CADTH Health Technology Review
Bevacizumab for the Treatment of Patients With Brain Radionecrosis
Rapid Review
Authors: Shannon Hill, Danielle MacDougall
Abbreviations
CI
confidence interval
FLAIR
fluid attention inversion recovery
Gd
gadolinium
HIT-6
Headache Impact Test-6
KPS
Karnofsky Performance Status
MIDAS
Migraine Disability Assessment Test
RCT
randomized controlled trial
SR
systematic review
Key Messages
This review identified limited evidence regarding the clinical effectiveness and safety of bevacizumab for patients with symptomatic brain radionecrosis after radiosurgery. These identified studies had several limitations, most notably due to the limited number of studies with control groups; therefore, the findings related to the effectiveness and safety in this population are uncertain.
For adult patients with symptomatic brain radionecrosis, treatment with bevacizumab may be associated with radiographic responses, a reduction in volumetric outcomes, an improvement in overall clinical and neurologic symptoms, an improvement in functional outcomes, and a reduction in corticosteroid use.
Limited evidence from 1 study suggests that treatment with bevacizumab may be associated with greater radiographic response, a reduction in volumetric outcomes, and clinical symptom improvement compared to treatment with corticosteroids. The recurrence of brain radionecrosis for patients who received bevacizumab compared to corticosteroids was similar between groups.
Commonly reported adverse events after patients with symptomatic brain radionecrosis were treated with bevacizumab included hypertension, proteinuria, edema, pulmonary embolism, and various thromboembolic events.
Context and Policy Issues
Brain radiation necrosis (hereafter referred to as radionecrosis) is a severe complication characterized by tissue death caused by radiation that may impact all or part of the brain tissue.1 Radionecrosis is most commonly associated with high-dose radiation treatment for primary or secondary brain tumours, but may also develop following radiotherapy to noncentral nervous system tumours that are in close proximity to brain tissues.1 It is estimated that the incidence of systematic brain radionecrosis is increasing due to the growing use of stereotactic radiosurgery and higher doses of radiation during initial therapy.1 In patients with brain metastases, the incidence of radionecrosis is between 5% and 25%.2 Risk factors associated with the occurrence of brain radionecrosis may include tumour volume, prescribed radiotherapy dose, fraction size, volume of normal brain irradiated, previous radiation exposure, and the use of concurrent therapy.2 Brain radionecrosis is largely diagnosed based on clinical symptoms and radiological presentation.1 Clinical symptoms may include neurologic deterioration and functional loss, which may progress to death.1 Conventional radiological imaging has limitations in differentiating between tumour progression and radionecrosis, but efforts have been made to improve imaging through MRI, magnetic resonance spectroscopy, and PET imaging.1,2
Symptomatic brain radionecrosis is typically treated with high-dose corticosteroids, such as dexamethasone.1,2 Corticosteroids help reduce inflammation signals and cytokines produced by the necrotic tissues, and may reduce potential blood brain barrier leaks.2 Because corticosteroids help reduce edema, most patients experience rapid clinical symptom improvements once steroids are initiated.2 Corticosteroid dosing varies depending on the type of corticosteroid and indication, but typically is prescribed at 4 mg to 8 mg per day.2 In some severe cases, surgical resection may be considered if treatment with corticosteroids proves unresponsive.1,2
Bevacizumab is an alternative treatment option for brain radionecrosis that has been used for colorectal, lung, brain, ovarian, cervical, and kidney cancers.3,4 Bevacizumab is a recombinant humanized monoclonal antibody that selectively binds to and neutralizes human vascular endothelial growth factor.5 Bevacizumab prevents human vascular endothelial growth factor from binding to endothelial cell surface receptors, and therefore regulates vascular permeability, which reduces edema caused by brain radionecrosis.3 Bevacizumab treatment is also an accessible option because it allows for relatively long dosing intervals due to its prolonged half-life and does not require continuous use.3
A Health Canada Notice of Compliance does not exist for bevacizumab for brain radionecrosis,5 and CADTH’s reimbursement review process does not typically review biosimilar drugs. The purpose of this report is to summarize and critically appraise the evidence related to the clinical effectiveness and safety of bevacizumab, to support decisions involved in the treatment of patients with symptomatic brain radionecrosis after radiosurgery.
Research Questions
What is the clinical effectiveness and safety of bevacizumab for patients with symptomatic brain radionecrosis after radiosurgery?
What is the comparative clinical effectiveness and safety of bevacizumab versus corticosteroids for patients with symptomatic brain radionecrosis after radiosurgery?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were bevacizumab and radionecrosis. No filters were applied to limit the retrieval by study type. Conference abstracts were excluded. Where possible, retrieval was limited to the human population. The search was completed on October 24, 2022, and limited to English-language documents published since January 01, 2012.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Q1 and Q2: Adult patients diagnosed with symptomatic brain radionecrosis after receiving radiosurgery for brain metastases |
Intervention | Q1 and Q2: Bevacizumab (any dose) |
Comparator | Q1: Placebo, no treatment, or no comparator Q2: Corticosteroids (e.g., dexamethasone) |
Outcomes | Q1 and Q2: Clinical effectiveness (e.g., progression-free survival, overall survival, response rate, duration of response, radionecrosis volume, symptom management and/or relief, quality of life) and safety (e.g., adverse events of grade 3 and grade 4, serious adverse events, mortality) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2012. Systematic reviews (SRs) in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)6 for SR, and the Downs and Black checklist7 for randomized and non-randomized studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
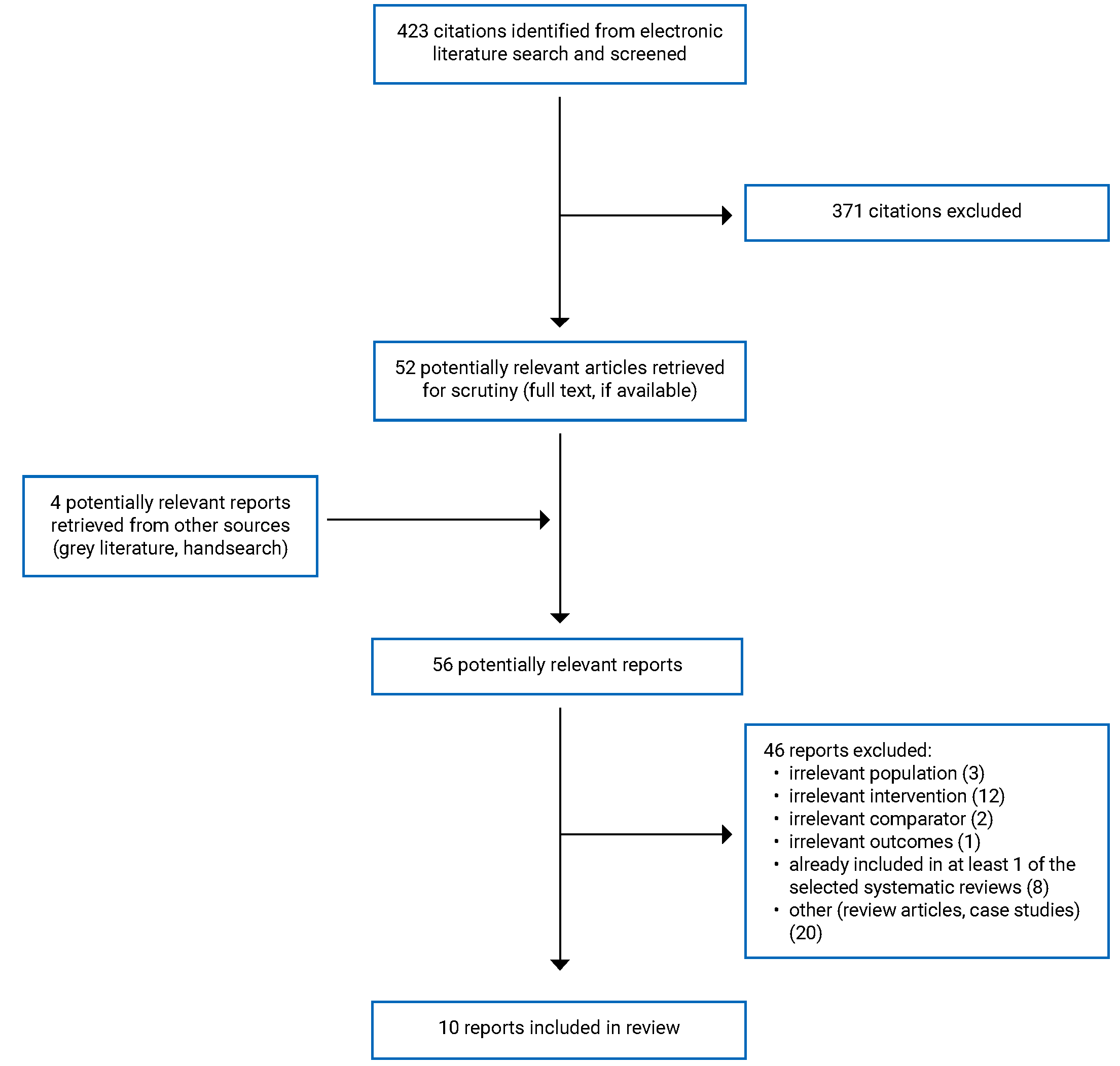
A total of 423 citations were identified in the literature search. Following screening of titles and abstracts, 371 citations were excluded and 52 potentially relevant reports from the electronic search were retrieved for full-text review. Four potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 46 publications were excluded for various reasons, and 10 publications met the inclusion criteria and were included in this report. These comprised 4 SRs and 6 non-randomized studies. Appendix 1 presents the PRISMA8 flow chart of the study selection.
Summary of Study Characteristics
Four SRs9-12 including 1 with meta-analysis9 and 6 non-randomized studies13-18 were included in this report.
Additional details regarding the characteristics of included publications are provided in Appendix 2. There was a large degree of overlap between the studies included in the SRs. The degree of overlap between SRs is presented in Appendix 5.
Study Design
Two SRs were published in 2021,9,10 1 SR was published in 2017,11 and 1 SR was published in 2013.12 The authors of 1 SR and meta-analysis included 12 non-randomized studies published up to August 2020.9 The authors of 1 SR included 12 primary studies comprised of 2 randomized controlled trials (RCT) and 10 non-randomized studies published up to March 2020.10 The authors of 1 SR included 21 primary studies comprised of 1 RCT and 20 non-randomized study published up to September 2016.11 The authors of 1 SR included 7 primary studies comprised of 1 RCT and 6 non-randomized studies published up to September 2012.12 The primary study overlap between these SRs is summarized in Appendix 5. Fourteen of the 31 primary studies were included in 2 or more SRs.
Two non-randomized studies were published in 2022,13,14 2 non-randomized studies were published in 2021,15,16 1 non-randomized study was published in 2017,17 and 1 non-randomized study was published in 2016.18 Four of the non-randomized studies were single-arm retrospective cohort studies that used historical patient data to compare the change in outcomes before and after treatment.13,15-17 Two of the non-randomized studies were single-arm prospective cohort studies that collected patient data prospectively to compare the change in outcomes before and after treatment.14,18 When reported, patient follow-up times varied across each study, but ranged from 6 months to 14.2 months.
Country of Origin
The included SRs were conducted in China,9,10 Italy,11 and the US.12
The included non-randomized studies were conducted in Canada,13 the US,14 China,15-17 and Japan.18
Patient Population
All 4 SRs included primary studies of patients with brain radionecrosis due to radiosurgery for brain metastases.9-12 The total number of patients included in the SRs ranged from 30 to 236, and the sample size of each included primary study ranged from 1 to 58.9-12
Each non-randomized study included patients who had undergone radiosurgery, were diagnosed with brain radionecrosis, and were subsequently treated with bevacizumab.13-18 The number of patients included in each non-randomized study ranged from 10 to 40, and the mean or median age of patients ranged from 35.1 years to 64 years.13-18
Interventions and Comparators
Consistent with the inclusion criteria for the current report, the identified SRs included primary studies that assessed the effectiveness of bevacizumab for the treatment of patients with brain radionecrosis due to radiosurgery for brain metastases.9-12 The dose and regimen of bevacizumab treatment varied across the studies, from 1 mg/kg to 15 mg/kg for up to 8 weeks.9-12 The comparators for the identified SRs included single-arm before and after treatment studies,9-12 corticosteroids,10 and placebo.10-12
Similarly, the identified non-randomized studies assessed the effectiveness of bevacizumab for the treatment of patients with brain radionecrosis due to radiosurgery for brain metastases.13-18 The dose and regimen of bevacizumab treatment varied across the studies, and ranged from 2.5 mg/kg to 10 mg/kg every 2 to 4 weeks for a maximum of 6 cycles.13-18 Each included non-randomized study was a single-arm before and after treatment study.13-18
Outcomes
The identified SRs reported outcomes related to the clinical effectiveness and safety of bevacizumab for the treatment of patients with brain radionecrosis after radiosurgery. Three SRs reported the number of patients that experienced a radiographic response to treatment.9-11 Each SR reported MRI findings related to volumetric changes associated with brain radionecrosis, measured through MRI T1 gadolinium (Gd) or T2 fluid attention inversion recovery (FLAIR) enhancement.9-12 Three SRs reported outcomes associated with neurologic symptom progression,9-11 while 1 SR reported unspecified clinical symptom progression.12 Two SRs reported outcomes associated with the Karnofsky Performance Status (KPS) score,9,10 which is a tool used to measure the functionality of patients with cancer, as well as their ability to perform ordinary tasks.19 Each SR reported outcomes related to corticosteroid use,9-12 specifically dexamethasone, for 3 of the identified SRs.9,10,12 Three SRs reported outcomes related to safety and adverse events, which included occurrence and symptoms of adverse events,9-11 as well as radionecrosis recurrence in 1 SR.10
Similarly, the identified non-randomized studies assess the clinical effectiveness and safety of bevacizumab for the treatment of patients with brain radionecrosis after radiosurgery. One single-arm retrospective cohort study reported outcomes related to the number of patients who experience a radiographic response to treatment.13 Five non-randomized studies reported MRI findings related to volumetric changes measured through MRI T1 Gd enhancement,13-17 while 4 non-randomized studied reported volumetric changes measured through MRI T2 FLAIR enhancement.13-16 One single-arm prospective cohort study reported MRI findings related to the efficacy of treatment specifically for perilesional edema remission.18 One single-arm prospective cohort study reported outcomes associated with neurologic symptom progression,14 while 1 single-arm retrospective cohort study reported unspecified clinical symptom progression.15 Four non-randomized studies reported outcomes associated with KPS score.14-16,18 Five non-randomized studies reported outcomes related to corticosteroid use,13-16,18 with 2 non-randomized studies reporting outcomes specifically for dexamethasone use.13,18 Five non-randomized studies reported outcomes related to safety and adverse events, which included occurrence and symptoms of adverse events,13-15,18 radionecrosis recurrence,14,17 overall survival,13 progression-free survival,13 and mortality.14,18
Summary of Critical Appraisal
An overview of the critical appraisal of the included studies is summarized in the following. Additional details regarding the strengths and limitations of the included publications are provided in Appendix 3.
Systematic Reviews
All 4 SRs provided clearly defined the research question, inclusion criteria, and provided adequate details of the included primary studies.9-12 Only 1 SR stated that review methods were established before the review was conducted and provided the PROSPERO registration number.10 Because 3 SRs did not state that the review methods were established before the review was conducted, it is challenging to determine if there were any deviations in the methods used that may impact validity. Three SRs included multiple database searches in their search strategy,9-11 while 1 SRs stated that only 1 database was used for the search strategy.12 Each included SR provided literature search terms and a search strategy, which may help determine reproducibility.9-12 None of the SRs restricted the time frame of their search,9-12 while 3 SRs did not restrict by study design, which may allow for reduced selection or publication bias;9,11,12 however, this may be impacted because each SR only included studies published in English.9-12 Two SRs indicated that literature search screening and data collection were done in duplicate, thus minimizing potential errors in data collection and synthesis.10,11 Only 2 SRs assessed the risk of bias of the included primary studies using appropriate techniques;9,10 however, it was unclear if risk of bias between primary studies was accounted for when interpreting the results of the review for each SR.9-12 It is unclear if risk of bias was assessed in 2 SRs, which may impact the ability to interpret the validity of findings for each study.11,12 Additionally, publication bias was not assessed in any of the SRs.9-12 One SR with MA included appropriate methods of statistical combination and measurement of heterogeneity (e.g., I2 statistics), and discussed heterogeneity in its findings when applicable.9 Three SRs did not provide adequate information related to the statistical analysis, presenting challenges in determining if appropriate statistical analyses were conducted for primary study outcomes.10-12 None of the SRs reported sources of funding for the included primary studies.9-12 Each SR disclosed any potential conflict of interest implications for the review,9-12 while 2 SRs disclosed if any funding was received for the review.9,10
Non-Randomized Studies
None of the included non-randomized studies had a separate control group, which creates a major challenge in determining the true measure of effect for the intervention; therefore, any findings from these studies should be interpreted with caution as uncontrolled factors may have influenced the findings.13-18 All 6 included non-randomized studies clearly defined the objective, outcomes, intervention, and characteristics of included patients.13-18 Each non-randomized study received ethical approval,13-18 while 1 study registered the protocol before conducting the study, which allows for greater confidence in determining if there were any deviations in the methods used.14 Five non-randomized studies clearly defined the patient inclusion criteria,13-15,17,18 while 1 non-randomized study did not define the patient inclusion or exclusion criteria, which may impact study reproducibility.16 Each non-randomized study clearly described the main findings,13-18 with 4 studies including appropriate measures of variability (range and 95% confidence intervals [CIs]).13-15,18 Four non-randomized studies used appropriate statistical tests to assess main outcomes and the outcomes measures used were valid and reliable.13-15,18 Two non-randomized studies did not provide adequate information related to the statistical tests used to assess the main outcomes, which may be create challenges for accurately interpreting the findings and could impact internal validity.16,17 Patient data were collected from the same population over the same period of time in each non-randomized study, and patient data were likely representative of the population from which they were recruited, which may help determine generalizability in similar popualtions.13-18 No evidence was provided in any of the non-randomized studies that indicated that the staff, places, and facilities may have been representative of the treatment the majority of the patients received.13-18 None of the identified non-randomized studies adequately identified principal confounders or account for possible confounding factors in the analysis, which may impact the true measure of effect for the intervention.13-18 Compliance with the intervention was reliable for each non-randomized study due to the nature of the intervention.13-18 Two non-randomized studies clearly accounted for patients lost to follow-up, with 1 study indicating that no patients were lost to follow-up.14,18 Due to the retrospective cohort study design of 4 of the non-randomized studies, there may be limitations to the data available for follow-up analysis, as these studies are limited by information captured in the past.13,15-17 Three non-randomized studies provided information related to any funding received for the study,14,15,18 while 5 non-randomized studies declared any potential conflict of interest implications.13,15-18
Summary of Findings
Four SRs9-12 (1 with an MA)9 and 6 non-randomized studies13-18 were identified regarding the clinical effectiveness and safety of bevacizumab for patients with symptomatic brain radionecrosis after radiosurgery. Appendix 4 presents the main study findings by outcome, which include radiographic response after treatment, MRI change after treatment, change in clinical symptoms, KPS score, corticosteroid use, and safety and adverse events. One SR included 2 primary studies with direct comparison outcomes for bevacizumab treatment versus placebo or corticosteroids.10 The other findings in this review from the SRs9-12 and non-randomized studies13-18 did not include a separate control group (i.e., relevant evidence was single-arm and uncontrolled). The findings from the controlled studies (i.e., versus placebo or versus corticosteroids) are presented separately from the findings, with no control group (i.e., no comparator), in the tables and text, when applicable.
There was some overlap in the primary studies that were included in the SRs. Findings from the SRs were reported using pooled estimates (either by MA or simple data pooling) or by individual primary study, based on how the data were presented in the SR. When feasible, to avoid duplication of the results, outcome data from an individual primary studies within SRs were only reported once; however, some of the pooled estimates from separate reviews may contain some of the same data. A citation matrix illustrating the degree of overlap is presented in Appendix 5.
Clinical Effectiveness and Safety of Bevacizumab for Patients With Symptomatic Brain Radionecrosis After Radiosurgery
All 4 SRs and 6 non-randomized studies reported outcomes for patients who received bevacizumab treatment for symptomatic brain radionecrosis after radiosurgery from single-arm uncontrolled studies,9-18 while 1 SR included 1 RCT that reported findings for patients who received bevacizumab compared to patients who received placebo.10 Three SRs presented overall results from pooled findings of included primary studies.9-11
Radiographic Response After Treatment
Bevacizumab Treatment Versus Placebo
One SR reported on 1 primary RCT that indicated that all patients who received bevacizumab treatment for brain radionecrosis experienced a radiographic response compared to none of the patients who received placebo.10 This finding was statistically significantly different (P = 0.013).10
Bevacizumab Treatment With No Control Group
Three SRs reported the number of patients who experienced a radiographic response for patients who received bevacizumab treatment.9-11 One SR defined a radiographic response as any reduction observed in radionecrosis or edema volume on MRI images.9 Three SRs that combined uncontrolled findings from primary studies and reported that 93%,9 84.7%,10 and 97.6%11 of patients who received bevacizumab treatment for brain radionecrosis experienced a radiographic response.
One single-arm retrospective cohort study reported that among 15 patients who received bevacizumab treatment for brain radionecrosis, 60% reported no radiographic response, while 33% and 7% reported a minimal or definite radiographic response, respectively.13
MRI Change After Treatment
MRI T1 Gd Enhancement Volume Change for Bevacizumab Treatment Versus Placebo
One SR reported on 1 primary RCT that indicated that patients who received bevacizumab treatment for brain radionecrosis were shown to have a 63% reduction in MRI T1 Gd enhancement volume compared to a 17% increase for patients who were given a placebo.10 This finding was statistically significantly different (P = 0.0058).10
MRI T1 Gd Enhancement Volume Change From Bevacizumab Treatment With No Control Group
All 4 SRs reported uncontrolled findings from primary studies for MRI T1 Gd enhancement volume changes after treatment with bevacizumab for patients with brain radionecrosis.9-12 Three SRs reported combined findings from primary studies and found that patients treated with bevacizumab showed a reduction in MRI T1 Gd enhancement volume, which ranged from a 26% to 100% reduction in volume.9-11 One SR with MA reported the pooled uncontrolled MRI T1 Gd enhancement volume findings across 6 included primary studies and reported a statistically significant reduction rate after patients were treated with bevacizumab for brain radionecrosis (i.e., 48.58% reduction; 95% CI, 38.32% to 58.85%; I2 = 80%; P < 0.001).9 One SR reported on 1 primary study that was not captured in the other included SRs, and found that MRI T1 Gd enhancement volume was reduced but did not report any numeric value associated with the reduction.12
Five single-arm cohort studies reported on MRI T1 Gd enhancement volume changes after treatment with bevacizumab for patients with brain radionecrosis.13-17
Three single-arm cohort studies reported the number of patients who experienced an MRI T1 Gd enhancement volume reduction, and found that 80%,14 95%,15 and 92.86%17 of included patients from each study experienced a volume reduction.
One single-arm retrospective cohort study reported a mean reduction of 3 cm3 (95% CI, 4.9 cm3 to 11.0 cm3) among patients after bevacizumab treatment, but no measure of statistical significance was reported.13 One single-arm retrospective cohort study14 reported that the median volume reduction difference after bevacizumab treatment was 12.1 cm3, with a 76% median reduction volume at 12 months, which was statistically significantly different (P = 0.012). One singe-arm retrospective cohort study reported that the reduction in MRI T1 volume from baseline was statistically significant at 1 month (48.4%), 3 months (74%), and 6 months (75%).15 One single-arm retrospective cohort study reported the mean MRI T1 Gd volume reduction to be 45% after treatment, but no measure of statistical significance was reported.16
MRI T2 FLAIR Enhancement Volume Change From Bevacizumab Treatment Versus Placebo
One SR reported on 1 primary RCT that indicated that patients who received bevacizumab treatment for brain radionecrosis had a 59% reduction in MRI T2 FLAIR volume compared to an increase of 14% in patients who were given a placebo.10 This findings was statistically significant (P = 0.0149).10
MRI T2 FLAIR Enhancement Volume Change From Bevacizumab Treatment With No Control Group
All 4 SRs reported MRI T2 FLAIR enhancement volume changes after treatment with bevacizumab for patients with brain radionecrosis.9-12 Three SRs reported combined findings from primary studies and found that patients treated with bevacizumab showed a reduction in MRI T2 FLAIR enhancement volume, which ranged from a 48% to 74% reduction in volume.9-11 One SR with MA reported the pooled uncontrolled MRI T2 FLAIR volume findings across 6 included primary studies and reported a statistically significant reduction rate of 62.017% (95% CI, 52.23% to 71.79%; P = 0.01).9 One SR reported on 1 primary study that was not captured in the other included SRs, and found that MRI T2 FLAIR volume was reduced but did not report any numeric value associated with the reduction.12
Four single-arm cohort studies reported on outcomes found through MRI T2 FLAIR enhancement volume changes after treatment with bevacizumab for patients with brain radionecrosis.13-16 Two single-arm cohort studies reported the number of patients who experienced an MRI T2 FLAIR volume reduction, and found that 90%14 and 95%15 of included patients from each study experienced a volume reduction. One single-arm retrospective cohort study reported a mean volume reduction of 27.9 cm3 (95% CI, 12.0 cm3 to 67.7 cm3) among patients after bevacizumab treatment, but no measure of statistical significance was reported.13 One single-arm prospective cohort study reported that the median vasogenic edema reduction difference between before bevacizumab treatment and after, as measured by MRI T2 FLAIR images, was 27.61 cm3, with a 70% median reduction at 12 months; however, this was not statistically significant (P = 0.086).14 One single-arm retrospective cohort study reported that the reduction in MRI T2 edema volume from baseline was statistically significant at 1 month (47.6%), 3 months (76.2%), and 6 months (66.3%) after bevacizumab treatment.15 One single-arm retrospective cohort study reported that the mean MRI T2 FLAIR volume after treatment was 26.1 cm3 with a mean volume reduction of 74%, but no measure of statistical significance was reported.16 One single-arm prospective cohort study reported a statistically significant rate of perilesional edema remission for patients who received bevacizumab treatment compared to those who received baseline measurements (78.9%; 95% CI, 62.7% to 90.4%; P < 0.001).18 Additionally, the median time to remission was 3.03 months (95% CI, 2.86 months to 3.85 months), the mean reduction in perilesional edema volume from baseline to 1 month after treatment was 63%, and the mean reduction in contrast-enhanced lesions from baseline to last treatment was 92.8%.
Change in Clinical Symptoms
Unspecified Clinical Symptoms for Bevacizumab Versus Placebo
One SR reported the findings from 1 primary RCT and found that the proportion of patients who experienced clinical improvement after bevacizumab treatment was 100% compared to 0 patients who received a placebo (n = 7 in both groups), but no measure of statistical significance was reported.10
Unspecified Clinical Symptoms From Bevacizumab Treatment With No Control Group
One SR reported on 1 primary study that was not captured in the other included SRs, and found that there was an improvement in clinical symptoms for the patients who received bevacizumab treatment but no numeric value was provided for this finding.12 One single-arm retrospective cohort study reported the overall change in symptomatic response for patients who received bevacizumab treatment.15 The authors reported that 2.5% of patients experienced progressed symptoms, 30% of patients experience stable symptoms, and 67.5% of patients experienced improved symptoms.15
Neurologic Symptoms
Three SRs that reported combined uncontrolled findings from primary studies, reported on the overall number of patients who experience a change in neurologic symptoms after treatment with bevacizumab for brain radionecrosis.9-11 Two SRs reported that 3.5%9 and 3.2%11 of included patients showed no response or worsened neurologic symptoms. Three SRs reported that 10%,9 9%,10 and 5.6%11 of included patients showed stable neurologic symptoms. Three SRs reported that 46%,9 79.7%,10 and 91.2%11 of included patients showed improved symptoms. Two SRs reported that 40%9 and 6%10 of included patients showed complete symptom resolution.
One single-arm prospective cohort study reported on the change in the Migraine Disability Assessment Test (MIDAS)20 and Headache Impact Test-621 at 3 months after bevacizumab treatment for patients without radionecrosis recurrence.14 Overall, the MIDAS score statistically significantly decreased (median decrease = 92%; range, 58% to 100%; P = 0.022) and the total Headache Impact Test-6 score statistically significantly decreased (median decrease = 24.8%; range, –14.1% to 39%; P = 0.02).14 The total days of headache statistically significantly decreased (median = 77%; range, –11% to 95%; P = 0.019).14 The MIDAS pain score reported a statistical significant decrease by 36% (median = 33%; range, –43% to 100%; P < 0.001).14
Karnofsky Performance Status Score
Two SRs reported the overall number of patients who experienced a change in the KPS score after bevacizumab treatment for brain radionecrosis.9,10 Both SRs reported that KPS scores improved in 80%9 and 78%10 of patients, while 1 SR reported that 22% of patients experienced stable or decreased KPS scores.10 Four single-arm cohort studies reported on the change in KPS scores from baseline in patients who were treated with bevacizumab for brain radionecrosis.14-16,18 One single-arm cohort study reported a median score increase of 10 points,14 1 single-arm cohort study reported a median post-treatment score of 70 points,15 and 1 single-arm cohort study reported a mean post-treatment score increase of 31.8 points overall.16 The study that reported an increase of 70 points was reported to be statistically significant,15 while the study that reported an increase of 10 points was reported as not statistically significant, and statistical significance for the increase in 31.8 points was not reported.14,16 One single-arm cohort study reported the number of patients who experienced an improvement in KPS score and found that overall, 42.1% of patients (95% CI, 21.8% to 54%) experienced an improvement, while 26.5% of those patients experience a score increase by 10%, and 15.8% experienced a score improvement by 20%.18 The number of patients who experienced a score improvement at last follow-up was 23.8% (95% CI, 8.2% to 47.2%).18 No measure of statistical significance was reported for these findings.
Corticosteroid Use
Dexamethasone
Three SRs reported uncontrolled findings related to the change in dexamethasone use after treatment with bevacizumab for brain radionecrosis.9,10,12 Two SRs reported that overall, 97%9 and 97.8%10 of patients reduced or discontinued dexamethasone after bevacizumab treatment. One SR reported a mean dexamethasone dose reduction of 9.08 mg,9 while another SR reported that the dexamethasone dose was reduced to 0 after bevacizumab treatment; however, it is unclear what the initial dexamethasone dose was.12 Two single-arm cohort studies reported on the change in dexamethasone use after treatment with bevacizumab. One single-arm retrospective cohort study reported that among the 9 patients who did receive dexamethasone treatment, 5 patients experienced a dose reduction after bevacizumab treatment, while 4 patients had no dose reduction.13 One single-arm prospective cohort study reported that 76.3% (95% CI, 59.8% to 88.6%) of patients experienced a reduction in dexamethasone after bevacizumab treatment.18 Additionally, the mean dexamethasone dose at 6 months post bevacizumab treatment was 0.6 mg per day and 0.8 mg per day at final follow-up compared to mean baseline measurements of 1.7 mg per day. No measure of statistical significance was presented for any of these findings.
Unspecified Corticosteroids
One SR reported that 97% of patients experienced a reduction of corticosteroid use, and the median decrease in corticosteroid dose was 8.6 mg (range = 0 mg to 24 mg)11; this finding did not include a control group. One single-arm prospective cohort study reported that the median decrease of days of corticosteroid use was 13 (range, 0 to 355); however, this was not statistically significant (P = 0.374).14 One single-arm retrospective cohort study reported that the mean time for half reduction dose of corticosteroids was 7 days (range, 2 to 22 days), while the mean reduced dose was 7.6 mg (0 mg to 20 mg). No measure of statistical significance was reported for this finding. One single-arm retrospective cohort study reported that the proportion of patients who discontinued corticosteroid use after treatment was 100%.16
Safety and Adverse Events
Reported Adverse Events
Two SRs reported the occurrence of adverse events.9,10 One SR included adverse events from 5 included primary studies and found that adverse events occurred in 9.5% to 100% of patients from each study.9 One SR included adverse events from 5 included primary studies and found that adverse events occurred in 17% to 33% of patients in 3 primary studies, while 2 primary studies reported 41 and 6 events.10 The reported adverse events from 3 SRs included hypertension, proteinuria, edema, mild allergy, arthralgia, dysgeusia, fatigue, urinary tract infection, pulmonary embolism, infection, headache, rash, fever, blurred vision, hyperglycemia, ischemic stroke, anemia, leukopenia, neutropenia, lymphocytopenia, aspiration pneumonia, pneumonia with severe sepsis, deep vein thrombosis, superior sagittal sinus thrombosis, and ischemic changes due to small vessel thrombosis.9-11 When reported, the severity of adverse events ranged from grade 1 to grade 3 or more.9-11
Four single-arm cohort studies reported the occurrence of adverse events.13-15,18 One single-arm retrospective cohort study reported that of 15 included patients, 4 patients reported an adverse event.13 One single-arm prospective cohort study reported that 6 of 10 included patients experienced serious adverse events, while 9 of 10 included patients experienced a treatment-emergent adverse event.14 One single-arm retrospective cohort study reported 0 adverse events out of 40 included patients.15 One single-arm prospective cohort study reported that adverse events occurred in 87.8% of patients, while grade 3 or higher adverse events occurred in 24.4% of those patients who experienced adverse events.18 The reported adverse events from the 4 single-arm cohort studies included deep vein thrombosis, pulmonary embolism, stroke, wound dehiscence, transient monocular blurred vision, transient diplopia, headache, blurred vision, leg cramps, fall, neck pain, numbness, seizures, traumatic fall, vomiting, hypertension, elevated alanine aminotransferase, convulsion, anemia, mucocutaneous hemorrhage, proteinuria, intracranial hemorrhage, and unexpected death.13-15,18 Only 1 single-arm cohort study reported that the severity of adverse events that was reported were grade 3 or higher.18
Radionecrosis Recurrence
One SR reported that 34% of patients who received bevacizumab for brain radionecrosis experienced radionecrosis recurrence.10 One primary RCT that compared patients who received bevacizumab to those who received a placebo for brain radionecrosis was included in the SR and reported that 3 of 7 patients treated with bevacizumab experienced radionecrosis recurrence; however, no comparison to the placebo group was carried out for this outcome because all patients in the placebo group experienced radionecrosis progression; therefore, patients were crossed over to the bevacizumab group.10 Two non-randomized studies reported that 20% and 84.6% of patients experienced radionecrosis recurrence after receiving bevacizumab.
Overall Survival and Progression-Free Survival
One single-arm prospective cohort study reported that the median overall survival from first treatment was 21.7 months, while the median overall survival from first MRI was 28.5 months in 15 patients who received bevacizumab for brain radionecrosis.13 In addition, the median progression-free survival from first treatment was 6.5 months in 15 patients who received bevacizumab for brain radionecrosis.13
Mortality
Two single-arm cohort studies reported the occurrence of all-cause mortality among patients who received bevacizumab for brain radionecrosis.14,18 One single-arm cohort study reported all-cause mortality in 0 of 10 included patients.14 One single-arm prospective cohort study reported that mortality occurred in 14.6% of included patients.18
Comparative Clinical Effectiveness and Safety of Bevacizumab Versus Corticosteroids for Patients With Symptomatic Brain Radionecrosis After Radiosurgery
One SR reported on 1 primary RCT that compared patients who received bevacizumab to patients who received unspecified corticosteroids for brain radionecrosis.10
Radiographic Response After Treatment
One RCT reported that a statistically significantly greater proportion of patients who received bevacizumab for brain radionecrosis experienced a radiographic response compared to patients who received corticosteroids (65.5% versus 31.5%; P < 0.001).10
MRI Change After Treatment
MRI T1 Gd Enhancement Volume Change
One RCT reported that patients who received bevacizumab for brain radionecrosis had a statistically significantly greater mean MRI T1 Gd enhancement volume reduction of 25.5%, compared to patients who received corticosteroids who had a mean reduction of 5% (P = 0.027).10
MRI T2 FLAIR Enhancement Volume Change
One RCT reported that patients who received bevacizumab for brain radionecrosis had a statistically significantly greater mean MRI T2 FLAIR enhancement volume reduction (i.e., 51.8%) compared to patients who received corticosteroids (i.e., 19.3%; P < 0.001).10
Change in Clinical Symptoms
Unspecified Clinical Symptoms
One RCT reported that 62.1% of patients who received bevacizumab for brain radionecrosis had an improvement in clinical symptoms compared to 42.6% of patients who received corticosteroids, which was statistically significantly greater (P = 0.039).10
Radionecrosis Recurrence
One primary RCT reported that 24.1% of patients who received bevacizumab for brain radionecrosis experienced a recurrence, compared to 24% of patients who received corticosteroids. No statistical significance measure was reported for this finding.
Limitations
The SRs identified in this report have limitations that should be considered while interpreting the results. Most notably, the quality of evidence included in the SRs is limited by study design, specifically with case studies, case series, or single-arm non-randomized studies. Thus, the quality of evidence that informed many of the outcomes in this review is unclear and may be at high risk of bias and uncertainty. Additionally, 2 of the SRs presented information from primary studies based on individual case outcomes, which creates challenges in appropriately controlling for information overlap in this report; as such, some findings may overlap with other outcomes across the SRs included in this review. There was also a large degree of heterogeneity within and across primary studies included in the SR, specifically related to cancer type and treatment protocols. Because of this heterogeneity, it is challenging to accurately compare outcomes across primary studies.
Similarly, all 6 included primary clinical studies were observational single-arm cohort studies (i.e., uncontrolled studies). Because of this study design, the primary clinical studies included in this report may be at high risk of bias and any finding associated with these studies should be interpreted with caution. The measure of clinical effect of the intervention is uncertain due to a lack of randomization, lack of separate control group, limited statistical analysis, and high potential for confounding factors associated with any findings. Findings may also be limited by heterogeneity across primary clinical studies regarding type of cancer and treatment protocol. The heterogeneity across primary clinical studies may also impact the generalizability of the reported findings to specific patient groups.
There was a lack of comparative evidence from the controlled studies included in this report. Only 1 study was included regarding the clinical effectiveness and safety of bevacizumab for brain radionecrosis compared to corticosteroids, which was included as a primary study in 1 SR. Details related to baseline patient characteristics and information related to treatment protocols were not provided, which may impact the ability to interpret the findings related to this comparison. In addition, 1 study was included that compared bevacizumab treatment to placebo, which was included as a primary study in 1 SR. This study included a small cohort and similarly lacked details related to baseline characteristics and treatment protocols, therefore impacting the ability to interpret findings related to this comparison. The other evidence included in this review was single arm (i.e., no control group), and either had no comparison (e.g., radiographic response to treatment) or reported the change from baseline within a single group. The limited evidence comparing outcomes in patients who received bevacizumab to a separate group of patients who did not receive bevacizumab highlights a potential gap in the evidence base and the overall ability to determine the measure of effects for bevacizumab treatment.
The generalizability of findings specifically from the primary studies included in the SRs may be challenging to determine because the time frame of included primary studies extends to 2007 and it is unknown if older findings may be applicable to the modern treatment landscape. Additionally, only 1 included non-randomized study was conducted in Canada.13 The majority of the included evidence related to the clinical effectiveness and safety of bevacizumab for brain radionecrosis was conducted in a variety of countries. Thus, it is unclear how generalizable the findings are to the Canadian context. This should be considered because management of cancer-related outcomes may vary between countries; therefore, may have different implications depending on the population and cultural context.
Conclusions and Implications for Decision- or Policy-Making
This report included 4 SRs (1 with an MA)9-12 and 6 non-randomized studies13-18 related to the clinical effectiveness and safety of bevacizumab for patients with brain radionecrosis after radiosurgery. One of these SRs also reported findings from 1 primary RCT related to the clinical effectiveness and safety of bevacizumab for patients with brain radionecrosis after radiosurgery compared to corticosteroids.10 Each included study specified that the population of interest included adult patients who received bevacizumab treatment for brain radionecrosis after radiosurgery for related brain metastases.9-18 Each study indicated the treatment protocol for bevacizumab, but this varied among studies. The dose of bevacizumab treatment ranged from 1 mg/kg to 15 mg/kg for up to 8 weeks, which may have included multiple cycles.9-18 No information was available related to the treatment protocol for patients who received croticosteroids.10
Based on the evidence summarized within this report, the majority of patients included in the SRs who received bevacizumab treatment for brain radionecrosis reported a radiographic response after treatment (based on evidence from single-arm studies, or compared to placebo)9-11 but findings from 1 single-arm cohort study showed that the majority of patients experienced no radiographic response.13 Evidence from all 4 SRs and 5 single-arm cohort studies reported that patients who received bevacizumab reported reductions in MRI T1 Gd enhancement volumes; the reductions ranged from 26% to 100% when compared to baseline measurements or placebo.9-17 Similarly, evidence from all 4 SRs and 4 single-arm cohort studies reported that patients who received bevacizumab reported reductions in MR1 T2 FLAIR enhancement volumes, which ranged from reductions of 11% to 96%, when compared to baseline measurements or placebo.9-16 The number of patients who experience radionecrosis recurrence after treatment with bevacizumab ranged from 20% to 85%, as reported in 1 SR (with single-arm evidence) and 2 single-arm cohort studies.10,14,17
Evidence from 2 SRs (that included single-arm studies or comparisons with placebo) and 1 single-arm cohort study reported that the majority of patients experienced clinical symptom improvement after receiving bevacizumab treatment.10,12,15 Single-arm evidence from 3 SRs reported that the majority of patients who received bevacizumab had an improvement in neurologic symptoms associated with brain radionecrosis (ranging from 85% to 96% of patients),9-11 and 1 single-arm cohort study reported a decrease in symptoms measured by standardized migraine and headaches tests.14 Single-arm evidence from 2 SRs and 4 cohort studies reported that the majority of patients who received bevacizumab had improvements in KPS scores, with 3 single-arm cohort studies reporting score improvements of 10 to 90 points.14-16
Single-arm evidence from 4 SRs and 5 cohort studies reported on the reduction or discontinuation of dexamethasone and other corticosteroid use, and indicated that the majority of patients discontinued or reduced their use after bevacizumab treatment (ranging from 55.5% to 100% of patients).9-16,18 Three SRs and 4 single-arm cohort studies reported outcomes related to adverse events, and stated that the proportion of patients who experienced an adverse event following bevacizumab treatment ranged from 0% to 100% of patients (based on studies with sample sizes ranging from 4 to 112 patients).9-11,13-15,18 Commonly reported adverse events included hypertension, proteinuria, edema, pulmonary embolism, and various thromboembolic events. When reported, the severity of adverse events ranged from grade 1 to grade 3.9-11,18 One single-arm cohort study reported that the median overall survival after first treatment and first MRI was 21.7 and 28.5 months, respectively, while the median progression-free survival was 6.5 month for patients treated with bevacizumab.13 Similarly, 2 single-arm cohort studies reported that all-cause mortality occurred in none of the 10 patients from 1 study and in 14.6% of patients in the other study who received bevacizumab treatment.14,18
When compared to patients who received corticosteroid treatment for brain radionecrosis, a statistically significantly larger proportion of patients who received bevacizumab experienced radiographic responses to treatment.10 In addition, patients who received bevacizumab had statistically significantly larger reductions in MRI T1 Gd and T2 FLAIR enhancement volumes, and a higher proportion of patients reported clinical improvements compared to those who received corticosteroids.10 The number of patients who experienced radionecrosis recurrence was similar in patients who received bevacizumab compared to corticosteroids.10 These findings are from 1 primary RCT included in 1 SR within this report.10
The limitations for the included literature (e.g., uncertain quality of primary studies included in the SRs, clinical heterogeneity of all included studies, the overall quality of included studies and potential high risk of bias, lack of statistical analyses, limited evidence from controlled studies, and limited Canadian context) should be considered when interpreting the findings of this report. The evidence from this report will help stakeholders in decision-making related to the use of bevacizumab for patients with brain radionecrosis. Further high-quality research that is specific to the Canadian context is needed to adequately assess the clinical effectiveness and safety of bevacizumab use in this patient population.
References
1.Chung C, Bryant A, Brown PD. Interventions for the treatment of brain radionecrosis after radiotherapy or radiosurgery. Cochrane Database Syst Rev. 2018;7:CD011492. PubMed
2.Vellayappan B, Tan CL, Yong C, et al. Diagnosis and management of radiation necrosis in patients with brain metastases. Front Oncol. 2018;8:395. PubMed
3.Zhuang H, Shi S, Yuan Z, Chang JY. Bevacizumab treatment for radiation brain necrosis: mechanism, efficacy and issues. Mol Cancer. 2019;18(1):21. PubMed
4.Cancer Care Ontario (CCO). Drug formulary: bevacizumab. 2022; https://www.cancercareontario.ca/en/drugformulary/drugs/infosheet/44071. Accessed 2022 Nov 14.
5.Avastin (bevacizumab): 25 mg/mL solution for injection in 100 mg and 400 mg vials [product monograph]. Mississauga (ON): Hoffmann-La Roche Limited; 2022 Apr 29: https://www.rochecanada.com/PMs/Avastin/Avastin_PM_E.pdf. Accessed 2022 Nov 14.
6.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
7.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
8.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
9.Khan M, Zhao Z, Arooj S, Liao G. Bevacizumab for radiation necrosis following radiotherapy of brain metastatic disease: a systematic review & meta-analysis. BMC Cancer. 2021;21(1):167. PubMed
10.Liao G, Khan M, Zhao Z, Arooj S, Yan M, Li X. Bevacizumab treatment of radiation-induced brain necrosis: a systematic review. Front Oncol. 2021;11:593449. PubMed
11.Delishaj D, Ursino S, Pasqualetti F, et al. Bevacizumab for the treatment of radiation-induced cerebral necrosis: a systematic review of the literature. J Clin Med Res. 2017;9(4):273-280. PubMed
12.Lubelski D, Abdullah KG, Weil RJ, Marko NF. Bevacizumab for radiation necrosis following treatment of high grade glioma: a systematic review of the literature. J Neurooncol. 2013;115(3):317-322. PubMed
13.Climans SA, Ramos RC, Jablonska PA, Shultz DB, Mason WP. Bevacizumab for cerebral radionecrosis: a single-center experience. Can J Neurol Sci. 2022:1-6. PubMed
14.Dashti SR, Kadner RJ, Folley BS, et al. Single low-dose targeted bevacizumab infusion in adult patients with steroid-refractory radiation necrosis of the brain: a phase II open-label prospective clinical trial. J Neurosurg. 2022:1-11. PubMed
15.Li J, He J, Cai L, et al. Bevacizumab as a treatment for radiation necrosis following stereotactic radiosurgery for brain metastases: clinical and radiation dosimetric impacts. Ann Palliat Med. 2021;10(2):2018-2026. PubMed
16.Weng Y, Shen J, Zhang L, et al. Low-dosage bevacizumab treatment: effect on radiation necrosis after gamma knife radiosurgery for brain metastases. Front Surg. 2021;8:720506. PubMed
17.Zhuang H, Yuan X, Yuan Z, Wang P. Indication of bevacizumab for cerebral radiation necrosis. Recent Pat Anticancer Drug Discov. 2017;12(3):272-277. PubMed
18.Furuse M, Nonoguchi N, Kuroiwa T, et al. A prospective, multicentre, single-arm clinical trial of bevacizumab for patients with surgically untreatable, symptomatic brain radiation necrosis†. Neurooncol Pract. 2016;3(4):272-280. PubMed
19.National Cancer Institute. Karnofsky Performance Status. 2022; https://www.cancer.gov/publications/dictionaries/cancer-terms/def/karnofsky-performance-status. Accessed 2022 Nov 11.
20.AstraZeneca Pharmaceuticals, LP. The Migraine Disability Assessment test. Chicago (IL): The National Headache Foundation; 2007: https://headaches.org/wp-content/uploads/2018/02/MIDAS.pdf. Accessed 2022 Nov 10.
21.QualityMetric Inc., GlaxoSmithKline Group of Companies. HIT-6™ Headache Impact Test. Red Deer (AB): Aspire Medicine; 2001: https://www.aspiremedicine.ca/wp-content/uploads/2020/10/HIT-6.pdf. Accessed 2022 Nov 10.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Relevant intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Khan et al. (2021)9 China Funding source: The Natural Science Foundation of Shenzhen (No.JCYJ20170307095828424); Shenzhen Health and Family Planning System Research Project (No.SZBC2017024) | Study design: SR with MA Last search date: August 2020 Number of included studies: 12 non-randomized studies | Eligibility criteria: Studies reporting the efficacy of bevacizumab for radionecrosis in patients with brain metastases after receiving radiotherapy for intracranial disease Total number of patients included: 89 Sample size (range): 1 to 21 | Intervention (dose range): Bevacizumab (1 mg/kg to 15 mg/kg) up to 6 weeks Comparator: Single arm before and after treatment studies | Outcomes:
Follow-up (range): 3.3 to 22.7 months |
Liao et al. (2021)10 China Funding source: Natural Science Foundation of Shenzhen (No. JCYJ20170307095828424) and Shenzhen Health and Family Planning System Research Project (No. SZBC2017024) | Study design: SR Last search date: March 2020 Number of included studies: 12 (2 RCTS and 10 non-randomized studies) | Eligibility criteria: Published RCTs and non-randomized studies with more than 5 participants that investigated the efficacy and safety of bevacizumab for the treatment of radiation-induced brain necrosis Total number of patients included: 236 Sample size (range): 6 to 58 | Intervention (dose range): Bevacizumab (1 mg/kg to 15 mg/kg) up to 6 weeks Comparators: Corticosteroids, placebo, and single arm before and after studies | Outcomes:
Follow-up (range): 8.1 to 22.7 months |
Delishaj et al. (2017)11 Italy Funding source: NR | Study design: SR Last search date: September 2016 Number of included studies: 21 (1 RCT and 20 non-randomized studies) | Eligibility criteria: Studies including patients with brain radionecrosis and treated with bevacizumab Total number of patients included: 125 Sample size (range): 1 to 24 | Intervention (dose range): Bevacizumab (5 mg/kg to 15 mg/kg) up to 4 weeks Comparator: Placebo or single arm before and after treatment studies | Outcomes:
Follow-up (median): 8 months |
Lubelski et al. (2013)12 US Funding source: NR | Study design: SR Last search date: September 2012 Number of included studies: 7 (1 RCT and 6 non-randomized studies) | Eligibility criteria: Clinical studies of patients with radionecrosis following radiation therapy for high-grade glioma and were treated with bevacizumab Total number of patients included: 30 Sample size (range): 1 to 8 | Intervention (dose range): Bevacizumab (5 mg/kg to 10 mg/kg) up to 8 weeks Comparator: Placebo or single arm before and after treatment studies | Outcomes:
Follow-up: NR |
KPS = Karnofsky Performance Status; NR = not reported; RCT = randomized controlled trial; SR = systematic review.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design and objective | Population characteristics | Relevant intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Climans et al. (2022)13 Canada Funding source: NR | Study design: Single-arm retrospective cohort study Objective: To understand the use of bevacizumab for cerebral radionecrosis regarding the magnitude of clinical benefits and toxicities | Eligibility criteria: Data from neuro-oncology patients diagnosed with radionecrosis and treated with bevacizumab between January 2017 and March 2021 were included Number of participants: 15 Median age: 55 Number of females (%): 10 (67%) Cancer type, n (%):
| Intervention (dose): Bevacizumab (7.5 mg/kg) every 3 weeks for up to 4 total doses Comparator: Single arm before and after treatment study | Outcomes:
Follow-up (median): 14.2 months |
Dashti et al. (2022)14 US Funding source: Norton Health care Foundation and UK Health care | Study design: Single-arm prospective cohort study Objective: To evaluate the safety and efficacy of a single targeted low-dose bevacizumab infusion in patients diagnosed with brain radionecrosis | Eligibility criteria: Adults with a KPS score of ≥ 70% and life expectancy of ≥ 3 months with at least 1 radionecrosis symptom Number of participants: 10 Mean age (SD): 35.1 (14.8) Number of females (%): 8 (80%) Cancer type, n (%): NR | Intervention (dose): Bevacizumab (2.5 mg/kg) Comparator: Single arm before and after treatment study | Outcomes:
Follow-up: 12 months |
Li et al. (2021)15 China Funding source: National Natural Science Foundation of China (NSFC) (No. 81703166), Natural Science Foundation of Guangdong Province (No. 2019A1515011943), China Postdoctoral Science Foundation (No. 2019M662974) and Science and Technology Program of Guangzhou (No. 202002030445), and Medical Scientific Research Foundation of Guangdong Province (A2020505 and A2020499). | Study design: Single-arm retrospective cohort study Objective: Evaluate the effects of bevacizumab as a treatment for brain radionecrosis following radiosurgery for brain metastases | Eligibility criteria: Patients diagnosed with brain metastases and radiographic radionecrosis who received bevacizumab for up to 6 months Number of participants: 40 Mean age (range): 55.5 (29 to 72) Number of females (%): 14 (35%) Cancer type, n (%):
| Intervention (dose): Bevacizumab (5 mg/kg) every 2 weeks or 10 mg/kg every 3 weeks Comparator: Single arm before and after treatment study | Outcomes:
Follow-up: 6 months |
Weng et al. (2021)16 China Funding source: NR | Study design: Single-arm retrospective cohort study Objective: To evaluate the efficacy of low-dose bevacizumab treatment for brain radionecrosis following Gamma Knife surgery in patients with brain metastases | Eligibility criteria: Patients treated with bevacizumab for cerebral radionecrosis caused by Gamma Knife surgery between January 2013 and December 2017 Number of participants: 22 Median age (range): 64 (48 to 79) Number of males (%): 11 (50%) Cancer type, n (%):
| Intervention: Bevacizumab (3 mg/kg) every 2 weeks for 2 to 4 courses Comparator: Single arm before and after treatment study | Outcomes:
Follow-up: 6 months |
Zhuang et al. (2017)17 China Funding source: NR | Study design: Single-arm retrospective cohort study Objective: To evaluate clinical data of patients with cerebral radionecrosis who received bevacizumab treatment | Eligibility criteria: Patients with primary or metastatic lesions with a history of radiotherapy and diagnosis of radionecrosis who underwent bevacizumab treatment from June 2011 to December 2014 Number of participants: 14 Median age (range): 56 (31 to 70) Number of females (%): 8 (57%) Cancer type, n (%):
| Intervention (dose): Bevacizumab (5 mg/kg) every 3 to 4 weeks for at least 3 cycles Comparator: Single arm before and after treatment study | Outcomes:
Follow-up: NA (chart review) |
Furuse et al. (2016)18 Japan Funding source: Health and Labour Sciences Research Grant administered by Japan’s Ministry of Health, Labour and Welfare (Clinical Trial on Development of New Drugs and Medical Devices, H24 to 006) | Study design: Single-arm prospective cohort study Objective: To evaluate the safety and efficacy of bevacizumab in patients with symptomatic brain radionecrosis | Eligibility criteria: Patients treated with radiotherapy for a tumour with perilesional edema caused by radionecrosis and a KPS score of ≥ 60 Number of participants: 38 Median age (range): 54.5 (17 to 73) Number of females (%): 16 (42.1%) Cancer type, n (%): Not specified | Intervention: Bevacizumab (5 mg/kg) every 2 weeks for up to 6 cycles Comparator: Single arm before and after treatment study | Outcomes:
Follow-up: 12 months |
KPS = Karnofsky Performance Status; NA = not applicable; NR = not reported; SD = standard deviation.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Systematic Reviews Using AMSTAR 26
Strengths | Limitations |
|---|---|
Khan (2021)9 | |
|
|
Liao (2021)10 | |
|
|
Delishaj (2017)11 | |
|
|
Lubelski (2013)12 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; RCT = randomized controlled trial.
Table 5: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist7
Strengths | Limitations |
|---|---|
Climans (2022)13 | |
|
|
Dashti (2022)14 | |
|
|
Li (2021)15 | |
|
|
Weng (2021)16 | |
|
|
Zhuang (2017)17 | |
|
|
Furuse (2016)18 | |
|
|
CI = confidence interval.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 6: Summary of Comparative Findings by Outcome — Radiographic Responses After Treatment
Outcome | Liao et al. (2021),10 SR | |||
|---|---|---|---|---|
Bevacizumab vs. corticosteroidsa | Bevacizumab vs. placebob | |||
Bevacizumab treatment | Corticosteroid treatment | Bevacizumab treatment | Placebo group | |
Sample size | 58 | 54 | 7 | 7 |
Proportion of patients with radiographic response | 65.5% | 31.5% | 100% | 0 |
P value | < 0.001 | 0.0013 | ||
SR = systematic review
aOutcomes based on 1 RCT (Xu et al. 2018)
bOutcomes based on 1 RCT (Levin et al. 2011)
Table 7: Summary of Uncontrolled Findings by Outcome — Radiographic Responses After Treatment
Outcome | Khan et al. (2021),9 SR with MA | Liao et al. (2021),10 SR | Delishaj et al. (2017),11 SR | Climans et al. (2022),13 Single-arm retrospective cohort study |
|---|---|---|---|---|
Sample size | 89 | 236 | 125 | 15 |
Overall number of patients with radiographic response, n (%) | 83 (93%) | 200 (84.7%) | 122 (97.6%) | — |
No response, n (%) | — | — | — | 9 (60%) |
Minimal response, n (%) | — | — | — | 5 (33%) |
Definite response, n (%) | — | — | — | 1 (7%) |
CI = confidence interval; MA = meta-analysis; RCT = randomized controlled study; SD = standard deviation; SR = systematic review.
Table 8: Summary of Comparative Findings by Outcome — MRI Change After Treatment
Outcome | Liao et al. (2021),10 SR | |||
|---|---|---|---|---|
Bevacizumab vs. corticosteroidsa | Bevacizumab vs. placebob | |||
Bevacizumab treatment | Corticosteroid treatment | Bevacizumab treatment | Placebo group | |
MRI T1 Gd Enhancement volume Change | ||||
Sample size | 58 | 54 | 7 | 7 |
Mean volume change | 25.5% (reduction) | 5% (reduction) | 63% (reduction) | 17% (increase) |
P value | 0.027 | 0.0058 | ||
MRI T2 FLAIR Enhancement volume Change | ||||
Sample size | 58 | 54 | 7 | 7 |
Mean volume change | 51.8% (reduction) | 19.3% (reduction) | 59% (reduction) | 14% (increase) |
P value | < 0.001 | 0.0149 | ||
SR = systematic review
aOutcomes based on 1 RCT (Xu et al. 2018)
bOutcomes based on 1 RCT (Levin et al. 2011)
Table 9: Summary of Uncontrolled Findings by Outcome — MRI Change After Treatment
Study citation and design | Sample size | Outcome | Result | P value | Notes |
|---|---|---|---|---|---|
MRI T1 Gd Enhancement volume Change | |||||
Khan et al. (2021)9 SR with MA | 89 | Mean volume reduction (SD) | 47.03% (24.4%) (reduction) | — | Mean volume reduction outcome was based on 12 included studies Pooled analysis was based on 6 included studies (n = NR) |
— | Pooled volume reduction rate (95% CI) | 48.58% (38.32% to 58.85%); I2 = 80% (reduction) | P < 0.001 | Pooled analysis was based on 6 included studies (n = NR) | |
Liao et al. (2021)10 SR | 236 | Median volume reduction (range) | 50% (26% to 80%) (reduction) | — | Median volume reduction outcome was based on 12 included studies |
Delishaj et al. (2017)11 SR | 94 | Median volume reduction | 64% (reduction) | — | Median volume reduction outcome was based on 9 included studies |
Range of mean volume reduction | 48.1% to 100% (reduction) | — | Range of mean volume reduction was based on 10 included studies | ||
Lubelski et al. (2013)12 SR | 1 | Change in volume | Reduction | — | Change in volume outcomes is based on 1 included study with 1 patient No numeric value was provided in the change in volume outcome |
Climans et al. (2022)13 Single-arm retrospective cohort study | 15 | Mean volume reduction (95% CI) | 3.0 cm3 (4.9 cm3 to 11.0 cm3) (reduction) | — | — |
Dashti et al. (2022)14 Single-arm prospective cohort study | 10 | > 25% volume reduction at 3 month follow-up, n (%; 95% CI) | 8 (80%; 44% to 98%) | — | Volume reduction was measured by MRI T1 images |
Median volume reduction at 12 months (range) | 76% (53% to 96%) (reduction) | — | |||
Median volume reduction difference (range) | 12.1 cm3 (−1.0 cm3 to 27.3 cm3) (reduction) | P = 0.012 | |||
Li et al. (2022)15 Single-arm retrospective cohort study | 40 | Number of patients with volume reduction, n (%) | 38 (95%) | — | — |
Reduction in volume at 1 month post treatment (range) | 48.4% (−18% to 92%) (reduction) | P < 0.001 | |||
Reduction in volume at 3 months post treatment (range) | 74% (8% to 95%) (reduction) | P < 0.001 | |||
Reduction in volume at 6 months post treatment (range) | 75% (−213% to 98.7%) (reduction) | P < 0.001 | |||
Weng et al. (2021)16 Single-arm retrospective cohort study | 22 | Mean volume after treatment (range) | 6.99 cm3 (0.7 cm3 to 20.6 cm3) | — | — |
Mean reduction after treatment | 45% (reduction) | — | |||
Zhuang et al. (2017)17 Single-arm retrospective cohort study | 14 | Volume reductions after treatment, n (%) | 13 (92.86%) | — | — |
MRI T2 FLAIR Enhancement volume Change | |||||
Khan et al. (2021)9 SR with MA | 89 | Mean volume reduction (SD) | 61.78% (23.2%) (reduction) | — | Mean volume reduction outcome was based on 12 included studies (n = 89) Pooled analysis was based on 6 included studies (n = NR) |
— | Pooled volume reduction rate (95% CI) | 62.017% (52.235% to 71.799%); I2 = 66.9% (reduction) | P = 0.01 | Pooled analysis was based on 6 included studies (n = NR) | |
Liao et al. (2021)10 SR | 236 | Median volume reduction (range) | 59% (48% to 74%) (reduction) | — | Median volume reduction outcome was based on 12 included studies |
Delishaj et al. (2017)11 SR | 84 | Median volume reduction | 60% (reduction) | — | Median volume reduction outcome was based on 9 included studies |
Range of mean volume reduction | 48.4% to 66% (reduction) | — | Range of mean volume reduction was based on 8 included studies | ||
Lubelski et al. (2013)12 SR | 1 | Change in volume | Reduction | — | Change in volume outcomes is based on 1 included study with 1 patient No numeric value was provided in the change in volume outcome |
Climans et al. (2022)13 Single-arm retrospective cohort study | 15 | Mean volume reduction (95% CI) | 27.9 cm3 (12.0 cm3 to 67.7 cm3) (reduction) | — | — |
Dashti et al. (2022)14 Single-arm prospective cohort study | 10 | > 25% vasogenic edema reduction at 3 month follow-up, n (%; 95% CI) | 9 (90%; 56% to 100%) | — | Vasogenic edema reduction was measured by MRI T2 FLAIR images |
Median vasogenic edema reduction at 12 months (range) | 70% (11% to 83%) (reduction) | — | |||
Median vasogenic edema reduction difference (range) | 27.61 cm3 (0.6 cm3 to −216.1 cm3) (reduction) | P = 0.086 | |||
Li et al. (2022)15 Single-arm retrospective cohort study | 40 | Number of patients with T2 edema volume reduction, n (%) | 38 (95%) | — | — |
Reduction in edema volume at 1 month post treatment (range) | 47.6% (−14% to 92.2%) (reduction) | P < 0.001 | |||
Reduction in edema volume at 3 months post treatment (range) | 76.2% (−40% to 96%) (reduction) | P < 0.001 | |||
Reduction in edema volume at 6 months post treatment (range) | 66.3% (−39% to 92%) (reduction) | P < 0.001 | |||
Weng et al. (2021)16 Single-arm retrospective cohort study | 22 | Mean volume after treatment (range) | 26.1 cm3 (5.6 cm3 to 60.8 cm3) | — | — |
Mean volume reduction after treatment | 74% (reduction) | — | |||
Furuse et al. (2016)18 Single-arm prospective cohort study | 38 | Rate of perilesional edema remission (95% CI) | 78.9% (62.7% to 90.4%) | P < 0.001 | Compared to baseline measurements |
Median time to remission from enrolment (95% CI) | 3.03 months (2.86 to 3.85 months) | — | |||
Mean reduction in perilesional edema volume from baseline to 1 month after treatment | 63% (reduction) | — | |||
Mean reduction in contrast-enhanced lesions from baseline to last treatment | 92.8% (reduction) | — | |||
CI = confidence interval; FLAIR = Fluid attention inversion recovery; Gd = gadolinium; MA = meta-analysis; NR = not reported; RCT = randomized controlled trial; SD = standard deviation; SR = systematic review.
Table 10: Summary of Comparative Findings by Outcome — Clinical Symptoms
Outcome | Liao et al. (2021),10 SR | |||
|---|---|---|---|---|
Bevacizumab vs. corticosteroidsa | Bevacizumab vs. placebob | |||
Bevacizumab treatment | Corticosteroid treatment | Bevacizumab treatment | Placebo group | |
Sample size | 58 | 54 | 7 | 7 |
Clinical symptom improvement, n (%) | 36 (62.1%) | 23 (42.6%) | 7 (100%) | 0 |
P value | 0.039 | — | ||
SR = systematic review.
aOutcomes based on 1 RCT (Xu et al. 2018)
bOutcomes based on 1 RCT (Levin et al. 2011)
Table 11: Summary of Uncontrolled Findings by Outcome — Clinical Symptoms
Outcome | Khan et al. (2021),9 SR with MA | Liao et al. (2021),10 SR | Delishaj et al. (2017),11 SR | Lubelski et al. (2013),12 SRa | Dashti et al. (2022),14 Single-arm prospective cohort study | Li et al. (2022),15 Single-arm retrospective cohort study |
|---|---|---|---|---|---|---|
Sample size | 85 | 133 | 125 | 1 | 8 | 40 |
Change in Unspecified Clinical Symptoms | ||||||
Change in overall clinical symptoms | — | — | — | Improvement | — | — |
Progressed symptoms, n (%) | — | — | — | — | — | 1 (2.5%) |
Stable symptoms, n (%) | — | — | — | — | — | 12 (30%) |
Improved symptoms, n (%) | — | — | — | — | — | 27 (67.5%) |
Change in Neurologic Symptoms | ||||||
No response or worsened symptoms, n (%) | 3 (3.5%) | — | 4 (3.2%) | — | — | — |
Stable symptoms, n (%) | 9 (10%) | 13 (9%) | 7 (5.6%) | — | — | — |
Improved symptoms, n (%) | 39 (46%) | 106 (79.7%) | 114 (91.2%) | — | — | — |
Complete symptom resolution, n (%) | 34 (40%) | 8 (6%) | — | — | — | — |
Total MIDAS score decrease | — | — | — | — | 84% | — |
Median (range); P value | — | — | — | — | 92% (58% to 100%); P = 0.022 | — |
Total MIDAS pain score decrease | — | — | — | — | 61% | — |
Median (range); P value | — | — | — | — | 33% (−43% to 100%); P < 0.001 | — |
Total decrease in days of headache | — | — | — | — | 61% | — |
Median (range); P value | — | — | — | — | 77% (−11% to 95%); P = 0.019 | — |
Total HIT-6 score decrease | — | — | — | — | 18.3% | — |
Median (range); P value | — | — | — | — | 24.8% (−14.1% to 39%); P value = 0.02 | — |
HIT-6 = Headache Impact Test – 6; MA = meta-analysis; MIDAS = Migraine Disability Assessment Test; SR = systematic review.
aChange in clinical symptom outcome is based on 1 included study with 1 patient. No numeric value was provided for this outcome.
Table 12: Summary of Findings by Outcome — Karnofsky Performance Status Score
Outcomes | Khan et al. (2021),9 SR with MA | Liao et al. (2021),10 SR | Dashti et al. (2022),14 Single-arm prospective cohort study | Li et al. (2021),15 Single-arm prospective cohort study | Weng et al. (2021),16 Single-arm retrospective cohort study | Furuse et al. (2016),18 Single-arm prospective cohort study |
|---|---|---|---|---|---|---|
Sample Size | 10 | 37 | 10 | 40 | 22 | 38 |
KPS score improvement | ||||||
n (%) | 8 (80%) | 29 (78%) | — | — | — | 16 (42.1%; 95% CI 21.8% to 54%) |
Improvement by 10%, n (%) | — | — | — | — | — | 10 (26.3%) |
Improvement by 20%, n (%) | — | — | — | — | — | 6 (15.8%) |
Improvement at last follow-up, n (%) | — | — | — | — | — | 5 (23.8%; 95% CI 8.2% to 47.2%) |
Median (range) | — | — | 10 points (−10 to 10); P = 0.232 | — | — | — |
Mean | — | — | — | 31.8 | — | — |
KPS score stable or decreased, n (%) | — | 8 (22%) | — | — | — | — |
KPS score post treatment, median (range) | — | — | — | 70 (60 to 90); P < 0.001 | — | — |
CI = confidence interval; KPS = Karnofsky Performance Status.
Notes: KPS score outcomes for Dashti et al. (2022), Li et al. (2021), Wend et al. (2021), and Furuse et al. (2016) were compared to pre-treatment or baseline measurements.
Table 13: Summary of Findings by Outcome — Corticosteroid Use
Study citation and design | Sample size | Outcome | Result | Notes |
|---|---|---|---|---|
Dexamethasone | ||||
Khan et al. (2021)9 SR with MA | 31 | Dose discontinuation or reduction, n (%) | 30 (97%) | Among patients who recorded dexamethasone dosage before and after bevacizumab treatment |
Mean dexamethasone dose reduction | 9.08 mg | |||
Liao et al. (2021)10 SR | 47 | Dose reduction, n (%) | 46 (97.8%) | Dexamethasone dose reduction outcome was based on 5 included studies |
Lubleksi et al. (2013)12 SR | 1 | Change in dose of dexamethasone after treatmenta | 0 mg | Change in volume outcomes is based on 1 included study with 1 patient |
Climans et al. (2022)13 Single-arm retrospective cohort study | 15 | Dose reduction, n (%) | 5 (33%) | Not applicable refers to patients who did not receive any dexamethasone treatment |
No dose reduction, n (%) | 4 (27%) | |||
Not applicable, n (%) | 6 (40%) | |||
Furuse et al. (2016)18 Single-arm prospective cohort study | 35 | Dose reduction, n (%; 95% CI) | 29 (76.3%; 59.8% to 88.6%) | Compared to baseline measures (mean = 1.7 mg/day) |
Mean dexamethasone dose at 6 months post treatment | 0.6 mg/day | |||
Mean dexamethasone dose at final follow-up | 0.8 mg/day | |||
Unspecified Corticosteroid | ||||
Delishaj et al. (2017)11 SR | NR | Proportion of patient that had a reduction of corticosteroid use | 97% | Corticosteroid use outcomes were based on 17 included studies |
Median decrease in corticosteroid dose (range) | 8.6 mg (0 to 24 mg) | |||
Dashti et al. (2022)14 Single-arm prospective cohort study | 10 | Median decrease of days of corticosteroid use (range); P value | 13 (0 to 355); P = 0.374 | During the 12 months follow-up after treatment |
Li et al. (2021)15 Single-arm retrospective cohort study | 40 | Mean time for half reduction dose, days (range) | 7 (2 to 22) | — |
Mean reduced dose (range) | 7.6 mg (0 to 20 mg) | |||
Weng et al. (2021)16 Single-arm retrospective cohort study | 22 | Discontinuation of corticosteroid use after treatment, n (%) | 22 (100%) | — |
CI = confidence interval; NR = not reported.
aBaseline dexamethasone dose was NR.
Table 14: Summary of Findings by Outcome — Safety and Adverse Events
Study citation and design | Primary study | Sample size | Number of adverse events reported, n (%) | Reported adverse event symptom; n (%) |
|---|---|---|---|---|
Khan et al. (2021)9 SR with MA | Tanigawa et al (2019) | 4 | 4 (100%) |
|
Zhuang et al. (2019) | 21 | 2 (9.5%) |
| |
Glitza et al. (2017) | 7 | 1 (14%) |
| |
Sadraei et al. (2015) | 17 | 5 (29%) |
| |
Zhuang et al. (2015) | 14 | 2 (14%) |
| |
Liao et al. (2021)10 SR | Xu et a. (2018) | 112 | 41b |
|
Yonezawa et al. (2014) | 9 | 3 (33%) |
| |
Wang et al. (2012) | 17 | 3 (18%) |
| |
Levin et al. (2011) | 11 | 6b |
| |
Torcuator et al. (2009) | 6 | 1 (17%) |
| |
Delishaj et al. (2017)11 SR | Not specified | NR | — |
|
Climans et al. (2022)13 Single-arm retrospective cohort study | — | 15 | — |
|
Dashti et al. (2022)14 Single-arm prospective cohort study | — | 10 | SAE, n (%) = 6 (60%) |
|
Any treatment-emergent AE, n (%) = 9 (90%) | — | |||
Li et al. (2021)15 Single-arm retrospective cohort study | — | 40 | 0 | — |
Furuse et al. (2016)18 Single-arm prospective cohort study | — | 41 | AE, n (%) = 36 (87.8%) |
|
Occurrence of Grade ≥ 3 AE, n (%) = 10 (24.4%) | — |
AE = adverse event; ALT = alanine aminotransferasel; DVT = deep vein thrombosis; MA = meta-analysis; NR = not reported; OS = overall survival; SAE = serious adverse events; SR = systematic review; UTI = urinary tract infection.
aGrade of adverse event was not specified.
bReported as number of events and only based on patients that received bevacizumab, including those initially randomized to placebo who crossed over to bevacizumab.
cThe number of patients experiencing the reported symptoms was NR.
dReported as more than 10% frequency.
Table 15: Summary of Comparative Findings by Outcome — Radionecrosis Recurrence
Outcome | Liao et al. (2021),10 SR | |||
|---|---|---|---|---|
Bevacizumab vs. corticosteroidsa | Bevacizumab vs. placebob | |||
Bevacizumab treatment | Corticosteroid treatment | Bevacizumab treatment | Placebo group | |
Sample size | 58 | 54 | 7 | NA |
Number of radionecrosis recurrence, n (%) | 14 (24.1%) | 13 (24%) | 3 (42.8%) | NA |
NA = not applicable; SR = systematic review.
aOutcomes based on 1 RCT (Xu et al. 2018)
bOutcomes based on 1 RCT (Levin et al. 2011). Comparison with the placebo group is not applicable as all patients in the placebo group had disease progression and were crossed over to the bevacizumab group.
Table 16: Summary of Uncontrolled Findings by Outcome — Radionecrosis Recurrence
Outcome | Liao et al. (2021),10 SR | Dashti et al. (2022),14 Single-arm prospective cohort study | Zhuang et al. (2017),17 Single-arm retrospective cohort study |
|---|---|---|---|
Sample size | 135 | 10 | 13 |
Number of radionecrosis recurrence, n (%) | 46 (34%) | 2 (20%) | 11 (84.6%)a |
95% CI | — | (3% to 56%) | — |
CI = confidence interval; NR = not reported; SR = systematic review.
aAmong patients who responded to first treatment.
Table 17: Summary of Findings by Outcome — Overall Survival and Progression-Free Survival
Outcome | Climans et al. (2022),13 Single-arm retrospective cohort study | Notes |
|---|---|---|
Sample size | 15 | — |
Median OS from first treatment (months) | 21.7 | — |
Median OS from first MRI (months) | 28.5 | — |
Median PFS from first treatment (months) | 6.5 | PFS was defined as freedom from tumour progression but not radionecrosis progression |
OS = overall survival; PFS = progression-free survival.
Table 18: Summary of Findings by Outcome — Mortality
Outcome | Dashti et al. (2022),14 Single-arm prospective cohort study | Furuse et al. (2016),18 Single-arm prospective cohort study |
|---|---|---|
Sample size | 10 | 41 |
Occurrence of all-cause mortality, n (%) | 0 | 6 (14.6%) |
Appendix 5: Overlap Between Included Systematic Reviews
Note that this appendix has not been copy-edited.
Table 19: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Khan (2021)9 | Liao (2021)10 | Delishaj (2017)11 | Lubelski (2013)12 |
|---|---|---|---|---|
Tanigawa et al. Respirol Case Rep. 2019; 7(7): e00454 | Yes | — | — | — |
Zhuang et al. Onco Targets Ther. 2019; 12: 8447 to 53 | Yes | Yes | — | — |
Li et al. Int J Radiat Oncol Biol Physics. 2018; 100(3): 621 to 9 | — | Yes | — | — |
Xu et al. Int J Radiat Oncol Biol Physics. 2018; 101(5): 1087 to 95 | — | Yes | — | — |
Glitza et al. Melanoma Res. 2017; 27(6): 580 to 4 | Yes | — | — | — |
Ma et al. J Craniofac Surg. 2017; 28(6): e569-e71 | Yes | — | — | — |
Zhuang et al. Oncotarget. 2016; 7(30): 48842 to 48849 | — | — | Yes | — |
Zhuang et al. Sci Rep. 2016; 6: 24364 | Yes | Yes | — | — |
Delishaj et al. Rare Tumors. 2015; 7(4): 6018 | — | — | Yes | — |
Sadraei et al. Am J Clin Oncol. 2015; 38(3): 304 to 10 | Yes | Yes | Yes | — |
Xian-Pan et al. J Cancer Res Ther. 2015; 11(2): 485 to 7 | Yes | — | Yes | — |
Bostrom et al. Strahlenther Onkol. 2014; 190(4): 416 to 421 | — | — | Yes | — |
Yonezawa et al. J Neuro-Oncol. 2014; 119(1): 101 to 9 | Yes | Yes | — | — |
Alessandretti et al. Case Rep Oncol. 2013; 6(3): 598 to 601 | Yes | — | Yes | — |
Boothe et al. Neuro-Oncology. 2013; 15(9): 127 to 63 | Yes | Yes | Yes | — |
Furuse et al. Jpn J Clin Oncol. 2013; 43(3): 337 to 41 | Yes | Yes | Yes | — |
DeSalvo et al. J Radiol Case Rep. 2012; 6(7): 9 to 16 | — | — | Yes | — |
Wang et al. Eur J Med Res. 2012; 17(1): 25 | Yes | Yes | Yes | Yes |
Arratibel-Echarren et al. Neurologia. 2011; 26(2): 74 to 80 | — | — | Yes | Yes |
Benoit et al. J Neurol. 2011; 258(2): 328 to 329 | — | — | Yes | — |
Furuse et al. J Neurooncol. 2011; 102(3): 471 to 475 | — | — | — | Yes |
Jeyaretna et al. J Clin Oncol. 2011; 29(7): e159 to 162 | — | — | Yes | — |
Levin et al. Int J Radiat Oncol Biol Physics. 2011; 79(5): 1487 to 95 | — | Yes | Yes | Yes |
Matuschek et al. Strahlemther Onkol. 2011; 187(2): 135 to 139 | — | — | Yes | Yes |
Nonoguchi et al. J Neurooncol. 2011; 105(2); 423 to 431 | — | — | Yes | — |
Sanborn et al. Clin Neurol Neurosurg. 2011; 113(9): 798 to 802 | — | — | Yes | — |
Liu et al. Int J Radiat Oncol Biol Phys. 2009; 75(4): 1148 to 1154 | — | — | Yes | — |
Torcuator et al. J Neurooncol. 2009; 94(1): 63 to 8 | — | Yes | Yes | Yes |
Wong et al. J Clin Oncol. 2008; 26(34): 5649 to 5650 | — | — | Yes | — |
Gonzalez et al. Int J Radiat Oncol Biol Physics. 2007; 67(2): 323 to 6 | — | Yes | Yes | Yes |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca