CADTH Health Technology Review
Mepivacaine Versus Bupivacaine for Patients Undergoing Total Joint Arthroplasty
Rapid Review
Authors: Shannon Hill, Melissa Severn, Carolyn Spry
Abbreviations
AM-PAC
Activity Measure for Post-Acute Care
CI
confidence interval
ED
emergency department
HOOS, JR
Hip disability and Osteoarthritis Outcome Score for Joint Replacement
LOS
length of stay
MA
meta-analysis
OR
odds ratio
RCT
randomized controlled trial
SR
systematic review
THA
total hip arthroplasty
TJA
total joint arthroplasty
TKA
total knee arthroplasty
Key Messages
Mepivacaine was found to have statistically significantly better results than bupivacaine for various specific measurements related to neurologic symptoms, mobility, length of stay, urinary retention, and adverse events and safety; however, for the overall evidence, the difference in outcomes between the 2 did not consistently reach the level of statistical significance.
The overall evidence for postoperative pain largely found no statistically significant difference between mepivacaine and bupivacaine, except for proportion of postoperative zero pain, where mepivacaine resulted in a statistically greater proportion of patients reporting zero pain postoperatively than bupivacaine.
Evidence was only identified for individuals who received either total hip arthroplasty or total knee arthroplasty, and thus the findings presented in this report may not be generalizable to other total joint reconstruction or replacement surgeries.
No evidence was identified regarding the cost-effectiveness or evidence-based guidelines for the use of mepivacaine versus bupivacaine for total joint arthroplasty.
Context and Policy Issues
Total joint arthroplasty (TJA) or total joint replacement is a surgical procedure to restore the function of a joint by removing parts of an arthritic or damaged joint and replacing them with prosthetic materials.1,2 Total hip arthroplasty (THA) and total knee arthroplasty (TKA) are the 2 most common arthroplasty procedures, but replacement surgery can be performed on other joints including the ankle, wrist, shoulder, and elbow.1 From 2020 to 2021, approximately 110,000 joint replacement surgeries were performed in Canada, with 55,300 and 55,285 of these surgeries being THA or TKA procedures, respectively.3 For the previous 10 years, the number of TJA surgeries increased each year in Canada, but the COVID-19 pandemic resulted in 20% fewer surgeries from 2020 to 2021.3 Recovery after TJA procedures may be painful and can result in limited mobility, depending on the location of the surgery.2 It is common for patients to stay in hospital for several days post-surgery, and adverse events may prolong total recovery time.2
Pain control for TJA is often multimodal and can include perioperative anesthesia, acetaminophen, and nonsteroidal anti-inflammatory drugs.4 Perioperative anesthesia is important for enhancing recovery pathways to minimize pain, and also offers benefits like early postoperative mobilization and decreased length of stay in hospital.5 Bupivacaine is a common perioperative anesthesia used in arthroplasty procedures and is indicated for local or regional anesthesia use.6 Bupivacaine for arthroplasty can be given as a hyperbaric solution or isobaric solution in a spinal administration; the anesthesia onset is rapid (approximately 5 minutes) and has a typical duration of 3 to 9 hours, but can last up to 72 hours.6-9 Hyperbaric bupivacaine solutions have a greater density than the cerebrospinal fluid, allowing for a quicker onset and shorter duration of motor and sensory block, whereas isobaric bupivacaine solutions have an equal density to the cerebrospinal fluid allowing for a slower onset and longer duration of action.10 Mepivacaine is another common perioperative anesthesia indicated for local or regional anesthesia use.11 It has a rapid onset of anesthesia (3 to 20 minutes), and a duration of 2 to 2.5 hours.11 The more rapid nature of mepivacaine has been reported to translate to quicker postoperative mobilization and shorter length of stay.7 It has also been noted that drowsiness and lassitude have not been commonly reported in mepivacaine use, and it has been shown to have preferable tissue compatibility with minimal irritation or tissue damage from administration.11
Because mepivacaine use provides more rapid anesthesia, there is question as to whether mepivacaine may be a more appropriate form of anesthetic for TJA than bupivacaine. The aim of the current report is to summarize the evidence regarding the clinical effectiveness, cost-effectiveness, and recommendations from evidence-based guidelines for the use of mepivacaine versus bupivacaine for patients undergoing TJA.
Research Questions
What is the comparative clinical effectiveness of mepivacaine versus bupivacaine for patients undergoing total joint arthroplasty?
What is the cost-effectiveness of mepivacaine versus bupivacaine for patients undergoing total joint arthroplasty?
What are the evidence-based guidelines for the use of mepivacaine for patients undergoing total joint arthroplasty?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, and the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were mepivacaine and joint arthroplasty. No filters were applied to limit the retrieval by study type. Conference abstracts were excluded from the search results. The search was completed on August 8, 2022, and limited to English-language documents published since January 1, 2017.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Patients undergoing total joint arthroplasty |
Intervention | Mepivacaine |
Comparator | Q1 and Q2: Bupivacaine Q3: Not applicable |
Outcomes | Q1: Clinical effectiveness (e.g., postoperative pain, postoperative length of stay, opioid use, return of motor function, safety [e.g., adverse events]) Q2: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained, incremental cost-effectiveness ratios) Q3: Recommendations regarding the administration and use of mepivacaine |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies, economic evaluations, evidence-based guidelines |
Q = question.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or they were published before 2017. Primary studies retrieved by the search were excluded if they were captured in at least 1 included systematic review.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)12 for systematic reviews and the Downs and Black checklist13 for randomized and non-randomized studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
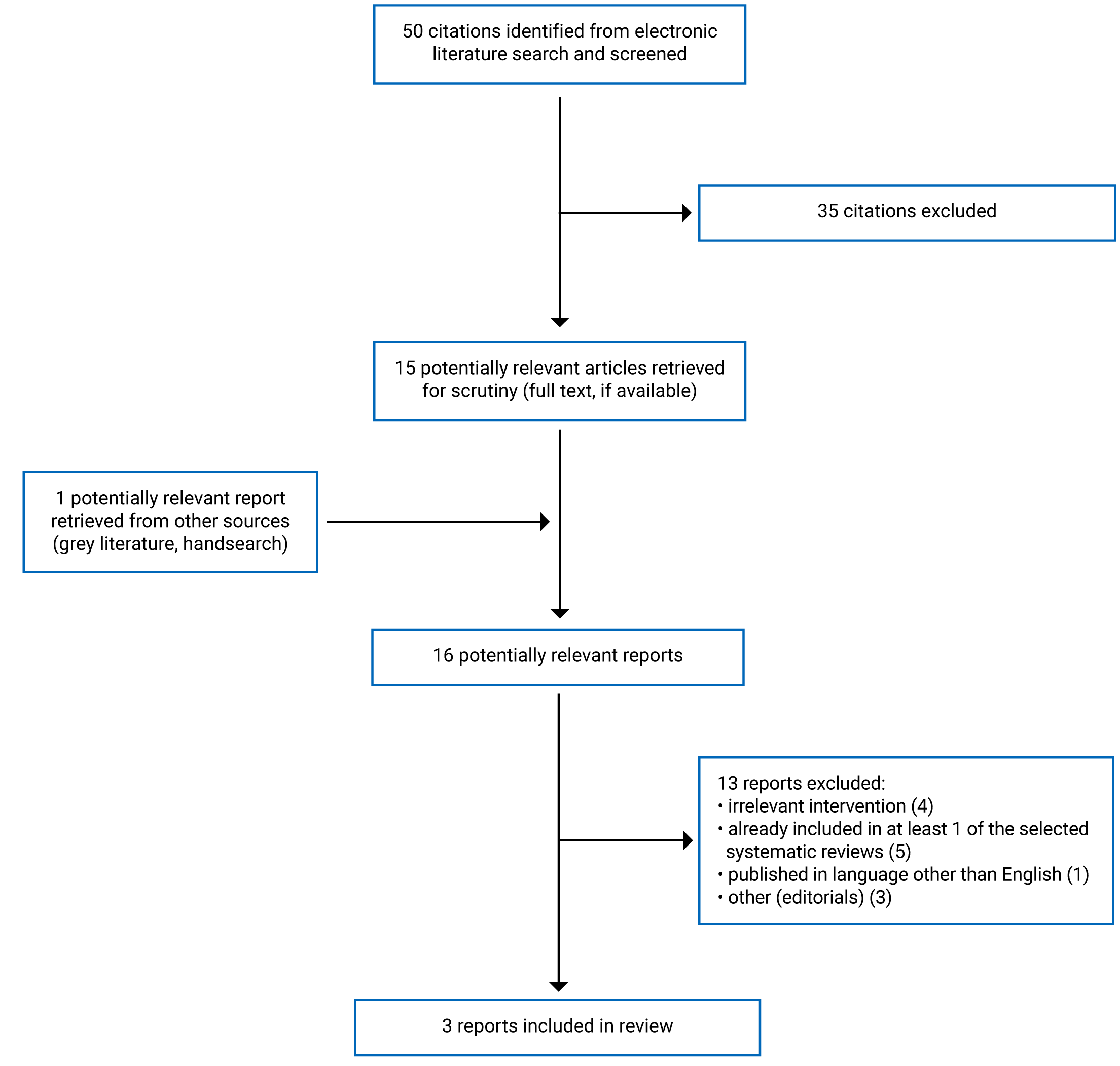
A total of 50 citations were identified in the literature search. Following screening of titles and abstracts, 35 citations were excluded and 15 potentially relevant reports from the electronic search were retrieved for full-text review. One potentially relevant publication was retrieved from the grey literature search for full-text review. Of the 16 potentially relevant articles, 13 publications were excluded for various reasons, and 3 publications met the inclusion criteria and were included in this report. These comprised 1 systematic review (SR) with meta-analysis (MA) and 2 non-randomized studies. Appendix 1 presents the PRISMA14 flow chart of the study selection.
Summary of Study Characteristics
One SR with MA15 and 2 non-randomized studies9,10 were included in this report.
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
The SR by Siddiqi et al. (2022)15 included 3 randomized controlled trials (RCTs) and 2 retrospective cohort studies in the MA. The search for relevant studies had no restrictions on time frame, but the included primary studies were published between 2018 and 2020.
Two non-randomized studies included in this report were published in 202210 and 2021.9 Both were retrospective cohort studies. One retrospective cohort study did not report follow-up findings after discharge, while 1 retrospective cohort study included follow-up times of 2 weeks, 6 weeks, and 3 months for applicable outcomes.9
Country of Origin
The SR15 and 2 retrospective cohort studies9,10 were conducted in the US.
Patient Population
The primary studies in the SR included patients who received spinal anesthesia for THA or TKA, with a total number of 1,550 patients included in the review.15 The primary studies of the SR either reported on both THA and TKA (1 RCT and 1 non-randomized study), only THA (1 RCT), or only TKA (1 RCT and 1 non-randomized study).15
One retrospective cohort study10 included patient data from 1,328 patients who underwent primary unilateral THA or TKA with spinal anesthesia performed at either an acute care hospital or affiliated ambulatory surgery centre from September 2020 to September 2021. The second retrospective cohort study9 included 141 patients who received spinal anesthesia for anterior approach THA from an ambulatory surgery centre between November 2018 and July 2020.
Interventions and Comparators
The primary studies of the SR15 compared mepivacaine and bupivacaine for spinal anesthesia in THA and TKA. The range of doses for 4 primary studies was 52.5 mg to 70 mg, and 10 mg to 12.5 mg, for mepivacaine and bupivacaine, respectively.15 Doses for 1 primary study were not reported. In addition, the number of patients that received mepivacaine and bupivacaine for each primary study ranged from 15 to 563 and 16 to 491, respectively.15
One retrospective cohort study10 compared mepivacaine and hyperbaric or isobaric bupivacaine. The mean dose and standard deviation for THA patients that received mepivacaine, hyperbaric bupivacaine, or isobaric bupivacaine was 63.4 (± 75.3) mg, 10.9 (± 1.7) mg, and 12.7 (± 2.1) mg, respectively.10 The mean dose and standard deviation for TKA patients that received mepivacaine, hyperbaric bupivacaine, or isobaric bupivacaine was 65.2 (± 54.5) mg, 10.7 (± 1.6) mg, and 11.0 (± 2.4) mg, respectively.10 The second retrospective cohort study9 compared 2% mepivacaine (40 to 60 mg) to 0.75% hyperbaric bupivacaine (10.5 mg to 15 mg) for spinal anesthesia in THA.
Outcomes
The SR15 assessed surgical outcomes related to time of full neurologic motor return, pain levels, mobility, postoperative length of stay in hospital (LOS), and complications, including transient neurologic symptoms and urinary retention.
One retrospective cohort study10 assessed LOS in days, postoperative day 0 ambulation, failed same-day discharge attempt, first mobility using the Activity Measure for Post-Acute Care (AM-PAC) 6-Clicks mobility score,16 first physical therapy documented ambulation distance, urinary retention, home discharge, 30-day readmission, and 30-day emergency department (ED) return. The second retrospective cohort study9 assessed time in each phase of care, pain scores (0 to 10 scale), pain medication received, time to ambulation, ambulation distance, time to controlled void, bethanechol doses, and postoperative nausea or vomiting. In addition, the second retrospective cohort study9 assessed pain (visual analogue scale) and Hip disability and Osteoarthritis Outcome Score for Joint Replacement (HOOS, JR) scores at 2 weeks, 6 weeks, and 3 months; and 90-day postoperative outcomes, including complications, ED visits, hospital readmissions, and reoperations.
Summary of Critical Appraisal
The SR15 clearly described the objective and provided details related to the literature search strategy, including time frame of the search, study designs included, and search terms applied, which allows for potential reproducibility for this review. The authors of the SR15 also indicated that manual screening of bibliographic references was done to identify any potentially relevant studies. The authors did not state if a research protocol was established before conducting the SR, which may make it challenging to determine if appropriate and reliable methods were followed to produce the findings of this study. It is unclear if literature screening, study selection, or data extraction was performed in duplicate, to minimize potential errors for study selection and data extraction. It was stated that risk of bias assessments for included primary studies was performed in duplicate using the Cochrane Collaboration Tool for RCTs and A Cochrane Risk of Bias Assessment Tool: for Non-Randomized Studies of Interventions. Each included study was reported to have a low risk of bias. Duplicate assessments may reduce missing or erroneous information in determining the risk of bias. The authors of this review did not provide a list of excluded studies, reasons for exclusion, and information related to funding for primary studies that were included in the review. Without this information, it is difficult to determine if relevant studies have been excluded, leading to increased risk of selection bias, or if there was a potential risk to editorial independence due to funding sources. Limited details of the study characteristics of the included studies were presented, which included information related to study year, design, population, intervention, comparison, dosing, results, and limitations. The authors of this review used appropriate methods for statistical analysis based on the Cochrane Handbook for Systematic Review of Interventions. They assessed heterogeneity using I2 statistics and Cochrane chi-square tests, and considered heterogeneity in the discussion of results for each reported outcome. This is helpful to interpret the reliability of results across studies. The MA compared results from both RCTs and non-randomized studies, but the author did not discuss how results should be interpreted due to the variation in study design. Given the reported low risk of bias of the included studies, no assessment of potential impact of risk of bias on the results of the MA was conducted. Finally, though the authors provided a conflict-of-interest declaration, they did not report funding information for this study.
The objective, main outcome, patient characteristics, and interventions received were clearly described in both retrospective cohort studies.9,10 One retrospective cohort study10 described principal confounders and used multivariate linear and regression models to compare outcomes while controlling for confounders. The other retrospective cohort study9 did not adequately describe principal confounders or control for confounders, but the authors noted that any confounding factors were unlikely to be significant. Because confounding factors were not controlled for, it is unclear if the reported finding could be solely attributed the interventions used. One retrospective cohort study10 did not adequately report details regarding included patients, if patient data were obtained from the same population, and the reasons for excluding patients, which may create concern over selection bias and impact generalizability of findings. The other retrospective cohort study9 did provide details related to patient recruitment and data use, and stated that patient data were drawn from the same population group at a single institution from 2018 to 2020. The study population appeared to be representative of the entire population from which they were recruited, and a justification was given for excluding any patient data. The main findings from both retrospective cohort studies9,10 were clearly described and included appropriate estimates of variability where applicable. Actual P values were also reported for both retrospective cohort studies, except where the P value was less than 0.001.9,10 Appropriate statistical analyses were used in both retrospective cohort studies for dichotomous, continuous, and multiple variables.9,10 In addition, 1 retrospective cohort study10 provided a subgroup analysis for same-day discharge groups and risk-adjust analysis to control for principal confounders. Providing appropriate statistical analyses helps determine accurate interpretation for main findings. Both retrospective cohort studies lack the randomization effect of RCTs to balance confounding factors across study groups and reduce associated risk of bias.9,10 Finally, both retrospective cohort studies reported that no funding was received to conduct their study.9,10 One retrospective cohort study10 reported no conflict of interest, while the other retrospective cohort study9 did declare potential conflicts of interest, and it appeared unlikely that funding and other interest inappropriately influenced the outcomes and interpretation of findings in either study.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
Appendix 4 presents the main study findings of the SR15 and 2 retrospective cohort studies.9,10 The findings are presented by main outcomes, which are neurologic symptoms (Table 6), mobility (Table 7), pain (Table 8), LOS (Table 9), urinary retention (Table 10), additional clinical outcomes (Table 11), and adverse events and safety (Table 12).
Clinical Effectiveness of Mepivacaine Versus Bupivacaine for Patients Undergoing TJA
One SR15 and 2 retrospective cohort studies9,10 were found regarding the clinical effectiveness of mepivacaine versus bupivacaine for patients undergoing TJA.
Neurologic Symptoms
The SR15 identified 3 studies that compared the time to postoperative motor function return for mepivacaine versus bupivacaine spinal anesthesia. The pooled overall effect for time to postoperative motor function return significantly favoured mepivacaine (154 minutes) compared to bupivacaine (170 minutes) with a mean difference of −27.34 (95% confidence interval [CI], −41.12 to −13.56; P = 0.0472; I2 = 0%).15 The SR15 also identified transient neurologic symptoms (defined as pain or abnormal sensation in the lower back, buttocks, and lower extremities) from 1 included study that reported transient neurologic symptoms in 10%, 11.3%, and 3.9% of patients treated with mepivacaine, hyperbaric bupivacaine, and isobaric bupivacaine, respectively. The difference between the groups was not statistically significant (P = 0.36).15 One retrospective cohort study9 reported that transient neurologic symptoms occurred in 2 patients who received bupivacaine versus none among those who received mepivacaine (P = 0.489).
Mobility
Four studies in the SR15 reported outcomes for mobilization distance on postoperative day 0, while 3 studies reported outcome for mobilization distance on postoperative day 1. Combined early mobilization for postoperative day 0 and day 1 was shown to be greater for the patients who received mepivacaine (94.2 ft) compared to patients who received bupivacaine (89.1 ft), with a mean difference of 5.1 ft (95% CI, −15 to 25.2).15 This difference was not statistically significant (P = 0.61) and the heterogeneity among studies was significant (I2 = 54%).15 One retrospective cohort study9 reported ambulation distances in postoperative recovery room for recipients of mepivacaine and bupivacaine. Mepivacaine recipients had a greater average ambulation distance (69 ft) compared to bupivacaine recipients (64.4 ft); however, this difference was not statistically significant (P = 0.611).
One retrospective cohort study10 reported the number of patients ambulated on postoperative day 0. The authors found that patients who received mepivacaine were more likely to be ambulated on postoperative day 0 compared to patients who received bupivacaine, for both THA and TKA procedures (P < 0.001 in each comparison). Mepivacaine still showed a greater likelihood than bupivacaine of patients ambulated on postoperative day 0, with an odds ratio (OR) of 2.391 (95% CI, 1.789 to 3.197; P < 0.001) after controlling for confounding factors.10 The authors also found significant differences in both THA and TKA procedures for first physical therapy ambulation distance for those who received mepivacaine compared to bupivacaine (P < 0.001).10 However, a subgroup analysis of same-day discharge patients did not find a statistically significant difference between mepivacaine and bupivacaine for first physical therapy ambulation distance, following either THA (P = 0.144) or TKA (P = 0.757).10 When controlling for confounding factors, patients who received mepivacaine had a greater first physical therapy ambulation distance with an OR of 21.785 (95% CI, 10.459 to 33.111; P < 0.001) compared to those who received bupivacaine.10 This retrospective cohort study10 also assessed AM-PAC 6-Clicks mobility scores and found that mepivacaine recipients and hyperbaric bupivacaine recipients has statistically significantly higher scores compared to isobaric bupivacaine recipients for those who underwent THA (P = 0.003), but not for those who underwent TKA (P = 0.607). A subgroup analysis for patients discharged the same day of procedure found that mepivacaine recipients had higher AM-PAC 6 Click mobility scores for both THA and TKA (P < 0.001 in each comparison).10 However, the difference between mepivacaine and bupivacaine for this outcome was not statistically significant after controlling for confounding factors (P = 0.192).10
One retrospective cohort study9 compared time to postoperative mobilization outcomes between mepivacaine and bupivacaine. No significant difference was found for the number of hours to ankle plantar or dorsiflexion (P = 0.502). However, mepivacaine recipients had a significant decrease in number of hours to sitting up (P < 0.001) and number of hours to ambulation (P < 0.001) compared to bupivacaine.9
Pain
Three studies in the SR15 reported on pain scores on postoperative day 0, while 4 studies reported on pain scores on postoperative day 1. Combined pain scores during the early postoperative period showed lower average pain scores for those who received mepivacaine (3.57) compared to those who received bupivacaine (3.68), with a mean difference of −0.1 (95% CI, −2.1 to 1.9).15 The difference was not statistically significant (P = 0.91), and no heterogeneity was detected between the studies for this assessment (I2 = 0). One retrospective cohort study9 reported postoperative pain outcomes from immediately after up to 5 hours after procedure, and found that bupivacaine recipients reported significantly lower postoperative pain scores at 1 hour (P < 0.001), 2 hours (P < 0.001), and 3 hours (P = 0.003) compared to mepivacaine recipients. Additionally, the authors reported outcomes for the proportion of patients who experienced zero pain immediately postoperative, up to 5 hours postoperative. The authors found that a significantly larger proportion of mepivacaine recipients reported zero postoperative pain at 1 hour (P = 0.010), 2 hours (P < 0.001), 3 hours (P = 0.006), 4 hours (P < 0.001), and 5 hours (P = 0.043) compared to bupivacaine recipients.9 There was no significant difference in postoperative pain scores for those who received mepivacaine or bupivacaine at 2 weeks (P = 0.308), 6 weeks (P = 0.386), or 3 months (P = 0.575).9 Mepivacaine recipients reported significantly higher pain scores at discharge compared to bupivacaine recipients (P = 0.004), and postoperative pain medication use was significantly higher in mepivacaine recipients compared to bupivacaine recipients (P < 0.001).9
Length of Stay
Three studies in the SR15 reported on overall LOS and found that mepivacaine recipients had a significantly lower mean LOS of 25.95 hours, compared to a mean LOS of 29.96 hours for bupivacaine recipients. The mean difference in overall LOS was −7.03 hours (95% CI, −10.02 to −4.04; P = 0.0057); however, the between-studies heterogeneity was high for this assessment (I2 = 53%).15 One retrospective cohort study10 reported that those who received mepivacaine showed significantly lower LOS days compared to those who received bupivacaine for both THA (P < 0.001) and TKA (P < 0.001) procedures. When controlling for confounders, LOS was significantly lower for those who received mepivacaine compared to those who received bupivacaine (OR = −0.421; 95% CI, −0.502 to −0.330; P < 0.001).10 In addition, the authors of this retrospective cohort study10 reported significantly higher numbers of 0-day LOS for those who received mepivacaine compared to those who received bupivacaine for both THA (P < 0.001) and TKA (P < 0.001) procedures. When controlling for confounding factors, those who received mepivacaine had higher odds of 0-day LOS, with an OR of 5.767 (95% CI, 4.357 to 7.634; P < 0.001).10 One retrospective cohort study9 reported the time spent in each ambulatory phase while in hospital and found a significantly lower number of hours for mepivacaine recipients in the postoperative phase (P < 0.001) and total facility time (P < 0.001) compared to bupivacaine recipients.
Urinary Retention
Five studies in the SR15 found that the incidence of postoperative urinary retention was significantly lower in those who received mepivacaine compared to those who received bupivacaine (P = 0.0181); however, there was moderate heterogeneity among studies reporting urinary retention as a postoperative complication (I2 = 49%). One retrospective cohort study10 reported no significant difference in the rates of urinary retention for mepivacaine recipients compared to bupivacaine recipients, for both THA (P = 0.097) and TKA (P = 0.734) procedures. Controlling for confounding factors, this did not change the statistical significance in the difference between mepivacaine and bupivacaine for this outcome (P = 0.452).10 Finally, 1 retrospective cohort study9 reported a significantly lower number of hours to controlled void for mepivacaine recipients compared to bupivacaine recipients (P < 0.001), and the number of patients who required bethanechol doses (used to manage voiding) was significantly lower with mepivacaine than with bupivacaine (P < 0.001).
Additional Clinical Outcomes
One retrospective cohort study10 found that significantly more patients who underwent THA and received mepivacaine were discharged to their homes compared to those who received bupivacaine (P = 0.001). No significant difference was observed for patients who underwent TKA and received either mepivacaine or bupivacaine (P = 0.106).10 When controlling for confounding factors, patients who received mepivacaine were more likely to be discharged home with an OR of 6.537 (95% CI, 1.540 to 27.743; P = 0.011) compared to patients who received bupivacaine.10
One retrospective cohort study9 found no significant difference between mepivacaine and bupivacaine in HOOS, JR scores, which measured hip disability and osteoarthritis outcomes for patients at 2 weeks (P = 0.990), 6 weeks (P = 0.704), and 3 months (P = 0.604) postoperative.
Adverse Events and Safety
One retrospective cohort study10 reported on the number of failed same-day discharge attempts between mepivacaine recipients compared to bupivacaine recipients and found no significant difference for both THA (P = 0.334) and TKA (P = 0.449) procedures. Similarly, when controlling for confounding factors, this difference between mepivacaine and bupivacaine for failed same-day discharge attempts was not statistically significant (OR = 0.801; 95% CI, 0.458 to 1.400; P = 0.436).10 The same retrospective cohort study10 reported that mepivacaine recipients had a significantly lower 30-day readmissions rate than bupivacaine recipients for TKA (P = 0.008), but not for THA (P = 0.699).10 The odds of a 30-day readmission was not significantly different in mepivacaine versus bupivacaine recipients after controlling for confounding factors (OR = 0.494; 95% CI, 0.226 to 1.083; P = 0.078).10 No significant difference was found for mepivacaine recipients compared to bupivacaine recipients for 30-day ED returns in either THA (P = 0.305) or TKA (P = 599) cohorts.10 The odds of 30-day ED returns was not significantly different between mepivacaine and bupivacaine recipients after adjusting for confounding factors (OR = 1.068; 95% CI, 0.552 to 2.067; P = 0.845).10
One retrospective cohort study9 reported on 90-day adverse events between mepivacaine recipients and bupivacaine recipients and found no difference between total complications (P = 1.00), ED visits (P = 1.00), hospital admissions (P = 1.00), and reoperations (P = 1.00). In addition, the retrospective cohort study9 found no statistically significant difference between mepivacaine and bupivacaine recipients in the incidence of postoperative nausea or vomiting (P = 0.223) and hypotension requiring treatment (P = 0.153).9
Cost-Effectiveness of Mepivacaine Versus Bupivacaine for Patients Undergoing TJA
No evidence was identified regarding the cost-effectiveness of mepivacaine versus bupivacaine for patients undergoing TJA; therefore, no summary can be provided.
Guidelines Regarding the Use of Mepivacaine Versus Bupivacaine for Patients Undergoing TJA
No evidence-based guidelines were identified regarding the use of mepivacaine for patients undergoing TJA; therefore, no summary can be provided.
Limitations
The main limitations were related to the generalizability and applicability of the findings. The SR15 reported findings for combined surgical outcomes, which included data from patients who underwent THA or TKA, but the authors did not provide a subgroup analysis for surgical outcomes related only to THA or TKA. This may be a concern for accurately interpreting findings and may impact generalizability depending on the arthroplasty procedure (e.g., findings for patients who only received THA may not be applicable to those who received TKA or may undergo another form of TJA). In addition, the authors reported considerable heterogeneity for mobility, LOS, and urinary retention outcomes, but did not provide details on how heterogeneity may impact findings for these outcomes.15 These limitations should be considered when interpreting findings drawn from the SR.
Although many outcomes (e.g., neurologic symptoms, mobility, pain, LOS, urinary retention, and adverse events and safety) were reported across multiple studies, there was a high degree of heterogeneity for the methods used to collect relevant outcome data, making it challenging to compare outcomes across the studies.
The included studies were all conducted in the US and therefore it is unclear how generalizable these findings may be to the Canadian context. In addition, this report could not identify evidence related to the cost-effectiveness of mepivacaine versus bupivacaine for patients undergoing TJA, or evidence-based guidelines providing recommendations regarding the use of mepivacaine versus bupivacaine for patients undergoing TJA.
Conclusions and Implications for Decision- or Policy-Making
This report identified 1 SR with MA15 and 2 retrospective cohort studies9,10 regarding the clinical effectiveness of mepivacaine versus bupivacaine for patients undergoing TJA.
The included studies provided findings for a variety of clinical outcomes regarding the use of mepivacaine compared to bupivacaine spinal anesthesia. These outcomes were found in similar populations, being adults who underwent either THA or TKA. Overall, some clinical evidence regarding the use of mepivacaine versus bupivacaine for patients undergoing TJA was identified that may be in favour of mepivacaine, depending on the outcome being measured. Patients who received mepivacaine for THA or TKA were shown to have significantly better neurologic symptom outcomes for postoperative motor function return.15 Mepivacaine recipients showed significantly better mobility outcomes for being ambulated on postoperative day 0,10 first physical therapy ambulation distance,10 AM-PAC 6-Clicks mobility scores for those who underwent THA,10 number of hours to sitting up,9 and number of hours to ambulation.9 Mepivacaine recipients showed significantly better pain outcomes when assessing zero postoperative pain at 1, 2, 3, 4, and 5 hours;9 however, no significant difference was found for combined pain scores during the early postoperative period.15 For those who did report having postoperative pain, bupivacaine was found to have significantly better outcomes for postoperative pain at 1, 2, and 3 hours.9 Mepivacaine recipients were shown to have significantly better outcomes for overall LOS,15 LOS days,10 0-day LOS,10 hours in postoperative phase,9 and total facility time.9 Mepivacaine recipients were shown to have significantly better urinary retention outcomes for number of urinary events,15 number of hours to controlled void,9 and number of patients who required bethanechol doses.9 Mepivacaine recipients were shown to have significantly better outcomes for home discharge outcomes when controlling for confounding factors.10 Mepivacaine recipients were shown to have significantly better 30-day readmission outcomes for patients who underwent TKA10; however, no difference was found for failed same-day discharge attempts,10 30-day readmissions when controlling for confounding factors,10 30-day ED returns,10 90-day adverse events,9 postoperative nausea or vomiting,9 and hypotension requiring treatment.9
These findings are based on reported outcomes found in the identified studies and should be interpreted with considerations for their methodological limitations and heterogeneity of outcome measurements. Given that the findings of these studies are only related to patients who have received either THA or TKA, the generalizability of the results for other TJA procedures is unknown. Patient satisfaction or quality of life measurements were not captured in any of the identified studies. Despite these concerns, the studies identified do provide multiple findings for major clinical outcomes related to neurologic symptoms, mobility, pain, LOS, urinary retention, and adverse events and safety that should be considered for future decisions around the use of mepivacaine. Future high-quality studies that also evaluate other forms of TJA, patient satisfaction with mepivacaine or bupivacaine, and changes in health-related quality of life would help stakeholders’ decisions concerning the use of either for TJA procedures. In addition, evidence on the cost-effectiveness and evidence-based recommendations for using mepivacaine versus bupivacaine in TJA are needed to inform treatment selection decisions for optimal patient outcomes.
References
1.Foran JRH. Total joint replacement. Rosemont (IL): American Academy of Orthopaedic Surgeons; 2021: https://orthoinfo.aaos.org/en/treatment/total-joint-replacement/. Accessed 2022 Aug 30.
2.Arthroplasty. Baltimore (MD): John Hopkins University; 2022: https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/arthroplasty. Accessed 2022 Aug 30.
3.Hip and knee replacements in Canada: CJRR annual report, 2020–2021. Ottawa (ON): Canadian Institute for Health Information; 2022: https://www.cihi.ca/sites/default/files/document/hip-knee-replacements-in-canada-cjrr-annual-report-2020-2021-en.pdf. Accessed 2022 Aug 30.
4.Erens GA, Walter B, Crowley M. Total hip arthroplasty. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2021: https://www.uptodate.com. Accessed 2022 Aug 30.
5.Amundson AW, Johnson RL. Anesthesia for total knee arthroplasty. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate.; 2022: https://www.uptodate.com. Accessed 2022 Aug 30.
6.Bupivacaine hydrochloride in dextrose injection USP: 7.5 mg / mL sterile hyperbaric solution local anesthetic for spinal use only [product monograph]. Oakville (ON): SteriMax; 2018 Mar 23: https://pdf.hres.ca/dpd_pm/00044528.PDF. Accessed 2022 Aug 30.
7.Kuhn AW, Lynch JR, Ahlers CG, Polkowski GG. Spinal anesthetic type and independent risk factors for postoperative urinary retention following total joint arthroplasty. J Surg Orthop Adv. 2020;29(4):225-229. PubMed
8.Collins JB, Song J, Mahabir RC. Onset and duration of intradermal mixtures of bupivacaine and lidocaine with epinephrine. Can J Plast Surg. 2013;21(1):51-53. PubMed
9.Calkins TE, McClatchy SG, Rider CM, Toy PC. Mepivacaine vs bupivacaine spinal anesthesia in total hip arthroplasty at an ambulatory surgery center. J Arthroplasty. 2021;36(11):3676-3680. PubMed
10.Stock LA, Dennis K, MacDonald JH, Goins AJ, Turcotte JJ, King PJ. Postoperative outcomes of mepivacaine vs. bupivacaine in patients undergoing total joint arthroplasty with spinal anesthesia. Arthroplasty. 2022;4(1):32. PubMed
11.Carbocaine 1% (10 mg/mL) and Carbocaine 2% (20 mg/mL) mepivacaine hydrochloride injection [product monograph]. Kirkland (QC): Pfizer Canada; 2017 Aug 2: https://pdf.hres.ca/dpd_pm/00041424.PDF. Accessed 2022 Aug 30.
12.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
13.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
14.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
15.Siddiqi A, Mahmoud Y, Secic M, et al. Mepivacaine versus bupivacaine spinal anesthesia for primary total joint arthroplasty: a systematic review and meta-analysis. J Arthroplasty. 2022;37(7):1396-1404.e1395. PubMed
16.6 Clicks functional measurement tool: why it’s drawing crowds at conferences far and wide. Cleveland (OH): Cleveland Clinic; 2017: https://consultqd.clevelandclinic.org/6-clicks-functional-measurement-tool-why-its-drawing-crowds-at-conferences-far-and-wide/. Accessed 2022 Aug 29.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Review
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics for included primary studies | Intervention and comparator | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Siddiqi et al. (2022)15 US Funding source: NR | Number of included studies: 5 (3 RCTs and 2 non-randomized studies) | Eligibility criteria: Patients who received spinal anesthesia for THA or TKA Total number of patients included: 1550 Sample size (range): 31 to 1054 | Intervention (dosage range): Mepivacaine (52.5 mg to 70 mg)a Comparator (dosage range): Bupivacaine (10 mg to 12 mg)a | Outcomes:
Follow-up: Follow-up details NR for included studies |
mg = milligram; NR = not reported; RCT = randomized controlled trial; THA = total hip arthroplasty; TKA = total knee arthroplasty.
aOne included study did not provide dosages for intervention or comparator.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design, setting, number of patients included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Stock et al. (2022)10 US Funding source: No funding | Study design: Retrospective cohort study Setting: Joint Replacement Centre N = 1328 | Eligibility criteria: Patients who received spinal anesthesia for primary unilateral THA or TKA from September 2020 to September 2021 Number of patients in each TJA cohort:
Mean age (SD):
| Intervention (mean dose for THA and TKA): Mepivacaine (63.4 mg; 65.2 mg) Comparator (mean dose for THA and TKA):
| Outcomes:
Follow-up: NA |
Calkins et al. (2021)9 US Funding source: No funding | Study design: Retrospective cohort study Setting: Ambulatory surgery centre N = 282 | Eligibility criteria: Patients who received spinal anesthesia for anterior approach THA between November 2018 and July 2020 Mean age (SD):
Number of females (%):
| Intervention (dosage): Mepivacaine (40 mg to 60 mg) Comparator (dosage): Hyperbaric bupivacaine (10.5 mg to 15 mg) | Outcomes:
Follow-up:
|
AM-PAC = Activity Measure for Post-Acute Care; ED = emergency department; HOOS, JR = Hip Disability and Osteoarthritis Outcome Score for Joint Replacement; mg = milligram; NA = not applicable; PONV = postoperative nausea/vomiting; SD = standard deviation; THA = total hip arthroplasty; TJA = total joint arthroplasty; TKA = total knee arthroplasty.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of the Systematic Review and Meta-Analysis Using AMSTAR 212
Strengths | Limitations |
|---|---|
Siddiqi et al. (2022)15 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess Systematic Reviews 2; PICO = patients, interventions, comparators, and outcomes; RCT = randomized controlled trial.
Table 5: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist13
Strengths | Limitations |
|---|---|
Stock et al. (2022)10 | |
|
|
Calkins et al. (2021)9 | |
|
|
ANOVA = analysis of variance.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 6: Summary of Findings by Outcome — Neurologic Symptoms
Study citation and design | Study Findings |
|---|---|
Postoperative Motor Function Return | |
Siddiqi et al. (2022)15 Systematic Review and Meta Analysis (outcome based on 3 included studies) | Combined values for N, Mean and SD for 3 included studies (minutes) Mepivacaine
Bupivacaine
Mean difference (95% CI) = -27.34 (-41.12 to -13.56); P = 0.0472; I2 = 0% |
Transient Neurologic Symptoms | |
Siddiqi et al. (2022)15 Systematic Review and Meta Analysis (outcome based on 1 included study) | Occurrence of transient neurologic symptoms (%) Mepivacaine: Occurrence = 10 Hyperbaric Bupivacaine: Occurrence = 11.3 Isobaric Bupivacaine: Occurrence = 3.9 P = 0.36 |
Calkins et al. (2021)9 Retrospective cohort study (N = 282) | Transient neurological symptoms Mepivacaine (n = 141): n (%) = 0 (0) Bupivacaine (n = 141): n (%) = 2 (1.4) P = 0.498 |
CI = confidence interval; N = number; SD = standard deviation.
Table 7: Summary of Findings by Outcome — Mobility
Study citation and design | Study Findings | |
|---|---|---|
Mobilization Distance Postoperative Day 0 | ||
Siddiqi et al. (2022)15 Systematic Review and Meta Analysis (outcome based on 4 included studies) | Combined total distance for 4 included studies (feet) Mepivacaine: Total = 195 Bupivacaine: Total = 300 Mean difference (95% CI) = 12.01 (-9.04 to 33.05); P = 0.26; I2 = 55% | |
Calkins et al. (2021)9 Retrospective cohort study (N = 282) | Ambulation distance in postoperative recovery room (feet) Mepivacaine (n = 141): Mean (SD) = 69 (30.4) Bupivacaine (n = 141): Mean (SD) = 64.4 (58.4) P = 0.661 | |
Mobilization Distance Postoperative Day 1 | ||
Siddiqi et al. (2022)15 Systematic Review and Meta Analysis (outcome based on 3 included studies) | Combined total distance for 3 included studies (feet) Mepivacaine: Total = 145 Bupivacaine: Total = 196 Mean difference (95% CI) = 5.04 (-24.38 to 34.46); P = 0.76; I2 = 54% | |
Number of Patients Ambulated Postoperative Day 0 | ||
Stock et al. (2022)10 Retrospective cohort study (N = 1328) | Unadjusted postoperative THA Mepivacaine (n = 232): n (%) = 196 (84.5) Hyperbaric Bupivacaine (n = 401): n (%) = 282 (70.3) Isobaric Bupivacaine (n = 34): n (%) = 19 (55.9) P < 0.001 | Unadjusted postoperative TKA Mepivacaine (n = 131): n (%) = 225 (85.9) Hyperbaric Bupivacaine (n = 502): n (%) = 328 (65.3) Isobaric Bupivacaine (n = 28): n (%) = 17 (60.7) P < 0.001 |
Subgroup analysis of mepivacaine vs. bupivacaine for same-day discharge patients THA Mepivacaine (n = 141): n (%) = 141 (100.0) Bupivacaine (n = 104): n (%) = 104 (100.0) P = NA | Subgroup analysis of mepivacaine vs. bupivacaine for same-day discharge patients TKA Mepivacaine (n = 138): n (%) = 138 (100.0) Bupivacaine (n = 59): n (%) = 59 (100.0) P = NA | |
Risk-adjusted mepivacaine vs. bupivacaine (n)a Mepivacaine: OR (95% CI) = 2.391 (1.789 to 3.197); P < 0.001 | ||
First Physical Therapy Ambulation Distance | ||
Stock et al. (2022)10 Retrospective cohort study (N = 1328) | Unadjusted postoperative THA (feet) Mepivacaine (n = 232): Mean (SD) = 184 (±84.84) Hyperbaric Bupivacaine (n = 401): Mean (SD) = 151 (±97.51) Isobaric Bupivacaine (n = 34): Mean (SD) = 142.55 (±114.21) P < 0.001 | Unadjusted postoperative TKA (feet) Mepivacaine (n = 131): Mean (SD) = 165.24 (±101.79) Hyperbaric Bupivacaine (n = 502): Mean (SD) = 134.57 (±98.89) Isobaric Bupivacaine (n = 28): Mean (SD) = 111.67 (±77.44) P < 0.001 |
Subgroup analysis of mepivacaine vs. bupivacaine for same-day discharge patients THA (feet) Mepivacaine (n = 141): Mean (SD) = 208.93 (±66.60) Bupivacaine (n = 104): Mean (SD) = 193.81 (±73.84) P = 0.144 | Subgroup analysis of mepivacaine vs. bupivacaine for same-day discharge patients TKA (feet) Mepivacaine (n = 138): Mean (SD) = 215.53 (±82.85) Bupivacaine (n = 59): Mean (SD) = 220.25 (±90.13) P = 0.757 | |
Risk-adjusted mepivacaine vs. bupivacaine (feet)a Mepivacaine: OR (95% CI) = 21.785 (10.459 to 33.111); P < 0.001 | ||
Activity Measure for Post-Acute Care 6-Clicks Mobility Score | ||
Stock et al. (2022)10 Retrospective cohort study (N = 1328) | Unadjusted postoperative THA score Mepivacaine (n = 232): Mean (SD) = 20.43 (±2.51) Hyperbaric Bupivacaine (n = 401): Mean (SD) = 20.48 (±2.75) Isobaric Bupivacaine (n = 34): Mean (SD) = 18.82 (±2.92) P = 0.003 | Unadjusted postoperative TKA score Mepivacaine (n = 131): Mean (SD) = 19.98 (±2.50) Hyperbaric Bupivacaine (n = 502): Mean (SD) = 20.13 (±2.75) Isobaric Bupivacaine (n = 28): Mean (SD) = 20.5 (±2.5) P = 0.607 |
Subgroup analysis of mepivacaine vs. bupivacaine for same-day discharge patients THA score Mepivacaine (n = 141): Mean (SD) = 20.16 (±2.38) Bupivacaine (n = 104): Mean (SD) = 21.26 (±2.28) P = 0.001 | Subgroup analysis of mepivacaine vs. bupivacaine for same-day discharge patients TKA score Mepivacaine (n = 138): Mean (SD) = 19.96 (±2.54) Bupivacaine (n = 59): Mean (SD) = 22.08 (±2.15) P < 0.001 | |
Risk-adjusted mepivacaine vs. bupivacaine scorea Mepivacaine: OR (95% CI) = -0.209 (-0.523 to 0.105); P = 0.192 | ||
Time to Postoperative Mobilization | ||
Calkins et al. (2021)9 Retrospective cohort study (N = 282) | Hours to ankle dorsi/plantar flexion Mepivacaine (n = 141): Mean (SD) = 1.6 (0.7) Bupivacaine (n = 141): Mean (SD) = 1.8 (1.2) P = 0.502 Hours to sitting up Mepivacaine (n = 141): Mean (SD) = 2.5 (0.7) Bupivacaine (n = 141): Mean (SD) = 3.3 (1.1) P < 0.001 Hours to ambulation Mepivacaine (n = 141): Mean (SD) = 3.2 (1.0) Bupivacaine (n = 141): Mean (SD) = 4.5 (1.6) P = < 0.001 | |
CI = confidence interval; N = number; NA = not applicable; OR = odds ratio; SD = standard deviation; THA = total hip arthroplasty; TKA = total knee arthroplasty; vs. = versus.
aRisk-adjusted comparison controls for age, body mass index, sex, American Society of Anesthesiologists score, and procedure type (THA or TKA).
Table 8: Summary of Findings by Outcome — Pain
Study citation and design | Study Findings |
|---|---|
Pain Postoperative Day 0 | |
Siddiqi et al. (2022)15 Systematic Review and Meta Analysis (outcome based on 3 included studies) | Combined total pain scores for 3 included studies (VASa) Mepivacaine: Total = 118 Bupivacaine: Total = 172 Mean difference (95% CI) = 1.44 (0.94 to 1.94); P = 0.75; I2 = 0% |
Calkins et al. (2021)9 Retrospective cohort study (N = 282) | Immediate postoperative pain (0-10 scale) Mepivacaine (n = 141): Mean (SD) = 0.1 (0.8) Bupivacaine (n = 141): Mean (SD) = 0.1 (0.8) P = 0.83 1-hour postoperative pain (0-10 scale) Mepivacaine (n = 141): Mean (SD) = 1.6 (2.7) Bupivacaine (n = 141): Mean (SD) = 0.6 (1.6) P < 0.001 2-hour postoperative pain (0-10 scale) Mepivacaine (n = 141): Mean (SD) = 1.7 (2.5) Bupivacaine (n = 141): Mean (SD) = 0.9 (1.9) P < 0.001 3-hour postoperative pain (0-10 scale) Mepivacaine (n = 141): Mean (SD) = 1.3 (2.1) Bupivacaine (n = 141): Mean (SD) = 0.9 (1.9) P = 0.003 4-hour postoperative pain (0-10 scale) Mepivacaine (n = 141): Mean (SD) = 0.8 (1.9) Bupivacaine (n = 141): Mean (SD) = 0.8 (1.7) P = 0.945 5-hour postoperative pain (0-10 scale) Mepivacaine (n = 141): Mean (SD) = 0.3 (1.0) Bupivacaine (n = 141): Mean (SD) = 0.7 (1.6) P = 0.099 |
Zero pain immediately postoperative (% only) Mepivacaine (n = 141): = 99% Bupivacaine (n = 141): = 99% P = 1.000 Zero pain at 1-hour postoperative (% only) Mepivacaine (n = 141): = 69% Bupivacaine (n = 141): = 86% P = 0.010 Zero pain at 2-hour postoperative (% only) Mepivacaine (n = 141): = 58% Bupivacaine (n = 141): = 79% P < 0.001 Zero pain at 3-hour postoperative (% only) Mepivacaine (n = 141): = 57% Bupivacaine (n = 141): = 73% P = 0.006 Zero pain at 4-hour postoperative (% only) Mepivacaine (n = 141): = 39% Bupivacaine (n = 141): = 61% P < 0.001 Zero pain at 5-hour postoperative (% only) Mepivacaine (n = 141): = 28% Bupivacaine (n = 141): = 45% P = 0.043 | |
Pain Postoperative Day 1 | |
Siddiqi et al. (2022)15 Systematic Review and Meta Analysis (outcome based on 4 included studies) | Combined total pain scores for 4 included studies (VASa) Mepivacaine: Total = 219 Bupivacaine: Total = 276 Mean difference (95% CI) = 0.04 (-0.32 to 0.39); P = 0.84; I2 = 0% |
Postoperative Pain at 2 Weeks, 6 weeks, and 3 Months | |
Calkins et al. (2021)9 Retrospective cohort study (N = 282) | Postoperative pain at 2 weeks (VASa) Mepivacaine: Mean = 2.2 Bupivacaine: Mean = 1.9 P = 0.308 Postoperative pain at 6 weeks (VASa) Mepivacaine: Mean = 1.6 Bupivacaine: Mean = 1.8 P = 0.386 Postoperative pain at 3 months (VASa) Mepivacaine: Mean = 1.3 Bupivacaine: Mean = 1.3 P = 0.575 |
Discharge Pain | |
Calkins et al. (2021)9 Retrospective cohort study (N = 282) | Discharge Pain (0-10 scale) Mepivacaine (n = 141): Mean (SD) = 1.1 (1.9) Bupivacaine (n = 141): Mean (SD) = 0.5 (1.2) P = 0.004 |
Pain Medication Use | |
Calkins et al. (2021)9 Retrospective cohort study (N = 282) | Morphine equivalents given (mg) Mepivacaine (n = 141): Mean (SD) = 7.8 (6.2) Bupivacaine (n = 141): Mean (SD) = 3.7 (5.8) P < 0.001 |
CI = confidence interval; mg = milligram; N = number; SD = standard deviation; VAS = visual analogue scale.
aScale range for VAS measurement was not reported.
Table 9: Summary of Findings by Outcome — Length of Stay
Study citation and design | Study Findings | |
|---|---|---|
Postoperative Length of Stay | ||
Siddiqi et al. (2022)15 Systematic Review and Meta Analysis (outcome based on 3 included studies) | Combined values for total, mean and SD for 3 included studies (hours) Mepivacaine
Bupivacaine
Mean difference (95% CI) = -7.03 (-10.02 to -4.04); P = 0.0057; I2 = 53% | |
Stock et al. (2022)10 Retrospective cohort study (N = 1328) | Unadjusted postoperative THA (days) Mepivacaine (n = 232): Mean (SD) = 0.43 (±0.59) Hyperbaric Bupivacaine (n = 401): Mean (SD) = 0.92 (±0.79) Isobaric Bupivacaine (n = 34): Mean (SD) = 1.12 (±1.00) P < 0.001 | Unadjusted postoperative TKA (days) Mepivacaine (n = 131): Mean (SD) = 0.51 (±0.59) Hyperbaric Bupivacaine (n = 502): Mean (SD) = 1.09 (±0.91) Isobaric Bupivacaine (n = 28): Mean (SD) = 1.00 (±0.61) P < 0.001 |
Risk-adjusted mepivacaine vs. bupivacaine (days)a Mepivacaine: OR (95% CI) = -0.421 (-0.502 to -0.330); P < 0.001 | ||
0 Day Length of Stay | ||
Stock et al. (2022)10 Retrospective cohort study (N = 1328) | Unadjusted postoperative THA Mepivacaine (n = 232): n (%) = 141 (60.8) Hyperbaric Bupivacaine (n = 401): n (%) = 96 (23.9) Isobaric Bupivacaine (n = 34): n (%) = 8 (23.5) P < 0.001 | Unadjusted postoperative TKA Mepivacaine (n = 131): n (%) = 138 (52.7) Hyperbaric Bupivacaine (n = 502): n (%) = 55 (11.0) Isobaric Bupivacaine (n = 28): n (%) = 4 (14.3) P < 0.001 |
Risk-adjusted mepivacaine vs. bupivacaine (n)a Mepivacaine: OR (95% CI) = 5.767 (4.357 to 7.634); P < 0.001 | ||
Time Spent in Each Ambulatory Phase | ||
Calkins et al. (2021)9 Retrospective cohort study (N = 282) | Preoperative unit (hours) Mepivacaine (n = 141): Mean (SD) = 1.5 (0.6) Bupivacaine (n = 141): Mean (SD) = 1.7 (0.5) P = 0.18 Operating room (hours) Mepivacaine (n = 141): Mean (SD) = 1.5 (0.2) Bupivacaine (n = 141): Mean (SD) = 1.6 (0.2) P = 0.25 Postoperative unit (hours) Mepivacaine (n = 141): Mean (SD) = 4.0 (1.1) Bupivacaine (n = 141): Mean (SD) = 5.7 (1.6) P < 0.001 Total facility time (hours) Mepivacaine (n = 141): Mean (SD) = 7.0 (1.3) Bupivacaine (n = 141): Mean (SD) = 8.8 (2.0) P < 0.001 | |
CI = confidence interval; N = number; OR = odds ratio; SD = standard deviation; THA = total hip arthroplasty; TKA = total knee arthroplasty; vs. = versus.
aRisk-adjusted comparison controls for age, body mass index, sex, American Society of Anesthesiologists score, and procedure type (THA or TKA).
Table 10: Summary of Findings by Outcome — Urinary Retention
Study citation and design | Study Findings | |
|---|---|---|
Postoperative Urinary Retention | ||
Siddiqi et al. (2022)15 Systematic Review and Meta Analysis (outcome based on 5 included studies) | Combined occurrence of urinary events (%) Mepivacaine: Occurrence = 7.15 Bupivacaine: Occurrence = 10.58 Overall difference (95% CI) = -3.43 (0.48 to 1.01); P = 0.0181; I2 = 49% | |
Stock et al. (2022)10 Retrospective cohort study (N = 1328) | Unadjusted postoperative THAa Mepivacaine (n = 232): n (%) = 3 (1.3) Hyperbaric Bupivacaine (n = 401): n (%) = 5 (1.2) Isobaric Bupivacaine (n = 34): n (%) = 2 (5.9) P = 0.097 | Unadjusted postoperative TKAa Mepivacaine (n = 131): n (%) = 2 (0.8) Hyperbaric Bupivacaine (n = 502): n (%) = 6 (1.2) Isobaric Bupivacaine (n = 28): n (%) = 0 (0.0) P = 0.734 |
Subgroup analysis of mepivacaine vs. bupivacaine for same-day discharge patients THAa Mepivacaine (n = 141): n (%) = 2 (1.4) Bupivacaine (n = 104): n (%) = 1 (1.0) P = 1.000 | Subgroup analysis of mepivacaine vs. bupivacaine for same-day discharge patients TKAa Mepivacaine (n = 138): n (%) = 0 (0.0) Bupivacaine (n = 59): n (%) = 1 (1.7) P = 0.299 | |
Risk-adjusted mepivacaine vs. bupivacaine (n)ab Mepivacaine: OR (95% CI) = 0.661 (0.225 to 1.942); P = 0.452 | ||
Calkins et al. (2021)9 Retrospective cohort study (N = 282) | Hours to controlled void Mepivacaine (n = 141): Mean (SD) = 3.1 (1.1) Bupivacaine (n = 141): Mean (SD) = 4.9 (1.6) P < 0.001 Required bethanechol Mepivacaine (n = 141): n (%) = 27 (19.1) Bupivacaine (n = 141): n (%) = 54 (38.3) P < 0.001 Straight urinary catheter use Mepivacaine (n = 141): n (%) = 0 (0) Bupivacaine (n = 141): n (%) = 0 (0) P = NA | |
CI = confidence interval; N = number; NA = not applicable; OR = odds ratio; SD = standard deviation; THA = total hip arthroplasty; TKA = total knee arthroplasty; vs = versus.
aUrinary retention was defined as any instance of postoperative straight or foley catheter use.
bRisk-adjusted comparison controls for age, body mass index, sex, American Society of Anesthesiologists score, and procedure type (THA or TKA).
Table 11: Summary of Findings by Outcome — Additional Clinical Outcomes
Study citation and design | Study Findings | |
|---|---|---|
Home Discharge | ||
Stock et al. (2022)10 Retrospective cohort study (N = 1328) | Unadjusted postoperative THA Mepivacaine (n = 232): n (%) = 232 (100) Hyperbaric Bupivacaine (n = 401): n (%) = 389 (97.0) Isobaric Bupivacaine (n = 34): n (%) = 31 (91.2) P = 0.001 | Unadjusted postoperative TKA Mepivacaine (n = 131): n (%) = 260 (99.2) Hyperbaric Bupivacaine (n = 502): n (%) = 486 (96.8) Isobaric Bupivacaine (n = 28): n (%) = 27 (96.4) P = 0.106 |
Subgroup analysis of mepivacaine vs. bupivacaine for same-day discharge patients THA Mepivacaine (n = 141): n (%) = 141 (100) Bupivacaine (n = 104): n (%) = 104 (100) P = NA | Subgroup analysis of mepivacaine vs. bupivacaine for same-day discharge patients TKA Mepivacaine (n = 138): n (%) = 138 (100) Bupivacaine (n = 59): n (%) = 59 (100) P = NA | |
Risk-adjusted mepivacaine vs. bupivacaine (n)x Mepivacaine: OR (95% CI) = 6.537 (1.540 to 27.743); P = 0.011 | ||
HOOS, JR | ||
Calkins et al. (2021)9 Retrospective cohort study (N = 282) | HOOS, JR at 2 weeks Mepivacaine: Mean = 71.5 Bupivacaine: Mean = 71.5 P = 0.990 HOOS, JR at 6 weeks: Mepivacaine: Mean = 78.6 Bupivacaine: Mean = 77.9 P = 0.704 HOOS, JR at 3 months Mepivacaine: Mean = 85.7 Bupivacaine: Mean = 84.5 P = 0.604 | |
CI = confidence interval; HOOS, JR = Hip Disability and Osteoarthritis Outcome Score for Joint Replacement; N = number; NA = not applicable; OR = odds ratio; THA = total hip arthroplasty; TKA = total knee arthroplasty; vs. = versus.
aRisk-adjusted comparison controls for age, body mass index, sex, American Society of Anesthesiologists score, and procedure type (THA or TKA).
Table 12: Summary of Findings by Outcome — Adverse Events and Safety
Study citation and design | Study Findings | |||
|---|---|---|---|---|
Failed Same-Day Discharge Attempt | ||||
Stock et al. (2022)10 Retrospective cohort study (N = 1328) | Unadjusted postoperative THA Mepivacaine (n = 232): n (%) = 14 (6.0) Hyperbaric Bupivacaine (n = 401): n (%) = 22 (5.5) Isobaric Bupivacaine (n = 34): n (%) = 4 (11.8) P = 0.334 | Unadjusted postoperative TKA Mepivacaine (n = 131): n (%) = 6 (2.3) Hyperbaric Bupivacaine (n = 502): n (%) = 17 (3.4) Isobaric Bupivacaine (n = 28): n (%) = 0 (0.0) P = 0.449 | ||
Risk-adjusted mepivacaine vs. bupivacaine (n)x Mepivacaine: OR (95% CI) = 0.801 (0.458 to 1.400); P = 0.436 | ||||
30-Day Readmission | ||||
Stock et al. (2022)10 Retrospective cohort study (N = 1328) | Unadjusted postoperative THA Mepivacaine (n = 232): n (%) = 4 (1.7) Hyperbaric Bupivacaine (n = 401): n (%) = 8 (2.0) Isobaric Bupivacaine (n = 34): n (%) = 0 (0.0) P = 0.699 | Unadjusted postoperative TKA Mepivacaine (n = 131): n (%) = 4 (1.5) Hyperbaric Bupivacaine (n = 502): n (%) = 30 (6.0) Isobaric Bupivacaine (n = 28): n (%) = 0 (0.0) P = 0.008 | ||
Subgroup analysis of mepivacaine vs. bupivacaine for same-day discharge patients THA Mepivacaine (n = 141): n (%) = 2 (1.4) Bupivacaine (n = 104): n (%) = 0 (0.0) P = 0.509 | Subgroup analysis of mepivacaine vs. bupivacaine for same-day discharge patients TKA Mepivacaine (n = 138): n (%) = 2 (1.4) Bupivacaine (n = 59): n (%) = 2 (3.4) P = 0.585 | |||
Risk-adjusted mepivacaine vs. bupivacaine (n)x Mepivacaine: OR (95% CI) = 0.494 (0.226 to 1.083); P = 0.078 | ||||
30-Day ED Return | ||||
Stock et al. (2022)10 Retrospective cohort study (N = 1328) | Unadjusted postoperative THA Mepivacaine (n = 232): n (%) = 5 (2.2) Hyperbaric Bupivacaine (n = 401): n (%) = 15 (3.7) Isobaric Bupivacaine (n = 34): n (%) = 0 (0.0) P = 0.305 | Unadjusted postoperative TKA Mepivacaine (n = 131): n (%) = 9 (3.4) Hyperbaric Bupivacaine (n = 502): n (%) = 15 (3.0) Isobaric Bupivacaine (n = 28): n (%) = 0 (0.0) P = 0.599 | ||
Subgroup analysis of mepivacaine vs. bupivacaine for same-day discharge patients THA Mepivacaine (n = 141): n (%) = 4 (2.8) Bupivacaine (n = 104): n (%) = 0 (0.0) P = 0.138 | Subgroup analysis of mepivacaine vs. bupivacaine for same-day discharge patients TKA Mepivacaine (n = 138): n (%) = 2 (3.6) Bupivacaine (n = 59): n (%) = 2 (3.4) P = 1.000 | |||
Risk-adjusted mepivacaine vs. bupivacaine (n)x Mepivacaine: OR (95% CI) = 1.068 (0.552 to 2.067); P = 0.845 | ||||
Total 90-Day Adverse Events | ||||
Calkins et al. (2021)9 Retrospective cohort study (N = 282) | Total complications Mepivacaine: n = 5 Bupivacaine: n = 5 P = 1.00 | ED Visits Mepivacaine: n = 4 Bupivacaine: n = 4 P = 1.00 | Hospital admissions Mepivacaine: n = 1 Bupivacaine: n = 1 P = 1.00 | Reoperations Mepivacaine: n = 1 Bupivacaine: n = 1 P = 1.00 |
Postoperative Nausea/Vomiting | ||||
Calkins et al. (2021)9 Retrospective cohort study (N = 282) | Postoperative nausea or vomiting Mepivacaine (n = 141): n (%) = 31 (22.0) Bupivacaine (n = 141): n (%) = 22 (15.6) P = 0.223 | |||
Hypotension Requiring Treatment | ||||
Calkins et al. (2021)9 Retrospective cohort study (N = 282) | Hypotension requiring treatment Mepivacaine (n = 141): n (%) = 13 (9.2) Bupivacaine (n = 141): n (%) = 6 (4.3) P = 0.153 | |||
CI = confidence interval; ED = emergency department; N = number; OR = odds ratio; THA = total hip arthroplasty; TKA = total knee arthroplasty; vs. = versus.
aRisk-adjusted comparison controls for age, body mass index, sex, American Society of Anesthesiologists score, and procedure type (THA or TKA).
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policymakers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, except for Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca