Peer-Reviewed Article
National and International Policies on the Use of Biosimilars: An Environmental Scan
Jaemin Kim, Jessica Arias, Scott Gavura
Ontario Health Provincial Drug Reimbursement Programs
Environmental Scan
Key Messages
Biosimilars are biologic drugs that are highly similar to their reference biologics that were already authorized for sale.
Interchangeability is a term used to describe when 1 drug can be exchanged for another and is expected to have the same clinical effect. Interchangeability may allow 1 medicine to be substituted for another at the time of dispensing (automatic substitution). However, the decision to allow automatic substitution is made by each jurisdiction according to its own regulations.
Interchangeability of a reference biologic (the originator product) and a biosimilar is a designation in the US and Finland. The US, France, Germany, Norway, and Australia allow automatic substitution between reference biologics and biosimilars, whereas other countries do not. Interchangeability is limited to select products in the US and Australia.
The countries included in this Environmental Scan (N = 13) endorse starting patients who have not yet received treatment on a biosimilar. Switching between reference biologics and biosimilars is generally allowed in all the countries included in this review; however, many jurisdictions prefer switching be clinician led with ongoing clinical monitoring of patients.
Practices such as target setting, quotas, and financial incentives, as well as guidelines and recommendations for prescription of biosimilars, can be effective ways to encourage biosimilar use. Mandatory switching is also implemented in 11 Canadian jurisdictions.
Extrapolation is the regulatory and scientific process of granting a clinical indication to a medicine without clinical efficacy and safety data to support that indication. Extrapolation of indications for reference biologics to biosimilars is reasonable, provided several factors are comparable: mechanism of action across indications, pharmacokinetics and biodistribution, safety, immunogenicity, and other factors that affect the safety and efficacy for each indication and patient population.
Pricing and procurement practices vary internationally. Some countries implement policies controlling the list price of a biosimilar (and its reference drug less commonly) at the time of biosimilar launch. Pricing policies include a free-pricing policy (i.e., manufacturers are free to set the price of biosimilars) and mandatory price reductions. Tendering is the most common practice in procurement to achieve lower prices and to increase biosimilar uptakes in 8 countries reviewed in this Environmental Scan.
Biosimilar-related policies and markets are rapidly evolving, so recent changes might have not been fully captured in this Environmental Scan. Therefore, caution is required in interpreting the findings.
Context and Policy Issues
The FDA defines a biosimilar as “a biological product that is highly similar to and has no clinically meaningful differences from an existing FDA-approved reference product” in terms of safety, purity, and potency. Biological products or biologics are derived from living organisms; they differ from traditional drugs in terms of structural complexities, manufacturing process, and regulatory requirements. As a result, biologics usually have a higher price than traditional drugs, which can create barriers to access. Biosimilars are designed to increase access for patients who need treatment with a biologic medicine.
Because biosimilars are biologic medicines, they differ from generic drugs in terms of their molecular size and structure as well as the complexity and cost of development. Biosimilars are typically larger and more complex molecules that are more complex to manufacture than generics, which are typically small molecules, and have significantly higher research and development costs and risks. Unlike generic drugs which contain identical ingredients to their reference products, biosimilars are highly similar but not identical to their reference biologics.
The introduction and use of biosimilars is an opportunity to significantly reduce spending on biologics. It is estimated that Canada could save $1.8 billion over 3 years on biologic drugs if biosimilar uptake was maximized and negotiated discounts were applied.1 Several jurisdictions within Canada have implemented policies that promote switching to biosimilars and, as a result, have reported savings within their health care systems.2,3 Understanding the various policies implemented across jurisdictions related to switching, interchangeability, pricing, and market distribution can support the implementation and uptake of biosimilars, further increasing savings to the health care system in general.
This Environmental Scan (ES) was conducted as part of the pan-Canadian Biosimilars Initiative, which is a collaboration between the Ontario Health Provincial Drug Reimbursement Programs (PDRP) and the pan-Canadian Pharmaceutical Alliance (pCPA). Findings of this ES can be used to inform recommendations on policy development and education for health care providers and patients.
Objective and Research Questions
The objective of this ES was to identify, synthesize, and understand national and international policies regarding biosimilar use. The research questions were:
What policies, programs, and/or strategies have been implemented in Canadian and in other international jurisdictions on interchangeability, switching, and substitution between reference biologics and biosimilars?
Do jurisdictions consider reference biologics interchangeable with biosimilars?
What are the circumstances that exempt patients from switching to a biosimilar drug?
What are the circumstances that determine the interchangeability (e.g., is it specific to a particular indication for use)?
What is the position of other jurisdictions on extrapolation of indications for biosimilars?
What practices have international jurisdictions put in place to improve or maintain the viability of biosimilars in the marketplace?
How have jurisdictions decided to divide the market?
What supply-side policies have been implemented regarding pricing and procurement?
What policies have been implemented to mitigate the impact of drug shortages?
Methods
Literature Search Method
A literature search was conducted using key resources, including Ovid MEDLINE, Ovid Embase, and Cochrane library. Searches were limited to the English language and articles published from January 1, 2011, to May 17, 2021.
Search updates were conducted in March 2022 (targeted web search only) and March 2023 (database search update with targeted web search).
Database-specific search strategies were developed using a combination of keywords and free-text terms with Boolean operators (“and” and “or”). The search terms are listed in Table 1 (refer to Appendix 1 for detailed search strategies).
Concepts | Search terms |
|---|---|
Biosimilars |
|
Reference biologics |
|
Interchangeability, switching, substitution |
|
Postmarket strategies |
|
A web-based search was conducted using the Google search engine and the CADTH Grey Matters checklist. The first 5 pages of results from the Google Advanced Search were visually scanned, and potentially relevant findings were downloaded.
Screening and Study Selection
One author independently screened the titles and abstracts for eligibility based on the criteria outlined in Table 2. Articles were included if they were English-language articles that described policies, practices, and/or programs on switching, substitution, and interchangeability of reference biologics and biosimilars or if they described postmarket strategies used in different jurisdictions.
Relevant articles and/or web sources from non–English-speaking jurisdictions were included only if they were translated to English. Details of the inclusion criteria of this ES are summarized in Table 2.
Studies that did not meet the inclusion criteria were excluded based on the title and abstract or, for web-based results, a limited review of the full text.
Table 2: Study Selection Criteria
Criteria | Details |
|---|---|
Publication type |
|
Jurisdictions of interest |
|
To be eligible, an article must have described at least 1 of the following criteria | |
1. Switching, interchangeability, substitution |
|
2. Postmarket strategies |
|
Synthesis Approach
Findings were summarized narratively. When summarizing the key characteristics of biosimilar policies outlined in research question 1, relevant findings were separated based on jurisdictions and key themes of information (i.e., interchangeability, switching, and substitution). Findings related to subsequent study objectives were grouped similarly for consistency.
Consultations and Feedback
Provincial and territorial drug plan and cancer agency representatives in Canada were invited to provide feedback on the draft report. No additional feedback was received before finalizing the draft.
Findings
The initial literature search (conducted on May 17, 2021) identified 2,430 citations.
Two published articles were identified from updated database search conducted on March 1, 2023. Twenty-nine references were included from web searches conducted in March 2022 and March 2023. The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow chart of the study selection process is presented in Appendix 2.
During the first update search (conducted in March 2023), we identified meaningful information on the biosimilar policies of Italy, Belgium, Sweden, and Denmark. Therefore, these countries were also included. A total of 13 countries were included in this report and relevant information on their policies is presented.
Research Question 1: Policies on Interchangeability, Substitution,
and Switching
Definition of Interchangeability Across Jurisdictions
There is variability in the definition and approaches to interchangeability among countries and regions; this report uses the term interchangeability or interchangeable as defined in each jurisdiction. The various definitions of interchangeability across jurisdictions are presented in Table 3.
Table 3: Definitions of Interchangeability Across Jurisdictions4
Jurisdiction | Regulatory authority | Health authority’s position on interchangeability | Statutory or legal definition of interchangeability | Implementation authority |
|---|---|---|---|---|
Australia | Therapeutic Goods Administration | No formal definition of interchangeability. However, “brands that can be substituted by the pharmacist are indicated in the Schedule of Pharmaceutical Benefits by an ‘a-flag’ (a small ‘a’). Only a-flagged medicines can be substituted by the pharmacist.”10 | No | Pharmaceutical Benefits Advisory Committee |
Canada | Health Canada | “…the term ‘interchangeability’ often refers to the ability for a patient to be changed from one drug to another equivalent drug, by a pharmacist, without the intervention of the prescriber who wrote the prescription. Health Canada’s authorization of a biosimilar is not a declaration of equivalence to the reference biologic drug. The authority to declare two products interchangeable rests with each province and territory according to its own rules and regulations.”11 | No | Individual provinces and territories |
European Union | EMA | “Interchangeability refers to the possibility of exchanging one medicine for another medicine that is expected to have the same clinical effect. The Heads of Medicines Agencies (HMA) and European Medicine Agency (EMA) consider that once a biosimilar is approved in the EU it is interchangeable, which means the biosimilar can be used instead of its reference product (or vice versa) or 1 biosimilar can be replaced with another biosimilar of the same reference product. Decisions regarding substitution (the practice of dispensing 1 medicine instead of another medicine without consulting the prescriber) are not within the remit of the EMA and are managed by individual member states.”9 | No | Member states |
US | FDA | FDA determines a biological product to be interchangeable with a reference product if the biological product “is biosimilar to the reference product” and “can be expected to produce the same clinical result as the reference product in any given patient” and “for a biological product that is administered more than once to an individual, the risk in terms of safety or diminished efficacy of alternating or switching between use of the biological product and the reference product is not greater than the risk of using the reference product without such alternation or switch.”8 | Yes (Biologics Price Competition and Innovation Act 2009) | Individual states |
EMA = European Medicines Agency; EU = European Union.
In all countries included in this review, the interchangeability of a biosimilar with its reference biologic is closely linked to substitution and nonmedical switching.4,5
The term switching in this report refers to the replacement of a reference biologic with a biosimilar. Two terms will be used in relation to switching: medical switching is a switch made by a physician in consultation with the patient and nonmedical switching is a switch mandated by health authorities without requiring the approval of the prescribing physician.7 Substitution or automatic substitution refers to replacing 1 biologic drug with a biosimilar at the pharmacy.
According to a survey conducted by WHO, interchangeability refers to switching in most countries6 (refer to Appendix 3). The survey results also indicated that most countries leave the switching decision to the prescribing physician’s discretion and do not allow automatic substitution.5,6
In the US, interchangeability is a designation to allow for substitution. The FDA is the only health authority that has a statutory and legal definition of interchangeability. Other jurisdictions, such as the European Union (EU) and the UK, have defined interchangeability in their guidance documents, but these definitions are not legally binding.4
In Europe, interchangeability refers to the possibility of exchanging 1 medicine for another expected to have the same effect. This replacement of a drug can occur based on a decision made by a physician (“switching”) or pharmacist (“automatic substitution”).4,5
Most EU member states included in this review (n = 8) leave treatment decisions (reference biologic or biosimilar) to the prescribing physician. As such, interchangeability in Europe is not synonymous with automatic substitution because it involves the prescriber.4
International Policies on Interchangeability, Substitution, and Switching: Summary by Jurisdiction
More than half of the countries included in this review (n = 7) do not allow automatic substitution of reference biologics with biosimilars, but most do recommend medical switching. Table 4 presents a snapshot of international policies on interchangeability, substitution, and switching. Details of each country’s policies are summarized subsequently. A summary of the policies is also presented in Appendix 4.
Table 4: International Jurisdictions’ Policies on Interchangeability, Substitution, and Switching
Jurisdiction | Interchangeability and substitution | Switching | |||
|---|---|---|---|---|---|
Interchangeability designation | Automatic substitution | Biosimilar use for patients who are treatment naive | Medical switching | Nonmedical switching | |
Australia | No | Yesa | Yes | Yes | Yesb |
Canada | No | No | Yes | Yes | Yesc |
Denmark | — | No | — | Yes | Yesd |
Finland | Yes | No | — | Yes | No |
France | No | Yese | Yes | Yes | No |
Germany | No | Yesf | Yes | Yes | No |
Italy | No | No | Yes | Yes | No |
The Netherlands | No | No | Yes | Yes | No |
New Zealand | No | No | — | Yes | No |
Norway | No | Yes | Yes | Yes | No |
Sweden | — | No | — | Yes | No |
UK | No | No | — | Yes | No |
US | Yes | Yesg | — | Yes | No |
Note: Cells with a dash indicate that no information was identified.
aDrugs that are “a” flagged only.
bFor metastasized bowel cancer treatment only.
cAlberta, British Columbia, New Brunswick, Northwest Territories, Nova Scotia, Ontario, Quebec, and Saskatchewan.
dAs a result of the national purchasing policy.
eTwo drugs only.
fStarting March 14, 2024.
gInterchangeable-designated drugs only.
United States
According to the Biologics Price Competition and Innovation (BPCI) Act in the US, a biosimilar can be designated as “interchangeable.”12 The US FDA requires clinical trials to evaluate the interchangeability of a biosimilar in which patients are switched back and forth between the reference biologic and a biosimilar.13-18
In 2019, The FDA finalized its biosimilar interchangeability guidelines.17 For a product to be considered an interchangeable biosimilar, the FDA requires the sponsor to perform a clinical study or studies involving multiple switches to demonstrate that the risk in terms of side effects or diminished efficacy is not greater than the risk of using the reference product without such switching. A switching study or studies should evaluate changes in treatment that result from 2 or more alternating exposures (switch intervals) to the proposed interchangeable product and to the reference product. A product designated as interchangeable by the FDA can be substituted with its reference product at the pharmacy level without any intervention of the prescribing medical practitioner, subject to state law.
To date, 5 biosimilar products have been approved for the interchangeable designation: Semglee (insulin glargine-yfgn, approved in July 2021), Cyltezo (adalimumab-adbm, approved in October 2021), Cimerli (ranibizumab-eqrn, approved in October 2022), Rezvoglar (insulin glargine-aglr, approved in November 2022), and Abrilada (adalimumab-afzb, approved in October 2023).19-23
Although the FDA grants an interchangeable designation to a biosimilar, the decision to implement automatic substitution at the pharmacy level is up to individual states. On April 22, 2021, Oklahoma became the final state to permit biosimilar substitution.24 All states have enacted laws that authorize pharmacists to dispense interchangeable products.4,13,25,26
State laws differ in the specifics, but biosimilars must be approved by the FDA as interchangeable before substitution can occur. Many state laws include provisions such as that patients must be notified of biosimilar substitution and prescribers can prevent substitution by noting “dispense as written” on the prescription. Each state also requires that pharmacists must communicate with the prescriber after a substitution is made.4,13,18,27,28
The state of Delaware requires the patient’s written consent before substitution, whereas several other states only require that package labelling on biosimilars must specify the name of the interchangeable biologic.29 In North Dakota, patients have the right to reject substitution, but they have to pay for the higher cost of the reference biologic.27
United Kingdom
There are no regulations and/or guidelines on interchangeability between biosimilars and reference biologics established by the regulatory authority in the UK. However, the National Health Service (NHS) guidance states, “Once authorised, biosimilar products are considered to be interchangeable with their reference product, which means a prescriber can choose the biosimilar medicine over the reference product (or vice versa) and expect to achieve the same clinical effect (therapeutic equivalence).”5
In November 2022, the UK Medicines and Healthcare products Regulatory Agency (MHRA) updated its 2021 guidance on biosimilars to allow interchangeability between biosimilars by adding the following statement, “A biosimilar product is considered to be interchangeable with another biosimilar to the same reference product.”30
Within this framework, interchangeability is subject to the consultation between prescribers and patients.5,30 Interchangeability in the UK refers to prescriber switching (between reference biologics and biosimilars) only.30 Substitution at the pharmacy level is prohibited.13
The British Biosimilar Association recommends switching to a less expensive biosimilar medicine at the prescriber level in consideration of the scientific evidence.13
European Union
On September 19, 2022, the EMA and the Heads of Medicines Agencies (HMA) issued a joint statement confirming that biosimilars approved in the EU are interchangeable with their reference drugs.31
EU member states will continue to decide which biological medicines are available for prescribing and whether automatic substitution is allowed at the pharmacy level.9,13,15,31
Countries such as France, Germany, and Norway allow automatic substitution and encourage switching in established patients undergoing treatment with a reference biologic with the consent of the patient.13
Several EU countries, such as Denmark, Finland, and the Netherlands, have issued national guidance on interchangeability.5,6 In Denmark, nonmedical switches have taken place due to the national purchase of biosimilars.32
France
France was the first European country to introduce a law in 2014 to permit substitution of biosimilars at the pharmacy level. The country passed the Social Security and Finance Bill that would allow automatic substitution for patients who are treatment naive; however, it was never implemented.13,25,33
On April 14, 2022, the French government published a ruling in the Journal officiel that permits pharmacists’ right to substitute biological drugs. Only 2 biological drugs, filgrastim (Neupogen) and pegfilgrastim (Neulasta), are eligible for automatic substitution currently.34
Germany
In November 2018, the German Health Ministry introduced a draft bill on safety in the supply of pharmaceuticals (The Gesetz für mehr Sicherheit in der Arzneimittelversor-gung bill), that aimed to provide a legal framework for the automatic substitution of biosimilars. It was originally set to be implemented in 2022.35,36
Following the publication of the law, the federal joint committee G-BA published its first draft of the rule in April 2022. However, with pushback from the Federal Association of the Pharmaceutical Industry and a group of biosimilar manufacturers, the cabinet passed the Financial Stabilisation of the Statutory Health Insurance System bill in August 2022, which would delay the biosimilar substitution initiative by a year.37
With a new regulation coming into effect on March 14, 2024, pharmacy substitution will be allowed between reference biologics and biosimilars, as well as between biosimilars.
The German Federal Agency (Paul-Ehrlich-Institut) promotes switching between biosimilars and reference biologics with proper clinical monitoring. The decision of switching is up to the prescribing physician.13
Italy
The Italian Medicines Agency (AIFA) stated that reference biologics and biosimilars can be considered interchangeable only on the basis of the clinician’s assessment.38,39
AIFA is of the position that the reference biologic and the biosimilar are different and alternative therapeutic options.39 However, AIFA indicated that biosimilars are the preferred option, especially for patients who are treatment naive.38 Automatic substitution is not allowed, and AIFA excluded biosimilars from the transparency lists (the lists indicate medicines reimbursed by the Italian National Health Service based on a reference price system).39
The decision to switch is entrusted to the prescribing physician only. Physicians can choose which product to use based on the patient’s need, clinical presentation, and the benefit-risk balance after consulting with the patient.39
The Netherlands
In 2015, the Dutch Medicine Board indicated their support for pharmaceutical substitution of biosimilars.25 However, a recent study (2021) confirmed that automatic substitution is not allowed in the country.40 The Medicine Evaluation Board in the Netherlands encourages biosimilar prescriptions for patients who are treatment naive but switching must be decided by physicians along with the involvement of the pharmacist and the patient. Adequate clinical monitoring is required after switching.13
Sweden
Similar to other European countries, medical switching is permitted but automatic substitution is prohibited.41,42 Most counties in Sweden recommend a switch for patients who are stable and informed.43
Finland
In May 2015, the Finnish Medicines Agency (Fimea) announced a recommendation for interchangeability of biosimilars with their reference biologics.44 Fimea is of the position that biosimilars licensed in the EU are interchangeable. For example, biosimilar filgrastim is designated as interchangeable in the country.25 Fimea specifically recommends that biosimilars are interchangeable only under the supervision of a health care professional.13,45
Switching is recommended with proper clinical monitoring and at the physician’s discretion.13,45 Automatic substitution is not allowed at the time of writing. Government proposals to introduce biosimilar substitution had been criticized by the pharmaceutical industry; however, implementation plans for substitution were published by a parliamentary health committee in February 2023.46,47
Norway
Similar to other European countries, physician-led medical switching is recommended with proper clinical monitoring. In 2017, the Norwegian Medicines Agency (NoMA) proposed an amendment to the Pharmacy Act to permit automatic substitution;13,36,48 it is now allowed in pharmacies in the country.49
Oceania
Australia
The Pharmaceutical Benefits Advisory Committee (PBAC) does not use the terms interchangeability or substitution.4 Biosimilars that have been “a” flagged by the PBAC can be replaced at the pharmacy level in consultation with the patient. As of June 2022, 15 biosimilars approved in the country have been “a” flagged.50 The prescriber can indicate “substitution is not permitted” for “a”-flagged biosimilars.4,51
Use of biosimilars is endorsed for patients who are treatment naive.13,52 Effective on June 1, 2021, the country has implemented nonmedical switching for metastatic bowel cancer treatment. The biologic treatment Avastin has been withdrawn from the Pharmaceutical Benefit Scheme and a biosimilar, Mvasi, has been listed. With this implementation, patients on treatment with Avastin will have to pay for the drug privately or switch to Mvasi.53
New Zealand
The New Zealand Medicines and Medical Devices Safety Authority (Medsafe) recommends that prescribing physicians make the decision to switch to a biosimilar.54 Switching decisions should be made based on clear communication and agreement with the patient.54-56 Any biologic medicines may not be substituted at the pharmacy without prescriber’s agreement.57
Policies on Interchangeability, Substitution, and Switching in Canadian Jurisdictions
Health Canada defines a biosimilar as “a biologic drug highly similar to a biologic drug that was already authorized for sale.”11 The authorization of a biosimilar is not a declaration of equivalence to the reference biologic product. Decisions on interchangeability are made by each province and territory.5 Health Canada is of the position that a switching decision should be made by the treating physician in consultation with the patient considering available clinical evidence and any relevant jurisdictional policies.58
All provinces and territories except Manitoba encourage using biosimilars in patients who are treatment naive by granting preferential status to certain biosimilars.32,59 This means patients prescribed certain biologics for the first time would be required to take its biosimilar to receive coverage by the public or private drug plan.
British Columbia was the first province to introduce a nonmedical switching policy that applies to the drugs listed in Appendix 5.32,60 This policy also supports extrapolation of indications (i.e., off-label use of biosimilars). For oncology drugs, as per the Oncology Biosimilars Utilization Policy, patients starting new treatment on bevacizumab, trastuzumab, or rituximab can only receive coverage for the biosimilar version.59,61
Alberta also introduced a similar policy that took effect on July 1, 2020 (refer to Appendix 5 for the drug list), followed by New Brunswick (announced on April 21, 2021). Patients who need to continue treatment with the reference biologic for medical reasons can apply for exceptional request.59
On May 18, 2021, Quebec announced a biosimilar initiative that requires patients who are treated with reference biologics to switch to biosimilar versions if available and do so on an ongoing basis. Exceptions apply to people who are pregnant, who must switch to a biosimilar 12 months after giving birth, and patients younger than 18 years. Patients who have experienced 2 or more treatment failures are also exempt and do not need to switch.59,62
Also in 2021, the government of the Northwest Territories announced a 6-month period to switch to biosimilars by June 20, 2022.63
On February 4, 2022, Nova Scotia became the fifth province to implement a nonmedical switching policy.59 Saskatchewan followed in October 2022.59,64
The Ontario Ministry of Health announced a biosimilar switching policy would be coming into effect on March 31, 2023, with a 9-month transition period.59 Newfoundland and Labrador and Yukon announced the same policy in March 2023. Prince Edward Island became the 11th jurisdiction to implement nonmedical switching in October 2023.
Figure 1 shows the timeline of biosimilar switching initiatives in jurisdictions in Canada.
Figure 1: Timeline of Biosimilar Switching Initiatives in Canada
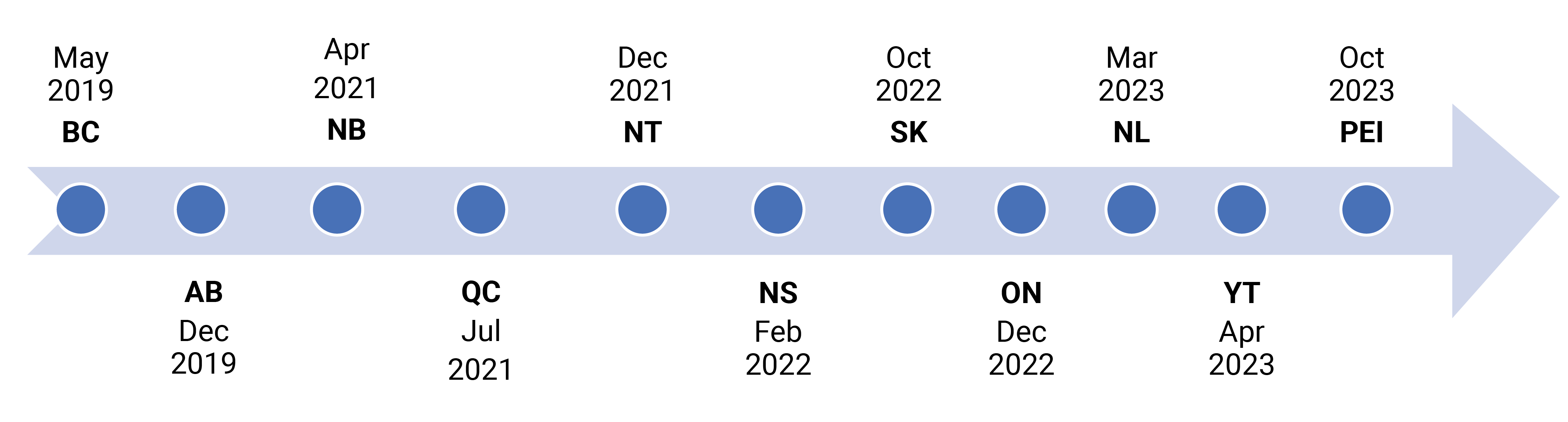
AB = Alberta; BC = British Columbia; NB = New Brunswick; NL = Newfoundland and Labrador; NS = Nova Scotia; NT = Northwest Territories; ON = Ontario; PEI = Prince Edward Island; QC = Quebec; SK = Saskatchewan; YT = Yukon.
Manitoba and Nunavut are the remaining jurisdictions without a biosimilar switching policy. Manitoba Health, Seniors and Active Living, has implemented a Tiered Biologics Reimbursement Policy since August 15, 2018. This policy only applies to new patients (who have not been treated previously with a biologic) and existing patients who have previously received biologic therapy but it was ineffective.59,65 Humira became a Tier 2 biologic drug in August 2021; patients new to this treatment only receive coverage for a biosimilar (refer to Appendix 6 for a tiered biologics reimbursement flow chart and the list of Tier 1 and Tier 2 products).
Appendix 7 presents the current state of biosimilar policies in provinces and territories in Canada.
International Policies (Demand-Side Policies) to Encourage Switching
To encourage switching to biosimilars, various policies, such as targets, quota, and financial incentives, have been implemented across European countries.32,66
France has a quota policy that a physician can prescribe reference biologics for a maximum 30% of their patients.32 The country also set a biosimilar target of 80% of market share by year 2022 as a part of the National Health Strategy in 2018. To reach this target, the French government implemented a pilot project to promote biosimilar uptake in 62 hospitals. Results show the biosimilar uptake rate has increased to 50%.67
There are several incentive programs targeted to hospital prescribers in France. The incentive programs include payment for performance programs (i.e., hospitals are awarded bonuses according to a score based on indicators such as biosimilar prescription rates) and gainsharing programs (i.e., sharing 20% of gains with hospital prescribers). Gainsharing is an incentive system based on sharing savings associated with biosimilar use (difference in price between reference drug and biosimilar) and investing these savings back into patient care.
Most recently, a new incentive program was implemented in France, targeting community-based practitioners in which prescribers can share gains up to 30% in 2022 and then 20% in 2023 by initiating treatment with a biosimilar or switching to a biosimilar.67,68 An incentive program targeting pharmacists is to be implemented soon which would allow for pharmacy-level substitution.67
Similar to France, the UK has set a target of 80% and offers incentives for prescribing biosimilars. For example, NHS England offers providers 1% of the contract value of biosimilars if they start 90% of new patients on a biosimilar and switch 80% of existing patients to a biosimilar.32
In addition to targets and incentives, the NHS implemented a best-value biological medicine policy, which adopts using best-value biological medicines (including biosimilars) in 90% of new patients within 3 months of launching a biosimilar. If more than 1 treatment is suitable, the best-value biological medicine should be chosen (considering transparently costed device training, any patient support programs offered by manufacturers, administration costs, and price per dose). If treatment decisions are not made based on this principle, the reasons should be documented and made available to commissioners if required.69,70
In Scotland, a biological medicines treatment cost comparator was developed and shared with regional health boards. It shows treatment costs of different agents and has encouraged biosimilar use within each health board. The 14 regional NHS health boards were also encouraged to put plans in place to switch patients to biosimilars.69
In Germany, physicians have to pay the amount exceeding a fixed budget produced by prescribing reference biologics.32 The uptake of biosimilars varies across regions, mainly due to regional-level biosimilar quotas as well as gainsharing contracts at the payer level.68,71 Gainsharing initiatives have been arranged between groups of physicians and insurers. For example, the BioLike initiative was launched by the insurer company Barmer GEK for gastroenterologists and rheumatologists in multiple regions, such as Hamburg, Saarland, Saxony, Schleswig-Holstein, Thuringia, and Westphalia-Lippe. This initiative allows for sharing the savings from tumour necrosis factor-alpha inhibitor biosimilar prescriptions between groups of prescribers and the insurer.68,71 Interviews with prescribers and insurers revealed that a monitoring or sanctioning system to regulate adherence to biosimilar quotas has been an effective driver of biosimilar uptake.68,71
In Sweden, most counties recommend the most cost-effective product, which is often a biosimilar.43 Gainsharing arrangements between local county councils and the central government has worked as an incentive for local hospitals. For reimbursed outpatient medicines, savings are shared between the central government and the counties, and the savings stay within the drug budgets of local hospitals. This has been an incentive to prescribe biosimilars at the hospital level.43,68
Finland adopted a similar approach as the NHS policy on best-value biological medicine. Physicians are obliged to prescribe the least expensive product if biosimilars are available. They are required to justify the selection of a more expensive alternative in the medical records.69,72
Other European countries have adopted guidelines and recommendations to encourage biosimilar use.69 For example, Denmark, Sweden, and Italy use guidelines and recommendations for switching to the biosimilar adalimumab for physicians about purchasing and formulary decisions. Germany has guidelines on economic prescribing to encourage physicians to prescribe biosimilars.
Appendix 8 summarizes the policies implemented across countries to encourage switching to biosimilars.
Extrapolation of Indications: Positions of International Jurisdictions and Canada
Regulatory Frameworks for Extrapolation
Extrapolation allows the approval of a biosimilar in an indication held by the reference biologic not directly studied in clinical trials of the biosimilar.73,74
In Europe, indications of a reference biologic can be approved for its biosimilar in the absence of specific clinical data generated with the biosimilar. The EMA states, “If a biosimilar is highly similar to a reference medicine and has comparable safety and efficacy in one therapeutic indication, safety and efficacy data may be extrapolated to other indications approved for the reference medicine.”9,16 All scientific evidence available from comparability studies must establish biosimilarity and address the specific aspects of the extrapolated indication. The following major criteria must be met for a biosimilar to be approved based on extrapolated safety and efficacy data.9
Mechanism of action: The mechanism of action of the active substance should be mediated by the same receptors in both the initial and the extrapolated indication.
Relevant study population: Comprehensive comparability studies must show that the biosimilar is highly similar to the reference medicine in a key indication in a population for which potential differences in clinical performance can be detected; equivalence and clinical comparative studies have been performed in the most sensitive therapeutic indication.
Extrapolation across different clinical settings: Data for a given indication may not be directly applicable in terms of safety or efficacy to an indication that falls within another therapeutic area where the mechanism of action may be different. In this case, additional studies may be needed.
Extrapolation of safety data: Safety data can only be extrapolated after a comparable safety profile has been established for the biosimilar in 1 therapeutic indication.
Extrapolation of immunogenicity data: Immunogenicity always requires justification because other factors (e.g., patients, disease, treatment-related factors) also have to be considered to determine immunogenicity.
The FDA is of the same position as the EMA regarding extrapolation. Biosimilars can be licensed for 1 or more additional indications of the reference biologic without the need for repeat clinical trials in each indication.12 Designation for extrapolation is based on assessment of scientific justification for each indication. Scientific justification may include (but is not limited to) assessment of potential differences with the mechanism of action across indications, pharmacokinetics and biodistribution, safety, immunogenicity, or other factors that affect safety and efficacy for each indication and patient population.16,17
FDA approvals typically allow for complete or near-complete extrapolation. However, active patent protections hinder a biosimilar’s ability to achieve complete label indications.17
Health Canada uses the term “Authorization of Indications” and has a similar approach as EMA and FDA. Authorization of indications is dependent on the demonstration of similarity between the biosimilar and reference biologic drug based on the data from clinical and nonclinical studies. With the established similarity, indications may be granted even if clinical trials are not conducted in each indication.75
Extrapolation in Practice
Although the regulatory authorities can approve a biosimilar for extrapolated indications, it has been challenged by many experts and clinicians. One example is the approval of biosimilar infliximab in Europe.16 The EMA approved biosimilar infliximab for extrapolation to all indications granted to the reference biologic based on 2 comparative trials in patients with ankylosing spondylitis and rheumatoid arthritis. Experts opposed the decision with the following arguments:
rheumatoid arthritis is not the most sensitive clinical condition (lower efficacy margin against placebo in rheumatoid arthritis), lower dose use in rheumatoid arthritis versus other therapeutic indications, use of infliximab in combination with methotrexate in rheumatoid arthritis
among the immune-mediated inflammatory diseases, patients with rheumatoid arthritis do not represent the most sensitive population for the development of immunogenic responses.
The EMA later recommended the implementation of a comparative randomized clinical trial of the biosimilar infliximab and its originator in patients with Crohn disease.
According to a survey study of the European Society for Medical Oncology, most prescribers had an appropriate understanding of extrapolation of indications, and overall responses indicated that they feel comfortable using a biosimilar in an extrapolated indication.76 However, the study did not show if clinicians actually prescribe biosimilars for extrapolated indications. One editorial article pointed out the example of biosimilar filgrastim (Zarzio) to describe the safety of a biosimilar in extrapolated indications.77 The confirmatory study was conducted in patients with breast cancer who had chemotherapy-induced neutropenia, and the use of biosimilar filgrastim was approved in Europe for other indications granted based on extrapolation. Related data and clinical experience demonstrated the safety and effectiveness of biosimilar filgrastim in patients with other tumour types who had chemotherapy-induced neutropenia. It also indicated that the drug was safe and effective in other extrapolated indications, such as stem cell mobilization.
Research Question 2: Biosimilar Policies Related to Pricing and Procurement
The uptake of biosimilars is influenced by multiple factors, but pricing is considered a significant driver of biosimilar use, especially in Europe.78 Wide variation exists among jurisdictions in the regulation of biosimilar list prices. There are 2 types of price regulations that have been commonly implemented among international jurisdictions:79
Direct price controls require manufacturers set the biosimilar price at a certain level relative to the price of the reference biologic drug (e.g., France, Italy, Belgium).
Some countries use reference pricing, in which manufacturers are free to set a biosimilar price but are limited by the reimbursement amount (e.g., Germany, the Netherlands, the US). Because patients are less willing to choose a drug with a high copayment, manufacturers are discouraged from setting a price higher than the reimbursement level. Using this system, therapeutically similar biologic drugs are grouped together (reference and biosimilar), and a single reimbursement level is set for the drugs in the cluster.
Biosimilar procurement policies vary across countries but tendering or direct contracting with manufacturers appear to be common.
Table 5 shows a snapshot of pricing and procurement policies that international jurisdictions have adopted. Details of each country’s policies are summarized in the International Policies on Pricing and Procurement section. A summary of these policies is presented in Appendix 9.
Table 5: International Policies on Pricing and Procurement
Jurisdiction | Pricing | Procurement | |||
|---|---|---|---|---|---|
Free pricinga (reference priceb or price ceiling may apply) | Direct price control (e.g., mandatory price cut) | National purchasing strategy | Regional- or hospital-level tendering | Other | |
Australia | — | Yes | — | Yes | — |
Belgium | — | Yes | — | Yes | — |
Denmark | Yes | — | Yes | — | — |
Finland | — | Yes | — | Yes | — |
France | — | Yes | Yes | — | — |
Germany | Yesc | — | — | Yes | — |
Italy | — | Yes | — | Yes | — |
The Netherlands | Yesc | — | — | Yes | — |
New Zealand | Yesd | — | No information identified | ||
Norway | Yese | — | Yes | — | — |
Sweden | Yes | — | Yes | Yes | — |
UK | Yese | — | Yes | Yes | — |
US | Yesc | — | — | — | Yesf |
aManufacturers can set the price of biosimilars, but conditions such as reference pricing or price ceiling apply.
bReference prices can be established based on external prices or internal prices. External reference pricing uses the price(s) of a medicine in 1 or several countries as a benchmark or reference price for the purpose of setting or negotiating the price of medicines in a given country. Internal reference pricing uses the price(s) of identical medicines or similar medicines or therapeutically equivalent treatments within a country to derive a benchmark or reference price.
cReference pricing is used to set the reimbursement limit.
dInternational reference pricing is used as a tool in price negotiations.
eA maximum price is imposed.
fHospitals purchase drugs directly from manufacturers, wholesalers, or group purchasing organizations.
International Policies on Pricing and Procurement
United States
There is no mandatory price cut at the launch of a biosimilar in the US. The Centers for Medicare & Medicaid Services sets the follow-on biologic drug reference price at wholesale acquisition cost, also known as the estimated list price. This is defined in federal law as an estimate of the price a wholesaler pays a manufacturer for drugs purchased from the wholesaler’s supplier, which is typically the manufacturer of the medicine, with 6% of the reference drug average sales price (ASP) added if this information is available. The ASP is defined in federal law, and it is the price measure used for Medicare Part B reimbursement.80
Although mandatory discounts are not required, reference drug discounts occur with increasing biosimilar competition across Medicare and private settings. Up to a 30% price reduction is generally expected.81
However, under the current market dynamics, pharmacy benefits management companies (third-party administrators of prescription drug programs on behalf of insurers) have a significant financial incentive to limit the uptake of biosimilars to continue the large rebate payments (refer to Appendix 10).
When a biosimilar is launched, the initial discount is typically around 15% to 20%. Unless insurers can switch all their patients to the biosimilar, the cost of the lost rebates on the patients who remain on the originator would not be offset by the value of the discount because the number of patients who start on the biosimilar is likely to be small. It also makes it difficult for biosimilar sponsors to launch volume-based rebates.
In other words, there is a disincentive to switch to the biosimilar for insurers because they would not want to lose the incumbent rebates paid on the reference biologics.80,82 To prevent providers from having a disincentive to prescribe biosimilars, the Biologic Price Competition and Innovation Act (BPCIA) requires Medicare payment for biosimilars to include a fixed percentage based on the more expensive reference biologic. Medicare implemented a new payment policy that pays a blended average sales price for all biosimilars that share a common reference biologic drug based on their blended ASP plus a fixed percentage of the reference biologic’s ASP.18 Most hospitals and physician offices purchase drugs directly from manufacturers and wholesalers or through group purchasing organizations.18,81 Some facilities are eligible to use the 340B Drug Discount Program, which is a program that creates a price ceiling for outpatient drugs based on Medicaid’s payment rate, to obtain biologics at reduced prices.18
United Kingdom
The UK has adopted a free pricing approach upon regulatory approval of drugs. The NHS list prices of biosimilars are governed by the terms of the voluntary pricing scheme (VPAS) that the manufacturers have opted.83 The VPAS sets price ceilings based on negotiations and manufacturer profit levels. This scheme limits manufacturer profit and overall NHS spending on branded medicines; excess profits must be repaid or additional discounts must be provided to the NHS.79,83
Reference drug manufacturers are not required to reduce their selling price at the launch of a biosimilar. There are no official mandatory discounts for biosimilars.41
In England, tendering occurs at the regional level, although it is centrally managed by NHS England. Tendering takes a multiple-winner approach in which a company has access to a greater or smaller part of the market depending on the competitiveness of the bid.84
France
Single-winner, price-driven tenders are conducted at the hospital and regional level in France.41,85 On average, tender contracts last 36 months, but the tender process reopens with the entry of a new biosimilar.85
The biosimilar price must be equal to or lower than the reference drug price. There is a mandatory list price cut for both reference biologics (20% to 30%) and biosimilars (30% to 40%).78,85
Biosimilar price is fixed upon negotiation between a manufacturer and the Economic Committee for Medicinal Product (Comité Economique des Produits de Santé [CEPS]).78 Typically, biosimilar prices are set 10% to 20% lower than the price of the reference biologic drug.
Germany
Multiwinner, open-house rebate tender systems exist in Germany. Tenders are conducted through regional Sickness Funds and hospitals. Sickness Funds are membership-based not-for-profit insurance companies (government-delegated) and function as the main payer. They are obliged to sign contracts with at least 2 companies to supply in each region.41,86
There is no mandatory price reduction of reference drugs at the launch of a biosimilar, but manufacturers must increase rebates to a sustainable level.41,86 Most insurance companies rely on the organization of “open-house rebate contracts (Open-House-Rabattverträge)” in which all suppliers of reference biologics and biosimilars can participate. Participants can sign a supply contract if they adhere to certain predefined conditions, such as mandatory discounts on list prices. These open-house rebate contracts have resulted in biosimilar discounts in the country. Discounts may be negotiated through tenders by individual Sickness Funds.78 However, some regulations apply in retail markets (e.g., originator rebate increase upon biosimilar launch).45,86
Relatively high price differences between biosimilars and reference drugs are a driver for biosimilar use in the country.87 The actual price difference between the biosimilar and the reference biologic is usually not known to prescribers. However, local Sickness Funds are aware of the magnitude of the discounted price differences, and they can endorse biosimilar use.71
Italy
Each regional health authority in Italy has a procurement mechanism for all hospital drugs. It is usually nonexclusive with a 24-month contract duration. Tenders can reopen at the market entry of biosimilars. Tenders usually allow a single winner when fewer than 3 manufacturers participate. When the tender includes more than 3 competitors, a multiwinner approach is taken.41,88
Biosimilars are included in the same drug class as their reference biologics (e.g., class A for essential drugs; class H for drugs used in hospital and specialist care).88 This ensures the physician’s prescriptive freedom and therapeutic continuity if needed (for patients already on the reference drug).39
Biosimilars must be priced at least 20% less than the price of the reference drugs after negotiations with AIFA.78,88 Final net prices are determined from subsequent contracting procedures so typically higher discounts are applied for the final retail price. The updated pricing guidelines (in 2021) allow more streamlined price and reimbursement negotiations for biosimilars included in class A or H.88 No mandatory reference drug price reduction is required at the launch of a biosimilar. However, mandatory net discounts apply for the reference biologics in the hospital sector (33.35% to 50%).41
The Netherlands
National tenders are not in place in the Netherlands. However, hospitals (sometimes in collaboration with an insurer) may choose to organize tenders for high-cost drugs.41 Tenders are run at the hospital level for inpatient drugs, whereas outpatient drug tenders are run by health insurance providers.89 Biosimilar pricing is regulated by the standard process for branded medicines.41 External reference pricing is used,45 and there is no mandatory list price reduction of the reference product and biosimilars.41,88
Belgium
Most biosimilars and reference products in Belgium are used in the hospital setting only. These drugs are procured by individual hospitals and hospital groups (usually via single-winner tendering).90 Biologic drugs in outpatient settings are directly negotiated and contracted between manufacturers and insurance providers.91
In 2018, mandatory price reduction measures were introduced for reference biologics with the entry of its biosimilar (minimum 20% up to 38% price reduction).90 Biosimilars are negotiated individually with the National Institute of Health and Disability (NIHDI), and they are allowed to launch at their reference drugs’ official prices. However, further discounts arise from tendering and contracting procedures.
Denmark
The Danish government negotiates the price of biologics through a centralized system (Amgros). The drug that wins the call for tender is purchased (de facto single-winner tender) with a 12-month contract duration.41 This national purchasing approach encouraged nonmedical switching for all patients in hospital settings.32,41 There is no official mandatory price reduction, and net prices are determined through tenders.41,45
Sweden
There is no mandatory list price reduction for reference drugs and biosimilars in Sweden.41 A maximum price is imposed in a retail setting, but no maximum price is imposed for hospital use.45
Tenders typically take a single-winner approach except for infliximab (split between patients who are treatment naive and those who are currently on treatment).41 The current purchasing mode within the national reimbursement system is facilitated by a rebate payment shared between the government, the county councils (payers), and, in some cases, health care institutions (providers).92
Moorkens et al. (2020)43 indicated that biosimilar use at the regional level depends on the extent of the rebated price differences, local guidelines, and gainsharing agreements. Outpatient medicines are reimbursed at the same price in all counties. However, procurement and pricing agreements occur differently in hospital settings at each county.
The managed entry agreement system provides an incentive to county councils to promote the uptake of the least expensive product, which often is a biosimilar. The entry agreement is led by the Dental and Pharmaceutical Benefits Agency (the agency). The agency and the Swedish Association of Local Authorities and Regions distribute a list of confidential drug prices to the payers (Drug and Therapeutics Committees of the county councils) who can make recommendations on which drugs to prescribe. Physicians only know a price ranking of products included in the entry agreement because rebates of these agreements are confidential.43 Prices can be renegotiated every 6 months in the event a company with a new product has applied for reimbursement. This mechanism may stimulate competition in hospital settings.43
Finland
Regional tenders in Finland are led by a group of local hospitals and typically have a single-winner approach with a 48-month contract duration. Tender contracts can reopen when a biosimilar enters the market (a couple of months after the marketing authorization).45
In Finland, the prices of reimbursable biologics are highly regulated, and the Pharmaceuticals Pricing Board sets the maximum wholesale prices for reimbursable medicinal products in outpatient care.
Biosimilar list prices are set approximately 30% less than the reference drug price.45,72 After mandatory price regulation began in 2017, the price reduction of reference drugs occurred when the first biosimilar entered the market.72
Norway
Hospital drugs in Norway are procured through national-level tenders organized by the Norwegian Drug Procurement Cooperation. Tenders are price-driven and typically have a single-winner approach with a 12-month contract duration.41,93 However, the Norwegian Pharmaceutical Industry Association has proposed allowing 2 winners if certain pricing criteria are met.94,95
For outpatient settings, biosimilars are distributed by 3 main pharmacy chains, and price negotiations are kept confidential.95
Reference biologic and biosimilar manufacturers are free to set a price less than the maximum sales price set by NoMA.41,95 There is no mandatory price reduction,41 and the price of hospital biosimilars (for inpatient use) is determined through tenders.
For outpatient biosimilars, progressive price discounts apply and increase over time with market competition and turnover of the drugs. However, price revisions can happen at the earliest 12 months after the last price cut when the turnover of the drugs exceeds a certain value.95
Australia
The Australian government has adopted a reference pricing policy by which it subsidizes therapeutically equivalent drugs up to the lowest priced drugs.96 PBAC takes a cost-minimization approach to approved biosimilars and prevents them from reaching a list price premium.97 The lowest-priced drug listed on the Pharmaceutical Benefit Scheme (e.g., a biosimilar) sets a benchmark price for the other brands of that drug.97,98
Statutory price reductions apply to the first listing of a bioequivalent or biosimilar brand of a pharmaceutical item.52,96,98 When biologic drugs are first approved, they are listed on the F1 formulary which consists of single-brand drugs. The prices of drugs on the F1 formulary are reduced on the 5-, 10-, and 15-year anniversaries of their listing. When a biosimilar enters the market, the reference biologic is moved to the F2 formulary, which consists of generics and biosimilars, and the original reference biologic is subject to a price reduction of up to 25%.98
The latest Strategic Agreement signed by the Generic and Biosimilar Medicines Association has increased the mandatory price cut for originators from 25% to 40% to now 25% to 60%.97
Procurement strategies differ across states and markets (i.e., hospital versus retail). In some hospitals, single-winner tenders are used to drive competition.97
New Zealand
According to a WHO case study, the Pharmaceutical Management Agency (Pharmac) of New Zealand directly negotiates conditions on drug price and supply with suppliers (manufacturers).99 For biosimilars, international reference pricing is used informally as a tool in price negotiations to determine a fair price.100
Pricing and Procurement Policies in Canada
The pCPA, on behalf of provincial, territorial, and federal drug plans, negotiates confidential price reductions for biosimilars.101
Biosimilar procurement practices differ across jurisdictions in Canada and may be centralized or conducted at the local hospital level. Jurisdictions within Canada may restrict their formulary listings to certain biosimilar brands or allow for the purchase of multiple brands.
Implications of Pricing and Procurement Strategies
Countries have implemented various pricing policies, such as direct control of the biosimilar list price (and sometimes also the originator) and use of a reference price.
Aggressive price control could result in unsustainable levels of price reduction, which may disincentivize market competition and lead to manufacturers’ withdrawal from the market. To prevent that, the Netherlands takes a progressive price discount approach in which biosimilars can launch at the reference price; subsequent reference pricing mechanisms set the conditions for both biosimilars and originators then competition is used to promote price discounts.
Pricing policies can set the baseline for the list price, and the discounted list price is subject to further reductions through procurement mechanisms.
Tendering is a commonly reported procurement strategy that affects biosimilar uptake among many jurisdictions. Hospital-, regional-, and national-level tendering occurs in countries such as Belgium, France, Germany, Italy, Norway, and the UK. It has been reported that tendering can be effective at obtaining higher price discounts for biosimilars.102
A national purchasing policy has also been reported to promote biosimilar use. Several European countries implemented a policy that the government will purchase the least expensive biologic (which is often a biosimilar) and limits the availability of the reference biologics.
Although there is no tendering for biosimilars in Canada, it has been reported that price negotiations led by the pCPA have resulted in a greater reduction in biosimilar prices than seen in tendering markets in European countries.102
However, with these contracting mechanisms resulting in additional price discounts, there is also a potential risk of excessive price erosion, causing manufacturers’ withdrawal from the market, which can potentially lead to drug supply shortages. This will be discussed further in the following section.
Research Question 3: Policies to Mitigate the Impact of Drug Shortages
Dranitsaris et al. (2017)103 discussed drug tendering in the context of drug supply and shortage, and highlighted some of the implications for biosimilar-related policies as follows:
Biologic drugs have a complex manufacturing process and are particularly vulnerable to drug shortages. Biosimilars have the potential to expand treatment options and help prevent drug shortages of biologic drugs by increasing the number of suppliers.
Tendering is a widely used strategy for procurement of biosimilars. However, drug suppliers may leave markets due to low pricing and reduced competition associated with tendering. This could potentially result in drug shortages.
To mitigate the risk of drug supply shortages, authorities should monitor whether tendering leads to decreased supplier options. European Biopharmaceutical Enterprises recommends tendering processes for biologics and biosimilars include a variety of selection criteria and that solely price-based tendering should be avoided.
A recent report on biosimilar policy sustainability presented recommendations for biosimilar contracting policies to minimize the risk of supply shortages.102 For instance, Norway encountered supply problems because of the single-winner tendering system so 2-winner tendering has been proposed as a solution to avoid supply shortage.102
The authors of the report suggested that multiwinner tendering helps improve predictability of supply volume which avoids any unforeseeable shortages. Transparency in supply (from the manufacturer side) and usage (from the health care system side) should also be considered across the supply chain so that manufacturers can enter the market with a sustainable drug price and commitment to a realistic level of supply.102
Limitations
The findings of this ES are an overview of biosimilar policies of national and international jurisdictions. However, this ES may not provide an entirely comprehensive review because the literature search used to inform the findings was limited (i.e., English-language articles published between 2011 and 2023).
Because this ES focused on the breadth of the evidence, the methodological quality of the included articles was not assessed. There was wide variability in article types, study designs, and data sources so each article has different levels of evidence strength.
Biosimilar policies may vary between oncology and non-oncology or by therapeutic areas. However, most articles included in this ES discussed policies without a distinction between oncology and non-oncology. In addition, biosimilar-related policies and markets are rapidly evolving, so recent changes might have not been fully captured in this ES. Therefore, caution is required in interpreting the findings of this ES.
Conclusion and Implications for Policy-Making
Although biosimilar use is growing in most jurisdictions, the uptake of biosimilars varies considerably across jurisdictions. This is primarily due to differences in policies and/or strategies implemented once a biosimilar enters the market. The findings of this ES highlight the major policies and strategies that can influence biosimilar utilization:
More than half of the 13 countries reviewed do not allow automatic substitution but most leave switching decisions to physicians. The majority of jurisdictions, especially EU member states, promote medical switching. A few countries and several provinces and territories in Canada have adopted policies for mandatory nonmedical switching.
Nonmedical switching policies are implemented typically through a reimbursement policy. A national purchasing strategy can also result in nonmedical switching at the hospital level.
To promote biosimilar use, jurisdictions have adopted several demand-side policies, such as target setting, quotas, financial incentives, and guidelines and recommendations for prescription of biosimilars. In some countries, the prescribing physician and/or hospital receives a financial incentive when they prescribe the least expensive biologic; other countries have implemented quota policies.
Pricing and tendering are the commonly used supply-side strategies as a driver for biosimilar uptake.
The potential benefits of biosimilars can vary among jurisdictions depending on their policies and practices. Cost-savings are often described as the key benefit of using biosimilars, but it is important to know how these savings will be used to improve health care. The lower price of biosimilars can improve the cost-effectiveness of the biologic therapy, which leads to increased patient access to biologic therapy.104 Medicines for Europe recommends policies called benefit-sharing models, in which part of the savings from the use of biosimilars is shared and reinvested for the benefit of patients, physicians, and payers. For example, at the University Hospital Southampton in the UK, the generated savings from a biosimilar switching program were reinvested in the expansion of the clinical team. In France, a pilot project to encourage biosimilar prescriptions was implemented and part of the savings generated by hospitals (30%) was shared with the care units. In Canada, the government of British Columbia indicated that they aim to improve drug plan sustainability with plans to reinvest the savings from biosimilars to expand coverage of treatments and add more drugs to their formulary.60 This reallocation of savings can improve patient access to health care resources (e.g., increased access to pharmacological treatment).104
The successful uptake of biosimilars will be driven by pricing policies that reduce costs to the entire health care system, strategies that demonstrate improvements to the health care system because of the cost-savings, and procurement practices that ensure a viable market. Policy-makers may consider setting price requirements for reference biologics and biosimilars, implementing tendering practices to achieve the best value, demonstrating how savings from biosimilars have been reinvested into the health care system, and ensuring procurement practices mitigate risks related to supply challenges.
References
1.Potential savings from biosimilars in Canada. Ottawa (ON): Patented Medicine Prices Review Board; 2018: http://www.pmprb-cepmb.gc.ca/CMFiles/NPDUIS/Potential_Savings_from_Biosimilars_in_Canada_Biosimilar_Workshop_e.pdf
2.Canada’s evolving market for biosimilars and what it means for payers. Ottawa (ON): Patented Medicine Prices Review Board; 2022: https://www.canada.ca/content/dam/pmprb-cepmb/documents/npduis/analytical-studies/posters/2022/BiosimilarsInCanada_Poster_EN_ISPOR2022.pdf
3.Government of British Columbia. B.C.’s biosimilars program expands. 2021: https://news.gov.bc.ca/releases/2021HLTH0067-000653. Accessed 2023 Mar 1.
4.Afzali A, Furtner D, Melsheimer R, Molloy PJ. The Automatic Substitution of Biosimilars: Definitions of Interchangeability are not Interchangeable. Adv Ther. 2021;38(5):2077-2093. PubMed
5.Kang H, Thorpe R, Knezevic I, et al. Regulatory challenges with biosimilars: an update from 20 countries. Ann N Y Acad Sci. 2021;1491(1):42-59. PubMed
6.GaBI: Generics and Biosimilar Initiative. Different approaches to the interchangeability of biosimilars. 2021: https://www.gabionline.net/biosimilars/research/Different-approaches-to-the-interchangeability-of-biosimilars. Accessed 2021 Aug 20.
7.Dufont I, Viel E, Gilbert S. At a glance: safety of switching biologics and their interchangeability. Quebec City (QC): Institut national d'excellence en santé et services sociaux; 2020: https://www.inesss.qc.ca/fileadmin/doc/INESSS/Rapports/Medicaments/CoupDoeil_switching_biologics_EN.pdf
8.Considerations in demonstrating interchangeability with a reference product guidance for industry. Silver Spring (MD): U.S. Food and Drug Administration; 2019: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/considerations-demonstrating-interchangeability-reference-product-guidance-industry. Accessed 2021 Oct 19.
9.Biosimilars in the EU - information guide for healthcare professionals. Amsterdam (NL): European Medicine Agency, European Commission; 2019: https://www.ema.europa.eu/en/documents/leaflet/biosimilars-eu-information-guide-healthcare-professionals_en.pdf
10.Australian Government Department of Health. Who chooses whether the biosimilar medicine or the reference biological medicine is used? 2019: https://www1.health.gov.au/internet/main/publishing.nsf/Content/biosimilar-hp-who-chooses-whether-biosimilar-medicine-or-reference-biological-medicine-is-used. Accessed 2021 Oct 19.
11.Health Canada. Biosimilar biologic drugs in Canada: fact sheet. 2019: https://www.canada.ca/en/health-canada/services/drugs-health-products/biologics-radiopharmaceuticals-genetic-therapies/applications-submissions/guidance-documents/fact-sheet-biosimilars.html
12.Alvarez DF, Wolbink G, Cronenberger C, Orazem J, Kay J. Interchangeability of Biosimilars: What Level of Clinical Evidence is Needed to Support the Interchangeability Designation in the United States? BioDrugs. 2020;34(6):723-732. PubMed
13.Rathore AS, Stevenson JG, Chhabra H, Maharana C. The global landscape on interchangeability of biosimilars. Expert Opin Biol Ther. 2021:1-16. PubMed
14.Esteban E, Bustos RH, García JC, Jáuregui E. Biosimilars: An Approach to some Current Worldwide Regulation Frameworks. Curr Clin Pharmacol. 2019;14(1):16-40. PubMed
15.Bennett CL, Schoen MW, Hoque S, et al. Improving oncology biosimilar launches in the EU, the USA, and Japan: an updated Policy Review from the Southern Network on Adverse Reactions. Lancet Oncol. 2020;21(12):e575-e588. PubMed
16.Blandizzi C, Meroni PL, Lapadula G. Comparing Originator Biologics and Biosimilars: A Review of the Relevant Issues. Clin Ther. 2017;39(5):1026-1039. PubMed
17.García JJ, Raez LE, Rosas D. A narrative review of biosimilars: a continued journey from the scientific evidence to practice implementation. Transl Lung Cancer Res. 2020;9(5):2113-2119. PubMed
18.Mulcahy AW, Hlavka JP, Case SR. Biosimilar Cost Savings in the United States: Initial Experience and Future Potential. Rand Health Q. 2018;7(4):3. PubMed
19.Jeremias S. Abrilada Approved as Second Interchangeable Humira Biosimilar. AJMC Center for Biosimilars. 2023: https://www.centerforbiosimilars.com/view/abrilada-approved-as-second-interchangeable-humira-biosimilar. Accessed 2024 Feb 26.
20.GaBI: Generics and Biosimilar Initiative. New insulin glargine and potential adalimumab interchangeable biosimilars. 2023: https://gabionline.net/biosimilars/news/new-insulin-glargine-and-potential-adalimumab-interchangeable-biosimilars. Accessed 2023 Jan 31.
21.U.S. Food and Drug Administration. FDA Approves First Interchangeable Biosimilar Insulin Product for Treatment of Diabetes. FDA News Release. 2021: https://www.fda.gov/news-events/press-announcements/fda-approves-first-interchangeable-biosimilar-insulin-product-treatment-diabetes. Accessed 2021 Aug 20.
22.Hagen T. FDA grants interchangeable status for Boehringer Ingelheim’s adalimumab biosimilar (Cyltezo). AJMC Center For Biosimilars. 2021: https://www.centerforbiosimilars.com/view/fda-grants-interchangeable-status-for-boehringer-ingelheim-s-adalimumab-biosimilar-cyltezo-. Accessed 2021 Oct 26.
23.Myshko D. FDA approves first interchangeable biosimilar to Lucentis. Formulary Watch. 2022: https://www.formularywatch.com/view/fda-approves-first-interchangeable-biosimilar-to-lucentis. Accessed 2023 Mar 28.
24.Safe Biologics: Alliance for Safe Biologics Medicines. Oklahoma becomes final state to permit biosimilar substitution. 2021: https://safebiologics.org/2021/05/oklahoma-becomes-final-state-to-permit-biosimilar-substitution/. Accessed 2021 Sep 16.
25.Chen B, Nagai S, Armitage JO, et al. Regulatory and Clinical Experiences with Biosimilar Filgrastim in the U.S., the European Union, Japan, and Canada. Oncologist. 2019;24(4):537-548. PubMed
26.Purvis L, McSpadden J. State biosimilar substitution laws could reduce consumer access and savings. AARP Public Policy Institute. 2022: https://www.aarp.org/pri/topics/health/prescription-drugs/state-biosimilar-substitution-laws-could-reduce-consumer-access.html
27.Yale K, Awosika O, Rengifo-Pardo M, Ehrlich A. Understanding State Regulation of Biosimilars and Effect on Prescribers. J Drugs Dermatol. 2017;16(10):995-1000. PubMed
28.Cauchi R. State Laws and Legislation Related to Biologic Medications and Substitution of Biosimilars. National Conference of State Legislatures. 2019: https://www.ncsl.org/research/health/state-laws-and-legislation-related-to-biologic-medications-and-substitution-of-biosimilars.aspx. Accessed 2021 Aug 20.
29.GaBI: Generics and Biosimilar Initiative. Delaware passes biosimilars substitution law. 2014: https://www.gabionline.net/policies-legislation/Delaware-passes-biosimilars-substitution-law. Accessed 2023 Mar 8.
30.GaBI: Generics and Biosimilar Initiative. UK updates guidance to allow biosimilars interchangeability. 2023: https://gabionline.net/guidelines/uk-updates-guidance-to-allow-biosimilars-interchangeability. Accessed 2023 Feb 1.
31.GaBI: Generics and Biosimilar Initiative. EMA calls for biosimilar interchangeability across the EU. 2022: https://www.gabionline.net/biosimilars/general/ema-calls-for-biosimilar-interchangeability-across-the-eu. Accessed 2022 Oct 4.
32.Dufont I, Viel E, Gilbert S. Safety of switching biologics and their interchangeability. Quebec City (QC): Institut national d'excellence en santé et services sociaux; 2020: https://www.inesss.qc.ca/fileadmin/doc/INESSS/Rapports/Medicaments/INESSS_Biosimilar_SK.pdf
33.Ordre National des Pharmacien. Biosimilars: the Social Security financing law for 2020 removes the right of substitution. 2020: https://www.ordre.pharmacien.fr/Communications/Les-actualites/Biosimilaires-la-loi-de-financement-de-la-Securite-sociale-pour-2020-supprime-le-droit-de-substitution. Accessed 2021 Sep 16.
34.Chaffin Z. Biosimilars could transform French healthcare. Le Monde. 2022: https://www.lemonde.fr/en/economy/article/2022/04/26/biosimilars-could-transform-french-healthcare_5981666_19.html. Accessed 2023 Mar 6.
35.GaBI: Generics and Biosimilar Initiative. Automatic pharmacist substitution of biosimilars in Germany. 2019: https://www.gabionline.net/policies-legislation/Automatic-pharmacist-substitution-of-biosimilars-in-Germany. Accessed 2021 Sep 16.
36.Barbier L, Mbuaki A, Simoens S, Declerck P, Vulto AG, Huys I. Regulatory Information and Guidance on Biosimilars and Their Use Across Europe: A Call for Strengthened One Voice Messaging. Front Med (Lausanne). 2022;9:820755. PubMed
37.Global Pricing News Alert: German cabinet passes “Financial Stabilisation of the Statutory Health Insurance System” bill. Eversana. 2022: https://www.eversana.com/2022/08/04/global-pricing-news-alert-german-cabinet-passes-financial-stabilisation-of-the-statutory-health-insurance-system-bill/. Accessed 2023 Mar 7.
38.Trifirò G, Marcianò I, Ingrasciotta Y. Interchangeability of biosimilar and biological reference product: updated regulatory positions and pre- and post-marketing evidence. Expert Opin Biol Ther. 2018;18(3):309-315. PubMed
39.Raffaelli EA, Massimino F. Biosimilars: considerations in light of the Italian legal framework. GaBI Journal. 2019;8(1):5-23.
40.Vogler S, Schneider P, Zuba M, Busse R, Panteli D. Policies to Encourage the Use of Biosimilars in European Countries and Their Potential Impact on Pharmaceutical Expenditure. Front Pharmacol. 2021;12:1479. PubMed
41.IQVIA. County scorecards for biosimilar sustainability - appendix. 2020: https://www.iqvia.com/insights/the-iqvia-institute/reports/country-scorecards-for-biosimilar-sustainability
42.Frisk P. Biosimilars in Sweden: comments on substitution. 2022: https://legemiddelverket.no/Documents/Om%20oss/Arrangementer/WGEMA/Presentasjoner%202022/Pia%20Frisk%20-%20Biosimilars%20SWE%20May%202022.pdf
43.Moorkens E, Simoens S, Troein P, Declerck P, Vulto AG, Huys I. Different Policy Measures and Practices between Swedish Counties Influence Market Dynamics: Part 2-Biosimilar and Originator Etanercept in the Outpatient Setting. BioDrugs. 2019;33(3):299-306. PubMed
44.GaBI: Generics and Biosimilar Initiative. Finnish drug regulator recommends interchangeability of biosimilars. 2015: https://www.gabionline.net/policies-legislation/Finnish-drug-regulator-recommends-interchangeability-of-biosimilars. Accessed 2021 Sep 17.
45.Market review - biosimilar medicine markets. Brussels (BE): Biosimilar Medicines; 2020: https://www.medicinesforeurope.com/wp-content/uploads/2021/03/Biosimilar%20Market%20Review-Final.pdf
46.Wallace D. Finnish biosimilar substitution proposals get pushback from industry. Pink Sheet: Pharma Intelligence. 2022: https://pink.pharmaintelligence.informa.com/GB152352/Finnish-Biosimilar-Substitution-Proposals-Get-Pushback-From-Industry. Accessed 2023 Mar 7.
47.Wallace D. Finland sees progress on biosimilar substitution plans. Pink Sheet: Pharma Intelligence. 2023: https://pink.pharmaintelligence.informa.com/GB152508/Finland-Sees-Progress-On-Biosimilar-Substitution-Plans. Accessed 2023 Mar 7.
48.Norwegian Medicines Agency. Switching between a reference product and a biosimilar - Legemiddelverket. Statens legemiddelverk. 2017: https://legemiddelverket.no/nyheter/switching-between-a-reference-product-and-a-biosimilar. Accessed 2021 Sep 16.
49.Norwegian Medicines Agency. Biosimilar medicines can be exchanged in pharmacies. Statens legemiddelverk. 2022: https://legemiddelverket.no/nyheter/biotilsvarende-legemidler-kan-byttes-i-apotek. Accessed 2023 Mar 7.
50.Biosimilar medicines subsidised on the Pharmaceutical Benefits Scheme. Melbourne (AU): Australian Government Department of Health; 2022: https://atep.edu.au/wp-content/uploads/2022/07/biosimilar-medicines-subsidised-on-the-pharmaceutical-benefits-scheme_0.pdf
51.GaBI: Generics and Biosimilar Initiative. Biosimilars in Australia – a-flagging and sustainability. 2021: https://www.gabionline.net/biosimilars/general/Biosimilars-in-Australia-a-flagging-and-sustainability. Accessed 2021 Sep 16.
52.Biosimilars uptake drivers. Melbourne (AU): Australian Government Department of Health; [no date][no date][no date][no datehttps://www.pbs.gov.au/general/biosimilars/biosimilar-uptake-drivers-q-and-a.pdf]:
53.Alliance for Safe Biologic Medicines. Australia begins forced switching of metastatic cancer patients. 2021: https://safebiologics.org/2021/07/australia-begins-forced-switching-of-metastatic-cancer-patients/. Accessed 2021 Aug 20.
54.New Zealand Medicines and Medical Devices Safety Authority. Biosimilars. 2014: https://www.medsafe.govt.nz/profs/riss/biosimilars.asp. Accessed 2021 Sep 14.
55.Pharmac. Biological and biosimilar medicines. 2020: https://pharmac.govt.nz/medicine-funding-and-supply/what-you-need-to-know-about-medicines/biological-and-biosimilar-medicines/. Accessed 2021 Sep 13.
56.GaBI: Generics and Biosimilar Initiative. New Zealand guidelines for biosimilars. 2014: https://www.gabionline.net/guidelines/New-Zealand-guidelines-for-biosimilars. Accessed 2021 Sep 13.
57.bpacNZ. Biosimilars: the future of prescribing biological medicines. 2020: https://bpac.org.nz/2020/biosimilars.aspx
58.Siu E, Tomalin A, West K, Anderson S, Wyatt G. An ever-evolving landscape: an update on the rapidly changing regulation and reimbursement of biosimilars in Canada. GaBI Journal. 2019;8(3):107-118.
59.Canadian Society of Intestinal Research. Provincial and territorial biologics policies. 2022: https://badgut.org/information-centre/a-z-digestive-topics/provincial-biologics-policies/. Accessed 2023 Mar 6.
60.Government of British Columbia. Biosimilars initiative for prescribers. 2024: https://www2.gov.bc.ca/gov/content/health/practitioner-professional-resources/pharmacare/prescribers/biosimilars-initiative-health-professionals. Accessed 2021 Sep 16.
61.BC Cancer. Biosimilar drugs. 2023: http://www.bccancer.bc.ca/health-professionals/clinical-resources/biosimilar-drugs. Accessed 2023 Mar 9.
62.List of medications. Quebec City (QC): Régie de l’assurance maladie; 2021: https://www.ramq.gouv.qc.ca/sites/default/files/documents/liste-med-2021-09-29-en_0.pdf
63.GaBI: Generics and Biosimilar Initiative. Northwest Territories, Canada announces biosimilars switching policy. 2022: https://gabionline.net/biosimilars/general/northwest-territories-canada-announces-biosimilars-switching-policy. Accessed Oct 17.
64.GaBI: Generics and Biosimilar Initiative. Canada’s Saskatchewan province introduces biosimilars switching policy. 2022: https://gabionline.net/biosimilars/general/canada-s-saskatchewan-province-introduces-biosimilars-switching-policy. Accessed 2023 Jan 31.
65.Tiered Biologics Reimbursement Policy. Winnipeg (MB): Government of Manitoba; 2023: https://www.gov.mb.ca/health/pharmacare/profdocs/tiered_biologics_specialty.pdf
66.GaBi: Generics and Biosimilar Initiative. Targets and incentives to encourage use of biosimilars. 2021: https://www.gabionline.net/reports/Targets-and-incentives-to-encourage-use-of-biosimilars. Accessed 2021 Aug 20.
67.GaBI: Generics and Biosimilar Initiative. Incentives promoting use of biosimilar medicines in France. 2022: https://gabionline.net/reports/incentives-promoting-use-of-biosimilar-medicines-in-france. Accessed 2023 Feb 1.
68.Barcina Lacosta T, Vulto AG, Turcu-Stiolica A, Huys I, Simoens S. Qualitative Analysis of the Design and Implementation of Benefit-Sharing Programs for Biologics Across Europe. BioDrugs. 2022;36(2):217-229. PubMed
69.Moorkens E, Godman B, Huys I, et al. The Expiry of Humira® Market Exclusivity and the Entry of Adalimumab Biosimilars in Europe: An Overview of Pricing and National Policy Measures. Front Pharmacol. 2020;11:591134. PubMed
70.Commissioning framework for biological medicines (including biosimilar medicines). London (GB): NHS England; 2017: https://www.england.nhs.uk/wp-content/uploads/2017/09/biosimilar-medicines-commissioning-framework.pdf
71.Moorkens E, Barcina Lacosta T, Vulto AG, et al. Learnings from Regional Market Dynamics of Originator and Biosimilar Infliximab and Etanercept in Germany. Pharmaceuticals. 2020;13(10):324. PubMed
72.Luukkanen SV, Tolonen HM, Airaksinen M, Saarukka LSM. The Price and Market Share Evolution of the Original Biologics and Their Biosimilars in Finland. BioDrugs. 2022;36(4):537-547. PubMed
73.Declerck P, Danesi R, Petersel D, Jacobs I. The Language of Biosimilars: Clarification, Definitions, and Regulatory Aspects. Drugs. 2017;77(6):671-677. PubMed
74.Li E, Lobaina E. Application of the FDA Biosimilar Extrapolation Framework to Make Off-Label Determinations. J Manag Care Spec Pharm. 2017;23(12):1227-1232. PubMed
75.Guidance document: information and submission requirements for biosimilar biologic drugs. Ottawa (ON): Government of Canada; 2016: https://www.canada.ca/en/health-canada/services/drugs-health-products/biologics-radiopharmaceuticals-genetic-therapies/applications-submissions/guidance-documents/information-submission-requirements-biosimilar-biologic-drugs-1.html. Accessed 2024 Mar 4.
76.Giuliani R, Tabernero J, Cardoso F, McGregor KH, Vyas M, de Vries EGE. Knowledge and use of biosimilars in oncology: a survey by the European Society for Medical Oncology. ESMO Open. 2019;4(2):e000460. PubMed
77.7Krendyukov A, Schiestl M. Extrapolation concept at work with biosimilar: a decade of experience in oncology. ESMO Open. 2018;3(2). PubMed
78.Ponzianelli A, Bendinelli N, Vilei C, et al. Biosimilars: An European Overview. Acta Scientific Pharmacology. 2020;1(2):8.
79.Renwick MJ, Smolina K, Gladstone EJ, Weymann D, Morgan SG. Postmarket policy considerations for biosimilar oncology drugs. Lancet Oncol. 2016;17(1):e31-e38. PubMed
80.Waxman H, Corr B, Sharp J, McDonald R, Kenyatta K. Getting to lower prescription drug prices: the key drivers of costs and what policymakers can do to address them. New York (NY): Commonwealth Fund; 2020: https://www.commonwealthfund.org/publications/fund-reports/2020/oct/getting-lower-prescription-drug-prices-key-drivers-costs
81.Wilsdon T, Pistollato M, Ross-Stewart K, Saada R, Barquin P. Unlocking the potential of biosimilars: a roadmap for biosimilar policy sustainability biosimilar policy landscape & sustainability assessment - United States of America. Roseland (NJ): Organon; 2022: https://biosimilarsroadmap.com/wp-content/uploads/sites/19/2022/07/CRA-Organon-Biosimilars-Country-Landscape-and-Sustainability-Assessment-USA-vSTC3.pdf
82.GaBI: Generics and Biosimilar Initiative. US drug contracting system is ‘rigged’ against biosimilars. 2018: https://www.gabionline.net/biosimilars/general/US-drug-contracting-system-is-rigged-against-biosimilars. Accessed 2021 Sep 16.
83.Wilsdon T, Pistollato M, Ross-Stewart K, Saada R, Barquin P. Unlocking the potential of biosimilars: a roadmap for biosimilar policy sustainability biosimilar policy landscape & sustainability assessment - United Kingdom. Roseland (NJ) Organon; 2022: https://biosimilarsroadmap.com/wp-content/uploads/sites/19/2022/07/CRA-Organon-Biosimilars-Country-Landscape-and-Sustainability-Assessment-GBR-vSTC.pdfj
84.Moorkens E, Vulto AG, Kent J, et al. A Look at the History of Biosimilar Adoption: Characteristics of Early and Late Adopters of Infliximab and Etanercept Biosimilars in Subregions of England, Scotland and Wales - A Mixed Methods Study. BioDrugs. 2021;35(1):75-87. PubMed
85.Wilsdon T, Pistollato M, Ross-Stewart K, Saada R, Barquin P. Unlocking the potential of biosimilars: a roadmap for biosimilar policy sustainability biosimilar policy landscape & sustainability assessment - France. Roseland (NJ): Organon; 2022: https://biosimilarsroadmap.com/wp-content/uploads/sites/19/2022/07/CRA-Organon-Biosimilars-Country-Landscape-and-Sustainability-Assessment-FRA-vSTC.pdf
86.Wilsdon T, Pistollato M, Ross-Stewart K, Saada R, Barquin P. Unlocking the potential of biosimilars: a roadmap for biosimilar policy sustainability biosimilar policy landscape & sustainability assessment - Germany. Roseland (NJ): Organon; 2022: https://biosimilarsroadmap.com/wp-content/uploads/sites/19/2022/07/CRA-Organon-Biosimilars-Country-Landscape-and-Sustainability-Assessment-DEU-vSTC.pdf
87.GaBI: Generics and Biosimilar Initiative. Influence of local policy measures and practices on biosimilar/originator market dynamics in Germany. 2021: https://www.gabionline.net/biosimilars/research/Influence-of-local-policy-measures-and-practices-on-biosimilar-originator-market-dynamics-in-Germany. Accessed 2021 Aug 20.
88.Wilsdon T, Pistollato M, Ross-Stewart K, Saada R, Barquin P. Unlocking the potential of biosimilars: a roadmap for biosimilar policy sustainability biosimilar policy landscape & sustainability assessment - Italy. Roseland (NJ): Organon; 2022: https://biosimilarsroadmap.com/wp-content/uploads/sites/19/2023/02/CRA-Organon-Biosimilars-Country-Landscape-and-Sustainability-Assessment-ITA-vSTC3.pdf
89.Wilsdon T, Pistollato M, Ross-Stewart K, Saada R, Barquin P. Unlocking the potential of biosimilars: a roadmap for biosimilar policy sustainability biosimilar policy landscape & sustainability assessment- Netherlands. Roseland (NJ): Organon; 2022: https://biosimilarsroadmap.com/wp-content/uploads/sites/19/2022/07/CRA-Organon-Biosimilars-Country-Landscape-and-Sustainability-Assessment-NLD-vSTC.pdf
90.Moorkens E, Vulto AG, Huys I. Biosimilars in Belgium: a proposal for a more competitive market. Acta Clinica Belgica. 2020;0(0):1-12. PubMed
91.Wilsdon T, Pistollato M, Ross-Stewart K, Saada R, Barquin P. Unlocking the potential of biosimilars: a roadmap for biosimilar policy sustainability biosimilar policy landscape & sustainability assessment- Belgium. Roseland (NJ): Organon; 2022: https://biosimilarsroadmap.com/wp-content/uploads/sites/19/2022/07/CRA-Organon-Biosimilars-Country-Landscape-and-Sustainability-Assessment-BEL-vSTC.pdf
92.IQVIA. County scorecards for biosimilar sustainability - Sweden. 2020: https://www.iqvia.com/-/media/iqvia/pdfs/institute-reports/country-scorecards-for-biosimilar-sustainability/iqvia-biosimilar-scorecard-sweden.pdf?la=en&hash=67D35C7056B02873F266E0BD270522B6
93.Mack A. Norway, biosimilars in different funding systems. What works? GaBI Journal. 2015;4(2):90-92.
94.County scorecards for biosimilar sustainability - Norway. 2020: https://www.iqvia.com/-/media/iqvia/pdfs/institute-reports/country-scorecards-for-biosimilar-sustainability/iqvia-biosimilar-scorecard-norway.pdf?la=en&hash=587B419F8E3AD460F607D9D84C2FECE0
95.Wilsdon T, Pistollato M, Ross-Stewart K, Saada R, Barquin P. Unlocking the potential of biosimilars: a roadmap for biosimilar policy sustainability biosimilar policy landscape & sustainability assessment - Norway. Roseland (NJ): Organon; 2022: https://biosimilarsroadmap.com/wp-content/uploads/sites/19/2022/07/CRA-Organon-Biosimilars-Country-Landscape-and-Sustainability-Assessment-NOR-vSTC.pdf
96.Williams G, Loveday C, McKie S. Pricing & reimbursement laws and regulations 2023. Global Legal Insights. 2021: https://www.globallegalinsights.com/practice-areas/pricing-and-reimbursement-laws-and-regulations/australia. Accessed 2021 Sep 15.
97.Wilsdon T, Pistollato M, Ross-Stewart K, Saada R, Barquin P. Unlocking the potential of biosimilars: a roadmap for biosimilar policy sustainability biosimilar policy landscape & sustainability assessment - Australia. Roseland (NJ): Organon; 2022: https://biosimilarsroadmap.com/wp-content/uploads/sites/19/2022/07/CRA-Organon-Biosimilars-Country-Landscape-and-Sustainability-Assessment-AUS-vSTC.pdf
98.NPS MedicineWise. Biologics, biosimilars and PBS sustainability. 2021: https://www.nps.org.au/news/biologics-biosimilars-and-pbs-sustainability. Accessed 2021 Sep 15.
99.Country pharmaceutical pricing policies: a handbook of case studies. Geneva (CH): World Health Organization; 2021: https://apps.who.int/iris/handle/10665/341188. Accessed 2023 Mar 15.
100.How is international reference pricing used within biosimilar pricing? Remap Consulting. 2022: https://remapconsulting.com/biosimilars/how-is-international-reference-pricing-used-within-biosimilar-pricing/. Accessed 2023 Mar 8.
101.GaBI: Generics and Biosimilar Initiative. Pricing and reimbursement of medicines in Canada. 2022: https://www.gabionline.net/generics/research/pricing-and-reimbursement-of-medicines-in-canada. Accessed 2024 Feb 22.
102.Wilsdon T, Pistollato M, Ross-Stewart K, Saada R, Barquin P. Biosimilars: A global roadmap for policy sustainability. Roseland (NJ): Organon; 2022: https://biosimilarsroadmap.com/wp-content/uploads/sites/19/2022/07/Biosimilars-A-global-roadmap-for-policy-sustainability-Final.pdf
103.Dranitsaris G, Jacobs I, Kirchhoff C, Popovian R, Shane LG. Drug tendering: drug supply and shortage implications for the uptake of biosimilars. Clinicoecon Outcomes Res. 2017;9:573-584. PubMed
104.Dutta B, Huys I, Vulto AG, Simoens S. Identifying Key Benefits in European Off-Patent Biologics and Biosimilar Markets: It is Not Only About Price! BioDrugs. 2020;34(2):159-170. PubMed
Appendix 1: Search Strategies
Note that this appendix has not been copy-edited.
Ovid MEDLINE
Search Strategy for Research Question 1
exp Biosimilar Pharmaceuticals/
(biosimilar* or “biosimilar medicine*” or “biosimilar agent*” or “biosimilar drug*” or “biosimilar pharmaceutical*”).tw,kw.
1 or 2
exp Biological Factors/
(“reference biologic*” or “biologic drug*” or “biologic agent*” or biopharmaceutical* or “biological medicinal product*” or originator*).tw,kw.
4 or 5
exp therapeutic equivalency/ or exp Drug Substitution/
(Interchangeab* or “drug substitut*” or “therapeutic equivalen*” or substitut* or switch* or replace* or equival* or equivalen* or bioequivalen* or alternat* or transition* or multiple switch* or switchback* or “automatic substitut*”).tw,kw.
7 or 8
(circumstance* or indication or “patient-related factor*” or Consideration* or decision* or RWE or “Real-world evidence” or “RWD” or “RW” or “real-world data” or “real-world” or “clinical practice” or efficac* or regulat* or unregulat* or policies or policy or law or laws).tw,kw.
9 and 10
3 and 6 and 11
(Jurisdiction* or provinc* or state$ or territor* or country or countries or county or counties or government* or “health authorit*” or “decision-maker*” or funder* or “health administrat*”).tw,kw.
12 and 13
limit 14 to (English language and yr=”2011-Current”)
Search Strategy for Research Question 2
exp Biosimilar Pharmaceuticals/
(biosimilar* or “biosimilar medicine*” or “biosimilar agent*” or “biosimilar drug*” or “biosimilar pharmaceutical*”).tw,kw.
1 or 2
exp Biological Factors/
(“reference biologic*” or “biologic drug*” or “biologic agent*” or biopharmaceutical* or “biological medicinal product*” or originator*).tw,kw.
4 or 5
Drug Industry/ec or Drug Industry/tr or Forecasting/
((Drug* or medication*) adj3 (shortage or supply or availability or available or disruption or demand or “supply chain” or vulnerability or “raw material shortage*” or “raw supply shortage*” or compliance or “production issue*” or “market issue*” or “company closure*”)).tw,kw.
(“Risk mitigation” or “mandatory nonmedical switching”).tw,kw.
7 or 8 or 9
3 and 6
1210 and 11
Drug approval/ or *Government Regulation/ or *Product Surveillance, Postmarketing/ or Delivery of Health Care/ec or *Health Policy/
(“Drug Cost*” or “cost containment” or “drug policy” or “drug policies” or generic* or “brand-name” or “marketed drug*”).tw,kw.
13 or 14
11 and 15
“supply and distribution”.hw,kf,fs,fx.
((payer* or tender* or price* or pricing or procure* or procuring or pharmac* or supply side* or supplier* or rebate* or quota* or funder* or funding* or pharmacy or reimburs* or clawback) adj2 (policy or policies or arrangement*)).tw,kw.
((“price discount” or discount$ or “mark-up”) adj2 (limit or prohibit* or control* or mandatory or adjust*)).tw,kw.
17 or 18 or 19
11 and 20
12 or 16 or 21
limit 22 to (English language and yr=”2011-Current”)
Search Strategy for Research Question 3
exp Biosimilar Pharmaceuticals/
(biosimilar* or “biosimilar medicine*” or “biosimilar agent*” or “biosimilar drug*” or “biosimilar pharmaceutical*”).tw,kw.
1 or 2
exp Biological Factors/
(“reference biologic*” or “biologic drug*” or “biologic agent*” or biopharmaceutical* or “biological medicinal product*” or originator*).tw,kw.
4 or 5
Drug Industry/ec or Drug Industry/tr or Forecasting/
((Drug* or medication*) adj3 (shortage or supply or availability or available or disruption or demand or “supply chain” or vulnerability or “raw material shortage*” or “raw supply shortage*” or compliance or “production issue*” or “market issue*” or “company closure*”)).tw,kw.
(“Risk mitigation” or “mandatory nonmedical switching”).tw,kw.
7 or 8 or 9
3 and 6
10 and 11
Drug approval/ or *Government Regulation/ or *Product Surveillance, Postmarketing/ or Delivery of Health Care/ec or *Health Policy/
(“Drug Cost*” or “cost containment” or “drug policy” or “drug policies” or generic* or “brand-name” or “marketed drug*”).tw,kw.
13 or 14
11 and 15
“supply and distribution”.hw,kf,fs,fx.
((payer* or tender* or price* or pricing or procure* or procuring or pharmac* or supply side* or supplier* or rebate* or quota* or funder* or funding* or pharmacy or reimburs* or clawback) adj2 (policy or policies or arrangement*)).tw,kw.
((“price discount” or discount$ or “mark-up”) adj2 (limit or prohibit* or control* or mandatory or adjust*)).tw,kw.
17 or 18 or 19
11 and 20
12 or 16 or 21
limit 22 to dt=20180801-20211231
limit 23 to english language
remove duplicates from 24
Ovid Embase
Search Strategy for Research Question 1
exp biosimilar agent/
(biosimilar* or “biosimilar medicine*” or “biosimilar agent*” or “biosimilar drug*” or “biosimilar pharmaceutical*”).tw,kw.
1 or 2
exp Biological Factors/
(“reference biologic*” or “biologic drug*” or “biologic agent*” or biopharmaceutical* or “biological medicinal product*” or originator*).tw,kw.
4 or 5
exp therapeutic equivalency/ or exp Drug Substitution/
(Interchangeab* or “drug substitut*” or “therapeutic equivalen*” or substitut* or switch* or replace* or equival* or equivalen* or bioequivalen* or alternat* or transition* or multiple switch* or switchback* or “automatic substitut*”).tw,kw.
7 or 8
(circumstance* or indication or “patient-related factor*” or Consideration* or decision* or RWE or “Real-world evidence” or “RWD” or “RW” or “real-world data” or “real-world” or “clinical practice” or efficac* or regulat* or unregulat* or policies or policy or law or laws).tw,kw.
9 and 10
3 and 6 and 11
limit 12 to (English language and yr=”2011-current”)
remove duplicates from 13
(“Case Reports” or letter or newspaper article).pt.
15 not 16
Search Strategy for Research Question 2
exp biosimilar agent/
(biosimilar* or “biosimilar medicine*” or “biosimilar agent*” or “biosimilar drug*” or “biosimilar pharmaceutical*”).tw,kw.
1 or 2
exp Biological Factor/
(“reference biologic*” or “biologic drug*” or “biologic agent*” or biopharmaceutical* or “biological medicinal product*” or originator*).tw,kw.
4 or 5
3 and 6
Drug Industry/ec or Drug Industry/tr or Forecasting/
((Drug* or medication*) adj3 (shortage or supply or availability or available or disruption or demand or “supply chain” or vulnerability or “raw material shortage*” or “raw supply shortage*” or compliance or “production issue*” or “market issue*” or “company closure*”)).tw,kw.
(“Risk mitigation” or “mandatory nonmedical switching”).tw,kw.
8 or 9 or 10
7 and 11
“Drug approval”/ or *”Government Regulation”/ or *”postmarketing surveillance”/ or “Health care delivery”/ec or *Health care policy/
(“Drug Cost*” or “drug-tendering process*” or “cost containment” or funding or funded or fund or pricing or reimbursement or “drug policy” or “drug policies” or generic* or “brand-name” or “marketed drug*”).tw,kw.
13 or 14
7 and 15
“supply and distribution”.fs,fx,ec.
((payer* or tender* or price* or pricing or procure* or procuring or pharmac* or supply side* or supplier* or rebate* or quota* or funder* or funding* or pharmacy or reimburs* or clawback) adj2 (policy or policies or arrangement*)).tw,kw.
((“price discount” or discount$ or “mark-up”) adj2 (limit or prohibit* or control* or mandatory or adjust*)).tw,kw.
17 or 18 or 19
7 and 20
12 or 16 or 21
limit 22 to (english language and yr=”2011-current”)
(“Case Reports” or letter or newspaper article).pt.
23 not 24
Remove duplicates from 25
Search Strategy for Research Question 3
exp biosimilar agent/
(biosimilar* or “biosimilar medicine*” or “biosimilar agent*” or “biosimilar drug*” or “biosimilar pharmaceutical*”).tw,kw.
1 or 2
exp Biological Factor/
(“reference biologic*” or “biologic drug*” or “biologic agent*” or biopharmaceutical* or “biological medicinal product*” or originator*).tw,kw.
4 or 5
3 and 6
Drug Industry/ec or Drug Industry/tr or Forecasting/
((Drug* or medication*) adj3 (shortage or supply or availability or available or disruption or demand or “supply chain” or vulnerability or “raw material shortage*” or “raw supply shortage*” or compliance or “production issue*” or “market issue*” or “company closure*”)).tw,kw.
(“Risk mitigation” or “mandatory nonmedical switching”).tw,kw.
8 or 9 or 10
7 and 11
“Drug approval”/ or *”Government Regulation”/ or *”postmarketing surveillance”/ or “Health care delivery”/ec or *Health care policy/
(“Drug Cost*” or “drug-tendering process*” or “cost containment” or funding or funded or fund or pricing or reimbursement or “drug policy” or “drug policies” or generic* or “brand-name” or “marketed drug*”).tw,kw.
13 or 14
7 and 15
“supply and distribution”.fs,fx,ec.
((payer* or tender* or price* or pricing or procure* or procuring or pharmac* or supply side* or supplier* or rebate* or quota* or funder* or funding* or pharmacy or reimburs* or clawback) adj2 (policy or policies or arrangement*)).tw,kw.
((“price discount” or discount$ or “mark-up”) adj2 (limit or prohibit* or control* or mandatory or adjust*)).tw,kw.
17 or 18 or 19
7 and 20
12 or 16 or 21
limit 22 to english language
limit 16 to em=201831-202152
(conference abstract or “Case Reports” or editorial or comment or letter or newspaper article).pt.
24 not 25
remove duplicates from 26
Cochrane Library
Search Strategy for Research Question 1
Biosimilar Pharmaceuticals.af.
(biosimilar* or “biosimilar medicine*” or “biosimilar agent*” or “biosimilar drug*” or “biosimilar pharmaceutical*”).tw,kw.
1 or 2
Biological Factors.af.
(“reference biologic*” or “biologic drug*” or “biologic agent*” or biopharmaceutical* or “biological medicinal product*” or originator*).tw,kw.
4 or 5
(therapeutic equivalency or Drug Substitution).af.
(Interchangeab* or “drug substitut*” or “therapeutic equivalen*” or substitut* or switch* or replace* or equival* or equivalen* or bioequivalen* or alternat* or transition* or multiple switch* or switchback* or “automatic substitut*”).tw,kw.
7 or 8
(circumstance* or indication or “patient-related factor*” or Consideration* or decision* or RWE or “Real-world evidence” or “RWD” or “RW” or “real-world data” or “real-world” or “clinical practice” or efficac* or regulat* or unregulat* or policies or policy or law or laws).tw,kw.
9 and 10
(Jurisdiction* or provinc* or state$ or territor* or country or countries or county or counties or government* or “health authorit*” or “decision-maker*” or funder* or “health administrat*”).tw,kw.
3 and 6 and 11 and 12
remove duplicates from 13
limit 14 to last 10 years
Search Strategy for Research Question 2
Biosimilar Pharmaceuticals.af.
(biosimilar* or “biosimilar medicine*” or “biosimilar agent*” or “biosimilar drug*” or “biosimilar pharmaceutical*”).tw,kw.
One or 2
Biological Factors.af.
(“reference biologic*” or “biologic drug*” or “biologic agent*” or biopharmaceutical* or “biological medicinal product*” or originator*).tw,kw.
Four or 5
Three and 6
(Drug Industry or Drug Industry or Forecast*).af.
((Drug* or medication*) adj3 (shortage or supply or availability or available or disruption or demand or “supply chain” or vulnerability or “raw material shortage*” or “raw supply shortage*” or compliance or “production issue*” or “market issue*” or “company closure*”)).tw,kw.
(“Risk mitigation” or “mandatory nonmedical switching”).tw,kw.
Eight or 9 or 10
Seven and 11
(“Drug approval*” or “Government Regulation*” or “postmarketing product surveillance” or “Delivery of Health Care” or “Health Policy”).af.
(“Drug Cost*” or “drug-tendering process*” or “cost containment” or funding or funded or fund or pricing or reimbursement or “drug policy” or “drug policies” or generic* or “brand-name” or “marketed drug*”).tw,kw.
Thirteen or 14
Seven and 15
“supply and distribution”.af.
((payer* or tender* or price* or pricing or procure* or procuring or pharmac* or supply side* or supplier* or rebate* or quota* or funder* or funding* or pharmacy or reimburs* or clawback) adj2 (policy or policies or arrangement*)).tw,kw.
((“price discount” or discount$ or “mark-up”) adj2 (limit or prohibit* or control* or mandatory or adjust*)).tw,kw.
Seventeen or 18 or 19
Seven and 20
Twelve or 16 or 21
remove duplicates from 22
limit 23 to past 10 years
Search Strategy for Research Question 3
Biosimilar Pharmaceuticals.af.
(biosimilar* or “biosimilar medicine*” or “biosimilar agent*” or “biosimilar drug*” or “biosimilar pharmaceutical*”).tw,kw.
1 or 2
Biological Factors.af.
(“reference biologic*” or “biologic drug*” or “biologic agent*” or biopharmaceutical* or “biological medicinal product*” or originator*).tw,kw.
4 or 5
3 and 6
(Drug Industry or Drug Industry or Forecast*).af.
((Drug* or medication*) adj3 (shortage or supply or availability or available or disruption or demand or “supply chain” or vulnerability or “raw material shortage*” or “raw supply shortage*” or compliance or “production issue*” or “market issue*” or “company closure*”)).tw,kw.
(“Risk mitigation” or “mandatory nonmedical switching”).tw,kw.
8 or 9 or 10
7 and 11
(“Drug approval*” or “Government Regulation*” or “postmarketing product surveillance” or “Delivery of Health Care” or “Health Policy”).af.
(“Drug Cost*” or “drug-tendering process*” or “cost containment” or funding or funded or fund or pricing or reimbursement or “drug policy” or “drug policies” or generic* or “brand-name” or “marketed drug*”).tw,kw.
13 or 14
7 and 15
“supply and distribution”.af.
((payer* or tender* or price* or pricing or procure* or procuring or pharmac* or supply side* or supplier* or rebate* or quota* or funder* or funding* or pharmacy or reimburs* or clawback) adj2 (policy or policies or arrangement*)).tw,kw.
((“price discount” or discount$ or “mark-up”) adj2 (limit or prohibit* or control* or mandatory or adjust*)).tw,kw.
17 or 18 or 19
7 and 20
12 or 16 or 21
remove duplicates from 22
limit 23 to yr=”2011 -Current”
Appendix 2: Study Selection Process
Note that this appendix has not been copy-edited.
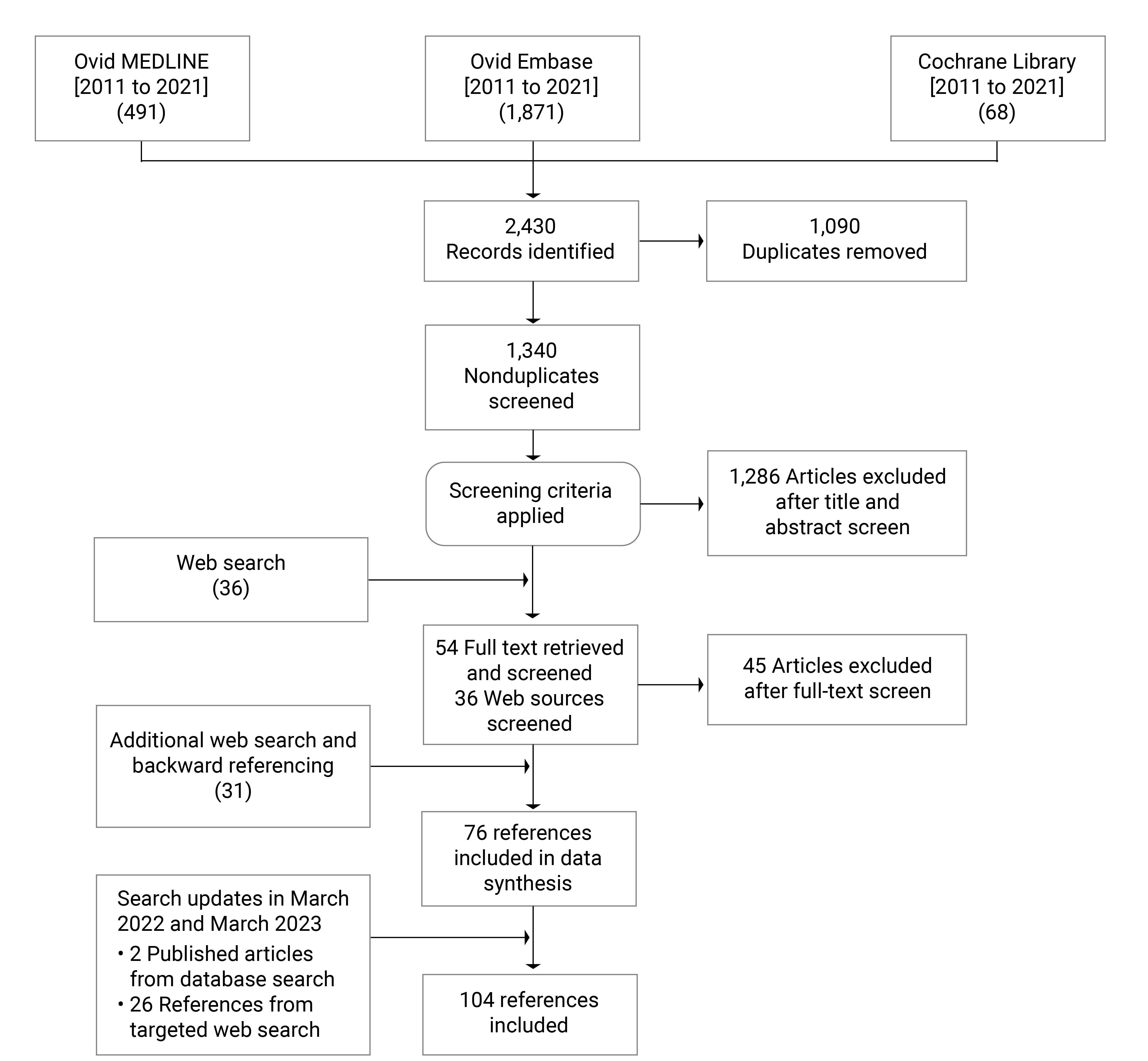
Appendix 3: Interchangeability of Biosimilars in International Jurisdictions
Note that this appendix has not been copy-edited.
In 2019, WHO conducted the survey in 18 countries and the EU. The survey was updated in 2020. Table 6 presents the survey results.5.
Table 6: Biosimilar Interchangeability in International Jurisdictions
Country | Interchangeability automatically accepted upon approval of the biosimilar | Depend on the clinical evidence provided by the biosimilar manufacturer | Depend on prescriber’s decision |
|---|---|---|---|
Brazil | — | Yes | Yes |
Canada | — | — | Yes |
China | — | — | Yes |
Cuba | — | Yes | — |
Egypt | — | — | Yes |
EU | — | — | Yes |
Ghana | — | Yes | Yes |
India | — | — | Yes |
Indonesia | — | — | Yes |
Iran | Yes | — | — |
Japan | Yes | — | — |
Jordan | — | — | Yes |
Malaysia | — | — | — |
Peru | — | Yes | — |
Republic of Korea | — | — | Yes |
Russia | — | Yes | — |
Singapore | — | — | Yes |
Thailand | — | — | Yes |
Zambia | — | Yes | Yes |
Appendix 4: Summary of International Policies on Interchangeability, Substitution, and Switching
Note that this appendix has not been copy-edited.
Table 7: International Policies on Interchangeability, Substitution, and Switching
Policies | Jurisdiction | Features/conditions |
|---|---|---|
Interchangeability designation | US | Regulations allow the FDA to designate biosimilars as interchangeable |
Finland | Filgrastim interchangeability designated | |
Automatic substitution | US | Interchangeability designated biosimilars only |
Germany | Pharmacy substitution is expected to be allowed in March 2024 | |
Australia | ‘a-flagged’ cases only (case-by-case basis) | |
France | Two drugs only (Neulasta and Neupogen) | |
Norway | Pharmacy substitution is allowed | |
Medical switching | US, UK, France, Germany, Italy, the Netherlands, Denmark, Sweden, Finland, Norway, Australia, New Zealand, Canada | Switching decisions are at the discretion of the prescribing physician |
Biosimilar use for patients who are treatment naive | Germany, France, Italy, the Netherlands, Norway, Australia, Canada | Regulations exist or authorities recommend prescribing biosimilars for patients who are treatment naive |
Nonmedical switching | Canada (BC, AB, QC, NB, NS, SK, NT, ON, NL, YT, PEI) | Exceptions apply |
Australia | Switching from Avastin to Mvasi (for metastatic bowel cancer treatment) | |
Denmark | National tendering resulted in nonmedical switching at hospital level |
Appendix 5: Nonmedical Switching Drug Lists
Note that this appendix has not been copy-edited.
Table 8: Nonmedical Switching in British Columbia — List of Drugs
Drug (reference product) | Biosimilar | Condition |
|---|---|---|
Adalimumab (Humira) | Amgevita Hadlima (for adults only) Hulio Hyrimoz Idacio |
|
Etanercept (Enbrel) | Brenzys Erelzi |
|
Infliximab (Remicade) | Inflectra Renflexis |
|
Rituximab (Rituxan) | Truxima Riximyob Ruxience™ |
|
Insulin glargine (Lantus) | Basaglar |
|
Insulin lispro originator (Humalog)c | Admelog | |
Insulin aspart (NovoRapid)d | Trurapi Kirsty | |
Enoxaparin (Elonox)e | Elonox, Elonox HP |
|
aOnly Brenzys was indicated for PsA at this time.
bRiximyo is not yet approved to treat GPA or MPA.
cCoverage extended until May 30, 2024.
dCoverage extended until November 30, 2024.
eBiosimilar listed June 1, 2023.
Table 9: Nonmedical Switching in Alberta — List of Drugs
Drug (reference product) | Biosimilar | Condition |
|---|---|---|
Adalimumab (Humira) | Amgevita Hadlima Hulio Hyrimoz Idacio |
|
Enoxaparin (Lovenox) | Inclunox Noromby Redesca |
|
Insulin lispro (Humalog) | Admelog |
|
Insulin aspart (NovoRapid) | Trurapi |
Appendix 6: Tiered Biologics Reimbursement in Manitoba
Note that this appendix has not been copy-edited.
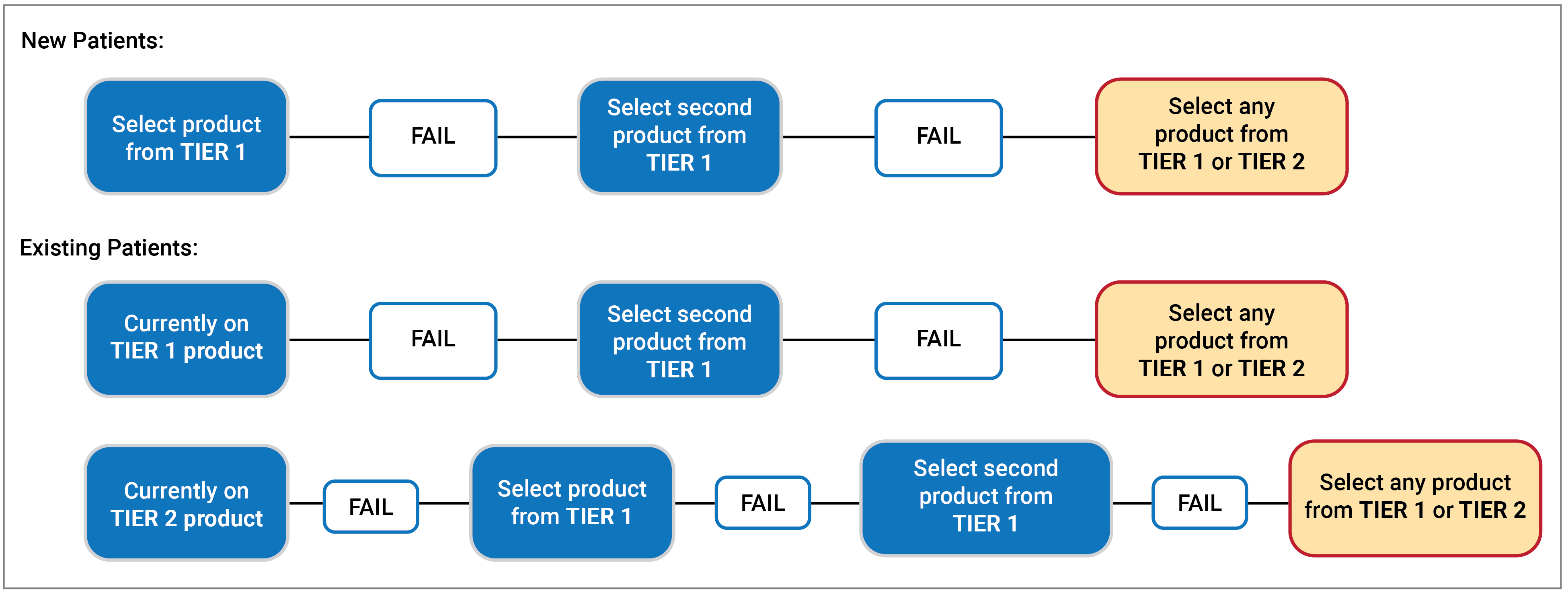
Table 10: List of Tier 1 and Tier 2 Products
Condition | Tier 1 | Tier 2 |
|---|---|---|
Gastroenterology | ||
Crohn and fistulizing Crohn disease | Abrilada (adalimumab) Amgevita (adalimumab) Avsola (infliximab) Brenzys (etanercept) Cimzia (certolizumab pegol) Cosentyx (secukinumab) Erelzi (etanercept) Hadlima (adalimumab) Hulio (adalimumab) Hyrimoz (adalimumab) Idacio (adalimumab) Inflectra (infliximab) Renflexis (infliximab) Simlandi (adalimumab) Simponi (golimumab) Yuflyma (adalimumab) | Enbrel (etanercept) Humira (adalimumab) Remicade (infliximab) |
Ulcerative colitis | Abrilada (adalimumab) Amgevita (adalimumab) Avsola (infliximab) Brenzys (etanercept) Cimzia (certolizumab pegol) Cosentyx (secukinumab) Erelzi (etanercept) Hadlima (adalimumab) Hulio (adalimumab) Hyrimoz (adalimumab) Idacio (adalimumab) Inflectra (infliximab) Renflexis (infliximab) Rinvoq (upadacitinib) Simlandi (adalimumab) Simponi (golimumab) Taltz (ixekizumab) Tremfya (guselkumab) Yuflyma (adalimumab) | Enbrel (etanercept) Humira (adalimumab) Remicade (infliximab) |
Dermatology | ||
Abrilada (adalimumab) Amgevita (adalimumab) Avsola (infliximab) Bimzelx (bimekizumab) Brenzys (etanercept) Cosentyx (secukinumab) Erelzi (etanercept) Hadlima (adalimumab) Hulio (adalimumab) Hyrimoz (adalimumab) Idacio (adalimumab) Ilumya (tildrakizumab) Inflectra (infliximab) Renflexis (infliximab) Siliq (brodalumab) Simlandi (adalimumab) Skyrizi (risankizumab) Taltz (ixekizumab) Tremfya (guselkumab) Yuflyma (adalimumab) | Enbrel (etanercept) Humira (adalimumab) Remicade (infliximab) Stelara (ustekinumab) | |
Rheumatology | ||
Ankylosing spondylitis | Abrilada (adalimumab) Amgevita (adalimumab) Avsola (infliximab) Brenzys (etanercept) Cimzia (certolizumab pegol) Cosentyx (secukinumab) Erelzi (etanercept) Hadlima (adalimumab) Hulio (adalimumab) Hyrimoz (adalimumab) Idacio (adalimumab) Inflectra (infliximab) Renflexis (infliximab) Simlandi (adalimumab) Simponi (golimumab) Yuflyma (adalimumab) | Enbrel (etanercept) Humira (adalimumab) Remicade (infliximab) |
Psoriatic arthritis | Abrilada (adalimumab) Amgevita (adalimumab) Avsola (infliximab) Brenzys (etanercept) Cimzia (certolizumab pegol) Cosentyx (secukinumab) Erelzi (etanercept) Hadlima (adalimumab) Hulio (adalimumab) Hyrimoz (adalimumab) Idacio (adalimumab) Inflectra (infliximab) Renflexis (infliximab) *Rinvoq (upadacitinib) Simlandi (adalimumab) Simponi (golimumab) Taltz (ixekizumab) Tremfya (guselkumab) Yuflyma (adalimumab) | Enbrel (etanercept) Humira (adalimumab) Remicade (infliximab) |
Rheumatoid arthritis | Abrilada (adalimumab) Actemra (tocilizumab) Amgevita (adalimumab) Avsola (infliximab) Brenzys (etanercept) Cimzia (certolizumab pegol) Erelzi (etanercept) Hadlima (adalimumab) Hulio (adalimumab) Hyrimoz (adalimumab) Idacio (adalimumab) Inflectra (infliximab) Kevzara (sarilumab) Olumiant (baricitinib) Orencia (abatacept) Renflexis (infliximab) Rinvoq (upadacitinib) Riximyo (rituximab) Ruxience (rituximab) Simlandi (adalimumab) Simponi (golimumab) Simponi IV (golimumab) Truxima (rituximab) Xeljanz (tofacitinib) Xeljanz XR (tofacitinib) Yuflyma (adalimumab) | Enbrel (etanercept) Humira (adalimumab) Kineret (anakinra) Remicade (infliximab) Rituxan (rituximab) |
Appendix 7: Biosimilar Policy Status in Canadian Jurisdictions
Note that this appendix has not been copy-edited.
Table 11: Biosimilar Policies in Canadian Jurisdictions
Province | Biosimilar Policies (as of March 2024) |
|---|---|
British Columbia |
|
Alberta |
|
Saskatchewan |
|
Manitoba |
|
Ontario |
|
Quebec |
|
New Brunswick |
|
Newfoundland and Labrador |
|
Nova Scotia |
|
Prince Edward Island |
|
Yukon |
|
Northwest Territories |
|
Nunavut |
|
Appendix 8: International Policies to Encourage Switching
Note that this appendix has not been copy-edited.
Table 12: Summary of International Policies to Encourage Switching
Policies | Jurisdiction | Key features |
|---|---|---|
Biosimilar prescription targets and quotas | UK | 80% of market share as a national target |
France | Physicians can prescribe reference biologics for maximum 30% of patients | |
Germany | Penalty for the amount exceeding certain percentage of prescriptions | |
Financial incentive | US | Financial incentives for prescribing physicians and/or hospitals |
UK | ||
France | ||
Payer-led incentive | The Netherlands | A grant/higher reimbursement paid by insurers to the hospitals that have an adalimumab biosimilar contract with disadvantageous conditions |
Gainsharing | Germany | Savings shared between groups of physicians and insurers |
Sweden | Savings shared between local county councils and the central government | |
Legislative measures/guidelines supporting biosimilar prescription | UK | Best value biological medicine policy requires the use of the most cost-effective biologic |
Germany, Belgium, France, Italy, Denmark, Finland, Sweden | Use of guidelines/recommendations to encourage biosimilar prescription |
Appendix 9: International Policies on Pricing and Procurement of Biosimilars
Note that this appendix has not been copy-edited.
Table 13: Biosimilar Pricing and Procurement in International Jurisdictions
Policies | Jurisdiction | Features/conditions | |
|---|---|---|---|
Procurement | National tenders | UK, France, Sweden, Denmark, Norway | National purchasing strategy |
Regional/hospital tenders | UK, Germany, Sweden, Italy, the Netherlands, Finland, Belgium | Tenders by health care trusts, local authorities, hospitals, or group of hospitals | |
Direct purchase | US | Direct purchase from manufacturers, wholesalers, or GPO | |
Pricing | Free pricing | UK | Price ceilings apply |
Norway | A maximum price is imposed | ||
US, Germany, the Netherlands, Sweden | Reference pricing is used | ||
Denmark | Price is determined through tenders | ||
Direct price control | France, Italy, Finland, Belgium, Australia | Mandatory price reduction exists | |
Appendix 10: Biologics Market Dynamics in the US
Note that this appendix has not been copy-edited.
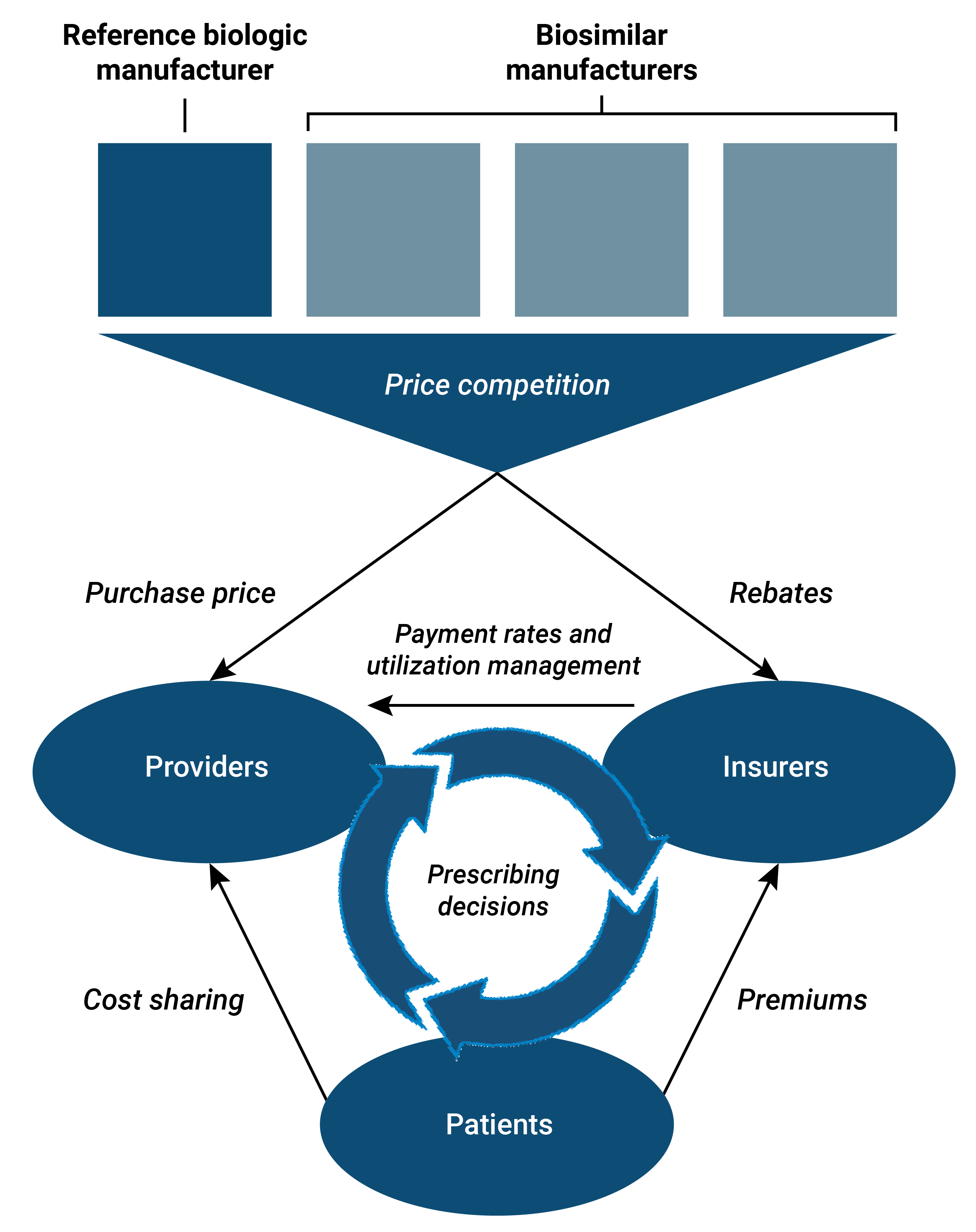
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca.