CADTH Health Technology Review
Cannabis for Opioid Use Disorder
Rapid Review
Authors: Eugenia Palylyk-Colwell, Sharon Bailey
Abbreviations
AE
adverse event
GRADE
Grading of Recommendations Assessment, Development, and Evaluation
MMT
methadone maintenance treatment
OAT
opioid agonist treatment
OUD
opioid use disorder
OTP
opioid treatment program
PEER
Patients, Experience, Evidence, Research
RCT
randomized controlled trial
UDS
urinary drug screen
Key Messages
Evidence is inconsistent and of very low to moderate quality for the clinical effectiveness of cannabis regarding treatment retention and adherence, craving and withdrawal symptoms, or illicit opioid or other substance use. There is lack of consensus in the included publications as to whether use of cannabis in opioid use disorder is beneficial or detrimental.
No evidence of an impact of cannabis on quality of life, functioning, satisfaction, relapse, hospitalizations, or overdoses in people with opioid use disorder was identified.
One evidence-based guideline developed by health care and allied health professionals in Canada strongly recommends against the use of cannabinoids for the treatment of opioid use disorder in the primary care setting due to no or inconclusive evidence.
Context and Policy Issues
Opioid use disorder (OUD) is a challenging form of addiction caused by the misuse of prescribed, diverted, or illicitly obtained opioids.1 It is a chronic, relapsing disorder that is often associated with increased opioid-related morbidity and death.1,2 In Canada, the opioid crisis and related harms continue to have a detrimental effect on affected individuals, their families, communities, and the health care system.3 From April 2018 to March 2019, OUD accounted for the highest rates of hospitalizations for opioid-related harms in Canada, exceeding those due to opioid-related poisoning (overdoses) and adverse drug reactions to prescribed opioids.4
A national clinical practice guideline for the management of OUD that was intended to promote the use of evidence-based treatments for the clinical management of OUD in Canada was published in 2018.2 The guideline strongly recommends the use of opioid agonist treatment (OAT) with buprenorphine-naloxone as the preferred first-line treatment for OUD with methadone used as a second-line treatment if patients fail to respond to buprenorphine-naloxone, or if the combination is not the preferred option.2 Alternative or adjunct treatment options include OAT with slow-release oral morphine, withdrawal management alone (without transition to OAT), psychosocial treatment interventions, or oral naltrexone.2 The use of cannabis for the management of OUD is not mentioned in the 2018 national guideline.
There has been growing interest in the use of cannabis for OUD to mitigate opioid withdrawal symptoms, reduce opioid consumption and cravings, improve OUD treatment retention, and to prevent relapses, overdoses, and opioid-related deaths.5 Cannabis is viewed as an appealing option because many of the barriers that prevent people with OUD accessing traditional OAT do not apply to cannabis due to its legalization in Canada.6 Due to emerging data and the relatively favourable safety profile of cannabis, further investigation of cannabis as a treatment option for OUD may be warranted.5 Use of cannabis for management of OUD, however, is not without risks (e.g., cognitive impairment, addiction potential, greater risk for other substance use disorders).7 For this reason, it is suggested that the evaluation of cannabis for OUD should be held to the same evidence base for efficacy, safety, and comparative effectiveness as has been required for other treatments that are used for the management of OUD.7
Given the increasing interest in the use of cannabis for OUD, questions have arisen concerning potential coverage of cannabis as a component of opioid treatment programs (OTPs). In consideration of this, a review of the clinical effectiveness of cannabis in OUD is needed to determine if cannabis could have a beneficial effect on treatment outcomes in people with OUD or mitigate serious consequences of OUD, such as hospitalizations or overdoses. Thus, the aim of this report is to summarize the evidence on the clinical effectiveness of cannabis for the management of OUD and to identify evidence-based guidelines to inform decisions about the use of cannabis for people with OUD in Canadian clinical practice.
Research Questions
What is the clinical effectiveness of cannabis for the management of opioid use disorder?
What are the evidence-based guidelines regarding the use of cannabis for the management of opioid use disorder?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, PsycInfo, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were OUD and cannabis as intervention. CADTH-developed search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, network meta-analyses, any types of clinical trials or observational studies, and guidelines. Comments, newspaper articles, editorials, and letters were excluded. Where possible, retrieval was limited to the human population. The search was also limited to English language documents published between January 1, 2017 and August 5, 2022.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2017. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded. Reports of primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic review. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)8 for systematic reviews, the Downs and Black checklist9 for non-randomized studies, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument10 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Criteria | Description |
|---|---|
Population | People with opioid use disorder |
Intervention | Cannabis, with or without other interventions (e.g., opioid agonist therapies, psychotherapy, counseling) |
Comparator | Q1: No treatment with cannabis, with or without other interventions (e.g., opioid agonist therapies, psychotherapy, counseling) Q2: Not applicable |
Outcomes | Q1: Clinical effectiveness (e.g., opioid use, quality of life, functioning, participant satisfaction, relapse, symptom severity, safety [e.g., adverse events]) Q2: Recommendations regarding best practices (e.g., appropriate patient populations, recommended treatment strategies) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies, evidence-based guidelines |
Summary of Evidence
Quantity of Research Available
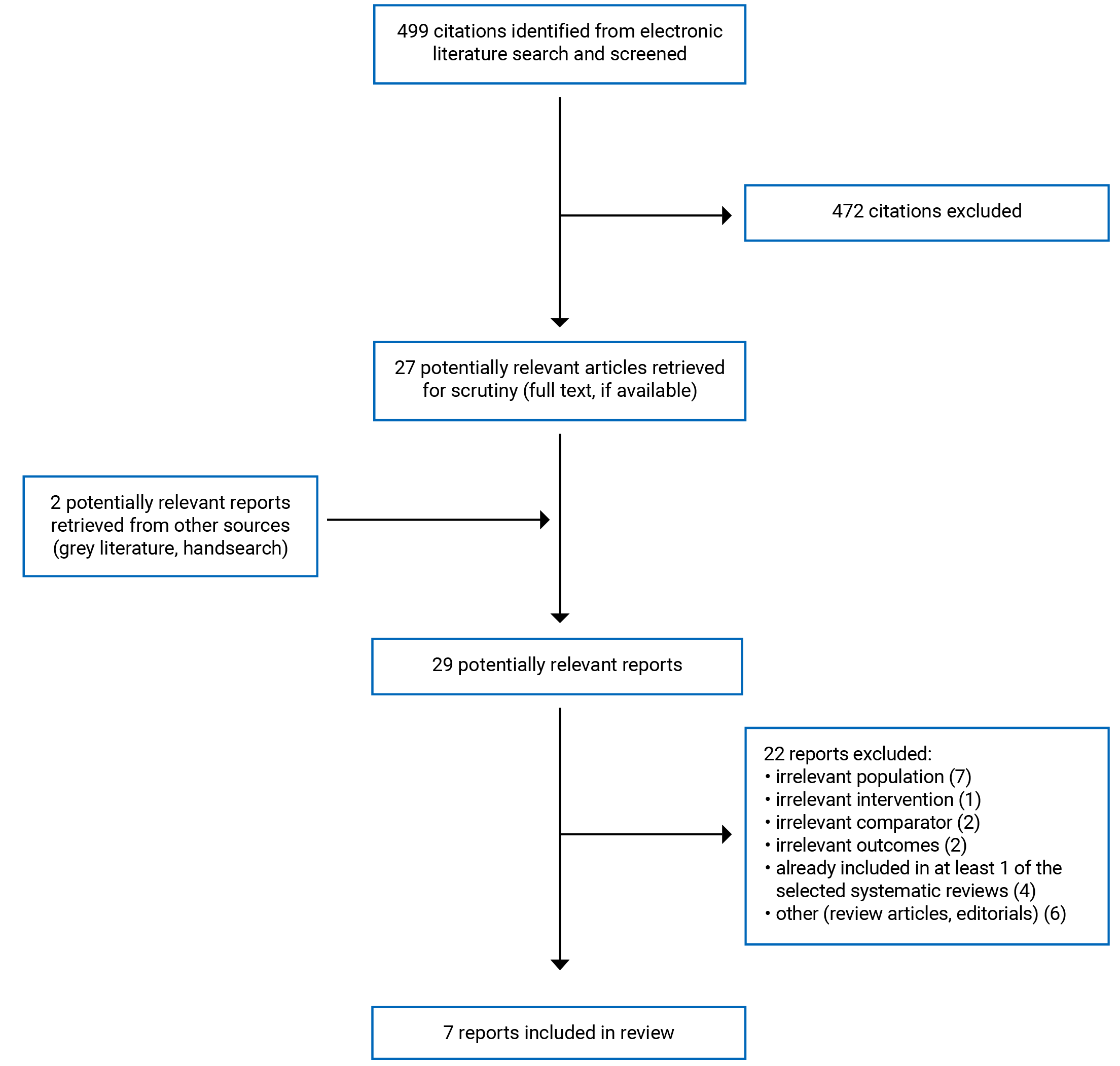
A total of 499 citations were identified in the literature search. Following screening of titles and abstracts, 472 citations were excluded and 27 potentially relevant reports from the electronic search were retrieved for full-text review. Two potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 22 publications were excluded for various reasons, and 7 publications met the inclusion criteria and were included in this report. These comprised 5 systematic reviews, 1 non-randomized study, and 1 evidence-based guideline. Appendix 1 presents the PRISMA11 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 6.
Summary of Study Characteristics
Five systematic reviews,12-16 1 non-randomized study,17 and 1 evidence-based guideline18 are included in this report.
Three systematic reviews12,13,15 had inclusion criteria that were broader than those of the current review. One systematic review12 included both human and animal studies as well as people with substance use disorders other than OUD, 1 systematic review13 examined the effects of co-occurring substances in addition to cannabis on treatment outcomes in people with OUD, and 1 systematic review15 evaluated the effects of cannabis on people with mental disorders in addition to those with opioid dependence. Only the subset of primary studies from these systematic reviews that met the inclusion criteria for the current review are presented in this report.
There were 4 primary studies19-22 identified in the literature search results that met the inclusion criteria for this review but were excluded due to their inclusion in the systematic reviews that have been included in the current report.
Additional details regarding the characteristics of the included publications are provided in Appendix 2.
There was some overlap in the primary studies included in the systematic reviews and the degree of overlap is summarized in Appendix 5.
Study Design
The primary studies included in the systematic reviews were mainly non-randomized studies (e.g., prospective cohort studies, retrospective cohort studies, retrospective chart reviews, cross-sectional studies, and secondary analyses of clinical trials) as well as a small number of randomized controlled trials (RCTs). A meta-analysis was attempted in 1 systematic review16 of the 5 included systematic reviews12-16; however, due to high heterogeneity the results could only be described qualitatively. In the 3 systematic reviews12,13,15 with broader inclusion criteria than those of the current review, there were 2 RCTs in each of 2 systematic reviews12,15 (i.e., 4 unique RCTs) and 1 RCT and 7 non-randomized studies in 1 systematic review13 that were relevant to the current review. Overall, the number of non-randomized studies included in the remaining 2 systematic reviews14,16 ranged from 23 to 41. The systematic reviews were published from 2019 to 2022 and the latest search dates were between July 2018 and February 2021. The follow-up in the primary studies included in the systematic reviews ranged from 1 hour to 11 years.
The 1 included non-randomized study,17 published in 2022, was a retrospective cohort study that was conducted at a single methadone maintenance treatment (MMT) clinic in patients with OUD, with or without a diagnosis of schizophrenia or chronic psychosis. Records for all patients (categorized as cannabis-users or non-users based on urinary drug screening [UDS]) admitted to the clinic over a 23-year period were studied to ascertain if there was a relationship between cannabis use, treatment retention, and survival status.
The 1 included evidence-based guideline,18 published in 2019, was developed by the Patients, Experience, Evidence, Research (PEER) group comprising members from various health care practices and locations in Canada with experience managing OUD. Evidence for the guideline was identified from a systematic review23 of systematic reviews and RCTs, which was current up to June 2018. The evidence was graded according to the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework and the recommendations, which were developed by consensus among the committee members, underwent an extensive peer-review process.
Country of Origin
The first authors of the included systematic reviews were from France,12 US,13 Canada,14,16 and Germany.15 The primary studies within the 3 systematic reviews12,13,15 with broad inclusion criteria that were relevant to the current review were from the US and Israel.
The authors of the non-randomized study17 were from Israel. The evidence-based guideline18 was developed by health care and allied health professionals in Canada.
Patient Population
For the current review, the terms: opioid dependence, heroin-use disorder, and people with substance use disorder where the substance was identified as opioids, or people who used opioids and were in an opioid treatment study were all considered synonymous with OUD. Two systematic reviews14,16 specifically enrolled people with OUD. The relevant patient populations in the remaining 3 systematic reviews included people with substance (opioid) use disorder,12 people who used opioids and were included in an original opioid treatment study in the US,13 and patients with opioid dependence.15 One systematic review13 included adults (3 18 years of age) whereas the remaining 4 systematic reviews did not specify an age range for inclusion. None of the 5 included systematic reviews reported details on baseline patient demographic or disease characteristics.
The 1 non-randomized study17 enrolled adult (3 18 years of age) people with OUD who were admitted to a MMT program with or without a diagnosis of schizophrenia/chronic psychosis and at least 1 attempt at residential treatment with the goal of total abstinence. Of the total enrolled, 50 (5.7%) people had schizophrenia/chronic psychosis whereas 827 (94.3%) people did not. Mean (SD) age at admission was approximately 39.6 (9.9 years), and the study population was predominantly male (74.6%) with a history of prior cannabis use (80.2%) and mean (SD) duration of opioid misuse of approximately 17.2 (10.0) years.
The target population in the included PEER guideline18 is patients with OUD who are treated in a primary care setting. The intended users of the guideline are primary care practitioners and patients with OUD.
Interventions and Comparators
For almost all clinical effectiveness outcomes considered in this report, comparisons in the non-randomized studies were between the use of cannabis and that of no use of cannabis (i.e., alone or in combination with other interventions such as methadone, buprenorphine, naltrexone, counseling, behavioural therapy, or mixed modalities). For the relevant RCTs identified in the 3 systematic reviews with broad inclusion criteria,12,13,15 2 RCTs evaluated cannabidiol 400 mg or 800 mg single doses versus placebo once daily for 3 consecutive days,12 and 2 RCTs evaluated dronabinol 30 mg/day versus placebo.15 For the remaining relevant RCT identified in 1 systematic review,13 although the intervention and comparator were buprenorphine and methadone, respectively, marijuana (cannabinoids) was evaluated as a co-occurring substance and predictor of treatment retention.
In the included non-randomized study,17 the comparison was between cannabis use versus no cannabis use.
The PEER guideline18 evaluated various pharmacotherapies for the treatment of OUD including buprenorphine-naloxone, methadone, naltrexone, and cannabis. Evidence for cannabis in OUD was derived from 1 RCT that compared dronabinol 30 mg/day versus placebo, which was also included in 1 systematic review15 that has been included in the current review.
Outcomes
The outcomes derived from the included systematic reviews and non-randomized study were treatment retention and adherence,13-17 craving and opioid withdrawal symptoms,12,14,15 illicit opioid, other substance, or polydrug use,13,14,16 psychological or physiologic responses,14,15 survival,17 criminal activity and risky behaviour,16 and safety.15
In general, the treatment outcomes measured in the primary studies were not well defined in the included systematic reviews. Treatment retention was typically measured as the proportion of people remaining in treatment at the end of the study.13 Treatment adherence was reported in only 1 systematic review14 and the method of determining adherence was either not defined in the publication or was inferred by UDS or pill count.
In 2 relevant RCTs included in 1 systematic review,12 craving was measured using a visual analogue scale, and positive and negative effects were measured using the Positive and Negative Affect Schedule following exposure to neutral and drug-related cues (e.g., videos, neutral objects, or heroin-related paraphernalia), although no further details were provided. In 1 relevant RCT included in 1 systematic review,15 the severity of opioid withdrawal symptoms was measured by the Subjective Opiate Withdrawal Scale. In 5 primary studies included in 1 systematic review14 the effects of cannabis versus no cannabis (measured by UDS or self-report) were assessed on opioid craving and withdrawal, but no details were provided on the severity of craving or withdrawal symptoms.
In 3 systematic reviews,13,14,16 that reported the impact of cannabis on illicit opioid, other substance, or polydrug use, outcomes were determined by positive UDS or self-reported drug use.
In 2 systematic reviews14,15 that reported psychological or physiologic responses, the primary studies ascertained cannabis use (or non-use) by UDS or self-report and the method of measurement of the responses were either not described or were determined by measuring vital signs during withdrawal sessions. The association between cannabis and criminal activity or risky behaviours was reported in 1 systematic review16; however, no details on how these data were derived was provided.
In the 1 non-randomized study,17 survival status of included patients was retrieved from the Israeli National Population Registry, which records all deaths in Israel.
In the 2 relevant RCTs included in 1 systemic review15 that reported on safety, adverse events (AEs) were reported by the study investigators or following once weekly review of medication tolerability with a research psychiatrist.
Clinical effectiveness evidence for cannabis considered for the PEER guideline18 comprised 1 RCT that was also included in 1 systematic review15 included in the current review.
Summary of Critical Appraisal
An overview of the critical appraisal of the included publications is summarized in the following text. Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Systematic Reviews
In all 5 systematic reviews,12-16 the review objective was clearly described and a PRISMA flow diagram detailing study selection, and adequate details on the included primary studies were provided. In 3 systematic reviews,12,14,16 the authors stated that the review was designed according to PRISMA guidelines, whereas in 1 systematic review,15 the authors stated that the review followed guidance from the Centre for Reviews and Dissemination and the Cochrane Collaboration. Following well established processes for developing and conducting systematic reviews increases transparency in the methodology and confidence that the systematic review was done appropriately.
Study protocols were registered in PROSPERO for 3 systematic reviews.14-16 For the other 2 systematic reviews,12,13 it was unclear if the review methods were established before the conduct of the review. Access to the review protocol and literature search strategy facilitates reproducibility of the reviews and apprises 1 to any protocol deviations that may have occurred. The research question and inclusion criteria included the components of PICO (population, intervention, comparator, outcome) in 3 systematic reviews,14-16 whereas in 2 systematic reviews,12,13 only the literature search terms were provided. In all but 1 systematic review,12 literature searches were conducted in multiple databases. It is possible that by not adhering to a PICO framework for study selection or by not searching multiple databases that important primary studies could have been missed.
Selection of studies was done independently by 2 reviewers (and disagreements resolved by an additional reviewer or by consensus) in 4 systematic reviews.13-16 Agreement rates between reviewers were reported in 2 systematic reviews.13,16 In 1 systematic review, there was no explanation provided pertaining to study selection.12 Lists of excluded studies were not provided in any of the included systematic reviews, although in 1 systematic review,15 the authors stated that a list of excluded studies was available upon request. Data extraction was performed independently by 2 or more reviewers according to standardized methods in 3 systematic reviews,13,15,16 with agreement rates between reviewers reported in 1 systematic review.13 In 1 systematic review,14 data extraction was done by 1 reviewer but was checked for accuracy and completeness by another reviewer, and in 1 systematic review12 the process for data extraction was not mentioned. By conducting study selection or data extraction in duplicate, the potential for errors in study selection and data abstraction are mitigated.
The risk of bias in individual primary studies was not assessed in 1 systematic review12; however, it was assessed separately by 2 reviewers in the other 4 systematic reviews,13-16 with each systematic review using a different instrument such as the Quality in Prognostic Studies tool,24 National Heart, Lung, and Blood Institute Quality Assessment Tool for Observational and Cross-Sectional Studies,25 the Cochrane Risk of Bias tool,26 and the Newcastle-Ottawa scale.27 In 1 systematic review,16 the overall quality of the evidence was assessed using GRADE methodology.28 All of the tools used to assess risk of bias have been published and are frequently used to assess the methodological quality and risk of bias in systematic reviews. In general, the risk of bias in the included primary studies was assessed as low to high and the quality of evidence as very low to moderate across the systematic reviews that assessed risk of bias and quality of evidence.
A meta-analysis of primary studies was planned in 1 systematic review16; however, due to high heterogeneity across included studies the authors opted to describe the individual studies and results qualitatively instead.
The source of funding of the individual primary studies was reported in 1 systematic review,15 but not the others. The source of funding and conflict of interest declarations by the authors were available for all included systematic reviews.
Non-Randomized Study
In the included non-randomized study,17 the objective, inclusion criteria, and patient characteristics were clearly reported, and the main study findings were presented with estimates of random variability, appropriate statistical testing, and actual P values. Included patients were representative of the entire population from which they were derived because the records for all patients with OUD admitted to the single centre (MMT clinic) of the study were analyzed. All patients were also followed up in a similar manner (i.e., 1 year from admission to the MMT clinic).
Patients, health care practitioners, and study authors were not blinded to the intervention. Moreover, the study was not randomized and there was no description of potential confounders. As a result, it is not known if potential confounders could have influenced the study results because due to lack of randomization it is not known if potential confounders were distributed equally across the included patients. This was a single centre study that derived information about patients treated over a 23-year time frame. Therefore, it is unclear if the treatment setting and patient population are representative of other treatment settings or current OTPs given expected clinical practice changes over this time period.
In this study, cannabis use was based on UDS; however, urine samples were analyzed for cannabis only during the 1st and 13th months of treatment. Patients were categorized as being cannabis-users or non-users based on a positive UDS at either of these time points. Measurement of cannabis use in this manner may not be representative of the overall pattern of cannabis use over the duration of the study and could either have under- or overestimated cannabis use in the study population.
Guideline
The included PEER guideline18 was of high quality. A rigorous guideline development process was undertaken including a systematic review that has been published.23 The objective, intended users, target population were clearly described and the guideline committee membership reflected various health care practices and locations across Canada with experience managing OUD. Key questions and recommendations were developed through consensus and the quality of the evidence was rated according to GRADE methodology.28 Draft recommendations underwent an extensive peer-reviewed process involving health care professionals and people with lived experience with OUD.
Summary of Findings
The main findings from the included systematic reviews12-16 and non-randomized study17 are summarized in this section. A detailed summary of the study findings by outcome is provided in Appendix 4. All included systematic reviews reported study findings as narrative summaries and not as quantitative summary estimates, therefore, the current report also includes narrative summaries of the findings. Although a meta-analysis was planned for 1 systematic review,16 the high heterogeneity in the included studies precluded the ability to do so and instead the authors described the included studies and their results qualitatively. There was some overlap in the primary studies that were included in the systematic reviews and so the narrative summaries from these systematic reviews may include some of the same studies. A citation matrix illustrating the degree of overlap is provided in Appendix 5.
Clinical Effectiveness of Cannabis for the Management of OUD
Evidence regarding the clinical effectiveness of cannabis for the management of OUD was available from 5 systematic reviews12-16 and 1 non-randomized study.17 Most of the evidence is derived from non-randomized studies (e.g., prospective cohort, retrospective cohort, cross-sectional studies, and secondary analyses of clinical trials) although there were 5 RCTs included among the primary studies in the systematic reviews.
No evidence on the clinical effectiveness of cannabis for the management of OUD on quality of life, functioning, participant satisfaction, relapse, or serious sequelae such as hospitalization or overdose was identified.
Treatment Retention and Adherence
Four systematic reviews13-16 and 1 non-randomized study17 reported on treatment retention in OTPs by people with OUD who used cannabis. One systematic review13 reported that based on 6 studies (1 RCT and 5 non-randomized), co-occurring use of marijuana statistically significantly reduced treatment retention. In another systematic review,15 based on 1 RCT that assessed dronabinol versus placebo, there was no statistically significant difference in treatment retention between groups. In most of the primary studies included in each of 2 systematic reviews,14,16 there was no statistically significant association between cannabis use and treatment retention. For example, in 1 systematic review,14 17 of 23 non-randomized studies reported no statistically significant association between cannabis use and treatment retention, whereas 5 studies suggested there was a negative effect of cannabis on treatment retention and 5 studies reported statistically significantly higher treatment retention in cannabis users, although there were inconsistencies between the latter studies related to the frequency of cannabis use. In the other systematic review,16 8 of 11 non-randomized studies reported no statistically significant association between cannabis use and treatment retention; however, 3 studies reported there was a statistically significant association between cannabis use and treatment retention. A subgroup analysis by country in this systematic review16 found cannabis use to be associated with decreased treatment retention in studies conducted in the US and with increased retention times in studies conducted in Israel. Although a meta-analysis had been planned in this systematic review16 to examine the effect of cannabis use on treatment retention, due to significant heterogeneity and high risk of bias among the studies, the authors chose not to do so, and the review concluded that there was no consensus among studies that cannabis use is associated with longer treatment retention.
Treatment adherence according to cannabis use in people with OUD was assessed in 1 systematic review.14 Based on 6 non-randomized studies; cannabis was not found to be statistically significantly associated with treatment adherence in 3 studies, whereas 1 study reported cannabis users were significantly more likely to adhere to treatment. The remaining 2 studies reported that based on an inverted U-shaped dose-response curve, intermittent cannabis users had statistically significantly improved adherence versus non-users or consistent users of cannabis.
In the non-randomized study,17 cumulative 1-year treatment retention was statistically significantly longer in patients in the study cohort who did not use cannabis compared with cannabis users. Among patients in the subset with schizophrenia or chronic psychosis, cumulative 1-year treatment retention did not differ between cannabis users and non users.
Craving and Opioid Withdrawal
Three systematic reviews12,14,15 reported on craving and opioid withdrawal symptoms in people with OUD who used cannabis. In 2 RCTs included in 1 systematic review,12 compared with placebo, use of cannabidiol for 3 consecutive days was associated with reduced cue-induced craving and anxiety and treatment effect lasted 7 days. Based on 5 non-randomized studies included in another systematic review,14 the effect of cannabis use on opioid craving or withdrawal was inconsistent, as 3 studies reported there was no statistically significant relationship and 2 studies reported a statistically significant reduction in at least 1 measurement of opioid withdrawal in cannabis users. In 1 placebo-controlled RCT in opioid dependent patients undergoing inpatient detoxification and naltrexone induction that was included in 1 systematic review,15 use of dronabinol was associated with statistically significant lower severity of withdrawal symptoms as measured by the Subjective Opiate Withdrawal Scale; however, rates of successful induction onto extended-release naltrexone did not differ between dronabinol and placebo.
Illicit Opioid, Other Substance, or Polydrug Use
Three systematic reviews13,14,16 reported on illicit opioid, other substance (e.g., alcohol, cocaine, or crack), or polydrug use in people with OUD who were cannabis-users versus non-users with mixed findings. In the first systematic review,13 based on 2 non-randomized studies, marijuana use was associated with a non-statistically significant increase in opioid abstinence outcomes in 1 study and a statistically significant increased likelihood of having a positive UDS for opioids in the other study. Overall, this systematic review found that co-occurring substance use was associated with negative treatment outcomes, regardless of the intervention used.13
The second systematic review14 included 11 non-randomized studies that examined the relationship between cannabis use and use of alcohol, cocaine/crack, and benzodiazepines during treatment in people with OUD. Of these, 3 studies reported a statistically significant increased use of alcohol among cannabis users. In 9 studies that examined use of cannabis and cocaine or crack, 5 studies found no correlation of cannabis use, 2 studies reported statistically significant increased use of cocaine in cannabis users, and 2 studies supported inverse relationships between the frequency of cannabis use and use of cocaine or crack. In 7 studies that examined benzodiazepine use among cannabis users, 3 studies reported statistically significant increased benzodiazepine use whereas 4 studies did not detect significant differences in the use of benzodiazepines according to cannabis use.
The third systematic review16 included 12 non-randomized studies that examined the relationship between cannabis use and continued or illicit opioid use in people with OUD receiving MMT. The results of these studies were inconsistent as 8 studies reported no statistically significant association between cannabis use and illicit or other opioid use, whereas 4 studies reported an association between cannabis use and illicit opioid or other drug use. Some of the included studies also reported on the association between cannabis use and other drug use (e.g., cocaine, benzodiazepines, alcohol, stimulants, etc.) but with highly inconsistent results. Although a meta-analysis was planned to examine the effects of cannabis use on continued opioid use, due to significant heterogeneity among the studies and high risk of bias, it was not possible to do so, and it was concluded that there was no consensus among studies that cannabis use is associated with reduced opioid use.16
Psychological or Physiologic Responses
Two systematic reviews14,15 reported on some measure of psychological or physiologic health in relation to cannabis use in patients with OUD. In 1 systematic review14 that included 6 non-randomized studies providing information for this outcome, 2 studies reported statistically significantly worse health indicators (e.g., poor appetite, poor physiologic functioning) in cannabis users and 4 studies did not find a significant relationship between cannabis and measures of psychological health. In the other systematic review,15 1 included RCT investigated the use of dronabinol versus placebo on physiologic outcomes. Use of dronabinol in patients undergoing withdrawal from oxycodone was associated with dose-dependent sustained sinus tachycardia along with anxiety and panic, as well as significant increases in heart rate compared to placebo.
Additional Clinical Outcomes
The non-randomized study17 examined survival status in relation to cannabis use in patients with OUD receiving MMT. Survival since admission to the MMT program did not statistically significantly differ according to cannabis use on admission.
One systematic review16 examined the association between cannabis use and criminal activity (based on 2 non-randomized studies) and on risky behaviour (e.g., HIV infection) based on 1 non-randomized study. For criminal activity, the 2 studies differed in that 1 study reported cannabis use was not associated with any differences in criminal activity and 1 study reported that cannabis use was a significant predictor of criminal activity at 12 months. For risky behaviours, 1 study reported that cannabis use was not related to any risk behaviours.
Safety
One systematic review15 included 2 RCTs that reported on AEs and safety associated with use of dronabinol. In 1 RCT, no significant differences in the frequency of AEs between dronabinol and placebo were observed; however, a post-hoc analysis of participants who also smoked marijuana regularly during the outpatient phase had lower rates of insomnia and anxiety and were more likely to complete the 8-week trial. users and non-users were observed. In the other RCT, use of dronabinol in people undergoing withdrawal from oxycodone was associated with dose-dependent serious AEs (e.g., sinus tachycardia, increased heart rate).
Guidelines Regarding the Use of Cannabis for the Management of OUD
The 1 included evidence-based guideline18 recommended against the use of cannabinoids for management of OUD (i.e., strong recommendation, very low-quality evidence). This recommendation was based on no systematic review evidence and very low-quality evidence from 1 RCT due to inconsistency, imprecision, and risk of bias.23
Limitations
Four13-16 of the 5 included systematic reviews were conducted using rigorous methodology and practices for systematic reviews; however, all are limited by the quality of the available evidence. The quality of the evidence was rated by the systematic review authors as very low to moderate and associated with a low to high risk of bias in the 4 systematic reviews13-16 that conducted risk of bias assessments. In a quality assessment according to GRADE conducted in 1 systematic review,16 it was noted that the overall quality of evidence was very low due to inconsistency, imprecision, and high risk of bias.
Most of the included evidence was derived from observational, non-randomized trials (e.g., prospective cohort, retrospective cohort, cross-sectional, and secondary analysis studies). Further, in most studies use of cannabis in people with OUD was not the focus of the study, but rather the concomitant use of cannabis was evaluated along with pharmacologic therapy (e.g., methadone, buprenorphine, naltrexone) or other treatment modalities for OUD. No meta-analyses of the available evidence could be conducted due to high heterogeneity among the primary studies, therefore, only narrative summaries (as opposed to quantitative summary estimates) are available for the assessment of clinical effectiveness of cannabis for OUD.16
One systematic review15 reported AE and safety data pertaining to dronabinol, an oral synthetic delta-9-tetrahydrocannabinol analogue and cannabinoid-1 receptor agonist. Dronabinol was approved for use as an antiemetic in Canada in the past, but its authorization was cancelled post-market and it is no longer commercially available in Canada.29
No evidence on the clinical effectiveness of cannabis for the management of OUD on quality of life, functioning, participant satisfaction, relapse, or serious sequelae such as hospitalization or overdose was identified.
An inherent drawback to investigating cannabis use as an intervention is the lack of standardization of the active ingredients contained in cannabis, as well as the dose, frequency of administration, route of administration, or source as these are highly variable. Many primary studies included in the systematic reviews did not differentiate between medical use or recreational use of cannabis. Further, in these studies cannabis use versus non-use was typically based on the results of UDS for cannabis or self-reporting. The frequency of UDS for cannabis and for opioids (as a measure of treatment adherence or to verify the use of illicit opioids) was often not reported. In the included non-randomized study,17 cannabis users and non users were categorized as such based on the results of a UDS obtained after the 1st and 13th month of MMT treatment. The results may not be representative of the overall pattern of cannabis use over the duration of the study and could likely under- or overestimate the frequency of cannabis use in the study population.
Two of the included systematic reviews14,16 were conducted by authors in Canada. Given that the included primary studies in these reviews were generally of low quality and associated with methodological limitations, inconsistency, and imprecision, it is difficult to determine if the results are generalizable to Canadian clinical practice.
There is a lack of RCT evidence that focuses on cannabis use as a specific intervention for the management of OUD. Moreover, there is also a lack of evidence-based guidelines to guide treatment decision-making in people with OUD, most likely due to the paucity of high-quality evidence for use of cannabis in OTPs.
Conclusions and Implications for Decision- or Policy-Making
This report summarizes the available evidence on the clinical effectiveness of cannabis for the management of OUD from 5 systematic reviews12-16 and 1 non-randomized study.17 One evidence-based guideline18 for the management of OUD in primary care is also included.
Overall, the evidence identified for the clinical effectiveness of cannabis in OUD is considered to be of very low to moderate quality and associated with high heterogeneity, inconsistency, imprecision, and risk of bias.13-16 Generally the authors of the systematic reviews included in this report12-16 are in agreement that there is no consensus that use of cannabis is associated with improved treatment outcomes in people with OUD or that the available evidence supports cannabis use in this setting as either beneficial or detrimental. Notably, these findings are aligned with a 2017 CADTH Rapid Response report on the use of medical cannabis in residential transition or addition programs in which no relevant literature regarding the clinical effectiveness, cost-effectiveness, or evidence-based guidelines regarding the use of medical cannabis in adults with addictions being treated in residential transition or addiction programs was found.30
The 1 evidence-based guideline18 identified in the current review was developed by a committee of health care and allied health professionals in Canada. The guideline recommends against the use of cannabinoids for the management of OUD in primary care (i.e., strong recommendation, very low-quality evidence) due to no or inconclusive RCT evidence identified for cannabinoids for OUD.23
The limitations of the included publications should be considered in the interpretation of the findings of this report. Most of the available evidence is derived from non-randomized, observational studies in which the objective was not to specifically investigate cannabis use versus non-use on treatment outcomes in people with OUD. In the future, well-designed RCTs that specifically evaluate a standardized form of cannabis (i.e., dose, route of administration, source) as a focused intervention in people with OUD are needed to inform the clinical effectiveness of cannabis for the treatment of people with OUD, which in turn will be beneficial for clinical and policy decisions.
The implications of increased access to medical and non-medical cannabis in Canada and other countries extend not only to coverage decisions regarding cannabis for people with OUD, but also to how cannabis use could impact prescribing practices and treatment approaches for people with OUD. People in OTPs may be required to undergo regular UDS or to enter into a treatment agreement. The concomitant use of cannabis could pose a treatment barrier if it is perceived that an individual is non-adherent with treatment due to a positive UDS or reported use of cannabis.14,23
References
1.Strain E. Opioid use disorder: epidemiology, pharmacology, clinical manifestations, course, screening, assessment and diagnosis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: http://www.uptodate.com. Accessed 2022 Sep 3.
2.Bruneau J, Ahamad K, Goyer M, et al. Management of opioid use disorders: a national clinical practice guideline. CMAJ. 2018;190(9):E247-e257. PubMed
3.Health Canada. Federal actions on opioids to date. 2022; https://www.canada.ca/en/health-canada/services/opioids/federal-actions/overview.html#a9. Accessed 2022 Sep 3.
4.Public Health Agency of Canada. Understanding a broader range of opioid-related hospitalziations in Canada. 2021; https://www.canada.ca/en/health-canada/services/opioids/data-surveillance-research/understanding-broader-range-opioid-related-hospitalizations.html. Accessed 2022 Sep 3.
5.Wiese B, Wilson-Poe AR. Emerging Evidence for Cannabis' Role in Opioid Use Disorder. Cannabis Cannabinoid Res. 2018;3(1):179-189. PubMed
6.Health Canada. Canada legalizes and strictly regulates cannabis. 2018; https://www.canada.ca/en/health-canada/news/2018/10/canada-legalizes-and-strictly-regulates-cannabis.html. Accessed 2022 Sep 3.
7.Humphreys K, Saitz R. Should Physicians Recommend Replacing Opioids With Cannabis? JAMA. 2019;321(7):639-640. PubMed
8.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
9.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
10.Agree Next Steps Consortium. The AGREE II Instrument. Hamilton (ON): AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2022 Sep 3.
11.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
12.Paulus V, Billieux J, Benyamina A, Karila L. Cannabidiol in the context of substance use disorder treatment: A systematic review. Addict Behav. 2022;132:107360. PubMed
13.Blondino CT, Gormley MA, Taylor DDH, et al. The Influence of Co-Occurring Substance Use on the Effectiveness of Opiate Treatment Programs According to Intervention Type. Epidemiol Rev. 2020;42(1):57-78. PubMed
14.Lake S, St Pierre M. The relationship between cannabis use and patient outcomes in medication-based treatment of opioid use disorder: A systematic review. Clin Psychol Rev. 2020;82:101939. PubMed
15.Hoch E, Niemann D, von Keller R, et al. How effective and safe is medical cannabis as a treatment of mental disorders? A systematic review. Eur Arch Psychiatry Clin Neurosci. 2019;269(1):87-105. PubMed
16.McBrien H, Luo C, Sanger N, et al. Cannabis use during methadone maintenance treatment for opioid use disorder: a systematic review and meta-analysis. CMAJ Open. 2019;7(4):E665-E673. PubMed
17.Volkov I, Schreiber S, Adelson M, Shoshan S, Peles E. Cannabis use is associated with lower retention in methadone maintenance treatment, but not among schizophrenic- and other chronically psychotic patients. J Addict Dis. 2022;40(2):183-191. PubMed
18.Korownyk C, Perry D, Ton J, et al. Managing opioid use disorder in primary care: PEER simplified guideline. Can Fam Physician. 2019;65(5):321-330. PubMed
19.Bagra I, Krishnan V, Rao R, Agrawal A. Does Cannabis Use Influence Opioid Outcomes and Quality of Life Among Buprenorphine Maintained Patients? A Cross-sectional, Comparative Study. J Addict Med. 2018;12(4):315-320. PubMed
20.Hurd YL, Spriggs S, Alishayev J, et al. Cannabidiol for the Reduction of Cue-Induced Craving and Anxiety in Drug-Abstinent Individuals With Heroin Use Disorder: A Double-Blind Randomized Placebo-Controlled Trial. Am J Psychiatry. 2019;176(11):911-922. PubMed
21.Franklyn AM, Eibl JK, Gauthier GJ, Marsh DC. The impact of cannabis use on patients enrolled in opioid agonist therapy in Ontario, Canada. PLoS ONE [Electronic Resource]. 2017;12(11):e0187633. PubMed
22.Zielinski L, Bhatt M, Sanger N, et al. Association between cannabis use and methadone maintenance treatment outcomes: an investigation into sex differences. Biol Sex Differ. 2017;8:8. PubMed
23.Korownyk C, Perry D, Ton J, et al. Opioid use disorder in primary care: PEER umbrella systematic review of systematic reviews. Can Fam Physician. 2019;65(5):e194-e206. PubMed
24.Hayden JA, van der Windt DA, Cartwright JL, Côté P, Bombardier C. Assessing bias in studies of prognostic factors. Ann Intern Med. 2013;158(4):280-286. PubMed
25.National Institutes of Health. National Heart, Lung, and Blood Institute. Study Quality Assessment Tools. https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools. Accessed September 2, 2022.
26.Cochrane Collaboration. Risk of bias tools. 2019; https://www.riskofbias.info/. Accessed 2022 Sep 2.
27.Bawor M, Dennis BB, Anglin R, Steiner M, Thabane L, Samaan Z. Sex differences in outcomes of methadone maintenance treatment for opioid addiction: a systematic review protocol. Syst Rev. 2014;3:45. PubMed
28.Guyatt GH, Oxman AD, Schünemann HJ, Tugwell P, Knottnerus A. GRADE guidelines: a new series of articles in the Journal of Clinical Epidemiology. J Clin Epidemiol. 2011;64(4):380-382. PubMed
29.Health Canada. Product Information for Marinol (dronabinol). 2022; https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=17209. Accessed 2022 Sep 3.
30.Medical cannabis in residential transition or addiction programs: a review of clinical and cost-efffectiveness and guidelines. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2017: https://www.cadth.ca/medical-cannabis-residential-transition-or-addiction-programs-review-clinical-and-cost. Accessed 2022 Sep 3.
31.Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. PubMed
32.A guideline developer's handbook. (SIGN publication no. 50). Edinburgh (GB): Scottish Intercollegiate Guidelines Network (SIGN); 2015: https://www.sign.ac.uk/media/1644/sign50_2015.pdf. Accessed 2022 Sep 3.
33.Zielinski L, Bhatt M, Eisen RB, et al. Association between cannabis use and treatment outcomes in patients receiving methadone maintenance treatment: a systematic review protocol. Syst Rev. 2016;5(1):139. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Review objective, search dates, Study designs and numbers of primary studies included | Population characteristics | Relevant intervention and comparator(s) | Relevant clinical outcomes, length of follow-up |
|---|---|---|---|---|
Paulus et al., (2022),12 France Funding: No specific grant from funding agencies in the public, commercial, or not-for-profit sectors | Review objective: To offer a comprehensive overview of animal and human studies regarding use of CBD on SUDs Search dates: Database inception to February 2021 Number of included studies: 40 (25 animal and 15 human); the 15 human studies were 9 RCTs, 4 crossover studies, and 2 case reports 2 RCTs were relevant to the present review | Human studies: People (age range NR) with SUD (i.e., tobacco, cannabis, alcohol, opioids, cocaine, and methamphetamine) Relevant Population: Drug abstinent individuals with heroin-use disorder | Intervention: CBD 400 mg or 800 mg once daily for 3 consecutive days Comparator: Placebo | Outcomes:
Follow-up: 1 hour to 7 days |
Blondino et al. (2020),13 United States Funding: NR | Review objective: To identify eligible opioid treatment studies in the US that assessed the relationship between co-occurring substance use and treatment outcome (i.e., opioid abstinence and treatment retention) Search dates: Database inception to November 28, 2018 Number of included studies: 34 including 7 RCTs, 6 prospective cohort and 21 retrospective cohort studies 8 studies (1 RCT, 1 prospective cohort, and 6 retrospective cohort studies) were relevant to the present review | People3 18 years who used opioids and were included in an original opioid treatment study conducted in the US that assessed and reported an association between the co-occurring substance use and treatment outcome | Intervention: Marijuana (as a co-occurring substance in the included studies) Comparator: NA | Outcomes:
Relevant Follow-up: 90 days to 3 years |
Lake et al. (2020),14 Canada Funding: Canadian Institutes of Health Research and the Pierre Elliott Trudeau Foundation | Review objective: To systematically search and review clinical and epidemiological literature to summarize the evidence on the impact of cannabis use on treatment outcomes for the 3 most common modalities of MOUD Search dates: Database inception to July 10, 2020 Number of included studies: 41 (14 prospective cohort studies, 13 secondary analyses of clinical trials, 9 retrospective chart reviews, and 5 cross-sectional studies) | People (age range NR) enrolled in community-based epidemiological or clinic-based (observational or experimental) human research that assessed cannabis use during methadone, buprenorphine, or naltrexone treatment for MOUD | Intervention: Plant-based cannabis Comparator: NA | Outcomes: Primary:
Secondary:
Follow-up: 30 days to 2 years |
Hoch et al., (2019),15 Germany Funding: Germany Ministry of Health | Review objective: To analyze efficacy and safety of cannabis-based medication (with or without additional medication and psychotherapy) for the treatment of patients with mental disorders Search dates:2006 to August 2018 Number of included studies: 4 SRs and 14 RCTs 2 RCTs were relevant to the present review | Patients (age range NR) with various mental disorders including dementia, cannabis and opioid dependence, psychoses or schizophrenia, general social anxiety, post-traumatic stress disorder, anorexia nervosa, ADHD, or Tourette’s disorder Relevant population: Patients with opioid dependence | Intervention: Dronabinol (titrated to 30 mg per day or up to 30 mg per session, decreased from 40 mg) Comparator: Placebo | Outcomes: Primary:
Secondary:
Follow-up: 8 to 12 weeks |
McBrein et al. (2019),16 Canada Funding: Catalyst Grant 155404 from the Canadian Institutes of Health Research | Review objective: To examine the relationship between cannabis use and opioid use during MMT Search dates: Database inception to July 12, 2018 Number of included studies: 23 (4 cross-sectional studies, 3 secondary analyses, 10 prospective cohort studies, and 6 retrospective cohort studies) Meta-analyses of illicit opioid use in 6 studies and of treatment retention in 4 studies were attempted | Patients (age range NR) with OUD receiving MMT | Intervention: Cannabis use Comparator: NA | Outcomes:
Follow-up: 12 weeks to 11 years |
ADHD = attention deficit hyperactivity disorder; AE = adverse event; CBD = cannabidiol; CO2 = carbon dioxide; HIV = HIV; HRQoL = health-related quality of life; MOUD = medication-based treatment of opioid use disorder; MMT = methadone maintenance treatment; NA = not applicable; NR = not reported; RCT = randomized controlled trial; SUD = substance use disorder; SR = systematic review.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design, setting | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Volkov et al. (2022),17 Israel Funding: Adelson Family Foundation | Single centre, retrospective cohort study MMT clinic in a medical centre (Tel-Aviv, Israel) | Patients 18 years and older diagnosed with OUD and at least one attempt at residential treatment with the goal of total abstinence admitted to a MMT clinic between June 1993 to December 2016, including patients with a lifetime DSM-IV-TR diagnosis of schizophrenia or chronic psychosis Sample size: 877 (50 [5.7%] patients with schizophrenia/psychosis and 827 [94.3%] study cohort patients with other mental disorders including opioid dependence) Mean (SD) age at admission: ~39.6 (9.9) years Male, n (%): 654 (74.6) Prior cannabis usea, n (%): 703 (80.2) Mean (SD) duration of opioid misuse: ~17.2 (10.0) years | Intervention: Cannabis use Comparator: No cannabis use | Outcomes:
Follow-up: 1 year |
DSM-IV-TR = Diagnostic and Statistical Manual of Mental Disorders, 4th edition, Text Revised; MMT = methadone maintenance treatment; OUD = opioid use disorder; SD = standard deviation.
aUrine test to assess prior cannabis use was done in the first month of treatment.
Table 4: Characteristics of Included Guideline
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
PEER Simplified Guideline (2019)18 | ||||||
Intended users: Primary care practitioners and patients with OUD Target population: Patients with OUD treated in primary care | Management of OUD in the primary care setting | Diagnosis, pharmacotherapy, prescribing practices, tapering, psychosocial (counseling), residential treatment, and comorbidities | Systematic review of SRs with additional RCT search for trials published after the most recent SR; observational studies were included if no SR or RCT were available Evidence was up to date as of June 2018 (but was generally limited to the past 5 to 10 years) | Evidence was rated according to GRADE | A guideline committee (N = 13) with members representing various practices and locations across Canada and experience managing OUD used an iterative process to determine key questions, develop practice recommendations, and refine/finalize the guideline and recommendations by consensus | Draft recommendations underwent an extensive peer-reviewed process involving 52 health care professionals and 5 people with lived experience |
GRADE = Grading of Recommendations Assessment, Development and Evaluation; NA = not applicable; NR = not reported; OUD = opioid use disorder; PEER = Patients, Experience, Evidence, Research; RCT = randomized controlled trial; SR = systematic review.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 5: Strengths and Limitations of Systematic Reviews Using AMSTAR 28
Strengths | Limitations |
|---|---|
Paulus et al. (2022)12 | |
The review authors stated that a systematic search was performed using PRISMA guidelines and the search terms were provided but no further details were given.31 There was adequate description of the interventions, outcomes/results, and research designs of included studies. The review authors declared conflict of interest (of which there were none). The source of funding for the review was provided. | The research question and inclusion criteria for the review did not include the components of PICO. Only the search terms used to select studies for inclusion were reported. No statement was made that the review methods were established before the conduct of the review. No explanation was provided pertaining to the selection of study designs. Only 1 database (PubMed) was searched. The search was limited to articles published in English or French but no justification for the restriction was provided. The process for selecting included and excluded studies was not described (e.g., if at least 2 reviewers independently selected studies and how disagreements were resolved). The process for extracting data was not described. No list of excluded studies was provided. There was limited description of the patient populations or comparators for included studies. There was no RoB assessment conducted. Sources of funding for individual studies were not reported. Although heterogeneity among included studies was noted as a limitation in the discussion of the review, the review authors did not assess or discuss heterogeneity when interpreting or discussing the results of the review. No assessment of publication bias was conducted. |
Blondino et al. (2020)13 | |
The review authors conducted a systematic literature search using 4 databases (MEDLINE/PubMed, Embase, PsychINFO, and CINAHL) and provided the search terms. Study selection was performed independently by 2 reviewers and any disagreements were resolved by a 3rd reviewer. Agreement rates between reviewers at each stage were high: 86.3% (titles), 88.9% (abstracts), and 87.4% (full-text articles) Data extraction was done according to a protocol and data extraction sheet and was performed independently by 4 authors. Extraction of study characteristics was completed with 87.5% agreement between authors and extraction of results and outcomes was completed with 92.8% agreement between authors. Included studies were described in adequate detail (i.e., population, intervention, comparators, outcomes, and study design) including RoB score for each included study. RoB was assessed using the Quality in Prognostic Studies tool by 2 authors who independently assessed RoB in 6 domains: study participation, study attrition, prognostic factor measurement, outcome measurement, study confounding, statistical analysis, and reporting.24 Each domain was assigned a numeric rating of low (1), moderate (2), or high (3) risk of bias so that studies with a low risk of bias had a final score of 6 to 8, moderate risk 9 to 12, and high risk > 13. Any disagreements were resolved by a 3rd author. The review authors declared conflict of interest (of which there were none). The source of funding for the review was provided. | The research question and inclusion criteria for the review did not include the components of PICO. Only the search terms used to select studies for inclusion were reported. No statement was made that the review methods were established before the conduct of the review. Although the types of study designs that were excluded were described (e.g., case studies, cost-effectiveness studies, study protocols, and studies assessing diagnostic or prognostic tools), no explanation was provided as to why these designs were excluded. No list of excluded studies was provided. The search was limited to articles published in English and human studies but no justification for the restrictions was provided. Sources of funding for individual studies were not reported. The review authors did not assess or discuss heterogeneity in the included studies when interpreting or discussing the results of the review. Although the potential for the review to suffer from publication bias was noted, no formal assessment of publication bias was conducted. Evidence was rated as having low to moderate risk of bias. |
Lake et al. (2020)14 | |
The review authors stated that the review was designed according to PRISMA guidelines.31 A review protocol was registered in PROSPERO (CRD42019125097). The review authors conducted a systematic literature search using 6 databases (MEDLINE, Embase, PsychINFO, Web of Science, CINAHL, and EBM reviews) and provided the search terms. The MEDLINE search strategy was provided as a supplementary file. The research question and inclusion criteria for the review followed the components of PICO. A preliminary scan and elimination of studies that did not clearly meet eligibility requirements was done by 1 author and then study selection was performed independently by 2 reviewers and any disagreements were resolved by consensus. Agreement rates between reviewers were not reported. Data extraction was done by 1 author using a standardized form and was assessed for accuracy and completeness by a 2nd reviewer. Quality assessment of included studies was assessed according to the National Institutes of Health’s National Heart, Lung, and Blood Institute (NHLBI) Quality Assessment Tool for Observational and Cross-Sectional Studies resulting in a final assessment of a study as poor, fair, or good.25 One author rated all studies and a second author independently rated the quality of a random sample of 13 studies (32% of included studies). Included studies were described in adequate detail (i.e., population, intervention, comparators, outcomes, and study design) including a quality score for each included study. The review authors declared conflict of interest (of which there were none). The source of the funding for the review was provided. | Although the types of study designs that were excluded were described (e.g., qualitative research, case reports, case series, ecological studies, descriptive studies, studies that did not use plant-based cannabis, or studies that assessed lifetime exposure to cannabis or did not operationalize cannabis exposure at the patient level), no explanation was provided as to why these designs were excluded. No list of excluded studies was provided. The search was limited to peer-reviewed articles published in English but no justification for the restrictions was provided. Sources of funding for individual studies were not reported. Although heterogeneity among included studies was noted as a limitation in the discussion of the review and reasons for lack of consistency explained, the review authors did not assess heterogeneity when interpreting the results of the review. No assessment of publication bias was conducted although given the generally non-significant cannabis-related results, the authors noted that the review was unlikely to be biased by selective reporting or unpublished null data. Evidence was rated as being of fair methodological quality and associated with a high degree of heterogeneity regarding the measurement of cannabis use. |
Hoch et al. (2019)15 | |
The review authors stated that the review followed guidance published by the Centre for Reviews and Dissemination and the Cochrane Collaboration. A review protocol was registered in PROSPERO (CRD42016053592). The review authors developed 3 detailed search strategies and searches were conducted using 5 databases (MEDLINE, PubMed, Embase, PsychINFO, and the Cochrane Library) and provided the search terms. The research question and inclusion criteria for the review followed the components of PICO. Search results and full-text articles were independently assessed by 2 reviewers and disagreements were resolved by consensus or referral to a 3rd reviewer. Data extraction was performed independently by 2 reviewers using a standardized form and disagreements were resolved by a 3rd reviewer. The authors stated that a list of excluded studies was available upon request. Quality assessment of included studies was assessed using the Cochrane RoB tool for systematic reviews and the SIGN checklist for RCTs.26,32 RoB assessment was performed independently by 2 reviewers and any disagreements resolved by a 3rd reviewer. Included studies were described in detail (i.e., population, intervention, comparators, outcomes, study design) including the source of individual study funding, along with a level of evidence and a RoB score. The authors stated that due to high heterogeneity of primary outcome measures, no aggregated data analysis was possible; however, the study results were interpreted considering sample size, level of evidence, RoB, and level of heterogeneity/homogeneity. The review authors declared conflict of interest (of which there were none). The source of the funding for the review was provided. | The types of study designs that were included or excluded in the review were not described although this information may be in the study protocol. No assessment of publication bias was conducted. Most included studies were rated as being of moderate quality. |
McBrein et al., (2019)16 | |
The review authors stated that the review was presented according to PRISMA guidelines.31 A review protocol was registered in PROSPERO (CRD42015029372) and has been published.33 The authors developed a detailed literature search strategy that was available as supplementary material and conducted searches using 6 databases (MEDLINE, PubMed, Embase, PsychINFO, CINAHL, and ProQuest Dissertations and Theses Global). The research question and inclusion criteria for the review followed the components of PICO. Search results and full-text articles were screened in duplicate at all stages by independent reviewers. Interrater agreement between reviewers was measured using the kappa statistic (κ). Data extraction was performed in duplicate by independent reviewers. Interrater agreement was deemed acceptable for both title/abstract (κ = 0.63, 95% CI, 0.57 to 0.69) and full-text screening (κ = 0.60, 95% CI, 0.45 to 0.74). RoB was assessed in duplicate by independent reviewers using the modified Newcastle-Ottawa Scale as all included studies were observational by design.27 The overall quality of the evidence was assessed using the GRADE framework.28 Included studies were described in sufficient detail (i.e., study design, intervention, outcomes, and findings). The review authors declared conflict of interest (of which there were none). The authors provided satisfactory explanations for the high heterogeneity among studies and considered the heterogeneity and RoB results when interpreting the results and discussing the study findings. The review authors declared conflict of interest (of which 1 author reported personal fees from Canadian Cannabis Clinics). The source of the funding for the review was provided. | Although the review authors identified the study designs that were included (i.e., observational and RCT studies), they did not list study designs that were excluded or the rationale for exclusion. The method for handling disagreements between reviewers for inclusion of studies, data extraction, or quality assessment was not reported. A list of excluded studies was not provided. The descriptions of included studies did not include the population or source of funding of the individual studies. The authors had planned to conduct a meta-analysis of primary studies and provide quantitative summary estimates; however, due to high heterogeneity the authors opted to describe the included studies and their results qualitatively instead. The I2 statistic was used to determine heterogeneity and a value of > 40% indicated high heterogeneity. Publication bias was not assessed. Evidence quality was rated as low with a high risk of bias. According to GRADE, the quality of evidence for illicit opioid use was very low and risk of bias was serious whereas for treatment retention, the quality of evidence was also very low, and risk of bias was not serious. |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; CI = confidence interval; CINAHL = Cumulative Index to Nursing and Allied Health Literature; EBM = evidence-based medicine; GRADE = Grading of Recommendations Assessment, Development, and Evaluation; PICO = population, intervention, comparator, outcome; PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-analyses; RCT = randomized controlled trial; RoB = risk of bias.
Table 6: Strengths and Limitations of the Primary Clinical Study Using the Downs and Black Checklist9
Strengths | Limitations |
|---|---|
Volkov et al. (2022)17 | |
Reporting
External validity
Internal validity
| Reporting
External validity
Internal validity
Power
|
AE = adverse event; CI = confidence interval; MMT = methadone maintenance treatment; OTP = opioid treatment program; OUD = opioid use disorder; SD = standard deviation.
Table 7: Strengths and Limitations of the Guideline Using AGREE II10
Item | PEER Simplified Guideline (2019)18 |
|---|---|
Domain 1: scope and purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes |
Domain 2: stakeholder involvement | |
4. The guideline development group includes individuals from all relevant professional groups. | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes |
6. The target users of the guideline are clearly defined. | Yes |
Domain 3: rigour of development | |
7. Systematic methods were used to search for evidence. | Yes |
8. The criteria for selecting the evidence are clearly described. | Yesa |
9. The strengths and limitations of the body of evidence are clearly described. | Yesa |
10. The methods for formulating the recommendations are clearly described. | Yesa |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes |
14. A procedure for updating the guideline is provided. | Unclear |
Domain 4: clarity of presentation | |
15. The recommendations are specific and unambiguous. | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes |
17. Key recommendations are easily identifiable. | Yes |
Domain 5: applicability | |
18. The guideline describes facilitators and barriers to its application. | Unclear |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes |
20. The potential resource implications of applying the recommendations have been considered. | No |
21. The guideline presents monitoring and/or auditing criteria. | No |
Domain 6: editorial independence | |
22. The views of the funding body have not influenced the content of the guideline. | No |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II.
aDetails pertaining to the systematic review and a comprehensive evidence review is available in a co-publication to the guidelines.23
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 8: Summary of Findings by Outcome — Treatment Retention and Adherence
Study citation and study design | Method of measurement | Results | Notes |
|---|---|---|---|
Blondino et al. (2020)13 Systematic review 6 included studies assessed the association between the co-occurring use of marijuana and treatment retention | Cannabis use: Positive UDS or self-reported frequency of cannabis use Treatment retention: Primary study reporting a decrease or increase in treatment retention |
|
|
Lake et al. (2020)14 Systematic review 27 included studies examined the association between cannabis use and treatment retention or stabilization. 6 included studies examined the association between cannabis use and treatment adherence | Cannabis use: Positive UDS or self-reported frequency of cannabis use Treatment retention: Primary study reporting retention times, association with early treatment drop-out or treatment discontinuation Treatment adherence: Either NR or by pill count or UDS | Treatment retention:
Treatment adherence:
|
|
Hoch et al. (2019)15 Systematic review 1 included RCT investigated dronabinol use and treatment retention | Cannabis use: Intervention (dronabinol) Treatment retention: Length of stay in 8-day inpatient detoxification program and 8-week outpatient program |
|
|
McBrein et al. (2019)16 Systemic review 11 included studies examined cannabis use and treatment retention for MMT | Cannabis use: Dichotomized cannabis use (use vs. non-use) as reported in primary study Treatment retention: Primary study reporting an increase or decrease in treatment retention |
|
|
Volkov et al. (2022)17 Retrospective cohort study | Cannabis use: Dichotomized cannabis use (use vs. non-use) Treatment retention: Proportion of patients in a MMT program at 1-year from admission |
|
|
CI = confidence interval; MMT = methadone maintenance treatment; OTP = opioid treatment program; NR = not reported; RCT = randomized clinical trial; SR = systematic review; UDS = urinary drug sample.
Table 9: Summary of Findings by Outcome — Craving and Opioid Withdrawal Symptoms
Study citation and study design | Method of measurement | Results | Notes |
|---|---|---|---|
Paulus et al. (2022)12 Systematic review 2 included RCTs examined the effect of CBD on opioid use in patients with OUD | Cannabis use: Intervention (cannabinoids) Craving and Symptoms: Exposure to neutral and drug-related cues (e.g., videos, neutral objects, or heroin-related paraphernalia) following CBD or placebo administration. Measurement of craving and anxiety responses were by VAS, positive and negative affects by the PANAS, as well as vital signs and measurement of salivary cortisol levels. |
|
|
Lake et al. (2020)14 Systematic review 5 included studies examined the association between cannabis use and opioid craving and withdrawal | Cannabis use: Positive UDS or self-reported frequency of cannabis use Craving and Symptoms: Primary study reported relationship between cannabis use and opioid craving or withdrawal, severity of withdrawal symptoms from chart review. |
|
|
Hoch et al., (2019)15 Systematic review 1 included RCT investigated dronabinol use and opioid withdrawal symptoms | Cannabis use: Intervention (dronabinol) Craving and Symptoms: Severity of opioid withdrawal symptoms measured by the SOES. |
|
|
CBD = cannabidiol; DB = double-blind; OUD = opioid use disorder; PANAS = Positive and Negative Affect Schedule; RCT = randomized controlled trial; SOES = Subjective Opiate Withdrawal Scale VAS = visual analogue scale.
Table 10: Summary of Findings by Outcome — Illicit Opioid, Other Substance, or Polydrug Use
Study citation and study design | Method of measurement | Results | Notes |
|---|---|---|---|
Blondino et al. (2020)13 Systematic review 2 included studies assessed the association between the co-occurring use of marijuana and opioid abstinence in OTPs | Cannabis use: Positive UDS or self-reported frequency of cannabis use Drug use: Primary study report of increased or decreased opioid abstinence |
|
|
Lake et al. (2020)14 Systematic review 11 included studies examined the relationship between cannabis use and other substance use during treatment | Cannabis use: Positive UDS or self-reported frequency of cannabis use Drug use: Primary study report of increased use of various substances or relapse |
|
|
McBrein et al. (2019)16 Systematic review 12 included studies examined the relationship between cannabis use and continued or illicit opioid use | Cannabis use: Dichotomized cannabis use (use vs. non-use) Drug use: Primary study report of illicit opioid or heroin use or reported relationship or association between cannabis and illicit opioid use |
|
|
MOUD = medication-based treatment of opioid use disorder; MMT = methadone maintenance treatment; OTP = opioid treatment program; OUD = opioid use disorder; SR = systematic review; UDS = urinary drug sample.
Table 11: Summary of Findings by Outcome — Psychological or Physiologic Responses
Study citation and study design | Method of measurement | Results | Notes |
|---|---|---|---|
Lake et al. (2020)14 Systematic review 6 included studies reported some measurement of physical, psychological, and/or general health outcome in relation to cannabis use during treatment | Cannabis use: Positive UDS or self-reported frequency of cannabis use Responses: Primary study reports of any measurement of physical, psychological, and/or general health relationship to cannabis use |
|
|
Hoch et al. (2019)15 Systematic review 1 included RCT investigated dronabinol use and physiologic outcomes | Cannabis use: Intervention (dronabinol) Responses: Measurement of heart rate, blood pressure, oxygen saturation, respiration rate and end-tidal CO2 levels during withdrawal sessions |
|
|
CO2 = carbon dioxide; RCT = randomized controlled trial; UDS = urinary drug sample.
Table 12: Summary of Findings by Outcome — Additional Clinical Outcomes
Study citation and study design | Method of measurement | Results | Notes | |
|---|---|---|---|---|
Survival | ||||
Volkov et al. (2022)17 Retrospective cohort study | Cannabis use: Dichotomized cannabis use (use vs. non-use) Survival: Patients’ survival status was retrieved from the Israeli National Population Registry which reports all deaths in the country. |
|
| |
Criminal Activity or Risky Behaviours | ||||
McBrein et al. (2019)16 Systematic review 2 included studies reported on the association between cannabis use and criminal activity 1 included study reported on cannabis use and risk of HIV infection | Cannabis use: Dichotomized cannabis use (use vs. non-use) Criminal activity or risk behaviour: Primary study report of association with the outcome. |
|
| |
CI = confidence interval; HIV = HIV; UDS = urinary drug sample.
Table 13: Summary of Findings by Outcome — Safety
Study citation and study design | Method of measurement | Results | Notes |
|---|---|---|---|
Hoch et al., (2019)15 Systematic review 2 included RCTs reported on AEs and safety associated with dronabinol use | Cannabis use: Intervention (dronabinol) Safety: Once weekly review of medication tolerability with a research psychiatrist and AEs and safety outcomes reported by study investigators. |
|
|
AE = adverse event; RCT = randomized controlled trial NA = not applicable; NR = not reported.
Table 14: Summary of Recommendations in Included Guideline
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
PEER Simplified Guideline (2019)18 | |
“We recommend against the use of cannabinoids for management of OUD.”18 (p 322) Supporting evidence: No SRs and 1 RCT were identified that met the inclusion criteria for the SR undertaken for the PEER simplified guideline. This RCT is included in the SRs included in this report (refer to Appendix 5). “Cannabinoids are also often proposed for treatment of OUD. However, we recommend against their use owing to absence of clinical benefit.”18 (p 327) “Bottom Line: Current evidence does not seem to suggest dronabinol significantly reduces withdrawal symptoms when patients undergo opioid detoxification. At best, it may help with withdrawal symptoms as a patient stops opioids without opioid antagonist therapy but due to confounding variables such as the ability to use withdrawal symptom treatment, it is unclear whether dronabinol directly lead to those benefits. Currently no randomized control trial evidence is available regarding opioid overdose related deaths. Additional research is needed, and future evidence will impact the conclusion made at this time.” (Appendix 1 Full Evidence Review, p 53)23 | Strong recommendation, very low-quality evidence No or inconclusive RCT evidence was identified for cannabinoids for OUD.23 “Quality of Evidence: VERY LOW due to inconsistency, imprecision, and risk of bias.”23 (p 53) |
OUD = opioid use disorder; PEER = Patients, Experience, Evidence, Research group.
Appendix 5: Overlap Between Included Systematic Reviews
Note that this appendix has not been copy-edited.
Table 15: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Paulus et al. (2022)12 | Blondino et al. (2020)13 | Lake et al. (2020)14 | Hoch et al. (2019)15 | McBrien et al. (2019)16 |
|---|---|---|---|---|---|
Abrahamson T et al. Subst Abuse 2016;37(1):104 to 109 | — | — | Yes | — | — |
Bagra I et al. J Addict Med 2018;12(4):315 to 320 | — | — | Yes | — | — |
Bell J et al. J Subst Abuse 1997;9:15 to 25 | — | — | — | — | Yes |
Best D et al., Drug Alcohol Rev 1999;18:31 to 38 | — | — | Yes | — | Yes |
Bleich AVI et al. Addiction 1999;94(10):1533 to 1540 | — | — | — | — | Yes |
Bisaga A et al., Drug Alcohol Depend 2015;154:38 to 45 | — | — | Yes | Yes | — |
Budney AJ et al. Addiction 1998;93(4):493 to 503 | — | — | Yes | — | — |
Chaudry ZA et al. Psychiatrist 2012;36:218 to 224 | — | — | Yes | — | — |
Church SH et al. Am J Drug Alcohol Abuse 2001;27(3):441 to 452 | — | — | Yes | — | — |
Dayal P et al. J Subst Use 2016;21:309 to 316 | — | — | Yes | — | — |
Eastwood B et al. Drug Alcohol Dep 2019;194:438 to 446 | — | — | Yes | — | — |
Epstein DH and Preston, KL. Am J Addict 2015;24(4):323 to 328 | — | — | Yes | — | — |
Epstein DH and Preston KL. Addiction 2003;98(3):269 to 279 | — | — | Yes | — | Yes |
Fareed A et al. J Addict Med 2014;8(5):345 to 350 | — | — | Yes | — | — |
Franklyn AM et al. PLoS One 2017;12(11):Article e0187633 | — | — | Yes | — | — |
Ghitza UE et al. Addict Behav 2007;106(7):1309 to 1318 | — | Yes | — | — | — |
Grella CE and Stein JA. Psychiatr Serv 2006;57(7):1007 to 1015 | — | Yes | — | — | — |
Hakansson A et al. J Addict 2016;8 | — | — | Yes | — | — |
Hill KP et al. Drug Alcohol Dep 2013;132(1 to 2):342 to 345 | — | — | Yes | — | — |
Hser YI et al. Addiction 2014;109(1):79 to 87 | — | Yes | Yes | — | |
Hurd YL et al. Am J Psychiat 2019;176(11):911 to 922 | Yes | — | — | — | — |
Hurd YL et al. Neurotherap 2015;12(4):807 to 815 | Yes | — | — | — | — |
Jarvis BP et al. J Subst Abuse Treat 2018;85:38 to 44 | — | — | Yes | — | — |
Jicha CJ et al. Drug Alcohol Dep 2015;157:179 to 183 | — | — | — | Yes | — |
Joe, GW. Addiction 1998;93:1177 to 1190 | — | Yes | Yes | — | Yes |
Klimas JK et al. Drug Alcohol Dep 2018;186:182 to 186 | — | — | Yes | — | — |
Kumar N et al. Am J Addict 2016;25(7):542 to 548 | Yes | — | — | — | |
Levine AR et al. J Subst Abuse Treat 2015;54:37 to 43 | — | — | Yes | — | Yes |
Lions CL et al. Drug Alcohol Dep 2014;135:1 to 8 | — | — | Yes | — | Yes |
Matson SC et al. J Addict Med 2014;8(3):176 to 182 | — | — | Yes | — | — |
Nava F et al, Prog Neuro-Psychopharmacol Biol Psychiat 2007;31(5):1089 to 1094 | — | — | Yes | — | Yes |
Nirenberg TD et al. Psychol Addict Behav 1996;10:222 to 227 | — | — | Yes | — | Yes |
Peles E et al. Drug Alcohol Dep 2018;185:112 to 119 | — | — | Yes | — | — |
Peles E et al. J Addict Dis 2008;27(4):11 to 25 | — | Yes | Yes | — | Yes |
Peles E et al. Drug Alcohol Dep 2006;82(3):211 to 217 | — | — | — | — | Yes |
Pierce JM et al. Am J Drug Alcohol Abuse 2009;35(1):48 to 53 | — | — | — | — | Yes |
Potter JS et al. J Stud Alcohol Drug 2013;74(4):605 to 613 | — | — | Yes | — | — |
Proctor SL et al. J Subst Use 2016;21:601 to 613 | — | Yes | Yes | — | Yes |
Raby WN et al. Am J Addict 2009;18(4):301 to 308 | — | — | Yes | — | — |
Roux P et al. Curr Pharm Design 2014;20(25):4097 to 4105 | — | — | Yes | — | — |
Roux P et al. Harm Red J 2011:8:31 | — | — | Yes | — | — |
Saxon AJ et al. Addiction 1996;91(8):1197 to 1209 | — | Yes | Yes | — | Yes |
Saxon AJ et al. Am J Addict 1993;2:201 to 211 | — | — | — | — | Yes |
Scavone JL et al. Am J Addict 2013;22(4):344 to 351 | — | — | Yes | — | Yes |
Schiff M et al. Addict Behav 2007;32(10):2108 to 2119 | — | — | Yes | — | Yes |
Shams I et al. BJPsych Open 2019;5(6):e91 | — | — | Yes | — | — |
Socias ME et al. Addiction 2018;113(12):2250 to 2258 | — | — | Yes | — | — |
Somers CJ and O’Connor J. Irish Med J 2012;105(9):295 to 298 | — | — | Yes | — | Yes |
Strain EC et al. Drug Alcohol Dep 1991;27(2):127 to 34 | — | — | — | — | Yes |
Wasserman DA et al. Drug Alcohol Dep 1998;52(3):183 to 192 | — | — | Yes | — | Yes |
Weizman T et al. Austr New Zealand J Psychiat 2004;38(1 to 2):42 to 46 | — | — | Yes | — | Yes |
White WL et al. J Pscychoactive Drug 2014;46(2):114 to 122 | — | — | Yes | — | Yes |
Zielinski L et al. Biol Sex Diff, 2017;8:8 | — | — | Yes | — | Yes |
Appendix 6: References of Potential Interest
Note that this appendix has not been copy-edited.
The following publications were identified because they provide additional information to corroborate the findings of this report (i.e., previous CADTH reports) or additional guidance on the management of OUD or the prescribing of cannabis for medical use.
Previous CADTH Reports
Medical cannabis in residential transition or addiction programs: a review of clinical and cost-effectiveness and guidelines. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2017: https://www.cadth.ca/medical-cannabis-residential-transition-or-addiction-programs-review-clinical-and-cost. Accessed 2022 Sep 3.
Guidelines and Recommendations
Busse JW, Vankrunkelsven P, Zeng L, at al. Medical cannabis or cannabinoids for chronic pain: a clinical practice guideline. BMJ. 2021;374:n2040. .PubMed
Bruneau J, Ahamad K, Goyer M, et al. Management of opioid use disorders: a national clinical practice guideline. CMAJ. 2018;190(9):E247-e257.
CRISM national guideline for the clinical management of opioid use disorder. Canadian Research Initiative on Substance Misuse; 2018: https://crism.ca/projects/opioid-guideline/. Accessed 2022 Sep 3.
Guidance in authorizing cannabis products within primary Care. Mississauga (ON): College of Family Physicians of Canada; 2021: https://www.cfpc.ca/CFPC/media/PDF/CFPC-Guidance-in-Cannabis-Within-Primary-Care.pdf. Accessed 2022 Sep 3.
National Institute for Health and Care Excellence. Cannabis-based medicinal products. (NICE guideline NG144) 2021; https://www.nice.org.uk/guidance/ng144. Accessed 2022 Sep 3.
Rieb LM, Samaan Z, Furlan AD, et al. Canadian Guidelines on Opioid Use Disorder Among Older Adults. Can Geriatr J. 2020;23(1):123-134. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca