CADTH Health Technology Review
Delayed Tuberculin Skin Testing
Rapid Review
Authors: Anusree Subramonian, Melissa Walter
Abbreviations
GRADE
Grading of Recommendations, Assessment, Development and Evaluations
IGRA
interferon gamma release assay
TB
tuberculosis
TST
tuberculin skin testing
Key Messages
With delayed tuberculin skin testing (TST) a single TST is performed to screen for tuberculosis (TB) infection 8 weeks after exposure to a known case of TB.
The clinical utility (i.e., clinical benefits and harms of testing) of delayed TST for identifying TB among close contacts with no known risks compared to testing immediately after and at 8 weeks after TB exposure is not known (no evidence was found).
It is not known if delayed TST is a cost-effective approach for identifying TB among close contacts with no known risks compared to testing immediately after and at 8 weeks after TB exposure (no evidence was found).
One evidence-based guideline developed in Canada does not provide specific recommendations regarding delayed TST in close contacts with no known risks of TB. However, the guideline authors discuss that a single TST at 8 weeks after TB exposure could be a practical option for medium-priority contacts (i.e., those with a lower risk to develop active disease). For high-priority contacts (i.e., those with the most exposure and highest risk to develop active disease), the authors propose testing immediately after exposure and a repeat test 8 weeks later.
Context and Policy Issues
Tuberculosis (TB) is a communicable disease caused by the bacillus Mycobacterium tuberculosis. It is 1 of the most common causes of death worldwide.1 Globally, WHO estimated that about 10 million individuals had active TB in 2019. In Canada, prevalence of TB is relatively low at around 4.6 to 5.1 people per 100,000 population.2 Indigenous Peoples and foreign-born Canadian residents experience a disproportionately higher burden of TB. For example, the incidence rate in the Inuit population is about 70 per 100,000 and that among foreign-born-Canadians is about 15 per 100,000 population.2
Spread from person to person through droplet or aerosol form, TB primarily affects the lungs; however, it can affect virtually all systems in the human body. With the advancement of medical science in the field of antibiotics, TB is curable with a treatment regime of 6 months, which can also prevent disease transmission.1 Post TB sequelae, the spectrum of conditions and complications in TB survivors, can lead to long-term disability and affect quality of life.3 Early identification and treatment of TB is crucial in disease management as well as in prevention of additional transmission.
When a TB case is diagnosed, contact investigation is essential in identifying active or latent infections. In Canada, contact investigations are initiated when a notification about a new infection is received by the public health authorities. Ideally, contact tracing interviews are conducted within 3 days and screening of high-priority contacts are arranged within 7 days. This would ensure early detection of TB infection in the contacts and preventive treatment, as required, can be provided to infected individuals.4 The contacts are prioritized based on location, duration of exposure and settings. High-priority contacts are the individuals with most exposure, at highest risk of progression to active TB. They include household contacts (e.g., living in the same house as index patient), household-like contacts (e.g., congregate settings such as jail, homeless shelter, or caregivers of index patient), and contacts in health care procedures with high risk of aerosol occurrence. Medium-priority contacts include those with a lesser risk of progression to active disease but have regular and frequent contact with index patient. They could include regular sexual partners not living in the same household, close friends, co-workers, or classroom contacts. Low priority contacts are casual occasional contacts with the least risk of progression to active disease.5
Presence of a TB infection can be identified using screening tests such as the TST or interferon gamma release assay (IGRA).6 TST is also known as purified protein derivative test or Mantoux test. The basis of TST is cell-mediated immunity against tuberculin antigens. In individuals who are infected with TB, administration of the purified protein derivative evokes a delayed-hypersensitivity reaction within 48 to 72 hours.6,7 This would result in swelling and induration at the injection site. TST is administered as an intradermal injection in the inner part of the forearm. Size of the subsequently developed induration is measured 48 to 72 hours later. Generally, at least 5 mm of induration is considered positive in high-risk individuals (e.g., persons living with HIV, known recent contact to patient with active TB).7 TST has several advantages and disadvantages. TST can be performed by a health care worker with minimal training even in remote locations, is inexpensive, and the results are relatively easy to measure. However, the main disadvantage of TST is that the patient needs to return to the test site in order for the results to be measured 2 to 3 days later. There is also inter-reader variability in measuring the induration, false-positive results possible due to cross reaction to other antigens, and a risk of adverse events.
Either TST or IGRA are recommended as screening tests for identifying TB infection. TST is recommended for serial or repeated testing in the context of a contact screening.7 This would require the individual to visit the test site or clinic multiple times - to receive the test and then to read the result over the course of several weeks. One of the main challenges with repeat testing is the drop-out rate between the tests, resulting in incomplete assessment of the contact.5 Delayed TST is proposed as a solution to this issue. In delayed TST, a single TST is administered 8 weeks post-exposure, rather than a TST to be administered immediately and then a second after 8 weeks post-exposure.
The purpose of this report is to summarize the evidence regarding the clinical utility, cost-effectiveness, and evidence-based guidelines regarding delayed TST in close contacts who have no known risk factors to require immediate testing.
CADTH has conducted a larger Condition Level Review on TB. A condition level review is an assessment that incorporates all aspects of a condition, including prevention, detection, treatment, and management. For more information on CADTH’s Condition Level Review of TB, please visit the project page (https://www.cadth.ca/tuberculosis).
Research Questions
What is the clinical utility of tuberculin skin testing at 8 weeks post-exposure to tuberculosis versus testing immediately after and at 8 weeks post-exposure to tuberculosis?
What is the cost-effectiveness of tuberculin skin testing at 8 weeks post-exposure to tuberculosis versus testing immediately after exposure and at 8 weeks post-exposure to tuberculosis?
What are the evidence-based guidelines informing the use of tuberculin skin testing at 8 weeks post-exposure to tuberculosis versus testing immediately after and at 8 weeks post-exposure to tuberculosis?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s Mesh (Medical Subject Headings), and keywords. The main search concepts were tuberculin skin testing, tuberculosis, and timing or delayed testing. Additional focused searches were also run on the concepts contact tracing or testing and tuberculosis, combined with CADTH-developed search filters to limit retrieval to guidelines; and on the concept tuberculin skin testing combined with CADTH-developed search filters to limit retrieval to health technology assessments, systematic reviews, meta-analyses, or indirect treatment comparisons. Where possible, retrieval was limited to the human population. The search was completed on August 2, 2022 and limited to English-language documents published since January 1, 2012.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Q1 to Q3: People of any age who are found to be close contacts of tuberculosis and have no known risk factors that require immediate testing |
Intervention | Q1 to Q3: Tuberculin skin testing at 8 weeks post-exposure |
Comparator | Q1 and Q2: Tuberculin skin testing immediately after and at 8 weeks post-exposure Q3: NA |
Outcomes | Q1: Clinical utility i.e., benefits (e.g., adherence to testing, patient satisfaction, etc.) and harms (missed diagnoses, missed opportunity for early treatment, activation of tuberculosis, etc.) Q2: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained) Q3: Evidence-based recommendations describing best clinical practice(s) |
Study designs | Health technology assessments, systematic reviews, randomized-controlled trials, non-randomized studies, economic evaluations, evidence-based guidelines |
NA = not applicable.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2012. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic reviews. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer following the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument8 as a guide. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
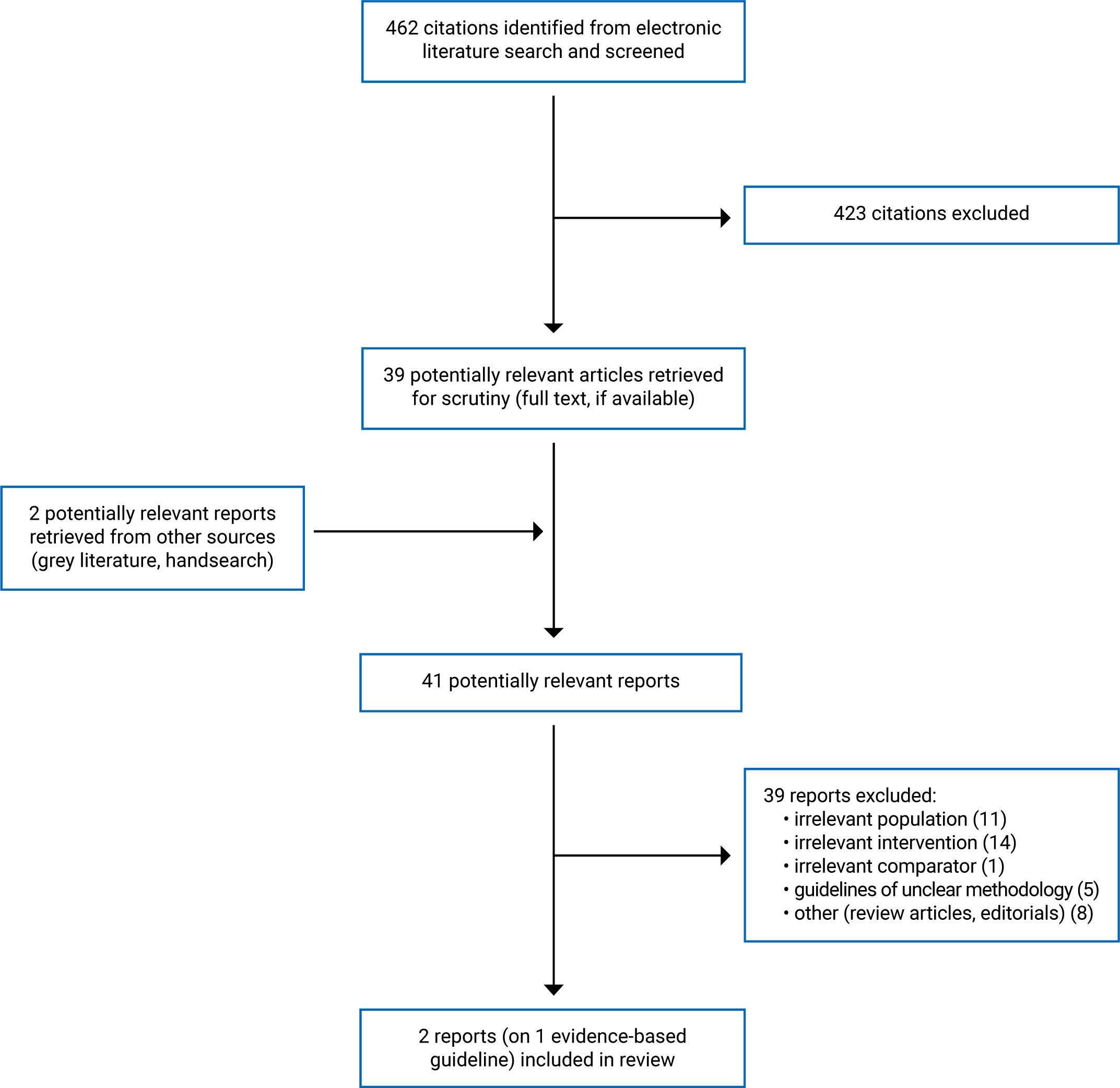
A total of 462 citations were identified in the literature search. Following screening of titles and abstracts, 423 citations were excluded and 39 potentially relevant reports from the electronic search were retrieved for full-text review. Two potentially relevant publications were retrieved from the grey literature search for full-text review. Of these 41 potentially relevant articles, 39 publications were excluded for various reasons, and 1 evidence-based guideline (across 2 publications5,7) met the inclusion criteria and was included in this report. Appendix 1 presents the PRISMA9 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
The evidence-based guideline included in the report was the Canadian Tuberculosis Standards (the Standards), 8th Edition.5,7 Two chapters of the Standards that were relevant to the current report were included.5,7 Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
The Standards guideline was developed by the Canadian Thoracic Society and the latest update was published in 2022.10 The Standards covered several aspects of TB such as epidemiology, prevention, diagnosis, and management. Each chapter was informed by literature searches conducted between March 2021 and July 2021. Recent studies and systematic reviews were prioritized while assessing the evidence base. Search strategies and inclusion criteria for the literature search were not reported. Although it was reported that the authors undertook risk of bias assessment of the identified evidence, no formal tools were used for this. The authors did not follow a formal Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach to evaluate the quality of the evidence due to the high number of recommendations. Each recommendation was developed by panel authors using consensus and finalized by the committee chair. A pre-defined framework was used to assign the strength of recommendation as well as the level of evidence. Recommendations were graded as strong (intervention should be followed) or conditional (intervention can be considered depending on the individual patient). Quality of evidence for each recommendation were assigned as good or poor depending on the type and volume of studies identified for each recommendation. Recommendation statements formulated based on consensus of expert opinion were reported as a good practice statement. Lastly, recommendations supported by federal, provincial, or territorial legislation were listed as regulations.10
Country of Origin
The guideline was developed in Canada.10
Patient Population
The target population of the guideline was all individuals who are at risk of TB or those confirmed to have latent or active TB. Relevant to the current report, the population was individuals who were close contacts of TB and have no known risk factors. They include high-priority (e.g., household contacts, contacts in congregate settings such as jails) and medium-priority (e.g., close friends, co-workers, classroom contacts).10
The intended users for the Standards were public health professionals, clinical specialists (e.g., internists, infectious disease specialists), primary care providers, and decision-makers.10
Interventions and Comparators
The Standards provided recommendations regarding a broad range of interventions relating to various aspects of prevention, diagnosis, and management of TB. TST in contacts after exposure to TB was the intervention relevant to the current report.5,7
Outcomes
The guideline did not report the specific outcomes considered during development and which outcomes were eligible during selection of supporting evidence.
Summary of Critical Appraisal
The details of the methodology and development of the Standards guideline were described in a separate document.10 The overall objective of the guideline was described, along with the population to which the guideline is meant to apply. They included all individuals with confirmed or at risk of active or latent TB. However, the health questions related to each recommendation were not specifically listed. The guideline authors were mostly clinical specialists from across Canada. Stakeholders such as public health professionals and policy advisors were also involved. The views and preferences of the target population were not sought. The intended users of the guideline were clearly described and were appropriate. The guideline was externally reviewed by topic experts before publication. A plan for future updates was outlined.
Overall, the rigour of development of the guideline had some limitations. Authors of each chapter conducted literature searches for identifying evidence. The authors did not report any methods for systematic search for evidence such as research questions, search strategy, or selection criteria. Therefore, the reproducibility of the evidence was low. No formal tools were used to assess the risk of bias of included evidence. GRADE process was not followed. However, an established framework was used to grade the recommendations and the level of evidence. Recommendation statements were formulated through consensus of authors. Factors such as risk-benefit profile, cost, and implement ability were considered in establishing the strength of recommendations.
The recommendation statements were specific and clearly identifiable. Since the scope of the guideline was large, different aspects of TB care (e.g., prevention, diagnosis, management, and public health concerns) were described in separate chapters. Only the chapters relevant to the current report were reviewed here.5,7
Regarding the intervention relevant to the current report, no formal recommendation statements were made in the guideline. A standard approach to the screening of high- and medium-priority contacts using TST was described. However, the link between these general statements and supporting evidence related to them was unclear.
Facilitators and barriers to the application of guideline were not described. Tools for implementing the guideline, as well as monitoring criteria were not described. It was unclear whether potential resource implications of the recommendations were considered. Thus, the practical applicability of the guideline was low. There was editorial independence while developing the guideline. Potential conflicts of interests of the authors were declared and addressed. The guideline was funded by the Public Health Agency of Canada and the Canadian Thoracic Society. The authors reported that there was no external funding.
Additional details regarding the strengths and limitations are provided in Appendix 3.
Summary of Findings
Clinical Utility of Delayed TST
No relevant evidence regarding the clinical utility of delayed TST at 8 weeks post-exposure to TB versus testing immediately after and at 8 weeks post-exposure to TB was identified; therefore, no summary can be provided.
Cost-Effectiveness of Delayed TST
No relevant evidence regarding the cost-effectiveness of delayed TST at 8 weeks post-exposure to TB versus testing immediately after and at 8 weeks post-exposure to TB was identified; therefore, no summary can be provided.
Guidelines Regarding the Use of Delayed TST
Appendix 4 presents the detailed recommendations and general statements relevant to the current report.
The Standards conditionally recommends TST in situations where a repeat testing might be necessary such as a contact investigation or to identify new TB infections in high-risk settings.7
No specific formal recommendation statements were made regarding delayed TST at 8 weeks post-exposure to TB.
However, a standard approach to screening and evaluation of contacts after exposure to TB was discussed.5 The authors stated that high-priority contacts should have repeated testing. Ideally, a TST is to be done immediately after exposure to TB, or as soon as the contacts of the known TB case are identified. A second TST is warranted at least 8 weeks after the exposure.5 In case of medium-priority contacts, the standards suggest that, a single round of screening after 8 weeks from last exposure is the practical option.5 Considering factors such as loss to follow-up for repeat testing, and the likelihood of detecting conversions, the authors suggested that if an initial screening cannot be arranged within 4 weeks of exposure, a single screening after 8 weeks is more efficient.5 Low priority casual contacts are not routinely screened. If they are investigated, a single TST 8 weeks or more from last day of exposure is suggested.5
It should be noted that since these suggestions were not formal recommendations, a strength of recommendation or level of evidence was not provided. The supporting evidence for these suggestions was unclear from the publication.
Limitations
No evidence regarding the clinical utility or cost-effectiveness of delayed TST compared to testing immediately after and at 8 weeks post-exposure to TB among close contacts with no known risk factors was identified. Only 1 evidence-based guideline was included in this report. There were no formal evidence-based recommendations for or against delayed TST at 8 weeks post-exposure compared to repeat testing in close contacts. The guideline also had methodological limitations as described in the previous section.
Conclusions and Implications for Decision- or Policy-Making
One evidence-based guideline by the Canadian Tuberculosis Standards was included in this report. No specific recommendation regarding delayed TST among close contacts with no known risk factors was provided in the guideline. General statements from the guideline suggested that a single test after 8 weeks from last contact to a TB case could be a practical approach in medium-priority contacts. In high-priority contacts such as household close contacts, repeat testing (i.e., TST as soon as contact is established, and a second test 8 weeks later), is the preferred strategy. However, these were not formal evidence-supported recommendations and therefore should be interpreted with caution. Additionally, the guideline had several methodological limitations. Whether the guideline authors conducted a systematic search for evidence was not reported in the publication. The practical applicability of the guideline was low due to limited details on implementation, resource considerations, and criteria for monitoring adherence.
No evidence regarding the clinical utility or cost-effectiveness of delayed TST compared to testing immediately after and at 8 weeks post-exposure to TB among close contacts with no known risk factors was identified.
Overall, due to a limited volume of evidence identified, and the methodological limitations of the Standards guideline, the evidence regarding delayed TST for close contacts of TB is limited and remains uncertain.
A previous CADTH report identified 14 guidelines regarding the identification of latent and active TB.11 Recommendations for selective TB identification strategies, testing for latent TB infection, and diagnosis of active TB were summarized in that report.11 CADTH has also published reports on screening for latent TB infections in specific groups, such as in occupational settings,11 in post-secondary institutions,12 in people with compromised immunity before biologic therapy,13 and in people with existing chronic conditions.14
References
1.Global tuberculosis report 2020. Geneva (CH): World Health Organization; 2020: https://www.who.int/publications/i/item/9789240013131. Accessed 2022 Aug 28.
2.Mounchili A, Perera R, Lee RS, Njoo H, Brooks J. Chapter 1: Epidemiology of tuberculosis in Canada. Canadian Journal of Respiratory, Critical Care, and Sleep Medicine. 2022;6(sup1):8-21.
3.Sotgiu G, Centis R, Migliori GB. Post-tuberculosis sequelae and their socioeconomic consequences: worth investigating. The Lancet Global Health. 2021;9(12):e1628-e1629. PubMed
4.WHO operational handbook on tuberculosis. Module 1: prevention - tuberculosis preventive treatment. Geneva (CH): World Health Organization; 2020: https://www.who.int/publications/i/item/9789240002906. Accessed 2022 Aug 31.
5.Rea E, Huard J, Lee R. Chapter 11: Tuberculosis contact investigation and outbreak management. Canadian Journal of Respiratory, Critical Care, and Sleep Medicine. 2022;6(sup1):167-183.
6.Pahal P, Sharma S. PPD skin test. [Updated 2022 Jan 24]. StatPearls. Treasure Island (FL): StatPearls Publishing; 2022: https://www.ncbi.nlm.nih.gov/books/NBK556037/. Accessed 2022 Aug 28.
7.Campbell JR, Pease C, Daley P, Pai M, Menzies D. Chapter 4: Diagnosis of tuberculosis infection. Canadian Journal of Respiratory, Critical Care, and Sleep Medicine. 2022;6(sup1):49-65.
8.Agree Next Steps Consortium. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2022 Aug 29.
9.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
10.Preface. Canadian Journal of Respiratory, Critical Care, and Sleep Medicine. 2022;6(sup1):1-7.
11.Identification of tuberculosis: a review of the guidelines. (CADTH rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/identification-tuberculosis-review-guidelines. Accessed 2022 Aug 31.
12.Screening for latent tuberculosis infection in post-secondary institutions: clinical utility, cost-effectiveness, and guidelines. (CADTH Rapid response report: summary of abstracts). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/screening-latent-tuberculosis-infection-post-secondary-institutions-clinical-utility-cost. Accessed 2022 Aug 31.
13.Latent tuberculosis infection testing in people with compromised immunity prior to biologic therapy: a review of diagnostic accuracy, clinical utility, and guidelines. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/latent-tuberculosis-infection-testing-people-compromised-immunity-prior-biologic-therapy-review. Accessed 2022 Aug 31.
14.Brett K, Severn M. CADTH health technology review: tuberculosis screening for people with chronic conditions. Can J Health Technol. 2021;1(5). https://www.cadth.ca/tuberculosis-screening-people-chronic-conditions. Accessed 2022 Aug 31.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Guideline
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
Intended users: Public health professionals, clinicians (e.g., primary care provider, infectious disease specialists), and decision-makers Target population: All individuals at risk of, or with confirmed active or latent TB | Prevention, screening, diagnosis, and management of TB Relevant to the current report: Delayed TST | NR | Authors conducted literature searches. Search strategy, inclusion criteria NR. A systematic review was not conducted. Authors conducted risk of bias of included studies and quality of assessment. However, no formal appraisal tools were used. GRADE process was not conducted. | Strength of recommendation was reflected as:
Level of evidence: Good = For diagnostic methods, 1 or more high quality RCT, 1 or more published SR of observational studies, or 2 or more observational studies are available as evidence. Poor = For diagnostic methods, 1 or more SR that concluded that the evidence was not high quality, 2 or more observational studies with low quality/ inconsistent results, or only 1 observational study available. | Recommendations were developed by chapter authors by consensus of the panel. Strength of recommendation was assigned based on the level of evidence available. | The guideline documents were reviewed internally within the committee. The key recommendations were presented at a meeting and sought feedback from all authors. External reviewers (topic experts) as well as members of the CRGC reviewed the chapters before publishing. |
CRGC = Canadian Respiratory Guidelines Committee: GRADE = Grading of Recommendations, Assessment, Development and Evaluations; NR = not reported; RC = randomized-controlled trial; SR = systematic review; TB = tuberculosis; vs. = versus.
Note: This table has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Table 3: Strengths and Limitations of Guideline Using AGREE II8
Item | |
|---|---|
Domain 1: Scope and purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | No |
3.The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes |
Domain 2: Stakeholder involvement | |
4.The guideline development group includes individuals from all relevant professional groups. | Partially |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | No |
6.The target users of the guideline are clearly defined. | Yes |
Domain 3: Rigour of development | |
7. Systematic methods were used to search for evidence. | No |
8. The criteria for selecting the evidence are clearly described. | No |
9. The strengths and limitations of the body of evidence are clearly described. | No |
10. The methods for formulating the recommendations are clearly described. | Partially |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Unclear |
12. There is an explicit link between the recommendations and the supporting evidence. | No |
13. The guideline has been externally reviewed by experts before its publication. | Yes |
14. A procedure for updating the guideline is provided. | Yes |
Domain 4: Clarity of presentation | |
15. The recommendations are specific and unambiguous. | Yes |
16. The different options for management of the condition or health issue are clearly presented. | NA |
17. Key recommendations are easily identifiable. | Yes |
Domain 5: Applicability | |
18. The guideline describes facilitators and barriers to its application. | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No |
20. The potential resource implications of applying the recommendations have been considered. | No |
21. The guideline presents monitoring and/or auditing criteria. | No |
Domain 6: Editorial independence | |
22. The views of the funding body have not influenced the content of the guideline. | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II.
Note that this table has not been copy-edited.
Appendix 4: Main Study Findings
Table 4: Summary of Recommendations in Included Guideline
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
Note: No specific recommendations regarding delayed TST were provided in the guideline. General statements regarding delayed TST in high and medium priority contacts reported in the guideline are provided below.
| NA |
IGRA = interferon gamma release assay; LTBI = latent tuberculosis infection; NA = not applicable; TB = tuberculosis; TST = tuberculin skin testing.
Note that this table has not been copy-edited.
Appendix 5: References of Potential Interest
Previous CADTH Reports
Wells C, Severn M. CADTH health technology review: incentives and support programs to improve adherence to tuberculosis treatment. Can J Health Technol. 2021;1(2). https://www.cadth.ca/incentives-and-support-programs-improve-adherence-tuberculosis-treatment. Accessed 2022 Aug 29. PubMed
Identification of tuberculosis: a review of the guidelines. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/identification-tuberculosis-review-guidelines. Accessed 2022 Aug 29.
Prevention of tuberculosis: a review of guidelines. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/prevention-tuberculosis-review-guidelines. Accessed 2022 Aug 29.
Contact tracing for potential exposure to tuberculosis: guidelines. (CADTH Rapid response report: summary of abstracts). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/contact-tracing-potential-exposure-tuberculosis-guidelines. Accessed 2022 Aug 29.
Interventions used to screen for tuberculosis: clinical effectiveness and guidelines. (CADTH Rapid response report: reference list). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/interventions-used-screen-tuberculosis-clinical-effectiveness-and-guidelines. Accessed 2022 Aug 29.
Interventions for the diagnosis of tuberculosis: clinical effectiveness and guidelines. (CADTH Rapid response report: reference list). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/interventions-diagnosis-tuberculosis-clinical-effectiveness-and-guidelines. Accessed 2022 Aug 29.
Systematic Reviews
Faust L, McCarthy A, Schreiber Y. Recommendations for the screening of paediatric latent tuberculosis infection in indigenous communities: a systematic review of screening strategies among high-risk groups in low-incidence countries. BMC Public Health. 2018;18(1):979. PubMed
Berti E, Galli L, Venturini E, de Martini M, Chiappini E. Tuberculosis in childhood: a systematic review of national and international guidelines. BMC Infect Dis. 2014;14 Suppl 1:S3. PubMed
Economic Evaluations
Sousa S, Rocha D, Silva JC, et al. Comparing the cost-effectiveness of two screening strategies for latent tuberculosis infection in Portugal. Pulmonology. 2021;27(6):493-499. PubMed
Guidelines and Recommendations
Alternate Population
Thanassi W, Behrman AJ, Reves R, et al. Tuberculosis screening, testing, and treatment of US health care personnel: ACOEM and NTCA Joint Task Force on Implementation of the 2019 MMWR Recommendations. J Occup Environ Med. 2020;62(7):e355-e369. PubMed
Bielecka T, Augustynowicz-Kopec E, Gonerko P, et al. Recommendations for the management of tuberculosis in children - KOMPASS TB. Part 1: Tuberculosis prevention. Advances in Respiratory Medicine. 2018;86(3). PubMed
Hauk L. Tuberculosis: guidelines for diagnosis from the ATS, IDSA, and CDC. Am Fam Physician. 2018;97(1):56-58. PubMed
Waring J, Waring J, National Tuberculosis Advisory Committee. National Tuberculosis Advisory Committee Guideline: management of tuberculosis risk in healthcare workers in Australia. Commun Dis Intell Q Rep. 2017;41(3):E199-E203. PubMed
Chiappini E, Lo Vecchio A, Garazzino S, et al. Recommendations for the diagnosis of pediatric tuberculosis. Eur J Clin Microbiol Infect Dis. 2016;35(1):1-18. PubMed
Getahun H, Matteelli A, Abubakar I, et al. Management of latent Mycobacterium tuberculosis infection: WHO guidelines for low tuberculosis burden countries. Eur Respir J. 2015;46(6):1563-76. PubMed
Krause V, National Tuberculosis Advisory Committee. Policy recommendation: latent tuberculosis infection screening and treatment in children in immigration detention. Commun Dis Intell Q Rep. 2015;39(4):E597-8. PubMed
Additional References
Isler MA, Rivest P, Mason J, Brassard P. Screening employees of services for homeless individuals in Montreal for tuberculosis infection. J Infect Public Health. 2013;6(3):209-15. PubMed
Communicable Disease Control Manual Chapter 4: tuberculosis. Assessment and follow-up of TB contacts. Vancouver (BC): BC Centre for Disease Control; 2019: http://www.bccdc.ca/resource-gallery/Documents/Communicable-Disease-Manual/Chapter%204%20-%20TB/8.0%20Assessment%20and%20Followup%20of%20TB%20Contacts.pdf. Accessed 2022 Aug 29.
Yukon communicable disease control – TB control. Chapter 10: contact investigation. Whitehorse (YT): Yukon Health and Social Services; 2015: https://yukon.ca/sites/yukon.ca/files/hss/hss-imgs/tbmanual-chapter10.pdf. Accessed 2022 Aug 29.
NWT tuberculosis manual. Section 9: contact tracing. Yellowknife (NT): Government of Northwest Territories Health and Social Services; 2014: https://www.hss.gov.nt.ca/professionals/sites/professionals/files/resources/tb-section-9-steps-contact-investigation.pdf. Accessed 2022 Aug 29.
Nolt D, Starke JR; AAP Committee on Infectious Diseases. Tuberculosis infection in children and adolescents: testing and treatment. Pediatrics. 2021;148(6):e2021054663. https://publications.aap.org/pediatrics/article/148/6/e2021054663/183445/Tuberculosis-Infection-in-Children-and-Adolescents. Accessed 2022 Aug 29. PubMed
WHO operational handbook on tuberculosis. Module 1: prevention - tuberculosis preventive treatment. Geneva (CH): World Health Organization; 2020: https://www.who.int/publications/i/item/9789240002906. Accessed 2022 Aug 31.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca