CADTH Health Technology Review
Bevacizumab for Recurrent Platinum-Sensitive Ovarian Cancer
Rapid Review
Authors: Sara D. Khangura, Jennifer Horton
Abbreviations
AUC
area under the curve
CI
confidence interval
CT
chemotherapy
HR
hazard ratio
HTA
health technology assessment
NR
not reported
NRS
nonrandomized study
ORR
objective response rate
OS
overall survival
PFI
platinum-free interval
PFS
progression-free survival
QoL
quality of life
RCT
randomized controlled trial
RECIST
Response Evaluation Criteria in Solid Tumours
SR
systematic review
VEGF
vascular endothelial growth factor
Key Messages
It was not clear from the studies in this review whether bevacizumab plus chemotherapy does or does not improve overall survival compared to chemotherapy alone (or with placebo) for recurrent platinum-sensitive ovarian cancer.
Most studies in this review found that bevacizumab plus chemotherapy results in longer progression-free survival than chemotherapy alone (or with placebo) for recurrent platinum-sensitive ovarian cancer.
Most studies in this review found that bevacizumab plus chemotherapy had a more beneficial effect on treatment response than chemotherapy alone (or with placebo) for recurrent platinum-sensitive ovarian cancer.
There was no difference in quality of life, based on 1 randomized controlled trial, and no clear differences in adverse events reported between bevacizumab plus chemotherapy or chemotherapy alone (or with placebo).
Context and Policy Issues
Ovarian is the deadliest of gynecological cancers,1-3 causing an estimated 1,950 deaths in Canada in 2022, with approximately 3,000 new cases diagnosed in the same year.4 Ovarian cancer ranks as the fifth most common cause of cancer mortality in women who live in Canada, with relative survival being lower than that for all other cancers combined.5
Given their similar clinical courses and responses to treatment, epithelial ovarian cancer is often considered collectively with cancers of the fallopian tube(s) and peritoneal region in research and health care.6 Treatment for primary epithelial ovarian cancer usually includes surgery with adjuvant chemotherapy (CT) — often a platinum-based CT, such as carboplatin and paclitaxel, or cisplatin and paclitaxel.1,6 Whereas most patients demonstrate some response to platinum-based CT in first-line therapy, disease recurrence occurs in more than 70% of patients.1,2,7 Importantly, the duration of treatment response to platinum-based CT observed in first-line therapy, before disease recurrence, is known as the platinum-free interval (PFI), and is a determining factor in the therapy used for the treatment of ovarian cancer recurrence. Patients with a PFI of fewer than 6 months are classified as platinum-resistant, whereas those who experience a PFI of 6 months or more are considered platinum-sensitive.6
Conventional treatment for recurrent, platinum-sensitive ovarian cancer has prioritized re-treatment with platinum-based CT;2 however, high rates of subsequent recurrence, development of drug resistance to platinum-based CT, and poor patient outcomes have resulted in the development and investigation of novel therapies intended to optimize the benefits of CT.3 One of these therapies targets tumour angiogenesis (i.e., the development of blood supply to the tumour, which is essential for its growth and metastasis).8-10 The use of anti–vascular endothelial growth factor (VEGF) drugs to reduce tumour angiogenesis has been the subject of oncological research for years,11 and in the context of ovarian cancer, bevacizumab is the anti-VEGF therapeutic that was first, and has been most widely, studied.8,12
Bevacizumab as an adjunct to CT has shown clinical effectiveness in primary and recurrent platinum-resistant ovarian cancer, whereas its role in recurrent platinum-sensitive ovarian cancer is less clear.13 While bevacizumab with CT was approved by the FDA in 2016 for the treatment of platinum-sensitive ovarian cancer,2 there are currently no jurisdictions in Canada that fund the use of bevacizumab for the treatment of recurrent platinum-sensitive ovarian cancer.
Given the benefit that bevacizumab offers to patients with primary and recurrent platinum-resistant ovarian cancer, this report aims to summarize the evidence regarding the clinical effectiveness of bevacizumab plus CT (followed by bevacizumab maintenance therapy) in the treatment of recurrent platinum-sensitive ovarian cancer.
Research Question
What is the clinical effectiveness of bevacizumab in combination with chemotherapy followed by bevacizumab maintenance therapy for patients who have recurrent ovarian cancer and are platinum sensitive?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were ovarian cancer, bevacizumab, and recurrence or platinum-sensitivity. Conference abstracts were excluded. The search was completed on April 3, 2023, and limited to English-language documents published since January 1, 2013.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. Reference lists of relevant systematic reviews (SRs) were also screened for potentially eligible studies. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Patients with histologically confirmed recurrent epithelial ovarian cancer and who are platinum sensitive Excluded: Patients who previously received anti–vascular endothelial growth factor–targeted therapy (e.g., bevacizumab) |
Intervention | Bevacizumab in combination with chemotherapy (e.g., carboplatin with gemcitabine, liposomal pegylated doxorubicin, and paclitaxel) followed by bevacizumab maintenance therapy |
Comparator | Chemotherapy (with placebo or alone) followed by placebo or no treatment in the maintenance phase |
Outcomes | Clinical benefits (e.g., overall survival, progression-free survival, response rate, quality of life) and harms (e.g., adverse events, treatment discontinuation) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, and if they were duplicate publications or conference abstracts. SRs in which all relevant primary studies were captured in other more recent or more comprehensive SRs were excluded. To ensure maximum coverage of relevant data, and account for overlap between eligible primary studies that were both identified by this review and summarized in eligible SRs, the original primary study reports were included and summarized, and SRs that reported no additional eligible primary studies were excluded (as described).
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Downs and Black checklist14 for randomized and nonrandomized primary studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
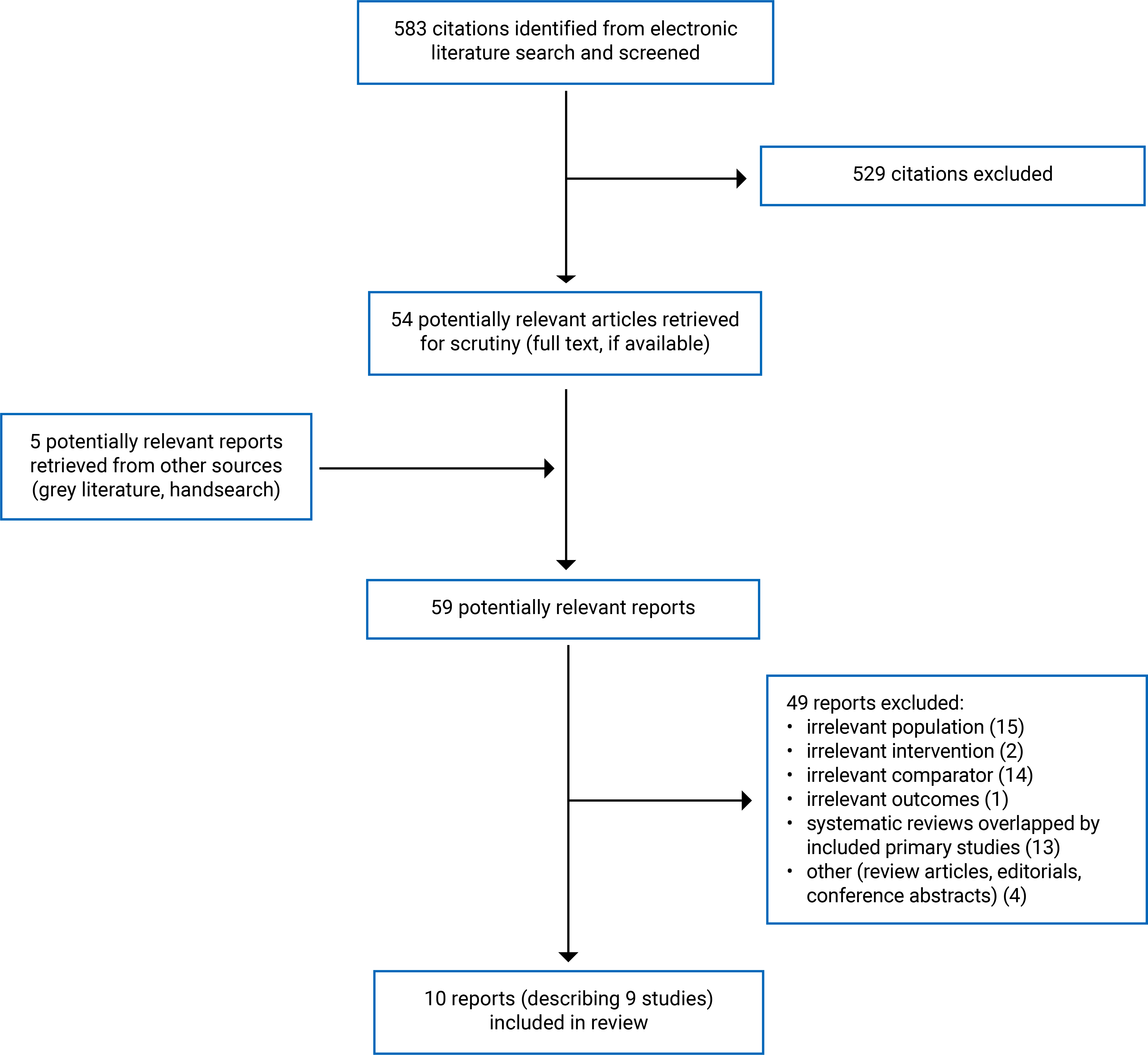
A total of 583 citations were identified in the literature search. Following screening of titles and abstracts, 529 citations were excluded and 54 potentially relevant reports from the electronic search were retrieved for full-text review. Five potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 49 publications were excluded for various reasons, and 10 publications (describing 9 eligible studies)15-24 met the inclusion criteria and were included in this report. These comprised 2 randomized controlled trials (RCTs) (reported in 3 publications) and 7 nonrandomized studies (NRSs). Appendix 1 presents the PRISMA25 flow chart of the study selection.
While this report summarizes 9 relevant primary clinical research studies (published in 10 papers), 13 eligible SRs and health technology assessments (HTAs) were also identified by the searches conducted for this review.13,26-37 Most of the SRs and HTAs had broader scope and research questions than those in this report (e.g., multiple types of ovarian and/or other cancers, or multiple types of anti-VEGF monoclonal antibody drugs). Across these 13 SRs and HTAs, only 2 RCTs eligible for inclusion in this report were identified; consequently, this report sought to summarize the available primary clinical study reports (including the 2 RCTs identified in the 13 SRs), which described more relevant and detailed information than was available in the 13 SRs.13,26-37
A table outlining these 13 SRs and HTAs, their publications of relevance to this report (i.e., the 2 RCTs with information published across 3 full-report publications15-17), and the overlap between publications is available in Appendix 5.
Additional references of potential interest are provided in Appendix 6.
Summary of Study Characteristics
Study Design
The 10 articles describing 9 primary clinical studies summarized in this report were published between 2012 and 2023.15-24 Two of the studies were RCTs (published across 3 reports)15-17 and 7 studies used nonrandomized retrospective designs.18-24
Both of the RCTs were multicentre, phase III clinical trials,15-17 and 1 of the RCTs used a double-blind study design.16,17 Of the 7 NRSs, 2 used a multicentre design,18,20 and 4 selected patients from a single treatment centre.19,21-23 One of the NRSs did not report information on the centre(s) from which patient data were drawn.24 Four of the NRSs used matched cohort designs21-24 with various patient characteristics of some potential relevance to this report, including age,23,24 duration of PFI,21-23 number of previous cycles of CT,21,24 tumour histology,21,23,24 and secondary surgical intervention.22 Finally, 2 of the NRSs made treatment comparisons using historical controls (i.e., data for patients in the control groups were taken from a different period in time than those for patients in the intervention groups).23,24
Country of Origin
Both of the RCT reports listed primary and other coauthors from the US.15-17 Whereas 1 of the RCT reports was clear about 67 study sites being located in the US (65 centres), Japan (1 centre), and South Korea (1 centre),15 the other RCT report did not provide information on the number or location(s) of study sites.16,17
Six of the 7 NRSs were located in Italy,18 Turkey,19 Korea,20,22 Brazil,21 and Japan.23 One NRS did not report the location of its research, but all of the coauthors of the paper were listed as being based in the US.24
Patient Population
All of the primary clinical studies included patients with ovarian cancer,15-24 with overall study sample sizes ranging between 3223 and 674 patients.15 Of the patients included in these overall study samples, all were eligible for inclusion in this report in 5 studies,16,17,20-23 whereas only subgroups of patients were eligible for inclusion in this report in 4 studies.15,18,19,24 Of the 4 studies with only subgroup data eligible for inclusion in this report, eligible subgroups ranged in size from 1124 to 638 participants.15
All 9 primary clinical studies included patients with recurrent platinum-sensitive ovarian cancer,15-24 with 4 studies specifying inclusion of other, related, types of cancers relevant to this report (i.e., primary peritoneal and/or fallopian tube cancer),15-19 and 2 studies that were specific in the subtype of ovarian cancer of interest, including patients with ovarian clear cell carcinoma20 and those with ovarian or peritoneal low-grade serous carcinoma.18
The mean or median ages of patients in the treatment groups across the eligible studies ranged from 5319 to 63 years.23 Other relevant features of eligible patients were reported with various frequency across the included studies, with 7 reporting on duration of PFI,15-18,20-23 5 describing secondary surgical intervention,16-18,20-22 and 5 reporting additional, potentially relevant patient characteristics.15-17,19,20,22
Of note, 1 of the NRSs reported overlap in some of its participants with those of the GOG-0213 trial (i.e., 38 patients in the intervention group and 4 in the control group).22 Similarly (though not reported), this study and a later study included in this review (published in 2022 by the same first author and describing 1 of the same institutions as a study centre from which patient data were drawn) appeared to have drawn data from the same institution, using an overlapping time frame and similar eligibility criteria, suggesting that some or all of the patients in these 2 included studies may have overlapped.20,22
Interventions and Comparators
All patients in the 9 included studies received either bevacizumab with CT, or CT alone (with or without placebo).15-24
Intervention
Dosages of bevacizumab were consistent across the 9 included studies. All patients to whom bevacizumab was administered received 15 mg/kg.15-24 There was a variety of CT drugs used in the intervention arms15-24 with 2 of the most common regimens including carboplatin (area under the curve [AUC] 5) plus paclitaxel (175 mg/m2)15,21-23 and gemcitabine (1,000 mg/m2) plus carboplatin (AUC 4)16,17,20,21 (with 1 study reporting the same latter combination containing carboplatin at a dose of AUC 522). Other carboplatin-containing CT regimens with dosages not reported included those with or without pegylated liposomal doxorubicin, gemcitabine, or docetaxel.18,19,24 One study reported the use of single-drug CTs (no dosages reported), including paclitaxel, cyclophosphamide, and doxorubicin.24
The 9 primary clinical studies also described a consistent duration of treatment cycle for all treatment groups of 3 weeks.15-24 Studies describing the planned number of treatment cycles for intervention groups reported 6 cycles (or more, depending on disease progression).15-17,23 Studies reporting the mean, median, and/or number of treatment cycles administered in the intervention groups across study follow-up18-22,24 ranged from a mean, median, or number of 6 cycles18,20-22 to 11 cycles.19
Bevacizumab maintenance therapy was reported in 7 of the included studies,15-17,19-23 whereas 2 did not specify whether bevacizumab maintenance therapy was administered.18,24 One study reported that bevacizumab maintenance therapy was administered to 65% of patients (with no information provided on maintenance therapy for the remaining 35% of patients).19
Control
As in the intervention groups, there was a variety of CT drugs used in the control groups of the included studies,15-24 with the most common CT regimens also including carboplatin (AUC 5) plus paclitaxel (175 mg/m2)15,21,23 or gemcitabine (1,000 mg/m2) plus carboplatin (AUC 4).16,17,21,23 Other carboplatin-containing CT regimens included those with or without pegylated liposomal doxorubicin, gemcitabine, paclitaxel, or docetaxel (dosages not reported).18,20,22,24 Other combination regimens with no dosages provided included camptothecin plus cisplatin,20 docetaxel plus cisplatin, and belotecan plus cisplatin.24 Other studies reported the use of single-drug CTs (with no dosages reported), including carboplatin, cyclophosphamide, doxorubicin,24 paclitaxel,22,24 camptothecin,20 topotecan,22,24 etoposide, navelbine, or pemetrexed.24 One study did not report any of the CT drugs used in the control group.19
Studies describing the planned number of CT-only treatment cycles for control groups reported 6 cycles.15-17,23 Studies describing the mean, median, or number of cycles administered to the control groups all reported 6 cycles.18,20-22 Two studies did not report the number of cycles planned or administered for the control group.19,24
One study in this report (i.e., the OCEANS trial) included the use of a placebo alongside the CT regimen.16,17 Similarly, the OCEANS trial was the only study included in this report that described the use of maintenance therapy in the control group of the study.16,17 The remaining studies did not describe use of a placebo or make mention of maintenance therapy in the control groups.15,18-24
Outcomes
Overall Survival
Outcomes of relevance to overall survival (OS) — including numbers and proportions of study patients who died, months of OS observed, 5-year OS, and hazard ratios (HRs) characterizing the effect of treatment assignment — were reported by 7 of the included studies.15,16,19-22,24
The 2 RCTs defined OS from the date of randomization to the date of death from any cause,15,16 and 3 of the NRSs reporting on OS defined it from the start date of treatment until death from disease or last follow-up,20 until disease progression or death by any cause,21 or until cancer-related death or end of the study.22 One study defined OS from the time of first recurrence until death or the last clinic visit.19 One NRS did not define OS.24
Three of the NRSs performed multivariate analyses to estimate HRs for the effect of treatment assignment on OS, adjusting for age,21 stage,22 histology,21,22 grade,22 PFI,20-22 secondary surgery,20,22 serum cancer antigen (CA) 125 levels at recurrence,20 and CCNE1 overexpression.21
Progression-Free Survival
Outcomes of relevance to progression-free survival (PFS) — including numbers and proportions of study patients whose disease progressed, months of PFS observed, or HRs characterizing the effect of treatment assignment — were reported by all of the 9 included studies.15,17-24 One RCT included some patients who had received bevacizumab in first-line therapy and presented main findings for PFS from this mixed population;15 however, some PFS data were available from a subgroup analyses of patients who had not received bevacizumab in first-line therapy, and these were included and summarized in this report. The other RCT presented findings for PFS generated from study investigators as well as those performed by an independent review committee;17 the latter of which were summarized in this report. One NRS matched some patients in the control group to those in the intervention group, reporting findings for PFS from both matched and unmatched analyses;23 data from both analyses were included in this report. Another NRS reported most findings for PFS from the entire study cohort, which included patients with both platinum-sensitive and platinum-resistant ovarian cancer;24 therefore, few relevant data describing PFS were available for inclusion and summary in this report.
The 2 RCTs defined PFS as observed events of disease progression occurring between the date of randomization to the date of disease progression, last contact, or death,15,17 and 6 of the NRSs defined it as events of disease progression occurring from the date of treatment initiation to the date of disease progression,18,20-24 death,18,21 or last contact.18 One study did not define PFS.19 Both RCTs described the use of standardized criteria (i.e., Response Evaluation Criteria in Solid Tumours [RECIST] to ascertain disease progression),15,17 as did 4 of the NRSs.19,20,22,23
Both RCTs and 4 of the NRSs performed multivariate analyses to estimate HRs for the effect of treatment assignment on PFS, adjusting for age,21 stage,22 histology,21,22 grade,22 PFI,16,17,20-22 secondary surgery,15-18,20,22 treatment-free interval before progression,15 serum CA 125 levels at recurrence,20 CCNE1 overexpression,21 and death.15
Treatment Response
Outcomes describing response to treatment — including complete response, partial response, stable disease, progressive disease, overall or objective response rate (ORR), and/or duration of response — were reported by 6 of the included studies summarized in this report.17,18,20,21,23,24 One NRS reported treatment response findings from the entire study cohort only (which included patients with both platinum-sensitive and platinum-resistant ovarian cancer);24 thus, no relevant data were available for inclusion and summary in this report.
Of the 5 eligible studies that included relevant data, 4 described complete response,18,20,21,23 5 described partial response,17,18,20,21,23 3 described stable disease,18,20,21 3 described progressive disease,18,20,21 4 described ORR,17,20,21,23 and 1 described duration of response.17 Four of the NRSs used RECIST criteria to characterize treatment response.18,20,21,23
Quality of Life
Patient-reported quality of life (QoL) was reported by 1 of the included RCTs.15 Data were collected at 5 points in time across study follow-up using the Function Assessment of Cancer Therapy (Ovary) trial outcome index (FACT-O TOI), including treatment side effect subscales specific to bevacizumab and surgery, as well as the physical functioning subscale of the Short Form (36) Health Survey (SF-36).15 Authors of the study reported that a 6-point difference in scores between groups would constitute a clinically meaningful difference.15 Of note, data for this outcome were only reported for the entire study cohort (including those who received bevacizumab in first-line therapy),15 but have been included and summarized in this report.
Safety
Toxicity, complications, and adverse events associated with treatment were reported by 5 of the included studies;15,16,19,23,24 though, 1 of the NRS reported findings only from the entire study cohort (which included patients with both platinum-sensitive and platinum-resistant ovarian cancer),24 which were therefore not eligible for inclusion in this report. The 4 studies reporting data of relevance tallied observed adverse events or major complications for each treatment group.15,16,19,23 Of these 4 studies, 3 used the Common Terminology Criteria for Adverse Events (CTCAE) to characterize adverse events.15,16,23 The remaining study did not describe methods for identification or categorization of the major complications that it reported.19 Both the RCTs specified that safety data were based on an as-treated approach (i.e., according to treatment received) as opposed to the intention-to-treat approach (i.e., according to the treatment group assignment) that was taken with the PFS and OS outcomes.15,16
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Summary of Critical Appraisal
Randomized Controlled Trials
The 2 RCTs included in this report were generally well-reported, with clear descriptions of the studies’ aims and objectives, patients, interventions, and outcomes, as well as estimates of random variability and actual P values.15-17 Both trials also reported observed adverse events.15,17 While both RCTs reported the use of multicentre designs,15-17 1 did not report information on the numbers or locations of treatment centres,16,17 which are details necessary to assess the study procedures. The other RCT did not include information on maintenance therapy in the control arm of the study.15
In general, information necessary to assess the external validity of the RCTs was either poorly or not reported (i.e., details regarding patient recruitment were not provided; for instance, the number of patients who refused to participate in the studies), and information necessary to assess the representativeness of the study patients, health care facilities, and treatment received to the broader population was not provided.15-17
The RCTs demonstrated several robust features supporting internal validity (i.e., by definition, patients were randomized to treatment assignments,15-17 which eliminates selection bias and distributes patient characteristics evenly across the treatment groups). One of the RCTs used a double-blind, placebo-controlled design,16,17 which is an important methodological feature that can reduce bias and supports the internal validity of the study. Both RCTs also used intention-to-treat analyses,15-17 which ensures that the randomized treatment assignment is retained, and that any patient loss to follow-up, treatment discontinuation, or other protocol deviations that occur across the study do not introduce bias.38 In addition, both trials recruited study patients across the same time frame,15-17 which is important for ensuring that the treatment received and other variables associated with the delivery of health care across time are comparable. Both of the RCTs also used survival analyses,15-17 which account for factors such as staggered entry into the study, recurrent events, and censoring.
In addition to these methodological strengths, several limitations were observed in both of the RCTs — 1 of which did not use a double-blind or placebo-controlled design,15 and also reported a protocol deviation partway through the study. Whereas eligible patients were initially excluded if they had prior exposure to bevacizumab in first-line therapy, this was modified later in the trial, allowing these patients with previous exposure to bevacizumab entry into the study,15 and introducing analytical risks and challenges associated with including 2 different populations in the study (i.e., potential risk of bias and impact on study power).39 In the other RCT, because there was no information reported about the study centres, it could not be determined whether patients in different treatment groups were recruited from the same or different centres,16,17 which is important for ensuring consistency in treatment exposures and essential for assessing internal validity.
Finally, study power calculations were performed and described for both RCTs; however, neither study observed enough events to satisfy the requirements of these power calculations.15-17
Nonrandomized Studies
The 7 NRSs included in this report demonstrated some strengths and several limitations.18-24 By nature of their designs, no randomization was performed in any of the studies, which introduces the risk of selection bias and can impact the internal validity of the study findings and conclusions. All of the NRSs used retrospective designs,18-24 which introduces potential bias and limitations associated with data that were not necessarily collected for research purposes (e.g., missing data, variation in treatment received, and/or unstandardized methods for data collection).
One of the strengths observed in the NRSs included generally clear reporting of study aims and objectives.18-24 And whereas most of the NRSs clearly reported essential details describing patients and outcomes,18-24 several studies did not provide detailed information describing the interventions that patients were administered (e.g., drugs, dosages, and/or treatment schedules were not reported for the control group).18-20,22,24 While it was clear in 4 of the included studies that the CT regimens used in both treatment groups were consistent, and therefore comparable,15-18,21 5 of the studies either did not clearly describe consistent or obviously comparable CT regimens across the treatment groups, introducing a potential risk to the internal validity of the findings and conclusions.19-24 And while 2 studies did not specify whether bevacizumab maintenance therapy was administered,18,24 all 7 of the NRSs provided no information on maintenance therapy in the control arms of the studies.18-24 Three of the NRSs described safety data (i.e., observations of adverse events;19,23,24 though, adverse event data were not eligible for inclusion in this report for 1 of these studies24), whereas 4 did not report this information.18,20-22
While 1 study reported information supporting the representativeness of the treatment that was administered to patients,18 the other studies did not provide the information necessary to assess external validity, making the representativeness of the patients and interventions to the broader population unclear.18-24
All18-23 but 124 of the studies were clear about drawing patient data from the same source(s), which is important for ensuring consistency in the treatment and health care received across the groups. Similarly, most of the NRSs described the use of patient data from across the same time frame for both treatment groups,18,20,21,23,24 whereas 2 described the use of historical controls,19,22 which constitutes a limitation. Patients treated at different time points may have had variable exposures or interventions that are not directly comparable, introducing a risk of confounding that could compromise the internal validity of findings and conclusions. Four of the NRSs used matched study designs,21-24 which can reduce the risk of confounding by ensuring that patients are more similar in their features and characteristics. Five of the NRSs used multivariate analyses to adjust for relevant covariates that could introduce a risk of confounding and compromise internal validity18-22 (e.g., age,21 PFI,20-22 and secondary surgery).18,22 Of note, while 1 of these studies reported the use of multivariate analyses, the covariates used were not specified.19 All of the 7 NRSs included in this report described the use of survival analyses,18-24 which account for such factors as staggered entry into the study, recurrent events, and censoring.
Other limitations observed include duplicate publication, as reported by 1 of the NRSs. In this study, 38 patients in the intervention group and 4 in the control group were also included previously in the GOG-0213 study.20 Of potential relevance to this was an apparent risk of duplicate publication across this study and another NRS included in this review22 (i.e., both papers reported the same first author, 1 of the same institutions from which data were drawn across an overlapping timeline, and both papers has similar patient eligibility criteria).20,22 While the duplication cannot be ascertained with certainty, these factors constitute a risk of duplicate publication, which can falsely inflate the apparent volume of available data, and has been described as scientific misconduct.40
Finally, whereas 4 of the NRSs reported their source(s) of funding,18,19,21,22 3 did not;20,23,24 it is essential that source(s) of funding be disclosed in the report of findings to allow for consideration of any potential conflict of interest or risk of bias.
Additional details regarding the strengths and limitations of the included studies are provided in Appendix 3.
Summary of Findings
Overall Survival
Most of the 7 studies in this review that reported on OS identified a statistically significant benefit of bevacizumab with CT as compared to CT only (or with placebo).15,16,19-22,24
Randomized Controlled Trials
Survival was investigated in both of the included RCTs at a median follow-up of 49.6 months for both treatment groups in the GOG-0213 trial,15 and a median follow-up of 57.5 months (95% confidence interval [CI], 0.3 to 73.9) for the entire study population in the OCEANS trial.16 Whereas the GOG-0213 study reported 189 patient deaths (62.4%) in the bevacizumab plus CT group and 179 patient deaths (59.1%) in the CT-only group,15 the OCEANS trial reported 353 patient deaths among the entire study population (72.9%);16 numbers of patients deaths between treatment groups were characterized as not statistically significantly different for both RCTs.15,16
Median months of OS were not reported for the subgroup of patients in the GOG-0213 study who had not received bevacizumab in first-line therapy.15 In the OCEANS trial, the bevacizumab group experienced 33.6 months (95% CI not reported [NR]) of OS and the CT-only group experienced 32.9 months (95% CI NR) of OS.16 While no statistical characterization of the difference between treatment groups in median months of OS was reported in the OCEANS trial, the authors stated in their conclusions that there was no statistically significant differences in OS observed between treatment groups.16 The lack of statistical significance in OS between treatment groups was further demonstrated in the report of hazard analyses, which generated an HR of 0.868 (95% CI, 0.707 to 1.066) in the GOG-0213 trial15 and 0.952 (95% CI, 0.771 to 1.176; P = 0.6479) in the OCEANS trial.16
Nonrandomized Studies
Of the 5 NRSs that analyzed OS,19-22,24 3 included the number of patient deaths observed across follow-up.20-22 One NRS reported 9 deaths in 52 patients from the bevacizumab and CT group, and 57 deaths in 104 patients in the CT-only group across a median follow-up of 35.6 months (range = 4.1 to 118.5).22 A statistical comparison of the treatment groups generated a P value of 0.016, indicating a benefit in favour of the bevacizumab and CT group.22 Another NRS observed 7 deaths in 36 patients to whom bevacizumab and CT were administered, and 46 deaths in 102 patients who were administered CT only, across a median 19.9 months of follow-up (with no statistical characterization of the difference between treatment groups reported).20 The third NRS described total deaths observed across the entire study cohort, reporting 61 patient deaths in 124 patients across a median of 40 months of follow-up (with no statistical characterization of the difference between treatment groups reported).21
Two NRSs reported data describing patients who experienced 5-year OS,19,22 with 1 study observing 68% of patients surviving to 5 years in the bevacizumab and CT group versus 64% of patients in the CT-only group (P = 0.28), indicating no statistically significant difference.19 The other study found that 51.5% of patients in the bevacizumab and CT group survived to 5 years, as compared to 42.8% of patients in the CT-only group (with no statistical characterization of the difference between groups reported).22
Data describing median months of OS were reported by 3 NRSs20,21,24 (though 1 provided only a P value characterizing the difference between treatment groups, and did not provide data specific to the observed months of OS for each of the groups [i.e., P = 0.8631], demonstrating no statistically significant difference24). One of the studies observed a median of 43.5 months (95% CI, 31.9 to 55.1) of OS in the bevacizumab and CT group as compared to 32.1 months (95% CI, 22.1 to 42.1) in the CT-only group, indicating a statistically significant difference in favour of bevacizumab and CT (i.e., P = 0.043).20 Another NRS found a median of 48.9 months (95% CI NR) of OS for patients to whom bevacizumab and CT was administered versus 51.9 months (95% CI NR) of OS for patients receiving CT only, demonstrating no statistically significant difference between the groups (i.e., P = 0.410).21
Three NRSs reported findings from multivariate hazard analyses for OS by treatment group,20-22 2 of which found HRs indicating a statistically significant benefit in favour of bevacizumab and CT,20,22 (i.e., HR = 0.435; 95% CI, 0.195 to 0.970,20 and HR = 0.39; 95% CI, 0.19 to 0.80).22 The third study found an HR of 0.70 (95% CI, 0.30 to 1.61), demonstrating no statistically significant difference between the treatment groups.21
Progression-Free Survival
While there was some variability across the 9 studies describing PFS in this report,15-24 most identified a statistically significant benefit in favour of bevacizumab with CT as compared to CT only (or with placebo).
Randomized Controlled Trials
Disease progression was observed in both of the included RCTs at a median follow-up of 49.6 months for each of the treatment groups in the GOG-0213 trial,15 and a median follow-up of 24 months for the entire study population in the OCEANS trial.17 Whereas the GOG-0213 study reported disease progression in 88% of patients in the bevacizumab plus CT group and 90.1% of patients in the CT-only group,15 the OCEANS trial reported disease progression in 338 patients from both treatment groups17 (with no characterization of the difference between treatment groups reported in either study for this parameter).
Median months of PFS observed in the bevacizumab plus CT groups for the RCTs, respectively, were 13.8 (95% CI NR) in the GOG-0213 study and 12.3 (95% CI, 10.7 to 14.6) in the OCEANS trial. For the CT-only and CT plus placebo groups, respectively, median months of PFS observed were 10.2 (95% CI NR) in the GOG-0213 trial15 and 8.6 (95% CI, 8.3 to 10.2) in the OCEANS study.17 While no statistical characterization of the difference between treatment groups in median months of PFS was reported in either trial, the lack of overlap in 95% CIs between treatment groups for the OCEANS trial data indicates a statistically significant benefit in favour of the patients who received bevacizumab plus CT in that study.17
Both RCTs also reported findings for PFS from multivariate analyses by treatment group, with the GOG-0213 study authors reporting a statistically significant HR in favour of the bevacizumab plus CT group of 0.63 (95% CI, 0.53 to 0.75),15 and the OCEANS authors similarly reporting a statistically significant HR finding that favoured bevacizumab plus CT (i.e., HR = 0.451; 95% CI, 0.351 to 0.580).17
Nonrandomized Studies
Of the NRS, 3 studies reported on the numbers of patients in whom disease progression was observed.20-22 Across a median follow-up of 19.9 months in 1 study (95% CI NR), disease progression was observed in 23 of 36 patients in the bevacizumab plus CT group, and 81 of 102 patients in the CT-only group.20 In another study, 23 of 52 patients in the bevacizumab plus CT group and 81 of 104 patients in the CT-only group experienced disease progression across a median follow-up of 35.6 months (range = 4.1 to 118.5).22 In the third study reporting on PFS, the duration of follow-up was not reported (i.e., median follow-up was reported for the OS outcome only), with the authors reporting a total of 84 patients in whom disease progression was observed across the entire study cohort of 124 patients (i.e., 67.7%).21
Data describing duration of PFS were reported by all 7 of the included NRS;18-24 however, 1 study reported median months of PFS for the bevacizumab plus CT group only,19 and another only reported a P value characterizing the statistical difference in duration of PFS between treatment groups.24 Of the 6 NRSs reporting on median months of PFS in patients to whom bevacizumab plus CT were administered, median months of PFS ranged from between 8.2 (95% CI NR)19 and 37.1 (95% CI, 13.42 to 40.56).18 Of the 5 NRSs reporting on median months of PFS in patients to whom CT-only was administered, median months of PFS ranged from between 6.31 (95% CI NR)23 and 16.0 (95% CI NR).21 Six of these studies also characterized the statistical difference in median PFS between treatment groups using P values,18,20-24 with 4 reporting a statistically significant benefit of bevacizumab plus CT as compared to CT only,18,20,22,23 and 2 reporting no statistically significant difference between the treatment groups.21,24
Five of the NRSs also reported findings from hazard analyses for PFS by treatment group, with HRs ranging from between 0.30 (95% CI, 0.15 to 0.80)18 and 0.54 (95% CI, 0.26 to 1.09).21 Four studies reported a statistically significant benefit in favour of bevacizumab plus CT,18,20,22,23 whereas 1 reported no statistical difference between treatment groups.21
Treatment Response
The RCT describing treatment response reported an ORR of 78.5% in patients to whom bevacizumab and CT were administered as compared to 57.4% in the group receiving CT plus placebo, indicating a statistically significant improvement in the bevacizumab and CT group (i.e., P < 0.001).17 Duration of response was reported as 10.4 months in the bevacizumab and CT group versus 7.4 months in the CT plus placebo group, generating an HR of 0.534 (95% CI, 0.408 to 0.698) and indicating a statistically significant improvement in patients receiving bevacizumab and CT.17
Of the 4 NRSs reporting data on treatment response,18,20,21,23 3 described ORRs for each of the treatment groups.20,21,23 Two of the studies reported a statistically significant improvement in ORR for the bevacizumab and CT groups (i.e., P = 0.0320 and P = 0.002),21 and the third did not characterize the difference between treatment groups, reporting only the proportions of study patients in whom ORR was observed (i.e., 92.3% in the bevacizumab and CT group versus 57.9% in the CT-only group).23
Quality of Life
The RCT that collected data and reported on QoL found an overall difference in mean scores between treatment groups of −0.37 (95% CI, −1.80 to 1.06; P = 0.62), demonstrating no statistically significant or clinically meaningful difference between the bevacizumab and CT as compared to the CT-only groups.15 Similarly, there was no statistically significant difference found between treatment groups at any point in time across the patient-reported QoL assessment.15
Safety
Both RCTs described the proportion of patients who experienced any adverse event of grade III or higher,15,16 with the GOG-0213 trial reporting these in 96% of patients to whom bevacizumab and CT were administered as compared to 86% of those to whom CT only was administered.15 The OCEANS trial observed any adverse event of grade III or higher in 90.3% of patients receiving bevacizumab and CT versus 82.4% in those who received CT plus placebo.16 Serious adverse events were also reported in both RCT reports, with 28% and 36.4% of patients in the bevacizumab and CT groups affected, respectively, in the GOG-0213 and OCEANS studies, and 11% and 25.3% of patients in the CT-only or CT plus placebo groups, respectively.15,16 Both trials also reported the proportions of patients with adverse events that led to treatment discontinuation, with 25% and 22.3% in the bevacizumab and CT groups in the GOG-0213 and OCEANS trials, respectively, and 11% and 4.7% in the CT-only and CT plus placebo groups, respectively.15,16 No statistical characterization of the differences in adverse events observed across the study treatment groups was reported for either trial.15,16
Both of the NRSs provided comparative statistics for the adverse events reported, with 1 NRS reporting no statistically significantly differences across the treatment groups in the proportions of patients experiencing any of the observed adverse events.19 The other NRS reported statistically significantly more cases of neutropenia, epistaxis, fatigue, and hypertension in the bevacizumab plus CT group as compared to the CT-only group; and statistically significantly more cases of alopecia in the CT-only group, with no other significant differences reported.23
Appendix 4 presents the main study findings with details describing all adverse events observed.
Limitations
Despite a large body of published literature describing bevacizumab and CT for the treatment of platinum-sensitive ovarian cancer, the base of high-quality evidence is not as large as multiple SRs13,26-37 (as well as this review) describe only 2 RCTs15-17 on the topic. Seven NRSs were also identified and included in this review, all of which were retrospective in their designs and many of which included mixed populations that were not all relevant to this topic (e.g., both primary and recurrent cases,18 or both patients who were platinum sensitive and those who were platinum resistant).19,24 One of the RCTs also included patients with mixed features (i.e., patients who had or had not been exposed to bevacizumab in first-line therapy).15 These mixed study populations and the retrospective, observational designs and methods used in the majority of studies included in this review limited the data available for summary in this report.
While most of the interventions and comparators used in some of the studies included in this report were consistent and clear, several did not clearly describe the interventions and/or comparators used (e.g., there were missing details concerning the CT drugs used,19 information was lacking for dosages and/or schedules,18-20,22,24 and a clear description of maintenance therapy in the intervention group was missing),18,24 which limited the certainty concerning the eligibility of the regimens and the potential impact of variability in these interventions on the findings and conclusions of the included studies. Importantly, any potential differences in CT regimens across the intervention and comparator groups were unclear in 5 of the included NRSs,19,20,22-24 which could compromise the comparability of the treatment groups in these studies.
Outcomes reported by the studies included in this report were reasonably consistent, with PFS15-24 and/or OS15-17,19-22,24 being featured in all of the studies. However, only 1 study collected patient-reported outcomes data describing QoL,15 which limits the extent to which patient-oriented outcomes can be described. Similarly, 4 of the included studies did not describe adverse events associated with treatment,18,20-22 which are critical for understanding the potential harms that an intervention may cause in the context of any benefit that may be observed.
Another important limitation noted in this report was the possibility of duplicate publication of data from patients who overlapped across several of the included studies (i.e., 1 NRS reported the inclusion of some patient data that was also reported previously in the GOG-0213 trial).22 Another NRS included in this report shared some of the study coauthors and included patients with similar eligibility from the same institution across an overlapping time frame with this study,20,22 suggesting the possibility of duplicate publication across these included studies, which could falsely inflate the appearance of relevant data.
Finally, while the studies included in this report were conducted in several countries and various regions around the world,15-24 none of the included studies were conducted in Canadian sites. This may affect the applicability of the summarized evidence to the Canadian population and health care context.
Conclusions and Implications for Decision- or Policy-Making
This review identified 9 eligible studies (reported across 10 publication), including 2 RCTs and 7 NRSs.15-24 All of the studies described comparisons between bevacizumab and CT versus CT only (with 1 RCT describing CT with a placebo in the comparison group) in patients with recurrent platinum-sensitive ovarian cancer.15-24 The outcomes described included PFS, OS, treatment response, QoL, and safety.15-24
All of the 9 studies included in this report described PFS, with 6 (including both RCTs) describing a statistically significant benefit of bevacizumab and CT as compared to CT alone or CT plus placebo,15,17,18,20,22,23 and 2 studies finding no statistically significant difference between the treatment groups.21,24 Similarly, of 3 studies describing response to treatment (including 1 RCT) and characterizing the statistical difference between treatment groups, all reported a benefit of bevacizumab and CT versus CT only or CT plus placebo.17,20,21 Of note, the value and importance of PFS as an outcome for informing decision-making has been called into consideration. As an end point initially intended to inform phase II trials, it can imply a direct measurement of survival where there is none, and does not account for patient-oriented outcomes, such as QoL.41 Thus, while a preponderance of evidence summarized in this review indicates a benefit of bevacizumab in terms of PFS, it is useful to consider the broader clinical and patient-oriented implications of this finding, as well as the utility and potential limitations of PFS as an outcome in support of policy-making and/or decision-making.
Conversely, OS was not found to differ statistically between the treatment groups in 5 of the 7 included studies summarized in this review (including both RCTs),15,16,19,21,24 whereas 2 studies did report a statistically significant benefit that favoured bevacizumab and CT as compared to CT only.20,22 The lack of effect of bevacizumab and CT on OS has been discussed elsewhere. A recent network meta-analysis concluded that, while antiangiogenic drugs (including bevacizumab and CT followed by bevacizumab maintenance therapy) may offer an OS benefit in high-risk primary and platinum-resistant ovarian cancer, their effectiveness in the platinum-sensitive setting is not clear based on a not statistically significant difference in comparison with CT alone.13 Two SRs and MAs have reported a marginal benefit of bevacizumab and CT in recurrent ovarian cancer; however, both patients who were platinum resistant and those who were platinum sensitive were included in these analyses, with neither group clearly driving the observed benefit.27,29
Bevacizumab was described by both of the RCT reports included in this review as having a known safety profile,15,16 and has been described in other literature as a drug with tolerable toxicity.3 This could help to explain the limited number of studies reporting safety data in this report (i.e., 4 of the studies published later in time did not report any information describing adverse events).18,20-22 Nonetheless, the relevant safety data that were summarized in this report15,16,19,23 (particularly the more fulsome data included in the RCT reports15,16), indicate that toxicity and harms caused by bevacizumab are important considerations that must be weighed against the potential benefits that patients may experience — including survival and QoL.
QoL was reported in 1 of the included RCTs, indicating no statistically or clinically meaningful difference between bevacizumab and CT as compared to CT alone.15 This is an important finding that would benefit from further investigation to better understand the impacts of bevacizumab on patient experiences, QoL, and impacts on daily life — particularly, as previously mentioned, because the available safety data summarized in this report indicate the potential for harms, and data on survival remain inconclusive. Future research investigating the benefits and harms of bevacizumab could address this gap by prioritizing and analyzing patient-oriented outcomes.
CADTH has completed previous work on the role of bevacizumab in ovarian cancer — a 2015 report recommended reimbursement of bevacizumab with CT for high-risk primary ovarian cancer,42 and a 2016 report recommended reimbursement of bevacizumab with CT for platinum-resistant ovarian cancer,43 though both recommendations were contingent on cost-effectiveness.42,43 Cost-effectiveness is a consideration that could support and inform policy- and decision-making concerning bevacizumab with CT in the recurrent platinum-sensitive ovarian cancer context. While some work has been done, including a Canadian cost-effectiveness analysis in the platinum-resistant setting44 and a cost-effectiveness study in the first-line therapeutic setting, cost-effectiveness data specific to recurrent platinum-sensitive disease would be useful to consider alongside the available clinical effectiveness data.
Future research may also benefit from investigation of more targeted populations, rather than mixed populations that combine, for instance, primary and recurrent ovarian cancer, or platinum-sensitive and platinum-resistant disease (i.e., given the variation in responses to treatment described in the literature,13,27,29 more focused research on platinum-sensitive disease — particularly studies using randomized, double-blind designs — will help elucidate the benefit and utility of bevacizumab for this patient population).
References
1.Yang L, Xie HJ, Li YY, Wang X, Liu XX, Mai J. Molecular mechanisms of platinum-based chemotherapy resistance in ovarian cancer (Review). Oncol Rep. 2022;47(4). PubMed
2.Bartoletti M, Pelizzari G, Gerratana L, et al. Bevacizumab or PARP-Inhibitors Maintenance Therapy for Platinum-Sensitive Recurrent Ovarian Cancer: A Network Meta-Analysis. Int. 2020;21(11):27. PubMed
3.Zhang W, Shen Z, Luo H, Hu X, Zheng L, Zhu X. The Benefits and Side Effects of Bevacizumab for the Treatment of Recurrent Ovarian Cancer. Curr Drug Targets. 2017;18(10):1125-1131. PubMed
4.Darren RB, Abbey P, Ryan RW, et al. Projected estimates of cancer in Canada in 2022. Can Med Assoc J. 2022;194(17):E601. PubMed
5.Navaneelan T, Ellison L. Ovarian cancer: Survival statistics. Catalogue no. 82-624-X. Ottawa (ON): Statistics Canada; 2015: https://www150.statcan.gc.ca/n1/pub/82-624-x/2015001/article/14212-eng.htm. Accessed 2023 Apr 23.
6.Coleman RL, Sabbitini P. Medical treatment for relapsed epithelial ovarian,fallopian tube, or peritoneal cancer: Platinum-sensitive disease. In: T.W. P, ed. UpToDate. Waltham (MA): UpToDate; 2023. Accessed 2023 Apr 12.
7.National Cancer Institute. When Ovarian Cancer Returns, Surgery May Be a Good Choice for Selected Patients. 2022; https://www.cancer.gov/news-events/cancer-currents-blog/2022/ovarian-cancer-return-surgery-desktop-iii#:~:text=In%20more%20than%207%20of,possible%20before%20starting%20chemotherapy%20again. Accessed 2023 Apr 25.
8.Liu Y, Luo Y, Cai M, et al. Anti-angiogenic therapy in ovarian cancer: current situation & prospects. Indian J Med Res. 2021;154(5):680-690. PubMed
9.Lugano R, Ramachandran M, Dimberg A. Tumor angiogenesis: causes, consequences, challenges and opportunities. Cell Mol Life Sci. 2020;77(9):1745-1770. PubMed
10.National Cancer Institute. NCI Dictionary of Cancer Terms: angiogenesis. https://www.cancer.gov/publications/dictionaries/cancer-terms/def/angiogenesis, 2023 Apr 24.
11.Duda DG, Batchelor TT, Willett CG, Jain RK. VEGF-targeted cancer therapy strategies: current progress, hurdles and future prospects. Trends Mol Med. 2007;13(6):223-230. PubMed
12.Bakir MS, Birge O, Karadag C, et al. Bevacizumab in recurrent ovarian cancer. Journal of BUON. 2021;26(4):1271-1278. PubMed
13.Helali AE, Wong CHL, Choi HCW, et al. A comprehensive systematic review and network meta-analysis: the role of anti-angiogenic agents in advanced epithelial ovarian cancer. Sci Rep. 2022;12(1):3803. PubMed
14.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
15.Coleman RL, Brady MF, Herzog TJ, et al. Bevacizumab and paclitaxel-carboplatin chemotherapy and secondary cytoreduction in recurrent, platinum-sensitive ovarian cancer (NRG Oncology/Gynecologic Oncology Group study GOG-0213): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2017;18(6):779-791. PubMed
16.Aghajanian C, Goff B, Nycum LR, Wang YV, Husain A, Blank SV. Final overall survival and safety analysis of OCEANS, a phase 3 trial of chemotherapy with or without bevacizumab in patients with platinum-sensitive recurrent ovarian cancer. Gynecol Oncol. 2015;139(1):10-16. PubMed
17.Carol A, Stephanie VB, Barbara AG, et al. OCEANS: A Randomized, Double-Blind, Placebo-Controlled Phase III Trial of Chemotherapy With or Without Bevacizumab in Patients With Platinum-Sensitive Recurrent Epithelial Ovarian, Primary Peritoneal, or Fallopian Tube Cancer. J Clin Oncol. 2012;30(17):2039-2045. PubMed
18.Musacchio L, Turinetto M, Arenare L, et al. Effect of bevacizumab in advanced low grade serous ovarian cancer: Data from the MITO 22 trial. Gynecol Oncol. 2023;172:72-77. PubMed
19.Akilli H, Rahatli S, Aliyeva K, Altundag O, Kuscu UE, Ayhan A. Survival in recurrent ovarian cancer patients before and after the bevacizumab era: an observational single-centre study. J Obstet Gynaecol. 2022;42(6):2230-2234. PubMed
20.Kim SI, Kim JH, Noh JJ, et al. Impact of bevacizumab and secondary cytoreductive surgery on survival outcomes in platinum-sensitive relapsed ovarian clear cell carcinoma: A multicenter study in Korea. Gynecol Oncol. 2022;166(3):444-452. PubMed
21.Ribeiro ARG, Salvadori MM, De Brot L, et al. Retrospective analysis of the role of cyclin E1 overexpression as a predictive marker for the efficacy of bevacizumab in platinum-sensitive recurrent ovarian cancer. Ecancermedicalscience. 2021;15 (no pagination). PubMed
22.Kim SI, Lee EJ, Lee M, et al. Recurrence patterns after bevacizumab in platinum-sensitive, recurrent epithelial ovarian cancer. Int J Gynecol Cancer. 2020;30(12):1943-1950. PubMed
23.Hirasawa T, Machida H, Iida T, Ikeda M, Shida M, Mikami M. Impact of Adding Bevacizumab to Paclitaxel + Carboplatin for Platinum-Sensitive Recurrent Epithelial Ovarian Cancer: A Propensity Score Matching Analysis. Tokai J Exp Clin Med. 2018;43(3):85-89. PubMed
24.Akers SN, Riebandt G, Miller A, Groman A, Odunsi K, Lele S. Bevacizumab for the treatment of recurrent ovarian cancer: a retrospective cohort study. Eur J Gynaecol Oncol. 2013;34(2):113-119. PubMed
25.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
26.Liu Y, Huang Y, Li J, et al. A comprehensive comparison of medication strategies for platinum-sensitive recurrent ovarian cancer: A Bayesian network meta-analysis. Front Pharmacol. 2022;13:1010626. PubMed
27.Liu S, Kasherman L, Fazelzad R, et al. The use of bevacizumab in the modern era of targeted therapy for ovarian cancer: A systematic review and meta-analysis. Gynecol Oncol. 2021;161(2):601-612. PubMed
28.Bevacizumab in the treatment of ovarian cancer. KCE Report 285. Brussels (Belgium): Belgian Health Care Knowledge Centre; 2021: https://kce.fgov.be/sites/default/files/2021-11/Download%20the%20report%20in%20English%20%28116%20p.%29.pdf. Accessed 2023 Apr 12.
29.Wang H, Xu T, Zheng L, Li G. Angiogenesis Inhibitors for the Treatment of Ovarian Cancer: An Updated Systematic Review and Meta-analysis of Randomized Controlled Trials. Int J Gynecol Cancer. 2018;28(5):903-914. PubMed
30.Wu YS, Shui L, Shen D, Chen X. Bevacizumab combined with chemotherapy for ovarian cancer: an updated systematic review and meta-analysis of randomized controlled trials. Oncotarget. 2017;8(6):10703-10713. PubMed
31.Yi S, Zeng L, Kuang Y, et al. Antiangiogenic drugs used with chemotherapy for patients with recurrent ovarian cancer: a meta-analysis. OncoTargets and therapy. 2017;10:973-984. PubMed
32.Li X, Zhu S, Hong C, Cai H. Angiogenesis inhibitors for patients with ovarian cancer: a meta-analysis of 12 randomized controlled trials. Curr Med Res Opin. 2016;32(3):555-562. PubMed
33.Li J, Zhou L, Chen X, Ba Y. Addition of bevacizumab to chemotherapy in patients with ovarian cancer: a systematic review and meta-analysis of randomized trials. Clin Transl Oncol. 2015;17(9):673-683. PubMed
34.Ding SS, Li L, Yu CX. Systematic evaluation of bevacizumab in recurrent ovarian cancer treatment. Journal of BUOn. 2014;19(4):965-972. PubMed
35.Aravantinos G, Pectasides D. Bevacizumab in combination with chemotherapy for the treatment of advanced ovarian cancer: a systematic review. J Ovarian Res. 2014;7:57. PubMed
36.Bevacizumab in combination with gemcitabine and carboplatin for treating the first recurrence of platinum-sensitive advanced ovarian cancer. London (UK): National Institute for Health and Care Excellence; 2013: https://www.nice.org.uk/guidance/ta285/documents/ovarian-fallopian-tube-and-primary-peritoneal-cancer-recurrent-advanced-platinumsensitive-or-partially-platinumsensitive-bevacizumab-evaluation-report. Accessed 2023 Apr 12.
37.Zhou M, Yu P, Qu X, Liu Y, Zhang J. Phase III trials of standard chemotherapy with or without bevacizumab for ovarian cancer: a meta-analysis. PLoS ONE. 2013;8(12):e81858. PubMed
38.McCoy CE. Understanding the Intention-to-treat Principle in Randomized Controlled Trials. West J Emerg Med. 2017;18(6). PubMed
39.Lösch C, Neuhäuser M. The statistical analysis of a clinical trial when a protocol amendment changed the inclusion criteria. BMC Med Res Methodol. 2008;8:16. PubMed
40.Werner MU. Salami-slicing and duplicate publication: gatekeepers challenges. Scand J Pain. 2021;21(2):209-211. PubMed
41.Gyawali B, Eisenhauer E, Tregear M, Booth CM. Progression-free survival: it is time for a new name. Lancet Oncol. 2022;23(3):328-330. PubMed
42.Avastin for Ovarian Cancer. Ottawa (ON): CADTH; 2015: https://www.cadth.ca/avastin-ovarian-cancer-details. Accessed 2023 Apr 24.
43.Avastin for Platinum-Resistant Ovarian Cancer. Ottawa (ON): CADTH; 2016: https://www.cadth.ca/avastin-platinum-resistant-ovarian-cancer-details. Accessed 2023 Apr 24.
44.Ball G, Xie F, Tarride JE. Economic Evaluation of Bevacizumab for Treatment of Platinum-Resistant Recurrent Ovarian Cancer in Canada. Pharmacoeconom Open. 2018;2(1):19-29. PubMed
45.Neyt M, Vlayen J, Devriese S, Camberlin C. First- and second-line bevacizumab in ovarian cancer: A Belgian cost-utility analysis. PLoS ONE. 2018;13(4):e0195134. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Randomized Controlled Trials | ||||
Coleman et al. (2017)15 i.e., Gynecologic Oncology Group (GOG) 0213 Trial Countries: US (primary location) with study centres in Japan and South Korea Funding sources: National Cancer Institute (NCI) grants to the Gynecologic Oncology Group (GOG) Administrative Office (CA 27469), the Gynecologic Oncology Group Statistical Office (CA 37517), NRG Oncology (1U10 CA180822), and NRG Operations (U10CA180868). Roche/Genentech supported the NCI-CRADA Study investigators received grant funding from Ann Rife Cox Chair in Gynecology; Judy Reis/Albert Pisani Ovarian Cancer Research Fund; Genentech/Roche; Chugai/Roche | Mutlicentre (N = 67), phase III randomized controlled trial (with randomization stratified by PFI) | Patients ≥ 18 years of age with recurrent, platinum-sensitive, epithelial ovarian, primary peritoneal, or fallopian tube cancer treated between 2007 and 2014 All patients observed in the study (including those exposed/not exposed to first-line therapy with bevacizumab), N = 674 Patients eligible for this report (including only those not exposed to first-line therapy with bevacizumab), n = 638 All patients in the intervention group*, N = 337:
All patients in the control group*, N = 337:
Eligible patients in the intervention group, N = 323:
Eligible patients in the comparator group, N = 315:
*While exposure to bevacizumab in first-line therapy is an exclusion criterion for this report, study characteristics data for this study include and describe the full study population, including those with previous exposure to bevacizumab | Intervention: Bevacizumab (15 mg/kg) + platinum-based CT i.e., paclitaxel (175 mg/m2) + carboplatin (AUC 5) every 3 weeks for 6 cycles, followed by bevacizumab maintenance therapy until disease progression or unacceptable toxicity Comparator: CT only i.e., paclitaxel (175 mg/m2) + carboplatin (AUC 5) every 3 weeks for 6 cycles (maintenance phase NR) | Outcomes: PFS i.e., date of randomization to the date of disease progression (ascertained using RECIST v. 1.1 criteria), last contact or death including multivariate analyses describing HR adjusted for surgery, treatment-free interval for progression or death OS i.e., date of randomization to the date of death from any cause Safety i.e., observations of adverse events using the CTCAE criteria (v. 3), including treatment discontinuation* QoL i.e., patient-reported surveys using the FACT-O TOI, including the TSE subscales specific to bevacizumab and SF-36 physical functioning subscale* Follow-up: Months (intervention group), median (IQR) = 49.6 (41.5 to 62.2) Months (control group), median (IQR) = 49.6 (40.8 to 59.3) *While these data include both patients with and without previous exposure to bevacizumab, they have been summarized in the report |
Aghajanian et al. (2015)16 Country: US (locations of study/treatment centers NR) Funding source: Study sponsor reported as Genentech | Mutlicentre (N = NR), phase III, double-blind randomized controlled trial (with randomization stratified by PFI and SCS) | Patients ≥ 18 years of age with platinum-sensitive recurrent ovarian, primary peritoneal, or fallopian tube cancer and were randomized to treatment groups between 2007 and 2010 All patients observed in the study, N = 484 Patients in the intervention group, N = 242:
Patients in the control group, N = 242:
| Intervention: Bevacizumab (15 mg/kg) + CT i.e., gemcitabine (1,000mg/m2) + carboplatin (AUC 4mg/mL/min) every 3 weeks for 6 to 10 cycles, followed by maintenance therapy with bevacizumab until disease progression or unacceptable toxicity Comparator: CT i.e., gemcitabine (1,000mg/m2) + carboplatin (AUC 4mg/mL/min) + placebo every 3 weeks for 6 to 10 cycles, followed by maintenance therapy with placebo until disease progression or unacceptable toxicity | Outcomes: OS i.e., date of randomization to the date of death from any cause Safety i.e., observations of adverse events within 30 days of treatment using the CTCAE criteria (v. 3) Follow-up (OS outcome): Months, median (range) = 57.5 (0.3 to 73.9) |
Aghajanian et al. (2012)17 Country: US (locations of study/treatment centers NR) Funding source: Reported as ‘None’; however, Genentech (South San Francisco, CA) is described as the study sponsor and supporter of the study | Outcomes: PFS i.e., date of randomization to the date of disease progression (ascertained using RECIST v. 1.1 criteria), or death from any cause including multivariate analyses describing HR adjusted for PFI and SCS OS (interim analyses only) i.e., date of randomization to the date of death from any cause* Treatment response i.e., PR, ORR and DOR Safety i.e., observations of adverse events using the NCICT criteria (v. 3)** Follow-up: Months, median = 24 *Because data for OS in this paper were described by the authors as immature and generated from an interim analysis, they are not included from this paper; rather, OS data are included in this report from the 2015 paper from the OCEANS trial *Because safety data in this paper were collected earlier in time than those reported in the 2015 OCEANS trial paper, they are not included from this paper; rather, safety data are included in this report from the 2015 paper from the OCEANS trial | |||
Non-randomized Studies | ||||
Musacchio et al. (2023)18 Country: Italy Funding source: AIRC grant numbers IG 2016 – ID. 18921 and IG 2021 – ID. 25932 projects – P.I. SP and CO-2018 to 12367051 (Ministero della Salute) P.I SP Ricerca Corrente grant M2/7 from Ministero della Salute | Multicentre, retrospective cohort | Patients with low grade serous carcinoma of the ovary and peritoneum who were treated between 2014 and 2021
Eligible patients in the intervention group, N = 16:
Eligible patients in the comparator group, N = 33:
| Intervention: Bevacizumab (15 mg/kg) + platinum-based CT i.e., carboplatin or carboplatin + PLD* or carboplatin + gemcitabine or carboplatin + paclitaxel (dosages NR) every 3 weeks for 6 cycles (maintenance therapy NR) Comparator: Platinum-based CT only i.e., carboplatin or carboplatin + PLD* or carboplatin + gemcitabine or carboplatin + paclitaxel (dosages NR) every 3 weeks for 6 cycles (maintenance phase NR) *Authors do not define the acronym; in other papers included in this review, this acronym is elaborated as ‘pegylated liposomal doxorubicin’ | Outcomes: PFS (i.e., time between the date of platinum-therapy start and the date of disease progression or death or last contact with patients who did not experience an event being censored on Jan 31, 2021) including multivariate analyses adjusted for SCS Treatment response using RECIST categories i.e., CR, PR, SD, PD Follow-up: NR |
Akilli et al. (2022)19 Country: Turkey Funding source: Reported as none. | Retrospective, single-centre, historically-controlled cohort | Patients with recurrent epithelial ovarian carcinoma, fallopian tube cancer and primary peritoneal carcinoma treated between 2007 and 2017.
Patients in the intervention group*, N = 200:
Patients in the comparator group*, N = 196:
Eligible patients in the intervention group, N = 126:
Eligible patients in the comparator group, N = 135:
*Patient characteristics data includes both platinum-sensitive and platinum resistant patients i.e., no characteristics data were reported for the eligible subgroup of platinum-sensitive patients which are relevant to this report | Intervention: Bevacizumab (15 mg/kg) + CT i.e., paclitaxel + carboplatin (dosages NR) every 3 weeks (median cycles administered = 11; range 4 to 52), followed by bevacizumab maintenance therapy*; this regimen became available at the study hospital after 2013 and informed the active intervention arm of the cohort. Comparator: CT only i.e., CT drugs, dosages and schedules NR (maintenance therapy NR); this undescribed regimen was reported as the standard of care before 2013 and informed the control arm of the cohort *Authors report that 65% of the patients receiving bevacizumab also received maintenance therapy, suggesting that 35% may not have received maintenance therapy with bevacizumab | Outcomes: PFS (classified according to RECIST criteria) OS (i.e., time of first recurrence until death or the last clinic visit) Safety i.e., observations of major complications Follow-up: Months, median (range) = 48.5 (2.8 to 120) |
Kim et al. (2022)20 Country: Korea Funding source: NR | Multicentre, retrospective cohort | Patients with platinum-sensitive, relapsed ovarian clear cell carcinoma treated between 2007 and 2021 All patients observed in the study and eligible for this report, N = 138 Patients in the intervention group, N = 36:
Patients receiving bevacizumab in first-line therapy, n (%) = 0 (0) SCS, n(%) = 12 (33.3) CT cycles, median (range) = 6 (3 to 9) Patients in the comparator group, N = 102:
| Intervention: Bevacizumab (15 mg/kg) + CT i.e., paclitaxel (175 mg/m2) + carboplatin (AUC 5) or gemcitabine (1000 mg/m2) + carboplatin (AUC 4) every 3 weeks (median cycles administered = 6; range = 3 to 9), followed by bevacizumab maintenance therapy until disease progression, unacceptable toxicity or patient refusal Comparator: CT only i.e., paclitaxel + carboplatin or docetaxel + carboplatin or pegylated liposomal doxorubicin + carboplatin or gemcitabine + carboplatin or camptothecin (i.e., topotecan, belotecan, and irinotecan) + cisplatin or camptothecin (i.e., topotecan, belotecan, and irinotecan) (dosages NR) every 3 weeks (median cycles administered = 6; range = 2 to 9); maintenance therapy NR | Outcomes: PFS (i.e., start date of treatment until disease progression as defined by RECIST v. 1.1), including multivariate analyses describing HR adjusted for PFI, serum CA-125 levels at recurrence and SCS OS (i.e., start date of treatment until death from disease or last follow-up), including multivariate analyses describing hazard ratios adjusted for PFI, serum CA-125 levels at recurrence and SCS Treatment response using RECIST version 1.1 categories i.e., CR, PR, SD, PD and OR Follow-up: Months, median = 19.9 |
Ribeiro et al. (2021)21 Country: Brazil Funding sources: São Paulo Research Foundation, grant number 2018/02314 to 6; ecancer, UK Charity number 1176307 | Single-centre, retrospective cohort with 1:1 patient-matched analyses (using PFI, number of previous cycles of CT and histology) | Patients with platinum-sensitive, recurrent ovarian carcinoma treated between 2007 and 2017 All patients observed in the study and eligible for this report, N = 124 Patients in the intervention group, n = 62:
Patients in the control group (matched 1:1 to patients in the intervention group), n = 62:
| Intervention: Bevacizumab (15 mg/kg) + CT i.e., carboplatin (AUC 4mg/mL/minute) + gemcitabine (1,000 mg/m2) or carboplatin (AUC 4mg/mL/minute) + doxorubicin (30 mg/m2) or carboplatin (AUC 5 mg/mL/minute) + paclitaxel (175 mg/m2); carboplatin was replaced by cisplatin (60 to 75 mg/m2) in patients experiencing hypersensitivity, every 3 weeks for an average of 6 cycles; bevacizumab maintenance therapy was continued, provided benefit with no serious adverse events were observed Comparator: CT only i.e., carboplatin (AUC 4mg/mL/minute) + gemcitabine (1,000 mg/m2) or carboplatin (AUC 4mg/mL/minute) + doxorubicin (30 mg/m2) or carboplatin (AUC 5 mg/mL/minute) + paclitaxel (175 mg/m2), every 3 weeks for an average of 6 cycles (carboplatin was replaced by cisplatin (60 to 75 mg/m2) in patients experiencing hypersensitivity); maintenance therapy NR | Outcomes: PFS (i.e., start date of treatment until disease progression or death by any cause), including multivariate analyses describing hazard ratios adjusted for age, histology, PFI and CCNE1 overexpression OS (i.e., start date of treatment until disease progression or death by any cause), including multivariate analyses describing hazard ratios adjusted for age, histology, PFI and CCNE1 overexpression Treatment response using RECIST v. 1.1 categories i.e., CR, PR was recorded as a response; SD, PD was recorded as no response; OR Follow-up: Median 40 months (95% CI NR) for OS; median time for overall study/other outcomes NR |
Kim et al. (2020)22 Country: Korea Funding source: Seoul National University (No. 800 to 20170249; 800 to 20180201) and Seoul National University Hospital (No. 0620173250) | Single-centre, retrospective cohort with 1:2 patient-matched analyses (using PFI and secondary surgical intervention) | Patients with platinum-sensitive, relapsed epithelial ovarian cancer treated between 2008 and 2019 All eligible patients observed in the study, N = 192 Patients in the intervention group, n = 52*:
Patients in the control group (matched 2:1 to patients in the intervention group), n = 104**:
*38 of these patients were also enrolled in the GOG-0213 trial **4 of these patient were also enrolled I the GOG-0213 trial | Intervention: Bevacizumab (15 mg/kg) + CT i.e., paclitaxel (175 mg/m2) + carboplatin (AUC 5) or gemcitabine (1000 mg/m2) + carboplatin (AUC 5) every 3 weeks (median cycles administered = 6, range 4 to 9), followed by bevacizumab maintenance therapy until disease progression, unacceptable toxicity, patient request or physician recommendation Comparator: CT only i.e., paclitaxel or docetaxel + carboplatin; docetaxel + cisplatin; gemcitabine + carboplatin; PLD + carboplatin; topotecan; or belotecan + cisplatin every 3 weeks (median cycles administered = 6, range 3 to 15); dosages NR; maintenance therapy NR | Outcomes: PFS i.e., start date of treatment to the date of disease progression (ascertained using RECIST v. 1.1 criteria) or last follow-up, including multivariate analyses adjusted for stage, histologic type, grade, PFI, and secondary surgery OS i.e., start date of treatment to the date of cancer-related death or end of the study, including multivariate analyses adjusted for stage, histologic type, grade, PFI, and secondary surgery Follow-up: Median (range) in months = 35.6 (4.1 to 118.5) |
Hirasawa et al. (2018)23 Country: Japan Funding source: NR | Single-centre, historically-controlled retrospective cohort with 1:1 patient-matched analyses (using age at recurrence, PFI, histology) | Patients with platinum-sensitive recurrent epithelial ovarian cancer treated between 2008 to 2013 (control group) or 2014 to 2017 (intervention group) All patients observed in the study (and eligible for inclusion in this report), N = 32 Patients in the intervention group, n = 13:
Patients in the control group (all, including those matched and unmatched to patients in the intervention group), n = 19:
Patients in the control group (matched 1:1 to patients in the intervention group), n = 13:
| Intervention: Bevacizumab (15 mg/kg) every + CT i.e., paclitaxel (175 mg/m2) + carboplatin (AUC 5) every 3 weeks for 6 cycles, followed by bevacizumab maintenance therapy until disease progression or unacceptable toxicity Comparator: CT only i.e., paclitaxel (175 mg/m2) + carboplatin (AUC 5) or gemcitabine (1000 mg/m2) + carboplatin (AUC 4) every 3 weeks for 6 cycles (maintenance therapy NR) | Outcomes: PFS i.e., start date of treatment to the day of disease progression (ascertained using RECIST v. 1.1 criteria) or death Treatment response using RECIST v. 1.1 i.e., CR, PR, ORR Safety using CTCAE v. 4 Follow-up: Median months, intervention group = 14.5 Median months, control group = 4.4 |
Akers et al. (2013)24 Country: US Funding source: NR | Retrospective cohort with 1:1 patient-matched analyses (using age, platinum response, histology, surgical outcome, grade, and number of previous chemotherapy regimens) | Patients with recurrent ovarian cancer treated between 2006 and 2009 All patients observed in the study (including both platinum-sensitive and platinum-resistant cases), N = 64 Patients eligible for this report (including only those who were platinum-sensitive), n = 11 Patients in the intervention group*, n = 32:
Patients in the comparator group*, n = 32:
Eligible patients in the intervention group, n = 7:
Eligible patients in the comparator group, n = 4:
*Patient characteristics data includes both platinum-sensitive and platinum resistant patients i.e., no characteristics data were reported for the eligible subgroup of platinum-sensitive patients which are relevant to this report | Intervention: Bevacizumab (15 mg/kg) + CT i.e., paclitaxel or cyclophosphamide or doxorubicin or carboplatin + gemcitabine (dosages NR), every 3 weeks followed by bevacizumab maintenance therapy until disease progression or unacceptable toxicity (mean cycles of bevacizumab administered = 7, range = 1 to 18; cycles of CT = NR); maintenance therapy NR* Comparator: CT only i.e., paclitaxel or cyclophosphamide or doxorubicin or carboplatin + gemcitabine or topotecan or etoposide or carboplatin or navelbine or pemetrexed or carboplatin + paclitaxel (dosages and schedules NR); maintenance therapy NR * *Information on interventions administered include both platinum-sensitive and platinum resistant patients i.e., no data were reported for the eligible subgroup of platinum-sensitive patients which are relevant to this report | Outcomes: PFS i.e., start date of treatment with bevacizumab or last cytotoxic chemotherapy until disease progression or last date of follow up OS (definition NR) Treatment response rate using RECIST criteria (i.e., CR, PR, SD, PD) or modified Rustin criteria* Safety, reported as adverse events observed* Follow-up: NR *These outcome data include both platinum-sensitive and platinum resistant patients i.e., no data were reported for the eligible subgroup of platinum-sensitive patients which are relevant to this review and so, are not included in the summary of findings for this report |
AUC = area under the curve; CA-125 = cancer antigen 125; CCNE1 = cyclin E1; CI = confidence interval; CR = complete response; CT = chemotherapy; CTCAE = Common Terminology Criteria for Adverse Event; DOR = duration of response; ECOG = Eastern Cooperative Oncology Group; FACT-O TOI = Function Assessment of Cancer Therapy (Ovary) trial outcome index; GOG = Gynecologic Oncology Group; HR = hazard ratio(s); IQR = inter-quartile range; kg = kilogram(s); m = metre(s); mg = milligram(s); mL = millitre(s); N/n = number(s); NCI = National Cancer Institute; NCICT = National Cancer Institute dosimetry system for CT; NR = not reported; OR = overall/objective response; ORR = overall/objective response rate; OS = overall survival; PD = progressive disease; PFI = platinum-free interval; PFS = progression free survival; PLD = pegylated liposomal doxorubicin; PR = partial response; QoL = quality of life; RECIST = Response Evaluation Criteria in Solid Tumours; SF-36 = short-form survey 36; SCS = secondary cytotoxic surgery; SD = stable disease; SD = standard deviations; TSE = treatment side effects; v = version
Note: This table has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Table 3: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist14
Strengths | Limitations |
|---|---|
Randomized Controlled Trials | |
Coleman (2017)15 — GOG-0213 Trial | |
Reporting
External validity
Internal validity
| External validity
Internal validity
Study power
|
Reporting
Internal validity
| External validity
Internal validity
Study power
|
Non-randomized studies | |
Musacchio (2023)18 | |
Reporting
External validity
Internal validity
| Reporting
External validity
Internal validity
|
Akilli (2022)19 | |
Reporting
Internal validity
| Reporting
External validity
Internal validity
|
Kim (2022)20 | |
Reporting
Internal validity
| Reporting
External validity
Internal validity
Other
|
Ribeiro (2021)21 | |
Reporting
Internal validity
| Reporting
External validity
Internal validity
|
Kim et al. (2020)22 | |
Reporting
Internal validity
| Reporting
External validity
Internal validity
Other
|
Hirasawa (2018)23 | |
Reporting
Internal validity
| Reporting
External validity
Internal validity
Other
|
Akers (2013)24 | |
Reporting
Internal validity
| Reporting
External validity
Internal validity
Other
|
CT = chemotherapy; GOG = Gynecological Oncology Group; HR = hazard ratio; NR = not reported; OS = overall survival; PFI = platinum-free interval; PFS = progression free survival; QoL = quality of life; VEGF = vascular endothelial growth factor
Note: This appendix has not been copy-edited.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 4: Summary of Findings by Outcome — Overall Survival
Study, Treatment Groups | Deaths, n (%) patients | 5 year OS, n (%) patients | Months of OS, median (95%CI) | (a)HR (95% CI) | ||
|---|---|---|---|---|---|---|
Randomized Controlled Trials | ||||||
Coleman (2017)15 GOG-0213 | ||||||
Bevacizumab + CT (303/323 evaluable) | 189 (62.4) | NR | NR | 0.868 (0.707 to 1.066) | ||
CT only (303/315 evaluable) | 179 (59.1) | NR | NR | |||
Group difference, P (significance at < 0.05) | NR | — | — | NR (NS) | ||
Aghajanian (2015)16 OCEANS Trial | ||||||
Bevacizumab + CT | 353 (72.9) | NR | 33.6 (NR) | 0.952 (0.771 to 1.176) | ||
CT only | NR | 32.9 (NR) | ||||
Group difference, P (significance at < 0.05) | NR (NS) | — | NR | 0.6479 (NS) | ||
Non-Randomized Studies | ||||||
Akilli (2022)19 | ||||||
Bevacizumab + CT | NR | NR (68) | NR | NR | ||
CT only | NR | NR (64) | NR | |||
Group difference, P (significance at < 0.05) | — | 0.28 (NS) | — | — | ||
Kim (2022)20 | ||||||
Bevacizumab + CT | 7 (NR) | NR | 43.5 (31.9 to 55.1) | 0.435 (0.195 to 0.970) | ||
CT only | 46 (NR) | NR | 32.1 (22.1 to 42.1) | |||
Group difference, P (significance at < 0.05) | NR | — | 0.043 (favours bevacizumab + CT) | 0.042 (favours bevacizumab + CT) | ||
Ribeiro (2021)21 | ||||||
Bevacizumab + CT | 61 (49.1) | NR | 48.9 (NR) | 0.70 (0.30 to 1.61) | ||
CT only | NR | 51.9 (NR) | ||||
Group difference, P (significance at < 0.05) | NR | — | 0.410 (NS) | 0.401 (NS) | ||
Kim (2020)22 | ||||||
Bevacizumab + CT | 9 (NR) | NR (51.5) | NR | 0.39 (0.19 to 0.80) | ||
CT only | 57 (NR) | NR (42.8) | NR | |||
Group difference, P (significance at < 0.05) | 0.016 (favours bevacizumab + CT) | NR | — | 0.010 (favours bevacizumab + CT) | ||
Akers (2013)24 | ||||||
Bevacizumab + CT | NR | NR | NR | NR | ||
CT only | NR | NR | NR | |||
Group difference, P (significance at < 0.05) | — | — | 0.8631 (NS) | — | ||
aHR = adjusted hazard ratio; CI = confidence interval; CT = chemotherapy; GOG = Gynecologic Oncology Group; HR = hazard ratio; N/n = number(s); NR = not reported; NS = not statistically significant; OS = overall survival; P = P value; PFS = progression free survival
Table 5: Summary of Findings by Outcome — Progression-Free Survival
Study, Treatment Groups | Disease progression, n (%) patients | Months of PFS, median (95%CI) | (a)HR (95% CI) |
|---|---|---|---|
Randomized Controlled Trials | |||
Coleman (2017)15 GOG-0213 | |||
Bevacizumab + CT (299/323 evaluable) | 263 (88.0) | 13.8 (NR) | 0.63 (0.53 to 0.75) |
CT only (285/315 evaluable) | 259 (90.1) | 10.2 (NR) | |
Group difference, P (significance at < 0.05) | NR | NR | NR (favours bevacizumab) |
Aghajanian (2012)17 OCEANS Trial (IRC results) | |||
Bevacizumab + CT | 338 (NR) | 12.3 (10.7 to 14.6) | 0.451 (0.351 to 0.580) |
CT only | 8.6 (8.3 to 10.2) | ||
Group difference, P (significance at < 0.05) | NR | NR | < 0.001 (favours bevacizumab) |
Non-Randomized Studies | |||
Musacchio (2023)18 | |||
Bevacizumab + CT | NR | 37.1 (13.42 to 40.56) | 0.30 (0.15 to 0.80) |
CT only | NR | 11.22 (8.26 to 15.63) | |
Group difference, P (significance at < 0.05) | — | 0.013 (favours bevacizumab + CT) | NR (favours bevacizumab + CT) |
Akilli (2022)19 | |||
Bevacizumab + CT | NR | 8.2 (NR) | NR |
CT only | NR | NR (NR) | |
Group difference, P (significance at < 0.05) | — | NR | — |
Kim (2022)20 | |||
Bevacizumab + CT | 23 (NR) | 15.4 (6.0 to 24.8) | 0.571 (0.354 to 0.921) |
CT only | 81 (NR) | 7.5 (6.1 to 8.9) | |
Group difference, P (significance at < 0.05) | NR | 0.042 (favours bevacizumab + CT) | 0.022 (favours bevacizumab + CT) |
Ribeiro (2021)21 | |||
Bevacizumab + CT | 84 (67) | 19.5 (NR) | 0.54 (0.26 to 1.09) |
CT only | 16.0 (NR) | ||
Group difference, P (significance at < 0.05) | NR | 0.22 (NS) | 0.084 (NS) |
Kim (2020)22 | |||
Bevacizumab + CT | 34 (NR) | 17.0 (14.4 to 19.5) | 0.47 (0.31 to 0.70) |
CT only | 94 (NR) | 12.4 (9.8 to 15.0) | |
Group difference, P (significance at < 0.05) | NR | 0.002 (favours bevacizumab + CT) | < 0.001 (favours bevacizumab + CT) |
Hirasawa (2018)23 | |||
Analyses including all controls | |||
Bevacizumab + CT | NR | 14.71 (NR) | NR |
CT only (all, n = 19) | NR | 6.73 (NR) | |
Group difference, P (significance at < 0.05) | — | 0.00721 (favours bevacizumab + CT) | — |
Analyses including only matched controls | |||
Bevacizumab + CT | NR | 14.71 (NR) | 0.304 (0.114 to 0.8121) |
CT only (matched subgroup, n = 13) | NR | 6.31 (NR) | |
Group difference, P (significance at < 0.05) | — | 0.00561 (favours bevacizumab + CT) | 0.01752 (favours bevacizumab + CT) |
Akers (2013)24 | |||
Bevacizumab + CT | NR | NR | NR |
CT only | NR | NR | |
Group difference, P (significance at < 0.05) | — | 0.4269 (NS) | — |
aHR = adjusted hazard ratio; CI = confidence interval; CT = chemotherapy; GOG = Gynecologic Oncology Group; HR = hazard ratio; IRC = independent review committee; N/n = number(s); NR = not reported; NS = not statistically significant; P = P value; PFS = progression free survival
Table 6: Summary of Findings by Outcome — Treatment Response
Study, Treatment Group | Complete Response, n (%) | Partial Response, n (%) | Stable Disease, n (%) | Progressive Disease, | Overall or Objective Response, n % | Duration of Response, months |
|---|---|---|---|---|---|---|
Randomized Controlled Trials | ||||||
Aghajanian (2012)17 OCEANS Trial | ||||||
Bevacizumab + CT | NR | 148 (61.2) | NR | NR | 190 (78.5) | 10.4 |
CT only | NR | 117 (48.3) | NR | NR | 139 (57.4) | 7.4 |
HR (95% CI) | NR | 0.534 (0.408 to 0.698) | ||||
Group difference, P (significance) | NR | < 0.001 (favours bevacizumab) | NR | |||
Non-Randomized Studies | ||||||
Musacchio (2023)18 | ||||||
Bevacizumab + CT (13/16 pt evaluable) | 5 (38) | 7 (53.8) | 1 (7.7) | NR | NR | NR |
CT only (29/33 pt evaluable) | 3 (10.3) | 9 (31) | 10 (34.5) | 7 (24.1) | NR | NR |
Group difference, P (significance) | NR | — | — | |||
Kim (2022)20 | ||||||
Bevacizumab + CT | 8 (22.2) | 11 (30.6) | 11 (30.6) | 6 (16.7) | NR (52.85) | NR |
CT only | 27 (26.5) | 6 (5.9) | 12 (11.8) | 57 (55.9) | NR (32.4) | NR |
Group difference, P (significance) | NR | 0.03 (favours bevacizumab) | — | |||
Ribeiro (2021)21 | ||||||
Bevacizumab + CT | NR | NR | NR | NR | NR (79.0 to 93.3) | NR |
CT only | NR | NR | NR | NR | NR (67.9) | NR |
Group difference, P (significance) | — | 0.002 (favours bevacizumab) | — | |||
Hirasawa (2018)23 | ||||||
Bevacizumab + CT | 9 (NR) | 3 (NR) | NR | NR | NR (92.3) | NR |
CT only (all, n = 19) | 3 (NR) | 8 (NR) | NR | NR | NR (57.9) | NR |
Group difference, P (significance) | NR | NR | — | — | NR | — |
CI = confidence interval; CT = chemotherapy; N/n = number(s); NR = not reported; NS = not statistically sigificant; P = P value
Table 7: Summary of Findings by Outcome — Quality of Life (FACT-O TOI)
Study, Treatment Groups | Mean scores (SE) | Overall treatment group difference in mean scores (95% CI) | ||||
|---|---|---|---|---|---|---|
Before cycle 1 | Before cycle 3 | Before cycle 6 | 6 months after cycle 1 | 12 months after cycle 1 | ||
Coleman (2017)15 GOG-0213 | ||||||
Bevacizumab + CT | 75.3 (0.9) | 73.4 (0.9) | 72.3 (1.0) | 77.2 (1.0) | 77.8 (1.0) | –0·37 (–1·80 to 1·06) |
CT only | 75.8 (0.8) | 74.2 (1.0) | 73.3 (1.0) | 77.1 (1.0) | 77.0 (1.1) | |
Group difference, P (significance at < 0.05) | NR (NS) | 0.351 (NS) | 0.276 (NS) | 0.897 (NS) | 0.479 (NS) | 0·62 (NS) |
CI = confidence interval; CT = chemotherapy; FACT-O TOI = Function Assessment of Cancer Therapy (Ovary) trial outcome index; GOG = Gynecologic Oncology Group; SE = standard error; NS = not statistically significant; P = P value
Table 8: Summary of Findings by Outcome — Adverse Events
Study citation | Adverse Event | Patient Affected, n (%) | Group difference, P (significance) | |
|---|---|---|---|---|
Intervention Group | Comparator Group | |||
Randomized Controlled Trials | ||||
Coleman (2017)15 GOG-0213 RCT | Any adverse event | NR | ||
Grade III or worse | 317 (96) | 282 (86) | ||
Serious adverse events | 92 (28) | 37 (11) | ||
Adverse events leading to treatment discontinuation | 82 (25) | 37 (11) | ||
Death (from PD or unknown cause) | 5 (2) | 0(0) | ||
Auditory | ||||
Grade I to II | 29 (3) | 23 (7) | ||
Grade III to V | 3 (1) | 0 (0) | ||
Allergy/immunology | ||||
Grade I to II | 100 (30) | 68 (21) | ||
Grade III to V | 32 (10) | 26 (8) | ||
Coagulation | ||||
Grade I to II | 6 (2) | 3 (1) | ||
Grade III to V | 6 (2) | 0 (0) | ||
Constitutional symptoms | ||||
Grade I to II | 258 (78) | 266 (81) | ||
Grade III to V | 29 (9) | 9 (3) | ||
Cardiac | ||||
Grade I to II | 126 (38) | 28 (9) | ||
Grade III to V | 46 (14) | 5 (2) | ||
Dermatology/skin | ||||
Grade I to II | 286 (87) | 277 (85) | ||
Grade III to V | 9 (3) | 1 (< 1) | ||
Endocrine | ||||
Grade I to II | 47 (14) | 33 (10) | ||
Grade III to V | 1 (< 1) | 0 (0) | ||
Gastrointestinal | ||||
Grade I to II | 259 (78) | 207 (91) | ||
Grade III to V | 38 (12) | 19 (6) | ||
Renal/genitourinary | ||||
Grade I to II | 58 (18) | 39 (12) | ||
Grade III to V | 5 (2) | 3 (1) | ||
Hemorrhage/bleeding | ||||
Grade I to II | 134 (41) | 24 (7) | ||
Grade III to V | 6 (2) | 3 (1) | ||
Blood/bone marrow | ||||
Grade I to II | 4 (12) | 63 (19) | ||
Grade III to V | 285 (86) | 259 (79) | ||
Infection | ||||
Grade I to II | 83 (25) | 70 (21) | ||
Grade III to V | 43 (13) | 19 (6) | ||
Lymphatics | ||||
Grade I to II | 44 (13) | 42 (13) | ||
Grade III to V | 0 (0) | 0 (0) | ||
Secondary malignancy | ||||
Grade I to II | 0 (0) | 0 (0) | ||
Grade III to V | 1 (< 1) | 1 (< 1) | ||
Musculoskeletal/soft tissue | ||||
Grade I to II | 70 (21) | 34 (10) | ||
Grade III to V | 6 (2) | 1 (< 1) | ||
Metabolic/laboratory | ||||
Grade I to II | 143 (43) | 102 (31) | ||
Grade III to V | 67 (20) | 32 (10) | ||
Neurology | ||||
Grade I to II | 235 (71) | 255 (78) | ||
Grade III to V | 29 (9) | 17 (5) | ||
Ocular/visual | ||||
Grade I to II | 72 (22) | 48 (15) | ||
Grade III to V | 3 (1) | 1 (< 1) | ||
Pulmonary/upper respiratory | ||||
Grade I to II | 173 (52) | 124 (38) | ||
Grade III to V | 14 (4) | 6 (2) | ||
Pain | ||||
Grade I to II | 222 (67) | 225 (69) | ||
Grade III to V | 50 (15) | 6 (2) | ||
Vascular | ||||
Grade I to II | 10 (3) | 2 (1) | ||
Grade III to V | 14 (4) | 4 (1) | ||
Aghajanian (2015)16 OCEANS RCT | Any adverse event | 247 (100) | 233 (100) | NR |
Grades III to V | 223 (90.3) | 192 (82.4) | ||
Grade V | 1 (0.4) | 1 (0.4) | ||
Serious | 90 (36.4) | 59 (25.3) | ||
Grades III to V | 76 (30.8) | 47 (20.2) | ||
Adverse events leading to study treatment discontinuation | 55 (22.3) | 11 (4.7 | ||
Special interest (any grade) | 233 (94.3) | 198 (85.0) | ||
Arterial thromboembolic event (any grade) | 6 (2.4) | 1 (0.4) | ||
CNS bleeding, any grade | 2 (0.8) | 2 (0.9) | ||
Non-CNS bleeding, grade ≥ III | 14 (5.7) | 2 (0.9) | ||
LV systolic dysfunction/CHF, grade ≥ III | 2 (0.8) | 2 (0.9) | ||
Fistula or abscess, any grade | 2 (0.8) | 0 (0) | ||
GI perforations | 2 (0.8) | 1 (0.4) | ||
Hypertension, grade ≥ III | 45 (18.2) | 2 (0.9) | ||
Febrile neutropenia | 4 (1.6) | 4 (1.7) | ||
Neutropenia, grade ≥ IV | 52 (21.1) | 51 (21.9) | ||
Proteinuria, grade ≥ III | 27 (10.9) | 2 (0.9) | ||
Posterior reversible encephalopathy syndrome (any grade) | 2 (0.8) | 0 (0) | ||
Venous thromboembolic event | 11 (4.5) | 6 (2.6) | ||
Wound healing complication | 2 (0.8) | 0 (0) | ||
Non-Randomized Studies | ||||
Akilli (2022)19 | Intestinal perforation | 2 (1) | 2 (1) | 0.4 (NS) |
Enterocutaneous fistula | 2 (1) | 0 (0) | 0.1 (NS) | |
Enterovaginal fistula | 3 (1.5) | 1 (0.5) | 0.5 (NS) | |
Gastrointestinal hemorrhage | 1 (0.5) | 0 (0) | 0.1 (NS) | |
Grade III to IV hematologic toxicity | 27 (13.7) | 22 (11) | 0.6 (NS) | |
Hirasawa (2018)23 (all controls included, n = 19) NRS | Hematologic toxicities | |||
Anemia | 9 (69.2) | 16 (84.2) | 0.401 (NS) | |
Thrombocytopenia | 5 (38.5) | 3 (15.8) | 0.219 (NS) | |
Neutropenia | 7 (53.8) | 18 (94.7) | 0.0102 (favours CT only) | |
Febrile neutropenia | 1 (7.7) | 0 (0) | 0.406 (NS) | |
Non-hematologic toxicities | ||||
Alopecia | 8 (61.5) | 18 (94.7) | 0.0289 (favours bevacizumab + CT) | |
Epistaxis | 7 (53.8) | 0 (0) | 0.00051 (favours CT only) | |
Fatigue | 3 (23.1) | 15 (78.9) | 0.00329 (favours CT only) | |
Hoarseness | 1 (7.7) | 0 (0) | 0.406 (NS) | |
Hypertension | 5 (38.5) | 0 (0) | 0.00639 (favours CT only) | |
Intestinal obstruction | 2 (15.4) | 0 (0) | 0.157 (NS) | |
Malaise | 1 (7.7) | 0 (0) | 0.406 (NS) | |
Mucositis oral | 1 (7.7) | 0 (0) | 0.406 (NS) | |
Proteinuria | 3 (23.1) | 0 (0) | 0.0577 (NS) | |
Sensory | 7 (53.8) | 9 (47.4) | 1 (NS) | |
Thromboembolic event | 1 (7.7) | 0 (0) | 0.406 (NS) | |
Intestinal perforation | 2 (1) | 2 (1) | 0.4 (NS) | |
Enterocutaneous fistula | 2 (1) | 0 (0) | 0.1 (NS) | |
Enterovaginal fistula | 3 (1.5) | 1 (0.5) | 0.5 (NS) | |
Gastrointestinal hemorrhage | 1 (0.5) | 0 (0) | 0.1 (NS) | |
Grade III to IV hematologic toxicity | 27 (13.7) | 22 (11) | 0.6 (NS) | |
Hematologic toxicities | ||||
Anemia | 9 (69.2) | 16 (84.2) | 0.401 (NS) | |
Thrombocytopenia | 5 (38.5) | 3 (15.8) | 0.219 (NS) | |
Neutropenia | 7 (53.8) | 18 (94.7) | 0.0102 (favours CT only) | |
Febrile neutropenia | 1 (7.7) | 0 (0) | 0.406 (NS) | |
Non-hematologic toxicities | ||||
Alopecia | 8 (61.5) | 18 (94.7) | 0.0289 (favours bevacizumab + CT) | |
Epistaxis | 7 (53.8) | 0 (0) | 0.00051 (favours CT only) | |
Fatigue | 3 (23.1) | 15 (78.9) | 0.00329 (favours CT only) | |
Hoarseness | 1 (7.7) | 0 (0) | 0.406 (NS) | |
Hypertension | 5 (38.5) | 0 (0) | 0.00639 (favours CT only) | |
Intestinal obstruction | 2 (15.4) | 0 (0) | 0.157 (NS) | |
Malaise | 1 (7.7) | 0 (0) | 0.406 (NS) | |
Mucositis oral | 1 (7.7) | 0 (0) | 0.406 (NS) | |
Proteinuria | 3 (23.1) | 0 (0) | 0.0577 (NS) | |
Sensory | 7 (53.8) | 9 (47.4) | 1 (NS) | |
Thromboembolic event | 1 (7.7) | 0 (0) | 0.406 (NS) | |
Intestinal perforation | 2 (1) | 2 (1) | 0.4 (NS) | |
Enterocutaneous fistula | 2 (1) | 0 (0) | 0.1 (NS) | |
Enterovaginal fistula | 3 (1.5) | 1 (0.5) | 0.5 (NS) | |
CHF = congestive heart failure; CT = chemotherapy; CNS = central nervous system; GI = gastrointestinal; GOG = Gynecologic Oncology Group; LVS = left ventricular; N/n = number(s); NR = not reported; NRS = non-randomized study; NR = not reported; NS = not statistically significant; P = P value; PD = progressive disease; RCT = randomized controlled trial
Appendix 5: Overlap Between Eligible Systematic Reviews
Table 9: Overlap in Relevant Primary Studies Between Eligible Systematic Reviews
Primary study citation | Helali (2022)13 | Liu (2022)26 | Liu (2021)27 | Wang (2018)29 | KCE 201745 | Wu (2017)30 | Yi (2017)31 | Li (2016) 32 | Li (2015)33 | Ding (2014)34 | Aravantinos (2014)35 | NICE (2013)36 | Zhou (2013)37 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
Gynecologic Oncology Group Study (GOG-0213) | |||||||||||||
Coleman, R. L. et al. Lancet Oncol. (2017) | Yes | Yes | Yes | — | — | — | — | — | — | — | — | — | — |
Coleman RL. et al. [abstract] Gynecol Oncol. 2015;137:3Y4 | — | — | — | Yes | — | — | — | — | — | — | — | — | — |
Coleman RL et al. [abstract] Presented at: Society of Gynecologic Oncology 2015 Annual Meeting on Women’s Cancer; March 28 to 31, 2015; Chicago, Illinois. Abstract 3. | — | — | — | — | Yes | Yes | Yes | — | — | — | — | — | — |
OCEANS Trial | |||||||||||||
Aghajanian, C. et al. Gynecol. Oncol. 139 (1) (2015) 10 to 16 | — | — | Yes | — | — | — | Yes | — | — | — | — | — | — |
Aghajanian, C. et al. J. Clin. Oncol. 30, 2039 to 2045 (2012) | Yes | Yes | Yes | Yes | Yes | Yes | — | Yes | Yes | Yes | Yes | Yes | Yes |
Aghajanian C et al. [abstract] Presented at the ESMO Congress, Vienna, Austria, 28 September – 2 October 2012. Abstract 9670. | — | — | — | — | — | — | — | — | — | — | Yes | — | — |
Note: This table has not been copy-edited.
Appendix 6: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
Avastin for Platinum-Resistant Ovarian Cancer. Ottawa (ON): CADTH. 2016. https://www.cadth.ca/avastin-platinum-resistant-ovarian-cancer-details Accessed 2023 Apr 24.
Avastin for Ovarian Cancer. Ottawa (ON): CADTH. 2015. https://www.cadth.ca/avastin-ovarian-cancer-details Accessed 2023 Apr 24.
Additional References
Comparisons between bevacizumab and poly ADP ribose polymerase inhibitors (PARP-I)
Olaparib plus bevacizumab for maintenance treatment of advanced ovarian, fallopian tube or primary peritoneal cancer. [TA693]. London (UK): National Institute of Health and Care Excellence. 2021. https://www.nice.org.uk/guidance/ta693/resources/olaparib-plus-bevacizumab-for-maintenance-treatment-of-advanced-ovarian-fallopian-tube-or-primary-peritoneal-cancer-pdf-82609438840261 Accessed 2023 Apr 24.
Bartoletti M, Pelizzari G, Gerratana L, et al. Bevacizumab or PARP-Inhibitors Maintenance Therapy for Platinum-Sensitive Recurrent Ovarian Cancer: A Network Meta-Analysis. Int J Mol Sci. 2020;21(11):3805. PubMed
Olaparib in combination with bevacizumab for ovarian, fallopian tube or primary peritoneal cancer – maintenance therapy. Newcastle upon Tyne (UK): National Institute for Health and Care Research Innovation Observatory. 2019. https://www.io.nihr.ac.uk/techbriefings/olaparib-in-combination-with-bevacizumab-for-ovarian-fallopian-tube-or-primary-peritoneal-cancer-maintenance-therapy/ Accessed 2023 Apr 23.
Pfisterer J, Shannon CM, Baumann K, et al. Bevacizumab and platinum-based combinations for recurrent ovarian cancer: a randomised, open-label, phase 3 trial. Lancet. 2020;21(5):699-709. PubMed
Contributor: Chris Kamel
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca