CADTH Health Technology Review
Occupational Therapy for Mental Health Conditions and Substance Use Disorders
Rapid Review
Authors: Zahra Jafari, Aleksandra Grobelna
Abbreviations
ADL
activities of daily living
COT
conventional occupational therapy
GOT
group occupational therapy
GSSP
grocery shopping skill program
IOT
individualized occupational therapy
MA
meta-analysis
MHC
mental health conditions
NMA
network meta-analysis
OT
occupational therapy
POT
psychosocial occupational therapy
PSST
psychosocial skills training
RCT
randomized controlled trial
RoB
risk of bias
SR
systematic review
SUD
substance use disorders
SZ
schizophrenia
TTM
Tree Theme Method
Key Messages
Occupational therapy interventions may be effective for reducing symptoms of depression and anxiety and improving function and participation with the interventions in adult patients diagnosed with depression and/or anxiety.
In patients with schizophrenia, occupational therapy interventions may improve social functioning, cognitive performance, executive function, and motivation; and reduce the duration and rate of rehospitalization.
We did not find any evidence regarding the clinical effectiveness of occupational therapy for the treatment of bipolar disorders, obsessive-compulsive disorder, and post-traumatic stress disorder that met the inclusion criteria for our review.
We did not find any evidence meeting our inclusion criteria about the cost-effectiveness of occupational therapy for the treatment of mental health conditions, as well as the clinical effectiveness and cost-effectiveness of occupational therapy for the treatment of substance use disorders.
Context and Policy Issues
WHO conceptualizes mental health as a “state of well-being in which the individual realizes his or her abilities, can cope with the normal stresses of life, can work productively and fruitfully and can contribute to his or her community”.1 Mental disorders (e.g., anxiety disorders, depression, bipolar disorder, post-traumatic stress disorder [PTSD], schizophrenia (SZ), eating disorders, and disruptive behaviour and dissocial disorders) are highly prevalent, in which 1 in every 8 people in the world lives with a mental disorder.2 In Canada, 1 in 3 people aged 15 and older may be affected by a mental illness during their lifetime; and every year, about 15% of Canadians use health services for a mental illness.3 According to WHO, “mental disorders may also be referred to as mental health conditions (MHC). The latter is a broader term covering mental disorders, psychosocial disabilities, and (other) mental states associated with significant distress, impairment in functioning, or risk of self-harm.”2 MHCs are generally characterized by “a combination of abnormal thoughts, perceptions, emotions, behaviour, and relationships with others, and 1 person in every 4 will suffer from a diagnosable MHC during their life.”4
MHCs can increase the risk for other diseases and add to the disease burden.5 In the Kohen and colleagues (2018) study5 investigating the mental health treatment gap in the region of Americas (Argentina, Brazil, Canada, Chile, Colombia, Guatemala, Mexico, Peru, and the US), mental and substance use disorders (SUD) contributed to 10.5% of the global burden of disease, and the weighted mean treatment gap, referring to the percentage of patients who may not receive treatment for moderate to severe disorders, ranged from 53.2% to 78.7%. As a growing public health concern, the findings of this study highlighted the treatment gap for mental health disorders in the Americas.5
The American Psychiatric Association defines SUDs as “a complex condition in which there is the uncontrolled use of a substance (e.g., alcohol, tobacco, or illicit drugs) despite harmful consequences.”6 Based on the estimate of the global burden of diseases due to SUDs between 1990 and 2016, SUDs contribute to 11.8 million deaths globally per year and 1.5% of the global disease burden.7 People with SUDs have a considerable burden of MHCs, in which more than half of the people with SUDs will experience an MHC during their lives.8
According to the Canadian Association of Occupational Therapists, “occupational therapy (OT) is a type of health care that helps to solve the problems that interfere with a person’s ability to do the things that are important to them including self-care (e.g., getting dressed, eating, and moving around the house), being productive (e.g., going to work or school, and participating in the community), and leisure activities (e.g., sports, gardening, and social activities).”9 OT practitioners are integral members of multidisciplinary health care teams and have the education, skills, and knowledge to provide OT interventions for people with MHCs10 or SUDs.11 Current evidence suggests that OT practitioners can help these populations to engage in meaningful occupations, participate in community living, and contribute to society.10,11 With respect to a wide range of MHCs and the extent of the treatment gap for those with mental disorders, as well as the diversity of pharmacological and non-pharmacological treatment options reported in the literature,12,13 the objective of this report was to summarize and critically appraise available evidence on the clinical effectiveness and cost-effectiveness of OT for the management of MHCs and SUDs.
Research Questions
What is the clinical effectiveness of occupational therapy for the treatment of mental health conditions?
What is the clinical effectiveness of occupational therapy for the treatment of substance use disorders?
What is the cost-effectiveness of occupational therapy for the treatment of mental health conditions?
What is the cost-effectiveness of occupational therapy for the treatment of substance use disorders?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy consisted of both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were occupational therapy, mental health, and substance use disorder. CADTH-developed search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, indirect treatment comparisons, and economic studies. The results of a focused search (with the main concepts appearing in the title or subject heading only) were also included. This search was limited to randomized and nonrandomized studies. Where possible, retrieval was restricted to the human population. The search was completed on February 23, 2023, and was limited to English-language documents published since January 1, 2018.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles, and abstracts were reviewed, and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Questions 1 and 3: Patients of any age with any of the following mental health conditions:
Questions 2 and 4: Patients of any age with substance use disorders |
Intervention | Occupational therapy in any health care setting |
Comparator | No occupational therapy, any comparator |
Outcomes | Questions 1 and 2: Clinical benefits (e.g., symptoms, quality of life) or harms (e.g., adverse events) Questions 3 and 4: Cost-effectiveness (e.g., cost per QALY gained, ICER) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies, economic evaluations |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before January 1, 2018.
Critical Appraisal of Individual Studies
One reviewer critically appraised systematic reviews (SRs) using the AMSTAR (A MeaSurement Tool to Assess Systematic Reviews 2) tool14 and randomized and nonrandomized primary studies using the Downs and Black checklist.15 For 1 SR with network meta-analysis (NMA), both the Questionnaire to Assess the Relevance and Credibility of an NMA16 and AMSTAR14 were used. Summary scores were not calculated for the studies; rather, the strengths and limitations observed among the included studies were summarized and described narratively Appendix 3.
Summary of Evidence
Quantity of Research Available
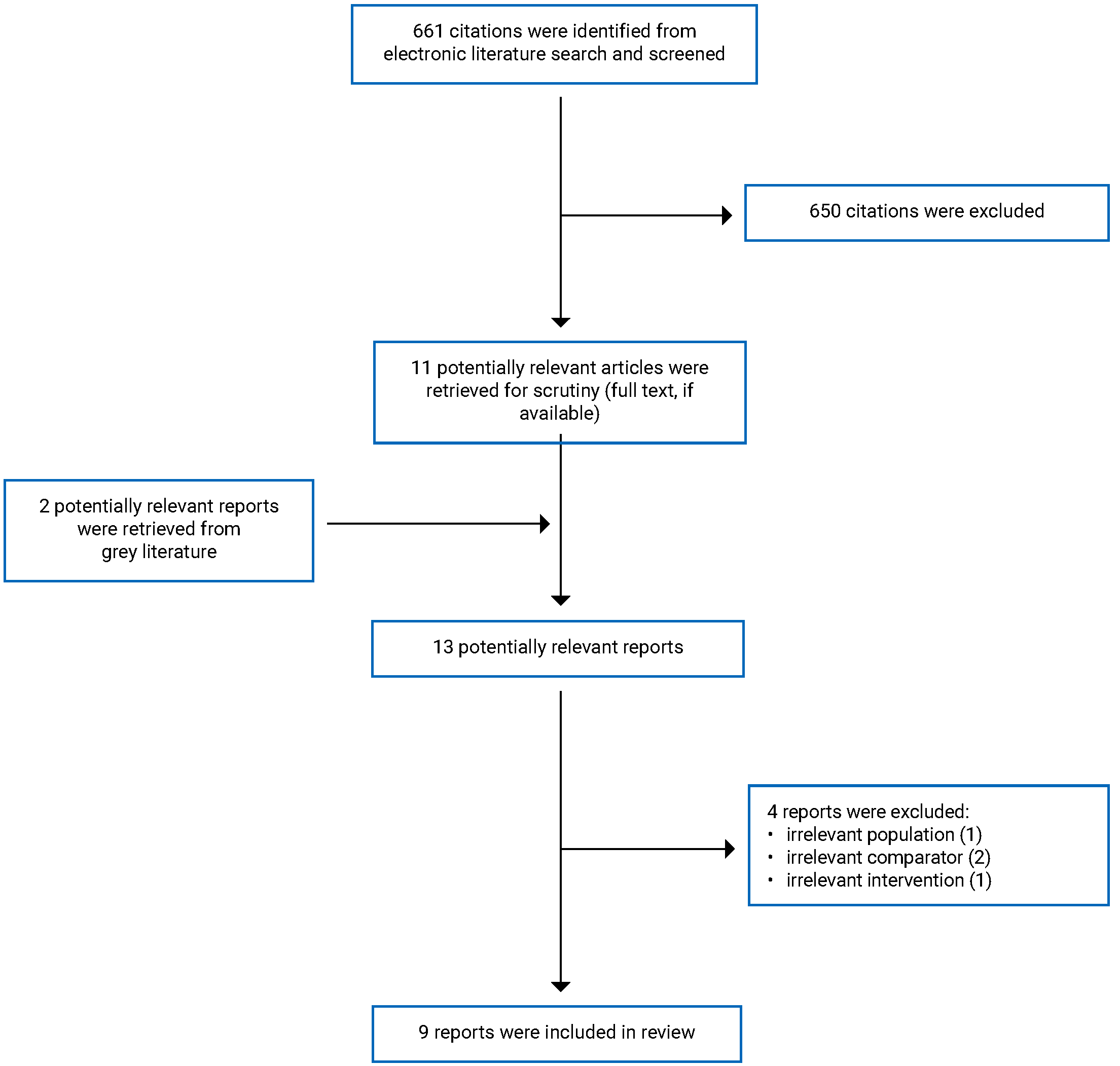
A total of 661 citations were identified in the literature search. Following the screening of titles and abstracts, 650 citations were excluded, and 11 potentially relevant articles from the electronic search were retrieved for full-text review. Two potentially relevant publications were identified from the grey literature search for full-text review. Of these 13 potentially relevant articles, 4 were excluded because of the irrelevant population, intervention, or comparator. Nine publications met the selection criteria and were included in this report.
Appendix 1 presents the PRISMA17 flow chart of the study selection. Additional references of potential interest are provided in Appendix 5.
Summary of the Study Characteristics
Nine peer-reviewed publications including 3 SRs13,18,19 and 6 primary studies20-25 were included in this report. Given the diversity of the 3 included SRs in terms of population, intervention, comparator, and outcome (i.e., PICO components), there was no overlap in their primary studies.
Additional details regarding the characteristics of the included publications are provided in Appendix 2 (Table 2 and Table 3).
Study Design
Of the 9 peer-reviewed publications that met the selection criteria for this report, 3 were SRs consisting of 1 SR and NMA (using Bayesian statistical analysis with informative prior distributions),13 1 SR and meta-analysis (MA),19 and 1 SR with a narrative synthesis of evidence.18 and 6 were primary studies including 3 randomized controlled trials (RCTs)20,22,25 and 3 prospective cohort studies.21,23,24 In the SR and NMA, of the 256 included studies, 5 RCTs reporting OT interventions were relevant to this report.
Country of Origin
Systematic Reviews
The authors of 1 SR and NMA (Watt et al. 2022),13 1 SR and MA (Noone et al. 2019),19 and 1 SR with the narrative synthesis of evidence (Christie et al. 2021)18 were based in Canada13 and the UK,18,19 respectively.
Primary Studies
Primary studies including 3 RCTs and 3 prospective cohort studies were conducted by authors from Japan (Shimada et al. 2022, Shimada et al. 2018),20,22 Sweden (Gunnarsson et al. 2018),25 Korea (Kim et al. 2020),23 Turkey (Karaman et al. 2020),24 and Japan (Shimada et al. 2019),21 respectively.
Patient Population
Systematic Reviews
In 1 SR and NMA13 describing the comparative efficacy of drug and nondrug interventions for reducing symptoms of depression, RCTs on patients with dementia aged 70 years or older who experienced depression as a neuropsychiatric symptom of dementia or had a diagnosis of a major depressive disorder were selected for review. In 1 SR and MA to assess the effectiveness of psychosocial interventions for depression and anxiety,19 8 RCTs on patients with dementia between 73 and 88 years who were diagnosed with depression or anxiety were included. In an SR to narratively describe the effectiveness of OT for improving function and participation in activities of everyday life (ADL),18 8 RCTs on adults aged 18 years with a primary diagnosis of depression, without a history of organic brain disorders or bipolar disorders, were selected for review.
Primary Studies
Six primary studies on the clinical effectiveness of various types of OT programs met the selection criteria to be included in this report,20-25 consisting of 1 study on adults with depression and/or anxiety disorders25 and 5 studies on patients diagnosed with SZ.20-24
In an RCT by Gunnarsson and colleagues (2018),25 patients were adults with depression and/or anxiety who were reporting problems with their everyday life, without a history of severe somatic illness or psychosis.
Shimada and colleagues published 3 papers on patients with SZ or schizoaffective disorders aged between 20 and 60 years who were newly hospitalized in a psychiatric hospital and discharged within 1 year. Patients with a diagnosis other than SZ or schizoaffective disorders, those with a history of cognitive delay, neurologic disorders, and/or significant drug or alcohol abuse, and patients with comorbid serious physical disorders were excluded from the study.
Kim and colleagues (2020)23 conducted a prospective cohort study in clinically stable patients with SZ aged between 19 and 55 years. Patients had at least 2 years of SZ diagnosis, and those with a history of severe impairments in social, psychological, and/or personal function, a diagnosis of other mental illnesses, or auditory, visual, and/or language impairments were excluded from the study. In the prospective cohort study by Karaman and colleagues (2020)24 included patients with SZ aged between 18 and 65 years, without additional psychiatric illnesses, active use of alcohol or substances, and being in a recurrent period.
Interventions and Comparators
Systematic Reviews
In an SR and NMA,13 of the 256 drugs, nondrug interventions, or any other interventions targeting symptoms of depression in patients with dementia in comparison with usual care or placebo, 5 studies included conventional OT (COT). In an SR and MA19 on patients with dementia, psychosocial interventions specifically targeting depression or anxiety symptoms were compared with usual care (including other psychosocial interventions relevant to OT practice) or waitlist controls. In an SR with a narrative synthesis of evidence18 on adults with a primary diagnosis of depression, OT (occupational, functional, and vocational interventions) was compared with non-OT alternative interventions (e.g., psychoeducation, cognitive behavioural therapy [CBT], medication, social activity, board games, and a creative writing course).
Primary Studies
In an RCT25 on adults with depression and/or anxiety disorders, the intervention was the Tree Theme Method (TTM), and the comparator was a conventional OT (COT) program. In the TTM intervention, the patient told their life story with a focus on activities in everyday life. Each session included a reflective dialogue between the patient and the OT. For the control group who received COT, the therapist defined what they meant by COT (i.e., best practice), to ensure that the treatment did not resemble the TTM intervention. The treatment plan included 5 sessions for both TTM and COT.
The other 5 primary studies were conducted on patients diagnosed with SZ. In 2 RCTs20,22 and 1 retrospective study,21 group OT (GOT) combined with individualized OT (IOT) and GOT alone were intervention and comparator, respectively. For GOT, occupational therapists provided support, such as consultations regarding living challenges, preparation support for discharge, available social resources, and community services. The IOT program aimed to facilitate proactive participation in treatment and improve outcomes. It consisted of a combination of effective psychosocial treatment programs relevant to OT practice such as motivational interviewing, self-monitoring, individualized visits, handicraft activities, individualized psychoeducation, and discharge planning. The treatment duration was 1 to 2 hours for 3 to 5 times per week, for a maximum of 3 months.
In a prospective cohort study,23 the effectiveness of a grocery shopping skill program (GSSP) was compared to no intervention (patients in the waiting list). The areas of GSSP intervention were skills for grocery shopping, identifying and selecting different food types, strategy integration, and selection of products for cooking. The waitlist control group received the same GSSP after the completion of the program for the intervention group. The intervention plan was provided for 4 weeks for both groups.
In the other prospective cohort study,24 2 intervention groups received either psychosocial skills training (PSST) or COT services. The control group included outpatients in the psychotic disorders clinic who received no treatment. The skill areas covered in PSST were developing communication skills and problem-solving skills, learning to deal with attention and memory problems, understanding psychosis and schizophrenia, understanding antipsychotic drug treatment and its side effects, evaluating the treatment, learning to deal with persistent symptoms, recognizing and monitoring warning signs, avoiding alcohol and drugs, “keeping away from the search for useless treatment,” 24 understanding how to deal with stress, increasing self-confidence, evaluating time and developing daily activities, making friends, and participating in social activities. The treatment plan consisted of 18 sessions completed between 10 to 18 weeks.
Outcomes
Systematic Reviews
Two SRs13,19 used standard questionnaires to assess depression (i.e., Geriatric Depression Scale [GDS] and/or Cornell Scale for Depression [CSD]) and/or anxiety (e.g., Hamilton Anxiety Scale [HAS], Rating Anxiety in Dementia [RAID], and Neuropsychiatric Inventory-Anxiety [NPI-A]). In the third SR,18 the outcome measures were standard questionnaires to assess occupational performance, level of function or participation in ADL, and/or satisfaction (i.e., Medical Outcomes Study-Short Form, WHO Quality of Life Scale, and Work Limitations Questionnaire [WLQ]). The SRs did not provide details on to interpret outcome measures (e.g., range of scores for each scale, the direction of improvement, or worsening).
Primary Studies
In 1 RCT,25 self-report questionnaires were used to assess changes in ADL and psychological symptoms including Canadian Occupational Performance Measurement (COPM), Satisfaction with Daily Occupations (SDO), Occupational Balance Questionnaire (OBQ), Symptom Checklist-90-R (SCL-90-R), Montgomery-Åsberg Depression Rating Scale (MADRS) (scores equal to or lower than 12, between 12 to 19, between 20 to 34, and equal to or higher than 35 were classified as no depression, mild depression, moderate depression, and severe depression, respectively), Hospital Anxiety and Depression Scale (HADS) (scores equal to or below 6, between 7 to 10, and equal to or higher than 11 were classified as no anxiety or depression, possible anxiety or depression, and probable severe anxiety or depression, respectively), Manchester Short Assessment of Quality of Life (MANSA), Client Satisfaction Questionnaire (CSQ), and Helping Alliance questionnaire (HAq-II).
In 2 RCTs on patients with SZ,20,22 several standard questionnaires were used to assess changes in social functioning, cognitive functioning, motivation, and satisfaction including Brief Assessment of Cognition in Schizophrenia (BACS) (the mean scores of the healthy participants were set to 0, and the standard deviations [SD] were set to 1), Schizophrenia Cognition Rating Scale (SCoRS) (higher ratings reflect more impairment), Social Functioning Scale (SFS) (a higher score indicates a higher level of social functioning), Global Assessment of Functioning (GAF) scale (a higher score indicates better functioning), Intrinsic Motivation Inventory (IMI) (a higher score reflects greater intrinsic motivation for a specified task), Morisky Medication on Adherence Scale-8 (MMAS-8) (a higher score indicates better adherence to the prescribed medications), and CSQ 8 (a higher score shows greater treatment satisfaction). In the same population, the authors also compared the 2 groups in the rate and period of rehospitalization after 2-year follow-up.21
In 1 prospective study on patients with SZ,24 social functioning was assessed using SFS, Personal and Social Performance Scale (PSP), General Psychopathology Scale (GPS), and Positive and Negative Syndrome Scale (PANSS) (a higher score indicates more severe symptoms of psychopathology). In the other prospective study on patients with SZ,23 the outcome measures were the Executive Function Performance Test (EFPT) (a higher score indicates more severe impairment in executive function), ADL index, and Montreal Cognitive Assessment (MoCA) (a score lower than 23 indicates cognitive impairment corresponding to mild cognitive impairment [MCI]).
Summary of the Critical Appraisal
Systematic Reviews
Of the 9 studies included in this report, 3 were SRs (Table 4) consisting of 1 SR and NMA on the comparative efficacy of a wide range of drug and nondrug interventions (including OT interventions in 5 studies) for reducing symptoms of depression in dementia,13 1 SR and MA on psychosocial interventions for reducing depression or anxiety in dementia,19 and 1 SR without quantitative analysis of the evidence on the effectiveness of OT for improving function and participation in ADL in adults with depression.18 We used a MeaSurement Tool to Assess Systematic Reviews (AMSTAR-2)14 to assess the quality of SRs and determine whether the most important elements of systematic review methodology were reported. Overall, except for a few limitations, particularly in 1 of the SRs,19 the 3 SRs included in this review had well-reported and appropriate methods.
The strengths of the 3 SRs were in defining the research question and inclusion and exclusion criteria, describing the study design of the selected primary studies, using a comprehensive literature search strategy, providing adequate detail about the included studies, following a robust selection method with duplicate screening and duplicate data extraction, using the Cochrane risk of bias (RoB) tool for assessing RoB in individual studies included in the SRs, and considering RoB in individual studies when interpreting the results. All 3 SRs13,18,19 included explanations for the heterogeneity observed in the results, publication bias, and the potential impact of studies with low sample sizes (or small study bias, which may have resulted in more extreme treatment effects).26 In 2 SRs including quantitative synthesis,13,19 the papers were clear in using appropriate methods for statistical combination of results, and discussed the potential impact of RoB in individual studies on the results of MA. Except for 1 SR,19 2 other SRs13,18 contained an explicit statement showing that the review methods were established before the conduct of the review, and they also provided a list of excluded studies and justified the exclusions. The sources of funding for the primary studies included in the review were not reported in all 3 SRs. Sources of funding for included primary studies are important for understanding the extent to which these may contribute to RoB in the findings of the studies and the interpretation of their results (e.g., studies funded by private industry are at a higher RoB in favour of the intervention under study).14 The SR by Noone and colleagues (2019)19 was unclear on sources of funding and any conflicts of interest that could impact the conduct and/or findings of the reviews. Overall, providing information about sources of funding and potential conflicts of interest in both primary studies included in the review and the SRs is essential evidence of transparency in the studies, which allows for assessing the potential impact of external factors on the reviews.
In addition to AMSTAR-2, the strength, and limitations of the NMA by Watt and colleagues (2021)13 were assessed using the Questionnaire to Assess the Relevance and Credibility of NMA (Table 5)
16 This questionnaire consists of 26 questions related to the relevance (i.e., the usefulness of NMA to inform health care decision-making) and credibility (including 5 subdomains: indirect comparison or NMA, analysis, reporting quality and transparency, interpretation, and conflict of interest) of NMA.16
The NMA by Watt and colleagues (2021)13 was considered sufficiently relevant, and the overall credibility domain of the NMA was judged as sufficient, based on the judgments of the 5 subdomains of the rating questionnaire. In this NMA, within-study randomization was considered for statistical analysis, both direct and indirect comparisons were available for pairwise contrasts, and agreement in treatment effects (i.e., consistency) was evaluated and discussed. Briefly, the authors provided a rationale for the choice of statistical analysis. A Bayesian random effects NMA in OpenBUGS was used for data analysis, and when more than 1 study existed for a treatment comparison, the Bayesian random effects pairwise MA was conducted. Further, informative prior distributions were implemented for all between-study heterogeneity variables, and vague prior distributions were implemented for trial baselines and treatment effects. The authors reported mean differences with a minimum clinically important difference derived using a distribution-based approach. To approximate the minimum clinically important difference, they derived estimates at 0.4 and 0.5 SDs of the pooled SD. Global inconsistency was assessed by comparing deviance and deviance information criterion statistics between consistency and inconsistency models. The loop-specific approach was used to assess local inconsistency in each closed network loop. The authors conducted subgroup analyses based on the following effect modifiers: study setting (residence in a nursing home or assisted living facility versus community or clinic setting), mean age of study population, the proportion of women (equal or lower than 50% or higher than 50%), whether standardized criteria were used to diagnose dementia, study size (omitting studies with less than 50 patients enrolled), dementia severity (mild-moderate or moderate-severe), and intervention duration (equal to or lower than 11 weeks or higher than 11 weeks). Sensitivity analyses were performed based on 2 components of the quality assessment that posed the greatest risk to the validity of study findings: missing outcome data and blinding of outcome assessment. A comparison-adjusted funnel plot was used to assess small study effects.
Primary Studies
The Downs and Black Checklist15 used for critical appraisal of the included primary studies consists of 5 sections (Table 6): reporting, external validity, internal validity, confounding, and power. In the following paragraphs, the strengths and weaknesses of the included primary studies are individually described in each of the 5 sections.
Reporting: Six primary studies including 3 RCTs20,22,23 and 3 prospective cohort studies21,23,24 were included in this report. The items that were clearly mentioned in the studies were: study objectives, main outcomes, characteristics of the patients included, interventions, main findings of the study, and estimate random variability in data for main outcomes. Except for 1 study,21 sources of funding were reported in all studies. Across the studies, the important adverse events consequential to the intervention and characteristics of patients lost to follow-up were only described in 122 and 2 studies21,24, respectively. In addition, except for 1 study,21 distributions of principal confounders in the study groups were not reported in the included studies, which could put the studies at risk of confounding bias.
External Validity: Except for 2 studies,20,22 it was unclear if the patients who were asked to participate in the study were representative of the entire population recruited (i.e., poor reporting of the source of the population). Moreover, in all studies, it was uncertain if the patients who were prepared to participate were representative of the recruited population. Most primary studies included in this report had a single-centre study design. The studies also didn’t provide adequate information about the estimate of the total population eligible to be recruited, which could limit their external validity.
Internal Validity: In the RCTs,20,22,23 trained evaluators or research assistants who were assigned to measure the main outcomes were blinded to the study groups. In addition, the main outcome measures were valid and reliable scales or questionnaires known in OT, psychology, or neuropsychiatry.
Confounding: None of the included studies reported the number of patients lost to follow-up. Except for 1 study,21 the statistical analysis section of the articles did not clearly report if adequate adjustments were considered for confounding that could affect the main findings. Thus, the primary studies included in this report were at risk of confounding bias. This type of bias can preclude finding a true intervention effect and may cause an inaccurate estimate (underestimate or overestimate) of the true association between exposure and an outcome.27
Power: Except for 2 studies,21,25 it was unclear that the studies were sufficiently powered to detect clinically significant effects. Overall, studies with small sample sizes are susceptible to inflated effect size estimates and publication bias, and they can reduce the chance of detecting a true effect.28
Additional details regarding the strengths and limitations of included publications are summarized in Appendix 3 (i.e., Table 4 for SRs, Table 5 for the NMA by Watt et al. 2021,13 and Table 6 for primary studies).
Summary of Findings
We identified 9 studies13,18-25 to address the research question on the clinical effectiveness of OT for MHCs. We did not find any studies that met inclusion criteria about the cost-effectiveness of OT for the treatment of MHCs, as well as the clinical effectiveness and cost-effectiveness of OT for the treatment of SUDs Appendix 4 presents the main outcomes of the included studies.
Effectiveness of OT in Reducing the Symptoms of Anxiety and/or Depression in Patients with Dementia
In the SR and NMA13 on the comparative efficacy of different interventions for reducing symptoms of depression in patients with dementia, the results of 5 RCTs reporting OT interventions showed the effectiveness of OT in improving the symptoms of depression compared to usual care. In this study, the minimum clinically important difference in symptom scores was estimated to be 2.0 at 0.4 SDs and 2.5 at 0.5 SDs. In MA, the standardized mean difference (SMD) with a 95% credible interval (Crl) (calculated based on the scores of the Cornell scale for depression in dementia) was −2.56 (−5.20 to 0.12), in favour of OT interventions. The probability of mean differences (MDs) higher than 0.4 SDs (i.e., probability of an important difference between treatment groups) was 64.8%. Similar results were observed in the NMA, as the SMD with 95% credible interval (Crl) was −2.59 (−4.70 to −0.40), and the probability of MDs higher than 0.4 SDs was 69.9%. In this NMA, both direct and indirect evidence was considered to assess consistency between direct and indirect comparisons, and a consistency rather than an inconsistency model provided a better model fit.
The findings of 1 SR and MA19 were in support of the effectiveness of psychosocial interventions relative to usual care or waitlist controls (i.e., multicomponent intervention, Tai Chi, problem adaptation therapy, and exercise and/or walking) in reducing symptoms of depression (n = 4 studies) and anxiety (n = 3 studies). According to the Q-Cochrane test, inconsistency index (I2) values between 0.0 to 39.9, 40.0 to 69.9, 70.0 to 89.9, and 90 to 100 correspond with mild, moderate, severe, and highly severe heterogeneity.29 In this SR, inconsistency index (I2) values for the anxiety 1-week postintervention as well as post-6-month follow-up were evidence of severe and moderate heterogeneity, respectively, showing that the findings should be interpreted with caution. (Table 7).
Effectiveness of COT for Improving Function and Participation in Adults with Anxiety and/or Depression
In an SR with the narrative synthesis of evidence from 6 primary studies on OT,18 it was concluded that strong evidence supported the OT return-to-work intervention effectiveness for improving depression symptomology. Evidence was not in support of COT lifestyle interventions for improving anxiety, suicidal ideation, and work participation.
In comparison between before and after intervention results, the findings of 1 RCT25 showed the effectiveness of both TTM and COT in improving ADL and reducing psychological symptoms (depression and anxiety), and no significant difference was found between TTM and COT (Table 8).
Effectiveness of OT for the Management of SZ
Social and Cognitive Functioning
The findings of 1 RCT22 on patients diagnosed with SZ showed higher effectiveness of GOT combined with IOT compared to GOT alone on cognitive functioning, motivation, medication adherence, and treatment satisfaction (Table 9). After 5-year follow-up, the superiority of GOT combined with IOT relative to GOT only was reported in all domains of social functioning (withdrawal and/or social engagement, interpersonal communication, prosocial activities, recreation, independence-competence, independence-performance, employment and/or occupation), 2 domains of cognitive functioning (verbal memory and brief assessment of cognition), all motivation scores (interest and/or enjoyment, value and/or usefulness, perceived choice, and intrinsic motivation inventory [IMI]), and treatment satisfaction.22
In 1 prospective cohort study in patients with SZ,24 in within group comparisons, both PSST and COT showed significant improvement in social functioning. The authors reported higher scores in SFS and Personal and Social Performance (PSP),scale and a reduced total score in the PANSS and GPS. In between-group comparisons, PSST demonstrated greater improvement compared to COT in all outcome measures (Table 10).
Rehospitalization
The authors (2019)21 also compared the 2 groups in the rate and period of rehospitalization after a 2-year follow-up and reported a significantly lower rate and shorter length of rehospitalization in patients who received GOT combined with IOT compared to GOT alone (Table 11).
Executive Function
In 1 prospective cohort study,23 patients with SZ who received GSSP combined with COT showed significantly better post-treatment scores in executive function and ADL compared to those receiving COT only (Table 12).
Limitations
Existing evidence had several limitations in response to the research questions of this review. We did not find any publications about the clinical effectiveness and cost-effectiveness of OT for the treatment of SUDs that met the inclusion criteria for our review. The evidence was also limited on the cost-effectiveness of OT for the treatment of MHCs. Specifically, the findings of this review are focused on the clinical effectiveness of OT for the treatment of MHCs limited to adult patients diagnosed with depression and/or anxiety, and SZ.
In the primary studies included in this report, patients were excluded if they had concurrent MHCs or SUDs. Although excluding patients with other accompanying conditions may be part of the study design in health research, there is a substantial overlap in MHCs and SUDs in clinical practice that should be taken into account.
There was no overlap among the relevant primary studies summarized in the SRs included in this report. Likewise, except for 3 publications on the same population in patients with SZ by Shimada and colleagues (2018, 2019, 2021),20-22 the included primary studies were widely varied in terms of the research question, population, and intervention of interest. The breadth of research questions likely reflects the diversity of interventions that could all reasonably be considered OT, as well as the diversity of patients and/or indications that could potentially be managed with OT. This variation in relevant evidence limits the extent to which the findings could be effectively synthesized.
The 3 SRs13,18,19 varied widely in terms of the types and quality of primary studies included in the review. For example, in 1 SR and NMA,13 the RoB in the OT interventions was rated as low, and no evidence of small study effects (the impact of low sample sizes on the findings) was identified. However, in 1 SR and MA, the authors discussed the limited quality of the included primary studies and the potential impact of small sample sizes on the results. In the third SR without MA,18 the overall quality of the included primary studies was reported as acceptable. Nonetheless, the methodological heterogeneity of the interventions precluding complete or partial MAs was discussed in all 3 SRs.
In general, OT interventions appear to be effective at reducing symptoms of depression and anxiety and improving function and participation in MHCs reviewed in this report (i.e., depression, anxiety, and/or schizophrenia). However, it is difficult to draw firm conclusions about the clinical effectiveness of OT in MHCs due to several research limitations of the selected studies such as not reporting adverse events consequential to the intervention, not reporting the characteristics of patients lost to follow-up, and poor reports of the source of population.
Conclusions and Implications for Decision- or Policy-Making
Evidence from 3 SRs13,18,19 and 1 RCT25 included in this report suggests that in adults with depression and/or anxiety, OT interventions13,25 and psychosocial interventions19 may be effective for reducing symptoms of depression and/or anxiety. In addition, OT interventions18 may be effective at improving function and participation in this patient population.
Of the 5 primary studies on patients with SZ, 3 studies (2 RCTs20,22 and 1 prospective cohort21) from a research group on the same population in Japan showed individualized OT adds value to group treatment in areas such as treatment satisfaction, cognitive function, and motivation, and reducing the period and rate of rehospitalization. The other 2 primary studies (2 prospective cohorts23,24) on patients with SZ were diverse in terms of the research question and interventions of interest. Briefly, these studies were in support of the higher effectiveness of PSST compared to COT in improving social functioning,24 the higher effectiveness of GSSP (a type of PSST) relative to COT in executive function and ADL.23 It could be concluded that, according to the studies selected for this report, specialized and/or tailored OT interventions may be more effective compared to conventional OT.
Overall, given the level of evidence (1 SR with NMA, 1 SR with MA, 1 SR with a narrative synthesis of evidence, 4 RCTs, and 3 prospective cohorts), the findings of this review are supportive of the clinical effectiveness of OT for the treatment of MHCs in adult patients with depression and/or anxiety and patients with SZ. Although the generalizability of the findings summarized in this report may be limited in their application to the Canadian context, as the included studies represented a broad range of populations by country of origin, the SR with NMA13 included in this report was published by a large group of Canadian authors, and another SR18 included primary studies conducted in Canada. Nonetheless, given the diversity of selected studies for this report in terms of research question and methodology, the extent to which studies from other cultures might contribute to the Canadian context remains unclear and requires further research.
With respect to the selection criteria for this review, we did not find any publications about the clinical effectiveness of OT for the treatment of SUDs, and the cost-effectiveness of OT for the treatment of both MHCs and SUDs. Future research may assist with decision-making in these areas.
References
1.World Health Organization. Mental health. 2022; https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response. Accessed 2023 Mar 8.
2.World Health Organization. Mental disorders. 2022; https://www.who.int/news-room/fact-sheets/detail/mental-disorders. Accessed 2023 Mar 9.
3.Government of Canada. Mental illness in Canada. 2020; https://health-infobase.canada.ca/datalab/mental-illness-blog.html. Accessed 2023 Mar 23.
4.Aoki Y, Yaju Y, Utsumi T, et al. Shared decision-making interventions for people with mental health conditions. Cochrane Database Syst Rev. 2022;11(11):Cd007297. PubMed
5.Kohn R, Ali AA, Puac-Polanco V, et al. Mental health in the Americas: an overview of the treatment gap. Rev Panam Salud Publica. 2018;42:e165. https://www.ncbi.nlm.nih.gov/pubmed/31093193. Accessed 2023 Mar 10. PubMed
6.American Psychiatric Association. What Is a substance use disorder? 2020; https://www.psychiatry.org/patients-families/addiction-substance-use-disorders/what-is-a-substance-use-disorder. Accessed 2023 Mar 10.
7.The global burden of disease attributable to alcohol and drug use in 195 countries and territories, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Psychiatry. 2018;5(12):987-1012. PubMed
8.Aas CF, Vold JH, Gjestad R, et al. Substance use and symptoms of mental health disorders: a prospective cohort of patients with severe substance use disorders in Norway. Subst Abuse Treat Prev Policy. 2021;16(1):20. PubMed
9.Canadian Association of Occupational Therapists. What is occupational theraphy? 2022; https://caot.ca/site/about/ot?nav=sidebar&banner=1. Accessed 2023 Mar 8.
10.Lannigan EG, Noyes S. Occupational therapy interventions for adults living with serious mental illness. Am J Occup Ther. 2019;73(5):7305395010p7305395011-7305395010p7305395015.
11.Stoffel VC, Moyers PA. An evidence-based and occupational perspective of interventions for persons with substance-use disorders. Am J Occup Ther. 2004;58(5):570-586. PubMed
12.Gartlehner G, Wagner G, Matyas N, et al. Pharmacological and non-pharmacological treatments for major depressive disorder: review of systematic reviews. BMJ Open. 2017;7(6):e014912. PubMed
13.Watt JA, Goodarzi Z, Veroniki AA, et al. Comparative efficacy of interventions for reducing symptoms of depression in people with dementia: systematic review and network meta-analysis. BMJ. 2021;372:n532. PubMed
14.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
15.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
16.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. PubMed
17.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
18.Christie L, Inman J, Davys D, Cook PA. A systematic review into the effectiveness of occupational therapy for improving function and participation in activities of everyday life in adults with a diagnosis of depression. J Affect Disord. 2021;282:962-973. PubMed
19.Noone D, Stott J, Aguirre E, Llanfear K, Spector A. Meta-analysis of psychosocial interventions for people with dementia and anxiety or depression. Aging Ment Health. 2019;23(10):1282-1291. PubMed
20.Shimada T, Inagaki Y, Shimooka Y, Kawano K, Tanaka S, Kobayashi M. Effect of individualized occupational therapy on social functioning in patients with schizophrenia: A five-year follow-up of a randomized controlled trial. J Psychiatr Res. 2022;156:476-484. PubMed
21.Shimada T, Ohori M, Inagaki Y, et al. Effect of adding individualized occupational therapy to standard care on rehospitalization of patients with schizophrenia: A 2-year prospective cohort study. Psychiatry Clin Neurosci. 2019;73(8):476-485. PubMed
22.Shimada T, Ohori M, Inagaki Y, et al. A multicenter, randomized controlled trial of individualized occupational therapy for patients with schizophrenia in Japan. PLoS ONE [Electronic Resource]. 2018;13(4):e0193869. PubMed
23.Kim YS, Park JH, Lee SA. Is a program to improve grocery-shopping skills clinically effective in improving executive function and instrumental activities of daily living of patients with schizophrenia? Asian J Psychiatr. 2020;48:101896. PubMed
24.Karaman IGY, Kasal MI, Ingec C, Yastibas C, Gulyuksel F, Gulec M. Effect of adjunct psychosocial skills training on social functioning of schizophrenia patients who get occupational therapy in a community mental health center: A comparative study. Noropsikiyatr. 2020;57(3):248-253. PubMed
25.Birgitta Gunnarsson A, Wagman P, Hedin K, Hakansson C. Treatment of depression and/or anxiety - outcomes of a randomised controlled trial of the tree theme method R versus regular occupational therapy. BMC Psychol. 2018;6(1):25. PubMed
26.Turner RM, Bird SM, Higgins JP. The impact of study size on meta-analyses: examination of underpowered studies in Cochrane reviews. PLoS One. 2013;8(3):e59202. PubMed
27.Skelly AC, Dettori JR, Brodt ED. Assessing bias: the importance of considering confounding. Evid Based Spine Care J. 2012;3(1):9-12. PubMed
28.Button KS, Ioannidis JP, Mokrysz C, et al. Power failure: why small sample size undermines the reliability of neuroscience. Nat Rev Neurosci. 2013;14(5):365-376. PubMed
29.Higgins J, Thomas J, Chandler J, et al. Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022). Cochrane; 2022.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, objective, funding source | Study designs and the number of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Christie et al. 202118 UK Funding source: No funding | Design: SR Total studies included: 6 Total studies relevant to this review: 6 (4 RCTs and 2 observational studies) | Population included: Adults with a primary diagnosis of depression Age in all included studies ≥ 18 years Sex: NR Exclusion criteria:
| Interventions included: OT (occupational, functional, and vocational interventions) Comparator: Non-OT alternative interventions | Outcome measure Standard questionnaires or scales assessing:
Follow-up: 3-month follow-up in 1 included study |
Watt et al. 202113 Canada Funding source: Alberta Critical Care Strategic Clinical Network | Design: SR and NMA Total studies included: 256 Total studies relevant to this review: 5 RCTs | Population included: Patients with depression as a neuropsychiatric symptom of dementia or who were diagnosed with a major depressive disorder. Age in all included studies ≥ 70 years Sex: At least 50% females Exclusion criteria:
| Interventions included: Drugs or nondrug interventions or any other interventions targeting symptoms of depression Interventions relevant to this review: OT Comparator: Usual care or placebo | Outcome measure Standard depression scales:
Follow-up: NR |
Noone et al. 201919 UK Funding source: NR | Design: SR and MA Total studies included: 8 Total studies relevant to this review: 8 RCTs | Population included: People with dementia diagnosed with depression or anxiety Age in all included studies was between 73 and 88 years Sex: Both males and females (statistics NR). Exclusion criteria: Pharmacological interventions | Interventions included: Psychosocial interventions that specifically targeted depression or anxiety symptoms. Comparator: Usual care or waitlist controls | Outcome: Standard scales assessing depression or anxiety Follow-up: 6-month follow-up in 5 included studies |
MA = meta-analysis; NMA = network meta-analysis; NR = not reported; OT = occupational therapy; RCT = randomized controlled trial; SR = systematic review.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, design, country, objective, funding source | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|
Shimada et al. (2022)20 Study design: RCT Country: Japan Funding source: No funding | Inpatients with SZ or schizoaffective disorders Number of patients (n), Age in year, mean (SD), range: Total: 102, 42.55 (10.54), NR:
Sex: number of males, n (%) Total: 54 (52.94)
| Intervention: GOT combined with IOT Comparator: GOT | Outcomes Primary outcome Social functioning: SFS Secondary outcomes Cognitive Functioning:
Motivation
Treatment satisfaction: CSQ-8 Follow-up: 5 years |
Karaman et al. (2020)24 Study design: Prospective cohort Country: Turkey Funding source: No funding | Patients diagnosed with SZ Number of patients (n), Age in year, mean (SD), range: Total: 62, 42.55 (10.54), NR
Sex: number of males (%) Total: 42 (67.74)
| Intervention: COT combined with PSST Comparator:
| Outcomes Changes in social functioning:
Follow-up: Ten to 18 weeks postbaseline |
Kim et al. 202023 Study design: Prospective cohort Country: Korea Funding source: The Soonchunhyang University Research Fund | Patients diagnosed with SZ Number of patients (n), Age in year, mean (SD), range: Total: 20, 42.55 (10.54), NR:
Sex: number of males (%) Total: 9 (45.0):
| Intervention: GSSP Comparator: No intervention | Outcomes Changes in: ADL Executive function: EFPT Global cognitive function: MoCA Follow-up: Four weeks postbaseline |
Shimada et al. (2019)21 Study design: Prospective cohort Country: Japan Funding source: NR | Patients with SZ or schizoaffective disorder who were discharged within 1 year from a psychiatric hospital. Number of patients (n), Age in year, mean (SD), range: Total: 109, 42.07 (10.66), 20 to 65:
Sex: number of males (%) Total: 55 (50.46):
| Intervention: GOT combined with IOT Comparator: GOT alone | Outcomes:
Follow-up: 2 years |
Gunnarsson et al. (2018)25 Study design: RCT Country: Sweden Funding source: Medical Research Council of Southeast Sweden Department of Research and Development, Kronoberg Region, Southern Health Care Region, Sweden | Adults with depression and/or anxiety disorders Age in year, mean (SD), range:
Sex: Both males and females (statistics NR). | Intervention: TTMa Comparator: COT | Outcomes Changes in: ADL Psychological symptoms:
Follow-up: Post 5 sessions of intervention |
Shimada et al. (2018)22 Study design: RCT Country: Japan Funding source: Japanese Association of OT | Patients diagnosed with SZ who were discharged within 1 year from a psychiatric hospital. Number of patients (n), Age in year, mean (SD), range Total: 136, 42.07 (10.66), 20 to 65:
Sex: number of males (%) Total: 67 (49.26):
| Intervention: GOT combined with IOT Comparator: GOT | Outcomes Cognitive Functioning:
Motivation:
Medication adherence: MMAS Treatment satisfaction: CSQ Follow-up: The time between baseline and discharge or 3-months posthospitalization |
ADL = activities of daily living; BACS = Brief Assessment of Cognition in Schizophrenia; CANTAB = Cambridge Neuropsychological Test Automated Battery; COPM = Canadian Occupational Performance Measurement; COT = conventional occupational therapy; CSQ = Client Satisfaction Questionnaire; EFPT = Executive Function Performance Test; GAF = Global Assessment of Functioning; GOT = group occupational therapy; GPS = General Psychopathology Scale; GSSP = grocery shopping skill program; HADS = Hospital Anxiety and Depression Scale; IMI = Intrinsic Motivation Inventory; IOT = individualized occupational therapy; LOTCA = Loewenstein Occupational Therapy Cognitive Assessment battery; MADR = Montgomery-Åsberg Depression Rating Scale; MANSA = Manchester Short Assessment of Quality of Life; MMAS = Morisky Medication on Adherence Scale; MMSE: mini-mental state examination; MoCA = Montreal Cognitive Assessment; OBQ = Occupational Balance Questionnaire; OT = occupational therapy; NR = not reported; POT = psychosocial occupational therapy; PSP = Personal and Social Performance Scale; PSST = psychosocial skills training; RCT = randomized controlled trial; SCL-90-R = Symptom Checklist-90-R; SCoRS = Schizophrenia Cognition Rating Scale; SD = standard deviation; SDO = Satisfaction with Daily Occupations; SFS = Social Functioning Scale; SZ = schizophrenia; TTM = Tree Theme Method.
aA client-centred occupational therapy intervention designed to increase the ability to cope with and enhance satisfaction with everyday life, both at home and at work.25
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Systematic Reviews Using a MeaSurement Tool to Assess Systematic Reviews 2 (AMSTAR 2)14
AMSTAR Item | Watt et al. (2021)13 | Christie et al. (2021)18 | Noone et al. (2019)19 |
|---|---|---|---|
1. Did the research questions and inclusion criteria for the review include the components of PICO? | Yes | Yes | Yes |
2. Did the report of the review contain an explicit statement that the review methods were established before the conduct of the review and did the report justify any significant deviations from the protocol? | Yes | Yes | No |
3. Did the review authors explain their selection of the study designs for inclusion in the review? | Yes | Yes | Yes |
4. Did the review authors use a comprehensive literature search strategy? | Yes | Yes | Yes |
5. Did the review authors perform study selection in duplicate? | Yes | Yes | Yes |
6. Did the review authors perform data extraction in duplicate? | Yes | Yes | Yes |
7. Did the review authors provide a list of excluded studies and justify the exclusions? | Yes | Yes | No |
8. Did the review authors describe the included studies in adequate detail? | Yes | Yes | Yes |
9. Did the review authors use a satisfactory technique for assessing the RoB in individual studies that were included in the review? | Yes | Yes | Yes |
10. Did the review authors report on the sources of funding for the studies included in the review? | No | No | No |
11. If meta-analysis was performed did the review authors use appropriate methods for the statistical combination of results? | Yes | NA | Yes |
12. If meta-analysis was performed, did the review authors assess the potential impact of RoB in individual studies on the results of the meta-analysis or other evidence synthesis? | Yes | NA | Yes |
13. Did the review authors account for RoB in individual studies when interpreting/ discussing the results of the review? | Yes | Yes | Yes |
14. Did the review authors provide a satisfactory explanation for, and discussion of, any heterogeneity observed in the results of the review? | Yes | Yes | Yes |
15. If they performed quantitative synthesis did the review authors carry out an adequate investigation of publication bias (small study bias) and discuss its likely impact on the results of the review? | Yes | NA | Yes |
16. Did the review authors report any potential sources of conflict of interest, including any funding they received for conducting the review? | Yes | Yes | No |
NA = not applicable; PICO = population, intervention, comparator, outcome; RoB = risk of bias.
Table 5: Strengths and Limitations of a NMA in Watt et al. (2021)13 Using a Questionnaire to Assess the Relevance and Credibility of NMA16
Items | Yes, no, or can’t answer |
|---|---|
Relevance | |
1. Is the population relevant? | Yes |
2. Are any critical interventions missing? | No |
3. Are any relevant outcomes missing? | No |
4. Is the context (e.g., settings and circumstances) applicable to your population? | Yes |
Credibility: Evidence base | |
5. Did the researchers attempt to identify and include all relevant RCTs? | Yes |
6. Do the trials for the interventions of interest form one connected network of randomized controlled trials? | Yes |
7. Is it apparent that poor-quality studies were included thereby leading to bias? | No |
8. Is it likely that bias was induced by selective reporting of outcomes in the studies? | No |
9. Are there systematic differences in treatment effect modifiers (i.e., baseline patient or study characteristics that impact the treatment effects) across the different treatment comparisons in the network? | No |
10. If yes (i.e., there are such systematic differences in treatment effect modifiers), were these imbalances in effect modifiers across the different treatment comparisons identified before comparing individual study results? | Yes |
Credibility: Analysis | |
11. Were statistical methods used that preserve within-study randomization? (No naive comparisons) | Yesa |
12. If both direct and indirect comparisons are available for pairwise contrasts (i.e., closed loops), was agreement in treatment effects (i.e., consistency) evaluated or discussed? | Yes |
13. In the presence of consistency between direct and indirect comparisons, were both direct and indirect evidence included in the network meta-analysis? | Yes |
14. With inconsistency or an imbalance in the distribution of treatment effect modifiers across the different types of comparisons in the network of trials, did the researchers attempt to minimize this bias with the analysis? | Yes |
15. Was a valid rationale provided for the use of random effects or fixed effect models? | Yes |
16. If a random-effects model was used, were assumptions about heterogeneity explored or discussed? | Yes |
17. If there are indications of heterogeneity, were subgroup analyses or meta-regression analysis with prespecified covariates performed? | Yes |
Credibility: Reporting quality and transparency | |
18. Is a graphical or tabular representation of the evidence network provided with information on the number of RCTs per direct comparison? | Yes |
19. Are the individual study results reported? | Yes |
20. Are results of direct comparisons reported separately from results of the indirect comparisons or network meta-analysis? | Yes |
21. Are all pairwise contrasts between interventions as obtained with the network meta-analysis reported along with measures of uncertainty? | Yes |
22. Is a ranking of interventions provided given the reported treatment effects and its uncertainty by the outcome? | Yes |
23. Is the impact of important patient characteristics on treatment effects reported? | Yes |
Credibility: Interpretation | |
24. Are the conclusions fair and balanced? | Yes |
Credibility: Conflict of Interest | |
25. Were there any potential conflicts of interest? | No |
26. If yes, were steps taken to address these? | Yes |
NA = not applicable; NR = not reported; RCTs = randomized controlled trials.
a“If item 11 is scored as a no resulting in a fatal flaw, the overall domain should be judged as fatally flawed and the network meta-analysis may have serious validity issues.”16
Detailed responses to questions related to “Analysis and Reporting Quality and Transparency” could be found in the Supplementary Data of Watt, et al. (2021) study.13
Table 6: Strengths and Limitations of Primary Clinical Studies Using the Downs and Black Checklist15
Downs and Black Checklist’s Items | Gunnarsson (2018)25 | Shimada (2018)22 | Shimada (2019)21 | Kim (2020)23 | Karaman (2020)24 | Shimada (2022)20 |
|---|---|---|---|---|---|---|
Reporting | ||||||
1. Is the objective of the study clear? | Yes | Yes | Yes | Yes | Yes | Yes |
2. Are the main outcomes clearly described in the Introduction or Methods? | Yes | Yes | Yes | Yes | Yes | Yes |
3. Are the characteristics of the patients included in the study clearly described? | Yes | Yes | Yes | Yes | Yes | Yes |
4. Are the interventions clearly described? | Yes | Yes | Yes | Yes | Yes | Yes |
5. Are the distributions of principal confounders in each group of subjects clearly described? | No | No | Yes | No | No | No |
6. Are the main findings of the study clearly described? | Yes | Yes | Yes | Yes | Yes | Yes |
7. Does the study estimate random variability in data for main outcomes? | Yes | Yes | Yes | Yes | Yes | Yes |
8. Have all the important adverse events consequential to the intervention been reported? | No | Yes | No | No | No | No |
9. Have characteristics of patients lost to follow-up been described? | No | No | Yes | No | Yes | No |
10. Have actual P values been reported for the main outcomes except for probability < 0.001? | Partially | Partially | Yes | No | Partially | Yes |
External validity | ||||||
11. Is the source of funding clearly stated? | Yes | Yes | No | Yes | Yes | Yes |
12. Were subjects who were asked to participate in the study representative of the entire population recruited? | Unclear | Yes | Unclear | Unclear | Unclear | Yes |
13. Were those subjects who were prepared to participate representative of the recruited population? | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
14. Were staff, places, and facilities where patients were treated representative of the treatment most received? | Yes | Yes | Yes | Yes | Yes | Yes |
Internal validity | ||||||
15. Was an attempt made to blind study subjects to the intervention? | NA | NA | NA | NA | NA | NA |
16. Was an attempt made to blind those measuring the main outcomes? | Yes | Yes | No | No | No | Yes |
17. If any of the results of the study were based on data dredging was this made clear? | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
18. Was the time period between intervention and outcome the same for intervention and control groups or adjusted for? | Yes | Yes | Yes | Yes | Yes | Yes |
19. Were the statistical tests used to assess the main outcomes appropriate? | Yes | Yes | Yes | Yes | Yes | Yes |
20. Was compliance with the interventions reliable? | Yes | Yes | Yes | Yes | Yes | Yes |
21. Were the main outcome measures used accurate? (Valid and reliable) | Yes | Yes | Yes | Yes | Yes | Yes |
Internal validity – confounding (selection bias) | ||||||
22. Were patients in different intervention groups recruited from the same population? | Yes | Yes | Unclear | Yes | Unclear | Yes |
23. Were study subjects in different intervention groups recruited over the same period of time? | Yes | Yes | Unclear | Yes | Unclear | Yes |
24. Were study subjects randomized to intervention groups? | Yes | Yes | NA | Yes | NA | Yes |
25. Was the randomized intervention assignment concealed from patients and staff until recruitment was complete? | Yes | Yes | NA | Yes | NA | Yes |
26. Was there an adequate adjustment for confounding in the analyses from which the main findings were drawn? | Unclear | Unclear | Yes | Unclear | Unclear | Unclear |
27. Were losses of patients to follow-up taken into account? | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
Power | ||||||
28. Was the study sufficiently powered to detect clinically important effects where the P value for a difference due to chance is < 5%? | Yes | Yes | Unclear | Unclear | Unclear | Unclear |
NA = not applicable
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 7: Summary of Findings by Outcome — Impact of Psychosocial Interventions on Symptoms of Depression and Anxiety in Patients with Dementia, Noone et al. (2019)19
Outcome | Number of included studies | Standardized mean difference (SMD), Random-Effects Model, 95% confidence interval (CI) | Test for overall effect | Test for heterogeneity | ||||
|---|---|---|---|---|---|---|---|---|
Z | Pa | Tau2 | Chi2 | P | I2 b | |||
Depression 1-week postintervention | 4 | −0.62 (−0.94 to −0.29) | 3.71 | 0.0002 | 0.00 | 2.35 | 0.50 | 0% |
Anxiety 1-week postintervention | 3 | −1.33 (−2.21 to −0.44) | 2.95 | 0.003 | 0.42 | 7.25 | 0.03 | 72% |
Anxiety 6-month follow-up | 2 | −1.06 (−2.05 to −0.07) | 2.11 | 0.04 | 0.33 | 2.81 | 0.09 | 64% |
aThere was a significant medium to large effect for psychosocial interventions in reducing depression.
bAccording to the Q-Cochrane test, I2 (inconsistency index) values between 0.0 to 39.9, 40.0 to 69.9, 70.0 to 89.9, and 90 to 100 correspond with mild, moderate, severe, and highly severe heterogeneity.29 I2 values for the second and third outcomes suggest that the effect may not be accurate and should be interpreted with caution.
Table 8: Summary of Findings by Outcome — Changes in Outcome Measures Before and After Interventions, Gunnarsson et al. (2018)25
Outcome measures | Tree theme method (TTM) (n = 12) | Conventional occupational therapy (COT) (n = 12) | P (between group comparisons) | ||||
|---|---|---|---|---|---|---|---|
Baseline median (IQR)a | After Intervention median (IQR) | P | Baseline median (IQR) | After Intervention median (IQR) | P | ||
Canadian occupational performance Measure (COPM) Performance Satisfaction | 4 (3, 5) 2 (2, 4) | 5 (3, 6) 4 (2, 6) | ≤ 0.01 ≤ 0.01 | 3 (3,5) 3 (2, 4) | 5 (3,6) 5 (3, 6) | ≤ 0.01 ≤ 0.01 | 0.60 0.59 |
Satisfaction with daily occupations (SDO) Activity level Satisfaction score | 7 (6, 8) 63 (50, 76) | 7 (6, 9) 65 (53, 77) | ≤ 0.01 0.21 | 8 (6, 9) 62 (53, 69) | 8 (6, 10) 64 (57, 72) | ≤ 0.01 0.02 | 0.65 0.34 |
Occupational balance questionnaire (OBQ) | 23 (17, 30) | 30 (21, 38) | ≤ 0.01 | 22 (15, 30) | 30 (21, 37) | ≤ 0.01 | 1.00 |
Symptom Checklist-90-R symptom scale Depression Anxiety | 83 (71, 91) 81(68, 93) | 73 (58, 87) 71 (53, 91) | ≤ 0.01 ≤ 0.01 | 81 (70, 91) 82 (67, 100) | 71 (57, 90) 78 (61, 93) | ≤ 0.01 0.01 | 0.34 0.73 |
Montgomery-Åsberg Depression Rating Scale (MADRS-S) | 25 (20, 30) | 20 (11, 29) | ≤ 0.01 | 25 (20, 32) | 20 (14, 27) | ≤ 0.01 | 0.43 |
Hospital Anxiety and Depression Scale (HADS) Anxiety Depression | 14 (10, 17) 10 (7, 13) | 12 (8, 15) 8 (3, 12) | ≤ 0.01 ≤ 0.01 | 14 (11, 16) 10 (7, 14) | 12 (9, 15) 7 (5, 11) | ≤ 0.01 ≤ 0.01 | 0.63 1.00 |
Manchester Short Assessment of QoL (MANSA) | 47 (37, 52) | 50 (38, 61) | 0.02 | 45 (35, 52) | 50 (39, 55) | 0.01 | 0.75 |
Client Satisfaction Questionnaire (CSQ) | NR | 26 (23, 30) | NA | NR | 26 (24, 30) | NA | 0.96 |
Helping Alliance questionnaire (HAq-II) Occupational therapist Patient | 86 (80, 92) 99 (93, 105) | 96 (90, 106) 106 (99, 111) | ≤ 0.01 ≤ 0.01 | 85 (80, 90) 95 (91, 101) | 94 (90, 102) 102 (94, 107) | ≤ 0.01 ≤ 0.01 | 0.99 0.96 |
IQR = interquartile range, NA = not applicable; NR = not reported.
aThe interquartile range (IQR) shows the difference between the 25th and 75th percentiles, including the central 50% of the observations.25
Table 9: Summary of Findings by Outcome — Outcome of Occupational Therapy for Patients with Schizophrenia, Shimada et al. (2018)22 and Shimada et al. (2022)20
Outcomes | Baseline | Post-treatment (3 months) | Follow-up (5 years) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
GOT and IOT (n = 48) | GOT (n = 54) | GOT and IOT (n = 48) | GOT (n = 54) | P | GOT and IOT (n = 48) | GOT (n = 54) | P | |||||||
Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |||
Social Functioning Scale (SFS)a | ||||||||||||||
Withdrawal and/or social engagement | 6.38 | 2.07 | 6.46 | 1.71 | NR | NR | NR | NR | NR | 9.65 | 1.83 | 7.89 | 1.96 | < 0.01 |
Interpersonal communication | 6.04 | 1.90 | 6.19 | 1.70 | NR | NR | NR | NR | NR | 9.31 | 2.21 | 7.59 | 2.05 | < 0.01 |
Prosocial activities | 12.96 | 6.50 | 17.09 | 7.90 | NR | NR | NR | NR | NR | 29.94 | 10.43 | 21.96 | 9.94 | < 0.01 |
Recreation | 18.25 | 5.39 | 20.35 | 5.63 | NR | NR | NR | NR | NR | 23.85 | 6.92 | 21.50 | 6.65 | < 0.01 |
Independence-competence | 20.56 | 6.02 | 19.11 | 6.75 | NR | NR | NR | NR | NR | 24.50 | 6.55 | 19.91 | 6.39 | < 0.01 |
Independence-performance | 17.27 | 4.76 | 16.86 | 4.52 | NR | NR | NR | NR | NR | 21.44 | 4.67 | 17.33 | 5.33 | < 0.01 |
Employment/occupation | 1.81 | 2.46 | 1.87 | 1.96 | NR | NR | NR | NR | NR | 4.46 | 0.20 | 2.46 | 2.36 | < 0.01 |
Total score | 83.27 | 20.99 | 86.87 | 18.66 | NR | NR | NR | NR | NR | 123.15 | 28.07 | 98.65 | 27.12 | < 0.01 |
Brief Assessment of Cognition in Schizophrenia (BACS) | ||||||||||||||
Verbal memory | −2.18 | 1.32 | −2.44 | 1.03 | −1.38 | 1.16 | −2.05 | 1.16 | < 0.01 | −1.32 | 1.12 | −2.17 | 1.18 | < 0.001 |
Working memory | −1.86 | 1.04 | −1.70 | 1.23 | −1.05 | 0.96 | −1.37 | 1.28 | 0.02 | −1.07 | 0.98 | −1.49 | 1.34 | 0.078 |
Verbal fluency | −1.32 | 1.09 | −1.20 | 0.98 | −0.93 | 0.97 | −1.19 | 0.96 | < 0.01 | −2.64 | 1.49 | −2.84 | 1.56 | 0.521 |
Attention | −2.67 | 1.27 | −2.54 | 1.26 | −1.88 | 1.05 | −2.21 | 1.15 | < 0.01 | −1.97 | 1.09 | −2.30 | 1.22 | 0.155 |
Composite scoreb | −2.30 | 0.95 | −2.29 | 0.97 | −1.51 | 0.76 | −1.87 | 0.88 | < 0.01 | −1.50 | 0.74 | −1.96 | 0.91 | 0.006 |
Intrinsic motivation inventory (IMI) | ||||||||||||||
Interest and/or enjoyment | 24.67 | 6.48 | 25.19 | 7.22 | 32.00 | 7.53 | 28.03 | 6.96 | < 0.01 | 32.58 | 6.38 | 28.04 | 6.23 | < 0.001 |
Value and/or usefulness | 23.38 | 8.27 | 23.25 | 8.35 | 30.37 | 7.54 | 26.91 | 7.63 | < 0.01 | 30.63 | 6.36 | 27.00 | 6.53 | 0.006 |
Perceived choice | 23.85 | 7.13 | 24.29 | 6.90 | 30.72 | 6.61 | 26.79 | 6.04 | < 0.01 | 29.79 | 5.68 | 26.44 | 4.99 | 0.002 |
Total score | 71.91 | 18.49 | 72.73 | 18.87 | 93.12 | 18.22 | 81.73 | 18.87 | < 0.01 | 93.04 | 14.52 | 81.48 | 15.91 | 0.002 |
Medication adherence | ||||||||||||||
Morisky medication adherence scale (MMSA-8) | 6.66 | 1.27 | 6.81 | 1.23 | 7.87 | 1.16 | 81.73 | 18.8 | < 0.01 | NR | NR | NR | NR | NR |
Treatment satisfaction | ||||||||||||||
Client satisfaction questionnaire (CSQ-8) | NR | NR | NR | NR | NR | NR | NR | NR | < 0.01 | 25.73 | 3.40 | 23.63 | 3.58 | 0.003 |
GOT = group occupational therapy; IOT = individualized occupational therapy; NR = not reported; OT = occupational therapy; SD = standard deviation.
aThe “social functioning scale (SFS)” was only reported in Schimada et al. (2022).
bThe composite score was calculated by averaging all the z-scores of the subscales in Brief Assessment of Cognition in Schizophrenia (BACS).
Table 10: Summary of Findings by Outcome — Social Functioning in Patients with schizophrenia Karaman et al. (2021)21
Social functioning scales, mean (standard deviation) | Psychosocial skills training (PPST) (n = 21) | Conventional occupational therapy (COT) (n = 22) | Control (n = 21) | P (between group-comparison) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
Before | After | P | Before | After | P | Before | After | P | ||
Positive and negative Syndrome Scale (PANSS) | 56.95 (12.25) | 50.19 (8.81) | P < 0.05 | 51.04 (7.24) | 40.68 (6.42) | P < 0.05 | 52.7 (12.00) | 51.66 (12.47) | P > 0.05 | < 0.05a |
General Psychopathology Scale (GPS) | 27.05 (5.55) | 24.62 (8.42) | P < 0.05 | 23.27 (4.35) | 19.18 (3.47) | P < 0.05 | 24.24 (6.19) | 26.00 (7.83) | P > 0.05 | < 0.05 |
Personal and Social Performance (PSP) | 51.20 (10.47) | 64.76 (9.41) | P < 0.05 | 58.00 (7.66) | 67.95 (7.66) | P < 0.05 | 52.62 (16.70) | 54.05 (17.29) | P > 0.05 | < 0.05 |
Patient-Social Functionality Scale (P-SFS) | 107.42 (24.40) | 82.28 (20.21) | P < 0.05 | 98.40 (28.19) | 109.13 (29.96) | P < 0.05 | 82.28 (20.21) | 84.52 (23.05) | P > 0.05 | < 0.05 |
aActual P values were not reported.
Table 11: Summary of Findings by Outcome — Rehospitalization Outcomes in Patients with Schizophrenia for 2-Year Follow-up, Shimada et al. (2019)21
Study groups | Total | GOT and IOT (n = 55) | GOT without IOT (n = 57) | P |
|---|---|---|---|---|
Rate of rehospitalization, n (%) | 56 (5.37) | 16 (28.57) | 40 (71.43) | < 0.001 |
Period of rehospitalization, day (standard deviation) | 278 (2,140) | NR | NR | < 0.001 |
GOT = group occupational therapy; IOT = individualized occupational therapy.
Table 12: Summary of Findings by Outcome — Executive Function and Activities of Daily Living of Patients with Schizophrenia, Kim et al. (2020)21
Cognitive measures, mean (standard deviation) | Grocery Shopping Skill Program (GSSP) (n = 10) | No intervention (n = 10) | P (between group comparison) | ||||
|---|---|---|---|---|---|---|---|
Before | After | P | Before | After | P | ||
Executive Function Performance Test (EFPT) | 54.10 (3.54) | 40.00 (1.88) | < 0.001 | 55.20 (5.86) | 54.10 (5.84) | > 0.05a | < 0.001 |
Activities of Daily Living (ADL) | 14.20 (1.68) | 20.10 (2.92) | < 0.001 | 19.90 (1.79) | 20.60 (2.27) | > 0.05 | < 0.05 |
Montreal Cognitive Assessment (MoCA) | 8.20 (1.61) | 12.50 (0.70) | < 0.001 | 9.60 (2.17) | 10.00 (1.70) | > 0.05 | < 0.001 |
aThe actual P value was not reported.
Appendix 5: References of Potential Interest
The following publications were identified because they may provide some information associated with this report, including SRs with alternative populations or interventions, RCTs with an alternative study design, and reviews (literature reviews or scoping reviews).
Systematic Reviews
Alternative Population
Cai Y, Li L, Xu C, Wang Z. The effectiveness of non-pharmacological interventions on apathy in patients with dementia: a systematic review of systematic reviews. Worldviews Evid Based Nurs. 2020;17(4):311-318. PubMed
Bahar-Fuchs A, Martyr A, Goh AM, Sabates J, Clare L. Cognitive training for people with mild to moderate dementia. Cochrane Database Syst Rev. 2019;3:CD013069. PubMed
Alternative Intervention
Novo A, Fonseca J, Barroso B, et al. Virtual reality rehabilitation's impact on negative symptoms and psychosocial rehabilitation in schizophrenia spectrum disorder: a systematic review. Healthcare (Basel). 2021 Oct 23;9(11):23. PubMed
Randomized Controlled Trials
Alternative Study Design (Study Protocols)
Pozzi C, Lanzoni A, Lucchi E, et al. Activity-based occupational therapy intervention for delirium superimposed on dementia in nursing home setting: a feasibility study. Aging-Clinical & Experimental Research. 2020;32(5):827-833. PubMed
Tran T, Donnelly C, Nalder EJ, Trothen T, Finlayson M. Occupational therapist-led mindfulness-based stress reduction for older adults living with subjective cognitive decline or mild cognitive impairment in primary care: a feasibility randomized control trial protocol. BMJ Open. 2020;10(6):e035299. PubMed
Walsh H, Fleming J, Silvestre Edo C, Bernabeu Guitart M, Murillo N. Occupational performance and multisensory stimulation during post-traumatic amnesia: An observational and randomized controlled trial protocol. Canadian Journal of Occupational Therapy - Revue Canadienne d Ergotherapie. 2019 Oct;86(4):326-337.
Martin-Fernandez J, Stevens N, Moriceau S, et al. Realist evaluation of the impact, viability and transferability of an alcohol harm reduction support programme based on mental health recovery: the Vitae study protocol. BMJ Open. 2022 08 11;12(8):e065361. PubMed
Reviews
Literature Reviews
Oyebode JR, Parveen S. Psychosocial interventions for people with dementia: An overview and commentary on recent developments. Dementia. 2019;18(1):8-35. PubMed
Scoping Reviews
Araya-Quintanilla F, Sepulveda-Loyola W, Cuyul-Vasquez I, et al. Recommendations and effects of rehabilitation programs in older adults after hospitalization for COVID-19: A scoping review. Am J Phys Med Rehabil. 2023;12:12. PubMed
Hoosain M, Plastow NA. Workplace-based occupational therapy for mental health in Africa: a scoping review protocol. BMJ Open. 2022;12(4):e054821. PubMed
Chimara M, van Niekerk L, van Biljon HM. Vocational rehabilitation for mental health service users with chronic mental illness in low-income to upper-middle-income countries: a scoping review protocol. BMJ Open. 2021;11(7):e047781. PubMed
Buresh M, Stern R, Rastegar D. Treatment of opioid use disorder in primary care. BMJ. 2021 05 19;373:n784.
Breslin L, Guerra N, Ganz L, Ervin D. Clinical utility of multisensory environments for people with intellectual and developmental disabilities: a scoping review. Am J Occup Ther. 2020;74(1):7401205060p7401205061-7401205060p7401205012.
Guidelines
Nacamura PAB, Marcon SS, Paiano M, et al. Guidelines to the families of mental health service users from the multi-professional team's perspective. Rev Bras Enferm. 2020;73(suppl 1):e20200389.iui. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as of the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, collecting, using, and disclosing by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca