Drugs, Health Technologies, Health Systems
Reimbursement Review
Cabozantinib
Requester: Public drug programs
Therapeutic area: Neuroendocrine tumours
Summary
What Are Locally Advanced or Metastatic Extrapancreatic or Pancreatic Neuroendocrine Tumours?
Neuroendocrine tumours (NETs), including extrapancreatic (epNET) and pancreatic (pNET) types, originate from secretory cells and can occur in various organs. These tumours can be functional, causing various symptoms, or nonfunctional. These tumours significantly impact individuals’ quality of life and their ability to perform daily activities.
In Canada, an Ontario-based study (2015) reported an increase in incidence from 2.46 per 100,000 to 5.86 per 100,000 over 15 years, with pNETs accounting for about 10% of cases.
What Are the Treatment Goals and Current Treatment Options for Locally Advanced or Metastatic Extrapancreatic or Pancreatic Neuroendocrine Tumours?
The treatment goals for patients with locally advanced or metastatic neuroendocrine tumours are to prolong life, delay disease progression, reduce cancer-related symptoms, prevent treatment complications, and improve or maintain patients’ functioning and quality of life.
Treatment approaches vary based on various factors, such as tumour grade, differentiation, functionality, and other factors for both epNETs and pNETs. The treatment options include the following:
For localized solid tumours: surgical resection is the first-line treatment.
For unresectable tumours, systemic therapy options include:
somatostatin analogues: initial therapy for unresectable metastatic disease or hormonal overproduction syndromes
targeted agents: options include everolimus, sunitinib, and cabozantinib for patients who have progressed on somatostatin analogues
chemotherapy agents: for example, capecitabine plus temozolomide
peptide receptor radionuclide therapy: generally considered after somatostatin analogues.
What Is Cabozantinib?
Cabozantinib is a tyrosine kinase inhibitor that is available as an oral tablet. Health Canada has approved cabozantinib for renal cell carcinoma, hepatocellular carcinoma, and differentiated thyroid carcinoma, but there is no indication for neuroendocrine tumours.
Why Did We Conduct This Review?
At the request of the participating public drug programs, we reviewed cabozantinib to inform a recommendation on whether it should be reimbursed for adults with locally advanced or metastatic extrapancreatic or pancreatic neuroendocrine tumours who have received at least 1 prior therapy.
How Did We Evaluate Cabozantinib?
We reviewed the clinical evidence on the beneficial and harmful effects and compared the costs of cabozantinib versus other treatments available in Canada or placebo in adults with locally advanced or metastatic extrapancreatic or pancreatic neuroendocrine tumours who have received at least 1 prior therapy.
The clinical evidence was identified through systematic searches for available studies.
The review was also informed by 1 clinician group submission and 1 patient group submission in response to our call for input, and by input from the participating public drug programs around issues that may impact their ability to implement a recommendation. We consulted 2 clinical experts in neuroendocrine tumours as part of the review process.
What Did We Find?
Clinical Evidence
We reviewed a phase III, multicentre, double-blinded, randomized controlled trial (the CABINET trial) comparing the efficacy and safety of cabozantinib with placebo in adults with locally advanced or metastatic extrapancreatic or pancreatic neuroendocrine tumours who have received at least 1 prior therapy.
Cabozantinib improved progression-free survival compared to placebo. Uncertainties arose from the early termination of the study (which might overestimate cabozantinib’s effect), small sample size, and limited information with which to appraise the potential for missing data. Clinical experts consulted by the review team indicated that the benefit was clinically meaningful.
The evidence was insufficient to demonstrate a benefit on overall survival for cabozantinib compared to placebo; there were wide confidence intervals that crossed the null, with the point estimate near the null for the pNET cohort. This may be influenced by the trial being underpowered for overall survival and the allowance of crossover from the placebo group to the cabozantinib group.
The trial only reported descriptive results with a high risk of bias regarding health-related quality of life, which is important to patients. Results of formal analyses of quality of life were not available. Based on the descriptive data on health-related quality of life, the overall health-related quality of life remained stable over time and was similar in both the cabozantinib and placebo groups among patients who completed questionnaires in the epNET and pNET cohorts.
Compared to the placebo group, patients in the cabozantinib group reported higher proportions of adverse events, serious adverse events, and discontinuation due to adverse events.
Evidence on the benefits and harms of cabozantinib as compared with other relevant comparators was unavailable.
Economic Evidence
Reimbursing cabozantinib for adults with locally advanced or metastatic extrapancreatic or pancreatic neuroendocrine tumours who have received at least 1 prior therapy is expected to increase costs to the public drug programs.
Abbreviations
177Lu
lutetium
AE
adverse event
CAPTEM
capecitabine and temozolomide
CI
confidence interval
ECOG
Eastern Cooperative Oncology Group
epNET
extrapancreatic neuroendocrine tumour
HR
hazard ratio
HRQoL
health-related quality of life
ITT
intention to treat
NET
neuroendocrine tumour
OS
overall survival
PFS
progression-free survival
pNET
pancreatic neuroendocrine tumour
PRRT
peptide receptor radionuclide therapy
QoL
quality of life
SSA
somatostatin analogue
Background
Introduction
The objective of the clinical review is to review and critically appraise the evidence on the beneficial and harmful effects of cabozantinib in the treatment of adults with locally advanced or metastatic extrapancreatic neuroendocrine tumours (epNETs) or pancreatic neuroendocrine tumours (pNETs) who have received at least 1 prior therapy. The focus will be placed on comparing cabozantinib to relevant comparators and identifying gaps in the current evidence. The economic review consists of a cost comparison of cabozantinib compared with relevant comparators for the same population. The comparators considered relevant to the reviews were somatostatin analogues (SSAs): lanreotide or octreotide, everolimus, sunitinib, streptozocin plus doxorubicin plus 5-fluorouracil, capecitabine plus temozolomide, lutetium (177Lu) dotatate, telotristat with an SSA, Y-90 microspheres, and placebo and/or standard of care.
Cabozantinib (Cabometyx) was previously reviewed by CDA-AMC as monotherapy for treating adults with locally advanced or metastatic differentiated thyroid carcinoma, and it was recommended for reimbursement with clinical criteria and/or conditions in November 2022.2 Additionally, in combination with nivolumab, it was recommended for reimbursement also with clinical criteria and/or conditions in November 2023 for treating adults with advanced or metastatic renal cell carcinoma who had no prior systemic therapy for metastatic disease.3
Table 1: Information on the Drug Under Review and on the CDA-AMC Review
Item | Description |
|---|---|
Information on the drug under review | |
Drug (product) | Cabozantinib, oral tablets (60 mg, 40 mg, or 20 mg) |
Relevant Health Canada indication | No indication for neuroendocrine tumours |
Mechanism of action | Cabozantinib inhibits multiple receptor tyrosine kinases, including AXL, FLT3, KIT, MER, MET, RET, ROS1, TIE-2, TRKB, TYRO3, and VEGF, which are involved in cell proliferation and angiogenesis |
Recommended dosage | NA |
Data protection status | Ends in 2027 |
Status of generic drugs/biosimilars | Two generics are under review by Health Canada |
Information on the CDA-AMC review | |
Requester | Oncology Working Group |
Indication under consideration for reimbursement | Adults with locally advanced or metastatic extrapancreatic or pancreatic neuroendocrine tumours who have received at least 1 prior therapy |
CDA-AMC = Canada’s Drug Agency; NA = not applicable; VEGF = vascular endothelial growth factor.
Sources of Information
The contents of the clinical review report are informed by studies identified through systematic literature searches and input received from interested parties.
Calls for patient group, clinician group, and industry input are issued for each nonsponsored reimbursement review. We received 1 patient group submission from the Canadian Neuroendocrine Tumour Society and 1 clinician group submission from the Commonwealth Neuroendocrine Tumour Research Collaboration, specifically the members who represent Canada. The Canadian Neuroendocrine Tumour Society summarized patient input data and provided evidence on patients’ experiences and perspectives of living with neuroendocrine cancer, including the Global NET Patient Survey (2017) by the International Neuroendocrine Cancer Alliance,4 the NET Patient Experiences and Perspectives Survey (2022) conducted online via SurveyMonkey, and qualitative interviews with neuroendocrine tumour (NET) patients and caregivers who have experience with cabozantinib. Several clinical experts provided input to support the review. The full submissions received are available on the project landing page in the consolidated input document.
Input from patient and clinician groups is considered throughout the review, including in the selection of outcomes to include in the clinical review and in the interpretation of the clinical evidence. Relevant patient and clinician group input is summarized in the Disease Background, Current Management, and Unmet Needs and Existing Challenges sections.
The drug programs provide input on each drug being reviewed through the reimbursement review process by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted for this review are summarized and provided to the expert committee in a separate document.
Each review team includes at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process. Two oncologists with expertise in the diagnosis and management of epNETs and pNETs participated as part of the review team, with representation from Ontario and Manitoba.
Disease Background
NETs are a diverse group of cancers originating from the secretory cells of the diffuse neuroendocrine system.5 pNETs are a subset of gastroenteropancreatic NETs and arise in the endocrine tissues of the pancreas.6 epNETs can occur in various organs such as the stomach, intestines, lungs, and esophagus.1 These tumours can be nonfunctional (i.e., unassociated with a hormonal syndrome) or functional (i.e., producing hormones that cause various clinical symptoms).1,6 NETs often are nonfunctional and present with nonspecific symptoms, leading to delays in diagnosis.7 A retrospective study in Ontario found that 20.8% of patients with NETs presented with metastatic disease at diagnosis.8
According to the input from the clinician group, NETs are 1 of the fastest-growing classes of cancers in Canada and worldwide. In Canada, an Ontario-based study reported an increase in incidence from 2.46 per 100,000 to 5.86 per 100,000 over 15 years from 1994 to 2009, with pNETs accounting for approximately 10% of cases.8 The estimated overall survival (OS) rates for patients with NETs are 68.3% at 3 years, 61.0% at 5 years, and 46.5% at 10 years.8 The primary tumour site and disease stage at diagnosis significantly affect OS. For nonmetastatic disease, the 10-year OS rate is 68.2%, whereas it is 17.5% for those with metastases at presentation and 18.7% for metastases after the initial diagnosis.8 For patients with pNETs, the estimated 10-year OS is about 30%.8 A collaborative team of experienced health care practitioners is essential for diagnosing and managing NETs. Diagnosis typically involves specialized pathological testing, imaging, and biochemical tests to confirm, categorize, and stage the disease.
According to the patient input for this review, NETs significantly negatively impact patients’ quality of life (QoL), causing symptoms like fatigue, diarrhea, and pain, which affect daily activities, emotional health, social life, and ability to work. Patients often experience a substantial negative impact on their energy and overall well-being and require various treatments to manage symptoms and disease progression.
Current Management
Treatment Goals
Per the input from the clinician group, current treatment goals for patients with locally advanced or metastatic epNETs or pNETs are to prolong life, delay disease progression, reduce cancer-related symptoms, prevent treatment complications, and improve or maintain patients’ functioning and QoL.
Given these treatment goals, clinical experts consulted by Canada’s Drug Agency (CDA-AMC) emphasized that progression-free survival (PFS) and health-related quality of life (HRQoL) are the most important outcomes for patients with NETs. They noted that the objective response rate is less relevant because HRQoL captures this measure. The experts indicated that assessing overall OS may be more challenging due to the protracted disease course, crossover between intervention and comparator groups, and small sample sizes in a trial setting.
Current Treatment Options
For locally advanced or metastatic epNETs or pNETs, treatment approaches vary based on tumour grade, differentiation, functionality, and the extent and location of the disease.9 According to the input from the clinician group, treatment options include surgical resection, intra-arterial hepatic therapy, and systemic therapy, including targeted agents, peptide receptor radionuclide therapy (PRRT), and chemotherapy when necessary. For localized solid tumours, surgery is typically the first-line treatment. For patients with metastatic disease, systemic drug therapies are used. Somatostatin analogues (SSAs) are generally the initial therapy for patients with unresectable metastatic disease or hormonal overproduction syndromes. For those who have progressed while on SSAs, treatment options include targeted agents like everolimus, sunitinib, and cabozantinib; chemotherapy such as capecitabine and temozolomide (CAPTEM); 177Lu dotatate; or PRRT for NETs that have advanced after first-line SSA therapy.
Key characteristics of cabozantinib are summarized with other treatments available for locally advanced or metastatic epNETs or pNETs in Table 1 in the Supplemental Material document (available on the project landing page).
Unmet Needs and Existing Challenges
Canadian members of the Commonwealth Neuroendocrine Tumour Research Collaboration reported that all patients with NETs eventually progress, developing metastases in multiple organ systems, which ultimately leads to death. However, there is generally a considerable period during which novel therapies can be applied. Current treatments are not effective or available for all patients, are poorly tolerated, and can lead to drug resistance. For example, PRRT is not universally funded for all patients with NETs across Canada, creating issues of inequity. Where funded, PRRT is available only at selected centres, requiring patients to travel, which negatively impacts the QoL of both patients and caregivers. Additionally, PRRT and chemotherapy regimens (e.g., CAPTEM) are associated with a higher risk of myelodysplastic syndromes and acute myeloid leukemia. Thus, there is a need for additional safe and effective treatment options for patients who have progressed or for whom current treatments are unsuitable for improving OS, slowing disease progression, and controlling hormonal symptoms.
Clinical experts also noted that all patients will eventually progress. Current treatments, such as SSAs and 177Lu dotatate, are not particularly effective and have significant side effects, highlighting a substantial unmet need for effective and well-tolerated treatment options in this patient population.
Considerations for Using the Drug Under Review
Contents within this section have been informed by input from the clinical experts consulted for the purpose of this review and from clinician groups. The following has been summarized by the review team.
Potential Place in Therapy
Cabozantinib is an oral small-molecule inhibitor of multiple tyrosine kinase inhibitors, including anti–vascular endothelial growth factor receptors, MET, AXL, and RET. This mechanism differs from other treatment options. Angiogenesis plays a key role in the pathogenesis of NETs. Experts highlighted that cabozantinib, as a multiple antiangiogenic agent, could potentially address the underlying disease process, improve patients’ QoL, and shift the current treatment paradigm for NETs, reducing the use of everolimus.
The clinician group agreed with the experts that cabozantinib would be an option for patients with advanced epNETs or pNETs who have received at least 1 prior therapy. They highlighted that it could become the standard of care for this population. In the pNET population, cabozantinib will replace the current use of everolimus or sunitinib in second-line treatment or in place of best supportive care. Given the limited funded treatment options for the epNET population, cabozantinib will replace the use of best supportive care.
Patient Population
Clinical experts consulted for this review consider adults with locally advanced or metastatic epNETs or pNETs who have experienced disease progression after at least 1 prior treatment or who are intolerant of the other therapies to be the most suited for cabozantinib treatment. The prior treatments include but are not limited to SSAs, 177Lu dotatate, or everolimus. Eligible patients also include those who are intolerant to the first-line treatments. Clinical experts highlighted that everolimus is not well tolerated, with side effects including hyperglycemia, pneumonitis, and other infections. Physician judgment, examinations, and diagnostic imaging (e.g., CT or MRI) are needed to assess disease progression. No companion test is required for initial cabozantinib treatment, and all patient groups are expected to benefit from cabozantinib, with no expected subgroup effects.
The clinician group agreed with the experts that the patient population best suited for cabozantinib should follow the eligibility criteria of the CABINET study.10 Cabozantinib is considered an additional line of treatment after progression on PRRT, sunitinib, or everolimus in pNETs and gastrointestinal NETs, and after everolimus for lung NETs. No patient populations are expected to be unsuitable for treatment. The clinician group also agrees that no specific diagnostic tests are required to initiate cabozantinib treatment.
Assessing the Response to Treatment
According to the clinical experts consulted for this review, patients undergoing treatment with cabozantinib may be assessed for treatment response via routine medical imaging every 2 to 3 months and routine clinical examination or blood work every month. The clinical experts consider clinically meaningful responses to include clinical and radiographic evidence of disease stability or progression, the maintenance or improvement of symptoms, and HRQoL.
The clinician group agrees with the clinical experts that clinical assessments (such as symptoms, QoL, or disease bulk) and radiographic information (size of lesions) should be used to evaluate patients’ responses to treatment.
Discontinuing Treatment
Treatment with cabozantinib would be discontinued due to evidence of disease progression based on RECIST (Response Evaluation Criteria in Solid Tumours), intolerable toxicities (e.g., fatigue, diarrhea, hypertension, weight loss, stomatitis, hand-foot syndrome, decreased appetite), or if radiation or surgery is required, according to the clinical experts.
The clinical group agreed with the experts that they would discontinue cabozantinib treatment if the disease progressed or the toxicity became unacceptable. The clinical group also pointed out that patient preference might be a reason for discontinuing cabozantinib.
Prescribing Considerations
The clinical experts consulted for this review stated that the initial cabozantinib prescription should be prescribed by clinicians with expertise in the management of NETs (e.g., medical oncologists or surgical oncologists) and that cabozantinib can be given in community settings.
The clinician group indicated that a collaborative team of health care providers experienced in managing NETs may be needed to manage and follow up on cabozantinib treatment. An oncologist-led multidisciplinary team may support using cabozantinib in the community setting and provide follow-up care.
Additional Considerations
The clinical experts consulted for this review noted that, in their experience, cabozantinib is better tolerated than other treatment options in this patient population.
Clinical Review
Methods
We conducted a systematic review to identify evidence for cabozantinib in the treatment of adults with locally advanced or metastatic epNETs or pNETs who have received at least 1 prior therapy (including but not limited to everolimus). Studies were selected according to the eligibility criteria in Table 2. We also considered long-term extension studies of included randomized controlled trials, indirect treatment comparisons that adhered to the eligibility criteria except for the study design criteria, and studies addressing gaps that did not meet the eligibility criteria but were considered to address important gaps in the systematic review evidence.
Relevant comparators included treatments used in clinical practice in Canada in the patient population under review. We included placebo as 1 of the relevant comparators because our preliminary scoping indicated that evidence comparing active treatments might not be available. Clinical experts also noted that treatment options are limited for patients with progressive NETs, especially for those with pNETs, after several prior treatments. We selected outcomes (and follow-up times) for review, considering clinical expert input and patient and clinician group input. Selected outcomes are those considered relevant to expert committee deliberations.
An information specialist conducted a literature search of key bibliographic databases, trial registries, and grey literature sources using a peer-reviewed search strategy. The initial search was completed on March 5, 2025, with alerts maintained until the Formulary Management Expert Committee meeting on July 17, 2025. Refer to the Supplemental Materials document for the detailed search strategies.
Detailed methods for literature searches, study selection, data extraction, and risk of bias appraisal are in Appendix 2 of the Supplemental Material.
Table 2: Systematic Review Eligibility Criteria
Criteria | Description |
|---|---|
Population | Adult patients with locally advanced or metastatic epNETs or pNETs who have received at least 1 prior therapy |
Intervention | Cabozantinib |
Comparator |
|
Outcomes | Efficacy:
Safety:
|
Study design | Phase III and IV RCTs |
AE = adverse events; HRQoL = health-related quality of life; RCT = randomized controlled trial; SAE = serious adverse event; SSA = somatostatin analogues; WDAE = withdrawal due to adverse events; Y-90 = yttrium 90.
Note: Although medullary thyroid carcinoma and small cell lung carcinoma are both neuroendocrine carcinomas, they are managed differently in clinical practice. Therefore, we excluded studies that focus on these 2 diseases.
Clinical Evidence
From the search for primary studies, we identified 218 unique records via the searches of databases and registers, of which we excluded 216 by title and abstract. We screened 2 records by full text and included 1 report of 1 study (the CABINET trial).10 We did not identify any potentially relevant records via other sources. No reports of long-term extensions of the included studies or studies addressing gaps were identified.
From the search for indirect treatment comparisons, we identified 118 unique records via the searches of databases, of which we excluded 115 by title and abstract. We screened 3 records by full text, of which none met the eligibility criteria by full-text screening. We did not identify any potentially relevant records via other sources.
A list of excluded studies, including reasons for exclusion, is in Appendix 2 in the Supplemental Material.
Systematic Review
Description of Studies
Study Characteristics
Characteristics of the included study (CABINET) are summarized in the following paragraphs. Additional details regarding the inclusion and exclusion criteria, interventions and comparators, and relevant outcome measures are in Appendix 3 in the Supplemental Material.
The CABINET trial by Chan et al. (2025)10 is a multicentre, phase III, double-blind (outcome assessors and participants), randomized controlled trial funded by the National Cancer Institute and Exelixis (the manufacturer), with additional support from the Alliance for Clinical Trials in Oncology and Alliance Foundation Trials programs. The trial was conducted at 62 sites in the US, with no sites in Canada.10 The trial aimed to evaluate the efficacy and safety of cabozantinib in adult patients with previously treated, progressive advanced epNET or pNET.
The CABINET trial10 included patients aged 18 or older with histologically confirmed, locally advanced, or metastatic well- or moderately differentiated NETs (epNETs or pNETs). Eligible patients had WHO tumour grades of 1 to 3 and an Eastern Cooperative Oncology Group (ECOG) performance status score of 0 to 2. They must have experienced disease progression (per RECIST 1.1 criteria) within 12 months before enrolment or unacceptable side effects after at least 1 FDA-approved therapy. The original protocol required that patients had prior therapy with everolimus, but a later amendment expanded the list of potential prior therapies owing to changes in the treatment landscape. These included somatostatin analogues, 177Lu dotatate; everolimus; temozolomide (with or without capecitabine); cisplatin plus etoposide or carboplatin plus etoposide (for epNETs), and sunitinib (for pNETs). Patients with poorly differentiated neuroendocrine carcinoma and high-grade neuroendocrine carcinoma without specified differentiation status were excluded.10 The inclusion and exclusion criteria were consistent across the 2 cohorts, focusing on patients with progressive disease despite prior therapies.10
The trial enrolled 298 patients, including 203 with epNETs and 95 with pNETs.10 Patients were randomly assigned in a 2:1 ratio to receive either 60 mg of cabozantinib or placebo orally daily. Randomization was stratified based on concurrent somatostatin analogue use and primary tumour site (midgut gastrointestinal and unknown primary versus non-midgut gastrointestinal, lung, or other sites) for the epNET cohort, and concurrent somatostatin analogue use and previous sunitinib therapy for the pNET cohort.10 To manage adverse events (AE), treatment interruption and dose reduction for cabozantinib (to 40 mg, then to 20 mg) and placebo were permitted.10 Participants could continue using somatostatin analogues if their dose has been stable for at least 2 months before enrolment. However, participants were prohibited from using full-dose oral anticoagulation and antiplatelet treatments, strong CYP3A4 inhibitors, or inducers. Considering the impact of cabozantinib on the corrected QT interval, drugs that prolong the corrected QT interval should be avoided if possible. Patients were unaware of their assigned treatment until disease progression, unacceptable toxic effects, or withdrawal of consent. In November 2020, a protocol amendment allowed patients receiving placebo to cross over to open-label cabozantinib after centrally confirmed progressive disease.10
There was no specific run-in period mentioned in the trial design.10 The trial was terminated early based on interim analysis results showing PFS benefit, with the data cut-off date for the final analyses being August 24, 2023.10 The primary end point was PFS, defined as the time from randomization to radiographic progressive disease (RECIST 1.1 by the investigator and confirmed in real time by blinded independent central review) or all-cause death. Patients were censored if they did not have postbaseline assessments, started new anticancer therapy before progression, were lost to follow-up, or reached the data cut-off without experiencing a PFS event. To evaluate tumour response and progression, participants underwent radiographic imaging every 12 weeks. Secondary end points of relevance included OS, defined as the time from randomization to death from any cause, and safety, measured by AE according to the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0. Patients without an OS event were censored at the date that they were last known to be alive. An optional correlative study also assessed the HRQoL using the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 and Quality of Life-gastrointestinal-related neuroendocrine tumours 21, but the results have not yet been made available.
Statistical Testing and Analysis Populations
The calculated sample size (210 for epNETs, 185 for pNETs) aimed to provide the trial with 90% power to detect a true hazard ratio (HR) for primary end point, PFS, of 0.583 in the epNET cohort and 0.568 in the pNET cohort.10 This was based on a stratified 1-sided log-rank test with an overall significance level of 0.025, corresponding to a 2-sided significance level of 0.05. For time-to-event analyses, the target sample size was event-driven. The trial required 164 progression events in the epNET cohort and 149 progression events in the pNET cohort.10
The trial included 2 interim analyses for futility after 33% and 66% of the projected progression events occurred in each cohort.10 For each interim analysis, 1-sided alpha spending of 0.001 for efficacy (PFS testing) was applied to control the type I error rate at a 1-sided alpha of 0.025. Other end points were uncontrolled for multiplicity and HRQoL was not inferentially tested. P values reported herein are 2-sided. In May 2023, the study investigators conducted protocol-specified interim analyses of PFS (second interim analysis for epNET cohort, first interim analysis for pNETs cohort) using local investigator assessment, followed by a blinded independent central review. Based on these interim results, the data and safety monitoring board recommended early trial termination. On August 24, 2023, the trial group assignments were unblinded, allowing all patients in the placebo group to receive cabozantinib. The trial used this time point as the data cut-off for the final analyses. The trial also conducted a prespecified OS analysis.
Efficacy analyses followed the intention-to-treat (ITT) principle, including all randomized patients in the analysis. Patients were assigned to the treatment group to which they were randomized, regardless of the actual treatment received. Safety analyses were based on the safety population, which included patients who were randomized and received any amount of protocol therapy. In the epNET cohort, the safety population had 2 fewer participants than the ITT population in each group. In the pNET cohort, the safety population had 1 fewer participant than the ITT population in the cabozantinib group and was the same as the ITT population in the placebo group.
Patient Disposition
Table 3 presents the patient disposition of the CABINET trial.10
Between October 2018 and August 2023, 203 patients with epNETs (cabozantinib: 134; placebo: 69) and 95 patients with pNETs (cabozantinib: 64; placebo: 31) were randomly assigned to receive cabozantinib or placebo.10 The ITT population included several misallocated patients: the epNET cohort had 7 patients with pNETs (4 in the cabozantinib group and 3 in the placebo group), and the pNET cohort had 3 patients with epNETs (2 in the cabozantinib group and 1 in the placebo group). Disease progression was the most common reason for discontinuing the assigned regimen in both the cabozantinib and placebo groups.10
Table 3: Patient Disposition in the ITT Population
Status, n (%) | epNET cohort (n = 203) | pNET cohort (n = 95) | ||
|---|---|---|---|---|
Cabozantinib, n | Placebo, n | Cabozantinib, n | Placebo, n | |
Eligible patients randomized | 134 | 69 | 64 | 31 |
Initiated treatment (safety population) | 132 | 67 | 63 | 31 |
Treatment discontinuation (% of eligible patients)a | 111 (83) | 60 (87) | 49 (77) | 29 (94) |
Reason for treatment discontinuation, n (% of randomized patients) | ||||
Disease progression | 52 (39) | 38 (55) | 28 (44) | 23 (74) |
AE | 34 (25) | 9 (13) | 10 (16) | 0 |
Withdrawn consent | 7 (5) | 4 (6) | 5 (8) | 4 (13) |
Death | 6 (4) | 4 (6) | 0 | 0 |
Other reason | 6 (4) | 3 (4) | 3 (5) | 2 (6) |
Alternative treatment | 5 (4) | 1 (1) | 1 (2) | 0 |
Other disease | 1 (1) | 1 (1) | 2 (3) | 0 |
AE = adverse event; epNET = extrapancreatic neuroendocrine tumour; ITT = intention to treat; pNET = pancreatic neuroendocrine tumour.
aThe reasons for discontinuation of the study were not clearly reported, except in cases in which patients withdrew consent.
Source: Supplementary appendix of Chan et al. (2025).10
Baseline Characteristics
In the epNET cohort, the median age was 66 years in both the cabozantinib (range: 28 to 86 years) and placebo groups (range: 30 to 82 years), and approximately 50% were female.10 Most patients (63% in the cabozantinib group and 52% in the placebo group) had an ECOG performance status score of 1, indicating that they had mild symptoms but were ambulatory. Primary tumour sites were mainly gastrointestinal (52% in the cabozantinib group and 67% in the placebo group) and in the lung (20% in the cabozantinib group and 17% in the placebo group), with 16% in the cabozantinib group and 3% in the placebo group having unknown primary sites. Most patients (64% in the cabozantinib group and 70% in the placebo group) had grade 2 tumours, and 31% in the cabozantinib group and 36% in the placebo group had functional tumours causing hormone syndromes. Nearly all patients (93% in both groups) had previously received somatostatin analogues, and a substantial portion had undergone PRRT with 177Lu dotatate (60% in the cabozantinib group and 59% in the placebo group) and everolimus (72% in the cabozantinib group and 64% in the placebo group).
In the pNET cohort, the median age was 60 years in the cabozantinib group (range: 29 to 79 years) and 64 years in the placebo group (range: 39 to 79 years), and 42% were female.10 A higher percentage of patients (55% in the cabozantinib group and 48% in the placebo group) had an ECOG performance status score of 0, indicating full activity without symptoms. Most patients (61% in both groups) had grade 2 tumours, 17% in the cabozantinib group and 16% in the placebo group had functional tumours. Nearly all patients (98% in the cabozantinib group and 97% in the placebo group) had received somatostatin analogues, and many had been treated with 177Lu dotatate (59% in the cabozantinib group and 58% in the placebo group), everolimus (80% in the cabozantinib group and 81% in the placebo group), and temozolomide-based therapy (67% in the cabozantinib group and 52% in the placebo group). Additionally, 28% of patients in the cabozantinib group and 22% in the placebo group had previously received sunitinib.
Table 5 of Appendix 4 presents additional baseline demographics and disease characteristics from the CABINET trial.10
Treatment Exposure and Concomitant Medications
In the epNET cohort, among the safety population, the median duration of cabozantinib treatment (n = 132) was 5.5 months, ranging from 0.2 to 32.4 months. Dose reductions due to AEs occurred in 66% of patients, with a median daily dose of 38.4 mg. For the placebo group (n = 67), the median duration was 2.8 months, ranging from 0.6 to 21.4 months. Dose reductions due to AEs occurred in 10% of patients, with a median daily dose of 59.0 mg. In the cabozantinib group, 45% of patients received subsequent anticancer therapy, while 67% of patients in the placebo group (including 20 [33%] who crossed over to open-label cabozantinib) received additional treatment (details are included in Supplementary Table 4 of Chen et al. 2025).10 More patients in the cabozantinib group (55%) received no additional therapy than in the placebo group (33%).
In the pNET cohort, among the safety population, the median duration of cabozantinib treatment (n = 63) was 8.3 months, ranging from 0.5 to 39.6 months. Dose reductions due to AEs occurred in 68% of patients, with a median daily dose of 37.9 mg. For the placebo group (n = 31), the median duration was 2.9 months, ranging from 0.5 to 11.2 months. Dose reductions due to AEs occurred in 19% of patients, with a median daily dose of 56.9 mg. In the cabozantinib group, 51% of patients received subsequent anticancer therapy, compared to 62% in the placebo group (including 12 [41%] who crossed over to open-label cabozantinib) (details are included in Supplementary Table 5 of Chen et al. 2025).10 More patients in the cabozantinib group (49%) received no additional therapy compared with the placebo group (38%).
More details on concomitant medications, including the timing of their initiation, were not provided.
Critical Appraisal
Table 10 of Appendix 5 in the Supplementary Material presents the results of the risk of bias appraisal of the included study.
Internal Validity
The CABINET trial protocol indicated that a randomization system was used to perform stratified permuted block randomization, suggesting a low risk of bias in the randomization process, though specific details of allocation concealment were unclear. Patient characteristics at baseline were relatively balanced in both the epNET and pNET cohorts, except that the cabozantinib group had a higher unknown primary tumour site in the epNET cohort. This may be attributable to chance, given the relatively small sample size. Clinical experts consulted by the review team did not expect an important impact of this imbalance on efficacy. The targeted sample sizes were 210 participants (164 events) for the epNET cohort and 185 participants (149 events) for the pNET cohort. However, the actual sample sizes were 203 participants (111 events) for the epNET cohort and 95 participants (57 events) for the pNET cohort, which is smaller than the targeted sample sizes or events, particularly for the pNET cohort. Despite not achieving the planned sample size, the trial had enough power to detect statistical differences between the 2 groups for PFS outcome. The small number of participants or events, particularly in the pNET cohort, could be associated with unstable treatment effect estimation in the analyses.
Although the trial was double-blind, the blinding process description was not fully explicit. Based on the publication, patients were blinded and the outcome assessor was likely blinded before the data cut-off date. Given that cabozantinib is linked to specific AEs like hypertension and diarrhea, this could potentially unblind patients and investigators. This potential for unblinding might influence subjective components of disease progression assessments (e.g., when doing the clinical evaluations and assessing the tumour size through measuring lesion size from medical imaging) and AE reporting, potentially biasing treatment efficacy and safety estimates. However, there is no clear evidence of unblinding and use of a blinded independent central review for PFS assessments enhanced the internal validity of the results. The trial presents treatment-related AEs rather than all AEs, which involves subjective interpretations of AE attribution by the investigator. There was no statement in the protocol about whether attribution occurred in a blinded manner.
The primary analyses (PFS and OS) were based on the ITT population, which is appropriate.10 In this trial, most patients discontinued the intervention (cabozantinib or placebo) due to disease progression or AEs, which aligns with clinical practice. The proportion of discontinuation of study treatment due to withdrawn consent (suggestive of trial discontinuation) or unknown reasons was small and similar between the 2 groups (Table 4). The trial’s statistical methods were generally appropriate, using stratified Cox regression models and Kaplan-Meier methods for the PFS and OS analysis. Because the trial did not report the results of testing the proportional hazards assumption, the validity of the assumption underlying the HRs from time-to-event analyses could not be comprehensively assessed.11 Visual inspection of the Kaplan-Meier plots suggests the assumption was likely met for PFS in both cohorts (Figures 1 and 2). However, Kaplan-Meier plots for OS did not separate at any point during follow-up (Figures 1 and 2). While the trial adjusted for multiplicity in the planned interim analysis for the primary outcome (i.e., PFS), it did not appear that adjustments were made for secondary outcomes (i.e., OS); however, these were not statistically significant. HRQoL was not tested statistically. The duration of follow-up was adequate to capture the benefit for PFS, although less so for OS or long-term safety outcomes. The trial relied on relative hazard estimations and medians (between-group difference not reported), without providing absolute risk estimations at relevant time points between the 2 groups to assist in further judging the clinical importance of time-to-event results.
In this trial, the epNET cohort included 7 patients with pNETs (4 in the cabozantinib group and 3 in the placebo group), and the pNET cohort included 3 patients with epNETs (2 in the cabozantinib group and 1 in the placebo group).10 Misallocating patients to incorrect cohorts could introduce bias, potentially skewing results. However, sensitivity analyses excluding these misallocated participants yielded consistent results with the primary analyses (Table 8 of Appendix 4).
Ending the trial early based on interim analysis results (the second interim analysis for epNET and the first interim analysis for pNETs) and the superior efficacy observed with cabozantinib could potentially overestimate the treatment effect.10,12 This decision might prevent the trial from assessing potential long-term benefits and fully capturing adverse effects. The trial’s power calculations were based on the primary end point (PFS),10 and findings regarding secondary end points (e.g., OS) may be underpowered. Allowing patients who received a placebo to crossover to the cabozantinib group is an important ethical consideration, but the crossover (20 in the epNET cohort and 12 in the pNET cohort) may diminish the ability to observe an OS benefit for cabozantinib in both cohorts. Participants in the placebo group who experienced disease progression and crossed over to open-label cabozantinib could influence HRQoL assessments and self-reported AEs.
The CABINET trial did not provide details on the proportion of patients who discontinued the trial or the censoring reasons for time-to-event end points. Therefore, we are unclear about how many patients might have been censored due to loss to follow-up or for moving to subsequent treatment before disease progression. Based on the provided disposition, this number appears to be low, but we cannot make a definitive conclusion about this for PFS, OS, and harm outcomes. The number of patients contributing data decreases substantially over time for HRQoL. The analysis of complete cases assumes that missing values occurred completely at random, which is not a reasonable assumption given the likely reasons for missing values (e.g., death).
Although the CABINET trial used PFS to assess the efficacy of cabozantinib as the primary outcome, the validity of PFS as a surrogate end point to predict an OS benefit among patients with NETs remains uncertain. One study using observational data reported that PFS was associated with improved OS among patients with metastatic NETs who received somatostatin analogues or everolimus.13 However, trial-based evidence specific to the treatment regimen of interest is not available.
External Validity
The CABINET trial included patients with histologically confirmed, locally advanced or metastatic well or moderately differentiated epNETs or pNETs.10 The trial included a well-defined patient population with clear inclusion and exclusion criteria, ensuring the findings’ applicability to the broader NET patient population.10 Patients with poor ECOG performance status (scores of 3 or higher) and those with poorly differentiated neuroendocrine carcinoma were not eligible, which may limit generalizability to patients with poorer performance status or more aggressive disease.
The trial was conducted at 62 sites in the US.10 The trial authors stated that the demographic characteristics of the trial participants are representative and generalizable to those with neuroendocrine tumours in the US and elsewhere,10 the mean age and sex were similar to a study conducted in Ontario in 2015.8 However, the trial participants may not fully represent the ethnic and demographic diversity seen in Canadian clinical practice or differ from Canadian medical centres in terms of access to supportive medications and procedures.
The trial used placebo as the comparator,10 which may not fully reflect clinical practice in Canada where active comparators such as everolimus or 177Lu dotatate are commonly used. The clinical experts consulted by the review team indicated that the choice of placebo was justified due to the lack of established efficacy of other therapies in patients with progressive disease, particularly for the epNET cohort. However, concerns arose for patients with pNETs because they have more treatment options than those with epNETs. We did not identify any studies comparing the efficacy and safety of cabozantinib and other active comparators.
The CABINET trial included patients who had treatments like PRRT, 177Lu dotatate, everolimus, and targeted therapies or allowed cointerventions such as somatostatin analogues,10 which aligns well with treatment practices in Canada, enhancing the results’ generalizability to settings in Canada. The trial did not use specific inclusion criteria, such as randomizing only patients who tolerated or adhered to treatment, enhancing generalizability to the wider patient population. In the trial, patients received regular monitoring and dose adjustments, which aligned with routine practice in Canada, according to clinical experts. In addition, cabozantinib was administered after progression on prior therapies and at a dose of 60 mg orally daily with dose reductions specified for managing AEs, which are appropriate and align with its use in clinical practice in Canada, where dose adjustments are made based on patient tolerance. Given that cabozantinib is used similarly for other indications, the intervention has good applicability to practice in Canada.
The primary outcome of PFS and secondary outcomes such as OS and safety outcomes in the trial10 are clinically relevant and important to patients. These outcomes reflect measures of both efficacy and harms, and the methods used for assessing these outcomes (e.g., RECIST 1.1 criteria) align with clinical practice in Canada. Due to the lack of formal statistical comparisons and the high risk of bias in HRQoL data, we cannot draw any definitive conclusions on this patient-important outcome.
Results
Efficacy
Table 4 presents the results for outcomes important to this review. The results of sensitivity analyses for efficacy outcomes are consistent with the primary analyses. Figure 1 and Figure 2 present the Kaplan-Meier plots for PFS and OS in the epNET and pNET cohorts. Key results include the following:
PFS: Compared to placebo, cabozantinib was associated with an HR of 0.38 (95% confidence interval [CI], 0.25 to 0.59) for disease progression or death in the epNET cohort and an HR of 0.23 (95% CI, 0.12 to 0.42) in the pNET cohort.10
OS: The evidence was insufficient to show meaningful differences between the cabozantinib and placebo groups in both the epNET and pNET cohorts. The 95% CIs were wide and overlapped with the null threshold (i.e., HR = 1) in both the epNET and pNET cohorts, with the pNET cohort having a particularly wide 95% CI.10
HRQoL: The overall HRQoL remained stable over time among participants who completed the EORTC QLQ-C30 questionnaire and seemed comparable between the 2 groups in both the epNET and pNET cohorts. However, the 95% CIs were wide and overlapping for the 2 groups, based on descriptive mean scores and 95% CIs.10 Formal analyses for HRQoL have not been reported in the included study.
Sensitivity analyses: The trial conducted sensitivity analyses, including PFS as assessed by investigators, accounting for the misallocation of patients into the incorrect disease cohort.10 These analyses yielded consistent results with the primary analysis in both the epNET and pNET cohorts.
Figure 1: PFS and OS in the epNET Cohorts
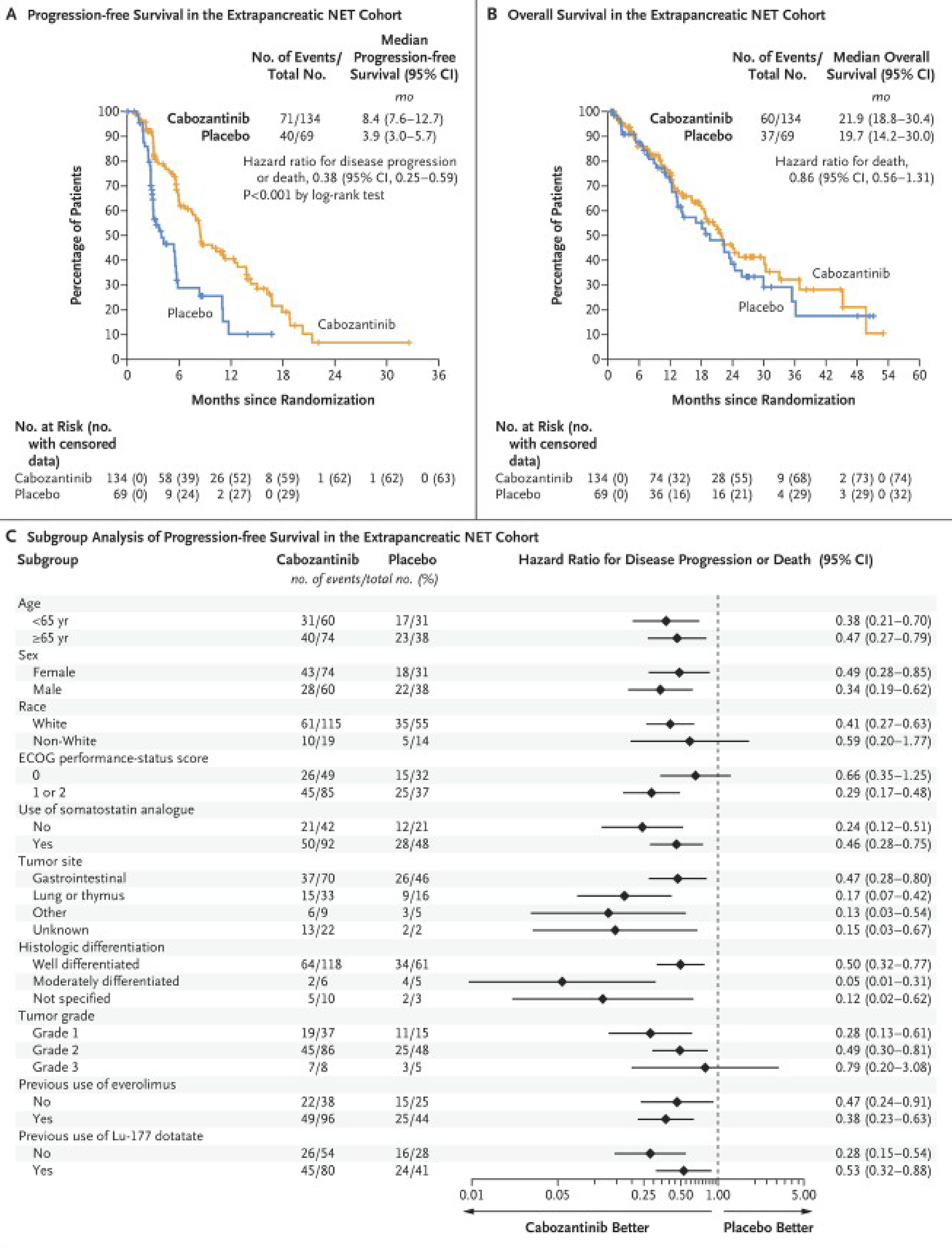
CI = confidence interval; ECOG = Eastern Cooperative Oncology Group; epNET = extrapancreatic neuroendocrine tumour; Lu-177 = lutetium dotatate; NET = neuroendocrine tumour; no. = number; OS = overall survival; PFS = progression-free survival; yr = year.
Source: From N Engl J Med, Chan JA, Geyer S, Zemla T, Knopp MV, Behr S, Pulsipher S, Ou FS, Dueck AC, Acoba J, Shergill A, Wolin EM, Halfdanarson TR, Konda B, Trikalinos NA, Tawfik B, Raj N, Shaheen S, Vijayvergia N, Dasari A, Strosberg JR, Kohn EC, Kulke MH, O’Reilly EM, Meyerhardt JA., Phase 3 Trial of Cabozantinib to Treat Advanced Neuroendocrine Tumors, 392(7), 653 to 665. Copyright © (2025) Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.10
Figure 2: PFS and OS in the pNET Cohorts
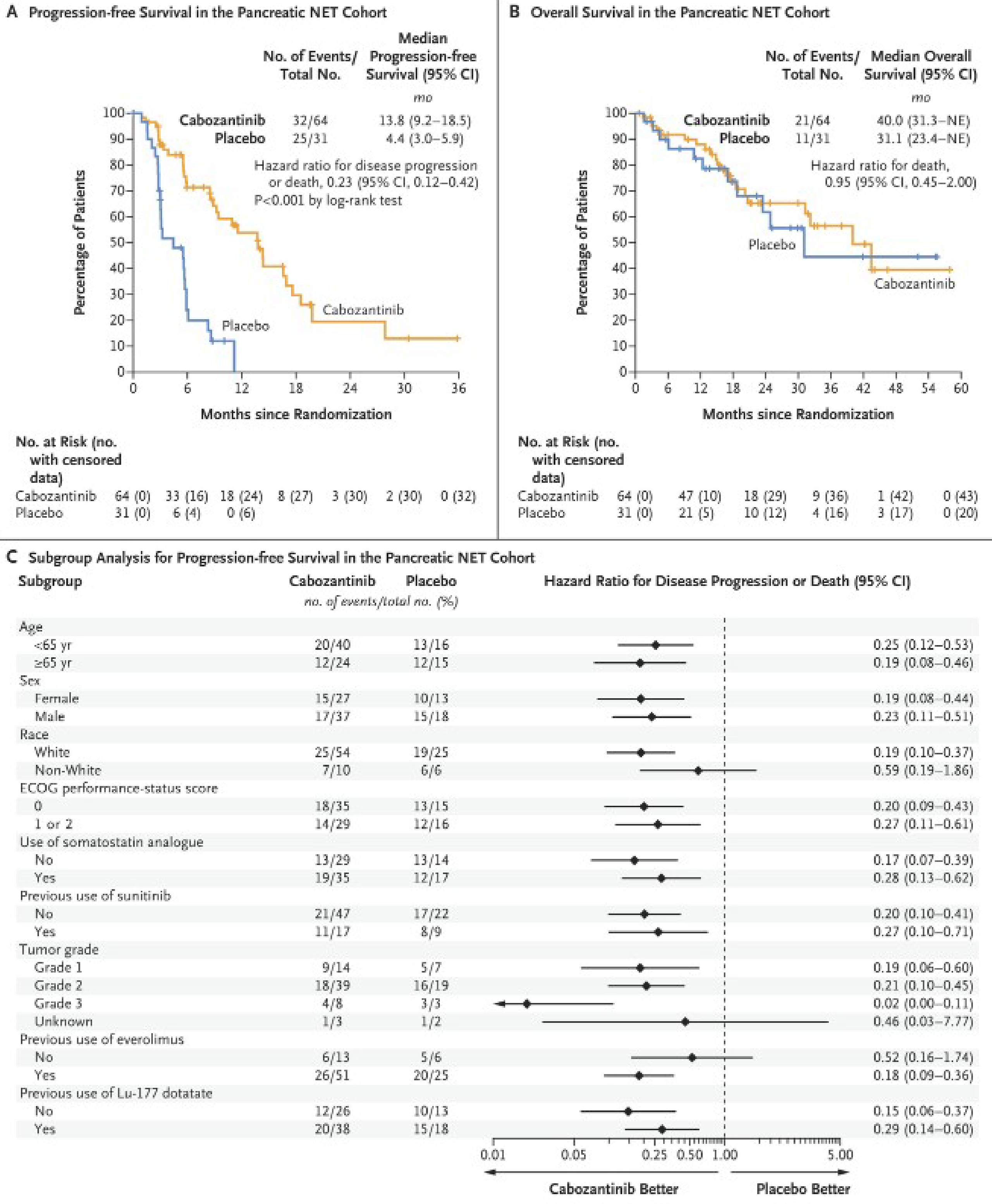
CI = confidence interval; ECOG = Eastern Cooperative Oncology Group; Lu-177 = lutetium dotatate; NET = neuroendocrine tumour; no. = number; OS = overall survival; PFS = progression-free survival; pNET = pancreatic neuroendocrine tumour; yr = year.
Source: From N Engl J Med, Chan JA, Geyer S, Zemla T, Knopp MV, Behr S, Pulsipher S, Ou FS, Dueck AC, Acoba J, Shergill A, Wolin EM, Halfdanarson TR, Konda B, Trikalinos NA, Tawfik B, Raj N, Shaheen S, Vijayvergia N, Dasari A, Strosberg JR, Kohn EC, Kulke MH, O’Reilly EM, Meyerhardt JA., Phase 3 Trial of Cabozantinib to Treat Advanced Neuroendocrine Tumors, 392(7), 653 to 665. Copyright © (2025) Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.10
Table 4: Summary of Key Efficacy Results Patient Disposition in the ITT Population
Variable | epNET cohort (n = 203) | pNET cohort (n = 95) | ||
|---|---|---|---|---|
Cabozantinib, n = 134 | Placebo, n = 69 | Cabozantinib, n = 64 | Placebo, n = 31 | |
PFSa | ||||
Patients with disease progression or death, n (%) | 71 (53) | 40 (58) | 32 (50) | 25 (81) |
Median (95% CI) time to event, months | 8.4 (7.6 to 12.7) | 3.9 (3.0 to 5.7) | 13.8 (9.2 to 18.5) | 4.4 (3.0 to 5.9) |
HR (95% CI) | 0.38 (0.25 to 0.59) | Reference | 0.23 (0.12 to 0.42) | Reference |
P value | < 0.001 | Reference | < 0.001 | Reference |
Median follow-up, months, (95% CI) | 10.2 (8.2 to 13.8) | 13.8 (10.1 to 19.7) | ||
OSb | ||||
Patients who died, n (%) | 60 (45) | 37 (54) | 21 (33) | 11 (35) |
Median (95% CI) time to event | 21.9 (18.8 to 30.4) | 19.7 (14.2 to 30.0) | 40.0 (31.3 to NE) | 31.1 (23.4 to NE) |
HR (95% CI) | 0.86 (0.56 to 1.31) | Reference | 0.95 (0.45 to 2.00) | Reference |
P value | NR | Reference | NR | Reference |
Median follow-up, months, (95% CI) | 24.2 (NR) | 23.1 (NR) | ||
HRQoLc | ||||
Descriptive results | The trial authors concluded that the overall HRQoL remained stable over time and was similar between the 2 groups in both cohorts. | |||
CI = confidence interval; epNET = extrapancreatic neuroendocrine tumour; HR = hazard ratio; HRQoL = health-related quality of life; ITT = intention to treat; NE = not estimable; NR = not reported; OS = overall survival; PFS = progression-free survival; pNET = pancreatic neuroendocrine tumour.
Notes: PFS were analyzed based on the ITT population.
OS and PFS: the trial calculated medians using the Kaplan-Meier method and constructed 95% CIs with the Brookmeyer-Crowley methodology. To estimate the HR, the trial used stratified Cox proportional hazards regression models, stratified by randomization strata, and tested the difference between groups using the stratified log-rank test.
HRQoL: HRQoL measures combined function and symptom scores to create a summary score. The study calculated descriptive means and 95% CIs; however, the full statistical analysis of HRQoL was not available.
aPFS: the time from randomization to radiographic progressive disease, according to Response Evaluation Criteria in Solid Tumours (RECIST) 1.1, as determined retrospectively by blinded independent central review or death from any cause.
bOS: time from randomization to death from any cause.
cHRQoL: measured by EORTC QLQ-C30 with higher scores = better HRQoL; reported the mean score and 95% CI; data were plotted in Supplementary Figure 5 of Chan et al. (2025).10
Source: Chan et al. (2025)10 and its supplementary appendix.
Harms
Table 5 presents the results for harm outcomes important to this review. Treatment-related AEs and serious AEs (judged by the investigator) and all Grade 5 AE (regardless of attribution) were reported. Any grade AEs and AEs of Grade 3 to 5 can be found in Table 6 to Table 9 within the Supplemental Materials. Key results include the following:
Compared to the placebo group, patients in the cabozantinib group had higher proportions of any grade treatment-related AEs, serious AEs, and withdrawals due to AEs. Specific AE leading to withdrawal were not reported. The results of planned statistical analyses (i.e., P values) for between-group differences were not reported.10
In the epNET cohort:
The most common (10% or more) treatment-related grade 3 or 4 adverse events were hypertension (21%), fatigue (13%), and diarrhea (11%).10 In contrast, the participants in the placebo group experienced these AEs at the following rates: 3% for hypertension, 7% for fatigue, and 4% for diarrhea.
Grade 5 events occurred in 9 patients (7%) in the cabozantinib group and 4 patients (6%) in the placebo group.10
In the pNET cohort:
The most common (10% or more) treatment-related grade 3 or 4 adverse events were hypertension (22%), fatigue (11%), and thromboembolic events (11%).10 In contrast, the participants in the placebo group experienced these AEs at the following rates: 10% for hypertension, 3% for fatigue, and 0% for thromboembolic events.
No grade 5 AEs were reported.10
Table 5: Summary of Key Safety Results
Safety outcomes | epNET cohort | pNET cohorta | ||
|---|---|---|---|---|
Cabozantinib, n = 132 | Placebo, n = 67 | Cabozantinib, n = 63 | Placebo, n = 31 | |
Treatment-related AEs, n (%) | 130 (98) | 55 (82) | 62 (98) | 26 (84) |
Treatment-related SAE (Grade 3 or higher AEs), n (%) | 82 (62) | 18 (27) | 41 (65) | 7 (23) |
WDAE | 34 (31) | 9 (15) | 10 (20) | 0 (0) |
Death due to AE | 9 (7) | 4 (6) | 0 | 0 |
AE = adverse event; epNET = extrapancreatic neuroendocrine tumour; pNET = pancreatic neuroendocrine tumour; SAE = serious adverse event; WDAE = withdrawal due to adverse events.
Note: The safety population included all patients who underwent randomization and received at least one dose of intervention or placebo.
aNo grade 5 AEs were reported in the pNET cohort.
Discussion
Efficacy
The CABINET trial examined the efficacy of cabozantinib in adults with locally advanced or metastatic epNETs or pNETs who had received at least 1 prior therapy.10 The trial reported relative hazard estimates and medians for assessing the efficacy of cabozantinib. The clinical experts consulted by the review team indicated that the observed benefit on PFS was clinically meaningful. Early termination based on interim analysis results could potentially overestimate the magnitude of the treatment effect. The small sample size, especially in the pNET cohort, and the limited ability to appraise the potential for missing data for both the epNET and pNET cohorts further contributes to uncertainty in effect estimations. Although cabozantinib showed improvements in PFS, the evidence was not sufficient to observe an OS difference between the trial groups at the time of analysis. The result may be influenced by the crossover of patients from the placebo group to cabozantinib and the high rate of subsequent anticancer therapies. It is unclear whether further follow-up would change the results.
Compared with other anti–vascular endothelial growth factor receptor-targeting tyrosine kinase inhibitors, such as sunitinib, axitinib, and pazopanib, cabozantinib is a multitarget tyrosine kinase inhibitor that includes MET and AXL, which may contribute to its efficacy.14 While sunitinib is approved for pNET, other inhibitors have shown activity but are not approved in Canada or elsewhere.15,16
The generalizability of the study results may be limited by the exclusion of certain patient subpopulations, such as those with poor physical performance scores (ECOG 3 or greater), poorly differentiated neuroendocrine carcinoma, and high-grade neuroendocrine carcinoma without specification of differentiation status. Clinical experts suggest that these patients might benefit from cabozantinib treatment, but further research is needed to support this. The use of a placebo rather than an active comparator may affect the interpretation of clinical relevance, as the efficacy of therapy for patients with advanced NETs after progression on prior treatments is not well established. No studies were identified that compared cabozantinib with other active comparators (e.g., sunitinib).
Clinician inputs from clinical experts and clinician groups emphasized the need for additional therapies for patients with advanced NETs. Additionally, the views of clinician groups and clinical experts highlight the importance of individualized treatment based on patient preferences and characteristics. Patient group input identified HRQoL, PFS, and OS as important outcomes. The improvement in PFS with cabozantinib supports an advantage for this outcome, but the uncertainty in the OS and HRQoL findings suggests a lack of clarity about whether it meets all the unmet clinical needs identified by interest-holders. HRQoL appeared to remain stable over time,10 which may be an important consideration for patients in terms of drug tolerance. However, the high risk of bias in HRQoL data indicates that we need to interpret the findings with caution. The clinical experts consulted for this review noted that, despite the AEs associated with cabozantinib, the stability and similarity in QoL between cabozantinib and placebo suggest some benefits for patients in the cabozantinib group.
Although OS benefit was not demonstrated, the clinical experts highlighted that this might be attributed to early trial termination upon meeting the primary end point, ethical crossover from the placebo arm to active treatment, and the indolent nature of epNETs and pNETs, which makes demonstrating OS benefit challenging. The clinical experts indicated that similar patterns have been seen in other NET trials, such as NETTER-1, in which PFS benefit did not translate into OS benefit.17 Clinical experts believed that conducting a larger trial with OS as the primary end point would not be feasible.
Harms
Cabozantinib treatment in patients with advanced NETs has been associated with a higher incidence of AEs compared to placebo. Common treatment-related AEs included hypertension, fatigue, diarrhea, and thromboembolic events.10 Grade 3 or higher AEs occurred in 62% or 65% of patients treated with cabozantinib, compared to 27% or 23% of patients receiving placebo in the epNET and pNET cohorts, respectively.10 Clinical experts suggest that although these safety issues are significant, they are generally manageable in clinical practice through dose modifications and supportive care measures. Patient group input highlights that despite the high incidence of AEs, patients may consider these harms acceptable if the drug provides significant clinical benefits.
Several limitations may affect the interpretation of safety results.10 Early termination of the trial based on interim analysis results precluded the ability to assess longer-term AEs.10 Using placebo rather than an active comparators may limit understanding of relative safety compared to other active treatments.10 The absence of long-term safety data and direct comparative data versus relevant active comparators are gaps in the current evidence.
Conclusion
The CABINET trial10 provides evidence that cabozantinib significantly improves PFS in adults with locally advanced or metastatic epNETs or pNETs that has progressed after prior therapies. This efficacy aligns with patient expectations for extended disease control. There is some uncertainty in the findings due to the interim nature of the analysis, small sample size, and limited ability to assess the impact of potential missing data. The evidence was insufficient to show a benefit of cabozantinib on OS. Longer follow-up for OS may be informative; however, allowance for crossover from placebo to cabozantinib will challenge the ability to observe a difference between groups. HRQoL was not analyzed statistically and was at risk of bias due to missing outcome data. The safety profile of cabozantinib, characterized by a high incidence of grade 3 or higher AEs such as hypertension, fatigue, and diarrhea, requires careful management and dose adjustments. The lack of data on specific populations, such as those with poor ECOG performance scores, leads to uncertain generalizability in these populations. We did not identify any studies comparing the efficacy and safety of cabozantinib and other active comparators in advanced or metastatic NETs.
Economic Review
The economic review consisted of a cost comparison for cabozantinib compared with everolimus, sunitinib, CAPTEM, and 177Lu dotatate for adults with locally advanced or metastatic extrapancreatic or pancreatic neuroendocrine tumours who have received at least 1 prior therapy. CAPTEM was considered a comparator only for pancreatic neuroendocrine tumours.
Based on public list prices, cabozantinib is expected to have a per-patient cost of $8,436 per 28 days. Everolimus, sunitinib, CAPTEM, and 177Lu dotatate are expected to have per-patient costs of $4,823, $4,650, $813, and $17,500 per 28 days, respectively (Table 11, Appendix 6). Therefore, the incremental costs of cabozantinib per patient per 28-day cycle are $3,613, $3,786, and $7,623 compared to everolimus, sunitinib, and CAPTEM, respectively. Compared to 177Lu dotatate, cabozantinib is associated with incremental savings of $9,064. As such, the impact of the reimbursement of cabozantinib for the treatment of locally advanced or metastatic extrapancreatic or pancreatic neuroendocrine tumours in patients who have received at least 1 prior therapy is contingent on which treatments are displaced. Additional items for consideration are provided in the following bullets:
According to the clinical review, evidence from the CABINET trial10 assessing the efficacy and safety of cabozantinib compared with placebo in adults with locally advanced or metastatic epNETs or pNETs whose disease has progressed after prior therapies suggests that cabozantinib improved PFS and increased the incidence of grade 3 or higher side effects. OS results were uncertain due to the short follow-up. No evidence was identified regarding the comparative efficacy and safety of cabozantinib versus other active comparators.
As of April 2025, cabozantinib is only available as a brand name product in Canada. There are 2 generics under review by Health Canada (Table 1).
No health care resource use outcomes were reported in the clinical trial.10
According to the clinical experts consulted for this review, cabozantinib is expected to have similar treatment-related health care resource use compared with other treatments available in Canada. They noted that 177Lu dotatate is a radioactive therapy that is only administered in a tertiary referral centre with dedicated nuclear medicine and/or radiation oncology and, therefore, it is expected that cabozantinib would have lower administration costs when compared with 177Lu dotatate.
Cabozantinib was previously reviewed by CDA-AMC for different indications only. CDA-AMC previously reviewed 177Lu dotatate (2022), everolimus (2016), and sunitinib (2012) for patients with NETs, for which positive recommendations for reimbursement were issued.
No Canadian cost-effectiveness studies were identified based on a literature search conducted on May 20, 2025.
Conclusion
The impact of the reimbursement of cabozantinib for the treatment of locally advanced or metastatic extrapancreatic or pancreatic neuroendocrine tumours in patients who have received at least 1 prior therapy is uncertain. Based on public list prices, cabozantinib would result in higher drug costs to the health system compared to most comparators (everolimus, sunitinib, and CAPTEM), with the exception of 177Lu dotatate, against which cabozantinib would result in lower costs. It is unknown whether there is a clinical benefit when comparing cabozantinib versus all relevant comparators.
References
1.Strosberg JR. Post TW, ed. Clinical characteristics of well-differentiated neuroendocrine tumors arising in the gastrointestinal and genitourinary tracts. UpToDate; 2025. Accessed February 12, 2025. http://www.uptodate.com/
2.CADTH. Drug Reimbursement Review: cabozantinib (Cabometyx) for differentiated thyroid carcinoma. 2022. Accessed February 12, 2025. https://www.cda-amc.ca/cabozantinib
3.CADTH. Drug Reimbursement Review: cabozantinib (Cabometyx) for advanced or metastatic renal cell carcinoma. 2023. Accessed February 12, 2025. https://www.cda-amc.ca/cabozantinib-0
4.Singh S, Granberg D, Wolin E, et al. Patient-Reported Burden of a Neuroendocrine Tumor (NET) Diagnosis: Results From the First Global Survey of Patients With NETs. J Glob Oncol. 2017;3(1):43-53. doi:10.1200/jgo.2015.002980 PubMed
5.Rindi G, Mete O, Uccella S, et al. Overview of the 2022 WHO Classification of Neuroendocrine Neoplasms. Endocr Pathol. 2022;33(1):115-154. doi:10.1007/s12022-022-09708-2 PubMed
6.Strosberg JR. Post TW, ed. Classification, clinical presentation, diagnosis, and staging of pancreatic neuroendocrine neoplasms. UpToDate; 2025. Accessed February 12, 2025. http://www.uptodate.com/
7.Basuroy R, Bouvier C, Ramage JK, Sissons M, Srirajaskanthan R. Delays and routes to diagnosis of neuroendocrine tumours. BMC Cancer. 2018;18(1):1122. doi:10.1186/s12885-018-5057-3 PubMed
8.Hallet J, Law CH, Cukier M, Saskin R, Liu N, Singh S. Exploring the rising incidence of neuroendocrine tumors: a population-based analysis of epidemiology, metastatic presentation, and outcomes. Cancer. 2015;121(4):589-97. doi:10.1002/cncr.29099 PubMed
9.Zhang JY, Kunz PL. Making Sense of a Complex Disease: A Practical Approach to Managing Neuroendocrine Tumors. JCO Oncol Pract. 2022;18(4):258-264. doi:10.1200/OP.21.00240 PubMed
10.Chan JA, Geyer S, Zemla T, et al. Phase 3 Trial of Cabozantinib to Treat Advanced Neuroendocrine Tumors. N Engl J Med. 2025;392(7):653-665. doi:10.1056/NEJMoa2403991 PubMed
11.Kuitunen I, Ponkilainen VT, Uimonen MM, Eskelinen A, Reito A. Testing the proportional hazards assumption in cox regression and dealing with possible non-proportionality in total joint arthroplasty research: methodological perspectives and review. BMC Musculoskelet Disord. 2021;22(1):489. doi:10.1186/s12891-021-04379-2 PubMed
12.Bassler D, Montori VM, Briel M, Glasziou P, Guyatt G. Early stopping of randomized clinical trials for overt efficacy is problematic. J Clin Epidemiol. 2008;61(3):241-6. doi:10.1016/j.jclinepi.2007.07.016 PubMed
13.Ter-Minassian M, Zhang S, Brooks NV, et al. Association Between Tumor Progression Endpoints and Overall Survival in Patients with Advanced Neuroendocrine Tumors. Oncologist. 2017;22(2):165-172. doi:10.1634/theoncologist.2016-0175 PubMed
14.Hyde AJ, Nassabein R, AlShareef A, et al. Eastern Canadian Gastrointestinal Cancer Consensus Conference 2018. Curr Oncol. 2019;26(5):e665-e681. doi:10.3747/co.26.5193 PubMed
15.Grillo F, Florio T, Ferraù F, et al. Emerging multitarget tyrosine kinase inhibitors in the treatment of neuroendocrine neoplasms. Endocr Relat Cancer. 2018;25(9):R453-R466. doi:10.1530/erc-17-0531 PubMed
16.Taboada RG, Cavalher FP, Rego JF, Riechelmann RP. Tyrosine kinase inhibitors in patients with neuroendocrine neoplasms: a systematic literature review. Ther Adv Med Oncol. 2024;16:17588359241286751. doi:10.1177/17588359241286751 PubMed
17.Strosberg JR, Caplin ME, Kunz PL, et al. (177)Lu-Dotatate plus long-acting octreotide versus high-dose long-acting octreotide in patients with midgut neuroendocrine tumours (NETTER-1): final overall survival and long-term safety results from an open-label, randomised, controlled, phase 3 trial. Lancet Oncol. 2021;22(12):1752-1763. doi:10.1016/s1470-2045(21)00572-6 PubMed
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.