CADTH Health Technology Review
Treatment Strategies for Sexual Dysfunction Associated With Psychotropic Medications
Rapid Review
Authors: Khai Tran, Jennifer Horton
Abbreviations
PDE-5
phosphodiesterase type 5
RCT
randomized controlled trial
SD
sexual dysfunction
Key Messages
For antipsychotic-related sexual dysfunction, 1 guideline recommends switching to aripiprazole or another non-hyperprolactinemic antipsychotic as the first option. Alternatively, the guideline recommends adjunctive treatment with aripiprazole, or switching to antipsychotics that have less impact on sexual function. Another guideline recommends adding estrogen or testosterone treatment to the antipsychotic medication to assist sexual dysfunction in women.
For antidepressant-related sexual dysfunction, 1 guideline recommends switching to agomelatine or to a non-serotonergic drug or fluvoxamine as first option. Alternatively, the guideline recommends switching to a partially non-serotonergic antidepressant, adding antidotes, or using vaginal lubricants.
Context and Policy Issues
A 2015 survey estimated that about 30% of inmates in federal Canadian prisons received prescriptions for psychotropic medications, compared with about 8% in the general population.1 Psychotropic medications, including antipsychotics and antidepressants, may cause sexual dysfunction (SD) in men and women.2 Sexual dysfunction associated with psychotropic medications in women may include low desire, reduced arousal, and pain, while erectile dysfunction, premature or delayed ejaculation, and low desire are the primary problems in men.3
There are 2 types of antipsychotics, typical and atypical antipsychotic drugs.4 Typical antipsychotics are first generation antipsychotic drugs developed in the 1950s, while second generation antipsychotic drugs developed in the 1990s are atypical antipsychotics.4 Typical antipsychotic drugs bind strongly to dopamine type 2 (D2) receptors, while atypical antipsychotic drugs have lower affinity for dopaminergic receptors.5 Both typical and atypical antipsychotics are associated with impairment of sexual functioning.6,7 However, some drugs may affect sexual function more than others.6,7 A systematic review with meta-analysis showed that quetiapine, ziprasidone, perphenazine, and aripiprazole were associated with frequencies of SD ranging from 16% to 27%, while olanzapine, risperidone, haloperidol, clozapine, and thioridazine were associated with higher frequencies of SD (i.e., 40% to 60%).8
Treatment with different antidepressant classes such as tricyclic antidepressants, serotonin-norepinephrine reuptake inhibitors, selective serotonin reuptake inhibitors, and monoamine oxidase inhibitors can lead to all types of sexual side effects.9 A meta-analysis on treatment-emergent SD related to antidepressants indicated that fluoxetine, paroxetine, citalopram, venlafaxine, and sertraline were associated with highest frequencies of total SD (70% to 80%).10 The frequencies of SD of mirtazapine, fluvoxamine, escitalopram, duloxetine, phenelzine, and imipramine varied from 25% to 45%.10 Other antidepressant drugs that had frequencies of SD comparable to or lower than placebo were moclobemide, agomelatine, amineptine, nefazodone, and bupropion.10
Most antipsychotics and some antidepressants are associated with elevation of plasma prolactin, termed hyperprolactinemia.11,12 Patients with hyperprolactinemia frequently have SD, osteoporosis, and even breast cancer.11 The secretion of prolactin is regulated by the inhibitory action of the D2 receptors in the hypothalamic infundibular system.12 Therefore, the use of psychotropic medications can lead to a decrease in dopamine and consequently an increase in prolactin, resulting in SD.12 Typical antipsychotics are responsible for hyperprolactinemia, termed prolactin-raising drugs, while atypical antipsychotics are unfrequently or transiently associated with increase in prolactin, termed prolactin-sparing drugs.12 Among antidepressant drugs, some tricyclics (e.g., clomipramine, trimipramine), selective serotonin reuptake inhibitors (e.g., sertraline, fluoxetine), and monoamine oxidase inhibitors (e.g., pargyline, clorgyline) can cause hyperprolactinemia.12 There are several guidelines with recommendations for the assessment and management of antipsychotic-induced hyperprolactinemia.13
Table 1 presents information regarding the frequencies of SD of various drug classes of antipsychotics and antidepressants, distinguishing the effect of the drugs on serum prolactin levels and the degree of prolactin elevation.
Sexual dysfunction caused by psychotropic medications is often overlooked in clinical practice.7,14 Given the frequency of psychotropic medication-induced SD, management of this adverse effect is important to prevent long-term nonadherence.7,15 Several strategies for the treatment of medication-associated SD have been proposed in the literature, include waiting for spontaneous remission, dose reduction, drug holiday (i.e., off medication for 2 to 3 days before sexual activity), nonpharmacologic interventions, switching to another medication, and adding a medication to reverse SD.2,15 However, it is unclear if there are any evidence-based guidelines that provide recommendations for treatment strategies for the management of SD induced by psychotropic medications.
This report aims to summarize the recommendations from evidence-based guidelines regarding the management of SD associated with psychotropic medications.
Table 1: Frequencies of Sexual Dysfunction Associated with Psychotropic Medications
Class | Drug | Effect on prolactin level (degree of elevationa) | Frequencies of sexual dysfunction, % |
|---|---|---|---|
Antipsychotics | |||
Typical | Haloperidol | Raising (high)16 | |
Typical | Chlorpromazine | Raising (moderate16) | Not identified |
Typical | Flupenthixol | Raising (not identified) | Not identified |
Typical | Fluphenazine | Raising (high16) | 7819 |
Typical | Loxapine | Raising (moderate16) | Not identified |
Typical | Methotrimeprazine | Raising (not identified) | Not identified |
Typical | Perphenazine | Raising (moderate16) | |
Typical | Pimozide | Raising (moderate16) | Not identified |
Typical | Prochlorperazine | Raising (not identified) | Not identified |
Typical | Trifluoperazine | Raising (moderate16) | 20 to 40 (male)20 varied with assessment questionnaire; 45 (female)21; 4718 |
Typical | Zuclopenthixol | Raising (not identified) | Not identified |
Atypical | Asenapine | Raising (moderate16) | Not identified |
Atypical | Brexpiprazole | Sparing (not identified) | 3.122 |
Atypical | Lurasidone | Sparing (none or low)16 | 1.923; < 102 |
Antidepressants | |||
NDRI | Bupropion | Sparing (none16) | 1010; placebo level2 |
TCA | Amitriptyline | Sparing (low16) | 5.724 |
TCA | Clomipramine | Raising (high16) | 50 to 702 |
TCA | Desipramine | Sparing (low16) | Not identified |
TCA | Trimipramine | Raising (not identified) | Not identified |
TCA | Doxepin | Sparing (not identified) | Not identified |
SNRI | Duloxetine | Raising (not identified) | |
TCA | Imipramine | Raising (not identified) | |
TeCA | Mirtazapine | Sparing (none16) | |
TCA | Nortriptyline | Sparing (none16) | |
Serotonin modulator | Trazodone | Sparing (none16) | |
SNRI | Venlafaxine | Raising (not identified) | |
Serotonin modulator | Vortioxetine | Sparing (not identified) | |
NDRI = norepinephrine dopamine reuptake inhibitor; SNRI = serotonin-norepinephrine reuptake inhibitor; TCA = tricyclic antidepressant; TeCA = tetracyclic antidepressant.
aHigh: > 50%; moderate: 25 to 50%; low: < 25%; none or low: rare reports.
Research Question
What are the evidence-based guidelines regarding the management of sexual dysfunction associated with psychotropic medications?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, PsycINFO, the Cochrane Database of Systematic Reviews, the International HTA Database, and the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were psychotropics, antidepressants, antipsychotics, and sexual dysfunction. CADTH-developed search filters were applied to limit retrieval to guidelines. Where possible, retrieval was limited to the human population. The search was completed on August 23, 2022, and limited to English-language documents published since January 1, 2012.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 2.
Criteria | Description |
|---|---|
Population | People with mental health conditions who are being treated with psychotropic medications (e.g., antidepressants, antipsychotics, anxiolytics) |
Intervention | Any strategies for the management of SD associated with psychotropic medications (e.g., switching to another psychotropic medication, modifying the dose of the psychotropic medication, treatment with additional pharmacotherapy [e.g., testosterone, levothyroxine, phosphodiesterase type 5 inhibitors]) |
Comparator | Not applicable |
Outcomes | Recommendations regarding best practices (e.g., which strategies are recommended or not recommended, treatment protocols) |
Study designs | Evidence-based guidelines |
SD = sexual dysfunction.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 2, or were published before 2012.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument30 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
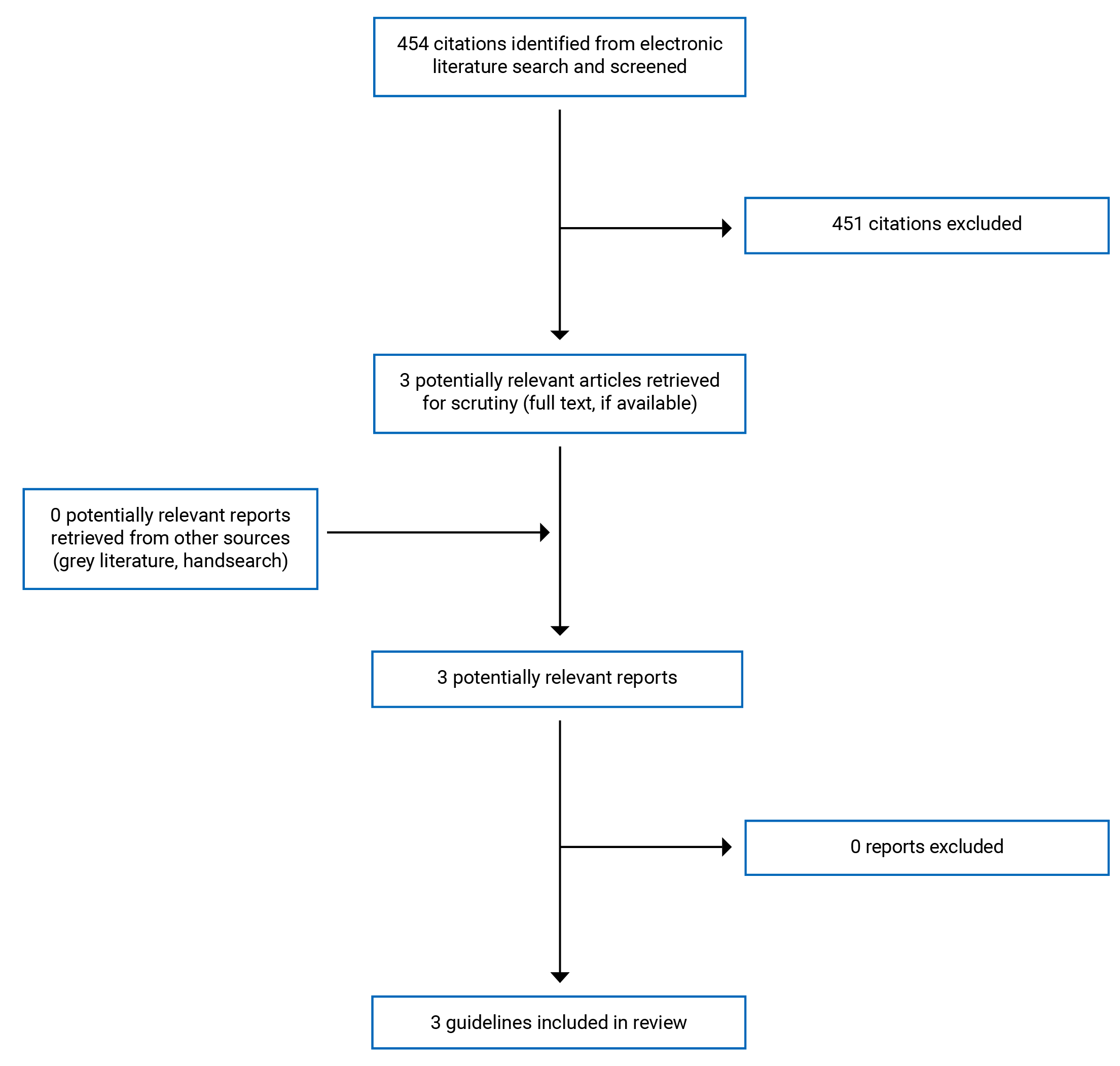
A total of 454 citations were identified in the literature search. Following screening of titles and abstracts, 451 citations were excluded and 3 potentially relevant reports from the electronic search were retrieved for full-text review. No potentially relevant publications were retrieved from the grey literature search for full-text review. All 3 potentially relevant articles (i.e., guidelines) met the inclusion criteria and were included in this report. Appendix 1 presents the PRISMA31 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
Additional details regarding the characteristics of included guidelines (Table 3) are provided in Appendix 2.
Study Design
The 2021 and 2019 guidelines by Montejo et al.7,14 provide clinical recommendations for management strategies of antipsychotic-related SD7 and antidepressant-related SD14 for clinicians prescribing antipsychotics and antidepressants, respectively. Both guidelines7,14 involved literature searches from 2 databases, and the evidence was summarized narratively. The major outcome considered in both guidelines was improvement in SD associated with antipsychotics7 or antidepressants.14 The level of evidence assigned to each recommendation was based on the Scottish Intercollegiate Guidelines Network Grading Review Group. Neither guideline7,14 reported on the process of developing the recommendations or the evaluation and guideline validation.
The 2016 guideline by Galletly et al.32 provides recommendations for the clinical management of schizophrenia and related disorders for all health professionals, including policy-makers, working in Australia and New Zealand. The working group planned the scope, and individual members drafted sections according to their areas of interest and expertise. The working group reviewed the manuscript, and discussion occurred via a series of teleconferences. When there was disagreement, the issue was discussed until consensus was reached. The level of evidence was assigned according to the Australian National Health and Medical Research Council criteria. Recommendations were considered as either evidence-based (when there was sufficient evidence on the topic) or consensus-based (when evidence was weak or lacking).
Country of Origin
Both guidelines by Montejo et al.7,14 were conducted by authors from Spain.
The guideline by Galletly et al.32 was conducted by authors from Australia.
Patient Population
The target population in the 2021 guideline by Montejo et al. was patients with psychoses,7 and the target population in the 2019 guideline by Montejo et al. was patients with depression.14
The target population in the guideline by Galletly et al.32 was patients with schizophrenia and related disorders, including schizoaffective disorder, schizotypal disorder, schizophreniform disorder, and acute transient psychotic disorder with symptoms of schizophrenia.
Interventions
The 2 guidelines by Montejo et al.7,14 provide management strategies for treatment-emergent SD in patients taking antipsychotics7 or antidepressants.14
The interventions and practices considered in the guideline by Galletly et al.32 include treatment and management of ultra-high-risk syndromes, first-episode psychoses, and prolonged psychoses, including psychoses associated with substance use.
Outcomes
The outcome in the 2 guidelines by Montejo et al.7,14 was improvement of SD associated with antipsychotics7 or antidepressants.14
The guideline by Galletly et al.32 considered all clinical outcomes related to early intervention, physical health, psychosocial treatments, cultural considerations, and improving vocation.
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of the included guidelines (Table 4) are provided in Appendix 3.
All 3 guidelines7,14,32 were explicit in terms of scope and purpose (i.e., objectives, health questions, and populations), and had clear presentation (i.e., specific, unambiguous, and easy-to-find key recommendations, with options for managing the different conditions or health issues). In terms of stakeholder involvement, the guideline by Galletly et al.32 clearly defined target users, the development groups, and public consultation groups, while both guidelines by Montejo et al.7,14 did not report the guideline development groups and the views and preferences of the target population. In both guidelines by Montejo et al.,7,14 literature was searched from 2 databases, the evidence was summarized narratively, and the level of evidence assigned to each recommendation was based on the Scottish Intercollegiate Guidelines Network Grading Review Group. The guideline by Galletly et al.32 did not report on the evidence collection, selection, and synthesis, but it provided the criteria for rating the levels of evidence for intervention studies. The recommendations in the guideline by Galletly et al.32 were not graded, but they were classified as evidence-based recommendations or consensus-based recommendations, depending on the availability and strength of the evidence. The strengths and limitations of the body of evidence, and methods of formulating the recommendations, were clearly described in the guideline by Galletly et al.,32 but not in both guidelines by Montejo et al.7,14 All 3 guidelines7,14,32 considered health benefits and risks of side effects in formulating the recommendations. None of the included guidelines7,14,32 provided a procedure for updating the guidelines. For applicability, the guideline by Galletly et al.,32 but not the guidelines by Montejo et al.,7,14 was explicit in terms of facilitators and barriers to application, advice and/or tools on how the recommendations can be put into practice, resource implications, and monitoring or auditing criteria. For editorial independence, all 3 guidelines7,14,32 reported competing interests of the authors or guideline development group members. Overall, the 2 guidelines by Montejo et al.7,14 were of low methodological quality, while the guideline by Galletly et al.32 was of moderate methodological quality.
Summary of Findings
Appendix 4 presents the summary of guideline recommendations (Table 5).
Guidelines Regarding the Management of SD Associated With Psychotropic Medications
Antipsychotic-Related SD
Two guidelines7,32 provided some management strategies for antipsychotic-related SD.
The guideline by Montejo et al.7 recommends switching to aripiprazole (Evidence Level A), or switching to a non-hyperprolactinemic antipsychotic drug such as quetiapine or ziprasidone (Evidence Level B), as the first option for all sexual dimensions including low sexual desire, orgasm retardation, anorgasmia, erectile dysfunction, and poor vaginal lubrication. Alternatively, the guideline7 recommends adding aripiprazole for low sexual desire, orgasm retardation, and anorgasmia (Evidence Level B), adding phosphodiesterase type 5 (PDE-5) inhibitors for erectile dysfunction (Evidence Level B), and using vaginal lubricants for poor vaginal lubrication (Evidence Level B). Other options are switching to olanzapine below 15 mg/day (Evidence Level B) or lowering the dose of the current antipsychotics (Evidence Level C) for all sexual dimensions.
The guideline by Galletly et al.32 recommends adding estrogen or testosterone treatment to the antipsychotic medication to address SD including lowered libido, poor vaginal lubrication, and anorgasmia in women with psychoses (evidence-based recommendation). In addition, although they are not evidence-based recommendations, the guideline32 provides management strategies for the side effects of antipsychotic drugs, including SD associated with hyperprolactinemia, in a table form. The guideline32 suggests that prolactin level should be evaluated, testing should be conducted to exclude pituitary tumour, and medication should be switched to a prolactin-sparing drug if symptoms of sexual and menstrual dysfunction exist.
Antidepressant-Related SD
The guideline by Montejo et al.14 provides some management strategies for antidepressant-related SD. As the first option, the guideline recommends switching to agomelatine (Evidence Level A), switching to non-serotonergic drugs such as bupropion or mirtazapine (Evidence Level B) for all sexual dimensions, or adding bupropion for low sexual desire (Evidence level B). Alternatively, the guideline14 recommends switching to desvenlafaxine (50 mg/day) or vortioxetine (< 15 mg/day) for all sexual dimensions (Evidence Level B). Other options are dose reduction in association with aripiprazole for low sexual desire, dose reduction for orgasm retardation, dose reduction or “weekend holiday” protocol for anorgasmia, adding PDE-5 inhibitors for erectile dysfunction, and dose reduction in addition with using vaginal lubricants for poor vaginal lubrication (Evidence Level C).
Limitations
The authors of both guidelines by Montejo et al.7,14 recognized that information on the best method of treatment for SD associated with psychotropic medications was scarce. For some strategies, such as waiting for spontaneous SD remission, dosage reduction, and add-on treatment, the evidence is not strong, as there is a lack of controlled studies to support these strategies.
The guideline by Galletly et al.32 has an evidence-based recommendation for the management of SD associated with antipsychotic medication in women with psychoses, but not men. The recommendation only suggests the use of antidotes or adjunctive treatment to improve SD in women, without examining other strategies.
Conclusions and Implications for Decision- or Policy-Making
This report identified 2 Spanish guidelines7,14 and 1 Australian guideline32 with low to moderate methodological quality.
For antipsychotic-related SD, the guideline by Montejo et al.7 recommends switching to aripiprazole or another non-hyperprolactinemic antipsychotic as the first option. If this is not possible, the guideline recommends adjunctive treatment with aripiprazole, switching to antipsychotics that have less impact on sexual function, or dose reduction. The guideline by Galletly et al.32 recommends adding estrogen or testosterone treatment to the antipsychotic medication to assist SD in women. This guideline also provides some management strategies for SD associated with hyperprolactinemia induced by antipsychotics.
For antidepressant-related SD, the guideline by Montejo et al.14 recommends switching to agomelatine or to a non-serotonergic drug (e.g., bupropion or mirtazapine) or fluvoxamine as first option. If this is not possible, the guideline recommends switching to a partially non-serotonergic antidepressant (e.g., desvenlafaxine or vortioxetine), adding antidotes such as PDE-5 inhibitors, using vaginal lubricants, or dose reduction.
Given that psychotropic medications can be often associated with SD, a delicate balance between prescribing an effective drug that improves psychotropic symptomatology and minimizing its impact on sexual function is important to improve patients’ quality of life and prevent treatment nonadherence. The identified guidelines provide some strategies for the management of antipsychotic- and antidepressant-related SD, emphasizing switching to drugs that have low impact on SD or using adjunctive treatment. While dose reduction was suggested as an alternative in 2 guidelines,7,14 this approach was neither recommended nor advisable. The recommendations of the included guidelines may be applicable to the Canadian context, provided that the recommended drugs are available and approved for use in Canada. Given the lack of strong evidence, more research is needed to obtain better evidence-based recommendations.
References
1.Brown GP, Stewart LA, Rabinowitz T, Boudreau H, Wright AJ. Approved and Off-Label Use of Prescribed Psychotropic Medications among Federal Canadian Inmates. Can J Psychiatry. 2018;63(10):683-691. PubMed
2.Lew-Starowicz M, Giraldi A. Impact of Psychotropic Medications on Sexual Functioning. In: Lew-Starowicz M GA, Krüger T, ed. Psychiatry and Sexual Medicine: Springer, Cham; 2021:353-371.
3.Laumann EO, Paik A, Rosen RC. Sexual dysfunction in the United States: prevalence and predictors. JAMA. 1999;281(6):537-544. PubMed
4.Typical and Atypical Antipsychotic Agents. 2022; https://www.goodtherapy.org/drugs/anti-psychotics.html, 2022 Sep 21.
5.Dazzan P, Morgan KD, Orr K, et al. Different effects of typical and atypical antipsychotics on grey matter in first episode psychosis: the AESOP study. Neuropsychopharmacology. 2005;30(4):765-774. PubMed
6.Park YW, Kim Y, Lee JH. Antipsychotic-induced sexual dysfunction and its management. World J Mens Health. 2012;30(3):153-159. PubMed
7.Montejo AL, de Alarcón R, Prieto N, Acosta JM, Buch B, Montejo L. Management Strategies for Antipsychotic-Related Sexual Dysfunction: A Clinical Approach. J Clin Med. 2021;10(2). PubMed
8.Serretti A, Chiesa A. A meta-analysis of sexual dysfunction in psychiatric patients taking antipsychotics. Int Clin Psychopharmacol. 2011;26(3):130-140. PubMed
9.Higgins A, Nash M, Lynch AM. Antidepressant-associated sexual dysfunction: impact, effects, and treatment. Drug Healthc Patient Saf. 2010;2:141-150. PubMed
10.Serretti A, Chiesa A. Treatment-emergent sexual dysfunction related to antidepressants: a meta-analysis. J Clin Psychopharmacol. 2009;29(3):259-266. PubMed
11.Peuskens J, Rubio G, Schreiner A. Dosing and switching of paliperidone ER in patients with schizophrenia: Recommendations for clinical practice. Annals of General Psychiatry. 2014;13(1). PubMed
12.Torre DL, Falorni A. Pharmacological causes of hyperprolactinemia. Ther Clin Risk Manag. 2007;3(5):929-951. PubMed
13.Grigg J, Worsley R, Thew C, Gurvich C, Thomas N, Kulkarni J. Antipsychotic-induced hyperprolactinemia: synthesis of world-wide guidelines and integrated recommendations for assessment, management and future research. Psychopharmacology. 2017;234(22):3279-3297. PubMed
14.Montejo AL, Prieto N, de Alarcón R, Casado-Espada N, de la Iglesia J, Montejo L. Management Strategies for Antidepressant-Related Sexual Dysfunction: A Clinical Approach. J Clin Med. 2019;8(10). PubMed
15.Clayton AH, Alkis AR, Parikh NB, Votta JG. Sexual Dysfunction Due to Psychotropic Medications. Psychiatric Clinics of North America. 2016;39(3):427-463. PubMed
16.Drugs that cause hyperprolactinemia. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: http://www.uptodate.com. Accessed 2022 Sep 6.
17.Bobes J, Garc APMP, Rejas J, et al. Frequency of sexual dysfunction and other reproductive side-effects in patients with schizophrenia treated with risperidone, olanzapine, quetiapine, or haloperidol: the results of the EIRE study. J Sex Marital Ther. 2003;29(2):125-147. PubMed
18.Mujahid MA, Sarkar AA, Monzur SE, et al. Factors associated with sexual side effects of antipsychotics in patients with psychotic disorders. Arch NIMH. 2020;3(2):21-24.
19.Kelly DL, Conley RR. A randomized double-blind 12-week study of quetiapine, risperidone or fluphenazine on sexual functioning in people with schizophrenia. Psychoneuroendocrinology. 2006;31(3):340-346. PubMed
20.Nebhinani N, Grover S, Avasthi A. Sexual dysfunction in male subjects receiving trifluoperazine, risperidone, or olanzapine: rates vary with assessment questionnaire. Prim Care Companion CNS Disord. 2012;14(2). PubMed
21.Reddy S, Menghal R, Rathi P, P. R. Empirical evaluation of olanzapine, risperidone, and trifluoperazine induced sexual dysfunction in female schizophrenic patients. International Journal of Psychology. 2019;11(1):14-19.
22.Clayton AH, Ivkovic J, Chen D, George V, Hobart M. Effect of Brexpiprazole on Prolactin and Sexual Functioning: An Analysis of Short- and Long-Term Study Data in Major Depressive Disorder. J Clin Psychopharmacol. 2020;40(6):560-567. PubMed
23.Clayton AH, Tsai J, Mao Y, Pikalov A, Loebel A. Effect of Lurasidone on Sexual Function in Major Depressive Disorder Patients With Subthreshold Hypomanic Symptoms (Mixed Features): Results From a Placebo-Controlled Trial. J Clin Psychiatry. 2018;79(5). PubMed
24.Chen LW, Chen MY, Lian ZP, et al. Amitriptyline and Sexual Function: A Systematic Review Updated for Sexual Health Practice. Am J Mens Health. 2018;12(2):370-379. PubMed
25.Jacobsen PL, Mahableshwarkar AR, Palo WA, Chen Y, Dragheim M, Clayton AH. Treatment-emergent sexual dysfunction in randomized trials of vortioxetine for major depressive disorder or generalized anxiety disorder: a pooled analysis. CNS Spectr. 2016;21(5):367-378. PubMed
26.Dueñas H, Brnabic AJ, Lee A, et al. Treatment-emergent sexual dysfunction with SSRIs and duloxetine: effectiveness and functional outcomes over a 6-month observational period. Int J Psychiatry Clin Pract. 2011;15(4):242-254. PubMed
27.Lee KU, Lee YM, Nam JM, et al. Antidepressant-Induced Sexual Dysfunction among Newer Antidepressants in a Naturalistic Setting. Psychiatry Investig. 2010;7(1):55-59. PubMed
28.Strohmaier J, Wüst S, Uher R, et al. Sexual dysfunction during treatment with serotonergic and noradrenergic antidepressants: clinical description and the role of the 5-HTTLPR. World J Biol Psychiatry. 2011;12(7):528-538. PubMed
29.Khazaie H, Rezaie L, Rezaei Payam N, Najafi F. Antidepressant-induced sexual dysfunction during treatment with fluoxetine, sertraline and trazodone; a randomized controlled trial. Gen Hosp Psychiatry. 2015;37(1):40-45. PubMed
30.Agree Next Steps C. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2022 Sep 6.
31.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
32.Galletly C, Castle D, Dark F, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the management of schizophrenia and related disorders. Australian and New Zealand Journal of Psychiatry. 2016;50(5):410-472. PubMed
Appendix 1: Selection of Included Studies
Note that this appendix has not been copy-edited.
Appendix 2: Characteristics of Included Publications
Table 3: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
Montejo et al. (2021)7 | ||||||
Intended users: Clinicians involved in prescribing antipsychotics to patients with psychosis Target population: Patients with psychosis | Management strategies for treatment-emergent SD in patients taking antipsychotics | Improvement of SD associated with antipsychotics | Literature search of 2 databases with no time limit. Key search terms were provided. Evidence was summarized narratively | Level of evidencea assigned based on the Scottish Intercollegiate Guidelines Network Grading Review Group | NR | NR |
Montejo et al. (2019)14 | ||||||
Intended users: Clinicians involved in prescribing antidepressants to patients with depression Target population: Patients with depression | Management strategies for treatment-emergent SD in patients taking antidepressants | Improvement of SD associated with antidepressants | Literature search of 2 databases with no time limit. Key search terms were provided. Evidence was summarized narratively | Level of evidencea assigned based on the Scottish Intercollegiate Guidelines Network Grading Review Group | NR | NR |
RANZCP, Galletly et al. (2016)32 | ||||||
Intended users: Health professionals working in Australia and New Zealand involved in the clinical management of schizophrenia and related disorders Target population: Patients with schizophrenia, schizoaffective disorder, schizotypal disorder, schizophreniform disorder and acute transient psychotic disorder with symptoms of schizophrenia | Treatment and management of ultra–high-risk syndromes, first-episode psychoses, and prolonged psychoses, including psychoses associated with substance use | All clinical outcomes related to early intervention, physical health, psychosocial treatments, cultural considerations, and improving vocation | NR | Level of evidence was assigned according to Australian NHMRC.b There are 2 types of recommendationsb | The working group planned the scope and individual members drafted sections according to their areas of interest and expertise. The working group reviewed the manuscript, and discussion occurred via a series of teleconferences. For disagreement, the issue was discussed until consensus was reached. | The draft was reviewed by experts in schizophrenia. The guideline was published in a peer-reviewed journal. |
NHMRC = National Health and Medical Research Council; NR = not reported; RANZCP = Royal Australian and New Zealand College of Psychiatrists; SD = sexual dysfunction.
aLevel of evidence:
A: Recommended (good evidence that the measure is effective, and the benefits far outweigh the harms).
B: Recommended (at least moderate evidence that the measure is effective, and the benefits outweigh the harms).
C: Neither recommended nor inadvisable (at least moderate evidence that the measure is effective; however, the level of benefit is very similar to the level of harm and a general recommendation cannot be justified).
bLevel of evidence:
I: A systematic review of level II studies.
II: A randomized controlled trial.
III-1: A pseudo-randomized controlled trial (i.e., alternate allocation or some other method).
III-2: A comparative study with concurrent controls.
III-3: A comparative study without concurrent controls.
bTypes of recommendations:
Evidence-based recommendations (EBR): Formulated when the working group judged that there was sufficient evidence on the topic.
Consensus-based recommendations (CBR): Formulated when evidence was weak or lacking.
Note that this appendix has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Guideline Using AGREE II30
Item | RANZCP, Galletly et al. (2016)32 | Montejo et al. (2021)7 | Montejo et al. (2019)14 |
|---|---|---|---|
Domain 1: Scope and purpose | |||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes |
3. The population (e.g., patients, public) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes |
Domain 2: Stakeholder involvement | |||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | NR | NR |
5. The views and preferences of the target population (e.g., patients, public) have been sought. | Yes | NR | NR |
6. The target users of the guideline are clearly defined. | Yes | Yes | Yes |
Domain 3: Rigour of development | |||
7. Systematic methods were used to search for evidence. | NR | Yes | Yes |
8. The criteria for selecting the evidence are clearly described. | NR | Yes | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Unclear | Unclear |
10. The methods for formulating the recommendations are clearly described. | Yes | NR | NR |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes | Yes | Yes |
14. A procedure for updating the guideline is provided. | NR | NR | NR |
Domain 4: Clarity of presentation | |||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes |
Domain 5: Applicability | |||
18. The guideline describes facilitators and barriers to its application. | Yes | NR | NR |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes | NR | NR |
20. The potential resource implications of applying the recommendations have been considered. | Yes | NR | NR |
21. The guideline presents monitoring and/or auditing criteria. | Yes | NR | NR |
Domain 6: Editorial independence | |||
22. The views of the funding body have not influenced the content of the guideline. | Unclear | No external funding | No external funding |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; NR = not reported; RANZCP = Royal Australian and New Zealand College of Psychiatrists.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 5: Summary of Recommendations in Included Guideline
Recommendations and supporting evidence | Quality of evidence and strength of recommendations | |
|---|---|---|
Montejo et al. (2021)7 | ||
Management strategies for antipsychotic-related SD | ||
First option: For low sexual desire, orgasm retardation, anorgasmia, erectile dysfunction, and decreased vaginal lubrication, switching to aripiprazole7 (p. 10) | Quality of evidence: A Strength of recommendation: Recommended | |
Switching to non-hyperprolactinemic antipsychotics, such as quetiapine or ziprasidone7 (p. 10) | Quality of evidence: B Strength of recommendation: Recommended | |
Supporting evidence: Six studies found that aripiprazole improved SD frequencies across all sexual dimensions (desire, arousal, and orgasm). Six other studies showed that switching to antipsychotics that have little effect on prolactin levels also improved SD. | ||
Alternatively: Adding aripiprazole (for low sexual desire, orgasm retardation, anorgasmia), adding PDE-5 inhibitors (for erectile dysfunction), and using vaginal lubricants (decreased vaginal lubrication)7 (p. 10) | Quality of evidence: B Strength of recommendation: Recommended | |
Switching to olanzapine below 15 mg/day for all sexual dimensions7 (p. 10) | Quality of evidence: B Strength of recommendation: Recommended | |
Lowering the dose of the current antipsychotic for all sexual dimensions7 (p. 10) | Quality of evidence: C Strength of recommendation: Neither recommended nor inadvisable | |
Supporting evidence: Seven studies have shown that adding aripiprazole concomitantly with other antipsychotics improved SD. Six studies have shown that, aside from aripiprazole, PDE-5 inhibitors improve erectile dysfunction. Two studies provided evidence for switching to olanzapine. For dose reduction, 1 study recommended decreasing the dose as first step in intervention, but 2 other studies found this strategy is not effective and may have a risk of relapse.7 | ||
Montejo et al. (2019)14 | ||
Management strategies for antidepressant-related SD | ||
First option: For low sexual desire, orgasm retardation, anorgasmia, erectile dysfunction, and scarce vaginal lubrication, switching to agomelatine14 (p. 12) | Quality of evidence: A Strength of recommendation: Recommended | |
Switching to a non-serotonergic drug, such as bupropion or mirtazapine, for all sexual dimensions14 (p. 12) | Quality of evidence: B Strength of recommendation: Recommended | |
Adding bupropion for low sexual desire14 (p. 12) | Quality of evidence: B Strength of recommendation: Recommended | |
Supporting evidence: One study comparing agomelatine with venlafaxine found that both drugs had similar antidepressant efficacy, but patients treated with agomelatine had better sexual function compared to those receiving venlafaxine. The evidence was further demonstrated in 3 double-blind placebo-controlled trials comparing agomelatine with paroxetine or escitalopram and placebo, showing that sexual problems in the agomelatine groups were comparable with placebo. Five studies showed that switching to other non-serotonergic drugs (e.g., agomelatine, bupropion, mirtazapine) can improve SD, although the therapeutic response to the switch needs to be carefully monitored. Three double-blind placebo-controlled trials found that the addition of bupropion improved sexual function; however, adding bupropion may worsen anxiety level in some patients.14 | ||
Alternatively: Switching to desvenlafaxine (50 mg/day) or vortioxetine (< 15 mg/day) for all sexual dimensions14 (p. 12) | Quality of evidence: B Strength of recommendation: Recommended | |
Dose reduction in association with aripiprazole (for low sexual desire), dose reduction (for orgasm retardation), dose reduction or “weekend holiday” protocol (for anorgasmia), adding PDE-5 inhibitors (for erectile dysfunction), and dose reduction in addition to using vaginal lubricants14 (p.12) | Quality of evidence: C Strength of recommendation: Neither recommended nor advisable | |
Supporting evidence: One observational study found that switching to desvenlafaxine reduced severe treatment-emergent SD from 93% to 76% and improved sexual desire and orgasm, but not sexual arousal. Another study showed that desvenlafaxine when prescribed as first option had lower frequency of SD (44%) compared to venlafaxine (74%) and duloxetine (75%). One study showed that dose reduction of a serotonergic drug may improve treatment-emergent SD but worsen the depressive symptoms.14 | ||
RANZCP, Galletly et al. (2016)32 | ||
For women with psychoses: “Consider adding oestrogen or testosterone treatment to antipsychotic medication to assist sexual dysfunction.”32 (p. 454) Supporting evidence: One randomized trial showed that adding estrogen or testosterone treatment to the antipsychotic medication may assist SD problems in postmenopausal and premenopausal women. | Level of evidence: II Type of recommendation: EBR | |
Management strategies for SD associated with hyperprolactinemia induced by antipsychotic drugs:
Not EBR. | NA | |
EBR = evidence-based recommendation; NA = not applicable; PDE-5 = phosphodiesterase type 5; RANZCP = Royal Australian and New Zealand College of Psychiatrists; SD = sexual dysfunction.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Review Articles
Clayton AH, Alkis AR, Parikh NB, Votta JG. Sexual Dysfunction Due to Psychotropic Medications. Psychiatric Clinics of North America. 2016;39(3):427-463. PubMed
Montejo AL, Montejo L, Navarro-Cremades F. Sexual side-effects of antidepressant and antipsychotic drugs. Curr Opin Psychiatry. 2015;28(6):418-423. PubMed
Clayton AH, Croft HA, Handiwala L. Antidepressants and sexual dysfunction: mechanisms and clinical implications. Postgrad Med. 2014;126(2):91-99. PubMed
La Torre A, Giupponi G, Duffy D, Conca A. Sexual dysfunction related to psychotropic drugs: a critical review--part I: antidepressants. Pharmacopsychiatry. 2013;46(5):191-199. PubMed
La Torre A, Conca A, Duffy D, Giupponi G, Pompili M, Grözinger M. Sexual dysfunction related to psychotropic drugs: a critical review part II: antipsychotics. Pharmacopsychiatry. 2013;46(6):201-208. PubMed
Higgins A, Nash M, Lynch AM. Antidepressant-associated sexual dysfunction: impact, effects, and treatment. Drug Healthc Patient Saf. 2010;2:141-150. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca