CADTH Health Technology Review
Intravenous Iron Isomaltoside for Patients With Iron Deficiency Undergoing Elective Surgery
Rapid Review
Authors: Keeley Farrell, Sharon Bailey
Abbreviations
EQ-VAS
EQ visual analogue scale
KCCQ
Kansas City Cardiomyopathy Questionnaire
NYHA
New York Heart Association
RCT
randomized controlled trial
SF-36v2
Short Form (36) Health Survey version 2
TAVI
transcatheter aortic valve implantation
Key Messages
The results of 1 randomized controlled trial did not find a difference in functional status (6-minute walk distance and New York Heart Association class), hand grip strength, or health-related quality of life for patients who underwent a transcatheter aortic valve implantation treated with iron isomaltoside versus placebo.
There was 1 (1.4%) hypersensitivity reaction and 1 (1.4%) episode of chest pain in patients treated with iron isomaltoside in the randomized controlled trial. Rates of other adverse events were similar between patients treated with iron isomaltoside and placebo.
Context and Policy Issues
Anemia is a condition in which the hemoglobin concentration in the blood is lower than normal leading to a decreased capacity of the blood to carry oxygen to tissues.1 Iron is an essential mineral involved in several important metabolic processes and is required for the production of hemoglobin.2,3 Iron deficiency anemia is the most common form of anemia and has a variety of causes including malabsorption, increased iron demand (e.g., pregnancy), chronic disease, and blood loss (e.g., menstruation, perioperative, hemodialysis).1,4 Preoperative iron deficiency may be associated with a higher prevalence of preoperative anemia, higher blood transfusion requirements, postoperative fatigue, and longer hospital stays.5 Preoperative anemia is associated with increased morbidity and mortality.6,7 The prevalence of preoperative anemia has been estimated to range between 5% and 76% depending on a number of factors (i.e., age of patient, nature of condition, type of operation).8
Current treatment options for iron deficiency include oral iron supplementation, IV iron supplementation, and red blood cell transfusion.5 Oral iron supplements are easily administered; however, they are associated with gastrointestinal side effects in up to 52% of patients.8 These side effects may reduce tolerance and adherence to oral iron supplementation.5 Red blood cell transfusion in surgical patients is associated with multiple risks, including infection, circulatory overload, thromboembolic events, prolonged hospitalization, impaired quality of life, and mortality.5 Initial IV iron preparations included high-molecular-weight iron dextran; however, it has since been phased out because of fatal anaphylactic-type reactions.8 Newer formulations of IV iron were developed to increase safety; these include iron sucrose, ferric gluconate, ferumoxytol, ferric carboxymaltose, and iron isomaltoside.8,9
Previous studies have evaluated the efficacy of iron isomaltoside (also known as ferric derisomaltose) for the treatment of iron deficiency anemia in a range of patient populations (i.e., mixed etiologies, chronic kidney disease, inflammatory bowel disease).4 The main safety concern for iron isomaltoside is the potential for hypersensitivity reactions.4 Iron isomaltoside may be a potential treatment option for iron deficiency in patients undergoing elective surgery. A review of the evidence for the efficacy and safety of iron isomaltoside in this patient population could aid decision-making around the use of this drug.
The purpose of this report is to review the clinical effectiveness of iron isomaltoside for patients with iron deficiency undergoing elective surgery.
Research Question
What is the clinical effectiveness of IV iron isomaltoside for patients identified as iron deficient undergoing elective surgery, including high blood loss surgery?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was iron isomaltoside. Comments, newspaper articles, editorials, letters, and conference abstracts were excluded. If possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2017, and August 30, 2022.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adult patients identified as iron deficient undergoing elective surgery (i.e., any surgery scheduled in advance of the operation) |
Intervention | IV iron isomaltoside (any dosage) |
Comparator | IV iron sucrose (e.g., Venofer); oral iron medications; placebo |
Outcomes | Clinical effectiveness (e.g., mortality and morbidity, length of hospital stay, comorbidities, need for blood transfusion, hemoglobin level, hemoglobin change, patient quality of life), safety (e.g., hypersensitivity, allergic reaction, rate of adverse events) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2017.
Critical Appraisal of Individual Studies
The included randomized controlled trial (RCT) was critically appraised by 1 reviewer using the Downs and Black checklist10 as a guide. A summary score was not calculated for the included study; rather, the strengths and limitations were described narratively.
Summary of Evidence
Quantity of Research Available
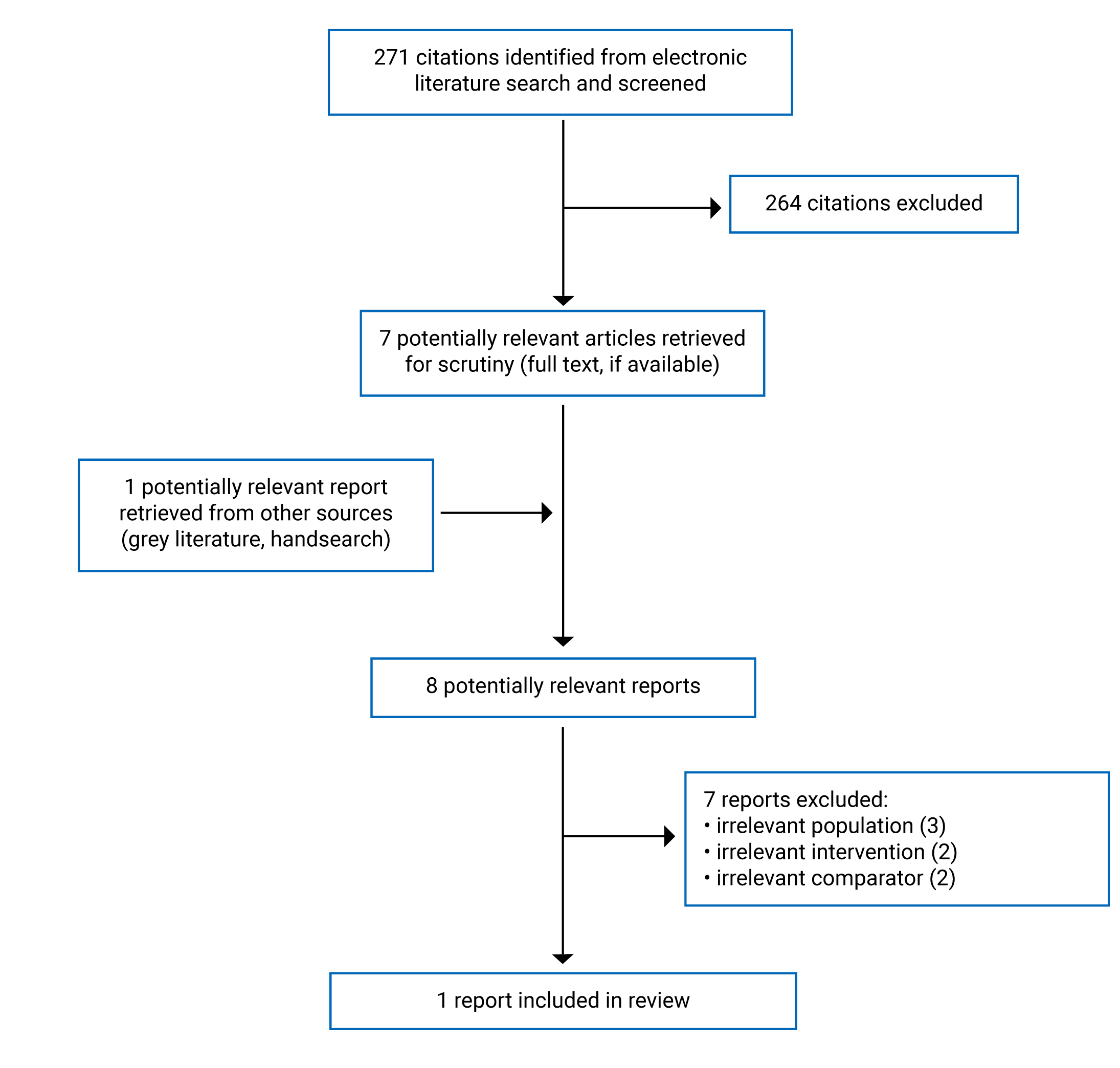
A total of 271 citations were identified in the literature search. Following screening of titles and abstracts, 264 citations were excluded and 7 potentially relevant reports from the electronic search were retrieved for full-text review. One potentially relevant publication was retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 7 publications were excluded for various reasons and 1 RCT met the inclusion criteria and was included in this report. The PRISMA11 flow chart of the study selection is presented in Appendix 1.
Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
One RCT12 was identified for inclusion in this report. Additional details regarding the characteristics of the included publication are provided in Appendix 2.
Study Design
The included study by Kvaslerud et al. (2022)12 was a single-centre, double-blind RCT.
Country of Origin
The RCT was conducted in Norway.12
Patient Population
The RCT by Kvaslerud et al. (2022)12 included 149 patients in the randomized population (74 in the iron isomaltoside group and 75 in the placebo group) and 104 patients in the modified intention-to-treat population (51 in the iron isomaltoside group and 53 in the placebo group). The inclusion criteria were adults aged 18 years or older with severe aortic stenosis and iron deficiency who were referred for non-emergency transcatheter aortic valve implantation (TAVI).12 The iron isomaltoside group included 51 patients with a mean age of 80.0 years.12 The patients in the iron isomaltoside group were 55% male and 22% had a history of smoking.12 The median EuroSCORE II in the iron isomaltoside group was 2.3%.12 The EuroSCORE is a risk model for predicting mortality after cardiac surgery with lower scores indicating lower predicted risk of mortality.13 The placebo group included 53 patients with a mean age of 79.2 years.12 The patients in the placebo group were 60% male and 36% had a history of smoking.12 The median EuroSCORE II in the placebo group was 2.1%.12
Interventions and Comparators
The intervention in the RCT was iron isomaltoside administered as a single IV infusion of 20 mg per kg body weight (rounded to the nearest 100 mg, maximum dose of 2,000 mg) dissolved in 100 mL sodium chloride 0.9%.12 The placebo group received a single IV infusion of 100 mL sodium chloride 0.9%.12 The iron isomaltoside and placebo were administered approximately 3 months before TAVI.
Outcomes
The primary outcome in the RCT was the 6-minute walk test (a measure of functional status) assessed 3 months after TAVI.12 The 6-minute walk test measures the distance a patient is able to walk over 6 minutes.12 Secondary outcomes were New York Heart Association (NYHA) class, health-related quality of life, muscle strength (hand grip strength), and adverse events. Health-related quality of life was assessed using the Kansas City Cardiomyopathy Questionnaire (KCCQ), the 3-level EQ-5D (EQ-5D-3L), the EQ visual analogue scale (EQ-VAS), and the Short Form (36) Health Survey version 2 (SF-36v2).12 The NYHA classification system categorizes patients into 1 of 4 classes with higher classes indicating worse functional status.14 The KCCQ is a 12-item form with 4 domains (physical limitation, symptom frequency, quality of life, and social limitation) with scores ranging from 0 to 100 (100 indicates the best health status and 0 indicates the worst).14 The EQ-5D indicates the degree of patient difficulty with 5 domains (mobility, self-care, usual activity, pain or discomfort, and anxiety or depression) with a score of 1 indicating perfect health, 0 equivalent to death, and lower than 0 indicating a state worse than death.14 The EQ-VAS is a global assessment of health status with scores ranging from 0 to 100 (0 indicates the worst health status).14 The SF-36v2 is a 36-item instrument that yields 8 scale scores and 2 summary scores (physical component summary and mental component summary) with higher scores indicating better health.15 Hand grip strength was measured using the Kern MAP hand-held dynamometer.12 The patients’ dominant hand was tested 3 times and the best result was used.12 A resistance of 40 kg was used for men and 20 kg for women.12
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
The objective, patient characteristics, interventions, and main findings were clearly described in the RCT by Kvaslerud et al. (2022)12 The characteristics of patients lost to follow-up were reported. A modified intention-to-treat analysis was used and approximately 30% of randomized patients in each treatment group were not included in the analysis.12 The authors stated that there was a higher dropout rate than expected because patients were enrolled in the study before a final decision about whether the patient would undergo TAVI.12 The baseline characteristics for excluded patients and those in the modified intention-to-treat analysis appeared similar overall; however, there appeared to be potential imbalances in some characteristics (e.g., more excluded patients with a history of smoking and chronic obstructive pulmonary disease).12 The RCT authors conducted sensitivity analyses for various scenario imputations for missing data and did not find an impact on the results for the primary outcome.12 All randomized patients were included in the safety analysis.12 Patients and investigators were blind to group allocation. Because iron isomaltoside is distinguishable from saline placebo, preparation and administration of the treatments was conducted by an unblinded third-party.12 The infusion stand, IV line, syringe, and injection site were covered, and the patient’s eyes were blinded while receiving the infusion.12 Blinding of patients and investigators aims to reduce the risk of performance bias and measurement bias. The main outcome measures were valid and reliable, and the statistical tests used were appropriate.12 Patients in different intervention groups were recruited from the same population. Patients were randomized to intervention groups using permuted blocks randomization.12 Randomization aims to balance the distribution of known and unknown confounders between treatment groups. The authors disclosed the funding source for the study and their potential conflicts of interest.
Summary of Findings
The main study findings are presented in Appendix 4.
Clinical Effectiveness of Iron Isomaltoside
Functional Status
There was no statistically significant difference in 6-minute walk distance assessed at 6-month follow-up (3 months after TAVI) between the iron isomaltoside and placebo groups in the RCT by Kvaslerud et al. (2022).12 There was no statistically significant difference in NYHA class at 6 months between the iron isomaltoside and placebo groups in the RCT.12
Muscle Strength
There was no statistically significant difference between patients treated with iron isomaltoside versus placebo in mean hand grip strength at 6 months in the RCT.12
Health-Related Quality of Life
There were no statistically significant differences in quality of life at 6 months assessed using the KCCQ, EQ-5D, and SF-36v2 between patients treated with iron isomaltoside versus those treated with placebo in the RCT.12
Safety
In the RCT, 37 (50.7%) serious adverse events occurred in the iron isomaltoside group and 49 (65.3%) in the placebo group.12 There was no statistically significant difference in serious adverse events between treatment groups. Two serious adverse events (1 hypersensitivity reaction and 1 episode of chest pain) in the iron isomaltoside group were deemed related to the study drug by the investigators.12 All other serious adverse events were deemed to be unrelated to the study drug, infusion procedure, or study testing.12 There were 3 (4.1%) mild infusion reactions in the iron isomaltoside group and 2 (2.7%) in the placebo group.12 There were 2 (2.7%) deaths in the iron isomaltoside group and 5 (6.7%) in the placebo group.12 There were 7 (9.6% of the iron isomaltoside group and 9.3% of the placebo group) infections treated with antibiotics in each of the treatment groups.12
Limitations
This report is limited by the quantity of relevant evidence. One relevant RCT was identified that compared iron isomaltoside to placebo in patients undergoing TAVI.12 No relevant studies were identified that compared iron isomaltoside to alternative therapies (i.e., IV iron sucrose, oral iron medications). Additionally, TAVI is a minimally invasive procedure, and no relevant evidence was identified that evaluated the efficacy and safety of iron isomaltoside in patients undergoing invasive surgical procedures.
The included RCT was not conducted in Canada.12 Therefore, it is unclear whether the results summarized in the report are generalizable to the Canadian setting.
Conclusions and Implications for Decision- or Policy-Making
This report comprised 1 RCT12 that evaluated iron isomaltoside for patients with iron deficiency undergoing TAVI.
Evidence from 1 RCT suggested there were no statistically significant differences between patients with iron deficiency undergoing TAVI treated with iron isomaltoside and placebo in 6-minute walk distance, NYHA class, hand grip strength, or health-related quality of life.12 In the RCT, 1 (1.4%) hypersensitivity reaction and 1 (1.4%) episode of chest pain were considered by investigators to be related to iron isomaltoside.12 All other serious adverse events were deemed to be unrelated to the study drug, infusion procedure, or study testing by investigators.12
CADTH has produced previous reports on IV iron preparations and iron isomaltoside specifically. A 2021 CADTH report aimed to summarize the evidence on the clinical effectiveness of iron isomaltoside for anemia due to pregnancy, menorrhagia, or other gynecological conditions.16 In 2020, the CADTH Canadian Drug Expert Committee recommended that “iron isomaltoside 1,000 (Monoferric) be reimbursed for the treatment of iron deficiency anemia in adult patients who have intolerance of or unresponsiveness to oral iron therapy with conditions.”17 Additionally, a 2019 CADTH report aimed to summarize the evidence on the clinical effectiveness, cost-effectiveness, and guidelines for IV iron preparations (e.g., iron isomaltoside, ferric carboxymaltose, iron sucrose) for patients with iron deficiency undergoing elective surgery.18 The report concluded that IV iron may result in better control of hemoglobin levels and fewer blood transfusions compared with no IV iron or usual care; however, between-group differences were not always statistically significant and the identified evidence was limited quality.18
Overall, the limited quantity of evidence makes it difficult to draw conclusions about the clinical effectiveness of iron isomaltoside for patients with iron deficiency undergoing elective surgery. Additional high-quality studies that compare iron isomaltoside with placebo or alternative therapies in patients with iron deficiency undergoing elective surgery (including invasive surgical procedures) would help stakeholders in decision-making around the use of iron isomaltoside.
References
1.Nutritional anaemias: tools for effective prevention and control. Geneva: World Health Organization; 2017: https://www.who.int/publications/i/item/9789241513067?sequence=1. Accessed 2022 September 26.
2.Kassianides X, Bhandari S. Hypophosphataemia, fibroblast growth factor 23 and third-generation intravenous iron compounds: a narrative review. Drugs Context. 2021;10. PubMed
3.Miller JL. Iron deficiency anemia: a common and curable disease. Cold Spring Harb Perspect Med. 2013;3(7). PubMed
4.Kassianides X, Bodington R, Bhandari S. An evaluation of ferric derisomaltose as a treatment for anemia. Expert Rev Hematol. 2021;14(1):7-29. PubMed
5.Gomez-Ramirez S, Bisbe E, Shander A, Spahn DR, Munoz M. Management of Perioperative Iron Deficiency Anemia. Acta Haematol. 2019;142(1):21-29. PubMed
6.Froessler B, Rueger AM, Connolly MP. Assessing the costs and benefits of perioperative iron deficiency anemia management with ferric carboxymaltose in Germany. Risk Manag Healthc Policy. 2018;11:77-82. PubMed
7.Goodnough LT, Maniatis A, Earnshaw P, et al. Detection, evaluation, and management of preoperative anaemia in the elective orthopaedic surgical patient: NATA guidelines. Br J Anaesth. 2011;106(1):13-22. PubMed
8.Ng O, Keeler BD, Mishra A, et al. Iron therapy for preoperative anaemia. Cochrane Database Syst Rev. 2019;12:CD011588. PubMed
9.Blumenstein I, Shanbhag S, Langguth P, Kalra PA, Zoller H, Lim W. Newer formulations of intravenous iron: a review of their chemistry and key safety aspects - hypersensitivity, hypophosphatemia, and cardiovascular safety. Expert Opin Drug Saf. 2021;20(7):757-769. PubMed
10.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
11.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
12.Kvaslerud AB, Bardan S, Andresen K, et al. Intravenous iron supplement for iron deficiency in patients with severe aortic stenosis scheduled for transcatheter aortic valve implantation: results of the IIISAS randomised trial. Eur J Heart Fail. 2022;24(7):1269-1279. PubMed
13.Nashef SAM, Roques F, Sharples LD, et al. EuroSCORE II. Eur J Cardiothorac Surg. 2012;41(4):734-745. PubMed
14.Greene SJ, Butler J, Spertus JA, et al. Comparison of New York Heart Association Class and Patient-Reported Outcomes for Heart Failure With Reduced Ejection Fraction. JAMA Cardiol. 2021;6(5):522-531. PubMed
15.Laucis NC, Hays RD, Bhattacharyya T. Scoring the SF-36 in Orthopaedics: A Brief Guide. J Bone Joint Surg Am. 2015;97(19):1628-1634. PubMed
16.Iron Isomaltoside for Anemia due to Pregnancy, Menorrhagia, or Other Gynecological Conditions. (CADTH Rapid response report: summary of abstracts). Ottawa (ON): CADTH; 2021: https://www.cadth.ca/iron-isomaltoside-anemia-due-pregnancy-menorrhagia-or-other-gynecological-conditions. Accessed 2022 September 26.
17.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: iron isomaltoside 1000 (Monoferric - Pharmacosmos A/S). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/sites/default/files/cdr/complete/SR0622%20Monoferric%20-%20CDEC%20Final%20%20Recommendation%20March%2027%2C%202020%20for%20posting.pdf. Accessed 2022 September 26.
18.Intravenous Iron Preparations for Patients Undergoing Elective Surgery: A Review of Clinical Effectiveness, Cost-Effectiveness, and Guidelines. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/intravenous-iron-preparations-patients-undergoing-elective-surgery-review-clinical-effectiveness. Accessed 2022 September 26.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Randomized Controlled Trial
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Kvaslerud et al. (2022)12 Norway Funding source: Pharmacosmos | Single-centre, double-blind, randomized controlled trial | Inclusion criteria: Adult patients aged 18 years or older with severe aortic stenosis and iron deficiency who were referred for non-emergency TAVI. Patients with hemoglobin < 10 g/dL or intravenous iron infusion within prior 6 months were excluded. Baseline characteristics: Iron group: 51 patients with a mean age of 80.0 years, 55% male, 22% with a history of smoking, and median EuroSCORE II of 2.3%. Placebo group: 53 patients with a mean age of 79.2 years, 60% male, 36% with a history of smoking, and median EuroSCORE II of 2.1%. | Intervention: iron isomaltoside administered as a single IV infusion of 20 mg/kg body weight (rounded to the nearest 100 mg, maximum dose of 2,000 mg) dissolved in 100 mL sodium chloride 0.9%. Comparator: a single intravenous infusion of 100 mL sodium chloride 0.9%. | Outcomes: 6-minute walk distance, health-related quality of life, NYHA class, muscle strength, adverse events Follow-up: 6 months |
NYHA = New York Heart Association; TAVI = transcatheter aortic valve implantation.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of the Randomized Controlled Trial Using the Downs and Black Checklist10
Strengths | Limitations |
|---|---|
Kvaslerud et al. (2022)12 | |
Objective, patient characteristics, interventions, and main findings clearly described Estimates of random variability (e.g., confidence intervals) were reported Characteristics of patients lost to follow-up were reported Adverse events were reported Patients and investigators were blind to group allocation The main outcome measures were valid and reliable Statistical tests used were appropriate Compliance with the intervention was reliable Patients in different intervention groups were recruited from the same population Patients were randomly allocated to intervention groups A sample size calculation was conducted a priori, and a sufficient number of patients were included The funding source for the study and potential conflicts of interest were disclosed | A modified intention-to-treat analysis was used and approximately 30% of randomized patients in each group were not included in the analysis The study was conducted in Norway and the results may not be generalizable to the Canadian population |
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 4: Summary of Findings of Kvaslerud et al. (2022)12 — Clinical Outcomes
Outcome | Iron isomaltoside (n = 51) | Placebo (n = 53) | Mean difference (95% CI) | P value | ||
|---|---|---|---|---|---|---|
Baseline | Follow-up | Baseline | Follow-up | |||
6-minute walk distance | ||||||
6-minute walk distance (m), mean (SD) | 355 (113) | 375 (132) | 367 (129) | 384 (128) | 2 (–21 to 25) | 0.86 |
NYHA class | ||||||
NYHA class, n (%) | ||||||
I | 1 (2) | 35 (69) | 2 (4) | 30 (57) | NR | 0.18 |
II | 27 (53) | 15 (29) | 27 (51) | 20 (40) | NR | — |
III | 22 (43) | 1 (2) | 23 (43) | 3 (6) | NR | — |
IV | 1 (2) | 0 | 1 (2) | 0 | NR | — |
Muscle strength | ||||||
Hand grip strength (kg), mean (SD) | 28.1 (10.1) | 27.9 (10.4) | 31.3 (11.5) | 31.5 (12.2) | –0.5 (–2.2 to 1.1) | 0.53 |
Health-related quality of life | ||||||
KCCQ overall summary score, median (IQR) | 69 (56 to 81) | 88 (71 to 95) | 64 (35 to 81) | 82 (65 to 94) | 0.6 (–6.4 to 7.7) | 0.86 |
KCCQ functional summary score, median (IQR) | 78 (56 to 86) | 88 (68 to 96) | 70 (50 to 86) | 89 (69 to 95) | –0.6 (–7.1 to 6.0) | 0.86 |
EQ-5D-3L index, median (IQR) | 0.83 (0.77 to 0.93) | 0.91 (0.82 to 0.97) | 0.81 (0.74 to 0.93) | 0.91 (0.78 to 0.97) | –0.001 (–0.4 to 0.4) | 0.97 |
EQ-5D VAS, median (IQR) | 67 (50 to 80) | 70 (48 to 84) | 50 (40 to 73) | 75 (60 to 85) | –7.8 (–16.5 to 0.86) | 0.077 |
SF-36v2 summary PCS, median (IQR) | 39 (33 to 47) | 45 (35 to 51) | 36 (31 to 44) | 43 (36 to 51) | –0.5 (–4.0 to 2.9) | 0.76 |
SF-36v2 summary MCS, median (IQR) | 51 (44 to 55) | 50 (44 to 56) | 48 (38 to 55) | 53 (43 to 56) | 3.0 (–0.2 to 6.3) | 0.067 |
CI = confidence interval; IQR = interquartile range; KCCQ = Kansas City Cardiomyopathy Questionnaire; NR = not reported; SD = standard deviation; SF-36v2 = Short Form (36) Health Survey version 2; NYHA = New York Heart Association; VAS = visual analogue scale.
Table 5: Summary of Findings of Kvaslerud et al. (2022)12 — Safety Outcomes
Outcome | Iron isomaltoside (n = 73) | Placebo (n = 75) | P value |
|---|---|---|---|
Adverse events, n | 53 | 66 | NR |
Serious adverse events, n | 37 | 49 | 0.071 |
Infections, n | |||
Intravenous treatment | 5 | 6 | NR |
Per oral treatment | 2 | 1 | NR |
Deaths, n | 2 | 5 | NR |
Infusion reactions, n | |||
Mild | 3 | 2 | NR |
Hypersensitivity reaction | 1 | 0 | NR |
Skin discoloration | 0 | 0 | NR |
NR = not reported.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
Quay T, Spry C. International Policies on Parenteral Iron. (CADTH Environmental scan no.89). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/international-policies-parenteral-iron-environmental-scan. Accessed 2022 September 26.
Non-Randomized Studies
Alternative Intervention or Comparator
Ploug M, Kroijer R, Qvist N, Knudsen T. Preoperative Intravenous Iron Treatment in Colorectal Cancer: Experience from Clinical Practice. J Surg Res. 2022;277:37-43. PubMed
Evans CR, Jones R, Phillips G, Greene G, Phillips M, Morris-Clarke R. Observational study of pre-operative intravenous iron given to anaemic patients before elective cardiac surgery. Anaesthesia. 2021;76(5):639-646. PubMed
Kam PM, Chu CW, Chan EM, Liu OL, Kwok KH. Use of intravenous iron therapy in colorectal cancer patient with iron deficiency anemia: a propensity-score matched study. Int J Colorectal Dis. 2020;35(3):521-527. PubMed
Review Articles
Schaefer B, Meindl E, Wagner S, Tilg H, Zoller H. Intravenous iron supplementation therapy. Mol Aspects Med. 2020;75:100862. PubMed
Grzywacz A, Lubas A, Fiedor P, Fiedor M, Niemczyk S. Safety and Efficacy of Intravenous Administration of Iron Preparations. Acta Pol Pharm. 2017;74(1):13-24. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca