CADTH Health Technology Review
Alternative Therapies to Immunoglobulin for Autoimmune Blistering Diseases
Rapid Review
Authors: Khai Tran, Melissa Walter
Abbreviations
BP
bullous pemphigoid
EADV
European Academy of Dermatology and Venereology
IVIg
IV immunoglobulin
PF
pemphigus foliaceus
PV
pemphigus vulgaris
RCT
randomized controlled trial
Key Messages
We did not find any evidence regarding the clinical effectiveness and safety of alternative treatments to IV immunoglobulin (IVIg) compared to IVIg or placebo for bullous pemphigoid (BP) or pemphigus vulgaris (PV) and pemphigus foliaceus (PF) that met our inclusion criteria for this review.
We identified 6 consensus guidelines presenting treatment algorithms for BP (3 guidelines) or PV and PF (3 guidelines). All guidelines recommend that IVIg may be used as a third-line treatment for severe or refractory cases.
For severe or refractory BP, other therapeutic options than IVIg include monoclonal antibodies, immunosuppressive drugs, immunoadsorption, and plasma exchange (3 guidelines).
For severe or refractory PV and PF, other therapeutic options than IVIg include immunosuppressive drugs, dapsone, immunoadsorption, plasma exchange, and IV corticosteroid pulse therapy (3 guidelines).
The evidence base supporting these guidelines was unclear; recommendations should be interpreted with caution.
Context and Policy Issues
Autoimmune blistering diseases are rare autoimmune diseases of the skin and/or mucous membrane, such as pemphigus and pemphigoid.1 Pemphigus is a group of rare, potentially life-threatening diseases that affect the outer layer of the skin (epidermis) and that are mediated by immunoglobulin G against structural proteins of the desmosomes at the cell-cell junctions, leading to the formation of fragile blisters that rupture easily and leave open sores that may become infected.2 Pemphigus encompasses 2 distinct forms that are caused by humoral autoimmune response: pemphigus vulgaris (PV) and pemphigus foliaceus (PF).2 PV is the most common form in which blisters develop deep in the epidermis in the area of the mouth, then spread to the skin and even the genitals.3 PF is a less severe type in which blisters occur in the superficial layers of the epidermis, form on the scalp and face first, and then spread to the chest and back.3 The annual incidence of pemphigus varies among countries and ethnicities, ranging from 0.6 cases per million in Switzerland (from 2001 to 2002) to 32.0 cases per million in Israel (from 1972 to 1977).4
Pemphigoid refers to a group of subepidermal autoimmune bullous diseases that are characterized by firm blisters and erosions of the skin or mucus membranes that usually will not rupture upon contact, due to autoantibodies against proteins of the hemidesmosomes at the epidermal-dermal junctions.2 Bullous pemphigoid (BP) is a common subtype of pemphigoid diseases that develop predominantly in the abdomen, back, arms, and legs.3 The annual incidence of BP in Europe varied from 2.5 cases per million to 42.8 cases per million.2 Incidence and prevalence data of both pemphigus and pemphigoid in Canada were not available. However, the 2003 record from Statistics Canada reported 15 deaths related to pemphigus and 15 deaths related to BP.5 Among pemphigus-related deaths, 1 was due to PV, 0 to PF, 10 to unspecified pemphigus, and 4 to other types.5 Death occurred mostly in people aged 80 and older.5
There is currently no cure for either pemphigus or pemphigoid; however, the cornerstone of treatment for the diseases is corticosteroids, which are administered topically or orally.3 Immunosuppressive drugs such as mycophenolate mofetil, azathioprine, or methotrexate may be used in combination with corticosteroids to reduce the overall dose of steroids.3 In severe or treatment-resistant cases, other therapies such as IV immunoglobulin (IVIg), rituximab, immunoadsorption, plasma exchange, cyclophosphamide, or pulse steroid therapy may be used.2 IVIg appears to be effective for refractory cases by reducing the levels of circulating autoantibodies associated with pemphigus and pemphigoid through catabolism.6,7
The demand for IVIg has been steadily increasing every year for the treatment of various autoimmune and inflammatory diseases. Due to the COVID-19 pandemic, which has had a strong impact on global blood and plasma collection, countries around the world are experiencing a decline in Ig products.8,9 The shortage of the Ig products, their high cost, and their increasing demand has made it necessary to reevaluate alternative treatment options.
The objective of this report is to summarize the evidence regarding the clinical effectiveness and safety of alternative treatments to IVIg, specifically rituximab, azathioprine, mycophenolate mofetil, cyclophosphamide, and leflunomide, compared to IVIg or placebo for PV, PF, and BP. This report also aims to summarize the recommendations from evidence-based guidelines regarding alternative treatments to IVIg for these populations.
Research Questions
What is the clinical effectiveness of alternative treatments to IVIg compared to IVIg or placebo for autoimmune blistering diseases?
What is the safety of alternative treatments to IVIg compared to IVIg or placebo for autoimmune blistering diseases?
What are the evidence-based guidelines regarding the use of alternative treatments to IVIg for autoimmune blistering diseases?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources, including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, and the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were rituximab, azathioprine, mycophenolate mofetil, cyclophosphamide, or leflunomide; and pemphigus or pemphigoid. An additional focused search for guidelines was conducted using the concepts pemphigus or pemphigoid, and CADTH-developed search filters were applied to this search to limit retrieval to guidelines. Retrieval was limited to the human population. The search was completed on April 12, 2023, and limited to English-language documents published since January 1, 2018.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Patients with autoimmune blistering diseases (i.e., pemphigus vulgaris, pemphigus foliaceus, and bullous pemphigoid) |
Intervention | Rituximab, azathioprine, mycophenolate mofetil, cyclophosphamide, leflunomide |
Comparator | Q1 to Q2: IV Immunoglobulin, placebo Q3: NA |
Outcomes | Q1: Clinical effectiveness (e.g., remission, rate of relapse, HRQoL) Q2: Safety (e.g., adverse events, severe adverse events) Q3: Recommendations regarding best practices (e.g., which alternative to use, dose and timing of treatment, indications) |
Study designs | Health technology assessments, systematic reviews, evidence-based guidelines |
HRQoL = health-related quality of life; NA = not applicable.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, or were published before 2018. Guidelines with unclear methodologies were excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument10 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
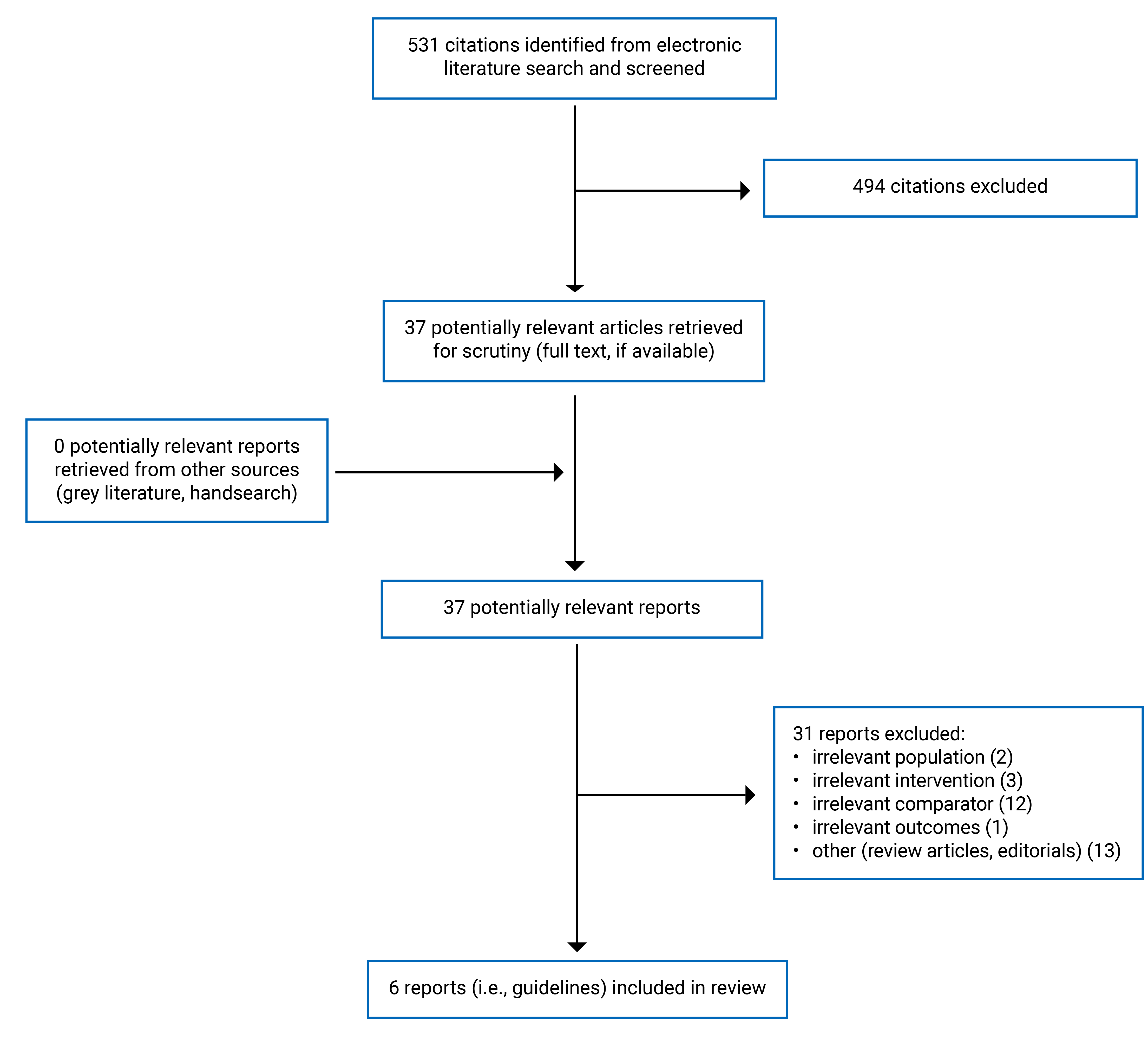
A total of 531 citations were identified in the literature search. Following screening of titles and abstracts, 494 citations were excluded and 37 potentially relevant reports from the electronic search were retrieved for full-text review. No potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 31 publications were excluded for various reasons, and 6 publications (i.e., guidelines) met the inclusion criteria and were included in this report. Appendix 1 presents the PRISMA11 flow chart of the study selection.
Summary of Study Characteristics
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
This report identified and included 6 guidelines, all of which were consensus guidelines for the management of BP12-14 or PV and PF15-17 that were based on information from existing guidelines. Guidelines for the management of BP were the European Academy of Dermatology and Venereology (EADV) guideline by Borradori et al. (2022),12 the Japanese guideline by Ujiie et al. (2019),13 and the Italian guideline by Cozzani et al. (2018).14 The 3 guidelines for the management of PV and PF were the Taiwanese Dermatology Association guideline by Chu et al. (2022),15 the EADV guideline by Joly et al. (2020),16 and the Italian guideline by Feliciani et al. (2018).17
The methods for evidence collection, selection, and synthesis were not reported; instead, expert panels reviewed and discussed evidence from previous guidelines. Specific methods for evaluating the quality of evidence that supports the recommendations were not reported in 5 guidelines.12,13,15-17 The quality of evidence in 1 guideline14 was assessed and given a grade ranging from 1 (i.e., randomized controlled trial [RCT]) to 5 (i.e., expert opinion).
The recommendations were made mostly through experts’ opinions. In each guideline, the working groups consisted of experts who reviewed the previous guideline recommendations, input their expert opinions, and prepared different versions of the statements until consensus was reached through voting. The methods for grading the strength of recommendations were not reported in 3 guidelines.14,15,17 Three guidelines12,13,16 provided the strength of each recommendation, which was voted by consensus. Two guidelines12,16 used syntax to grade the strength of recommendations ranging from highest (“is recommended” for strong recommendations) to lowest (“is not recommended” for negative recommendations). One guideline13 labelled its recommendations from A (strongly recommended) to D (recommended not to implement).
Country of Origin
The guidelines were conducted by authors from Europe,12,16 Taiwan,15 Japan,13 and Italy.14,17
Patient Population
The target population in the included guidelines was patients with BP12-14 or patients with PV or PF.15-17
The intended users in all included guidelines were health professionals who are involved in the patients’ management.
Interventions
The included guidelines12-17 considered diagnostic steps and treatment algorithms for the management of BP or PV and PF.
Outcomes
The included guidelines12-17 considered all clinical outcomes related to diagnosis, treatment, and monitoring of the diseases.
Summary of Critical Appraisal
All included guidelines12-17 were explicit in terms of scope and purpose (i.e., objectives, health questions, and populations), and clearly presented recommendations (i.e., they were specific, unambiguous, and it was easy to find key recommendations, with options for managing the different conditions or health issues). Recommendations were in the forms of treatment algorithms for specific conditions that were easy to follow.12-17 In terms of stakeholder involvement, all included guidelines12-17 clearly defined their target users and their development groups. However, it was unclear if the views and preferences of the patients were sought in all guidelines.12-17 In all included guidelines,12-17 recommendations were formulated through consensus based on information from previous guidelines, current evidence, and experts’ opinions. However, methods for evidence collection, criteria for selection, and methods for evidence synthesis were not provided. Therefore, it is unclear if the search and selection of relevant evidence was comprehensive, and the evidence base supporting the recommendations is uncertain. The procedures for updating the guidelines were not reported in all guidelines.12-17 None of the guidelines clearly described facilitators and barriers to application, advice and/or tools on how the recommendations can be put into practice, resource implications, or monitoring or auditing criteria.12-17 For editorial independence, all guidelines12-17 reported on the competing interests of guideline development group members, but did not report if the views of the funding body had any influence on the content of the guidelines. Overall, all the included guidelines were limited in terms of rigour of development, reporting, and applicability, which reduced certainty in the findings.
Additional details regarding the strengths and limitations of the included guidelines12-17 are provided in Appendix 3.
Summary of Findings
Clinical Effectiveness of Alternative Treatments to IVIg Compared to IVIg or Placebo for Autoimmune Blistering Diseases
No relevant health technology assessments or systematic reviews were identified regarding the clinical effectiveness of alternative treatments to IVIg for BP or PV and PF.
Safety of Alternative Treatments to IVIg Compared to IVIg or Placebo for Autoimmune Blistering Diseases
No relevant health technology assessments or systematic reviews were identified regarding the clinical safety of alternative treatments to IVIg for BP or PV and PF.
Guidelines Regarding the Use of Alternative Treatments to IVIg for Autoimmune Blistering Diseases
Appendix 4 presents the summary of recommendations from the included guidelines. All the identified guidelines (3 for BP12-14 and 3 for PV and PF)15-17 provided treatment algorithms that included options for first-line treatment, second-line treatment, and third-line treatment for treatment-resistant or hard-to-treat cases. Topical and oral corticosteroids were the first choice of treatments for BP, while systemic corticosteroids and rituximab were the first-line therapies for PV and PF. As IVIg was 1 of the options for third-line treatment or treatment-resistant cases, other third-line treatment options in each guideline were considered alternative treatments to IVIg and are discussed here.
Details of stepladder treatments, including first-line and second-line treatments in each guideline, are presented in Appendix 4 for BP or PV and PF, respectively.
Treatment Management of BP
The guideline from the EADV by Borradori et al. (2022)12 recommends that immunosuppressants such as methotrexate, azathioprine, or mycophenolate may be used as add-on therapy to corticosteroids in treatment-recalcitrant BP (i.e., resistant to 0.75 mg/kg per day of prednisone). In this guideline, IVIg is considered as a therapeutic option for recalcitrant BP, but not for severe BP, corticosteroid-dependent, or relapsing BP. Other therapeutic options in the same group with IVIg were rituximab, omalizumab, dupilumab, and immunoadsorption. The strength of both recommendations was labelled as “may be recommended,” which is the rating assigned if the evidence was derived from small RCTs, nonrandomized prospective multicentre studies, or large retrospective multicentre studies.
The Japanese guideline by Ujiie et al. (2019)13 describes options for the management of moderate, severe, and treatment-resistant BP, including IVIg and other therapies. It recommends oral steroids as first-line treatment, and that additional treatments may be considered if sufficient efficacy could not be achieved with oral steroids. These treatments include immunosuppressants (e.g., azathioprine, mizoribine, oral cyclophosphamide, cyclosporine, mycophenolate mofetil, methotrexate), methyl prednisolone pulse therapy, IVIg, plasma exchange, cyclophosphamide pulse therapy, tetracycline or minocycline plus nicotinamide, dapsone, and superpotent topical corticosteroids (e.g., clobetasol propionate). This guideline did not differentiate therapies based on the severity of the disease (i.e., moderate, severe, and treatment-resistant BP were grouped together and discussed collectively). Based on the level of evidence (not reported), the strength of recommendations for additional treatments to oral steroids was either labelled as C1, indicating that these therapeutic options “may be implemented,” or not reported.
The Italian guideline by Cozzani et al. (2018)14 recommends several therapeutic options for treatment-resistant BP, despite several weeks of intensive therapy with combined topical and oral steroids. These were immunosuppressants (such as methotrexate, azathioprine, mycophenolate), IVIg, immunoadsorption, rituximab, omalizumab, cyclophosphamide, and plasma exchange. This guideline did not report the strength of the recommendations but provided the level of evidence for each treatment option, ranging from level 1 (highest) to level 5 (lowest). Relevant to this report, recommendations for superpotent topical corticosteroids and plasma exchange were based on level 1 evidence, and recommendations for rituximab, omalizumab, and immunoadsorption were based on level 4 evidence.
Overall, recommendations from 3 guidelines12-14 for BP showed that IVIg is reserved for treatment-resistant or hard-to-treat cases, and the alternative therapies to IVIg include monoclonal antibodies (e.g., rituximab, omalizumab, dupilumab), immunosuppressive drugs (e.g., azathioprine, mycophenolate mofetil, cyclophosphamide, methotrexate), immunoadsorption, and plasma exchange.
Treatment Management of PV and PF
The Taiwanese guideline by Chu et al. (2022)15 recommends several third-line therapeutic options for patients who did not respond to azathioprine as second-line therapy. These were oral cyclophosphamide, methotrexate, mycophenolate mofetil, immunoadsorption, IVIg, and plasma exchange. This guideline was formulated based on information from previous consensus guidelines, and it did not classify the treatment options based on disease severity. The level of evidence or the strength of the recommendations were not reported.
The European EADV guideline by Joly et al. (2020)16 listed 3 treatments options that may be recommended as add-on therapy to rituximab or immunosuppressants in patients with severe or refractory pemphigus (PF or PV) who did not respond to rituximab or immunosuppressant therapy. These were IVIg, IV corticosteroid pulse therapy, and immunoadsorption. The strength of the recommendation was labelled as “may be recommended” as the evidence was derived from small RCTs, nonrandomized prospective multicentre or large retrospective multicentre studies.
The Italian guideline by Feliciani et al. (2018)17 recommended several therapeutic options as adjuvant to systemic corticosteroids in the third-line treatment of treatment-resistant pemphigus. These were IVIg, immunoadsorption, cyclophosphamide, methotrexate, or dapsone. The recommendations were formulated based on an existing French guideline for the management of pemphigus that was published in 2011. This guideline did not report the level of evidence or the strength of the recommendations.
Overall, recommendations from 3 guidelines15-17 for pemphigus showed that IVIg is used only in third-line treatment or treatment-resistant PV and PF, and the alternative therapies to IVIg include immunosuppressive drugs (e.g., cyclophosphamide, mycophenolate mofetil), immunoadsorption, plasma exchange, IV corticosteroid pulse therapy, methotrexate, and dapsone.
Limitations
The included guidelines had several limitations. First, because of the rarity of the diseases and few clinical studies with high degree of evidence, recommendations were made mostly by expert consensus, relying on their clinical experience and perspectives when supporting evidence was limited or not available. Second, there were some differences in recommendations from different guidelines that reflect incomplete knowledge on the optimal treatment modalities, probably due to the paucity of high-level evidence. For instance, IVIg is reserved for treatment-recalcitrant BP in the EADV guideline,12 while it is considered when sufficient efficacy cannot be achieved with oral steroids in moderate, severe, or treatment-resistant cases in the Japanese guideline.13 This would lead to the divergent expert opinion on a number of questions, which would need to be clarified with future studies. Third, the recommendations did not address potential side-effects of the proposed drugs. Also, patient preferences or experiences were not sought and considered while formulating the recommendations. Fourth, there were no clear recommendations for alternative therapies to IVIg specifically; instead, the drugs or therapies were grouped together with IVIg as therapeutic options for third-line treatment or hard-to-treat cases. This may lead to the assumption that those drugs or therapies are equivalent in treatment efficacy and safety.
Conclusions and Implications for Decision- or Policy-Making
No relevant literature was identified to answer the first 2 research questions; therefore, conclusions could not be provided regarding the clinical effectiveness and safety of alternative therapies to IVIg compared to IVIg or placebo for BP or PV and PF.
Six consensus guidelines were identified, 3 for the treatment of BP12-14 and 3 for the treatment of PV and PF.15-17 Recommendations in all included guidelines were in the forms of treatment algorithms in which lists of drugs were classified in a stepladder from first choice to third choice or for hard-to-treat cases. In both BP and PV or PF conditions, IVIg was reserved as a last option in severe or refractory cases. For BP, other therapeutic options to IVIg in the third-line category included monoclonal antibodies (e.g., rituximab, omalizumab, dupilumab), immunosuppressive drugs (e.g., azathioprine, mycophenolate mofetil, methotrexate, cyclophosphamide), immunoadsorption, and plasma exchange. For PV and PF, other therapeutic options to IVIg included immunosuppressive drugs (i.e., cyclophosphamide, mycophenolate mofetil, methotrexate), dapsone, immunoadsorption, plasma exchange, and IV corticosteroid pulse therapy. Although those therapies were listed together with IVIg for third-line treatment, their comparative efficacy and safety with IVIg or among each other remain unclear and have not been addressed in the guidelines. In addition, the methods reporting for these consensus-based guidelines was limited, and the evidence base supporting the recommendations is uncertain. Therefore, extreme caution should be taken when considering any of those therapies as alternatives to IVIg. Safety is the most important factor and should be carefully considered when choosing a therapy to replace IVIg. Future studies are needed to clarify the comparative clinical effectiveness and safety of alternative treatments to IVIg for autoimmune blistering diseases, and to support the development of robust evidence-based guidance for their use.
References
1.Ellebrecht CT, Maseda D, Payne AS. Pemphigus and Pemphigoid: From Disease Mechanisms to Druggable Pathways. J Invest Dermatol. 2022;142(3 Pt B):907-914. PubMed
2.Egami S, Yamagami J, Amagai M. Autoimmune bullous skin diseases, pemphigus and pemphigoid. J Allergy Clin Immunol. 2020;145(4):1031-1047. PubMed
3.NORD – National Organization for Rare Disorders. Pemphigus and Pemphigoid. 2019; https://rarediseases.org/rare-diseases/pemphigus/. Accessed 2023 May 1.
4.Schmidt E, Kasperkiewicz M, Joly P. Pemphigus. Lancet. 2019;394(10201):882-894. PubMed
5.Causes of death. Chapter XII: Diseases of the skin and subcutaneous tissue (L00 to L99), by age group and sex, Canada. Ottawa (ON): Statistics Canada; 2003: https://www150.statcan.gc.ca/n1/en/pub/84-208-x/2005002/t/4200018-eng.pdf?st=DG4toT6D. Accessed 2023 May 11.
6.Hertl M, Eming R. Management of refractory pemphigus vulgaris and pemphigus foliaceus. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2023: http://www.uptodate.com/. Accessed 2023 May 1.
7.Murrell D, Ramirez-Quizon M. Management and prognosis of bullous pemphigoid. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2023: http://www.uptodate.com/. Accessed 2023 May 1.
8.N’Kaoua E, Attarian S, Delmont E, et al. Immunoglobulin shortage: Practice modifications and clinical outcomes in a reference centre. Rev Neurol (Paris). 2022;178(6):616-623. PubMed
9.Novaretti MC, Dinardo CL. Clinical applications of immunoglobulin: update. Rev Bras Hematol Hemoter. 2011;33(3):221-230. PubMed
10.Agree Next Steps Consortium. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2023 May 1.
11.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
12.Borradori L, Van Beek N, Feliciani C, et al. Updated S2 K guidelines for the management of bullous pemphigoid initiated by the European Academy of Dermatology and Venereology (EADV). J Eur Acad Dermatol Venereol. 2022;36(10):1689-1704. PubMed
13.Ujiie H, Iwata H, Yamagami J, et al. Japanese guidelines for the management of pemphigoid (including epidermolysis bullosa acquisita). J Dermatol. 2019;46(12):1102-1135. PubMed
14.Cozzani E, Marzano AV, Caproni M, Feliciani C, Calzavara-Pinton P. Bullous pemphigoid: Italian guidelines adapted from the EDF/EADV guidelines. G Ital Dermatol Venereol. 2018;153(3):305-315. PubMed
15.Chu CY, Lee CH, Lee HE, et al. Taiwanese dermatological association (TDA) consensus for the management of pemphigus. J Formos Med Assoc. 2022;21:21. PubMed
16.Joly P, Horvath B, Patsatsi A, et al. Updated S2K guidelines on the management of pemphigus vulgaris and foliaceus initiated by the european academy of dermatology and venereology (EADV). J Eur Acad Dermatol Venereol. 2020;34(9):1900-1913. PubMed
17.Feliciani C, Cozzani E, Marzano AV, Caproni M, Di Zenzo G, Calzavara-Pinton P. Italian Guidelines in Pemphigus - adapted from the European Dermatology Forum (EDF) and European Academy of Dermatology and Venerology (EADV). G Ital Dermatol Venereol. 2018;153(5):599-608. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
EADV, Borradori et al. (2022)12 | ||||||
Intended users: Health professionals involved in the patient’s management including dermatologists, general practitioners, specialized nurses, and all other specialists. Target population: Patients with BP. | Management of BP including diagnostic steps and therapeutic management. | All new relevant knowledge on clinical practice, and evidence about benefits of novel diagnostic and therapeutic interventions and outcomes. | NR | Quality of evidence: NR Strength of recommendation: syntaxa was used for specific recommendations based on the levels of evidence. | The EADV Task force appointed a writing group to:
| The manuscript was revised by different European patient organizations. The revised version was finally passed to the EDF for final consensus. The guideline was published in peer-reviewed journal. |
TDA, Chu et al. (2022)15 | ||||||
Intended Users: Health professionals involved in management of pemphigus. Target Population: Patients with PV and PF. | Management of pemphigus including assessment of disease severity and therapeutic management. | All outcomes related to diagnosis, treatment, and monitoring of pemphigus. | NR | Quality of evidence: NR Strength of recommendation: NR | A panel of pemphigus experts:
| Published in peer-reviewed journal. |
EADV, Joly et al. (2020)16 | ||||||
Intended Users: Health professionals involved in the patient’s management including dermatologists, general practitioners, specialized nurses, and all other specialists whose expertise might be necessary based on the clinical context. Target Population: Patients with PV and PF | Management of PV and PF including diagnostic steps and therapeutic management. | All new relevant knowledge on clinical practice, and evidence about benefits of novel diagnostic and therapeutic interventions and outcomes. | NR | Quality of evidence: NR Strength of recommendation: syntaxa was used for specific recommendations based on the levels of evidence. | The EADV Task force appointed a writing group to:
| The manuscript was revised by different European patient organizations. The revised version was finally passed to the EDF for final consensus. The guideline was published in peer-reviewed journal. |
Ujiie et al. (2019)13 | ||||||
Intended Users: Health professionals involved in management of pemphigoid (including epidermolysis bullosa acquisita) Target Population: Patients with pemphigoid (including epidermolysis bullosa acquisita) | Management of pemphigoid including diagnostic steps and therapeutic management. | All outcomes related to diagnosis, treatment, and monitoring of pemphigoid. | NR | Quality of evidence: NR Strength of recommendation: labelled as A (strongly recommended); B (recommended); C1 (may be implemented); C2 (due to scant evidence, not actively recommended); D (recommended not to implement). | The Committee set clinical questions and described recommendations based on evidence-based medicine derived form Japanese and international sources. The guidelines were established mostly based on the opinions of the Committee. Details of the recommendation development and evaluation were not reported. | The guideline was published in peer-reviewed journal. |
Cozzani et al. (2018)14 | ||||||
Intended Users: Health professionals involved in the patient’s management including dermatologists, general practitioners, specialized nurses, and all other specialists. Target Population: Patients with BP. | Management of BP including diagnostic steps and therapeutic management. | All outcomes related to diagnosis, treatment, and monitoring of BP. | NR | Quality of evidence: labelled from 1 to 5b Strength of recommendation: NR | Not described in published articles. | The guideline was published in peer-reviewed journal. |
Feliciani et al. (2018)17 | ||||||
Intended Users: Health professionals involved in the patient’s management including dermatologists, general practitioners, specialized nurses, and all other specialists. Target Population: Patients with pemphigus (e.g., PV and PF). | Management of PV and PF including diagnostic steps and therapeutic management. | All outcomes related to diagnosis, treatment, and monitoring of pemphigus. | NR | Quality of evidence: NR Strength of recommendation: NR | A working group (group of experts):
| The revised version was finally passed to the EDF for final consensus of the EDF members. The guideline was published in peer-reviewed journal. |
BP = bullous pemphigoid; EADV = European Academy of Dermatology and Venereology; EDF = European Dermatology Forum; NR = not reported; PF = pemphigus foliaceus; PV = pemphigus vulgaris; TDA = Taiwanese Dermatological Association.
Note: This table has not been copy-edited.
aSyntax used for specific recommendations: “is recommended”: strong recommendations from large randomized prospective multicentre studies; “may be recommended”: recommendations from small randomized or non-randomized prospective multicentre or large retrospective multicentre studies; “may be considered”: recommendations pending from case series, or small retrospective single-centre studies. It also has been used when a consensus could not be reached among experts; “is not recommended”: negative recommendation.
bLevel of evidence: Level 1: randomized prospective single-centre or multicentre study. In case that in the latter the intervention is shown effective and not contradicted by other studies, it is considered validated; Level 2: randomized prospective single-centre study (in case of poor methodological quality), retrospective multicentre study; Level 3: case series, retrospective single-centre study; Level 4: anecdotal case reports; Level 5: expert opinion.
Appendix 3: Critical Appraisal of Included Publications
Note that this table has not been copy-edited.
Table 3: Strengths and Limitations of Guidelines Using AGREE II10
Item | EADV, Borradori et al. (2022)12 | TDA, Chu et al. (2022)15 | EADV, Joly et al. (2020)16 | Ujiie et al. (2019)13 | Cozzani et al. (2018)14 | Feliciani et al. (2018)17 |
|---|---|---|---|---|---|---|
Domain 1: scope and purpose | ||||||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes | Yes | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes | Yes | Yes | Yes |
Domain 2: stakeholder involvement | ||||||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes | Yes | Yes | Yes | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
6. The target users of the guideline are clearly defined. | Yes | Yes | Yes | Yes | Yes | Yes |
Domain 3: rigour of development | ||||||
7. Systematic methods were used to search for evidence. | No | No | No | No | No | No |
8. The criteria for selecting the evidence are clearly described. | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
9. The strengths and limitations of the body of evidence are clearly described. | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
10. The methods for formulating the recommendations are clearly described. | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
12. There is an explicit link between the recommendations and the supporting evidence. | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
13. The guideline has been externally reviewed by experts before its publication. | Yes | Yes | Yes | Yes | Yes | Yes |
14. A procedure for updating the guideline is provided. | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
Domain 4: clarity of presentation | ||||||
15. The recommendations are specific and unambiguous. | Yes (Treatment algorithm) | Yes (Treatment algorithm) | Yes (Treatment algorithm) | Yes (Treatment algorithm) | Yes (Treatment algorithm) | Yes (Treatment algorithm) |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes | Yes | Yes | Yes |
Domain 5: applicability | ||||||
18. The guideline describes facilitators and barriers to its application. | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
20. The potential resource implications of applying the recommendations have been considered. | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
21. The guideline presents monitoring and/or auditing criteria. | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
Domain 6: editorial independence | ||||||
22. The views of the funding body have not influenced the content of the guideline. | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes | Yes | Yes | Yes | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II.
Appendix 4: Main Study Findings
Note that this table has not been copy-edited.
Table 4: Summary of Recommendations in Included Guidelines for Bullous Pemphigoid EADV, Borradori et al. (2022)
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
EADV, Borradori et al. (2022)12 | |
Mild and moderate BP (BPDAI < 20 and 20 ≤ BPDAI < 57, respectively) | |
First choice | |
| Quality of evidence: NR Strength of recommendation: May be considered (recommendation pending) |
| Quality of evidence: NR Strength of recommendation: Is recommended (strong recommendation) |
Second choice | Quality of evidence: NR Strength of recommendation: May be recommended (recommendation) |
| |
Severe BP (BPDAI ≥ 57) | |
Note: In patients who do not achieve control within 1 to 3 weeks, dose of prednisone can be increase up to 0.75 mg/kg or add superpotent topical corticosteroids.d | Quality of evidence: NR Strength of recommendation: Is recommended (strong recommendation) |
Corticosteroid-dependent or relapsing BP | |
Combination with and/or introduction of conventional immunosuppressantse
| Quality of evidence: NR Strength of recommendation: May be considered (recommendation pending) |
In patients with poor general condition and/or contraindications to immunosuppressive drugs:
| Quality of evidence: NR Strength of recommendation: May be considered (recommendation pending) |
Treatment-recalcitrant BP (resistant to 0.75 mg/kg/day prednisone) | |
Combination with and/or introduction of conventional immunosuppressants:
| Quality of evidence: NR Strength of recommendation: May be considered (recommendation pending) |
Other therapeutic options:
| Quality of evidence: NR Strength of recommendation: May be considered (recommendation pending) |
BP = bullous pemphigoid; BPDAI = Bullous Pemphigoid Disease Activity Index; EADV = European Academy of Dermatology and Venereology; IVIg = IV immunoglobulin; NR = not reported; RCT = randomized controlled trial.
aTopical treatment was supported by 2 RCTs showing that topical corticosteroids improved BP patients’ outcome.
bA prospective observational multicenter study indicated that a 0.5 mg/kg/day prednisone is effective in patients with mild and moderate BP.
cNo consensus could be reached among experts regarding the use of doxycycline and dapsone in BP. Dapsone may be considered in patients with contraindications to oral corticosteroids or immunosuppressive treatments, with mild and moderate BP.
dEvidence from a multicenter observational study showed that increase the dose of prednisone up to 0.75 mg/kg or add topical corticosteroids in addition to 0.5 mg/kg prednisone is a therapeutic option in patients who do not achieve control within 1 to 3 weeks.
eEvidence on immunosuppressive drugs (i.e., methotrexate, azathioprine, mycophenolate) for patients with relapse BP who are not adequately controlled by topical or oral corticosteroids was supported by 3 RCTs and 1 retrospective observational study.
fA case study suggested that omalizumab may be considered in patients who are contraindicated to immunosuppressive drugs.
gThe beneficial effect of rituximab (anti-CD20 monoclonal antibody) in difficult-to-treat cases of BP was demonstrated in 2 case series and 1 retrospective chart review study.
hAn open retrospective series suggested the potential efficacy of dupilumab in BP.
iIn an RCT add-on therapy with IVIg, 2 g/kg/day in BP cases with no improvement on prednisolone ≥ 0.4 mg/kg/day showed a trend toward a beneficial effects.
jOne case series and 1 narrative review provided beneficial evidence of immunoadsorption as adjuvant treatment of severe/refractory BP.
Table 5: Summary of Recommendations in Included Guidelines for Bullous Pemphigoid, Ujiie et al. (2019)
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
Ujiie et al. (2019)13 | |
Mild BP | |
Topical therapy (steroid ointment, antibiotic-containing ointment, zinc oxide ointment)a | Quality of evidence: NR Strength of recommendation: NR |
Tetracycline (500 to 2000 mg/day) or minocycline (100 to 200 mg/day) + nicotinamide (500 to 2000 mg/day)b | Quality of evidence: NR Strength of recommendation: C1 (may be implemented) |
Dapsone 25 to 100 mg/day, concomitantly used with topical steroid therapyc | Quality of evidence: NR Strength of recommendation: C1 (may be implemented) |
Oral steroid: 0.2 to 0.3 mg/kg/day prednisolonec | Quality of evidence: NR Strength of recommendation: B (recommended) |
Moderate, severe and treatment resistant casesd | |
Oral steroid: 0.5 to 1 mg/kg/day prednisolone | Quality of evidence: NR Strength of recommendation: B (recommended) |
If sufficient efficacy cannot be achieved with oral steroids, considered additional treatments as followed: | |
Immunosuppressants:
| Quality of evidence: NR Strength of recommendation: C1 (may be implemented) |
Methyl prednisolone pulse therapy: 0.5 to 1 g/day for 3 days. | Quality of evidence: NR Strength of recommendation: C1 (may be implemented) |
IVIg therapy: 400 mg/kg/day intravenously for 5 days. | Quality of evidence: NR Strength of recommendation: C1 (may be implemented) |
Plasma exchange | Quality of evidence: NR Strength of recommendation: NR |
Cyclophosphamide pulse therapy: IV injection once per day (500 to 1000 mg/m2 body surface area) | Quality of evidence: NR Strength of recommendation: NR |
Rituximab | Quality of evidence: NR Strength of recommendation: NR |
Tetracycline or minocycline + nicotinamide | Quality of evidence: NR Strength of recommendation: C1 (may be implemented) |
Dapsone | Quality of evidence: NR Strength of recommendation: C1 (may be implemented) |
Superpotent topical corticosteroid (clobetasol propionate) | Quality of evidence: NR Strength of recommendation: NR |
BP = bullous pemphigoid; BPDAI = Bullous Pemphigoid Disease Activity Index; EADV = European Academy of Dermatology and Venereology; IVIg = IV immunoglobulin; NR = not reported; RCT = randomized controlled trial.
aAn RCT reported that, in mild and moderate cases, the systemic topical application of clobetasol propionate twice a day is effective.
bEvidence from a previous guideline suggested that a combination therapy of tetracycline (or minocycline) and nicotinamide was effective in some patients with mild BP. It is standard to use topical steroid in combination.
cEvidence supporting dapsone and oral steroid was not reported.
dSupporting evidence on treatment recommendations for moderate, severe, and treatment resistant cases was not reported.
Table 6: Summary of Recommendations in Included Guidelines for Bullous Pemphigoid, Cozzani et al. (2018)
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
Cozzani et al. (2018)14 | |
Localized or limited disease with mild activity | |
First choice | |
| Quality of evidence: Level 1, validated Strength of recommendation: NR |
Second choice | |
| Quality of evidence: Level 1 to 3, not validated Strength of recommendation: NR |
Treatment-resistant BP | |
| Quality of evidence: Level 1 to 3 Strength of recommendation: NR |
| Quality of evidence: Level 3 Strength of recommendation: NR |
| Quality of evidence: Level 4 Strength of recommendation: NR |
| Quality of evidence: Level 4 Strength of recommendation: NR |
| Quality of evidence: Level 3 Strength of recommendation: NR |
| Quality of evidence: Level 1 Strength of recommendation: NR |
BP = bullous pemphigoid; BPDAI = Bullous Pemphigoid Disease Activity Index; EADV = European Academy of Dermatology and Venereology; IVIg = IV immunoglobulin; NR = not reported; RCT = randomized controlled trial.
aEvidence from 2 RCTs suggested that clobetasol propionate was an effective treatment for mild BP.
bTwo systematic reviews and 1 narrative review provided evidence for the effectiveness of tetracyclines plus nicotinamide for the treatment of BP.
cFindings of a retrospective study showed that combination of low-dose methotrexate and superpotent topical steroids may result in protracted control of BP in carefully selected patients.
dFindings of a retrospective study support treatment of BP with dapsone.
eTwo RCTs and 3 retrospective studies provided evidence for the use of immunosuppressants for treatment of BP.
fOne case series suggested that IVIg may be a useful therapeutic alternative to conventional modalities for selected BP patients.
gOne case report and 1 narrative review suggested that immunoadsorption might be a safe and effective adjuvant treatment in severe and recalcitrant BP.
hFindings of 3 case series suggested that rituximab and omalizumab may be effective in treatment-resistant BP.
IFindings of case series suggested that low-dose oral cyclophosphamide might be an effective treatment of BP.
jFindings of 1 RCT suggested that plasma exchange allows a substantial saving of corticosteroids in the management of BP.
Table 7: Summary of Recommendations in Included Guidelines for Pemphigus Vulgaris and Pemphigus Foliaceus, TDA, Chu et al. (2022)
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
TDA, Chu et al. (2022)15 | |
First-line treatment | |
| Quality of evidence: NR Strength of recommendation: NR |
Second-line treatment | |
| Quality of evidence: NR Strength of recommendation: NR |
Third-line treatment | |
| Quality of evidence: NR Strength of recommendation: NR |
EADV = European Academy of Dermatology and Venereology; IVIg = IV immunoglobulin; NR = not reported; PDAI = Pemphigus Disease and Area Index; PF = pemphigus foliaceus; PV = pemphigus vulgaris; TDA = Taiwanese Dermatology Association; RCT = randomized controlled trial.
aThe use of systemic corticosteroids as one of the first-line therapies was supported by evidence from 2 previous guidelines.
bA network meta-analysis showed that rituximab was the most effective of the seven steroid-sparing adjuvants used for pemphigus treatment. One case series and 1 RCT showed that when rituximab was combined with corticosteroids, patients experienced better improvement and had a higher chance of disease improvement with when compared with corticosteroids alone. One systematic review and meta-analysis showed the effectiveness of rituximab in achieving complete remission of pemphigus.
cOne retrospective observational study suggested that azathioprine could serve as a good choice of maintenance therapy for patients who had received rituximab as first-line or add-on therapy.
dEvidence from a previous guideline supported the use of oral cyclophosphamide as alternative to azathioprine or mycophenolate mofetil in refractory cases with second line-treatment. Because of its potential toxicity, it is best reserved for patients with recalcitrant or severe PV.
eEvidence from a previous guideline supported the use of methotrexate, an immunomodulatory and corticosteroid-sparing agent, as a third-line treatment.
fEvidence from a previous guideline supported the use of mycophenolate mofetil as an alternative to azathioprine.
gEvidence from a previous guideline supported the use of immunoadsorption as third-line treatment.
hEvidence from a previous guideline supported the use of IVIg in concomitant with immunosuppressive adjuvants for treatment of pemphigus.
iEvidence from a previous guideline supported the use of plasma exchange as another alternative in refractory cases.
Table 8: Summary of Recommendations in Included Guidelines for Pemphigus Vulgaris and Pemphigus Foliaceus, EADV, Joly et al. (2020)
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
EADV, Joly et al. (2020)16 | |
Mild PF (PDAI ≤ 15) | |
First-line treatment | |
| Quality of evidence: NR Strength of recommendation: May be considered (recommendation pending) |
Second-line treatment | |
| Quality of evidence: NR Strength of recommendation: May be recommended (recommendation) |
Mild PV (PDAI ≤ 15) | |
First-line treatment | |
| Quality of evidence: NR Strength of recommendation: Is recommended (strong recommendation) |
Second-line treatment | |
| Quality of evidence: NR Strength of recommendation: Is recommended (strong recommendation) |
Moderate and severe types of PV and PF (15 < PDAI ≤ 45 and PDAI > 45, respectively) | |
First-line treatmente | |
| Quality of evidence: NR Strength of recommendation: Is recommended (strong recommendation) |
Severe/refractory PV and PF | |
| Quality of evidence: NR Strength of recommendation: May be recommended (recommendation) |
EADV = European Academy of Dermatology and Venereology; IVIg = IV immunoglobulin; NR = not reported; PDAI = Pemphigus Disease and Area Index; PF = pemphigus foliaceus; PV = pemphigus vulgaris; TDA = Taiwanese Dermatology Association; RCT = randomized controlled trial.
aEvidence from a report of 9 cases showed that dapsone could be used as initial treatment of mild PF. Dapsone is often combined with topical corticosteroids.
bA retrospective cohort study showed that patients relapsed with dapsone alone need a systemic corticosteroid treatment.
cTwo case series suggested that rituximab alone or associated with oral corticosteroids was an effective treatment for pemphigus.
dEvidence from 2 RCTs showed that systemic corticosteroid therapy alone or with an immunosuppressive drug (azathioprine or mycophenolate) as corticosteroid-sparing agent was an effective treatment for pemphigus, particularly in patients with an increased risk of corticosteroid side-effect related to prolonged use of corticosteroids, or there is no possibility to treat with rituximab.
eTwo RCTs and 1 cost study provided evidence to support for first-line treatment in patients with moderate and severe pemphigus.
fAn RCT showed that IVIg was an effective and safe treatment for patients with pemphigus who are relatively resistant to systemic steroids.
gA case-control study showed that high-dose pulse administration of glucocorticoids is a potentially effective therapy to be considered in the treatment of patients with severe pemphigus vulgaris.
hFindings from 2 case series showed that the combination of immunoadsorption with rituximab, pulsed dexamethasone, azathioprine, or mycophenolate mofetil might be effective in treatment of difficult-to-treat pemphigus.
Table 9: Summary of Recommendations in Included Guidelines for Pemphigus Vulgaris and Pemphigus Foliaceus, Feliciani et al. (2018)
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
Feliciani et al. (2018)17 | |
First-line treatment | |
| Quality of evidence: NR Strength of recommendation: NR |
Second-line treatment with adjuvant to systemic corticosteroids | |
| Quality of evidence: NR Strength of recommendation: NR |
Third-line treatment with adjuvant to systemic corticosteroids | |
| Quality of evidence: NR Strength of recommendation: NR |
EADV = European Academy of Dermatology and Venereology; IVIg = IV immunoglobulin; NR = not reported; PDAI = Pemphigus Disease and Area Index; PF = pemphigus foliaceus; PV = pemphigus vulgaris; TDA = Taiwanese Dermatology Association; RCT = randomized controlled trial.
aFindings of 3 case series and 1 consensus document suggested that rituximab may be an effective treatment of refractory pemphigus.
bAn RCT found that IVIg was an effective and safe treatment for patients with pemphigus who are relatively resistant to systemic steroids.
cOne case series, 1 retrospective study and 1 consensus document provided evidence for the effectiveness of immunoadsorption in difficult-to-treat pemphigus.
dOne prospective cohort study and 1 case report highlighted the potential role of cyclophosphamide therapy for pemphigus.
eOne retrospective cohort study showed that methotrexate was an effective and safe adjuvant therapy for PV.
fAn RCT demonstrated a trend to efficacy of dapsone as a steroid-sparing drug in maintenance-phase PV.
Appendix 5: References of Potential Interest
Review Articles
Guignant M, Tedbirt B, Murrell DF, et al. How Do Experts Treat Patients with Bullous Pemphigoid around the World? An International Survey. JID Innov. 2022;2(4):100129. PubMed
Khalid SN, Khan ZA, Ali MH, Almas T, Khedro T, Raj Nagarajan V. A blistering new era for bullous pemphigoid: A scoping review of current therapies, ongoing clinical trials, and future directions. Ann Med Surg (Lond). 2021;70:102799. PubMed
Zhao W, Wang J, Zhu H, Pan M. Comparison of Guidelines for Management of Pemphigus: a Review of Systemic Corticosteroids, Rituximab, and Other Immunosuppressive Therapies. Clin Rev Allergy Immunol. 2021;61(3):351-362. PubMed
Patel PM, Jones VA, Murray TN, Amber KT. A Review Comparing International Guidelines for the Management of Bullous Pemphigoid, Pemphigoid Gestationis, Mucous Membrane Pemphigoid, and Epidermolysis Bullosa Acquisita. Am J Clin Dermatol. 2020;21(4):557-565. PubMed
Contributor: Elizabeth Carson
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca