CADTH Health Technology Review
Real-Time Continuous Glucose Monitoring: A Review of Guidelines
Rapid Review
Authors: Angela M. Barbara, Aleksandra Grobelna
Abbreviations
AACE
American Association of Clinical Endocrinology
ADA
American Diabetes Association
AGREE
Appraisal of Guidelines for Research and Evaluation
CGM
continuous glucose monitoring
isCGM
intermittently scanned continuous glucose monitoring
NICE
National Institute for Health and Care Excellence
rtCGM
real-time continuous glucose monitoring
RCT
randomized controlled trial
SMBG
self-monitoring of blood glucose
Key Messages
Six evidence-based guidelines regarding the use of real-time continuous glucose monitoring in people living with type 1 or type 2 diabetes were included in this report. Three included guidelines were of high quality, while 3 guidelines were of moderate quality due to unclear reporting of methodological details.
Four evidence-based guidelines strongly recommended the use of real-time continuous glucose monitoring in adults for the management of type 1 diabetes, based on intermediate- to high-quality evidence.
Four guidelines recommended real-time continuous glucose monitoring for adults living with type 2 diabetes, based on low- to high-quality evidence.
Three guidelines strongly recommended the use of real-time continuous glucose monitoring in children and young people living with type 1 diabetes, based on intermediate- to high-quality evidence.
One guideline recommended real-time continuous glucose monitoring for children and young people with type 2 diabetes, based on expert consensus rather than evidence of clinical effectiveness.
Context and Policy Issues
Diabetes is a chronic condition in which the body is not able to produce enough insulin and/or properly use insulin.1 The body needs insulin to use sugar as an energy source.1 Type 1 diabetes is an autoimmune condition in which the insulin-producing beta cells of the pancreas are destroyed by the immune system.1 Type 1 diabetes is often diagnosed in childhood and common presenting symptoms include frequent urination, excessive thirst, weight loss, and diabetic ketoacidosis (a potentially life-threatening complication of diabetes in which acids called ketones build up to dangerous levels in the body).2,3 In addition, hypoglycemia-related changes can have a negative impact on the quality of life of people with type 1 diabetes and lead to hypoglycemia fears.4 Type 2 diabetes is a condition that occurs when the body does not make enough insulin and/or does not respond to the insulin it makes.1 In the early stages of type 2 diabetes, there may be no symptoms or only mild symptoms that can go unnoticed.5 When symptoms are present, they can include frequent urination, excessive thirst and hunger, fatigue, blurry vision, slow-healing wounds, and tingling, pain, or numbness in the hands and/or feet.5
Approximately 3 million Canadians have diagnosed diabetes.6 The most common type of diabetes in adults is type 2 diabetes, accounting for approximately 90% of adults living with diabetes in Canada.7 In children and youth aged younger than 20 years in Canada, type 1 diabetes accounts for at least 85% of diabetes cases.6
All people living with type 1 diabetes and some people with type 2 diabetes need to take insulin to keep blood glucose levels within the target range.1,8 There are many ways insulin therapy can be delivered, including multiple daily injections and insulin pumps.8 Blood glucose monitoring is used in combination with insulin therapy to adjust insulin doses and maintain glucose control.9 The traditional method for blood glucose monitoring is self-monitoring of blood glucose (SMBG) using a glucometer (also called capillary blood glucose monitoring).10 SMBG requires a fingerstick to take a blood sample, which can be painful and time-consuming.11 Some people living with diabetes find it difficult to practice SMBG at the recommended rates (e.g., 6 to 10 times per day).9 Additionally, nocturnal or asymptomatic hypoglycemia (low blood glucose) may not be recognized through SMBG.11 Severe hypoglycemia can lead to coma or death.11
Continuous glucose monitoring (CGM) systems continuously measure the glucose concentration in the interstitial fluid and transfer the data to a receiver which displays the results.11 These devices represent an alternative to SMBG for people living with diabetes. CGM systems typically consist of 3 components: a sensor inserted into the deepest layer of the skin, a transmitter attached to the sensor, and a receiver (monitor or smartphone) that displays the results.11,12 There are 2 types of CGM systems available for personal use: real-time CGM (rtCGM) and intermittently scanned CGM (isCGM, also known as flash glucose monitoring).11 rtCGM systems (e.g., Dexcom G6, Guardian Connect) measure the glucose values and automatically display a recent value.11 rtCGM devices have the capability for alerts and alarms for current and/or impending glycemic events, such as hyperglycemia or hypoglycemia.13 Some older rtCGM systems (e.g., Dexcom G5) require daily calibration with SMBG, whereas newer devices (e.g., Dexcom G6) do not.13,14 The rtCGM sensor application site is typically the abdomen or gluteus area.11,15
Diabetes is regarded as a burdensome disease for health care systems because of the time and resource costs related to the management of diabetes and its complications.6 The direct cost to the Canadian health care system for type 1 and type 2 diabetes was $3.8 million in 2020 and is estimated to climb to $4.9 million in 2030.16 The financial burden of rtCGM use in patients is also high.17 Many people in Canada with diabetes pay more than 3% of their income, or more than $1,500 per year, for prescribed medications, devices, and supplies; these out-of-pocket costs affect treatment adherence.16
In 2022, CADTH reviewed the clinical and cost-effectiveness of CGM in 3 rapid reviews: rtCGM compared to isCGM for people with diabetes,18 rtCGM compared to SMBG for people with type 1 diabetes,19 and rtCGM versus SMBG for people with type 2 diabetes.20 The purpose of this rapid review is to summarize and critically appraise evidence-based guidelines regarding the use of rtCGM in people living with type 1 or type 2 diabetes.
Research Question
What are the evidence-based guidelines regarding the use of real-time continuous glucose monitoring in adult and pediatric populations living with type 1 or type 2 diabetes?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, and the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were continuous glucose monitoring (CGM), real-time continuous glucose monitoring (rtCGM), type 1 diabetes, and type 2 diabetes. No filters were applied to limit the retrieval by study type. Comments, newspaper articles, editorials, letters, and conference abstracts were excluded.
Where possible, retrieval was limited to the human population. The search was completed on July 12, 2022, and limited to English-language documents published since January 1, 2017.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | People living with type 1 or type 2 diabetes |
Intervention | Real-time continuous glucose monitoring |
Comparator | Not applicable |
Outcomes | Recommendations regarding the appropriate use of real-time continuous glucose monitoring for adults and pediatric populations living with type 1 or type 2 diabetes (e.g., considerations for the implementation and use of real-time continuous glucose monitoring for adults and pediatric populations respectively) |
Study designs | Evidence-based guidelines |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1 or were published before 2020. Guidelines for pregnant people living with type 1 or type 2 diabetes were excluded. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument21 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
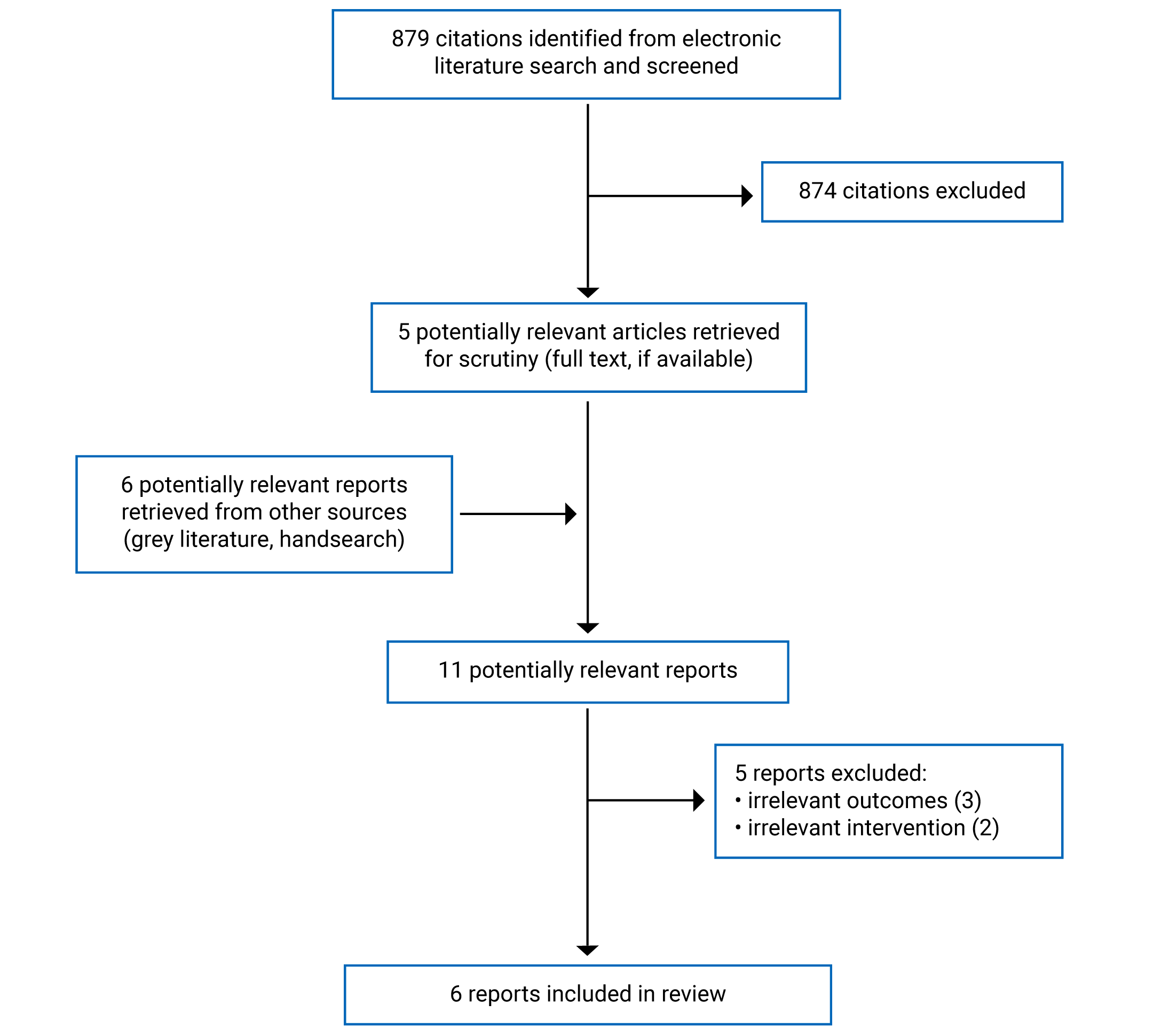
A total of 879 citations were identified in the literature search. Following screening of titles and abstracts, 874 citations were excluded and 5 potentially relevant reports from the electronic search were retrieved for full-text review. Six potentially relevant publications were retrieved from the grey literature search for full-text review. Of these 11 potentially relevant articles, 5 publications were excluded for various reasons, and 6 evidence-based guidelines met the inclusion criteria and were included in this report. Appendix 1 presents the PRISMA22 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
Six evidence-based guidelines10,23-27 were included in this report.
Five guidelines10,23-25,27 reported their methodology in separate publications.28-31 These documents were used to supplement the information summarized in this report.
Study Design
The American Diabetes Association (ADA) Standards of Medical Care for Diabetes23 were updated in 2022. An extensive literature search was performed, and relevant literature was reviewed through July 1, 2021, with critical updates through August 1, 2021 considered. Recommendations were revised based on new evidence, new considerations for standard of care practices, or to clarify prior recommendations or revise wording to match the strength of the published evidence. Recommendations were assigned letter ratings depending on the quality of the evidence: A for well-conducted randomized controlled trials (RCTs) that are adequately powered or have compelling non-experimental evidence; B for well-conducted cohort studies or case-control studies; C for poorly controlled or uncontrolled studies or conflicting evidence with the weight of evidence supporting the recommendation; or E for expert census or clinical experience. The ADA Standards of Care23 were reviewed by ADA’s clinical staff leadership, and underwent annual review and approval by the board of directors.
The 3 National Institute for Health and Care Excellence (NICE) guidelines10,24,25 were updated in 2022 and informed by systematic reviews of clinical effectiveness and cost-effectiveness. Systematic searches until May 2021 for relevant RCTs, systematic reviews of RCTs, and economic evaluations were undertaken. The NICE guidelines10,24,25 used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach to evaluate the quality of the evidence. The quality of evidence was graded from very low to high, and reflected the strength of recommendations in the wording (i.e., “offer/advise” was used for strong recommendations with clear evidence of benefit, while “consider” was used if the evidence was less certain). The committee discussed the evidence and drafted the recommendations. The committee moved from the evidence to each recommendation and discussed any issues that influenced their decision-making. In line with the GRADE principles on “evidence to decisions”, summaries of the discussions described the relative value placed on outcomes, benefits and harms, resource use, and the overall quality of the evidence.10,24,25
The American Association of Clinical Endocrinology (AACE) guideline26 was published in 2021 and informed by systematic searches between January 2012 and February 2021 for systematic reviews, RCTs, and non-randomized studies. Levels of evidence were assigned to included studies according to established AACE evidence ratings: strong (RCT or meta-analysis of only RCTs), intermediate (meta-analysis of non-randomized studies, network meta-analysis, non-randomized studies, epidemiological studies), or weak (discovery science, economic studies, case series, case reports, preclinical studies, basic science).26 These ratings informed the confidence and strength of evidence in aggregate for each recommendation: grades A (very strong), B (strong), C (not strong), and D (primarily based on expert opinion). Clinical questions provided the framework for the guidelines with answers in the form of recommendations. Final recommendations were based on discussion and unanimous consensus.26
The 2021 Diabetes Canada guideline on glucose monitoring in adults and children with diabetes27 was an update to the 2018 recommendations for monitoring glycemic control. This 2021 report was developed based on a systematic search of the literature published from November 2017 to October 2020 to retrieve relevant articles published since the last literature search of the original report. The full-text citations and critical appraisal reports were prepared by the McMaster Evidence Review and Synthesis Team and reviewed by the expert working group, who graded the evidence and drafted the revised recommendations. Evidence levels were designated as follows: 1A for evidence obtained from a systematic review or meta-analysis of high-quality RCTs or an appropriately designed RCT with adequate power to answer the research question; 1B for a non-randomized clinical trial or cohort study with indisputable results; 2 for an RCT or systematic review that does not meet level 1 criteria; 3 for a non-randomized clinical trial or cohort study or systematic review or meta-analysis of non-randomized trials or cohort studies; and 4 for other studies. Grading of recommendations was based on the level of the best evidence: A (the best evidence was at level 1); B (level 2); C (level 3); and D (required best evidence at level 4 or consensus). The steering committee reviewed the cited evidence independently and suggested revisions to the draft recommendations and the text.27 Final recommendations were unanimously approved by the steering committee.27
Country of Origin
The ADA guideline23 and AACE guideline26 were designed for use in the US. The 3 NICE guidelines10,24,25 were intended to be applied in England. The Diabetes Canada guideline27 was developed for Canada.
Patient Population
The target populations of 3 guidelines23,26,27 were adults and children living with diabetes. The other 3 guidelines targeted adults with type 1 diabetes,10 adults with type 2 diabetes,25 and children and young people with type 1 diabetes.10
The intended users of 5 guidelines10,23,24-26 were health care professionals and other key stakeholders. For the NICE guidelines,10,24,25 the intended users also included people living with type 1 or type 2 diabetes, and their families and carers. The intended users of the Diabetes Canada guideline27 were not explicitly reported, but can be deduced to be people living with diabetes and their health care providers.27
Interventions and Comparators
Recommendations that specified rtCCM in the 6 guidelines10,23-27 were included. Five guidelines10,23-26 made recommendations regarding any CGM systems, which include rtCGM and isCGM. Due to the large number and nature of these recommendations (e.g., general usage, patient education, discussing patient concerns),10,23-26 only specific recommendations regarding the use of rtCGM were considered relevant for this report.
In the evidence synthesis for all guidelines,10,23-27 the comparator was SMBG.
rtCGM was also compared to isCGM in the evidence synthesis for all guidelines.10,23-27 isCGM systems (e.g., FreeStyle Libre) measure glucose levels every minute and store 1 value every 15 minutes. isCGM systems need to be actively scanned to display glucose information.11 Only the most recent 8 hours of data are retained in isCGM systems and, therefore, the person using the system must scan the sensor at least every 8 hours to avoid data gaps.13
Outcomes
The primary outcomes in the 3 NICE guidelines10,24,25 were hemoglobin A1C, time spent in target glucose range estimates, hypoglycemia, glycemic variability, mortality, and diabetic ketoacidosis. Secondary outcomes were other adverse events, mental health outcomes, awareness of hypoglycemia, adherence, and quality of life.10,24,25 The 3 NICE guidelines10,24,25 also considered cost-effectiveness.
Three guidelines23,26,27 did not report on the outcomes considered during development, or if and which outcomes were eligible during selection of supporting evidence; however, evidence on hemoglobin A1C,23,26,27 time in range estimates,26,27 hypoglycemia,23,26,27 quality of life,23,26,27 and adverse events (e.g., severe hypoglycemia,26,27 hospitalizations,23 emergency department visits23) were mentioned in the recommendations and/or supporting evidence.23,26,27
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Summary of Critical Appraisal
An overview of the critical appraisal of the included guidelines is summarized in the following text. Additional details regarding the strengths and limitations of the included guidelines are provided in Appendix 3.
With respect to scope and purpose, all guidelines10,23-27 provided a clear description of their objectives and specified the target populations. The clinical research questions covered by the guidelines were reported in 4 guidelines,10,24-26 but not in the ADA23 and Diabetes Canada27 guidelines.
The guideline development groups were comprised of clinical and methodological experts from multidisciplinary areas for all guidelines.10,23-27 The NICE guidelines10,24,25 included at least 2 lay members (patients with type 1 or type 2 diabetes and caregivers) on their guideline committees, and sought involvement from people with type 1 or 2 diabetes who use health and care services, family members, caregivers, and the public. For 3 guidelines,23,26,27 the views and preferences of the target population were not sought and there was no mention of patient, parent, or caregiver representation or consultation.23,26,27
With respect to rigour of guideline development, systematic methods were used to search for evidence in all guidelines.10,23-27 The NICE guidelines10,24,25 provided full details of the strategy used to search for evidence. The ADA and Diabetes Canada guidelines23,27 provided very brief details of their methodology; specifically, the undertaking of a literature review and the search time frame. However, it was not specified how the literature review process was carried out (e.g., databases searched, main search terms, inclusion criteria, how relevant studies were selected) in these 2 guidelines.23,27 The authors of the AACE guideline26 conducted literature searches in 1 database (i.e., PubMed), which may have resulted in omission of relevant information.
The link between the individual recommendations and supporting evidence was not completely evident in 5 guidelines.10,23-27 Rather, each report10,23-27 provided a section on the overall evidence for CGM or rtCGM. Therefore, the reasoning used to reach the individual recommendations was not always clear. Four guidelines10,24-26 were externally reviewed by experts before publication, but 2 guidelines did not report how the guideline was validated.23,27
All guidelines10,23-27 provided specific, unambiguous, and easily identifiable recommendations. The potential resource implications of applying the recommendations were considered in 4 guidelines,10,24-26 but not in the ADA23 and Diabetes Canada27 guidelines.
Four guidelines10,24-26 described their procedure for updating their guidelines. While it was reported that the ADA guideline23 underwent an annual review, the procedure for guideline updates was not explicitly described.
Regarding editorial independence, it was uncertain whether the views of the funding body influenced the content of the included guidelines.10,23-27 For each guideline,10,23-27 the funding was provided by the professional organization (i.e., ADA, NICE, AACE, Diabetes Canada) that was responsible for creating the guidelines, and there was no explicit statement that the views of the funding body had not influenced the guideline. However, all guidelines10,23-27 reported the competing interests of their authors.
In summary, the 3 NICE guidelines10,24,25 followed a detailed process for developing the recommendations based on the criteria outlined in the AGREE II instrument.21 The methodology of the AACE guideline26,27had some limitations. The ADA23 and Diabetes Canada27 guidelines did not report sufficient detail regarding the methodology used for developing their recommendations.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
Guidelines
Appendix 4 presents the main study findings and authors’ conclusions.
Recommendations Regarding the Use of rtCGM for Adults With Type 1 Diabetes
The ADA Standards of Care23 recommended rtCGM for adults with type 1 diabetes for diabetes management based on level A evidence (well-conducted and adequately powered RCTs; strength of recommendation not reported).
The NICE guideline for adults with type 1 diabetes10 made a strong recommendation for the use rtCGM (level of evidence not reported). The NICE guideline10 also strongly recommended the use of SMBG if a person could not or did not want to use rtCGM (level of evidence not reported).
The Diabetes Canada guideline27 recommended rtCGM for adults with type 1 diabetes who were willing and able to use rtCGM devices on a near-daily basis (grade A recommendation, based on well-conducted RCTs). rtCGM was recommended versus SMBG (grade A recommendation, based on well-conducted RCTs) and isCGM (grade B recommendation, based on low- to moderate-quality RCTs).
The AACE guideline26 strongly recommended rtCGM over isCGM for persons with diabetes (type not specified) with problematic hypoglycemia who required predictive alarms/alerts based on low- to intermediate-quality evidence. The AACE guideline26 also very strongly recommended rtCGM for persons aged 65 years and older with insulin-requiring diabetes (type not specified), based on intermediate-quality evidence.
Recommendations Regarding the Use of rtCGM for Adults With Type 2 Diabetes
The ADA Standards of Care23 recommended rtCGM for adults with type 2 diabetes for diabetes management, based on level A evidence (strength of recommendation not reported).
The NICE guideline for adults with type 2 diabetes25 recommended rtCGM as an alternative to isCGM if available for the same or lower cost, based on evidence indicating that the benefit was less than certain.
The Diabetes Canada guideline27 recommended rtCGM for adults with type 2 diabetes using basal-bolus therapy who had not achieved their hemoglobin A1C target and were willing and able to use rtCGM devices (grade A recommendation, based on well-conducted RCTs).
The AACE guideline26 strongly recommended rtCGM over isCGM for persons with diabetes (type not specified) with problematic hypoglycemia who required predictive alarms/alerts based on low- to intermediate-quality evidence. The AACE guideline26 also very strongly recommended rtCGM for persons 65 years of age and older with insulin-requiring diabetes (type not specified) based on intermediate-quality evidence.
Recommendations Regarding the Use of rtCGM for Children and Adolescents With Type 1 Diabetes
The ADA Standards of Care23 recommended rtCGM for youth with type 1 diabetes for diabetes management, based on level B evidence (well-conducted cohort studies).
The NICE guideline for children and young people with type 1 diabetes24 made a strong recommendation for the use of rtCGM (level of evidence not reported). The NICE guideline also made a strong recommendation for offering children and young people with type 1 diabetes a choice of rtCGM device, with a list of factors to consider when choosing a device (e.g., device accuracy, access to specific technologies, fear of hypoglycemia, device calibration, predictability of child or young person’s activity, and blood glucose levels). The NICE guideline24 also strongly recommended the use of isCGM for children and young people with type 1 diabetes who were unable to use rtCGM or expressed a clear preference for isCGM (level of evidence not reported). A strong recommendation was also made for the use capillary blood glucose monitoring for persons who could not or did not want to use rtCGM or isCGM (level of evidence not reported).24
The Diabetes Canada guideline27 recommended rtCGM for children with type 1 diabetes who were willing and able to use rtCGM devices on a near daily basis (grade A recommendation, based on well-conducted RCTs).
Recommendations Regarding the Use of rtCGM for Children and Adolescents With Type 2 Diabetes
The ADA Standards of Care23 recommended rtCGM for youth with type 2 diabetes for diabetes management, based on expert consensus or clinical expertise (in the absence of evidence from clinical studies).
Other Recommendations
The ADA Standards of Care23 recommended that rtCGM be used as close to daily as possible for maximum benefit, based on level A evidence. The ADA guideline23 also recommended periodic use of rtCGM or isCGM in circumstances where continuous use was not appropriate, desired, or available. The level of evidence supporting this recommendation was reported as C (poorly controlled or uncontrolled studies, or conflicting evidence), but the evidence itself was not reported.23
Limitations
Four guidelines10,23,25,27 recommended rtCGM for people who had the ability to use rtCGM devices. For examples, the ADA Standards of Care23 made recommendations for adults and youth “who are capable of using devices safely (either by themselves or with a caregiver)” and the NICE guidelines for adults with type 110 and type 2 diabetes25 made recommendations for alternatives to rtCGM for people who “cannot use” rtCGM.10 However, there was no further information or guidance provided in the guideline documents regarding how the clinician should determine if patients meet these requirements.10,23,25
CGM technologies are changing very quickly with increasing overlap between rtCGM and isCGM, as features such as predictive alerts or alarms (available in rtCGM devices) are added to newer isCGM devices.10 The guideline authors acknowledged this, and therefore did not make recommendations on using specific devices, as such recommendations would soon be out of date.10,23,24
The Diabetes Canada guideline23 was developed for the Canadian context, but was assessed as having a number of limitations due to incomplete reporting of the methods. The other 5 guidelines10,23-26 were developed for use in the US23,26 or England10,24,25; therefore, the generalizability of the recommendations to the Canadian context was unclear.
Conclusions and Implications for Decision- or Policy-Making
This report comprised 6 evidence-based guidelines10,23-27 regarding the use of rtCGM in people living with type 1 or type 2 diabetes.
Of the included guidelines, 410,23,26,27 recommended the use of rtCGM by adults, including seniors (who are at significantly higher risk for severe hypoglycemia compared to younger people),23,26 for the management of type 1 diabetes. This recommendation is aligned with the findings of the 2022 CADTH report on the clinical effectiveness and cost-effectiveness of rtCGM in type 1 diabetes.19 The report concluded that rtCGM may have been favoured over SMBG in improving hemoglobin A1C, time in range outcomes, and severe hypoglycemia in adults with type 1 diabetes. The CADTH report19 also found that rtCGM may be more cost-effective in the long term compared to SMBG in adults with type 1 diabetes.19
Four guidelines23,25-27 recommended the use of rtCGM by adults with type 2 diabetes. This recommendation reflects the results of the 2022 CADTH report on the effectiveness of type 2 diabetes that rtCGM20 may provide positive effects on hemoglobin A1C, with low rates of severe adverse events. However, the CADTH report found that rtCGM was not cost-effective compared to SMBG in people with type 2 diabetes.20
Three guidelines23,24,27 recommended the use of rtCGM for children and young people with type 1 diabetes. This also reflects the findings of the 2022 CADTH report on the effectiveness of type 1 diabetes19 that rtCGM may provide positive effects on hemoglobin A1C, time in range, time above range, and treatment satisfaction in children and pediatric patients with type 1 diabetes.
Overall, the strength of these recommendations ranged from less than certain to very strong and were based on evidence that ranged in quality from very low to high.10,23,26,27 The quality of the clinical and cost-effectiveness evidence of rtCGM (as assessed by systematic review authors) was also found to range from very low to high-quality in the 2 CADTH reports on type 1 and type 2 diabetes.19,20 Recommendations emphasized patient choice and suggested that adherence to rtCGM was likely to be higher if the device was matched to a person’s needs and preferences.10,23-25,27
The authors of the Diabetes Canada guideline27 and the NICE guideline for children and young people24 acknowledged that there was a lack of evidence on the clinical effectiveness of rtCGM in children and young people with type 2 diabetes. The CADTH report on the clinical and cost-effectiveness of rtCGM in type 2 diabetes20 also reported no evidence in pediatric patients. Diabetes Canada27 and NICE24 did not make recommendations for the use of rtCGM for children and young people with type 2 diabetes. Rather the NICE guideline24 made a recommendation for research on continuous glucose monitoring in children and young people living with type 2 diabetes. On the other hand, the ADA guideline23 recommended rtCGM for youth with type 2 diabetes based on expert consensus and/or clinical expertise, in the absence of evidence of clinical effectiveness.
Five guidelines23,24,25,26,27 recommended rtCGM more favourably than isCGM for diabetes management. The NICE guideline for adults with type 1 diabetes10 recommended both rtCGM and isCGM, due to the very low certainty of the evidence on comparative clinical effectiveness between the 2 CGM technologies.
In general, there was agreement across guidelines on the use of rtCGM for the management of type 1 and 2 diabetes in adults and pediatric populations. However, the variation in the strengths of recommendations and heterogeneity in the quality of evidence should be considered when interpreting the findings of this report. Guidelines developed with rigorous methodology that are specific to the Canadian context would provide additional guidance in use of rtCGM for diabetes management in a more local context.
References
1.Public Health Agency of Canada. Diabetes facts. 2012; https://www.canada.ca/en/public-health/services/chronic-diseases/diabetes/diabetes-facts.html. Accessed 2022 Jul 6.
2.DiMeglio LA, Evans-Molina C, Oram RA. Type 1 diabetes. Lancet. 2018;391(10138):2449-2462. PubMed
3.Center for Disease Control and Prevention. Diabetic ketoacidosis. 2021; https://www.cdc.gov/diabetes/basics/diabetic-ketoacidosis.html. Accessed 2022 Jul 6.
4.Hermanns N, Kubiak T, Kulzer B, Haak T. Emotional changes during experimentally induced hypoglycaemia in type 1 diabetes. Biol Psychol. 2003;63(1):15-44. PubMed
5.Artasensi A, Pedretti A, Vistoli G, Fumagalli L. Type 2 diabetes mellitus: a review of multi-target drugs. Molecules. 2020;25(8):1987. PubMed
6.Ontario health technology assessment series: Continuous monitoring of glucose for type 1 diabetes: A health technology assessment. Ontario Health Technology Assessment Series. 2018;18(2):1-160. PubMed
7.Public Health Agency of Canada. Diabetes in Canada. 2017; https://www.canada.ca/en/public-health/services/publications/diseases-conditions/diabetes-canada-highlights-chronic-disease-surveillance-system.html. Accessed 2022 Jul 6.
8.Shah RB, Patel M, Maahs DM, Shah VN. Insulin delivery methods: past, present and future. Int J Pharm Investig. 2016;6(1):1-9. PubMed
9.McGill JB, Ahmann A. Continuous glucose monitoring with multiple daily insulin treatment: outcome studies. Diabetes Technol Ther. 2017;19(S3):S-3-S-12. PubMed
10.Type 1 diabetes in adults: diagnosis and management. NICE guideline [NG17]. London (UK): National Institute for Health and Care Excellence; 2022. Accessed 2022 Jul 6.
11.Freckmann G. Basics and use of continuous glucose monitoring (CGM) in diabetes therapy. Journal of Laboratory Medicine. 2020;44(2):71-79.
12.Galindo RJ, Aleppo G. Continuous glucose monitoring: The achievement of 100 years of innovation in diabetes technology. Diabetes Res Clin Pract. 2020;170:108502. PubMed
13.Edelman SV, Argento NB, Pettus J, Hirsch IB. Clinical implications of real-time and intermittently scanned continuous glucose monitoring. Diabetes Care. 2018;41(11):2265-2274. PubMed
14.Thabit H, Prabhu JN, Mubita W, et al. Use of factory-calibrated real-time continuous glucose monitoring improves time in target and HbA1c in a multiethnic cohort of adolescents and young adults with type 1 diabetes: The MILLENNIALS study. Diabetes Care. 2020;43(10):2537-2543. PubMed
15.Faccioli S, Del Favero S, Visentin R, et al. Accuracy of a CGM Sensor in Pediatric Subjects With Type 1 Diabetes. Comparison of Three Insertion Sites: Arm, Abdomen, and Gluteus. J Diabetes Sci Technol. 2017;11(6):1147-1154. PubMed
16.Diabetes in Canada Backgrounder. Ottawa (ON): Diabetes Canada; 2020: https://www.diabetes.ca/DiabetesCanadaWebsite/media/Advocacy-and-Policy/Backgrounder/2020_Backgrounder_Canada_English_FINAL.pdf. Accessed 2022 Jul 11.
17.Parkin CG, Graham C, Smolskis J. Continuous Glucose Monitoring Use in Type 1 Diabetes: Longitudinal Analysis Demonstrates Meaningful Improvements in HbA1c and Reductions in Health Care Utilization. J Diabetes Sci Technol. 2017;11(3):522-528. PubMed
18.Intermittently Scanned and Real-Time Continuous Glucose Monitoring for People With Diabetes. Ottawa (ON): CADTH; 2022: https://www.cadth.ca/intermittently-scanned-and-real-time-continuous-glucose-monitoring-people-diabetes.
19.Real Time Continuous Glucose Monitoring for People Living with Type 1 Diabetes. Ottawa (ON): CADTH; 2022: https://www.cadth.ca/real-time-continuous-glucose-monitoring-people-living-type-1-diabetes. Accessed 2022 Nov 6.
20.Real Time Continuous Glucose Monitoring for People Living with Type 2 Diabetes. Ottawa (ON): CADTH; 2022: https://www.cadth.ca/real-time-continuous-glucose-monitoring-people-living-type-2-diabetes. Accessed 2022 Nov 6.
21.Agree Next Steps C. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2022 Jul 6.
22.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
23.Draznin B, Aroda VR, Bakris G, et al. 7. Diabetes Technology: Standards of Medical Care in Diabetes-2022. Diabetes Care. 2022;45(Supplement_1):S97-S112. PubMed
24.Diabetes (type 1 and type 2) in children and young people: diagnosis and management. NICE guidance [NG18]. London (UK): National Institute for Health and Care Excellence; 2022: https://www.nice.org.uk/guidance/ng18/resources/diabetes-type-1-and-type-2-in-children-and-young-people-diagnosis-and-management-pdf-1837278149317. Accessed 2022 Jun 27.
25.Type 2 diabetes in adults: management. NICE guideline [NG28]. London (UK): National Institute for Health and Care Excellence; 2022: https://www.nice.org.uk/guidance/ng28. Accessed 2022 Jun 27.
26.Grunberger G, Sherr J, Allende M, et al. American Association of Clinical Endocrinology clinical practice guideline: the use of advanced technology in the management of persons with diabetes mellitus. Endocr Pract. 2021;27(6):505-537. PubMed
27.Cheng AY, Feig DS, Ho J, et al. Blood glucose monitoring in adults and children with diabetes: Update 2021. Can J Diabet. 2021;45(7):580-587. PubMed
28.Developing NICE guidelines: the manual. [PMG20]. London (UK): National Institute for Health and Care Excellence; 2022: https://www.nice.org.uk/process/pmg20/resources/developing-nice-guidelines-the-manual-pdf-72286708700869. Accessed 2022 Jun 24.
29.American Diabetes Association. Professional Practice Committee: Standards of Medical Care in Diabetes—2022. Diabetes Care. 2022;45:S3.
30.American Diabetes Association. Introduction: Standards of medical care in diabetes—2022. Diabetes Care. 2022;45(Suppl.1):S1-S2. PubMed
31.Sherifali D, Rabi D, Houlden R. Diabetes Canada clinical practice guidelines expert committee. Can J Diabet. 2018;42:S6-S9.
32.Type 1 diabetes in children and young people: diagnosis and management. NICE guideline NG[18]. London (UK): National Institute for Health and Care Excellence; 2022: https://www.nice.org.uk/guidance/ng18/evidence/b-continuous-glucose-monitoring-in-children-and-young-people-with-type-1-diabetes-pdf-11011942190. Accessed 2022 Jul 02.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
Intended users: Clinicians, researchers, policy-makers, and other interested individuals with components of diabetes care, general treatment goals, and tools to evaluate quality of care Target population: Patients with diabetes, including children from birth to 11 years of age and adolescents aged 12 to 18 years, and older adults (aged 65 years and older) | Diabetes technology for patients with diabetes Relevant intervention: rtCGM |
| Evidence collected using a systematic literature review, with critical updates | Ratings depended on quality of evidence in support of the recommendation:
| Existing recommendations were updated based on new evidence, new considerations for standard of care practices, or, in some cases, to clarify the prior recommendations or revise wording to match the strength of the published evidence. The literature review is supplemented with input from ADA staff and the medical community at large. Annual review and approval by the ADA board of directors, which includes health care professionals, scientists, and lay people. Review by the ADA scientific and medical staff. | Feedback by the larger clinical community was welcome, and readers were invited to comment online. |
Intended users: Health care professionals, including those working in dental services; commissioners and providers; children and young people with T1D and T2D, and their families and carers Target population: Children and young people (aged < 18 years) with T1D and T2D | Diagnosis and management of T1D and T2D in children and young people Relevant intervention: rtCGM |
| Evidence collected using a systematic evidence review of clinical and cost-effectiveness | Evidence quality was assessed using the GRADE approach. Strength of recommendation was reflected in the wording:
| The committee discussed the evidence and drafted the recommendations. The committee moved from the evidence to each recommendation discussed any issues influenced their decision-making. In line with the GRADE principles on “evidence to decisions”, summaries of the discussions described the relative value placed on outcomes, benefits and harms, resource use, and the overall quality of the evidence, as well as other considerations. | Registered stakeholders comment on the draft scope and draft guideline. NICE formally responds to comments from stakeholders, and these responses are published on the NICE website. Regular consultation allows organizations and individuals to comment on the recommendations. Once published, the guidelines are regularly checked, and updated in light of new evidence or intelligence, if necessary. |
NICE N18 guideline, 202210,28 | ||||||
Intended users: Health care professionals, including those working in dental services; commissioners and providers; adults with T1D, and their families and carers Target population: Adults with T1D (aged ≥ 18 years) | Diagnosis and management of T1D in adults Relevant intervention: rtCGM |
| Evidence collected using a systematic evidence review of clinical and cost-effectiveness | Evidence quality was assessed using the GRADE approach. Strength of recommendation was reflected in the wording:
| The committee discussed the evidence and drafted the recommendations. The committee moved from the evidence to each recommendation discussed any issues influenced their decision-making. In line with the GRADE principles on “evidence to decisions”, summaries of the discussions described the relative value placed on outcomes, benefits and harms, resource use, and the overall quality of the evidence, as well as other considerations. | Registered stakeholders comment on the draft scope and draft guideline. NICE formally responds to comments from stakeholders, and these responses are published on the NICE website. Regular consultation allows organizations and individuals to comment on the recommendations. Once published, the guidelines are regularly checked, and updated in light of new evidence or intelligence, if necessary. |
Intended users: Health care professionals, including those working in dental services; commissioners and providers; adults with T2D, and their families and carers Target population: Adults with T2D (aged ≥ 18 years) | Management of T2D in adults Relevant intervention: rtCGM |
| Evidence collected using a systematic evidence review of clinical and cost-effectiveness | Evidence quality was assessed using the GRADE approach. Strength of recommendation was reflected in the wording:
| The committee discussed the evidence and drafted the recommendations. The committee moved from the evidence to each recommendation discussed any issues influenced their decision-making. In line with the GRADE principles on “evidence to decisions”, summaries of the discussions described the relative value placed on outcomes, benefits and harms, resource use, and the overall quality of the evidence, as well as other considerations. | Registered stakeholders comment on the draft scope and draft guideline. NICE formally responds to comments from stakeholders, and these responses are published on the NICE website. Regular consultation allows organizations and individuals to comment on the recommendations. Once published, the guidelines are regularly checked, and updated in light of new evidence or intelligence, if necessary. |
AACE guideline, 202126 | ||||||
Intended users: Clinicians, diabetes care teams, health care professionals, other stakeholders Target population: People with diabetes | Use of advanced technology in the management of person with diabetes mellitus Relevant intervention: rtCGM |
| Evidence collected through comprehensive literature reviews | Grades for strength of recommendation:
Levels of evidence:
| To develop the recommendations, the task force discussed the evidence found in the literature. When the task force determined guidance to be necessary despite a lack of available supporting literature, a recommendation was developed based on expert opinion and consensus of task force authors’ collective experience, knowledge, and judgment. The recommendation grades and grades for strength of evidence were confirmed through discussion and consensus. The final guideline document was also discussed to achieve unanimous consensus for each recommendation. | Drafts of the guidelines were reviewed and approved by all task force members, external reviewers, oversight committee, AACE board of directors, and peer reviewers for the journal Endocrine Practice. |
Intended users: Clinicians, health care professions Target population: Adults, children, adolescents, and pregnant women with diabetes | Blood glucose monitoring in adults and children with diabetes Relevant intervention: rtCGM |
| Evidence collected through systematic literature reviews | Criteria for assigning levels of evidence to published studies:
Criteria for assigning grades of recommendations for clinical practice:
| The expert working group reviewed the citations, graded the evidence, drafted the revised recommendations, and created the initial draft of the preamble document to accompany the revised recommendations. The steering committee reviewed the cited evidence independently and suggested revisions to the draft recommendations and the text. The grading of the recommendations ware reviewed independently by the Independent Methods Review co-chair. The finalized recommendations were unanimously approved by the steering committee. | NR |
AACE = American Association of Clinical Endocrinology; ADA = American Diabetes Association; AGREE II = Appraisal of Guidelines for Research and Evaluation II; CEBM = Centre for Evidence-Based Medicine; DKA = diabetic ketoacidosis; ED = emergency department; GRADE = Grading of Recommendations, Assessment, Development, and Evaluation; MA = meta-analysis; NICE = National Institute for Health and Care Excellence; NMA = network meta-analysis; NRS = non-randomized study; QoL = quality of life; RCT = randomized controlled trial; rtCGM = real-time continuous glucose monitoring; SAE = severe adverse events; SMBG = self-monitoring of blood glucose; T1D = type 1 diabetes; T2D = type 2 diabetes; TIR = time in range.
Note that this table has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Guidelines Using AGREE II21
Item | ADA guideline, 202223 | NICE N17 guideline, 202210 | NICE NG 18 guideline, 202224 | NICE N28 guideline, 202225 | AACE guideline, 202126 | Diabetes Canada, 202127 |
|---|---|---|---|---|---|---|
Domain 1: Scope and purpose | ||||||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | No | Yes | Yes | Yes | Yes | No |
3. The population (e.g., patients, public) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes | Yes | Yes | Yes |
Domain 2: Stakeholder involvement | ||||||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes | Yes | Yes | Yes | Yes |
5. The views and preferences of the target population (e.g., patients, public) have been sought. | No | Yes | Yes | Yes | No | No |
6. The target users of the guideline are clearly defined. | Yes | Yes | Yes | Yes | Yes | Partially |
Domain 3: Rigour of development | ||||||
7. Systematic methods were used to search for evidence. | Yes | Yes | Yes | Yes | Yes | Yes |
8. The criteria for selecting the evidence are clearly described. | No | Yes | Yes | Yes | Partially | Partially |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Yes | Yes | Yes | Yes | Yes |
10. The methods for formulating the recommendations are clearly described. | No | Yes | Yes | Yes | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Partially1 | Partially1 | Partially1 | Partially1 | Yes | Partially1 |
13. The guideline has been externally reviewed by experts prior to its publication. | No | Yes | Yes | Yes | Yes | No |
14. A procedure for updating the guideline is provided. | No | Yes | Yes | Yes | Yes | No |
Domain 4: Clarity of presentation | ||||||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes | Yes | Yes | Yes |
Domain 5: Applicability | ||||||
18. The guideline describes facilitators and barriers to its application. | No | Yes | Yes | Yes | No | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No | Partially | Partially | Partially | Yes | No |
20. The potential resource implications of applying the recommendations have been considered. | No | Yes | Yes | Yes | Yes | No |
21. The guideline presents monitoring and/or auditing criteria. | No | Yes | Yes | Yes | No | No |
Domain 6: Editorial independence | ||||||
22. The views of the funding body have not influenced the content of the guideline. | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes | Yes | Yes | Yes | Yes |
AACE = American Association of Clinical Endocrinology; ADA = American Diabetes Association; AGREE II = Appraisal of Guidelines for Research and Evaluation II; NICE = National Institute for Health and Care Excellence.
1The supporting evidence is presented in a separate section on CGM or rtCGM, but not linked to the individual recommendations.
Appendix 4: Summary of Recommendations in Included Guidelines
Note that this appendix has not been copy-edited.
Table 4: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Strength of recommendations and level of evidence |
|---|---|
ADA guideline, 202223 | |
Recommendations for blood glucose monitoring in diabetes care Recommendation 7.11: “Real-time continuous glucose monitoring A or intermittently scanned continuous glucose monitoring B should be offered for diabetes management in adults with diabetes on multiple daily injections or continuous subcutaneous insulin infusion who are capable of using devices safely (either by themselves or with a caregiver). The choice of device should be made based on patient circumstances, desires, and needs.” (p. S100) Supporting evidence: Multiple RCTs were performed using rtCGM devices, and the results were largely positive in terms of reducing hemoglobin A1C levels and/or episodes of hypoglycemia as long as participants regularly wore the devices. The initial RCTs were primarily done in adults with T1D on CSII and/or MDI. The primary outcome was met and showed benefit in adults of all ages including seniors. In adults with T1D, 3 RCTs compared isCGM and rtCGM. In 2 of the studies, the primary outcome was a reduction in time spent in hypoglycemia, and rtCGM showed benefit compared with isCGM. In the other study, the primary outcome was improved TIR, and rtCGM also showed benefit compared with isCGM. A retrospective analysis also showed improvement in TIR comparing rtCGM with isCGM. RCT data on rtCGM use in individuals with T2D on MDI and mixed therapies have consistently shown reductions in hemoglobin A1C but not a reduction in rates of hypoglycemia. The improvements in T2D largely occurred without changes in insulin doses or other diabetes medications. Retrospective data from rtCGM use in a Veterans Affairs population with TID and T2D treated with insulin show that use of rtCGM significantly lowered hemoglobin A1C and reduced rates of emergency department visits or hospitalizations for hypoglycemia, but did not significantly lower overall rates of emergency department visits, hospitalizations, or hyperglycemia. | Strength of recommendation: NR Level of evidence: A (clear evidence from well-conducted RCTs that are adequately powered) |
Recommendation 7.12: “Real-time continuous glucose monitoring A or intermittently scanned continuous glucose monitoring C can be used for diabetes management in adults with diabetes on basal insulin who are capable of using devices safely (either by themselves or with a caregiver). The choice of device should be made based on patient circumstances, desires, and needs.” (p. S100) Supporting evidence: Refer to evidence for Recommendation 7.11 RCT data on rtCGM use in individuals with T2D on basal insulin have consistently shown reductions in hemoglobin A1C but not a reduction in rates of hypoglycemia. | Strength of recommendation: NR Level of evidence: A |
Recommendation 7.13: “Real-time continuous glucose monitoring B or intermittently scanned continuous glucose monitoring E should be offered for diabetes management in youth with type 1 diabetes on multiple daily injections or continuous subcutaneous insulin infusion who are capable of using the device safely (either by themselves or with a caregiver). The choice of device should be made based on patient circumstances, desires, and needs.” (p. S100) Supporting evidence: In 3 RCTs in youth with T1D on CSII and/or MDI, data were less consistent than in adults with T1D. | Strength of recommendation: NR Level of evidence: B (supporting evidence from well-conducted cohort studies) |
Recommendation 7.14: “Real-time continuous glucose monitoring or intermittently scanned continuous glucose monitoring should be offered for diabetes management in youth with type 2 diabetes on multiple daily injections or continuous subcutaneous insulin infusion who are capable of using devices safely (either by themselves or with a caregiver). The choice of device should be made based on patient circumstances, desires, and needs.” (p. S100) Supporting evidence: NR | Strength of recommendation: NR Level of evidence: E (expert consensus or clinical experience) |
Recommendation 7.15: “In patients on multiple daily injections and continuous subcutaneous insulin infusion, rt CGM devices should be used as close to daily as possible for maximal benefit. A” (p. S100) Supporting evidence: Multiple RCTs were performed using rtCGM devices, and the results were largely positive in terms of reducing hemoglobin A1C levels and/or episodes of hypoglycemia as long as participants regularly wore the devices. | Strength of recommendation: NR Level of evidence: A |
Recommendation 7.17: “Periodic use of real-time or intermittently scanned continuous glucose monitoring or use of professional continuous glucose monitoring can be helpful for diabetes management in circumstances where continuous use of continuous glucose monitoring is not appropriate, desired, or available. C” (pages S100 to S101) Supporting evidence: NR | Strength of recommendation: NR Level of evidence: C (supportive evidence from poorly controlled or uncontrolled studies or conflicting evidence with the weight of evidence supporting the recommendation) |
NICE N17 guideline, 202210 | |
Recommendations for management of adults with T1D: CGM Recommendation 1.6.10: “Offer adults with type 1 diabetes a choice of real-time continuous glucose monitoring (rtCGM) or intermittently scanned continuous glucose monitoring (isCGM, commonly referred to as 'flash'), based on their individual preferences, needs, characteristics, and the functionality of the devices available.” (p. 18) Supporting evidence: The committee agreed that there was enough evidence in key outcomes, such as hemoglobin A1C, time in range, and severe or nocturnal hypoglycemia, to demonstrate that rtCGM provided clinical benefits over standard SMG. However, they considered the evidence for rtCGM compared with isCGM was not good enough in terms of quality or sample size to clearly show clinical benefits of 1 technology over the other. The health economic modelling found that, when benefit of reduced fear of hypoglycemia with CGM was included, both rtCGM and isCGM were cost-effective for the full population of adults with T1D compared with standard SMBG. | Strength of recommendation: Reflected in the wording:
Level of evidence: Reported in separate publication of evidence review for guideline, but not reported for each recommendation or in guideline document. |
Recommendation 1.6.14: “If a person cannot use or does not want rtCGM or isCGM, offer capillary blood glucose monitoring.” (p. 20) Supporting evidence: NR | |
NICE NG 18 guideline, 202224 | |
Recommendations for management of T1D in children and young people: CGM Recommendation 1.2.60: “Offer real-time continuous glucose monitoring (rtCGM) to all children and young people with type 1 diabetes, alongside education to support children and young people and their families and carers to use it.” (p. 15) Supporting evidence: The evidence on rtCGM showed it led to a decrease in hemoglobin A1C and an increase in time in range. This reflected the committee’s experience in clinical practice. Because the evidence showed similar benefits of rtCGM for children and young people as for adults, the committee extrapolated the cost-effectiveness results from adults, concluding that rtCGM was cost-effective in this population. | Strength of recommendation: Reflected in the wording:
Level of evidence: Reported in separate publication of evidence review for guideline,32 but not reported for each recommendation or in guideline document. |
Recommendation 1.2.61: “Offer intermittently scanned continuous glucose monitoring (isCGM, commonly referred to as 'flash') to children and young people with type 1 diabetes aged 4 years and over who are unable to use rtCGM or who express a clear preference for isCGM.” (pages 15 to 16) Supporting evidence: Since the same clinical benefits were not found for isCGM in children and young people as in adults, the committee agreed those cost-effectiveness findings could not be extrapolated, so they could not conclude that isCGM was a cost-effective technology for the full population of children and young people. They therefore agreed that isCGM should be restricted to children and young people who were unable or did not want to use rtCGM, or who preferred isCGM. Children and young people who preferred isCGM were likely to have better adherence with this type of device, so it would provide more benefit. | |
Recommendation 1.2.62: “Offer children and young people with type 1 diabetes a choice of rtCGM device, based on their individual preferences, needs, characteristics, and the functionality of the devices available. See box 1 for examples of factors to consider as part of this discussion.” (p. 16) Supporting evidence: NR | |
Recommendation 1.2.66: “If a person cannot use or does not want rtCGM or isCGM, offer capillary blood glucose monitoring.” (p. 18) Supporting evidence: NR | |
NICE N28 guideline, 202225 | |
Recommendations for management of adults with T2D: CGM Recommendation 1.6.19: “Consider real-time continuous glucose monitoring (rtCGM) as an alternative to isCGM for adults with insulin-treated type 2 diabetes if it is available for the same or lower cost.” (p. 12) Supporting evidence: There was no evidence that rtCGM was cost-effective for people with T2D, so the committee agreed it could not be recommended for all adults with T2D (whether or not they used insulin). They noted, however, that prices of rtCGM had reduced over the past few years, and if this continued to happen there may come a time when it was no more expensive than isCGM. rtCGM would be an appropriate alternative for people who met the criteria for isCGM. | Strength of recommendation: Reflected in the wording:
Level of evidence: Reported in separate publication of evidence review for guideline, but not reported for each recommendation or in guideline document. |
Recommendation 1.6.22: “If a person is offered rtCGM or isCGM but cannot or does not want to use any of these devices, offer capillary blood glucose monitoring.” (p. 13) Supporting evidence: Although many people will choose CGM if offered, there are some people who either cannot be offered it or do not want to use it. Because it was still important for these people to monitor their blood glucose levels, the committee made a recommendation to reinforce the importance of offering capillary blood glucose monitoring instead. | |
AACE Guideline, 202126 | |
Recommendations for the use of advanced technology in the management of people with diabetes mellitus When is one method of CGM (rtCGM vs isCGM) preferred over the other? Recommendation 2.3.1: “rtCGM should be recommended over isCGM to persons with diabetes with problematic hypoglycemia (frequent/severe hypoglycemia, nocturnal hypoglycemia, hypoglycemia unawareness) who require predictive alarms/alerts; however, the lifestyle of persons with diabetes and other factors should also be considered.” (pages 519 to 520) Supporting evidence: Studies comparing rtCGM and isCGM were sparse. Available evidence showed that rtCGM was superior to isCGM, when these systems did not include threshold alarms, in reducing hypoglycemia and improving TIR in adults with T1D with normal hypoglycemia awareness. Apart from hypoglycemia risk, reviews suggested that rtCGM may be preferred for persons with diabetes who were physically active or had busy lifestyles that would inhibit frequent scanning of an isCGM sensor, required uninterrupted monitoring by parents/caregivers, chose to use advanced insulin delivery technologies, or could not achieve desired glycemic targets with isCGM. | Strength of recommendation: Grade B (strong) Level of evidence: Low-intermediate strength of evidence |
In what settings or special situations is use of diabetes technologies beneficial? Recommendation 2.10.2: “rtCGM is recommended for persons ≥65 years old with insulin-requiring diabetes to achieve improved glycemic control, reduce episodes of severe hypoglycemia, and improve QoL; however, glycemic goals should be individualized due to increased comorbidities and reduced capacity to detect and counter-regulate against severe hypoglycemia in this population.” (p. 523) Supporting evidence: Older persons with diabetes were at a significantly higher risk for severe hypoglycemia than younger individuals. Investigations in the use of CGM within this population have been shown to detect and reduce hypoglycemia, reduce hemoglobin A1C, and improve QoL. In a 2020 RCT, 203 older adults (≥ 60 years) were randomized to use CGM or SMBG. At 6 months, CGM was associated with a decrease in severe hypoglycemia compared with SMBG, showing statistically significant reductions in severe hypoglycemia incidence rates compared with SMBG. The use of CGM was also associated with reductions in the percentage of time spent < 70 mg/dL versus increases with SMBG use. The investigators of a subgroup analysis of T1D and T2D trial cohorts assessed changes in glycemic status among rtCGM versus SMBG users and reported statistically significant hemoglobin A1C reduction with rtCGM versus SMBG use. | Strength of recommendation: Grade A (very strong) Level of evidence: Intermediate strength of evidence |
Diabetes Canada, 202127 | |
Blood glucose monitoring in adults and children with diabetes Recommendation 5: In individuals with type 1 diabetes using basal-bolus insulin therapy or CSII, who are willing and able to use these devices on a nearly daily basis: rtCGM should be used to: i – reduce hemoglobin A1C and increase TIR ii – reduce duration and incidence of hypoglycemia iii – improve aspects of diabetes-specific quality of life (in adults) iv – increase treatment satisfaction (in adults using CSII). (p. 584) Supporting evidence: For people living with T1D who use basal-bolus injection therapy or CSII, rtCGM has been shown to reduce hemoglobin A1C and increase glucose TIR, while simultaneously reducing duration and incidence of hypoglycemia in adults and children. These glycemic benefits of rtCGM have been demonstrated in trials recruiting adults and children with hemoglobin A1C at target (< 7.5%) or above target; and in trials which included adults at or above target. rtCGM has been shown to reduce biochemical (i.e., not necessarily symptomatic) hypoglycemia in adults. rtCGM has also been shown to improve quality of life and hypoglycemia distress in adults with T1D. Two of 3 RCTs that included children as young as 6 years, comparing rtCGM to CBG testing, showed lower hemoglobin A1C and less TBR in both adults and children, but this was not seen in pediatric participants in the other study, which had very low use of rtCGM and was under-powered to detect differences in hypoglycemia. Lower hemoglobin A1C with rtCGM in children may depend on time spent using CGM since further analysis of pediatric subjects in this latter trial showed use of rtCGM for 6 or more days per week improved hemoglobin A1C by –0.8% at 12 months. Characteristics such as younger age, and higher frequency of CBG testing prior to rtCGM, may help predict those who are more likely to use rtCGM consistently. Another study in younger children (ages 4 to 10 years) did not show any change or differences in hemoglobin A1C or CGM parameters between groups, although the use of rtCGM was associated with a high degree of parental satisfaction with rtCGM. These findings underscore a fear of hypoglycemia, which is reflected in more conservative recommended glucose targets. | Strength of recommendation: i, ii – Grade A (best evidence was Level 1) iii, iv – Grade B (best evidence was Level 2) Level of evidence: i, ii – 1A (SR or MA of high-quality RCTs, or appropriately designed RCT with adequate power) iii, iv – 2 (low-quality RCT or systematic overview) |
Recommendation 6: In adults with type 1 diabetes with impaired awareness of hypoglycemia or recent severe hypoglycemia: a – rtCGM should be used to reduce incidence of hypoglycemia and severe hypoglycemic events compared with CBG testing b – rtCGM is recommended to reduce time in hypoglycemia compared with isCGM. (p. 584) Supporting evidence: rtCGM has been shown to reduce episodes of severe hypoglycemia in adults with a history of severe hypoglycemia or impaired awareness of hypoglycemia using MDI. Two studies have directly compared rtCGM with isCGM in adults with T1D. rtCGM users spent more TIR and less time below range than isCGM users in a 5-week RCT in adults with normal awareness of hypoglycemia using MDI or CSII. In an 8-week study of individuals with impaired awareness of, or recent severe hypoglycemia using MDI, rtCGM reduced time in hypoglycemia and fear of hypoglycemia, which was not seen with isCGM. Superiority of rtCGM to protect from hypoglycemia in this high-risk population was supported in the extension phase of this study, where switching to rtCGM was associated with significant reduction in TBR in subjects originally randomized to isCGM. | Strength of recommendation: a – Grade A b – Grade B Quality of evidence: a – 1A b – 2 |
Recommendation 7: In adults with type 2 diabetes using basal-bolus insulin therapy who have not achieved their hemoglobin A1C target, who are willing and able to use these devices on a nearly daily basis:
Supporting evidence: For people living with T2D using basal-bolus injection therapy, a randomized controlled trial of 158 subjects demonstrated that the use of rtCGM reduced hemoglobin A1C to a greater extent than usual care, with more time spent in the target range and less time spent above range at 24 weeks. | Strength of recommendation: Grade A Quality of evidence: 1A |
AACE = American Association of Clinical Endocrinology; ADA = American Diabetes Association; CBG = capillary blood glucose; CGM = continuous glucose monitoring; CSII = continuous subcutaneous insulin infusion; isCGM = intermittently scanned continuous glucose monitoring; MA = meta-analysis; MDI = multiple daily injection; NICE = National Institute for Health and Care Excellence; NR = not reported; QoL = quality of life; RCT = randomized controlled trial; rtCGM, real-time continuous glucose monitoring; SMBG = self-monitoring of blood glucose; SR = systematic review; T1D = type 1 diabetes; T2D = type 2 diabetes; TBR = time below range; TIR = time in range.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
Intermittently Scanned and Real-Time Continuous Glucose Monitoring for People with Diabetes. Ottawa (ON): CADTH. 2022 https://www.cadth.ca/intermittently-scanned-and-real-time-continuous-glucose-monitoring-people-diabetes
Flash Glucose Monitoring and Continuous Glucose Monitoring for People with Diabetes in Acute Care Settings. Ottawa (ON): CADTH. 2021 https://www.cadth.ca/flash-glucose-monitoring-and-continuous-glucose-monitoring-people-diabetes-acute-care-settings
Continuous Glucose Monitoring for Patients with All Diabetes Types: Clinical Effectiveness and Guidelines. Ottawa (ON): CADTH. 2018 https://www.cadth.ca/continuous-glucose-monitoring-patients-all-diabetes-types-clinical-effectiveness-and-guidelines
Self-Monitoring of Blood Glucose Frequency for Patients with Hypoglycemia Unawareness: A Review of Clinical Effectiveness and Guidelines. Ottawa (ON): CADTH. 2017 https://www.cadth.ca/self-monitoring-blood-glucose-frequency-patients-hypoglycemia-unawareness-review-clinical
Other Guideline Documents
Borot S, Benhamou PY, Atlan C, et al. Practical implementation, education and interpretation guidelines for continuous glucose monitoring: A French position statement. Diabetes Metab. 2018;44(1):61-72. PubMed
Danne T, Nimri R, Battelino T, et al. International Consensus on Use of Continuous Glucose Monitoring. Diabetes Care. 2017;40(12):1631-1640. PubMed
Kesavadev J, Misra A, Saboo B, et al. Time-in-range and frequency of continuous glucose monitoring: Recommendations for South Asia. Diabetes Metab Syndr. 2022;16(1):102345. PubMed
Petrie JR, Peters AL, Bergenstal RM, Holl RW, Fleming GA, Heinemann L. Improving the Clinical Value and Utility of CGM Systems: Issues and Recommendations: A Joint Statement of the European Association for the Study of Diabetes and the American Diabetes Association Diabetes Technology Working Group. Diabetes Care. 2017;40(12):1614-1621. PubMed
Guideline Documents, Methodology Not Reported
Borot S, Benhamou PY, Atlan C, et al. Practical implementation, education, and interpretation guidelines for continuous glucose monitoring: A French position statement. Diabetes Metab. 2018;44(1):61-72. PubMed
Review Articles
Pettus J, Edelman SV. Recommendations for Using Real-Time Continuous Glucose Monitoring (rtCGM) Data for Insulin Adjustments in Type 1 Diabetes. J Diabetes Sci Technol. 2017;11(1):138-147. PubMed
Ziegler R, von Sengbusch S, Kroger J, et al. Therapy Adjustments Based on Trend Arrows Using Continuous Glucose Monitoring Systems. J Diabetes Sci Technol. 2019;13(4):763-773. PubMed
Additional Reference
Bruttomesso D, Laviola L, Avogaro A, et al. The use of real time continuous glucose monitoring or flash glucose monitoring in the management of diabetes: A consensus view of Italian diabetes experts using the Delphi method. Nutrition, Metabolism and Cardiovascular Diseases. 2019;29(5):421-431. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca