CADTH Health Technology Review
Mesalamine for the Treatment of Crohn Disease
Rapid Review
Authors: Keeley Farrell, Jennifer Horton
Abbreviations
CDAI
Crohn’s Disease Activity Index
IBDQ
Inflammatory Bowel Disease Questionnaire
RCT
randomized controlled trial
Key Messages
Evidence suggested high-dose mesalamine was more likely to induce remission in patients with mild to moderate active Crohn disease than placebo. There was no significant difference between low-dose mesalamine and placebo for induction of remission.
Evidence comparing mesalamine to budesonide on remission was mixed. There was some evidence suggesting that high-dose budesonide was more likely to induce remission in patients with mild to moderate active Crohn disease than low-dose mesalamine. However, no significant differences were observed between budesonide and mesalamine at comparable doses (high or low), and when high-dose mesalamine was compared with low-dose budesonide.
Evidence suggested unspecified corticosteroids were more likely to induce remission in patients with mild to moderate active Crohn disease than mesalamine.
Evidence suggested there were no differences in withdrawals due to adverse events for mesalamine versus placebo, budesonide, or corticosteroids. Limited evidence suggested there were no significant differences in pancreatitis between patients with active Crohn disease treated with mesalamine versus azathioprine.
No evidence was identified that evaluated the clinical effectiveness of mesalamine for the treatment of severe active Crohn disease.
Context and Policy Issues
Inflammatory bowel disease includes both Crohn disease and ulcerative colitis.1 Crohn disease is a chronic inflammatory condition that impacts the gastrointestinal tract.2 It is a lifelong condition and patients can experience periods of active disease that alternate with periods of remission.3 Crohn disease can affect any part of the digestive tract from mouth to anus.3 However, it occurs most frequently in the terminal ileum, ileocecal region, colon, and perianal region.3 Common symptoms of Crohn disease can include diarrhea, abdominal pain, rectal bleeding, fever, weight loss, and fatigue.2 Crohn disease is associated with increased risk of mortality from digestive conditions as well as increased risk of all-cause mortality compared to the general population.4 Crohn disease can present at any time from early childhood to late adulthood; however, more than 80% of patients are diagnosed before the age of 40 years.5 The number of people living with Crohn disease in Canada was estimated to be 135,000 in 2018.1
For patients with active Crohn disease, 1 of the goals of treatment is induction of remission. Current treatment options for Crohn disease include aminosalicylates (e.g., mesalamine, sulfasalazine), corticosteroids (e.g., budesonide, prednisone, prednisolone), immunosuppressants (e.g., azathioprine, methotrexate), and biologic agents (e.g., infliximab, adalimumab, vedolizumab).4 In Canada, many drug programs require patients with Crohn disease to have failed therapy on a first-line option before being eligible for reimbursement of a biologic.6
Mesalamine is an established treatment in ulcerative colitis; however, there is uncertainty around its efficacy in Crohn disease.7 Evidence of the comparative effectiveness of mesalamine for the treatment of active Crohn disease versus other available treatment options could aid decision-making around place in therapy for this drug.
The aim of the current report is to summarize the evidence regarding the clinical effectiveness of mesalamine versus no treatment or placebo and versus alternative therapies for the treatment of active Crohn disease.
Research Questions
What is the clinical effectiveness of mesalamine versus no treatment or placebo for the treatment of active Crohn disease?
What is the clinical effectiveness of mesalamine versus alternative therapies for the treatment of active Crohn disease?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were mesalamine and Crohn disease. CADTH-developed search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, or indirect treatment comparisons; and randomized controlled trials or controlled clinical trials. Where possible, retrieval was limited to the human population. The search was completed on June 24, 2022. It was limited to English-language documents published since January 1, 2017.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults with active Crohn disease |
Intervention | Mesalamine (also known as 5-aminosalicylic acid or mesalazine) |
Comparator | Q1: No treatment/placebo Q2: Alternative therapies (limited to corticosteroids [e.g., budesonide, prednisone, prednisolone] and immunosuppressants [e.g., azathioprine, methotrexate]) |
Outcomes | Clinical effectiveness (e.g., induction of remission, maintenance of remission, safety [e.g., adverse events]) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or they were published before 2017. Articles that compared mesalamine to therapies other than corticosteroids or immunosuppressants (such as biologic agents) were excluded. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded.8
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)9 for systematic reviews, the “Questionnaire to assess the relevance and credibility of a network meta-analysis”10 for network meta-analyses, and the Downs and Black checklist11 for randomized studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
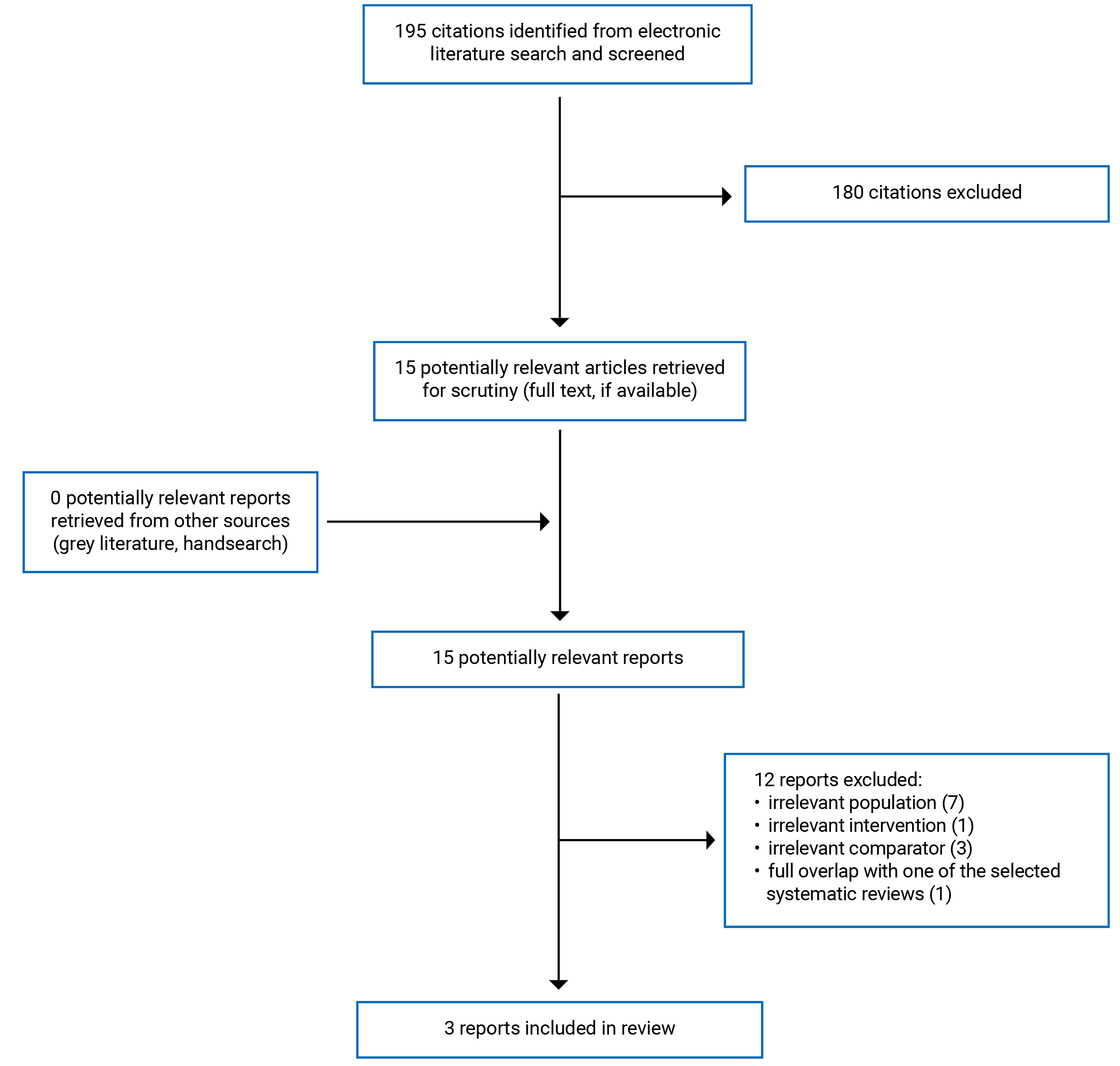
A total of 195 citations were identified in the literature search. Following screening of titles and abstracts, 180 citations were excluded and 15 potentially relevant reports from the electronic search were retrieved for full-text review. No potentially relevant publications were retrieved from the grey literature search. Of these potentially relevant articles, 12 publications were excluded for various reasons, and 3 publications met the inclusion criteria and were included in this report. These comprised 2 systematic reviews and 1 randomized controlled trial (RCT). Appendix 1 presents the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)12 flow chart of the study selection. Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
In total, 1 systematic review,13 1 systematic review with a network meta-analysis,14 and 1 RCT15 were included in this report.
Both systematic reviews13,14 had broader inclusion criteria than the present report. Specifically, the systematic review by Gordon et al. (2021)13 included patients of any age, and the eligible comparators included any pharmacological agent. Eligible interventions for the systematic review by Coward et al. (2017)14 included olsalazine, balsalazide, and sulfasalazine. Only the characteristics and results of the subset of relevant studies are described in the present report.
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
The systematic review by Gordon et al. (2021)13 included 25 RCTs (1 of which is relevant to the present report). The search criterion was RCTs published up to and including October 29, 2019.13 The systematic review by Gordon et al. (2021)13 included a meta-analysis; however, the results from the meta-analysis are not presented in this report, as only 1 relevant RCT was included in the systematic review. The systematic review and network meta-analysis by Coward et al. (2017)14 included 22 RCTs (9 of which are relevant to the present report). The authors identified RCTs from existing Cochrane reviews and an updated search with a time frame from January 2004 until November 2015.14 A Bayesian random-effects model was used for the network meta-analysis.14
The RCT by Yokoyama et al. (2018)15 was a multi-centre, double-blind study.
Country of Origin
One of the systematic reviews was conducted by authors in the UK.13 The systematic review with network meta-analysis was conducted by authors in Canada.14
The RCT was conducted in Japan.15
Patient Population
Seventy-two adults with active Crohn disease were included in the relevant RCT of the systematic review by Gordon et al. (2021)13 They were randomized to receive azathioprine or mesalamine, with an equal number of patients (n = 36) in each group.13 The baseline Crohn’s Disease Activity Index (CDAI) scores of patients in the relevant RCT were not reported. The systematic review and network meta-analysis included studies of adults (≥ 18 years) with active Crohn disease.14 The baseline CDAI scores of patients in the relevant RCTs ranged from 150 to 450.14
The RCT by Yokoyama et al. (2018)15 included 112 patients aged 15 years or older with active Crohn disease, with a CDAI score between 180 and 400. The patients were randomized to receive budesonide or mesalamine. The budesonide group included 56 patients with a mean age of 38 years and a mean CDAI score of 255.15 The mesalamine group included 56 patients with a mean age of 36 years and a mean CDAI score of 263.15
Interventions and Comparators
In the relevant RCT included in the systematic review by Gordon et al. (2021),13 azathioprine (2 to 3 mg/kg/day) was the intervention versus mesalamine (3.2 g/day) as comparator.13 The relevant interventions in the systematic review and network meta-analysis were low-dose mesalamine (< 2.4 g/day) and high-dose mesalamine (≥ 2.4 g/day).14 The relevant comparators were placebo, low-dose budesonide (≤ 6 mg/day), high-dose budesonide (> 6 mg/day), and unspecified corticosteroids.14
In the RCT, the intervention was oral budesonide 9 mg once daily and the comparator was oral mesalamine 1 g 3 times per day.15 Patients in the intervention group also received matched-placebo for mesalamine 3 times per day, and those in the comparator group received matched-placebo for budesonide once daily.15
Outcomes
The systematic review by Gordon et al. (2021)13 assessed incidence of pancreatitis and pancreatitis-related mortality.
The systematic review with network meta-analysis14 and the RCT15 assessed remission. The systematic review defined remission as a CDAI score below 150,14 whereas the RCT defined it as a CDAI score of 150 or lower.15 The CDAI is a score that represents the severity of disease activity in patients with Crohn disease.16 It is calculated based on an assessment of patient symptoms.16 CDAI values below 150 indicate non-active disease, values of 150 or higher indicate active disease, and values greater than 450 indicate severe disease.16 The primary outcome in the RCT was remission at week 8 defined as a CDAI score of 150 or lower. It was assessed for noninferiority of budesonide to mesalamine.15 The noninferiority margin was set as a 10% between-group difference.15 The systematic review with network meta-analysis14 also assessed withdrawals due to adverse events.
Secondary efficacy outcomes of the RCT included change in CDAI score, clinical improvement defined as remission (CDAI score ≤ 150) or a decrease in CDAI score of 100 or more from baseline, clinical improvement defined as remission (CDAI score ≤ 150) or a decrease in CDAI score of 70 or more from baseline, disease-specific health-related quality of life, and adverse events.15 Disease-specific health-related quality of life was assessed using the Inflammatory Bowel Disease Questionnaire (IBDQ). The IBDQ is a 32-item questionnaire with questions divided into 4 dimensions (bowel symptoms, systemic symptoms, emotional function, and social function).17 Scores range from 32 to 224 with higher scores representing better quality of life.17
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Systematic Reviews
Both systematic reviews had clear objectives and study eligibility criteria.13,14 Gordon et al. (2021)13 established the review methods and registered their protocol before conducting the review. The authors of the Coward et al. (2017)14 systematic review did not state whether the review methods were established before conducting the review. Thus, it is unknown if the methods were adjusted in a way that could introduce potential bias after the review had begun. Both systematic reviews used comprehensive literature search methods. The literature searches were conducted in multiple databases and trial registries, the search strategies were provided, and no language restrictions were used.13,14 In the Gordon et al. (2021)13 systematic review, the reference lists of included studies were handsearched for additional articles. In the Coward et al. (2017)14 systematic review, experts in the field were consulted to identify additional studies. A list of excluded studies and justifications for exclusion were provided in the Gordon et al. (2021)13 systematic review. A full list of the excluded studies was not provided in the Coward et al. (2017)14 systematic review; however, reasons for exclusion were provided. Study selection was performed in duplicate in the Gordon et al. (2021)13 systematic review. In the Coward et al. (2017)14 systematic review, abstract screening was performed in duplicate; however, the authors did not state whether full-text screening was performed in duplicate. Performing study selection in duplicate reduces errors and the potential risk of biases due to an individual’s selective preference for some studies. In both systematic reviews, data extraction was performed independently by at least 2 reviewers. The interventions and comparators of the included primary studies were described in adequate detail in both systematic reviews.13,14 The age of patients was not reported individually by included primary study in either systematic review. The countries where included studies were conducted were also not reported in either systematic review. Additionally, the length of follow-up of the included studies was not reported in the Gordon et al. (2021)13 systematic review. The risk of bias in the included studies was assessed using appropriate methods in both systematic reviews.13,14 The authors of the Gordon et al. (2021)13 systematic review declared that they had no conflicts of interest and reported the funding source for the review. The authors of the Coward et al. (2017)14 systematic review disclosed their potential conflicts of interest; however, they did not state whether any funding was received for the review.
Network Meta-Analysis
The systematic review by Coward et al. (2017)14 included a network meta-analysis that had several methodological strengths. The interventions of interest formed 1 connected network of RCTs. A random-effects model was used, and heterogeneity was assessed. Multiple sensitivity analyses were conducted to explore any sources of heterogeneity. There was no statistical inconsistency between direct and indirect evidence. The findings of the network meta-analysis were clearly reported. One limitation of the network meta-analysis was that some of the included primary studies were assessed as being at unclear risk of bias and 1 study was assessed as being at high risk of bias. An additional limitation was that there were several potential effect modifiers (e.g., disease severity at enrolment, disease location, concomitant medication, previous intestinal resections) that were not adjusted for. Imbalances in effect modifiers across studies can result in biased effect estimates.
Randomized Controlled Trial
The objective, patient characteristics, interventions, and main findings of the included RCT were clearly described.15 More patients discontinued the study in the mesalamine group. Eleven patients discontinued in the mesalamine group, and 6 patients discontinued in the budesonide group.15 The recruitment method for the study participants was not described; therefore, it is unclear whether the sample is representative of the source population. The study participants were blind to the intervention they received. The authors state that the study was double-blind; however, details on blinding of the investigators were not provided (e.g., process used to ensure investigators were blind to treatment assignment, and whether investigators were blinded the entire duration of the study).15 The main outcome measures used were valid and reliable, and adverse events were reported. A power calculation was conducted a priori, and an adequate number of patients was recruited to the study. Patients were stratified according to whether they were receiving concomitant azathioprine or 6-mercaptopurine and then randomized in a 1:1 ratio to the treatment and control groups.15 The randomization scheme was generated by a third party.15 The funding source for the study was reported and the authors disclosed their potential conflicts of interest.15
Summary of Findings
Appendix 4 presents the main study findings.
Clinical Effectiveness of Mesalamine
Evidence regarding the clinical effectiveness of mesalamine for the treatment of active Crohn disease was available from 1 systematic review,13 1 systematic review with a network meta-analysis,14 and 1 RCT.15
Remission
There was a statistically significant difference in induction of remission in favour of high-dose mesalamine versus placebo overall, and in a subgroup analysis of patients with CDAI scores from 150 to 450 at enrolment in the network meta-analysis.14 The network meta-analysis suggested there was a statistically significant difference in induction of remission in favour of high-dose budesonide versus low-dose mesalamine.14 There was a statistically significant difference in induction of remission in favour of corticosteroids versus both high-dose and low-dose mesalamine.14 There were no statistically significant differences in induction of remission for low-dose mesalamine versus placebo or low-dose budesonide, and for high-dose mesalamine versus high-dose or low-dose budesonide.14
In the RCT there were no statistically significant differences in remission rates for mesalamine versus budesonide at weeks 2, 4, or 8.15
CDAI Score
In the RCT, the proportion of patients with clinical improvement (defined as a CDAI score ≤ 150, a CDAI score decrease from baseline ≥ 100, or a CDAI score decrease from baseline ≥ 70) was numerically higher in the budesonide group than the mesalamine group at weeks 2, 4, and 8; however, the statistical significance of these results was not reported.
There were no significant differences between treatment groups in the decrease in mean CDAI score from baseline to weeks 2, 4, and 8.15
Quality of Life
In the RCT, mean IBDQ scores improved from baseline to weeks 2, 4, 8, and 10 in both the mesalamine and budesonide groups.15 Improvements were numerically higher in the budesonide group; however, the statistical significance of these results was not reported.15
Pancreatitis
The systematic review reported no significant differences in pancreatitis events between the mesalamine and azathioprine groups (1 RCT).13 There was 1 pancreatitis event in the azathioprine group and none in the mesalamine group.13 The systematic review reported no deaths resulting from azathioprine-induced or mesalamine-induced pancreatitis (1 RCT).13
Adverse Events
There were no significant differences in withdrawals due to adverse events for mesalamine versus placebo, budesonide, or corticosteroids in the network meta-analysis.14
In the RCT, 1 patient in the mesalamine group and no patients in the budesonide group experienced severe adverse events.15 One patient in the mesalamine group and 3 patients in the budesonide group experienced 1 or more serious adverse events.15 The investigators did not consider any of the serious adverse events to be related to the study drug.15 Four patients in each treatment group discontinued treatment due to adverse events.15
Limitations
Limited evidence was identified that compared mesalamine to immunosuppressants for the treatment of active Crohn disease. The relevant RCT included in the systematic review by Gordon et al. (2021)13 compared mesalamine to an immunosuppressant (azathioprine); however, only safety outcomes were reported in the systematic review. Additionally, the relevant RCTs included in the systematic review by Coward et al. (2017)14 and the RCT by Yokoyama et al. (2018)15 included patients with mild to moderate active Crohn disease. No evidence was identified that evaluated the effectiveness of mesalamine for the treatment of severe active Crohn disease.
The scope of this report included comparisons of mesalamine to placebo, corticosteroids, and immunosuppressants. Studies that evaluated mesalamine versus additional treatment options, such as biologic agents, were not included in this report.
The baseline CDAI scores of patients in the relevant RCTs differed per individual study and ranged from 150 to 450 in the systematic review and network meta-analysis.14 The mean CDAI score and distribution of scores between treatment groups were not reported for the included primary studies.14 If scores were concentrated on either end of this range, it could impact the generalizability of the findings from this systematic review. Additionally, imbalance in CDAI scores between treatment groups could impact the results.
The included RCT was not conducted in Canada.15 The countries of the primary studies included in the systematic reviews were not specified.13,14 Therefore, it is unclear whether the results summarized in the report are generalizable to Canada.
The relevant primary studies summarized in the included systematic reviews were of variable methodological quality.13,14 The authors of the Gordon et al. (2021)13 systematic review rated the relevant RCT as being at high risk of bias. The authors of the Coward et al. (2017)14 systematic review rated multiple relevant RCTs as being at unclear risk of bias and 1 relevant RCT as being at high risk of bias.
Conclusions and Implications for Decision- or Policy-Making
This report comprised 1 systematic review,13 1 systematic review with a network meta-analysis,14 and 1 RCT15 that evaluated mesalamine for the treatment of active Crohn disease.
Evidence from the network meta-analysis suggested there was a statistically significant difference in the induction of remission in favour of high-dose mesalamine versus placebo, and in favour of high-dose budesonide versus low-dose mesalamine.14 Results of the network meta-analysis also indicate a statistically significant difference in the induction of remission in favour of unspecified corticosteroids versus both high-dose and low-dose mesalamine.14 However, the network meta-analysis indicated no significant difference in the induction of remission for low-dose mesalamine versus placebo or for high-dose mesalamine versus high-dose or low-dose budesonide.14 Similarly, results from the RCT indicated there was no significant difference in remission rate for mesalamine versus budesonide.15
There were no significant differences in withdrawals due to adverse events for mesalamine versus placebo, budesonide, or corticosteroids in the network meta-analysis.14 The systematic review by Gordon et al. (2021)13 reported no significant differences in pancreatitis events between the mesalamine and azathioprine groups and no deaths due to drug-induced pancreatitis (1 RCT). In the RCT, 4 patients in each treatment group discontinued treatment due to adverse events.15 One patient in the mesalamine group and 3 patients in the budesonide group experienced 1 or more serious adverse events and the investigators did not consider any of the serious adverse events to be related to the study drug.15
The scope of this report did not include comparisons of mesalamine to biologic agents; however, a 2019 CADTH Optimal Use Report addressed several policy questions around the reimbursement criteria for biologic therapy for patients with Crohn disease.6 Several policy options were suggested in the report, including permitting first-line biologic treatment for patients with fistulizing Crohn disease.6
High-quality studies that evaluate the comparative effectiveness of mesalamine versus other treatment options, including immunosuppressants or biologic agents in patients with severe Crohn disease, would help health care decision-makers re-evaluate the place in therapy of mesalamine in the treatment of active Crohn disease.
References
1.Kaplan GG, Bernstein CN, Coward S, et al. The Impact of Inflammatory Bowel Disease in Canada 2018: Epidemiology. J Can Assoc Gastroenterol. 2019;2(Suppl 1):S6-S16. PubMed
2.Veauthier B, Hornecker JR. Crohn's Disease: Diagnosis and Management. Am Fam Physician. 2018;98(11):661-669. PubMed
3.Mills SC, von Roon AC, Tekkis PP, Orchard TR. Crohn's disease. BMJ Clin Evid. 2011;2011.
4.Panaccione R, Steinhart AH, Bressler B, et al. Canadian Association of Gastroenterology Clinical Practice Guideline for the Management of Luminal Crohn's Disease. JCAG. 2019;2(3):e1-e34. PubMed
5.Freeman HJ. Natural history and long-term clinical course of Crohn's disease. World J Gastroenterol. 2014;20(1):31-36. PubMed
6.Appropriate Pharmacotherapy for Inflammatory Bowel Disease. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/hta-he/ho0003-he0018-ibd-ou360.pdf. Accessed 19 Jul 2022.
7.Iacucci M, de Silva S, Ghosh S. Mesalazine in inflammatory bowel disease: a trendy topic once again? Can J Gastroenterol. 2010;24(2):127-133. PubMed
8.Damiao A, de Azevedo MFC, Carlos AS, Wada MY, Silva TVM, Feitosa FC. Conventional therapy for moderate to severe inflammatory bowel disease: A systematic literature review. World J Gastroenterol. 2019;25(9):1142-1157. PubMed
9.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
10.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. PubMed
11.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
12.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
13.Gordon M, Grafton-Clarke C, Akobeng A, et al. Pancreatitis associated with azathioprine and 6-mercaptopurine use in Crohn’s disease: a systematic review. Frontline gastroenterol. 2021;12(5):423-436. PubMed
14.Coward S, Kuenzig ME, Hazlewood G, et al. Comparative Effectiveness of Mesalamine, Sulfasalazine, Corticosteroids, and Budesonide for the Induction of Remission in Crohn's Disease: A Bayesian Network Meta-analysis. Inflamm Bowel Dis. 2017;23(3):461-472. PubMed
15.Yokoyama T, Ohta A, Motoya S, et al. Efficacy and Safety of Oral Budesonide in Patients with Active Crohn's Disease in Japan: A Multicenter, Double-Blind, Randomized, Parallel-Group Phase 3 Study. Inflamm. 2018;2(3):154-162. PubMed
16.Freeman HJ. Use of the Crohn's disease activity index in clinical trials of biological agents. World J Gastroenterol. 2008;14(26):4127-4130. PubMed
17.Pallis AG, Mouzas IA, Vlachonikolis IG. The inflammatory bowel disease questionnaire: a review of its national validation studies. Inflamm Bowel Dis. 2004;10(3):261-269. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews and Network Meta-Analysis
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Gordon et al. (2021)13 UK National Institute of Health and Care Research Cochrane Programme Grant | Study design: systematic review and meta-analysis Included studies: 25 RCTs, including 1 relevant to this report | Studies of patients of any age with Crohn disease undergoing therapy for induction or maintenance of remission. Relevant population: adults with active Crohn disease. Baseline CDAI scores for patients in the included studies were not reported. | Eligible interventions: azathioprine, 6-mercaptopurine Eligible comparators: placebo, no intervention, any other pharmacological agent Relevant intervention: azathioprine (2 to 3 mg/kg/day) Relevant comparator: mesalamine (3.2 g/day) | Outcomes: incidence of pancreatitis, pancreatitis-related mortality Follow-up: ≥3 months |
Coward et al. (2017)14 Canada NR | Study design: systematic review and network meta-analysis Included studies: 22 RCTs, including 9 relevant to the present report | Studies of adults (≥18 years) with Crohn disease. Studies of patients in post-operative remission were excluded. Baseline CDAI scores of patients in the relevant RCTs ranged from 150 to 450. | Eligible interventions: aminosalicylates (mesalamine, olsalazine, balsalazide, and sulfasalazine), unspecified corticosteroids, budesonide Eligible comparators: placebo, aminosalicylates (mesalamine, olsalazine, balsalazide, and sulfasalazine), unspecified corticosteroids, budesonide Relevant interventions: low-dose mesalamine (<2.4 g/day), high-dose mesalamine (≥2.4 g/day) Relevant comparators: placebo, low-dose budesonide (≤6 mg/day), high-dose budesonide (>6 mg/day), unspecified corticosteroids | Outcomes: induction of remission, withdrawals due to adverse events Follow-up: 8 to 17 weeks |
CDAI = Crohn’s Disease Activity Index; NR = not reported; RCT = randomized controlled trial.
Table 3: Characteristics of Included Randomized Controlled Trial
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Yokoyama et al. (2018)15 Japan AstraZeneca | Multi-centre, double-blind, RCT | Inclusion criteria: Patients aged 15 years or older with a diagnosis of active Crohn disease verified by X-ray, endoscopy, or histology affecting the ileum, ileocecal region, and/or ascending colon. Patients needed to have a CDAI score between 180 and 400 during the screening phase. Baseline characteristics: Budesonide group: 56 patients with a mean age of 38 years, 66% male, mean disease duration 8.6 years, mean CDAI score 255 Mesalamine group: 56 patients with a mean age of 36 years, 77% male, mean disease duration 7.8 years, mean CDAI score 263 | Intervention: oral budesonide 9 mg once daily and matched-placebo for mesalamine 3 times per day Comparator: oral mesalamine 1 g 3 times per day and matched-placebo for budesonide once daily | Outcomes: rate of remission, change in CDAI score, clinical improvement, disease-specific health-related quality of life, adverse events Follow-up: 8-week treatment period and 2-week dose tapering period (10 weeks total) |
CDAI = Crohn’s Disease Activity Index; RCT = randomized controlled trial.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Systematic Reviews and Network Meta-Analysis Using AMSTAR 29 and the ISPOR Questionnaire10
Strengths | Limitations |
|---|---|
Gordon et al. (2021)13 | |
Clear objective and inclusion criteria that included components of population, intervention, comparator, and outcomes The research methods were established prior to conducting the review and the protocol was registered The choice of study designs included in the review (i.e., RCTs) was explained The literature search was conducted in multiple databases and trial registries, the search strategy was provided, no language restrictions were used, reference lists of included studies were handsearched for additional articles Study selection and data extraction were performed independently by 2 reviewers List of excluded studies and justifications for exclusion were provided The interventions and comparators used in the included primary studies were described in detail The risk of bias in included primary studies was assessed independently by 2 reviewers using a satisfactory technique The funding source was reported, and the authors declared that they had no conflicts of interest | Some details of included primary studies were lacking (i.e., countries, age of patients, length of follow-up) Sources of funding for individual studies included in the review were not reported The relevant included primary study was assessed as being at high risk of bias by the systematic review’s authors |
Coward et al. (2017)14 | |
Clear objective and inclusion criteria that included components of population, intervention, comparator, and outcomes The choice of study designs included in the review (i.e., RCTs) was explained The literature search was conducted in multiple databases and trial registries, the search strategy was provided, no language restrictions were used, experts in the field were consulted to identify additional studies Abstract screening was performed in duplicate; however, it is unclear whether full-text screening was performed in duplicate Data extraction was performed independently by 3 reviewers The interventions, comparators, and time frame for follow-up of the included primary studies were described in detail The risk of bias in included primary studies was assessed independently by 3 reviewers using a satisfactory technique The authors disclosed their potential conflicts of interest Network meta-analysis The interventions of interest formed 1 connected network of RCTs Statistical methods were used that preserve within-study randomization There was no statistical evidence of inconsistency found between direct and indirect evidence A random-effects model was used, and heterogeneity was assessed Multiple sensitivity analyses were conducted to explore heterogeneity The findings were clearly reported | The authors did not state whether the research methods were established prior to conducting the review Full list of excluded studies was not provided however, reasons for exclusion were provided Some details of included primary studies were lacking (e.g., countries, age of patients) The authors do not state whether any funding was received for the review Network meta-analysis Multiple included primary studies were assessed as being at unclear risk of bias and 1 study was assessed as high risk of bias There are several potential effect modifiers (e.g., disease severity at enrolment, disease location, concomitant medication, previous intestinal resections) that were not adjusted for |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; ISPOR = International Society for Pharmacoeconomics and Outcomes Research.
Table 5: Strengths and Limitations of Randomized Controlled Trial Using the Downs and Black Checklist11
Strengths | Limitations |
|---|---|
Yokoyama et al. (2018)15 | |
Objective, patient characteristics, interventions, and main findings clearly described Estimates of random variability (e.g., confidence intervals) were reported Study participants were blind to the intervention they received Patients, care providers, and care setting were representative of the population and setting of interest The authors state that the study was double-blind however, details on blinding of investigators were not provided The main outcome measures were valid and reliable Adverse events were reported Participants were randomly allocated to intervention groups A power calculation was conducted a priori to determine sample size The funding source was reported, and the authors disclosed their potential conflicts of interest | More patients discontinued the study in the mesalamine group with may have led to an underestimate of the effect of mesalamine Recruitment method for study participants was not described The study was conducted in Japan and the results may not be generalizable to the Canadian population |
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 6: Summary of Findings of Included Systematic Reviews and Network Meta-Analysis
Study citation and study design | Subgroup | Comparison | Detailed findings |
|---|---|---|---|
Induction of remission | |||
Coward et al. (2017)14 SR and NMA (9 RCTs) | Overall | Low-dose mesalamine vs. placebo | OR = 1.05 (95% CrI, 0.49 to 2.45) OR>1 favours mesalamine |
High-dose mesalamine vs. placebo | OR = 2.11 (95% CrI, 1.39 to 3.31) OR>1 favours mesalamine | ||
Low-dose budesonide vs. low-dose mesalamine | OR = 1.45 (95% CrI, 0.50 to 3.97) OR>1 favours budesonide | ||
Low-dose budesonide vs. high-dose mesalamine | OR = 0.73 (95% CrI, 0.34 to 1.50) OR>1 favours budesonide | ||
High-dose budesonide vs. low-dose mesalamine | OR = 3.02 (95% CrI, 1.25 to 6.78) OR>1 favours budesonide | ||
High-dose budesonide vs. high-dose mesalamine | OR = 1.52 (95% CrI, 0.97 to 2.28) OR>1 favours budesonide | ||
Corticosteroids vs. low-dose mesalamine | OR = 3.64 (95% CrI, 1.50 to 8.34) OR>1 favours corticosteroids | ||
Corticosteroids vs. high-dose mesalamine | OR = 1.83 (95% CrI, 1.16 to 2.88) OR>1 favours corticosteroids | ||
Patients with CDAI from 150 to 450 at enrolment | Low-dose mesalamine vs. placebo | OR = 1.10 (95% CrI, 0.41 to 3.05) OR>1 favours mesalamine | |
High-dose mesalamine vs. placebo | OR = 2.23 (95% CrI, 1.15 to 4.16) OR>1 favours mesalamine | ||
High-dose budesonide vs. low-dose mesalamine | OR = 2.91 (95% CrI, 0.93 to 8.37) OR>1 favours budesonide | ||
High-dose budesonide vs. high-dose mesalamine | OR = 1.45 (95% CrI, 0.82 to 2.52) OR>1 favours budesonide | ||
Corticosteroids vs. low-dose mesalamine | OR = 2.98 (95% CrI, 0.96 to 8.62) OR>1 favours corticosteroids | ||
Corticosteroids vs. high-dose mesalamine | OR = 1.49 (95% CrI, 0.82 to 2.66) OR>1 favours corticosteroids | ||
Withdrawals due to adverse events | |||
Coward et al. (2017)14 SR and NMA (9 RCTs) | Overall | Low-dose mesalamine vs. placebo | OR = 1.74 (95% CrI, 0.33 to 8.99) OR<1 favours mesalamine |
High-dose mesalamine vs. placebo | OR = 1.07 (95% CrI, 0.36 to 3.43) OR<1 favours mesalamine | ||
Low-dose budesonide vs. low-dose mesalamine | OR = 0.20 (95% CrI, 0.01 to 2.36) OR<1 favours budesonide | ||
Low-dose budesonide vs. high-dose mesalamine | OR = 0.32 (95% CrI, 0.02 to 2.57) OR<1 favours budesonide | ||
High-dose budesonide vs. low-dose mesalamine | OR = 0.53 (95% CrI, 0.10 to 3.50) OR<1 favours budesonide | ||
High-dose budesonide vs. high-dose mesalamine | OR = 0.86 (95% CrI, 0.32 to 2.54) OR<1 favours budesonide | ||
Corticosteroids vs. low-dose mesalamine | OR = 1.26 (95% CrI, 0.19 to 8.65) OR<1 favours corticosteroids | ||
Corticosteroids vs. high-dose mesalamine | OR = 2.02 (95% CrI, 0.63 to 6.49) OR<1 favours corticosteroids | ||
Incidence of pancreatitis | |||
Gordon et al. (2021)13 SR (1 RCT) | Patients with active disease | Azathioprine vs. mesalamine | • Pancreatitis events o Azathioprine group: 1/36 o Mesalamine group: 0/36 • OR = 3.08 (95% CI, 0.12 to 78.27; P value = 0.49) o OR<1 favours azathioprine |
Pancreatitis-related mortality | |||
Gordon et al. (2021)13 SR (1 RCT) | Patients with active disease | Azathioprine vs. mesalamine | There were no reported deaths resulting from azathioprine-induced or mesalamine-induced pancreatitis. |
CDAI = Crohn’s Disease Activity Index; CI = confidence interval; CrI = credible interval; NMA = network meta-analysis; OR = odds ratio; RCT = randomized controlled trial; SR = systematic review.
Table 7: Summary of Findings of Yokoyama et al. (2018)15 — Remission Rate and CDAI
Outcome | Time point | Treatment group | |
|---|---|---|---|
Budesonide (n=56) | Mesalamine (n=56) | ||
Remission rate, % | Week 2 | 12.5 | 10.7 |
Difference (90% CI), P value | NR (NR), 0.768 | ||
Week 4 | 21.4 | 12.5 | |
Difference (90% CI), P value | NR (NR), 0.208 | ||
Week 8 | 30.4 (n = 17) | 25.0 (n = 14) | |
Difference (90% CI), P value | 5.4 (–8.5 to 18.9), 0.526 | ||
Proportion of patients with clinical improvement (CDAI score ≤150 or a CDAI score decrease from baseline ≥100), %a | Week 2 | 25.0 | 17.9 |
Week 4 | 33.9 | 19.6 | |
Week 8 | 42.9 | 30.4 | |
Proportion of patients with clinical improvement (CDAI score ≤150 or a CDAI score decrease from baseline ≥70), %a | Week 2 | 33.9 | 19.6 |
Week 4 | 39.3 | 23.2 | |
Week 8 | 48.2 | 32.1 | |
Decrease in mean CDAI score from baselineb | Weeks 2, 4, and 8 | NR | NR |
P value | NS | ||
CDAI = Crohn’s Disease Activity Index; CI = confidence interval; NR = not reported; NS = not significant.
aDifference (90% CI), P values were not reported.
bResults for this outcome were presented in a figure and exact values could not be ascertained.
Table 8: Summary of Findings of Yokoyama et al. (2018)15 — Additional Outcomes
Outcome | Detailed findings |
|---|---|
Quality of life (IBDQ) | Mean IBDQ scores improved from baseline to weeks 2, 4, 8, and 10 in both treatment groups. Improvements were numerically higher in the budesonide group (the level of statistical significance was not reported). |
Adverse events |
|
CDAI = Crohn’s Disease Activity Index; IBDQ = Inflammatory Bowel Disease Questionnaire.
Appendix 5: References of Potential Interest
Previous CADTH Reports
Biologics versus Immunomodulators or Antibiotics for the Management of Fistulizing Crohn’s Disease: A Review of Comparative Clinical Effectiveness and Cost-Effectiveness. Ottawa (ON): CADTH. 2019. https://www.cadth.ca/biologics-versus-immunomodulators-or-antibiotics-management-fistulizing-crohns-disease-review Accessed 19 Jul 2022.
Sequencing of Pharmacological Management of Crohn’s Disease and Ulcerative Colitis: A Review of Guidelines. Ottawa (ON): CADTH. 2019. https://www.cadth.ca/sequencing-pharmacological-management-crohns-disease-and-ulcerative-colitis-review-guidelines Accessed 19 Jul 2022.
Early Biologic Treatment versus Conventional Treatment for the Management of Crohn’s Disease: A Review of Comparative Clinical Effectiveness and Cost-Effectiveness. Ottawa (ON): CADTH. 2019. https://www.cadth.ca/early-biologic-treatment-versus-conventional-treatment-management-crohns-disease-review-comparative Accessed 19 Jul 2022.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca