CADTH Health Technology Review
Octreotide Long-Acting Release and Everolimus for Recurrent Meningiomas
Rapid Review
Authors: Zahra Jafari, Jennifer Horton
Abbreviations
AE
adverse events
CI
confidence interval
CNS
central nervous system
LAR
long-acting release
OE
octreotide long-acting release in combination with everolimus
OS
overall survival
PFS
progression-free survival
RCT
randomized controlled trial
RT
radiotherapy
ST
systemic therapy or treatment
Key Messages
The systematic search resulted in 1 single-arm prospective study and 1 retrospective cohort study. No relevant randomized controlled trials, systematic reviews, or evidence-based guidelines were identified that met the criteria for this review.
Evidence was limited, inconsistent, and of low quality for the clinical effectiveness of octreotide long-acting release in combination with everolimus in patients with recurrent meningiomas.
The quantity and quality of current publications were not sufficient to draw a conclusion in support of or against the clinical effectiveness of octreotide long-acting release in combination with everolimus relative to other systematic therapies in patients with recurrent meningiomas.
Additional research is required to inform decision-making in this context.
Context and Policy Issues
According to the Brain Tumours Registry of Canada (2019),1 between 2013 and 2017 of tumours of the meninges, meningioma was the most common tumour, consisting of 23.8% of all central nervous system (CNS) tumours and 37.5% of all non-malignant CNS tumours. In addition, females had higher rates of tumours of the meninges than males. With an estimated incidence of 2.3 to 8.3 in 100.000 individuals, meningiomas are the most common primary brain tumours in the US.2
A WHO classification for CNS brain tumours grades meningioma based on clinical outcomes as WHO I, WHO II, and WHO III, representing benign, atypical, and anaplastic meningiomas, respectively.3 Although most meningiomas are benign (70% to 80%) and slow-growing, atypical and anaplastic meningiomas are more aggressive with a tendency for recurrence, worse clinical outcomes, and higher disease-specific mortality.3 The rate of recurrence and the risk of transformation to malignancy is dependent on the histopathological type of meningioma. Prompt diagnosis and understanding of the severity of the tumour play a prominent role in the management of the disease.4 Current evidence suggests individualizing indications for treatment and with consideration for factors such as age, comorbidity, life expectancy, patient preference, histologic grade, molecular factors, tumour location, and extent of resection.5
Surgical resection and/or radiotherapy (RT) are common therapeutic interventions for patients with meningioma.6 However, complete surgical resection might not be possible in patients with the tumour located in an anatomically challenging position. For such patients, RT might be used alone or following subtotal surgical resection. In addition, few studies report the benefits of these interventions, and the tumours may recur in many patients depending on surgical resection, RT series, and other effective variables.6 Although subsequent surgical resections may be suggested for patients with a recurrence, they might not be a viable option for some patients, such as those with skull base tumours. Where further surgical resections or RT are not recommended, systemic therapy (ST) may be considered. To date, a variety of STs has been used for treating recurrent meningioma (e.g., chemotherapy, hormonal therapy, targeted therapies, and biologic drugs), but the response rate and the efficacy of systemic drugs have not been yet promising.5
Therapeutic alternatives are limited for aggressive and recurrent meningiomas.7 According to an in vitro study, the combination of octreotide long-acting release (LAR) and everolimus may have an additive antiproliferative effect on recurrent meningiomas.8 Generics octreotide LAR and everolimus are available in Canada. However, a Health Canada Notice of Compliance does not exist for either octreotide9 or everolimus10 in patients with recurrent meningiomas, and CADTH’s reimbursement review process does not typically review generic drugs. In August 2022, CADTH published a reference list on this topic that identified some relevant studies.11 The objective for this report was to systematically summarize and critically appraise the evidence regarding the clinical effectiveness of octreotide LAR, a somatostatin agonist, in combination with everolimus, a mechanistic target of rapamycin (mTOR) inhibitor, in patients with recurrent meningioma.
Research Question
What is the clinical effectiveness of octreotide long-acting release in combination with everolimus in patients with recurrent meningiomas?
Methods
Literature Search Methods
This report is based on a literature search developed for a previous CADTH report.11 For the previous report, a limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy consisted of both controlled vocabularies, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were meningiomas, octreotide, and everolimus. No filters were applied to limit the retrieval by study type. Where possible, retrieval was limited to the human population. The search was completed on August 17, 2022; and was limited to English-language documents published since January 1, 2017.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before January 1, 2017.
Critical Appraisal of Individual Studies
The included publications met the selection criteria and were critically appraised by 1 reviewer using the Downs and Black checklist12 for randomized and non-randomized studies. Summary scores were not calculated for the studies; rather, the strengths and limitations of each publication were described narratively as detailed in Appendix 3.
Criteria | Description |
|---|---|
Population | Patients diagnosed with recurrent meningiomas |
Intervention | Octreotide long-acting release in combination with everolimus |
Comparator | Other therapies (i.e., hydroxyurea, bevacizumab, sunitinib, imatinib), octreotide alone, everolimus alone, no comparator |
Outcomes | Clinical effectiveness, including benefits (i.e., progression-free survival, overall survival, response rate, duration of response, quality of life), and harms (i.e., safety [e.g., adverse events of ≥ grade 3 and grade 4], mortality) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies |
Summary of Evidence
Quantity of Research Available
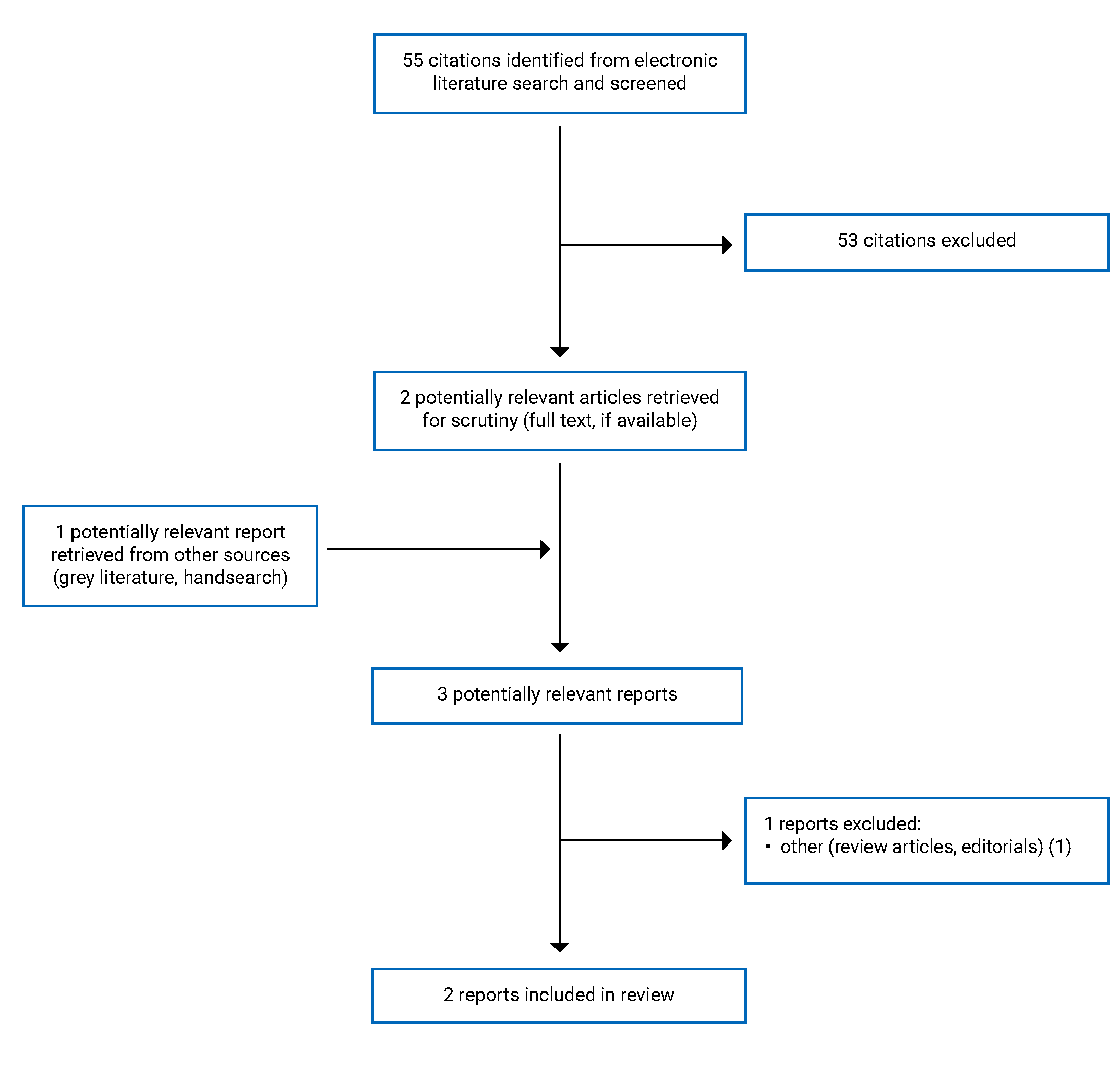
A total of 55 citations was identified in the literature search. Following the screening of titles and abstracts, 53 citations were excluded and 2 potentially relevant reports from the electronic search were retrieved for full-text review. One potentially relevant publication was retrieved from the grey literature search for full-text reviews. Of these potentially relevant articles, 1 review publication was excluded, and 2 non-randomized studies that met the inclusion criteria were included in this report. Appendix 1 presents the PRISMA13 flow chart of the study selection.
Additional references of potential interest that did not meet the inclusion criteria are provided in Appendix 5.
Summary of Study Characteristics
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
One of the 2 included non-randomized studies (authored by Graillon and colleagues) was a single-arm prospective phase II study on octreotide LAR in combination with everolimus (OE) published in 2020.7
The second study was a retrospective cohort study by Cardona and colleagues14 comparing the effectiveness of OE versus sunitinib for recurrent aggressive meningiomas in patients with recurrent or refractory meningiomas at 2 reference centres. It was published in 2019.
Country of Origin
The single-arm prospective study was conducted in France7, and the retrospective cohort study was performed in Colombia.14
Patient Population
The prospective phase II study by Graillon and colleagues included 20 patients: 11 (55%) females and 9 (45%) males, with a mean age of 55 years (range 30 to 75). Patients had a Karnofsky performance status of at least 50% and histologically confirmed meningioma of grade 1 (n = 2, 10%), grade 2 (n = 10, 50%), or grade 3 (n = 8, 40%), who were ineligible for further surgery and/or RT. The Karnofky performance test is a standard scale ranging from 0 (death) to 100 (no evidence of disease, no symptoms) for measuring the ability of patients with cancer to perform ordinary tasks.15 In addition, a documented progression based on 2 different MRIs confirming an increase in 2-dimensional tumour area of at least 5% per 3 months or at least 10% for 6 months before inclusion was required. The history of ST was acceptable. A life expectancy of greater than 3 months and adequate hematologic, renal and hepatic functions were also required. What adequate amount means for these measures was not reported in the article. Four patients had neurofibromatosis type 2 (NF2) germline mutation. The location of tumours was convexity, parasagittal (21, 60%); skull base (9, 26%); and intraventricular (4, 11%).
The retrospective cohort study (2019)14 was based on a review of records of 31 patients, including 22 (71%) females and 9 males (29%), with a mean age of 55 years (range 22 to 88). The included patients had WHO II or WHO III recurrent or refractory meningiomas and had received ST if they had 1 to 5 previous relapses. The most prevalent histology was anaplastic meningioma, which was reported in 20 (65%) patients. A total of 8 (26%) patients had multicentric diseases. Bone involvement was present in nearly half of the patients, and brain invasion was reported in 13 (41.2%) patients with grade III tumours. The location of tumours was anterior fossa (13, 42%), parasagittal (8, 26%), middle fossa (5, 16%), convexity (4, 13%), and posterior fossa (1, 3%).
Interventions and Comparators
In the prospective study,7 everolimus was orally administrated at a fixed dosage of 10 mg per day. Doses could be decreased by 5 mg in case of adverse events (AE). In addition, 30 mg octreotide was administered monthly by an intramuscular injection until tumour progression. The study duration was 1 year, which was extended to 3 years in case of disease stabilization.
In the retrospective cohort study,14 patients were treated with OE (30 mg intramuscular octreotide every 28 days in combination with10 mg oral everolimus per day), oral sunitinib (50 mg per day for days 1 to 28 of 42 days), or bevacizumab (10 mg/kg IV on days 1 and 15). The median time elapsed between RT and the beginning of the first line of ST was 22.9 months (95% CI, 1.8 to 189.0).
The retrospective cohort study was unclear about the intervention groups and the number of patients in the study groups. Notably, the information provided in the abstract and methods and/or results was not consistent. Two study groups were identifiable based on treatment sequences (representing 1st, 2nd, and 3rd lines). The groups were OE, sunitinib, and bevacizumab; and sunitinib, OE, and bevacizumab in the abstract, but everolimus, sunitinib, and bevacizumab; and sunitinib, everolimus, and bevacizumab in the methods and results section of the paper. In addition, according to the abstract, a total of 14 patients received OE, 11 received sunitinib, and the remaining 6 received other second-line drugs (N = 31). However, based on the results, 19 patients received everolimus or OE, and 11 patients received sunitinib (N = 30).
Outcomes
In the prospective study,7 patients were clinically evaluated monthly. Cerebral MRI was performed at inclusion and then every 3 months until progression for all patients. The determination of progression was assessed using the Response Assessment in Neuro-Oncology (RANO) criteria.16 Based on the RANO criteria in the intention-to-treat (ITT) population analysis, the 6-month progression-free survival rate (PFS6) was the primary end point of this study. The PFS6 is estimated to be 11% to 15% in untreated recurrent meningiomas, and treatment is considered of interest if PFS6 exceeds 35%.17 The study hypothesized that OE could improve this rate by up to 40%. A per-protocol (PP) population was defined as the population that fulfilled the inclusion and exclusion criteria and underwent at least 2 months of treatment. The maximum tumour diameter, 2-dimensional tumour area, and 3D volume were assessed. Patients with a treatment duration of less than 2 months, missing data, non-measurable initial volume, or very high tumour growth rate (> 300%/3 months) were excluded from the growth rate substudy. Safety was evaluated based on the National Cancer Institute’s Common Terminology Criteria for Adverse Event version 4.0. In summary, PFS6, overall survival (OS), response rate, tumour growth rate, and safety were the outcomes reported.
In the retrospective cohort study,14 patients were evaluated by physical examination every 3 weeks and MRI scans every 8 weeks. Assessment of response was based on RANO criteria.16 Routine laboratory studies were assessed each month or earlier if medically indicated. Toxicities were graded according to the National Cancer Institute’s Common Terminology Criteria for Adverse Events, version 4.0. Every therapy was discontinued after disease progression or toxicity. Overall, PFS rate, OS rate, response rate, and safety (i.e., toxicities) were reported as outcomes.
Summary of Critical Appraisal
The prospective study7 provided adequate information on the main objective, outcomes assessed, patient characteristics, and interventions received. The main findings were analyzed and described using the Kaplan–Meier method with a 95% confidence interval (CI), and the results were presented with actual probabilities. The incidence of AEs also was reported in detail. The study setup consisted of accurate (valid and reliable) outcome measures, and evidence of the risk of false positives was not observed. Moreover, the description of the staff, places, and facilities associated with treatment were representative of the treatment administered. However, the study didn’t report the estimates of random variability (e.g., range or standard deviation [SD]) in the data for the main outcomes. The generalizability of the outcomes and the ability for assessing comparative effectiveness were unknown given that the outcomes were derived from a single-arm prospective study in a cohort that might not be representative of the eligible population. The impact of potential confounding factors (e.g., health history, other diseases, drug history, drug interactions, age at onset of illness, socioeconomic status, and the extent of support network) on the outcomes was not described. In addition, the investigators did not perform a sample size calculation and it was unknown if the study was adequately powered to identify statistically significant differences for all outcomes.
In the retrospective cohort study,14 the objective and patient characteristics were properly described. The main findings were assessed using the Kaplan–Meier method and the Log-Rank test with 95% CI, and the results were presented along with actual probabilities. The staff, places, and facilities associated with treatment were representative of the procedures received by patients. However, the information provided in the abstract and the body of the article was inconsistent, and the study reporting was unclear about treatment sequences (i.e., study groups) and the number of patients in the study groups. The estimates of random variability (e.g., range or SD) in the data for the main outcomes were not reported. The outcomes were likely to be affected by confounding factors due to selection bias because of limitations in recruiting patients into the different intervention groups. For example, the treatment selection was based on some factors such as AE profile, patient preferences, and the availability of insurers). Other examples of confounding factors not considered in this study were: crossover after progression or intolerability of the first line of medication, a low and variable number of patients in the sequences and/or lines of treatment, the variable time on medication, and the previous exposure to a medication. Toxicities were reported as the only AEs and other potential AEs were not described. Moreover, the investigators did not report a sample size calculation and it was unknown if the study was adequately powered to identify statistically significant differences for all outcomes. Overall, the outcomes of the study may not have enough generalizability to the population of interest.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
Appendix 4 presents the main findings of the 2 included studies.7,14
The findings are presented by main outcomes consisting of PFS rate (Table 4), OS rate (Table 5), tumour growth rate (Table 6), response rate (Table 7), and treatment safety (Table 8).
Clinical Effectiveness of Octreotide LAR in Combination With Everolimus in Recurrent Meningioma
PFS Rate
In the prospective study,7 in the ITT population analysis, the PFS6 rate was 55% (95% CI, 31.3 to 73.5) with a median of 6.6 months (95% CI, 2.7 to 15.0), and the 12-month PFS rate (PFS12) was 30% (95% CI, 12.2 to 50.1). In PP analysis, the PFS6 and PSF12 rates were 61.1% (95% CI, 35.3 to 79.2) and 33.3% (95% CI, 13.6 to 54.5), respectively.
In the retrospective cohort study,14 no statistically significant difference was found in PFS between the treatment with OE (median = 12.1 months; 95% CI, 9.2 to 21.1) and sunitinib (median = 9.1 months; 95% CI, 6.8 to 6.8) (P = 0.43).
OS Rate
In the prospective study,7 6-month and 12-month OS rates in ITT analysis were 90% (95% CI, 65.6 to 97.4) and 75% (95% CI, 50.0 to 88.7), respectively.
In the retrospective cohort study,14 the median OS for the cohort after initiating medical treatment was 37.3 months (95% CI, 28.5 to 42.1). The OS of the group treated with the OE, sunitinib, and bevacizumab sequence was 6.5 months longer than the OS of the group treated with the sunitinib, OE, and bevacizumab sequence. The difference was statistically significant (36.0 versus 29.5, P = 0.0001). Other variables, such as the extension of the initial surgery, the time between diagnosis and the start of medical treatment (higher or lower than 20 months), the number of recurrences, age, and sex had no statistically significant impact on the OS rate.
Tumour Growth Rate
In the prospective study,7 the median preinclusion surface growth rate per 3 months was 42% (range: 10% to 269%), during a median follow-up of 21 months. The volume growth rate was compared before inclusion and during treatment by independent MRI reviews. Patients with tumour progression at 3 months were considered for the 6-month analysis. A statistically significant decrease (> 50%, P = 0.0002) in the volume growth rate was observed in 78% of patients (21 out of 27 tumours) at 3 months, with a reduction in mean and median growth rates from 43.5% and 16.6% before treatment to 4.2% and 0.0% after treatment, respectively. In addition, at 6 months, a statistically significant decrease (P = 0.0003) in the volume growth rate was found in 67% of patients (12 out of 18 tumours) with reduced mean and median growth rate from 49.0% and 19.2% before treatment to 5.0% and 0.48% after treatment, respectively. In addition, long-term (i.e., > 2 years) tumour growth control was reported in 3 patients.
Response Rate
In the prospective study,7 no complete or partial response was observed in compliance with the RANO criteria, except for the disappearance of 2 separate subcutaneous nodules in 1 patient.
In the retrospective cohort study,14 stable disease and partial responses were reported for 6 (43%) and 4 (28.6%) of OE patients, respectively; and 7 (63.6%) and 4 (36.4%) of sunitinib patients, respectively.
Treatment Safety
In the prospective study,7 stomatitis (i.e., swelling and redness of the mouth lining) was reported in 11 (55%) patients, including 3 with grade III AEs requiring discontinuation of both drugs in 1 patient and discontinuation of everolimus alone in another patient. Other AEs were asthenia and fatigue 9 (45%), hypercholesterolemia 9 (45%), abdominal pain and diarrhea 8 (40%), cutaneous rash 6 (30%), hypertriglyceridemia 6 (30%), hyperglycemia and diabetes 5 (25%), aspartate aminotransferase/alanine aminotransferase (ASAT/ALAT) increase 4 (20%), nausea and vomiting 3 (15%), neutropenia 2 (15%), pneumopathy 1 (5%), and cholelithiasis 1 (5%).
In the retrospective cohort study,14 all patients in the 2 treatment sequences experienced a level of toxicity. Irrespective of the line of treatment, the most common side effects were grade 1 or 2 fatigue (12 [86%]) and grade 1 or 2 edema (2 [14%]) for OE, and grade 1 or 2 fatigue (7 [73%]) and hypothyroidism (2 [18%]) for those exposed to sunitinib. Moreover, treatment with sunitinib led to grade 3 fatigue and a dose reduction in 3 (9.7%) patients; and exposure to bevacizumab was associated with deep vein thrombosis in 2 (6.4%) patients.
Limitations
Only 2 observational, non-randomized trials (i.e., a prospective single-arm study7 and a retrospective cohort review of records14) were identified on the clinical effectiveness of OE in patients with recurrent meningiomas. In the single-arm trial,7 20 patients received the intervention of interest and were followed for 6 and 12 months. Because of the absence of a control treatment (i.e., no comparator), single-arm studies are not appropriate for demonstrating the comparative benefit of an intervention.18 In the retrospective cohort study,14 the effectiveness of OE versus sunitinib was assessed by reviewing the records of 31 patients non-randomly divided into treatment groups, which might not be representative of the eligible population. The study was unclear over the sequences and lines of treatment as well as the number of patients in study groups. Both studies were unclear regarding how the sample size was calculated and had heterogeneity in patients in terms of tumour grade and location and the history of surgery, RT, radiosurgery, and/or chemotherapy might have affected the outcomes. These limitations are concerns for accurately interpreting the results and may have an impact on the generalizability of the findings.
Overall, an insufficient number of studies and a lack of high-quality evidence, especially RCTs, create uncertainties about the validity and generalizability of the treatment outcomes with OE in patients with refractory or recurrent meningiomas. In addition, the 2 studies were conducted in France and Colombia. It is unclear how generalizable these findings may be to the Canadian context.
Conclusions and Implications for Decision- or Policy-Making
This report summarizes the available evidence on the clinical effectiveness of OE for patients diagnosed with recurrent meningiomas from 1 single-arm prospective study7 and 1 retrospective cohort review of patients’ medical records.14 Whereas, the findings of the single-arm study were in support of improved PFS and OS rates and a reduced tumour growth rate, and results from the retrospective cohort study14 suggested that OE and sunitinib had similar efficacy and safety profiles. In addition, a range of AEs such as stomatitis, asthenia, abdominal pain, hypercholesterolemia, cutaneous rash,7 fatigue, and edema14 in exposure to OE, and fatigue and hypothyroidism in exposure to sunitinib14 were reported.
Besides being non-randomized, both included studies were relatively small (i.e., with 31 patients or less) and patients were unlikely to be representative of the patient population for whom the interventions may be indicated. Therefore, there are concerns about the risk of selection bias, low generalizability of the findings, and uncertainty of the power of the studies to determine statistically significant differences in treatment effect between the interventions.
Overall, the evidence identified for the clinical effectiveness of OE is considered to be of low quality and associated with high heterogeneity, inconsistency, imprecision, and risk of bias.7,14 Because of the limited number of relevant studies and the low quality of existing evidence, it is hard to draw a conclusion regarding the clinical effectiveness of OE for patients with recurrent meningiomas.
Additional research with rigorous methodological approaches, such as well-designed and sufficiently powered RCTs, is needed to reduce uncertainty, inconsistency, and the risk of bias in the current available evidence, improve the generalizability of findings, and support stakeholders with decision-making regarding the use of OE in patients with recurrent meningiomas in the Canadian context.
References
1.Walker E, Zakaria D, Yuan Y, Yasmin F, Shaw A, Davis F. Brain Tumour Registry of Canada (BTRC): Incidence (2013-2017) and Mortality (2014-2018) Report. Brain Tumour Registry of Canada; 2019: https://braintumourregistry.ca/incidence-report. Accessed 2022 Nov 3.
2.Ostrom QT, Gittleman H, Fulop J, et al. CBTRUS Statistical Report: Primary Brain and Central Nervous System Tumors Diagnosed in the United States in 2008-2012. Neuro Oncol. 2015;17(Suppl 4):iv1-iv62. PubMed
3.Wilson TA, Huang L, Ramanathan D, et al. Review of Atypical and Anaplastic Meningiomas: Classification, Molecular Biology, and Management. Front Oncol. 2020;10:565582. PubMed
4.Pearson BE, Markert JM, Fisher WS, et al. Hitting a moving target: evolution of a treatment paradigm for atypical meningiomas amid changing diagnostic criteria. Neurosurg Focus. 2008;24(5):E3. PubMed
5.Brastianos PK, Galanis E, Butowski N, et al. Advances in multidisciplinary therapy for meningiomas. Neuro Oncol. 2019;21(Suppl 1):i18-i31. PubMed
6.Rogers L, Barani I, Chamberlain M, et al. Meningiomas: knowledge base, treatment outcomes, and uncertainties. A RANO review. J Neurosurg. 2015;122(1):4-23. PubMed
7.Graillon T, Sanson M, Campello C, et al. Everolimus and Octreotide for Patients with Recurrent Meningioma: Results from the Phase II CEVOREM Trial. Clinical Cancer Research. 2020;26(3):552-557. PubMed
8.Graillon T, Defilles C, Mohamed A, et al. Combined treatment by octreotide and everolimus: Octreotide enhances inhibitory effect of everolimus in aggressive meningiomas. J Neurooncol. 2015;124(1):33-43. PubMed
9.Sandostatin (octreotide): 50mcg/mL, 100 mcg/mL, 200 mcg/mL ocreotide (as acetate) solution for subcutaneous injection or intravenous injection [product monograph]. Dorval (QC): Novartis Pharmaceuticals Canada Inc.; 2021 Apr 19.
10.AFINITOR (everolimus) and AFINITOR DISPERZ: 2.5mg, 5mg, 10mg, oral tablets [product monograph]. Dorval (QC): Novartis Pharmaceuticals Canada Inc. 2021 Nov 30.
11.Octreotide Long Acting Release and Everolimus for Recurrent Meningiomas. Ottawa (ON): CADTH; 2022: https://www.cadth.ca/octreotide-long-acting-release-and-everolimus-recurrent-meningiomas. Accessed 2022 Nov 3.
12.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
13.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700. PubMed
14.Cardona AF, Ruiz-Patino A, Zatarain-Barron ZL, et al. Systemic management of malignant meningiomas: A comparative survival and molecular marker analysis between Octreotide in combination with Everolimus and Sunitinib. PLoS ONE. 2019;14(6):e0217340. PubMed
15.Schag CC, Heinrich RL, Ganz PA. Karnofsky performance status revisited: reliability, validity, and guidelines. J Clin Oncol. 1984;2(3):187-193. PubMed
16.Huang RY, Bi WL, Weller M, et al. Proposed response assessment and endpoints for meningioma clinical trials: report from the Response Assessment in Neuro-Oncology Working Group. Neuro Oncol. 2019;21(1):26-36. PubMed
17.Kaley T, Barani I, Chamberlain M, et al. Historical benchmarks for medical therapy trials in surgery- and radiation-refractory meningioma: a RANO review. Neuro Oncol. 2014;16(6):829-840. PubMed
18.Cucherat M, Laporte S, Delaitre O, et al. From single-arm studies to externally controlled studies. Methodological considerations and guidelines. Therapie. 2020;75(1):21-27. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Graillon et al. (2020)7 France Funding: French National Cancer Institute funding (PHRCK 2013) | A prospective, single-arm study | N = 20 Age = 55 years (30 to 75) Female n = 11 (55%) Number of growing tumours NF2 patients = 20 Non-NF2 patients = 15 Tumour grade, n (% patients) Grade I = 2 (10) Grade II = 10 (50) Grade III = 8 (40) Tumour location, n (% tumours) Convexity, parasagittal = 21 (60) Skull base = 9 (26) Intraventricular = 4 (11) Previous surgery, n (%) One = 2 (10) Multiple = 18 (90) Previous radiotherapy or radiosurgery, n (%) None 1 (5) One 10 (50) Multiple 9 (45) Previous chemotherapy, n (%) Yes = 5 (25) No = 15 (75) | Intervention: Everolimus was orally administrated at a fixed dosage of 10 mg/day. Doses could be decreased by 5 mg in case of an adverse event. 30 mg octreotide long-acting release was administrated monthly by an intramuscular injection until tumour progression. The study duration was 1 year. It was extended to 3 years in case of disease stabilization. Comparator: NA | Outcomes: • Six-month PFS • OS • Tumour growth rate • Response rate • Safety (i.e., AEs) Follow-up: Median = 21 months |
Cardona et al. (2019)14 Colombia Funding: Andre’s F. Cardona | A retrospective cohort study | N = 31 Age = 55 years (28 to 88) Female n = 22 (71%) Tumour grade, n (% patients, 95% CI) Grade II = 11 (35, 19 to 52) Grade III = 20 (65, 48 to 81) Tumour location, n (% tumours, 95% CI) Anterior fossa = 13 (42, 25 to 59) Parasagittal = 8 (25, 10 to 41) Middle fossa = 5(16, 3 to 29) Convexity = 4 (13, 11 to 25) Posterior fossa = 1 (3, 0 to 9) Previous recurrence, n (%, 95% CI) 1 = 4 (13, 11 to 25) 2 = 9 (29, 13 to 45) 3 = 10 (32, 16 to 49) 4 = 5 (16, 3 to 29) 5 = 3 (10, 0 to 20) Previous surgery, n (%, 95% CI) 1 = 2 (6, 0 to 15) 2 = 19 (61, 44 to 78) 3 = 6 (19, 5 to 33) 4 = 1 (3, 0 to 9) 5 = 3 (10, 0 to 20) Multicentricity = 8 (26) The extent of resection, n (%, 95% CI) Total = 14 (45, 27 to 62) Subtotal = 17 (55, 37 to 72) | Intervention: Treatment with: OE (as 30 mg octreotide intramuscular injection every 28 days plus 10 mg oral everolimus per day), Su (50 mg taken by mouth per day for days 1 to 28 of 42 days), or Bev (10 mg/kg IV, days 1 and 15). Treatment had 2 different sequences:
Every therapy was discontinued after disease progression or toxicity. Comparator: Su | Outcomes: • PFS • OS • Response rate • Safety (i.e., AEs) Follow-up: Median = 31.8 months |
AEs = adverse events; Bev = bevacizumab; CI = confidence interval; NA = not applicable; NF2 = neurofibromatosis type 2; OE = octreotide long-acting release in combination with everolimus; OS = overall survival; PFS = progression-free survival rate; Su = sunitinib.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist12
Strengths | Limitations |
|---|---|
Grallon et al. (2020)7 | |
The objective, main outcomes assessed, patient characteristics, and interventions received were clearly described in the introduction and/or methods sections. The source of funding was clearly stated. Accurate (valid and reliable) outcome measures used. The main findings were clearly analyzed and described using the Kaplan–Meier method with 95% CI. The results included actual probabilities. AEs were reported in detail. Evidence of data dredging or the risk of false positives was not observed. The staff, places, and facilities associated with treatment were representative of the treatment procedure completed. | The study was unclear regarding the impact of potential confounding factors (e.g., health history, other diseases, drug history, drug interactions, age at onset of illness, socioeconomic status, and the extent of support network) on the outcomes. Because of not reporting a sample size calculation, it was unknown if the study was adequately powered to identify statistically significant differences for all outcomes. The outcomes might have limited generalizability to patients with recurrent meningiomas because of a relatively small size, foreign-based, and single-centre study design. Assessing comparative effectiveness could be difficult because of the study design (i.e., a single-arm study) and the probability of unclear method of patient selection and the potentially high risk of selection bias. |
Cardona et al. (2019)14 | |
The objective and patient characteristics were clearly described in the introduction and/or methods sections. The source of funding was clearly stated. Accurate (valid and reliable) outcome measures used. The main findings were analyzed using the Kaplan–Meier method and the Log-Rank test with 95% CI. The results included actual probabilities. Toxicities were reported as AEs. The staff, places, and facilities associated with treatment were representative of the treatment received by the patients. | The risk of selection bias given that the treatment selection was based on factors such as AE profile, patient preference (oral or IV administration, etc.), and the availability of insurers. The study was unclear about treatment sequences and the number of patients in study groups (i.e., inconsistency in the information provided in the abstract and methods and/or results). Although toxicities were reported, it was unclear if all important AEs were considered. The role of several principal confounding factors and the method for adjusting survival curves for confounders were not described, therefor there was a high risk of confounding bias. Examples of confounding factors were crossover after progression or intolerability of the first line of medication, the low and variable number of patients in the sequences or lines of treatment, the variable time during which a patient received the medication, and the previous exposure to the medication. Limitations such as ambiguity in treatment sequences and the number of patients in study groups, as well as not considering the impact of several confounding factors might have affected the outcomes. No information was provided about the fidelity and completeness of patients’ records. A sample size calculation was not reported in the article, and it was unknown if the study was adequately powered to identify statistically significant differences for all outcomes. |
AEs = adverse events; CI = confidence interval.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 4: Summary of Findings by Outcome — PFS
Study citation and design | Method of measurement | End point | Result |
|---|---|---|---|
Graillon et al. (2020)7 Prospective, single-arm study | ITT population analysis |
| N = 20
|
PP analysis |
| N = 18
| |
Cardona et al. (2019)14 Retrospective cohort study | Results No statistically significant difference between octreotide long-acting release in combination with everolimus (median PFS = 12.1 months; 95% CI, 9.2 to 21.1) and sunitinib (median PSF = 9.1 months; 95% CI, 6.8 to 16.8) (P = 0.43) | ||
CI = confidence interval; ITT = intention-to-treat; PFS = progression-free survival rate; PFS6 = PFS at 6 months; PFS12 = PFS at 12 months; PP = Per-protocol.
Table 5: Summary of Findings by Outcome — OS
Study citation and design | Method of measurement | Time point | Results |
|---|---|---|---|
Graillon et al. (2020)7 Prospective, single-arm study | ITT population analysis |
| N = 20
|
Cardona et al. (2019)14 Retrospective cohort study | Results
| ||
Bev = bevacizumab; CI = confidence interval; ITT = intention-to-treat; OE = octreotide long-acting release in combination with everolimus; OS = Overall survival rate; OS6 = OS at 6 months; OS12 = OS at 12 months; Su = sunitinib.
Table 6: Summary of Findings by Outcome — Tumour Growth Rate
Study citation and design | Method of measurement | Time point | Result | P value |
|---|---|---|---|---|
Graillon et al. (2020)7 Prospective, single-arm study | MRI | Reduced tumour volume | A major decrease (> 50%):
| 0.0002 0.0003 |
Long-term tumour growth control (i.e., > 2 years) | Observed in 3 patients | NA |
MRI = MRI; NA = not applicable; NF2 = neurofibromatosis type 2; SSTR2A = somatostatin receptor subtype 2A.
Table 7: Summary of Findings by Outcome — Response Ratea
Study citation and design | Study findings |
|---|---|
Graillon et al. (2020)7 Prospective, single-arm study |
|
Cardona et al. (2019)14 Retrospective cohort study | Stable disease and partial response in the first line of treatment
|
aAssessed according to the RANO criteria.16
Table 8: Summary of Findings by Outcome — Safety
Study citation and design | Study findings |
|---|---|
Graillon et al. (2020)7 Prospective, single-arm study |
|
Cardona et al. (2019)14 Retrospective cohort study |
|
AEs = adverse events; OE = octreotide long-acting release in combination with everolimus.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
The following publications were identified because they provide additional information associated with the topic of this report (i.e., previous CADTH reports) or additional guidance on ST or multidisciplinary therapy for relapsed/refractory meningioma.
Previous CADTH Reports
Octreotide Long-Acting Release and Everolimus for Recurrent Meningiomas. Ottawa (ON): CADTH. 2022. https://www.cadth.ca/octreotide-long-acting-release-and-everolimus-recurrent-meningiomas Accessed 2022 Nov 3.
Combination Therapy for the Treatment of Central Nervous System Malignancies: Clinical Effectiveness and Guidelines. Ottawa (ON): CADTH. 2019. https://www.cadth.ca/combination-therapy-treatment-central-nervous-system-malignancies-clinical-effectiveness-and Accessed 2022 Nov 3.
Review Articles
Brastianos PK, Galanis E, Butowski N, et al. Advances in multidisciplinary therapy for meningiomas. Neuro Oncol. 2019;21(Suppl 1):i18-i31. PubMed
Dasanu CA, Alvarez-Argote J, Limonadi FM, Codreanu I. Bevacizumab in refractory higher-grade and atypical meningioma: the current state of affairs. Expert Opin Biol Ther. 2019;19(2):99-104. PubMed
Dasanu CA, Samara Y, Codreanu I, Limonadi FM, Hamid O, Alvarez-Argote J. Systemic therapy for relapsed/refractory meningioma: Is there potential for antiangiogenic agents? J Oncol Pharm Pract. 2019;25(3):638-647. PubMed
Zhao L, Zhao W, Hou Y, et al. An Overview of Managements in Meningiomas. Front Oncol. 2020;10:1523. PubMed
Graillon T, Tabouret E, Chinot O. Chemotherapy and targeted therapies for meningiomas: what is the evidence? Curr Opin Neurol. 2021;34(6):857-867. PubMed
Maggio I, Franceschi E, Tosoni A, et al. Meningioma: not always a benign tumor. A review of advances in the treatment of meningiomas. CNS Oncol. 2021;10(2):Cns72. PubMed
McFaline-Figueroa JR, Kaley TJ, Dunn IF, Bi WL. Biology and Treatment of Meningiomas: A Reappraisal. Hematol Oncol Clin North Am. 2022;36(1):133-146. PubMed
Pellerino A, Bruno F, Palmiero R, et al. Clinical Significance of Molecular Alterations and Systemic Therapy for Meningiomas: Where Do We Stand? Cancers (Basel). 2022;14(9). PubMed
In Vitro Study
Graillon T, Romano D, Defilles C, et al. Octreotide therapy in meningiomas: in vitro study, clinical correlation, and literature review. Journal of Neurosurgery. 2017;127(3):660-669. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca