CADTH Health Technology Review
Exercise-Based Interventions for the Presurgical Management of Knee Osteoarthritis: A Rapid Qualitative Review
Rapid Review
Authors: Jamie Anne Bentz, Jennifer Horton, Danielle MacDougall
Abbreviations
ECHTA
Equity Checklist for Health Technology Assessment
GLA:D
Good Life With Osteoarthritis in Denmark
GP
general practitioner
OA
osteoarthritis
Key Messages
One reviewer conducted a thematic synthesis of 16 studies focused on the perspectives, expectations, and experiences of people living with knee osteoarthritis (OA) regarding accessing and engaging with presurgical interventions for managing knee OA incorporating individual and/or group-based exercise.
People with knee OA held various beliefs regarding the safety and usefulness of presurgical exercise-based interventions for the condition, often informed by interactions with health care providers early in their knee OA journey. Negative beliefs about exercise could make people apprehensive about engaging in it, while positive beliefs motivated initial access and engagement.
Intrinsic, personal, and extrinsic contexts could influence people’s beliefs about presurgical exercise-based interventions and their ability and motivation to access, use, and ultimately benefit from them. People experiencing intrinsic motivation, self-efficacy, and a natural tendency toward physical activity, and those who did not experience symptoms or comorbidities interfering with exercise, described accessing and engaging in these interventions as easier. Initial access also depended largely on the nature of interactions with health care providers early in their knee OA journey. Some people reported difficulty accessing or engaging in these interventions when they had competing commitments or lacked sufficient funds, insurance coverage, equipment, and appropriate physical environments.
People with knee OA generally reported feeling motivated by and benefiting from interventions that were structured, had an educational component, contained appropriately challenging but easily mastered exercises tailored to their contexts and needs, and included either in-person or virtual guidance from an exercise expert. They tended to find encouragement and motivation through group-based exercises. Some also reported feeling externally motivated by technologies sending automated reminders, motivations, and feedback regarding their physical activity. Many experienced positive outcomes after engaging in these interventions, which improved their quality of life, encouraged positive beliefs about exercise, and promoted continued use.
Decision-makers interested in promoting equity in access, use, and benefit may consider publicly funding exercise-based interventions that can be tailored to individuals’ needs; may be delivered either in-person or virtually; can be offered outside of working hours; include exercises that are easy to execute while tending to other commitments; and use affordable equipment suitable for a range of body types.
Context and Policy Issues
OA, also known as degenerative joint disease, is the most common type of arthritis and a leading cause of disability worldwide.1 Approximately 3.9 million people aged 20 or older in Canada (13.6%) live with diagnosed OA, with prevalence increasing as the population grows and ages.1 The condition has a substantial impact on the Canadian economy. Pain and functional limitations may lead to the inability to participate in employment, reduced working hours, or workplace modifications.2,3 Sharif et al.4 estimated that lost productivity due to OA will cost the Canadian economy $17.5 billion a year by 2031. The cost of treating OA in Canada is estimated to reach $7.6 billion a year by 2031, approximately $2.8 billion of which will be attributed to total joint replacement surgeries.5
With the knee joint being the most common location of OA, an estimated 22.9% of people aged 40 or older live with knee OA worldwide.6-8 Knee OA is characterized by the degeneration and loss of articular cartilage, a connective tissue that absorbs shock and reduces friction between bones.9,10 Damage and loss of articular cartilage ultimately lead to changes that affect the whole knee joint, causing stiffness, reduced range of motion, swelling and inflammation, and pain.10 The causes of knee OA are complex, with risk factors including, but not limited to, increased age, female sex, genetic predisposition, high bone density, race and ethnicity, and hormonal factors.7,8,10-12 Injuries resulting from repetitive or excessive loads on the knee joint due to high-impact sports, workplace activities, joint misalignment, or living with overweight or obesity also may contribute to its development.8,10
Knee OA significantly impacts a person’s physical and psychosocial well-being and is associated with lower mental health and health-related quality of life.2,3,13 Pain, reduced mobility, and a loss of trust or confidence in the body’s capabilities can interrupt, deter, or necessitate modifications to daily activities, which may result in decreased independence and restrict social activities.2,3 Experiencing pain and reduced functional ability can also cause emotionally distressing feelings of loss, inadequacy, frustration, irritability, depression, embarrassment, a reduced sense of control, and fear for the future.2,3
Of note, surgical interventions for knee OA are reserved for cases with symptoms not sufficiently managed with evidence-based nonsurgical interventions, including exercise-based therapies, a first-line treatment for mild to severe knee OA.14,15 Exercise for managing knee OA may incorporate strengthening, aerobic, neuromuscular, and mind-body exercises, such as tai chi and yoga.14,15
Given the increasing prevalence of knee OA, its significant psychosocial and economic impacts, and the costs associated with surgical interventions, demand for exercise-based interventions for its management will likely increase. Research qualitatively examining the perspectives, expectations, and experiences of people with knee OA regarding accessing and engaging with presurgical exercise-based therapies for their condition contributes helpful evidence for informing decision-making regarding their provision, funding, and implementation in Canadian jurisdictions.
Since people living with knee OA already report difficulties engaging in activities of daily living and social opportunities because of pain, reduced mobility, and loss of confidence in the body’s ability, it is possible that living with the condition may already impede a person’s eagerness and ability to access, use, and ultimately benefit from exercise-based interventions for its management.2,3 However, some people living with knee OA might experience additional difficulties accessing, using, and benefiting from exercise-based interventions due to disparities in historical, social, institutional, and environmental disadvantage, as well as discrimination. Remaining analytically open to equity considerations may help to understand whether, how, and why some groups may experience such inequities to inform funding and implementation decisions that consider and address them.
This rapid qualitative review provides a nuanced understanding and synthesis of the perspectives, expectations, and experiences of people living with knee OA regarding accessing and engaging with presurgical interventions for knee OA that incorporate individual and/or group-based exercise. Additionally, it will explore considerations regarding equity in accessing, using, and experiencing benefit from these interventions, as detailed in these perspectives, expectations, and experiences.
Research Question
What are the perspectives, expectations, and experiences of people living with knee OA regarding accessing and engaging with presurgical interventions for the management of knee OA that incorporate individual and/or group-based exercise?
In addition to the primary research question, the reviewer paid particular attention to considerations regarding equity in accessing, using, and experiencing benefit from individual and/or group-based exercise interventions for the presurgical management of knee OA, as detailed by people living with knee OA.
Methods
Literature Search Methods
The literature search used for this report was developed and conducted for a previous CADTH reference list examining the qualitative evidence available on the perspectives, expectations, and experiences of people with knee OA regarding presurgical management of the condition.16 For the previous report, a limited search was conducted by an information specialist on key resources, including MEDLINE, CINAHL, and Scopus. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. An intervention of interest in the previous report was Goodlife with Osteoarthritis in Denmark (GLA:D) programming. This exercise-based intervention targets hip and knee OA through structured, individualized education and neuromuscular training sessions.17 For this reason, a supplemental search was conducted, with the main search concept being the GLA:D program. No filters were applied to limit the retrieval by study type. The searches were completed on December 14, 2022, and were limited to English-language documents published since January 1, 2018.
Selection Criteria and Methods
To select studies included in the current qualitative evidence synthesis, the reviewer (also the analyst for the current review) screened the titles and abstracts of the citations included in the previous reference list (n = 24) and the references of potential interest included its appendix (n = 8). To select the studies included in the previous CADTH reference list,16 another reviewer screened the titles and abstracts of the citations captured in the literature search.
For this review, the full texts of potentially relevant articles identified from those included in the reference list were retrieved. The reviewer assessed the full texts and selected articles for inclusion in the current qualitative evidence synthesis based on the criteria presented in Table 1. Of note, the selection criteria for the original reference list differed from that of the current review in that the phenomenon of interest was broader than that of the current review, including any intervention used for the presurgical management of knee OA. The evaluation criteria for the original reference list, then, were perspectives on, expectations of, and experiences with accessing and undergoing these interventions.
Table 1: Selection Criteria for the Current Qualitative Evidence Synthesis
Criteria | Description |
|---|---|
Sample | Adults aged ≥ 18 years living with knee osteoarthritis who are not yet eligible for (or have not yet accessed) surgical interventions for the condition |
Phenomenon of interest | Presurgical interventions for knee osteoarthritis that incorporate individual and/or group-based exercise |
Design | Any qualitative design |
Evaluation | Perspectives on, expectations of, and experiences with accessing and undergoing presurgical interventions for knee osteoarthritis management that incorporate individual and/or group-based exercise |
Research type | Primary qualitative studies; qualitative component of mixed-methods studies (excluding surveys) |
For this review, individual or group-based exercise interventions were defined as those involving or seeking to enhance engagement with strengthening, aerobic, neuromuscular, and/or mind-body exercises intended to manage knee OA. Interventions of interest included exercise interventions that were self-directed or supervised (e.g., by a health care professional or physical trainer) and delivered over any medium (e.g., by phone, videoconference, or in-person). Literature detailing experiences with weight management programs intended to manage knee OA was included if these interventions had an exercise component.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1. Additionally, articles were excluded if they were published in languages other than English or duplicate publications.
Critical Appraisal of Individual Studies
To critically appraise the included studies, the reviewer of the current rapid qualitative review used the optimized version of the Critical Appraisal Skills Programme (CASP) tool.18 This tool promotes an efficient and systematic appraisal that acknowledges, accepts, and considers the diverse philosophical underpinnings of qualitative inquiry and the varied approaches and methods they inform.18 The reviewer used the optimized CASP tool’s 11 items as prompts for engaged and critical reflection about the trustworthiness and rigour of the included studies. They did not exclude articles based on their quality but instead critically appraised the included studies to provide readers with insight into their limitations and strengths. The results of the critical appraisal are summarized narratively and reported in Table 3 in Appendix 3.
Data Analysis
One reviewer independently synthesized the qualitative data using Thomas and Harden’s thematic synthesis.19 The analysis focused on exploring the perspectives, expectations, and experiences of people living with knee OA regarding accessing and engaging with presurgical interventions for the management of knee OA that incorporate individual and/or group-based exercise.
To begin the analysis, the reviewer first familiarized themselves with the studies by reading and rereading them in their entirety while making marginal notes and memos on initial thoughts and insights in a Microsoft Word document. These initial notes and memos included reflections to promote reflexivity, descriptions prompting familiarization with the content, and responses to questions listed in the optimized CASP tool to facilitate critical appraisal.
After making these initial notes and memos, the reviewer used NVivo20 to begin line-by-line coding of the text.19 They coded lines located under the “findings” and “results” sections of the included citations, assigning codes according to meaning and content.19 Only text relevant to the perspectives, expectations, and experiences of accessing and engaging with presurgical interventions for the management of knee OA incorporating individual or group-based exercise were coded. During line-by-line coding, the reviewer assigned the initial codes inductively19 but remained attuned to areas of interest identified in the research questions. Of note, given the variability of interventions of interest, the reviewer sought to capture common characteristics or features of the perspectives, expectations, and experiences of those accessing and engaging with exercise-based interventions broadly, rather than perspectives, expectations, and experiences regarding each intervention separately.
After line-by-line coding, the reviewer employed a constant comparative method to compare codes across codes and studies.19,21 At this stage, the reviewer examined all coded text to determine whether they had consistently interpreted the codes or if additional levels of coding were needed.19 They created descriptive themes as appropriate to capture the meanings of groups of initial codes.19 Then, they considered the connections and relationships between these descriptive themes to produce analytical themes.19
In addition, during the analysis, the reviewer used considerations detailed in the Scoping and Evaluation phases of Benkhalti et al.’s Equity Checklist for Health Technology Assessment (ECHTA)22 to inform which concepts to remain sensitive to during the analysis to capture equity considerations. They conceptualized inequities as differences between social groups that are unnecessary, avoidable, unfair, and unjust regarding the ability to access, utilize, and experience benefit (i.e., self-perceived improvement in physical, social, and psychological well-being) from available exercise-based interventions for the management of knee OA.22,23 The reviewer remained attuned to potential inequities in access, utilization, and benefit, and whether distribution disparities or institutional biases and care processes contributed to inequities.22 Instead of using dimensions of equity as a coding framework, the reviewer used these elements as concepts to prompt sensitivity to data allowing for the exploration, description, and reporting of how equity considerations related to the experiences of accessing and engaging with exercise-based therapies for knee OA management.
Reflexivity
To uphold qualitative best practice, before screening the citations and throughout the analytical process, the reviewer practised reflexivity by creating memos about their prior experiences, assumptions, and knowledge relevant to knee OA and exercise-based interventions used to manage it.21 They used these memos to reflect upon how their previous understandings might influence and inform their analysis, and challenged assumptions or interpretations not grounded in the data.
Summary of Evidence
Quantity of Research Available
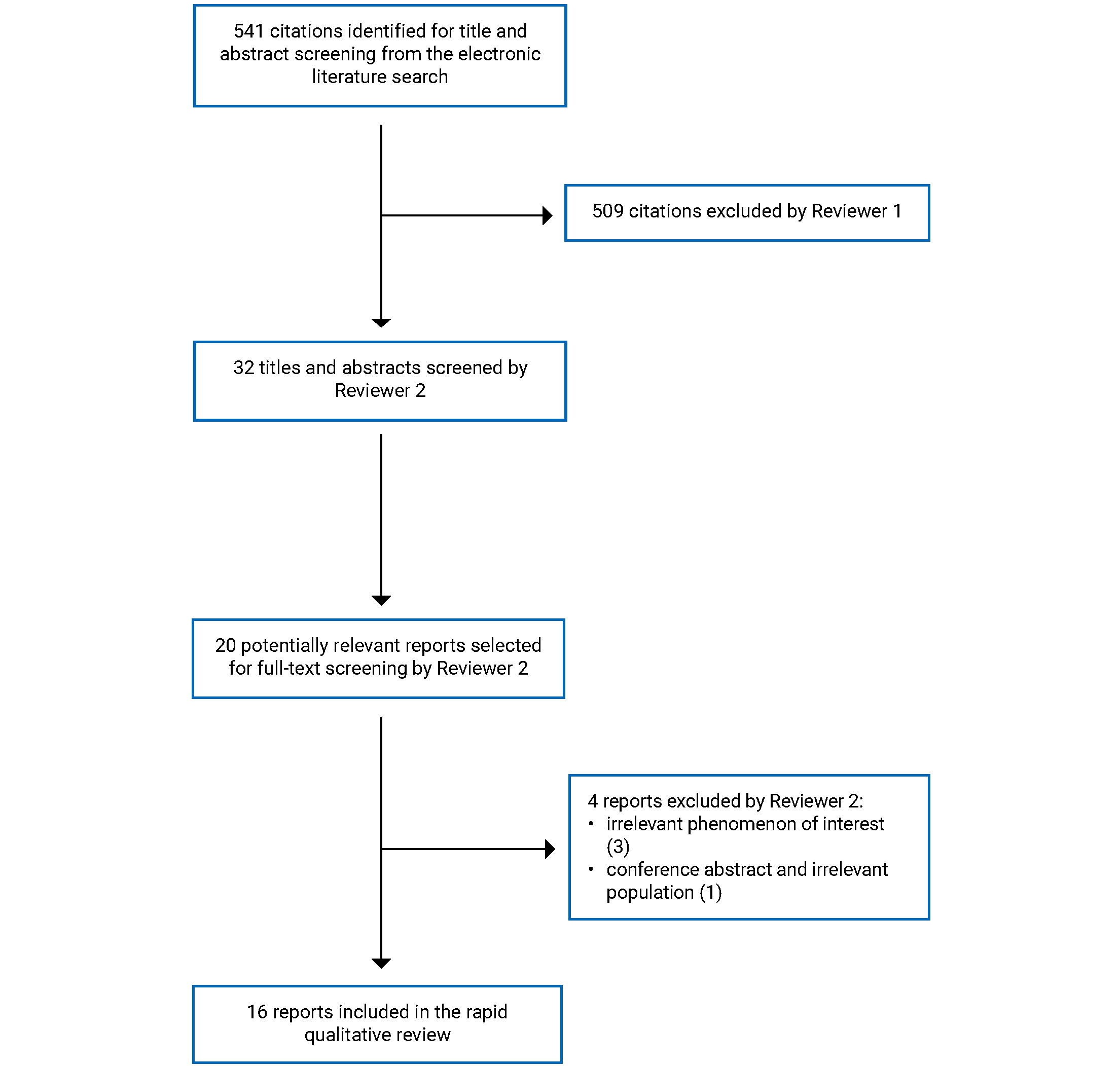
The literature search identified a total of 541 citations. One reviewer excluded 509 articles following title and abstract screening. After screening the remaining 32 potentially relevant titles and abstracts, another reviewer (i.e., the reviewer conducting the current qualitative evidence synthesis) excluded 12 citations and selected 20 potentially relevant reports for full-text review. Of these potentially relevant articles, they excluded 4 publications for various reasons and included 16 in the synthesis. Appendix 1 presents the PRISMA24 flow chart of the study selection.
Summary of Study Characteristics
Study Designs and Methods of Data Collection and Analysis
Of the 16 included studies, all were qualitative studies.25-40 The authors of 5 studies reported specific qualitative methodologies underpinning their studies, including Batista et al.25 and Wallis et al.39 using phenomenological approaches; Ezzat et al.27 using interpretive description; Leese et al.32 using supra-analysis; and Yeh et al.40 using a qualitative description approach. Of the remaining 11 studies, the authors reported methods of data collection and analysis but did not specify an overarching methodology informing these methods.
The authors of 15 studies analyzed data obtained through semistructured interviews,25-34,36-40 and the authors of 1 study collected data using focus groups.35
For their analytical approach, the authors of 7 studies reported using thematic analysis,27,29,30,34,36,37,39 2 used a form of qualitative content analysis,35,40 and 1 used methods borrowed from both thematic analysis and content analysis.25 The authors of 1 study reported using systematic text condensation26 and the authors of 1 study reported using phenomenographic analysis.32 Additionally, the authors of 3 studies used analytical methods informed by grounded theory approaches,28,31,38 and the authors of 1 study used methods borrowed from thematic analysis, constructivist grounded theory, and longitudinal qualitative analysis.33
Settings and Participant Characteristics
Seven of the studies were conducted in Australia,27,29,30,34,36,37,39 2 in Sweden,26,35 and 1 each in Canada,32 the UK,33 the Netherlands,28 Italy,25 Japan,38 and Taiwan.40 The authors of 1 study were affiliated with an institution in the US, although they did not explicitly report whether they conducted their study in this country.31
The authors of 5 studies recruited participants from both urban or metropolitan and suburban or regional settings,25,29,34,37,38 and the authors of 3 studies recruited exclusively from major urban or metropolitan locations.30,32,39 The authors of 3 studies reported the regions, states, or provinces they sampled from, but did not provide information about the rurality of their sample.26,33,35,36 Yeh et al.40 reported recruiting from “one medical center and two regional hospitals” in northwestern Taiwan. Finally, the authors of 3 studies neither explicitly reported a region they recruited from nor the rurality of their sample.27,28,31 Most of the authors had recruited their participants from clinical trials or randomized control trials investigating exercise-based interventions for managing knee and/or hip OA.27-35,39
The studies included a combined total of 392 people living with knee OA, including 3 people living with hip and knee OA. Three studies also included a combined total of 22 people reporting their hip as the joint primarily affected by OA.25,26,35 Additionally, Knoop et al.28 included physiotherapists (n = 11) and dieticians (n = 5), and Lawford et al.30 included physical therapists (n = 7) in their samples. Sample sizes ranged from 938 to 11840 participants.
The authors of the included citations reported that 272 (65.7%) of the combined total of 414 study participants living with knee and/or hip OA identified as female or as women. The reported ages of participants ranged from 40 to 89 years.25-30,32,34,36-40 The authors of 1 study only reported including participants aged 45 years to 75 years or older.33
Only Ledingham et al.31 reported the race or ethnicity of their participants, of which 9 were Black (36%), 12 were white (48%), and 4 were other unspecified races or ethnicities (16%).
Presurgical Exercise-Based Interventions Experienced
Five of the included studies did not investigate experiences of a particular exercise-based intervention but instead broadly reported participants’ experiences accessing or engaging with any exercise, or physiotherapy care, used for managing knee OA.25,36-38,40 Of the studies reporting experiences of particular interventions, 4 explored the experiences of interventions with an exercise-based component delivered or monitored in-person,28,33,39 4 with exercise-based components delivered or monitored virtually or digitally,26,29,34,35 and 2 with exercise-based components monitored or delivered to some people in-person and others virtually or to all persons via a hybrid medium.27,31,32 One study did not clearly report the medium through which the exercise-based component was monitored or delivered.28 Nine studies explored experiences of interventions that were guided by or had the option of being guided by an exercise expert.26-33,39 Three studies reported the experiences of interventions incorporating, or having the option of incorporating, group-based exercise.27,31,39
Appendix 2 provides additional details regarding the included studies’ designs, methods, settings, participants, and exercise-based interventions explored.
Summary of Critical Appraisal
Of the 16 included studies, all were of moderate to high quality. Appendix 3 reports details about the strengths and limitations of the included studies, which are summarized here.
Most limitations in the included studies related to incongruencies noted between the studies’ philosophical underpinnings, methodologies, and methods. Congruence between these elements enhances the credibility of a study’s findings, as it indicates that researchers have the knowledge and skills necessary to conduct qualitative inquiry.41 The reviewer noted possible dissonance between philosophical underpinnings, methodologies, and/or methods in all but 5 of the included citations.31,32,35,38,40
A qualitative approach was appropriate for addressing the stated research objectives of all 16 studies.
By transparently reporting the methods they used, researchers enhance the rigour of their study by providing readers insights into whether their methods were sufficiently reasonable and appropriate.42 Except in 3 cases,27,29,39 all authors explicitly reported the methods used to recruit and select their participants. The authors of 1 study did not report their justification as to why they used a random sampling technique, which is not typically considered best practice in qualitative inquiry.28 Otherwise, all authors detailing their recruitment strategies reported using a purposeful sampling approach appropriate for gaining access to relevant experiential experts. Additionally, all authors reported the number and characteristics of their participants. This enhanced the theoretical transferability of the studies’ findings by providing information allowing readers to compare settings and participants to their own context.
All authors described the methods they used for data collection, although the authors of 6 studies did not report the length of their interviews or focus groups,29,30,33,34,36,37 and the authors of 1 study did not report the medium through which they collected data.32 The authors of 13 out of 16 studies reported a particular analytical approach guiding the methods used for data analysis,26-32,34-38,40 with all but 136 providing sufficient detail to show that the methods used were appropriately rigorous and aligned with the cited approach.
All authors provided a statement of ethical approval. The authors of 10 studies also detailed the nature of the relationship between the researchers and participants,25-27,29-31,34,35,38,40 and the authors of 5 studies explicitly reported using reflexive practices or how their values may have influenced the research process.25-27,31,34,39 All studies also explicitly discussed methods used to enhance the credibility of their findings (e.g., pilot-testing interview guides, sampling until theoretical saturation, using multiple analysts, and member checking). However, in 10 cases, these methods were incongruent with their stated ontological, epistemological, or methodological assumptions.25-30,34,36,37,39
Analytical Findings
The thematic synthesis yielded 3 interrelated analytical themes: beliefs about presurgical exercise, which underpinned and influenced initial access to and utilization of exercise-based interventions; intrinsic, personal, and extrinsic contexts, which influenced beliefs regarding, access to, and the utilization of exercise; and experiences of the content, structure, and outcomes of exercise-based interventions, which intersected with contextual realities, and influenced beliefs about, and the utilization of, exercise.
Beliefs About Presurgical Exercise
People living with knee OA expressed various understandings and beliefs regarding the safety, usefulness, and potential benefit of presurgical exercise-based interventions, which underpinned and influenced their initial access to and utilization of them.
Negative Beliefs About Presurgical Exercise
Some people living with knee OA expressed apprehension about engaging in presurgical exercise-based interventions because of their negative beliefs about them.25,30,33,36,38,39 Some believed that exercise was boring or unenjoyable.30,33,39 Others assumed that physical activity or exercise had caused their knee OA, or would further strain and damage the knee joint and worsen symptoms of pain or crepitus.25,30,33,38,39 Moreover, some people with knee OA anticipated that presurgical exercise would not be worthwhile because it would cause neither benefit nor harm, or because nothing could prevent the assumed inevitability of continued joint deterioration and the fate of needing surgery.25,36,39 Relatedly, some believed exercise could only be useful postoperatively, where it could “help with the recovery process following the intervention [surgery].”39
Some people with knee OA developed these negative beliefs about presurgical exercise after interactions with health care providers who had advised them to avoid some or all exercise, or informed them they could do nothing for their condition besides “learning to live with it,” managing pain with medications, and eventually (and inevitably) having surgery.25,36,37,39 Others believed exercise-based interventions would be useless because they had not experienced improved symptoms despite being physically active, leading them to believe “the knees have gone too far for the exercises to be much good.”36 People’s experiences of symptoms like pain or their knees clicking with movement could also inform their beliefs in the presumed hopelessness of exercise, as they interpreted these symptoms as clues that their knee joint had deteriorated to a “bone on bone” state beyond the point at which any intervention but surgery could be helpful.39
Positive Beliefs About Presurgical Exercise
Not all people with knee OA held negative beliefs about exercise before engaging in exercise-based interventions.25,26,36-40 In some cases, positive beliefs about exercise coexisted with assumptions about the inevitability of surgery. Some people living with knee OA believed, often again because of discussions with their health care providers, that presurgical exercise could delay their need for surgery or prepare the body for a smoother postoperative recovery.25,26,37 When viewing exercise as only useful for delaying or preparing for surgery, however, some people reported disengaging in exercise-based interventions when they received a scheduled surgery date, with 1 noting, “I feel that the end of this problem is near. That’s why I’m not performing the exercises as I should anymore.”25,26
Some, however, believed exercise would benefit them outside of its relationship to surgery. Many people described their symptoms of knee OA (e.g., pain, joint clicking and crepitus, and reduced mobility) and associated sequelae (e.g., disrupted sleep, reduced ability to engage in activities of daily living, reduced independence, and adverse impacts on social relationships and quality of life) as factors that motivated them to initially access and engage with presurgical exercise-based interventions.26,37 Inherent to this motivation was the belief and expectation that exercise could and would alleviate these symptoms and their associated consequences.25,26,36,39 Other positive beliefs or expectations regarding exercise-based interventions included: that exercise would facilitate weight loss; that exercise was generally an inherent need of the body; and that exercise would be an intervention they could see in action, “not like taking supplements with hyaluronic acid, those [supplements] you do not see what they do.”25,38,40
Intrinsic and Personal, and Extrinsic Contexts
Intrinsic and personal, and extrinsic contexts within which people experienced exercise-based interventions intersected with and influenced beliefs about exercise and the experiences of exercise-based interventions.
Intrinsic and Personal Contexts
People with knee OA experienced self-efficacy (i.e., the belief in their ability to engage in exercise-based interventions successfully), intrinsic motivation (i.e., the drive to exercise even in the absence of external motivators, also referred to as “willpower” or “determination”), a natural tendency toward incorporating physical activity in their lives, and the ability to problem-solve or use coping activities (e.g., mindfulness in the context of physically challenging activities) as intrinsic phenomena and personal characteristics facilitating their initial and continued engagement in exercise-based interventions.25,28,31,33,39
Personal health conditions and states also influenced their motivation to initiate and engage in exercise. As previously discussed, symptoms of knee OA could inspire people to access exercise-based interventions.25,26,36,37,39 As detailed later, experiencing improvement in these symptoms because of these interventions encouraged continued engagement in them.30,33,34 However, experiencing knee pain related to OA, symptoms caused by other comorbidities (e.g., injuries, mental health conditions, respiratory infections, or cancer), and fatigue could also impede motivation and the physical ability to exercise.25,30,36,39 Additionally, while some people living with knee OA and overweight or obesity believed their body weight made exercising more physically challenging, they also expected exercise to help manage their weight, which would subsequently reduce stress on their joints and improve their exercise capabilities.28,40 However, some people living with obesity experienced inequities in using exercise-based interventions as prescribed because the equipment required to do so did not account for and work with their body types.30
Extrinsic Contexts
Extrinsic contexts were the external circumstances or settings within which people accessed and engaged with exercise-based interventions for knee OA. The nature and impact of social interactions occurring within exercise-based interventions are detailed under the “Experiences of the Content, Structure, and Outcomes of Exercise-Based Interventions” theme.
Early Interactions With and Access to Health Care Providers
Interactions with providers within the health care system often led to people’s initial introductions to and engagement with exercise-based interventions. To access these interventions, people living with the condition first had to receive a diagnosis of knee OA through a health care provider, typically a general practitioner (GP).36,37 Many people living with knee OA reported that, while desiring or valuing the concept of specific OA management instructions from their health care providers, their GPs did not offer such instruction and generally were not active in their OA care beyond providing their initial diagnosis, prescribing and advising them to use pain medications, or referring them to other providers.25,34,36,38
Without clear instructions and direction from their GPs, people with knee OA consulted other health care providers (e.g., rheumatologists, orthopedic surgeons, or sports medicine physicians), acquaintances, and the internet to search for information on how to best manage their knee OA.25,37 The sometimes conflicting information from these different sources led some to believe that there were no set guidelines for OA management and that even health care professionals based management decisions on intuition or subjective attitudes.25 As 1 person living with OA noted, “There is an almost religious way of thinking about how to deal with the pathology. It is not an exact science; when you choose the physicians, you choose the treatment.”25
Lacking clear and consistent management instructions from their GPs, some people with knee OA self-directed their management using a “trial and error” approach, which often included engaging in physical activity or accessing care from an exercise expert (typically a physiotherapist) through referrals made by a GP, another medical provider, or themselves.25,36,37 As previously detailed, beliefs regarding the safety and usefulness of exercise, often gained through initial interactions with health care professionals, could influence people with knee OA’s decisions to incorporate exercise into their OA management plans.25,26,30,33,36-40 Most of the included studies described experiences of exercise-based interventions supervised, instructed, and guided by physiotherapists, physical therapists, or exercise scientists.25,27-34,36,37,39 As detailed under the “Experiences of the Content, Structure, and Outcomes of Exercise-Based Interventions” theme, people with knee OA generally positively experienced and ascribed great value to the guidance, supervision, and support offered by these professionals in the context of exercise-based interventions.25-27,29,31-37,39
Funding
Despite being valued, even conveniently located and geographically accessible exercise experts were not accessible to all people with knee OA due to costs associated with accessing care from them.25,28,36,37 People with knee OA discussed concerns about funding mainly in the context of physiotherapy-based interventions, which many described as particularly expensive, and reported funding at least partially with public or private insurance.25,28,36,37 A minority reported they intended to continue physiotherapy after running out of insurance coverage, as they had the means to pay out-of-pocket and considered it a “good investment.”36,37 Many, however, described their engagement with physiotherapy as dependent on at least partial insurance coverage and planned to cease using this intervention when this coverage ran out.25,28,36,37 Even with partial coverage, some found it challenging to afford the out-of-pocket costs of physiotherapy not covered by insurance.28 Relatedly, Nelligan et al.34 reported that while some people with knee OA thought paying out-of-pocket for an exercise-based intervention could act as an incentive for people to continue engaging in it “so long as it wasn’t too expensive,” most believed that private insurers or government initiatives should subsidize costs so more people could access it.34
Competing Commitments
People living with knee OA reported that engaging in exercise-based interventions could be difficult due to competing commitments, such as work and caregiving responsibilities that, like exercise, required using finite time and energy.25,30,32,33,35,39
People with knee OA had differing perceptions regarding their agency to choose exercise in the context of competing commitments. One person with knee OA described as a “busy mother” by Leese et al. upheld that engaging in exercise was a choice informed by the value she ascribed to exercise relative to her other commitments: “I wasn’t invested that I absolutely had to do, come hell or high water, these steps so I’d be like yeah, I just didn’t walk very much today.”32 In contrast to this perspective, another person indicated that external commitments removed his ability to exercise agency: “We are trapped into a spiral in which work, we can say, takes up a lot of energy and a lot of time, and then that time is taken away from us.”25 With a similar outlook, some nonretired individuals living with OA reported that traditional OA treatment programs were typically scheduled during working hours, making them difficult for younger people to access.35
Physical Environment
People with knee OA also described how tools within and characteristics of their environment facilitated effective and continued use of exercise-based interventions. Facilitating tools included appropriate shoes, assistive devices (e.g., canes or walking sticks), exercise equipment (e.g., weights, elliptical trainers, and cycle machines), and medications to control pain.31,37,39 Others mentioned how having a physical space dedicated to exercise in their home facilitated engagement in exercise.31,33 As 1 person noted, “It was an easy process for me, because I had everything laid out. I kept my bag right there in the kitchen, so while I’m in the kitchen, before I start my day, I would just do my exercises.”31 Others spoke of how finding and accessing a suitable physical environment outside their home, such as flat or soft ground, helped them exercise effectively.39
However, not everyone had access to facilitating tools or physical environments. As previously detailed, some people living with obesity experienced difficulty engaging in and receiving maximum benefit from prescribed exercises because the equipment available to them was inappropriate for their body types.30 Some people with knee OA living in smaller residences reported not having the space to exercise at home, so they preferred having the option to exercise in alternative locations.27 Additionally, climate and geographical factors could influence people’s motivation and ability to engage in exercise-based interventions. Some participating in exercise outdoors described how their engagement in physical activity depended on the weather, reporting they felt unmotivated and physically unable to tolerate exercise during storms or heat.39 Similarly, in the context of a walking program, some experienced that living in a hilly area impeded their ability to exercise.39
Experiences of the Content, Structure, and Outcomes of Exercise-Based Interventions
Experiences of the content, structure, and outcomes of presurgical exercise-based interventions for knee OA intersected with the previously detailed contextual realities, and influenced beliefs about and the utilization of the interventions.
Appreciation for Structured Interventions
Many people living with knee OA valued structured interventions, that is, those prescribing specific exercises to perform at certain frequencies, often within a particular time frame.26,31,39 People appreciated the specific instructions and expectations of structured interventions, which differed from the nonexistent, nonspecific, or contradictory instructions many had received from health care providers elsewhere in their knee OA journey.25,26,39 In addition to providing specific instructions and expectations, structured interventions could also serve as a source of external motivation during and after completing the self-directed or guided intervention program.39 As 1 person stated, “It [a walking program] got me off my backside. I’m a lazy person and it just made me do it.”39 To motivate themselves to continue exercising in the context of self-directed exercise or after structured programs had ended, some people with knee OA described self-creating exercise routines (e.g., by designating a place and time to conduct exercise each day), which they experienced as helping them continue to make exercise a part of their daily lives.31
Appreciation for Educational Components
Many people in the included studies also engaged in interventions with an educational component delivered before or during exercise, which they tended to appreciate and value.26-35,37 These educational components provided people with knee OA information about the causes and pathophysiology of their condition, the safety and potential benefits of exercise, and how to conduct it properly.26,28,29,31,33,34 Participants felt they benefited from and were motivated by educational or instructional materials that were credible (i.e., informed by exercise experts or evidence), clear and easy to understand (i.e., delivered in plain and accessible language), and easily accessed as often as needed.26,34 When doing exercise-based interventions without the visual supervision of an exercise expert, they particularly appreciated having videos, photographs, and written materials or instructional manuals to reference.29,34
Referencing their experience of the educational component of the exercise-based intervention they received, 1 person with knee OA stated, “It was a shock when I heard that I have OA, because I was young and believed that I should be very cautious. But now it was explained that this is not the case, and that I can still do almost anything.”28 As exemplified in this quote, the educational components of exercise-based interventions sometimes changed people’s negative beliefs about exercise, thus fostering their motivation and confidence to engage in it.28,29,31,33
Ease of Engagement and Individual Tailoring
People living with knee OA often positively experienced and expressed appreciation for exercise-based interventions that were appropriately challenging in intensity or variety but also mentally, physically, and logistically easy to engage with and master.26-31,33-35,39 Some people with knee OA reported losing interest or stopping engagement with exercise-based interventions they experienced as too challenging or not challenging enough.26,28,30,34,35,39 Experiencing exercises as physically and technically easy, however, supported mastery, sometimes after few or no supervised sessions with an exercise expert, which, in turn, promoted a sense of self-efficacy.27-29,34,39 Some people with knee OA also appreciated how they could engage in easily-executed exercises while tending to other tasks like cooking or cleaning.29 Exercises challenging enough to maintain interest but easy enough to allow for self-efficacy and incorporation into everyday activities facilitated longer-term engagement in exercise, even after formal support and supervision ceased.27,28,31,34
While appreciating structured interventions, people living with knee OA also valued interventions tailored to their individual needs and capabilities.26,28,29,31,33-35,37 This tailoring ensured that interventions were appropriately challenging yet easy enough to promote self-efficacy, interest, motivation, and progress.28,29,31,33,34 Some people with knee OA independently tailored interventions by pacing, skipping, or adding to exercises prescribed by a structured program.31,34,39 As 1 person noted, “I thought about it [the prescribed exercises] and said, ‘I can’t do this.’ But then I said, ‘But no. Let me give it a shot and just try to do it,’ and [pause] it’s not like I gotta be vigorous with it, just take my time.”31 Self-tailoring required knowing and recognizing one’s limitations, being motivated to continue despite them, conceptualizing prescribed activities as modifiable, and negotiating how to conduct them accordingly. While some people did this knowing, motivating, conceptualizing, and negotiating for themselves, these processes were often facilitated or made possible by interacting with or watching other people and technologies.26,28,29,31-35,37,39
Guidance by Exercise Experts
Many people living with knee OA valued the guidance, supervision, and support offered by physiotherapists, physical therapists, and exercise scientists (together referred to here as “exercise experts”) in the context of exercise-based interventions.25-27,29,31-37,39 They perceived these exercise experts as having the knowledge and expertise to teach them how to perform exercises safely and beneficially; therefore, they valued the education, instructions, encouragement, reassurance, and corrections these professionals provided.26-33,35,39 People with knee OA also appreciated their exercise experts’ use of timely, easy-to-understand, respectful, focused, encouraging, warm, and open methods of communication and interaction and their tendency to listen and respond to their individual needs, even in the context of group-based interventions.25,26,29-31,33,37,39 They experienced these communication and interaction styles as promoting an efficient and complete understanding of information and a therapeutic alliance characterized by a mutual connection, trust, respect, and understanding.26,29-31,33,37,39
Within these therapeutic alliances grounded in effective and respectful communication, people with knee OA felt valued as human beings in ways many had not when interacting with other health care providers.25,33,37 Some described sensing that their exercise experts were invested in “knowing” them as individuals, which allowed them to feel safe disclosing potentially sensitive information.31,33,35,37 They perceived that this information sharing allowed their experts to identify problems and tailor interventions to address their needs.31,33,35,37 As 1 person described: “I think [the physiotherapist] understands that better than my doctors, because he’s worked by my side with me, he’s supported me, it’s more intimate. He’s been keen to help resolve the problems, rather than doing, what I call a supermarket shelf, one size fits all program. He’s really worked hard to try and work out what’s best in my circumstance.”37 Strong therapeutic alliances also prompted them to feel more accountable to their exercise experts and, in turn, the exercises they decided upon together.30,31,33
The information, guidance, encouragement, intervention tailoring, and accountability experienced within interactions with their exercise experts promoted the belief in and experience of exercise as safe, beneficial, and achievable, which fostered self-efficacy and motivation to engage in it.27,29-33,39 As 1 person stated, “I knew exactly what the expectation was in terms of getting it [the exercise] done correctly and for safety’s sake…it made a big difference, ‘cause to go home and not be sure exactly how to do…the steps…that in itself for me is stressful.”31 Ascribing great value to expert guidance and support, many people with knee OA appreciated or wanted more frequent interactions with and monitoring from their experts.26,29,31,33,35,39 In some cases, when these interactions ceased, so did their engagement with exercise-based interventions.28,30,33
The medium through which people interacted with their exercise experts influenced the experience and perceived benefit they obtained from these interactions. People with knee OA were initially skeptical of virtually-delivered interventions, questioning whether it would be possible to receive guidance without visual and/or physical contact with their expert or remain motivated to participate in their homes.26,27,29 In some cases, people receiving virtual guidance did experience these and other challenges. People receiving instruction exclusively through asynchronous virtual chats or telephone, for example, noted they would have appreciated the reassurance of even 1 face-to-face session where their exercise expert could visually monitor their exercises and provide corrections as needed.26,29,35 Other challenges experienced with virtual interactions included learning to use the technologies or platforms required, delays in obtaining meeting links, and “technology hiccups” such as dropped connections.27 However, people with knee OA generally experienced these challenges as annoying but easy to overcome.27
Despite these challenges, many people with knee OA reported positive experiences virtually interacting with their exercise experts. Perhaps most appreciated was the perceived flexibility, convenience, accessibility, and comfort of virtual interactions.26,27,29 With the freedom to engage in interactions where they wanted, people experienced greater comfort during interactions and saved money and time they otherwise would have spent commuting, facilitating their ability to access guided interventions despite competing commitments.26,27,29 Location flexibility also reduced inequities in accessing guided interventions that people living in rural and remote locations would have otherwise experienced had the services only been offered in a distant location they could not have easily or realistically commuted to.29 In addition to these benefits, people with knee OA believed their exercise experts gave them more undivided, focused attention during virtual interactions, which allowed them to “get right down to talking.”29 With some exceptions, most people interacting with exercise experts via videoconference believed these experts had enough visual information to instruct them effectively.27 Some interacting with their exercise experts exclusively over the telephone also had positive experiences despite the lack of visual interaction, with 1 person stating, “You know what? I found [telephone care] just as good if not better.”29 People positively experiencing telephone interactions reported that the relative anonymity of the medium encouraged their sharing of personal information and that their exercise experts had “excellent visual skills” that allowed them to provide effective feedback based only on verbal descriptions.29
Group-Based Exercise as Motivating
People with knee OA reported feeling comforted and encouraged by sharing their experiences with others who lived with and truly understood the condition.38 Those participating in group-based interventions reported that watching others with OA provided a point of reference that allowed them to situate their capabilities and progress and made them feel less alone in their experience.31 As 1 person noted, “It was encouraging… you could just see that there’s a whole range of abilities, and you sort of start to see like that you aren’t weird, or something like that.”31 Viewing others with their condition accomplishing challenging exercises could be motivating because it gave them hope that they, too, could be successful.31 Exercising alongside others also fostered a sense of camaraderie and accountability, which those with low intrinsic motivation experienced as especially important.31,33 As 1 person described, “It’s more motivating when you’re doing it [exercise] with someone else…if it’s just me, I don’t, I don’t care about me. [laughs] But it’s different, I’d care about someone else.”
Interactions With Technologies
In some cases, people living with knee OA interacted with technology that provided automated reminders to engage in exercise, motivating messages, and/or information about their activity levels relative to their goals.26,31,32,34,35,39 With some exceptions, people generally experienced these technologies as annoying but helpful reminders and sources of external motivation.26,31,32,34,35,39 In some cases, this motivation stemmed from the knowledge that these technologies would relay information to their exercise experts or the research team from whom they desired favourable judgment.31 Receiving automated notifications from these technologies could also make people feel cared for and connected to these persons.31
However, people with knee OA also sometimes anthropomorphized technologies, so they became sources of encouragement, motivation, and accountability, similar to how interactions with humans could.31,32,34 One person living with knee OA, for example, noted, “[The Fitbit] is happy when I do 10 000 steps…just like a friend supporting me, encouraging me… a Fitbit helps me feel less alone…it’s huge for me because you know most of my life I’ve not had a lot of support and so support is huge, just huge.”32 Others described feeling the need to appease technologies monitoring and providing feedback on their performance, feeling “judged” and “graded” by them and subsequently “pressured,” “forced,” or “nagged” to uphold a certain level of activity deemed acceptable to them.31,32,34
Many people with knee OA also found the quantifiable information about their activity levels that these technologies provided useful and motivating.32,35 When considered alongside experiences like pain, they could use this information to understand their bodies’ limits and capabilities better so they could set realistic exercise goals.35 With these goals set, they could use the quantitative information as evidence validating their need for rest.35 People also used this information to prove to their exercise experts that they had been accountable to exercise plans.32 People experienced glitches where the technologies did not accurately measure their activity levels as sources of frustration because of the lost “credit” for their efforts and a potential threat to their experts’ trust.32,35 One person emphasized that exercise experts should believe their client’s accounts of their physical activity in cases where they claimed their technologies had not provided accurate measurements.32
People experienced automated information and feedback about their activity levels relative to their activity goals in different ways.32,34,35 Knowing they were close to their goals could motivate some people with knee OA to “make that extra effort” to meet them.32,35 When meeting or exceeding goals, some experienced feelings of gratification and accomplishment, which enhanced their overall motivation to continue exercising, but also, as 1 person noted, could inspire exercise beyond their safe limits.32,35 Some people who perceived themselves as naturally active and intrinsically motivated were unaffected or positively impacted by alerts that they had not met their activity goals.32 Others, however, reported experiencing negative feelings, such as guilt, shame, and anxiety.34,35 Some people found negative feedback useless or “a reminder of the bleeding obvious.”34 In most cases, however, people with knee OA experienced these negative emotions and the desire to avoid them as motivators to continue engaging with exercise.34,35
Unlike that delivered by a human, information and feedback sent by these technologies did not recognize or account for people’s contexts (e.g., injuries, illnesses, or necessary sedentary activities), interests, and sources of motivation.31,32,34,35 This sometimes resulted in people receiving notifications that shamed them for factors perceived as beyond their control, resulting in frustration rather than motivation.34 Additionally, some people with knee OA felt the repetitive information delivered by these technologies became redundant, especially as they established exercise habits and no longer relied on the technologies as external motivators.31,32 Others — including those with high intrinsic motivation, a natural tendency for exercise, or little interest in technologies — ascribed little value to the automated information provided by the technologies even at baseline.32,35 As 1 of these people stated, “When this six months is over, I’ll take the Fitbit and throw it away because it has no relevance to my life…I know what I’m doing and I don’t care what this little machine tells me.”32 Other challenges or concerns people had when interacting with technologies included difficulties initially setting them up and worries that unauthorized individuals or organizations may gain access to the information they collected.35
The Experience of and Meanings Ascribed to Outcomes
Many people with knee OA reported experiencing positive outcomes after engaging in presurgical exercise-based interventions.26-31,33,34,36,39 These included improvement in knee OA symptoms (e.g., pain, joint stiffness and swelling, and reduced mobility), which led to greater functioning and independence, less reliance on pain medications, engagement in and enjoyment of activities they could no longer do before, and a delay in the need for surgery.26-31,33,34,36,39 As 1 person recounted, “This program has had an absolute crucial role in the fact that I can manage my everyday life as well as I can now.”26 Besides reduced OA symptoms, some people reported experiencing additional “bonus” physical benefits, such as weight loss or improved sleep.34,39 Experiencing these physical benefits and desiring to retain them encouraged continued motivation in exercise, even after structured exercise-based interventions ended.30,33,34
People also experienced psychosocial benefits. As they engaged in exercise successfully while learning to work safely through pain, they reported fearing pain less and gaining confidence in their body’s capability to endure and benefit from exercise.27,31,39 Their newfound belief in exercise as a safe, beneficial, and achievable intervention for managing knee OA provided people with hope for a future where they could achieve new goals: “Now I want to travel…I want to be able to walk and climb places that I want to see. My goal is I want to get there. And [I can] by doing the exercises or stretches.”27 Relatedly, people often discovered they were capable of more than they initially believed, which increased their self-efficacy regarding their ability to live with and manage their knee OA and engagement in more physical activity.27,29,34,39 Some people also reported that their moods and social lives improved with exercise, which provided them with opportunities to interact with people they otherwise would not have.39
Although rarely reported in the included citations, some people experienced no benefit or adverse outcomes due to exercise-based interventions.26,33 Experiencing no physical improvement in knee OA symptoms did not always mean people disregarded interventions as potentially useful.26 Some ascribed the lack of benefit to factors other than the intervention, stating, for example, “The reason that it didn’t help me is probably because I started too late.”26 For others, however, a lack of experienced improvement in symptoms could hinder their desire to continue exercising.33 Additionally, some people with knee OA continued to hold negative perceptions or apprehensions about exercise after engaging in exercise-based interventions. These included the conceptualization that “all exercise is boring” and continued concerns regarding exercising in pain or their ability to engage in physical activity safely and effectively.31,33
Limitations
This review has limitations that may reduce the trustworthiness of its findings. While the reviewer deemed all included citations to be of moderate to high quality, all had limitations impacting the potential trustworthiness of their findings, most of which related to incongruencies between their ontological and epistemological underpinnings, methodologies, and methods. Furthermore, since most of the included studies recruited participants from clinical trials, it is also possible that the perspectives and experiences detailed in this review are from people who were more inclined to know about, be interested in, and motivated to engage with these interventions than the general population.
It is also important to note that the initial search strategy, created for another report, was not built explicitly to capture equity considerations regarding presurgical exercise-based interventions for managing knee OA.22 Therefore, it is possible that relevant equity considerations are missing from this report and that the voices of people especially likely to experience inequities in accessing, utilizing, and benefiting from these interventions were underrepresented in this review.
Additionally, 1 reviewer conducted the initial title and abstract screening, from which a second reviewer selected relevant citations. This second reviewer also acted as the sole analyst for the thematic synthesis of the 16 included citations, which they conducted and reported within a limited time frame. These methods increased the likelihood of missing relevant citations or analytical findings.
Of note, when writing their analytical findings, the analyst encountered 1 additional relevant article by Wallis et al.43 that was captured by the literature search but not the initial title and abstract screening, and was therefore not included in the current review. This citation was an Australian study with a general qualitative design exploring barriers and enablers for referral to and participation in GLA:D.43 Among the participants interviewed were 7 people living with knee OA and 10 living with both knee and hip OA.43 The next section discusses Wallis et al.’s43 findings in relation to those of the current review. Of note, the study’s findings align with and add to those of the current review.
Conclusions and Implications for Decision- or Policy-Making
This thematic synthesis of 16 studies focused on the perspectives, expectations, and experiences of people living with knee OA regarding accessing and engaging with presurgical interventions for managing knee OA incorporating individual and/or group-based exercise.
It found that people with knee OA held various beliefs regarding the safety and usefulness of presurgical exercise-based interventions for managing the condition. Negative beliefs could hinder, and positive beliefs could motivate, access and use of these interventions, a finding also noted by Wallis et al.43 Many people with knee OA developed initial beliefs about presurgical exercise following interactions with health care providers, including GPs. These findings highlight how people’s initial access of and engagement with exercise-based interventions may at least partially depend on the knowledge and attitudes of the health care providers they interact with in the early stages of their knee OA journey. Additionally, people with knee OA desired clear and detailed instructions from their GPs regarding how to best manage the condition; however, they often experienced this instruction as limited and inconsistent with that obtained from other providers and sources. Participants in Wallis et al.’s study investigating barriers and facilitators to participation in GLA:D reported the same phenomenon.43 Additionally, they suggested that GPs receive education about GLA:D so more people with OA could gain knowledge about it and access it.43 It may be helpful for decision-makers contemplating the public funding of an exercise-based intervention for managing knee OA to determine whether health care providers in their jurisdiction have easy access to practice guidelines and educational resources detailing its potential benefits. Such resources may ensure that more people with knee OA can make informed decisions regarding, and gain referrals to, the intervention.
This review also found that intrinsic, personal, and extrinsic contexts could influence people’s beliefs about presurgical exercise-based interventions and their ability and motivation to access, use, and ultimately benefit from them. People with high intrinsic motivation and self-efficacy, a natural tendency toward exercise and problem-solving, and who did not experience symptoms or comorbidities interfering with exercise tended to find accessing and remaining engaged in presurgical exercise-based interventions easier. In contrast, those with health care providers who shared negative or inconsistent information about exercise, with competing commitments demanding their time and energy, who lacked adequate personal funds and insurance, and who did not have appropriate tools and physical environments to engage in exercise experienced difficulties accessing, remaining motivated, and continuing to engage with these interventions. Of note, Wallis et al. reported similar contexts as impacting participation in GLA:D and added to the personal contexts described in the reviewed literature by reporting “language background” as a barrier to participation.43 They did not, however, elaborate further on how language background influenced the experience of this exercise-based intervention.43
This review also found that experiences of the content, structure, and outcomes of presurgical exercise-based interventions intersected with contextual realities and influenced beliefs about and the utilization of exercise. The findings under this theme provide decision-makers with insights into the types of interventions people with knee OA will likely be motivated by, and experience benefit from. These may include interventions that are structured; include an educational component to foster positive beliefs and self-efficacy regarding exercise; can be tailored, so they are appropriately challenging but easily mastered; and are guided either in-person or virtually by an exercise expert that can provide education, instruction, support, encouragement, motivation for accountability, and tailoring. Wallis et al.43 similarly reported supervision and feedback received from physiotherapists during and after GLA:D as key enablers to continued participation in it. People with knee OA, especially those lacking intrinsic motivation, also reported finding encouragement and motivation through group-based exercises. Some also reported feeling annoyed but externally motivated and sometimes validated by technologies sending automated reminders, motivations, and feedback regarding their exercise. However, a lack of tailoring limited the perceived benefit of these automated messages.
The current review found that many people with knee OA experienced positive physical, psychological, and social outcomes of exercise-based interventions, which Wallis et al.43 reported as well. These outcomes constructively impacted quality of life, encouraging positive beliefs about exercise and promoting its continued use. However, the findings of this review and Wallis et al.’s study43 also indicate that some people with knee OA may experience inequities in accessing and using exercise-based interventions and ultimately experiencing these benefits. These include people less likely to have access to GPs or exercise experts (e.g., people in rural and remote communities);44 those at risk of having limited time available for exercise (e.g., single working parents);45 those lacking adequate private health insurance coverage (e.g., people who are unemployed or retired); those lacking access to appropriate exercise equipment (e.g., people with low income or those living with overweight and obesity); and people lacking physical environments or space suitable for exercise (e.g., people living in smaller residences). Publicly funding exercise-based interventions may help ensure access to those without private insurance or who cannot afford to pay out-of-pocket. Interventions promoting equity of access and use may include those that can be delivered either in-person (e.g., for those without suitable home environments) or virtually (e.g., for those unable to afford transportation, living in rural and remote communities, or with time poverty); are offered outside of working hours; and include exercises that are easy to execute while tending to other commitments. Decision-makers may also consider whether the interventions under review require the use of equipment and, if so, whether this equipment is appropriate for a range of body types and available to those who cannot pay out-of-pocket for it.
References
1.Osteoarthritis in Canada Ottawa (ON): Public Health Agency of Canada; 2020: https://www.canada.ca/content/dam/phac-aspc/documents/services/publications/diseases-conditions/osteoarthritis/osteoarthritis-factsheet.pdf. Accessed 2023 Feb 6.
2.Wride JM, Bannigan K. ‘If you can’t help me, so help me God I will cut it off myself…’ The experience of living with knee pain: a qualitative meta-synthesis. Physiotherapy. 2018;104(3):299-310. PubMed
3.Wallis JA, Taylor NF, Bunzli S, Shields N. Experience of living with knee osteoarthritis: a systematic review of qualitative studies. BMJ Open. 2019;9(9):e030060. PubMed
4.Sharif B, Garner R, Hennessy D, Sanmartin C, Flanagan WM, Marshall DA. Productivity costs of work loss associated with osteoarthritis in Canada from 2010 to 2031. Osteoarthr Cartil. 2017;25(2):249-258. PubMed
5.Sharif B, Kopec J, Bansback N, et al. Projecting the direct cost burden of osteoarthritis in Canada using a microsimulation model. Osteoarthr Cartil. 2015;23(10):1654-1663. PubMed
6.Turkiewicz A, Petersson IF, Björk J, et al. Current and future impact of osteoarthritis on health care: a population-based study with projections to year 2032. Osteoarthr Cartil. 2014;22(11):1826-1832. PubMed
7.Cui A, Li H, Wang D, Zhong J, Chen Y, Lu H. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClinicalMedicine. 2020;29-30:100587. PubMed
8.March L, Cross M. Epidemiology and risk factors for osteoarthritis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: www.uptodate.com. Accessed 2023 Jan 31.
9.Hsu H, Siwiec RM. Knee Osteoarthritis. Treasure Island (FL): StatPearls Publishing; 2022.
10.Berteau JP. Knee Pain from Osteoarthritis: Pathogenesis, Risk Factors, and Recent Evidence on Physical Therapy Interventions. J Clin Med. 2022;11(12):07.
11.Hussain SM, Cicuttini FM, Alyousef B, Wang Y. Female hormonal factors and osteoarthritis of the knee, hip and hand: a narrative review. Climacteric. 2018;21(2):132-139. PubMed
12.Hartley A, Sanderson E, Granell R, et al. Using multivariable Mendelian randomization to estimate the causal effect of bone mineral density on osteoarthritis risk, independently of body mass index. Int J Epidemiol. 2022;51(4):1254-1267. PubMed
13.Park HM, Kim HS, Lee YJ. Knee osteoarthritis and its association with mental health and health-related quality of life: A nationwide cross-sectional study. Geriatr Gerontol Int. 2020;20(4):379-383. PubMed
14.Deveza LA, Bennell K. Management of moderate to severe knee osteoarthritis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: www.uptodate.com. Accessed 2023 Jan 31.
15.Deveza LA, Bennell K. Management of knee osteoarthritis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: www.uptodate.com. Accessed 2023 Jan 31.
16.Presurgical management for people with knee osteoarthritis. (CADTH reference list). Ottawa (ON): CADTH; 2022: https://www.cadth.ca/sites/default/files/pdf/htis/2022/RA1247%20Presurgical%20Knee%20OA%20mgmt%20Final.pdf. Accessed 2023 Jan 31.
17.Thalund Grønne D, Ris Hansen I, Kongsted A, Roos E, Hartvigsen J, Thorgaard Skou S. GLA:D Denmark Annual Report 2020 Odense (DK): University of Southern Denmark; 2021 https://gladinternational.org/wp-content/uploads/2021/08/Annual-Report-2020-eng-v349-GLAD-Denmark.pdf. Accessed 2023 Feb 7.
18.Long HA, French DP, Brooks JM. Optimising the value of the critical appraisal skills programme (CASP) tool for quality appraisal in qualitative evidence synthesis. Res Methods Med Health Sci. 2020;1(1):31-42.
19.Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. 2008;8(1):45. PubMed
20.NVivo qualitative data analysis [software] [computer program]. Doncaster (AU): QRS International Pty Ltd 2015.
21.Charmaz K. Constructing grounded theory 2nd ed. London (UK): Sage Publications Ltd 2014.
22.Benkhalti M, Espinoza M, Cookson R, Welch V, Tugwell P, Dagenais P. Development of a checklist to guide equity considerations in health technology assessment. Int J Technol Assess Health Care. 2021;37(1):e17. PubMed
23.Whitehead M. The concepts and principles of equity and health. Int J Health Serv. 1992;22(3):429-445. PubMed
24.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
25.Battista S, Manoni M, Dell'Isola A, Englund M, Palese A, Testa M. Giving an account of patients' experience: A qualitative study on the care process of hip and knee osteoarthritis. Health Expect. 2022;25(3):1140-1156. PubMed
26.Cronström A, Dahlberg LE, Nero H, Ericson J, Hammarlund CS. 'I would never have done it if it hadn't been digital': a qualitative study on patients' experiences of a digital management programme for hip and knee osteoarthritis in Sweden. BMJ Open. 2019;9(5):e028388. PubMed
27.Ezzat AM, Bell E, Kemp JL, et al. “Much better than I thought it was going to be”: Telehealth delivered group-based education and exercise was perceived as acceptable among people with knee osteoarthritis. Osteoarthr Cartil Open. 2022;4(3):100271. PubMed
28.Knoop J, de Joode JW, Brandt H, Dekker J, Ostelo R. Patients' and clinicians' experiences with stratified exercise therapy in knee osteoarthritis: a qualitative study. BMC Musculoskelet Disord. 2022;23(1):559. PubMed
29.Lawford BJ, Delany C, Bennell KL, Hinman RS. “I was really sceptical...But it worked really well”: a qualitative study of patient perceptions of telephone-delivered exercise therapy by physiotherapists for people with knee osteoarthritis. Osteoarthr Cartil. 2018;26(6):741-750. PubMed
30.Lawford BJ, Bennell KL, Allison K, Schwartz S, Hinman RS. Challenges With Strengthening Exercises for Individuals With Knee Osteoarthritis and Comorbid Obesity: A Qualitative Study With Patients and Physical Therapists. Arthritis Care Res (Hoboken). 2022;74(1):113-125. PubMed
31.Ledingham A, Cohn ES, Baker KR, Keysor JJ. Exercise adherence: beliefs of adults with knee osteoarthritis over 2 years. Physiother. 2020;36(12):1363-1378. PubMed
32.Leese J, MacDonald G, Backman CL, Townsend A, Nimmon L, Li LC. Experiences of Wearable Technology by Persons with Knee Osteoarthritis Participating in a Physical Activity Counseling Intervention: Qualitative Study Using a Relational Ethics Lens. JMIR Mhealth Uhealth. 2021;9(11):e30332. PubMed
33.Moore AJ, Holden MA, Foster NE, Jinks C. Therapeutic alliance facilitates adherence to physiotherapy-led exercise and physical activity for older adults with knee pain: a longitudinal qualitative study. J Physiother. 2020;66(1):45-53. PubMed
34.Nelligan RK, Hinman RS, Teo PL, Bennell KL. Exploring Attitudes and Experiences of People With Knee Osteoarthritis Toward a Self-Directed eHealth Intervention to Support Exercise: Qualitative Study. JMIR Rehabil Assist Technol. 2020;7(2):e18860. PubMed
35.Ostlind E, Ekvall Hansson E, Eek F, Stigmar K. Experiences of activity monitoring and perceptions of digital support among working individuals with hip and knee osteoarthritis - a focus group study. BMC Public Health. 2022;22(1):1641. PubMed
36.Sutton L, Jose K, Hansen E, et al. Navigating the maze of osteoarthritis treatment: A qualitative study exploring the experience of individuals with osteoarthritis in Tasmania, Australia. Musculoskelet. 2022;12:12. PubMed
37.Teo PL, Bennell KL, Lawford B, Egerton T, Dziedzic K, Hinman RS. Patient experiences with physiotherapy for knee osteoarthritis in Australia-a qualitative study. BMJ Open. 2021;11(3):e043689. PubMed
38.Uritani D, Ikeda A, Shironoki T, et al. Perceptions, beliefs, and needs of Japanese people with knee osteoarthritis during conservative care: a qualitative study. BMC Musculoskelet Disord. 2021;22(1):754. PubMed
39.Wallis JA, Webster KE, Levinger P, Singh PJ, Fong C, Taylor NF. Perceptions about participation in a 12-week walking program for people with severe knee osteoarthritis: a qualitative analysis. Disabil Rehabil. 2019;41(7):779-785. PubMed
40.Yeh WL, Tsai YF, Hsu KY, Chen DW, Wang JS, Chen CY. Weight control in older adults with knee osteoarthritis: a qualitative study. BMC Musculoskelet Disord. 2020;21(1):504. PubMed
41.Lincoln YS, Guba EG. But is it rigorous? Trustworthiness and authenticity in naturalistic evaluation. New Dir Program Eval. 1986;1986(30):73-84.
42.Tracy S. Qualitative Quality: Eight “Big-Tent” Criteria for Excellent Qualitative Research. Qual Inq. 2010;16:837-851.
43.Wallis JA, Ackerman IN, Brusco NK, et al. Barriers and enablers to uptake of a contemporary guideline-based management program for hip and knee osteoarthritis: A qualitative study. Osteoarthr Cartil Open. 2020;2(4):100095. PubMed
44.Liu X, Seidel JE, McDonald T, et al. Rural-Urban Disparities in Realized Spatial Access to General Practitioners, Orthopedic Surgeons, and Physiotherapists among People with Osteoarthritis in Alberta, Canada. Int J Environ Res Public Health. 2022;19(13):7706. PubMed
45.Spinney J, Millward H. Time and Money: A New Look at Poverty and the Barriers to Physical Activity in Canada. Soc Indic Res. 2010;99(2):341-356.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Studies
Author, year, country | Aims/objectivesa | Methodology/design, sampling, data collection method, data analysis method | Description of exercise-based intervention | Setting | Inclusion criteria and sample size | Participant characteristicsb |
|---|---|---|---|---|---|---|
Battista et al. (2022)25 Italy | To investigate how patients with OA experience their disease and care process, highlighting potential elements that can enhance or spoil it, to optimize their quality of care | Descriptive phenomenology Purposeful, maximum variation sampling; access to participants was gained through health care providers specializing rheumatic and musculoskeletal disease rehabilitation and snowball sampling; sampling completed once reaching “data saturation” (as determined by 2 analysts) Semistructured interviews (approximately 60 minutes each) conducted via videoconference Thematic analysis and methods borrowed from content analysis | Participants were asked to describe their perspectives on and experiences with “physical activity” intended to manage their OA. | Participants were recruited from urban and suburban locations in the northern part of the country (cities NR) | Individuals (N = 11) with physician-diagnosed knee and/or hip OA who could speak Italian and were willing to participate | Age: Mean 60.8 years (range, 45 years to 73 years) 54.5% (n = 6) female; 45.5% (n = 5) male Health literacy/education: NR Income/employment status/SES: 63.6% (n = 7) not retired; 36.4% (n = 4) retired Race/ethnicity (self-reported): NR Other relevant information: 45.5% (n = 5) living with hip OA; 27.3% (n = 3) living with knee and hip OA; 27.3% (n = 3) living with knee OA |
Cronström et al. (2019)26 Sweden | To investigate the experiences of a digital management program for hip and knee OA, including education and exercise as well as an option to chat with an assigned physical therapist for feedback, questions, and support | Qualitative design (specific methodology NR) Purposeful, maximum variation sampling; participants were recruited after their enrolment in a digital OA management program; “data collection stopped when no further information was added” (p. 3) Semistructured interviews (30 to 40 minutes) conducted face-to-face (n = NR), by Skype (n = NR), or by telephone (n = NR) Systematic text condensation | Participants had engaged in a 6-week, digitally-delivered, non–group-based OA management program (Joint Academy) incorporating education on physical activity and individualized neuromuscular exercises of increasing difficulty. While enrolled in the program, participants had the option to chat asynchronously with an assigned physical therapist to obtain feedback and ask questions. | The study was conducted at a regional hospital in the southern part of the country | Individuals (N = 19) with confirmed hip or knee OA who could speak and understand Swedish | Age: Mean 65 years (range, 45 years to 80 years) 52.6% (n = 10) female; 47.4% (n = 9) male Health literacy/education: NR Income/employment status/SES: 52.6% (n = 10) retired; additional information NR Race/ethnicity (self-reported): NR Other relevant information: 52.6% (n = 10) living with hip OA; 47.3% (n = 9) living with knee OA |
Ezzat et al. (2022)27 Australia | To understand patient perceived acceptability of participating in a telehealth-delivered, group-based education and exercise-therapy program for knee OA | Interpretive description Participants were recruited by email from an ongoing clinical trial; sampling methods otherwise NR Semistructured interviews (mean = 24 minutes; range, 11 to 40 minutes) conducted in-person (n = 16) or by videoconference (n = 3) Inductive thematic analysis | Participants had engaged in a physiotherapist-led, standardized but individualized group education and supervised neuromuscular exercise-therapy program (GLA:D); participants had received GLA:D either via telehealth (57.9%; n = 11) or in-person (42.1%; n = 8). All participants had completed 12 exercise-therapy sessions. | City or region NR | Individuals (N = 19) aged 40 years or older with a primary clinical diagnosis of knee OA; with sufficient English language abilities to participate in the clinical trial; and who lived within a 10-kilometre radius of a clinical site offering GLA:D | Age: Mean 62 years (range, 49 years to 72 years) 63.2% (n = 12) female; additional information NR Health literacy/education: NR Income/employment status/SES: NR Race/ethnicity (self-reported): NR |
Knoop et al. (2022)28 Netherlands | To explore the experiences with stratified exercise therapy in knee OA from the patient’s, physiotherapist’s, and dietician’s perspectivec | Qualitative design (specific methodology NR) Participants of the qualitative study were randomly sampled from the experimental arm of an RCT Semistructured interviews (15 to 30 minutes) conducted via the telephone Open, axial, and selective coding “of the Grounded Theory Approach” | Participants had received stratified physiotherapist-delivered exercise therapy with protocolized interventions tailored to 3 patient subgroups. The high muscular strength subgroup received education and home exercises; the low muscle strength subgroup received education, home exercises, and muscle strength training; and the subgroup living with obesity received education, adapted muscle strength, and aerobic training. The number of exercise sessions delivered ranged from 3 to 18, with those with high muscle strength receiving the fewest and those living with obesity receiving the most sessions. | City or region NR, but all authors are situated in Amsterdam | Individuals (N = 15) meeting clinical criteria for knee OA 5 participants each from the following subgroups: high muscular strength; low muscular strength; and living with obesity | Age: Mean 61.9 years (range, 45 years to 78 years) 86.7% (n = 13) female; 13.3% (n = 2) male Health literacy/education: NR Income/employment status/SES: NR Race/ethnicity (self-reported): NR |
Lawford et al. (2018)29 Australia | To explore people’s perceptions of exercise therapy delivered by physiotherapists via telephone for their knee OA | Qualitative design (otherwise NR) Participants were recruited from the intervention arm of an RCT (which had recruited participants through advertisements distributed via social media, community locations, consumer organizations, medical clinics, radio, and newspapers, and through a previous volunteer database); authors reported collecting data until reaching “theoretical saturation;” sampling methods otherwise NR Semistructured interviews (length NR) conducted over the telephone “Thematic approach” (described in the cited approach as “thematic analysis”) | Over a period of 6 months, participants had received 5 to 10 phone calls from a physiotherapist. During the calls, physiotherapists collaborated with participants to create an individualized strengthening program and physical activity plan, monitored their progress, provided education about knee OA and the benefits of exercise, provided behavioural change support, and adjusted the program and goals as necessary. | Participants were recruited from metropolitan (n = 12) and regional (n = 8) areas | Individuals (N = 20) who met NICE clinical criteria for knee OA; had average knee pain of ≥ 4 on an 11-point scale; had a history of knee pain lasting at least 3 months; and who had received exercise advice and support from a physiotherapist via telephone over a 6-month period | Age: Mean, 58.8 years (range, 47 years to 79 years) 65% (n = 13) female; 35% (n = 7) male Health literacy/education: 30% (n = 6) some tertiary training; 25% (n = 5) graduated from university or polytechnic postgraduate study; 20% (n = 4) postgraduate study; 20% (n = 4) 3 years or more of high school; less than 3 years of high school (n = 1) Income/employment status/SES: 40% (n = 8) retired; 35% (n = 7) employed full-time; 25% (n = 5) employed part-time Race/ethnicity (self-reported): NR |
Lawford et al. (2022)30 Australia | To explore challenges associated with implementing a home-based strengthening exercise program for individuals with knee OA and comorbid obesityc | Qualitative design (specific methodology NR) Purposeful, maximum variation sampling; Participants were recruited from an RCT (which had recruited participants through advertisements distributed via social media, community locations, consumer organizations, medical clinics, radio, and newspapers, and through a previous volunteer database); authors reported collecting data until reaching “theoretical saturation” Semistructured interviews (length NR) conducted over the phone “Inductive thematic approach” (described in the cited approach as “thematic analysis”) | Participants had attended 5 individual physical therapy sessions over 12 weeks. The physical therapists provided education about exercise and taught participants an exercise program and instructed them to perform at home 4 times per week. 10 participants received a weight bearing program, while 12 received a non–weight-bearing program. The physical therapists progressed or modified the programs based on their assessment of the participants. | Melbourne | People (N = 22) aged 50 years or greater living with knee OA and comorbid obesity | Age: Mean (± SD) 63 years (± 7.0 years) 59.1% (n = 13) female; 40.9% (n = 9) male Health literacy/education: NR Income/employment status/SES: 54.5% (n = 12) employed; 45.5% (n = 10) not employed Race/ethnicity (self-reported): NR |
Ledingham et al. (2020)31 NR | To explore experiences, feelings, and perspectives related to long-term adherence to exercise among adults with painful knee OA participating in a 2-year RCT, and identify factors that influenced long-term adherence to exercise | Qualitative design (otherwise NR) Purposeful, maximum variation sampling; participants were recruited from an RCT; the authors reported reaching “data saturation” after analyzing data of 25 participants Semistructured interviews (mean length 41 minutes; range, 28 to 61 minutes) conducted in-person Analytical approaches informed by constructivist grounded theory | Participants engaged in an in-person, group-based, 6-week, twice weekly strength training exercise class led by a physical therapist or exercise scientist and an assistant. Classes included education and postural awareness advice, a walking warm-up followed by side-stepping exercises, and progressive strengthening exercises. Participants were instructed to continue performing the exercises 3 times per week at home after completing the class. All participants received a weekly non-interactive telephone message reminding them to continue their exercises. 56% (n = 14) also received twice monthly calls from a telephone-linked communication system (BOOST) delivering tailored exercise motivation messages. | Setting NR, but all authors are affiliated with institutions in Boston, Massachusetts | Community-dwelling adults (N = 25) aged 50 years or older with self-reported doctor-diagnosed knee OA and knee pain | Age: Mean (± SD) 67.3 years (± 6.1 years; range, 57 years to 79 years) 84% (n = 21) female; additional information NR Health literacy/education: NR Income/employment status/SES: NR Race/ethnicity (self-reported): 36% (n = 9) Black; 48% (n = 12) white; 16% (n = 4) “other” |
Leese et al. (2021)32 Canada | To explore everyday ethical issues experienced by people with knee OA in their relationships with themselves and physical therapists while using a physical activity wearable | Secondary analysis (supra-analysis) of semistructured interview data originally obtained for the qualitative component of an RCT The authors selected the data obtained from 21 of the 56 interviews conducted for the previous primary qualitative study for inclusion in their secondary analysis using principles of purposeful, maximum variation sampling; data collection ceased when the research team agreed their findings were sufficiently varied to describe a range of experiences relevant to the research objectives The data used in the secondary analysis were originally obtained via in-depth, semistructured interviews (lasting 60 to 90 minutes); medium NR Analytical methods informed by phenomenographic analysis | Participants interviewed for the primary qualitative study had received a technology-enabled counselling intervention to increase moderate to vigorous physical activity. The intervention consisted of a 1.5-hour session during which participants received 15 minutes of group-based education about physical activity, a physical activity wearable, and individual counselling with a physiotherapist trained in motivational interviewing. Participants wore the wearable activity tracker (which tracked physical activity data and reported it on a medium viewable by the participant and physical therapist) for 24 hours a day except while in water. The physical therapist reviewed participants’ physical activity data during 4 biweekly scheduled phone calls. | Vancouverd | Interview data included in the secondary analysis were collected from adults (N = 21) living in Vancouver with a physician-confirmed diagnosis of knee OA or who passed 2 criteria for early OA (i.e., being aged 50 years or older with knee pain lasting more than 28 separate or consecutive days during the previous year) | Age: Mean 61.2 years (range, 40 years to 82 years) 61.9% (n = 13) female; 38.1% (n = 8) male Health literacy/education: Educational levels ranged from high school graduate (n = 4) to a bachelor’s degree or above (n = 11) Income/employment status/SES: Annual household income ranged from under CA$12,000 (n = 1) to more than CA$100,000 (n = 4) Race/ethnicity (self-reported): NR |
Moore et al.(2020)33 UK | To investigate the following questions: 1.What are people’s experiences and perceived impact of physiotherapist-led exercise interventions for knee pain attributable to OA? 2.What barriers and facilitators to change in exercise and physical activity behaviour exist over time? | Longitudinal qualitative study (specific methodology NR) Purposeful, maximum variation sampling; participants were recruited from the intervention arms of an RCT (which recruited participants from up to 100 general practices and their associated physiotherapy services); sampling continued until reaching “data saturation” Semistructured interviews (length NR) conducted in-person at 2 points in time: first, shortly following the intervention period of the RCT, and then approximately 12 months after the intervention period of the RCT; conducted in-person Thematic analysis (the authors also cited methods inspired by constructivist grounded theory and longitudinal qualitative analysis) | Participants received physiotherapist-led sessions incorporating advice and exercise; 1 “usual care” group (n = 10) received up to 4 treatment sessions consisting of advice and exercise over 12 weeks. A second “individually-tailored exercise” group (n = 8) received 6 to 8 sessions consisting of individualized, supervised, and progressed lower limb exercises over 12 weeks. A third “targeted exercise adherence” group (n = 12) had 8 to 10 contacts with a physiotherapist over 6 months and transitioned from lower limb exercise to general physical activity. | RCT participants were recruited from the West Midlands North and North West regions in the country | Individuals (N = 30) aged 45 years or older with knee pain and/or stiffness in one or both knees who met criteria for a clinical diagnosis of OA 22 of the 30 participants interviewed shortly after the intervention period also participated in the 12-month follow-up interviews | Age: 16.7% (n = 5) aged 45 to 54 years; 30% (n = 9) aged 55 to 64 years; 26.7% (n = 8) aged 65 to 74 years, 26.7% (n = 8) aged 75 years or older 50% (n = 15) female; 50% (n = 15) male Health literacy/education: NR Income/employment status/SES: NR Race/ethnicity (self-reported): NR |
Nelligan et al. (2020)34 Australia | To explore the attitudes and experiences of people with knee OA who accessed a self-directed e-health intervention and the features perceived as useful to facilitate self-directed exercise | Qualitative design (specific methodology NR) Purposeful, maximum variation sampling; Participants were recruited from the intervention arm of an RCT (which originally recruited through social media, online newspapers, and a volunteer database); sample size was dictated by “theoretical saturation” Semistructured interviews (length NR) conducted via the telephone Thematic analysis | Participants received access to a website (“My Knee Exercise”) that contained educational information about knee OA, exercise, and general physical activity. The website also prescribed a 24-week lower limb strengthening exercise program (with exercises to be completed 3 times per week). The exercise program was supported by a corresponding 24-week automated SMS program developed using behaviour change theory. Participants received weekly automated text messages prompting them to self-report how many exercise sessions they had completed in the previous week. They received automated responses based on their reported level of adherence. Additionally, they received regular text messages containing behaviour change technique suggestions. | Participants resided in locations across all states and territories except for the Northern Territory 56.3% (n = 9) resided in regional areas; 43.8% (n = 7) resided in metropolitan areas | Individuals (n = 16) with knee OA who had accessed the 24-week e-health intervention designed to support exercise participation as part of a RCT | Age: Mean 62.6 years (range, 48 years to 75 years) 50% (n = 8) female; 50% (n = 8) male Health literacy/education: 56.3% (n = 9) had completed tertiary education; 43.8% (n = 7) had completed secondary education Income/employment status/SES: 50% (n = 8) retired; 25% (n = 4) employed part-time; 25% (n = 4) employed full-time Race/ethnicity (self-reported): NR |
Ostlind et al. (2022)35 Sweden | To explore the experiences of using a wearable activity tracker to monitor physical activity and the general perceptions of digital support in OA care among individuals of working age with hip and knee OA | Qualitative design (specific methodology NR) Combination of purposeful and convenience sampling; participants were recruited from the intervention arm of an RCT 3 semistructured focus groups (60 to 75 minutes) with 6 participants each, conducted in-person Qualitative content analysis | All participants received education about OA, self-management, and exercise in group-based lectures. Then, they used a wearable activity tracker and its associated app to monitor and receive feedback on their physical activity over 12 weeks. | Data were collected in the southern part of the country (additional information NR) | People (N = 18) of working age living with knee or hip OA who had worn a physical activity tracker 12 weeks to monitor their physical activity | Age: Mean (± SD) 58 years (± 6.0 years) 72.2% (n = 13) self-identified as women; other information NR Health literacy/education: 50% (n = 9) reported having a postsecondary education; additional information NR Income/employment status/SES: 50% (n = 9) reported engaging in sedentary work; additional information NR Race/ethnicity (self-reported): NR Other relevant information: 61.1% (n = 11) reported the knee joint as the most affected by OA; 38.9% (n = 7) reported the hip joint as most affected by OA |
Sutton et al. (2022)36 Australia | To explore the experience of people living with OA in Tasmania, Australia; to gain an understanding of their navigation of the health system; and to explore their beliefs and understandings of the role of exercise and joint replacement surgery for the management of OA | Qualitative design (specific methodology NR) Purposeful sampling; Participants were recruited through targeted advertisements on social media and contact with people who had expressed interest in other research studies within the institution (Menzies Institute for Medical Research); sampling ceased when “interviews were not eliciting any new ideas” Semistructured interviews (length NR) conducted over telephone (n = 6) or in-person (n = 20) Thematic analysis | As part of the interview guide, participants were asked to describe their perspectives on and experiences with exercise for the management of knee OA. | Tasmania | People (N = 26) aged 45 years or older with a diagnosis of knee OA from a health professional | Age: Mean 66 years (SD or range NR) 80.8% (n = 21) female; additional information NR Health literacy/education: NR Income/employment status: 50% lived in an area with an IRSADd score greater than the 90th percentile of Tasmania; 23% in an area with an IRSAD score greater than the 50th percentile of Tasmania Race/ethnicity (self-reported): NR |
Teo et al. (2021)37 Australia | To explore the experiences of people who had recently received physiotherapy care for their knee OA in Australia and how these experiences aligned with the national Clinical Care Standard for knee OA | Qualitative design (specific methodology NR) Purposeful, convenience sampling; participants were recruited via Facebook and a research volunteer database; sample size determined by “data saturation” Semistructured interviews (length NR) conducted via telephone Thematic analysis | Participants had received physiotherapy care for their knee OA in the past 6 months. The interview guide contained questions asking participants about their experiences regarding exercise-based interventions delivered by their physiotherapists. | Participants were recruited from all 6 states and 2 territories of the country 79.2% (n = 19) of participants resided in major cities; 12.5% (n = 3) in outer regional locations; and 8.3% (n = 2) in inner regional locations | Adults (N = 24) meeting the NICE criteria for knee OA who had consulted a physiotherapist about their knee OA in the 6 months before the study | Age: Mean (± SD), 63.5 years (± 9.8 years; range, 49 years to 81 years) 75% (n = 18) female; additional information NR Health literacy/education: 20.8% (n = 5), reported having 3 or more years of high school; 20.8% (n = 5) reported having some tertiary training; 29.2% (n = 7), reported graduated from university or polytechnic; 29.2% (n = 7) reported having any postgraduate education Income/employment status/SES: 12.5% (n = 3) worked full-time; 29.2% (n = 7), worked part-time; 12.5% (n = 3) were unable to work due to health reasons; 45.8% (n = 11) were retired Race/ethnicity (self-reported): NR |
Uritani et al. (2021)38 Japan | To clarify how Japanese people with knee OA experience and perceive their symptoms and disabilities, and how they face them during conservative care | Qualitative design (specific methodology NR) Purposeful, maximum variation sampling; access to participants was obtained through orthopedic surgeons, physical therapists, and a health promotion program cooperating with the study and the study’s author; data collection continued until reaching theoretical saturation Semistructured interviews (60 to 90 minutes) conducted in-person; all interviews were conducted 1-on-1, with the exception of 1 interview conducted with 2 participants who were a couple Analytical methods informed by constructivist grounded theory | When asked to describe how they deal with knee pain and difficulty in moving, some participants spoke of their experiences with exercise as an intervention. | Participants resided in different regions in the country; places of recruitment included a hospital in a suburban area (n = 6), a clinic in an urban area (n = 2), and a health care program in a suburban area (n = 1) | Individuals (N = 9) aged > 50 years residing in Japan with a confirmed diagnosis of knee OA in 1 or both knees and a self-reported experience of pain or disability | Age: Mean (± SD): 74.3 years (± 5.5 years; range, 67 years to 80 years) 77.8% (n = 7) women; 22.2% (n = 2) men Health literacy/education: NR Income/employment status/SES: Housewife, retired from previous profession (n = 3); housewife (n = 2); housewife and volunteer worker (n = 1); volunteer worker, retired (n = 1); carpenter (n = 1); part-time university lecturer (n = 1) Race/ethnicity (self-reported): NR |
Wallis et al. (2019)39 Australia | To explore the perceptions of people with severe knee OA and increased cardiovascular risk about participating in a walking program | Phenomenological approach (specific approach NR) Participants were recruited from the intervention arm of an RCT (which recruited participants from a metropolitan health service’s OA clinic); sampling methods otherwise NR Semistructured interviews (averaging 15 minutes) conducted face-to-face Thematic analysis; qualitative data were triangulated with quantitative data from the RCT | Participants engaged in a moderate intensity 12-week walking program of 70 km per week, with each session lasting at least 10 minutes. Each participant had a planning session with a physiotherapist before starting the program. The physiotherapist supervised 1 walking session per week, and these supervised sessions were delivered either 1-on-1 or in a group setting (based on each participant’s preference). | Region or geographic location NR; however, participants had received care at a metropolitan health service clinic | Individuals (N = 21) older than 50 years of age who attended a metropolitan health service’s hip and knee OA clinic, were diagnosed radiographically with severe knee OA, and had at least moderate cardiovascular risk (i.e., at least stage 2 of the Adult Exercise Screening Tool) | Age: Mean 67.1 years (range, 51 to 84 years) 57.1% (n = 12) male; 42.9% (n = 9) female Health literacy/education: NR Income/employment status/SES: 61.9% (n = 13) reported being retired; 14.3% (n = 3) reported working part-time; 9.5% (n = 2) reported working full-time; 9.5% (n = 2) reported not working; 4.8% (n = 1) reported working casually Race/ethnicity (self-reported): NR |
Yeh et al. (2020)40 Taiwan | To understand weight-control strategies, facilitators of, and barriers toward weight control in older adults with knee OA who preferred not to undergo physician-recommended total knee arthroplasty | Qualitative description Purposeful, convenience sampling; access to participants was gained through physicians or nurses in outpatient orthopedic surgical clinics; sampling and data collection continued until reaching “data saturation” Semistructured interviews (20 to 60 minutes) conducted face-to-face Content analysis | Participants were asked to describe their thoughts of, experiences with, and needs related to exercise and home-based exercise training in the context of weight management (intended to manage knee OA). | Participants were recruited from 1 medical centre and 2 regional hospitals in the northwestern region of the country | Individuals (N = 118) that had been diagnosed with knee OA, were aged ≥ 55 years, did not feel comfortable undergoing physician-recommended total knee arthroplasty, and were able to understand and speak Mandarin Chinese | Age: Mean (± SD) 70.8 years (± 7.2 years, range 56 years to 89 years) Female, 67.8% (n = 80); male, 32.2% (n = 38) Health literacy/education: 10.2% (n = 12) reported being illiterate; 55.9% (n = 66) had completed primary school; 15.3% (n = 18) had completed junior high school; 14.4% (n = 17) had completed senior high school; 4.2% (n = 5) had college education or above Income/employment status/SES: 83.9% (n = 99) reported not currently working; 16.1% (n = 19) reported working Race/ethnicity (self-reported): NR Additional relevant information: 93.2% (n = 110) had not previously received knee arthroplasty; 6.8% (n = 8) had previously received knee arthroplastyf |
BOA = Better Management of Patients With Osteoarthritis; GLA:D = Good Life With Osteoarthritis: Denmark; IRSAD = The Index of Relative Socio-economic Disadvantage; NICE = National Institute for Health and Care Excellence; NR = not reported; OA = osteoarthritis; QSE = quadriceps strengthening exercise; RCT = randomized control trial; SES = socioeconomic status; SMS = short messaging service.
Note: All non-integers have been rounded to the nearest 10th.
aThe aims and objectives of the studies are reported in the words of their authors.
bThe reporting of participant characteristics in this table uses the terms used by the authors of the included citations. Of note, while none of the authors reported including people identifying as genders other than men or women, it is possible this was because of limitations in how they collected and reported their demographic data.
cThis study also included participants who were health care providers. Only information relevant to the subsample of participants living with OA are reported in this table.
dThe primary data used to inform the secondary analysis were collected at this location.
eHigher IRSAD scores are indicative of greater socioeconomic advantage and vice versa.
fStudy included as the majority of participants had not received knee arthroplasty in the past.
Note that this appendix has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Critical Appraisal Using the Optimized CASP18 Tool
Strengths | Limitations |
|---|---|
Battista et al. (2022)25 | |
|
|
Cronström et al. (2019)26 | |
|
|
Ezzat et al. (2022)27 | |
|
|
Knoop et al. (2022)28 | |
|
|
Lawford et al. (2018)29 | |
|
|
Lawford et al. (2022)30 | |
|
|
Ledingham et al. (2020)31 | |
|
|
Leese et al. (2021)32 | |
|
|
Moore et al. (2020)33 | |
|
|
Nelligan et al. (2020)34 | |
|
|
Ostlind et al. (2022)35 | |
|
|
Sutton et al. (2022)36 | |
|
|
Teo et al. (2021)37 | |
|
|
Uritani et al. (2021)38 | |
|
|
Wallis et al. (2019)39 | |
|
|
Yeh et al. (2020)40 | |
|
|
CASP = Critical Appraisal Skills Programme; NR = not reported; RCT = randomized control trial.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca