CADTH Health Technology Review
Bladder Scanners in Personal Care Homes
Rapid Review
Authors: Qiukui Hao, Quenby Mahood
Abbreviations
RCT
randomized controlled trial
SD
standard deviation
MMSE
mini-mental state examination score
QoL
quality of life
USAPV
ultrasound-assisted prompted
CPV
conventional prompted voiding
GDS
Geriatric Depression Scale
SF-36
36-Item Short Form Survey
SF-12v2
Short Form 12 item (version 2) Health Survey
EQ-5D
EuroQoL-5D
ADL
Activities of Daily Living
Key Messages
For older adults with incontinence in a personal care home setting, using a bladder scanner to assist traditional urinary incontinence care may reduce the amount of daytime urine loss and use of incontinence pads without increasing caregivers’ care burden.
Adding a bladder scanner to urinary incontinence care may not impact patient quality of life, mental state, depression, physical function, and level of motivation.
These findings were based on 2 studies, 1 of which lacked a control group and did not directly measure the effect of adding a bladder scanner to urinary incontinence care on patients’ urine loss. This may limit our confidence in the findings.
We did not find any studies that reported on the effect of using bladder scanners in the personal care setting on rates of catheterization, emergency department visits, urinary tract infections, or other harms. We also did not identify any cost-effectiveness studies or evidence-based guidelines that met inclusion criteria for this report.
Context and Policy Issues
In Canada, the population is rapidly aging; 1 in 10 people living in Canada will be aged 65 or older by 2036. For adults at the age of 65, life expectancy for males is 17.4 years and 20.8 years for females.1 The demand for personal care homes or nursing for older adults has been steadily increasing and new residents in these facilities were older and had more comorbidities and functional impairment.2 Many residents in these long-term care facilities are not born in Canada and did not speak English as their first language, which makes the health care in these facilities more complex and challenging.3
Personal care homes generally provide comprehensive care for older adults with disability, cognitive impairment, and other chronic illnesses, but they receive far less attention than other acute health care settings.4 At least 50% of residents in these facilities experience urinary incontinence,5,6 which is an essential indicator of the quality of life in older adults.7,8 Older adults with incontinence are at a relatively higher risk of acute urinary retention that needs to be addressed in the emergency department due to lower abdominal pain and distress.9,10
Traditionally, medical history and physical examinations are important for the diagnosis of acute urinary retention and conventional prompted voiding care was used for urinary incontinence management by prompting older residents to void after regularly asking the older adults every 2 or 3 hours whether they had the desire to void. Ultrasound plays an important role in the management of urinary tract diseases as a diagnostic aid or care assistant,11 particularly for individuals who may not be able to respond to prompted voiding and provide accurate medical history. For example, either bladder ultrasound or catheterization is required for the diagnosis of acute urinary retention.12 If a bladder ultrasound is immediately available, bladder ultrasound is a good first choice over catheterization, as it is noninvasive and more comfortable for people and if the results are normal, catheterization could be avoided.12
Bladder scanners are portable ultrasound devices and can be used to measure bladder volume, including postvoid residual (PVR) volume, and provide 3-dimensional bladder images. A health technology assessment published in 2006 by Health Quality Ontario suggested that portable bladder scanners were acceptable in the older population; however, evidence regarding the clinical effectiveness of bladder scanners for long-term care facility settings was limited.13 Previous studies determined that using bladder scanners had acceptable sensitivity, specificity and excellent test-retest and interrater reliability for obtaining the PVR among nursing home residents with incontinence.14
The cost of bladder scanners might be a barrier to their application in the long-term care setting.14 Furthermore, nursing knowledge, training, scopes of practice, and related education also affect its widespread use in these settings.15-17 To support the decision-making about bladder scanners in personal care homes, we prepared this Rapid Response report to summarize available studies and evidence-based guidelines regarding the clinical effectiveness and cost-effectiveness of bladder scanners in these specific settings.
Research Questions
What is the clinical effectiveness of bladder scanners for personal care homes?
What is the cost-effectiveness of bladder scanners for personal care homes?
What are the evidence-based guidelines regarding the use of bladder scanners for personal care homes?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, Cumulative Index to Nursing and Allied Health Literature (CINAHL), the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were bladder and scans and portability or personal care homes. CADTH-developed search filters were applied to limit retrieval to guidelines for an additional search of the concepts bladder and scans. The search was completed on January 19, 2023 and limited to English-language documents published since January 1, 2013. Conference abstracts were omitted from the search results.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles, and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Residents of personal care homes (i.e., residential facilities with 24-hour nursing care for predominantly older persons with chronic illness or disability) |
Intervention | Bladder scanner (i.e., portable ultrasound device that measure the volume of urine in the bladder) |
Comparator | Q1 and Q2: No bladder scanner Q3: Not applicable |
Outcomes | Q1: Clinical benefits (e.g., reduction in emergency department transfers or visits, reduction in catheterization, health-related quality of life) and harms (e.g., patient discomfort, urinary tract infection, health care-acquired infection) Q2: Cost-effectiveness (e.g., cost per QALY gained, ICER) Q3: Recommendations regarding use of bladder scanners in personal care homes (e.g., best practices, contraindications) |
Study designs | Q1: Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies. Q2: Economic evaluations Q3: Evidence-based guidelines |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Exclusion Criteria
Publications were excluded if they did not meet the eligible criteria outlined in Table 1. Duplicate publications, studies published before 2013, or non-English publications were excluded. Studies with unclear settings, expert opinions or guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
One reviewer critically appraised the included studies using the Downs and Black checklist18 for randomized and nonrandomized studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
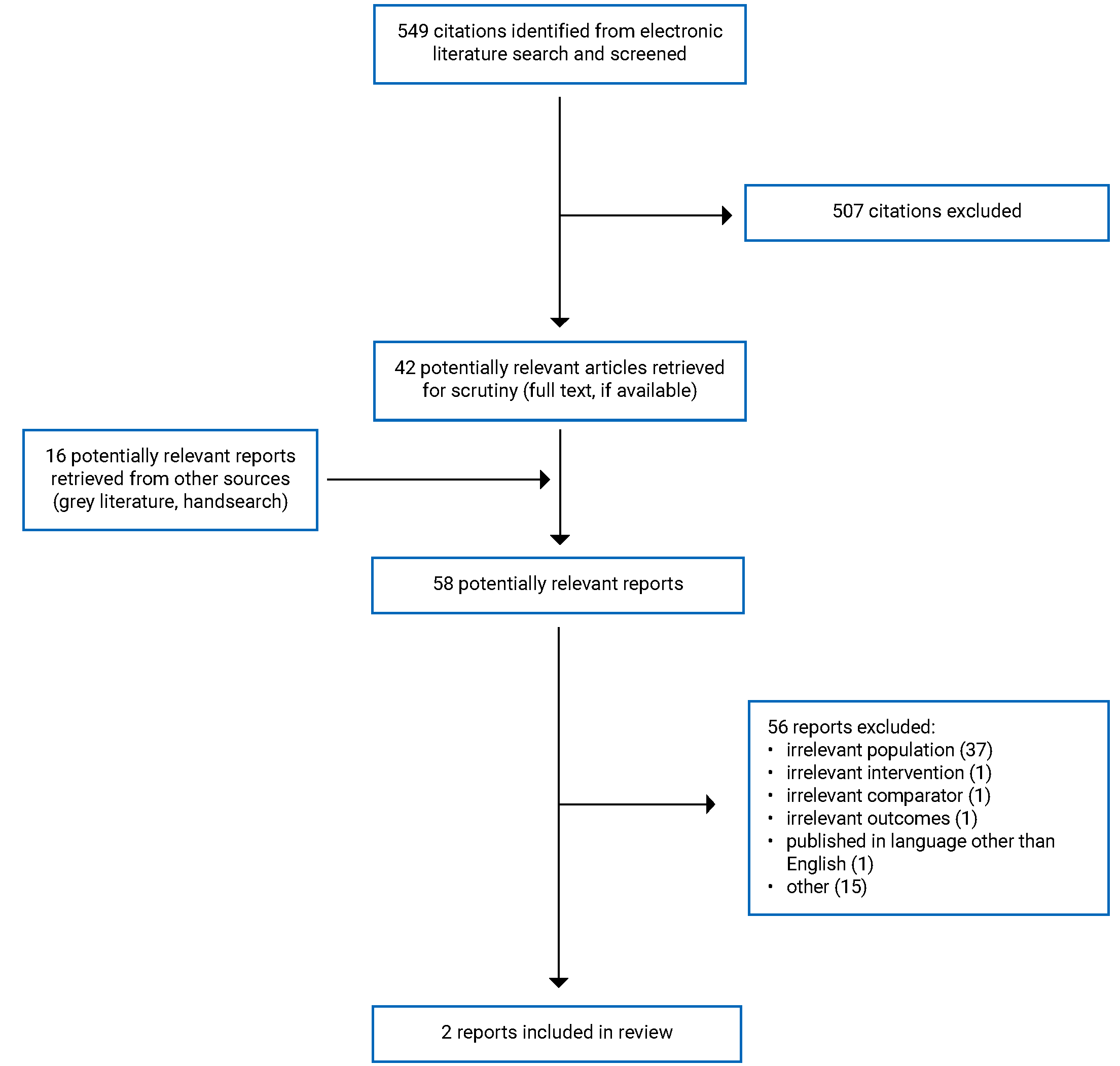
A total of 549 citations were identified in the literature search. Following the screening of title and abstracts, 507 citations were excluded and 42 potentially relevant reports from the electronic search were retrieved for full-text screening. Sixteen potentially relevant publications were retrieved from the grey literature search for full-text screening. Of these 58 potentially relevant articles, 56 were excluded for various reasons. This report includes 2 primary studies (one randomized controlled trial [RCT] and 1 before-and-after study).19,20 Appendix 1 presents the PRISMA flow chart21 of the study selection. Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
This report included 2 primary clinical studies.19,20 We did not identify any systematic reviews, health technology assessments, economic evaluation reports or evidence-based guidelines that met inclusion criteria. Additional details regarding the characteristics of included publications are provided in Appendix 2 (Table 2).
Study Design
Two primary clinical studies conducted in Japanese personal care homes (study authors originally used “nursing home” to describe study setting) were included in this report.19,20 One study was a cluster RCT published in 201919; the other was an uncontrolled before-and-after study published in 2016.19 The cluster RCT randomized 13 personal care homes into the intervention (n = 7) and the control group (n = 6) with a ratio of 1:1 in western and eastern parts of Japan.19 Two of the 13 personal care homes did not provide eligible older residents (one each for the intervention and the control group), leaving 11 eligible personal care homes (n = 5 for the intervention group and n = 6 for the control group) in this study.
Country of Origin
Both eligible studies were conducted in Japan.19,20 The cluster RCT enrolled 13 personal care homes from the western and eastern parts of Japan.19 The uncontrolled before-and-after study included 6 personal care homes in the Kanto area of Japan.20
Patient Population
The publications identified for this report included older adults (65 years or older) with urinary incontinence residing in personal care homes. For patients in the cluster RCT, 62/80 (77.5%) of patients were female with a median age of 85 years, a median Carlson comorbidity index of 3, a median mini-mental state examination score (MMSE) of 15, and 40 of 80 (50%) of patients were almost fully dependent and required extensive assistance in daily activities from their caregiver.19 For patients in the uncontrolled before-and-after study, 59 of 77 (76.6%) were female with a mean age of 84.1 years, and 41 of 77 (53%) of patients were almost fully dependent on their caregiver.19 The caregivers of patients also participated in the 2 studies with a median age of 42 in the RCT intervention group and a median age of 36 years in the RCT control group; and a mean age of 36 years in the before-after study; their professional career was around 11 years in the cluster RCT and 6 years in the uncontrolled before-and-after study.19,20
Interventions and Comparators
The intervention was ultrasound-assisted prompted voiding (USAPV) care using a portable ultrasound device for 8 weeks in the cluster RCT.19 First, caregivers calculated the patient participant’s optimal intravesical urine volume for voiding by the sum of the mean values of voided volume and residual volume. Then, caregivers used the portable ultrasound device regularly to monitor the urine volume in the bladder every 2 to 3 hours and prompted the patients to void when the intravesical urine volume was more than 75% of the individually precalculated bladder capacity. The comparator was the conventional prompted voiding care without residual urine volume measurement. Patients in the comparator group were regularly asked every 2 to 3 hours by their caregiver if they desired to void and prompted patients to void when the response was yes. The uncontrolled before-and-after study used a similar intervention to the cluster RCT for 12 weeks and compared the outcomes to baseline values in the same group.20
Outcomes
The cluster RCT19 reported the following as their primary outcome measures for efficacy: the change in the amount of urine loss during the day measured by weighing the incontinence pads and quality of life (QoL) measured by EQ-5D (ranging from −0.59 to 1.00 with higher scores indicating better QoL)22 from baseline to the end of the intervention. The secondary outcomes in this study included the score of mental state measured by MMSE (ranging from 0 to 30 with higher scores indicating better function),23 depression measured by the Geriatric Depression Scale (GDS, ranging from 0 to 30, with higher scores indicating greater severity of depression),24 physical function measured by the Barthel index (ranging from 0 to 100, with higher scores indicating greater physical function)25 and “level of motivation” measured by the vitality index (ranging from 0 to 10 with higher scores indicating greater motivation level).26 The study also reported the change in caregivers’ QoL measured by SF-12v2 (ranging from 0 to 100, with higher scores indicating better QoL)27 and mental stress for care burden with the visual analogue scale (ranging from 0: not stressful at all to 100: very stressful).
The primary outcome of the uncontrolled before-and-after study20 was the change in absorbent cost from the week before baseline to the end of the study. Absorbent cost (the cost to the facility for incontinence pads) was used as a surrogate measure of incontinence; a reduction in cost would be interpreted as a reduction in the use of incontinence pads and associated incontinence (urine loss). The activities of daily living (ADL) of patients were measured by the vitality index, which is a validated tool consisting of 5 subscales: walking, communication, feeding, toileting, and rehabilitation (total score: 0 to 10 with higher scores indicating greater ADL). The study also reported the change in the QoL of caregivers measured by SF-36 with 8 subscales (ranging from 0 to 100 with higher scores indicating better QoL).
Summary of Critical Appraisal
Cluster RCT
The cluster RCT clearly reported study objectives and process, inclusion and exclusion criteria, intervention and comparator, participant characteristics, outcome measures, and the main findings.19 The RCT did not have patients lost to follow-up during the intervention and indicated good adherence to the intervention. The study assessed the impacts of the intervention on QoL and care burdens, which may be important outcomes to consider for decision-making. The cluster RCT was a preregistered clinical trial (No. UMIN000017963) with the study protocol available for the public28 and reported all planned outcomes in the protocol. In the analysis, to adjust for some potential confounding factors, the researchers calculated a propensity score and adjusted the score in the final model. The study was funded by an academic association in Japan, which may have little influence on potential publication bias. Additionally, the RCT included 13 personal care homes in the geographical cluster of western and eastern parts of Japan, which probably had a good representation for Japanese personal care homes.
Several methodology limitations need to be mentioned in the cluster RCT.19 First, the study may have been underpowered in detecting an important difference in QoL. The study authors also did not consider intracluster correlation for sample size calculation, which underestimated the required sample size for the daytime urine loss outcome. According to the underestimated calculation based on relative rate of urine loss reduction, the study required 92 patients. However, the study only included 80 patients who met the eligibility criteria and reported results for absolute daytime urine loss. Second, this study was an open-label study, which did not attempt to use blinding during the study. Considering the practical issues of the study, blinding patients and caregivers would be difficult to achieve. To help reduce the performance bias, the outcome assessors should have been blinded to treatment allocation. Third, the study randomized at the cluster level, but their analysis was based on the individual patients and did not assess the cluster mean for outcomes at baseline across different clusters, which was recommended for the analysis of cluster randomized trials.29 The daytime urine loss at baseline was significantly higher in the intervention group than in the control group (median 300 mL versus 150 mL, P < 0.05), which suggests that patients in the intervention group experienced more incontinence at baseline. This may result in a bias to favour the intervention. Fourth, the final logistic regression model to evaluate the effect of the intervention (the propensity score-adjusted odds ratio) needed to be clarified. The dependent variable in the model seems to be individuals whose daytime urine loss decreased by more than 25%, but the independent variable was unclear in the model. The study authors did not report the propensity score-adjusted odds ratio for improving urine loss in the result section.
Uncontrolled Before-and-After Study
The uncontrolled before-and-after study clearly reported study objectives, inclusion and exclusion criteria, intervention details, participant characteristics, outcome measures and the main findings.20 The study did not have patients lost to follow-up during the intervention and indicated good adherence to the intervention. The study assessed the impact of the intervention on caregivers’ QoL and ADL for patients, which may be important considerations for decision-making. The study was funded by an academic association in Japan, which may have little influence on potential publication bias.
There are several methodology limitations in the before-and-after study.20 First, the sampling methods needed to be clearer. The study seems to have used convenience sampling of personal care homes, which may have reduced sample generalizability to other settings. Second, the study did not report the sample size calculation. It is unclear whether the study had enough power to detect statistically significant changes in patients’ ADL and caregivers’ QoL. Third, due to the nature of the study, the study did not have a control group. It is difficult to attribute the before-and-after changes to the effect of the intervention. The study reported the absorbent cost as their primary outcome, which was a surrogate outcome for the effectiveness of using a bladder scanner for the management of incontinence. It is possible that factors beyond the amount or severity of patient incontinence could have contributed to levels of incontinence pad use or purchasing. Fourth, the study used the paired t-test to compare the weekly absorbent cost across baseline, 4 weeks, 8 weeks and 12 weeks, which would increase the type I error. For repeat measures without missing data, a better statistical method would be repeat repeated measures ANOVA.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3 (Table 3).
Summary of Findings
A cluster RCT and an uncontrolled before-and-after study reported the clinical effectiveness of using bladder scanners (portable ultrasound devices) to assist conventional urinary incontinence care for older personal home residents and assess the impact on their caregivers.19,20 No relevant evidence was available for the cost-effectiveness of bladder scanners for personal care homes and no eligible guidelines were identified in this report.
Appendix 4 presents the main study findings.
Clinical Effectiveness of Bladder Scanners for Personal Care Homes
Daytime Urine Loss
A cluster RCT included older personal home residents (n = 80) with urinary incontinence and compared the changes in daytime urine loss between intervention and control groups as 1 of the primary outcomes.19 The study found that the absolute decrease from baseline in daytime urine loss at the end of treatment (8 weeks) was statistically significantly greater in the USAPV group than conventional prompted voiding (CVP) group, in both adjusted and unadjusted analyses (Table 4).
Absorbent Cost
One uncontrolled before-and-after study 20 evaluated absorbent costs incurred by a personal care home before and after the implementation of a USAPV protocol as a surrogate measure of USAPV effectiveness to manage urinary incontinence. This study reported a statistically significant reduction of 11.8% in weekly absorbent cost from baseline to the end of the USAPV intervention. The study also reported 40 of 77 (51.9%) patients with reduced absorbent cost and 3 of 77 (3.9%) patients being pad-free at the end of the USAPV intervention. Patients with fair bladder function showed statistically significantly greater cost reduction from baseline than patients with poor bladder function. Patients with care-needs levels 1 to 3 tended to have a greater relative cost reduction than patients with care-needs levels 4 to 5 (almost dependent in physical function), but the difference was not statistically significant (Table 5).
Other Patient Outcomes
The other primary outcome for the eligible cluster RCT was patients’ QoL measured by EQ-5D.19 The study found that there was no statistically significant change in patients’ QoL from baseline within the USAPV group (P = 0.42) and within the CPV group (P = 0.72) (Table 6). The study also reported that the changes from baseline in patients’ mental state (measured by MMSE), depression level (measured by GDS) and physical function (measured by Barthel index) were not statistically significant within either the USAPV group or the CPV group (Table 7, Table 8, Table 9).19 Both included studies evaluated patients’ motivation and ADL (measured by the vitality index) and reported no statistically significant differences from baseline within the USAPV group19,20 or within the CPV group19 (Table 10).
Caregiver QoL
Two studies19,20 reported the impacts of USAPV on caregivers’ QoL measured by SF-12v2 or SF-36. The uncontrolled before-and-after study20 reported that the management of urinary incontinence using USAPV statistically increased care worker’s QoL in role emotional and mental health subscales of SF-36 from baseline to the end of treatment. However, the cluster RCT did not find statistically significant changes from baseline to the end of treatment within the USAPV group and within the CPV group19 (Table 11).
Care Burden
A cluster RCT19 reported that there was no statistically significant increase in caregivers’ care burden (measured by a visual analogue scale [VAS], 0 to 100, a higher score indicated more care burden) from baseline within the USAPV group; whereas, there was a statistically significant increase in caregivers’ care burden from baseline within the control group. However, the change in caregivers’ care burden from baseline was not statistically significantly different between the USAPV group and the CPV group (Table 12).
Cost-Effectiveness of Bladder Scanners for Personal Care Homes
No cost-effectiveness evidence regarding bladder scanners for personal care homes was identified; therefore, no summary can be provided.
Evidence-Based Guidelines Regarding the Use of Bladder Scanners for Personal Care Homes
No evidence-based guidelines regarding bladder scanners for personal care homes was identified; therefore, no summary can be provided.
Limitations
The body of evidence that was identified to address the clinical effectiveness research question was limited, consisting of 1 cluster RCT and 1 uncontrolled before-and-after study.19,20 All participants in the 2 eligible studies were from Japanese personal care homes and the uncontrolled before-and-after study was the precursor to the RCT. Both studies were conducted by the same Japanese research team. It seems that both studies included personal care homes in which all caregivers had adequate knowledge of portable bladder scanners and with good resources for potential ultrasound training or supervision; similar results may not be expected for other settings with fewer resources. Certainty in the effectiveness findings for the intervention from the uncontrolled before-and-after study was limited due to the study design.20 Only 1 RCT was identified to examine the effectiveness of the intervention in this report.19 All available evidence was limited to Japan. The generalizability to personal care homes or other settings in Canada was also unclear.
All eligible patients for the included studies had urinary incontinence and most of them (more than 70%) were female.19,20 The generalizability of findings to populations with other conditions (e.g., urinary retention) or to older males was unclear. Both studies followed patients up to the end of the treatment (either 8 or 12 weeks). The long-term effects of using portable ultrasound or whether the effects of the intervention can be maintained were not assessed.
When interpreting the evidence, only statistical significance was identified and considered; minimal important differences for all outcome measures were not reported. No evidence was identified that evaluated bladder scanners with respect to potential harms (e.g., patient discomfort, urinary tract infection, health care-acquired infection) and for preventing emergency department visits or catheterization. Finally, no evidence for the cost-effectiveness of bladder scanners for personal care homes and evidence-based guidelines regarding bladder scanners for personal care homes were identified.
Conclusions and Implications for Decision- or Policy-Making
A cluster RCT19 and an uncontrolled before-and-after study20 were identified to address the clinical effectiveness of bladder scanners for personal care homes. The 2 studies provided limited evidence suggesting that using a bladder scanner to assist prompted voiding care to manage urinary incontinence (for 8 weeks or 12 weeks) reduces patients’ daytime urine loss and absorbent cost without increasing caregivers’ care burden. However, there were no statistically significant differences in any patient important outcome measures (QoL, mental state, depression, physical function and level of motivation) between baseline and the end of the treatment or between the intervention and control groups. The uncontrolled before-and-after study had significant limitations in study design and the methodologies, such as convenience sampling, and inappropriate statistical analysis methods.20
All studies were conducted in Japan, and the generalizability of the evidence to Canadian personal care homes was unclear. No evidence was identified for potential harms or for preventing emergency department visits or catheterization. No evidence regarding the cost-effectiveness and evidence-based guideline of bladder scanners for personal care homes was identified that met the inclusion criteria for this report.
Indirect evidence from hospital or postoperative settings may be helpful for decision-making. For example, Donaldson and colleagues reported that PVR volume measured by bladder scanners can be used for decision-making and cost-effectiveness analysis for health care utilization (ambulatory office emergency visits) among postoperative patients.30 Chen and colleagues reported that using portable bladder scanners reduced the incidence of urinary tract infections for patients with acute ischemic stroke.31
In addition to the clinical evidence, decision-makers may wish to consider whether local health care providers’ or caregivers’ knowledge of ultrasound, the related cost for the device and potential training, or other practical issues impact the application of bladder scanners. The local prevalence of urinary incontinence, people’s values and preferences on daytime urine loss, and local absorbent costs may also affect the application of the available evidence.
The current report identified some research gaps in the body of evidence regarding using bladder scanners for personal care homes. Providing robust evidence on the impact of bladder scanners for the management of acute urinary retention and on other outcomes, like catheterization and emergency department transfers, will require future studies with enough statistical power and using robust designs.
References
1.Sheets DJ, Gallagher EM. Aging in Canada: state of the art and science. Gerontologist. 2013;53(1):1-8. PubMed
2.Ng R, Lane N, Tanuseputro P, et al. Increasing complexity of new nursing home residents in Ontario, Canada: a serial cross-sectional study. J Am Geriatr Soc. 2020;68(6):1293-1300. PubMed
3.Estabrooks CA, Squires JE, Carleton HL, Cummings GG, Norton PG. Who is looking after Mom and Dad? Unregulated workers in Canadian long-term care homes. Can J Aging. 2015;34(1):47-59. PubMed
4.Feder J, Komisar HL, Niefeld M. Long-term care in the United States: an overview. Health Aff (Millwood). 2000;19(3):40-56. PubMed
5.Offermans MP, Du Moulin MF, Hamers JP, Dassen T, Halfens RJ. Prevalence of urinary incontinence and associated risk factors in nursing home residents: a systematic review. Neurourol Urodyn. 2009;28(4):288-294. PubMed
6.Shaw C, Cahill J, Wagg A. The current state of continence in Canada: a population representative epidemiological survey. Can J Urol. 2020;27(4):10300-10305. PubMed
7.Corrado B, Giardulli B, Polito F, Aprea S, Lanzano M, Dodaro C. The impact of urinary incontinence on quality of life: a cross-sectional study in the metropolitan city of Naples. Geriatrics (Basel). 2020;5(4):96. PubMed
8.Dubeau CE, Simon SE, Morris JN. The effect of urinary incontinence on quality of life in older nursing home residents. J Am Geriatr Soc. 2006;54(9):1325-1333. PubMed
9.Pannill FC, 3rd, Williams TF, Davis R. Evaluation and treatment of urinary incontinence in long term care. J Am Geriatr Soc. 1988;36(10):902-910. PubMed
10.Billet M, Windsor TA. Urinary retention. Emerg Med Clin North Am. 2019;37(4):649-660. PubMed
11.Southgate SJ, Herbst MK. Ultrasound of the urinary tract. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022: https://www.ncbi.nlm.nih.gov/books/NBK535381/. Accessed 2023 Jan 16.
12.Barrisford GW, Steele GS. Acute urinary retention. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: http://www.uptodate.com. Accessed 2022 Dec 21.
13.Medical Advisory Secretariat. Portable bladder ultrasound: an evidence-based analysis. Ont Health Technol Assess Ser. 2006;6(11):1-51. PubMed
14.Ouslander JG, Simmons S, Tuico E, et al. Use of a portable ultrasound device to measure postvoid residual volume among incontinent nursing home residents. J Am Geriatr Soc. 1994;42(11):1189-1192. PubMed
15.Christianson TM, Hoot TJ, Todd M. Understanding nursing knowledge of continence care and bladder scanner use in long-term care: an evaluation study. Gerontol Geriatr Med. 2021;7:23337214211046090. PubMed
16.Ostaszkiewicz J, Tomlinson E, Hunter K. The effects of education about urinary incontinence on nurses' and nursing assistants' knowledge, attitudes, continence care practices, and patient outcomes: a systematic review. J Wound Ostomy Continence Nurs. 2020;47(4):365-380. PubMed
17.Wilson A, Renee Dugger D, Ehlman K, Eggleston B. Implementation science in nursing homes: a case study of the integration of bladder ultrasound scanners. Ann Longterm Care. 2015;23(6). https://www.hmpgloballearningnetwork.com/site/altc/articles/implementation-science-nursing-homes-case-study-integration-bladder-ultrasound-scanners. Accessed 2023 Feb 8.
18.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
19.Suzuki M, Miyazaki H, Kamei J, et al. Ultrasound-assisted prompted voiding care for managing urinary incontinence in nursing homes: a randomized clinical trial. Neurourol Urodyn. 2019;38(2):757-763. PubMed
20.Suzuki M, Iguchi Y, Igawa Y, et al. Ultrasound-assisted prompted voiding for management of urinary incontinence of nursing home residents: efficacy and feasibility. Int J Urol. 2016;23(9):786-790. PubMed
21.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
22.EuroQol Group. EuroQol: a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199-208. PubMed
23.Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189-198. PubMed
24.Yesavage JA, Brink TL, Rose TL, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. 1982;17(1):37-49. PubMed
25.Mahoney FI, Barthel DW. Functional evaluation: the Barthel Index. Md State Med J. 1965;14:61-65. PubMed
26.Toba K, Nakai R, Akishita M, et al. Vitality Index as a useful tool to assess elderly with dementia. Geriatr Gerontol Int. 2002;2(1):23-29.
27.Al Omari O, Alkhawaldeh A, ALBashtawy M, Qaddumi J, Holm MB, AlOmari D. A review of the Short Form Health Survey-Version 2. J Nurs Meas. 2019;27(1):77-86. PubMed
28.Ultrasound-assisted prompted voiding for incontinent elderly living in geriatric health services facilities. UMIN Clinical Trials Registry. 2015; https://center6.umin.ac.jp/cgi-open-bin/ctr_e/ctr_his_list.cgi?recptno=R000020774. Accessed 2020 Feb 3.
29.Hooper R, Forbes A, Hemming K, Takeda A, Beresford L. Analysis of cluster randomised trials with an assessment of outcome at baseline. BMJ. 2018;360:k1121. PubMed
30.Donaldson K, Woll A, Jansen SM, Edenfield A, Swift S, Heisler CA. A cost-effectiveness analysis of postvoid-void residual bladder scan thresholds in the postoperative setting. Int Urogynecol J. 2022;33(10):2727-2733. PubMed
31.Chen SC, Chen PY, Chen GC, Chuang SY, Tzeng IS, Lin SK. Portable bladder ultrasound reduces incidence of urinary tract infection and shortens hospital length of stay in patients with acute ischemic stroke. J Cardiovasc Nurs. 2018;33(6):551-558. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Objective and Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Suzuki et al. (2019)19 Japan Funding source: Japanese Society of Geriatric Urology | Objective: To determine whether ultrasound-assisted prompted voiding (USAPV) care is more efficacious than conventional prompted voiding (CPV) care for managing urinary incontinence in nursing homes Study design: Cluster randomized clinical trial | Clusters In 13 nursing homes from western and eastern Japan, no patients were enrolled from 2 of 13 (one nursing home each for intervention and control group), leaving 11 nursing homes providing eligible residents from 2015 to 2016. Nursing home residents Inclusion criteria: (1) aged 65 years and older; (2) care-needs level of 1 (mild) to 5 (severe) defined by the Japanese Long-Term Care Insurance system; (3) using pads or diapers because of urinary incontinence; (4) postvoid residual urine volume of less than 300 mL. Exclusion criteria: serious consciousness disorder, acute phase disease end-of-life care, or a mass in the lower abdomen (e.g., pelvic tumour, pelvic cystic disease, and abnormal ascites detected by ultrasonography). Number of participants: n = 80 (45 in USAPV group and 35 in CPV group) Median age: 85 years, range from 81 to 90 years Sex: 73% female in USAPV group and 83% in CPV group Caregivers Fifty care workers and 49 with completed data, median age: 42 years for intervention group and 36 years for comparator group | Eight weeks for both intervention and comparator Intervention: USAPV: Caregivers regularly monitored the urine volume in the bladder every 2 to 3 using a ultrasound device and prompted the participants to void when the volume was more than 75% of the individually prefixed bladder capacity. Comparator: CPV: Caregivers regularly asked the residents every 2 to 3 hour whether they had a desire to void and prompted them to void when the response was yes. | Outcomes: Nursing home residents
Caregivers:
Follow-up: 8 weeks |
Suzuki et al. (2016)20 Japan Funding source: Japanese Society of Geriatric Urology | Objective: To assess the efficacy and feasibility of ultrasound-assisted prompted voiding for the management of urinary incontinence in nursing homes. Study design: nonrandomized single-arm study | Nursing home residents Incontinent older adults residing in 6 nursing homes in the Kanto area of Japan between November 2011-December 2012 Exclusion criteria: individuals with severe consciousness disorder, acute phase diseases or end-of-life care. Number of participants: n = 77 (38 with poor bladder function and 39 with fair bladder function) Median age: 84.1 years, Sex: 76.6% female Care workers: n = 36 (mean age: 36 years with 58.3% women) with completed data of 47 participating care workers | All patients received the CPV care for 1 week and subsequently underwent the intervention for 12 weeks. Intervention: USAPV: Certified staff care workers (under the supervision of attending physicians and nurses) regularly monitored the intravesical urinary volume using an ultrasound device; when the volume had reached 75% of the optimal volume, the participant was prompted to void in a toilet. Comparator: Single-arm study without comparator group. | Outcomes:
Follow-up: 12 weeks |
ADL = Activities of Daily Living; CPV = conventional prompted voiding; EQ-5D = EuroQoL-5D; GDS = Geriatric Depression Scale; MMSE = Mini-Mental State Examination; NA = not applicable; NR = not reported; QoL = Quality of life; SF-12v2 = Short Form 12 item (version 2) Health Survey; SF-36 = 36-Item Short Form Survey; USAPV = ultrasound-assisted prompted voiding.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist18
Strengths | Limitations |
|---|---|
Suzuki (2019)19 | |
Randomized controlled trial | |
The objectives and process of the study were clearly described. Inclusion and exclusion criteria were clearly described. The characteristics of nursing home residents (e.g., age, sex, care-needs levels, comorbidity index, function measures, daytime voided volume, and urine loss at baseline) were clearly described for each group. The outcomes measures were clearly described in the methods section The intervention and comparator were clearly described. The distribution of principal confounders in each group of patients were provided in Table 1. The main findings of the study were clearly described. The estimates of the random variability (interquartile range) for the main outcomes were provided. The care burdens of caregivers were measured by a visual analogue scale. The actual P values were reported. The patients are likely representative of nursing home residents in Japan. A propensity score was used to adjust the imbalance of baseline characteristics between 2 groups. No patients were lost to follow-up. The length of follow-up was the same between intervention and control groups. A sample size calculation considering effect size, type I error, power and dropout rate was provided. The randomized sequence was adequately generated using a random number table. The clinical trial was preregistered (Number: UMIN000017963) with the study protocol available for the public.28 Reported all planned outcomes in the publication (compared with the outcomes in the protocol suggesting). | The randomized sequence concealment was unclear. The methods to calculate the sample size missed the intracluster correlation (the correlation between the outcomes of 2 individuals from the same cluster). The study did not attempt to use a blind method (e.g., at least blind the outcome assessor) to reduce the risk of bias. The sample size (n = 80) is smaller than the expected sample size (n = 92) based on the relative rate reduction of urine loss, but the primary outcomes were absolute reduction in daytime urine loss and QOL. Although the authors reported propensity score-adjusted P values, 2 baseline characteristics of nursing home residents (Barthel index and daytime urine loss) were statistically different between the intervention and control groups. The unit of analysis was individual residents and did not consider the cluster distribution (mean and variability). The model construction used to evaluate the effect of the intervention was unclear. The definitions of adverse events were unclear and were not mentioned in the methods section or study protocol. This study enrolled nursing homes from Japan; the generalizability to Canada was unclear. |
Suzuki (2016)20 | |
Nonrandomized study (Before-and-after study) | |
The objectives of the study are clearly described. Inclusion and exclusion criteria were clearly described. The characteristics of patients (e.g., age, sex, care-needs levels) were clearly described. The outcome measures were clearly described in the methods section using validated questionnaires. The intervention was clearly described. The main findings of the study were clearly described. The estimates of the random variability (interquartile range) for the main outcomes were provided. The actual P values were reported. | The sampling method was not clearly reported. The study did not conduct sample size calculation. No control groups. The absorbent cost was a surrogate outcome for the effectiveness of using a bladder scanner for the management of incontinence. The distributions for outcome data were not examined. The statistical analysis (paired t-test) is inappropriate for comparing weekly cost of absorbents. The unit of cost measurement (¥, Japanese Yen?) was unclear. The definitions of adverse events were unclear and were not mentioned in the methods section. This study enrolled 6 nursing homes in Japan; the generalizability to Canada was unclear. |
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 4: Summary of Findings by Outcome — Daytime Urine Loss
Statistic parameters | Suzuki (2019)19 | |
|---|---|---|
Intervention (USAPV) | Control (CPV) | |
Pre-treatment median [IQR] (g) | 300 [195 to 470] | 150 [120 to 270] |
After treatment median [IQR] (g) | 250 [100 to 438] | 180 [100 to 320] |
P value for comparing pre- and after treatment | 0.008 | 0.90 |
Median change [IQR] (g) | −80.0 [-175 to + 24] | −9.0 [-60 to + 80] |
Raw P value for comparing changes of the 2 groups | 0.018 | |
Propensity score-adjusted P value for comparing changes of the 2 groups | 0.048 | |
CPV = conventional prompted voiding; g = gram; IQR = Interquartile range; USAPV = ultrasound-assisted prompted voiding.
Table 5: Summary of Findings by Outcome — Absorbent Cost
Statistic parameters | Suzuki (2016)20 |
|---|---|
Intervention (USAPV) | |
Pre-treatment cost, ¥/week/person | 1,239 |
Posttreatment cost, ¥/week/person | 1,093 |
Posttreatment cost reduction from baseline, % | 11.8 |
P value for comparing baseline and after treatment | 0.006 |
Patients with reduced absorbent cost, n/N (%) | 40/77 (51.9) |
Patients being pad-free, n/N (%) | |
4 weeks | 2/77 (2.9) |
8 weeks | 2/77 (2.9) |
12 weeks | 3/77 (3.9) |
Posttreatment cost reduction from baseline inpatient subgroups, % | |
Patients with fair bladder function (n = 39) | 19.5 |
Patients with poor bladder function (n = 38) | 3.7 |
P value for comparing fair and poor bladder function | 0.037 |
Patients with care-needs levels 1 to 3 (n = 36) | 15.7 |
Patients with care-needs levels 4 to 5 (n = 41) | 4.3 |
P value for comparing care-needs 1 to 3 and 4 to 5 levels | 0.381 |
N = total sample; n = sample in the subgroup; USAPV = ultrasound-assisted prompted voiding; ¥ = Japanese Yen.
Table 6: Summary of Findings by Outcome — Patients’ QoL Measured by EQ-5D
Statistic parameters | Suzuki (2019)19 | |
|---|---|---|
Intervention (USAPV) | Control (CPV) | |
Pre-treatment median [IQR] (g) | 0.533 [0.204 to 0.605] | 0.596 [0.485 to 0.676] |
After treatment median [IQR] (g) | 0.533 [0.200 to 0.613] | 0.596 [0.459 to 0.670] |
P value for comparing pre- and after treatment | 0.42 | 0.72 |
Median change [IQR] (g) | NR | NR |
P value for comparing changes of the 2 groups | NR | |
CPV = conventional prompted voiding; EQ-5D = EuroQoL-5D (ranging from −0.594 to 1 with higher scores indicating better QOL); IQR = Interquartile range; NR = not reporte; SF-12v2 = Short Form 12 item (version 2) Health Survey; USAPV = ultrasound-assisted prompted voiding.
Table 7: Summary of Findings by Outcome — Patients’ Mental State Measured by MMSE
Statistic parameters | Suzuki (2019)19 | |
|---|---|---|
Intervention (USAPV) | Control (CPV) | |
Pre-treatment median [IQR] | 15 [8 to 18] | 17 [8 to 22] |
After treatment median [IQR] | 14 [9 to 18] | 17 [ 9 to 21] |
P value for comparing baseline and after treatment | 0.36 | 0.89 |
Median change [IQR] | NR | NR |
P value for comparing changes | NR | |
CPV = conventional prompted voiding; IQR = Interquartile range; MMSE = Mini-mental state examination (ranging from 0 to 30 with higher scores indicating better function); NR = not reported; USAPV = ultrasound-assisted prompted voiding.
Table 8: Summary of Findings by Outcome — Patients’ Depression Level Measured by GDS
Statistic parameters | Suzuki (2019)19 | |
|---|---|---|
Intervention (USAPV) | Control (CPV) | |
Pre-treatment median [IQR] | 8 [4 to 11] | 6 [4 to 10] |
After treatment median [IQR] | 8 [5 to 10] | 7 [4 to 10] |
P value for comparing baseline and after treatment | 0.19 | 0.44 |
Median change [IQR] | NR | NR |
P value for comparing changes | NR | |
CPV = conventional prompted voiding; GDS = Geriatric depression score (ranging from 0 to 30 with higher scores indicating greater severity of depression); IQR = Interquartile range; NR = not reported; USAPV = ultrasound-assisted prompted voiding.
Table 9: Summary of Findings by Outcome — Patients’ Physical Function Measured by Barthel Index
Statistic parameters | Suzuki (2019)19 | |
|---|---|---|
Intervention (USAPV) | Control (CPV) | |
Pre-treatment median [IQR] | 30 [20 to 45] | 45 [35 to 55] |
After treatment median [IQR] | 33 [19 to 45] | 45 [30 to 512] |
P value for comparing baseline and after treatment | 0.82 | 0.65 |
Median change [IQR] | NR | NR |
P value for comparing changes | NR | |
CPV = conventional prompted voiding; IQR = Interquartile range; NR = not reported; USAPV = ultrasound-assisted prompted voiding.
Note: Barthel index ranges from 0 to 100 with higher scores indicating greater physical function.
Table 10: Summary of Findings by Outcome — Patients’ Level of Motivation or ADL Measured by Vitality Index
Statistic parameters | Suzuki (2019)19 | Suzuki (2016)20 | |
|---|---|---|---|
Intervention (USAPV) | Control (CPV) | Intervention (USAPV) | |
Pre-treatment median [IQR] | 6 [5 to 8] | 6 [5 to 8] | NR |
After treatment median [IQR] | 6 [5 to 8] | 6 [5 to 8] | NR |
Pre-treatment mean | NR | NR | 6.96 |
After treatment mean | NR | NR | 6.76 |
P value for comparing baseline and after treatment | 0.52 | 0.68 | 0.236 |
Median change [IQR] | NR | NR | NR |
P value for comparing changes | NR | NA | |
CPV = conventional prompted voiding; IQR = Interquartile range; NR = not reported; NA = not applicable; USAPV = ultrasound-assisted prompted voiding.
Note: Vitality index ranges from 0 to 10 with higher scores indicating greater motivation level or ADL level.
Table 11: Summary of Findings by Outcome — Caregivers’ QOL
Statistic parameters | Suzuki (2019)19 | Suzuki (2016)20 | |
|---|---|---|---|
Intervention (USAPV) | Control (CPV) | Intervention (USAPV) | |
SF-12v2 | |||
Physical component summary | |||
Baseline median [IQR] | 50.4 [35.5 to 54.5] | 50.3 [47.9 to 53.9] | NR |
After treatment median [IQR] | 50.4 [44.5 to 58.1] | 49.7 [43.3 to 57.0] | NR |
P value for comparing baseline and after treatment | 0.17 | 0.68 | NR |
Median change [IQR] | NR | NR | NR |
P value for comparing changes | NR | NR | |
Mental component summary | |||
Baseline median [IQR] | 52.3 [47.8 to 54.7] | 49.1 [45.2 to 53.4] | NR |
After treatment median [IQR] | 49.9 [45.3 to 52.0] | 51.1 [45.1 to 56.3] | NR |
P value for comparing baseline and after treatment | 0.15 | 0.60 | NR |
Median change [IQR] | NR | NR | NR |
P value for comparing changes | NR | — | NR |
Role or social component summary | |||
Baseline median [IQR] | 45.8 [32.0 to 55.6] | 48.4 [35.9 to 52.9] | NR |
After treatment median [IQR] | 43.8 [38.6 to 50.7] | 52.2 [39.0 to 50.1] | NR |
P value for comparing baseline and after treatment | 0.76 | 0.93 | NR |
Median change [IQR] | NR | NR | NR |
P value for comparing changes | NR | — | NR |
SF-36 | |||
Mental health | |||
Baseline mean (SD) | NR | NR | 60.1 (20.8) |
After treatment mean (SD) | NR | NR | 68.2 (15.5) |
P value for comparing baseline and after treatment | NR | NR | 0.007 |
Role emotional | |||
Baseline mean (SD) | NR | NR | 80.8 (19.2) |
After treatment mean (SD) | NR | NR | 89.6 (12.7) |
P value for comparing baseline and after treatment | NR | NR | 0.020 |
Physical functioning | |||
Baseline mean (SD) | NR | NR | 87.7 (14.1) |
After treatment mean (SD) | NR | NR | 87.4 (15.5) |
P value for comparing baseline and after treatment | NR | NR | 0.872 |
Role physical | |||
Baseline mean (SD) | NR | NR | 85.3 (15.7) |
After treatment mean (SD) | NR | NR | 89.4 (12.9) |
P value for comparing baseline and after treatment | NR | NR | 0.274 |
Bodily pain | |||
Baseline mean (SD) | NR | NR | 61.5 (24.6) |
After treatment mean (SD) | NR | NR | 69.1 (18.2) |
P value for comparing baseline and after treatment | NR | NR | 0.058 |
General health perceptions | |||
Baseline mean (SD) | NR | NR | 60.7 (17.6) |
After treatment mean (SD) | NR | NR | 60.8 (18.8) |
P value for comparing baseline and after treatment | NR | NR | 0.0937 |
Vitality | |||
Baseline mean (SD) | NR | NR | 52.5 (17.9) |
After treatment mean (SD) | NR | NR | 58.7 (17.7) |
P value for comparing baseline and after treatment | NR | NR | 0.057 |
Social functioning | |||
Baseline mean (SD) | NR | NR | 79.2(20.9) |
After treatment mean (SD) | NR | NR | 85.8(17.7) |
P value for comparing baseline and after treatment | NR | NR | 0.076 |
CPV = conventional prompted voiding; IQR = Interquartile range; NR = not reported; SD = Standard deviation; SF-12v2 = Short Form 12 item (version 2) Health Survey (ranging from 0 to 100 with higher scores indicating better QOL); SF-36 = 36-Item Short Form Survey (ranging from 0 to 100 with higher scores indicating better QOL); USAPV: ultrasound-assisted prompted voiding.
Table 12: Summary of Findings by Outcome — Change in Caregivers’ Care Burden Measured by VAS
Statistic parameters | Suzuki (2019)19 | |
|---|---|---|
Intervention (USAPV) | Control (CPV) | |
Pre-treatment median [IQR] | 50.5 [46.5 to 83.8] | 58.0 [49.5 to 76.0] |
After treatment median [IQR] | 52.5 [41.5 to 87.5] | 75.0 [63.0 to 84.0] |
P value for comparing baseline and after treatment | 0.17 | 0.010 |
Median change [IQR] | 0 [-5 to + 14] | + 9 [-1.5 to + 25] |
P value for comparing changes between group | 0.10 | |
CPV = conventional prompted voiding; IQR = Interquartile range; NR = not reported; USAPV = ultrasound-assisted prompted voiding; VAS = visual analogue scale (ranged from 0: not stressful at all to 100: very stressful).
Appendix 5: References of Potential Interest
Economic Evaluations in Postoperative Setting
Donaldson K, Woll A, Jansen SM, Edenfield A, Swift S, Heisler CA. A cost-effectiveness analysis of post-void residual bladder scan thresholds in the postoperative setting. Int Urogynecol J. 2022;33(10):2727-2733. PubMed
Prieto J. Optimising the use of bladder ultrasound scanners to improve the quality and safety of patient care and reduce costs: an economic assessment to establish the best, most cost-efficient way to manage the provision and use of bladder ultrasound scanners in a hospital NHS trust. London (UK): Royal College of Nursing; 2016: https://www.rcn.org.uk/-/media/Royal-College-Of-Nursing/Documents/Professional-Development/Research/Innovations/Burdetters-Case-Studies/Jacqui-Prieto-Case-Study.pdf. Accessed 2023 Feb 8.
Previous CADTH Reports
Portable ultrasound for patients with non-urgent conditions: clinical and cost-effectiveness. Ottawa (ON): CADTH; 2011: https://www.cadth.ca/sites/default/files/pdf/htis/oct-2011/RA0556-000%20Portable%20Ultrasound.pdf. Accessed 2023 Feb 8.
Bladder scanner use prior to catheterization: a clinical review. Ottawa (ON): CADTH; 2008: https://www.cadth.ca/sites/default/files/pdf/htis/Bladder%20Scanner%20Use%20Prior%20to%20Catheterization%20A%20Clinical%20Review.pdf. Accessed 2023 Feb 8.
Guidelines and Recommendations
Johansson RM, Malmvall BE, Andersson-Gare B, et al. Guidelines for preventing urinary retention and bladder damage during hospital care. J Clin Nursing. 2013;22(3-4):347-355. PubMed
Review Articles
Jorge BM, Mazzo A, Amado Martins JC, Dias Henriques FM, Ferreira Cassini M. The person with urinary retention: student perception and scientific evidence on the use of portable ultrasound scanners. Revista de Enfermagem Referência. 2017;4(12):19-26.
Additional References
Schallom M, Prentice D, Sona C, et al. Accuracy of measuring bladder volumes with ultrasound and bladder scanning. Am J Crit Care. 2020;29(6):458-467. PubMed
Chen SC, Chen PY, Chen GC, Chuang SY, Tzeng IS, Lin SK. Portable bladder ultrasound reduces incidence of urinary tract infection and shortens hospital length of stay in patients with acute ischemic stroke. J Cardiovasc Nurs. 2018;33(6):551-558. PubMed
Cho MK, Noh EJ, Kim CH. Accuracy and precision of a new portable ultrasound scanner, the Biocon-700, in residual urine volume measurement. Int Urogynecol J. 2017;28(7):1057-1061. PubMed
Guidelines for eligible expenditures for long-term care homes. Toronto (ON): Government of Ontario; 2017: https://www.ltchomes.net/LTCHPORTAL/Content/Snippets/Guideline_for_Eligible_Expenditures_for_LTCHs_Final_Version__2.0_ADM_Approved_FINAL-s.pdf. Accessed 2023 Feb 8.
Thanagumtorn K. Accuracy of post-void residual urine volume measurement using an ultrasound bladder scanner among postoperative radical hysterectomy patients. J Med Assoc Thai. 2016;99(10):1061-1066. PubMed
Wilson A, Dugger R, Ehlman K, Eggleston B. Implementation science in nursing homes: a case study of the integration of bladder ultrasound scanners. Ann Longterm Care. 2015;23(6). https://www.hmpgloballearningnetwork.com/site/altc/articles/implementation-science-nursing-homes-case-study-integration-bladder-ultrasound-scanners. Accessed 2023 Feb 8.
Daurat A, Choquet O, Bringuier S, Charbit J, Egan M, Capdevila X. Diagnosis of postoperative urinary retention using a simplified ultrasound bladder measurement. Anesth Analg. 2015;120(5):1033-1038. PubMed
Iwatsubo E, Suzuki M, Igawa Y, Homma Y. Individually tailored ultrasound-assisted prompted voiding for institutionalized older adults with urinary incontinence. Int J Urol. 2014;21(12):1253-1257. PubMed
Lai KY, Chan WK, Ho WF, Leung CS, Li YK. Application of bladder scan in ambulatory management protocol for acute urinary retention with presumed diagnosis of benign prostatic hypertrophy. Hong Kong J Emerg Med. 2014;21(5):300-307.
Ung KA, White R, Mathlum M, Mak-Hau V, Lynch R. Comparison study of portable bladder scanner versus cone-beam CT scan for measuring bladder volumes in post-prostatectomy patients undergoing radiotherapy. J Med Imaging Radiat Oncol. 2014;58(3):377-383. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca