CADTH Health Technology Review
Platelet-Rich Plasma Injections for Lower Back Pain
Rapid Review
Authors: Qiukui Hao, Melissa Walter
Abbreviations
CI
confidence interval
LBP
lower back pain
NRS
numerical rating scale
ODI
Oswestry Disability Index
OR
odds ratio
PRP
platelet-rich plasma
PRPIs
platelet-rich plasma injections
RCTs
randomized controlled trials
RR
risk ratio
SMD
standardized mean difference
VAS
visual analogue scale
Key Messages
Platelet-rich plasma injections (PRPIs) might be better than other injections (including steroid injections) for patients with lower back pain in reducing pain and enhancing patient satisfaction, without increasing the risk of major complications or serious adverse events.
For patients with low back pain who received PRPI, disability measures were lower up to 6 months after treatment than before PRPI, while MRI findings were unchanged from baseline.
The included systematic reviews did not report any major complications or serious adverse events related to PRPIs.
We did not find any studies reporting on the comparisons between PRPI and other conservative treatments such as non-steroidal anti-inflammatory drugs, exercise, or physiotherapy that met the inclusion criteria for this report.
Context and Policy Issues
Lower back pain (LBP) is a syndrome rather than a disease. LBP is characterized as pain in the region at the back of the body from the lower edge of the twelfth rib to the lower gluteal folds, with or without pain extending to 1 or both legs that persists for at least 1 day.1 Chronic LBP refers to pain that persists for more than 12 weeks, even after receiving treatment for its potential causes.2 LBP is a common and complex musculoskeletal problem and is the leading cause of disability or absence from work globally.1,3,4 People in all age groups, from children to older adults, can be affected by LBP. Approximately 60% to 80% of people experience LBP at some point during their lifetime.5 The point prevalence of activity-limiting LBP was about 7.3%, responsible for 60.1 million disability-adjusted life-years in 2015.4
The prevalence of LBP increases with age and peaks around 80 to 89 years.3 The age-adjusted prevalence of LBP was higher in females than males.3 Due to population increase and aging, LBP-induced years lived with disability, related costs, and health care use have increased substantially and will continue to increase in coming decades.4 Although most LBP episodes will recover within 4 to 6 weeks with little or no serious consequence,4,6,7 around 30% of people will suffer from at least 1 recurrent episode within 1 year after recovery.4 Similar epidemiology data and clinical features for LBP were reported in a Canadian national population health survey.6 In Canada, about 3% of people visited the emergency department with back pain from 2009 to 2015 in the largest emergency department in Atlantic Canada; among those with back pain, over 60% of patients were diagnosed with LBP.8
Only a small proportion of people with LBP had exact causes, such as vertebral fracture, infections, inflammatory disorders, or malignant disease.4 These types of disease-specific LBP need specific medical attention and management targeting the cause. However, most people with LBP cannot find the specific source of the pain. Multiple factors, including issues with intervertebral discs, facet joints, or vertebral end plates can cause nonspecific LBP.4 Lifestyle factors like smoking, obesity, and low levels of physical activity may also contribute to this type of pain, as well as psychological factors and pain-processing mechanisms.4 Identifying the risk factors of LBP is important for treatment.
There are numerous treatment options available for LBP, including pharmacological and non-pharmacological therapies.9 Current guidelines suggest physical (mainly exercise), psychological interventions, and self-management strategies such as education, advice to remain active, or applying superficial heat, while these guidelines do not strongly emphasize surgery or injections.7,10 The effectiveness, safety, and cost-effectiveness are crucial considerations for choosing emerging interventions. Despite the emergence of injectable interventions for patients with LBP, they have not been widely implemented in clinical practice due to inconsistent or low-quality evidence regarding their clinical effectiveness and safety, and were not recommended by guidelines.7,10,11
Platelet-rich plasma (PRP) is an injectable biologic product, which consists of a higher concentration of the patient’s platelets in a small amount of plasma than in peripheral blood.12 Clinicians have used PRP to treat various conditions for over 30 years,12 including musculoskeletal disorders,13 surgical wounds,14 thin endometrium,15 premature ovarian failure,16 and acne scars.17 PRP contains numerous growth factors in platelet granularities such as fibroblast growth factor, transforming growth factors beta-1, angiogenesis factor, and growth factor.12 The exact mechanisms by which PRP and its components can treat these diseases are not yet clear, but they might be involved in tissue repair, pain relief, and regenerative processes.13-17
PRPIs are becoming 1 potential intervention for patients with LBP.18 Based on a nonsystematic literature review,19 several observational studies have reported the effectiveness of PRPIs; however, there is lack of high-quality clinical trials in this population. Given the uncertain and developing evidence base for PRPIs, the objective of this report is to evaluate the recent evidence on the clinical effectiveness and safety of PRPIs for the treatment of LBP in adults.
Research Question
What is the clinical effectiveness of platelet-rich plasma injections for the treatment of lower back pain in adults?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources, including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, and a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were platelet-rich plasma injections and back pain. Conference abstracts were excluded. Retrieval was limited to the human population. The search was completed on April 27, 2023 and limited to English-language documents published since January 1, 2018.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first screening level, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1. For this report, we considered a review to be a systematic review if it indicated that the evidence was searched for systematically and had clear inclusion and exclusion criteria.
Criteria | Description |
|---|---|
Population | Adults with lower back pain |
Intervention | Platelet-rich plasma injections |
Comparator | Usual care (e.g., no treatment with platelet-rich plasma injections, exercise or physiotherapy, cortisone injections, non-steroidal anti-inflammatory drugs) |
Outcomes | Clinical benefits (e.g., pain, function, mobility, quality of life, patient satisfaction) and harms (e.g., adverse events) |
Study designs | Health technology assessments and systematic reviews |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2018. Systematic reviews and health technology assessments in which all relevant primary studies were captured in at least 1 other more recent or more comprehensive systematic review were excluded.
Critical Appraisal of Individual Studies
The included systematic reviews were critically appraised by 1 reviewer using A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2).20 Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
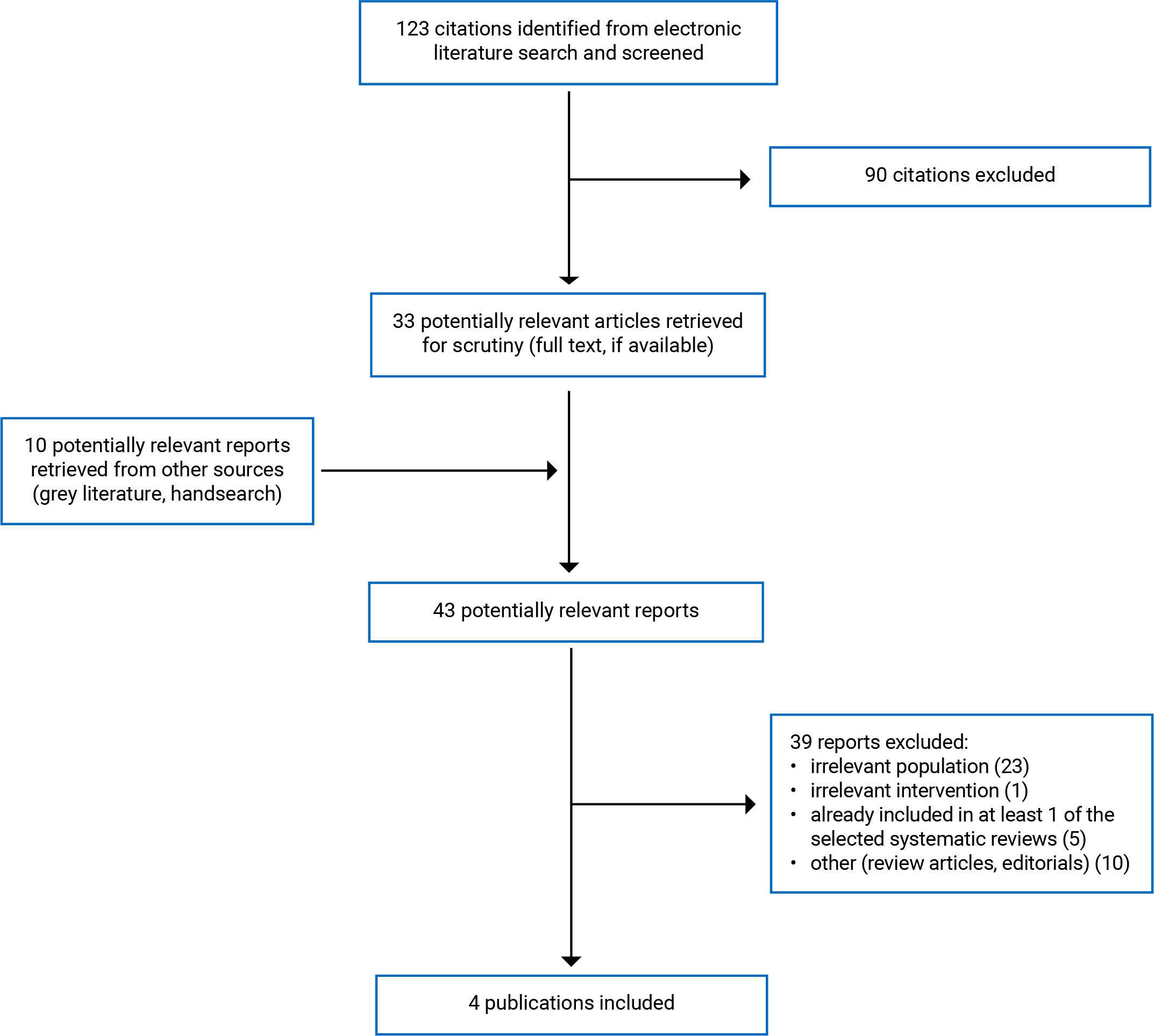
A total of 123 citations were identified in the literature search. Following screening of titles and abstracts, 90 citations were excluded and 33 potentially relevant reports from the electronic search were retrieved for full-text review. Ten potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 39 publications were excluded for various reasons, and 4 systematic reviews met the inclusion criteria and were included in this report. Appendix 1 presents the PRISMA21 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 6.
Summary of Study Characteristics
We included 4 systematic reviews in this report.22-25 Two23,25 of the 4 systematic reviews had broader inclusion criteria on interventions than the present report. Specifically, both systematic reviews23,25 included both PRPIs and mesenchymal stem cell interventions. Only the subset of studies reporting on PRPIs was relevant to this rapid review and are described in the remainder of our report. Additional details regarding the characteristics of included publications are provided in Appendix 2.
Appendix 5 includes a table describing the overlap in relevant primary studies in the included systematic reviews.
Study Design
Two22,25 of 4 systematic reviews included single-arm meta-analyses comparing the outcome after treatment to baseline, 1 systematic review24 included the meta-analyses comparing PRPIs to control interventions, and 1 systematic review23 summarized the findings from primary studies narratively and did not conduct a meta-analysis. The number of primary studies involving PRPIs that were included in the systematic reviews ranged from 3 to 15 primary studies,22,25 which comprised randomized controlled trials (RCTs), observational studies, and case reports. One systematic review25 was published in 2018, 1 systematic review24 was published in 2020, 1 systematic review23 was published in 2022 and 1 systematic review22 was published in 2023 with the search up to April 18, 2022. We found 1 systematic review24 that consisted of 3 RCTs, which were also included in another systematic review.25 We utilized both systematic reviews24,25 because the former compared PRPI interventions to control interventions in their meta-analyses,24 while the latter had a wider range of studies but only conducted single-arm meta-analyses.25
Country of Origin
Of the 4 systematic reviews, 2 systematic reviews22,24 were from China, 1 systematic review was from Italy,23 and 1 systematic review was from the US.25 One systematic review22 presented the countries or regions of included primary studies. Of the 6 studies within this systematic review, 3 RCTs were conducted in the US and 3 observational studies were conducted in Japan, India, and the US.22
Patient Population
Two22,23 of 4 systematic reviews22-25 involved patients with chronic discogenic LBP. One review included patients with LBP but did not report the type or duration of LBP.24 One review included patients with LBP and lower extremity pain (duration not reported).25 The number of included patients in 3 systematic reviews22-24 ranged from 127 to 198. The mean age of patients in primary studies within 2 systematic reviews22,24 ranged from 33 years to 52.91 years and age was not reported in the 2 remaining systematic reviews.23,25 In 2 systematic reviews, the percentage of males ranged from 39% to 80%22,24 and was not reported in the other 2 systematic reviews.23,25
Interventions and Comparators
One systematic review24 compared the effectiveness and safety of PRPIs to control injections without PRPIs, which included anesthetic, steroids, or contrast agents. The remaining 3 systematic reviews22,23,25 reported the before and after changes for receiving PRPIs without a comparator group. PRPI sites or routes of administration were reported as intradiscal,22,25 sacroiliac joint,24,25 intra-articular,24,25 and epidural injection.25 One systematic review23 did not report the site of the injection for PRP, but reported the injected PRP volumes ranged from 1 mL to 3 mL, when reported.23,24 None of the systematic reviews22-25 clearly reported the types of PRP used (pure or leucocyte PRP), the frequencies of the injections, treatment history, and the co-interventions for LBP.
Outcomes
All 4 systematic reviews reported or discussed pain outcomes.22-25 Pain was assessed by the visual analogue scale (VAS) or numerical rating scale (NRS). In 2 systematic reviews,22,24 the VAS or NRS were reported in a 10-point scale, while the scale of pain measures was clear in the other 2 systematic reviews.23,25 The disability was assessed in 2 systematic reviews22,25 by Oswestry Disability Index (ODI),22 Functional Rating Index, or Roland-Morris Disability Questionnaire.25 The pain or disability scales used in individual studies were not reported in detail, including their psychometric properties and interpretation scores such as what direction represents improvement or worsening, or minimal important difference. Three systematic reviews22-24 mentioned adverse events or major complications. One systematic review23 described the MRI changes after PRPIs treatment. One systematic review24 also reported the rate of patient satisfaction. Three systematic reviews reported the mean or median duration of follow-up,22-24 which ranged from 1 week to 60 weeks. The remaining systematic review did not report the duration of follow-up.25
Summary of Critical Appraisal
In all 4 systematic reviews,22-25 the objective was clearly described, multiple databases were searched, keywords or medical subject terms or keywords of the search and study selection flow charts were provided, the review authors declared no conflicts of interest, lists of included articles were presented and the study characteristics were described. None of the systematic reviews provided lists of excluded articles or assessed the sources of funding in individual studies. Despite searching in multiple databases, 3 systematic reviews22-24 did not report performing a grey literature search and 2 systematic reviews23,25 did not report searching the Embase database specifically. These limitations may result in missing some studies (unpublished or studies conducted in Europe) or mis-identification of potential publication bias.
At least 2 reviewers independently performed the article selection and data extraction in 1 systematic review.23 Two reviewers independently selected articles in 2 systematic reviews,22,25 but it was unclear how the data extraction was performed. In the fourth systematic review,24 it was unclear how article selection and data extraction were conducted. The possibility of inappropriate inclusion or exclusion or errors in data extraction cannot be ruled out. Although 3 systematic reviews22-24 assessed the risk of bias of included individual studies and reported study quality, they did not assess the potential impact of study risk of bias on the interpretation of results. One systematic review23 authors judged that only 1 out of 7 primary studies had high-quality (low risk of bias);in another systematic review22, some meta-analyses only included 1 or 2 primary observational studies; therefore, the results of these analyses may be driven by individual studies with high risk of bias. One systematic review25 evaluated the grading of evidence, considering the quality of included individual studies and stratified the assessment according to PRPI sites. However, the review25 did not include an outcome-specific assessment of evidence, making it challenging to interpret the reported level of evidence. In 2 systematic reviews22,25 with substantial statistical heterogeneity, no analysis was conducted to explore the observed heterogeneity.
The systematic review by Peng et al. (2023)22 included a single-arm meta-analysis to compare the changes in pain and disability outcomes between post-PRPI treatment and baseline and calculated incidence rates for improvement; this analysis was methodologically flawed. The review authors22 calculated the incidence rate for improvement in outcome measures of over 30% or 50% based on the pooled odds ratio (OR) in their meta-analysis. The formula used to calculate the incidence rate was “incidence rate= OR/(1+OR)” and the results were reported as percentages. To accurately calculate the incidence rate, 1 must consider the new events, the population at risk, and a time frame, and report it as events per people-year. Reporting the incidence rate results based on a pooled OR is unreliable. Alternatively, the systematic review authors could have extracted the proportion of patients who experienced a 30% or 50% decrease in pain or disability and use appropriate proportional meta-analysis to get a pooled proportion.26
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
One included systematic review24 compared PRPIs and controls interventions without PRPIs. Two systematic reviews22,25 included data from RCTs or observational studies on patients who received PRPI and conducted meta-analyses of data from the intervention arm alone. The fourth systematic review23 provided narrative summaries of the findings of the individual studies that were included (1 out of 7 included individual studies had a control group and the details of control were unclear). Appendix 4 presents the main study findings. Due to some overlap in the studies included in the 2 systematic reviews with single-arm meta-analyses22,25 the pooled estimates from the 2 systematic reviews may contain some of the same individual study data (Appendix 5).
Clinical Effectiveness of PRPI
Pain Scores
All included systematic reviews22-25 reported pain scores after PRPI in people with LBP, and generally demonstrated statistically significant reductions from baseline or compared to a control. One systematic review24 reported that PRPI was statistically significantly more effective than the control group in reducing pain scores within 8 weeks. However, the method of measurement for the pain scores was unclear. Two systematic reviews22,25 reported the pooled estimates of post-PRPI pain scores at various time points from single-arm meta-analysis. These systematic reviews reported that pain scores were statistically reduced at 1 month,22 2 months,22 6 months,22,25 and 12 months25 after PRPI compared with before PRPI with substantial statistical heterogeneity (I2 = 77% to 98%). However, the comparisons of pain scores between post-PRPI time points were not statistically significant.22 For PRP administered by lumbar facet joint injection, intra-articular injection and sacroiliac joint injection, the systematic review by Sanapati et al. (2018)25 provided a narrative summary of findings for each study in tables, indicating that most studies reported positive effects of PRPI on pain (i.e., pain decreased). One systematic review23 reported the findings from 4 primary studies in which pain scores were numerically lower after PRPI treatment (unclear time point) compared with before PRPI treatment. However, it is unclear what methods were used to measure pain scores and the time frame for outcome measures.
The systematic review by Sanapati et al. (2018)25 also reported the level of evidence, but failed to specify it based on the outcomes (pain or disability). PRP treatment administered through lumbar disc injection has a level III (fair) evidence in reducing pain.25 However, for lumbar facet joint, intra-articular injection, and sacroiliac joint injection, the level of evidence was level IV (limited).25 In this review,25 level III (fair) evidence was defined as “evidence obtained from at least one relevant high quality nonrandomized trial or observational study with multiple moderate or low-quality observational studies” and level IV (limited) was defined as “evidence obtained from multiple moderate or low-quality relevant observational studies” (page 519, Table 1).
Number of Patients With Pain Relief
One systematic review24 reported that PRPI was statistically significantly more effective than the control group in improving the rate of patients who experienced at least 50% pain relief at 3 months. Another systematic review22 reported the calculated incidence rates based on pooled odds ratios for patients who experienced more than 30% and 50% pain relief after PRPI treatment compared with before PRPI treatment at 1 month, 2 months, and 6 months, with more than half of patients reaching at least 30% of pain relief at any measured time points. However, the reliability of these incidence rates is questioned due to the use of flawed methods or formulas.
Disability
Two systematic reviews22,25 reported disability outcomes. One systematic review22 evaluated the incidence rates of patients who experienced a 30% or 50% decrease from baseline in disability score after PRPI treatment. This review reported 40.2% of patients reaching at least a 30% decrease in disability score at 2 months, and 53.9% reaching at least a 50% decrease in disability score at 6 months. However, we had concerns regarding the accuracy of the findings due to the utilization of incorrect methods or formulas in this review. The second review25 reported that the disability scores were numerically lower after PRPI treatment at 3 months or 6 months than before PRPI treatment.
Patient Satisfaction
One systematic review reported that PRPI can statistically significantly enhance patient satisfaction rates compared to control interventions.24 The details of the outcome measure, such as the time it was taken, the tool used to assess patient satisfaction and its psychometric properties, and whether the outcome assessors were blinded to group allocation, were not provided.
Adverse Events
All 4 systematic reviews22-25 considered adverse events, and 1 review24 provided a meta-analysis on adverse events. Based on the meta-analysis,24 there was no statistical difference in adverse events between patients in the PRPI treatment group and the control group. Two systematic reviews reported that no serious adverse events or complications occurred.22,23 In the fourth systematic review,25 adverse events were considered for some individual studies in tables, and PRPIs did not appear to have serious safety concerns. However, the definitions of considered adverse events were not provided.
Other Outcomes
One systematic review based on 2 individual studies noted that, for most patients, there were no significant changes in hydration level, height of the intervertebral disc, and disc bulging in MRI after PRPI intervention compared to before PRPI intervention.23
Limitations
There are some methodological limitations in the body of evidence presented. In this report, we identified 4 systematic reviews22-25 to answer the research question on clinical effectiveness of PRPIs. Two22,25 of these reviews used single-arm meta-analysis to provide before-after comparisons of outcomes in within the PRPI group, while 1 systematic review23 narratively summarized the findings of the included primary studies. Only 1 systematic review24 included a meta-analysis comparing PRPI to the control group. Most of the primary studies included in these reviews were observational studies, with only a small number of RCTs (3 RCTs per systematic review in 2 systematic reviews22,24). The sample sizes of included systematic reviews22-24 were relatively small, with fewer than 200 patients. For the results from before-after comparison, observational studies or RCTs with high risk of bias, we cannot conclusively determine that the changes in the outcome measure are solely caused by the PRPI intervention, and there may be potential selection bias, recall bias, or performance bias. None of the systematic reviews conducted subgroup analysis or meta-regression to investigate the observed statistical heterogeneity. Moreover, 1 systematic review22 employed flawed methods to calculate the incidence rate.
The body of evidence also has issues with unclear reporting. All included systematic reviews22-25 did not provide a comprehensive description of the types of PRPI used such as pure or leucocyte PRP or the frequencies of the injections. In addition, the treatment history or co-interventions with the PRPIs intervention were not clearly provided. We are unclear about the psychometric properties for disability measures, the definition of the patient satisfaction and adverse events. Thus, the interpretations of evidence regarding these outcomes were limited.
We also noted some evidence gaps in this report. There was no systematic review conducted that considered the patients' perspective by comparing the observed mean difference with the tool’s minimal important difference in their statistical findings. Moreover, no systematic review was found that reported the comparisons between PRPI and other conservative treatments such as non-steroidal anti-inflammatory drugs, exercise or physiotherapy in the current report. The primary studies of 1 included systematic review22 were conducted in Asia and the US. Thus, the generalizability of these findings to settings in Canada is uncertain.
Conclusions and Implications for Decision- or Policy-Making
Four systematic reviews22-25 were identified to address the clinical effectiveness of PRPI for patients with LBP. These studies provided evidence from RCTs, before and after studies, and case reports to suggest that patients with LBP treated with PRPI had statistically significantly reduced pain (up to 12 months) or disability scores (up to 6 months) compared to before PRPI treatment. One systematic review24 that included 3 RCTs reported that PRPI may be better than control injections (including steroid injections) for patients with LBP in reducing pain scores within 8 weeks, improving the number of patients who experienced at least 50% pain relief at 3 months, and enhancing patient satisfaction, without increasing the adverse event rate. No major complications or adverse effects related to PRPIs were reported in all included systematic reviews.22-25 Due to the potential bias of observational studies and before-after designs, these findings need to be interpreted with caution.
Individuals with LBP typically require a range of interventions, both pharmacological and non-pharmacological interventions.9 One systematic review23 only included patients who did not respond to conservative treatment and had MRI evidence of disc degeneration. Other included systematic reviews22,24,25 did not clearly report the indication for starting PRPI treatment. Additionally, the definition of conservative treatment was unclear, leaving uncertainty about whether all individuals need an MRI or conservative treatment before further intervention with PRPI.
The prognosis of patients with LBP is relatively good in that most patients can recover with other treatment such as exercise or physiotherapy;4,6,7,9 however, we did not identify any studies comparing PRPI with exercise or physiotherapy that met our inclusion criteria. We may need such comparative studies to fully assess the benefits of adding PRPI to usual care or other interventions. When there is acceptable variability in population and intervention characteristics, conducting a systematic review with network meta-analysis may be helpful to get the relative effect of PRPI versus other active interventions. Considering the current limitations of the body of evidence, primary studies with robust design and adequate sample size that address the relative effects of PRPI versus other treatments are also needed. The accessibility and cost of PRPI, and the values or preferences of patients regarding injections can also play a significant role in the decision-making process.
References
1.Hoy D, March L, Brooks P, et al. The global burden of low back pain: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis. 2014;73(6):968-974. PubMed
2.Meucci RD, Fassa AG, Faria NM. Prevalence of chronic low back pain: systematic review. Rev Saude Publica. 2015;49:1. PubMed
3.Wu A, March L, Zheng X, et al. Global low back pain prevalence and years lived with disability from 1990 to 2017: estimates from the Global Burden of Disease Study 2017. Ann Transl Med. 2020;8(6):299. PubMed
4.Hartvigsen J, Hancock MJ, Kongsted A, et al. What low back pain is and why we need to pay attention. Lancet. 2018;391(10137):2356-2367. PubMed
5.Freburger JK, Holmes GM, Agans RP, et al. The rising prevalence of chronic low back pain. Arch Intern Med. 2009;169(3):251-258. PubMed
6.Guideline for the evidence-informed primary care management of low back pain. 2nd ed. Calgary (AB): Toward Optimized Practice (TOP); 2011: https://www.cfpc.ca/CFPC/media/Resources/Pain-Management/Low_Back_Pain_Guidelines_Oct19.pdf. Accessed 2023 May 05.
7.Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet. 2017;389(10070):736-747. PubMed
8.Edwards J, Hayden J, Asbridge M, Magee K. The prevalence of low back pain in the emergency department: a descriptive study set in the Charles V. Keating Emergency and Trauma Centre, Halifax, Nova Scotia, Canada. BMC Musculoskelet Disord. 2018;19(1):306. PubMed
9.Chou R. Subacute and chronic low back pain: Nonpharmacologic and pharmacologic treatment. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2023: http://www.uptodate.com. Accessed 2023 Apr 25.
10.Foster NE, Anema JR, Cherkin D, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet. 2018;391(10137):2368-2383. PubMed
11.Buchbinder R, van Tulder M, Öberg B, et al. Low back pain: a call for action. Lancet. 2018;391(10137):2384-2388. PubMed
12.Everts P, Onishi K, Jayaram P, Lana JF, Mautner K. Platelet-Rich Plasma: New Performance Understandings and Therapeutic Considerations in 2020. Int J Mol Sci. 2020;21(20). PubMed
13.Martínez-Martínez A, Ruiz-Santiago F, García-Espinosa J. Platelet-rich plasma: myth or reality? Radiologia (Engl Ed). 2018;60(6):465-475. PubMed
14.Bolton L. Platelet-Rich Plasma: Optimal Use in Surgical Wounds. Wounds. 2021;33(8):219-221. PubMed
15.Streit-Ciećkiewicz D, Kołodyńska A, Futyma-Gąbka K, Grzybowska ME, Gołacki J, Futyma K. Platelet Rich Plasma in Gynecology-Discovering Undiscovered-Review. Int J Environ Res Public Health. 2022;19(9). PubMed
16.Sharara FI, Lelea LL, Rahman S, Klebanoff JS, Moawad GN. A narrative review of platelet-rich plasma (PRP) in reproductive medicine. J Assist Reprod Genet. 2021;38(5):1003-1012. PubMed
17.Emer J. Platelet-Rich Plasma (PRP): Current Applications in Dermatology. Skin Therapy Lett. 2019;24(5):1-6. PubMed
18.Akeda K, Yamada J, Linn ET, Sudo A, Masuda K. Platelet-rich plasma in the management of chronic low back pain: a critical review. J Pain Res. 2019;12:753-767. PubMed
19.Mohammed S, Yu J. Platelet-rich plasma injections: an emerging therapy for chronic discogenic low back pain. J Spine Surg. 2018;4(1):115-122. PubMed
20.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
21.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
22.Peng B, Xu B, Wu W, Du L, Zhang T, Zhang J. Efficacy of intradiscal injection of platelet-rich plasma in the treatment of discogenic low back pain: A single-arm meta-analysis. Medicine (Baltimore). 2023;102(10):e33112. PubMed
23.Di Martino A, Barile F, Fiore M, Ruffilli A, Faldini C. Are injectable regenerative therapies effective in the treatment of degenerative disc disease? A systematic review. J Neurosurg Sci. 2022;66(5):399-405. PubMed
24.Xuan Z, Yu W, Dou Y, Wang T. Efficacy of Platelet-rich Plasma for Low Back Pain: A Systematic Review and Meta-analysis. J Neurol Surg A Cent Eur Neurosurg. 2020;81(6):529-534. PubMed
25.Sanapati J, Manchikanti L, Atluri S, et al. Do Regenerative Medicine Therapies Provide Long-Term Relief in Chronic Low Back Pain: A Systematic Review and Metaanalysis. Pain Physician. 2018;21(6):515-540. PubMed
26.Barker TH, Migliavaca CB, Stein C, et al. Conducting proportional meta-analysis in different types of systematic reviews: a guide for synthesisers of evidence. BMC Med Res Methodol. 2021;21(1):189. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Peng et al. (2023)22 China Funding source: National Natural Science Foundation of China and Changsha City | Study design: systematic review with single-arm meta-analysis Number of included and relevant studies: 6 | Patients with discogenic LBP Number of patients: 127 (number in the individual studies ranged from 14 to 29) Sex: male (n = 8 to 14, 45% to 60%) Mean age: from 33 to 47.5 years. Disease duration: one study reported a median of 90 days; for other studies over 3 or 6 months. | Intervention: intradiscal injection of PRP Comparator: Baseline scores in the same group | Outcomes:
Follow-up: from 1 week to 60 weeks |
DI Martino et al. (2022)23 Italy Funding source: the authors declared no conflict of interest. | Study design: systematic review of RCTs, observational studies, and/or case reports without meta-analysis Number of included studies: 17 (7 were relevant to the current report). | Patients with discogenic LBP, failure of conservative treatment, MRI evidence of disc degeneration Number of patients: 198 Sex: NR Mean age: NR Disease duration: at least 3 to 6 months | Intervention: Autologous PRP (volume injected between 1 mL and 3 mL). Comparator: 1 individual study had a control group without comparator details and for other studies, the comparator was baseline score in the same group | Outcomes:
Follow-up: from 2 months to 12 months |
Xuan et al. (2020)24 China Funding source: the authors declared no conflict of interest. | Study design: systematic review of RCTs Number of included and relevant studies: 3 | Patients with LBP Number of patients: 131 (number in the individual studies ranged from 40 to 46) Sex: males in the intervention group: n = 10 to 16, proportion = 43% to 80%; in the control group: n = 9 to16, proportion = 39% to 80%. Mean age: from 35 to 52.91 years Disease duration: NR | Intervention: intra-articular injection with PRP; Ultrasound-guided sacroiliac joint injection with 3 mL leukocyte-free PRP with 0.5 mL calcium chloride; Intradiscal injection. Comparator: Intra-articular injection with local anesthetic/ corticosteroid; ultrasound-guided sacroiliac joint injection with 1.5 mL methylprednisolone (40 mg/mL); Intradiscal contrast drug. | Outcomes:
Follow-up: from within 8 weeks to 1 year |
Sanapati et al. (2018)25 US Funding source: the authors declared no conflict of interest. | Study design: systematic review of RCTs, observational studies and case reports with single-arm meta-analysis Number of included studies: 21 (15 were relevant to the current report). | Patients with LBP and lower extremity pain Number of patients: NR Sex: NR Mean age: NR Disease duration: NR | Intervention: PRP (lumbar disc injections, epidural injections, lumbar facet intra-articular injections, sacroiliac joint injection) Comparator: Baseline scores in the same group | Outcomes:
Follow-up: NR |
NA = not applicable; NR = not reported; ODI = Oswestry Disability Index; RDQ = Roland-Morris Disability Questionnaire; NRS = Numerical Rating Scale; RCTs = randomized controlled trials; PRP = platelet-rich plasma; LBP = lower back pain; VAS = visual analogue scale.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Systematic Reviews Using AMSTAR 220
Strengths | Limitations |
|---|---|
Peng et al. (2023)22 | |
The purpose of the study was clearly described. The intervention, comparator, and study designs of the individual study for inclusion were clearly described. The protocol of this review was prospectively registered in the INPLASY (202240108). Multiple databases were searched (PubMed, Embase, Cochrane Library, Clinical Trials databases and Chinese databases). Medical subject terms, related entry terms, and search strategy for PubMed were provided. The authors manually searched reference lists of retrieved studies and related reviews. A flow chart of study selection was provided. The details of included studies were described. The review authors assessed risk of bias for included RCTs using Cochrane Risk of Bias Assessment Tool and for included observational studies using the Newcastle–Ottawa Scale. The full-text screening and risk of bias assessments were clearly described and conducted by 2 reviewers independently. The review authors declared no conflicts of interest. | A grey literature search was not reported. The list of excluded studies was not provided. The review authors did not report the funding sources for eligible studies. It is unclear if the study data extractions were performed by 2 authors independently. The review authors did not assess the potential impact of risk of bias in individual studies on result interpretations. The review authors used the wrong formula, incidence rate = OR/ (1+OR), to calculate the incidence rate and related confidence intervals for improvement in outcome measures. The review authors use inappropriate methods for the statistical combination of results. No explanation provided for the observed heterogeneity in the results. Publication bias was not assessed. Sensitivity analyses were not conducted. |
DI Martino et al. (2022)23 | |
The purpose of the study was clearly described. Multiple databases were searched (PubMed, Medscape, MEDLINE, Google Scholar, and Cochrane databases). Keywords used in the search were provided. References from the identified articles were checked. A flow chart of study selection was provided. The review authors assessed the risk of bias in included studies using the quality index checklist developed by Downs and Black. The study selection processes were clearly described and conducted by 2 reviewers. The data extraction process was prepared and agreed upon by 3 independent authors. The review authors declared no conflicts of interest. | The outcomes and study designs of the individual study were not clearly described. Embase was not searched. The full search strategy was not available. A grey literature search was not reported. The review authors did not assess the risk of bias for eligible studies and potential publication bias. The list of excluded studies was not provided. The review authors did not report the funding sources for eligible studies. The review authors did not assess the potential impact of risk of bias in individual studies on result interpretations. |
Xuan et al. (2020)24 | |
The purpose of the study was clearly described. The study designs of the individual study for inclusion were clearly described. Multiple databases were searched (PubMed, Embase, Web of Science, EBSCO, and the Cochrane Library). Keywords in the search were provided. The authors hand-searched the reference lists of the retrieved studies and the relevant reviews. A flow chart of study selection was provided. The details of included studies in were adequately described. The review authors assessed the risk of bias for eligible studies using the Jadad scale. The review authors use appropriate methods for the statistical combination of results. The review authors declared no conflicts of interest. | The diagnostic criteria of LBP, disease durations, and background therapies were not clearly described. A grey literature search was not reported. We are unclear if the study selection process, the data extractions, and risk of bias assessments were performed by 2 authors independently. The list of excluded studies was not provided. The reported figures and main text showed inconsistencies in the direction of the treatment effect on pain relief at 3 months and patient satisfaction. The review authors did not report the funding sources for eligible studies. |
Sanapati et al. (2018)25 | |
The purpose of the study was clearly described. Multiple databases were searched (PubMed, Cochrane library, US National Guideline Clearing house, and Clinical trials). The authors also searched the references of the previous systematic reviews and cross references, and other sources such as non-indexed journals and abstracts. The search strategy was provided. A flow chart of study selection was provided. The full-text screening and risk of bias assessments were clearly described and conducted by 2 reviewers independently. The review authors assessed the risk of bias for eligible studies using multiple tools, including the Cochrane review rating system, Interventional Pain Management Techniques -- Quality Appraisal of Reliability and Risk of Bias Assessment Tool for RCTs and observational studies. The authors provided the level of evidence according to the best-evidence synthesis and multiple available criteria, including the Cochrane Review criteria and the United States Preventive Task Force criteria. The review authors declared no conflicts of interest. | The intervention and outcome measures of the individual study were not clearly described. Embase was not searched. It is unclear if the study data extractions were performed by 2 authors independently. The review authors did not assess potential publication bias. The list of excluded studies was not provided. The review authors did not report the funding sources for eligible studies. The confidence interval stated in the main text regarding the mean difference in pain scores from baseline to the 12-month follow-up does not match the figures presented in the related Figure 3. No analysis was conducted to explore the observed statistical heterogeneity. |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; NA = not applicable; NR = not reported; OR = odds ratio; RCTs = randomized controlled trials.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 4: Summary of Findings by Outcome — Pain
Author (year) and study design | Results | |||||
|---|---|---|---|---|---|---|
Time points | Statistics | Effect size | Method of measurement | P | Notes | |
Pain scores | ||||||
Peng et al. (2023)22 Systematic review with 6 articles: 3 RCTs and 3 perspective cohort studies | 1 month | Pooled SMD (95% CI) | −1.04 (−1.89 to −0.20) | VAS or NRS with 10-point scale | 0.02 | Before-after intradiscal PRPI, from meta-analysis with 3 studies |
2 months | Pooled SMD (95% CI) | −1.33 (−2.20 to −0.46) | VAS or NRS with 10-point scale | 0.003 | Before-after intradiscal PRPI, from meta-analysis with 3 studies | |
6 months | Pooled SMD (95% CI) | −1.42 (−2.25 to −0.59) | VAS or NRS with 10-point scale | 0.0008 | Before-after intradiscal PRPI, from meta-analysis with 4 studies | |
1 month vs. 2 months | Pooled SMD (95% CI) | −0.20 (0.55 to 0.14) | VAS or NRS with 10-point scale | 0.25 | Unclear methods | |
1 month vs. 6 months | Pooled SMD (95% CI) | −0.13 (−0.48 to 0.21) | VAS or NRS with 10-point scale | 0.45 | Unclear methods | |
2 months vs. 6 months | Pooled SMD (95% CI) | 0.06 (−0.28 to 0.41) | VAS or NRS with 10-point scale | 0.72 | Unclear methods | |
DI Martino et al. (2022)23 Systematic review with 7 relevant articles | NR | NR | Before: 7.1 ± 1.2 After: 1.8 ± 2 | VAS with unclear scale | NR | Reported by Akeda et al. (2011) |
NR | NR | Before: 66 ± 13.2 After: 43.3 ± 25.7 | VAS with unclear scale | NR | Reported by Navani et al. (2016) and Levi et al. (2016) | |
NR | NR | Before: 84 ± 11 After: 8 ± 17 | VAS with unclear scale | NR | Reported by Kirchner et al. (2016) | |
NR | Mean with unclear variability measure | Before: 75 ± 13 After: 32 ± 24 | VAS with unclear scale | NR | Reported by Akeda et al. (2017) | |
Xuan et al. (2020)24 Systematic review with 3 RCTs | Within 8 weeks | Pooled MD (95% CI) | −1.47 (−2.12 to −0.81) | NR | < 0.0001 | Intervention-control, from meta-analysis with 2 studies |
Sanapati (2018)25 Systematic review with 15 relevant articles | 6 months | Pooled MD (95% CI) | −40.63 (−68.07 to −13.19) | VAS or NRS ranges from 0 to 100 | 0.004 | Before-after the lumbar disc PRPI, from meta-analysis with 5 studies |
12 months | Pooled MD (95% CI) | −36.41 (−52.31 to −20.51) | VAS or NRS ranges from 0 to 100 | < 0.001 | Before-after the lumbar disc PRPI, from meta-analysis with 3 studies | |
6 months | Pooled MD (95% CI) | −60.28 (−79.27 to −41.29) | Unclear tool ranges from 0 to 100 | < 0.001 | Before-after the epidural PRPI, from meta-analysis with 3 studies | |
Over 50% pain relief (pain score decreased > 50% from baseline) | ||||||
Peng et al. (2023)22 Systematic review with 6 articles: 3 RCTs and 3 perspective cohort studies | 1 month | Incidence rates (95% CI) | 51.0% (0.17 to 0.84) | NA | NR | Before-after, transferred from OR |
2 months | Incidence rates (95% CI) | 53.1% (0.21 to 0.83) | NA | NR | Before-after, transferred from OR | |
6 months | Incidence rates (95% CI) | 51.9% (0.41 to 0.63) | NA | NR | Before-after, transferred from OR | |
Xuan et al. (2020)24 Systematic review with 3 RCTs (2 included in the meta-analysis) | 3 months | Pooled risk ratio (95% CI) | 4.14 (2.22 to 7.74) | NA | < 0.001 | Intervention-control, from meta-analysis with 2 studies |
Over 30% pain relief (pain score decreased > 30% from baseline) | ||||||
Peng et al. (2023)22 Systematic review with 6 articles: 3 RCTs and 3 perspective cohort studies | 1 month | Incidence rates (95% CI) | 57.3% (0.32 to 0.80) | NA | NR | Before-after, transferred from pooled OR |
2 months | Incidence rates (95% CI) | 50.7% (0.19 to 0.82) | NA | NR | Before-after, transferred from pooled OR | |
6 months | Incidence rates (95% CI) | 65.6% (0.48 to 0.80) | NA | NR | Before-after, transferred from OR | |
CI = confidence interval; NA = not applicable; NR = not reported; VAS = Vvsual analogue scale; NRS = Numerical Rating Scale; RCTs = randomized controlled trials; PRP = platelet-rich plasma; LBP = lower back pain; MD = mean difference; SMD = standardized mean difference.
Table 5: Summary of Findings by Outcome — Disability
Author (year) and study design | Results | |||||
|---|---|---|---|---|---|---|
Time points | Statistics | Effect size | Method of measurement | P | Notes | |
Disability score Changes | ||||||
aDI Martino et al. (2022)23 Systematic review with 7 relevant articles | Baseline; 3 months; 6 months | NR | Baseline: 27.9 ± 8.5 3 months: 10.5 6 months: 8.5 ± 8.81 | ODI with unclear scale | NR | Reported by Kumar et al. (2015); PRP epidural injections |
Baseline; 3 months; 6 months | NR | Baseline: 22.0 ± 8.3 3 months: 11.2 ± 10.2 6 months: 11.7 ± 9.2 | ODI with unclear scale | NR | Reported by Becker et al. (2007); PRP epidural injections | |
Baseline; 3 months | NR | Baseline: 49.2 ± 9.624 3 months: 29.5 ± 11.65 | ODI with unclear scale | NR | Reported by Bhatia and Chopra (2016); PRP epidural injections | |
Disability score decreased by 30% from the baseline | ||||||
Peng et al. (2023)22 Systematic review with 6 articles: 3 RCTs and 3 perspective cohort studies | 2 months | Incidence rates (95% CI) | 40.2% (0.26 to 0.56) | ODI with unclear scale | NR | Before-after, transferred from pooled OR |
Disability score decreased by 50% from the baseline | ||||||
Peng et al. (2023)22 Systematic review with 6 articles: 3 RCTs and 3 perspective cohort studies | 6 months | Incidence rates (95% CI) | 53.9% (0.42 to 0.67) | ODI with unclear scale | NR | Before-after, transferred from pooled OR |
CI = confidence interval; NR = not reported; ODI = Oswestry Disability Index; RDQ = Roland-Morris Disability Questionnaire.
aData from appendix table 11 in the included systematic review.23
Table 6: Summary of Findings by Outcome — Patient Satisfaction
Author (year) and study design | Results | |||||
|---|---|---|---|---|---|---|
Time points | Statistics | Effect size | Method of measurement | P | Notes | |
Xuan et al. (2020)24 Systematic review with 3 RCTs (2 included in the meta-analysis) | NR | Pooled RR (95% CI) | 1.91 (1.04 to 3.53) | NA | 0.04 | Intervention vs. control “offers relatively good patient satisfaction.” (page 531) |
CI = confidence interval; NA = not applicable; NR = not reported; RR = risk ratio.
Table 7: Summary of Findings by Outcome — Adverse Events
Author (year) and study design | Results | |||||
|---|---|---|---|---|---|---|
Time points | Statistics | Effect size | Method of measurement | P | Notes | |
Xuan et al. (2020)24 Systematic review with 3 RCTs (2 included in the meta-analysis) | NR | Pooled RR (95% CI) | 1.92 (0.94 to 3.91) | NA | 0.07 | Intervention vs. control |
CI = confidence interval; NA = not applicable; NR = not reported; RR = risk ratio.
Appendix 5: Overlap Between Included Systematic Reviews
Note that this appendix has not been copy-edited.
Table 8: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Peng (2023)22 | Di Martino (2022)23 | Xuan (2020)24 | Sanapati (2018)25 |
|---|---|---|---|---|
Goyal T, Paswan AK, et al. J Musculoskelet Res. 2022; 25:2250009. | Yes | — | — | — |
Zielinski MA, Evans NE, et al. Pain Physician. 2022; 25:29 to 34. | Yes | — | — | — |
Jain D, Goyal T, et al.Pain Med. 2020; 21:2719 to 25. | Yes | — | — | — |
Navani A, Ambach MA, et al. IPM Reports. 2018; 2:111 to 118. | — | — | — | Yes |
Akeda K, Ohishi K, et al. Asian Spine J. 2017; 11(3):380 to 9. | Yes | Yes | — | Yes |
Centeno C, Markle J, et al. J Exp Orthop. 2017; 4:38 | — | — | — | Yes |
Ko GD, Mindra S, et al. J Back Musculoskelet Rehabil. 2017; 30:363 to 370. | — | — | — | Yes |
Singla V, Batra YK, et al. Pain Pract. 2017; 17(06):782 to 791. | — | — | Yes | Yes |
Wu J, Zhou J, et al. Pain Pract. 2017; 17(07):914 to 924. | — | — | Yes | Yes |
Bhatia R, Chopra G, et al. J Clin Diagn Res. 2016; 10:UC05-UC07. | Yes | |||
Kirchner F and Anitua E. J Craniovertebr Junction Spine2016; 7:250 to 256. | — | Yes | — | Yes |
Levi D, Horn S, et al. Pain Med. 2016; 17(6):1010 to 22. | Yes | Yes | — | Yes |
Monfett M, Harrison J, et al. Int Orthop. 2016; 40:1321 to 1328. | — | — | — | Yes |
Tuakli-Wosornu YA, Terry A, et al. PM R. 2016; 8(01): 1 to 10. | Yes | Yes | Yes | Yes |
Wu J, Du Z, et al. Pain Phys. 2016; 8;19(8;11):617 to 625 | — | — | — | Yes |
Kumar R, Goni VG, et al. Asian Spine J. 2015; 9:916 to 922. | — | — | — | Yes |
Navani A and Gupta D. Tech Region Anesth Pain Management. 2015; 19:54 to 59 | — | — | — | Yes |
Navani A and Hames A. Tech Region Anesth Pain Management. 2015; 19(1 to 2):38 to 44. | — | Yes | — | — |
Bodor M, Toy A, et al. Lecture Notes in Bioengineering. 2014; Berlin: Springer, no page information. | — | Yes | — | — |
Akeda K, Imanishi T, et al. Spine J Meet Abstr. 2011; No page information. | — | Yes | — | — |
Becker C, Heidersdorf S, et al. Spine (Phila Pa 1976). 2007; 32:1803 to 1808. | — | — | — | Yes |
“—” = Not included.
Appendix 6: References of Potential Interest
Systematic Reviews – all relevant primary studies were captured in at least one other more comprehensive systematic review
Schneider BJ, Hunt C, Conger A, et al. The effectiveness of intradiscal biologic treatments for discogenic low back pain: a systematic review. Spine J. 2022;22(2):226-237. PubMed
Ambrosio L, Vadala G, Russo F, et al. Interventional Minimally Invasive Treatments for Chronic Low Back Pain Caused by Lumbar Facet Joint Syndrome: A Systematic Review. Global Spine J. 2023 May;13(4):1163-1179. PubMed
Daste C, Laclau S, Boisson M, et al. Intervertebral disc therapies for non-specific chronic low back pain: a systematic review and meta-analysis. Ther Adv Musculoskelet Dis. 2021;13:1759720X211028001.
Chang MC, Park D. The Effect of Intradiscal Platelet-Rich Plasma Injection for Management of Discogenic Lower Back Pain: A Meta-Analysis. J Pain Res. 2021;14:505-512. PubMed
Randomized Controlled Trials
Singh G, Talawar P, Kumar A, Sharma R, Purohit G, Bhandari B. Effect of autologous platelet-rich plasma (PRP) on low back pain in patients with prolapsed intervertebral disc: A randomised controlled trial. Indian J Anaesth. 2023;67(3):277-282. PubMed
Zhang J, Liu D, Gong Q, Chen J, Wan L. Intradiscal Autologous Platelet-Rich Plasma Injection for Discogenic Low Back Pain: A Clinical Trial. Biomed Res Int. 2022;2022:9563693. PubMed
Won SJ, Kim DY, Kim JM. Effect of platelet-rich plasma injections for chronic nonspecific low back pain: A randomized controlled study. Medicine (Baltimore). 2022;101(8):e28935. PubMed
Schepers MO, Groot D, Kleinjan EM, Pol MM, Mylenbusch H, Klopper-Kes AHJ. Effectiveness of intradiscal platelet rich plasma for discogenic low back pain without Modic changes: A randomized controlled trial. Interventional Pain Medicine. 2022;1(1):100011.
Goyal T, Paswan AK, Jain D, Verma N, Dubey RK. Comparative Evaluation Of Efficacy Of Percutaneous Intradiscal Radiofrequency Ablation And Platelet Rich Plasma Injection For Discogenic Low Back Pain: A Prospective Randomized Trial. Journal of Musculoskeletal Research. 2022;25(3).
Akeda K, Ohishi K, Takegami N, et al. Platelet-Rich Plasma Releasate versus Corticosteroid for the Treatment of Discogenic Low Back Pain: A Double-Blind Randomized Controlled Trial. J Clin Med. 2022;11(2):07.
Abo Elfadl GM, Elawamy AM, Abedalmohsen AM, El Sayed AAE, Bahloul M, Ismail EA. Prophylactic use of platelet-rich plasma for post-spinal low back pain following gynecological surgery: a randomized clinical trial. Braz J Anesthesiol. 2021;05:05.
Jain D, Goyal T, Verma N, Paswan AK, Dubey RK. Intradiscal Platelet-Rich Plasma Injection for Discogenic Low Back Pain and Correlation with Platelet Concentration: A Prospective Clinical Trial. Pain Med. 2020;21(11):2719-2725. PubMed
Non-Randomized Studies
Singh C, Yadav S, Loha S, Prakash S, Paswan AK. Comparison of intra-articular lumbar facet joint injection of platelet-rich plasma and steroid in the treatment of chronic low back pain: A prospective study. Journal of Orthopaedics, Trauma and Rehabilitation. 2023.
Machado ES, Ambach MA, Caldas JM, Wei JJ, Bredemeier M. Personalized multitarget biologic injection in the spine: prospective case series of multitarget platelet-rich plasma for low back pain. Regen Med. 2022;17(1):11-22. PubMed
Akeda K, Takegami N, Yamada J, et al. Platelet-Rich Plasma-Releasate (PRPr) for the Treatment of Discogenic Low Back Pain Patients: Long-Term Follow-Up Survey. Medicina (Kaunas). 2022;58(3):16. PubMed
Additional References
Wang F, Cheung CW, Wong SSC. Regenerative medicine for the treatment of chronic low back pain: a narrative review. J Int Med Res. 2023;51(2):3000605231155777. PubMed
Patel A, Koushik S, Schwartz R, et al. Platelet-Rich Plasma in the Treatment of Facet Mediated Low Back Pain: A Comprehensive Review. Orthop Rev (Pavia). 2022;14(4):37076. PubMed
Note: excluded as not a systematic review as defined for Rapid response.
Hauser RA, Matias D, Woznica D, Rawlings B, Woldin BA. Lumbar instability as an etiology of low back pain and its treatment by prolotherapy: A review. J Back Musculoskeletal Rehabil. 2022;35(4):701-712. PubMed
Chou R, Fu R, Dana T, Pappas M, Hart E, Mauer KM. Interventional Treatments for Acute and Chronic Pain: Systematic Review. (Comparative Effectiveness Review No. 247). Rockville (MD): Agency for Healthcare Research and Quality (AHRQ); 2021. https://effectivehealthcare.ahrq.gov/sites/default/files/product/pdf/cer-247-interventional-treatments-acute-chronic-pain_0.pdf. Accessed 2023 May 03.
Baig MZ, Abdullah UEH, Muhammad A, Aziz A, Syed MJ, Darbar A. Use of Platelet-Rich Plasma in Treating Low Back Pain: A Review of the Current Literature. Asian Spine J. 2021;15(1):117-126. PubMed
Urits I, Viswanath O, Galasso AC, et al. Platelet-Rich Plasma for the Treatment of Low Back Pain: a Comprehensive Review. Curr Pain Headache Rep. 2019;23(7):52. PubMed
Darrow M, Shaw B, Nicholas S, Li X, Boeger G. Treatment of unresolved lower back pain with platelet-rich plasma injections. Cogent Medicine. 2019;6(1):1-10.
Akeda K, Yamada J, Linn ET, Sudo A, Masuda K. Platelet-rich plasma in the management of chronic low back pain: a critical review. J Pain Res. 2019;12:753-767. PubMed
Mohammed S, Yu J. Platelet-rich plasma injections: an emerging therapy for chronic discogenic low back pain. J Spine Surg. 2018;4(1):115-122. PubMed
Contributor: Elizabeth Carson
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca