CADTH Health Technology Review
Tocilizumab for Neuromyelitis Optica Spectrum Disorder
Rapid Review
Authors: Qiukui Hao, Aleksandra Grobelna
Abbreviations
AQP4
aquaporin 4
ARR
annualized relapse rate
AZA
azathioprine
CI
confidence interval
EDSS
Expanded Disability Status Scale
HR
hazard ratio
IVMP
IV methylprednisolone
logMAR
logarithm of the minimum angle of resolution
MMF
mycophenolate mofetil
NMOSD
neuromyelitis optica spectrum disorder
OCT
optical coherence tomography
OR
odds ratio
SMD
standardized mean difference
TCZ
tocilizumab
Key Messages
Patients with neuromyelitis optica spectrum disorder treated with tocilizumab may experience decreased risks of relapse or disability progression compared to before treatment, but it is uncertain whether these changes can be entirely attributed to tocilizumab (TCZ) treatment.
TCZ might be better than azathioprine for patients with neuromyelitis optica spectrum disorder in reducing relapse risk.
TCZ might improve or have no impact on pain and fatigue measures for patients with neuromyelitis optica spectrum disorder.
Adverse events were common during TCZ treatment, but patients treated with TCZ may experience adverse events at a similar or lower rate to those treated with azathioprine.
One evidence-based guideline suggests that TCZ can be used as 1 of the second-line drugs to prevent long-term relapse for patients with neuromyelitis optica spectrum disorder who have no response to other immunosuppressants.
We did not find any studies that compared TCZ to other immunosuppressants or any studies on the cost-effectiveness of TCZ for treating neuromyelitis optica spectrum disorder that met the inclusion criteria for this report.
Context and Policy Issues
Neuromyelitis optica spectrum disorder (NMOSD) (also named neuromyelitis optica or Devic disease) is a rare and relapsing chronic autoimmune disease of the central nervous system characterized by demyelination and axonal damage primarily targeting astrocytes in optic nerves and the spinal cord.1 Neuroimaging characteristics (observed by MRI) and aquaporin-4(AQP4) autoantibodies are important in NMOSD diagnosis and the differential diagnosis from multiple sclerosis and myelin oligodendrocyte glycoprotein antibody-associated diseases.1 The NMOSD incidence (0.037 to 0.73 per 100,000 person-years) and prevalence (0.7 to 10 per 100,000 persons) vary across studies, with the incidence and prevalence reported to be the highest in Afro-Caribbean regions and lowest in Australia and New Zealand.2 In British Columbia, Canada, the mean incidence of NMOSD ranged from 0.14 to 0.60 per 100,000 person-years from 1986 to 2020 in Asian populations.3 Sex and ethnic groups were identified as influencing factors for these epidemiological data.
The median age of NMOSD onset is 32 to 41 years, with the peak incidence in middle-aged adults (30 to 59 years), but it also can affect children and older adults.1,2 The prevalence of NMOSD among females was reported as 2.3 to 7.6 times greater than that among males.2 People with NMOSD suffer from a wide range of symptoms that include severe visual loss, physical disability, pain, bladder dysfunction, intractable vomiting and hiccoughs, or other non-disease-specific symptoms (e.g., muscle, trunk, or leg pain).1 The features of clinical manifestations for NMOSD typically reflect the acute episodes of optic neuritis (optic nerve inflammation), transverse myelitis (spinal cord inflammation), and area postrema syndrome.4 Unlike multiple sclerosis, patients with NMOSD are unlikely to experience a secondary progressive phase of the disease; however, relapse and attacks are closely related to disability and death.1 Over half of the patients with NMOSD will be disabled and approximately one-third of patients will have died within 5 years after the first attack if the disease is left untreated.5
Acute attacks for NMOSD include the first attack and subsequent acute relapses defined as the worsening of original symptoms or the onset of new related symptoms that last for at least 24 hours and occur more than 30 days after the previous attack.6 Severe acute attacks can lead to paraplegia (paralysis of the legs), blindness, respiratory failure, or long-term disabilities.6 The most important goals of the management for NMOSD are to prevent disability and mortality by reducing the duration and severity of acute attacks or the risk of consequential relapses after the first attack.4,6 For all patients with suspected NMOSD acute attack, several clinical practice guidelines recommend a high-dose glucocorticoid pulse as the first-line intervention and plasma exchange as the second-line treatment. Considering relapses could result in accumulated neurologic deficits closely related to poor prognosis, long-term immunotherapy (at least 5 years or lifetime treatment) is generally used once the diagnosis of NMOSD is made or after the management of the acute attacks.7
For long-term immunotherapies, available options include humanized monoclonal antibodies, azathioprine (AZA), mycophenolate mofetil (MMF), methotrexate, mitoxantrone, and oral glucocorticoids.7 Health Canada–approved the humanized monoclonal antibodies eculizumab and satralizumab as immunosuppressive drugs for preventing relapse in people with NMOSD.8 However, due to inconsistency in the limited available evidence, the current clinical practice guidelines have not established the optimal immunotherapies and treatment durations.7 Some clinicians prescribe the off-label use of tocilizumab (TCZ) or rituximab for patients with NMOSD as alternative immunosuppressive drugs.7
TCZ is a humanized monoclonal antibody against the interleukin-6 (IL-6) receptor that is approved in Canada for the treatment of moderately to severely active rheumatoid arthritis.9,10 TCZ also can be used in patients hospitalized with Covid-19 pneumonia and other diseases.11 In patients with NMOSD, IL-6 can stimulate abnormal B-cell response and increase AQP4 autoantibodies that play a crucial role in immunopathogenesis and astrocyte injury.12 TCZ as 1 of the IL-6 inhibitors, had demonstrated immunological effects on immune cells and in reducing the AQP4 antibody levels,13 suggesting it may be a promising immunotherapy option for this condition. The purpose of this report is to review the clinical effectiveness and cost-effectiveness of TCZ for patients with NMOSD compared to alternative pharmacological therapies or no treatment. We also summarized relevant evidence-based guidelines regarding the use of TCZ in patients with NMOSD.
Research Questions
What is the clinical effectiveness of tocilizumab for patients with neuromyelitis optica spectrum disorder compared to alternative pharmacological therapies?
What is the clinical effectiveness of tocilizumab for patients with neuromyelitis optica spectrum disorder compared to no treatment?
What is the cost-effectiveness of tocilizumab for patients with neuromyelitis optica spectrum disorder?
What are the evidence-based guidelines regarding the use of tocilizumab for the treatment of patients with neuromyelitis optica spectrum disorder?
Methods
Literature Search Methods
A literature search was conducted by an information specialist on key resources, including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were tocilizumab and neuromyelitis optica spectrum disorder (NMOSD). No filters were applied to limit the retrieval by study type. Where possible, retrieval was limited to the human population. The search was completed on February 2, 2023 and was limited to English-language documents published since January 1, 2018.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Patients (of any age) with neuromyelitis optica spectrum disorder |
Intervention | Tocilizumab (any dose) |
Comparator | Q1 and Q3: Any alternative pharmacological therapies (e.g., immunosuppressant therapies or corticosteroids including satralizumab, azathioprine, mycophenolate mofetil, methotrexate, cyclophosphamide, cyclosporine, prednisone, eculizumab, rituximab) Q2 and Q3: Placebo or no treatment Q4: Not applicable |
Outcomes | Q1 and Q2: Clinical benefits (e.g., mortality, time to first relapse, relapse rate, disability [e.g., Kurtzke Expanded Disability Status Scale measure], health-related quality of life, functionality, symptom severity) and harms (e.g., rate of adverse events) Q3: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained, incremental cost-effectiveness ratio) Q4: Recommendations regarding best practices (e.g., appropriate patient populations, guidance regarding treatment protocols for tocilizumab use) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies, economic evaluations, evidence-based guidelines |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1. We also excluded duplicate publications and citations that were published before 2018. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic reviews or reported the impacts of the intervention only on immune cells. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A Measurement Tool to Assess systematic Reviews 2 (AMSTAR 2)14 for systematic reviews, the Downs and Black checklist15 for randomized and non-randomized studies, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument16 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
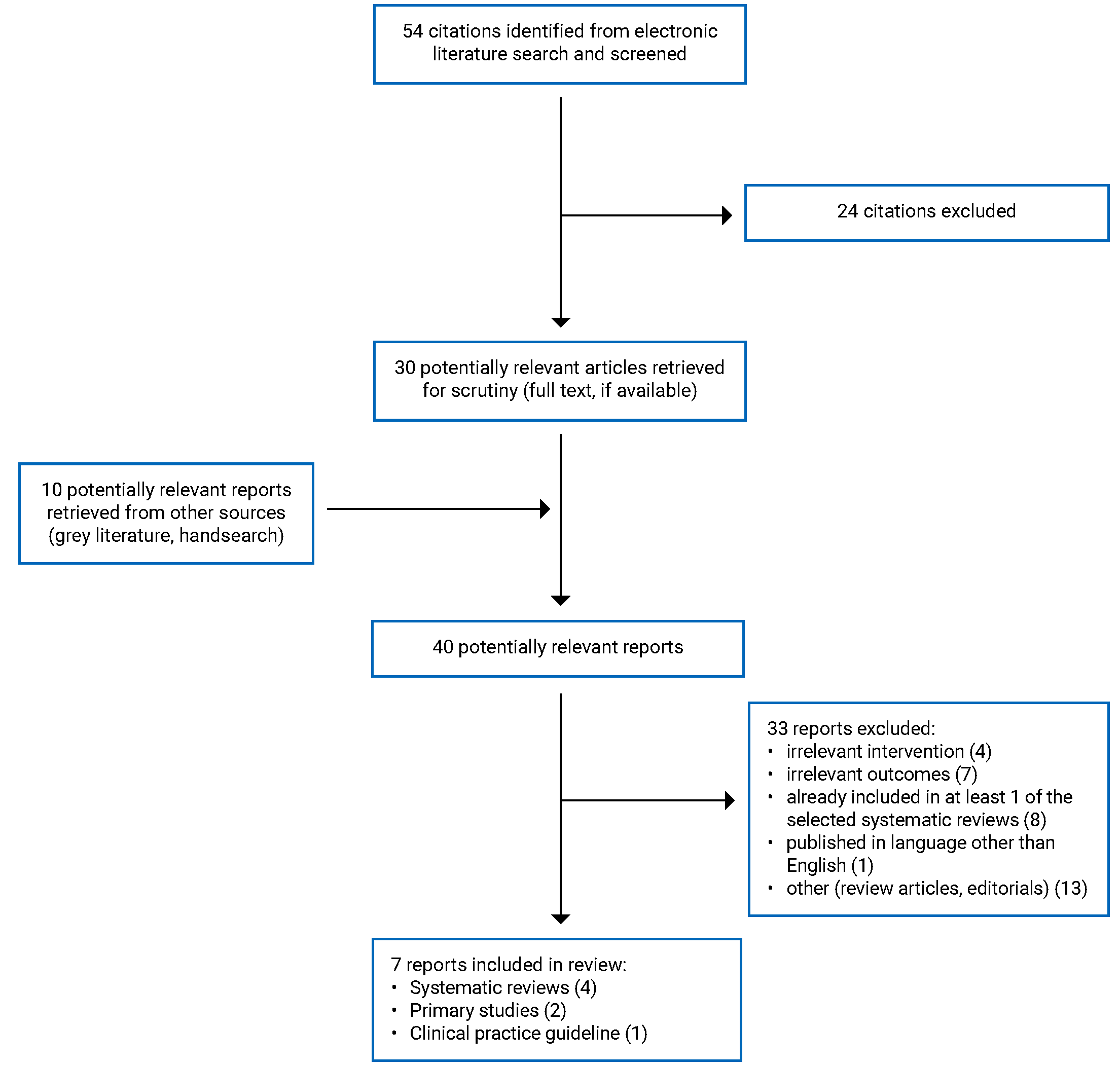
A total of 54 citations were identified in the literature search. Following the screening of titles and abstracts, 24 citations were excluded, and 30 potentially relevant reports from the electronic search were retrieved for full-text review. Ten potentially relevant publications were retrieved from the grey literature search for a full-text review. Of these potentially relevant articles, 33 publications were excluded for various reasons, and 7 publications met the inclusion criteria and were included in this report. These comprised 4 systematic reviews, 2 non-randomized studies, and 1 evidence-based guideline. Appendix 1 presents the PRISMA17 flow chart of the study selection. Additional references of potential interest are provided in Appendix 6.
Summary of Study Characteristics
Four systematic reviews,18-21 2 non-randomized studies,22,23 and 1 evidence-based guideline24 were included. Three systematic reviews19-21 had broader inclusion criteria on interventions; only the subset of studies reporting on TCZ and its comparison were relevant to the current report. We only described the characteristics and results of this subset in this report. Appendix 5 includes a table describing the overlap in relevant primary studies in the included systematic reviews. Given this overlap, the summary of the systematic reviews in this report may repeat some primary study findings. Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
Three18-20 of 4 systematic reviews included meta-analyses and 1 systematic review21 summarized the findings from primary studies narratively but did not conduct a meta-analysis. The number of primary studies involving TCZ that were included in the systematic reviews ranged from 7 to 27 primary studies, which comprised retrospective observational studies, case reports, and 1 randomized controlled trial (RCT). One review18 provided an indirect comparison of TCZ (7 primary studies) and AZA (19 primary studies) for 1 outcome using pooled effect size based on the test of interaction.25 Three systematic reviews18,20,21 included the same RCT (TANGO trial), which compared TCZ and AZA.26 Two systematic reviews20,21 were published in 2021, 1 systematic review19 was published in 2022 and the fourth systematic review18 was published in 2023 with the search up to July 21, 2022.
Two observational studies with a retrospective before-after design were published in 202323 and 2021.22 One study23 retrospectively collected data for NMOSD patients treated with TCZ and compared the changes between baseline and after treatment. This study also employed adjusted logistic regression models to identify risk factors for relapse. The second study22 included NMOSD patients treated with TCZ, AZA, and rituximab and healthy controls. This study compared the differences between baseline and after treatment within each treatment group or across the 3 drug groups as well as the difference between NMOSD patients and the healthy controls on optical coherence tomography (OCT) measures.
One evidence-based clinical practice guideline was included from Latin America.24 The guideline development group comprised experts in neurology who were involved in the diagnosis and care of NMOSD patients and conducted a systematic literature search (from 1990 to 2019) to identify relevant evidence. The ratings of the quality of evidence and strength of recommendations were not reported. The RAND-UCLA methodology for reaching formal consensus was used, and the recommendations were formulated based on formal consensus and voting processes.24 The grade (i.e., appropriate, inappropriate, or uncertain) and proportion of expert agreement for recommendation statements were provided as outputs of the voting processes.
Country of Origin
Of the 4 systematic reviews,18-21 2 systematic reviews were from Nepal,20,21 the third systematic review was from China,18 and the fourth systematic review21 was from the US. One systematic review20 presented the countries or regions of included primary studies. Of the 7 relevant studies, the RCT was conducted in 6 centres in China and the 6 observational studies were conducted in Germany, Spain, France, Japan, and the US.20
The 2 observational studies22,23 were single-centre studies that were conducted in the same hospital in China; and a group from Latin American developed the clinical practice guideline.24
Patient Population
All 4 systematic reviews18-21 involved patients with NMOSD, and the number of included patients ranged from 59 to 1,078. The age of patients ranged from 12 years to 68 years with mean age ranging from 29 years to 50 years in primary studies included in 1 systematic review;20 mean ages were 42 years (TCZ studies) and 37 years (AZA studies) in the second systematic review;18 the mean age ranged from 29 to 50 in the primary studies included in the third systematic review;19 and age was not reported in the fourth systematic review.21 The study populations were predominantly female in 3 systematic reviews18-20, with the proportion of females ranging from 86% to 92%. The fourth systematic review21 did not report the proportion of females. The proportion of patients with AQP4-positive serotype ranged from 14% to 100% across primary studies in 1 systematic review,19 40% to 100% in the second review,20 and was reported as 85.8% in patients with TCZ treatment in the third systematic review and 81.3% for the fourth systematic review.18 One review20 noted that AZA and mycophenolate mofetil were the most common add-on drugs for TCZ, while the remaining systematic reviews18,19,21 did not report the add-on drugs.
The 2 non-randomized studies22,23 included adults with NMOSD. The first study included 65 adult patients with a median age of 44.23 The second study22 included 50 adults with NMOSD and 10 healthy controls with an age range of 18 years to 75 years (mean age from 41 years to 53 years for patients with NMOSD and 44 for healthy controls). The proportion of females was 90% or over for both studies.22,23 The proportion of patients with AQP4-IgG seropositive was 83% in 1 study,23 while all patients were AQP4-IgG seropositive in the second study.22
The included clinical practice guideline was for the management of patients with NMOSD.24 The intended users of the guideline were clinicians involved in the care of patients with NMOSD. There was no pediatrician in the guideline development panel; therefore, pediatric patients with NMOSD may not have been considered in this guideline.
Interventions and Comparators
Two systematic reviews18,21 compared the effectiveness and safety of TCZ and AZA, and the remaining 2 systematic reviews19,20 compared the before-and-after changes for TCZ without a comparator group. Two systematic reviews18,19 did not report the dosage and route of administration of TCZ. The other 2 systematic reviews20,21 reported TCZ can be administrated with IV with a dosage of 6 mg/kg to 8 mg/kg every 4 or 6 weeks, or subcutaneously with a dose of 162 mg every 1 to 2 weeks, and AZA can be administered orally with a dosage of 2 to 3 mg/kg per day.
One eligible retrospective observational study23 included patients who were regularly administered IV TCZ (8 mg/kg) every 4, 6 or 8 weeks and compared outcomes before-and-after treatment. The second retrospective observational study22 compared the before-after change scores of OCT measures across 3 drug interventions: IV TCZ (8 mg/kg/month), oral AZA (2 mg/kg/day to 3 mg/kg/day) and IV rituximab (dosage depending on the proportion of CD19+ B-cells in peripheral blood mononuclear cells) and healthy controls.
The included guideline24 considered most treatments for NMOSD that includes TCZ, AZA, eculizumab, inebilizumab, satralizumab, cyclophosphamide, mitoxantrone, IV methylprednisolone, plasmapheresis, mycophenolate mofetil, and rituximab.
Outcomes
All 4 systematic reviews18-21 reported relapse-related outcomes and disability status. Two systematic reviews20,21 reported adverse events and death. One systematic review21 also reported MRI-related disease activity, AQP-4 antibody titres, pain and fatigue (each measured by a numerical rating scale with an unreported range). The specific outcomes for relapse included: annualized relapse rate (ARR), relapse-free rate, hazard risk for relapse and time to first relapse. Disability status was assessed by the Expanded Disability Status Scale (EDSS)27 and ambulatory status. EDSS is a formal scale with possible scores ranging from 0 to10 with higher scores indicating greater disability, while ambulatory status was not a formal scale with the following options: unrestricted, restricted, wheelchair, cane, or walker.28 The mean or median follow-up duration ranged from 16 months to 78.9 months in 1 systematic review,18 12 months to 31 months in the second systematic review,19 12 months to 31.8 months in the third systematic review,20 and 3 months to 80 months in the fourth systematic review.21
One retrospective observational before-and-after study23 reported relapse-related outcomes (including ARR, relapse-free rate, time to the first relapse and risk factors for relapse), disability status, and adverse events with a median follow-up of 34 months. The other retrospective observational study22 reported the changes in visual acuity measures and imaging features (OCT) with a median follow-up ranging from 13 months to 14.6 months.
The included guideline24 considered the relapse risk, disability, and safety outcomes. For some recommendation statements, the costs were considered.
Summary of Critical Appraisal
Systematic Reviews
In all 4 systematic reviews,18-21 the objective was clearly described, multiple databases were searched, keywords of the search and study selection flow charts were provided, the review authors declared no conflicts of interest, lists of included articles were presented and the study characteristics were described. None of the systematic reviews18-21 provided lists of excluded articles or assessed the funding sources in individual studies. Two systematic reviews18,21 did not report performing a grey literature search. These limitations may result in the inappropriate exclusion of some studies, missing some unpublished studies or misidentification of potential publication bias. In 1 systematic review,20 article selection and data extraction were done independently by 2 reviewers. In 2 systematic reviews,18,21 it was unclear how article selection and data extraction were conducted. In the fourth systematic review,19 the article selection was done independently by 2 reviewers, but it was unclear how the data extraction was performed, The possibility of missing some relevant articles or errors in data extraction cannot be ruled out. Although 3 systematic reviews18-20 assessed the risk of bias of included individual studies (and reported study quality to be “satisfactory” or “Newcastle-Ottawa Scale score ranged from 5 to 7” for observational studies [1 systematic review20 presented the overall rating for 6 individual studies: 5 high risk of bias and 1 low risk of bias]; with “some concerns” in risk of bias for the included RCT), they did not assess the potential impact of study risk of bias on the interpretation of results. One systematic review21 did not assess the risk of bias of included individual studies, so the quality of these studies is unknown. The results may be driven by individual studies with high risk of bias.
One systematic review18 compared the effectiveness of TCZ and AZA, but only included the TCZ arm of the TANGO trial and left the direct comparison between the 2 drugs out of the pooled analysis. Instead, the systematic review authors pooled data from single-arm trials of TCZ and AZA, and then used the Douglas G test of interaction25 to compare the difference in ARR between the 2 drug groups. This method did not adjust potential confounding factors and cannot take the advantage of randomization in the primary RCT, which only can provide indirect evidence and is likely an inappropriate analysis method for indirect comparisons. This systematic review18 also misinterpreted the P values for effect size and used a fixed-effect model for meta-analysis with moderate heterogeneity, which will result in a narrow confidence interval and in favour of interventions that compared a random-effect model. One systematic review21 summarized findings from individual studies narratively, and some outcome measures (fatigue and ambulatory status) were not validated.
Among the 3 systematic reviews18,20,21 that included the TANGO trial (which provided the only direct comparison between TCZ and AZA among all included primary studies), 2 systematic reviews18,20 assessed the risk of bias for the TANGO trial. One systematic review20 reported the TANGO trial had a high risk of bias in the deviation from the intended intervention domain and an unclear risk of bias in the missing outcome data domain based on Cochrane’s risk of bias tool. This RCT was assessed as having “some concerns” by systematic review authors. The other systematic review18 reported that 2 stars for “selection,” 1 star for “comparability,” an 3 stars for “outcome” based on the Newcastle-Ottawa Scale (no further information was available about how the risk of bias assessments were conducted and the meaning of the risk of bias).
Retrospective Observational Studies
The 2 retrospective observational studies22,23 clearly reported study objectives, inclusion and exclusion criteria, intervention details, participant characteristics, outcome measures, and the main findings. The 2 studies used appropriate statistical analysis methods for comparing changes before-and-after the intervention. Both studies22,23 were funded by academic institutions in China, which may have little influence on potential publication bias. Neither study22,23 conducted sample size calculations, which may result in underpowering for detecting the changes in visual acuity or pain measures. One study23 used a before-after design without a control group. Due to the nature of the design, it is difficult to attribute the before-and-after changes to the effect of TCZ. In this study,23 the authors did not describe the secondary outcome measures well (disability and pain) and the covariates in the logistic regression models. In the other study,22 the authors did not provide detailed information on changes in visual acuity measures, the number of eyes in each drug group, and the covariates in the generalized estimating equations.
Evidence-Based Guideline
The critical appraisal of the included clinical practice guideline24 was performed in a previous CADTH report on rituximab for NMOSD.29 More details about the quality of the guideline can be found in the reports. Briefly, the guideline had clear descriptions of scope, population, target users, guideline developers, and was externally peer-reviewed. The guideline had a transparent literature search and recommendation development methods based on consensus and voting, but the evidence assessment and strength of the recommendations were unclear. Although several authors declared the conflicts of interest, how these were addressed is unclear.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
Three included systematic reviews18,20,21 included the TANGO trial, which was an RCT that compared TCZ and AZA.26 Two reviews18,20 only included data from the TCZ arm of the trial, and the third systematic review21 included data from the 2 arms; however, they included the interim analysis for the TANGO trial as the final results of this trial were not available at that time. The directions of all reported outcomes in the interim analysis were the same as the final trial result report. In this report, we summarized the main findings of the trial based on the final report26 rather than the interim analysis. Appendix 4 presents the main study findings.
Due to some overlap in the studies included in the systematic reviews (Appendix 5), the pooled estimates from these systematic reviews may contain some of the same data. For the systematic reviews without a meta-analysis that narratively summarized the findings on the same outcome,20,21 to avoid duplication of results, outcome data from an individual primary study are only reported once.
Clinical Effectiveness of TCZ
Relapse-Related Outcomes
Four systematic reviews18-21 reported on ARR, mostly based on findings from single-arm trials. Three systematic reviews18-20 showed that pooled estimates of ARR were statistically significantly reduced after TCZ treatment compared with before TCZ treatment. One systematic review21 reported mean or median changes in ARR for the individual included studies and showed that ARR values were numerically lower after TCZ treatment than before TCZ treatment. The included before-after study23 also showed that the ARR values were statistically significantly reduced after TCZ treatment compared with before TCZ treatment. One systematic review18 reported that ARR was statistically significantly lower with TCZ than AZA, based on indirect comparisons of pooled TCZ and AZA findings from separate, single-arm studies. Moderate to substantial statistical heterogeneities were found in this systematic review18 for TCZ and AZA arms.
One systematic review21 (presenting findings from the TANGO trial26) and 1 before-after study23 reported relapse-free rates. The proportion of patients who were relapse-free was 76.9% from 1 observational study with a median follow-up of 34.1 months after TCZ treatment.23 The systematic review21 narratively summarized the findings of 2 individual included case series and reported 70.3% of patients were relapse-free after TCZ treatment with an unclear follow-up period. The proportion of patients who were relapse-free at the end of the study (up to 92 weeks of follow-up) was statistically significantly higher in the TCZ arm (89%) compared with the AZA arm (56%) in the TANGO trial.26 The before-after study23 showed that the median time to first relapse was 62 weeks for patients treated with TCZ, and identified an infusion interval of more than 4 weeks and pGFAP greater than 220 pg/mL as statistically significant risk factors for relapse with very wide confidence intervals (i.e., low precision). There was a trend for TCZ monotherapy to increase the risk of relapse, but this did not reach statistical significance.
Disability
Three systematic reviews18-20 reported that pooled estimates of EDSS were statistically significantly reduced after TCZ treatment compared with before TCZ treatment. Moderate statistical heterogeneities were found in 2 systematic reviews.18,19 One systematic review21 narratively summarized EDSS findings from 10 observational studies (case reports included) and reported 6 individual studies with “significant” EDSS improvement, 2 studies with “mild” improvement, and 2 studies with “unchanged” in EDSS after TCZ treatment. Levels of EDSS improvement were not otherwise defined by systematic review authors. This systematic review also narratively summarized the difference in EDSS between patients treated with TCZ and AZA from the TANGO trial. Presenting findings from the TANGO trial publication,26 there was a statistically significantly lower disability progression rate measured by EDSS in the TCZ group than in the AZA group after 12 weeks of treatment (5 of59 versus 15 of 59, HR: 0.288; 95% CI, 0.105 to 0.759; P = 0.0087). The study authors concluded the same at 24 weeks of treatment; however, the statistical test results for comparing the 2 groups on disability progression were inconsistent within the trial publication at this time point (2 of 59 versus 5 of 59, HR: 0.221; 95% CI, 0.047 to 1.042; P = 0.0309 in the main text; P = 0.0004 in Table 2). The TANGO trial considered the minimally important difference for EDSS as validated for patients with multiple sclerosis (i.e., “disability progression” was defined as an increase in EDSS of at least 1.0 if baseline score was 5.5 or less; at least of 0.5 if baseline score was great than 5.5). The included before-after study23 also showed that the median EDSS scores were statistically significantly reduced after TCZ treatment compared with before treatment both for AQP4-antibody positive and negative patients.
One systematic review21 identified a case series (with 12 patients) that reported on ambulatory status and found that most patients (n = 9) had stable ambulatory status after TCZ treatment.
Adverse Events
Two systematic reviews20,21 and 1 before-and-after study23 reported adverse events in patients with NMOSD who received TCZ treatment. One systematic review20 showed that the pooled estimate of the proportion of patients with any adverse events was 56%, and the proportion of patients with serious adverse events was 11%. One systematic review21 that included findings from the TANGO trial reported that the proportions of patients with at least 1 adverse event were 97% (61% treatment-related adverse events as determined by the trial authors) in the TCZ arm and 95% (83% treatment-related adverse events as determined by the trial authors) in the AZA arm and the proportions of patients with at least 1 serious adverse event was 8% and 15%, respectively (without statistical test). The serious adverse events included pneumonia, herpes zoster infection, deep vein thrombosis, basal ganglia hemorrhage, and myelitis.
Mortality
One systematic review21 identified 3 deaths. One occurred in 1 of the included observational studies, and 2 occurred in the TANGO trial (1 for each arm). The trial and the systematic review authors noted these deaths are unlikely related to the treatment.
Pain and Fatigue
One systematic review21 and 1 before-after study reported on pain outcomes measured by the numerical rating scale. The systematic review showed that pain scores were numerically lower after 12 months of TCZ treatment compared with before TCZ treatment (without statistical test). However, the before-after study23 reported the pain score remained unchanged after TCZ treatment (median follow-up of 34.1 months) compared with before TCZ treatment (without statistical test). Based on findings from individual included studies, 1 systematic review21 reported that the general fatigue scores (no details on the measures) were numerically lower after TCZ treatment compared with before TCZ treatment (without statistical test).
Other Outcomes
One observational study22 reported eye- and vision-related outcomes in patients with NMOSD who were treated with TCZ, rituximab, or AZA and compared the changes in eye measures between patients and heathy controls. This study concluded that there were no changes in LogMAR visual acuity or low-contrast letter acuity either in NMOSDON+ eyes (eyes with a history of acute optic neuritis attack) or NMOSDON- eyes (eyes without a history of acute optic neuritis attack) after TCZ, AZA and rituximab treatment compared with baseline. No data were reported to support conclusions on visual acuity. The study also reported OCT measures of eyes and noted that patients treated with TCZ and rituximab did not display macular ganglion cell complex or peripapillary retinal nerve fibre layer thinning in NMOSDON- eyes, while patients treated with AZA showed statistically significant macular ganglion cell complex or peripapillary retinal nerve fibre layer thinning in NMOSDON- eyes. NMOSD patients treated with AZA showed statistically significant greater thinning in macular ganglion cell complex or peripapillary retinal nerve fibre layer measures compared with patients treated with TCZ and rituximab in NMOSDON- eyes. These measures may serve as indicators of retinal ganglion cell loss.
One systematic review21 also reported MRI-related disease activity measures and AQP4-and myelin oligodendrocyte glycoprotein antibody titres in patients with NMOSD after TCZ treatment but noted that the 2-antibody status was not correlated with a higher risk of relapse.
Cost-Effectiveness of TCZ
No cost-effectiveness evidence regarding TCZ for patients with NMOSD was identified; therefore, no summary can be provided.
Evidence-Based Guidelines Regarding the Use of TCZ
The clinical practice guidelines24 from Latin America presents statements on various treatments for patients with NMOSD, described in detail in a previous CADTH report.29 For long-term relapse prevention, the guideline recommends the early start of immunosuppressant treatments to reduce disease activity and prevent NMOSD attacks. Immunosuppressant treatments addressed by this guideline include AZA, MMF, rituximab, TCZ, eculizumab, satralizumab, inebilizumab, and oral steroids.
TCZ is suggested as 1 of the second-line treatment options for patients who have no response to other immunosuppressants to prevent long-term relapse prevention (Appropriate, 90% agreement). Eculizumab, inebilizumab, and satralizumab also can be used under these conditions; the guideline did not favour a particular humanized monoclonal antibody for second-line therapy. When starting immunosuppressant treatment (AZA, MMF, or rituximab), oral steroid tapering or maintained therapy were suggested in this guideline; however, this guideline did not mention whether adding TCZ should be combined with the oral steroid therapy. This guideline did not report the strength of the recommendations or the quality of evidence informing the recommendations, though the authors cited the TANGO trial26 and 1 observational study to support the statement regarding TCZ. The 2 studies were captured by systematic reviews included in this report.
Limitations
Although we identified 4 systematic reviews18-21 and 2 retrospective observational studies22,23 to answer the research question on the clinical effectiveness of TCZ, most included primary studies in these systematic reviews were uncontrolled before-after studies or case reports, except for 1 RCT. This RCT (with “some concerns” according to systematic review authors20) overlapped among 3 systematic reviews, and an overlap matrix of relevant primary studies (Appendix 5) reveals that more recent systematic reviews do not substantially build on the evidence base. Due to the nature of the observational studies, potential selection bias, recall bias or performance bias in the body of evidence cannot be ruled out. Potentially inappropriate indirect comparisons of pooled estimates may amplify the bias. The quantity and quality of evidence regarding pain and fatigue were limited. The death events (n = 3) were low among included studies, and the comparison of TCZ and other immunosuppressants on mortality was not determined.
TCZ and other antibodies are usually expensive compared with traditional oral drugs (e.g., AZA), and patients underwent prolonged infusion intervals mainly due to economic burden.23 Cost-effectiveness will be essential for future decision-making. However, we did not find any cost-effectiveness studies of TCZ among patients with NMOSD.
Most eligible patients for the included studies were adults and most (over 80%) of them are female, which reflects the prevalence of NMOSD worldwide.2 However, the data did not allow us to comment on the subgroup effects of the pediatric population and the male population. When applying the evidence to these minor populations, one might need to consider the applicability of the evidence to the target population. The management of patients with NMOSD involved many drugs and the usual care may differ across different studies. Observational studies, especially for uncontrolled before-after studies, may not account for these differences, and it is unclear to what extent the difference in outcome measures between studies can be attributed to different usual care therapies. The variabilities in add-on drugs, treatment intervals, or comorbidities in the primary studies were probably some reasons for the observed heterogeneity in the pooled estimates. The current report did not identify comparisons of TCZ versus other immunosuppressant treatments such as satralizumab, MMF, methotrexate, cyclophosphamide, cyclosporine, prednisone, eculizumab, inebilizumab, and rituximab. Furthermore, the identified guideline24 did not address the place in therapy for TCZ relative to other second-line treatment options. Together, it remains unclear which patients may benefit from TCZ compared to alternative immunosuppressant therapies, particularly other humanized monoclonal antibodies.
The primary studies of the included systematic reviews18-21 were conducted in Asia, Europe, and the US. The clinical practice guideline24 was from Latin America and considered the local cost in Latin America. Thus, the generalizability of these findings to settings in Canada is uncertain.
Conclusions and Implications for Decision- or Policy-Making
Four systematic reviews18-21 and 2 observational studies22,23 were identified to address the clinical effectiveness of TCZ for patients with NMOSD. Evidence from before-and-after studies without a control group suggests that patients treated with TCZ had statistically significantly reduced ARR and EDSS compared with before TCZ treatment. Evidence from 2 systematic reviews18,21 indicated that TCZ may be better than AZA to manage patients with NMOSD in reducing the relapse risk and increasing the relapse-free rate. However, these findings were based on a single RCT26 and an indirect comparison of pooled findings from single-arm trials, which did not account for confounding variables. One before-and-after study23 without a control group, identified infusion interval of more than 4 weeks and pGFAP greater than 220 pg/mL as risk factors for relapse, but the confidence intervals were very wide (i.e., low precision). Using TCZ may slow disability progression compared with AZA; however, some observational studies showed the EDSS scores were unchanged after TCZ treatment. The adverse events were common during the treatment. However, the proportion of adverse events was similar between TCZ and AZA, and the proportions of treatment-related adverse events and serious adverse events were numerically higher in the AZA group than in the TCZ group. The serious adverse events included pneumonia, herpes zoster infection, deep vein thrombosis, basal ganglia hemorrhage, and myelitis. Based on a retrospective study,22 TCZ treatments may have little or no impact on visual acuity function but may have some benefits in OCT measures. The impacts of TCZ on pain and fatigue were inconsistent: some studies in 1 included systematic review21 showed numerically lower scores (pain and fatigue), while another study23 with a longer follow-up did not show any changes in pain measure scores.
One evidence-based clinical practice guideline24 from Latin America suggests that TCZ can be used for patients with NMOSD who have no response to other immunosuppressants to prevent long-term relapse. However, this guideline did not report the strength of the recommendation or the quality of evidence informing the recommendation. The available evidence identified for this report suggests TCZ can be potentially used before AZA when considering the relapse outcomes and disability status, but the quality of evidence was low. Future guidelines may need to consider all related evidence regarding benefits and harms to make transparent and trustworthy recommendations. Considering the limitations of the body of evidence, such as the limitation of observational studies with before-and-after study designs without a control group, and the potentially inappropriate indirect comparison of pooled estimates, these findings should be interpreted with caution. In addition, the generalizability of the evidence to settings in Canada or minor NMOSD populations (e.g., pediatric, male) was unclear.
Cost-effectiveness will be helpful for decision- or policy-making. However, no evidence regarding the cost-effectiveness of TCZ for patients with NMOSD was identified that met the inclusion criteria for this report. TCZ requires IV or subcutaneous administration; patients’ values or preferences regarding injection and oral medicine also may affect the decision-making.30
To compare the clinical effectiveness of TCZ to other pharmacological therapies or no treatment, we should consider both direct and indirect evidence. The evidence synthesis by 1 included systematic review18 omitted the direct comparison from the TANGO trial that directly compared TCZ versus AZA. To help decision-making regarding the use of TCZ for NMOSD, we need to consider it relative to other immunosuppressant treatments, including other humanized monoclonal antibodies recommended for second-line therapy. However, an available systematic review with network meta-analysis31 did not include TCZ. When possible, given the availability of trials that address the relative effects of AZA versus other treatments, a systematic review with network meta-analysis may be helpful to answer the question. Future primary studies with a robust methodology, such as those with prospective designs or RCTs, comparing TCZ with other immunosuppressants, are also required.
References
1.Glisson CC. Neuromyelitis optica spectrum disorders (NMOSD): clinical features and diagnosis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2023: https://www.uptodate.com/contents/neuromyelitis-optica-spectrum-disorders-nmosd-clinical-features-and-diagnosis. Accessed 2023 Mar 3.
2.Papp V, Magyari M, Aktas O, et al. Worldwide incidence and prevalence of neuromyelitis optica: a systematic review. Neurology. 2021;96(2):59-77. PubMed
3.Lee JD, Guimond C, Yee IM, et al. Incidence of multiple sclerosis and related disorders in Asian populations of British Columbia. Can J Neurol Sci. 2015;42(4):235-241. PubMed
4.Huda S, Whittam D, Bhojak M, Chamberlain J, Noonan C, Jacob A. Neuromyelitis optica spectrum disorders. Clin Med (Lond). 2019;19(2):169-176. PubMed
5.Wingerchuk DM, Hogancamp WF, O'Brien PC, Weinshenker BG. The clinical course of neuromyelitis optica (Devic's syndrome). Neurology. 1999;53(5):1107-1114. PubMed
6.Ma X, Kermode AG, Hu X, Qiu W. NMOSD acute attack: understanding, treatment and innovative treatment prospect. J Neuroimmunol. 2020;348:577387. PubMed
7.Glisson CC. Neuromyelitis optica spectrum disorders (NMOSD): treatment and prognosis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2023: https://www.uptodate.com/contents/neuromyelitis-optica-spectrum-disorders-nmosd-treatment-and-prognosis. Accessed 2023 Mar 3.
8.Pharmacoeconomic report: satralizumab (enspryng): (Hoffmann-La Roche Limited): indication: neuromyelitis optica spectrum disorder. (CADTH Common Drug Review). Ottawa (ON): CADTH; 2021: https://www.ncbi.nlm.nih.gov/books/NBK583281/. Accessed 2023 Mar 3.
9.Scott LJ. Tocilizumab: a review in rheumatoid arthritis. Drugs. 2017;77(17):1865-1879. PubMed
10.CADTH Canadian Drug Expert Committee recommendation: tocilizumab (actemra - Hoffmann-La Roche Limited): indication: giant cell arteritis. Ottawa (ON): CADTH; 2018: https://www.ncbi.nlm.nih.gov/pubmed/30427624. Accessed 2023 Mar 3.
11.Ghosn L, Chaimani A, Evrenoglou T, et al. Interleukin-6 blocking agents for treating COVID-19: a living systematic review. Cochrane Database Syst Rev. 2021;3(3):CD013881. PubMed
12.Chihara N, Aranami T, Sato W, et al. Interleukin 6 signaling promotes anti-aquaporin 4 autoantibody production from plasmablasts in neuromyelitis optica. Proc Natl Acad Sci U S A. 2011;108(9):3701-3706. PubMed
13.Liu Y, Zhang H, Zhang TX, et al. Effects of tocilizumab therapy on circulating B Cells and T helper cells in patients with neuromyelitis optica spectrum disorder. Front Immunol. 2021;12:703931. PubMed
14.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
15.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
16.Agree Next Steps Consortium. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2023 Mar 3.
17.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
18.Tang Q, Yao M, Huang Y, Bian J, Wang Y, Ji W. A comparison of the efficacy of tocilizumab versus azathioprine for neuromyelitis optica spectrum disorder: a study protocol for systematic review and meta-analysis. Medicine (Baltimore). 2023;102(4):e32748. PubMed
19.Luitel P, Ghimire A, Upadhyay D, Ojha R. Efficacy of monoclonal antibodies in neuromyelitis optica: an updated systematic review with meta-analysis. Clin Exp Neuroimmunol. 2022;13(4):194-207.
20.Kharel S, Shrestha S, Ojha R, Guragain N, Ghimire R. Safety and efficacy of interleukin-6-receptor inhibitors in the treatment of neuromyelitis optica spectrum disorders: a meta-analysis. BMC Neurol. 2021;21(1):458. PubMed
21.Lotan I, McGowan R, Levy M. Anti-IL-6 therapies for neuromyelitis optica spectrum disorders: a systematic review of safety and efficacy. Curr Neuropharmacol. 2021;19(2):220-232. PubMed
22.Zeng P, Du C, Zhang R, et al. Optical coherence tomography reveals longitudinal changes in retinal damage under different treatments for neuromyelitis optica spectrum disorder. Front Neurol. 2021;12:669567. PubMed
23.Yang S, Zhang C, Zhang TX, et al. A real-world study of interleukin-6 receptor blockade in patients with neuromyelitis optica spectrum disorder. J Neurol. 2023;270(1):348-356. PubMed
24.Carnero Contentti E, Rojas JI, Cristiano E, et al. Latin American consensus recommendations for management and treatment of neuromyelitis optica spectrum disorders in clinical practice. Mult Scler Relat Disord. 2020;45:102428. PubMed
25.Altman DG, Bland JM. Interaction revisited: the difference between two estimates. BMJ. 2003;326(7382):219. PubMed
26.Zhang C, Zhang M, Qiu W, et al. Safety and efficacy of tocilizumab versus azathioprine in highly relapsing neuromyelitis optica spectrum disorder (TANGO): an open-label, multicentre, randomised, phase 2 trial. Lancet Neurol. 2020;19(5):391-401. PubMed
27.Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology. 1983;33(11):1444-1452. PubMed
28.Lotan I, Charlson RW, Ryerson LZ, Levy M, Kister I. Effectiveness of subcutaneous tocilizumab in neuromyelitis optica spectrum disorders. Mult Scler Relat Disord. 2019;39:101920. PubMed
29.Banerjee S, Butcher R. Rituximab for the treatment of neuromyelitis optica spectrum disorder. (CADTH Health Technology Review). Can J Health Technol. 2021;1(2). https://www.cadth.ca/sites/default/files/pdf/htis/2021/RD0058%20Rituximab%20for%20NMOSD%20Final.pdf. Accessed 2023 Mar 3.
30.González-González JG, Diaz Gonzalez-Colmenero A, Millan-Alanis JM, et al. Values, preferences and burden of treatment for the initiation of GLP-1 receptor agonists and SGLT-2 inhibitors in adult patients with type 2 diabetes: a systematic review. BMJ Open. 2021;11(7):e049130. PubMed
31.Huang W, Wang L, Zhang B, Zhou L, Zhang T, Quan C. Effectiveness and tolerability of immunosuppressants and monoclonal antibodies in preventive treatment of neuromyelitis optica spectrum disorders: a systematic review and network meta-analysis. Mult Scler Relat Disord. 2019;35:246-252. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that these tables have not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Tang et al. (2023)18 China Funding source: No funding and conflicts of interest disclosed. | Study design: systematic review of primary studies was registered on PROSPERO (CRD42022346673) Number of included studies: 27 | Patients with NMOSD meeting the diagnostic criteria in 2006 or 2015 TCZ: N = 148 (number in the individual studies ranged from 3 to 59) AZA: N = 930 (number in individual studies ranged from 13 to 119) Sex: female predominance (TCZ: n = 136, 92%; AZA: n = 802, 86%) Mean age of onset: TCZ: 42.3 years; AZA: 37.5 years Mean disease duration: TCZ: 5.5 to 10.7 years AZA: 0.6 to 15 years AQP4 antibody positivity: TCZ: 85.8%; AZA unclear. | Intervention: TCZ Dosage: NR Route of administration: NR Comparator: AZA Dosage: NR Route of administration: NR | Outcomes:
Mean or median follow-up:
|
Luitel et al. (2022)19 Nepal Funding source: the authors declared no conflict of interest. | Study design: systematic review of primary studies Number of included studies: 36 articles (8 were relevant to the current report). | Patients with NMO (any age, sex or nationality) N = 59 (number in individual studies ranged from 3 to 14) Sex: female predominance (n = 51, 86%) Mean age: ranging from 29 to 50 Mean disease duration: 1.9 to 6.8 years AQP4 antibody positivity: 14% to 100% | Intervention: Monoclonal antibodies (TCZ was relevant to the current report) TCZ dosage: NR Route of administration: NR Comparator: no comparator group | Outcomes:
Mean or median follow-up: 12 to 31 months |
Kharel et al. (2021)20 Nepal Funding source: None | Study design: systematic review of primary studies was registered on PROSPERO (CRD42021226900) Number of included studies: 9 articles in qualitative synthesis and 7 articles in quantitative synthesis (7 were relevant to the current report). | Patients with NMOSD or NMO (any age or nationality) N = 98 (number in individual studies ranged from 3 to 59) Sex: female predominance (n = 90, 92%) Age ranging from 12 to 68 years; Mean age: ranging from 29 to 50 Mean disease duration: 2.3 to 8.2 years AQP4 antibody positivity: 40% to 100% | Intervention: IL-6 receptor inhibitors (TCZ was relevant to the current report) TCZ dosage: IV 6mg or 8 mg/kg/4 or 6 weeks or subcutaneous dose of 162mg every 1 to 2 weeks. Add-on drugs: AZA and mycophenolate mofetil were most common Comparator: no comparator group | Outcomes:
Mean or median follow-up: 12 to 31.8 months |
Lotan et al. (2021)21 US and Israel Funding source: None | Study design: systematic review of primary studies including case reports. Number of included studies: 25 articles (19 were relevant to the current report: 12 case reports; 6 case series; 1 RCT). | Patients with NMOSD N = 230 (number in individual studies ranged from 1 to 118) Sex: NR Mean age: NR Mean disease duration: NR AQP4 antibody positivity: 81.3% | Intervention: anti-IL-6 monoclonal antibody: TCZ and satralizumab (TCZ was relevant to the current report) IV 6mg-8 mg/kg/4 or 6 weeks or subcutaneous dose of 162mg every 1 to 2 weeks. Comparator: AZA: oral medicine, dose of 2 to 3 mg/kg/day; no comparator group | Outcomesa:
Mean or median follow-up: 3 to 80 months |
AQP4 = aquaporin 4; ARR = annualized relapse rate; AZA = azathioprine; EDSS = Expanded Disability Status Scale; MOG = myelin oligodendrocyte glycoprotein; NA = not applicable; NMO = neuromyelitis optica; NMOSD = neuromyelitis optica spectrum disorder; NR = not reported; TCZ = tocilizumab.
aThe systematic review included the interim analysis for the RCT due to the final results of this study have not been published, in this table, the RCT data from the final publication.26
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Yang et al. (2023)23 China Funding source: National Natural Science Foundation of China and Tianjin Province | Retrospective case series with before-and-after comparisons | Adults (18+ years) diagnosed with NMOSD based on the 2015 international panel for Neuromyelitis Optica Diagnosis criteria and received TCZ treatment. Exclusion criteria: patients who were treated with other immunosuppressants within the expected pharmacodynamics effect window before TCZ initiation; B-cell count < lower limit of normal; patients with a history of clinically significant infection, with heart, liver, or kidney insufficiency or with tumour disease currently or within past 5 years. Sex: 92.3% females Age at disease onset: median (IQR): 44.2 (40.6, 47.8) AQP4-IgG positivity: 54 (83.1%) Number of patients: n = 65 | Intervention: TCZ (IV 8 mg/kg; infusion interval 4 weeks, 6 weeks or 8 weeks) Comparator: No comparator group | Outcomes:
Follow-up: median (IQR): 34.1 (25.5 to 39.3) months |
Zeng et al. (2021)22 China Funding source: National Natural Science Foundation of China and Tianjin Province | Retrospective observational study | Confirmed diagnosis of AQP4-IgG seropositive NMOSD patients based on the 2015 international consensus criteria and complete clinical and OCT imaging data with a minimum 1-year follow-up. Age: 18 to 75 years Exclusion criteria: less than 6 months after ON onset; experienced a new ON attract during follow-ups; spherical equivalent > 2 diopters; intraocular pressure > 21 mm Hg; history of ocular surgery, laser treatment, or ocular trauma or other ocular diseases other than cataract, such as glaucoma, uveitis, or retinal diseases; history of; systemic diseases. Sex: 49 females in the patient group and 9 females in the healthy control group. Number of participants: 50 patients and 10 healthy controls. | Intervention: TCZ (IV infusion at the dose of 8 mg/kg/month) Rituximab (IV, dose according to the proportion of B-cells) AZA (oral medicine at the dose of 2 to 3 mg/kg/day) Comparators: Within group (change from baseline) and between-group (TCZ, rituximab, AZA) comparisons Healthy controls without any intervention | Outcomes:
Follow-up (median):
|
AZA = azathioprine; IQR = Interquartile range; logMAR = logarithm of the minimum angle of resolution; OCT = optical coherence tomography; ON = Optic neuritis; TCZ = tocilizumab.
Table 4: Characteristics of Included Guideline
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
Carnero Contentti et al. (2020)24 | ||||||
Intended users: Clinicians involved in the management of patients with NMOSD in Latin America Target population: patients with NMOSD in Latin America | NMOSD diagnosis, prognosis, management and treatment. Interventions include IVMP, oral steroids, PLEX, AZA, MMF, RTX, tocilizumab, eculizumab, inebilizumab, satralizumab, and mitoxantrone | Relapse risk, disability, safety and local cost in Latin America. | A systematic search of the literature, without language restrictions, was carried out on MEDLINE and Embase from (1990 to 2019) Methods for evidence synthesis were unclear. | NR | The guideline development panel comprised experts who were involved in the diagnosis and care of NMOSD patients in neurology in different regions of Latin America. To achieve consensus, the RAND/UCLA methodology of reaching formal consensus was used through iterative ratings with feedback from representatives and professionals.a A steering group (2 chairpersons and a project manager) developed a list of proposals and submitted them to the rating group (8 professionals). The rating group voted for statements based on published evidence. The consensus was defined as 70% agreement among the group. For statements in which there was no consensus, 2 further rounds of voting were conducted. Then the steering group draft the initial version of the guideline and submitted it to peer review and finalized the guideline. | The guideline report was externally peer-reviewed. |
AZA = azathioprine; IVMP = IV methylprednisolone; MMF = mofetil mycophenolate; NMOSD = neuromyelitis optica spectrum disorder; NR = not reported; PLEX = plasmapheresis; RTX = rituximab.
aRAND/UCLA methodology is an appropriateness method developed by RAND corporation and the University of California Los Angeles.
Appendix 3: Critical Appraisal of Included Publications
Note that these tables have not been copy-edited.
Table 5: Strengths and Limitations of Systematic Reviews Using AMSTAR 214
Strengths | Limitations |
|---|---|
Tang et al. (2023)18 | |
The purpose of the study was clearly described. The protocol of this review was prospectively registered in the PROSPERO. Multiple databases were searched (PubMed, MEDLINE, Embase and CENTRAL databases). Medical subject headings and related entry terms were provided. A flow chart of study selection was provided. The details of included studies were adequately described. The review authors assessed the RoB for eligible studies using the Newcastle-Ottawa Scale. Publication bias were assessed using the Egger test and funnel plots. Sensitivity analyses were conducted. The review authors reported no conflicts of interest. | The intervention, comparator, and study designs of the individual study for inclusion were not clearly described. The full search strategy was not available. A grey literature search was not reported. The study selection process and data extraction were unclear. The list of excluded studies was not provided. The review authors did not report the sources of funding for eligible studies. The fixed-effect model was used for meta-analysis, but with moderate heterogeneity, the random-effect model would be more appropriate. The review authors did not assess the potential impact of RoB in individual studies on result interpretations. The review authors misinterpreted the statistical combinations and referred to wrong p values for pooled effect size. No explanation for the observed heterogeneity in the results. No direct comparison data were included from the TANGO randomized controlled trial. |
Luitel et al. (2022)19 | |
The purpose of the study was clearly described. The study designs of the individual study for inclusion were clearly described. Multiple databases were searched (PubMed, Scopus, Embase, Google Scholar). Medical subject headings and related entry terms were provided. The search strategy was provided. A grey literature search (unpublished study) and screening the references of the included studies and the previous systematic review were conducted. A flow chart of study selection was provided. The study selection process was clearly described and conducted by 2 reviewers. The details of included studies in were adequately described. The review authors assessed the RoB for eligible studies using the JBI Quality Appraisal Tool. The review authors use appropriate methods for statistical combination of results. Publication bias were assessed using the Egger test and funnel plots. Sensitivity analyses were conducted. The review authors provided explanations for the observed heterogeneity. The review authors declared no conflicts of interest. | The diagnostic criteria of NMOSD were not clearly described. It was unclear if the data extractions were conducted by 2 authors independently. The list of excluded studies was not provided. The review authors did not report the sources of funding for eligible studies. The review authors did not assess the potential impact of RoB in individual studies on results interpretation. |
Kharel et al. (2021)20 | |
The purpose of the study was clearly described. The study designs of the individual study for inclusion were clearly described. Multiple databases (PubMed, Embase and the Cochrane Library) were searched. Medical subject headings for PubMed, Emtree terms for Embase were used in the search strategy. Keywords and the search strategies were described. The search was broadened to include preprint server, thesis repositories, expert inquiries. Additional search including manual searching of reference lists was conducted. The review authors assessed the RoB: Cochrane Collaboration’s RoB tool for RCT; NOS for observational studies. The review authors use appropriate methods for statistical combination of results. Publication bias were assessed using the Egger test and the visual inspection of funnel plots. Sensitivity analyses were conducted to check the robustness of results. A flow chart of study selection was provided. The study selection process, data extraction and RoB assessment were clearly described and conducted independently by 2 reviewers. The details of included studies in were adequately described. The review authors explored possible reasons of observed heterogeneity using meta-regression. The review authors declared no conflicts of interest. | The diagnostic criteria of NMOSD were not clearly described. The list of excluded studies was not provided. The review authors did not report the sources of funding for eligible studies. The review authors did not assess the potential impact of RoB in individual studies on the results of the meta-analysis and results interpretation. |
Lotan et al. (2021)21 | |
The purpose of the study was clearly described. Multiple databases were searched (PubMed, Embase and web of science databases). Medical subject headings and keywords were provided. A flow chart of study selection was provided. The details of included studies were adequately described. The review authors reported no conflicts of interest. | The intervention, comparator, outcomes, and study designs of the individual study for were not clearly described. The full search strategy was not available. A grey literature search was not reported. The study selection process and data extraction were unclear. The review authors did not assess the RoB for eligible studies and potential publication bias. The list of excluded studies was not provided. The review authors did not report the sources of funding for eligible studies. The review authors did not assess the potential impact of RoB in individual studies on result interpretations. Fatigue and ambulatory status measures were not validated. |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; ISPOR = International Society for Pharmacoeconomics and Outcomes Research; NA = not applicable; NR = not reported. RoB = risk of bias; RCT = randomized controlled trial; NOS = Newcastle-Ottawa Scale.
Table 6: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist15
Strengths | Limitations |
|---|---|
Yang et al. (2023)23 | |
The objectives of the study were clearly described. Inclusion and exclusion criteria were clearly described. The characteristics of participants (e.g., age, sex, disease duration) were clearly described. The primary outcome measures were clearly described. The intervention was clearly described. The main findings of the study were clearly described. The statistical analysis (paired t-test and Wilcoxon signed-rank test) was appropriate for comparing before-and-after outcomes. The adjusted ORs were calculated using the multivariable logistic regression model. The estimates of the variability (IQR or 95% CI) for the main outcomes were provided. The actual P values were reported. | The study did not conduct sample size calculations. No control groups. The secondary outcome measures (disability and pain) and the definitions of adverse events were unclear and were not mentioned in the methods section. In the adjusted logistic regression models, the covariates or confounding factors were unclear. |
Zeng et al. (2021)22 | |
The objectives of the study were clearly described. Inclusion and exclusion criteria were clearly described. Baseline characteristics of participants (e.g., age, sex, disease duration, follow-up time, visual acuity) were clearly described. The OCT measures were clearly described. The intervention was clearly described. The main findings of the study were clearly described. The statistical analysis considered the intereye correlation and used a generalized estimating equation analysis, which was appropriate for related measures. The actual change scores and P values for OCT measures were reported. | The study did not conduct sample size calculations. The number of eyes included in the analysis for each drug was unclear. The changes in visual acuity measures were not well described. OCT measures are surrogate outcomes for visual function. The covariates in the generalized estimating equation were unclear. |
IQR = interquartile range; OCT = Optical Coherence Tomography; ORs = odds ratios; CI = confidence interval.
Table 7: Strengths and Limitations of Guideline Using AGREE II16
Item | Guideline (2020)24 |
|---|---|
Domain 1: Scope and purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Not explicit but implied. |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes |
Domain 2: Stakeholder involvement | |
4. The guideline development group includes individuals from all relevant professional groups. | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes |
6. The target users of the guideline are clearly defined. | Yes |
Domain 3: Rigour of development | |
7. Systematic methods were used to search for evidence. | Yes |
8. The criteria for selecting the evidence are clearly described. | No |
9. The strengths and limitations of the body of evidence are clearly described. | No |
10. The methods for formulating the recommendations are clearly described. | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | To some extent but lacked details. |
12. There is an explicit link between the recommendations and the supporting evidence. | Unclear |
13. The guideline has been externally reviewed by experts before its publication. | Yes |
14. A procedure for updating the guideline is provided. | No |
Domain 4: Clarity of presentation | |
15. The recommendations are specific and unambiguous. | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes |
17. Key recommendations are easily identifiable. | Yes |
Domain 5: Applicability | |
18. The guideline describes facilitators and barriers to its application. | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No |
20. The potential resource implications of applying the recommendations have been considered. | No |
21. The guideline presents monitoring and/or auditing criteria. | No |
Domain 6: Editorial independence | |
22. The views of the funding body have not influenced the content of the guideline. | The authors reported that they did not receive any specific grant for the research. |
23. Competing interests of guideline development group members have been recorded and addressed. | Conflicts of interest were declared but it was unclear how they were addressed; several authors had received grants and/or consultation fees from pharmaceutical manufacturers. |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; NA = not applicable; NR = not reported.
Appendix 4: Main Study Findings
Note that these tables have not been copy-edited.
Table 8: Summary of Findings by Outcome — Relapse Risk
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
Group (number of studies or participants) or variables | Statistics | Effect size | I2 (%) | Notes | |
ARR | |||||
Tang et al. (2023)18 Systematic review with 27 articles | TCZ (8 studies) | Pooled SMD (95% CI) | −1.27 (−1.52 to −1.03) | 52.7 | Before-after |
AZA (15 studies) | Pooled SMD (95% CI) | −1.01 (−1.12 to −0.90) | 83.4 | Before-after | |
Comparison between TCZ and AZA pooled SMD | P value | 0.0314 | NA | Based on Douglas G test of interaction.25 | |
Luitel et al. (2022)19 Systematic review with 8 relevant articles | TCZ (6 studies) | Pooled SMD (95% CI) | −2.45 (−3.13 to −1.77) | 0 | Before-after |
Kharel et al. (2021)20 Systematic review with 7 relevant articles | TCZ (7 studies) | Pooled MD (95% CI) | −2.20 (−2.71 to −1.68) | 0 | Before-after |
Lotan (2021)21 Systematic review with 19 relevant articles | TCZ (5 case series) | Mean or median | Before: 1.8 to 3 After: 0 to 0.6 | NA | Before-after; authors concluded “Significant reduction” (no statistical tests reported) |
Yang (2023)23 Before-and-after study | TCZ (65 patients) | Median (range) | Before: 1.9 (0.1 to 6.3); After: 0.1 (0 to 1.4) | NA | P < 0.001 |
Relapse-free rate | |||||
Lotan et al. (2021)21 Systematic review with 19 relevant articlesa | TCZ (64 cases from case report) | n (%) | 45 (70.3%) | NA | NA |
TANGO: TCZ arm (n = 56) | n (%) | 50 (89%) | NA | NA | |
TANGO: AZA arm (n = 52) | n (%) | 29 (56%) | NA | NA | |
Comparison between TCZ and AZA within TANGO | HR (95% CI) | 0.188 (0.076 to 0.463) | NA | NA | |
Yang (2023)23 Before-after study | 65 patients | n (%) | 76.9% | NA | NA |
Time to first relapse | |||||
Yang (2023)23 Before-after study | 65 patients | Median (range), weeks | 62 (16 to 168) | NA | NA |
Risk factors for relapse | |||||
Yang (2023)23 Before-and-after study | AQP4-ab (+) | OR (95% CI) | 6.2 (0.4 to 92.0) | NA | NA |
Concomitant autoimmune disease | OR (95% CI) | 1.8 (0.4 to 9.2) | NA | NA | |
Infusion interval > 4 weeks | OR (95% CI) | 10.7 (1.6 to 71.4) | NA | NA | |
pGFAP > 220 pg/mL | OR (95% CI) | 20.6 (3.3 to 129.4) | NA | NA | |
TCZ monotherapy vs. TCZ plus corticosteroids | OR (95% CI) | 11.4 (0.8 to 166.4) | NA | NA | |
Age of disease onset (decades) | OR (95% CI) | 0.8 (0.5 to 1.5) | NA | NA | |
AQP4-ab = aquaporin antibody; ARR = annualized relapse rate; AZA = azathioprine; CI = confidence interval; HR = hazard ratio; IQR = interquartile range; MD = mean difference; NA = not applicable; NR = not reported; OR = odds ratio; pGFAP = plasma glial fibrillary acidic protein; SMD = standardized mean difference, TCZ = tocilizumab.
aThe systematic review included the interim analysis for the RCT as the final results of this study were not yet published. In this table, the RCT data are reported from the final publication.26
Table 9: Summary of Findings by Outcome — Disability
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
Treatment (number of studies or participants) | Statistics | Effect size | I2 (%) | Notes | |
EDSS | |||||
Tang et al. (2023)18 Systematic review with 27 articles | TCZ (8 studies) | Pooled SMD (95% CI) | −0.84 (−1.08 to −0.60) | 45.6 | Before-after |
Luitel et al. (2022)19 Systematic review with 8 relevant articles | TCZ (7 studies) | Pooled SMD (95% CI) | −1.10 (−1.75 to −0.44) | 51 | Before-after |
Kharel et al. (2021)20 Systematic review with 7 relevant articles | TCZ (4 studies) | Pooled MD (95% CI) | −0.79 (−1.89 to 0.31) | 0 | Before-after |
Lotan et al. (2021)21 Systematic review with 19 relevant articles | TCZ (10 studies) | Number of studies | Significant improvement (n = 6); Mild improvement (n = 2); Unchanged (n = 2) | NA | Before-after |
Yang et al. (2023)23 Before-after study | TCZ in AQP4-ab (+) patients (n = 54) | Median (range) | Before: 5.75 (1 to 8.5) After: 3.5 (0 to 8) | NA | P < 0.001 |
TCZ in AQP4-ab (-) patients (n = 11) | Median (range) | Before: 5 (1.5 to 6.0) After: 2.5 (0 to 5.5) | NA | P = 0.043 | |
Ambulatory status (no measurement details) | |||||
Lotan et al. (2021)21 Systematic review with 19 relevant articles | TCZ (12 cases from case series) | Number of patients | Improved ambulatory status (n = 2); stable state (n = 9) | NA | Before-after |
CI = confidence interval; EDSS = Expanded Disability Status Scale; MD = mean difference; NA = not applicable; NR = not reported. SMD = standardized mean difference TCZ = tocilizumab.
Table 10: Summary of Findings by Outcome — Adverse Events
Variable | Kharel 202120 Systematic review with 7 relevant articles | Lotan (2021)21 Systematic review with 19 relevant articlesa | Yang (2023)23 Before-after study | |||
|---|---|---|---|---|---|---|
Point estimate | 95% CI | Observational studies N = NR | TANGO RCT TCZ arm N = 59 | TANGO RCT AZA arm N = 59 | N = 65 | |
Any adverse events | ||||||
Overall proportions (%) | 56 | 27 to 85 | NR | 97 | 95 | NR |
Upper respiratory tract infections (n) | 49 | 3 | 17 | 23 | 8 | |
UTI (n) | 43 | 9 | 17 | 21 | 11 | |
Hypercholesterolemia (n) | 13 | 9 | NR | NR | 7 | |
Leucopenia or neutropenia (n) | 12 | 11 | 4 | 23 | NR | |
Fatigue (n) | 20 | 1 | 13 | 6 | 15 | |
Anemia (n) | 9 | 6 | 16 | 21 | NR | |
Hepatotoxicity or elevated liver enzymes (n) | NR | 3 | 18 | 27 | 28 | |
Nausea (n) | NR | 1 | 8 | 19 | NR | |
Infusion-related reactions (n) | NR | 2 | NR | NR | 5 | |
Any treatment-related adverse events (determined by study authors) | ||||||
Proportions (%) | NR | NR | 61 | 83 | NR | |
Serious adverse events | ||||||
Overall proportions (%) | 11 | 5 to 17 | NR | 8 | 15 | NR |
Pneumonia (n) | NR | NR | 2 | 1 | 3 | |
Herpes Zoster (n) | NR | NR | 1 | 2 | 4 | |
DVT (n) | NR | 1 | 1 | 1 | NR | |
Basal ganglia hemorrhage (n) | NR | NR | 1 | 0 | NR | |
Myelitis (n) | NR | NR | 1 | 0 | NR | |
Other serious adverse events (n) | NR | NR | 0 | 7 | NR | |
Death | ||||||
Death (n) | NR | 1 | 1 | 1 | NR | |
AZA = azathioprine; CI = confidence interval; DVT = deep vein thrombosis; NA = not applicable; NR = not reported; RCT = randomized controlled trial; SMD = standardized mean difference TCZ = tocilizumab; UTI = urinary tract infection.
aThe systematic review included the interim analysis for the RCT as the final results of this study were not yet published. In this table, the RCT data are reported from the final publication.26
Table 11: Summary of Findings by Outcome — Pain and Fatigue
Author (year) and study design | Resultsa | ||||
|---|---|---|---|---|---|
Number of patients | Pre-treatment, mean, SD or median, IQR | 6 months, mean, SD | After-treatment, mean, SD or median, IQR | Follow-up | |
Pain assessed by numerical rating (no measurement details) | |||||
Lotan et al. (2021)21 Systematic review with 19 relevant articles | 7 | 3.0 ± 1.3 | 1.3 ± 1.3 | 0.9 ± 1.2 | 12 months |
19 | 3.2 ± 2.2 | NR | 1.7 ± 2.6 | NR | |
8 | 6.5 (5.0 to 7.0) | NR | 2.5 (0.3 to 4.5) | NR | |
Yang et al. (2023)23 Before-after study | 34 | 2 (1.5 to 3.5) | NR | 2.5 (1.5 to 4.0) | 34.1 months |
Fatigue assessed by numeric levels (no measurement details) | |||||
Lotan et al. (2021)21 Systematic review with 19 relevant articles | 7 | 6.1 ± 2.0 | 3.0 ± 1.3 | 0.9 ± 1.2 | 12 months |
19 | 4.4 ± 2.9 | NR | 2.3 ± 1.8 | NR | |
IQR = interquartile range; NA = not applicable; NR = not reported; SD = standard deviation.
aP values for comparisons were not available.
Table 12: Summary of Findings by Outcome — Optical Coherence Tomography Measures
Eyes compared | Patients with NMOSD | Healthy controls (HC) | ||
|---|---|---|---|---|
Tocilizumab (TCZ) | Rituximab (RTX) | Azathioprine (AZA) | ||
n | 20 | 12 | 18 | 10 |
mGCC thickness | ||||
NMOSDON+ eyes at baseline, μm (SD) | 66.91 (8.23) | NA | ||
NMOSDON+ eyes change from baseline, Beta coefficient (95% CI) | −1.77 (−3.44, −0.09) | −2.03 (−3.58, −0.48) | −1.79 (−2.22, −1.37) | NA |
P value for the change from baseline | 0.041 | 0.017 | < 0.001 | NA |
NMOSDON- eyes at baseline, μm (SD) | 91.92 (3.52) | NA | ||
NMOSDON- eyes change from baseline, Beta coefficient (95% CI) | −0.19 (−0.87, 0.48) | 0.00 (−0.31, 0.32) | −0.84 (−1.50, −0.18) | NA |
P value for the change from baseline | 0.549 | 0.980 | 0.017 | NA |
Healthy eyes at baseline, μm (SD) | NA | NA | NA | 97.53 (2.32) |
Healthy eyes changes from baseline, Beta coefficient (95% CI) | NA | NA | NA | 0.00 (−0.31, 0.32) |
P value for the change from baseline | NA | NA | NA | 0.980 |
P value for the change of between-group | NMOSDON+ eyes: TCZ, RTX, AZA, NS; NMOSDON- eyes: TCZ and AZA: P < 0.05; AZA and HC P < 0.01. | |||
FLV | ||||
NMOSDON+ eyes at baseline, % (SD) | 6.83 (4.54) | NA | ||
NMOSDON+ eyes change from baseline, Beta coefficient (95% CI) | −0.66 (−2.26, 0.94) | −6.15 (−6.65, −4.34) | 1.20 (−2.40, 4.80) | NA |
P value for the change from baseline | 0.392 | 0.001 | 0.4 | NA |
NMOSDON- eyes at baseline, % (SD) | 1.16 (1.63) | NA | ||
NMOSDON- eyes change from baseline, Beta coefficient (95% CI) | −0.06 (−0.25, 0.07) | 0.06 (−0.39, 0.60) | −0.21 (−0.54, 0.86) | NA |
P value for the change from baseline | 0.498 | 0.898 | 0.793 | NA |
Healthy eyes at baseline, %(SD) | NA | NA | NA | 0.45 (0.49) |
Healthy eyes changes from baseline, Beta coefficient (95% CI) | NA | NA | NA | 0.01 (−0.26, 0.27) |
P value for the change from baseline | NA | NA | NA | 0.965 |
P value for the change of between-group | NR | |||
Global pRNFL | ||||
NMOSDON+ eyes at baseline, μm (SD) | 71.88 (12.94) | NA | ||
NMOSDON+ eyes change from baseline, Beta coefficient (95% CI) | −2.07 (−0.75, −3.39) | −2.18 (−0.36, −4.00) | −2.37 (−0.98, −3.75) | NA |
P value for the change from baseline | 0.005 | 0.023 | 0.003 | NA |
NMOSDON- eyes at baseline, μm (SD) | 110.50 (6.94) | NA | ||
NMOSDON- eyes change from baseline, Beta coefficient (95% CI) | −1.67 (−3.73, 0.40) | −2.67 (−6.45, 1.11) | −5.34 (−2.87, −7.82) | NA |
P value for the change from baseline | 0.108 | 0.147 | < 0.001 | NA |
Healthy eyes at baseline, % (SD) | NA | NA | NA | 112.40 (8.10) |
Healthy eyes changes from baseline, Beta coefficient (95% CI) | NA | NA | NA | −0.23 (−1.69, 2.15) |
P value for the change from baseline | NA | NA | NA | 0.796 |
P value for the change of between-group | NMOSDON+ eyes: TCZ, RTX, AZA, NS; NMOSDON- eyes: TCZ and AZA: P < 0.05; AZA and HC P < 0.001. | |||
Total macular volume | ||||
NMOSDON+ eyes at baseline, mm3 (SD) | 6.30 (0.30) | NA | ||
NMOSDON+ eyes change from baseline, Beta coefficient (95% CI) | −0.12 (−0.22, −0.01) | −0.15 (−0.21, −0.08) | −0.12 (−0.20, −0.04) | NA |
P value for the change from baseline | 0.028 | 0.001 | 0.006 | NA |
NMOSDON- eyes at baseline, mm3 (SD) | 6.93 (0.27) | NA | ||
NMOSDON- eyes change from baseline, Beta coefficient (95% CI) | −0.04 (−0.08, −0.01) | −0.07 (−0.14, 0.00) | −0.09 (−0.14, −0.04) | NA |
P value for the change from baseline | 0.105 | 0.059 | 0.003 | NA |
Healthy eyes at baseline, mm3 (SD) | NA | NA | NA | 7.23 (0.37) |
Healthy eyes changes from baseline, Beta coefficient (95% CI) | NA | NA | NA | 0.00 (−0.06,0.04) |
P value for the change from baseline | NA | NA | NA | 0.738 |
P value for the change of between-group | NMOSDON+ eyes: TCZ, RTX, AZA: NS; NMOSDON- eyes TCZ, RTX, AZA: NS; AZA and HC: P < 0.05. | |||
Cup area in optic disc | ||||
NMOSDON+ eyes at baseline, mm2 (SD) | 1.19 (0.67) | NA | ||
NMOSDON+ eyes change from baseline, Beta coefficient (95% CI) | 0.08 (−0.01, 0.16) | 0.07 (0.01, 0.12) | 0.14 (0.02, 0.26) | NA |
P value for the change from baseline | 0.010 | 0.019 | 0.023 | NA |
NMOSDON- eyes at baseline, mm2 (SD) | 0.62 (0.31) | NA | ||
NMOSDON- eyes change from baseline, Beta coefficient (95% CI) | 0.04 (0.01, 0.08) | 0.03 (−0.03,0.08) | 0.04 (−0.02, 0.10) | NA |
P value for the change from baseline | 0.026 | 0.269 | 0.175 | NA |
Healthy eyes at baseline, mm2 (SD) | NA | NA | NA | 0.61 (0.37) |
Healthy eyes changes from baseline, Beta coefficient (95% CI) | NA | NA | NA | 0.03 (−0.01, 0.07) |
P value for the change from baseline | NA | NA | NA | 0.129 |
P value for the change of between-group | NR | |||
Cup volume in optic disc | ||||
NMOSDON+ eyes at baseline, mm3 (SD) | 0.24 (0.17) | NA | ||
NMOSDON+ eyes change from baseline, Beta coefficient (95% CI) | 0.03 (0.00, 0.06) | 0.05 (0.016, 0.08) | 0.02 (−0.00, 0.05) | NA |
P value for the change from baseline | 0.038 | 0.006 | 0.020 | NA |
NMOSDON- eyes at baseline, mm3 (SD) | 0.10 (0.07) | NA | ||
NMOSDON- eyes change from baseline, Beta coefficient (95% CI) | −0.00 (−0.03, 0.02) | 0.00 (−0.02, 0.03) | 0.01 (−0.01, 0.03) | NA |
P value for the change from baseline | 0.711 | 0.694 | 0.468 | NA |
Healthy eyes at baseline, mm3 (SD) | NA | NA | NA | 0.10 (0.09) |
Healthy eyes changes from baseline, Beta coefficient (95% CI) | NA | NA | NA | 0.01 (−0.03, 0.05) |
P value for the change from baseline | NA | NA | NA | 0.588 |
P value for the change of between-group | NR | |||
Rim area in optic disc | ||||
NMOSDON+ eyes at baseline, mm2 (SD) | 1.18 (0.44) | NA | ||
NMOSDON+ eyes change from baseline, Beta coefficient (95% CI) | −0.10 (−0.21, 0.02) | −0.07 (−0.12, 0.02) | −0.14 (−0.27, −0.02) | NA |
P value for the change from baseline | 0.103 | 0.050 | 0.024 | NA |
NMOSDON- eyes at baseline, mm2 (SD) | 1.52 (0.28) | NA | ||
NMOSDON- eyes change from baseline, Beta coefficient (95% CI) | −0.03 (−0.06, 0.01) | −0.01 (−0.09, 0.03) | −0.18 (−0.50, 0.13) | NA |
P value for the change from baseline | 0.098 | 0.474 | 0.234 | NA |
Healthy eyes at baseline, mm2 (SD) | NA | NA | NA | 1.70 (0.34) |
Healthy eyes changes from baseline, Beta coefficient (95% CI) | NA | NA | NA | −0.05 (−0.11, 0.01) |
P value for the change from baseline | NA | NA | NA | 0.087 |
P value for the change of between-group | NR | |||
Rim volume in optic disc | ||||
NMOSDON+ eyes at baseline, mm3 (SD) | 0.08 (0.07) | NA | ||
NMOSDON+ eyes change from baseline, Beta coefficient (95% CI) | −0.01 (−0.02, 0.000) | −0.01 (−0.02, 0.000) | −0.01 (−0.02, 0.00) | NA |
P value for the change from baseline | 0.031 | 0.028 | 0.041 | NA |
NMOSDON- eyes at baseline, mm3 (SD) | 0.18 (0.07) | NA | ||
NMOSDON- eyes change from baseline, Beta coefficient (95% CI) | −0.01 (−0.03, 0.00) | −0.01 (−0.02, 0.00) | −0.01 (−0.02, 0.00) | NA |
P value for the change from baseline | 0.096 | 0.074 | 0.087 | NA |
Healthy eyes at baseline, mm3 (SD) | NA | NA | NA | 0.23 (0.12) |
Healthy eyes changes from baseline, Beta coefficient (95% CI) | NA | NA | NA | −0.01 (−0.02, 0.00) |
P value for the change from baseline | NA | NA | NA | 0.055 |
P value for the change of between-group | NR | |||
CI = confidence interval; FLV = focal loss volume; mGCC = macular ganglion cell complex; NA = not applicable; NMOSD = neuromyelitis optica spectrum disorder; NR = not reported; NS = not statistically significant; pRNFL = peripapillary retinal nerve fibre layer thickness; SD = standard deviation; TCZ = tocilizumab; μm = micrometres.
Table 13: Summary of Findings by Outcome — Other outcomes
Study citation and study design | Outcomes | Result | Notes |
|---|---|---|---|
Lotan et al. (2021)21 Systematic review with 19 relevant articles | MRI-related disease activity measures | No new or enhancing MRI lesions (9 articles) Improvement in lesion volume in the brain and the spinal cord (3 articles) 1 article reported no new or enhancing lesions in 6 patients with spinal cord MRI and 3 patients with brain MRI available during the TCZ treatment, but 2 patients with active spinal cord lesions. 1 article noted 1 new lesion in 10 available brain MRIs (10%) and 2 lesions in 9 available spinal MRIs (22.2%). | NA |
AQP4-and MOG-antibody Titres | Decreased AQP4 antibody titres: 6 articles Persistently elevated titres: 2 articles Among 4 AQP4 seropositive patients, 1 patient became seronegative, 2 patients had lower AQP4 antibody titres and 1 had persistently elevated titres. Among 10 MOG-positive NMOSD patients, 2 became seronegative and 1 MOG Ab titre remained persistently elevated and 7 not reported. | “TCZ effect on AQP4- and MOG-antibody status was not correlated with a higher risk of relapse.” |
AQP4 = aquaporin 4; MRI = NA = not applicable; NR = not reported. SMD = standardized mean difference; TCZ = tocilizumab.
Table 14: Summary of Recommendations in Included Guidelines
Recommendations | Expert agreement |
|---|---|
Carnero Contentti et al. (2020)24 | |
“Early start of IST [immunosuppressant treatment] treatments to reduce disease activity and therefore to prevent NMOSD attacks is recommended (p. 8).” | Appropriate, 100% agreement |
“Tocilizumab can be used in NMOSD patients showing no response to other immunosuppressants in clinical practice (p. 13).” | Appropriate, 90% agreement |
IST = immunosuppressant treatment; NMOSD = neuromyelitis optica spectrum disorder.
Appendix 5: Overlap Between Included Systematic Reviews
Note that this table has not been copy-edited.
Table 15: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Tang et al. (2023)18 | Luitel et al. (2022)19 | Kharel et al. (2021)20 | aLotan et al. (2021)21 |
|---|---|---|---|---|
Ringelstein M, et al. Neurology(R) neuroimmunology and neuroinflammation. 2022;9(1): No page information. | Yes | No | No | No |
Du C, et al. l Frontiers in immunology. 2021;12: 660230. | Yes | No | No | No |
Zhang C, et al. The Lancet Neurology. 2020;19(5): 391 to 401. | Yes | No | Yes | Yesb |
Rigal J, et al. Multiple sclerosis and related disorders. 2020;46:102483 | Yes | Yes | Yes | No |
Lotan I, et al. Multiple sclerosis and related disorders.2019;39:101920. | Yes | Yes | Yes | Yes |
Ayzenberg I, et al. JAMA neurology. 2013;70(3):394 to 397. | Yes | Yes | Yes | Yes |
Araki M, et al. Neurology. 2014;82(15):1302 to 1306. | Yes | Yes | Yes | Yes |
Ringelstein M, et al. l JAMA neurology. 2015;72(7):756 to 763. | Yes | Yes | Yes | Yes |
Dalla Costa G, et al. Multiple Sclerosis Journal. 2015 21 (S11): 654 to 779. | No | Yesc | No | No |
Dalla Costa G, et al. Multiple Sclerosis Journal. 2019: 279089; P729 | No | Yesc | No | Yes |
Carreón Guarnizo E, et al. Neurologia. 2019: S0213 to 4853(19)30033 to 7. | No | Yes | Yes | Yes |
Ringelstein, M. Multiple sclerosis journal; 2019: No page information | No | No | No | Yesd |
Araki, M. Neurochemistry International. 2019;130:104315 | No | No | No | Yesd |
aLotan et al. 2021 also included 12 relevant articles that were not included in the other 3 systematic reviews and are therefore not presented in this table.
bIncluded interim analysis presented in conference abstract.
cConference abstract.
dUpdated case series.
Appendix 6: References of Potential Interest
Previous CADTH Reports
Rituximab for the treatment of neuromyelitis optica spectrum disorder. (Health Technology Review). Ottawa (ON): CADTH: 2021 Feb 9: https://www.cadth.ca/rituximab-treatment-neuromyelitis-optica-spectrum-disorder. Accessed 2023 Mar 3.
Clinical review report: eculizumab (soliris). Alexion Pharma Canada Corp. Indication: neuromyelitis optica spectrum disorder. (CADTH Common Drug Review). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/sites/default/files/cdr/clinical/sr0640-soliris-nmosd-clinical-review-report.pdf. Accessed 2023 Mar 3.
Clinical review report: satralizumab (enspryng): (Hoffmann-La Roche Limited). Indication: neuromyelitis optica spectrum disorder. Ottawa (ON): CADTH; 2021: https://www.cadth.ca/sites/default/files/cdr/clinical/sr0663-enspryng-clinical-review-report.pdf. Accessed 2023 Mar 3.
Systematic Reviews
Xie Q, Zheng T, Sun M, Sun J, Wang M. A meta-analysis to determine the efficacy and safety of tocilizumab in neuromyelitis optica spectrum disorders. Mult Scler Relat Disord. 2020;45:102421. PubMed
Kastrati K, Aletaha D, Burmester GR, et al. A systematic literature review informing the consensus statement on efficacy and safety of pharmacological treatment with interleukin-6 pathway inhibition with biological DMARDs in immune-mediated inflammatory diseases. RMD Open. 2022;8(2):09. PubMed
Randomized Controlled Trials
Zhang C, Zhang M, Qiu W, et al. Safety and efficacy of tocilizumab versus azathioprine in highly relapsing neuromyelitis optica spectrum disorder (TANGO): an open-label, multicentre, randomised, phase 2 trial. Lancet Neurol. 2020;19(5):391-401. PubMed
Additional References
Ringelstein M, Ayzenberg I, Lindenblatt G, et al. Interleukin-6 receptor blockade in treatment-refractory MOG-IgG-associated disease and neuromyelitis optica spectrum disorders. Neurol Neuroimmunol Neuroinflamm. 2022;9(1):01. PubMed
Rigal J, Pugnet G, Ciron J, Lepine Z, Biotti D. Off-label use of tocilizumab in neuromyelitis optica spectrum disorders and MOG-antibody-associated diseases: a case-series. Mult Scler Relat Disord. 2020;46:102483. PubMed
Lotan I, Charlson RW, Ryerson LZ, Levy M, Kister I. Effectiveness of subcutaneous tocilizumab in neuromyelitis optica spectrum disorders. Mult Scler Relat Disord. 2019;39:101920. PubMed
Du C, Zeng P, Han JR, et al. Early initiation of tocilizumab treatment against moderate-to-severe myelitis in neuromyelitis optica spectrum disorder. Front Immunol. 2021;12:660230. PubMed
Carreon Guarnizo E, Hernandez Clares R, Castillo Trivino T, et al. Experience with tocilizumab in patients with neuromyelitis optica spectrum disorders. Neurologia (Engl Ed). 2022;37(3):178-183. PubMed
Xie Q, Sun M, Sun J, Zheng T, Wang M. New progress in the treatment of neuromyelitis optica spectrum disorder with monoclonal antibodies (review). Exp Therapeutic Medicine. 2021;21(2):148. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca