CADTH Health Technology Review
Alternative Therapies to Immunoglobulin for Multifocal Motor Neuropathy
Rapid Review
Authors: Khai Tran, Jennifer Horton
Abbreviations
Ig
immunoglobulin
IVIg
intravenous immunoglobulin
MMN
multifocal motor neuropathy
Key Messages
We did not find any evidence regarding the clinical effectiveness and safety of alternative treatments to IV Immunoglobulin (IVIg) compared to IVIg or placebo for multifocal motor neuropathy that met our inclusion criteria for this review.
We did not find any evidence-based guidelines regarding the use of alternative treatments to IVIg for multifocal motor neuropathy that met the criteria for this review.
Context and Policy Issues
Multifocal motor neuropathy (MMN) is a rare disorder in which focal areas of multiple motor nerves are attacked by the immune system.1 It is slowly progressive and characterized by asymmetric weakness of the limbs without affecting sensory nerves.1 The prevalence of the disease is estimated to be 0.6 to 2 per 100,000 population in North America and Europe.1 It involves upper limbs more than lower limbs, and occurs more frequently in males than females, with a ratio of 2.7 to 1.1 Disease onset can occur between the ages of 20 to 70 years, with a mean age onset 40 years.1,2 MMN is diagnosed by nerve conduction studies showing multifocal conduction block on electrophysiological testing.1 However, some patients with MMN have no detectable conduction block.1 Other findings that support the diagnosis of MMN are the abnormal A waves on electrodiagnostic studies, axonal sprouting on motor nerve biopsies, and increased signal intensities on T2-weighted magnetic resonance images of the brachial plexus, a network of nerves that sends signals from the from the spinal cord to the shoulder, arm, and hand.1 Thirty percent to 80% of patients with MMN have elevated serum anti-GM1 (ganglioside-monosialic acid) antibodies.1 These antibodies are, however, not specific to MMN and can be found in other immune-mediated neuropathies.2
Immunoglobulins (Ig) are therapeutic products purified from pooled blood plasma from healthy donors.3 Ig can be administered through intramuscular, IV or subcutaneous injection.3 IV Ig (IVIg) is a treatment option for MMN.4 A recent systematic review has found that initial therapy with IVIg may improve muscle strength and functional disability compared with placebo in many patients with MMN.5 Dosing of IVIg is usually initiated at a total of 2 g/kg given over 2 to 5 days (e.g., 0.4 g/kg daily for 5 consecutive days).4 Maintenance IVIg dose ranges from 0.4 g/kg once weekly to 2 g/kg every 8 weeks depending on response and tolerance.4
The demand for Ig has been steadily increasing every year for the treatment of various autoimmune and inflammatory diseases including MMN.6,7 Due to the COVID-19 pandemic that has had a strong impact on global blood and plasma collection, countries around the world are experiencing a decline in Ig products.6 The shortage of the Ig products together with their increasing demand has made it necessary to re-evaluate alternative treatment options. Alternative treatments to IVIg for MMN include immunomodulating drugs such as cyclophosphamide, rituximab, mycophenolate mofetil, beta-interferon, cyclosporin, azathioprine, infliximab, corticosteroids, and plasma exchange.2,8 The clinical effectiveness of some of these alternative treatments remains unclear or controversial.2,8,9
The objective of this report is to summarize the evidence regarding the clinical effectiveness and safety of alternative treatments to IVIg, specifically corticosteroids and plasma exchange, compared to IVIg or placebo for MMN. This report also aims to summarize the recommendations from evidence-based guidelines regarding alternative treatments to IVIg given to this population.
Research Questions
What is the clinical effectiveness of alternative treatments to IVIg compared to IVIg or placebo for MMN?
What is the safety of alternative treatments to IVIg compared to IVIg or placebo for MMN?
What are the evidence-based guidelines regarding the use of alternative treatments to IVIg for MMN?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concept was multifocal motor neuropathy, with relevant MeSH focused to the “drug therapy” subheading. A supplemental search was conducted for multifocal motor neuropathy with CADTH-developed search filters applied to limit retrieval to guidelines. The search was completed on March 24, 2023 and limited to English-language documents published since January 1, 2018.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Patients with multifocal motor neuropathy |
Intervention | Corticosteroids (e.g., prednisolone), plasma exchange |
Comparator | Q1 to Q2: IV immunoglobulin, placebo Q3: Not applicable |
Outcomes | Q1: Clinical benefits (e.g., improvement in disability, change in muscle strength, resolution of conduction block, health-related quality of life) Q2: Harms (e.g., adverse events, severe adverse events) Q3: Recommendations regarding best practices (e.g., which alternative to use, dose and timing of treatment, indications) |
Study designs | Health technology assessments, systematic reviews, evidence-based guidelines |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, or were published before 2018.
Summary of Evidence
Quantity of Research Available
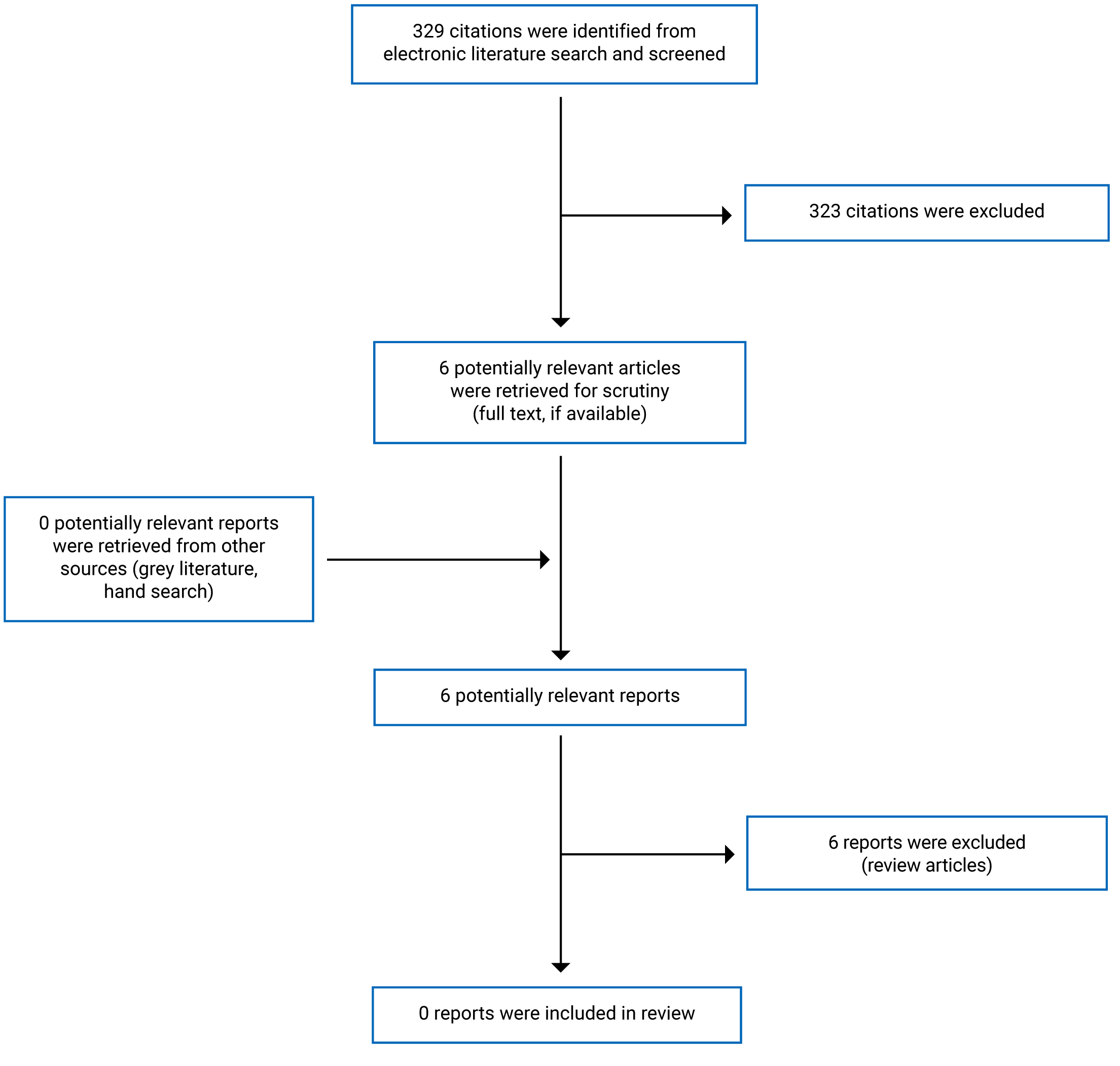
A total of 329 citations were identified in the literature search. Following screening of titles and abstracts, 323 citations were excluded and 6 potentially relevant reports from the electronic search were retrieved for full-text review. No potentially relevant publications were retrieved from the grey literature search for a full-text review. None of these 6 potentially relevant articles met the inclusion criteria and they were excluded from this report for various reasons. Appendix 1 presents the PRISMA10 flow chart of the study selection.
Summary of Findings
No relevant health technology assessments, systematic reviews, or evidence-based guidelines were identified regarding the clinical effectiveness, or recommendations for alternative treatments to IVIg (i.e., corticosteroids, plasma exchange) compared to IVIg or placebo for MMN; therefore, no summary can be provided.
Limitations
No relevant health technology assessments, systematic reviews, or evidence-based guidelines were identified that met the criteria for this review. This report may be limited by the literature search time frame (i.e., 2018 onward). It is unknown whether there is relevant literature published more than 5 years ago.
Conclusions and Implications for Decision- or Policy-Making
No relevant literature was identified to answer the research questions; therefore, conclusions could not be provided regarding the clinical effectiveness and safety, or recommendations on the use of alternative treatments to IVIg for MMN.
Recent nonsystematic reviews2,8,9 have reported that older studies conducted in the 1990s have shown that steroids and plasma exchange were ineffective in MMN, and might result in clinical worsening in some cases. Thus, it is unlikely that these therapies can be considered as alternative treatments to IVIg for MMN during drug shortages. The lack of published evidence may have precluded the formation of appropriate guidelines on the treatment options in MMN. Until new available clinical evidence and guidelines for alternative treatments to IVIg for MMN are available, especially steroids and plasma exchange, their place in clinical practice remains unclear.
References
1.Lange DJ, Robinson-Papp J. Multifocal motor neuropathy. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2023: http://www.uptodate.com/. Accessed 2023 Mar 28.
2.Yeh WZ, Dyck PJ, van den Berg LH, Kiernan MC, Taylor BV. Multifocal motor neuropathy: controversies and priorities. J Neurol Neurosurg Psychiatry. 2020;91(2):140-148. PubMed
3.Novaretti MC, Dinardo CL. Immunoglobulin: production, mechanisms of action and formulations. Rev Bras Hematol Hemoter. 2011;33(5):377-382. PubMed
4.Hameed S, Cascella M. Multifocal Motor Neuropathy. Treasure Island (FL): StatPearls Publishing; 2022: https://www.ncbi.nlm.nih.gov/books/NBK554524/. Accessed 2023 Mar 28.
5.Keddie S, Eftimov F, van den Berg LH, Brassington R, de Haan RJ, van Schaik IN. Immunoglobulin for multifocal motor neuropathy. Cochrane Database Syst Rev. 2022;1:CD004429. PubMed
6.N'Kaoua E, Attarian S, Delmont E, et al. Immunoglobulin shortage: Practice modifications and clinical outcomes in a reference centre. Rev Neurol (Paris). 2022;178(6):616-623. PubMed
7.Novaretti MC, Dinardo CL. Clinical applications of immunoglobulin: update. Rev Bras Hematol Hemoter. 2011;33(3):221-230. PubMed
8.Lawson VH, Arnold WD. Multifocal motor neuropathy: a review of pathogenesis, diagnosis, and treatment. Neuropsychiatr Dis Treat. 2014;10:567-576. PubMed
9.Briani C, Cocito D, Campagnolo M, Doneddu PE, Nobile-Orazio E. Update on therapy of chronic immune-mediated neuropathies. Neurol Sci. 2022;43(Suppl 2):605-614. PubMed
10.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
Appendix 1: Selection of Included Studies
Contributor: Elizabeth Carson
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca