CADTH Health Technology Review
Canakinumab for Adult-Onset Still Disease
Rapid Review
Authors: Khai Tran, Monika Mierzwinski-Urban
Abbreviations
AE
adverse event
AOSD
adult-onset Still disease
CRP
C-reactive protein
DMARD
disease-modifying antirheumatic drug
ESR
erythrocyte sedimentation rate
IL
interleukin
NSAID
nonsteroidal anti-inflammatory drug
SJIA
systemic juvenile idiopathic arthritis
SR
systematic review
TNF
tumour necrosis factor
Key Messages
This review identified limited evidence from 2 systematic reviews about the clinical effectiveness and safety of canakinumab for patients with adult-onset Still disease (AOSD). Most studies in the systematic reviews on AOSD did not have a control group; therefore, the findings related to the effectiveness and safety of canakinumab in this population are uncertain.
For adults with AOSD, treatment with canakinumab may be associated with a complete or partial response to treatment, corticosteroid-sparing effect, and a decrease or normalization of key laboratory parameters, such as leukocyte count, erythrocyte sedimentation rate, and serum levels of ferritin and C-reactive protein, compared with baseline.
In adults with AOSD, limited evidence suggested there was no statistically significant difference between canakinumab and placebo in articular manifestations.
Adverse events associated with canakinumab treatment included infections, leukopenia, musculoskeletal and connective tissue disorders, skin disorders, thoracic and mediastinal disorders, gastrointestinal disorders, and site injection reactions. Severe adverse events included macrophage activation syndrome, hepatocytotoxicity, and serious infections that led to discontinuation of treatment.
No studies were found comparing canakinumab and alternative pharmacologic treatments for AOSD.
No studies were found on the cost-effectiveness of canakinumab for the treatment of AOSD.
No evidence-based guidelines were found on the use of canakinumab for the treatment of ASOD.
Context and Policy Issues
Adult-onset Still disease (AOSD) is a multisystem autoinflammatory disorder of unknown etiology.1 AOSD is a rare disease with a low prevalence of 1 to 34 cases per 1 million people, which is slightly more common in females than in males.2 The incidence of AOSD varies between 0.16 and 0.6 new cases per 100,000 people worldwide.3,4 Although AOSD appears to have a bimodal age distribution (typically observed in patients between the ages of 15 and 25 years and between the ages of 35 to 45 years), older patients with AOSD have been reported.5
Clinical features of AOSD include high-spiking fever, skin rash, arthritis, lymphadenopathy, and hepatosplenomegaly.6 However, life-threatening complications, such as severe multiorgan inflammation or systemic hyperinflammation with macrophage activation syndrome, may also occur.7 Although highly unspecific, patients with AOSD are likely to have an elevated erythrocyte sedimentation rate (ESR) and elevated levels of C-reactive protein (CRP), serum ferritin, blood neutrophils, and liver enzymes.4,8 Based on the clinical and laboratory manifestations, patients with AOSD can be divided into 2 distinct groups: those with predominantly systemic clinical features (e.g., fever and skin rash) and those with chronic arthritis similar to rheumatoid arthritis.8 Due to the lack of diagnostic markers and its heterogeneous clinical features, diagnosis of AOSD is mainly based on exclusion of conditions such as infections, malignancy, or other rheumatic diseases. Diagnosis of AOSD is guided by classification criteria proposed by Yamaguchi et al.9 and Fautrel et al.10
AOSD is considered the adult form of systemic juvenile idiopathic arthritis (SJIA), which affects children aged 16 years and younger, because both share common clinical and biological features.11 Therefore, it is accepted that Still disease includes both SJIA and AOSD, a continuum concept based on age.11 The pathogenesis of AOSD remains unclear; however, AOSD is associated with high levels of some proinflammatory cytokines, such as interleukin (IL)-1 beta, IL-6, IL-18, tumour necrosis factor (TNF) alpha, and interferon gamma.6 Increased knowledge of the pivotal role of these proinflammatory cytokines has led to the design and development of biologic drugs as inhibitors to those cytokines for AOSD treatment.3
Nonsteroidal anti-inflammatory drugs (NSAIDs) and corticosteroids are usually prescribed as first-line treatments for AOSD.12 In case of failure or adverse reactions with these agents, conventional disease-modifying antirheumatic drugs (DMARDs), such as cyclosporin A, azathioprine, leflunomide, hydroxychloroquine, or methotrexate, are prescribed as second-line drugs.12 If AOSD is refractory to first- and second-line drugs, IL-1 beta, IL-6, and TNF-alpha antagonists are the biologic drugs of choice for treatment.
There are 3 IL-1 inhibitors (anakinra, rilonacept, and canakinumab) currently available on the market.13 Anakinra is a nonglycosylated recombinant soluble antagonist of IL-1 receptor that inhibits both IL-1 alpha and IL-1 beta by binding to IL-1 receptor, with a half-life of 4 to 6 hours.4,14 Rilonacept is a dimeric fusion protein, with the extracellular domain of both IL-1 receptor component that binds circulating IL-1 beta.4,14 Its half-life is 6.3 to 8.6 days.4,14 Canakinumab, a fully human monoclonal antibody selective inhibitor of IL-1 beta, has a half-life of 21 to 28 days.4,14 All 3 drugs are administered subcutaneously; however, due to different half-lives, the injections of these drugs are given at different intervals: anakinra is given daily, rilonacept is given weekly, while canakinumab is given every 4 weeks.14 Thus, a potential advantage of canakinumab over other IL-1 inhibitors is related to its longer half-life that allows for a monthly subcutaneous injection, which may reduce site reactions.4,15
Canakinumab has been licensed by the US FDA,4,16 the European Medicine Agency,4,17 and Health Canada18 for treatment of autoinflammatory syndromes in adults, adolescents, and children, including cryopyrin-associated periodic syndromes, familial Mediterranean fever, TNF receptor–associated periodic syndrome, hyperimmunoglobulinemia D syndrome or mevalonate kinase deficiency, and Still disease (SJIA and AOSD). The approval of canakinumab for the treatment of Still disease is based on the concept that SJIA and AOSD are a single disease with a different age of onset,11 and there is increasing evidence on the use of canakinumab in the management of AOSD that is refractory to corticosteroids and DMARDs.4 For treatment of SJIA, the average annual drug cost of canakinumab based on the manufacturer’s submitted price was $208,000 for patients who weigh 37 kg or less and $416,000 for patients who weigh 38 kg or more.19 To support decision-making about canakinumab for the treatment of AOSD, it is important to evaluate clinical effectiveness and cost-effectiveness of canakinumab compared with no treatment or alternative pharmacologic interventions.
This report aims to summarize the clinical effectiveness of AOSD compared with no treatment or alternative pharmacologic interventions. The report also aims to summarize the cost-effectiveness of canakinumab for the treatment of AOSD, and the recommendations from evidence-based guidelines regarding the use of canakinumab for the treatment of AOSD.
Research Questions
What is the clinical effectiveness of canakinumab for the treatment of AOSD compared to alternative pharmacologic interventions?
What is the clinical effectiveness of canakinumab for the treatment of AOSD compared to placebo or no treatment?
What is the cost-effectiveness of canakinumab for the treatment of AOSD?
What are the evidence-based guidelines regarding the use of canakinumab for the treatment of AOSD?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were canakinumab and adult-onset Still disorder. No filters were applied to limit the retrieval by study type. Conference abstracts were excluded. The search was completed on January 30, 2023, and limited to English-language documents published since January 1, 2018.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Patients with adult-onset Still disease |
Intervention | Canakinumab (any dose) |
Comparator | Q1, Q3: Alternative pharmacological interventions (e.g., corticosteroids, conventional or biologic DMARDs, NSAIDs) Q2, Q3: Placebo or no treatment Q4: Not applicable |
Outcomes | Q1, Q2: Clinical benefits (e.g., symptom severity, symptom remission, pain reduction, safety, patient satisfaction, health-related quality of life) and harms (e.g., adverse events) Q3: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained, incremental cost-effectiveness ratio) Q4: Recommendations regarding the use of canakinumab for adult-onset Still disease (e.g., appropriate treatment regimen, treatment delivery, dosage) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies, economic evaluations, evidence-based guidelines |
DMARD = disease-modifying antirheumatic drug; NSAID = nonsteroidal anti-inflammatory drug.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1 or were published before 2018. Systematic reviews (SRs) in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Measurement Tool to Assess Systematic Reviews 2 (AMSTAR 2)20 for SRs. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
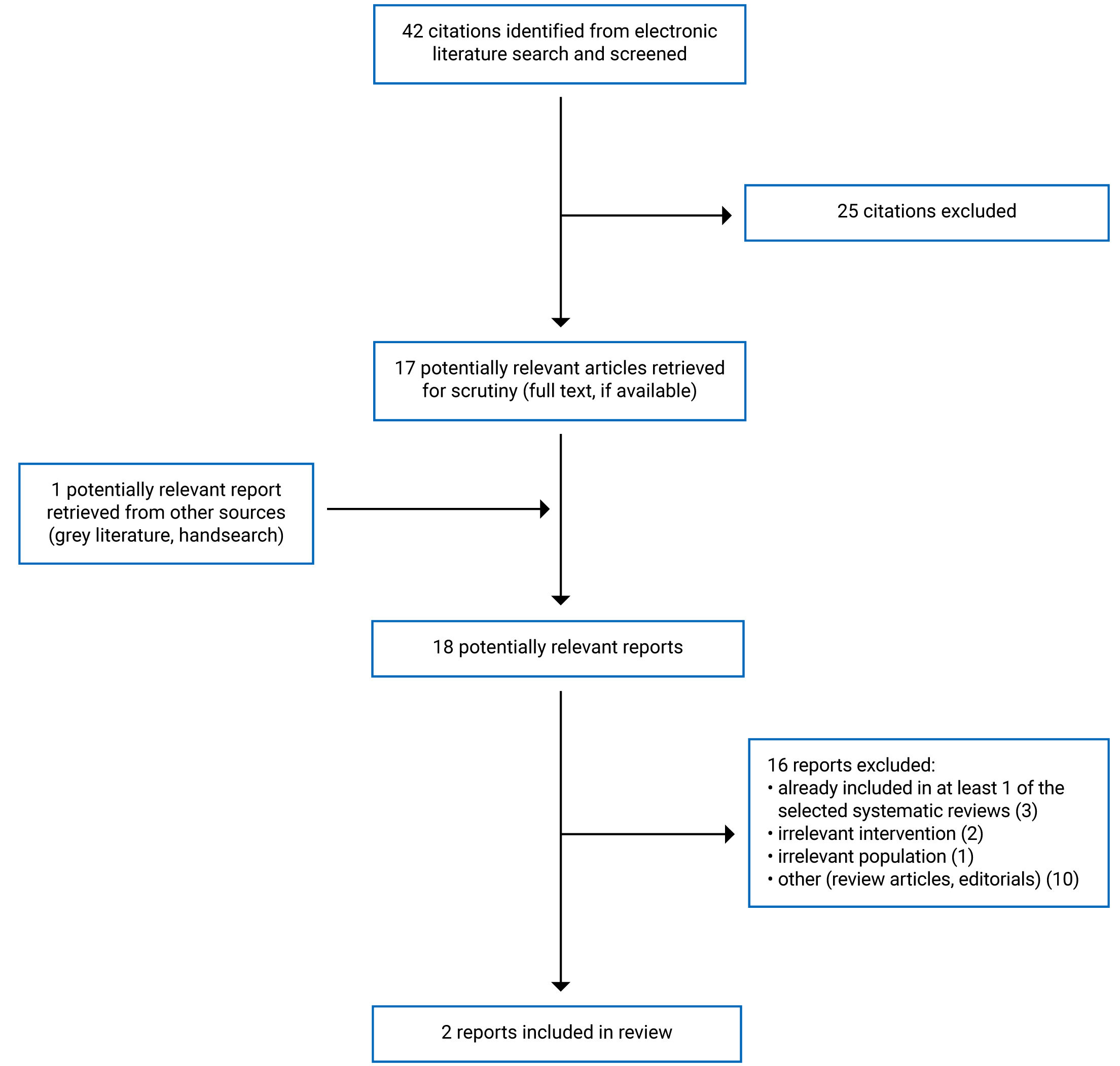
A total of 42 citations were identified in the literature search. Following screening of titles and abstracts, 25 citations were excluded and 17 potentially relevant reports from the electronic search were retrieved for full-text review. One potentially relevant publication was retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 16 publications were excluded for various reasons, and 2 publications, which were 2 SRs, met the inclusion criteria and were included in this report. Appendix 1 presents the PRISMA21 flow chart of the study selection.
Summary of Study Characteristics
Additional details regarding the characteristics of 2 included SRs22,23 are provided in Appendix 2.
Study Design
The SR by Cota-Arce et al. (2021)22 identified and included 17 studies published from 2012 to 2021. These were 7 case reports, 4 case series, 4 retrospective observational studies without a control group, 1 placebo-controlled phase II trial, and 1 pooled analysis study. A total of 144 patients were included for narrative synthesis. The authors did not describe any methods of pooling the results.
The SR by Kedor et al. (2021)23 identified and included 9 studies published from 2016 to 2021. These were 4 case series, 4 retrospective observational studies, and 1 placebo-controlled phase II trial. A total of 110 patients were included for narrative synthesis. The authors did not describe any methods of pooling the results.
Both SRs22,23 had 5 primary studies (i.e., 4 single-arm studies and 1 randomized controlled trial [RCT]) that overlapped with each other. The overlap in relevant primary studies between included SRs22,23 is presented in Appendix 5. In the single-arm studies, outcomes were compared from baseline to the end of canakinumab treatment.
Country of Origin
The SRs were conducted by authors from Mexico22 and Germany.23 The primary studies included in both SRs22,23 were conducted by authors from US, Italy, France, Sweden, Switzerland, the Netherlands, Turkey, Germany, and Greece.
Patient Population
The studies included in the SR by Cota-Arce et al. (2021)22 reported 144 patients with an age range between 16 and 72 years. There were more females (63.7%) than males (36.3%). Almost all patients (99.3%) had AOSD that had an inadequate clinical response with previous treatments, including NSAIDs, steroids, conventional DMARDs, or biologic drugs (e.g., anakinra, tocilizumab, TNF-alpha inhibitors).
The studies included in the SR by Kedor et al. (2021)23 had a total of 110 patients refractory to previously treated with NSAIDs, steroids, DMARDs, or biologic drugs. Patients’ age was not reported. There were more females (66%) than males (34%).
In the RCT included in both SRs,22,23 patients who were treated with NSAIDs, glucocorticoids, or conventional DMARDs required a stable dose before randomization and throughout the study treatment period (i.e., ≥ 2 weeks for NSAIDs, ≥ 1 week of ≤ 10 mg/day for prednisolone equivalent, and ≥ 6 weeks for conventional DMARDs). For biologic drugs, a washout period between 1 week to 9 months was required. It was unclear whether canakinumab with conventional DMARDs were co-administered to patients in the single-arm studies.
Interventions and Comparators
All observational studies (i.e., case reports, case series, and retrospective observational studies) included the 2 SRs,22,23 which were single-arm, before-and-after studies (i.e., did not include a control group), comparing canakinumab treatment with no treatment at baseline. The phase II trial included in both SRs22,23 compared canakinumab with placebo. Duration of treatment was 1 month to 18 months among studies in the SR by Cota-Arce et al. (2021)22 and 3 months to 43 months among studies in the SR by Kedor et al. (2021).23 Across studies included in both SRs,22,23 the dosage of canakinumab varied from 150 mg to 300 mg every 4 weeks.
Outcomes
The main outcomes evaluated in both SRs22,23 were degree of remission, reduction or discontinuation of corticosteroid use, laboratory values (e.g., leukocytosis, ESR, CRP, and ferritin), and adverse events (AEs) occurring during canakinumab therapy. The degree of remission was classified as complete response (i.e., the resolution of all manifestations (e.g., articular manifestations) or symptoms that the patient presented at baseline, including spiking fever, skin rash, arthralgia, arthritis, lymphadenopathy, hepatosplenomegaly, leukocytosis, and altered laboratory values), partial response (i.e., patients had clinical improvement, but not fulfilling the criteria for complete response), and no response (i.e., neither clinical nor laboratory improvements were observed).
Articular manifestations were assessed using the Disease Activity Score 28 (DAS28), a combined index that measures disease activity in patients with rheumatoid arthritis based on a count of 28 swollen and tender joints, which evaluates a patient’s response to treatment with a score ranging from 0 to 9.4. An absolute level of disease activity can be selected as a clinically meaningful goal for therapeutic intervention, with a value of 3.2 or less defined as the threshold for a low disease activity state and less than 2.6 as the threshold for remission.24 A reduction in the DAS28 score by 0.6 represents a moderate improvement; a reduction of more than 1.2 represents a major improvement.24 The DAS28-ESR is calculated based on erythrocyte sedimentation rate, while DAS28-CRP is calculated based on C-reactive protein.24
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Both SRs22,23 narratively synthesized the findings from their included studies. The intervention, population, and study design were clearly stated in their inclusion criteria. Due to rarity of the disease, the SR by Cota-Arce et al. (2021)22 was opened up to all study designs, including case reports, case series, observational studies, RCTs, and pooled analyses, whereas the SR by Kedor et al. (2021)23 excluded case reports. The review question, search strategy, and inclusion and exclusion criteria were clearly stated in both SRs.22,23 In the search strategy, both SRs22,23 used at least 2 databases. The authors of both SRs22,23 declared that the work of the review received no funding from any sources. Potential conflicts of interest were declared by the authors of both SRs.22,23
In the SR by Cota-Arce et al. (2021),22 duplicate study selection and data extraction and risk-of-bias assessment of the included studies were performed. The Cochrane risk-of-bias tool was used to assess the quality of the RCTs, and the adapted version of the Newcastle-Ottawa Scale was used to assess the quality of observational studies without a control group. The level of evidence of each publication was determined using the Oxford Centre for Evidence-Based Medicine tool. All of these would give a clear understanding regarding the quality of evidence reported by the SR.
In contrast, the SR by Kedor et al. (2021)23 did not use duplicate study selection and data extraction for data collection, and it is unclear whether this may have biased the selection of included studies. In this SR,23 the risk of bias of the included primary studies (i.e., case series, retrospective observational studies, and RCT) and the quality of the evidence from the included studies were not assessed. Not assessing the risk of bias of the included studies and the quality of evidence fails to establish transparency of evidence synthesis results and findings.
There were several shortcomings in both SRs.22,23 The comparators, outcomes, and time frame for follow-up were not prespecified. Establishment of a protocol before the review was not reported. This would have some risks in reporting bias. There was no plan established to investigate causes of heterogeneity among included studies. Because the search strategy did not include searching of the reference lists of the included studies, search trial registries, and search for grey literature, it is possible that some relevant studies may have been missed. A list of excluded studies was not provided.
The SR by Cota-Arce et al. (2021)22 was judged to be of moderate methodological quality because it fulfilled some components of study design and data collection in the quality assessment of a SR. The SR22 narratively synthesized the data with a clear description of the quality of evidence. The SR22 had some limitations in data synthesis. The SR by Kedor et al. (2021)23 was judged to be of low methodological quality because it had some shortcomings in study design, data collection, quality assessment of the included studies, and data synthesis.
Summary of Findings
Appendix 4 presents the main study findings.
Clinical Effectiveness of Canakinumab for the Treatment of AOSD Compared With Alternative Pharmacologic Interventions
No studies comparing canakinumab with alternative pharmacologic interventions for the treatment of AOSD were identified; therefore, no summary can be provided.
Clinical Effectiveness of Canakinumab for the Treatment of AOSD Compared With no Treatment or Placebo
Because both SRs22,23 had 5 primary studies that overlapped, the summary of findings from each SR might contain some of the same data.
Remission
The SR by Cota-Arce et al. (2021)22 evaluated the degree of remission from baseline to after treatment for 99 patients with AOSD and found a complete response in 68 patients (68.7%) and a partial response in 16 patients (16.2%); 15 patients (15.1%) had AOSD that showed no clinical improvement or were excluded due to AEs at the end of observation. The SR by Kedor et al. (2021)23 reported that among 110 patients with AOSD from single-arm studies, there was a complete response in 76 patients (69%) and partial response in 19 patients (17%); 15 patients (14%) had AOSD that showed no clinical improvement or were excluded due to AEs at the end of observation.
Articular Manifestations
Findings from a phase II RCT included in both SRs,22,23 12 of 18 patients (67%) in the canakinumab group and 7 of 17 patients (41%) in the placebo group showed a reduction in DAS28-ESR score of more than 1.2 points at week 12, which represents a major improvement in articular manifestations. However, the difference in the DAS28-ESR response rate was not statistically significant between groups (P = 0.18).
Corticosteroid Use
The SR by Cota-Arce et al. (2021)22 reported that, of 64 patients from single-arm studies who were treated with canakinumab in combination with prednisone or methyl prednisone, 13 patients (20.3%) had corticosteroid-sparing effect and 29 patients (45.3%) discontinued the use of corticosteroids at the end of follow-up. The SR by Kedor et al. (2021)23 reported that, of 81 patients from 6 single-arm studies, 33 patients (40.7%) stopped or weaned corticosteroids and 16 patients (20%) reduced the use of corticosteroids at the end of follow-up compared with baseline.
Laboratory Values
The SR by Cota-Arce et al. (2021)22 reported that 73.7% (42 of 57 patients) treated with canakinumab from 7 studies had leukocytosis resolved and presented normal white blood cell counts at the end of the observation period. For other parameters, 88.9% (56 of 63 patients) had ESR within the normal range, 87.4% (76 of 87 patients) had normal serum ferritin levels, and 95.4% (62 of 65 patients) had normal CRP levels at the end of the observation period.
The SR by Kedor et al. (2021)23 reported similar results. Four case series reported that patients had ESR, CRP, and/or serum ferritin levels that were substantially reduced or returned to the normal range following canakinumab therapy compared to baseline. In an observational study in which 4 patients were subsequently switched to canakinumab after their AOSD failed to respond to anakinra, the elevated levels of serum ferritin, ESR, and CRP returned to normal ranges in 3 of 4 patients. One observational study of 50 patients reported a substantial improvement in most investigated parameters, including leukocytosis and ESR, CRP, and ferritin levels, after canakinumab therapy.
However, in the phase II RCT (reported in both SRs), there were no statistically significant differences in serum ESR, CRP, and ferritin levels between the canakinumab and placebo groups; however, the numerical findings and the actual P values were not reported in either SR.
Adverse Events
The SR by Cota-Arce et al. (2021)22 reported that patients in 11 studies (6 case reports, 2 case series, and 3 retrospective observational studies) did not experience any AEs following canakinumab therapy. Common AEs reported in other single-arm studies in patients treated with canakinumab were infections and infestations (23.3%), musculoskeletal and connective tissue disorders (19.5%), gastrointestinal disorders (14.2%), such as abdominal pain, nausea, and diarrhea, general disorders, and administration site conditions (9.5%), and respiratory, thoracic, and mediastinal disorders (6.2%). There were 18 severe AEs, including macrophage activation syndrome episodes and serious infections. One patient died due to macrophage activation syndrome. Nine of 69 patients (13%) stopped canakinumab treatment due to AEs.
The SR by Kedor et al. (2021)23 reported that patients in 3 case series did not experience any AEs. A case series study of 11 patients reported a case of the reactivation of latent tuberculosis 9 months after first injection of canakinumab. In a case series of 10 patients, 1 patient developed leucopenia, 1 patient developed a herpes zoster infection during treatment with canakinumab. Three of 13 patients in an uncontrolled observational study had herpes zoster reactivation, prostatitis, and mild leukopenia, respectively. In an uncontrolled observational study of 50 patients treated with canakinumab, there were 2 cases of severe pneumonia, 1 of which led to treatment cessation. Ten of 50 patients (20%) experienced infections: 5 in respiratory tract, 2 in the lower urinary tract, 1 fungal infection in the oral cavity, 1 fungal infection in the external genital area, and 1 mild skin and soft tissue infection. Three of 50 patients (6%) had drug-related leukopenia.
In the phase II RCT included in both SRs,22,23 4 patients in the canakinumab group presented 1 of the following serious AEs: hepatocytotoxicity, patella-femoral pain syndrome, hypotonia, and deep vein thrombosis. Both SRs reported a higher number of common AEs in the canakinumab group compared with the placebo group that were musculoskeletal and connective tissue disorders, infections and infestations, gastrointestinal disorders, skin and subcutaneous tissue disorders, and general disorders and administration site conditions; however, neither SR reported the numerical findings. It was reported that after calculating the exposure times in the canakinumab group and the placebo group, the authors of the RCT concluded that the AE rate per 100 patient-years of exposure was similar in both groups.
Cost-Effectiveness of Canakinumab for the Treatment of AOSD
No studies evaluating the cost-effectiveness of canakinumab for the treatment of AOSD were identified; therefore, no summary can be provided.
Guidelines Regarding the Use of Canakinumab for the Treatment of AOSD
No evidence-based guidelines regarding the use of canakinumab for the treatment of AOSD were identified; therefore, no summary can be provided.
Limitations
One of the major limitations of the included SRs22,23 was that the available evidence was limited with low quality. Most of the studies included in the SRs22,23 were case reports, small case series, and noncontrolled retrospective observational studies. The quality of those studies was expected to be of low quality due to their study design (i.e., uncontrolled single-arm studies). Indeed, the levels of evidence in most of those studies were judged to be low by the authors of the SR by Cota-Arce et al. (2021)20 (but not assessed in the other included SR). The results in those studies are susceptible to various forms of bias that threatened the internal and external validity. The results observed in those studies might not be attributed to canakinumab alone because there are many confounding factors that were not controlled. Only 1 phase II randomized placebo-controlled trial with a relatively small population (17 patients in the canakinumab group versus 14 patients in the placebo group) was included in the SRs.22,23 In addition, the lack of an activity score specific for AOSD, the lack of comparative arms in most studies, and the variety of parameters reported make it difficult to quantitatively synthesize.
In all the studies included in the SRs, canakinumab was introduced to patients for whom previous treatment with 1 or more previous biologic agents had failed. There were no clinical data identified in this report regarding the use of canakinumab for the treatment of DMARDs-naive patients; therefore, no summary can be provided regarding the use canakinumab as a first-line treatment for AOSD. Many patients were given canakinumab in combination with conventional DMARDs to minimize steroid exposure and its related AEs. It is therefore unclear whether the effects observed were attributed to canakinumab alone or to the combination of conventional DMARDs and canakinumab.
The dosage of canakinumab administration was different across the studies, varying from 150 mg to 300 mg every 4 weeks. Treatment duration across studies also varied from 1 month to 43 months. Long-term follow-up data were lacking.
Most of the primary studies included in the SRs were conducted by authors from countries with a similar disease management as Canada, such as the US, France, Italy, Sweden, the Netherlands, Germany, and Greece. Thus, the results of canakinumab treatment of patients with AOSD may be applicable to the Canadian context.
Also, specific guidelines and economic evaluation studies are lacking.
Conclusions and Implications for Decision- or Policy-Making
This report identified 2 SRs,22,23 providing limited evidence on the effectiveness and safety of canakinumab compared with placebo or before treatment in patients with AOSD. Because there are 5 primary studies overlapped between the SRs,22,23 the summary of findings from each SR might contain some of the same data. Evidence comparing clinical effectiveness of canakinumab with alternative pharmacologic interventions was not identified. Also, no evidence was identified regarding the cost-effectiveness of canakinumab, or recommendations from evidence-based guidelines regarding the use of this biologic drug for the treatment of AOSD.
The majority of data for treatment of AOSD with canakinumab were derived from empirical observations through case reports, case series, and uncontrolled retrospective observational studies (i.e., these studies reported clinical outcomes within groups of patients, but did not make between-group comparisons), showing that its use led to a complete or partial response to treatment, corticosteroid-sparing effect, and decrease or normalization of some key laboratory parameters such as leukocyte count, ESR, and serum levels of ferritin and CRP. For safety, most of AEs reported were infection and infestations, leukopenia, musculoskeletal and connective tissue disorders, skin and subcutaneous disorders, thoracic and mediastinal disorders, gastrointestinal disorders, and site injection reactions. Serious AEs included macrophage activation syndrome, hepatocytotoxicity, and serious infections. However, in the phase II RCT included in both SRs, the difference in change of DAS28 scores (i.e., articular manifestations) between the canakinumab and placebo groups did not reach statistical significance.
Because the majority of the evidence on canakinumab treatment in both SRs22,23 was derived from studies with low-quality study design, such as case reports, case series, and uncontrolled observational studies, together with other limitations, the clinical effectiveness and safety of canakinumab for AOSD treatment remains unclear. Thus, controlled clinical trials comparing the clinical effectiveness of various biologic drugs would improve our understanding of the effectiveness of canakinumab compared with other available treatments. An economic evaluation on the cost-effectiveness of canakinumab compared with other drugs are needed to understand the cost-effectiveness of canakinumab for AOSD treatment. In addition, evidence-based guidelines are needed to provide recommendations regarding the use of canakinumab for AOSD; these would be useful to inform clinicians and policy-makers involved in providing care for patients with AOSD.
References
1.Bywaters EG. Still's disease in the adult. Ann Rheum Dis. 1971;30(2):121-133. PubMed
2.Zhou S, Qiao J, Bai J, Wu Y, Fang H. Biological therapy of traditional therapy-resistant adult-onset Still's disease: an evidence-based review. Ther Clin Risk Manag. 2018;14:167-171. PubMed
3.Macovei LA, Burlui A, Bratoiu I, et al. Adult-onset Still's disease-a complex disease, a challenging treatment. Int J Mol Sci. 2022;23(21). PubMed
4.Galozzi P, Baggio C, Bindoli S, Oliviero F, Sfriso P. Development and role in therapy of canakinumab in adult-onset Still's disease. Front Pharmacol. 2018;9:1074. PubMed
5.Maruyama A, Kokuzawa A, Yamauchi Y, et al. Clinical features of elderly-onset adult-onset Still's disease. Mod Rheumatol. 2021;31(4):862-868. PubMed
6.Sfriso P, Bindoli S, Galozzi P. Adult-onset Still's disease: molecular pathophysiology and therapeutic advances. Drugs. 2018;78(12):1187-1195. PubMed
7.Efthimiou P, Kadavath S, Mehta B. Life-threatening complications of adult-onset Still's disease. Clin Rheumatol. 2014;33(3):305-314. PubMed
8.Maria AT, Le Quellec A, Jorgensen C, Touitou I, Rivière S, Guilpain P. Adult onset Still's disease (AOSD) in the era of biologic therapies: dichotomous view for cytokine and clinical expressions. Autoimmun Rev. 2014;13(11):1149-1159. PubMed
9.Yamaguchi M, Ohta A, Tsunematsu T, et al. Preliminary criteria for classification of adult Still's disease. J Rheumatol. 1992;19(3):424-430. PubMed
10.Fautrel B, Zing E, Golmard JL, et al. Proposal for a new set of classification criteria for adult-onset still disease. Medicine (Baltimore). 2002;81(3):194-200. PubMed
11.Jamilloux Y, Gerfaud-Valentin M, Martinon F, Belot A, Henry T, Sève P. Pathogenesis of adult-onset Still's disease: new insights from the juvenile counterpart. Immunol Res. 2015;61(1-2):53-62. PubMed
12.Gerfaud-Valentin M, Jamilloux Y, Iwaz J, Sève P. Adult-onset Still's disease. Autoimmun Rev. 2014;13(7):708-722. PubMed
13.Giampietro C, Fautrel B. Anti-interleukin-1 agents in adult onset Still's disease. Int J Inflam. 2012;2012:317820. PubMed
14.Sfriso P, Bindoli S, Doria A, Feist E, Galozzi P. Canakinumab for the treatment of adult-onset Still's disease. Expert Rev Clin Immunol. 2020;16(2):129-138. PubMed
15.Tomelleri A, Campochiaro C, De Luca G, Farina N, Cavalli G, Dagna L. Canakinumab injection for the treatment of active Still's disease, including adult-onset Still's disease. Expert Opin Orphan Drugs. 2021;9(3):77-86.
16.Novartis. Novartis ILARIS® (canakinumab) receives FDA approval for new indication to treat Adult-Onset Still’s Disease (AOSD). 2020 Jun 16; https://www.novartis.com/us-en/news/media-releases/novartis-ilaris-canakinumab-receives-fda-approval-new-indication-treat-adult-onset-stills-disease-aosd. Accessed 2023 Feb 27.
17.European Public Assessment Report (EPAR): Ilaris (canakinumab). Amsterdam (NL): European Medicines Agency; 2022: https://www.ema.europa.eu/en/medicines/human/EPAR/ilaris. Accessed 2023 Feb 27.
18.Ilaris (canakinumab): 150 mg/1 mL for subcutaneous injection [product monotraph]. Dorval (QC): Novartis Pharmaceuticals Canada Inc; 2022 Nov 10: https://www.ask.novartispharma.ca/download.htm?res=ilaris_scrip_e.pdf&resTitleId=785. Accessed 2023 Feb 15.
19.Drug Reimbursement Review pharmacoeconomic report: canakinumab (Ilaris) for the treatment of active systemic juvenile idiopathic arthritis in patients aged 2 years and older. Ottawa (ON): CADTH; 2016 Nov: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0463_Ilaris_sJIA_PE_Report.pdf. Accessed 2023 Mar 6.
20.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
21.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
22.Cota-Arce JM, Cota J, De Leon-Nava MA, et al. Efficacy and safety of canakinumab in the treatment of adult-onset Still's disease: a systematic review. Semin Arthritis Rheum. 2021;51(6):1282-1290. PubMed
23.Kedor C, Tomaras S, Baeumer D, Feist E. Update on the therapy of adult-onset Still's disease with a focus on IL-1-inhibition: a systematic review. Ther Adv Musculoskelet Dis. 2021;13. PubMed
24.Wells G, Becker JC, Teng J, et al. Validation of the 28-joint Disease Activity Score (DAS28) and European League Against Rheumatism response criteria based on C-reactive protein against disease progression in patients with rheumatoid arthritis, and comparison with the DAS28 based on erythrocyte sedimentation rate. Ann Rheum Dis. 2009;68(6):954-960. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this table has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, duration of treatment |
|---|---|---|---|---|
Cota-Arce et al. (2021)22 Country: Mexico Funding source: No funding received for this study. | Systematic review 17 studies (2012 to 2021) having 144 patients were included for narrative synthesis:
| Patients with AOSD previously treated with NSAIDS, steroids, conventional DMARDs, or biological agents (anakinra, tocilizumab, TNF-alpha inhibitors). Age: 16 to 72 years % Female: 63.7 99.3% of patients had inadequate clinical response or active disease with systemic or arthritic manifestations. | Intervention: Canakinumab (4 mg/kg per month; 150 mg per month; 300 mg per month; 2 injections of 150 mg separated by 1 week) Comparator: Placebo or before treatment In the RCT included in the SR, patients who were treated with NSAIDs, glucocorticoids or conventional DMARDs required a stable dose prior to randomization and throughout study treatment period. (≥ 2 weeks for NSAIDs, ≥ 1 week of ≤ 10 mg/day prednisolone equivalent, and ≥ 6 weeks conventional DMARDs). For biological agents, a washout period between 1 week to 9 months was required. | Outcomes:
Duration of treatment: 1 month to 18 months |
Kedor et al. (2021)23 Country: Germany Funding source: No funding received for this study. | Systematic review 9 studies (2016 to 2021) having 110 patients were included for narrative synthesis:
| Patients with AOSD previously treated with NSAIDS, steroids, conventional DMARDs, or biological agents. Age: NR % Female: 66 | Intervention: Canakinumab (300 mg per month; 150 mg per month, 150 mg every 2 weeks; 4 mg/kg per month) Comparator: Placebo or before treatment In the RCT included in the SR, patients who were treated with NSAIDs, glucocorticoids or conventional DMARDs required a stable dose prior to randomization and throughout study treatment period. (≥ 2 weeks for NSAIDs, ≥ 1 week of ≤ 10 mg/day prednisolone equivalent, and ≥ 6 weeks conventional DMARDs). For biological agents, a washout period between 1 week to 9 months was required. | Outcomes:
Duration of treatment: 3 months to 43 months |
AE = adverse event; AOSD = adult-onset Still disorder; CRP = C-reactive protein; DAS = Disease Activity Score; DMARD = disease-modifying antirheumatic drug; ESR = erythrocyte sedimentation rate; NR = not reported; NSAID = nonsteroidal anti-inflammatory drug; RCT = randomized controlled trial.
aComplete response – The resolution of all manifestations or symptoms that the patient presented at baseline, including spiking fever, shin rash, arthralgia, arthritis, lymphadenopathy, hepatosplenomegaly, leukocytosis, and altered laboratory values.
bPartial response – Patients had clinical improvement, but not fulfilling the criteria for complete response.
cNo response – Neither clinical nor laboratory improvements were observed.
Appendix 3: Critical Appraisal of Included Publications
Note that this table has not been copy-edited.
Table 3: Strengths and Limitations of Systematic Reviews Using AMSTAR 220
Strengths | Limitations |
|---|---|
Cota-Arce et al. (2021)22 | |
|
|
Kedor et al. (2021)23 | |
|
|
AMSTAR 2 = A Measurement Tool to Assess Systematic Reviews 2; RCT = randomized controlled trial.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 4: Summary of Findings by Outcome — Remission
Parameters | Cota-Arce et al. (2021)22 | Kedor et al. (2021)23 |
|---|---|---|
Patients on treatment with Canakinumab, N | 99 | 110 |
Response to treatment, % | ||
Complete | 68.7 | 69 |
Partial | 16.2 | 17 |
Nonea | 15.1 | 14 |
ACR = American College of Rheumatology; CRP = C-reactive protein; AE = adverse event; DAS = Disease Activity Score; ESR = erythrocyte sedimentation rate; RCT = randomized controlled trial; SR = systematic review.
aPatients showed no clinical improvement or were excluded due to AEs.
Table 5: Summary of Findings by Outcome — Articular Manifestations22,23
Parameter | Canakinumab | Placebo | P value |
|---|---|---|---|
DAS28-ESRa response (reduction of ≥ 1.2), n (%) | 12 (67) | 7 (41) | 0.18 |
DAS = Disease Activity Score; ESR = erythrocyte sedimentation rate.
aThe DAS28, a combined index that measures disease activity in patients with rheumatoid arthritis, is based on a count of 28 swollen and tender joints, with a score ranging from 0 to 9.4, which is used to evaluate patient’s response to treatment. An absolute level of disease activity can be selected as a clinically meaningful goal for therapeutic intervention; with a value of ≤3.2 defined as the threshold for a low disease activity state and <2.6 as the threshold for remission.24 A DAS28 reduction by 0.6 represents a moderate improvement; a reduction more than 1.2 represents a major improvement.24 DAS28(ESR) is calculated based on erythrocyte sedimentation rate.24
Table 6: Summary of Findings by Outcome — Corticosteroid Use
Parameters | Cota-Arce et al. (2021)22 | Kedor et al. (2021)23 |
|---|---|---|
Reduced steroid use, % (n of N) | 20.3 (13 of 64) | 20.0 (16 of 81) |
Stopped steroid use, % (n of N) | 45.3 (29 of 64) | 40.7 (33 of 81) |
Table 7: Summary of Findings by Outcome — Laboratory Values
Parameters | Cota-Arce et al. (2021)22 | Kedor et al. (2021)23 |
|---|---|---|
Leukocytosis resolved or improved, % (n of N) | 73.7 (42 of 57) | 100 (50 of 50) |
ESR decreased or normalized, % (n of N) | 88.9 (56 of 63) | 97.7 (86 of 88) |
CRP decreased or normalized, % (n of N) | 95.4 (62 of 65) | 97.4 (75 of 77) |
Serum ferritin decreased or normalized, % (n of N) | 87.4 (76 of 87) | 98.6 (72 of 73) |
CRP = C-reactive protein; ESR = erythrocyte sedimentation rate; NSS = not statistically significant; RCT = randomized controlled trial; vs. = versus.
Note: The findings summarized in this table are based on uncontrolled, single-arm studies summarized in the SRs. In the RCT included in both SRs, differences between canakinumab and placebo groups in ESR, CRP, and serum ferritin levels were reported as not reaching statistical significance, but neither SR reported the numerical findings, nor did they report the actual probability values for these comparisons.
Table 8: Summary of Findings by Outcome — Adverse Events
Adverse events | Cota-Arce et al. (2021)22 | Kedor et al. (2021)23 |
|---|---|---|
None | 6 case reports, 2 case series and 3 retrospective observational studies reported no AEs. | 3 case series reported no AEs. |
Common adverse events | 210 AEs reported in 47.9% (69 of 114) patients.
|
|
Severe adverse events | 18 SAEs: MAS episodes and serious infections. | Severe pneumonia: 4% (2 of 50) |
Treatment cessation due to AEs, % (n/N) | 13% (9 of 69) | 2% (1 of 50) |
Death | 1 patient due to MAS episode. | — |
AE = adverse event; MAS = macrophage activation syndrome; RCT = randomized controlled trial; SAE = severe AE.
Note: The findings in this table are based on the uncontrolled, single-arm studies summarized in the SRs. In the RCT included in both SRs, it was reported that a higher number of AEs were observed in the canakinumab group than in the placebo group, however, numerical findings for the comparisons were not reported in either SR. However, the AE rate per 100 patient-years of exposure was similar in both groups. Common AEs were musculoskeletal and connective tissue disorders, infections and infestations, gastrointestinal disorders, skin and subcutaneous tissue disorders, general disorders, and administration site conditions. Four patients presented 1 of the following severe AEs: hepatotoxicity, patella-femoral pain syndrome, hypotonia, and deep vein thrombosis.
Appendix 5: Overlap Between Included Systematic Reviews
Note that this table has not been copy-edited.
Table 9: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation (country of origin) | Cota-Arce et al. (2021)22 | Kedor et al. (2021)23 |
|---|---|---|
Kontzias A, Efthimiou P. Semin Arthritis Rheum 2012;42:201-5. (US) | Yes | — |
Banse C et al. Jt Bone Spine 2013;80:653-5. (France) | Yes | — |
Eriksson PER et al. J Rheumatol 2013;40:1632-3. (Sweden) | Yes | — |
Barsotti S et al. J Clin Rheumatol 2014;20:121. (Italy) | Yes | — |
Lo Gullo A et al. Jt Bone Spine 2014;81:376-7. (Italy) | Yes | — |
Rossi-Semerano L et al. Orphanet J Rare Dis 2015;10:1-11. (France) | Yes | — |
Colafrancesco S, et al. Front Pharmacol 2017;8:369. (Italy) | Yes | Yes |
Feist E et al. Clin Exp Rheumatol 2018;36:668-75. (Germany) | Yes | — |
Schwartz C et al. BMJ Case Rep 2018;2018:1-5. (US) | Yes | — |
Breillat P et al. Ann Intern Med 2018;168:455-6. (France) | Yes | |
Cavalli G et al. Arthritis Res Ther 2019;21:1-2. (Italy) | Yes | Yes |
Chamseddin B et al. J Cutan Pathol 2019;46:528-31. (US) | Yes | — |
Kiltz U et al. Ann Rheum Dis 2020;79:E10. (Switzerland) | Yes | — |
Khairoun M et al. Neth J Med 2020;78:136-41. (the Netherlands) | Yes | — |
Kedor C et al. Ann Rheum Dis 2020;79:1090-7. (Germany) | Yes | Yes |
Vitale A et al. Mediators Inflamm 2020;2020. (Italy) | Yes | Yes |
Laskari K et al. Semin Arthritis Rheum 2021;51:137-43. (Greece) | Yes | Yes |
Tomelleri A et al. J Ann Rheum Dis 2020; 79: 851-852. (Italy) | — | Yes |
Ugurlu SGG et al.: case series [Abstract]. Arthritis Rheumatol 2018; 70(Suppl. 10). (Turkey) | — | Yes |
Vitale A et al. Front Pharmacol 2016; 7: 380. (Italy) | — | Yes |
Campochiaro CTA et al. [Abstract]. Arthritis Rheumatol 2019; 71(Suppl. 10). (Italy) | — | Yes |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca