CADTH Reimbursement Review
Tisagenlecleucel (Kymriah)
Sponsor: Novartis Pharmaceuticals Canada Inc.
Therapeutic area: Relapsed or refractory follicular lymphoma
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Ethics Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
allo-SCT
allogeneic stem cell transplant
auto-SCT
autologous stem cell transplant
BR
bendamustine plus rituximab
CAR
chimeric antigen receptor
CI
confidence interval
CNS
central nervous system
CR
complete remission
CRR
complete remission rate
CRS
cytokine release syndrome
DoR
duration of remission
EAS
efficacy analysis set
ECOG PS
Eastern Cooperative Oncology Group Performance Status
ELLyE
Ensemble Leucemie Lymphomes Espoir
EMA
European Medicines Agency
EQ VAS
EQ visual analogue scale
EQ-5D-3L
3-Level ED-5D
ESS
effective sample size
FACT-Lym
Functional Assessment of Cancer therapy-Lymphoma
FL
follicular lymphoma
FLIPI
The Follicular Lymphoma International Prognostic Index
GELF
Groupe d'Etude des Lymphomes Folliculaires
HPF
high power field
HR
hazard ratio
HRQoL
health-related quality of life
ICU
intensive care unit
IRC
independent review committee
ITC
indirect treatment comparison
KM
Kaplan-Meier
LC
Lymphoma Canada
LD
lymphodepleting
LDH
lactate dehydrogenase
mAb
monoclonal antibody
MAIC
matching-adjusted indirect comparison
MCID
minimally clinically important differences
NE
not estimable
NHL
non-Hodgkin lymphoma
NOC/c
Notice of Compliance with conditions
O-CHOP
obinutuzumab plus cyclophosphamide plus doxorubicin plus vincristine plus prednisone
ORR
overall response rate
OS
overall survival
PFS
progression-free survival
PI3K
phosphoinositide 3-kinase
POD24
progression of disease within 24 months of first-line treatment
PR
partial response
PRO
patient-reported outcome
PRR
partial response rate
QoL
quality of life
r/r
relapsed or refractory
R2
rituximab plus lenalidomide
R-CHOP
rituximab plus cyclophosphamide plus doxorubicin plus vincristine plus prednisone
RCT
randomized controlled trial
R-CVP
rituximab plus cyclophosphamide plus vincristine plus prednisone
R-GDP
rituximab plus gemcitabine plus dexamethasone plus cisplatin
R-ICE
rituximab plus ifosfamide plus carboplatin plus etoposide
SAE
serious adverse event
SCT
hematopoietic stem cell transplant
SF-36
36-Item Short Form Survey
SOC
standard of care
VAS
visual analogue scale
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information on Application Submitted for Review
Item | Description |
|---|---|
Information on drug submitted for review | |
Drug product | Tisagenlecleucel (Kymriah) 1.2 × 106 to 6.0 × 108 CAR-positive viable T cells suspended in 1 or more patient-specific infusion bags for single-dose, one-time, IV administration |
Sponsor | Novartis Pharmaceuticals Canada Inc. |
Indication | For the treatment of adults with relapsed or refractory grade 1, 2, or 3a follicular lymphoma after 2 or more lines of systemic therapy |
Reimbursement request | As per indications |
Health Canada approval status | NOC/c |
Health Canada review pathway | Priority review |
NOC date | December 19, 2022 |
Recommended dose | 0.6 to 6.0 × 108 CAR-positive viable T cells (nonweight based) |
CAR = chimeric antigen receptor; NOC/c = Notice of Compliance with conditions.
Introduction
Follicular lymphoma (FL) is the second most common subtype of non-Hodgkin lymphoma (NHL) in Western countries and is characterized by follicular clusters or patterns of follicle centre B cells in a lymph node, bone marrow, or spleen.1-3 FL is a relapsing and remitting disease, characterized by recurrent disease progression, shorter remission periods, and decreased survival (i.e., overall survival [OS] or progression-free survival [PFS]) with each treatment course.4-7 Even though FL manifests as an indolent clinical course over many years in general, most patients eventually develop increasingly resistant disease, resulting in patients with relapsed or refractory (r/r) FL having reduced treatment options and poor prognoses.4,8 Many patients with indolent FL may survive for decades, although a significant proportion of patients experience aggressive disease, which results in approximately 20% of affected patients dying 2 to 3 years after diagnosis.9 Although Canada-specific mortality data for FL could not be identified, in 2022, it was projected that there will be 3,000 deaths due to NHL in Canada.10 Patients with r/r FL experience significant health-related quality of life (HRQoL) impairment.11,12 The overall prevalence of FL was estimated to be 1 per 3,000 people.13 Despite being a rare disease, FL is considered to be among the most prevalent of the lymphomas due to its chronicity and incurability in its advanced stages.4,5,14,15 The overall incidence of FL is also low, with rates ranging from 2.2 to 3.5 per 100,000 new cases per year in Asia, Australia, Europe, and the US.16 According to a survey conducted in the US, the percentage of patients relapsing and receiving subsequent treatments was estimated to be 41%, 40%, and 30% for patients who received 1 line, 2 lines, and 3 lines of treatment, respectively.17
Staging of FL describes the extent to which the disease has spread in the body: stage I FL involves 1 node or a group of adjacent nodes or single extranodal lesions without nodal involvement; stage II FL involves 2 or more nodal groups on the same side of the diaphragm and limited contiguous extranodal involvement; stage III FL involves nodes on both sides of the diaphragm and nodes above the diaphragm with spleen involvement; stage IV FL has additional noncontiguous extralymphatic involvement.18 Grading of FL is determined by the number of large FL cells (also known as centroblasts) and reflects the aggressiveness of the tumour: grade 1 FL has 0 to 5 centroblasts per high power field (HPF); grade 2 FL has 6 to 15 centroblasts per HPF; and grade 3 FL has more than 15 centroblasts per HPF. Grade 3 FL has been subdivided into grade 3a (centrocytes are present) and grade 3b (solid sheets of centroblasts present).18 Grade 1, 2, and 3a FLs are generally considered to be low grade or slow growing, whereas grade 3b FL is faster growing.
The main goals of treatment are to cure the lymphoma in patients with stage I to II FL, and to extend remission in patients with stage III to IV FL.19,20 Once a diagnosis of FL is confirmed, the gold standard for the management of asymptomatic patients with indolent FL is watchful waiting.17 For small, localized symptomatic FL, radiotherapy is considered the standard of care (SOC).21,22 For grade 1, 2, and 3a FL, the preferred chemoimmunotherapy regimen is bendamustine plus rituximab (BR).20,23,24 In frail and older adults, rituximab monotherapy, a chemotherapy-free approach, is the preferred first-line regimen, according to European and North American guidelines.25,26 However, some Canadian centres do not have access to rituximab monotherapy. Instead, these physicians would keep patients on BR for several treatment cycles or for as long as possible. Beyond first-line treatment, there is currently no gold standard for the care of the r/r FL population. In terms of treatment options for second-line regimens for r/r FL, combined immunochemotherapy is the preferred treatment strategy, such as obinutuzumab, cyclophosphamide, doxorubicin hydrochloride, vincristine sulphate, and prednisone (O-CHOP).20 Hematopoietic stem cell transplant (SCT) may be considered in young and fit patients with no comorbidities in the second-line setting. Autologous stem cell transplant (auto-SCT) is more common than allogeneic stem cell transplant (allo-SCT) in this population. However, only a small subset of patients with FL would be eligible for transplant in the second-line setting.
Patients with r/r FL in the third-line setting and beyond are heavily pretreated and have advanced disease. A heterogenous mix of immunochemotherapy (for most patients) and SCT (for a minority of patients) are the current treatment options in this hard-to-treat population. In recent years, chimeric antigen receptor (CAR) T-cell therapy has emerged as another form of immunotherapy for the treatment of blood cancers, including lymphomas. Although promising results have been reported for the CAR T-cell therapies for advanced stage lymphomas, severe adverse effects related to CAR T-cell therapy, such as cytokine release syndrome (CRS) and neurologic toxicities, have also been reported.27
Tisagenlecleucel (Kymriah) is a second-generation autologous CAR T-cell therapy directed at the cell-surface protein CD19, which is only expressed on B cells or their precursors and not on hematopoietic stem cells or non-B-cell tissues. On December 19, 2022, tisagenlecleucel received a Notice of Compliance with conditions (NOC/c) from Health Canada for adults with r/r grade 1, 2, or 3a FL after 2 or more lines of systemic therapy.28 The recommended dose of tisagenlecleucel for the indicated population is 0.6 to 6.0 × 108 CAR-positive viable T cells (nonweight based) suspended in 1 or more patient-specific infusion bags for a single-dose, one-time, IV administration.28
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups that responded to CADTH’s call for input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
One patient group, Lymphoma Canada (LC), provided input to the tisagenlecleucel submission. LC is a national Canadian registered charity. It collected input from patients with r/r FL through an online anonymous survey conducted from November 2022 to January 2023. Of the 44 respondents, only 1 had experience with tisagenlecleucel. In addition, LC obtained patient feedback from a French patient organization called Ensemble Leucemie Lymphomes Espoir (ELLyE). ELLyE collected feedback from 162 patients on CAR T-cell therapy, including 19 who had experience with tisagenlecleucel from January 2019 to September 2020 in France.
Based on the patient input, FL has significant negative impact on a patient’s physical and psychosocial well-being, affecting everyday life, work, and family.
Patients indicated that there is a need for more therapeutic options that provide longer disease remission, lead to a longer life span, and improve quality of life (QoL). They also indicated that all patients in Canada should have easy access to new therapies.
Patients who had experience with tisagenlecleucel indicated that the drug is effective; adverse events (AEs) were reported but were manageable.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The clinical panel indicated that for patients with FL, the most important treatment goals are to prolong survival (for both OS and PFS) and improve QoL. However, patients with r/r FL relapse after frontline therapies or are refractory to available treatments, which subsequently affects their long-term PFS and QoL. In addition, some patients may not tolerate current treatments well, due to AEs or complications associated with SCT.
The clinical panel noted that many factors (e.g., patient characteristics, previous treatments, treatment effects and toxicity, whether a treatment is reimbursed by drug plans, disease progression and transformation, and patient preference) need to be considered before deciding which treatment to provide. Watch and wait is a common approach for many patients with FL, even after disease relapse. Patients who need active treatments typically receive bendamustine or a rituximab-based therapy (such as BR; rituximab, cyclophosphamide, vincristine sulphate, plus prednisone [R-CVP]; rituximab, cyclophosphamide, doxorubicin hydrochloride [hydroxydaunorubicin], vincristine sulphate [Oncovin], plus prednisone [R-CHOP]; or rituximab plus lenalidomide [R2]). Patients with relapsed disease after the treatment with chemoimmunotherapy, particularly those who progress within 2 years, may receive auto-SCT if they are suitable candidates. After all these treatments, some patients maintain the indolent status and some transform to large cell lymphoma. The clinical panel suggested that tisagenlecleucel be used as a third-line treatment or beyond for patients with r/r FL. There are not many options available for patients at this stage.
The clinical panel indicated that although a more selective population would be suitable for treatment with CAR T-cell therapy in clinical trials of r/r FL, in practice, CAR T-cell therapy can be used in a broader patient population (for example, patients with certain comorbidities or disease status). In clinical practice, suitable patients can be identified based on clinical judgment, which combines medical history, laboratory and imaging findings, and often a lymph node biopsy. The panel noted that patients who are likely to benefit from other available treatments or who have an Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 3 or higher are least suitable for tisagenlecleucel. The panel also noted that there is not a specific patient characteristic that can be used to predict which patient will respond better to tisagenlecleucel and which will not.
The panel indicated that in clinical practice, patients are evaluated and followed in a manner similar to that described in the clinical trials of FL. Remission and survival are measured. Physical exams and imaging exams are routinely conducted to assess the patient’s response to CAR T-cell therapy.
The panel suggested that meaningful responses to treatment with tisagenlecleucel would be not only a high complete remission rate (CRR), but also durability of treatment response and long-term PFS and OS. The panel noted that after CAR T-cell therapy, clinicians will assess treatment response (e.g., with CT scan) at 3 months, or sooner if needed.
The panel emphasized that a multidisciplinary team, which involves hematologists, infectious disease specialists, neurologists, an intensive care unit (ICU) team, and other specialists, is required to diagnose, treat, and monitor patients who receive tisagenlecleucel and to ensure the safe and effective delivery of this treatment.
Clinician Group Input
Two clinician groups provided input for the review of tisagenlecleucel: Cell Therapy Transplant Canada, and the Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee.
In general, the clinician group input was consistent with the input provided by the experts consulted by CADTH for the tisagenlecleucel review. It also suggested that tisagenlecleucel be used in patients with r/r FL who are not eligible to receive an allo-SCT or auto-SCT as third-line therapy or beyond. In addition, CD19 CAR T-cell therapy, including tisagenlecleucel, will only be considered in patients without significant organ dysfunction, according to the clinician group.
The clinician group noted that assessment of response to treatment should be based on the standard lymphoma response criteria, and clinical exams and imaging scans, such as CT and PET, should be performed. Outcomes such as remission rates, PFS, patient safety, as well as HRQoL should be measured.
Drug Program Input
Input was obtained from the drug programs that participate in the CADTH reimbursement review process. The following were identified as key factors that could potentially impact the implementation of a CADTH recommendation for tisagenlecleucel:
considerations for initiation of therapy
considerations for prescribing of therapy
generalizability
care provision issues
system and economic issues.
The clinical experts consulted by CADTH provided advice on the potential implementation issues raised by the drug programs.
Clinical Evidence
Pivotal Studies and Randomized Controlled Trial Evidence
Description of Studies
One clinical study, ELARA (formerly known as Study E2202),29 was included in the systematic review. The ELARA study (N = 98) is a phase II, open-label, single-arm study that evaluated the efficacy and safety of tisagenlecleucel in patients with r/r grade 1, 2, or 3a FL after 2 or more lines of systemic therapy. The primary end point was CRR assessed by independent review committee (IRC) through 24 months. Secondary end points included overall response rate (ORR), OS, PFS, duration of response (DoR), and HRQoL (assessed by Functional Assessment of Cancer Therapy-Lymphoma [FACT-Lym], 36-Item Short Form Survey [SF-36], and 3-Level EQ-5D [EQ-5D-3L]). Data up to 30 months of follow-up were available at the time of this review (data cut-off date was March 29, 2022). The median age observed in the overall r/r FL population was 57 years (range, 29 to 73 years). More males (68.1%) were enrolled than females (31.9%), and most patients (84.0%) were white. Almost all patients (97.0%) had a baseline ECOG PS of 0 or 1. Most patients also had grade 1 or 2 disease (90.4%) and stage III or IV disease (80%). Enrolled patients received a median of 4 (range, 2 to 13) prior lines of treatments. Of the 98 included patients, 77.6% were refractory to their last line of antineoplastic therapy. The proportion of patients who progressed in the 24 months after first-line anti-CD20 monoclonal antibody (mAb)–containing therapy was 64.9%.
Efficacy Results
At the data cut-off date of March 29, 2022, among the 97 patients who were treated with tisagenlecleucel, the CRR was 68.1% (95% confidence interval [CI], 57.7% to 77.3%), ORR was 86.2% (95% CI, 77.5% to 92.4%), and partial response rate (PRR) was 18.1% (95% CI, not reported) at 24-month follow-up per IRC assessment. The results from local assessment were consistent with the IRC assessment. Median DoR was not reached with tisagenlecleucel at the respective median follow-up times in the ELARA trial.
In the ELARA trial, median OS was not reached at the 24-month follow-up (cut-off date of March 29, 2022). Thirteen deaths had occurred in the study, and the OS rate was 87.7% (95% CI, 78.3% to 93.2%) at 24 months and 82.6% (95% CI, 70.2% to 90.2%) at 30 months.
The median PFS per IRC was not reached at the time of the data cut-off (March 29, 2022), and there were 38 PFS events in total (disease progression or death). The PFS rate was 77.8% (95% CI, 67.7% to 85.1%) at 6 months, 67.2% (95% CI, 56.3% to 75.9%) at 12 months, and 57.4% (95% CI, 46.2% to 67.0%) at 24 months.
Over time, there were no notable changes in the proportion of patients reported to have improved, stable, or deteriorated FACT-Lym and SF-36 scores after tisagenlecleucel infusion. Overall, 70% to 88% of patients reported no deterioration in HRQoL based on FACT-Lym and SF-36 scores at 12 months, with similar trends observed at 18 months and 24 months. Results of the EQ-5D-3L visual analogue scale (VAS) score showed that HRQoL was maintained from baseline after the tisagenlecleucel infusion. The mean EQ VAS score was 69.4 at baseline, which increased to 72.5 at 6 months, 75.9 at 12 months, and 71.9 at 24 months. However, these results should be interpreted with caution because the 24-month results were based on approximately half of the patients enrolled in the study.
Harms Results
At the data cut-off date of March 29, 2022, of the 97 patients evaluable for safety, 99% experienced at least 1 AE. The most commonly reported AEs for patients any time after infusion were CRS (49.5%), neutropenia (43.3%), anemia (25.8%), diarrhea (25.8%), headache (23.7%), decreased white blood cell count (22.7%), pyrexia (18.6%), thrombocytopenia (18.6%), fatigue (17.5%), nausea (17.5%), decreased neutrophil count (17.5%), constipation (16.5%), and hypogammaglobulinemia (15.5%). Serious adverse events (SAEs) were reported in 46.4% patients any time after infusion. The most commonly reported SAEs included CRS (19.6%), pneumonia (10.3%), and febrile neutropenia (8.2%). There were 13 deaths (13.4% of patients) reported after tisagenlecleucel infusion in the ELARA study: 7 patients died due to the study indication (after progression of the underlying disease) and 6 died for other reasons (AEs for 5 patients and euthanasia for 1 patient).
In terms of AEs of special interest, more than 40% of patients experienced any-grade CRS (49.5%), hematological disorders such as cytopenias (78.4%), and infections (55.7%). Across hematological disorders such as cytopenias, at least 25% of the patients reported neutropenia (43.3%) or anemia (25.8%). Overall, the majority of patients (74.2%) experienced hematological events of grade 3 or higher. Infections occurring any time after infusion were reported in 54 patients (55.7%), 16 of whom (16.5%) had infections suspected to be related to tisagenlecleucel. Most of the patients had either grade 1 or 2 infections, while 21.6% of patients had infections of grade 3 or higher (9.0% of whom had AEs suspected to be related to tisagenlecleucel). Death due to infection (pneumonia) was reported in 1 patient. Any-grade serious neurologic adverse reactions were reported in 12 patients (12.4%), 10 of whom experienced these events in the 8 weeks after tisagenlecleucel infusion. Grade 3 or 4 AEs considered to be serious were reported in 3 patients (3.1%), 1 of whom recovered.
According to the clinical experts consulted by CADTH, the safety profile of tisagenlecleucel is consistent with that of other CAR T-cell therapies, and no unexpected safety signals were observed in the ELARA trial.
Table 2: Summary of Key Results From the ELARA Trial
Outcomes | ELARA |
|---|---|
Efficacy (EAS, N = 94) | |
OS | |
Death, n | 13 |
Rate, % (95% CI) | 24-month OS rate: 87.7 (78.3 to 93.2) 30-month OS rate: 82.6 (70.2 to 90.2) |
KM median OS, months (95% CI) | Not reached (34.5 to NE) |
PFS | |
Events, n | 38 |
Rate, % (95% CI) | Local assessment 6-month PFS rate: 78.0 (68.0 to 85.2) 12-month PFS rate: 67.8 (57.1 to 76.4) 24-month PFS rate: 57.4 (46.2 to 67.0) IRC assessment 6-month PFS rate: 77.8 (67.7 to 85.1) 12-month PFS rate: 67.2 (56.3 to 75.9) 24-month PFS rate: 57.4 (46.2 to 67.0) |
KM median PFS, months (95% CI), range | IRC assessment At FU of 24 months: not reached (18.2 to NE) |
CRR, n (%) [95% CI] | Local assessment: 69 (73.4) [63.3 to 82.0] IRC assessment: 64 (68.1) [57.7 to 77.3] |
ORR, n (%) [95% CI] | Local assessment: 85 (90.4) [82.6 to 95.5] IRC assessment: 81 (86.2) [77.5 to 92.4] |
DoR range, months, KM median (95% CI) | Not reached |
Safety (safety analysis set, N = 97) | |
Patients with ≥ 1 AE, n (%) | 96 (99.0) |
Patients with ≥ 1 SAE, n (%) | 45 (46.4) |
Death, n (%) | 13 (13.4) |
Notable harms, n (%) | |
Any CRS | 48 (49.5) |
Serious neurologic AEs | 12 (12.4) |
Hematological disorders, including cytopenias | 76 (78.4) |
Prolonged depletion of normal B cells or agammaglobulinemia, any grade | 18 (18.6) |
Infection | 54 (55.7) |
AE = adverse event; CI = confidence interval; CRR = complete remission rate; CRS = cytokine release syndrome; DoR = duration of response; EAS = efficacy analysis set; FU = follow-up; IRC = independent review committee; KM = Kaplan-Meier; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; SAE = serious adverse event.
Source: ELARA Clinical Study Report.29 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Critical Appraisal
The single-arm, noncomparative design of the ELARA study is 1 of its key limitations. Interpreting the results of studies with this design is difficult because it may not be apparent whether the results are from the effect of the intervention, a placebo effect, or the effect of natural history. Although it is acknowledged that this study design has so far predominated in the evaluation of CAR T-cell therapies for advanced cancers across a variety of tumour types, and there may be practical limitations to conducting a randomized controlled trial (RCT) in patients with r/r FL, there is no clear rationale that makes a RCT infeasible. Subsequently, the lack of a comparator makes it difficult to determine whether the magnitude of the treatment effect would be replicated in a larger comparative trial or in the real world. Another limitation of the ELARA study is the relatively small sample size and selective study population.
Follow-up time was likely sufficient for assessing tumour response and safety outcomes associated with tisagenlecleucel in general. However, the follow-up duration was not long enough to fully capture the effects on OS and PFS, and thus these results are considered immature. In addition to the duration of the study and the noncomparative design, subsequent treatments make it difficult to interpret the OS and PFS results. The survival results (OS, PFS) should be considered in the context of subsequent treatments, because it may be difficult to tell which treatment has more impact on patient’s survival, especially when there is a lack of comparative data in the ELARA study.
The ELARA trial had an open-label design, which can result in a bias in the measurement of subjectively assessed outcomes, such as response, PFS, HRQoL, and AEs. In addition, the study presented patient-reported outcomes (PROs) and HRQoL data up to 24 months; however, there is a risk of attrition bias and drawing conclusions on a select population because the analyses at 24 months were based on half of the study population from baseline and the results could be biased to favour tisagenlecleucel.
According to the clinical experts consulted by CADTH, the ELARA study population generally represents the patients in Canada with r/r FL who would be receiving tisagenlecleucel. However, the clinical experts noted that patients seen in clinical practice would include those with a poorer performance status (the ELARA study only included patients with an ECOG PS of 0 or 1), those who had received prior CD19-targeted therapy, and those with more comorbidities.
Long-Term Extension Studies
There was no long-term extension study submitted by the sponsor.
Indirect Comparisons
Description of Studies
One indirect treatment comparison (ITC) was submitted by the sponsor and included in CADTH’s clinical review.31 Due to the lack of a common comparator, the sponsor conducted an unanchored matched-adjusted indirect comparison (MAIC) to estimate the comparative ORR, CRR, OS, and PFS between tisagenlecleucel and axicabtagene ciloleucel (2 × 106 CAR T cells per kg) in patients with r/r FL after 2 or more lines of therapy. Although the comparator treatment used in the MAIC has not yet been reviewed by the CADTH pan-Canadian Oncology Drug Review Expert Review Committee for this patient population, the ITC was used to inform the sponsor's pharmacoeconomic model and, therefore, reviewed by the clinical team. The MAIC was based on individual data from patients who received tisagenlecleucel in the ELARA study and aggregate-level data from patients who received axicabtagene ciloleucel in the ZUMA-5 study.
Efficacy Results
The MAIC analysis compared 52 patients who received efficacy-evaluable, nonbridging chemotherapy in the ELARA study and 86 patients in the efficacy-evaluable set in the ZUMA-5 study who had at least 24 months of follow-up. Compared to axicabtagene ciloleucel, the MAIC estimated a response difference for tisagenlecleucel in ORR of –3.03% (95% CI, –13.67% to 7.61%) and in CRR of –5.03% (95% CI, –23.85% to 13.80%). Compared to axicabtagene ciloleucel, the MAIC analysis estimated the hazard of death and disease progression for tisagenlecleucel to be 0.49 (95% CI, 0.16 to 1.49) and 0.84 (95% CI, 0.37 to 1.90), respectively.
Harms Results
The 53 patients who received infused nonbridging chemotherapy in the ELARA study and the 124 patients in the infused set of the ZUMA-5 study were included in the MAIC of safety outcome. At least 1 AE of any grade was reported in 44.6% of patients in the ELARA study and 78.2% of patients in the ZUMA-5 study. AEs of grade 3 or higher were reported in no patients in the ELARA study and in 6.5% of patients in the ZUMA-5 study. Management of CRS with corticosteroids was documented in 3.0% and 15.3% of patients in the ELARA and ZUMA-5 studies, respectively. CRS management with tocilizumab was documented in 9.9% and 45.2% of patients in the ELARA and ZUMA-5 studies, respectively. Neurologic events of any grade were documented in 9.5% of patients in the ELARA study and in 56.5% of patients in the ZUMA-5 study. Neurologic events of grade 3 or higher were reported in 0.19% and 15.32% of patients in the ELARA and ZUMA-5 studies, respectively.
Critical Appraisal
For an unanchored MAIC to produce unbiased treatment-effect estimates, adjustment for all effect modifiers and prognostic variables in the analysis is needed. However, MAICs are rarely able to overcome the strict assumption and the bias resulting from missing covariates is very difficult to quantify. Key methodological differences between the ELARA and ZUMA-5 studies that could not be adjusted for and failure to match on key covariates may have confounded the study results. Furthermore, MAICs cannot account for unknown cross-trial differences; thus, MAIC estimates are susceptible to bias from unknown confounding. An evaluation of potential bias from residual confounding was not reported; therefore, the magnitude of this bias in the relative treatment-effect estimates is unclear. There is also concern about the loss of precision in the results, given the reduction in the effective sample size (ESS). Overall, the direction of bias could not be determined due to the abovementioned limitations, and the CADTH team could not draw any strong conclusions from the MAIC. Outcomes other than treatment response and survival that are important to patients, clinicians, and drug plans (e.g., HRQoL and symptoms) were not analyzed in the MAIC.
Studies Addressing Gaps in the Pivotal and RCT Evidence
Two studies provided additional context to the effectiveness and safety of tisagenlecleucel for the treatment of r/r FL. Tisagenlecleucel was compared to standard chemotherapy in 1 study (ELARA versus ReCORD-FL),32 and the second study was a single-arm, noncomparative trial.33
ELARA Versus ReCORD-FL
Description of Studies
In the absence of a direct head-to-head comparison of tisagenlecleucel to SOC, the sponsor compared the treatment effect of tisagenlecleucel observed in the ELARA study to SOC, defined as standard chemotherapy as documented in the ReCORD-FL study. The ReCORD-FL study is a noninterventional, multicentre, retrospective chart review conducted by the sponsor to provide patient-level data that could be used to form a historical control group with which to compare standard chemotherapy in the ELARA study. Patient-level data were collected from patients treated for r/r FL between 1998 and 2020 from 10 sites across Europe and North America, including 1 Canadian site (n = 12). Where feasible, the ReCORD-FL study adopted the same inclusion and exclusion criteria as the ELARA study. Propensity score matching was used to achieve an approximate balance on the number of prior lines of therapy while balancing other key baseline prognostic variables between the ELARA and ReCORD-FL studies. The distribution of the weighted time-to-event end points of OS and PFS were estimated using a Kaplan-Meier (KM) analysis, whereas hazard ratios (HRs) were estimated using Cox proportional hazard regression. At the data cut-off, 97 patients with r/r FL in the ELARA study (March 29, 2022) and 143 patients in the ReCORD-FL study (December 31, 2021) were included. After weighting, patients in the ELARA (n = 97) and ReCORD-FL (ESS = 47.5) studies had a mean age of 55.4 years and 56.5 years, respectively, were mostly male (67% to 72%), and just more than a third had documented prior auto-SCT therapy. Approximately 68% and 70.2% of patients in the ELARA and ReCORD-FL studies, respectively, were documented as double refractory, and 77.3% and 63.9%, respectively, were documented as refractory to last prior therapy.
Efficacy Results
At the data cut-off, death events were observed in 13.4% of patients in the ELARA study and 45.2% of patients in the ReCORD-FL study. Median OS was not estimable (NE) in the ELARA study. For patients in the ReCORD-FL study, the median OS was 36.6 months (95% CI, 25.8 months to NE). The KM estimate for OS at 24 months was 90.8% (95% CI, 84.7% to 96.9%) and 64.8% (95% CI, 49.5% to 80.0%) for ELARA and ReCORD-FL, respectively. Compared to standard chemotherapy, tisagenlecleucel was associated with an estimated risk reduction in death of 72% (hazard ratio [HR] = 0.28; 95% CI, 0.07% to 0.49%).
At the data cut-off, disease progression was observed in 42.3% of patients in the ELARA study and 63.7% of patients in the ReCORD-FL study. Median PFS was NE in the ELARA study. For patients in the ReCORD-FL study, median PFS was 11.5 months (95% CI, 5.9 to 35.6 months). The KM estimate for PFS at 24 months was 58.6% (95% CI, 48.6% to 68.6%) and 38.3% (95% CI, 22.7% to 53.8%) in the ELARA and ReCORD-FL studies, respectively. Compared to standard chemotherapy, tisagenlecleucel was associated with an estimated risk reduction in death or starting a new anticancer therapy of 47% (HR = 0.53; 95% CI, 0.25% to 0.81%).
Harms Results
Harms outcomes were not compared between the ELARA and ReCORD-FL studies.
Critical Appraisal
The nonrandomized comparison of the ELARA and ReCORD-FL studies makes interpretation of the efficacy of tisagenlecleucel relative to standard chemotherapy challenging. To mitigate potential differences in baseline prognostic factors related to OS and PFS, inclusion and exclusion criteria from the ELARA study were applied to the ReCORD-FL study, and eligible patients in the ReCORD-FL study were systematically selected based on highest propensity scores. Moreover, a comparison of weighting by odds was conducted to assess the causal effects of prescribing tisagenlecleucel versus chemotherapy. However, several inclusion and exclusion criteria in the ELARA study could not be applied to the ReCORD-FL study. Moreover, prognostic factors considered important by the clinical experts consulted by CADTH for the purpose of this review, such as baseline ECOG PS and Follicular Lymphoma International Prognostic Index (FLIPI) scores, were not included in the propensity model. Consequently, there is uncertainty around the treatment effects of tisagenlecleucel relative to standard chemotherapy due to selection bias and unmeasured and residual confounding that cannot be entirely ruled out. Baseline characteristics after weighting were well balanced, as evidenced by absolute mean differences of less than 25%. However, the complete baseline demographic and disease characteristics of patients in the 2 studies were not reported after matching. Therefore, it is unclear what effect the weighting had on the balance of other relevant patient characteristics. The applications of weights resulted in a reduced ESS of 45.7, in which 52% of enrolled patients in the ReCORD-FL study were lost. The reduction in sample size may contribute to imprecision, leading to uncertainty of the results. Regarding the PFS efficacy outcome, date of disease progression was not available for most patients in the ReCORD-FL study. Moreover, radiographic assessment of disease progression tends to be less frequent in the real-world setting than in clinical trial protocols. Accordingly, the date of disease progression was considered at the time a new anticancer therapy was initiated in both the ReCORD and ELARA studies for comparative analysis of PFS, and censoring was redefined to occur at the last contact date, rather than the last assessment date, in the ELARA study to avoid bias due to timing of assessment. Uncertainty about outcome assessment is further compounded due to inconsistencies in assessment across patients included in the ReCORD-FL study. Because assessment of patients in the ReCORD-FL study was not planned according to a uniform protocol, physicians may have used subjective criteria to assess clinical response. Based on input from the clinical experts, the patients included in the comparison of the ELARA and ReCORD-FL studies appeared to be younger than what is typically seen in the clinical setting. The clinical experts noted that the selected anticancer treatments were appropriate SOC regimens. However, whether the change in PFS definition for the purpose of efficacy comparison between the ELARA and ReCORD-FL studies is an appropriate surrogate for the standard definition of PFS is uncertain.
Study by Schuster et al.
Description of Study
The study by Schuster et al. (2017)33 was a single-centre, single-arm, phase IIa clinical trial conducted in the US. The objective of this study was to estimate the efficacy of a single infusion of tisagenlecleucel in patients with NHL and r/r CD19+ lymphomas after chemotherapy. Patients were eligible if they had CD19+ diffuse large B-cell lymphoma or FL with no curative treatment options, a limited prognosis (< 2 years of anticipated survival), and a partial response or stable disease after the most recent therapy. Patients with FL were eligible if they had measurable disease less than 2 years after the second line of immunochemotherapy (excluding single-drug monoclonal antibody therapy). A total of 15 patients with r/r FL were enrolled in this study, 14 of whom received the tisagenlecleucel treatment. Median age of the 14 patients was 59 years (range, 43 to 72 years). There was an equal distribution of male and female patients (50%). All patients (100%) had a baseline ECOG PS of 0 or 1. Overall, 64% of the patients had grade 1 to 2 FL and 86% had stage IV FL. Regarding prior therapy, patients received a median of 5.0 (range, 2 to 10) prior lines of treatment. The intervention of interest in this study is tisagenlecleucel, which was administered as a one-time, single infusion of CD19 CAR T cells by IV injection (total dose of 1 to 5 × 108 CD19 CAR T cells). The median total dose of tisagenlecleucel was 5.00 × 108 (range, 1.79 × 108 to 5.00 × 108), and the median dose of tisagenlecleucel per kilogram of body weight was 5.79 × 106 (range = 3.08 × 106 to 8.87 × 106). The median number of days from apheresis to infusion was 39 (range, 27 to 145). All 14 patients with FL received lymphodepleting (LD) chemotherapy before the tisagenlecleucel infusion. The primary outcome in the study by Schuster et al. was ORR at 3 months in patients with NHL. The secondary outcomes were CRR, PRR, DoR, OS, PFS, and time to next treatment.
Efficacy Results
In the study by Schuster et al., the median OS was not reached at either 28.6 or 49.0 months of median follow-up, and the OS rate was 93% at 28.6 months median follow-up. The median PFS was also not reached at 28.6 months; however, a decline was observed at longer follow-ups (median PFS was 32.4 months and 26.2 months at median follow-ups of 49 months and 60 months, respectively). The estimated progression-free probabilities were 77%, 70%, and 43% at median follow-ups of 11.4 months, 28.6 months, and 60 months, respectively. The study by Schuster et al. assessed the response rate at shorter follow-ups (3 months and 6 months). This study reported an ORR of 79% at both assessment points. The CRR was 50% at 3 months and 71% at both 6 months and 49 months. The median DoR was not reached with tisagenlecleucel at the respective median follow-up times. PROs have not been included in the study by Schuster et al.
Harms Results
The main AEs were CRS of any grade and of grade 3 or 4, which were experienced by 42.9% and 14.3% of patients with FL, respectively. Tisagenlecleucel was administered as a single-time infusion; therefore, no patients discontinued treatment in the study by Schuster et al. One patient with FL who had encephalopathy had progressive neurologic deterioration that resulted in death. Data for other AEs of special interest were only reported for the overall NHL population in the study be Schuster et al. Eleven patients (39%) reported neurologic toxicities, including encephalopathy in 3 patients (27%), delirium in 2 patients (18%), and tremor in 2 patients (18%). In addition, cognitive disturbance, confusion, involuntary movements, and memory impairment were each reported in 1 patient (9%).
Critical Appraisal
The main limitations of the study be Schuster et al. are the single-arm design, the lack of a comparator, and the open-label nature, which limit the interpretation of effect. Moreover, the sample size calculation for this study was based on the overall NHL population and was not specific to the FL subgroup, which could limit detection of the magnitude of effect among the FL subgroup.
In terms of generalizability, this study was conducted in the US, which may have a different health system and different treatment conditions than Canada. The patient population in this study had a baseline ECOG PS of 0 or 1. It is not clear if the results are generalizable to patients with a poorer performance status.
Conclusions
Evidence from a single-arm study (ELARA) suggests that treatment with tisagenlecleucel is associated with clinically important tumour responses, including complete remission, in adults with r/r FL after 2 or more lines of systemic therapy. There is insufficient evidence — in part due to the limited follow-up duration of the trial — to determine the effects of tisagenlecleucel on OS and PFS. Results of PROs suggest that a patient’s QoL could be maintained; however, 24-month HRQoL data were based on only about 50% of the baseline population. It is unclear if treatment with tisagenlecleucel would improve HRQoL. The harms associated with the tisagenlecleucel infusion are consistent with its mechanism of action, and no unexpected safety signals observed.
The CADTH clinical assessment identified limitations of the sponsor’s comparison of the ELARA and ReCORD-FL studies and the sponsor-conducted MAIC (including small sample sizes, heterogeneity across study designs and populations, and the inability to adjust for all potential effect modifiers and prognostic variables), which substantially limited the ability to interpret the relative treatment effects observed for tisagenlecleucel, standard chemotherapy, and axicabtagene ciloleucel.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of tisagenlecleucel (1.2 × 106 to 6.0 × 108 CAR-positive viable T cells for IV use) in the treatment of adults with r/r grade 1, 2, or 3a FL after 2 or more lines of systemic therapy.
Disease Background
The contents of this section have been informed by materials submitted by the sponsor and clinical expert input. The following information has been summarized and validated by the CADTH review team.
NHL accounts for approximately 90% of the cancers that affect the lymphocytes.34 FL is the second most common subtype of NHL in Western countries and is characterized by follicular clusters or patterns of follicle centre B cells in a lymph node, bone marrow, or spleen.1-3 Staging of FL describes the extent to which the disease has spread in the body: stage I FL involves 1 node or a group of adjacent nodes or single extranodal lesions without nodal involvement; stage II FL involves 2 or more nodal groups on the same side of the diaphragm and limited contiguous extranodal involvement; stage III FL involves nodes on both sides of the diaphragm and nodes above the diaphragm with spleen involvement; and stage IV FL has additional noncontiguous extralymphatic involvement.18 Grading of FL is determined by the number of large FL cells (also known as centroblasts) and reflects the aggressiveness of the tumour: grade 1 FL has 0 to 5 centroblasts per HPF; grade 2 FL has 6 to 15 centroblasts per HPF; and grade 3 FL has more than 15 centroblasts per HPF. Grade 3 FL has been subdivided into grade 3a (centrocytes are present) and grade 3b (solid sheets of centroblasts present).18 Grade 1, 2, and 3a FLs are generally considered to be low grade or slow growing, whereas grade 3b FL is faster growing. In the early stages, most patients experience few symptoms and slow disease progression.1,35 The most common signs or symptoms in these stages are painless swelling or enlargement of 1 or more groups of lymph nodes in the neck, armpit, or groin that does not resolve with time.1,35 Although usually painless, the swollen lymph nodes may cause compression of organs, restricted movement, and disfigurement.11,19,36 In advanced stages, patients can experience fever, night sweats, and weight loss, as well as bone marrow involvement that results in bruising or bleeding, leucocytosis, thrombocytosis, thrombocytopenia, and leucopenia.13,36-39 FL is a relapsing and remitting disease, characterized by recurrent disease progressions, shorter remission periods, and decreased survival (i.e., OS or PFS) with each treatment course.4-7 Even though FL manifests as an indolent clinical course over many years in general, patients can still present with aggressive disease, which relapses more rapidly or is refractory to treatment, or the FL can undergo histologic transformation to a more aggressive type of lymphomas (e.g., 10% to 70% of FL transforms to diffuse large B-cell lymphoma over time, with a risk of 2% to 3% per year).40-43 Most patients eventually develop increasingly resistant disease, resulting in reduced treatment options and poor prognosis for patients with r/r FL.4,8 Many patients with indolent FL may survive for decades, although a significant proportion of patients experience aggressive disease, which results in approximately 20% of affected patients dying within 2 to 3 years of diagnosis.9 Patients who relapse within 12 months of SCT or progress within 24 months have an extremely poor prognosis.44 Although Canada-specific mortality data for FL could not be identified, in 2022, it was projected that there would be 3,000 deaths due to NHL in Canada.10 Results of a retrospective analysis conducted in a single centre in the US showed that among patients with FL who had received multiple lines of treatment, median OS was 11.7 years, 8.8 years, and 5.3 years for patients who received the second-line, third-line, and fourth-line treatments, respectively.6 Compared with disease-free and newly diagnosed patients, those with r/r FL suffer from more significant HRQoL impairment.11,12
In general, patients present with asymptomatic lymphadenopathy manifesting as painless superficial small to medium-sized lymph nodes that are typically present for many years before a FL diagnosis is established.34,40 Thus, most patients are diagnosed at an advanced stage (i.e., 66% to 70% of patients are initially diagnosed at stage III or IV, which is considered incurable but treatable).45 Most patients are usually diagnosed with advanced FL during the sixth decade of life, although approximately 25% of patients are diagnosed when they are younger than 40 years.46 After diagnosis, FL is staged to determine the extent and distribution of the disease and to guide treatment decision-making. The most common method for staging lymphoma is the Ann Arbor staging system.19,35,47 A grade is also assigned to the lymphoma: low grade is typically used to describe indolent or slow-growing tumours, and intermediate or high-grade is used to describe aggressive or fast-growing lymphomas.35 One of the tools used most widely to estimate the prognosis of patients with FL is the FLIPI, which considers age (older than 60 years versus 60 years or younger), Ann Arbor stage (III to IV versus I to II), number of involved nodal areas (more than 4 versus no greater than 4), hemoglobin level (lower than 120 g/L versus 120 g/L or higher), and serum lactate dehydrogenase concentration (above normal versus normal or below).48
The overall prevalence of FL is estimated to be 1 per 3,000 people, according to the Orphanet database.13 Despite being a rare disease, FL is considered to be among the most prevalent of the lymphomas due to chronicity and incurability in its advanced stages.4,5,14,15 The overall incidence of FL is also low, with rates ranging from 2.2 to 3.5 per 100,000 new cases per year in Asia, Australia, Europe, and the US.16 According to a survey conducted in the US, the percentage of patients relapsing and receiving subsequent treatments is estimated to be 41%, 40%, and 30% for patients who have received first-line, second-line, and third-line treatments, respectively.17
Standards of Therapy
The contents of this section have been informed by materials submitted by the sponsor and clinical expert input. The following information has been summarized and validated by the CADTH review team.
The treatment goals for FL vary, depending upon the stage of the FL and individual patient factors. In general, available treatments for stage I to II FL have curative potential; however, for most patients with advanced stage III to IV FL, no curative therapies are available. Therefore, the main goals of treatment are to cure the lymphoma in patients with stage I to II FL and to extend remission in patients with stage III to IV FL.19,20
Once a diagnosis of FL is confirmed, the gold standard for the management of asymptomatic patients with indolent FL is watchful waiting, also known as watch and wait.23,49 On average, 49% of patients newly diagnosed with FL can be managed with a watchful waiting approach, based on the opinion of Canadian clinical experts consulted by the sponsor.17 According to the clinical experts consulted by CADTH, watch and wait is a common practice for many patients with FL, even after disease relapse.
First-Line Treatments
For small, localized symptomatic FL, radiotherapy is considered the SOC, according to North American and European guidelines.19,20,50 This is supported by several provincial guidelines in Canada.21,22 For grade 1, 2, and 3a FLs, the preferred chemoimmunotherapy regimen is BR, based on high-level evidence of efficacy and favourable tolerability in this population.20,23,24 In frail and older adults, rituximab monotherapy, a chemotherapy-free approach, is the preferred first-line regimen, according to European and North American guidelines.25,26 However, some Canadian centres do not have access to rituximab monotherapy. Instead, physicians keep patients on BR for several treatment cycles or for as long as possible. Beyond first-line treatment, there is currently no gold standard for the care of the r/r FL population.
Second-Line Treatments
Treatment options for second-line regimens for r/r FL depend on several factors, including level of fitness, prior treatment, and length of time to relapse.20 Combined immunochemotherapy, such as O-CHOP, is the preferred treatment strategy in this population.20 According to the clinicians consulted by the sponsor, SCT may be considered in young and fit patients with no comorbidities in the second-line setting. Auto-SCT is given more often than allo-SCT in this population. However, only a small subset of FL patients would be eligible for transplant as a second-line option. SCT is limited by highly selective eligibility criteria and typically reserved for younger, medically fit patients with chemotherapy-sensitive disease.20,25,51,52 The clinical experts consulted by CADTH agreed with these strategies.
Third-Line Treatments
FL is a relapsing disease with continued unmet needs in adults with r/r FL after 2 or more lines of therapy, despite available established therapies. Patients with r/r FL in the third-line setting and beyond represent a heavily pretreated and advanced stage patient population. The SOC in Canada in the third-line setting for patients with r/r FL is heterogenous and varies across the regions. Based on Canadian clinician input, a heterogenous mix of immunochemotherapy (for most patients) and SCT (for a minority of patients) are the current treatment options in this hard-to-treat population.
Treatments in this setting may include SCT; however, there is controversy with regard to the clinical benefit of SCT in patients with r/r FL, and both allo-SCT and auto-SCT may be associated with significant mortality and morbidity.20,25,51-53 Although SCT has been included in the treatment algorithm diagram for r/r FL in the third-line setting, it is expected that the number of patients with r/r FL eligible for SCT in the third-line setting will be small.
According to clinicians consulted by the sponsor, most patients in the third-line setting will keep recycling combined immunochemotherapy that might have been used in previous lines, including the following regimens (which are the most frequently used options in Canada): R-CVP, R-CHOP, O-CHOP, R-GDP (rituximab, gemcitabine, dexamethasone, and cisplatin), BR, and R-ICE (rituximab, ifosfamide, carboplatin, and etoposide). While used by some physicians in their clinical practice, the R2 immunomodulatory regimen is currently not officially indicated for the treatment of FL in Canada, per the latest Canadian product monograph for lenalidomide.54 Furthermore, although no official Health Technology Assessment submission has been made by the sponsor to Canadian health technology assessment agencies, CADTH conducted a health technology review of R2 in r/r B-cell NHL and concluded that available evidence remains limited.55 According to Canadian clinicians’ input, there is somewhat limited access to R2 in some provinces. In the third-line setting and beyond, idelalisib, a phosphoinositide 3-kinase (PI3K) inhibitor, is indicated for the treatment of patients with r/r FL in Canada.56 However, idelalisib is not publicly reimbursed across Canada and is inaccessible at some sites, according to several clinicians.57 Furthermore, it is generally at the bottom of the treatment list due to important side effects and is used as a palliative treatment. In recent years, CAR T-cell therapy has emerged as another form of immunotherapy for the treatment of blood cancers, including lymphomas. Although promising results have been reported for the CAR T-cell therapies in patients with advanced stage lymphomas, severe adverse effects related to CAR T-cell therapy, such as CRS and neurologic toxicities, are also reported.27 One CAR T-cell product, axicabtagene ciloleucel, was recently approved by Health Canada (September 2022), with an NOC/c for the treatment of adults with r/r grade 1, 2, or 3a FL after 2 or more lines of systemic therapy.58 Note that at the time of this report, axicabtagene ciloleucel has not been reviewed by CADTH for the current indication, and it has not been publicly funded for this indication.
In clinical practice, a patient’s response to treatment is commonly assessed using the Lugano classification,59 in which fluorodeoxyglucose PET/CT was incorporated into the initial Ann Arbor staging system for fluorodeoxyglucose-avid lymphomas.
Drug Under Review
Tisagenlecleucel is a second-generation autologous CAR T-cell therapy directed at the cell-surface protein CD19, which is only expressed on B cells or their precursors, and not on hematopoietic stem cells or non-B-cell tissues. The CAR comprises a murine single-chain antibody fragment that recognizes CD19 and is fused to intracellular signalling domains from 4 to 1BB (CD137) and cluster of differentiation 3 (CD3) zeta. The CD3 zeta component is critical for initiating T-cell activation and antitumour activity, whereas 4 to 1BB enhances the expansion and persistence of tisagenlecleucel. CD19 is expressed throughout most stages of normal B-cell differentiation (early pre-B to mature B cells) and is present in a wide range of B-lymphoid malignancies that span different stages of B-cell differentiation. Targeting CD19 by genetically modifying a patient’s own T cells to express an anti-CD19 directed CAR has been shown to effectively treat various advanced B-cell malignancies. Upon binding to CD19-expressing cells, the CAR transmits a signal to promote T-cell expansion, activation, target-cell elimination, and persistence of tisagenlecleucel.28
On December 19, 2022, tisagenlecleucel received an NOC/c from Health Canada for adults with r/r grade 1, 2, or 3a FL after 2 or more lines of systemic therapy.28 For 1 of the conditions for the authorization of tisagenlecleucel, the sponsor committed to undertake a randomized phase III trial of patients with r/r FL. Patients will be randomized to tisagenlecleucel or the investigator’s choice of treatment in line with the SOC. The primary end point will be PFS, and OS and ORR will be the secondary end points.60
Per the warnings and precautions in the tisagenlecleucel product monograph, “Treatment should only be administered in a treatment facility with personnel fully trained and approved for the care of patients receiving Kymriah infusion therapy. Fully trained staff will administer the Kymriah infusion using precautions for immunosuppressed patients.” The recommended dose of tisagenlecleucel for the indicated population is 0.6 to 6.0 × 108 CAR-positive viable T cells (nonweight based) suspended in 1 or more patient-specific infusion bags for a single-dose, one-time, IV administration.28
Key characteristics of tisagenlecleucel and another CAR T-cell therapy, axicabtagene ciloleucel, which is indicated for adults with r/r FL, are summarized in Table 3. Other comparators for tisagenlecleucel, such as immunochemotherapy and SCT, are not included in this table.
Table 3: Key Characteristics of Tisagenlecleucel and Axicabtagene Ciloleucel
Characteristic | Tisagenlecleucel | Axicabtagene ciloleucel |
|---|---|---|
Mechanism of action | CD19-directed genetically modified autologous T-cell immunotherapy | |
Indicationa | For the treatment of adults with refractory or relapsed grade 1, 2, or 3a FL after 2 or more lines of systemic therapy | |
Route of administration | IV infusion for one-time treatment | |
Recommended dose | Recommended dose: 0.6 to 6.0 × 108 CAR-positive viable T cells | Target dose: 2 × 106 positive viable CAR-positive viable T cells per kg body weight to a maximum of 2 × 108 CAR-positive viable T cells for patients ≥ 100 kg |
Serious adverse effects or safety issues |
|
|
AE = adverse event; CAR = chimeric antigen receptor; CRS = cytokine release syndrome: FL = follicular lymphoma.
aHealth Canada indication (NOC/c).
Sources: Product monographs for tisagenlecleucel28 and axicabtagene ciloleucel.58
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups. The full original patient input(s) received by CADTH have been included in the stakeholder section at the end of this report.
One patient group, LC, provided input to the submission. LC is a national Canadian registered charity. It collected input from patients with r/r FL through an online anonymous survey from November 2022 to January 2023. Of the 44 respondents, only 1 had experience with tisagenlecleucel. Skipping logic was built into the survey so that respondents were asked questions only relevant to them. In addition, LC obtained patient feedback from a French patient organization called ELLyE. ELLyE collected feedback from 162 patients on CAR T-cell therapy, including 19 who had experience with tisagenlecleucel, from January 2019 to September 2020 in France.
LC Survey
Most of the respondents to the LC survey were female, living in Canada, aged 55 years to 74 years, and had been diagnosed with FL 9 to 10 years before the survey.
At the time of diagnosis of FL, the most common symptoms are enlarged lymph nodes and fatigue, followed by indigestion, abdominal pain, bloating, body aches, and pain. Patients mentioned that a low immunoglobulin level has a significant negative impact in everyday life. The most common psychosocial impacts reported were stress of cancer diagnosis, anxiety, and fear of progression or relapse. FL has a negative impact on the ability to work, visit family and friends, travel, and contribute financially to household expenses. Some patients mentioned that because of their compromised immune system, they are worried about getting COVID and must limit their social interactions.
In terms of experiences with currently available treatments, 44%, 24%, and 15% of the respondents (n = 34) received 1, 2, and 3 lines of treatment, respectively. The most common treatment received by respondents was chemotherapy. Important side effects of treatment reported were fatigue, low activity level, hair loss, and neuropathy. Seventy percent of patients had access to treatment locally, with various levels of difficulty based on the location and waiting time. Absence from work, drug costs, and travel costs are financial aspects of lymphoma treatment for patients.
Patients also had problems with long waiting times to be diagnosed, see a specialist, have a biopsy, and have an MRI or CT scan.
Patients indicated that there is a need for more therapeutic options that provide longer disease remission, a longer life span, and improve QoL. Respondents indicated that new therapies should be available to all patients in Canada, and that patients should not have to travel to another province to get the treatment. Some respondents think it would be better to get stem cell or CAR T-cell treatments as a first-line treatment or in the earlier stages of the disease, when QoL has not been affected very much and the chances of successful therapy is higher. One patient suggested a more integrative approach to cancer treatment that included natural medicine.
Only 1 respondent in the 75- to 84-year age group had experience with tisagenlecleucel. The respondent has been in remission for more than 2 years at the time of survey. Although this patient had side effects, such as neutropenia, thrombocytopenia, decreased appetite, and anemia, the patient would recommend this therapy to other patients with r/r FL.
ELLyE Survey
Of the 19 patients (5 female and 14 male) who had been treated with tisagenlecleucel, information on the number of prior lines of treatments was available for the 14 patients who received tisagenlecleucel as a second-line (n = 6) or later-line treatment (n = 8). The most common prior treatment, received by 11 patients, was chemotherapy with or without immunotherapy.
The main concern of this group of patients was the impact of FL on their own QoL and that of their loved ones, such as fatigue, nausea, weight loss, anxiety, disrupted social life, and being dependent. The patients were also concerned about the financial and distance implications of travelling to get treatment in France.
Some patients indicated that the benefits from CAR T-cell therapy included “complete remission,” “treatment of pain,” and “hope of recovery to follow.”
The patient group input suggested that in both Canada and France, CAR T-cell therapy should be provided at an earlier stage of disease or as an earlier line of therapy.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). In addition, as part of the tisagenlecleucel review, a panel of 4 clinical experts from across Canada was convened to characterize unmet therapeutic needs, assist in identifying and communicating situations in which there are gaps in the evidence that could be addressed through the collection of additional data, promote the early identification of potential implementation challenges, gain further insight into the clinical management of patients living with a condition, and explore the potential place in therapy of the drug (e.g., potential reimbursement conditions). A summary of this panel discussion is presented in the following.
Unmet Needs
The clinical panel indicated that for patients with FL, the most important goals of an ideal treatment are to prolong survival (both OS and PFS) and improve the patient’s QoL. However, patients with r/r FL relapse after frontline therapies or are refractory to available treatments, which subsequently affects their long-term PFS and QoL. In addition, some patients may not tolerate current treatments well due to the related AEs or complications associated with SCT. The clinical panel indicated that the greatest unmet needs for treatments such as tisagenlecleucel are in patients who progress in the 2 years after initial therapy, those who have already received SCT, and those who have been double refractory to chemotherapy and rituximab (implying limited treatment options).
Place in Therapy
The clinical panel noted that the treatment algorithm for adults with r/r FL is complicated. Many factors (e.g., patient characteristics, previous treatments, treatment effects and toxicity, whether a treatment is reimbursed by drug plans, disease progression and transformation, and patient preference) need to be considered before deciding which treatment to provide. Watch and wait is a common approach for many patients with FL, even after disease relapse. Patients who need active treatments typically receive bendamustine or rituximab-based therapies such as BR, R-CVP, R-CHOP, or R2. PI3K inhibitors are rarely used. Patients with relapsed disease after treatment with chemoimmunotherapy, particularly those who progress within 2 years, may receive auto-SCT if they are suitable candidates. After all these treatments, some patients maintain indolent status and some transform to large cell lymphoma; therefore, the proportion of patients who may be treated with CAR T-cell therapy is small. The clinical panel suggested that tisagenlecleucel be used as third-line or later-line treatments for patients with r/r FL. These patients usually have a treatment response that lasts less than 6 months from their previous treatment (medication or SCT). There are not many options available for the patients at this stage. CAR T-cell therapy would be considered due to its different mechanism of action.
The clinical panel noted that an auto-SCT is not mandatory before tisagenlecleucel can be given, because this is not the SOC in Canada.
For patients who have received previous CD19-targeted therapy, there is a lack of evidence to suggest whether the use of tisagenlecleucel is appropriate.
Patient Population
The clinical panel indicated that in practice, CAR T-cell therapy is used in a broader patient population than that enrolled in clinical trials, where a more selective population is recruited. For example, the panel noted that suitable patients for treatment with tisagenlecleucel would be those with acceptable organ function rather than those with excellent organ function, which is generally required for an auto-SCT. In clinical practice, suitable patients can be identified based on clinical judgment, which combines medical history, laboratory and imaging findings, and often a lymph node biopsy. When determining the suitability of tisagenlecleucel for a patient, the bulk of disease and rapid disease progression are among the factors that need to be taken into account.
The panel noted that patients who are likely to benefit from other available treatments or who have an ECOG PS of 3 or higher are least suitable for treatment with tisagenlecleucel.
The panel also noted that there is not a specific patient characteristic that can be used to predict who will respond to tisagenlecleucel and who will not.
Assessing the Response to Treatment
The panel indicated that in clinical practice, patients who receive treatments for FL, including CAR T-cell therapy, are evaluated and followed in a manner similar to that described the clinical trials of investigational treatments for FL. Remission and survival are measured. Physical exams and imaging exams are routinely conducted to assess the patient’s response to CAR T-cell therapy.
The panel suggested that meaningful responses to treatment with tisagenlecleucel would be not only a high CRR, but also the durability of treatment response and long-term PFS and OS. In addition, the clinicians are interested in knowing if the treatment is cost-effective.
The panel noted that after CAR T-cell therapy, the clinicians will assess the treatment response (e.g., with a CT scan) at 3 months, or sooner if needed.
Patients Who Go Through Pretreatment but Do Not Receive Tisagenlecleucel
The panel noted that it is rare for patients with FL to go through pretreatment but not receive tisagenlecleucel. If this happens, it can be due to rapid disease progression in the interim or to the emergence of major complications, such as a new myocardial infarction or stroke. Manufacturer failure is another reason for this situation.
When it happens, the cell therapy product can be manufactured again. If patients do not receive tisagenlecleucel after going through pretreatment, most can progress in the 6 months after their previous treatment, assuming these are high-risk patients. There are limited treatment options available for them. Palliative chemotherapy can be given. Other options may include radiation therapy, more chemotherapy, novel drugs, or a clinical trial, depending on a patient’s clinical status.
Subsequent Therapy After Tisagenlecleucel Failure
The panel indicated that in the case of a relapse after infusion with tisagenlecleucel, patients may participate in a clinical trial. In the absence of a clinical trial, they may try a chemoimmunotherapy that they haven’t been exposed to.
Prescribing Considerations
The panel emphasized that a multidisciplinary team, involving hematologists, infectious disease specialists, neurologists, an ICU team, and other specialists, is required to diagnose, treat, and monitor patients who receive tisagenlecleucel to ensure the safe and effective delivery of this treatment.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups. The full original clinician group inputs received by CADTH have been included in the stakeholder section at the end of this report.
Two clinician groups provided input for the review of tisagenlecleucel: Cell Therapy Transplant Canada, and the Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee.
Unmet Needs
The clinician group indicated that poor overall response rates and short remission intervals are the main challenges in the treatment of patients with FL in the third-line setting and beyond. The chemoimmunotherapeutic strategies, when used a second time around, will result in a lack of efficacy and can be toxic for older patients, which adversely affects QoL. Allo-SCT is an option with curative potential, but the number of eligible patients is minimal. Another option, auto-SCT, which has excellent responses, is often used as a second-line or third-line treatment, but it is not appropriate for patients who are refractory to chemotherapy. Because most patients with FL are not eligible for SCT as a third-line therapy or beyond, CD19-targeted CAR T-cell therapy may be an option for these patients.
Place in Therapy
The clinician groups suggested that tisagenlecleucel be used in patients with r/r FL who are not eligible to receive allo-SCT or auto-SCT in the third-line setting or beyond. In addition, CD19 CAR T-cell therapy, including tisagenlecleucel, will only be considered in patients without significant organ dysfunction in their opinion. The clinician groups believed that CAR T-cell therapy will shift the current treatment paradigm but will not change the current approach to the use of auto-SCT or allo-SCT.
Patient Population
The clinician groups considered the following patients to be eligible for tisagenlecleucel:
adults with FL (grade 1, 2, or 3a) refractory to 2 or more lines of systemic therapy that includes an anti-CD20 monoclonal antibody and an alkylating drug
adults with FL (grade 1, 2, or 3a) who relapse after the second line of therapy, including auto-SCT for those who are eligible for transplant.
The clinician groups considered the following patients to be ineligible for tisagenlecleucel:
patients previously treated with allo-SCT or with active central nervous system (CNS) involvement
patients with any suspicion of disease transformation (grade 3b FL or diffuse large B-cell lymphoma), based on a recent biopsy
patients who previously received CD19-directed therapy.
The clinician groups indicated that significant organ-specific issues (liver, renal, pulmonary), as well as active and/or uncontrolled infection and uncontrolled autoimmune disease, may be reasons not to pursue CAR T-cell therapy. The use of CAR T-cell therapy might be preferred before auto-SCT in some patients.
Assessing Response to Treatment
The clinician groups noted that assessment of response to treatment should be based on standard lymphoma response criteria identified with clinical exams and imaging scans such as CT and PET. Outcomes such as remission rates, PFS, patient safety, and HRQoL should be measured.
Discontinuing Treatment
Not applicable.
Prescribing Conditions
The clinician groups indicated that CAR T-cell therapy in Canada is currently provided in cell therapy centres that are approved by Health Canada. Approval from the Foundation for the Accreditation of Cellular Therapy is also an important consideration. A foundation-approved transplant centre will have the necessary standard of programs and policies to safely provide CAR T-cell treatment. Institutional experience, trained CAR T-cell health care providers, tumour boards, and data collection capabilities are also required. Within an institution, infectious disease, ICU, or emergency department involvement, as well as specific expertise from the neurology service, need to be in place. To use tisagenlecleucel, a specific centre must have successfully completed an onboarding process that includes red cell microparticle dry runs, stem cell processing, and apheresis audits, as well as specific legal agreements.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
There was no direct comparator in the phase II information submitted by the sponsor. PAG notes that current treatments for r/r FL after 2 lines of systemic therapy vary and can include a CD20-targeted medication (rituximab, obinutuzumab) plus various chemotherapy backbones if they were not used previously (e.g., GDP, ICE), lenalidomide plus rituximab, and SCT. | Comment from the drug programs to inform pERC deliberations. |
Considerations for initiation of therapy | |
The Health Canada indication for tisagenlecleucel is specific to r/r grade 1, 2, and 3a FL after 2 or more prior lines of systemic therapy. The ELARA trial excluded grade 3b FL. Are patients with r/r grade 3b FL eligible for treatment with tisagenlecleucel? | The clinical experts indicated that grade 3b FL accounts for a small proportion of all FL, and it behaves more like DLBCL. Usually, patients with grade 3b FL have been excluded from clinical trials and there is a lack of good evidence. The unmet need is greater in this particular patient population, which has a poor prognosis. Although it is unclear whether tisagenlecleucel should be given to these patients, the clinical experts assumed that tisagenlecleucel may be as effective in this subset as other CAR T-cell therapies that have been approved for use in patients with grade 3b FL and DLBCL. |
If recommended for reimbursement, will patients with the following characteristics be excluded from treatment with tisagenlecleucel?
What about other types of low-grade lymphoma (e.g., marginal zone, Waldenstrom’s macroglobulinemia, MALT lymphoma)? | The clinical experts indicated that some of these patients can be treated with tisagenlecleucel in clinical practice:
The clinical experts noted that in clinical practice, the following patients should not be treated with tisagenlecleucel:
|
What bridging therapies can be considered for tisagenlecleucel in patients with r/r FL? | The clinical experts noted that in practice, radiation would be used as bridging therapy for localized FL. Steroids, rituximab, R2, and chemotherapies are also used in clinical practice. |
Is there sufficient evidence to support re-treatment with tisagenlecleucel in the case of disease relapse? | The clinical experts indicated that in clinical practice, there is a lack of trial data to support re-treatment with tisagenlecleucel in patients with disease relapse. |
Considerations for prescribing of therapy | |
The manufacturer indicates that tisagenlecleucel can be given in either the inpatient or outpatient setting, provided it is a CAR T-cell certified centre. | Comment from the drug programs to inform pERC deliberations. |
Delivery of tisagenlecleucel must take place at specialized treatment centres that are accredited and certified by the manufacturer. There continues to be limited access to CAR T-cell services in Canada. Although access is expanding, interprovincial travel and out-of-country funding remains necessary in many parts of Canada. Due to geographical site limitations, patients may need to travel for treatment that requires interprovincial agreements to ensure equitable access. | Comment from the drug programs to inform pERC deliberations. |
Generalizability | |
Should patients who recently started third-line systemic therapy be allowed to switch to CAR T-cell therapy, provided all other criteria are met? | The clinical experts indicated that if a patient responds to third-line systemic therapy and does not have progressive disease, there is no need to switch to CAR T-cell therapy. However, if progressive disease is a concern, a patient would be allowed to switch to CAR T-cell therapy, provided all other criteria are met. |
Funding algorithm (oncology only) | |
Treatments for r/r FL vary and are characterized by a complex therapeutic space with multiple lines of therapy, subpopulations that respond differently to the treatment, or competing products. | Comment from the drug programs to inform pERC deliberations. |
Care provision issues | |
CRS is sometimes managed with tocilizumab. The product monograph for tisagenlecleucel indicates that 2 doses of tocilizumab should be onsite before the tisagenlecleucel infusion is started and that additional doses can be administered within 8 hours, if needed. In the event of a tocilizumab shortage, is there another treatment that can be used to manage CRS? | The clinical experts noted that when tocilizumab is not available, other treatments used to manage CRS can include steroids, siltuximab, and anakinra (interleukin-1 receptor inhibitor). However, the experts pointed out that a shortage of tocilizumab is unlikely in practice. |
Premedication with acetaminophen and diphenhydramine 30 to 60 minutes before tisagenlecleucel infusion is recommended. Systemic corticosteroids should be avoided. | Comment from the drug programs to inform pERC deliberations. |
Other care provision issues: patients need to stay within 2 hours of travel of a qualified clinical facility for at least 4 weeks after infusion. | Comment from the drug programs to inform pERC deliberations. |
System and economic issues | |
The feasibility of adoption (including budget impact) must be addressed. Given the anticipated patient volumes, PAG is concerned that existing capacity may not be able to meet demand. | Comment from the drug programs to inform pERC deliberations. |
There have been significant manufacturing delays for tisagenlecleucel. How does the delayed turnaround time impact the clinical effectiveness of tisagenlecleucel? | The clinical experts indicated that manufacturing delays are a significant clinical problem, especially for the patients who progress quickly and have more disease burden. In such cases, tisagenlecleucel may not be as effective as it is for patients who do not have disease progression. In addition, some patients may not be able to receive tisagenlecleucel after leukapheresis and bridging therapies. |
CAR = chimeric antigen receptor; CNS = central nervous system; CRS = cytokine release syndrome; DLBCL = diffuse large B-cell lymphoma; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FL = follicular lymphoma; GDP = gemcitabine, dexamethasone, and cisplatin; ICE = ifosfamide, carboplatin, and etoposide; MALT = mucosa-associated lymphoid tissue; PAG = Provincial Advisory Group; pERC = CADTH pan-Canadian Oncology Drug Review Expert Review Committee; r/r = relapsed or refractory; R2 = lenalidomide plus rituximab; SCT = stem cell transplant.
Clinical Evidence
The objective of CADTH’s Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of tisagenlecleucel in the treatment of adults with r/r grade 1, 2, or 3a FL after 2 or more lines of systemic therapy. The focus will be placed on comparing tisagenlecleucel to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of tisagenlecleucel is presented in 3 sections, and CADTH’s critical appraisal of the evidence is included after each section. The first section, the Systematic Review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. The second section includes indirect evidence from the sponsor. The third section includes additional studies that were considered by the sponsor to address important gaps in the pivotal and RCT evidence.
Included Studies
Clinical evidence from the following is included in the CADTH review and appraised in this document:
1 pivotal study (ELARA29)
1 ITC (study comparing tisagenlecleucel and axicabtagene ciloleucel31)
2 additional studies addressing gaps in evidence (Schuster et al. [2017],33 and a study comparing tisagenlecleucel with SOC32).
Pivotal Studies and RCT Evidence
The contents of this section have been informed by materials submitted by the sponsor. The following information has been summarized and validated by the CADTH review team.
Description of Studies
Characteristics of the included studies are summarized in Table 5.
Table 5: Details of Evidence Identified by the Sponsor
Characteristics | ELARA |
|---|---|
Designs and populations | |
Study design | Multicentre, international, open-label, single-arm, phase II trial |
Locations | 30 sites in 12 countries (Australia, Austria, Belgium, France, Germany, Italy, Japan, Netherlands, Norway, Spain, UK, US) |
Patient enrolment datesa | Start date: November 2018 End date: May 2025 |
Nonrandomized (N) | 97 |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Tisagenlecleucel Dose: 0.6 to 6.0 × 108 CAR-positive viable T cells ROA: IV (single infusion) |
Comparator(s) | NA |
Study duration | |
Screening phase | Mean: 83.9 (SD = 25.50) days Median: 77 (IQR = 69 to 75; range, 45 to 157) days |
Time from enrolmentb to tisagenlecleucel infusion | Mean: 51.8 (SD = 20.93) days Median: 46 (IQR = 38 to 57, range, 23 to 127) days |
Treatment phase | Single-dose, one-time infusion |
Follow-up phase | 24 months |
Outcomes | |
Primary end point | CRR per IRC in the EAS through 24 months |
Secondary and exploratory end points | Secondary: ORR (at 24 months) PRR (at 24 months) DoR (at 24 months) PFS (at 6, 12, and 24 months) OS (at 24 and 30 months) Safety (at 24 months) PROs (at 24 months) Exploratory: Time to next antilymphoma therapy (at 24 months) |
Publication status | |
Publications | Fowler et al. (2022),61 Fowler et al. (2021),62,63 Schuster et al. (2021),64 Fowler et al. (2020),65 Hao et al. (2021),66 Schuster et al. (2021),67-70 Thieblemont (2021),71,72 Author (2021),73 Author (2022),74 NCT0356846175 |
Allo-SCT = allogeneic stem cell transplant; CAR = chimeric antigen receptor; CNS = central nervous system; CRR = complete response rate; DoR = duration of response; EAS = efficacy analysis set; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FL = follicular lymphoma; IQR = interquartile range; IRC = independent review committee; NA = not applicable; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; PRO = patient-reported outcome; PRR = partial response rate; ROA = route of administration; SD = standard deviation; SCT = hematopoietic stem cell transplant;.
aDates reported are the study start and end dates from the Clinicaltrials.gov record.
bEnrolment was defined as the point when the patient met all inclusion and/or exclusion criteria and the patient’s leukapheresis product was received and accepted by the manufacturing facility.
Source: ELARA Clinical Study Report.29 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
ELARA is a multicentre, international, open-label, single-arm phase II trial. The objective was to determine the efficacy, safety, pharmacokinetics (also referred to as cellular kinetics), and PROs of tisagenlecleucel in adults with r/r FL after 2 or more lines of systemic therapy. The ELARA study design included 3 sequential phases: screening, pretreatment, and treatment and follow-up, as illustrated in Figure 1. During the screening phase and before study enrolment, a patient’s blood mononuclear cells were collected via leukapheresis. In the pretreatment phase, patients could undergo optional bridging therapy to control their leukemia and LD chemotherapy. The treatment and follow-up phases involved a tisagenlecleucel one-time IV infusion and safety and efficacy follow-up that lasted at least 24 months. For all patients who received an infusion of tisagenlecleucel, additional survival follow-up was to be performed to determine survival status every 3 months. Efficacy was evaluated using PET, CT, or MRI, based on Lugano classification response criteria.59 Efficacy was evaluated at months 3, 6, 9, 12, 18, and 24 after infusion, and every 6 months thereafter until end of study, which was defined as the point when all patients completed their month 24 evaluation or discontinued prematurely. Onsite assessments were to be performed any time disease progression or relapse was suspected, until disease progression or relapse, the start of new anticancer therapies, death, loss to follow-up, or withdrawal of consent. The primary efficacy end point was CRR per IRC through 24 months.
Data reported in this review are for the most recent data cut-off date of March 29, 2022 (corresponding with the date when 90 patients had completed follow-up of 24 months from infusion or discontinued earlier). A prior data cut-off of March 29, 2021 was conducted (corresponding with the date that 90 patients had completed follow-up of 12 months from infusion or discontinued earlier).
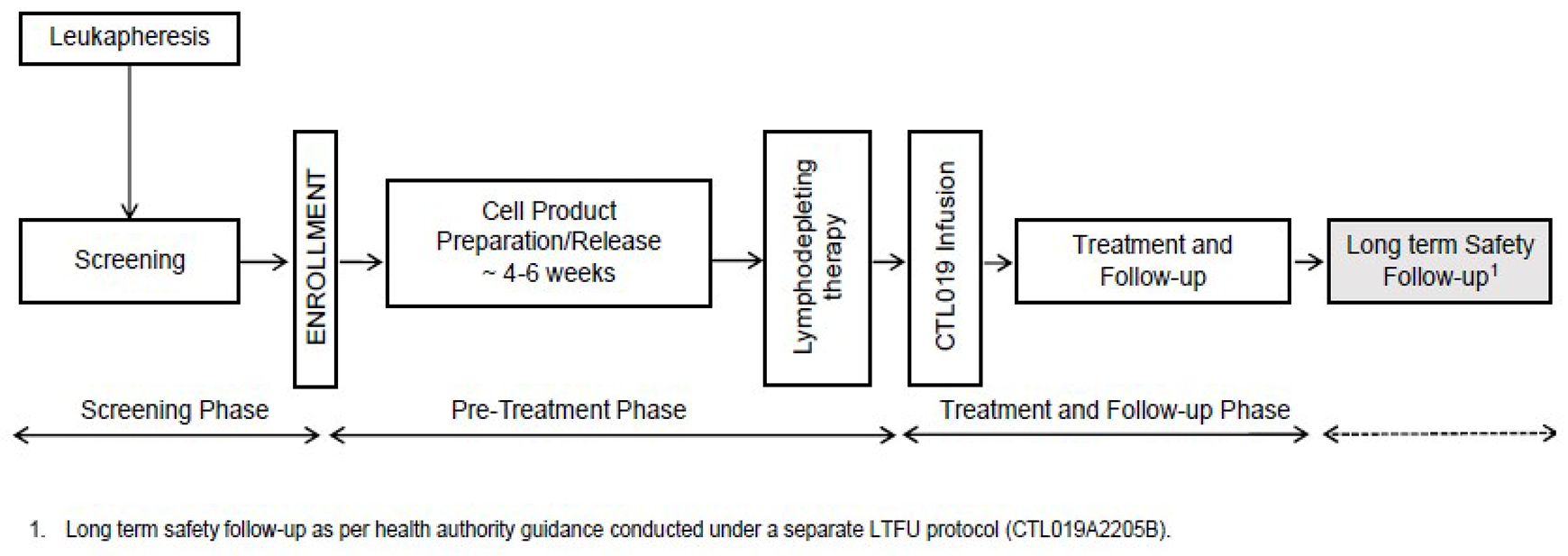
Populations
Inclusion and Exclusion Criteria
Patients eligible for inclusion in this study were required to be at least 18 years of age and to have histologically confirmed r/r FL (grade 1, 2, or 3a) by central pathology review. The FL had to meet at least 1 of the following criteria:
refractory to a second or later line of systemic therapy (including an anti-CD20 antibody and an alkylating drug) or relapsed within 6 months of completion of a second or later line of systemic therapy
relapsed during anti-CD20 antibody maintenance (following at least 2 lines of therapies) or within 6 months of maintenance completion
relapsed after auto-SCT
radiographically measurable disease at screening
ECOG PS of 0 or 1 at screening
a leukapheresis product of nonmobilized cells accepted for manufacturing.
Key exclusion criteria were evidence of histologic transformation and/or grade 3b FL and prohibited prior therapies, including prior anti-CD19 or anti-CD20 therapy, gene therapy, adoptive T-cell therapy, or allo-SCT. Patients who had active CNS abnormalities were excluded from the ELARA trial as well.
Interventions
The recommended dose of tisagenlecleucel in the ELARA trial was 0.6 to 6.0 × 108 CAR-positive viable T cells administered as a one-time, single IV infusion. Prior to tisagenlecleucel infusion, all patients were required to receive LD chemotherapy. This step was to be omitted in cases of significant cytopenia (e.g., white blood cell count < 1,000 cells/μL, absolute lymphocyte count < 200 cells/μL) or any condition that, in the investigator’s opinion, precluded LD chemotherapy. LD chemotherapy was started 1 week before tisagenlecleucel infusion so that the CAR-positive viable T cells could be administered 2 to 6 days after completion of the LD chemotherapy. The chemotherapy start date varied based on the selected chemotherapy. For LD chemotherapy, cyclophosphamide-based regimens were the preferred drugs due to the vast experience with the use of these drugs in the facilitation of adoptive immunotherapy. The first option as a LD regimen was:
fludarabine (25 mg/m2 IV daily for 3 doses) plus cyclophosphamide (250 mg/m2 IV daily for 3 doses starting with the first dose of fludarabine).
If there was previous grade 4 hemorrhagic cystitis with cyclophosphamide or if a patient had resistance to a previous cyclophosphamide-containing regimen, then the following regimen was allowed:
bendamustine 90 mg/m2 IV daily for 2 days.
No other regimen was allowed for LD chemotherapy.
Bridging Therapy
Of the 97 patients infused, 44 (45.4%) patients received optional antineoplastic bridging therapy before tisagenlecleucel infusion. The most common drugs (in ≥ 5% of patients) were rituximab (21.6%), dexamethasone (11.3%), gemcitabine (10.3%), oxaliplatin (7.2%), prednisolone (7.2%), etoposide (6.2%), cyclophosphamide (5.2%), and vincristine (5.2%). In 5 patients, only corticosteroids were administered as bridging therapy. Further, 2 patients received bridging radiotherapy: 1 patient received only radiotherapy and the other patient received radiotherapy and corticosteroids.
Lymphodepleting Chemotherapy
All 97 infused patients received LD chemotherapy before the tisagenlecleucel infusion. Most patients (92 [94.8%]) received fludarabine plus cyclophosphamide, whereas the remaining 5 (5.2%) patients received bendamustine.
Prior to tisagenlecleucel infusion, a minimum of 2 doses of tocilizumab per patient and emergency equipment had to be confirmed as available and had to be available for infusion within 2 hours for the management of CRS-related AEs.
All patients (n = 97) who received tisagenlecleucel also received concomitant medications (Table 6). As reported by Anatomic Therapeutic Chemical class, most patients received anilides (57.7%), sulfonamides plus trimethoprim, (54.6%), nucleosides plus nucleotides (49.5%), proton pump inhibitors (37.1%), and colony-stimulating factors (37.1%). In all, 17 (17.5%) patients in the infused set received anticytokine medication for CRS-related AEs.
Table 6: Concomitant Medication Use by ATC Class and Preferred Term in the ELARA Study
Exposure | Tisagenlecleucel, n (%) (N = 97) |
|---|---|
Concomitant medications received | 97 (100.0) |
Anilides | 56 (57.7) |
Antivirals | 32 (33.0) |
Benzodiazepine derivatives | 22 (22.7) |
Colony-stimulating factors | 36 (37.1) |
Combinations of penicillins, including beta-lactamase inhibitors | 27 (27.8) |
Combinations of sulfonamides and trimethoprim, including derivatives | 53 (54.6) |
Fluoroquinolones | 22 (22.7) |
Heparin group | 33 (34.0) |
Natural opium alkaloids | 26 (26.8) |
Nucleosides and nucleotides, excluding reverse transcriptase inhibitors | 48 (49.5) |
Osmotically acting laxatives | 26 (26.8) |
Other antiepileptics | 27 (27.8) |
Potassium | 25 (25.8) |
Preparations that inhibit uric acid production | 48 (49.5) |
Proton pump inhibitors | 36 (37.1) |
Triazole derivatives | 33 (34.0) |
Propulsives | 29 (29.9) |
Serotonin (5-HT3) antagonists | 33 (34.0) |
Solutions that affect the electrolyte balance | 25 (25.8) |
ATC = Anatomical Therapeutic Chemical.
Notes: In the ELARA study, concomitant treatments with n ≥ 20 are only included from a long list of therapies in the E2202 Clinical Study Report; the cut-off date was March 29, 2022.
Concomitant medications on or after the start of study treatment or starting before and continuing after the start of study treatment are summarized. A medication or therapy can be included in more than 1 ATC class.
Source: ELARA Clinical Study Report.29 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Outcomes
The efficacy end points assessed in this Clinical Review Report are provided in Table 7 and are subsequently summarized. Summarized end points are based on those included in the sponsor’s Summary of Clinical Evidence, as well as those identified as important to this review, according to stakeholders, such as clinical experts, clinician groups, or patient groups.
Table 7: Outcomes Summarized From the ELARA Study
Outcome measures | Time point | End point |
|---|---|---|
CRR | At 24 months | Primary |
ORR | At 24 months | Secondary |
DoR | At 24 months | Secondary |
OS (rate) | At 24 and 30 months | Secondary |
OS (median) | At 24 months | Secondary |
PFS (rate) | At 6, 12 and 24 months | Secondary |
PFS (median) | At 24 months | Secondary |
AEs | At 24 months | Secondary |
PROs | At 12 and 24 months | Secondary |
AE = adverse event; CRR = complete response rate; DoR = duration of response, ORR = overall response rate, OS = overall survival; PFS = progression-free survival; PRO = patient-reported outcome.
Note: There was no key secondary outcome and secondary outcomes were not tested, according to a prespecified statistical hierarchy or adjusted for multiple comparisons. The analysis of all primary and all secondary outcomes were performed using the efficacy analysis set.
Source: ELARA Clinical Study Report.29 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Definitions of the various outcomes reported in the ELARA study are as follows:
CRR was defined as the proportion of patients with a best overall response of complete response (CR) recorded from tisagenlecleucel infusion until progressive disease or the start of new anticancer therapy, whichever came first.
ORR was defined as the proportion of patients with a best overall disease response of CR or partial response (PR).
DoR was defined as the time from the date of first documented disease response (CR or PR) to the date of first documented progression or death due to FL. If a patient did not have an event before the earliest censoring event, DoR was censored at the date of the last adequate assessment on or before the earliest censoring event.
PFS was defined as the time from the date of tisagenlecleucel infusion to the date of first documented progression or death due to any cause. If a patient did not have an event, PFS was censored at the date of the last adequate assessment. The censoring reasons could be any of the following:
ongoing without an event
lost to follow-up
withdrew consent
new anticancer therapy (including SCT if the patient proceeded to SCT after tisagenlecleucel infusion)
event documented after at least 2 missing tumour assessments
adequate assessments no longer available.
PFS was also analyzed as the time from enrolment to the date of progression or death due to any reason in the enrolled set.
OS was defined as the time from the date of tisagenlecleucel infusion to the date of death due to any reason. If a death was not observed by the data cut-off date, OS was censored at the date of last contact. The distribution function of OS was estimated using the KM method. OS was also analyzed as the time from enrolment to the date of death due to any reason for in the enrolled set.
Posttisagenlecleucel AE summaries included all AEs that started or worsened during the postinfusion period (i.e., within 8 weeks of the first tisagenlecleucel infusion, 8 weeks to 1 year after tisagenlecleucel infusion, more than1 year after the first tisagenlecleucel infusion, and any time after the tisagenlecleucel infusion. The postinfusion period was the main period of safety reporting.
PROs included FACT-Lym, SF-36, and EQ-5D-3L, and were assessed at baseline and postbaseline scheduled assessments.
The FACT-Lym is a questionnaire designed to assess HRQoL in patients with lymphoma. It consists of a generic core HRQoL instrument (FACT-G) and a cancer-site-specific module (Lym-S). The FACT-G has 27 statements that patients need to rate on a 5-point scale (not at all, a little, somewhat, quite a bit, very much). The statements cover 5 subscales (physical well-being, social/family well-being, emotional well-being, functional well-being, and additional concerns). The Lym-S module consists of 15 statements patients need to rate on an identical 5-point scale specific for NHL. This scale is designed for patient self-administration. Higher scores demonstrate improvement in QoL. Minimally clinically important differences (MCIDs) were estimated to range from 5.5 to 11 for the FACT-Lym trial outcome index, 3 to 7 for the FACT-G total score, 2.9 to 5.4 for the FACT-Lym subscale score, and 6.5 to 11.2 for FACT-Lym total score.76
The SF-36 is a widely used and extensively studied generic instrument to measure HRQoL among healthy patients and patients with acute and chronic conditions. It consists of 8 subscales that can be scored individually: physical functioning, role-physical, bodily pain, general health, vitality, social functioning, role-emotional, and mental health. Two overall summary scores, the physical component summary and the mental component summary, also can be computed. The SF-36 has proven useful in monitoring general and specific populations, comparing the relative burden of different diseases, differentiating the health benefits produced by different treatments, and screening individual patients.29 There were no FL-specific MCIDs identified for the SF-36 in the literature; however, an absolute score increase of 3 to 5 points for both the physical component summary and mental component summary was reported as a MCID across various conditions, such as idiopathic pulmonary fibrosis and colitis.77,78
The EQ-5D-3L is a widely used, self-administered questionnaire designed to assess health status in adults. The measure is divided into 2 distinct sections. The first section includes 1 item addressing each of 5 dimensions (mobility, self-care, usual activity, pain/discomfort, and anxiety/depression). Patients rate each of these items, from no problem, some problem, or extreme problem. A composite health index is then defined by combining the levels for each dimension. The second section of the questionnaire measures self-rated (global) health status using a vertically oriented VAS, where 100 represents the best possible health state and 0 represents the worst possible health state. Respondents are asked to rate their current health by placing a mark along this continuum. The recall period is “today,” and the questionnaire requires approximately 5 to 10 minutes to complete. In the ELARA study, only the change in VAS scores were reported. No disease-specific MCID for the EQ-5D-3L VAS score in patients with FL was reported; however, in the general population an increase in the VAS score of 10.9 was considered to indicate improved health.29,79
Statistical Analysis
A prior study of idelalisib in patients with r/r FL after 2 lines of therapy reported an observed CRR of 14%.80 This result was used as the null hypothesis for the ELARA study because idelalisib was the therapy with best CRR among the approved and widely used treatment options in this setting at the time the trial was being planned. Therefore, based on the null hypothesis of a CRR of 15% or less and assuming an underlying CRR of 30% for tisagenlecleucel, 90 patients in the primary analysis would provide at least 90% cumulative power to demonstrate statistical significance, using a 2-look Lan-DeMets group sequential design with O’Brien-Fleming type boundary and an exact CI at a 1-sided cumulative 0.025 level of significance, if the underlying CRR is 30%. In this setting, a CRR of 23.3% (21 of 90 patients) was needed to claim success. Therefore, assuming that 20% of enrolled patients will not be infused for reasons such as manufactory failure or worsening of the patient’s condition, at least 113 patients needed to be enrolled to ensure that 90 patients were treated and available for the primary analysis.
All statistical analyses were performed using data collected up to the cut-off date of March 29, 2022. The analysis of the primary outcome was performed by testing the null hypothesis of a CRR of 15% or less at a 1-sided cumulative 2.5% level of significance (i.e., P ≤ 0.15 for H0 versus P > 0.15 for Ha). The 15% was derived from the CRR from approved PI3K inhibitors for the treatment of FL that relapsed after 2 prior systemic therapies based on single-arm, open-label, phase II studies. The CRR was analyzed at an interim analysis (using the interim efficacy analysis set [EAS]) and the primary analysis (EAS) of a group sequential design. The CRR was summarized along with 2-sided exact Clopper-Pearson CIs, with coverage level determined by the O’Brien-Fleming type alpha-spending approach, according to Lan and DeMets (1983).81 The study was considered successful if the lower bound of the 2-sided exact CI for ORR was greater than 15%, so that the null hypothesis that the CRR was less than or equal to 15% could be rejected. Patients who were of unknown clinical response were treated as nonresponders.
PFS, OS, and DoR were estimated using the KM method. The median OS and the proportion of patients alive at 3, 6, 12, 18, and 24 months, with 95% CIs, were presented. The median PFS and the proportion of patients without an event at 3, 6, 9, and 12 months, with 95% CIs, were presented. The ORR was summarized along with the 2-sided 95% exact Clopper-Pearson CIs. DoR was summarized for patients with a CR only, as well as for those with a CR or PR. The median response duration, as well as proportion of patients without event at 3, 6, 9, and 12 months, with 95% CIs, were presented.
Reporting of AEs (except for CRS) was based on MedDRA version 25.0 and Common Terminology Criteria for Adverse Events (CTCAE) version 4.03. There was no key secondary outcome and secondary outcomes were not tested, according to a prespecified statistical hierarchy, or adjusted for multiple comparisons. All analyses of secondary outcomes were performed using the EAS. For PROs, summary scores were calculated and descriptive statistics and change from baseline of the summary scores of each domain were derived from all available data at the time of the analysis, using the EAS.
Sensitivity Analyses
The analysis of the primary outcome was performed on the enrolled set, the tisagenlecleucel-infused set, and the per-protocol set using the same methodology, and on the modified EAS and the EAS, which excluded patients who achieved a CR at the radiologic assessment at baseline per IRC. Consistent results were observed when CRR was analyzed across the different analysis sets, and the results were consistent with those of the EAS.
The secondary outcomes included ORR, DoR, PFS, OS, safety, and PROs. IRC assessment was used in the main analysis of secondary outcomes that involved disease response. All analyses of the secondary efficacy outcomes were performed on the EAS. In addition, selected analyses were performed for the tisagenlecleucel-infused set and/or for the enrolled set.
Subgroup Analyses
The following prespecified subgroups of interest were used for the supporting efficacy analysis of the primary outcome:
age (< 65 years, ≥ 65 years)
sex (male, female)
race (Asian, Black or African American, white, Native Hawaiian or Other Pacific Islander or American Indian, Alaska Native)
ethnicity (Hispanic or Latino, not Hispanic or Latino)
FLIPI (low or intermediate, high)
histological grade (1, 2, 3a)
number of prior lines of antineoplastic therapy (≤ 2 lines, 3 or 4 lines, > 4 lines)
PI3K inhibitor use (naive, pretreated)
prior SCT therapy (yes, no) and relapse (12 months or less from SCT, more than 12 months from SCT)
disease status to last line of prior antineoplastic therapy (refractory, relapsed)
progression of disease within 24 months of first-line treatment (POD24) with anti-CD20
mAb-containing therapy (yes, no)
bulky disease at baseline (defined per IRC as imaging showing any nodal or extranodal tumour mass that is > 7 cm in diameter or the involvement of at least 3 nodal sites, each with a diameter > 3 cm) (yes, no)
bridging therapy (yes, no)
lactate dehydrogenase (LDH) at study entry (≤ upper limit of normal, > upper limit of normal)
R2 use lenalidomide plus rituximab in same regimen (naive, pretreated)
US sites (yes, no)
total metabolic tumour volume at baseline (low tumour burden [tumour volume ≤ 510 cm3], high tumour burden [tumour volume > 510 cm3]
double refractory, defined as patients who failed to respond or relapsed within 6 months of therapy with anti-CD20 and alkylating drugs, any regimen (yes, no)
Of these subgroups, the ones relevant to the CADTH review (i.e., that may have important prognostic, confounding, effect modification influence on outcomes) based on clinician input are age, FLIPI score, number of prior lines of antineoplastic therapy, prior SCT, POD24, bulky disease, bridging therapy, and LDH at study entry.
Handling of missing values: Patients in this study who are of unknown clinical response were treated as nonresponders. Other missing data were simply noted as missing on appropriate tables and/or listings.
Table 8: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
CRR (primary end point) | Testing the null hypothesis of the CR being ≤ 15% at a 1-sided cumulative 2.5% level of significance | NA | Patients who were of unknown clinical response were treated as nonresponders Missing data are noted as missing on appropriate tables and/or listings | Enrolled set, tisagenlecleucel-infused set, and PPS, using the same methodology as that of the definitions of the outcomes |
OS, PFS, DoR (secondary end points) | Kaplan-Meier method | NA | Patients who were of unknown clinical response were treated as nonresponders Missing data are noted as missing on appropriate tables and/or listings | Enrolled set, tisagenlecleucel-infused set, and PPS, using the same methodology as that of the definitions of the outcomes |
CR = complete response; CRR = complete response rate; DoR = duration of response; NA = not applicable; OS = overall survival; PFS = progression-free survival; PPS = per-protocol set.
Source: ELARA Clinical Study Report.29 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Data Cut-off Dates
In the ELARA trial, analyses were conducted at various cut-off dates.
The data cut-off for the interim analysis was May 26, 2020, when 52 patients who received a tisagenlecleucel infusion had either been followed for 6 months or discontinued earlier.
The prespecified data cut-off for the primary analysis was September 28, 2020, when 94 patients had been followed for at least 6 months or discontinued earlier. This analysis was used for Health Authority interactions.
An extended follow-up analysis (data cut-off of March 29, 2021) was conducted after 90 patients who received a tisagenlecleucel were followed for at least 12 months or discontinued earlier, and was the basis for registration applications.
The 24-month follow-up analysis, with a data cut-off of March 29, 2022, was conducted after approximately 90 patients who received a tisagenlecleucel infusion and were followed for 24 months or discontinued earlier. Results of this analysis were presented in the current review.
Note that on the primary data cut-off date (September 28, 2020), the primary end point (CRR determined by IRC based on Lugano classification response criteria) was met, with a CRR of 66.0% (95% CI, 55.5% to 75.4%). The lower bound of the 95% CI was greater than 15%. The results were consistent across all data cut-off dates. The observed benefits were maintained at later data cut-off dates, including March 29, 2022.29
Analysis Populations
The analysis populations in the ELARA trial are summarized in Table 9.
The EAS consisted of all patients who received tisagenlecleucel and had measurable disease at baseline per IRC. This analysis set was used for all efficacy analyses of the primary and secondary outcomes.
The safety set consisted of all patients who received tisagenlecleucel. This analysis set was used for all safety analyses.
Table 9: Analysis Populations of the ELARA Study
Population | Definition | Application |
|---|---|---|
Screened set | All patients who signed the consent and were screened for the study. | Used for all disposition data. |
Enrolled set | All patients enrolled in the study. Enrolment was defined as the point at which the patient meets all inclusion and/or exclusion criteria, and the patient’s leukapheresis product was received and accepted by the manufacturing facility. | Used for all baseline and demographic summaries and listings and for sensitivity analyses. |
Tisagenlecleucel-infused set | All patients who received tisagenlecleucel. | Same as safety analysis set. used for sensitivity analyses. |
EAS | All patients who received tisagenlecleucel and had measurable disease at baseline per IRC. Nonmeasurable disease at baseline was defined as the absence of index lesions at baseline disease evaluation (i.e., no disease at baseline). | Used for all efficacy analyses of the primary and secondary outcomes, per protocol. |
mEAS | Same as for EAS, except refers to first 90 patients who received tisagenlecleucel and had measurable disease at baseline per IRC. The first 90 patients were followed for 12 months after infusion or discontinued earlier. | Earlier analysis, with a data cut-off of March 29, 2021. |
PPS | Subset of patients in the EAS who had a diagnosis of relapsed or refractory follicular lymphoma at baseline and received the recommended dose. | Used for sensitivity analyses. |
Safety analysis set | All patients who received tisagenlecleucel. | Used for all safety analyses. |
EAS = efficacy analysis set; IRC = independent review committee; mEAS = modified efficacy analysis set; PPS = per-protocol set.
Source: ELARA Clinical Study Report.29 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Results
Patient Disposition
A summary of patient disposition in the ELARA trial is provided in Table 10.
A total of 119 patients were screened by the data cut-off (March 29, 2022). Of these, 98 (82.4%) patients were enrolled and 21 (17.6%) patients were excluded. All but 1 enrolled patients (n = 97) received their tisagenlecleucel infusion. Of the 98 patients enrolled, 73 (74.5%) patients were in follow-up at the time of the data cut-off and 25 (25.5%) patients had discontinued the study. The most common reason for discontinuation was death (i.e., 13 [13.3%] patients).
Table 10: Summary of Patient Disposition From the ELARA Study
Patient disposition | ELARA (N = 119) |
|---|---|
Total screened, N | 119 |
Completed screening phase, enrolled, n (%) | 98 (82.4) |
Patients did not meet at least 1 inclusion and/or exclusion criterion and/or did not complete screening, n (%) | 21 (17.6) |
Reason for screening failure, N (%) | |
Physician decision not to continue | 1 (0.8) |
Screen failure | 19 (16.0) |
Patient decision not to continue | 1 (0.8) |
Total patients enrolled, N | 98 |
Infused, n (%) | 97 (99.0) |
Discontinued from study, n (%) | 25 (25.5) |
Reason for discontinuation, n (%) | |
Death | 13 (13.3) |
Physician decision | 7 (7.1) |
Patient decision | 4 (4.1) |
Lost to follow-up | 1 (1.0) |
Rapid progression of lymphoma | — |
Inadequate T-cell count for collection or manufacturing failure | — |
EAS, n (%) | 94 (95.9) |
PPS, n (%) | 85 (86.7) |
Safety analysis set, n (%) | 97 (99.0) |
EAS = efficacy analysis set, PPS = per-protocol set.
Source: ELARA Clinical Study Report.29 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Baseline Characteristics
In total, 98 patients were enrolled in this study and 97 received treatment with tisagenlecleucel.
The baseline characteristics of the included study population in the ELARA trial are detailed in Table 11.
At the data cut-off date of March 29, 2022, a total of 94 patients with r/r FL had received a one-time, single infusion of tisagenlecleucel. The median age observed in the overall r/r FL population was 57 years (range, 29 to 73 years). More males (68.1%) were enrolled than females (31.9%), and most patients (84.0%) were white. Almost all patients (97%) had a baseline ECOG PS of 0 or 1. Most patients also had grade 1 to 2 (90.4%) and stage III to IV (80%) disease. In terms of prior therapies, enrolled patients had received a median of 4 (range, 2 to 13) prior lines of treatments. All of the included patients (n = 98; 100%) received prior therapy with an anti-CD20 mAb and alkylating drugs, and 36.7% of the patients received prior SCT. Of the 98 included patients, 77.6% were refractory to the last line of antineoplastic therapy. The proportion of patients who progressed within 24 months of first-line anti-CD20 mAb-containing therapy was 64.9%.
The previous therapies received by patients in the ELARA trial are summarized in Table 12.
Table 11: Summary of Patient Baseline Characteristics in the ELARA Trial
Characteristic | EAS (N = 94) |
|---|---|
Age, years | |
Mean (SD) | 56.4 (10.54) |
Median (range) | 57 (29 to 73) |
Q1 to Q3 | 49.0 to 65.0 |
Sex, n (%) | |
Male | 64 (68.1) |
Female | 30 (31.9) |
Stage, n (%) | |
I | 5 (5.3) |
II | 13 (13.8) |
III | 20 (21.3) |
IV | 55 (58.5) |
Missing | 1 (1.1) |
Ann Arbor stage, n (%) | |
I | NR |
II | NR |
III | NR |
IV | NR |
Grade, n (%) | |
Grade 1 or 2 | 85 (90.4) |
Grade 3a | 9 (9.6) |
FLIPI, n (%) | |
Low | 17 (18.1) |
Intermediate | NR |
High | NR |
Prior therapy | |
Mean (SD) | 3.9 (1.81) |
Median (range) | 4.0 (2 to 13) |
25th to 75th percentile | 2.0 to 5.0 |
Number of prior lines of antineoplastic therapy, n (%) | |
2 | 24 (25.5) |
3 or 4 | 43 (45.7) |
> 4 | 27 (28.7) |
ECOG PS, n (%) | |
0 | 53 (56.4) |
1 | 38 (40.4) |
2 | 3 (3.2)a |
Race, n (%) | |
White | 79 (84.0) |
Asian | 11 (11.7) |
Black or African American | 1 (1.1) |
Missing | 3 (3.2) |
Elevated LDH > ULN, n (%) | |
Yes | 41 (43.6) |
No | 53 (56.4) |
Bulky disease, n (%) | |
Yes | 62 (66.0) |
No | 32 (34.0) |
POD24, n (%) | |
Yes | 61 (64.9) |
No | 33 (35.1) |
EAS = efficacy analysis set; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FLIPI = Follicular Lymphoma International Prognostic Index; LDH = lactate dehydrogenase; NR = not reported; POD24 = progression of disease within 24 months of first-line treatment; Q1 = first quartile; Q3 = third quartile; SD = standard deviation; ULN = upper limit of normal.
aThese 3 patients had an ECOG PS of 2 recorded just before receiving tisagenlecleucel infusion, and not at the time of signing the informed consent form.
Source: ELARA Clinical Study Report.29 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Table 12: Summary of FL Therapies Administered Prior to Tisagenlecleucel in the ELARA Trial
Prior therapy to which disease was refractory | Receipt of prior therapy, n (%) |
|---|---|
Anti-CD20 mAb | 98 (100.0) |
Refractory to anti-CD20 mAb | 85 (86.7) |
POD24 from first-line anti-CD20 mAb-containing therapy | 61 (62.2) |
Alkylating drugs | 98 (100.0) |
Refractory to alkylating drug | 70 (71.4) |
PI3K inhibitors | 21 (21.4) |
Refractory to PI3K inhibitors | 14 (14.3) |
Refractory to anti-CD20 mAb (any regimen) + alkylating drug (any regimen) | 67 (68.4) |
Refractory to anti-CD20 mAb (any regimen) + alkylating drug (any regimen) + Pi3k inhibitors (any regimen) | 10 (10.2) |
Refractory to anti-CD20 mAb (any regimen) + alkylating drug (any regimen) + lenalidomide (any regimen) | 17 (17.3) |
Prior SCT | 36 (36.7) |
Relapsed ≤ 12 months after autologous SCT | 15 (15.3) |
FL = follicular lymphoma; mAb = monoclonal antibody; PI3K = phosphoinositide 3-kinase; POD24 = progression of disease within 24 months of first-line treatment; SCT = hematopoietic stem cell transplant.
Source: ELARA Clinical Study Report.29 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Exposure to Study Treatments
As tisagenlecleucel is given as a single-dose, one-time IV infusion, all patients who were infused in the ELARA trial received 100% of the dose. The median time from enrolment to infusion is summarized in Table 13. In the ELARA trial, 97 patients received tisagenlecleucel treatment with a median duration of 46 days (range, 23 to 127 days) from enrolment to treatment infusion.
Table 13: Overview of Time to Infusion in the ELARA Trial
Exposure | Tisagenlecleucel (N = 97) |
|---|---|
Total, patient-weeks or patient-years | NA |
Exposure, mean (SD) | NA |
Time to infusion, days, median (range) | 46 (23 to 127)a |
Adherence, % | 100 |
NA = not applicable; SD = standard deviation.
aTime from enrolment to tisagenlecleucel infusion.
Source: ELARA Clinical Study Report.29 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
The recommended tisagenlecleucel dose range in the ELARA study was 0.6 to 6.0 × 108 CAR-positive viable T cells. All except 4 patients received tisagenlecleucel within the targeted dose range. The median dose administered was 2.06 × 108 CAR-positive viable T cells (range, 0.1 to 6.0 × 108 cells). The median total viable cell count was 12 × 108 cells (range, 0.4 to 34.0 × 108 cells).
Overall, 22 (22.7%) patients received at least 1 new antineoplastic medication after the tisagenlecleucel infusion, mostly of whom had stable disease or progressive disease (Table 14). Regarding the types of subsequent therapy, most patients received lenalidomide (12.4%) and/or rituximab (11.3%) after the infusion.
Upon CADTH’s request, the sponsor specified that in the ELARA study, no patients received a subsequent auto-SCT, while 4.12% of the patients have received a subsequent allo-SCT.
Table 14: Antineoplastic Medication Received After Tisagenlecleucel Infusion in the ELARA Trial
Exposure | Tisagenlecleucel, n (%) (N = 97) |
|---|---|
At least 1 medication | 22 (22.7) |
Anthracyclines and related substances (doxorubicin) | 1 (1.0) |
Antineoplastic drugs (copanlisib) | 2 (2.1) |
Combinations of antineoplastic drugs (cyclophosphamide with doxorubicin hydr/08193401/) | 1 (1.0) |
Folic acid analogues (methotrexate) | 1 (1.0) |
Glucocorticoids (dexamethasone) | 1 (1.0) |
Glucocorticoids (prednisolone) | 1 (1.0) |
Glucocorticoids (prednisone) | 1 (1.0) |
Investigational drug | 7 (7.2) |
Rituximab | 11 (11.3) |
Loncastuximab tesirine | 1 (1.0) |
Nivolumab | 1 (1.0) |
Obinutuzumab | 1 (1.0) |
Cyclophosphamide | 3 (3.1) |
Bendamustine | 2 (2.1) |
Ifosfamide | 2 (2.1) |
Melphalan | 1 (1.0) |
Trofosfamide | 1 (1.0) |
Other antineoplastic drugs (idelalisib) | 5 (5.2) |
Other immunosuppressants (lenalidomide) | 12 (12.4) |
Platinum compounds (carboplatin) | 1 (1.0) |
Podophyllotoxin derivatives (etoposide) | 3 (3.1) |
Protein kinase inhibitors (ibrutinib) | 1 (1.0) |
Protein kinase inhibitors (zanubrutinib) | 1 (1.0) |
Purine analogues (fludarabine) | 2 (2.1) |
Vinca alkaloids and analogues (vincristine) | 1 (1.0) |
Note: A medication can be included in more than 1 ATC class.
Source: ELARA Clinical Study Report.29 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Efficacy
Response Rates
Response rates with tisagenlecleucel used in the third-line setting for patients with r/r FL are provided in Table 15.
In the ELARA trial, among the 97 patients who were treated with tisagenlecleucel, the CRR was 68.1% (95% CI, 57.7% to 77.3%), the ORR was 86.2% (95% CI, 77.5% to 92.4%), and the PRR was 18.1% (95% CI, NR) at 24-month follow-up per IRC assessment. The median duration of follow-up was 28.85 months from the time of the infusion to the data cut-off.29 The results from local assessment were consistent with the IRC assessment.
Table 15: Summary of Response Rates in the ELARA Trial
Response rates at 24 months | Tisagenlecleucel (N = 97) |
|---|---|
Number of patients contributing to the analysis | 94 (EAS) |
ORR, n (%) [95% CI] | Local assessment: 85 (90.4) [82.6 to 95.5] |
IRC assessment: 81 (86.2) [77.5 to 92.4] | |
CRR, n (%) [95% CI] | Local assessment: 69 (73.4) [63.3 to 82.0] |
IRC assessment: 64 (68.1) [57.7 to 77.3] | |
PRR, n (%) [95% CI] | Local assessment: 16 (17.0) [NR] |
IRC assessment: 17 (18.1) [NR] | |
Stable disease rate, n (%) [95% CI] | Local assessment: 3 (3.2) [NR] |
IRC assessment: 3 (3.2) [NR] | |
PD rate, n (%) [95% CI] | Local assessment: 6 (6.4) [NR] |
IRC assessment: 9 (9.6) [NR] |
CI = confidence interval; CRR = complete response rate; EAS = efficacy analysis set; IRC = independent review committee; NR = not reported; ORR = overall response rate; PD = progressive disease; PRR = partial response rate.
Source: ELARA Clinical Study Report.29 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Results of the predefined sensitivity analyses were similar to those in the primary analysis of CRR per IRC assessment. The CRR per local assessment was 73.4% (95% CI, 63.3% to 82.0%), which was consistent with the IRC assessment. In addition, consistent results with the EAS were observed when CRR was analyzed using different analysis sets (i.e., enrolled set, tisagenlecleucel-infused set, and per-protocol set).
Results of the prespecified subgroup analyses were consistent with the primary analysis of CRR. The CRRs across the subgroups ranged from 40.0% to 84.8%, which were similar to the overall study population in the EAS. Results in the subgroups of age, FLIPI score, number of prior lines of therapies, prior SCT use, POD24 status, bulky disease, bridging therapy, and LDH level at baseline are presented in Table 36 in Appendix 1. These subgroups are considered clinically important by the experts consulted for this review.
Duration of Response
Median DoR was not reached with tisagenlecleucel at the median follow-up time in ELARA (Table 16). The median duration of follow-up was 20.7 months (range, 0 to 29.6 months).
Overall Survival
The ELARA study reported median OS and OS event rates with tisagenlecleucel at different time points (Table 17).
In the ELARA trial, median OS was not reached at the 24- month follow-up (cut-off date of March 29, 2022). Thirteen deaths occurred in the study, and the OS rate was 87.7% (95% CI, 78.3% to 93.2%) and 82.6% (95% CI, 70.2% to 90.2%) at 24 and 30 months, respectively.
Table 16: Summary of DoR in the ELARA Trial
Duration of response | Tisagenlecleucel (N = 97) |
|---|---|
Number of patients contributing to the analysis | 81 (EAS) |
Median DoR follow-up time (range), months | 20.7 (0 to 29.6) |
DoR (median in months) | Both local and IRC: not reached |
CI = confidence interval; DoR = duration of response; EAS = efficacy analysis set; IRC = independent review committee.
Source: ELARA Clinical Study Report.29 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Table 17: Summary of OS in the ELARA Trial
Outcomes | Tisagenlecleucel (N = 97) |
|---|---|
Number of patients contributing to the analysis | 94 (EAS) |
Median OS follow-up time (range), months | 24.3 (1.8 to 36.4) |
Rate, % (95% CI) | 24-month OS rate: 87.7 (78.3 to 93.2) 30-month OS rate: 82.6 (70.2 to 90.2) |
Median (95% CI) | At FU of 24 months: not reached (34.5 to NE) |
CI = confidence interval; EAS = efficacy analysis set; FU = follow-up; NE = not estimable; OS = overall survival.
Source: ELARA Clinical Study Report.29 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Progression-Free Survival
Median PFS and PFS event rates with tisagenlecleucel are summarized in Table 18. The PFS rate with tisagenlecleucel was evaluated at multiple time points and data cut-off dates, ranging from 6 months to 24 months.
In the ELARA trial, the median PFS per IRC was not reached at the time of the data cut-off (March 29, 2022) and there were 38 PFS events in total (disease progression or death). The PFS rate was 77.8% (95% CI, 67.7% to 85.1%), 67.2% (95% CI, 56.3% to 75.9%), and 57.4% (95% CI, 46.2% to 67.0%) at 6, 12, and 24 months, respectively.
Fifty-six patients were censored from the analysis for the following reasons: 51 patients were ongoing without an event, 3 patients started new anticancer therapy other than SCT, 1 patient withdrew their consent, and 1 patient was lost to follow-up.
PFS results assessed by the local investigator were consistent with IRC assessment.
Table 18: Summary of PFS in the ELARA Trial
Outcomes | Tisagenlecleucel (N = 97) |
|---|---|
Number of patients contributing to the analysis | 94 (EAS) |
Median PFS FU time (range), months | 20.9 (0 to 31.4) |
PFS rate, % (95% CI) | Local assessment 6-month PFS rate: 78.0 (68.0 to 85.2) 12-month PFS rate: 67.8 (57.1 to 76.4) 24-month PFS rate: 57.4 (46.2 to 67.0) IRC assessment 6-month PFS rate: 77.8 (67.7 to 85.1) 12-month PFS rate: 67.2 (56.3 to 75.9) 24-month PFS rate: 57.4 (46.2 to 67.0) |
Median PFS, months (95% CI) | IRC assessment At 24-month FU: not reached (18.2, NE) |
CI = confidence interval; EAS = efficacy analysis set; FU = follow-up; IRC = independent review committee; NE = not estimable; PFS = progression-free survival.
Source: ELARA Clinical Study Report.29 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Patient-Reported Outcomes
In the ELARA trial, PROs were assessed in the EAS (n = 94) to evaluate the impact of tisagenlecleucel on patients’ HRQoL. Three PRO instruments were used to capture impact on QoL: FACT-Lym, SF-36, and EQ-5D-3L. As previously reported, MCIDs were estimated to range from 5.5 to 11 for the FACT-Lym trial outcome index, 3 to 7 for FACT-G total score, 2.9 to 5.4 for the FACT-Lym subscale score, and 6.5 to 11.2 for the FACT-Lym total score.76 For SF-36, MCIDs were estimated to be 3 for both the physical component and the mental component scores.77
FACT-Lym and SF-36 Questionnaires
Over time, there were few notable changes in the proportion of patients reporting improved, stable, or deteriorated FACT-Lym or SF-36 scores after the tisagenlecleucel infusion (Figure 2). Overall, 70% to 88% of patients reported no deterioration in QoL based on the FACT-Lym and SF-36 scores at 12 months, with similar trends observed at 18 and 24 months.
Figure 2: Proportion of Patients Who Deteriorated, Improved, or Did Not Change on FACT-Lym and SF-36 Questionnaires (EAS)
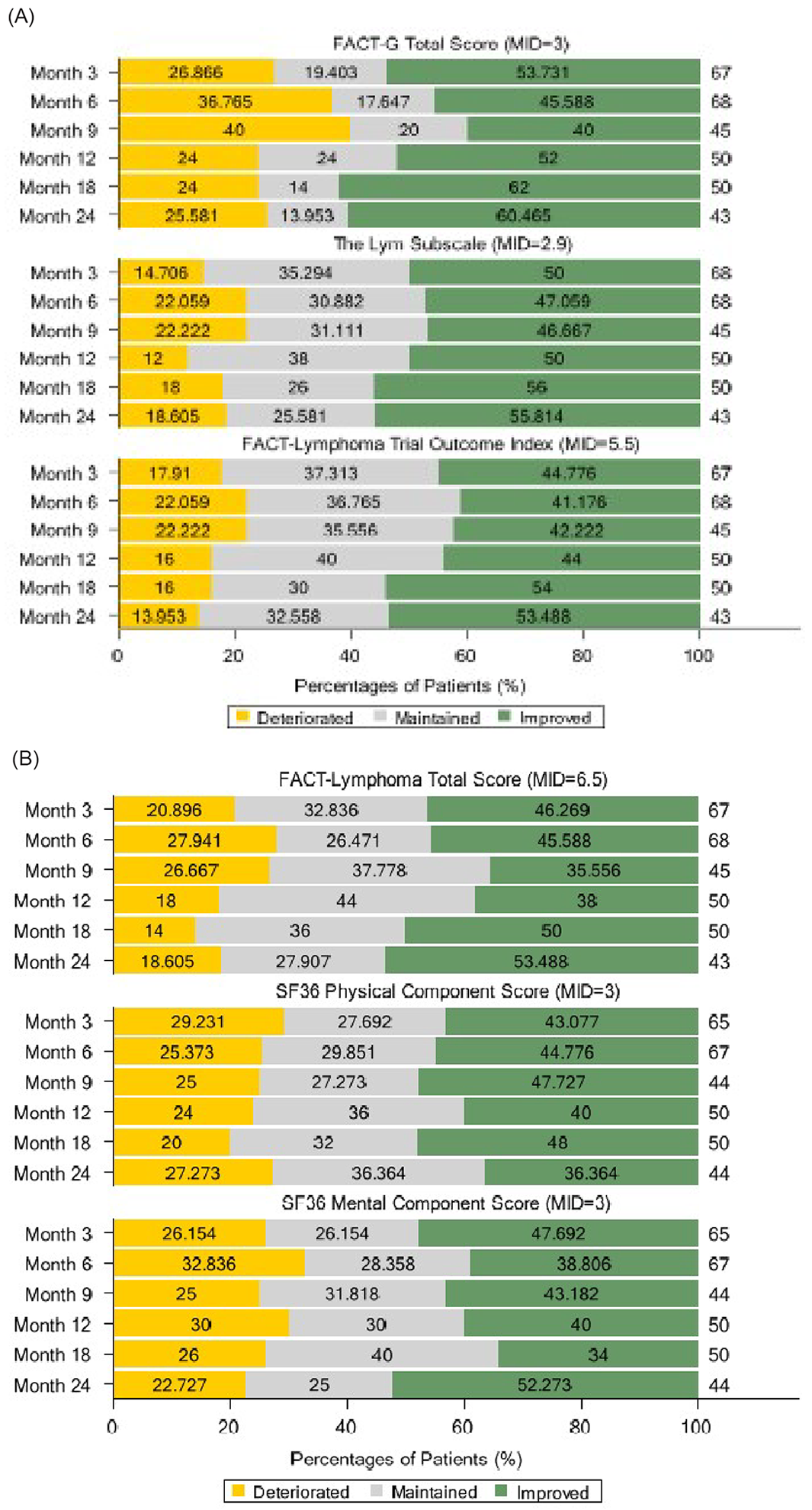
EAS = efficacy analysis set; FACT = Functional Assessment of Cancer Therapy; Lym = lymphoma; MID = minimally important differences; SF-36 = 36-Item Short Form Survey.
Source: ELARA Clinical Study Report.29
EQ-5D-3L Questionnaire
Results of the EQ-5D-3L VAS score showed that HRQoL was maintained from baseline after the tisagenlecleucel infusion. The mean EQ VAS score was 69.4 at baseline and increased to 72.5 at 6 months, 75.9 at 12 months, and 71.9 at 24 months (Table 19). The 24-month results were based on approximately half of the population at baseline.
Table 19: EQ VAS Score and Change From Baseline by Visit in the ELARA Trial (EAS)
Time point | Statistics | EQ VAS score |
|---|---|---|
Baseline | n | 76 |
Mean (SD) | 69.4 (20.97) | |
Median (minimum to maximum) | 74.5 (10 to 100) | |
Month 3 | n | 64 |
Mean (SD) | 75.5 (20.41) | |
Median (minimum to maximum) | 80.0 (8 to 100) | |
Month 3 change from baseline | n | 60 |
Mean (SD) | 3.4 (23.70) | |
Median (minimum to maximum) | 5.5 (–83 to 69) | |
Month 6 | n | 63 |
Mean (SD) | 72.5 (19.77) | |
Median (minimum to maximum) | 74.0 (21 to 100) | |
Month 6 change from baseline | n | 58 |
Mean (SD) | 3.7 (18.63) | |
Median (minimum to maximum) | 3.5 (–60 to 50) | |
Month 12 | n | 50 |
Mean (SD) | 75.9 (19.15) | |
Median (minimum to maximum) | 80.0 (19 to 100) | |
Month 12 change from baseline | n | 44 |
Mean (SD) | 5.8 (13.55) | |
Median (minimum to maximum) | 3.5 (–29 to 50) | |
Month 18 | n | 49 |
Mean (SD) | 76.5 (18.01) | |
Median (minimum to maximum) | 78.0 (25 to 100) | |
Month 18 change from baseline | n | 43 |
Mean (SD) | 6.8 (12.64) | |
Median (minimum to maximum) | 7.0 (–15 to 58) | |
Month 24 | n | 43 |
Mean (SD) | 71.9 (19.78) | |
Median (minimum to maximum) | 75.0 (19 to 100) | |
Month 24 change from baseline | n | 36 |
Mean (SD) | 3.8 (18.17) | |
Median (minimum to maximum) | 4.5 (–68 to 45) |
EAS = efficacy analysis set; VAS = visual analogue scale; SD = standard deviation.
Source: ELARA Clinical Study Report.29 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Harms
In the ELARA study, all safety outcomes were reported in the safety analysis set (i.e., all patients who received an infusion of tisagenlecleucel). After the one-time infusion of tisagenlecleucel, patients were followed for up to 24 months in the ELARA study. Refer to Table 20 for harms data.
Adverse Events
Of the 97 patients evaluable for safety, 99% experienced any-grade AEs.
The most common AEs reported in at least 15% of patients any time after the infusion were CRS (49.5%), neutropenia (43.3%), anemia (25.8%), diarrhea (25.8%), headache (23.7%), decreased white blood cell count (22.7%), pyrexia (18.6%), thrombocytopenia (18.6%), fatigue (17.5%), nausea (17.5%), decreased neutrophil count (17.5%), constipation (16.5%), and hypogammaglobulinemia (15.5%).
Serious Adverse Events
A total of 46.4% of patients experienced an SAE at any time after the infusion. The most commonly reported SAEs included CRS (19.6%), pneumonia (10.3%), and febrile neutropenia (8.2%).
Withdrawal Due to Adverse Events
Not applicable.
Mortality
There were 13 deaths (13.4% of patients) reported after the tisagenlecleucel infusion in the ELARA study; 7 patients died from the study indication (i.e., progression of the underlying disease) and 6 from other causes (AEs for 5 patients and euthanasia for 1 patient).
Notable Harms
In terms of AEs of special interest, more than 40% of patients experienced any-grade CRS (49.5%), hematological disorders that included cytopenias (78.4%), and infections (55.7%). Most patients experienced CRS (n = 47) within 8 weeks of the tisagenlecleucel infusion. All CRS events except 1 (fatal, grade 5) were of low-grade severity (grade 1 or 2).
Across hematological disorders that included cytopenias, at least 25% of patients reported neutropenia (43.3%) or anemia (25.8%). Overall, the majority of patients (74.2%) experienced hematological events of grade 3 or higher.
Infections occurring any time after the infusion were reported in 54 patients (55.7%), 16 of whom (16.5%) had infections suspected to be related to tisagenlecleucel. Most of the patients had either grade 1 or 2 infections, although infections of grade 3 or higher were reported in 21.6% of patients (9.0% of whom had AEs suspected to be related to tisagenlecleucel). Death due to infection (pneumonia) was reported in 1 patient.
Any-grade serious neurologic adverse reactions were reported in 12 patients (12.4%), 10 of whom experienced these events within 8 weeks of tisagenlecleucel infusion. Grade 3 or 4 AEs considered serious were reported in 3 patients (3.1%), 1 of whom recovered.
Table 20: Summary of Harms in the ELARA Study (Safety Analysis Set)
Event | Tisagenlecleucel (N = 97) |
|---|---|
Patients with at least 1 AE, n (%) | 96 (99.0) |
AEs with a frequency > 10%, n (%) | |
Cytokine release syndrome | 48 (49.5) |
Neutropenia | 42 (43.3) |
Anemia | 25 (25.8) |
Diarrhea | 25 (25.8) |
Headache | 23 (23.7) |
Decreased white blood cell count | 22 (22.7) |
Pyrexia | 18 (18.6) |
Thrombocytopenia | 18 (18.6) |
Fatigue | 17 (17.5) |
Nausea | 17 (17.5) |
Decreased neutrophil count | 17 (17.5) |
Constipation | 16 (16.5) |
Hypogammaglobulinemia | 15 (15.5) |
Febrile neutropenia | 14 (14.4) |
Cough | 12 (12.4) |
Arthralgia | 11 (11.3) |
Back pain | 11 (11.3) |
Pneumonia | 11 (11.3) |
Decreased lymphocyte count | 10 (10.3) |
Decreased platelet count | 10 (10.3) |
Any AE, grade ≥ 3, n (%) | 79 (81.4) |
Patients with at least 1 SAE, n (%) | 45 (46.4) |
Cytokine release syndrome | 19 (19.6) |
Pneumonia | 10 (10.3) |
Febrile neutropenia | 8 (8.2) |
Pyrexia | 3 (3.1) |
Acute respiratory failure | 2 (2.1) |
Basal cell carcinoma | 2 (2.1) |
COVID-19 | 2 (2.1) |
Encephalopathy | 2 (2.1) |
Neutropenia | 2 (2.1) |
Pleural effusion | 2 (2.1) |
Squamous cell carcinoma | 2 (2.1) |
Infusion-related reaction | 2 (2.1) |
Any SAE, grade ≥ 3, n (%) | 32 (33.0) |
Patients who stopped treatment due to AEs, n (%) | NA |
Deaths, n (%) | 13 (13.4) |
Study indication (disease progression) | 7 (7.2) |
Other reasons | 6 (6.2) |
Adverse event | 5 (5.2) |
bladder transitional cell carcinoma | 1 (1.0) |
cytokine release syndrome | 1 (1.0) |
metastatic squamous cell carcinoma | 1 (1.0) |
pneumonia | 1 (1.0) |
postprocedural complication | 1 (1.0) |
euthanasia | 1 (1.0) |
AEs of special interest, n (%) | N = 97 |
CRS, any grade | 48 (49.5) |
CRS, grade ≥ 3 | 1 (1.0) |
Serious neurologic AE, any grade | 12 (12.4) |
Serious neurologic AE, grade ≥ 3 | 3 (3.1) |
Hematological disorders, including cytopenias, any grade | 76 (78.4) |
Hematological disorders, including cytopenias, grade ≥ 3 | 72 (74.2) |
Infections, any grade | 54 (55.7) |
Infections, grade ≥ 3 | 21 (21.6) |
Prolonged depletion of normal B cells or agammaglobulinemia, any grade | 18 (18.6) |
Prolonged depletion of normal B cells or agammaglobulinemia, grade ≥ 3 | 1 (1.0) |
AE = adverse event; CRS = cytokine release syndrome; NA = not applicable; SAE = serious adverse event.
Source: ELARA Clinical Study Report.29 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Critical Appraisal
Internal Validity
The single-arm, noncomparative study design of the ELARA study is 1 of its key limitations. Interpreting the results of studies with this design is difficult because it may not be apparent whether the results are from the effect of the intervention, a placebo effect, or the effect of natural history. It is acknowledged that this study design has so far predominated in the evaluation of CAR T-cell therapies for advanced cancers across a variety of tumour types. It is also acknowledged that there may be practical limitations to conducting an RCT in patients with r/r FL (beyond first-line treatment), such as decreasing population size with subsequent lines of therapy and lack of a gold-standard treatment in these later lines of treatment. However, there is no clear rationale that makes an RCT infeasible, and a search of clinicaltrials.gov showed that patients are being recruited into phase III RCTs comparing a CAR T-cell product with SOC therapy in patients with r/r FL (after first-line therapy).82 Some of the limitations of the single-arm design in determining the benefits of tisagenlecleucel are mitigated by the following. First, the hypothesis testing for the primary outcome of CRR was established against the response rate derived from studies of available PI3K inhibitors for the treatment of r/r FL. The clinical experts consulted by CADTH confirmed that a CRR of 15% was a clinically relevant threshold, and noted that any treatment that achieves a 30% CRR in the third or later line of treatment is considered a good therapy. Second, the primary assessment of CRR was done by IRC and confirmed by investigator assessment, providing internal validation of the tumour response results. And third, given that patients enrolled in the study primarily had failed 3 or more lines of prior therapies for FL, the achieved clinically important CRR observed in the ELARA study is likely valid. However, the lack of a comparator makes it difficult to determine whether the magnitude of the treatment effect would be replicated in a larger comparative trial or in the real-world.
Another limitation of the ELARA study is the relatively small sample size and the selective study population. For example, patients were excluded if they had an ECOG PS of 2 or had received prior anti-CD19 therapy or prior allo-SCT. Ninety-eight patients were enrolled, and 94 received treatment with tisagenlecleucel and were included in the primary analyses. The small sample size could restrict data interpretation, particularly for subgroup analyses, although the method of sample size and power calculation was justified. In addition, the statistical analyses for efficacy were based on the EAS population, which excluded patients who were enrolled and underwent apheresis but were subsequently unable to receive tisagenlecleucel. This approach is not aligned with the intention-to-treat principle, nor does it reflect the expected clinical practice population. This would potentially overestimate the benefit of tisagenlecleucel. However, because 94 of 98 enrolled patients were included in the EAS population, the impacts on the validity of the results from this analysis approach are minimal.
Follow-up time was likely sufficient for assessing tumour response and safety outcomes associated with tisagenlecleucel in general. However, median OS and median PFS were not reached at the 24-month follow-up, nor was the corresponding upper limit of the 95% CI, suggesting that the follow-up duration was not long enough to fully capture the effects on OS and PFS, so these results are considered immature. In addition to the duration of the study and the noncomparative design, subsequent treatments make it difficult to interpret the OS and PFS results. After the infusion of tisagenlecleucel, 23% of the patients received at least 1 subsequent antineoplastic medication and 4% received an allo-SCT. The survival results (OS, PFS) should be considered in the context of subsequent treatments because it may be difficult to tell which treatment had more of an impact on a patient’s survival, especially when there was a lack of comparative data in the ELARA study.
The ELARA trial was open-label, which can result in a bias in the measurement of subjectively assessed outcomes such as response, PFS, HRQoL, and AEs. As noted previously, response rates were assessed by IRC in addition to the investigators, which likely reduced the risk of bias in these outcome measures. As well, the tumour response results were consistent across the various assessment methods. PROs and HRQoL results are at risk of performance and detection bias related to the lack of patient and investigator blinding, although the extent and direction of the bias are uncertain.
The study presented PRO and HRQoL data up to 24 months; however, there is a risk of attrition bias and drawing conclusions on a select population because the analyses at 24 months were based on half of the study population from baseline and the results could be biased in favour of tisagenlecleucel.
External Validity
According to the clinical experts consulted by CADTH, the population of the ELARA study generally represents patients in Canada with r/r FL who would be receiving tisagenlecleucel. However, the clinical experts noted that patients seen in clinical practice would include those with poorer performance status (the ELARA study only included patients with an ECOG PS 0 or 1), those who received prior CD19-targeted therapy, and those who have more comorbidities. After screening, the procedures and cointerventions (including manufacturing process, depleting chemotherapy, bridging therapy, and posttisagenlecleucel interventions) were consistent with those adopted in the Canadian setting, although some discrepancies exist, per the clinical experts. The results of the ELARA study can be generalized to the patient population in Canada.
According to the clinical experts consulted by CADTH, the efficacy outcomes used in this study are clinically relevant and important for clinical trials of patients with r/r FL. Because ELARA was an open-label trial, all patients knew about the treatment that they received. This would have some impact on PROs such as HRQoL, but would be less likely to affect objective outcomes such as survival and response rates.
In addition, lack of long-term data on patient survival and response rates is another limitation, given that FL is an indolent and slowly progressive disease. Clinical benefits of the treatment, especially survival benefits and improvement in HRQoL, need to be evaluated in the longer term.
Long-Term Extension Studies
There are no long-term extension studies submitted by the sponsor for this review.
Other Relevant Evidence
This section includes additional relevant studies that were included in the sponsor’s submission to CADTH and were considered to address important gaps in the evidence included in the Systematic Review.
Results of 2 non-RCTs that may have addressed evidence gaps are presented in the Studies Addressing Gaps in the Pivotal and RCT Evidence section.
Indirect Evidence
The contents of this section have been informed by materials submitted by the sponsor. The following information has been summarized and validated by the CADTH review team.
Objectives for the Summary of Indirect Evidence
The objective of this section is to summarize and critically appraise available indirect evidence comparing tisagenlecleucel to other relevant treatments for r/r FL after 2 or more lines of therapy relevant to the Canadian clinical practice setting.
Description of Indirect Comparison
The efficacy and safety of tisagenlecleucel has been previously assessed in the ELARA study,29 whereas its efficacy against standard chemotherapy was compared in the ReCORD-FL study.32 However, no head-to-head comparison of tisagenlecleucel against other advanced treatments for r/r FL after 2 or more lines of therapy was available for this review. Due to this gap in evidence, 1 sponsor-conducted ITC in the form of a MAIC of tisagenlecleucel versus axicabtagene ciloleucel was reviewed.31
Study Selection Method
Study selection criteria and key aspects of the methods used for the systematic review are summarized in Table 21.
Based on the prespecified eligibility criteria detailed in Table 21, the sponsor conducted a systematic literature search of clinical trials and observational studies to identify relevant comparators approved for the treatment of adults with r/r FL after 2 or more lines of therapy. The literature search included all studies published between 1998 and June 2022, based on the approval of rituximab in November 1997 (US) and June 1998 (EU) for FL. However, only studies published from 2014 onward, coinciding with the introduction of the new Lugano response criteria, were considered for inclusion.59,83 Systematic literature searches were conducted of multiple electronic databases, including MEDLINE, Embase, the Cochrane Central Register of Controlled Trials, and the Cochrane Database of Systematic Reviews. In addition, abstracts from 5 relevant conference proceedings from 2019 to 2022 were hand-searched, and the reference lists of previously published systematic reviews and meta-analyses were screened.
The study screening, selection, and data extraction were conducted by 2 independent reviewers. Studies identified from the systematic literature search were first screened based on the title and abstract. A full-text screening was then carried out for studies selected at the title and abstract screening stage. A third reviewer was involved to resolve any discrepancies during the title, abstract, and full-text review. A list of excluded studies was reported, with reasons for exclusion. Two independent reviewers extracted data and assessed the risk of bias of the included studies using the National Institute for Health and Care Excellence and the Downs and Back checklist to determine the quality of reporting of RCTs and nonrandomized trials, respectively.84,85
Table 21: Study Selection Criteria and Methods for ITCs Submitted by the Sponsor
Characteristics | Indirect comparison |
|---|---|
Population | Adults 18 years and older with confirmed diagnosis of r/r FL |
Intervention | Tisagenlecleucel |
Comparator |
|
Outcome |
|
Study designs | The following phase II or phase III study designs were eligible for inclusion:
|
Publication characteristics |
|
Inclusion criteria | For inclusion in the overall SLR evidence, the study must have the following information available for abstraction:
For selection of historic controls, studies must have the following available for abstraction:
|
Exclusion criteria |
For selection of historic controls:
|
Databases searched | The following key biomedical database were searched from January 1998 to June 2022:
In addition to these databases, abstracts from 5 relevant conference proceedings were hand-searched for the previous 3 years (2019 to 2022). Furthermore, bibliographic screening of previously published SLRs and meta-analyses was conducted to identify any data gaps |
Selection process | All the records retrieved from the literature search (using a multistring search strategy) were screened based on the abstract supplied with each citation. Each citation was screened by 2 independent reviewers, and any discrepancies between reviewers were reconciled by a third independent reviewer. Citations that did not match the eligibility criteria were excluded at this first-level screening; where unclear, citations were included. Duplicates of citations (due to overlap in the coverage of databases) were also excluded at the abstract screening stage. Full-text copies of all references that could potentially meet the eligibility criteria were downloaded. The eligibility criteria were applied to the full-text citations. Each full text article was screened by 2 independent reviewers, and any discrepancies between reviewers reconciled by a third independent reviewer. |
Data extraction process | Data presented in the studies still included after this stage were extracted to data extraction grids. Where more than 1 publication describing a single trial was identified, the data were compiled into a single entry in the data extraction grid. Each publication was referenced in the data extraction grid to recognize that more than 1 publication may have contributed to the entry. Data from included studies were extracted in parallel by 2 independent reviewers, with reconciliation of any differences by a third independent reviewer. |
Quality assessment | Assessment of the quality of reporting of the included evidence was carried out using the following checklists:
|
Auto-SCT = autologous stem cell transplant; CDSR = Cochrane Database of Systematic Reviews; CENTRAL = Cochrane Central Register of Controlled Trials; CR = complete response; CRR = complete response rate; EU = European Union; FL = follicular lymphoma; FLIPI = Follicular Lymphoma International Prognostic Index; ITC = indirect treatment comparison; NHL = non-Hodgkin lymphoma; NICE = National Institute for Health and Care Excellence; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; PR = partial response; RCT = randomized controlled trial; r/r = relapsed/refractory; SCT = stem cell transplant; SLR = systematic literature review.
Source: Clinical Study Report for sponsor-submitted MAIC.31 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Objectives
The objective of the sponsor-submitted MAIC was to compare the efficacy and safety of tisagenlecleucel to axicabtagene ciloleucel in patients with r/r FL after 2 or more lines of therapy. Of note, axicabtagene ciloleucel received a NOC/c from Health Canada for the treatment of adults with r/r grade 1, 2, or 3a FL after 2 or more lines of systemic therapy on September 29, 2022,86 and to date has not been reviewed by the CADTH pan-Canadian Oncology Drug Review Expert Review Committee for this patient population. The MAIC was reviewed by a CADTH clinical team because it was used to inform the sponsor's pharmacoeconomic model.
Study Selection Methods
A total of 4,865 records were screened by abstract, followed by a full-text screening of 1,133 articles. Of these, 132 unique studies published between January 1998 and June 2022 were extracted for clinical review. To be eligible for inclusion in the ITC, the population, outcomes, and the study design of studies identified from the systematic literature review were required to be aligned with those of the ELARA trial conducted by the sponsor. Moreover, comparators were only considered relevant if they had been reviewed to be approved or recommended interventions and met the following parameters:
comparator treatments were regulatory approved regimens or recommended as treatments by evidence-based clinical guidelines
studies included a sample size of more than 30 patients
studies reported data for PFS (e.g., median or rate).
Using those parameters, 42 of the 132 studies were considered for inclusion in the ITC. Of these, 14 studies were conducted as clinical trials (9 single-arm trials, 3 RCTs, and 2 non-RCTs) and 28 were observational studies. The interventions assessed across these studies included Pi3K inhibitors (idelalisib, copanlisib, duvelisib), CAR T-cell therapies (axicabtagene ciloleucel; tisagenlecleucel), R2, mosunetuzumab, tazemetostat, rituximab and/or chemotherapy, SOC in general, and stem cells transplants (auto-SCT or allo-SCT).
These 42 studies were then assessed to determine if diagnosis, clinical management, and response criteria assessment were similar to those applied in the ELARA trial. As a result, 12 studies were excluded due to a publication date before the introduction of the new 2014 Lugano response criteria. After applying the study selection criteria and key aspects of the methods for the systematic review summarized in Table 21, 8 studies were considered to be potential comparator studies: 4 that assessed PI3K inhibitors (2 assessed idelalisib, 1 assessed copanlisib, and 1 assessed duvelisib),80,87-89 and 1 each assessed CAR T-cell therapy (axicabtagene ciloleucel),90 mosunetuzumab,91 salvage therapy after auto-SCT relapse,92 and SOC.93 Interventions that were considered not to be relevant to the Canadian clinical setting were excluded. For example, idelalisib, although indicated for the treatment of patients with r/r FL in Canada, is not publicly reimbursed across Canada and is inaccessible at some sites, according to input the sponsor received from several clinicians.57 Furthermore, copanlisib, duvelisib, and mosunetuzumab are not currently commercialized for treatment of FL in Canada.
The sponsor determined that axicabtagene ciloleucel was the only advanced therapy relevant to the Canadian clinical context. Accordingly, 1 study met the criteria as a comparator treatment to tisagenlecleucel for inclusion in the ITC: ZUMA-5.94
MAIC Analysis Methods
A summary of the methods of analysis for the MAIC is presented in Table 23. An unanchored MAIC approach was selected for the indirect comparison between tisagenlecleucel and axicabtagene ciloleucel due to a lack of common comparator.31 Individual patient-level data from the ELARA study (data cut-off date of March 29, 2022) and aggregated data from the ZUMA-5 study (axicabtagene ciloleucel; data cut-off date of March 31, 2021) were used.29,61,94
The covariates used for match-adjustment were informed by clinical experts consulted by the sponsor and against European Medicines Agency (EMA) recommendation based on importance. Relevant baseline prognostic factors were included in the MAIC if they were commonly and consistently reported in both the ELARA and ZUMA-5 studies. The prognostic factors considered and included in the propensity score model are detailed in Table 22. The covariates included in the MAIC were age (≥ 65 years versus < 65 years); sex (male versus female); race (white versus nonwhite [from original source]); ECOG PS (> 1 versus 1); Ann Arbor stage (IV versus III versus I to II); FLIPI score (≥ 3 versus 2 versus 0 to 1); high tumour bulk per Groupe d'Etude des Lymphomes Folliculaires (GELF) criteria (yes versus no); prior line of therapy (≥ 3 versus < 3); refractory to most recent regimen (yes versus no); POD24 from first anti-CD20 mAb-containing therapy; and prior auto-SCT.
Table 22: Prognostic Factors of Efficacy Outcomes in Patients With r/r FL Considered and Included in the MAIC of Tisagenlecleucel vs. Axicabtagene Ciloleucel
Prognostic factors | Input from clinical experts | EMA recommendations | Inclusion in ITC |
|---|---|---|---|
Demographic | |||
Agea | Important | Recommended | Included |
Sexa | Not important | Recommended | Included |
Racea | Not important | Recommended | Included |
Region | Not important | Recommended as a supplementary factor when race is not available | Excludedb |
Disease stage and tumour size | |||
Histological transformation | Very important | Not evaluated | Excludedc |
FL grade | Not important | Not evaluated | Excludedd |
Ann Arbor stagea | Not important | Recommended | Included |
Bulky massa | Less important | Not evaluated | Included |
Lesion size | Not important | Not evaluated | Excludedd |
Nodal size involvement | Not important | Recommended | Excludedd |
Marrow involvement | Not important | Not evaluated | Excludedd |
Performance statusa | Important | Recommended | Included |
Lab measures, symptoms, comorbidities | |||
Elevated LDH | Important | Recommended on the overall category, but no details on individual variables | Excludedd |
Hemoglobin | Not important | Excludedd | |
Hepatic dysfunction | Not important | Excludedd | |
Lymphoma symptoms | Less important | Excludedd | |
Other disease characteristics | |||
FLIPI scorea | Very important | Recommended | Included |
Time since diagnosis | Not evaluated | Recommended | Excludedd |
Prior treatment history | |||
Number of prior treatmentsa | Important | Recommended | Included |
Prior rituximab | Not important | Not evaluated | Excludedd |
Prior fludarabine | Not important | Not evaluated | Excludedd |
Prior bendamustine | Not important | Not evaluated | Excludedd |
Prior anthracycline | Not important | Not evaluated | Excludedd |
Prior auto-SCTa | Not important | Recommended | Included |
Relapsed/refractory status to systemic therapies | |||
POD24a | Important | Recommended | Included |
Relapsed or refractory to last treatment (0.5 years)a | Very important | Recommended on the overall category, but no details on individual variables | Included |
Disease refractory to 2 or more regimens | Not evaluated | Excludedd | |
Double refractory | Not evaluated | Excludede | |
Chemoresistant | Very important | Excludedd | |
Measures specific to CAR T cells | |||
Lymphodepleting regimen | Not important | Not evaluated | Excludedd |
Bridging chemotherapya | Not evaluated | Not evaluated | Included |
Auto-SCT = autologous stem cell transplant; CAR = chimeric antigen receptor; EMA = European Medicines Agency; FL = follicular lymphoma; FLIPI = follicular lymphoma international prognostic index; ITC = indirect treatment comparison; LDH = lactate dehydrogenase; MAIC = matching-adjusted indirect treatment comparison; POD24 = progression of disease within 24 months of first line of treatment; r/r = relapsed or refractory; vs. = versus.
aCovariates included in the MAIC were age (≥ 65 years vs. < 65 years); sex (male vs female); race (white vs. nonwhite [from original source]); ECOG PS (> 1 vs. 1); Ann Arbor stage (IV vs. III vs. I to II); FLIPI score (≥ 3 vs. 2 vs. 0 to 1); high tumour bulk per GELF criteria (yes vs. no); prior lines of therapy (≥ 3 vs < 3); refractory to most recent regimen (yes vs. no); POD24 from first anti-CD20 mAb-containing therapy; and prior auto-SCT.
bRegion was excluded because race was included in the MAIC.
cInclusion criteria for both the ELARA and ZUMA-5 studies.
dNo data available in the ZUMA-5 publication.
eDefinition of double refractory unavailable in the ZUMA-5 publication.
Source: Clinical Study Report for sponsor-submitted MAIC.31 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Baseline characteristics in the ELARA and ZUMA-5 studies were balanced by assigning weights to selected ELARA patients, such that:
weighted mean baseline characteristics in the selected ELARA patients exactly matched those reported for patients in the ZUMA-5 study
each individual patient weight was equal to the patient’s estimated odds (relative propensity) of being in the ZUMA-5 study versus the ELARA study, given the patient’s baseline characteristics.
Weights were determined from a logistic regression model for the propensity of inclusion in the ZUMA-5 versus ELARA study, with all matched-on-baseline characteristics included as independent variables in the model. Because only summary statistics for baseline characteristics were available for the ZUMA-5 study, the logistic model was estimated using the methods of moments approach as opposed to the maximum likelihood approach.95-97 Baseline characteristics between the ELARA infused set nonbridging chemotherapy subgroup and the ZUMA-5 infused set after matching were compared using the Wald test.
Weighted ORR and CRR were calculated for the ELARA efficacy-evaluable set nonbridging chemotherapy subgroup using the same weights that were applied to match average baseline characteristics. Wald tests were used to compared ORR and CRR efficacy results between the ELARA and ZUMA-5 studies after matching.
Weighted median PFS, weighted median OS, and corresponding 95% Cis were calculated using the Nelson-Aalen estimator for the ELARA efficacy-evaluable set nonbridging subgroup, incorporating the same weights used to match baseline characteristics. The PFS and OS curves for the ZUMA-5 study were reconstructed using the Guyot method. A weighted long-rank test was performed for the comparison of the survival curves; the curve was unweighted for the ZUMA-5 study and weighted for the ELARA study. The HR and corresponding 95% CI were estimated using a weighted Cox proportional hazard model after matching.
The following safety outcomes were assessed in the MAIC: CRS, tocilizumab and corticosteroid use for CRS management, and neurologic events. Weighted CRS, tocilizumab and corticosteroid use for CRS management, and neurologic events were calculated for the ELARA infused set nonbridging chemotherapy subgroup, incorporating the same weights used to match baseline characteristics. Wald tests were used to compare safety outcomes in the ELARA and ZUMA-5 studies after matching.
Weights were only applied to ELARA patients for whom individual patient data were available; weighting did not impact the efficacy or safety outcomes reported for the ZUMA-5 efficacy-evaluable and ZUMA-5 infused sets, respectively, which were based on published aggregate data.
Table 23: MAIC Analysis Methods for Tisagenlecleucel vs. Axicabtagene Ciloleucel
Methods | Description |
|---|---|
Analysis methods | MAIC |
Patient data | Individual patient-level data from the ELARA study for tisagenlecleucel and aggregated patient characteristics data from the ZUMA-5 study for axicabtagene ciloleucel |
Covariates identified as important by clinical experts consulted by sponsor or based on EMA recommendation | Very important or recommended:
Important or recommended:
Less important or recommended:
Not important or recommended:
Not evaluated or recommended:
|
Outcomes | ORR CRR OS PFS |
Safety | CRS Tocilizumab and corticosteroid use for CRS management Neurologic events |
Sensitivity analysis | All infused patients in the ELARA study with and without nonbridging chemotherapy matched with the ZUMA-5 infused set |
Subgroup analysis | With vs. without bridging therapy |
Auto-SCT = autologous stem cell transplant; CRR = complete response rate; CRS = cytokine release syndrome; FL = follicular lymphoma; FLIPI = Follicular Lymphoma International Prognostic Index; LDH = lactate dehydrogenase; MAIC = matching-adjusted indirect treatment comparison; ORR = overall response rate; OS = overall survival; POD24 = progression of disease within 24 months of first-line of treatment; vs. = versus.
aCovariates included in MAIC.
Source: Clinical Study Report for sponsor-submitted MAIC.31 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Summary of Included Studies
The sponsor-submitted MAIC included 2 single-arm, open-label, multicentre phase II trials: ELARA and ZUMA-5. The ITC included individual patient-level data for nonbridging chemotherapy patients who received tisagenlecleucel in the ELARA study (n = 53) and aggregated data with patients who received axicabtagene ciloleucel in the ZUMA-5 study (n = 124).
A detailed description of the ELARA study is provided in the Pivotal Studies and RCT Evidence section of this clinical report. Briefly, patients were enrolled if they had r/r disease after at least 2 lines of systemic therapy or during or within 6 months of anti-CD20 mAb maintenance, or if they relapsed after auto-SCT. Optional bridging chemotherapy before tisagenlecleucel infusion was allowed. Patients received fludarabine-based or bendamustine-based LD chemotherapy before tisagenlecleucel infusion. The primary efficacy end point in the ELARA study was CRR assessed by a central IRC. ORR, PFS, OS, and safety outcomes were evaluated in the ELARA study as secondary end points. As of the March 29, 2022, data cut-off date, a total of 98 patients were enrolled and, among them, 97 patients were infused with tisagenlecleucel. The following patient sets from the ELARA study were used in the comparison of tisagenlecleucel with axicabtagene ciloleucel for the primary analysis:
the ELARA infused set nonbridging chemotherapy subgroup (n = 53), which included patients who had received tisagenlecleucel infusion in the ELARA trial who did not receive bridging chemotherapy. This cohort was used for matching with axicabtagene ciloleucel on baseline characteristics and comparing safety outcomes.
the ELARA efficacy-evaluable set nonbridging chemotherapy subgroup (n = 52), which included patients who had received tisagenlecleucel infusion in ELARA trial who did not receive bridging chemotherapy and who had measurable disease at baseline per IRC. This cohort was used for comparing efficacy outcomes.
ZUMA-5 is an ongoing pivotal single-arm, open-label, multicentre, phase II study aimed to assess the efficacy and safety of axicabtagene ciloleucel in adults with r/r indolent NHL, including FL and marginal zone lymphoma. Patients were enrolled if they had r/r disease after at least 2 lines of treatment with combination chemoimmunotherapy, which must have included an anti-CD20 mAb-containing therapy combined with an alkylating drug. Patients underwent leukapheresis and received conditioning chemotherapy (cyclophosphamide at 500 mg/m2 per day and fludarabine at 30 mg/m2 per day on days −5, −4, and −3) followed by a single infusion of axicabtagene ciloleucel (2 × 106 CAR T cells per kg) on day 0. Bridging chemotherapy before axicabtagene ciloleucel infusion was used in 2 (1.6%) of 124 infused patients as of the March 12, 2020, data cut-off date. Patients received LD chemotherapy with fludarabine and cyclophosphamide before axicabtagene ciloleucel infusion. The primary efficacy end point in the ZUMA-5 study was ORR assessed by a central IRC. CRR, PFS, OS, and safety outcomes were evaluated in the ZUMA-5 study as secondary end points. Aggregate data for baseline characteristics were obtained directly from the ZUMA-5 publication,94 and aggregate data for efficacy and safety outcomes were obtained directly from the American Society of Hematology 2021 ZUMA-5 publication.98 As of the March 31, 2021, data cut-off, a total of 157 patients with r/r indolent NHL were enrolled. Among the 149 infused patients, 124 (83.2%) patients had r/r FL. The following patient sets from the ZUMA-5 study were used in the primary comparison with ELARA patients:
the ZUMA-5 infused set (n = 124), which included axicabtagene ciloleucel–infused patients with r/r FL. This cohort was used as the reference for ELARA patients to match to, and for comparing safety outcomes.
The ZUMA-5 efficacy-evaluable set (n = 86), which included axicabtagene ciloleucel–infused patients with r/r FL who had at least 24 months of follow-up. This cohort was used for comparing efficacy outcomes.
Fifty-three infused, nonchemotherapy bridging patients from the ELARA study were matched with 124 infused patients in the ZUMA study. Baseline characteristics of patients in the ELARA and ZUMA-5 studies before and after matching are summarized in Table 24. After matching, all matched-on-baseline characteristics were balanced in the ELARA and ZUMA- 5 studies. Patients included in the MAIC were mainly younger than 65 years (69.4%), male (59.9%), and white (92.7%). In regard to disease severity at baseline, 37.1% of patients had an ECOG PS of 1; 36.3% and 49.2% were assessed as having stage III and stage IV disease, respectively, on the Ann Arbor staging system; 38.7% and 43.6% had a FLIPI score of 2 and 3 or greater, respectively; and 51.6% were classified as having high tumour bulk based on the GELF criteria. Regarding prior therapies, 62.9% of a patients had 3 or more lines of prior therapy and 24.2% had prior auto-SCT. Overall, 67.7% of patients were refractory to their most recent regimen and 54.8% were POD24 from first anti-CD20 mAb-containing therapy.
Table 24: Patient Characteristics of the ELARA Nonbridging Chemotherapy Subgroup and the Zuma-5 Infused Set
Baseline characteristics | Before matching | After matching | ||
|---|---|---|---|---|
ELARA (N = 53) | ZUMA-5 (N = 124) | ELARA (N = 53) | ZUMA-5 (N = 124) | |
Age, years | ||||
≥ 65 years, n (%) | 14 (26.42) | 38 (30.65) | NE (30.65) | NE (30.65) |
Sex, n (%) | ||||
Male | 33 (62.26) | 73 (58.87) | NE (58.87) | NE (58.87) |
Race, n (%) | ||||
White | 49 (92.45) | 115 (92.74) | NE (92.74) | NE (92.74) |
ECOG PS, n (%) | ||||
1 | 18 (33.96) | 46 (37.10) | NE (37.10) | NE (37.10) |
Anne Arbor stage, n (%) | ||||
III | 15 (28.30) | 45 (36.29) | NE (36.29) | NE (36.29) |
IV | 26 (49.06) | 61 (49.19) | NE (49.19) | NE (49.19) |
FLIPI score (%) | ||||
2a | 11 (20.75) | 48 (38.71) | NE (38.71) | NE (38.71) |
≥ 3 | 26 (49.06) | 54 (43.55) | NE (43.55) | NE (43.55) |
GELF criteria, n (%) | ||||
High tumour bulk | 30 (56.60) | 64 (51.61) | NE (51.61) | NE (51.61) |
Prior therapies | ||||
≥ 3 prior lines of therapies, n (%)a | 44 (83.02) | 78 (62.90) | NE (62.90) | NE (62.90) |
Prior auto-SCT, n (%) | 19 (35.85) | 30 (24.19) | NE (24.19) | NE (24.19) |
Response to prior therapies, n (%) | ||||
POD24 from first anti-CD20 mAb-containing therapy | 34 (64.15) | 68 (54.84) | NE (54.84) | NE (54.84) |
Refractory to most recent regimen | 38 (71.70) | 84 (67.74) | NE (67.74) | NE (67.74) |
Auto-SCT = autologous stem cell transplant; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FLIPI = Follicular Lymphoma International Prognostic Index; GELF = Groupe d’Etude des Lymphomes Folliculaires; mAb = monoclonal antibody; NE = not estimable; POD24 = progression of disease within 24 months of first-line of treatment.
aDenotes P value < 0.05. P values were calculated using the Wald test.
Source: Clinical Study Report for sponsor-submitted MAIC.31 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Results
The MAIC analysis compared 52 ELARA efficacy-evaluable nonbridging chemotherapy patients to 86 patients in the ZUMA-5 efficacy-evaluable set. After-matching efficacy results are presented.
Treatment Response
Comparisons of ORR and CRR between the ELARA nonbridging chemotherapy subgroup and the ZUMA-5 study are summarized in Table 25.
The ORR was 91.2% (95% CI, 76.2% to 97.1%) and 94.2% (95% CI, 87.0% to 98.1%) for patients in the ELARA and ZUMA-5 studies, respectively. The ORR difference between the ELARA and ZUMA-5 studies was –3.03 (95% CI, –13.7% to 7.6%). The CRR was 74.0% (95% CI, 54.4% to 8.2%) and 79.1% (95% CI, 69.0% to 8.1%) for patients in the ELARA and ZUMA-5 studies, respectively. The CRR difference between the ELARA and ZUMA-5 studies was –5.0% (95% CI, –23.9% to 13.8%).
Sensitivity analyses comparing ORR and CRR between the ELARA infused set that included those with and without nonbridging chemotherapy and the ZUMA-5 study were consistent to the primary MAIC analysis.
Table 25: Comparisons of ORR and CRR Between the ELARA Efficacy-Evaluable Nonbridging Chemotherapy Subgroup and the ZUMA-5 Efficacy-Evaluable Set After Matching
Response | ELARA (N = 52) | ZUMA-5 (N = 86) |
|---|---|---|
ORR, % (95% CI) | ||
Rate | 91.16 (76.21 to 97.07) | 94.19 (86.95 to 98.09) |
Response difference | –3.03 (–13.67 to 7.61) | Reference |
P valuea | 0.58 | — |
CRR, % (95% CI) | ||
Rate | 74.04 (54.41 to 87.21) | 79.07 (68.95 to 87.10) |
Response difference | –5.03 (–23.85 to 13.80) | Reference |
P valuea | 0.60 | — |
CI = confidence interval; CRR = complete response rate; ORR = overall response rate.
aP values were calculated using the Wald test.
Source: Clinical Study Report for sponsor-submitted MAIC.31 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Overall Survival
KM curves comparing PFS in the ELARA to ZUMA-5 studies are presented in Figure 3.
Median OS was not estimated for either the ELARA study or the ZUMA-5 study. The hazard of death for tisagenlecleucel compared to axicabtagene ciloleucel was 0.49 (95% CI, 0.16 to 1.49; P = 0.21).
Sensitivity analysis of OS between the ELARA infused set that included those with and without nonbridging chemotherapy and the ZUMA-5 study documented an HR of 0.34 (95% CI, 0.14 to 0.84).
Progression-Free Survival
KM curves comparing PFS in the ELARA to ZUMA-5 studies are presented in Figure 4.
Median time of PFS was 36.6 months (95% CI, 25.7 to 29.6 months) for in the ZUMA-5 study. Median PFS was not estimated for tisagenlecleucel. The hazard of disease progression or death for tisagenlecleucel compared to axicabtagene ciloleucel was 0.84 (95% CI, 0.37 to 1.90).
Sensitivity analysis of PFS between the ELARA infused set that included patients with and without nonbridging and the ZUMA-5 study noted an HR of 1.17 (95% CI, 0.63 to 2.18).
Figure 3: KM Curves and HRs for OS Comparing the ELARA Efficacy-Evaluable Set Nonbridging Chemotherapy Subgroup and the ZUMA-5 Efficacy-Evaluable Set After Matching
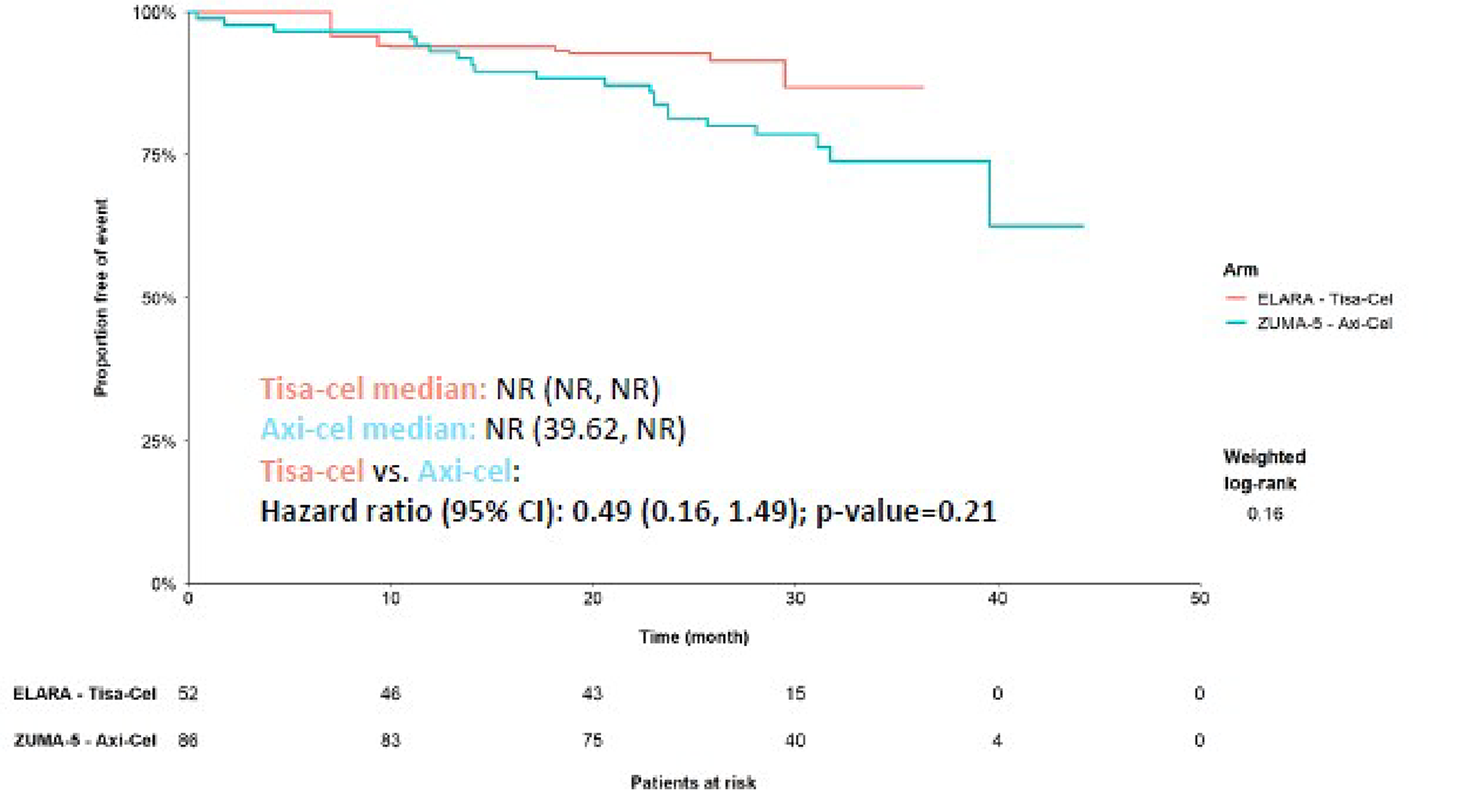
Axi-cel = axicabtagene ciloleucel; CI = confidence interval; HR = hazard ratio; KM = Kaplan-Meier; NR = not reported; OS = overall survival; Tisa-cel = tisagenlecleucel.
Note: The OS curve for the ZUMA-5 trial was reconstructed using the Guyot method. The median OS and 95% CI were estimated using the Nelson-Aalen estimator and log transformation.
Source: Clinical Study Report for sponsor-submitted MAIC.31
Figure 4: KM Curves and HRs of PFS Comparing the ELARA Efficacy-Evaluable Set Nonbridging Chemotherapy Subgroup and the ZUMA-5 Efficacy-Evaluable Set After Matching
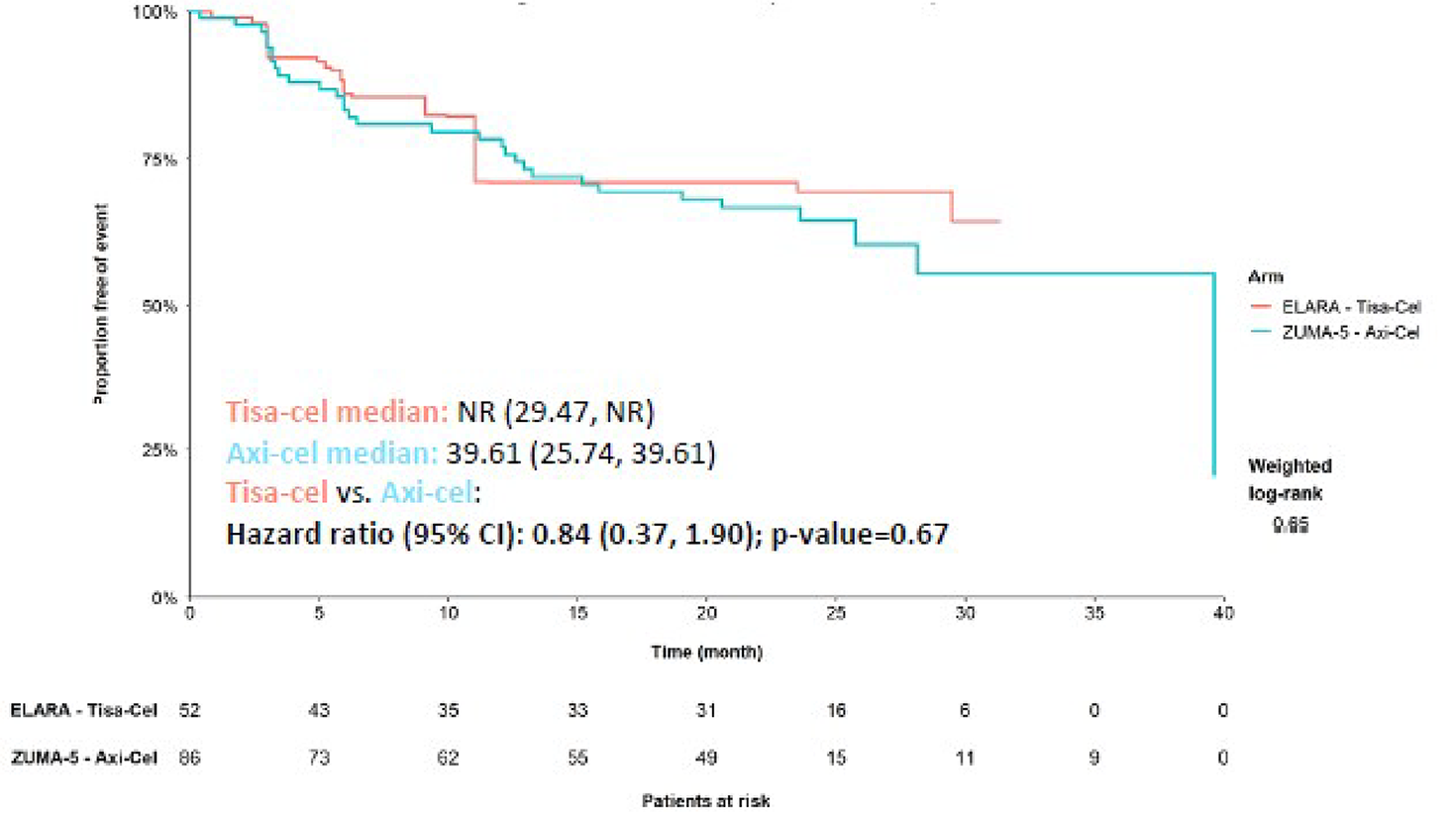
Axi-cel = axicabtagene ciloleucel; CI = confidence interval; HR = hazard ratio; KM = Kaplan-Meier; NR = not reported; PFS = progression-free survival; Tisa-cel = tisagenlecleucel.
Note: The PFS curve for the ZUMA-5 trial was reconstructed using the Guyot method. The median PFS and 95% CI were estimated using the Nelson-Aalen estimator and log transformation.
Source: Clinical Study Report for sponsor-submitted MAIC.31
Harms
Fifty-three ELARA infused nonbridging chemotherapy patients and 124 patients in the ZUMA-5 infused set were included in the MAIC of safety outcome. Harms outcomes in the ELARA infused set nonbridging chemotherapy subgroup and the ZUMA-5 study after matching are summarized in Table 26.
At least 1 AE of any grade was reported in 44.6% of patients in the ELARA study and 78.2% of patients in the ZUMA-5 study, for a response difference of –33.7% (95% CI, –54.0% to –13.3%). AEs of grade 3 or above were reported in no patients in the ELARA study and in 6.5% of patients in the ZUMA-5 study, for a response difference of –6.4% (95% CI, –10.8% to –2.1%).
The management of CRS with corticosteroids was documented in 3.0% of patients in the ELARA study and 15.3% in the ZUMA-5 study, for a response difference of –12.3% (95% CI, –21.0% to –3.6%). CRS management with tocilizumab was documented in 9.9% of patients in the ELARA study and 45.2% of patients in the ZUMA-5 study, for a response difference of –35.3% (95% CI, –47.8% to –22.7%).
Neurologic events of any grade were documented in 9.5% of patients in the ELARA study and 56.5% of patients in the ZUMA-5 study, for a response difference of –47.0% (95% CI, –61.9 to –32.1). Neurologic events of grade 3 and above were reported among 0.19% of patients in the ELARA study and 15.3% of patients in the ZUMA-5 study, for a response difference of –15.1% (95% CI, –21.5% to –8.8%).
Sensitivity analysis comparing safety outcomes between the ELARA infused set that included patients with and without nonbridging chemotherapy and the ZUMA-5 study were consistent with the primary MAIC analysis.
Table 26: Comparison of Safety Outcomes Between the ELARA Infused Set Nonbridging Chemotherapy Subgroup and the ZUMA-5 Infused Set After Matching
Outcome | ELARA infused set (N = 53) | ZUMA-5 infused set (N = 124) |
|---|---|---|
At least 1 AE, % (95% CI) | ||
All grades | 44.56 (27.14 to 63.43) | 78.23 (69.92 to 85.13) |
Response difference | –33.67 (54.01 to 13.32) | Reference |
≥ Grade 3 | 0.00 (0.00 to 0.00) | 6.45 (2.83 to 12.32) |
Response difference | –6.45 (–10.78 to 2.13) | Reference |
CRS management, % (95% CI) | ||
Corticosteroid | 3.03 (0.41 to 19.07) | 15.32 (9.48 to 22.89) |
Response difference | –12.29 (–20.98 to –3.60) | Reference |
Tocilizumab | 9.91 (3.89 to 23.0) | 45.16 (36.21 to 54.35) |
Response difference | –35.25 (–47.76 to –22.74) | Reference |
Neurologic events, % (95% CI) | ||
All grade | 9.48 (2.51 to 29.91) | 56.45 (47.26 to 65.33) |
Response difference | –46.97 (–61.85 to –32.09) | Reference |
≥ Grade 3 | 0.19 (0.03 to 1.44) | 15.32 (9.48 to 22.89) |
Response difference | –15.13 (–21.48 to –8.78) | Reference |
AE = adverse event; CI = confidence interval; CRS = cytokine release syndrome.
Source: Clinical Study Report for sponsor-submitted MAIC.31 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Critical Appraisal
The MAIC was based on studies identified from a sponsor-conducted systematic review of treatments for FL in adults.99 The systematic review was comprehensive, involving multiple electronic databases, clinical registries, and supplementary manual searches. By following the PRISMA guidelines, the systematic review minimized error and bias in the study selection process. The reasons for study exclusion were reported, and selection and data extraction process were well defined. Although the risk of bias of the comparator trial was assessed, this rating was not detailed in the systematic review.
The MAIC was limited by important methodological differences between the ELARA and ZUMA-5 studies that could not be matched in the analyses. These differences are summarized in Table 27. As previously described, eligibility criteria in the ELARA study required patients to be r/r FL after 2 or more lines of systemic therapy, during or within 6 months of anti-CD20 mAb maintenance, or relapsed after auto-SCT. However, the eligibility criteria for the ZUMA-5 study did not include the 6-month caveat. Moreover, the definition of refractory differed; in the ELARA study, refractory was defined as failure to respond to previous treatment or progressive disease within 6 months of prior therapy completion, and in the ZUMA-5 study, patients were considered refractory on progression within 6 months of completion of the most recent prior treatment. Of note, although re-treatment was not permitted in the ELARA study, it was allowed in the ZUMA-5 study. Overall, 11 (8.9%) patients in the ZUMA-5 infused set received re-treatment. Due to a lack of access to ZUMA-5 individual patient data, the MAIC was unable to account for these factors. Finally, the definition of neurologic event in the ELARA study was more detailed than that used in the ZUMA-5 study. According to the clinical experts consulted by CADTH for this review, safety outcomes would bias neurologic event results toward the ZUMA-5 study due to difference in definitions.
The choice to conduct an unanchored MAIC was appropriately justified by the lack of a common comparator between the ELARA and ZUMA-5 studies. However, for an unanchored MAIC to produce unbiased treatment-effect estimates, all effect modifiers and prognostic variables need to be adjusted in the analysis. The covariates used for match-adjustment in the sponsor-submitted MAIC were informed by consultation with clinical experts experienced in the treatment of patients with r/r FL and EMA recommendations. A total of 31 covariates were identified as having some importance by the clinical experts or were recommended by the EMA. However, the MAIC was unable to adjust for all baseline characteristics of interest; only observed factors commonly and consistently reported in both studies were included for adjustment. In the end, the final MAIC matched on 11 variables (age, sex, race, ECOG PS, Ann Arbor stage, FLIPI score, high tumour bulk, prior lines of therapy, refractoriness to the most recent regimen, progression of disease within 12 months of first-line treatment from first anti-CD20 mAb-containing therapy, and prior auto-SCT). Of concern was the absence of matching on a number of prognostic factors considered important by the clinical experts and EMA, including nodal site involvement, LDH, lymphoma symptoms, chemoresistance, and time since diagnosis, because no data were available in the ZUMA-5 publication. Further compounding the issue was the differences in samples used for adjustment among the infused set and those used for efficacy comparison in the efficacy-evaluable set. The limitation would likely be more apparent in the ZUMA-5 study, given the larger sample size difference between the infused set (n = 124) and the efficacy-evaluable set (n = 86). Although the analysis assumed that patient characteristics in the ELARA infused set were comparable to those in the efficacy-evaluable set, the assumption was not validated. This difference has the likely potential to bias the results in favour of tisagenlecleucel. As the MAIC failed to meet the core assumption that all effect-modifier and prognostic factors were accounted for, conclusions about the effect of tisagenlecleucel relative to axicabtagene ciloleucel could not be drawn, owing to unknown amounts of residual bias.100,101 As noted by the National Institute for Health and Care Excellence (NICE) Decision Support Unit technical guidance, the failure of this assumption leads to an unknown amount of bias in the unanchored estimate.95
A sensitivity analysis was conducted to compare patients with and without bridging chemotherapy from the ELARA with ZUMA-5 studies. However, due to the lack of details about how the sensitivity analysis was conducted and how the 2 populations compared, the CADTH review team was unable to comment on the results with any certainty.
Unadjusted and matched-adjusted baseline covariates were reported. Baseline characteristics after matching were well balanced, with almost perfect matching for the covariates included in the MAIC. However, the complete baseline demographic and disease characteristics for patients in both trials were not reported after matching; only the balance of patient characteristics relevant to the covariates used in the matching were reported. Therefore, it is unclear what effect the matching had on the balance of other relevant patient characteristics.
The application of weight resulted in a reduced ESS of 26 patients, in which 51.9% of enrolled patients in the ELARA study were lost. The reduction in ESS suggests poor population overlap, with the results being heavily influenced by a subset of patients from the ELARA study, which may not be representative of the entire sample. The reduction in sample size may contribute to imprecision, increasing the uncertainty of the results.
Baseline characteristics and clinical results from the comparator study were derived from aggregate patient data, further limiting the interpretability of the MAIC results. Published KM curves pooled data over different covariates that may affect survival. A major limitation of the KM extraction method used in MAICs is the inability to derive separate KM curves for different subgroups or to model the joint effects of covariates and treatment.102 As a result, the treatment effects estimated may be impacted by aggregation bias.102 Furthermore, the precision of data extraction from KM curves is often dependent on the quality of the initial input (e.g., clear versus blurry figures) and depth of information provided in the original publications.
Of note, the MAIC assessed the end points of CRR, ORR, OS and PFS, as well as harms. Other efficacy end points of interest to patients and clinical experts, such as HRQoL, were not investigated.
Table 27: Assessment of Homogeneity for MAIC
Characteristics | Description and handling of potential effect modifiers |
|---|---|
Disease severity | Before matching, the proportion of patients with a FLIPI score of 2 (20.75% vs. 38.71%; P < 0.05) was significantly lower in the ELARA infused set nonbridging chemotherapy subgroup than in the ZUMA-5 infused set. After matching, disease severity was balanced between studies. |
Treatment history | In the ELARA study, 45.4% of patients received bridging chemotherapy before tisagenlecleucel infusion. In the ZUMA-5 study, 1.6% of patients received bridging chemotherapy before axicabtagene ciloleucel infusion. Only patients who received nonbridging chemotherapy were included in the MAIC. The proportion of patients with ≥ 3 prior lines of therapy (83.0% vs. 62.9%; P < 0.05) was significantly higher in the ELARA infused set nonbridging chemotherapy subgroup. After matching, patient characteristics were balanced. |
Trial eligibility criteria | In the ELARA study, adults were enrolled if they had r/r FL after 2 or more lines of systemic therapy, during or within 6 months of anti-CD20 mAb maintenance, or relapsed after auto-SCT. Optional bridging chemotherapy before tisagenlecleucel infusion was allowed. Patients would receive fludarabine-based or bendamustine-based LD chemotherapy before tisagenlecleucel infusion. In the ZUMA-5 study, adults were enrolled if they had r/r FL after 2 or more lines of treatment with combination chemoimmunotherapy, which must have included an anti-CD20 mAb-containing therapy combined with an alkylating drug. Bridging chemotherapy before axicabtagene ciloleucel infusion was not used in most patients. For the MAIC, patients who received bridging therapy in the ZUMA-5 study were excluded from analysis. |
Definition of refractory | In the ELARA study, refractory was defined as a failure to respond to previous treatment (stable disease or progressive disease as the best response) or progressive disease within 6 months of prior therapy completion. In the ZUMA-5 study, refractory was defined as progression within 6 months of completion of the most recent prior treatment. According to the clinical experts, the definition of refractory may be considered equivalent in the ELARA and ZUMA-5 studies. |
Definition of POD24 | In the ELARA study, POD24 was defined as primary refractory or progression of disease within 24 months of initiation of a first-line anti-CS20 mAb-containing treatment. In the ZUMA-5 study, POD24 was defined as progression within 24 months of initiation of a first-line anti-CD20 mAb-containing treatment. According to the clinical experts, the definition of POD24 may be considered equivalent in the ELARA and ZUMA-5 studies. |
Definitions of efficacy end point | Both the ELARA and ZUMA-5 studies had similar definitions for ORR, PFS and OS. Responses in both studies were evaluated against the Lugano classification by a central IRC. |
Timing of end point evaluation | In the ELARA study, the best overall disease response was identified from the time of tisagenlecleucel infusion until progressive disease or the start of a new anticancer therapy. In the ZUMA-5 study, the time period during which response was assessed was not clearly documented. |
Definition of safety end points | Both the ELARA and ZUMA-5 studies based CRS grading and management on the Lee scale.103 The definition of a neurologic event differed between the studies: In the ELARA study, a neurologic event was primarily reflective of encephalopathy and delirium, and may present clinically as signs and symptoms of varying severity, including confusion, disorientation, agitation, aphasia, somnolence, and tremors. In severe cases, seizures, motor weakness, incontinence, impaired consciousness, increased intracranial pressure, and cerebral edema may be concurrent to, following the resolution of, or in the absence of CRS. In the ZUMA-5 study, a neurologic event was defined based on the study by Topp et al. (2015),104 and included cranial nerve disorders, deliria (including confusion), disturbances in thinking and perception, encephalopathies, mental impairment disorders, movement disorders (including parkinsonism), neurologic disorders not otherwise classified, neuromuscular disorders, personality disorders and disturbances in behaviour, psychiatric disorders not otherwise classified, and seizures (including subtypes). |
Auto-SCT = autologous stem cell transplant; CRS = cytokine release syndrome; FL = follicular lymphoma; FLIPI = Follicular Lymphoma International Prognostic Index; IRC = independent review committee; LD = lymphodepleting; mAb = monoclonal antibody; MAIC = matching-adjusted indirect treatment comparison; ORR = overall response rate; OS = overall survival; POD24 = progression of disease within 24 months of first-line treatment; r/r = relapsed or refractory.
Source: Sponsor-submitted MAIC of ELARA vs. ZUMA-5.31 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Studies Addressing Gaps in the Pivotal and RCT Evidence
The contents of this section have been informed by materials submitted by the sponsor. The information has been summarized and validated by the CADTH review team.
The sponsor indicated that for ethical and practical reasons, novel therapies such as CAR T-cell therapy for rare diseases have typically been evaluated in single-arm trials, which results in a lack of direct comparative evidence with a control group (e.g., SOC or usual care).29,33,61,80,94,105 Further, a single-arm design is supported by the rarity of patients with r/r FL, the lack of an established SOC for r/r FL, and low response rates for currently available therapies in this high-risk population. These complicating factors make the identification of a relevant comparator difficult. Consultations with both the FDA and the EMA on the clinical development program and registration strategy for tisagenlecleucel in r/r FL resulted in agreement on the study design, primary and secondary end points, and on the statistical analysis methods undertaken in the ELARA study. For the tisagenlecleucel submission, the pivotal study, ELARA, was a single-arm trial; therefore, the lack of a control group constitutes an important evidence gap. To address this evidence gap, a retrospective cohort study, ReCORD-FL, was undertaken in adults with grade 1, 2, or 3a r/r FL after 2 or more lines of therapy to construct a historic cohort of control patients to augment current and future single-arm trials in the r/r FL setting.93
In addition, the pivotal ELARA study provided efficacy outcomes with up to 30 months of follow-up. Longer-term efficacy data and safety data are needed to explore the treatment effect of tisagenlecleucel in the study population. Therefore, results of the study be Schuster et al. (2017)33 are summarized in this review.
Table 28: Summary of Gaps in the Evidence
Gap in pivotal and RCT evidence | Studies that address gaps | |
|---|---|---|
Study description | Summary of key results | |
Lack of a control or comparator treatment group | A retrospective cohort study via medical record review of adults with grade 1, 2, or 3a FL who were r/r after ≥ 2 lines of therapy, including an anti-CD20 and an alkylator. | This study provides information on important outcomes such as CRR, ORR, TNT-D, EFS, and OS from 187 patients who received standard of care for r/r FL in the third-line setting and beyond, providing a valuable source of control data. |
Short-term follow-up | A single-centre, single-arm study of patients with non-Hodgkin lymphoma, including r/r FL. | This study provides information on ORR, CRR, OS, PFS, DoR, and safety for 28 patients (14 with r/r FL) who received tisagenlecleucel. Data are available up to 60 months, thus providing a valuable source of long-term data. |
CRR = complete remission rate; DoR = duration of response; EFS = event-free survival; FL = follicular lymphoma; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; r/r = relapsed or refractory; RCT = randomized controlled trial; TNT-D = time to next treatment or death.
Description of the ELARA and ReCORD-FL Trials
In the absence of direct head-to-head comparisons of tisagenlecleucel to SOC, the sponsor compared the treatment effect of tisagenlecleucel as observed in the ELARA study to SOC, defined as standard chemotherapy, as documented in the retrospective ReCORD-FL cohort study.
The ELARA study (n = 98) is an ongoing, single-arm, open-level, multicentre, phase II study assessing the efficacy and safety of tisagenlecleucel in adults with r/r FL after 2 or more lines of therapy. A detailed description of the ELARA study is provided in the Studies Addressing Gaps in the Pivotal and RCT Evidence section of this clinical report. The ReCORD-FL study (n = 187) is a noninterventional, multicentre, retrospective chart review conducted by the sponsor with the purpose of providing patient-level data for a historical control group to compare with standard chemotherapy data in the ELARA trial. The study scheme for the ReCORD-FL study is illustrated in Figure 5. Patient-level data were collected from patients treated for r/r FL between 1998 and 2020 from 10 sites in Europe and North America, including 1 Canadian site (n = 12). The medical records of patients with r/r FL were abstracted and provided by physicians or their designates who have been or are treating patients with FL. Clinical outcomes were measured from the start of each observed line of therapy until the earliest of death, the last available follow-up, or the data cut-off date. Anonymized patient data were entered into an electronic data collection form using a secure web-based data collection portal. Data were collected or derived at 3 time points:
from the initial diagnosis of FL (the earliest was in 1998) through the study index date
at the time of the study index date (between January 2, 2000, and December 31, 2018)
from the study index date until the earliest of the following: death, last available record and/or follow-up, or December 31, 2020.
Figure 5: The ReCORD-FL Study Scheme
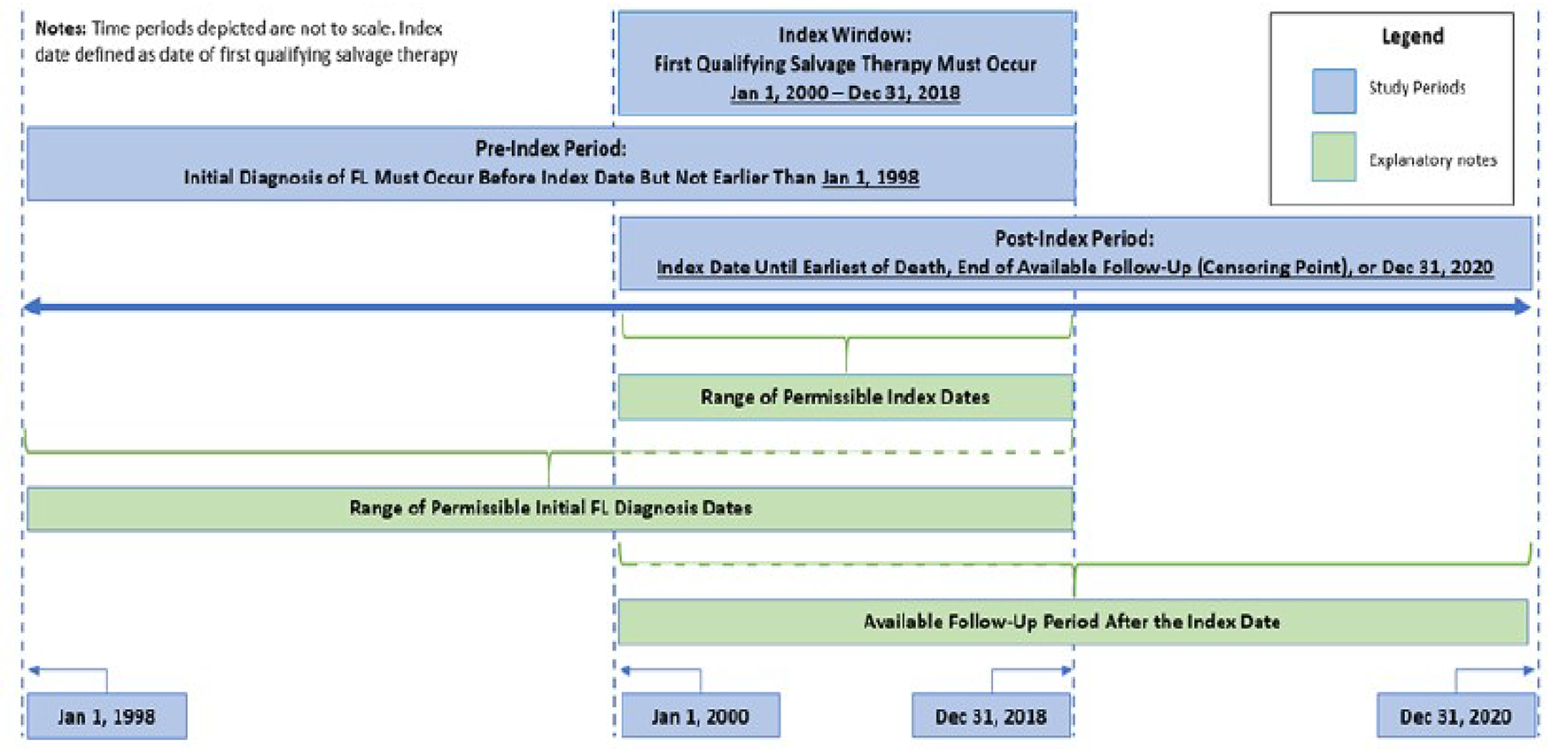
FL = follicular lymphoma.
Source: Clinical Study Report for ELARA versus ReCORD.32
Populations
Where feasible, the ReCORD-FL study adopted the same inclusion and exclusion criteria as the ELARA study. For inclusion into the ReCORD-FL study, patients 18 years and older were required to meet 1 of the following criteria defining r/r FL:
refractory to a second line or later line of systemic therapy (including an anti-C20 antibody and an alkylating drug) or relapse within 6 months of completion of a second line or later line of systemic therapy
relapse during anti-C20 antibody maintenance (after at least 2 lines of therapies) or within 6 months of maintenance completion
relapse after auto-SCT.
Moreover, patients must have initiated at least 1 additional line of systemic therapy after first meeting the criteria for r/r FL; have at least 3 months of available follow-up data after the index date, unless the patient died in the 3 months after the index date; were confirmed histologically as having grade 1, 2, or 3a disease at the time of the index date; have an index date during the period between January 1, 2000, and December 31, 2018, with an initial diagnosis of FL occurring before the index date but not earlier than January 1, 1998; and have an ECOG PS of 0 or 1 at the time of the index date. Of note, eligible patients may have been living or deceased at the time of data abstraction. Patients were excluded if the following criteria were noted at or before the study index date: evidence of histological transformation; grade 3b FL; prior anti-CD19 therapy; prior gene therapy; prior adoptive T-cell therapy; prior allo-SCT; active CNS involvement by malignancy; active neurologic autoimmune or inflammatory disorders; and any enrolment in a CAR T-cell trial.
Of note, not all inclusion and exclusion criteria in the ELARA study were adopted in the ReCORD-FL study. Notable inclusion and exclusion criteria that were not feasible to apply in the ReCORD-FL study are summarized in Table 29.
Table 29: ELARA Inclusion and Exclusion Criteria Not Feasible to Apply in the ReCORD-FL Study
Criteria not feasible to apply | Reason |
|---|---|
Inclusion criteria | |
Radiographically measurable disease at baseline defined as:
| Data from radiography and other imagining studies are usually not captured to this level of detail in real-word medical records for patients with FL |
Adequate pulmonary function defined as:
| Data are usually not captured in real-word medical records for patients with FL |
Must have leukapheresis product of nonmobilized cells accepted for manufacturing | Not applicable in the ReCORD-FL study, as this does not apply to a non-CAR T-cell treatment regimen |
Patients have the following lab values during the screening phase: absolute number of CD3+ T cells > 150/mm3 (> 0.15 × 109/L) | Not applicable in the ReCORD-FL study as these data are not routinely available as a standard-of-care laboratory values |
Exclusion criteria | |
Prescence of active or prior hepatitis B or C, as indicated by serology | Low completeness has generally been expected for lab results |
Presence of HIV antibody | Low completeness has generally been expected in medical records |
Uncontrolled acute life-threatening bacterial, viral, or fungal infection | Low completeness has generally been expected in medical records |
Cardiac or cardiac repolarization abnormality, including any of the following:
| Low completeness has generally been expected in medical records |
Previous or concurrent malignancy with the following exceptions:
| Low completeness has generally been expected in medical records |
AV = atrioventricular; ECHO = echocardiogram; FL = follicular lymphoma; LVEF = left ventricular ejection fraction; MI = myocardial infarction; MRA = coronary magnetic resonance angiography; MUGA = multigated acquisition; NYHA = New York Hearts Association.
Source: Clinical Study Report for ELARA vs. ReCORD.32
Interventions
Tisagenlecleucel
Tisagenlecleucel as administered in the ELARA study is described in detail in the Pivotal Studies and RCT Evidence section.
Standard of Care
SOC included treatment with chemotherapy, anti-CD20 antibody monotherapy, a PI3K inhibitor, high-dose chemotherapy as salvage therapy for auto-SCT or allo-SCT, or radioimmunotherapy. A chemotherapy mix that included auto-SCT at the index date or later was also accepted as SOC. In addition, other cancer-directed systemic therapies, including investigational drugs, except for CAR T-cell therapy, were considered. Watch and wait was not considered a relevant therapy option for the purpose of this study. Previous treatment with other FL-targeting medications, such as PI3K inhibitors, was permitted if patients recovered from all treatment-related AEs.
Outcomes
Overall Survival
OS was defined as time to death from any cause. OS was censored at the last date the patient was known to be alive if no death had been observed at the time of analysis.
Progression-Free Survival
Dates of disease progression were not available for most patients in the ReCORD-FL study. Accordingly, a comparison analysis of PFS was performed by considering death or initiation of new anticancer therapy for patients in both the ReCORD-FL and ELARA studies. Patients were censored at the date of last contact if no progression, death, or new anticancer therapy initiation occurred.
Statistical Analysis
Selection of Eligible Line of Chemotherapy
It was noted that patients in the ReCORD-FL study may meet inclusion and exclusion criteria at the start of more than 1 line of therapy. A propensity score, operationalized as the probably of being enrolled in the ELARA study conditional on observed variables measured at the start of the line of therapy, was estimated for each patient at each eligible line of therapy in the ReCORD-FL study. This approach was used to achieve an approximate balance of the number of prior lines of therapy while also balancing other key baseline prognostic variables between the ELARA and ReCORD-FL studies. Covariates were considered relevant for adjustment if deemed to have some level of importance (less important to very important) by clinical experts consulted by the sponsor or if recommended by the EMA and aligned with health authorities. Relevant baseline prognostic factors were included in the propensity score model if they were commonly and consistently reported in both the ELARA and ReCORD-FL studies. Prognostic factors considered and included in the propensity score model are detailed in Table 30. The covariates included in the final propensity model were age at treatment initiation (continuous variable); region (Europe or North America); sex (female or male); history of auto-SCT (yes or no); number of previous lines of systematic treatment (> 4 or 2 to 4); disease stage at FL diagnosis and initiation of treatment (continuous variable); sites of nodal involvement at treatment initiation (> 4 or ≤ 4); double refractory (yes or no); and progression of disease within 24 months of first-line treatment (yes or no).
Table 30: Prognostic Factors of Efficacy Outcomes in Patients With r/r FL Considered and Included in the Propensity Score Model for the ITC of Tisagenlecleucel vs. SOC
Prognostic factors | Input from clinical experts | EMA recommendations | Inclusion in ITC |
|---|---|---|---|
Demographic | |||
Agea | Important | Recommended | Included |
Sexa | Not important | Recommended | Included |
Race | Not important | Recommended | Excludedb |
Regiona | Not important | Recommended as a supplementary factor when race is not available | Included |
Disease stage and tumour size | |||
Histological transformation | Very important | Not evaluated | Excludedc |
FL grade | Not important | Not evaluated | Excludedd |
Ann Arbor stage | Not important | Recommended | Included |
Bulky mass | Less important | Not evaluated | Excludedb |
Lesion size | Not important | Not evaluated | Excludedb |
Nodal size involvementa | Not important | Recommended | Included |
Marrow involvement | Not important | Not evaluated | Excludedb |
Performance status | Important | Recommended | Excludedd |
Lab measures, symptoms, comorbidities | |||
Elevated LDH | Important | Recommended on the overall category, but no details on individual variables | Excludedd |
Hemoglobin | No important | Excludedd | |
Hepatic dysfunction | No important | Excludedb | |
Lymphoma symptoms | Less important | Excludedb | |
Other disease characteristics | |||
FLIPI score | Very important | Recommended | Excludedd,e |
Time since diagnosisa | Not evaluated | Recommended | Included |
Prior treatment history | |||
Number of prior treatmentsa | Important | Recommended | Included |
Prior auto-SCTa | Not important | Recommended | Included |
Relapsed/refractory status to systemic therapies | |||
POD24a | Important | Recommended | Included |
Relapsed/refractor to last treatment (0.5 years) | Very important | Recommended on the overall category but not details on individual variables | Excludedf |
Disease refractory to 2 or more regiments | Not evaluated | ||
Chemoresistant | Very important | ||
Double refractorya | Not evaluated | Included |
Auto-SCT = autologous stem cell transplant; EMA = European Medicines Agency; FL = follicular lymphoma; FLIPI = Follicular Lymphoma International Prognostic Index; ITC = indirect treatment comparison; LDH = lactate dehydrogenase; POD24 = progression of disease within 24 months of first-line of treatment; r/r/ = relapsed or refractory; SOC = standard of care.
aCovariates included in the propensity score model were age at treatment initiation (continuous variable); region (Europe or North America); sex (female or male); history of auto-SCT (yes or no); number of previous lines of systematic treatment (> 4 or 2 to 4); disease stage at initial FL diagnosis and initiation of treatment (continuous variable); sites of nodal involvement at treatment initiation (> 4 or ≤ 4); double refractory (yes or no); and POD24 (yes of no).
bNo data available in the ReCORD-FL study.
cExclusion criteria.
dMissing data in the ReCORD-FL study.
eThree of the 5 risk factors of the FLIPI score were included in the propensity score model (age, number of nodal sites, and disease stage).
fExcluded because double refractory already captures refractoriness status, and included in the propensity score model.
Source: Clinical Study Report for comparison of ELARA vs. ReCORD-FL.32 (Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.30)
For each line of therapy, a patient’s propensity score was conditional on the values of their covariates at baseline for that line of therapy. One eligible line of therapy per patient was systematically selected to correspond with the patient’s highest propensity score. Accordingly, for each patient in the ReCORD-FL study, the eligible line of therapy was selected, at which time key baseline prognostic factors were mostly closely aligned with those in the ELARA study. After the selection of 1 line of therapy for each patient in the ReCORD-FL study, patients with a selected line of any chemotherapy, including monotherapy or combination therapy with or without anti-CD20 body, were included in the comparison of SOC in the ReCORD-FL study versus tisagenlecleucel in the ELARA study.
Estimates of Comparison
Estimates of the treatment effect were based on the comparison of patients from the ELARA study and patients from the ReCORD-FL study. Propensity scores were recalculated to ensure that baseline prognostic values were balanced in the 2 groups. The point estimates of propensity scores were based on a logistic regression adjusted for the included covariates listed in Table 30. The model was fitted using maximum likelihood estimation. Using the propensity score estimates, the odds of a patient in the ReCORD-FL study being enrolled in the ELARA study was calculated, given their baseline variables at the selected line of chemotherapy.
The time-to-event end point of OS and PFS were evaluated from the start of enrolment in the ELARA study and from the start date of the selected line of therapy in the ReCORD-FL study. The weighting by odds method was used in the comparison analysis.106 The distribution of the weighted time-to-event end points were estimated using KM analysis, whereas HRs were estimated using Cox proportional hazard regression. Patients from the ELARA study were assigned a weight of 1, and patients from the ReCORD-FL study were assigned a weight equal to their odds of being enrolled in the ELARA study. The median survival time proportion of patients without an event at 6, 12, 18, and 24 months, as well as corresponding HRs, were also calculated. Bootstrap 95% CIs were provided.
Results
Patient Disposition
Baseline Characteristics
Baseline characteristics in the ELARA and ReCORD-FL studies before and after weighting are summarized in Table 31.
After weighting, included patients from the ELARA (N = 97) and ReCORD-FL (ESS = 45.7) studies appeared balanced on age, sex, prior auto-SCT, number of previous lines of therapies, disease stage at initial diagnosis, time between diagnosis and treatment, sites of nodal involvement, double refractoriness, and POD24. Patients were, on average, middle aged (mean age, 55.4 to 56.5 years), mainly male (67% to 72%), and just more than a third were documented to have had prior auto-SCT therapy. Approximately 68.0% and 70.2% of patients in the ELARA and ReCORD-FL studies, respectively, were documented as double refractory. Approximately 82% of patients in the ReCORD-FL study were refractory to the last prior therapy compared to 73% of patients in the ELARA study, whereas approximately 11% to 40% of patients in the ReCORD-FL study had intermediate or low FLIPI scores, compared to 21% to 19% of patients in the ELARA study.
Table 31: Comparison of Baseline Characteristics in the ELARA Study and the ReCORD-FL Study Before and After Weighting
Baseline variables | ELARA | ReCORD-FL | |||
|---|---|---|---|---|---|
Before weighting | After weighting | ||||
Point estimate | SMD | Point estimate | SMD | ||
N | 97 | 78 | — | 99.8a | — |
Included in PS modellingb | |||||
Age at treatment initiation (years) | |||||
Mean (SD) | 56.5 (10.4) | 58.2 (12.6) | 0.144 | 55.4 (12.2) | 0.096 |
Range | 29 to 73 | 25 to 84 | — | 25 to 84 | — |
Age at treatment initiation, n (%) | |||||
< 65 years | 73 (75.3) | 51 (65.4) | 0.217 | 76.7 (76.9) | 0.039 |
≥ 65 years | 24 (24.7) | 27 (34.6) | 0.217 | 23.0 (23.1) | 0.039 |
Sex, n (%) | |||||
Female | 32 (33.0) | 35 (44.9) | 0.246 | 27.8 (27.9) | 0.111 |
Male | 65 (67.0) | 43 (55.1) | 0.246 | 72.0 (72.1) | 0.111 |
Region, n (%) | |||||
Europe | 44 (45.4) | 49 (62.8) | 0.356 | 39.7 (39.8) | 0.113 |
RoW | 53 (54.6) | 29 (37.2) | 0.356 | 60.1 (60.2) | 0.113 |
Prior auto-SCT, n (%) | |||||
Yes | 36 (37.1) | 25 (32.1) | 0.107 | 37.3 (37.3) | 0.005 |
No | 61 (62.9) | 53 (67.9) | 0.107 | 62.5 (62.7) | 0.005 |
Number of previous lines of systemic treatment | |||||
Mean (SD) | 3.9 (1.8) | 3.4 (2.0) | 0.245 | 3.9 (2.1) | 0.022 |
Range | 2 to 13 | 2 to 10 | — | 2 to 10 | — |
Number of previous lines of systemic treatment, n (%) | |||||
≤ 4 | 69 (71.1) | 63 (80.8) | 0.227 | 75.6 (75.7) | 0.104 |
> 4 | 28 (28.9) | 15 (19.2) | 0.227 | 24.2 (24.3) | 0.104 |
Disease stage at initial FL diagnosis, n (%) | |||||
I | 6 (6.2) | 4 (5.1) | 0.046 | 4.4 (4.4) | 0.081 |
II | 13 (13.4) | 7 (9.0) | 0.141 | 7.9 (7.9) | 0.178 |
III | 21 (21.6) | 13 (16.7) | 0.127 | 27.2 (27.2) | 0.130 |
IV | 57 (58.8) | 54 (69.2) | 0.219 | 60.3 (60.5) | 0.035 |
Months between initial FL diagnosis and initiation of treatment | |||||
Mean (SD) | 77.3 (56.3) | 64.9 (47.2) | 0.238 | 73.2 (52.2) | 0.075 |
Range | 6.4 to 355.4 | 2.8 to 55.0 | — | 2.8 to 255 | — |
Number of nodal involvements at treatment initiation, n (%) | |||||
≤ 4 | 39 (40.2) | 39 (50.0) | 0.198 | 36.6 (36.7) | 0.072 |
> 4 | 58 (59.8) | 39 (50.0) | 0.198 | 63.2 (63.3) | 0.072 |
Double refractory, n (%) | |||||
Yes | 66 (68.0) | 58 (74.4) | 0.140 | 70.1 (70.2) | 0.048 |
No | 31 (32.0) | 20 (25.6) | 0.140 | 29.7 (29.8) | 0.048 |
POD24, n (%) | |||||
Yes | 61 (62.9) | 45 (57.7) | 0.106 | 63.8 (63.9) | 0.022 |
No | 36 (37.1) | 33 (42.3) | 0.106 | 36.0 (36.1) | 0.022 |
Baseline variables not included in PS modelling | |||||
Refractory status to last prior therapy, n (%) | |||||
Yes | 75 (77.3) | 66 (84.6) | 0.187 | 82.3 (82.4) | 0.128 |
No | 21 (21.6) | 12 (15.4) | 0.162 | 17.5 (17.6) | 0.103 |
Missing | 1 (1.0) | 0 | 0.144 | 0.0 | 0.144 |
FLIPI score, n (%) | |||||
High | 59 (60.8) | 50 (64.1) | 0.068 | 65.1 (65.2) | 0.091 |
Intermediate | 20 (20.6) | 12 (15.4) | 0.137 | 10.8 (10.8) | 0.272 |
Low | 18 (18.6) | 4 (5.1) | 0.425 | 4.0 (4.0) | 0.473 |
Missing | 0 | 12 (15.4) | 0.603 | 19.9 (20.0) | 0.706 |
Auto-SCT = autologous stem cell transplant; FL = follicular lymphoma; FLIPI = Follicular Lymphoma International Prognostic Index; POD24 = progression of disease within 24 months of first-line treatment; PS = propensity score; RoW = rest of world; SD = standard deviation; SMD = standard mean difference.
aSample size after weighting (i.e., sum of weights) was 99.8 for the ReCORD-FL study and the effective sample size was 45.7.
bBecause double refractoriness and last prior therapy refractory status both capture refractoriness status, only 1 prognostic factor (double refractoriness) was included in the propensity model. Furthermore, refractoriness to last prior therapy was already very well balanced (SMD < 0.25) before weighting. FLIPI score was excluded from the model on the basis of missingness (12 [15%] additional chemotherapy-treated patients would be excluded from the analysis if FLIPI were included in the model). Considering that 3 of the 5 risk factors of the FLIPI score are already included in the model (age, number of nodal sites, disease stage), which achieved excellent balance with absolute SMDs < 0.25, FLIPI (without missing values) was also well balanced in the cohorts before weighting and, thus, to conserve sample size, FLIPI score was excluded.
Source: Clinical Study Report for comparison of ELARA vs. ReCORD-FL.32 (Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Exposure to Study Treatments
Median follow-up time, defined as time to death or last follow-up date, was 26.2 months for patients who received tisagenlecleucel in the ELARA study and 26.2% in patients who received chemotherapy in the ReCORD-FL study.
Among the patients included from the ReCORD-FL study, the most frequent (> 5%) regimens were BR (14.1%), bendamustine monotherapy (7.7%), cyclophosphamide plus fludarabine plus rituximab (6.4%), R-ICE (6.4%), and R-CHOP (5.1%).
Efficacy
Overall Survival
Comparison of OS between the ELARA and ReCORD-FL studies is summarized in Table 32. KM plots for OS are illustrated in Figure 6.
After weighting, death events were observed in 13.4% of patients in ELARA study and 45.2% of patients in ReCORD-FL study at the time of data cut-off. Median OS was not estimable (NE) for ELARA study. Among patients in ReCORD-FL study, the median OS was 36.6 months (95% CI, 25.8 to NE) after weighting. The KM estimate for OS at 24 months was 90.8% (95% CI, 84.7 to 96.9) and 64.8% (95% CI, 49.5 to 80.0) for ELARA and ReCORD-FL studies, respectively. Compared to standard chemotherapy, tisagenlecleucel was associated with an estimated risk reduction in death of 72% (HR = 0.28; 95% CI, 0.07 to 0.49).
Table 32: Comparison of OS in the ELARA Study and the ReCORD-FL Study Before and After Weighting
Outcome | ReCORD-FL | ELARA | |
|---|---|---|---|
Before weighting | After weighting | ||
N | 78 | 99.8a | 97 |
Kaplan-Meier analysis | |||
Events (%) | 34 (43.6) | 45.1 (45.2) | 13 (13.4) |
Median, 95% CI (months) | 66.3 (33.9 to NE) | 35.6 (25.8 to NE) | NA (35.5 to NE) |
OS rates (95% CI) | |||
6 months | 85.2 (77.5 to 93.2) | 82.7 (69.6 to 95.9) | 100 (100 to 100) |
12 months | 73.7 (63.6 to 83.8) | 70.1 (55.3 to 84.9) | 96.6 (93.0 to 100) |
18 months | 69.3 (58.6 to 80.0) | 65.5 (50.3 to 80.7) | 93.2 (87.9 to 98.5) |
24 months | 67.8 (56.9 to 78.6) | 64.8 (49.5 to 80.0) | 90.8 (84.7 to 96.9) |
Cox proportional hazard model | |||
Before weighting HR (95% CI) | Reference | — | 0.28 (0.07 to 0.49) |
After weighting HR (95% CI) | — | Reference | 0.34 (0.09 to 0.59) |
CI = confidence interval; HR = hazard ratio; NA = not available; NE = not estimable; OS = overall survival.
Note: Data cut-off dates were March 29, 2022, for the ELARA study and December 31, 2021, for the ReCORD-FL study.
aSample size after weighting (i.e., sum of weights) was 99.8 for the ReCORD-FL study and the effective sample size was 45.7.
Source: Clinical Study Report for comparison of ELARA vs. ReCORD-FL.32 (Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Progression-Free Survival
The PFS comparison of the ELARA and ReCORD-FL studies is summarized in Table 33. KM plots for PFS after weighting are illustrated in Figure 7.
After weighting, disease progression events (i.e., death or the start of a new anticancer therapy) were observed in 42.3% of patients in the ELARA study and 63.7% of patients in the ReCORD-FL study at the time of data cut-off. Median PFS was NE for the ELARA study. Among patients in the ReCORD-FL study, median PFS was 11.5 months (95% CI, 5.9 to 35.6 months). The KM estimate for PFS at 24 months was 58.6% (95% CI, 48.6% to 68.6%) and 38.3% (95% CI, 22.7% to 53.8%) for the ELARA and ReCORD-FL studies, respectively. Compared to standard chemotherapy, tisagenlecleucel was associated with an estimated risk reduction in disease progression of 47% (HR = 0.53; 95% CI, 0.25 to 0.81).
Figure 6: KM Curves of OS in the ELARA and ReCORD-FL Studies After Weighting
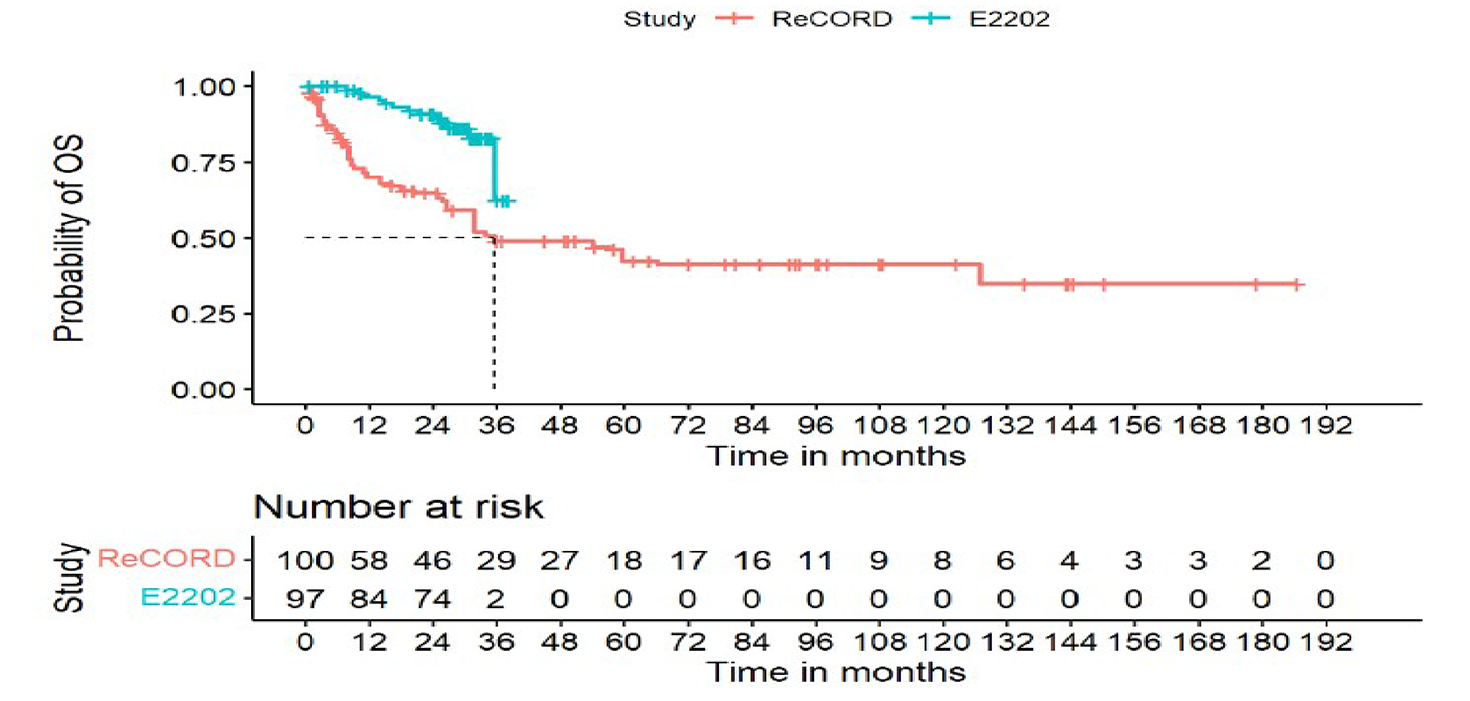
E2202 = the ELARA study; KM = Kaplan-Meier; NE = not estimable; OS = overall survival.
Note: Data cut-off dates were March 29, 2022, for the ELARA study and December 31, 2021, for the ReCORD-FL study. Sample size after weighting (i.e., sum of weights) was 99.8 for the ReCORD-FL study and the effective sample size was 45.7.
Source: Clinical Study Report for comparison of ELARA versus ReCORD-FL.32 (Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.)
Table 33: Comparison of PFS in the ELARA Study and the ReCORD-FL Study Before and After Weighting
Outcome | ReCORD-FL | ELARA | |
|---|---|---|---|
Before weighting | After weighting | ||
N | 78 | 99.8a | 97 |
PFS rates, % (95% CI) | |||
6 months | 71.3 (61.3 to 81.3) | 62.3 (46.0 to 78.6) | 85.3 (78.2 to 92.3) |
12 months | 57.4 (46.3 to 68.5) | 49.2 (33.2 to 65.2) | 70.5 (61.5 to 79.6) |
18 months | 50.4 (39.0 to 61.7) | 43.6 (27.5 to 59.6) | 62.9 (53.2 to 72.7) |
24 months | 47.3 (35.8 to 58.8) | 38.3 (22.7 to 53.8) | 58.6 (48.6 to 68.6) |
Cox proportional hazard model | |||
Before weighting HR (95% CI) | Reference | — | 0.69 (0.38 to 1.0) |
After weighting HR (95% CI) | — | Reference | 0.53 (0.25 to 0.81) |
CI = confidence interval; HR = hazard ratio; PFS = progression-free survival.
Notes: Data cut-off dates were March 29, 2022, for the ELARA study and December 31, 2021, for the ReCORD-FL study.
aSample size after weighting (i.e., sum of weights) was 99.8 for the ReCORD-FL study and the effective sample size was 45.7.
Source: Clinical Study Report for comparison of ELARA vs. ReCORD-FL.32 (Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Figure 7: KM Curves of PFS in the ELARA and ReCORD-FL Studies After Weighting
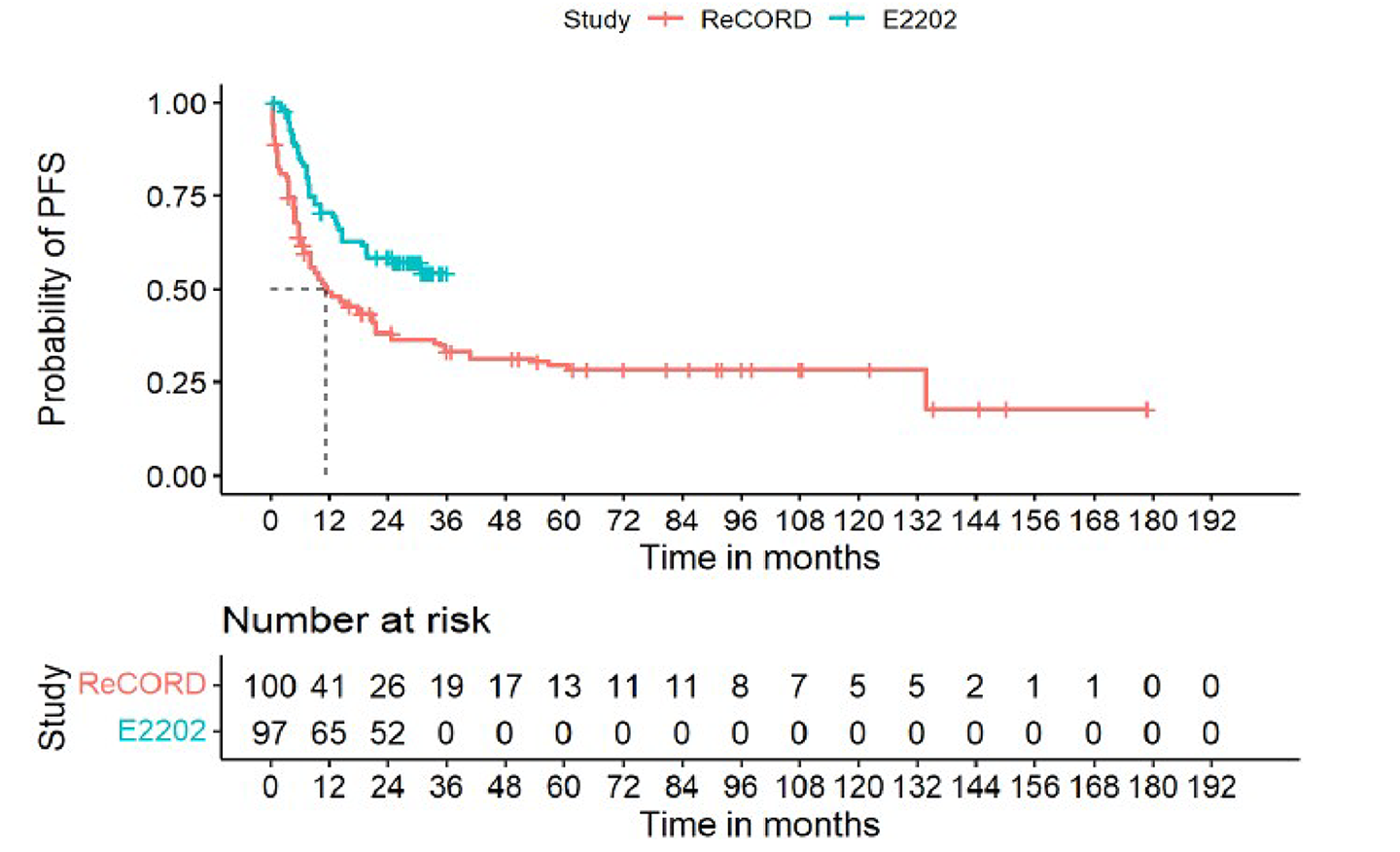
E2202 = the ELARA study; KM = Kaplan-Meier; PFS = progression-free survival.
Notes: Data cut-off dates were March 29, 2022, for the ELARA study and December 31, 2021, for the ReCORD-FL study. Sample size after weighting (i.e., sum of weights) was 99.8 for the ReCORD-FL study and the effective sample size was 45.7.
Source: Clinical Study Report for comparison of ELARA versus ReCORD-FL.32 (Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Harms
Harms outcomes were not compared between the ELARA and ReCORD-FL studies.
Critical Appraisal
Internal Validity
The nonrandomized comparison of the ELARA and ReCORD-FL studies makes interpretation of the efficacy and safety of tisagenlecleucel challenging. To mitigate potential differences in baseline prognostic factors related to OS and PFS, the inclusion and exclusion criteria of the ELARA study were applied to the ReCORD-FL study, and eligible patients from the ReCORD-FL study were systematically selected based on the highest propensity scores. Moreover, comparisons by weighting by odds were conducted to assess the causal effects of prescribing tisagenlecleucel versus chemotherapy. However, important prognostic factors such as baseline ECOG PS and FLIPI scores were not included in the propensity model. Also, important exclusion criteria — as noted by the clinical experts consulted by CADTH for the purpose of this review — specific to the ELARA study, such as the exclusion of patients with a cardiac or cardiac repolarization abnormality and a previous or concurrent malignancy, could not be applied to the ReCORD-FL study. Consequently, there is uncertainty around the treatment effects of tisagenlecleucel relative to standard chemotherapy due to selection bias and unmeasured and residual confounding that cannot be entirely ruled out.
Unadjusted and match-adjusted baseline covariates were reported. Baseline characteristics after matching were well balanced, as evidenced by absolute mean differences of less than 25%. However, the complete baseline demographic and disease characteristics for patients in both trials were not reported after matching; only the balance of patient characteristics relevant to the covariates used in the matching was reported. It was noted that there were differences in the reported characteristics between the cohorts before the weights were applied, indicating heterogeneity. Therefore, it is unclear what effect the matching had on the balance of other relevant patient characteristics. The application of weights resulted in a reduced ESS of 45.7; the reduction in ESS in the primary analysis contributes to imprecision in the estimates, leading to uncertainty of the results.
Standard procedures define PFS as the time to first documented disease progression or death from any cause. However, the date of disease progression was not available for most patients in the ReCORD-FL study. Moreover, radiographic assessment of disease progression is less frequent (or not performed at all) in the real-world setting than in clinical trial protocols. Accordingly, for a comparative analysis of PFS, the date of disease progression was considered at the time a new anticancer therapy was started in both the ReCORD-FL and ELARA studies. Accordingly, censoring was redefined to occur at the last contact date, rather than the last assessment date, in ELARA study to avoid bias related to the timing of assessment. However, due to the inherent limitations of retrospective studies, the accuracy of the date of last contact is uncertain. The validity of using the date of a new anticancer therapy as a surrogate for disease progression is uncertain. Uncertainty about outcome assessment is further compounded by inconsistencies in the assessment of patients included in the ReCORD-FL study. Because the assessment of patients included in the ReCORD-FL study was not planned in the uniform protocol, physicians may have used subjective criteria to assess clinical response or disease progression.
External Validity
Based on input from the clinical experts, the patients included in the comparison of the ELARA and ReCORD-FL studies appeared to be younger than what is typically seen in the clinical setting. The clinical experts noted that the selected anticancer treatments were appropriate SOC regimens. However, whether the change in PFS for the purpose of efficacy comparison between the ELARA and ReCORD-FL studies is appropriate is uncertain.
Description of the Schuster Study
The study by Schuster et al. (2017)33 was conducted at a single centre in the US. This study reported data from a cohort of patients with FL (n = 14) enrolled in a single-arm, phase IIa clinical trial conducted in patients with NHL and r/r CD19+ lymphomas after chemotherapy. The objective of this study was to estimate the efficacy of tisagenlecleucel in patients with NHL. As a part of the FL subgroup, a total of 15 patients with r/r FL were enrolled, of whom 14 received tisagenlecleucel. This was a pilot study designed to test the central hypothesis of antitumour responses of CD19 CAR T-cell infusions in patients with advanced B-cell NHL. At entry, the suitability of each patient’s T cells for CD19 CAR T-cell manufacturing was determined, and those who had adequate T cells went for leukapheresis. Purified T cells were transduced with CD19-BB-zeta. After leukapheresis at the discretion of physician, patients received bridging therapy followed by staging and LD chemotherapy.
Details of the Schuster et al. study are summarized in Table 34.
Table 34: Details of the Schuster et al. Study
Characteristics | Schuster et al. study |
|---|---|
Objective | To report the efficacy results of tisagenlecleucel therapy in cohorts of patients with r/r diffuse large B-cell lymphoma or FL, and to provide up to 3 years of follow-up data |
Study design | Single-centre, open-label, single-arm, phase IIa trial |
Locations | Single site in the US |
Patient enrolment datesa | Start date: February 2014 End date: September 2020 |
Nonrandomized (N) | 14 (in the FL single-arm cohort) |
Inclusion criteria | Adults with CD19+ diffuse large B-cell lymphoma or FL with no curative treatment options, a limited prognosis (< 2 years of anticipated survival), and a partial response to or stable disease after the most recent therapy Measurable progression of disease less than 2 years after the second line of immunochemotherapy (excluding single-drug monoclonal antibody therapy) |
Exclusion criteria | NR |
Intervention | Tisagenlecleucel Dose:
ROA: IV (single infusion) |
Comparator(s) | NA |
Screening phase | NR |
Time since enrolmentb to tisagenlecleucel infusion | NR |
Treatment phase | Single-dose, one-time infusion |
Follow-up phase | 28.6 months (Schuster et al. [2017]33) 49 months (Chong et al. [2019]107) 60.7 months (Chong et al. [2021]108) |
Primary end point | ORR at 3 months |
Secondary and exploratory end points | Secondary:
|
Publications | Schuster et al. (2017),33 Chong et al. (2019),107 Chong et al. (2021),108 Chong et al. (2016),109 Levine et al. (2015),110 Schuster et al. (2015),111-113 Schuster et al. (2014),114 Schuster et al. (2016),115 NCT02030834116 |
CAR = chimeric antigen receptor; CRR = complete response rate; DoR = duration of response; FL = follicular lymphoma; mFU = median follow-up; NA = not applicable; NR = not reported; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; PRR = partial response rate; ROA = route of administration; TTNT = time to next treatment.
aDates reported are the study start and end dates from the clinicaltrials.gov record for each trial.
bEnrolment was defined as the point when the patient met all inclusion and/or exclusion criteria and the patient’s leukapheresis product was received and accepted by the manufacturing facility.
Sources: Schuster et al.33 and NCT02030834.116 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Populations
Patients eligible for inclusion in this study were required to have CD19+ diffuse large B-cell lymphoma or FL with no curative treatment options (e.g., allo-SCT or auto-SCT), with a limited prognosis (several months to < 2 years of anticipated survival) and a PR or stable disease after the most recent therapy. Patients with FL were eligible if they had measurable progression of disease less than 2 years after the second line of immunochemotherapy (excluding single-drug monoclonal antibody).
Interventions
Tisagenlecleucel was administered as a one-time, single infusion of CD19 CAR T cells by IV injection (total dose of 1 to 5 × 108 cells).33
Bridging Therapy
In the overall study population, 10 of 28 patients received bridging therapy after apheresis and before LD chemotherapy; however, the specific number of patients with FL who received bridging therapy was not provided.
Lymphodepleting Chemotherapy
The LD chemotherapy received by 14 patients included bendamustine in 6 patients, cyclophosphamide plus fludarabine in 1 patient, radiation plus cyclophosphamide in 3 patients, cyclophosphamide alone in 2 patients, carboplatin plus gemcitabine in 1 patient, and modified EPOCH (doxorubicin, etoposide, cyclophosphamide, but no prednisone or vincristine) in 1 patient.
Outcomes
The primary outcome in the Schuster et al. (2017)33 study was ORR at 3 months in patients with NHL, based on the 1999 International Working Group response criteria. The secondary outcomes included CRR, PRR, DoR, OS, PFS, safety, and time to next treatment.
Statistical Analysis
The primary outcome of ORR and the associated 95% CIs were calculated based on binomial distribution. PFS and DoR were estimated using the KM methodology. The median survival time and rate of survival with 95% CIs were calculated at different time points. The handling of missing data and sensitivity analyses have not been reported in this study.
Sample Size and Power Calculation
Sample size of the Shuster et al. study was estimated based on a response rate of 50% (15 of 30 patient responses), with 95% CIs of the true response rate being more than 30%. Even though the population of interest in this study was patients with FL, the sample size calculation was based on the overall NHL population.
Results
Patient Disposition
A total of 15 patients with r/r FL were enrolled, of whom 14 received tisagenlecleucel treatment. One patient did not receive the treatment because of rapid disease progression.
Baseline Characteristics
Among the 14 patients who received treatment with tisagenlecleucel, the median age was 59 years (range, 43 to 72 years). There was equal distribution of male and female patients (50% each). The median lines of prior therapy was 5.0 (range, 2 to 10 lines). Overall, 12 patients (86%) were at the advanced stage of disease, which is defined as stage III or IV, according to the modified Ann Arbor staging system. In 4 patients (28%), bone marrow was involved. Elevated LDH was recorded in 9 patients (64%). All patients (100%) had a baseline ECOG PS of 0 or 1. Eight of 14 patients (57%) had double refractory FL, which was defined as disease in which progressive or stable disease was considered to be the best response to chemotherapy (stable disease was defined as disease that is less than 12 months in duration after the patient has undergone at least 4 cycles of first-line therapy or 2 cycles of second-line, third-line, or later line therapies) or relapsed in the 12 months after auto-SCT. Patients must have received an anti-CD20 mAb (unless they had negative test results for CD20) and an anthracycline as 1 of their previous treatment regimens. Three patients (21%) had received prior auto-SCT and 1 patient (7%) had received prior allo-SCT.33
Exposure to Interventions
As tisagenlecleucel is given as a single-dose, one-time IV infusion, all patients who were infused in the included studies received 100% of the dose. The median number of days from apheresis to tisagenlecleucel infusion was 39 (range, 27 to 145 days).33 The median total dose of tisagenlecleucel in the overall study population was 5.00 × 108 cells (range, 1.79 × 108 to 5.00 × 108 cells) and the median dose of tisagenlecleucel per kilogram of body weight was 5.79 × 106 cells (range, 3.08 × 106 to 8.87 × 106 cells). No information pertaining to concomitant medications, cointerventions, or subsequent treatments was reported.
Efficacy
In the Schuster et al. study, the response rates were analyzed at 3 months and 6 months. This study reported an ORR of 79% at both assessment points. The CRR was 50% at 3 months and 71% at both 6 months and 49 months.
The median OS was not reached at either 28.6 months or 49 months of median follow-up, and the rate was 93% at 28.6 months of median follow-up. Median PFS was also not reached at 28.6 months; however, a decline was observed at longer follow-up (i.e., median PFS was 32.4 months and 26.2 months at a median follow-up of 49 months and 60 months, respectively). The estimated progression-free probabilities were 77%, 70%, and 43% at median follow-up of 11.4 months, 28.6 months, and 60 months, respectively. The median DoR was not reached at the respective median follow-up time.33,107-109
Key efficacy results are summarized in Table 35.
Table 35: Summary of Key Efficacy Outcomes in the Schuster et al. Study
Outcomes | Tisagenlecleucel (N = 14) |
|---|---|
Overall survival | |
Number of patients contributing to the analysis | 14 |
Rate, n (%) | At 28.6 months of mFU: 13 (93) |
Median (95% CI), months | At 49 months of mFU: not reached (27.2 to NE) |
Progression-free survival | |
Number of patients contributing to the analysis | 14 |
Rate, n (%) [95% CI] | At 11.4 months of mFU: 11 (77) [45 to 92] At 28.6 months of mFU: 10 (70) At 60 months of mFU: 6 (43) [18 to 66] |
Median (95% CI), months | At 28.6 months of mFU: not reached At 49 months of mFU: 32.4 (3.5 to NE) |
Response rates | |
Number of patients contributing to the analysis | 14 |
ORR, n (%) | At 3 months of mFU: 11 (79) At 60.7 months of mFU: 11 (79) |
CRR, n (%) | At 3 months of mFU: 7 (50) At 6 months of mFU: 10 (71) At 49 months of mFU: 10 (71) At 60.7 months of mFU: 10 (71) |
Duration of response | |
Number of patients contributing to the analysis | 12 patients at 28.6 mFU; 11 patients at 49 mFU |
DoR, months, median (95% CI) | At 28.6 months of mFU: not reached At 49 months of mFU: not reached (9.5 to NE) At 60 months of mFU: not reached (9.5 to NE) |
CI = confidence interval; CRR = complete response rate; DoR = duration of response; mFU = median follow-up; NE = not estimable; ORR = overall response rate.
Sources: Schuster et al. (2017),33 Chong et al. (2019),107 Chong et al. (2021),108 and Chong et al. (2016).109 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Harms
Adverse Events
Overall, 6 patients (42.9%) with FL experienced any-grade CRS, 2 (14.3%) of whom reported grade 3 or 4 CRS.109
Serious Adverse Events
Refer to the Adverse Events and Notable Harms sections for CRS and neurologic toxicities.
Withdrawal Due to Adverse Events
Tisagenlecleucel was administered as a one-time infusion; therefore, no patients discontinued treatment in the Schuster et al. study.
Mortality
One death was reported during the study in a patient with FL and progressive neurologic deterioration who had encephalopathy.
Notable Harms
CRS was reported in 6 patients: 4 patients had grade 2 CRS; 1 patient had grade 3 CRS, and 1 patient had grade 4 CRS.
Data for other AEs of special interest were only reported for the overall NHL population in the Schuster et al. study. Eleven patients (39%) reported neurologic toxicities, including encephalopathy in 3 patients (27%), delirium in 2 patients (18%), and tremor in 2 patients (18%). In addition, cognitive disturbance, confusion, involuntary movements, and memory impairment were each reported in 1 patient (9%).
Critical Appraisal
Internal Validity
The main limitations of the Schuster et al. study are the single-arm design, lack of comparator, and open-label nature of the study, which limit interpretation of the treatment effect attributable to tisagenlecleucel. Moreover, the sample size calculation for this study was based on the overall NHL population and was not specific to the FL subgroup, which could limit the detection of magnitude of the effect among the FL subgroup.
External Validity
In terms of generalizability, this study was conducted in the US, which may have a different health system and treatment conditions than Canada.
The patient population in this study had a baseline ECOG PS of 0 or 1. It is not clear if the results are generalizable to patients with a poorer performance status.
Discussion
Summary of Available Evidence
One clinical study, ELARA, was included in the systematic review. The ELARA study is a phase II, open-label, single-arm study that evaluated the efficacy and safety of tisagenlecleucel in patients with r/r grade 1, 2, or 3a FL after 2 or more lines of systemic therapy. The primary end point was CRR per IRC through 24 months. Secondary end points included ORR, OS, PFS, DoR, and HRQoL. A total of 94 of the 98 patients enrolled in the ELARA study received tisagenlecleucel and were included in the primary efficacy analyses. Data with up to 30 months of follow-up were available at the time of this review (data cut-off date of March 29, 2022). The median age observed in the overall r/r FL population was 57 years (range, 29 to 73 years). More males (68.1%) were enrolled than females (31.9%), and most patients (84.0%) were white. Almost all patients (97.0%) had a baseline ECOG PS of 0 or 1. Most patients also had grade 1 or 2 (90.4%) and stage III or IV (80.0%) disease. Enrolled patients had received a median of 4 (range, 2 to 13) prior lines of treatments. Of the 98 included patients, 77.6% were refractory to the last line of antineoplastic therapy. The proportion of patients who progressed within 24 months of first-line anti-CD20 mAb-containing therapy was 64.9%.
One sponsor-submitted ITC was summarized and critically appraised. Although the comparator treatment used in the MAIC has not yet been reviewed by the CADTH pan-Canadian Oncology Drug Review Expert Review Committee for this indication, the ITC was used to inform the sponsor’s pharmacoeconomic model and therefore was reviewed by the clinical team. The sponsor performed a MAIC to estimate the ORR, CRR, OS, and PFS of tisagenlecleucel relative to axicabtagene ciloleucel in patients with r/r FL after 2 more line of therapies. The MAIC included 2 single-arm, open-label, multicentre phase II trials, and was based on individual data from patients who received tisagenlecleucel in the ELARA study and on aggregate data from patients who received axicabtagene ciloleucel in the ZUMA-5 study, which was identified during a systematic review of r/r FL anticancer therapies.
The sponsor also provided an additional study in which patients in the ELARA study were matched with patients included in the retrospective cohort ReCORD-FL study to provide comparator efficacy data for tisagenlecleucel versus standard chemotherapy.
In addition, a single-centre, single-arm study (by Schuster et al.) evaluating the effectiveness and safety of tisagenlecleucel in patients with NHL (including 14 patients with r/r FL) was reviewed. OS and PFS data with up to 60 months of follow-up were reported.
Interpretation of Trial Results
Efficacy
CRR was the primary outcome in the ELARA study. The CRR per IRC was 68.1% (95% CI, 57.7% to 77.3%) in the treated population. The results of sensitivity analyses based on various analysis sets and subgroup analyses based on various patient characteristics at baseline supported the primary analysis of CRR. The clinical experts consulted by CADTH indicated that the results of the CRR was clinically important based on their clinical experience in treating patients with r/r FL.
Survival outcomes were identified by CADTH with input from patient groups and clinicians as some of the most important efficacy outcomes to assess treatment effect in patients with r/r FL. Prolonged survival may be correlated with high response rates (e.g., ORR and CRR); patients who achieve a CR after CAR T-cell therapy have a better prognosis (e.g., more favourable survival) than those who do not respond well but this is not always the case, per the clinical experts. In a meta-analysis evaluating the relationship between response rates and median PFS in patients with NHL (including FL, which accounted for 23% of the study population), a strong correlation between response rates and PFS was found (the coefficient of determination [r2] was 0.78 for ORR versus median PFS and 0.74 for CRR versus median PFS). The results were similar in the subgroup of patients with r/r FL and treatment-naive FL.117 In another meta-analysis examining the correlation between response and survival outcomes, a moderate correlation was observed between CRR and median PFS in patients with FL (r2 = 0.69). In this study, the authors noted that because the median OS was usually not reached in clinical trials of NHL, limiting the data, none of the median OS-related correlation analysis results were evaluable.118
At the data cut-off of March 29, 2022, based on the 30-month data in the ELARA study, the survival rate was 82.6% (95% CI, 70.2% to 90.2%) in the EAS, whereas the median OS was not reached at the time of analysis. Another survival outcome, PFS, measures the length of time from tisagenlecleucel infusion to the date of disease progression or death from any cause. The proportion of patients who remained progression-free at 24 months was 57.4% (95% CI, 46.2% to 67.0%). According to the clinical experts consulted by CADTH, the survival data look promising in patients with r/r FL. However, given that the OS data and the PFS data are immature (30 months of data thus far), it is still too early to determine the impact of tisagenlecleucel on a patient’s longer-term survival. In addition, the survival benefit gained from treatment with tisagenlecleucel compared to currently available treatments for r/r FL could not be claimed due to the noncomparative design of the ELARA study. It is also worth considering the OS in patients with FL who do not receive CAR T-cell therapy when interpreting these results. Results from a retrospective analysis conducted in a single centre in the US showed that among patients with FL who had received multiple lines of treatment, median OS was 11.7 years, 8.8 years, and 5.3 years for patients who received the second-line, third-line, and fourth-line treatments, respectively. In this study, recurrent uses of single-drug rituximab (9% to 31%), alkylator-based chemotherapy (22% to 26%), and radiotherapy alone or radioimmunotherapy (10% to 18%) were common in second-line to sixth-line therapy. Ten percent of treated patients received SCT during the course of their therapy (auto-SCT, 6%; allo-SCT, 4%). Investigational therapies (not specified and unclear whether a CAR T-cell product was used) ranged from 8% to 22% when second-line or later therapy was required.6
After tisagenlecleucel infusion, some patients received subsequent antineoplastic medications (23.0%) or allo-SCT (4.1%) when they were considered to have stable disease or progressive disease. It is unknown how subsequent therapy with allo-SCT and other cancer treatments would impact a patient’s survival or response to tisagenlecleucel treatment.
HRQoL was an outcome indicated as important by patients with r/r FL, as well as clinicians. HRQoL is also useful in contextualizing the impacts of other efficacy outcomes and harms. Although the findings related to HRQoL based on the 3 tools from the ELARA study suggested that a patient’s HRQoL at baseline was maintained at 24 months, firm conclusion regarding the effect of tisagenlecleucel on HRQoL could not be made due to the large amount of missing data (at 24 months, HRQoL data were available in only half of the baseline population). It is unclear if treatment with tisagenlecleucel is associated with improved HRQoL based on the available evidence.
Due to lack of direct comparative evidence, results from the sponsor-submitted MAIC suggest that ORR, CRR, OS, and PFS associated with tisagenlecleucel treatment are similar to those outcomes associated with axicabtagene ciloleucel treatment. However, definitive conclusions related to the response and survival benefits of tisagenlecleucel, compared to axicabtagene ciloleucel, cannot be drawn from the MAIC analysis due to methodological limitations, including trial design differences that could not be adjusted for in the analysis; adjustment on only a limited number of potential prognostic factors and effect modifiers; and small sample sizes.
Results of a comparison between tisagenlecleucel and standard chemotherapy (from the ReCORD-FL study, which was a noninterventional, multicentre, retrospective chart review used as an external comparator) suggested that, compared to standard chemotherapy, tisagenlecleucel was associated with improved OS and PFS. However, interpretation of the comparative results is limited by the potential for selection bias and residual confounding despite propensity score matching. Therefore, the statistical inference from the comparison of the ELARA to ReCORD-FL studies has low reliability and validity and the results are highly uncertain.
Results of a small single-arm study by Schuster et al. reported favourable CRR per IRC assessment (71% at 49 months), a 93% OS rate at 29-month follow-up, and a 43% PFS rate at 60-month follow-up. Interpretation of the study findings is also limited due to the study design.
Harms
At the data cut-off date of March 29, 2022, all 97 patients in the safety analysis set of the ELARA study reported at least 1 AE. The most common AEs reported were CRS, neutropenia, anemia, diarrhea, headache, decreased white blood cell count, pyrexia, thrombocytopenia, fatigue, nausea, decreased neutrophil count, constipation, and hypogammaglobulinemia. Most of these AEs are symptoms of CRS, which is a usual but severe AE associated with CAR T-cell therapy. A total of 46.4% of patients experienced any SAE. The most commonly reported SAEs included CRS, pneumonia, and febrile neutropenia. There were 13 deaths reported after tisagenlecleucel infusion in the ELARA study (13.4% of patients; 7 patients died from the study indication and 6 from other causes). In terms of AEs of special interest, more than 40% of patients experienced any-grade CRS (49.5%), hematological disorders including cytopenias (78.4%), and infections (55.7%). According to the clinical experts consulted by CADTH, the safety profile of tisagenlecleucel is consistent with other CAR T-cell therapies, and no unexpected safety signals were observed in the ELARA study.
Fifty-three ELARA patients who received infused nonbridging chemotherapy and 124 patients in the ZUMA-5 infused set were included in the MAIC of safety outcomes. At least 1 AE of any grade was reported in 44.6% of patients in the ELARA study and in 78.2% of patients in the ZUMA-5 study. AEs of grade 3 or above were reported in no patients in the ELARA study and in 6.5% of patients in the ZUMA-5 study. Management of CRS with corticosteroids was documented in 3.0% and 15.3% of patients in the ELARA and ZUMA-5 studies, respectively. CRS management with tocilizumab was documented in 9.9% and 45.2% of patients in the ELARA and ZUMA-5 studies, respectively. Neurologic events of any grade were documented in 9.5% of patients in the ELARA study and in 56.5% of patients in the ZUMA-5 study, respectively. Neurologic events of grade 3 or above were reported among 0.19% and 15.32% of patients in the ELARA and ZUMA-5 studies, respectively. Based on the MAIC, tisagenlecleucel appears to have a better toxicity profile than axicabtagene ciloleucel. However, due the previously described limitations of the MAIC analysis, including the application of different definitions of neurologic events in the ELARA and ZUMA-5 studies, the results from the comparative harms analyses between tisagenlecleucel and axicabtagene ciloleucel were associated with too much uncertainty to draw a definitive conclusion.
Harms outcomes were not compared between the ELARA and ReCORD-FL studies.
In the Schuster et al. study, CRS of any grade and of grade 3 or 4 was recorded in 42.9% and 14.3% of patients with r/r FL, respectively. Other harm outcomes were reported for the overall population with NHL in this study, and results specific for patients with r/r FL were not reported.
Conclusion
Evidence from a single-arm study (ELARA) suggests that treatment with tisagenlecleucel is associated with clinically important tumour responses, including complete remission, in adults with r/r FL after 2 or more lines of systemic therapy. There is insufficient evidence — in part due to the limited follow-up duration of the trial — to determine the effects of tisagenlecleucel on OS and PFS. PROs suggest that a patient’s QoL could be maintained; however, 24-month HRQoL data were based on only about 50% of the baseline population. It is unclear if treatment with tisagenlecleucel would improve HRQoL. The harms associated with the tisagenlecleucel infusion are consistent with its mechanism of action, and no unexpected safety signals observed.
The CADTH clinical assessment identified limitations of the sponsor’s comparison of the ELARA and ReCORD-FL studies and the sponsor-conducted MAIC (including small sample sizes, heterogeneity across study designs and populations, and the inability to adjust for all potential effect modifiers and prognostic variables), which substantially limited the ability to interpret the relative treatment effects observed for tisagenlecleucel, standard chemotherapy, and axicabtagene ciloleucel.
References
1.Canadian Cancer Society. Follicular lymphoma. 2022; https://cancer.ca/en/cancer-information/cancer-types/non-hodgkin-lymphoma/what-is-non-hodgkin-lymphoma/follicular-lymphoma. Accessed 2022 Oct 03.
2.American Cancer Society. Types of B-cell lymphomas. About non-Hodgkin lymphoma 2022; https://www.cancer.org/cancer/non-hodgkin-lymphoma/about/b-cell-lymphoma.html. Accessed 2022 Oct 03.
3.Freedman A, Friedberg JW. Histologic transformation of follicular lymphoma. Waltham (MA): UpToDate; 2022: www.uptodate.com. Accessed 2023 Feb 17.
4.Link BK, Day BM, Zhou X, et al. Second-line and subsequent therapy and outcomes for follicular lymphoma in the United States: data from the observational National LymphoCare Study. Br J Haematol. 2019;184(4):660-663. PubMed
5.Hubel K, Salles G, Marcus R, Zinzani PL, Dreyling M. New treatment options in advanced stage follicular lymphoma. Hemasphere. 2018;2(6):e156. PubMed
6.Batlevi CL, Sha F, Alperovich A, et al. Follicular lymphoma in the modern era: survival, treatment outcomes, and identification of high-risk subgroups. Blood Cancer J. 2020;10(7):74. PubMed
7.Rivas-Delgado A, Magnano L, Moreno-Velázquez M, et al. Response duration and survival shorten after each relapse in patients with follicular lymphoma treated in the rituximab era. Br J Haematol. 2019;184(5):753-759. PubMed
8.Johnson PW, Rohatiner AZ, Whelan JS, et al. Patterns of survival in patients with recurrent follicular lymphoma: a 20-year study from a single center. J Clin Oncol. 1995;13(1):140-147. PubMed
9.Klyuchnikov E, Bacher U, Kroger NM, et al. Reduced-intensity allografting as first transplantation approach in relapsed/refractory grades one and two follicular lymphoma provides improved outcomes in long-term survivors. Biol Blood Marrow Transplant. 2015;21(12):2091-2099. PubMed
10.Brenner DR, Poirier A, Woods RR, et al. Projected estimates of cancer in Canada in 2022. CMAJ. 2022;194(17):E601-607. PubMed
11.Pettengell R, Donatti C, Hoskin P, et al. The impact of follicular lymphoma on health-related quality of life. Ann Oncol. 2008;19(3):570-576. PubMed
12.Price M, Ravelo A, Sae-Hau M, et al. Patient-reported disease burden in chronic lymphocytic leukemia, diffuse large B-cell lymphoma, and follicular lymphoma: results from a national patient advocacy survey. J Clin Oncol. 2019;37(15_suppl):e18198.
13.Orphanet. Follicular lymphoma (ORPHA:545). 2010; https://www.orpha.net/consor/cgi-bin/Disease_Search.php?lng=EN&data_id=8750&Disease_Disease_Search_diseaseGroup=Follicular-lymphoma&Disease_Disease_Search_diseaseType=Pat&Disease(s)/group%20of%20diseases=Follicular-lymphoma&title=Follicular%20lymphoma&search=Disease_Search_Simple. Accessed 2022 Oct 03.
14.Morton LM, Wang SS, Devesa SS, Hartge P, Weisenburger DD, Linet MS. Lymphoma incidence patterns by WHO subtype in the United States, 1992-2001. Blood. 2006;107(1):265-276. PubMed
15.Kahl BS, Yang DT. Follicular lymphoma: evolving therapeutic strategies. Blood. 2016;127(17):2055-2063. PubMed
16.Cerhan JR. Epidemiology of follicular lymphoma. Hematol Oncol Clin North Am. 2020;34(4):631-646. PubMed
17.Drug Reimbursement Review sponsor submission: Kymriah (tisagenlecleucel), target of 0.6 to 6.0*108 CAR-positive viable T-cells (non-weight based) and cell suspension in patient-specific single infusion bag for intravenous infusion [internal sponsor's package]. Dorval (QC): Novartis Pharmaceuticals Canada Inc.; 2023 Feb 08.
18.Freedman A, Aster JC. Clinical manifestations, pathologic features, diagnosis,and prognosis of follicular lymphoma. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: www.uptodate.com. Accessed 2023 Feb 17.
19.Dreyling M, Ghielmini M, Rule S, et al. Newly diagnosed and relapsed follicular lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2021;32(3):298-308. PubMed
20.NCCN Guidelines. B-cell lymphomas, version 5.2022. Plymouth Meeting (PA): National Comprehensive Cancer Network; 2022: https://www.nccn.org/. Accessed 2022 Oct 04.
21.Guideline Resource Unit. Clinical practice guideline on lymphoma, version 16. Edmonton (AB): Cancer Care Alberta, Alberta Health Services; 2021: https://www.albertahealthservices.ca/assets/info/hp/cancer/if-hp-cancer-guide-lyhe002-lymphoma.pdf. Accessed 2022 Oct 05.
22.BC Cancer. Hodgkin lymphoma. (Cancer management manual: lymphoma, chronic leukemia, myeloma). Vancouver (BC): Provincial Health Services Authority; 2013: http://www.bccancer.bc.ca/health-professionals/clinical-resources/cancer-management-manual/lymphoma-chronic-leukemia-myeloma/hodgkin-lymphoma#Treatment. Accessed 2022 Oct 05.
23.Kuruvilla J, Assouline S, Hodgson D, et al. A Canadian evidence-based guideline for the first-line treatment of follicular lymphoma: joint consensus of the Lymphoma Canada Scientific Advisory Board. Clin Lymphoma Myeloma Leuk. 2015;15(2):59-74. PubMed
24.Lymphoma Canada. Follicular lymphoma guidelines. 2015; http://www.lymphoma.ca/medpath/#md:cid=1&md:viewname=dashboardTreeView&ca:viewname=CADefault&ca:id=404&car:viewname=CourseActivityResourcesEmpty&cat:viewname=CourseActivityTreeActivityByType. Accessed 2022 Oct 05.
25.Robinson SP, Canals C, Luang JJ, et al. The outcome of reduced intensity allogeneic stem cell transplantation and autologous stem cell transplantation when performed as a first transplant strategy in relapsed follicular lymphoma: an analysis from the Lymphoma Working Party of the EBMT. Bone Marrow Transplant. 2013;48(11):1409-1414. PubMed
26.Buske C, Hutchings M, Ladetto M, et al. ESMO Consensus Conference on malignant lymphoma: general perspectives and recommendations for the clinical management of the elderly patient with malignant lymphoma. Ann Oncol. 2018;29(3):544-562. PubMed
27.National Cancer Institute. CAR T cells: enginneering patients' immune cells to treat their cancers. 2022; https://www.cancer.gov/about-cancer/treatment/research/car-t-cells. Accessed 2023 Apr 8.
28.Kymriah (tisagenlecleucel): 1.2 x 106 to 6.0 x 108 CAR-positive viable T cells, cell suspension in infusion bag, for intravenous use [product monograph]. Dorval (QC): Novartis Pharmaceuticals Canada Inc.; 2022 Dec 19.
29.Clinical Study Report: CCTL019E2202. A phase II, single arm, multicenter open label trial to determine the efficacy and safety of tisagenlecleucel (CTL019) in adult patients with refractory or relapsed follicular lymphoma, version 1.0 [internal sponsor's report]. Dorval (QC): Novartis Pharmaceuticals Canada Inc.; 2022 Aug 12.
30.Kymriah (tisagenlecleucel) for treatment of adult patients with refractory or relapsed follicular lymphoma after two or more lines of therapy [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Kymriah (tisagenlecleucel) cell suspension in infusion bag, 1.2 x 106 to 6.0 x 108 CAR-positive viable T cells for intravenous use. Dorval (Quebec): Novartis Pharmaceuticals Canada Inc.; 2023 Feb 08.
31.Matching-adjusted indirect treatment comparisons of efficacy and safety of tisagenlecleucel versus axicabtagene ciloleucel among adult patients with relapsed/refractory follicular lymphoma [internal sponsor's report] In: Drug Reimbursement Review sponsor submission: Kymriah (tisagenlecleucel), target of 0.6 to 6.0*108 CAR-positive viable T-cells (non-weight based) and cell suspension in patient-specific single infusion bag for intravenous infusion. Dorval (QC): Novartis Pharmaceuticals Canada Inc.; 2022 Aug.
32.Indirect comparison of study E2202 (data cut-off: March 2022) versus ReCORD standard of care / chemotherapy-treated patients in relapsed/refractory follicular lymphoma [internal sponsor's report] In: Drug Reimbursement Review sponsor submission: Kymriah (tisagenlecleucel), target of 0.6 to 6.0*108 CAR-positive viable T-cells (non-weight based) and cell suspension in patient-specific single infusion bag for intravenous infusion. Dorval (QC): Novartis Pharmaceuticals Canada Inc.; 2022 Sep.
33.Schuster SJ, Svoboda J, Chong EA, et al. Chimeric Antigen Receptor T Cells in Refractory B-Cell Lymphomas. N Engl J Med. 2017;377(26):2545-2554. PubMed
34.Shankland KR, Armitage JO, Hancock BW. Non-Hodgkin lymphoma. Lancet. 2012;380(9844):848-857. PubMed
35.Understanding NHL: a patient's guide to non-Hodgkin lymphoma. Mississauga (ON): Lymphoma Canada; 2020: https://z9a2f9c2.rocketcdn.me/wp-content/uploads/2020/05/2020430-NHL-Interior-WEB.pdf. Accessed 2022 Oct 04.
36.Kohrt HEK, Ugarte A. Follicular Lymphoma: a guide for patients - information based on ESMO clinical practice guidelines, v.2014.1 Lugano (CH): ESMO; 2014: https://www.esmo.org/content/download/52236/963497/1/EN-Follicular-Lymphoma-Guide-for-Patients.pdf. Accessed 2022 Oct 03.
37.Salles GA. Clinical features, prognosis and treatment of follicular lymphoma. Hematology Am Soc Hematol Educ Program. 2007;2007(1):216-225. PubMed
38.Conlan MG, Armitage JO, Bast M, Weisenburger DD. Clinical significance of hematologic parameters in non-Hodgkin's lymphoma at diagnosis. Cancer. 1991;67(5):1389-1395. PubMed
39.Freedman A. Follicular lymphoma: 2018 update on diagnosis and management. Am J Hematol. 2018;93(2):296-305. PubMed
40.Freedman A. Follicular lymphoma: 2014 update on diagnosis and management. Am J Hematol. 2014;89(4):429-436. PubMed
41.Casulo C, Byrtek M, Dawson KL, et al. Early relapse of follicular lymphoma after rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone defines patients at high risk for death: an analysis from the National LymphoCare Study. J Clin Oncol. 2015;33(23):2516-2522. PubMed
42.Casulo C, Burack WR, Friedberg JW. Transformed follicular non-Hodgkin lymphoma. Blood. 2015;125(1):40-47. PubMed
43.Seymour JF, Marcus R, Davies A, et al. Association of early disease progression and very poor survival in the GALLIUM study in follicular lymphoma: benefit of obinutuzumab in reducing the rate of early progression. Haematologica. 2019;104(6):1202-1208. PubMed
44.Singh D, Singh A, Mukkamalla SKR. Relapsed and refractory follicular lymphoma. In: [Internet] S, ed. Treasure Island (FL): StatPearls Publishing; 2023: https://www.ncbi.nlm.nih.gov/books/NBK589677/. Accessed 2023 Apr 21.
45.Sarkozy C, Maurer MJ, Link BK, et al. Cause of death in follicular lymphoma in the first decade of the rituximab era: a pooled analysis of French and US cohorts. J Clin Oncol. 2019;37(2):144-152. PubMed
46.Jaglowski SM, Linden E, Termuhlen AM, Flynn JM. Lymphoma in adolescents and young adults. Semin Oncol. 2009;36(5):381-418. PubMed
47.Carbone PP, Kaplan HS, Musshoff K, Smithers DW, Tubiana M. Report of the Committee on Hodgkin's Disease Staging Classification. Cancer Res. 1971;31(11):1860-1861. PubMed
48.Solal-Céligny P, Roy P, Colombat P, et al. Follicular lymphoma international prognostic index. Blood. 2004;104(5):1258-1265. PubMed
49.NCCN Guidelines for Patients. Follicular lymphoma. Plymouth Meeting (PA): National Comprehensive Cancer Network; 2022: https://www.nccn.org/patients/guidelines/content/PDF/nhl-follicular-patient.pdf. Accessed 2022 Oct 04.
50.Lopez-Guillermo A, Caballero D, Canales M, et al. Clinical practice guidelines for first-line/after-relapse treatment of patients with follicular lymphoma. Leuk Lymphoma. 2011;52 Suppl 3:1-14. PubMed
51.Klyuchnikov E, Bacher U, Woo Ahn K, et al. Long-term survival outcomes of reduced-intensity allogeneic or autologous transplantation in relapsed grade 3 follicular lymphoma. Bone Marrow Transplant. 2016;51(1):58-66. PubMed
52.Smith SM, Godfrey J, Ahn KW, et al. Autologous transplantation versus allogeneic transplantation in patients with follicular lymphoma experiencing early treatment failure. Cancer. 2018;124(12):2541-2551. PubMed
53.Sarkozy C, Trneny M, Xerri L, et al. Risk factors and outcomes for patients with follicular lymphoma who had histologic transformation after response to first-line immunochemotherapy in the PRIMA trial. J Clin Oncol. 2016;34(22):2575-2582. PubMed
54.Teva-Lenalidomide (lenalidomide as lenalidomide hydrochloride monohydrate) 2.5 mg, 5 mg, 10 mg, 15 mg, 20 mg, and 25 mg oral capsules [product monograph]. Toronto (ON): Teva Canada Limited; 2022 Sep 13: https://pdf.hres.ca/dpd_pm/00067563.PDF. Accessed 2023 Aug 28.
55.Khangura SD, Ryce A. Lenalidomide plus rituximab chemotherapy for relapsed or refractory indolent B-cell Non-Hodgkin lymphomas. Can J Health Technol. 2021;1(11). 10.51731/cjht.2021.203. Accessed 2022 Nov 01.
56.Zydelig (idelalisib): 150 mg and 100 mg, oral tablet [product monograph]. Mississauga (ON): Gilead Sciences Canada, Inc.; 2020 Aug 18: https://pdf.hres.ca/dpd_pm/00057731.PDF. Accessed 2023 Aug 28.
57.pCODR Expert Review Committee (pERC) final recommendation: idelalisib (Zydelig - Gilead Sciences, Inc). Ottawa (ON): CADTH; 2016 Sep 29: https://www.cadth.ca/sites/default/files/pcodr/pcodr_idelalisib_zydelig_fl_fn_rec.pdf. Accessed 2022 Oct 31.
58.Yescarta (axicabtagene ciloleucel): target of 2 × 106 chimeric antigen receptor (CAR)-positive viable T cells per kg body weight with a maximum of 2 × 108 CAR-positive viable T cells, csuspension in patient-specific single infusion bag, for intravenous infusion [product monograph]. Mississauga (ON): Gilead Sciences Canada, Inc.; 2022 Oct 13: https://pdf.hres.ca/dpd_pm/00067754.PDF. Accessed 2023 Aug 28.
59.Cheson BD, Fisher RI, Barrington SF, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J Clin Oncol. 2014;32(27):3059-3068. PubMed
60.Qualifying notice for Kymriah. Ottawa (ON): Health Canada; 2022: https://www.canada.ca/en/health-canada/services/drugs-health-products/drug-products/notice-compliance/conditions/qualifying-notice-kymriah-263500.html. Accessed 2023 May 25.
61.Fowler NH, Dickinson M, Dreyling M, et al. Tisagenlecleucel in adult relapsed or refractory follicular lymphoma: the phase 2 ELARA trial. Nat Med. 2022;28(2):325-332. PubMed
62.Fowler NH, Dickinson M, Ghosh M, et al. Assessment of healthcare resource utilization and costs in patients with relapsed or refractory follicular lymphoma undergoing CAR-T cell therapy with tisagenlecleucel: results from the Elara study. Blood. 2021;138(Supplement 1):3533-3533.
63.Fowler NH, Dickinson M, Martinez‐Lopez J, et al. Patient‐reported quality of life (Qol) following tisagenlecleucel (Tisa‐Cel) infusion in adult patients (Pts) with relapsed/refractory follicular lymphoma (R/R Fl). Hematol Oncol. 2021;39(S2):358-361.
64.Schuster SJ, Dickinson M, Dreyling M, et al. Efficacy and Safety of Tisagenlecleucel (Tisa‐Cel) in Adult Patients (Pts) with Relapsed/Refractory Follicular Lymphoma (R/R Fl): Primary Analysis of the Phase 2 Elara Trial. Hematol Oncol. 2021;39(S2):139-141.
65.Fowler NH, Dickinson M, Dreyling M, et al. Efficacy and safety of tisagenlecleucel in adult patients with relapsed/refractory follicular lymphoma: interim analysis of the phase 2 Elara trial. Blood. 2020;136(Supplement 1):1-3.
66.Hao Y, Hsu W-C, Parzynski CS, et al. Comparison of Clinical Outcomes Among Patients with Relapsed/Refractory Follicular Lymphoma Treated with Tisagenlecleucel in the Elara Trial Versus a Real-World External Control Arm of Patients Treated with Standard of Care. Blood. 2021;138(Supplement 1):2419.
67.Schuster SJ, Dickinson M, Dreyling M, et al. V484: Efficacy and safety of Tisagenlecleucel (Tisa-cel) in adult patients (Pts) with relapsed/refractory follicular lymphoma (r/r FL): primary analysis of the phase 2 ELARA trial. Oncol Res Treat. 2021;44(Suppl 2):104-105.
68.Schuster SJ, Dickinson M, Dreyling M, et al. IBCL-195: primary analysis of the phase 2 ELARA trial: tisagenlecleucel efficacy and safety in adult patients with relapsed/refractory follicular lymphoma (r/r FL). Clin Lymphoma Myeloma Leuk. 2021;21(Suppl 1):S403-S404.
69.Schuster SJ, Dickinson MJ, Dreyling MH, et al. Efficacy and safety of tisagenlecleucel (Tisa-cel) in adult patients pPts) with relapsed/refractory follicular lymphoma (r/r FL): primary analysis of the phase 2 Elara trial. J Clin Oncol. 2021;39(15_suppl):7508.
70.Schuster SJ, Dickinson M, Dreyling M, et al. S210: Efficacy and safety of tisagenlecleucel in adult patients with relapsed/refractory follicular lymphoma: primary analysis of the phase 2 Elara trial. Hemasphere. 2021;5(S2):62.
71.Thieblemont C. Efficacy of tisagenlecleucel in adult patients with high-risk relapsed/refractory follicular lymphoma: subgroup analysis of the phase II ELARA study. Presented at: ASH 2021 Meeting, 2021 Dec 11-14; Atlanta (GA). 2021.
72.Thieblemont C, Dickinson M, Martinez-Lopez J, et al. Efficacy of tisagenlecleucel in adult patients (pts) with high-risk relapsed/refractory follicular lymphoma (r/r FL): subgroup analysis of the phase II ELARA study. Blood. 2021;138(Supplement 1):131.
73.Efficacy and safety of tisagenlecleucel in adult patients with relapsed/refractory follicular lymphoma: Interim analysis of the phase 2 ELARA trial. Clin Adv Hematol Oncol. 2021;19(1 Suppl 2):12.
74.Author. Tisagenlecleucel Is Safe and Effective in Relapsed/Refractory Follicular Lymphoma. Cancer Discov. 2022;12(3):OF4. PubMed
75.Novartis Pharmaceuticals. NCT03568461: Efficacy and safety of tisagenlecleucel in adult patients with refractory or relapsed follicular lymphoma (ELARA). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2022: https://clinicaltrials.gov/ct2/show/NCT03568461. Accessed 2022 Nov 30.
76.Harrison CN, Mesa RA, Kiladjian JJ, et al. Health-related quality of life and symptoms in patients with myelofibrosis treated with ruxolitinib versus best available therapy. Br J Haematol. 2013;162(2):229-239. PubMed
77.Swigris JJ, Brown KK, Behr J, et al. The SF-36 and SGRQ: validity and first look at minimum important differences in IPF. Respir Med. 2010;104(2):296-304. PubMed
78.Irvine EJ. Quality of life of patients with ulcerative colitis: past, present, and future. Inflamm Bowel Dis. 2008;14(4):554-565. PubMed
79.Stark RG, Reitmeir P, Leidl R, Konig HH. Validity, reliability, and responsiveness of the EQ-5D in inflammatory bowel disease in Germany. Inflamm Bowel Dis. 2010;16(1):42-51. PubMed
80.Salles G, Schuster SJ, de Vos S, et al. Efficacy and safety of idelalisib in patients with relapsed, rituximab- and alkylating agent-refractory follicular lymphoma: a subgroup analysis of a phase 2 study. Haematologica. 2017;102(4):e156-e159. PubMed
81.Lan KKG, Demets DL. Discrete sequential boundaries for clinical trials. Biometrika. 1983;70(3):659-663.
82.ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine: https://clinicaltrials.gov/ct2/home. Accessed 2023 Apr 13.
83.Johnson SA, Kumar A, Matasar MJ, Schoder H, Rademaker J. Imaging for staging and response assessment in lymphoma. Radiology. 2015;276(2):323-338. PubMed
84.National Institute for Health and Care Excellence. Appendix B: methodology checklist: systematic reviews and meta-analyses. (The guidelines manual) 2012; https://www.nice.org.uk/process/pmg6/resources/the-guidelines-manual-appendices-bi-2549703709/chapter/appendix-b-methodology-checklist-systematic-reviews-and-meta-analyses. Accessed 2023 Apr 19.
85.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
86.Qualifying notice for Yescarta. Ottawa (ON): Health Canada; 2022: https://www.canada.ca/en/health-canada/services/drugs-health-products/drug-products/notice-compliance/conditions/qualifying-notice-yescarta-256106.html. Accessed 2023 Apr 19.
87.Flinn IW, Miller CB, Ardeshna KM, et al. DYNAMO: a phase II study of duvelisib (IPI-145) in patients with refractory indolent non-Hodgkin lymphoma. J Clin Oncol. 2019;37(11):912-922. PubMed
88.Leppä S, Santoro A, Demeter J, et al. Long-term follow-up of patients (pts) with relapsed or refractory (r/r) follicular lymphoma (FL) treated with copanlisib. J Clin Oncol. 2019;37(15_suppl):7553-7553.
89.Eyre TA, Osborne WL, Gallop-Evans E, et al. Results of a multicentre UK-wide compassionate use programme evaluating the efficacy of idelalisib monotherapy in relapsed, refractory follicular lymphoma. Br J Haematol. 2018;181(4):555-559. PubMed
90.Jacobson C, Chavez JC, Sehgal AR, et al. Primary analysis of Zuma-5: a phase 2 study of axicabtagene ciloleucel (Axi-Cel) in patients with relapsed/refractory (r/r) indolent non-hodgkin lymphoma (iNHL). Blood. 2020;136(Supplement 1):40-41.
91.Budde LE, Sehn LH, Matasar M, et al. Safety and efficacy of mosunetuzumab, a bispecific antibody, in patients with relapsed or refractory follicular lymphoma: a single-arm, multicentre, phase 2 study. Lancet Oncol. 2022;23(8):1055-1065. PubMed
92.Sesques P, Bourcier J, Golfier C, et al. Clinical characteristics and outcomes of relapsed follicular lymphoma after autologous stem cell transplantation in the rituximab era. Hematol Oncol. 2020;38(2):137-145. PubMed
93.Salles G, Schuster SJ, Fischer L, et al. A retrospective cohort study of treatment outcomes of adult patients with relapsed or refractory follicular lymphoma (ReCORD-FL). Hemasphere. 2022;6(7):e745. PubMed
94.Jacobson CA, Chavez JC, Sehgal AR, et al. Axicabtagene ciloleucel in relapsed or refractory indolent non-Hodgkin lymphoma (ZUMA-5): a single-arm, multicentre, phase 2 trial. Lancet Oncol. 2022;23(1):91-103. PubMed
95.Phillippo DM, Ades AE, Dias S, Palmer S, Abrams KR, Welton NJ. NICE DSU technical support document 18: methods for population-adjusted indirect comparisons in submission to NICE. Sheffield (UK): Decision Support Unit, ScHARR, University of Sheffield; 2016: https://www.sheffield.ac.uk/media/34216/download?attachment. Accessed 2023 Aug 28.
96.Signorovitch JE, Sikirica V, Erder MH, et al. Matching-adjusted indirect comparisons: a new tool for timely comparative effectiveness research. Value Health. 2012;15(6):940-947. PubMed
97.Signorovitch JE, Wu EQ, Yu AP, et al. Comparative effectiveness without head-to-head trials: a method for matching-adjusted indirect comparisons applied to psoriasis treatment with adalimumab or etanercept. Pharmacoeconomics. 2010;28(10):935-945. PubMed
98.Neelapu SS, Chavez JC, Sehgal AR, et al. Long-term follow-up analysis of zuma-5: A phase 2 study of axicabtagene ciloleucel (AXI-CEL) in patients with relapsed/refractory (R/R) indolent non-hodgkin lymphoma (INHL). Blood. 2021;138(SUPPL 1):93.
99.SLR to assess clinical efficacy, safety, patient-reported outcomes, and epidemiology associated with the third line treatment for relapsed and/or refractory follicular lymphoma [internal sponsor's report] In: Drug Reimbursement Review sponsor submission: Kymriah (tisagenlecleucel), target of 0.6 to 6.0*108 CAR-positive viable T-cells (non-weight based) and cell suspension in patient-specific single infusion bag for intravenous infusion. Dorval (QC): Novartis Pharmaceuticals Canada Inc.; 2022.
100.Phillippo DM, Ades AE, Dias S, Palmer S, Abrams KR, Welton NJ. Methods for population-adjusted indirect comparisons in health technology appraisal. Med Decis Making. 2018;38(2):200-211. PubMed
101.Phillippo DM, Dias S, Elsada A, Ades AE, Welton NJ. Population adjustment methods for indirect comparisons: a review of National Institute for Health and Care Excellence technology appraisals. Int J Technol Assess Health Care. 2019;35(3):221-228. PubMed
102.Guyot P, Ades AE, Ouwens MJ, Welton NJ. Enhanced secondary analysis of survival data: reconstructing the data from published Kaplan-Meier survival curves. BMC medical research methodology. 2012;12:9. PubMed
103.Lee DW, Gardner R, Porter DL, et al. Current concepts in the diagnosis and management of cytokine release syndrome. Blood. 2014;124(2):188-195. PubMed
104.Topp MS, Gökbuget N, Stein AS, et al. Safety and activity of blinatumomab for adult patients with relapsed or refractory B-precursor acute lymphoblastic leukaemia: a multicentre, single-arm, phase 2 study. The Lancet Oncology. 2015;16(1):57-66. PubMed
105.Neelapu SS, Locke FL, Bartlett NL, et al. Axicabtagene ciloleucel CAR T-cell therapy in refractory large b-cell lymphoma. N Engl J Med. 2017;377(26):2531-2544. PubMed
106.Williamson E, Morley R, Lucas A, Carpenter J. Propensity scores: from naive enthusiasm to intuitive understanding. Stat Methods Med Res. 2012;21(3):273-293. PubMed
107.Chong EA, Svoboda J, Nasta SD, et al. CD19-directed CAR T cell therapy (CTL019) for relapsed/refractory diffuse large B-cell and follicular lymphomas: four year outcomes. Hematol Oncol. 2019;37:137-138.
108.Chong EA, Ruella M, Schuster SJ, Lymphoma Program Investigators at the University of Pennsylvania. Five-year outcomes for refractory B-cell lymphomas with CAR T-cell therapy. N Engl J Med. 2021;384(7):673-674. PubMed
109.Chong EA, Svoboda J, Nasta SD, et al. Chimeric antigen receptor modified T cells directed against CD19 (CTL019) in patients with poor prognosis, relapsed or refractory CD19+ follicular lymphoma: prolonged remissions relative to antecedent therapy. Blood. 2016;128(22):1100.
110.Levine BL, Svoboda J, Nasta SD, et al. Chimeric antigen receptor modified T cells directed against CD19 (CTL019) induce clinical responses in patients with relapsed or refractory CD19+ lymphomas. Cytotherapy. 2015;17(6):S13.
111.Schuster SJ, Svoboda J, Dwivedy Nasta S, et al. Sustained remissions following chimeric antigen receptor modified T Cells directed against CD19 (CTL019) in patients with relapsed or refractory CD19+ lymphomas. Blood. 2015;126(23):183.
112.Schuster SJ, Svoboda J, Nasta SD, et al. 139: Phase II trial of chimeric antigen receptor modified T cells directed against CD19 in relapsed/refractory diffuse large B cell, follicular, and mantle cell lymphomas. In: Oral presentations. Hematol Oncol. 2015;33(S1):175-176.
113.Schuster SJ, Svoboda J, Nasta S, et al. Phase IIa trial of chimeric antigen receptor modified T cells directed against CD19 (CTL019) in patients with relapsed or refractory CD19+ lymphomas. J Clin Oncol. 2015;33(15_suppl):8516.
114.Schuster SJ, Svoboda J, Dwivedy Nasta S, et al. Phase IIa trial of chimeric antigen receptor modified T cells directed against CD19 (CTL019) in patients with relapsed or refractory CD19+ lymphomas. Blood. 2014;124(21):3087.
115.Schuster SJ, Svoboda J, Nasta S, et al. Recovery of humoral immunity in patients with durable complete responses following chimeric antigen receptor modified t cells directed against CD19 (CTL019). J Clin Oncol. 2016;34(15_suppl):7564.
116.University of Pennsylvania. NCT02030834: Phase IIa study of redirected autologous T cells engineered to contain anti-CD19 attached to TCRz and 4-signalling domains in patients with chemotherapy relapsed or refractory CD19+ lymphomas. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2023: https://clinicaltrials.gov/ct2/show/NCT02030834. Accessed 2022 Nov 30.
117.Mangal N, Salem AH, Li M, Menon R, Freise KJ. Relationship between response rates and median progression-free survival in non-Hodgkin's lymphoma: a meta-analysis of published clinical trials. Hematol Oncol. 2018;36(1):37-43. PubMed
118.Zhu R, Lu D, Chu YW, et al. Assessment of Correlation Between Early and Late Efficacy Endpoints to Identify Potential Surrogacy Relationships in Non-Hodgkin Lymphoma: a Literature-Based Meta-analysis of 108 Phase II and Phase III Studies. The AAPS journal. 2017;19(3):669-681. PubMed
Appendix 1: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Table 36: Summary of Subgroup Analyses of CRR per IRC in the ELARA Study (EAS)
CRR in subgroups | Tisagenlecleucel |
|---|---|
Rates in n (%) (95% CI) (Data at 24 mos) | |
Number of patients contributing to the analysis | 94 |
Age < 65 years (n = 70) ≥ 65 years (n = 24) | 45 (64.3) (51.9 to 75.4) 19 (79.2) (57.8 to 92.9) |
FLIPI Low/intermediate (n = 37) High (n = 57) | 29 (78.4) (61.8 to 90.2) 35 (61.4) (47.6 to 74.0) |
Number of prior lines of therapy 2 (n = 24) 3 to 4 (n = 43) > 4 (n = 27) | 14 (58.3) (36.6 to 77.9) 35 (81.4) (66.6 to 91.6) 15 (55.6) (35.3 to 74.5) |
Prior SCT Yes (n = 35) No (n = 59) | 22 (62.9) (44.9 to 78.5) 42 (71.2) (57.9 to 82.2) |
POD24 Yes (n = 61) No (n = 33) | 36 (59.0) (45.7 to 71.4) 28 (84.8) (68.1 to 94.9) |
Bulky disease Yes (n = 61) No (n = 33) | 40 (64.5) (51.3 to 76.3) 24 (75.0) (56.6 to 88.5) |
Bridging therapy Yes (n = 44) No (n = 50) | 28 (63.6) (47.8 to 77.6) 36 (72.0) (57.5 to 83.8) |
LDH at study entry ≤ ULN (n = 53) > ULN (n = 41) | 39 (73.6) (59.7 to 84.7) 25 (61.0) (44.5 to 75.8) |
CI = confidence interval; CRR = complete response rate; EAS = Efficacy analysis set; FLIPI = Follicular Lymphoma International Prognostic Index; LDH = lactate dehydrogenase; IRC = independent review committee; mos = months; POD24 = progression of disease within 24 months from first-line treatment; ULN = upper limit of the normal.
Source: ELARA Clinical Study Report.29 (Note: Details from table have been taken from the sponsor’s Summary of Clinical Evidence.30)
Pharmacoeconomic Review
Abbreviations
AE
adverse event
auto
autologous
BR
rituximab plus bendamustine
CAR
chimeric antigen receptor
CRS
cytokine release syndrome
FL
follicular lymphoma
ICER
incremental cost-effectiveness ratio
ICU
intensive care unit
KM
Kaplan-Meier
LY
life-year
MAIC
matching-adjusted indirect comparison
OCCI
Ontario Case Costing Initiative
O-CHOP
obinutuzumab plus cyclophosphamide plus doxorubicin plus vincristine plus prednisone
OS
overall survival
PFS
progression-free survival
PSM
partitioned survival model
QALY
quality-adjusted life-year
r/r
relapsed or refractory
R2
rituximab plus lenalidomide
R-CHOP
rituximab plus cyclophosphamide plus doxorubicin plus vincristine plus prednisone
RCT
randomized controlled trial
R-CVP
rituximab plus cyclophosphamide plus vincristine plus prednisone
R-GDP
rituximab plus gemcitabine plus dexamethasone plus cisplatin
R-ICE
rituximab plus ifosfamide plus carboplatin plus etoposide
SCT
stem cell transplant
SOC
standard of care
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Tisagenlecleucel (Kymriah), cell suspension of CAR-positive viable T cells, for IV infusion |
Submitted price | Tisagenlecleucel, cell suspension of 0.6 to 6.0 × 108 cells (nonweight-based dose): $450,000 per one-time infusion |
Indication | Adults with r/r grade 1, 2, or 3a FL after 2 or more lines of systemic therapy |
Health Canada approval status | NOC/c |
Health Canada review pathway | Priority review |
NOC date | December 19, 2022 |
Reimbursement request | As per indication |
Sponsor | Novartis Pharmaceuticals Canada Inc. |
Submission history | Previously reviewed: yes (through CADTH’s Health Technology Review process) Indications: acute lymphoblastic leukemia and diffuse large B-cell lymphoma Recommendation date: January 15, 2019 Recommendation (issued by Health Technology Expert Review Panel): reimburse with clinical criteria and/or conditions |
CAR = chimeric antigen receptor; FL = follicular lymphoma; NOC/c = Notice of Compliance with conditions; r/r = relapsed or refractory.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Partitioned survival model |
Target population | Adults with r/r grade 1, 2, or 3a FL after 2 or more lines of systemic therapy |
Treatment | Tisagenlecleucel |
Comparators | SOC, axicabtagene ciloleucel SOC is composed of chemotherapy (89%) and auto-SCT (11%) Chemotherapy includes 6 different regimens:
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (30 years) |
Key data sources |
|
Submitted results | ICER = $95,025 per QALY gained compared with SOC (incremental costs = $364,298; incremental QALYs = 3.83) Dominant compared with axicabtagene ciloleucel (incremental costs = savings $40,488; incremental QALYs = 1.17) |
Key limitations |
|
CADTH reanalysis results |
|
Auto-SCT = autologous stem cell transplant; BR = rituximab plus bendamustine; CAR = chimeric antigen receptor; FL = follicular lymphoma; ICER = incremental cost-effectiveness ratio; LY = life-year; MAIC = matching-adjusted indirect comparison; O-CHOP = obinutuzumab plus cyclophosphamide plus doxorubicin plus vincristine plus prednisone; OS = overall survival; PFS = progression-free survival; QALY = quality-adjusted life-year; R2 = rituximab plus lenalidomide; R-CHOP = rituximab plus cyclophosphamide plus doxorubicin plus vincristine plus prednisone; R-CVP = rituximab plus cyclophosphamide plus vincristine plus prednisone; R-GDP = rituximab plus gemcitabine plus dexamethasone plus cisplatin; R-ICE = rituximab plus ifosfamide plus carboplatin plus etoposide; r/r = relapsed or refractory; SOC = standard of care; WTP = willingness to pay.
Conclusions
Evidence from the ELARA single-arm trial suggests that treatment with tisagenlecleucel (Kymriah) may be associated with clinically important tumour responses, including complete remission, in adults with relapsed or refractory (r/r) follicular lymphoma (FL) after 2 or more lines of systemic therapies. However, there is insufficient evidence — in part due to the limited follow-up duration of the trial — to determine the effects of tisagenlecleucel on overall survival (OS) and progression-free survival (PFS). The CADTH clinical assessment identified limitations with the sponsor’s comparison of the ELARA trial to the ReCORD-FL study, which substantially limited the ability to interpret the relative treatment effects observed between tisagenlecleucel and standard-of-care (SOC) treatment. Indeed, important prognostic factors were excluded from the propensity model that matched patients receiving tisagenlecleucel in the ELARA trial with those receiving SOC in the ReCORD-FL study. Moreover, important exclusion criteria specific to the ELARA trial, such as previous or concurrent malignancy, could not be applied to the ReCORD-FL study. Of note, the CADTH clinical review indicated that the propensity score matching method employed by the sponsor to compare tisagenlecleucel with SOC resulted in a reduced effective sample size (whereby the majority of patients in the ReCORD-FL study were lost), which may further contribute to imprecision. Consequently, the clinical review concluded there is uncertainty around the treatment effects of tisagenlecleucel relative to SOC due to selection bias and unmeasured and residual confounding that cannot be entirely ruled out.
Given the magnitude of uncertainty surrounding OS for tisagenlecleucel, its comparative efficacy against SOC, and the durability of such a benefit, CADTH was unable to derive a robust base case estimate of cost-effectiveness. Moreover, given the duration of the ELARA trial (i.e., 38 months), in contrast to the model’s time horizon (i.e., 30 years), it is important to note that the majority of the quality-adjusted life-year (QALY) benefit (83%) realized by patients receiving tisagenlecleucel was derived from the period beyond which there are observed trial data (i.e., extrapolated period). To address this, CADTH conducted separate reanalyses involving 2 different parametric assumptions of treatment effect waning for OS: (A) an exponential distribution that assumes a 17.5-year postinfusion treatment effect before waning; and (B) a log-normal distribution that assumes a 7.9-year postinfusion effect before waning.
Results from CADTH reanalysis A and reanalysis B were generally aligned; tisagenlecleucel is not cost-effective at a $50,000 willingness-to-pay (WTP) threshold compared to SOC. In CADTH reanalysis A (assuming that the treatment effect would wane 17.5 years after infusion), tisagenlecleucel was associated with an incremental cost-effectiveness ratio (ICER) of $193,516 per QALY gained compared to SOC. In CADTH reanalysis B (assuming that the treatment effect would wane 7.9 years after infusion), tisagenlecleucel was associated with an ICER of $434,036 per QALY gained compared to SOC. The estimated ICERs were higher than the sponsor’s base case value, driven primarily by an adjustment of tisagenlecleucel’s parametric distribution of OS. In line with clinical expert advice, these reanalyses achieved more plausible OS curves in the absence of robust long-term evidence, while still conferring a benefit with tisagenlecleucel. CADTH notes that both reanalyses assume that life expectancy increases for patients receiving tisagenlecleucel relative to current SOC (2.65 and 1.15 years of life gained with tisagenlecleucel in reanalysis A and B, respectively). In the absence of randomized controlled trial (RCT) evidence, the true comparative impact of tisagenlecleucel on OS relative to SOC is uncertain. These estimates may therefore overestimate the incremental benefits associated with tisagenlecleucel relative to current SOC.
Assuming that PFS and OS outcomes from the nonrandomized comparison between the ELARA and ReCORD-FL study can be replicated in the real-world setting and that extensions in life occur relative to current SOC, a price reduction of between 71% and 82% would still be required for tisagenlecleucel to be cost-effective at a WTP threshold of $50,000 per QALY gained. This would mean a reduction in the one-time price of tisagenlecleucel from $450,000 to between $130,500 and $81,000. This range reflects the uncertainty around long-term survival extrapolation, as analyzed in CADTH reanalyses A and B.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
One patient group, Lymphoma Canada, provided input from data collected with 2 surveys. The first was conducted from January 2019 to September 2020 in France and comprised 162 patients receiving autologous chimeric antigen receptor (CAR) T-cell therapy (19 of whom had experience with tisagenlecleucel). The second was conducted from November 2022 to January 2023 in Canada and comprised 44 patients with r/r FL (1 of whom had experience with tisagenlecleucel). The most important outcomes for patients included delaying disease progression and achieving long-term remission, with the ultimate objective of improving survival; reducing side effects from treatments; preserving independence to minimize the burden on caregivers; and maintaining quality of life. For survey respondents with experience with current treatment options, the majority had received 1 line of therapy (44%), followed by 2 lines (24%) and 3 lines (15%), for which chemoimmunotherapy was the most commonly prescribed treatment. The majority of patients surveyed received a regimen of rituximab plus cyclophosphamide plus doxorubicin plus vincristine plus prednisone (R-CHOP) or of rituximab plus bendamustine (BR). Important side effects of chemotherapy included fatigue, low activity level, hair loss, and neuropathy. In addition, patients emphasized the need for therapies that can be administered at a hospital located near home to minimize travel time and burden on caregivers. The patient living in Canada who had experience with tisagenlecleucel had to travel out of province for treatment. That patient, who experienced side effects that included neutropenia, thrombocytopenia, decreased appetite, and anemia, has been in remission for more than 2 years.
Registered clinician input was received from 2 groups: Cell Therapy Transplant Canada, and the Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee. According to clinician input, the current pathway of care for patients with r/r FL after 2 or more lines of systemic therapy is chemoimmunotherapy and autologous (auto) or allogeneic stem cell transplant (SCT). Chemoimmunotherapy is likely less efficacious among re-treated patients. Although few patients are eligible, allogeneic SCT may have curative potential, whereas auto-SCT may not be appropriate among chemo-refractory patients. Clinicians advocated that tisagenlecleucel be used in patients with r/r FL who are not eligible to receive SCT in the third-line setting. Clinicians consider that tisagenlecleucel could shift the current treatment paradigm by replacing chemoimmunotherapy in the third-line setting, but will likely not replace auto-SCT or allogenic SCT among eligible patients. Clinician input also indicated that tisagenlecleucel may be used in advance of autologous SCT among patients who have a chemotherapy-refractory history. Furthermore, it was noted that tisagenlecleucel should only be considered in relatively fit patients without significant comorbidities. Patients with uncontrolled infections, severe organ dysfunction, and poor performance status should be excluded.
Participating drug plans noted concerns that the existing capacity may not be able to meet the anticipated demand in Canada. Given the requirement for specialized and accredited centres in which the therapy can be administered, access to CAR T-cell therapy may further require interprovincial travel and, without full coverage of interprovincial reimbursement, may impact equitable access across Canada. The evidence surrounding CAR T-cell re-treatment was noted to be an important area of uncertainty. Finally, drug plans queried whether alternate treatments could be used to treat cytokine release syndrome (CRS) in the event of a tocilizumab shortage.
Several of these concerns were addressed in the sponsor’s model:
The impact of disease and treatment on a patient’s quality of life was captured with utility values. Adverse events (AEs) were incorporated as disutilities in the analyses.
The SOC modelled by the sponsor reflected the current treatments available to patients with r/r FL.
In addition, CADTH addressed some of these concerns as follows:
Based on clinical expert judgment, subsequent therapies for patients receiving tisagenlecleucel and SOC were aligned with the expected treatment mix in Canadian clinical practice.
Therapies that may be available in the future (i.e., axicabtagene ciloleucel), as well as therapies that are currently used off-label (i.e., a regimen of rituximab plus lenalidomide [R2]) for this indication were explored as comparators in pairwise scenario analyses.
CADTH was unable to address the following concerns raised from stakeholder input:
Capacity is not explicitly considered in the model. The sponsor assumes all patients with r/r FL have access to tisagenlecleucel, if required, and that the manufacturing time is similar to that observed in the trial.
Accessing axicabtagene ciloleucel may require interprovincial travel. These costs were not considered in the analysis, given the heterogeneity across provinces in terms of policies for interprovincial billings. Furthermore, given the public payer perspective, patient-borne interprovincial travel costs were not included as it was considered outside the scope of this review’s perspective.
Economic Review
The current review is for tisagenlecleucel for adults with r/r grade 1, 2, or 3a FL after 2 or more lines of systemic therapy.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of tisagenlecleucel compared with SOC and axicabtagene ciloleucel. Aligned with the Health Canada–indicated population, the modelled population comprised adults with r/r grade 1, 2, or 3a FL after 2 or more lines of systemic therapy.1
Tisagenlecleucel is a second-generation autologous CAR T-cell therapy directed at the cell-surface protein CD19, which is present in a wide range of B-lymphoid malignancies, including FL.1 It is available as a single-dose cell suspension for infusion, containing a target nonweight-based dose of 0.6 to 6.0 × 108 cells.2 The sponsor’s submitted price for tisagenlecleucel is $450,000 per infusion, not including costs associated with pretreatment (i.e., leukapheresis and cryopreservation, bridging chemotherapy, and lymphodepleting chemotherapy), hospitalization related to inpatient administration, and postinfusion intensive care unit (ICU) stays.1
The comparators for this analysis included SOC and axicabtagene ciloleucel. For SOC, 89% of patients received chemotherapy and 11% underwent auto-SCT.1 The treatment cost associated with chemotherapy was estimated as a weighted average of 6 chemotherapy regimens: rituximab plus cyclophosphamide plus vincristine plus prednisone (R-CVP); rituximab plus cyclophosphamide plus doxorubicin plus vincristine plus prednisone (R-CHOP); obinutuzumab plus cyclophosphamide plus doxorubicin plus vincristine plus prednisone (O-CHOP); rituximab plus gemcitabine plus dexamethasone plus cisplatin (R-GDP); rituximab plus bendamustine (BR); and rituximab plus ifosfamide plus carboplatin plus etoposide (R-ICE).1
Based on clinician-informed proportions of patients on each chemotherapy regimen and the average number of cycles per regimen, the sponsor estimated the annual drug cost of chemotherapy to be $33,743.1 The sponsor estimated the cost of auto-SCT to be $129,326, which incorporated the auto-SCT procedure cost (including stem cell harvesting), as well as follow-up costs from postprocedure day 27 to postprocedure day 100.1 The SOC composite cost was estimated as a weighted average of chemotherapy and auto-SCT costs ($46,729).1 For axicabtagene ciloleucel, a one-time acquisition cost of $485,000 was considered, with the same outpatient administration cost, average length of hospitalization, and ICU stays for reasons other than CRS as tisagenlecleucel.1 Vial-sharing was not incorporated by the sponsor.
The clinical outcomes modelled were PFS and OS.1 The economic outcomes of interest were QALYs and life-years (LYs). The economic evaluation was conducted over a lifetime time horizon (30 years), from the perspective of the Canadian public health care payer.1 Costs and outcomes were discounted at 1.5% per annum.1
Model Structure
The sponsor used a partitioned survival model (PSM) to capture all costs and outcomes associated with tisagenlecleucel and comparators. The model included 3 health states — progression-free, progressive disease, and death — and transitions between health states occurred on a weekly cycle length (Figure 1).1 The proportion of patients in the progression-free, progressive disease, and death states was estimated over time, based on OS and PFS curves, which were informed by the ELARA and ZUMA-5 single-arm trials, as well as the ReCORD-FL retrospective cohort study.1 The proportion of patients with progressive disease (i.e., in the postprogression state) was estimated as the difference between the proportion of living patients (estimated from the OS curve) and the proportion of patients in the progression-free state (estimated from the PFS curve). PFS was defined as the time from the date of enrolment to the date of first documented progression or death from any cause.1 Patients began in the progression-free health state and, over time, could progress to either the progressive disease health state or the death state.1 Patients in the progressive disease health state could either remain in this health state or transition to the death state (i.e., patients could not return to the progression-free health state).1
Model Inputs
Baseline patient characteristics were derived from the ELARA trial, a phase II, single-arm, multicenter, open-label trial investigating the efficacy and safety of tisagenlecleucel among patients with r/r grade 1, 2, or 3a FL (n = 97).1 The average patient in the modelled cohort, which the sponsor assumed reflected the patient population in Canada, was 57 years old, weighed 79 kg, and was more likely to be male (67%) than female.3 These characteristics were derived from the enrolled patient population of the ELARA trial and were used to inform the drug dosage regimens and the age-specific and sex-specific distribution of mortality risk in the general population.1
Clinical efficacy parameters used to characterize tisagenlecleucel, axicabtagene ciloleucel, and SOC, including OS and PFS, were derived from various data sources. For tisagenlecleucel, inputs were based on the ELARA single-arm trial (data cut-off: March 29, 2022).3 For axicabtagene ciloleucel, inputs were derived from efficacy-evaluable patients in the ZUMA-5 single-arm trial (i.e., patients with > 24 months of follow-up) (data cut-off: March 31, 2021).4 For SOC, inputs were informed from the chemotherapy subgroup of the ReCORD-FL study, which was an observational study that constructed a historical control cohort of patients with r/r FL treated with usual therapies in routine practice and who met inclusion criteria similar to that used in the ELARA and ZUMA-5 trials.5 Specifically, OS and PFS for SOC were informed by individual patient-level data from the chemotherapy subgroup of the ReCORD-FL study, whereby patients were weighted to be comparable with the ELARA enrolled trial population using propensity score matching.1 In addition, the sponsor submitted a matched-adjusted indirect comparison (MAIC) that assessed the efficacy and safety of axicabtagene ciloleucel relative to tisagenlecleucel in patients with r/r FL after 2 or more lines of therapy using the ZUMA-5 and ELARA trials, which informed OS and PFS for axicabtagene ciloleucel.
Notably, the sponsor distinguished between the efficacy estimated in the interpolated period (i.e., up to the longest follow-up time in the ELARA trial at the March 2022 data cut-off [38 months]) and the extrapolated period (i.e., beyond 38 months and across the model’s lifetime horizon [30 years]).1 In the interpolated period, the sponsor used a dependent parametric model with a generalized-gamma distribution to estimate OS and PFS for tisagenlecleucel and SOC, and an independent model with a log-normal distribution to estimate OS and PFS for axicabtagene ciloleucel.1 In the extrapolated period, the sponsor assumed that there would be no difference in the rate of survival decline between tisagenlecleucel and its comparators.1 Hence, beyond month 38, the OS and PFS curves for patients receiving tisagenlecleucel and axicabtagene ciloleucel were adjusted by the relevant transition probabilities derived from the ReCORD-FL study. Survival distributions were selected based on the Akaike information criterion and the Bayesian information criterion, as well as visual inspection.1
Utility values were derived from an analysis of 3-Level EQ-5D index data collected in the ELARA trial, with Canadian tariffs applied.6 The model assigned utility values to the progression-free and progressive disease health states using pooled utility estimates across treatments.1 The sponsor calculated utility values of 0.845 and 0.841 for the progression-free and progressive disease states, respectively. Trial-based utility scores were adjusted using age-related utility decrements, based on an algorithm developed by Ara et al. (2010)7 to align estimates with those of the general population in the same age band as the ELARA trial. The model incorporated disutilities associated with AEs that qualified as grade 3 or higher with a rate of at least 5% in any of the treatments considered.1 AE rates were informed by the ELARA trial (for tisagenlecleucel),3 the literature (for SOC),8-10 and the ZUMA-5 trial (for axicabtagene ciloleucel).4 AE disutilities were derived from the National Institute for Health and Care Excellence (NICE) appraisal of idelalisib in refractory FL.11 Patients receiving tisagenlecleucel and axicabtagene ciloleucel therapies were assumed to incur additional treatment disutilities associated with all grades of CRS and ICU stays not due to CRS, which were derived from the ELARA and ZUMA-5 trials, respectively.1 Patients receiving SCT either in the initial third line of therapy or as a subsequent therapy in the fourth-line were assumed to incur additional disutility, derived from Guadagnolo et al. (2006).12
Costs captured in the model included pretreatment costs (i.e., drug acquisition, drug administration, and hospitalization associated with pretreatment), treatment costs (i.e., drug acquisition, drug administration, and hospitalization associated with treatment), follow-up medical costs before progression (i.e., physician visits, CT scans, and laboratory tests), subsequent treatment costs in the fourth-line setting, follow-up medical costs in the postprogression state, AE management costs, and terminal care costs.1 Drug-acquisition costs for tisagenlecleucel were based on the sponsor’s submitted price.1 The dosing modelled for tisagenlecleucel is consistent with that described in the Overview section. Drug-acquisition costs were sourced from the IQVIA database, and dosing schedules were based on chemotherapy regimen monographs from Cancer Care Ontario.13
For tisagenlecleucel, the model separately estimated costs for patients who proceeded with infusion (99%) and patients who did not; patients who discontinued before infusion were assumed to incur the costs of SOC after leukapheresis. For axicabtagene ciloleucel, all patients were assumed to receive the infusion, based on the ZUMA-5 trial. Prior to CAR T-cell infusion, patients receiving tisagenlecleucel and axicabtagene ciloleucel underwent leukapheresis and cryopreservation, bridging chemotherapy, and lymphodepleting chemotherapy. Pretreatment costs were applied in the first cycle of the model. The cost of leukapheresis ($1,589) and cryopreservation ($268), which were applied to all patients receiving CAR T-cell therapies, were estimated from the Ontario Case Costing Initiative (OCCI)14 and the INESSS appraisal of tisagenlecleucel in diffuse large B-cell lymphoma,15 respectively. The cost of bridging chemotherapy was assumed to be equal to 1 cycle of (gemcitabine-oxaliplatin plus rituximab [or R-GemOx]) ($4,781), which was applied to 45% of patients receiving tisagenlecleucel and to 1% of patients receiving axicabtagene ciloleucel, based on the proportions observed in the respective clinical trials.1 The cost of lymphodepleting chemotherapy was based on 2 regimens: fludarabine plus cyclophosphamide ($985), and bendamustine ($3,500). Given that the dosing schedule and proportion of patients receiving each regimen were informed by the ELARA and ZUMA-5 trials, weighted costs were modelled for tisagenlecleucel and axicabtagene ciloleucel.1 Hospitalization and ICU inputs for tisagenlecleucel and axicabtagene ciloleucel were estimated based on the respective trials, where 86% and 100% of patients received the infusion in an inpatient setting, respectively. Costs typically associated with ongoing monitoring were obtained from the Canadian Institute for Health Information’s Patient Cost Estimator for an inpatient hospitalization.16
For patients receiving SOC, treatment costs included chemotherapy (89%) and auto-SCT (11%), as reported in the ReCORD-FL study.5 The treatment costs associated with comparators were as previously described. The sponsor assumed that a proportion of patients receiving R-CVP (27%), R-CHOP (8%), O-CHOP (18%), and R-ICE (25%) would receive chemotherapy in an inpatient setting. Auto-SCT procedure costs were obtained from the Interprovincial Health Insurance Agreements Coordinating Committee.17
The total weighted costs of subsequent therapy differed by prior treatment (i.e., those who received CAR T-cell therapy versus SOC as third-line therapy) and were applied as a one-off cost in the first model cycle after progression (Table 14). Treatment monitoring costs and health care resource use costs were sourced from the Ontario Ministry of Health Schedule of Benefits for Laboratory and Physician Services.18 Treatment-specific AE costs were estimated based on the literature and data from OCCI14 and applied as a one-time cost in the first model cycle. All patients who transitioned to death were assumed to incur terminal care costs ($71,012) in the last cycle before death, based on the study by de Oliveira et al. (2016).19
Summary of Sponsor’s Economic Evaluation Results
The sponsor conducted the base case using a probabilistic sensitivity analysis with 5,000 simulations. The deterministic and probabilistic results were similar. The probabilistic findings are presented in the following.1
Base Case Results
Compared with SOC, tisagenlecleucel was associated with an incremental QALY gain of 3.83 and an incremental cost of $364,298, resulting in an ICER of $95,025 per QALY.1 In addition, axicabtagene ciloleucel was dominated by tisagenlecleucel (i.e., tisagenlecleucel was associated with an incremental QALY gain of 1.17 and a cost savings of $40,488 relative to axicabtagene ciloleucel) (Table 3).1
The sponsor’s analysis predicted that tisagenlecleucel was associated with a longer duration of life than SOC or axicabtagene ciloleucel (i.e., incremental LYs of 4.84 and 1.46, respectively). Given the duration of the ELARA trial (i.e., 38 months), in contrast to the model’s time horizon (i.e., 30 years), it is important to note that the majority of the QALY benefit (83%) realized by patients receiving tisagenlecleucel was derived during the period beyond which there are observed trial data (i.e., extrapolated period). Moreover, the sponsor’s analysis predicted that 30% of patients treated with tisagenlecleucel would be alive at the end of the 30-year time horizon, when the average patient in the modelled cohort would have reached 87 years of age. The key cost driver among patients receiving CAR T-cell therapy was the cost of drug acquisition, accounting for 80% and 81% of the total costs incurred by patients receiving tisagenlecleucel and axicabtagene ciloleucel, respectively. Due to the aforementioned sponsor’s assumption that patients on SOC would be receiving CAR T-cell therapies in subsequent treatment lines (fourth-line and beyond), the main cost driver in the SOC arm, which accounted for 28% of its total expected cost, was drug acquisition.
Tisagenlecleucel was cost-effective at a WTP threshold of $50,000 per QALY in 58% of the iterations when compared to SOC, and in 81% of the iterations when compared to axicabtagene ciloleucel. The sponsor’s submitted analysis is based on the publicly available prices for all drug treatments. Additional results from the sponsor-submitted economic evaluation base case are presented in Appendix 3.
Table 3: Summary of the Sponsor’s Economic Evaluation Results, Probabilistic
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER ($/QALY) |
|---|---|---|---|---|---|
Tisagenlecleucel vs. SOC | |||||
SOC | $191,496 | Reference | 7.22 | Reference | Reference |
Tisagenlecleucel | $555,793 | $364,298 | 11.05 | 3.83 | $95,025 |
Tisagenlecleucel vs. axicabtagene ciloleucel | |||||
Axicabtagene ciloleucel | $596,281 | Reference | 9.88 | Reference | Reference |
Tisagenlecleucel | $555,793 | –$40,488 | 11.05 | 1.17 | Dominant |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care.
Note: Given that the sponsor's comparative efficacy data were derived from separate studies (i.e., the ReCORD-FL chart review for tisagenlecleucel vs. SOC, and a MAIC for tisagenlecleucel vs. axicabtagene ciloleucel), a sequential analysis is inappropriate. Therefore, only pairwise probabilistic results are presented.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analyses Results
The sponsor assessed several model parameters and assumptions in probabilistic scenario analyses, which included assuming hazard nonproportionality between tisagenlecleucel and SOC in the interpolated period (i.e., until month 38); applying hazard ratios derived from the ReCORD-FL study and a MAIC to estimate OS and PFS for SOC and axicabtagene ciloleucel relative to tisagenlecleucel in the interpolated period (i.e., until month 38); using natural mortality adjusted for the standardized mortality rate to inform OS in the extrapolated period (i.e., beyond month 38); and using historical control data from the ReCORD-FL study to inform OS and PFS in the extrapolated period beyond month 60. When fitting an independent model to estimate OS and PFS for tisagenlecleucel and SOC, the ICER increased to $127,218 per QALY. In contrast, when natural mortality adjusted for the standardized mortality rate was used to inform OS in the extrapolated period, the ICER decreased to $75,528 per QALY. All other scenarios resulted in ICERs ranging between $76,283 and $94,228 per QALY.1
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
Dependent model assumption for PFS and OS between tisagenlecleucel and SOC is improbable. In the interpolated period (first 38 months), the sponsor used a dependent parametric model to estimate OS and PFS for tisagenlecleucel and SOC, and an independent model to estimate OS and PFS for axicabtagene ciloleucel. CADTH notes that dependent models may be applied with a proportional hazards (PH) model that assumes that the effect of the treatment coefficient is to multiply the hazard by a constant, as well as with an accelerated failure time (AFT) model that assumes that the effect of the treatment coefficient is to accelerate or decelerate the natural history of the disease by a constant. In using a dependent AFT model to characterize the comparative efficacy of tisagenlecleucel and SOC (i.e., single parametric model with treatment coefficient), the sponsor assumed that treatment with tisagenlecleucel would have a multiplicative effect on survival time, consistent across the lifetime horizon of the model. As such, an acceleration factor was considered between tisagenlecleucel and SOC; that is, the treatment coefficient uniformly shifted the survival curves for tisagenlecleucel (relative to SOC) forward. As a second-generation autologous CAR T-cell therapy directed at the cell-surface protein CD19, a pathway that is currently unaddressed by available treatments for r/r grade 1, 2, or 3a FL after 2 or more lines of systemic therapy, tisagenlecleucel represents a different class of therapy with a unique mechanism of action. CADTH notes that it is not ideal to apply a dependent model to Kaplan-Meier (KM) data for 2 treatment arms when the respective studies assess the efficacy of treatments with different mechanisms of action and, consequently, different patterns of event hazards over time. As such, it is improbable that a single functional form will match both the tisagenlecleucel and SOC study arms successfully.20 Moreover, joint models may introduce bias to the estimated survival in both arms, given that the parameter estimates inevitably deviate from the best fit for either arm.21
CADTH notes that to fit a dependent model, the PH or AFT assumption must be assessed. The PH assumption was assessed for OS and PFS between the ELARA trial and the ReCORD-FL chemotherapy subgroup after weighting. The sponsor conducted log-cumulative hazard plots and tested the correlation of scaled Schoenfeld residuals with rank-ordered time, which showed that the PH assumption was violated for both clinical outcomes. Because Schoenfeld residuals represent the difference between the observed treatment covariate and the expected, given the risk set at that time, they should be flat and centred around zero. Conversely, when ranked by event time, the plots of the Schoenfeld residuals conducted for OS and PFS between the ELARA and ReCORD-FL studies show a distinct pattern (Figure 2 and Figure 3). Moreover, the significant correlation of residuals with time (P = 0.001 for OS; P = 0.038 for PFS) is interpreted as a violation of the PH assumption. CADTH notes that the sponsor did not provide evidence that the AFT assumption was evaluated (e.g., through survival time quantile-quantile plots between tisagenlecleucel and SOC) in their clinical and pharmacoeconomic submissions.
Nevertheless, it is worth mentioning that even if the PH or AFT assumptions were appropriate for the interpolated period, uncertainty remains as to whether the assumptions would hold for the extrapolated period. In light of this, CADTH notes that the appropriateness of a dependent model can only be assumed if a credible argument, based on the epidemiology of the disease and the mechanism of action of the interventions, is provided by the sponsor and validated by clinical experts. CADTH sought expert clinical advice, which confirmed that the unique mechanism of action offered by tisagenlecleucel places it in a different therapy class than current SOC, rendering both the PH and AFT assumptions highly improbable.
CADTH conducted a reanalysis by applying independent parametric models to estimate OS and PFS for tisagenlecleucel and SOC.
Approach to modelling PFS and OS in the extrapolated period is uncertain, given the lack of long-term efficacy data. The sponsor used distinct approaches to estimate PFS and OS for tisagenlecleucel and comparators in the interpolated period (i.e., first 38 months) and the extrapolated period (i.e., beyond month 38 and across the 30-year lifetime horizon of the model). In the submitted pharmacoeconomic report, the sponsor suggested that after 38 months, the model assumed there was no difference in the mortality rate (for OS) or PFS rate across all treatments,1 which does not reflect the model. In the extrapolated period, the sponsor assumed that there would be no difference in the rate of decline for OS or PFS between tisagenlecleucel, SOC, and axicabtagene ciloleucel. In so doing, the OS and PFS parametric distributions for tisagenlecleucel and axicabtagene ciloleucel were adjusted by the respective transition probabilities derived from the ReCORD-FL cohort study for the SOC arm. Hence, the sponsor assumed that the difference between treatments achieved by month 38 would be maintained across the lifetime horizon of the model. Implicit in this modelling approach is the optimistic assumption that the incremental benefit observed for tisagenlecleucel relative to SOC and axicabtagene ciloleucel at month 38 would be sustained indefinitely (i.e., no treatment waning).
CADTH notes that this assumption is highly uncertain, particularly when considering that no head-to-head evidence of tisagenlecleucel is currently available against either SOC or axicabtagene ciloleucel for this indication. It is also worth noting that, as an ongoing trial, the ELARA data analyzed at the March 29, 2022, cut-off represents an interim analysis. Evidence suggests that the clinical benefit of cancer drugs demonstrated in primary publications is often different than that compared with updated mature data. A recent study comparing projected survival based on parametric extrapolations with observed survival based on updated data of 32 trials, identified through FDA oncology approvals, revealed that extrapolations based on initial KM curves had low precision compared with updated KM curves.22 Moreover, imprecision increases with the increasing length of time required for extrapolation and the size of the censored population. Given this, CADTH contends that the assumption of sustained incremental benefit for tisagenlecleucel relative to comparators across the model’s 30-year lifetime horizon represents substantial uncertainty and likely influences the pharmacoeconomic results. Although the clinical experts consulted by CADTH indicated that a benefit with tisagenlecleucel relative to SOC was plausible, the magnitude and duration of such a benefit is uncertain in the absence of more robust evidence.
CADTH conducted a reanalysis using parametric models based on ELARA and ZUMA-5 trial data to extrapolate the PFS and OS of tisagenlecleucel and axicabtagene ciloleucel, respectively, for the entire duration of the model.
The impact of tisagenlecleucel on long-term PFS and OS is highly uncertain. The sponsor’s base case predicted a survival advantage with tisagenlecleucel compared to SOC and axicabtagene ciloleucel (incremental LYs of 4.84 and 1.46, respectively); however, 84% of that advantage was accrued in the period beyond which there are observed trial data. Moreover, the sponsor’s analysis projected that 30% of patients treated with tisagenlecleucel would be alive at the end of the 30-year time horizon, when the average patient in the modelled cohort would have reached 87 years of age. At the ELARA interim analysis reviewed by the CADTH clinical team (data cut-off: March 29, 2022), PFS and OS data for tisagenlecleucel were immature, as neither the median PFS nor the median OS had been reached. CADTH notes that in the absence of mature data, the extent to which the parametric distributions overestimate or underestimate the true incremental LYs is uncertain. In addition, the sponsor’s base case predicted that tisagenlecleucel extended LYs gained in the progression-free and the progressive disease states relative to SOC (3.7 and 1.1, respectively), indicating that treatment with tisagenlecleucel is associated with reductions in the rate of postprogression mortality. Specifically, 23% of the incremental survival attributed to tisagenlecleucel, relative to SOC, is due to a drug benefit that begins after the treatment has stopped controlling the disease. However, as the postprogression mortality transition is not modelled directly in the PSM approach, it is not possible to establish from the model whether this effect was supported by the trial data or was generated entirely during extrapolation.
CADTH sought clinical expert advice to validate the PFS and OS extrapolations derived from different parametric distributions for each treatment strategy based on clinical plausibility. According to clinical expert judgment, the OS and PFS curves for SOC (generated with the generalized-gamma distribution) produced 15-year extrapolations that were within range of the observed ReCORD-FL KM estimates, as well as 20-year and 30-year extrapolations that were aligned with biological plausibility. In contrast, the clinical experts consulted by CADTH emphasized the lack of evidence to support the use of parametric distributions that predict a sustained long-term OS and PFS benefit favouring tisagenlecleucel over SOC. According to the experts, although the ELARA trial findings appeared favourable and clinically important (and a survival benefit with tisagenlecleucel was deemed plausible), the magnitude and durability of such a benefit was highly uncertain in the absence of longer-term or head-to-head evidence. The experts indicated that given the degree of uncertainty surrounding the durability of the treatment effect of tisagenlecleucel relative to SOC, it is clinically plausible for the OS curve of tisagenlecleucel to converge with that of SOC within the model’s lifetime horizon. In addition, the clinical experts noted that the sponsor’s base case OS extrapolation, which estimated that 29% of patients treated with tisagenlecleucel would be alive at 87 years (i.e., the end of the 30-year lifetime horizon), was highly optimistic.
In light of these limitations, CADTH conducted 2 reanalyses with different assumptions of treatment effect durability that sought to address the uncertainty in long-term clinical outcomes. In reanalysis A, the OS of patients receiving tisagenlecleucel was modelled using the exponential distribution; the OS for tisagenlecleucel was capped by the OS for SOC at 17.5 years, when the survival curves would have otherwise crossed. In reanalysis B, the OS of patients receiving tisagenlecleucel was modelled using the log-normal distribution; the OS for tisagenlecleucel was capped by the OS for SOC at 7.9 years, when the survival curves would have otherwise crossed. The generalized-gamma distribution was maintained for the PFS extrapolations of tisagenlecleucel and SOC in each reanalysis. In line with clinical expert advice, these reanalyses achieved more plausible OS curves in the absence of long-term evidence, while still conferring a benefit with tisagenlecleucel.
PSM does not capture the efficacy associated with subsequent therapy. The sponsor used a PSM to capture all costs and outcomes associated with tisagenlecleucel and SOC. Although the PSM has routinely been used to model oncology treatments, there are numerous limitations documented related to its use.23,24 Based on clinical expert opinion, the sponsor assumed that 45% of patients who fail SOC in the third-line setting would incur the cost of CAR T-cell therapy in the fourth-line setting (i.e., 28% would receive tisagenlecleucel and 17% would receive axicabtagene ciloleucel). However, the efficacy benefit of subsequent treatments among patients who receive SOC was not explicitly modelled. Upon CADTH’s request, the sponsor specified that 13% of patients in the ReCORD-FL chemotherapy subgroup received CAR T-cell therapy as subsequent treatment. Thus, there is a misalignment between the subsequent therapy observed among the ReCORD-FL patients (whose outcomes are used to derive the OS for SOC) and the subsequent therapy usage assumed by the sponsor in the model. Although it was possible to alter the distribution of subsequent therapies in line with clinical expert judgment, doing so only impacted the cost of subsequent therapy and not the underlying OS estimates for SOC. That is, the sponsor assumed that 45% of patients who received SOC incurred the high costs associated with receiving CAR T-cell therapy as a fourth-line treatment without experiencing the full extent of the survival benefit associated with it. This assumption reduced the incremental cost and increased the incremental benefit of tisagenlecleucel relative to SOC, thereby introducing a cost-effectiveness bias in favour of tisagenlecleucel.
CADTH could not fully address this limitation, owing to the structure of the model. However, to decrease the underlying bias, CADTH conducted a reanalysis assuming that 13% of patients who receive SOC as third-line therapy would subsequently receive CAR T-cell therapy in the fourth-line setting. This is aligned with the observed proportion of patients in the ReCORD-FL chemotherapy subgroup who received CAR T-cell therapy as subsequent therapy.
Exclusion of costs related to CAR T-cell therapy. In the sponsor’s base case, costs related to a CAR T-cell therapy eligibility assessment were excluded. Feedback from the clinical experts consulted by CADTH noted that the upfront costs of assessment for CAR T-cell therapy eligibility would include those associated with MRIs, PET scans, bone marrow transplants, lumbar punctures, and bloodwork. Should tisagenlecleucel be reimbursed, this assessment cost would be incurred by all adults with r/r grade 1, 2, or 3a FL after 2 or more lines of systemic therapy, regardless of whether they would go on to receive CAR T-cell therapy. In addition, the pretreatment cost of leukapheresis considered by the sponsor ($1,589) for patients receiving CAR T-cell therapy was underestimated. CADTH consulted the OCCI for apheresis costs and obtained a cost of $5,426 for stem cell apheresis (code 1.LZ.58.HX; data not available for leukapheresis specifically due to limited events).25 This underestimated the costs incurred by patients receiving tisagenlecleucel relative to SOC, thereby biasing the results of the economic analysis in favour of the drug under review.
CADTH conducted a reanalysis that included the additional CAR T-cell therapy eligibility assessment cost and the updated costs associated with apheresis.
The selection of comparators is not supported by current clinical practice. The sponsor included axicabtagene ciloleucel in the analysis, citing its approval by Health Canada. At the time of the present review, axicabtagene ciloleucel did not meet any of the 3 criteria for relevant comparators: reimbursement by at least 1 participating drug plan, currently used off-label, and a positive recommendation from CADTH.26 However, a submission to CADTH for axicabtagene ciloleucel was received for the treatment of adults with r/r grade 1, 2, or 3a FL after 2 or more lines of systemic therapy during the present review, indicating that the product may be available in the future.27 Therefore, CADTH included the comparison of tisagenlecleucel and axicabtagene ciloleucel as a scenario analysis only. The sponsor submitted a MAIC between tisagenlecleucel and axicabtagene ciloleucel, which was appraised by CADTH (refer to the Clinical Review Report for the complete appraisal). Results from the sponsor-submitted MAIC suggested that the OS and PFS associated with tisagenlecleucel are comparable to the OS and PFS associated with axicabtagene ciloleucel. Moreover, the CADTH clinical team noted that definitive conclusions related to the response and survival benefits of tisagenlecleucel, compared to axicabtagene ciloleucel, could not be drawn from the MAIC analysis due to methodological limitations, including trial design differences that could not be adjusted for in the analyses, adjustment on only a limited number of potential prognostic factors and effect modifiers, and the small effective sample sizes in the analyses.
In addition, the sponsor omitted the R2 regimen from the base case analysis, despite evidence that this therapy is prescribed by some oncologists in current Canadian clinical practice.1 During the review process, both the participating drug plans and the clinical expert panel convened by CADTH indicated that the R2 regimen is used off-label for the treatment of adults with r/r grade 1, 2, or 3a FL after 2 or more lines of systemic therapy in Canada. However, the sponsor did not provide sufficient information regarding the comparison of tisagenlecleucel and R2 as part of its clinical and pharmacoeconomic submission.
CADTH excluded axicabtagene ciloleucel as a comparator in the reanalysis.
CADTH conducted a scenario analysis that compared tisagenlecleucel with axicabtagene ciloleucel. Given that conclusions about the comparative effect of tisagenlecleucel relative to axicabtagene ciloleucel could not be drawn, CADTH assumed efficacy equivalence of the CAR T-cell therapies.
As the relevant clinical evidence for the R2 regimen could not be appraised, CADTH conducted a scenario analysis that assumed efficacy equivalence of tisagenlecleucel and the R2 regimen.
Poor modelling practices were employed. The sponsor’s submitted model included numerous IFERROR statements, resulting in situations in which the parameter value was overwritten with an alternative value without alerting the user to the automatized overwriting. The systematic use of IFERROR statements rendered thorough auditing of the sponsor’s model impractical, as it remains unclear whether the model ran inappropriately by overriding errors. In addition, CADTH noted that when selecting an option from a dropdown list, an unprompted change would be triggered in an unrelated dropdown list, which complicated the validation process.
CADTH was unable to address this limitation, noting that a thorough validation of the submitted model was not possible.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation
Sponsor’s key assumption | CADTH comment |
|---|---|
The sponsor estimated the cost of auto-SCT to be $129,326, which incorporates the auto-SCT procedure cost (including stem cell harvesting), as well as follow-up costs from day 27 to day 100 after the procedure. This was based on basic block rates from the Interprovincial Health Insurance Agreements Coordinating Committee17 and follow-up costs from a Canadian source.28 | Uncertain. CADTH notes that the basic block rate for an adult auto-SCT (> 72 hours) is $77,956, which comprises all facility costs (including inpatient and diagnostic costs) and a maximum length of stay of 16 days.17 There is uncertainty regarding the average number of days for which postprocedure follow-up costs should be considered. Although the sponsor’s auto-SCT cost input reflects follow-up costs up to 100 days after the procedure, assuming no follow-up costs beyond 16 days after the procedure does not impact the ICER of tisagenlecleucel relative to SOC. |
The sponsor assumed that among patients receiving CAR T-cell therapies, the proportions receiving pretreatment with bridging chemotherapy would differ according to the specific CAR T-cell therapy received (i.e., 45% for tisagenlecleucel vs. 1% for axicabtagene ciloleucel). These proportions were derived from the ELARA and ZUMA-5 trials, respectively. | Not appropriate. Based on clinical expert feedback, the proportion of patients receiving bridging therapy before CAR T-cell infusion is likely to be similar across CAR T-cell products in real-world clinical practice. However, modifying this assumption does not have a substantial impact on tisagenlecleucel’s ICER relative to axicabtagene ciloleucel. |
Based on the ELARA trial, the model estimated costs separately for patients who proceeded with the tisagenlecleucel infusion (99%) and those who did not. For axicabtagene ciloleucel, all patients (100%) were assumed to have received a CAR T-cell infusion based on the infused population from the ZUMA-5 trial. | Uncertain. Based on clinical expert feedback, the rates of tisagenlecleucel and axicabtagene ciloleucel infusion may be impacted by both patient characteristics and implementation considerations. The time needed to manufacture and infuse CAR T-cell therapies beyond that observed in the ELARA and ZUMA-5 trials may impact the proportion of patients who could receive a CAR T-cell infusion. |
auto-SCT = autologous stem cell transplant; CAR = chimeric antigen receptor; ICER = incremental cost-effectiveness ratio; SOC = standard of care.
CADTH Reanalyses of the Economic Evaluation
Base Case Results
CADTH reanalyses involved changes to model parameter values and assumptions, in consultation with clinical experts. The following changes were made to address several limitations of the economic model: applying independent models to estimate the OS and PFS of tisagenlecleucel and SOC; using parametric distributions based on ELARA and ZUMA-5 trial data to extrapolate the OS and PFS of tisagenlecleucel and axicabtagene ciloleucel for the entire lifetime horizon of the model; including a CAR T-cell eligibility assessment cost and updating pretreatment costs associated with apheresis; aligning subsequent therapies among patients receiving SOC in the third-line setting with the observed proportion of patients in the ReCORD-FL chemotherapy subgroup; and excluding axicabtagene ciloleucel as a comparator. However, given the magnitude of uncertainty surrounding OS for tisagenlecleucel, its comparative efficacy against SOC, and the durability of such a benefit, CADTH was unable to derive a robust base case estimate of cost-effectiveness. CADTH conducted separate reanalyses that involved different parametric assumptions for the treatment effect of tisagenlecleucel. In reanalysis A, tisagenlecleucel’s OS was modelled using the exponential distribution, and in reanalysis B, tisagenlecleucel’s OS was modelled using the log-normal distribution. These changes are summarized in Table 5.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. Dependent model assumption for PFS and OS between tisagenlecleucel and SOC is improbable | Dependent models used to estimate the OS and PFS of tisagenlecleucel and SOC | Independent models used to estimate the OS and PFS of tisagenlecleucel and SOC |
2. Approach to modelling PFS and OS in the extrapolated period is uncertain, given the lack of long-term efficacy data | Beyond month 38, the OS and PFS curves for tisagenlecleucel and axicabtagene ciloleucel were adjusted for transition probabilities derived from the ReCORD-FL study | Parametric distributions based on ELARA and ZUMA-5 trial data were used to extrapolate the PFS and OS of tisagenlecleucel and axicabtagene ciloleucel for the duration of the model |
3. Exclusion of CAR T-cell–related costs |
|
|
4. Partitioned survival model does not capture the efficacy associated with subsequent therapy | Therapy mix in the fourth-line for patients who receive SOC in the third line:
| Therapy mix in the fourth-line for patients who receive SOC in the third line:
|
5. Impact of tisagenlecleucel on long-term PFS and OS is uncertaina |
|
|
6. Impact of tisagenlecleucel on long-term PFS and OS is uncertaina |
|
|
CADTH re-analysis A | Reanalyses 1 + 2 + 3 + 4 + 5 | |
CADTH re-analysis B | Reanalyses 1 + 2 + 3 + 4 + 6 | |
Auto-STC = autologous stem cell transplant; CAR = chimeric antigen receptor; OS = overall survival; PFS = progression-free survival; SOC = standard of care; SCT = stem cell therapy.
aCADTH reanalyses 5 and 6 (which change the tisagenlecleucel parametric distribution of OS to exponential and log-normal, respectively) require that reanalyses 1 and 2 be performed concurrently; that is, to change the tisagenlecleucel parametric distribution, the model must be independent and the extrapolation method parametric.
Results from CADTH reanalyses A and B were generally aligned; tisagenlecleucel is not cost-effective at a $50,000 WTP threshold, compared to SOC. In CADTH reanalysis A (assuming that the treatment effect would wane 17.5 years after infusion), tisagenlecleucel was associated with an ICER of $193,516 per QALY compared to SOC (incremental costs = $420,926; incremental QALYs = 2.18). In CADTH reanalysis B (assuming that the treatment effect would wane 7.9 years after infusion), tisagenlecleucel was associated with an ICER of $434,036 per QALY compared to SOC (incremental costs = $420,063; incremental QALYs = 0.97). The probability that tisagenlecleucel was cost-effective at a WTP threshold of $50,000 per QALY was 0.1% and 0.0% in reanalyses A and B, respectively.
The estimated ICERs were higher than the sponsor’s base case value, driven primarily by adjustment of tisagenlecleucel’s parametric distribution for OS and the omission of the dependent model assumption. In line with clinical expert advice, these reanalyses achieved more plausible OS curves in the absence of long-term evidence, while still conferring a survival benefit with tisagenlecleucel. CADTH reanalyses predicted that 19% of patients treated with tisagenlecleucel would be alive at the end of the model’s lifetime horizon, when the average patient in the cohort would have reached 87 years of age. In both reanalyses, most incremental QALYs were due to improvements in LYs. Furthermore, 71% (reanalysis A) and 40% (reanalysis B) of QALYs gained by patients receiving tisagenlecleucel were derived from the extrapolated period beyond which there are observed trial data. The key cost driver among patients receiving tisagenlecleucel (78%) and patients receiving SOC (38%) was related to drug-acquisition costs in both reanalyses.
CADTH reanalyses are based on the publicly available prices for all drug treatments. Full results are available in Appendix 4.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results (Deterministic)
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor base case (deterministic) | SOC | $182,744 | 7.31 | Reference |
Tisagenlecleucel | $551,987 | 11.27 | $93,289 | |
CADTH reanalysis 1: dependent model assumption | SOC | $171,151 | 7.40 | Reference |
Tisagenlecleucel | $556,958 | 10.59 | $121,047 | |
CADTH reanalysis 2: long-term extrapolation | SOC | $182,727 | 7.32 | Reference |
Tisagenlecleucel | $551,776 | 11.65 | $85,068 | |
CADTH reanalysis 3: CAR T-cell costs | SOC | $186,498 | 7.31 | Reference |
Tisagenlecleucel | $558,854 | 11.27 | $94,075 | |
CADTH reanalysis 4: subsequent therapy | SOC | $148,454 | 7.31 | Reference |
Tisagenlecleucel | $551,987 | 11.27 | $101,952 | |
CADTH reanalysis 5: tisagenlecleucel OS (exponential)a | SOC | $171,132 | 7.41 | Reference |
Tisagenlecleucel | $558,048 | 9.45 | $189,092 | |
CADTH reanalysis 6: tisagenlecleucel OS (log-normal)a | SOC | $171,132 | 7.41 | Reference |
Tisagenlecleucel | $556,769 | 8.44 | $371,990 | |
CADTH reanalysis A: (1 + 2 + 3 + 4 + 5) | SOC | $146,643 | 7.41 | Reference |
Tisagenlecleucel | $564,915 | 9.45 | $204,417 | |
CADTH reanalysis B: (1 + 2 + 3 + 4 + 5 + 6) | SOC | $146,643 | 7.41 | Reference |
Tisagenlecleucel | $563,636 | 8.44 | $402,237 | |
CADTH reanalysis A (probabilistic) | SOC | $148,479 | 7.34 | Reference |
Tisagenlecleucel | $569,405 | 9.51 | $193,516 | |
CADTH reanalysis B (probabilistic) | SOC | $148,479 | 7.34 | Reference |
Tisagenlecleucel | $568,542 | 8.30 | $434,036 |
CAR = chimeric antigen receptor; ICER = incremental cost-effectiveness ratio; OS = overall survival; QALY = quality-adjusted life-year; SOC = standard of care.
Note: Given that axicabtagene ciloleucel is not currently a relevant comparator, the CADTH reanalysis focused on the pairwise comparison of tisagenlecleucel to SOC.
aCADTH reanalyses 5 and 6 (which change the tisagenlecleucel parametric distribution of OS to exponential and log-normal, respectively) require that reanalyses 1 and 2 be performed concurrently; that is, to change the tisagenlecleucel parametric distribution, the model must be independent and the extrapolation method parametric.
Scenario Analysis Results
CADTH undertook price reduction analyses based on the sponsor’s results and CADTH’s reanalyses. Results of CADTH reanalysis A suggested that a price reduction of 71% would be required to achieve cost-effectiveness of tisagenlecleucel relative to SOC at a $50,000 per QALY threshold. In CADTH reanalysis B, a price reduction of 82% would be required (Table 7).
Table 7: CADTH Price Reduction Analyses
Analysis | ICERs for tisagenlecleucel vs. SOC ($/QALY) | ||
|---|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis A | CADTH reanalysis B |
No price reduction | $93,287 | $204,417 | $402,237 |
10% | $82,034 | $182,649 | $359,272 |
20% | $70,781 | $160,881 | $316,307 |
30% | $59,528 | $139,113 | $273,342 |
40% | $48,275 | $117,345 | $230,377 |
50% | $37,022 | $95,577 | $187,413 |
60% | $25,769 | $73,809 | $144,448 |
70% | $14,516 | $52,041 | $101,483 |
80% | $3,263 | $30,273 | $58,518 |
90% | Dominant | $8,505 | $15,553 |
100% | Dominant | Dominant | Dominant |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care.
CADTH undertook 2 scenario analyses for each of the CADTH reanalyses, outlined as follows:
comparing tisagenlecleucel with axicabtagene ciloleucel in light of the fact that a submission for axicabtagene ciloleucel was received for this indication during the present review
comparing tisagenlecleucel with the R2 regimen, given that participating drug plans and the clinical expert panel convened by CADTH noted its off-label use for this patient population in current Canadian clinical practice.
In the first scenario, CADTH assumed efficacy equivalence between CAR T-cell therapies, given that conclusions about the comparative effect of tisagenlecleucel relative to axicabtagene ciloleucel could not be drawn because of the unknown amounts of residual bias in the sponsor-submitted MAIC. Tisagenlecleucel was the dominant strategy in both reanalysis A and reanalysis B (incremental costs = –$37,013 to –$37,026; incremental QALYs = 0); that is, tisagenlecleucel generated cost savings for the same number of QALYs gained.
In the second scenario, CADTH assumed efficacy equivalence between tisagenlecleucel and the R2 regimen, owing to the fact the sponsor did not provide any information regarding the MAIC of tisagenlecleucel compared with the R2 regimen as part of its clinical and pharmacoeconomic submission. Tisagenlecleucel was the dominated strategy in both reanalysis A and reanalysis B (incremental costs = $387,426 to $386,806; incremental QALYs = 0); that is, tisagenlecleucel generated higher costs for the same number of QALYs gained.
The results of these analyses are presented in Table 16.
Issues for Consideration
Travel-associated costs: Travel costs and the requirement for time spent away from work was not considered. The sponsor’s implementation plan indicated that not all provinces or territories will have a site to provide tisagenlecleucel.29 For jurisdictions that do not currently have a site to provide tisagenlecleucel, there will be a need for patients to travel out of province for treatment. Furthermore, it was noted by clinical experts that some provinces do not have the capacity to assess patients’ eligibility for CAR T-cell therapy. The implementation plan suggests that the sponsor will coordinate travel and lodging logistics for patients and their caregivers who arrive to receive treatment and who need to remain in proximity to the qualified treatment centre for a maximum of 2 weeks before the infusion and 4 weeks after the infusion.29 The sponsor states that the program is intended to support adherence to tisagenlecleucel’s monitoring requirements by providing financial support to cover transportation-related expenses and lodging costs for patients and their caregivers during the pretreatment and treatment periods when they are required to stay in close proximity to the qualified treatment centre. If this patient support program is not operationalizable and travel expenses (e.g., travel, lodging, food) have to be absorbed by the patient or public payer, this may impact access to tisagenlecleucel. Disparities in funding and treatment access may vary, depending on the province or territory, and the requirement for access to a tertiary care centre for the delivery of tisagenlecleucel may have equity of access implications that were not substantively considered in the economic submission.
Manufacturing delays: The sponsor noted that in the ELARA trial, the median duration from enrolment to treatment infusion was 46 days (range, 23 to 127 days).3 However, the sponsor did not provide any information with regard to the median duration from leukapheresis to enrolment. Hence, the median time from apheresis collection to final product delivery (i.e., when tisagenlecleucel would be ready to be infused back into the patient) is unknown. A recent real-world study conducted in the US based on 3 commercial claims databases revealed that the median time from leukapheresis to CAR T-cell infusion was 26 to 27 days.30 However, CADTH clinical expert feedback noted the potential for greater variability in manufacturing time in the Canadian real-world setting, given that apheresis collection would be conducted at a broad network of pan-Canadian treatment sites, with manufacturing conducted across the border in the US.31 Clinical expert feedback emphasized that manufacturing delays are a significant clinical problem, especially among patients who progress relatively fast and have a higher disease burden. In the context of manufacturing delays, tisagenlecleucel would not be as effective among fast-progressors as it would among patients who do not have disease progression. Moreover, the sponsor noted that if there were delays of more than 4 weeks between completion of lymphodepleting chemotherapy and tisagenlecleucel infusion (and the white blood cell count were > 1,000 cells/µL), patients would need to be re-treated with lymphodepleting chemotherapy before being infused. Costs arising from manufacturing delays were not considered in the economic model.
Manufacturing failures: Issues pertaining to manufacturing are important to the successful delivery of CAR T-cell therapies. Manufacturing failure may occur due to an inadequate number of T-cells in the apheresed product, poor selection of T-cells on day 0 of manufacturing, or irreversibly impaired T-cells (i.e., no response to stimulation in culture), microbial contamination, equipment-related cell loss, high endotoxin level, and accidents. The sponsor notes that the tisagenlecleucel manufacturing success rate in the ELARA trial was 100%; hence, the impact of manufacturing failure was not considered in the submitted economic model. It is worth noting that having a leukapheresis product of nonmobilized cells accepted for manufacturing was part of the inclusion criteria for patients enrolled in the ELARA trial. As such, the rate of manufacturing failure that could be expected in real-world practice is unknown. However, manufacturing failures of CAR T-cell therapies are not uncommon and have been previously observed in trials of tisagenlecleucel32 and other CAR T-cell products.33,34 There may be additional costs associated with manufacturing failures, including increased hospital stays while a second sample is prepared, if possible. In addition, manufacturing failures may affect patient outcomes due to treatment delays or compromised doses.
Capacity constraints: The implementation plan indicated that, as of April 2022, the sponsor has manufactured and delivered clinical and commercial batches of tisagenlecleucel for more than 6,900 patients at more than 370 sites worldwide. The sponsor did not state its current annual capacity to produce therapy for patients in Canada. The sponsor did not consider potential capacity constraints in the submitted economic evaluation.
High resource and administrative burden: To be able to treat patients with tisagenlecleucel, specialized centres need to be trained and accredited by the manufacturer. Obtaining and maintaining this accreditation process can result in a high resource burden, including the development of various protocols and supporting yearly audits. In addition, this treatment has the added complexity of needing coordination between patient care and product preparation by an external manufacturer. Because there are likely multiple CAR T-cell therapies being administered by specialized centres, there will be a need to manage various protocols for the preparation and delivery of each product type, which can increase the overall administrative burden.
Shortage of drugs to manage CRS: CRS tends to be managed with tocilizumab, which is in relatively short supply in Canada. Tocilizumab has been listed on the Drug Shortages Canada website due to its use in COVID-19 treatment. Health Canada has previously declared a Tier 3 shortage of tocilizumab, a designation reserved for shortages that will have the greatest potential impact on Canada’s health care system.35 The use of siltuximab has been considered by some clinicians in the event of a severe shortage of tisagenlecleucel, although this treatment is currently only publicly funded by the Alberta drug formulary.36 A shortage of treatments for CRS may affect tisagenlecleucel use because of the risk of CRS associated with CAR T-cell therapy. This is especially relevant, as 46.4% of patients in the ELARA trial experienced any SAE) after infusion, with the most commonly reported SAE being CRS (19.6%).
Future treatments: Clinical experts indicated that Canadian hospitals are in the midst of growing their capacity to manufacture CAR T-cell products in the future. In particular, the BC Cancer Immunotherapy Program in British Columbia has developed in-house expertise and the infrastructure to manufacture CAR T-cells for the treatment of blood cancers. In fact, more than 50 patients with end-stage leukemia and lymphoma in British Columbia and Ontario have received CAR T-cell therapy manufactured by the BC Cancer Immunotherapy Program as part of CLIC-01, a phase I/II pan-Canadian clinical trial.37 Clinical expert feedback noted that the price of CAR T-cell therapy produced in this setting would be substantially lower than CAR T-cell therapy developed by the pharmaceutical industry.
Sequential use of CAR T-cell products: Evidence for the sequential use of CAR T-cell therapies does not exist; thus, the cost-effectiveness and budget impact of the sequential use of CAR T-cell products is unknown.
Overall Conclusions
Evidence from the ELARA single-arm trial suggests that treatment with tisagenlecleucel may be associated with clinically important tumour responses, including complete remission, in adults with r/r FL after 2 or more lines of systemic therapy. However, there is insufficient evidence — in part due to the limited follow-up duration of the trial — to determine the effects of tisagenlecleucel on OS and PFS. The CADTH clinical assessment identified limitations of the sponsor’s comparison of ELARA to ReCORD-FL data, which substantially limited the ability to determine the relative treatment effects observed for tisagenlecleucel and SOC. Indeed, important prognostic factors were excluded from the propensity model that matched patients receiving tisagenlecleucel in the ELARA trial with those receiving SOC in the ReCORD-FL study. Moreover, important exclusion criteria specific to the ELARA trial, such as the exclusion of patients with previous or concurrent malignancy, could not be applied to the ReCORD-FL study. Of note, the CADTH clinical review indicated that the propensity score matching method employed by the sponsor to compare tisagenlecleucel with SOC resulted in a reduced effective sample size (whereby the majority of patients in the ReCORD-FL study were lost) that may have further contributed to imprecision. Consequently, the clinical review concluded there is uncertainty around the treatment effects of tisagenlecleucel relative to SOC due to selection bias and unmeasured and residual confounding that cannot be entirely ruled out.
Given the magnitude of uncertainty surrounding OS for tisagenlecleucel, its comparative efficacy against SOC, and the durability of such a benefit, CADTH was unable to derive a robust base case estimate of cost-effectiveness. Moreover, given the duration of the ELARA trial (i.e., 38 months) in contrast to the model’s time horizon (i.e., 30 years), it is important to note that the majority of the QALY benefit (83%) realized by patients receiving tisagenlecleucel was derived from the period beyond which there are observed trial data (i.e., extrapolated period). To address this, CADTH conducted 2 separate reanalyses involving different parametric assumptions of treatment effect: in reanalysis A, tisagenlecleucel’s OS was modelled using the exponential distribution (assuming 17.5 years of treatment effect after infusion before waning); and in reanalysis B, tisagenlecleucel’s OS was modelled using the log-normal distribution (assuming 7.9 years of treatment effect after infusion before waning). In addition, the following changes were made consistently in reanalyses A and B to address limitations of the economic model: applying independent models to estimate the OS and PFS of tisagenlecleucel and SOC; using parametric distributions based on ELARA and ZUMA-5 trial data to extrapolate the OS and PFS of tisagenlecleucel and axicabtagene ciloleucel; including a CAR T-cell eligibility assessment cost and updating pretreatment costs associated with apheresis; aligning subsequent therapies among patients receiving SOC in the third-line setting with the observed proportion of patients in the ReCORD-FL chemotherapy subgroup; and excluding axicabtagene ciloleucel as a comparator.
Results from CADTH reanalysis A and reanalysis B were generally aligned: tisagenlecleucel is not cost-effective at a $50,000 WTP threshold compared to SOC. In CADTH reanalysis A (assuming 17.5 years of treatment effect after infusion before waning), tisagenlecleucel was associated with an ICER of $193,516 per QALY gained compared to SOC (incremental costs = $420,926; incremental QALYs = 2.18). In CADTH reanalysis B (assuming 7.9 years of treatment effect after infusion before waning), tisagenlecleucel was associated with an ICER of $434,036 per QALY gained compared to SOC (incremental costs = $420,063; incremental QALYs = 0.97). The estimated ICERs were higher than the sponsor’s base case values, driven primarily by adjustment of tisagenlecleucel’s parametric distribution of OS. In line with clinical expert advice, these reanalyses achieved plausible OS curves in the absence of robust long-term evidence, while still conferring a benefit with tisagenlecleucel . CADTH notes that both reanalyses assume life expectancy increases for patients receiving tisagenlecleucel relative to current SOC (2.65 years and 1.15 years of life gained in reanalysis A and reanalysis B, respectively). However, in the presence of nonrandomized evidence, the true comparative impact of tisagenlecleucel on OS relative to SOC remains uncertain. The CADTH reanalyses assume that the impacts of residual confounding that could influence the nonrandomized comparison between ELARA and ReCORD-FL data are limited, and that their findings could be replicated in real-world clinical practice. Both assumptions are highly uncertain. Hence, given the available evidence, the estimates presented in the CADTH reanalyses likely represent the upper bounds of the incremental gains that may be realized from this therapy.
A price reduction of 71% or 82% would be required for tisagenlecleucel to be cost-effective at a WTP threshold of $50,000 per QALY gained, conditional on tisagenlecleucel’s long-term impact on OS relative to SOC. This would mean a reduction in the one-time price of tisagenlecleucel, from $450,000 to $130,500 and $81,000, respectively. This range reflects the uncertainty around long-term survival extrapolation, as analyzed in CADTH reanalyses A and B. CADTH undertook 2 scenario analyses on each of the CADTH reanalyses to incorporate the comparison of tisagenlecleucel to axicabtagene ciloleucel and R2. In the first scenario, CADTH compared tisagenlecleucel with axicabtagene ciloleucel, given that a submission for axicabtagene ciloleucel was received for this indication during the present review. Tisagenlecleucel was the dominant strategy in both reanalyses (incremental costs = –$37,013 to –$37,026; incremental QALYs = 0); that is, tisagenlecleucel generated cost savings for the same number of QALYs gained. In the second scenario, CADTH compared tisagenlecleucel with R2, given that participating drug plans and clinical expert feedback noted its off-label use for this patient population in current Canadian clinical practice. Tisagenlecleucel was the dominated strategy in both reanalyses (incremental costs = $387,426 to $386,806; incremental QALYs = 0); that is, tisagenlecleucel generated higher costs for the same number of QALYs gained.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Kymriah (tisagenlecleucel), 1.2 x 106 to 6.0 x 108 CAR-positive viable T cells, cell suspension in infusion bag, for intravenous use. Dorval (QC): Novartis Pharmaceuticals Canada Inc.; 2023 Feb 08.
2.Kymriah (tisagenlecleucel): 1.2 x 106 to 6.0 x 108 CAR-positive viable T cells, cell suspension in infusion bag, for intravenous use [product monograph]. Dorval (QC): Novartis Pharmaceuticals Canada Inc.; 2022 Dec 19.
3.Clinical Study Report: CCTL019E2202. A phase II, single arm, multicenter open label trial to determine the efficacy and safety of tisagenlecleucel (CTL019) in adult patients with refractory or relapsed follicular lymphoma, version 1.0 [internal sponsor's report]. Dorval (QC): Novartis Pharmaceuticals Canada Inc.; 2022 Aug 12.
4.Kite a Gilead Company. A phase 2 multicenter study of axicabtagene ciloleucel in subjects with relapsed/refractory indolent non-hodgkin lymphoma (ZUMA-5). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2023: https://www.clinicaltrials.gov/ct2/show/NCT03105336. Accessed 2023 Mar 04.
5.Salles G, Schuster SJ, Fischer L, et al. A retrospective cohort study of treatment outcomes of adult patients with relapsed or refractory follicular lymphoma (ReCORD-FL). Hemasphere. 2022;6(7):e745. PubMed
6.Bansback N, Tsuchiya A, Brazier J, Anis A. Canadian valuation of EQ-5D health states: preliminary value set and considerations for future valuation studies. PLoS One. 2012;7(2):e31115. PubMed
7.Ara R, Brazier JE. Populating an economic model with health state utility values: moving toward better practice. Value Health. 2010;13(5):509-518. PubMed
8.Sehn LH, Chua N, Mayer J, et al. Obinutuzumab plus bendamustine versus bendamustine monotherapy in patients with rituximab-refractory indolent non-Hodgkin lymphoma (GADOLIN): a randomised, controlled, open-label, multicentre, phase 3 trial. Lancet Oncol. 2016;17(8):1081-1093. PubMed
9.Zinzani PL, Chen R, Armand P, et al. Pembrolizumab monotherapy in patients with primary refractory classical hodgkin lymphoma who relapsed after salvage autologous stem cell transplantation and/or brentuximab vedotin therapy: KEYNOTE-087 subgroup analysis. Leuk Lymphoma. 2020;61(4):950-954. PubMed
10.van Oers MH, Klasa R, Marcus RE, et al. Rituximab maintenance improves clinical outcome of relapsed/resistant follicular non-Hodgkin lymphoma in patients both with and without rituximab during induction: results of a prospective randomized phase 3 intergroup trial. Blood. 2006;108(10):3295-3301. PubMed
11.National Institute for Health and Care Excellence. Idelalisib for treating refractory follicular lymphoma (Technology appraisal guidance TA604) 2019; https://www.nice.org.uk/guidance/ta604. Accessed 2023 Aug 25.
12.Guadagnolo BA, Punglia RS, Kuntz KM, Mauch PM, Ng AK. Cost-effectiveness analysis of computerized tomography in the routine follow-up of patients after primary treatment for Hodgkin's disease. J Clin Oncol. 2006;24(25):4116-4122. PubMed
13.Cancer Care Ontario (CCO). GDP Regimen: gemcitabine-dexamethasone-Platinol® (CISplatin). CCO Formulary 2019; https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/46166. Accessed 2023 Aug 25.
14.Ontario Case Costing Initiative (OCCI): ambulatory care 2017/2018 by procedure. Toronto (ON): Ontario Health and Long-Term Care; 2017: https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi. Accessed 2022 Dec.
15.Institut national d'excellence en sante et en services sociaux. Tisagenlecleucel for the treatment of relapsed or refractory diffuse large B-cell lymphoma: appendicies. Quebec (QC): INESSS; 2019: https://www.inesss.qc.ca/fileadmin/doc/INESSS/Rapports/Therapies_cellulaires/INESSS_Kymriah_Annexes_LDGCB.pdf. Accessed 2023 Aug 25.
16.Canadian Institute for Health Information (CIHI). Patient Cost Estimator. 2022; https://www.cihi.ca/en/patient-cost-estimator. Accessed 2022 Mar 10.
17.Interprovincial Health Insurance Agreements Coordinating Committee (IHIACC). Final - Interprovincial Billing Rates for Designated High Cost Transplants Effective for Discharges on or After April 1, 2022. Organ Transplants. Toronto (ON): Ontario Ministry of Health, Ontario Ministry of Long-Term Care; 2022: https://files.ontario.ca/moh-2023-2024-rates-high-cost-procedures-en-2023-03-24.pdf. Accessed 2023 Aug 25.
18.Trapani D, Tay-Teo K, Tesch ME, et al. Implications of oncology trial design and uncertainties in efficacy-safety data on health technology assessments. Curr Oncol. 2022;29(8):5774-5791. PubMed
19.de Oliveira C, Pataky R, Bremner KE, et al. Phase-specific and lifetime costs of cancer care in Ontario, Canada. BMC Cancer. 2016;16(1):809. PubMed
20.Royston P, Parmar MK. Restricted mean survival time: an alternative to the hazard ratio for the design and analysis of randomized trials with a time-to-event outcome. BMC Med Res Methodol. 2013;13:152. PubMed
21.Bagust A, Beale S. Survival analysis and extrapolation modeling of time-to-event clinical trial data for economic evaluation: an alternative approach. Med Decis Making. 2014;34(3):343-351. PubMed
22.Everest L, Blommaert S, Chu RW, Chan KKW, Parmar A. Parametric survival extrapolation of early survival data in economic analyses: a comparison of projected versus observed updated survival. Value Health. 2022;25(4):622-629. PubMed
23.Woods B, Sideris E, Palmer S, Latimer N, Soares M. Partitioned survival analysis for decision modelling in health care: a critical review. (NICE DSU technical support document 19). Sheffield (GB): Decision Support Unit, ScHARR University of Sheffield; 2017: https://www.sheffield.ac.uk/nice-dsu/tsds/partitioned-survival-analysis. Accessed 2023 Aug 25.
24.Woods BS, Sideris E, Palmer S, Latimer N, Soares M. Partitioned survival and state transition models for healthcare decision making in oncology: where are we now? Value Health. 2020;23(12):1613-1621. PubMed
25.Ontario Case Costing Initiative (OCCI). Toronto (ON): Ontario Health and Long-Term Care; 2017: https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi. Accessed 2023 Aug 25.
26.Procedures for CADTH Rembursement Reviews, version 15. Ottawa (ON): CADTH; 2023: https://www.cadth.ca/sites/default/files/Drug_Review_Process/CADTH_Drug_Reimbursement_Review_Procedures.pdf. Accessed 2023 Feb.
27.Drug Reimbursement Review: axicabtagene ciloleucel (Yescarta) for the treatment of adult patients with relapsed or refractory grade 1, 2 or 3a follicular lymphoma (FL) after two or more lines of systemic therapy [in-progress]. Ottawa (ON): CADTH; 2023: https://www.cadth.ca/axicabtagene-ciloleucel-0. Accessed 2023 Apr 19.
28.Holbro A, Ahmad I, Cohen S, et al. Safety and cost-effectiveness of outpatient autologous stem cell transplantation in patients with multiple myeloma. Biol Blood Marrow Transplant. 2013;19(4):547-551. PubMed
29.CADTH Reimbursement Review Implementation Planning for Cell or Gene Therapy. Ottawa (ON): CADTH; 2020: https://www.cadth.ca/sites/default/files/Drug_Review_Process/CADTH_Implementation_Plan_Template.docx. Accessed 2023 Aug 25.
30.Keating SJ, Gu T, Jun MP, McBride A. Health care resource utilization and total costs of care among patients with diffuse large B cell lymphoma treated with chimeric antigen receptor T cell therapy in the United States. Transplant Cell Ther. 2022;28(7):404 e401-404 e406.
31.Novartis. Novartis expands Kymriah® manufacturing footprint with first-ever approved site for commercial CAR-T cell therapy manufacturing in Asia. 2020; https://www.novartis.com/news/media-releases/novartis-expands-kymriah-manufacturing-footprint-first-ever-approved-site-commercial-car-t-cell-therapy-manufacturing-asia. Accessed 2023 Apr 11.
32.Schuster SJ, Svoboda J, Chong EA, et al. Chimeric antigen receptor T cells in refractory B-cell lymphomas. N Engl J Med. 2017;377(26):2545-2554. PubMed
33.Axicabtagene ciloleucel for diffuse large B-cell lymphoma: economic report. (CADTH optimal use report vol. 9, no. 1d). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/pdf/car-t/ct0002-axicabtagene-ciloleucel-economic-report-redacted.pdf. Accessed 2023 Aug 25.
34.Drug Reimbursement Review clinical, pharmacoeconomic, ethics, and stakeholder input reports: lisocabtagene maraleucel (Breyanzi) for relapsed or refractory large B-cell lymphoma. Can J Health Technol. 2022;2(10). 10.51731/cjht.2022.461. Accessed 2023 Aug 25.
35.Verma AA, Pai M, Saha S, et al. Managing drug shortages during a pandemic: tocilizumab and COVID-19. CMAJ. 2021;193(21):E771-E776. PubMed
36.DeltaPA. Ottawa (ON): IQVIA; 2021: https://www.iqvia.com/. Accessed 2022 Feb 28.
37.BC Cancer. CLIC-01 clinical trial: building BC Cancer’s capabilities in cutting-edge immunotherapy. 2023; http://www.bccancer.bc.ca/about/news-stories/stories/clic-01-clinical-trial-building-bc-cancer%E2%80%99s-capabilities-in-cutting-edge-immunotherapy. Accessed 2023 Apr 11.
38.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2022; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2023 Feb.
39.Rinvoq (upadacitinib): 15 mg, 30 mg, 45 mg extended-release oral tablets [product monograph]. St-Laurent (QC): AbbVie; 2023 Jul 19: https://www.abbvie.ca/content/dam/abbvie-dotcom/ca/en/documents/products/RINVOQ_PM_EN.pdf. Accessed 2022 Oct 01.
40.Indirect comparison of Study E2202 (data cut-off: March 2022) versus ReCORD standard of care / chemotherapy-treated patients in relapsed/refractory follicular lymphoma [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Kymriah (tisagenlecleucel), 1.2 x 106 to 6.0 x 108 CAR-positive viable T cells, cell suspension in infusion bag, for intravenous use. Dorval (QC): Novartis Pharmaceuticals Canada Inc.; 2022 Sep.
41.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Kymriah (tisagenlecleucel), 1.2 x 106 to 6.0 x 108 CAR-positive viable T cells, cell suspension in infusion bag, for intravenous use. Dorval (QC): Novartis Pharmaceuticals Canada Inc.; 2023 Feb 08.
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts and participating drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison for r/r Grade 1, 2, or 3a FL After 2 or More Lines of Systemic Therapy (Gene Therapy)
Treatment | Strength / concentration | Form | Price | Recommended dosage | Cost per cycle or 1-time use | Cost per 28 days |
|---|---|---|---|---|---|---|
CAR T-Cell Therapy | ||||||
Tisagenlecleucel (Kymriah) | See dosage | Suspension for IV infusion | 450,000.0000a | Target nonweight-based dose of 0.6 to 6.0 × 108 cells (one-time infusion) | 450,000 | NA |
Table 9: CADTH Cost Comparison for r/r Grade 1, 2, or 3a FL After 2 or More Lines of Systemic Therapy (Chemotherapy, SCT)
Treatment | Strength / concentration | Form | Price | Recommended dosage | Cost per cycle or 1-time use | Cost per 28 days |
|---|---|---|---|---|---|---|
Chemotherapy | ||||||
R-CVP | ||||||
Rituximab (biosimilar) | 10 mg/mL | 100 mg vial for IV infusion | 297.0000b | 21-day cycles: 375 mg/m2 on day 1c | 2,079 | 2,772 |
Cyclophosphamide (Procytox) | 20 mg/mL | 500 mg vial 1,000 mg vial 2000 mg vial for IV infusion | 93.1400 168.8300 310.6000 | 21-day cycles: 750 mg/m2 IV on day 1c | 262 | 349 |
Vincristine (generic) | 1 mg/mL | 1 mg vial 2 mg vial 5 mg vial for IV infusion | 30.6000 62.0000 153.0000 | 21-day cycles: 1.4 mg/m2 IV (max 2 mg) on day 1c | 62 | 83 |
Prednisone (generic) | 50 mg | Tablet | 0.1735 | 21-day cycles: 100 mg orally dailyc | 7 | 10 |
R-CVP regimen cost (21-day cycle) | 2,410 | 3,214 | ||||
R-CHOP | ||||||
Rituximab (biosimilar) | 10 mg/mL | 100 mg vial for IV infusion | 297.0000b | 21-day cycles: 375 mg/m2 on day 1c | 2,079 | 2,772 |
Cyclophosphamide (Procytox) | 20 mg/mL | 500 mg vial 1,000 mg vial 2000 mg vial for IV infusion | 93.1400 168.8300 310.6000 | 21-day cycles: 750 mg/m2 IV on day 1c | 262 | 349 |
Doxorubicin (generic) | 2 mg/mL | 10 mg vial 50 mg vial for IV infusion | 50.0000 250.0000 | 21-day cycles: 50 mg/m2 IV on Day 1c | 455 | 607 |
Vincristine (generic) | 1 mg/mL | 1 mg vial 2 mg vial 5 mg vial for IV infusion | 30.6000 62.0000 153.0000 | 21-day cycles: 1.4 mg/m2 IV (max 2 mg) on day 1c | 62 | 83 |
Prednisone (generic) | 50 mg | Tablet | 0.1735 | 21-day cycles: 100 mg orally on days 1 to 5c | 2 | 2 |
R-CHOP regimen cost (21-day cycle) | 2,860 | 3,813 | ||||
O-CHOP Induction | ||||||
Obinutuzumab (Gazyva) | 25 mg/mL | 1,000 mg vial for IV infusion | 5,275.5000 | 21-day cycles: 1,000 mg IV on days 1, 8, and 15c | 15,827 | 21,102 |
Cyclophosphamide (Procytox) | 20 mg/mL | 500 mg vial 1,000 mg vial 2000 mg vial for IV infusion | 93.1400 168.8300 310.6000 | 21-day cycles: 750 mg/m2 IV on day 1c | 262 | 349 |
Doxorubicin (generic) | 2 mg/mL | 10 mg vial 50 mg vial for IV infusion | 50.0000 250.0000 | 21-day cycles: 50 mg/m2 IV on day 1c | 455 | 607 |
Vincristine (generic) | 1 mg/mL | 1 mg vial 2 mg vial 5 mg vial for IV infusion | 30.6000 62.0000 153.0000 | 21-day cycles: 1.4 mg/m2 IV (max 2 mg) on day 1c | 62 | 83 |
Prednisone (generic) | 50 mg | Tablet | 0.1735 | 21-day cycles: 100 mg orally on days 1 to 5c | 2 | 2 |
O-CHOP Induction cost (21-day cycle) | 16,607 | 22,143 | ||||
O-CHOP Maintenance | ||||||
Obinutuzumab (Gazyva) | 25 mg/mL | 1,000 mg vial for IV infusion | 5,275.5000 | 21-day cycles: 1,000 mg IV on day 1c | 5,276 | 7,034 |
Cyclophosphamide (Procytox) | 20 mg/mL | 500 mg vial 1,000 mg vial 2000 mg vial for IV infusion | 93.1400 168.8300 310.6000 | 21-day cycles: 750 mg/m2 IV on day 1c | 262 | 349 |
Doxorubicin (generic) | 2 mg/mL | 10 mg vial 50 mg vial for IV infusion | 50.0000 250.0000 | 21-day cycles: 50 mg/m2 IV on day 1c | 455 | 607 |
Vincristine (generic) | 1 mg/mL | 1 mg vial 2 mg vial 5 mg vial for IV infusion | 30.6000 62.0000 153.0000 | 21-day cycles: 1.4 mg/m2 IV (max 2 mg) on day 1c | 62 | 83 |
Prednisone (generic) | 50 mg | Tablet | 0.1735 | 21-day cycles: 100 mg orally on days 1 to 5c | 2 | 2 |
O-CHOP Maintenance cost (21-day cycle) | 6,056 | 8,075 | ||||
R-GDP | ||||||
Rituximab (biosimilar) | 10 mg/mL | 100 mg vial for IV infusion | 297.0000b | 21-day cycles: 375 mg/m2 on day 1c | 2,079 | 2,772 |
Gemcitabine (generic) | 40 mg/mL | 1,000 mg vial 2000 mg vial with lyophilized powder for infusion | 270.0000 540.0000 | 21-day cycles: 1,000 mg/m2 days 1 and 8c | 1,080 | 1,440 |
Dexamethasone (generic) | 4 mg | Tablet | 0.3046 | 21-day cycles: 40 mg days 1 to 4c | 12 | 16 |
Cisplatin (generic) | 1 mg/mL | 50 mg vial 100 mg vial with solution for injection | 135.0000 270.0000 | 21-day cycles: 75 mg/m2 on day 1c | 405 | 540 |
R-GDP regimen cost (21-day cycle) | 3,576 | 4,768 | ||||
R-ICE | ||||||
Rituximab (biosimilar) | 10 mg/mL | 100 mg vial for IV infusion | 297.0000b | 21-day cycles: 375 mg/m2 on day 1c | 2,079 | 2,772 |
Ifosfamide (Ifex) | 50 mg/mL | 1,000 mg vial 3,000 mg vial with powder for solution | 138.3400 423.6399 | 21-day cycles:1,667 mg/m2 on days 1 to 3c | 1,245 | 1,660 |
Carboplatin (generic) | 10 mg/mL | 50 mg vial 150 mg vial 450 mg vial 600 mg vial for injection | 70.0000 210.0000 600.0000 775.0020 | 21-day cycles: AUC 5 on day 1; maximum dose for AUC 5 is 750 mgc | Max: 985 | 1,313 |
Etoposide (generic) | 20 mg/mL | 100 mg vial 200 mg vial 500 mg vial for injection | 75.0000 150.0000 375.0000 | 21-day cycles: 100 mg/m2 on days 1 to 3c | 450 | 600 |
R-ICE regimen cost (21-day cycle) | 4,759 | 6,345 | ||||
BR | ||||||
Bendamustine (generic) | 5 mg/mL | 25 mg vial 100 mg vial with powder for solution | 296.8800 1,062.5000 | 28-day cycles: 90 mg/m2 days 1 and 2c | 3,906 | 3,906 |
Rituximab (biosimilar) | 10 mg/mL | 100 mg vial for IV infusion | 297.0000b | 28-day cycles: 375 mg/m2 on day 1c | 2,079 | 2,079 |
BR regimen cost (21-day cycle) | 5,985 | 5,985 | ||||
R2 | ||||||
Rituximab (biosimilar) | 10 mg/mL | 100 mg vial for IV infusion | 297.0000b | 28-day cycles: (Cycle 1): 375 mg/m2 on days 1, 8, 15, and 22; (Cycles 2 to 5): 375 mg/m2 on day 1 | Induction: 8,316 Maintenance: 2,079 | Induction: 8,316 Maintenance: 2,079 |
Lenalidomide (generic) | 10 mg 20 mg | Capsule | 90.2500 100.7500 | 28-day cycles: 20 mg capsule daily on days 1 to 21c | 2,116 | 2,116 |
R2 induction regimen cost (21-day cycle) | 10,432 | 10,432 | ||||
R2 maintenance regimen cost (21-day cycle) | 4,195 | 4,195 | ||||
Stem Cell transplant (SCT) | ||||||
Autologous SCT (< 72 hours) | Adult autologous stem cell transplant (< 72 hours)- includes all facility costs including inpatient and diagnostic costs | 36,645d per transplant | NA | |||
Autologous SCT (> 72 hours) | Adult autologous stem cell transplant (> 72 hours)- includes all facility costs including inpatient and diagnostic costs | 77,956e per transplant | NA | |||
Allogeneic SCT (non-MUD patients) | Adult allogeneic stem cell transplant - includes all facility costs including inpatient and diagnostic costs - excludes matched unrelated donor (MUD) patients | 179,392d per transplant | NA | |||
Allogeneic SCT (MUD patients) | Adult allogeneic stem cell transplant - includes all facility costs including inpatient and diagnostic costs - matched unrelated donor (MUD) patients | 216,542d per transplant | NA | |||
Note: All prices are wholesale from IQVIA Delta PA (accessed February 2023), unless otherwise indicated, and do not include dispensing fees. Calculations assume a patient body weight of 75 kg and a body surface area of 1.8 m2.
aSponsor’s submitted price.1
bOntario Drug Benefit Formulary or Exceptional Access Program list price38 (accessed February 2023).
cCancer Care Ontario Formulary: Regimens database.39
dInterprovincial Billing Rates for Designated High Cost Transplants Effective for Discharges on or After 1, 2022.17 The cost includes all facility costs associated with a single transplant episode including inpatient and diagnostic costs.
eInterprovincial Billing Rates for Designated High Cost Transplants Effective for Discharges on or After 1, 2022.17 The cost includes all facility costs associated with a single transplant episode including inpatient and diagnostic costs, with a maximum length of stay of 16 days.
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | The sponsor included axicabtagene ciloleucel in the analysis citing its approval by Health Canada. Axicabtagene ciloleucel does not meet any of the 3 criteria for relevant comparators: (1) reimbursed by at least one participating drug plan, (2) currently used off-label, and (3) received positive recommendation from CADTH. The sponsor excluded the R2 regimen (lenalidomide + rituximab) from the base case analysis, despite the fact that the therapy is used off-label for the treatment of adult patients with r/r grade 1, 2, or 3a FL after 2 or more lines of systemic therapy in Canada. |
Model has been adequately programmed and has sufficient face validity | No | The sponsor’s model was not thoroughly debugged. For instance, CADTH remarks that when selecting an option within a dropdown list, an unprompted change would be triggered in an unrelated dropdown list, which complicated the validation process. |
Model structure is adequate for decision problem | No | The PSM further introduces structural assumptions about the relationship between PFS and OS (i.e., nonmutually exclusive curves), which is potentially problematic since they are likely dependent outcomes. Clinical expert opinion suggested that survival is linked to the occurrence of progressive disease and thus the transition probability to death should vary for patients within the progression-free state compared to those in the progressive disease state. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment. |
FL = follicular lymphoma; OS = overall survival; PFS = progression-free survival; R2 regimen = combination of lenalidomide + rituximab.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
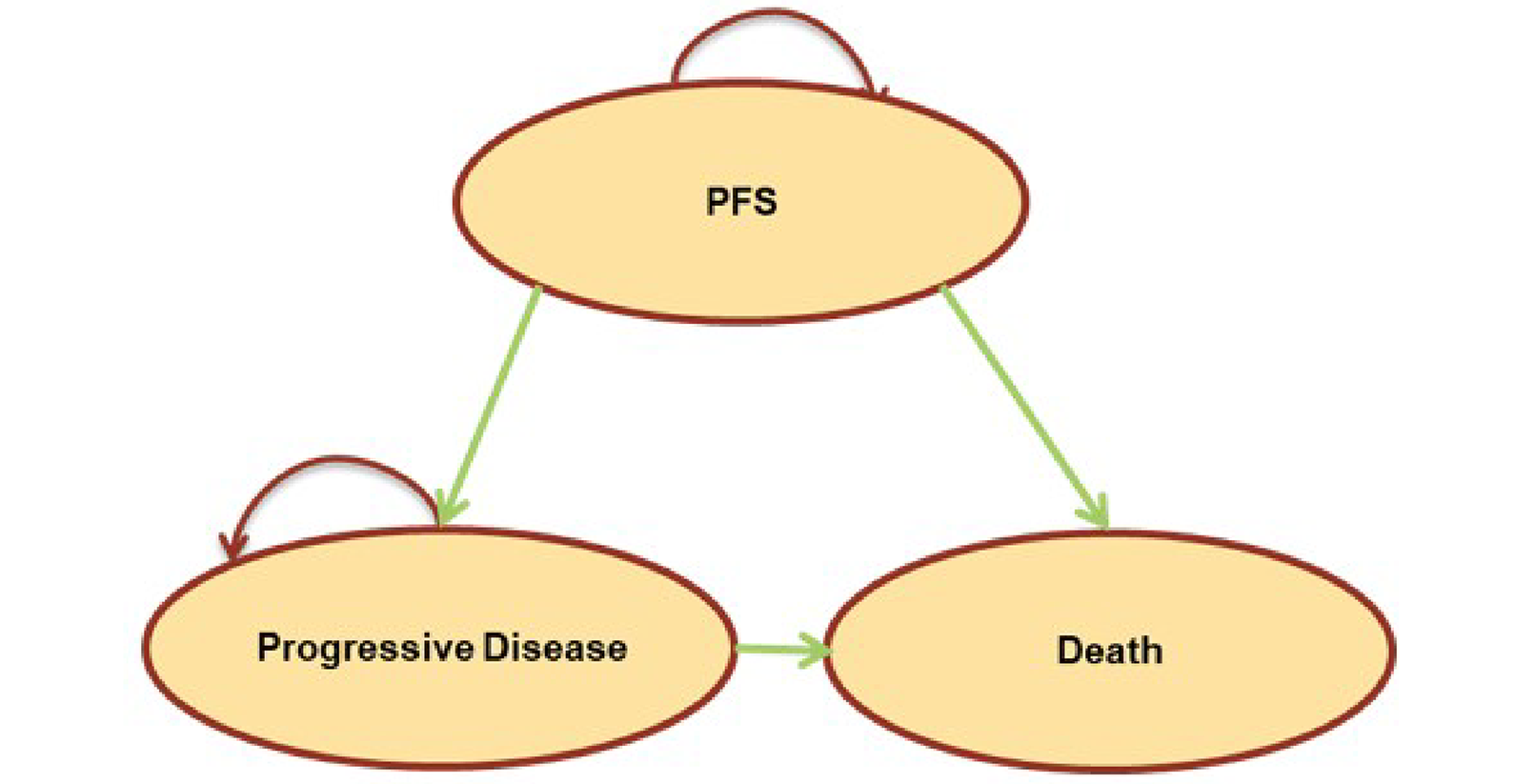
Detailed Results of the Sponsor’s Base Case
Table 11: Distribution of Subsequent Therapy
Subsequent therapy in 4L | Initial 3L treatment regimen on which patients have progressed | |
|---|---|---|
CAR T cell (Tisagenlecleucel/axicabtagene ciloleucel) | SOC (Chemotherapy/auto-SCT) | |
SOC | 58% | 25% |
Chemotherapy | 38% | 8% |
Autologous SCT | 4% | 3% |
Allogeneic SCT | 17% | 14% |
CAR T cell | 0% | 45% |
Tisagenlecleucel | 0% | 28% |
Axicabtagene ciloleucel | 0% | 17% |
No active treatment | 26% | 14% |
Clinical trial | 16% | 16% |
auto-SCT = autologous stem cell transplant; CAR = chimeric antigen receptor; SCT = stem cell transplant; SOC = standard of care.
Source: Sponsor’s pharmacoeconomic submission.1
Table 12: Disaggregated Results of the Sponsor’s Base Case
Parameter | Tisagenlecleucel | SOC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 13.99 | 9.15 | 4.84 |
Preprogression | 9.28 | 5.57 | 3.71 |
Postprogression | 4.72 | 3.58 | 1.13 |
Discounted QALYs | |||
Total | 11.05 | 7.22 | 3.83 |
Preprogression | 7.37 | 4.40 | 2.96 |
Postprogression | 3.71 | 2.83 | 0.89 |
Disutility due to SCT | −0.01 | −0.01 | 0.00 |
Disutility due to AE | −0.02 | 0.00 | −0.01 |
Discounted costs ($) | |||
Total | $555,793 | $191,496 | $364,298 |
Pre-treatment | $7,540 | $0 | $7,540 |
Drug/procedure | $5,117 | $0 | $5,117 |
Administration | $309 | $0 | $309 |
Hospitalization | $2,114 | $0 | $2,114 |
Treatment | $463,247 | $56,371 | $406,876 |
Drug/procedure | $446,771 | $53,784 | $392,988 |
Administration | $107 | $1,867 | -$1,761 |
Hospitalization | $16,369 | $720 | $15,649 |
AEs | $8,167 | $894 | $7,273 |
Follow-up cost before progression | $6,180 | $2,270 | $3,910 |
Subsequent treatment | $16,962 | $70,895 | -$53,934 |
Medical cost postprogression | $10,106 | $7,678 | $2,428 |
Terminal care | $43,592 | $53,388 | -$9,796 |
ICER ($/QALY) | $95,025 | ||
AE = adverse events; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; SCT = stem cell transplant; SOC = standard of care.
Figure 2: Assessment of the Proportional Hazard Assumption for the ELARA Trial vs. the ReCORD-FL Chemotherapy Subgroup After Weighting, Schoenfeld Residuals for OS
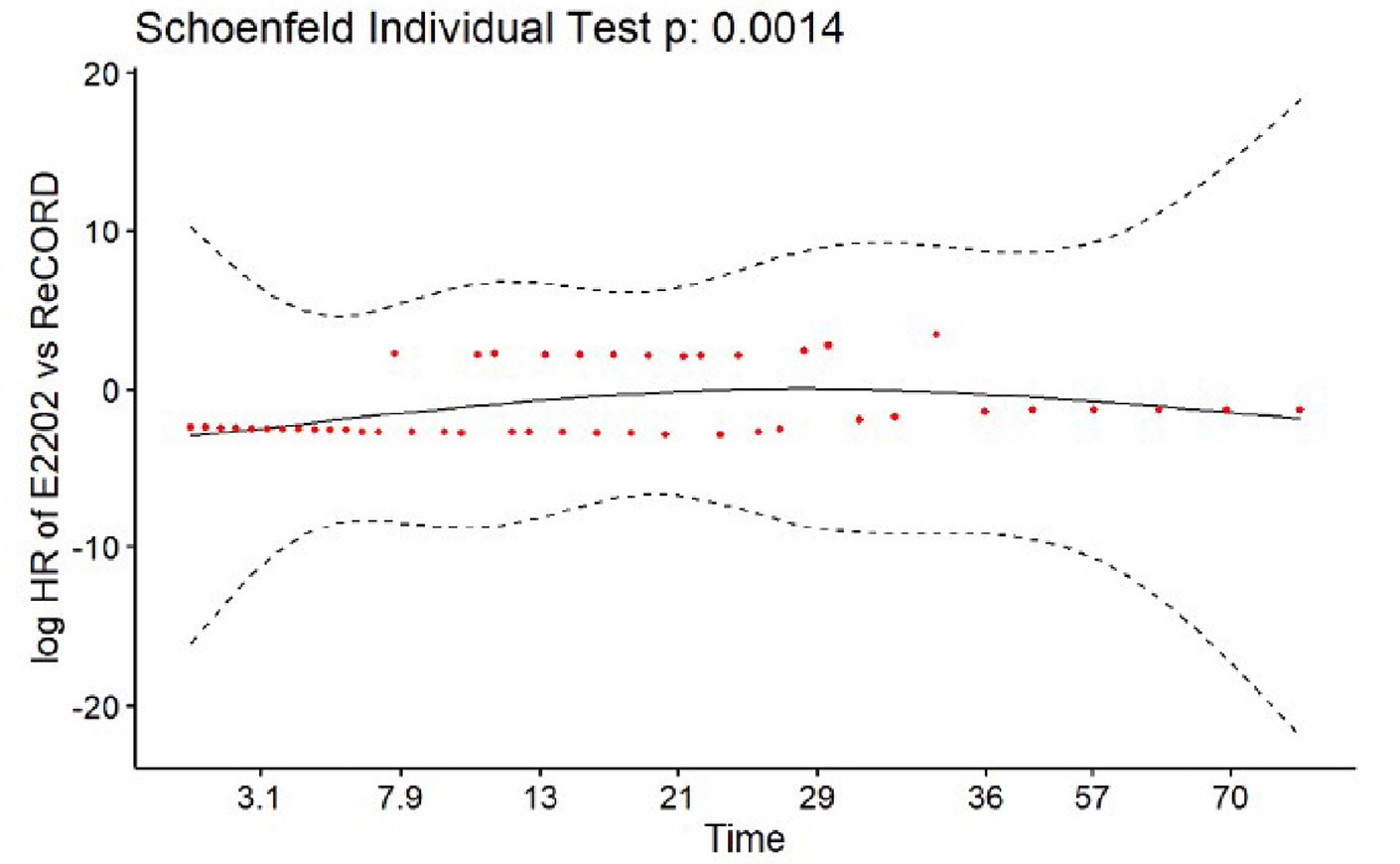
Source: Sponsor’s study report: “Indirect Comparison of Study E2202 (data cut-off: March 2022) versus ReCORD Standard of Care / Chemotherapy-Treated Patients in Relapsed/Refractory Follicular Lymphoma.”40
Figure 3: Assessment of the Proportional Hazard Assumption for the ELARA Trial vs. the ReCORD-FL Chemotherapy Subgroup After Weighting, Schoenfeld Residuals for PFS
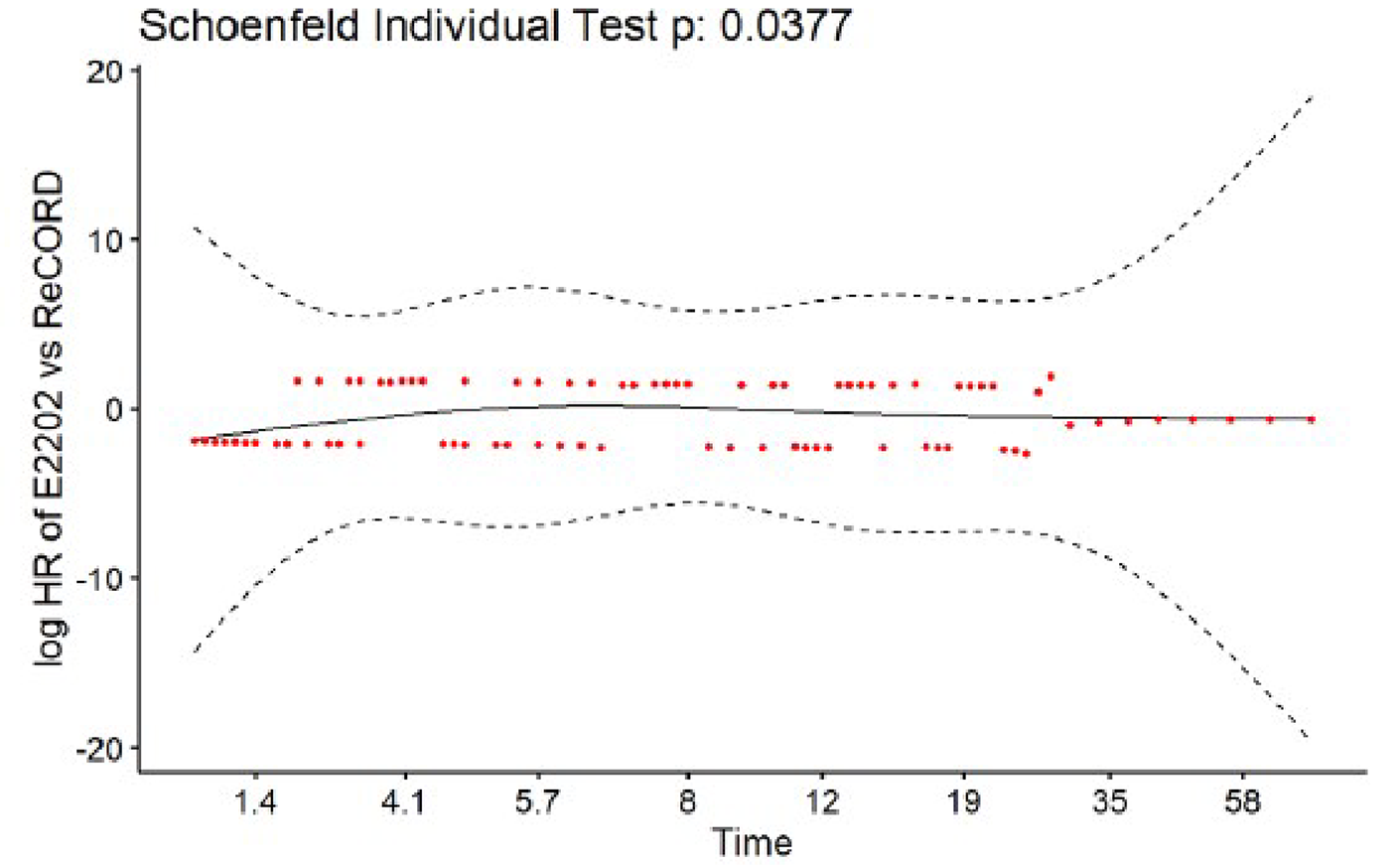
Source: Sponsor’s study report: “Indirect Comparison of Study E2202 (data cut-off: March 2022) versus ReCORD Standard of Care / Chemotherapy-Treated Patients in Relapsed/Refractory Follicular Lymphoma.”40
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Figure 4: OS for SOC and Tisagenlecleucel in CADTH Reanalyses A and B
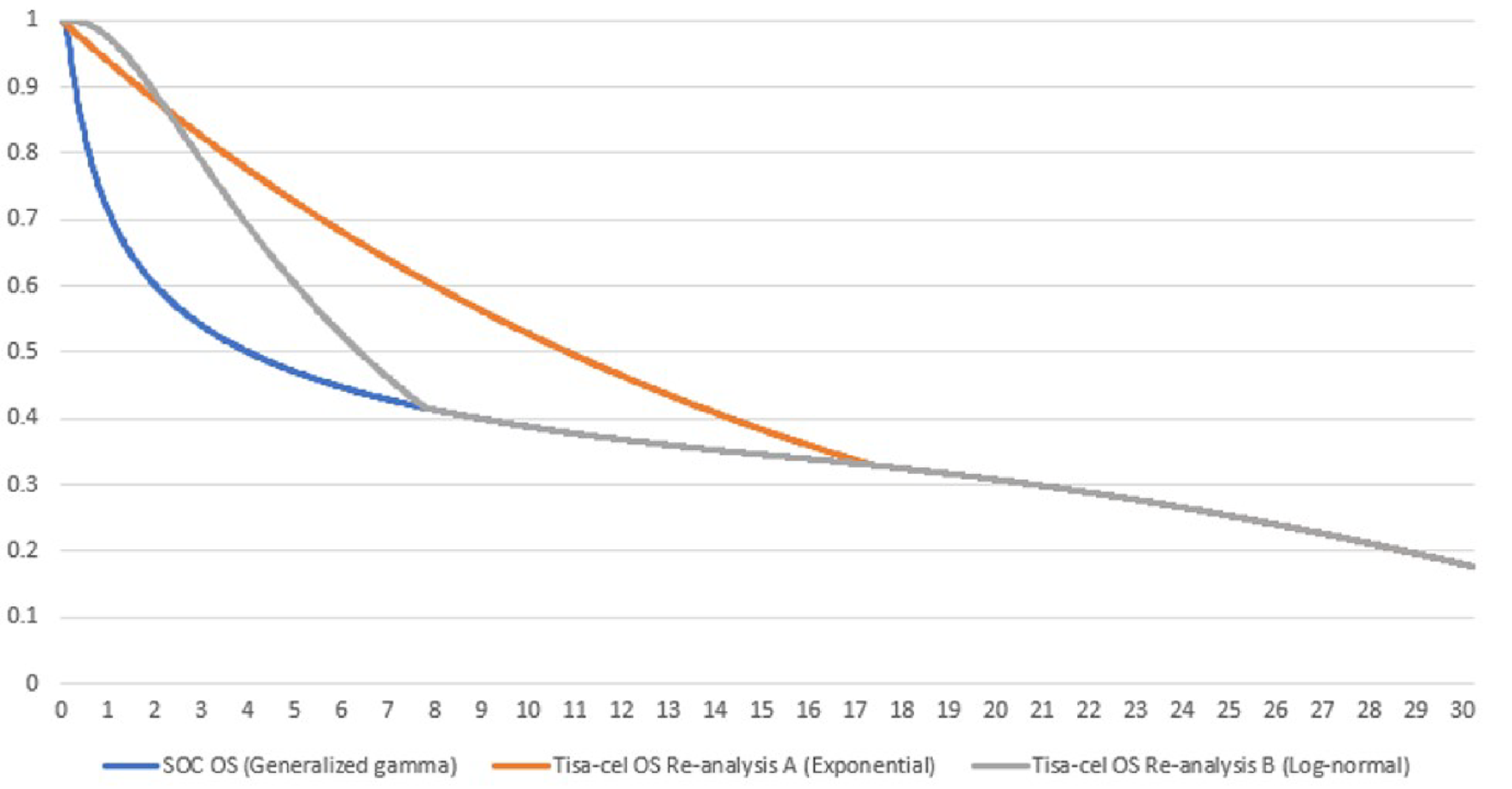
OS = overall survival; SOC = standard of care.
Source: Sponsor’s pharmacoeconomic submission.1
Table 13: Disaggregated Summary of CADTH’s Reanalysis A
Parameter | Tisagenlecleucel | SOC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 11.94 | 9.29 | 2.65 |
Preprogression | 8.45 | 5.96 | 2.49 |
Postprogression | 3.49 | 3.33 | 0.16 |
Discounted QALYs | |||
Total | 9.51 | 7.34 | 2.18 |
Preprogression | 6.73 | 4.73 | 2.00 |
Postprogression | 2.81 | 2.62 | 0.19 |
Disutility due to SCT | −0.01 | −0.01 | −0.01 |
Disutility due to AE | −0.02 | 0.00 | −0.01 |
Discounted costs ($) | |||
Total | $569,405 | $148,479 | $420,926 |
Pre-treatment | $14,352 | $0 | $14,352 |
Drug/procedure | $11,929 | $0 | $11,929 |
Administration | $309 | $0 | $309 |
Hospitalization | $2,114 | $0 | $2,114 |
Treatment | $463,277 | $59,377 | $403,900 |
Drug/procedure | $446,802 | $56,790 | $390,012 |
Administration | $107 | $1,867 | -$1,761 |
Hospitalization | $16,369 | $720 | $15,649 |
AEs | $8,167 | $894 | $7,273 |
Follow-up cost before progression | $5,827 | $2,474 | $3,353 |
Subsequent treatment | $19,956 | $25,436 | -$5,480 |
Medical cost postprogression | $7,483 | $7,136 | $347 |
Terminal care | $50,342 | $53,162 | -$2,820 |
ICER ($/QALY) | $193,516 | ||
AE = adverse events; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; SCT = stem cell transplant; SOC = standard of care.
Table 14: Disaggregated Summary of CADTH’s Reanalysis B
Parameter | Tisagenlecleucel | SOC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 10.44 | 9.29 | 1.15 |
Preprogression | 8.25 | 5.96 | 2.29 |
Postprogression | 2.18 | 3.33 | −1.14 |
Discounted QALYs | |||
Total | 8.30 | 7.34 | 0.97 |
Preprogression | 6.57 | 4.73 | 1.84 |
Postprogression | 1.76 | 2.62 | −0.86 |
Disutility due to SCT | −0.01 | −0.01 | −0.01 |
Disutility due to AE | −0.02 | 0.00 | −0.01 |
Discounted costs ($) | |||
Total | $568,542 | $148,479 | $420,063 |
Pre-treatment | $14,352 | $0 | $14,352 |
Drug/procedure | $11,929 | $0 | $11,929 |
Administration | $309 | $0 | $309 |
Hospitalization | $2,114 | $0 | $2,114 |
Treatment | $463,277 | $59,377 | $403,900 |
Drug/procedure | $446,802 | $56,790 | $390,012 |
Administration | $107 | $1,867 | -$1,761 |
Hospitalization | $16,369 | $720 | $15,649 |
AEs | $8,167 | $894 | $7,273 |
Follow-up cost before progression | $5,753 | $2,474 | $3,279 |
Subsequent treatment | $20,367 | $25,436 | -$5,069 |
Medical cost postprogression | $4,684 | $7,136 | -$2,452 |
Terminal care | $51,941 | $53,162 | -$1,221 |
Indirect costs | $0 | $0 | $0 |
ICER ($/QALY) | $434,036 | ||
AE = adverse events; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; SCT = stem cell transplant; SOC = standard of care.
Scenario Analyses
Table 15: Scenario Analyses Conducted on CADTH Reanalyses A and B
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
CADTH re-analysis A: Exponential OS for Tisagenlecleucel | SOC | $148,479 | 7.34 | Reference |
Tisagenlecleucel | $569,405 | 9.51 | $193,516 | |
CADTH re-analysis B: Log-normal OS for Tisagenlecleucel | SOC | $148,479 | 7.34 | Reference |
Tisagenlecleucel | $568,542 | 8.30 | $434,036 | |
CADTH re-analysis A - Scenario 1: Tisagenlecleucel vs. Axicabtagene ciloleucel | Tisagenlecleucel | $569,405 | 9.51 | Reference |
Axicabtagene ciloleucel | $606,431 | 9.51 | Dominant | |
CADTH re-analysis B - Scenario 1: Tisagenlecleucel vs. Axicabtagene ciloleucel | Tisagenlecleucel | $568,542 | 8.30 | Reference |
Axicabtagene ciloleucel | $605,555 | 8.30 | Dominant | |
CADTH re-analysis A - Scenario 2: Tisagenlecleucel vs. R2 | R2 | $181,979 | 9.53 | Reference |
Tisagenlecleucel | $569,405 | 9.53 | Dominated | |
CADTH re-analysis B - Scenario 2: Tisagenlecleucel vs. R2 | R2 | $181,736 | 8.32 | Reference |
Tisagenlecleucel | $568,542 | 8.32 | Dominated |
ICER = incremental cost-effectiveness ratio; LY = life-year; OS = overall survival; QALY = quality-adjusted life-year; R2 = regimen combining lenalidomide and rituximab; SOC = standard of care.
Appendix 5: Submitted BIA and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 16: Summary of Key Takeaways
Key Takeaways of the BIA |
|---|
|
Summary of Sponsor’s BIA
The sponsor submitted a budget impact analysis (BIA) to estimate the incremental 3-year budget impact of reimbursing tisagenlecleucel for the treatment of adult patients with r/r grade 1, 2, or 3a FL after 2 or more lines of systemic therapy, as per its Health Canada indication.41 The analysis was performed from the perspective of the Canadian public drug plan formulary. The sponsor estimated the budget impact by comparing 2 scenarios: a reference scenario that estimated the total costs associated with SOC for the treatment of adult patients with r/r grade 1, 2, or 3a FL after 2 or more lines of systemic therapy; and a new drug scenario, where CAR T-cell therapies (including tisagenlecleucel and axicabtagene ciloleucel) are funded in the third-line setting.41 SOC was composed of a mix of chemoimmunotherapy (i.e., R-CVP; R-CHOP; O-CHOP; R-GDP, R-ICE, BR) and SCT. The sponsor estimated the eligible population using an epidemiology-based approach, leveraging data from multiple sources in the scientific literature and assumptions based on clinical expert input. The sponsor included drug-acquisition costs, as well as those associated with pre-treatment pertaining to CAR T-cell therapies (i.e., leukapheresis, cryopreservation, bridging and lymphodepleting therapies). The dosing modelled for tisagenlecleucel reflected the product monograph. Key inputs to the BIA are documented in Table 19.
Key assumptions made by the sponsor include:
42% of patients with FL would be on watchful waiting at the time of diagnosis, and 10% among them would be eligible for treatment annually.
41%, 40%, and 30% of patients with FL who received a first-, second-, and third-line treatment would relapse and receive subsequent therapy, respectively.
Axicabtagene ciloleucel would be listed on Canadian public drug plans (PDPs) by the time tisagenlecleucel is evaluated by CADTH. Hence, the sponsor included axicabtagene ciloleucel as a comparator for both third- and fourth-line settings in the BIA model.
4% and 15% of patients in the eligible population would seek treatment through clinical trials for investigational therapies in third- and fourth-line settings, respectively (at no additional cost to drug plans).
27% of patients receiving tisagenlecleucel and comparators in third line would not seek active treatment in later lines.
Pre-treatment regimens and the proportion of patients receiving each therapy (i.e., leukapheresis, cryopreservation, bridging and lymphodepleting chemotherapies) before CAR T-cell infusion were based on the ELARA and ZUMA-5 clinical trials, and assumed reflective of Canadian clinical practice.
Table 17: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as Year 1 / Year 2 / Year 3 if appropriate) |
|---|---|
Target Population | |
Adult population in Canada | 30,074,400 |
Annual incidence rate of NHL | 0.03% |
Annual mortality rate of NHL | 0.01% |
Prevalence of NHL | 22,302 |
Proportion of NHL that are FL | 25.0% |
Proportion of patients on watchful waiting | 42.4% |
Proportion of patients requiring treatment | 10.3% |
Proportion of treated patients | 57.6% |
1L, 2L, and 3L transformed FL rate | 1.4% |
Proportion of patients who relapse and are treated in 1L Proportion of patients who relapse and are treated in 2L Proportion of patients who relapse and are treated in 3L | 41.0% 40.0% 30.0% |
Number of patients eligible for tisagenlecleucel in 3L | 560 / 154 / 162 |
Number of patients eligible for tisagenlecleucel in 4L | 168 / 46 / 49 |
Market Uptake (3 years) | |
Uptake in 3L (reference scenario) SOC Clinical trials Axicabtagene ciloleucel Uptake in 4L (reference scenario) SOC Clinical trials Axicabtagene ciloleucel No active treatment | 89.1% / 86.6% / 84.5% 4.0% / 5.0% / 6.0% 6.9% / 8.4% / 9.5% 54.1% / 52.2% / 51.1% 15.0% / 15.0% / 15.0% 3.8% / 5.7% / 6.9% 27.0% / 27.0% / 27.0% |
Uptake in 3L (new drug scenario) Tisagenlecleucel SOC Clinical trials Axicabtagene ciloleucel Uptake in 4L (new drug scenario) Tisagenlecleucel SOC Clinical trials Axicabtagene ciloleucel No active treatment | 11.1% / 13.6% / 15.5% 78.0% / 73.0% / 69.0% 4.0% / 5.0% / 6.0% 6.9% / 8.4% / 9.5% 6.2% / 9.3% / 11.1% 48.0% / 43.0% / 40.0% 15.0% / 15.0% / 15.0% 3.8% / 5.7% / 6.9% 27.0% / 27.0% / 27.0% |
Cost of treatment (per patient) | |
Tisagenlecleucel (one-time) Acquisition Leukapheresis and cryopreservation Bridging therapy (weighted) Lymphodepleting chemotherapy (weighted) | $ 450,000 $ 1,858 $ 2,169 $ 1,115 |
SOC Chemotherapy (weighted) Autologous SCT Allogenic SCT | $ 33,743 (annual) $ 101,392 (one time) $ 216,542 (one time) |
Axicabtagene ciloleucel (one-time) Acquisition Leukapheresis Bridging therapy (weighted) Lymphodepleting chemotherapy (weighted) | $ 485,000 $ 1,589 $ 59 $ 1,915 |
1L = first-line; 2L = second-line; 3L = third line; 4L = fourth-line; FL = follicular lymphoma; NHL = non-Hodgkin’s lymphoma; SOC = standard of care.
Summary of the Sponsor’s BIA Results
Results of the sponsor’s base case BIA suggest that the incremental expenditures associated with the reimbursement of tisagenlecleucel for the Health Canada–indicated population of adult patients with r/r grade 1, 2, or 3a FL after 2 or more lines of systemic therapy would be $30,834,589 in Year 1, $10,675,787 in Year 2, and $12,831,841 in Year 3, for a 3-year cumulative total of $54,342,216, under the drug plan perspective.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Projected market size is underestimated: The sponsor assumed that 41% of patients with FL would relapse and continue with subsequent treatment in the second-line setting. CADTH notes that the expert input elicited by the sponsor is based on clinical practice as observed in the US, where the proportion of patients with FL who receive second-line therapy is potentially restricted by accessibility issues inherent to a predominantly private health care system. Indeed, clinical experts convened by CADTH indicated that the proportion of patients who relapse and continue with subsequent therapy in second-line would be higher in Canadian clinical practice. As such, CADTH maintains that the estimate obtained from US-based oncologists may underestimate the proportion of patients who receive second-line therapy in Canada.
CADTH conducted a reanalysis by assuming that 55% of patients with FL would relapse and continue with subsequent treatment in the second-line setting.
CADTH conducted a scenario analysis, in which the sponsor’s original assumption that 41% of patients with FL would relapse and continue treatment in second-line was incorporated.
Projected market share of tisagenlecleucel is underestimated: The sponsor assumed that tisagenlecleucel would have a market share of 11.1%, 13.6% and 15.5% in Years 1, 2, and 3, respectively. Clinical expert feedback emphasized that the sponsor’s market share projections were substantially lower than they would anticipate in practice if a therapy like tisagenlecleucel were to be funded in third line. This aligned with the feedback received from registered clinician groups in Canada who noted that tisagenlecleucel was expected to shift the current treatment paradigm by replacing chemoimmunotherapy as a new preferred treatment for patients with r/r grade 1, 2, or 3a FL after 2 or more lines of systemic therapy. Indeed, clinicians advocated for tisagenlecleucel to be used in patients with r/r FL who are not eligible to receive SCT in the third-line setting.
CADTH conducted a re-analysis by adjusting the projected market share of tisagenlecleucel to 22.3%, 27.2% and 30.9% in Years 1, 2, and 3, respectively based on feedback sought from clinical experts.
Inclusion of axicabtagene ciloleucel as a comparator is not supported by current clinical practice. The sponsor included axicabtagene ciloleucel in the budget impact analysis citing its approval by Health Canada. At the time of the present review, axicabtagene ciloleucel does not meet any of the 3 criteria for relevant comparators: (1) reimbursed by at least 1 participating drug plan, (2) currently used off-label, and (3) received positive recommendation from CADTH. However, a submission for axicabtagene ciloleucel was received for the treatment of adult patients with r/r grade 1, 2, or 3a FL after 2 or more lines of systemic therapy during the present review, indicating that the product may be available in the future.
CADTH conducted a re-analysis that excluded axicabtagene ciloleucel as a comparator. Of note, axicabtagene ciloleucel’s market share in the submitted third- and fourth-line reference scenarios were redistributed to SOC, while its market share in the third- and fourth-line new drug scenarios were redistributed to tisagenlecleucel.
CADTH performed an exploratory analysis that included axicabtagene ciloleucel as a comparator in the third- and fourth-line new drug scenarios in light of the advanced notification of a submission for this product.
Exclusion of R2 as a comparator is not supported by current clinical practice: The sponsor omitted the R2 regimen (lenalidomide + rituximab) from the budget impact analysis, despite evidence that the therapy is prescribed by some oncologists in current Canadian clinical practice. In fact, during the review process, both the participating drug plans and the clinical expert panel convened by CADTH indicated that the R2 regimen is used off-label for the treatment of adult patients with r/r grade 1, 2, or 3a FL after 2 or more lines of systemic therapy in Canada. The sponsor provided functionality in their model to consider the R2 regimen.
CADTH explored the addition of the R2 regimen as a comparator and notes this did not impact the incremental budget impact given that tisagenlecleucel was not assumed to capture market share from R2.
Exclusion of CAR T-cell–related costs: The pre-treatment cost of leukapheresis considered by the sponsor ($1,589) for patients receiving CAR T-cell therapy was underestimated. CADTH consulted the Ontario Case Costing Initiative (OCCI) for apheresis costs and obtained a cost of $5,426 for stem cell apheresis (code 1.LZ.58.HX).25 In addition, the sponsor failed to consider the upfront costs of assessment of CAR T-cell therapy eligibility, which would include costs associated with MRIs, PET scans, bone marrow transplants, lumbar punctures, and bloodwork. Should tisagenlecleucel be reimbursed, this assessment cost would be incurred by all adult patients with r/r grade 1, 2, or 3a FL after 2 or more lines of systemic therapy (regardless of whether they would go on to receive CAR T-cell therapy).
CADTH conducted a re-analysis that included updated costs associated with leukapheresis.
As CAR T-cell eligibility assessment costs are nonnegligible and would be applied uniformly across all patients starting treatment in the third-line setting, CADTH included them in a scenario analysis undertaken from a health care system perspective.
CADTH Reanalyses of the BIA
CADTH conducted reanalyses of the BIA by increasing the proportion of patients with FL who would relapse and continue with treatment in second-line, adjusting the projected share of tisagenlecleucel, excluding axicabtagene ciloleucel as a comparator, including the R2 regimen as a comparator, and updating CAR T-cell pre-treatment costs.
Table 18: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. Projected market size (i.e., proportion of patients with FL who would relapse and continue with treatment in 2L) | 41% | 55% |
2. Projected market share of tisagenlecleucel |
|
|
3. Axicabtagene ciloleucel as relevant comparator | Axicabtagene ciloleucel included. | Axicabtagene ciloleucel excluded. |
4. CAR T-cell pre-treatment costs | Cost associated with apheresis ($1,589) is underestimated. | Updated cost associated with apheresis ($5,426). |
CADTH base case | Reanalysis 1 + 2 + 3 + 4 | |
The results of the CADTH stepwise re-analysis are presented in summary format in Table 19 and a more detailed breakdown is presented in Table 20. Based on the CADTH base case, the estimated budget impact associated with the reimbursement of tisagenlecleucel for the treatment of r/r grade 1, 2, or 3a FL after 2 or more lines of systemic therapy is expected to be $109,216,203 in year 1, $37,814,864 in year 2, and $45,452,416 in year 3, with a 3-year total of $192,483,483.
Table 19: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $54,342,216 |
CADTH re-analysis 1 | $72,898,095 |
CADTH re-analysis 2 | $108,684,433 |
CADTH re-analysis 3 | $87,856,691 |
CADTH re-analysis 4 | $54,834,732 |
CADTH base case | $192,483,483 |
BIA = budget impact analysis.
CADTH conducted additional scenario analyses to address remaining uncertainty, using the CADTH base case. Results are provided in Table 18.
Assuming that axicabtagene ciloleucel would be a comparator in the third- and fourth-line new drug scenarios in light of the submission for this product.
Exploring the budget impact associated with the reimbursement of tisagenlecleucel from a broader health care system perspective.
Applying CAR T-cell eligibility assessment costs uniformly across all patients starting treatment in third line within a scenario analysis undertaken from a health care system perspective.
Assuming that 41% of patients with FL would relapse and continue with subsequent treatment in second-line.
Table 20: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $27,175,045 | $53,863,009 | $16,140,223 | $17,895,317 | $87,898,549 |
New drug | $27,175,045 | $84,697,598 | $26,816,009 | $30,727,158 | $142,240,765 | |
Budget impact | $0 | $30,834,589 | $10,675,787 | $12,831,841 | $54,342,216 | |
CADTH base case | Reference | $39,365,515 | $49,747,268 | $13,588,265 | $14,171,215 | $77,506,748 |
New drug | $39,365,515 | $158,963,471 | $51,403,130 | $59,623,631 | $269,990,231 | |
Budget impact | $0 | $109,216,203 | $37,814,864 | $45,452,416 | $192,483,483 | |
CADTH scenario analysis 1: Inclusion of axicabtagene ciloleucel as a comparator | Reference | $39,365,515 | $76,148,267 | $22,726,573 | $25,158,451 | $124,033,291 |
New drug | $39,365,515 | $159,623,654 | $51,628,930 | $59,898,281 | $271,150,864 | |
Budget impact | $0 | $83,475,386 | $28,902,357 | $34,739,830 | $147,117,573 | |
CADTH scenario analysis 2: Health care perspectivea | Reference | $44,197,393 | $55,855,715 | $15,254,888 | $15,904,093 | $87,014,696 |
New drug | $44,623,415 | $174,866,918 | $56,431,979 | $65,378,909 | $296,677,806 | |
Budget impact | $426,022 | $119,011,203 | $41,177,091 | $49,474,816 | $209,663,110 | |
CADTH scenario analysis 3: Inclusion of CAR T-cell eligibility costs (Health care perspective) | Reference | $44,197,393 | $55,855,715 | $15,254,888 | $15,904,093 | $87,014,696 |
New drug | $46,939,932 | $177,795,453 | $57,238,184 | $66,224,772 | $301,258,409 | |
Budget impact | $2,742,540 | $121,939,738 | $41,983,296 | $50,320,679 | $214,243,713 | |
CADTH scenario analysis 4: 71% price reduction | Reference | $39,365,515 | $49,747,268 | $13,588,265 | $14,171,215 | $77,506,748 |
New drug | $39,365,515 | $73,354,888 | $21,652,569 | $23,824,596 | $118,832,052 | |
Budget impact | $0 | $23,607,620 | $8,064,303 | $9,653,380 | $41,325,304 | |
CADTH scenario analysis 5: 82% price reduction | Reference | $39,365,515 | $49,747,268 | $13,588,265 | $14,171,215 | $77,506,748 |
New drug | $39,365,515 | $60,091,586 | $17,043,327 | $18,278,266 | $95,413,180 | |
Budget impact | $0 | $10,344,319 | $3,455,061 | $4,107,051 | $17,906,431 | |
CADTH scenario analysis 6: 41% of patients relapse and continue treatment in second line | Reference | $29,345,202 | $37,084,327 | $10,129,434 | $10,563,997 | $57,777,758 |
New drug | $29,345,202 | $118,500,042 | $38,318,697 | $44,446,707 | $201,265,445 | |
Budget impact | $0 | $81,415,715 | $28,189,262 | $33,882,710 | $143,487,687 |
BIA = budget impact analysis; CAR = chimeric antigen receptor.
aHealth care perspective includes medical follow-up in pre- and postprogression stages, as well as management of adverse events.
Ethics Review
Abbreviations
ALL
acute lymphoblastic leukemia
CAR
chimeric antigen receptor
CRS
cytokine release syndrome
DLBCL
diffuse large B-cell lymphoma
FL
follicular lymphoma
ICU
intensive care unit
MAIC
matching-adjusted indirect comparison
MCL
mantle cell lymphoma
MM
multiple myeloma
r/r
relapsed or refractory
SCT
stem cell transplant
Supplementary Ethical Considerations: Tisagenlecleucel for Follicular Lymphoma
Ethical considerations relevant to chimeric antigen receptor (CAR) T-cell therapies in the treatment of hematological cancers are described in the section entitled Summary Report: Ethical Considerations in the Use of CAR T-Cell Therapies for Hematological Cancers. Ethical considerations specific to the use of tisagenlecleucel for the treatment of adults with relapsed or refractory (r/r) grade 1, 2, or 3a follicular lymphoma (FL) after 2 or more lines of systemic therapy have also been identified from a review of patient input, clinician group input, and drug program input, as well as consultation with clinical experts engaged by CADTH for this review and CADTH clinical and economic reviewers:
Patient experiences and treatment options for FL: As described in detail in the CADTH Clinical Review Report, FL is a subtype of non-Hodgkin B-cell lymphoma that presents as an indolent (or slow growing) cancer. As a result, many patients with FL are asymptomatic and may not require intervention beyond surveillance for many years after diagnosis. However, most patients with FL will eventually develop increasingly resistant or refractory disease, characterized by recurrent disease progression, shorter remission periods, and decreased survival. Patients with r/r FL have limited third-line therapeutic options, especially if they are ineligible for stem cell transplant (SCT) and have a need for therapies with fewer toxicities and a more durable response. Patients who become chemotherapy refractory have no remaining therapeutic options available and thus have an unmet need for treatment that can delay disease progression.
Clinical decision-making for r/r FL: Clinical experts consulted by CADTH during this reimbursement review noted that as a disease, FL presents heterogeneously among patients with respect to symptoms and severity of disease. They discussed how this presented challenges for clinicians tasked with determining the best therapeutic course of action. For example, although many patients present with indolent FL or have long remission periods between treatments, others may present with a more aggressive form of the disease that requires immediate therapeutic intervention or they may become chemotherapy refractory. Although tisagenlecleucel is proposed for use beyond second-line therapy in patients with FL, clinical experts noted that there are other third-line therapies available to treat FL. Owing to the heterogeneity of FL and the availability of other third-line therapies, the clinical experts discussed how the decision to recommend tisagenlecleucel for the treatment of FL would include a consideration of all available therapeutic options, as well as a patient’s individual presentation of the disease and circumstances. Shared decision-making may be part of this process, given the range of therapies available and an individualized risk-benefit calculus.
Evidentiary uncertainties related to tisagenlecleucel for FL: The safety and efficacy of tisagenlecleucel in the treatment of adults with r/r FL after 2 or more lines of systemic therapy was evaluated in the pivotal phase II, open-label, single-arm ELARA trial. As noted in the CADTH Clinical Review Report, treatment with tisagenlecleucel is associated with clinically important tumour responses, including complete remission, but the ELARA trial did not yield long-term safety and efficacy data or comparative effectiveness data. To address the gap in comparative data, and as described in detail in the clinical report, the sponsor provided 1 sponsor-conducted matching-adjusted indirect comparison (MAIC) of tisagenlecleucel and axicabtagene ciloleucel (another CAR T-cell therapy) and 1 retrospective cohort study, which was used to compare the treatment effect of standard chemotherapy to tisagenlecleucel. However, the CADTH clinical assessment identified methodological limitations of both studies (including small sample sizes, heterogeneity across study designs and populations, and the inability to adjust for all potential effect modifiers and prognostic variables), which substantially limited the ability to interpret the relative treatment effects observed for tisagenlecleucel and axicabtagene ciloleucel or standard chemotherapy. The clinical experts noted that given the availability of other therapeutic options for the treatment of FL beyond second-line therapies, they would prefer to have a higher level of evidence — including long-term efficacy outcomes and comparative effectiveness data collected from a phase III trial — to inform clinical decision-making with respect to tisagenlecleucel. Moreover, they emphasized the importance of having comparative effectiveness data, given the availability of alternative treatments for this patient population, and the fact that CAR T-cell therapy is highly costly, resource intensive, and administratively burdensome, which presents significant opportunity costs for publicly funded oncology and non-oncology drug budgets and health care systems.
Jurisdictional inequities: Clinical experts also noted that variability in funding for FL treatments, and oncological drugs more broadly, across Canadian jurisdictions could result in inequities in access to tisagenlecleucel were it reimbursed in a piecemeal manner for patients in Canada.
Summary Report: Ethical Considerations in the Use of CAR T-Cell Therapies for Hematological Cancers
Summary
Normative and empirical literature on CAR T-cell therapies, as well as past CADTH ethics reports of CAR T-cell therapies for hematological cancers, were reviewed to summarize the ethical considerations associated with the use of CAR T-cell therapies for the treatment of hematological cancers.
Ethical considerations arising in the context of hematological cancers include the unmet need for durable, life-prolonging treatment for patients with r/r disease, as well as disparities in the incidence, diagnosis, treatment, and outcomes in hematological cancers, especially they way these affect patients from racialized, marginalized, and low socioeconomic groups and those residing in rural areas.
Ethical considerations arising in the evidence used to evaluate CAR T-cell therapies indicate limitations in the representativeness of clinical trial populations, the absence of long-term safety and efficacy data, and the absence of comparative effectiveness data. Uncertainty about the magnitude of clinical benefit presents challenges for the pharmacoeconomic assessment of CAR T-cell therapies and the assessment of opportunity costs, and may expose payers to greater financial risks. Budget forecasting may underestimate the overall budget impact of reimbursing CAR T-cell therapies if they are implemented fairly and as needed.
Ethical considerations arise with respect to the potential benefits and harms related to the use and delivery of CAR T-cell therapies. Several access considerations arise in the context of CAR T-cell therapies in Canada, including those related to geographical access, especially as they may disproportionately impact racialized, marginalized, and low socioeconomic groups and those lacking caregiver support, as well as inequities that may arise during referral or treatment. Considerations related to privacy and cultural-sensitive practices also arise in the context of cell and tissue ownership, as do considerations related to informed consent, shared decision-making, and balanced communication related to CAR T-cell therapies.
Ethical considerations for health systems include challenges associated with the capacity to manufacture and deliver CAR T-cell therapy and scale CAR T-cell centres across Canada due to the complex infrastructure and personnel requirements. Fair priority-setting criteria are required if demand for therapy exceeds manufacturing or delivery capacity. The reimbursement of high-cost, resource-intensive therapies such as CAR T-cell therapies presents opportunity costs for health systems within and beyond the hematological-oncological cancer space. Resources for health information infrastructure may be required to support post-market surveillance, the collection of real-world evidence, and the implementation of alternative pricing or financing models.
Objectives
This report summarizes the ethical considerations common to the use of CAR T-cell therapies for the treatment of children and adults with hematological cancers in Canada, as identified in the normative and empirical literature on CAR T-cell therapies and informed by previous CADTH ethics reports of CAR T-cell therapies for hematological cancers. These reports addressed ethical considerations related to CAR T-cell therapies in the context of acute lymphoblastic leukemia (ALL), diffuse large B-cell lymphoma (DLBCL), FL, mantle cell lymphoma (MCL), and multiple myeloma (MM).1-8 Past CADTH reports draw on published literature, consultation with clinical experts, consideration of input from patient groups, clinician groups, and drug programs, and collaboration with clinical and pharmacoeconomic review teams at CADTH. Domains of interest in this summary report include ethical considerations related to the therapeutic context of hematological cancers, the evidentiary basis and use of CAR T-cell therapies, and health systems. In the context of this report, any reference to CAR T-cell therapy refers to CAR T-cell therapies used to treat hematological cancers.
Key Ethical Considerations
Therapeutic Context: Hematological Cancers
Patient and caregiver experiences, as well as diagnostic and treatment pathways, vary across the different hematological cancers for which CAR T-cell therapies are available or are under development (e.g., ALL, DLBCL, FL, MCL, MM). Nonetheless, common ethical considerations are reported across indications, including those related to the high unmet needs of the patient population and equity issues related to disparities in diagnosis, treatment, and outcomes of these cancers. Presently, CAR T-cell therapies are reimbursed, or are under consideration for reimbursement, as second-line, third-line, and fourth-line therapies for patients with r/r disease, for whom there are few or no available alternative treatments or for whom alternative treatments have failed. As a result, patients eligible for CAR T-cell therapy are usually characterized as having a high unmet need for durable, life-prolonging therapy.
Published literature, which is largely reported from the US, indicates that there are disparities in diagnosis, treatment, and outcomes across hematological cancers, especially for racialized, marginalized, and low socioeconomic groups and those residing in rural areas or far from tertiary care centres, and sometimes across age groups.1,2,5-8 Published literature concerning the distribution, incidence, treatment, and outcomes of hematological cancers in Canada is more limited, in part due to gaps in the collection of age-, sex-, and race-related demographic data in Canadian health information databases.9,10 This may limit a contextualized understanding of cancer-related disparities observed in Canada and its subnational jurisdictions.1
The clinical experts consulted during previous CADTH reimbursement reviews indicated that geography (residence in rural areas and/or far from tertiary centres) and socioeconomic status could impact the distribution of diagnosis, treatment, and outcomes for hematological cancers in Canada.1,2 They noted that disparities are more likely to be observed in access to primary care before diagnosis than once a patient is actively followed in the cancer care system. However, even in cancer care, requirements to travel and leave one’s support system and costs associated with travel, time off work, or childcare, as well as inconsistent funding and support across Canadian jurisdictions, can differentially impact patients’ and caregivers’ decision-making about treatment and care, including for CAR T-cell therapies, as will be discussed later. Disparities in outcomes between age groups have also been reported in Canada, as adults older than 70 years may have fewer therapeutic options if they are considered ineligible for common second-line or third-line treatments for hematological cancers, including allogenic SCT and autologous SCT.2
Evidence and Evaluation of CAR T-Cell Therapies
Ethical Considerations in Clinical Trial Data
During reimbursement review, CAR T-cell therapies have usually been evaluated with phase I/II or II, single-arm, open-label trials that offer only limited certainty about short-term therapeutic safety and efficacy and lack head-to-head comparative effectiveness and long-term safety, efficacy, and survival data.1-8 Uncertainty about the magnitude and duration of clinical benefit presents challenges for the assessment of clinical benefits and harms.11 Clinical experts consulted during previous CADTH reimbursement reviews of CAR T-cell therapies noted that the risks associated with evidentiary uncertainty for particular therapies are partially mitigated by the growing body of evidence on CAR T-cell therapies as a therapeutic class, which facilitates earlier identification and response to adverse events.1,2 Evidence-generating measures, such as active post-market surveillance, are required to better understand the risk-benefit profile and cost-effectiveness of CAR T-cell therapies in practice,12 and to inform the clinical and policy decision-making that serves the interests of patients and the public.11,13,14
The extent to which participants in CAR T-cell therapy trials are representative of patients in clinical practice in Canada varies. CAR T-cell therapy trials have generally tended to exclude patients with an Eastern Cooperative Oncology Group Performance Status (ECOG PS) greater than 1, which may not be reflective of clinical practice.1,2,6 Further, trials tend to include patients with a median age lower than that observed in practice, which may present challenges for the applicability of results to patients who are older and exclude patients with HIV or hepatitis B.1,6 CAR T-cell therapy trials also tend to include disproportionately higher rates of patients who are white than from other racial or ethnic groups, irrespective of disease incidence within the patient population.1,2,6 Indeed, racial and socioeconomic disparities in access to, and inclusion in, clinical trials have been reported in clinical trials for CAR T-cell therapies in the US (where most CAR T-cell trials are conducted).15,16 For example, participants who were African American and Black were underrepresented in clinical trials of 5 CAR T-cell products across 7 indications for hematological cancers, and are often underrepresented in clinical trials for cancer therapies across hematological indications more generally.1,6-8,15 This may potentially exacerbate existing health disparities observed in these populations15 and lead to a limited understanding of, and hinder efforts to, eliminate the racial and ethnic disparities observed in disease outcomes for these populations.17
The underrepresentation of racial, ethnic, and other marginalized groups, as well as women, in clinical trials has been identified as a common issue in clinical trials generally. Underrepresentation in trial participation is ethically concerning, as diverse clinical trial participation contributes to building trust in medical research and institutions (which can impact a patient’s willingness to pursue treatment), promotes fairness for potential participants and their communities, and produces higher-quality biomedical knowledge.18 Clinical experts consulted by CADTH in a previous reimbursement review were uncertain about the clinical implications of the underrepresentation of racial or ethnic groups in CAR T-cell trials.1 However, demographically representative clinical trial data for CAR T-cell therapies may help to determine whether therapeutic efficacy varies between subgroups and whether nontherapeutic factors (such as caregiver support or socioeconomic status) have an impact on effectiveness and clinical outcomes in the real world.1,19 Greater support is required to facilitate equitable access to clinical trial participation and to CAR T-cell treatment centres,15,18 and it is important to consider how trial participant selection may privilege certain groups and disadvantage others where demand for CAR T-cell therapy and trial participation exceed supply.11,20
Ethical Considerations in Economic Models
The lack of long-term safety, efficacy, and survival data, as well as head-to-head comparative effectiveness data, at the time of a reimbursement review has implications for the pharmacoeconomic assessment of CAR T-cell therapies, as it limits the ability to accurately model and assess cost-effectiveness.1,21,22 Uncertainty about pharmacoeconomic assessments, which are used to support the ethical principles of stewardship and public accountability in resource allocation,3 has implications for resource allocation at a health systems level, because it hinders assessments of opportunity costs (or forgone benefits) associated with the reimbursement and resourcing of CAR T-cell therapies over other resources.1,6,23 Data collection for long-term safety, efficacy, and comparative effectiveness may support more the robust pharmacoeconomic assessments used to inform reimbursement recommendations and decisions.23
Concerns about evidentiary limitations in pharmacoeconomic assessments and health-system sustainability have prompted consideration of alternative pricing and reimbursement models (e.g., value-based agreements, outcome-based pricing) as potential risk-sharing mechanisms that could possibly help mitigate the risks that payers face when reimbursing high-cost therapies, including CAR T-cell therapies, based on uncertain clinical and pharmacoeconomic evidence.6,23-28 Although not currently used in Canada for the reimbursement of CAR T-cell therapies, risk-sharing payment models have been used in other jurisdictions (especially in Europe).24 However, they way such financial arrangements are designed has ethical implications for the distribution of their potential benefits and burdens (e.g., for patients, the public, patients, payers, and manufacturers).28 For example, the way the value of a drug is defined, such as which surrogate outcomes are selected to evaluate efficacy, impacts how financial risks are distributed between manufacturers and payers.
The budget impact of implementing a CAR T-cell therapy may be underestimated if the estimated uptake does not reflect expected demand by patients and clinicians. In the absence of challenges related to manufacturing and delivery capacity, which will be discussed later, CAR T-cell therapies that are reimbursed are expected to be widely adopted by clinicians and patients, resulting in a high expected budget impacted.1 Higher budget impacts may present challenges for health systems with respect to the consideration of opportunity costs and fair resource allocation within and beyond the reimbursement of hematological-oncological therapies.6
Use of CAR T-Cell Therapies
Potential Benefits and Harms in the Use and Delivery of CAR T-Cell Therapies
CAR T-cell therapies have the potential to expand access to therapeutic options for patients without alternative options, including those who are ineligible for SCT (e.g., patients who are still sufficiently healthy to receive CAR T-cell therapy but not to undergo SCT, patients who could not find a suitable match for allogeneic SCT, and patients who exceed the age cut-offs for SCT). As a result, CAR T-cell therapies may offer equity-related advantages by expanding therapeutic options for older patients and for patients who are Black, Indigenous, and racialized, who may be underrepresented in SCT registries and thus unable to find adequate matches for allogeneic SCT in a timely manner.2,29 CAR T-cell therapies may offer additional practical advantages over existing therapies, especially for patients residing in rural or remote regions or with mobility issues, as they require a single infusion and treatment period, and as a durable therapy, may offer the first treatment-free window for patients with some cancers (e.g., MM).1,30,31
Nonetheless, most CAR T-cell therapies lack long-term safety and efficacy data at the time of reimbursement review, which limits the assessment of clinical benefits and harms. In practice, the balance of potential risks and benefits associated with CAR T-cell therapy is assessed relative to available alternative therapeutic options and to a patient’s condition (which in the case of refractory/r cancer, may have a poor prognosis).1,11,32,33 CAR T-cell therapies bear the risk of severe toxicities, including cytokine release syndrome (CRS) and other adverse events. Moreover, shortages or inconsistent availability of treatments (e.g., tocilizumab) used to treat patients who develop adverse events (e.g., CRS) after CAR T-cell therapy could impact the safe administration of these therapies.4
Although the long-term safety of CAR T-cell therapies remains uncertain, clinical experts consulted in previous reimbursement reviews noted that the safety of CAR T-cell therapies has improved as clinicians have become more experienced at administering treatment and identifying and responding to adverse events.1,2 This suggests that the safety of CAR T-cell therapies is context-dependent, where safety and efficacy may be impacted by the level of experience of the treating team and centre and the availability of supportive resources.12 The collection of post-market data and real-world evidence related to the use of novel CAR T-cell therapies could contribute to a more robust understanding of the real-world safety and efficacy of CAR T-cell therapies, and the balance of risks and benefits, in diverse clinical practice settings and communities.
Equitable Access to CAR T-Cell Therapies
The safe and effective administration of CAR T-cell therapies presently requires administration in a limited number of accredited treatment centres equipped with specialized infrastructure and highly trained providers, which are currently localized in large urban centres in Canada. As a result, access to CAR T-cell therapies may be moderated by geographic and financial barriers. Patients residing far from treatment centres (including in other provinces or territories) must travel to access treatment and spend more than a month near the treatment centre for pre-infusion and post-infusion treatment and care.1-3 The financial and psychosocial burdens resulting from geographic distance may impact patients’ therapeutic decision-making (e.g., patients opting for noncurative or inferior treatments to avoid leaving their communities or spending an extended time in hospital).1
Disparities in access to CAR T-cell therapies have been widely reported in the US context, including across race, geography (residence), and socioeconomic status.34,35 Geographic disparities in access to CAR T-cell therapies are especially salient in Canada, and especially for populations residing in rural and Northern communities or in provinces and territories without CAR T-cell centres, given Canada’s vast geography and the limited number of established and proposed CAR T-cell centres.1,2 In the Canadian context, race-based disparities in access should be considered, as they impact Indigenous people — especially in light of their disproportionately increased representation in rural and Northern communities — as well as other marginalized people or groups.1,2 At the same time, CAR T-cell therapies may offer access-related advantages over, and be less burdensome than, existing treatments, as they only required a single treatment period.1,31 Ensuring equitable access to high-quality care across Canada may also require considering what, if anything, might be owed to patients who are eligible for, but opt not to pursue, effective therapeutic options, such as CAR T-cell therapy, due to geographic or other barriers.1
Presently in Canada, most jurisdictions provide some support for accommodation and/or food-related expenses for people who reside a certain distance from an infusion centre, whereas fewer provide support for travel costs.1 CAR T-cell manufacturers may offer programs for financial and/or accommodation support for required travel, but often include distance-related eligibility cut-offs, which could leave gaps in coverage for some patients or provide insufficient support to cover all costs borne by patients and caregivers.1,2,6,36 Adequate financial support for patients and caregivers may be important for facilitating equitable access to CAR T-cell therapies by mitigating cost-related barriers that are exacerbated by geography (e.g., costs associated with travel, accommodations, and lost income for patients and caregivers who reside outside of cities with CAR T-cell treatment facilities).1,6
Referral practices can also impact access to CAR T-cell therapies in Canada.6,12,37,38 Not only do patients require access to primary care, to be referred for CAR T-cell therapy, physicians must be aware of available therapies and eligibility criteria, as well as the processes involved in making a referral to a treatment centre (which could be located in a different jurisdiction).1,2 Providers less confident in their knowledge about CAR T-cell therapies may be less likely to refer,37 and racial and ethnic disparities observed in the distribution of patients receiving CAR T-cell therapy may be, in part, explained by disparities in referral patterns in primary care rather than in treatment practices in cancer care.38 Accordingly, it is important to have clear and equitable referral practices, educate clinicians about CAR T-cell therapies and referral processes, facilitate communication between clinicians and treatment centres, and provide systems-level supports for clinicians practising outside the large metropolitan centres where CAR T-cell centres are located.1,2 Eligibility for CAR T-cell therapy presently requires patients to have already undergone and failed several lines of therapy, but not all patients may have had access to, or been eligible for, earlier lines of therapy for reasons outside of their or their providers’ control; this may present a barrier to access to CAR T-cell therapy for a subset of patients.1,31
Cell Ownership
The collection and storage of patients’ cells during CAR T-cell manufacturing may raise questions related to patient privacy and cell ownership, particularly when manufacturers are outside of Canadian jurisdictions.1,6,39 It is important to recognize that tissue and genetic materials are valued differently by different cultural groups (e.g., Indigenous groups internationally), and that informed consent processes need to clearly detail cell processing and ownership, as well as how remaining cells that are not infused will be handled or disposed of.40 Consultation with diverse groups has been identified as essential to CAR T-cell research and implementation to ensure that cell handling and disposal practices, as well as educational and consent materials, are sensitive to the needs and values of diverse patients and communities.6,39,40 In the Canadian context, attention should be paid to understanding Indigenous communities’ values and practices with respect to cell and tissue ownership and governance (e.g., with reference to guidance such as the First Nations principles of OCAP [ownership, control, access, possession]).41
Considerations for Informed Consent
Processes should be in place to ensure that patients (and caregivers) are apprised of the unique risks of, and evidentiary uncertainties related to, CAR T-cell therapies to support robust and ongoing, iterative informed consent, including as patients transition between care settings.6,42-45 Robust consent processes should recognize both the unique vulnerabilities of patients with cancer who have limited or no alternative therapeutic options, and who may be exposed to hype or the underreporting of treatment-related harms or uncertainties related to CAR T-cell therapies, as well as their autonomous decision-making capacity.4,6,8 The term “cure” should be avoided in discussions to avoid misleading or promoting false hope for therapies for which long-term clinical effectiveness remains unknown.46 The balance of potential risks and benefits associated with CAR T-cell therapy should be assessed in a process of shared decision-making by patients, providers, and caregivers. For CAR T-cell therapies approved for use in pediatric populations, it is important to recognize the unique vulnerability of children who are reliant on parents or caregivers for decision-making, as well as broader support. Depending on age or determined level of competency, minors may have a more active role in consent or assent to treatment, supported by age-appropriate educational materials about the potential benefits and harms of CAR T-cell therapy to facilitate family-based discussions.43,45 Discussions related to the preservation of fertility may also be important for adolescents and young adults considering CAR T-cell therapy.2 Studying and considering patient reported outcomes and patient experiences may better facilitate shared decision-making about the use of CAR T-cell therapies.12 Additional resources, including the use of translators and the provision of age-appropriate and language-appropriate educational materials for patients and caregivers, may be required to support patient decision-making.45
Health Systems
Manufacturing and Health Systems Capacity
There are at least 2 challenges related to CAR T-cell therapy delivery in Canada: manufacturing and health systems capacity.12 The first concerns the capacity to manufacture and supply CAR T-cell therapies, and for timely coordination between manufacturers and CAR T-cell centres for limited manufacturing slots and a multiweek preparatory and manufacturing period (e.g., stabilizing patients’ conditions before apheresis, manufacturing and treatment, coordinating bridging therapy, apheresis, and the transport of cells). As each step in the complex sequence of manufacturing and delivery requirements for CAR T-cell therapy represents an opportunity for disruption or delay, it may be important to consider the development of contingency plans to ensure a stable supply.1,47 Patients may be harmed by delays in access to therapy, because they have to be in sufficiently stable and in good health to remain eligible for, and to be able to withstand, treatment.1,31 The proliferation of CAR T-cell therapies also presents a growing administrative burden for centres, which must maintain resource-intensive accreditations and manage multiple protocols for the preparation and delivery of a growing number of therapies.1 The possibility of domestic, local CAR T-cell manufacturer in hospital and research settings is currently under investigation in the CLIC-01 clinical trial in British Columbia.48 Although still nascent, the potential use of a local CAR T-cell manufacturer in the future may expedite access to CAR T-cell therapies for patients (including eliminating the time required to transport cells to and from international manufacturing facilities) and is expected to be less costly and more cost-effective than the price of CAR T-cell therapies produced by pharmaceutical manufacturers.48
The second challenge concerns the health systems capacity required to meet the therapeutic demand for CAR T-cell therapies in Canada due to the complex infrastructure and personnel requirements.6,39 For example, implementation requires tertiary medical centres with specialized expertise, specialized training for staff, infrastructure modifications, close interactions among experienced inpatient, intensive care unit (ICU), outpatient, and emergency personnel and facilities, and the identification of and planning for patients before and after treatment. The implementation of an increasing number of CAR T-cell therapies for a growing number of indications may exacerbate existing health systems capacity challenges. Presently, there are a limited number of pediatric and adult CAR T-cell centres in Canada, which are localized in large urban centres in only some provinces. Although access in provinces and territories lacking CAR T-cell centres is managed through interjurisdictional agreements, the distribution of CAR T-cell centres in Canada could present a barrier for access to treatment for patients residing far from, or in jurisdictions without, CAR T-cell facilities. As a result, it is important to consider the allocation of CAR T-cell centres in a way that reflects regional, rural-urban, and sociodemographic equity.6,49
Although not currently used, outpatient delivery of CAR T-cell therapies has been suggested as a potential mechanism to address capacity limitations and expand access to a greater number of patients by circumventing limitations in inpatient capacity (e.g., health human resources, hospital beds, ICU capacity, apheresis facilities) and to reduce health systems costs.1,49 However, outpatient delivery would increase the need for patients to have access to social supports and a reliable caregiver, because the responsibility for care would be shifted largely onto patients and caregivers and away from trained health care personnel and health systems.1 Thus, a shift to outpatient delivery could potentially exacerbate burdens and the resulting inequities associated with accessing CAR T-cell therapies for patients and caregivers in lower socioeconomic strata and residing far from CAR T-cell centres, as is already observed in the context of SCTs.1 Outpatient delivery would still require significant health systems resources to deliver safe follow-up care for patients presenting with severe side effects or requiring ongoing care, emphasizing the need to invest in the infrastructure required to implement CAR T-cell therapies.6,39
Resource Allocation in the Context of Capacity Limitations
Insufficient supply or capacity to deliver CAR T-cell therapies raises ethical questions related to distributive justice (e.g., Who should be prioritized for access to a particular CAR-T-cell therapy, and why?), as well as procedural justice (e.g., who should decide how to allocate limited resources and capacity? What constitutes a fair allocation process?).1,3,20,47,50 Fair decision-making processes and priority-setting criteria are required to inform the prioritization of patients for access to CAR T-cell therapies within and across indications to facilitate the equitable allocation of limited resources in Canada.1-8 Indeed, as multiple CAR T-cell therapies become available for single indications, criteria may also be required to determine whether to use 1 therapy over another,31 or whether patients would be eligible (and if so, under what conditions) for re-treatment with CAR T-cell therapy. The development of pan-Canadian priority-setting criteria for prioritizing access to CAR T-cell therapies and/or pan-Canadian coordination could facilitate fair resource allocation processes, accountability in decision-making, equitable pan-Canadian access to CAR T-cell therapies, reduce decision-making burden for clinicians, and reduce inefficiencies as a result of duplicated efforts.1,3,50 Consideration of manufacturing and health systems capacity implications may be required if CAR T-cell therapies demonstrate long-term curative potential, which could prompt the use of CAR T-cell therapy in earlier lines of treatment and, thus, for a greater number of patients.11
Funding, Opportunity Costs, and Data Infrastructure
The reimbursement and implementation of CAR T-cell therapies, which are highly expensive and resource intensive, raises concerns about the sustainability of the Canadian health care system1,6,12 and stewardship, or the responsible use of health resources based on available evidence.3 Reimbursing and implementing CAR T-cell therapies presents opportunity costs (or forgone benefits for other treatments or health care services) for fixed health care budgets in which not all services or therapies can be reimbursed, both within hematological and oncological therapies and in other therapeutic classes.12,14,23,42,51,52 Additionally, it presents opportunity costs for health systems resources (e.g., hospital beds, ICU capacity, access to clinical specialists) due to the resource-intensive nature of CAR T-cell therapies.1,3 As discussed previously, uncertainty in the clinical evidence and pharmacoeconomic models used to evaluate CAR T-cell therapies limits the ability to accurately assess the magnitude of benefit of CAR T-cell therapies relative to other treatments or services, and thus to inform an understanding of whether the benefits and burdens associated with funding some therapies or services but not others are distributed fairly.23 Clear and transparent decisions about the expansion of access to CAR T-cell therapies in the context of existing systems constraints, competing health care priorities, and long-term health systems sustainability are required to support fair decision-making and sustain patient and public trust.1,11,26,42 Although, as discussed previously, alternative pricing and reimbursement models may potentially help attenuate the risks faced by payers reimbursing therapies based on uncertain clinical and pharmacoeconomic evidence, it is still important to recognize that CAR T-cell therapies would still remain very expensive and resource intensive from a health systems perspective.1
From a health systems perspective, it is also important to consider the clinical and health informatics infrastructure and resources required to collect the data needed to implement novel funding models and post-market surveillance.14,39
Conclusion
CAR T-cell therapies are being introduced as second-line, third-line, and fourth-line therapies for the treatment of various hematological cancers (e.g., ALL, DLBCL, FL, MCL, MM). Published empirical and normative literature, as well as past CADTH ethics reviews of CAR T-cell therapies, were reviewed to identify the ethical considerations relevant to the use of CAR T-cell therapies for the treatment of hematological cancers. Ethical considerations in the context of hematological cancers include the need for an effective, durable treatment that prolongs life, as well as existing disparities in the incidence, diagnosis, treatment, and outcomes for racialized, marginalized, and low socioeconomic groups, although more data are required to inform a greater understanding of disparities in the Canadian context. Clinical trials assessing CAR T-cell therapies may not be fully representative of the patient population in Canada (e.g., across race, age, functional status) and lack long-term safety and efficacy data and comparative effectiveness data. The lack of long-term and comparative clinical data limits the certainty of pharmacoeconomic assessments, which poses challenges for the assessment of opportunity costs, and may expose payers to greater financial risks. The way alternate pricing or funding arrangements are designed has implications of the distribution of the potential benefits and risks associated with the reimbursement of high-cost therapies based on uncertain clinical and pharmacoeconomic evidence. Underestimates in the demand for CAR T-cell therapy can lead to underestimates in the total budget impact of reimbursing and implementing CAR T-cell therapies.
The implementation of CAR T-cell therapies to clinical practice raises several access-related considerations, given a limited delivery capacity and resulting geographic barriers to access; notably, barriers to access may disproportionately impact racialized, marginalized, and low socioeconomic groups, as well as those lacking caregiver support. The reimbursement and implementation of an increasing number of CAR T-cell therapies raises several ethical considerations for health systems, including challenges associated with scaling CAR T-cell delivery across Canada due to the complex and resource-intensive infrastructure and personnel requirements. A possible shift to outpatient delivery in the future may expand access to CAR T-cell therapies, but may also shift responsibility for care onto patients and caregivers, and may disproportionately burden patients without robust caregiver support. The development of fair, consistent criteria to prioritize access to CAR T-cell therapy would facilitate equitable access across Canada, especially if demand exceeds manufacturing or delivery capacity (e.g., the growing number of CAR T-cell therapies and use in earlier lines of therapy if CAR T-cell therapies demonstrate curative potential may exacerbate demand). Additionally, the high cost of implementing CAR T-cell therapies presents a challenge for health care budgets and raises questions about the systems-level opportunity costs (both within and beyond the oncological space) of reimbursing CAR T-cell therapies.
The absence of long-term and comparative evidence for the safety and efficacy of CAR T-cell therapies necessitates robust post-market surveillance to better understand the risk-benefit profile, as well as cost-effectiveness, of CAR T-cell therapies in practice. Moreover, where possible, post-market surveillance and the use of real-world evidence may contribute to a better understanding of how the safety and efficacy of CAR T-cell therapies in clinical practice may be impacted by nonclinical factors, and whether this has an impact on how the benefits and burdens associated with the use of this therapy are distributed fairly across diverse demographic subgroups of patients with hematological cancers in Canada.
References
1.Drug Reimbursement Review clinical, pharmacoeconomic, and ethics reports: ciltacabtagene autoleucel (Carvykti) for the treatment of adult patients with multiple myeloma, who have received at least three prior lines of therapy, including aproteasome inhibitor, an immunomodulatory agent and ananti-CD38 antibody, and who are refractory to their last treatment. Can J Health Technol. 2023;3(8). 10.51731/cjht.2023.706. Accessed 2023 Aug 24.
2.Drug Reimbursement Review clinical, pharmacoeconomic, and ethics reports: brexucabtagene autoleucel (Tecartus) for the treatment of adult patients with relapsed or refractory B-cell precursor acute lymphoblastic leukemia (ALL). Can J Health Technol. 2023;3(6). 10.51731/cjht.2023.668. Accessed 2023 Aug 24.
3.Tisagenlecleucel for acute lymphoblastic leukemia and diffuse large b-cell lymphoma: ethics and implementation report. (CADTH optimal use report; vol.8, no.3d). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/pdf/car-t/op0538-tisagenlecleucel-ethics-and-implementation-jan2019.pdf. Accessed 2023 Aug 24.
4.Axicabtagene ciloleucel for large B-cell lymphoma: ethics and implementation report. (CADTH optimal use report; vol. 9, no. 1e). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/pdf/car-t/ct0002-ipe-report.pdf. Accessed 2023 Aug 24.
5.Drug Reimbursement Review clinical, pharmacoeconomic, and ethics reports: brexucabtagene autoleucel (Tecartus) for mantle cell lymphoma. Can J Health Technol. 2021;1(11). 10.51731/cjht.2021.187. Accessed 2023 Aug 24.
6.Drug Reimbursement Review clinical, pharmacoeconomic, and ethics reports: axicabtagene ciloleucel (Yescarta) for treatment of adult patients with relapsed or refractory large B-cell lymphoma (LBCL), who are candidates for autologous stem cell transplant (ASCT). Can J Health Technol. 2023;3(6). 10.51731/cjht.2023.667. Accessed 2023 Aug 24.
7.Drug Reimbursement Review clinical, pharmacoeconomic, ethics, and stakeholder input reports: lisocabtagene maraleucel (Breyanzi) for relapsed or refractory large B-cell lymphoma. Can J Health Technol. 2022;2(10). 10.51731/cjht.2022.461. Accessed 2023 Aug 24.
8.Drug Reimbursement Review clinical, pharmacoeconomic, and ethics reports: idecabtagene vicleucel (Abecma) for multiple myeloma. Can J Health Technol. 2022;2(2). 10.51731/cjht.2022.250. Accessed 2023 Aug 24.
9.Tsang M, Le M, Ghazawi FM, et al. Multiple myeloma epidemiology and patient geographic distribution in Canada: a population study. Cancer. 2019;125(14):2435-2444. PubMed
10.Mohyuddin GR, Sinnarajah A, Gayowsky A, Chan KKW, Seow H, Mian H. Quality of end-of-life care in multiple myeloma: a 13-year analysis of a population-based cohort in Ontario, Canada. Br J Haematol. 2022;199(5):688-695. PubMed
11.Imbach KJ, Patel A, Levine AD. Ethical considerations in the translation of CAR-T cell therapies. Cell Gene Ther Insights. 2018;4(4):295-307.
12.Gagelmann N, Sureda A, Montoto S, et al. Access to and affordability of CAR T-cell therapy in multiple myeloma: an EBMT position paper. Lancet Haematol. 2022;9(10):e786-e795. PubMed
13.Buitrago J, Adkins S, Hawkins M, Iyamu K, Oort T. Adult survivorship: considerations following CAR T-Cell therapy. Clin J Oncol Nurs. 2019;23(2):42-48. PubMed
14.Atilla E, Kilic P, Gurman G. Cellular therapies: day by day, all the way. Transfus Apher Sci. 2018;57(2):187-196. PubMed
15.Al Hadidi S, Schinke C, Thanendrarajan S, Zangari M, van Rhee F. Enrollment of Black participants in pivotal clinical trials supporting US Food and Drug Administration approval of chimeric antigen receptor-T cell therapy for hematological malignant neoplasms. JAMA Netw Open. 2022;5(4):e228161. PubMed
16.Alqazaqi R, Schinke C, Thanendrarajan S, et al. Geographic and racial disparities in access to chimeric antigen receptor-T cells and bispecific antibodies trials for multiple myeloma. JAMA Netw Open. 2022;5(8):e2228877. PubMed
17.Marinac CR, Ghobrial IM, Birmann BM, Soiffer J, Rebbeck TR. Dissecting racial disparities in multiple myeloma. Blood Cancer J. 2020;10(2):19. PubMed
18.Schwartz AL, Alsan M, Morris AA, Halpern SD. Why diverse clinical trial participation matters. N Engl J Med. 2023;388(14):1252-1254. PubMed
19.Knight JM, Hackett E, Szabo A, et al. Associations between socioeconomic status and bispecific LV20.19 CAR T-cell therapy outcomes. Haematologica. 2023;108(2):588-593. PubMed
20.Jecker NS, Wightman AG, Rosenberg AR, Diekema DS. From protection to entitlement: selecting research subjects for early phase clinical trials involving breakthrough therapies. J Med Ethics. 2017;43(6):391-400. PubMed
21.CAR T-cell therapy: perceived need versus actual evidence. Lancet Oncol. 2018;19(10):1259. PubMed
22.Jonsson B, Hampson G, Michaels J, Towse A, von der Schulenburg JG, Wong O. Advanced therapy medicinal products and health technology assessment principles and practices for value-based and sustainable healthcare. Eur J Health Econ. 2019;20(3):427-438. PubMed
23.Choi G, Shin G, Bae S. Price and prejudice? The value of chimeric antigen receptor (CAR) T-cell therapy. Int J Environ Res Public Health. 2022;19(19):12366. PubMed
24.Goncalves E. Value-based pricing for advanced therapy medicinal products: emerging affordability solutions. Eur J Health Econ. 2022;23(2):155-163. PubMed
25.Holmes H. Barriers to patient access to CAR-T therapy in the community setting. From: Journal of Clinical Pathways. 2018; https://www.texasoncology.com/who-we-are/media-center/in-the-news/news-articles/2018/june/barriers-to-patient-access-to-car-t-therapy-in-the. Accessed 2023 Aug 24.
26.de Lima Lopes G, Nahas GR. Chimeric antigen receptor T cells, a savior with a high price. Chin Clin Oncol. 2018;7(2):21. PubMed
27.Brigand T, Prokupkova A, Muller G, ECL Access to Medicines Task Force. CAR-T cell therapies: how much for survival? Brussels (BE): Association of European Cancer Leagues; 2018: https://www.cancer.eu/wp-content/uploads/2018/06/CAR-T-ECL-Article_Final_20062018.pdf. Accessed 2023 Aug 24.
28.Kannarkat JT, Good CB, Parekh N. Value-based pharmaceutical contracts: value for whom? Value Health. 2020;23(2):154-156. PubMed
29.Apostolidou E, Lachowiez C, Juneja HS, et al. Clinical outcomes of patients with newly diagnosed acute lymphoblastic leukemia in a county hospital system. Clin Lymphoma Myeloma Leuk. 2021;21(11):e895-e902. PubMed
30.Cohen AD, Hari P, Htut M, et al. Patient perceptions regarding ciltacabtagene autoleucel treatment: qualitative evidence from interviews with patients with relapsed/refractory multiple myeloma in the CARTITUDE-1 study. Clin Lymphoma Myeloma Leuk. 2023;23(1):68-77. PubMed
31.Goldfinger M, Shah N, Cooper DL. Chimeric antigen receptor T-cell therapy for patients with multiple myeloma-a call for equal opportunity. JAMA Oncol. 2023;9(3):297-298. PubMed
32.Kuehn BM. The promise and challenges of CAR-T gene therapy. JAMA. 2017;318(22):2167-2169. PubMed
33.Chimeric antigen receptor T-cell therapy for B-cell cancers: effectiveness and value - final evidence report. Boston (MA): Institute for Clinical and Economic Review (ICER); 2018: https://icer.org/wp-content/uploads/2020/10/ICER_CAR_T_Final_Evidence_Report_032318.pdf. Accessed 2023 Aug 24.
34.Ahmed N, Shahzad M, Shippey E, et al. Socioeconomic and racial disparity in chimeric antigen receptor T cell therapy access. Transplant Cell Ther. 2022;28(7):358-364. PubMed
35.Emole J, Lawal O, Lupak O, Dias A, Shune L, Yusuf K. Demographic differences among patients treated with chimeric antigen receptor T-cell therapy in the United States. Cancer Med. 2022;08:08.
36.Snyder S, Albertson T, Garcia J, Gitlin M, Jun MP. Travel-related economic burden of chimeric antigen receptor T cell therapy administration by site of care. Adv Ther. 2021;38(8):4541-4555. PubMed
37.Blue B. Socioeconomic and racial disparity in chimeric antigen receptor T cell (CART) therapy access. Transplant Cell Ther. 2022;28(7):345-346. PubMed
38.Molina A, Muffly L. CT-095 disparities and incomplete capture of race/ethnicity data in adults with hematologic malignancies referred for cellular therapies. Clin Lymphoma Myeloma Leuk. 2022;22(Suppl 2):S433-S434.
39.Lamprecht M, Dansereau C. CAR T-cell therapy: update on the state of the science. Clin J Oncol Nurs. 2019;23(2):6-12. PubMed
40.Weinkove R, George P, Ruka M, Haira TH, Giunti G. Chimeric antigen receptor T-cells in New Zealand: challenges and opportunities. N Z Med J. 2021;134(1542):96-108. PubMed
41.First Nations Information Governance Centre (FNIGC). The First Nations Principles of OCAP®. https://fnigc.ca/ocap-training/. Accessed 2023 Aug 24.
42.Cossu G, Birchall M, Brown T, et al. Lancet Commission: stem cells and regenerative medicine. Lancet. 2018;391(10123):883-910. PubMed
43.Mahadeo KM, Khazal SJ, Abdel-Azim H, et al. Management guidelines for paediatric patients receiving chimeric antigen receptor T cell therapy. Nat Rev Clin Oncol. 2019;16(1):45-63. PubMed
44.Darrow JJ, Sarpatwari A, Avorn J, Kesselheim AS. Practical, legal, and ethical issues in expanded access to investigational drugs. N Engl J Med. 2015;372(3):279-286. PubMed
45.McConville H, Harvey M, Callahan C, Motley L, Difilippo H, White C. CAR T-cell therapy effects: review of procedures and patient education. Clin J Oncol Nurs. 2017;21(3):E79-E86.
46.Bach PB, Giralt SA, Saltz LB. FDA approval of tisagenlecleucel: promise and complexities of a $475 000 cancer drug. JAMA. 2017;318(19):1861-1862. PubMed
47.Couzin-Frankel J. For experimental cancer therapy, a struggle to ensure supply keeps up with demand. Science 2017; https://www.sciencemag.org/news/2017/06/experimental-cancer-therapy-struggle-ensure-supply-keeps-demand. Accessed 2023 Aug 24.
48.Kekre N, Hay KA, Webb JR, et al. CLIC-01: Manufacture and distribution of non-cryopreserved CAR-T cells for patients with CD19 positive hematologic malignancies. Front Immunol. 2022;13:1074740. PubMed
49.Snyder S, Chung KC, Jun MP, Gitlin M. Access to chimeric antigen receptor T cell therapy for diffuse large B cell lymphoma. Adv Ther. 2021;38(9):4659-4674. PubMed
50.Unguru Y, Fernandez CV, Bernhardt B, et al. An ethical framework for allocating scarce life-saving chemotherapy and supportive care drugs for childhood cancer. J Natl Cancer Inst. 2016;108(6):djv392. PubMed
51.Gumer JM. A new frontier in the fight against cancer (that is, for those who can afford it): the approval and cost of CAR T-cell therapies. Voices Bioeth. 2018;4. https://journals.library.columbia.edu/index.php/bioethics/article/view/6024/2987. Accessed 2023 Aug 24.
52.Gonzalez-Vicent M, Sanz J, Fuster JL, et al. Autoimmune hemolytic anemia (AIHA) following allogeneic hematopoietic stem cell transplantation (HSCT): a retrospective analysis and a proposal of treatment on behalf of the Grupo Espanol De Trasplante de Medula Osea en Ninos (GETMON) and the Grupo Espanol de Trasplante Hematopoyetico (GETH). Transfus Med Rev. 2018;32(3):179-185. PubMed
Stakeholder Input
Patient Input
Lymphoma Canada
About Lymphoma Canada
Lymphoma Canada is a national Canadian registered charity whose mission it is to empower patients and the lymphoma community through education, support, advocacy, and research. Based out of Mississauga (ON), we collaborate with patients, caregivers, healthcare professionals, and other organizations and stakeholders, to promote early detection, find new and better treatments for lymphoma patients, help patients access those treatments, learn about the causes of lymphoma, and work together to find a cure. Resources are provided in both English and French. www.lymphoma.ca
Information Gathering
The data presented in this submission was collected from two online anonymous patient surveys. Lymphoma Canada created and advertised a survey which was available from November 15, 2022, to January 20, 2023. The link was promoted via e-mail to patients registered in the LC national emailing list and made available via social media outlets, including Twitter, Instagram, and Facebook accounts. The survey had a combination of multiple choice, rating, and open-ended questions. Skipping logic was built into the survey so that respondents were asked questions only relevant to them. Open-ended responses were noted in this report verbatim, to provide a deeper understanding of patient perspectives. 44 responses were collected. Information from this survey was largely used to identify the main areas of concern for patients with relapsed or refractory FL, as only one respondent indicated experience with Kymriah. No Canadian centers facilitated clinical trials for Kymriah, which prompted Lymphoma Canada to reach out to other national lymphoma patient organizations to collect drug-specific information for this indication.
In addition to the patient survey we promoted, information contained in this submission included patient feedback from a French patient organization called Ensemble Leucemie Lymphomes Espoir (ELLyE). ELLyE kindly shared with Lymphoma Canada results of a patient survey they created to gather experience on CAR-T cell therapy (including Kymriah) for a health technology assessment in France. The survey was first created in January 2019, then updated in January 2020. Promotion of the link included posts on social media and the support of hematologists to their lymphoma patients. 162 responses were collected between January 2019 and September 2022, 19 specifically commented on their experience with Kymriah.
Ensemble Leucemie Lymphomes Espoir (ELLyE). ELLyE is an association of patients and relatives under the French law of 1901 specialized in lymphomas, chronic lymphocytic leukemia and Waldenström disease. Their mission is based on four main criteria: information, support, action, and research. To carry out its missions, ELLyE relies on a team of professionals and volunteers with a wide range of skills, as well as on a scientific advisory board with diverse but recognized profiles in the field of hematological malignancies. https://www.ellye.fr/
Disease Experience
LC Survey
Of the 44 respondents that completed the virtual survey created by Lymphoma Canada, the majority lived in Canada (n = 33), were between age of 55 and 74 (n = 23), and self-identified as female (n = 23). Most patients that completed the survey were diagnosed with follicular lymphoma 9-10 years ago (n = 18). More information on demographics can be found in Tables 1-4.
Table 1: Country of Respondents From Lymphoma Canada Survey
Respondents | CAN | USA | Skipped | Total |
|---|---|---|---|---|
Patients with follicular lymphoma | 33 | 1 | 10 | 44 |
Table 2: Age Range of Respondents From Lymphoma Canada Survey
Respondents | Age (years old) | Skipped | Total | ||||
|---|---|---|---|---|---|---|---|
35-44 | 45-54 | 55-64 | 65-74 | 75-84 | |||
Patients with follicular lymphoma | 1 | 3 | 11 | 12 | 7 | 10 | 44 |
Table 3: Gender of Respondents From Lymphoma Canada Survey
Respondents | Gender | |||
|---|---|---|---|---|
Female | Male | Skipped | Total | |
Patients with follicular lymphoma | 23 | 11 | 8 | 44 |
Table 4: Number of Years Ago Respondents Were Diagnosed With Follicular Lymphoma, From Lymphoma Canada Survey
Respondents | Years | Skipped | Total | ||||
|---|---|---|---|---|---|---|---|
<1 | 1-2 | 3-5 | 5-8 | 9-10 | |||
Patients with follicular lymphoma | 1 | 7 | 7 | 7 | 18 | 4 | 40 |
Respondents from the LC survey were asked to rate the severity of their physical symptoms on a scale of 1 (no impact) to 5 (significant negative impact), both during the time of diagnosis (40 respondents answered) and on their current quality of life (38 respondents answered). At the time of diagnosis respondents rated enlarged lymph nodes and fatigue (20%, n = 8 for both) as the most common symptom rated as a 5. This was followed by indigestion, abdominal pain, or bloating (17.5%, n = 7) and bodily aches and pains (15%, n = 6). When asked about the symptoms which currently impact their everyday life, respondents rated low immunoglobulin levels (8%, n = 3) as a significant negative impact.
Respondents of the LC survey were also asked questions about the psychosocial impacts they experienced at the time of diagnosis (40 respondents answered) and on their current quality of life (38 respondents answered). The most common answers for initial diagnosis were stress of diagnosis (88%, n = 35), anxiety/worry (75%, n = 30), and fear of progression (65%, n = 26). Similar concerns were reported by follicular lymphoma patients on current quality of life, including fear of progression/relapse (63%, n = 24), stress of having cancer (45%, n = 17), and anxiety/worry (45%, n = 17).
When patients were asked about the impact of their follicular lymphoma symptoms on current daily activities and quality of life, 38 respondents provided feedback. The most common factors rated as a significant negative impact (5 out of 5) was the ability to go to work, school or volunteer and visit with family and friends (18%, n = 7 for both). The ability to travel (16%, n = 6) and contribute financially to household expenses (10%, n = 4) were also significant impacts on the day-to-day lives of those that responded to the LC survey.
A few quotes from the LC survey are included below depict actual patient representations of the daily activities and current QoL of this patient population:
“I am so grateful to have two remissions, to enjoy my life, to be with my precious grandchildren who were born after my successful treatment. Covid has added stress because my immunity is lower. I feel that I am a lucky woman and if I relapse again, I hope I will have successful treatment. I attend virtual conferences, have taken mindfulness classes, joined a women’s art group and had hope and joy. Relapse is still a fear.”
“I am very fortunate that I knew how to advocate for myself, so I got chemotherapy and am in remission. I am fortunate that I was able to work full time during my radiation and 2.5 years of chemotherapy. As a health care professional, I see the toll cancer can take on those diagnosed. This makes me even more appreciative that I have good health and a good job.”
“A bit concerned about getting COVID as I'm not sure how sick I'd get. So, I'm probably a bit more careful than most people. I always wear my mask when shopping or attending indoor events. I make an exception when visiting family and close friends. Have had my 2 original COVID shots as well as three boosters.”
“My lymphoma diagnosis has contributed to my retirement 2 years earlier than I had planned for. This has significant ramifications on my retirement income with 2 years of non-contribution.”
“I have much less energy; I limit social interactions due to my compromised immune system.”
Experiences With Currently Available Treatments
LC Survey
Of the 44 total respondents, 34 patients that completed Lymphoma Canada’s survey included details about their treatments, side effects, and access of medical care. Most respondents received only one line of treatment (44%, n = 15). 24% had received two lines of therapy (24%, n = 8) and 15% had received three lines of therapy (15%, n = 5). In Table 5, the most common treatments received by follicular lymphoma patients are included. Overall, patients that completed this survey received various forms of chemotherapy (CHOP, CVP).
Table 5: Most Common Treatments Received by Respondents From Lymphoma Canada Survey
Line of Therapy | Treatment | Number of respondents |
|---|---|---|
1 | CHOP + Rituximab | 8 |
1 | Bendamustine + Rituximab | 8 |
1 | CVP + Rituximab | 2 |
1 | Chemotherapy (unspecified) | 2 |
1 | Bendamustine | 2 |
2 | Rituximab | 5 |
2 | Radiation | 4 |
2 | Bendamustine + Rituximab | 3 |
3 | Radiation | 2 |
3 | Ibrutinib | 1 |
CHOP = Cyclophosphamide, Hydroxydaunorubicin, Oncovin, Prednisone; CVP = cyclophosphamide, vincristine sulfate, prednisone
Patients from the LC survey rated treatment-related fatigue (24%, n = 8), immediate side effects of treatment (21%, n = 7) and low activity level (21%, n = 7) as significant negative impacts (5 out of 5) experienced during treatment. Most common physical symptoms experienced with previous treatments were fatigue (76%, n = 26), hair loss (44%, n = 15), and neuropathy (41%, n = 14).
Regarding access to treatment, 19 of 27 respondents (70%) were able to access their lymphoma treatment locally and 18 of 32 patients reported no difficulty (56%) or little difficulty (22%, n = 7) based on location and waiting time. The largest factors which contributed to financial implications when receiving lymphoma treatment included absence from work (56%, n = 13), drug costs (35%, n = 8), and travelling costs (35%, n = 8) of 23 respondents that provided feedback.
Below are direct quotes from respondents which comment on difficulties when accessing lymphoma treatment:
“My oncologist is over-booked and over-worked. I had to wait a long time to be diagnosed, six months to see a specialist, followed by a one year wait for an MRI, followed by two months until the specialist called me in for the results. He had not read the results ahead of time and was stunned and just kept repeating, "You have so many lymph nodes." Even though he didn't say I had cancer, I knew, and this was not the best way to hear the news. Then a wait to get an MRI, and a wait to see the surgeon and then again for the biopsy. After that, another long wait for results, followed by a long wait to get an appointment with an oncologist.”
“The biopsy and assessment of the tumour took the longest time. It was 5 months from the start of the growth to the first chemo treatment. Definitely too long.”
“Waiting time for guided CT biopsies as well as PET scan.”
“Alternate therapies like nutritional supplements.”
“Probably CART and stem cell as it cannot be done in Kelowna.”
Improved Outcomes
LC Survey
Respondents in the LC survey were asked to rate, on a scale of 1 -5 (1 = not important; 5 = extremely important), the importance of various factors when receiving a new drug or therapy to treat their follicular lymphoma (34 provided input). Aspects such as longer disease remission, longer life span and improved quality of life were the most important outcomes for this patient population (refer to Table 6).
Table 6: Importance of Treatment Outcomes or Factors When Receiving a New Treatment, by Respondents of the Lymphoma Canada Survey
Treatment outcome or factor | Percentage of respondents with rating of 5 | Number of respondents |
|---|---|---|
Longer disease remission | 79% | 27 |
Allow me to live longer | 79% | 27 |
Improve quality of life and perform daily activities | 59% | 20 |
Control disease symptoms | 18% | 6 |
Normalize blood counts | 18% | 6 |
Interestingly, 82% of 34 respondents (n = 28) voted they would be willing to tolerate side effects to access new treatments if the side effects were not very severe and short-term. In addition, 71% of patients (n = 24 of 34) indicate there is a need for more therapeutic options to treat follicular lymphoma. Collectively, this evidence demonstrates patients favour having a variety of options regarding their treatment, so they can live longer, with less symptoms, and an improved quality of life. 55% of respondents (n = 19 of 34) also reported it is extremely important (10 out of 10) to have a choice when deciding their treatment option, based on various factors including side effects, expected outcomes and financial implications.
A few quotes are included below to demonstrate what is important to follicular lymphoma patients regarding outcomes:
“I would be willing to go through side effects, knowing there would be an improved outcome.”
“New therapies should be available to all Canadians, not just those in certain provinces. You should not have to travel out of province to get treatment.”
“I understand how hard it is to make new therapies available in socialized medicine, but there must be some way to give people more options. It would be nice to see clinical trials more broadly accessible. Surely the government can work with drug companies to make this happen. When you’re diagnosed, you feel desperate to have a chance at survival without severe side effects. The patient needs to have some choice in order to have some sense of control. I would also like to see more integrative approaches to cancer treatment - with doctors and specialists in natural medicine working together for the benefit of their patients.”
“We need more emphasis on trying to find out before the patient gets any treatment if it will work. I don't like seeing that you have to fail three times before a lifesaving treatment is allowed to be given. By that time the body and quality of life has been affected and possibly ruins the chances of getting a stem cell or CAR T therapy. Research that looks at why a patient will respond or not respond to a certain treatment needs to be continually investigated.”
“I’ve had Car T and I am doing well. I think this should be looked at as a therapy earlier on in the diagnosis. Possibly when you experience your second remission.”
Experience With Drug Under Review
LC Survey
Of the 44 respondents to Lymphoma Canada surveys, only 1 respondent had experience with the drug to which this submission relates. This patient identified as female, 75-84 years old, was diagnosed 5-8 years ago, and treated with Kymriah for their third treatment through a compassionate access program. Based on their response, out of province travel was required and they have been in-remission for over two years now. Please refer below for feedback received on this patient’s experience with CAR-T and Kymriah:
“My responses are based on my current status. I am post Car t Therapy and restricted to travel etc. for a considerable time period. I require my vaccinations etc once again and until I get my immunity built up, I am limited with whom I see and interact with. I have received my first Covid shot, and flu shot over again and now waiting until I can have a pneumonia shot (at 6 months post Car t.) after 6 months I then begin the basic immunity shots. This will take upwards to a year…so they tell me!! I am alive and well!”
This respondent also reported side effects of neutropenia, thrombocytopenia, decreased appetite and anemia while receiving treatment and was admitted into hospital to manage side effects. This patient selected “yes” when asked if they would recommend this therapy to other patients with relapsed or refractory follicular lymphoma.
In this survey another patient commented: “Please approve CAR-T and similar new therapies as first-line treatments that are less toxic and have less adverse side effects compared to the current treatments like chemotherapy.”
ELLyE Survey
Based on the survey results provided by ELLyE, 19 patients indicated they had been treated with Kymriah in France. Of these respondents 11 were patients, 7 were relatives filling out the survey on behalf of their loved one. The patient demographics included 5 females and 14 males, with most receiving Kymriah in their second line of treatment (n = 6) and most common prior treatment was chemotherapy with or without immunotherapy (n = 11). Refer to Tables 7-9 below.
Table 7: Age Range of Respondents From ELLyE Survey
Respondents | >35 | Age (years old) | Skipped | Total | ||||
|---|---|---|---|---|---|---|---|---|
35-44 | 45-54 | 55-64 | 65-74 | 75-84 | ||||
Patients with follicular lymphoma | 5 | 1 | 1 | 5 | 2 | 2 | 3 | 19 |
Table 8: Number of Treatments Received by Respondents From ELLyE Survey
Line of Therapy | Number of respondents |
|---|---|
2 | 6 |
3 | 4 |
4 | 2 |
4 or more | 2 |
Table 9: Most Common Treatments Received by Respondents From ELLyE Survey
Type of therapy | Number of respondents |
|---|---|
Stem Cell Transplant | 2 |
Chemotherapy With or Without Antibody | 11 |
Surgery | 1 |
Immunotherapy (Monotherapy) | 1 |
Numerous patients from the ELLyE survey commented on the quality of life of themselves and their loved ones during their treatment with Kymriah and its associated prior chemotherapy treatments:
“Fatigue, nausea, weight loss, latent anxiety of my relatives”
“My husband manages all the family life and my meals. I was very dependent.”
“Very disrupted social life; physical level: fatigue, nausea (weight loss that had to be regained between each treatment), tiredness. My husband took care of all the shopping (I didn't go to the stores anymore because of the risk of infection), the meals during the two days after each treatment because the nausea was then very intense (vomiting sometimes), at the psychological level: upheaval due to the announcement of the diagnosis and then to the announcement of a partial response to the treatment while we were waiting for a complete response “
“A life in parenthesis, no more outings, no more parties, no vacations, a permanent anxiety linked to the wait for the results of various exams, a total loss of confidence in life since we only have bad news for 2 years. Very great support from family and friends”
“Great fatigue impossible to have a normal life very difficult for the caregiver because the patient is little accompanied when chemotherapy is not effective.”
“It is a struggle for the patient and his family on the physical level too much fatigue, very hard on the financial side especially as a non-resident foreigner.”
When asked about the benefits gained from CAR-T therapy several patients left the following comments:
“Complete remission.”
“Treatment of pain.”
“Hope of recovery to follow.”
Other factors indicated in the survey that were of concern to patients receiving CAR-T in France was the distance and financial implications of travelling to receive treatment.
“Difficulty of circulation between the western suburbs and the east of Paris, congested ring road, very expensive cabs”
“I had to rent an apartment in Lyon to accompany my husband (700€). I found myself alone in a city where I knew no one with my husband who was going through a terrible ordeal.”
“Difficult at the financial level, the train journeys were at the patient's expense, as were the hotels and the compulsory cabs because of the difficulty in walking. It is very difficult to follow a treatment far from home, especially as the patient has little support.”
Both in Canada and France, there is a consensus that this therapy should be provided at an earlier stage/line of therapy. For timely and equitable access, Canadian lymphoma patients should be able to receive CAR-T therapy locally and not be expected to travel to receive treatment. Local access, within each province, will significantly improve the patient experience by reducing the fear and risk of getting sick while travelling and improve quality of life by keeping patients close to their caregivers and support systems.
Companion Diagnostic Test
Not applicable.
Anything Else?
Not applicable.
Conflict of Interest Declaration — Lymphoma Canada
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission?
No.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
Yes, ELLyE (France) provided results of their patient survey on Kymriah.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 10: Financial Disclosures for Lymphoma Canada
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Gilead | — | — | — | X |
Novartis | — | — | X | — |
Bristol Myers Squibb | — | — | X | — |
Clinician Input
Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee
About Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee
OH-CCO’s Cancer Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs (PDRP) and the Systemic Treatment Program.
Information Gathering
Information is gathered via emails.
Current Treatments and Treatment Goals
Current standard of care involves chemotherapy, chemo-immunotherapy, autologous stem cell transplant, and in selected patients allogeneic stem cell transplant. Radiation may also be used for symptom control and in very palliative scenarios. The disease course can be quite variable with some patients having very long remissions between therapies and others behaving in a more refractory manner.
Treatment goal is mostly palliative with some curative intent with alloSCT. There are some reports of very long term remissions following autologous stem cell transplantation. Most important goals are delay disease progression, improve health-related quality of life, and alleviate symptoms.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Patients eventually becomes chemotherapy refractory and there are no treatment options afterwards. Also repeated courses of cytotoxic therapy can be associated with marrow damage (i.e., MDS) which then limits the ability to treat further and adversely affects quality of life. CART therapy would not be expected to have long-term marrow damage issues. Although data is early, we wonder whether CART therapy might be potentially curative for some patients, compared with the currently available therapies.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
3L therapy would be an appropriate time to consider CAR T-cell therapy given the benefit of available treatment is lower. It is uncertain at this time whether this may replace autologous stem cell transplant. We suspect that CART may be tried in advance of autologous stem cell transplant in those patients who have a more chemotherapy-refractory history for their follicular lymphoma.
There will be a prevalent FL population that would be eligible for this CAR-T therapy at the time of implementation.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Most suitable patients would be as per the clinical trial population. Exclusion may include severe organ dysfunction and poor performance status, uncontrolled infections.
Despite being excluded in the pivotal study, we would like to consider CAR-T in selected patients who had received prior CD19- directed therapy or allogeneic stem cell transplant. CART therapy might be preferred to be used prior to autologous stem cell transplantation in some patients.
There should be some flexibility around ECOG or KPS status.
There is an existing CAR-T therapy network in Ontario that can handle patient referrals.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
As per standard lymphoma response criteria.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Not applicable as this is a single infusion. Some patients may become ineligible for therapy during CAR-T cell manufacturing.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
Centres that have expertise in CAR T-cell therapy.
Conflict of Interest Declarations — Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
OH-CCO provided secretariat function to the group.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Declaration for Clinician 1
Name: Dr. Tom Kouroukis
Position: Lead, OH-CCO Hem DAC
Date: 20-01-2023
Table 11: COI Declaration for Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 2
Name: Dr. Pierre Villeneuve
Position: Member, OH-CCO Hem DAC
Date: 06-01-2023
Table 12: COI Declaration for Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee — Clinician 2
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Cell Therapy Transplant Canada
About Cell Therapy Transplant Canada
Cell Therapy Transplant Canada (CTTC; www.cttcanada.org) is a member-led, national, multidisciplinary organization providing leadership and promoting excellence in patient care, research and education in the field of hematopoietic stem cell transplant and cell therapy.
We are the professional society representing the stem cell transplant community in Canada, including physician, nursing, laboratory, and allied health professionals, along with an active family and caregiver group.
Information Gathering
The proposed submission was drafted by a CTTC physician member and then shared with two committees – our Board of Directors, and our standing committee of program directors, representing the cell therapy and stem cell transplant programs across Canada. These two committees were provided an opportunity to review this report and provide input.
Current Treatments and Treatment Goals
Follicular Lymphoma is the most common subtype of indolent non-Hodgkin lymphoma (NHL) including approximately 1400 new cases in Canada per year. The median age of diagnosis is 65 and the condition is mainly incurable. Patients will receive multiple lines of therapy over time with progressively lower overall response rates (ORR) and shorter treatment-free intervals. FL is a heterogeneous malignancy often presenting with diffuse lymphadenopathy, bone marrow involvement, splenomegaly and on occasion extra nodal involvement. Patients may be asymptomatic with advanced stage disease. It is important to note that initial therapy may be surveillance and well-defined criteria of when to initiate treatment are defined by the Groupe d'Etude des Lymphomes Folliculaires (GELF) or the British National Lymphoma Investigation (BNLI). Thus, the presence of disease does not warrant immediate therapy. Therapeutic choices may vary depending on the biology of the disease (pace of progression, indicators POD24, FLIPI) as well as patient specific factors such as age, comorbidities and preference. Canadian treatment guidelines have been developed based on large phase three studies, at least for front-line (1L) and second-line (2L). Front line patients will typically receive chemo-immunotherapy (BR) (Rummel MJ, Lancet 2013) along with R-maintenance (2 years) (Salles G, Lancet 2011). Few patients presenting with limited stage newly diagnosed FL may be treated with involved field radiation therapy alone. Frail patients may receive palliative single agent chemotherapy or Rituximab monotherapy. Approximately 15-20% of FL patients will demonstrate early relapse/progression while still receiving induction therapy or within 6 months of completing Rituximab. Such patients may receive chemotherapy (CHOP) in combination with Obinatuzimab (Gadolin trial, Sehn LH, Lancet Oncology 2016; PFS and OS benefit). It should be noted that FL patients may transform into large cell NHL at any point in their disease course and treatment for these patients may include consideration of salvage (platinum-based) chemotherapy followed by an autologous stem cell transplant (SCT). Otherwise autografts for FL are generally performed for fit patients with chemo-sensitive disease in 2nd or 3rd line.
Treatment of FL in third line is challenging for patients that are not suitable for SCT. Treatment response and duration are limited with currently available therapies. In Canada, treating physicians will often repurpose chemo-immunotherapy approaches (R-GDP, R-CVP). Two other regimens may be considered: (i) idelalisib (Delta study, Furman RR, NEJM 2014) which has significant immune-related and infectious complications or (ii) R-2 (Revlimid/Rituximab) –currently no Health Canada indication. A few young fit patients may be considered for an allogeneic SCT in 4L.
For the proposed indication (adult patients with R/R FL after two lines of therapy) Tisagenlecleucel has the potential to address current gaps including access to therapies that demonstrate superior complete response rates (CRR 68%) that are durable (77.8% of CRR remain in remission at 24m) with a low level of long-term toxicities. With excellent disease control, it is anticipated that disease dependent quality of life measures will/may also improve. The CTTC continually aims to ensure the Canadian landscape for cell-based therapy remains at a high level. This is accomplished through our association including webinars, a general annual meeting and the support of multiple multi-disciplinary working groups (pharmacy, SCT nursing, social work, quality teams). To date we have focused on autologous and allogeneic SCT and remain committed to these effective therapies for eligible patients. Tisagenlecleucel represents an exciting new treatment option in this field.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
In Canada treatment of FL patients in 3L or beyond is limited by two fundamental challenges that include: (i) poor ORRs and (ii) short remissions or treatment-free intervals. This in part relates to the disease biology that demonstrates recurrent progressions with increasingly shorter durations of relapse-free intervals following each line of therapy. The current treatment options in 3L FL typically involve re-purposing chemo-immunotherapeutic strategies that when used “a second time around” lack efficacy and can be toxic for an older target population. While allogeneic SCT remains a potential option with curative potential, the number of eligible patients is minimal. Autologous SCT may be indicated also, with excellent responses often used in 2L or 3L, but only suitable for chemosensitive patients (i.e. not appropriate for chemorefractory patients). Despite these options the vast majority of FL patients at 3L+ are not eligible for either form of transplant. CD19-CAR-T therapy may be an option for a proportion of these patients (i.e., not suitable for an autograft but may be considered for a CAR-T approach). This may be the case with a 4-1BB co-stimulatory based CD19 CAR-T platform, which demonstrates a lower level of grade 3-4 CRS (0%), and grade 3-4 ICANS (1%) and can be considered in the outpatient setting. From this, a single infusion of CD19 CAR-T cells appears to provide a high level of response that is durable based on the most recent ELARA data.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
We would envision/advocate Tisagenleuclucel be positioned in patients not/ or no longer eligible to receive an allogenic or autologous SCT with relapsed or refractory FL at 3L or beyond. Other currently available therapies in non-transplant eligible FL 3L+ may include chemo-immunotherapy (R-GDP, R-CVP), R-2 or idelalisib. The latter two are typically used infrequently due to unacceptable side effects or access in the absence of a HC indication (NOC). Given a novel mechanism including sustained chimeric CD19 attack, CAR-T is clearly effective in patients who have previously received at least two prior lines of treatment for FL. The high rates of ORR/CRR and durable responses are remarkable when compared to other non-cellular based therapies. CAR-T will cause a shift in the current treatment paradigm, but we do not believe it will change the current approach to use of autologous and allogenic SCT for eligible patients. CD19 CAR-T will only be considered in relatively “fit” patients without significant co-morbidities (organ dysfunction).
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Eligible patients will include adults (>18y) with FL (grade 1,2 or 3A) either refractory to 2 or more lines of systemic therapy that includes an anti-CD20 monoclonal antibody and an alkylating agent or who relapse following 2L therapy including an autologous SCT, for those who are transplant-eligible. Patients previously treated with an allogeneic SCT or with active CNS involvement would be ineligible. Any suspicion of disease transformation (FL 3B or DLBCL) would be excluded from this specific indication but may go on to CD19-CAR-T under a different indication. A recent lymph node biopsy may be required to exclude transformation (increased LDH, unstable tumor growth). Patients who previously received CD19-directed therapy may not be eligible for FL Tisagenleceucel.
As an expanding number of CTTC cell therapy centers gain experience in the use of CD19-41BB CAR-T for R/R DLBCL (since 2020), there has been a learning curve specifically involving patient selection as it pertains to disease (biology) and fitness. Significant organ-specific issues (liver, renal/CrCl, pulmonary) as well as active/uncontrolled infection and uncontrolled autoimmune disease may be reasons not to pursue CAR-T. By far ECOG/performance status (0, 1) has emerged as a critical factor in terms of both efficacy and cumulative toxicity. Based on the current use of Tisagenlecleucel in large cell NHL, centers have devised established and effective referral processes, intake of consults as well as specific recommendations for post d30 care (antimicrobial prophylaxis, vaccinations, disease monitoring). The treatment platform/design for FL vs DLBCL are essentially identical. Moreover, centers that have on-boarded know how to properly collect cells, process/ship them, perform lympho-depletion and manage CAR-T patients post infusion. The ability to safely perform this procedure in the “outpatient” setting may have considerable advantages for institutional bed capacity. This collective Canadian experience will be incorporated into the effective “roll out” of CAR-T for FL.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
Data from ELARA indicates a remarkable ORR of 86% with 68% of patients achieving a CRR. Less than 10% of patients demonstrated progressive disease. The ability to determine or measure response are well defined and part of current routine clinical practice (clinical exam, CT and PET). Perhaps more impressive is the ongoing durability of responders following a single cell infusion with a PFS rate not yet met at 29 months of follow-up. Given the demographics of FL, patient safety is critical. In the absence of a clear efficacy advantage, 41BB-driven CD19 CAR-T may have a superior toxicity profile with very low incidence of ICANS. The ability to control disease with prolonged deep response should translate into a better quality of life. On the other hand, prolonged cumulative toxicity may have adverse effects and it will be important to study these parameters. Efficacy and toxicity monitoring will be completed through the CIBMTR who are a key stakeholder of the CTTC and Canadian transplant community.
What factors should be considered when deciding to discontinue treatment with the drug under review?
As a single infusion, treatment discontinuation is less of a consideration. However, this highlights the importance of patient selection and deciding which patients are more or less likely to derive clinical benefit or experience significant toxicity.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
CAR-T therapy in Canada currently includes Cell Therapy centers that are Health Canada approved (at a minimum). FACT approval is also an important consideration. A FACT-approved transplant center will have the necessary SOPs/policies to safely perform CAR-T. Institutional experience, trained CAR-T HCPs / tumor boards and data collection capabilities are also required. Within an institution, infectious disease, ICU/ER involvement as well as specific expertise from Neurology service need to be in place. To be able to use Tisagenleucleucel, a specific center must have successfully completed an onboarding process that includes RMP, dry runs, stem cell processing and apheresis audits as well as specific legal agreements. Many of these centers are already familiar with the use of this product in other indications (B-cell ALL, DLBCL)
Additional Information
No additional information is pertinent.
Conflict of Interest Declarations — Cell Therapy Transplant Canada
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission?
No help from outside the clinician group was obtained.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
No help from outside the clinician group was obtained.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Declaration for Clinician 1
Name: Mona Shafey
Position: Clinical Associate Professor, University of Calgary; Medical Director, Alberta Blood & Marrow Transplant Program
Date: 12-Jan-2023
Table 13: COI Declaration for Cell Therapy Transplant Canada — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Novartis | X | — | — | — |
Kite/Gilead | X | — | — | — |
Declaration for Clinician 2
Name: Terrance Comeau
Position: Director, New Brunswick Cellular Therapy Program
Date: 13-Jan-2023
Table 14: COI Declaration for Cell Therapy Transplant Canada — Clinician 2
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Kite | X | — | — | — |
Declaration for Clinician 3
Name: Gizelle Popradi
Position: Director, Stem Cell Transplant Program, McGill University Health Center
Date: 13-Jan-2023
Table 15: COI Declaration for Cell Therapy Transplant Canada — Clinician 3
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Novartis | — | X | — | — |
Kite/Gilead | — | X | — | — |
Declaration for Clinician 4
Name: Kelly Davison
Position: Assistant Professor, Department of Medicine, McGill University
Date: 19-Jan-2023
Table 16: COI Declaration for Cell Therapy Transplant Canada — Clinician 4
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Novartis | X | — | — | — |
Kite/Gilead | X | — | — | — |
BMS | X | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.