CADTH Health Technology Review
Copper and Ceruloplasmin Tests for Children With Global Developmental Delay and Intellectual Disability
Rapid Review
Authors: Zahra Jafari, Carolyn Spry
Abbreviations
GDD
global developmental delay
ID
intellectual disability
IEM
inborn errors of metabolism
MD
Menkes disease
TIDE
treatable intellectual disability endeavour
WD
Wilson disease
Key Messages
No evidence was identified regarding the diagnostic test accuracy or clinical utility of copper and ceruloplasmin tests compared to other tests or criteria to detect Wilson disease and Menkes disease in children with global development delay and intellectual disability that met the criteria for this review.
No evidence-based guidelines were found on the use of copper and ceruloplasmin tests for children with global developmental delay and intellectual disability that met the criteria for this review.
Context and Policy Issues
Global developmental delay (GDD) and intellectual disability (ID) affect up to 3% of the pediatric population.1 GDD and ID are phenotypically and genetically heterogeneous and a specific diagnosis may not be achieved in many patients.2 The diagnosis of GDD is limited to children younger than 5 years old, but later they may progress in which to meet diagnostic criteria for ID and represent the same population.3 Because of overlaps in etiological diagnoses of GDD and ID, investigations for a definitive diagnosis of both disorders are similar.3 Depending on the research design, objectives, and severity of GDD/ID in studies, etiological diagnosis of GGD/ID is widely variable.3 Based on the Diagnostic and Statistical Manual of Mental Disorders (DSM-5),4 the reports of an identifiable cause for severe ID and mild ID are up to 80%5 and 24%,6 respectively. Common etiological diagnoses for GDD/ID are prenatal intrinsic factors (e.g., genetic, central nervous system malformation, metabolic), prenatal extrinsic factors (e.g., teratogens, toxins, infections), perinatal factors (e.g., asphyxia, prematurity, neonatal complications), and postnatal factors (e.g., neglect, psychosocial environment, infections, trauma, toxins).3,7 Given the crucial role of early detection for initiating primary rehabilitation services and treatment, an integrative approach for etiological evaluation of patients within general pediatricians in coordination with other medical specialists is essential.3
To guide physicians toward an understanding of etiology that optimizes therapeutic yield, the American Academy of Pediatrics, the American Academy of Neurology and the British Columbia-based Treatable Intellectual Disability Endeavour (BC TIDE) protocol have each proposed multitiered investigations for GDD/ID.3 The existing recommendations or protocols intend to simplify the investigation of GDD/ID by limiting tests that are time-consuming or not clinically relevant and support the efficient use of limited health care resources.3 In 2018, the Canadian Pediatric Society published a statement to provide a framework for the clinical investigation of GDD/ID.3 The key elements of investigation recommended in this statement were formal vision and hearing tests, chromosomal microarray, Fragile-X DNA test, and first-tier test for treatable inborn errors of metabolism (IEM). Brain imaging was recommended in the presence of specific neurologic findings.3
IEM is not a common cause of GDD/ID.1 However, early screening may detect IEM before the phenotype evolves to more severe neurologic and/or systemic symptoms and allow for earlier treatment leading to improved health outcomes.1 To facilitate earlier diagnosis of potentially treatable GDD/ID, beginning in 2012, community-based pediatricians in BC were provided with information on the TIDE first-tier screening protocol and encouraged to widely screen children with unexplained GDD/ID with or without neurologic features and other comorbid symptoms typically occurring in IEM.1 The rationale was that some IEM might present with GDD/ID as the only feature before the manifestation of neurologic features.8 In the protocol, the copper and ceruloplasmin tests were aimed to identify Wilson disease (WD) and Menkes disease (MD). In a recent retrospective study, Vallance and colleagues (2021)1 compared the test volume and diagnostic yield of the BC TIDE first-tier screening tests for IEM 7 years before (2006 to 2012) and 7 years after (2013 to 2019) the protocol implementation.1 Following this retrospective study, the BC Children’s Hospital provided guidance in which the screening of some tests, including copper and ceruloplasmin, were no longer recommended since they had no contribution to the diagnostic yield, and no children with WD or MD were also identified.1,9
The trace metal copper is essential for a variety of biologic processes. However, excessive amounts of copper are extremely toxic, and the concentration of copper is kept under tight control in the body.10 The copper-transporting P-type adenosine triphosphatase (ATPases) ATP7A and ATP7B are characterized as central regulators of cellular copper metabolism. Mutations in ATP7A or ATP7B disrupt the homeostatic copper balance, leading to copper deficiency (e.g., MD) or copper overload (e.g., WD), respectively.10 WD, first described by Samuel Wilson in 1912, is a rare autosomal recessive metabolic disorder (estimated prevalence of 1 per 40,000 to 50,000)11 caused by mutations in the ATP7B copper transporter gene.12 There is no gold standard for the diagnosis of WD, and it is often delayed due to the non-specific clinical features and the need for a combination of clinical and laboratory tests for diagnosis.12,13 The neurologic manifestations of the disease include variable combinations of dysarthria, dystonia, tremor, and choreoathetosis, and misdiagnosis and delay in treatment can progress to hepatic failure or severe neurologic disability and death.13
MD is an X-linked, fatal, multisystemic disorder of copper metabolism that mostly affects males.14 Previous estimates of the prevalence of MD based on confirmed clinical patients vary from 1 in 40,000 to 1 in 354,507.15 However, in a recent study based on a genome aggregation database from a large diverse population, the predicted birth prevalence of MD or ATP7A-related disorders was reported as high as 1 in 8,664 live male births.15 MD results from mutations in the ATP7A gene, often intragenic mutations, or partial gene deletions.14 ATP7A contributes to the delivery of copper to the secreted copper enzymes and the export of surplus copper from cells.14 Progressive neurodegeneration, connective tissue disturbances, and peculiar kinky hair are the main disease manifestations.14 The severity of MD is considerably variable ranging from classical MD to occipital horn syndrome as the most severe and mild forms, respectively.16 Patients with severe form usually die before the third year of life.14 No cure exists for the disease, but very early copper-histidine treatment may correct some of the neurologic symptoms.14
Given the wide range of etiologies involved in GDD/ID, as well as the potential role of IEM as diagnostic biomarkers of WD and MD, the objectives of this report were to systematically summarize and critically appraise current literature regarding the diagnostic test accuracy of copper and ceruloplasmin tests for detecting WD and MD in children with GDD/ID, the clinical utility of copper and ceruloplasmin tests for children with GDD/ID, and evidence-based guidelines on the use of copper and ceruloplasmin tests for children with GDD/ID.
Research Questions
What is the diagnostic test accuracy of copper and ceruloplasmin tests (to detect Wilson disease and/or Menkes disease) for children with global development delay and intellectual disability?
What is the clinical utility of copper and ceruloplasmin tests for children with global development delay and intellectual disability?
What are the evidence-based guidelines regarding the use of copper and ceruloplasmin tests for children with global development delay and intellectual disability?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Library, the University of York Centre for Reviews and Dissemination databases, the websites of Canadian and major international health technology agencies, as well as focused internet search. The search strategy comprised both controlled vocabularies, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were developmental disabilities, copper, ceruloplasmin, and testing. The search was conducted in 2 parts. No filters were applied to limit the retrieval by study type for research questions 1 and 2. For question 3, a search filter was applied to a broader search of developmental disabilities, copper, and ceruloplasmin to limit retrieval to guidelines. Comments, newspaper articles, editorials, and letters were excluded. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2017, and November 14, 2022.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Children with global developmental delay and intellectual disability. |
Intervention | Specific copper and ceruloplasmin tests, i.e., serum copper; blood ceruloplasmin levels/serum ceruloplasmin concentration. |
Comparator | Q1: Leipzig criteria for Wilson disease; genetic testing for ATP7A (Wilson disease); or genetic testing for ATP7B (Menkes disease); no comparator. Q2: No testing; no comparator. Q3: Not applicable. |
Reference standard | Q1: Wilson disease: Leipzig criteria, genetic testing for ATP7A, or liver biopsy; Menkes disease: genetic testing for ATP7B or liver biopsy. Q2 and Q3: Not applicable. |
Outcomes | Q1: Diagnostic test accuracy (e.g., sensitivity, specificity, positive predictive value, negative predictive value). Q2: Clinical utility (e.g., time to treatment, morbidity, the incidence of Wilson disease and/or Menkes disease, mortality, quality of life, referrals, unnecessary follow-up). Q3: Recommendations regarding the use of copper and ceruloplasmin tests for children with GDD/ID. |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies, evidence-based guidelines. |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before January 1, 2017.
Summary of Evidence
Quantity of Research Available
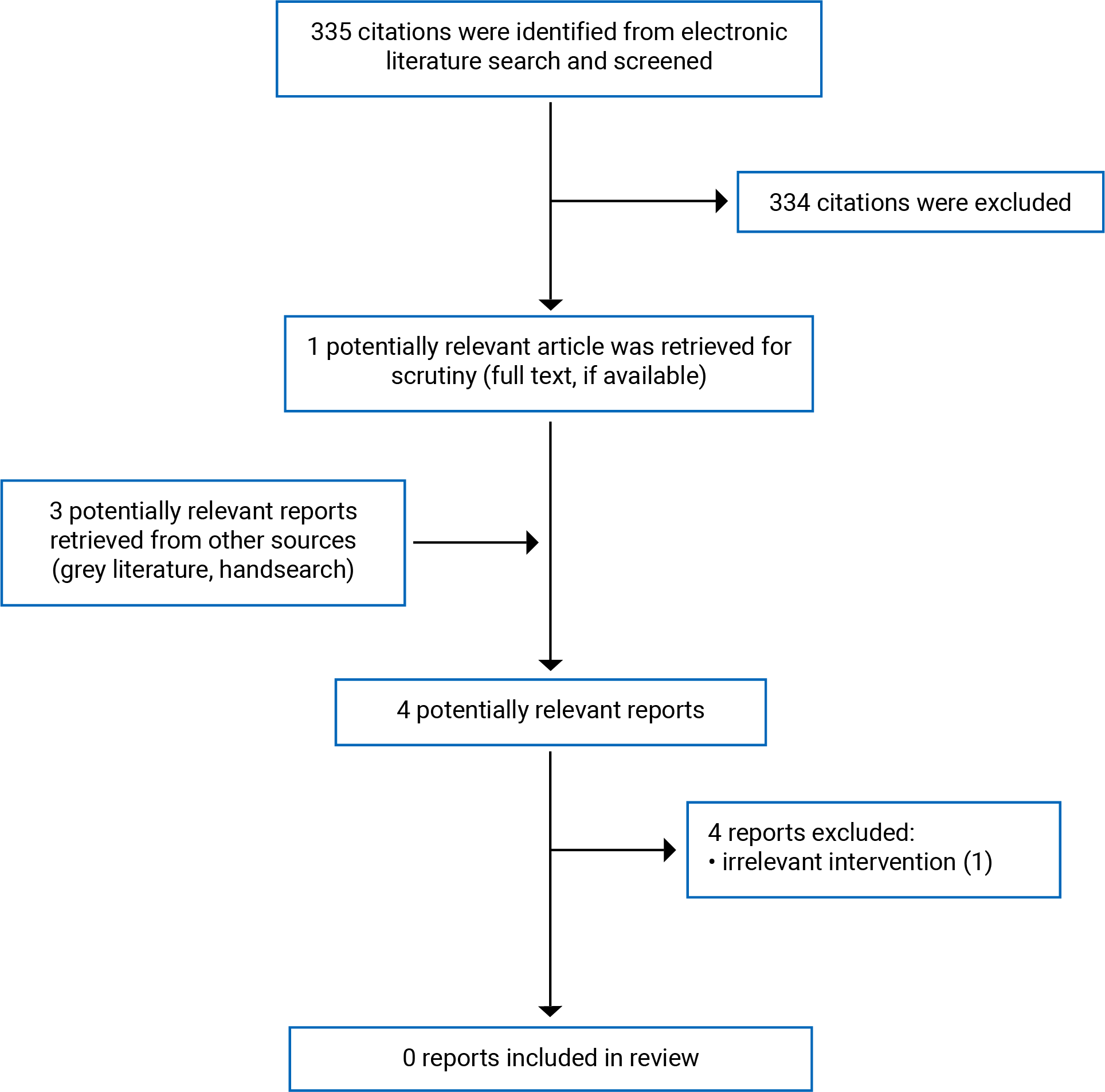
A total of 335 citations were identified in the literature search. Following the screening of titles and abstracts, 334 citations were excluded and 1 potentially relevant report from the electronic search was retrieved for full-text review. Three potentially relevant publications were retrieved from the grey literature search for full-text reviews. Of these 4 potentially relevant articles, all were excluded for various reasons, and no publications met the inclusion criteria to be included in this report. Appendix 1 presents the PRISMA17 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 2.
Summary of Findings
Diagnostic Test Accuracy of Copper and Ceruloplasmin Tests
No relevant literature was identified regarding the diagnostic test accuracy of copper and ceruloplasmin tests compared to other tests or criteria to detect WD and MD in children with GDD/ID; therefore, no summary can be provided.
Clinical Utility of Copper and Ceruloplasmin Tests
No relevant literature was identified concerning the clinical utility of copper and ceruloplasmin tests for children with GDD/ID; therefore, no summary can be provided.
Evidence-Based Guidelines
No evidence-based guidelines were identified on the use of copper and ceruloplasmin tests for children with GDD/ID; therefore, no summary can be provided.
Limitations
No relevant literature was identified regarding both the diagnostic test accuracy of copper and ceruloplasmin tests compared to other tests or criteria to detect WD and MD in children with GDD/ID and the clinical utility of copper and ceruloplasmin tests in children with GDD/ID. In addition, no evidence-based guidelines that met the criteria for this review were identified on the use of copper and ceruloplasmin tests for children with GDD/ID either.
Conclusions and Implications for Decision- or Policy-Making
Overall, there was a lack of evidence regarding the use of copper and ceruloplasmin tests for children with GDD/ID. Therefore, no conclusion can be provided regarding the diagnostic test accuracy of copper and ceruloplasmin tests compared to other tests or criteria to detect WD and MD in children with GDD/ID as well as the clinical utility of copper and ceruloplasmin tests in children with GDD/ID. Comprehensive research with rigorous methodological approaches is required for decision-making in this context.
References
1.Vallance H, Sinclair G, Rakic B, Stockler-Ipsiroglu S. Diagnostic yield from routine metabolic screening tests in evaluation of global developmental delay and intellectual disability. Paediatr Child Health. 2021;26(6):344-348. PubMed
2.Vasudevan P, Suri M. A clinical approach to developmental delay and intellectual disability. Clin Med (Lond). 2017;17(6):558-561. PubMed
3.Bélanger SA, Caron J. Evaluation of the child with global developmental delay and intellectual disability. Paediatr Child Health. 2018;23(6):403-419. PubMed
4.Association. AP. Neurodevelopmental disorders. In: Diagnostic and statistical manual of mental disorders. 5th ed ed. Washington, DC American Psychatric Publishing; 2013:31-87.
5.van Karnebeek CD, Stockler-Ipsiroglu S. Early identification of treatable inborn errors of metabolism in children with intellectual disability: The Treatable Intellectual Disability Endeavor protocol in British Columbia. Paediatr Child Health. 2014;19(9):469-471. PubMed
6.Shaffer LG. American College of Medical Genetics guideline on the cytogenetic evaluation of the individual with developmental delay or mental retardation. Genet Med. 2005;7(9):650-654. PubMed
7.Jimenez-Gomez A, Standridge SM. A refined approach to evaluating global developmental delay for the international medical community. Pediatr Neurol. 2014;51(2):198-206. PubMed
8.van Karnebeek CD, Shevell M, Zschocke J, Moeschler JB, Stockler S. The metabolic evaluation of the child with an intellectual developmental disorder: diagnostic algorithm for identification of treatable causes and new digital resource. Mol Genet Metab. 2014;111(4):428-438. PubMed
9.First-Tier Metabolic Testing: Evidence-Based Practice Change Recommendation. In: BC Children's Hospital.2021: https://www.childhealthbc.ca/sites/default/files/2021_bcch_tide_communication_pediatricians_first-tier-metabolic-testing_april10.pdf. Accessed 24 Nov, 2022.
10.de Bie P, Muller P, Wijmenga C, Klomp LW. Molecular pathogenesis of Wilson and Menkes disease: correlation of mutations with molecular defects and disease phenotypes. J Med Genet. 2007;44(11):673-688. PubMed
11.Sandahl TD, Laursen TL, Munk DE, Vilstrup H, Weiss KH, Ott P. The Prevalence of Wilson's Disease: An Update. Hepatology. 2020;71(2):722-732. PubMed
12.Ryan A, Nevitt SJ, Tuohy O, Cook P. Biomarkers for diagnosis of Wilson's disease. Cochrane Database Syst Rev. 2019;2019(11). PubMed
13.Lorincz MT. Wilson disease and related copper disorders. Handb Clin Neurol. 2018;147:279-292. PubMed
14.Tümer Z, Møller LB. Menkes disease. Eur J Hum Genet. 2010;18(5):511-518. PubMed
15.Kaler SG, Ferreira CR, Yam LS. Estimated birth prevalence of Menkes disease and ATP7A-related disorders based on the Genome Aggregation Database (gnomAD). Mol Genet Metab Rep. 2020;24:100602. PubMed
16.Tümer Z, Horn N. Menkes disease. In: Roach E, Miller V, eds. Neurocutaneous Syndromes Cambridge: Cambridge University Press; 2004 222–233.
17.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: References of Potential Interest
The following publications were identified because they provide some information associated with this report, such as the evaluation of children with GDD/ID, the accuracy of copper and ceruloplasmin tests in WD, the efficacy of different diagnostic tests for identifying WD, and IEM in children with autism spectrum disorders.
Systematic Reviews
Alternative Population
Salman HM, Amin M, Syed J, et al. Biochemical testing for the diagnosis of Wilson's disease: A systematic review. J Clin Lab Anal. 2022;36(2):e24191. PubMed
Guidelines
Alternative Population
Nagral A, Sarma MS, Matthai J, et al. Wilson's Disease: Clinical Practice Guidelines of the Indian National Association for Study of the Liver, the Indian Society of Pediatric Gastroenterology, Hepatology and Nutrition, and the Movement Disorders Society of India. J Clin Exp Hepatol. 2019;9(1):74-98. PubMed
Socha P, Janczyk W, Dhawan A, et al. Wilson's Disease in Children: A Position Paper by the Hepatology Committee of the European Society for Paediatric Gastroenterology, Hepatology and Nutrition. J Pediatr Gastroenterol Nutr. 2018;66(2):334-344. PubMed
Non-Randomized Studies
Unclear Population and Intervention
Vallance H, Sinclair G, Rakic B, Stockler-Ipsiroglu S. Diagnostic yield from routine metabolic screening tests in evaluation of global developmental delay and intellectual disability. Paediatr Child Health. 2021;26(6):344-348. PubMed
Note: The objective of this retrospective study was to determine the test volume and diagnostic yield of IEM in unexplained children with GDD/ID. In this study, the records of 4 metabolic (plasma amino acids; urine organic acids; dried blood spot acylcarnitines; and urine purine, pyrimidine, and certain metabolites) and 5 chemistry (ammonia, copper, ceruloplasmin, homocysteine, and lactate) tests before (2006 to 2012) and after (2013 to 2019) the implementation of the BC TIDE first-tier screening protocol were reviewed. Due to some methodological limitations, this study was not eligible for inclusion in this Rapid Review. Notably, the article provided no information about the demographic characteristics and clinical indication of the study population, children with GDD/ID. In addition, the chemistry tests, including copper and ceruloplasmin, were not considered for estimating the test volume and were not generally reported since they were conducted in laboratories across the BC and were not readily searchable for authors. Therefore, the relevance of this study to the clinical utility of copper and ceruloplasmin tests in GDD/ID was unclear.
Alternative Population
El Fotoh W, El Naby SAA, Abd El Hady NMS. Autism Spectrum Disorders: The Association with Inherited Metabolic Disorders and Some Trace Elements. A Retrospective Study. CNS Neurol Disord Drug Targets. 2019;18(5):413-420. PubMed
Tang NL, Hui J, Huang D, et al. Reference intervals of spot urine copper excretion in preschool children and potential application in pre-symptomatic screening of Wilson disease. Pathology. 2020;52(4):439-446. PubMed
Lu X, Li S, Zhang W, et al. Assessment of the diagnostic value of serum ceruloplasmin for Wilson's disease in children. BMC Gastroenterol. 2022;22(1):124. PubMed
Sonia ZF, Rukunuzzaman M, Karim MB, Yasmin A, Alam R. Efficacy of Different Diagnostic Test for Identifying Wilson's Disease. Mymensingh Medical Journal: MMJ. 2022;31(1):117-123. PubMed
Review Articles
Alternative Population
Zigman T, Petkovic Ramadza D, Simic G, Baric I. Inborn Errors of Metabolism Associated With Autism Spectrum Disorders: Approaches to Intervention. Front Neurosci. 2021; 15:673600. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as of the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca