CADTH Health Technology Review
Low-Dose Ipilimumab in Combination With Nivolumab or Pembrolizumab for the Treatment of Advanced Melanoma
Rapid Review
Authors: Tara Cowling, Heather Neilson, Ransi Nayakarathna, Quenby Mahood
Abbreviations
irAE
immune-related adverse event
pCODR
pan-Canadian Oncology Drug Review
pERC
pCODR Expert Review Committee
Key Messages
The review did not find any studies exclusively on the clinical effectiveness and safety of low-dose ipilimumab in combination with nivolumab for the treatment of advanced melanoma that met the criteria for this review.
The review found limited evidence, from 1 single-arm phase II trial of 70 adults and 1 retrospective cohort study of 9 adults, on the clinical benefits and safety of low-dose ipilimumab in combination with pembrolizumab (or nivolumab for an unspecified number of patients in the retrospective cohort study) for the treatment of advanced melanoma.
In the single-arm study, 20 of 70 enrolled patients (29%) achieved a confirmed response, including 5 complete (7.2%) and 15 partial responses (21.4%). In the retrospective cohort study, 3 of 9 patients (33%) achieved a partial response.
The review did not find any studies on the cost-effectiveness of low-dose ipilimumab in combination with nivolumab or pembrolizumab for the treatment of advanced melanoma that met our criteria for this review.
Context and Policy Issues
In 2021 in Canada, approximately 8,700 people were diagnosed with melanoma skin cancer and 1,250 people were expected to die from this disease.1 The 5-year survival rate for people with stage 4 melanoma — when melanoma has spread to other, distant sites in the body, also known as metastatic or advanced melanoma — is 15% to 20%.2 Patients who experience this condition have reported placing high value on controlling their disease progression, death, pain, and other symptoms; they have also reported that the benefits of treatment outweigh the risks of side effects.3
In Canada, the current treatment for advanced melanoma includes, but is not limited to, immunotherapy with drugs such as ipilimumab (Yervoy), nivolumab (Opdivo), and pembrolizumab (Keytruda). Ipilimumab is a recombinant human immunoglobulin G1 monoclonal antibody, also known as a CTLA-4-blocking antibody or anti-CTLA-4. Ipilimumab binds to CTL-4, a down-regulator of T-cell activation pathways that enhances the T-cell antitumour response.4 Nivolumab, a fully human monoclonal immunoglobulin G4 antibody, and pembrolizumab, a humanized monoclonal antibody, are immune checkpoint inhibitors, also known as anti-PD-1 drugs. Both nivolumab and pembrolizumab block PD-1 activity through binding to the PD-1 receptor on T-cells.5,6 This binding prevents other ligands from binding, thereby releasing inhibition of the T-cell antitumour immune response.5 Research has shown that the combination of ipilimumab and nivolumab results in a greater enhancement of T-cell function than does either treatment alone.4
Health Canada has issued a Notice of Compliance for each drug as follows:
Ipilimumab is approved as a single drug (3 mg/kg) or in combination with nivolumab (1 mg/kg) for the treatment of adult patients with unresectable or metastatic melanoma who have not received prior systemic therapy for unresectable or metastatic melanoma. This combination should be administered on the same day every 3 weeks for the first 4 doses or until unacceptable toxicity, whichever occurs earlier. After completion, nivolumab should be administered as a single drug (anti-PD-1 maintenance) for as long as clinical benefit is observed or until treatment is no longer tolerated by the patient.7,8
Nivolumab is approved as monotherapy for the treatment of unresectable or metastatic melanoma in patients who have not received prior systemic therapy for unresectable or metastatic melanoma; for patients who experienced disease progression following ipilimumab (and a BRAF inhibitor for patients who are BRAF V600 positive); and as adjuvant therapy for patients with advanced melanoma after complete resection.8
Pembrolizumab is approved as monotherapy for the treatment of unresectable or metastatic melanoma in patients who have not received prior treatment with ipilimumab (patients who are BRAF V600 positive may have received prior BRAF inhibitor therapy); and for patients who experienced disease progression following ipilimumab therapy (and a BRAF or MEK inhibitor for patients who are BRAF V600 positive).9
These approvals do not address second-line therapy for patients who complete anti-PD-1 monotherapy but later experience disease progression, or patients who receive an anti-PD-1 drug in the adjuvant setting but later experience a relapse (Figure 1). While the combination of ipilimumab (3 mg/kg) and anti-PD-1 drugs could be an effective option, grade 3 to 4 treatment-related adverse events have been reported in more than 50% of patients receiving this combination.10 In addition, a CADTH pan-Canadian Oncology Drug Review (pCODR) indicated that the costs of these drugs per patient over 28 days are $1,825 for nivolumab and $32,480 for ipilimumab.3 An alternative option may be to combine a lower dose of ipilimumab (1 mg/kg) with an anti-PD-1 therapy (nivolumab or pembrolizumab). However, the clinical effectiveness, safety, and cost-effectiveness of this combination are unknown.

This report adds to previous CADTH reports on immunotherapy for advanced melanoma. A 2019 Reference List, based on literature published between 2014 and 2019,11 and a 2019 Technology Review12 found no relevant evidence of the clinical effectiveness of nivolumab, pembrolizumab, or the combination of ipilimumab and nivolumab in patients who progressed after anti-PD-1 adjuvant therapy. A 2018 Technology Review focused on ipilimumab monotherapy after patient progression on pembrolizumab or nivolumab. In that report, the results from 3 retrospective nonrandomized studies suggested some response from ipilimumab but a high rate of adverse events among patients who received ipilimumab.13 Two reports from 2012 and 2014 were reimbursement recommendations by the pCODR Expert Review Committee (pERC). In the 2012 report, the committee recommended reimbursement for ipilimumab monotherapy as treatment for patients who received prior systemic therapy;14 in the 2014 report, the committee recommended ipilimumab as first-line treatment for adults.15
The objective of the current report is to summarize evidence regarding the clinical effectiveness, safety, and cost-effectiveness of low-dose ipilimumab (1 mg/kg) in combination with nivolumab or pembrolizumab for patients with advanced melanoma who completed anti-PD-1 monotherapy and later progressed, or those who received an anti-PD-1 drug in the adjuvant setting and later relapsed. Therefore, the focus of this report is on anti-PD-1 drugs as second-line treatment (Figure 1).
Research Questions
Among adult patients who progressed after treatment with anti-PD-1 monotherapy or relapsed within 6 months of treatment with an anti-PD-1 drug in the adjuvant setting:
What is the clinical effectiveness of low-dose ipilimumab in combination with nivolumab for the treatment of advanced melanoma?
What is the clinical effectiveness of low-dose ipilimumab in combination with pembrolizumab for the treatment of advanced melanoma?
What is the cost-effectiveness of low-dose ipilimumab in combination with nivolumab for the treatment of advanced melanoma?
What is the cost-effectiveness of low-dose ipilimumab in combination with pembrolizumab for the treatment of advanced melanoma?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including Medline and Embase via Ovid, the Cochrane Library, the University of York Centre for Reviews and Dissemination databases, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were ipilimumab (Yervoy) and nivolumab (Opdivo) or pembrolizumab (Keytruda) and advanced melanoma. Search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, network meta-analyses, any types of clinical trials or observational studies, and economic studies. Where possible, retrieval was limited to the human population. Conference abstracts were omitted from the search results. The search was completed on June 2, 2022, and was limited to English-language documents published since January 1, 2017.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adult patients with advanced melanoma who have progressed after treatment with anti-PD-1 monotherapy or have relapsed within 6 months of treatment with an anti-PD-1 drug in the adjuvant setting |
Intervention | Q1 and Q3: Four cycles of low-dose ipilimumab (1 mg/kg) in combination with nivolumab (3 mg/kg or maximum of 480 mg) with or without anti-PD-1 maintenance Q2 and Q4: Four cycles of low-dose ipilimumab (1 mg/kg) in combination with pembrolizumab (2 mg/kg or maximum of 200 mg) with or without anti-PD-1 maintenance |
Comparator | Standard care or no treatment, ipilimumab (3 mg/kg) alone or in combination with nivolumab or pembrolizumab |
Outcomes | Q1 and Q2: Clinical effectiveness (e.g., progression-free survival, overall survival, response rate, duration of response, quality of life, safety [e.g., adverse events of ≥ grade 3 and grade 4, serious adverse events, deaths]) Q3 and Q4: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained, incremental cost-effectiveness ratios) |
Study designs | Health technology assessments, systematic reviews, randomized-controlled trials, non-randomized studies, economic evaluations |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2017. Other exclusion criteria included studies involving other interventions (e.g., surgery) combined with the interventions of interest, and studies focused on comorbid disease populations (e.g., autoimmune diseases).
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Downs and Black checklist16 applicable to randomized and nonrandomized studies. Summary scores were not calculated for the included study; rather, the strengths and limitations of the included publication were described narratively.
Summary of Evidence
Quantity of Research Available
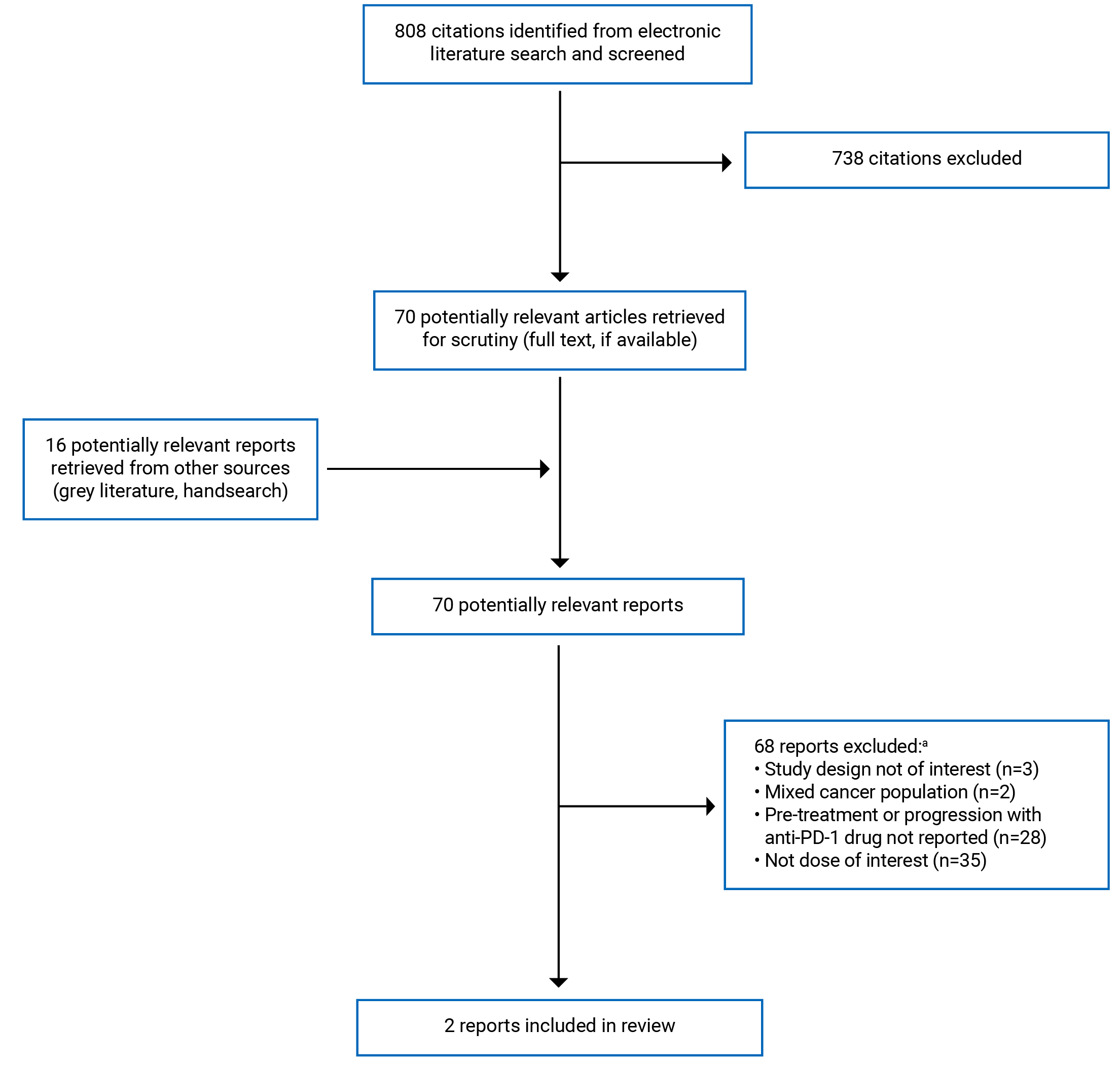
A total of 808 citations were identified in the literature search. Following screening of titles and abstracts, 738 citations were excluded and 70 potentially relevant reports from the electronic search were retrieved for full-text review. Sixteen potentially relevant publications were retrieved from the grey literature search for full-text review. Of potentially relevant articles, 68 publications were excluded for various reasons, and 2 publications, both nonrandomized studies,17,18 met the inclusion criteria and were included in this report. Appendix 1 presents the PRISMA19 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
Two publications met the eligibility criteria and were included in this report.17,18 Details regarding the characteristics of these publications are provided in Appendix 2.
Study Design
The first included study was a nonrandomized, open-label, single-arm, phase II clinical trial. The objective of the study was to examine the efficacy of pembrolizumab plus low-dose ipilimumab in advanced melanoma in patients, refractory to an anti-PD-1 or PD-L1 antibody.17 The second study was a retrospective cohort study. The objective of the study was to investigate the safety and efficacy of low-dose ipilimumab plus anti-PD-1 therapy in the second line or above setting.18
Country of Origin
The single-arm phase II trial17 recruited patients from 7 medical centres across the US, and the retrospective cohort study18 included patients from Germany.
Patient Population
The single-arm phase II trial17 examined 70 adult patients with unresectable or metastatic melanoma and known BRAF mutation status. Patients had experienced disease progression during treatment with an anti-PD-1 or anti-PD-L1 antibody immediately before accrual to the study or experienced disease progression within 6 months of receiving an adjuvant anti-PD-1 antibody without intercurrent therapy.
The retrospective cohort study18 examined 9 adult patients with unresectable stage III or IV melanoma. In total, 6 of the 9 patients (66.7%) were in stage M1c or M1d at the initiation of combined immunotherapy. None of the patients had a BRAF V600 mutation. All patients had relevant comorbidities or had experienced severe immune-related side effects during previous immunotherapy.
Interventions and Comparators
The single-arm phase II trial17 involved participants who received pembrolizumab (200 mg) intravenously along with low-dose ipilimumab (1 mg/kg) intravenously once every 3 weeks for 4 doses, potentially followed by maintenance with pembrolizumab (200 mg) intravenously once every 3 weeks for up to 2 years. Patients who attained a complete response, confirmed on at least 2 scans after a minimum of 24 weeks of study treatment, could discontinue treatment early. No dose reductions of pembrolizumab or ipilimumab were permitted. As this was a single-arm study, there was no comparator treatment group.
The retrospective cohort study18 examined the safety profile and efficacy of low-dose ipilimumab (1 mg/ kg) combined with anti-PD-1 immunotherapy in patients who progressed after anti-PD-1 monotherapy. Seven of 9 patients received anti-PD-1 maintenance therapy, either with nivolumab or pembrolizumab; the median number of doses was 7.5 (range = 2 to 17).
Outcomes
The primary outcome in the single-arm phase II trial17 was the objective response rate from pembrolizumab and low-dose ipilimumab following initial progression on an anti-PD-1 or anti-PD-L1 antibody in advanced melanoma. Secondary outcomes were progression-free survival (defined as time on study treatment until immune-related progressive disease, clear clinical progression, or death), and safety. Exploratory outcomes included the associations of baseline tumour gene expression patterns with clinical outcomes. Although not prespecified end points in the study protocol, overall survival (defined as the time from enrolment to death from any cause) and duration of response (defined as the time from first evidence of response until disease progression or death) were also assessed.
The primary outcome of the retrospective cohort study18 was the rate of severe (grade 3 to 5) immune-related adverse events (irAEs), graded according to National Cancer Institute’s Common Terminology Criteria for Adverse Events (version 5.0). These events were assessed from the first dose of combined immunotherapy to November 1, 2020. Safety was assessed based on the frequency and severity of irAEs, and whether treatment discontinuation or death occurred. Exploratory outcomes included resistance to previous PD-1–based immunotherapy and following response to combined immunotherapy; best overall response, progression-free survival, and overall survival were also examined as outcomes.
Summary of Critical Appraisal
The 2 included nonrandomized studies were critically appraised using the Downs and Black tool.16 The following summary highlights the strengths and limitations from each study, with additional details provided in Appendix 3.
A number of strengths were identified for the 2 included studies.17,18 Both studies addressed clearly focused research objectives. In both studies the outcomes were measured objectively, the follow-up period of participants was sufficiently long, and statistical tests for assessing the main outcomes were appropriate. The single-arm phase II trial17 had well-defined eligibility criteria for the study population, whereas the retrospective cohort study’s inclusion and exclusion criteria18 were not adequately described.
In terms of methodological limitations, both studies had nonrandomized, single-arm designs and the retrospective cohort study18 had a limited number of participants (n = 9). Therefore, both studies were prone to selection bias and neither study accounted for confounding factors. Due to the lack of a control group, randomization, and blinding, there is an inability to distinguish between the effect of the treatment, a placebo effect, and the effect of natural history. In addition, it is difficult to interpret the magnitude of response without a frame of reference for comparison, such as the effect of ipilimumab alone.
Furthermore, the single-arm phase II study excluded patients who were refractory to an anti-PD-1 or anti-PD-L1 antibody and experienced high-grade toxicity; therefore, the authors noted that observed toxicity rates may have been subject to selection bias. The study authors also noted a lack of formal consensus on how they defined progression on an anti-PD-1 or anti-PD-L1 antibody at the time of study.17
Given the methodological limitations of these 2 studies, the results reported should be interpreted with caution.
Summary of Findings
A summary of findings is presented in the following text according to the research questions posed by this report. Appendix 4 presents the main study findings and authors’ conclusions.
Clinical Effectiveness of Low-Dose Ipilimumab in Combination With Nivolumab
One retrospective cohort study was identified that assessed the clinical effectiveness of low-dose ipilimumab combined with either nivolumab or pembrolizumab in 9 adult patients with advanced melanoma who had a history of disease progression following immunotherapy.18 The number of patients who received nivolumab (as opposed to pembrolizumab) in combination therapy was unspecified; therefore, the results of this study are presented in the Clinical Effectiveness of Low-Dose Ipilimumab in Combination With Pembrolizumab section, where this limitation is noted.
No studies were identified that exclusively assessed the clinical effectiveness of low-dose ipilimumab combined with nivolumab in adult patients with advanced melanoma who progressed after treatment with anti-PD-1 monotherapy or relapsed within 6 months of treatment with an anti-PD-1 drug in the adjuvant setting; therefore, no summary can be provided.
Clinical Effectiveness of Low-Dose Ipilimumab in Combination With Pembrolizumab
Two studies were identified that reported on the clinical effectiveness of low-dose ipilimumab in combination with pembrolizumab.17,18 The trials were both nonrandomized studies of patients with advanced melanoma refractory to an anti-PD-1 or anti-PD-L1 antibody.
In the single-arm phase II trial,17 60 of 70 patients had received prior treatment with an anti-PD-1 antibody monotherapy and 10 patients had prior treatment with an anti-PD-1 or anti-PD-L1 antibody–based combination therapy, with a median of 4.8 months on a prior anti-PD-1 or anti-PD-L1 antibody treatment. In the retrospective cohort study,18 9 patients had prior treatment with an anti-PD-1 therapy for a median duration of 5.3 months.
In the retrospective cohort study of 9 patients, the combination therapy either included nivolumab or pembrolizumab as the anti-PD-1 drug; the number of patients who received pembrolizumab (as opposed to nivolumab) was unspecified.18
Response
In the single-arm phase II trial,17 20 of 70 enrolled patients (29%) achieved a confirmed response (95% confidence interval [CI], 18.4 to 40.6), including 5 complete (7.2%) and 15 partial responses (21.4%). Among patients who responded, the median duration of response was 16.6 months (95% CI, 7.9 to not reached). Responses were observed across all clinical subgroups, including patients with elevated lactate dehydrogenase levels and brain and liver metastases, and patients who progressed on an anti-PD-1 or anti-PD-L1 antibody in the adjuvant setting. Fifteen percent of responses (2 of 13) were among patients who progressed on a prior anti-PD-1 or anti-PD-L1 antibody within 6 months, although responses were also observed among those with longer prior treatment. Additionally, these responses occurred predominantly among patients with intermediate to non-T-cell–inflamed and PD-L1–negative tumours.
In the retrospective cohort study,18 3 of 9 patients had a partial response (accounting for the objective response rate of 33.3%) and the disease control rate was 66.7%. The number of patients who received pembrolizumab (as opposed to nivolumab) was unspecified.
Progression-Free Survival
The median progression-free survival was 5 months (95% CI, 2.8 to 8.3) in the single-arm phase II trial17 and 5.7 months in the retrospective cohort study.18 In the latter study, the number of patients who received pembrolizumab (as opposed to nivolumab) was unspecified.
Overall Survival
The median overall survival was 24.7 months (95% CI, 5.2 to not reached) in the single-arm phase II trial17 and 21.6 months in the retrospective cohort study.18 In the latter study, the 12-month overall survival rate was 79% (95% CI, 56.9% to 100%); the number of patients who received pembrolizumab (as opposed to nivolumab) was unspecified.18
Adverse Events
In the single-arm phase II trial,17 grade 3 to 4 adverse events—most commonly colitis, diarrhea, rash, and transaminase elevations—occurred in 27% of patients.
In the retrospective cohort study,18 5 of 9 patients (55.6%) experienced irAEs of any grade. Grade 3 irAEs occurred in 3 of 9 patients (33.3%). No patients experienced a grade 4 or 5 irAE. The number of patients who received pembrolizumab (as opposed to nivolumab) was unspecified.
Cost-Effectiveness of Low-Dose Ipilimumab in Combination With Nivolumab
No studies were identified that assessed the cost-effectiveness of low-dose ipilimumab combined with nivolumab in adult patients with advanced melanoma who progressed after treatment with anti-PD-1 monotherapy or relapsed within 6 months of treatment with an anti-PD-1 drug in the adjuvant setting; therefore, no summary can be provided.
Cost-Effectiveness of Low-Dose Ipilimumab in Combination With Pembrolizumab
No studies were identified that assessed the cost-effectiveness of low-dose ipilimumab combined with pembrolizumab in adult patients with advanced melanoma who progressed after treatment with anti-PD-1 monotherapy or relapsed within 6 months of treatment with an anti-PD-1 drug in the adjuvant setting; therefore, no summary can be provided.
Limitations
There are several limitations worth noting. First, there was no evidence identified on the cost-effectiveness of low-dose ipilimumab in combination with nivolumab or pembrolizumab, respectively. In addition, the evidence on clinical effectiveness was limited to only 2 studies with a low number of participants.17,18
In terms of generalizability to the Canadian context, the single-arm phase II trial17 included participants from 7 medical centres across the US, and the retrospective cohort study included 9 patients from Germany. Although patients living in Canada were not included in these studies, the characteristics of the patient population would not necessarily be different, but the delivery of care in other countries, including treatment pathways for patients with melanoma and lack of comparison to the standard of care in Canada, may limit generalizability.18 Furthermore, the low-dose regimen is not currently approved for use in Canada.
Due to the limitations related to volume of evidence, methodological concerns, and generalizability, caution should be used when interpreting the results of these 2 studies.
Conclusions and Implications for Decision- or Policy-Making
Two studies met the inclusion criteria of this review, comprising a single-arm phase II trial of 70 patients17 and a retrospective cohort study of 9 patients.18 All patients were adults with advanced melanoma who had experienced progression or relapse following anti-PD-1 therapy. Both studies reported on the clinical effectiveness of low-dose ipilimumab combined with pembrolizumab (or nivolumab in the retrospective cohort study18), and both included some patients who received anti-PD-1 maintenance for up to 2 years (7 of 9 patients received anti-PD-1 maintenance therapy in the retrospective cohort study; an unknown number of patients received maintenance therapy in the single-arm phase II trial). No evidence was identified that met the eligibility criteria in this report for studying the cost-effectiveness of low-dose ipilimumab combined with either pembrolizumab or nivolumab.
In general, the combination of low-dose ipilimumab and pembrolizumab (or nivolumab) was associated with antitumour activity and tolerability. Response rates ranged from 29%17 to 33%,18 and among responders, the median duration of response was 16.6 months.17 Adverse event rates (grade 3 to 4 or 3+) ranged from 27%17 to 33%.18 The median progression-free survival ranged from 5 months17 to 5.7 months.18 The overall survival ranged from 21.6 months18 to 24.7 months.17
Additional studies that did not meet the eligibility criteria are provided in Appendix 5. Notably, a phase IIIb and IV randomized trial of nivolumab plus low- versus high-dose ipilimumab in adult patients (n = 360), known as the CheckMate 511 Trial, did not have an eligible patient population given that all patients were previously untreated.20 Moreover, an international retrospective cohort study of patients resistant to anti-PD-1 drugs who received ipilimumab alone or ipilimumab plus anti-PD-1 therapy (n = 355) did not have an eligible intervention given that the dose of ipilimumab was 3 mg/kg.21
Previous, related CADTH reports have been published in this population but with different interventions of interest (e.g., ipilimumab monotherapy13-15), a higher dose of ipilimumab (e.g., 3 mg/kg13-15), or in the first-line treatment setting.15 Another related CADTH report was nonspecific to dose.12 The sparse evidence for the clinical effectiveness of low-dose ipilimumab in combination with nivolumab for the treatment of advanced melanoma is consistent with the lack of evidence noted previously by CADTH, based on literature published up to and including 2019.11,12
This report offers limited evidence regarding the clinical effectiveness of low-dose ipilimumab in combination with nivolumab or pembrolizumab following treatment with anti-PD-1 monotherapy, and no evidence was identified regarding the cost-effectiveness of these treatments. Future studies are needed with robust study designs, such as randomized-controlled trials with a higher number of recruited patients, in the second-line setting, that include patient populations of those in Canada and a comparator treatment group that is the Canadian standard of care, to address the clinical and cost-effectiveness of low-dose ipilimumab in combination with pembrolizumab or nivolumab.
References
1.Canadian Cancer Statistics Advisory Committee, Canadian Cancer Society, Statistics Canada, Public Health Agency of Canada. Canadian cancer statistics. Toronto, ON: Canadian Cancer Society; 2021: www.cancer.ca/Canadian-Cancer-Statistics-2021-EN. Accessed 2022 Jun 20.
2.Canadian Cancer Society. Survival statistics for melanoma skin cancer. 2022; https://cancer.ca/en/cancer-information/cancer-types/skin-melanoma/prognosis-and-survival/survival-statistics.
3.Pan-Canadian Oncology Drug Review. pCODR Expert Review Committee (pERC) final recommendation for Nivolumab (Opdivo) plus Ipilimumab (Yervoy) for metastatic melanoma. Ottawa (ON): PCODR; 2017: https://www.cadth.ca/sites/default/files/pcodr/pcodr_opdivo_yervoy_metmela_fn_rec.pdf. Accessed 2022 Jun 20.
4.Ipilimumab: drug information. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: www.uptodate.com. Accessed 2022 Jun 3.
5.Nivolumab: drug information. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: www.uptodate.com. Accessed 2022 Jun 3.
6.Pembrolizumab: drug information. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: www.uptodate.com. Accessed 2022 Jun 3.
7.Yervoy (ipilimumab for injection): intravenous infusion, 5 mg i;ilimumab/mL, 10 mL and 40 mL vials, antineoplastic [product monograph including patient medication information]. Montreal, Canada: Bristol-Myers Squibb Canada Co.; 2012: https://www.bms.com/assets/bms/ca/documents/productmonograph/YERVOY_EN_PM.pdf.
8.Opdivo: nivolumab for injection: intravenous infusion, 10 mg nivolumab/ml, 40 mg and 100 mg single use vials: antineoplastic (anatomical therapeutic chemical index code: L01XC17) [product monograph, including patient information]. Montreal, Canada: Bristol-Myers Squibb Canada Co.; 2015: https://www.bms.com/assets/bms/ca/documents/productmonograph/OPDIVO_EN_PM.pdf.
9.Keytruda (pembrolizumab): powder for solution for infusion 50 mg, solution for infusion 100 mg/4mL vial, antineoplastic agent, monoclonal antibody [product monograph including patient medication information]. Kirkland, QC: Merck Canada Inc.; 2017: https://pdf.hres.ca/dpd_pm/00040232.PDF. Accessed 2022 Jun 20.
10.Hodi FS, Chapman PB, Sznol M, et al. Safety and efficacy of combination nivolumab plus ipilimumab in patients with advanced melanoma: results from a North American expanded access program (CheckMate 218). Melanoma Res. 2021;31(1):67-75. PubMed
11.Cancer immunotherapy after adjuvant immunotherapy: clinical effectiveness and guidelines. (CADTH rapid response report: reference list). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/pdf/htis/2019/RA1056%20Cancer%20Immunotherapies%20Final.pdf. Accessed 2022 Jun 20.
12.Dosing and timing of immuno-oncology drugs (CADTH Technology Review). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/dosing-and-timing-immuno-oncology-drugs. Accessed 2022 Jul 5.
13.Metastatic melanoma gap analysis (CADTH Technology Review). Ottawa (ON): CADTH; 2018: https://www.cadth.ca/sites/default/files/pdf/HE0004_Metastatic_Melanoma_Gap_Analysis_TR_Final.pdf. Accessed 2022 Jun 20.
14.Pan-Canadian Oncology Drug Review. pCODR Expert Review Committee (pERC) final recommendation for ipilimumab (Yervoy) for advanced melanoma. Ottawa (ON): pCODR; 2012: https://www.cadth.ca/sites/default/files/pcodr/pcodr-yervoy-adv-mel-fn-rec.pdf. Accessed 2022 Jun 20.
15.Pan-Canadian Oncology Drug Review. pCODR Expert Review Committee (pERC) final recommendation for ipilimumab (Yervoy) for first line advanced melanoma. Ottawa (ON): pCODR; 2014: https://www.cadth.ca/sites/default/files/pcodr/pcodr-yervoy1st-fn-rec.pdf. Accessed 2022 Jun 20.
16.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
17.Olson DJ, Eroglu Z, Brockstein B, et al. Pembrolizumab plus ipilimumab following anti-PD-1/L1 failure in melanoma. J Clin Oncol. 2021;39(24):2647-2655. PubMed
18.Klee G, Kurzhals J, Hagelstein V, et al. Low-dose ipilimumab combined with anti-PD-1 immunotherapy in patients with metastatic melanoma following anti-PD-1 treatment failure. Melanoma Res. 2021;31(5):464-471. PubMed
19.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009;6(7):e1000100. PubMed
20.Lebbé C, Meyer N, Mortier L, et al. Evaluation of two dosing regimens for nivolumab in combination with ipilimumab in patients with advanced melanoma: results from the phase IIIb/IV CheckMate 511 Trial. J Clin Oncol. 2019;37(11):867-875. PubMed
21.Pires da Silva I, Ahmed T, Reijers ILM, et al. Ipilimumab alone or ipilimumab plus anti-PD-1 therapy in patients with metastatic melanoma resistant to anti-PD-(L)1 monotherapy: a multicentre, retrospective, cohort study. Lancet Oncol. 2021;22(6):836-847. PubMed
Appendix 1: Selection of Included Studies
Note that this appendix has not been copy-edited.
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Olson et al. (2021),17 United States, Merck Investigator Studies Program | Open-label, single-arm phase II trial | 70 adult patients with unresectable or metastatic melanoma with known BRAF mutation status. Median patient age was 64 years (range: 27-87); 47 of 70 patients (67%) were male. 62 patients (89%) had cutaneous melanoma; 20 patients (29%) had BRAF V600 mutations; 34 patients (49%) had M1c or M1d disease; 22 patients (31%) had elevated serum lactate dehydrogenase concentrations. All patients had experienced disease progression during treatment with an anti-PD-1/L1 antibody immediately before accrual to the study or disease progression within 6 months of adjuvant anti-PD-1 antibody without intercurrent therapy. Patients had previous grade 3-4 toxicity from anti-PD-1/L1 antibody therapy leading to treatment discontinuation; patients with active CNS metastases were excluded. | Pembrolizumab (200 mg) intravenously along with low-dose ipilimumab (1 mg/kg) intravenously once every 3 weeks for four doses, followed by pembrolizumab intravenously 200 mg once every 3 weeks for up to 2 years | Primary: Objective response rate of pembrolizumab with low-dose ipilimumab following initial progression on an anti-PD-1/L1 antibody in advanced melanoma. Secondary: Progression-free survival (defined as time on study treatment until immune related progressive disease, clear clinical progression, or death) and safety. Exploratory: Associations of baseline tumor gene expression patterns with clinical outcomes. Additional: Overall survival (time from enrollment to death from any cause) and duration of response (defined as the time from first evidence of response until disease progression or death) Follow-up: up to 2 years |
Klee et al. (2021),18 Germany, source of funding not reported | Retrospective cohort | 9 patients with inoperable stage III (n=2) or IV (n=7) metastatic melanoma. 6 of 9 patients (66.7%) were in M-stage M1c or M1d at the initiation of combined immunotherapy. None of the patients had a BRAF V600 mutation. 6 patients had cutaneous melanoma, 2 had melanoma of unknown primary and one patient had mucosal melanoma. Average patient age was 79.4 ± 8.03 years; 6 of 9 (66.7%) were male. All patients had relevant co-morbidities or had experienced severe irAEs during previous immunotherapy. All patients had a history of disease progression following immunotherapy | Ipilimumab (1 mg/kg) with nivolumab 3 mg/kg or pembrolizumab 200 mg every 3 weeks for four doses. After four doses of combined immunotherapy staging examinations (computer tomography/MRI) were performed to assess treatment response. Following combined immunotherapy, patients received anti-PD-1 monotherapy with nivolumab or pembrolizumab or were switched to another therapy. | Primary: Rate of severe (grade 3–5) irAEs. irAEs were graded according to National Cancer Institute Common Terminology Criteria for Adverse Events (version 5.0), assessed from the first dose of combined immunotherapy to 1 November 2020. Safety was assessed based on the frequency of irAEs, their severity and whether they led to treatment discontinuation or death. Exploratory: resistance to previous PD-1-based immunotherapy, clinical outcomes following response to combined immunotherapy, including best overall response, progression-free survival, and overall survival Follow-up: median 13.1 months |
BRAF = BRAF 600, a specific mutation in the BRAF gene; irAE = immune-related adverse events; PD-1 = programmed cell death-1; PD-L1 = programmed cell death ligand-1.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist16
Strengths | Limitations |
|---|---|
Olson et al. (2021)17 | |
|
|
Klee et al. (2021)18 | |
|
|
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Table 4: Summary of Findings of Included Primary Clinical Studies
Main study findings | Authors’ conclusion |
|---|---|
Olson et al. (2021)17 | |
| “The combination of pembrolizumab plus low-dose ipilimumab demonstrated significant antitumor activity and tolerability in a multicenter clinical trial. This study demonstrated long-term responses, suggesting that durable survival—a hallmark of immunotherapy activity—may be possible even after failure of an anti-PD-1/L1 antibody (p. 2653).”17 |
Klee et al. (2021)18 | |
| “Dual inhibition of anti-cytotoxic T-lymphocyte–associated antigen 4 (with low-dose ipilimumab) and PD-1 may be a useful treatment option for patients with advanced melanoma who have progressed following anti-PD-1 monotherapy. The irAE profile may also be more favorable than that seen with standard IPI3+NIVO1 therapy. As a result, this dosing regimen could be considered for selected patient populations, for example, elderly patients, patients with multiple co-morbidities or those who have suffered from severe irAEs during previous immunotherapy.” (p.470) |
irAE = immune-related adverse events; irRECIST = immune-related Response Evaluation Criteria in Solid Tumors; PD-L1 = programmed cell death ligand-1.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
Cancer immunotherapy after adjuvant immunotherapy: clinical effectiveness and guidelines. (CADTH Rapid Response Report: Reference List). Ottawa, ON: CADTH;2019: https://www.cadth.ca/sites/default/files/pdf/htis/2019/RA1056%20Cancer%20Immunotherapies%20Final.pdf. Accessed 2022 Jun 23.
Dosing and timing of immune-oncology drugs. (CADTH Technology Review: Optimal Use 360 Report). Ottawa, ON: CADTH; 2019: https://www.cadth.ca/dosing-and-timing-immuno-oncology-drugs. Accessed 2022 Jul 5.
Metastatic melanoma gap analysis. (CADTH Technology Review; no.9). Ottawa, ON: CADTH; 2018: https://www.cadth.ca/sites/default/files/pdf/HE0004_Metastatic_Melanoma_Gap_Analysis_TR_Final.pdf. Accessed 2022 Jun 23.
Yervoy for first line advanced melanoma: details. (CADTH Reimbursement Review). Ottawa, ON: CADTH; 2014: https://www.cadth.ca/yervoy-first-line-advanced-melanoma-details. Accessed 2022 Jun 23.
Yervoy for advanced melanoma: details. (CADTH Reimbursement Review). Ottawa, ON: CADTH; 2012: https://www.cadth.ca/yervoy-advanced-melanoma-details. Accessed 2022 Jun 23.
Review Articles
Karlsson AK, Saleh SN. Checkpoint inhibitors for malignant melanoma: a systematic review and meta-analysis. Review. Clin Cosmet Investig Dermatol. 2017;10:325-339. PubMed
Additional References
Higher dose of ipilimumab (3 mg/kg)
Friedman CF, Spencer C, Cabanski CR, et al. Ipilimumab alone or in combination with nivolumab in patients with advanced melanoma who have progressed or relapsed on PD-1 blockade: clinical outcomes and translational biomarker analyses. J Immunother Cancer. 2022;10(1):01. PubMed
Pires da Silva I, Ahmed T, Reijers ILM, et al. Ipilimumab alone or ipilimumab plus anti-PD-1 therapy in patients with metastatic melanoma resistant to anti-PD-(L)1 monotherapy: a multicentre, retrospective, cohort study. Lancet Oncol. 2021;22(6):836-847. PubMed
Ineligible due to previous treatment
Lebbé C, Meyer N, Mortier L, et al. Evaluation of two dosing regimens for nivolumab in combination with ipilimumab in patients with advanced melanoma: results from the phase IIIb/IV CheckMate 511 trial. J Clin Oncol. 2019;37(11):867-875. PubMed
Kirchberger MC, Moreira A, Erdmann M, Schuler G, Heinzerling L. Real world experience in low-dose ipilimumab in combination with PD-1 blockade in advanced melanoma patients. Oncotarget. 2018;9(48):28903-28909. PubMed
Long GV, Atkinson V, Cebon JS, et al. Standard-dose pembrolizumab in combination with reduced-dose ipilimumab for patients with advanced melanoma (KEYNOTE-029): an open-label, phase 1b trial. Lancet Oncol. 2017;18(9):1202-1210. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca