CADTH Health Technology Review
Therapeutic Support for Pressure Injuries
Rapid Review
Authors: Thyna Vu, Nicole Askin
Abbreviations
AMSTAR 2
A MeaSurement Tool to Assess systematic Reviews 2
EQ-5D-5L
EuroQol 5-Dimensions 5-Levels
HR
Hazard ratio
ICU
Intensive care unit
ITT
Intention-to-treat
LTC
Long-term care
NMA
Network meta-analysis
PU-QoL-UI
Pressure Ulcer Quality of Life Utility Instrument
PUSH
Pressure ulcer scale for healing
RCT
Randomized controlled trial
RoB
Risk of bias
RR
Risk ratio
SR
Systematic review
Key Messages
Reactive air surfaces, alternating-pressure (active) air surfaces, and reactive gel surfaces may be more effective at preventing pressure injuries compared to foam surfaces. The clinical effectiveness of therapeutic support surfaces to prevent pressure injuries may be influenced by the care setting (e.g., long-term care, acute care, intensive care units) as well as follow-up time.
An overview of reviews with a network meta-analysis did not find any significant differences between different types of support surfaces on time to pressure injury. However, limited evidence suggests there may be a difference between foam surfaces, compared to other types of foam surfaces.
Specialized skin protection cushions may also help to prevent pressure injuries compared to standard foam cushions, though there may be no difference between different types of air cushions.
It was unclear if there are significant differences between support surfaces for the treatment of pressure injuries. Authors of an overview of reviews stated that reactive air surfaces may be more effective than foam surfaces, but this was not statistically significant.
Limited evidence was identified regarding adverse events and health-related quality of life, as well as for pediatric patients.
Limited evidence was identified for support surfaces other than mattresses, beds, and overlays (e.g., cushions), as well as therapeutic small devices for prevention of pressure injuries. No studies were identified for therapeutic small devices for treatment.
Context and Policy Issues
Pressure injuries (also referred to as pressure ulcers, pressure sores, decubitus ulcers, or bed sores) are wounds to the skin and underlying tissue caused by rubbing (friction) or prolonged pressure.1 People with mobility problems or who lie in bed for long periods of time (e.g., following a surgical procedure) are at risk of developing pressure injuries.1 Comorbidities that can affect the skin or ability to heal can also increase risk of developing pressure injuries, including diabetes, cardiovascular disease, renal disease, and immunosuppression.2 Pressure injuries are painful and can lead to the development of serious infections including sepsis; they are also associated with lower health-related quality of life, longer length of stay in hospital, and greater risk of mortality.3,4 Systematic reviews have estimated the prevalence of pressure injuries to be 0.56 to 230 per 1,000 in the community or general population,5 and 128 per 1,000 for hospitalized adults.6 Canadian studies assessing various settings, including acute care, long-term care (LTC), home, tertiary care, and complex continuing care, have estimated the prevalence to be 128 to 292 per 1,000, and some have reported higher prevalence in LTC and complex continuing care facilities, compared to acute care or home settings.7
Interventions that are used to prevent or treat pressure injuries include support surfaces (specific types of beds or bed systems, overlays, and mattresses), as well as therapeutic small devices.1 Both support surfaces and therapeutic small devices are designed to relieve or redistribute pressure on the body, increasing blood flow to the tissues and relieve distortion of the skin and soft tissue and thus prevent or treat pressure injuries.1,8 There are many types of support surfaces with different features. For example, support surfaces may be powered (i.e., operate with electricity) or not, or made of different materials (e.g., air cells, foam materials, gel materials), or designed to improve the skin microclimate.1 Examples of therapeutic small devices include total contact casting, which uses a cast to support the foot and lower leg, redistributing pressure over the sole of the foot and reducing pressure; and cast walkers, which hold the ankle at a 90-degree angle, also reducing pressure on the forefoot.8 Another type of therapeutic small device is purpose-designed positioning devices, which assist with body positioning and thus redistribute pressure.9
Understanding what interventions are effective at preventing and treating pressure injuries will help health care providers understand best practices and improve patient outcomes. Thus, this report aims to summarize the clinical effectiveness of therapeutic support surfaces and therapeutic small devices for patients who have developed or are at risk of developing a pressure injury.
Research Questions
What is the clinical effectiveness of using therapeutic support surfaces for patients who have developed a pressure injury or are at risk of developing a pressure injury?
What is the clinical effectiveness of using therapeutic small devices for patients who have developed a pressure injury or are at risk of developing a pressure injury?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, Cochrane Library, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were pressure injuries and therapeutic support surfaces/devices. Search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses or network meta-analyses, randomized controlled trials, controlled clinical trials, and non-randomized studies. Comments, newspaper articles, editorials, and letters were excluded. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2017, and July 18, 2022.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Q1, Q2: Patients (of any age) who have developed a pressure injury or are at risk of developing a pressure injury |
Intervention | Q1: Therapeutic support surfaces Q2: Therapeutic small devices |
Comparator | Q1: Alternative surfaces; no treatment Q2: Standard of care; no treatment |
Outcomes | Q1, Q2: Clinical effectiveness (e.g., injury prevention, injury relief, length of time to heal, patient quality of life, hospitalizations, hospital length of stay, safety, adverse events) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2020. Studies that focused on bundled interventions or intraoperative interventions were excluded. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded. Primary studies retrieved by the search were excluded if they were captured in at least 1 included overview and/or systematic review.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)10 for systematic reviews, the “Questionnaire to assess the relevance and credibility of a network meta-analysis”11 for network meta-analyses, and the Downs and Black checklist12 for randomized and non-randomized studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
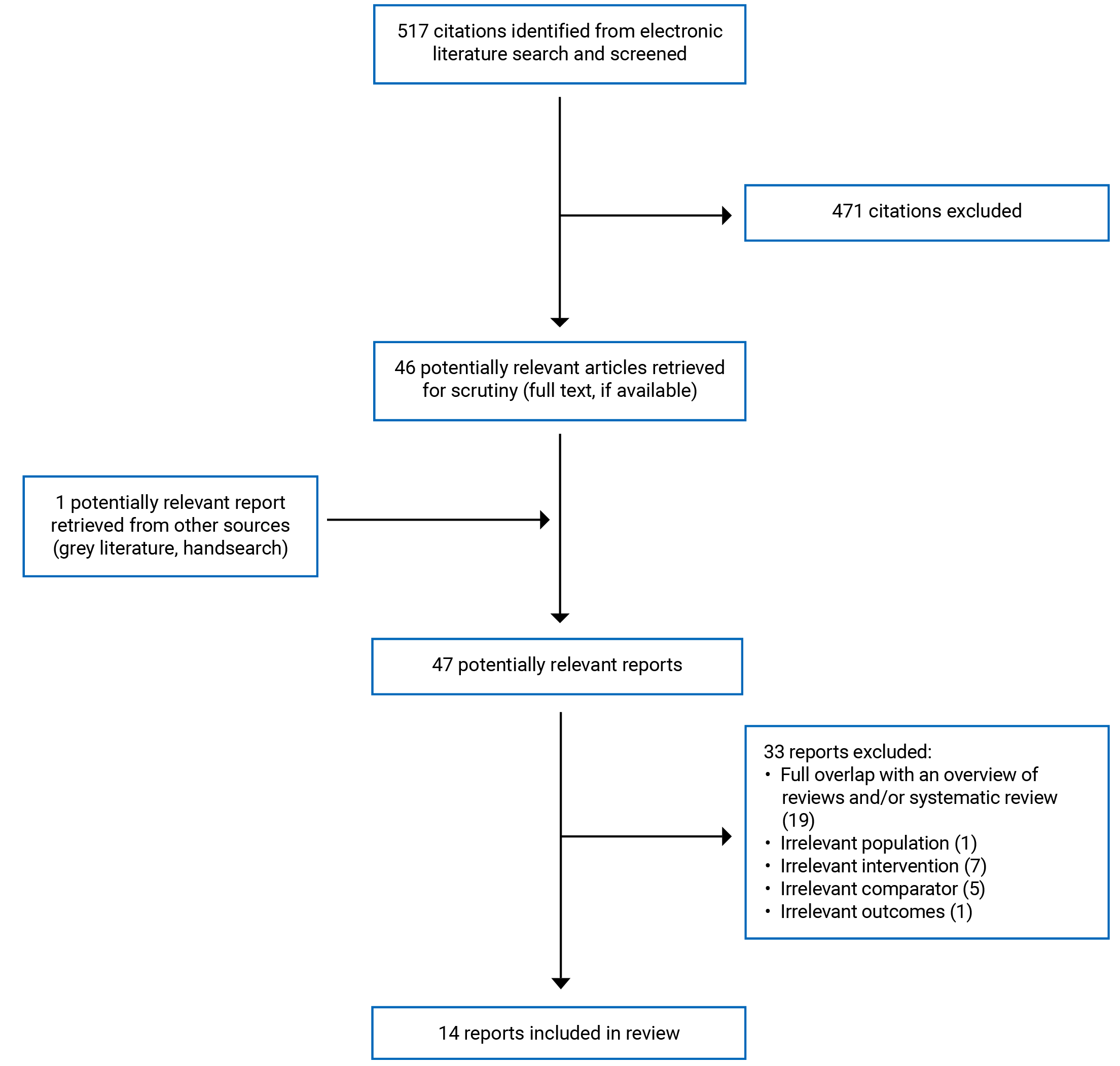
A total of 517 citations were identified in the literature search. Following screening of titles and abstracts, 471 citations were excluded and 46 potentially relevant reports from the electronic search were retrieved for full-text review. One potentially relevant publication was retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 33 publications were excluded for various reasons, and 14 publications met the inclusion criteria and were included in this report. These comprised 1 overview of reviews, 5 systematic reviews (SRs), 2 randomized controlled trials (RCTs), and 6 non-randomized studies. Appendix 1 presents the PRISMA13 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 6.
Summary of Study Characteristics
One overview of reviews with a network meta-analysis (NMA),1 5 SRs14-18 including 2 with meta-analyses,16,18 2 RCTs,19,20 and 6 non-randomized studies21-26 were included in this report.
Three SRs15,16,18 had broader inclusion criteria than this report: 2 SRs16,18 included a range of interventions to prevent pressure injuries other than therapeutic support surfaces or therapeutic small devices, while 1 SR15 included studies that reported on alternative outcomes (e.g., measures of pressure relief using pressure mapping). Only the subset of relevant studies will be described in this report. The overview of reviews1 and 1 SR14 focused on support surfaces (beds, overlays, and mattresses), 1 SR15 focused on wheelchair pressure-relieving cushions, and 1 SR17 focused on pressure-redistributing static chairs. The SR of pressure-redistributing static chairs did not identify any relevant primary studies.17
Additional details regarding the characteristics of included publications are provided in Appendix 2. There was some overlap of studies included in the overview of reviews and SRs, and the degree of overlap is summarized in Appendix 5.
Study Design
This report includes 1 overview of reviews with an NMA,1 5 SRs14-18 (2 with meta-analyses16,18), 2 RCTs,19,20 and 6 non-randomized studies.21-26 There was some overlap of studies included in the overview of reviews and SRs, and the degree of overlap is summarized in Appendix 5.
The overview of reviews1 did not state their search range, but was published in August 2021 and included Cochrane reviews published up to 2021. The reviews were eligible if they only included RCTs. They identified a total of 69 RCTs, and conducted NMAs for 3 outcomes using a Frequentist approach and random-effects model. They also presented the direct pairwise comparisons where available. For the 3 outcomes, the number of RCTs included in each network and number of network contrasts were:
prevention — pressure injury incidence: 40 RCTs, with 78 network contrasts
prevention — time to pressure injury development: 10 RCTs, with 15 network contrasts
treatment — proportion of patients with completely healed pressure injuries: 4 RCTs, with 6 network contrasts.
One SR17 searched until June 2021, and 2 SRs16,18 reported their search was updated to the end of 2019. The remaining 2 SRs14,15 did not report the date ranges covered by their searches or when they conducted their searches. Three SRs16-18 were restricted to RCTs only, while 2 SRs14,15 included RCTs and non-randomized studies. Two SRs16,18 had broader inclusion criteria than this report: 1 SR had 8 relevant RCTs,16 and the other SR had 29 relevant RCTs.18
The 2 RCTs were published in 202219 and 2020,20 and the non-randomized studies were published in 202121,22 and 2020.23-26 Within the non-randomized studies, study designs included cross-sectional,21 before-after cohort,22,25 retrospective observational cohort using health administrative data,23 prospective observational cohort,24 and prospective observational cohort with a historical control.26 When reported, follow-up times varied across studies, and ranged from 3 days to 18 months.
Country of Origin
The first author of the overview of reviews was from the UK,1 and the first authors of the SRs were from Australia,16,18 Indonesia,14 the UK,17 and the US.15 The primary studies included in these reviews came from Australia, Belgium, Brazil, Canada, China, Denmark, Finland, France, Germany, Iran, Italy, Japan, Netherlands, South Korea, Sweden, Turkey, the UK, and the US.1,16,18
The RCTs were conducted in and enrolled patients from Australia19 and China,20 and the non-randomized studies were conducted in and enrolled patients from Belgium,22 Denmark,25 Finland,23 Taiwan,24 the UK,21 and the US.26
Patient Population
Most included studies were restricted to adults. One non-randomized study21 focused on children. Another non-randomized study24 did not explicitly restrict to adults or report the age range, but reported a mean age of over 60 years.
The overview of reviews1 and 1 SR17 did not restrict by setting, including acute care and other hospital settings, LTC settings, and intensive care units (ICUs). This SR17 also focused on patients who remained seated for extended periods of time. Two SRs,14,16 1 RCT,19 and 2 non-randomized studies23,24 focused on patients in the ICU. One SR18 and 2 non-randomized studies21,25 focused on patients in acute hospital settings. Two non-randomized studies22,26 focused on nursing home or LTC residents.
Interventions and Comparators
Two SRs16,18 included a broader range of interventions, assessing multiple types of interventions to prevent pressure injuries; only the results from interventions relevant to this report are presented and discussed.
The overview of reviews,1 3 SRs,14,16,18 and 6 non-randomized studies21-26 assessed therapeutic support surfaces, specifically beds, mattresses, and/or overlays, comparing to other support surfaces. One SR15 compared wheelchair pressure-relieving cushions to other types of cushions, and another SR17 compared any type of pressure-redistributing static chair to any comparator. One RCT20 compared a special postoperative cushion to standard of care (conventional sponge pads). Two SRs16,18 and 1 RCT19 assessed heel protection devices (e.g., heel-offloading boots) compared to standard care (pillow, standard pressure-redistributing surface, or defined as “per admitting ward”) or an alternative protection device.
Most included studies assessed the interventions for prevention. The overview of reviews1 also assessed these interventions for treatment of pressure injuries. One non-randomized study22 had assessed a therapeutic support surface in 2 groups (1 group for prevention, the other group for treatment), but did not have a comparator group for the prevention group; thus, only the results for the treatment group are summarized in this report.
Outcomes
For preventive interventions, relevant reported outcomes from the overview of reviews and SRs included incidence of pressure injury,1,14-18 time to pressure injury development,1 health-related quality of life,1,17 and adverse events.1,17 Health-related quality of life was measured using the 100-point visual analogue scale, EuroQol 5-Dimensions 5-Levels (EQ-5D-5L) questionnaire, or Pressure Ulcer Quality of Life Utility Instrument (PU-QoL-UI). From the primary clinical studies, similar outcomes were reported, including incidence of pressure injury,19,20,23-26 time to pressure injury development,19,23 pressure damage,21 severity of pressure injuries that developed,19 and adverse events.20
For treatment interventions, relevant reported outcomes from the overview of reviews included proportion of patients with completely healed pressure injuries, time to completely healed pressure injuries, and adverse events.1 One non-randomized study assessed changes in pressure injury state based on the Pressure Ulcer Scale for Healing (PUSH) tool.22
Summary of Critical Appraisal
An overview of the critical appraisal of the included publications is summarized in the following text. Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Overview of Reviews
In the overview of reviews with NMA,1 the protocol was published before the review, the inclusion criteria were clearly defined, the selection of reviews was described and presented in a flow chart, a list of included primary studies was provided, and characteristics of the included studies were described. The authors of the overview of reviews conducted study selection and risk of bias (RoB) assessment of the reviews independently, incorporated RoB assessment into the analysis, and declared their funding and potential conflicts of interest. They also reported the RoB assessments of the RCTs done by the Cochrane reviews’ authors. RCTs that had been excluded from the Cochrane reviews were re-screened to assess if any could contribute data to the NMA, and 1 additional RCT was added. As this RCT had not undergone RoB assessment previously, the overview of review’s authors assessed its RoB and used the Cochrane risk of bias tool. The authors did not provide a justification for why only Cochrane reviews were eligible. As this overview focused only on Cochrane reviews, other SRs were excluded, so it is possible some relevant primary studies were not included. Data extraction was conducted by 1 review author and checked by a second author, and it is not clear if they checked agreement or calculated a kappa score; thus, the potential for errors in data extraction is unclear.
For the NMAs, a rationale was provided for their choice of model (Frequentist approach with random-effects model), as the authors stated they assumed there is an average effect size for a range of similar populations. Indirect evidence was obtained from comparisons of treatments with a common comparator. Issues related to units of analysis, missing data, and transitivity assumptions were addressed, and if heterogeneity was identified, the certainty of evidence was downgraded. The NMAs included RCTs at unclear or high RoB, with a wide range of follow-up durations and multiple types of care settings. Pre-planned subgroup analyses based on 4 characteristics (RoB, care setting, baseline skin status, and follow-up duration) were done if a network had substantial heterogeneity (using the I2 measure, with P < 0.10 indicating heterogeneity due to the χ2 test’s low power) and if there were sufficient studies. For pressure injury incidence, subgroup analyses indicated that care setting and follow-up time may be contributing to heterogeneity. For time to pressure injury, there was substantial heterogeneity, but the prespecified subgroup analysis could not be done due to few studies; therefore, it is unclear what factors were driving the heterogeneity for this outcome. The authors reported no heterogeneity for proportion of patients with completely healed pressure injuries.
Sensitivity analyses were conducted to assess the impact of missing data for 2 outcomes (incidence of pressure injury and proportion of patients with healed pressure injuries), which did not substantially change the results. This analysis was not done for time to healing, which authors stated was due to the nature of the outcome. Primary studies were extracted from the included reviews; thus, there was no over-representation of primary studies. For all 3 outcomes, network estimates and direct pairwise estimates were provided, and network diagrams were also presented. Funnel plots were also presented and did not indicate publication bias for any outcome. Authors may have overstated some findings, including stating that specific interventions may lead to improved outcomes when the network contrast was not statistically significant.
Systematic Reviews
One SR15 reported some details in supplementary materials that could not be accessed at the time of writing this report, including the PRISMA flow chart and descriptions of included studies; therefore, it was not possible to critically appraise these parts of the review. Another SR17 did not have any included studies; a critical appraisal of its planned methods is summarized in the following text.
All 5 included SRs14-18 had clearly defined research questions and inclusion criteria, and searched multiple databases. Four SRs14,16-18 stated that 2 review authors determined study inclusion (1 SR14 specified that title-abstract screening was done by 1 author), and that they searched reference lists of the studies that were included after screening. Data extraction was done by 2 authors in 2 SRs,16,18 and by 1 author in 1 SR.14 Four SRs14,16-18 stated they used or planned to use the Cochrane risk of bias assessment tool for RoB assessment, with 1 SR14 stating they also used the Oxford Centre for Evidence-Based Medicine guidelines to assess quality; 3 SRs16-18 stated RoB assessment was done by 2 authors. One SR15 did not provide details about how many authors conducted screening or data extraction, or about how RoB analysis was done. Three SRs that identified relevant studies14,16,18 did not provide details about the included patients (e.g., mean age, proportion of male or female patients); for 1 SR,15 it is unclear if these characteristics are reported in detail in their supplementary materials.
Four SRs15-18 stated their conflicts of interest, and 3 SRs16-18 stated the funding received for the review. Four SRs14,16-18 stated their protocol was published in advance. None of the reviews explained their selection of study designs, with 3 SRs16-18 limited to only RCTs. None of the reviews indicated that they had searched grey literature or contacted experts in the field.
Two SRs16,18 conducted meta-analyses if there were at least 2 sufficiently similar primary studies. One SR18 defined this as studies with the same intervention type and were similar with respect to population, intervention, comparator, outcome, and setting; the other SR16 did not define “sufficiently similar,” although both SRs share the same first author and thus may have used the same definition. Both included only RCTs and specified that they used random-effects models. For both SRs,16,18 all relevant primary studies were at unclear or high RoB, with moderate to substantial heterogeneity; both also could not assess publication bias due to the limited number of studies. The heterogeneity may have been due to several factors, such as the small number of studies, small sample sizes, differences between interventions, and inclusion of studies at high or unclear RoB.
Randomized Controlled Trials
Both RCTs19,20 clearly described their objective, outcomes, patient inclusion criteria, and interventions of interest; both recruited patients for both groups from the same population over the same time period and used appropriate statistical tests. Both also declared their funding source and if there were potential conflicts of interest. One RCT19 clearly described their main findings including the 95% confidence intervals, conducted a sample size calculation, and specified that they used the intention-to-treat (ITT) principle. For the other RCT,20 the outcome of interest for this report was not reported in detail, and it is not reported if they conducted a sample size calculation or used the ITT approach. One RCT19 reported that approximately 10% of the recruited patients were lost to follow-up for both the intervention and control groups, which may have introduced attrition bias. The other RCT20 did not report that any patients were lost to follow-up.
One RCT19 reported that they blinded the statistician who conducted the data analysis; this was not reported by the other RCT.20 It is likely that due to the nature of the intervention, the patients and most research staff could not have been blinded to group assignment. Lack of blinding has the potential to introduce detection and/or performance biases; however, the study that did not report any blinding only assessed objective outcomes.
Non-Randomized Studies
The objective, main outcomes, and interventions were clearly described by all 6 non-randomized studies.21-26 Five studies21-24,26 described the characteristics of the included patients. Four studies23-26 reported their outcomes in detail, including the 95% confidence interval and/or exact P values. It is unclear from all 6 studies21-26 if all adverse events that occurred were reported. Due to lack of randomization, it is possible the findings from these studies may be biased due to confounding. Only 1 study24 incorporated some potential confounding variables into their adjusted regression model; the other studies did not provide any lists of potential confounders. Three studies21-23 reported both their funding and potential conflicts of interest; 1 study24 reported their funding source but not potential conflicts of interest, while 2 studies25,26 did not report their funding or conflicts of interest.
Summary of Findings
Clinical Effectiveness of Therapeutic Support Surfaces
One overview of reviews with an NMA,1 3 SRs14,16,18 (2 with meta-analyses16,18), and 5 non-randomized studies21,23-26 were identified regarding the clinical effectiveness of beds, mattresses, and/or overlays to prevent pressure injuries, while 2 SRs15,16 and 1 RCT20 reported on cushions or chairs to prevent pressure injuries. Additional details are available in Appendix 4 by outcome: pressure injury incidence (Table 6), time to pressure injury (Table 7), adverse events (Table 8), and health-related quality of life (Table 9).
Prevention With Therapeutic Support Surfaces — Beds, Mattresses, and Overlays
As the overview of reviews with an NMA1 reported on many comparisons (27 direct comparisons and 78 network contrasts), this summary focuses on key comparisons as reported by the overview’s authors. Key comparisons were defined as comparisons between support surfaces that the authors stated are likely widely used: alternating-pressure (active) air surfaces, reactive air surfaces, foam surfaces, reactive sheepskin surfaces, and reactive gel surfaces. The NMA’s network comparisons found that reactive air surfaces, alternating-pressure (active) air surfaces, and reactive gel surfaces may reduce pressure injury incidence compared to foam surfaces. However, it is unclear if there is a significant difference between other key comparisons. All NMA findings agreed with the results of corresponding pairwise direct analyses where available. The authors also reported that alternating-pressure (active) air surfaces, reactive water surfaces, and reactive sheepskin surfaces may reduce risk compared to standard hospital surfaces, but noted these findings should be interpreted with caution, as what is considered “standard” may vary between studies.
Three SRs14,16 (2 with meta-analyses16,18) had considerable overlap of included primary studies with the overview of reviews, but focused separately on the ICU14,16 and acute care settings,18 while the overview of reviews’ NMA1 pooled studies from various settings. Thus, the results of these SRs are presented, as they may indicate differences between settings. The SR with meta-analysis of acute care patients18 included 24 RCTs for support surfaces, and 23 overlapped with the overview of reviews. The authors conducted meta-analyses for 3 types of support surfaces (active, reactive, and sheepskin) and reported that with ITT analyses, only sheepskin was associated with a significantly lower risk of pressure injury compared to standard care (a standard hospital mattress, with or without additional reactive surfaces). Subgroup meta-analyses did not find a significant difference between active and reactive support surfaces; compared to standard mattresses, active surfaces were found to be better, and reactive surfaces may also be better with borderline significance based on per-protocol analyses, but ITT analyses were not significant.18 The SR with meta-analysis of ICU patients16 included 5 RCTs assessing support mattresses; all were also included in the overview of reviews.1 They reported that for ICU patients, there was no statistically significant difference between 2 types of active support surfaces based on 1 RCT (a mattress with optional pulsation and low air loss features, compared to a continuous/alternating low-pressure control mattress), or between 2 types of reactive surfaces based on 1 RCT (2 viscoelastic foam mattresses); 2 RCTs reported lower pressure injury incidences for reactive surfaces compared to standard mattresses, but the pooled risk ratio (RR) was not statistically significant. Another SR14 also assessed support surfaces for adult ICU patients, including RCTs and non-randomized studies; as all the RCTs were included in the overview1 and/or the previously-described SR,16 only the results from the 4 non-randomized studies are summarized. Significantly fewer pressure injuries were found when alternating-pressure air mattresses were used compared to foam mattresses, and with low air loss mattresses compared to air pressure mattresses. No significant difference was found between viscoelastic foam mattresses versus air pressure mattresses, or alternating-pressure air mattresses versus alternating-pressure air overlays.14
Five non-randomized studies were identified that assessed a variety of interventions and comparators. Two studies had similar interventions and comparators, comparing a pressure-redistributing foam mattress24 or pressure-relieving mattresses21 to a non-pressure-relieving foam mattress24 or standard mattress21; an observational cohort24 found the intervention to be associated with reduced pressure injuries, while the cross-sectional study21 did not find a significant difference. Two studies assessed overlays.25,26 One observational study25 assessed the introduction of 2 types of static overlays in a hospital setting. During the implementation period, 123 patients used an overlay and none developed a pressure injury; however, statistical analyses did not find a significant difference in pressure injury incidence between the pre- and post-implementation periods. Another cohort study26 assessed a low-profile alternating-pressure overlay with a non-powered pressure redistribution mattress, which was associated with a significantly fewer pressure injuries when compared to a historical control (no overlay, mattress only). An observational cohort study23 found 1 type of support surface (a non-alternating, dynamic, minimum pressure air mattress system, with a double-cell structure and reactive adjustment technology) was associated with a significantly lower risk of developing pressure injuries compared to 6 other types of support surfaces.
Time to pressure injury development was assessed by the overview of reviews with NMA1 and 1 non-randomized study.24 The overview of reviews’ NMA reported that reactive air surfaces likely reduce hazard of developing pressure injuries compared to foam surfaces, though this network contrast was not statistically significant. All other comparisons with foam surfaces did not provide clear evidence of an effect on pressure injuries. In their summary of reviews, the evidence was unclear as to whether reactive air surfaces differ in the hazard of developing new pressure injuries compared to alternating-pressure (active) air surfaces; the mixed-effects estimate from the NMA had a comparable hazard ratio (HR) to the direct comparison, but with a wider confidence interval that contains HR = 1 due to data sparseness in the network as opposed to the direct evidence which excluded the null. The authors speculated that, for this contrast, the direct comparison may be more reliable. The overview of reviews1 and 1 non-randomized study24 also compared between 2 types of foam mattresses, and both reported there may be significant differences between types of foam mattresses.
The overview of reviews1 assessed adverse events, and identified 5 comparisons. The authors reported that all data offered low or very low certainty evidence due to issues like RoB, imprecision, and/or inconsistency, and it was unclear if there were any differences in adverse event rates between the identified comparisons. They also assessed health-related quality of life and identified 2 comparisons. They reported that there may be little to no difference between reactive sheepskin surfaces and standard hospital surfaces in LTC settings, and it is unclear if there is a difference between alternating-pressure (active) air surfaces and foam surfaces at 90 days in acute care and LTC settings.
Prevention with Therapeutic Support Surfaces — Cushions and Chairs
One SR15 assessed wheelchair pressure-relieving cushions compared to cushions made of different materials, although only 3 primary studies reported clinical outcomes (incidence of pressure injuries). Two studies compared multiple-compartment air cushions to single-compartment air cell cushions, and neither study reported a statistical difference in incidence of pressure injuries between groups. The third RCT15 compared a skin protection cushion (consisting of air, gel, or contoured foam) to a segmented (flat) foam cushion, which review authors reported is standard care. The skin protection cushion was associated with fewer pressure injures under the ischial tuberosities, but there was no significant difference for incidence of pressure injuries under the ischial tuberosities and sacrum. Another SR16 identified 1 RCT that compared tragacanth gel cushions to standard foam cushions for adult patients in the trauma ICU, and measured the days to developing a pressure injury. This study found that the tragacanth gel cushions led to a statistically significant delay in developing of pressure injuries.
One RCT20 compared a special postoperative cushion to conventional sponge pads for patients following a percutaneous nephrolithotomy, and found patients who used the specially designed cushion had a lower incidence of pressure injuries. They were also the only study to report on adverse events for this intervention type, and found that the incidence of renal hemorrhage due to improper postoperative position and rate of tube folding of the renal fistula were lower with the special postoperative cushion. One SR16 with 1 relevant RCT also reported on effect of pressure-redistributing cushions on time to pressure injury development for patients in the ICU. They found that compared to a standard foam cushion, a tragacanth gel cushion was associated with a statistically significant increase in mean days to injury, though the difference was just over 1 day.
One SR17 focused on pressure-redistributing static chairs but did not identify any RCTs that met their criteria, and thus could not provide a summary of whether these chairs can help to prevent or manage pressure injuries.
Treatment With Therapeutic Support Surfaces
The overview of reviews with an NMA1 and 1 non-randomized study22 were identified regarding the clinical effectiveness of support surfaces (beds, mattresses, and/or overlays) to treat pressure injuries. Additional details are available in Appendix 4 by outcome: proportion of patients with fully healed pressure injuries (Table 10), time to pressure injury healing (Table 11), change in skin status (Table 12), and adverse events (Table 13).
The overview of reviews with an NMA1 compared different types of therapeutic support surfaces on the proportion of patients with healed pressure injuries. The authors concluded that more people with pressure injuries may heal completely with a reactive air surface than a foam surface; however, this statement should be interpreted with caution since the network contrast and direct pairwise comparison were not statistically significant. All other comparisons were uncertain. All network contrasts aligned with direct pairwise comparisons where available.
The overview of reviews1 assessed adverse events, and concluded that it is unclear if there are any differences in adverse event rates between any of the identified comparisons.1
One non-randomized before-after study22 assessed the impact of fully automated pulsating support system air mattresses, comparing patients’ skin status as measured by the PUSH tool at baseline and after 30 days. The authors stated that most pressure injuries did not deteriorate and 4 pressure injuries completely epithelialized (healed), though deterioration was also observed.
Clinical Effectiveness of Therapeutic Small Devices
Prevention With Therapeutic Small Devices
Two SRs16,18 and 1 RCT19 reported on the clinical effectiveness of heel protection devices (e.g., heel-offloading boots) on pressure injury incidence. Additional details are available in Appendix 4 by outcome: pressure injury incidence (Table 14) and time to pressure injury development (Table 15).
Three RCTs from the 2 SRs,16,18 as well as an additional RCT,19 compared similar heel protection devices (heel protector, heel-offloading boot, or heel suspension boot) to standard of care or pillows in the ICU or hospital nursing units: all reported significantly lower incidence of pressure injuries in the intervention group. One SR18 also identified 2 additional RCTs. One RCT compared a foot waffle to a hospital pillow: the incidence of pressure injuries was lower in the foot waffle group, but it was not statistically significant. The second RCT compared between a foot waffle, egg crate, and bunny boot, and reported that incidence was comparable across all 3 groups.18
Two RCTs18,19 (1 from a SR18) reported on time to pressure injury development. One RCT18 found no difference between a foot waffle device versus hospital pillow, while the other RCT19 found a lower HR with a heel-offloading boot than standard practice (pillows).
Treatment With Therapeutic Small Devices
No studies were identified that reported on therapeutic small devices for treatment of pressure injuries; therefore, no summary can be provided.
Summary of Findings in LTC Settings
From the identified studies summarized above, the overview of reviews1 and 2 non-randomized studies22,26 provided evidence regarding the clinical effectiveness of therapeutic support surfaces in LTC settings.
The overview of reviews1 and 1 non-randomized study26 assessed therapeutic support surfaces to prevent pressure injuries. The overview of reviews’1 narrative summary reported that for people in LTC settings, therapeutic support surfaces associated with a reduced incidence of pressure injury were:
reactive air surfaces and alternating-pressure (active) air surfaces, compared to foam surfaces
reactive air surfaces, compared to alternating-pressure (active) air surfaces.
One non-randomized study26 reported that using a low-profile alternating-pressure overlay with a pressure-redistributing mattress was associated with significantly lower incidence of pressure injuries, compared to the mattress without the overlay, over an average of 4.5 months. The overview of reviews1 also identified RCTs that assessed health-related quality of life and that included patients in LTC settings. They concluded there may be little to no difference between reactive sheepskin surfaces and standard hospital surfaces, and it is unclear if there is a difference between alternating-pressure (active) air surfaces and foam surfaces at 90 days.
One RCT from the overview of reviews1 and 1 non-randomized study22 assessed therapeutic support surfaces for treatment of pressure injuries. The RCT reported that compared to foam surfaces, people using reactive air surfaces may be more likely to have healed pressure injuries.1 The non-randomized study22 assessed a full automated pulsating support system air mattress and reported that after 30 days, most pressure injuries remained stable, a few improved, and 1 deteriorated.
Limitations
There are several limitations that prevent definitive conclusions regarding the clinical effectiveness of therapeutic support surfaces and therapeutic small devices for the prevention or treatment of pressure injuries.
The overview of reviews1 and SRs14-18 noted many of their included primary studies were at unclear or high RoB. Due to the nature of the intervention, blinding of the patients and most study personnel is not possible. While 1 RCT19 stated they blinded the statistician who conducted the data analysis, it is unclear if similar measures were taken by other studies, which may have resulted in performance or detection bias for subjective outcomes. The sample size was also low for many primary studies included in the overview and/or SRs. Many of the included primary studies from the overview of reviews and SRs were published more than 10 years ago, and it is unclear if their findings are generalizable to newer surfaces and devices, as well as to modern settings.
There was considerable heterogeneity across studies, with different care settings, follow-up durations, and types of interventions being compared. Due to the many types of support surfaces identified, although this report identified a large volume of primary studies, most pairwise comparisons only had 1 to 3 primary studies, and results may have varied due to differences in care setting. The overview of reviews and SRs were not always consistent in how they classified different types of support surfaces; for example, the overview of reviews1 compared 12 types including different types of reactive surfaces (e.g., air, gel) while another SR18 grouped together all reactive support surfaces. Comparisons to standard surfaces may also include a range of surface types, as what is considered standard may vary by place and time.1 Although potential differences between different care settings (acute and ICU) was partially assessed by 2 focused SRs,16,18 these reviews were also based largely on the same RCTs as the overview of reviews and at unclear or high RoB.
Adverse events were reported by the overview of reviews1 and 1 RCT.20 Authors of the overview stated that little is known about differences in adverse event rates between different therapeutic support surfaces for treatment or intervention.1 It is also unclear if no adverse events occurred or if they were not reported in the other included studies. As potential harms were not discussed by most included studies, the results may be biased toward favouring the intervention.
The overview of reviews with NMA1 had sparse data for all 3 networks, which resulted in considerable uncertainty. The authors may also have overinterpreted some results despite this uncertainty, such as stating some interventions may lead to improved outcomes when the comparison was not statistically significant.
Many of the included studies in this report focused on therapeutic support surfaces for prevention. There were few studies regarding therapeutic support surfaces for treatment, or for therapeutic small devices for prevention, and thus the findings for these interventions should be interpreted with caution. There were also no studies identified for therapeutic small devices for treatment. Most studies also focused on adult patients with only 1 non-randomized study focused on pediatric patients,21 so it is unclear if the findings are generalizable to children or adolescents.
The included studies were conducted from a wide range of countries. Only 5 RCTs from the overview of reviews1 (including 1 RCT that also overlapped with a SR16) were conducted in Canada, and all focused on therapeutic support surfaces to prevent pressure injuries. Thus, it is unclear how generalizable these findings are to the Canadian context, or to specific geographical, ethnic, or cultural groups in Canada, particularly regarding therapeutic support surfaces for treating pressure injuries, and therapeutic small devices for prevention or treatment.
Conclusions and Implications for Decision- or Policy-Making
This report identified 1 overview of reviews with NMA,1 5 SRs14-18 (2 with meta-analyses16,18), 2 RCTs,19,20 and 6 non-randomized studies21-26 regarding the use of therapeutic support surfaces to prevent or treat pressure injuries, or therapeutic small devices to prevent pressure injuries. Most the identified evidence included in this report were focused on adults, regarding the use of therapeutic support surfaces (particularly mattresses, beds, or overlays) to prevent pressure injuries. No relevant evidence was identified regarding the use of therapeutic small devices to treat pressure injuries.
For the clinical effectiveness of therapeutic support surfaces including mattresses, beds, and overlays to prevent pressure injuries, the overview of reviews’ NMA found that alternating-pressure (active) air surfaces and reactive gel surfaces may reduce pressure injury incidence compared to foam surfaces.1 An SR with meta-analysis focused on acute care patients,18 which largely overlapped with the overview of reviews, reported that sheepskin reactive surfaces were associated with reduced incidence of pressure injuries; standard surfaces, compared to active or reactive support surfaces, led to mixed results depending on the type of analysis (ITT or per-protocol). Two SRs of ICU patients14,16 (1 with a meta-analysis16) were identified and also largely overlapped with the overview of reviews. The SR with meta-analysis16 reported that reactive surfaces may reduce pressure injury compared to standard mattresses, though the meta-analysis of 2 studies was not statistically significant. Non-randomized studies from the other SR14 reported that alternating-pressure air mattresses were better than foam mattresses and low air loss mattresses were superior to air pressure mattresses. Mixed results were found for the identified non-randomized studies comparing pressure-relieving mattresses compared to standard mattresses21,24 and for overlays,25,26 which may be due to differences between studies (e.g., care setting). One non-randomized study23 indicated that a non-alternating, dynamic, minimum pressure air mattress system with a double-cell structure and reactive adjustment technology may reduce incidence of pressure injuries compared to other surfaces. The overview of reviews1 and 1 SR16 did not find significant differences between different types of active surfaces or reactive surfaces for pressure injury incidence or time to pressure injury, though there may be differences between different types of foam surfaces on time to pressure injury development.1,24 Only the overview of reviews1 reported on adverse events and health-related quality of life, and identified limited studies: it is uncertain if there are differences in adverse event rates between different support surfaces, and the effect on health-related quality of life is also unclear.
For the clinical effectiveness of cushions to prevent pressure injuries, from a SR15 assessing wheelchair pressure-relieving cushions, 2 studies did not find a significant difference between multiple-compartment air cell cushions and single-compartment air cell cushions; 1 study compared a skin protection cushion to a standard foam cushion and found no significant difference was found between incidence of all pressure injuries. Another SR16 identified 1 RCT where tragacanth gel cushions led to a delay in developing pressure injuries compared to standard foam cushions. One RCT20 also reported that their specially designed postoperative cushion also led to lower incidence of pressure injuries and reduced adverse events compared to conventional sponge pads.
For the clinical effectiveness of therapeutic support surfaces including mattresses, beds, and overlays to treat pressure injuries, the authors of the overview of reviews1 indicated that reactive air surfaces may be more effective than foam surfaces for treating pressure injuries; however, the network comparison and direct pairwise comparison were not statistically significant, so this should be interpreted with caution. It is also unclear if any other comparisons were clinically significant. Limited evidence was identified for adverse events, so it is unclear if there are differences in adverse event rates between types of therapeutic support surfaces. One non-randomized study22 found mixed results for fully automated pulsating support system air mattresses.
For the clinical effectiveness of therapeutic small devices including mattresses, beds, and overlays to prevent pressure injuries, the authors suggested that compared to standard care (e.g., pillows), heel protection devices may reduce pressure injury incidence16,19; however, evidence was limited and a meta-analysis18 reported that the pooled RR was not statistically significant. Findings were also mixed for time to pressure injury development.18,19 One RCT found no differences between a bunny boot, egg crate, or foot waffle.18
Overall, this review found some evidence to suggest that certain types of therapeutic support surfaces may help to prevent pressure injuries, such as active and reactive support surfaces compared to foam surfaces. There were comparatively fewer studies identified that assessed therapeutic support surfaces for treatment: authors of the overview of reviews stated that reactive air surfaces may be more effective than foam surfaces, but this finding should be interpreted with caution as it was not statistically significant. Two SRs and 1 RCT were identified regarding therapeutic small devices, and suggested that heel protection devices such as heel-offloading boots may lead to reduced pressure injuries compared to a pillow, although this finding should also be interpreted with caution due to limited evidence and a non-significant meta-analysis. The effects on these interventions for prevention or treatment on health-related quality of life and adverse events are unclear. Another gap is for pressure-redistributing static chairs, based on 1 SR17 that did not identify any relevant RCTs.
The methodological limitations of the included literature should be considered when interpreting the findings from this report, including small sample sizes, various sources of heterogeneity, many primary studies at unclear or high RoB, and limited reporting on adverse events. Further research set in Canada to assess benefits and harms for these interventions — through adequately powered and high-quality RCTs, particularly for therapeutic small devices for the treatment of pressure injuries — is warranted.
References
1.Shi C, Dumville JC, Cullum N, et al. Beds, overlays and mattresses for preventing and treating pressure ulcers: an overview of Cochrane Reviews and network meta-analysis. Cochrane Database Syst Rev. 2021;8:CD013761. PubMed
2.McNichol L, Mackey D, Watts C, Zuecca N. Choosing a support surface for pressure injury prevention and treatment. Nursing. 2020;50(2):41-44. PubMed
3.Hospital Harm Improvement Resource: Pressure Ulcer. Ottawa (ON): Canadian Patient Safety Institute; 2021: https://www.patientsafetyinstitute.ca/en/toolsResources/Hospital-Harm-Measure/Documents/Resource-Library/HHIR%20Pressure%20Ulcer.pdf. Accessed 2022 Jul 29.
4.Essex HN, Clark M, Sims J, Warriner A, Cullum N. Health-related quality of life in hospital inpatients with pressure ulceration: Assessment using generic health-related quality of life measures. Wound Repair Regen. 2009;17(6):797-805. PubMed
5.Cullum N, Buckley H, Dumville J, et al. Wounds research for patient benefit: a 5-year programme of research. Programme Grants Appl Res. 2016;4(13).
6.Li Z, Lin F, Thalib L, Chaboyer W. Global prevalence and incidence of pressure injuries in hospitalised adult patients: A systematic review and meta-analysis. Int J Nurs Stud. 2020;105:103546. PubMed
7.Houghton PE. Wound Prevalence in Canada: Reflection after 20 Years. Vol 19. North York (ON): Wound Care Canada; 2021: https://www.woundscanada.ca/docman/public/wound-care-canada-magazine/wcc-2021-v20-n1/2150-wcc-summer-2021-v19n1-final-p-46-57-wound-prevalence-reflection/file. Accessed 2022 Jul 29.
8.Fibreglass Total Contact Casting, Removable Cast Walkers, and Irremovable Cast Walkers to Treat Diabetic Neuropathic Foot Ulcers: A Health Technology Assessment. Toronto (ON): Health Quality Ontario; 2017: http://www.hqontario.ca/Portals/0/Documents/evidence/reports/hta-fibreglass-1709-en.pdf. Accessed 2022 Jul 29.
9.Kapp S, Gerdtz M, Gefen A, Prematunga R, Santamaria N. An observational study of the maintenance of the 30° side-lying lateral tilt position among aged care residents at risk of developing pressure injuries when using the standard care pillow and a purpose-designed positioning device. Int Wound J. 2019;16(5):1080-1086. PubMed
10.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
11.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. PubMed
12.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
13.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
14.Bambi AA, Yusuf S, Irwan AM. Reducing the Incidence and Prevalence of Pressure Injury in Adult ICU Patients with Support Surface Use: A Systematic Review. Adv Skin Wound Care. 2022;35(5):263-270. PubMed
15.Damiao J, Gentry T. A systematic review of the effectiveness of pressure relieving cushions in reducing pressure injury. Assist Technol. 2022:1-5. PubMed
16.Lovegrove J, Fulbrook P, Miles S, Steele M. Effectiveness of interventions to prevent pressure injury in adults admitted to intensive care settings: A systematic review and meta-analysis of randomised controlled trials. Aust Crit Care. 2022;35(2):186-203. PubMed
17.Stephens M, Bartley C, Dumville JC. Pressure redistributing static chairs for preventing pressure ulcers. Cochrane Database Syst Rev. 2022;2:CD013644. PubMed
18.Lovegrove J, Fulbrook P, Miles SJ, Steele M. Effectiveness of interventions to prevent pressure injury in adults admitted to acute hospital settings: A systematic review and meta-analysis of randomised controlled trials. Int J Nurs Stud. 2021;122:104027. PubMed
19.Barakat-Johnson M, Lai M, Stephenson J, et al. Efficacy of a heel offloading boot in reducing heel pressure injuries in patients in Australian intensive care units: A single-blinded randomised controlled trial. Intensive Crit Care Nurs. 2022;70:103205. PubMed
20.Xue J, Yang Q. Clinical application of a special postoperative position cushion for patients after percutaneous nephrolithotomy: a randomized trial. Ann. 2021;10(2):1861-1865. PubMed
21.Marufu TC, Setchell B, Cutler E, et al. Pressure injury and risk in the inpatient paediatric and neonatal populations: A single centre point-prevalence study. J Tissue Viability. 2021;30(2):231-236. PubMed
22.Raepsaet C, Zwaenepoel E, Manderlier B, et al. A Fully Automated Pulsating Support System for Pressure Injury Prevention and Treatment in 10 Belgium Nursing Homes: An Observational Study. Journal of Wound, Ostomy, & Continence Nursing. 2021;48(2):115-123. PubMed
23.Ahtiala M, Kivimäki R, Laitio R, Soppi E. Effect of mattress deployment on pressure ulcer development: a real-world observational cohort experience. Vol 11. London (UK): Wounds International; 2020: https://www.directhealthcaregroup.com/app/uploads/effect-of-mattress-deployment-on-pressure-ulcer-development-a-realworld-observational-cohort-experience-1.pdf. Accessed 2022 Jul 29.
24.Bai DL, Liu TW, Chou HL, Hsu YL. Relationship between a pressure redistributing foam mattress and pressure injuries: An observational prospective cohort study. PLoS ONE [Electronic Resource]. 2020;15(11):e0241276. PubMed
25.Horup MB, Soegaard K, Kjolhede T, Fremmelevholm A, Kidholm K. Static overlays for pressure ulcer prevention: a hospital-based health technology assessment. Br J Nurs. 2020;29(12):S24-S28. PubMed
26.Stone A. Preventing Pressure Injuries in Nursing Home Residents Using a Low-Profile Alternating Pressure Overlay: A Point-of-Care Trial. Adv Skin Wound Care. 2020;33(10):533-539. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Overview of Reviews, Systematic Reviews, and Network Meta-Analyses
Study citation, country, funding source | Objective, last search date, study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Relevant clinical outcomes, length of follow-up |
|---|---|---|---|---|
Overview of Reviews | ||||
Shi et al. (2021)1 UK Funding source: NIHR | Last search date: NR Number of included studies: 6 reviews, including
Number of primary RCTs and network contrasts in the NMA:
| Prevention:
Treatment:
| Interventions: Support surfaces (specialized medical devices designed to relieve or redistribute pressure on the body or both, to prevent and treat pressure ulcers) Comparator: Any other support surface; reference comparator for NMA was foam surfaces | Prevention outcomes:
Prevention studies follow-up (range): 3 days to 7 months (median: 14 days) Treatment outcomes:
Treatment studies follow-up (range): 7 days to 18 months (median: 37.5 days) |
Systematic Reviews | ||||
Bambi et al. (2022)14 Indonesia Funding: NR | Last search date: NR Number of included studies: 8 (4 RCTs, 2 cohort studies, 2 quasi-experimental studies) | Eligibility criteria: Adult ICU patients Total participants: NR Sample size (range): 52 to 1,654 Mean age: NR % female: NR | Intervention: Active or reactive support surfaces Comparator: Any support surface | Outcome: Pressure injury incidence Follow-up (range): 7 to 30 days |
Damiao and Gentry (2022)15 US Funding: NR | Last search date: NR Number of included studies: 17 (3 relevant to this report: 2 RCTs, 1 non-randomized studies) | Eligibility criteria: NRa | Intervention: Wheelchair pressure-relieving cushions Comparator(s): Cushions made of different materials | Outcome: Development of pressure injury Follow-up: 1 study followed patients for 35 days; NR for 2 studies |
Lovegrove et al. (2022)16 Australia Funding: The Prince Charles Hospital Foundation (scholarship) | Last search date: end of 2019 Number of included studies: 26 RCTs (7 relevant: support surfaces = 6; heel protection devices = 1)b | Eligibility criteria: Adult patients in ICU settings Total participants: NR Sample size (range): NR Mean age: NR % female: NR | Relevant interventions: Support surfaces or heel protection devices Comparators: Alternative surfaces, standard care | Outcome: Pressure injury incidence Follow-up: NR for most studies, up to 2 weeks where reported |
Stephens et al. (2022)17 UK Funding: NIHR | Last search date: June 23, 2021 Number of included studies: 0 RCTs | Eligibility criteria: Adults who remain seated for extended periods of time, in any care setting | Intervention: Any type of pressure-redistributing static chair Comparator: Any comparator, e.g., standard chairs, other types of pressure-redistributing chairs | Outcomes: • Pressure injury incidence • Health-related quality of life • Adverse events Follow-up: NA |
Lovegrove et al. (2021)18 Australia Funding: The Prince Charles Hospital Foundation (scholarship) | Last search date: end of 2019 Number of included studies: 45 RCTs Number of relevant RCTs: 28 (support surfaces = 24; heel protection devices = 4) b | Eligibility criteria: Adult patients in acute hospital settings Total participants: NR Sample size (range): NR Mean age: NR % female: NR | Relevant interventions: Support surfaces or heel protection devices Comparators: Alternative surfaces, standard care | Outcome: Pressure injury incidence Follow-up: NR for most studies; when reported, ranges from 5 days to 60 days, or to discharge |
ICU = intensive care unit; ITT = intention to treat; NA = not applicable; NIHR = National Institute for Health Research; NMA = network meta-analysis; NR = not reported; RCT = randomized controlled trial.
aThe supplementary materials could not be accessed at the time of writing this report; it is unclear if additional details about the population characteristics are presented in the supplementary materials or not reported.
bMany of the primary RCTs included in the systematic reviews by Lovegrove et al. related to support surfaces were also included in the overview of reviews. Five out of 7 studies (6 related to support surfaces) included by Lovegrove et al. (2022)16 are covered in the overview, while 23 out of 28 studies (24 related to support surfaces) by Lovegrove et al. (2021)18 are covered in the overview.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design and setting | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Randomized Controlled Trial | ||||
Barakat-Johnson et al. (2022)19 Australia Funding: No funding; in-kind support was provided by each facility to conduct the study. | Single-blinded RCT ICU | Eligibility criteria: Adult ICU patients at high risk of developing a pressure injury (Waterlow score ≥ 15 or Braden scale ≤ 12) but without pre-existing heel pressure injuries (N = 394) Mean (SD) age: 60.1 (16.7) Age range: 16.7 to 94.8 % female: 33.2% | Intervention: Heel-offloading boot (Prevalon™ boot) Comparator: Standard hospital pillow or Posey® Heel Protector boot | Outcome:
Follow-up: 28 days from admission |
Xue and Yang (2020)20 China Funding: National Social Science Foundation of China, Innovation Platform’s Open Foundation of Education Department in Hunan, Provincial Department of Health, PI, General Project, China. | RCT Hospital, Department of Urology | Eligibility criteria: Patients who underwent percutaneous nephrolithotomy (N = 450) Number of female patients: 221 Mean (SD) age: 47.03 (8.9) Age range: 18 to 76 | Intervention: Special postoperative position cushion with a sacrococcygeal pad and a back pad Comparator: Conventional hip sponge pads | Outcomes:
Follow-up: NR; patients typically need 5 to 7 days of rest after this procedure |
Non-Randomized Studies | ||||
Marufu et al. (2021)21 UK Funding: None | Cross-sectional study Children’s hospital | Eligibility criteria: Children allotted to a pediatric or neonatal bed in June/July 2020 (N = 88) Median (range) age: 0.85 (0 to 17.5) % female: 42.0% | Relevant intervention: Pressure-relieving mattress Comparator: Standard mattress | Relevant outcome: Pressure damage Follow-up: NA |
Raepsaet et al. (2021)22 Belgium Funding: Care of Sweden AB, Tranemo, Sweden | Cohort (before-after comparison) Nursing homes | Eligibility criteria: Adults residing in a nursing home (Total N = 40; relevant [treatment] = 18) Mean (SD) age: 86 (7.56) % female: 85% | Intervention: A fully automated pulsating support system air mattress Comparator: Before-after | Relevant outcomes: Changes in pressure injury state Follow-up: 30 days |
Ahtiala et al. (2020)23 Finland Funding source: Turku University Hospital Foundation | Retrospective observational cohort ICU | Eligibility criteria: Adult patients admitted to the ICU from 2010 to 2015 (N = 8,956 included in analysis) Mean (range) age: 61.4 (18 to 95) % female: 36.1% | Intervention: Non-alternating, dynamic, minimum pressure air mattress system, with a double-cell structure and reactive adjustment technology Comparators:
| Outcomes:
Follow-up: Study assessed 6 years of data (2010 to 2016) |
Bai et al. (2020)24 Taiwan Funding source: Ministry of Science and Technology, Taiwan; Yuan Ze University, Taiwan | Observational prospective cohort ICU | Eligibility criteria: ICU patients from November 2017 to September 2018 with risk off developing a pressure injury (N = 254) Mean age: 64.05 % female: 38.6% Risk of developing a pressure injury, based on Braden pressure injury risk assessment score:
| Intervention: Pressure-redistributing foam mattress Comparator: Non-pressure redistributing foam mattress | Outcomes: Development of pressure injuries Follow-up: until discharge |
Horup et al. (2020)25 Denmark Funding: NR | Observational study (pre-post implementation) University hospital – geriatric and orthopedic wards | Eligibility criteria: Patients admitted during the 7 months before introducing static overlays, and 6 months after overlays were introduced (N = 1,557) Mean age: NR % female: NR | Interventions (chosen during the post-implementation period based on risk score with the Braden scale and clinical assessment):
Comparators:
|
|
|
|
|
|
|
ICU = intensive care unit; LTC = long-term care; NR = not reported; RCT = randomized controlled trial.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Systematic Reviews and Network Meta-Analyses Using AMSTAR 210 and the ISPOR Questionnaire11
Strengths | Limitations |
|---|---|
Overview of Reviews | |
Shi et al. (2021)1 | |
|
|
Systematic Reviews | |
Bambi et al. (2022)14 | |
|
|
Damiao et al. (2022)15 a | |
|
|
Lovegrove et al. (2022)16 | |
|
|
Stephens et al. (2022)17 | |
|
|
Lovegrove et al. (2021)18 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; ISPOR = International Society for Pharmacoeconomics and Outcomes Research; NMA = network meta-analysis; RCT = randomized controlled trial; SR = systematic review.
aSome details, including the PRISMA flow chart and descriptions of included studies, were presented in supplementary materials that could not be accessed at the time of writing this report; thus, it is not possible to critically appraise these components.
Table 5: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist12
Strengths | Limitations |
|---|---|
Randomized Controlled Trials | |
Barakat-Johnson (2022)19 | |
|
|
Xue and Yang (2020)20 | |
|
|
Non-Randomized Studies | |
Marufu et al. (2021)21 | |
|
|
Raepsaet et al. (2021)22 | |
|
|
Ahtiala et al. (2020)23 | |
|
|
Bai et al. (2020)24 | |
|
|
Horup et al. (2020)25 | |
|
|
Stone et al. (2020)26 | |
|
|
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 6: Summary of Findings for Therapeutic Support Surfaces for Prevention – Pressure Injury Incidence
Comparison (intervention vs. comparator) | Study design and citation | Study findings |
|---|---|---|
Reactive air surfaces vs. foam surfaces | Shi et al. (2021)1 Overview of reviews with NMA | RR (95% CI) from NMA: 0.46 (0.29 to 0.75) |
Alternating-pressure (active) air surfaces vs. foam surfaces | Shi et al. (2021)1 Overview of reviews with NMA | RR (95% CI) from NMA: 0.63 (0.42 to 0.93) |
Reactive gel surfaces vs. foam surfaces | Shi et al. (2021)1 Overview of reviews with NMA | RR (95% CI) from NMA: 0.47 (0.22 to 1.01) |
Reactive gel surfaces vs. reactive air surfaces | Shi et al. (2021)1 Overview of reviews with NMA | RR (95% CI) from NMA: 1.02 (0.48 to 2.16) |
Reactive sheepskin surfaces vs. foam surfaces | Shi et al. (2021)1 Overview of reviews with NMA | RR (95% CI) from NMA: 0.58 (0.32 to 1.05) |
Reactive sheepskin surfaces vs. reactive air surfaces | Shi et al. (2021)1 Overview of reviews with NMA | RR (95% CI) from NMA: 1.25 (0.62 to 2.53) |
Reactive sheepskin surfaces vs. alternating (active) air surfaces | Shi et al. (2021)1 Overview of reviews with NMA | RR (95% CI) from NMA: 0.93 (0.48 to 1.78) |
Reactive sheepskin surfaces vs. reactive gel surfaces | Shi et al. (2021)1 Overview of reviews with NMA | RR (95% CI) from NMA: 1.23 (0.51 to 2.96) |
Alternating-pressure (active) air surfaces vs. reactive air surfaces | Shi et al. (2021)1 Overview of reviews with NMA | RR (95% CI) from NMA: 1.35 (0.82 to 2.20) |
Reactive gel surfaces vs. alternating-pressure (active) air surfaces | Shi et al. (2021)1 Overview of reviews with NMA | RR (95% CI) from NMA: 0.76 (0.34 to 1.66) |
Reactive gel surfaces followed by foam surfaces vs. foam surfaces | Shi et al. (2021)1 Overview of reviews with NMA | RR (95% CI) from NMA: 2.88 (0.70 to 11.83) |
Standard hospital surfaces vs. reactive air surfaces | Shi et al. (2021)1 Overview of reviews with NMA | RR (95% CI) from NMA: 2.31 (1.41 to 3.79) |
Reactive gel surfaces followed by foam surfaces vs alternating-pressure (active) air surfaces | Shi et al. (2021)1 Overview of reviews with NMA | RR (95% CI) from NMA: 4.60 (1.18 to 17.86) |
Standard hospital surfaces vs. alternating-pressure (active) air surfaces | Shi et al. (2021)1 Overview of reviews with NMA | RR (95% CI) from NMA: 1.71 (1.13 to 2.60) |
Reactive gel surfaces followed by foam surfaces vs. reactive gel surfaces | Shi et al. (2021)1 Overview of reviews with NMA | RR (95% CI) from NMA: 6.09 (1.27 to 29.20) |
Standard hospital surfaces vs. reactive gel surfaces | Shi et al. (2021)1 Overview of reviews with NMA | RR (95% CI) from NMA: 2.27 (1.10 to 4.66) |
Reactive gel surfaces followed by foam surfaces vs. reactive sheepskin surfaces | Shi et al. (2021)1 Overview of reviews with NMA | RR (95% CI) from NMA: 4.96 (1.10 to 22.33) |
Standard hospital surfaces vs. reactive sheepskin surfaces | Shi et al. (2021)1 Overview of reviews with NMA | RR (95% CI) from NMA: 1.85 (1.11 to 3.07) |
Reactive gel surfaces followed by foam surfaces vs. reactive water surfaces | Shi et al. (2021)1 Overview of reviews with NMA | RR (95% CI) from NMA: 6.68 (1.31 to 34.11) |
Reactive surface vs. standard mattress | Lovegrove et al. (2022)16 SR with NMA (2 RCTs)a | ITT meta-analysis: RR (95% CI) = 0.24 (0.04 to 1.46) Both studies were statistically significant, with lower PI incidence in the reactive surface group than standard mattress group. |
Two types of active support surfaces (optional pulsation and low air loss features vs. a continuous/alternating low-pressure control mattress) | Lovegrove et al. (2022)16 SR (1 relevant RCT)a | PI incidence was not significantly different (P = 0.35, per protocol) |
Two types of reactive surfaces | Lovegrove et al. (2022)16 SR (1 RCT) a | PI incidence was not significantly different (P = 0.44, per protocol) |
Viscoelastic foam mattress vs. air pressure mattress | Bambi et al. (2022)14 SR (1 relevant non-randomized study – quasi-experiment) | RR (95% CI) after 7 days = 1.5 (0.2 to 2.6) |
Low air loss mattress vs. air pressure mattress | Bambi et al. (2022)14 SR (1 cohort study) | PI incidence after 5 days: • Low air loss mattress: 0% • Air pressure mattress: 18.0% • P = 0.046 |
Alternating-pressure air mattress vs. alternating-pressure air overlays | Bambi et al. (2022)14 SR (1 quasi-experimental study) | RR (95% CI) after > 14 days = 0.89 (0.42 to 1.83) |
Alternating-pressure air mattress vs. foam mattress | Bambi et al. (2022)14 SR (1 quasi-experimental study) | PI incidence after 21 days: • Alternating-pressure air mattress: 18.8% • Foam mattress: 48.5% P = 0.011 |
Active support surfaces vs. any comparator | Lovegrove et al. (2021)18 SR with MAa | ITT (6 RCTs): RR (95% CI) = 0.79 (0.59 to 1.06) PP (7 RCTs): RR (95% CI) = 0.54 (0.35 to 0.83) |
Reactive support surfaces vs. any comparator | Lovegrove et al. (2021)18 SR with MAa | ITT (5 RCTs): RR (95% CI) = 0.55 (0.24 to 1.26) PP (4 RCTs): RR (95% CI) = 0.53 (0.30 to 0.95) |
Sheepskin surfaces vs. any comparator | Lovegrove et al. (2021)18 SR with MA (2 RCTs)a | ITT: RR (95% CI) = 0.42 (0.22 to 0.78) |
Active support surfaces vs. reactive support surfaces | Lovegrove et al. (2021)18 SR with MAa | ITT (3 RCTs): RR (95% CI) = 0.86 (0.72 to 1.02) PP (3 RCTs): RR (95% CI) = 0.77 (0.55 to 1.08) |
Active surfaces compared to standard mattress | Lovegrove et al. (2021)18 SR with MA (2 RCTs)a | PP: RR (95% CI) = 0.31 (0.17 to 0.58) |
Reactive surfaces compared to standard mattress | Lovegrove et al. (2021)18 SR with MAa | ITT (3 RCTs): RR (95% CI) = 0.38 (0.07 to 2.08) PP (3 RCTs): RR (95% CI) = 0.39 (0.16 to 0.99) |
Pressure-relieving mattress vs. standard mattress | Marufu et al. (2021)21 Non-randomized study (cross-sectional study, N = 88) | Protective mattress, compared to standard mattress, was not associated with risk reduction for pressure damage (P = NR), but was associated with risk reduction in skin assessment classification: OR (95% CI) = −0.39 (−0.66 to −0.1) |
Non-alternating, dynamic, minimum pressure air mattress system, with a double-cell structure and reactive adjustment technology vs. polyurethane foam | Ahtiala et al. (2020)23 Non-randomized study (real-world observational cohort, N = 8,956) | HR (95% CI) for preventing pressure injuries until discharge = 3.330 (2.537 to 4.370) Mean (range) days until discharge: 3.6 (0 to 64) |
Non-alternating, dynamic, minimum pressure air mattress system, with a double-cell structure and reactive adjustment technology vs. one-cell, dynamic, low-pressure air mattress system | Ahtiala et al. (2020)23 Non-randomized study (real-world observational cohort, N = 8,956) | HR (95% CI) for preventing pressure injuries until discharge = 2.866 (2.235 to 3.677) Mean (range) days until discharge: 3.6 (0 to 64) |
Non-alternating, dynamic, minimum pressure air mattress system, with a double-cell structure and reactive adjustment technology vs. alternating dynamic air mattress, every fourth cell | Ahtiala et al. (2020)23 Non-randomized study (real-world observational cohort, N = 8,956) | HR (95% CI) for preventing pressure injuries until discharge = 2.693 (1.931 to 3.757) Mean (range) days until discharge: 3.6 (0 to 64) |
Non-alternating, dynamic, minimum pressure air mattress system, with a double-cell structure and reactive adjustment technology vs. alternating dynamic air mattress, with 20 cells within the cell system cycle time 15 minute | Ahtiala et al. (2020)23 Non-randomized study (real-world observational cohort, N = 8,956) | HR (95% CI) for preventing pressure injuries until discharge = 5.066 (2.346 to 10.940) Mean (range) days until discharge: 3.6 (0 to 64) |
Non-alternating, dynamic, minimum pressure air mattress system, with a double-cell structure and reactive adjustment technology vs. alternating/continuous low-pressure, dynamic air mattress, with 24 cells | Ahtiala et al. (2020)23 Non-randomized study (real-world observational cohort, N = 8,956) | HR (95% CI) for preventing pressure injuries until discharge = 3.410 (1.493 to 7.785) Mean (range) days until discharge: 3.6 (0 to 64) |
Non-alternating, dynamic, minimum pressure air mattress system, with a double-cell structure and reactive adjustment technology vs. complete therapy bed | Ahtiala et al. (2020)23 Non-randomized study (real-world observational cohort, N = 8,956) | HR (95% CI) for preventing pressure injuries until discharge = 2.877 (1.057 to 7.830) Mean (range) days until discharge: 3.6 (0 to 64) |
Pressure-redistributing foam mattress vs. non-pressure redistributing foam mattress | Bai et al. (2020)24 Non-randomized study (observational prospective cohort, N = 254) | Pressure injury incidence during ICU stay (mean length of stay in days = 8.9):
Difference in severity of pressure injuries was statistically non-significant (P = 0.280) |
Static overlays (high-density viscoelastic foam overlay, or thermoplastic polyurethane) vs. no overlay (standard mattress or alternating air mattress only) | Horup et al. (2020)25 Non-randomized study (before-after implementation, N = 1,557) | Mean length of stay in days = 6 days No patients on the overlays (n = 123) developed pressure injuries. No significant difference was found for pressure injury incidence in the periods before and after implementing the overlays (n = 1557; P = 0.874). |
Low-profile alternating-pressure support surface vs. standard of care (non-powered pressure redistribution mattress only) | Stone (2020)26 Non-randomized study (historical control, based on retrospective review) | Mean (SD; range) days spent on the overlay: 140.9 (94.1; 7 to 258) Pressure injury incidence:
|
Intervention – Pressure-Relieving Cushions | ||
Multi-component air cushion vs. single-compartment air cushion | Damiao and Gentry (2022)15 SR (1 RCT, 1 non-randomized study – prospective observational) | Neither study found a statistically significant difference. |
Skin protection cushion (consisting of air, gel, or contoured foam) vs. segment (flat) foam cushion | Damiao and Gentry (2022)15 SR (1 RCT) | There were fewer pressure injuries to the ischial tuberosities in the skin protection cushion group (P = 0.04), but no significant difference when considering pressure injuries for the ischial tuberosities and sacrum (P = 0.14). |
Tragacanth gel cushion vs. standard foam cushion | Lovegrove et al. (2022)16 SR (1 RCT) | Shakibamehr et al., 2019:
|
Special position cushion with a sacrococcygeal pad and a back pad vs. conventional hip sponge pad | Xue and Yang (2021)20 RCT | Incidence of postoperative pressure injuries was lower in the intervention group (P = 0.05) during hospital stay. |
CI = confidence interval; ITT = intention to treat; NMA = network meta-analysis; OR = odds ratio; PP = per-protocol; RR = risk ratio; RCT = randomized controlled trial; SR = systematic review.
aThe SRs by Lovegrove et al. largely overlap with the overview of reviews by Shi et al1: from the RCTs relevant to this report and this outcome, Lovegrove et al. (2022)16 has 1 unique study, while Lovegrove et al. (2021)18 overlaps entirely with the overview. Their meta-analyses results are presented here due to their focus on specific care settings (ICU and acute care, respectively), as the overview of reviews did not conduct analyses by different care settings, and this may be a cause of heterogeneity.
Table 7: Summary of Findings for Therapeutic Support Surfaces for Prevention – Time to Pressure Injury Development
Comparison (Intervention vs. comparator) | Study design and citation | Outcome |
|---|---|---|
Intervention – Support Surfaces (Mattresses, Beds, Overlays) | ||
Reactive sheepskin surfaces vs. standard hospital surfaces | Shi et al. (2021)1 Overview of reviews with NMA | HR (95% CI) from NMA = 0.45 (0.21 to 0.94) |
Foam surfaces vs. standard or undefined hospital surfaces | Shi et al. (2021)1 Overview of reviews with NMA | HR (95% CI) from NMA = 0.70 (0.32 to 1.54) |
Alternating-pressure (active) air surfaces vs. reactive air surfaces | Shi et al. (2021)1 Overview of reviews with NMA | HR (95% CI) from NMA = 2.25 (0.58 to 8.75) Direct pairwise HR (95% CI): 2.25 (1.05 to 4.83)a |
Alternating-pressure (active) air surfaces vs. foam surfaces | Shi et al. (2021)1 Overview of reviews with NMA | HR (95% CI) from NMA = 0.45 (0.17 to 1.16) |
Reactive air surfaces vs. foam surfaces | Shi et al. (2021)1 Overview of reviews with NMA | HR (95% CI) from NMA = 0.20 (0.04 to 1.05) |
Reactive sheepskin vs. foam surface | Shi et al. (2021)1 Overview of reviews with NMA | HR (95% CI) from NMA = 0.64 (0.22 to 1.88) |
Alternating-pressure (active) air surfaces vs. reactive sheepskin surfaces | Shi et al. (2021)1 Overview of reviews with NMA | HR (95% CI) from NMA = 0.71 (0.17 to 2.95) |
Reactive air surfaces vs. reactive sheepskin surfaces | Shi et al. (2021)1 Overview of reviews with NMA | HR (95% CI) from NMA = 0.31 (0.04 to 2.26) |
Alternating-pressure (active) air surfaces vs. standard hospital surfaces | Shi et al. (2021)1 Overview of reviews with NMA | HR (95% CI) from NMA = 0.31 (0.09 to 1.06) |
Reactive air surfaces vs. standard hospital surfaces | Shi et al. (2021)1 Overview of reviews with NMA | HR (95% CI) from NMA = 0.14 (0.02 to 0.87) |
Alternating-pressure (active) air surfaces vs. another type of alternating-pressure (active) air surfaces | Shi et al. (2021)1 Overview of reviews (2 RCTs, N = 2581) | Both studies indicated no clear difference of developing a pressure injury at up to 60 days. |
Foam surfaces vs. other types of foam surfaces | Shi et al. (2021)1 Overview of reviews (2 RCTs, N = 146) | Direct comparison, HR (95% CI):
|
Bai et al. (2020)24 Non-randomized study (observational prospective cohort, N = 254) | Mean days to pressure injury:
| |
Reactive air surfaces vs. another type of reactive air surfaces | Shi et al. (2021)1 Overview of reviews (1 RCT, N = 123) | Reported no significant difference |
Intervention – Pressure-Redistributing Cushions | ||
Tragacanth gel cushion vs. standard foam cushion | Lovegrove et al. (2022)16 SR (1 relevant RCT, N = 100) | Shakibamehr et al., 2019 – mean (SD) days to erythema (pressure injury):
|
CI = confidence interval; HR = hazard ratio; ICU = intensive care unit; NMA = network meta-analysis; PP = per-protocol; RCT = randomized controlled trial; SR = systematic review.
aThe network contrast of reactive air surfaces vs. alternating-pressure air surfaces has a wide confidence interval with the review authors state is due to data sparseness, and they state they consider the direct pairwise comparison to be more reliable, so both are presented in the table. For all other network contrasts, there were no substantial differences between the results of the NMA and pairwise analyses.
Table 8: Summary of Findings for Therapeutic Support Surfaces for Prevention – Adverse Events
Comparison | Author (Year), study design, length of follow-up | Setting | Outcome(s) |
|---|---|---|---|
Intervention – Mattress, Beds, Overlays | |||
Alternating-pressure (active) air surfaces vs. foam surfaces | Shi et al. (2021)1 Overview of reviews (3 relevant RCTs) | Acute and LTC | Two studies reported similar rates of adverse events between both groups; the third study reported 1 death but did not specify which group. |
Alternating-pressure (active) air surfaces vs. another type of alternating-pressure (active) air surface | Shi et al. (2021)1 Overview of reviews (1 relevant RCT) | Acute and LTC | Study reported total number of adverse events but did not report data by treatment vs. control group. |
Foam surfaces vs. reactive air surfaces | Shi et al. (2021)1 Overview of reviews (1 relevant RCT) | Acute | Counts of adverse events were reported for each group. The review authors stated it is unclear if there is a difference. |
Foam surfaces vs. undefined surfaces (Bedcare) | Shi et al. (2021)1 Overview of reviews (1 relevant RCT) | LTC | No adverse events were reported in either group. |
Reactive gel surfaces compared with undefined surfaces (Aiartex) | Shi et al. (2021)1 Overview of reviews (1 relevant RCT) | LTC | Study indicated no adverse events. |
Intervention – Cushion | |||
Special postoperative position cushion with a sacrococcygeal pad and a back pad vs. conventional hip sponge pads | Xue and Yang (2021)20 RCT | Hospital | Incidence of renal hemorrhage due to improper postoperative position and rate of tube folding of the renal fistula were lower in the intervention group than comparator group (P = 0.05). |
LTC = long-term care; NR = not reported; RCT = randomized controlled trial.
Table 9: Summary of Findings for Therapeutic Support Surfaces for Prevention – Health-Related Quality of Life
Comparison | Author (Year), study design, length of follow-up | Setting | Outcome(s) |
|---|---|---|---|
Intervention – Mattress, Beds, Overlays | |||
Alternating-pressure (active) air surfaces vs. foam surfaces | Shi et al. (2021)1 Overview of reviews (1 relevant RCT) Follow-up: 90 days | Acute and LTC | Mean difference (95% CI):
|
Reactive sheepskin surfaces vs. undefined 'standard hospital surfaces' | Shi et al. (2021)1 Overview of reviews (1 relevant RCT) Follow-up: NR | LTC | Mean score on visual analogue scale:
|
EQ-5D-5L = EuroQol 5-Dimensions 5-Levels; LTC = long-term care; NR = not reported; PU-QoL-UI = Pressure Ulcer Quality of Life Utility Instrument; RCT = randomized controlled trial.
Table 10: Summary of Findings for Therapeutic Support Surfaces for Treatment – Proportion of Patients With Healed Pressure Injuries
Comparison (Intervention vs. comparator) | Study design and citation | Outcome |
|---|---|---|
Intervention – Mattress, Beds, Overlays | ||
Reactive water surface vs. alternative pressure (active) air surface | Shi et al. (2021)1 Overview of reviews with NMA | RR (95% CI) from NMA = 1.03 (0.27 to 3.98) |
Reactive water surface vs. reactive air surface | Shi et al. (2021)1 Overview of reviews with NMA | RR (95% CI) from NMA = 0.76 (0.48 to 1.19) |
Reactive water surface vs. foam surface | Shi et al. (2021)1 Overview of reviews with NMA | RR (95% CI) from NMA = 1.00 (0.72 to 1.38) |
Alternating-pressure (active) air surface vs. reactive air surface | Shi et al. (2021)1 Overview of reviews with NMA | RR (95% CI) from NMA = 0.74 (0.19 to 2.82) |
Alternating-pressure (active) air surface vs. foam surface | Shi et al. (2021)1 Overview of reviews with NMA | RR (95% CI) from NMA = 0.97 (0.26 to 3.58) |
Reactive air surface vs. foam surface | Shi et al. (2021)1 Overview of reviews with NMA | RR (95% CI) from NMA = 1.32 (0.96 to 1.80) |
Alternating-pressure (active) air surfaces compared with another type of alternating-pressure (active) air surface | Shi et al. (2021)1 Overview of reviews (3 RCTs) | All RCTs reported no statistically significant differences for improvement, healing, or number of healed heel ulcers. |
Reactive gel surfaces vs. undefined reactive surfaces (Aiartex) | Shi et al. (2021)1 Overview of reviews (1 RCT) | Direct pairwise RR (95% CI) = 1.58 (0.41 to 6.11) |
CI = confidence interval; LTC = long-term care; NA = not applicable; NMA = network meta-analysis; NR = not reported; RCT = randomized controlled trial; RR = risk ratio.
Table 11: Summary of Findings for Therapeutic Support Surfaces for Treatment – Status of Pressure Injury
Comparison | Author (Year), study design, follow-up | Setting | Outcome(s) |
|---|---|---|---|
Fully automated pulsating support system air mattress (before-after comparison) | Raepsaet et al. (2021)22 Multicenter cohort study Follow-up: 30 days | Nursing homes | Mean (range) PUSH score:
Most existing pressure injuries did not deteriorate and some improved (reduced PUSH score), but deterioration was also seen. No statistical tests were conducted. |
PUSH = Pressure Ulcer Scale for Healing.
Table 12: Summary of Findings for Therapeutic Support Surfaces for Treatment – Time to Pressure Injury Healing
Comparison (Intervention vs. comparator) | Study design and citation | Setting(s) | HR (95% CI) | Certainty of evidence |
|---|---|---|---|---|
Reactive air surfaces vs. foam surfaces | Shi et al. (2021)1 Overview of reviews (1 RCT) Median follow-up: 37.5 days | LTC | 2.66 (1.34 to 5.17) | Low |
CI = confidence interval; HR = hazard ratio; LTC = long-term care; NR = not reported; RCT = randomized controlled trial.
Table 13: Summary of Findings for Therapeutic Support Surfaces for Treatment – Adverse Events
Comparison | Author (Year), study design | Setting | Outcome(s) |
|---|---|---|---|
Alternating-pressure (active) air surfaces vs. foam surfaces | Shi et al. (2021)1 Overview of reviews (1 RCT) | Acute care | No major adverse events attributed to support surfaces. Uncertain if there is a difference. |
Foam surfaces vs. reactive water surfaces | Shi et al. (2021)1 Overview of reviews (1 RCT) | LTC | Defined by primary study authors as eczema, maceration, and pain; incidence or difference between groups not reported by review authors. Uncertain if there is a difference. |
Reactive air surfaces vs. foam surfaces | Shi et al. (2021)1 Overview of reviews (2 RCTs) | Acute care | Both studies did not clearly suggest any difference in adverse events. Uncertain if there is a difference. |
Alternating-pressure (active) air surfaces compared with another type of alternating-pressure (active) air surface | Shi et al. (2021)1 Overview of reviews (4 RCTs) | Acute and LTC | Studies largely reported death data but did not state other adverse events, outcome data were not pooled. Uncertain if there is a difference. |
Reactive air surfaces vs. undefined standard hospital surfaces | Shi et al. (2021)1 Overview of reviews (2 RCTs) | Acute and LTC | Review authors did not pool data due to different definitions of adverse events. Uncertain if there is a difference. |
Reactive gel surfaces vs. undefined reactive surfaces (Aiartex) | Shi et al. (2021)1 Overview of reviews (1 RCT) | LTC | Review authors did not pool data due to different definitions of adverse events. Uncertain if there is a difference. |
CI = confidence interval; HR = hazard ratio; LTC = long-term care; RCT = randomized controlled trial.
Table 14: Summary of Findings for Therapeutic Small Devices for Prevention – Pressure Injury Incidence
Comparison (Intervention vs. comparator) | Study design and citation | Outcome |
|---|---|---|
Heel protector for offloading heels vs. pillows | Lovegrove et al. (2022)16 SR (1 RCT) | Meyers, 2017 – pressure injury incidence:
|
Heel protection devices vs. standard care (per admitting ward, standard pressure-redistributing support surface) or pillow | Lovegrove et al. (2021)18 SR with MA | ITT (3 RCTs): RR (95% CI) = 0.64 (0.22 to 1.87) PP (2 RCTs): RR (95% CI) = 0.38 (0.21 to 0.67) |
Heel-offloading boot vs. standard practice (pillows) | Barakat-Johnson et al. (2022)19 Single-blinded RCT | OR (95% CI) = 0.0883 (0.0104 to 0.749). Severity of observed pressure injuries were:
|
Bunny boot vs. egg crate vs. foot waffle | Lovegrove et al. (2021)18 SR (1 RCT) | Gilcreast et al., 2005:
|
CI = confidence interval; ITT = intention-to-treat; MA = meta-analysis; OR = odds ratio; RCT = randomized controlled trial; RR = risk ratio; SR = systematic review.
Table 15: Summary of Findings for Therapeutic Small Devices for Prevention – Time to Pressure Injury Development
Comparison (Intervention vs. comparator) | Study design and citation | Outcome |
|---|---|---|
Foot waffle device vs. heel elevation with a hospital pillow | Lovegrove et al. (2021)18 SR (1 RCT) | Tymec et al., 1997 – mean days to pressure injury:
|
Heel-offloading boot vs. standard practice (pillows) | Barakat-Johnson et al. (2022)19 Single-blinded RCT | HR (95% CI) = 0.0896 (0.0110 to 0.727) “hazard of ICU-acquired heel PI [pressure injury] from admission to ICU was 11.2 times less in the intervention group than in controls” (p.6) |
CI = confidence interval; HR = hazard ratio; ICU = intensive care unit; RCT = randomized controlled trial.
Appendix 5: Overlap Between Included Systematic Reviews
Note that this appendix has not been copy-edited.
Table 16: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Shi et al., 20211 | Bambi et al., 202214 | Damiao et al., 202215 | Lovegrove et al., 202216 | Lovegrove et al., 202118 |
|---|---|---|---|---|---|
Allman et al. Ann Intern Med 1987;107(5):641‐8. | Yes | – | – | – | – |
Andersen et al. Acta Dermatovener (Stockholm) 1982;63:227 to 30 | Yes | – | – | – | Yes |
Aronovitch et al. Ostomy Wound Manage 1999;45(3):34 to 44. | Yes | – | – | – | Yes |
Bååth et al. Appl Nurs Res 2015;30, 170 to 175 | – | – | – | – | Yes |
Ballard K. Prof Nurse 1997;13(1):27 to 32. | Yes | – | – | – | – |
Beeckman et al. Int. J Nurs Stud 2019;97:105 to 13. | Yes | – | – | – | – |
Bennett et al. J Am Geriatr Soc 1998;46(5):569 to 76. | Yes | – | – | – | Yes |
Berthe et al. Acta Chirurgica Belgica 2007;107(2):155 to 61. | Yes | – | – | – | Yes |
Bharucha et al. J Wound Ostomy Cont Nurs 2018;45(4), 310 to 6. | – | – | – | – | Yes |
Black et al. J Wound Ostomy Cont Nurs 2012;39:267 to 73 | – | Yes | – | – | – |
Bliss et al. BMJ 1967;1(5537):394 to 7 | Yes | – | – | – | – |
Bliss. Age Aging 1995;24:297 to 302 | Yes | – | – | – | – |
Brienza et al. J Am Geriatr Soc 2010;58(12), 2308 to 2314. | – | – | Yes | – | – |
Brienza et al. J Am Geriatr Soc 2018;66(9), 1752 to 1759. | – | – | Yes | – | – |
Bueno de Camargo et al. Crit Care Res Pract 2018;2018:Article ID 3712067. | Yes | Yes | – | Yes | – |
Cassino et al. Acta Vulnologica 2013;11(1):15 to 21. | Yes | – | – | – | – |
Cassino et al. Minerva Chirurgica 2013;68(1):105 to 16. | Yes | – | – | – | – |
Cavicchioli et al. J Wound Care 2007;16(7):285 to 9. | Yes | – | – | – | – |
Cobb et al. TriService Nursing Research Program (TSNRP) 1997. | Yes | – | – | – | Yes |
Collier. J Wound Care 1996;5(5):207 to 11 | Yes | – | – | – | – |
Conine et al. Rehabilitation Nurs 1990;15(3):133 to 7. | Yes | – | – | – | – |
Cooper et al. J Wound Care 1998;7(8):374 to 6 | Yes | – | – | – | Yes |
Daechsel et al. Arch Phys Med Rehabil 1985;66(4):246 to 8. | Yes | – | – | – | – |
Day et al. Decubitus 1993;6(1):32 to 43. | Yes | – | – | – | – |
Demarre et al. Int J Nurs Stud 2012;49(4):416 to 26. | Yes | Yes | – | – | Yes |
Devine. J Tissue Viability 1995;5(3):94 to 8. | Yes | – | – | – | – |
Donnelly et al. J Wound Care 2011;20 (7), 309 to 318. | – | – | – | – | Yes |
Evans et al. J Wound Care 2000;9(4):181 to 6. | Yes | – | – | – | – |
Ewing et al. Australian Nurses' | Yes | – | – | – | – |
Ferrell et al. JAMA 1993;269(4):494 to 7 | Yes | – | – | – | – |
Feuchtinger et al. J Clin Nurs 2006;15(2):162 to 7 | Yes | – | – | – | – |
Finnegan et al. J Tissue Viability 2008;17(1):2 to 9 | Yes | – | – | – | – |
Gilcreast et al. J. Wound Ostomy Cont. Nurs. 2005; 32 (2), 112 to 120. | – | – | – | – | Yes |
Gray et al. J Tissue Viability 1994;4(4):128 to 32. | Yes | – | – | – | Yes |
Gray et al. J Wound Care 2000;9(1):29 to 31. | Yes | – | – | – | Yes |
Gray et al. Wounds UK 2008;4(4):124 to 8. | Yes | – | – | – | – |
Grindley et al. Br J Nurs (Mark Allen Publishing) 1996;5(21):1303 to 10. | Yes | – | – | – | – |
Groen et al. Journal of Wound Care 1999;8(7):333 to 5. | Yes | – | – | – | – |
Gunningberg et al. Journal of Wound Care 2000;9(10):455 to 60. | Yes | – | – | – | Yes |
Hampton. Br J Nurs (Mark Allen Publishing) 1997;6(3):167 to 70. | Yes | – | – | – | – |
Hofman et al. Lancet (London, England) 1994;343(8897):568 to 71 | Yes | – | – | – | Yes |
Hoshowsky et al. Res Nurs Health 1994;17(5):333 to 9 | Yes | – | – | – | – |
Inman et al. JAMA 1993;269(9):1139 to 43 | Yes | – | – | Yes | – |
IRCT2015110619919N3. 2016 | Yes | – | – | – | – |
Jiang et al. Adv Skin Wound Care 2020;33(3):1 to 9 | – | Yes | – | – | – |
Jiang et al. Int J Clin Exp Med 2014;7(9):2820 to 7. | Yes | Yes | – | – | Yes |
Jolley et al. Med J Aust 2004;180(7):324 to 7. | Yes | – | – | – | Yes |
Kemp et al. Res Nurs Health 1993;16(2):89 to 96 | Yes | – | – | – | – |
Laurent. 3rd European Conference for Nurse Managers, 1997 Oct; Brussels (Belgium) 1998 | Yes | – | – | – | – |
Lazzara et al. Decubitus 1991;4(4):42 to 4, 46, 48. | Yes | – | – | – | – |
Malbrain et al. J Tissue Viability 2010;19(1):7 to 15 | Yes | – | – | – | – |
Manzano et al. J Adv Nurs 2013;69:2099 to 106. | – | Yes | – | – | – |
Marvaki et al. Cureus 2020;12:e8785. | – | Yes | – | – | – |
McGowan et al. Primary Intention 2000:127 to 34. | Yes | – | – | – | Yes |
Meaume et al. J Wound Care 2017; 26(9), 537 to 544. | – | – | Yes | – | – |
Meyers. J Wound, Ostomy Cont Nurs 2017;44(5):429e33. | – | – | – | Yes | – |
Mistiaen P et al. Wound Repair Regen 2010;18(6):572 to 9. | Yes | – | – | – | – |
Mulder et al. J Geriatric Dermatology 1994;2(3):87 to 91. | Yes | – | – | – | – |
Munro et al. Geriatr Nurs 1989;10:190 to 2. | Yes | – | – | – | – |
Nixon et al. Health Technology Assessment (Winchester, England) 2006;10(22):1 to 163. | Yes | – | – | – | Yes |
Nixon et al. Health Technology Assessment (Winchester, England) 2019;23(52):1 to 176. | Yes | – | – | – | Yes |
Nixon et al. Int J Nurs Stud 1998;35(4):193 to 203 | Yes | – | – | – | – |
Ozyurek et al. Clin Nurse Spec 2015;29(4):210 to 7 | Yes | Yes | – | Yes | – |
Park et al. J Wound Ostomy Continence Nurs 2017;44(5):440 to 4. | Yes | – | – | – | Yes |
Phillips. Br J Nurs (Mark Allen Publishing) 1999;8(21):1447 to 52 | Yes | – | – | – | – |
Price et al. J Wound Care 1999;8(4):187 to 90. | Yes | – | – | – | Yes |
Pring et al. J Wound Care 1998;7(4):177 to 9. | Yes | – | – | – | – |
Rafter. Br J Nurs 2011;20(11):32. | Yes | – | – | – | – |
Ricci et al. EWMA Journal 2013;13(1):27 to 32. | Yes | – | – | – | – |
Rosenthal et al. Arch Phys Med Rehabil 2003;84(12):1733 to 42. | Yes | – | – | – | – |
Russell et al. Adv Skin Wound Care 2003;16(6):317 to 27. | Yes | – | – | – | Yes |
Russell et al. Ostomy Wound Manage 2000;46(2):46 to 51,54 to 5. | Yes | – | – | – | Yes |
Sanada et al. J Tissue Viability 2003;13(3):112 to 4, 116, 118. | Yes | – | – | – | Yes |
Santy et al. Report to Northern and Yorkshire Regional Health Authority 1994. | Yes | – | – | – | – |
Sauvage et al. J Wound Care 2017;26(6):304 to 12. | Yes | – | – | – | – |
Schultz et al. AORN Journal 1999;70(3):434, 437 to 40, 443 to 9 | Yes | – | – | – | – |
Shakibamehr et al. J Caring Sci 2019;8(1):45e9. https://doi.org/10.15171/jcs.2019.007. | – | – | – | Yes | – |
Sideranko et al. Res Nurs Health 1992;15(4):245 to 51. | Yes | – | – | – | – |
Stapleton. Geriatr Nurs (London, England) 1986;6(2):23 to 5. | Yes | – | – | – | – |
Strauss et al. J Fam Pract 1991;33(1):52 to 9. | Yes | – | – | – | – |
Takala et al. Clin Intensive Care 1996;7(5):228 to 35. | Yes | – | – | Yes | – |
Taylor. Br J Nurs (Mark Allen Publishing) 1999;8(12):771 to 4,776 to 8. | Yes | – | – | – | – |
Theaker et al. Anaesthesia 2005;60(4):395 to 9 | Yes | – | – | Yes | – |
Tymec et al. Adv. Wound Care 1997; 10 (1), 39 to 44. | – | – | – | – | Yes |
Van Leen et al. Adv Skin Wound Care 2018;31(1):1 to 5. | Yes | – | – | – | – |
Van Leen et al. J Tissue Viability 2011;20(1):30 to 4. | Yes | – | – | – | – |
Van Leen et al. Wounds 2013;25(10):287 to 92. | Yes | – | – | – | – |
Vanderwee et al. Age Aging 2005;34(3):261 to 7. | Yes | – | – | – | Yes |
Vermette et al. Wounds 2012;24(8):207 to 14. | Yes | – | – | – | Yes |
Vyhlidal et al. Appl Nurs Res 1997;10(3):111 to 20. | Yes | – | – | – | – |
Whitney et al. J Gerontol Nurs 1984;10(9):20 to 1, 24 to 5 | Yes | – | – | – | – |
Whittingham. J Tissue Viability 1999;9(3):104 | Yes | – | – | – | – |
Note: The systematic review by Stephens et al. (2022)17 is not included in this table since they did not identify any relevant studies.
Appendix 6: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
Off-Loading Devices for People with Diabetic Neuropathic Foot Ulcers: A Rapid Qualitative Review. Ottawa (ON): CADTH, 2020. https://www.cadth.ca/loading-devices-people-diabetic-neuropathic-foot-ulcers-rapid-qualitative-review. Accessed 2022 Jul 22.
Lateral Rotation Mattresses for the Prevention and Treatment of Pressure Injuries: Clinical Effectiveness and Guidelines. Ottawa (ON): CADTH, 2019. https://www.cadth.ca/lateral-rotation-mattresses-prevention-and-treatment-pressure-injuries-clinical-effectiveness-and. Accessed 2022 Jul 22.
Mattresses or Overlays Used in Palliative End-of-Life Care: Clinical Evidence and Guidelines. Ottawa (ON): CADTH, 2019. https://www.cadth.ca/mattresses-or-overlays-used-palliative-end-life-care-clinical-evidence-and-guidelines. Accessed 2022 Jul 22.
Non-Pharmacological Prevention of Pressure Injuries: An Environmental Scan. Ottawa (ON): CADTH, 2019. https://www.cadth.ca/non-pharmacological-prevention-pressure-injuries-environmental-scan. Accessed 2022 Jul 22.
Health Technology Assessments
Published Before 2020
Fibreglass total contact casting, removable cast walkers, and irremovable cast walkers to treat diabetic neuropathic foot ulcers: a health technology assessment. Toronto (ON): Health Quality Ontario, 2017. Accessed 2022 Aug 08. http://www.hqontario.ca/Portals/0/Documents/evidence/reports/hta-fibreglass-1709-en.pdf
Systematic Reviews
Published Before 2020
Gaspar S, Peralta M, Marques A, Budri A, Gaspar de Matos M. Effectiveness on hospital-acquired pressure ulcers prevention: a systematic review. Int. Wound J. 2019;16(5):1087-1102. PubMed
Maki-Turja-Rostedt S, Stolt M, Leino-Kilpi H, Haavisto E. Preventive interventions for pressure ulcers in long-term older people care facilities: A systematic review. J. Clin. Nurs. 2019;28(13-14):2420-2442. PubMed
Rae KE, Isbel S, Upton D. Support surfaces for the treatment and prevention of pressure ulcers: a systematic literature review. J. Wound Care. 2018;27(8):467-474. PubMed
Shi C, Dumville JC, Cullum N. Support surfaces for pressure ulcer prevention: A network meta-analysis. PLoS ONE [Electronic Resource]. 2018;13(2):e0192707. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca