CADTH Health Technology Review
Removable Rigid Dressings for the Post-Operative Management of Leg Amputations
Rapid Review
Authors: Thyna Vu, Robyn Butcher
Abbreviations
AGREE II
Appraisal of Guidelines for Research and Evaluation II
AMSTAR 2
MeaSurement Tool to Assess systematic Reviews 2
DoD
Department of Defense
GRADE
Grading of Recommendations Assessment, Development, and Evaluation
LLA
lower limb amputation
PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
RCT
randomized controlled trial
RRD
removable rigid dressing
SR
systematic review
VA
Veteran Affairs
VRA
Netherlands Society of Physical and Rehabilitation Medicine
Key Messages
Two systematic reviews and 1 randomized controlled trial provided evidence on the clinical effectiveness and safety of removable rigid dressings compared to soft dressings.
Overall, there was limited evidence suggesting that removable rigid dressings had beneficial or neutral effects compared to soft dressings, and both types of dressings were associated with few adverse events.
Limitations that may reduce the certainty of the evidence include small sample sizes, lack of randomization in non-randomized studies, lack of blinding, and selective reporting.
Three evidence-based guidelines based on low-quality evidence were identified that provided recommendations related to removable rigid dressings. The Australian, Dutch, and US guidelines recommend the rigid dressings for transtibial amputations, although Australian and Dutch guidelines specified removable rigid dressings. The Dutch guideline recommends against the use of rigid dressings for transfemoral amputations.
No evidence was identified on the cost-effectiveness of removable rigid dressings compared to alternative dressings.
Context and Policy Issues
People may require a lower limb amputation (LLA) for a variety of causes, including non-traumatic conditions, such as diabetes peripheral vascular disease, and congenital deficiencies, or traumatic cases, such as injuries.1 LLAs may be minor, defined as at the ankle, foot, or toe; or major, which includes through-knee, below-knee (transtibial) and above-knee (transfemoral) amputation.2 Estimates of LLA vary by type, as well as by country, time frame, and other factors. Worldwide, estimates range from 1.5 to 9,600 per 100,000 people, with higher incidence among people with diabetes.3 The incidence of LLA per 100,000 individuals is estimated to be 24 in the US, and 26 in the UK.3,4 A Canadian retrospective study using data from 2006 to 2012 reported that the incidence of LLA per 100,000 was 22.9 overall; 7.1 for transtibial amputations, and 5 for transfemoral amputations, which had declined slightly from about 6 per 100,000.5 Although the incidence of major LLAs in Canada has been stable or slightly declining over time,2,5 as populations age and the number of people with diabetes and/or peripheral artery disease increase, the number of people who will undergo major LLA may also increase. Understanding how to best provide care following an LLA can help to achieve optimal long-term health outcomes.6
Post-surgery management aims to provide a clean healing environment, reduce swelling and pain, protect the limb from external trauma, reduce incidence of knee flexion contractions, reduce hospital length of stay, reduce time to casting for a prosthesis, and allow for quicker return to daily living activities.6 One aspect of post-surgery management is the choice of dressing used. Dressings used following LLAs include soft dressings, non-removable rigid dressings, and removable rigid dressings (RRDs); each with different features, advantages, and disadvantages.6 Soft dressings are relatively low-cost, easy to apply, and allow for the wound to be checked if needed.1,6 However, they are associated with greater risk of injury from external trauma and increased risk of knee flexion contractures.6 They also have a tendency to fall off more easily, and could place uneven pressures on the residual limb, if not applied correctly, which may inhibit healing.6 In contrast, rigid dressings can provide more protection to the limb from external trauma; however, they are more difficult to apply.6,7 The use of non-removable rigid dressings has decreased in clinical practice due to inaccessible wound site for inspection, and a high risk of wound dehiscence (splitting or re-opening of the surgical incision) for people with ischemic disease.6 An RRD is a type of rigid dressing that can also be easily removed to provide access to the wound site if needed without requiring a new cast be made after the inspection; however, they may also have a higher risk of knee flexion contractures compared to non-removable rigid dressings.1,6 The choice of dressing used seems to vary between sites, based on factors such as training and local practice patterns.6
The objective of this report is to identify and summarize current evidence regarding the clinical effectiveness, cost-effectiveness, and recommendations from evidence-based guidelines of RRDs versus alternative dressings for the post-operative management of people who underwent leg amputation.
Research Questions
What is the clinical effectiveness of removable rigid dressings versus alternative dressings for the post-operative management of people who underwent leg amputation?
What is the cost-effectiveness of removable rigid dressings versus alternative dressings for the post-operative management of people who underwent leg amputation?
What are the evidence-based guidelines regarding the use of removable rigid dressings for the post-operative management of people who underwent leg amputation?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were lower extremity amputation and dressings. No filters were applied to limit the retrieval by study type. The search was completed on May 6, 2022 and limited to English-language documents published since January 1, 2012.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | People with leg amputations (transtibial or transfemoral) |
Intervention | Removable rigid dressings |
Comparator | Q1 to Q2: Alternative dressings (e.g., non-removable rigid dressings, soft dressings, stump shrinkers, compression bandages) Q3: Not applicable |
Outcomes | Q1: Clinical effectiveness (e.g., healing time, length of time from amputation to prosthetic fitting, residual limb size, quality of life, pain, comfort, swelling, safety [e.g., rates of adverse events]) Q2: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained) Q3: Recommendations regarding best practices (e.g., appropriate patient populations, cleaning, and maintenance protocols) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies, economic evaluations, evidence-based guidelines |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2012.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)8 for systematic reviews, the Downs and Black checklist9 for randomized and non-randomized studies, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument10 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
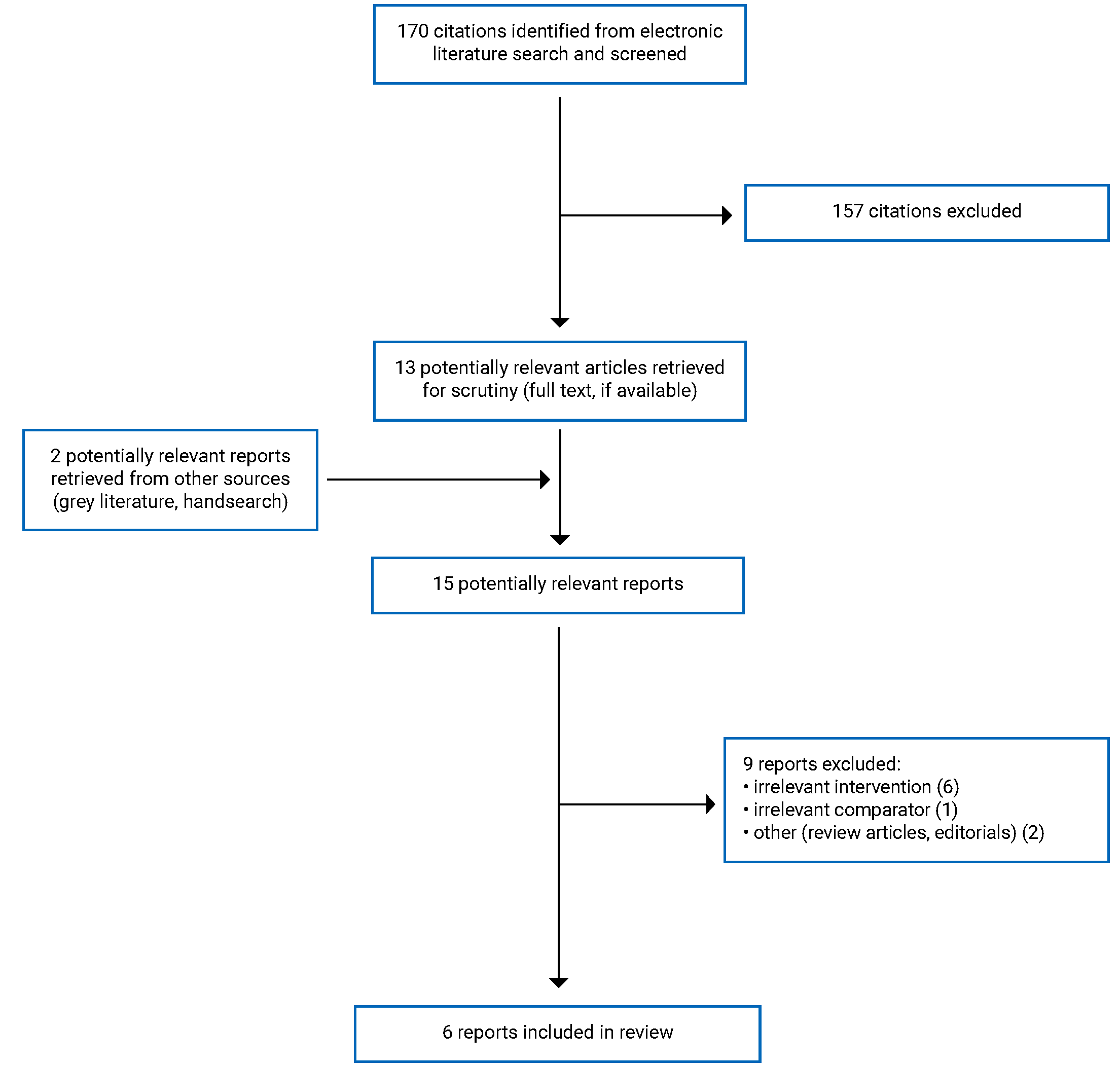
A total of 170 citations were identified in the literature search. Following screening of titles and abstracts, 157 citations were excluded and 13 potentially relevant reports from the electronic search were retrieved for full-text review. Two potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 9 publications were excluded for various reasons, and 6 publications met the inclusion criteria and were included in this report. These comprised 2 systematic reviews (SRs) with meta-analyses, 1 randomized controlled trial (RCT), and 3 evidence-based guidelines. Appendix 1 presents the PRISMA11 flow chart of the study selection. Additional references of potential interest are provided in Appendix 6.
Summary of Study Characteristics
Two SRs with meta-analyses1,12 1 RCT,13 and 3 evidence-based guidelines14-16 were included in this report. Both SRs1,12 had broader inclusion criteria for the intervention than this review, comparing rigid dressings (including RRDs). However, both focused on transtibial amputations and had narrower comparator criteria limited to soft dressings.1,12 Where meta-analyses included studies not relevant to this report, only data from the individual studies were reported. Only the primary clinical studies that met the inclusion criteria are presented in this report. There was some overlap in the studies included in the SRs, and the degree of overlap is summarized in Appendix 5.
Two of the guidelines15,16 also addressed broader inclusion criteria, providing guidance related to amputation of lower extremities in general. One guideline14 was specific to RRDs. Only the recommendations related to the usage of RRDs are presented in this report. The literature search used by the Agency for Clinical Innovation’s guideline14 was reported in a separate document,17 used to supplement the information about the guideline in this report.
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
Both SRs1,12 conducted meta-analyses and searched multiple databases, and at least 1 clinical trial registry. The number of relevant primary studies ranged from 1 to 4 RCTs and 1 to 3 non-randomized studies.1,12 The latest literature search dates were between December 201312 and December 2018.1
The included RCT was a single-centre, single-blinded study using data from 2017 to 2018.13 The patients were randomized using block-of-4 randomization, and were not blinded. However, the assessor measuring outcomes was blinded to patients’ group assignment. The investigators performed a sample size calculation and used an intention-to-treat approach to analyze data.13
All 3 included evidence-based guidelines used systematic literature searches of multiple databases.14-16 All noted that the quality of evidence was low, and thus the recommendations were weak in strength or based on expert opinion.14-16
The guideline by the Agency for Clinical Innovation14 used different quality assessment tools for different types of studies (AMSTAR for SRs, a modified version of Downs and Black for primary clinical studies, and a tool adapted from the STROBE statement for practitioner survey studies). Aside from assessing evidence quality, they did not provide a guideline development methodology.
The guideline by the US Department of Veteran Affairs (VA) and Department of Defense (DoD)15 was an update to a previously published guideline. The VA and DoD guideline used the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) methodology to assess the quality of the literature and consulted with a focus group of people with LLA to provide patient perspectives. Experts gathered at a meeting to develop and update recommendations, and the draft guideline was reviewed by experts from inside and outside the federal sector.
The guideline by Geertzen et al.16 was developed by the Netherlands Society of Physical and Rehabilitation Medicine (VRA) and used evidence-based guideline development forms to assess the quality of identified literature. Details about the guideline development methodology were not provided, though they stated that in addition to the scientific evidence, they also considered patient preferences, availability of special techniques or expertise, organizational aspects, social consequences, and costs when developing the recommendations.
Country of Origin
The SRs were conducted by authors from Singapore1 and Australia.1,12 The primary studies of the SRs that were relevant to this report were from Australia, France, Thailand, the Netherlands, and the US.1,12 The included RCT13 was conducted in Thailand.
The evidence-based guidelines were developed by the New South Wales (Australia) government’s Agency for Clinical Innovation,14 the US’s VA and DoD,15 and the Netherlands Society of Physical and Rehabilitation Medicine.16 The VA and DoD guideline15 states that its intended population of interest are adults eligible for care within the VA and DoD health care delivery systems. The other 2 guidelines14,16 do not specify which country they are meant to be applied to; however, it is likely they are intended for use in the countries in which they were developed.
Patient Population
Both SRs1,12 included people who had undergone transtibial amputations; 1 SR1 stated that if studies included transtibial and transfemoral amputations, it was included if at least 75% of patients had transtibial amputation. The relevant RCTs in the SRs had sample sizes between 23 and 56, while the relevant non-randomized studies had between 15 and 104.1,12 One SR1 did not have age restrictions, and reported details for the individual studies, where for the relevant studies, the mean age ranged from approximately 57 to 73 years, and the proportion of male patients ranged from 42% to 80%. The other SR12 was restricted to adults and did not report demographic details for the individual studies.
The RCT13 was restricted to adults (defined as patients 18 years or older). From the sample of 25, including 5 people who dropped out, the mean age was 53.65 years, and 64% of patients were men. Patients in the intervention group did not differ significantly from the patients in the control group on age, sex, cause of amputation, duration after amputation, or baseline residual limb volume.
The evidence check for the Australian guideline14 considered amputations generally, though their review question specific to post-operative dressings focused on LLAs. The VA and DoD,15 and Dutch guidelines16 provide recommendations for individuals with LLAs. For the recommendations regarding the type of dressing, the Australian,14 VA, and DoD15 guidelines provide guidance for people with transtibial amputation, while the Dutch guideline16 provides recommendations following transtibial and transfemoral amputation.
Interventions and Comparators
Both SRs1,12 compared rigid dressings to soft dressings; but not all their primary studies focused on RRDs. One SR1 included 9 studies, 5 of which compared RRDs to soft dressings; the other SR12 included 6 studies, 4 of which compared RRDs to soft dressings. The RCT13 compared RRDs to elastic bandages, which is a type of soft dressing.
The follow-up time varied across studies, possibly due to the use of time-to-event assessment approach, for which follow-up ended once an outcome was achieved. One SR1 reported the follow-up time for individual studies, with durations of up to 8 weeks for the studies relevant to this report. The other SR12 did not report follow-up time for individual studies. In the RCT, the follow-up time was over 2 months for some patients.13 In this report, short-term is defined as up to 1 month, while medium-term is defined as 1 to 3 months.
Recommendations that specified RRDs were included in 2 guidelines.14,16 One guideline15 provided a recommendation for rigid or semi-rigid dressings, without specifying removable or non-removable; however, they referred to RRDs in the evidence discussion, which may indicate their recommendation includes RRDs.
Outcomes
Both SRs1,12 reported clinical effectiveness and safety outcomes. The clinical outcomes reported in the SRs included changes in swelling (measured in cm3),1 time to wound healing,1 time to no pain,1 time to walking,1 length of hospital stay,1 time to prosthetic fitting or casting,12 and complications or adverse effects (proportion of events per group).1,12 Where available, the SR by Kwah et al.1 grouped the outcomes as short- or medium-term; they also presented a range of complications, including those related to the skin (i.e., wound infections or breakdown, stump revisions, further amputations, pressure areas) and not skin-related (i.e., deaths, chest infections, medical complications, falls, pain). The other SR12 reported 2 types of skin-related complications (i.e., progression to transfemoral amputation, and wound infection).
The RCT13 also reported on clinical effectiveness and safety outcomes. Their primary outcome was time to residual limb maturation, which the authors defined as the time when the volume of the residual limb had stabilized (i.e., not changed more than 10% since the last assessment), soft tissue atrophy had occurred, and the residual limb had developed into a cylindrical shape. Their secondary outcomes included complications (recorded by medical record or patient self-report) and patient satisfaction (using a 5-point Likert scale, where a higher score indicated greater satisfaction).
The 3 included evidence-based guidelines considered efficacy outcomes (e.g., wound healing, time to prosthetic fitting, changes in functional status),14-16 and 2 guidelines considered safety-related outcomes (e.g., falls, complications).14,15
Summary of Critical Appraisal
An overview of the critical appraisal of included publications is presented in the following section. Additional details regarding the strengths and limitations of included publications are provided in Appendix 3 for the SRs (Table 5), primary clinical study (Table 6), and guidelines (Table 7).
Systematic Reviews
Both SRs1,12 clearly stated their research question and inclusion criteria. The primary studies included I the SRs1,12 were identified from searches in multiple databases and at least 1 trial registry, performed within 24 months of the review’s completion. One SR1 published the methods in advance; the other SR12 did not report if a protocol had been published before the review being conducted. Thus, for 1 SR12 it is unclear if there were any significant protocol deviations which may impact the interpretation of their findings. One SR1 described the selection of articles, presented a flow chart, and listed both included and excluded studies, but the other SR12 did not report such details. Providing details about the literature search increases the reproducibility of the review. None of the SRs explained their method of study selection.1,12 Due to these limitations, it is unclear if the selection process could capture all relevant studies.
In 1 SR,1 2 reviewers independently conducted the study selection, assessed the risk of bias of included primary studies, and extracted data using a piloted form. In the other SR12 the authors did not state if study selection was performed in duplicate, which may also increase the risk of not capturing all relevant studies. Data extraction was not performed in duplicate, and it is unclear how data was extracted. Thus, the potential for data extraction errors could not be assessed.
Both SRs1,12 assessed the quality of included studies. One SR1 used criteria from the Cochrane Handbook for Systematic Reviews of Interventions to assess risk of bias, while the other SR12 used the Cochrane trial quality review criteria. One SR1 reported level of risk for different domains; all relevant studies were scored as having high or unclear risk for at least some types of biases, though a few studies were judged as low risk of bias for some domains. They also reported a GRADE score for each outcome and concluded that all reported outcomes had very low certainty.1 The other SR12 summarized the method of randomization, blinding, attrition bias, and statistical analyses for each study, and concluded that most papers in the review were of low-quality.
Meta-analyses were conducted by both SRs.1,12 One SR1 conducted multiple meta-analyses for different outcomes, using appropriate statistical methods.1
Both SRs1,12 reported the funding received by the review authors. One SR1 stated the funding was for their review, while the other SR12 acknowledged the funding was received by their department. The review authors in 1 SR1 reported no conflicts of interest, while the other SR12 did not report conflicts of interests.
Randomized Controlled Trials
The included RCT13 clearly reported their objective, intervention, and findings. The authors described the randomization method and reported baseline characteristics of all randomized patients, including those who dropped. The patients were recruited at the same site over the same time, and the treatment site was likely representative of typical care. However, it is unclear if the patients were representative of the population due to the relatively small sample size.
The main outcome was assessed with appropriate statistical tests based on the intention-to-treat population and adjusted for different follow-up lengths.13 The outcome assessor was blinded to the patients’ group assignment.13 Patients were not blinded; however, blinding was not feasible for them due to the nature of the intervention. Though the lack of blinding is unlikely to significantly affect objective outcomes such as stump volume; a potential exists for performance bias of subjective outcomes, such as self-reported satisfaction or complications.
Although the number of patients was smaller than what the authors predetermined in a sample size calculation, a post-study statistical analysis indicated that the study had 80% power to detect differences in treatment effect between the study groups.13 From the 25 randomized patients, 5 dropped out (2 from the RRD group, 3 from the control group). The reported reasons for dropping out were inconvenience, diagnosis of cancer or congestive heart failure.13
The authors reported their funding, stating they were supported by a university grant, though it is unclear if this grant was specifically for this study. They also did not report on conflicts of interest.13
Guidelines
All 3 included guidelines14-16 provided clear details regarding their scope and purpose, including their target users. the recommendations were also easy to identify. Only the US guideline15 clearly stated that their guideline development group included people from all relevant professional groups, although the Dutch guideline16 indicated that patient views or preferences had been considered, while the Australian guideline14 reported a consensus among expert clinicians and professional organizations regarding a preference of rigid dressings over soft dressings. All the guidelines used systematic literature searches for evidence, described their selection criteria and quality of evidence, and presented the recommendations in a way that made them easy to identify.14-16 Two guidelines15,16 ranked their recommendations as weak; while the Australian guideline14 did not report strength of recommendations, referring to them as expert consensus.
Two guidelines14,16 provided unambiguous recommendations regarding RRDs following transtibial amputations. The Dutch guideline16 provided a recommendation based on expert opinion against rigid dressings for people after a transfemoral amputation. Similarly, the US guideline15 recommends rigid dressings without specifying removable or non-removable, though the evidence summary supporting the recommendation specified RRDs. All guidelines reported some details regarding rigour of development, though none described how the recommendations were formulated or provided a procedure for updating the guidelines.14-16 Two guidelines15,16 were externally reviewed; the Australian guideline14 did not state if their guideline underwent external review. Overall, the guidelines did not provide advice for how to put the recommendations into practice, or monitoring and/or auditing criteria.14-16 The US and Dutch guidelines15,16 considered the availability of needed resources (potential facilitators or barriers), and resource use or costs (potential resource implications) when developing the guidelines. For both of these guidelines,15,16 the authors declared no conflicts of interest or reported that competing interests had been recorded and addressed. The Australian guideline14 did not state they considered facilitators, barriers, or resource use, and they did not provide conflicts of interest information. For all 3 guidelines, it is unlikely the funding body influenced the guideline’s recommendations.14-16
Summary of Findings
Appendix 4 presents the main study findings of the included SRs1,12 and RCT13 by outcome. The outcomes of interest reported were changes in swelling (Table 8), participant satisfaction (Table 9), time to events (Table 10), and complications (Table 11). Appendix 4 also presents the summary of guideline recommendations14-16 (Table 12). There was some overlap in the included SRs: 1 RCT was included in both SRs, with the citation matrix illustrating the overlap presented in Appendix 5 (Table 13). To avoid duplication of reporting, the outcome data from this RCT is reported only once as part of 1 SR.
Clinical Effectiveness of Removable Rigid Dressings
Change In Swelling
One SR1 identified 3 studies that assessed the change in swelling as measured by the stump volume in cm3. All 3 studies assessed within 1 month (short-term) and 2 also assessed the outcome from 1 to 3 months (medium-term). The meta-analyses found that that in the short-term, RRD was associated with a statistically significantly faster decrease in swelling compared to soft dressings. However, in the medium-term, there difference between the groups was not statistically significantly. This suggests that compared to using soft dressings, using RRDs may be associated with a faster reduction in swelling in the short-term, but not in the medium-term.
Patient Satisfaction
The RCT13 assessed patient satisfaction on a 5-point Likert scale, where a higher score indicated greater satisfaction, which might indicate patients’ adherence to the treatment. They found that the mean scores were 4.45 and 4.11 for the RRD and elastic bandages groups, respectively, indicating a similar levels of patient satisfaction without a statistically significant difference between the devices.13
Time-Related Outcomes
One SR1 reported on the length of hospital stay, time to wound healing, time to no pain, and time to walking. For each outcome, 1 relevant study of the SR reported data. Compared to soft dressing, RRD was associated with shorter time from amputation to wound healing and length of hospital stay. No significant difference between groups was found for time from amputation to no pain and time from amputation to walking.
Time to fitting or casting the prosthesis was assessed by 1 SR12 and 1 RCT.13 While this SR12 conducted a meta-analysis for this outcome, it included studies not relevant to this report (grouping RRDs with non-removable rigid dressings); thus, only data from the individual relevant studies, and not the meta-analyses, are included in this report. The SR12 identified 4 relevant studies, 2 of which reported a statistically significantly shorter time to casting in the RRD group than the soft dressing group, while the other 2 reported no statistically significant difference between the 2 groups. The RCT13 reported on time to residual limb maturation, assuming that once limb maturation was achieved, it was time for prosthetic casting. The RCT13 found that the RRD group had a significantly shorter time to residual limb maturation than the group treated with elastic bandages, even after adjusting for the time since amputation. Thus, time to fitting or casting had mixed results across the identified studies.
Complications
A variety of complications were reported by the studies included in this report. The RCT13 reported that, overall, there were no complications in the RRD group; whereas 3 out of 12 patients experienced complications in the elastic bandages group. This difference was not statistically significant.
Both SRs1,12 and the RCT13 reported skin-related complications (e.g., wound infection or breakdown or trauma, skin irritation, progression to transfemoral amputation or further amputation, pressure areas). In general, skin-related complication rates were numerically similar across both the RRD and soft dressing groups, except for progression to re-amputation, reported by a retrospective cross-sectional study reported by 1 SR12 with 5% with RRD compared to 17% with soft dressing. A RCT in the other SR1 also assessed revisions to transfemoral amputation, and found it occurred for 4% and 8% of patients in the RRD and soft dressings groups, respectively. The included RCT13 identified 2 (approximately 17%) skin-related complications in the elastic bandages group compared to none in the RRD group. The level of statistical significance was not reported or observed for any of the comparisons.
One SR1 reported non-skin-related complications including deaths, medical complications, and falls. One or 2 RCTs in the SR reported for each of the outcomes, with none showing statistically significant differences between the RRD and soft dressing groups. Pooled analysis found that approximately 18% of patients in the soft dressings group experienced falls compared to 13% in the RRD group.1 For the other assessments, the complication rates were less than 15% in both groups. The RCT13 reported that 1 participant in the elastic bandages group had a knee flexion contracture, compared to none in the RRD group.
Cost-Effectiveness of Removable Rigid Dressings
No cost-effectiveness studies of RRDs versus alternative dressings for the post-operative management of people who underwent leg amputation were identified; therefore, no summary can be provided.
Guidelines
The Australian guideline14 recommends the use of RRDs for people who have undergone a transtibial amputation, based on an evidence review finding RRDs were associated with improved outcomes. The developers noted a lack of RCTs and poor quality of evidence due to risk of biases in available studies. They did not provide a strength rating for the recommendation.
The US VA and DoD clinical guideline15 recommends that a rigid or semi-rigid dressing be used as soon as possible post-amputation for transtibial amputation, with rigid post-operative dressings preferred if limb protection is a priority. The strength of the recommendation was rated as weak. While the recommendation itself does not specify RRDs, the authors refer to previous research specific to RRDs in the discussion section; implying that the recommendation may apply to RRDs.
The Dutch guideline16 states that a RRD may be considered for people with a transtibial amputation if 1 wishes to use a rigid dressing and regular wound monitoring is indicated. The literature search for post-operative management identified 2 studies comparing RRDs with soft dressings. The guideline does not recommend rigid dressings for people following transfemoral amputation. They also state that following transfemoral amputation, the current post-operative management using stump dressing (light elastic bandages or stump stockings) can be maintained. While this recommendation does not specify RRDs, it implies that specified alternative dressings are recommended over all types of rigid dressings for patients who undergo transfemoral amputation. Both recommendations were graded as based on expert opinion.
Limitations
Several limitations were identified that prevent definitive conclusions regarding the clinical effectiveness of RRDs compared to other dressings for leg amputations. Most primary clinical studies included in the SRs1,12 and RCT13 had relatively small sample sizes: all the RCTs had less than 100 patients, and only 1 non-randomized study had a sample size of more than 100. These studies varied in the outcomes they assessed, and several outcomes of interest to this review only had data from a single study. Although pooled analyses were available for a few outcomes, they also had relatively few patients (between 45 and 76) in total. Thus, many of the presented results are based on relatively small sample sizes.
Both SRs1,12 included RCTs and non-randomized studies. One SR12 did not report details regarding the individual studies’ population. The included primary clinical studies also had varying levels of risk of bias.1,12 Some methodological limitations reported by the SRs were related to risk of selection bias in non-randomized studies,1,12 lack of allocation concealment,1 incomplete outcome data,1,12 selective reporting,1 inappropriate statistical tests,12 and lack of power analysis or sample size calculation.12 Non-blinding of patients could have led to performance bias, but due to the nature of the intervention, it is unlikely that participant blinding would have been possible. Quality issues from the primary studies can cause uncertainty in the findings presented by the SRs. The RCT was also limited by lack of blinding of the patients.13 Across all the included primary clinical studies, only 2 published in in the past 10 years; thus, it is unclear if some findings from the older studies would still apply today, given changes in technology care delivery (e.g., if newer RRDs are better and may have improved outcomes compared to older RRDs, or if changes in post-amputation care that could affect the clinical benefits of RRDs).
Some of the guidelines were unclear as they referred to rigid dressings without specifying RRDs.15,16 All guidelines14-16 were based on low- or poor-quality evidence, and have weak15,16 or unranked recommendations.14
Evidence for clinical effectiveness was available for limited to transtibial amputation and comparisons of RRDs to soft dressings, with none of the included primary studies compared RRDs to other types of dressings (e.g., non-removable rigid dressings). In addition, none of the included studies were conducted in Canada, and none of the guidelines were specifically intended for use in Canada. Thus, the generalizability of the findings and recommendations to the Canadian context are unknown, due to differences between countries regarding health care systems and availability of resources.
Conclusions and Implications for Decision- or Policy-Making
This rapid review was conducted to examine the clinical effectiveness and cost-effectiveness of RRDs compared to alternative dressings, as well as summarize guidelines regarding the use of RRDs. A previous CADTH report from 201218 addressed a similar topic, comparing RRDs to non-removable rigid dressings for people following leg amputation. That report found limited evidence (from 1 RCT published in 2008) indicating no significant differences in clinical effectiveness or adverse events between RRDs and non-removable rigid dressings, but it did not identify ang evidence regarding cost-effectiveness or recommendations from evidence-based guidelines.18
The current report includes 2 SRs1,12 1 RCT,13 and 3 evidence-based guidelines.14-16 The SRs and RCT provide evidence regarding the clinical effectiveness and safety of RRDs compared to soft dressings for people who had a transtibial amputation.1,12,13 Evidence comparing the clinical effectiveness of RRDs to alternative dressings for people following a transfemoral amputation was not identified. In addition, no evidence was identified regarding the cost-effectiveness of RRDs compared to alternative dressings for people with a leg amputation.
There was limited evidence to suggest that in the short-term (less than 1 month), using RRDs may lead to greater reduction in swelling, shorter time to wound healing, and shorter length of hospital stay compared to using soft dressings.1 However, over the medium-term (1 to 3 months), no significant differences were found between RRDs and soft dressings regarding change in swelling, time from amputation to no pain, and time to walking.1 The evidence was mixed regarding the time to fitting or casting the prosthesis.12,13 A variety of complications were reported and they occurred at generally similar rates for both the RRD and soft dressing groups.1,12,13 The statistical significance of the differences in the rate of complications were not reported or observed for any comparison. Thus, this review found that overall, RRDs had a beneficial or neutral effect on clinical outcomes compared to soft dressings with similar adverse events rates. However, these results should be interpreted with caution due to the small sample sizes and other methodological limitations.
Two identified guidelines14,16 recommended using RRDs for transtibial amputations whereas 1 guideline15 recommends rigid dressings, without specifying RRDs. One guideline recommends against the using rigid dressings for transfemoral amputations.16 All the guidelines were based on low-quality evidence and the strength of recommendations was not graded or ranked as weak.
Due to the limitations of the included studies in this report, there is insufficient evidence to provide definitive conclusions about the clinical effectiveness of RRDs compared to alternative dressings following leg amputation. More robust research from well-designed studies, including research set in Canada, is required to provide evidence on the clinical effectiveness and cost-effectiveness of RRDs for people following a leg amputation.
References
1.Kwah LK, Webb MT, Goh L, Harvey LA. Rigid dressings versus soft dressings for transtibial amputations. Cochrane Database Syst Rev. 2019;6:CD012427. PubMed
2.Hussain MA, Al-Omran M, Salata K, et al. Population-based secular trends in lower-extremity amputation for diabetes and peripheral artery disease. Can Med Assoc J. 2019;191(35):E955-E961. PubMed
3.Moxey PW, Gogalniceanu P, Hinchliffe RJ, et al. Lower extremity amputations — a review of global variability in incidence. Diabet Med. 2011;28(10):1144-1153. PubMed
4.Ahmad N, Thomas GN, Gill P, Chan C, Torella F. Lower limb amputation in England: prevalence, regional variation and relationship with revascularisation, deprivation and risk factors. a retrospective review of hospital data. J R Soc Med. 2014;107(12):483-489. PubMed
5.Imam B, Miller WC, Finlayson HC, Eng JJ, Jarus T. Incidence of lower limb amputation in Canada. Can J Public Health. 2017;108(4):e374-e380. PubMed
6.Reichmann JP, Stevens PM, Rheinstein J, Kreulen CD. Removable rigid dressings for postoperative management of transtibial amputations: a review of published evidence. Pm R. 2018;10(5):516-523. PubMed
7.Sumpio B, Shine SR, Mahler D, Sumpio BE. A comparison of immediate postoperative rigid and soft dressings for below-knee amputations. Ann Vasc Surg. 2013;27(6):774-780. PubMed
8.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
9.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
10.Agree Next Steps Consortium. The AGREE II instrument. Hamilton (ON): AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2022 Jun 7.
11.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
12.Churilov I, Churilov L, Murphy D. Do rigid dressings reduce the time from amputation to prosthetic fitting? A systematic review and meta-analysis. Ann Vasc Surg. 2014;28(7):1801-1808. PubMed
13.Koonalinthip N, Sukthongsa A, Janchai S. Comparison of removable rigid dressing and elastic bandage for residual limb maturation in transtibial amputees: a randomized controlled trial. Arch Phys Med Rehabil. 2020;101(10):1683-1688. PubMed
14.Guide to the use of post-operative rigid dressings for transtibial amputations. St Leonards (AU): Agency for Clinical Innovation; 2017: https://aci.health.nsw.gov.au/__data/assets/pdf_file/0006/360492/RMC-Guide.pdf Accessed 2022 May 11.
15.VA/DoD clinical practice guideline for rehabilitation of individuals with lower limb amputation. Washington (DC): Department of Veterans Affairs and Department of Defense; 2017: https://www.healthquality.va.gov/guidelines/Rehab/amp/VADoDLLACPG092817.pdf Accessed 2022 Jun 7.
16.Geertzen J, van der Linde H, Rosenbrand K, et al. Dutch evidence-based guidelines for amputation and prosthetics of the lower extremity: amputation surgery and postoperative management. Part 1. Prosthet Orthot Int. 2015;39(5):351-360. PubMed
17.Tivey D, Duncan J, Scarfe A, Lambert R, Cameron A. Amputee care standards. Glebe (AU): Sax Institute; 2015: https://www.saxinstitute.org.au/publications/evidence-check-library/amputee-care-standards/. Accessed 2022 May 18.
18.Removable rigid dressings for leg amputation: a review of the clinical effectiveness, cost effectiveness and guidelines. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2012: https://www.cadth.ca/sites/default/files/pdf/htis/feb-2012/RC0325%20Amputation%20Dressings%20Final.pdf Accessed 2022 May 12.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews and Meta-Analyses
Study citation, country, funding source | Study designs, study objectives, search dates, number of primary studies | Population characteristics | Intervention and comparator | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Kwah et al. (2019)1 Singapore Funding source: National Institute for Health Research, via the Cochrane Infrastructure funding to Cochrane Wounds | SR and MA of RCTs and quasi-RCTs (studies with quasi-randomized allocation procedures) Objective: To determine if rigid dressings are more effective than soft dressings for wound healing following transtibial amputation. Search dates: Up to December 2018 Number of included studies: 9 Number of relevant studies: 5 (4 RCT, 1 NRS) | People who had a transtibial amputation Sample sizes from relevant studies: 15 to 56 Mean age from relevant studies: 57 to 73 % male from relevant studies: 42 to 80% | Eligible intervention: Rigid dressings Relevant intervention: RRD Comparator: Soft dressing | Outcomes:
Follow-up: up to 8 weeks |
Churilov et al. (2014)12 Australia Funding source: the Victoria Government, particularly the Operational Infrastructure Support Grant | SR and MA of RCTs and cross-sectional studies Objective: To determine if rigid dressings are more effective than soft dressings for wound healing following transtibial amputation Search dates: Up to December 2013 Number of included studies: 6 Number of relevant studies: 4 (1 RCT, 3 NRS) | Adults who had an amputation of the lower limb Sample sizes from relevant studies: 50 to 104 Mean age from relevant studies: NR % male from relevant studies: NR | Eligible intervention: Rigid dressings Relevant intervention: RRD Comparator: Soft dressing | Outcomes:
Follow-up: NR; only reported mean time from amputation to casting or fitting, which varied from 19 to 76 days by study and group. |
MA = meta-analysis; NR = not reported; NRS = non-randomized studies; RCT = randomized controlled trial; RRD = removable rigid dressing; SR = systematic review.
Table 3: Characteristics of Included Primary Clinical Study
Study citation, country, funding source | Study design and setting | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Randomized controlled trial | ||||
Koonalinthip et al. (2019)13 Thailand Funding source: Ratchadapisek Sompoch Endowment Fund Chulalongkorn University (grant no. RA61/002). | Study design: Single-centre, single-blinded (assessor-blinded) RCT Setting: Department of Rehabilitation Medicine, King Chulalongkorn Memorial Hospital Sample size calculation: Yes Intention-to-treat analysis: Yes | Adults (18+ years) who had a transtibial amputation from July 2017 to February 2018 (n = 25, including 5 who dropped out). Mean (SD) age in years:
% male:
Cause of amputation (%):
Mean (SD) duration after trauma in days:
Mean (SD) baseline residual limb volume in cm3:
| Intervention: RRD Comparator: EB | Outcomes:
Follow-up: Until the residual limb matured; at least 1 participant followed for over 150 days. |
DM = diabetes mellitus; EB = elastic bandage; RCT = randomized controlled trial; RRD = removable rigid dressing; SD = standard deviation.
aResidual limb maturation defined as: the volume of the residual limb had stabilized (volume did not change more than 10% from previous assessment), soft tissue atrophy occurred, and residual limb had been molded into a cylindrical shape. (p.1684).13
Table 4: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice, major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|
New South Wales (Australia)’s Agency for Clinical Innovation (2017)14 | |||||
Intended users: Clinicians managing patients who have undergone an amputation Target population: Individuals with lower limb amputation | Intervention: RRDs Outcomes: Swelling, wound healing, protection from potential trauma, shape for prosthetic fitting, pain control | Conducted a systematic review that searched PubMed, EMBASE (Ovid), EBM reviews including Cochrane Database of Systematic Reviews, Database of Abstracts of Reviews of Effects (DARE), Cochrane Central Register of Controlled Trials (CENTRAL), ACP Journal Club, Cochrane Methodology Register, Health Technology Assessment and NHS Economic Evaluation Database (NHSEED – Ovid), and CINAHL. | The evidence was graded based on the study design type, level of risk of confounding and bias, and probability of causal relationship. | The guideline refers to the systematic review’s identified evidence (findings and quality). Two reviews were rated as ‘good’ quality and 3 were ‘poor’, and the included primary studies were also rated and varied. They state that despite some limitations of the literature, emergent research suggests RRDs are associated with better clinical outcomes and thus they recommend RRDs be used. Details about process used by the development group to arrive at the recommendation were not provided. | NR |
US Department of Veterans Affairs and US Department of Defense (2017)15 | |||||
Intended users: Veterans Affairs and Department of Defense health care providers Target population: Adults (18+) with lower limb amputation treated in any Veterans Affairs and Department of Defense clinical setting | Intervention: Rigid or semi-rigid dressings Outcomes: Time from amputation to prosthetic fitting, wound healing rate, mobility, edema volume, residual limb healing time, hospitalization time, infection rate | Conducted a systematic review that searched the Cochrane Database of Systematic Reviews, CINAHL, EMBASE, Health Technology Assessment Database, MEDLINE/ PreMEDLINE, PsychINFO, PubMed (in-process and Publisher records), and AHRQ. Selection criteria included being a clinical study or systematic review and meeting inclusion criteria for any of the key questions. | Used the GRADE methodology to assess the evidence and assigned the strength for each recommendation. | The guideline development process included formulating and prioritizing the key questions, conducting a systematic review, convening a face-to-face meeting, and drafting the guideline. After assessing the evidence quality, the working group had an in-person meeting to discuss and interpret the evidence review findings, review recommendations from the previous guideline, and develop new clinical recommendations. Each recommendation was given a strength rating by the working group based on an evidence to recommendations framework. A focus group of patients provided patient perspectives to inform the recommendation development. Following the meeting, the working group drafted the updated guideline. | Experts from inside and outside the federal sector reviewed the draft guideline. Their comments or edits were incorporated based on panel consensus and consistency with the evidence review. |
Netherlands Society of Physical and Rehabilitation Medicine, Geertzen et al. (2014)16 | |||||
Intended Users: Health care providers Target Population: Adults undergoing amputation of a lower extremity, particularly people with vascular disease | Intervention: Rigid dressings, including RRDs Outcome: Number of days to prosthesis fitting, time required for wound healing, function, adverse events (e.g., contractures) | Conducted a systematic search of the Cochrane Library, MEDLINE, Embase, PsychINFO, and CINAHL up to January 2011. Selection criteria included comparative studies with robust evidence (meta-analyses, systematic reviews, RCTs, controlled trials). If these were unavailable, further comparative cohort studies, comparative case-control studies or non-comparative studies were searched. Case reports were also used to help with opinion-forming for certain key questions. | Quality was assessed using evidence-based guideline development assessment forms; selected articles were graded by quality and low-quality articles were excluded. | Recommendations were developed based on scientific evidence, as well as other important considerations including patient preferences, availability of special techniques or expertise, organizational aspects, social consequences, and costs. | NR |
AHRQ = Agency for Healthcare Research and Quality; GRADE = Grading of Recommendations Assessment, Development and Evaluation (methodology); NR = not reported; RCT = randomized controlled trial; RRD = removable rigid dressings.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 5: Strengths and Limitations of Systematic Reviews and Meta-Analyses Using AMSTAR 28
Strengths | Limitations |
|---|---|
Kwah et al. (2019)1 | |
The research question and inclusion criteria were clearly stated and included the population, intervention, comparator, and outcomes. The methods were established before the review and published in advance (CD012427), and deviations from the protocol were reported. The review authors used a comprehensive search strategy including searching 7 databases, providing keywords and/or search strategy, searching reference lists of included studies, trial or study registries, and grey literature. The literature search was conducted within 24 months of the review’s completion, and thus should include studies that were recently published relative to the review’s completion date. The 2 review authors independently screened titles, abstracts, and full-text publications. The 2 review authors independently extracted data using a data extraction form that was piloted, with disagreements resolved by discussion or arbitration by a third review author. A list of excluded studies was provided, including justifications for the exclusions. The included studies were described in adequate detail and assessed for risk of bias in multiple domains. Risk of bias and GRADE assessments were performed independently by the 2 review authors. Sources of funding for the included studies were searched for by reviewers and reported where available. Appropriate methods were used for statistical combination of results in the meta-analysis. A sensitivity analysis that excluded studies with a high or unclear risk of bias for random sequence generation, concealed allocation, blinding of outcome assessor and incomplete outcome data was conducted. The reviewers discussed the likely impact of risk of bias on the review results. The review authors’ conflicts of interest and their funding source were reported. | The review authors did not explain their selection of study designs included in the review. It is unclear if content experts were consulted. Publication restrictions (study designs, languages) were not justified. Causes of heterogeneity were not investigated. Although the authors planned to do so, they stated that due to the small number of included studies, they could not. Separate estimates for RCTs and NRSs (quasi-RCTs) were not reported. Graphical or statistical tests were not performed for publication bias. |
Churilov et al. (2014)12 | |
The research question and inclusion criteria were clearly stated and included the population, intervention, comparator, and outcomes. The methods provided included the objective, search strategy, inclusion and exclusion criteria, and risk of bias assessment. The review authors used a comprehensive search strategy including searching 3 databases and 1 trial registry, providing keywords and/or search strategy and searching reference lists of included studies. The literature search was conducted within 24 months of the review’s completion, and thus should include studies that were recently published relative to the review’s completion date. However, the systematic review was published 8 years ago (in 2014), and the advantage of its literature search’s recency may not apply today. The number of excluded studies and their reasons for exclusion were provided. Data extraction was not performed in duplicate; however, 1 reviewer extracted, and another reviewer assessed the extracted data. The included studies were assessed for risk of bias using the Cochrane trial quality review criteria, including type of study, randomization, blinding, attrition bias, statistical analyses used, and power analysis. The authors investigated sources of heterogeneity in the results and discussed the likely impact on the review. Funding received by the review authors was reported. | The review authors did not state they had established the review methods before conducting the review. The methods did not state their plan for investigating causes of heterogeneity. It is unclear if there were any protocol deviations. The search strategy did not state if they searched grey literature or consulted content experts. Publication restrictions were not justified including the study designs included in the review. It is not stated if study selection was performed in duplicate. A list of excluded studies was not provided. Separate estimates for RCTs and NRSs were not reported. Some details about the included studies were not provided, including the mean age and proportion of male patients for each included study. Risk of bias in individual studies was not accounted for in the discussion of the results. Sources of funding for the included studies were not reported. Conflicts of interest were not reported. |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; GRADE = Grading of Recommendations, Assessment, Development, and Evaluation; NRS = non-randomized study; RCT = randomized controlled trial.
Table 6: Strengths and Limitations of Clinical Study Using the Downs and Black checklist9
Strengths | Limitations |
|---|---|
Randomized controlled trial | |
Koonalinthip et al. (2020)13 | |
Reporting: The objective, main outcomes, patient characteristics, interventions of interest, and main findings were clearly described. The treatment and control groups did not differ significantly at baseline based on reported characteristics. The number of patients who dropped out was reported, including their reasons for dropping out. Adverse events were reported. Actual P values were reported. External validity: Everyone at the site who had a transtibial amputation was screened for enrollment in this study. Therefore, patients may be representative of the population from which they were recruited. The proportion of people who were asked to participate and agreed was stated. The staff and facilities where treatment occurred was representative of the treatment typically provided. Internal validity – bias: Patients were assessed by a staff who was blinded to the intervention. Analyses adjusted for different follow-up lengths. The main outcomes used were valid and reliable, and assessed with appropriate statistical tests. Internal validity – confounding: Patients in all groups were recruited from the same population and over the same period. Patients were randomized to intervention groups using block-of-4 randomization. The randomized intervention assignment was concealed from the staff who assessed patients. Analyses were conducted using the intention-to-treat approach. Other: A sample size calculation was performed. While the number of patients was smaller than the calculated size, the statistical power after data analysis was 80%. It is unclear if this calculation includes the number of people who dropped out. | Reporting: 20% of randomized patients dropped out, though the intervention and comparator groups had similar proportions of patients who dropped out. External validity: As the sample size was relatively small (N = 25) and patients were recruited from a single-centre, patients may not be representative of the population from which they were recruited. It is not clear if the distribution of confounding factors was the same in the study sample and source population. Internal validity – bias: Patients were not blinded to the intervention; however, it is unlikely this would have been possible due to the nature of the intervention. Compliance with the intervention was not assessed. |
Table 7: Strengths and Limitations of Guidelines Using AGREE II10
Item | Agency for Clinical Innovation (2017)14 | US VA and DoD (2019)15 | VRA, Geertzen et al. (2015)16 |
|---|---|---|---|
Domain 1: Scope and purpose | |||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes |
Domain 2: Stakeholder involvement | |||
4. The guideline development group includes individuals from all relevant professional groups. | Unclear | Yes | Unclear |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Unclear | Yes | Yes – patient preferences noted as important when making recommendations. |
6. The target users of the guideline are clearly defined. | Yes | Yes | Yes |
Domain 3: Rigour of development | |||
7. Systematic methods were used to search for evidence. | Yes | Yes | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes | Yes | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Yes | Yes |
10. The methods for formulating the recommendations are clearly described. | No | No | No |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | Yes |
13. The guideline has been externally reviewed by experts prior to its publication. | Unclear | Yes | Yes – published in a peer-reviewed journal. |
14. A procedure for updating the guideline is provided. | No | No | No |
Domain 4: Clarity of presentation | |||
15. The recommendations are specific and unambiguous. | Yes | Unclear – the relevant recommendation does not specify RRDs, but refers to RRDs in the supporting evidence. | Partially yes – 1 recommendation specifically refers to RRDs, but another recommendation refers to rigid dressings – it is unclear if this includes RRDs. |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes |
Domain 5: Applicability | |||
18. The guideline describes facilitators and barriers to its application. | No | Partial yes – their evidence to recommendation framework includes considering if interventions are generally available and variability in resourcing requirements. | Partial yes – they stated they considered availability of special techniques or expertise and organizational aspects when developing the recommendations. |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No | No | No |
20. The potential resource implications of applying the recommendations have been considered. | No | Yes – their evidence to recommendation framework includes considering costs of resource use. | Yes – they stated they considered social consequences and costs when developing the recommendations. |
21. The guideline presents monitoring and/or auditing criteria. | No | No | No |
Domain 6: Editorial independence | |||
22. The views of the funding body have not influenced the content of the guideline. | Likely yes – the systematic review was conducted by an independent, not-for-profit organization that receives its core funding from the local government. The guideline was developed by an agency that is part of the New South Wales government. | Likely yes – funding for this guideline was NR, but disclosure statements were used to identify any potential conflicts of interest by the project team members, and none were identified. | Likely yes – the guidelines were developed by the VRA, the authors declared no conflicts of interest, and funding came from the Quality Foundation of Dutch Medical Specialists. |
23. Competing interests of guideline development group members have been recorded and addressed. | No | Yes | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; DoD = Department of Defense; NR = not reported; RRD = removable rigid dressing; VA = Veteran Affairs; VRA = Netherlands Society of Physical and Rehabilitation Medicine.
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Table 8: Summary of Findings by Outcome — Change in Swelling (Stump volume in cm3)
Details | Kwah et al. (2019)1 – SR with MA (2 RCTs, 1 quasi-RCT) | ||||||
|---|---|---|---|---|---|---|---|
Hidayati et al. (2013) – RCT | Janchai et al. (2008) – RCT | Mueller (1982) – quasi-RCT | Pooled analysis | ||||
RRD | Soft dressing | RRD | Soft dressing | RRD | Soft dressing | ||
Short-term (less than 1 month) | |||||||
N | 12 | 11 | 12 | 14 | 8 | 8 | |
Mean change in swelling (cm3) | 133.3 | 94.6 | 42.7 | 21.9 | 70.6 | 31.2 | — |
Standard deviation | 6.2 | 33.6 | 62.7 | 118.5 | 21.3 | 49 | — |
Weight (%) | 39.82 | 12.73 | 47.45 | 100 | |||
MD (95% CI) | 38.78 (−1.64 to 79.2) | 20.84 (−50.65 to 92.33) | 39.5 (2.48 to 76.52) | 38.84 (11.33 to 62.34) | |||
Heterogeneity | — | — | — | Tau2 = 0; Chi2 = 0.22, df = 2 (P = 0.9); I2 = 0% | |||
Overall effect | — | — | — | Z = 2.83 (P = 0) | |||
Medium-term (1 to 3 months) | |||||||
N | 12 | 11 | 11 | 11 | NR | NR | |
Mean change in swelling (cm3) | 87.9 | 106.5 | 79.9 | 83 | NR | NR | — |
Standard deviation | 70.6 | 76.2 | 103.3 | 113.1 | NR | NR | — |
Weight (%) | 69.34 | 30.66 | — | 100 | |||
MD (95% CI) | −18.53 (−78.71 to 41.65) | −3.13 (−93.64 to 87.38) | — | −13.81 (−63.92 to 36.31) | |||
Heterogeneity | — | — | — | Tau2 = 0; Chi2 = 0.08, df = 1 (P = 0.78); I2 = 0% | |||
Overall effect | — | — | — | Z = 0.54 (P = 0.59) | |||
CI = confidence interval; MA = meta-analysis; MD = mean difference; NR = not reported; RCT = randomized controlled trial; RRD = removable rigid dressing; SR = systematic review.
Table 9: Summary of Findings by Outcome — Participant Satisfaction
Study citation and study design | Study details and outcomes | RRD (n = 13) | Elastic bandage (n = 12) | P value |
|---|---|---|---|---|
Koonalinthip et al. (2020)13 RCT | Mean participant satisfaction on a 5-point Likert Scale:
| 4.45 | 4.11 | 0.312 |
RCT = randomized controlled trial; RRD = removable rigid dressing.
Table 10: Summary of Findings by Outcome — Time to Events
Study citation and design | For SRs: individual clinical study citation, design, and details | RRD | Soft dressing | Effect estimate (95% CI) | P value | ||
|---|---|---|---|---|---|---|---|
N | Outcome | N | Outcome | ||||
Time from amputation to wound healing in days | |||||||
Kwah et al. (2019)1 SR (1 RCT) | Vigier et al., 1999 (RCT) | 28 | Mean (SD) = 71.2 (31.7) | 28 | Mean (SD) = 96.8 (54.9) | MD = −25.6 (−49.08 to −2.12) | NR |
Time from amputation to no pain in days | |||||||
Kwah et al. (2019)1 SR (1 RCT) | Hidayati et al., 2013 (RCT) | 12 | Mean (SD) = 4.8 (2) | 11 | Mean (SD) = 5.2 (2.3) | MD = −0.35 (−2.11 to 1.41) | NR |
Time from amputation to walking in days | |||||||
Kwah et al. (2019)1 SR (1 RCT) | Vigier et al., 1999 (RCT) | 28 | Mean (SD) = 30.3 (16.2) | 28 | Mean (SD) = 33.3 (9.5) | MD = −3 (−9.96 to 3.96) | NR |
Length of hospital stay in days | |||||||
Kwah et al. (2019)1 SR (1 RCT) | Vigier et al., 1999 (RCT) | 28 | Mean (SD) = 99.8 (22.4) | 28 | Mean (SD) = 129.9 (48.3) | MD = −30.1 (−49.82 to −10.38) | NR |
Time to residual limb maturationa or prosthetic casting/fitting in days | |||||||
Churilov et al. (2014)12 SR (1 RCT, 3 NRSs) | Deutsch et al., 2005 (RCT) Type of RRD: Below-knee Outcome: Time to fitting | 26 | NR | 24 | NR | SMD = 0.04 (−0.57 to 0.65) | NR |
Taylor et al., 2008 (NRS: retrospective cross-sectional study) Type of RRD: Below-knee Outcome: Time to casting | 28 | NR | 37 | NR | SMD = −0.47 (−0.97 to 0.03) | NR | |
Ladenheim et al., 2007 (NRS: retrospective cross-sectional study) Type of RRD: Below-knee Outcome: Time to casting | 76 | NR | 28 | NR | SMD = −0.52 (−0.96 to −0.08) | NR | |
van Velzen et al., 2005 (NRS: retrospective cross-sectional study) Type of RRD: Above-knee Outcome: Time to casting | 39 | NR | 31 | NR | SMD = −1.15 (−1.66 to −0.64) | NR | |
Koonalinthip et al. (2020)13 b RCT Outcome: Time to limb maturation | – | 13 | Median (IQR) = 28 (17 to 51) | 12 | Median (IQR) = 54 (30 to 77) | aHRc = 3.3234 (1.083 to 10.203) | 0.036 |
aHR = adjusted hazard ratio; CI = confidence interval; IQR = interquartile range; MD = mean difference; NR = not reported; NRS = non-randomized study; RCT = randomized controlled trial; RRD = removable rigid dressing; SD = standard deviation; SMD = standardized mean difference.
aLimb maturation was defined by study authors as when the volume of the residual limb had stabilized (volume did not change more than 10% from previous assessment), soft tissue atrophy occurred, and residual limb had been molded into a cylindrical shape. (p.1684) The authors stated they assumed that once limb maturation was achieved, it was time for prosthetic casting.
bKoonalinthip et al.’s control group was elastic bandages, a type of soft dressing.
cAdjusted hazard ratio accounts for the time since amputation.
Note: A MD or SMD value of > 0 denotes a longer time to prosthetic casting or fitting for the intervention (RRD) compared to the control (soft dressing) group, while a value of < 0 denotes a shorter time for the RRD group compared to control.
Table 11: Summary of Findings by Outcome – Complications
Outcome | Study citation and design | For SRs: Clinical study and study details, or pooled analysis | Proportion of events in RRD group | Proportion of events in soft dressing group | Effect estimate, RR (95% CI) | P value |
|---|---|---|---|---|---|---|
All types | ||||||
All types of complications | Koonalinthip et al. (2020)13 RCT | – | 0/13 | 3/12 | NR | 0.096 |
Skin-related complications | ||||||
All types of skin-related complications | Kwah et al. (2019)1 SR (2 RCTs, 1 quasi-RCT) | Deutsch et al., 2005 (RCT) | 1/26 | 2/24 | 0.46 (0.04 to 4.77) | NR |
Janchai et al., 2008 (RCT) | 1/12 | 1/14 | 1.17 (0.08 to 16.72) | NR | ||
Mueller, 1982 (quasi-RCT) | 0/7 | 0/8 | Not estimable | NR | ||
Koonalinthip et al. (2020)13 RCT | – | 0/13 | 2/12 a | NR | NR | |
Progression to TFA or re-amputation | Kwah et al. (2019)1 SR (1 RCT) | Deutsch et al., 2005 (RCT) Outcome: revisions to TFA | 1/26 | 2/24 | 0.46 (0.04 to 4.77) | NR |
Churilov et al. (2014)12 SR (1 NRS) | Van Velzen et al., 2005 (NRS: retrospective cross-sectional)a Outcome: Progression to “re-amputation” | NR; 5% | NR; 17% | NR | NR | |
Wound breakdown or trauma or infection | Kwah et al. (2019)1 SR (2 RCTs) | Deutsch et al., 2005 (RCT) | 1/26 | 2/24 | 0.46 (0.04 to 4.77) | NR |
Janchai et al., 2008 (RCT) | 1/12 | 1/14 | 1.17 (0.08 to 16.72) | NR | ||
Churilov et al. 2014)12 SR (1 NRS) | Van Velzen et al., 2005 (NRS: retrospective cross-sectional) | NR | NR | NR | No significant difference in “wound problems.” | |
Koonalinthip et al. (2020)13 RCT | – | 0/13 | 2/12 b | NR | NR | |
Pressure areas | Kwah et al. (2019)1 SR (1 NRS) | Mueller, 1982 (NRS: quasi-RCT) | 0/7 | 0/8 | Not estimable | NR |
Non-skin related | ||||||
All non-skin-related complications | Kwah et al. (2019)1 SR (2 RCTs) | Deutsch et al., 2005 (RCT) | 3/26 | 3/24 | 0.92 (0.21 to 4.14) | NR |
Janchai et al., 2008 (RCT) | 1/12 | 1/14 | 1.17 (0.08 to 16.72) | NR | ||
Deaths | Kwah et al. (2019)1 SR (1 RCT) | Deutsch et al., 2005 (RCT) | 3/26 | 3/24 | 0.92 (0.21 to 4.14) | NR |
Medical complicationsc | Kwah et al. (2019)1 SR (1 RCT) | Deutsch et al., 2005 (RCT) | 2/26 | 0/24 | 4.63 (0.23 to 91.81) | NR |
Falls | Kwah et al. (2019)1 SR (2 RCTs) | Deutsch et al., 2005 (RCT) | 4/26 | 6/24 | 0.62 (0.2 to 1.92) | NR |
Janchai et al., 2008 (RCT) | 1/12 | 1/14 | 1.17 (0.08 to 16.72) | NR | ||
Pooled analysis (Deutsch and Janchai) | 5/38 | 7/38 | 0.68 (0.24 to 1.93) Heterogeneity: Tau2 = 0; Chi2 = 0.19, df = 1(P = 0.66); I2 = 0% Z = 0.73 (P = 0.47) | NR | ||
Knee flexion contracture | Koonalinthip et al. (2020)13 RCT | – | 0/13 | 1/12 | NR | NR |
CI = confidence interval; NR = not reported; NRS = non-randomized study; RCT = randomized controlled trial; RR = risk ratio; RRD = removable rigid dressing; SD = soft dressing; TFA = transfemoral amputation.
aThe reporting is unclear for this outcome because there are differences in how the related data were reported in different tables of the SR and in this specific study. Thus, the accuracy of the reported percentage of complications is unclear.
bIncludes skin irritation (n = 1) and wound dehiscence (n = 1).
cMedical complications include outcomes like organ failure or illness not directly related to residual wound healing. (p.31).1
Table 12: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Strength of recommendations and quality of evidence |
|---|---|
New South Wales (Australia)’s Agency for Clinical Innovation (2017)14 | |
Recommendations: Recommends the use of a RRD for patients who have undergone a transtibial amputation. Supporting evidence: A commissioned systematic review identified 5 systematic reviews and an additional 6 primary studies, and found RRDs were consistently associated with faster wound healing compared to soft dressings. RRDs were also associated with lower rates of surgical revision, and reduced time from amputation to several outcomes (wound healing, initial prosthetic casting, and independent walking) for people with transtibial amputation. However, there was a notable lack of randomized trials, inconsistent outcome measures, failure to blind outcome assessors, and risk of biases. | Strength of recommendation: NR Quality of evidence: Poor |
US Veteran Affairs and Department of Defense (2017)15 | |
Recommendations: Recommends the use of rigid (or semi-rigid dressings) after transtibial amputations, with a preference for rigid dressings if limb protection is a priority. Supporting evidence: Refers to evidence that supports RRDs or semi-rigid removable dressings over soft dressings, including reduced acute post-amputation edema volume, faster healing time, and reduced hospitalization time. (p.33). | Strength of recommendation: Weak for Quality of evidence: Low |
Netherlands Society of Physical and Rehabilitation Medicine (VRA), Geertzen et al. (2015)16 | |
Recommendations:
Supporting evidence: In a systematic literature search for post-operative management, 2 studies were identified that assessed RRDs. One RCT compared a vacuum-formed RRD to a conventional rigid dressing after TTA and had similar results for time to prosthetic fitting and patients’ function with their prosthesis. The other RCT compared RRDs to soft dressings and found residual limb volume was smaller in the RRD group at 2 weeks, but no difference was found at 4 weeks. Supporting evidence against rigid dressings for TFA was not provided; the guideline states this is based on the working group’s opinion. | Strength of recommendations: Level 4 – Expert opinion. Quality of evidence:
|
GRADE = Grading of Recommendations Assessment, Development and Evaluation; KD = knee-disarticulation; NR = not reported; RRD = removable rigid dressing; TFA = transfemoral amputation; TTA = transtibial amputation.
Appendix 5: Overlap Between Included Systematic Reviews
Note that this appendix has not been copy-edited.
Table 13: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Kwah et al. (2019)1 | Churilov et al. (2014)12 |
|---|---|---|
Deutsch et al. Prosthet Orthot Int. 2005;29(2):193 to 200. | Yes | Yes |
Hidayati et al. Med J Indones. 2013;22:16 to 21. | Yes | No |
Janchai et al. J Med Assoc Thai. 2008;91(9):1441 to 6. | Yes | No |
Mueller. Phys Ther. 1982;62(10):1438 to 41 | Yes | No |
Vigier et al. Arch Phys Med Rehabil. 1999;80(10):1327 to 30. | Yes | No |
Taylor et al. Prosthet Orthot Int. 2008;32:223 to 30 | No | Yes |
Ladenheim et al. J Prosthet Orthot. 2007;19: 2 to 5. | No | Yes |
van Velzen et al. Prosthet Orthot Int. 2005;29:3 to 12 | No | Yes |
Appendix 6: References of Potential Interest
Previous CADTH Reports
Rigid dressings for edema management for leg amputation: a review of clinical and cost-effectiveness. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2017; https://www.cadth.ca/sites/default/files/pdf/htis/2017/RC0933-RigidDressing-Final.pdf Accessed 2022 May 12.
Removable Rigid Dressings for Leg Amputation: A Review of the Clinical Effectiveness, Cost Effectiveness and Guidelines. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2012; https://www.cadth.ca/sites/default/files/pdf/htis/feb-2012/RC0325%20Amputation%20Dressings%20Final.pdf Accessed 2022 May 12.
Review Articles
Reichmann JP, Stevens PM, Rheinstein J, Kreulen CD. Removable rigid dressings for postoperative management of transtibial amputations: a review of published evidence. Pm R. 2018;10(5):516-523. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca