CADTH Health Technology Review
Oral Feeding for Preterm Infants on Respiratory Support
Rapid Review
Authors: Khai Tran, Sharon Bailey
Abbreviations
CPAP
continuous positive airway pressure
HFNC
high-flow nasal cannula
Key Messages
No health technology assessments or systematic reviews were identified regarding the clinical effectiveness of oral feeding in preterm infants while on continuous positive airway pressure or high-flow nasal cannula.
No evidence-based guidelines were identified regarding oral feeding in preterm infants while on continuous positive airway pressure or high-flow nasal cannula that met the criteria for this review.
Context and Policy Issues
Preterm birth, defined as babies born alive before 37 weeks of pregnancy, occurs in about 8% of pregnancies in Canada every year.1 It is the leading cause of infant morbidity and mortality, and it is estimated to cost the Canadian health care system more than 8 billion dollars per year.2 As preterm infants have immature respiratory control mechanisms, non-invasive ventilation, such as nasal continuous positive airway pressure (CPAP) and high-flow nasal cannula (HFNC), is often required.3
Enteral feeding, also known as tube feeding, which directly delivers nutrition to the stomach or small intestine,4 is usually started in the first 2 to 5 days for very preterm infants (i.e., infants born at less than 32 weeks gestation) whose swallowing mechanisms have not fully matured to ensure that the infant receives appropriate nutrition.5 The maturation of suck, swallow, and breath coordination occurs in preterm infants around 33 to 36 weeks of gestation, at which time oral feeding — including breast feeding, bottle feeding, and cup feeding — can be initiated.6 Initiation of oral feeding before a preterm infant’s swallowing mechanism has become fully established can lead to aspiration.7,8 However, research has shown that delays in transition from tube feeding to oral feeding may lead to delayed oral motor development, prolonged hospital stays, and persistent feeding disorders.9,10
As non-invasive ventilation mechanisms provide access to the mouth, oral feeding is increasingly provided to preterm infants receiving nasal CPAP and HFNC with an attempt to optimize nutrition, support neurodevelopment outcomes, and reduce hospital length of stay.11,12 However, the safety of oral feeding in preterm infants while on non-invasive ventilation is unknown.13,14 Nasal CPAP has been shown to inhibit the swallow reflex in adults.15,16 HFNC may also impact swallowing safety by affecting the airway protection mechanisms in neonatal and adult populations.14,17 Thus, oral feeding to preterm infants while receiving nasal CPAP and HFNC may not be free from adverse events.
The objective of this report is to summarize the evidence regarding the clinical effectiveness of oral feeding compared with alternative feeding strategies such as enteral feeding in preterm infants while on nasal CPAP and HFNC. This report also aims to summarize the recommendations from evidence-based guidelines regarding oral feeding given to this population.
Research Questions
What is the clinical effectiveness of oral feeding while on continuous positive airway pressure or high-flow nasal cannula in preterm infants?
What are the evidence-based guidelines regarding oral feeding while on continuous positive airway pressure or high-flow nasal cannula in preterm infants?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cumulative Index to Nursing and Allied Health Literature (CINAHL), the Cochrane Database of Systematic Reviews, the international HTA database, and the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were preterm infants, artificial respiration, and feeding methods. CADTH-developed search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, network meta-analyses, and guidelines. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2017, and September 26, 2022.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Preterm infants (< 37 weeks) requiring respiratory support |
Intervention | Q1 to Q2: Oral feeding while on CPAP or HFNC |
Comparator | Q1: Alternative feeding strategies while on CPAP or HFNC (i.e., enteral feeding) Q2: NA |
Outcomes | Q1: Clinical effectiveness (e.g., length of stay, transition to oral feeding, weight gain) Q2: Guidelines and recommendations on best practices (e.g., assessing readiness, transition strategies) |
Study designs | Health technology assessments, systematic reviews, evidence-based guidelines |
CPAP = continuous positive airway pressure; HFNC = high-flow nasal cannula; NA = not applicable; Q = question.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, or if they were published before 2017.
Summary of Evidence
Quantity of Research Available
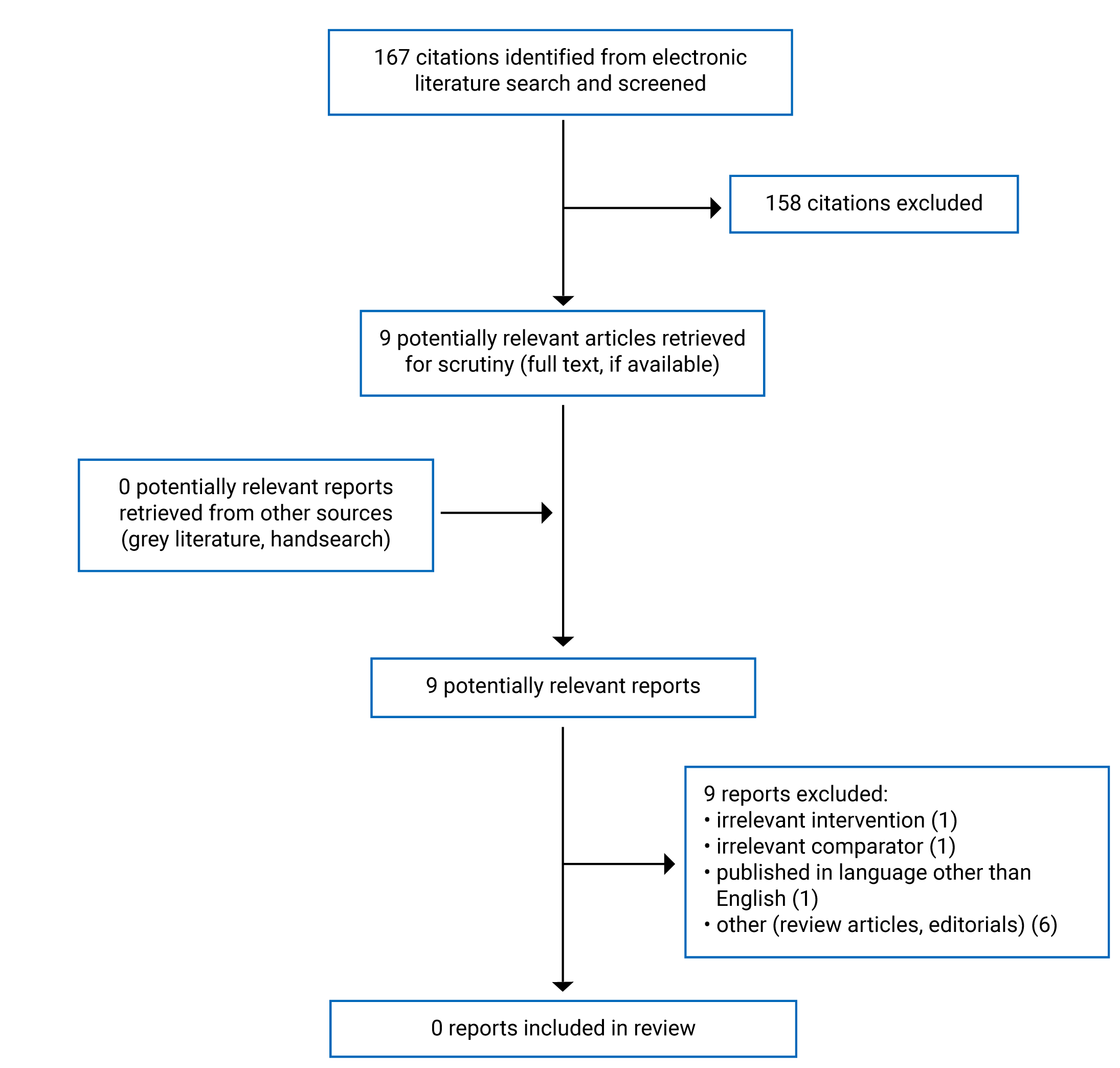
A total of 167 citations were identified in the literature search. Following screening of titles and abstracts, 158 citations were excluded and 9 potentially relevant reports from the electronic search were retrieved for full-text review. No potentially relevant publications were retrieved from the grey literature search for full-text review. None of these 9 potentially relevant articles met the inclusion criteria and they were excluded from this report for various reasons. Appendix 1 presents the PRISMA18 flow chart of the study selection.
Summary of Findings
No relevant health technology assessments, systematic reviews, or evidence-based guidelines were identified regarding the clinical effectiveness of or recommendations for oral feeding while on CPAP or HFNC in preterm infants; therefore, no summary can be provided.
Limitations
No relevant health technology assessments, systematic reviews, or evidence-based guidelines were identified that met the criteria for this review. This report is limited by the parameters for the search, such as the time frame (i.e., from 2017 onward) and the study designs for the clinical effectiveness question (i.e., only health technology assessments and systematic reviews were searched). It unknown whether there is literature that was published more than 5 years ago or that used a different study design (e.g., randomized controlled trials, non-randomized studies) that was excluded due to the limitations of the search.
Conclusions and Implications for Decision- or Policy-Making
Conclusions could not be drawn regarding the clinical effectiveness of and recommendations for oral feeding while on nasal CPAP or HFNC in preterm infants because no relevant literature was identified to answer the research questions.
Further research is needed to determine the efficacy and safety of oral feeding in comparison with alternative feeding strategies such as enteral feeding in preterm infants while on nasal CPAP or HFNC. Likewise, evidence-based guidelines are needed to provide recommendations on feeding strategies for preterm infants while on respiratory support.
References
1.Statistics Canada. Preterm live births in Canada, 2000 to 2013. 2016; https://www150.statcan.gc.ca/n1/pub/82-625-x/2016001/article/14675-eng.htm. Accessed 2022 October 3.
2.Lim G, Tracey J, Boom N, et al. CIHI survey: Hospital costs for preterm and small-for-gestational age babies in Canada. Healthc Q. 2009;12(4):20-24. PubMed
3.Morley SL. Non-invasive ventilation in paediatric critical care. Paediatr Respir Rev. 2016;20:24-31. PubMed
4.Mayo Clinic. Home enteral nutrition. 2021; https://www.mayoclinic.org/tests-procedures/home-enteral-nutrition/about/pac-20384955. Accessed 2022 October 17.
5.Bozzetti V, De Angelis C, Tagliabue PE. Nutritional approach to preterm infants on noninvasive ventilation: An update. Nutrition. 2017;37:14-17. PubMed
6.Mizuno K, Ueda A. The maturation and coordination of sucking, swallowing, and respiration in preterm infants. J Pediatr. 2003;142(1):36-40. PubMed
7.Thoyre SM, Holditch-Davis D, Schwartz TA, Melendez Roman CR, Nix W. Coregulated approach to feeding preterm infants with lung disease: effects during feeding. Nurs Res. 2012;61(4):242-251. PubMed
8.Davis NL, Liu A, Rhein L. Feeding immaturity in preterm neonates: Risk factors for oropharyngeal aspiration and timing of maturation. J Pediatr Gastroenterol Nutr. 2013;57(6):735-740. PubMed
9.Lainwala S, Kosyakova N, Power K, et al. Delayed achievement of oral feedings is associated with adverse neurodevelopmental outcomes at 18 to 26 months follow-up in preterm infants. Am J Perinatol. 2020;37(5):483-490. PubMed
10.Jadcherla SR, Wang M, Vijayapal AS, Leuthner SR. Impact of prematurity and co-morbidities on feeding milestones in neonates: A retrospective study. J Perinatol. 2010;30(3):201-208. PubMed
11.Shetty S, Hunt K, Douthwaite A, Athanasiou M, Hickey A, Greenough A. High-flow nasal cannula oxygen and nasal continuous positive airway pressure and full oral feeding in infants with bronchopulmonary dysplasia. Arch Dis Child Fetal Neonatal Ed. 2016;101(5):F408-411. PubMed
12.Dalgleish SR, Kostecky LL, Blachly N. Eating in “SINC”: Safe Individualized Nipple-Feeding Competence, a quality improvement project to explore infant-driven oral feeding for very premature infants requiring noninvasive respiratory support. Neonatal Netw. 2016;35(4):217-227. PubMed
13.Coletti KD, Bagdure DN, Walker LK, Remy KE, Custer JW. High-flow nasal cannula utilization in pediatric critical care. Respir Care. 2017;62(8):1023-1029. PubMed
14.Wilkinson DJ, Andersen CC, Smith K, Holberton J. Pharyngeal pressure with high-flow nasal cannulae in premature infants. J Perinatol. 2008;28(1):42-47. PubMed
15.Nishino T, Sugimori K, Kohchi A, Hiraga K. Nasal constant positive airway pressure inhibits the swallowing reflex. Am Rev Respir Dis. 1989;140(5):1290-1293. PubMed
16.Ferrara L, Bidiwala A, Sher I, et al. Effect of nasal continuous positive airway pressure on the pharyngeal swallow in neonates. J Perinatol. 2017;37(4):398-403. PubMed
17.Dodrill P, Gosa M, Thoyre S, et al. First, do no harm: A response to “Oral Alimentation in Neonatal and Adult Populations Requiring High-Flow Oxygen via Nasal Cannula”. Dysphagia. 2016;31(6):781-782. PubMed
18.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
Appendix 1: Selection of Included Studies
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca