CADTH Health Technology Review
Airway Pressure Release Ventilation for Acute Respiratory Distress Syndrome: An Update
Rapid Review
Authors: Keeley Farrell, Jennifer Horton
Abbreviations
RCT
randomized controlled trial
PaO2/FiO2
partial pressure of oxygen/ fraction of inspired oxygen
Key Messages
Evidence suggested there was no significant difference in mortality between patients with or at risk of acute respiratory distress syndrome treated with airway pressure release ventilation versus other mechanical ventilation strategies.
The evidence of the clinical effectiveness of airway pressure release ventilation in patients with or at risk of acute respiratory distress syndrome is uncertain for several outcomes (length of intensive care unit stay, oxygenation, ventilator-free days, mean arterial pressure). Evidence from some studies suggested there was a significant benefit favouring airway pressure release ventilation versus other mechanical ventilation strategies for these outcomes, other studies suggested there was a significant benefit favouring other mechanical ventilation strategies, and some studies found no significant differences between treatment groups.
Results from 1 study suggested there were no significant differences in incidence of acute respiratory distress syndrome between patients treated with airway pressure release ventilation versus pressure-controlled synchronized intermittent mandatory ventilation and pressure support.
Evidence suggested there was no significant difference in tracheostomy between patients with or at risk of acute respiratory distress syndrome treated with airway pressure release ventilation versus control. In 1 study significantly more patients treated with airway pressure release ventilation experienced severe hypercapnia than those treated with low tidal volume ventilation.
One guideline suggests considering the use of airway pressure release ventilation in patients without severe acute respiratory distress syndrome.
Context and Policy Issues
Acute respiratory distress syndrome is a life-threatening condition resulting from fluid buildup in the lungs leading to an acute, widespread, inflammatory lung injury.1 The condition has a variety of causes including pneumonia, aspiration, sepsis, pancreatitis, and trauma,1 and main symptoms are severe shortness of breath and rapid breathing.2 Acute respiratory distress syndrome is associated with high mortality rates ranging from 35% to 46% depending on the severity of lung injury at onset.1 The incidence rate in Canada was estimated to be 27.6 cases per 100,000 person-years from October 2010 to December 2012.3,4
Treatment of acute respiratory distress syndrome is generally supportive and can include mechanical ventilation, prevention of complications such as venous thromboembolism, and nutritional support, while addressing the underlying cause of the condition.3 Mild cases of acute respiratory distress syndrome may respond to noninvasive ventilation; however, most patients require sedation, intubation, and ventilation.3 A range of mechanical ventilation strategies can be used to treat patients with acute respiratory distress syndrome. These can include pressure-controlled ventilation, volume-controlled ventilation, extracorporeal membrane oxygenation, low tidal volume ventilation, and airway pressure release ventilation.5,6
Airway pressure release ventilation is a mechanical ventilation mode that uses continuous positive airway pressure to maintain adequate lung volume and a time cycled release phase to aid with carbon dioxide removal.5,7 It was introduced to improve oxygenation and potentially decrease the incidence of barotrauma (injury to the body due to change in air pressure), and could have a role in preventing acute respiratory distress syndrome.7 Patients on airway pressure release ventilation are able to breathe spontaneously throughout both the continuous positive airway pressure and time cycled release phase.5
The aim of the current report is to summarize the clinical evidence and evidence-based guidelines regarding the use of airway pressure release ventilation for patients with or at risk of acute respiratory distress syndrome that have been published since the 2018 CADTH report.8
Research Questions
What is the clinical effectiveness of airway pressure release ventilation in adult inpatients at risk of or with acute respiratory distress syndrome?
What are evidence-based guidelines informing the use of airway pressure release ventilation in adult inpatients at risk of or with acute respiratory distress syndrome?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were airway pressure release ventilation, acute respiratory distress syndrome, intensive care units, and emergency units. No filters were applied to limit the retrieval by study type. Where possible, retrieval was limited to the human population. The search was completed on July 25, 2022 and limited to English-language documents published since January 1, 2017.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. As an update to a previous CADTH report, articles were included if they were made available since the previous search date and were not included in the 2018 CADTH report.8 The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adult inpatients at risk of or with acute respiratory distress syndrome in the ICU or ER |
Intervention | Airway pressure release ventilation |
Comparator | Q1: ARDSnet (low tidal volume conventional ventilation); open lung ventilation; extracorporeal membrane oxygenation; prone ventilation; standard care; no comparator Q2: No comparator |
Outcomes | Q1: Clinical effectiveness (e.g., oxygenation, hemodynamics, regional blood flow, patient comfort and length of mechanical ventilation, survival, etc.) Q2: Recommendations regarding initiating, managing and/or weaning airway pressure release ventilation; recommendations regarding expiratory time |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies, evidence-based guidelines |
ARDS = acute respiratory distress syndrome; ER = emergency room; ICU = intensive care unit.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, or they were duplicate publications. Systematic reviews in which all relevant studies were captured in more comprehensive systematic reviews were excluded.9 Primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic reviews. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)10 for systematic reviews, the Downs and Black checklist11 for randomized studies, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument12 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
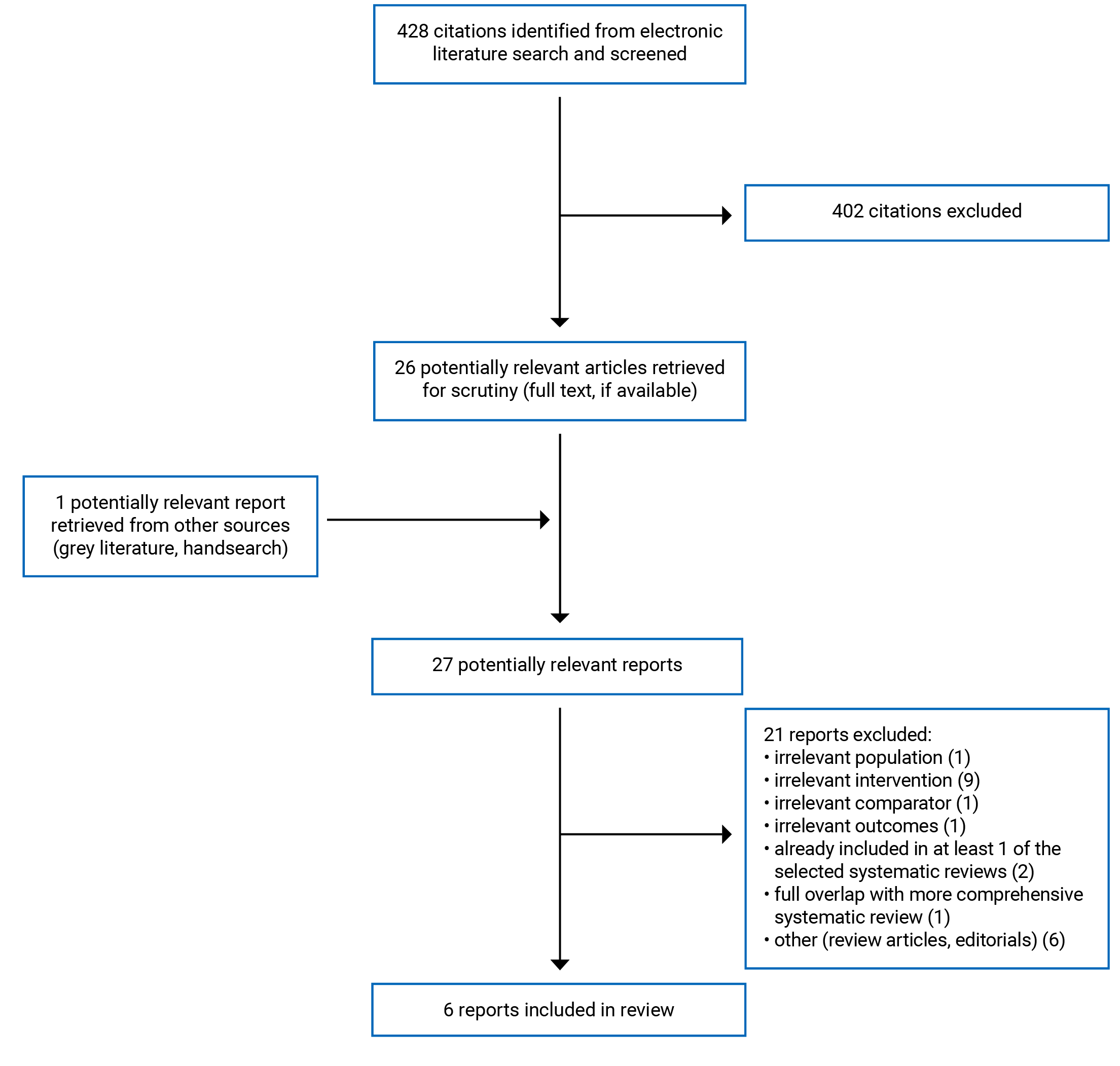
A total of 428 citations were identified in the literature search. Following screening of titles and abstracts, 402 citations were excluded and 26 potentially relevant reports from the electronic search were retrieved for full-text review. One potentially relevant publication was retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 21 publications were excluded for various reasons, and 6 publications met the inclusion criteria and were included in this report. These comprised 3 systematic reviews, 2 randomized controlled trials (RCTs), and 1 evidence-based guideline. Appendix 1 presents the PRISMA13 flow chart of the study selection.
Summary of Study Characteristics
In total 3 systematic reviews,14-16 2 RCTs17,18 and 1 guideline19 were included in this report. The 3 systematic reviews14-16 included meta-analyses; however, they all included results from studies that are not relevant to the present report. Therefore, the results of the meta-analyses are not described in this report.
All the systematic reviews included primary studies that were already described in the previous CADTH report8 on this topic (and therefore, are not discussed in the current report). Two of the systematic reviews15,16 did not specify the study settings in the inclusion criteria (i.e., intensive care unit or emergency room) and the study settings for the included studies were not described. Therefore, only studies that included intensive care, unit-related outcomes (i.e., length of intensive care unit stay, mortality in the intensive care unit) were considered relevant to the present report. Only the characteristics and results of the subset of relevant studies will be described in this report.
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
The systematic review by Chen et al. (2021)14 included 6 RCTs in total, 4 of which are relevant to the present report. The literature search was conducted up to August 8, 2019 and no restrictions were imposed based on date of publication.14 The systematic review by Sun et al. (2020)15 included 14 studies in total (7 RCTs and 7 retrospective studies), 8 of which are relevant to the present report (5 RCTs, 2 2-arm retrospective studies, and 1 single-arm retrospective study). The literature search was conducted January 23, 2019 and no restrictions were imposed based on date of publication.15 The systematic review by Zhong et al. (2020)16 included 7 RCTs in total, 4 of which are relevant to the present report. The literature search was conducted up to March 2019 and no restrictions were imposed based on date of publication.16
All the systematic reviews14-16 had overlap in their included primary studies. Four primary studies were included in more than 1 systematic review. A citation matrix depicting the overlap between the included systematic reviews is provided in Appendix 5.
Both included RCTs were single-centre studies.17,18 The RCT by Ibarra-Estrada et al. (2022)17 was single-blind (investigators and data analysts were blinded). The RCT by Küçük et al. (2022)18 was open label.
The German Society for Anesthesiology and Intensive Care Medicine guideline was published in 2019.19 A systematic literature search was conducted to identify guidelines, systematic reviews, meta-analyses, RCTs, and non-randomized studies.19 The body of evidence for each question was evaluated according to the Grading of Recommendations, Assessment, Development and Evaluation criteria. There were 5 categories for quality of evidence ratings (no relevant evidence, very low, low, moderate, high).19 The members of the guideline group voted for or against each recommendation. Each recommendation was assigned a strength based on the quality of evidence and clinical judgment. There were 3 categories of recommendation strength (no recommendation, weak recommendation, strong recommendation).19
Country of Origin
All the systematic reviews were conducted by authors from China.14-16 The relevant studies included in the systematic reviews by Chen et al. (2021)14 and Sun et al. (2020)15 were conducted in China, US, Finland, Japan, and Germany. The countries where the included primary studies were conducted were not specified in the systematic review by Zhong et al. (2020).16
The RCT by Ibarra-Estrada et al. (2022)17 was conducted in Mexico. The RCT by Küçük et al. (2022)18 was conducted in Turkey.
The guideline group for the German Society for Anesthesiology and Intensive Care Medicine guideline19 included scientific societies from Germany, Austria, and Switzerland.
Patient Population
The systematic review by Chen et al. (2021)14 included studies of critically ill adults with acute respiratory distress syndrome admitted to the intensive care unit. The systematic reviews by Sun et al. (2020)15 and Zhong et al. (2020)16 included studies of adults with acute respiratory distress syndrome and did not specify the settings of the included studies. Therefore, only primary studies with intensive care, unit-related outcomes were considered relevant to the present report.
The RCT by Ibarra-Estrada et al. (2022)17 included adults with COVID-19 and acute respiratory distress syndrome who had received less than 24 hours of endotracheal mechanical ventilation. The airway pressure release ventilation group consisted of 45 patients (71% male) with a mean age of 55 years and a mean partial pressure of oxygen/ fraction of inspired oxygen (PaO2/FiO2) ratio of 140.17 The low tidal volume group consisted of 45 patients (69% male) with a mean age of 57 years and a mean PaO2/FiO2 ratio of 149.17 The RCT by Küçük et al. (2022)18 included patients aged 18 to 85 years who required invasive mechanical ventilation but were not initially diagnosed with acute respiratory distress syndrome and had been staying in the intensive care unit for 24 hours or more. The airway pressure release ventilation group included 32 patients (8 female, 24 male) with a median age of 50 years and a median lung injury prediction score of 8.5.18 The pressure-controlled synchronized intermittent mandatory ventilation plus pressure support group included 33 patients (4 female, 29 male) with a median age of 54 years and a median lung injury prediction score of 9.18
The intended users of the German Society for Anesthesiology and Intensive Care Medicine guideline19 are critical care teams. The target population for the guideline is patients with acute respiratory insufficiency.19 The guideline defines patients with acute respiratory insufficiency as those with acute respiratory distress syndrome as well as patients who require mechanical ventilation or extracorporeal procedures due to acute hypoxemic or hypercapnic respiratory insufficiency.19
Interventions and Comparators
All the systematic reviews included primary studies that used airway pressure release ventilation as the intervention.14-16 In the systematic review by Chen et al. (2021),14 the comparators in the relevant primary studies were synchronized intermittent mandatory ventilation and pressure-controlled synchronized intermittent mandatory ventilation with pressure support.14 For the systematic review by Sun et al. (2020),15 the comparators in the relevant primary studies were low tidal volume ventilation, pressure control ventilation, assist-control ventilation, and synchronized intermittent mandatory ventilation.15 The comparators in the relevant primary studies of the systematic review by Zhong et al. (2020)16 were low tidal volume ventilation modes, including volume control ventilation, pressure-control ventilation, and synchronized intermittent mandatory ventilation.16
The intervention used in both RCTs was airway pressure release ventilation.17,18 In the RCT by Ibarra-Estrada et al. (2022)17 all patients received a 12-hour stabilization period of protective low tidal volume ventilation. The initial settings on airway pressure release ventilation were as follows: high pressure (inspiratory pressure) had a maximum allowed level of 30 cm H2O; low pressure was set at 0 cm H2O; inspiratory time was initiated at 4 seconds; and expiratory time was set at 0.4 to 0.6 seconds. The expiratory flow termination was maintained between 50% and 75% (of the peak flow).17 The comparator was low tidal volume ventilation.17 The settings were a tidal volume of 6 mL/kg of predicted body weight, with lower limit of 4 mL/kg of predicted body weight in case of plateau pressure greater than 30 cm H2O, and upper limit of 8 mL/ kg of predicted body weight if needed to manage patient-ventilator interactions or acidosis.17
In the RCT by Küçük et al. (2022),18 all patients were ventilated using the conventional method until they could be evaluated. The standard initial settings for airway pressure release ventilation were Thigh (prolonged time)/Tlow (release time) of 4/0.8 seconds. The high pressure was set to plateau airway pressure value (if patient was paralyzed) or mean airway pressure in the previous conventional method as reference.18 Low pressure was always set to 0 cm H2O.18 Tlow range was adjusted as 0.4 seconds to 1.2 seconds.18 The comparator was pressure-controlled synchronized intermittent mandatory ventilation with pressure support.18 The pressure level was adjusted to get a tidal volume of 6 to 8 mL/kg of predicted body weight.18 Optimal positive end-expiratory pressure between 5 cm and 10 cm H2O was applied to all patients in the comparator group by titration according to the oxygen requirement.18
The German Society for Anesthesiology and Intensive Care Medicine guideline considered mechanical ventilation and extracorporeal gas exchange interventions.19 The relevant recommendation in the guideline was on airway pressure release ventilation and biphasic positive airway pressure, described as “pressure-controlled ventilation with the possibility of spontaneous breathing in the inspiration and expiration phases”.19
Outcomes
The reported outcomes in the included studies were mortality,14-18 length of intensive care unit stay,15-18 oxygenation (PaO2/FiO2),14-16 tracheostomy,15,17,18 ventilator-free days by day-28,16,17 mean arterial pressure,14,16 days of mechanical ventilation,15,17 extubation,17,18 incidence of acute respiratory distress syndrome,18 length of hospital stay,18 sedation requirement,18 barotrauma,17 severe hypercapnia,17 and deep vein thrombosis.17
The outcomes considered in the German Society for Anesthesiology and Intensive Care Medicine guideline were benefits, risks, clinical experience, patient preferences, and mandatory resources required.19
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Systematic Reviews
All the systematic reviews had clear objectives and inclusion criteria that included components of population, intervention, comparator, and outcomes.14-16 None of the systematic review authors stated whether the review methods were established before conducting the review. Without a pre-established protocol, it is unclear how to determine if the methods were adjusted in a way that could introduce bias after the review had begun. All of the literature searches were conducted in multiple databases and the keywords used were provided.14-16 The literature search for the systematic review by Chen et al. (2021)14 had no language restrictions. The authors of the Sun et al. (2020)15 systematic review also searched a trial registry and grey literature. Providing details of these elements of the search strategy increases its reproducibility. Study selection was performed independently by 2 reviewers in all the systematic reviews.14-16 Performing study selection in duplicate helps reduce the risk of bias in study selection. None of the systematic reviews provided a list of the excluded studies; however, they provided the reasons for exclusion in flow charts of study selection.14-16 Unjustified exclusion of studies could bias the results of the review. Data extraction was performed in duplicate in 2 of the systematic reviews.14,16 The authors of the Sun et al. (2020)15 systematic review do not state whether data extraction was performed in duplicate. Performing data extraction in duplicate increases the likelihood of completeness and accuracy of data capture. The populations, interventions, comparators, and outcomes of the included primary studies were described in adequate detail in all the systematic reviews.14-16 None of the systematic reviews specified the time frame for follow-up of the included primary studies. The settings (i.e., whether patients were in the intensive care unit or emergency room) of the included primary studies were not specified in the Sun et al. (2020)15 and Zhong et al. (2020)16 systematic reviews. Additionally, the countries where the included studies were conducted were not specified in the Zhong et al. (2020)16 systematic review. The risk of bias of the included primary studies was assessed using validated tools in all the systematic reviews. However, in the Sun et al. (2020)15 systematic review the results of the risk of bias assessment (e.g., quality ratings) were not provided. All the systematic reviews reported their funding sources and stated that the authors had no conflicts of interest.14-16
Randomized Controlled Trials
The study objective, patient characteristics, interventions, and main findings were clearly described in both RCTs.17,18 The main outcome measures used were valid and reliable, and the statistical tests used were appropriate in both the RCTs. Commonly known adverse events were reported in both studies. Patients were not blind to the intervention they received in either of the RCTs. In the Ibarra-Estrada et al. (2022)17 RCT investigators and data analysts were blind to group allocation. In the Küçük et al. (2022)18 RCT investigators were not blind to group allocation. Objective outcomes such as mortality and length of intensive care unit stay are unlikely to be influenced by blinding. In both RCTs patients from different intervention groups were recruited from the same population. Patients were randomized to intervention groups in a 1:1 ratio using block randomization in both studies.17,18 Randomization aims to balance the distribution of known and unknown confounders between treatment groups. In the Küçük et al. (2022)18 RCT, the investigators conducted a sample size calculation a priori to determine the number of patients to adequately power the study. In the Ibarra-Estrada et al. (2022)17 RCT a sample size calculation was conducted a priori; however, the study did not recruit the required number of patients in each group because the safety monitoring board stopped the trial early due to episodes of barotrauma, higher incidence of hypercapnia, and trends in mortality in the airway pressure release ventilation group.17 Therefore, the RCT did not reach the anticipated power estimated through sample size calculation and it is unclear in the study was sufficiently powered to detect a significant difference between the intervention groups for all outcomes. The statistical analysis did not adjust for multiplicity in either RCT. Adjusting for multiplicity is important for studies that assess multiple outcomes due to the potential inflation of the type I error rate. The authors of the Ibarra-Estrada et al. (2022)17 RCT disclosed their potential conflicts of interest; however, they did not state whether they received any funding for the study. The authors of the Küçük et al. (2022)18 RCT stated that they did not have any conflicts of interest and no funding was received for the study.
Guideline
The full version of the German Society for Anesthesiology and Intensive Care Medicine guideline was not available in English and therefore, this critical appraisal is based on a review of the summary document.19 Further detail related to some of the critical appraisal domains may have been provided in the full version of the guidelines.
The objective, health questions covered by the guideline, target population, and target users were clearly described.19 The guideline development group included individuals from relevant professional groups.19 The authors stated that patient preferences were taken into account in making the recommendations; however, details were not provided on how this information was sought. The literature search was conducted in multiple databases, however, other details of the search strategy (e.g., keywords used, number of authors who performed study selection, etc.) were not provided.19 The inclusion and exclusion criteria for selecting evidence were not adequately provided. The strengths and limitations of the body of evidence were discussed. The guideline group voted on recommendations; however, no description is provided of the voting process used and there is no discussion of the alignment between the voting and the final recommendations.19 Both the benefits and risks of interventions were considered when formulating the recommendations. There was an explicit link between the relevant recommendation and the supporting evidence; however, additional details such as the number of studies of each design were not provided. The guideline did not describe an external review process.19 The guideline authors state that the next review of the guideline is scheduled for 2022 but details on the procedure for updating the guideline were not provided.19 The recommendation regarding airway pressure release ventilation was specific and unambiguous. The recommendations were placed through the body of the guidelines and the key recommendations were not easily identifiable.19 Combining all the recommendations into a table or using bold text would have made them easier to identify. The guideline identified the funding source and included an explicit statement that the funder did not influence literature selection and evidence assessment.19 The conflicts of interest for the guideline development group were disclosed.
Summary of Findings
Appendix 4 presents the main study findings. There was some overlap in the primary studies that were included in the systematic reviews; therefore, to avoid duplication of results, outcome data from an individual primary study are only reported once.
Clinical Effectiveness of Airway Pressure Release Ventilation
Length of Intensive Care Unit Stay
Two systematic reviews15,16 and 1 RCT17 reported mixed evidence for the effect of airway pressure release ventilation on length of intensive care unit stay in patients with acute respiratory distress syndrome. In the systematic review by Sun et al. (2020)15 results from 2 of the included studies (1 RCT, 1 retrospective study) suggested there was no statistically significant difference in length of intensive care unit stay for airway pressure release ventilation versus other mechanical ventilation strategies (low tidal volume, synchronized intermittent mandatory ventilation) and another included RCT found a statistically significant difference in favour of synchronized intermittent mandatory ventilation. In the systematic review by Zhong et al. (2020)16 results from 1 included RCT suggested no statistically significant difference in length of intensive care unit stay between airway pressure release ventilation and low tidal volume ventilation; however, results from 2 other included RCTs suggested there was a statistically significant difference in favour of airway pressure release ventilation versus low tidal volume ventilation.
Evidence from the RCT by Ibarra-Estrada et al. (2022)17 suggested no statistically significant difference between airway pressure release ventilation and low tidal volume ventilation in length of intensive care unit stay in patients with acute respiratory distress syndrome and COVID-19.
Evidence from the RCT by Küçük et al. (2022)18 suggested there was a statistically significant difference in length of intensive care unit stay in favour of airway pressure release ventilation versus pressure-controlled synchronized intermittent mandatory ventilation and pressure support in patients at risk of acute respiratory distress syndrome.
Mortality
Evidence from the relevant primary studies included in 3 systematic reviews14-16 and 1 RCT17 suggested there was no statistically significant difference in mortality for patients with acute respiratory distress syndrome treated with airway pressure release ventilation versus other mechanical ventilation strategies.
Evidence from the RCT by Küçük et al. (2022)18 suggested there was no statistically significant difference in 28-day mortality between patients at risk of acute respiratory distress syndrome treated with airway pressure release ventilation versus pressure controlled synchronized intermittent mandatory ventilation and pressure support.
Oxygenation
Three systematic reviews14-16 reported mixed evidence for the effect of airway pressure release ventilation on oxygenation in patients with acute respiratory distress syndrome. Evidence from 3 RCTs included in the systematic reviews suggested there was no statistically significant difference in oxygenation for airway pressure release ventilation versus other mechanical ventilation strategies (synchronized intermittent mandatory ventilation, low tidal volume ventilation) and evidence from 2 RCTs included in the systematic reviews suggested there was a statistically significant difference in favour of airway pressure release ventilation versus synchronized intermittent mandatory ventilation.14,16
Ventilator-Free Days
One systematic review16 and 1 RCT17 reported mixed evidence for the effect of airway pressure release ventilation on ventilator-free days in patients with acute respiratory distress syndrome. Results from the systematic review by Zhong et al. (2020)16 suggested there was a statistically significant difference in ventilator-free days in favour of airway pressure release ventilation versus synchronized intermittent mandatory ventilation (2 RCTs) and pressure-control ventilation (1 RCT). Results from the systematic review suggested no statistically significant difference in ventilator-free days for airway pressure release ventilation versus volume control ventilation (1 RCT).16 Evidence from the Ibarra-Estrada et al. (2022)17 RCT suggested no statistically significant difference in ventilator-free days between airway pressure release ventilation and low tidal volume ventilation.
Mean Arterial Pressure
Evidence for the effect of airway pressure release ventilation on mean arterial pressure in patients with acute respiratory distress syndrome from 2 systematic reviews14,16 was mixed. Evidence from the systematic review by Zhong et al. (2020)16 suggested that there was a statistically significant difference in the mean arterial pressure in favour of airway pressure release ventilation versus synchronized intermittent mandatory ventilation (2 RCTs). One RCT in the systematic review by the Chen et al. (2021)14 found no statistically significant difference in mean arterial pressure between airway pressure release ventilation and synchronized intermittent mandatory ventilation and another RCT in the systematic review found a statistically significant difference in favour of airway pressure release ventilation versus synchronized intermittent mandatory ventilation.
Additional Clinical Outcomes
The systematic review by Sun et al. (2020)15 reported on days of mechanical ventilation in patients with acute respiratory distress syndrome; however, it did not report the statistical significance of the results. In the systematic review the days of mechanical ventilation were numerically higher in the airway pressure release ventilation group in some of the identified studies (2 RCTs, 1 retrospective study), the same in both groups in 1 retrospective study and numerically higher in the control group in 1 RCT.15 In the RCT by Ibarra-Estrada (2022),17 there was no statistically significant difference in days of mechanical ventilation or extubation between airway pressure release ventilation versus low tidal volume ventilation in patients with acute respiratory distress syndrome and COVID-19.
In the RCT by Küçük et al. (2022)18 there was no statistically significant difference in incidence of acute respiratory distress syndrome, length of hospital stay, sedation requirement, vasopressor or inotrope requirement, or extubation between patients at risk of acute respiratory distress syndrome treated with airway pressure release ventilation versus pressure controlled synchronized intermittent mandatory ventilation and pressure support.
Safety Outcomes
The systematic review by Sun et al. (2020)15 reported on tracheostomy; however, it did not report on the statistical significance of the results. The systematic review reported that the number of patients with acute respiratory distress syndrome who received a tracheostomy was numerically higher in the control group versus the airway pressure release ventilation group (1 RCT, 1 retrospective study).15 In the RCT by Ibarra-Estrada (2022)17 there was no statistically significant difference in tracheostomy, barotrauma, or deep vein thrombosis between airway pressure release ventilation versus low tidal volume ventilation in patients with acute respiratory distress syndrome and COVID-19. Significantly more patients treated with airway pressure release ventilation experienced severe hypercapnia than those treated with low tidal volume ventilation in the RCT by Ibarra-Estrada (2022).17
In the RCT by Küçük et al. (2022),18 there was no statistically significant difference in tracheostomy between patients at risk of acute respiratory distress syndrome treated with airway pressure release ventilation versus those treated with pressure controlled synchronized intermittent mandatory ventilation and pressure support.
Guidelines Regarding the Use of Airway Pressure Release Ventilation
The German Society for Anesthesiology and Intensive Care Medicine guideline gives a weak recommendation to consider using airway pressure release ventilation and biphasic positive airway pressure (i.e., pressure-controlled ventilation with the possibility of spontaneous breathing in the inspiratory and expiratory phases) in patients without severe acute respiratory distress syndrome.19 The recommendation is based on evidence from small randomized and observational studies that the guideline authors rated as low quality.19
Limitations
Limited evidence was identified that evaluated airway pressure release ventilation in patients at risk of acute respiratory distress syndrome. Only 1 RCT18 of patients at risk of acute respiratory distress syndrome was identified and included in this report. The other included studies evaluated airway pressure release ventilation in patients who had been diagnosed with acute respiratory distress syndrome.14-17 Additionally, limited evidence regarding the safety of airway pressure release ventilation was identified.
Only 1 guideline was identified that included a recommendation on the use of airway pressure release ventilation in patients without severe acute respiratory syndrome. The was based on low quality evidence and was rated by the guideline authors as a weak recommendation.19
The included literature was of variable in methodological quality. Chen et al. (2021)14 assessed the included primary studies in their systematic review as being at unclear risk of bias. Zhong et al. (2020)16 rated all primary studies included in their systematic review as being at high risk of performance bias. The authors of the Sun et al. (2020)15 did not provide details on their quality assessment of the included primary studies. Due to the nature of the intervention, blinding of patients is not possible and therefore, studies are at risk of performance bias.
None of the relevant primary studies included in 2 of the systematic reviews14,15 or the 2 included RCTs17,18 were conducted in Canada. The countries where the included primary studies were conducted were not specified in the systematic review by Zhong et al. (2020).16 Additionally, the German Society for Anesthesiology and Intensive Care Medicine guideline19 is not specific to Canada. Therefore, it is unclear whether the results summarized in this report are generalizable to the Canadian context. Further, the RCT by Ibarra-Estrada et al. (2022)17 was conducted in the intensive care unit of a specialized COVID-19 centre and the results may not be generalizable to other settings.
Conclusions and Implications for Decision- or Policy-Making
This report comprised 3 systematic reviews,14-16 2 RCTs,17,18 and 1 evidence-based guideline.19
A range of mechanical ventilation strategies were used as comparators in the included systematic reviews14-16 and RCTs.17,18 Overall, the evidence regarding the clinical effectiveness of airway pressure release ventilation versus other mechanical ventilation strategies was mixed. Results from the relevant primary studies included in the systematic reviews14-16 and RCTs17,18 suggested there was no significant difference in mortality between patients treated with airway pressure release ventilation versus other mechanical ventilation strategies. Results from the included studies varied for several outcomes (length of intensive care unit stay, oxygenation, ventilator-free days, mean arterial pressure). For length of intensive care unit stay evidence from some studies suggested there was a statistically significant difference in favour airway pressure release ventilation versus other mechanical ventilation strategies, other studies suggested there was a statistically significant difference in favour of other mechanical ventilation strategies, and some studies found no statistically significant differences in these outcomes between groups.14-18 For the other outcomes (oxygenation, ventilator-free days, mean arterial pressure) evidence from some studies suggested there was a statistically significant difference in favour airway pressure release ventilation versus other mechanical ventilation strategies; whereas others found no statistically significant differences between groups.14-17 Results from 1 RCT suggested there was no statistically significant difference in incidence of acute respiratory distress syndrome between patients treated with airway pressure release ventilation versus control (pressure controlled synchronized intermittent mandatory ventilation and pressure support).18
Evidence from 2 RCTs suggested there was no significant difference in tracheostomy between airway pressure release ventilation versus control in patients with or at risk of acute respiratory distress syndrome. In 1 RCT, significantly more patients treated with airway pressure release ventilation experienced severe hypercapnia than those treated with low tidal volume ventilation.17
The German Society for Anesthesiology and Intensive Care Medicine guideline suggests considering the use of pressure-controlled ventilation with the possibility of spontaneous breathing in the inspiratory and expiratory phases (i.e., airway pressure release ventilation and biphasic positive airway pressure) in patients without severe acute respiratory distress syndrome.19
A 2018 CADTH report8 on this topic identified 5 primary clinical studies (2 RCTs, 1 retrospective cohort study, and 2 single-arm studies) that evaluated airway pressure release ventilation in patients with or at risk of acute respiratory distress syndrome. Overall, the results of the included studies favoured airway pressure release ventilation, however, the studies had important limitations as outlined in the previous CADTH report.8 These included the lack of blinding in the RCTs, the single-arm design of 2 of the non-randomized studies, and the lack of formal statistical comparisons and lack of specification of what ventilation modes were used in the control group in the retrospective cohort study.8
Due to the heterogenous results as well as the range of different comparators used in the included studies, it is difficult to draw conclusions around the clinical effectiveness of airway pressure release ventilation for the treatment of patients with acute respiratory distress syndrome. Additionally, limited evidence was identified that evaluated airway pressure release ventilation in patients at risk of acute respiratory distress syndrome. One evidence-based guideline was identified that suggests considering the use of airway pressure release ventilation in patients without severe acute respiratory distress syndrome.19 Future high-quality studies that focus on the comparative efficacy and safety of airway pressure release ventilation versus specific alternative ventilation strategies would help stakeholders in decision-making around the use of this intervention.
References
1.Fan E, Brodie D, Slutsky AS. Acute Respiratory Distress Syndrome: Advances in Diagnosis and Treatment. Jama. 2018;319(7):698-710. PubMed
2.Acute Respiratory Distress Syndrome (ARDS). Victoria (BC): HealthLink BC. 2021. https://www.healthlinkbc.ca/illnesses-conditions/lung-and-respiratory-conditions/acute-respiratory-distress-syndrome-ards. Accessed 2022 Aug 30.
3.Saguil A, Fargo MV. Acute Respiratory Distress Syndrome: Diagnosis and Management. Am Fam Physician. 2020;101(12):730-738. PubMed
4.Parhar KKS, Zjadewicz K, Soo A, et al. Epidemiology, Mechanical Power, and 3-Year Outcomes in Acute Respiratory Distress Syndrome Patients Using Standardized Screening. An Observational Cohort Study. Ann Am Thorac Soc. 2019;16(10):1263-1272. PubMed
5.Banavasi H, Nguyen P, Osman H, Soubani AO. Management of ARDS - What Works and What Does Not. Am J Med Sci. 2021;362(1):13-23. PubMed
6.Epelbaum O, Aronow WS. Mechanical ventilation in the acute respiratory distress syndrome. Hosp Pract (Minneap). 2017;45(3):88-98. PubMed
7.Mallory P, Cheifetz I. A comprehensive review of the use and understanding of airway pressure release ventilation. Expert Rev Respir Med. 2020;14(3):307-315. PubMed
8.Airway Pressure Release Ventilation for Acute Respiratory Distress Syndrome: Clinical Effectiveness and Guidelines. Ottawa (ON): CADTH. 2018. https://www.cadth.ca/airway-pressure-release-ventilation-acute-respiratory-distress-syndrome-clinical-effectiveness-and. Accessed 2022 Aug 30.
9.Othman F, Alsagami N, Alharbi R, Almuammer Y, Alshahrani S, Ismaeil T. The efficacy of airway pressure release ventilation in acute respiratory distress syndrome adult patients: A meta-analysis of clinical trials. Ann Thorac Med. 2021;16(3):245-252. PubMed
10.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
11.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
12.Agree Next Steps C. The AGREE II Instrument. Hamilton, ON: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2022 Aug 30.
13.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
14.Chen C, Zhen J, Gong S, Yan J, Li L. Efficacy of airway pressure release ventilation for acute respiratory distress syndrome: a systematic review with meta-analysis. Ann Palliat Med. 2021;10(10):10349-10359. PubMed
15.Sun X, Liu Y, Li N, You D, Zhao Y. The safety and efficacy of airway pressure release ventilation in acute respiratory distress syndrome patients: A PRISMA-compliant systematic review and meta-analysis. Medicine (Baltimore). 2020;99(1):e18586. PubMed
16.Zhong X, Wu Q, Yang H, et al. Airway pressure release ventilation versus low tidal volume ventilation for patients with acute respiratory distress syndrome/acute lung injury: a meta-analysis of randomized clinical trials. Ann Transl Med. 2020;8(24):1641. PubMed
17.Ibarra-Estrada MA, Garcia-Salas Y, Mireles-Cabodevila E, et al. Use of Airway Pressure Release Ventilation in Patients With Acute Respiratory Failure Due to COVID-19: Results of a Single-Center Randomized Controlled Trial. Crit Care Med. 2022;50(4):586-594. PubMed
18.Kucuk MP, Ozturk CE, Ilkaya NK, Kucuk AO, Ergul DF, Ulger F. The effect of preemptive airway pressure release ventilation on patients with high risk for acute respiratory distress syndrome: a randomized controlled trial. Braz J Anesthesiol. 2022;72(1):29-36. PubMed
19.Fichtner F, Moerer O, Weber-Carstens S, et al. Clinical Guideline for Treating Acute Respiratory Insufficiency with Invasive Ventilation and Extracorporeal Membrane Oxygenation: Evidence-Based Recommendations for Choosing Modes and Setting Parameters of Mechanical Ventilation. Respiration. 2019;98(4):357-372. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Chen et al. (2021)14 China Funding source: Zhejiang Provincial Program for the Zhejiang Medical and Health Science and Technology Program | Study design: systematic review and meta-analysis Included studies: 6 RCTs in total, 4 RCTs relevant to the present report | Inclusion criteria: studies of critically ill adults (aged ≥ 18 years) with ARDS admitted to the ICU. Baseline characteristics for patients in the relevant RCTs were reported individually by study and appeared to be balanced between treatment groups. | Intervention: Airway pressure release ventilation Comparators: Traditional mechanical ventilation modes (i.e., synchronized intermittent mandatory ventilation, low tidal volume ventilation, controlled mechanical ventilation, assistant-control ventilation) | Outcomes: 28-day mortality, oxygenation index, mean arterial pressure, airway peak pressure Follow-up: NR |
Sun et al. (2020)15 China Funding source: Fujian provincial Health and Family Planning Young and Middle-Aged Talents Training Project; Changji Hui Autonomous Prefecture Science and Technology Plan Project | Study design: systematic review and meta-analysis Included studies: 14 studies in total (7 RCTs and 7 retrospective studies); 5 RCTs, 2 two-arm retrospective studies, and 1 single-arm retrospective study relevant to the present report | Inclusion criteria: studies of adults with ARDS. Relevant population: adult patients with ARDS in the ICU Baseline characteristics were reported individually by study and appeared to be balanced between treatment groups. | Intervention: airway pressure release ventilation Comparators: low tidal volume ventilation, pressure control ventilation, pressure support ventilation, assist-control ventilation, synchronized intermittent mandatory ventilation | Outcomes: mortality in ICU, duration of ICU stay, oxygenation, days of ventilation, tracheostomy Follow-up: NR |
Zhong et al. (2020)16 China Funding source: Provincial Science and Technology Department Project in Sichuan | Study design: systematic review and meta-analysis Included studies: 7 RCTs in total, 4 RCTs relevant to the present report | Inclusion criteria: studies of adults (aged ≥ 18 years) with ARDS (defined as PaO2/FiO2 < 300 mm Hg). Relevant population: adult patients with ARDS in the ICU. Baseline characteristics were reported individually by study and appeared to be balanced between treatment groups. | Intervention: airway pressure release ventilation Comparator: low tidal volume ventilation | Outcomes: hospital mortality, ventilator-free days, mean arterial pressure, oxygenation, length of ICU stay, pneumothorax Follow-up: NR |
ARDS = acute respiratory distress syndrome; ICU = intensive care unit; NR = not reported; PaO2/FiO2 = partial pressure of oxygen/ fraction of inspired oxygen; RCT = randomized controlled trial.
Table 3: Characteristics of Included Randomized Controlled Trials
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Ibarra-Estrada et al. (2022)17 Mexico Funding source: NR | Single-centre, single-blind RCT | Inclusion criteria: Adults (aged ≥ 18 years) with COVID-19 and ARDS (defined as PaO2/FiO2 < 300 mm Hg) who have received less than 48 hours of endotracheal mechanical ventilation. Baseline characteristics: APRV group: 45 patients with a mean age of 55 years, 71% male, mean PaO2/FiO2 ratio of 140, mean APACHE II score of 14.3. LTV group: 45 patients with a mean age of 57 years, 69% male, mean PaO2/FiO2 ratio of 149, mean APACHE II score of 15.3. | Intervention: APRV Comparator: low tidal volume ventilation | Outcomes: ventilator-free days, days of mechanical ventilation, length of ICU stay, extubation, tracheostomy, barotrauma, severe hypercapnia, deep vein thrombosis, mortality Follow-up: 28 days |
Küçük et al. (2022)18 Turkey Funding source: none | Single-centre, open-label RCT | Inclusion criteria: Patients (aged 18 to 85 years) who required invasive mechanical ventilation but were not initially diagnosed with ARDS with a LIPS > 7 and stayed in the ICU for > 24 hours. Baseline characteristics: APRV group: 32 patients (8 female, 24 male) with a median age of 50 years, median LIPS of 8.5, median APACHE II of 17, median SOFA of 7. P-SIMV-PS group: 33 patients (4 female, 29 male) with a median age of 54 years, median LIPS of 9, median APACHE II of 17, median SOFA of 6. | Intervention: APRV Comparator: P-SIMV-PS | Outcomes: incidence of ARDS, mortality, length of ICU stay, sedation requirement, length of hospital stay, tracheostomy, extubation Follow-up: 28 days |
APACHE II = Acute Physiology and Chronic Health Evaluation II; APRV = airway pressure release ventilation; ARDS = acute respiratory distress syndrome; ICU = intensive care unit; LIPS = Lung Injury Prediction Score; LTV = low tidal volume; NR = not reported; PaO2/FiO2 = partial pressure of oxygen/ fraction of inspired oxygen; P-SIMV-PS; Pressure-controlled Synchronized Intermittent Mandatory Ventilation + Pressure Support; RCT = randomized controlled trial; SOFA = Sequential Organ Failure Assessment.
Table 4: Characteristics of Included Guideline
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
German Society for Anesthesiology and Intensive Care Medicine (2019)19 | ||||||
Intended users: critical care teams Target population: patients with acute respiratory insufficiency | Mechanical ventilation and extracorporeal gas exchange | Benefits and risks, clinical experience, patient preferences, mandatory resources | Questions were developed using the Patient Intervention Control Outcome structure. A systematic literature search was then conducted in multiple databases. The literature was selected based on predefined criteria. Current guidelines, systematic reviews and meta-analyses were examined first. RCTs and lower-quality studies were evaluated in the absence of meta-analyses. | Meta-analyses and systematic reviews were critically appraised according to the criteria of the Scottish Intercollegiate Guidelines Network. The body of evidence for each question was summarized and evaluated according to the GRADE criteria. There were 5 categories for quality of evidence ratings (no relevant evidence, very low, low, moderate, high). | The guideline group consisted of 59 mandate holders from 21 scientific societies from Germany, Austria, and Switzerland. The members of the guideline group voted for or against each recommendation individually in the first stage and in a second stage voted as their role of mandate holders of 1 of the 21 scientific societies. The strength of each recommendation was assigned based on the benefits and risks of a specific therapy as well as clinical experience, patient preferences, and an assessment of mandatory resources. There were 3 categories of recommendation strengths (no recommendation, weak recommendation, and strong recommendation). | NR |
GRADE = Grading of Recommendations, Assessment, Development and Evaluation; NR = not reported; RCT = randomized controlled trial.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 5: Strengths and Limitations of Systematic Reviews Using AMSTAR 210
Strengths | Limitations |
|---|---|
Chen et al. (2021)14 | |
The systematic review has a clear objective and inclusion criteria that included components of population, intervention, comparator, and outcomes The choice of study designs (i.e., RCTs) included in the systematic review was explained Search was conducted in multiple databases, keywords used were provided, and there were no language restrictions Study selection and data extraction were performed independently by 2 reviewers Population, interventions, comparators, and outcomes of included primary studies were described in adequate detail The risk of bias of included primary studies was assessed using a satisfactory technique Funding source for the systematic review was reported Authors stated that they had no conflicts of interest | The authors do not state whether the review methods were established before conducting the systematic review. A list of excluded studies was not provided, however, the reasons for exclusion were provided. Time frame for follow-up of included primary studies not specified. Sources of funding for individual studies included in the systematic review not reported. |
Sun et al. (2020)15 | |
The systematic review has a clear objective and inclusion criteria that included components of population, intervention, comparator, and outcomes The choice of study designs (i.e., RCTs and non-randomized studies) included in the systematic review was explained Search was conducted in multiple databases and a trial registry, grey literature was searched, and keywords used were provided Study selection was performed independently by 2 reviewers Population, interventions, comparators, and outcomes of included primary studies were described in adequate detail The risk of bias of included primary studies was assessed independently by 2 reviewers using a satisfactory technique Funding sources for the systematic review were reported Authors stated that they had no conflicts of interest | The authors do not state whether the systematic review methods were established before conducting the review The authors do not state whether data extraction was performed in duplicate A list of excluded studies was not provided, however, the reasons for exclusion were provided Time frame for follow-up and settings (i.e., whether patients were in the ICU) of included primary studies not specified Sources of funding for individual studies included in the systematic review not reported The authors state that they assessed risk of bias in the included studies, however, do not provide their quality ratings for the studies |
Zhong et al. (2020)16 | |
The systematic review has a clear objective and inclusion criteria that included components of population, intervention, comparator, and outcomes The choice of study designs (i.e., RCTs) included in the systematic review was explained Search was conducted in multiple databases and keywords used were provided Study selection and data extraction were performed independently by 2 reviewers Population, interventions, comparators, and outcomes of included primary studies were described in adequate detail The risk of bias of included primary studies was assessed independently by 2 reviewers using a satisfactory technique Funding source for the systematic review was reported Authors stated that they had no conflicts of interest | The authors do not state whether the systematic review methods were established before conducting the review A list of excluded studies was not provided, however, the reasons for exclusion were provided Time frame for follow-up, countries, and settings (i.e., whether patients were in the ICU) of included primary studies not specified Sources of funding for individual studies included in the systematic review not reported |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; ICU = intensive care unit; RCT = randomized controlled trial.
Table 6: Strengths and Limitations of Randomized Controlled Trials Using the Downs and Black Checklist11
Strengths | Limitations |
|---|---|
Ibarra-Estrada et al. (2022)17 | |
The objective, patient characteristics, interventions, and main findings clearly described Commonly known adverse events reported There was a similar number of patients lost to follow-up in each group Baseline characteristics appeared to be balanced between treatment groups The main outcome measures were valid and reliable Statistical tests used were appropriate Investigators and data analysts were blind to group allocation Patients in different intervention groups were recruited from the same population over the same period Patients were randomized to intervention groups in a 1:1 ratio using the permuted blocks technique The authors disclosed their potential conflicts of interest | Patients were not blind to the intervention they received Three patients in the intervention group and 2 patients in the control group were crossed over to the opposite group Statistical analysis did not adjust for multiplicity A sample size calculation was conducted a priori, however, the study did not recruit the required number of patients in each group because the trial was stopped early by the safety monitoring board The funding source for the study was not reported The study was conducted in the ICU of a specialized COVID-19 centre and the results may not be generalizable to other settings The study was conducted in Mexico and the results may not be generalizable to the Canadian population |
Küçük et al. (2022)18 | |
The objective, patient characteristics, interventions, and main findings clearly described Commonly known adverse events reported There was a similar number of patients lost to follow-up in each group Baseline characteristics appeared to be balanced between treatment groups The main outcome measures were valid and reliable Statistical tests used were appropriate Compliance with the interventions was reliable Patients in different intervention groups were recruited from the same population Patients were assigned to intervention groups in a 1:1 ratio using block randomization A sample size calculation was conducted a priori, and an adequate number of patients was recruited The authors stated that they had no conflicts of interest No funding was received for the study | The study used an open-label design The period for patient recruitment was not specified Statistical analysis did not adjust for multiplicity The study was conducted in Turkey and the results may not be generalizable to the Canadian population |
ICU = intensive care unit.
Table 7: Strengths and Limitations of Guideline Using AGREE II12
Item | German Society for Anesthesiology and Intensive Care Medicine (2019)19 |
|---|---|
Domain 1: scope and purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes |
Domain 2: stakeholder involvement | |
4. The guideline development group includes individuals from all relevant professional groups. | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Unclear |
6. The target users of the guideline are clearly defined. | Yes |
Domain 3: rigour of development | |
7. Systematic methods were used to search for evidence. | Partially |
8. The criteria for selecting the evidence are clearly described. | Partially |
9. The strengths and limitations of the body of evidence are clearly described. | Yes |
10. The methods for formulating the recommendations are clearly described. | Partially |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Partially |
13. The guideline has been externally reviewed by experts before its publication. | Unclear |
14. A procedure for updating the guideline is provided. | Partially |
Domain 4: clarity of presentation | |
15. The recommendations are specific and unambiguous. | Yes |
16. The different options for management of the condition or health issue are clearly presented. | NA |
17. Key recommendations are easily identifiable. | No |
Domain 5: applicability | |
18. The guideline describes facilitators and barriers to its application. | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No |
20. The potential resource implications of applying the recommendations have been considered. | No |
21. The guideline presents monitoring and/or auditing criteria. | No |
Domain 6: editorial independence | |
22. The views of the funding body have not influenced the content of the guideline. | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; NA = not applicable.
Note: The full version of the guideline was not available in English, therefore, the critical appraisal of the guideline was based on a summary document.19
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 8: Summary of Findings by Outcome — Length of ICU Stay
Study citation and study design Subgroup | Intervention used in control group | Method of measurement | APRV | Control | Comparison (95% CI) | Notes | P value |
|---|---|---|---|---|---|---|---|
Patients with ARDS | |||||||
Length of ICU stay (days) | |||||||
Sun et al. (2020)15 SR (1 RCT, Maxwell et al. 2010) | LTV | Mean (SD) | 16.47 (12.83) | 14.18 (13.26) | SMD = 0.17 (−0.32 to 0.67) | SMD < 0 favours APRV | NS |
Sun et al. (2020)15 SR (1 retrospective study, Liu et al. 2009) | SIMV | Mean (SD) | 35 (49) | 31 (38) | SMD = 0.09 (−0.45 to 0.64) | SMD < 0 favours APRV | NS |
Sun et al. (2020)15 SR (1 single-arm retrospective study, Dart et al. 2005) | NA | Mean (SD) | 17 (7) | NA | NA | — | NA |
Sun et al. (2020)15 SR (1 RCT, Varpula et al. 2004) | SIMV | Mean (SD) | 11.9 (1.7) | 10.7 (1.4) | SMD = 0.76 (0.24 to 1.29) | SMD < 0 favours APRV | Significant |
Zhong et al. (2020)16 SR (1 RCT, Hirshberg et al. 2018) | LTV (VC) | Mean (SD) | 6.47 (4.5) | 10.5 (11.24) | Mean difference = −4.03 (−9.76 to 1.70) | Mean difference < 0 favours APRV | NS |
Zhong et al. (2020)16 SR (1 RCT, Putensen et al. 2001) | LTV (PCV) | Mean (SD) | 23 (2) | 30 (2) | Mean difference = −7.00 (−8.43 to −5.57) | Mean difference < 0 favours APRV | Significant |
Zhong et al. (2020)16 SR (1 RCT, Zhou XZ et al. 2017) | LTV (SIMV) | Mean (SD) | 7.09 (1.42) | 10.87 (2.11) | Mean difference = −3.78 (−4.69 to −2.78) | Mean difference < 0 favours APRV | Significant |
Ibarra-Estrada et al. (2022)17 RCT | LTV | Median (IQR) | 9 (7 to 16) | 12 (8 to 17) | NR | — | 0.17 |
Patients at risk of ARDS | |||||||
Length of ICU stay (days) | |||||||
Küçük et al. (2022)18 RCT | — | — | — | — | — | — | — |
Overall | P-SIMV+PS | NA | NR | NR | NR | Length of ICU stay was higher in the control group | 0.019 |
Surviving patients | P-SIMV+PS | Median (min-max) | 11 (2 to 58) | 23.5 (10 to 81) | NR | — | 0.027 |
APRV = airway pressure release ventilation; ARDS = acute respiratory distress syndrome; CI = confidence interval; ICU = intensive care unit; IQR = interquartile range; LTV = low tidal volume; NA = not applicable; NR = not reported; NS = not significant; PCV = pressure control ventilation; P-SIMV+PS = Pressure controlled Synchronized Intermittent Mandatory Ventilation + Pressure Support; RCT = randomized controlled trial; SD = standard deviation; SIMV = synchronized intermittent mandatory ventilation; SMD = standard mean difference; SR = systematic review; VC = volume control.
Table 9: Summary of Findings by Outcome — Mortality
Study citation and study design | Intervention used in control group | Method of measurement | APRV | Control | Comparison (95% CI) | Notes | P value |
|---|---|---|---|---|---|---|---|
Patients with ARDS | |||||||
28-day mortality | |||||||
Chen et al. (2021)14 SR (1 RCT, Ota et al. 2009) | SIMV | Number of events/total | 5/17 | 24/40 | RR = 0.49 (0.23 to 1.07) | RR < 1 favours APRV | NS |
Chen et al. (2021)14 SR (1 RCT, Varpula et al. 2004) | SIMV | Number of events/total | 5/30 | 5/28 | RR = 0.93 (0.30 to 2.88) | RR < 1 favours APRV | NS |
Chen et al. (2021)14 SR (1 RCT, Varpula et al. 2003) | P-SIMV+PS | Number of events/total | 2/18 | 3/15 | RR = 0.56 (0.11 to 2.90) | RR < 1 favours APRV | NS |
Ibarra-Estrada et al. (2022)17 RCT | LTV | Number of events (%) | 35 (78) | 27 (60) | NR | — | 0.07 |
Mortality in ICU | |||||||
Sun et al. (2020)15 SR (1 retrospective study, Gonzalez et al. 2010) | A/C | Number of events (%) | 65 (27) | 514 (41) | NR | — | NR |
Sun et al. (2020)15 SR (1 RCT, Maxwell et al. 2010) | LTV | Number of events (%) | 2 (6) | 2 (6) | RR = 1.03 (0.15 to 6.89) | RR < 1 favours APRV | NS |
Sun et al. (2020)15 SR (1 retrospective study, Liu et al. 2009) | SIMV | Number of events (%) | 6 (31) | 23 (58) | RR = 0.65 (0.30 to 1.40) | RR < 1 favours APRV | NS |
Death during hospitalization | |||||||
Zhong et al. (2020)16 SR (1 RCT, Hirshberg et al. 2018) | LTV (VC) | Number of events/total | 6/18 | 10/17 | OR = 0.35 (0.09 to 1.39) | OR < 1 favours APRV | NS |
Zhong et al. (2020)16 SR (1 RCT, Zhou XZ et al. 2017) | LTV (SIMV) | Number of events/total | 5/30 | 10/30 | OR = 0.40 (0.12 to 1.36) | OR < 1 favours APRV | NS |
Zhong et al. (2020)16 SR (1 RCT, Putensen et al. 2001) | LTV (PCV) | Number of events/total | 3/15 | 4/15 | OR = 0.69 (0.12 to 3.79) | OR < 1 favours APRV | NS |
Patients at risk of ARDS | |||||||
28-day mortality | |||||||
Küçük et al. (2022)18 RCT | P-SIMV+PS | Number of events (%) | 14 (43.8) | 17 (51.5) | NR | — | 0.705 |
A/C = assist-control ventilation; APRV = airway pressure release ventilation; ARDS = acute respiratory distress syndrome; CI = confidence interval; ICU = intensive care unit; LTV = low tidal volume; NR = not reported; NS = not significant; OR = odds ratio; PCV = pressure control ventilation; P-SIMV+PS = Pressure controlled Synchronized Intermittent Mandatory Ventilation + Pressure Support; RCT = randomized controlled trial; RR = relative risk; SIMV = synchronized intermittent mandatory ventilation; SR = systematic review; VC = volume control.
Table 10: Summary of Findings by Outcome — Oxygenation
Study citation and study design | Intervention used in control group | Method of measurement | APRV | Control | Comparison (95% CI) | Notes | P value |
|---|---|---|---|---|---|---|---|
Patients with ARDS | |||||||
Oxygenation (PaO2/FiO2) | |||||||
Chen et al. (2021)14 SR (1 RCT, Song et al. 2016) | SIMV | Mean (SD) | 240.3 (66.82) | 288.83 (85.25) | Mean difference = −48.53 (−112.10, 15.04) | Mean difference > 0 favours APRV | NS |
Chen et al. (2021)14 SR (1 RCT, Ota et al. 2009) | SIMV | Mean (SD) | 255.2 (70.7) | 180.5 (65.2) | Mean difference = 74.70 (35.49 to 113.91) | Mean difference > 0 favours APRV | Significant |
Chen et al. (2021)14 SR (1 RCT, Varpula et al. 2004) | SIMV | Mean (SD) | 150 (55) | 164.4 (10.5) | Mean difference = −14.40 (−34.46 to 5.66) | Mean difference > 0 favours APRV | NS |
Sun et al. (2020)15 SR (1 retrospective study, Liu et al. 2009) | SIMV | NA | NR | NR | NR | Oxygenation increased in patients with severe ARDS treated with APRV | NR |
Sun et al. (2020)15 SR (1 single-arm retrospective study, Dart et al. 2005) | NA | NA | NR | NA | NA | APRV significantly improved oxygenation | NR |
Oxygenation index (PaO2/FiO2) on day 3 | |||||||
Zhong et al. (2020)16 SR (1 RCT, Hirshberg et al. 2018) | LTV (VC) | Mean (SD) | 172 (98) | 162 (34) | Mean difference = 10.00 (−39.66 to 59.66) | Mean difference > 0 favours APRV | NS |
Zhong et al. (2020)16 SR (1 RCT, Zhou XZ et al. 2017) | LTV (SIMV) | Mean (SD) | 210.81 (32.01) | 181.02 (27.81) | Mean difference = 29.79 (14.62 to 44.96) | Mean difference > 0 favours APRV | Significant |
APRV = airway pressure release ventilation; ARDS = acute respiratory distress syndrome; CI = confidence interval; ICU = intensive care unit; LTV = low tidal volume; NA = not applicable; NR = not reported; NS = not significant; PaO2/FiO2 = partial pressure of oxygen/ fraction of inspired oxygen; RCT = randomized controlled trial; SD = standard deviation; SIMV = synchronized intermittent mandatory ventilation; SR = systematic review; VC = volume control.
Table 11: Summary of Findings by Outcome — Ventilator-Free Days
Study citation and study design | Intervention used in control group | Method of measurement | APRV | Control | Comparison (95% CI) | Notes | P value |
|---|---|---|---|---|---|---|---|
Patients with ARDS | |||||||
Ventilator-free days by day 28 | |||||||
Zhong et al. (2020)16 SR (1 RCT, Hirshberg et al. 2018) | LTV (VC) | Mean (SD) | 15.33 (19.31) | 6 (14.55) | Mean difference = 9.33 (−1.96 to 20.62) | Mean difference > 0 favours APRV | NS |
Zhong et al. (2020)16 SR (1 RCT, Zhou XZ et al. 2017) | LTV (SIMV) | Mean (SD) | 19.08 (5.08) | 14.76 (4.31) | Mean difference = 4.32 (1.94 to 6.70) | Mean difference > 0 favours APRV | Significant |
Zhong et al. (2020)16 SR (1 RCT, Varpula et al. 2004) | LTV (SIMV) | Mean (SD) | 13.4 (1.7) | 12.2 (1.5) | Mean difference = 1.20 (0.38 to 2.02) | Mean difference > 0 favours APRV | Significant |
Zhong et al. (2020)16 SR (1 RCT, Putensen et al. 2001) | LTV (PCV) | Mean (SD) | 13 (7.75) | 7 (7.75) | Mean difference = 6.00 (0.45 to 11.55) | Mean difference > 0 favours APRV | Significant |
Ibarra-Estrada et al. (2022)17 RCT | LTV | Median (IQR) | 3.7 (0 to 15) | 5.2 (0 to 19) | NR | — | 0.28 |
APRV = airway pressure release ventilation; ARDS = acute respiratory distress syndrome; CI = confidence interval; IQR = interquartile range; LTV = low tidal volume; NA = not applicable; NR = not reported; NS = not significant; PCV = pressure control ventilation; RCT = randomized controlled trial; SD = standard deviation; SIMV = synchronized intermittent mandatory ventilation; SR = systematic review; VC = volume control.
Table 12: Summary of Findings by Outcome — Mean Arterial Pressure
Study citation and study design | Intervention used in control group | Method of measurement | APRV | Control | Comparison (95% CI) | Notes | P value |
|---|---|---|---|---|---|---|---|
Patients with ARDS | |||||||
Mean arterial pressure (mmHg) | |||||||
Chen et al. (2021)14 SR (1 RCT, Song et al. 2016) | SIMV | Mean (SD) | 89.9 (19.4) | 90.7 (9.75) | Mean difference = −0.80 (−14.03 to 12.43) | Mean difference > 0 favours APRV | NS |
Chen et al. (2021)14 SR (1 RCT, Varpula et al. 2004) | SIMV | Mean (SD) | 86 (2.65) | 84 (2.71) | Mean difference = 2.00 (0.62 to 3.38) | Mean difference > 0 favours APRV | Significant |
Mean arterial pressure (mmHg) on day 3 | |||||||
Zhong et al. (2020)16 SR (1 RCT, Zhou XZ et al. 2017) | LTV (SIMV) | Mean (SD) | 87.01 (7.14) | 82.12 (6.51) | Mean difference = 4.89 (1.43 to 8.35) | Mean difference > 0 favours APRV | Significant |
Zhong et al. (2020)16 SR (1 RCT, Varpula et al. 2004) | LTV (SIMV) | Mean (SD) | 83 (2.53) | 79 (1.87) | Mean difference = 4.00 (2.83 to 5.17) | Mean difference > 0 favours APRV | Significant |
APRV = airway pressure release ventilation; ARDS = acute respiratory distress syndrome; CI = confidence interval; ICU = intensive care unit; LTV = low tidal volume; NR = not reported; NS = not significant; PaO2/FiO2 = partial pressure of oxygen/ fraction of inspired oxygen; RCT = randomized controlled trial; SD = standard deviation; SIMV = synchronized intermittent mandatory ventilation; SR = systematic review.
Table 13: Summary of Findings by Outcome — Additional Clinical Outcomes
Study citation and study design Subgroup | Intervention used in control group | Method of measurement | APRV | Control | P value |
|---|---|---|---|---|---|
Patients with ARDS | |||||
Days of mechanical ventilation | |||||
Sun et al. (2020)15 SR (1 RCT, Maxwell et al. 2010) | LTV | Mean (SD) | 10.49 (7.23) | 8 (4.01) | NR |
Sun et al. (2020)15 SR (1 retrospective study, Gonzalez et al. 2010) | A/C | Median (range) | 3 (2 to 5) | 3 (2 to 7) | NR |
Sun et al. (2020)15 SR (1 retrospective study, Liu et al. 2009) | SIMV | Mean (SD) | 27 (39) | 23 (20) | NR |
Sun et al. (2020)15 SR (1 RCT, Varpula et al. 2004) | SIMV | Mean (SD) | 13.4 (1.7) | 12.2 (1.5) | NR |
Sun et al. (2020)15 SR (1 RCT, Putensen et al. 2001) | PCV | Mean (SD) | 15 (2) | 21 (2) | NR |
Ibarra-Estrada et al. (2022)17 RCT | LTV | Median (IQR) | 9 (6 to 14) | 10 (8 to 15) | 0.28 |
Extubation | |||||
Ibarra-Estrada et al. (2022)17 RCT | LTV | Number of events (%) | 13 (29) | 20 (44) | 0.12 |
Patients at risk of ARDS | |||||
Incidence of ARDS | |||||
Küçük et al. (2022)18 RCT | — | — | — | — | — |
Overall | P-SIMV+PS | Number of events (%) | 1 (3.1) | 5 (15.2) | 0.197 |
Length of hospital stay (days) | |||||
Küçük et al. (2022)18 RCT | — | — | — | — |
|
Surviving patients | P-SIMV+PS | Median (min-max) | 25.5 (8 to 79) | 33 (17 to 85) | 0.297 |
Sedation requirement | |||||
Küçük et al. (2022)18 RCT | — | — | — | — | — |
Overall | P-SIMV+PS | Number of patients (%) | 23 (71.9) | 30 (91.0) | 0.061 |
Surviving patients | P-SIMV+PS | Total/day – median (min-max) | 3 (1 to 18) | 6.5 (2 to 65) | 0.170 |
Vasopressor/inotrope requirement | |||||
Küçük et al. (2022)18 RCT | — | — | — | — | — |
Overall | P-SIMV+PS | Number of patients (%) | 23 (71.9) | 23 (69.7) | 1.0 |
Surviving patients | P-SIMV+PS | Total/day – median (min-max) | 6.5 (1 to 14) | 2 (1 to 15) | 0.093 |
Extubation | |||||
Küçük et al. (2022)18 RCT | — | — | — | — | — |
Overall | P-SIMV+PS | Number of patients (%) | 17 (53.1) | 19 (57.6) | 0.911 |
APRV = airway pressure release ventilation; ARDS = acute respiratory distress syndrome; CI = confidence interval; IQR = interquartile range; LTV = low tidal volume; P-SIMV+PS = Pressure controlled Synchronized Intermittent Mandatory Ventilation + Pressure Support; RCT = randomized controlled trial; SD = standard deviation.
Table 14: Summary of Findings by Outcome — Additional Safety Outcomes
Study citation and study design Subgroup | Intervention used in control group | Method of measurement | APRV | Control | P value |
|---|---|---|---|---|---|
Patients with ARDS | |||||
Tracheostomy | |||||
Sun et al. (2020)15 SR (1 RCT, Maxwell et al. 2010) | LTV | Number of events (%) | 19 (NR) | 21 (NR) | NR |
Sun et al. (2020)15 SR (1 retrospective study, Gonzalez et al. 2010) | A/C | Number of events (%) | 46 (NR) | 105 (NR) | NR |
Ibarra-Estrada et al. (2022)17 RCT | LTV | Number of events (%) | 9 (20) | 15 (33) | 0.15 |
Barotrauma | |||||
Ibarra-Estrada et al. (2022)17 RCT | LTV | Number of events (%) | 4 (9) | 4 (9) | 1.0 |
Severe hypercapnia | |||||
Ibarra-Estrada et al. (2022)17 RCT | LTV | Number of events (%) | 19 (42) | 7 (15) | 0.009 |
Deep vein thrombosis | |||||
Ibarra-Estrada et al. (2022)17 RCT | LTV | Number of events (%) | 6 (13) | 4 (9) | 0.73 |
Patients at risk of ARDS | |||||
Tracheostomy | |||||
Küçük et al. (2022)18 RCT | — | — | — | — | — |
Overall | P-SIMV+PS | Number of events (%) | 2 (6.3) | 5 (15.2) | 0.427 |
A/C = assist-control ventilation; APRV = airway pressure release ventilation; ARDS = acute respiratory distress syndrome; LTV = low tidal volume; NR = not reported; P-SIMV+PS = Pressure controlled Synchronized Intermittent Mandatory Ventilation + Pressure Support; RCT = randomized controlled trial.
Table 15: Summary of Recommendations in Included Guideline
Recommendations and supporting evidence | Quality of evidence and strength of recommendation |
|---|---|
German Society for Anesthesiology and Intensive Care Medicine (2019)19 | |
Recommendation: “Weighing the potential clinical benefits and the lack of evidence for relevant harm, we suggest to consider the use of pressure-controlled ventilation with the possibility of spontaneous breathing in the inspiratory and expiratory phases in patients without severe ARDS. Further, the individual patients’ particular medical conditions (e.g., increased ICP) should be considered as contraindication for spontaneous breathing. (p. 363)”19 Supporting evidence: Recommendation was informed by small randomized and observational studies in heterogeneous patient cohorts. Some observed benefits of minute volume-assisted ventilation modes enabling spontaneous breathing observed in the studies included a reduced need for sedation with fewer hemodynamic side effects, less delirium and cognitive dysfunction, and earlier mobilization to counteract muscular inactivity atrophy. | Quality of evidence: Low (“Higher-quality studies are likely to influence the confidence of the guideline group in the estimated effect or to change the estimate [p. 360]”)19 Strength of recommendation: Weak (“Weak confidence in the relation between desired and undesired effects or weak predominance of benefits or risks [p. 360]”)19 |
ARDS = acute respiratory distress syndrome; ICP = intracranial pressure.
Appendix 5: Overlap Between Included Systematic Reviews
Note that this appendix has not been copy-edited.
Table 16: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Chen et al. (2021)14 | Sun et al. (2020)15 | Zhong et al. (2020)16 |
|---|---|---|---|
Varpula T, et al. Acta Anaesthesiol Scand. 2004;48:722 to 31. | Yes | Yes | Yes |
Varpula T, et al. Acta Anaesthesiol Scand. 2003;47:516 to 24. | Yes | Yes | — |
Song S, et al. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2016;28:15 to 21. | Yes | — | — |
Ota K, et al. Crit Care Med. 2009;37:A190. | Yes | — | — |
Hirshberg EL, et al. Crit Care Med. 2018;46:1943 to 52. | — | Yes | Yes |
Putensen C, et al. Am J Respir Crit Care Med. 2001;164:43 to 9. | — | Yes | Yes |
Gonzalez M, et al. Intensive Care Med. 2010;36:817 to 27. | — | Yes | — |
Maxwell RA, et al. J Trauma. 2010;69:501 to 10. discussion 511. | — | Yes | — |
Liu L, et al. Hiroshima J Med Sci. 2009;58:83 to 8. | — | Yes | — |
Dart BW, et al. J Trauma. 2005;59:71 to 6. | — | Yes | — |
Zhou XZ. Chin J Lung Dis. 2017;10:431 to 5. | — | — | Yes |
Yes = indicates the primary study was included within the systematic review.
— = indicates the primary study was not included within the systematic review.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca