CADTH Health Technology Review
Sotrovimab for the Treatment of COVID-19
Rapid Review
Authors: Zahra Jafari, Danielle MacDougall
Abbreviations
CT
cycle threshold
HR
hazard ratio
ICU
intensive care unit
mAb
monoclonal antibody
NPS
nasopharyngeal swab
OR
odds ratio
PCR
polymerase chain reaction
SARS-CoV-2
severe acute respiratory syndrome coronavirus 2
VL
viral load
VOC
variants of concern
Key Messages
Sotrovimab may not have clinical effectiveness in treating Omicron subvariant BA.2.
This finding generally aligns with the Health Canada and WHO recommendations and the findings of previously published in vitro studies against the use of sotrovimab for Omicron subvariants, except for BA.1.
Given the limited number and observational, nonrandomized design of the included studies, and the absence of evidence on the clinical effectiveness of sotrovimab for outpatients with confirmed COVID-19 Omicron subvariants BA.3 to BA.5, it was difficult to draw a firm conclusion about the clinical effectiveness of sotrovimab for Omicron subvariants.
Context and Policy Issues
COVID-19, which is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has spread globally and posed a major challenge to health care systems worldwide.1 Although the implementation of mass vaccination campaigns has markedly reduced the health care burden associated with COVID-19,2 the vaccination rate differs considerably across countries, and some evidence demonstrates reduced efficacy of vaccines against new viral variants of concern (VOC).3,4 Therapeutic drugs directed against SARS-CoV-2 have been developed to impede COVID-19 progression, especially in patients with a higher likelihood of experiencing severe outcomes.2 Among existing drugs, neutralizing monoclonal antibodies (mAbs) target the spike protein of SARS-CoV-2 that mediates viral entry into host cells.5
In 2021, based on the results of randomized placebo-controlled trials indicating the efficacy of some mAbs in preventing COVID-19 progression,6-8 drug regulatory authorities including Health Canada (July 30, 2021)9 and the US FDA10 granted emergency use authorization (EUA) status for sotrovimab 500 mg to treat early COVID-19 in patients at high risk of progression. Sotrovimab (other names: VIR-7831, GSK4182136; sold under the brand name Xevudy) is a human-neutralizing immunoglobulin G (Ig G) mAb that inhibits SARS-CoV-2 replication.11 According to the last update of the Canadian Product Monograph for sotrovimab (September 14, 2021),12 this drug is indicated for the treatment of mild to moderate COVID-19, confirmed by direct SARS-CoV-2 viral testing, in adults and adolescents (≥ 12 years of age, weighing at least 40 kg) who are at high risk for progressing to hospitalization and/or death. Sotrovimab is not authorized for use in patients who are hospitalized due to COVID-19, who require oxygen therapy due to COVID-19, or who require an increase in baseline oxygen flow rate due to COVID-19 (in those on chronic oxygen therapy due to underlying non–COVID-19 related comorbidity).12 Prior to the Omicron variant surge, a phase III, randomized, placebo-controlled study13 reported a statistically significant reduction in the composite end point of hospitalization or death when sotrovimab was given within 5 days of symptom onset.
Since the emergence of COVID-19, the evolution of SARS-CoV-2 and the spread of multiple variants have compromised the efficacy of COVID-19 therapeutics and vaccines.1 On November 30, 2021, the US government SARS-CoV-2 Interagency Group (SIG) classified Omicron as a VOC.14 The Delta variant (B.1.617.2) reached almost 90% of all viral sequences submitted to the Global Initiative on Sharing All Influenza Data (GISAID) by October 2021, and Omicron (including B.1.1.529, BA.1, BA.1.1, BA.2, BA.3, BA.4, and BA.5 lineages) has become the dominant variant circulating globally, accounting for more than 98% of viral sequences after February 2022.15 Omicron’s mutations have increased its transmissibility and immune system evasion while compromising the efficacy of some anti–SARS-CoV-2 mAbs.3,13,16 In 2022, several in vitro studies reported a substantial reduction of sotrovimab’s in vitro neutralization activity against the Omicron BA.2, BA.4, and BA.5 subvariants, while it was still susceptible against the Omicron BA.1 and BA.1.1 subvariants.17-19 According to these in vitro findings, the last update of the recalls and safety alerts of Health Canada (April 14, 2022),20 the US National Institute of Health (NIH) COVID-19 treatment guidelines on anti-SARS-CoV-2 mAbs (August 18, 2022),21 WHO’s Living Guideline (Therapeutics and COVID-19, September 15, 2022),22 and several Canadian guidelines,23 the use of sotrovimab for the treatment of COVID-19 is not recommended. Overall, a Health Canada Notice of Compliance does not exist for sotrovimab in patients with COVID-19, and a previous CADTH report (September 2021) identified no relevant evidence regarding the clinical effectiveness of sotrovimab for the treatment of patients with COVID-19.24 Given the rapidly growing number of publications reporting the clinical effectiveness of mAbs drugs for the treatment of COVID-19, and the changing epidemiology of Omicron subvariants with potentially different effectiveness of sotrovimab, the objective of this report was to systematically review and critically summarize current evidence of the clinical effectiveness of sotrovimab for patients with COVID-19 Omicron subvariants.
Research Question
What is the clinical effectiveness of sotrovimab for the COVID-19 Omicron variant or subvariants?
Methods
Literature Search Methods
The literature search strategy used in this report is an update of a strategy developed for a previous CADTH report.24 For the current report, a limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, and Canadian and major international health technology agencies, as well as a focused internet search. No filters were applied to limit retrieval by study type. The initial search was limited to English-language documents published between March 1, 2019, and August 30, 2021. For the current report, database searches were rerun on December 15, 2022, to capture any articles published or made available since the initial search date. The search for major health technology agencies was also updated to include documents published since August 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. As an update to a previous CADTH report,24 articles were included if they were made available since the previous search date and met the selection criteria for this report. The final selection of full-text articles was based on the selection criteria presented in Table 1. Studies with mixed Omicron subvariant populations were eligible for inclusion; studies that reported only on the Omicron subvariant BA.1 were excluded. Studies that did not confirm the Omicron subvariant in patients were included if data collection took place during a time period in which the Omicron variant or subvariants were dominant, as reported by study authors.
Criteria | Description |
|---|---|
Population | Patients (aged 12 years and older) with confirmed COVID-19 Omicron subvariants BA.2 to BA.5 Include: organ transplant recipients, immunocompromised patients Exclude: patients with cancer |
Intervention | Sotrovimab alone or in combination with other therapies |
Comparator | No treatment, placebo, or other active treatments (e.g., monoclonal antibodies) |
Outcomes | Clinical benefits (e.g., mortality, hospitalization, ICU admission, hospital length of stay, severity of clinical symptoms, viral load, mechanical ventilation) and harms (e.g., adverse events) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before August 1, 2021.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Downs and Black checklist25 for randomized and nonrandomized studies. Summary scores were not calculated for the studies; rather, the strengths and limitations of each publication were described narratively as detailed in Appendix 3.
Summary of Evidence
Quantity of Research Available
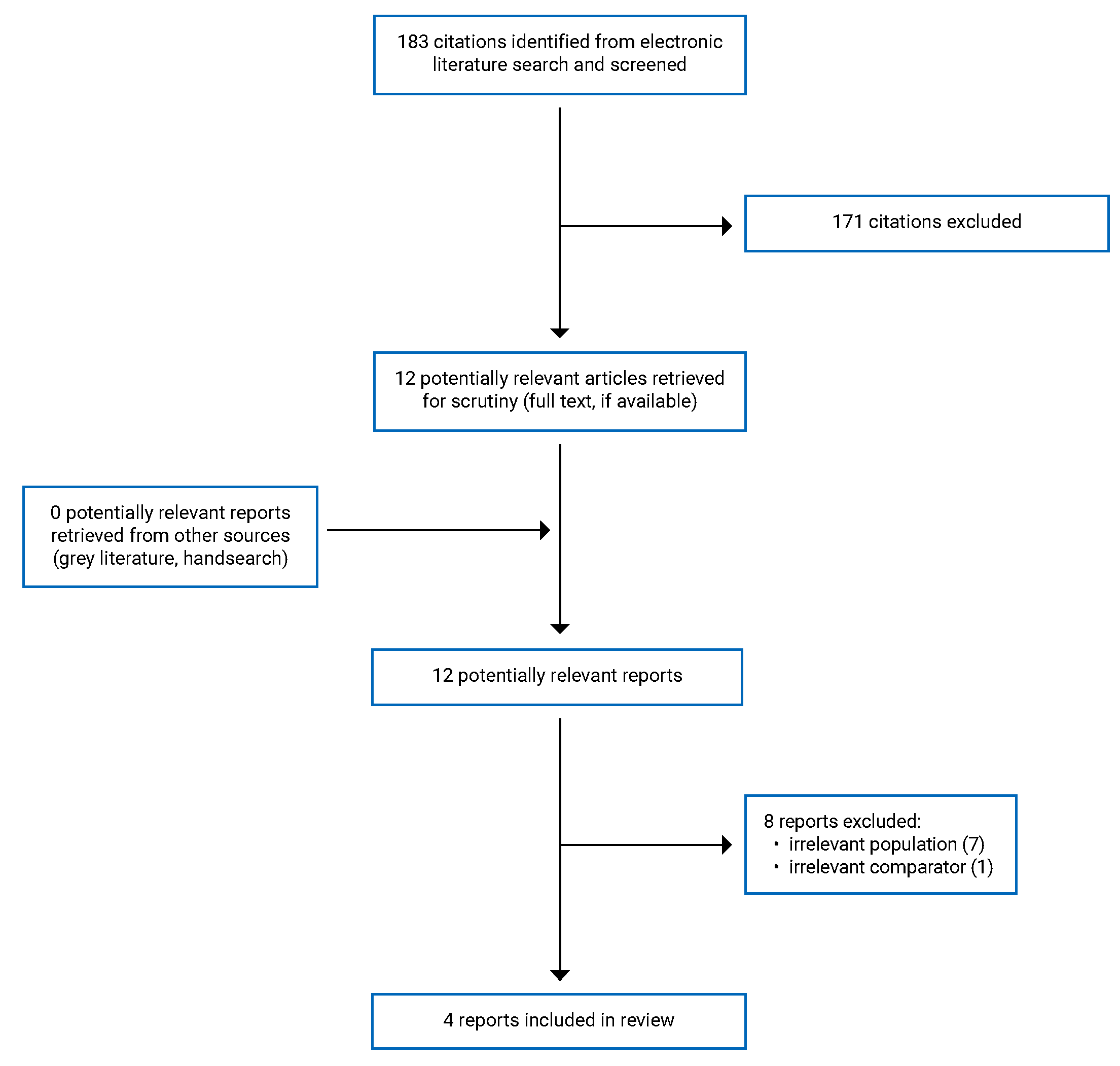
A total of 339 citations — 183 from article search results (peer-reviewed publications) and 156 from preprint search results (non–peer-reviewed preprints) — were identified in the literature search. Following screening of titles and abstracts in peer-reviewed articles, 171 citations were excluded and 12 potentially relevant reports from the electronic search were retrieved for full-text review. No potentially relevant publications were retrieved from the grey literature search for full-text review. Of the 12 potentially relevant articles, 8 were excluded for various reasons (i.e., irrelevant population or no comparator), and 4 publications26-29 met the selection criteria and were included in this report. Non–peer-reviewed preprints were not considered for this report. Appendix 1 presents the PRISMA30 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 5, including a short list of preprints that met the selection criteria but were not included in this report, since they were non–peer-reviewed preprints.
Summary of Study Characteristics
Three nonrandomized retrospective studies26-28 and 1 nonrandomized prospective study29 reporting the clinical effectiveness of sotrovimab in patients with confirmed COVID-19 during the surge of Omicron subvariants were included in this report.
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
The 4 publications included were observational, nonrandomized studies: 3 retrospective26-28 and 1 prospective.29
Country of Origin
The 3 retrospective studies were conducted by authors based in the UK,28 Germany,26 and Qatar,27 and the prospective study29 was conducted by authors based in Italy.
Patient Population
In a retrospective cohort study with the OpenSAFELY platform by Zheng et al. (2022),28 adult patients with non-severe COVID-19 confirmed with positive polymerase chain reaction (PCR) test results, who were at high risk of severe outcomes from COVID-19, were investigated. Data collection was performed at 2 time periods in England: first, between December 16, 2021, and February 10, 2022, when Omicron BA.1 was the predominant subvariant; and second, between February 16, 2022, and May 1, 2022, when Omicron BA.2 was the predominant subvariant. In this study, patients with onset of COVID-19 symptoms within the previous 5 days who belonged to at least 1 of the following high-risk cohorts were included in the study: Down syndrome, solid cancer, hematological disease, stem cell transplant, renal disease, liver disease, immune-mediated inflammatory disorders, primary immune deficiencies, HIV and/or AIDS, solid organ transplant, and/or rare neurologic conditions. Patients with signs of recovery, who required admission to the hospital for COVID-19, or who required supplemental oxygen for the management of COVID-19-related symptoms were excluded from the study.
In a single-centre, retrospective, matched cohort study by Woo et al. (2022),26 all hospitalized adults at the University Medical Center Hamburg-Eppendorf with confirmed SARS-CoV-2 Omicron subvariants between December 2021 and June 2022 were studied. The VOC type for different subvariants was tested using several high-throughput TaqMan-based quantitative PCR (qPCR) panels based on the detection of multiple mutations in the viral spike protein. A total of 860 patients were divided into 4 subgroups consisting of patients who received antiviral treatment and the matched control groups who did not receive antiviral treatment: patients treated with sotrovimab in the regular ward, sotrovimab combined with remdesivir in the regular ward, sotrovimab in the intensive care unit (ICU), and sotrovimab combined with remdesivir in the ICU. To minimize confounding from sex; age; comorbid conditions; treatment with dexamethasone; vaccination status; and history of coronary heart disease, chronic pulmonary disease, diabetes mellitus with or without end-organ damage, and chronic kidney disease, a propensity score was generated for each patient. Using a nearest-neighbour matching algorithm, patients in the treatment group were matched with patients who did not receive antiviral treatment at a 1:6 ratio for patients treated in the regular ward and at a 1:1 ratio for patients admitted to the ICU. To account for disease severity, the matching was performed separately for patients treated in regular wards and for patients admitted to the ICU. The exclusion criteria were not reported in the article.
In a retrospective matched (1:2) cohort study, Zaqout et al. (2022)27 reported the outcomes of all outpatients in the resident population of Qatar aged 50 years or older, who tested positive for SARS-CoV-2 using PCR or rapid antigen testing and were at risk for progression to severe symptoms. During the Omicron wave in Qatar, more than 70% of incident patients had BA.2 infections.31 The remaining patients mostly had BA.1, with “marginal” Delta incidence (13.7%).27 The data were collected between December 2021 and June 2022, and the number of patients in the sotrovimab and control groups was 345 and 583, respectively. The sotrovimab and control groups were matched (1:2 ratio) in sex, age, nationality, COVID-19 vaccination status, previous infection status, comorbid conditions, and epidemic phase. The control group consisted of patients who were offered treatment but opted not to receive it. Patients with symptoms of severe COVID-19 (oxygen saturation level < 90% or required oxygen supplements) within 7 days of diagnosis or before receiving sotrovimab were excluded from the study.
In a single-centre, prospective, nonrandomized study by Mazzotta et al. (2022),29 all consecutive patients between December 21, 2021, and March 15, 2022, with confirmed mild to moderate SARS-CoV-2 Omicron (BA.1 or BA.2) diagnosis, who met the Italian Medicine Agency (Agenzia Italiana del Farmaco [AIFA]) criteria for early treatment with mAbs or antiviral agents were enrolled. Of 568 patients enrolled, 521 patients were included who received 1 of the lines of treatment, including sotrovimab, molnupiravir, nirmatrelvir combined with ritonavir, or remdesivir, and had a viral load measured on days 1 and 7. Overall, 469 patients (90%) were vaccinated, 81 patients (15%) had negative baseline serology, and the median time from symptom onset to the first day of treatment was 3 days (2 to 4 days). Exclusion criteria were not reported in the article.
Interventions and Comparators
In the retrospective cohort study by Zheng et al. (2022),28 the authors aimed to compare the effectiveness of sotrovimab and molnupiravir in preventing severe outcomes of COVID-19 in adult patients in the community who were at high risk of severe outcomes. In the first period of data collection (between December 16, 2021, and February 10, 2022, when Omicron BA.1 was the predominant subvariant in England), 3,331 and 2,689 patients were treated with sotrovimab and molnupiravir, respectively. In the second period of data collection (between February 16, 2022, and May 1, 2022, when Omicron BA.2 was the predominant subvariant in England), 5,979 and 11,970 patients were treated with sotrovimab and molnupiravir, respectively.
In the single-centre, retrospective, matched cohort study by Woo et al. (2022),26 the authors aimed to investigate in-hospital mortality for patients with Omicron subvariants who were treated with sotrovimab, with or without remdesivir, compared to matched control groups who did not receive treatment. Treatment regimens were either a single 500 mg IV infusion of sotrovimab, or a single 500 mg IV infusion of sotrovimab combined with a 3-day course of remdesivir (200 mg on day 1, followed by 100 mg daily on days 2 and 3).
In the retrospective matched cohort study by Zaqout et al. (2022),27 the authors aimed to compare the effectiveness of sotrovimab versus no treatment in reducing the progression to severe symptoms from COVID-19 during a time period when the BA.2 subvariant was dominant. The intervention was a single 500 mg IV infusion of sotrovimab over 30 minutes within 7 days of infection, and the comparator was a group of eligible patients who opted not to receive the treatment.
In the single-centre, prospective, nonrandomized study by Mazzotta et al. (2022),29 the authors aimed to compare the in vivo viral load reduction in nasopharyngeal swabs (NPSs) collected on day 1 and day 7 from outpatients with mild to moderate symptoms with confirmed BA.1 or BA.2 Omicron subvariants treated with sotrovimab, molnupiravir, nirmatrelvir combined with ritonavir, or remdesivir. The treatment allocation was based on drug availability, time from symptom onset, and the presence of comorbidities as defined by the AIFA criteria. The dosage and administration route of drugs (IV infusion or oral consumption) were not described in the article.
Outcomes
In the retrospective cohort study by Zheng et al. (2022),28 the primary outcome was COVID-19–related admission to hospital or death within 28 days post-treatment. The secondary outcomes were hospital admission or death from all causes within 28 days post-treatment and hospital admission or death from COVID-19 within 60 days of the start of treatment.
In the single-centre, retrospective, matched cohort study by Woo et al. (2022),26 the only outcome measure was the in-hospital mortality rate. The follow-up period post-treatment was not reported.
In the retrospective matched cohort study by Zaqout et al. (2022),27 the odds of progression to severe symptoms of COVID-19 were the outcome measure, and the follow-up period post-treatment was not reported.
In the single-centre, prospective, nonrandomized study by Mazzotta et al. (2022),29 the primary end point was log2 viral load variation from day 1 to day 7. SARS-CoV-2 load in NPSs was assessed using the Abbott Alinity m RealTime System (Abbott Laboratories, Wiesbaden, Germany), and expressed as log2 of cycle threshold (CT) values. The secondary end point was the proportion of negative NPSs on day 7 and the occurrence of clinical failure defined as hospitalization due to the development of severe COVID-19 or death from any cause within 30 days post-treatment.
Summary of Critical Appraisal
In the retrospective, population-based, cohort study authored by Zheng et al. (2022),28 the objective, the main outcomes to be measured, the characteristics of the included patients, the interventions of interest, the distribution of principal confounders in each group of patients to be compared, and the main findings were described. In this study, patients in the 2 intervention groups (sotrovimab and molnupiravir) were recruited from the same population over the same period of time. Thus, it was likely that the patients were representative of the eligible population to be included. The main outcome measures used were accurate, and the statistical tests used to assess the main outcomes were appropriate. The authors used the Cox proportional hazards model to determine the risk of admission to the hospital or death from COVID-19 within 28 days post-treatment, and to lower the risk of selection bias, the analyses were adjusted for the impact of potential confounders (e.g., demographic information, high-risk cohort categories, vaccination status, calendar time [or calendar week to count for trends in prescriptions and incidence of COVID-19 outcomes], body mass index, and comorbidities). However, the authors didn’t report the dosage and administration route of sotrovimab and molnupiravir (IV infusion or oral consumption) and the characteristics of patients lost to follow-up. In addition, it should be noticed that studies relying on large datasets for data extraction are at risk of selection bias due to factors such as inconsistency in administrative data recording, misclassification bias in outcome events, and missing data.
In the single-centre, retrospective, matched cohort study by Woo et al. (2022),26 the objective, the main outcomes to be measured, the characteristics of the included patients, the interventions of interest, and the main outcomes were described. To determine the in-hospital mortality rate for the different treatment groups (sotrovimab or sotrovimab combined with remdesivir in the regular ward or ICU), principal confounders (i.e., sex, age, comorbid conditions, immunosuppression, and past treatment with dexamethasone) were described. To reduce the risk of selection bias, patients in different intervention groups were recruited from the same population and at the same period; and the staff, places, and facilities associated with treatment were representative of the treatment procedure completed. However, the treatment groups were not adjusted for vaccination status, since this information was not available for all patients, and the study had no regular follow-up after hospital discharge. Because of the study design (i.e., a single-centre study), the included patients might not have been representative of the entire population eligible to be considered, which makes the generalizability of the findings uncertain. The limitations of retrospective studies for data extraction (e.g., inconsistency in administrative data recording, and missing data) and the risk of selection bias also should be acknowledged.
In the retrospective matched cohort study by Zaqout et al. (2022),27 the objective, the main outcomes to be measured, the characteristics of the included patients, the intervention of interest, and the main outcomes were described. To estimate the effectiveness of sotrovimab compared to no treatment in reducing progression to severe outcomes from COVID-19, the 2 study groups were matched (1:2) for principal confounders (i.e., sex, age, nationality, vaccination status, prior infection status, comorbid conditions, and epidemic phase). The main outcome measure (progression to severe symptoms of COVID-19) was defined according to WHO guidelines and was appropriate. In this study, the source of data was all eligible patients for sotrovimab treatment in the resident population of Qatar, and the study groups were recruited from the same population, at the same time period. Thus, the study groups included were representative of the entire population from which they were recruited. The statistical tests used to assess the main outcomes (the adjusted odds ratios) were appropriate, and the staff, places, and facilities associated with treatment were representative of the treatment procedure completed. However, the characteristics of patients lost to follow-up and the follow-up time period post-treatment were not reported, leading to uncertainty in the main outcome measure. In addition, the limitations of a retrospective design for data extraction (e.g., inconsistency in administrative data recording, misclassification bias in outcome events, and missing data) and the risk of selection bias should be considered.
In the single-centre, nonrandomized, prospective study by Mazzotta et al. (2022),29 the objective, the main outcomes to be measured, the characteristics of the included patients, and the interventions of interest were described. The authors used weighted marginal linear regression models to adjust the impact of principal confounders (i.e., the calendar month of infusion, immunodeficiency at the time of infusion, and duration of symptoms) on the outcomes. The main findings, the estimates of random variability for the main outcomes, and actual P values were reported; and the staff, places, and facilities associated with treatment were representative of the completed treatment procedure. However, the dosage and administration route of the 4 drugs administered (sotrovimab, molnupiravir, nirmatrelvir combined with ritonavir, or remdesivir), and the characteristics of patients lost to follow-up, were not reported. The study findings might have been influenced by selection bias given a nonrandomized design, and treatment allocation based on drug availability, time from symptoms onset, and presence of comorbidities. In addition, given the source of data limited to a single centre, the patients might not have been representative of the entire population eligible to be included, and the generalizability of findings was uncertain.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
The main findings of 4 observational, nonrandomized studies (3 retrospective26-28 and 1 prospective)29 during the surge of the Omicron variant are summarized in this section.
Appendix 3 presents the main findings of the included studies and the authors’ conclusions.
Hospital Admission or Death From COVID-19
In the retrospective, cohort study by Zheng et al. (2022),28 the outcomes were reported in 2 time frames, between December 16, 2021, and February 10, 2022, when Omicron BA.1 was the predominant subvariant (period 1 of data collection) and between February 16, 2022, and May 1, 2022, when Omicron BA.2 was the predominant subvariant (period 2 of data collection). The 2 groups treated with sotrovimab and molnupiravir were not different in baseline characteristics (age, sex, ethnicity, high-risk cohorts, immune-mediated inflammatory diseases, body mass index, diabetes, chronic cardiac disease, hypertension, chronic respiratory disease, vaccination). In the following sections, the outcomes of these 2 time periods are reported separately.
Period 1, Primary Outcome: Admission to Hospital or Death Within 28 Days Post-Treatment
Among 6,020 patients treated with sotrovimab or molnupiravir, 87 (1.45%) were admitted to the hospital or died of COVID-19: 32 (0.96%) in the sotrovimab group and 55 (2.05%) in the molnupiravir group. Of these 87 patients, 25 (0.42%) died of COVID-19 during 28 days of follow-up: 7 in the sotrovimab group and 18 in the molnupiravir group. Among 78 patients who were admitted to the hospital for COVID-19, fewer than 5 out of 29 patients in the sotrovimab group and 11 out of 49 in the molnupiravir group received critical care. The median duration of stay in the hospital was 6 days (range, 2 to 18) for the sotrovimab group and 7.5 days (range, 4 to 12) for the molnupiravir group. After adjusting for the impact of demographic information, high-risk cohort categories, vaccination status, calendar time, body mass index, and other comorbidities (using Cox proportional hazards models), treatment with sotrovimab was associated with a substantially lower risk of severe outcomes versus treatment with molnupiravir (hazard ratio [HR] = 0.54; 95% confidence interval [CI], 0.33 to 0.88; P = 0.01). Consistent results were found in propensity score weighted Cox models (HR = 0.50; 95% CI, 0.31 to 0.81; P = 0.005), and when the analysis was restricted to patients who were fully vaccinated (HR = 0.53; 95% CI, 0.31 to 0.90; P = 0.02).
Period 1, Secondary Outcome: Admission to Hospital or Death Within 60 Days Post-Treatment
Ninety-five patients (1.58%) were admitted to the hospital or died of COVID-19 during 60 days of follow-up post-treatment: 34 in the sotrovimab group and 61 in the molnupiravir group. The results of stratified Cox regression showed a significantly lower risk in the sotrovimab group versus the molnupiravir group (HR ranging from 0.46 to 0.51 in models 1 to 4; P < 0.05). During 28 days of follow-up after the start of treatment, 250 patients (4.17%) were admitted to the hospital or died of any cause: 127 (3.83%) in the sotrovimab group and 123 (4.58%) in the molnupiravir group. The stratified Cox regression showed no significant difference in the risk of admission to the hospital or death from all causes between the sotrovimab and molnupiravir groups (HR ranging from 0.84 to 0.96 in models 1 to 4; P > 0.05).
Period 2, Primary Outcome: Admission to Hospital or Death Within 28 Days Post-Treatment
Among 7,949 patients, 97 (1.22%) were admitted to the hospital or died of COVID-19: 57 (0.95%) in the sotrovimab group and 40 (2.03%) in the molnupiravir group. Of these 97 patients, 28 (0.35%) died of COVID-19: 9 in the sotrovimab group and 19 in the molnupiravir group. Using both stratified Cox regression (HR = 0.44; 95% CI, 0.27 to 0.71; P = 0.001) and propensity score weighted Cox model (HR = 0.53; CI 95%, 0.32 to 0.86; P = 0.010), treatment with sotrovimab was associated with a substantially lower risk of admission to the hospital or death from COVID-19 versus treatment with molnupiravir.
Authors’ conclusion: In routine care of adult patients in England with COVID-19 Omicron subvariants BA.1 and BA.2 in the community, with a high risk of severe outcomes from COVID-19, those who received sotrovimab were at a lower risk of severe outcomes compared to those treated with molnupiravir.
In the retrospective matched cohort study by Zaqout et al. (2022),27 the adjusted odds ratio (AOR) of progression to severe symptoms of COVID-19 requiring hospitalization in patients receiving sotrovimab treatment was 2.67 (95% CI, 0.60 to 11.91). In the analysis restricted to a subgroup of patients at a higher risk of severe forms of COVID-19, the AOR of progression to severe symptoms of COVID-19 with sotrovimab treatment was 0.65 (95% CI, 0.17 to 2.48). By restricting this analysis to the Omicron-dominated epidemic phase (86.3% Omicron variant versus 13.7% Delta variant in total), the AOR of progression to severe symptoms of COVID-19 with sotrovimab treatment was 0.88 (95% CI, 0.16 to 4.89).
Authors’ conclusion: In a setting dominated by the BA.2 subvariant, sotrovimab had no protective effect compared to no treatment in reducing COVID-19 severity.
In the single-centre, nonrandomized, prospective study by Mazzotta et al. (2022),29 a higher proportion of chronic respiratory disease (P < 0.001), liver disease (P < 0·001), and immunodeficiency (P = 0.010) was observed on day 1 in patients who received sotrovimab compared to other treatments (i.e., nirmatrelvir combined with ritonavir, molnupiravir, and remdesivir). The rate of COVID-19–related hospitalization or death from any cause within 30 days follow-up post-treatment was 9 out of 568 total registered patients, including 7 out of 226 (3.1%) in the sotrovimab group (5 with BA.1 and 2 with BA.2) and 2 out of 87 (2.3%) in the irmatrelvir combined with ritonavir group (2 with BA.1).
Authors’ conclusion: Sotrovimab had a higher rate of COVID-19-related hospitalization or death from any cause within 30 days following the start of treatment versus other treatments.
In-Hospital Mortality Rate
In the single-centre, retrospective, matched cohort study by Woo et al. (2022),26 after propensity score matching, the study groups (sotrovimab, sotrovimab combined with remdesivir, and no treatment in the regular ward or ICU) did not differ in sex; age; comorbid status; treatment with dexamethasone; vaccination status; or history of coronary heart disease, chronic pulmonary disease, diabetes mellitus with or without end-organ damage, and chronic kidney disease. However, the in-hospital mortality rate did not differ between the sotrovimab and control groups (6.7% [n = 4] versus 2.8% [n = 10]; P = 0.11), and between the sotrovimab combined with remdesivir group and the control group (4.5% [n = 1] versus 3.0% [n = 4]; P = 0.72). In the ICU, the rate of congestive heart failure was lower in the sotrovimab group versus the control group (67.8% [n = 59] versus 85.1% [n = 74]; P = 0.012), and chemotherapy was required less in the sotrovimab group versus the control group (77.0% [n = 67] versus 100% [n = 87]; P < 0.001). However, in the in-hospital mortality rate, no significant difference was identified between the sotrovimab and control groups (41.4% [n = 36] versus 27.6% [n = 24]; P = 0.09), and between sotrovimab in combination with remdesivir and the control groups (31.2% [n = 5] versus 32.3% [n = 31]; P = 0.91). In addition, the study authors reported that the in-hospital mortality rate was not statistically different among patients with Omicron BA.1, BA.2, and BA.4 and/or BA.5 subvariants in all subgroups; however, the data to support this finding were not provided in the publication.
Authors’ conclusion: Sotrovimab adds no clinical benefit for hospitalized patients with COVID-19 Omicron subvariants.
Viral Load
In the single-centre, nonrandomized, prospective study by Mazzotta et al. (2022),29 BA.1 and BA.2 subvariants were detected in 378 (73%) and 143 (27%) patients, respectively. The baseline mean viral load (VL) was 4.12 (standard deviation = 0.27) log2 CT (4.16 for BA.1 and 4.01 for BA.2). The proportion of total patients with CT less than or equal to 40 on day 7 was 6.7% (35 out of 521: 31 infected with BA.1 and 4 with BA.2). CT values greater than or equal to 40 cycles are considered negative results.29 Sotrovimab had better VL-reducing activity than remdesivir against BA.1 (P = 0.008) but not BA.2. Nirmatrelvir combined with ritonavir significantly reduced VL compared to other drugs, including sotrovimab, both in the BA.1 and the BA.2 subvariants (P ≤ 0.001). Molnupiravir was superior to sotrovimab in reducing VL in BA.2 (P < 0.001), but not BA.1.
Authors’ conclusion: Among 4 drugs administered for the treatment of outpatients with Omicron subvariants BA. 1 and BA.2, sotrovimab only had better VL-reducing activity compared with remdesivir against BA.1.
Overall Conclusion Based on the Included Studies
In outpatients with confirmed COVID-19 Omicron subvariant BA.2, 1 retrospective study reported a lower risk of admission to the hospital or death from COVID-19 within 28 days of follow-up in treatment with sotrovimab versus molnupiravir.28 Two other studies on outpatients with Omicron subvariants reported no statistically significant differences between sotrovimab and comparators in post-treatment VL (versus nirmatrelvir combined with ritonavir, molnupiravir, and remdesivir),29 or COVID-19 severity (versus no treatment).27 In addition, in a single-centre, retrospective study on hospitalized patients with Omicron subvariants, no difference was observed between sotrovimab and no treatment for in-hospital mortality rate.26
Limitations
Despite the availability of high-quality papers reporting the outcomes of different drugs including mAbs and sotrovimab for the treatment of outpatients with COVID-19 before the Omicron surge, the number of publications on the clinical effectiveness of sotrovimab for Omicron subvariants was limited. For this review, we found 4 studies reporting the clinical effectiveness of sotrovimab against Omicron subvariants compared to other drugs28,29 or no treatment.26,27 All 4 studies had an observational, nonrandomized design, including 3 retrospective studies26-28 and 1 prospective study.29 Despite considering matched control groups in 2 studies26,27 and using statistical adjustments for the impact of some potential confounders in 2 other studies,28,29 the studies were neither blinded nor randomized. Therefore, the risks of selection bias and confounding were possible, and the impact of unmeasured or uncontrolled confounding could not be excluded. Two included studies were single-centre reports26,29 and 1 study27 was limited to the small population of Qatar. Because of the design of these studies, the patients might not have been representative of the entire population eligible to be included, and the generalizability of the findings was uncertain. Overall, retrospective studies are more at risk of selection bias due to missing data32 and potential inconsistencies in data recording and data extraction.33 In addition, the reporting of findings in a mixed population of multiple Omicron subvariants and the absence of publications reporting the clinical effectiveness of sotrovimab in subvariants BA.3 to BA.5 in outpatients with confirmed COVID-19 is a limitation that adds to uncertainty about the clinical effectiveness of sotrovimab for specific Omicron subvariants. Moreover, the studies were conducted by authors from 3 European countries26,28,29 and 1 Asian27 country, and the generalizability of the findings to the population in Canada is uncertain.
Conclusions and Implications for Decision- or Policy-Making
This report summarizes the findings of studies on the clinical effectiveness of sotrovimab for Omicron subvariants compared to other drugs28,29 or no treatment.26,27 Of 4 included observational studies, 3 were not in support of the clinical effectiveness of sotrovimab in treating the Omicron BA.2 subvariant.27-29 One study on outpatients with confirmed COVID-19 subvariants BA.1 and BA.2 reported a lower risk of admission to the hospital or death from COVID-19 after treatment with sotrovimab compared with molnupiravir.28 In 2 other studies on outpatients with Omicron BA.2, it was shown that sotrovimab may not be effective in reducing VL relative to other drugs (including nirmatrelvir combined with ritonavir, molnupiravir, and remdesivir),29 or decreasing COVID-19 severity compared to no treatment.27 In addition, 1 study on hospitalized patients with Omicron subvariants reported no significant difference in mortality rates with sotrovimab treatment compared with no treatment.26 These findings are generally aligned with previously published in vitro findings showing that sotrovimab retains most of the neutralization activity against Omicron BA.1, but it may be ineffective against Omicron BA.2.3,34 In addition, there was a limited number (N = 4) of studies that were relevant to this report, which may have been due in part to the recency of the evidence base and the existence of recommendations against the use of sotrovimab for patients with COVID-19 since April 2022.20-22 Nonetheless, because of the limited number (N = 4) and the observational, nonrandomized design of included studies, the absence of evidence on the clinical effectiveness of sotrovimab on outpatients with confirmed Covid-19 subvariants BA.3 to BA.5, as well as finding no eligible study conducted in Canada, it was difficult to draw any firm conclusions about the clinical effectiveness of sotrovimab for Omicron subvariants in the Canadian context. Additional research with rigorous methodological approaches can reduce uncertainty and the risk of bias in current evidence, improve the generalizability of findings, and support stakeholders with decision-making regarding the clinical effectiveness of sotrovimab for Omicron subvariants.
References
1.Piccicacco N, Zeitler K, Ing A, et al. Real-world effectiveness of early remdesivir and sotrovimab in the highest-risk COVID-19 outpatients during the Omicron surge. J Antimicrob Chemother. 2022;77(10):2693-2700. PubMed
2.Mazzaferri F, Mirandola M, Savoldi A, et al. Exploratory data on the clinical efficacy of monoclonal antibodies against SARS-CoV-2 Omicron variant of concern. Elife. 2022;11. PubMed
3.Planas D, Saunders N, Maes P, et al. Considerable escape of SARS-CoV-2 Omicron to antibody neutralization. Nature. 2022;602(7898):671-675. PubMed
4.Dejnirattisai W, Huo J, Zhou D, et al. SARS-CoV-2 Omicron-B.1.1.529 leads to widespread escape from neutralizing antibody responses. Cell. 2022;185(3):467-484.e415. PubMed
5.Benton DJ, Wrobel AG, Xu P, et al. Receptor binding and priming of the spike protein of SARS-CoV-2 for membrane fusion. Nature. 2020;588(7837):327-330. PubMed
6.Gupta A, Gonzalez-Rojas Y, Juarez E, et al. Early Treatment for Covid-19 with SARS-CoV-2 Neutralizing Antibody Sotrovimab. N Engl J Med. 2021;385(21):1941-1950. PubMed
7.Dougan M, Nirula A, Azizad M, et al. Bamlanivimab plus Etesevimab in Mild or Moderate Covid-19. N Engl J Med. 2021;385(15):1382-1392. PubMed
8.Weinreich DM, Sivapalasingam S, Norton T, et al. REGEN-COV Antibody Combination and Outcomes in Outpatients with Covid-19. N Engl J Med. 2021;385(23):e81. PubMed
9.Health Canada. Regulatory decision summary - PrSotrovimab. 2021; https://covid-vaccine.canada.ca/info/regulatory-decision-summary-detailTwo.html?linkID=RDS00836. Accessed 2023 Jan 11.
10.Fact sheet for healthcare providers: emergency use authorization (EAU) of sotrovimab. Silver Spring (MD): U.S. Food and Drug Administration (FDA); 2022: https://www.fda.gov/media/149534/download#:~:text=FDA%20has%20authorized%20the%20emergency,to%20severe%20COVID%2D19%2C%20including. Accessed 2023 Jan 11.
11.Deng J, Heybati K, Ramaraju HB, Zhou F, Rayner D, Heybati S. Differential efficacy and safety of anti-SARS-CoV-2 antibody therapies for the management of COVID-19: a systematic review and network meta-analysis. Infection. 2022:1-15. PubMed
12.Sotrovimab for injection: 500 mg/8 mL (62.5 mg/mL) single use vial, solution for infusion [product monograph]. Mississauga (ON): GlaxoSmithKline Inc.; 2021 Sep 14: https://ca.gsk.com/media/6587/sotrovimab_pm_en.pdf. Accessed 2023 Jan 23.
13.Chen P, Nirula A, Heller B, et al. SARS-CoV-2 Neutralizing Antibody LY-CoV555 in Outpatients with Covid-19. N Engl J Med. 2021;384(3):229-237. PubMed
14.SARS-CoV-2 variant classifications and definitions. (COVID-19). Atlanta (GA): Centers for Disease Control and Prevention (CDC); 2022: https://www.cdc.gov/coronavirus/2019-ncov/variants/variant-classifications.html. Accessed 2023 Jan 12.
15.World Health Organization (WHO). Tracking SARS-CoV-2 variants. 2022; https://www.who.int/activities/tracking-SARS-CoV-2-variants. Accessed 2022 Dec 19.
16.Fact sheet for healthcare providers: emergency use authorization (EUA) for bebtelovimab. Silver Spring (MD): U.S. Food and Drug Administration (FDA); 2022: https://www.fda.gov/media/156152/download. Accessed 2023 Jan 23.
17.Yamasoba D, Kosugi Y, Kimura I, et al. Neutralisation sensitivity of SARS-CoV-2 omicron subvariants to therapeutic monoclonal antibodies. Lancet Infect Dis. 2022;22(7):942-943. PubMed
18.Wang Q, Guo Y, Iketani S, et al. Antibody evasion by SARS-CoV-2 Omicron subvariants BA.2.12.1, BA.4 and BA.5. Nature. 2022;608(7923):603-608. PubMed
19.Cao Y, Yisimayi A, Jian F, et al. BA.2.12.1, BA.4 and BA.5 escape antibodies elicited by Omicron infection. Nature. 2022;608(7923):593-602. PubMed
20.Health professional risk communication: sotrovimab for injection - risk of treatment failure due to circulation of SARS-CoV-2 Omicron BA.2 subvariant. (Recalls and safety alerts). Ottawa (ON): Health Canada; 2022: https://recalls-rappels.canada.ca/en/alert-recall/sotrovimab-injection-risk-treatment-failure-due-circulation-sars-cov-2-omicron-ba2. Accessed 2022 Dec 20.
21.COVID-19 Treatment Guidelines Panel. Anti-SARS-CoV-2 monoclonal antibodies. In: Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. Bethesda (MD): National Institutes of Health (NIH); 2022: https://files.covid19treatmentguidelines.nih.gov/guidelines/section/section_111.pdf. Accessed 2022 Dec 19.
22.Therapeutics and COVID-19: living guideline. Geneva (Switzerland): World Health Organization; 2022: https://www.who.int/publications/i/item/WHO-2019-nCoV-therapeutics-2023.1. Accessed 2023 Jan 09.
23.Pharmacological therapies for COVID-19. (CADTH health technology review). Ottawa (ON): CADTH; 2022: https://www.cadth.ca/sites/default/files/ou-tr/HC0031%20COVID%20Drug%20Guidelines.pdf. Accessed 2023 Jan 23.
24.Sotrovimab for the treatment of COVID-19. (CADTH health technology review: rapid review). Ottawa (ON): CADTH; 2021: https://www.cadth.ca/sites/default/files/covid-19/RC1384%20Sotrovimab%20for%20COVID%20Final.pdf. Accessed 2023 Jan 23.
25.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
26.Woo MS, Brehm TT, Fischer M, et al. Sotrovimab in Hospitalized Patients with SARS-CoV-2 Omicron Variant Infection: a Propensity Score-Matched Retrospective Cohort Study. Microbiol Spectr. 2022:e0410322. PubMed
27.Zaqout A, Almaslamani MA, Chemaitelly H, et al. Effectiveness of the neutralizing antibody sotrovimab among high-risk patients with mild-to-moderate SARS-CoV-2 in Qatar. Int J Infect Dis. 2022;124:96-103. PubMed
28.Zheng B, Green ACA, Tazare J, et al. Comparative effectiveness of sotrovimab and molnupiravir for prevention of severe covid-19 outcomes in patients in the community: observational cohort study with the OpenSAFELY platform. BMJ. 2022;379:e071932. PubMed
29.Mazzotta V, Cozzi Lepri A, Colavita F, et al. Viral load decrease in SARS-CoV-2 BA.1 and BA.2 Omicron sublineages infection after treatment with monoclonal antibodies and direct antiviral agents. J Med Virol. 2022:e28186. PubMed
30.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700. PubMed
31.Altarawneh HN, Chemaitelly H, Ayoub HH, et al. Effects of Previous Infection and Vaccination on Symptomatic Omicron Infections. N Engl J Med. 2022;387(1):21-34. PubMed
32.Ayilara OF, Zhang L, Sajobi TT, Sawatzky R, Bohm E, Lix LM. Impact of missing data on bias and precision when estimating change in patient-reported outcomes from a clinical registry. Health Qual Life Outcomes. 2019;17(1):106. PubMed
33.Weinger MB, Slagle J, Jain S, Ordonez N. Retrospective data collection and analytical techniques for patient safety studies. J Biomed Inform. 2003;36(1-2):106-119. PubMed
34.Cameroni E, Bowen JE, Rosen LE, et al. Broadly neutralizing antibodies overcome SARS-CoV-2 Omicron antigenic shift. Nature. 2022;602(7898):664-670. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Primary Observational Clinical Studies
Study citation, country, aim, funding source | Study design, date of data collection | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Zheng et al. (2022)28 Country: UK Aim: To compare sotrovimab and molnupiravir in preventing admission to the hospital or death from COVID-19 Funding source:
| A retrospective cohort study with the OpenSAFELY platforma Date of data collection:
Sample size calculation: No | Adult patients with COVID-19 confirmed with positive PCR test results, who were at high risk of severe outcomes from COVID-19. Disease severity: Non-severe symptoms of COVID-19 Total sample size: Period 1: 6,020 (mean age = 52 years, 59% female)
Period 2: 7,949 (mean age 58.8 years)
Inclusion criteria:
Exclusion criteria:
| Intervention: Sotrovimab Comparator: Molnupiravir | Outcomes: Primary outcome: COVID-19-related admission to the hospital or death within 28 days post-treatment. Secondary outcomes:
Follow-up: Within 28 or 60 days post-treatment |
Woo et al. (2022)26 Country: Germany Aim: To investigate the in-hospital mortality rate from COVID-19 in hospitalized patients with Omicron subvariants compared to control groups Funding source: NR | A single-centre, retrospective matched cohort study Date of data collection: between December 2021 and June 2022 Sample size calculation: No | Hospitalized adults with confirmed SARS-CoV-2 Omicron subvariants Disease severity: Hospitalized patients with COVID-19 Total number of patients: 860
Exclusion criteria: NR | Intervention:
Comparator: Patients with SARS-CoV-2 Omicron subvariants who did not receive antiviral treatment were matched with the treatment groups in the regular ward (1:6) and ICU (1:1). | Outcomes:
|
Zaqout et al. (2022)27 Country: Qatar Aim: To compare the effectiveness of sotrovimab vs. no treatment in reducing the progression to severe COVID-19 symptoms Funding source:
| A retrospective matched (1:2) cohort study Date of data collection: Between December 2021 and June 2022 Sample size calculation: No | All eligible outpatients aged ≥ 50 years (70% assumed with BA.2 subvariant), who tested positive for SARS-CoV-2 using PCR or rapid antigen tests and were at risk of progression to severe symptoms. Disease severity: Non-severe symptoms The number of matched patients (1:2) in the sotrovimab and control groups:
Exclusion criteria: Symptoms of severe COVID-19 including oxygen saturation level < 90% or requiring oxygen supplements within 7 days of diagnosis or before receiving sotrovimab | Intervention: A single 500 mg IV infusion of sotrovimab over 30 minutes within 7 days of infection Comparator: Eligible patients who opted not to receive treatment. The sotrovimab and control groups were matched (1:2) in sex, age, nationality, COVID-19 vaccination status, previous infection status, comorbidity conditions, and epidemic phase. | Outcomes:
Follow-up: NR |
Mazzotta et al. (2022)29 Country: Italy Aim: To study viral load decrease in BA.1 and BA.2 Omicron subvariants after treatment with sotrovimab vs. other drugs Funding:
| A single-centre, nonrandomized prospective study Date of data collection: Between 21 December 2021 and 15 March 2022 Sample size calculation: No | All consecutive patients during the study time period with confirmed SARS-CoV-2 Omicron (BA.1 or BA.2) diagnosis Disease severity: Mild to moderate COVID-19 Total number of patients: 521 (median age = 66 years, 45% female, 90% vaccinated) including 371 (73%) BA.1 and 143 (27%) BA.2
Inclusion criteria: Outpatients who met the Scientific Committee of the Italian Medicine Agency criteria for early treatment by mAbs or antiviral agents Exclusion criteria: NR | Intervention:
Treatment allocation was subject to drug availability, time from symptoms onset, and presence of comorbidities as defined by the Italian Medicine Agency criteria. Comparator: No placebo or control group. The 4 interventions were compared together. | Outcomes:
Follow-up: A telephone visit 30 days post-treatment |
ICU = intensive care unit; NPS = nasopharyngeal swab; NR = not reported; PCR = polymerase chain reaction; SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
aOpenSAFELY is a data analytics platform created on behalf of the UK National Health Service (NHS) for the analysis of electronic health records in response to urgent COVID-19 research questions.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist25
Strengths | Limitations |
|---|---|
Zheng et al. (2022),28 a retrospective cohort study | |
The objective, the main outcomes to be measured, the characteristics of the included patients, and the interventions of interest were described. The distribution of principal confounders in each group of patients was described. The main findings, estimates of random variability for the main outcomes, and actual P values were reported. In the 2 intervention groups (sotrovimab and molnupiravir), patients were recruited from the same population within the same period of time. As such, the patients were likely representative of the eligible population to be considered. Evidence of data dredging in the main outcomes was not observed. The main outcome measures used were accurate. The statistical tests used to assess the main outcomes were appropriate. The Cox proportional hazards models were applied to determine the risk of admission to the hospital or death from COVID-19 within 28 days post-treatment. The analyses were adjusted for some potential confounders including demographic information, high-risk cohort categories, vaccination status, calendar time, body mass index, and comorbidities. The source of funding was reported. | Drug dosage and administration route (IV infusion or oral consumption) were not reported. The characteristics of patients lost to follow-up were not reported. The limitations of using large datasets for data extraction (such as inconsistency in administrative data recording, misclassification bias in outcome events, and missing data) and potential risks for selection bias should be considered. |
Woo et al. (2022),26 a single-centre, retrospective matched cohort study | |
The objective, the main outcomes to be measured, the characteristics of the included patients, and the interventions of interest were described. To compare 4 treatment subgroups in the in-hospital mortality rate from COVID-19, principal confounders (i.e., sex, age, comorbid conditions, immunosuppression, and past treatment with dexamethasone) were considered. The main findings, estimates of random variability for the main outcomes, and actual P values were reported. The staff, places, and facilities associated with treatment were representative of the treatment procedure completed. The statistical tests used to assess the main outcomes were appropriate. Using a nearest-neighbour matching algorithm, patients in the treatment group were matched with patients who did not receive antiviral treatment. Evidence of data dredging in the main outcomes was not observed. | Vaccination status was not available for all patients, and the study groups were not adjusted for this potential confounding factor. The study had no regular follow-up after hospital discharge. Thus, only in-hospital mortality rate but not overall survival was reported. The characteristics of patients lost to follow-up were not reported. Because of a single-centre study design, the patients might not have been representative of the entire population eligible to be included, and the generalizability of findings was uncertain. The limitations of retrospective studies in data extraction (including inconsistency in administrative data recording, misclassification bias in outcome events, and missing data) and the risk of selection bias should be acknowledged. The source of funding was not reported. |
Zaqout et al. (2022),27 a retrospective matched cohort study | |
The objective, the main outcomes to be measured, the characteristics of the included patients, and the interventions of interest were described. The treatment (sotrovimab) and no treatment (control) groups were matched (1:2) in principal confounders, including sex, age, nationality, vaccination status, prior infection status, comorbidity conditions, and epidemic phase. The main findings, estimates of random variability for the main outcomes, and actual P values were described. The main outcome measures used were accurate. The study groups (sotrovimab and no treatment) were recruited from the same population (all eligible patients in the resident population of Qatar), at the same time period. As such, the patients were likely representative of the eligible population to be considered. The staff, places, and facilities associated with treatment were representative of the treatment procedure completed. The statistical tests used to assess the main outcomes (adjusted odds ratios) were appropriate. Evidence of data dredging in the main outcomes was not observed. The source of funding was stated. | The follow-up period post-treatment was not reported, leading to uncertainty in the main outcome measure. The characteristics of patients lost to follow-up were not reported. The limitations of retrospective studies in data extraction (including inconsistency in administrative data recording, misclassification bias in outcome events, and missing data) and the risk of selection bias should be considered. |
Mazzotta et al. (2022),29 a single-centre, nonrandomized prospective study | |
The objective, the main outcomes to be measured, the characteristics of the included patients, and the interventions of interest were described. The main outcome measures used were accurate. In statistical analysis, the impact of principal confounding factors (calendar month of infusion, immunodeficiency at time of infusion, and duration of symptoms) was adjusted by modelling the treatment assignment (via the inverse probability of weighting), the outcome (via regression adjustment), or both (doubly robust methods). The main findings, estimates of random variability for the main outcomes, and actual P values were reported. Evidence of data dredging in the main outcomes was not observed. The staff, places, and facilities associated with treatment were representative of the treatment procedure completed. The source of funding was reported. | Drug dosage and administration route (IV infusion or oral consumption) were not reported. The outcomes might have been influenced by selection bias due to a nonrandomized design, and treatment allocation based on drug availability, time from symptoms onset, and presence of comorbidities. Because of a single-centre study design, the patients might not have been representative of the entire population eligible to be included, and the generalizability of findings was uncertain. The characteristics of patients lost to follow-up were not reported. |
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 4: Summary of Findings of Included Primary Observational Clinical Studies
Study citation, study design, study aim | Main findings | Author’s conclusions |
|---|---|---|
Zheng et al. (2022)28 Study design: A retrospective, cohort study with the OpenSAFELY platform Aim: To compare sotrovimab and molnupiravir in preventing admission to the hospital or death from COVID-19 | Period 1: Between December 16, 2021, and February 10, 2022, when Omicron BA.1 was the predominant subvariant in England.
Period 2 of data collection between February 16, 2022, and May 1, 2022, when Omicron BA.2 was the predominant subvariant in England
| In routine care of adult patients in England with COVID-19 in the community with a high risk of severe outcomes from COVID-19, patients with Omicron subvariants BA.1 and BA.2 who received sotrovimab were at a lower risk of severe outcomes from COVID-19 vs. patients treated with molnupiravir. |
Woo et al. (Dec 2022)26 Study design: A single-centre, retrospective cohort study Aim: To investigate the in-hospital mortality rate from COVID-19 in hospitalized patients with Omicron subvariants compared to control groups |
| In hospitalized patients with Omicron subvariants, despite a lower rate of congestive heart failure and immunosuppressive therapy, sotrovimab led to no benefit in reducing the in-hospital mortality rate vs. no treatment. |
Zaqout et al. (2022)27 Study design: A retrospective matched cohort study Aim: To compare the effectiveness of sotrovimab vs. no treatment in reducing the progression to severe COVID-19 symptoms |
| No evidence was identified showing the protective effect of sotrovimab vs. no treatment in reducing COVID-19 severity in a setting dominated by the BA.2 subvariant. |
Mazzotta et al. (2022)29 Study design: A single-centre, nonrandomized prospective study Aim: To study viral load decrease in BA.1 and BA.2 Omicron subvariants after treatment with sotrovimab vs. other drugs |
| In reducing VL, sotrovimab was not effective against BA.2 subvariant. Nirmatrelvir combined with ritonavir and molnupiravir showed antiviral activity against BA.2. Sotrovimab had the highest proportion of COVID-19-related hospitalization or death from any cause within 30 days of follow-up post-treatment (7 out of 9 patients in total). |
AOR = adjusted odds ratio; CI = confidence interval; CT = cycle threshold; HR = hazard ratio; ICU = intensive care unit; VL = viral load.
aCT values ≥ 40 cycles are considered negative results.29
Appendix 5: References of Potential Interest
Previous CADTH Reports
Sotrovimab for the treatment of COVID-19. (CADTH health technology review: rapid review). Ottawa (ON): CADTH; 2021: https://www.cadth.ca/sites/default/files/covid-19/RC1384%20Sotrovimab%20for%20COVID%20Final.pdf. Accessed 2023 Jan 23.
The following publications were identified because they provide some information associated with this report, such as non–peer-reviewed preprints reporting the outcomes of treatment with sotrovimab in the context of Omicron subvariants; as well as guidelines, recommendations, or monographs regarding the treatment of patients with COVID-19, including the use of sotrovimab.
Non–Peer-Reviewed Preprints
Cheng M, Reyes C, Satram S, et al. Real-world Effectiveness of Sotrovimab for the Early Treatment of COVID-19 During SARS-CoV-2 Delta and Omicron Waves in the United States [non peer-reviewed preprint]. medRxiv. 2022: doi: 10.1101/2022.1109.1107.22279497. https://europepmc.org/article/ppr/ppr542871. Accessed 2022 Dec 15.
Degli Antoni M, Giagulli C, Messali S, et al. Potential Benefit of Early Treatment with Sotrovimab in Patients With High Risk for Severe COVID-19 Carrying BA.2 Infection [non peer-reviewed preprint]. Preprints.org. 2022: doi: 10.20944/preprints202207.200223.v202201. http://europepmc.org/abstract/PPR/PPR519510. Accessed 2022 Dec 15.
Yoshida J, Shiraishi K, Noda H, et al. Sotrovimab neutralizing SARS-CoV-2: Risk factors for post-infusion clinical events [non peer-reviewed preprint]. Res Sq. 2022: doi: 10.21203/rs.21203.rs-1495310/v1495311. http://europepmc.org/abstract/PPR/PPR473840. Accessed 2022 Dec 15.
Guidelines and Recommendations
Singh AK, Singh A, Singh R, Misra A. An updated practical guideline on use of molnupiravir and comparison with agents having emergency use authorization for treatment of COVID-19. Diabetes Metab Syndr. 2022 Feb;16(2):102396. PubMed
COVID-19 updates: NIH outpatient treatment guidelines. Med Lett Drugs Ther. 2022 02 21;64(1644):32. PubMed
Bartoletti M, Azap O, Barac A, et al. European society of clinical microbiology and infectious diseases guidelines for coronavirus disease 2019: an update on treatment of patients with mild/moderate disease. Clin Microbiol Infect. 2022 Dec;28(12):1578-1590. PubMed
Homer CS, Roach V, Cusack L, et al. The National COVID-19 Clinical Evidence Taskforce: pregnancy and perinatal guidelines. Med J Aust. 2022 11 06;217 Suppl 9:S14-S19. PubMed
White H, McDonald SJ, Barber B, et al. Care for adults with COVID-19: living guidelines from the National COVID-19 Clinical Evidence Taskforce. Med J Aust. 2022 10 03;217(7):368-378. PubMed
COVID-19 Treatment Guidelines Panel. Anti-SARS-CoV-2 monoclonal antibodies. In: Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. Bethesda (MD): National Institutes of Health (NIH); 2022: https://files.covid19treatmentguidelines.nih.gov/guidelines/section/section_111.pdf. Accessed 2022 Dec 19.
COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. Bethesda (MD): National Institutes of Health (NIH); 2022: https://files.covid19treatmentguidelines.nih.gov/guidelines/archive/covid19treatmentguidelines-12-06-2022.pdf. Accessed 2022 Dec 20.
Therapeutics and COVID-19: living guideline. Geneva (Switzerland): World Health Organization; 2022: https://www.who.int/publications/i/item/WHO-2019-nCoV-therapeutics-2023.1. Accessed 2023 Jan 09.
Monographs
Sotrovimab for injection: 500 mg/8 mL (62.5 mg/mL) single use vial, solution for infusion [product monograph]. Mississauga (ON): GlaxoSmithKline Inc.; 2021 Sep 14: https://ca.gsk.com/media/6587/sotrovimab_pm_en.pdf. Accessed 2023 Jan 23.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca