CADTH Health Technology Review
Concurrent or Sequential Administration of Drugs for COVID-19 and Influenza
Rapid Review
Authors: Shannon Hill, Sharon Bailey
Abbreviations
HTA
health technology assessment
PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Key Messages
With the continued COVID-19 pandemic and the resurgence of seasonal influenza, there is the potential that some populations may need drugs for the prevention and/or treatment of COVID-19 and/or influenza at the same time (i.e., concurrent use) or close together (i.e., sequential use).
No evidence was identified regarding the clinical effectiveness, safety, or evidence-based guidelines for the concurrent or sequential use of cilgavimab and tixagevimab, nirmatrelvir and ritonavir, and/or oseltamivir that met the criteria for this review.
Context and Policy Issues
The COVID-19 pandemic has prompted concerns over the circulation of respiratory co-infections, specifically with COVID-19 and influenza. In Canada, approximately 3.9 million cases of COVID-19 have been reported since the beginning of the pandemic in 2020, while influenza accounts for approximately 12,200 hospitalizations and 3,500 deaths each year.1,2 During the 2019 to 2020 influenza season in Canada and other northern hemisphere countries, influenza activity dropped in March 2020 due to the implementation of strict public health measures designed to limit the spread of COVID-19.3,4 During the 2020 to 2021 influenza season in Canada, the test positivity rate of influenza A and B was 0.0015 (95% CI, 0.001 to 0.002) compared to the pre-pandemic test positivity rate of 0.0028 (95% CI, 0.001 to 0.007).4 With the easing of COVID-19 public health restrictions in Canada, there has been a resurgence of seasonal influenza and a continued prevalence of COVID-19.3 The concern of potential respiratory co-infections with COVID-19 and influenza has raised the question of appropriate, effective, and safe treatment in people with or at high risk of coinfection with COVID-19 and influenza. In addition, there is concern over the proper use of preventive therapy for people who may be at risk of poor outcomes if infected with COVID-19, whether that may influence therapeutic and prophylactic treatment considerations if those individuals are infected by COVID-19 and/or influenza, or if they are a close contact of an individual with influenza.
In Canada, there are separate pharmacological options available for the prevention and treatment of COVID-19 and influenza. Cilgavimab and tixagevimab (commonly known as Evusheld) is a long-acting antibody combination therapy approved for use in Canada in April 2022.5 Cilgavimab and tixagevimab is used as a pre-exposure prophylaxis for COVID-19 in adults and adolescents who cannot receive the vaccine due to a severe allergy, or are immunocompromized and may not have an adequate response to the vaccine.5 Cilgavimab and tixagevimab is administered as 2 separate sequential intramuscular injections (i.e., 1 injection for cilgavimab and 1 injection for tixagevimab) that may provide protection for 6 to 9 months.5,6 Nirmatrelvir and ritonavir (commonly known as Paxlovid) is an oral antiviral treatment authorized for adults with mild to moderate COVID-19 who are at high risk for progression to severe COVID-19 (e.g., advanced age, people who are immunocompromized, people who have comorbidities).7 Nirmatrelvir and ritonavir treatment includes two 150 mg doses of nirmatrelvir and one 100 mg dose of ritonavir taken twice daily for 5 days.7,8 Oseltamivir (commonly known as Tamiflu) is a neuraminidase inhibitor antiviral treatment option for influenza.9 Oseltamivir may be offered to patients aged 1 year or older who have been symptomatic for no more than 2 days, and may also be used as a preventive measure for adults and children aged 1 year or older who are in close contact with symptomatic influenza patients.9 For the treatment of symptomatic influenza, oseltamivir should be taken twice daily for 5 days.9 For preventive measures, oseltamivir should be taken once daily for 10 days.9
These prevention and treatment options for COVID-19 and influenza may be complex, and different variations of either prevention or treatment (or both) regimens may be needed depending on the patient indication. As a result, there is concern for regimen overlap, not only for people with or at high risk of infection with COVID-19 and influenza, but also those who may be at risk of poor outcomes if infected with COVID-19 who have been exposed to or infected with influenza (with or without COVID-19 infection). The objective of this report is to summarize the evidence regarding the clinical effectiveness, safety, and recommendations from evidence-based guidelines for the concurrent or sequential administration of cilgavimab and tixagevimab, nirmatrelvir and ritonavir, and/or oseltamivir.
Research Questions
What is the clinical effectiveness and safety of concurrent administration of cilgavimab and tixagevimab, nirmatrelvir and ritonavir, and/or oseltamivir?
What is the clinical effectiveness and safety of sequential administration of cilgavimab and tixagevimab, nirmatrelvir and ritonavir, and/or oseltamivir?
What are the evidence-based guidelines regarding concurrent administration or sequential administration of cilgavimab and tixagevimab, nirmatrelvir and ritonavir, and/or oseltamivir?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were COVID-19, influenza, oseltamivir, cilgavimab/tixagevimab, and nirmatrelvir/ritonavir. CADTH-developed search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, indirect treatment comparisons, and guidelines. Conference abstracts were excluded. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2020 and June 28, 2022.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Q1 to 3: Adults infected with COVID-19 or at risk of poor outcomes if infected with COVID-19 and/or influenza |
Intervention | Q1: Concurrent administration of cilgavimab and tixagevimab, nirmatrelvir and ritonavir, and/or oseltamivir Q2: Sequential administration of cilgavimab and tixagevimab, nirmatrelvir and ritonavir, and/or oseltamivir Q3: Concurrent administration or sequential administration of cilgavimab and tixagevimab, nirmatrelvir and ritonavir, and/or oseltamivir |
Comparator | Q1 to 2: Cilgavimab and tixagevimab, nirmatrelvir and ritonavir, and/or oseltamivir not administered concurrently or in sequence Q3: Not applicable |
Outcomes | Q1 to 2: Clinical effectiveness (e.g., mortality, clinical symptoms, safety [e.g., adverse events]) Q3: Recommendations regarding concurrent or sequential administration of cilgavimab and tixagevimab, nirmatrelvir and ritonavir, and/or oseltamivir (e.g., dosing intervals for optimal administration and effect, appropriate and/or inappropriate populations) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies, evidence-based guidelines |
Q = question.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2020. Guidelines with unclear methodology were also excluded.
Summary of Evidence
Quantity of Research Available
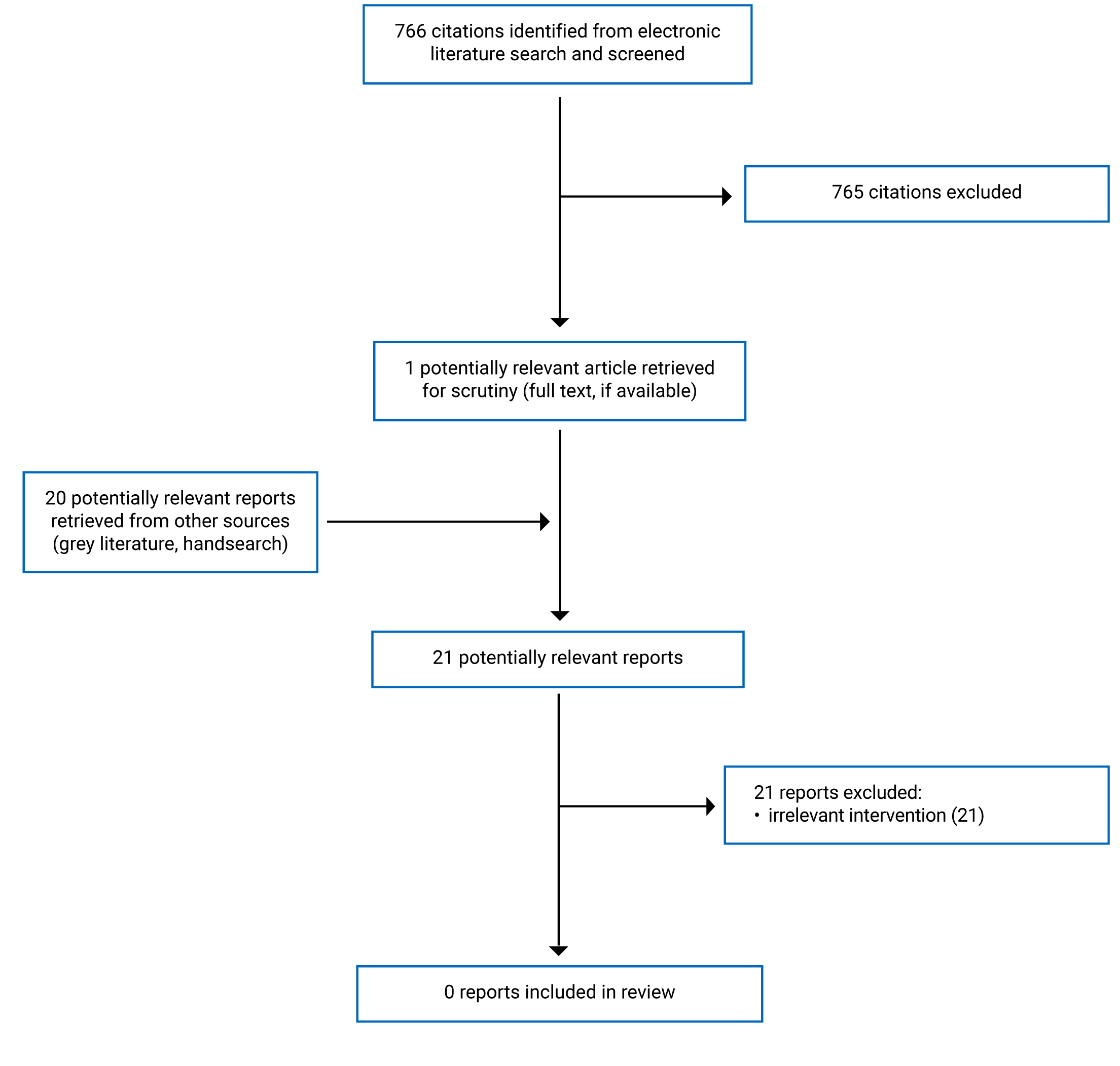
A total of 766 citations were identified in the literature search. Following screening of titles and abstracts, 765 citations were excluded and 1 potentially relevant report from the electronic search was retrieved for full-text review. In addition, 20 potentially relevant publications were retrieved from the grey literature search for full-text review. Of these 21 potentially relevant articles, all were excluded for various reasons; no publications met the inclusion criteria to be included in this report. Appendix 1 presents the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)10 flow chart of the study selection. Additional references of potential interest are provided in Appendix 2.
Summary of Findings
Clinical Effectiveness of Concurrent Administration
No relevant literature was identified regarding the clinical effectiveness and safety of concurrent administration of cilgavimab and tixagevimab, nirmatrelvir and ritonavir, and/or oseltamivir; therefore, no summary can be provided.
Clinical Effectiveness of Sequential Administration
No relevant literature was identified regarding the clinical effectiveness and safety of the sequential administration of cilgavimab and tixagevimab, nirmatrelvir and ritonavir, and/or oseltamivir; therefore, no summary can be provided.
Guidelines
No evidence-based guidelines were identified regarding concurrent or sequential administration of cilgavimab and tixagevimab, nirmatrelvir and ritonavir, and/or oseltamivir; therefore, no summary can be provided.
Limitations
No relevant literature was identified regarding the clinical effectiveness and safety of concurrent or sequential administration of cilgavimab and tixagevimab, nirmatrelvir and ritonavir, and/or oseltamivir. Additionally, no evidence-based guidelines were identified regarding concurrent or sequential administration of cilgavimab and tixagevimab, nirmatrelvir and ritonavir, and/or oseltamivir. This report may be limited by the time frame used for literature searches (extended only to 2020); however, based on the nature of this topic as it relates to COVID-19, it is unlikely that there would be relevant literature that was published before 2020.
Conclusions and Implications for Decision- or Policy-Making
No relevant literature or evidence-based guidelines were identified regarding the concurrent or sequential administration of cilgavimab and tixagevimab, nirmatrelvir and ritonavir, and/or oseltamivir; therefore, no conclusions regarding the clinical effectiveness, safety, or evidence-based guidelines can be provided.
The continued COVID-19 pandemic and the resurgence of influenza has highlighted the potential complexity for patient management strategies when considering prevention and treatment regimens for COVID-19 and/or influenza. At the time this review was completed, the drug monographs for cilgavimab and tixagevimab, nirmatrelvir and ritonavir, and oseltamivir do not mention any considerations for drug interactions with one another.11-13 Further research examining the clinical effectiveness and safety of concurrent or sequential administration of cilgavimab and tixagevimab, nirmatrelvir and ritonavir, and/or oseltamivir is required to investigate the potential impact on patients infected with COVID-19 and influenza, people infected with COVID-19 and exposed to influenza, and people at high-risk of poor outcomes if infected with COVID-19 who have been exposed to or infected with influenza (with or without a COVID-19 infection).
The lack of published evidence precludes the creation of appropriate guidance for health care providers to refer to for the care of this patient population. COVID-19 is an evolving landscape, and future preventive and treatment options may become available that could impact, alter, or expand concurrent or sequential administration of drugs.
References
1.Government of Canada. COVID-19 epidemiology update. 2022; https://health-infobase.canada.ca/covid-19/. Accessed 2022 Jul 13.
2.Government of Canada. Flu (influenza): for health professionals. 2022; https://www.canada.ca/en/public-health/services/diseases/flu-influenza/health-professionals.html. Accessed 2022 Jul 13.
3.Aoki FY, Papenburg J, Mubareka S, Allen UD, Hatchette TF, Evans GA. 2021–2022 AMMI Canada guidance on the use of antiviral drugs for influenza in the COVID-19 pandemic setting in Canada. J Assoc Med Microbiol Infect Dis Can. 2022;7(1):1-7.
4.Groves HE, Piche-Renaud PP, Peci A, et al. The impact of the COVID-19 pandemic on influenza, respiratory syncytial virus, and other seasonal respiratory virus circulation in Canada: A population-based study. Lancet Reg Health Am. 2021;1:100015. PubMed
5.Government of Canada. Summary Basis of Decision - Evusheld - Health Canada. 2020; https://covid-vaccine.canada.ca/info/summary-basis-decision-detailTwo.html?linkID=SBD00589. Accessed 2022 Jul 12.
6.Tixagevimab and Cilgavimab (Evusheld) (CADTH Drug implementation advice). Ottawa (ON): CADTH; 2022: https://www.cadth.ca/sites/default/files/hta-he/HD0008-Evusheld.pdf. Accessed 2022 Aug 2.
7.Government of Canada. Summary Basis of Decision - Paxlovid - Health Canada. 2022; https://covid-vaccine.canada.ca/info/summary-basis-decision-detailTwo.html?linkID=SBD00577. Accessed 2022 Jul 12.
8.Nirmatrelvir and Ritonavir (Paxlovid) (CADTH Drug implementation advice). Ottawa (ON): CADTH; 2022: https://www.cadth.ca/sites/default/files/pdf/HD0007%20Paxlovid_Final.pdf. Accessed 2022 Aug 2.
9.Aoki FY, Allen UD, Mubareka S, Papenburg J, Stiver H G, Evans GA. Use of antiviral drugs for seasonal influenza: Foundation document for practitioners—Update 2019. J Assoc Med Microbiol Infect Dis Can. 2019;4(2):60-82.
10.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
11.Evusheld: tixagevimab and cilgavimab injection solution, 100 mg/mL (tixagevimab) and 100 mg/mL (cilgavimab), intramuscular use, anti-SARS-CoV-2 spike protein monoclonal antibodies [product monograph]. Mississauga (ON): AstraZeneca Canada Inc; 2022: https://pdf.hres.ca/dpd_pm/00065403.PDF. Accessed 2022 Aug 2.
12.Paxlovid: nirmatrelvir tablets; ritonavir tablets, 150 mg nirmatrelvir; 100 mg ritonavir co-packaged for oral use [product monograph]. Kirkland (QC): Pfizer Canada ULC; 2022: https://pdf.hres.ca/dpd_pm/00066256.PDF. Accessed 2022 Aug 2.
13.Tamiflu: oseltamivir capsule, 30 mg, 45 mg and 75 mg oseltamivir (as oseltamivir phosphate), oseltamivir powder for oral suspension, 6 mg/mL oseltamivir (as oseltamivir phosphate) when reconstituted, antiviral agent [product monograph]. Mississauga (ON): Hoffmann-La Roche Limited; 2017: https://pdf.hres.ca/dpd_pm/00038482.PDF. Accessed 2022 Aug 2.
Appendix 1: Selection of Included Studies
Appendix 2: References of Potential Interest
Note that this appendix has not been copy-edited.
Guidelines and Recommendations
Concurrent or Sequential Treatment Not Specified
Agarwal A, Rochwerg B, Lamontagne F, et al. A living WHO guideline on drugs for Covid-19. BMJ 2020;370:m3379. https://www.bmj.com/content/bmj/370/bmj.m3379.full.pdf. Accessed 2022 Jul 6. See: Nirmatrelvir/ritonavir (Update 9, published 22 April 2022), pages 7 and 8.
Review Articles
Rios P, Radhakrishnan A, Antony J, et al. Effectiveness and safety of antiviral or antibody treatments for coronavirus [non peer-reviewed preprint]. medRxiv; 2020: doi: 10.1101/2020.03.19.20039008. https://www.medrxiv.org/content/10.1101/2020.03.19.20039008v2. Accessed 2022 Jul 6.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca