Drugs, Health Technologies, Health Systems
Reimbursement Review
Bevacizumab
Requester: Public drug programs
Therapeutic area: Endometrial cancer
Summary
What Is Endometrial Cancer?
Endometrial cancer is the most common type of uterine cancer and originates in the lining of the uterus. It is the most common gynecological cancer.
For 2025, there was a projected 8,600 new cases and 1,700 deaths from endometrial cancer in Canada.
What Are the Treatment Goals and Current Treatment Options for Endometrial Cancer?
The goal of therapy for patients with recurrent or metastatic endometrial cancer is to improve overall survival (OS), improve progression-free survival (PFS), and improve symptoms as a cure is rarely achievable.
Therapeutic approaches for recurrent or metastatic endometrial cancer are mainly driven by molecular profile and disease stage. Surgery remains the first-line intervention unless it is not possible due to disease burden or other comorbidities.
Treatment options for recurrent or metastatic disease include chemotherapy alone, chemotherapy combined with immunotherapy including dostarlimab or pembrolizumab, chemotherapy combined with trastuzumab for HER2-positive tumours, or hormonal therapy. Pembrolizumab monotherapy is specifically recommended for recurrent deficient mismatch repair tumours, and pembrolizumab plus lenvatinib for proficient mismatch repair tumours in later treatment lines.
What Is Bevacizumab and Why Did Canada’s Drug Agency Conduct This Review?
Bevacizumab is a humanized antiangiogenic monoclonal antibody that stops the growth of tumour cells by inhibiting VEGF. At the time this review was conducted, Health Canada has not approved bevacizumab for the treatment of endometrial cancer.
At the request of the participating public drug programs, Canada’s Drug Agency (CDA-AMC) reviewed bevacizumab to inform a recommendation on whether it should be reimbursed in combination with chemotherapy for second or later lines of therapy for patients with recurrent or metastatic endometrial cancer.
How Did CDA-AMC Evaluate Bevacizumab?
CDA-AMC reviewed the clinical evidence on the beneficial and harmful effects and compared costs of bevacizumab in combination with chemotherapy versus other treatments used in Canada for second or later lines of therapy for patients with recurrent or metastatic endometrial cancer. The comparators considered relevant to the review were platinum doublet chemotherapy (carboplatin plus paclitaxel, carboplatin plus docetaxel, cisplatin plus doxorubicin), pembrolizumab monotherapy, pembrolizumab and lenvatinib, dostarlimab with carboplatin and paclitaxel, and trastuzumab with carboplatin and paclitaxel.
The clinical evidence was identified through a systematic search for available studies.
The review was also informed by 1 clinician group submission in response to our call for input, and by input from the participating public drug programs around issues that may impact their ability to implement a recommendation. Two gynecologic oncologists with representation from the Atlantic region and the Prairies were consulted as part of the review process.
What Were the Findings?
Clinical Evidence
CDA-AMC reviewed the evidence from 1 phase II randomized controlled trial (MITO END-2 trial) comparing bevacizumab plus carboplatin and paclitaxel to carboplatin and paclitaxel in patients with advanced or recurrent endometrial cancer.
The evidence was insufficient to show a difference in OS or PFS for bevacizumab plus carboplatin and paclitaxel compared with carboplatin and paclitaxel alone. The results for PFS were limited by risk of bias due to the open-label design. The results for both OS and PFS were affected by imprecision (wide 95% confidence intervals crossing null) and indirectness (i.e., the study population does not directly align with the population of interest).
Between-group differences (95% confidence interval) for overall response rate and disease control rate were not reported nor statistically tested which challenged meaningful conclusions.
No evidence to inform how bevacizumab combined with platinum-based chemotherapy affects patients’ health-related quality of life.
The harms reported in MITO END-2 trial were consistent with the known safety profile of bevacizumab.
No comparative evidence was identified on the relative treatment effects of bevacizumab combined with platinum-based chemotherapy versus other comparator treatments.
Economic Evidence
Reimbursing bevacizumab for adults with recurrent or metastatic endometrial cancer after disease progression on at least 1 line of therapy is expected to generally reduce costs to the public drug programs compared to most regimens.
Abbreviations
AE
adverse event
AUC
area under the curve
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
dMMR
deficient mismatch repair
HRQoL
health-related quality of life
MMR
mismatch repair
MSI
microsatellite instability
ORR
overall response rate
OS
overall survival
PFS
progression-free survival
pMMR
proficient mismatch repair
SAE
serious adverse event
Background
Introduction
The objective of the Clinical Review is to review and critically appraise the evidence on the beneficial and harmful effects of bevacizumab in combination with chemotherapy in the second or later lines of therapy for patients with recurrent or metastatic endometrial cancer. The focus will be placed on comparing bevacizumab combined with platinum-based chemotherapy to relevant comparators in clinical practice in Canada and identifying gaps in the current evidence. The economic review consists of a cost comparison for bevacizumab combined with platinum-based chemotherapy compared with relevant comparators for the same population. The comparators considered relevant to the reviews were platinum doublet chemotherapy (carboplatin plus paclitaxel, carboplatin plus docetaxel, cisplatin plus doxorubicin), pembrolizumab monotherapy, pembrolizumab and lenvatinib, dostarlimab with carboplatin and paclitaxel, and trastuzumab with carboplatin and paclitaxel.
Table 1: Information on the Drug Under Review and on the CDA-AMC Review
Item | Description |
|---|---|
Information on the drug under review | |
Drug | Bevacizumab, 100 mg and 400 mg vials (25 mg/mL solution for injection) |
Relevant Health Canada indication | Not applicable |
Mechanism of action | Humanized antiangiogenic monoclonal antibody that stops the growth of tumour cells by inhibiting vascular endothelial growth factor, leading to inhibition of angiogenesis (i.e., growth of new blood vessels) and reduced blood supply to tumour cells |
Data protection status | No information found in the Register of Innovative Drugs |
Status of biosimilars | Several biosimilar products are currently available on the market in Canada. |
Information on the CDA-AMC review | |
Requester | Oncology Working Group |
Indication under consideration for reimbursement | Bevacizumab in combination with chemotherapy in the second or later lines of therapy for patients with recurrent or metastatic endometrial cancer. |
CDA-AMC = Canada’s Drug Agency.
Context for the Review
The Oncology Working Group indicated there is an interest in clinical practice to use bevacizumab in combination with chemotherapy in the second or later lines of therapy in the treatment of patients with recurrent or metastatic endometrial cancer. At the request of the participating public drug programs, Canada’s Drug Agency (CDA-AMC) reviewed bevacizumab to inform a recommendation on whether it should be reimbursed for this indication.
Submission History for the Drug Under Review
CDA-AMC previously reviewed bevacizumab through the reimbursement review process for several oncology therapeutic areas, including cervical cancer, ovarian cancer, colorectal cancer, lung cancer, hepatocellular carcinoma, and glioblastoma multiforme.
Sources of Information
The contents of the Clinical Review report are informed by studies identified through systematic literature searches and input received from interested parties (clinician group and drug programs), and input from clinical experts consulted for this review.
Calls for patient group, clinician group, and industry input are issued for each Non-Sponsored Reimbursement Review. We received 1 clinician group submission from Ontario Health (Cancer Care Ontario) Gynecology Cancer Drug Advisory Committee, which gathered the input through emails. There were no submissions from patient groups or industry. The full submission received is available on the project landing page in the consolidated input document.
Input from the clinician group is considered throughout the review, including in the selection of outcomes to include in the Clinical Review and in the interpretation of the clinical evidence. Relevant input is summarized in the Disease Background, Current Management, and Unmet Needs and Existing Challenges sections.
The drug programs provide input on each drug being reviewed through the reimbursement review process by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted for this review are summarized and provided to the expert committee in a separate document.
Each review team includes at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process. Two specialists with expertise in the diagnosis and management of endometrial cancer participated as part of the review team, with representation from the Atlantic region and the Prairies.
Disease Background
Endometrial cancer is the most common type of uterine cancer and originates in the lining of the uterus (i.e., endometrium).1 More than 95% of uterine cancers are endometrial cancer.2 The age-standardized incidence rate in 2020 was 34.8 per 100,000.3 Projected data for uterine cancer for 2025 in Canada was 8,600 new cases and 1,700 deaths.4 Endometrial cancer is more often diagnosed among females who are postmenopausal, with an average age of diagnosis of 65 years.1,5
Endometrial cancer is associated with numerous symptoms that substantially impair physical functioning and HRQoL. The most common symptom of endometrial cancer is abnormal or unusual vaginal bleeding, which may be periodic or continuous.6 Additional signs and symptoms include pain or feeling of pressure in the pelvis, lower abdomen, back or legs, urinary and bowel dysfunction, and unintentional weight loss.6 Symptoms such as menopausal-like effects, sexual dysfunction, anxiety, depression, and long-term side effects of chemotherapy result in a decline of quality of life.1,5
Diagnosis of endometrial cancer is based on clinical assessments to evaluate tumour location, size, and spread, supported by radiological imaging and histopathological analysis of biopsy samples to determine histological type, grade, and molecular profile. The prognosis of endometrial carcinoma is determined primarily by disease stage, grade, histology and molecular classification. To determine the stage of endometrial cancer, clinicians often rely on the International Federation of Gynecology and Obstetrics (FIGO) system, which is based on the tumour size, degree of spread to lymph nodes, and metastasis to distant organs.7 In Canada, the overall 5-year net survival for endometrial cancer is 82%.8 It is important to note that survival varies greatly with each type or subtype of tumour and the stage of endometrial cancer.8
Molecular testing during endometrial biopsy is an important basis for clinical treatment decisions and risk assessment. Mismatch repair (MMR) protein expression and microsatellite instability (MSI) are key biomarkers for evaluating DNA repair functionality.9,10 Endometrial cancer is categorized as MSI-high, MSI-low, or microsatellite stable based on MSI testing, and MMR, proficient mismatch repair (pMMR), or deficient mismatch repair (dMMR) based on MMR testing.9,10 Additional molecular tests are also recommended to assess for other molecular subtypes such as mutations in p53, POLE, and estrogen receptor and HER2 expression.9,10
Current Management
Treatment Goals
The clinical experts noted that the goal of therapy for patients with recurrent or metastatic endometrial cancer is to improve overall survival (OS), improve progression-free survival (PFS), and improve symptoms as a cure is rarely achievable.
Current Treatment Options
Although surgery, chemotherapy, hormonal treatment, and radiation have been the main treatment for decades, molecular profiling and precision-based approaches for tumours are rapidly becoming a part of treatment strategies. Therapeutic approaches for recurrent or metastatic endometrial cancer are individualized based on molecular profile and disease stage. Treatment is tailored according to molecular subtype (e.g., dMMR or pMMR, HER2 status) and the patient’s overall health. Quality of life and symptom control play major roles in decision-making in advanced or recurrent disease.
Surgery is the preferred first-line intervention for comprehensive staging and cytoreduction. The clinical experts consulted by CDA-AMC indicated that surgery offers the best outcomes unless the patient is not a surgical candidate due to endometrial cancer disease burden or other comorbidities. For stage III endometrial cancers, adjuvant treatment after surgery is tailored based on molecular profile, stage, and residual disease. Current treatment options could include chemotherapy and radiation, chemotherapy plus immunotherapy such as dostarlimab or pembrolizumab, or hormonal therapy. Platinum-based chemotherapy with carboplatin and paclitaxel are the backbone regimens. Other combination chemotherapies are carboplatin and docetaxel.
Treatment options for metastatic disease are also tailored based on molecular profile and location of disease. They include chemotherapy alone, chemotherapy combined with immunotherapy including dostarlimab or pembrolizumab, chemotherapy combined with trastuzumab, or hormonal therapy. In recurrent endometrial cancer, pembrolizumab monotherapy is specifically recommended for dMMR tumours, and pembrolizumab plus lenvatinib for pMMR tumours. For patients with HER2-positive tumours, trastuzumab combined with chemotherapy is preferred over other regimens.
Radiation therapy is used for adjuvant settings to provide local control or at time of recurrence especially if the cancer is confined to the pelvis, or for palliation. Hormonal therapy with progestins such as medroxyprogesterone or megestrol are used for patients with hormone-sensitive tumours.
Unmet Needs and Existing Challenges
Patients with advanced or recurrent endometrial cancer tend to have a poor prognosis and certain targeted therapies are limited by their tumours’ molecular profile. If a patient is not a candidate for available immunotherapy due to underlying health conditions (i.e., comorbidities) then their treatment options are very limited. Currently, there are no effective therapies available for patients who progress on first-line or second-line treatment. In patients whose disease does not respond to chemotherapy or recurs quickly after initial treatment, currently available treatment options (apart from immunotherapy for dMMR tumours) have poor response rates and additional treatment options are needed. There is a treatment gap in pMMR tumours and p53 mutated tumours that have progressed after chemotherapy.
Considerations for Using the Drug Under Review
Contents within this section have been informed by input from the clinical experts consulted for the purpose of this review and from clinician groups. The following has been summarized by the review team.
Place in Therapy
Bevacizumab would be an alternative drug available for endometrial cancer that specifically targets VEGF, a separate disease pathway different from currently available therapies. Bevacizumab would provide an alternative to lenvatinib which tends to be poorly tolerated and can only be given with pembrolizumab for patients with no contraindications to immunotherapy. The clinical experts mentioned that bevacizumab could be used in combination with chemotherapy and then as maintenance therapy. Bevacizumab may be useful in situations with ascites or pleural effusion.
Patient Populations
Patients who would likely benefit most would be those with p53 mutated advanced disease with pMMR status. Poorly differentiated tumours without HER2 positivity have the greatest need for intervention with drugs similar to bevacizumab, as the disease responds poorly to standard therapies and has short progression-free intervals. These patients are generally identified based on surgical pathology or biopsy reports when surgery is not an option. However, there are currently no reliable objective biomarkers or companion diagnostic tests to predict which tumour types benefit most specifically from bevacizumab treatment.
Assessing the Response to Treatment
Clinical experts noted that a clinically meaningful response to bevacizumab in advanced or recurrent endometrial cancer includes having disease stability, which is less than 20% tumour growth with no new lesions, or tumour shrinkage with improved PFS of at least 3 months. Symptom improvement, such as reduced ascites or less pain, may accompany response but varies by disease site. Routine clinical assessments during treatment include performance status evaluation, and imaging studies as per clinician discretion. Treatment continuation typically depends on evidence of disease stability or clinical improvement, as judged by follow-up imaging and symptom control.
Discontinuing Treatment
Treatment discontinuation should be considered if disease progression or intolerable side effects occur. Disease progression is defined as an increase of 20% or greater in target lesions or new sites of disease. Substantial side effects could include fistula development, uncontrolled hypertension or proteinuria, venous thromboembolism, arterial thrombosis, hemorrhage, or bowel perforation.
Prescribing Considerations
Patients should be assessed by either a gynecologic oncologist or medical oncologist trained to treat gynecologic cancers to ensure best treatment selection as endometrial cancer treatment is very specific to molecular profiling. Treatment can be safely delivered in outpatient clinics, including in rural and remote sites as the risk of infusion reaction is very low and treatment is quick and easy to deliver. Patients should be monitored for hypertension, proteinuria, poor wound healing, fistula development, venous and arterial thromboembolism, bleeding, and impaired renal function. Patients with known renal dysfunction or hypertension should be closely monitored. Those at risk of bowel perforation or fistula should be informed of the signs and symptoms that would signal that it is necessary to seek urgent assessment.
Clinical Review
Methods
The review team conducted a systematic review to identify evidence for bevacizumab in combination with chemotherapy in second or later lines of therapy for patients with recurrent or metastatic endometrial cancer. Studies were selected according to the eligibility criteria in Table 2. Long-term extension studies of included randomized controlled trials, indirect treatment comparisons that adhered to the eligibility criteria (except for the study design criteria), and studies addressing gaps that did not meet the eligibility criteria but were considered to address important gaps in the systematic review evidence were included.
Relevant comparators included treatments used in clinical practice in Canada in the patient population under review. Clinical expert input and clinician group input were considered when selecting outcomes (and follow-up times) for review. Selected outcomes are those considered relevant to expert committee deliberations. Detailed methods for the literature searches, study selection, data extraction, and risk of bias appraisal are included in the Supplemental Material (available on the project landing page) in Appendix 1.
Table 2: Systematic Review Eligibility Criteria
Criteria | Description |
|---|---|
Population | Adult patients with recurrent or metastatic endometrial cancer after disease progression on at least 1 line of therapy |
Intervention | Bevacizumab combined with platinum doublet chemotherapya |
Comparator |
|
Outcomes | Efficacy outcomes:
Safety:
|
Study design | Phase II, III and IV RCTs |
AE = adverse event; HRQoL = health-related quality of life; SAE = serious adverse event
aMost commonly used platinum doublet chemotherapies are carboplatin and paclitaxel, carboplatin and docetaxel, cisplatin, and doxorubicin.
Clinical Evidence
Following a systematic search of primary studies, the review team identified 501 unique records via the searches of databases and registers, of which 493 were excluded by title and abstract. The review team screened 8 records by full text and included 1 report of 1 study (the MITO END-2 trial).11 There were no reports of long-term extensions of the included study.
From the search for indirect treatment comparisons, the review team identified 133 unique records via the searches of databases and registers, of which none met the eligibility criteria during title and abstract screening. No potentially relevant records were identified via other sources.
A list of excluded studies, including reasons for exclusion, is included in Appendix 1 in the Supplemental Material.
Systematic Review
Description of Study
Study Characteristics
Characteristics of the included study are summarized in Table 3. Additional details pertaining to the eligibility criteria are in Lorusso et al. (2019).11
The MITO-END2 trial enrolled patients in 16 sites in Italy between April 2012 and June 2014. Patients were randomized to a 1:1 ratio to observe approximately 89 PFS events including recurrence, progression, or death. Stratification criteria were cancer type (endometrioid versus nonendometrioid endometrial cancer), advanced stage III and IV versus recurrent disease, and the number of previous chemotherapy lines (0 versus 1).
Doses administered were as follows in the bevacizumab plus carboplatin and paclitaxel group: carboplatin area under the curve (AUC) 5 and paclitaxel 175 mg/m2 plus bevacizumab 15 mg/kg every 21 days for 6 to 8 cycles; and bevacizumab 15 mg/kg maintenance every 3 weeks until disease progression, unacceptable toxicity, or patient’s refusal. The 3 initial bevacizumab doses were administered first over 90 minutes, then over 60 minutes, and then over 30 minutes afterwards. The over 30 minutes administration was maintained if well tolerated. In the carboplatin and paclitaxel group, the combination of carboplatin AUC 5 and paclitaxel 175 mg/m2 was used.
Table 3: Characteristics of Study Included in the Systematic Review
Study name, design, and sample size | Key inclusion criteria | Key exclusion criteria | Intervention and comparator | Relevant end points |
|---|---|---|---|---|
Lorusso et al. (2019) MITO END-2 trial Phase II multicentre (Italy), open-label RCT N = 108 |
|
| Intervention: Bevacizumab plus carboplatin and paclitaxel until disease progression, unacceptable toxicity or patient’s refusal. Comparator: Carboplatin and paclitaxel until disease progression, unacceptable toxicity or patient’s refusal. | Primary end point:
Secondary end points:
Other end points:
|
ALP = alkaline phosphatase; ALT = alanine aminotransferase; ANC = absolute neutrophil count; AST = aspartate aminotransferase; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-EN24 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire – Endometrial Cancer Module; RCT – randomized controlled trial; ULN = upper limit of normal.
aAdequate renal and hepatic function defined as: total serum bilirubin ≤ institutional ULN unless patient has Gilbert syndrome in which case direct bilirubin must be < ULN for the institution, AST and/or ALT ≤ 2.5 x ULN for the institution or ≤ 5 x ULN if liver metastases are present, ALP < 1.5 x ULN for the institution (if > 1.5 x ULN, then ALP liver fraction must be < 1.5 ULN) and serum creatinine ≤ 1.5 x ULN for the institution (or calculated creatinine clearance ≥ 50 mL/min/1.73 m2).
bAdequate bone marrow function, defined as: total leukocytes 3.0 × 109/L, ANC 1.5 × 109/L, and platelet count 100 × 109/L.
Source: Lorusso et al. (2019).11
Statistical Testing and Analysis Populations
In the MITO END-2 trial, a total of 89 PFS events were required to achieve 80% power to detect a 0.70 proportional hazard ratio with a 1-sided log-rank test at a 20% significance level, with an expectation of enrolling 108 patients and assuming the loss to follow-up to be less than 10%. Sample size assumptions were based on a median PFS of 12 months in advanced or recurrent endometrial cancer, as reported in Miller et al. (2012).12
There was no mention of control for multiple comparisons in the trial publication.
Efficacy analysis included all patients who were enrolled and the intention-to-treat population, regardless of whether they received treatment. Forty-nine patients in the standard treatment arm and 47 in the experimental arm represented the population with measurable or nonmeasurable disease, evaluable for response analysis. The safety population included all patients who received at least 1 chemotherapy cycle.
Log-rank tests were used to test for substantial treatment differences between the groups. Hazard ratios (HRs) and 95% confidence intervals (CIs) were estimated but the method was not reported. Interim unplanned futility analysis and final analysis using the Breslow or Generalized Wilcoxon test was performed post hoc to further explore the differences in PFS between treatments. The trial investigators used the Breslow test based on a claim of different velocity of the occurrence of progression events between the unplanned futility analysis and final analysis, and crossing of the survival curves.
Patient Disposition
In the MITO END-2 trial, 110 patients were screened for eligibility. There were 2 patients who did not meet eligibility criteria, thus 108 patients were randomized to receive either bevacizumab plus carboplatin and paclitaxel (n = 54) or carboplatin and paclitaxel (n = 54). Two patients refused treatment, 1 in each arm. A total of 106 patients, 53 patients in the bevacizumab plus carboplatin and paclitaxel arm and 53 patients in the carboplatin and paclitaxel arm received treatment.
No information was provided about overall treatment discontinuations nor discontinuations from the study. Similarly, there was no information on protocol deviations.
Baseline Characteristics
Patients’ baseline characteristics from the study population in the MITO END-2 trial are presented in Table 4.
Treatment Exposure and Concomitant Medications
Treatment exposures are presented in Table 5. The median number of treatment cycles of carboplatin and paclitaxel in the bevacizumab plus carboplatin and paclitaxel group was 6 (range, 1 to 8). Fourteen patients (26%) in the bevacizumab plus carboplatin and paclitaxel group required chemotherapy dose reductions.
No information on concomitant medications was reported in the trial. Additionally, no information was provided on subsequent treatments.
Table 4: Summary of Baseline Characteristics From Studies Included in the Systematic Review
Characteristic | Bevacizumab plus carboplatin and paclitaxel (N = 54) | Carboplatin and paclitaxel (N = 54) |
|---|---|---|
Age, median (range), years | 63 (28 to 81) | 65 (32 to 80) |
ECOG PS score, n (%) | ||
0 | 46 (85) | 44 (81) |
1 or 2 | 8 (15) | 10 (19) |
Disease status, n (%) | ||
Advanced | 19 (35) | 19 (35) |
Recurrent | 34 (63) | 33 (61) |
Histology, n (%) | ||
Endometrioid | 37 (72) | 38 (70) |
Serous or clear cell | 11 (20) | 7 (13) |
Grading, n (%) | ||
Grade 1 or 2 | 23 (43) | 19 (35) |
Grade 3 | 25 (46) | 28 (52) |
Previous treatment, n (%) | ||
Chemotherapy | 11 (20) | 15 (28) |
Radiotherapy | 23 (42) | 26 (48) |
Comorbidities, n (%) | ||
Hypertension | 23 (43) | 29 (54) |
Renal | 1 (2) | 2 (4) |
Diabetes | 5 (9) | 4 (7) |
ECOG PS = Eastern Cooperative Oncology Group Performance Status.
Source: Lorusso et al. (2019).11
Characteristic | Bevacizumab plus carboplatin and paclitaxel (N = 53) | Carboplatin and paclitaxel (N = 53) |
|---|---|---|
Number of cycles of carboplatin and paclitaxel per patient, median (range) | 6 (1 to 8) | 6 (1 to 8) |
Patients with > 6 carboplatin and paclitaxel cycles, n (%) | 13 (25) | 15 (28) |
Number of cycles of bevacizumab per patient, median (range) | 12 (1 to 38) | 0 |
Delays for toxicity, n (%) | 17 (39) | 17 (31) |
Chemotherapy dose reductions, n (%) | 14 (26) | 14 (26) |
Discontinuations for toxicity, n (%) | 10 (18) | 2 (4) |
During chemotherapy phase | 6 | 2 |
During maintenance phase | 4 | NA |
NA = not applicable.
Source: Lorusso et al. (2019).11
Critical Appraisal
Internal Validity
The MITO END-2 trial was described as randomized, with limited additional details provided. The implementation of stratification suggests that a computerized randomization schedule was used, which is appropriate. Details regarding allocation concealment were not reported, leaving uncertainty about whether the randomization sequence remained blinded until participants were assigned to treatment groups. If the allocation sequence was not concealed, risk of bias would be introduced in the randomization process. Due to the relatively small sample size, prognostic balance may not have been reached (i.e., between-group differences may arise due to chance), and some differences between treatment groups for baseline characteristics were observed. There were slight imbalances between groups in disease grade 1 or 2 (higher in the bevacizumab plus carboplatin and paclitaxel group) versus 3, previous chemotherapy and radiotherapy treatment (lower in the bevacizumab plus carboplatin and paclitaxel group), and coexisting hypertension (higher in the bevacizumab plus carboplatin and paclitaxel group). However, the clinical experts consulted by CDA-AMC did not expect the observed imbalances to substantially affect the results of the trial or systematically favour 1 treatment group over the other. The evaluation of response occurred in patients with measurable disease, and there is increased risk that randomization was not fully upheld in this population because the existence of measurable disease was not a stratification factor.
The trial was open label by design, therefore the patients, caregivers, and study investigators were aware of the assigned treatments. When trials are not blinded, there is concern for bias being introduced due to deviations from the intended interventions. Similar exposure to the study treatments across groups provides some reassurance that this source of potential bias may be limited. Toxicity-related discontinuations were higher in the bevacizumab plus carboplatin and paclitaxel group (18%) compared to the carboplatin and paclitaxel group (4%), which may be aligned with clinical expectations, given the increased occurrence of severe adverse events (SAEs) within the bevacizumab plus carboplatin and paclitaxel group. The use of concomitant medications was not described in the publication, therefore it is unknown whether there may be differences across groups that could impact the results.
The efficacy outcomes collected in the study (OS, PFS, objective response rate [ORR]) are standard in oncology trials. Responses were evaluated according to the Response Evaluation Criteria in Solid Tumours Version 1.1 criteria in patients with measurable disease. Use of the Response Evaluation Criteria in Solid Tumours Version 1.1 criteria and a set assessment schedule may assist in the consistency of tumour assessments. However, patients who reported clinical deterioration were also considered as progressing even in the absence of radiologic confirmation. Additionally, the measurement of PFS and ORR was based on unblinded investigator assessments rather than a blinded independent central review. Because assessment of response involves subjective interpretations of scans, reliance on investigator evaluations and patient self-report of deterioration introduces risk of bias in measurement of the outcome for ORR and PFS.13 This risk of bias would likely favour the bevacizumab plus carboplatin and paclitaxel group. Similarly, there is a risk of bias in the reporting of subjective harms, although the possible direction is difficult to determine. The evaluation of OS is objective and not affected by this potential source of bias.
As might be expected for a phase II trial, which are typically designed to evaluate preliminary efficacy and characterize safety, the trial employed lenient significance thresholds (P < 0.20) and there was no control for multiple comparisons (i.e., risk of type I error is increased). Nevertheless, statistical testing of the primary end point (PFS) did not reach statistical significance. The power assumptions reported in the methods of the publication were not fully aligned with the analysis approach; the use of a 2-sided log-rank test rather than the planned 1-sided test, would have resulted in reduced power under the same assumptions. While the proportional hazards assumption was not tested, the Kaplan-Meier curves show that it was violated. There was some separation in favour of bevacizumab plus carboplatin and paclitaxel shortly after randomization, which remained until the curves crossed at about 130 weeks (30 months). The authors made a post hoc decision to retest PFS using the Breslow test which places increased weight on earlier events when a greater proportion of patients remain at risk. While the authors report statistical significance (i.e., P < 0.20), this analysis has limitations and may be considered hypothesis generating. Implementation of post hoc statistical tests after reviewing the data introduces high risk of bias, there is an increased risk of type I error, and the P value remains nonsignificant at a conventional significance level (i.e., P < 0.05). Crossing of the PFS curves late in follow-up should not be overinterpreted, as it may reflect statistical uncertainty. Few patients remain at risk at this time point which would render the effect estimates highly unstable.
The trial was not specifically powered to detect an OS difference and fewer than one-half of OS events had accrued at the time of the analysis. The hazards for OS are also nonproportional and longer follow-up would be needed to further characterize the potential for long-term benefit, as the Kaplan-Meier curves do not separate until relatively late (around 100 weeks [23 months]). Estimates of median OS also occur late in the survival curve when there has been an important degree of censoring and the number of patients remaining at risk is low (particularly in the bevacizumab plus carboplatin and paclitaxel group). This indicates that the estimates of the median are unreliable and could differ to an important degree from the true medians. As is common in oncology trials, effects on OS reflect the effect of the investigational treatment as well as subsequent treatments. Given that the subsequent treatments used by patients in the trial were not reported, it is not possible to judge whether these reflect current clinical practice in Canada nor what the impact of these might be on the results. While PFS is a surrogate end point which may be used to predict future OS, it has not been validated as a surrogate outcome for OS or health-related quality of life (HRQoL). Therefore, any benefit in PFS may not translate to clinically meaningful patient benefits in terms of length and quality of survival.14,15 Given that the PFS analysis did not reach statistical significance, its value in predicting a future OS improvement is limited.
The reporting of patient disposition was limited and there was no description of missing data handling nor the possible proportions of missing data. Censoring reasons were also not reported which challenged any meaningful assessment of the potential for informative censoring in the time to event analyses. The limited reporting in the publication does not allow for a comprehensive appraisal of the potential for risk of bias due to missing outcome data. There was also incomplete reporting of the results which challenges clinical interpretation. Between-group differences in PFS and OS probabilities with 95% CIs at clinically relevant time points were not reported. Statistical evaluation of response rates was also not reported, nor were descriptive comparisons across groups with measures of precision. Although HRQoL and symptom outcomes were planned to be assessed using the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 and European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire – Endometrial Cancer Module, the trial investigators reported they were unable to analyze patient-reported outcomes data due to low response rates. The missing data limits understanding of how treatment with bevacizumab plus carboplatin and paclitaxel affects patient’s quality of life in the population with endometrial cancer. Although the trial was registered, a clear documentation of the statistical analysis plan was not identified by the CDA-AMC review team.
External Validity
The MITO END-2 trial was conducted in 16 sites in Italy. Racial characteristics were not reported. While the study was conducted in Italy, the clinical experts indicated that the findings from the study were applicable to the population in Canada. The clinical experts consulted during the review indicated that the study inclusion criteria, which specified patients had to have confirmed advanced stage III or IV, or recurrent endometrial cancer, is consistent with what would be expected in clinical practice. The clinical experts noted that carcinosarcomas, which are an aggressive form of endometrial cancer, have a similar clinical behaviour as serous carcinoma. Unlike the trial which excluded patients with carcinosarcomas, physicians typically manage carcinosarcoma cases as endometrial cancer and do not restrict treatment based on this histological type. More than 80% of patients had an Eastern Cooperative Oncology Group Performance Status score of 0 which appeared high to the clinical experts for patients who have advanced stage or recurrent disease.
To be included in the trial, patients were not required to have progressed on a previous line of treatment. About 20% to 28% of patients had previous chemotherapy and about twice as many (42% to 48%) had previous external radiation therapy. While it may be reflective of the standard of care for endometrial cancer in Italy where the trial was conducted, the trial data suggests that the population may include patients having no previous chemotherapy and/or radiation. However, the publication did not specify the full extent of pretreatment, number of prior lines of therapy, and other possible treatments for endometrial cancer (e.g., surgery, hormonal therapy) that may have been used in the selected patient population. It is not clear whether some patients were able to undergo surgery at any point during induction or maintenance treatment as that could influence stability of the tumour and delay progression. Therefore, the trial results which are based on a substantial proportion of patients without prior carboplatin plus paclitaxel chemotherapy, may not be entirely applicable to the population outlined in the reimbursement request (i.e., second line or later) nor to a population that is heavily pretreated as is common in the recurrent or metastatic setting.
According to the clinical experts, patients would be administered bevacizumab plus carboplatin and paclitaxel in line with the MITO END-2 trial (i.e., carboplatin AUC 5 plus paclitaxel 175 mg/m2 and bevacizumab 15 mg/kg every 21 days for 6 to 8 cycles plus bevacizumab 15 mg/kg maintenance every 3 weeks until disease progression or unacceptable toxicity or patient’s refusal).
Although platinum-based chemotherapies, particularly the carboplatin and paclitaxel combination therapy, are widely used in Canada as standard of care in advanced endometrial cancer, the clinical experts noted additional therapies used in practice including monotherapies such as pembrolizumab, combination therapies (i.e., pembrolizumab and lenvatinib, dostarlimab with carboplatin and paclitaxel, trastuzumab with carboplatin and paclitaxel) and hormonal therapies. No studies were identified that compared bevacizumab in combination with platinum-based chemotherapy versus these relevant comparators in the advanced or metastatic setting.
Results
Efficacy
Results for outcomes important to this review are presented in Table 6. The median follow-up at the time of the final analysis was 60 months (range not reported).
Table 6: Summary of Key Efficacy Results
Outcome | Bevacizumab plus carboplatin and paclitaxel (N = 54) | Carboplatin and paclitaxel (N = 54) |
|---|---|---|
OS | ||
Events, n (%) | 22 (40.7) | 25 (46.3) |
Censored, n (%) | NR | NR |
Median OS, months (95% CI) | 40 (35.7 to 44.2) | 29.7 (21.7 to 37.7) |
HR (95% CI)a | 0.71 (0.31 to 1.36) | |
P valueb | 0.239 | |
PFS | ||
Events, n (%) | 46 (85.2) | 40 (74.1) |
Censored, n (%) | NR | NR |
Median, months (95% CI) | 13.7 (7.5 to 20.0) | 10.5 (7.2 to 13.5) |
HR (95% CI)a | 0.846 (0.5 to 1.3) | |
P valueb | 0.437 | |
Response | ||
Number of evaluable patients for response analysis | 47 | 49 |
Overall response rate, n (%)c | 35 (74.4) | 26 (53.1) |
Complete response, n (%) | 21 (44.7) | 9 (18.4) |
Partial response, n (%) | 14 (29.8) | 17 (34.7) |
Stabilized disease, n (%) | 10 (21.2) | 20 (40.1) |
Progressive disease, n (%) | 2 (4.2) | 3 (6.1) |
6-months disease control rate, n (%)d | 49/54 (90.7) | 38/54 (70.4) |
12-months disease control rate, n (%)d | 29/54 (53.7) | 24/54 (44.4) |
CI = confidence interval; HR = hazard ratio; NR = not reported; OS = overall survival; PFS = progression-free survival.
aStatistical model not described in the publication.
bTwo-sided log-rank test
cThe overall response rate includes complete and partial responses.
dThe disease control rate includes complete and partial responses as well as stabilized disease.
Source: Lorusso et al. (2019).11
Pagebreak
Key results include the following:
The evidence was insufficient to demonstrate a difference in OS or PFS between the bevacizumab plus carboplatin and paclitaxel and carboplatin and paclitaxel groups.
ORR was 74.4% in the bevacizumab plus carboplatin and paclitaxel treatment group and 53.1% in the carboplatin and paclitaxel group. No between-group difference (95% CI) nor statistical testing was reported.
Although HRQoL outcomes measures, the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 and the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire – Endometrial Cancer Module, were prespecified, they were not analyzed or reported in the publication because of a low patient response to the questionnaires.
Figure 1: Kaplan-Meier Plot of OS
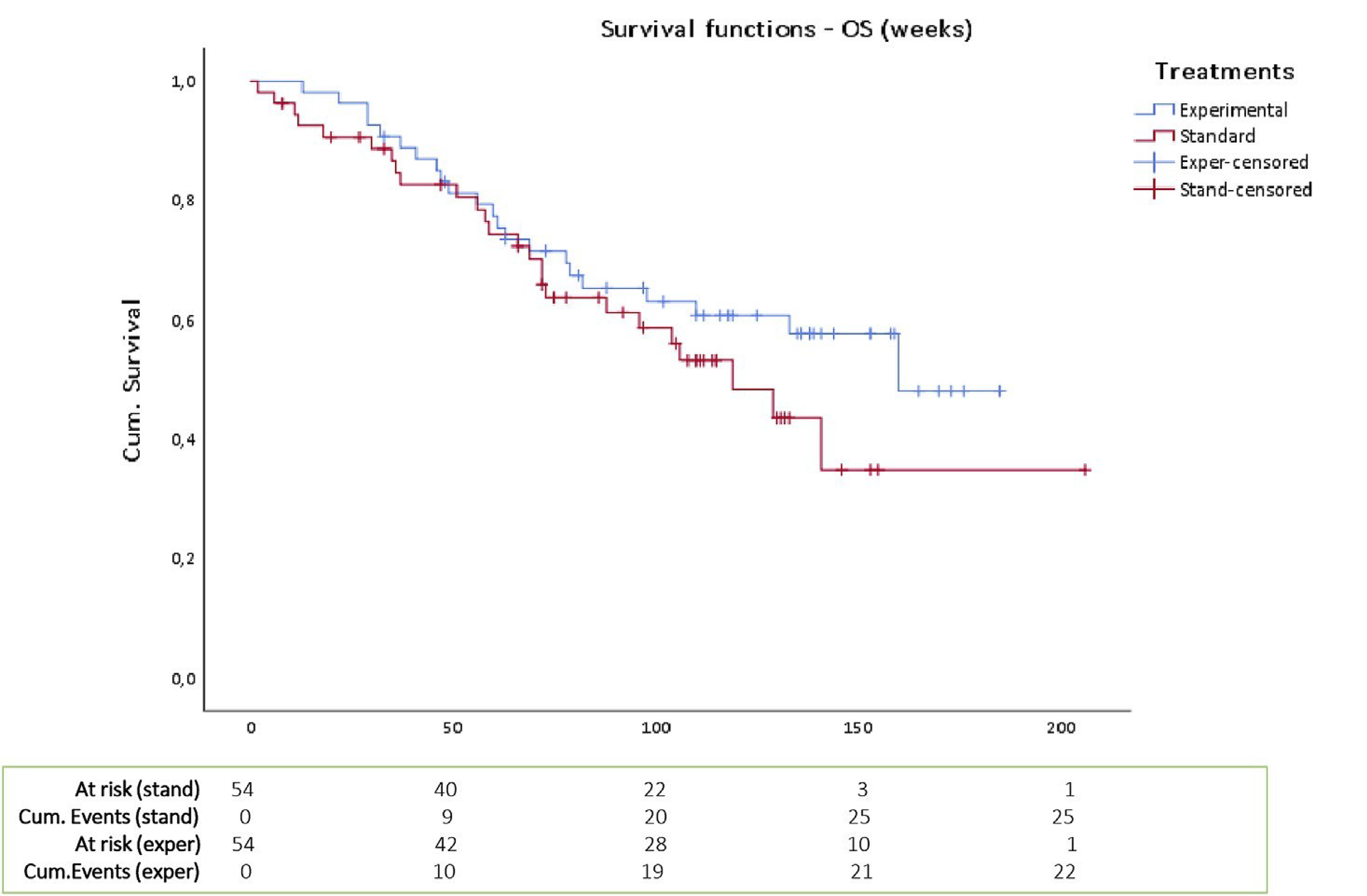
OS = overall survival.
Source: Lorusso et al. (2019).11 Reprinted from Gynecologic Oncology (155), Lorusso et al. Carboplatin-paclitaxel compared to Carboplatin-Paclitaxel-Bevacizumab in advanced or recurrent endometrial cancer: MITO END-2 - a randomized phase II trial, Pages No. 409 to 410, Copyright 2025, with permission from Elsevier.
Figure 2: Kaplan-Meier Plot of PFS
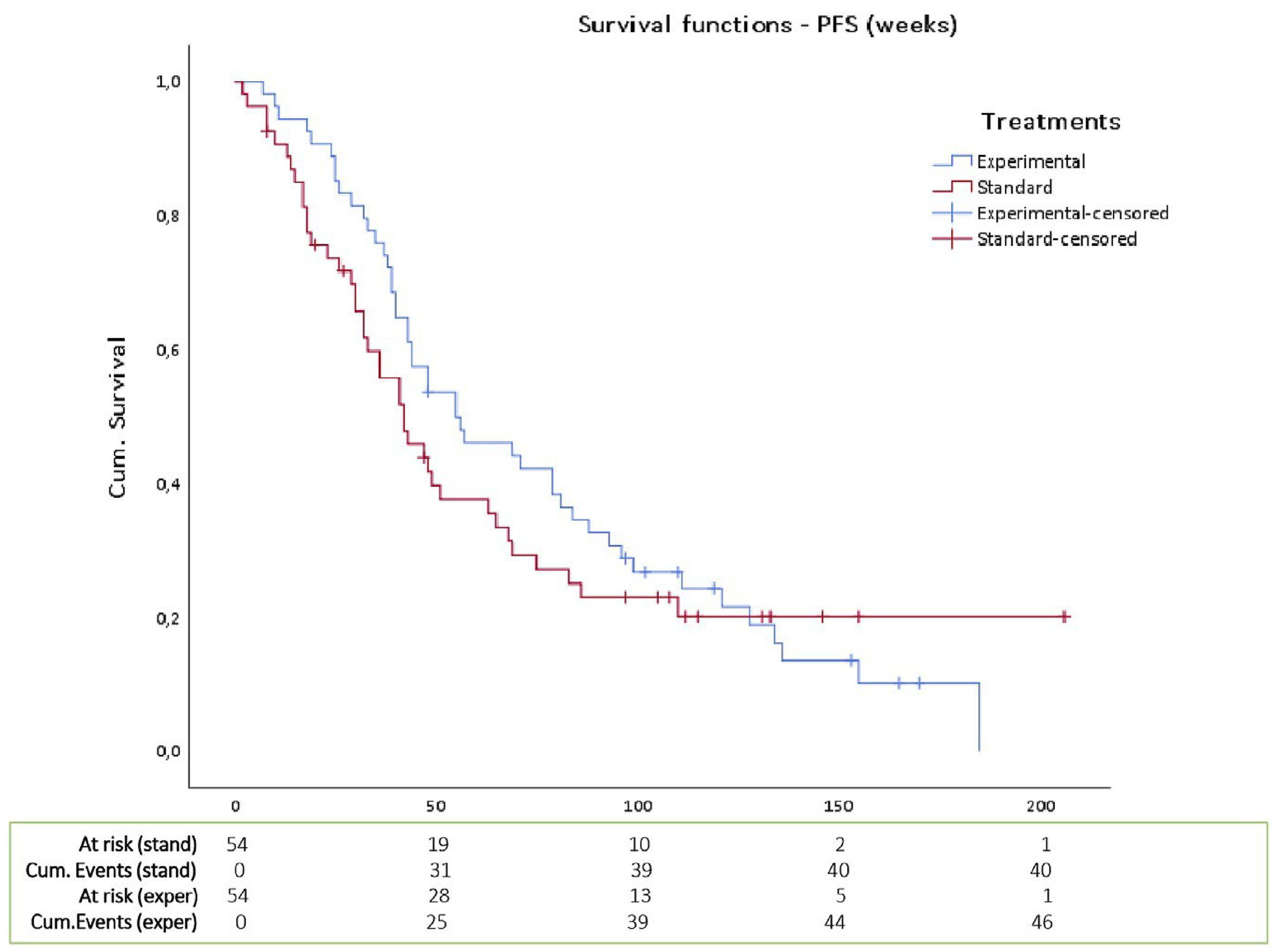
PFS = progression-free survival.
Source: Lorusso et al. (2019).11 Reprinted from Gynecologic Oncology (155), Lorusso et al., Carboplatin-paclitaxel compared to Carboplatin-Paclitaxel-Bevacizumab in advanced or recurrent endometrial cancer: MITO END-2 - a randomized phase II trial, Pages No. 409 to 410, Copyright 2025, with permission from Elsevier.
The total number of patients with grade 3 or higher AEs was not reported. For bevacizumab plus carboplatin and paclitaxel versus carboplatin and paclitaxel:
The most common grade 3 or higher hematological AEs were neutropenia (56.6% versus 46.3%), leukopenia (28.3% versus 27.8%), and anemia (11.3% versus 11.1%).
The proportion of patients with grade 3 or higher arterial (11.1% versus 1.9%) or venous thromboembolic events (7.4% versus 0%) was higher in the bevacizumab plus carboplatin and paclitaxel arm compared with the carboplatin and paclitaxel arm.
The proportion of patients with grade 3 or higher gastrointestinal fistulas was 5.5% versus 0%.
The proportion of patients with grade 2 or higher myocardial ischemia was 3.7% versus 1.9%, and arrhythmia was 1.9% versus 0%.
New onset grade 2 or higher hypertension was experienced by 20.7% of patients treated with bevacizumab plus carboplatin and paclitaxel compared to no patients in the carboplatin and paclitaxel arm. No worsening of baseline or pre-existing hypertension was reported.
A higher proportion of patients treated with bevacizumab plus carboplatin and paclitaxel (18%) compared with carboplatin and paclitaxel (4%) experienced discontinuations due to AEs.
No deaths coded as AEs were reported in the trial.
Outcome | Bevacizumab plus carboplatin and paclitaxel (N = 53) | Carboplatin and paclitaxel (N = 53) |
|---|---|---|
Patients with ≥ 1 SAEs | ||
SAEs, n (%) | 16 (30.2) | 7 (13.2) |
Patients with ≥ 1 grade ≥ 3 AEs, n (%) | ||
Anemia | 6 (11.3) | 6 (11.1) |
Leukopenia | 15 (28.3) | 15 (27.8) |
Neutropenia | 30 (56.6) | 25 (46.3) |
Febrile neutropenia | 3 (5.6) | 0 |
Thrombocytopenia | 3 (5.6) | 0 |
Asthenia | 5 (9.4) | 1 (1.9) |
Nausea | 1 (1.9) | 0 |
Renal toxicity | 1 (1.8) | 0 |
Thromboembolic events | 6 (11.1) | 1 (1.9) |
Arterial | 2 (3.7) | 1 (1.9) |
Venous | 4 (7.4) | 0 |
Fistulas | 2 (3.7) | 0 |
Grade ≥ 2 AEs, n (%) | ||
Grade ≥ 2 hypertension | 11 (20.7) | 0 |
Grade ≥ 2 cardiac toxicity | ||
Myocardial ischemia | 2 (3.7)a | 1 (1.9) |
Arrhythmia | 1 (1.9) | 0 |
Grade 2 dyspnea | 1 (1.9) | 2 (3.7) |
Grade 2 neurologic confusional state | 3 (5.5) | 0 |
Grade 2 hemorrhage | 0 | 1 (1.9) |
Discontinuation due to AEs, n (%) | ||
Discontinuation due to AEs | 10 (18) | 2 (4) |
AE = adverse event; SAE = serious adverse event.
aOne patient in the bevacizumab plus carboplatin and paclitaxel treatment arm had a clinically significant reduction in left ventricular ejection fraction.
Source: Lorusso et al. (2019).11
Discussion
Efficacy
The input from the clinician group and clinical experts consulted by CDA-AMC indicated that there are limited effective therapies for patients with endometrial cancer who progress on first-line or second-line treatments.
A single phase II open-label trial (MITO END-2) of bevacizumab plus carboplatin and paclitaxel versus carboplatin and paclitaxel alone conducted among patients (n = 108) with advanced stage III or IV or recurrent endometrial cancer in Italy provided evidence for this review. Phase II clinical trials are typically designed to evaluate preliminary efficacy and characterize safety. Several features of the trial design and conduct are consistent with this exploratory nature, including limited protocol information and statistical analysis plan, small sample size, lack of blinding, lenient significance thresholds, and no adjustment for multiple comparisons. In light of these limitations, the trial was not designed to confirm efficacy.
Evidence from the MITO END-2 trial was insufficient to demonstrate a difference in PFS when patients received bevacizumab plus carboplatin and paclitaxel compared to carboplatin and paclitaxel alone. Interpretation of the effect estimates was limited by a risk of bias due to the open-label design, violation of the proportional hazards assumption, and substantial imprecision (wide CIs crossing the null). The probability of PFS at clinically relevant time points was not reported. Review of the point estimates alone suggests an approximately 3-month increase in the median PFS with the addition of bevacizumab plus carboplatin and paclitaxel, which the clinical experts consulted by the review team believed was clinically meaningful. However, these results need to be interpreted in the context of the failed hypothesis test and other sources of uncertainty (including risk of bias). A between-group difference in the medians (with 95% CI) was not reported, restricting any appraisal of imprecision. The within-group medians were associated with wide 95% CIs which almost completely overlapped across the treatment groups, indicating high uncertainty about the potential difference between groups.
The evidence was insufficient to demonstrate a difference in OS with bevacizumab plus carboplatin and paclitaxel compared to carboplatin and paclitaxel alone. The trial was not specifically powered to detect an OS difference and fewer than one-half of the total OS events had accrued at the time of the analysis. Longer follow-up would be needed to further characterize the potential for long-term benefit, as the Kaplan-Meier curves did not separate until relatively late (around 100 weeks [23 months]). The clinical experts consulted by the review team believed that the difference in reported point estimates of median OS for bevacizumab plus carboplatin and paclitaxel versus carboplatin and paclitaxel was suggestive of clinical benefit. However, these results similarly need to be interpreted in light of the failed hypothesis test and other important limitations. The median in each group occurs in the tail of the Kaplan-Meier curve when there is increased censoring and the number of patients at risk is low (particularly in the bevacizumab plus carboplatin and paclitaxel group). This means that the reported medians are not reliable and that the true medians could differ to an important degree from what is reported in the trial publication.
The study also reported on ORR, another surrogate end point. The development of conclusion about this outcome was limited by a lack of statistical comparison or reporting of between-group differences and CIs. Though there were plans to investigate the impact of bevacizumab plus carboplatin and paclitaxel on HRQoL in the MITO END-2 trial, the results were not reported. The study authors indicated that this was due to few patients completing the questionnaires. Therefore, the effect of bevacizumab combined with platinum-based chemotherapy on patient-reported outcomes in the study is unknown. Similarly, there was no evidence to inform on the potential benefit of bevacizumab plus carboplatin and paclitaxel versus other relevant comparators used in clinical practice in Canada.
Patients with 1 previous line of platinum-based chemotherapy were eligible for the MITO END-2 trial but this was not a requirement for inclusion, and patients with more than 1 previous line were excluded. Some characteristics of the included patients were reflective of the expected patient population who may be treated with bevacizumab plus carboplatin and paclitaxel in Canada (i.e., those with advanced stage III or IV disease). However, there was some misalignment between the study population and the reimbursement request which may reduce the applicability of the results. For example, the study included patients with advanced endometrial cancer in first-line treatment which is not part of the reimbursement request. Also, the degree and types of previous treatments was unclear in the trial population.
The study authors suggested that further investigation is needed to better understand the potential efficacy of bevacizumab plus carboplatin and paclitaxel in patients with endometrial cancer. In particular, enrolment of a larger sample size and a more homogeneous group of patients with advanced endometrial cancer (e.g., based on molecular characteristics) may be able to inform on the population who may be most likely to experience benefit from bevacizumab plus carboplatin and paclitaxel.
Harms
Results from the MITO END-2 trial indicate that the proportion of patients in the bevacizumab plus carboplatin and paclitaxel arm who experienced SAEs was higher than the carboplatin and paclitaxel arm (30% versus 13%), as was the proportion who discontinued treatment due to AEs (18% versus 4%).
The addition of bevacizumab to carboplatin and paclitaxel was associated with a higher incidence of certain cardiovascular AEs of special interest, such as grade 3 or higher arterial or venous thromboembolism, grade 2 or higher myocardial ischemia, and new onset grade 2 or higher hypertension. There was also a higher incidence of fistulas in the bevacizumab plus carboplatin and paclitaxel group compared to the carboplatin and paclitaxel group. The clinical experts highlighted that these AEs are known risks of bevacizumab. They explained that the longer duration of exposure to bevacizumab induction and maintenance therapy could partially explain the higher rates of some AEs and discontinuation due to AEs in the bevacizumab arm. According to the experts, the occurrence of substantial AEs are typical reasons to stop or discontinue treatment.
The rates of hematological toxicities including neutropenia, leukopenia, anemia were similar between treatment groups, with neutropenia being slightly higher in the bevacizumab plus carboplatin and paclitaxel arm. The clinical experts noted that the hematological AEs can likely be attributed to the carboplatin and paclitaxel chemotherapy backbone used in both arms.
The clinical experts expressed that the AEs were as expected and aligned with the known safety profile of bevacizumab. There were no reports of deaths coded as AEs.
Conclusion
Treatment options for recurrent or metastatic endometrial cancer after disease progression on at least 1 line of therapy are currently limited. One phase II randomized controlled trial (MITO END-2) provided evidence for the efficacy and safety of bevacizumab plus carboplatin and paclitaxel compared with carboplatin and paclitaxel alone in the treatment of advanced or recurrent endometrial cancer. In this trial, the evidence was insufficient to show a difference between bevacizumab plus carboplatin and paclitaxel and carboplatin and paclitaxel alone for OS and PFS. ORR was not tested statistically and between-group differences with CIs were not reported. Due to several sources of uncertainty (risk of bias, imprecision, and differences between the trial population and specific population of interest), definitive conclusions about the potential benefit of bevacizumab plus carboplatin and paclitaxel compared to carboplatin and paclitaxel alone could not be drawn. Data on HRQoL were collected but not presented, leaving the potential effect of bevacizumab plus carboplatin and paclitaxel unknown. As suggested by the study authors, a larger trial with a more refined patient population is needed to better understand which patients may derive benefit from treatment with bevacizumab plus carboplatin and paclitaxel. Characterization of harms in the study was compatible with the known safety profile of bevacizumab. No comparative evidence was identified on the relative treatment effects of bevacizumab plus carboplatin and paclitaxel versus other comparator treatments.
Economic Review
Methods
The economic review consisted of a cost comparison for bevacizumab combined with platinum doublet chemotherapy compared with comparators for adults with recurrent or metastatic endometrial cancer after disease progression on at least 1 line of therapy.
Based on public list prices, bevacizumab is expected to have a cost ranging from $975 to $1,948 per patient per 28-day cycle based on different doses for bevacizumab (7.5 mg/kg to 15 mg/kg every 21 days). When bevacizumab is added to chemotherapy (i.e., carboplatin plus paclitaxel or docetaxel, and cisplatin plus doxorubicin), the average cost of the regimen ranges from $2,321 to $8,928 depending on the bevacizumab dose and chemotherapy regimen (refer to Appendix 1 in the Supplemental Material). Pembrolizumab monotherapy and pembrolizumab plus lenvatinib are expected to have per patient costs of $11,733 and $17,408 per 28-day cycle, respectively. Dostarlimab plus chemotherapy (i.e., carboplatin plus paclitaxel) is expected to have patient costs ranging from $13,375 to $20,075 per 28-day cycle. Trastuzumab plus chemotherapy (i.e., carboplatin plus paclitaxel) is expected to have per patient costs ranging from $2,564 to $9,939 per 28-day cycle. Bevacizumab plus chemotherapy (i.e., carboplatin plus paclitaxel or docetaxel, and cisplatin plus doxorubicin) is less costly than pembrolizumab monotherapy (incremental savings of $2,805 to $9,412), pembrolizumab plus lenvatinib (incremental savings of $8,480 to $15,087), dostarlimab plus chemotherapy (incremental savings of $11,147 to $17,754), and trastuzumab plus chemotherapy (incremental savings of $1,011 to $6,943) per 28 days depending on cycle and chemotherapy drugs used. Bevacizumab plus chemotherapy is more costly than chemotherapy alone. As such, the impact of the reimbursement of bevacizumab for adults with locally advanced or metastatic endometrial cancer after disease progression on at least 1 line of therapy is contingent on which treatments are displaced. Additional items for consideration include:
According to the Clinical Review, evidence from the MITO END-2 trial was insufficient to show a difference in OS and PFS for bevacizumab plus chemotherapy (i.e., carboplatin plus paclitaxel) compared to chemotherapy alone (i.e., carboplatin plus paclitaxel).11 The ORR and disease control rate were unknown due to insufficient evidence. No evidence was identified regarding the comparative efficacy and safety of bevacizumab plus chemotherapy versus other active comparators.
As of December 2025, there are multiple biosimilars of bevacizumab currently marketed in Canada.
No health care resource use outcomes were reported in the clinical trial. According to the clinical experts consulted for this review, bevacizumab plus chemotherapy is expected to have similar treatment-related health care resource use compared with other treatments available in Canada. They noted that pembrolizumab is administered over a short infusion time and, therefore, it is expected that bevacizumab would have higher monitoring and treatment administration costs than pembrolizumab. However, compared with dostarlimab and trastuzumab, bevacizumab is expected to have similar monitoring costs. Clinical experts emphasized the need to consider differences among subgroups when assessing the treatments, since subgroup response to treatment regimens vary greatly.
While bevacizumab has been previously reviewed by CDA-AMC for cervical and ovarian cancer, all receiving positive recommendations, bevacizumab has not been previously reviewed by CDA-AMC for this indication. As of December 2025, there are no drugs under review by CDA-AMC for endometrial cancer.
No cost-effectiveness studies conducted in Canada that included bevacizumab for adults with recurrent or metastatic endometrial cancer after disease progression on at least 1 line of therapy were identified based on a literature search conducted on September 9, 2025, with alerts maintained until the Formulary Management Expert Committee (FMEC) meeting on January 22, 2026.
Conclusion
The reimbursement of bevacizumab for the treatment of recurrent or metastatic endometrial cancer after disease progression on at least 1 line of therapy is expected to decrease overall drug acquisition costs compared to most regimens, depending on the cycle, but increase drug acquisition costs compared with chemotherapy alone. Based on the Clinical Review conclusions, bevacizumab is expected to have a similar length of life compared with chemotherapy alone; however, there was no statistically significant evidence that it extends the length of life. Bevacizumab is expected to have reduced safety when compared with chemotherapy. The comparative efficacy of bevacizumab plus chemotherapy with other comparators is unknown, as it has not yet been assessed in the published literature.
Given that bevacizumab, when added to chemotherapy, is more costly than chemotherapy alone and does not extend life, bevacizumab may not be a cost-effective option compared with chemotherapy alone. Bevacizumab plus chemotherapy is less costly than most comparator regimens, but its comparative effect is unknown; thus, its relative cost-effectiveness is unknown. A cost-effectiveness analysis would be required to determine the cost-effectiveness of bevacizumab plus chemotherapy relative to other comparator treatments.
References
1.Makker V, MacKay H, Ray-Coquard I, et al. Endometrial cancer. Nature reviews Disease primers. 2021;7(1):88. PubMed
2.Canadian Cancer Society. Endometrial carcinoma. 2025. Accessed October 27, 2025. https://cancer.ca/en/cancer-information/cancer-types/uterine/what-is-uterine-cancer/endometrial-carcinoma
3.Ontario Health (Cancer Care Ontario). Ontario Cancer Statistics 2024. Ontario Health; 2025. Accessed October 27, 2025. https://www.cancercareontario.ca/sites/ccocancercare/files/assets/OCS2024.pdf
4.Canadian Cancer Statistics Advisory Committee in collaboration with the Canadian Cancer Society, Statistics Canada, and the Public Health Agency of Canada. Canadian Cancer Statistics 2025. Canadian Cancer Society; 2025. Accessed December 12, 2025.
5.Ferrandina G, Petrillo M, Mantegna G, et al. Evaluation of quality of life and emotional distress in endometrial cancer patients: a 2-year prospective, longitudinal study. Gynecol Oncol. 2014;133(3):518-525. PubMed
6.Canadian Cancer Society. Symptoms of uterine cancer. 2025. Accessed October 27, 2025. https://cancer.ca/en/cancer-information/cancer-types/uterine/signs-and-symptoms
7.American Cancer Society. Endometrial cancer stages. 2025. https://www.cancer.org/cancer/types/endometrial-cancer/detection-diagnosis-staging/staging.html
8.Canadian Cancer Society. Survival Statistics for Uterine Cancer. 2024. Accessed October 27, 2025. https://cancer.ca/en/cancer-information/cancer-types/uterine/prognosis-and-survival/survival-statistics
9.Corr B, Cosgrove C, Spinosa D, Guntupalli S. Endometrial cancer: molecular classification and future treatments. BMJ Medicine. 2022;1(1):e000152. doi: 10.1136/bmjmed-2022-000152 PubMed
10.Yang Y, Wu SF, Bao W. Molecular subtypes of endometrial cancer: Implications for adjuvant treatment strategies. Int J Gynaecol Obstet. 2024;164(2):436-459. doi: 10.1002/ijgo.14969 PubMed
11.Lorusso D, Ferrandina G, Colombo N, et al. Carboplatin-paclitaxel compared to Carboplatin-Paclitaxel-Bevacizumab in advanced or recurrent endometrial cancer: MITO END-2 - A randomized phase II trial. Gynecol Oncol. 2019;155(3):406-412. doi: 10.1016/j.ygyno.2019.10.013 PubMed
12.Miller D, Filiaci V, Fleming G, et al. Late-Breaking Abstract 1: Randomized phase Ill noninferiority trial of first line chemotherapy for metastatic or recurrent endometrial carcinoma: A Gynecologic Oncology Group study. 2012:771.
13.Dello Russo C, Navarra P. Local Investigators Significantly Overestimate Overall Response Rates Compared to Blinded Independent Central Reviews in Uncontrolled Oncology Trials: A Comprehensive Review of the Literature. Front Pharmacol. 2022;13:858354. doi: 10.3389/fphar.2022.858354 PubMed
14.Booth CM, Eisenhauer EA, Gyawali B, Tannock IF. Progression-Free Survival Should Not Be Used as a Primary End Point for Registration of Anticancer Drugs. J Clin Oncol. 2023;41(32):4968-4972. doi: 10.1200/JCO.23.01423 PubMed
15.Yarza R, Barquin A, Caruso G, et al. Progression-free survival as a surrogate of overall survival in metastatic or recurrent endometrial cancer: an EORTC gynecologic cancer group study. Int J Gynecol Cancer. 2025;35(11):102115. doi: 10.1016/j.ijgc.2025.102115 PubMed
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.