Drugs, Health Technologies, Health Systems
Reimbursement Recommendation
Trabectedin
Reimbursement request: In combination with doxorubicin as first-line treatment for advanced unresectable or metastatic uterine or soft tissue leiomyosarcoma
Requester: Public drug programs
Final recommendation: Reimburse with conditions
Summary
What Is the Reimbursement Recommendation for Trabectedin?
The Formulary Management Expert Committee (FMEC) recommends that trabectedin in combination with doxorubicin be reimbursed as first-line treatment for patients with advanced unresectable or metastatic uterine or soft tissue leiomyosarcoma, provided certain conditions are met.
What Are the Conditions for Reimbursement?
Trabectedin in combination with doxorubicin may be reimbursed for the treatment of adult patients aged 18 years or older with histologically confirmed leiomyosarcoma who have not previously received chemotherapy in the locally advanced or metastatic setting. A price reduction for trabectedin may be required.
Why Did CDA-AMC Make This Recommendation?
FMEC reviewed the Canada’s Drug Agency (CDA-AMC) report, which included a review of the clinical evidence, specifically 1 randomized controlled phase III trial (LMS04) comparing trabectedin in combination with doxorubicin versus doxorubicin in previously untreated advanced or metastatic uterine or soft tissue leiomyosarcoma and a cost comparison of trabectedin in combination with doxorubicin versus other treatments used in Canada. FMEC also considered input received from 1 patient group, the Canadian Cancer Society, and 1 clinician group, the Ontario Health (Cancer Care Ontario) Gynecological Cancer Drug Advisory Committee.
Based on the CDA-AMC assessment of the health economic evidence, which consisted of a cost comparison table, reimbursement of trabectedin in combination with doxorubicin is associated with higher drug acquisition costs to publicly funded drug programs than relevant comparators, based on publicly available list prices. The cost-effectiveness of trabectedin in combination with doxorubicin compared to relevant comparators is unknown. A price reduction may therefore be required.
FMEC concluded that it is uncertain regarding if trabectedin in combination with doxorubicin demonstrates acceptable clinical value versus appropriate comparators. While trabectedin in combination with doxorubicin demonstrated improved progression-free survival by blinded independent central review compared to doxorubicin monotherapy, and possibly other survival benefits, the magnitude of effect is uncertain. The reimbursement conditions were further developed based on significant unmet clinical needs, distinct social and ethical considerations, economic considerations, and impacts on health systems of soft tissue and uterine leiomyosarcoma.
Therapeutic Landscape
What Is Soft Tissue or Uterine Leiomyosarcoma?
Soft tissue sarcomas are a heterogeneous group of rare tumours. Leiomyosarcoma is the most frequent subtype of soft tissue sarcoma, originating in smooth muscle such as the gastrointestinal tract, large blood vessels, or the uterus. Patients with soft tissue sarcomas commonly present with a gradually enlarging, painless mass and may develop symptoms such as pain, paresthesia, or edema. Patients with uterine leiomyosarcomas can experience no symptoms or abnormal uterine bleeding, abdominal distention or pain, or pelvic pain or pressure. Common sites of metastases include the liver, lung, upper abdomen, and pelvis. Approximately 30% of patients with newly diagnosed uterine leiomyosarcoma present with distant metastatic disease.
In 2024, an estimated 1,700 people in Canada were diagnosed with soft tissue sarcoma and 660 died from the disease. In Norway, the incidence of uterine leiomyosarcoma from 2000 to 2012 was 0.86 per 100,000 people, according to the Cancer Registry of Norway.
What Are the Current Treatment Options?
Pharmacological treatments for advanced unresectable or metastatic soft tissue or uterine leiomyosarcoma include doxorubicin monotherapy, gemcitabine-docetaxel, and doxorubicin-ifosfamide.
What Is the Treatment Under Review?
Trabectedin is an antineoplastic drug that binds to DNA and triggers a cascade of events that leads to apoptosis and tumour cell death. Available as a 1 mg per vial powder for IV administration via central line, trabectedin is approved by Health Canada to be used with pegylated liposomal doxorubicin for patients with platinum-sensitive ovarian cancer or relapsed ovarian cancer. Trabectedin is also approved for the treatment of patients with metastatic liposarcoma or leiomyosarcoma after failure of prior anthracycline and ifosfamide chemotherapy. The use of trabectedin in combination with nonpegylated doxorubicin in the first-line treatment of soft tissue and uterine leiomyosarcoma is considered off-label.
Why Did We Conduct This Review?
Clinicians from a provincial sarcoma disease site group and a gynecology-oncology disease site group have requested that trabectedin in combination with doxorubicin be funded, given the emerging evidence and unmet needs in unresectable or metastatic leiomyosarcoma. The data protection for trabectedin ended on May 13, 2018, with 1 generic currently under review by Health Canada. This drug is therefore eligible for nonsponsored reimbursement review, per the Procedures for Reimbursement Reviews. At the request of participating public drug programs, we reviewed the efficacy and safety of trabectedin in combination with doxorubicin as first-line treatment for adults with advanced unresectable or metastatic soft tissue or uterine leiomyosarcoma.
Input From Interested Parties
One patient group, the Canadian Cancer Society, highlighted that individuals with leiomyosarcoma require timely and equitable access to affordable treatments that improve survival, prolong disease remission, and improve health-related quality of life with minimal side effects. The patient group also highlighted that, because the disease is rare and its presentation is heterogeneous, these patients do not always receive timely and accurate diagnosis. Therefore, they also cannot receive timely and appropriate treatment through specialized health care providers. There are also challenges to maintaining their quality of life.
One clinician group, the Ontario Health (Cancer Care Ontario) Gynecological Cancer Drug Advisory Committee, advocated for patients with leiomyosarcoma to access new treatments that can delay disease progression with reduced intolerance and toxicity.
Public drug plans inquired about the evidence for trabectedin in combination with doxorubicin to inform a recommendation on whether it should be reimbursed for adults with advanced unresectable or metastatic soft tissue or uterine leiomyosarcoma. The public drug plans outlined implementation questions related to treatment eligibility and potential costs.
Disclaimer: The perspectives shared by people with lived experience who present to the committee reflect their individual experiences and are not necessarily representative of all people with the same condition or course of treatment. Their insights provide valuable context about what a patient, support person, or caregiver might go through when facing this condition or treatment, helping to inform the committee’s deliberations. These narratives complement other forms of evidence and input and should be considered as part of a broader understanding of the condition and treatment under review. When gender or gendered pronouns are used in these narratives, they are included with the permission of the individual.
Summary of Deliberation
The Formulary Management Expert Committee (FMEC) deliberated on all domains of value of the deliberative framework before developing their recommendation: clinical value, unmet clinical need, distinct social and ethical considerations, economic considerations, and impacts on health systems. For further information on the domains of value, please refer to the Expert Committee Deliberation at Canada’s Drug Agency document.
FMEC considered the following key discussion points, organized by the 5 domains of value.
Clinical Value
FMEC concluded that it is uncertain whether trabectedin in combination with doxorubicin demonstrates acceptable clinical value versus appropriate comparators in the setting in Canada.
Through reflection on the input from patient groups or insights shared by the person with lived experience, FMEC members noted the following important patient values or perspectives: patients seek treatments that improve survival, prolong remission, and improve health-related quality of life with minimal side effects.
FMEC members highlighted the following discussion points:
Based on the LMS04 trial, there was prolonged progression-free survival (PFS) with trabectedin in combination with doxorubicin versus doxorubicin alone (12 months versus 6 months; hazard ratio for progression or death = 0.37 [95% CI, 0.26 to 0.53]). The probability of PFS at 2 years was 30% in the trabectedin-doxorubicin group versus 3% in the doxorubicin group. Time to overall survival (OS) was a median of 33 months in the trabectedin-doxorubicin group versus 24 months in the doxorubicin group (hazard ratio = 0.65; 95% CI, 0.44 to 0.95); probability of OS at 2 years was 68% in the trabectedin-doxorubicin group versus 49% in the doxorubicin group.
FMEC acknowledged some uncertainty in the magnitude of OS benefit with trabectedin in combination with doxorubicin due to confidence intervals that indicate the possibility of no difference when compared with doxorubicin. Furthermore, the evidence was insufficient to demonstrate a difference in objective response rate between treatment groups due to a lack of reported data.
However, FMEC also heard from clinical experts that 1 key benefit of trabectedin in combination with doxorubicin is its ability to improve the patient’s candidacy for surgical resection and the ability to receive debulking surgeries throughout the disease journey. These surgical opportunities likely contribute to the survival benefits for patients.
FMEC discussed concerns regarding the harms of treatment with trabectedin-doxorubicin versus doxorubicin, including serious adverse events (AEs) (50% versus 27%, respectively), AEs of grade 3 or 4 (97% versus 56%), and withdrawals due to AEs (9% versus 4%). Notably, there was a higher incidence and severity of hematologic events (e.g., neutropenia, febrile neutropenia, and thrombocytopenia) in the combination treatment group compared with the doxorubicin group. Finally, there was a higher incidence of liver toxicity in the combination treatment group. Although AEs were higher in the trabectedin in combination with doxorubicin group, FMEC noted that deaths at the primary analysis occurred in 57% of patients in the trabectedin in combination with doxorubicin group compared with 67% of patients in the doxorubicin group.
FMEC discussed that the study’s comparator aligns with 1 of several treatment options in clinical practice. In addition to doxorubicin used in the LMS04 trial, gemcitabine-docetaxel and doxorubicin-ifosfamide are available in the first-line setting for leiomyosarcoma in Canada.
Unmet Clinical Need
FMEC concluded that there is a significant clinical need arising from advanced or metastatic soft tissue or uterine leiomyosarcoma despite available treatments.
Through reflection on the input from patient groups or insights shared by the person with lived experience, FMEC members noted the following important patient values or perspectives: the need for increased awareness about leiomyosarcoma, improved diagnostic protocols, and effective therapies with fewer side effects.
FMEC members highlighted the following discussion points:
Given the heterogeneity and rarity of leiomyosarcoma, including uterine leiomyosarcoma (with an estimated incidence of 0.86 per 100,000 people); the need to receive a timely and accurate diagnosis; and the limited access to specialized health care providers for receiving timely and appropriate treatment, latitude for uncertainty in clinical evidence should be considered.
The treatment of patients with unresectable or metastatic soft tissue sarcoma is palliative in intent. Available chemotherapy options include single drugs (e.g., pegylated liposomal doxorubicin or gemcitabine) or combination anthracycline-based regimens (doxorubicin plus ifosfamide, gemcitabine plus docetaxel, or doxorubicin plus dacarbazine); these treatments do not significantly modify the disease trajectory and demonstrate low objective response rates, and AEs are common.
Soft tissue sarcomas are rare tumours. The 5-year OS of metastatic soft tissue sarcoma is estimated to range from 15% to 25%, with a median survival of 12 to 24 months. Uterine leiomyosarcoma is an aggressive tumour with a high risk of relapse and a poor prognosis, regardless of disease stage at presentation.
FMEC also noted that most patients were willing to tolerate more severe or frequent side effects if treatments offered a significant improvement in survival or quality of life or longer remissions.
Distinct Social and Ethical Considerations
FMEC concluded that trabectedin in combination with doxorubicin would not address a significant nonclinical need arising from advanced or metastatic soft tissue or uterine leiomyosarcoma despite available treatments.
FMEC did not identify any important measures that should be implemented to ensure that the use of trabectedin in combination with doxorubicin addresses relevant social and ethical implications.
Through reflection on the input from patient groups or insights shared by the person with lived experience, FMEC members noted the following important patient values and perspectives: there is a lack of awareness that leiomyosarcoma and the need for self-advocacy (e.g., to obtain tests, treatments, and referrals) add to the burden of the disease. Patients residing in rural locations or small provinces face additional geographical challenges in accessing specialized treatment centres, which results in a greater financial burden due to travel and time away from work.
FMEC members highlighted the following discussion points:
Despite available treatments, multiple nonclinical needs exist, including considerations related to parenteral therapy, specialized care providers, and treatment centres. There is also a need for travel for treatment, and there is a treatment burden placed on the patient, their family, and their caregivers.
Economic Considerations
FMEC concluded that there are economic considerations that would be important to address when implementing the reimbursement of trabectedin in combination with doxorubicin.
FMEC members highlighted the following discussion points:
The per-patient, per 28-day cost of trabectedin in combination with doxorubicin is higher than the costs of doxorubicin monotherapy, docetaxel plus gemcitabine, and doxorubicin plus ifosfamide.
Compared to doxorubicin monotherapy, trabectedin in combination with doxorubicin has improved PFS and may have improved OS.
Doxorubicin makes up approximately 45% of therapies used in Canada for this population; therefore, the committee noted that the available evidence is relevant to approximately 45% of patients.
The comparative clinical effectiveness of docetaxel plus gemcitabine and doxorubicin plus ifosfamide is unknown.
The cost-effectiveness of trabectedin relative to any comparators is unknown.
Given the extent of uncertainty due to the lack of data and the incremental cost of trabectedin, a price reduction is warranted.
Trabectedin is available only as a branded product in Canada (Yondelis). As of June 10, 2025, there were no generic versions of trabectedin available and no pan-Canadian Pharmaceutical Alliance negotiations. One generic submission is under review by Health Canada.
Additional cost implications not included in the calculation of drug administration costs include:
potentially higher costs associated with AEs, such as liver toxicity and febrile neutropenia when compared to doxorubicin monotherapy
potentially higher costs of treatment due to the administration of granulocyte colony-stimulating factor for primary prophylaxis of febrile neutropenia when compared to doxorubicin monotherapy and docetaxel plus gemcitabine
potentially lower costs of hospitalizations or outpatient visits related to better drug tolerance compared to doxorubicin plus ifosfamide.
Impacts on Health Systems
FMEC did not identify any impacts on health systems that are important to address when implementing treatment with trabectedin in combination with doxorubicin.
FMEC members highlighted the following discussion points:
The treatment duration is longer with trabectedin in combination with doxorubicin. For example, doxorubicin is administered as a 10- to 15-minute infusion, followed by trabectedin as a 3-hour infusion every 3 weeks for 6 cycles followed by trabectedin every 3 weeks for up to 17 cycles. The comparator of doxorubicin monotherapy is expected to be administered as a 10- to 15-minute infusion every 3 weeks for up to 6 cycles in both initial and maintenance therapy.
However, given the rarity of leiomyosarcoma, it is anticipated that treatment with trabectedin in combination with doxorubicin will have minimal impact on health systems.
Figure 1: Recommendation Pathway
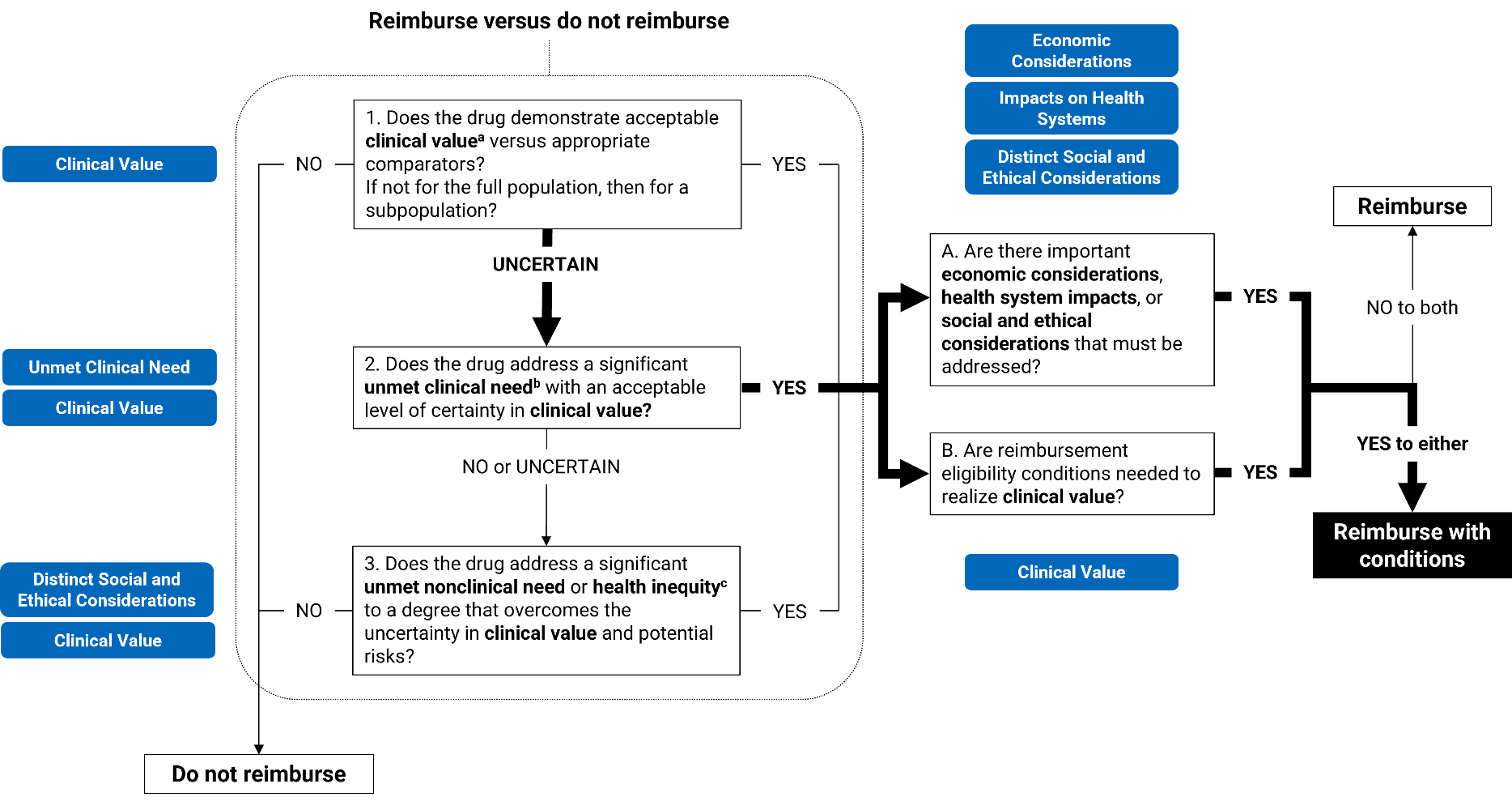
aAcceptable clinical value refers to at least comparable clinical value (if the drug is expected to be substitutive treatment) or added clinical value (if the drug is expected to be additive treatment) versus appropriate comparators.
bSignificant unmet clinical need depends on all of the following: severity of the condition, availability of effective treatments, and challenges in evidence generation due to the rarity of the condition or ethical issues.
cUnmet nonclinical need and health inequity are key components within the distinct and social ethical considerations domain of value.
Full Recommendation
With a vote of 7 to 0, FMEC recommends that trabectedin in combination with doxorubicin, for the treatment of advanced unresectable or metastatic uterine or soft tissue leiomyosarcoma in adults, be reimbursed if the conditions presented in Table 1 are met.
Table 1: Conditions, Reasons, and Guidance
Reimbursement condition | Reason | Implementation guidance |
|---|---|---|
Initiation | ||
1. Trabectedin-doxorubicin may be initiated in patients with locally advanced or metastatic uterine or soft tissue leiomyosarcoma who meet all of the following criteria: 1.1. aged 18 years or older 1.2. have not previously received chemotherapy in the locally advanced and/or metastatic setting. | Evidence from the LMS04 trial demonstrated that treatment with trabectedin-doxorubicin resulted in a clinical benefit in patients with these characteristics. | The diagnosis of leiomyosarcoma should be histologically confirmed. Eligible patients may include those who have received prior surgery, radiotherapy, or hormone therapy. |
2. Patients should have good performance status. | Patients with an ECOG performance status of 0 to 1 were included in the LMS04 trial. | Patients should have good performance status as determined by the treating clinician. |
Discontinuation and renewal | ||
3. Trabectedin-doxorubicin should be discontinued in 1 of the following situations: 3.1. disease progression 3.2. unacceptable toxicities. | Consistent with clinical practice, patients in the LMS04 trial discontinued treatment upon disease progression or significant AEs. In the LMS04 trial, patients were monitored with imaging (CT or MRI) every 6 weeks during treatment and at 3 weeks after the last treatment cycle. During maintenance treatment, imaging was conducted every 9 weeks until disease progression or up to 12 months. | Patients should be monitored for clinical response as per standard local practice. |
Prescribing | ||
4. Prescribing should be limited to clinicians with expertise in the diagnosis and management of sarcomas. Treatment should be delivered and supervised in institutions with appropriate monitoring of systemic therapy. | This will ensure that appropriate treatment is prescribed for patients and AEs are optimally managed. | — |
5. Trabectedin-doxorubicin should only be reimbursed when started as a combination therapy. | Trabectedin was initiated in combination with doxorubicin in the LMS04 trial. | — |
Pricing | ||
6. A price reduction may be required | The reimbursement of trabectedin-doxorubicin is expected to increase overall drug acquisition costs. No evidence was identified regarding the cost-effectiveness of trabectedin relative to its comparators. A cost-effectiveness analysis would be needed to determine whether trabectedin is cost-effective. Price reductions may be required, given that trabectedin-doxorubicin is associated with higher drug acquisition costs and potential clinical benefit vs. doxorubicin, but unknown benefit relative to other active comparators. | — |
AE = adverse events; ECOG = Eastern Cooperative Oncology Group; vs. = versus.
Feedback on Draft Recommendation
CDA-AMC received 1 clinician group feedback submission from the Ontario Health (Cancer Care Ontario) Gynecological Cancer Drug Advisory Committee as well as feedback from the public drug programs on the draft recommendation. The clinician group was largely in support of the recommendation. Both groups requested clarity on the re-treatment with trabectedin monotherapy. Editorial changes have been incorporated. Further clarification was also made that the consideration of trabectedin in the second-line setting was not the focus of this review.
FMEC Information
Members of the committee: Dr. Emily Reynen (Chair), Dr. Zaina Albalawi, Dr. Hardit Khuman, Ms. Valerie McDonald, Dr. Bill Semchuk, Dr. Jim Silvius, Dr. Marianne Taylor, Dr. Maureen Trudeau, Dr. Dominika Wranik. Two guest specialists from the Prairies participated in this review.
Regrets: One expert committee member did not attend the meeting.
Meeting date: July 17, 2025
Conflicts of interest: None
Special thanks: CDA-AMC extends our special thanks to the individuals who presented directly to FMEC and to patient organizations representing the community of those living with leiomyosarcoma, including the Canadian Cancer Society, Sasha Frost, and Leeann Noye.
Note: CDA-AMC makes every attempt to engage with people with lived experience as closely to the indication and treatments under review as possible; however, at times, CDA-AMC is unable to do so and instead engages with individuals with similar treatment journeys or experience with comparators under review to ensure lived experience perspectives are included and considered in reimbursement reviews. CDA-AMC is fortunate to be able to engage with individuals who are willing to share their treatment journey with FMEC.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.