CADTH Health Technology Review
Transanal Total Mesorectal Excision for Adults With Rectal Cancer
Rapid Review
Authors: Angela M. Barbara, Anusree Subramonian, Jennifer Horton
Abbreviations
CI
confidence interval
CRM
circumferential resection margin
DRM
distal resection margin
ICER
incremental cost-effectiveness ratio
LaTME
laparoscopic total mesorectal excision
NHS
National Health Service
RCT
randomized controlled trial
QALY
quality-adjusted life year
SR
systematic review
TaTME
transanal total mesorectal excision
TME
total mesorectal excision
Key Messages
Transanal total mesorectal excision may result in lower rates of conversion to open procedure and a better circumferential resection margin compared with laparoscopic total mesorectal excision in adults with rectal cancer.
Transanal total mesorectal excision may be comparable to laparoscopic total mesorectal excision for cancer recurrence, survival, death, and short-term safety outcomes in adults with rectal cancer.
Total mesorectal excision may be more cost-effective than laparoscopic and open total mesorectal excision in adults with rectal cancer, but this is uncertain.
Context and Policy Issues
Colorectal cancer is projected to be the fourth most-diagnosed cancer in 2022 in Canada.1 It is also the second-leading cause of cancer death, accounting for 11% of all cancer deaths.1 Rectal cancer is a subset of colorectal cancer, with symptoms that include changes in bowel habits, rectal bleeding, and weight loss.2 The 5-year survival of patients with advanced rectal cancer is 58%.3 The treatment of rectal cancer can be challenging because what works for 1 patient may not work for another.3 Surgery is 1 of the main therapies for rectal cancer, with the primary goal of complete removal of the tumour.4 The stage, size, and location of the tumour, and the patient’s characteristics (e.g., sex, body mass index, skeletal morphology) can affect the choice of surgical approach for rectal cancer.4
Total mesorectal excision (TME), which involves the complete removal of the rectum and surrounding lymphatic tissue,5 is the standard of care for tumours in the distal to middle rectum.6 TME can be performed with open or laparoscopic techniques.2 Conventional open surgery is a procedure in which the surgeon makes a large incision to access the surgery site.7,8 In contrast, laparoscopic surgery is a less-invasive and more advanced procedure in which a laparoscope is used to make a much smaller incision.7-9 Laparoscopic TME (LaTME) can be complicated by certain factors, such as a narrow pelvis, obesity, or large tumours, which can reduce the surgeon’s ability to access the distal part of the rectum.5,10 In such cases, a laparoscopic procedure would need to be converted to the more invasive open TME procedure, which may result in worse short-term post-surgical outcomes.2
Transanal endoscopic surgery is a technique that offers access to rectal cancers through the anus.11 Transanal total mesorectal excision (TaTME) is a surgical procedure that combines the transanal endoscopic surgery approach with the LaTME procedure. The TaTME approach is a minimally invasive surgery for rectal cancer which may facilitate access to tumours that are not amenable to the laparoscopic approach (e.g., patients who are obese, patients who have a narrow pelvis).4 For distal and middle rectal cancers, the TaTME surgical treatment facilitates reaching tumours in the distal part of the rectum through the transanal approach and tumours in the middle rectum laparoscopically.4
A previous CADTH report on this topic12 found strong evidence based on 5 moderate- to high-quality systematic reviews (SRs) and 6 low- to moderate-quality non-randomized studies that suggested that TaTME was clinically effective and safe for patients with rectal cancer based on the assessment of short-term outcomes compared with LaTME. However, the report had insufficient evidence about the comparative clinical effectiveness of TaTME versus LaTME over the long term or TaTME versus open TME, and it had no cost-effectiveness evidence for either of the comparisons.12
The purpose of the current report is to review and critically appraise recent evidence pertaining to the clinical effectiveness and the cost-effectiveness of TaTME for adults with rectal cancer compared with conventional open TME or LaTME
Research Questions
What is the clinical effectiveness of transanal total mesorectal excision for adults with rectal cancer?
What is the cost-effectiveness of transanal total mesorectal excision for adults with rectal cancer?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources, including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were TaTME and rectal cancer. No filters were applied to limit the retrieval by study type. If possible, retrieval was limited to the human population. The search was completed on September 16, 2022, and was limited to English-language documents published since January 1, 2020.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2020. SRs in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded; the references of these SRs are provided in Appendix 6. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs. Non-randomized studies were excluded.
Criteria | Description |
|---|---|
Population | Q1 and Q2: Adults with rectal cancer (any location in the rectum: high, mid, or low) |
Intervention | Q1 and Q2: Transanal total mesorectal excision |
Comparator | Q1 and Q2: Conventional open total mesorectal excision or laparoscopic total mesorectal excision |
Outcomes | Q1: Clinical effectiveness (e.g., conversion to open procedure, reoperation, perioperative morbidity, readmission, length of hospital stay, recurrence of cancer [locoregional or systemic], disease-free survival, circumferential resection margin, positive resection margin, completeness and quality of mesorectal excision, health-related quality of life), and harms (e.g., adverse events, infection, anastomotic leak, incisional hernia, injury to the urethra and bladder, ileus, complication rate, blood loss, mortality) Q2: Cost-effectiveness (e.g., quality-adjusted life-year, incremental cost-effectiveness ratio) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, economic evaluations |
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)13 for SRs, the Downs and Black checklist14 for randomized studies, and the Drummond checklist15 for economic evaluations. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
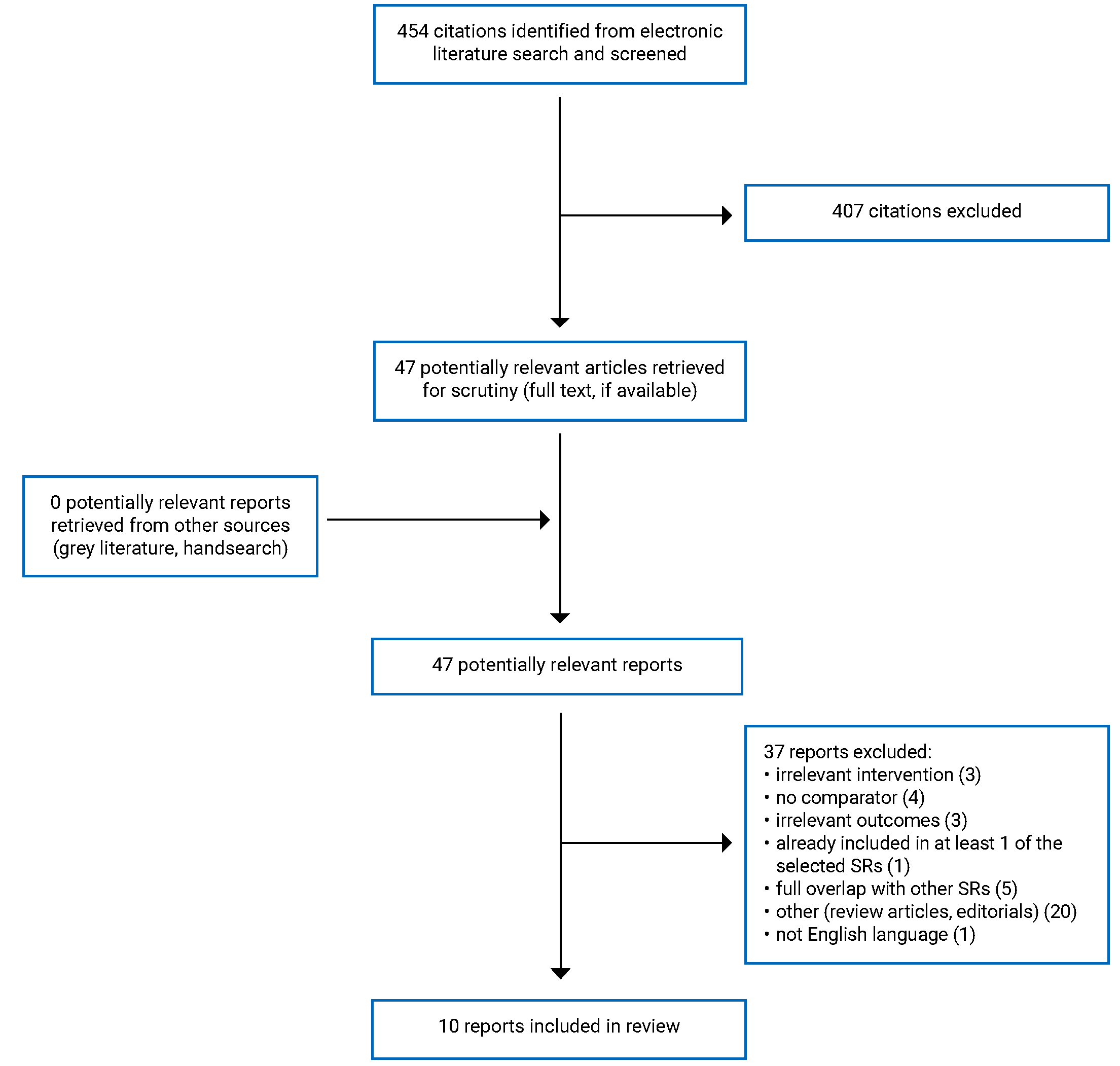
A total of 454 citations were identified in the literature search. Following screening of titles and abstracts, 407 citations were excluded and 47 potentially relevant reports from the electronic search were retrieved for full-text review. A grey literature search found no potentially relevant publications for full-text review. Of these potentially relevant articles, 37 publications were excluded for various reasons, and 10 publications met the inclusion criteria and were included in this report. These comprised 8 SRs, 1 randomized controlled trial (RCT), and 1 economic evaluation. The PRISMA16 flow chart of the study selection is presented in Appendix 1.
Additional references of potential interest are provided in Appendix 6.
Summary of Study Characteristics
Eight SRs,17-24 1 RCT,25 and 1 economic evaluation26 were included in this report.
Two SRs18,24 also assessed other surgical interventions (e.g., robotic TME). For those 2 SRs,18,24 only the subset of primary studies meeting our inclusion criteria were presented here.
The prospective cohort study by Wasmuth et al. (2020)27 was of special interest to potential users of this review. However, it did not meet our inclusion criteria because it was a non-randomized study. However, the study27 was included in 1 SR24 that has been included in this report.
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
This report includes 8 SRs with meta-analyses17-24 that were published between 2021 and 2022. The relevant primary studies in the SRs ranged between 7 and 26. These primary studies were either parallel RCTs or comparative non-randomized studies (prospective or retrospective cohort studies and matched case-control studies). The latest literature search dates were between January 2019 and November 2021.
There was some overlap in the primary studies included in the SRs; the degree of overlap is summarized in Appendix 5.
The RCT25 was an open-label, noninferiority trial performed at 16 hospitals in 10 provinces in China from April 2016 to June 2021.
One economic evaluation26 by the National Institute for Health and Care Excellence National Guideline Alliance was included in this report. It was a cost-effectiveness analysis, using the public perspective (i.e., National Health Service [NHS] and personal and social services, both in the UK) with a lifetime horizon. A partitioned survival analysis approach was used for the analysis. The model considered 3 health states: alive without progressed disease, alive with progressed disease, and death. The clinical data were sourced from an evidence review conducted by the National Institute for Health and Care Excellence National Guideline Alliance, which was presented in the same publication.26 Cost data, including treatment costs and procedure costs, were obtained from the NHS. Equipment costs and quality-of-life estimates were obtained from the published literature. Several assumptions were used in the model. Estimate of occurrence of complication (e.g., surgical site infection) after TaTME procedure was assumed to be equivalent to that of the laparoscopic surgery. It was assumed that the complications have only short-term impact on quality of life. Patients were assumed to be treated with 6 cycles of systemic chemotherapy. For TaTME, the systemic chemotherapy and palliative costs were set to zero. The costs were based on 2016–2017 values (£), with a discount rate of 3.5%, and a willingness-to-pay (WTP) threshold of £20,000 per quality-adjusted life-year (QALY).26
Country of Origin
The first authors of the SRs were from Australia,20 China,17,22 Italy,18 Morocco,23 Russia,19 and South Korea.21,24 The primary studies in 7 SRs17,19-24 relevant to this report were conducted in Belgium, China, Denmark, France, Hong Kong, Italy, Poland, Russia, South Korea, Spain, Taiwan, the Netherlands, and the US. One SR18 did not report where the included studies were conducted.
The authors of the RCT25 were from China, where the trial was conducted.
The cost-effectiveness analysis was conducted in the UK.26
Patient Population
All 8 SRs17-24 included adults with rectal cancer. The RCT25 included adults with stages I to III rectal cancer.
The cost-effectiveness analysis26 was based on a clinical evidence review involving adults with non-metastatic rectal cancer.
Interventions and Comparators
The intervention was TaTME, and the comparator was LaTME in all 8 SRs17-24and the RCT.25 One SR24 also included 2 primary studies in which the comparator was LaTME or open TME.
The intervention of interest in the cost-effectiveness analysis26 was the TaTME procedure. The relevant comparators considered in the model were open surgery and laparoscopic surgery.
Outcomes
All 8 SRs17-24 and the RCT25 reported on various intraoperative, oncological, pathological, and postoperative outcomes.
Three SRs21-23 and the RCT25 reported on conversion to open procedure. Conversion in LaTME was defined as when the procedure was completed with open surgery.21,22 Conversion in TaTME was defined as a case in which the procedure was completed by open surgery or the TME was performed by the transanal approach, but the conversion occurred at the transabdominal phase.21
Intraoperative blood loss was investigated by 2 SRs21,22 and the RCT.25 Intraoperative complications were reported by 1 SR22 and the RCT,25 which defined intraoperative complications as unexpected surgical adverse events occurring during surgery (e.g., iatrogenic injury of the blood vessels, bowel, or other organs; hemorrhage; subcutaneous emphysema; and CO2 embolism). The length of hospital stay was reported by 3 SRs21-23 and the RCT.25 One SR21 reported readmission and reoperation.21 The RCT25 also reported secondary surgery.
One SR18 assessed local recurrence. Two SRs19,24 assessed both local and distant recurrence. Three SRs18,19,24 reported overall and disease-free survival.
Positive circumferential resection margin (CRM) or CRM involvement was investigated by 5 SRs17,18,21,23,24 and the RCT.25 Positive or clear CRM was defined as tumour-free at a distance of at least 1 mm from the mesorectal fascia.18,25 CRM length was reported by 2 SRs.21,22 Positive digital resection margin (DRM) was reported by 4 SRs17,18,21,23 and the RCT.25 DRM was defined as more than 1 mm between the closest tumour to the cut edge of the tissue.25 DRM length was reported by 2 SRs.21,22
Incompleteness of TME was assessed by 3 SRs17,21,24 and the RCT.25 Completeness or quality of TME was reported by 3 SRs18,22,23 and the RCT.25 The SR by Milone et al. (2022)18 assessed completeness of TME using the Quirke criteria.18 In the SR by Ziati et al. (2021)23 and the RCT,25 TME quality was considered complete or nearly complete. Harvested lymph nodes were reported by 4 SRs17,21-23 and the RCT.25
Two SRs19,20 assessed health-related quality of life using the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30). This is a validated scale that measures the quality of life in cancer patients by through 30 questions about 5 functional aspects (physical, role, emotional, cognitive, and social), 8 symptoms (fatigue, nausea, pain, dyspnea, loss of appetite, insomnia, constipation and diarrhea, financial strain), and global health status.18-20 Two SRs18,19 reported health-related quality of life using the EQ Visual Analogue Scale, which records the patient’s self-rated health and can be used as a quantitative measure of health outcome that reflects the patient’s own judgment. The complementary EQ-5D 3 Levels descriptive system comprises 5 dimensions: mobility, self-care, usual activities, pain and discomfort, and anxiety and depression. Each dimension has 3 levels: no problems, some problems, and extreme problems.19
Mortality was reported by 3 SRs18,21,22 and the RCT.25 Postoperative complications were reported by 4 SRs18,20,22,23 and the RCT.25 Two SRs18,22 used the Clavien-Dindo classification to rank postoperative complications, in which grades I and II were categorized as minor and grades III to V were classified as major complications. In the RCT,25 specific postoperative complications were diagnosed according to ether an image-based physical evaluation or obvious clinical evidence, and then were stratified by the Clavien-Dindo classification system.
The RCT25 also assessed incision infection and abdominal and pelvic infection. Anastomotic leakage was reported by 2 SRs18,23 and the RCT.25 Anastomotic leakage was defined as clinical evidence of a defect of the integrity of the intestinal wall at the anastomotic site or presence of a pelvic abscess adjacent to the anastomosis.25 Ureter or urethral injury was reported by 1 SR,21 and intestinal obstruction was reported by 1 SR21 and the RCT25
The outcome of the included economic evaluation26 was incremental cost-effectiveness ratio (ICER) reported as cost per QALY.
Summary of Critical Appraisal
Systematic Reviews
All included SRs17-24 were generally well conducted, but with several limitations. In all SRs,17-24 the review objective was clearly stated, a literature search was conducted using multiple databases, a list of the included primary studies was presented, the characteristics of the included studies were described, the risk of bias of included studies was assessed, and potential publication bias was investigated.
One SR18 had a published protocol and another SR21 registered its review in PROSPERO. No pre-published protocol was referenced in any of the other 6 SRs,17,19,20,22-24 and it is unclear if they had methods that were established a priori. Six SRs17,19-21,23,24 included clear statements regarding the use of Preferred Reporting Items for Systematic Reviews and Meta Analyses (PRISMA) statement standards for the conduct of the SRs and meta-analyses.16 One SR19 used Cochrane SR methodology.28
Study selection and data extraction was completed by 2 reviewers in 3 SRs.18,19,24 Five SRs17,20-23 did not report how study selection was performed but did report that data extraction was performed independently by 2 reviewers. Therefore, the potential for errors in study selection cannot be ruled out in these reviews. A list of excluded studies was not presented in any of the included SRs.17-24 In the absence of justifications for excluding studies, it is unclear if the selection process captured all the relevant studies.
The SR by Li et al. (2022)17 reported on whether personnel, patients, and outcome assessors were blinded in the included RCTs. One of the 2 RCTs in the SR17 included blinded study personnel and participants; outcome assessors were not blinded in either trial.17 Unblinded studies are at an increased risk for bias.
Seven SRs17,19-24 assessed the quality of included non-randomized studies using the Newcastle-Ottawa scale, and 1 SR18 used the ROBINS-I (Risk Of Bias In Non-randomized Studies of Interventions). Three SRs17,20,22 assessed the quality of included RCTs with the Jadad scale, and 1 SR18 used the Cochrane RoB 2 tool. All SRs assessed between-study heterogeneity using I2 measure of inconsistency. Clear criteria for the selection of a random- or fixed-effect model for the meta-analyses were provided in 4 SRs.17-19,21,22,24 Random-effect meta-analyses were performed in 2 SRs20,23 with no clear rationale provided for the use of the random-effect model compared with the fixed-effect model.
Three SRs17,19,20 did not report the study designs of non-randomized trials (e.g., prospective observational study). Reporting of study designs was possibly inaccurate in another SR.18 For example, an included primary study identified by the original authors as a matched case-control study was described by 2 SRs as a retrospective study17 or a retrospective cohort study,18 suggesting reporting errors.
Four SRs19,21,23,24 were limited by including only non-randomized studies and no RCTs. In these SRs,19,21,23,24 all non-randomized studies were pooled in meta-analyses, regardless of study design (e.g., cohort, case-control). The other 4 SRs17,18,20,22 included a mix or RCTs and non-randomized studies. In these SRs,17,18,20,22 RCTs and non-randomized studies were pooled in meta-analyses. The Cochrane Handbook for Systematic Reviews of Interventions28 recommends that different observational study designs, or observational and randomized studies, should not be combined in a meta-analysis because this causes increased heterogeneity.28
In 7 SRs,17-22,24 the authors provided a statement on conflict of interest. In 1 SR,23 the authors did not declare whether they had any conflicts of interest.
Randomized Controlled Trial
The included RCT25 clearly reported the objective, interventions, and findings. The authors described the randomization method and reported baseline characteristics of all randomized participants, including those who dropped out. The participants were recruited at 16 centres, and the treatment sites were likely representative for receiving TME for rectal cancer. However, all participating centres were in China; therefore, their findings may not be generalizable to Canadian settings.
The primary outcomes were 3-year disease-free survival and 5-year overall survival.25 Sample size calculation was conducted based on the primary outcomes, and the required sample size was achieved at the desired 80% power to detect differences in treatment effect between intervention groups. However, as of the time of publication,25 data on disease-free survival or overall survival were expected at a future date and were not reported in the article.
The early analysis was pre-planned, and the reported outcomes were assessed with appropriate statistical tests. Blinding of patients, study personnel, and outcome assessors was not feasible due to the nature of the intervention. Interoperative and postoperative outcomes were assessed by the participating surgeons. Pathological outcomes were evaluated by 2 specialized pathologists in each participating centre in a blinded manner. All outcomes were reviewed by the Chinese Transanal Endoscopic Collaborative (group that launched the RCT).25
Economic Evaluation
The research question and the objective of the cost-effectiveness analysis26 were clearly described. The type of analysis, perspectives, and time horizon were described and were appropriate for the purpose. The interventions and comparators considered in the model were also appropriate, and the comparators were alternate approaches to the intervention of interest. A partitioned survival analysis model was used for the analysis. In a partitioned survival analysis model, patients belong in 1 of the mutually exhaustive health states, which is determined by overall survival curves. This decision modelling tool is commonly used for economic analyses of interventions for advanced cancers.29 The rationale for this model was described well. The health states were distinct and covered all probable scenarios after the treatment. The sources of data used in the model were clear. The clinical estimates were based on results from an SR of clinical effectiveness with detailed methodology. The clinical effectiveness SR had well-defined eligibility criteria and a comprehensive literature search. Meta-analyses were conducted to quantitatively synthesize the evidence. Cost data, including procedure costs and equipment costs, were sourced from reputable source. Results of the base-case analysis were clearly reported. Deterministic sensitivity analyses were conducted to identify which factors influenced the cost-effectiveness. A cost-effectiveness acceptability curve was presented. The conclusions of the analysis were presented well with appropriate caveats.
However, the analysis was not without limitations. Although a detailed critique of the partitioned survival analysis model is beyond the scope of this report, a major limitation of the model is that mutually exhaustive health states were assumed when, in reality, this may not be true.29 There was a lack of clinical data for TaTME for some outcomes (e.g., complications).26 The authors used assumptions to fill in these gaps. For example, occurrence of surgical site infection for TaTME was assumed to be equivalent to the laparoscopic approach. Complications were assumed to have only short-term effects on quality of life. The costs of systemic chemotherapy and palliative care were set to zero for TaTME. The validity of these assumptions in real-life settings were unclear. For the outcome overall survival, the effect estimate from the clinical review was not statistically significant because the confidence interval passed the point of no effect. However, a point estimate of the hazard ratio was used in the analytic model, which showed increased survival and reduced recurrence with TaTME. It is likely that TaTME was associated with lower QALYs and increased costs than what was considered in the model, since there could be no change in overall survival with TaTME. This could affect result of the analysis in favour of the comparators. Additionally, the authors conducted a sensitivity analysis by using only statistically significant results, which found that TaTME was no longer the optimal approach. Considering the assumptions and these limitations, the validity of the results may be low, and should be interpreted with caution. When reporting results of the analysis, numerical ICERs for each treatment option were not reported, which made independent assessment of the results challenging. It was unclear whether the WTP threshold was appropriate for the settings. Finally, the study was conducted in the UK from the perspective of the NHS.26 The generalizability of the findings to Canadian settings is unclear.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
There was some overlap in the primary studies that were included in the SRs.17-24 Therefore, to minimize duplication of reporting, meta-analyses for a clinical effectiveness outcome in 1 SR were not reported if all included studies were captured in a more recent or more comprehensive meta-analysis in another SR. If study outcomes were included in 1 of the meta-analyses, they were reported only in the pooled estimates (and not the individual study level results). Appendix 4 presents the main study findings.
Clinical Effectiveness of Transanal Total Mesorectal Excision for Adults With Rectal Cancer
Conversion to Open Procedure
Evidence from 2 SRs21,22 and the RCT25 indicated that TaTME was associated with a statistically significant lower rate of conversion to open procedure compared with LaTME. Heterogeneity among the included studies was zero in 1 SR21,22 and not important in the other SRs,21,22 indicating that the results were consistent across studies in both SRs.21,22
Intraoperative Blood Loss
Two SRs21,22 reported no statistically significant difference in intraoperative blood loss between the TaTME and LaTME groups. There was moderate to substantial heterogeneity in the analyzed studies. The RCT25 found that intraoperative estimated blood loss was comparable between TaTME and LaTME.
Interoperative Complications
One SR22 and the RCT25 reported that intraoperative complication rates were not significantly different between the TaTME and LaTME groups. There was no heterogeneity among the studies in the SR.22
Length of Hospital Stay
Two SRs21,22 and the RCT25 reported no significant differences in length of hospital stay between the TaTME and LaTME groups. Both SRs21,22 found substantial heterogeneity in hospital stay between studies included in the meta-analysis.
Readmission
One SR21 reported no statistically significant difference in readmissions between the TaTME and LaTME groups, and moderate heterogeneity.
Reoperation
One SR21 reported no statistically significant difference in reoperations between the TaTME and LaTME groups. There was no heterogeneity between included studies. The RCT25 reported that 4.4% of patients in the TaTME group and 3.5% of patients in the LaTME group required secondary surgery within 30 days after surgery because of anastomotic leakage, anastomotic bleeding, intestinal obstruction, abdominal or pelvic infection, or intraperitoneal bleeding.
Recurrence of Cancer
Two SRs19,24 found no statistically significant difference in local recurrence of cancer between the TaTME group and the open TME or LaTME groups. One of these SRs24 reported substantial heterogeneity in local recurrence. This heterogeneity was due to 1 prospective observational study (Wasmuth et al. [2020]). In contrast, another SR18 reported that local recurrence was statistically significantly lower in the TaTME group compared with the open TME or LaTME groups based on 1 included retrospective observational study.
Two SRs19,24 reported no statistically significant differences in distant cancer recurrence between the TaTME group and the open TME or LaTME groups.
Disease-Free Survival
Two SRs18,24 reported that disease-free survival was not statistically significantly different in the TaTME group compared with the open TME or LaTME groups.
Overall Survival
Two SRs18,24 reported no statistically significant differences in overall survival between the TaTME group and the open TME or LaTME groups.
Circumferential Resection Margin
Two SRs17,24 showed that the positive CRM was statistically significantly lower in the TaTME group compared with the LaTME group. A third SR18 reported that clear CRM was not statistically significantly different between the TaTME and LaTME groups. Li et al. (2022)17 performed a subgroup analysis by study design in their SR and found a statistically significant difference in positive CRM only when 2 included RCTs were pooled. In the subgroup analyses of the prospective observational studies and of the retrospective observational studies, there were no statistically significant differences in the positive CRM between the TaTME and LaTME groups. The RCT25 reported no statistically significant difference in positive CRM between the TaTME and LaTME groups.
Two SRs21,22 reported no statistically significantly difference in length of CRM between the TaTME group and the open TME or LaTME groups, but there was notable heterogeneity.
Distal Resection Margin
Three SRs17,18,23 and the RCT25 reported that positive DRM was not statistically significantly different between the TaTME and LaTME groups.
Two SRs21,22 reported no statistically significant differences in length of DRM between TaTME and open TME or LaTME. One SR21 reported high heterogeneity among studies, and the other SR22 reported no heterogeneity.
Completeness or Quality of Mesorectal Excision
One SR17 reported the findings for mesorectum incompleteness in 3 different ways. Two different effect estimates were reported in the text and in a forest plot. Although both effect estimates indicated a significant difference in favour of TaTME compared with LaTME, the authors reported narratively that there was no significant difference in the mesorectum incompleteness rate observed between the TaTME and LaTME groups.17 Therefore, the results from this SR are unclear.17
Findings from the other SRs18,21,24 found no statistically significant differences in completeness of mesorectum between the TaTME and LaTME groups. The RCT25 reported no statistically significant difference in specimen quality of mesorectum excision between the TaTME and LaTME groups. The quality of the TME specimen was complete and nearly complete in all cases; none of the patients in the trial had an incomplete TME.25
Harvested Lymph Nodes
One SR17 found no significant difference in the number of harvested lymph nodes observed between the TaTME and LaTME groups; however, the heterogeneity was substantial.17 One cohort study in another SR21 and the RCT25 also reported no statistically significant differences in number of harvested lymph nodes between the TaTME and LaTME groups.
Health-Related Quality of Life
Three SRs18-20 reported that overall or global measures of health-related quality of life were not statistically significantly different between the TaTME and LaTME groups.
Mortality
Perioperative mortality was assessed in 1 SR,22 and was found to be not statistically significantly different between the TaTME and LaTME groups. There was no heterogeneity in the analyzed studies.
The results from 2 SRs18,21 and the RCT25 indicated no statistically significant differences in 30-day post-operative mortality between the TaTME and LaTME groups. The RCT25 reported that 1 patient in the TaTME group died of septic shock as a result of abdominal infection, and 1 patient in the LaTME group died of a cerebrovascular accident.25 One SR21 reported that 1 patient in the TaTME group died and 3 patients in the LaTME group died (causes of death were not reported).
Postoperative Complications
One SR18 found no statistically significant difference in minor complications assessed 30 days post-surgery between the TaTME and LaTME groups. Two SRs21,22 reported no statistically significant differences in major complications between the TaTME and LaTME groups, and another SR23 also found no statistically significant differences between TaTME in LaTME in postoperative complications. There was no heterogeneity in studies analyzed in 3 SRs.18,21,22 In the RCT,25 there was no statistically significant difference in the overall postoperative complication rate between the TaTME and LaTME groups. Based on the Clavien-Dindo classification of surgical complications, the severity of surgical complications between the 2 groups did not differ.25 Another SR20 found no statistically significant difference in complications requiring surgery between the TaTME and LaTME groups.
Anastomotic Leak
Two SRs18,21 and the RCT25 found no statistically significant difference in the rate of anastomotic leakage between the TaTME and LaTME groups.
Infection
The RCT25 reported no statistically significant differences in the rates of incisional infection and abdominal or pelvic infection between the TaTME and LaTME groups.
Urethral Injury
One SR21 found no statistically significant difference in ureter or urethral injury between the TaTME and LaTME groups.
Intestinal Obstruction
One SR21 reported no statistically significant difference in intestinal obstruction between the TaTME and LaTME groups. However, the RCT25 reported a statistically significantly lower rate of intestinal obstruction in the TaTME group compared with the LaTME group.
Cost-Effectiveness of Transanal Total Mesorectal Excision for Adults With Rectal Cancer
The authors of the cost-effectiveness analysis26 reported that, at a WTP threshold of £20,000 per QALY, TaTME was the most cost-effective (dominant) option compared with open surgery and laparoscopic surgery. TaTME was the least expensive option, with the highest QALY among all compared approaches in the base-case analysis. The numerical ICERs of each approach were not reported. The authors also noted that these results were based on the effect estimate for overall survival associated with TaTME, which was obtained from their clinical effectiveness review.26 However, the estimates were not statistically significant. When a sensitivity analysis using only statistically significant estimates was conducted, laparoscopic surgery was found to be the most cost-effective approach. In most other scenarios, TaTME remained the most cost-effective option.
The cost-effectiveness acceptability curve of the base-case analysis showed that that TaTME was the most cost-effective option compared with open surgery and laparoscopic surgery at various WTP thresholds. At a WTP threshold of £20,000 per QALY, the probability of TaTME being the cost-effective option was 86% compared with 2% and 13% for open surgery and laparoscopic surgery, respectively.26
Limitations
The majority of the clinical effectiveness evidence supporting the SRs was derived from retrospective observational studies with few participants (less than 100). Of a total of 46 primary studies in the 8 SRs,17-24 3 were RCTs, whereas the rest were non-randomized studies. The limited number of RCTs included reduces the quality of evidence because observational studies have inherent biases due to potential confounding factors, such as sex, body mass index, American Society of Anesthesiologists classification, tumour stage, distance from anal verge, and neoadjuvant chemoradiotherapy.
Due to the nature of the intervention, blinding was generally not feasible in all primary studies. Lack of blinding particularly effects subjective outcomes, such as health-related quality of life.
Heterogeneity in pooled analyses was reported for several outcomes (interoperative blood loss, hospital stay, local recurrence, CRM length, DRM length, harvested lymph nodes). Heterogeneity may have resulted from the pooling of different study designs, different numbers of surgeons who performed the procedures, different experiences with the surgical procedures, and variable lengths of follow-up. Inconsistency causes uncertainty in the findings presented in the SRs. Also, the evidence in the SRs focused on short-term rather than long-term outcomes.
TaTME was developed as a surgical alternative for specific subgroups of patients (e.g., patients with obesity; male patients with bulky distal tumours; patients with a narrow pelvis).4,30 However, evidence on using TaTME in these subgroups of patients was not available in the studies included in this report. Inconsistency between the results of 3 SRs17,18,24 and the RCT25 was observed for positive CRM. There was also inconsistency between the results of 1 SR21 and the RCT25 for intestinal obstruction following surgery. These conflicting findings may present challenges to interpretation. However, none of the results were in direct opposition to each other (i.e., a statistically significant positive association compared with a statistically significant negative association).
The cost-effectiveness evidence was based on 1 economic evaluation26 with several limitations as detailed in the Critical Appraisal section. There was uncertainty about the validity of increased survival with TaTME because the clinical data supporting the analysis were inconclusive, and assumptions regarding complications and costs of TaTME were unclear. Overall, the evidence from the cost-effectiveness analysis was uncertain.
None of the SRs, primary studies within the SRs,17-24 RCT,25 or economic evaluation26 were conducted by authors in Canada. It is unclear if the clinical effectiveness and cost-effectiveness findings are generalizable to Canadian clinical practice.
Conclusions and Implications for Decision- or Policy-Making
This report was based on 8 SRs,17-24 1 RCT,25 and 1 economic evaluation26 that explored the clinical effectiveness of TaTME compared with LaTME or open TME for adults with rectal cancer. The results of the SRs17-24 were based on many moderate- to high-quality non-randomized studies and some moderate- to high-quality RCTs (as assessed by the review authors). The clinical effectiveness of TaTME was primarily compared with LaTME, which reflects the current shift from the conventional open approach to the minimally invasive laparoscopic technique.17,20,21,26,31
Overall, the evidence regarding clinical effectiveness suggests that TaTME has lower rates of conversion21,22 and positive CRM17,21,22,24 compared with LaTME or open TME. For other assessed outcomes, the evidence indicates that TaTME was as clinically effective and safe compared with LaTME or open TME for patients with rectal cancer. Specifically, no statistically significant differences were found between TaTME and LaTME or open TME for intraoperative blood loss,21,22 intraoperative complications,22,25 hospital stay,21,22,25 readmission,21 reoperation,21,25 local and distant recurrence,19,24 overall and disease-free survival,18,19,24 CRM length,21,22 DRM,17,18,22,23,25 DRM length,21,22 completeness or quality of TME,18,21-25 harvested lymph nodes,17,21,25 global health-related quality of life,18-20 mortality,18,21,22,25 postoperative complications,18,20-22,25 and anastomotic leakage.21,22,24
TaTME may be cost-effective compared with open TME and LaTME. However, the only available evidence was from 1 economic evaluation26 based in the UK, and the findings were uncertain.
Based on the available evidence, it may be reasonable to expect that TaTME may be an effective and safe alternative to LaTME and/or open TME for the treatment of patients with rectal cancer. However, the limitations of the included literature should be considered when interpreting the findings of this report. Large-scale clinical trials with longer follow-up periods are required to better determine the effect of TaTME on long-term outcomes. Future economic evaluations conducted from the Canadian perspective may be helpful to further inform clinical and policy decisions.
References
1.Brenner DR, Poirier A, Woods RR, et al. Projected estimates of cancer in Canada in 2022. CMAJ. 2022;194(17):E601-E607. PubMed
2.Vennix S, Pelzers L, Bouvy N, et al. Laparoscopic versus open total mesorectal excision for rectal cancer. Cochrane Database Syst Rev. 2014(4).
3.Prashad A, Mitchell M, Argent-Katwala M, Daly C, Earle CC, Finley C. Pan-Canadian standards for cancer surgery. Can J Surg. 2019;62(4 Suppl 3):S171. PubMed
4.Bleday R, Shibata D. Radical resection of rectal cancer. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2021: http://www.uptodate.com. Accessed 2022 Oct 20.
5.Delibegovic S. Introduction to total mesorectal excision. Medical Archives. 2017;71(6):434. PubMed
6.De Rosa M, Wynn G, Rondelli F, Ceccarelli G. Transanal total mesorectal excision for rectal cancer: State of the art. Mini-invasive Surgery. 2020;4:34.
7.Surgery Center of Anchorage. Open Surgery vs Laparoscopic Surgery: Which Is the Best Procedure? 2022; https://www.farnorthsurgery.com/blog/open-surgery-vs-laparoscopic-surgery#:~:text=Difference%20between%20Open%20Surgery%20and%20Laparoscopic%20Surgery&text=Open%20surgery%20is%20a%20traditional,of%20one%2Dquarter%20or%20less. Accessed 2022 Oct 19.
8.Kuhry E, Schwenk W, Gaupset R, Romild U, Bonjer J. Long-term outcome of laparoscopic surgery for colorectal cancer: a cochrane systematic review of randomised controlled trials. Cancer Treat Rev. 2008;34(6):498-504. PubMed
9.Carr BM, Lyon JA, Romeiser J, Talamini M, Shroyer ALW. Laparoscopic versus open surgery: a systematic review evaluating Cochrane systematic reviews. Surg Endosc. 2019;33(6):1693-1709. PubMed
10.Neiva GIBdM, da Silva P, Soares FA, et al. Tansanal total mesorectal excision (TaTME): systematization and mediated results in 10 patients. Journal of Coloproctology (Rio de Janeiro). 2020;40(1):50-55.
11.Saur N, Bleier J. Transanal endoscopic surgery (TES). In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2020: https://www.uptodate.com. Accessed 2022 Oct 13.
12.Transanal Total Mesorectal Excision for Adult Patients with Rectal Cancer: A Review of Clinical Effectiveness and Cost-Effectiveness. Ottawa (ON): CADTH; 2020: https://www.cadth.ca/transanal-total-mesorectal-excision-adult-patients-rectal-cancer-review-clinical-effectiveness-and. Accessed 2022 Oct 13.
13.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
14.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
15.Higgins JPT, Green S, editors. Figure 15.5.a: Drummond checklist (Drummond 1996). Cochrane handbook for systematic reviews of interventions. London (GB): The Cochrane Collaboration; 2011: http://handbook-5-1.cochrane.org/chapter_15/figure_15_5_a_drummond_checklist_drummond_1996.htm. Accessed 2022 Oct 24.
16.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
17.Li L, Wang T, Hu D, et al. Pathologic outcomes of transanal versus laparoscopic total mesorectal excision for rectal cancer: a meta-analysis of 26 studies. Int J Colorectal Dis. 2022;37(5):1063-1071. PubMed
18.Milone M, Adamina M, Arezzo A, et al. UEG and EAES rapid guideline: Systematic review, meta-analysis, GRADE assessment and evidence-informed European recommendations on TaTME for rectal cancer. Surg Endosc. 2022;36(4):2221-2232. PubMed
19.Alimova I, Chernyshov S, Nagudov M, Rybakov E. Comparison of oncological and functional outcomes and quality of life after transanal or laparoscopic total mesorectal excision for rectal cancer: a systematic review and meta-analysis. Tech Coloproctol. 2021;25(8):901-913. PubMed
20.Choy KT, Yang TWW, Prabhakaran S, Heriot A, Kong JC, Warrier SK. Comparing functional outcomes between transanal total mesorectal excision (TaTME) and laparoscopic total mesorectal excision (LaTME) for rectal cancer: a systematic review and meta-analysis. Int J Colorectal Dis. 2021;36(6):1163-1174. PubMed
21.Kwon SH, Joo YI, Kim SH, et al. Meta-analysis of transanal versus laparoscopic total mesorectal excision for rectal cancer: a 'New Health Technology' assessment in South Korea. Ann Surg Treat Res. 2021;101(3):167-180. PubMed
22.Ren J, Luo H, Liu S, Wang B, Wu F. Short- and mid-term outcomes of transanal versus laparoscopic total mesorectal excision for low rectal cancer: a meta-analysis. Ann Surg Treat Res. 2021;100(2):86-99. PubMed
23.Ziati J, Souadka A, Benkabbou A, et al. Transanal total mesorectal excision for patients with rectal cancer: a Systematic review and meta-analysis. Gulf J Oncolog. 2021;1(35):66-76. PubMed
24.Moon JY, Lee MR, Ha GW. Long-term oncologic outcomes of transanal TME compared with transabdominal TME for rectal cancer: a systematic review and meta-analysis. Surg Endosc. 2022;36(5):3122-3135. PubMed
25.Liu H, Zeng Z, Zhang H, et al. Morbidity, Mortality, and Pathologic Outcomes of Transanal Versus Laparoscopic Total Mesorectal Excision for Rectal Cancer Short-term Outcomes From a Multicenter Randomized Controlled Trial. Ann Surg. 2022;11:11. PubMed
26.National Guideline Alliance part of the Royal College of Obstetricians Gynaecologists. Optimal surgical technique for rectal cancer: Colorectal cancer (update). Evidence review C3. London (UK): National Institute for Health and Care Excellence; 2020: https://www.ncbi.nlm.nih.gov/books/NBK559937/. Accessed 2022 Oct 24.
27.Wasmuth HH, Faerden AE, Myklebust TA, et al. Transanal total mesorectal excision for rectal cancer has been suspended in Norway. Br J Surg. 2020;107(1):121-130. PubMed
28.Cochrane handbook for systematic reviews of interventions. In: Higgins JP, Thomas J, Chandler J, et al., eds. version 6.3 (updated February 2022). Chichester (UK): John Wiley & Sons; 2022: https://training.cochrane.org/handbook. Accessed 2022 Oct 24.
29.Woods B SE, Palmer S, Latimer N, Soares M. . Technical Support Document 19. Partitioned Survival Analysis for Decision Modelling in Health Care: A Critical Review. Sheffield (UK): NICE Decision Support Unit; 2017: https://www.sheffield.ac.uk/nice-dsu/tsds/partitioned-survival-analysis. Accessed 2022 Oct 20.
30.Rouanet P, Mourregot A, Azar CC, et al. Transanal endoscopic proctectomy: an innovative procedure for difficult resection of rectal tumors in men with narrow pelvis. Dis Colon Rectum. 2013;56(4):408-415. PubMed
31.Lo Bianco S, Lanzafame K, Piazza CD, Piazza VG, Provenzano D, Piazza D. Total mesorectal excision laparoscopic versus transanal approach for rectal cancer: A systematic review and meta-analysis. Ann Med Surg (Lond). 2022;74:103260. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Li et al. (2022)17 China Funding source: Natural Science Foundation of Gansu Province, Gansu Health Scientific Research Project, Fundamental Research Funds for the Central Universities, Institute Scientific Research Fund Project/Youth Project | Objective: To identify the pathologic outcomes provided by TaTME compared with LaTME in the treatment of low or middle rectal cancer treatment. Databases searched: PubMed, Cochrane Library, Embase Last search date: November 1, 2021 Relevant included studies: 26 studies (2 RCTs, 24 NRS) | Inclusion criteria: RCTs, prospective or retrospective studies comparing TaTME with LaTME in patients who underwent rectal cancer surgery Excluded: Reviews, case reports, noncomparable data, and repeat publications | Intervention: TaTME Comparator: LaTME | Outcomes: CRM, DRM, mesorectum incompleteness, harvested lymph nodes |
Milone et al. (2022)18 Italy Funding source: European Association for Endoscopic Surgery | Objective: To develop evidence-informed recommendations on the use of TaTME vs. laparoscopic in patients with rectal cancer. Databases searched: Medline, Embase, OpenGrey Last search date: January 30, 2021 Relevant included studies: 16 studies (1 RCT, 15 NRS) | Inclusion criteria: Adult patients with adenocarcinoma of the rectum Excluded: Single incision and open surgery | Intervention: TaTME Comparator: LaTME | Outcomes: Recurrence, survival, CRM, DRM, TME completeness, quality of life, mortality, complications, anastomotic leak |
Moon et al. (2022)24 South Korea Funding source: Fund of Biomedical Research Institute, Jeonbuk National University Hospital | Objective: To conduct a systematic review and meta-analysis to evaluate survival outcomes and recurrence rates of TaTME compared with transabdominal TME in patients with rectal cancer. Databases searched: PubMed, Cochrane CENTRAL, Embase Last search date: April 7, 2020 Relevant included studies: 10 NRS | Inclusion criteria: Patients with rectal cancer who were treated with TaTME or transabdominal TME (all surgical modalities such as open, laparoscopic, and robotic surgery) Excluded: Patients with stage IV or recurred rectal cancer; patients who received abdominoperineal resection; had no extractable data and authors were unavailable to provide additional information; case series with < 10 patients | Intervention: TaTME Comparator: LaTME or Open TME | Outcomes: Recurrence, survival, CRM, TME incompleteness, anastomotic leak |
Alimova et al. (2021)19 Russia Funding source: NR | Objective: To compare long-term oncological and functional outcomes after TaTME and LaTME for rectal cancer. Databases searched: PubMed, Cochrane Database of Systematic Reviews Last search date: February 8, 2020 Relevant included studies: 10 NRS | Inclusion criteria: Patients diagnosed with rectal cancer Excluded: Lack of sufficient data or outcomes of interest; duplicate publication; abdominoperineal resections; and non-comparative studies, reviews, meta-analyses, letters, case reports or conference abstracts | Intervention: TaTME Comparator: LaTME | Outcomes: Recurrence, survival, length of hospital stay, quality of life |
Choy et al. (2021)20 Australia Funding source: NR | Objective: To assess comparative functional outcomes following TaTME and LaTME, with a focus on anorectal and genitourinary outcomes. Databases searched: PubMed, Embase, MEDLINE, Cochrane Library Last search date: August 31, 2020 Relevant included studies: 7 studies (1 RCT, 6 NRS) | Inclusion criteria: NR Excluded: Non-English studies, letters, perspectives, conference abstracts, or studies focusing on pediatric patients were excluded | Intervention: TaTME Comparator: LaTME | Outcomes: Quality of life, complications |
Kwon et al. (2021)21 South Korea Funding source: National Evidence-based Healthcare Collaborating Agency in South Korea | Objective: To compare the safety and efficacy between TaTME and LaTME Databases searched: Medline, Embase, Cochrane Library, Korean databases (KoreaMed, KMbase, KISTI, KISS, RISS) Last search date: August 31, 2019 Included studies: 16 NRS | Inclusion criteria: Patients diagnosed with rectal cancer; cohort studies Excluded: Reviews, letters, editorials, commentaries, conference abstract, and clinical reports; studies with sample size < 20 in each group; languages other than English; inappropriate data; duplicate patient series; inadequate technique for intervention or comparator; and nonhuman research | Intervention: TaTME Comparator: LaTME | Outcomes: Conversion to open procedure, intraoperative blood loss, length of hospital stay, readmission, reoperation, CRM, DRM, TME incompleteness, harvested lymph nodes, mortality, complications, anastomotic leak, urethral injury, internal obstruction |
Ren et al. (2021)22 China Funding source: Medical Science and Technology Research Fund of Guangdong Province, China | Objective: To conduct a meta-analysis of TaTME and LaTME comparative studies for low rectal cancer to provide a basis to evaluate the safety and efficacy of the procedure. Databases searched: China National Knowledge Infrastructure, Chinese BioMedical Database, PubMed, Embase, Cochrane CENTRAL, Wanfang Database Last search date: May 2020 Relevant included studies: 10 studies (2 RCTs, 8 NRS) | Inclusion criteria: Patients diagnosed with low rectal cancer (distance of tumour from anal verge < 7 cm) Excluded: Studies with benign lesions only, or no distinct group of malignant rectal tumour, studies on other surgical methods, studies in languages other than English or Chinese, and correspondences, letters, case reports, reviews, meta-analysis, and conference abstracts | Intervention: TaTME Comparator: LaTME | Outcomes: Conversion to open procedure, intraoperative blood loss, length of hospital stay, recurrence, CRM, DRM, TME quality, harvested lymph nodes, mortality, complications, anastomotic leak, internal obstruction |
Ziati et al. (2021)23 Morocco Funding source: NR | Objective: To evaluate short-term oncological and perioperative outcomes of TaTME compared to LaTME for rectal cancer. Databases searched: Medline (PubMed) Last search date: January 1, 2019 Relevant included studies: 12 NRS | Inclusion criteria: Patients who were diagnosed with rectal cancer based on pathological examination Excluded: Duplicate or repeat studies, meta-analysis, non-comparative studies, conference abstracts, expert opinions, editorials, letters and commentaries, nonhuman research, interventions on cadavers, reports on robotic TaTME, articles with other languages than French and English, no TME group as a control, studies with benign lesions only, studies on transanal endoscopic microsurgery or other local excision | Intervention: TaTME Comparator: LaTME | Outcomes: Conversion to open procedure, length of hospital stay, CRM, DRM, TME completeness, harvested lymph nodes, complications, anastomotic leak |
CENTRAL = Central Register of Controlled Trials; CRM = circumferential resection margin; DRM = distal resection margin; LaTME = laparoscopic total mesorectal excision; NR = not reported; NRS = non-randomized studies; TaTME = transanal total mesorectal excision; TME = total mesorectal excision.
Table 3: Characteristics of the Included Primary Clinical Study
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Liu et al. (2022)25 China Funding source: Sun Yat Yat-sen University Clinical Research 5010 Program, Science and Technology Projects in Guangzhou, China Postdoctoral Science Foundation, Guangdong Basic and Applied Basic Research Foundation | Study design: RCT Setting: 16 centres in 10 Chinese provinces Objective: To assess the surgical safety and oncological outcomes of TaTME vs LaTME in patients with rectal cancer | Inclusion criteria: Patients aged 18 to 75 years; had an ASA class I-III; had clinical stage I-III rectal adenocarcinoma below peritoneal reflection based on preoperative imaging; and were expected to undergo a sphincter-sparing procedure via TME principles for curative intent. Excluded: Patients who had T1 cancers that could be locally resected; had CRM involvement as indicated by preoperative MRI; had tumours with ingrowth in the internal sphincter or levator ani; and had contraindications for surgery. Number of patients: TaTME, N = 544; LaTME; N = 545 Median age (IQR), years: TaTME = 58 (50 to 67); LaTME = 60 (52 to 67) % Female: TaTME = 34; LaTME = 39. | Intervention: TaTME Comparator: LaTME | Outcomes: Conversion to open procedure, intraoperative blood loss, hospital length of stay, CRM, DRM, TME completeness, harvested lymph nodes, mortality complications, infection, anastomotic leak Follow-up: 5 yearsa |
ASA = American Society of Anesthesiologists; CRM = circumferential resection margin; DRM = distal resection margin; LaTME = laparoscopic total mesorectal excision; IQR = inter-quartile range; RCT = randomized controlled trial; TaTME = transanal total mesorectal excision; TME = total mesorectal excision.
aAt the time of publication, data on 3-year and 5-year outcomes was not yet available. The publication reported on initial study findings.
Table 4: Characteristics of Included Economic Evaluation
Study citation country, funding source | Type of analysis, time horizon, perspective | Population characteristics | Intervention and comparator(s) | Approach | Source of clinical, cost, and utility data used in analysis | Main assumptions |
|---|---|---|---|---|---|---|
NICE NG151 Evidence Review26 UK Funding source: NICE | Analysis: cost-effectiveness analysis Time horizon: Lifetime (36 years) Perspective: public health care payer perspective (NHS and Personal Social Services) WTP threshold: £20,000 per QALY | Adults with non-metastatic rectal cancer. Population data were obtained from the clinical evidence review of 28 studies | Relevant intervention: TaTME Comparator: Open surgery, laparoscopic resection, robotic surgery Outcomes: overall survival, local recurrence, complications | Partitioned survival analysis approach Discount rate 3.5% | Clinical data were sourced from the evidence review component of the report. Cost data were sourced from NHS reference costs 2016/17 Equipment costs from another cost-effectiveness analysis of prostate cancer (Ramsay et al., 2012) QoL estimates were obtained from Rao et al., 2017 | Complication estimate of TaTME was assumed to be equivalent to laparoscopic the approach. Estimate on local recurrence of TaTME was assumed as RR = 0.54 due to lack of clinical evidence. Complications were assumed to have a short impact on QoL and morbidity. Patients were assumed to be treated with 6 cycles of systemic chemotherapy. For TaTME, the systemic chemotherapy and palliative costs were set to zero |
NHS = National Health Service; NICE = National Institute of Health and Care Excellence; NG = NICE guidance; NR = not reported; QALY = quality-adjusted life-years; QoL = quality of life; RR = relative risk; TaTME = transanal total mesorectal excision; WTP = willingness to pay threshold.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 5: Strengths and Limitations of Systematic Reviews Using AMSTAR 213
Strengths | Limitations |
|---|---|
Li et al. (2022)17 | |
The research question and inclusion criteria included the components of PICO. The searches were conducted in multiple databases, key search terms were provided, and additional references were search for in identified paper bibliographies. Adequate details about the included studies were described. All the data were extracted by 2 investigators independently. Disagreements in data extraction were determined by the third author. The Jadad scale was used to assess quality in individual RCTs, and the NOS was used for individual NRSs. Appropriate methods were used for meta-analyses Authors assessed the potential impact of quality in individual studies on the results of the meta-analyses. Authors included heterogeneity in their interpretation of the clinical effectiveness results of the review. Authors investigated possible publication bias using funnel plots. Authors reported their funding source and declared no conflicts of interest. | It is unclear if the review methods were established before the conduct of the review. Trial registries and grey literature were not searched. Authors did not provide justification for eligible study designs. The literature search strategy was not presented. It was unclear if study selection was performed by a sole reviewer or in duplicate. A list of excluded studies with justifications for exclusion was not provided. Follow-up for primary studies were not reported. Sources of funding for individual studies included in the review were not reported. Data from both RCTs and NRS were pooled in meta-analyses; and subgroup analysis by study design was performed for only 1 outcome (CRM). |
Milone et al. (2022)18 | |
The research question and inclusion criteria included the components of PICO. There was an explicit statement that the review methods were established before the conduct of the review. The searches were conducted in multiple databases, key search terms were provided. Open Grey and trial registries were also searched. Comprehensive literature search strategies and detailed methods were available in the Appendix files online. Study selection was completed by 2 reviewers independently and conflicts were resolved by discussion. Outcome data were extracted by 1 author and cross checked by a second author and disagreements were resolved by discussion. Adequate details about the included studies were described. The risk of bias assessment was performed using Cochrane ROB-2 for RCTs and the ROBINS-I for NRS. Appropriate methods were used for meta-analyses. Authors included inconsistency in their interpretation of the findings of the review. Authors reported their funding source. Authors declared no direct conflicts of interest. Indirect conflicts were documented and managed as per GIN standards. | Authors did not provide justification for eligible study designs. A list of excluded studies with justifications for exclusion was provided. Follow-up for primary studies were not reported. Sources of funding for individual studies included in the review were not reported. The authors reported that the included NRS were all cohort studies. However, the titles of some study publications indicated they were case-control studies. Therefore, the reporting of study designs may not be accurate. Data from 1 RCT and NRS were pooled in meta-analyses. It was not possible to check for small study effect either visually by inspecting the symmetry of the funnel plot or statistically by applying the Egger’s test because of an inadequate number of studies for most outcomes. |
Moon et al. (2022)24 | |
The research question and inclusion criteria included the components of PICO. The searches were conducted in multiple databases, key search terms were provided, and further articles were checked manually to retrieve additional studies. Adequate details about the included studies were described. Follow-up for primary studies were reported. Article titles and abstracts were screened, and full texts were independently reviewed by 2 reviewers. Any differences in judgment regarding inclusion were resolved through discussion between the reviewers. The NOS was used to assess methodological quality of the included NRSs. Appropriate methods were used for meta-analyses. Authors assessed the potential impact of quality in individual studies on the results of the meta-analyses. Authors included heterogeneity in their interpretation of the results of the review. Authors investigated publication bias using funnel plots. Authors reported their funding source and declared no conflicts of interest. | Although the authors refer to the study protocol, there is not reference to its publication or registration. Therefore, it is unclear if the review methods were established before the conduct of the review. Trial registries and grey literature were not searched. Authors did not provide justification for eligible study designs. The literature search strategy was not presented. NRS only were included, which could be biased due to inherent confounding. A list of excluded studies with justifications for exclusion was not provided. Sources of funding for individual studies included in the review were not reported. |
Alimova et al. (2021)19 | |
The research question and inclusion criteria included the components of PICO. The searches were conducted in multiple databases, key search terms were provided, and reference lists of selected publications were hand-searched for additional relevant studies. Study selection and data extraction was completed by 2 authors independently. Adequate details about the included studies were described. The NOS was used to evaluate the quality of the individual NRSs. Appropriate methods were used for meta-analyses. Authors assessed the potential impact of quality in individual studies on the results of the meta-analyses. Authors considered heterogeneity in their interpretation of the results of the review. Authors declared no conflicts of interest. | It is unclear if the review methods were established before the conduct of the review. Trial registries and grey literature were not searched. Authors did not provide justification for eligible study designs. The literature search strategy was not presented. NRSs only were included, which could be biased due to inherent confounding. A list of excluded studies with justifications for exclusion was not provided. Sources of funding for individual studies included in the review were not reported. Authors did not investigate publication bias as there were less than 10 studies in each analysis, in accordance with Cochrane guidelines. |
Choy et al. (2021)20 | |
The aim of the review was clearly stated. The interventions and outcomes clearly stated. The searches were conducted in multiple databases, key search terms were provided, and cited references in each retrieved paper were checked for relevance. Data extraction was performed independently by 2 reviewers. Any discrepancies were resolved by consensus and discussion between the 2 reviewers and the supervising author. Adequate details about the included studies were described. The Jadad scale was used to assess quality in individual RCTs, and the NOS was used for NRSs. Authors assessed the potential impact of quality in individual studies on the results of the meta-analyses. Appropriate methods were used for meta-analyses. Authors considered heterogeneity in their interpretation of the results. Authors investigated publication bias using Egger’s test. Authors declared no conflicts of interest. | It is unclear if the review methods were established before the conduct of the review. The inclusion criteria were not clearly stated. Trial registries and grey literature were not searched. Authors did not provide justification for eligible study designs. The literature search strategy was not presented. It was unclear if study selection was performed by a sole reviewer or in duplicate. Follow-up for primary studies were not reported. A list of excluded studies with justifications for exclusion was not provided. Sources of funding for individual studies included in the review were not reported. Data from both RCTs and NRSs were pooled in the meta-analyses. |
Kwon et al. (2021)21 | |
The research question and inclusion criteria included the components of PICO. An explicit statement was provided that the review methods were established before the conduct of the review (registered in PROSPERO). The searches were conducted in multiple databases and key search terms were provided. Data extraction was performed by 2 reviewers. Any disagreements were settled by consensus-based discussion between the 2 reviewers. Adequate details about the included studies were described. The NOS was used to assess methodological quality and risk of bias of the included studies. Appropriate methods were used for meta-analyses. Authors considered heterogeneity in their interpretation of the results of the review. Authors investigated publication bias using funnel plots. Authors reported their funding source and declared their conflicts of interest. | Trial registries and grey literature were not searched. Authors did not provide justification for eligible study designs. The literature search strategy was not presented. It was unclear if study selection was performed by a sole reviewer or in duplicate. Follow-up for primary studies were not reported. Sources of funding for individual studies included in the review were not reported. A list of excluded studies with justifications for exclusion was not provided. |
Ren et al. (2021)22 | |
The research question and inclusion criteria included the components of PICO. The searches were conducted in multiple databases and key search terms were provided. Data were extracted independently by 2 investigators and any disagreements were resolved by consulting another author. Adequate details about the included studies were described. The Jadad scale was used to assess quality in individual RCTs, and the NOS was used for individual NRS. Appropriate methods were used for meta-analyses. Authors considered heterogeneity in their interpretation of the results of the review. Authors investigated publication bias using funnel plots. Authors reported their funding source and declared no potential conflicts of interest. | It was unclear if the review methods were established before the conduct of the review. Trial registries and grey literature were not searched. Authors did not provide justification for eligible study designs. The literature search strategy was not presented. It was unclear if study selection was performed by a sole reviewer or in duplicate. Follow-up for primary studies were not reported. Sources of funding for individual studies included in the review were not reported. A list of excluded studies with justifications for exclusion was not provided. |
Ziati et al. (2021)23 | |
The research question and inclusion criteria included the components of PICO. The searches were conducted in MEDLINE (PubMed), and key search terms were provided. Data were extracted independently by 2 investigators. Adequate details about the included studies were described. The NOS was used to evaluate the quality in individual NRS. Appropriate methods were used for meta-analyses. Authors considered heterogeneity in their interpretation of the results of the review. Authors investigated publication bias using funnel plots. | It was unclear if the review methods were established before the conduct of the review. Trial registries and grey literature were not searched. Authors did not provide justification for eligible study designs. The literature search strategy was not presented. It was unclear if study selection was performed by a sole reviewer or in duplicate. NRSs only were included, which could be biased due to inherent confounding. Follow-up for primary studies were not reported. Sources of funding for individual studies included in the review were not reported. A list of excluded studies with justifications for exclusion was not provided. Authors did not report about funding for the systematic review The authors did not declare whether they had potential conflicts of interest. |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; CRM = circumferential resection margin; GIN = Guidelines International Network; NRS = non-randomized study; NOS = Newcastle-Ottawa Scale; NRS = non-randomized studies; PICO = population/participants, intervention, comparison, outcomes; ROB-2 = Risk of Bias tool for randomized trials, version 2; RCT = randomized controlled trial; ROBINS-I = Risk Of Bias In Non-randomized Studies - of Interventions.
Table 6: Strengths and Limitations of the Clinical Study Using the Downs and Black Checklist14
Strengths | Limitations |
|---|---|
Liu et al. (2022)25 | |
Reporting: The objective, outcomes, patient characteristics, interventions of interest, and main findings were clearly described. Estimates of the random variability (e.g., IQR, confidence intervals) in the data for the main outcomes were reported. Adverse events were reported. The number of randomized participants in each intervention group that withdrew from the study (9 vs. 10) and their reasons were reported (did not receive intervention as randomized because withdrew consent, underwent another operation, or found distant metastases intraoperatively). Actual P values were reported The number of participants in each intervention group excluded (5 vs. 2) from the modified intention-to-treat analysis and reasons for their exclusion were reported (postoperative pathology not rectal cancer, improper consent, patient refusal). External validity: Potential participants screened for enrolment and eligibility were verified by the CTESC Research Committee. Therefore, participants may be representative of the population from which they were recruited. The eligibility of the surgeons performing the interventions was reported. Internal validity – bias: The pathological outcomes were assessed by 2 specialized pathologists in each participating centres in a blinded manner. The outcomes used were accurate and assessed with appropriate statistical tests. All outcomes were reviewed by the CTESC Research committee every 3 months. Surgical practice was standardized in both intervention groups. Surgical quality control was maintained by using unedited videos of all surgeries. These videos were reviewed by the CTESC Research Committee and feedback was regularly provided to the study investigators. Internal validity – confounding: Participants were randomized to intervention groups using 1:1 randomization by a centralized web-based system with stratification by centre. Power: A sample size calculation was performed. The study was adequately powered at 80% to detect 3-year disease-free survival and 5-year overall survival. | External validity: The proportion of people who were asked to participate and agreed was not stated. Significantly higher rate of inter-sphincteric resection was found in patients who received TaTME, and the sacrifice of the internal sphincter could potentially have impaired functional outcomes. All participating centres were in China. Therefore, the findings may not be applicable to Canada. Internal validity – bias: The surgeons and patients were not masked to the treatment allocation; however, it is unlikely this would have been feasible due to the nature of the intervention. Other: Conflicts of interest were not reported. |
CTESC = Chinese Transanal Endoscopic Surgery Collaborative; IQR = inter-quartile range; TaTME = transanal total mesorectal excision.
Table 7: Strengths and Limitations of the Economic Evaluation Using the Drummond Checklist15
Strengths | Limitations |
|---|---|
NICE NG151 Evidence Review26 | |
The research question and its economic importance were stated. The type of analysis, perspectives, and time horizon were clearly stated and was appropriate. The interventions and comparators of interest were reported and were appropriate. The rationale for choosing comparators were clearly described. Sources of data used in the analysis were reported. The clinical effectiveness was estimated by the authors by conducting a systematic review and meta-analysis. The methods and results of the systematic review was included in the publication. Sources of cost and quality of life data were reported. They were appropriate and valid. The primary outcome measure was ICER (cost per QALY) which was appropriate for the research question. Currency and price data along with discount rates were reported. The analysis was done using a partitioned survival analysis model. The choice of model and its parameters were described. Deterministic sensitivity analysis was conducted in addition to the base-case analysis to evaluate the various factors included in the model. Incremental analysis was reported. A cost-effectiveness acceptability curve was provided. Conclusions drawn from the data and the results were reported clearly. They were accompanied by appropriate caveats. | The health states in the model are considered mutually independent in the partitioned survival analysis model. It is unclear whether the health states are mutually exclusive in real world settings. There were several assumptions for the analysis of TaTME vs laparoscopic or open surgery to cover for the missing data. For example, the authors assumed that occurrence of surgical site infection with TaTME would be equivalent to the laparoscopic approach. For TaTME, costs of systemic chemotherapy and palliative care were set to zero. The validity of these assumptions in real-life settings was unclear. There was a lack of clinical evidence for outcomes such as complications. The clinical review found that overall survival with TaTME was not significantly different from laparoscopic approach. However, a point estimate that showed increased survival with TaTME was considered in the economic model. Use of an estimate favouring TaTME when there is no difference could skew the results in favour of TaTME. When only statistically significant results were used in the sensitivity analysis, the results were no longer favourable to TaTME. Numerical ICERs for each approach were not reported. The study was conducted for UK settings. The generalizability of results to Canadian settings was unclear. |
HR = hazard ratio; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-years; TaTME = transanal total mesorectal excision.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 8: Summary of Findings by Outcome — Intraoperative Outcomes
Study citation | Study design | Outcome | Outcome results | Effect estimate (95% CI) | P value | |
|---|---|---|---|---|---|---|
TaTME group | LaTME group | |||||
Conversion to open procedure | ||||||
Kwon et al. (2021)21 | SR and MA (13 NRS) | Conversion rates, # events/total | 12 of 839 | 76 of 899 | RR = 0.19 (0.11 to 0.34) I2 = 0% | < 0.001 |
Ren et al. (2021)22 | SR and MA (2 RCTs, 8 NRS) | Conversion to open procedure. # events/total | 6 of 378 | 29 of 394 | OR = 0.25 (0.11 to 0.54) I2 = 9% | 0.001 |
Liu et al. (2022)25 | RCT | Conversion, # events/total (%) | 0 of 544 | 6 of 545 (1.1%) | NR | 0.03 |
Intraoperative blood loss | ||||||
Kwon et al. (2021)21 | SR and MA (6 NRS) | Interoperative blood loss | NR n = 203 | NR n = 259 | MD = −8.37 (−27.82 to 11.08) I2 = 48% | 0.40 |
Ren et al. (2021)22 | SR and MA (3 NRS) | Interoperative blood loss | NR n = 104 | NR n = 133 | MD = 13.99 (−16.39 to 44.37) I2 = 66% | 0.37 |
Liu et al. (2022)25 | RCT | Intraoperative blood loss, median mL (IQR) | 50 (40 to 100) | 50 (40 to 100) | NR | 0.29 |
Intraoperative complications | ||||||
Ren et al. (2021)22 | SR and MA (1 RCT, 6 NRS) | Intraoperative complications, # events/total | 17 of 255 | 9 of 242 | OR = 1.90 (0.84 to 12.46) I2 = 0% | 0.12 |
Liu et al. (2022)25 | RCT | Intraoperative complications, # events/total (%) | 26 of 544 (4.8%) | 33 of 545 (6.1%) | Difference = −1.3% (−4.2% to 1. 1.7%) | 0.42 |
Length of hospital stay | ||||||
Kwon et al. (2021)21 | SR and MA (12 NRS) | Hospital stay | NR n = 810 | NR n = 870 | MD = −0.51 (−1.43 to 0.41) I2 = 88% | 0.28 |
Ren et al. (2021)22 | SR (1 NRS) | Hospital stay, mean days (SD) | 10.3 (1.4) n = 39 | 9.6 (4.6) n = 64 | MD = −0.41 (−1.81 to 1.01) I2 = 79% | NSS |
Liu et al. (2022)25 | RCT | Postoperative hospital stay, median days (IQR) | 8.0 (7.0 to 10.0) | 9.0 (7.0 to 10.0) | NR | 0.22 |
Readmission | ||||||
Kwon et al. (2021)21 | SR and MA (7 NRS) | Readmission, # events/total | 100 of 646 | 112 of 680 | RR = 0.90 (0.70 to 1.15) I2 = 49% | 0.40 |
Reoperation | ||||||
Kwon et al. (2021)21 | SR and MA (5 NRS) | Reoperation, # events/total | 17 of 209 | 19of 243 | RR = 0.86 (0.45 to 1.61) I2 = 0% | 0.63 |
Liu et al. (2022)25 | RCT | Secondary surgery within 30 days after surgery, # events/total (%) | 24 of 454 (4.4%) | 19 of 455 (3.5%) | NR | NR |
CI = confidence interval; IQR = inter-quartile range; LaTME = laparoscopic total mesorectal excision; MA = meta-analysis; MD = mean difference; NR = not reported; NRS = non-randomized study; NSS = not statistically significant; OR = odds ratio; RCT = randomized controlled trial; RR = risk ratio; SD = standard deviation; SR = systematic review; TaTME = transanal total mesorectal excision.
Table 9: Summary of Findings by Outcome — Oncological outcomes
Study citation | Study design | Outcome | Outcome results | Effect estimate (95% CI) | P value | |
|---|---|---|---|---|---|---|
TaTME group | Open or LaTME group | |||||
Local recurrence | ||||||
Milone et al. (2022)18 | SR (1 NRS) | Local recurrence (Follow-up 3 years) | NR n = 710 | HR = 0.4 (0.23 to 0.69) | SS | |
Moon et al. (2022)24 | SR and MA (11 NRS) | Local recurrence; # events/total | 33 of 529 | 54 of 1,637 | RR = 1.12 (0.43 to 2.89) I2 = 66% | 0.82 |
Alimova et al. (2021)19 | SR and MA (7 NRS) | Local recurrence; # events/total | 4 of 188 | 7 of 217 | OR = 0.78 (0.22 to 2.79) I2 = 0% | 0.71 |
Distant recurrence | ||||||
Moon et al. (2022)24 | SR and MA (5 NRS) | Distant recurrence; # events/total | 15 of 163 | 20 of 166 | RR = 0.75 (0.40 to 1.41) I2 = 0% | 0.38 |
Alimova et al. (2021)19 | SR and MA (3 NRS) | Distant metastasis rate; # events/total (%) | 7of 98 (7.1%) | 13 of 98 (13.3%) | OR = 0.53 (0.19 to 1.47) I2 = 0% | 0.23 |
CI = confidence interval; HR = hazard ratio; LaTME = laparoscopic total mesorectal excision; MA = meta-analysis; NR = not reported; NRS = non-randomized study; OR = odds ratio; RR = risk ratio; SR = systematic review; SS = statistically significant; TaTME = transanal total mesorectal excision.
Table 10: Summary of Findings by Outcome — Survival
Study citation | Study design | Outcome | Outcome results | Effect estimate (95% CI) | P value | |
|---|---|---|---|---|---|---|
TaTME group | Open or LaTME group | |||||
Overall survival | ||||||
Milone et al. (2022)18 | SR (1 NRS) | Overall survival (Follow-up 3 years) | NR n = 710 | HR = 0.74 (0.53 to 1.03) | NSS | |
Moon et al. (2022)24 | SR and MA (6 NRS) | Overall survival (2 to 5 years), # events/total | 24 of 279 | 36 of 1,637 | RR = 0.65 (0.39 to 1.08) I2 = 0% | 0.10 |
Disease-free survival | ||||||
Milone et al. (2022)18 | SR (1 NRS) | Disease-free survival (Follow-up 3 years) | NR n = 710 | HR = 0.81 (0.65 to 1.02) | NSS | |
Moon et al. (2022)24 | SR and MA (6 NRS) | Disease-free survival (2 to 5 years), # events/total | 49 of 279 | 72 of 1,637 | RR = 0.75 (0.54 to 1.04) I2 = 0% | 0.09 |
CI = confidence interval; HR = hazard ratio; I2 = LaTME = laparoscopic total mesorectal excision; NR = not reported; NRS = non-randomized study; NSS = not statistically significant; RR = risk ratio; SR = systematic review; TaTME = transanal total mesorectal excision.
Table 11: Summary of Findings by Outcome — Pathological Outcomes
Study citation | Study design | Outcome | Outcome results | Effect estimate (95% CI) | P value | |
|---|---|---|---|---|---|---|
TaTME group | Open or LaTME group | |||||
CRM | ||||||
Li et el. (2022)17 | SR and MA (2 RCTs, 23 NRS) | Positive CRM, # events/total (All studies) | 76 of 1,642 | 111 of 1,890 | OR = 0.72 (0.53 to 0.98) I2 = 0% | 0.04 |
SR and MA (2 RCTs) | Positive CRM (Subgroup analysis by study design) | NR n = 82 | NR n = 82 | OR = 0.20 (0.05 to 0.74) I2 = 0% | 0.02 | |
SR and MA (4 prospective NRS) | NR n = 125 | NR n = 128 | OR = 2.70 (0.51 to 14.24) I2 = 0% | 0.24 | ||
SR and MA (19 retrospective NRS) | NR n = 1,435 | NR n = 1,680 | OR = 0.76 (0.55 to 1.04) I2 = 0% | 0.09 | ||
Milone et al. (2022)18 | SR and MA (1 RCT, 11 NRS) | Clear CRM (tumour-free CRM at a distance of at least 1 mm) | NR n = 1,909 | OR = 1.36 (0.88 to 2.08) | NSS | |
Moon et al. (2022)24 | SR and MA (8 NRS) | CRM involvement, # events/total | 15of 317 | 37 of 338 | RR = 0.48 (0.27 to 0.87) I2 = 0% | 0.001 |
Ziati et al. (2021)23 | SR (1 NRS) | Positive CRM, # events/total | 14 of 367 | 38 of 1,176 | OR = 1.19 (0.64 to 2.22) | NSS |
Liu et al. (2022)25 | RCT | Positive CRM # events/total (%) | 5 of 544 (0.9%) | 5 of 545 (0.9%) | NR | > 0.99 |
CRM length | ||||||
Kwon et al. (2021)21 | SR and MA (4 NRS) | Length of CRM | NR n = 147 | NR n = 127 | MD = 1.64 (−1.32 to 4.60) I2 = 97% | 0.28 |
Ren et al. (2021)22 | SR and MA (6 NRS) | CRM distance | NR n = 241 | NR n = 241 | MD = 1.67 (−0.42 to 3.75) I2 = 94% | 0.12 |
DRM | ||||||
Li et el. (2022)17 | SR and MA (2 RCTs, 13 NRS) | DRM involvement | 25 of 720 | 32 of 812 | OR = 0.82 (0.49 to 1.37) I2 = 0% | 0.44 |
Milone et al. (2022)24 | SR and MA (1 RCT, 7 NRSs) | Clear DRM (tumour-free DRM at a distance of at least 1 mm) | NR n = 1,521 | OR = 1.36 (0.88 to 2.08) | NSS | |
Liu et al. (2022)25 | RCT | Positive DRM, # events/total (%) | 2 of 544 (0.4%) | 4 of 545 (0.7%) | NR | 0.69 |
DRM length | ||||||
Kwon et al. (2021)21 | SR and MA (9 NRS) | Length of DRM | NR n = 339 | NR n = 394 | MD = 1.88 (−2.96 to 6.73) I2 = 87% | 0.45 |
Ren et al. (2021)22 | SR and MA (8 NRS) | DRM distance | NR n = 314 | NR n = 322 | MD = −0.09 (−0.22 to 3.75) I2 = 0% | 0.17 |
TME incompleteness | ||||||
Li et el. (2022)17 | SR and MA (2 RCTs, 5 NRS) | Mesorectum incompleteness, # events/total | 80 of 1,047 | 115 of 1,237 | OR = 0.56 (0.39 to 0.80)a I2 = 9%a OR = 0.64 (0.46 to 0.88)b I2 = 9%b | 0.001a 0.006b |
Moon et al. (2022)24 | SR and MA (8 NRS) | TME incompleteness, # events/total | 20 of 288 | 25 of 262 | RR = 0.88 (0.50 to 1.55) I2 = 0% | 0.66 |
Kwon et al. (2021)21 | SR and MA (11 NRS) | Incompleteness of mesorectum, # events/total | 45 of 382 | 39 of 354 | RR = 1.00 (0.70 to 1.45) I2 = 10% | 0.98 |
Liu et al. (2022)25 | RCT | Number of incomplete mesorectal excision, # events/total | 0 of 544 | 0 of 545 | NR | > 0.99 |
TME completeness or quality | ||||||
Milone et al. (2022)18 | SR and MA (1 RCT, 6 NRS) | Completeness of TME, assessed using the Quirke criteria | NR n = 1,407 | OR = 1.9 (0.81 to 4.44) | NSS | |
Ziati et al. (2021)23 | SR and MA (8 NRS) | Macroscopic quality of the mesorectum (complete and nearly complete), # events/total (%) | 321 of 356 (90.2%) | 290 of 344 (84.3%) | OR = 1.29 (0.61 to 2.70) I2 = 40% | 0.51 |
Liu et al. (2022)25 | RCT | Number of complete total mesorectum excision, # events/total (%) | 539 of 544 (99.1%) | 544 of 545 (99.1%) | NR | > 0.99 |
Harvested lymph nodes | ||||||
Li et el. (2022)17 | SR and MA (1 RCT, 15 NRS) | Harvested lymph nodes | NR n = 727 | NR n = 792 | OR = 0.43 (−0.97 to 1.83) I2 = 62% | 0.54 |
Kwon et al. (2021)21 | SR (1 NRS) | Harvested lymph nodes, mean (SD) | 22 (22) n = 40 | 19.5 (6.5) n = 20 | MD = 2.50 (−4.89 to 9.89) | NSS |
Liu et al. (2022)25 | RCT | Number of harvested lymph nodes, median (IQR) | 14 (10 to 19) | 15 (11 to 20) | NR | 0.15 |
CI = confidence interval; CRM = circumferential resection margin; DRM = digital resection margin; IQR = inter-quartile range; LaTME = laparoscopic total mesorectal excision; MA = meta-analysis; MCC = matched case-control; MD = mean difference; NR = not reported; NRS = non-randomized study; NSS = not statistically significant; OR = odds ratio; RCT = randomized controlled trial; RR = risk ratio; SR = systematic review; TaTME = transanal total mesorectal excision.
aFindings reported in the narrative text of the document.
bFindings reported in Figure 5 forest plot of mesorectum incompleteness risk ratios.
Table 12: Summary of Findings by Outcome — Health-Related Quality of Life
Study citation | Study design | Outcome | Outcome results | Effect estimate (95% CI) | P value | |
|---|---|---|---|---|---|---|
TaTME group | LaTME group | |||||
Alimova et al. (2021)19 | SR (1 NRSa) | EQ-5D-3L VAS, mean (95% CI) (Follow-up 6.6 months)b | 75.6 (69.9 to 81.3) n = 27 | 79.1 (72.8 to 85.3) n = 27 | NR | 0.40 |
EQ-5D-3L index, mean (95% CI) (Follow-up 6.6 months)b | 88.1 (83.1 to 93.1) n = 27 | 92.8 (88.2 to 97.4) n = 27 | NR | 0.159 | ||
Choy et al. (2021)20 | SR (1 NRSa) | EORTC QLQ C30 Global health status (0 to 100, higher score = better health-related QoL), mean | 79.6 n = 27 | 83.6 n = 27 | NR | 0.208 |
SR (1 NRSc) | 77.72 n = 49 | 79.86 n = 36 | NR | 0.625 | ||
SR (1 NRSd) | 73.96 n = 16 | 72.62 n = 15 | NR | 0.874 | ||
CI = confidence interval; EORTC QLQC30 = European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EQ-5D-3L = EQ-5D 3 Levels; LaTME = laparoscopic total mesorectal excision; NR = not reported; NRS = non-randomized study; TaTME = transanal total mesorectal excision; QoL = quality of life; SR = systematic review; VAS = visual analogue scale.
aVeltcamp et al. (2019a).
b.Length of follow-up was reported in the SR by Milone et. (2022).
cBjoern et al. (2019).
dMora et al. (2018).
Table 13: Summary of Findings by Outcome — Mortality
Study citation | Study design | Outcome | Outcome results | Effect estimate (95% CI) | P value | |
|---|---|---|---|---|---|---|
TaTME group | LaTME group | |||||
Mortality | ||||||
Milone et al. (2022)18 | SR and MA (11 NRS) | 30-day or in-hospital mortality | NR n = 1,859 | OR = 0.27 (0.08 to 0.88) | SS | |
Kwon et al. (2021)21 | SR and MA (4 NRS) | Mortality within 30 days, # events/total | 1 of 425 | 3 of 422 | RR = 0.40 (0.06 to 2.76) I2 = 0% | 0.35 |
Ren et al. (2021)22 | SR and MA (8 NRS) | Perioperative mortality, # events/total | 1 of 307 | 1 of 319 | RR = 0.81 (0.11 to 6.16) I2 = 0% | 0.84 |
Liu et al. (2022)25 | RCT | 30-day mortality, # events/total | 1 of 454 | 1 of 455 | Difference = 0.0 (−2.4 to 2.4) | > 0.99 |
CI = confidence interval; LaTME = laparoscopic total mesorectal excision; MA = meta-analysis; NR = not reported; NRS = non-randomized studies; OR = odds ratio; RCT = randomized controlled trial; RR = risk ratio; SR = systematic review; SS = statistically significant; TaTME = transanal total mesorectal excision.
Table 14: Summary of Findings by Outcome — Harms
Study citation | Study design | Outcome | Outcome results | Effect estimate (95% CI) | P value | |
|---|---|---|---|---|---|---|
TaTME group | LaTME group | |||||
Postoperative complications | ||||||
Milone et al. (2022)18 | SR and MA (11 NRS) | 30-day minor complications (Clavien-Dindo ≤ 3) | NR n = 486 | OR = 0.87 (0.52 to 1.44) | NSS | |
Choy et al. (2021)20 | SR and MA (1 RCT, 2 NRS) | Complications requiring surgery, # event/total | 9 of 79 | 14 of 70 | OR = 0.58 (0.23 to 1.42) I2 = 0% | 0.332 |
Kwon et al. (2021)21 | SR and MA (9 NRS) | Major complications (Clavien-Dindo classification ≥ 3), # event/total | 33 of 312 | 45 of 317 | OR = 0.75 (0.50 to 1.13) I2 = 0% | 0.17 |
Ren et al. (2021)22 | SR and MA (2 RCTs, 6 NRS) | Major morbidity (Clavien-Dindo classification ≥ 3), # event/total | 36 of 309 | 40 of 296 | OR = 0.83 (0.51 to 1.35) I2 = 0% | 0.45 |
Ziati et al. (2021)23 | SR and MA (8 NRS) | Postoperative complications, # event/total (%) | 70 of 297 (23.6%) | 92 of 372 (24.7%) | OR = 0.85 (0.57 to 1.25) I2 = 2% | 0.41 |
Liu et al. (2022)25 | RCT | All postoperative complications within 30 days after surgery, # event/total (%) | 73 of 544 (13.4%) | 66 of 545 (12.1%) | Difference = 1.2 (−2.8 to 5.2) | 0.53 |
30-day minor complications (Clavien-Dindo < 3), # event/total (%) | 47 of 544 (8.6%) | 45 of 455 (8.3%) | NR | 0.86 | ||
30-day major complications (Clavien-Dindo ≥ 3), # event/total (%) | 26 of 544 (4.8%) | 21 of 455 (3.9%) | ||||
Infection | ||||||
Liu et al. (2022)25 | RCT | Incisional infection, # event/total (%) | 1 of 544 (0.2%) | 1 of 545 (0.2%) | Difference = 0.0 (−2.4 to 2.4) | > 0.99 |
Abdominal or pelvic infection, # event/total (%) | 8 of 455 (1.5%) | 6 of 455 (1.1%) | Difference = 0.3 (−1.5 to 2.1) | 0.61 | ||
Anastomotic leak | ||||||
Milone et al. (2022)18 | SR and MA (8 NRS) | Anastomotic leakage | NR n = 1,657 | OR = 0.94 (0.82 to 1.63) | NSS | |
Kwon et al. (2021)21 | SR and MA (8 NRS) | Anastomotic leakage, # event/total | 24 of 317 | 25 of 372 | RR = 1.01 (0.59 to 1.72) I2 = 0% | 0.97 |
Liu et al. (2022)25 | RCT | Anastomotic leakage within 30 days after surgery, # event/total (%) | 39 of 544 (6.2%) | 29 of 545 (5.3%) | Difference = 1.9 (−1.1 to 5.0) | 0.21 |
Urethral injury | ||||||
Kwon et al. (2021)21 | SR and MA (2 NRS) | Ureter or urethral injury, # event/total | 1 of 446 | 2 of 496 | RR = 0.83 (0.10 to 6.63) I2 = 0% | 0.86 |
Intestinal obstruction | ||||||
Kwon et al. (2021)21 | SR and MA (8 NRS) | Intestinal obstruction, # event/total | 24 of 317 | 25 of 372 | RR = 1.01 (0.59 to 1.72) I2 = 0% | 0.97 |
Liu et al. (2022)25 | RCT | Intestinal obstruction within 30 days after surgery, # event/total (%) | 10 of 544 (1.8%) | 22 of 545 (4.0%) | Difference = −2.2 (−4.5 to 0.3) | 0.05 |
CI = confidence interval; LaTME = laparoscopic total mesorectal excision; MA = meta-analysis; NR = not reported; NRS = non = randomized studies; NSS = not statistically significant; OR = odds ratio; RCT = randomized controlled trial; RR = risk ratio; SR = systematic review; TaTME = transanal total mesorectal excision.
Table 15: Summary of Findings of Included Economic Evaluation
Main study findings | Authors’ conclusion |
|---|---|
NICE NG151 Evidence Review26 | |
The study examined the cost-effectiveness of TaTME compared to laparoscopic surgery or open surgery for rectal cancer. Cost-effectiveness analysis was conducted using a partitioned survival analysis approach, on a lifetime horizon and from a public payer perspective. WTP threshold = £20,000 per QALY Results of the base-case analysis: TaTME (reference) Total cost = £9,812 Total QALY = 11.15 TaTME vs, laparoscopic surgery Total cost = £11,042; incremental cost = £1,230 Total QALY = 10.34; incremental QALY = –0.81 ICER (TaTME vs. laparoscopic surgery): Cost per QALY NR TaTME was dominant TaTME vs. open surgery Total cost = £11,963; incremental cost = £2,151 Total QALY = 9.08; incremental QALY = –2.07 ICER (TaTME vs. open surgery): Cost per QALY NR TaTME was dominant The base case results showed that TaTME is the most cost-effective option, with the lowest total cost and highest QALY. The authors noted that the results for TaTME were based on effect estimates OS (HR = 0.5, 95% CI = 0.20 to 1.24) and local recurrence (RR = 0.54). The effect estimates for OS was not statistically significant (CI cross the value of no effect) Results of the deterministic sensitivity analysis: TaTME was the most cost-effective strategy in most of the modelled scenarios. Scenarios when laparoscopic was the optimal strategy: When only the statistically significant changes were considered in the model When OS with TaTME was considered equal to that with laparoscopic surgery When upper HR of TaTME was considered in the model Scenario when open surgery was the optimal surgery: When upper HR of TaTME and laparoscopic surgery were considered in the model. In all other scenarios, TaTME was found to be the optimal approach. The cost-effectiveness acceptability curve: At the WTP threshold of £20,000 per QALY, the probability of various approaches being the most cost-effective strategy were: TaTME - 86% Laparoscopic surgery - 13% Open surgery - 2% The CEAC showed that the probability of TaTME being cost-effective option was 86% starting from a WTP threshold of £6,000 per QALY and remained so with increase in WTP thresholds. The probability of laparoscopic surgery becoming cost-effective was less than 25% at £2,000 per QALY and decreased to around 13% when WTP threshold was £8,000 per QALY. The probability of laparoscopic surgery becoming cost-effective was around 12% at £1,000 per QALY and decreased to 2% when WTP threshold was £1,000 per QALY. | “A speculative analysis comparing the open, laparoscopic, robotic and TaTME approaches suggests that the TaTME may be cost-effective. However, the lack of clear data as well as the assumptions required to run this four-way comparison severely limit the conclusions that can be drawn from the analysis. (p.198)”26 |
CEAC = cost-effectiveness acceptability curve; CI = confidence interval; HR = hazard ratio; ICER = incremental cost-effectiveness ratio; NG = NICE guidance; NICE = National Institute for Health and Care Excellence; NR = not reported; OS = overall survival; QALY = quality-adjusted life-years; RR = relative risk; TaTME = transanal total mesorectal excision; WTP = willingness to pay.
Appendix 5: Overlap Between Included Systematic Reviews
Note that this appendix has not been copy-edited.
Table 16: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Li et al. (2022)17 | Milone et al. (2022)18 | Moon et al. (2022)24 | Alimova et al. (2021)19 | Choy et al. (2021)19 | Kwon et al. (2021)21 | Ren et al. (2021)22 | Ziati et al. (2021)23 |
|---|---|---|---|---|---|---|---|---|
Burghgraef et al. Ann Surg Oncol. 2022;29(3):19–1920. | Yes | — | — | — | — | — | — | — |
Matsuda et al. Surg Endosc. 2021;35(2):971–8. | — | Yes | — | — | — | — | — | — |
Ren et al. Asian J Surg. 2021; 44(1):181–5. | Yes | Yes | — | — | — | — | Yes | — |
Ye et al. Eur J Oncol. 2021; 47(5):1019–25. | Yes | — | — | — | — | — | — | — |
Zeng et al. Surg Endoscopy. 2021;36(6):3902–10. | Yes | — | — | — | — | — | — | — |
Alhanafy et al. Dis Colon Rectum. 2020;63(11):1500–10. | Yes | — | — | — | — | — | — | — |
Bjoern and Perdawood. Coloproctol. 2020;24:231–6. | — | — | — | Yes | — | — | — | — |
Foo et al. Dis Colon Rectum. 2020;63(4):497–503. | — | — | — | — | Yes | — | — | — |
de Lacy et al. BMC Cancer. 2020;20(1):677. | — | Yes | — | — | — | — | — | — |
Wasmuth et al. Br J Surg. 2020;107:121–30. | — | — | Yes | — | — | — | — | |
Zeng et al. Surg Endoscopy. 2020;34(9):3956–62. | — | Yes | — | — | — | — | — | — |
Zuhdy et al. J Laparoendosc Adv Surg Tech A. 2020; 30(7):769–76. | Yes | — | — | — | — | — | — | — |
Alamali et al. Dan Med J. 2019;66:A5555. | — | — | — | — | — | Yes | — | — |
Bjoern et al. J Gastrointest Surg. 2019;23(8):1623–30. | Yes | — | — | Yes | Yes | Yes | — | Yes |
Chen P and Yang S. Dis Colon Rect. 2019;62:e191. | — | — | Yes | — | — | — | — | — |
Chen YT et al. Asian J Surg. 2019;42(6):674 –80. | Yes | — | Yes | Yes | — | Yes | Yes | Yes |
Detering et al. J Am Coll Surg. 2019;228(3):235–44e1. | Yes | Yes | — | — | — | Yes | — | — |
Dou et al. Zhonghua Wei Chang Wai Ke Za Zhi, 2019;22:246–54. | — | — | — | — | Yes | — | — | — |
Mo et al. Chin J Oper Proc Gen Surg. 2019;13:155–8. | — | — | — | — | — | — | Yes | — |
Perdawood et al. Scand J Surg. 2019;108(1):49–54. | Yes | — | — | — | — | Yes | — | — |
Roodbeen et al. Surg Endosc. 2019;33(8):2459–67. | Yes | Yes | — | — | — | Yes | Yes | Yes |
Rubinkiewsicz et al. BMC Surg. 2019;19(1):79–87. | Yes | Yes | — | Yes | Yes | Yes | — | — |
Sparreboom et al. Colorectal Dis. 2019;21(7):767–74. | Yes | — | — | — | — | Yes | — | — |
Veltcamp Helbach et al. Surg Endosc. 2019a;33(1):79–87. | Yes | Yes | — | Yes | Yes | Yes | — | Yes |
Veltcamp Helbach et al. Surg Endosc. 2019b;33(1):94–102. | — | — | — | — | — | — | — | — |
Chang and Kiu. J Laparoendosc Adv Surg Tech. 2018;28(4):365–9. | Yes | — | — | — | — | Yes | — | Yes |
Denost et al. Surgical Endoscopy. 2018; 32(3):1486–94. | — | — | Yes | — | — | — | — | — |
ESCP. Colorectal Dis 20 Suppl. 2018; 6:33–46. | — | — | — | — | — | — | — | Yes |
Gordeyev et al. Eur Surg. 2018;51:13–8. | — | Yes | Yes | — | — | — | — | — |
Mege et al. Colorectal Dis. 2018;20(6):O143–51. | Yes | — | Yes | Yes | — | Yes | Yes | Yes |
Mora et al. Cir. 2018;86(2):140–7. | — | — | — | — | Yes | — | — | — |
Perdawood et al. Surg Endosc. 2018;32(5):2312–21. | — | Yes | — | — | — | — | — | Yes |
Persiani et al. Dis Colon Rectum. 2018;61(7):809–16. | Yes | — | — | — | — | Yes | — | Yes |
Rubinkiewsicz et al. Cancer Manag Res. 2018;10:5239–45. | — | Yes | — | — | — | — | Yes | — |
Lelong et al. J Am Coll Surg. 2017;224(5):917–25. | Yes | — | Yes | Yes | — | Yes | Yes | — |
Xu et al. World J Gastroenterol. 2017;23:5798–808. | — | — | Yes | — | — | — | — | — |
Chen CC et al. Ann Surg Oncol. 2016;23(4):1169–76. | Yes | Yes | — | — | — | Yes | — | Yes |
Chouillard et al. Tech Coloproctol; 2016:20(8):537–44. | Yes | — | — | — | — | — | — | — |
Marks et al. Tech Coloproctol. 2016;20(7):467–73. | — | Yes | Yes | Yes | — | — | — | — |
Rasulov et al. Tech Coloproctol. 2016; 20(4):227–34. | Yes | — | — | — | — | Yes | — | Yes |
de'Angelis et al. Langenbecks Arch Surg. 2015;400(8):945–59. | Yes | Yes | Yes | Yes | — | — | Yes | — |
Fernández-Hevia et al. Ann Surg. 2015; 261(2):221–7. | Yes | Yes | — | — | — | Yes | — | Yes |
Kanso et al. Dis Colon Rectum. 2015;58(7):637–44. | Yes | — | — | — | — | — | Yes | — |
Denost et al. Ann Surg. 2014;260(6):993–9. | Yes | — | — | — | — | — | Yes | — |
Velthuis et al. Surg Endosc. 2014; 28(12):3494–9. | Yes | Yes | — | — | — | — | — | — |
ESCP = 2017 European Society of Coloproctology collaborating group
Appendix 6: References of Potential Interest
Previous CADTH Reports
Transanal Total Mesorectal Excision for Adult Patients with Rectal Cancer: A Review of Clinical Effectiveness and Cost-Effectiveness. Ottawa (ON): CADTH. 2020. https://www.cadth.ca/transanal-total-mesorectal-excision-adult-patients-rectal-cancer-review-clinical-effectiveness-and
Systematic Reviews
Full Overlap of Primary Studies With Included Systematic Reviews
Aubert M, Mege D, Panis Y. Total mesorectal excision for low and middle rectal cancer: laparoscopic versus transanal approach-a meta-analysis. Surg Endosc. 2020;34(9):3908-3919. PubMed
Hajibandeh S, Hajibandeh S, Eltair M, et al. Meta-analysis of transanal total mesorectal excision versus laparoscopic total mesorectal excision in management of rectal cancer. Int J Colorectal Dis. 2020;35(4):575-593. PubMed
Lo Bianco S, Lanzafame K, Piazza CD, Piazza VG, Provenzano D, Piazza D. Total mesorectal excision laparoscopic versus transanal approach for rectal cancer: A systematic review and meta-analysis. Ann Med Surg (Lond). 2022;74:103260. PubMed
van der Heijden JAG, Koeter T, Smits LJH, et al. Functional complaints and quality of life after transanal total mesorectal excision: a meta-analysis. Br J Surg. 2020;107(5):489-498. PubMed
Wang X, Zheng Z, Yu Q, et al. Impact of Surgical Approach on Surgical Resection Quality in Mid- and Low Rectal Cancer, A Bayesian Network Meta-Analysis. Front Oncol. 2021;11:699200. PubMed
No Comparator
Casey L, Larach JT, Waters PS, et al. Application of minimally invasive approaches to pelvic exenteration for locally advanced and locally recurrent pelvic malignancy - A narrative review of outcomes in an evolving field. Eur J Surg Oncol. 2022;17:17. PubMed
Lau SYC, Choy KT, Yang TWW, et al. Defining the learning curve of transanal total mesorectal excision: a systematic review and meta-analysis. ANZ J Surg. 2022;92(3):355-364. PubMed
Wasmuth HH, Gachabayov M, Bokey L, et al. Statistical, Clinical, Methodological Evaluation of Local Recurrence Following Transanal Total Mesorectal Excision for Rectal Cancer: A Systematic Review. Dis Colon Rectum. 2021;64(7):899-914. PubMed
Economic Evaluations
Comparative Cost-Analysis
Di Candido F, Carvello M, Keller DS, et al. A comparative cost analysis of transanal and laparoscopic total mesorectal excision for rectal cancer. Updates Surg. 2021;73(1):85-91. PubMed
Review Articles
Guo Z, Ji X, Wang S, et al. Clinical Status and Future Prospects of Transanal Total Mesorectal Excision. Front. 2021;11:752737.
Vannijvel M, Wolthuis AM. Limitations and Concerns with Transanal Total Mesorectal Excision for Rectal Cancer. Clin. 2022;35(2):141-145. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca