CADTH Health Technology Review
Multiple Prosthetic Sockets for Lower Limb Amputations
Rapid Review
Authors: Calvin Young, Quenby Mahood
Abbreviations
AGREE
Appraisal of Guidelines for Research and Evaluation
BDI
Beck Depression Inventory
RCT
randomized controlled trial
TAPES
Trinity Amputation and Prosthetic Experience Scales
VAS
visual analogue scale
Key Messages
Clinicians may provide people being fitted for a prosthesis with temporary test prosthetic sockets to solicit feedback on their shape and comfort. The feedback can then be incorporated into the final design of the prosthesis, allowing customization based on the individual’s experience.
Limited evidence suggests that providing people with lower limb amputation a test socket before fitting a permanent socket may improve mobility and function, pain while walking, and prosthetic satisfaction, as well as decrease the frequency of admissions.
One guideline recommends the postoperative use of a prosthesis as soon as possible after transtibial amputation and that custom-made prostheses are preferable to prefabricated prostheses.
Additional high-quality evidence is needed to better understand the most appropriate use of multiple prosthetic sockets in people with lower limb amputation.
Context and Policy Issues
Amputation is the surgical removal or loss of a body part due to injury or disease. Common reasons for amputation include trauma, cancer, peripheral vascular disease, severe infection, neuropathy, and complications of diabetes.1,2 While they may be considered medically necessary to control disease or prevent mortality, lower limb amputations are associated with mobility issues, psychological distress, and decreased quality of life.3,4
In Canada, the annual rate of lower limb amputation is approximately 25 people per 100,000.5,6 While amputation impacts people of any age, sex, or gender, the incidence of lower limb amputation is disproportionally higher in males and those older than 75 years.5,6 Care related to amputation, rehabilitation, and the long-term management of people with lower limb amputation is associated with significant use of health care resources.6-9
Postoperative care that aims to maximize mobility, enables activities of daily living, and controls comorbid conditions is important to the rehabilitation process in people with lower limb amputation.4,10 Once surgical wounds have sufficiently healed, it may be appropriate to initiate prosthesis fitting. There are many different approaches to prosthesis fitting that can be considered, particularly when designing the prosthetic socket. The socket is the interface between the individual’s residual limb and the prosthesis, and can be above or below the knee, depending on whether the amputation was transfemoral or transtibial. Proper fit of the socket is critical, as inappropriate fit can cause pain, stress, skin irritation or breakdown, and pressure sores.11 Achieving optimal socket fit is challenging as the shape and size of the residual limb fluctuates as it matures due to muscle atrophy, post-operative edema, and residual limb muscle activity.12
One strategy to potentially increase socket fit is to use interim prosthetic sockets (also known as test sockets, check sockets, or preparatory sockets) that can be adjusted and modified based on user feedback. Typically made of thermoplastic materials that are readily adjustable by prosthetists, interim sockets can be used in the recovery phase to enable early mobilization.13,14 Once the surgical wound is completely healed and the residual limb has stabilized to a more permanent shape, a definitive socket (also known as a permanent socket) intended for long-term use can be designed and manufactured based on the changes made to the interim socket.13
Clinicians and policy-makers may be faced with complex decisions regarding the use of multiple prosthetic sockets for people with lower limb amputations. To ensure these decisions can be made in consideration of the available evidence, the objective of this report is to summarize the published literature regarding the clinical effectiveness of multiple prosthetic sockets for people with lower limb amputations. Additionally, evidence-based guidelines that provide recommendations regarding the use of multiple prosthetic sockets for people with lower limb amputations will be reviewed.
Research Questions
What is the clinical effectiveness of multiple prosthetic sockets for people with lower limb amputations?
What are the evidence-based guidelines regarding the use of multiple prosthetic sockets for people with lower limb amputations?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including Medline, Cumulative Index to Nursing and Allied Health Literature (CINAHL), the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were amputation, lower limbs, prosthetics, and sockets. A CADTH-developed search filter was applied to limit retrieval to guidelines for a secondary search for the concepts amputation, lower limbs, and prosthetics. The search was conducted on May 24, 2022, and limited to English-language documents published since January 1, 2012.
A supplementary literature search was conducted to address additional research questions related to the use of prosthetic sockets in people with lower limb amputation that were outside the scope of this Rapid Review. The methodology and findings of this search are available in Appendix 6.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | People with lower limb amputations (transtibial or transfemoral) |
Intervention | Multiple prosthetic sockets (e.g., volume check socket, ambulatory test socket, test socket, temporary socket, interim socket, preparatory socket, definitive socket, check socket) fitted over the course of preparatory and definitive prosthetic treatment |
Comparator | Q1: Single definitive prosthetic socket; no comparator Q2: Not applicable |
Outcomes | Q1: Clinical effectiveness (e.g., residual limb volume, mobility, balance, comfort, pain, swelling, edema, skin breakdown [e.g., ulcers, blisters], quality of life, patient satisfaction) Q2: Recommendations regarding best practices (e.g., types of sockets for preparatory and definitive prosthetics, optimum number of sockets required) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies, evidence-based guidelines |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2012. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: the Downs and Black checklist15 for non-randomized studies and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument16 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
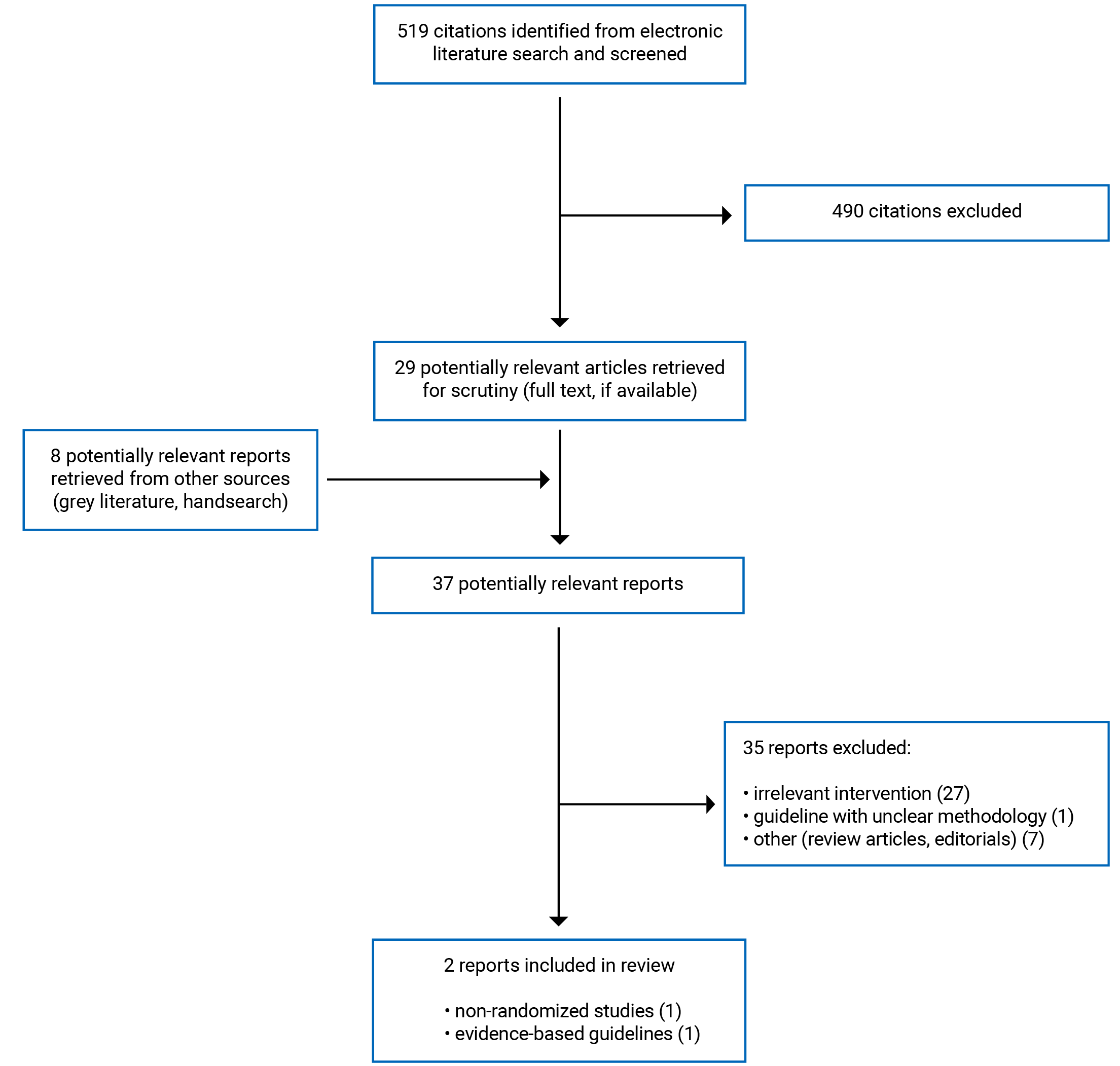
A total of 519 citations were identified in the literature search. Following screening of titles and abstracts, 490 citations were excluded and 29 potentially relevant reports from the electronic search were retrieved for full-text review. Eight potentially relevant publications were identified from the grey literature for full-text review. Of these 37 potentially relevant articles, 35 publications were excluded for various reasons, and 2 publications that met the inclusion criteria were included in this report. These comprised 1 non-randomized study17 and 1 evidence-based guideline.18 Appendix 1 presents the PRISMA19 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
One non-randomized study17 and 1 evidence-based guideline18 met the selection criteria and were included in this review. No relevant health technology assessments, systematic reviews, or randomized controlled trials (RCTs) were identified. Detailed study characteristics are provided in Table 2 and Table 3 in Appendix 2.
Study Design
The non-randomized study17 was a single-centre, retrospective cohort study. The study was carried out between January 2016 and May 2017.
The evidence-based guideline18 was developed by a group of Dutch researchers affiliated with various institutions in the Netherlands, led by the Netherlands Society of Physical and Rehabilitation Medicine. The guidelines were informed by evidence retrieved using systematic searches in 5 electronic databases, including the Cochrane Library, Medline, Embase, PsycINFO, and CINAHL. The systematic searches were supplemented by manual literature searches. The searches were conducted up to January 2011 and were limited to articles published in Dutch, English, German, and French. Eligible study designs varied by topic and were dependent on the types of available literature (e.g., if robust systematic reviews or RCTs were available, data from observational studies were not considered). The individual studies were assigned a level based on their methodological quality between A1 (higher quality) and D (lower quality). Recommendations were assigned a level of evidence using EBRO (Dutch evidence-based guideline development) criteria. Levels of evidence ranged between level 1 (based on a systematic review of at least 2 independent, high-quality RCTs or at least 2 independent, high-quality RCTs with consistent results) and level 4 (based on expert opinion). A clear description of the methods used to formulate recommendations (e.g., consensus, voting) was not provided.
Country of Origin
The retrospective cohort study17 was conducted in Turkey. The guideline18 was assumed to be intended for use in the Netherlands.
Patient Population
The retrospective cohort study17 included data from 88 individuals, between the ages of 18 and 70 years, who received a lower limb prosthesis for transtibial or transfemoral amputation at the study centre, had used their prosthesis for at least 6 months, and who underwent lower limb amputation for acquired reasons. People who had bilateral lower limb amputation or who underwent lower limb amputation due to reasons such as tumours, congenital anomalies, infections, burns, and poliomyelitis, were excluded. The mean age of study participants was 40.31 years in the test socket group and 38.89 years in the no test socket group. The proportion of female participants was 38.6%. Mean body mass index was 26.05 kg/m2 in the test socket group and 25.97 kg/m2 in the no test socket group. Of the 88 participants, 63 (71.6%) had transtibial amputation and 25 (28.4%) had transfemoral amputation. The time since amputation and the reasons for amputation were not reported.
For the included guideline,18 the target population is people with lower limb amputation. The intended users of the guideline18 are clinicians involved in providing care for people with amputation and prostheses of the lower extremity.
Interventions and Comparators
Participants of the retrospective cohort study17 were divided into 2 groups: those who received a test socket and those who did not receive a test socket. The test sockets were temporary sockets used shortly after amputation. While the test socket resembled the permanent (i.e., definitive) socket, they were manufactured using thermoplastic material that could be adjusted based on user feedback. Once a final shape was obtained, the permanent socket was designed according to the changes made to the test socket. Participants in the no test socket group had a permanent socket designed without the use of a test socket.
The guideline18 made recommendations on a wide range of interventions that can be provided to individuals through the post-amputation rehabilitation process (e.g., physical therapy, psychological therapies, exercise), including prostheses. Relevant to the current report, there are recommendations specific to interim prostheses that can be used in the early postoperative phase, before the fitting of a definitive prosthesis.
Outcomes
The retrospective cohort study17 reported on various measures of clinical effectiveness, including measures of mobility and function, pain, depressive symptoms, participant satisfaction, and other clinical outcomes (i.e., prosthesis delivery time, frequency of admissions to the study clinic).
Measures of mobility and function included duration of daily prosthesis use, daily walking distance with prosthesis, time to complete a 10-metre walk test on a flat surface, time to complete a 10-step climbing up test, time to complete a 10-step climbing down test, time to complete a 10-metre walking up an 8% slope test, and time to complete a 10-metre walking down an 8% slope test.
Pain was assessed at rest and while walking using the visual analogue scale (VAS). Participants were asked to indicate their level of pain on a 10 cm scale that ranged from 0 (no pain) to 10 (very severe pain).17 The VAS tool is widely used to assess pain in research and has shown promising validity in many clinical settings and patient populations.20-22
Depressive symptoms were measured using the Beck Depression Inventory (BDI). The BDI is a 21-question multiple-choice self-report inventory where each answer is rated on a 4-point scale ranging from 0 to 3. A total score is calculated by adding the values from each item.17 Total scores range from 0 to 63, with higher scores indicating more severe depressive symptoms. Like the VAS, the BDI is widely used in research and has promising validity in many patient populations.23-25
Participant satisfaction was assessed with the Turkish version of the Trinity Amputation and Prosthetic Experience Scales (TAPES). The TAPES contains 3 subscales, including:
the psychosocial adjustment subscale, which is scored on a 5-point Likert scale; total scores range from 5 to 75, with higher scores representing higher levels of psychosocial adjustment17
the activity restriction subscale, which is scored on a 3-point Likert scale; total scores range from 12 to 36, with higher scores representing higher levels of activity restriction17
the prosthesis satisfaction subscale, which is scored on a 5-point Likert scale; total scores range from 10 to 50, with higher scores representing higher levels of prosthesis satisfaction.17
The Turkish version of the TAPES has demonstrated validity and reliability in Turkish people with unilateral lower limb amputation (i.e., the population examined in the retrospective cohort study).17,26
Additional clinical outcomes assessed in the retrospective cohort study17 included prosthesis delivery time and frequency of admission to the study clinic within 3 months. Clear descriptions of these outcomes were not provided. For prosthesis delivery time, it was assumed that this was the time between initial prosthesis measurement and final delivery, but this was unclear. Similarly, the authors reported on the frequency of admissions to the study clinic within 3 months, but it was unclear what time frame was being evaluated (e.g., whether it was the 3 months following amputation or prosthesis delivery, or another time frame).
The authors of the included guideline18 appeared to consider many different outcomes when formulating recommendations relevant to the current report, including time to final prosthesis fitting, edema, measures of mobility, risk for complications, and time to complete stump healing, as these were the outcomes summarized from the cited literature.
Summary of Critical Appraisal
The methodological quality of the included studies17,18 is presented here. Additional details regarding the strengths and limitations of the included publications are provided in Appendix 3, Table 4 and Table 5.
Non-Randomized Studies
The methodological quality of the retrospective cohort study17 was assessed using the Downs and Black checklist.15 The study17 had clearly described objectives, intervention, comparator, outcomes, and main findings. Additionally, the authors clearly described the patient eligibility criteria (i.e., inclusion and exclusion criteria), reported estimates of random variability (e.g., standard deviations), and provided exact P values (rather than simply reporting whether a result was statistically significant or not). Baseline demographic data, such as age, gender, weight, height, body mass index, education level, occupation, and type of amputation, were described and were tested for statistically significant differences between intervention groups. For all these demographic characteristics, there were no statistically significant differences between those who received a test socket and those who did not. Robust reporting of these study characteristics and results increases the reproducibility of the study. Additional methodological strengths were that compliance with the assigned intervention was reliable, outcome measures were valid, and authors declared their sources of support (i.e., departmental sources) and that they had no potential conflicts of interest. Finally, the study participants, care providers, and care settings appeared to be representative of the population and care setting of interest, increasing the external validity of the study.17
As for methodological limitations, assignment of patients to receive a test socket or no test socket was not done at random. It is possible that prognostic factors, patient preference, and clinician discretion were factors in determining which treatment participants received, increasing the risk of bias due to confounding. Additionally, the timing of outcome assessment was poorly reported. It was unclear how much time had passed between prosthesis fitting, with or without a test socket, and outcome measurement. It was possible that the timing of outcome measurement was not consistent between treatment groups, potentially leading to biased results (i.e., if some participants had more time to adjust to their definitive prosthesis, they may have performed better on tests for mobility and physical function). It was also unclear whether the outcomes reported in the study17 were all collected as part of routine follow-up assessments and retrieved from medical records, or if some outcomes were measured after initiating the study. Furthermore, participants and outcome assessors of the retrospective cohort study17 were aware of the intervention received by the participant; therefore, there was a risk of bias in either direction depending on the perceptions and expectations of those involved, particularly due to the subjective nature of the assessed outcomes. There was a lack of reporting of adverse events, and it was unlikely that all important adverse events that may have been a consequence of the intervention (e.g., skin ulcers, blisters) were recorded. Additionally, the authors of the study17 conducted tests for statistical significance for many outcomes without adjustment for multiplicity. Therefore, there may be potential type I error rate inflation. The findings of the study are also at risk for reporting bias as the authors did not register a protocol outlining their intentions before completing the study. Finally, the generalizability of the findings from the retrospective cohort study17 to Canadian settings was unclear given it was conducted at a single centre in Turkey.
Overall, the non-randomized study17 was of low methodological quality due to the limitations related to study design, poor reporting, and risk of bias due to confounding and other sources.
Evidence-Based Guidelines
The methodological quality of the guideline18 was assessed using the AGREE II instrument.16 The guideline18 provided clear descriptions of its scope, objective, target population (i.e., people with lower limb amputation), and target users (i.e., clinicians involved in providing care for people with amputation and prostheses of the lower extremity). The name, affiliated institution, and geographic location of the authors were provided; however, the professional discipline or area of expertise of each author and their role in the guideline development group were not reported. Therefore, it was unclear if individuals from all relevant professional groups were consulted while drafting the recommendations. Similarly, while the authors stated that important aspects such as patient preferences, financial costs, and potential facilitators and barriers of applying recommendations were considered when drafting the guidelines, the methods used to incorporate these considerations were not reported. It was unclear what impact these considerations may have had on the recommendations. The authors used systematic methods to search for evidence to inform their recommendations, considered the benefits and risks of various interventions when drafting recommendations, and there was an explicit link between the recommendations and the supporting evidence. These methodological strengths increase the credibility of the recommendations. However, there was a lack of reporting on the criteria for selecting studies (e.g., there was limited description of inclusion and exclusion criteria, it was unclear if studies were screened in duplicate), the methods used for formulating the recommendations, and the procedure for updating the guideline. As a result, the reproducibility of the guideline18 is low. Furthermore, the guideline18 did not include a description of facilitators and barriers to guideline application, advice or tools on how the recommendations can be put into practice, and did not present monitoring or auditing criteria, decreasing the usability of the guideline.18 Finally, the guideline18 appeared to have editorial independence as the authors declared that they had no conflicts of interest and the views of the funding body (i.e., the Quality Foundation of Dutch Medical Specialists) did not seem to have any influence on the content of the guidelines.
Summary of Findings
The overall findings of the included studies are highlighted in the following text. Detailed summaries of the main findings by outcome are available in Appendix 4 (Table 6 to Table 11).
Clinical Effectiveness of Multiple Prosthetic Sockets
Mobility and Function
The retrospective cohort study17 found that participants with transtibial or transfemoral amputation who used a test socket before final prosthesis fitting had increased painless daily walking distance, took less time to complete a 10-step climbing up test, and took less time to complete a 10-metre walk test up an 8% slope at follow-up when compared to those who did not use a test socket before final prosthesis fitting. There were no statistically significant differences between participants with transtibial or transfemoral amputation in the test socket and no test socket groups for other measures of mobility and function at follow-up, including duration of daily prosthesis use, time to complete a 10-metre walk test on a flat surface, time to complete a 10-step climbing down test, and time to complete a 10-metre walk test down an 8% slope.
Pain
Participants in the test socket group who had transtibial or transfemoral amputation experienced statistically significantly less pain while walking at follow-up (measured with the VAS) compared to participants in the no test socket group of the retrospective cohort study.17 There were no significant differences in resting pain (measured with the VAS) between the test socket and no test socket groups in people with transtibial or transfemoral amputation at follow-up.
Depression
Findings from the retrospective cohort study17 suggested that there were no statistically significant differences in depressive symptoms (measured with the BDI) at follow-up between participants with transtibial or transfemoral amputation in the test socket and no test socket groups.
Participant Satisfaction
Participant satisfaction was assessed in the retrospective cohort study17 using the TAPES. According to the results for each of the TAPES subscales, participants with transtibial or transfemoral amputation in the test socket group had higher psychosocial adjustment, lower physical activity restriction, and higher prosthesis satisfaction than participants in the no test socket group at follow-up.
Other Clinical Outcomes
The authors of the retrospective cohort study17 concluded that participants with transtibial or transfemoral amputation in the test socket group had a lower frequency of admissions to the study clinic within 3 months but had longer mean prosthesis delivery times.
Guidelines
The guideline18 included 3 relevant recommendations related to the use of multiple prosthetic sockets for people with lower limb amputation.
The first recommendation stated that the postoperative use of (interim) prosthesis as soon as possible after transtibial amputation appears to result in fewer complications and revisions and a shorter time to fitting of the final prosthesis. The authors considered the findings of 4 comparative studies evaluating the effect of the timing of prosthesis fitting when formulating this recommendation.
The second recommendation stated that universal interim prostheses are less suitable for first provision, as they are not optimally adapted to the specific situation of the patient’s stump. This recommendation was based on expert opinion, as no evidence to inform this statement was identified.
The third recommendation stated that a custom-made prosthesis (not necessarily the final prosthesis) provided as early as possible in the postoperative phase is preferable to universal prefab prosthesis. This recommendation was based on expert opinion, as no evidence to inform this statement was identified.
Limitations
There was no evidence identified related to the use of multiple prosthetic sockets in people younger than 18 years or older than 70 years; thus, the clinical effectiveness of multiple prosthetic sockets in children and older adults was unclear. This is an important limitation given the high incidence of lower limb amputation in people older than 70 years.5,6
A limited quantity of evidence addressing the clinical effectiveness of multiple prosthetic sockets for people with lower limb amputations was identified. The clinical evidence summarized in this review was from 1 retrospective cohort study17 that included a limited number of participants (88 individuals). The identified evidence has limited generalizability. For example, the included retrospective cohort study17 examined 1 protocol for the use of a temporary test socket before designing and manufacturing the permanent socket in people with transtibial or transfemoral amputation. The clinical effectiveness of this protocol is not likely representative of all multiple prosthetic socket protocols used to manage people from the time of amputation to the final prosthesis fitting, as these protocols may be highly variable. Additionally, the retrospective cohort study17 was conducted in Turkey, and the applicability of its findings to Canadian settings is unclear.
The authors of the retrospective cohort study17 did not describe minimal clinically important difference values for any outcomes measured using questionnaires, tools, or scales (e.g., pain assessed using the VAS, depressive symptoms assessed using BDI scores). It was unclear if any of the reported statistically significant differences in outcomes assessed using these measures translate into clinically meaningful differences.
The relevant recommendations from the included guideline18 were based on low-quality evidence or expert opinion, due to the absence of research addressing the authors’ topics of interest. Additionally, no recommendations were identified regarding the optimal number of sockets that should be provided during the preparatory and definitive prosthesis treatment phases.
Conclusions and Implications for Decision- or Policy-Making
This review identified 1 non-randomized study17 and 1 evidence-based guideline18 regarding the use of multiple prosthetic sockets for people with lower limb amputation.
Findings from the low-quality non-randomized study17 suggested that people with lower limb amputation who use a temporary test socket to inform the design of the permanent prosthesis may experience improvements to some measures of mobility and function (i.e., painless daily walking distance, time to complete a 10-step climbing up test, time to complete a 10-metre walk test up an 8% slope), less pain while walking, increased prosthesis satisfaction, and fewer clinic admissions compared to those who are fitted for their permanent prosthesis without the use of a test socket. There were no statistically significant differences between participants who received a test socket and participants who did not receive a test socket for the remaining outcomes examined in the study,17 including severity of depressive symptoms, resting pain, and certain measures of mobility and function (i.e., duration of daily prosthesis use, time to complete a 10-metre walk test on a flat surface, time to complete a 10-step climbing down test, and time to complete a 10-metre walk test down an 8% slope). The evidence-based guideline18 recommends the postoperative use of a prosthesis as soon as possible after transtibial amputation. In addition, the guideline18 recommends custom-made prostheses (not necessarily the final version) over prefab prostheses as early as possible in the postoperative phase.
The limitations of the included literature should be considered when interpreting the findings of this report. These limitations include the low quality of the non-randomized study17 and of the evidence informing relevant recommendations from the guideline;18 the unclear clinical significance of the statistically significant between-group findings from the non-randomized study;17 and the paucity of literature on children, older adults, and from Canadian settings. Future higher-quality research is warranted to address some of the knowledge gaps regarding the clinical effectiveness of multiple prosthetic sockets that are identified in this review. Additional evidence-based guidelines, particularly those intended for use in Canadian settings, may be helpful to clinicians and policy-makers involved in providing care for people with lower limb amputation and for whom multiple prosthetic sockets may be appropriate.
References
1.Kayssi A, de Mestral C, Forbes TL, Roche-Nagle G. A Canadian population-based description of the indications for lower-extremity amputations and outcomes. Can J Surg. 2016;59(2):99-106. PubMed
2.Ovadia SA, Askari M. Upper extremity amputations and prosthetics. Semin Plast Surg. 2015;29(1):55-61. PubMed
3.Sahu A, Sagar R, Sarkar S, Sagar S. Psychological effects of amputation: a review of studies from India. Ind Psychiatry J. 2016;25(1):4-10. PubMed
4.Pran L, Baijoo S, Harnanan D, Slim H, Maharaj R, Naraynsingh V. Quality of life experienced by major lower extremity amputees. Cureus. 2021;13(8):e17440. PubMed
5.Essien SK, Kopriva D, Linassi AG, Zucker-Levin A. Trends of limb amputation considering type, level, sex and age in Saskatchewan, Canada 2006-2019: an in-depth assessment. Arch Public Health. 2022;80(1):10. PubMed
6.Imam B, Miller WC, Finlayson HC, Eng JJ, Jarus T. Incidence of lower limb amputation in Canada. Can J Public Health. 2017;108(4):e374-e380. PubMed
7.Dillingham TR, Pezzin LE, Shore AD. Reamputation, mortality, and health care costs among persons with dysvascular lower-limb amputations. Arch Phys Med Rehabil. 2005;86(3):480-486. PubMed
8.Aljarrah Q, Bakkar S, Aleshawi A, et al. Analysis of the peri-operative cost of non-traumatic major lower extremity amputation in Jordan. Clinicoecon Outcomes Res. 2020;12:13-21. PubMed
9.Al-Thani H, Sathian B, El-Menyar A. Assessment of healthcare costs of amputation and prosthesis for upper and lower extremities in a Qatari healthcare institution: a retrospective cohort study. BMJ Open. 2019;9(1):e024963. PubMed
10.Kovac I, Neven K, Ognjen Ž, et al. Rehabilitation of lower limb amputees. Period Biol. 2015;117:147-159.
11.Turner S, McGregor AH. Perceived effect of socket fit on major lower limb prosthetic rehabilitation: a clinician and amputee perspective. Arch Rehabil Res Clin Transl. 2020;2(3):100059. PubMed
12.Sanders JE, Fatone S. Residual limb volume change: systematic review of measurement and management. J Rehabil Res Dev. 2011;48(8):949-986. PubMed
13.Gerschutz MJ, Haynes ML, Nixon D, Colvin JM. Strength evaluation of prosthetic check sockets, copolymer sockets, and definitive laminated sockets. J Rehabil Res Dev. 2012;49(3):405-426. PubMed
14.Gordon R, Magee C, Frazer A, Evans C, McCosker K. An interim prosthesis program for lower limb amputees: comparison of public and private models of service. Prosthet Orthot Int. 2010;34(2):175-183. PubMed
15.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
16.Agree Next Steps Consortium. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2022 June 21.
17.Aydin A, Caglar Okur S. Effects of test socket on pain, prosthesis satisfaction, and functionality in patients with transfemoral and transtibial amputations. Med Sci Monit. 2018;24:4031-4037. PubMed
18.Geertzen J, van der Linde H, Rosenbrand K, et al. Dutch evidence-based guidelines for amputation and prosthetics of the lower extremity: Rehabilitation process and prosthetics: part 2. Prosthet Orthot Int. 2015;39(5):361-371. PubMed
19.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
20.Bijur PE, Silver W, Gallagher EJ. Reliability of the visual analog scale for measurement of acute pain. Acad Emerg Med. 2001;8(12):1153-1157. PubMed
21.Delgado DA, Lambert BS, Boutris N, et al. Validation of digital visual analog scale pain scoring with a traditional paper-based visual analog scale in adults. J Am Acad Orthop Surg Glob Res Rev. 2018;2(3):e088. PubMed
22.Gallagher EJ, Liebman M, Bijur PE. Prospective validation of clinically important changes in pain severity measured on a visual analog scale. Ann Emerg Med. 2001;38(6):633-638. PubMed
23.Beck AT, Steer RA, Carbin MG. Psychometric properties of the Beck Depression Inventory: twenty-five years of evaluation. Clin Psychol Rev. 1988;8(1):77-100.
24.Richter P, Werner J, Heerlein A, Kraus A, Sauer H. On the validity of the Beck Depression Inventory: a review. Psychopathology. 1998;31(3):160-168. PubMed
25.Sharp LK, Lipsky MS. Screening for depression across the lifespan: a review of measures for use in primary care settings. Am Fam Physician. 2002;66(6):1001-1008. PubMed
26.Topuz S, Ülger Ö, Yakut Y, Gül Şener F. Reliability and construct validity of the Turkish version of the Trinity Amputation and Prosthetic Experience Scales (TAPES) in lower limb amputees. Prosthet Orthot Int. 2011;35(2):201-206. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Non-Randomized Study
Study citation, country, funding source | Objective and study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Aydın and Çağlar Okur (2018)17 Turkey Funding source: Departmental sources. Authors were affiliated with the Department of Prosthetics and Orthotics, Dicle University Medical School, Diyarbakir, Turkey and the Department of Physical Therapy and Rehabilitation, Sadi Konuk Research Hospital, Istanbul, Turkey. | Objective: To assess the outcomes of patients who received a lower limb prosthesis with or without a test socket. Study design: Single-centre, retrospective cohort study. | Included: People between the ages of 18 and 70 years who received a lower limb prosthesis for transtibial or transfemoral amputations at the study centre were included if they used their prostheses for at least 6 months and underwent lower limb amputation for acquired reasons. Excluded: People who had bilateral lower limb amputation, who underwent lower limb amputation due to reasons such as tumours, congenital anomalies, infections, burns, and poliomyelitis, and who had silicone linear, active, and passive vacuum suspension systems. Number of participants: 88 (44 in the test socket group; 44 in the no test socket group). Mean age (SD): 40.31 (12.08) years in the test socket group; 38.89 (11.53) years in the no test socket group. Gender: 36.36% female in the test socket group; 40.90% female in the no test socket group. Mean BMI (SD): 26.05 (2.69) kg/m2 in the test socket group; 25.97 (2.65) kg/m2 in the no test socket group. Amputation level: 72.72% transtibial and 27.27% transfemoral in the test socket group; 70.45% transtibial and 29.54% transfemoral in the no test socket group. | Intervention: Multiple prosthetic sockets. Following amputation, test sockets that were fitted and adjusted based on the user’s feedback were used during the early phase of rehabilitation. Permanent sockets were designed according to the changes made to the test sockets and were provided to the participants. Comparator: Single definitive prosthetic socket. Participants were provided with a permanent socket that was designed without a test socket. | Clinical outcomes:
Follow-up: Outcomes were assessed at a single time point. The time between initial prosthesis use and outcomes assessment was unclear. |
BDI = Beck Depression Inventory; BMI = body mass index; SD = standard deviation; TAPES = Trinity Amputation and Prosthesis Experience Scales; VAS = visual analogue scale.
Note that this appendix has not been copy-edited.
Table 3: Characteristics of Included Guideline
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, synthesis, and quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|
Geertzen et al. (2015)18 | |||||
Intended users: Clinicians involved in providing care for people with amputation and prosthetics of the lower extremity. Target population: People with lower limb amputation. | Interventions that can be provided to patients through the post-amputation rehabilitation process (e.g., physical therapy, psychological therapies, exercise), including prostheses. | Recommendations made in the guideline considered many different outcomes, including time to final prosthesis fitting, edema, walking performance, prosthesis function, patient satisfaction, comfort, and costs. | Evidence collection: Systematic literature searches were conducted in the Cochrane Library, MEDLINE, Embase, PsycINFO and CINAHL. Additional manual searches were also conducted. Literature searches were conducted up to January 2011. Evidence selection: Publications that addressed topics of interest were retrieved from the literature searches. Eligible study designs varied by topic and were dependent on the types of available literature (e.g., if robust systematic reviews or RCTs were available, data from observational studies were not considered). The number of reviewers involved in the article selection process was NR. Evidence synthesis: Findings from relevant studies were narratively summarized. Evidence quality assessment: The methodological quality of individual studies was assessed; however, the methods used were poorly reported (studies were assigned a level between A1 and D depending on their design and quality). | The methods used by the guideline development group to produce recommendations were NR. Recommendations were assigned a level of evidence using EBRO (Dutch evidence-based guideline development) criteria. Levels of evidence ranged between level 1 (based on a systematic review of at least 2 independent high quality RCTs or at least 2 independent high quality RCTs with consistent results) and level 4 (based on expert opinion). | NR. |
NR = not reported; RCT = randomized controlled trial.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of the Non-Randomized Study Using the Downs and Black Checklist15
Strengths | Limitations |
|---|---|
Aydın and Çağlar Okur (2018)17 | |
The objectives, intervention, comparator, and main outcomes were clearly described. Participant eligibility criteria were provided. Participant characteristics (e.g., age, gender, BMI, amputation level, education, occupation) were clearly described. The main findings of the study were clearly described Estimates of random variability (e.g., standard deviations) and actual P values were reported. Due to the nature of the study (i.e., a retrospective chart review of patients with follow-up data), no participants were lost to follow-up. Study participants, care providers, and setting appeared to be representative of the population and care setting of interest. Compliance with the intervention was reliable. Outcome measures were valid. The authors declared that they had no potential conflicts of interest. Sources of support were disclosed (departmental sources). | Intervention assignment was not done at random. It was likely that prognostic factors, patient preference, and clinician discretion were factors in determining which treatment participants received, increasing the risk of bias due to confounding. The timing of outcome assessment was not reported (i.e., the amount of time between prosthesis fitting, with or without a test socket, and outcome measurement). It was likely that the time since intervention was not consistent between treatment groups, potentially biasing the results. Participants and outcome assessors were aware of the intervention received by the participant. It was unclear if outcome data were retrieved from medical records or were measured by the study authors after initiating the study It was unlikely that all important adverse events that may have been a consequence of the intervention were recorded. No power calculation was performed; and it is unknown whether the study may have been insufficiently powered to detect statistically significant differences in some of the outcomes of interest. This is particularly concerning in the transfemoral amputation group, which had a small sample size (n = 25). Tests for statistical significance were conducted for many outcomes without adjustment for multiplicity. Therefore, there may be potential inflation of the type I error rate. There was no registered protocol for the study. Therefore, the findings are at risk for reporting bias as it was not possible to confirm whether outcomes were reported according to a pre-specified plan. Single-centre study (conducted in Turkey); the generalizability to Canadian settings was unclear. |
BMI = body mass index.
Table 5: Strengths and Limitations of the Guideline Using AGREE II16
AGREE II Item | Geertzen et al. (2015)18 |
|---|---|
Domain 1: Scope and Purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes |
Domain 2: Stakeholder Involvement | |
4. The guideline development group includes individuals from all relevant professional groups. | Unclear |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Unclear |
6. The target users of the guideline are clearly defined. | Yes |
Domain 3: Rigour of Development | |
7. Systematic methods were used to search for evidence. | Yes |
8. The criteria for selecting the evidence are clearly described. | No |
9. The strengths and limitations of the body of evidence are clearly described. | No |
10. The methods for formulating the recommendations are clearly described. | No |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes |
13. The guideline has been externally reviewed by experts before its publication. | No |
14. A procedure for updating the guideline is provided. | No |
Domain 4: Clarity of Presentation | |
15. The recommendations are specific and unambiguous. | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes |
17. Key recommendations are easily identifiable. | Yes |
Domain 5: Applicability | |
18. The guideline describes facilitators and barriers to its application. | Unclear |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No |
20. The potential resource implications of applying the recommendations have been considered. | Unclear |
21. The guideline presents monitoring and/or auditing criteria. | No |
Domain 6: Editorial Independence | |
22. The views of the funding body have not influenced the content of the guideline. | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II.
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Table 6: Summary of Findings by Outcome — Mobility and Function
Study citation and design | Study Findings |
|---|---|
Duration of daily prosthesis use | |
Aydın and Çağlar Okur (2018)17 Retrospective cohort study (N = 88) | Participants with transtibial amputation – mean value (SD)
Participants with transfemoral amputation – mean value (SD)
|
Painless daily walking distance with prosthesis | |
Aydın and Çağlar Okur (2018)17 Retrospective cohort study (N = 88) | Participants with transtibial amputation – mean value (SD)
Participants with transfemoral amputation – mean value (SD)
|
Time to complete 10-metre walking on a flat surface | |
Aydın and Çağlar Okur (2018)17 Retrospective cohort study (N = 88) | Participants with transtibial amputation – mean value (SD)
Participants with transfemoral amputation – mean value (SD)
|
Time to complete 10-step climbing up | |
Aydın and Çağlar Okur (2018)17 Retrospective cohort study (N = 88) | Participants with transtibial amputation – mean value (SD)
Participants with transfemoral amputation – mean value (SD)
|
Time to complete 10-step climbing down | |
Aydın and Çağlar Okur (2018)17 Retrospective cohort study (N = 88) | Participants with transtibial amputation – mean value (SD)
Participants with transfemoral amputation – mean value (SD)
|
Time to complete 10-metre walking up at an 8% slope | |
Aydın and Çağlar Okur (2018)17 Retrospective cohort study (N = 88) | Participants with transtibial amputation – mean value (SD)
Participants with transfemoral amputation – mean value (SD)
|
Time to complete 10-metre walking down at an 8% slope | |
Aydın and Çağlar Okur (2018)17 Retrospective cohort study (N = 88) | Participants with transtibial amputation – mean value (SD)
Participants with transfemoral amputation – mean value (SD)
|
SD = standard deviation.
aStatistically significant.
Table 7: Summary of Findings by Outcome — Pain
Study citation and design | Study Findings |
|---|---|
Resting pain | |
Aydın and Çağlar Okur (2018)17 Retrospective cohort study (N = 88) | Participants with transtibial amputation – mean VAS score (SD)
Participants with transfemoral amputation – mean VAS score (SD)
|
Pain while walking | |
Aydın and Çağlar Okur (2018)17 Retrospective cohort study (N = 88) | Participants with transtibial amputation – mean VAS score (SD)
Participants with transfemoral amputation – mean VAS score (SD)
|
SD = standard deviation; VAS = visual analogue scale.
Note: VAS scores range from 0 (no pain) to 10 (very severe pain).17
aStatistically significant.
Table 8: Summary of Findings by Outcome — Depression
Study citation and design | Study Findings |
|---|---|
Depressive symptoms | |
Aydın and Çağlar Okur (2018)17 Retrospective cohort study (N = 88) | Participants with transtibial amputation – mean BDI score (SD)
Participants with transfemoral amputation – mean BDI score (SD)
|
BDI = Beck Depression Inventory; SD = standard deviation.
Note: BDI scores range from 0 to 3 for each item with total score ranging from 0 to 63. A higher score represents more severe depressive symptoms.17
aStatistically significant.
Table 9: Summary of Findings by Outcome — Participant Satisfaction
Study citation and design | Study Findings |
|---|---|
Prosthesis satisfaction | |
Aydın and Çağlar Okur (2018)17 Retrospective cohort study (N = 88) | Participants with transtibial amputation – mean TAPES subscale score (SD)
Participants with transfemoral amputation – mean TAPES subscale score (SD)
|
SD = standard deviation; TAPES = Trinity Amputation and Prosthesis Experience Scales.
Note: The TAPES scale contains 3 subscales. The psychosocial adjustment subscale is scored on a 5-point Likert scale, with total scores ranging from 5 to 75. A higher score represents higher level of psychosocial adjustment. The activity restriction subscale is scored on a 3-point Likert scale, with total scores ranging from 12 to 36. A higher score represents higher level of activity restriction. The prosthesis satisfaction subscale is scored on a 5-point Likert scale, with total scores ranging from 10 to 50. A higher score represents higher level of prosthesis satisfaction.17
aStatistically significant.
Table 10: Summary of Findings by Outcome — Other Clinical Outcomes
Study citation and design | Study Findings |
|---|---|
Prosthesis delivery time | |
Aydın and Çağlar Okur (2018)17 Retrospective cohort study (N = 88) | Participants with transtibial amputation – mean value (SD)
Participants with transfemoral amputation – mean value (SD)
|
Frequency of admissions to the study clinic within 3 months | |
Aydın and Çağlar Okur (2018)17 Retrospective cohort study (N = 88) | Participants with transtibial amputation – mean value (SD)
Participants with transfemoral amputation – mean value (SD)
|
SD = standard deviation.
aStatistically significant.
Table 11: Summary of Relevant Recommendations in Included Guideline
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
Geertzen et al. (2015)18 | |
Relevant recommendations: 1. “Postoperative use of a prosthesis as soon as possible after transtibial amputation appears to result in fewer complications and revisions and a shorter time to fitting of a prosthesis (Level 3) (p. 368).”18
2. “Universal interim prostheses are less suitable for first provision (Level 4) (p. 369).”18
3. “A custom-made prosthesis (not necessarily the final version), as early as possible in the postoperative phase, is preferable to a pre-fab prosthesis (Level 4) (p. 369).”18
| Studies were categorized based on their methodological quality using the following criteria: Level A1:
Level A2:
Level B:
Level C:
Level D:
Recommendations were assigned a level of evidence using EBRO (Dutch evidence-based guideline development) criteria, which categorizes conclusions as being based on: Level 1: Study of level A1 or at least two independently conducted studies of level A2, with consistent results Level 2: One study of level A2 or at least two independently conducted studies of level B Level 3: One study of level B or C Level 4: Expert opinion |
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
Microprocessor-controlled knee prosthetics for individuals with transfemoral amputation. (CADTH reference list). Ottawa (ON): CADTH; 2021: https://www.cadth.ca/sites/default/files/pdf/htis/2021/RA1164%20Microprocessor%20knees%20Final.pdf. Accessed 2022 June 22.
Elevated vacuum suspension systems for adults with amputation: a review of clinical effectiveness, cost-effectiveness, and guidelines. (CADTH rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/sites/default/files/pdf/htis/2020/RC1224%20EVSS%20Final.pdf. Accessed 2022 June 22.
3D printed prosthetic socket liners for patients requiring a limb prosthetic device: clinical effectiveness and safety. (CADTH rapid response report: reference list). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/pdf/htis/2019/RA1032%203D%20Printed%20Prosthetics%20Final.pdf. Accessed 2022 June 22.
Osseointegrated prosthetic implants for lower limb amputation: a review of clinical effectiveness, cost-effectiveness and guidelines. (CADTH rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2017: https://www.cadth.ca/sites/default/files/pdf/htis/2017/RC0856%20Osseointegrated%20Prosthetic%20Implants%20Final.pdf. Accessed 2022 June 22.
Guidelines and Recommendations — Unclear Methodology
Centers for Medicare & Medicaid Services. Lower Limb Prosthetic Workgroup consensus document. Health technology assessment. Baltimore (MD): Centers for Medicare & Medicaid Services; 2017: https://www.cms.gov/Medicare/Coverage/DeterminationProcess/downloads/LLP_Consensus_Document.pdf. Accessed 2022 June 22.
Review Articles
Griffet J. Amputation and prosthesis fitting in paediatric patients. Orthop Traumatol Surg Res. 2016 Feb;102(1 Suppl):S161-175. PubMed
Appendix 6: Supplementary Search for Additional Resources
Note that this appendix has not been copy-edited.
A customized supplement to this report is provided to help inform health care decision-making and addresses a specific set of questions that may be of potential interest but were out of scope for the review.
Research Questions
What are the different types of sockets that are standard practice for preparatory treatment and definitive prosthetic treatment?
What is the optimum number of sockets required for a preparatory and definitive prosthetic treatment?
What are all the current terms used for prosthetic sockets and how are these defined?
Methods
Literature Search Methods
A targeted literature search was conducted by an Information Specialist in Medline, Cumulative Index to Nursing and Allied Health (CINAHL), Scopus, as well as a focused Internet search. The search was completed on June 8, 2022 and was limited to English language documents published since January 1, 2017.
Selection Criteria and Methods
One reviewer screened literature search results (titles and abstracts) and selected publications that potentially addressed the research questions. Full texts of study publications were not reviewed.
Results
Systematic Reviews
Brodie Mc, Murray Lc, McGarry A. Transfemoral prosthetic socket designs: a review of the literature. Journal Prosthet Orthot. 2022;34(2):e73-e92.
Note: Describes the available evidence for various transfemoral socket designs.
Al Shuaili N, Aslani N, Duff L, McGarry A. Transtibial prosthetic socket design and suspension mechanism: a literature review. J Prosthet Orthotics. 2019;31(4):224-245.
Note: Discusses the advantages and disadvantages of various transtibial prosthetic socket designs and suspension mechanisms.
Narrative Reviews
Olsen J, Turner S, Chadwell AE, Dickinson A, Ostler C, Armitage L, et al. The impact of limited prosthetic socket documentation: a researcher perspective. Front Rehabilit Sci. 2022;3:853414. https://www.frontiersin.org/articles/10.3389/fresc.2022.853414/full. Accessed 2022 June 22.
Note: Highlights the lack of published information on prosthetic socket manufacturing and evaluation in clinical trials from a research perspective. Information on temporary check sockets is provided.
Wang M, Nong Q, Liu Y, Yu H. Design of lower limb prosthetic sockets: a review. Expert Rev Med Devices. 2022 Jan;19(1):63-73. doi: 10.1080/17434440.2022.2020094. Epub 2021 Dec 31. PMID: . PubMed
Note: This review outlines the key factors that can affect lower limb prosthetic socket use and describes a classification scheme for categorizing socket types.
Safari R. Lower limb prosthetic interfaces: clinical and technological advancement and potential future direction. Prosthet Orthot Int. 2020 Dec;44(6):384-401. PubMed
Note: Describes the advancements made in lower limb prosthetic socket designs over the last 50 years and discusses potential directions for future research.
Paterno L, Ibrahimi M, Gruppioni E, Menciassi A, Ricotti L. Sockets for limb prostheses: a review of existing technologies and open challenges. IEEE Trans Biomed Eng. 2018;65(9):1996-2010. doi: 10.1109/TBME.2017.2775100. Epub 2018 Jan 23. PubMed
Note: Describes the main parameters that affect the prosthetic interface and provides a classification of the different socket types proposed in the literature. Advantages and disadvantages of various prosthetic socket types are also described.
Guidelines and Recommendations
Stevens PM, Depalma RR, Wurdeman SR. Transtibial socket design, interface, and suspension: a clinical practice guideline. J Prosthet Orthotics. 2019;31(3):172-178.
Note: Includes recommendations regarding the different types of transtibial socket designs. Descriptions of patellar tendon bearing and total surface bearing sockets are provided.
VA/DoD clinical practice guideline for rehabilitation of individuals with lower limb amputation. Washington(DC); Department of Veteran Affairs; Department of Defence; 2017: https://www.healthquality.va.gov/guidelines/Rehab/amp/VADoDLLACPG092817.pdf. Accessed 2022 June 22.
Note: Includes information related to the design of prosthetic sockets for people with lower limb amputation. Recommendation #15 suggests there is insufficient evidence to recommend for or against any particular socket design.
Additional Resources
Martin JH, Borraez AS, Bustos CR, Ortiz, FP, Castro PM. Dynamic socket design for transtibial prosthesis. In: Bennani S, Lakhrissi Y, Khaissidi G, Mansouri A, Khamlichi Y, eds. WITS 2020. Lecture Notes in Electrical Engineering. Vol 745. Singapore: Springer; 2022: https://link.springer.com/chapter/10.1007/978-981-33-6893-4_44. Accessed 2022 June 22.
Selvam PS, Sandhya M, Chandrasekaran K, Hepzibah Rubella D, Karthikeyan S. Prosthetics for lower limb amputation. In. Arazpour M, ed. Prosthetics and Orthotics. London (UK): IntechOpen; 2021: https://www.intechopen.com/chapters/76822. Accessed 2022 June 22.
Note: The different types of prostheses and their components for people with lower limb amputation are discussed. Sections 6.1.1 and 6.1.2 provide information on temporary and permanent prostheses, respectively.
Stokosa J. Prosthesis parts. Merck Manual: Consumer Version. Kenilworth (NJ): Merck & Co.; 2021: https://www.merckmanuals.com/home/special-subjects/limb-prosthetics/prosthesis-parts. Accessed 2022 June 22. Note: This consumer manual provides an overview of the different parts of a prosthesis.
Stokosa J. Limb prosthesis preparation. Merck Manual: Consumer Version. Kenilworth (NJ): Merck & CO.; 2021: https://www.merckmanuals.com/home/special-subjects/limb-prosthetics/limb-prosthesis-preparation. Accessed 2022 June 22.
Note: The procedure for preparing limbs for prostheses is discussed. There is a section on how preparatory prostheses can be used early in the rehabilitation process.
Horizon Orthotic & Prosthetic Experience (HOPE). Custom prosthetic sockets 101. 2019; https://hopekc.com/custom-prosthetic-sockets-101-kansas-city-area-prosthetic-specialists/. Accessed 2022 June 22.
Note: The different types of prosthetic sockets and the qualities of an effective custom prosthetic socket are discussed.
Life as an amputee: lower limb amputees. Ottawa (ON): War Amps; 2019: https://www.waramps.ca/pdf/english-site/ways-we-help/living-with-amputation/life-as-an-amputee-lower-limb.pdf. Accessed 2022 June 22.
Note: A resource that discusses life with lower limb amputation. Includes an appendix that defines many technical terms, including check (test)/diagnostic socket.
Orfit. The history of the check socket. 2018; https://www.orfit.com/blog/the-history-of-the-check-socket/. Accessed 2022 June 22.
Note: Briefly describes the history of check sockets.
Godfrey BS. Lower limb prosthetics. PM&R KnowledgeNow. 2019; https://now.aapmr.org/lower-limb-prosthetics/. Accessed 2022 June 22.
Note: Describes the different types of sockets for lower limb prostheses.
Physiopedia. Lower limb prosthetic sockets and suspension systems. 2022; https://www.physio-pedia.com/Lower_Limb_Prosthetic_Sockets_and_Suspension_Systems. Accessed 2022 June 22.
Note: Describes the process for socket casting, creating a positive mould, and rectification. The use of a “check”/test/diagnostic socket is also discussed.
War Amps. Technical terms. 2022; https://www.waramps.ca/ways-we-help/living-with-amputation/#Terms. Accessed 2022 June 22.
Note: A glossary of technical terms commonly used in the field of prosthetics, including check/diagnostic socket.
Limbs4Life. Glossary of terms. 2022; https://www.limbs4life.org.au/prosthetics/glossary-of-terms. Accessed 2022 June 22.
Note: A glossary of terms commonly used by clinicians who provide care to people with amputation, including check socket.
References Published Before 2017
Al-Fakih EA, Abu Osman NA, Mahmad Adikan FR. Techniques for interface stress measurements within prosthetic sockets of transtibial amputees: a review of the past 50 years of research. Sensors (Basel). 2016;16(7):20. PubMed
Note: Discusses the evolution of transtibial socket design, advantages and disadvantages of patellar tendon bearing and total surface bearing sockets, and the role of check sockets.
Yoo S. Advancements in lower limb prosthetics (sockets and suspensions). [video]. Moss Rehab. Einstein Healthcare Network. 2016; https://www.youtube.com/watch?v=8b0h5w6hZ0o
Note: Covers many topics relevant to lower limb prostheses, including prosthetic anatomy, socket types, and suspension systems.
Johnson K, Davis AJ. Lower extremity prosthetic sockets and suspension systems. In: Spires MC, Kelly BM, Davis AJ, eds. New York: Springer Publishing Company: https://connect.springerpub.com/content/book/978-1-6170-5114-2/part/part01/chapter/ch06. Accessed 2022 June 22.
Note: Discusses lower and upper extremity restoration and rehabilitation and serves as a reference for practitioners to support clinical decision-making.
Sanders JE, Fatone S. Residual limb volume change: systematic review of measurement and management. J Rehabil Res Dev. 2011;48(8):949-986. .PubMed
Note: Systematic review that assesses what is known about the measurement and management of residual limb volume change in people with lower limb amputation. Initial (preparatory or interim) prostheses are discussed.
Schuch CM. Transfemoral amputation: prosthetic management. In: Bowker HK, Michael JW, eds. Atlas of Limb Prosthetics: Surgical Prosthetic, and Rehabilitation Principles. Rosemont (IL): American Academy of Orthopedic Surgeons; 2002: https://www.oandplibrary.org/alp/chap20-02.asp. Accessed 2022 June 22.
Note: There is a section on transfemoral socket designs that provides an overview of the different types of socket designs and when they may be indicated for use.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca.