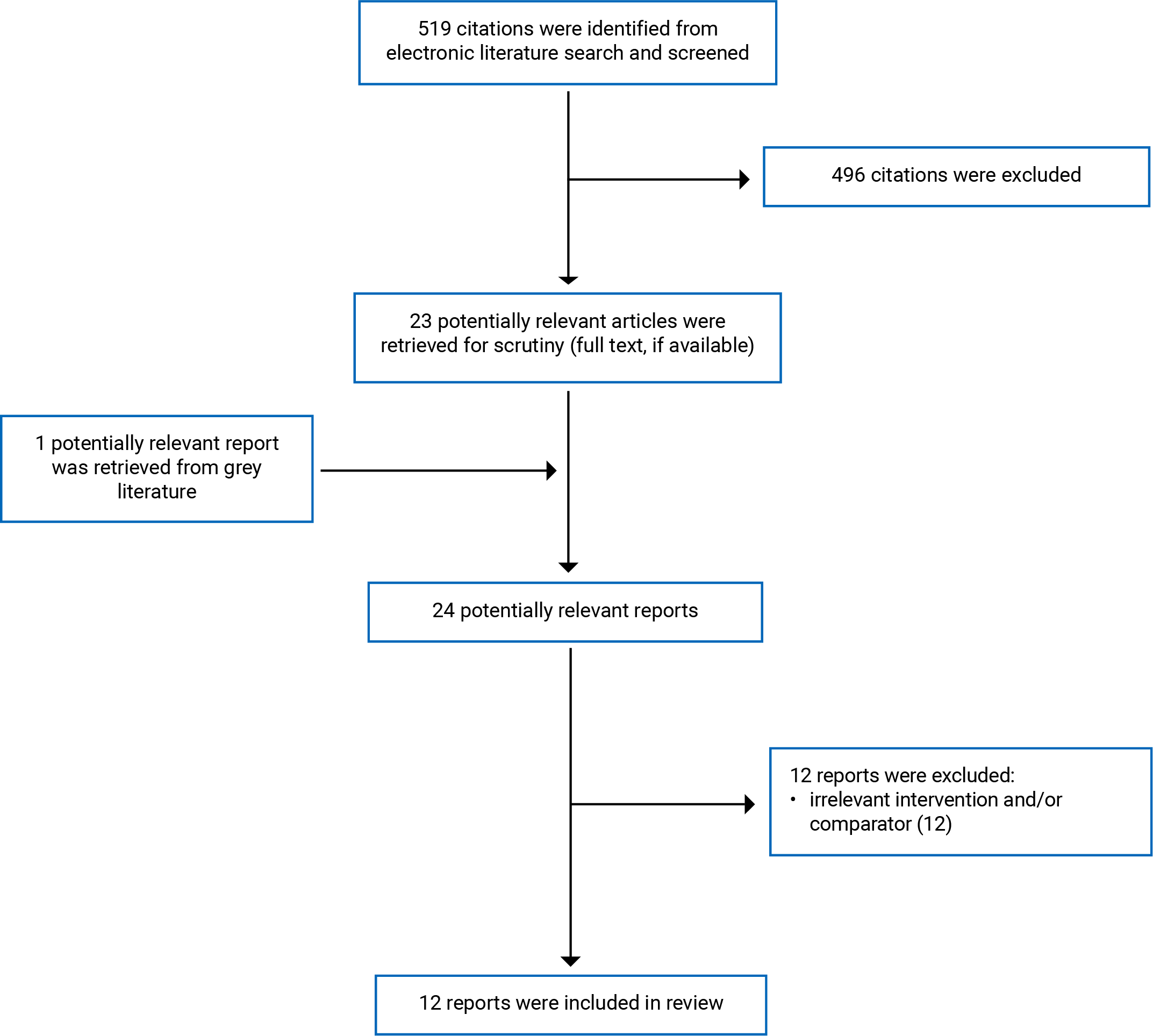
A total of 519 citations were identified in the literature search. Following the screening of titles and abstracts, 496 citations were excluded and 23 potentially relevant articles from the electronic search were retrieved for full-text review. One potentially relevant publication was identified from the grey literature search for full-text reviews. Of these 24 potentially relevant articles, 12 were excluded because of the irrelevant intervention and/or comparator, and 122-5,14,21-27 met the selection criteria and were included in this report.
Appendix 1 presents the PRISMA28 flow chart of the study selection. Additional references of potential interest are provided in Appendix 5.
Summary of the Study Characteristics
Twelve peer-reviewed publications, including 1 SR with MA,14 8 observational studies,3-5,21-25 1 economic evaluation (i.e., cost-effectiveness study),27 and 2 guidelines2,26 were included in this report.
Additional details regarding the characteristics of the included publications are provided in Appendix 2 (Table 2, Table 3, Table 4, and Table 5).
Study Design
Of the 12 peer-reviewed publications that met the selection criteria for this report, 8 were observational studies3-5,21-25 (including 5 retrospective studies,4,21-25 2 prospective observational trials,3,5 and 1 analysis of a placebo RCT3) comparing patients who received riluzole with patients who did not receive riluzole or who received a placebo. The other 4 publications were 1 SR of RCTs with MA (search date from the databases’ inception to April 2011),14 1 cost-utility analysis,27 and 2 guidelines.2,26 For the study with cost-utility analysis, costs were quantified based on the health care sector and societal perspectives, and 5-year and 10-year time horizons were examined. A total of 4 reference case models were provided, representing the health care sector and societal perspectives at 5 years and 10 years. The cost-effectiveness threshold was set at $100,000 per quality-adjusted life-year (QALY) gained in the US context.27
Country of Origin
The authors of 1 SR with MA,14 1 economic evaluation,27 and 2 guidelines2,26 were based in the US,14,27 Sweden,26 and Canada.2 Eight observational studies3-5,21-25 were conducted in the US,21 UK,4 Iran,5 China,3 Austria,25 Taiwan,23 and Italy.24
Patient Population
In 1 SR with MA14 on patients who were diagnosed with ALS, of the 4 RCTs included, 1 study involved adults aged older than 75 years.29 The age range in other studies and the sex ratio in all included studies were not reported.
All 8 primary studies3-5,21-25 were carried out on male and female adults with a probable or definite ALS diagnosis. The studies had variable patient inclusion criteria related to age,21,22 riluzole use,3-5,21-25 Amyotrophic Lateral Sclerosis Functional Rating Scale (ALSFRS) score at baseline,21,22 and time from onset to enrolment.21,22 The exclusion criteria were not reported in the studies.
In 1 economic evaluation study,27 a cost-utility analysis was conducted on the information of patients with ALS treated with riluzole in the authors’ institution.
Both guidelines2,26 included in this report were focused on patients diagnosed with ALS.
Interventions and Comparators
In 1 SR with MA,14 the intervention and comparator were treatment with oral riluzole and a placebo, respectively.
In all 8 primary studies,3-5,21-25 the intervention was riluzole and the comparators were no treatment with riluzole3,5,21-25 or a placebo.4
In the economic evaluation study,27 the intervention was riluzole and the comparator was usual supportive care for ALS, without riluzole use.
In the revised guideline of the European Federation of Neurological Associations (EFNS) on the clinical management of ALS,26 among a wide range of controlled therapeutic interventions, riluzole was the drug intervention relevant to this report. In the guideline on Canadian best practice recommendations for the management of ALS, among a variety of interventions included in the guideline (such as disease-modifying therapies; multidisciplinary care; respiratory management; nutritional management; medication alignment; interventions to manage venous thromboembolism, difficulty speaking, and other symptoms; exercise; cognition and behaviour management interventions; caregiver support, and palliative care), riluzole was 1 of the disease-modifying therapies relevant to this report.2
Outcomes
In 1 SR and MA,14 the primary outcome was a pooled hazard ratio (HR) based on percent mortality (or tracheostomy) for riluzole versus a placebo over all time points up to 12 months. Secondary outcomes were survival at 12 months and muscle strength and function evaluated by modified Norris Scales and adverse events (AE).
Outcome measures reported in the primary studies were survival rate,4,21,23-25 stage-specific risk of progression based on King and Fine’til 9 (FT9) staging methods,22 long-term (e.g., ranged from 36 months21 to 200 months3,25) riluzole effectiveness based on ALSFRS,3 and QoL using the ALS Assessment Questionnaire (ALSAQ-40).5
The ALSAQ-40 is a 40-item questionnaire, specifically designed to evaluate QoL in patients with ALS. The questionnaire contains 40 items divided into 5 sections, representing 5 distinct areas of health: mobility (10 items), activities of daily living (10 items), eating and drinking (3 items), communication (7 items), and emotional functioning (10 items). The questions refer to the patient’s condition during the past 2 weeks and the answers are given on a 5-point Likert scale, providing a summary score from 0 (best health status) to 100 (worst health status).30
In the economic evaluation study,27 the primary outcome was to examine the cost-effectiveness of riluzole in the treatment of ALS in regard to recent advances in disease staging and understanding of stage-specific drug effects. The authors used the FT9 staging method of ALS for estimating costs and utilities, and health states were described using the 3-Level EQ-5D.
Costs at 2018 prices obtained at the author’s institution from patients with ALS were disaggregated into recurring costs (RCs) and “one-off” transition and/or “tollgate” costs (TCs). Distributions of transition probabilities and utility weights were informed by direct estimation, whereas lognormal distributions were used for stage-specific RCs and TCs.
In the revised report of the EFNS task force on the clinical management of ALS,31 updating EFNS’s guidelines on the clinical management of ALS and identifying areas for further research were the main outcomes. In the guideline on Canadian best practice recommendations for the management of ALS,2 the primary outcome was to summarize best practice recommendations for the care and management of patients living with ALS in Canada, including all stages of the disease. This guideline aimed to establish a national standard to improve the quality of care for patients, families, and caregivers living with ALS.
Summary of the Critical Appraisal
Systematic Reviews
Of the 12 studies included in this report, 1 was an SR with MA to examine the efficacy of riluzole in prolonging survival, in delaying the use of tracheostomy to sustain survival, and to assess the efficacy of riluzole upon functional health.14 We used the a Measurement Tool to Assess Systematic Reviews (AMSTAR-2) checklist15 to evaluate the quality of the SR and determine whether the most important elements of the SR methodology were reported (Table 6).
The strengths of the SR were in defining the research question and inclusion and exclusion criteria, describing the study design of the selected primary studies, using a comprehensive literature search strategy, conducting study selection and data extraction in duplicate, using a satisfactory tool for assessing the risk of bias (RoB) in primary studies (based on the Cochrane Handbook for Systematic Reviews of Interventions) and reporting potential sources of conflict of interest. The methods for data synthesis to evaluate the time-to-tracheostomy primary outcome, which involved pooling weighted average HRs for each primary study, were appropriate. The authors applied life table methods to obtain summary survival curves for combined treated and combined control participants across different studies and doses, and the median survival for treated and control participants was estimated by interpolation from the survival curves. However, the SR did not include an explicit statement showing that the systematic search protocol was established before the conduct of the review and did not provide a list of excluded studies and justify the exclusions. The authors also did not describe the selected primary studies in detail, investigate publication bias (small study bias) in individual studies, and discuss its potential impact on the results of MA. Thus, the potential impact of studies with low sample sizes (which could result in more extreme treatment effects)32 on the findings was unclear. In addition, the SR did not report the sources of funding for the primary studies included in the review. Sources of funding for included primary studies are important for understanding the extent to which these may contribute to RoB in the findings, and the interpretation of their results (e.g., studies funded by private industry are at a higher RoB in favour of the intervention under study33).
Primary Studies
The Downs and Black Checklist used for critical appraisal of the included primary studies consists of 5 sections (Table 7): reporting, external validity, internal validity, confounding, and power. In the following paragraphs, the strengths and weaknesses of the included primary studies are described for each of the 5 sections.
Reporting: The items clearly described or reported in the 8 observational, nonrandomized studies3 to 5,21 to 25 (i.e., 5 retrospective studies,4,21-25 2 prospective observational trials,3,5 and 1 analysis of a placebo RCT3) included in this report were study objectives, characteristics of the patients (except 1 study5), interventions, estimated random variability in data for main outcomes (except 1 study25), actual P values for the main outcomes (except 1 study5), and characteristics of patients lost to follow-up. The main findings were not clearly described in 4 studies,4,5,21,22 and the distribution of potential confounders (e.g., sex, age, and disease characteristics) were not reported in 5 studies.3-5,23
External validity: Staff, places, and facilities described in the studies were representative of the procedures provided to patients, and funding sources were reported in most studies (except 3 studies).5,23,24 The primary studies included in this report were unclear if the patients who were asked to participate in the studies were representative of the entire population recruited (i.e., poor reporting of the source of the population).
Internal validity: The main outcome measures and statistical tests used for data analysis were clearly described in the studies (except for the unclear appropriateness of analyses in 2 studies).5,23 However, the studies did not report any information about adherence to medications. Thus, the number of patients who did not follow the prescribed regimen was unknown.
Confounding: In all studies it was unclear if losses of patients to follow-up were considered in statistical analyses, and it was unclear in most studies3-5,22,24 whether statistical analyses were adequately adjusted for potential confounding factors.
Power: Sample size and power calculation were not reported in the studies, and it was unclear if they were sufficiently powered to detect clinically significant effects, such as the survival advantage of riluzole in later stages of the disease25 and its impact on QoL.5
Additional details regarding the strengths and limitations of the included publications are summarized in Appendix 3.
Economic Evaluation
The 36-item Drummond checklist17 (Table 8) was used for critical appraisal of 1 study on the cost-effectiveness of riluzole for ALS included in this report.27 The areas questioned in the reporting checklist are related to the research question, description of the study and intervention, study design, measurements, valuation of costs and consequences, potential discounting, incremental analysis, presentation of results with uncertainty and sensitivity analyses, and discussion of results in the context of policy relevance and existing literature. The authors used appropriate self-reported measures of patients’ physical function (specifically, ALSFRS-Revised [ALSFR-R] scores) and QoL (EQ-5D scores) over time, along with the FT9 staging of ALS, to estimate costs and utilities using Markov models. The time horizons considered for these estimates were 5 years and 10 years, and the main model assumptions appeared to be appropriate;27 however, they did not provide adequate details of the patients from whom valuations were obtained, and productivity changes and their relevance to the study question. Productivity changes (losses) may contribute to a large proportion of costs of health conditions in an economic evaluation from a societal perspective,34 and using an appropriate methodology for measuring and valuing these productivity costs is essential.35 However, there is currently a lack of methodological consensus on how productivity losses should be measured and valued.34
Guidelines
The Appraisal of Guidelines for Research and Evaluation (AGREE) II Reporting Checklist18 (Table 9) was used for the critical appraisal of the 2 guidelines2,26 included in this report. The checklist is a tool to improve the completeness of reporting in clinical practice guidelines and is intended to provide guidance to guideline developers, guideline users, guideline funders, peer reviewers, and journal editors about the essential components of a high-quality practice guideline.36 The checklist entails 6 quality domains (scope and purpose, stakeholder involvement, rigour and development, clarity of presentation, applicability, and editorial independence) and 23 key items.36 The areas clearly described or reported in the 2 guidelines2,26 were overall objectives; main questions; target patients; the guideline development groups, including individuals from relevant health care professionals; the target users of the guidelines; the methods for formulating the recommendations; and the consideration of health benefits, side effects, and risks in formulating the recommendations. In both guidelines, key recommendations were easily identifiable, recommendations were specific and unambiguous, and different options for the management of patients with ALS were clearly presented. In addition, both guidelines included statements demonstrating that the views of the funding bodies have not influenced the content of the guideline, and competing interests of guideline development group members were mentioned. However, facilitators and barriers to the applications and monitoring and/or auditing criteria were the areas not covered in the guidelines. In the guideline developed by Shoesmith et al. (2020),2 it was unclear if a systematic method was used to search for evidence, and both guidelines were uncertain if the views of patients with ALS were sought. The guideline developed by Andersen et al. (2012)26 was unclear in several aspects, such as explaining how the quality of evidence supporting the recommendations was assessed and providing a link between the recommendations and their supporting evidence to ensure transparency and support the credibility of the recommendations. In addition, the guideline did not specify a procedure for updating its recommendations and did not indicate whether it underwent external expert review before publication. External review by subject matter experts is important to ensure the guideline’s rigour, accuracy, and relevance to the field.37
Summary of Findings
We identified 12 studies, including 1 SR with MA14 and 8 observational studies3-5,21-25 (5 retrospective studies,4,21-25 2 prospective observational trials,3,5 and 1 analysis of a placebo RCT3) on the clinical effectiveness of riluzole for patients with ALS, 1 study27 on the cost-effectiveness of riluzole for patients with ALS, and 2 evidence-based guidelines2,26 regarding the use of riluzole for the treatment of patients with ALS.
Appendix 4 presents the main outcomes of the included studies.
Clinical Effectiveness of Riluzole for Patients With ALS
Tracheostomy-Free Survival
In 1 SR with MA14 that reported pooled HRs, riluzole 100 mg per day was associated with a 9% gain in the probability of 1-year tracheostomy-free survival (49% in the placebo group and 58% in the riluzole group) and increased median tracheostomy-free survival from 11.8 months to 14.8 months compared to a placebo (Table 10). Improved survival time from disease onset to death or tracheostomy was not statistically significant in the Georgoulopoulou et al. (2013) study (Table 14).24
Survival
In the SR with MA,14 the pooled HR of mortality at 12 months with riluzole 100 mg was lower in patients who received riluzole than in those who received placebo. In the Thakore et al. (2022) study,21 median survival was significantly longer (i.e., 2 months) in patients treated with riluzole than in patients who did not receive riluzole, and 1-year treatment was associated with improved median survival by 1.9 months (Table 11). In the Georgoulopoulou et al. (2013) study,24 a significantly longer median survival time from onset to death (43 months versus 31 months) was reported in patients receiving riluzole than in patients not receiving riluzole (Table 14). A higher survival time23 (Table 13) and a survival advantage only for the initial treatment period or the early stage of the disease25 (Table 12) compared to no treatment with riluzole were reported in 2 other studies. In summary, the identified studies all reported a survival advantage for patients who received treatment with riluzole compared with those who did not.
Stage-Specific Risk of Progression
In the Thakore et al. (2020) study,22 adjustments were made for age and ALSFRS-R slope at the initial visit, and the probability of progression (represented by the transition from early to late stages and death based on the King and FT9 staging methods) with and without riluzole was evaluated. The reported HRs for both staging methods suggested the effectiveness of riluzole in reducing the risk of transitioning between different stages of ALS; however, the statistical significance of these findings was not reported (Table 15). Likewise, in the Fang et al. (2018) study,4 the time at stage 4 was significantly longer for patients receiving riluzole than for those receiving a placebo (Table 16).
Function and Muscle Strength
In 1 SR with MA,14 there was a small beneficial effect (i.e., a statistically significantly slower rate of decline) for riluzole versus a placebo on both bulbar and limb function (Table 10), but not on muscle strength (mean difference for rate of decline of muscle strength = −1.88; 95% confidence interval, −5.79 to 2.03).
Functional ability rated by ALSFRS and ALSFRS-R in 1 study3 showed significantly higher scores, which represented better functional ability, in patients treated with riluzole compared to patients not treated with riluzole (Table 17).
Adverse Events
In 1 SR with MA,14 there were increases in a few nonserious AEs (i.e., nausea, asthenia, and a 3-fold increase in serum alanine transferase), which were mostly reversible after stopping the drug (Table 10).
Quality of Life
QoL was assessed in 1 study5 in which no significant differences were found between patients treated with riluzole and patients not treated with riluzole from baseline to 12 months (Table 18).
Cost-Effectiveness of Riluzole for Patients With ALS
In the economic evaluation study,27 from the health care sector perspective at the 5-year horizon, riluzole use contributed to 0.182 QALY gained at a cost difference of $12,348 ($5,403 riluzole cost; $8,870 RC and –$1,925 TC differences), demonstrating an incremental cost-effectiveness ratio of $67,658 per QALY. The study findings supported the cost-effectiveness of riluzole to treat ALS at the $100,000 per QALY threshold at generic drug costs (Table 19), and a conclusion of cost-effectiveness was maintained for analyses with a 10-year time horizon and from the societal perspective. Table 20 demonstrates the health state utility weights and costs (in dollars per month) by stage reported in this study.
Guidelines Regarding Riluzole Use for Patients With ALS
The authors of the 2 guidelines included in this report recommend that (Table 21):
Patients with ALS should be offered treatment with riluzole 50 mg twice daily (based on evidence from RCTs), except for patients with progressive muscular atrophy, primary lateral sclerosis, or hereditary spastic paraplegia (based on expert consensus [EC]).26
Treatment with riluzole is recommended soon after the diagnosis of ALS (based on EC), given its effectiveness in enhancing survival time by a median duration of 3 months.2
Patients taking riluzole should be monitored for AEs (based on EC). In cases where patients experience fatigue while taking riluzole, the consideration of reducing or discontinuing the medication may be appropriate (based on EC and evidence from observational, nonrandomized studies).2
Limitations
The primary studies3-5,21-25 included in this report were at RoB from several aspects, such as not reporting the distribution of potential confounders (e.g., sex, age, and disease characteristics),3-5,23,27 compliance with the medications (riluzole), if losses of patients to follow-up were considered in statistical analyses,3-5,21-25 if the statistical analyses were adequately adjusted for potential confounding factors,3-5,22,24,27 and if statistical analyses were sufficiently powered to detect clinically significant effects. We did not find any studies that compare riluzole’s clinical effectiveness with alternative pharmacological drugs in patients with ALS.
In terms of the cost-effectiveness of riluzole for ALS, we did not identify any Canadian economic analyses that met the inclusion criteria for this review. In addition, the cost evaluation study included in this report27 was based on US health care perspectives, and the relevance of the information reported in this study to the Canadian health care system is unclear.
Conclusions and Implications for Decision- or Policy-Making
We reviewed a total of 9 studies (1 SR with MA14 and 8 primary studies3-5,21-25) on the clinical effectiveness of riluzole in patients with ALS compared to those not receiving riluzole3,21-25 or those who received a placebo.4,5,14 According to the SR with MA published in 2012,14 riluzole 100 mg was associated with 3 months longer median tracheostomy-free survival time than a placebo. Additionally, 6 studies published between 2013 and 2022 reported improved survival time21,23-25 and reduced risk of disease progression at different stages4,22 in patients treated with riluzole compared to those not receiving treatment22 or receiving a placebo.4
The SR and MA included in this report14 found that the AEs associated with riluzole were generally minor and reversible, such as nausea, asthenia, and an increase in serum alanine transferase. In addition, CADTH sought input from 1 patient with lived experience of early treatment with riluzole, who identified slowing disease progression and minimal side effects as priority outcomes for ALS treatment, which were aligned with the findings reported in this review.
Regarding functional ability, limited evidence suggests a small beneficial effect of riluzole compared to placebo on both bulbar and limb function,14 as well as improved functional ability compared to no treatment.3 In addition, we identified 1 study that reported no significant difference in QoL between treatment with riluzole and a placebo.5
We did not find any studies on the clinical effectiveness of riluzole for patients with ALS compared to alternative pharmacological therapies.
The findings of 1 economic evaluation study published in 202027 showed riluzole’s cost-effectiveness to treat ALS at the $100,000 per QALY threshold at generic drug cost, from a US health care system perspective.
According to 2 evidence-based guidelines,2,26 treatment with riluzole (50 mg twice daily) is recommended to treat ALS and should be initiated upon diagnosis,2,26 except for patients with progressive muscular atrophy, primary lateral sclerosis, or hereditary spastic paraplegia.26 While the guidelines did not comment on treatment delivery or implementation considerations in detail, the patient contributor to this report expressed a preference for the oral medication form due to its convenience (compared to infusions). The patient also highlighted potential barriers to access, such as the risk of losing medication access when requiring full-time continuous positive airway pressure (CPAP) therapy due to declining health.
The findings of the studies included in this report support the clinical effectiveness (i.e., longer survival time; reduced risk of disease progression; and minor, reversible AEs) of riluzole versus no treatment or a placebo for patients with ALS and suggest early treatment soon after disease diagnosis. Also, riluzole might be cost-effective at generic drug costs,27 though additional economic evaluation studies from a Canadian health care perspective are required to reach firm conclusions about the cost-effectiveness of riluzole for ALS and to facilitate informed decision-making. Furthermore, it is important to note that there are ongoing trials investigating the use of add-on drugs in conjunction with riluzole (Appendix 5) that have the potential to influence the role of riluzole in the treatment approach for ALS in the future. These additional interventions and the ongoing research highlight the dynamic nature of ALS treatment and the possibility of evolving treatment strategies beyond riluzole monotherapy.
References
1.Amyotrophic Lateral Sclerosis Society of Canada. New Canadian investments in ALS research reflect growing knowledge about the disease and increasing likelihood of effective treatments being developed. Toronto (ON): ALS Society of Canada; 2016 Nov 23: https://als.ca/blogs/new-canadian-investments-als-research-reflect-growing-knowledge-disease-increasing-likelihood-effective-treatments-developed/. Accessed 2023 May 25.
2.Shoesmith C, Abrahao A, Benstead T, et al. Canadian best practice recommendations for the management of amyotrophic lateral sclerosis. CMAJ. 2020;16(192). PubMed
3.Chen L, Liu X, Tang L, Zhang N, Fan D. Long-term use of riluzole could improve the prognosis of sporadic amyotrophic lateral sclerosis patients: a real-world cohort study in China. Front Aging Neurosci. 2016;8:246. PubMed
4.Fang T, Al Khleifat A, Meurgey JH, et al. Stage at which riluzole treatment prolongs survival in patients with amyotrophic lateral sclerosis: a retrospective analysis of data from a dose-ranging study. Lancet Neurol. 2018;17(5):416-422. PubMed
5.Shamshiri H, Fatehi F, Abolfazli R, et al. Trends of quality of life changes in amyotrophic lateral sclerosis patients. J Neurol Sci. 2016;368:35-40. PubMed
6.Tysnes OB, Holmøy T, Indrekvam S, Fondenæs O. Ventilation of patients with amyotrophic lateral sclerosis. Tidsskriftet den Norske Legeforening. 2021 May 14: https://tidsskriftet.no/en/2021/05/kronikk/ventilation-patients-amyotrophic-lateral-sclerosis. Accessed 2023 Jun 5.
7.Gladman M, Dharamshi C, Zinman L. Economic burden of amyotrophic lateral sclerosis: a Canadian study of out-of-pocket expenses. Amyotroph Lateral Scler Frontotemporal Degener. 2014;15(5-6):426-432. PubMed
8.Zarate CA, Manji HK. Riluzole in psychiatry: a systematic review of the literature. Expert Opin Drug Metab Toxicol. 2008;4(9):1223-1234. PubMed
9.Bensimon G, Lacomblez L, Meininger V. A controlled trial of riluzole in amyotrophic lateral sclerosis. ALS/Riluzole Study Group. N Engl J Med. 1994;330(9):585-591. PubMed
10.Lacomblez L, Bensimon G, Leigh PN, Guillet P, Meininger V. Dose-ranging study of riluzole in amyotrophic lateral sclerosis. Amyotrophic Lateral Sclerosis/Riluzole Study Group II. Lancet. 1996;347(9013):1425-1431. PubMed
11.Health Canada. Notice of compliance [NOC] information: APO-Riluzole. 2022: https://health-products.canada.ca/noc-ac/nocInfo?no=28030. Accessed 2023 May 18.
12.Health Canada. Product information. APO-Riluzole. 2023: https://health-products.canada.ca/dpd-bdpp/info?lang=eng&code=83784. Accessed 2023 May 18.
13.PrAPO-Riluzole, riluzole tablets, USP, riluzole 50 mg [product monograph]. Toronto (ON): APOTEX INC; 2012: https://pdf.hres.ca/dpd_pm/00017738.PDF. Accessed 2023 May 18.
14.Miller RG, Mitchell JD, Moore DH. Riluzole for amyotrophic lateral sclerosis (ALS)/motor neuron disease (MND). Cochrane Database Syst Rev. 2012;2012(3):CD001447. PubMed
15.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
16.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
17.Higgins JPT, Green S, editors. Figure 15.5.a: Drummond checklist (Drummond 1996). Cochrane handbook for systematic reviews of interventions. London (GB): The Cochrane Collaboration; 2011: http://handbook-5-1.cochrane.org/chapter_15/figure_15_5_a_drummond_checklist_drummond_1996.htm. Accessed 2023 May 18.
18.Agree Next Steps C. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2023 May 18.
19.CADTH framework for patient engagement in health technology assessment. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/cadth-framework-patient-engagement-health-technology-assessment. Accessed 2023 May 26.
20.Staniszewska S, Brett J, Simera I, et al. GRIPP2 reporting checklists: tools to improve reporting of patient and public involvement in research. BMJ. 2017;358:j3453. PubMed
21.Thakore NJ, Lapin BR, Mitsumoto H, Pooled Resource Open-Access Als Clinical Trials Consortium. Early initiation of riluzole may improve absolute survival in amyotrophic lateral sclerosis. Muscle Nerve. 2022;66(6):702-708. PubMed
22.Thakore NJ, Lapin BR, Pioro EP. Stage-specific riluzole effect in amyotrophic lateral sclerosis: a retrospective study. Amyotroph Lateral Scler Frontotemporal Degener. 2020;21(1-2):140-143. PubMed
23.Lee CT, Chiu YW, Wang KC, et al. Riluzole and prognostic factors in amyotrophic lateral sclerosis long-term and short-term survival: a population-based study of 1149 cases in Taiwan. J Epidemiol. 2013;23(1):35-40. PubMed
24.Georgoulopoulou E, Fini N, Vinceti M, et al. The impact of clinical factors, riluzole and therapeutic interventions on ALS survival: a population based study in Modena, Italy. Amyotroph Lateral Scler Frontotemporal Degener. 2013;14(5-6):338-345. PubMed
25.Cetin H, Rath J, Fuzi J, et al. Epidemiology of amyotrophic lateral sclerosis and effect of riluzole on disease course. Neuroepidemiology. 2015;44(1):6-15. PubMed
26.Andersen PM, Abrahams S, Borasio GD, et al. EFNS guidelines on the clinical management of amyotrophic lateral sclerosis (MALS): revised report of an EFNS task force. Eur J Neurol. 2012;19(3):360-375. PubMed
27.Thakore NJ, Pioro EP, Udeh BL, Lapin BR, Katzan IL. A cost-effectiveness framework for amyotrophic lateral sclerosis, applied to riluzole. Value Health. 2020;23(12):1543-1551. PubMed
28.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
29.Bensimon G, Lacomblez L, Delumeau JC, Bejuit R, Truffinet P, Meininger V. A study of riluzole in the treatment of advanced stage or elderly patients with amyotrophic lateral sclerosis. J Neurol. 2002;249(5):609-615. PubMed
30.Green C, Kiebert G, Murphy C, et al. Patients' health-related quality-of-life and health state values for motor neurone disease/amyotrophic lateral sclerosis. Qual Life Res. 2003;12(5):565-574. PubMed
31.Shaw JW, Johnson JA, Coons SJ. US valuation of the EQ-5D health states: development and testing of the D1 valuation model. Med Care. 2005;43(3):203-220. PubMed
32.Turner RM, Bird SM, Higgins JP. The impact of study size on meta-analyses: examination of underpowered studies in Cochrane reviews. PLoS One. 2013;8(3):e59202. PubMed
33.Fabbri A, Lai A, Grundy Q, Bero LA. The influence of industry sponsorship on the research agenda: a scoping review. Am J Public Health. 2018;108(11):e9-e16. PubMed
34.Jiang S, Wang Y, Si L, et al. Incorporating productivity loss in health economic evaluations: a review of guidelines and practices worldwide for research agenda in China. BMJ Glob Health. 2022;7(8). PubMed
35.Koopmanschap M, Burdorf A, Jacob K, Meerding WJ, Brouwer W, Severens H. Measuring productivity changes in economic evaluation: setting the research agenda. PharmacoEcon. 2005;23(1):47-54. PubMed
36.AGREE reporting checklist. 2023: https://www.agreetrust.org/resource-centre/agree-reporting-checklist/. Accessed 2023 May 16.
37.Leung L. Validity, reliability, and generalizability in qualitative research. J Family Med Prim Care. 2015;4(3):324-327. PubMed
38.Cedarbaum JM, Stambler N, Malta E, et al. The ALSFRS-R: a revised ALS functional rating scale that incorporates assessments of respiratory function. BDNF ALS Study Group (Phase III). J Neurol Sci. 1999;169(1-2):13-21. PubMed
39.Clinical review report: edaravone (radicava) (Mitsubishi Tanabe Pharma Corporation): indication: for the treatment of Amyotrophic Lateral Sclerosis (ALS). Appendix 4, validity of outcome measures.: Ottawa (ON): CADTH; 2019 https://www.ncbi.nlm.nih.gov/books/NBK542356/. Accessed 2023 Jun 5.
40.Balendra R, Al Khleifat A, Fang T, Al-Chalabi A. A standard operating procedure for King's ALS clinical staging. Amyotroph Lateral Scler Frontotemporal Degener. 2019;20(3-4):159-164. PubMed
41.Bowden CL, Mintz J, Tohen M. Multi-state outcome analysis of treatments (MOAT): application of a new approach to evaluate outcomes in longitudinal studies of bipolar disorder. Mol Psychiatry. 2016;21(2):237-242. PubMed
42.Maverick J. Recurring expenses vs. non-recurring expenses: what's the difference? Investopedia. 2021: https://www.investopedia.com/ask/answers/072815/what-difference-between-recurring-and-nonrecurring-general-and-administrative-expenses.asp. Accessed 2023 Jun 5.
43.Brainin M, Barnes M, Baron JC, et al. Guidance for the preparation of neurological management guidelines by EFNS scientific task forces: revised recommendations 2004. Eur J Neurol. 2004;11(9):577-581. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of the Included Systematic Review
Study citation, country, objective, funding source | Study designs and the number of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Miller et al. (2012)14 US Funding source:
| Design: Systematic review and MA Total studies included: 4 RCTs Total studies relevant to this review: 4 RCTs | Population included: Adults diagnosed with amyotrophic lateral sclerosis Age in all included studies: Older than 75 yrs in 1 study and NR in 3 studies Total number of patients: 1477
Sex: NR Exclusion criteria:
| Interventions included: Riluzole (100 mg) Comparator: Placebo | Outcome measure: Primary outcome: Tracheostomy-free survival over all time points with riluzole vs. placebo Secondary outcome:
Follow-up: 12 months in 4 RCTs included in MA |
MA = meta-analysis; NR = not reported; RCT = randomized controlled trial.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, design, country, funding source | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|
Thakore et al. (2022)21 Design: Retrospective Country: US Funding source: No funding. | Patients with ALS. Number of patients (n), Age in year, mean (SD), range: Total: 4,778, NR, NR
Sex: number of males, n (%) Total: 2,997 (75.44)
Inclusion criteria: Patients with information on
Exclusion criteria: NR | Intervention: Riluzole Comparator: No treatment with riluzole | Outcomes: Survival rate Follow-up: 36 months |
Thakore et al. (2020)22 Design: Retrospective Country: US Funding source: No funding. | Patients with ALS. Number of patients (n), Age in year, mean (SD), range: Total: 1,903, NR, NR
Sex: number of males, n (%) Total: 1,032 (64.74)
Inclusion criteria: Patients with information on
Exclusion criteria: NR | Intervention: Riluzole Comparator: No treatment with riluzole | Outcomes: Stage-specific risk of progression based on King and FT9 (Fine’til 9) staging methods Follow-up: 36 months |
Fang et al. (2018)4 Design: Retrospective analysis of a randomized controlled trial (RCT) Country: UK Funding source: NIHR Maudsley Biomedical Research Centre, The European Union Joint Programme on Neurodegeneration, and the King’s Summer Undergraduate Studentship. | Patients with ALS. Number of patients (n), Age in year, mean (SD), range: Total: 959, NR, NR
Sex: number of males, n (%) NR Inclusion criteria: Patients with probable or definite ALS diagnosis Exclusion criteria: NR | Intervention: Riluzole (100 mg per day) Comparator: Placebo | Outcomes: Survival rate Follow-up: 800 days |
Chen et al. (2016)3 Design: Prospective observational study Country: China Funding source: National Natural Science Foundation of China | Patients with ALS. Number of patients (n), Age in year, mean (SD), range: Total: 1,540, NR, NR
Sex: number of males, n (%) Total: NR
Inclusion criteria:
Exclusion criteria: NR | Intervention: Riluzole (50 mg, twice per day) Comparator: Patients not on riluzole | Outcomes:
Follow-up: Every 3 month follow-up up to 200 months |
Shamshiri et al. (2016)5 Design: Prospective observational study Country: Iran Funding source: NR | Patients with ALS. Number of patients (n), Age in year, mean (SD), range: Total: 132, NR, NR
Sex: number of males, n (%) NR Inclusion criterion: Patients with probable or definite ALS diagnosis Exclusion Criteria: NR | Intervention: Riluzole Comparator: Patients not on riluzole | Outcomes: Quality of life (QoL) assessed by ALS Assessment Questionnaire (ALSAQ-40) Follow-up: 1 year |
Cetin et al. (2015)25 Design: Retrospective Country: Austria Funding source: No funding. | Patients with ALS. Number of patients (n), Age in year, mean (SD), range: Total: 911, 64.50, NR
Sex: number of males, n (%) Total: NR
Inclusion criteria:
Exclusion criteria: Age below 20 years | Intervention: Riluzole (100 mg per day) Comparator: Patients not on riluzole | Outcomes: Survival rate Follow-up: 200 months |
Georgoulopoulou et al. (2013)24 Design: Retrospective Country: Taiwan Funding source: NR | Patients with ALS. Number of patients (n), Age in year, mean (SD), range: Total: 193, NR, NR
Sex: number of males, n (%) Total: 102 (52.84)
Inclusion criteria: Patients diagnosed with ALS Exclusion criteria: NR | Intervention: Riluzole Comparator: Patients not on riluzole | Outcomes: Survival rate Follow-up: 168 months |
Lee et al. (2013)23 Design: Retrospective Country: Taiwan Funding source: NR | Patients with ALS. Number of patients (n), Age in year, mean (SD), range: Total: 1,149, 56.27 (14.15), NR
Sex: number of males, n (%) Total: 715 (62.23)
Inclusion criteria: Patients diagnosed with ALS Exclusion criteria: NR | Intervention: Riluzole (100 mg per day) Comparator: Patients not on riluzole | Outcomes: Survival rate Follow-up: 120 months |
ALS = amyotrophic lateral sclerosis; ALSFRS = amyotrophic lateral sclerosis functional rating scale; ALSFRS-R = revised amyotrophic lateral sclerosis functional rating scale; NR = not reported; SD = standard deviation.
Table 4: Characteristics of the Included Economic Evaluation
Study citation, country, funding source | Type of analysis, time horizon, perspective | Population characteristics | Intervention and comparator(s) | Approach | Source of clinical, cost, and utility data used in the analysis | Main assumptions |
|---|---|---|---|---|---|---|
Thakore et al. (2020)27 US Funding source: Internal NICORE (Neurologic Institute Center for Outcomes Research and Evaluation, Cleveland Clinic) grant | aAnalysis: cost-utility analysis Time horizon: 5 and 10 years Perspective: US Health care sector and societal perspectives with a willingness to pay threshold of USD $100,000 per QALY. | Patients treated with riluzole in a prospective cohort study | Intervention: Riluzole Comparator: Usual supportive care for ALS, without riluzole use. | A cost-effectiveness framework using Markov models with 1 month cycles by FT9a stage (stage 0 to 4) State transition probability matrices were estimated from the Pooled Resource Open-Access ALS Clinical Trials (PRO-ACT) database. | Self-reported measures of patients’ physical function over time (ALSFRS-R) and quality of life (EQ-5D)b were obtained at the authors’ institution from patients with ALS. FT9 staging of ALS was used for the estimation of costs and utilities based on ALSFRS-R dataa Cost inputs included physician, outpatient facility, and home health care costs. | For analyzing treatment cost, the efficacy of all (bioequivalent) formulations of riluzole was assumed to be identical. Because an early diagnosis was unlikely (FT9 stage 0), treatment was assumed to start in FT9 stage 1. |
ALS = amyotrophic lateral sclerosis; ALSFRS-R = revised ALS functional rating scale; EQ-5D = European Quality of Life 5 Dimension scale; FT9 = Fine’til 9; QALY = quality-adjusted life-year.
aFT9 is a novel staging method derived from the revised ALS functional rating scale (ALSFRS-R). It is a widely used 12-question, 5-level instrument comprised of 4 sub-scores (bulbar, fine motor, gross motor, and respiratory; 3 questions each). FT9 counts the number of ALSFRS-R sub-scores that are 9 or less (12 is normal).38
bThe EQ-5D is a brief, multi-attribute, preference-based health status measure. This measure consists of five health dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression), with each dimension specifying either three (EQ-5D-3L) or five levels (EQ-5D-5L) of severity, and is completed by a patient or respondent.31
Table 5: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations for development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
Andersen et al. (2012)26 | ||||||
Intended users: Clinicians Target population: Patients with ALS | Existing management options for ALS Interventions relevant to this report: Riluzole | Updating European Federation of Neurological Associations (EFNS) guidelines on the clinical management of ALS Identifying areas where further research is needed. | A literature search in 14 databases with no constraints on language or publication status. | NR | Recommendations were reached by consensus. Each pair of investigators prepared a written analysis that was communicated and discussed by email with the other members of the task force. A combined draft was then written by the chairman and circulated to the task force for further discussions. All recommendations had to be agreed by all members of the task force unanimously. | NR |
Shoesmith et al. (2020)2 | ||||||
Intended Users: Clinicians, allied health professionals, and primary care providers Target Population: Patients with ALS | Existing management options for ALS Interventions relevant to this report: Riluzole | Outlining best practice recommendations for the care and management of patients living with ALS in Canada, including all stages of the disease. | A literature search in 4 databases. Forty-seven clinical questions were selected based on ranking by experts. | The quality of evidence was orderly classified from 1 to 4 by the working group. | Recommendations were reached by consensus. The working group met regularly at face-to-face meetings and through regular group teleconferences. Each topic group drafted preliminary guideline statements for each clinical question. The draft statements were reviewed by the working group and refined on an iterative basis, ideally until consensus was obtained. There was consensus on all statements and no vote was held. | In the first round, the executive draft summary was reviewed and commented on by the Canadian ALS Research Network (including all multidisciplinary ALS clinics in Canada) and topic experts external to the working group representing gastroenterology, respirology, palliative care, and physiatry. In the second round, key stakeholders within each provincial ALS Society were asked to review and comment on the revised executive draft summary. |
ALS = amyotrophic lateral sclerosis; NR = not reported.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 6: Strengths and Limitations of the Included Systematic Review Using a MeaSurement Tool to Assess Systematic Reviews 2 (AMSTAR 2)15
Checklist’s Items | Miller et al. (2012)14 |
|---|---|
1. Did the research questions and inclusion criteria for the review include the components of PICO? | Yes |
2. Did the report of the review contain an explicit statement that the review methods were established before the conduct of the review and did the report justify any significant deviations from the protocol? | No |
3. Did the review authors explain their selection of the study designs for inclusion in the review? | Yes |
4. Did the review authors use a comprehensive literature search strategy? | Yes |
5. Did the review authors perform study selection in duplicate? | Yes |
6. Did the review authors perform data extraction in duplicate? | Yes |
7. Did the review authors provide a list of excluded studies and justify the exclusions? | No |
8. Did the review authors describe the included studies in adequate detail? | No |
9. Did the review authors use a satisfactory technique for assessing the RoB in individual studies that were included in the review? | Yes |
#10. #Did the review authors report on the sources of funding for the studies included in the review? | No |
11. If meta-analysis was performed did the review authors use appropriate methods for the statistical combination of results? | Yes |
12. If meta-analysis was performed, did the review authors assess the potential impact of RoB in individual studies on the results of the meta-analysis or other evidence synthesis? | Unclear |
13. Did the review authors account for RoB in individual studies when interpreting/ discussing the results of the review? | Yes |
14. Did the review authors provide a satisfactory explanation for, and discussion of, any heterogeneity observed in the results of the review? | Yes |
15. If they performed quantitative synthesis did the review authors carry out an adequate investigation of publication bias (small study bias) and discuss its likely impact on the results of the review? | No |
16. Did the review authors report any potential sources of conflict of interest, including any funding they received for conducting the review? | Yes |
NA = not applicable; PICO = population, intervention, comparator, outcome; RoB = risk of bias.
Table 7: Strengths and Limitations of Primary Clinical Studies Using the Downs and Black Checklist16
Checklist’s Items | Thakore (2022)21 | Thakore (2020)22 | Fang (2018) 4 | Chen (2016)3 | Shamshiri (2016)5 | Cetin (2015)25 | Lee (2013)23 | Georgoulopoulou (2013)24 |
|---|---|---|---|---|---|---|---|---|
1. Is the objective of the study clear? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
2. Are the main outcomes clearly described in the Introduction or Methods? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No |
3. Are the characteristics of the patients included in the study clearly described? | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes |
4. Are the interventions clearly described? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
5. Are the distributions of principal confounders in each group of subjects clearly described? | No | No | No | No | No | No | No | No |
6. Are the main findings of the study clearly described? | No | No | No | Yes | No | Yes | Yes | Yes |
7. Does the study estimate random variability in data for main outcomes? | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes |
8. Have all the important adverse events consequential to the intervention been reported? | No | No | No | No | No | No | No | No |
9. Have characteristics of patients lost to follow-up been described? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
10. Have actual P values been reported for the main outcomes except for probability < 0.001? | Yes | Partially | Yes | Yes | No | Yes | Yes | Partially |
11. Is the source of funding clearly stated? | Yes | Yes | Yes | Yes | No | Yes | No | No |
12. Were subjects who were asked to participate in the study representative of the entire population recruited? | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
13. Were those subjects who were prepared to participate representative of the recruited population? | NA | NA | NA | Unclear | Unclear | NA | NA | NA |
14. Were staff, places, and facilities where patients were treated representative of the treatment most received? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
15. Was an attempt made to blind study subjects to the intervention? | NA | NA | NA | NA | NA | NA | NA | NA |
16. Was an attempt made to blind those measuring the main outcomes? | NA | NA | NA | NA | NA | NA | NA | NA |
17. If any of the results of the study were based on data dredging was this made clear? | No | No | No | No | No | No | No | No |
18. Was the time period between intervention and outcome the same for intervention and control groups or adjusted for? | Yes | Yes | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
19. Were the statistical tests used to assess the main outcomes appropriate? | Yes | Yes | Yes | Yes | Partially | Yes | Unclear | Yes |
20. Was compliance with the interventions reliable? | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
21. Were the main outcome measures used accurate (Valid and reliable)? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
22. Were patients in different intervention groups recruited from the same population? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
23. Were study subjects in different intervention groups recruited over the same period of time? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
24. Were study subjects randomized to intervention groups? | No | No | No | No | No | No | No | No |
25. Was the randomized intervention assignment concealed from patients and staff until recruitment was complete? | NA | NA | NA | NA | NA | NA | NA | NA |
26. Was there an adequate adjustment for confounding in the analyses from which the main findings were drawn? | Yes | Unclear | Unclear | Unclear | Unclear | Yes | Yes | No |
27. Were losses of patients to follow-up taken into account? | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
28. Was the study sufficiently powered to detect clinically important effects where the P value for a difference due to chance is < 5%? | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
NA = not applicable.
Table 8: Strengths and Limitations of the Included Economic Evaluation Study Using the Drummond Checklist17
Checklist’s Items | Thakore et al. (2020)27 |
|---|---|
1. The research question is stated. | Yes |
2. The economic importance of the research question is stated. | Yes |
3. The viewpoint(s) of the analysis are clearly stated and justified. | Yes |
4. The rationale for choosing alternative programs or interventions compared is stated. | Unclear |
5. The alternatives being compared are clearly described. | Yes |
6. The form of economic evaluation used is stated. | Yes |
7. The choice of form of economic evaluation is justified in relation to the questions addressed. | Yes |
Data collection | |
8. The source(s) of effectiveness estimates used are stated. | Yes |
9. Details of the design and results of the effectiveness study are given (if based on a single study). | Yes |
10. Details of the methods of synthesis or meta-analysis of estimates are given (if based on a synthesis of a number of effectiveness studies). | NA |
11. The primary outcome measure(s) for the economic evaluation are clearly stated. | Yes |
12. Methods to value benefits are stated. | Yes |
13. Details of the subjects from whom valuations were obtained were given. | No |
14. Productivity changes (if included) are reported separately. | Partially |
15. The relevance of productivity changes to the study question is discussed. | No |
16. Quantities of resource use are reported separately from their unit costs. | Yes |
17. Methods for the estimation of quantities and unit costs are described. | Yes |
18. Currency and price data are recorded. | Yes |
19. Details of currency of price adjustments for inflation or currency conversion are givena | Yes |
20. Details of any model used are given. | Yes |
21. The choice of model used and the key parameters on which it is based are justified. | Yes |
Analysis and interpretation of results | |
22. Time horizon of costs and benefits is stated. | Yes |
23. The discount rate(s) is stated. | Yes |
24. The choice of the discount rate(s) is justifieda | Yes |
25. An explanation is given if costs and benefits are not discounted. | NA |
26. Details of statistical tests and confidence intervals are given for stochastic data. | Yes |
27. The approach to sensitivity analysis is given. | Yes |
28. The choice of variables for sensitivity analysis is justified. | Yes |
29. The ranges over which the variables are varied are justified. | partially |
30. Relevant alternatives are compared. | Yes |
31. Incremental analysis is reported. | Yes |
32. Major outcomes are presented in a disaggregated as well as aggregated formb | Yes |
33. The answer to the study question is given. | Yes |
34. Conclusions follow from the data reported. | Yes |
35. Conclusions are accompanied by the appropriate caveats. | Yes |
NA = not applicable.
aAnnual discount was set at 3% for expenses and utilities. Costs were adjusted to the year 2018 using the Health care Personal Consumption Expenditures chain-type price index.
Table 9: Strengths and Limitations of Guidelines Using the AGREE II Checklist18
Checklist’s Items | Andersen et al. (2012)14 | Shoesmith et al. (2020)2 |
|---|---|---|
Domain 1: Scope and Purpose | ||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes |
Domain 2: Stakeholder Involvement | ||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Unclear | Unclear |
6. The target users of the guideline are clearly defined. | Yes | Yes |
Domain 3: Rigour of Development | ||
7. Systematic methods were used to search for evidence. | Yes | Unclear |
8. The criteria for selecting the evidence are clearly described. | Yes | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | No | Partially |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Unclear | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Unclear | Yes |
14. A procedure for updating the guideline is provided. | Partially | NA |
Domain 4: Clarity of Presentation | ||
15. The recommendations are specific and unambiguous. | Yes | Yes |
16. The different options for the management of the condition or health issue are clearly presented. | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes |
Domain 5: Applicability | ||
18. The guideline describes the facilitators and barriers to its application. | No | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No | Yes |
20. The potential resource implications of applying the recommendations have been considered. | No | Yes |
21. The guideline presents monitoring and/or auditing criteria. | No | No |
Domain 6: Editorial Independence | ||
22. The views of the funding body have not influenced the content of the guideline. | Yes | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes |
NA = not applicable.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 10: Summary of Evidence for Riluzole in Amyotrophic Lateral Sclerosis (ALS) in a Systematic Review and Meta-analysis by Miller et al. (2012)14
Outcomes | Assumed riska | Corresponding risk | Relative effect, (95% confidence interval) | Total number of patients (studies) | Quality of the evidence | Comments |
|---|---|---|---|---|---|---|
Placebo | Riluzole (95% CI) | |||||
Pooled HR of mortality or tracheostomy at 12 months with riluzole 100 mg | 510 events per 1000 patients | 419 per 1000 (367 to 475) | HR = 0.83 (0.70 to 1.00) | 1282 (3) | High | The relative effect showed a 3-month increase in median survival from 11.80 to 14.80 months. |
The mortality rate at 12 months with riluzole 100 mg | 440 events per 1000patients | 343 per 1000 (286 to 405) | RR = 0.78 (0.65 to 0.92) | 799 (3) | High | — |
Rate of decline of Norris Scaleb - Norris Limb with riluzole 100 mg and 12-month follow-up | 23.10 point per year the weighted mean rate of decline | The mean rate of decline in the intervention groups was 3.94 point slower (7.25 to 0.64 slower) | NR | 731 (3) | High | The pooled data showed a slower decline of limb function in the riluzole group. |
Rate of decline of Norris Scale - Norris bulbar with riluzole 100 mg and 12-month follow-up | 11.10 point per year weighted mean rate of decline | The mean rate of decline in the intervention groups was 2.06 slower (3.86 to 0.27 slower) | NR | 742 (3) | High | The pooled data showed a slower decline of bulbar function in the riluzole group. |
AE: nausea | 91 events per 1000 patients | 142 per 1000 (96 to 207) | RR = 1.55 (1.06 to 2.28) | 801(3) | High | — |
AE: asthenia | 116 events per 1000 patients | 175 per 1000 (124 to 246) | RR = 1.5 (1.07 to 2.12) | 801 (3) | High | — |
AE: three-fold increase in alanine transferase | 49 events per 1000 patients | 129 per 1000 (78 to 211) | RR = 2.62 (1.59 to 4.31) | 801 (3) | High | — |
AE = adverse event; HR = hazard ratio; NR + not reported; RR = risk ratio.
aAssumed risk refers to the median control group risk across studies. The corresponding risk (and its 95% confidence interval) was based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% confidence interval).14
bThe Norris Scale is a comprehensive tool used for assessing the functional capacity of individuals with ALS, encompassing two distinct sections. The first section is known as the Norris Limb Scale, which comprises 21 items focused on activities of daily living (ADLs) pertaining to the extremities. These items encompass tasks such as gripping, buttoning, zipping, and standing up. The second section, known as the Norris Bulbar Scale, consists of 13 items specifically designed to evaluate bulbar function, which includes speech and swallowing abilities. Each item is assigned an ordinal 4-point scale, with corresponding values and functional scores of “normal” (3 points), “somewhat impaired” (2 points), “inadequate” (1 point), and “cannot do at all” (0 points). The maximum score achievable for the Norris Limb Scale and Norris Bulbar Scale is 63 and 39, respectively.39
Table 11: Summary of Findings by Outcome — Impact of Early Initiation of Riluzole on Median Survival in Thakore et al. (2022)21
Outcomes | Riluzole (n = 3,446) | No riluzole (n = 1,332) | P value |
|---|---|---|---|
Median survival period (months) | 22.60 | 20.20 | < 0.001 |
The impact of delayed riluzole initiation by 1 year | Reduced median survival from the onset by 1.90 months (40.10 to 38.20 months) | ||
Table 12: Summary of Findings by Outcome — Survival Time (day) in Cetin et al. (2015)25
Outcomes | Riluzole (n = 1,125) mean (CI 95%) | No riluzole (n = 415) mean (CI 95%) | P value |
|---|---|---|---|
Group 1 (≤ 0.20)a | 1,255 (1,105 to 1,404) | 908 (829 to 987) | 0.010b |
Group 2 (0.21 to 0.40) | 1,089 (910 to 1,268) | 908 (829 to 987) | 0.09 |
Group 3 (0.41 to 0.60) | 794 (240 to 1,348) | 829 (449 to 1,209) | 0.77 |
Group 4 (0.61 to 0.80) | 582 (433 to 731) | 829 (449 to 1,209) | 0.28 |
Group 5 (≥ 0.81) | 601 (518 to 684) | 829 (449 to 1,209) | 0.026 |
aTo evaluate a possible time-dependent effect of riluzole therapy, the patients were classified into five groups according to their therapy ratio. The groups were defined as the duration of riluzole therapy in days divided by the survival time from diagnosis in days. The duration of riluzole therapy was calculated as the total dosage of prescribed pills divided by the defined daily dose for riluzole (i.e., 100 mg).
bRiluzole therapy was associated with a survival advantage only for the initial treatment period.
Table 13: Summary of Findings by Outcome — Survival Time in Lee et al. (2015)23
Outcomes | Riluzole (n = 698) OR (CI 95%) | No riluzole (n = 451) OR (CI 95%) | P value |
|---|---|---|---|
Survival time (months) | 0.457 (0.297 to 0.748) | 1.00 | 0.002 |
CI = confidence interval; OR = odds ratio.
Table 14: Summary of Findings by Outcome — Survival Time in Georgoulopoulou et al. (2013)24
Outcomes | Riluzole (n = 133) Median (CI 95%) | No Riluzole (n = 60) Median (CI 95%) | P value |
|---|---|---|---|
Survival time (months to death) | 43 (37 to 51) | 31 (25 to 46) | < 0.01 |
Survival time (months to tracheostomy) | 38 (35 to 43) | 31 (25 to 46) | 0.11 |
CI = confidence interval.
Table 15: Summary of Findings by Outcome — Stage-Specific Riluzole Effect in Thakore et al. (2020)22
Outcomes | HR | Outcomes | HR |
|---|---|---|---|
Transition in King's stagesa | Fine’til 9 (FT9) stagesb | ||
Stages 1 to 2 | 0.81 | Stages 1 to 2 | 0.84 |
Stages 2 to 3 | 0.82 | Stages 3 to 4 | 0.71 |
Stage 4 to death | 0.57 | Stage 4 to death | 0.67 |
HR = hazard ratio.
aThe King’s staging system consists of 5 disease stages, with stage 5 being death. Stages 1 to 3 are based on the number of brain regions involved in the disease, measured by symptoms of weakness, wasting, spasticity, dysphagia, or dysarthria. Stage 4 is a nutritional failure, defined by the requirement for gastrostomy, or respiratory failure, defined by the requirement for non-invasive ventilation (NIV).40
bFine’til 9 (FT9) is a novel staging method derived from the revised amyotrophic lateral sclerosis functional rating scale (ALSFRS-R). It is a widely used 12-question, 5-level instrument comprised of 4 sub-scores (bulbar, fine motor, gross motor, and respiratory; 3 questions each). Each function is scored from 4 (normal) to 0 (no ability), with a maximum total score of 48 and a minimum total score of 0. FT9 sums the number of ALSFRS-R sub-scores that are 9 or less (12 is considered normal).27
Table 16: Summary of Findings by Outcome — Stage at Which Riluzole Treatment Prolongs Survival in Fang et al. (2018)4
Outcomes | Hazard ratio | P value |
|---|---|---|
A longer stage 4 in patients with 100 mg per day riluzole compared to a placebo | 0.55, 95% CI, 0.36 to 0.83 | 0.037 |
A longer stage 4 in multistate outcome analysis of treatments (MOAT)a with 100 mg per day riluzole compared to a placebo | 0.638, 95% CI, 0.464 to 0.878 | 0.006 |
aMulti-state Outcome Analysis of Treatments (MOAT) is a method for survival analysis that partitions total survival time into clinically distinct periods operationally defined by cut points on rating scales.41
Table 17: Summary of Findings by Outcome — Long-Term Riluzole Effectiveness in Chen et al. (2016)3
Outcomes | Riluzole (n = 1,125) | No Riluzole (n = 415) | P value |
|---|---|---|---|
Body-mass index (BMI) (mean, 95% CI, Kg/m2) | 23.3, 23.0 to 23.6 | 22.6, 22.4 to 22.9 | < 0.0005 |
ALSFRS score | 34.0 (7.0) | 32.0(9.0) | < 0.0005 |
ALSFRS-R score | 42.0 (7.0) | 40.0 (9.0) | < 0.0005 |
ALSFRS = Amyotrophic Lateral Sclerosis Functional Rating Scale; ALSFRS-R = Revised Amyotrophic Lateral Sclerosis Functional Rating Scale; IQR = Interquartile range.
Table 18: Summary of Findings by Outcome — Quality of Life in Shamshiri et al. (2016)5
Outcomesa | Riluzole (n = NR) | No riluzole (NR) | P value |
|---|---|---|---|
Baseline | 88.62 (43.74) | 83.79 (37.840 | > 0.05b |
Month 6 | 95.73 (44.65) | 96.70 (36.70) | > 0.05 |
Month 12 | 108.16 (43.04) | 114.15 (34.81) | > 0.05 |
NR = not reported.
aQuality of life was assessed using Amyotrophic Lateral Sclerosis (ALS) Assessment Questionnaire (ALSAQ-40). This 40-item questionnaire has been specifically designed to evaluate the quality of life of ALS patients.
bActual P values were not reported.
Table 19: Summary of Findings of the Economic Evaluation Study — Cost-Effectiveness of Riluzole for Amyotrophic Lateral Sclerosis by Thakore et al. (2020)27
Outcomes | Treatment | Residual QALYs | Treatment cost | Health care sector perspective | Societal perspective | ||||
|---|---|---|---|---|---|---|---|---|---|
Cumulative recurrent costsa | Cumulative transition/ tollgate costsb | ICER (cost/QALY) | Cumulative recurrent costs | Cumulative transition/ tollgate costs | ICER (cost/QALY) | ||||
Cost-effectiveness | Model I | Model II | |||||||
5-year horizon | Riluzole | 1.671 | $5,403 | $73,206 | $36,776 | $67,658 | $234,527 | $50,189 | $59,756 |
No riluzole | 1.488 | $0 | $64,335 | $38,702 | $226,075 | $53,138 | |||
Difference | 0.182 | $5,403 | $8,870 | -$1,925 | -$8,452 | -$2,949 | |||
— | Model III | Model IV | |||||||
10-year horizon | Riluzole | 1.889 | $6,145 | $85,057 | $40,745 | $70,258 | $393,005 | $56,236 | $69 217 |
No riluzole | 1.608 | $0 | $70,716 | $41,512 | $378,557 | $57,402 | |||
Difference | 0.281 | $6,145 | $14,541 | -$767 | $14,448 | -$1,166 | |||
ICER = indicates incremental cost-effectiveness ratio; QALY = quality-adjusted life-years.
“Recurring costs” (RCs) refer to ongoing expenses that are incurred on a regular basis, typically at fixed intervals. These costs are repeated periodically, such as monthly, quarterly, or annually.42
“One-off” transition or “tollgate” costs (TCs) are expenses associated with a specific event or milestone during a project's lifecycle. These costs are typically incurred during the transition from one phase to another or at key checkpoints within a project.42
Table 20: Summary of Findings of the Economic Evaluation Study — Health state utility weights and costs ($ per month) by stage in Thakore et al. (2020)27
Outcomes | Stage 1 | Stage 2 | Stage 3 | Stage 4 | Comments |
|---|---|---|---|---|---|
Heath state utilities EQ-5D weights (standard error) | 0.743 (0.013) | 0.629 (0.009) | 0.541 (0.012) | 0.464 (0.015) | Stage 0 weight = 0.789 (Estimates from 1868 observations obtained from 678 patients.) |
Total health care sector RC | 1,232 | 1,808 | 2,464 | 3,350 | — |
Total societal monthly RC (HCA) | 2,531 | 4,336 | 5,787 | 7,469 | Absenteeism included in RC, not under TC by HCA. Absenteeism cost of $3,031 per month was incurred even after death. |
Total societal monthly RC by (FCM) | 1,232 | 2171 | 3189 | 4,438 | Absenteeism included in TC, not under RC by FCM. |
Total cumulative health care sector TC | 491 | 10,073 | 22,656 | 44,479 | Costs applied to stages 0 to 1, 1 to 2, 2 to 3, 3 to 4, and 4 to death transitions were 245.5; 5,036.5; 11, 082.5; 17,203.0; 10,911.5; respectively. |
Total cumulative societal TC (HCA) | 491 | 10,073 | 27,758 | 54,683 | Costs applied to stages 0 to 1, 1 to 2, 2 to 3, 3 to 4, and 4 to death transitions were 245.5; 5,036.5; 13,633.5; 22,305.0; 20,462.5; respectively. |
Total cumulative societal TC (FCM) | 4,388 | 16,568 | 35,552 | 63,776 | Costs applied to stages 0 to 1, 1 to 2, 2 to 3, 3 to 4, and 4 to death transitions were 2,194; 8,284; 15,582;,23,604; 21,112; respectively. |
ALS = amyotrophic lateral sclerosis; DME = durable medical equipment; FCM = friction cost method; GT = gastric tube; HCA = human capital approach; RC = recurring costs; TC = transition/tollgate cost.
Table 21: Summary of Recommendations in the Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
aAndersen et al. (2012)26 | |
“Patients with ALS should be offered treatment with riluzole 50 mg twice daily (p. 366)”. | Level A |
“Irrespective of familial disposition, all patients with symptomatic progressive motor neuron disorders (MND) and carrying a superoxide dismutase type 1 (SOD1) gene mutation should be offered treatment with riluzole (p. 366). | GCPP |
“Patients with progressive muscular atrophy, primary lateral sclerosis or hereditary spastic paraplegia should as a rule not be treated with riluzole (p. 366)”. | GCPP |
bShoesmith et al. (2020)2 | |
Riluzole prolongs survival by a median duration of 3 months. | Level A |
Riluzole should be initiated soon after the diagnosis of ALS. | Level EC |
“Regular monitoring of potential adverse effects of riluzole is important (p. E1454).” In patients developing fatigue while taking riluzole, reducing or discontinuing the drug may be considered. | Level EC Level C |
Riluzole is effective with the progression of the disease, including the development of respiratory insufficiency. | Level EC |
“Patients and healthcare authorities should be educated on the rationale for patient attendance at a multidisciplinary clinic (page E1454).” The education contributes to increased use of riluzole, percutaneous feeding tubes, and non-invasive ventilation (NIV) support. | Level B |
ALS = amyotrophic lateral sclerosis; EC = expert consensus; GCPP = good clinical practice point.
aExisting evidence was evaluated according to the recommendations of the European Federation of Neurologic Societies (EFNS) resulting in level A, B, or C recommendations.43 Where there was a lack of evidence but consensus was clear, the authors stated their opinion as “good clinical practice points” (GCPP).14
bCriteria developed for rating levels of evidence in guideline recommendations by Shoesmith et al. (2020)2: A = at least 2 consistent class I studies; B = at least 1 class I study or 2 consistent class II studies; C = at least 1 class II study or 2 consistent class III studies; EC = expert consensus among Canadian ALS clinical experts where evidence meeting criteria for Level A through Level C is lacking. The authors applied the following criteria for rating therapeutic studies: Class I — randomized controlled clinical trial (RCT) in a representative population; masked or objective outcome assessment; relevant baseline characteristics are presented and substantially equivalent between treatment groups, or there is an appropriate statistical adjustment for differences; also required are concealed allocation, primary outcome(s) clearly defined, exclusion and inclusion criteria clearly defined, adequate accounting for dropouts (with at least 80% of enrolled participants completing the study) and crossovers with numbers sufficiently low to have minimal potential for bias. Class II — cohort study meeting criteria a–d (see class I) or an RCT that lacks 1 or 2 criteria b–d (see class I); all relevant baseline characteristics are presented and substantially equivalent among treatment groups, or it is appropriate; statistical adjustment for differences; masked or objective outcome assessment. Class III — controlled studies (including well-defined natural history controls or patients serving as their own controls); a description of major confounding differences between treatment groups that could affect the outcome; outcome assessment masked, objective, or performed by someone who is not a member of the treatment team. Class IV — did not include patients with the disease; did not include patients receiving different interventions; undefined or unaccepted interventions or outcome measures; no measures of effectiveness or statistical precision were presented or calculable.
Appendix 5: References of Potential Interest
The following publications were identified because they may provide additional information associated with this report.
Primary Studies
Alternative Intervention and/or Comparator
Chen PC, Hsieh YC, Huang CC, Hu CJ. Tamoxifen for amyotrophic lateral sclerosis: A randomized double-blind clinical trial. Medicine (Baltimore). 2020;99(22):e20423. PubMed
Ludolph AC, Schuster J, Dorst J, et al. Safety and efficacy of rasagiline as an add-on therapy to riluzole in patients with amyotrophic lateral sclerosis: a randomized, double-blind, parallel-group, placebo-controlled, phase 2 trial. Lancet Neurol. 2018;17(8):681-688. PubMed
Nagata E, Ogino M, Iwamoto K, et al. Bromocriptine mesylate attenuates amyotrophic lateral sclerosis: a phase 2a, randomized, double-blind, placebo-controlled research in Japanese patients. PLoS ONE. 2016;11(2):e0149509. PubMed
Elia AE, Lalli S, Monsurro MR, et al. Tauroursodeoxycholic acid in the treatment of patients with amyotrophic lateral sclerosis. Eur J Neurol. 2016;23(1):45-52. PubMed
Shibuya K, Misawa S, Kimura H, et al. A single-blind randomized controlled clinical trial of mexiletine in amyotrophic lateral sclerosis: efficacy and safety of sodium channel blocker phase II trial. Amyotroph Lateral Scler Frontotemporal Degener. 2015;16(5-6):353-358. PubMed
Dupuis L, Dengler R, Heneka MT, et al. A randomized, double-blind, placebo-controlled trial of pioglitazone in combination with riluzole in amyotrophic lateral sclerosis. PLoS ONE. 2012;7(6):e37885. PubMed
Verstraete E, Veldink JH, Huisman MH, et al. Lithium lacks effect on survival in amyotrophic lateral sclerosis: a phase IIb randomized sequential trial. J Neurol, Neurosurg Psychiatry. 2012;83(5):557-564. PubMed
Witzel S, Maier A, Steinbach R, et al. Safety and effectiveness of long-term intravenous administration of edaravone for treatment of patients with amyotrophic lateral sclerosis. JAMA Neurol. 2022;79(2):121-130. PubMed
Favero FM, Voos MC, Castro I, Caromano FA, Oliveira ASB. Epidemiological and clinical factors impact on the benefit of riluzole in the survival rates of patients with ALS. Arq Neuropsiquiatr. 2017;75(8):515-522. PubMed
No Comparator
Inoue-Shibui A, Kato M, Suzuki N, et al. Interstitial pneumonia and other adverse events in riluzole-administered amyotrophic lateral sclerosis patients: a retrospective observational study. BMC Neurol. 2019;19(1):72. PubMed
Stevic Z, Kostic-Dedic S, Peric S, et al. Prognostic factors and survival of ALS patients from Belgrade, Serbia. Amyotroph Lateral Scler Frontotemporal Degener. 2016;17(7-8):508-514. PubMed
Current Trials on Add-On Drugs to Riluzole
AB Science. NCT03127267: Efficacy and Safety of Masitinib Versus Placebo in the Treatment of ALS Patients. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2023: https://clinicaltrials.gov/ct2/show/NCT03127267. Accessed 2023 Jun 09.
Corestem, Inc. NCT04745299: Evaluation the efficacy and safety of mutiple lenzumestrocel (Neuronata-R® Inj.) treatment in patients with ALS (ALSummit). Bethesda (MD): U.S. National Library of Medicine; 2022: https://clinicaltrials.gov/ct2/show/NCT04745299?term=NCT04745299&draw=2&rank=1. Accessed 2023 Jun 09.
Sanofi. NCT05237284: Phase 2 Study for SAR443820 in Participants With Amyotrophic Lateral Sclerosis (ALS) (HIMALAYA). Bethesda (MD): U.S. National Library of Medicine; 2023: https://clinicaltrials.gov/ct2/show/NCT05237284?term=NCT05237284&draw=2&rank=1. Accessed 2023 Jun 09.
InFlectis BioScience. NCT05508074: Treatment Combining Riluzole and IFB-088 in Bulbar Amyotrophic Lateral Sclerosis (TRIALS Protocol). Bethesda (MD): U.S. National Library of Medicine; 2022: https://clinicaltrials.gov/ct2/show/NCT05508074?term=NCT05508074&draw=2&rank=1. Accessed 2023 Jun 09.
Reviews
Johnson SA, Fang T, De Marchi F, et al. Pharmacotherapy for amyotrophic lateral sclerosis: a review of approved and upcoming agents. Drugs. 2022;82(13):1367-1388. PubMed
Neupane P, Thada PK, Singh P, et al. Investigating edaravone use for management of Amyotrophic Lateral Sclerosis (ALS): a narrative review. Cureus. 2023;15(1):e33746. PubMed
Song Y, Jia Q, Guan X, et al. Herbal medicine for amyotrophic lateral sclerosis: a systematic review and meta-analysis. Front Pharmacol. 2022;13:946548. PubMed
Andrews JA, Jackson CE, Heiman-Patterson TD, Bettica P, Brooks BR, Pioro EP. Real-world evidence of riluzole effectiveness in treating amyotrophic lateral sclerosis. Amyotrophic Lateral Sclerosis & Frontotemporal Degeneration. 2020;21(7-8):509-518. PubMed
Appendix 6: Guidance for Reporting Involvement of Patients and the Public (Version 2) Short-Form Reporting Checklist
Note that this appendix has not been copy-edited.
Table 22: Patient Involvement in Riluzole for the Treatment of ALS
Section and topic | Items | Reported in section |
|---|---|---|
Aim | A patient living with ALS, who is currently taking riluzole, was engaged during the writing of this report. He shared his experience, thoughts, perspectives, and priorities to help contextualize the information gathered from the literature search. The purpose of the engagement was to offer a unique perspective of the treatment to allow for a more nuanced understanding of the literature and to add context to the findings reported in the literature. | Key Messages |
Methods | A request for engagement was disseminated through a relevant patient advocacy group, and an individual responded expressing interest. After giving informed consent, the patient participated in a semi-structured dialogue with a Patient Engagement Officer and the Research Officer authoring this report via a one-hour video call. A summary of the engagement discussion was prepared by the Patient Engagement Officer and shared with the patient, who confirmed that the contents reflected his experience and the discussion. This summary was subsequently shared with the Research Officer, who was able to refer to it while considering the evidence compiled during the literature search. | Methods |
Results of engagement | The researchers were made aware of the importance of two specific outcomes that mattered to the patient. In particular, the patient identified the need for minimal and manageable side effects and an effective slowing of disease progression. | Key Messages |
Discussion and conclusions | The patient contributor was highly engaged in the dialogue, openly sharing his personal experience living with ALS, his diagnosis and symptoms, treatment experience, and perspectives on riluzole. He reported a high degree of satisfaction with riluzole, stating that he did not experience noticeable side effects. He reported that it is not causing harm and has the potential to be offering a benefit, so is a wise decision to take. He recommended that other people with ALS could benefit from riluzole. He appreciates that riluzole is an oral medication, preferring that to an infusion for convenience. He prefers minimizing time spent in the hospital or clinic whenever possible. The patient reported barriers to access, including losing access to the medication if there is a decline in health to the point of requiring full-time continuous positive airway pressure (CPAP) therapy. | Conclusions and Implications for Decision- or Policy-Making |
Reflections/critical perspective | The success of patient engagement in the review is related to several factors. First, the patient was supported by a Patient Engagement Officer. Second, the Research Officer was receptive to patient involvement and consulted the summary of the engagement during their consideration of the clinical evidence. Finally, compensation was offered for patient collaborators’ time and expertise. Limitations to our approach include our method of engagement through video calls. ALS can impact the ability to speak or write, making it difficult to communicate. This was mitigated by offering the patient different ways to engage, including by video call or in writing via email. In this instance, the individual chose a video call as his preferred method of engagement. Another limitation of our approach is that people need reliable internet access and access to a phone, computer, or tablet to contribute to CADTH’s work, which may exclude some voices. | Conclusions and Implications for Decision- or Policy-Making |
ALS = amyotrophic lateral sclerosis.
Contributors: Elizabeth Carson, Adeline Markarian, Farhana Shivji
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as of the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, collecting, using, and disclosing by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca.