CADTH Health Technology Review
Diacetylmorphine for Adults With Opioid Dependence
Rapid Review
Authors: Khai Tran, Danielle MacDougall
Abbreviations
CRISM
Canadian Research Initiative in Substance Misuse
DAM
diacetylmorphine
HDM
hydromorphone
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
MMT
methadone maintenance therapy
NAOMI
North American Opiate Medication Initiative
QALY
quality-adjusted life year
SALOME
Study to Assess Long-term Opioid Maintenance Effectiveness
Key Messages
Injectable diacetylmorphine might provide more benefits and lower costs compared with oral methadone maintenance therapy in patients with severe opioid use disorder.
The Canadian Research Initiative in Substance Misuse guideline recommends that both injectable diacetylmorphine and hydromorphone should be considered as treatment options for individuals with severe, treatment-refractory opioid use disorder and ongoing illicit injection opioid use, and that the injectable opioid agonist treatment should have an end date to transition to an oral opioid agonist treatment.
No recent studies on the clinical effectiveness of diacetylmorphine for injection in comparison with methadone or buprenorphine were identified.
No cost-effectiveness studies of injectable diacetylmorphine compared with buprenorphine were identified.
Context and Policy Issues
Opioid dependence has devastating consequences for individuals, families, and society. Between January 2016 and September 2021, 26,690 Canadians died from opioid-related toxicity.1 In 2021, there were approximately 20 opioid toxicity deaths per day in Canada compared with 7 deaths per day in 2016 and 12 deaths per day in 2018.1 Almost all (98%) of those deaths were accidental, and 88% of these accidental deaths occurred in British Columbia, Alberta, or Ontario.1 From January 2016 to September 2021, there were 29,228 hospitalizations due to opioid-related poisoning in Canada and 12,977 hospitalizations due to stimulant-related poisoning.1 Opioid-related poisoning hospitalizations increased by 27% in the first year of pandemic (April 2020 to March 2021) compared with the previous year (April 2019 to March 2020).1
Maintenance therapy with oral opioid agonist treatment medications, such as methadone or buprenorphine, can be effective in decreasing drug use and preventing mortality and illegal activity in many individuals with opioid use disorder.2 However, a subset of individuals with severe opioid use disorder who used to inject opioids may not benefit from oral maintenance treatment, therefore alternative approaches are needed.3 In 2009, the North American Opiate Medication Initiative (NAOMI) trial conducted in Canada found that injectable diacetylmorphine (DAM) was more effective than oral methadone maintenance therapy (MMT) for higher retention and response rates in addiction treatment, and reduction in rates of illicit opioid use or illegal activity in long-term users of injectable heroin.4 However, DAM had more serious adverse events compared with oral MMT.4 At that time, DAM was not available in Canada.5 A subsequent trial, the Study to Assess Long-term Opioid Maintenance Effectiveness (SALOME), was designed to find an acceptable alternative to DAM, and showed that injectable hydromorphone (HDM) was noninferior to injectable DAM and had fewer adverse events.6 Health Canada has recently approved DAM as an injectable opioid agonist therapy for adult patients with severe opioid use disorder who use injectable opioids and have failed previous opioid agonist therapy, including oral MMT.7 DAM is delivered in a supervised setting due to its risk of serious adverse events, such as overdose and seizure.4,7 Injectable DAM can be provided in combination with oral MMT to prevent withdrawal symptoms.7
This report aims to summarize the evidence on the clinical effectiveness and cost-effectiveness of DAM for injection versus methadone or buprenorphine for adults with opioid dependence. Additionally, this report also aims to summarize the recommendations from evidence-based guidelines regarding the use of DAM for injection for adults with opioid dependence.
Research Questions
What is the clinical effectiveness of DAM for injection versus methadone or buprenorphine for adults with opioid dependence?
What is the cost-effectiveness of DAM for injection versus methadone or buprenorphine for adults with opioid dependence?
What are the evidence-based guidelines regarding the use of DAM for injection for adults with opioid dependence?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were injectable diacetylmorphine and opioid dependence. No filters were applied to limit the retrieval by study type. Conference abstracts were excluded. If possible, retrieval was limited to the human population. The search was completed on June 1, 2022, and limited to English-language documents published since January 1, 2017.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults with opioid dependence |
Intervention | Diacetylmorphine for injection |
Comparator | Q1 and Q2: Methadone or buprenorphine (any formulations, including buprenorphine-naloxone) Q3: Not applicable |
Outcomes | Q1: Clinical benefits and harms (e.g., retention in treatment, illicit drug use, overdose rates, mortality, health-related quality of life, social functioning [e.g., attendance at school or work], emotional and psychological functioning [e.g., anxiety, depression, sleep], adverse events) Q2: Cost-effectiveness (e.g., incremental cost per health benefit or QALY gained) Q3: Recommendations regarding best practices (e.g., appropriate patient populations and clinical settings, treatment protocols [e.g., dosing and frequency], recommended safeguards, strategies to mitigate harms, adverse events, and misuse) |
Study designs | Health technology assessments, systematic reviews, randomized-controlled trials, non-randomized studies, economic evaluations, evidence-based guidelines |
Q = question; QALY = quality-adjusted life-year.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1 or they were published before 2017. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: The Drummond checklist8 for economic evaluations, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument9 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
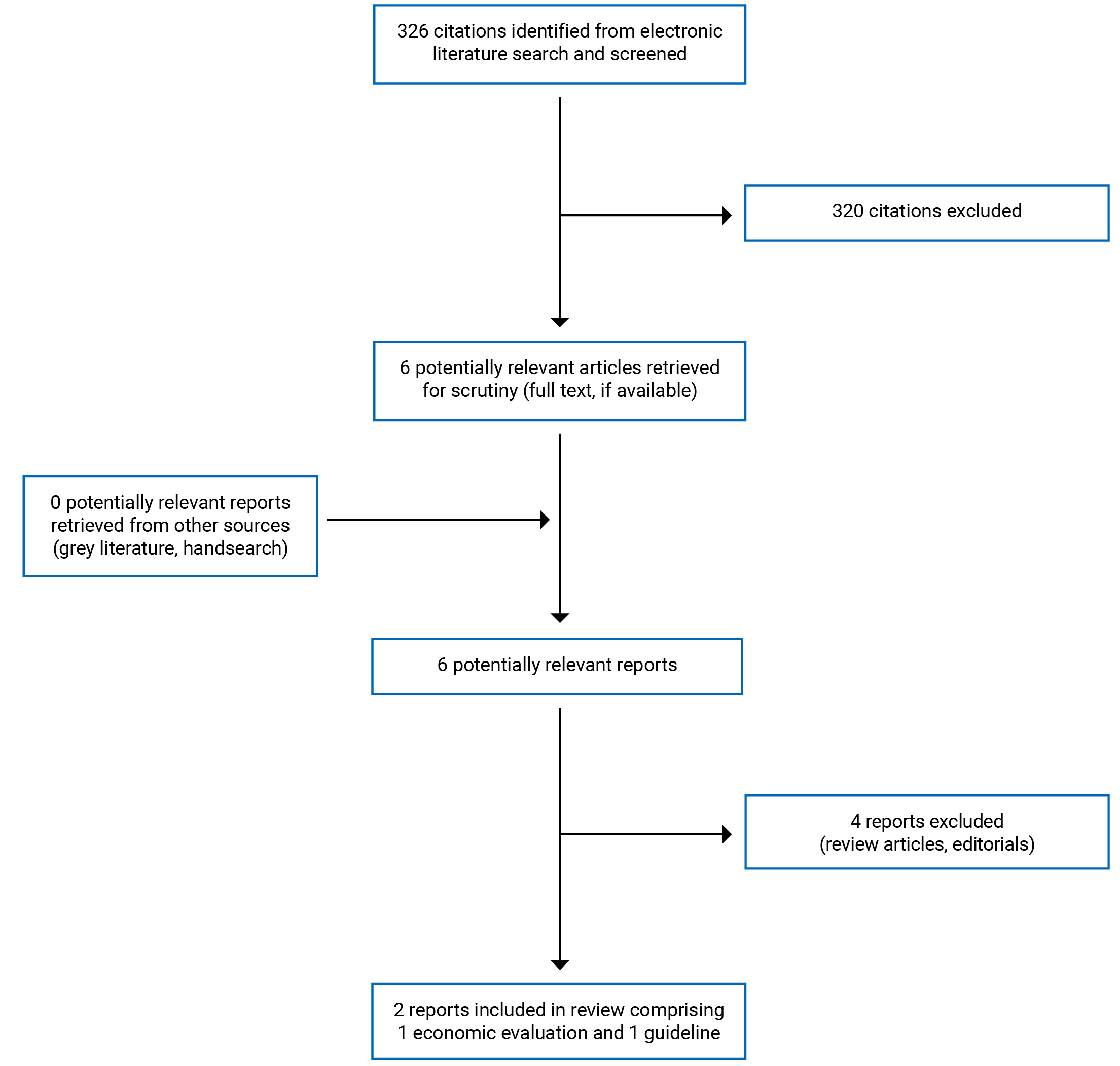
A total of 326 citations were identified in the literature search. Following screening of titles and abstracts, 320 citations were excluded and 6 potentially relevant reports from the electronic search were retrieved for full-text review. No potentially relevant publications were retrieved from the grey literature search for full-text review. Of these 6 potentially relevant articles, 4 publications were excluded for various reasons, and 2 publications met the inclusion criteria and were included in this report. These comprised 1 economic evaluation study and 1 evidence-based guideline. The Preferred Reporting Items for Systematic Reviews and Meta Analyses (PRISMA)10 flow chart of the study selection is presented in Appendix 1.
Summary of Study Characteristics
Additional details regarding the characteristics of the included economic evaluation study11 (Table 2) and evidence-based guideline12 (Table 3) are provided in Appendix 2.
Study Design
The economic evaluation study by Bansback et al. (2018)11 used an existing semi–Markov cohort model13 to assess the cost-effectiveness of HDM or DAM compared with oral MMT for treatment of severe opioid use disorder in adults. The clinical data were from the SALOME6 and NAOMI4 trials, and data from an 11-year population study of methadone recipients in British Columbia.14 The SALOME trial6 found that HDM was noninferior to DAM for all clinical outcomes, with the exception that HDM had lower rates of adverse events compared to DAM. The NAOMI trial4 found DAM to be superior to oral MMT. A mixed treatment comparison approach was used to compare HDM and DAM with oral MMT. Resource use included utilization of drugs, non-protocol visits the health professionals, and other health care resources (hospitalizations, and criminal involvement and charges). All costs were calculated by multiplying resource use by respective costs, adjusted to 2015 Canadian dollars, and discounted at 5% per year. Health-related quality of life (HRQoL) was incorporated in terms of utility values on a scale from 0 (death) to 1 (full health), combined with life-years to generate quality-adjusted life-years (QALYs), which was discounted at 5%. The analyses were conducted from a Canadian societal perspective over a 50-year life-time horizon. A series of scenario analyses including the Ministry of Health perspective were conducted to explore the sensitivity of the results to specific parameter uncertainty, alternative assumptions, and sources of data.
The included evidence-based guideline12 was developed by the Canadian Research Initiative in Substance Misuse (CRISM), which provides recommendations on defining the patient population considered for injectable opioid agonist treatment and outlining considerations for medication selection and length of treatment. A systematic search of the literature was conducted, and the quality of evidence and the strength of recommendations were assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach.
Country of Origin
The economic evaluation study11 and the guideline12 was conducted by authors from Canada.
Patient Population
Patients considered in the economic evaluation study11 were from the cohorts of adults with severe opioid use disorder from the SALOME trial6 and the NAOMI trial.4 In the SALOME trial,6 patients had mean age of 44 years, 70% were men and 30% were women, and the average duration of usage was described as “15 years of injecting street heroin.” In the NAOMI trial,4 patients had mean age of 40 years, 61% were men and 39% were women, and the average duration of usage was 17 years of injection-drug use.
The target population of the CRISM guideline12 is adults with severe opioid use disorder, while the intended users are Canadian health professionals with clinical recommendations and guidance for the treatment of severe opioid use disorder with injectable opioid agonist treatment.
Interventions and Comparators
HDM was compared with DAM using within-trial analysis from the SALOME study,6 and HDM was indirectly compared with oral MMT using DAM as a common comparator from the NAOMI trial.4
The CRISM guideline12 formulated its recommendations concerning the injectable opioid agonist treatment (i.e., DAM or HDM).
Outcomes
The outcomes in the economic evaluation study11 were incremental costs, QALYs, and incremental cost-effectiveness ratio (ICER), which was calculated as the incremental cost per QALY change.
Major outcomes considered in the CRISM guideline12 were high retention rates, reduction of street opioid use, and adverse events.
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3 (Table 4).
The economic evaluation study by Bansback et al. (2018)11 clearly stated the objective, the economic importance of the research question, the rational for choosing the alternative comparators (i.e., DAM versus oral MMT, HDM versus oral MMT, and HDM versus DAM), and the type of economic evaluation (i.e., cost-effectiveness analysis) that was conducted. An existing semi–Markov cohort model for the purposes of the life-time analysis was further developed with a societal perspective. For data collection, the study clearly stated the source of effectiveness estimates with details of the design and findings (i.e., from 2 clinical trials, and data from an 11-year population study of methadone recipients in British Columbia), and the resource use and costs. The study clearly stated the outcome measures for economic evaluation (i.e., incremental costs, QALYs, and ICER). A Markov model was presented with all parameters used in the analysis. For the analysis and interpretation of results, the study clearly stated the time horizon of costs and benefits, statistical tests and confidence intervals, justification for the choice of variables for sensitivity analysis, and the ranges over which the variables were varied. A 5% discounting rate was applied for all costs and QALYs with a 50-year life-time horizon. The study reported incremental analysis and presented major outcomes in a disaggregated as well as aggregated form. Probabilistic analysis was used to estimate the means and 95% confidence intervals (CIs) of total costs, QALYs, and ICERs to reflect parameter uncertainty. The conclusion in the study was based on the data reported and was accompanied by the appropriate caveats. Overall, the study was of good methodological quality with respect to the study design, data collection, and analysis and interpretation of results.
The CRISM guideline12 was explicit in terms of scope and purpose (i.e., objectives, health questions, and populations), and had clear presentation (i.e., specific and unambiguous recommendations, different options for management of the condition or health issue, and easy to find key recommendations). In terms of stakeholder involvement, the guidelines clearly defined target users and the development groups. The views and preferences of the target population (e.g., patients, public) were sought. For rigour of development, the guideline reported systematic methods used to search for evidence, criteria for selecting evidence, explicit links between recommendations and the supporting evidence, and methods of formulating the recommendations. The guideline considered health benefits, side effects, and risks in formulating the recommendations, and it was externally peer-reviewed before publication. The guideline assessed the quality of evidence and graded the level of recommendations using the GRADE tool. For clarity, the recommendations in the guideline are specific and unambiguous, provide different options for management of the condition, and are easily identifiable. For applicability, the guideline was explicit in terms of facilitators and barriers to application, advice on how the recommendations can be put into practice, and resource implications (e.g., considering costs in recommendations). For editorial independence, the guideline reported competing interests of the guideline development group members and that the views of the funding body did not have influence on the content of the guidelines. Overall, the guideline was of good methodological quality.
Summary of Findings
The main study findings and authors’ conclusions are presented in Appendix 4.
Clinical Effectiveness of DAM for Injection for Adults With Opioid Dependence
No clinical studies comparing the clinical effectiveness of DAM for injection versus methadone or buprenorphine for adults with opioid dependence were identified; therefore, no summary can be provided.
Cost-Effectiveness of DAM for Injection for Adults With Opioid Dependence
Because the comparisons of HDM with DAM and HDM with oral MMT were not in scope in this review, only the cost-effectiveness results of DAM compared with oral MMT are presented here. Results for the comparisons of HDM with DAM and HDM with oral MMT are presented in Table 6 of Appendix 4.
The model results suggested that injectable DAM provided 3.5 additional years of life compared with oral MMT (18.4 years versus 14.9 years). When combining life-years with quality of life, the injectable DAM strategy provided a greater benefit in comparison to the oral MMT strategy (8.4 QALYs versus 7.4 QALYs; difference = 1.0 QALY). For total costs, DAM was less expensive compared with oral MMT ($1.01 million versus $1.15 million; difference = –$0.14 million) during the life-time. More than 90% of the cost was attributable to involvement in property and violent crime, and less than 3% attributable to treatment. The DAM strategy had a decrease in criminal charges for property crime per person-year of 0.5 compared with MMT and had 5.4 fewer involvements with property crimes per person-year (9.6 versus 15.0). Therefore, injectable DAM was considered to dominate oral MMT (ICER = dominates; 95% CI, dominates to 306.8) due to more benefit and less cost. Probabilistic analysis showed that injectable DAM had a 75% probability of dominating oral MMT. The results were consistent with all scenarios, with the exception of the Ministry of Health perspective.
Guidelines
The CRISM guideline12 provided 3 key recommendations based on the existing literature on injectable opioid agonist treatment. First, the guideline recommends that injectable opioid agonist treatment should be considered for individuals with severe, treatment-refractory opioid use disorder and ongoing illicit injection opioid use. This recommendation was rated conditional based on moderate quality of evidence. Second, the guideline suggests that both DAM and HDM are acceptable treatment options for individuals who are likely to benefit from injectable opioid agonist treatment. This recommendation was considered strong despite low quality of evidence, based on expert consensus, clinical experience in British Columbia, low risk of adverse events of HDM compared with DAM, and the unavailability of prescribed DAM in Canada at that time. Third, the guideline recommends that injectable opioid agonist treatment should be provided as an open-ended treatment, with decisions to transition to oral opioid agonist treatment. This recommendation was considered strong despite low quality of evidence based on the risk of fentanyl-contaminated illicit opioid use and WHO’s recommendation for opioid agonist treatment as an open-ended treatment.
Limitations
The economic evaluation study11 had several limitations. First, not all data were able to capture costs related to possession or dealing of drugs, disorderly conduct, sex work, driving violations, or illegal activities. Including these costs may further improve the cost-savings from treatment with DAM or HDM. Second, the study made several assumptions for transitions between treatment states that were beyond the trial data. However, various scenario analyses found that all were insensitive to the assumptions. Third, other oral opioid agonist treatment strategies such as buprenorphine or slow-release morphine, which are important options to improve the effectiveness of opioid agonist treatment, were not included in the model analysis and their inclusion in the model could affect the results on the cost-effectiveness of DAM or HDM. Lack of accessibility of these agents may limit the generalizability of rates of retention included in the model. Fourth, the model assumed only 1 state for relapse (defined by opioid use outside of treatment) and the individual left the treatment during relapse. In reality, some people may decide to remain on treatment despite relapse, and those who stay in treatment may have health advantage over those who do not.
The included guideline12 recognized that the recommendations were made based on the low- to moderate-quality evidence because of the low number of studies and the discrepancy in evidence supporting each medication (i.e., DAM and HDM).
This review did not identify recent studies on the clinical effectiveness of DAM for injection in comparison with methadone or buprenorphine.
Conclusions and Implications for Decision- or Policy-Making
This report identified 1 economic evaluation study11 and 1 evidence-based guideline12 conducted by authors in Canada. The economic evaluation study results suggested that injectable DAM might provide more benefits and lower costs compared with oral MMT in patients with severe opioid use disorder. The majority (> 90%) of cost-saving was largely from reduced involvement in criminal activity. The findings of this economic evaluation study11 on the comparison of DAM with oral MMT were inconsistent with those in previous studies in Canada and Europe.13,15,16 No cost-effectiveness studies of injectable DAM compared with buprenorphine were identified. The CRISM guideline12 provided 3 key recommendations on the patient populations considered for injectable opioid agonist treatment, medication selection, and treatment end date. The guideline recommends that both injectable DAM and HDM should be considered as treatment options for patients with severe, treatment-refractory opioid use disorder and ongoing illicit injection opioid use, and that the injectable opioid agonist treatment should have an end date to transition to oral opioid agonist treatment. The findings from the economic evaluation study and the recommendations of the CRISM guideline may be applicable to the Canadian context despite some limitations. Future studies are needed to compare the clinical effectiveness and cost-effectiveness of injectable DAM with other opioid agonist treatment strategies such as buprenorphine, slow-release morphine, or agents with any formulations.
References
1.Opioid- and Stimulant-related Harms in Canada. Ottawa (ON): Public Health Agency of Canada (PHAC); 2022: https://health-infobase.canada.ca/substance-related-harms/opioids-stimulants/. Accessed 2022 Jun 13.
2.Mattick RP, Breen C, Kimber J, Davoli M. Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence. Cochrane Database Syst Rev. 2014;2:CD002207. PubMed
3.Strang J, Groshkova T, Uchtenhagen A, et al. Heroin on trial: systematic review and meta-analysis of randomised trials of diamorphine-prescribing as treatment for refractory heroin addiction†. Br J Psychiatry. 2015;207(1):5-14. PubMed
4.Oviedo-Joekes E, Brissette S, Marsh DC, et al. Diacetylmorphine versus methadone for the treatment of opioid addiction. N Engl J Med. 2009;361(8):777-786. PubMed
5.Fletcher J. Canada in breach of ethical standards for clinical trials. CMAJ. 2014;186(1):11. PubMed
6.Oviedo-Joekes E, Guh D, Brissette S, et al. Hydromorphone Compared With Diacetylmorphine for Long-term Opioid Dependence: A Randomized Clinical Trial. JAMA Psychiatry. 2016;73(5):447-455. PubMed
7.Diacetylmorphine hydrochloride (diamorphine hydrochloride): 200 mg powder per vial or 5 g powder per vial for intramuscular and intravenous injection [product monograph]. Montreal (QC): Pharmascience Inc.; 2022 Feb 14: https://pdf.hres.ca/dpd_pm/00064756.PDF. Accessed 2022 Jun 13.
8.Higgins JPT, Green S, editors. Figure 15.5.a: Drummond checklist (Drummond 1996). Cochrane handbook for systematic reviews of interventions. London (GB): The Cochrane Collaboration; 2011: http://handbook-5-1.cochrane.org/chapter_15/figure_15_5_a_drummond_checklist_drummond_1996.htm. Accessed 2022 Jun 13.
9.Agree Next Steps Consortium. The AGREE II Instrument. Hamilton (ON): AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2022 Jun 13.
10.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
11.Bansback N, Guh D, Oviedo-Joekes E, et al. Cost-effectiveness of hydromorphone for severe opioid use disorder: findings from the SALOME randomized clinical trial. Addiction. 2018;113(7):1264-1273. PubMed
12.Fairbairn N, Ross J, Trew M, et al. Injectable opioid agonist treatment for opioid use disorder: a national clinical guideline. CMAJ. 2019;191(38):E1049-E1056. PubMed
13.Nosyk B, Guh DP, Bansback NJ, et al. Cost-effectiveness of diacetylmorphine versus methadone for chronic opioid dependence refractory to treatment. CMAJ. 2012;184(6):E317-328. PubMed
14.Nosyk B, MacNab YC, Sun H, et al. Proportional hazards frailty models for recurrent methadone maintenance treatment. Am J Epidemiol. 2009;170(6):783-792. PubMed
15.Dijkgraaf MG, van der Zanden BP, de Borgie CA, Blanken P, van Ree JM, van den Brink W. Cost utility analysis of co-prescribed heroin compared with methadone maintenance treatment in heroin addicts in two randomised trials. BMJ. 2005;330(7503):1297. PubMed
16.Byford S, Barrett B, Metrebian N, et al. Cost-effectiveness of injectable opioid treatment v. oral methadone for chronic heroin addiction. Br J Psychiatry. 2013;203(5):341-349. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of the Included Economic Evaluation
Study citation country, funding source | Type of analysis, time horizon, perspective | Population characteristics | Intervention and comparator(s) | Approach | Source of clinical, cost, and utility data used in analysis | Main assumptions |
|---|---|---|---|---|---|---|
Bansback et al. (2018)11 Canada Canadian Institutes for Health Research, Providence Health Care, the InnerChange Foundation, Providence Health Care Research Institute, St. Paul’s Hospital Foundation, and Vancouver Coastal Health | Cost-effectiveness analysis Time horizon: 50 years (life-time analysis) Perspective: Canadian’s societal perspective | Cohorts of adults with severe opioid use disorder from the SALOME trial and the NAOMI trial SALOME trial (HDM [n = 100] vs. DAM [n = 102]):
NAOMI trial (DAM [n = 115] vs. oral MMT [n = 111]):
| SALOME trial: HDM vs. DAM NAOMI trial: DAM vs. oral MMT DAM was used as common comparator | An existing semi–Markov model was further developed for the analysis. The model included treatment (HDM, DAM or MMT), relapse (defined by opioid use outside of treatment), abstinence from any opioids and death. Transition between health states could occur every 30 days. Probabilistic analysis was used to estimate the means, 95% CIs of total costs, QALYs and ICERs. | Clinical data were from the SALOME and NAOMI trials, and data from an 11-year population study of methadone recipients in British Columbia. Resource use: utilization of drugs, non-protocol visits the health professionals, other health care resources (hospitalizations, and criminal involvement and charges) All costs were calculated by multiplying resource use by respective costs, adjusted to 2015 Canadian dollars, and discounted at 5% per year. HRQoL was incorporated in terms of utility values on a scale from 0 (death) to 1 (full health), combined with life-years to generate QALYs, and discounted at 5%. | The demographic and clinical characteristics of the cohorts of adults with severe opioid use disorder were similar to those of the SALOME trial population and the NAOMI trial population. The mortality rate in the HDM state was the same as in the DAM state. |
CI = confidence interval; DAM = diacetylmorphine; HDM = hydromorphone; HRQoL = health-related quality of life; ICER = incremental cost-effectiveness ratio; MMT = methadone maintenance treatment; NAOMI = North American Opiate Medication Initiative; QALY = quality-adjusted life-year; SALOME = Study to Assess Long-term Opioid Medication Effectiveness; vs. = versus.
Note that this appendix has not been copy-edited.
Table 3: Characteristics of the Included Guideline
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
CRISM, Fairbairn et al. (2019)12 | ||||||
Intended users: Canadian health professionals with clinical recommendations and guidance for the treatment of severe opioid use disorder with injectable opioid agonist treatment Target population: Adults with severe opioid use disorder | Injectable opioid agonist treatment (DAM or HDM) | High retention rates, reduction of street opioid use, and adverse events. | The evidence from literature was systematically identified. The medical writer reviewed, selected, and compiled evidence, including cost-effectiveness data, for the co-chairs and the guideline review panel. | Quality of evidencea was rated using GRADE. | Key questions were developed by the guideline review committee co-chairs in conjunction with the medical writer. Strength recommendationsb were graded using GRADE tool. | The draft guideline recommendations were internally reviewed by the committee, and the feedback was addressed by the medical writer and committee co-chairs. The guideline was externally reviewed by the National Injectable Opioid Agonist Treatment Operational Guidance Review Committee. Ten international experts and 1 family member affected by opioid use disorder reviewed and provided input on the final draft. The guideline was published in a peer-reviewed journal. |
CRISM = Canadian Research Initiative in Substance Misuse; DAM = diacetylmorphine; GRADE = Grading of Recommendations Assessment, Development and Evaluation; HDM = hydromorphone.
aHigh level of evidence: Very confident that the true effect lies close to that of the estimate of the effect. Moderate level of evidence: Moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low level of evidence: Confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low level of evidence: Very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect.
bStrong recommendation for patients: Most people in your situation would want the recommended course of action and only a small proportion would not; you should request discussion with your care provider if the intervention is not offered. Strong recommendation for clinicians: Most patients should receive the recommended course of action; as an example, in this scenario, an algorithm or decision-making tool would not be necessary — the benefits of the recommended course of action would clearly outweigh any advantages of alternative interventions. Strong recommendation for health care administrators: The recommendation can be adopted as a policy in most situations. Moderate strength recommendation for patients: Most people in your situation would want the recommended course of action, but many would not. Moderate strength recommendation for clinicians: You should recognize that different choices will be appropriate for different patients and that you must help each patient to arrive at a management decision consistent with his or her values and preferences; in this scenario, an algorithm or decision-making tool would be advantageous to determine the best course of action. Moderate strength recommendation for health care administrators: Policy-making will require substantial debate and involvement of many stakeholders.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of the Economic Evaluation Using the Drummond Checklist8
Strengths | Limitations |
|---|---|
Bansback et al. (2018)11 | |
Study design | |
The study aimed to evaluate the cost-effectiveness of HDM compared with DAM and MMT. DAM was used as common comparator, so HDM was directly compared with DAM and indirectly compared with MMT. The study also compared DAM with MMT. The economic importance of the research question was stated that medically prescribed DAM is not available in Canada without special access due to regulatory and political reasons. The viewpoint of the analysis is stated that the model was constructed from a societal perspective. The rational for choosing the alternative interventions and the alternatives being compared was clearly described. The SALOME trial was used to directly compare HDM with DAM, and the NAOMI trial was used to indirectly compared HDM with MMT. The study used an existing semi–Markov cohort model for the purposes of the analysis. | Other oral opioid agonist treatment strategies such as buprenorphine or slow-release morphine were not included in the model analysis. |
Data collection | |
The authors clearly stated the source of clinical efficacy data, which were obtained from 2 clinical trials, and data from an 11-year population study of methadone recipients in British Columbia. Details of the clinical effectiveness of the 2 trials were given. The primary end points for the economic evaluation were incremental costs, QALYs, and ICER from a societal perspective. The costs incorporated and resources used were clearly described. All costs were calculated by multiplying resource use by respective costs, adjusted to 2015 Canadian dollars, and discounted at 5% per year. Details of the model used were given. Key parameters incorporated into the model were clearly described. | Not all cost data were captured. |
Analysis and interpretation of results | |
A 50-year time horizon was used for the life-time analysis. All costs were adjusted to 2015 Canadian dollars and discounted at 5% per year. The study was explicit in terms of details of statistical tests and confidence intervals, approach to sensitivity analysis, choice of variables for sensitivity analysis, ranges over which the variables were varied, and incremental analysis. Major outcomes are presented in a disaggregated as well as aggregated form. Probabilistic analysis was used to estimate the means and 95% CIs of total costs, QALYs and ICERs to reflect parameter uncertainty. The results of the study answered the research question. The conclusion was made based on reported data. The conclusion was accompanied by the appropriate caveats. | The model assumed only 1 state for relapse (defined by opioid use outside of treatment) and the individual left the treatment when being relapse. |
CI = confidence interval; DAM = diacetylmorphine; HDM = hydromorphone; ICER = incremental cost-effectiveness ratio; MMT = methadone maintenance treatment; NAOMI = North American Opiate Medication Initiative; QALY = quality-adjusted life-year; SALOME = Study to Assess Long-term Opioid Medication Effectiveness.
Table 5: Strengths and Limitations of the Guideline Using AGREE II9
Item | CRISM, Fairbairn et al. (2019)12 |
|---|---|
Domain 1: Scope and purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes |
3. The population (e.g., patients, public) to whom the guideline is meant to apply is specifically described. | Yes |
Domain 2: Stakeholder involvement | |
4. The guideline development group includes individuals from all relevant professional groups. | Yes |
5. The views and preferences of the target population (e.g., patients, public) have been sought. | Yes |
6. The target users of the guideline are clearly defined. | Yes |
Domain 3: Rigour of development | |
7. Systematic methods were used to search for evidence. | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes |
14. A procedure for updating the guideline is provided. | Yes |
Domain 4: Clarity of presentation | |
15. The recommendations are specific and unambiguous. | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes |
17. Key recommendations are easily identifiable. | Yes |
Domain 5: Applicability | |
18. The guideline describes facilitators and barriers to its application. | Yes |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes |
20. The potential resource implications of applying the recommendations have been considered. | Yes |
21. The guideline presents monitoring and/or auditing criteria. | Unclear |
Domain 6: Editorial independence | |
22. The views of the funding body have not influenced the content of the guideline. | No |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; CRISM = Canadian Research Initiative in Substance Misuse.
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Table 6: Summary of Findings of the Included Economic Evaluation
Main study findings | Authors’ conclusion |
|---|---|
Bansback et al. (2018)11 | |
Life-years:
QALYs (95% CI):
Total costs (95% CI) during life-time:
ICER (95% CI):
Probability of dominating MMT:
Involvement of property crimes per person-year:
Decrease in criminal charges for property crime per person-year compared to MMT:
For the comparison between DAM and MMT, the results were consistent in all scenarios, with the exception of the perspective taken (i.e., Ministry of Health). For the comparison between HDM and MMT, the results were consistent in all scenarios, with the exception of the price of medication and the perspective taken. | “In conclusion, our study finds that injectable HDM treatment is less costly and more beneficial than methadone treatment during a life-time predominantly through reducing the costs of involvement in violent and property criminal activity. In jurisdictions where DAM treatment is not available, not providing HDM treatment would add to the societal costs.”11 (p. 1271) |
CI = confidence interval; DAM = diacetylmorphine; Dd = dominated; Ds = dominates; HDM = hydromorphone; ICER = incremental cost-effectiveness ratio; MMT = methadone maintenance treatment; QALY = quality-adjusted life-year; vs. = versus.
Table 7: Summary of Recommendations in the Included Guideline
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
CRISM, Fairbairn et al. (2019)12 | |
Injectable opioid agonist treatment: “Injectable opioid agonist treatment should be considered for individuals with severe, treatment-refractory opioid use disorder and ongoing illicit injection opioid use.”12 (p. E1053) Two SRs with MAs support this recommendation. | Level of evidence: Moderate Strength of recommendation: Conditional |
Medication selection: “For patients who are determined to be likely to benefit from injectable opioid agonist treatment, both diacetylmorphine and hydromorphone are acceptable treatment options.”12 (p. E1053) Two SRs support this recommendation. | Level of evidence: Low Strength of recommendation: Strong |
Treatment end date: “Injectable opioid agonist treatment should be provided as an open-ended treatment, with decisions to transition to oral opioid agonist treatment made collaboratively with the patient.”12 (p. E1053) Two post-RCT observational cohort studies support this recommendation. | Level of evidence: Low Strength of recommendation: Strong |
CRISM = Canadian Research Initiative in Substance Misuse; MA = meta-analysis; SR = systematic review.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Review Articles
Ontario Agency for Health Protection and Promotion (Public Health Ontario), Leece P, Tenenbaum M. Evidence brief: effectiveness of supervised injectable opioid agonist treatment (siOAT) for opioid use disorder. Toronto (ON): Queen’s Printer for Ontario; 2017: https://www.publichealthontario.ca/-/media/documents/e/2017/eb-effectiveness-sioat.pdf?sc_lang=en. Accessed 2022 Jun 13.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca