CADTH Health Technology Review
Chloroprocaine for Spinal or Epidural Anesthesia
Rapid Review
Authors: Zahra Jafari, Carolyn Spry
Abbreviations
AMSTAR
A Measurement Tool to Assess Systematic Reviews
CP
chloroprocaine
LA
local anesthesia
MA
meta-analysis
NMA
network meta-analysis
RCT
randomized controlled trials
RR
risk ratio
SR
systematic review
TNS
transient neurologic symptoms
Key Messages
Compared to alternative local anesthetic drugs, chloroprocaine may result in a shorter or equal onset of sensory and motor blocks and recovery from sensory and motor blocks.
Compared to alternative local anesthetic drugs, chloroprocaine has a shorter time to unaided ambulation, time to independent urination, and time to discharge.
Chloroprocaine may have better or equal clinical effectiveness than alternative drugs for spinal or epidural local anesthesia.
Compared to alternative local anesthetic drugs, chloroprocaine may cause higher rates of adverse events. However, due to inconsistency in evidence, it was difficult to draw any firm conclusions in this regard, suggesting further investigation for decision-making.
We did not find any evidence regarding the cost-effectiveness of chloroprocaine compared to other local anesthetic drugs and evidence-based guidelines for using chloroprocaine for patients requiring spinal or epidural anesthesia that met the inclusion criteria for the present review.
Context and Policy Issues
Spinal and epidural anesthesia are procedures to deliver local anesthetics in or around the spine (lumbar level) that numb parts of the body to block pain.1 For epidural local anesthesia (LA), the drug is injected around the spinal cord into the epidural space, just outside the sac of cerebrospinal fluid (CSF). A small tube (catheter) is often left in place to receive more anesthetic drugs during or after the procedure if required. For spinal LA, the drug is injected into the CSF around the spinal cord only once (without a catheter placed) and rapidly begins to take effect.1 Overall for LA, anesthetics with rapid onset and fast regression (recovery or resolution) of sensory and motor blocks that allow for a quick recovery and fast discharge with minimal side effects are preferred.2
Because of the unique short duration of action, intense block, fast resolution of both sensory and motor blocks, quick recovery, and suitability for day-case surgery, lidocaine has an attractive pharmacokinetic profile for spinal anesthesia.2,3 However, due to concerns about lidocaine’s adverse events (AEs), such as hypotension, urinary retention, and transient neurologic symptoms (TNS), its widespread clinical use has been limited.2,4 The symptoms of TNS can appear within a few hours up to 24 hours after full recovery and may last up to 2 to 5 days.3 These symptoms consist of pain originating in the gluteal region and radiating to both lower extremities. Irrespective of dose or concentration, all forms of lidocaine are associated with TNS, and the cause of this painful condition is still unknown.3
Bupivacaine, introduced in the 1960s, is the most commonly used alternative to lidocaine. As an alternative, bupivacaine has a lower incidence of TNS but may have a longer recovery duration.5 In addition, bupivacaine might cause unpredictable, dose-dependent levels of LA and lead to complications, such as hemodynamic instability (insufficient blood flow in the body)3 and urinary retention.6
Chloroprocaine (CP) is a derivative of procaine indicated for spinal and epidural neuraxial anesthesia with a rapid onset of action and elimination by plasma cholinesterase metabolism.7 The obstetric setting is the most common application for CP, where it is used to provide fast-onset epidural anesthesia for urgent or emergent Caesarean delivery.7 Due to concerns about neurotoxicity related to preservatives, CP was withdrawn from the market in the 1980s; and reintroduced into clinical practice in 2004 with a new formulation without preservatives.3 Recently, the preservative-free 2-CP has regained popularity because of its desirable pharmacokinetic properties, such as very fast onset, a quick recovery time, and lower incidence of TNS.3,8
Due to a shortage of raw materials and a combination of corporate decisions by the CP manufacturer, preservative-free CP was removed from the market in Canada in 2012.9 CP is still manufactured and broadly available in the US and Europe under the trade names Clorotekal, Nesacaine, and Ampres.10 According to the Canadian Anesthesiologists’ Society (CAS),11 Health Canada–approved the importation of preservative-free CP to Canada in January 2021, but accessibility is limited by foreign supply.10 Given supply challenges, the question arises as to whether CP should be preferred over alternatives for spinal or epidural LA. With respect to recent changes to the use of chloroprocaine in Canada, it is unclear if chloroprocaine should be included in regular formulary use. This report aimed to summarize and critically appraise available evidence of the clinical effectiveness and cost-effectiveness of CP compared to alternative anesthetic drugs used for spinal or epidural LA, as well as the evidence-based guidelines for using CP for patients requiring spinal or epidural LA.
Research Questions
What is the clinical effectiveness of chloroprocaine for patients requiring spinal or epidural local anesthesia?
What is the cost-effectiveness of chloroprocaine for patients requiring spinal or epidural local anesthesia?
What are the evidence-based guidelines for the use of chloroprocaine for patients requiring spinal or epidural local anesthesia?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were epidural anesthesia, spinal anesthesia, and chloroprocaine. No filters were applied to limit retrieval by study type. The search was completed on March 27, 2023 and limited to English-language documents published since January 1, 2018.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first screening level, titles, and abstracts were reviewed, and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Patients (any age) requiring spinal or epidural local anesthesia |
Intervention | Chloroprocaine (any dose) |
Comparator | Q1 and Q2: Alternative anesthetic drugs used for spinal or epidural local anesthesia (e.g., bupivacaine, lidocaine, mepivacaine, ropivacaine, procaine, tetracaine) Q3: Not applicable |
Outcomes | Q1: Clinical effectiveness (e.g., pain relief, duration of pain relief, time to ambulation, length of stay, patient satisfaction, health-related quality of life) and safety (e.g., complications, rate of adverse events, mortality) Q2: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained, incremental cost-effectiveness ratio) Q3: Recommendations regarding the best use of chloroprocaine for spinal or epidural local anesthesia (e.g., appropriate administration, patient population, appropriate dose) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, economic evaluations, evidence-based guidelines |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in, were duplicate publications, or were published before January 1, 2018.
Critical Appraisal of Individual Studies
One reviewer critically appraised systematic reviews (SRs) using a Measurement Tool to Assess Systematic Reviews (AMSTAR-2) tool12 and randomized controlled trials (RCTs) using the Downs and Black checklist.13 For SRs with network meta-analysis (NMA), both AMSTAR12 and a Questionnaire to Assess the Relevance and Credibility of an NMA14 were used. Summary scores were not calculated for the studies; the strengths and limitations observed among the included studies were summarized and described narratively in Appendix 3.
Summary of Evidence
Quantity of Research Available
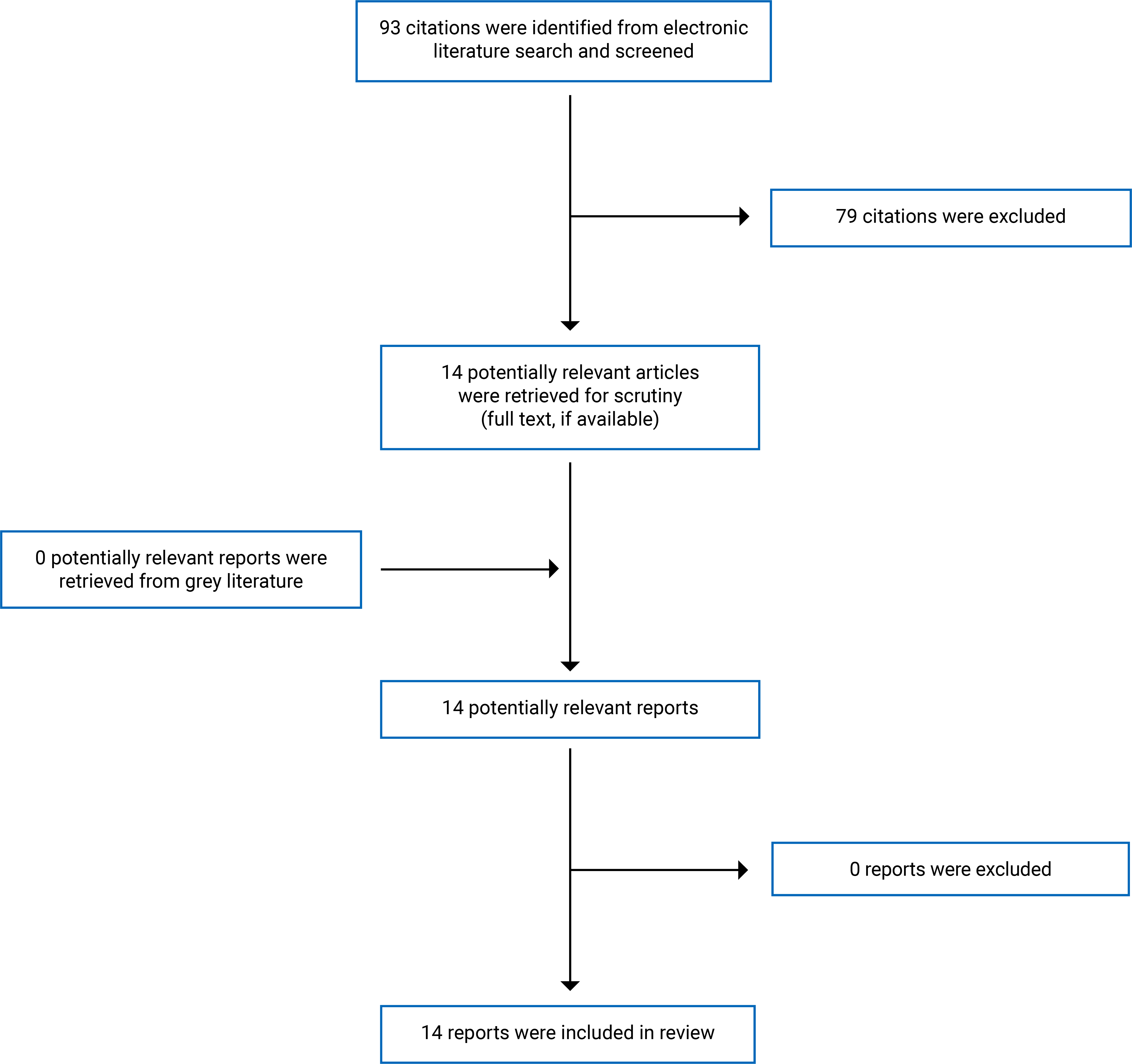
A total of 93 citations were identified in the literature search. Following the screening of titles and abstracts, 79 citations were excluded and 14 potentially relevant articles from the electronic search were retrieved for full-text review. No potentially relevant publication was identified from the grey literature search for full-text review. Fourteen publications2-4,6,15-24 met the selection criteria and were included in this report.
Appendix 1 presents the PRISMA25 flow chart of the study selection. Additional references of potential interest are provided in Appendix 5.
Summary of the Study Characteristics
Fourteen peer-reviewed publications2-4,6,15-24 including 2 SRs with NMA,3,21 1 SR with MA,2 and 11 RCTs4,6,15-20,22-24 were included in this report. Given the diversity of the 3 included SRs in terms of population, intervention, comparator, and outcome (i.e., PICO components), except for 1 RCT included in 2 SRs,2,3 no more overlaps were identified in the 3 SRs.2,3,21
Additional details regarding the characteristics of the included publications are provided in Appendix 2 (Table 2 and Table 3).
Study Design
Of the 14 peer-reviewed publications2-4,6,15-24 that met the selection criteria for this report, 11 were RCTs.4,6,15-20,22-24
The other 3 publications were SRs consisting of 1 SR with NMA based on a graph theoretical approach within a frequentist framework for indirect and mixed comparisons,3 1 SR with NMA using Bayesian statistical analysis for direct and indirect comparisons,21 and 1 SR with MA using a random effect model for statistical analysis.2
Country of Origin
Systematic Reviews
The authors of 2 SRs with NMA3,21 and 1 SR with MA2 were based in the UK, US, and Switzerland, respectively.
Primary Studies
Eleven RCTs4,6,15-20,22-24 were conducted by authors from India,4,6,16,18,20,22,23 China,24 Netherlands,15 Belgium,17 and US.19
Patient Population
Systematic Reviews
In 1 SR and NMA21 on the choice of local anesthetic for epidural Caesarean section, RCTs on women with epidural Caesarean section were selected for review. Of the 24 RCTs included, 5 RCTs used 2-CP 3% epidurally for surgical anesthesia.
In 1 SR and NMA3 to compare lidocaine with other types of local anesthetics in the frequency of TNS after spinal LA, RCTs and quasi-RCTS on adults undergoing surgery were considered for review. Of 24 RCTs, 2 RCTs26,27 used 2-CP for spinal LA.
In 1 SR and MA2 to compare the clinical outcomes of spinal 2-CP with low-dose bupivacaine, 4 RCTs on adults with lower extremity and abdominal surgery were included.
Primary Studies
Patients with various types of surgeries received spinal4,6,15-20,22,23 or epidural24 LA, including different ambulatory surgeries,16 perineal surgery or gynecological procedures,4,6,22 knee arthroscopy,15,17,24 ureteroscopic lithotripsy surgery,20 inguinal hernia repair surgery,18 lower abdominal or lower limb surgeries,23 and women undergoing cervical cerclage surgery.19
Interventions and Comparators
Systematic Reviews
In the SR and NMA by Reschke et al. (2020)21 to rank the speed of onset of the 6 local anesthetics for epidural Caesarean section, 2-CP 3% was compared with bupivacaine 0.5%, lidocaine 2%, lidocaine 2% plus bicarbonate, l-bupivacaine 0.5%, and ropivacaine 0.75%.
In the SR and NMA by Forget et al. (2019),3 the frequency of TNS with lidocaine was compared with other types of LA, including 2‐CP, bupivacaine, prilocaine, mepivacaine, procaine, ropivacaine, and levobupivacaine.
In the SR and MA by Saporito et al. (2019),2 the clinical outcomes of spinal 2-CP (40 or 50 mg) were compared with low-dose bupivacaine (less than 10 mg).
Primary Studies
Intervention: Except for 1 study with epidural LA,24 spinal LA was used in all primary studies.4,6,15-20,22,23 The studies used various percentages and doses of CP for LA consisting of 1-CP 1% (40 mg),6,20 2-CP 1% (30 mg),4,22 CP 1% (50 mg),17 2-CP 1% (40 mg),15,16,23 2-CP 1% (40 mg) combined with saline (0.025 mg);18 2-CP 3% (30 mg),24 or 2-CP 3% (50 mg) combined with fentanyl (0.015 mg).19
Comparators: The interventions that were compared with CP were: bupivacaine 5% with different doses (10 mg,6,16 20 mg,20 15 mg,4 or 10.5 mg18), prilocaine 2% (50 mg),17 levobupivacaine 5% (15 mg),22 prilocaine 2% (40 mg),15 lidocaine 2% (30 mg),24 2-CP (40 mg) combined with fentanyl (0.025 mg),18 2-CP 1% (40 mg) combined with buprenorphine (0.06 mg);23 or hyperbaric bupivacaine 0.75% (9 mg) combined with fentanyl (0.015 mg).19
Outcomes
Systematic Reviews
The outcome measures in 2 SRs with NMA3,21 and 1 SR with MA2 were speed of anesthesia onset and AEs,21 presence of TNS,3 onset time, block duration, time to ambulation, and time to discharge2 after spinal or epidural LA with CP compared to other drugs.
Primary Studies
The outcome measures used in the primary studies were the onset of sensory block,6,15,16,18-20,23,24,28 resolution (recovery or regression) of sensory block,6,15,17-20,23,24,28 onset of motor block,4,16,18,20,23,28 resolution of motor block,4,6,16,18-20,23,24,28 time to maximum sensory block,6 time to unaided ambulation,16,20,23,28 time to independent urination (spontaneous voiding),4,15,17,20,23,28 time for first analgesic dose,23 time to discharge,15,16,19,20 patient satisfaction,19 TNS,19 and other AEs (hypotension or urinary retention).4,17,18,24
Patients underwent spinal anesthesia in the sitting position at the L3-L44,6,15-19,22,23 or L4-L516,19,20,23 interspace (lumbar level) in the sitting position for the spinal LA, and L2–L3 interspace in the supine position for epidural LA.24 In all selected primary studies,4,6,15-20,22-24 patients were placed supinely following injection, and the sensory level was assessed every few minutes (e.g., 2 minutes) to pinprick until a constant level was achieved for 2 consecutive tests. Motor block was assessed every few minutes (e.g., 2 minutes) using the Bromage score (0 = no block, full straight leg raise possible; 1 = unable to raise straight leg, 2 = unable to flex knee but able to flex ankle; and 3 = no motor movement, complete motor block).29
In 1 study,19 patients were telephoned on the first postoperative day and asked to rate their satisfaction with the anesthetic (complete, adequate, or inadequate) and report any complaints of TNS (e.g., abnormal sensations such as hypoesthesia or dysesthesia in the gluteal region and radiating to the lower extremities), back pain, or headache.
Summary of the Critical Appraisal
SRs
Of the 14 studies included in this report, 3 were SRs (Table 4) consisting of 2 SRs with NMA3,21 and 1 SR with MA.2 We used the AMSTAR-2 checklist12 to evaluate the quality of SRs and determine whether the most important elements of the SR methodology were reported. In addition, we used the Questionnaire to Assess the Relevance and Credibility of NMAs14 to assess the strengths and limitations of the 2 SRs with NMA3,21 (Table 5). This questionnaire consists of 26 questions related to the relevance (i.e., the usefulness of NMA to inform health care decision-making) and credibility (including 5 subdomains: indirect comparison or NMA, analysis, reporting quality, and transparency, interpretation, and conflict of interest) of NMAs.14
The strengths of the 3 SRs were in defining the research question and inclusion and exclusion criteria, describing the study design of the selected primary studies, using a comprehensive literature search strategy, conducting study selection and data extraction in duplicate, using a satisfactory tool for assessing the risk of bias (RoB) in primary studies, and reporting potential sources of conflict of interest. In 2 SRs,2,21 the systematic search protocol was established before the conduct of the review. Two SRs2,21 did not list excluded studies and justify the exclusions. The SR with NMA21 on the choice of local anesthetic for epidural Caesarean section had several limitations. The authors did not adequately describe the selected primary studies, investigate publication bias (small study bias) and discuss its potential impact on the outcomes, interpret the potential impact of RoB in primary studies included in MA, and describe heterogeneity observed in MA results. For the NMA,21 the authors used the Markov Chain Monte Carlo algorithm to derive inferences from the random-effects Bayesian network, the Metmeta package to evaluate the assumptions of transitivity (i.e., the similarity of treatment effect distribution across primary studies) and consistency (of direct and indirect estimates), and meta-regression to assess the interactions of 2 covariates with the onset of surgical LA. The NMA21 was limited in including sufficient detail about the rationale for the use of random effects, conducting within-study randomization and assessing agreement in treatment effects (consistency) in statistical methods, assessing and discussing heterogeneity with subgroup analyses, and if all pairwise contrasts between interventions were reported along with measures of uncertainty.
Forget et al. (2019)3 conducted an SR with NMA to determine the frequency of TNS in adult surgical patients after spinal LA with lidocaine compared to other types of LA. Due to expected methodological and clinical heterogeneities across the included studies resulting in varying effect sizes between studies of pairwise comparisons, the authors used an inverse variance weighting for summary statistics and a random-effect model for statistical analyses. The included studies were analyzed based on a graph theoretical approach within a frequentist framework, and the competing treatments were ranked by P scores. The planned subgroup analyses were not conducted due to the low number of TNS events.
Both SRs with NMA,3,21 especially the Reschke et al. (2020) study,21 didn’t provide enough details from a statistical method standpoint, which made it challenging to evaluate this evidence. The NMA by Reschke et al. (2020)21 did not include sufficient detail about Bayesian statistical analyses, and the paper did not cite standard methods for NMA. Likewise, the graph theoretical approach referenced by Forget et al. (2019)3 did not appear to be a standard approach to NMA, and the authors did not provide adequate detail to explain the implications of this approach.
Primary Studies
The Downs and Black Checklist13 used for critical appraisal of the included primary studies consists of 5 sections (Table 6): reporting, external validity, internal validity, confounding, and power. In the following paragraphs, the strengths and weaknesses of the included primary studies are described in each of the 5 sections.
Reporting: The items clearly described in the 11 RCTs4,6,15-20,22-24 were: study objectives, main outcomes, characteristics of the patients, interventions, main findings of the study, estimated random variability in data for main outcomes, and the distributions of principal confounders. All studies reported funding sources. The typical examples of confounders in RCTs (e.g., sex, age, and disease characteristics)30 were clearly described in the selected studies. The rate of AEs was a secondary outcome measure in 5 studies4,17-19,24 and not an outcome measure in 6 studies.6,15,16,20,22,23
External Validity: Staff, places, and facilities reported in the studies were representative of the procedures provided to patients. All studies reported receiving no specific funding. It was unclear if the patients who were asked to participate in the study were representative of the entire population recruited (i.e., poor reporting of the source of the population).
Internal Validity: All RCTs were double-blinded, except for 2 studies16,18 that were not blind to those measuring the outcomes or were unclear. The main outcome measures and statistical tests (except for one study)22 used for data analysis were clearly described in the studies.
Confounding: Patients were randomized to intervention groups, and randomization was concealed from patients and staff. Patients in different intervention groups were recruited from the same population, but it was unclear whether participants were recruited over the same period of time. Data collection was conducted during ambulatory surgery, and there was no loss of patients for follow-up.
Power: Of the 11 selected RCTs, sample size and power calculation were reported in 8 studies.4,15-19,22,23 In 3 studies,6,20,24 it was unclear if they were sufficiently powered to detect clinically significant effects.
Additional details regarding the strengths and limitations of the included publications are summarized in Appendix 3.
Summary of Findings
We identified 14 studies including 2 SRs with NMA,3,21 1 SR with MA,2 and 11 RCTs4,6,15-20,22-24 regarding the clinical effectiveness of CP for patients with spinal or epidural LA. We did not find any studies that met the inclusion criteria regarding the cost-effectiveness of CP compared to other local anesthetics or evidence-based guidelines for using CP for patients requiring spinal or epidural LA.
Appendix 4 presents the main outcomes of the included studies.
Onset of Sensory Block
In 1 SR and NMA21 on the choice of local anesthetic for epidural Caesarean section, the mean onset of surgical LA from fastest to slowest was: lidocaine 2% with bicarbonate; 2-CP 3%; lidocaine 2%; ropivacaine 0.75%; bupivacaine 0.5%; bupivacaine 0.5% (Table 7).
The onset of sensory block was reported in 9 RCTs (Table 8).6,15,16,18-20,23,24,28 Four studies found that the onset of sensory block for CP was significantly shorter compared to bupivacaine,6,20 levobupivacaine,22 and prilocaine.15 In 1 study, the onset of sensory block for CP combined with saline was also shorter compared to both CP combined with fentanyl and bupivacaine.18 In 3 studies, the sensory block onset with CP was similar to bupivacaine,16 prilocaine,23 and lidocaine.24 Likewise in 1 study,19 the onset of sensory block was similar for CP combined with fentanyl and bupivacaine combined with fentanyl.
Onset of Motor Block
In 1 SR and MA,2 2-CP had a shorter motor block onset compared to a low dose (10 mg or less) of hyperbaric bupivacaine (Table 10).
Motor block onset was reported in 9 RCTs.4,6,15,16,18,20,23,24,28 Four studies found the onset of motor block was significantly shorter for CP compared to bupivacaine4,6,20 and prilocaine.15 This measure was also shorter for CP combined with saline compared to both CP combined with fentanyl and bupivacaine.18 While, 4 studies found similar results for CP relative to bupivacaine,16 prilocaine,23 levobupivacaine,22 and lidocaine.24
Resolution of the Sensory Block
The resolution of sensory block was reported in 7 RCTs.6,16,18-20,22,23 This measure was significantly shorter for CP compared to bupivacaine,6,20 prilocaine,17 and levobupivacaine;22 as well as for CP combined with fentanyl compared to bupivacaine combined with fentanyl19 and for CP combined with saline compared to both CP combined with fentanyl and bupivacaine.18 In 1 study, the CP sensory block resolution was similar to prilocaine’s.23
Resolution of the Motor Block
Motor block resolution was reported in 10 RCTs.4,6,15,16,18-20,22-24 Seven studies found a significantly shorter resolution of the motor block for CP compared to bupivacaine,4,6,16,20 prilocaine,15 levobupivacaine,22 and lidocaine.24 One study also reported a shorter motor block resolution for CP combined with saline compared to both CP combined with fentanyl and bupivacaine.18 However, 2 studies19,23 found no difference in the motor block resolution for CP compared to other alternatives, including CP compared to prilocaine,23 and CP combined with fentanyl compared to bupivacaine combined with fentanyl.19
Time to Maximum Sensory Block
Time to maximum sensory block was reported in 3 RCTs.6,19,22 This measure was found to be shorter for CP compared to bupivacaine in 1 study,6 and was reported similar for CP and levobupivacaine22 and CP combined with fentanyl and bupivacaine combined with fentanyl19 in 2 studies.19,22
Time to Discharge
In 1 SR and MA,2 time to discharge was significantly shorter for 2-CP compared to low-dose hyperbaric bupivacaine (Table 10).
Time to discharge was reported in 4 RCTs,15,16,19,20 all confirming a shorter time to discharge for CP compared to bupivacaine16,19 and prilocaine,15 as well as for CP combined with fentanyl compared to bupivacaine combined with fentanyl.19
Time to Unaided Ambulation
In 1 SR and MA,2 a significantly shorter time to ambulation was reported for 2-CP compared to low-dose hyperbaric bupivacaine (Table 10).
Time to unaided ambulation was reported in 4 RCTs,16,20,22,23 3 demonstrated a shorter time to unaided ambulation for CP compared to bupivacaine16 and levobupivacaine,22 and 1 showed no significant difference between CP and prilocaine.23
Time to Independent Urination
Time to unaided ambulation was reported in 6 RCTs,4,15,17,20,22,23 all confirming a shorter time to independent urination for CP compared to bupivacaine,4,20 prilocaine,15,17,23 and levobupivacaine.22
Patient Satisfaction
Patient satisfaction was reported in 1 study,19 demonstrating no difference between CP combined with fentanyl and bupivacaine combined with fentanyl.
Adverse Events
In 1 SR with NMA21 on the choice of local anesthetic for epidural Caesarean section, l-bupivacaine 0.5% was least likely to cause hypotension and 2-CP 3% was most likely to cause hypotension. Loss of surgical LA requiring intra-operative supplementation was most likely after 2-CP 3% and least likely after ropivacaine 0.75% (Table 7).
In 1 SR with NMA3 to compare lidocaine with other types of LA, the risk ratio (RR) of TNS was 80% to 90% lower for bupivacaine, levobupivacaine, prilocaine, procaine, and ropivacaine compared to lidocaine. The RR of TNS for 2-CP and mepivacaine did not differ from lidocaine (Table 11).
In RCTs included in the present report, AEs were reported in 5 studies17-19,24 showing no difference between CP with both prilocaine17 and lidocaine24 in hypotension and with bupivacaine in TNS19 and urinary retention.18 In addition, in 1 RCT, no patient with hypotension was reported with CP, while 20% was reported in patients anesthetized with bupivacaine.4
Limitations
All publications selected for this report focused on CP's clinical effectiveness for patients requiring spinal or epidural anesthesia. We did not find any publications that met the inclusion criteria on the cost-effectiveness of CP compared to other types of LA and evidence-based guidelines for using CP for patients requiring spinal or epidural anesthesia.
Of the 11 RCTs,4,6,15-20,22-24 more than half of the studies (n = 7, 64.0%) were conducted by authors in India,4,6,16,18,20,22,23 and other studies were carried out in China,24 Netherlands,15 Belgium,17 and the US.19 We did not find any relevant studies conducted in Canada, which might be influenced, at least in part, by the withdrawal of preservative-free CP from the market in Canada in 2012.9 Thus, the generalizability of these findings to the cross-Canada context is uncertain.
In 3 SRs with MA or NMA,2,3,21 except for 1 primary study27 included in 2 SRs,2,3 no overlapping studies were identified in the 3 SRs.2,3,21 Likewise, the 9 RCTs included in the review varied widely in terms of population characteristics (e.g., patients with perineal surgery,4,6,22,24 gynecological procedure,6 cervical cerclage surgery,19 ureteroscopic lithotripsy surgery,20 knee arthroscopy,15,17 inguinal hernia repair surgery,18 general ambulatory surgeries,16 lower abdominal or lower limb surgeries23), CP percentage (e.g., 1%,4,6,15-18,20,22,23 3%,19,24) and dosage (e.g., 30 mg,4,22,24 40 mg,6,15,16,18,20,23 50 mg,17,19) used, and the comparators (spinal bupivacaine 5% [10 mg,6,16 10.5 mg,18 15 mg,4 or 20 mg20], bupivacaine 0.75% [9 mg],19 prilocaine 2% [40 mg15 or 50 mg17], levobupivacaine 5% [15 mg],22 2-CP 1% [40 mg] combined with buprenorphine [0.06 mg],23 and epidural lidocaine 2% [30 mg]24). This variation in relevant evidence limits how much the findings can be effectively synthesized.
The 2 SRs with NMA,3,21 especially the SR by Reschke et al. (2020),21 didn’t provide adequate statistical details, which made evaluating this evidence challenging. Overall, this NMA21 had several methodological limitations that make the strength of the conclusions less certain. The 9 RCTs selected for this review did not have serious methodological concerns, except for not clearly describing the source of the study population and if the patients in intervention and control groups were recruited over the same period of time.
In the SR and NMA by Forget et al. (2019),3 only 226,27 out of the 24 RCTs included in the NMA used 2-CP for spinal LA.26 This NMA reported similar RRs of TNS for 2-CP to lidocaine. In another SR with NMA,21 loss of surgical anesthesia requiring intra-operative supplementation and hypotension during Caesarean section were more likely with 2-CP 3% compared to other local anesthetics. However, the RCTs17-19,24 included in the present report showed no difference between CP with alternative drugs for spinal LA in hypotension,17,24 TNS,19 and urinary retention.18 In addition, the rate of hypotension with CP was zero compared to 20% with bupivacaine in 1 RCT.4 Given the inconsistency in the literature, it was difficult to draw a conclusion about the rate of AEs with CP relative to alternative drugs for LA, suggesting further studies are needed.
Conclusions and Implications for Decision- or Policy-Making
The studies selected for this report supported better or equal clinical effectiveness for CP compared to other alternatives for spinal or epidural LA on several outcomes. For example, several studies found a shorter time for the onset of sensory block,6,15,20-22 the onset of motor block,2,4,6,15,20 recovery from the sensory block,6,17-20,22 and recovery from motor block4,6,16,18,20,22,24 with CP compared to alternative drugs for LA. In addition, in all studies reporting time to unaided ambulation2,16,20,22,23 (except 1 study with similar results for CP and prilocaine),23 time to independent urination,4,15,17,20,22,23 and time to discharge,2,15,16,19,20 CP was associated with a shorter time relative to other local anesthetics. Thus, it could be concluded that CP may result in better or equal clinical effectiveness compared to alternative drugs for spinal or epidural LA.
However, due to inconsistency in evidence, it was difficult to draw any firm conclusions about the safety of CP for spinal or epidural LA, corroborating the need for additional studies to assist with decision-making. In addition, the publications included in this report represented a broad range of study populations by country of origin, mostly by authors based in India. Thus, the extent to which studies from other cultures might contribute to the cross-Canada context remains unclear and requires further research.
We did not find any publications regarding the cost-effectiveness of CP compared to other types of LA or evidence-based guidelines for the use of CP for patients requiring spinal or epidural LA that met the inclusion criteria for this review.
References
1.Spinal and epidural anesthesia. MedLine Plus. Bethesda (MD): National Library of Medicine; 2023: https://medlineplus.gov/ency/article/007413.htm. Accessed 2023 Apr 17.
2.Saporito A, Ceppi M, Perren A, et al. Does spinal chloroprocaine pharmacokinetic profile actually translate into a clinical advantage in terms of clinical outcomes when compared to low-dose spinal bupivacaine? A systematic review and meta-analysis. J Clin Anesth. 2019;52:99-104. PubMed
3.Forget P, Borovac JA, Thackeray EM, Pace NL. Transient neurological symptoms (TNS) following spinal anaesthesia with lidocaine versus other local anaesthetics in adult surgical patients: a network meta-analysis. Cochrane Database Syst Rev. 2019;12:CD003006. PubMed
4.Khare A, Thada B, Yadav D, Mathur V, Singh M. A randomized double blind study to compare 1% 2-chloroprocaine and 0.5% hyperbaric bupivacaine in spinal anesthesia for infra-umbilical surgeries. Anaesth Pain Intensive Care. 2019;23(2):162-167.
5.Nair GS, Abrishami A, Lermitte J, Chung F. Systematic review of spinal anaesthesia using bupivacaine for ambulatory knee arthroscopy. Br J Anaesth. 2009;102(3):307-315. PubMed
6.Agrawal B, Akhtar P, Panda AK. Comparison of 1% chloroprocaine alone to 1% chloroprocaine with clonidine during daycare surgeries under spinal anesthesia. Int J Pharm Clin Res. 2022;14(4):262-269.
7.Tonder S, Togioka B, Maani C. Chloroprocaine. Treasure Island (FL): StatPearls; 2023: https://www.ncbi.nlm.nih.gov/books/NBK532901/. Accessed 2023 Apr 10.
8.Eng HC, Ghosh SM, Chin KJ. Practical use of local anesthetics in regional anesthesia. Curr Opin Anaesthesiol. 2014;27(4):382-387. PubMed
9.Szerb JJ. Reviving older drugs to deal with anesthesia drug shortages. Can J Anaesth. 2015;62(10):1042-1044. PubMed
10.Szerb J, Abbass SA, Banfield J, Uppal V. A survey assessing the need for spinal chloroprocaine to provide subarachnoid neuraxial anesthesia for short-duration surgeries in Canada. Can J Anaesth. 2021;68(7):1096-1099. PubMed
11.CAS Anesthesia News. Vol. 37(2) Toronto (ON): Canadian Anesthesiologists' Society; 2022: https://www.cas.ca/CASAssets/Documents/Anesthesia-News/CASnewsletterSummer2022.pdf. Accessed 2023 Apr 10.
12.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
13.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
14.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. PubMed
15.Wesselink E, Hurk GJD, Vegt RV, et al. Chloroprocaine versus prilocaine for spinal anesthesia in ambulatory knee arthroscopy: a double-blind randomized trial. Reg Anesth Pain Med. 2019;21. [Online ahead of print]. PubMed
16.Singh B, Anand A, Attri JP. A prospective open-label randomized controlled trial to compare intrathecal 1% 2-chloroprocaine versus 0.5% bupivacaine in ambulatory elective surgeries. Anesth Essays Res. 2020;14(2):266-270. PubMed
17.Guntz E, Vasseur C, Ifrim D, Louvard A, Fils JF, Kapessidou Y. Intrathecal chloroprocaine or hyperbaric prilocaine for ambulatory knee surgery? A prospective randomized study. J Exp Orthop. 2021;8(1):15. PubMed
18.Tiwari A, Singh S, Singh M, Sanghwan M. Comparison of bupivacaine and 2-chloroprocaine with and without fentanyl for subarachnoid block in inguinal hernia repair surgery: a randomised controlled study. J Clin Diagn Res. 2021;15(9):UC01-UC04.
19.Lee A, Shatil B, Landau R, Menon P, Smiley R. Intrathecal 2-chloroprocaine 3% versus hyperbaric bupivacaine 0.75% for cervical cerclage: a double-blind randomized controlled trial. Anesth Analg. 2022;134(3):624-632. PubMed
20.Sugumar M, Singh AK, Rath A, Reena, Jayanthi A. A comparative study of isobaric 1% chloroprocaine with 0.5% isobaric bupivacaine for ureteroscopic lithotripsy under spinal anaesthesia: a prospective randomised study. Cureus. 2022;14(4):e24633. PubMed
21.Reschke MM, Monks DT, Varaday SS, Ginosar Y, Palanisamy A, Singh PM. Choice of local anaesthetic for epidural caesarean section: a Bayesian network meta-analysis. Anaesthesia. 2020;75(5):674-682. PubMed
22.Bhaskara B, Shruthi S, Ramachandraiah R. A study to evaluate intrathecal 1% chloroprocaine and 0.5% levobupivacaine in perianal surgeries: a prospective randomized study. Anesth Essays Res. 2020;14(3):406-411. PubMed
23.Siddaiah J, Pujari VS, Madalu AS, Bevinaguddaiah Y, Parate LH. A comparative study on the effect of addition of intrathecal buprenorphine to 2-chloroprocaine spinal anesthesia in short duration surgeries. J Anaesthesiol Clin Pharmacol. 2019;35(4):533-539. PubMed
24.Yang Z, Li D, Zhang K, Yang F, Li M, Wang L. Comparison of epidural anesthesia with chloroprocaine and lidocaine for outpatient knee arthroscopy. J Orthop Surg. 2019;27(3):2309499019865534. PubMed
25.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
26.Casati A, Fanelli G, Danelli G, et al. Spinal anesthesia with lidocaine or preservative-free 2-chlorprocaine for outpatient knee arthroscopy: a prospective, randomized, double-blind comparison. Anesth Analg. 2007;104(4):959-964. PubMed
27.Teunkens A, Vermeulen K, Van Gerven E, Fieuws S, Van de Velde M, Rex S. Comparison of 2-chloroprocaine, bupivacaine, and lidocaine for spinal anesthesia in patients undergoing knee arthroscopy in an outpatient setting: a double-blind randomized controlled trial. Reg Anesth Pain Med. 2016;41(5):576-583. PubMed
28.Bhaskara B, Prabhakar SA, Rangadhamaiah R. Intrathecal 1% 2-chloroprocaine with fentanyl in comparison with ropivacaine (0.5%) with fentanyl in day care perianal surgery: prospective randomized comparative study. Anesth Essays Res. 2019;13(3):471-475. PubMed
29.Craig D, Carli F. Bromage motor blockade score - a score that has lasted more than a lifetime. Can J Anaesth. 2018;65(7):837-838. PubMed
30.Spieth PM, Kubasch AS, Penzlin AI, Illigens BM, Barlinn K, Siepmann T. Randomized controlled trials - a matter of design. Neuropsychiatr Dis Treat. 2016;12:1341-1349. PubMed
31.Hespanhol L, Vallio CS, Costa LM, Saragiotto BT. Understanding and interpreting confidence and credible intervals around effect estimates. Braz J Phys Ther. 2019;23(4):290-301. PubMed
32.9.2.2.2. Measures of relative effect: the risk ratio and odds ratio. In: Higgins JPT, Green S, eds. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0. London (UK): The Cochrane Collaboration; 2011.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this table has not been copy-edited.
Table 2: Characteristics of the Included Systematic Reviews (SRs)
Study citation, country, objective, funding source | Study designs and the number of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Reschke et al. (2020)21 US Funding source: No funding | Design: SR with NMA Total studies included: 24 RCTs Total studies relevant to this review: 5 RCTs on 2-CP 3% | Population included: 1,280 women with epidural Caesarean section Age in all included studies: NR Sex: Female Exclusion criteria: NR | Interventions included: Epidural 2-CP 3% Comparator:
| Outcome measure:
Follow-up: Intra-operative follow-up (no long-term follow-up postoperation) |
Forget et al. (2019)3 UK Funding source: No funding | Design: SR with NMA Total studies included: 24 RCTs and quasi-RCTS Total studies relevant to this review: 2 RCT on 2-CP | Population included: 2,226 adults undergoing surgery Age in all included studies: NR Sex: NR Exclusion criteria:
| Interventions included: Spinal lidocaine Comparator: Other local anesthetics
| Outcome measure: Presence of transient neurologic symptoms (TNS) Follow-up: 24 hours postspinal anesthesia |
Saporito et al. (2019)2 Switzerland Funding source: No funding | Design: SR with MA Total studies included: 4 RCTs Total studies relevant to this review: 4 RCTs on 2-CP | Population included: Adults with lower extremity and abdominal surgery Age in all included studies: NR Sex: NR Exclusion criteria: Studies with poor methodological quality. | Interventions included: Spinal 2-CP Comparator: Low-dose bupivacaine (10 mg or less) | Outcome:
Follow-up: Intra-operative follow-up (no long-term follow-up postoperation) |
CP = chloroprocaine; MA = meta-analysis; NMA = network meta-analysis; NR = not reported; RCT = randomized controlled trial; SR = systematic review.
Table 3: Characteristics of Included Randomized Controlled Trials (RCTs)
Study citation, design, country, objective, funding source | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|
Agrawal et al. (2022)6 Country: India Funding source: No funding. | Patient with short-duration elective ambulatory perineal surgery or gynecological procedure. Number of patients (n), Age in year, mean (SD), range: Total: 120, NR, 18 to 60
Sex: number of males, n (%) Total: 88 (75.44)
Inclusion criterion:
Exclusion Criteria:
| Intervention: Spinal 1-CP 1% (40 mg) Comparator: Spinal bupivacaine 5% (10 mg) | Outcomes:
Follow-up: During surgery and before discharge |
Lee et al. (2022)19 Country: US Funding source: No funding | Women undergoing cervical cerclage surgery. Number of patients (n), Age in year, mean (SD), range: Total: 41, NR, NR
Sex: number of males, n (%) Total: 41 (100) Inclusion criterion:
Exclusion Criteria:
| Intervention: Spinal 2-CP 3% (50 mg) combined with fentanyl (0.015 mg) Comparator: Spinal hyperbaric bupivacaine 0.75% (9 mg) combined with fentanyl (0.015 mg) | Outcomes:
Follow-up: 1 day (phone call on the first postoperative day) |
Sugumar et al. (2022)20 Country: India Funding source: No funding. | Patients with ureteroscopic lithotripsy surgery. Number of patients (n), Age in year, mean (SD), range: Total: 60, NR, 18 to 50
Sex: number of males, n (%) Total: 35 (58.33)
Inclusion criterion:
Exclusion Criteria:
| Intervention: Spinal CP 1% (40 mg) Comparator: Spinal bupivacaine 5% (20 mg) | Outcomes:
Follow-up: During surgery and before discharge |
Guntz et al. (2021)17 Country: Belgium Funding source: No funding. | Patients with knee arthroscopy. Number of patients (n), Age in year, mean (SD), range: Total: 80, NR, 18 to 80
Sex: number of males, n (%) NR Inclusion criterion:
Exclusion Criteria:
| Intervention: Spinal CP 1% (50 mg) Comparator: Spinal hyperbaric prilocaine 2% (50 mg) | Outcomes:
Follow-up: During surgery and before discharge |
Tiwari et al. (2021)18 Country: India Funding source: No funding. | Male patients with inguinal hernia repair surgery. Number of patients (n), Age in year, mean (SD), range: Total: 102, NR, 18 to 65
Sex: number of males, n (%) Total: 102 (100) Inclusion criterion:
Exclusion Criteria:
| Intervention: Spinal 2-CP 1% (40 mg) combined with saline (0.025 mg) Comparator: Spinal
| Outcomes:
Follow-up: During surgery and before discharge |
Bhaskara et al. (2020)22 Country: India Funding source: No funding. | Patients who underwent perianal surgeries. Number of patients (n), Age in year, mean (SD), range: Total: 60, NR, 18 to 55
Sex: number of males, n (%) NR Inclusion criterion:
Exclusion Criteria:
| Intervention: Spinal CP 1% (30 mg) Comparator: Spinal levobupivacaine 5% (15 mg) | Outcomes:
Follow-up: During surgery and before discharge |
Singh et al. (2020)16 Country: India Funding source: No funding. | Patients who underwent ambulatory surgeries. Number of patients (n), Age in year, mean (SD), range: Total: 60, NR, 18 to 60
Sex: number of males, n (%) Total: 22 (36.66)
Inclusion criterion:
Exclusion Criteria:
| Intervention: Spinal 2-CP 1% (40 mg) Comparator: Spinal hyperbaric bupivacaine 5% (10 mg) | Outcomes:
Follow-up: During surgery and before discharge |
Khare et al. (2019)4 Country: India Funding source: No funding. | Patients who underwent perianal surgeries. Number of patients (n), Age in year, mean (SD), range: Total: 90, NR, 18 to 60
Sex: number of males, n (%) Total: 68 (75.55)
Inclusion criterion:
Exclusion Criteria:
| Intervention: Spinal 2-CP 1% (30 mg) Comparator: Spinal hyperbaric bupivacaine 5% (15 mg) | Outcomes:
Follow-up: During surgery and before discharge |
Siddaiah et al. (2019)23 Country: India Funding source: No funding. | Patients undergoing lower abdominal or lower limb surgeries. Number of patients (n), Age in year, mean (SD), range: Total: 90, NR, 18 to 60
Sex: number of males, n (%) Total: 38 (42.22)
Inclusion criterion:
Exclusion Criteria:
| Intervention: Spinal 2-CP 1% (40 mg) Comparator: Spinal 2-CP 1% (40 mg) combined with buprenorphine (0.06 mg) | Outcomes:
Follow-up: During surgery and before discharge |
Wesselink et al. (2019)15 Country: The Netherlands Funding source: No funding. | Patients undergoing knee arthroscopy. Number of patients (n), Age in year, mean (SD), range: Total: 150, NR, 18 years and older
Sex: number of males, n (%) Total: 85 (56.66)
Inclusion criterion:
Exclusion Criteria:
| Intervention: Spinal 2-CP 1% (40 mg) Comparator: Spinal prilocaine 2% (40 mg) | Outcomes:
Follow-up: During the surgery and before discharge |
Yang et al. (2019)24 Country: China Funding source: No funding. | Patients undergoing knee arthroscopy. Number of patients (n), Age in year, mean (SD), range: Total: 80, NR, 18 to 60
Sex: number of males, n (%) Total: 80 (56.66)
Inclusion criterion:
Exclusion Criteria:
| Intervention: Epidural 2-CP 3% (30 mg) Comparator: Epidural lidocaine 2% (30 mg) | Outcomes:
Follow-up: During the surgery and before discharge |
AE = adverse events, ASA = American Society of Anesthesiologists, BMI = body mass index, CP = chloroprocaine, Kg/m2 = kilogram per square metre, LA = local anesthesia, NR = not reported, SD = standard deviation.
Appendix 3: Critical Appraisal of Included Publications
Note that this table has not been copy-edited.
Table 4: Strengths and Limitations of Systematic Reviews Using a MeaSurement Tool to Assess Systematic Reviews 2 (AMSTAR 2)12
Checklist’s items | Reschke et al. (2020)21 | Forget et al. (2019)3 | Saporito et al. (2019)2 |
|---|---|---|---|
1. Did the research questions and inclusion criteria for the review include the components of PICO? | Yes | Yes | Yes |
2. Did the report of the review contain an explicit statement that the review methods were established before the conduct of the review and did the report justify any significant deviations from the protocol? | Yes | Yes | No |
3. Did the review authors explain their selection of the study designs for inclusion in the review? | Yes | Yes | Yes |
4. Did the review authors use a comprehensive literature search strategy? | Yes | Yes | Yes |
5. Did the review authors perform study selection in duplicate? | Yes | Yes | Yes |
6. Did the review authors perform data extraction in duplicate? | Yes | Yes | Yes |
7. Did the review authors provide a list of excluded studies and justify the exclusions? | No | Yes | No |
8. Did the review authors describe the included studies in adequate detail? | No | Yes | Yes |
9. Did the review authors use a satisfactory technique for assessing the RoB in individual studies that were included in the review? | Yes | Yes | Yes |
10. Did the review authors report on the sources of funding for the studies included in the review? | Yes | Yes | Yes |
11. If meta-analysis was performed did the review authors use appropriate methods for the statistical combination of results? | Unclear | Yes | Yes |
12. If meta-analysis was performed, did the review authors assess the potential impact of RoB in individual studies on the results of the meta-analysis or other evidence synthesis? | Unclear | Yes | Yes |
13. Did the review authors account for RoB in individual studies when interpreting/ discussing the results of the review? | No | Yes | Partially |
14. Did the review authors provide a satisfactory explanation for, and discussion of, any heterogeneity observed in the results of the review? | Partially | Yes | Partially |
15. If they performed quantitative synthesis did the review authors carry out an adequate investigation of publication bias (small study bias) and discuss its likely impact on the results of the review? | No | Yes | Yes |
16. Did the review authors report any potential sources of conflict of interest, including any funding they received for conducting the review? | Yes | Yes | Yes |
NA = not applicable; PICO = population, intervention, comparator, outcome; RoB = risk of bias.
Table 5: Strengths and Limitations of Systematic Reviews with Network Meta-Analyses (NMA) Using a Questionnaire to Assess the Relevance and Credibility of NMA14
Checklist’s items | Reschke et al. (2020)21 | Forget et al. (2019)3 |
|---|---|---|
Yes, No, or CNA | ||
Relevance | ||
1. Is the population relevant? | Yes | Yes |
2. Are any critical interventions missing? | No | No |
3. Are any relevant outcomes missing? | No | No |
4. Is the context (e.g., settings and circumstances) applicable to your population? | Partially | Yes |
Credibility: Evidence base | ||
5. Did the researchers attempt to identify and include all relevant RCTs? | Yes | Yes |
6. Do the trials for the interventions of interest form one connected network of randomized controlled trials? | Yes | Yes |
7. Is it apparent that poor-quality studies were included thereby leading to bias? | CNA | No |
8. Is it likely that bias was induced by selective reporting of outcomes in the studies? | No | No |
9. Are there systematic differences in treatment effect modifiers (i.e., baseline patient or study characteristics that impact the treatment effects) across the different treatment comparisons in the network? | CNA | No |
10. If yes (i.e., there are such systematic differences in treatment effect modifiers), were these imbalances in effect modifiers across the different treatment comparisons identified before comparing individual study results? | CNA | NA |
Credibility: Analysis | ||
11. Were statistical methods used that preserve within-study randomization? (No naive comparisons) | No | Yesa |
12. If both direct and indirect comparisons are available for pairwise contrasts (i.e., closed loops), was agreement in treatment effects (i.e., consistency) evaluated or discussed? | No | CNA |
13. In the presence of consistency between direct and indirect comparisons, were both direct and indirect evidence included in the network meta-analysis? | Yes | Yes |
14. With inconsistency or an imbalance in the distribution of treatment effect modifiers across the different types of comparisons in the network of trials, did the researchers attempt to minimize this bias with the analysis? | CNA | Yes |
15. Was a valid rationale provided for the use of random effects or fixed effect models? | No | Yes |
16. If a random effects model was used, were assumptions about heterogeneity explored or discussed? | No | Yes |
17. If there are indications of heterogeneity, were subgroup analyses or meta-regression analysis with prespecified covariates performed? | Yes | No |
Credibility: Reporting quality and transparency | ||
18. Is a graphical or tabular representation of the evidence network provided with information on the number of RCTs per direct comparison? | Yes | Yes |
19. Are the individual study results reported? | Yes | Yes |
20. Are results of direct comparisons reported separately from results of the indirect comparisons or network meta-analysis? | CNA | Yes |
21. Are all pairwise contrasts between interventions as obtained with the network meta-analysis reported along with measures of uncertainty? | No | CNA |
22. Is a ranking of interventions provided given the reported treatment effects and its uncertainty by the outcome? | Yes | Yes |
23. Is the impact of important patient characteristics on treatment effects reported? | No | No |
Credibility: Interpretation | ||
24. Are the conclusions fair and balanced? | CNA | Yes |
Credibility: Conflict of interest | ||
25. Were there any potential conflicts of interest? | No | No |
26. If yes, were steps taken to address these? | NA | NA |
CAN = cannot answer; NA = not applicable; NR = not reported; RCTs = randomized controlled trials.
a“If item 11 is scored as a “no” resulting in a fatal flaw, the overall domain should be judged as fatally flawed and the network meta-analysis may have serious validity issues.”14
Table 6: Strengths and Limitations of Randomized Controlled Trials Using the Downs and Black Checklist13
Checklist’s items | Agrawal (2022)6 | Lee (2022)19 | Sugumar (2022)20 | Guntz (2021)20 | Tiwari (2021)18 | Singh (2020)16 | Bhaskara (2020)22 | Khare (2019)4 | Siddaiah (2019)23 | Wesselink (2019)15 | Yang (2019)24 |
|---|---|---|---|---|---|---|---|---|---|---|---|
Reporting | |||||||||||
1. Is the objective of the study clear? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
2. Are the main outcomes clearly described in the Introduction or Methods? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
3. Are the characteristics of the patients included in the study clearly described? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
4. Are the interventions clearly described? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
5. Are the distributions of principal confounders in each group of subjects clearly described? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
6. Are the main findings of the study clearly described? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
7. Does the study estimate random variability in data for main outcomes? | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes |
8. Have all the important adverse events consequential to the intervention been reported? | NA | Partiallya | NA | Partially | Partially | NA | NA | Partially | NA | NA | Partially |
9. Have characteristics of patients lost to follow-up been described? | NA b | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
10. Have actual P values been reported for the main outcomes except for probability < 0.001? | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | No |
External validity | |||||||||||
11. Is the source of funding clearly stated? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
12. Were subjects who were asked to participate in the study representative of the entire population recruited? | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
13. Were those subjects who were prepared to participate representative of the recruited population? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
14. Were staff, places, and facilities where patients were treated representative of the treatment most received? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
Internal validity | |||||||||||
15. Was an attempt made to blind study subjects to the intervention? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
16. Was an attempt made to blind those measuring the main outcomes? | Yes | Yes | Yes | Yes | Unclear | No | Yes | Yes | Yes | Yes | Yes |
17. If any of the results of the study were based on data dredging was this made clear? | No | No | No | No | No | No | No | No | No | No | No |
18. Was the time period between intervention and outcome the same for intervention and control groups or adjusted for? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
19. Were the statistical tests used to assess the main outcomes appropriate? | Yes | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes |
20. Was compliance with the interventions reliable? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
21. Were the main outcome measures used accurate (Valid and reliable)? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
Internal validity – Confounding (selection bias) | |||||||||||
22. Were patients in different intervention groups recruited from the same population? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
23. Were study subjects in different intervention groups recruited over the same period of time? | Unclear | Yes | Unclear | Unclear | Yes | Unclear | Yes | Unclear | Unclear | Unclear | Unclear |
24. Were study subjects randomized to intervention groups? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
25. Was the randomized intervention assignment concealed from patients and staff until recruitment was complete? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
26. Was there an adequate adjustment for confounding in the analyses from which the main findings were drawn? | Yes | Yes | Yes | Yes | Unclear | No | Yes | Yes | Yes | Yes | Yes |
27. Were losses of patients to follow-up considered? | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
Power | |||||||||||
28. Was the study sufficiently powered to detect clinically important effects where the P value for a difference due to chance is < 5%? | Unclear | Yes | Unclear | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Unclear |
NA = not applicable.
aThe rate of adverse events (AEs) was a secondary outcome measure in 5 studies.4,17-19,24
bNo loss of follow-up was reported in the selected studies.
Appendix 4: Main Study Findings
Note that this table has not been copy-edited.
Table 7: Summary of Findings by Outcome — Summary of Evidence for Epidural Anesthesia for Caesarean Section in a Systematic Review and Network Meta-analysis by Reschke et al. (2020)21
Outcomes | Value with worst drug (OR or mean, 95% Crl) | Value with best drug (OR or mean, 95% Crl) | Relative effect (OR or mean, 95% Crl) | Number of women (number of trials) | Comments |
|---|---|---|---|---|---|
Onset of surgical anesthesia | Bupivacaine 0.5% (19.8, 17.3 to 22.4) min | Lidocaine 2% (3.90, 1.8 to 6.0) | 6.4 (3.3 to 9.7) min | 1,280 (24) | Mean of onset for 2-CP 3% = 5.7 (3.0 to 8.3) min |
Intra-operative hypotension | 2-CP 3% (516, 438 to 594) per 1,000 | l-bupivacaine 0.5% (315, 236 to 407) per 1,000 | 0.52 (0.20 to 1.26) | 807 (14) | 2-CP3% OR (CrI) vs. l-bupivacaine 0.5% = 0.84 (0.24 to 2.86) |
Intra-operative supplementation | 2-CP 3% (250, 112 to 569) per 1,000 | Ropivacaine 0.75% (48, 19 to118) per 1,000 | 0.05 (0.00 to 0.76) | 886 (15) | 2-CP 3% OR (Crl) vs. Ropivacaine 75% = 0.05 (0.003 to 0.76) |
CP = chloroprocaine; Crl = credible interval; OR = odds ratio.
aCredible interval (CrI) reflects the Bayesian 95% confidence interval showing a 95% probability that the true estimate lie within the interval.31
Table 8: Summary of Findings by Outcome of 5 Studies — Clinical Effectiveness of Chloroprocaine Compared to Alternative Local Anesthetics
Variables | Agarwal et al. (2022)6 | Lee et al. (2022)19 | Sugumar et al. (2022)20 | Guntz et al. (2021)17 | Tiwari et al. (2021)18 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
Mean (SD) | P | Median (IQR) | P | Mean (SD) | P | Mean (SD) | P | Mean (SD) | P | |||||||
C (n = 60) | B (n = 60) | C + F (n = 60) | B + F (n = 60) | C (n = 30) | B (n = 30) | C (n = NR) | Pril (n = NR) | C + S (n = 34) | C + F (n = 34) | B (n = 34) | ||||||
Onset of sensory block (min) | 4.26 (1.64) | 4.29 (1.92) | 0.02 | 4 (2 to 6) | 4 (2 to 8) | 0.67 | 5.06 (0.82) | 6.24 (1.07) | < 0.001 | NR | NR | NR | 2.68 (0.58) | 4.04 (0.99) | 3.59 (0.61) | < 0.001 |
Onset of motor block (min) | 5.26 (0.29) | 5.32 (0.46) | 0.02 | NR | NR | NR | 6.83 (0.83) | 8.84 (0.84) | < 0.001 | NR | NR | NR | 3.37 (0.66) | 4.99 (1.01) | 4.57 (0.79) | < 0.001 |
Resolution of sensory block (min) | 153.06 (19.38) | 194.32 (21.86) | < 0.001 | 143 (116 to 162) | 198 (152 to 263) | 0.002 | 66.80 (4.69) | 191.50 (8.72) | < 0.001 | 169.0 (56.10) | 248.0 (59.40) | < 0.001 | 100.68 (25.510 | 133.65 (8.71) | 209.94 (51.76) | < 0.001 |
Resolution of motor block (min) | 169.52 (19.76) | 197.36 (21.39) | < 0.001 | 109 (88 to 148) | 112 (97 to 143) | 0.66 | 64.60 (5.88) | 175.33 (9.09) | < 0.001 | NR | NR | NR | 92.56 (24.310 | 107.74 (11.52) | 192.29 (47.56) | < 0.001 |
Time to maximum sensory block | 12.06 (3.24) | 13.38 (3.82) | 0.01 | T8 | T8 | 0.56 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
Time to discharge (min) | NR | NR | NR | 158 (137 to 188) | 229 (186 to 332) | 0.005 | 211.0 (24.0) | 441.60 (34.8) | < 0.001 | NR | NR | NR | NR | NR | NR | NR |
Time to unaided ambulation (min) | NR | NR | NR | NR | NR | NR | 210.60 (24.24) | 441.60 (34.80) | < 0.001 | NR | NR | NR | NR | NR | NR | NR |
Time to independent urination (min) | NR | NR | NR | NR | NR | NR | 2.84 (0.59) | 5.53 (0.57) | < 0.001 | 203.00 (57.60) | 287.30 (47.20) | < 0.001 | NR | NR | NR | NR |
Patient satisfaction | NR | NR | NR | 16/1/0a | 14/3/0 | 0.60 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
TNS | NR | NR | NR | 0 | 0 | 1.00 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
Hypotension | NR | NR | NR | NR | NR | NR | NR | NR | NR | 0 | 2 | 0.329 | NR | NR | NR | NR |
Urinary retention | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | 0 | 0 | 2 | > 0.05 |
B = bupivacaine, C = chloroprocaine, F = fentanyl, IQR = interquartile range, L = levobupivacaine, Lid = lidocaine, NR = not reported, Pril = prilocaine, S = saline, SD = standard deviation, TNS = transient neurologic symptoms.
aNumber of patients who rated their satisfaction with the anesthetics as 1 = complete, 2 = adequate, or 3 = inadequate.19
Table 9: Summary of Findings by Outcome of 6 Studies — Clinical Effectiveness of Chloroprocaine Compared to Alternative Anesthetic Drugs
Variables | Singh et al. (2020)16 | Bhaskara et al. (2020)22 | Khare et al. (2019)4 | Siddaiah et al. (2019)23 | Wesselink et al. (2019)15 | Yang et al. (2019)24 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
Mean (SD) | P | Mean (SD) | P | Mean (SD) | P | Mean (SD) | P | Median (IQR) | P | Mean (SD) | P | |||||||
C (n = 30) | B (n = 30) | C (n = 30) | L (n = 30) | C (n = 45) | B (n = 45) | C | Pril | C | Pril | C | Lid | |||||||
Onset of sensory block (min) | 5 | 7 | > 0.05 | 2.27 (0.52) | 3.37 (0.49) | < 0.001 | NR | NR | NR | 3.11 (1.53) | 2.93 (0.94) | 0.507 | 2 (2 to 4) | 4 (2 to 6) | 0.010 | 9.40 (92.2) | 9.70 (3.10) | > 0.05 |
Onset of motor block (min) | 8 | 9 | > 0.05 | 1.43 (0.50) | 1.57 (0.50) | 0.302 | 3.70 (0.60) | 4.10 (0.60) | 0.001 | 4.69 (2.07) | 4.16 (1.68) | 0.182 | 120 (90 to 135) | 165 (135 to 190) | <0.001 | 74.30 (15.1) | 73.70 (21.1) | > 0.05 |
Resolution of sensory block (min) | NR | NR | NR | 59.00 (8.75) | 126.83 (20.1) | < 0.001 | NR | NR | NR | 67.47 (19.3) | 72.0 (8.36) | 0.153 | NR | NR | NR | NR | NR | NR |
Resolution of motor block (min) | 88 | 150 | < 0.05 | 50.67 (5.68) | 181.00 (27.8) | < 0.001 | 71.16 (12.30) | 160.7 (14.8) | < 0.001 | 67.16 (21.7) | 70.84 (9.91) | 0.303 | 60 (60 to 82) | 75 (60 to 90) | 0.004 | 76.10 (16.3) | 85.90 (18.8) | < 0.05 |
Time to maximum sensory block | NR | NR | NR | T8 (T8 to T10) | T6 (T6 to T10) | 0.536 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
Time to discharge (min) | 180 | 365 | < 0.05 | NR | NR | NR | NR | NR | NR | NR | NR | NR | 222 (72) | 282 (42) | <0.001 | NR | NR | NR |
Time to unaided ambulation (min) | 130 | 220 | < 0.05 | 88.33 (9.13) | 206.67 (27.2) | < 0.001 | NR | NR | NR | 84.02 (18.9) | 85.80 (8.06) | 0.563 | NR | NR | NR | NR | NR | NR |
Time to independent urination (min) | 160 | 350 | < 0.05 | 79.83 (10.13) | 152.3 226.9 | < 0.001 | 199.40 (19.20) | 464.9 (30.3) | < 0.001 | 204.42 (81.3) | 269.42 (157) | 0.016 | 198 (60) | 258 (42) | <0.001 | NR | NR | NR |
Time for first analgesic dose | 100 | 250 | < 0.05 | NR | NR | NR | NR | NR | NR | 359.1 (253) | 855.8 (667) | < 0.001 | NR | NR | NR | NR | NR | NR |
Patient satisfaction | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
TNS | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
Hypotension | NR | NR | NR | NR | NR | NR | 0 | 9 | 0.002 | NR | NR | NR | NR | NR | NR | 1 | 2 | > 0.05 |
Urinary retention | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
B = bupivacaine, C = chloroprocaine, F = fentanyl, IQR = interquartile range, L = levobupivacaine, Lid = lidocaine, NR = not reported, Pr = prilocaine, S = saline, SD = standard deviation, TNS = transient neurologic symptoms.
Table 10: Summary of Findings by Outcome — Clinical Effectiveness of 2-Chloroprocaine Compared to Bupivacaine in a Systematic Review and Network Meta-analysis by Saporito et al. (2019)2
Outcomes | Pooled mean difference (min) | P valuea |
|---|---|---|
Motor block regression | −57.00 | 0.015 |
Sensory block regression | −140.30 | < 0.001 |
Time to ambulation | −84.60 | < 0.001 |
Time to discharge | −88.60 | < 0.001 |
Onset time | −1.10 | 0.118 |
aCompared to a low dose bupivacaine, spinal 2-chloroprocaine was associated with significantly faster motor and sensory block regression, and shorter time to ambulation and discharge.
Table 11: Summary of Findings by Outcome — The Risk Ratio of Transient Neurologic Symptoms (TNS) After Spinal Local Anesthesia in a Systematic Review and Network Meta-Analysis by Forget et al. (2019)3
Local anesthetics | Number of studies included in the analysis | Risk ratioa | Confidence interval |
|---|---|---|---|
Bupivacaine | 12 | 0.16 | 0.09 to 0.28 |
2‐chloroprocaine | 2 | 0.09 | 0.01 to 1.51a |
Mepivacaine | 4 | 1.01 | 0.18 to 5.82 |
Levobupivacaine | 2 | 0.13 | 0.02 to 0.69 |
Prilocaine | 4 | 0.18 | 0.07 to 0.49 |
Procaine | 2 | 0.14 | 0.04 to 0.52 |
Ropivacaine | 2 | 0.10 | 0.01 to 0.78 |
aRisk ratio (or relative risk) is the ratio of the risk of an event (here transient neurologic symptoms [TNS]) in 2 or more groups.32 According to Forget et al. (2019),3 in local anesthesia with 2-chloroprocaine and Mepivacaine, the RR of TNS might be as high as 1.51 and 5.82, respectively, showing no difference with lidocaine.
Appendix 5: References of Potential Interest
The following publications were identified because they may provide additional information associated with this report.
Systematic Reviews
Alternative Research Question
Yung EM, Abdallah FW, Todaro C, Spence E, Grant A, Brull R. Optimal local anesthetic regimen for saddle block in ambulatory anorectal surgery: an evidence-based systematic review. Reg Anesth Pain Med. 2020 09;45(9):733-739.
Nonrandomized Controlled Trials
Bhaskara B, Shruthi S, Ramachandraiah R. A study to evaluate intrathecal 1% chloroprocaine and 0.5% levobupivacaine in perianal surgeries: a prospective randomized study. Anesth Essays Res. 2020;14(3):406-411. PubMed
Herndon CL, Martinez R, Sarpong NO, Geller JA, Shah RP, Cooper HJ. Spinal anesthesia using chloroprocaine is safe, effective, and facilitates earlier discharge in selected fast-track total hip arthroplasty. Arthroplast Today. 2020;6(3):305-308. PubMed
Mims SC, Zanolli NC, Fuller M, Habib AS. Intrathecal bupivacaine versus chloroprocaine for transvaginal cervical cerclage placement: a retrospective cohort study. Int J Obstet Anesth. 2022;50:103276. PubMed
Gebhardt V, Hausen S, Weiss C, Schmittner MD. Using chloroprocaine for spinal anaesthesia in outpatient knee-arthroscopy results in earlier discharge and improved operating room efficiency compared to mepivacaine and prilocaine. Knee Surg Sports Traumatol Arthrosc. 2019;27(9):3032-3040. PubMed
Gebhardt V, Kiefer K, Bussen D, Weiss C, Schmittner MD. Retrospective analysis of mepivacaine, prilocaine and chloroprocaine for low-dose spinal anaesthesia in outpatient perianal procedures. Int J Colorectal Dis. 2018;33(10):1469-1477. PubMed
Animal Studies
Walker SM, Malkmus S, Eddinger K, et al. Evaluation of neurotoxicity and long-term function and behavior following intrathecal 1% 2-chloroprocaine in juvenile rats. Neurotoxicology. 2022 01;88:155-167. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as of the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, collecting, using, and disclosing by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca