CADTH Health Technology Review
Liposuction for Lymphedema
Rapid Review
Authors: Anusree Subramonian, Melissa Severn
Abbreviations
CCT
controlled compression therapy
HRQoL
health-related quality of life
ISL
International Society of Lymphology
LVA
lymphaticovenular anastomosis
IPG
interventional procedures guidance
MA
meta-analysis
NICE
National Institute of Health and Care Excellence
SR
systematic review
VLNT
vascularized lymph node transfer
Key Messages
Liposuction with controlled compressive therapy was associated with higher volume reduction compared with controlled compression therapy alone. This finding was from a low- to moderate-quality meta-analysis of 2 prospective cohort studies. The certainty of the evidence is very low.
Liposuction was associated with higher improvement in health-related quality of life compared with no treatment. However, the associated data were not reported to enable an independent corroboration of this finding, and the evidence was uncertain.
Overall, the evidence regarding the clinical effectiveness of liposuction compared with no treatment was very uncertain because it came from a small number of studies with methodological limitations and poor reporting.
Two guidelines recommended the use of liposuction for the treatment of lymphedema.
Context and Policy Issues
Lymphedema is an accumulation of protein-rich lymphatic fluid resulting in tissue swelling.1,2 It results from injury or damage to the lymphatic system and can affect any body part. Primary lymphedema is caused by genetic lymphatic dysplasia or congenital underdevelopment of the lymphatic system. Secondary lymphedema occurs secondary to extrinsic damage to the lymphatic system because of causes such as cancer, cancer treatment, trauma, infections, or other diseases.1,3 Lymphedema can cause lifelong impediment in several aspects of life, such as quality of life and mobility.2 Experts in Canada estimate that approximately 1 million people living in Canada are affected by lymphedema, but the exact prevalence is unclear.4 An epidemiological study on the prevalence and impact of lymphedema found that, in Canada, lower extremity lymphedema was more common than upper extremity lymphedema.3
The International Society of Lymphology (ISL) developed a staging criterion for lymphedema based on clinical presentation and severity.5,6 ISL staging ranges from stage 0 (subclinical stage with no swelling and lymphatic system changes) to stage III (hard, fibrotic tissue with associated skin changes). Severity of lymphedema is assessed based on the excess volume or volume increase compared with the contralateral side.6
Several options are available for the management of lymphedema, including conservative and surgical approaches.6 The conservative approach includes complete (or complex) decongestive therapy, controlled compression therapy (CCT), manual lymphatic drainage, use of compression garments, skin care, nutrition, and exercise. Surgical options include physiologic microsurgical procedures such as lymphaticovenular anastomosis (LVA) and vascularized lymph node transfer (VLNT), surgical debulking, liposuction, or even amputation in rare cases.6
Liposuction is the procedure of removing the hypertrophied adipose tissue that often occurs with the chronic accumulation of lymphatic fluid within the tissues.7 Conservative treatment, such as complete decongestive therapy and CCT, and microsurgical procedures do not remove the adipose tissue. Therefore, it has been postulated that liposuction, which removes the adipose tissue, combined with postoperative compression can result in complete reduction of excess fluid volume in late-stage lymphedemas.7
A recent CADTH reference list included a list of publications that evaluated the clinical effectiveness of liposuction as well as evidence-based guidelines regarding the use of liposuction for the management of lymphedema.8 The aim of the current report is to summarize and critically appraise the publications identified in that CADTH report. Thus, the purpose of this report is to summarize the evidence regarding the clinical effectiveness of liposuction for the management of lymphedema compared with either no treatment or to alternate treatment options. An additional objective of this report is to summarize the recommendations from evidence-based guidelines regarding the use of liposuction in lymphedema.
Research Questions
What is the clinical effectiveness of liposuction compared with no treatment for the treatment of lymphedema?
What is the clinical effectiveness of liposuction compared with alternative treatments for the treatment of lymphedema?
What are the evidence-based guidelines regarding the use of liposuction for the treatment of lymphedema?
Methods
Literature Search Methods
The literature search strategy used in this report is an update of 1 developed for a previous CADTH report.8 For the current report, a limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, Canadian and major international health technology agencies, as well as a focused internet search. No filters were applied to limit the retrieval by study type. The initial search was limited to English-language documents and was completed on June 23, 2022. For the current report, database searches were rerun on September 7, 2022, to capture any articles added to the databases since the initial search date. The search of major health technology agencies was also updated to include documents published since June 2022.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Individuals with lymphedema |
Intervention | Liposuction (any type) |
Comparator | Q1: No treatment Q2: Alternative treatments (e.g., wrapping and/or compression, drainage, combined decongestive therapy [e.g., manual lymphatic drainage and wearing compression garments]) Q3: Not applicable |
Outcomes | Q1 and Q2: Clinical effectiveness (e.g., reduced swelling, pain, bruising or discomfort; easier ambulation; improved quality of life) and safety Q3: Recommendations regarding best practices (e.g., appropriate populations or clinical settings, strategies to minimize adverse events) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies, evidence-based guidelines |
Q = question.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2017. Systematic reviews (SRs) in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded.9,10 Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs.11,12
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)13 for SRs, the Downs and Black checklist14 for randomized and nonrandomized studies, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument15 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
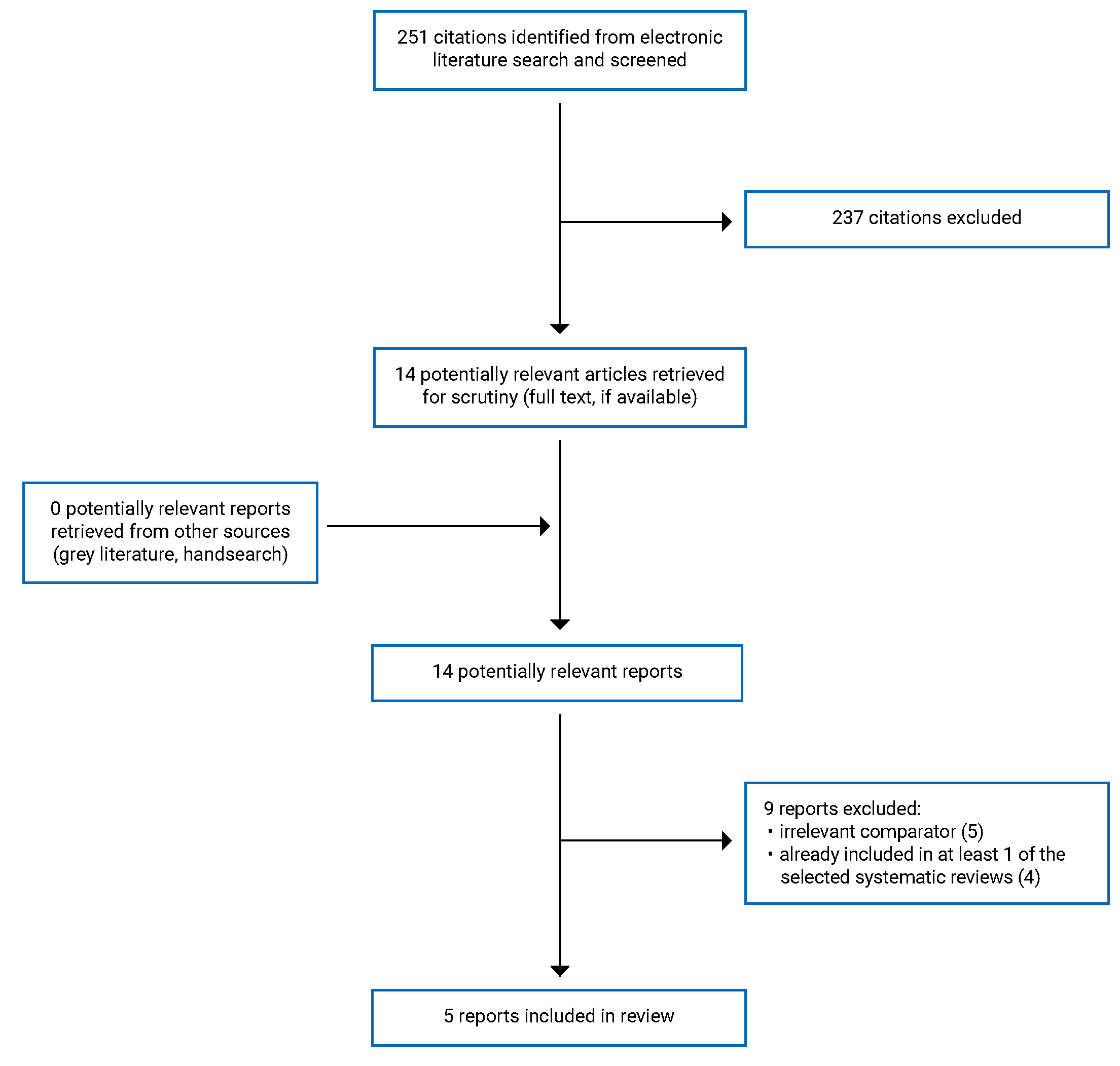
A total of 251 citations were identified in the literature search. Following screening of titles and abstracts, 237 citations were excluded and 14 potentially relevant reports from the electronic search were retrieved for full-text review. No potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 9 publications were excluded for various reasons, and 5 publications met the inclusion criteria and were included in this report. These comprised 3 SRs,16-18 1 nonrandomized study,19 and 1 evidence-based guideline.20 One of the included SRs, (by Chang et al.)16 also provided some additional evidence-based recommendations. The findings of the SR16 and the recommendations from that publication are summarized separately in this report. The methodology of the SR and evidence-based guideline were also critically appraised separately. Thus, evidence from 3 SRs16-18 (116 with a meta-analysis [MA] and evidence-based recommendations), 1 nonrandomized study,19 and 1 evidence-based guideline20 were summarized in this report.
The Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA)21 flow chart of the study selection is presented in Appendix 1 .
Additional references of potential interest are provided Appendix 6.
Summary of Study Characteristics
Three SRs,16-18 1 nonrandomized study,19 and 1 evidence-based guideline20 were included in this report. All 3 SRs had broader inclusion criteria than the present review.16-18 Several surgical and non-surgical interventions for lymphedema were considered as eligible interventions and comparators. For example, Chang et al.16 considered multiple surgical interventions such as liposuction and VLNT as well as interventions for the prevention of secondary lymphedema. Only the characteristics and results of the subset of relevant studies will be described in this report.
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
The SRs were published in 202116,17 and 2019.18 In all SRs, the authors searched multiple electronic databases to identify relevant studies.16-18 Trial registries and bibliographies were searched in 2 SRS.17,18 All SRs included randomized controlled trials and nonrandomized studies. Two SRs16,18 also included other study designs, such case series and case reports. The number of primary studies included in the 3 SRs were 6616 (15 relevant to the current report), 2517 (7 relevant to the current report), and 2618 (3 relevant to the current report). There was considerable overlap of primary studies across the SRs.16-18 A table outlining the overlap of primary studies is provided in Appendix 5.
Two of the SRs provided a narrative synthesis of results from the included primary studies.17,18 An MA was not conducted in either SR.
In the third SR, Chang and colleagues conducted an MA to quantitatively synthesize the results using the random-effect MA for several outcomes.16 The authors proposed recommendations based on the evidence identified in the SR, following the Grading of Recommendations, Assessment, Development and Evaluation criteria (GRADE) approach. The SR and recommendations were conducted as part of a consensus conference by the American Association of Plastic Surgeons. The recommendations were graded as strong (grade 1) if the benefits of an intervention outweighed the risks or weak (grade 2) if the risk-benefit profile was less then favourable. The quality of evidence supporting the recommendations were grouped as “A, B, or C” from the highest to lowest quality of evidence, respectively.16 However, additional details were not available from the publication.
An interventional procedures guideline (IPG) by NICE, published in 2022, was included in this report.20 Evidence backing the recommendations was sourced from a rapid review22 of literature conducted by the guideline development committee. Systematic literature search was conducted for the rapid review to identify SRs, randomized and nonrandomized studies, and case series. Recommendations were formulated based on this evidence, as well as on professional opinion from specialist advisors. Recommendations were classified as “standard arrangement” (good-quality evidence, adequate literature available, and a favourable risk-benefit profile), “special arrangement” (evidence uncertain, often given for emerging procedures, physician should communicate the uncertainties to the patient), “research only” (experimental procedure, high level of uncertainty in the evidence), or “do not use” (lack of efficacy or significant safety concerns).20,23
Last, 1 nonrandomized study by Brazio and Nguyen published in 2021 was included in this report. This was a retrospective medical record review study of patients with lymphedema who were treated at the study hospital from 2016 to 2019.19
Country of Origin
The authors of the SRs were from Australia17 and the US.16,18 The retrospective study by Brazio and Nguyen was conducted in the US.19 The IPG was developed in the UK.20
Patient Population
The populations of interest in 2 SRs were adults with secondary lymphedema16 or all individuals with lymphedema,17 irrespective of the location. The number of patients across the relevant included studies in the SRs was 643 for the SR by Chang et al.16 and 238 for the SR by Tang et al.17 The majority of patients in the 2 SRs had upper extremity lymphedema. The population of interest in the third SR was patients with head and neck lymphedema secondary to cancer treatment.16-18 There were a total of 40 patients with submental lymphedema from the 3 relevant studies of the SR.18 The stage of lymphedema in the relevant primary studies was not reported in any of the SRs.16-18
Brazio and Nguyen19 enrolled 21 patients with ISL stage I to III upper or lower extremity lymphedema, 19 of whom had secondary lymphedema. The mean age of the participants was 55.4 years (range = 25 to 75 years). The exclusion criteria were absence of a normal contralateral limb for comparison, 2 or fewer limb volume measurements, and noncompliance.
The intended users of the NICE IPG20 were health care professionals, and the target population was patients with chronic lymphedema. The target population in the guideline by Chang et al.16 was patients with or at high risk of developing lymphedema. Intended users were not clearly described but were probably health care professionals. The relevant population to the current report were patients with lymphedema.
Interventions and Comparators
The relevant intervention in the SRs was liposuction with or without other treatments.16-18 The interventions reported by the primary studies included in the SRs were liposuction, liposuction plus CCT, liposuction plus LNT, liposuction plus LVA, or liposuction plus compression garments.16-18 Additional details about the type of liposuction or usage of concurrent compression therapy were not reported in the SRs. The comparators in the relevant primary studies were CCT, LVA, LNT, rehabilitation program, or no treatment. Most of the relevant primary studies were single-arm studies with no comparator.16-18
In the retrospective medical record review study by Brazio and Nguyen,19 the intervention was liposuction plus a physiologic operation (LVA or VLNT). The comparator was physiologic operation only. The study participants were grouped into 4 treatment arms based on the treatment received and the order in which the treatments were offered, as follows: liposuction then physiologic operation (n = 2), physiologic operation then liposuction (n = 2), simultaneous liposuction and physiologic operation (n = 11), and physiologic operation only (n = 6). The treatment groups were assigned based on the clinical presentation and stage of lymphedema. Patients with more fibroadipose components and severe excess volume were offered dry liposuction first followed by a physiologic operation, whereas those with a milder presentation (e.g., reversible swelling, mostly pitting edema) received the physiologic procedure first. In the latter group, patients with suboptimal outcomes were given a lymph-sparing liposuction procedure after the physiologic operation. Simultaneous liposuction (lymph-sparing) and physiologic operation was offered to patients with a mixed presentation. All patients were managed with a combination of compressive garments, manual lymphatic drainage, elevation, and sequential mechanical compression before the operations.
The intervention of interest in the NICE IPG20 was liposuction for chronic lymphedema. Chang et al.16 considered all surgical interventions for the prevention and treatment of lymphedema. The relevant intervention to the current report was liposuction for the treatment of lymphedema.16
Outcomes
Reduction of excess limb volume was an outcome in the SR by Chang et al.16 and the nonrandomized study by Brazio and Nguyen.19 This outcome was measured either as percentage reduction in limb volume or as the amount of volume reduction in millilitres. The SR by Tang et.al,17 measured health-related quality of life (HRQoL) outcomes, assessing both disease-specific HRQoL and generic HRQoL.17 Incidence of cellulitis was considered in in the SR by Chang et al.16 and the nonrandomized study by Brazio and Nguyen.19 Use of compression garment (duration and level of compression) was evaluated in the nonrandomized study.19
The NICE IPG20,22 considered efficacy outcomes, such as sustained reduction in limb volume, improvement in HRQoL, and reduction in the incidence of cellulitis, as well as safety outcomes (e.g., pain, post-operative infections, venous thromboembolism).
Summary of Critical Appraisal
A narrative summary of strengths and limitations of included studies is provided in this section. One of the included studies was an SR with evidence-based guidelines.16 The 2 components of this publication are critically appraised separately. Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Systematic Review
Three SRs were included in the current report.16-18 All clearly reported their objective and inclusion criteria and included components of population, intervention, comparator, and outcomes. The authors searched multiple electronic databases to identify eligible studies within 24 months of completion of the reviews. Characteristics of the included primary studies were described in adequate detail in the SRs. In 2 SRs,16,17 the risk of bias of the included primary studies were assessed using tools appropriate for the study designs. In the SR by Chang et al.,16 MAs were conducted to quantitatively pool the individual study results using a random-effects MA approach. The authors assessed between-study heterogeneity using the I2 statistic. In situations in which high heterogeneity was observed, they investigated the sources by visual inspection. Subgroup analysis was conducted based on the location of lymphedema.16 In the other 2 SRs,17,18 the authors reported that MA was not conducted due to high heterogeneity17,18 and paucity of evidence.18 These seemed appropriate considering the evidence. The authors of all SRs declared that there were no conflicts of interest that could influence the conduct of the review or the interpretation of the findings.16-18 There was no external funding for any of the SRs.16-18
The SRs had several methodological weaknesses, which could lower the internal and external validity of the results.16-18 It was unclear whether protocols were established before the conduct of any of the SRs, and a published protocol was not available for any of them.16-18 In all SRs, it was unclear whether the study selection, data extraction, and critical appraisal of the included studies were conducted in duplicate by independent reviewers. By performing these steps in duplicate, accuracy and objectivity could be ensured. A list of excluded studies and the reason for exclusion were not provided in any of the SRs.16-18 In 1 SR,18 the Cochrane Risk of Bias tool was used to assess the quality of all included studies (RCTs, nonrandomized studies, case series). Several domains of that tool are not applicable to nonrandomized studies or case series (e.g., randomization, blinding); therefore, it is unclear if the risk of bias assessment was comprehensive for all included studies. In 2 SRs,17,18 numerical results or comparative data from the individual studies were not reported, making it challenging to interpret the results to adequately answer the research questions. In the SR with MA by Chang et al.,16 the potential impact of the risk of bias of the pooled studies on the results of meta-analyses was not discussed. The sources of funding for the individual studies were not reported in any of the included SRs.16-18 Last, the quality and findings of the SRs were dependent on the quality of the included studies. With the inclusion of case series and even case reports (whose quality is low or unclear), the validity and generalizability of the overall results of the SRs is very low.16-18
Nonrandomized Study
The nonrandomized study by Brazio and Nguyen19 had a clear objective. The main outcomes were reported in the methods section, and they were appropriate for the study objective. The inclusion and exclusion criteria were clear. The interventions and comparators were clearly described, along with the concurrent treatments received by all patients. Participants in all groups received the respective treatments during the same period from the same centre. The staff, places, and facilities where the patients were treated were likely representative of the treatment majority of patients would receive.
However, the study had several major limitations lowering the overall validity and reliability of the results.19 The study was a retrospective medical record review. There was no randomized allocation or blinding of patients or outcome assessors, which could introduce selection bias. Allocation to treatment type (physiologic operation, liposuction, or simultaneous) was determined based on patients’ clinical presentation and severity. For example, patients with relatively milder mild to moderate excess volume were offered physiologic operation first, and those with predominantly fibroadipose components were offered liposuction. These baseline differences in clinical severity and treatment could have influenced study findings and lowered the internal validity of the results. The authors reported that patients in all treatment groups were followed up for a similar period of time. However, the overall range of the follow-up periods was wide (250 to 808 days); variations in patients’ lifestyle, activities, and exposures over such a long time could have affected outcomes. The reporting of study results had some limitations. Simple outcome data for some study findings, especially the between-group comparisons, were presented in figures which were challenging to interpret. Effect estimates, confidence intervals (CIs), and P values for between-group comparisons were not reported. Results for each outcome were challenging to extract and interpret. The total number of patients screened for study eligibility, and details about the excluded patients were not described. It is unclear whether the study participants were representative of the source population. It was not clear whether a sample size calculation was performed; therefore, it is unknown whether the study was adequately powered to detect significant differences between the groups if present. Finally, because this was a retrospective medical record review study, only patients with adequate follow-up data were enrolled in the study. Thus, it is unknown if missing data from patients who were not included in the study could have changed the outcomes significantly.
Evidence-Based Guidelines
Two guidelines were included in this report.16,20 The scope and purpose of the guidelines were described. The publications defined the target population of the guidelines clearly. For the NICE IPG, the guideline development group included individuals from relevant professional groups, and patient groups were consulted.23 The target users of the guideline were clear. The guideline by Chang et al.16 was unclear about stakeholder involvement and the guideline development group, and its target users were not described (although likely to be health care professionals).16
Both guidelines used systematic methods to search for evidence. In the NICE IPG,20 a rapid review of literature was conducted.22 Clear inclusion and exclusion criteria, and appropriate search strategies, were used to identify evidence. The method of formulating recommendations was provided. The health benefit and risks of the intervention were considered. The guidelines were externally reviewed by experts before publication, and a procedure for updating the guideline was provided. Recommendations were graded based on the volume and quality of the supporting evidence. The criteria for these classifications were clear.20,23 In the guideline by Chang et al.,16 an SR was conducted to gather evidence for the guidelines. However, the method of formulating recommendations was unclear. The strengths and limitations of the supporting SR were summarized in the earlier section. An explicit link between the evidence and the recommendations were not provided. It was not reported whether the guideline was reviewed by experts before publication. No information on updating the guideline was provided. Although the grading of recommendations and the level of evidence was provided, the criteria for classifying the quality of evidence were not reported.16
The NICE IPG was clear in presentation.20 The recommendations were unambiguous and clearly identifiable, and different options of disease management were considered. In the guideline by Chang et al.,16 the recommendations were easy to identify, and alternate treatment options were presented. Neither guideline described facilitators and barriers to applying the reccommendations.16,20 Tools and advice for implementing the recommendations were not clear in either guideline. Although there was a partial discussion in the NICE IPG20 about resource implications of the implementation of guidelines, such considerations were not mentioned in the guideline by Chang et al.16 Similarly, monitoring or auditing criteria for the recommendations were provided in the NICE IPG,20 but not in the guideline by Chang et al.16
Editorial independence was ensured in the NICE IPG20 by way of recording and addressing conflicts of interests of the authors. It was declared that the views of the finding body did not influence the content of the guideline. However, these factors were not reported or addressed in the guideline by Chang et al.16
Overall, the guideline by Chang et al.16 was limited in presentation, stakeholder involvement, applicability, rigour, and clarity of development. Although the NICE IPG was based on a rapid review of the literature, the methodology was rigorous, comprehensive, and clearly presented.20
Summary of Findings
Results from the included studies are summarized here by outcome. The main study findings are presented in Appendix 4.
Clinical Effectiveness of Liposuction Compared With No Treatment
Reduction in Limb Volume
No relevant evidence was identified regarding the clinical effectiveness of liposuction compared with no treatment for the outcome reduction in limb volume.
The SR with MA by Chang et al.16 reported findings from MAs of case series studies comparing limb volumes before and after liposuction procedures. The findings suggested that liposuction procedure was associated with significant reduction in limb volumes postoperatively. Subgroup analyses showed similar results for upper and lower extremity lymphedema. The evidence was uncertain because of a lack of a comparator and the inherent methodological limitations of case series studies.
Cellulitis
Chang et al.16 reported results from 1 case series study of 10 patients about the preoperative and postoperative incidence of cellulitis. The incidence of cellulitis decreased from 7 patients (out of 10) before liposuction to 1 patient after the procedure. The odds ratio of this change was 21 (95% CI, 1.78 to 248.10). Due to the wide CI and the low sample size (N = 10), the certainty of this finding is likely very low.
Health-Related Quality of Life
One RCT (included in 2 SRs17,18) comparing liposuction to no treatment evaluated disease-specific HRQoL in 20 patients with head and neck lymphedema. The authors reported a statistically significant improvement in the liposuction group compared with the no treatment group; however, they did not report the comparative data.
One SR17 reported on HRQoL outcome before and after liposuction procedure. The authors of the SR summarized findings from 4 studies that compared preoperative HRQoL with HRQoL after liposuction. The authors reported that liposuction was associated with significant improvement in several domains of disease-specific as well as generic HRQoL, although numerical data and comparative effect sizes were not reported.
Clinical Effectiveness of Liposuction Compared With Alternative Treatments
Reduction in Limb Volume
The SR with MA by Chang et al. compared liposuction plus CCT with CCT alone in patients with stage II upper extremity lymphedema.16 Results from 2 analyses (data from 2 studies for each) suggested that, compared with CCT alone, liposuction plus CCT is associated with significantly higher percentage of volume reduction and a significantly higher amount of volume lost. There was no heterogeneity as indicated by I2 = 0%.
In the nonrandomized study (N = 21), Brazio and Nguyen19 compared liposuction plus physiologic procedures with physiologic procedures only and found no significant differences between the groups in percentage reduction of limb volume. However, data for this comparison were not reported. The study also had methodological limitations mainly due to baseline differences in disease severity and presentation between the groups. The clinical importance of the findings is unknown.
Cellulitis
In the retrospective study, Brazio and Nguyen19 reported that there were 2 incidences of a mild surgical site infection (cellulitis) after the VLNT procedure, which were resolved with treatment.
Health-Related Quality of Life
One SR17 included HRQoL results from 1 study of liposuction plus CCT versus CCT alone. The study authors reported that at 6 to 12 months after liposuction plus CCT there were “improvements” with pain, swelling, and difficulties with activities of daily living, measured using the visual analogue scale. For patients who received CCT alone, the authors reported that there were no changes or lesser changes in these outcomes. However, the authors did not provide any supporting data for an independent assessment. Results of generic HRQoL measured using other questionnaires, such as the Hospital Anxiety and Depression Scale and Psychological General Well-Being Index, also showed some within-group improvement for the treatment and comparison groups. However, no data were reported, so these finding should be interpreted with caution.
One prospective nonrandomized study (reported in 1 SR17) compared HRQoL after liposuction with conservative rehabilitation program using the Lymphedema Quality of Life Inventory. The results found that patients in both groups reported improvements in HRQoL. However, it was unclear whether a between-group comparison was conducted.
Use of a Compression Garment
In the retrospective study, Brazio and Nguyen19 reported that the duration of compression garment use per day decreased after liposuction or physiologic procedure. The level of compression (definition unclear) did not change within group from before to after surgery. However, a between-group comparison was not reported.
Guidelines Regarding the Use of Liposuction
The NICE IPG20 recommends that the liposuction procedure can be used if standard arrangements are in place for clinical governance, consent, and audit. The supporting rapid review found evidence from 2 SRs (1 with MA) and 5 before-and-after studies, and the guideline authors reported adequate evidence for the efficacy and safety of liposuction for chronic lymphedema.22 The guideline development committee also noted that the liposuction procedure should be advised when lymphedema persists after conservative management, and it should generally be done only once per limb. They also noted that the procedure is not curative, and the patient would need to wear compression garments for life.20
The SR and guideline by Chang et al.16 recommend that debulking procedures such as liposuction are “effective in addressing the nonfluid component such as fat involving lymphedema”16 (strong recommendation with low-quality evidence). The authors also recommended that although there is a role for liposuction plus a physiologic procedure, the timing of each procedure is unclear (strong recommendation with low-quality evidence).
Limitations
The findings of this report are limited by the quality of the evidence identified. The 3 SRs,16-18 1 nonrandomized study,19 and evidence-based guideline20 had several limitations as described in the Summary of Critical Appraisal section. Most of the studies included in the SRs were single-arm studies or case reports. Therefore, there was a paucity in comparative evidence relevant to the current report. No relevant studies were identified about the effectiveness of liposuction compared with alternative treatments such as manual lymphatic drainage or complete decongestive therapy. Safety outcomes of the liposuction procedure were not examined in the identified studies.
The evidence-based guidelines16,20 did not provide specific recommendations regarding the strategies to minimize adverse events, appropriate clinical settings, or criteria for selecting patients with lymphedema for liposuction. The guidelines also highlighted the paucity of well-designed comparative studies. The nonrandomized study was not conducted in Canada.19 It was not reported whether the studies included in the SRs16-18 were conducted in Canada, and neither guideline16,20 was specific to Canada. Therefore, the generalizability of the findings of this report to Canadian settings is not clear.
Conclusions and Implications for Decision- or Policy-Making
This report is an upgrade of a 2022 CADTH report,8 and the aim was to summarize the evidence regarding the clinical effectiveness and guidelines regarding liposuction for the treatment of lymphedema. Three SRs16-18 (1 with an MA and evidence-based guideline16), 1 nonrandomized study,19 and 1 evidence-based guideline20 were included in this report. The SRs had several limitations arising from including low-quality, single-arm studies and case series studies as well as methodological weakness (e.g., lack of clarity about study selection in duplicate by independent reviewers, issues with reporting results).16-18 The nonrandomized study19 had low internal validity because of baseline differences in patients in each treatment group. The NICE IPG20 was based on a rapid review of the literature, and the guideline by Chang et al.16 had less rigorous development and poor presentation.
Overall, although the SRs17,18 showed that liposuction is associated with a higher improvement in HRQoL compared with no treatment, there were limitations with reporting and the lack of comparative data make the evidence uncertain. After the liposuction procedure, patients reported significant volume reduction and improved HRQoL compared with before surgery. However, the evidence was from single-arm studies and case series studies, and no comparative outcome data were reported.17 One MA found that liposuction plus CCT was associated with a higher reduction of excess volume compared with CCT alone.16 In the nonrandomized study,19 no significant differences were found between liposuction and physiologic procedure in reducing excess volume. HRQoL improvement with liposuction compared with alternate treatments was uncertain from the evidence because comparative outcome data were not reported.17 Overall, the findings of this report should be interpreted with caution in light of the limitations.
The NICE IPG20 recommended the use of liposuction for lymphedema if standard arrangements are in place for clinical governance, consent, and audit. Based on low-quality evidence from an SR,16 1 guideline strongly recommended that liposuction is indicated to reduce the nonfluid component of lymphedema. However, the recommendations from both guidelines were based on evidence with methodological limitations. The generalizability to Canadian settings was unclear.
Overall, the evidence regarding the clinical effectiveness of liposuction for lymphedema is of low to moderate quality and of low certainty. Decision-makers should interpret the evidence with caution. Future well-designed comparative studies are warranted to evaluate the clinical effectiveness and safety of liposuction compared with other treatments for lymphedema.
References
1.Underwood E, Woods M, Riches K, Keeley V, Wallace A, Freeman J. Lymphedema Research Prioritization Partnership: A Collaborative Approach to Setting Research Priorities for Lymphedema Management. Lymphat Res Biol. 2019;17(3):356-361. PubMed
2.CDC. Lymphedema. 2022; https://www.cdc.gov/cancer/survivors/patients/lymphedema.htm. Accessed 2022 Oct 2.
3.Keast DH, Moffatt C, Janmohammad A. Lymphedema Impact and Prevalence International Study: The Canadian Data. Lymphat Res Biol. 2019;17(2):178-186. PubMed
4.Keast D, Towers A. The rising prevalence of lymphedema in Canada: A continuing dialogue. 2017: http://canadalymph.ca/wp-content/uploads/2015/04/PATHWAYS-Spring-2017-The-rising-prevalence-of-lymphedema-in-Canada.pdf. Accessed 2022 Oct 2.
5.International Society of Lymphology. The diagnosis and treatment of peripheral lymphedema. 2009 Concensus Document of the International Society of Lymphology. Lymphology. 2009;42(2):51-60. PubMed
6.Armer JM, Hulett JM, Bernas M, Ostby P, Stewart BR, Cormier JN. Best Practice Guidelines in Assessment, Risk Reduction, Management, and Surveillance for Post-Breast Cancer Lymphedema. Curr Breast Cancer Rep. 2013;5(2):134-144. PubMed
7.Schaverien MV, Munnoch DA, Brorson H. Liposuction Treatment of Lymphedema. Semin Plast Surg. 2018;32(1):42-47. PubMed
8.Clark M, Horton J. Liposuction for Lymphedema: CADTH Reference List. Ottawa CADTH; 2022: https://www.cadth.ca/liposuction-lymphedema. Accessed 2022 Oct 2.
9.Carl HM, Walia G, Bello R, et al. Systematic Review of the Surgical Treatment of Extremity Lymphedema. J Reconstr Microsurg. 2017;33(6):412-425. PubMed
10.Forte AJ, Huayllani MT, Boczar D, Ciudad P, Manrique O. Lipoaspiration and Lymph Node Transfer for Treatment of Breast Cancer-related Lymphedema: A Systematic Review. Cureus. 2019;11(11):e6096. PubMed
11.Alamoudi U, Taylor B, MacKay C, et al. Submental liposuction for the management of lymphedema following head and neck cancer treatment: a randomized controlled trial. J Otolaryngol Head Neck Surg. 2018;47(1):22. PubMed
12.Leppäpuska IM, Suominen E, Viitanen T, et al. Combined Surgical Treatment for Chronic Upper Extremity Lymphedema Patients: Simultaneous Lymph Node Transfer and Liposuction. Ann Plast Surg. 2019;83(3):308-317. PubMed
13.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
14.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
15.Agree Next Steps C. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2022 Oct 2.
16.Chang DW, Dayan J, Greene AK, et al. Surgical Treatment of Lymphedema: A Systematic Review and Meta-Analysis of Controlled Trials. Results of a Consensus Conference. Plast Reconstr Surg. 2021;147(4):975-993. PubMed
17.Tang NSJ, Ramakrishnan A, Shayan R. Quality-of-life outcomes after operative management of primary and secondary lymphoedema: a systematic review. ANZ J Surg. 2021;91(12):2624-2636. PubMed
18.Tyker A, Franco J, Massa ST, Desai SC, Walen SG. Treatment for lymphedema following head and neck cancer therapy: A systematic review. Am J Otolaryngol. 2019;40(5):761-769. PubMed
19.Brazio PS, Nguyen DH. Combined Liposuction and Physiologic Treatment Achieves Durable Limb Volume Normalization in Class II-III Lymphedema: A Treatment Algorithm to Optimize Outcomes. Ann Plast Surg. 2021;86(5S Suppl 3):S384-s389.
20.NICE. Liposuction for chronic lymphoedema. Interventional procedures guidance [IPG723]. London: National Institute for Health and Care Excellence; 2022: https://www.nice.org.uk/guidance/ipg723. Accessed 2022 Sep 2.
21.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
22.NICE. Interventional procedure overview of liposuction for chronic lymphoedema. London: National Institute for Health and Care Excellence; 2022: https://www.nice.org.uk/guidance/ipg723/evidence/overview-final-pdf-11067086989. Accessed 2022 Sep 16.
23.NICE. Interventional procedures programme manual (PMG 28). London: National Institute for Health and Care Excellence; 2022: https://www.nice.org.uk/process/pmg28/chapter/introduction. Accessed 2022 Sep 16.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Chang et al. (2021)a16 US, Canada Funding source: NR | Systematic review and meta-analysis of RCTs, nonrandomized cohort studies, and case series Total number of included primary studies = 66 Number of relevant primary studies = 15 | Adult patients with secondary lymphedema Number of participants: 643 Lymphedema location: UEL, n = 430 (12 studies) LEL, n = 187 (4 studies) Mixed (UEL or LEL) n = 26 (1 study) | Eligible intervention: Surgical interventions for the treatment of lymphedema (e.g., liposuction, vascular LNT, lymphaticovenular anastomosis), surgical interventions for the prevention of secondary lymphedema Relevant intervention: Liposuction (with compression therapy) Liposuction + CCT: 4 studies Liposuction + LNT: 2 studies Liposuction + compression garment: 8 studies Liposuction + LVA: 1 study Eligible comparator: Surgery (e.g., liposuction, vascular lymph node transplantation, lymphaticovenular anastomosis), compression therapy (e.g., graduated compression stockings, sequential compression devices) Relevant comparator: Surgery (e.g., liposuction, vascular lymph node transplantation, lymphaticovenular anastomosis), compression therapy (e.g., graduated compression stockings, sequential compression devices). Single-arm studies were also included in the SR. CCT: 2 studies LVA: 1 study LNT: 1 study No comparator (single arm): 11 studies | Outcomes: volume reduction, reduction in limb circumference, surgical complications, discontinuation of other lymphedema interventions, patient reported outcomes (e.g., QoL) Follow-up: Ranged from 6 months to 60 months across the included relevant primary studies |
Tang et al. (2021)17 Australia Funding source: NR | Systematic review of RCTs and nonrandomized studies Total number of included primary studies = 25 Number of relevant primary studies = 7 | Individuals with lymphedema Number of participants: 238 Lymphedema location: UEL, n = 162 (5 studies) LEL, n = 47 (2 studies) Head and neck: 29 (2 studies) Stage of lymphedema: NR | Eligible intervention: Any form of surgical intervention for lymphedema. Relevant intervention: Liposuction Liposuction: 5 studies Liposuction + CCT: 2 studies Eligible comparator: “appropriate control” Relevant comparator: no treatment, CCT, rehabilitation program No treatment: 1 study CCT: 1 study Rehabilitation program: 1 study No comparator (single arm): 4 studies | Outcomes: Disease-specific HRQoL. Generic HRQoL, patient satisfaction. Follow-up: Ranged from 1 month to 12 months across the included relevant primary studies. |
Tyker et al. (2019)18 US Funding source: No external funding received | Systematic review of RCTs, nonrandomized studies, case series and case reports. Total number of included primary studies = 26 Number of relevant primary studies = 3 | Patients with head and neck lymphedema following chemotherapy, radiation therapy or surgical removal of a head and neck cancer. Number of participants, n = 40 Lymphedema location: submental area, n = 40 (3 studies) | Eligible intervention: All lymphedema drainage interventions (e.g., manual lymph drainage, liposuction, chemotherapeutics) Relevant intervention: Liposuction (3 studies) Eligible comparator: Any lymphedema drainage intervention. Studies with no control group were included. Relevant comparator: No treatment: 1 study No comparator (single arm): 2 studies | Outcomes: improvement in lymphedema, self-reported improvement in appearance and distress reduction, objective observer score, patient satisfaction Follow-up: 6 months across the included relevant studies |
CCT = controlled compression therapy; HRQoL = health-related quality of life; ISL = International Society of Lymphology; LEL = lower extremity lymphedema; NR = not reported; LNT = lymph node transfer: LVA = lymphovenular anastomosis QoL = quality of life; RCT = randomized controlled trial; SR = systematic review; UEL = upper extremity lymphedema.
aThis publication also reported evidence-based recommendations by a consensus panel. Additional details about the development of recommendations are provided in Table 4.
Table 3: Characteristics of Included Primary Clinical Study
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Brazio and Nguyen(2021)19 US Funding source: None received | Retrospective medical record review study. | Patients with stage I to III lymphedema Number of participants, n = 21(2 with primary lymphedema; 19 with secondary lymphedema) Liposuction then physiologic, n = 2 Physiologic then liposuction, n = 2 Simultaneous, n = 11 Physiologic only, n = 6 Mean age: 55.4 years (range 25 to 75 years) Sex: 3 were males? (14.2%) The physiologic only group had predominantly stage I disease. Liposuction first group: had patients with higher stages of lymphedema and higher excess limb volume. The physiologic then liposuction group had stage II disease. Simultaneous group: all participants had stage II disease. | Intervention: Liposuction with or without physiologic operation (LVA or VLNT) Comparator: Physiologic operation only (LVA or VLNT) Participants in both groups were managed with a combination of compressive garments, MLD, elevation, and sequential mechanical compression before the surgery. Treatment groups were assigned based on the clinical presentation and stage of lymphedema. Patients with more fibroadipose component and severe volume excess were offered liposuction first, whereas those with a milder presentation received physiologic first. Simultaneous liposuction and physiologic was offered to patients with a mixed presentation. | Primary outcome: Percent reduction of excess limb volume as compared with unaffected contralateral limb Secondary outcomes: Compression garment class and duration of use; cellulitis; surgical complications Follow-up: Mean follow-up period 334 days (range 250 to 808 days). Follow-up was considered ended if patients underwent any other type of operation on the same limb. |
LVA = lymphaticovenular anastomosis; MLD = manual lymphatic drainage; VLNT = vascularized lymph node transfer.
Table 4: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
Intended users: Health care professionals Target population: Patients with chronic lymphedema | Liposuction for chronic lymphedema | Efficacy outcomes: Sustained reduction in limb volume, improvement in QoL, reduced incidence of cellulitis Safety outcomes: pain, postoperative infections, bleeding, venous thromboembolism, fat embolism, fluid overload | Evidence was obtained from a rapid review of literature as well as professional opinion | Each study identified in the rapid review were assessed separately. Recommendations are classified as -Standard arrangements: When the evidence is valid, relevant and of good quality, adequate literature available, consistent evidence, benefits within reasonable timelines, favourable risk-benefit profile. Special arrangement: When there are significant uncertainties in the evidence regarding the efficacy and safety of the procedure. Often provided for emerging procedures. The clinician should tell the patient about the uncertainties. Research Only: When the procedure is experimental, high level of uncertainty in evidence, or resolution of the uncertainties is required before routine use. Do not use: When there no efficacy or significant safety issues. | Recommendations were formulated by the multidisciplinary Interventional procedures advisory committee based on the evidence from rapid review and professional opinion from specialist advisors. | Draft recommendations were posted for consolation or feedback from the public, patient organizations, medical device companies, professional organizations, and other stakeholders. Recommendations are finalized by the committee after discussions. |
Chang et al. (2021)a16 | ||||||
Intended users: NR Target population: Patients with lymphedema, or at high- risk of developing lymphedema | Surgical interventions for the prevention and treatment of lymphedema Relevant intervention: Liposuction for the treatment of lymphedema | Reduction of limb volume, reduction in limb circumference, surgical complications, ability to continue conservative interventions (e.g., pressure therapy), QoL | Evidence collected using a systematic evidence review of clinical effectiveness (refer to Table 2 for additional details) | Evidence quality was assessed using the GRADE approach. Recommendations were graded as Strong (grade I- benefit outweigh risks) or weak (grade II- uncertain risk-benefit profile). Quality of evidence was graded as A, B, or C (details NR) | A consensus panel involving individuals with content and methodological expertise developed the recommendation statements. The statements were developed considering benefits, risks, and burdens of the intervention. Additional details NR | NR |
GRADE = Grading of Recommendations, Assessment, Development and Evaluations; NR = not reported; QoL = quality of life.
aThe characteristics of the guideline component of the publication is presented here. The characteristics of the systematic review was presented in Table 2.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 5: Strengths and Limitations of Systematic Reviews Using AMSTAR 213
Strengths | Limitations |
|---|---|
Chang et al. (2021)16 | |
The objective and inclusion criteria of the report were clearly reported and included components of population, intervention, comparator, and outcomes. Multiple electronic databases were searched. Search strategy was provided. Search was conducted within 24 months of publication. Characteristics and results of included studies were provided in adequate detail. Risk of bias in the individual studies were assessed using Cochrane Risk of Bias tool (for RCTs) and the Newcastle Ottawa Scale (for observational studies). The results of quality assessment were reported in the publication. Meta-analyses (MAs) were conducted to quantitatively synthesize the results. Appropriate methods were used. MA was conducted using a random-effects model. Heterogeneity was assessed using I2 statistic. In case of high heterogeneity, authors mentioned that potential sources of it were investigated using visual inspection, as well as sensitivity analysis. Subgroup analysis by location of lymphedema was conducted. Authors reported that there were no conflicts of interest related to the interventions considered in the SR. A funding source was not reported. | It was not mentioned whether the review protocol was established before the conduct of the review. All study designs, including case series, were eligible for inclusion. The rationale for this was unclear from the publication. Additional searching in the form of grey lit search and bibliographic search was not conducted. Trial registries were not searched. It was unclear whether content experts were consulted. It was unclear whether study selection, data extraction and risk of bias assessment was conducted in duplicate by at least 2 reviewers. A list of excluded studies, and reason for exclusion was not provided. Sources of funding for the studies were not reported. Several of the MAs had high heterogeneity. Results of sensitivity analyses, if conducted, were not reported. Potential impact of risk of bias on the results of meta-analysis was not discussed. Publication bias was not assessed. |
Tang et al. (2021)17 | |
The objective and inclusion criteria of the report were clearly reported and included components of population, intervention, and outcomes. Multiple electronic databases including trial registries were searched. A bibliographic search was conducted. Search strategy was provided. Search was conducted within 24 months of publication. Characteristics and results of included studies were provided in adequate detail. The various questionnaires used to measure HRQoL across the studies were detailed clearly. Risk of bias in the individual studies were assessed using the USPSTF Quality rating criteria, and the Agency for Health care Research and Quality criteria. The authors reported that most of the included studies were rated as moderate to good quality considering the study design. A meta-analysis was not conducted. However, the authors discussed the heterogeneity across the studies and the potential reasons for them. Authors reported that there were no conflicts of interest related to the interventions considered in the SR. A funding source was not reported. | It was not mentioned whether the review protocol was established before the conduct of the review. The comparator was mentioned as “appropriate control” and did not list individual comparators of interest. It was unclear which specific comparators, if any, that they searched for. All study designs including RCTs and NRSs were eligible for inclusion. The rationale for this was unclear from the publication. Study selection, and data extraction were not conducted in duplicates. It was unclear whether risk of bias assessment was conducted in duplicate, but unlikely. A list of excluded studies, and reason for exclusion was not provided. Lack of reporting numerical data from individual studies could make interpretation of results challenging. Sources of funding for the studies were not reported. |
Tyker et al. (2019)18 | |
The objective and inclusion criteria of the report were clearly reported and included components of population, intervention, and outcomes. The rationale for including non-comparative (single-arm) studies were provided. It was appropriate. Multiple electronic databases including trial registries were searched. A bibliographic search was conducted. Search strategy was provided. Search was conducted within 24 months of publication. Characteristics of included studies were provided in adequate detail. Risk of bias in the individual studies were assessed using the Cochrane Risk of Bias tool, which is validated for RCTs. Level of evidence for each of the interventions of interest were assessed using the Oxford Centre for Evidence-based Medicine criteria. A meta-analysis was not conducted. The reason for not conducting a quantitative synthesis was provided (e.g., heterogenous data, paucity of evidence), It was reasonable. Authors reported that there were no conflicts of interest related to the interventions considered in the SR. No external funding was received for the SR. | It was not mentioned whether the review protocol was established before the conduct of the review. It was unclear whether study selection, data extraction and risk of bias assessment was conducted in duplicate by at least 2 reviewers. A list of excluded studies, and reason for exclusion was not provided. Simple outcome data from individual primary studies were not reported. Findings of the studies were presented narratively without numerical results. Cochrane Risk of Bias tool is not intended to be used for nonrandomized studies. Several of its domains (e.g., randomization, blinding) are not applicable to NRSs. Therefore, it was unclear whether the risk of bias assessment is comprehensive. Sources of funding for the studies were not reported. |
AMSTAR 2 = A Measurement Tool to Assess systematic Reviews 2; HRQoL = health-related quality of life; MA = meta-analysis; NRS = nonrandomized studies; RCT = randomized controlled trial; SR = systematic review; USPSTF = United States Preventive Services Task Force.
Table 6: Strengths and Limitations of Clinical Study Using the Downs and Black Checklist14
Strengths | Limitations |
|---|---|
Brazio and Nguyen(2021)19 | |
The study objectives were mentioned. The main study outcomes were reported in the methods section. They were valid and appropriate for the study objective. Interventions and comparators were clear. The surgical procedures were described in detail. Concomitant treatments given to all patients pre-surgery were described. The staff, places, and facilities where the patients were treated were likely representative of the treatment majority of patients would receive. | The study was a retrospective chart review. There were no randomization or blinding. The baseline characteristics of the study participants differed considerably across the groups. Treatment (physiologic operation, liposuction or simultaneous) were different for patients based on their clinical presentation and lymphedema staging. Simple outcome data for some of the study findings, especially the between-group comparisons, were not presented clearly. Effect estimates, confidence intervals, and p values for between-group comparisons were not reported. Results for each outcome were challenging to extract. Potential surgical complications other than cellulitis were not described. The total number of patients from which the study participants were sourced were not described. It is unclear whether the study participants were representative of them. It is unclear whether patients in all treatment groups were followed up for a similar period of time. However, the overall range of follow-up period was wide (250 to 808 days). It was unclear whether power calculation was performed. Therefore, it is unknown if the study was adequately powered to detect significant differences between the groups if present. Since this was a retrospective chart review study, no patients were lost to follow-up. Rather, only patients with adequate follow-up data were enrolled in the study. It is possible that there were other patients who were lost to follow- up and thus not captured in the study, could have had different outcomes. |
Table 7: Strengths and Limitations of Guidelines Using AGREE II15
Item | Chang et al. (2021)16 | |
|---|---|---|
Domain 1: Scope and purpose | ||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes |
3. The population (e.g., patients, public) to whom the guideline is meant to apply is specifically described. | Partially | Yes |
Domain 2: Stakeholder involvement | ||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Unclear |
5. The views and preferences of the target population (e.g., patients, public) have been sought. | Yes | No |
6. The target users of the guideline are clearly defined. | Yes | No |
Domain 3: Rigour of development | ||
7. Systematic methods were used to search for evidence. | Yes a | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | No | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes | No |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Partially (the authors mentioned this but how is unclear) |
12. There is an explicit link between the recommendations and the supporting evidence. | Partially | No |
13. The guideline has been externally reviewed by experts before its publication. | Yes | NR |
14. A procedure for updating the guideline is provided. | Yes | No |
Domain 4: Clarity of presentation | ||
15. The recommendations are specific and unambiguous. | Yes | No |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Partially (other interventions are evaluated too) |
17. Key recommendations are easily identifiable. | Yes | Yes |
Domain 5: Applicability | ||
18. The guideline describes facilitators and barriers to its application. | No | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No | No |
20. The potential resource implications of applying the recommendations have been considered. | Partially | No |
21. The guideline presents monitoring and/or auditing criteria. | Yes | No |
Domain 6: Editorial independence | ||
22. The views of the funding body have not influenced the content of the guideline. | Yes | NR |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | NR |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; IPG = interventional procedures guidance; NICE = National Institute for Health care Excellence: NR = not reported.
aA rapid literature review with systematic methods was conducted to identify the evidence.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 8: Summary of Findings by Outcome — Reduction in Limb Volume
Author (year) and study design | Stage and location of lymphedema | Number of participants | Method of measurement | Result |
|---|---|---|---|---|
Liposuction + CCT vs. CCT alone | ||||
Chang et al. (2021)16 SR with MA 2 NRS | ISL II, UEL | n = 48 | Percentage reduction in limb volume | Random-effects MA of 2 studies (n = 48) Mean Difference (95% CI) = 63.95 (49.57 to 78.33), P < 0.00001, statistically significant favouring liposuction I2 = 0% |
Chang et al. (2021)16 SR with MA 2 NRS | ISL II, UEL | n = 69 | Reduction in limb volume (mL) | Random-effects MA of 2 studies (n = 69) Mean Difference in volume reduction (95% CI) = –895.81 (–1,140.063 to –650.98), P < 0.00001, statistically significant favouring liposuction I2 = 0% |
Liposuction vs. physiologic operation | ||||
Brazio and Nguyen(2021)19 Retrospective chart review study | LEL and UEL, Stage I to III | 21 | Percentage reduction of excess volume | At follow-up (mean follow-up period 334 days), all treatment groups showed normal or near-normal limb volume. Mean reduction in excess volume was 82% to 106% across the groups. The group with simultaneous liposuction and physiologic operation reported lowest reduction in excel volume at the end of follow-up (82%). The authors reported that there were no significant differences between the groups (data NR). |
Compared to preoperative volume | ||||
Chang et al. (2021)16 SR with MA 2 Case series | ISL II to III, UEL | 75 | Percentage reduction in limb volume | Random-effects MA of 2 studies Mean Difference in volume reduction (95% CI) = 28.68 (6.06 to 51.29) P < 0.01, statistically significant favouring liposuction I2 = 96% |
ISL II to III, LEL | 88 | Percentage reduction in limb volume | Random-effects MA of 2 studies Mean Difference in volume reduction (95% CI) = 29.23 (5.56 to 52.90) P < 0.02, statistically significant favouring liposuction I2 = 86% | |
ISL II to III, UEL and LEL | 163 | Percentage reduction in limb volume | Random-effects MA of 2 studies Mean Difference in volume reduction (95% CI) = 26.29 (18.64 to 34.24) P < 0.00001, statistically significant favouring liposuction I2 = 91% | |
Chang et al. (2021)16 SR with MA 6 Case series | ISL I to III, UEL | 207 | Reduction in limb volume (mL) | Random-effects MA of 5 studies Mean Difference in volume reduction (95% CI) = 1,294.16 (460.47 to 2,127.85) P < 0.002, statistically significant favouring liposuction I2 = 99% |
ISL I to III, LEL | 49 | Reduction in limb volume (mL) | Random-effects MA of 3 studies Mean Difference in volume reduction (95% CI) = 2,736.60 (1,767.00 to 3,706.20) P = 0.0001, statistically significant favouring liposuction I2 = N/A (results from only 1 study) | |
ISL I to III, UEL and LEL | 256 | Reduction in limb volume (mL) | Random-effects MA of 6 studies Mean Difference in volume reduction (95% CI) = 1,524.93 (748.84 to 2,301.01), P = 0.0001, statistically significant favouring liposuction I2 = 79.5% | |
CI = confidence interval; ISL = International Society of Lymphology; LEL = lower extremity lymphedema; MA = meta-analysis; NR = not reported; NRS = nonrandomized studies; RCT = randomized controlled trial; SR = systematic review; UEL = upper extremity lymphedema.
Table 9: Summary of Findings by Outcome — Cellulitis
Author (year) and study design | Stage and location of lymphedema | Number of participants | Result |
|---|---|---|---|
Liposuction compared to physiologic operation | |||
Brazio and Nguyen(2021)19 Retrospective study | LEL and UEL, ISL Stage I to III. | 21 | 2 incidences of mild surgical site infection after VLNT (one in simultaneous group, one in physiologic first group) |
Compared to preoperative cellulitis | |||
Chang et al. (2021)16 SR with MA 1 Case series | LEL and UEL ISL stage NR | 10 | Pre-op and post-op cellulitis Incidence of cellulitis, % Preoperative = 70% (7/10) Post-operative = 10% (1/10) OR (95% CI) = 21 (1.78 to 248.10), statistically significant favouring liposuction |
CI = confidence interval; ISL = International Society of Lymphology; LEL = lower extremity lymphedema; MA = meta-analysis; NR = not reported; OR = odds ratio; SR = systematic review; UEL = upper extremity lymphedema; VLNT = vascularized lymph node transfer.
Table 10: Summary of Findings by Outcome — Use of Compression Garment
Author (year) and study design | Stage and location of lymphedema | Number of participants | Method of measurement | Result |
|---|---|---|---|---|
Liposuction compared to physiologic operation | ||||
Brazio and Nguyen(2021)19 Retrospective study | LEL and UEL, Stage I to III. | 21 | Duration of compression garment use | Reported as similar between groups. Mean duration of use 500 days (range 56 to 1,027 days). Overall duration of compression among all participants: Pre-op 12.5 hours per day Post-op (at last follow-up): 7.5 hours per day P = 0.003. Between-group comparison NR |
Level of compression garment | The authors reported that the level of compression did not change within groups from pre-op to follow-up significantly. Between-group comparison NR | |||
LEL = lower extremity lymphedema; UEL = upper extremity lymphedema; NR = not reported.
Table 11: Summary of Findings by Outcome — Disease-Specific HRQoL
Author (year) and study design | Stage and location of lymphedema | Method of measurement | Number of participants | Result |
|---|---|---|---|---|
Liposuction vs. no treatment | ||||
Tang et al. (2021)17 SR 1 study | Neck | MBOE DAS59 | 20 | Alamoudi et al. (2018): MBOE and DAS 59: Statistically significant improvement in the liposuction group compared to control group in all 5 questions of both questionnaires. (Data NR) |
Liposuction + CCT compared to CCT alone | ||||
Tang et al. (2021)17 SR 1 study | UEL | VAS | 49 | Brorson et al., 2006: At 12 months, liposuction group showed “improvements” in pain, swelling and difficulties with ADL. “No change” in control group. At 6 months and 12 months, liposuction group showed “improvement” in QoL related to reduced mobility, swollen arm, heavy arm, and fatigue. “lesser changes” in the control group. (Data NR) |
Liposuction compared to rehabilitation program | ||||
Tang et al. (2021)17 SR 1 study | UEL, LEL | LyQLI | 68 | Klernas et al., 2018: Liposuction group showed “statistically significant” improvement in some domains. Control group also showed improvement to a “limited extent.” (Data NR) |
Compared to preoperative HRQoL | ||||
Tang et al. (2021)17 SR 2 studies | Neck | MBOE, DAS 59 | 9 | Brake et al., 2014: MBOE: “Statistically significant improvement” after liposuction compared to pre-op control group in all 5 questions. (Data NR) DAS 59: “Statistically significant improvement” after liposuction compared to pre-op control group in the domain of general self-consciousness of appearance. No significant improvement in other domains. (Data NR) |
UEL | VAS | 11 | Schaverien et al., 2012: The VAS scores were 64.60 and 81.20 at pre op and at 3 months post-op, respectively. The improvement was “statistically insignificant.” (Data NR) | |
ADL = activities of daily living; DAS59 = Derriford appearance scale; HRQoL = health-related quality of life; LEL = lower extremity lymphedema; LyQLI = lymphedema quality of life inventory; MBOE = modified blepharoplasty outcomes evaluation; NR = not reported; QoL = quality of life; SR = systematic review; UEL = upper extremity lymphedema; VAS = visual analogue scale.
Table 12: Summary of Findings by Outcome — Generic HRQoL
Author (year) and study design | Stage and location of lymphedema | Method of measurement | Number of participants | Result |
|---|---|---|---|---|
Liposuction + CCT compared to CCT alone | ||||
Tang et al. (2021)17 SR 1 study | UEL | HADS, NHP, PGWB | 49 | Brorson et al., 2006: HADS: At 6 months, liposuction group showed “decreased anxiety.” Control group showed “increased anxiety” at 12 months. (Data NR) PGWB: Liposuction group: showed “improvements” in total score, and general health. “No changes” in control group. (Data NR) |
Compared to preoperative HRQoL | ||||
Tang et al. (2021)17 SR 3 studies | UEL, LEL | PSFS | 21, | Boyages et al., 2015: At 6 months, “improvements” in all patients were noted in several domains. Unclear whether the improvements were significant. |
UEL | SF-36 | 60 | Hoffner et al., 2017: At 1 month, 3 months, and 12 months post-op, there were “significant increase” in one or more domains of the questionnaire. (Data NR) | |
UEL | HADS | 11 | Schaverien et al., 2012: At 3 months, there was reduction in anxiety (9.09 to 4.60) and depression (5.73 to 1.70). Unclear whether the improvements were significant. (Data NR) | |
HADS = Hospital Anxiety and Depression Scale; HRQoL = health-related quality of life; LEL = lower extremity lymphedema; NHP = Nottingham health profile; NR = not reported; PGWB = Psychological General Well-Being; PSFS = patient specific functional scale; SF-36 = medical outcomes 36-item short-form survey; SR = systematic review; UEL = upper extremity lymphedema.
Table 13: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
“Evidence on the efficacy and safety of liposuction for chronic lymphoedema is adequate. The evidence on safety shows that the potential risks include venous thromboembolism, fat embolism, and fluid overload. This procedure can be used provided that standard arrangements are in place for clinical governance, consent, and audit. (p.2)”20 Supporting evidence: Evidence from 2 SRs (1 with MA), and 5 before-and-after studies were identified in the rapid review of literature.22 | Standard arrangement recommendation Definition: A procedure is recommended for use with standard arrangements for clinical governance, consent, and audit when the evidence meets the following criteria: a) the evidence is valid, relevant and of good quality b) adequate quantity of literature is available c) sufficiently consistent results across the literature are present d) evidence show benefits of the procedure within an appropriate timeline e) the procedure has a favourable risk-benefit profile. |
Additional comments from the IPG committee: (Not evidence-based)
| N/A |
Chang et al. (2021)16 | |
“Debulking procedures such as liposuction are effective in addressing nonfluid component such as fat involving lymphedema (p.990).”16 Supporting evidence: Unclear. Results of the accompanying SR with MA are presented earlier. | Grade 1C (Strong recommendation with low-quality evidence) |
“There is a role for liposuction combined with physiologic procedures, although the timing of each procedure is currently unresolved.(p.990)”16 Supporting evidence: Unclear. Result of the accompanying SR with MA are presented elsewhere in this report. | Grade 1C (Strong recommendation with low-quality evidence) |
IPG = interventional procedures guidance; MA = meta-analysis; NA = not applicable; NICE = National Institute for Health care Excellence; SR = systematic review; NR = not reported.
Appendix 5: Overlap Between Included Systematic Reviews
Note that this appendix has not been copy-edited.
Table 14: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Chang et al. (2021)16 | Tang et al. (2021)17 | Tyker et al. (2019)18 |
|---|---|---|---|
Agarwal R, et al. Eur J Plast Surg. 1998;21:113 to 117. | Yes | — | — |
Alamoudi U, et al. J Otorlaryngol Head Neck Surg. 2018;47(1):22. | — | Yes | Yes |
Boyages J, et al. Ann Surg Oncol. 2015;22(3):S1263-S1270. | Yes | Yes | — |
Brake MK, et al. Otorlaryngol Head Neck Surg. 2014;151:221 to 225. | — | Yes | Yes |
Brorson H, et al. Lymphology. 1998;31:156 to 172. | Yes | — | — |
Brorson H, et al. Lymphology. 2006;39:8 to 25. | Yes | Yes | — |
Campisi CC, et al. Ann Plast Surg. 2017;78:184 to 190. | Yes | — | — |
Chang K, et al. Zhonghyua Wai Ke Za Zhi. 2017;55:274 to 278. | Yes | — | — |
Damstra RJ, et al. Br J Surg.2009;96:859 to 864. | Yes | — | — |
Granzow JW, et al. Ann Surg Oncol. 2014;21:1189 to 1194. | Yes | — | — |
Hoffner M, et al. Lymphat Res Biol. 2017;15:87 to 98. | Yes | Yes | — |
Hoffner M, et al. Plast Reconstr Surg Glob Open. 2018; 6:e1912. | Yes | — | — |
Klernas P, et al. Lymphat Res Biol. 2018;16:300 to 308. | — | Yes | — |
Lamprou DA, et al. Br J Surg. 2017;104: 84 to 89. | Yes | — | — |
Leppapuska IM, et al. Ann Plast Surg. 2019;83:308 to 317. | Yes | — | — |
Nicoli F, et al. Lasers Med Sci. 2015;30:1377 to 1385. | Yes | — | — |
Qi F, et al. Microsurgery. 2009;29:29 to 34. | Yes | — | — |
Schaverien MV, et al. J Plast Reconstr Aesthet Surg. 2021;65:935 to 942. | Yes | Yes | — |
Taylor SM, et al. Otolarynhol Head Neck Surg. 2012;146(6):1028 to 1030. | — | — | Yes |
Yes = indicates that the primary study was included in the systematic review; — = indicates that the primary study was not included in the systematic review.
Appendix 6: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
Liposuction for lipedema: 2022 Update. https://www.cadth.ca/liposuction-lipedema-2022-update
Systematic Review With Unclear Comparator
Ciudad P, Manrique OJ, Bustos SS, et al. Single-stage VASER-assisted liposuction and lymphatico-venous anastomoses for the treatment of extremity lymphedema: a case series and systematic review of the literature. Gland Surg. 2020;9(2):545-557. doi:10.21037/gs.2020.01.13 PubMed
Nonrandomized Studies
Klernäs P, Johnsson A, Boyages J, Brorson H, Munnoch A, Johansson K. Quality of Life Improvements in Patients with Lymphedema After Surgical or Nonsurgical Interventions with 1-Year Follow-Up. Lymphat Res Biol. 2020;18(4):340-350. doi:10.1089/lrb.2018.0065 PubMed
Chollet C, Malloizel-Delaunay J, Cabarrou B, et al. Liposuction-assisted brachioplasty in breast cancer-related lymphedema: Impact on volume reduction and quality of life. J Plast Reconstr Aesthet Surg. 2021;74(7):1633-1701. doi:10.1016/j.bjps.2020.11.025 PubMed
Review Articles
Ciudad P, Sabbagh MD, Agko M, et al. Surgical Management of Lower Extremity Lymphedema: A Comprehensive Review. Indian J. 2019 Jan;52(1):81-92. PubMed
Additional References
Stewart CJ, Munnoch DA. Liposuction as an effective treatment for lower extremity lymphoedema: A single surgeon's experience over nine years. J Plast Reconstr Aesthet Surg. 2018 02;71(2):239-245. PubMed
Garza R, 3rd, Skoracki R, Hock K, Povoski SP. A comprehensive overview on the surgical management of secondary lymphedema of the upper and lower extremities related to prior oncologic therapies. BMC Cancer. 2017 Jul 05;17(1):468. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca