CADTH Reimbursement Review
Ciltacabtagene Autoleucel (Carvykti)
Sponsor: Janssen Inc.
Therapeutic area: Relapsed or refractory multiple myeloma
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Ethics Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
aPFS
adjusted progression-free survival
ATO
average treatment effect in the overlap population
ATT
average treatment effect in the treated population
BCMA
B-cell maturation antigen
CAR
chimeric antigen receptor
CD
cluster of differentiation
CI
confidence interval
cilta-cel
ciltacabtagene autoleucel
CMRG
Canadian Myeloma Research Group
CR
complete response
CRS
cytokine release syndrome
CyBord
cyclophosphamide-bortezomib-dexamethasone
DOR
duration of response
DRd
daratumumab-lenalidomide-dexamethasone
ECOG
Eastern Cooperative Oncology Group
EORTC
European Organisation for Research and Treatment of Cancer
EQ-5D-5L
5-level EQ-5D
ESS
effective sample size
HR
hazard ratio
HRQoL
health-related quality of life
ICANS
immune effector cell–associated neurotoxicity syndrome
IMiD
immunomodulatory drug
IMWG
International Myeloma Working Group
IPD
individual patient data
IPTW
inverse probability of treatment weighting
IPW
inverse probability weighting
IRC
independent review committee
ISS
International Staging System
ITC
indirect treatment comparison
ITT
intention-to-treat
LDH
lactate dehydrogenase
MID
minimally important difference
mITT
modified intention-to-treat
MM
multiple myeloma
M protein
monoclonal protein
MRD
minimal residual disease
NE
not estimable
NOC
Notice of Compliance
NR
not reached
OIS
Oncology Information Service
OR
odds ratio
ORR
overall response rate
OS
overall survival
PD
progressive disease
PFS
progression-free survival
PGIC
Patient Global Impression of Change
PGIS
Patient Global Impression of Severity
PHA
proportional hazards assumption
PI
proteasome inhibitor
PR
partial response
PRO
patient-reported outcome
QLQ-C30
Quality of Life Questionnaire Core 30
QLQ-MY20
Quality of Life Questionnaire Myeloma Module
RCT
randomized controlled trial
r/r
relapsed or refractory
RWCP
real-world clinical practice
rwPFS
real-world progression-free survival
SAE
serious adverse event
sCR
stringent complete response
SCT
stem cell transplant
SD
standard deviation
SMD
standardized mean difference
TEAE
treatment-emergent adverse event
TTNT
time to next treatment
TTR
time to response
VGPR
very good partial response
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Ciltacabtagene autoleucel (Carvykti), cell suspension in infusion bag, 0.5 × 106 to 1.0 × 106 CAR-positive viable T cells per kg body weight with a maximum of 1 × 108 CAR-positive viable T cells, for IV infusion |
Indication | For the treatment of adult patients with multiple myeloma, who have received at least 3 prior lines of therapy, including a proteasome inhibitor, an immunomodulatory drug, and an anti-CD38 antibody, and who are refractory to their last treatment |
Reimbursement request | As per indication |
Health Canada approval status | NOC/c |
Health Canada review pathway | Advance consideration under NOC/c |
NOC date | February 9, 2023 |
Sponsor | Janssen Inc. |
CAR = chimeric antigen receptor; NOC/c = Notice of Compliance with Conditions.
Source: Product monograph.1
Introduction
Multiple myeloma (MM) is a plasma cell cancer caused by the growth of cancer cells in the bone marrow. It was estimated that 4,000 people in Canada would be diagnosed with MM in 2022 and that 1,650 would die from MM, with slightly more cases occurring in males than females.2 Although new therapies have been introduced that can improve a patient’s overall survival (OS) and progression-free survival (PFS), MM remains an incurable condition.3 Some estimates suggest that the median survival for patients with MM is just more than 5 years and, during this time, patients can receive 4 lines of therapy or more.3,4 Patients with MM will ultimately relapse and, according to the clinical experts consulted by CADTH for this review, are usually assessed on a monthly basis following therapy to monitor for relapse. Indications for relapse include a rise in monoclonal (M) protein in the serum or urine or rise in serum free light chain ratio, or development of CRAB symptoms (hypercalcemia, renal insufficiency, anemia, or new bone lesions) or extramedullary plasmacytomas.5 The median OS for patients with relapsed or refractory (r/r) MM is approximately 13 months.6
The treatment landscape for MM has changed significantly in the past number of years, with the emergence of new therapies in newly diagnosed and r/rMM settings.3 At relapse, the clinical experts consulted by CADTH noted that treatment for patients depends on patient factors, including age, comorbidities, and previous treatments. According to the clinical experts consulted by CADTH as well as the clinical guidelines, regimens containing carfilzomib or pomalidomide are typically reserved for relapse after daratumumab-based regimens in the third line or after.7 Other options in the fourth line of therapy and beyond include oral palliative chemotherapy and alkylating drugs, such as cyclophosphamide.7 The clinical experts consulted by CADTH noted that belantamab mafodotin is another option available to patients; however, this treatment is available only through special access and is not used frequently. In November 2022, the FDA requested the withdrawal of belantamab mafodotin from US markets based on the outcomes of the pivotal clinical trial (DREAMM-3), which did not meet the requirements of the FDA’s Accelerated Approval regulations.8 Selinexor was recommended for reimbursement with conditions by CADTH in July 2022, in combination with bortezomib and dexamethasone for the treatment of adult patients with MM who have received at least 1 prior therapy; however, funding negotiations are still ongoing. Despite an array of therapies, MM remains an incurable disease and patients eventually relapse and their disease becomes refractory to available treatments.6
The clinical experts and clinician groups consulted by CADTH agreed there is an unmet need for treatments beyond the third line that prolong survival, delay disease progression, improve quality of life, and minimize side effects. The clinical experts consulted by CADTH also noted there is a need for treatments to be tolerable for patients with comorbidities and that require a shorter treatment duration and lead to a longer treatment-free interval to reduce the treatment burden on this heavily pretreated patient population with a limited lifespan.
The sponsor’s reimbursement request is for the treatment of adult patients with MM who have received at least 3 prior lines of therapy, including a proteasome inhibitor (PI), an immunomodulatory drug (IMiD), and an anti–cluster of differentiation 38 (CD38) antibody, and whose disease is refractory to their last treatment. Ciltacabtagene autoleucel (cilta-cel) underwent review by Health Canada through advance consideration under its Notice of Compliance with Conditions (NOC/c) and received a NOC/c on February 9, 2023. It has not been previously reviewed by CADTH. It is recommended that cilta-cel be provided as a single-dose infusion at a dose of 0.5 to 1.0 × 106 chimeric antigen receptor (CAR)-positive viable T cells per kg of body weight, with a maximum dose of 1 × 108 CAR-positive viable T cells per single infusion.1
The objective of this report was to perform a systematic review of the beneficial and harmful effects of cilta-cel for the treatment of adult patients with r/rMM who have received at least 3 prior lines of therapy, including a PI, an IMiD, and an anti-CD38 antibody. Of note, this CADTH Reimbursement Review was conducted before issuance of a Health Canada NOC/c and the scope was based on the anticipated indication.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups that responded to CADTH’s call for patient input and from the clinical experts consulted by CADTH for the purpose of this review.
Patient Input
One patient group, Myeloma Canada, provided input for the review of cilta-cel. Two online surveys were conducted, and a total of 200 patients and 26 caregivers provided complete responses to the patient and caregiver survey, respectively. Patient respondents indicated that their ability to work was most significantly impacted by the symptoms associated with myeloma, followed by the ability to travel and exercise, as well as their mental health. Travel cost was identified as the most significant financial implication of treatment, and the majority of patient respondents indicated they required support from a caregiver for the management of MM or treatment-related symptoms. From the perspective of the caregiver respondents, the ability to travel was most significantly impacted by caring for an individual with MM, followed by the ability to work and spend time with family and friends. Most patient respondents reported experiencing at least some side effects associated with maintenance therapy after receiving a stem cell transplant (SCT), as well as some negative impact on their overall well-being and quality of life due to the side effects associated with maintenance therapy; in turn, as reported by Myeloma Canada, these side effects had a negative impact on caregivers’ duties.
The patient respondents identified infections as the most important aspect of myeloma to control. They further indicated that mobility and kidney problems were aspects of myeloma that were important to control. The patient respondents reported that future treatment for MM should improve quality of life, have tolerable side effects, achieve remission, and extend survival without the need for continuous treatment. Patient respondents also highlighted the need for the accessibility and portability of treatments and a supportive and communicative care team. Patient respondents further noted the importance of access to alternative newer treatments and minimal trips to the hospital or community treatment centre.
Of the respondents who reported no experience with CAR T-cell therapy, the majority of patients and caregivers indicated that an estimated minimum of 1 to 2 years of extended life without requiring any drugs to control myeloma was extremely desirable; 2 patients indicated this was not desirable. Of note, this desirability is dependent on the severity of side effects and quality of the extended life. With respect to the side effects associated with cilta-cel, survey respondents who did not have experience with CAR T-cell therapy felt that cytokine release syndrome (CRS) would be the most troublesome side effect, followed by neutropenia, fever, and neuropathy.
Clinician Input
Input From the Clinical Experts Consulted by CADTH
The clinical experts consulted by CADTH highlighted that the most important goals of treatment for patients with r/rMM are prolonging survival, delaying disease progression, improving quality of life, and minimizing side effects. The clinical experts also highlighted that there is an unmet need for treatments beyond the third line that are tolerable for patients with comorbidities. The clinical experts noted that it is beneficial for any treatment to require a shorter treatment duration and lead to a longer treatment-free interval to reduce the treatment burden on this heavily pretreated patient population with a limited lifespan. In addition, the clinical experts highlighted that patients’ immune systems become weaker after multiple prior lines of therapy, thereby creating a need for treatments that are tolerated in later lines of therapy. As well, the experts noted that from the time of diagnosis, patients with high-risk disease have poor responses to treatment, which is worsened in the relapsed–refractory setting. Therefore, there is a great need for therapies that show some improved activity in people with high-risk disease. Patients who relapse quickly after prior lines of therapy (e.g., < 2 years) are also likely to have a very poor prognosis and thus are in great need of a novel intervention.
The clinical experts agreed that the majority of patients with r/rMM would eventually be eligible for cilta-cel, with the exception of patients who have died before reaching the fourth line or who are ineligible for CAR T-cell therapy due to severe disease progression or poor functional status. Eligible patients would include those who have “adequate” organ function, i.e., sufficient for them to be able to tolerate CRS and immune effector cell–associated neurotoxicity syndrome (ICANS) (definition of adequate organ function should be broad and left to the discretion of the treating centres), and who have a good Eastern Cooperative Oncology Group (ECOG) Performance Status (PS) (i.e., score of 2 or less). In the absence of sufficient evidence to guide patient selection for cilta-cel treatment, the experts suggested that patients who have a short life expectancy (< 2 months), have progressive disease (PD) that is poorly controlled, are unable to move to a larger centre for 1 month, or who have poor functional status (ECOG PS > 2), may not be suitable for cilta-cel. The clinical experts noted that the major barrier to uptake would be capacity, as the demand for CAR T-cell therapy may be greater than the existing capacity in Canada.
The clinical experts reported that response to treatment Is typically assessed by regular monitoring that is part of the management of patients with r/rMM. The clinical experts noted that, in some cases, patients may go through pretreatment (i.e., apheresis and conditioning chemotherapy) but not receive cilta-cel. In those cases, the patients would receive supportive care until the acute crisis is resolved. If patients were to deteriorate substantially between apheresis and time of infusion, one may not proceed with cilta-cel infusion. The clinical experts reported that cilta-cel treatment can be provided by oncologists or hematologists in a specialized setting that has adequate infrastructure for cell therapy and access to excellent clinical support and multidisciplinary care, including critical and specialist care (e.g., intensive care unit, neurology, nephrology) to manage toxicities, as well as laboratory support to handle and process samples.
Clinician Group Input
The views of the clinician groups were consistent with the views of the clinical experts consulted by CADTH. Two clinician groups provided input for the review of cilta-cel: the Canadian Myeloma Research Group (CMRG) represented by 20 clinicians, and the Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee represented by 1 clinician. The clinical groups added that antibody drug conjugates, bispecific antibodies, and cellular therapies that are directed against B-cell maturation antigen (BCMA) on myeloma cells are positioned to fill the triple class–exposed or refractory space but are not currently available in Canada. Both groups indicated that patients with an ECOG PS of 0 to 2, minimal or no comorbidities, low tumour burden, and adequate organ function and blood counts would be the most likely to have the best outcomes.
Drug Program Input
The Provincial Advisory Group identified the following jurisdictional implementation issues: eligible patient population, eligibility for re-treatment, and concerns related to accessing clinical specialists and/or special settings. The clinical experts consulted by CADTH weighed evidence from the CARTITUDE-1 study and other clinical considerations to provide responses to the Provincial Advisory Group’s drug program implementation questions. Refer to Table 4 for more details.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
CARTITUDE-1 is a phase Ib/II, single-arm clinical trial of cilta-cel in patients with r/rMM who have received at least 3 prior lines of therapy, including a PI, an IMiD, and an anti-CD38 antibody. The main cohort described throughout this review included 113 enrolled patients and was conducted in 16 sites in the US. Of the 113 patients who underwent apheresis, 97 patients received cilta-cel infusion: 29 (30%) in phase Ib and 68 in phase II (70%). As of the final data cut-off date of January 11, 2022, there were 66 patients (58%) receiving ongoing follow-up. An additional cohort comprising 9 patients participated in 4 sites in Japan and is hereafter referred to as the Japanese cohort.
The primary objective for the phase Ib study was to characterize the safety of cilta-cel and confirm the recommended phase II dose. The primary objective for the phase II study was to evaluate the efficacy of cilta-cel through overall response rate (ORR) (at least a partial response [PR] or better) as assessed by an independent review committee (IRC). The ORR and its 2-sided 95% Clopper-Pearson exact confidence interval (CI) were assessed, and the P value from a 1-sided exact binomial test for the null hypothesis of an ORR of 30% or less was provided. Secondary end points included very good partial response (VGPR) or better rate, duration of response (DOR), minimal residual disease (MRD) negativity rate, time to response (TTR), PFS, OS, and health-related quality of life (HRQoL). An exploratory objective was to characterize the impact of the treatment process on health care resource utilization. The study was funded by Janssen Research & Development.
Four Clinical Study Reports were provided in the sponsor’s submission: the primary analysis report with a clinical data cut-off date of September 1, 2020,9 the safety and efficacy update reports with a clinical data cut-off date of February 11, 2021,10 and the final analysis report with a clinical data cut-off date of January 11, 2022. The final analysis report was used throughout this report unless otherwise specified.11 Results from phases Ib and II were pooled together, as the study procedures and criteria were consistent between both phases.
After enrolment, patients underwent apheresis, received conditioning treatment, and then received the cilta-cel infusion. Of all patients who were enrolled and received apheresis, 97 (86%) received cilta-cel. Bridging therapy to maintain disease stability was administered to 73 patients (75.3%) between apheresis and initiation of the conditioning regimen. No patients who received bridging therapy achieved complete response (CR) while on bridging therapy; thus, all were eligible to receive cilta-cel. The median number of CAR-positive viable T cells infused was 54.3 × 106 cells (range of 23.5 × 106 to 93.1 × 106 cells) with a median of 0.709 × 106 cells/kg administered (range, 0.51 × 106 to 0.95 × 106 cells/kg). Patients were followed up on days 3, 7, 10, 14, 21, 28, 42, 56, 78, and 100. After day 101, they were followed up every 28 days until study completion, defined as 2 years after the last patient has received their initial dose. Three patients were re-treated with cilta-cel.
The mean age of patients was 62 years (standard deviation [SD] = 8.38), and the majority of patients were younger than 65 years (62 patients; 64%) and white (69 patients; 71%), with an ECOG PS of 1 (54 patients; 56%) and International Staging System (ISS) stage I MM at baseline (61 patients; 63%). With regard to cytogenetic risk, 23 patients (24%) were high risk at baseline. All patients received at least 3 prior lines of MM therapy, with a median of 6 prior lines (range, 3 to 18). The most common prior antineoplastic drugs used were daratumumab in 94 patients (97%) and bortezomib in 92 patients (95%), and the most common IMiDs were lenalidomide in 96 patients (99%) and pomalidomide in 89 patients (92%). Almost all patients (96 patients; 99%) had disease that was refractory to the last line of prior therapy, and 85 patients (88%) had disease that was triple-refractory, i.e., refractory to the 3 major classes of therapeutic drugs (PI, IMiD, and anti-CD38 monoclonal antibody).
Efficacy Results
The key efficacy results of the CARTITUDE-1 trial are summarized in Table 2. As of the January 11, 2022, data cut-off, after a median follow-up of 27.7 months (range, 1.5 to 40.4), the median OS was not reached (NR). Among all treated patients (i.e., patients who received cilta-cel at the targeted recommended phase II dose; N = 97), there were 30 deaths (31%), and the 24-month OS rate was ||||| |||| ||| |||| || |||||. Among all enrolled patients (N = 113), the 24-month OS rate was ||||| |||| ||| |||| || |||||. Median PFS was also NR. Among all treated patients, || patients (||%) experienced PFS events, and the estimated 24-month PFS rate was ||||| |||| ||| |||| || |||||. Among all enrolled patients (N = 113), the 24-month PFS rate was ||||| |||| ||| |||| || |||||. ORR in the all-treated analysis set was 97.9% (95% CI, 92.7 to 99.7), stringent CR (sCR) was reached by 80 patients (82.5%; 95% CI, 73.4 to 89.4), VGPR by 12 patients (12.4%; 95% CI, 6.6 to 20.6), and PR by 3 patients (3.1%; 95% CI, 0.6 to 8.8). In the all-enrolled analysis set (n = 113), the ORR was 84.1% (95% CI, 76.0 to 90.3). The ORR results from the patient subgroups of interest were consistent with the primary analysis; however, the analysis was limited by small sample sizes. Median DOR was NR. Among all treated patients, the estimated probability that patients remained in response at 12 months was ||||| |||| ||| |||| || |||||; at 24 months it was ||||| |||| ||| |||| || ||||| and at 30 months it was ||||| |||| ||| |||| || |||||. Of the 61 patients with evaluable samples, 56 patients (91.8%; 95% CI, 81.9 to 97.3) achieved MRD negativity in bone marrow at 10−5 sensitivity following treatment with cilta-cel. Median time to first response (for patients with PR or better) was 0.95 months (range, 0.9 to 10.7) and mean time to first response was 1.4 months (SD = 1.54). Median time to best response was 2.6 months (range, 0.9 to 17.8) and median time to CR or better was 2.9 months (range, 0.9 to 17.8).
The European Organisation for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire Core 30 (QLQ-C30) completion rate at baseline was 92.6% (63 patients) and declined to 83.1% (54 patients), and 65.0% (39 patients) at day 100 and day 156, respectively. The EORTC QLQ-C30 suggested improvements over time compared with baseline, with decreases observed only initially on day 7 for global health status, physical functional scale, and fatigue symptom scale. This initial worsening is consistent with the potential onset of cilta-cel adverse events (AEs) related to CRS.12 There appeared to be consistent improvement in the pain symptom scale from baseline. The EORTC Quality of Life Questionnaire Myeloma Module (QLQ-MY20) completion rate at baseline was |||||% (|| patients) and declined to ||% (|| patients) at day 100. The EORTC QLQ-MY20 suggested improvements over time compared with baseline. The 5-level EQ-5D (EQ-5D-5L) completion rate at baseline was 92.6% (63 patients) and declined to ||% (|| patients) and ||||% (|| patients) at day 100 and day 156, respectively. The EQ-5D-5L suggested an initial decrease in both utility score and visual analogue score at day 7 followed by continuous improvement through day 100. The Patient Global Impression of Severity (PGIS) completion rate at baseline was 93% (63 patients) and declined to 78% (53 patients) and 57% (39 patients) at day 100 and day 156, respectively. Severity of pain assessed by PGIS was consistently reported as lower than baseline through day 352. Patient Global Impression of Change (PGIC) was only completed post infusion from day 28, where 67% of patients reported improvement, and the proportion increased to 87% by day 100, where the completion rate was 79% (54 patients).
In the Japanese cohort from the CARTITUDE-1 study (n = 9), the median follow-up was 8.5 months and the ORR was 100% (95% CI, 66.4 to 100). In the all-treated analysis set (n = 9), all DOR, PFS, and OS data were censored at the clinical data cut-off; therefore, median DOR, PFS, and OS were NR. The 9-month PFS rate was 100% and the estimated 12-month OS rate was 100%.
Harms Results
The key harms reported in the CARTITUDE-1 trial are summarized in Table 2. All patients in the all-treated analysis set (N = 97) experienced at least 1 AE, with || patients (||%) experiencing at least 1 grade 4 AE. The most common any-grade AEs were neutropenia (96%), CRS (95%), anemia (81%), and thrombocytopenia (80%). A total of 53 patients (55%) experienced at least 1 serious AE (SAE), with 30 patients (31%) experiencing a grade 3 or 4 SAE and 6 patients (6%) experiencing a grade 5 SAE. The most common SAEs were CRS (21%), pneumonia (6%), sepsis (5%), and ICANS (5%).
Between apheresis and the start of the conditioning treatment, 8 patients out of 113 (7%) died. Overall, 101 patients received the conditioning regimen, and 97 patients went on to receive cilta-cel. Out of the 4 patients who received the conditioning regimen but did not receive cilta-cel, 1 patient died. Out of all treated patients, 30 patients (30.9%) died: 16 due to AEs and 14 due to disease progression. No patients died within 30 days of the initial cilta-cel infusion, and 2 patients (2.1%) died within 100 days. Only 6 patients (6.2%) had a treatment-emergent adverse event (TEAE) leading to death that was considered to be related to cilta-cel; the remaining 10 deaths were not considered by the study investigators to be related to cilta-cel.
The notable harms identified in the CADTH protocol included CRS, neurologic toxicities, cytopenia, and secondary hypogammaglobulinemia. A total of 92 patients (95%) experienced CRS, with 4 patients (4%) experiencing a grade 3 or 4 CRS and 1 patient (1%) experiencing a grade 5 CRS complicated by secondary hemophagocytic lymphohistiocytosis. A total of 21 patients (22%) experienced CAR T-cell neurotoxicity, including || patients (10%) at grade 3 or 4. A total of 16 patients (17%) experienced ICANS, including 2 patients (2%) at grade 3 or 4. Other neurotoxicity was reported in 13 patients (13%), including 9 patients (9%) at grade 3 or 4. A total of 96 patients (99%) had experienced at least 1 grade 3 or 4 cytopenic AE, and the majority were transient, with recovery to grade 2 or better within the first 60 days following cilta-cel infusion. A total of 12 patients (12.4%) experienced hypogammaglobulinemia, including 2 patients (2.1%) with grade 3 or 4 events.
In the Japanese cohort, all 9 patients experienced at least 1 AE, and 8 (88.9%) experienced at least 1 grade 3 or 4 AE. Grade 3 or 4 cytopenias were reported in 8 patients (88.9%). Grade 1 or 2 CRS was reported in 8 patients (88.9%), and SAEs were reported in 1 patient (neutropenia, thrombocytopenia, fatigue, and CRS). No patient experienced CAR T-cell neurotoxicity (including ICANS or other neurotoxicity). No death was reported during the study.
Table 2: Summary of Key Results From the CARTITUDE-1 Trial (All-Treated Analysis Set With January 11, 2022, Data Cut-Off)
Outcome | CARTITUDE-1 (phase Ib + phase II) N = 97 |
|---|---|
OSa | |
Number of events (%) | 30 (30.9) |
Median, months (95% CI) | NE |
12-month OS rate % (95% CI) | |||| ||||| || ||||| |
24-month OS rate % (95% CI) | |||| ||||| || ||||| |
30-month OS rate % (95% CI) | |||| ||||| || ||||| |
PFSa | |
Number of events (%) | 43 (44.3%) |
Median, months (95% CI) | NE (24.54 to NE) |
12-month PFS rate % (95% CI) | |||| ||||| || ||||| |
24-month PFS rate % (95% CI) | |||| ||||| || ||||| |
30-month PFS rate % (95% CI) | |||| ||||| || ||||| |
ORRb | |
Overall response (sCR + CR + VGPR + PR), n (%) | 95 (97.9) |
95% CI for % | 92.7 to 99.7 |
VGPR or better (sCR + CR + VGPR), n (%) | 92 (94.8) |
95% CI for % | 88.4 to 98.3 |
sCR, n (%) | 80 (82.5) |
95% CI for % | 73.4 to 89.4 |
VGPR, n (%) | 12 (12.4) |
95% CI for % | 6.6 to 20.6 |
PR, n (%) | 3 (3.1) |
95% CI for % | 0.6 to 8.8 |
DORa | |
Number of events (%) | 42 (44.2) |
Median, months (95% CI) | NE (23.3 to NE) |
12-month DOR rate % (95% CI) | |||| ||||| || ||||| |
24-month DOR rate % (95% CI) | |||| ||||| || ||||| |
30-month DOR rate % (95% CI) | |||| ||||| || ||||| |
TTR | |
N | 95 |
Time to first responsec (months), mean (SD) | 1.4 (1.54) |
Median (range) | 0.95 (0.9 to 10.7) |
Time to best response (months), mean (SD) | ||| |||||| |
Median (range) | 2.6 (0.9 to 17.8) |
Harms, n (%) | |
TEAEs | 97 (100.0) |
SAEs | || |||||| |
Deaths | 30 (30.9) |
Notable harms | |
Cytopenia | 96 (99) |
Cytokine release syndrome | 92 (94.8) |
≥ Grade 3 | 5 (5.2) |
Neurotoxicity | 21 (21.6) |
ICANS | 16 (16.5) |
Other neurotoxicities | 13 (13.4) |
Hypogammaglobulinemia | 12 (12.4) |
CI = confidence interval; CR = complete response; DOR = duration of response; ICANS = immune effector cell–associated neurotoxicity syndrome; NE = not estimable; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; PR = partial response; SAE = serious adverse event; sCR = stringent complete response; SD = standard deviation; TEAE = treatment-emergent adverse event; TTR = time to response; VGPR = very good partial response.
aEstimated using the Kaplan-Meier method.
bResponse was assessed by an independent review committee, based on International Myeloma Working Group consensus criteria (2016). Percentages are calculated with the number of patients in the all-treated analysis set as denominator. Exact 95% CIs are provided.
cResponse is defined as PR or better.
Source: CARTITUDE-1 Clinical Study Report.9-11
Critical Appraisal
Internal Validity
CARTITUDE-1 was an open-label, single-arm phase Ib/II study in the US (16 centres) and Japan (4 centres). The primary limitation of CARTITUDE-1 was the absence of a comparator group against which the benefits and harms of cilta-cel could be compared. Single-arm trials are generally not considered as confirmatory for efficacy and are subject to several limitations that complicate their interpretation.13 ORR was tested against a predetermined hypothesis; however, there was no adjustment for multiplicity across the various analyses of the outcome (i.e., the various data cut-offs), so there is an increased risk of type I error. Results for the other outcomes (e.g., DOR, OS, PFS) were descriptive only. This trial does not provide any information for the effects of cilta-cel relative to the available comparator treatments used in Canada. According to the FDA assessment of the CARTITUDE-1 trial, end points such as OS and PFS are uninterpretable due to the lack of a comparator arm and were neither reviewed nor included in the FDA label.14 A limited number of patients were included in the all-treated analysis set (n = 97) and all-randomized analysis set (n = 113) of CARTITUDE-1. The magnitude of the treatment effect estimates observed in a small study sample may not be replicable in a larger study sample or generalizable to the target population in real-world clinical practice (RWCP).
It cannot be firmly concluded to what extent the improvements in ORR observed in patients would translate into OS benefits. ORR is accepted by the FDA as directly attributable to drug effect in “single-arm trials conducted in patients with refractory tumours where no available therapy exists.”15
The interpretation of efficacy in the all-treated analyses are at risk of bias in favour of cilta-cel. The population excludes patients (n = 16; 14%) who were enrolled and underwent apheresis but were subsequently unable to receive cilta-cel because they died or their disease progressed, or due to AEs or other reasons (e.g., patient choice). This population is not reflective of expected clinical practice and overrepresents the healthiest patients. Analyses based on the all-enrolled population are considered most appropriate for estimating the effect of assignment to treatment. As expected, when both were presented, the results of analyses of the all-treated population were more favourable compared with those of the all-enrolled population. Out of the 113 patients who underwent apheresis, 12 patients, including 8 patients who had died, did not receive the conditioning treatment. The clinical experts noted that, although this is common in r/rMM, the proportion of deaths is unusual, given how relatively healthy the trial population was. Only 3 patients were re-treated with cilta-cel; thus, there is not enough information to draw conclusions regarding re-treatment.
No subgroup analysis was specified in the study protocol a priori and, while the results for ORR were consistent with the primary analysis results across the patient subgroups of interest, the analysis was limited by the small sample size of some groups, such as patients who received prior allogeneic SCT.
The trial was open label, which can result in a risk of bias in the measurement of the outcomes, particularly for subjective outcomes such as ORR, PFS, HRQoL, and subjective harms. To reduce the risk of directional bias in reported outcomes, response outcomes were assessed by the investigators, an IRC, and a validated computer algorithm. The use of IRC may have mitigated this risk by following recommendations for end points based on tumour measurements.15 In addition, although the EORTC QLQ-C30 and EQ-5D-5L are comprehensive and widely used instruments designed to measure HRQoL, neither are currently validated for patients with r/rMM. Further, results for all HRQoL measures were at risk of bias due to missing data, particularly at longer follow-up (e.g., data for the EORTC QLQ-C30 were missing for ||% of all treated patients at day 100 and for ||% of patients by day 156). In addition to a diminishing sample size, the patients reporting HRQoL outcomes later in the study are expected to be the healthiest among the population. Given that the trial was nonrandomized, the impact of cilta-cel on patient-reported outcomes (PROs) in relation to other therapies is unknown.
Findings from the Japanese cohort of the CARTITUDE-1 trial were consistent with results from the main cohort; however, it only included 9 patients, which limits the interpretation of cohort findings.
External Validity
According to the clinical experts consulted by CADTH for this review, the demographic and disease characteristics of the CARTITUDE-1 study population9 were generally reflective of the population of patients in Canada with r/rMM. The mean age of patients in the trial was 62 years, which is younger than the mean age of 70 years at the time of diagnosis in Canada.16 If there was no access to less toxic bispecific therapies, the clinical experts would have expected a slightly larger proportion of patients to be older than 75 years of age (15% versus the trial’s 8%). However, clinicians can currently access these bispecific therapies through special access programs and would prioritize the older patient population for these therapies, making the trial’s age proportions reflective of the current population demographics. All patients met the inclusion criteria of an ECOG PS of 0 or 1 during screening, but 4 patients (4%) deteriorated to ECOG 2 on or before cilta-cel infusion. The clinical experts considered it common for patients to deteriorate after apheresis. The clinical experts also mentioned they would have expected potentially more patients with extramedullary plasmacytomas present past the third line of therapy, as this would denote worse disease, but that the 13% proportion in the trial is acceptable. They would have also expected a slightly higher proportion of patients to be of high cytogenetic risk (30% versus the trial’s 24%).
The clinical experts consulted by CADTH mentioned that the creatinine clearance required for inclusion in the trial (≥ 40 mL/min/1.73 m2) is higher than the level used to indicate poor kidney function in clinical practice (≥ 30 mL/min/1.73 m2). They also mentioned that including patients with an ECOG of 2 or less (rather than the trial’s criteria of < 2) would better align with clinical practice needs. One of the trial exclusion criteria is any prior therapy that targeted BCMA, which the clinical experts found concerning, as some clinicians would likely be giving their patients belantamab mafodotin, available through compassionate access, in their management of MM. The clinical experts noted that these patients may still respond well to CAR T-cell therapy17 and should not be excluded from cilta-cel eligibility.
With regard to prior therapy used by patients in the trial, the clinical experts noted that potentially all patients would have disease that is refractory to daratumumab within the first 3 lines of therapy (compared with 97% of patients in the trial). They also noted that selinexor is currently used as a bridging therapy in the US, but no patients had used selinexor in the trial, as selinexor (combined with dexamethasone and bortezomib) was not approved during the time of the trial.18 Finally, they noted it was surprising that 19% of patients had used anakinra for treating CRS, since it is rarely used in Canadian practice; however, they also noted this may have been due to a global shortage of tocilizumab.
The clinical experts consulted by CADTH for this review did not have any major concerns with the end points used in the CARTITUDE-1 trial. They considered OS, HRQoL, and PFS as the most important outcomes, which were secondary end points in the trial. It was noted that MRD negativity rate is not routinely used in clinical practice. All outcomes in the protocol were important to patients, clinicians, and drug plans; although they were evaluated, this trial provides no information about the efficacy and harms of cilta-cel relative to treatments that would otherwise be used in this patient population in clinical practice.
This study was a multicentre trial in the US. The clinical experts indicated there are few concerns to generalizing the findings from the pivotal study within the Canadian clinical setting.
Other Relevant Evidence
LEGEND-2 Trial
The sponsor also provided long-term (2-year and 4-year) data from LEGEND-2, a phase I, single-arm, open-label study (N = 74) conducted in 4 registered sites in China in patients with r/rMM who had received at least 3 prior lines of treatment. The cilta-cel CAR T-cell drug product studied in CARTITUDE-1 (produced in the US) and the LCAR-B38M CAR T-cell drug product studied in the LEGEND-2 study (produced in China), express an identical CAR protein targeting BCMA but were produced using different manufacturing and scale-up processes.19 Unlike cilta-cel, the LCAR-B38M CAR T-cell dose was split into 3 infusions administered over 7 days, with the number of CAR T cells administered increasing with each infusion. Patients were not required to have received an anti-CD38 antibody in prior therapy, and only 2 patients (2.7%) had received prior anti-CD38 antibody therapy. Patients with a history of allogeneic SCT were excluded from the trial.
The median age of patients was 54.5 years (range, 27 to 74), with a higher proportion of men (61%), and with a median time since initial MM diagnosis of 4 years (range, 1 to 9). LEGEND-2 provided longer-term safety and efficacy follow-up than the CARTITUDE-1 trial, with an additional median follow-up of 20.1 months. In the LEGEND-2 trial 4-year analysis, median follow-up time from dosing to cut-off was 47.8 months (range, 0.4 to 60.7). Median OS was not yet reached, but the 24-month OS rate was ||||% (95% CI, |||| || ||||), and the median PFS was 18 months (95% CI, 10.6 to 25.6). The ORR by sponsor assessment was 87.8% (95% CI, 78.2 to 94.3), with 54 patients (73%) achieving CR, 6 patients (8%) achieving PR, and 5 patients (7%) achieving VGPR. Median DOR was 23.26 months (95% CI, 13.04 to 32.69). The median time for initial response was 1.0 months (range, 0.4 to 3.5), and the median time for best response was 3.3 months (range, 0.4 to 28.5). All patients experienced at least 1 TEAE within 100 days post infusion, with AEs of grade 3 or greater in 45 patients (61%). The most common AEs were pyrexia in 68 patients (92%) and CRS in 68 patients (92%), and only 7 patients (10%) experienced a CRS of grade 3 or greater. Of the 74 patients in the analysis, 34 deaths (46%) were reported.
Critical Appraisal of LEGEND-2
LEGEND-2 was an open-label, single-arm phase I study conducted only in China (4 centres). The cilta-cel CAR T-cell drug product studied in CARTITUDE-1 (produced in the US) and the LCAR-B38M CAR T-cell drug product studied in the LEGEND-2 study (produced in China) express an identical CAR protein targeting BCMA, but were produced using different manufacturing and scale-up processes.19 The primary limitation was the absence of a comparator group against which the treatment benefits and harms of the LCAR-B38M CAR T-cell drug product could be compared. As such, there is no evidence of the effect of LCAR-B38M relative to available comparator therapies from this trial. The study protocol mentioned the use of a computerized algorithm and IRC for disease status evaluation; however, the findings are reported based on sponsor assessment (based on uniform medical reviews of source hospital medical records), leading to an increased risk of bias in the measurement of the outcome likely favouring LCAR-B38M. HRQoL was not assessed as an end point in this phase I study. The clinical experts consulted by CADTH for this review noted that the baseline characteristics of the LEGEND-2 study population would be closer to patients who are in the second line of therapy (younger and with limited use of daratumumab), rather than the fourth line of therapy and beyond. Moreover, because exposure to an anti-CD38 antibody was not required (only 2 patients had received prior anti-CD38 antibody therapy), this study population does not fully align with the reimbursement criteria for this review. The experts also mentioned that the low proportion of patients with neurotoxicity as an AE (only 1 patient) was not aligned with the results of CARTITUDE-1.
Comparative Observational Evidence for Cilta-Cel Versus Real-World Clinical Practice
The sponsor-submitted evidence consisted of 2 reports of 3 observational studies to compare cilta-cel with relevant treatment comparators in RWCP: CARTITUDE-1 versus LocoMMotion and CARTITUDE-1 versus real-world cohorts.20,21
CARTITUDE-1 Versus LocoMMotion20
The first sponsor-submitted report was an observational study comparing the effectiveness of cilta-cel (from CARTITUDE-1) versus RWCP as observed in the LocoMMotion prospective cohort study using individual patient data (IPD), with propensity score weighting and regression modelling in an attempt to adjust for known confounders. The following outcomes were planned to be assessed: clinical response (ORR, VGPR, CR or better, MRD), PFS, time to next treatment (TTNT), OS, PROs, safety, and resource utilization.20
The CARITUDE-1 study consisted of 113 patients who underwent apheresis and made up the intention-to-treat (ITT) population, and 97 patients who were treated with cilta-cel (modified ITT [mITT]). The selected LocoMMotion cohort consisted of 248 patients in the ITT population and 170 patients in the mITT population. After weighting, the effective ITT and mITT population size of the LocoMMotion cohort was 118 and 108 patients, respectively.
Following adjustment, the conditional hazard ratio (HR) for OS was 0.32 (95% CI, 0.17 to 0.58) in the ITT population (median OS = not estimable (NE) [95% CI, 31.47 to NE months] versus 11.76 months [95% CI, 7.16 to NE months]), and conditional HR was 0.20 (95% CI, 0.09 to 0.41) in the mITT population (median OS = NE [95% CI, NE to NE] versus 11.33 months [95% CI, 5.45 to NE months]), both favouring cilta-cel.
For PFS, the conditional HR between treatment groups was 0.19 (95% CI, 0.11 to 0.32) in the ITT population (median PFS = 28.03 months [95% CI, 20.11 to NE months] versus 4.07 months [95% CI, 2.86 to 5.09 months]) and conditional HR was 0.15 (95% CI, 0.08 to 0.29) in the mITT population (median PFS = NE [95% CI, 24.54 to NE months] versus 2.73 months [95% CI, 2.37 to 3.68 months]), both favouring cilta-cel.
For ORR, observed proportions in the ITT and mITT populations were 84.1% and 97.9% for cilta-cel, and 29.8% and 42.9% for RWCP from LocoMMotion, respectively. The inverse probability weighting (IPW)-estimated odds ratio (OR) was 22.00 (95% CI, 11.14 to 43.35) in the ITT population and 103.87 (95% CI, 24.17 to 446.37) in the mITT population, both in favour of cilta-cel.
Overall, there was a variation in study design (phase Ib/II open-label trial versus an observational and noninterventional study), heterogeneity between cohorts before and after adjustment, as well as uncertainty of the results due to the assumptions made and residual confounding. This limits the ability to draw strong conclusions about the comparative efficacy of cilta-cel with other treatments in this clinical setting, where no effective standard of care is available. Given the adjustment of the LocoMMotion population to the CARTITUDE-1 population, the generalizability of the results is similar to that of CARTITUDE-1. Additionally, there was a total of 92 unique regimens received in RWCP in the LocoMMotion study, which may not be reflective of Canadian clinical practice, and there were no Canadian investigative sites included in either the CARTITUDE-1 or LocoMMotion studies, which may impact the generalizability of the results to patients in Canada.
CARTITUDE-1 Versus Real-World Cohorts21
The other sponsor-submitted report included 2 observational studies to compare cilta-cel treatment with the real-world treatments received by patients for triple class–exposed r/rMM. In both studies, propensity score weighting was used in an attempt to adjust for known confounders.21 One analysis compared the IPD from CARTITUDE-1 with the IPD from a cohort of patients in the long term follow-up of 3 global r/rMM clinical trials of daratumumab (POLLUX, CASTOR, and EQUULEUS; hereinafter referred to as the daratumumab trial cohort). The other analysis compared the IPD from CARTITUDE-1 with the IPD for a CARTITUDE-1-like cohort of real-world patients receiving current treatment paradigms using data from the Flatiron Health database (hereinafter referred to as the Flatiron cohort). Outcomes included in the analyses consisted of ORR, CR rate or better, PFS, and OS. The outcomes of CR and VGPR were not evaluated in the Flatiron database; therefore, an assessment of ORR and CR rate or better was not possible.
The CARTITUDE-1 trial included 113 patients in the ITT population and 97 patients in the mITT population. A total of 351 and 288 patients were included in the daratumumab trial cohort in the ITT and mITT populations, respectively. After propensity score weighting, the base-case effective sample size (ESS) of the daratumumab trial cohort ITT and mITT populations was 212 and 116, respectively. In the Flatiron cohort, 229 and 196 patients made up the ITT and mITT populations, respectively. After adjustment, the ESS for the Flatiron cohort was 192 in the ITT population and 80 in the mITT population.
The HRs for OS for the comparison of cilta-cel with RWCP in the daratumumab trial cohort were 0.25 (95% CI, 0.17 to 0.38) and 0.20 (95% CI, 0.13 to 0.31) for the ITT population (median OS = NR [95% CI, 31.47 to NE months] versus 8.05 months [95% CI, 6.34 to 11.30 months]) and mITT population (median OS = NR [95% CI, NE to NE months] versus 10.90 months [95% CI, 8.18 to 16.20 months]), respectively, in favour of cilta-cel. The HRs for OS for the comparison of cilta-cel with RWCP in the Flatiron cohort were 0.32 (95% CI, 0.19 to 0.52) and 0.25 (95% CI, 0.14 to 0.43) for the ITT population (median OS = NR [95% CI, 31.47 to NE months] versus 12.30 months [95% CI, 9.72 to 15.50 months]) and mITT population (median OS = NR [95% CI, NE to NE] versus 13.20 months [95% CI, 9.17 to 21.30 months]), respectively, in favour of cilta-cel.
The HR for PFS for cilta-cel versus RWCP in the daratumumab trial cohort was 0.26 (95% CI, 0.18 to 0.37) in the ITT population (median PFS = ||||| |||||| |||| ||| ||||| || ||| ||| |||| |||||| |||| ||| ||||| ||||||| and 0.24 (95% CI, 0.16 to 0.35) in the mITT population, with a median PFS of NR (95% CI, 24.54 to NR) versus 5.32 months (95% CI, 2.76 to 8.31), in favour of cilta-cel. Results for adjusted PFS (aPFS), and real-world PFS (rwPFS) were consistent with the overall PFS analysis for the daratumumab trial cohort. The aPFS HR for cilta-cel versus RWCP in the Flatiron cohort was 0.22 (95% CI, 0.15 to 0.33) in the ITT population (median = aPFS, ||||| |||||| |||| ||| ||||| || ||| ||| |||| |||||| |||| ||| |||| || |||||| and 0.18 (95% CI, 0.12 to 0.26) in the mITT population, with a median aPFS of NR (95% CI, 24.54 to NR), versus 4.53 months (95% CI, 2.86 to 6.77), also in favour of cilta-cel. In the Flatiron cohort, the rwPFS HR was 0.22 (95% CI, 0.15 to 0.33) in the ITT population |||||| |||||| |||| ||| ||||| || ||| ||| |||| |||||| |||| ||| |||| || ||||||| and 0.18 (95% CI, 0.10 to 0.23) in the mITT population, with an rwPFS HR of NR (95% CI, 24.54 to NR) versus 5.88 months (95% CI, 4.01 to 8.48). After inverse probability of treatment weighting (IPTW), the OR for ORR comparing cilta-cel with RWCP was 22.55 (95% CI, 10.72 to 52.03) in the ITT population and 127.35 (95% CI, 34.24 to 850.09) in the mITT population. Results for ORR were not available in the comparison with the Flatiron cohort.
Results of the base-case analyses and sensitivity analyses were consistent across end points, analysis populations, and across data sources, favouring cilta-cel over RWCP in both the daratumumab trial cohort and the Flatiron cohort for all outcomes. For all outcomes, the magnitude of effect for cilta-cel was notably large compared with RWCP; however, the results were associated with wide 95% CIs, highlighting losses to precision and reducing the ability to draw strong conclusions about the magnitude of the effect. There were important differences in the design of the included studies that limit the ability to draw strong conclusions about the efficacy of cilta-cel compared with RWCP. This includes the differences in study design (phase Ib and II single-arm trial versus published literature from 3 clinical trials comprising 2 phase III randomized controlled trials [RCTs] and 1 phase Ib open-label RCT, and a real-world cohort from electronic health records), which could not be adjusted for in the analysis using propensity scoring methods. As well, there was notable heterogeneity in populations before adjustment and the potential for residual confounding following adjustment, and small sample sizes and wide 95% CIs, highlighting losses to precision.
Other Observational Studies Identified in the Literature Search
In total, 3 published articles met the CADTH predefined inclusion criteria for this review: CARTITUDE-1 versus the Monoclonal Antibodies in Multiple Myeloma: Outcomes After Therapy Failure (MAMMOTH),22 CARTITUDE-1 versus Therapie Monitor,23 and a meta-analysis of observational studies.24
CARTITUDE-1 Versus MAMMOTH22
This was an observational study using IPD from the CARTITUDE-1 trial and the MAMMOTH cohort to evaluate the efficacy of cilta-cel versus real-world therapies for the outcomes of ORR, PFS, and OS. Propensity score matching was used to attempt to adjust for confounding.22
The populations for CARTITUDE-1 consisted of 113 patients in the ITT population and 97 patients in the mITT population. Corresponding populations identified from MAMMOTH included 190 and 122 patients in the ITT and mITT populations, respectively. The matched populations included 95 patients in the ITT population in each cohort, and 69 patients in the mITT cohort. In the propensity score matched analysis, results for PFS and OS favoured patients in CARTITUDE-1 compared with the matched MAMMOTH population (HR = 0.11; 95% CI, 0.05 to 0.22) and HR = 0.20 (95% CI, 0.10 to 0.39). For ORR, 80 patients (84%) achieved an ORR in CARTITUDE-1 versus 27 patients (28%) in the MAMMOTH (OR = 13.4; 95% CI, 6.6 to 27.3) ITT analysis. Results for the mITT population were also consistent with the ITT population.
In general, the results of the analyses demonstrated a clinical benefit over RWCP from MAMMOTH; however, the reduced sample sizes from propensity score matching, unexplored heterogeneity, and wide 95% CIs resulted in uncertainty in the results and the magnitude of the observed effects. Given the methodological differences across studies and the risk of bias due to residual confounding, the comparison with external, historical, real-world data is nonconfirmatory and should only be viewed as exploratory.
CARTITUDE-1 Versus Therapie Monitor23
This observational study evaluated OS and TTNT for patients in CARTITUDE-1 versus patients receiving real-world treatments registered in the Therapie Monitor database in Germany maintained by the Oncology Information Service (OIS).23 IPD from both cohorts was used for comparison for the outcomes of OS and TTNT (as proxy for PFS), and propensity score weighting was used to attempt to adjust known confounders.
The ITT and mITT populations for CARTITUDE-1 consisted of 113 and 97 patients, and the ITT and mITT populations of Therapie Monitor consisted of 222 and 174 patients, respectively. After weighting, the ESS for the ITT population was not reported and the ESS for the mITT population was 42 patients. In the ITT population for OS, cilta-cel was favoured over RWCP (HR = 0.14, 95% CI, 0.07 to 0.25). For TTNT, cilta-cel was also favoured over RWCP from Therapie Monitor (HR = 0.13; 95% CI, 0.07 to 0.24). Results for OS and TTNT in the mITT population were consistent with the ITT population; however, the 95% CIs were wider (OS HR = 0.26 [95% CI, 0.08 to 0.84]; TTNT HR = 0.24 [95% CI, 0.09 to 0.67]).
All analysis methods were appropriate and suggested similar results favouring cilta-cel over RWCP; however, the results of the present analysis were associated with uncertainty, given the reduced sample sizes, the lack of adjustment for potential confounding factors, the notable heterogeneity in patient populations that remained for 6 of 9 key variables after adjustment, and the wide 95% CIs, particularly for the mITT population, resulting in greater uncertainty of the results.
Meta-Analysis of Observational Studies24
A frequentist, random-effects meta-analysis of observational studies evaluating cilta-cel versus physicians’ choice of treatment was identified in the published literature.24 The studies included in the meta-analysis consisted of all studies summarized here and included publications for the comparison of CARTITUDE-1 with LocoMMotion, the Flatiron cohort, the daratumumab trial cohort, the MAMMOTH cohort, and the OIS database. Outcomes included OS, PFS, and ORR. No analyses of ORR were conducted in the all–index dates analyses.
In the ITT population, including all eligible index dates, the overall HR for cilta-cel compared with RWCP was 0.26 (95% CI, 0.15 to 0.47) for OS and 0.22 (95% CI, 0.1 to 0.49) for PFS. Results for the mITT population were consistent with the ITT population. The OR for ORR in the ITT population was 13.94 (95% CI, 4.88 to 39.84), while in the mITT population, the OR for ORR was 86.22 (95% CI, 17.96 to 413.88) in favour of cilta-cel.
While the comparisons of cilta-cel with external cohorts from multiple studies provided a large evidence base for comparison, there were important limitations in this evidence, including methodological differences across the data sources that could not be adjusted for in the analysis using propensity scores, and a risk of confounding (due to the inability to adjust for important prognostic factors and/or differences remaining in the distribution of prognostic factors across cohorts after adjustment). Pooling via meta-analysis could not overcome the limitations of the individual studies; rather, meta-analysis may compound the bias. Results of the included observational comparisons were consistently in favour of cilta-cel over RWCP for all outcomes assessed. Similarly, the results of the meta-analysis were in favour of cilta-cel for OS, PFS, and TTNT for both the all–index dates and first–index dates analyses in both the ITT and mITT populations and in all sensitivity analyses; however, the 95% CIs were often wide, suggesting some imprecision, unexplained heterogeneity, and uncertainty in the magnitude of the effects.
Conclusions
One sponsor-submitted phase Ib/II, single-arm, open-label trial (CARTITUDE-1) provided evidence regarding the efficacy and safety of cilta-cel for patients with r/rMM who had received at least 3 prior lines of therapy. This trial design is not intended to be confirmatory for efficacy. In general, the clinical experts consulted by CADTH considered the ORR results to be clinically meaningful, especially when compared with currently available therapies. The nonrandomized design of CARTITUDE-1 made interpreting the PFS and OS events attributable to cilta-cel challenging; according to the FDA, CARTITUDE-1 could not inform OS or PFS. The results for HRQoL remained inconclusive due to a number of important limitations. A phase I long-term LCAR-B38M trial (LEGEND-2), based only in China, showed similar findings. All patients experienced at least 1 AE, and almost half experienced an SAE. The clinical experts noted that, in their experience, cilta-cel appeared to be less toxic than other therapies available in the fourth line and beyond. They remarked that the proportion of patients who experienced grade 3 or greater CRS or ICANS and who would require specialized intensive care was relatively low.
The comparative evidence came from observational comparisons using IPD from CARTITUDE-1 and real-world cohorts using propensity scores to adjust for known confounders. Although cilta-cel was favoured for all outcomes assessed, these findings must be interpreted in the context of the methodological limitations of these studies. Propensity score methods can only adjust or match on known and measured confounders and cannot account for unknown, unmeasured, or unmeasurable confounders, nor for differences in study design across comparators. Tests for residual confounding were not conducted in any of the studies, so the results are at risk of bias due to confounding. The generalizability of the results may be limited, since patients in the comparator arms received treatments that are not currently standard of care in Canada.
Introduction
Disease Background
MM is a plasma cell cancer caused by the growth of cancer cells in the bone marrow. It was estimated that 4,000 people in Canada would be diagnosed with MM in 2022 and that 1,650 would die from MM, with slightly more cases occurring in men than women.2 While new therapies have been introduced that can improve a patient’s OS and PFS, MM remains an incurable condition.3 Some estimates suggest that the median survival for patients with MM is just more than 5 years and, during this time, patients can receive 4 lines of therapy or more.3-5 Median OS for patients with r/rMM is approximately 13 months.6
MM is a heterogenous condition typically affecting older adults around the age of 65 years, and patients’ outcomes can be dependent on many factors, including their disease stage, prognostic indicators, and early treatment of symptomatic disease to limit or avoid organ damage.25 Typically, when MM is suspected clinically in patients they are tested for the presence of M proteins, although a small proportion of patients (approximately 2%) may present without any evidence of M protein.26
Patients with MM will ultimately relapse, and progression is usually identified by a rise in M protein in the serum or urine or rise in serum free light chain ratio.5 The clinical experts consulted by CADTH for this review noted that these levels are usually assessed on a monthly basis following therapy to monitor for relapse. Other indications of relapse include development of CRAB symptoms (hypercalcemia, renal insufficiency, anemia, or new bone lesions) or extramedullary plasmacytomas.5
With respect to prognosis, the International Myeloma Working Group (IMWG) defines high-risk cytogenetic features to include at least 1 of the following:
t(4;14), t(14;16), t(14;20), del(17p), or gain (1q) detected by fluorescence in situ hybridization (FISH)
nonhyperdiploid karyotype, high-risk gene expression profile signature, and del(13) detected by conventional cytogenetics.
In addition, 2 clinical features are associated with aggressive disease: elevated lactate dehydrogenase (LDH) and evidence of circulating plasma cells on routine peripheral smear examination (plasma cell leukemia).27 The preferred staging system for MM is the Revised ISS, which uses serum beta2-microglobulin, serum albumin, serum LDH, and bone marrow FISH results to stratify patients into 3 risk groups:
stage I: beta2-microglobulin of less than 3.5 mg/L, serum albumin of 3.5g/dL or greater, normal LDH, and no del(17p), t(4;14), t(14;16) by FISH
stage II: neither stage I nor III
stage III: beta2-microglobulin of 5.5 mg/L or greater, elevated LDH, and/or del(17p), t(4;14), t(14;16) by FISH.27
IMWG defines r/rMM as disease that is “nonresponsive while on salvage therapy or progresses within 60 days of last therapy in patients who have achieved minimal response or better at some point previously before then progressing in their disease course.”28
Standards of Therapy
The treatment landscape for MM has changed significantly in the past number of years with the emergence of new therapies in newly diagnosed and r/rMM settings.3
According to the clinical experts, initial therapy for patients depends on whether they are eligible or ineligible for transplant at diagnosis. Initial treatment for patients who are eligible for transplant includes induction therapy for 4 months with cyclophosphamide, bortezomib, and cyclophosphamide-bortezomib-dexamethasone (CyBord), according to the clinical experts. Patients undergo induction followed by treatment with melphalan and SCT, followed by consolidation therapy with lenalidomide-bortezomib-dexamethasone in some jurisdictions (depending on local practices and funding). According to the clinical experts, patients then continue with lenalidomide maintenance therapy until disease progression, which is standard across all Canadian jurisdictions.
The clinical experts noted that for patients who are transplant-ineligible, daratumumab-lenalidomide-dexamethasone (DRd) is the most commonly used treatment; other treatment options include lenalidomide-bortezomib-dexamethasone, lenalidomide-dexamethasone, and CyBord, although CyBord is used less frequently in current practice due to approvals that include lenalidomide-based regimens. Daratumumab-based regimens, such as DRd or daratumumab-bortezomib-melphalan-prednisone, were stated to be expected to be used more frequently going forward due to recent positive recommendations from CADTH and funding approvals across jurisdictions. The clinical experts expected that daratumumab-based regimens would be the preferred front-line option, with DRd as the most likely choice.
The clinical experts noted that at relapse, treatment depends on patient factors, including age, comorbidities, and previous treatments. In the second-line treatment setting, a second transplant may be an option for transplant-eligible patients, although the clinical experts stated it is not a common approach because of available alternatives; however, patients with long responses to the first transplant will often be considered for a second transplant if their age and comorbidities are not contraindications. The clinical experts stated that most patients will receive a daratumumab-containing regimen, likely DRd or daratumumab-bortezomib-dexamethasone; patients whose disease is refractory to lenalidomide would usually receive daratumumab-bortezomib-dexamethasone, while those who previously received bortezomib would receive DRd. Current treatment practices suggest using bortezomib or another PI after treatment with lenalidomide.7 The clinical experts further noted that isatuximab-based regimens were another option for patients, especially for those who are not eligible for daratumumab-based regimens, but these are currently not funded in Canada. The clinical experts state that isatuximab-based regimens would likely not be effective for patients who progress on a daratumumab-based regimen.
The clinical experts stated that pomalidomide-based regimens were considered in the third or fourth line of therapy, which is in line with clinical guidelines.7 Regimens containing carfilzomib were acknowledged to be available to patients in the second line, although these regimens are typically reserved for relapse after daratumumab-based regimens in the third line or after. Other options in the fourth line of therapy and beyond include oral palliative chemotherapy or alkylating drugs such as cyclophosphamide. The clinical experts consulted by CADTH noted that belantamab mafodotin is another option that could be available to patients; however, this treatment is only available through special access and is not used frequently. In November 2022, the FDA requested the withdrawal of belantamab mafodotin from US markets based on the outcomes of the pivotal clinical trial (DREAMM-3), which did not meet the requirements of the US FDA Accelerated Approval regulations.8 Selinexor was recently reviewed by CADTH in combination with bortezomib and dexamethasone for the treatment of adult patients with MM who have received at least 1 prior therapy and received a recommendation for reimbursement with conditions; however, funding negotiations are still ongoing. The treatment practices described by the clinical experts also align with recommended regimens by National Comprehensive Cancer Network guidelines.29
Despite an array of therapies, MM remains an incurable disease and patients eventually relapse and their disease becomes refractory to available treatments.6 The clinical experts and clinician groups consulted by CADTH agreed there is an unmet need for treatments beyond the third line that prolong survival, delay disease progression, improve quality of life, and minimize side effects. The clinical experts consulted by CADTH also noted there is a need for treatments to be tolerable, especially for patients with comorbidities and to require a shorter treatment duration and a longer treatment-free interval to reduce the treatment burden on this heavily pretreated patient population with a limited lifespan.
Drug
Cilta-cel is a BCMA-directed genetically modified autologous CAR T-cell immunotherapy. This personalized cellular therapy uses the patient’s own T cells in a process that includes T-cell collection, genetic modification of cells, cell infusion, and patient follow-up.30 These T cells are activated upon binding to the targeted cells (cells expressing BCMA), resulting in their lysis.
Cilta-cel was first approved by the FDA on February 28, 2022, for the treatment of adult patients with r/rMM after 4 or more prior lines of therapy, including a PI, an IMiD, and an anti-CD38 monoclonal antibody. It was approved by the European Medicines Agency on March 24, 2022, for the treatment of adult patients with r/rMM who have received at least 3 prior therapies, including an IMiD, a PI, and an anti-CD38 antibody, and who have demonstrated disease progression on the last therapy. Of note, this CADTH Reimbursement Review was conducted before issuance of a Health Canada Notice of Compliance with Conditions and the scope was based on the anticipated indication. The anticipated indication and the sponsor’s initial reimbursement request was for the treatment of adult patients with r/rMM who have received at least 3 prior lines of therapy, including a PI, an IMiD, and an anti-CD38 antibody. Cilta-cel underwent review by Health Canada through advance consideration under its Notice of Compliance with Conditions Policy. The Notice of Compliance with Conditions was issued on February 9, 2023. The approved indication is for the treatment of adult patients with MM who have received at least 3 prior lines of therapy, including a PI, an IMiD, and an anti-CD38 antibody and whose disease is refractory to their last treatment.1 The sponsor’s final reimbursement request was as per the indication. Cilta-cel has not been previously reviewed by CADTH.
Cilta-cel is a single-dose, 1-time treatment in a patient-specific infusion bag containing a suspension of CAR-positive viable T cells. The dose is 0.5 × 106 to 1.0 × 106 CAR-positive viable T cells per kg of body weight, with a maximum dose of 1 × 108 CAR-positive viable T cells per single infusion. Cilta-cel should be administered by experienced health professionals at qualified treatment centres.1
Key characteristics of cilta-cel and other therapies in the fourth line and beyond, as indicated in CADTH’s provisional funding algorithm,31 are presented in Table 3.
Table 3: Key Characteristics of Cilta-Cel and Other Therapies in Fourth Line and Beyond
Characteristic | Cilta-cel | Selinexora | Proteasome inhibitors (carfilzomib) | Immunomodulatory drugs (pomalidomide) |
|---|---|---|---|---|
Mechanism of action | BCMA-directed genetically modified autologous CAR T-cell immunotherapy. | Selinexor is a compound that specifically blocks XPO1, a nuclear export protein that transports cargo proteins within the cell. XPO1 inhibition by selinexor leads to reduction of cancer cells. | Proteasome inhibition leads to accumulation of misfolded protein in ER, resulting in apoptosis and inhibition of cell proliferation. | Immunomodulatory and antineoplastic activity; inhibits proliferation and induces apoptosis of hematopoietic tumour cells. |
Indicationb | For the treatment of adult patients with MM, who have received at least 3 prior lines of therapy, including a PI, an IMiD and an anti-CD38 antibody, and whose disease is refractory to their last treatment. | In combination with bortezomib and dexamethasone for the treatment of adult patients with MM who have received at least 1 prior therapy. | Carfilzomib: In combination with dexamethasone alone (Kd), for patients relapsed MM who have received 3 prior lines of therapy. | Pomalidomide: In combination with dexamethasone for patients with MM for whom both bortezomib and lenalidomide have failed and who have received at least 2 prior regimens and demonstrated disease progression on the last regimen. |
Route of administration | IV infusion | Orally | IV infusion | Orally |
Recommended dose | Single infusion of 0.5 to 1.0 × 106 CAR-positive viable T cells per kg body weight | 100 mg once weekly Treatment continued until disease progression or unacceptable toxicity |
Treatment continued until disease progression or unacceptable toxicity | Pd: 4 mg once daily, days 1 to 21 of each 28-day cycle Treatment continued until disease progression or unacceptable toxicity |
Serious adverse effects or safety issues | Cytokine release syndrome, neurologic toxicities (including ICANS), hemophagocytic lymphohistiocytosis or macrophage activation syndrome. Cilta-cel should be administered by experienced health professionals at qualified treatment centres. | Fatigue, severe or life-threatening hyponatremia, nausea, vomiting, diarrhea, anorexia or weight loss, thrombocytopenia, neutropenia, infections, dizziness, cataracts | Infusion reactions, TLS Infections, cardiac disorders, venous thrombosis, hypertension, hemorrhage, thrombocytopenia, hepatoxicity, hepatitis B reactivation, posterior reversible encephalopathy syndrome, PML, acute renal failure, pulmonary toxicity | Neutropenia, thrombocytopenia, infections, DVT and PE, hepatoxicity, anaphylaxis, hepatitis B reactivation, severe rash (SJS, TEN, DRESS), TLS, teratogenic effects |
Other | None | Currently under negotiations | Premedication for carfilzomib recommended with dexamethasone (at least 30 minutes prior), to reduce incidence and severity of infusion reactions | Antithrombotic prophylaxis recommended |
BCMA = B-cell maturation antigen; CAR = chimeric antigen receptor; CD38 = cluster of differentiation 38; DRESS = drug rash with eosinophilia and systemic symptoms; DVT = deep venous thrombosis; ER = endoplasmic reticulum; ICANS = immune effector cell–associated neurotoxicity syndrome; IMiD = immunomodulatory drug; Kd = carfilzomib-dexamethasone; MM = multiple myeloma; Pd = pomalidomide-dexamethasone; PE = pulmonary embolism; PI = proteasome inhibitor; PML = progressive multifocal leukoencephalopathy; SJS = Stevens-Johnson syndrome; TEN = toxic epidermal necrolysis; TLS = tumour lysis syndrome; XPO1 = exportin 1.
aSelinexor received a recommendation for reimbursement with conditions from CADTH on July 29, 2022. Funding negotiations are still ongoing, and it has not yet been publicly funded.
bHealth Canada–approved indication.
Source: PrPomalyst product monograph,32 Carvykti™ product monograph,1 Xpovio Product Monograph,33 PrKrypolis® Product Monograph34 Canadian Pharmacists Association.35
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups. The full original patient input received by CADTH has been included in the stakeholder section at the end of this report.
One patient group, Myeloma Canada, provided input for the review of cilta-cel. Myeloma Canada supports Canadians with myeloma to access new and innovative therapies. Two online surveys were conducted by Myeloma Canada from August 28 to September 29, 2022. A total of 200 patients across Canada and outside of Canada (France and Trinidad and Tobago) provided complete responses to the patient survey (with some missing responses for each question). A total of 26 caregivers across Canada provided complete responses to the caregiver survey. All survey respondents were required to have relapsed or refractory myeloma, received at least 1 prior line of therapy, or been caring for a patient who met these criteria.
Patient respondents indicated that their ability to work was most significantly impacted by the symptoms associated with myeloma, followed by the ability to travel and exercise. Of note, patient respondents highlighted the significant impact that myeloma had on their mental health. A total of 34% of patient respondents identified travel cost as the most significant financial implication of treatment, followed by drug cost and parking cost (28% each), lost income due to absence from work or disability (27%), and lost income and pension due to early retirement (20%) (N = 198). The majority of patient respondents (58%) indicated they required support from a caregiver for the management of myeloma or treatment-related symptoms (N = 197).
From the perspective of the caregiver respondents, the ability to travel was most significantly impacted by caring for an individual with MM, followed by the ability to work and spend time with family and friends. According to caregiver respondents, drug cost was the most significant implication of caring for an individual who was receiving treatment for myeloma (46%), followed by parking cost (42%), and travel cost (39%) (N = 26).
Patient respondents (36%) reported experiencing some side effects associated with maintenance therapy after receiving SCT, while 29% of patient respondents reported significant side effects (N = 188). Furthermore, 50% of patient respondents reported some negative impact on their overall well-being and quality of life due to the side effects associated with maintenance therapy. Caregiver respondents (31%) reported some negative impact on their duties as a caregiver due to the side effects associated with maintenance therapy experienced by the individual whom they were caring for (N = 26).
One patient respondent reported experience with “ide-cel, bb2121” and 2 patient respondents reported experience with other CAR T-cell therapy, not specified. One patient indicated that the CAR T-cell therapy they received was extremely effective in helping to control their myeloma, was very effective in improving their quality of life, and the side effects were very tolerable. After receiving CAR T-cell therapy, the patient reported a treatment interruption period of 1 to 3 months, which was somewhat important to them. Overall, the patient indicated the CAR T-cell therapy met their expectations in the treatment of their myeloma. The 1 other patient respondent indicated they were awaiting to receive their CAR T-cell therapy in fall 2022.
One patient and 1 caregiver respondent reported experience with cilta-cel. The patient indicated that they received treatment with cilta-cel once in 2015 and once in 2021, and their myeloma had relapsed, and they were currently receiving a new treatment. After receiving cilta-cel, their treatment interruption period (i.e., period when they did not require any drugs to control disease) was 4 to 7 months, which was somewhat important to the patient. The patient indicated cilta-cel was effective in helping to control their myeloma, and its associated side effects were tolerable. According to the patient, the following associated side effects were bearable: thrombocytopenia, neutropenia, neuropathy, nausea, leukopenia, lymphopenia, diarrhea, constipation, and anemia. Overall, the patient felt that treatment with cilta-cel improved their quality of life and met their expectations in the treatment of their myeloma.
The caregiver respondent indicated that the patient they cared for received cilta-cel less than 3 months ago and was currently in remission. After receiving cilta-cel, the patient’s treatment interruption period was 1 to 3 months, which was extremely important to the caregiver. The caregiver indicated that cilta-cel was extremely effective in helping to control the myeloma and felt less care was required as their caregiver. According to the caregiver, the following associated side effects were difficult to care for: CRS, neurotoxicity, thrombocytopenia, neutropenia, neuropathy, lymphopenia, diarrhea, and constipation.
Of the patient respondents without experience with CAR T-cell therapy, 27% received 3 lines of therapy, 23% received 2 lines of therapy, 18% received 1 line of therapy, 20% received 4 or more lines of therapy, and 12% were uncertain (N = 197). In response to the risk associated with waiting for modified T cells to be reintroduced when preparing to receive CAR T-cell therapy, most patient respondents (40%) without experience with CAR T-cell therapy indicated they would be concerned that their myeloma would relapse but they can live with the wait, while 30% indicated they would be willing to take the risk, 27% were uncertain and would discuss with their health care provider, and 1% would be unwilling to take the risk (N = 145). With respect to the side effects associated with cilta-cel, the survey respondents who did not have experience with CAR T-cell therapy felt that CRS would be the most troublesome side effect, followed by neutropenia, fever, and neuropathy. Among the patient respondents without experience with CAR T-cell therapy, 26% would consider cilta-cel as their next treatment option; 50% were uncertain (N = 145). These patient respondents further highlighted the importance of not having to continue with ongoing treatment after receiving CAR T-cell therapy despite the associated risks.
The patient respondents identified infections as the most important aspect of myeloma to control. They further indicated that mobility and kidney problems were aspects of myeloma that were important to control. Patient respondents reported that future treatment for MM should improve quality of life, have tolerable side effects, achieve remission, and extend survival without the need for continuous treatment. Patient respondents also highlighted the need for accessibility and portability of treatments and a supportive and communicative care team. Patient respondents further noted the importance of access to alternative newer treatments and minimal trips to the hospital or community treatment centre. Of the respondents who reported no experience with CAR T-cell therapy, 74% of patients (N = 143) and 60% of caregivers (N = 15) indicated that an estimated minimum of 1 to 2 years of extended life without requiring any drugs to control myeloma was extremely desirable; 2 patients indicated this was not desirable. Of note, this desirability is dependent on the severity of side effects and quality of the extended life.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). In addition, as part of the cilta-cel review, a panel of 3 clinical experts from across Canada was convened to characterize unmet therapeutic needs, assist in identifying and communicating situations where there are gaps in the evidence that could be addressed through the collection of additional data, promote the early identification of potential implementation challenges, gain further insight into the clinical management of patients living with a condition, and explore the potential place in therapy of the drug (e.g., potential reimbursement conditions). A summary of this panel discussion is also presented subsequently.
Unmet Needs
The clinical experts highlighted that the most important goals of treatment for patients with r/rMM are prolonging survival, delaying disease progression, improving quality of life, and minimizing side effects. Treatments for r/rMM are changing rapidly, and the treatment regimens vary across treatment centres in Canada, depending on drug availability. After diagnosis with MM, the lines of therapy that patients will go through depend on whether or not they are transplant-eligible. Front-line therapy determines which therapies are selected for the subsequent lines of therapy, as patients’ disease becomes increasingly refractory to treatment options as patients proceed through treatment lines. Choice of therapy also depends on the patients’ functional status and comorbidities, for example, carfilzomib may not be a good choice for patients with cardiac issues. The clinical experts noted that clinicians try not to reuse the same drugs in subsequent lines of therapy. Therefore, after 3 lines of therapy, the majority of patients will be triple-refractory and will need new families of drugs such as selinexor or antibody drug conjugates (belantamab mafodotin), which are not currently funded in Canada (selinexor in combination with bortezomib and dexamethasone has recently received a recommendation for reimbursement with conditions from CADTH. The price is currently being negotiated and belantamab mafodotin is available through compassionate patient access). There is a need for treatments beyond the third line that are tolerable for patients with comorbidities. The clinical experts also noted that it is beneficial for any treatment to require a shorter treatment duration and lead to a longer treatment-free interval to reduce the treatment burden on this heavily pretreated patient population with a limited lifespan.
The clinical experts also highlighted that patients’ immune systems become weaker after multiple lines of therapy, thereby creating a need for therapies that are tolerated in later lines of therapy. As well, the experts noted that from the time of diagnosis, patients with high-risk disease have poor responses to treatment, which is worsened in the relapsed–refractory setting. Therefore, there is a great need for therapies that show some improved activity in people with high-risk disease. Patients who relapse quickly after prior lines of therapy (e.g., < 2 years) are also likely to have a very poor prognosis and thus are in great need of a novel intervention.
Place in Therapy
The clinical experts agreed that the majority of patients with r/rMM would eventually be eligible for cilta-cel, with the exception of those patients who will have died before reaching the fourth line or who will be ineligible for CAR T-cell therapy due to severe disease progression or poor functional status. The clinical experts noted that the major barrier to uptake would be capacity, as the demand for CAR T-cell therapy may be greater than the existing capacity in Canada. The clinical experts anticipated that the demand for cilta-cel for the present indication may exceed the demand for CAR T-cell therapy for patients with relapsed or refractory large B-cell lymphoma because these patients often relapse aggressively with progression that is harder to control; whereas, for patients with MM, the relapse is slower and easier to predict and control.
Patient Population
The clinical experts noted that the CARTITUDE-1 trial enrolled a broad sample of patients with r/rMM, including older patients and patients with multiple prior lines of therapy. Eligible patients would include those who have “adequate organ” function to be able to tolerate cytokine release syndrome and ICANS (definition of adequate organ function should be broad and left to the discretion of the treating centres) and who have a good ECOG PS (i.e., ≤ 2). The experts noted it would be difficult to limit cilta-cel treatment by specific patient or disease characteristics, because even patients in high-risk groups (e.g., high cytogenetic risk) appeared to benefit in the CARTITUDE-1 trial. In the absence of sufficient evidence to guide patient selection for cilta-cel treatment, the experts suggested that patients who have a short life expectancy (< 2 months), have poorly controlled PD, are unable to move to a larger centre for 1 month, or have poor functional status (ECOG > 2) may not be suitable for cilta-cel. It was also noted by the clinical experts that some patients may have a contraindication to cilta-cel, for example, patients with poor renal function may be less tolerant to CRS.
Assessing Response to Treatment
The clinical experts reported that response to treatment is typically assessed by regular monitoring that is part of the management of patients with r/rMM. This includes biochemical measurement once a month of M proteins or free light chain ratios and imaging such as PET scans that is performed less frequently. The experts noted that response is typically assessed monthly, at first. In stable patients, intervals between response assessments may be extended to every 2 to 3 months. The clinical experts defined clinically meaningful response to treatment as a durable response that is better than PR, a reduction in the severity of disease symptoms (e.g., fatigue, breathlessness), and PFS that is at least 12 months in duration. The experts agreed that, with current treatments beyond the third line, the average duration of PFS is approximately 9 to 12 months.
Discontinuing Treatment
The clinical experts noted that in some rare cases, patients may go through pre-treatment (i.e., apheresis and conditioning chemotherapy) but not receive cilta-cel. This may be due to manufacturing issues (which would be unusual), or unexpected clinical deterioration, such as severe infection. In these cases, the patients would receive supportive care until the acute crisis is resolved. If patients were to deteriorate substantially between apheresis and time of infusion, one may not proceed with cilta-cel infusion.
The clinical experts reported that for patients who relapse following CAR T-cell therapy, the subsequent therapy would depend on which therapies the patient had already received. However, the experts acknowledge that almost half of these patients may not be eligible for any subsequent therapy due to poor functional status or rapidly progressing disease and would only receive supportive care. The clinical experts noted that some patients may be eligible for enrolment in clinical trials.
Prescribing Conditions
The clinical experts reported that cilta-cel treatment can be provided by oncologists or hematologists in a specialized setting that has adequate infrastructure for cell therapy and access to excellent clinical support and multidisciplinary care, including critical and specialist care (e.g., intensive care unit, neurology, nephrology) to manage toxicities, as well as laboratory support to handle and process samples. They noted that it would be especially important to be in a setting where CRS would be quickly diagnosed and managed. The clinical experts discussed that eventually, after years of experience with CAR T-cell therapy, there may be potential for providing cilta-cel in an outpatient setting, but this is not currently a viable option.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups. The full original clinician group inputs received by CADTH have been included in the stakeholder section at the end of this report.
Two clinician groups provided input for the review of cilta-cel: CMRG, represented by 20 clinicians, and Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee, represented by 1 clinician. The CMRG is a Canada-wide network of researchers aiming to develop better treatments for extending life of patients with myeloma, enhancing the quality of life for those living with myeloma and related disorders, and working to find a cure for these diseases and other plasma cell disorders. The Ontario Health (Cancer Care Ontario) Drug Advisory Committees provide evidence-based clinician and health system guidance on drug-related issues in support of Cancer Care Ontario’s mandate.
Unmet Needs
Both clinician groups identified the following treatment goals:
control the disease and its associated sequalae (i.e., bone destruction and pain, renal failure, hypercalcemia, and low blood counts) by achieving an antimyeloma response
maintain control of myeloma and its manifestations for as long as possible (i.e., maximize PFS)
improve OS.
Additional treatment goals identified by the CMRG included:
minimize adverse effects of treatment
optimize quality of life by adequately controlling the disease and minimizing toxicity with the aim to tailor the treatment approach to the individual patient.
According to the CMRG, fourth-line treatment options are limited. A pomalidomide- or carfilzomib-based regimen may be used if it was not used in third line. A regimen of bortezomib plus steroids may be used; however, it is associated with a short PFS and cannot be revisited in many jurisdictions if the patient is refractory to PIs. Cyclophosphamide can be added to many regimens or used with steroids as a doublet therapy; however, the cumulative lifetime exposure to cyclophosphamide in a patient is limited to 1 to 2 years due to its associated risks. This risk may further restrict the use of alternative alkylating drugs such as melphalan. As such, palliation, best supportive care, and local radiotherapy are often pursued within the context of the publicly funded system. Additional treatment options in Ontario identified by the Hematology Cancer Drug Advisory Committee were Special Access Program drugs (i.e., selinexor-dexamethasone, with or without bortezomib or belantamab). Of note, the CMRG indicated that antibody drug conjugates, bispecific antibodies, and cellular therapy that are directed against BCMA on myeloma cells are positioned to fill the triple class–exposed or refractory space but are not currently available in Canada.
The CMRG emphasized that myeloma remains incurable, and patients eventually become refractory to all available funded drugs. The clinician group further highlighted the most important unmet need is in patients with advanced disease who have received multiple lines of treatment and received the 3 major classes of drugs (triple-class–exposed or triple-class–refractory disease), including a PI, an IMiD, and an anti-CD38 antibody. Advanced disease progression and short DOR can lead to poor quality of life, advanced caregiver burden, and a shortened lifespan. The Hematology Cancer Drug Advisory Committee further indicated that the low response rate associated with currently available treatment options is an unmet need.
Place in Therapy
The CMRG advocated for cilta-cel to be used in patients with triple class–exposed or triple class–refractory myeloma, with cilta-cel to be used in sequence after other lines of therapy (i.e., after failure of multiple drugs). Consequently, cilta-cel is not expected to impact the sequencing of drugs earlier in the disease course or lead to a major change in the treatment algorithms before patients becoming triple-refractory. Instead, cilta-cel is expected to lead to a major shift in the current treatment paradigm for patients with advanced MM disease who previously received 3 lines of therapy. The Hematology Cancer Drug Advisory Committee suggested cilta-cel would fit into the current treatment paradigm, as per the clinical trial.
Patient Population
The CMRG suggested that the least suitable patients for treatment with cilta-cel would be frail, with rapidly proliferating disease, ongoing infection, significant organ dysfunction, and/or pre-existing pancytopenia. Patients whose disease is progressing at a rate anticipated to allow them to remain stable and relatively well during the 4- to 5-week period required for CAR T-cell processing would be the best suited for this treatment to avoid death before cell therapy product delivery. The Hematology Cancer Drug Advisory Committee suggested that patients with an ECOG PS of 0 to 2 and acceptable comorbidities would be the best suited for this treatment. The CMRG further suggested that patients with good PS, minimal or no comorbidities, low tumour burden, and adequate organ function and blood counts would be the most likely to have the best outcomes. Of note, the CMRG indicated that patients with other disease-related adverse prognostic factors, such as extramedullary disease and high-risk cytogenetics, do not fare significantly worse and should be eligible for cilta-cel.
Assessing Response to Treatment
The CMRG indicated that response to treatment is based on the M protein marker in the serum and/or urine, bone marrow biopsy and, in some instances, imaging studies; the MRD is an emerging parameter. The Hematology Cancer Drug Advisory Committee indicated that improved survival, disease control, and symptom improvement are used to determine treatment response. The CMRG indicated that a clinically meaningful response correlates with at least a partial remission per the IMWG consensus criteria (i.e., improvement in symptoms, energy, and ability to perform activities of daily living). The CMRG stated that responses are typically assessed every 1 to 3 months depending on clinical stability and treatment regimen used.
Discontinuing Treatment
Considerations regarding drug discontinuation are not applicable in the context of a single infusion of cilta-cel. Both clinician groups suggested that a major medical facility, tertiary hospital, or transplant centre with expertise in cellular therapies for hematologic malignancies is an appropriate setting for treatment with cilta-cel.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
If capacity limitations exist, how would you prioritize which patients should be offered cilta-cel? | The clinical experts acknowledge this is a difficult question, as all patients are likely to benefit from this therapy. They agree that 1 important factor is to determine which patients would have the best, most durable response to treatment. In the absence of sufficient evidence to guide patient selection for cilta-cel treatment, the experts suggested that patients who have a short life expectancy (< 2 months), poorly controlled progressive disease, are unable to move to a larger centre for 1 month, or who have poor functional status (ECOG > 2), may not be suitable for cilta-cel. The clinical experts noted that the major barrier to uptake would be capacity, as the demand for CAR T-cell therapy may be greater than the existing capacity in Canada. There was some disagreement on whether or not patients in cytogenetic high-risk groups should be prioritized for cilta-cel, as they have lower efficacy results but are less likely to benefit from other therapies. |
Similar to other CAR T-cell products wherein CADTH recommended only a 1-time dose, is there sufficient evidence to support re-treatment? If there is sufficient evidence, what is the minimum time interval between the first dose and the re-treatment dose? | Only 3 patients were re-treated with cilta-cel in the CARTITUDE-1 trial; thus, there is not enough information to draw conclusions regarding re-treatment. The clinical experts agreed there is insufficient evidence to support re-treatment. |
According to the inclusion criteria of the CARTITUDE-1 trial, patients had to have an ECOG Performance Status of 0 or 1. Should cilta-cel be used in patients with an ECOG Performance Status > 1? | The clinical experts felt it would be reasonable to generalize the CARTITUDE-1 results to patients with an ECOG Performance Status of 2. |
Is there a time-limited need to consider patients who were not able to access anti-CD38 (e.g., patients previously treated with the RVd regimen whose disease ended up being refractory to both lenalidomide and bortezomib)? | The clinical experts agreed it is important to include those patients who have not had the 3 families of treatment due to issues with access. The clinical experts noted they would not expect outcome of cilta-cel to be inferior in these patients compared with patients who met the CARTITUDE-1 eligibility criteria. |
Is it safe to administer cilta-cel in the outpatient setting?
| The clinical experts agreed it was safest to administer cilta-cel in a specialized, inpatient setting. They noted that eventually (with time and experience) it may be possible to identify patients who are less likely to develop severe complications such as grade 3 or 4 cytokine release syndrome, and that those patients may be treated in an outpatient setting such as those programs already in place for complex, malignant hematology for patients with acute leukemia that have resources similar to a transplant program that provide outpatient autologous transplant. |
CAR = chimeric antigen receptor; CD = cluster of differentiation; cilta-cel = ciltacabtagene autoleucel; ECOG = Eastern Cooperative Oncology Group; ICU = intensive care unit; RVd = lenalidomide-bortezomib-dexamethasone.
Clinical Evidence
The clinical evidence included in the review of cilta-cel is presented in 3 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor and indirect evidence selected from the literature that met the selection criteria specified in the review. The third section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review. Of note, no indirect evidence was submitted by the sponsor or identified in the literature that met the eligibility criteria for the review; however, estimates of the comparative efficacy of cilta-cel relative to physicians’ choice of treatment were available from the observational studies submitted by the sponsor and identified in the literature.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of cilta-cel cell suspension for IV infusion, 0.5 × 106 to 1.0 × 106 CAR-positive viable T cells per kg body weight (maximum 1 × 108 CAR-positive viable T cells) for the treatment of adult patients with r/rMM, who have received at least 3 prior lines of therapy including a PI, an IMiD, and an anti-CD38 antibody.
Methods
Studies selected for inclusion in the systematic review include pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 5. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Of note, the systematic review protocol presented subsequently was established before the granting of a Notice of Compliance from Health Canada.
Table 5: Inclusion Criteria for the Systematic Review
Critieria | Description |
|---|---|
Patient population | Adult patients with relapsed or refractory multiple myeloma who have received at least 3 prior lines of therapy, including a proteasome inhibitor, an immunomodulatory drug, and an anti-CD38 antibody Subgroups:
|
Intervention | Ciltacabtagene autoleucel (cilta-cel) cell suspension for IV infusion, 0.5 × 106 to 1.0 × 106 CAR-positive viable T cells per kg body weight (maximum 1 × 108 CAR-positive viable T cells) |
Comparators | A combination of 1 or more of the following:
|
Outcomes | Efficacy outcomes
Harms outcomes
|
Study design | Published and unpublished phase II, III, or IV trials |
AE = adverse event; CAR = chimeric antigen receptor; CD = cluster of differentiation; HRQoL = health-related quality of life; ICU = intensive care unit; SAE = serious adverse event, WDAE = withdrawal due to adverse event.
aSelinexor received a recommendation for reimbursement with conditions from CADTH on July 29, 2022. It is currently under negotiations and has not been publicly funded yet.
The literature search was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.36
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Published literature was identified by searching the following bibliographic databases: MEDLINE All via Ovid and Embase via Ovid. All Ovid searches were run simultaneously as a multifile search. Duplicates were removed first using Ovid deduplication for multifile searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was cilta-cel. The clinical trials registries searched were the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. See Appendix 1 for the detailed search strategies.
The initial search was completed on October 24, 2022. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee (pERC) on March 8, 2023.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool for Searching Health-Related Grey Literature checklist.37 Included in this search were the websites of regulatory agencies (FDA and European Medicines Agency). Google was used to search for additional internet-based materials. See Appendix 1 for more information on the grey literature search strategy.
A focused literature search for indirect treatment comparisons (ITCs) dealing with MM was run in MEDLINE All on October 24, 2022. No limits were applied to the search.
Findings From the Literature
A total of 2 studies were identified from the literature for inclusion in the systematic review (Figure 1). A list of excluded studies is presented in Appendix 2.
Table 6: Details of Included Studies
Detail | CARTITUDE-1 |
|---|---|
Designs and populations | |
Study design | Phase Ib/II, open-label, multicentre study |
Locations | US (16 centres) and Japan (4 centres) |
Patient enrolment dates |
|
Data cut-off dates |
|
Enrolled (N) | 113 (received apheresis) |
Treated (N) | 97 |
Main inclusion criteria |
|
Main exclusion criteria |
|
Drugs | |
Intervention |
|
Comparator(s) | None |
Duration | |
Phase | |
Screening | Within 28 days of apheresis |
Apheresis | On day of enrolment |
Conditioning regimen | Day −7 to day −5 |
Infusion | Day 1 |
Follow-up |
|
Outcomes | |
Primary end point | ORR: Proportion of patients who achieve a partial response or better according to the IMWG response criteria, as assessed via IRC |
Secondary and Exploratory end points | Secondary end points:
Exploratory end points:
|
Safety end points |
|
Notes | |
Publications | Cohen et al. (2022),39 Berdeja et al. (2021),30 Martin et al. (2022),40 Martin et al. (2022),12 Cohen et al. (2022),41 Ri et al. (2022)42 |
AE = adverse event; BCMA = B-cell maturation antigen; CAR = chimeric antigen receptor; CD = cluster of differentiation; cilta-cel = ciltacabtagene autoleucel; CR = complete response; CRS = cytokine release syndrome; ECOG = Eastern Cooperative Oncology Group; EORTC = European Organisation for Research and Treatment of Cancer; EQ-5D-5L = 5-level EQ-5D; HRQoL = health-related quality of life; IMiD = immunomodulatory drug; IMWG = International Myeloma Working Group; IRC = independent review committee; LPD = last patient dosed; MM = multiple myeloma; NYHA = New York Heart Association; ORR = overall response rate; PBMC = peripheral blood mononuclear cells; PD = progressive disease; PGIC = Patient Global Impression of Change; PGIS = Patient Global Impression of Severity; PI = proteasome inhibitor; QLQ-C30 = Quality of Life Questionnaire Core 30; QLQ-MY20 = Quality of Life Questionnaire Myeloma Module; SAE = serious adverse event; sCR = stringent complete response; VGPR = very good partial response.
Source: CARTITUDE-1 Clinical Study Report.11
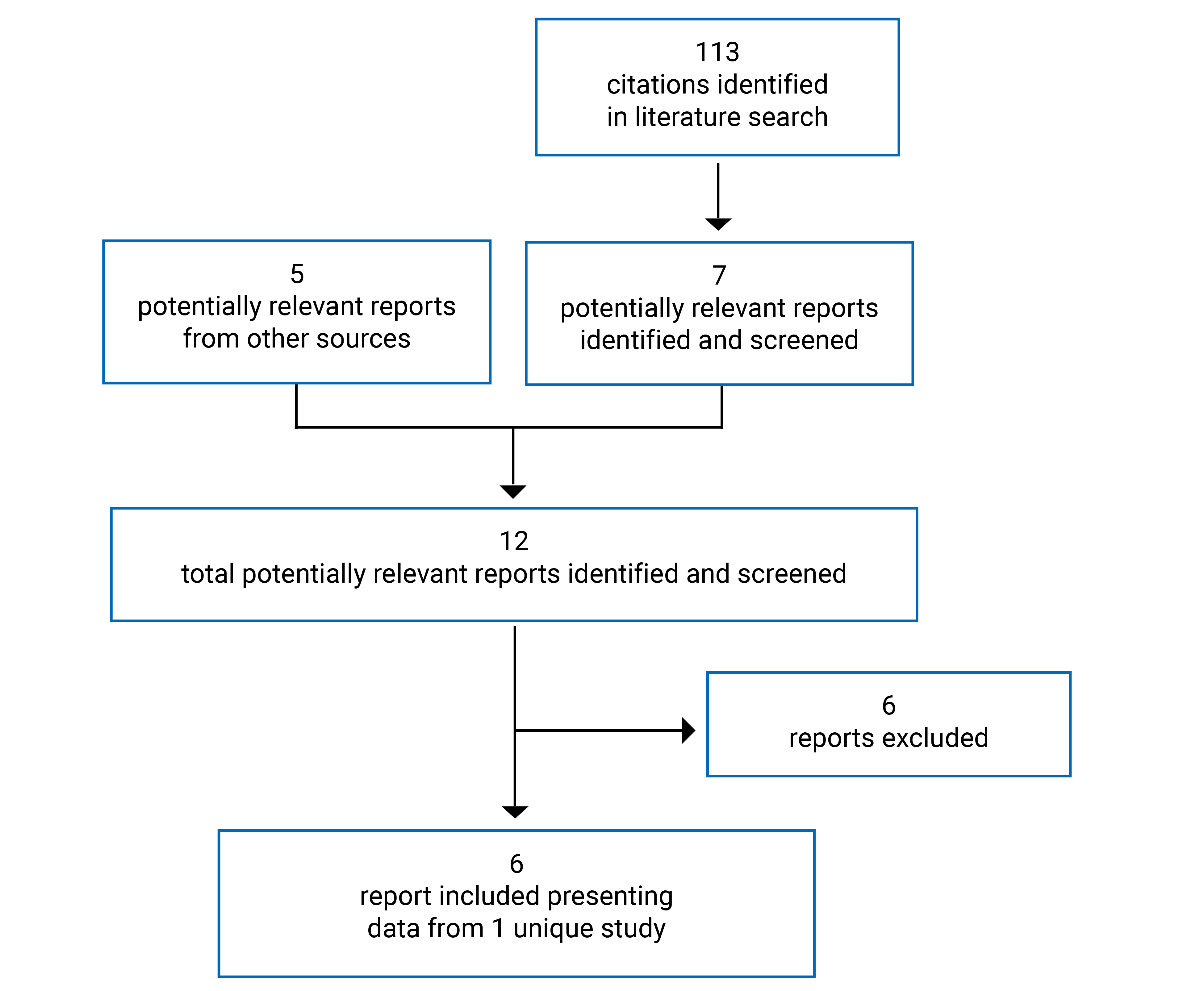
Description of Studies
CARTITUDE-1 is a phase Ib/II, single-arm clinical trial (N = 113) of cilta-cel in patients with r/rMM who have received at least 3 prior lines of therapy, including a PI, an IMiD, and an anti-CD38 antibody. In the trial, 97 patients received the full conditioning regimen followed by cilta-cel infusion. The main cohort described throughout this review included 113 enrolled patients and was conducted in 16 sites in the US.
The primary objective for the phase Ib study was to characterize the safety of cilta-cel and confirm the recommended phase II dose. The primary objective for the phase II study was to evaluate the efficacy of cilta-cel through ORR (PR or better) as assessed by an IRC. Secondary outcomes included VGPR or better rate, DOR, MRD negativity rate, TTR, PFS, OS, and HRQoL assessments. An exploratory objective was to characterize the impact of the treatment process on health care resource utilization. The study was funded by Janssen Research & Development. Patients were enrolled from 17 sites in the US. An additional cohort of patients from 4 sites in Japan was enrolled after the global program concluded, referred to as the Japanese cohort. No Canadian sites were included.
After enrolment, patients underwent apheresis, received conditioning treatment, and then received the cilta-cel infusion. Patients were followed up on days 3, 7, 10, 14, 21, 28, 42, 56, 78, and 100. After day 101, they were followed up every 28 days until study completion, defined as 2 years after the last patient has received their initial dose. AEs were reported until 100 days after last administration of any study treatment or until the start of subsequent systemic anticancer therapy if earlier. AEs that were considered to be related to study drug after 100 days, were reported until the end of the study. Long-term follow-up would continue for up to 15 years in a follow-up study.
A summary of the design of the CARTITUDE-1 study is shown in Figure 2. There were 4 Clinical Study Reports provided in the sponsor’s submission: a primary analysis report with a clinical data cut-off date of September 1, 2020,9 safety and efficacy update reports with a clinical data cut-off date of February 11, 2021,10 and a final analysis report with a clinical data cut-off date of January 11, 2022.11 Unless otherwise specified, the data presented are from the final Clinical Study Report with a data cut-off date of January 11, 2022, as findings were generally consistent over time.
Populations
Inclusion and Exclusion Criteria
Key inclusion and exclusion criteria for the CARTITUDE-1 study are shown in Table 66. Adult patients (aged ≥ 18 years) with a documented diagnosis of MM and documented disease progression were eligible if they had received at least 3 prior lines of therapy or were double refractory to a PI and an IMiD, and received a PI, an IMiD, and an anti-CD38 antibody. Patients were eligible if they had an ECOG PS of 0 or 1 and creatinine clearance of 40 mL/min/1.73 m2 or greater. Patients who had undergone prior treatment with CAR T-cell therapy, any therapy targeted to BCMA, or prior antitumour therapy were excluded, as were most patients diagnosed or treated for invasive malignancies other than MM. Patients with cardiac conditions within 6 months of enrolment were also excluded.
Figure 2: Schematic Overview of the Study Flow Chart
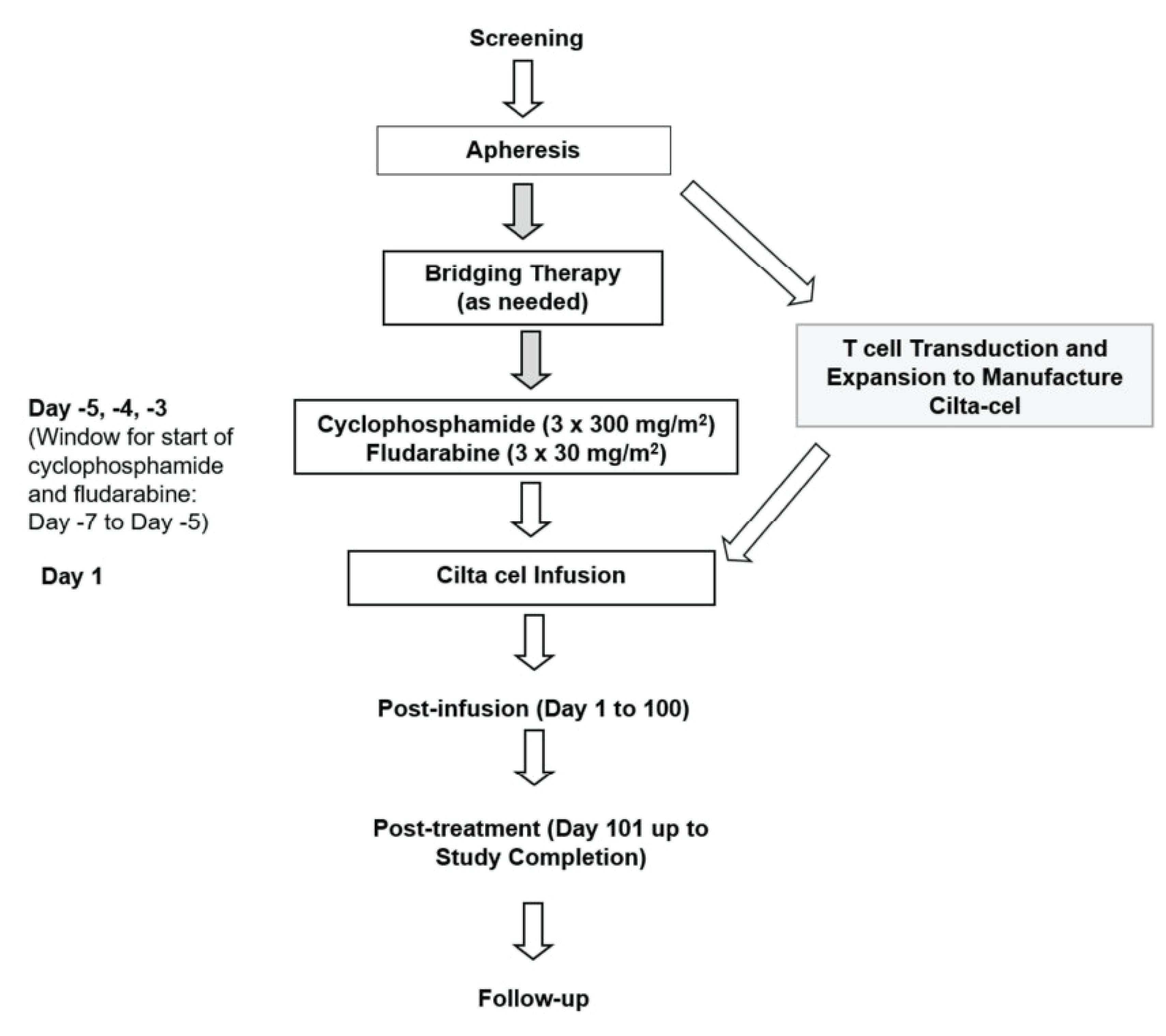
Cilta cel = ciltacabtagene autoleucel.
Source: CARTITUDE-1 Clinical Study Report.11
Baseline Characteristics
The baseline demographic and disease characteristics of all patients who received cilta-cel are presented in Table 7. The mean age of patients was 62 years (SD = 8.4 years), and the majority were younger than 65 years (62; 64%), male (57 patients; 59%), and white (69 patients; 71%), with an ECOG PS of 1 (54 patients; 56%) at infusion and ISS stage I at baseline (61 patients; 63%). With regard to cytogenetic risk, 23 patients (24%) were high risk at baseline. The majority of patients had received a prior transplant (87 patients; 90%). All patients received at least 3 prior lines of MM therapy with a median of 6 prior lines (range, 3 to 18), and approximately half had received more than 5 lines of therapy (49 patients; 51%). Prior to enrolment, all patients received a PI, an IMiD, and an anti-CD38 antibody therapy. The most common antineoplastic drugs used were daratumumab in 94 patients (97%) and bortezomib in 92 patients (95%), and the most common IMiDs used were lenalidomide in 96 patients (99%) and pomalidomide in 89 patients (92%).
Table 7: Summary of Baseline Characteristics (All-Treated Analysis Set)
Characteristic | CARTITUDE-1 (N = 97) |
|---|---|
Age, mean (SD), years | 62.0 (8.38) |
< 65 | 62 (63.9) |
65 to 75 | 27 (27.8) |
> 75 | 8 (8.2) |
Sex, male, n (%) | 57 (58.8) |
Race, n (%) | |
American Indian or Alaska Native | 1 (1.0) |
Asian | 1 (1.0) |
Black or African American | 17 (17.5) |
Native Hawaiian or Other Pacific Islander | 1 (1.0) |
White | 69 (71.1) |
Other | 8 (8.2) |
Weight, mean (SD), kg | 79.2 (16.69) |
ECOG Performance Status,a n (%) | |
0 | 39 (40.2) |
1 | 54 (55.7) |
2 | 4 (4.1) |
Type of myeloma by immunofixation, n (%) | |
Immunoglobulin G | 57 (58.8) |
Immunoglobulin A | 8 (8.2) |
Immunoglobulin M | 2 (2.1) |
Immunoglobulin D | 2 (2.1) |
Light chain | 24 (24.7) |
Kappa | 15 (15.5) |
Lambda | 9 (9.3) |
Biclonal | 4 (4.1) |
Type of measurable disease, n (%) | |
Serum only | 49 (50.5) |
Serum and urine | 6 (6.2) |
Urine only | 11 (11.3) |
Serum FLC only | 30 (30.9) |
Not evaluable | 1 (1.0) |
ISS staging at study baseline,b n (%) | |
I | 61 (62.9) |
II | 22 (22.7) |
III | 14 (14.4) |
Time since initial MM diagnosis to enrolment, years | |
Mean (SD) | 6.82 (3.617) |
Median (range) | 5.94 (1.6 to 18.2) |
Number of lytic bone lesions, n (%) | |
None | 28 (28.9) |
1 to 3 | 18 (18.6) |
4 to 10 | 15 (15.5) |
> 10 | 36 (37.1) |
Extramedullary plasmacytomas present, n (%) | 13 (13.4) |
% Plasma cells, bone marrow biopsy or aspirate,c n (%) | |
≤ 30 | 58 (60.4) |
> 30 to < 60 | 17 (17.7) |
≥ 60 | 21 (21.9) |
Bone marrow cellularity by biopsy, n (%) | |
Hypercellular | 25 (29.4) |
Normocellular | 35 (41.2) |
Hypocellular | 16 (18.8) |
Indeterminate | 9 (10.6) |
Cytogenetic risk at study baseline,d n (%) | |
Standard risk | 68 (70.1) |
High risk | 23 (23.7) |
Del(17p) | 19 (19.6) |
T(4;14) | 3 (3.1) |
T(14;16) | 2 (2.1) |
Unknown | 6 (6.2) |
Tumour BCMA expression (%), mean (SD) | 76.3 (16.44) |
Patients with 1 or more neurological history, n (%) | 72 (74.2) |
Prior therapy, n (%) | |
Prior transplant | 87 (89.7) |
Autologous | 87 (89.7) |
Allogenic | 8 (8.2) |
Number of lines of prior therapies, mean (SD) | ||| |||||| |
Median (range) | 6 (3 to 18) |
Category | |
3 | 17 (17.5) |
4 | || |||||| |
5 | || |||||| |
> 5 | 49 (50.5) |
Prior therapy | |
Dexamethasone | 97 (100) |
Lenalidomide | 96 (99.0) |
Daratumumab | 94 (96.9) |
Bortezomib | 92 (94.8) |
Pomalidomide | 89 (91.8) |
Carfilzomib | 83 (85.6) |
Melphalan | 80 (82.5) |
Cyclophosphamide | 63 (64.9) |
Ixazomib | 29 (29.9) |
Etoposide | 28 (28.9) |
Doxorubicin | 27 (27.8) |
Cisplatin | 24 (24.7) |
Elotuzumab | 23 (23.7) |
Thalidomide | 21 (21.6) |
BCMA = B-cell maturation antigen; ECOG = Eastern Cooperative Oncology Group; FISH = fluorescence in situ hybridization; FLC = free light chain; ISS = International Staging System; MM = multiple myeloma; SD = standard deviation.
aLast nonmissing ECOG Performance Status score on or before date of cilta-cel infusion (all patients met the inclusion criterion of ECOG Performance Status 0 or 1 during screening).
bISS staging was derived based on serum beta2-microglobulin and albumin.
cMaximum value from bone marrow biopsy and bone marrow aspirate was selected if both results were available. There was 1 patient with a nonevaluable bone marrow biopsy or /aspirate.
dCytogenic risk abnormalities were based on central FISH testing or local FISH and karyotype testing if central FISH was not available.
Source: CARTITUDE-1 Clinical Study Report.11
Refractory Status
A summary of refractory status to prior MM therapies is presented in Table 8. Almost all patients (96 patients; 99%) had disease that was refractory to the last line of prior therapy, and 85 patients (88%) had disease that was triple-refractory (i.e., refractory to the 3 major classes of therapeutic drugs [PI, IMiD, and anti-CD38 monoclonal antibody]). Forty-one patients (42.3%) were refractory to 5 or more drugs.
Table 8: Summary of Refractory Status to Prior MM Therapy (All-Treated Analysis Set)
Refractory status | CARTITUDE-1 (N = 97) |
|---|---|
PI + IMiD + anti-CD38 antibody, n (%) | 85 (87.6) |
Any PI, n (%) | 87 (89.7) |
Any IMiD, n (%) | 95 (97.9) |
Any anti-CD38 antibody, n (%) | 96 (99.0) |
At least 2 PIs + at least 2 IMiDs + 1 anti-CD38 antibody, n (%) | 41 (42.3) |
Refractory to last line of prior therapy, n (%) | 96 (99.0) |
Refractory to, n (%) | |
Bortezomib | 66 (68.0) |
Carfilzomib | 63 (64.9) |
Ixazomib | 27 (27.8) |
Lenalidomide | 79 (81.4) |
Pomalidomide | 81 (83.5) |
Thalidomide | 8 (8.2) |
Daratumumab | 94 (96.9)a |
Isatuximab | 7 (7.2) |
TAK-079b | 1 (1.0) |
Elotuzumab | 19 (19.6) |
Panobinostat | 8 (8.2) |
CD = cluster of differentiation; IMiD = immunomodulatory drug; MM = multiple myeloma; PI = proteasome inhibitor.
aTwo additional patients had disease that was refractory to other anti-CD38 antibodies.
bTAK-079 is an investigational anti-CD38 antibody.
Source: CARTITUDE-1 Clinical Study Report.11
Interventions
Randomization was not used in this study, and all patients who met the inclusion and exclusion criteria and were enrolled received apheresis. No blinding procedures were used in this open-label study.
On the day of study enrolment, eligible patients underwent apheresis to allow collection of peripheral blood mononuclear cells (target of 6 × 109 peripheral blood mononuclear cells; range, 2 to 20 × 109). Cilta-cel was manufactured specifically for each patient using their own T cells collected during apheresis. Batches were manufactured between August 3, 2018, and October 25, 2019. Patients who were clinically indicated to receive bridging therapy, to maintain disease stability while cilta-cel was manufactured, received it following preapproval from the sponsor. Bridging therapy was administered between the time of apheresis and the first dose of the conditioning regimen; 73 patients (75%) received bridging therapy, consisting of dexamethasone in 62 patients (64%), bortezomib in 26 patients (27%), cyclophosphamide in 22 patients (23%), and pomalidomide in 21 patients (22%). If a patient reached CR after bridging therapy, they were considered no longer eligible to receive cilta-cel.
Four weeks after apheresis, patients received a conditioning regimen of IV cyclophosphamide (300 mg/m2) and fludarabine (30 mg/m2) in 3 daily doses to induce lymphodepletion and promote CAR T expansion.
Day 1 occurred 5 to 7 days later, on the day of cilta-cel infusion. Patients were first premedicated with 50 mg of diphenhydramine (or the equivalent) and 650 mg to 1,000 mg of acetaminophen (or the equivalent). Cilta-cel was then administered as a single infusion dose of 0.75 × 106 CAR-positive viable T cells/kg (range of 0.5 × 106 to 1.0 × 106 CAR-positive viable T cells/kg, with a maximum total dose of 1.0 × 108).
Apheresis, conditioning, and infusion of cilta-cel was done in the controlled environment of a qualified clinical site under the direct observation of qualified study site personnel.
Re-treatment with cilta-cel was considered for patients who met the following criteria: PD after a best response of minimal response or better; no ongoing grade 3 or higher hematologic toxicity; no ongoing grade 2 nonhematologic toxicity (with the exception of nausea, vomiting, hair loss, and constipation); and at least 6 months between the first cilta-cel infusion and detection of PD. To be eligible for re-treatment with cilta-cel, patients had to meet the eligibility criteria for the study. A maximum of 1 re-treatment was allowed per patient. Bridging therapy before re-treatment could be considered based on a patient’s clinical status and the timing of the availability of the cilta-cel infusion, following approval from the sponsor.
Outcomes
The efficacy end points identified in the CADTH review protocol that were assessed in the clinical trial included in this review are summarized subsequently. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 3.
The primary objective for the phase Ib of the CARTITUDE-1 study was to characterize the safety of cilta-cel and confirm the recommended phase II dose. The primary objective for phase II was to evaluate the efficacy of cilta-cel through ORR. ORR was defined as the proportion of patients who achieved a PR or better (calculated as sCR + CR + VGPR + PR), according to the IMWG response criteria as assessed by an IRC before the end-of-study date.28 All response criteria used in this study are described in Table 37 in Appendix 4. PR is defined as a 50% or greater reduction of serum M protein and reduction in 24-hour urinary M protein by 90% or greater or reduced to less than 200 mg/24 hours; otherwise (if not measurable), it was defined as a decrease of 50% or greater in the difference between involved and uninvolved free light chain levels. If neither of these was measurable, a 50% or greater reduction in bone marrow plasma cells was sufficient as an alternative to M protein, provided the baseline percentage was 30% or greater. In addition to the previous criteria, if present at baseline, a reduction of 50% or greater in the size of soft-tissue plasmacytomas was also required.
Disease evaluations were performed by a central laboratory and ORR was assessed by IRC. The agreement between the IRC’s determination and the assessment by a validated computer algorithm developed by the sponsor was provided. This computer algorithm had been published previously as part of a pivotal study of daratumumab, bortezomib, and dexamethasone in MM.43 A sensitivity analysis of ORR was also conducted, based upon investigator assessment.
Secondary outcomes were also assessed by an IRC and included a response rate of VGPR or better, DOR, TTR, PFS, OS, MRD negativity rate, and HRQoL.
VGPR or better response rate was defined as the proportion of patients with a response of VGPR or better, according to the IMWG criteria (calculated as sCR + CR + VGPR).
DOR was calculated among responders (response of PR or better) from the date of initial documentation of a response of PR or better to the date of first documented evidence of PD, as defined in the IMWG criteria. Relapse from CR by positive immunofixation or trace amount of M protein was not considered disease progression. Disease evaluation continued beyond relapse, from CR until disease progression was confirmed. The outcome was censored for patients who did not progress at the last disease evaluation before the start of subsequent antimyeloma therapy.
TTR was defined as the time between the initial cilta-cel infusion date and the first efficacy analysis where the patient met the criteria for a response of PR or better. The outcome was censored for patients with no response either at the date of disease progression or at the last evaluation of disease before the start of subsequent antimyeloma therapy.
PFS was defined as the time between the initial cilta-cel infusion date and the date of first documented disease progression (defined in the IMWG criteria) or death due to any cause, whichever occurred first. The outcome was censored for patients whose condition had not progressed and who were still alive at the last disease evaluation before the start of subsequent antimyeloma therapy.
OS was defined as the time between the initial cilta-cel infusion date and the date of the patient’s death. The outcome was censored for patients who were still alive (or with unknown vital status) at the final calendar date of follow-up.
MRD negativity was assessed by comparing baseline bone marrow aspirates to post-treatment samples by next generation flow cytometry and/or next generation sequencing. Samples were collected at day 28 and every 6 months subsequently, regardless of the status of disease determined by the results of the blood and urine measures.
HRQoL was assessed in patients enrolled in phase II of the study using the EORTC QLQ-C30, the EORTC QLQ-MY20, EQ-5D-5L utility and EQ-5D Visual Analogue Scale scores, PGIC, and PGIS. Baseline assessments were completed at screening; subsequent assessments were conducted at day 7, day 28, day 56, day 78, day 100, and then every 28 days up to study completion. Meaningful and sustained improvement in scores compared with baseline were evaluated using established meaningful change thresholds. These thresholds were calculated using the PGIS and the PGIC, which are single items to assess overall HRQoL. A detailed discussion and critical appraisal of the HRQoL measure is provided in Appendix 3.
The EORTC QLQ-C30 consists of 30 questions that are scored to create 5 multi-item functional scales (physical, role, cognitive, emotional, and social), 3 multi-item symptom scales (fatigue, pain, and nausea and vomiting) and 6 single-item symptom scales (dyspnea, loss of appetite, insomnia, constipation, diarrhea, and financial difficulties).44 All the scales and single-item measures range in score from 0 to 100. Raw scores for each scale are computed as the average of the items that contribute to a particular scale. Scale sum scores are transformed so that a high score on the functional scales represents a high or healthy level of functioning, a high score on the symptom scales represents a high level of symptomatology, and a high score on the global health status represents a high HRQoL.45 The recall period for the EORTC QLQ-C30 was 1 week. In terms of construct validity, the subscales for pain, fatigue, physical and global quality of life were able to discriminate between patients who improved versus patients who were stable/deteriorated.46 In terms of internal consistency the Cronbach alpha ranged from 0.54 to 0.89 for all subscales, including in patients with r/rMM.47-50 Mean score changes of 6 to 17 in the QLQ-C30 were considered to be important to patients with MM,51 and a change of 8 and 12 points in patients who improved and deteriorated, respectively, on the global quality of life score was considered to be important to patients.52
The EORTC QLQ-MY20 was designed to be used with the EORTC QLQ-C30 to address issues of more relevance to patients with myeloma.53 Four single items from the EORTC QLQ-MY20 were used to assess emotional health status (feel restless or agitated, thinking about your illness, worried about dying, worried about health in the future). The recall, response options, and interpretation of the scores for the EORTC QLQ-MY20 are similar to those for the QLQ-C30. In terms of validity, when scales were compared between patients with a higher versus a lower ECOG PS, only the disease symptoms, treatment side effects, and body image scales demonstrated differences between patient groups according to their PS.53 Reliability was not assessed in patients with MM. When assessed for responsiveness to change, the scale scores for disease symptoms and body image decreased over time with treatment, while the scale scores for treatment side effects increased.53 The estimated minimally important differences (MIDs) for each subscale are the following: 10 points in disease symptoms, 10 points in side effects of treatment, 13 points in body image, and 9 points in future perspective.54
The EQ-5D-5L is a 5-item questionnaire that assesses 5 domains, including mobility, self-care, usual activities, pain/discomfort, and anxiety/depression, plus a visual analogue scale rating for “health today,” with anchors ranging from 0 (worst imaginable health state) to 100 (best imaginable health state). The scores from these 5 domains are computed to a single utility score ranging from 0 to 1. Validity, reliability, and responsiveness were not assessed and the MID was not estimated in patients with MM.
The PGIS is a single item in which patients are asked to rate the severity of their current pain on a 5-point verbal rating scale. The PGIC is a single item in which patients are asked to rate the change in their overall health status using a 7-point verbal rating scale and was only administered post infusion.
Semistructured interviews were conducted with patients enrolled in phase II of the trial at screening, on day 100, and approximately 6 months post infusion to inform their experiences with treatment. Patients in the Japanese cohort did not participate in the interviews.
Safety and tolerability were assessed using the incidence AEs, SAEs, and deaths and laboratory abnormalities, all of which were reported from the time a signed and dated informed consent form was obtained until day 100 or the start of any subsequent systemic anticancer therapy (whichever is earlier). After day 100, only AEs considered related to cilta-cel were reported until the end of the study. All neurotoxicity and hepatitis B virus reactivation events, as well as second primary malignancy, were reported during the first year after cilta-cel infusion, regardless of the date of onset.
AEs were reported using the National Cancer Institute Common Terminology Criteria for Adverse Events version 5.0 guidelines with the exception of CRS and ICANS (or cell-related encephalopathy syndrome [CRES]). In phase Ib, CRS was graded according to criteria outlined by Lee et al. (2014)55 and in phase II, CRS grading was updated to the ASTCT consensus grading system.56 Therefore, CRS events were re-evaluated according to the new standard to allow evaluation across the entirety of the study. On the other hand, CRES (assessed in phase Ib) was replaced by ICANS in an update of the Medical Dictionary for Regulatory Activities before phase II. ICANS is derived from immune effector cell–associated encephalopathy scores that were not collected from all patients in phase Ib; therefore, the complete evaluation of ICANS across the study was not possible.
Health resource utilization was collected for all phase II patients throughout the study until day 180 (± 7 days) and included number and duration of medical care encounters, including surgeries, radiographic diagnostics, laboratory tests, and other selected inpatient and outpatient procedures; duration of hospitalization, including duration by ward (e.g., intensive care unit); number and type of diagnostic and therapeutic tests and procedures; and outpatient medical encounters and treatments.
Statistical Analysis
In phase Ib of the study, no formal statistical hypothesis testing was performed. At least 24 and up to 50 patients were planned to be enrolled in the phase Ib part of the study to confirm the recommended phase II dose and assess safety. With 24 treated patients, if the true incidence rate of certain AEs identified as potential risks was 10%, the probability of observing at least 1 patient experiencing the event would be more than 90%. The AEs identified as potential risks include CRS, cytopenias, tumour lysis syndrome, and infections. In phase II of the study, the null hypothesis tested was an ORR for cilta-cel of 50%. At the time of the protocol, the sponsor asserted that for the therapies available to treat patients with r/rMM (including daratumumab), the reported ORR is 30% or less. Enrolling 60 patients would lead to approximately 90% power to declare that the ORR was higher than 30% at the 1-sided significance level of 0.05. The ORR was estimated empirically and 2-sided 95% CIs were calculated on the basis of the exact binomial distribution. The study was to be considered successful if the lower bound of the 95% CI exceeded 30%. For the Japanese cohort, with a sample size of at least 8 patients, the probability of observing an ORR of greater than 30% is at least 80%, assuming the ORR is 50%. The median event time and survival probability curve for DOR, OS, PFS, and TTR were estimated using the Kaplan-Meier method among patients who achieved a response during the study. The durability of MRD-negative status was characterized by quantifying rates of MRD-negative status (10–5) sustained for at least 6 or 12 months. The scores for all HRQoL assessments were summarized descriptively at relevant time points. Data from the qualitative interviews were analyzed using content analysis, and qualitative themes were presented.
A sensitivity analysis of ORR was performed based on the patients in the mITT analysis set (i.e., those who received cilta-cel) who received a product that met all of the prespecified release criteria. The agreement on ORR as assessed by an IRC compared with the validated computerized algorithm developed by the sponsor, was evaluated using the kappa statistic with a 95% CI. A sensitivity analysis was also conducted for ORR based on the investigators’ assessments.
The first analysis of the primary end point was conducted at 6 months after the last patient had received cilta-cel (data cut-off date of September 1, 2020). The analysis of VGPR or better rate, DOR, PFS, and OS were conducted for the same cut-off date. Updated analyses were undertaken 12 months after the last patient received their initial dose of cilta-cel (data cut-off date of February 11, 2021), and at the end of the study (i.e., 2 years after the last patient received their initial dose) (data cut-off date of January 11, 2022). No control for multiplicity for the statistical hypothesis testing for ORR was conducted.
Subgroup analyses of the primary outcome were conducted stratifying patients based on age, sex, race, total CAR T-positive cells infused, baseline ECOG PS, baseline ISS staging, number of prior lines of therapy, SCT history, disease type, refractory status, cytogenic risk group, baseline bone marrow plasma cells, baseline BCMA expression, and study site. The following subgroups aligned with the subgroups prespecified in the protocol for this CADTH review and are the only ones reported in the efficacy section: cytogenic risk group, SCT history (allogeneic and autologous), and number of prior lines of therapy.
Protocol Changes
The major changes to the study protocol are summarized as follows:
In amendment 1 (August 20, 2018; n = 2), additional safety information was collected.
In amendment 2 (March 11, 2019; n = 21), the number of patients enrolled in phase Ib was expanded, the CRS and neurotoxicity management guidelines were updated, and the CRS and neurotoxicity grading systems were updated to align with new guidelines.
In amendment 3 (July 30, 2019; n = 64), the study was transitioned into the phase II portion, the role of the IRC was added, and an assessment of medical resource utilization was added.
In amendment 4 (March 20, 2020; n = 113), other neurotoxicities as a safety risk were added, and additional monitoring and risk-minimization measures for cilta-cel were implemented.
A COVID-19 appendix (April 30, 2020; n = 113) was added to provide guidance on study conduct as a result of the COVID-19 pandemic.
Analysis Populations
The efficacy population in the CARTITUDE-1 trial included all patients who received cilta-cel at the recommended phase II dose level or, equivalently, all treated patients from phase Ib and phase II of the trial (n = 97). Efficacy outcomes were also estimated in the all-enrolled analysis set (n = 113), which included all patients enrolled (i.e., who underwent apheresis), regardless of whether they received cilta-cel. HRQoL outcomes were only assessed among treated patients in phase II (n = 68). The population used for safety outcome analyses was all treated patients from phase Ib and phase II (n = 97).
Results
There were 4 Clinical Study Reports provided in the sponsor’s submission:
primary analysis report with a clinical data cut-off date of September 1, 20209
safety and efficacy update reports with a clinical data cut-off date of February 11, 202110
final analysis report with a clinical data cut-off date of January 11, 2022, which was used throughout this report unless otherwise specified.11
Patient Disposition
Patient disposition for the US cohort of the CARTITUDE-1 study is presented in Table 9. Of the ||| patients screened, a total of 113 patients were enrolled and underwent apheresis. Of the 113 patients who underwent apheresis, 12 patients (11%) did not receive conditioning treatment due to death (8 patients; 7%), disease progression (2 patients; 2%), and withdrawal of consent (2 patients; 2%). Of the 101 patients who received conditioning treatment, 4 did not receive cilta-cel infusion because they refused (2 patients; 2%), experienced an AE (1 patient; 1%), or died (1 patient; 1%). A total of 97 patients received cilta-cel infusion, 29 (30%) in phase Ib and 68 in phase II (70%). As of the final data cut-off date of January 11, 2022, 66 patients (58%) were receiving ongoing follow-up.
Protocol Violations
At the time of the data cut-off date of February 11, 2021, out of all enrolled patients (n = 113), a total of || patients (|||%) had protocol deviations: || patients (|||%) received a disallowed concomitant treatment and || patient (|||%) required assessment of extramedullary plasmacytoma that was not performed according to schedule, as per protocol.
Table 9: Patient Dispositionsa
Disposition | CARTITUDE-1 |
|---|---|
Screened, N | ||| |
Enrolled, N | 113 |
Underwent apheresis, n (%) | 113 (100) |
Received conditioning regimen, n (%) | 101 (89.4) |
Underwent apheresis but did not receive conditioning regimen, n (%) | 12 (10.6) |
Death | 8 (7.1) |
Disease progression | 2 (1.8) |
Withdrawal of consent | 2 (1.8) |
Received cilta-cel infusion, n (%) | 97 (85.8) |
Phase Ib | 29 |
Phase II | 68 |
Received conditioning regimen but did not receive cilta-cel infusion, n (%) | 4 (3.5) |
Adverse event | 1 (0.9) |
Patient refused | 2 (1.8) |
Death | 1 (0.9) |
mITT,a N | 97 |
Ongoing follow-upb | 66 (58.4) |
Discontinued after cilta-cel infusionb | || |||||| |
Death | 30 (26.5) |
Withdrawal by patient | | ||||| |
Cilta-cel = ciltacabtagene autoleucel; mITT = modified intention-to-treat.
aIncludes all patients who received cilta-cel at the targeted recommended phase II dose level.
bAs of the data cut-off on January 11, 2022.
Source: CARTITUDE-1 Clinical Study Report.11
Exposure to Study Treatments
For all treated patients, with regard to the conditioning regimen, the median cumulative dose of cyclophosphamide infusion was 897.8 mg/m2 (range, 748 mg/m2 to 946 mg/m2); for fludarabine infusion, it was 89.6 mg/m2 (range, 45 mg/m2 to 95 mg/m2). Bridging therapy to maintain disease stability was administered to 73 patients (75.3%) between apheresis and initiation of the conditioning regimen (PIs in 44 [45%] patients; IMiDs in 26 [27%] patients; and anti-CD38 antibodies in 15 [16%] patients). No patients who received bridging therapy achieved CR while on bridging therapy, and all were eligible to receive cilta-cel, as per the study protocol. The median time from apheresis to cilta-cel infusion was 47 days (range, 41 to 167 days). The median number of CAR-positive viable T cells infused was 54.3 × 106 cells (range, 23.5 × 106 to 93.1 × 106 cells) with a median of 0.709 × 106 cells/kg administered (range, 0.51 × 106 to 0.95 × 106 cells/kg). The median duration of cilta-cel infusion was 19 minutes (range, 5 to 71 minutes).
In the Japanese cohort, all patients received the conditioning regimen of 300 mg/m2 cyclophosphamide and 30 mg/m2 fludarabine daily for 3 days. Of all 9 patients, 8 patients received a cilta-cel infusion at the target dose of 0.75 × 106 CAR-positive viable T cells/kg (range of 0.5 × 106 to 1.0 × 106 CAR-positive viable T cells/kg) and 1 patient received a below-target dose range of cilta-cel (0.41 × 106 CAR-positive viable T cells/kg).42
Dose Delays and Modifications
There were || patients (||||%) who experienced a delay in administration of cyclophosphamide or fludarabine conditioning due to an AE among || patients (||||%) and for other reasons among || patients (||||%), such as personal reasons, re-apheresis, rapid disease progression, and so forth. Cilta-cel infusion was delayed for || patient (|||%) to ||| days after lymphodepletion due to a positive rhinovirus test and interrupted for || patients (|||%) to flush the line. No infusions were delayed, interrupted, or aborted due to AEs.
Concomitant Medications
Prophylactic antivirals were prescribed for || patients (||%), most commonly acyclovir for || patients (||%). Prophylactic antibiotics were prescribed for || patients (||%), most commonly levofloxacin for || patients (||%). Prophylactic antifungals were prescribed for || patients (||%), most commonly fluconazole for || patients (||%).
All patients received concomitant medications during treatment. The most common medications were nucleosides and nucleotides (|| patients; ||||%), anilides (|| patients; ||||%), and interleukin inhibitors (|| patients; ||||%). All other concomitant medications are presented in Table 10.
Medications used to manage CRS were prescribed for 88 patients (91%) and included paracetamol (70 patients; 72.2%), tocilizumab (67 patients; 69.1%), cefepime (27 patients; 27.8%), sodium chloride solution (23 patients; 23.7%), dexamethasone (20 patients; 20.6%), and anakinra (18 patients; 18.6%).
Medications used to manage ICANS were prescribed for 16 patients (17%) and included dexamethasone (9 patients; 9%), tocilizumab (4 patients; 4%), and anakinra (3 patients; 3%).
Prior to cilta-cel infusion, transfusion of blood products was required for || patients (||||%) with || patients (||||%) who required packed red blood cells and || patients (||||%) who required platelets. Following cilta-cel infusion, transfusion of blood products was required for || patients (||||%); || patients (||||%) required packed red blood cells and || patients (||||%) required platelets, including for AEs in || patients (||||%). Growth factors were required for || patients (||||%), with filgrastim being the most commonly used in || patients (||||%).
Table 10: Other Concomitant Medicationsa
Other concomitant medication, n (%) | CARTITUDE-1 (phase Ib + phase II) N = 97 |
|---|---|
Nucleosides and nucleotides, excluding reverse transcriptase inhibitors | || |||||| |
Anilides | || |||||| |
Interleukin inhibitors | || |||||| |
Serotonin (5-HT3) antagonists | || |||||| |
Colony stimulating factors | || |||||| |
Fluoroquinolones | || |||||| |
Fourth-generation cephalosporins | || |||||| |
Salt solutions | || |||||| |
Imidazole and triazole derivatives | || |||||| |
Benzodiazepine derivatives | || |||||| |
Preparations inhibiting uric acid production | || |||||| |
Potassium | || |||||| |
Other antiepileptics | || |||||| |
Natural opium alkaloids | || |||||| |
Combinations of sulfonamides and trimethoprim, including derivatives | || |||||| |
Note: Concomitant medications by preferred anatomical therapeutic chemical class (> 50% of patients).
aAs of data cut-off September 1, 2022.
Source: CARTITUDE-1 Clinical Study Report.9
Subsequent Antimyeloma Therapy
As of the January 11, 2022, data cut-off date, among all treated patients, a total of || patients (||||%) received subsequent antimyeloma therapy. There were || patients (|||%) who received radiotherapy and || patients (|||%) who received an autologous transplant. The majority of patients received dexamethasone (|| patients; ||||%). With regard to other neoplastic drugs, || patients (||||%) received selinexor, || patients (|||%) received carfilzomib, and ||| patients (|||%) received bortezomib. With regard to monoclonal antibodies, || patients (||||%) received belantamab mafodotin and |||| patients (|||%) received daratumumab. Other treatments received included cyclophosphamide for || patients (||||%), cisplatin for || patients (|||%), etoposide for || patients (|||%), and pomalidomide for || patients (|||%). There were || patients (|||%) re-treated with cilta-cel.
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported subsequently. See Appendix 3 for detailed efficacy data.
Overall Survival
As of the January 11, 2022, data cut-off, after a median follow-up of 27.7 months (range, 1.5 to 40.4 months) the median OS was still NR. Among all treated patients, there were 30 deaths (31%), and the 24-month OS rate was ||||| |||| ||| |||| || |||||. Among all enrolled patients (N = 113), the 24-month OS rate was ||||| |||| ||| |||| || |||||.
A summary of OS for all treated patients and the corresponding Kaplan-Meier plot are shown in Table 11 and Figure 3, respectively.
In the Japanese cohort (N = 9), as of the clinical cut-off date of February 11, 2021, the median follow-up was 8.5 months and median OS was NR. The estimated 12-month OS rate was 100%.
Health-Related Quality of Life
Only patients in phase II of the CARTITUDE-1 study (n = 68) completed HRQoL assessments, and these were reported only in the primary Clinical Study Report at the September 1, 2020, data cut-off.9
Table 11: Overall Survival (All-Treated Analysis Set With January 11, 2022, Data Cut-Off)
Overall survivala | CARTITUDE-1 (phase Ib + phase II) N = 97 |
|---|---|
Number of events (%) | || |||||| |
Median OS, months (95% CI) | || |
6-month OS rate, % (95% CI) | |||| ||||| || ||||| |
12-month OS rate, % (95% CI) | |||| ||||| || ||||| |
18-month OS rate, % (95% CI) | |||| ||||| || ||||| |
21-month OS rate, % (95% CI) | |||| ||||| || ||||| |
24-month OS rate, % (95% CI) | |||| ||||| || ||||| |
27-month OS rate, % (95% CI) | 70.4 (60.1 to 78.6) |
30-month OS rate, % (95% CI) | |||| ||||| || ||||| |
CI = confidence interval; NE = not estimable; OS = overall survival.
aEstimated using the Kaplan-Meier method.
Source: CARTITUDE-1 Clinical Study Report.11
Figure 3: Kaplan-Meier Plot for Overall Survival (All-Treated Analysis Set With January 11, 2022, Data Cut-Off)

Note: Figure was redacted at the sponsor’s request.
EORTC Quality of Life Questionnaire Core 30
The EORTC QLQ-C30 completion rate at baseline was 92.6% (63 patients) and declined to 83.1% (54 patients) and 65.0% (39 patients) at day 100 and day 156, respectively. The EORTC QLQ-C30 showed improvements over time compared with baseline, with decreases observed initially on day 7 for global health status (Figure 4), physical functional scale (Figure 5), and fatigue symptom scale (Figure 7). This initial worsening is consistent with the potential onset of cilta-cel AEs related to CRS.12 There was consistent improvement in the pain symptom scale from baseline (Figure 6).
Meaningful improvement determined by a 1-point improvement on the PGIC assessment is described in Table 12. Data were available for 56 patients (82%) at day 28 and 52 patients (76%) at day 100. At day 100, 29 patients (53.7%) reported meaningful improvements in their global health status, 29 patients (57.7%) reported meaningful improvements in physical functioning, 39 patients (72.2%) reported meaningful improvement in pain symptoms, and 28 patients (53.8%) reported meaningful improvement in fatigue.
Table 12: Meaningful Change by Day (Anchor-Based) in EORTC QLQ-C30 Scales (All-Treated Analysis Set With September 1, 2020, Data Cut-Off)
Day | CARTITUDE-1 (phase II) N = 68,a n | Patients who achieved meaningful change,b n (%) | |||
|---|---|---|---|---|---|
Global health status scale | Physical functional scale | Pain symptom scales | Fatigue symptom scales | ||
Day 28 | 56 | 28 (50.0) | 13 (23.2) | 28 (50.0) | 21 (37.5) |
Day 56 | 55 | 35 (63.6) | 31 (56.4) | 22 (40.0) | 29 (52.7) |
Day 78 | 50 | 33 (66.0) | 28 (56.0) | 23 (46.0) | 32 (64.0) |
Day 100 | 54 | 29 (53.7) | 30 (57.7) | 39 (72.2) | 28 (53.8) |
cilta-cel = ciltacabtagene autoleucel; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; MID = minimally important difference; PGIC = Patient Global Impression of Change.
aPercentages are based on the number of patients with nonmissing data before cilta-cel infusion and post cilta-cel infusion assessment.
bFor anchor-based MID, PGIC is used as an anchor and MID is estimated as the mean change score for the patients who improved by 1 point on the PGIC (“A little better now”) from before cilta-cel infusion to each visit during the postinfusion period.
Source: CARTITUDE-1 Clinical Study Report.9
Figure 4: Mean (± SE) of EORTC QLQ-C30 Global Health Status Scale Over Time (All-Treated Analysis Set With September 1, 2020, Data Cut-Off)
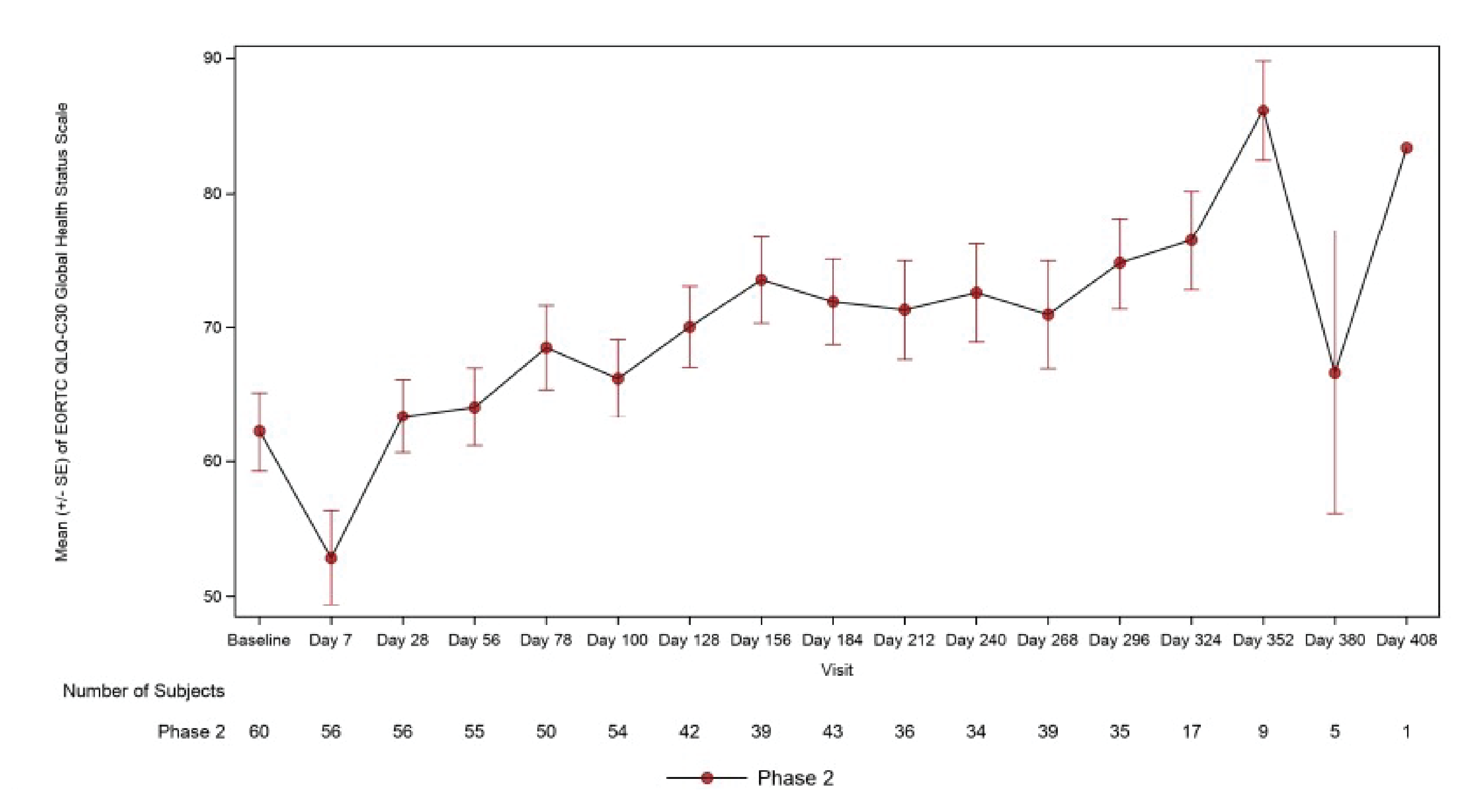
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; SE = standard error.
Source: CARTITUDE-1 Clinical Study Report.9
Figure 5: Mean (± SE) of EORTC QLQ-C30 Physical Functional Scale Over Time (All-Treated Analysis Set With September 1, 2020, Data Cut-Off)
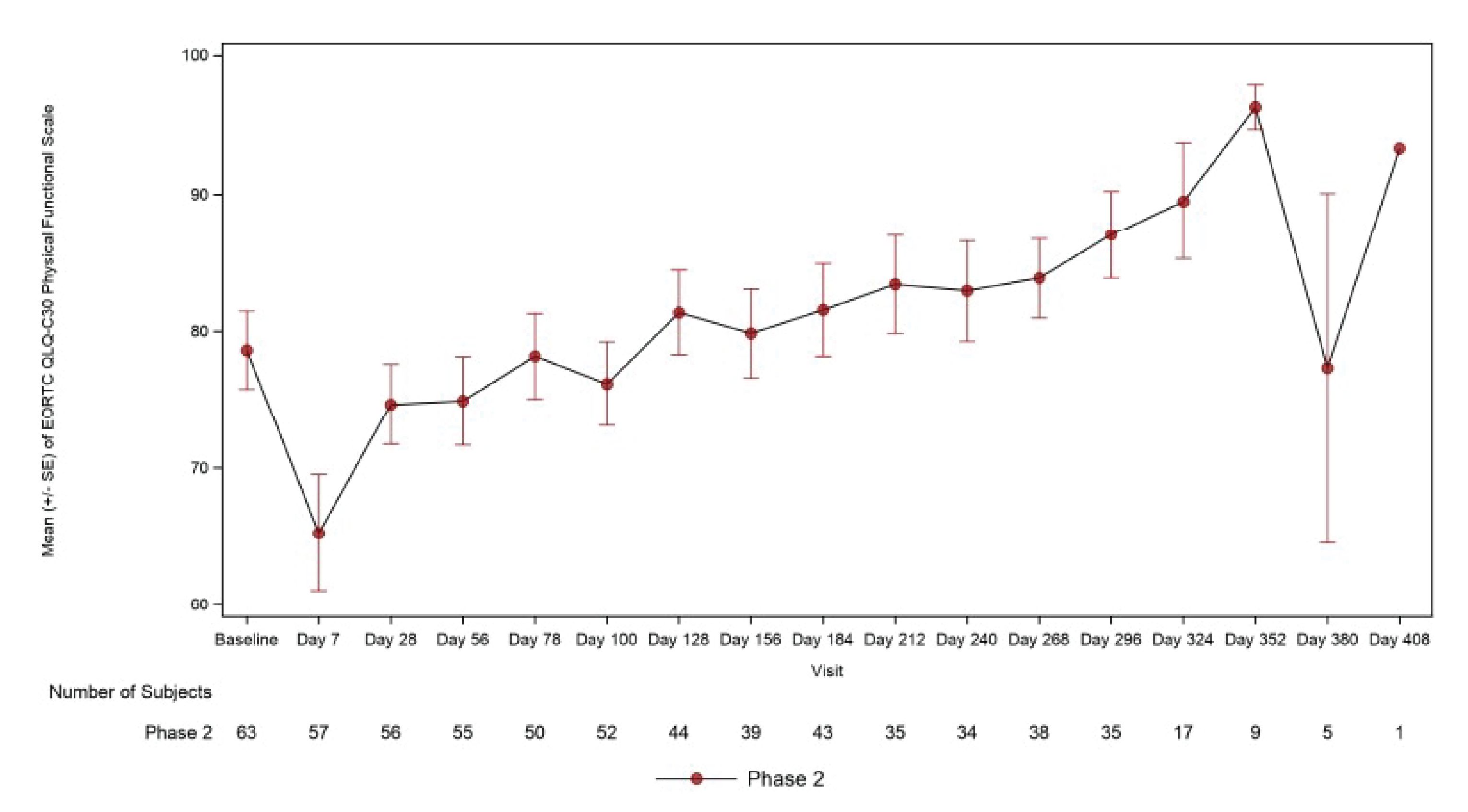
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; SE = standard error.
Source: CARTITUDE-1 Clinical Study Report.9
Figure 6: Mean (± SE) of EORTC QLQ-C30 Pain Symptom Scale Over Time (All-Treated Analysis Set With September 1, 2020, Data Cut-Off)
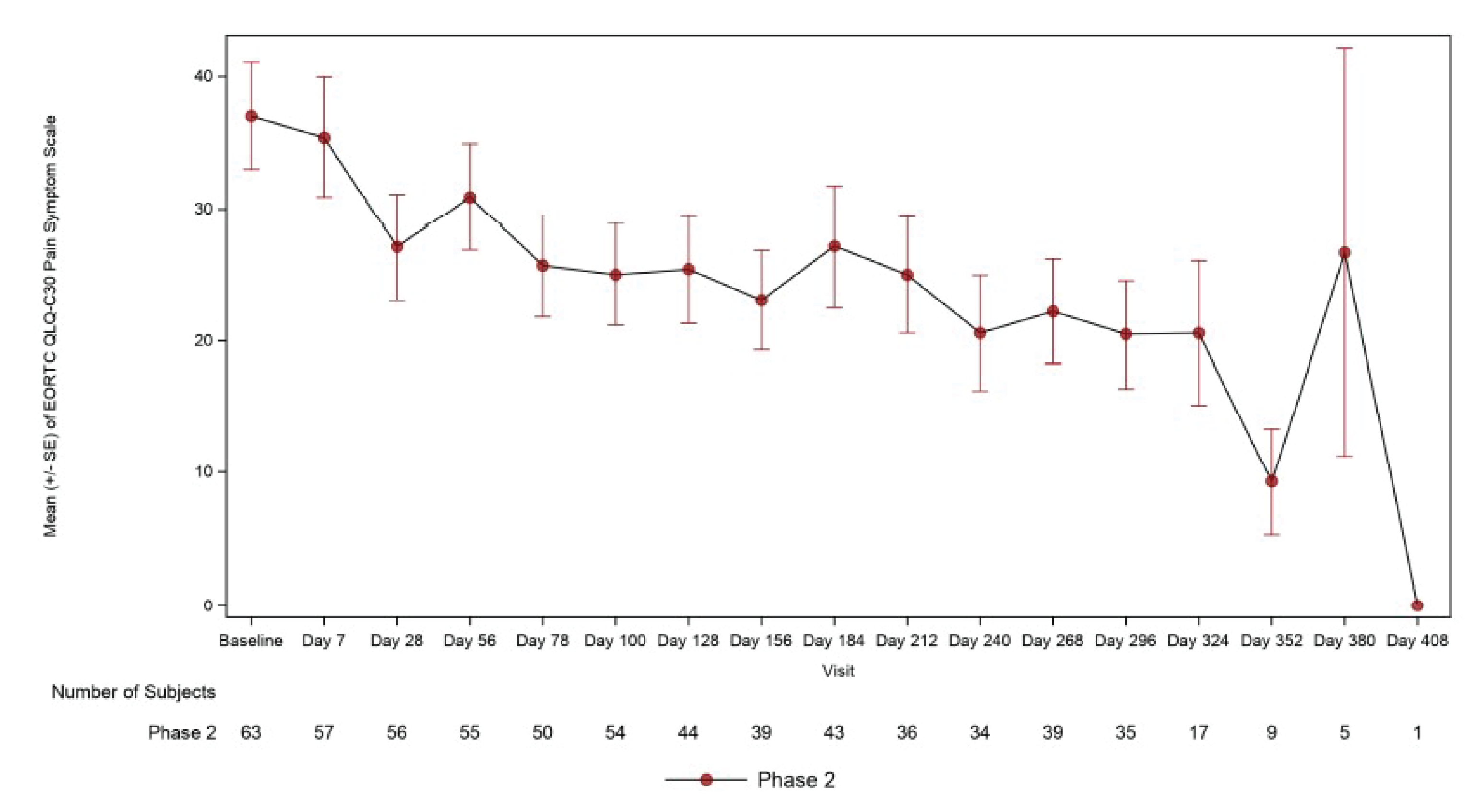
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; SE = standard error.
Source: CARTITUDE-1 Clinical Study Report.9
Figure 7: Mean (± SE) of EORTC QLQ-C30 Fatigue Symptom Scale Over Time (All-Treated Analysis Set With September 1, 2020, Data Cut-Off)
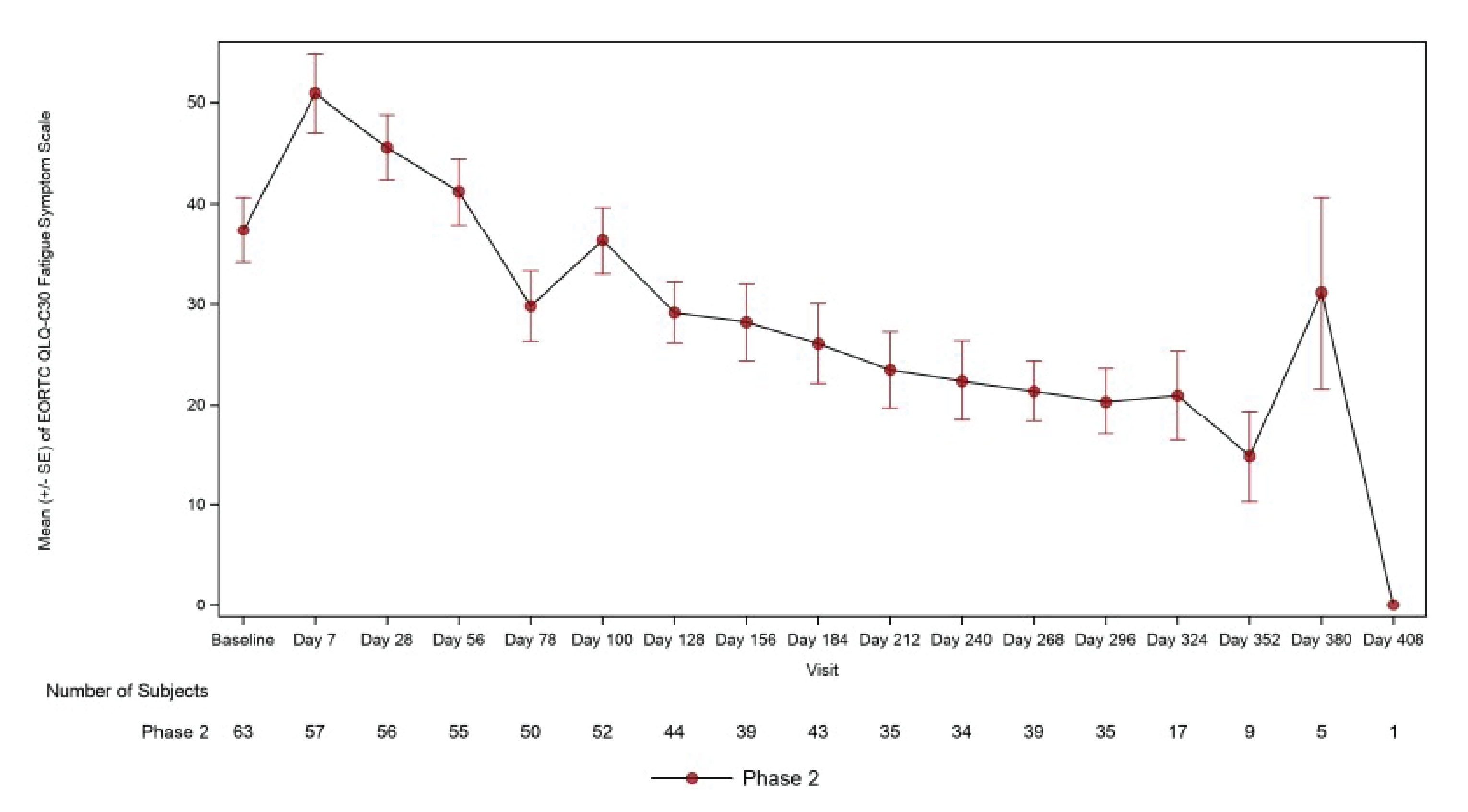
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; SE = standard error.
Source: CARTITUDE-1 Clinical Study Report9
EORTC Quality of Life Questionnaire Myeloma Module
The EORTC QLQ-MY20 completion rate at baseline was |||||% (|| patients) and declined to ||% (|| patients) at day 100. Clinically meaningful changes defined by literature-based MIDs of 10 points57 are presented in Table 13.
At day 100, 43 patients (81.1%) reported meaningful improvements regarding feeling restless or agitated, 27 patients (50.9%) reported improvements regarding thinking about illness, 22 patients (41.5%) reported improvements regarding being worried about dying, and 17 patients (32.1%) reported improvements regarding being worried about their health in the future.
At day 100, 35 patients (66.0%) achieved meaningful improvement in the future perspective scale, and patients showed consistent improvement over time compared with baseline through day 380, as shown in Figure 8.
Table 13: Meaningful Change (Literature-Based)a in EORTC QLQ-MY20 and Future Perspective Subscale (All-Treated Analysis Set With September 1, 2020, Data Cut-Off)
Day | CARTITUDE-1 (phase II) N = 68,a n | Patients who achieved meaningful change,b n (%) | ||||
|---|---|---|---|---|---|---|
Restless or agitated | Thinking about illness | Worried about dying | Worried about health in the future | Future perspective scale | ||
Day 7 | 57 | 41 (71.9) | 15 (26.3) | 20 (35.1) | 15 (26.3) | 28 (49.1) |
Day 28 | 55 | 50 (90.9) | 21 (38.2) | 19 (34.5) | 23 (41.8) | 33 (60.0) |
Day 56 | 55 | 45 (81.8) | 26 (47.3) | 21 (38.2) | 23 (41.8) | 33 (60.0) |
Day 78 | 49 | 40 (81.6) | 25 (51.0) | 20 (40.8) | 26 (53.1) | 36 (73.5) |
Day 100 | 53 | 43 (81.1) | 27 (50.9) | 22 (41.5) | 17 (32.1) | 35 (66.0) |
EORTC QLQ-MY20 = 20-item European Organisation for Research and Treatment of Cancer Myeloma Module.
aPercentages are based on the number of patients with nonmissing data before cilta-cel infusion and infusion assessment.
bFor literature-based minimally important difference, 10 points is used.57
Source: CARTITUDE-1 Clinical Study Report.9
Five-Level EQ-5D
The EQ-5D-5L completion rate for the utility score at baseline was 92.6% (63 patients) and declined to 78% (53 patients) and 57.3% (39 patients) at day 100 and day 156, respectively. The completion rates for the EQ visual analogue scale were similar. There was an initial decrease in both utility score and visual analogue score at day 7 followed by continuous improvement through day 100, as shown in Figure 9 and Figure 10.
Figure 8: Mean (± SE) of EORTC QLQ-MY20 Future Perspective Scale Over Time (All-Treated Analysis Set With September 1, 2020, Data Cut-Off)
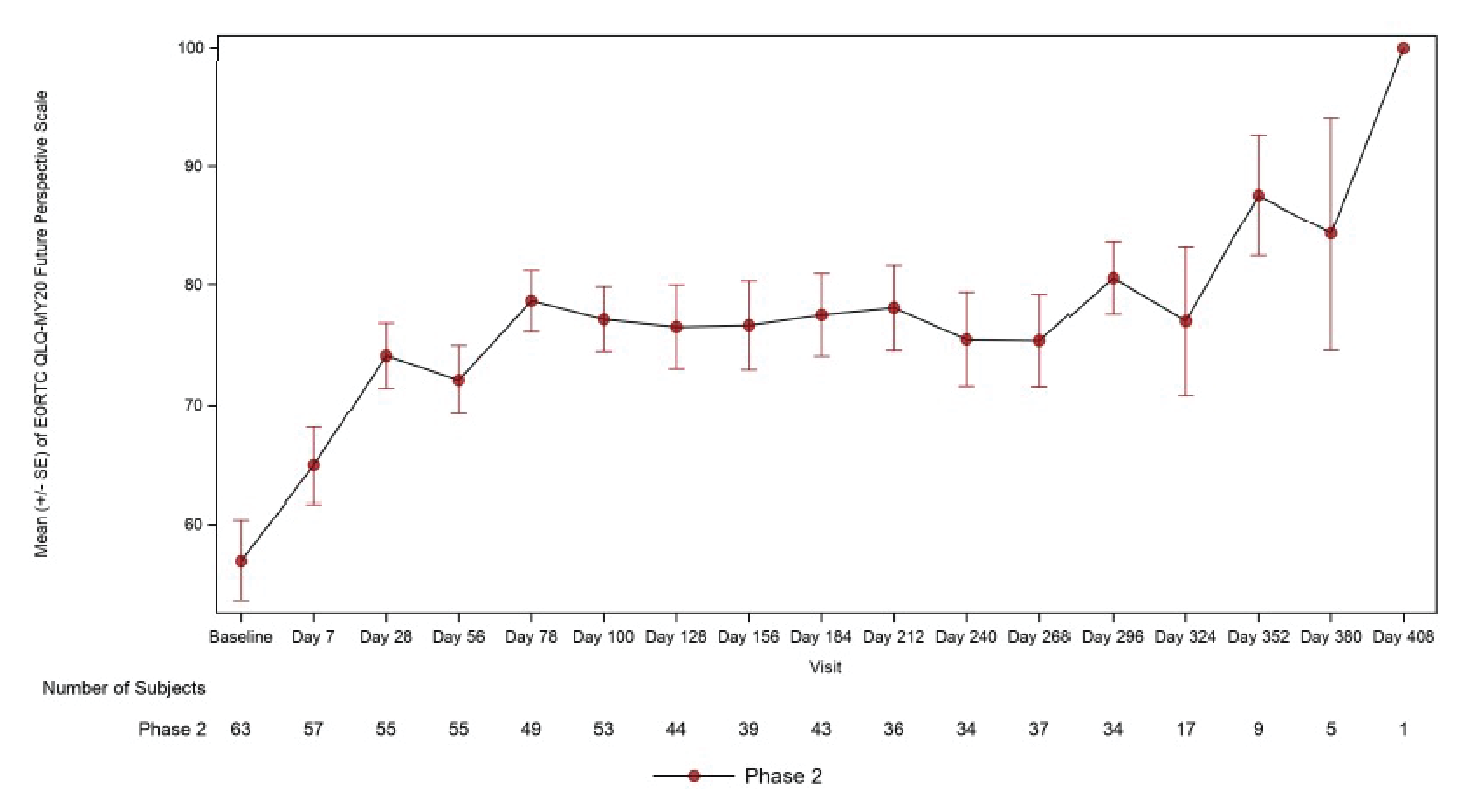
EORTC QLQ-MY20 = European Organisation for Research and Treatment of Cancer Myeloma Module; SE = standard error.
All the scores are presented in the range of 0 to 100 after linear transformation from raw scores (in the range of 1 to 4). A higher score for restlessness or agitation indicates worse health, whereas the higher score for the future perspectives, including worry about death and health in the future and thinking about illness, indicates better outcome.
Source: CARTITUDE-1 Clinical Study Report.9
Figure 9: Mean (± SE) of EQ-5D-5L Utility Score Over Time (All-Treated Analysis Set With September 1, 2020, Data Cut-Off)

Note: Figure was redacted at the sponsor’s request.
Figure 10: Mean (± SE) of EQ Visual Analogue Scale Over Time (All-Treated Analysis Set With September 1, 2020, Data Cut-Off)

Note: Figure was redacted at the sponsor’s request.
Patient Global Impression of Severity and Patient Global Impression of Change
The PGIS completion rate at baseline was 93% (63 patients) and declined to 78% (53 patients) and 57% (39 patients) at day 100 and day 156, respectively. Severity of pain was consistently reported as lower than baseline through day 352. PGIC was only completed post infusion from day 28, when the completion rate was 76% (52 patients), where 67% of patients reported improvement and the proportion increased to 74% by day 56, 86% by day 78, and 87% by day 100. PGIC completion rate at day 100 was 79% (54 patients).
Qualitative Interviews
Out of 27 patients who completed interview 1 before treatment, 23 patients completed interview 2 (on day 100 ± 30 days), and 24 patients completed interview 3 (on day 184 ± 30 days). Patient experiences from interviews 2 and 3 are reported in Table 14. In interview 1, pain and fatigue were the most commonly reported symptoms (85% and 74% respectively), considered to have the greatest impact on patients’ lives and identified as the symptoms patients would most like to see improved. After cilta-cel therapy, the proportion of patients in interviews 2 and 3 who reported pain (22% and 29% respectively) and fatigue (35% and 21% respectively) decreased.
Before treatment, the most common expectations of cilta-cel treatment reported by patients were remission (41%), extended life expectancy (15%), less treatment (11%), and cure (11%). In interviews 2 and 3, respectively, 78% and 92% of patients reported their expectations of cilta-cel were met or exceeded. In interviews 2 and 3, respectively, 52% and 71% of patients perceived their experience with cilta-cel as exclusively better than their previous treatment experiences.
Table 14: Patient Experiences After Cilta-Cel Treatment From the Qualitative Interviews
Topic | Patient experiences |
|---|---|
Symptoms | “Yes. I feel more energy. I feel more energy to be active… But I noticed that after the T-cell treatment, after maybe like a couple of months, my fatigue level has gone down. I’m at a…point now where I can stay up throughout the day.” Male, 46, second interview. “The changes mean a lot because living in pain and being tired, or just being careful, walking gingerly, that stuff was like a new normal and it bothered me because I know within myself I wasn’t like that.” Male, 46 years, third interview. “It’s just amazing to me. My neck doesn’t hurt and my back. I had such back issues and that doesn’t hurt anymore. So yes. It’s amazing.” Female, 71 years, third interview. |
HRQoL | “Well, I can now do, I can exercise, I can walk, I can do all my regular activities without any problem…” Female, 77 years, interview second interview. “Well, you know, like I said, I’m able to do more in terms of, if it’s doing things around the house that I wasn’t able to do before.” Male, 67 years, third interview. “I feel better. So definitely change in terms of feeling better about being able to go out and enjoy, enjoy life a little more.” Female, 52 years, third interview. “I’ve been dealing with the, the pain and the nausea from the chemo and stuff, and…just six months of a break is huge.” Male, 54 years, third interview. |
Experiences of cilta-cel and comparisons with previous treatments | “It was pretty easy, too. Like, I was surprised at how easy it was to get the cells taken out. Get them back in and…it was just like a transfusion.” Female, 56 years, second interview. “I got real tired of staying in the hospital for 10 days, especially after my fever broke… When I was running the fever… I guess I was happy to be there, but after the fever broke…I had nothing to do, and I wasn’t really happy about being there for 10 days.” Female, 66 years, second interview. “The only negative thing…was the fact that you have to be hospitalized for, in my case, 14 days.” Male, 64 years, second interview. It’s a lot easier and I feel better. And I would take this any day over, like getting the chemo and all that stuff. Yes. I would definitely do this again.” Female, 46 years, second interview. “All through treatments, chemo, I still had no energy. I wasn’t getting my energy back. It was pretty much consistent, the same. That never changed, but when I had this done, the CAR T-cell, each day progressively got better.” Male, 61 years, third interview. |
CAR = chimeric antigen receptor; cilta-cel = ciltacabtagene autoleucel; HRQoL = health-related quality of life.
Source: Cohen et al. (2022)41 and CARTITUDE-1 Clinical Study Report.9
Progression-Free Survival
As of the January 11, 2022, data cut-off, after a median follow-up of 27.7 months (range, 1.5 to 40.4 months), the median PFS based on IRC assessment was still NR. Among all treated patients, 43 patients (44%) experienced PFS events, and the 24-month PFS rate was ||||| |||| ||| |||| || |||||. Among all enrolled patients (N = 113), the 24-month PFS rate was ||||| |||| ||| |||| || ||||). A summary of PFS for the all-treated analysis set and the corresponding Kaplan-Meier plot are shown in Table 15 and Figure 11.
Table 15: PFS (All-Treated Analysis Set With January 11, 2022, Data Cut-Off)
PFSa | CARTITUDE-1 (phase Ib + phase II) N = 97 |
|---|---|
Number of events (%) | || ||||||| |
Median PFS, months (95% CI) | || ||||||| ||| |
6-month PFS rate % (95% CI) | |||| ||||| || ||||| |
12-month PFS rate % (95% CI) | |||| ||||| || ||||| |
18-month PFS rate % (95% CI) | |||| ||||| || ||||| |
21-month PFS rate % (95% CI) | |||| ||||| || ||||| |
24-month PFS rate % (95% CI) | |||| ||||| || ||||| |
27-month PFS rate % (95% CI) | 54.9 (44.0 to 64.6) |
30-month PFS rate % (95% CI) | |||| ||||| || ||||| |
CI = confidence interval; NE = not estimable; PFS = progression-free survival.
aEstimated using the Kaplan-Meier method.
Source: CARTITUDE-1 Clinical Study Report.11
Figure 11: Kaplan-Meier Plot for PFS Based on IRC Assessment (All-Treated Analysis Set With January 11, 2022, Data Cut-Off)

Note: Figure was redacted at the sponsor’s request.
In the Japanese cohort, at the clinical cut-off date of February 11, 2021, the median follow-up was 8.5 months and the ORR was 100% (95% CI, 66.4 to 100). In the all-treated analysis set (n = 9), all DOR, PFS, and OS data were censored at the clinical cut-off; therefore, median DOR, PFS, and OS were NR. The 9-month PFS rate was 100% and the estimated 12-month OS rate was 100%.42
Health Resource Utilization
Health resource utilization was reported supplementary to the assessment of safety, and findings were not included in the Clinical Study Reports. The sponsor clarified that since there were a lot of missing data points, a report was not developed.58
Overall Response Rate and Very Good Partial Response or Better Rate
ORR as assessed by the IRC was the primary end point in the CARTITUDE-1 trial. In the final data analysis with a data cut-off of January 11, 2022, ORR in the all-treated analysis set (n = 97) was 97.9% (95% CI, 92.7 to 99.7; P < 0.0001) as presented in Table 16. Stringent CR was reached by 80 patients (82.5%; 95% CI, 73.4 to 89.4), VGPR by 12 patients (12.4%; 95% CI, 6.6 to 20.6), and PR by 3 patients (3.1%; 95% CI, 0.6 to 8.8). In the all-enrolled analysis set (n = 113), the ORR was 84.1% (95% CI, 76.0 to 90.3). Stringent CR was reached by 80 patients (70.8%; 95% CI, 61.5 to 79.0), VGPR by 12 patients (10.6%; 95% CI, 5.6 to 17.8), and PR by 3 patients (2.7%; 95% CI, 0.6 to 7.6).
Subgroup analysis results were available only for the February 11, 2021, data cut-off. Results were consistent with the primary analysis results across the patient subgroups of interest, as shown in Table 17.
As part of the sensitivity analyses, the ORR was consistent across all assessment methods. ORR by computerized algorithm was 93.8% (95% CI, 87.0 to 97.7) and by investigator assessment was 96.9% (95% CI, 91.2 to 99.4). VGPR or better as assessed by the IRC for the all-treated analysis set was 94.8% (95% CI, 88.4 to 98.3), as shown in Table 16. For all patients enrolled (n = 113), the VGPR or better rate as assessed by an IRC was 81.4% (95% CI, 73.0 to 88.1).
Among the 3 patients who were re-treated with cilta-cel, best response by IRC and by investigator assessment was PD for 1 patient and stable disease for 2 patients. Best response by computer algorithm was stable disease for all 3 patients. All 3 patients had experienced PD by clinical cut-off, with PD occurring on day 32, day 41, and day 57, respectively, after re-treatment by IRC assessment, computerized algorithm, and investigator assessment. In the Japanese cohort, at the clinical cut-off date of February 11, 2021, the ORR was 100% (95% CI, 66.4 to 100).42
Duration of Response
At the January 11, 2022, data cut-off, median DOR by IRC assessment was NR. For the previous data cut-off on February 11, 2021, median DOR for all patients treated was |||| |||||| |||| ||| |||| |||||| || |||. Among all treated patients, the estimated probability that patients remained in response at 12 months was ||||| |||| ||| |||| || |||||; at 24 months it was ||||| |||| ||| |||| || ||||| and at 30 months it was ||||| |||| ||| |||| || |||||. A summary of DOR for all treated patients and the corresponding Kaplan-Meier plot are shown in Table 18 and Figure 12, respectively.
As part of the sensitivity analyses, median DOR as assessed by computerized algorithm was NR in the current analysis (95% CI, |||| |||||| || ||). The probability that patients remained in response after 24 months based on assessment by computerized algorithm was ||||| |||| ||| ||||| || ||||||.
At the clinical cut-off date of February 11, 2021, median DOR was NR in the Japanese cohort.42
Table 16: Overall Best Response (All-Treated Analysis Set With January 11, 2022, Data Cut-Off)
Overall best responsea | CARTITUDE-1 (phase Ib + phase II) N = 97 | |
|---|---|---|
n (%) | 95% CI for % | |
Best response | ||
sCR | 80 (82.5) | 73.4 to 89.4 |
CR | 0 | NE |
VGPR | 12 (12.4) | 6.6 to 20.6 |
PR | 3 (3.1) | 0.6 to 8.8 |
Overall response (sCR + CR + VGPR + PR) | 95 (97.9) | 92.7 to 99.7 |
P valueb | < 0.0001 | |
VGPR or better (sCR + CR + VGPR) | 92 (94.8) | 88.4 to 98.3 |
CR or better (sCR + CR) | 80 (82.5) | 73.4 to 89.4 |
CI = confidence interval; CR = complete response; NE = not estimable; PR = partial response; sCR = stringent complete response; VGPR = very good partial response.
aResponse was assessed by an independent review committee based on International Myeloma Working Group consensus criteria (2016). Percentages are calculated with the number of patients in the all-treated analysis set as denominator. Two-sided 95% Clopper-Pearson exact 95% CIs are provided.
bOne-sided P value from exact binomial test for the null hypothesis of overall response rate ≤ 30% is presented. P value was not adjusted for multiplicity.
Source: CARTITUDE-1 Clinical Study Report.11
Table 17: Subgroup Analyses of ORR Based on IRC Assessment (All-Treated Analysis Set With February 11, 2021, Data Cut-Off)
Subgroups | CARTITUDE-1 (phase Ib + phase II) n = 97 | ||
|---|---|---|---|
N | ORR n (%) | 95% CI for % | |
Cytogenetic risk groups | |||
High-risk | 23 | 23 (100) | 85.2 to 100 |
Standard risk | 68 | 66 (97.1) | 89.8 to 99.6 |
Number of lines of prior therapy (grouping 1) | |||
≤ 4 lines | 33 | 32 (97.0) | 84.2 to 99.9 |
> 4 lines | || | || |||||| | |||| || ||| |
Number of lines of prior therapy (grouping 2) | |||
3 lines | 17 | 17 (100) | 80.5 to 100 |
> 3 lines | 80 | 78 (97.5) | 91.3 to 99.7 |
Prior autologous stem cell transplant | |||
Yes | 87 | 85 (97.7) | 91.9 to 99.7 |
No | 10 | 10 (100) | 69.2 to 100 |
Prior allogeneic stem cell transplant | |||
Yes | || | | |||||| | |||| || |||| |
No | || | || |||||| | |||| || ||| |
CI = confidence interval; IRC = independent review committee; ORR = overall response rate.
Source: CARTITUDE-1 Clinical Study Report.10
Table 18: DOR on IRC Assessment (All-Treated Analysis Set With January 11, 2022, Data Cut-Off)
Duration of responsea | CARTITUDE-1 (phase Ib + phase II) N = 97 |
|---|---|
Number of events (%) | || |||||| |
Median DOR, months (95% CI) | NE (23.3 to NE) |
6-month DOR rate, % (95% CI) | |||| ||||| || ||||| |
12-month DOR rate, % (95% CI) | |||| ||||| || ||||| |
18-month DOR rate, % (95% CI) | |||| ||||| || ||||| |
21-month DOR rate, % (95% CI) | |||| ||||| || ||||| |
24-month DOR rate, % (95% CI) | |||| ||||| || ||||| |
27-month DOR rate, % (95% CI) | |||| ||||| || ||||| |
30-month DOR rate, % (95% CI) | |||| ||||| || ||||| |
CI = confidence interval; DOR = duration of response; IRC = independent review committee; NE = not estimable.
aEstimated using the Kaplan-Meier method.
Source: CARTITUDE-1 Clinical Study Report.11
Figure 12: Kaplan-Meier Plot for DOR on IRC Assessment (All-Treated Analysis Set With January 11, 2022, Data Cut-Off)

Note: Figure was redacted at the sponsor’s request.
Minimal Residual Disease Negativity Rate
At the January 11, 2022, data cut-off, compared with the previous data cut-off of February 11, 2021, there was no change to the proportion of patients who achieved MRD negativity in their bone marrow at 10−5 sensitivity following treatment with cilta-cel (Table 19). Of the 61 treated patients (63%) with evaluable samples, 56 (91.8%; 95% CI, 81.9 to 97.3) achieved MRD negativity in bone marrow at 10−5 sensitivity following treatment with cilta-cel.
Table 19: MRD Negativity Rate at 10−5 in Bone Marrow for Patients With Evaluable Sample (All-Treated Analysis Set With January 11, 2022, Data Cut-Off)
MRD negativity rate | CARTITUDE-1 (phase Ib + phase II) n = 61 | |
|---|---|---|
n (%) | 95% CI for % | |
MRD negativity and ≥ CRa | || |||||| | |||| || |||| |
MRD negativity and ≥ VGPRb | || |||||| | |||| || |||| |
Overall MRD negativity ratec | 56 (91.8) | 81.9 to 97.3 |
CI = confidence interval; CR = complete response; MRD = minimal residual disease; VGPR = very good partial response.
aOnly MRD assessments (10−5 testing threshold) within 3 months of achieving CR or stringent CR until death, progression, or subsequent therapy (exclusive) are considered.
bOnly MRD assessments (10−5 testing threshold) within 3 months of achieving ≥ VGPR until death, progression, or subsequent therapy (exclusive) are considered.
cOut of 61 patients with evaluable samples, i.e., patients with an identifiable clone at baseline and who had sufficient cells to be tested at a sensitivity level of 10−5 in a post-treatment sample.
Source: CARTITUDE-1 Clinical Study Report.10,11
Time to Response
At the January 11, 2022, data cut-off, the responders in the all-treated population (n = 95) had a median time to first response (for patients with PR or better) of 0.95 months (range, 0.9 to 10.7), and the mean time to first response was 1.4 months (SD = 1.54). Median time to best response was 2.6 months (range, 0.9 to 17.8), and median time to CR or better was 2.9 months (range, 0.9 to 17.8). These results represent an improvement in the response of 2 patients compared with the previous data cut-off of February 11, 2021. Findings are presented in Table 20.
As part of the sensitivity analyses, similar findings were observed when TTR was assessed by computer algorithm in the all-treated analysis set.
Table 20: TTR Based on IRC (All-Treated Analysis Set With January 11, 2022, Data Cut-Off)
TTR | CARTITUDE-1 (phase Ib + phase II) N = 97 |
|---|---|
Time to first responsea (months) | |
N | 95 |
Mean (SD) | ||| |||||| |
Median (range) | 0.95 (0.9 to 10.7) |
Time to best response (months) | |
N | 95 |
Mean (SD) | ||| |||||| |
Median (range) | 2.6 (0.9 to 17.8) |
Time to CR or better (months) | |
N | 80 |
Mean (SD) | ||| |||||| |
Median (range) | 2.9 (0.9 to 17.8) |
CR = complete response; IRC = independent review committee; PR = partial response; SD = standard deviation; TTR = time to response.
aResponse of PR or better.
Source: CARTITUDE-1 Clinical Study Report.11
Harms
Only those harms identified in the review protocol are reported subsequently. Refer to Table 21 for detailed harms data from the January 11, 2022, data cut-off. Safety was analyzed in all treated patients.
Adverse Events
All patients (n = 97) experienced at least 1 TEAE, with || patients (||%) experiencing at least 1 grade 4 TEAE. The most common TEAEs were neutropenia (96%), CRS (95%), anemia (81%), and thrombocytopenia (80%).
At least 1 TEAE with a maximum severity of at least grade 3 or higher occurred in all patients. The most common grade 3 or higher TEAEs were neutropenia (95%), anemia (68%), and leukopenia (61%).
Serious Adverse Events
A total of || patients (||%) experienced at least || SAE, with || patients (||%) experiencing a grade 3 or 4 SAE and || patients (||%) experiencing a grade 5 SAE. The most common SAEs were CRS (||%), pneumonia (||%), sepsis (||%), and ICANS (||%).
Withdrawal Due to Adverse Events
There was || patient who withdrew due to an AE after receiving conditioning treatment but before receiving cilta-cel infusion.
Mortality
Between apheresis and the start of the conditioning treatment, 8 patients out of 113 (7%) died. Overall, 101 patients received the conditioning regimen, and 97 patients went on to receive cilta-cel. Out of the 4 patients who received the conditioning regimen but did not receive cilta-cel, 1 patient died. Of all treated patients, a total of 30 patients (30.9%) died during the study: 16 due to AEs and 14 due to disease progression. ||||||| || ||| || total deaths occurred after the start of subsequent therapy, including || || || deaths due to PD and 4 of the 16 deaths due to AEs. No patients died within 30 days of the initial cilta-cel infusion, and 2 patients (2.1%) died within 100 days. Only 6 patients (6.2%) had a TEAE leading to death that was considered to be related to cilta-cel; the remaining 10 deaths were not considered to be related to cilta-cel by the study investigators.
Notable Harms
The notable harms identified in the CADTH protocol included CRS, neurologic toxicities, cytopenia, and secondary hypogammaglobulinemia.
Cytokine Release Syndrome
There was no change in the findings related to CRS between the initial analysis at the September 1, 2020, data cut-off and the final analysis at the January 11, 2022, data cut-off. A total of 92 patients (95%) experienced CRS with 4 patients (4%) experiencing a grade 3 or 4 CRS and 1 patient (1%) experiencing grade 5 CRS complicated by secondary hemophagocytic lymphohistiocytosis. The median time from cilta-cel infusion to CRS onset was 7 days (range, 1 to 12), with 82 patients (90%) experiencing onset of CRS after the third day from cilta-cel infusion. The median duration of CRS was 4 days (range, 1 to 14), with 81 patients (88%) experiencing CRS for 7 days or fewer. This is excluding the patient who experienced grade 5 CRS who experienced it for 97 days.
Other Neurologic Toxicities
A total of 21 patients (22%) experienced CAR T-cell neurotoxicity, including 10 patients (10%) at grade 3 or 4. A total of 16 patients (17%) experienced ICANS, including 2 patients (2%) at grade 3 or 4. Other neurotoxicity was reported in 13 patients (13%), including 9 patients (9%) at grade 3 or 4.
Cytopenia
No analysis for cytopenia was performed for the January 11, 2022, data cut-off. As of the February 11, 2021, data cut-off, 96 patients (99%) had experienced at least 1 grade 3 or 4 cytopenic AE. The majority of these AEs were transient, with recovery to grade 2 or better within the first 60 days following cilta-cel infusion, except for 25 (out of 60) patients with thrombocytopenia, 10 (out of 95) patients with neutropenia, and 8 (out of 96) patients with lymphopenia.
Hypogammaglobulinemia
A total of 12 patients (12.4%) experienced hypogammaglobulinemia, including 2 patients (2.1%) with grade 3 or 4 events.
Table 21: Summary of Harms (All-Treated Analysis Set With January 11, 2022, Data Cut-Off)
Harms | CARTITUDE-1 (phase Ib + phase II) (N = 97) |
|---|---|
Patients with ≥ 1 AE, n (%) | |
Total TEAEs | 97 (100.0) |
Grade 3 | 7 (7.2) |
Grade 4 | 84 (86.6) |
Grade 5 | 6 (6.2) |
Most common eventsa | |
Neutropenia | 93 (95.9) |
Cytokine release syndrome | 92 (94.8) |
Anemia | 79 (81.4) |
Thrombocytopenia | 77 (79.4) |
Leukopenia | 60 (61.9) |
Lymphopenia | 51 (52.6) |
Fatigue | 36 (37.1) |
Cough | 34 (35.1) |
Hypocalcemia | 31 (32.0) |
Hypophosphatemia | 30 (30.9) |
Diarrhea | 29 (29.9) |
Decreased appetite | 28 (28.9) |
AST increased | 28 (28.9) |
Nausea | 27 (27.8) |
Hypoalbuminemia | 27 (27.8) |
ALT increased | 24 (24.7) |
Hyponatremia | 22 (22.7) |
Constipation | 21 (21.6) |
Hypokalemia | 20 (20.6) |
Chills | 20 (20.6) |
Pyrexia | 20 (20.6) |
Patients with ≥ 1 SAE, n (%) | |
Total SAEs | 53 (54.6) |
Grade 3 or 4 | 30 (30.9) |
Grade 5 | 6 (6.2) |
Most common eventsb | |
Cytokine release syndrome | 20 (20.6) |
Pneumonia | 6 (6.2) |
Sepsis | 5 (5.2) |
ICANS | 5 (5.2) |
Deaths, n (%) | |
Total deaths | 30 (30.9) |
Due to disease progression | 14 (14.4) |
Due to AEs | 16 (16.5) |
Due to TEAEs | 6 (6.2) |
Sepsis and/or septic shock | 2 (2.1) |
CRS or HLH | 1 (1.0) |
Lung abscess | 1 (1.0) |
Respiratory failure | 1 (1.0) |
Neurotoxicity | 1 (1.0) |
Notable harms, n (%) | |
Cytopenia | 96 (99) |
Cytokine release syndrome | 92 (94.8) |
≥ Grade 3 | 5 (5.2) |
Neurotoxicity | 21 (21.6) |
ICANS | 16 (16.5) |
Other neurotoxicities | 13 (13.4) |
Hypogammaglobulinemia | 12 (12.4) |
AE = adverse event; ALT = alanine aminotransferase; AST = aspartate aminotransferase; CRS = cytokine release syndrome; HLH = hemophagocytic lymphohistiocytosis; ICANS = immune effector cell–associated neurotoxicity syndrome; SAE = serious adverse event; TEAE = treatment-emergent adverse event.
aFrequency > 20%.
bFrequency > 5%.
Source: CARTITUDE-1 Clinical Study Report.9-11
In the Japanese cohort, at the clinical cut-off date of February 11, 2021, all 9 patients experienced at least 1 AE, and 8 (88.9%) experienced at least 1 grade 3 or 4 AE. Grade 3 or 4 cytopenias were reported in 8 patients (88.9%). Grade 1 or 2 CRS was reported in 8 patients (88.9%) and SAEs were reported in 1 patient (neutropenia, thrombocytopenia, fatigue, and CRS). No patient experienced CAR T-cell neurotoxicity (including ICANS or other neurotoxicity). No deaths were reported during the study.42
Critical Appraisal
Internal Validity
CARTITUDE-1 was an open-label, single-arm phase Ib and II study in the US (16 centres) and Japan (4 centres).
The primary limitation of CARTITUDE-1 was the absence of a comparator group against which the benefits and harms of cilta-cel could be compared. Single-arm trials are generally not considered as confirmatory for efficacy and are subject to several limitations that complicate their interpretation; for example, it is not possible to distinguish between the effect of cilta-cel and a placebo effect or natural history of the disease in the absence of a frame of reference for comparison.13 ORR was tested against a predetermined hypothesis based on the sponsor’s assertion that at the time of the protocol for available therapies to treat r/rMM (including daratumumab), the reported ORR was 30%. However, for ORR, there was no adjustment for multiplicity across the various analyses of the outcome (i.e., the various data cut-offs), so there is an increased risk of type I error. Results for the other outcomes (e.g., DOR, OS, PFS) were descriptive only. This trial does not provide any information for the effects of cilta-cel relative to the available comparator treatments used in Canada. According to the FDA assessment of the CARTITUDE-1 trial, end points such as OS and PFS are uninterpretable due to the lack of a comparator arm and were neither reviewed nor included in the label. The FDA assessment noted that a single-arm study design was chosen for CARTITUDE-1, given the perceived lack of equipoise to randomize patients between cilta-cel and any of the currently available therapy options in this target population.14 There were a limited number of patients included in the all-treated analysis set (n = 97) and all-randomized analysis set (n = 113) of CARTITUDE-1. The magnitude of the treatment effect estimates observed in a small study sample may not be replicable in a larger study sample or generalizable to the target population in RWCP.
ORR was the primary end point and CARTITUDE-1 achieved the predetermined threshold for a positive outcome (lower limit of the 95% CI for ORR > 30%). It cannot be firmly concluded to what extent the improvements in ORR observed in patients would translate into OS benefits. ORR is accepted by the FDA as directly attributable to drug effect in “single-arm trials conducted in patients with refractory tumours where no available therapy exists.”15 In this trial, OS was not considered a primary or key secondary end point. However, the end point of OS is often considered important for oncology trials and was considered an important outcome by the clinical experts and patients. At the time of the final analysis, median OS was NR.
The interpretation of efficacy in the all-treated analyses is at risk of bias in favour of cilta-cel. The population excluded patients (n = 16; 14%) who were enrolled and underwent apheresis but were subsequently unable to receive cilta-cel because they died or their disease progressed, or due to AEs or other reasons (e.g., patient choice). This population is not reflective of expected clinical practice and overrepresents the healthiest patients. Analyses based on the all-enrolled population are considered most appropriate for estimating the effect of assignment to treatment. As expected, when both were presented, the results of analyses of the all-treated population were more favourable compared with those of the all-enrolled population. Out of the 113 patients who underwent apheresis, 12 patients did not receive the conditioning treatment, including 8 patients who died. The clinical experts noted that, although this is common in r/rMM, the proportion of deaths is unusual, given how relatively healthy the trial population was.
Only 3 patients were re-treated with cilta-cel; thus, there is not enough information to draw conclusions regarding re-treatment.
A subgroup analysis was not specified in the study protocol a priori, and while results for ORR were consistent with the primary analysis results across patient subgroups of interest, the analysis was limited by the small sample size of some groups, such as patients who received prior allogeneic SCT.
The trial was open label, which can result in a risk of bias in the measurement of the outcomes, particularly for subjective outcomes such as ORR, PFS, HRQoL, and subjective harms. Objective measurements of outcomes, such as OS, would not be reported with measurement bias due to the open-label design of the trial. To reduce the risk of directional bias in reported outcomes, response outcomes were assessed by the investigators, an IRC, and a validated computer algorithm. The results were consistent across the various assessment methods; any bias would likely be in favour or cilta-cel. Outcomes like HRQoL and subjective harms, which were self-reported by patients, are at risk of optimism bias, although the extent and direction of bias are uncertain.
With regard to the MRD negativity rate, there was a large amount of missing data, as only 61 patients had evaluable samples at the final data cut-off, limiting the interpretation of these findings.
In addition, although the EORTC QLQ-C30 and EQ-5D-5L are comprehensive and widely used instruments designed to measure HRQoL in the general population as well as in patient groups with diverse chronic diseases, neither are currently validated for patients with r/rMM. Further, results for all HRQoL measures were at risk of bias due to missing data, particularly at longer follow-up (e.g., data were missing for 44% of all treated patients for the EORTC QLQ-C30 at day 100 and for 60% of patients by day 156). In addition to a diminishing sample size, the patients reporting HRQoL outcomes later in the study are expected to be the healthiest among the population. Given that the trial was nonrandomized, the impact of cilta-cel on PROs in relation to other therapies is unknown.
Findings from the Japanese cohort of the CARTITUDE-1 trial were consistent with results from the main cohort; however, it only included 9 patients, which limits interpretation of cohort findings.
External Validity
According to the clinical experts CADTH consulted for this review, the CARTITUDE-1 study population is considered reflective of the requested reimbursement population. The following considerations are of importance regarding the external validity of the study.
Population: According to the clinical experts consulted by CADTH for this review, the demographic and disease characteristics of the CARTITUDE-1 study population9 were generally reflective of the population of patients in Canada with r/rMM. The mean age of patients in the trial was 62 years, which is younger than the mean age at the time of diagnosis of 70 years in Canada.16 If there was no access to less toxic bispecific therapies, clinical experts would have expected a slightly larger proportion of patients to be older than 75 years old (15% versus the trial’s 8%). However, clinicians can currently access these bispecific therapies through special access programs and would prioritize the older patient population for these therapies, making the trial’s age proportions reflective of the current population demographics. All patients met the inclusion criteria of ECOG 0 or 1 during screening, but 4 patients (4%) deteriorated to ECOG 2 on or before cilta-cel infusion. The clinical experts considered it common for patients to deteriorate after apheresis. The clinical experts also mentioned they would have expected potentially more patients with extramedullary plasmacytomas present past third line of therapy, as this would denote worse disease, but that the 13% proportion in the trial is acceptable. They would have also expected a slightly higher proportion of patients to be of high cytogenetic risk (30% versus the trial’s 24%).
The clinical experts consulted by CADTH mentioned that the creatinine clearance required for inclusion in the trial (≥ 40 mL/min/1.73 m2) is higher than the level used to indicate poor kidney function in clinical practice (≥ 30 mL/min/1.73 m2). They also mentioned that including patients with ECOG ≤ 2 (rather than the trial’s criteria of < 2) would better align with clinical practice needs. One of the trial exclusion criteria of CARTITUDE-1 was any prior therapy that is targeted to BCMA, which the clinical experts found concerning as some clinicians would likely be giving their patients belantamab mafodotin, available through compassionate access, in their management of MM. The clinical experts noted that these patients may still respond well to CAR T-cell therapy17 and should not be excluded from cilta-cel eligibility.
With regard to prior therapy used by patients in the trial, the clinical experts noted that potentially all patients would have disease that is refractory to daratumumab within the first 3 lines of therapy (compared with 97% of patients in the trial). They also noted that selinexor is currently used as a bridging therapy in the US, but no patients had used selinexor in the trial, as selinexor (combined with dexamethasone and bortezomib) was not approved during the time of the trial.18 Finally, they noted that it was surprising that 19% of patients had used anakinra for treating CRS since it is rarely used in Canadian practice; however, they also noted this may have been due to a global shortage of tocilizumab.
End points: The clinical experts consulted by CADTH for this review did not have any major concerns with the end points used in the CARTITUDE-1 trial. They considered OS, HRQoL, and PFS as the most important outcomes, which were secondary end points in the trial. It was noted that MRD negativity rate is not routinely used in clinical practice. All outcomes in the protocol were important to patients, clinicians, and drug plans; although they were evaluated, this trial provides no information about the efficacy and harms of cilta-cel relative to treatments that would otherwise be used in this patient population in clinical practice.
Setting: This study was a multicentre trial in the US. The clinical experts indicated that there are few concerns to generalizing the findings from the pivotal study within the Canadian clinical setting.
Indirect Evidence
A focused literature search for ITCs dealing with MM was run in MEDLINE All (1946-) on October 24, 2022. No limits were applied to the search. The literature search for ITCs identified 113 articles; however, no relevant ITCs were identified.
In total, 3 relevant articles were identified within the search for ITCs,22-24 which are summarized in the Other Relevant Evidence Section. These studies were not included by the sponsor for consideration as they did not reflect Canadian clinical practice; however, the CADTH review team considered them relevant to the current review.
Other Relevant Evidence
Long-Term Data From the LEGEND-2 Study
The sponsor provided long-term (2 year and 4 year) data from LEGEND-2, a phase I, single-arm, open-label study conducted in 4 registered sites in China in patients with r/rMM who had received at least 3 prior lines of treatment. These data were presented in a Clinical Study Report (data cut-off, November 26, 2019)19 and a published manuscript (data cut-off, May 25, 2021).59 LEGEND-2 provided a longer-term safety and efficacy follow-up than the CARTITUDE-1 trial with an additional 20.1-month median follow-up; median follow-up time was 47.8 months in LEGEND-2 (May 25, 2021, data cut-off date) and 27.7 months in the CARTITUDE-1 trial (January 11, 2022, data cut-off date).
The cilta-cel CAR T-cell drug product studied in CARTITUDE-1 (produced in the US) and the LCAR-B38M CAR T-cell drug product studied in the LEGEND-2 study (produced in China) express an identical CAR protein targeting BCMA but were produced using different manufacturing and scale-up processes.19
Methods
LEGEND-2 is a phase I, single-arm, open-label, multicentre study with 74 patients who were enrolled and received at least 1 injection of the LCAR-B38M CAR T-cell drug product. An overview of the LEGEND-2 trial design is presented in Figure 13 and is similar to the study design for CARTITUDE-1 with some exceptions. Unlike CARTITUDE-1, lymphodepletion was performed using cyclophosphamide 300 mg/m2 or cyclophosphamide 250 mg/m2 plus fludarabine 25 mg/m2.
Also, unlike cilta-cel, the LCAR-B38M CAR T-cell dose was split into 3 infusions administered over 7 days, with the number of CAR T cells administered increasing with each infusion. The median total number of T cells infused was ||||||||| ||||||| || || ||||||, and the body weight–adjusted median total number of viable T cells administered was ||||||||||| ||||||| |||| || |||||||||||.
AEs were graded using National Cancer Institute Common Terminology Criteria for Adverse Events version 4.03. Similar to CARTITUDE-1, efficacy was assessed by the criteria of response according to IMWG consensus recommendations, including ORR, DOR for responders, OS, and PFS. With regard to statistical analysis, 2-sided 95% exact CIs based on binomial distribution were calculated for each response category. Median DOR, PFS, and OS and corresponding 95% CIs were calculated using Kaplan-Meier methods.
Populations
Baseline patient characteristics of all treated patients are presented in Table 22. The median age of patients was 54.5 years (range, 27 to 74), with a higher proportion of men (61%) and with a median time since initial MM diagnosis of 4 years (range, 1 to 9). Inclusion criteria for refractory disease were defined as being resistant to at least 3 prior regimens (which must include bortezomib or thalidomide) or as other circumstances identified by clinical doctors. Patients in the trial received a median of 3 prior lines of MM therapy (range, 1 to 9) including 54 patients (73%) who received a PI therapy, 65 patients (88%) who received an IMiD drug, and 48 patients (65%) who received both PI and IMiD drugs. Patients were not required to have received an anti-CD38 antibody in prior therapy and only 2 patients (2.7%) had received prior anti-CD38 antibody therapy.
Patients with a history of allogeneic SCT were excluded from the trial, and 18 patients (24%) had a history of prior autologous SCT.
Figure 13: Schematic Overview of the LEGEND-2 Study Flow Chart
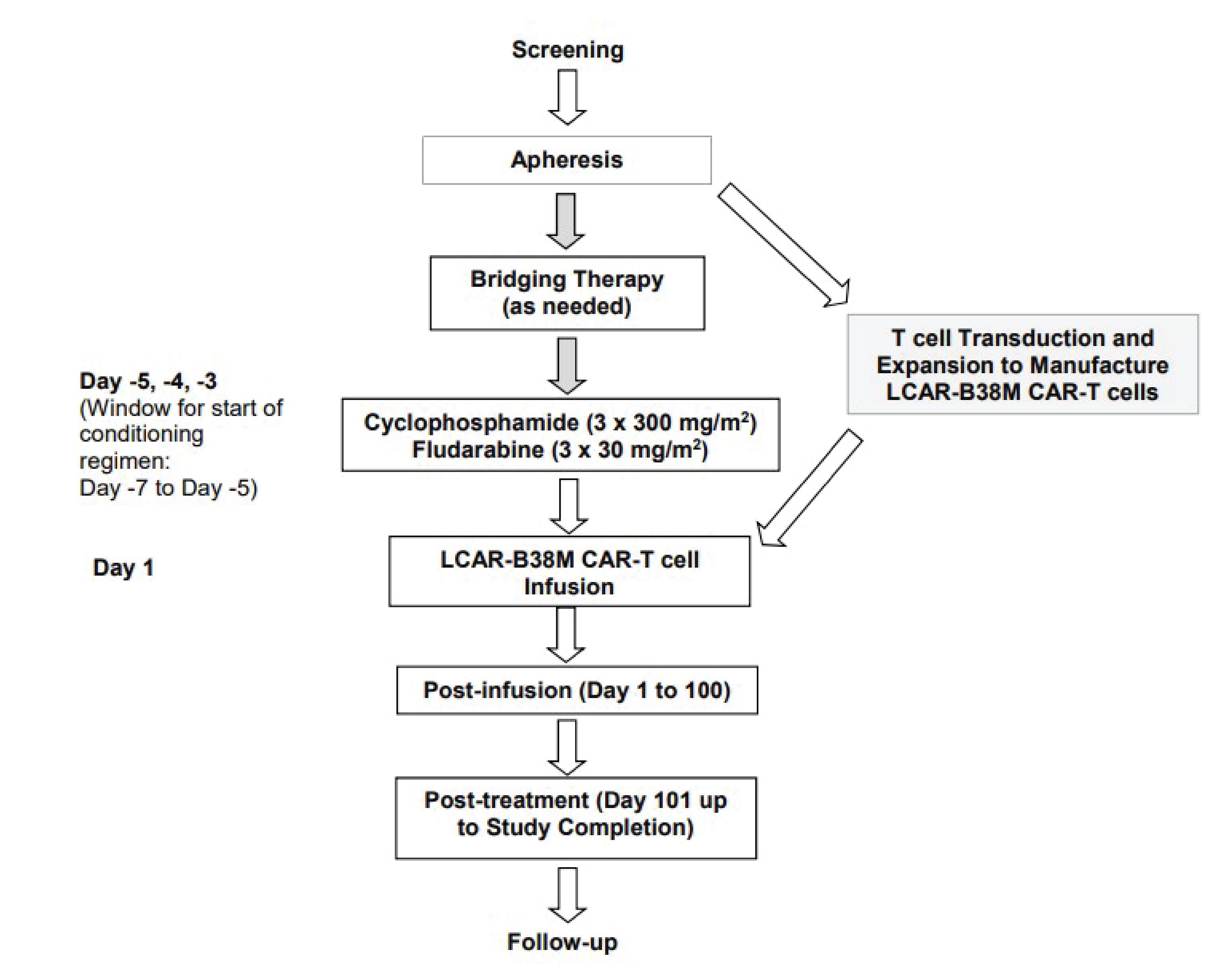
CAR = chimeric antigen receptor; ECOG = Eastern Cooperative Oncology Group.
Note: For patients aged > 70 years and ECOG = 1, cyclophosphamide may be reduced to 250 mg/m2 per investigator’s judgment with approval from the sponsor. Fludarabine dose may be reduced to 25 mg/m2 if the patient’s creatinine clearance is 40 mL/min/1.73 m2 to 70 mL/min/1.73 m2, or per the investigator’s judgment, with approval from the sponsor.
Table 22: Baseline Patient Characteristics in LEGEND-2 (All-Treated Analysis Set)
Characteristic | LEGEND-2 (N = 74) |
|---|---|
Demographics and baseline characteristics | |
Age, mean (SD), years | |||| |||||| |
< 65 | || |||||| |
65 to 74 | || |||||| |
≥ 75 | ||| |
Sex, male n (%) | 45 (60.8) |
Race, n (%) | |
Asian | 73 (98.6) |
White | 1 (1.4) |
Weight, mean (SD), kg | 63.7 (10.78) |
ECOG Performance Status, n (%) | |
0 | 10 (13.5) |
1 | 19 (25.7) |
2 | 1 (1.4) |
Missing | 44 (59.5) |
Type of myeloma by immunofixation, n (%) | |
Immunoglobulin G | || |||||| |
Immunoglobulin A | || |||||| |
Immunoglobulin D | | ||||| |
Light chain | || |||||| |
Kappa | | ||||| |
Lambda | || |||||| |
ISS staging at study baseline, n (%) | |
I | 33 (44.6) |
II | 14 (18.9) |
III | 21 (28.4) |
Unknown | 6 (8.1) |
Time since initial MM diagnosis to enrolment, years | |
Mean (SD) | ||| ||||| |
Median (range) | 4 (1 to 9) |
Prior therapies for MM | |
Number of prior lines of therapy, mean (SD) | |
Mean (SD) | ||| ||||| |
Median (range) | 3 (1 to 9) |
Prior transplant, n (%) | 18 (24.3) |
Prior PI, n (%) | 54 (73.0) |
Bortezomib | 53 (71.6) |
Carfilzomib | 3 (4.1) |
Prior IMiD, n (%) | 65 (87.8) |
Thalidomide | 47 (63.5) |
Lenalidomide | 35 (47.3) |
Pomalidomide | 3 (4.1) |
Prior PI and prior IMiD, n (%) | 48 (64.9) |
Prior monoclonal antibodies | 2 (2.7) |
Prior daratumumab | 1 (1.4) |
Prior isatuximab | 1 (1.4) |
ECOG = Eastern Cooperative Oncology Group; IMiD = immunomodulatory drug; ISS = International Staging System; MM = multiple myeloma; PI = proteasome inhibitor; SD = standard deviation.
Patient Disposition
In the LEGEND-2 trial, 86 patients were screened for eligibility, and 74 were enrolled and received at least 1 infusion of LCAR-B38M CAR T cells. By the November 26, 2019, data cut-off, 32 patients had died and 42 patients remained in follow-up. By the May 25, 2021, data cut-off (median follow-up, 47.8 months; range, 0.4 to 60.7), 2 more patients had died, 1 was lost to follow-up, and 39 patients remained in the study.59
Exposure to Study Treatments
All 74 patients received lymphodepletion chemotherapy with cyclophosphamide, and 8 patients (10.8%) also received fludarabine in their lymphodepletion regimen. The CAR T-cell treatment was divided into a 3-dose regimen administered over 7 days. Of the 74 patients enrolled, || (||%) received all 3 infusions. |||||||| patients did not follow the 3-dose regimen, including ||| patients (||||%) who received a single infusion on day 1.
Efficacy
In the 2-year analysis of LEGEND-2 with the November 26, 2019, data cut-off, median follow-up time from dosing to cut-off was 30.4 months (range, 0.4 to 42.8). In the 4-year analysis with the May 25, 2021, data cut-off, median follow-up time from dosing to cut-off was 47.8 months (range, 0.4 to 60.7). Median OS was not yet reached in both analyses, and on the November 26, 2019, cut-off the 24-month OS rate was ||||% (95% CI, |||| || ||||) for all patients. At the May 25, 2021, data cut-off, the estimated 24-month OS rate was 63.4% (95% CI not reported). The Kaplan-Meier estimated median PFS was 18 months (95% CI, 10.6 to 25.6) for all patients treated. HRQoL, MRD negativity rate, TTR, and health care utilization were not assessed in this study.
Findings on ORR and DOR are presented in Figure 14. At the May 25, 2021, data cut-off ORR by sponsor assessment was 87.8% (95% CI, 78.2 to 94.3), with 54 patients (73%) achieving CR, 6 patients (8%) achieving PR, and 5 patients (7%) achieving VGPR. Median DOR was 23.26 months (95% CI, 13.04 to 32.69). The median time to initial response using Kaplan-Meier was 1.0 months (range, 0.4 to 3.5) and the median time to best response was 3.3 months (range, 0.4 to 28.5).
Harms
A summary of harms in the LEGEND-2 study is presented in Table 23. All patients experienced at least 1 TEAE within 100 days post infusion, with AEs of grade 3 or greater in 45 patients (61%). The most common AEs were pyrexia in 68 patients (92%) and CRS in 68 patients (92%), and only 7 patients (10%) experienced CRS of grade 3 or greater. Of the 74 patients in the analysis, 34 deaths (46%) were reported as of the May 25, 2021, data cut-off, including 28 deaths (38%) due to disease progression.
Critical Appraisal
Internal Validity
LEGEND-2 was an open-label, single-arm phase I study of LCAR-B38M, a CAR product molecularly identical to cilta-cel, that was conducted in China (4 centres). The inclusion criteria in LEGEND-2 did not require prior therapy with an anti-CD38 antibody and excluded patients with a history of allogeneic SCT.
The primary limitation of LEGEND-2 was the absence of a comparator group against which the benefits and harms of the LCAR-B38M CAR T-cell drug product could be compared. As such, the estimation of the effects of treatment relative to current standards of practice is not possible. Further, single-arm trials are generally not considered as confirmatory for efficacy and do not allow for causal conclusions. The study protocol mentioned the use of a computerized algorithm and an IRC for disease status evaluation. However, findings are reported based on sponsor assessment (based on uniform medical reviews of source hospital medical records); thus, there is a risk of bias in the measurement of the outcome due to the open-label design, likely in favour of LCAR-B38M. Due to the open-label design of the trial, the reported response outcome measures (i.e., ORR, DOR, PFS) and subjective harms are at risk of bias due to the measurement of these outcomes (since the patients and investigators who measured or reported the outcomes were aware of the treatment received). For response outcomes, the bias would likely be in favour of the LCAR-B38M CAR T-cell drug product; known, subjective harms may have been overestimated. As per CARTITUDE-1, end points such as OS and PFS are uninterpretable at the population level due to the lack of a comparator arm.
With regard to the study treatment, there were 8 patients (11%) who received fludarabine in addition to the protocol-specified lymphodepletion chemotherapy with cyclophosphamide monotherapy. The sponsors reported no major differences in findings between both groups of patients. In addition, there were 18 patients (24%) who did not receive the protocol-specified 3-dose standard regimen: 9 patients (11%) in 1 site received a single infusion and 9 patients (11%) received 2, 4, or 7 infusions. The reasons for this deviation were not specified. As such, the estimated rates of ORR and OS describe a heterogenous treatment regimen and are difficult to compare with the CARTITUDE-1 study.
External Validity
The clinical experts consulted by CADTH for this review noted that the baseline characteristics of the LEGEND-2 study population would be closer to patients who are in the second line of therapy rather than the fourth line and beyond. No patients were older than 75 years of age, which is not reflective of Canadian clinical practice. The experts noted there was limited use of daratumumab in previous lines of therapy. Moreover, because exposure to an anti-CD38 antibody was not required, this study population is less relevant to this reimbursement review. The study took place in China, with no participating Canadian sites. For these reasons, the generalizability of the results to current Canadian clinical practice may be limited. The cilta-cel CAR T-cell drug product studied in CARTITUDE-1 (produced in the US) and the LCAR-B38M CAR T-cell drug product studied in the LEGEND-2 study (produced in China) express an identical CAR protein targeting BCMA but were produced using different manufacturing and scale-up processes.
HRQoL, MRD negativity rate, TTR, and health care utilization were not assessed as end points in this phase I study.
Comparative Observational Evidence for Cilta-Cel Versus RWCP
Due to the lack of evidence from RCTs comparing cilta-cel with relevant comparator treatments, the sponsor submitted 2 reports consisting of 3 observational studies comparing cilta-cel with relevant treatment comparators using IPD from CARTITUDE-1 and the US Flatiron longitudinal database, long-term follow-up of 3 daratumumab clinical trials, and the LocoMMotion prospective cohort study. As the treatment assignments across studies were not randomized, propensity score weighting was used to adjust for potential confounding variables.20,21
An additional 3 relevant studies were identified during screening of the search results for ITCs: 2 observational studies that used propensity score weighting to adjust for confounding, and 1 meta-analysis of observational evidence.22-24 Although the sponsor remarked in its submission that these studies were not relevant to the review, the CADTH review team included them because they estimate the effects of cilta-cel in the requested reimbursement population relative to the comparators defined in the predetermined protocol.
The objective of this section is to summarize and critically appraise the methods and findings of the sponsor-submitted observational studies as well as the evidence identified in the published literature.
Table 23: Summary of Harms in LEGEND-2 (All-Treated Analysis Set With May 25, 2021, Data Cut-Off)
Harms | LEGEND-2 (N = 74) | |
|---|---|---|
Any grade | Grade ≥ 3 | |
Any TEAE | 74 (100) | 45 (60.8) |
Pyrexia | 68 (91.9) | 11 (14.9) |
Cytokine release syndrome | 68 (91.9) | 7 (9.5)a |
Leukopenia | 32 (43.2) | 19 (25.7) |
Thrombocytopenia | 31 (41.9) | 14 (18.9) |
Increased AST | 28 (37.8) | 15 (20.3) |
Anemia | 22 (29.7) | 11 (14.9) |
Hypotension | 14 (18.9) | 4 (5.4) |
Increased ALT | 13 (17.6) | 0 |
Cough | 13 (17.6) | 1 (1.4) |
Neurotoxicity | 1 (1.4) | 0 |
AST = aspartate transaminase; ALT = alanine aminotransferase; TEAE = treatment-emergent adverse event.
aOne patient died 13 days post treatment due to grade 5 cytokine release syndrome.
Source: Zhao et al. (2022).59 Reprinted in accordance with Attribution 4.0 International (CC BY 4.0) Creative Commons — Attribution 4.0 International — CC BY 4.0.
Description of the Studies
Sponsor-Submitted Observational Studies
The sponsor-submitted evidence consisted of 2 observational studies to compare cilta-cel with relevant treatment comparators in RWCP.20,21
One sponsor-submitted report was an observational study comparing the effectiveness of cilta-cel (from CARTITUDE-1) versus RWCP as observed in the LocoMMotion prospective cohort study using propensity score weighting and regression modelling to adjust for confounding between the treatment and outcomes of clinical response (ORR, VGPR, CR or better, MRD), PFS, TTNT, OS, PROs, safety, and resource utilization.20
The other sponsor-submitted report included 2 observational studies to compare cilta-cel with real-world treatments for patients with triple class–exposed r/rMM. In both studies, propensity score weighting was used to adjust for potential confounding variables21:
1 analysis comparing the IPD from CARTITUDE-1 with the IPD from a cohort of patients in the long term follow-up of 3 global r/rMM clinical trials of daratumumab (POLLUX, CASTOR, and EQUULEUS), hereinafter referred to as the daratumumab trial cohort.
1 analysis comparing the IPD from CARTITUDE-1 with a CARTITUDE-1–like cohort of real-world patients receiving current treatment paradigms using data from the Flatiron Health database (hereinafter referred to as the Flatiron cohort).
Outcomes included in the second report included clinical response outcomes (ORR, CR or better), PFS, TTNT, and OS.
Figure 14: LEGEND-2 4-Year Data on ORR and DOR (All-Treated Analysis Set With May 25, 2021, Data Cut-Off)
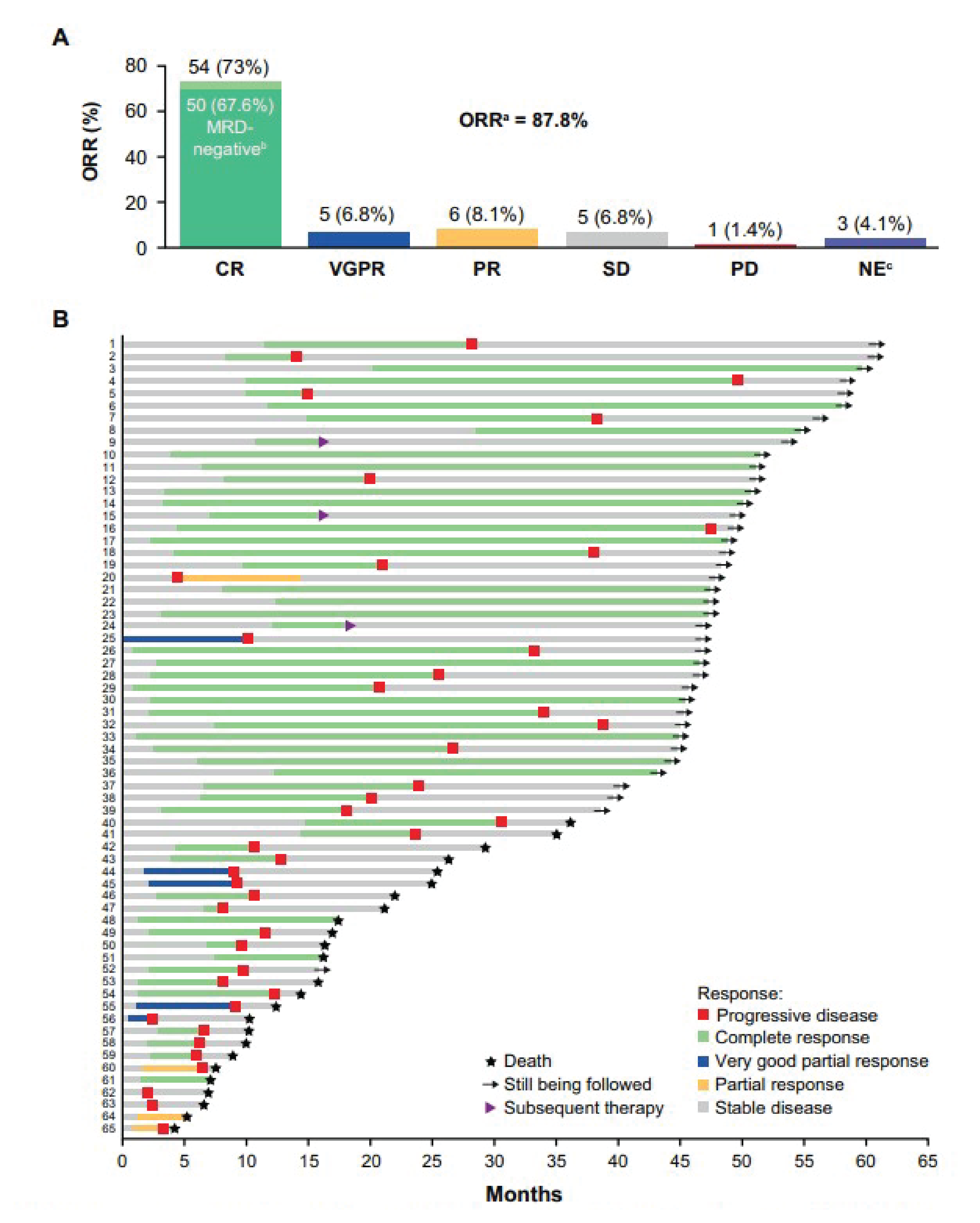
CR = complete response; CRS = cytokine release syndrome; MRD = minimal residual disease; NE = not evaluable; ORR = overall response rate; PD = progressive disease; PR = partial response; SD = stable disease; TLS = tumour lysis syndrome; VGPR = very good partial response.
Note: (A) Top portion of the figure presents best response in all patients. (B) Bottom portion of the figure presents duration of response in patients with a response.
a ORR includes patients with ≥ PR.
b Eight-colour flow cytometry with cell count up to 500,000 cells.
c One patient died of pulmonary embolism or acute coronary syndrome before evaluation, 1 patient died on day 13 due to CRS and TLS, and 1 patient received chemotherapy before first assessment and was censored.
Source: Zhao et al. (2022).59 Reprinted in accordance with Attribution 4.0 International (CC BY 4.0) Creative Commons — Attribution 4.0 International — CC BY 4.0.
Observational Evidence Identified in the Literature
In total, 3 published articles met the inclusion criteria predefined by CADTH for this review:
An observational study using IPD from the CARTITUDE-1 trial and the MAMMOTH cohort to evaluate the efficacy of cilta-cel versus real-world therapies for the outcomes of ORR, PFS, and OS. Propensity score matching was used to balance observed confounding variables.22
An observational study evaluating OS and TTNT for patients in CARTITUDE-1 versus patients receiving real-world treatments registered in the Therapie Monitor database in Germany maintained by the OIS.23 Propensity score weighting was used to adjust for potential confounding variables.
A meta-analysis of observational studies evaluating cilta-cel versus physicians’ choice of treatment.24 The studies included in the meta-analysis consisted of all studies summarized here and included publications for the comparison of CARTITUDE-1 to LocoMMotion, the Flatiron cohort, the daratumumab trial cohort, the MAMMOTH cohort, and the OIS database.
Sponsor-Submitted Observational Studies
Methods for Sponsor-Submitted Observational Study of CARTITUDE-1 Versus LocoMMotion20
Objective: The objective of the study was to evaluate the comparative efficacy of cilta-cel versus RWCP, as defined by the LocoMMotion prospective cohort study, within a population similar to the cilta-cel trial.20
Study selection methods: IPD from 2 sources were included in the sponsor’s study: CARTITUDE-1 and LocoMMotion. Features of the data sources included in the study are summarized in Table 24. Given that CARTITUDE-1 is a single-arm trial, an external control arm was used to assess the efficacy of cilta-cel versus available treatments for the management of patients with triple class–exposed MM who have received at least 3 prior regimens, including a PI, an IMiD, and an anti-CD38 monoclonal antibody. The LocoMMotion (NCT04035226) study was a prospective, noninterventional, multinational study that was designed as an external control arm for the CARTITUDE-1 study. Eligibility criteria for the LocoMMotion study and outcome definitions were aligned with the CARTITUDE-1 trial to recruit similar patient populations and to enable comparisons between the study populations. LocoMMotion documented RWCP patterns in patients whose disease progressed following treatment with PIs, IMiDs, and anti-CD38 monoclonal antibodies. In total, 248 patients were included across 76 sites in Europe and the US.
Comparisons of cilta-cel from the CARTITUDE-1 study (January 2022, clinical cut-off) with the RWCP of the LocoMMotion study (May 2021, clinical cut-off) were conducted using IPD from both studies within the described ITT population. In CARTITUDE-1, the ITT population included the patients who underwent apheresis (N = 113), which was the index date. For the comparator group from the LocoMMotion study, the ITT population included patients who were enrolled in the study (N = 248), with an index date defined as date of treatment initiation. Secondary analyses using the mITT populations were also conducted, with the mITT for CARTITUDE-1 consisting of patients who received cilta-cel at the targeted recommended phase II dose (N = 97), with the infusion date as the index date. The mITT for LocoMMotion consisted of a subset of patients from the ITT population who were alive and had not progressed within the number of days equal to the mean duration from apheresis to cilta-cel infusion, as observed in CARTITUDE-1, after the start of treatment (N = 170). The index date was defined as the date of treatment initiation plus the mean duration from apheresis to cilta-cel infusion as observed in CARTITUDE-1 (mean of 52 days).
The outcomes compared between CARTITUDE-1 and LocoMMotion that were included in the sponsor report consisted of the following:
Clinical response outcomes, including:
ORR, defined as the proportion of patients who achieved a PR or better according to the IMWG criteria; response after the start of subsequent therapy or re-treatment with cilta-cel was not considered.
VGPR or better rate, defined as the proportion of patients who achieve an sCR, CR, or VGPR according to the IMWG criteria; response after the start of subsequent therapy or re-treatment with cilta-cel was not considered.
CR or better rate, defined as the proportion of patients who achieve a sCR or a CR according to the IMWG criteria; response after the start of subsequent therapy or re-treatment with cilta-cel was not considered.
MRD negativity, defined as the proportion of patients who had negative MRD by bone marrow aspirate at any time point after the initial dose of the treatment regimen initiated at baseline and before disease progression or starting subsequent therapy or re-treatment with cilta-cel. Minimal residual disease positive patients included those for whom all tested samples were found to be MRD -positive or ambiguous. Patients with missing or unevaluable MRD status were considered as MRD -positive. MRD negativity was assessed at 10−4, 10−5, and 10−6.
PFS, defined as the time from the index date to the date of the first documented disease progression, as defined in the IMWG criteria, or death due to any cause, whichever occurred first. For patients who had not progressed and were alive, data were censored at the last disease evaluation before the start of any subsequent antimyeloma therapy or the re-treatment of cilta-cel.
OS, defined as the time from the index date to the date of the patient’s death. If the patient was alive or the vital status was unknown, then the patient’s data were censored at the date the patient was last known to be alive. Patients who died after consent withdrawal were considered as having an OS event.
PRO end points, including the EQ visual analogue scale and the EORTC QLQ-C30 Global Health Status, collected for CARTITUDE-1 at screening, days 7, 28, 56, 78, and 100 after infusion, and every 28 days thereafter. For LocoMMotion, PRO end points were collected at screening, days 1 and 7 of cycle 1, and at day 1 of every subsequent cycle. The index date for CARTITUDE-1 was the date of the infusion. As baseline PROs were assessed at screening only, screening values were used to impute values at infusion. For LocoMMotion, the index date was day 1. No adjusted analyses were conducted on the PRO end points; thus, the comparisons are not included in this report.
Safety end points, including any TEAEs, TEAEs of special interest (CRS, tumour lysis syndrome, neurotoxicity, and second primary malignancy), TEAEs leading to death, TEAEs by System Organ Class and Preferred Term, serious TEAEs, and severe TEAEs (Common Terminology Criteria for Adverse Events grade ≥ 3). No adjusted analyses were conducted on the safety outcomes; thus, the comparisons are not included in this report.
Other outcomes including other PROs, medical resource use, TTNT, clinical benefit rate, DOR, and TTR were planned to be analyzed, but were not evaluated in the report submitted by the sponsor.
Analysis methods: Outcome assessments were performed by the investigator and by an IRC in both the CARTITUDE-1 and LocoMMotion studies. The results presented in the sponsor-submitted report are based on the IRC assessments.
Potential prognostic variables in patients with triple class–exposed r/rMM were identified a priori through a review of the published literature and in consultation with clinical expert input. Potentially important prognostic factors consisted of the following: age, sex, race, body weight, baseline ISS disease stage, MM type, years since initial MM diagnosis, creatinine clearance, selected hematology laboratory analytes (hemoglobin, platelets, absolute lymphocyte count, white blood cell count, absolute neutrophil count), selected chemistry laboratory analytes (aspartate aminotransferase, alanine aminotransferase, alkaline phosphatase, creatinine clearance), albumin, beta2-microglobulin, ECOG PS, number of prior lines of therapy, number of prior lines of therapy by number of years since diagnosis, prior exposure or refractoriness to commonly used MM drugs, prior treatment with radiation, cytogenetic risk, level of refractoriness, type of measurable disease, time since disease became refractory, refractory to previous lines of therapy (yes or no), LDH, history of prior SCT, number of lytic bone lesions, extramedullary disease, and percentage of plasma cells in bone marrow. The prognostic strength of a factor was assessed by univariate regression, and the population differences were assessed using standardized mean differences (SMDs), where an SMD greater than 0.2 at the covariate level was considered indicative of an imbalance between groups. This rank-ordered list was presented to and validated by external clinical experts consulted by the authors of the study. The ranking was updated as required until a consensus was reached on the final rank-ordered list of factors.
A total of 17 covariates considered to be prognostic factors were established. The covariates included in the primary propensity score and outcome regression models were refractory status, ISS stage, time to progression (prior line), extramedullary disease, number of prior lines, years since diagnosis, average duration of prior lines, age, hemoglobin (g/dL), LDH (units/L), creatinine clearance (mL/min), ECOG PS, sex, and MM type. Covariates of race, history of transplant, and cytogenetic risk were considered important, but were not included. Race and history of transplant were reported by the sponsor to have a minimal impact on results but represented a source of imbalance for other baseline variables. While cytogenetic risk is known to be an important predictive factor, the sponsor noted that coverage in LocoMMotion was low (37.9% missing), despite the fact it was a required variable to be collected in the study.
Analysis Methods
Two statistical methods were used in the analyses, based on the predefined process, adapted from the National Institute for Health and Care Excellence Decision Support Unit Technical Support Document 17,60 a propensity score–weighted estimator and multivariable regression model.
Table 24: Key Study Design Features of Data Sources Included in the Sponsor-Submitted Observational Study — CARTITUDE-1 Versus LocoMMotion
Characteristics | CARTITUDE-1 | LocoMMotion |
|---|---|---|
Study design | Open-label, single-arm, phase Ib and II | Prospective observational, multinational cohort study |
Locations | 16 study sites in the US | 76 study sites (63 in Europe, 13 in the US) |
N analyzed | 113 (ITT), 97 (mITT) | 248 (ITT), 170 (mITT) |
Data cut-off | January 2022 | May 2021 |
Follow-up | Postinfusion period: Day 1 to day 100 Post-treatment period: Day 101 to end of study (2 years after last patient received initial dose) | NR |
Inclusion criteria |
|
|
Exclusion criteria |
| Must not be pregnant or must not plan to become pregnant within the study period |
Treatments | Ciltacabtagene autoleucel | Standard care based on clinical practice |
End points |
|
|
BCMA = B-cell maturation antigen; CAR T = chimeric antigen receptor T cell; CD = cluster of differentiation; CNS = central nervous system; CR = complete response; DOR = duration of response; ECOG = Eastern Cooperative Oncology Group; HRQoL = health-related quality of life; IMiD = immunomodulatory drug; IMWG = International Myeloma Working Group; ITT = intention-to-treat; LOT = line of therapy; mITT = modified intention-to-treat; MM = multiple myeloma; MRD = minimal residual disease; NR = not reported; ORR = overall response rate; OS = overall survival; PD = progressive disease; PFS = progression-free survival; PI = proteasome inhibitor; PK = pharmacokinetics; r/rMM = relapsed or refractory multiple myeloma; TTNT = time to next treatment; TTR = time to response; VGPR = very good partial response.
Propensity score weighting: Propensity scores were estimated using logistic regression specifying the binary treatment indicator as the dependent variable and selected baseline covariates as explanatory variables. The predicted propensity scores were then used to derive weights for each patient using the estimand-specific weighting formulas. IPW was used to reweight imbalanced baseline characteristics that were dissimilar between the CARTITUDE-1 and LocoMMotion cohorts. The primary analysis estimated the average treatment effect in the treated population (ATT) using IPW (IPW-ATT). Diagnostic metrics, including the degree of balance achieved by the different propensity score methods as measured by SMDs before and after weighting, and the achievement of overlap in estimated propensity scores in the distribution of the 2 treated cohorts, were considered when selecting an optimal propensity scoring method.
For secondary outcomes (including PFS, OS, and other measures), weighted Cox proportional hazards models were used to estimate the causal HR and corresponding 95% CIs. For some dichotomized outcomes (including ORR, VGPR or better, CR or better, and MRD negativity), weighted logistic regression models were used to estimate the OR and corresponding 95% CIs. The reported ORs were subsequently transformed to estimate response rate ratios.
Regression models: Multivariable regressions models were specified, including a treatment indicator and baseline covariates for adjustment in the model.
For time-to-event outcomes (including PFS, OS, TTNT, time to first response, DOR, and other measures), unweighted Cox proportional hazards models adjusting for covariates were used to estimate conditional HRs and their corresponding 95% CIs. For binary outcomes (including ORR, VGPR or better, CR or better, and MRD negativity), unweighted logistic regression models adjusting for covariates were used to estimate treatment effects in terms of conditional causal ORs and 95% CIs to determine the comparative efficacy of cilta-cel versus the LocoMMotion cohort.
Sensitivity analyses: In addition to the primary IPW-ATT approach, a sensitivity analysis using an alternative weighting formula for deriving the average treatment effect for the overlap population (ATO) was also conducted. Sensitivity analyses also explored the stability of the methods, wherein additional variables (race, history of prior transplant, cytogenetic risk) were included in the calculation of propensity scores.
Analysis of PRO end points: PRO end points were analyzed using a mixed-model for repeated measures, with change from baseline as the outcome and treatment, baseline value, visit, and treatment and visit interaction as fixed effects. However, given the inability to interpret unadjusted comparisons as treatment effects over time, the results were not included in the CADTH summary and appraisal.
Missing data: Complete data were available for CARTITUDE-1. For LocoMMotion, variables with a proportion of missing values of less than 25% (ISS, 12.5%; hemoglobin, 10.1%; LDH, 23.8%; creatinine clearance, 5.2%; ECOG, 1.2%; MM type, 16.5%) were imputed using the multiple imputation with chained equations approach.
Proportional hazards assumption: The proportional hazards assumption (PHA) for survival outcomes was assessed based on visual inspection of the log-cumulative hazard plot, visual inspection of the Schoenfeld residuals plot, and performance of the Grambsch-Therneau test with a P value of less than 0.05 considered to indicate a violation of the assumption. In cases where evidence was found that the PHA was violated, the sponsor considered alternative summaries of treatment effect, such as the restricted mean survival time, although results were not reported.
Results of the Sponsor-Submitted Observational Study: CARTITUDE-1 Versus LocoMMotion
Summary of Included Studies
Baseline covariates for ITT and mITT populations in the CARTITUDE-1 and LocoMMotion cohorts before and after IPW-ATT are summarized in Table 25. The CARITUDE-1 study consisted of 113 patients who underwent apheresis and made up the ITT population, and 97 patients who were treated with cilta-cel (mITT). Patients were selected from LocoMMotion based on the eligibility criteria for CARTITUDE-1. In total, 248 patients were enrolled into the LocoMMotion trial (ITT), and 170 patients were alive and progression-free after 52 days (mITT). After weighting, the effective ITT and mITT population size of the LocoMMotion cohort were 118, and 108 patients, respectively.
Prior to adjustment, there were numerous pairwise imbalances (SMD > 0.2) in baseline characteristics between CARTITUDE-1 and LocoMMotion cohorts. In the ITT population, CARTITUDE-1 enrolled more patients with pentuple refractory disease compared with the LocoMMotion population (||||% versus ||||%), and LocoMMotion included more patients with disease that was less than double (||||% versus ||||%) and triple (|||% versus ||||%) refractory. Compared with the LocoMMotion cohort, the CARTITUDE-1 group also consisted of more patients with:
ISS stage I disease (||||% versus ||||%) and fewer with ISS stage III disease (||||% versus ||||%)
a creatinine clearance of 90 mL/min or greater (||||% versus ||||%) and fewer with a creatinine clearance of less than 60 mL/min (||||% versus ||||%)
an ECOG PS of 0 (||||% versus ||||%) rather than 1
the immunoglobulin G type of MM (||||% versus ||||%) rather than non–immunoglobulin G type.
Other differences were observed for age, average duration of prior lines of therapy, time to progression on prior lines of therapy, and number of prior lines of therapy. Similar differences were observed in the mITT population, although differences were also observed for LDH and hemoglobin levels.
After adjustment, although there were no imbalances with an SMD greater than 0.2, observable differences remained in the ITT populations with regard to pentuple refractory status (||||% versus ||||%) and quadruple refractory status |||||% versus ||||||| years since diagnosis (< 6 years, ||||% versus ||||%; ≥ 6 years, ||||% versus ||||%), and hemoglobin (< 12 g/dL, ||||% versus ||||%; ≥ 12 g/dL, ||||% versus ||||%). In the mITT populations, observable differences remain in pentuple refractory status (||||% versus ||||%) and quadruple refractory status (||||% versus ||||%), extramedullary disease (||||% versus ||||||), age (≥ 65 years, ||||% versus ||||%), and ECOG PS (||, ||||% versus ||||%; ||, ||||% versus |||||).
Cytogenetic risk was considered an important risk factor; however, it was not included in the base-case analyses due to a high level of missingness in the LocoMMotion cohort (37.9% missing). When reported, there was a notable difference in the proportion of patients at a standard risk (ITT, ||||% versus ||||%; mITT, ||||% versus ||||%) and high risk (ITT, ||||% versus ||||%; mITT, |||% versus ||||%) between CARTITUDE-1 and LocoMMotion populations. Sensitivity analyses were conducted for both the ITT and mITT populations, including cytogenetic risk, race, and history of autologous SCT, for which the balance between groups was reduced based on the proportion of variables with an SMD greater than 0.2. Additional sensitivity analyses using IPW-ATO reweighting achieved the desired balance between groups in the selected prognostic variables.
Table 25: Overview of Patient Characteristics Before and After IPW-ATT
Ranked baseline covariates | ITT population | mITT population | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
CARTITUDE-1 | LocoMMotion before IPW-ATT | SMD | LocoMMotion after IPW-ATT | SMD | CARTITUDE-1 | LocoMMotion before IPW-ATT | SMD | LocoMMotion after IPW-ATT | SMD | |
Sample size, N | ||| | ||| | ||| | ||| | ||| | || | ||| | ||| | ||| | ||| |
Refractory status, % | ||||||||||
≤ Double | |||| | |||| | |||| | |||| | |||| | |||| | |||| | |||| | ||| | |||| |
Triple | ||| | |||| | ||| | ||| | |||| | ||| | ||||
Quadruple | |||| | |||| | |||| | |||| | |||| | |||| | ||||
Pentuple | |||| | |||| | |||| | |||| | |||| | |||| | ||||
ISS stage, % | ||||||||||
I | |||| | |||| | |||| | |||| | |||| | |||| | |||| | |||| | |||| | |||| |
II | |||| | |||| | |||| | |||| | |||| | |||| | ||||
III | |||| | |||| | |||| | |||| | |||| | |||| | ||||
Time to progression (prior line), % | ||||||||||
< 3 months | |||| | |||| | ||||| | |||| | |||| | |||| | |||| | ||||| | |||| | |||| |
≥ 3 months | |||| | |||| | |||| | |||| | |||| | |||| | ||||
Extramedullary disease, % | ||||||||||
Yes | |||| | |||| | ||||| | |||| | |||| | |||| | |||| | ||||| | |||| | |||| |
No | |||| | |||| | |||| | |||| | |||| | |||| | ||||
Number of prior lines, % | ||||||||||
≤ 4 | |||| | |||| | |||| | |||| | ||||| | |||| | |||| | |||| | |||| | ||||| |
5+ | |||| | |||| | |||| | |||| | |||| | |||| | ||||
Years since diagnosis, % | ||||||||||
< 6 | |||| | |||| | ||||| | |||| | ||||| | |||| | |||| | ||||| | |||| | ||||| |
≥ 6 | |||| | |||| | |||| | |||| | |||| | |||| | ||||
Average duration of prior lines, % | ||||||||||
< 8.14 months | |||| | |||| | |||| | |||| | |||| | |||| | ||| | |||| | |||| | |||| |
8.14 to < 11.76 months | |||| | |||| | |||| | |||| | |||| | |||| | ||||
11.76+ months | |||| | |||| | |||| | |||| | |||| | |||| | ||||
Age, % | ||||||||||
< 65 years | |||| | |||| | ||||| | |||| | |||| | |||| | |||| | ||||| | |||| | |||| |
≥ 65 years | |||| | |||| | |||| | |||| | |||| | |||| | ||||
Hemoglobin (g/dL), % | ||||||||||
< 12 | |||| | |||| | |||| | |||| | |||| | |||| | |||| | ||||| | |||| | |||| |
≥ 12 | |||| | |||| | |||| | ||| | |||| | ||| | ||||
LDH (units/L), % | ||||||||||
< 280 | |||| | |||| | ||||| | |||| | |||| | |||| | |||| | ||||| | |||| | |||| |
≥ 280 | |||| | |||| | |||| | |||| | |||| | |||| | ||||
Creatinine clearance (mL/min), % | ||||||||||
< 60 | |||| | |||| | |||| | |||| | |||| | |||| | |||| | |||| | |||| | |||| |
60 to 90 | |||| | |||| | |||| | |||| | |||| | |||| | ||||
≥ 90 | |||| | |||| | |||| | |||| | |||| | |||| | ||||
ECOG Performance Status, % | ||||||||||
0 | |||| | |||| | ||||| | |||| | ||||| | |||| | |||| | ||||| | |||| | ||||| |
1 | |||| | |||| | |||| | |||| | |||| | |||| | ||||
Gender, % | ||||||||||
Male | |||| | |||| | ||||| | |||| | |||||| | |||| | |||| | ||||| | |||| | |||| |
Female | |||| | |||| | |||| | |||| | |||| | |||| | ||||
MM type, % | ||||||||||
IgG | |||| | |||| | ||||| | |||| | |||| | |||| | |||| | ||||| | |||| | |||| |
Non-IgG | |||| | |||| | |||| | |||| | |||| | |||| | ||||
ATT = average treatment effect in the treated population; ECOG = Eastern Cooperative Oncology Group; IgG = immunoglobulin G; IPW = inverse probability of treatment weighting; ITT = intention-to-treat; ISS = International Staging System; LDH = lactate dehydrogenase; MM = multiple myeloma; RWCP = real-world clinical practice; SMD = standardized mean difference.
Note: The preweighting and postweighting distributions of demographics by intervention group are shown. SMDs > 0.2 were considered to indicate differences between groups.
Source: Sponsor-submitted indirect treatment comparison.20
Table 26 outlines the real-world treatment regimens received in LocoMMotion. Patients received a total of 291 treatment regimens in their RWCP line of interest for a total of 92 unique regimens. Therefore, patients could be counted in more than 1 regimen if they received more than 1 combination in their treatment before progression or death. The 9 most frequently used regimens comprised 51.9% of all patients, and 43 patients (17.3%) received a regimen that was not received by any other patient in the sample.
Table 26: Treatment Regimens in the LocoMMotion Cohort
Treatment | Frequency (N = 248) |
|---|---|
Carfilzomib-dexamethasone | 34 (13.7%) |
Cyclophosphamide-dexamethasone-pomalidomide | 33 (13.3%) |
Dexamethasone-pomalidomide | 28 (11.3%) |
Dexamethasone-ixazomib-lenalidomide | 14 (5.6%) |
Bortezomib-dexamethasone-panobinostat | 11 (4.4%) |
Bendamustine-bortezomib-dexamethasone | 7 (2.8%) |
Carfilzomib-cyclophosphamide-dexamethasone | 7 (2.8%) |
Dexamethasone-elotuzumab-pomalidomide | 6 (2.4%) |
Dexamethasone-lenalidomide | 6 (2.4%) |
Other | 145 (58%) |
Source: Sponsor-submitted indirect treatment comparison.20
Results
Overall survival: Results comparing OS between CARTITUDE-1 and LocoMMotion before and after adjustment are summarized in Table 27. The median OS for CARTITUDE-1 was NE (95% CI, 31.47 to NE) in the ITT population, and NE (95% CI, NE to NE) for the mITT population. The median OS for LocoMMotion RWCP estimated using IPW-ATT weighting was ||||| |||||| |||| ||| |||| || ||| in the ITT population, and 11.33 months (95% CI, 5.45 to NE) in the mITT population. Following adjustment, the conditional HR for OS was 0.32 (95% CI, 0.17 to 0.58) in the ITT population and 0.20 (95% CI, 0.09 to 0.41) in the mITT population, both favouring cilta-cel.
Results for additional analyses of OS using regression modelling, sensitivity analyses using IPW-ATO weights, and including additional variables (race, history of prior transplant, cytogenetic risk) are summarized in Figure 17. Results for these analyses were consistent with the primary analysis.
The log-cumulative hazard plot and Schoenfeld residuals plots for each outcome were visually inspected and there was no evidence of violation of the PHA before significant patient drop-off. For OS, the Grambsch-Therneau test was nonsignificant, indicating the PHA to be appropriate.
Health-related quality of life: No adjusted analyses of PRO end points were conducted; therefore, the results of PRO end points are not summarized in this report.
Table 27: Unadjusted and Adjusted Kaplan-Meier Estimated OS (ITT and mITT Populations)
Study | Unadjusted | Adjusted (ATT) | ||||
|---|---|---|---|---|---|---|
Median OS, months (95% CI) | 12-month OS rate, % (95% CI) | 15-month OS rate, % (95% CI) | Median OS, months (95% CI) | 12-month OS rate, % (95% CI) | 15-month OS rate, % (95% CI) | |
ITT population | ||||||
CARTITUDE-1 | NE (31.47 to NE) | ||||| |||||||| |||||| | ||||| |||||||| |||||| | NE (31.47 to NE) | ||||| |||||||| |||||| | ||||| |||||||| |||||| |
LocoMMotion | 12.39 (10.28 to NE) | 51.75 (44.15 to 58.83) | ||||| |||||||| |||||| | ||||| ||||||| ||| | ||||| |||||||| |||||| | ||||| |||||||| |||||| |
mITT population | ||||||
CARTITUDE-1 | NE (NE to NE) | ||||| |||||||| |||||| | ||||| ||||||| |||||| | NE (NE to NE) | ||||| |||||||| |||||| | ||||| ||||||| |||||| |
LocoMMotion | NE (12.12 to NE) | ||||| |||||||| |||||| | ||||| |||||||| |||||| | 11.33 (5.45 to NE) | ||||| |||||||| |||||| | ||||| |||||||| |||||| |
ATT = average treatment effect in the treated population; CI = confidence interval; HR = hazard ratio; ISS = international staging system; ITT = intention-to-treat; LOT = line of therapy; mITT = modified intention-to-treat; MM = multiple myeloma; NE = not estimable; OS = overall survival.
Note: Adjusted results correspond to the fully adjusted scenario, which adjusted for refractory status, ISS stage, time to progress on last regimen, extramedullary disease, number of prior LOTs, years since MM diagnosis, average duration of prior LOTs, age, hemoglobin, lactate dehydrogenase, creatinine clearance, Eastern Cooperative Oncology Group Performance Status, sex, and MM type.
Source: Sponsor-submitted indirect treatment comparison.20
Progression-free survival: Results comparing the PFS estimates for CARTITUDE-1 and LocoMMotion are summarized in Table 28. The median PFS for CARTITUDE-1 was 28.03 months (95% CI, 20.11 to NE) in the ITT population, and NE (95% CI, 24.54 to NE) for the mITT population. The median PFS for LocoMMotion RWCP using IPW-ATT weighting was 4.07 months (95% CI, 2.86 to 5.09) in the ITT population, and 2.73 months (95% CI, 2.37 to 3.68) in the mITT population. Following adjustment, the conditional HR for PFS between treatment groups was 0.19 (95% CI, 0.11 to 0.32) in the ITT population and 0.15 (95% CI, 0.08 to 0.29) in the mITT population, both favouring cilta-cel.
Results for additional analyses of PFS using regression modelling, sensitivity analyses using IPW-ATO weights, and including additional variables (race, history of prior transplant, cytogenetic risk) are summarized in Figure 17. Results for these analyses were consistent with the primary analysis.
The log-cumulative hazard plot and Schoenfeld residuals plots for each outcome were visually inspected and there was no evidence of violation of the PHA before significant patient drop-off. For PFS, the Grambsch-Therneau test was nonsignificant, indicating the PHA to be appropriate.
Table 28: Unadjusted and Adjusted Kaplan-Meier Estimated PFS (ITT and mITT Populations)
Study | Unadjusted | Adjusted (ATT) | ||||
|---|---|---|---|---|---|---|
Median PFS, months (95% CI) | 12-month PFS rate, % (95% CI) | 15-month PFS rate, % (95% CI) | Median PFS, months (95% CI) | 12-month PFS rate, % (95% CI) | 15-month PFS rate, % (95% CI) | |
ITT population | ||||||
CARTITUDE-1 | ||||| |||||||| ||| | ||||| |||||||| |||||| | ||||| |||||||| |||||| | ||||| |||||||| ||| | ||||| |||||||| |||||| | ||||| |||||||| |||||| |
LocoMMotion | 4.63 (3.88 to 5.62) | 19.88 (13.65 to 26.97) | ||||| |||||||| |||||| | |||| ||||||| ||||| | ||||| ||||||| |||||| | ||||| ||||||| |||||| |
mITT population | ||||||
CARTITUDE-1 | NE (24.54 to NE) | ||||| |||||||| |||||| | ||||| |||||||| |||||| | NE (24.54 to NE) | ||||| |||||||| |||||| | ||||| |||||||| |||||| |
LocoMMotion | 4.34 (3.65 to 5.55) | ||||| |||||||| |||||| | ||||| |||||||| |||||| | |||| ||||||| ||||| | ||||| ||||||| |||||| | ||||| ||||||| |||||| |
ATT = average treatment effect in the treated population; CI = confidence interval; ISS = international staging system; ITT = intention-to-treat; LOT = line of therapy; mITT = modified intention-to-treat; MM = multiple myeloma; NE = not estimable; PFS = progression-free survival.
Note: Adjusted results correspond to the fully adjusted scenario, which adjusted for refractory status, ISS stage, time to progress on last regimen, extramedullary disease, number of prior LOTs, years since MM diagnosis, average duration of prior LOTs, age, hemoglobin, lactate dehydrogenase, creatinine clearance, Eastern Cooperative Oncology Group Performance Status, sex, and MM type.
Source: Sponsor-submitted indirect treatment comparison.20
Clinical response outcomes: Results comparing CARTITUDE-1 and LocoMMotion for clinical response outcomes, including ORR and VGPR, are summarized in Table 29. In CARTITUDE-1, the ORR for observed proportions in the ITT and mITT populations for cilta-cel were 84.1% and 97.9%, respectively. In LocoMMotion, the ORR in the ITT and mITT populations for RWCP were 29.8% and 42.9%, respectively. The IPW-estimated OR was 22.00 (95% CI, 11.14 to 43.35) in the ITT population and 103.87 (95% CI, 24.17 to 446.37) in the mITT population, both in favour of cilta-cel. For VGPR, observed proportions within the ITT and mITT populations for response rates of VGPR or better were 81.4% and 94.8% from CARTITUDE-1, and 12.5% and 17.6% for LocoMMotion. The IPW-estimated OR was 39.08 (95% CI, 18.19 to 83.98) in the ITT population and 91.55 (95% CI, 32.63 to 256.89) in the mITT population, both in favour of cilta-cel. For both the ITT and mITT populations, no analyses of a response rate of CR or better and MRD negativity were conducted due to the small number of observed values in the LocoMMotion cohort. Observed response rates of CR or better in the cilta-cel and LocoMMotion cohorts were 70.8% and 0.4% in the ITT population and 82.5% and 0.6% in the mITT population. As 2 bone marrow samples were required for evaluation of MRD negativity, the base for the calculation could not be estimated for the ITT population in CARTITUDE-1, while 0 patients were MRD-negative in the ITT population in LocoMMotion. In the mITT population of CARTITUDE-1, 91.8% patients had evaluable MRD-negative samples, while MRD negativity was not evaluable in the mITT population in LocoMMotion.
Results for additional analyses of ORR and VGPR using regression modelling, sensitivity analyses using IPW-ATO weights, and including additional variables (race, history of prior transplant, cytogenetic risk) are summarized in Figure 16. Results for these analyses were consistent with the primary analysis.
Table 29: Summary of Observed and Adjusted Comparisons for Response Outcomes
Outcome | CARTITUDE-1, % | LocoMMotion, % | Adjusted RWCP, % (95% CI) | Observed OR (95% CI) | IPW-ATT adjusted OR (95% CI) | Response rate ratio (95% CI) |
|---|---|---|---|---|---|---|
ITT population | ||||||
ORR | 84.1% | 29.8% | 19.0 (13 to 27) | 12.41 (7.00 to 22.00) | 22.00 (11.14 to 43.35) | 4.34 (2.69 to 6.00) |
≥ VGPR | 81.4% | 12.5% | 10.0 (6 to 17) | 30.67 (16.74 to 56.17) | 39.08 (18.19 to 83.98) | 8.08 (3.63 to 12.53) |
mITT population | ||||||
ORR | 97.9% | 42.9% | 31 (23 to 41) | 63.12 (15.06 to 264.53) | 103.87 (24.17 to 446.37) | 3.12 (2.24 to 4.00) |
≥ VGPR | 94.8% | 17.6% | 17 (11 to 25) | 85.87 (32.14 to 229.39) | 91.55 (32.63 to 256.89) | 5.67 (3.25 to 8.08) |
ATT = average treatment effect in the treated population; CI = confidence interval; IPW = inverse probability weighting; ITT = intention-to-treat; LOT = line of therapy; mITT = modified intention-to-treat; MM = multiple myeloma; OR = odds ratio; ORR = overall response rate; RWCP = real-world clinical practice; VGPR = very good partial response.
Note: Adjusted comparisons account for refractory status, International Staging System stage, time to progression on prior line, presence of extramedullary disease, number of prior LOTs, years since MM diagnosis, average duration of prior LOTs, patient age and sex, hemoglobin at index date, lactate dehydrogenase at index date, creatinine clearance at index date, Eastern Cooperative Oncology Group Performance Status, and MM type.
Source: Sponsor-submitted indirect treatment comparison.20
Time to response: No results for TTR were included in the study comparing CARTITUDE-1 and LocoMMotion.
Safety: Only unadjusted comparisons of AEs from the CARTITUDE-1 and LocoMMotion studies were reported, and no adjusted analyses were conducted; therefore, harms results are not summarized in this report.
Critical Appraisal of Sponsor-Submitted Observational Study: CARTITUDE-1 Versus LocoMMotion
Given the lack of a comparator arm in the CARTITUDE-1 trial, the use of external real-world data to emulate a control arm was justified. The prospective, real-world LocoMMotion cohort was selected as an external control arm representing RWCP for this analysis based on its inclusion and exclusion criteria and enrolled population, which aimed to reduce the potential for selection bias and heterogeneity between populations by emulating a theoretical RCT for cilta-cel within the CARTITUDE-1 population.
In general, there was variation in the design of the CARTITUDE-1 and LocoMMotion studies, primarily that CARTITUDE-1 was a phase Ib/II, open-label trial while LocoMMotion was an observational and noninterventional study. Both studies were open label, so there is a risk of bias in the measurement of subjective outcomes, primarily for the response outcomes as well as harms and HRQoL, though harms and HRQoL results were not included in this report. In both studies, IRC was used for response outcomes; thus, the risk of bias may be reduced. Objective outcomes, including OS, should be unaffected by the open-label designs. The LocoMMotion cohort represented a broad population from Europe and the US, whereas the results from CARTITUDE-1 are drawn from US patients only. It is uncertain whether there are differences in clinical practice, or availability of treatments by region, and the direction and magnitude of potential biases remains unclear. Additionally, there were no Canadian investigative sites included in either the CARTITUDE-1 or LocoMMotion studies, which may impact the generalizability of the results to patients in Canada. Both the ITT and mITT populations were analyzed in the study. Analyses using the ITT population were considered more appropriate for comparisons, given that the mITT population excluded patients who progressed or died in the first 47 or 52 days. As such, the ITT population was more appropriate to estimate the effect of treatment assignment, while the mITT analyses were at a greater risk of bias due to the elimination of patients who were sicker, likely favouring cilta-cel. Regardless, outcomes were consistent across the ITT and mITT populations. An additional source of heterogeneity between the CARTITUDE-1 study and the LocoMMotion study affecting the generalizability of the results was the prior regimens received by patients in LocoMMotion. A total of 92 distinct regimens were used as prior treatment. Given the numerous prior treatment regimens, lack of analyses by type of prior regimen, and irrelevancy of many treatment regimens to Canadian clinical practice, the results of the study may not be generalizable to the population of patients in Canada.
As previously mentioned, the inclusion criteria for the LocoMMotion study were designed to match the inclusion criteria for the CARTITUDE-1 trial. Despite this, there was notable heterogeneity in the populations of the CARTITUDE-1 and LocoMMotion studies. The external validity of the results is generally in line with those from the CARTITUDE-1 study, given that the comparator population was adjusted for similarity to patients from CARTITUDE-1. Patients included in the CARTITUDE-1 trial were younger than those included in RWCP (i.e., patients included in LocoMMotion). Additionally, all patients had an ECOG PS of 0 or 1. Thus, the findings cannot be generalized to patients with an ECOG PS of 2 or more; however, as noted for the CARTITUDE-1 trial, the clinical experts consulted by CADTH considered generalizing to patients with an ECOG PS of 2 to be acceptable. A comprehensive list of potential prognostic covariates was identified through a review of the published literature and in discussion with clinical experts in the field consulted by the study authors. A total of 17 different potential prognostic factors were identified and 15 were considered and ranked in the analyses. Though covariates were ranked in order from most to least likely to influence the outcome of interest, the specific methods of ranking were not provided; thus, it is unclear what criteria were used to determine rank. Prior to adjustment, the baseline covariates for prognostic factors demonstrated considerable heterogeneity in refractory status, ISS stage, time to progression on prior lines of therapy, number of prior lines of therapy, duration of prior lines of therapy, age, creatinine clearance, ECOG PS, and MM type. Comparisons with externally generated cohorts are limited by the availability of information important to the analysis; indeed, the sponsor noted that due to significant missingness of data, covariates of race, history of transplant, and cytogenetic risk were not included in the adjustment. A sensitivity analysis of baseline covariate adjustment was conducted; however, results for the analyses including these covariates were not presented; thus, the impact of their exclusion remains unknown. Moreover, cytogenetic risk was considered a particularly important prognostic factor by the clinical experts consulted by CADTH; thus, its omission from the analyses must be considered. As with all nonrandomized studies, the potential for residual confounding for unobserved patient characteristics cannot be ruled out. Following adjustment, some heterogeneity remained, particularly in the mITT population, for refractory status, extramedullary disease, age, and ECOG PS.
Several assumptions were made in the analyses. The sponsor considered any patients with missing or unevaluable MRD status to be MRD-positive; in CARTITUDE-1, patients who died after consent withdrawal were considered as having an OS event. No consideration was given to the impact these assumptions had on the results, and no sensitivity or scenario analyses were conducted for these assumptions.
Multiple comparative analyses (propensity score weighting [IPW] and regression modelling) were performed for the ITT and mITT populations for CARTITUDE-1 versus the LocoMMotion study. The primary analysis method using IPW was considered appropriate, given the use of an external control arm and the need to adjust for confounding variables. Sensitivity analyses balancing baseline covariates using the ATO approach were also conducted, where perfect balance was achieved between treatment groups. The results of the adjusted treatment comparisons were consistent across end points, favouring cilta-cel over RWCP from the LocoMMotion study, with 95% CIs that did not include the null threshold. However, there was notable imprecision in all cases, as demonstrated by the wide 95% CIs, reflecting uncertainty in the magnitude of the effect. Though the reason for this imprecision was not hypothesized, it may be due to the small sample size of the CARTITUDE-1 trial, the observed heterogeneity between the populations, and potential endogeneity.
No adjusted analyses were conducted for HRQoL and safety outcomes and only naive comparisons of these outcomes from the CARTITUDE-1 and LocoMMotion trials were provided. As such, no conclusions can be drawn on the impact of cilta-cel on HRQoL or the comparative safety of cilta-cel versus current treatment options due to the risk of confounding.
Overall, given the phase Ib and phase II nature of the CARTITUDE-1 trial and the lack of a comparator arm, the ability to reach definitive conclusions on the comparative efficacy of cilta-cel was limited. Additionally, the heterogeneity between cohorts after adjustment, as well as the uncertainty of the results due to the assumptions made and the potential for residual confounding, limits the ability to draw strong conclusions about the comparative efficacy of cilta-cel versus other treatments. Given the adjustment of the LocoMMotion population to the CARTITUDE-1 population, the generalizability of the results is similar to that of CARTITUDE-1, which has previously been described in detail.
Methods of the Sponsor-Submitted Observational Study: CARTITUDE-1 Versus Real-World Cohorts21
Objectives
The objective of the sponsor-submitted observational study was to evaluate the comparative effectiveness of cilta-cel versus physicians’ choice as assessed in either the long-term follow-up of POLLUX, CASTOR, and EQUULEUS or Flatiron Health’s MM cohort registry.
Study Selection Methods
The data sources included in the report submitted by the sponsor included the IPD from the CARTITUDE-1 trial (data cut-off January 2022), the long-term follow-up of the global r/rMM daratumumab clinical trials (POLLUX, CASTOR, and EQUULEUS), and Flatiron Health’s longitudinal database. A flow chart depicting the selection of patients from each cohort is displayed in Figure 15.
CARTITUDE-1 was an open-label, single-arm, phase Ib and II trial; thus, observational comparisons using external control arms were conducted using CARTITUDE-1 as the index trial. All patients in the ITT and mITT population of the CARTITUDE-1 study were eligible for inclusion. The ITT population in CARTITUDE-1 included all patients who underwent apheresis, with the index date defined as the date of apheresis. The mITT population in CARTITUDE-1 consisted of all participants who received cilta-cel at the target dose, with the index date defined as the date of cilta-cel infusion. The ITT and mITT populations in CARTITUDE-1 consisted of 113 and 97 patients, respectively. The median follow-up period in CARTITUDE-1 as of the January 2022, data cut-off was 29 months for the ITT population and 27.7 months for the mITT population.
The first observational study aimed to compare patients treated with cilta-cel from the CARTITUDE-1 study and RWCP from the long-term follow-up for 3 trials of the anti-CD38 monoclonal antibody daratumumab (POLLUX, CASTOR, and EQUULEUS), hereinafter referred to as the daratumumab trial cohort. The POLLUX and CASTOR trials were both phase III, open-label RCTs, while the EQUULEUS study was an open-label, phase Ib study. To ensure similarity between CARTITUDE-1 and the daratumumab cohort, only those patients who satisfied key eligibility criteria for CARTITUDE-1 were included. These trials were selected considering various design and population characteristics, particularly the patient population, which included patients who were triple class–exposed and received at least 1 additional treatment following triple-class exposure (i.e., received ≥ 3 prior lines of therapy), with an ECOG PS less of than 2, a creatinine level of 2 mg/dL or less, and who had progressed on or within 12 months of the most recent line of therapy. These studies had also completed their primary analysis, had follow-up data available at least 6 months after primary database lock, and had provided subsequent therapy information, including line of therapy, best response, and progression status. Patients from these trials were included in the sponsor’s observational study from the point in time during their follow-up, when they fulfilled key eligibility criteria for CARTITUDE-1. Patients from both the daratumumab-based arms and the control arms (for participants who received an anti-CD38 monoclonal antibody as subsequent therapy during follow-up) were evaluated for inclusion in the study. The ITT population in the daratumumab trial cohort consisted of all participants who satisfied the eligibility criteria, with the index date defined as the start of each eligible line of therapy. The mITT population in the daratumumab trial cohort excluded eligible treatment lines, during which disease progression or death occurred within 47 days of initiating the respective line of therapy to account for the median of 47 days between apheresis and infusion in CARTITUDE-1. The index date was defined as the start of each eligible line of therapy plus 47 days. The ITT population from the daratumumab trial cohort included 351 patients (632 eligible lines of therapy), while the mITT population included 288 patients (434 eligible lines of therapy). The data cut-off for the updated analysis (2022) was June 2021, for CASTOR, September 2021, for POLLUX, and ranged from 2017 to 2019 for EQUULEUS, corresponding to an overall median follow-up of 23.9 months across all the eligible lines of therapy received after meeting the eligibility criteria.
The Flatiron Health longitudinal database represents a repository of patient-level electronic health records from community-based oncology clinics and academic centres in the US. Patients in the MM cohort registry were selected from the full Flatiron database who satisfied key eligibility criteria of CARTITUDE-1 and included the following criteria: newly diagnosed with MM (International Classification of Diseases, Ninth Revision [ICD-9] 203.0x or Tenth Revision [ICD-10] C90.0x or C90) and at least 2 documented clinical visits on or after January 1, 2011. All patients were required to be triple class–exposed with at least 1 additional treatment after triple-class exposure (i.e., received ≥ 3 prior lines of therapy). Patients were also required to have an ECOG PS of less than 2 and evidence of PD on or within 12 months of the most recent line of therapy or discontinuation of the core treatment within 60 days. The ITT and mITT populations in the Flatiron MM cohort were similar to the daratumumab trial cohort described previously. The ITT population consisted of 229 patients (482 eligible lines of therapy), and the mITT consisted of 196 patients (336 eligible lines of therapy). Patients included in the ITC initiated eligible lines of therapy between February 2016, and December 2019, and were followed until February 2021, to match the follow-up in CARTITUDE-1, corresponding to a median follow-up period of 21.9 months.
Figure 15: Flow Chart of Patient Selection in the Sponsor-Submitted Observational Study

Note: Figure was redacted at the sponsor’s request.
Outcomes evaluated in the sponsor-submitted report included ORR, CR or better rate, PFS (as well as aPFS, PFS, and rwPFS, as appropriate), and OS. The outcomes of CR and VGPR were not evaluated in the Flatiron database; therefore, an assessment of ORR and the rate of CR or better was not possible. The outcomes were defined as follows:
OS: In all cohorts, OS was defined as the time from the index data to the date or death. If a patient was alive or their vital status was not known, they were censored at the date they were last known to be alive. Since only the month and year of death were available in the Flatiron cohort, the middle of the month was used as the date of death. Patients in CARTITUDE-1 who died after consent withdrawal were considered as having an OS event.
aPFS: In all cohorts, an aPFS event was defined as disease progression, switch to subsequent treatment, or death due to any cause, whichever occurred first. For patients who experienced both disease progression and a subsequent treatment, the switch to subsequent treatment was considered the event. The duration was calculated as the time from index date to switch to a subsequent treatment postprogression, progression without subsequent treatment, or death, whichever occurred first. Patients who had not experienced an event were censored at their last disease evaluation. All events were ascertained by IRC in CARTITUDE-1 and by the investigator in the other cohorts.
rwPFS: In the daratumumab and Flatiron cohorts, rwPFS was defined as disease progression, switch to subsequent treatment, or death due to any cause, whichever occurred first. Duration was calculated as the time from the index data to the date of progression, start of next treatment, or death, whichever occurred first, with the date of last follow-up used in censoring. The rwPFS was ascertained by the investigator. In the analysis of rwPFS, events in CARTITUDE-1 were defined as per aPFS, described previously.
ORR: In both CARTITUDE-1 and the daratumumab cohort, ORR was defined as the proportion of patients who achieved a PR or better response according to IMWG criteria; ORR was assessed via IRC in CARTITUDE-1 and by the investigator in the daratumumab cohort. Patients in CARTITUDE-1 who experienced a response after the start of a subsequent therapy or re-treatment with cilta-cel were not considered.
CR or better rate: In both CARTITUDE-1 and the daratumumab cohort, a response rate of CR or better was defined as the percentage of patients achieving CR or sCR according to IMWG criteria. CR or better rate was assessed via IRC in CARTITUDE-1 and by the investigator in the daratumumab cohort.
Analysis Methods
Using the IPD from the CARTITUDE-1 trial, comparative efficacy versus RWCP (from the daratumumab trial cohort and the Flatiron cohort) was assessed using IPTW. The main analyses consisted of IPTW with ATT weighting, allowing for reweighting of the RWCP from the daratumumab trial and Flatiron cohorts to align with CARTITUDE-1. An initial analysis was conducted in 2021, with an updated analysis conducted in April 2022. As previously mentioned, 2 analytic populations were considered: the ITT and mITT populations.
A list of potentially important prognostic factors was created by consulting studies from a literature review as well as by collecting input from clinical experts consulted by the sponsor; however, few details were provided. The sponsor noted that a total of 15 of the identified prognostic factors were available in CARTITUDE-1. In consultation with the clinical experts consulted by the sponsor, the available prognostic factors were ranked from most to least important using an evidence-informed process considering both the strength of the prognostic factor in terms of PFS and OS and the degrees of imbalance between populations. Ranked prognostic factors in order of importance included refractory status, cytogenetic profile, ISS stage, presence of total plasmacytoma, time to progression on last regimen, number of prior lines of therapy, years since diagnosis, age, hemoglobin, LDH levels, prior SCT, ECOG status, race, sex, and type of MM. All relevant prognostic factors, with the exception of LDH and plasmacytoma, were available in the daratumumab trial cohort and the Flatiron cohort. The clinical experts consulted by the sponsor also agreed on a minimum set of factors that should be adjusted for in all analyses, which included the first 8 factors in the list.
The base-case analysis versus the daratumumab trial cohort weighted patients on the following factors: refractory status, cytogenetic profile, ISS stage, total plasmacytoma, time to progression on last regimen, number of prior lines of therapy, years since MM diagnosis, and age. The fully adjusted scenario also included hemoglobin, prior SCT, ECOG score, race, sex, and type of MM, in addition to the base-case variables. The base-case scenario versus the Flatiron cohort weighted patients on the following factors: refractory status, cytogenetic profile, ISS stage, time to progression on last regimen, number of prior lines of therapy, years since MM diagnosis, and age. The fully adjusted scenario also included hemoglobin, LDH, prior SCT, ECOG score, race, sex, and type of MM, in addition to the base-case variables.
The base case adjusted for the minimum set of factors deemed important by clinicians and considered all treatment lines initiated after becoming eligible (i.e., all index dates). Patients from the daratumumab trial cohort and the Flatiron cohort were able to be included at the earliest line of therapy initiated after all key eligibility criteria were met. This differed from the CARTITUDE-1 clinical trial, in which patients may have received additional lines of therapy between the time at which they first met all eligibility criteria and the time at which they were enrolled into the clinical trial. To account for this difference, patients in the physicians’ choice of treatment cohort who received multiple subsequent therapies after meeting eligibility criteria contributed multiple observations (corresponding to all eligible lines of therapy) to the current analysis, provided they met eligibility criteria at the beginning of each line of therapy. In such cases, a patient had multiple index dates, with 1 for each eligible line of therapy.
Regression models: Multivariable regressions were conducted including a binary treatment indicator (cilta-cel or RWCP) and covariates for adjustment in the model.
For time-to-event outcomes (e.g., PFS, aPFS, PFS or rwPFS, and OS), an unweighted Cox proportional hazards model adjusting for the relevant covariates was used to derive an HR and 95% CIs. For the comparison with Flatiron, an unweighted logistic regression adjusting for the relevant covariates was used to derive an OR and 95% CIs for binary outcomes (e.g., ORR and ≥ CR rate). The variance was estimated using a robust sandwich variance estimator specifying the participant identifier to account for participants with multiple index dates.
Sensitivity analyses: A range of sensitivity and exploratory analyses was conducted to assess the impact of modifying the participant populations, statistical methods, handling of missing data, eligible lines of therapy, and variables adjusted for in the analyses for the daratumumab trial cohort and the Flatiron cohort. The sensitivity analyses for the comparisons versus the daratumumab trial cohort and Flatiron cohort included IPTW analyses with ATT weighting (not doubly robust), multivariable regression, propensity score matching (1:1 nearest neighbour or optimal matching), and IPTW analyses with average treatment effect weighting (doubly robust). An exploratory analysis including only patients’ first eligible line of therapy was also conducted. Additional sensitivity analyses conducted for the Flatiron cohort comparison included the exclusion of observations with missing values for covariates of interest and the application of additional inclusion criteria from CARTITUDE-1 to the real-world cohort (11 + hemoglobin ≥ 8 g/dL and platelets ≥ 50 × 109/L).
Missing data: Missing values were imputed in the same way between CARTITUDE-1 and the daratumumab trial cohort and the Flatiron cohort. In CARTITUDE-1, prognostic factors were assessed at the time of apheresis for the ITT population and at the time of infusion for the mITT population, if available. If unavailable, the closest reported value before the index date was used. For the RWCP cohorts, which used different index dates, the time of assessment depended on the index date being used. For the CARTITUDE-1 population, the only variable requiring imputation was ISS stage (ITT population only). Values for the mITT were used for missing data at enrolment. If unavailable, mode value was used to impute missingness. For the RWCP cohort from the daratumumab trial cohort, the last observation was carried forward for variables (e.g., ECOG, cytogenetic profile), which was only assessed at the time of initial entry into the daratumumab clinical trials. Missing values for ISS stage were imputed using the mode value. For the RWCP cohort from Flatiron, imputation was required for ISS stage, hemoglobin, LDH, and ECOG PS. The last recorded value before the index date was used. Beta2-microglobulin values were used to impute missingness in ISS. A sensitivity analysis was conducted to assess the impact of imputation by only including complete cases for all variables except ECOG PS, which were preserved in the sensitivity analyses.
Proportional hazards assumption: The PHA for survival outcomes was assessed based on visual inspection of the log-cumulative hazard plot, visual inspection of the Schoenfeld residuals plot, and performance of the Grambsch-Therneau test with a P value of less than 0.05 considered to indicate a violation of the assumption.
Results of the Sponsor-Submitted ITC
Summary of Included Studies
As previously noted, the sponsor-submitted observational study compared the IPD from the CARTITUDE-1 trial with data from 3 daratumumab clinical trials (POLLUX, CASTOR, and EQUULEUS) and with a MM-specific population from the Flatiron cohort. Characteristics of the patients included in the observational study from each cohort are summarized in Table 30. The SMDs for covariates before and after weighting in the ITT and mITT populations between CARTITUDE-1 and the daratumumab trial cohort are summarized in Figure 18 and Figure 19, and the Flatiron cohort is summarized in Figure 20 and Figure 21 of Appendix 3.
The CARTITUDE-1 trial included 113 patients in the ITT population and 97 patients in the mITT population. A total of 351 and 288 patients were included in the daratumumab trial cohort in the ITT and mITT populations, respectively. After propensity score weighting, including covariates of refractory status, ISS stage, cytogenetic profile, time to progression on last regimen, extramedullary plasmacytomas, number of prior lines of therapy, years since MM diagnosis, and age, the base-case ESS of the daratumumab trial cohort was 212 in the ITT population and 116 in the mITT population. In the Flatiron cohort, 229 and 196 patients made up the ITT and mITT populations, respectively. After adjustment for the same covariates in the daratumumab trial cohort except for extramedullary plasmacytomas, the ESS for the Flatiron cohort was 192 in the ITT population and 80 in the mITT population.
Prior to weighting, there were notable differences (SMD > 0.2) between the CARTITUDE-1 and daratumumab trial populations in pentuple refractory status (||||% versus ||||%) versus triple or quadruple refractory status (||||% versus ||||%), time to progression on last therapy (> 4 months, ||||% versus ||||%), presence of extramedullary plasmacytosis (||||% versus |||%), number of prior lines of therapy (≤ 4, ||||% versus ||||%), years since MM diagnosis (> 6 years, ||||% versus ||||%), age (< 65 years, ||||% versus ||||%), hemoglobin level (≥ 12 g/dL, ||||% versus ||||%), and prior SCT (no, ||||% versus ||||%), with only moderate (SMD between 0.1 and 0.2) to small (SMD < 0.1) differences in remaining variables. After weighting, notable differences remained only for the variable of hemoglobin. For the mITT populations, notable differences before weighting were observed for refractory status, cytogenetic profile, time to progression on last regimen, extramedullary plasmacytomas, number of prior lines of therapy, age, hemoglobin level, prior SCT, and race. After weighting, differences remained for variables of extramedullary plasmacytomas, hemoglobin, prior SCT, and race.
Compared with the Flatiron cohort, there were notable differences in ISS stage (stage I, ||||% versus ||||%; stage II, ||||% versus ||||%; stage III, ||||% versus ||||%), cytogenetic profile (standard risk, ||||% versus ||||%; high risk, ||||% versus ||||%), time to progression on the prior line (≤ 4 months; ||||% versus ||||%), years since diagnosis (< 6 years, ||||% versus ||||%), age (< 65 years, ||||% versus ||||%), prior SCT (no, ||||% versus ||||%), and ECOG PS (ECOG 0, ||||% versus ||||%; ECOG 1, ||||% versus ||||%). After weighting, substantial differences remained for the variable of prior SCT, with moderate differences for LDH level and ECOG PS.
Table 30: Baseline Covariates Before and After Weighting; ITT and mITT Populations
Ranked baseline covariates | ITT population | mITT population | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
CARTITUDE-1 | Daratumumab trial cohorta | Flatiron cohortb | CARTITUDE-1 | Daratumumab trial cohort | Flatiron cohort | |||||
Before IPW-ATT | After IPW-ATT | Before IPW-ATT | After IPW-ATT | Before IPW-ATT | After IPW-ATT | Before IPW-ATT | After IPW-ATT | |||
N or ESS | ||| | ||| | ||| | ||| | ||| | || | ||| | || | ||| | || |
Refractory status, %d | ||||||||||
Triple or quadruple | || |||||| | ||| |||||| | || |||||| | || |||||| | || |||||| | || |||||| | ||| |||||| | || |||||| | || |||||| | || |||||| |
Pentuple | || |||||| | || |||||| | ||| |||||| | ||| |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| |
Other | || |||||| | || ||||| | || |||||| | || |||||| | || ||||| | || |||||| | || ||||| | | |||||| | || |||||| | | ||||| |
ISS stage, % | ||||||||||
I | || |||||| | ||| |||||| | ||| |||||| | || |||||| | ||| |||||| | || |||||| | ||| |||||| | || |||||| | || |||||| | || |||||| |
II | || |||||| | ||| |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| |
III | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || ||||| | | |||||| | || |||||| | || |||||| |
Time to progression (prior line), % | ||||||||||
≤ 4 months | || |||||| | || |||||| | ||| |||||| | || |||||| | ||| |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| |
> 4 months | || |||||| | ||| |||||| | || |||||| | ||| |||||| | || |||||| | || |||||| | ||| |||||| | || |||||| | ||| |||||| | || |||||| |
Extramedullary disease, %f,g | ||||||||||
Yes | || |||||| | || ||||| | ||| |||||| | || | || | || |||||| | || ||||| | || |||||| | || | || |
No | || |||||| | ||| |||||| | || |||||| | || | || | || |||||| | ||| |||||| | || |||||| | || | || |
Number of prior lines, % | ||||||||||
≤ 4 | || |||||| | ||| |||||| | || |||||| | || |||||| | || |||||| | || |||||| | ||| |||||| | || |||||| | || |||||| | || |||||| |
> 4 | || |||||| | ||| |||||| | ||| |||||| | ||| |||||| | ||| |||||| | || |||||| | || |||||| | || |||||| | ||| |||||| | || |||||| |
Years since diagnosis, % | ||||||||||
< 6 | || |||||| | ||| |||||| | ||| |||||| | ||| |||||| | ||| |||||| | || |||||| | ||| |||||| | || |||||| | ||| |||||| | || |||||| |
≥ 6 | || |||||| | ||| |||||| | || |||||| | || |||||| | || |||||| | || |||||| | ||| |||||| | || |||||| | || |||||| | || |||||| |
Age, % | ||||||||||
< 65 years | || |||||| | ||| |||||| | ||| |||||| | || |||||| | ||| |||||| | || |||||| | ||| |||||| | || |||||| | || |||||| | || |||||| |
≥ 65 years | || |||||| | ||| |||||| | || |||||| | ||| |||||| | || |||||| | || |||||| | ||| |||||| | || |||||| | ||| |||||| | || |||||| |
Hemoglobin (g/dL), % | ||||||||||
< 12 | || |||||| | ||| |||||| | ||| |||||| | ||| |||||| | ||| |||||| | || |||||| | ||| |||||| | || |||||| | ||| ||||||| | || |||||| |
≥ 12 | || |||||| | ||| |||||| | ||| |||||| | || |||||| | || |||||| | | ||||| | ||| |||||| | || |||||| | || ||||||| | || |||||| |
LDH (units/L), % | ||||||||||
< 280 | || |||||| | || | || | ||| |||||| | ||| |||||| | || |||||| | || | || | ||| ||||||| | || |||||| |
≥ 280 | || |||||| | || | || | || |||||| | || |||||| | || |||||| | || | || | || ||||||| | || |||||| |
ECOG Performance Status, % | ||||||||||
0 | || |||||| | ||| |||||| | || |||||| | || |||||| | || |||||| | || |||||| | ||| |||||| | || |||||| | || ||||||| | || |||||| |
1 | || |||||| | ||| |||||| | ||| |||||| | ||| |||||| | ||| |||||| | || ||||||| | ||| |||||| | || |||||| | ||| ||||||| | || |||||| |
Sex, % | ||||||||||
Male | || |||||| | ||| |||||| | ||| |||||| | ||| |||||| | ||| |||||| | || |||||| | ||| |||||| | || |||||| | ||| |||||| | || |||||| |
Female | || |||||| | ||| |||||| | || |||||| | ||| |||||| | || |||||| | || |||||| | ||| |||||| | || |||||| | || |||||| | || |||||| |
MM type, % | ||||||||||
IgG | || |||||| | ||| |||||| | || |||||| | ||| |||||| | ||| |||||| | || |||||| | ||| |||||| | || |||||| | ||||||||| | || |||||| |
Light chain | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| |
Other | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| |
Race | ||||||||||
White | || |||||| | ||| |||||| | ||| |||||| | ||| |||||| | ||| |||||| | || |||||| | ||| |||||| | || |||||| | ||| |||||| | || |||||| |
Black or African American | || |||||| | || ||||| | || ||||| | || |||||| | || |||||| | || |||||| | || ||||| | | ||||| | || |||||| | || |||||| |
NR or other | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | | |||||| | || |||||| | || |||||| |
Prior SCT | ||||||||||
No | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| |
Yes | || |||||| | ||| |||||| | ||| |||||| | ||| |||||| | ||| |||||| | || |||||| | ||| |||||| | || |||||| | ||| |||||| | || |||||| |
Cytogenetic profile | ||||||||||
High risk | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| |
Standard risk | || |||||| | ||| |||||| | ||| |||||| | ||| |||||| | ||| |||||| | || |||||| | ||| |||||| | || |||||| | ||| |||||| | || |||||| |
Unknown | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | | ||||| | || |||||| | | ||||| | || |||||| | | ||||| |
CD = cluster of differentiation; ECOG = Eastern Cooperative Oncology Group; ESS = effective sample size; IgG = immunoglobulin G; IMiD = immunomodulatory drug; IMWG = International Myeloma Working Group; IPW-ATT = average treatment effect in the treated population estimated by inverse probability weighting; ISS = International Staging System; ITT = intention-to-treat; mITT = modified intention-to-treat; LDH = lactate dehydrogenase; LOT = line of therapy; MM = multiple myeloma; NR = not reported; PI = proteasome inhibitor; RWCP = real-world clinical practice; SCT = stem cell transplant.
aBase-case results adjusted for refractory status, ISS stage, cytogenetic profile, time to progression on last regimen, extramedullary plasmacytomas, number of prior LOTs, years since MM diagnosis, and age.
bBase-case results adjusted for refractory status, ISS stage, cytogenetic profile, time to progression on last regimen, number of prior LOTs, years since MM diagnosis, and age.
cESS was rounded to whole number.
dRefractoriness was defined as discontinuation of the drug of interest within 60 days and starting a different drug in the next line or starting a new drug within 60 days after end of previous treatment (Flatiron cohort), described on the case report form as progressive disease or relapsed, per investigator assessment (post-daratumumab trials cohort) and according to IMWG consensus criteria (CARTITUDE-1). Penta (pentuple) refractory was defined as refractory to at least 2 IMiDs, 2 PIs, and an anti-CD38 monoclonal antibody, while triple or quadruple refractory was defined as refractory to 2 IMiDs and 1 PI, or 2 PIs and 1 IMiD, or 2 IMiDs and 2 PIs.
eISS was imputed for 47 participants in the daratumumab trial cohort and 56 patients in the Flatiron cohort.
fIncludes extramedullary plasmacytomas and soft-tissue components of bone-based plasmacytomas in the Flatiron cohort.
gIn the daratumumab trial cohort. Refers to soft-tissue mass that is not in contact with bone; does not include bone-based plasmacytomas.
hHemoglobin was imputed for 1 patient in the Flatiron cohort.
iLDH was imputed for 57 patients in the Flatiron cohort.
jFour patients had an ECOG status of 2 at infusion and were grouped in this category.
kECOG was imputed for 49 patients in the Flatiron cohort.
Source: Sponsor-submitted indirect treatment comparison.21
Table 31 outlines the real-world treatment regimens received in the daratumumab trial and Flatiron cohorts, presented in a hierarchy, capturing the mutually exclusive prevalence of each treatment as a single-drug therapy or in combination with any of the treatments listed in the subsequent rows of the table. The most commonly used treatment alone or in combination with other treatments was pomalidomide in the daratumumab trial cohort (ITT, 20.0%; mITT, 23.5%), while the most commonly used treatment alone or in combination with other treatments in the Flatiron cohort was carfilzomib (ITT, 27.8%; mITT, 29.2%).
Table 31: Treatment Regimens in the Daratumumab Trial and Flatiron Cohorts Across All Eligible Lines of Therapy
Treatment | Daratumumab trial cohort | Flatiron cohort | ||
|---|---|---|---|---|
||||||||||||||||||||||| | Frequency (mITT; observations = 378)a | ||||||||| ||||| |||| ||||| | Frequency (mITT; observations = 336)a | |
Carfilzomib | || |||||| | 66 (17.5) | ||| |||||| | 98 (29.2) |
Pomalidomide | ||| |||||| | 89 (23.5) | || |||||| | 69 (20.5) |
Daratumumab | || ||||| | 13 (3.4) | || ||||| | 28 (8.3) |
Ixazomib | || ||||| | 17 (4.5) | || ||||| | 20 (6.0) |
Elotuzumab | | ||||| | 4 (1.1) | || ||||| | 21 (6.3) |
Bortezomib | || |||||| | 63 (16.7) | || ||||| | 30 (8.9) |
Lenalidomide | || ||||| | 36 (9.5) | || ||||| | 7 (2.1) |
Panobinostat | | ||||| | 0 (0.0) | | ||||| | 1 (0.3) |
Selinexor | | ||||| | 3 (0.8) | || ||||| | 11 (3.3) |
Isatuximab | | ||||| | 2 (0.5) | | ||||| | 0 (0.0) |
Thalidomide, or melphalan, or cyclophosphamide | || |||||| | 51 (13.5) | || ||||| | 15 (4.5) |
Dexamethasone | || ||||| | 6 (1.6) | || ||||| | 5 (1.5) |
Others | || ||||| | 28 (7.4) | || ||||| | 31 (9.2) |
ITT = intention-to-treat; mITT = modified intention-to-treat.
aFor each treatment, the number and percent represent the participants who received that treatment as a single-drug therapy or in combination with any of the other treatments listed in the subsequent rows.
Source: Sponsor-submitted indirect treatment comparison.21
Results
Overall survival: Base-case results for OS are summarized in Table 32. The HRs for OS for the comparison of cilta-cel with RWCP in the daratumumab trial cohort were |||| (95% CI, |||| || ||||) and 0.20 (95% CI, 0.13 to 0.31) for the ITT and mITT populations, respectively, in favour of cilta-cel, with a median OS in the ITT population trial that was NR (95% CI, 31.47 to NE) in CARTITUDE-1 compared with 8.05 months (95% CI, 6.34 to 11.30) for RWCP in the daratumumab trial cohort and, in the mITT population, a median OS that was NR (95% CI, NE to NE) in CARTITUDE-1 compared with 10.90 months (95% CI, 8.18 to 16.20) in the daratumumab trial cohort.
The HRs for OS for the comparison of cilta-cel with RWCP in the Flatiron cohort were 0.32 (95% CI, 0.19 to 0.52) and 0.25 (95% CI, 0.14 to 0.43) for the ITT and mITT populations, respectively, in favour of cilta-cel, with a median OS that was NR (95% CI, 31.47 to NE) compared with 12.30 months (95% CI, 9.72 to 15.50) in the ITT populations of the CARTITUDE-1 and RWCP populations from Flatiron, and a median OS that was NR (95% CI, NE to NE) in CARTITUDE-1 compared with 13.20 months (95% CI, 9.17 to 21.30) in the mITT population from Flatiron. The results for the sensitivity analyses and the exploratory analyses considering only the patients’ first eligible line of therapy in the RWCP cohort were consistent with the main analyses.
Table 32: Summary of ITC Base-Case Results for OS
OS | ITT | mITT | ||
|---|---|---|---|---|
CARTITUDE-1 | RWCP ESS (N) | CARTITUDE-1 | RWCP ESS (N) | |
Daratumumab trial cohort (RWCP) | ||||
Sample size, N | ||| | ||| | || | ||| |
OS | ||||
HR (95% CI) | |||| |||||| ||||| | |||| |||||| ||||| | ||
P value | ||||||| | ||||||| | ||
Flatiron cohort (RWCP) | ||||
Sample size, N | ||| | ||| | || | || |
OS | ||||
HR (95% CI) | |||| |||||| ||||| | |||| |||||| ||||| | ||
P value | ||||||| | ||||||| | ||
CI = confidence interval; cilta-cel = ciltacabtagene autoleucel; ESS = effective sample size; HR = hazard ratio; ITC = indirect treatment comparison; ITT = intention-to-treat; mITT = modified intention-to-treat; OS = overall survival; RWCP = real-world clinical practice.
Note: HR < 1 indicates favourable treatment effect for cilta-cel.
Source: Sponsor-submitted ITC.21
Visual inspection of the log-cumulative hazard plots and Schoenfeld residuals plot for OS in the ITT and mITT populations in the comparisons of the CARTITUDE-1 with the daratumumab trial cohort and the Flatiron cohort did not show any clear evidence of violation before significant participant drop-off. The Grambsch-Therneau test for proportional hazards was conducted and found to be nonsignificant.
Health-related quality of life: No HRQoL results were analyzed in the study comparing CARTITUDE-1 and the daratumumab trial cohort or Flatiron cohort.
Progression-free survival: The results for PFS, aPFS, and rwPFS following IPTW are summarized in Table 33. The HR for PFS for cilta-cel versus RWCP in the daratumumab trial cohort was 0.26 (95% CI, 0.18 to 0.37) in the ITT population (median PFS, ||||| |||||| |||| ||| ||||| || ||| ||| |||| |||||| |||| ||| ||||| ||||||, and 0.24 (95% CI, 0.16 to 0.35) in the mITT population (median PFS, || |||| ||| ||||| || ||| ||| |||| |||||| |||| ||| |||| || |||||) in favour of cilta-cel.
Results for aPFS were consistent with the overall PFS analysis for the daratumumab trial cohort with an HR of 0.25 (95% CI, 0.17 to 0.36) in the ITT population (median aPFS, ||||| |||||| |||| ||| ||||| || ||| ||| |||| |||||| |||| ||| |||| || ||||||| ||| |||| |||| ||| |||| || ||||| in the mITT population (median aPFS = NR; 95% CI, ||||| || ||| ||| |||| |||||| |||| ||| || || || |||||), in favour of cilta-cel. The aPFS HR for cilta-cel versus RWCP in the Flatiron cohort was 0.22 (95% CI, 0.15 to 0.33) in the ITT population (median aPFS = 28.02 months [95% CI, 21.32 to NR months] versus 4.07 months [95% CI, 3.06 to 5.16 months]) and 0.18 (95% CI, 0.12 to 0.26) in the mITT population (median aPFS = NR [95% CI, 24.54 to NR months] versus 4.53 months [95% CI, 2.86 to 6.77 months]), also in favour of cilta-cel.
The HR for rwPFS for cilta-cel versus RWCP in the daratumumab trial cohort was 0.18 (95% CI, 0.13 to 0.25) in the ITT population (median rwPFS = ||||| |||||| |||| ||| ||||| || ||| ||| |||| |||||| |||| ||| ||||| |||||), and 0.18 (95% CI, 0.12 to 0.26) in the mITT population (median rwPFS, || |||| ||| ||||| || ||| ||| |||| |||||| |||| ||| |||| || |||||), both in favour of cilta-cel. Compared with the Flatiron cohort, the HR for rwPFS was 0.22 (95% CI, 0.15 to 0.33) in the ITT population, with a median rwPFS of 28.02 months (95% CI, 20.11 to NR months) versus 3.48 months (95% CI, 2.89 to 4.57 months), respectively, and an HR for rwPFS of 0.18 (95% CI, 0.10 to 0.23) in the mITT population, with a median rwPFS of NR (95% CI, 24.54 to NR months) versus 5.88 months (95% CI, 4.01 to 8.48 months), respectively.
The results for the sensitivity analyses and the exploratory analyses considering only patients’ first eligible line of therapy in the physicians’ choice cohort were consistent with the main analyses.
Table 33: Summary of ITC Base-Case Results for PFS Outcomes
PFS | ITT | mITT | ||
|---|---|---|---|---|
CARTITUDE-1 | RWCP ESS (N) | CARTITUDE-1 | RWCP ESS (N) | |
Daratumumab trial cohort (RWCP) | ||||
Sample size, N | ||| | ||| | || | ||| |
PFS | ||||
HR (95% CI) | |||| |||||| ||||| | |||| |||||| ||||| | ||
I and II | ||||||| | ||||||| | ||
Adjusted PFS | ||||
HR (95% CI) | |||| |||||| ||||| | |||| |||||| ||||| | ||
P value | ||||||| | ||||||| | ||
PFS vs. real-world PFS | ||||
HR (95% CI) | |||| |||||| ||||| | |||| |||||| ||||| | ||
P value | ||||||| | ||||||| | ||
Flatiron cohort (RWCP) | ||||
Sample size, N | ||| | ||| | || | || |
Adjusted PFS | ||||
HR (95% CI) | |||| |||||| ||||| | |||| |||||| ||||| | ||
P value | ||||||| | ||||||| | ||
PFS vs. real-world PFS | ||||
HR (95% CI) | |||| |||||| ||||| | |||| |||||| ||||| | ||
P value | ||||||| | ||||||| | ||
CI = confidence interval; ESS = effective sample size; HR = hazard ratio; ITC = indirect treatment comparison; ITT = intention-to-treat; mITT = modified intention-to-treat; PFS = progression-free survival; RWCP = real-world clinical practice.
HR < 1 indicates favourable treatment effect for cilta-cel.
Source: Sponsor-submitted ITC.21
Visual inspection of the log-cumulative hazard plots and Schoenfeld residuals plot for PFS in the ITT and mITT populations in the comparisons of the CARTITUDE-1 and daratumumab trial cohort did not show any clear evidence of violation before significant participant drop-off. The Grambsch-Therneau test for proportional hazards was conducted and found to be nonsignificant in the ITT population; however, in the mITT population, a potential violation of the PHA was reported (P = 0.012).
For aPFS, the daratumumab trial cohort did not show any clear evidence of violation of the PHA before significant participant drop-off in both the ITT and mITT populations. In the ITT population, the Grambsch-Therneau test was nonsignificant, indicating the PHA to be appropriate while, in the mITT population, a potential violation in the PHA was reported (P = 0.0063). In the Flatiron cohort, visual inspection of the log-cumulative hazard plots and Schoenfeld residuals plot in the ITT and mITT did not show any clear evidence of violation before significant participant drop-off. The Grambsch-Therneau test for proportional hazards was found to be nonsignificant.
For rwPFS, the daratumumab trial cohort did not show any clear evidence of violation of the PHA before significant participant drop-off in both the ITT and mITT populations. In the ITT population, the Grambsch-Therneau test was nonsignificant, indicating the PHS to be appropriate while, in the mITT population, a potential violation in the PHA was reported (P = 0.032). In the Flatiron cohort, visual inspection of the log-cumulative hazard plots and Schoenfeld residuals plot in the ITT and mITT did not show any clear evidence of violation before significant participant drop-off. The Grambsch-Therneau test for proportional hazards was found to be nonsignificant.
Clinical response outcomes: As previously noted, an ORR and a CR or better rate were not available in the comparison with the Flatiron cohort. Results for clinical response outcomes for cilta-cel compared with RWCP from the daratumumab trial cohort are summarized in Table 34. After IPTW, the OR for ORR comparing cilta-cel with RWCP was 22.55 (95% CI, 10.72 to 52.03) in the ITT population and 127.35 (95% CI, 34.24 to 850.09) in the mITT population. For the CR or better rate, the OR for cilta-cel compared with RWCP after IPTW in the ITT population was |||||| (95% CI, |||||| || ||||||||) and was |||||| (95% CI, |||||| || ||||||||) in the mITT population. The results for the sensitivity analyses and the exploratory analysis considering only patients’ first eligible line of therapy in the physicians’ choice cohort were consistent with the main analysis.
Table 34: Summary of Base-Case Results for ORR and Complete Response or Better Rate
Cilta-cel vs. | ITT | mITT | ||
|---|---|---|---|---|
CARTITUDE-1 | RWCP ESS (N) | CARTITUDE-1 | RWCP ESS (N) | |
Daratumumab trial cohort (RWCP) | ||||
Sample size, N | ||| | ||| | || | ||| |
ORR | ||||
OR (95% CI) | ||||| ||||||| |||||| | |||||| ||||||| ||||||| | ||
P value | ||||||| | ||||||| | ||
Relative risk (95% CI) | |||| |||| | |||| |||| | ||
CR or better rate | ||||
OR (95% CI) | |||||| |||||||| ||||||||| | |||||| |||||||| ||||||||| | ||
P value | ||||||| | ||||||| | ||
Relative risk (95% CI) | ||||| |||| | |||||| |||| | ||
CI = confidence interval; cilta-cel = ciltacabtagene autoleucel; CR = complete response; ESS = effective sample size; ITC = indirect treatment comparison; ITT = intention-to-treat; mITT = modified intention-to-treat; OR = odds ratio; ORR = overall response rate; RWCP = real-world clinical practice.
Note: OR > 1 indicates favourable treatment effect for cilta-cel.
Source: Sponsor-submitted ITC.21
Time to response: No results for TTR were included in the study comparing CARTITUDE-1 and the daratumumab trial cohort or Flatiron cohort.
Safety: No results for safety were included in the study comparing CARTITUDE-1 and the daratumumab trial cohort or Flatiron cohort.
Critical Appraisal of the Sponsor-Submitted Study: CARTITUDE-1 Versus Real-World Cohorts
Two IPTW analyses were submitted by the sponsor in an attempt to emulate a hypothetical RCT: 1 comparing cilta-cel with RWCP using IPD from patients who were enrolled in the POLLUX, CASTOR, and EQUULEUS trials, and 1 comparing cilta-cel with RWCP using IPD from patients in the Flatiron Health database. In both IPTW analyses, CARTITUDE-1 was used as the index trial. No systematic search was conducted to identify the comparator studies. Instead, the sponsor noted that the POLLUX, CASTOR, and EQUULEUS trials were selected for the daratumumab trial cohort based on the population of patients and the consideration that these existing studies had completed their primary analysis. The Flatiron Health database was selected to apply patient characteristics of CARTITUDE-1 to create an external cohort of real-world patients; no other rationale was provided. As these comparator cohorts were not selected using a systematic approach, there is a risk of selection bias. It is not possible to know whether the results may have differed if data from different r/rMM studies or databases had been used. Numerous therapies were used in the RWCP groups from the daratumumab trial cohort and the Flatiron cohort, many of which were not relevant to Canadian clinical practice. Additionally, the treatment regimens reported in the included sources were from 2017; the clinical experts consulted by CADTH noted that clinical practice has changed since the enrolment of patients reported in these sources; thus, they may not be reflective of current treatment standards and may introduce bias in the RWCP estimates, as patients undergoing third-line treatment today may be worse off than patients who underwent third-line treatment at the time of the data collection for this study.
There were important differences in the design of the included studies that limit the ability to draw strong conclusions about the efficacy of cilta-cel compared with RWCP based on adjusted comparisons with the daratumumab trial cohort and the Flatiron cohort. CARTITUDE-1 was a phase Ib/II single-arm trial, whereas the comparators included published literature from 3 clinical trials (2 phase III RCTs and 1 phase Ib open-label RCT), and a real-world cohort from electronic health records in the US. Although the daratumumab trials were RCTs, patients selected from this cohort and the Flatiron cohort were included in the analysis retrospectively. Data analyzed retrospectively from databases and medical records are prone to unique biases (e.g., selection bias, confounding) compared with those collected from prospective interventional studies (like RCTs and single-arm trials) that cannot be controlled for using IPTW methods. Further, in an attempt to mitigate bias in the measurement of the subjective response outcomes (e.g., CR, PFS) due to the open-label design, these outcomes were ascertained via IRC in the CARTITUDE-1 trial. The same outcomes in the daratumumab and Flatiron cohorts were ascertained via the investigators, thus the risk of bias in the measurement of these is increased relative to the same outcomes measured in CARTITUDE-1. Such methodological differences could not be adjusted for in the analyses and the magnitude and direction of any resulting bias is uncertain.
Two different populations were analyzed in the submitted IPTW: the ITT population and the mITT population, varying by the index date, where the ITT included all patients in CARTITUDE-1 who underwent apheresis and the mITT population included only patients who received cilta-cel infusion. Analyses using the ITT population were considered most appropriate for measuring the effect of assignment to the intervention and would result in the lowest risk of bias in effect estimates. There was evidence of heterogeneity between the ITT and mITT populations of CARTITUDE-1 and the daratumumab trial and Flatiron cohorts. After adjustment, differences remained across treatment groups for hemoglobin levels, prior SCT, race, and type of MM. There were also notable differences between CARTITUDE-1 and the Flatiron cohort in ISS stages, cytogenetic risk profile, time to progression on last treatment, years since diagnosis, ECOG PS, and prior SCT, with notable differences in LDH levels. After adjustment, some differences remained in LDH levels, prior SCT, and ECOG PS. Therefore, there remains a risk of confounding due to imbalances in the distribution of prognostic factors across the cohorts.
In the IPTW analyses for the daratumumab trial cohort and the Flatiron cohort, propensity scoring methods were considered appropriate, and important factors were considered in the calculation of weights. After weighting, the ESS of the daratumumab trial cohort and Flatiron cohort in the ITT populations were reduced by 39.6% and 16.2% from the included population, respectively. The ESS of the mITT populations of the daratumumab trial cohort and Flatiron cohort was reduced by 59.7% and 59.2%, respectively. All adjusted sample sizes represent substantial losses in the precision of effect estimates. Thus, there was potentially considerable heterogeneity between CARTITUDE-1 and the real-world cohorts among the variables included in the weighting process, which is an important limitation of the relative treatment effect estimates.
Numerous sensitivity and exploratory analyses were conducted to evaluate different methods of weighting, eligible lines of therapy, and which variables were included for adjustment. Most often, these sensitivity analyses adjusting the statistical method resulted in similar findings. Based on the inclusion criteria, patients in the comparator arms may have met eligibility criteria at more than 1 time point. As a result, base-case analyses were conducted considering all eligible lines of therapy, while exploratory analyses were conducted that only allowed patients to be included on their first eligible line of therapy. Either choice of inclusion criteria was considered appropriate; however, considering that patients in CARTITUDE-1 may have been beyond the fourth line of therapy at the time of inclusion in the trial, the first eligible line of treatment could be considered more appropriate. As such, the interpretation of the results presented using all lines of therapy as a comparator require care, due to the potential of unmeasured time-varying confounding. In all cases, the results of these exploratory analyses were consistent with those that considered all eligible lines.
Results of the base-case analyses and sensitivity analyses were consistent across end points, analysis populations, and across data sources, favouring cilta-cel over RWCP in both the daratumumab trial cohort and the Flatiron cohort for all outcomes. Several outcomes important to patients and clinicians, including AEs and HRQoL, were not included in the analyses. For all outcomes, the magnitude of effect for cilta-cel was notably large over RWCP; however, results were associated with wide 95% CIs for time-to-event outcomes and clinical response outcomes, highlighting losses to precision and reducing the ability to draw strong conclusions about the magnitude of the effect. Overall, given the adjustment of the daratumumab trial cohort and the Flatiron cohort to the CARTITUDE-1 population, the generalizability of the results is similar to that of CARTITUDE-1, which has previously been described in detail.
Observational Studies Identified in the Literature
Costa et al. (2022): CARTITUDE-1 Versus MAMMOTH22
In the absence of a direct comparator in the CARTITUDE-1 study, an observational study to evaluate and compare the efficacy of cilta-cel with real-world data extracted from the MAMMOTH study was conducted. Study and patient characteristics of CARTITUDE-1 have been described previously. The MAMMOTH study was a multicentre, retrospective collaboration of 14 academic institutions in the US that investigated the natural history and outcomes of patients with MM refractory to anti-CD38 monoclonal antibodies. Data from the MAMMOTH study were collected between January 2017, and June 2018. From the 275 patients included in the MAMMOTH dataset, a total of 190 patients were identified to be similar to the CARTITUDE-1 population and went on to receive additional treatment other than CAR T-cell therapy. Demographic and disease characteristics that were available in both cohorts were used to determine eligibility. The median duration of follow-up was 12.4 months (interquartile range, 10.6 to 15.2 months).
Both ITT and mITT populations were considered in the analyses comparing CARTITUDE-1 and MAMMOTH. The ITT and mITT populations for CARTITUDE-1 consisted of 113 patients in the ITT population and 97 patients in the mITT population (mirroring those in the sponsor-submitted evidence). Corresponding populations identified from MAMMOTH included 190 and 122 patients in the ITT and mITT populations, respectively. The ITT population from MAMMOTH included all patients who met the eligibility criteria for CARTITUDE-1. The index date was defined as the start date of the first therapy after meeting the inclusion criteria. The mITT population from MAMMOTH included a subset of the ITT population who had not died or progressed within 47 days; the index date was 47 days after the start of the first therapy after meeting the inclusion criteria. The efficacy end points included in the analysis consisted of ORR, PFS, and OS. End points for the CARTITUDE-1 study have previously been defined. The ORR for the MAMMOTH cohort was defined as the proportion of patients who achieved a PR or better according to IMWG criteria based on investigator assessment for the first subsequent therapy after meeting the inclusion criteria. PFS and OS in MAMMOTH were defined in the same manner as for CARTITUDE-1; however, for PFS in the MAMMOTH study, the date of initiation of a subsequent line of therapy was considered date of progression from prior therapy in some instances.
The analyses were performed according to a prespecified statistical analysis plan according to the authors, although the protocol was not cited. The nearest-neighbour 1:1 propensity score matching was done without replacement by setting the caliper at 0.05. Additionally, analyses using the stabilized IPTW were conducted to quantify treatment effect among the treated population. To satisfy the positivity assumption, only patients with overlapping propensity scores from the CARTITUDE-1 and MAMMOTH cohorts were included in the outcome analyses. Baseline covariates from CARTITUDE-1 were shared with MAMMOTH investigators without any outcome information, and propensity score models were specified without the knowledge of the outcomes. Propensity scores were calculated with the following covariates: age; sex; ethnicity (white versus other); ISS stage III (versus I, II, or unknown); time from diagnosis to index date; number of prior lines of therapy; prior autologous SCT; presence of high-risk cytogenetic abnormalities in any prior sample (t[4;14], t[14;16], del[17p]), refractoriness to bortezomib, ixazomib, carfilzomib, lenalidomide, pomalidomide, or anti-CD38 monoclonal antibody; triple-class refractoriness; penta-drug exposure (to bortezomib or ixazomib plus carfilzomib plus lenalidomide plus pomalidomide plus anti-CD38 monoclonal antibody); and penta-drug refractoriness. To compare ORR using the 1:1 matching, a logistic regression model stratified by matched pairs with treatment indicator as the only covariate was used to estimate the treatment effect in terms of the OR (95% CI). For PFS and OS analyses, a stratified Cox proportional hazards model using treatment indicator as the only covariate was used to estimate the HR (95% CI). For comparison of ORR using the weighted approaches, a weighted logistic regression model was employed that contained only a treatment group indicator to estimate the treatment effect in terms of the OR (95% CI) using a robust variance estimator. Weighted Kaplan-Meier estimates were used to describe the distributions of PFS and OS. A weighted Cox proportional hazards model using the ATT approach was applied to estimate the HR with 95% Wald-type CI using a robust sandwich variance estimator.
Prior to matching, there were notable imbalances in baseline characteristics between the CARTITUDE-1 and MAMMOTH cohorts. Compared with patients from the MAMMOTH (N = 190) study, the ITT population of the CARTITUDE-1 trial (N = 113) included:
enrolled patients who were older (mean age 65 years versus 61.7 years)
fewer patients with ISS stage III disease (15% versus 28%)
had a longer time from diagnosis to treatment (mean 6.4 years versus 5.3 years)
a higher proportion of patients with prior autologous SCT (88% versus 74%)
a higher proportion of patients with disease that was refractory to:
pomalidomide (85% versus 72%)
carfilzomib (70% versus 59%)
a lower proportion who were refractory to bortezomib or ixazomib (75% versus 84%)
a lower proportion of patients with disease that was triple-class refractory (88% versus 98%) but a higher proportion with disease that was penta drug–exposed (80% versus 58%) and penta drug–refractory (40% versus 31%).
In the 1:1 matching, 95 patients each from CARTITUDE-1 and MAMMOTH ITT were matched.
The RWCP treatments received as next therapy in the MAMMOTH cohort consisted of pomalidomide (34%), anti-CD38 monoclonal antibodies (24%), carfilzomib (19%), and cytotoxic chemotherapy (35%). In the mITT population, differences between CARTITUDE-1 (N = 97) and MAMMOTH (N = 122) before matching were observed for the variables of mean age (62 years versus 64.8 years); proportion of patients who were ISS stage III (14% versus 26%); mean number of prior lines of therapy (6.3 versus 5.7); mean years from diagnosis to therapy (6.8 versus 5.5); prior autologous SCT (90% versus 74%); the proportion of patients with disease refractory to bortezomib or ixazomib (75% versus 86%), carfilzomib (65% versus 55%), lenalidomide (81% versus 89%), pomalidomide (84% versus 71%); and the proportion of patients who were triple-class refractory (87% versus 98%) and penta drug–exposed (77% versus 57%). Balance was achieved across characteristics following matching in both the ITT and mITT populations.
In the propensity score matched analysis, in the ITT analysis, 80 patients (84%) achieved ORR in CARTITUDE-1 versus 27 patients (28%) in MAMMOTH (OR = 13.4; 95% CI, 6.6 to 27.3). The rate of CR or better was 60% compared with 2%, and 81% compared with 7% of patients who experienced VGPR or better. Results for PFS and OS favoured patients in CARTITUDE-1 compared with the matched MAMMOTH population (HR for PFS = 0.11; 95% CI, 0.05 to 0.22; and HR for OS = 0.20; 95% CI, 0.10 to 0.39). The 12-month PFS rate in CARTITUDE-1 was 73% (95% CI, 64% to 83%) compared with 12% (95% CI, 6% to 21%) in MAMMOTH, and the 12-month OS rate was 83% (95% CI, 76% to 91%) for CARTITUDE-1 compared with 39% (95% CI, 30% to 51%) for MAMMOTH. Results for the mITT population (weighted n = 69) were also consistent with the ITT population. Results for the additional analyses using stabilized IPTW and weighted ATT methods were consistent with the propensity score matched analysis.
Critical appraisal of Costa et al. (2022): Given the design of the CARTITUDE-1 trial, the propensity score matched analysis from the MAMMOTH study comparing cilta-cel with patients receiving RWCP was appropriate; however, given that no methods were reported for systematically identifying and selecting the MAMMOTH cohort for the external comparator, there is a risk of selection bias. There were differences in the study design of the 2 included studies: the MAMMOTH study was a retrospective study evaluating natural history in patients with MM, while CARTITUDE-1 was a single-arm clinical trial; thus, there are concerns with data availability, outcome assessment, and measurements. Outcomes in CARTITUDE-1 were adjudicated by an IRC while, in MAMMOTH, outcomes were assessed by the investigator. Data from the MAMMOTH study were collected between January 2017, and June 2018. The clinical experts consulted by CADTH noted that clinical practice has changed since the data collection period and therefore the results may not be representative of current effectiveness estimates for the comparator group. It was also unclear what treatment regimens were received by patients in the MAMMOTH study. Overall, the matched populations included 95 patients in the ITT population in each cohort and 69 patients in each mITT cohort, which represented a reduction of 16% and 29% from the original CARTITUDE-1 populations and a reduction of 50% and 43% from the MAMMOTH populations. The use of the ITT population for the primary analysis is considered the most appropriate, given that it measures the effect of assignment to the intervention.
Many relevant variables were considered in the calculation of propensity scores; however, it was not apparent whether these factors were selected via any systematic process. Therefore, it is unclear whether the included prognostic factors represent a comprehensive list, and there was no testing performed for residual confounding; thus, there may be a risk of bias. The authors noted that other important variables could not be gathered in MAMMOTH, including myeloma phenotype, ECOG PS, comorbidities, and cytopenias. While matching is considered appropriate, it results in reduced sample sizes, reducing the generalizability of the results. In general, the results of the analyses of the data from CARTITUDE-1 were supportive of cilta-cel, demonstrating a substantial clinical benefit over the RWCP results from MAMMOTH; however, the reduced sample sizes from propensity score matching, unexplored heterogeneity, and wide 95% CIs resulted in uncertainty in the results and the magnitude of the observed effects. Given the methodological differences across studies and resulting cohorts, as well as the risk of bias due to residual confounding, the comparison with external, historical, real-world data are nonconfirmatory and should only be viewed as exploratory. This published study was funded by the manufacturer of cilta-cel; financial conflicts of interest have the potential to impact the design, analysis, conduct, and reporting of research.
Merz et al. (2021): CARTITUDE-1 Versus Therapie Monitor23
Due to the study design of CARTITUDE-1, adjusted comparisons using IPD from CARTITUDE-1 were compared with IPD for triple class–exposed patients from the Therapie Monitor patient registry in Germany, run by OIS, to compare the effectiveness of cilta-cel versus the currently available therapies in RWCP. The CARTITUDE-1 trial has previously been described. Therapie Monitor includes data on approximately 4,000 patients with r/rMM from a representative sample of 108 German centres. The Therapie Monitor database was initiated in January 2016, and is maintained by OIS. Patients enrolled in Therapie Monitor who fulfilled the same key eligibility criteria as in CARTITUDE-1 were selected retrospectively for inclusion in the analyses. Certain CARTITUDE-1 eligibility criteria could not be applied because they were outside of the scope of Therapie Monitor, e.g., absence of cardiac conditions and absence of prior history of central nervous system involvement or signs of meningeal involvement of MM. All treatment lines initiated after a patient met eligibility criteria were used for analysis as long as patients fulfilled the eligibility criteria for CARTITUDE-1 at the start of the respective line of therapy. The ITT and mITT of CARTITUDE-1 have previously been described. The populations included in the ITT and mITT of Therapie Monitor were defined as described for the observational study submitted by the sponsor (CARTITUDE-1 versus LocoMMotion); where the ITT was composed of all eligible lines of therapy meeting the eligibility criteria (n = 312), and the mITT was composed of patients with an event or who were censored within 52 days after treatment initiation (the average duration between apheresis and infusion in CARTITUDE-1, n = 223). Two outcomes were compared between cilta-cel and RWCP: OS and TTNT. TTNT was used as a proxy for PFS in the OIS database. Outcome definitions were aligned between CARTITUDE-1 and Therapie Monitor. OS was defined as the time from the index date to the date of death; patients who were alive or of unknown vital status were censored at the last date they were known to be alive. TTNT was defined as the time from the index date to the initiation of the next line of therapy or death, whichever occurred first. Patients who were alive and did not initiate a next line of therapy were censored at the last date they were known to be alive.
Potential prognostic factors were identified via literature reviews and consultation with clinical experts, although few details of these methods were reported. Clinical experts ranked the potential prognostic factors identified in the literature in order of expected importance. The following factors, available in both data sources, were included in the analyses: refractory status, revised ISS stage at the index date, time to progression on the last prior line, number of prior lines of treatment, ECOG PS, age at index date, sex, average duration of prior lines, and years since diagnosis. The prognostic strength of these factors was explored using univariate and multivariate regression and imbalances were assessed using SMDs, where values greater than 0.2 were considered indicative of important differences. Total plasmacytomas was not available in Therapie Monitor, so it was not included in the analyses, despite being considered prognostic. Since comorbidities were collected more generally in Therapie Monitor, these were also not considered in the analyses.
The methods used for this analysis have been previously described and matched those of the study comparing CARTITUDE-1 and the LocoMMotion study described in the sponsor-submitted indirect evidence. Briefly, IPD from both CARTITUDE-1 and Therapie Monitor were pooled to conduct the analyses. First, the propensity score for each patient was estimated using a multivariable logistic regression model. Second, different sets of weights were derived and were used in the weighted analyses. The primary analysis method was the IPW-ATT approach, and an IPW-ATO approach was also conducted. The effectiveness of cilta-cel versus RWCP was estimated using inverse probability weights and multivariable Cox proportional hazards regression models. The variance was estimated using a robust sandwich variance estimator to account for the clustering of multiple treatment lines within patients. To estimate HRs and their 95% CIs, a weighted Cox proportional hazards model was used. The appropriateness of the PHA was judged via visual inspection of the log-cumulative hazard plot and the Schoenfeld residuals plots, and via performance of the Grambsch-Therneau test. A visual inspection of the shapes of the curves over time was also undertaken.
The ITT cohort consisted of 113 patients from CARTITUDE-1 and 222 patients for Therapie Monitor (312 treatment lines). The mITT cohort included 97 patients for CARTITUDE-1 and 174 patients for Therapie Monitor (223 treatment lines). A total of 33 unique treatment regimens were used in the Therapie Monitor cohort, the most common being ixazomib plus lenalidomide and dexamethasone (18%), pomalidomide and dexamethasone (15%), melphalan and prednisone (11%), elotuzumab plus lenalidomide and dexamethasone (8%), and bortezomib and dexamethasone (7%). Baseline characteristics were available only for the mITT population. There was notable heterogeneity between cohorts before adjustment, with 8 of 9 variables having an SMD greater than 0.2, indicating differences across cohorts. In the mITT population of the CARTITUDE-1 study (n = 97), 42.3% of patients had penta-refractory disease, while 0.4% of patients had penta-refractory disease in Therapie Monitor (n = 223). Other notable differences for CARTITUDE-1 versus Therapie Monitor included ISS stage (stage I, 34.0% versus 1.3%; stage II, 58.5% versus 42.6%; stage III, 7.2% versus 56.1%), number of prior lines of therapy (≤ 4, 34.0% versus 86.5%; > 4, 66.0% versus 13.5%), and age (< 65 years, 63.9% versus 14.3%), ECOG PS of 0 (40.2% versus 11.2%) or 1 (59.8% versus 88.8%), time to progression on last treatment (< 4 months, 49.5% versus 21.1%; ≥ 4 months, 50.5% versus 78.9%), time since diagnosis (< 6 years, 46.4% versus 85.7%; ≥ 6 years, 53.6% versus 14.3%), and average duration of prior therapy (8.14 months to < 11.76 months, 22.7% versus 33.2%; 11.76 months to < 17.61 months, 27.8% versus 34.5%; and > 17.61 months, 28.9% versus 17.0%). After IPW-ATT weighting, the sample size of the Therapie Monitor cohort reduced to 42 patients, and differences remained in 6 of 9 baseline characteristics, including refractory status, ISS stage, ECOG status, age, and average duration of prior lines of therapy, with new imbalances in sex. Weighting via IPW-ATO achieved perfect balance across the selected prognostic covariates.
In the ITT population, after IPW-ATT adjustment, the HR for OS comparing cilta-cel and RWCP favoured cilta-cel (HR = 0.14; 95% CI, 0.07 to 0.25). In the IPW-ATO and multivariable Cox proportional hazards regression models, cilta-cel was also favoured over RWCP (HR = 0.26 [95% CI, 0.13 to 0.54] and HR = 0.29 [95% CI, 0.15 to 0.58], respectively). For TTNT, all analyses favoured cilta-cel over RWCP from Therapie Monitor, with HRs of 0.13 (95% CI, 0.07 to 0.24) for IPW-ATT, 0.24 (95% CI, 0.12 to 0.49) for IPW-ATO, and 0.20 (95% CI, 0.11 to 0.39) using multivariable Cox proportional hazards regression models. Results for OS and TTNT in the mITT population were consistent with the ITT population; however, the 95% CIs were wider (OS: HR = 0.26 [95% CI, 0.08 to 0.84], HR = 0.31 [95% CI, 0.12 to 0.79], and HR = 0.16 [95% CI, 0.06 to 0.42]; TTNT: HR = 0.24 [95% CI, 0.09 to 0.67], HR = 0.26 [95% CI, 0.11 to 0.59], and HR = 0.15 [95% CI, 0.07 to 0.33]) using IPW-ATT, IPW-ATO, and multivariable Cox proportional hazards regression models, respectively.
Critical appraisal of Merz et al. (2021): Key critical appraisal points of the observational study conducted by Merz et al., 2021, include the differences in study design, and the heterogeneity across populations and prior treatments. This study was initiated and supported by the sponsor of cilta-cel. The data analysis, interpretation, and the writing of the manuscript were funded and conducted by the sponsor. As previously noted, the CARTITUDE-1 trial was a noncomparative study; thus, the creation of an external cohort arm was justified. The comparator cohort was generated from CARTITUDE-1-like patients from the Therapie Monitor database in Germany; however, due to the limited information available in the Therapie Monitor database, some of the eligibility criteria from CARTITUDE-1 could not be applied, impacting the comparability of these groups, and adding a risk of selection bias to this cohort, given that patients were not systematically selected. There are potential variations in clinical practice and standard of care for patients in Germany; thus, the results may not be generalizable to the population of patients in Canada. Additionally, patients received a total of 33 distinct regimens in the comparator group. No analyses by type of prior regimen were conducted, and many of the regimens received were irrelevant to Canadian clinical practice; thus, the results of the analyses may not be generalizable to the population of patients in Canada. Moreover, the clinical experts consulted by CADTH noted that clinical practice has changed since the enrolment of patients from Therapie Monitor; therefore, the data may not be representative of current effectiveness estimates for RWCP. Potential prognostic factors were identified by literature review and clinical expert input; however, no information on the process or selection was provided; thus, it was unclear if the list of potential prognostic factors was comprehensive. Before the weighting of important baseline characteristics and potential prognostic factors, there were notable differences between populations, which mostly remained following the application of weights, so the results are at risk of bias due to confounding. It was noted that many variables were out of the scope of the Therapie Monitor dataset and therefore could not be adjusted for including extramedullary plasmacytomas, detailed comorbidities, or cytogenetic risk, further contributing to the risk of bias due to confounding. The reduction in sample size for the Therapie Monitor cohort was substantial, indicating a substantial loss of precision and that the results are being heavily influenced by a subset of the sample. It is largely reflective of the large degree of heterogeneity in prognostic characteristics across the cohorts. All analysis methods were appropriate and suggested similar results, favouring cilta-cel over RWCP; however, the results of the present analysis were associated with uncertainty, given the reduced sample sizes, the notable heterogeneity in patient populations, and the wide 95% CIs, particularly for the mITT population, resulting in greater uncertainty of the results.
Costa et al. (2022): Meta-Analysis of Observational Studies24
Numerous observational studies have been conducted comparing the cilta-cel results from CARTITUDE-1 with physicians’ choice of treatment in the real world using IPD. As such, the study by Costa et al., 2022, pooled observational studies evaluating cilta-cel versus various compositions of RWCP in patients with triple class–exposed r/rMM via a meta-analysis to derive a single summary effect estimate on the effectiveness of cilta-cel.
No systematic search was conducted to identify relevant studies. In total, 5 observational studies examining the comparative effectiveness of cilta-cel versus RWCP were sponsored and published by Janssen and included in the meta-analysis. The 5 observational studies included in the meta-analysis are also described previously and included:
the IPW analysis of cilta-cel versus the daratumumab trial cohort using an earlier data cut-off (September 2019, for POLLUX and CASTOR, and a range of data cut-offs from 2017 to 2019 for EQUULEUS) than that provided in the analysis submitted by the sponsor and described previously, which represents a longer follow-up time for patients from the daratumumab trial cohort
the IPW analysis of cilta-cel versus the Flatiron cohort
the IPW analysis of cilta-cel versus the LocoMMotion trial
the IPW analysis of cilta-cel versus the Therapie Monitor database from Germany
the propensity score matching analysis of cilta-cel versus the MAMMOTH cohort.
To determine whether included studies were sufficiently similar to be included in a meta-analysis, characteristics relating to the analytical methods, included populations, and outcomes were considered. First, the included observational studies were assessed to determine whether the RWCP populations were aligned with CARTITUDE-1. The included observational studies were also assessed regarding the definitions for the index dates used for each population (i.e., all index dates versus first index dates). The observational study comparing CARTITUDE-1 versus MAMMOTH reported only results corresponding to the first index dates, whereas all other observational studies included both first index date and all index dates. The results for CARTITUDE-1 versus LocoMMotion were considered as both first and all index dates for the purpose of this meta-analysis based on the prospective nature of the LocoMMotion study. All the observational studies analyzed both the ITT and mITT populations. Additional population considerations for including studies in the meta-analysis were the individual weighted baseline characteristics for the ITT and mITT populations and whether the analyses were doubly robust or not (i.e., whether the baseline characteristics used for weighting were also adjusted for in the regression model). Only observational studies that evaluated commonly reported effectiveness end points were pooled in a meta-analysis. Meta-analyses were feasible only if results were available from more than 2 observational studies for a particular outcome. As such, 4 outcomes, including OS, PFS, TTNT, and ORR, were included in the analyses. Only results for OS, PFS, and ORR were of interest to this review. All outcomes were similarly defined across each observational study, except for the definition of PFS, which differed in the observational comparison of CARTITUDE-1 versus LocoMMotion. All other observational studies incorporated a switch to subsequent treatment as a proxy for progression when assessing PFS, whereas the LocoMMotion study did not. In each observational study, analyses using IPW-ATT weighting was used, which the authors noted resulted in comparative effect estimates that were reflective of the CARTITUDE-1 population.
Frequentist, random-effects meta-analyses were conducted using comparative effect estimates from each individual observational study. Larger weights were assigned to more precise estimates. To account for the inclusion of CARTITUDE-1 multiple times in the meta-analysis, a robust variance estimation was used. Statistical heterogeneity was tested by τ2, and heterogeneity across studies was evaluated using the I2 statistic. Sensitivity analyses were conducted to evaluate the effect of differences in patient populations, analytical methods, and study design between included observational studies where, in each analysis, 1 specification was modified. The first sensitivity analysis excluded the comparison of CARTITUDE-1 and Therapie Monitor due to the residual heterogeneity in prognostic factors in the adjusted analyses. The second sensitivity analysis excluded the comparison of CARTITUDE-1 and LocoMMotion because LocoMMotion was the only comparator that was prospective in design.
Baseline characteristics for the individual studies have previously been summarized, and many differences were noted across all comparisons. The included observational studies reported results that adjusted for 9 to 14 baseline characteristics, depending on data availability in each analysis. Only 2 observational studies reported results that were doubly robust. In general, after weighting, the baseline characteristics in the RWCP groups were aligned with the CARTITUDE-1 population; however, some small or moderate differences remained after adjustment in all ITCs.
Overall, the results in the ITT and mITT analyses were similar. In the analysis of the ITT population, including all eligible index dates, the overall HR for cilta-cel compared with RWCP was 0.26 (95% CI, 0.15 to 0.47) for OS, and 0.22 (95% CI, 0.1 to 0.49) for PFS. No analyses of ORR were conducted in the all–index dates analyses. When conducting the analyses using only the first index date, results were consistent with all index dates for the outcomes of OS and PFS. The OR for ORR in the ITT population was 13.94 (95% CI, 4.88 to 39.84) while, in the mITT population, the OR for ORR was 86.22 (95% CI, 17.96 to 413.88) in favour of cilta-cel. Results of all sensitivity analyses removing the Therapie Monitor database and the LocoMMotion cohort were consistent with the primary analyses. Statistical heterogeneity measured by I2 ranged between 0% and 77% across all analyses and end points, suggesting some unexplored heterogeneity with respect to the magnitude of the effects estimated across the various comparisons for OS and PFS.
Critical appraisal of Costa et al. (2022) meta-analysis of observational studies: The comparative effectiveness of cilta-cel has previously been estimated in a number of observational studies that have been funded and supported by the sponsor and manufacturer of cilta-cel. Critical appraisal points for the individual studies must be considered when interpreting the results of this meta-analysis. For this meta-analysis, no comprehensive literature search or selection procedure was reported for identifying relevant studies; rather, studies known to and conducted by that sponsor were included. As a result, the meta-analysis may be at a risk of selection bias, though it is unlikely that any studies were missed, given the lack of evidence available for cilta-cel. The comparator studies in the meta-analysis included numerous real-world treatment regimens; however, these regimens were not reported and, as noted for the individual studies, include regimens not relevant to Canadian clinical practice. While the comparisons of cilta-cel with external RWCP cohorts from multiple studies provided a large evidence base for comparison, there were important limitations in this evidence, including methodological differences across the data sources that could not be adjusted for using propensity scores, and a risk of confounding (due to the inability to adjust for important prognostic factors and/or differences remaining in the distribution of prognostic factors across cohorts after adjustment). Pooling via meta-analysis could not overcome the limitations of the individual studies; rather, meta-analysis may compound the bias.
In all cases, analyses by ITT and mITT population were conducted, with definitions generally consistent across studies. However, there were differences across studies, as the mean value of 52 days between apheresis and cilta-cel infusion was used in the mITT population for comparisons with Therapie Monitor and LocoMMotion, while the median of 47 days between apheresis and cilta-cel infusion was used in the mITT population for comparisons of CARTITUDE-1 to MAMMOTH, the daratumumab trial cohort, and the Flatiron cohort. As previously noted, analyses using the ITT population were considered more appropriate for estimating the effect of treatment assignment, while the mITT analyses were at a greater risk of bias due to the elimination of patients who progressed or died in the first 47 or 52 days, thus likely favouring cilta-cel.
The random-effects model was appropriate for incorporating the expected heterogeneity across the studies. In the present meta-analysis, as noted by the I2 and τ2 values, there was generally some statistical heterogeneity in the ITT and mITT populations for the outcomes of OS and PFS. Heterogeneity remained following the preplanned sensitivity analyses, which adjusted the index dates (first versus all index dates) and removing various studies (OIS and LocoMMotion) from the analyses, which could not be explained by the authors.
There were differences in the point estimates and 95% CIs reported from the individual studies versus those used in the meta-analysis. Though the differences were not substantial, the reason for the differences in the values used is unclear and the impact on the results remains unknown. The results of the reported observational studies were consistently in favour of cilta-cel over RWCP. Similarly, the results of the present meta-analysis were in favour of cilta-cel for OS, PFS, and TTNT for both the all–index and first–index dates analyses in both the ITT and mITT populations and in all sensitivity analyses; however, the 95% CIs were often wide, suggesting some imprecision, unexplained heterogeneity, and uncertainty in the magnitude of the effects.
Summary
In total, 4 reports of 5 observational studies and 1 meta-analysis of observational studies were included in the indirect evidence. Two reports were submitted by the sponsor; these included an observational comparison of CARTITUDE-1 and the LocoMMotion study, and 2 observational studies comparing CARTITUDE-1 with patients included in the long-term follow-up of 3 daratumumab trials and patients from the Flatiron Health database in the US. All studies used propensity score weighting in an attempt to adjust for confounding. Three studies that met the eligibility criteria for this review were identified in the CADTH literature search: an observational comparison of CARTITUDE-1 with the MAMMOTH study, an observational comparison of CARTITUDE-1 with the Therapie Monitor database in Germany, and a meta-analysis of published observational studies evaluating the comparative effectiveness of cilta-cel. As noted, these studies met the predefined CADTH criteria for inclusion in this review; however, according to the sponsor, the comparisons of CARTITUDE-1 with the daratumumab trial cohort, the MAMMOTH study, and the Therapie Monitor database were not eligible for submission, as they include comparator therapies that do not reflect current practice of care in Canada. While true, the comparator in each analysis was a basket of treatments considered physicians’ choice, reflecting RWCP, and analyses were not conducted by individual treatment regimen; thus, they are eligible for inclusion. Each included observational study conducted a comparison of cilta-cel using IPD from CARTITUDE-1 versus RWCP using IPD from a different source, including patients from the US and multiple European countries.
There was significant heterogeneity in design and population characteristics between the CARTITUDE-1 trial and the real-world data sources used to generate external control arms. The propensity scoring methods used by the individual studies can only adjust or match on known and measured confounders and cannot account for unknown, unmeasured, or unmeasurable confounders. Across a number of the included studies, the authors were unable to match on all CARTITUDE-1 eligibility criteria, were not able to weight or match on all potentially relevant prognostic factors and, in some cases, important imbalances remained in the distribution of prognostic factors even after propensity score adjustment. Testing for residual confounding was not conducted in any of the included studies; thus, there is a risk of bias due to confounding in these analyses. The magnitude and direction of any bias is unknown. Retrospective studies do not typically have rigorous processes of data collection and adjudication like those in a clinical trial and are often subject to missing or incomplete data. Due to the lack of comparator, the single-arm CARTITUDE-1 study and subsequent comparisons with RWCP are not suitable to conclude a treatment effect on survival outcomes (OS or PFS), and the comparisons with external data are nonconfirmatory and can only be interpreted in an exploratory, supportive manner.
Overall, there was consistency in the direction of effects of all included observational studies that demonstrated the effectiveness of cilta-cel across all outcomes, which suggests some credibility of the findings for RWCP; however, all studies were funded and supported by the sponsor. Financial conflicts of interest have the potential to impact the design, analysis, conduct, and reporting of research. Additional limitations of the observational studies include the small sample sizes, which were further reduced by matching and adjustment methods, the heterogeneity in population characteristics before and after adjustment, and imprecise estimates due to the moderately wide 95% CIs, all of which limit the interpretability of the comparative effectiveness results. Additionally, no safety or HRQoL outcomes were included in any of the studies; thus, safety and HRQoL with cilta-cel relative to other available treatments remain unknown. Though the results suggest that cilta-cel is superior to treatments used in RWCP, the comparative efficacy estimates remain uncertain.
Discussion
Summary of Available Evidence
The CADTH systematic review included 1 pivotal phase Ib/II trial (CARTITUDE-1).
The CARTITUDE-1 study is an ongoing phase Ib/II open-label, single-arm, multicentre study conducted in the US and Japan of cilta-cel in patients with r/rMM who have received at least 3 prior lines of therapy. Of 113 patients enrolled who received apheresis, 97 were treated with a single infusion of cilta-cel: 29 patients in phase Ib and 68 patients in phase II. Three patients were re-treated with cilta-cel.
The primary outcome was ORR, which was defined as the proportion of patients who achieved a PR or better according to the IMWG criteria. OS, PFS, DOR, TTR, VGPR or better rate, and MRD negativity were assessed as secondary outcomes. HRQoL was assessed as a secondary outcome in patients enrolled in phase II of the study.
The CARTITUDE-1 trial enrolled adult patients with a documented diagnosis of MM, an ECOG PS of less than 2, documented disease progression during or within 12 months of their last line of therapy, and who had received 3 or more prior lines of therapy or whose disease was double refractory to a PI and an IMiD and who had received a PI, an IMiD, and an anti-CD38 antibody. Patients with a history of prior treatment with CAR T-cell therapy or any therapy that is targeted to BCMA were excluded.
CARTITUDE-1 is a single-arm trial with a relatively small number of patients and no comparator group; thus, causal conclusions cannot be drawn, particularly for OS and PFS, which are considered noninterpretable. Other limitations include a large amount of missing data for PROs and a risk of bias in the measurement of some outcomes, such as subjective harms.
Other relevant evidence included long-term (2-year and 4-year) findings from the sponsor-submitted LEGEND-2 phase I, single-arm, open-label study (N = 74) conducted in 4 centres in China. An additional 4 reports of 5 observational studies (2 sponsor-submitted reports and 2 published reports) comparing cilta-cel with RWCP using IPD from CARTITUDE-1 and various external cohorts were included. Propensity score weighting or matching was used to adjust for potential confounding variables across the cohorts. One published meta-analysis, which included data from the 5 aforementioned observational studies, was also included.
Interpretation of Results
Efficacy
Among patients who received cilta-cel in the CARTITUDE-1 study,11 the ORR was 97.9% (95% CI, 92.7 to 99.7) with sCR reached by 82.5% (95% CI, 73.4 to 89.4) of patients, which was considered clinically meaningful by the clinical experts consulted by CADTH. The experts mentioned that it was rare for patients to achieve an sCR after a second line of therapy. According to the FDA assessment of the CARTITUDE-1 trial, end points such as OS and PFS are uninterpretable due to the lack of a comparator arm.14 Median OS and PFS were NR by the final data analysis, but the 30-month probability of OS and PFS was 69% and 55%, respectively, which was considered promising by the clinical experts. To put these results in context, the experts mention that the median OS and PFS for current therapies available in the fourth line and beyond is 9 to 12 months.61 The median DOR was NR in the final analysis; however, the probability that patients remained in response at 30 months was 51%, which was considered remarkable by the clinical experts as, to their knowledge, no other therapy for r/rMM has achieved a similar DOR so far. The clinical experts and patients also mentioned that DOR was an important outcome for MM as clinicians try to evaluate how much time patients have until their next line of therapy. Median time to first response was 0.95 months (range, 0.9 to 10.7) and median time to best response was 2.6 months (range, 0.9 to 17.8), which is consistent with TTR in other therapies for MM according to the clinical experts (expected range of 2 to 3 months). Of the patients with evaluable samples (63% of those treated), 92% achieved MRD negativity, which supports the duration and depth of response; however, this measure is not routinely used in clinical practice, according to the clinical experts, and the results are at risk of bias due to missing data. Only 3 patients were re-treated with cilta-cel in the trial; thus, there is insufficient evidence to draw conclusions about re-treatment.
Patient input identified quality of life as 1 of the most important factors of treatment. In the CARTITUDE-1 study, the HRQoL tools were not validated in the population of patients with r/rMM and there was an increasing amount of missing data following transfusion. After 28 days of infusion, there was a steady improvement in global health status and the physical and emotional functional scales and a decline in symptom-based scores over time. The clinical experts postulated that the majority of treatment-related AEs may have resolved by day 28, and that the single-infusion nature of the therapy could potentially explain the improvement in HRQoL over time. The experts emphasize that this is an advantage of cilta-cel compared with most current therapies that require repeated clinical visits and maintenance therapy. Patient input identified travel cost as the most significant financial implication of treatment.
The clinical experts identified selinexor (combined with dexamethasone and bortezomib) as a relevant comparator for transplant-ineligible patients but noted that, currently, there is no available comparative evidence for cilta-cel. Selinexor in combination with bortezomib and dexamethasone received a recommendation for reimbursement with conditions from CADTH in July 2022, but funding negotiations are still ongoing, and it is not yet funded in Canada.
Health care resource utilization (e.g., days in hospital, days in the intensive care unit) was considered an important outcome to both patients and clinicians and, although it was assessed as an exploratory outcome in the CARTITUDE-1 trial, a report was not developed by the sponsor due to multiple missing data points. As such, it is not possible to draw any conclusions about the effect of cilta-cel relative to other available therapies on health care resource utilization.
The primary limitation of the LEGEND-2 trial was the absence of a comparator group against which the treatment benefits and harms of the LCAR-B38M CAR T-cell drug product could be compared. Moreover, because exposure to an anti-CD38 antibody was not required (only 2 patients had received prior anti-CD38 antibody therapy), this study population does not fully align with the reimbursement criteria for this review.
There was significant heterogeneity in design and population characteristics between the CARTITUDE-1 trial and the real-world data sources used to generate external control arms. The propensity scoring methods cannot account for unknown, unmeasured, or unmeasurable confounders. Additional limitations of the observational studies include the small sample sizes, which were further reduced by matching and adjustment methods, the heterogeneity in population characteristics before and after adjustment, and imprecise estimates due to the moderately wide 95% CIs, all of which limit the interpretability of the comparative effectiveness results. Testing for residual confounding was not conducted in any of the included studies. Thus, there is a risk of bias due to confounding in these analyses. The magnitude and direction of any bias is unknown. Though the results suggest that cilta-cel is superior to the treatments used in RWCP, the comparative efficacy estimates remain uncertain.
Harms
All patients in the CARTITUDE-1 trial experienced at least TEAE, 91 patients (94%) experienced at least 1 grade 3 or 4 AE, and 6 patients (6%) experienced at least 1 grade 5 AE. A total of || patients (||%) experienced at least || SAE, with || patients (||%) experiencing a grade 3 or 4 SAE and || patients (||%) experiencing a grade 5 SAE. A total of 30 patients (||||%) died: || due to AEs and 14 due to disease progression. Only 6 patients (6.2%) had a TEAE with an outcome of death. A total of 92 patients (95%) experienced CRS, with 4 patients (4%) experiencing grade 3 or 4 CRS and 1 patient (1%) experiencing grade 5 CRS complicated by secondary hemophagocytic lymphohistiocytosis. A total of 21 patients (22%) experienced CAR T-cell neurotoxicity, including 10 patients (10%) at grade 3 or 4. A total of 16 patients (17%) experienced ICANS, including 2 patients (2%) at grade 3 or 4. Other neurotoxicity was reported in 13 patients (13%), including 9 patients (9%) at grade 3 or 4. A total of 96 patients (99%) had experienced at least 1 grade 3 or 4 cytopenic AE, with the majority resolving to grade 2 within 60 days of infusion. A total of 12 patients (12.4%) experienced hypogammaglobulinemia, including 2 patients (2.1%) with grade 3 or 4 events.
No safety or HRQoL outcomes were included in any of the observational studies, so no firm conclusions can be drawn about the safety of cilta-cel relative to available comparator treatments.
The clinical experts noted that, in their experience, cilta-cel appeared to be less toxic than other therapies available in the fourth line and beyond. They remarked that the proportion of patients who experienced CRS and ICANS that was grade 3 or more, and who would require specialized intensive care, was relatively low. However, out of the 113 patients who underwent apheresis, 12 patients did not receive the conditioning treatment, including 8 patients who died. The clinical experts noted that, although this is common in r/rMM, the proportion of deaths appears unusual, given the relatively healthy trial population.
In the sponsor-submitted LEGEND-2 trial, the clinical experts noted that the high proportion of patients with CRS of grade 3 or higher (7 patients; 10%) was unusual, but that the management of CRS has advanced since the study was conducted. They also mentioned the low proportion of patients with neurotoxicity as an AE (only 1 patient), which is not consistent with the results of the pivotal trial and known harms of cilta-cel.
Conclusions
One sponsor-submitted phase Ib/II, single-arm, open-label trial (CARTITUDE-1) provided evidence regarding the efficacy and safety of cilta-cel for patients with r/rMM who had received at least 3 prior lines of therapy. This trial design is not intended to be confirmatory for efficacy. In general, the clinical experts consulted by CADTH considered the ORR results to be clinically meaningful, especially when compared with currently available therapies. The nonrandomized design of CARTITUDE-1 made interpreting PFS and OS events attributable to cilta-cel challenging; according to the FDA, CARTITUDE-1 could not inform OS or PFS. The results for the HRQoL remained inconclusive due to a number of important limitations. A phase I long-term LCAR-B38M trial (LEGEND-2), based only in China showed similar findings. All patients experienced at least 1 AE, and almost half experienced an SAE. The clinical experts noted that cilta-cel appeared to be less toxic than the other therapies available in the fourth line and beyond, in their experience. They remarked that the proportion of patients who experienced CRS and ICANS that was grade 3 or more, and who would require specialized intensive care, was relatively low.
The comparative evidence came from observational comparisons using IPD from CARTITUDE-1 and real-world cohorts, using propensity scores to adjust for known confounders. Although cilta-cel was favoured for all outcomes assessed, these findings must be interpreted in the context of the methodological limitations of these studies. Propensity score methods can only adjust or match on known and measured confounders and cannot account for unknown, unmeasured, or unmeasurable confounders, nor for differences in study design across comparators. Tests for residual confounding were not conducted in any of the studies, so the results are at risk of bias due to confounding. The generalizability of the results may be limited, since patients in the comparator arms received treatments that are not currently standard of care in Canada.
References
1.Carvykti™ (ciltacabtagene autoleucel): Cell suspension in infusion bag, 0.5-1.0x106 CAR-positive viable T-cells per kg body weight with a maximum of 1x108 CAR-positive viable T-cells, for intravenous infusion [product monograph]. Toronto: Janssen Inc.; 2023.
2.Canadian Cancer Society. Multiple Myeloma: Incidence and Mortality. 2022; https://cancer.ca/en/cancer-information/cancer-types/multiple-myeloma/statistics#:~:text=Incidence%20and%20mortality&text=It%20is%20estimated%20that%20in,970%20will%20die%20from%20it. Accessed 13 Dec 2022.
3.Mikhael J, Ismaila N, Cheung MC, et al. Treatment of Multiple Myeloma: ASCO and CCO Joint Clinical Practice Guideline. Journal of Clinical Oncology. 2019;37(14):1228-1263. PubMed
4.Canadian Cancer Society. Survival statistics for multiple myeloma. 2021: https://cancer.ca/en/cancer-information/cancer-types/multiple-myeloma/prognosis-and-survival/survival-statistics#:~:text=In%20Canada%2C%20the%205%2Dyear,for%20at%20least%205%20years. Accessed 2022 Nov 15.
5.Rajkumar SV. Multiple myeloma: Overview of management Waltham (MA): UpToDate; 2022: https://www.uptodate.com. Accessed 2022 Oct 12.
6.Carvykti: EPAR Assessment report EMA/594558/2022. Amsterdam: European Medicines Agency; 2022: https://www.ema.europa.eu/en/documents/assessment-report/carvykti-epar-public-assessment-report_en.pdf. Accessed 14 Dec 2022.
7.NCCN Guidelines: Multiple Myeloma Plymouth Meeting (PA): National Comprehensive Cancer Network; 2022 Sep 14.
8.GSK. GSK provides an update on Blenrep (belantamab mafodotin-blmf) US marketing authorization. 2022; https://us.gsk.com/en-us/media/press-releases/gsk-provides-an-update-on-blenrep-belantamab-mafodotin-blmf-us-marketing-authorization/. Accessed 14 Dec 2022.
9.Clinical Study Report: 68284528MMY2001. CARTITUDE-1: A Phase 1b-2, Open-Label Study of JNJ-68284528, a Chimeric Antigen Receptor T cell (CAR-T) Therapy Directed Against BCMA in Subjects with Relapsed or Refractory Multiple Myeloma [internal sponsor's report]. Data cut-off date September 1, 2020. Primary Analysis. USA: Janssen Research & Development 2020.
10.Clinical Study Report: 68284528MMY2001. CARTITUDE-1: A Phase 1b-2, Open-Label Study of JNJ-68284528, a Chimeric Antigen Receptor T cell (CAR-T) Therapy Directed Against BCMA in Subjects with Relapsed or Refractory Multiple Myeloma [internal sponsor's report]. Data cut-off date February 11, 2021. Safety & Efficacy Update. USA: Janssen Research & Development 2021.
11.Clinical Study Report: 68284528MMY2001. CARTITUDE-1: A Phase 1b-2, Open-Label Study of JNJ-68284528, a Chimeric Antigen Receptor T cell (CAR-T) Therapy Directed Against BCMA in Subjects with Relapsed or Refractory Multiple Myeloma [internal sponsor's report]. Data cut-off date January 11, 2022. Final Analysis. USA: Janssen Research & Development 2022.
12.Martin T, Lin Y, Agha M, et al. Health-related quality of life in patients given ciltacabtagene autoleucel for relapsed or refractory multiple myeloma (CARTITUDE-1): a phase 1b-2, open-label study. Lancet Haematol. 2022;07:07.
13.Evans SR. Clinical trial structures. J Exp Stroke Transl Med. 2010;3(1):8-18. PubMed
14.FDA. BLA Clinical Review and Evaluation BLA 125746.0, ciltacabtagene autoleucel. 2021; https://www.fda.gov/vaccines-blood-biologics/carvykti. Accessed 15 Dec 2022.
15.FDA. Clinical Trial Endpoints for the Approval of Cancer Drugs and Biologics Guidance for Industry. 2018; https://www.fda.gov/media/71195/download. Accessed 30 Nov 2022.
16.Tsang M, Le M, Ghazawi FM, et al. Multiple myeloma epidemiology and patient geographic distribution in Canada: A population study. Cancer. 2019;125(14):2435-2444. PubMed
17.Ferreri CJ, Hildebrandt MAT, Hashmi H, et al. Idecabtagene Vicleucel (Ide-cel) Chimeric Antigen Receptor (CAR) T-Cell Therapy in Patients with Relapsed/Refractory Multiple Myeloma (RRMM) Who Have Received a Prior BCMA-Targeted Therapy: Real World, Multi-Institutional Experience. Blood. 2022;140(Supplement 1):1856-1858.
18.US Food & Drug Administration. FDA approves selinexor for refractory or relapsed multiple myeloma. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-selinexor-refractory-or-relapsed-multiple-myeloma. Accessed 11 Jan 2023.
19.Legend Biotech HK Limited, Janssen Research & Development. Clinical Study Report: NCT03090659. LEGEND-2: LCAR-B38M CAR-T cells in treating subjects with relapsed or refractory multiple myeloma [internal sponsor's report]. 2020.
20.Janssen EMEA. Adjusted Comparison of ciltacabtagene autoleucel (JNJ-68284528) versus standard of care in tri-exposed multiple myeloma patients based upon data from CARTITUDE-1 and the LocoMMotion Study (MMY4001) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: ciltacabtagene autoleucel. Toronto: Janssen Inc. 2022 Sep 23. 2022.
21.Janssen Research & Development. Adjusted treatment comparison to evaluate the comparative efficacy of ciltacabtagene autoleucel in CARTITUDE-1 versus physician’s choice of treatment in the long-term follow-up of POLLUX, CASTOR and EQUULEUS, and in Flatiron Health’s longitudinal database, for the treatment of patients with multiple myeloma with prior exposure to a proteasome inhibitor, an immunomodulatory agent and an anti-CD38 monoclonal antibody [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: ciltacabtagene autoleucel. Toronto: Janssen Inc. 2022 Sep 23. 2022.
22.Costa LJ, Lin Y, Cornell RF, et al. Comparison of Cilta-cel, an Anti-BCMA CAR-T Cell Therapy, Versus Conventional Treatment in Patients With Relapsed/Refractory Multiple Myeloma. Clinical lymphoma, myeloma & leukemia. 2022;22(5):326-335. PubMed
23.Merz M, Goldschmidt H, Hari P, et al. Adjusted Comparison of Outcomes between Patients from CARTITUDE-1 versus Multiple Myeloma Patients with Prior Exposure to PI, Imid and Anti-CD-38 from a German Registry. Cancers. 2021;13(23):29. PubMed
24.Costa LJ, Hari P, Berdeja JG, et al. Meta-analysis of ciltacabtagene autoleucel versus physician's choice therapy for the treatment of patients with relapsed or refractory multiple myeloma. Curr Med Res Opin. 2022;38(10):1759-1767. PubMed
25.Bergstrom DJ, Kotb R, Louzada ML, Sutherland HJ, Tavoularis S, Venner CP. Consensus Guidelines on the Diagnosis of Multiple Myeloma and Related Disorders: Recommendations of the Myeloma Canada Research Network Consensus Guideline Consortium. Clin Lymphoma Myeloma Leuk. 2020;20(7):e352-e367. PubMed
26.Rajkumar SV. Multiple myeloma: 2020 update on diagnosis, risk-stratification and management. Am J Hematol. 2020;95(5):548-567. PubMed
27.Laubach J. Multiple myeloma: Staging and prognostic studies. Waltham (MA): UpToDate 2022 May 26. Accessed Oct 12, 2022.
28.Rajkumar SV, Harousseau J-L, Durie B, et al. Consensus recommendations for the uniform reporting of clinical trials: report of the International Myeloma Workshop Consensus Panel 1. Blood, The Journal of the American Society of Hematology. 2011;117(18):4691-4695. PubMed
29.Multiple myeloma. Plymouth Meeting (PA): National Comprehensive Cancer Network; 2022: https://www.nccn.org/professionals/physician_gls/pdf/myeloma.pdf. Accessed 2022 Mar 3.
30.Berdeja JG, Madduri D, Usmani SZ, et al. Ciltacabtagene autoleucel, a B-cell maturation antigen-directed chimeric antigen receptor T-cell therapy in patients with relapsed or refractory multiple myeloma (CARTITUDE-1): a phase 1b/2 open-label study. Lancet. 2021;398(10297):314-324. PubMed
31.CADTH. Multiple Myeloma: Provisional Funding Algorithm 2022: https://www.cadth.ca/sites/default/files/pdf/PH0014%20Rapid%20Algorithm%20Report%20Multiple%20Myeloma.pdf. Accessed 2023 Jan 12.
32.Pomalyst® (pomalidomide), capsules, 1 mg, 2 mg, 3 mg and 4 mg (oral) [product monograph]. Mississauga (ON) Celgene Inc.; 2018: https://pdf.hres.ca/dpd_pm/00043809.PDF. Accessed 14 Dec 2022.
33.Xpovio (selinexor): tablets, 20 mg, oral [product monograph]. Oakville (ON): FORUS Therapeutics Inc; 2021.
34.Kyprolis® (carfilzomib): vial, 10, 30, 60 mg, injection [product monograph]. Mississauga (ON): Amgen Canada Inc.; 2019: https://pdf.hres.ca/dpd_pm/00051989.PDF. Accessed 14 Dec 2022.
35.Canadian Pharmacists Association. e-CPS. 2022: https://www.e-therapeutics.ca. . Accessed 30 Nov 2022.
36.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. Journal of clinical epidemiology. 2016;75:40-46. PubMed
37.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 28 Oct 2022.
38.Janssen Research & Development. A Study of JNJ-68284528, a Chimeric Antigen Receptor T Cell (CAR-T) Therapy Directed Against B-Cell Maturation Antigen (BCMA) in Participants With Relapsed or Refractory Multiple Myeloma (CARTITUDE-1). Identifier: NCT03548207. Bethesda (MD): ClinicalTrials.gov; 2018: https://www.clinicaltrials.gov/ct2/show/NCT03548207. Accessed 14 Dec 2022.
39.Cohen AD, Parekh S, Santomasso BD, et al. Incidence and management of CAR-T neurotoxicity in patients with multiple myeloma treated with ciltacabtagene autoleucel in CARTITUDE studies. Blood Cancer J. 2022;12(2):32. PubMed
40.Martin T, Usmani SZ, Berdeja JG, et al. Ciltacabtagene Autoleucel, an Anti-B-cell Maturation Antigen Chimeric Antigen Receptor T-Cell Therapy, for Relapsed/Refractory Multiple Myeloma: CARTITUDE-1 2-Year Follow-Up. Journal of Clinical Oncology. 2022:JCO2200842. PubMed
41.Cohen AD, Hari P, Htut M, et al. Patient Perceptions Regarding Ciltacabtagene Autoleucel Treatment: Qualitative Evidence From Interviews With Patients With Relapsed/Refractory Multiple Myeloma in the CARTITUDE-1 Study. Clinical Lymphoma Myeloma and Leukemia. 2022. PubMed
42.Ri M, Suzuki K, Ishida T, et al. Ciltacabtagene autoleucel in patients with relapsed/refractory multiple myeloma: CARTITUDE-1 (phase 2) Japanese cohort. Cancer Sci. 2022;02:02.
43.Palumbo A, Chanan-Khan A, Weisel K, et al. Daratumumab, bortezomib, and dexamethasone for multiple myeloma. New England Journal of Medicine. 2016;375(8):754-766. PubMed
44.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. JNCI: Journal of the National Cancer Institute. 1993;85(5):365-376. PubMed
45.Fayers PM. Interpreting quality of life data: population-based reference data for the EORTC QLQ-C30. Eur J Cancer. 2001;37(11):1331-1334. PubMed
46.Kvam AK, Wisloff F, Fayers PM. Minimal important differences and response shift in health-related quality of life; a longitudinal study in patients with multiple myeloma. Health Qual Life Outcomes. 2010;8:79. PubMed
47.Danaher EH, Ferrans C, Verlen E, et al. Fatigue and physical activity in patients undergoing hematopoietic stem cell transplant. Oncol Nurs Forum. 2006;33(3):614-624. PubMed
48.Molassiotis A, Wilson B, Blair S, Howe T, Cavet J. Unmet supportive care needs, psychological well‐being and quality of life in patients living with multiple myeloma and their partners. Psychooncology. 2011;20(1):88-97. PubMed
49.Ringdal K, Ringdal GI, Kaasa S, et al. Assessing the consistency of psychometric properties of the HRQoL scales within the EORTC QLQ-C30 across populations by means of the Mokken Scaling Model. Qual Life Res. 1999;8(1-2):25-43. PubMed
50.Wisløff F, Eika S, Hippe E, et al. Measurement of health-related quality of life in multiple myeloma. Nordic Myeloma Study Group. Br J Haematol. 1996;92(3):604-613. PubMed
51.Kvam AK, Fayers P, Wisloff F. What changes in health-related quality of life matter to multiple myeloma patients? A prospective study. Eur J Haematol. 2010;84(4):345-353. PubMed
52.Kvam AK, Fayers PM, Wisloff F. Responsiveness and minimal important score differences in quality-of-life questionnaires: a comparison of the EORTC QLQ-C30 cancer-specific questionnaire to the generic utility questionnaires EQ-5D and 15D in patients with multiple myeloma. Eur J Haematol. 2011;87(4):330-337. PubMed
53.Cocks K, Cohen D, Wisloff F, et al. An international field study of the reliability and validity of a disease-specific questionnaire module (the QLQ-MY20) in assessing the quality of life of patients with multiple myeloma. Eur J Cancer. 2007;43(11):1670-1678. PubMed
54.Sully K, Trigg A, Bonner N, et al. Estimation of minimally important differences and responder definitions for EORTC QLQ-MY20 scores in multiple myeloma patients. Eur J Haematol. 2019;103(5):500-509. PubMed
55.Lee DW, Gardner R, Porter DL, et al. Current concepts in the diagnosis and management of cytokine release syndrome. Blood, The Journal of the American Society of Hematology. 2014;124(2):188-195. PubMed
56.Lee DW, Santomasso BD, Locke FL, et al. ASTCT consensus grading for cytokine release syndrome and neurologic toxicity associated with immune effector cells. Biology of Blood and Marrow Transplantation. 2019;25(4):625-638. PubMed
57.Sully K, Trigg A, Bonner N, et al. Estimation of minimally important differences and responder definitions for EORTC QLQ‐MY20 scores in multiple myeloma patients. Eur J Haematol. 2019;103(5):500-509. PubMed
58.Janssen Canada response to November 23, 2022 DRR request for additional information regarding cilta-cel DRR review [internal additional sponsor's information]. Toronto, ON: Janssen Canada; 2022.
59.Zhao WH, Wang BY, Chen LJ, et al. Four-year follow-up of LCAR-B38M in relapsed or refractory multiple myeloma: a phase 1, single-arm, open-label, multicenter study in China (LEGEND-2). J Hematol Oncol. 2022;15(1):86. PubMed
60.Faria R, Hernandez Alava M, Manca A, Wailoo AJ. NICE DSU technical support document 17: The use of observational data to inform estimates of treatment effectiveness in technology appraisal: Methods for comparative individual patient data. Sheffield (GB): Decision Support Unit, ScHARR; 2015: https://www.sheffield.ac.uk/sites/default/files/2022-02/TSD17-DSU-Observational-data-FINAL.pdf. Accessed 22 Nov 2022.
61.Gandhi UH, Cornell RF, Lakshman A, et al. Outcomes of patients with multiple myeloma refractory to CD38-targeted monoclonal antibody therapy. Leukemia. 2019;33(9):2266-2275. PubMed
62.Janssen Research & Development. Clinical Study Protocol: 68284528MMY2001. CARTITUDE-1: A Phase 1b-2, Open-Label Study of JNJ-68284528, a Chimeric Antigen Receptor T cell (CAR-T) Therapy Directed Against BCMA in Subjects with Relapsed or Refractory Multiple Myeloma [internal sponsor's report]. 2022.
63.Fayers PM, Aaronson NK, Bjordal K, et al. The EORTC QLQ-C30 Scoring Manual (3rd Edition). Brussels (BE): European Organisation for Research and Treatment of Cancer; 2001: https://www.eortc.org/app/uploads/sites/2/2018/02/SCmanual.pdf. Accessed 2022 Nov 28.
64.EORTC Quality of Life. Questionnaires: Core. https://qol.eortc.org/core/. Accessed 2022 Nov 28.
65.Osborne TR, Ramsenthaler C, Siegert RJ, Edmonds PM, Schey SA, Higginson IJ. What issues matter most to people with multiple myeloma and how well are we measuring them? A systematic review of quality of life tools. Eur J Haematol. 2012;89(6):437-457. PubMed
66.Cocks K, King MT, Velikova G, et al. Evidence-based guidelines for interpreting change scores for the European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30. Eur J Cancer. 2012;48(11):1713-1721. PubMed
67.van Reenen M JB, Stolk E, Boye K, Herdman M, Kennedy-Martin M, Kennedy-Martin T, Slaap B. EQ-5D-5L User Guide Version 3.0. 2019: https://euroqol.org/publications/user-guides. Accessed 2022 Nov 04.
68.Stewart AK, Dimopoulos MA, Masszi T, et al. Health-related quality-of-life results from the open-label, randomized, phase III ASPIRE trial evaluating carfilzomib, lenalidomide, and dexamethasone versus lenalidomide and dexamethasone in patients with relapsed multiple myeloma. J Clin Oncol. 2016;34(32):3921. PubMed
69.Dimopoulos MA, Moreau P, Palumbo A, et al. Carfilzomib and dexamethasone versus bortezomib and dexamethasone for patients with relapsed or refractory multiple myeloma (ENDEAVOR): a randomised, phase 3, open-label, multicentre study. Lancet Oncol. 2016;17(1):27-38. PubMed
70.Facon T, Lee JH, Moreau P, et al. Phase 3 study (CLARION) of carfilzomib, melphalan, prednisone (KMP) v bortezomib, melphalan, prednisone (VMP) in newly diagnosed multiple myeloma (NDMM). Clinical Lymphoma, Myeloma and Leukemia. 2017;17(1):e26-e27.
Appendix 1: Literature Search Strategy
Note this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946 to present)
Embase (1974 to present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: October 24, 2022
Alerts: Biweekly search updates until project completion
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits:
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
.fs | Floating subheading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
# | Truncation symbol for one character |
? | Truncation symbol for one or no characters only |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Keyword heading word |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.mp | Mapped term |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
.yr | Publication year |
.jw | Journal title word (MEDLINE) |
.jx | Journal title word (Embase) |
freq = # | Requires terms to occur # number of times in the specified fields |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multidatabase Strategy
(ciltacabtagene* or cilta-cel* or Carvykti* or JNJ-68284528 or JNJ68284528 or WHO 11131 or WHO11131 or LCAR-B38M or LCARB38M or jnj 4528 or jnj4528 or 0L1F17908Q).ti,ab,kf,ot,hw,rn,nm.
1 use medall
*ciltacabtagene autoleucel/
(ciltacabtagene* or cilta-cel* or Carvykti* or JNJ-68284528 or JNJ68284528 or WHO 11131 or WHO11131 or LCAR-B38M or LCARB38M or jnj 4528 or jnj4528).ti,ab,kf,dq.
3 or 4
(conference abstract or conference review).pt.
5 not 6
7 use oemezd
2 or 8
remove duplicates from 9
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- ciltacabtagene OR “cilta-cel” OR Carvykti OR “JNJ-68284528” OR JNJ68284528 OR “WHO 11131” OR WHO11131 OR “LCAR-B38M” OR LCARB38M OR “jnj 4528” OR jnj4528]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the WHO. Targeted search used to capture registered clinical trials.
[Search -- ciltacabtagene OR “cilta-cel” OR Carvykti OR “JNJ-68284528” OR JNJ68284528 OR “WHO 11131” OR WHO11131 OR “LCAR-B38M” OR LCARB38M OR “jnj 4528” OR jnj4528]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search -- ciltacabtagene OR “cilta-cel” OR Carvykti OR “JNJ-68284528” OR JNJ68284528 OR “WHO 11131” OR WHO11131 OR “LCAR-B38M” OR LCARB38M OR “jnj 4528” OR jnj4528]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search -- ciltacabtagene OR “cilta-cel” OR Carvykti OR “JNJ-68284528” OR JNJ68284528 OR “WHO 11131” OR WHO11131 OR “LCAR-B38M” OR LCARB38M OR “jnj 4528” OR jnj4528]
Grey Literature
Search dates: October 12 to October 18, 2022
Keywords: [Search -- ciltacabtagene OR “cilta-cel” OR Carvykti OR “JNJ-68284528” OR JNJ68284528 OR “WHO 11131” OR WHO11131 OR “LCAR-B38M” OR LCARB38M OR “jnj 4528” OR jnj4528]
Limits: None
Updated: Search updated before the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Open-Access Journals
Appendix 2: Excluded Studies
Note this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
Cohen, A. D., et al. (2022). “Efficacy and safety of cilta-cel in patients with progressive MM after exposure to other BCMA-targeting agents.” Blood 12: 12. | Review article |
Usmani, S. Z., et al. (2022). “MM-181 CARTITUDE-1: Two-Year Post Last Patient in (LPI) Results From the Phase 1b/2 Study of Ciltacabtagene Autoleucel (Cilta-Cel), a B-Cell Maturation Antigen (BCMA)-Directed Chimeric Antigen Receptor T (CAR-T) Cell Therapy, in Patients With Relapsed/Refractory Multiple Myeloma (RRMM).” Clinical lymphoma, myeloma & leukemia 22 Suppl 2: S410-S411. | Conference abstract of included CSR |
Davis, J., et al. (2022). “Idecabtagene vicleucel versus ciltacabtagene autoleucel: a Sophie's choice for patients with relapsed refractory multiple myeloma.” Expert Review of Hematology 15(6): 473-475. | Review article |
Krejci, M., et al. (2022). “CAR-T cells for the treatment of relapsed/refractory multiple myeloma in 2022: efficacy and toxicity.” Neoplasma 69(5): 1008-1018. | Review article |
Rodriguez-Otero, P. and J. F. San Miguel (2022). “Post-CAR-T Cell Therapy (Consolidation and Relapse): Multiple Myeloma.” Springer chapter 34: 173-176. | Review article |
Mi, J. Q., et al. (2022). “Phase II, Open-Label Study of Ciltacabtagene Autoleucel, an Anti-B-Cell Maturation Antigen Chimeric Antigen Receptor-T-Cell Therapy, in Chinese Patients With RRMM (CARTIFAN-1).” Journal of clinical oncology: official journal of the American Society of Clinical Oncology: JCO2200690. | Population (receiving anti-CD38 antibody was not a requirement) |
BCMA = B-cell maturation antigen; CAR-T = chimeric antigen receptor T cell; MM = multiple myeloma; RRMM = relapsed/refractory multiple myeloma.
Appendix 3: Detailed Outcome Data
Note this appendix has not been copy-edited.
Figure 16: Summary of Adjusted Comparisons for CARTITUDE-1 Versus LocoMMotion for Clinical Response Outcomes

ATO = average treatment effect in the overlap population; ATT = average treatment effect in the treated population; CI = confidence interval; IPW = inverse probability weighting; ITT = intention-to-treat; mITT = modified intention-to-treat; OR = odds ratio; RWCP = real-world clinical practice.
Notes: Figure was redacted at the sponsor’s request.
a) Summary of adjusted comparisons for ORR; b) Summary of adjusted comparisons for ≥ VGPR.
Source: Sponsor-submitted indirect treatment comparison.20
Figure 17: Summary of Adjusted Comparisons for CARTITUDE-1 Versus LocoMMotion for Time-to-Event Outcomes

ATO = average treatment effect for the overlap population; ATT = average treatment effect in the treated population; CI = confidence interval; HR = hazard ratio; IPW = inverse probability weighting; ITT = intention-to-treat; mITT = modified intention-to-treat; RWCP = real-world clinical practice.
Notes: Figure was redacted at the sponsor’s request.
a) Summary of adjusted comparisons for PFS; b) summary of adjusted comparisons for OS; c) summary of adjusted comparisons for TTNT.
Source: Sponsor-submitted indirect treatment comparison.20
Figure 18: Balance of Covariates Before and After ATT Weighting for (A) Base-Case Scenario and (B) Fully Adjusted Scenario for CARTITUDE-1 Versus the Daratumumab Trial Cohort (ITT Population)
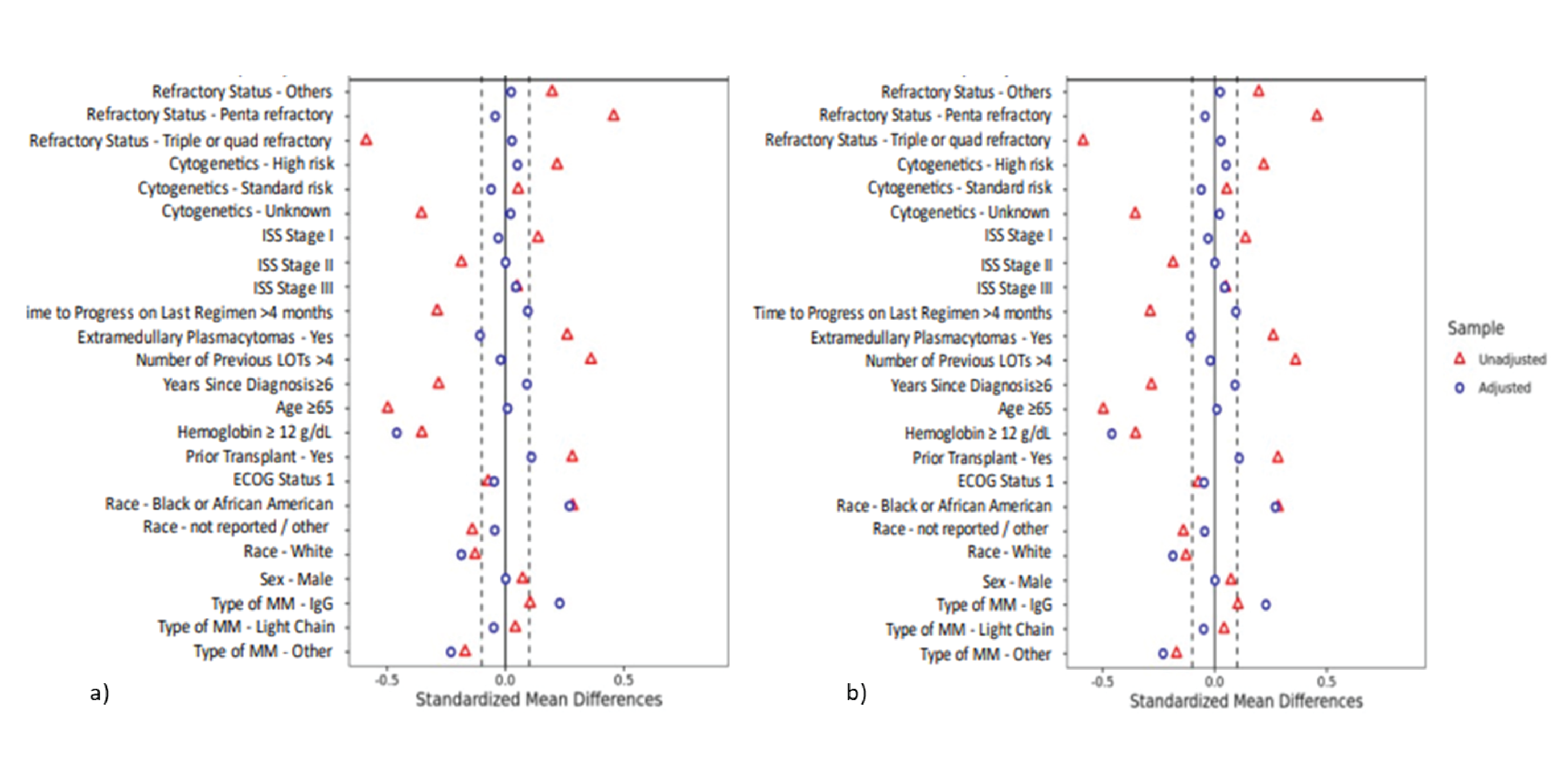
ATT = average treatment effect in the treated; ECOG = Eastern Cooperative Oncology Group; ISS = International Staging System; ITT = intention-to-treat; LOT = line of therapy; MM = multiple myeloma.
Notes: a) Balance of covariates before and after weighting in the base-case scenario, which adjusted for refractory status, ISS stage, cytogenetic profile, time to progression on last regimen, extramedullary plasmacytomas, number of prior LOTs, years since MM diagnosis, and age.
b) Balance of covariates before and after weighting in the fully adjusted scenario, which adjusted for all variables in the base case, plus hemoglobin, prior stem cell transplant, ECOG score, race, sex, and type of MM.
Source: Sponsor-submitted indirect treatment comparison.21
Figure 19: Balance of Covariates Before and After ATT Weighting for (A) Base-Case Scenario and (B) Fully Adjusted Scenario for CARTITUDE-1 Versus the Daratumumab Trial Cohort (mITT Population)

ATT = average treatment effect in the treated; ECOG = Eastern Cooperative Oncology Group; ISS = International Staging System; ITT = intention-to-treat; LOT = line of therapy; MM = multiple myeloma.
Notes: Figure was redacted at the sponsor’s request.
a) Balance of covariates before and after weighting in the base-case scenario, which adjusted for refractory status, ISS stage, cytogenetic profile, time to progression on last regimen, extramedullary plasmacytomas, number of prior LOTs, years since MM diagnosis, and age.
b) Balance of covariates before and after weighting in the fully adjusted scenario, which adjusted for all variables in the base case, plus hemoglobin, prior stem cell transplant, ECOG score, race, sex, and type of MM.
Source: Sponsor-submitted indirect treatment comparison.21
Figure 20: Balance of Covariates Before and After ATT Weighting for (A) Base-Case Scenario and (B) Fully Adjusted Scenario for CARTITUDE-1 Versus the Flatiron Cohort (ITT Population)

ATT = average treatment effect in the treated; ECOG = Eastern Cooperative Oncology Group; ISS = International Staging System; LOT = line of therapy; MM = multiple myeloma.
Notes: Figure was redacted at the sponsor’s request.
a) Base-case results adjusted for refractory status, ISS stage, cytogenetic profile, time to progression on last regimen, number of prior LOTs, years since MM diagnosis, and age.
b) The fully adjusted scenario adjusted for all variables in the base case, plus hemoglobin, LDH, prior SCT, ECOG score, race, sex, and type of MM.
Source: Sponsor-submitted indirect treatment comparison.21
Figure 21: Balance of Covariates Before and After ATT Weighting for (A) Base-Case Scenario and (B) Fully Adjusted Scenario for CARTITUDE-1 Versus the Flatiron Cohort (mITT Population)

ATT = average treatment effect in the treated; ECOG = Eastern Cooperative Oncology Group; ISS = International Staging System; LOT = line of therapy; MM = multiple myeloma.
Notes: Figure was redacted at the sponsor’s request.
a) Base-case results adjusted for refractory status, ISS stage, cytogenetic profile, time to progression on last regimen, number of prior LOTs, years since MM diagnosis, and age.
b) The fully adjusted scenario adjusted for all variables in the base case, plus hemoglobin, LDH, prior SCT, ECOG score, race, sex, and type of MM.
Source: Sponsor-submitted indirect treatment comparison.21
Appendix 4: Description and Appraisal of Outcome Measures
Note this appendix has not been copy-edited.
Aim
To define the criteria for response to MM treatment
To describe the following outcome measures and review their measurement properties, including validity, reliability, responsiveness to change, and the MID:
EORTC QLQ-C30
EORTC QLQ-MY20
EQ-5D-5L
Findings
Criteria for response to MM treatment are defined in Table 37. The findings on reliability, validity, responsiveness, and the MID of each outcome measure are summarized in Table 38.
Table 37: Criteria for Response to MM Treatment
Response | Response criteria |
|---|---|
Stringent complete response | CR as defined subsequently, plus
|
CRa |
|
VGPRa |
|
PR |
|
MR |
|
Stable disease | Not meeting criteria for sCR, CR, VGPR, PR, MR, or progressive disease |
Progressive diseasec | Any 1 or more of the following criteria:
|
CR = complete response; FLC = free light chain; MR = minimal response; PC = plasma cell; PR = partial response; sCR = stringent complete response; SPD = sum of the products of the maximal perpendicular diameters of measured lesions; VGPR = very good partial response.
Note: All response categories (CR, sCR, VGPR, PR, MR, and progressive disease) require 2 consecutive assessments made at any time before the institution of any new therapy; CR, sCR, VGPR, PR, MR, and stable disease categories also require no known evidence of progressive or new bone lesions if radiographic studies were performed. VGPR and CR categories require serum and urine studies regardless of whether disease at baseline was measurable on serum, urine, both, or neither. Radiographic studies are not required to satisfy these response requirements. Bone marrow assessments need not be confirmed. For progressive disease, serum M-component increases of ≥ 1 g/dL are sufficient to define relapse if lowest M-component is ≥ 5 g/dL.
aClarifications to the criteria for coding CR and VGPR in patients in whom the only measurable disease is by serum FLC levels: CR in such patients indicates a normal FLC ratio of 0.26 to 1.65 in addition to CR criteria listed earlier. VGPR in such patients requires a ≥ 90% decrease in the difference between involved and uninvolved FLC levels. For patients achieving VGPR by other criteria, a soft-tissue plasmacytoma must decrease by more than 90% in the sum of the maximal perpendicular diameter (SPD) compared with baseline.
bIn some cases it is possible that the original M protein light chain isotype is still detected on immunofixation, but the accompanying heavy-chain component has disappeared; this would not be considered as a CR even though the heavy-chain component is not detectable, since it is possible that the clone evolved to one that secreted only light chains. Thus, if a patient has immunoglobulin A lambda myeloma, then to qualify as CR there should be no immunoglobulin A detectable on serum or urine immunofixation; if free lambda is detected without immunoglobulin A, then it must be accompanied by a different heavy-chain isotype (immunoglobulin G, immunoglobulin M, and so forth).
cClarifications to the criteria for coding progressive disease: bone marrow criteria for progressive disease are to be used only in patients without measurable disease by M protein and by FLC levels; “25% increase” refers to M protein, and FLC, and does not refer to bone lesions, or soft-tissue plasmacytomas and the “lowest response value” does not need to be a confirmed value.
Source: CARTITUDE-1 clinical study protocol.62
Table 38: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EORTC QLQ-C30 | A cancer-specific, patient-reported outcomes measure that is commonly used in oncology clinical trials to evaluate HRQoL. The core questionnaire consists of 30 questions that are scored to create 5 multi-item functional scales (physical, role, emotional, cognitive, social), 3 multi-item symptom scales (fatigue, nausea and vomiting, pain), 6 single-item symptom scales (dyspnea, insomnia, appetite loss, constipation, diarrhea, financial difficulties), and a global health status/QoL scale.44,63 Presently, Version 3.0 of the questionnaire is the most current version and was used in the CARTITUDE-1 study.64 A 1-week recall period was used in CARTITUDE-111 to assess function and symptoms. Most items have 4 response options (“not at all,” “a little,” “quite a bit,” “very much”), with scores on these items ranging from 1 to 4, respectively. For the global health status/QoL scale, a 7-point Likert-type scale is used, with anchors between 1 (very poor) and 7 (excellent).63 The raw scores for each scale are computed as the average of the items that contribute to a particular scale. Each raw scale score is then converted to a standardized score that ranges from 0 to 100 using a linear transformation, with a higher score reflecting better function on the function scales, greater symptoms on the symptom scales, and better quality of life.63 Thus, a decline in score on the symptom scale would reflect an improvement, whereas an increase in score on the function and QoL scales would reflect an improvement.63 | Osborne et al.65 conducted a systematic literature review of validated HRQoL tools in MM. For EORTC QLQ-C30, the sample included patients with newly diagnosed MM, relapsed MM, mixed disease stages of MM and treatment experiences, and treated with HSCT.65 For the purposes of this review, data specific to only patients treated with HSCT were not reported subsequently. Validity: For construct validity, the subscales for pain, fatigue, physical and global QoL were able to discriminate between patients (mixed disease stages and treatment experiences, including 69 patients (29%) with relapsed/progression) who improved vs. patients who were stable/deteriorated (N = 239).46 All subscales, with the exception of the single-item diarrhea scale, were able to discriminate between patients with newly diagnosed MM according to their performance and response status (N = 484).50 Reliability: For internal consistency, the Cronbach alpha ranged from 0.54 to 0.89 for all subscales in patients with newly diagnosed MM, mixed disease stages and treatments, and treated with HSCT.47-50 Responsiveness: Responsiveness of the subscales to change over time varied depending on the sample population (listed previously) studied.65 To assess responsiveness, Kvam et al.52 used the global rating of change to identify whether patients with mixed disease stages and treatments changed over time. Of note, 69 patients (29%) had relapsed/progression disease.a,52 For the global QoL scale, the SRMb in patients who reported improvement and deterioration over a period of 3 months was 0.32 and 0.57, respectively (N = 239). In patients rating themselves as unchanged, the SRM was negligible.52 Note, results should be interpreted with caution as 86 patients (36%) did not receive treatment during the study52 (i.e., any change was not due to treatment). | Cocks et al.66 examined 118 published studies on various types of cancer, such as breast, lung, or head and neck, and used clinician expert input to determine meaningful differences and magnitude of change in the QLQ-C30. A small change was considered a subtle, clinically relevant change.66 Note, patients with MM were not included in the meta-analysis.66 Based on the meta-analysis estimates, the thresholds for no difference (trivial change) in the subscales were as follows (any difference larger than this trivial change would be considered important)66:
From the systemic review of validated HRQoL tools in MM conducted by Osborne et al.,65 the following estimated MIDs were reported for patients with mixed disease stages and treatments: Mean score changes of 6 to 17 in the QLQ-C30 were considered to be important to patientsc (N = 239).51 Of note, changes in the patient’s internal standard of measurement over time (i.e., response shift) may impact the estimated MID in MM; in particular, in patients with deteriorating disease.46 A change of 8 and 12 points in patients who improved and deteriorated, respectively, on the global QoL score was considered to be important to patientsd (N = 239).52 |
EORTC QLQ-MY20 | A 20-item myeloma module intended for use only in conjunction with the EORTC QLQ-C30. The module consists of 3 multi-item subscales, disease symptoms, side effects of treatment, and future perspective, and 1 single-item subscale, body image.65 In CARTITUDE-1,11 4 single items were administered from the EORTC QLQ-MY20 to assess emotional health status (feel restless or agitated, thinking about your illness, worried about dying, worried about health in the future). The recall period, response options, and interpretation used in CARTITUDE-1 were similar to the QLQ-C30 described previously.11 | Osborne et al.65 conducted a systematic literature review of validated HRQoL tools in MM. For EORTC QLQ-MY20, the sample included patients with newly diagnosed MM and patients who were diagnosed with MM for greater than 1 year.65 Validity: After removing the social support scale (4 items) in the QLQ-MY24 due to the ceiling effects, the psychometric properties of the resultant QLQ-MY20 were evaluated by Cocks et al.53 Patients had to be in a clinical trial at the time of this field study and had either newly diagnosed MM (N = 225) or relapsed/refractory MM (N = 15).53 For known-groups comparison, the QLQ-MY20 scale scores for patients with a WHO performance status of 0, 1, or 2 (N = 200) were compared with patients with a WHO performance status of 3 or 4 (N = 25) at baseline. Only the disease symptoms, treatment side effects, and body image scales demonstrated differences between patient groups according to their performance status (0/1/2 vs. 3/4).53 Reliability: Not assessed in patients with MM. Responsiveness: In addition to validity, Cocks et al.53 evaluated the responsiveness of QLQ-MY20. Details of the study are described previously in the validity section. Treatment received in the patient’s respective clinical trial could have been chemotherapy, transplant, or bisphosphonates. For responsiveness to change, the scale scores at baseline were compared with follow-up (during or on completion of the respective trial treatment) for 137 patients (57%) who achieved at least partial response. The scale scores for disease symptoms and body image decreased over time with treatment, while the scale scores for treatment side effects increased.53 | Sully et al.54 estimated the MID and responder definition in the QLQ-MY20 by triangulating (plotting on a forest plot) the estimates derived from the qualitative-based analysese using patient interviews (newly diagnosed MM, 10 patients; relapsed/refractory MM, 10 patients) and the anchor-f and distribution-g based analyses using existing clinical trial datah of patients with newly diagnosed and relapsed or refractory MM (newly diagnosed, 726 patients; relapsed/refractory, 1,421 patients). Additionally, the anchor-based estimates were summarized with a correlation-weighted average.54 These methods yielded the following estimated MIDs (the smallest difference in the mean scores between groups that is considered to clinically meaningful)54:
|
EQ-5D-5L | A generic measure of health status comprised of 2 parts. The descriptive system assesses health in 5 dimensions (mobility, self-care, usual activities, pain/discomfort and anxiety/depression).67 Each dimension has 5 increasing levels of severity/response (no problems, slight problems, moderate problems, severe problems and unable to/extreme problems). A unique health state profile is generated as a 5-digit code (e.g., 12345 indicates no problems with mobility, slight problems with self-care, moderate problems with usual activities, severe pain or discomfort, and extreme anxiety or depression).67 The health state can be converted to a summary index score based on societal (countries/regions) preference weights for the health state. Index scores range from less than 0 (negative values represent worse than dead, which is represented by 0) to 1 (full health), with higher scores representing higher health utility.67 Patient’s perceived health status on that day is also rated using the VAS, ranging from 0 (worst imaginable health) to 100 (best imaginable health).67 | Validity: Not assessed in patients with MM. Reliability: Not assessed in patients with MM. Responsiveness: Not assessed in patients with MM. | Not estimated in patients with MM. |
EORTC = European Organisation for Research and Treatment of Cancer; HRQoL = health-related quality of life; HSCT = hematopoietic stem cell transplant; ICC = intraclass correlation coefficient; MID = minimal important difference; MM = multiple myeloma; PFS = progression‐free survival; QLQ-C30 = Quality of Life Questionnaire Core 30; QLQ-MY20 = 20-item Quality of Life Questionnaire Myeloma Module; QLQ-MY24 = 24-item Quality of Life Questionnaire Myeloma Module; QoL = quality of life; SRM = standardized response mean; VAS = visual analogue scale.
aThe European Group for Blood and Marrow transplant criteria for response were used to determine the patients’ disease phase.52
bTo assess the magnitude of the difference in scores between patients who improved, deteriorated, and remained stable, SRMs were calculated and compared against the Cohen rule of thumb for interpreting the magnitude of mean differences in HRQoL scores: 0.20 represents a small change, 0.50 a moderate change, and > 0.80 a large change.52
cThe MIDs were estimated using 1) anchor-based approach; anchored to a structured quality-of-life interview (response options were improved, deteriorated, or unchanged) and 2) distribution-based approach; based on the standard deviations of baseline scores, as well as the receiver operating characteristic curve method.51
dThe MIDs were estimated using 1) anchor-based approach; anchored to a structured quality-of-life interview (response options were improved, deteriorated, or unchanged) and 2) distribution-based approach; based on the standard deviations of baseline scores.52
eQualitative-based analyses were performed using patient interviews (newly diagnosed and relapsed/refractory) that were conducted to understand what constitutes a meaningful change in the concepts evaluated by the QLQ-MY20.54
fAnchor-based MIDs were estimated by calculating the mean change score of patients who improved and deteriorated based on anchor definitions. Anchors were selected based on conceptual overlap with any of the QLQ‐MY20 scales. Patient‐reported anchors were the EORTC QLQ‐C30 global health status (QoL) scale and Functional Assessment of Cancer Therapy‐Gynecologic Oncology Group Neurotoxicity. Clinical anchors were the Eastern Cooperative Oncology Group Performance Status, matched AEs, and peripheral neuropathy‐related AEs. Anchor-based responder definitions were estimated by plotting receiver operating characteristic curves for each anchor-scale combination to discriminate between patients who changed vs. remained stable.54
gDistribution-based estimates of half the standard deviation and 1 standard error of measurement at baseline were calculated.54
hData were pooled across 3 clinical trials: ASPIRE,68 ENDEAVOUR,69 and CLARION.70 These were phase III, randomized, open-label studies comparing carfilzomib‐based regimens, with a primary end point of PFS in patients with relapsed or refractory as well as newly diagnosed MM ineligible for transplant.54
Pharmacoeconomic Review
Abbreviations
AE
adverse event
ASCT
autologous stem cell transplant
CAR
chimeric antigen receptor
ECOG
Eastern Cooperative Oncology Group
ICER
incremental cost-effectiveness ratio
ITC
indirect treatment comparison
IVIG
IV immunoglobulin
LY
life-year
OOS
out of specification
OS
overall survival
PFS
progression-free survival
QALY
quality-adjusted life-year
r/rMM
relapsed or refractory multiple myeloma
SOC
standard of care
VBA
value-based agreement
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Ciltacabtagene autoleucel (Carvykti), suspension of CAR-positive viable T cells, for IV infusion |
Submitted price | Ciltacabtagene autoleucel (Carvykti) 0.5 × 106 to 1.0 × 106 CAR-positive viable T cells per kg: $632,455 per administration |
Indication | For the treatment of adult patients with multiple myeloma who have received at least 3 prior lines of therapy, including a proteasome inhibitor, an immunomodulatory drug, and an anti-CD38 antibody, and who are refractory to their last treatment. |
Health Canada approval status | NOC/c |
Health Canada review pathway | Advance consideration under NOC/c |
NOC date | February 9, 2023 |
Reimbursement request | As per indication |
Sponsor | Janssen Inc. |
Submission history | Previously reviewed: No |
CAR = chimeric antigen receptor; NOC = Notice of Compliance; NOC/c = Notice of Compliance with Conditions.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation |
|
Target population | Adult patients with r/rMM who have received at least 3 prior lines of therapy, including a proteasome inhibitor, an immunomodulatory drug, and an anti-CD38 antibody |
Treatment | Ciltacabtagene autoleucel |
Comparators | Weighted basket comparator (SOC) consisting of:
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (20 years) |
Key data source |
|
Submitted results | ICER = $187,779 per QALY (incremental costs, $469,538; incremental QALYs, 2.50) |
Key limitations |
|
CADTH reanalysis results |
|
CAR = chimeric antigen receptor; ICER = incremental cost-effectiveness ratio; ITC = indirect treatment comparison; LY = life-year; OOS = out of specification; OS = overall survival; PFS = progression-free survival; QALY = quality-adjusted life-year; r/rMM = relapsed or refractory multiple myeloma; SOC = standard of care; WTP = willingness to pay.
Conclusions
The CADTH Clinical Review noted that the CARTITUDE-1 trial, although limited by its open-label design and absence of a comparator group, resulted in overall survival (OS) and progression-free survival (PFS) results that were considered clinically meaningful by the clinical experts consulted by CADTH. Due to a lack of a comparator treatment in the trial, comparative efficacy data were derived from the sponsor-submitted indirect treatment comparison (ITC). The CADTH Clinical Review highlighted numerous limitations with the ITC including various biases and unresolved heterogeneity. Overall, the Clinical Review concluded that the ITC and other indirect evidence were not suitable to conclude a treatment effect on survival outcomes between existing therapies and ciltacabtagene autoleucel (OS or PFS), and the comparisons with external data are nonconfirmatory and can only be interpreted in an exploratory, supportive manner.
Given the magnitude of uncertainty surrounding OS for ciltacabtagene autoleucel and its comparative efficacy against standard of care (SOC), CADTH was unable to derive a robust base-case estimate of cost-effectiveness. Feedback CADTH received from clinical experts noted long-term OS extrapolation was highly uncertain as there is limited long-term data on the durability of ciltacabtagene autoleucel effectiveness with regard to progression and overall survival in the multiple myeloma (MM) population. To address this, CADTH conducted 2 reanalyses. In both reanalyses, CADTH addressed key limitations with respect to costs related to chimeric antigen receptor (CAR) T-cell therapy, immunoglobulin costs, out of specification (OOS) product costs, subsequent therapy uptake, and utility values. However, these reanalyses differed in the assumptions surrounding OS. CADTH reanalysis A assumed long-term progression and mortality rates for those who received ciltacabtagene autoleucel remain fairly constant 2 years post CAR T-cell infusion. This assumes that the OS and PFS hazard rates seen in the CARTITUDE-1 trial do not change substantially over time. CADTH reanalysis B assumed increasing progression and mortality rates over time. This could occur if the rate of relapse for patients receiving ciltacabtagene autoleucel increases over time, for example.
In CADTH reanalysis A (long-term OS and PFS hazard rates remain close to constant over time), the incremental cost-effectiveness ratio (ICER) for ciltacabtagene autoleucel was $201,901 per quality-adjusted life-year (QALY) compared with SOC (incremental costs: $517,233; incremental QALYs: 2.56; incremental life-years [LYs]: 3.16). In CADTH reanalysis B (OS and PFS hazard rates increase over time due to increasing relapse rates), ciltacabtagene autoleucel was associated with an ICER of $286,972 per QALY compared with SOC (incremental costs: $521,954; incremental QALYs: 1.82; incremental LYs: 2.26). CADTH notes that both analyses assume substantial life expectancy increases for patients receiving ciltacabtagene autoleucel relative to current SOCs. In the absence of evidence from a randomized controlled trial, the true comparative impact of ciltacabtagene autoleucel on OS relative to SOC is highly uncertain. These estimates may therefore substantially overestimate the incremental benefits associated with ciltacabtagene autoleucel relative to current standards of care.
Assuming PFS and OS outcomes from CARTITUDE-1 are replicated in a real-world setting and large extensions in life occur relative to current SOC, a price reduction of 72% to 80% would still be required for ciltacabtagene autoleucel to be cost-effective at a willingness-to-pay (WTP) threshold of $50,000 per QALY. This range reflects uncertainty around long-term survival extrapolation, as analyzed in CADTH reanalysis A and B. CADTH notes that although health care resources associated with CAR T-cell delivery and adverse event (AE) management in the CADTH reanalyses are substantial (approximately $72,000 per infused patient), based on expert feedback, these costs may still be underestimated. Further price reductions may therefore be required to account for potentially higher health care system costs associated with delivering CAR T-cell therapy.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
One patient group, Myeloma Canada, provided input for the review of ciltacabtagene autoleucel. Myeloma Canada conducted online surveys with 200 patients and 26 caregivers; all except 2 patients were from Canada. Patients reported having been treated with between 1 and 6 prior lines of therapy. The most important aspect of myeloma for patients to control was infections, while mobility and kidney problems were also noted as very important. MM affected patients’ ability to work the most, followed by ability to travel and exercise. The most important factors for patients associated with a new treatment were quality of life, manageable side effects, effectiveness, accessibility and portability of treatment, and having a supportive care team. One patient and 1 caregiver had experience with ciltacabtagene autoleucel. The patient received 2 separate treatments with ciltacabtagene autoleucel, 6 years apart, upon resurgence of their myeloma. The patient reported their treatment as “effective,” while the caregiver noted the treatment to be “extremely effective” for the person for whom they provide care. The patient noted ciltacabtagene autoleucel had improved their overall quality of life, but it was too early to determine its effect on health outcomes.
CADTH received input from 2 registered clinician groups, the Canadian Myeloma Research Group and the Ontario Health Hematology Cancer Drug Advisory Committee. Current treatment options are variable; in general, if a patient receives a certain type of therapy in a prior line, they would receive a different type of therapy in subsequent lines. Treatment options include bortezomib-based induction (cyclophosphamide-bortezomib-dexamethasone, lenalidomide-bortezomib-dexamethasone), melphalan plus autologous stem cell transplant (ASCT), daratumumab-based regimens (e.g., cyclophosphamide-bortezomib-dexamethasone plus daratumumab), pomalidomide and dexamethasone (± cyclophosphamide), and carfilzomib and dexamethasone (± cyclophosphamide). The place in therapy for ciltacabtagene autoleucel would be in patients whose disease has relapsed after having already received 3 lines of therapy. As the drug is used late in the current lines of myeloma treatment, it is not expected to influence treatment sequencing, but the clinicians noted it would be expected to lead to a treatment paradigm shift for patients with advanced disease.
The drug plan input received for this review indicated that relevant comparators in a third-line and greater setting included pomalidomide-dexamethasone (± cyclophosphamide) and carfilzomib-dexamethasone (± cyclophosphamide). The plans had questions about which patients would be prioritized in the event of capacity limitations, and whether there was sufficient evidence to support re-treatment with ciltacabtagene autoleucel. The plans noted access considerations for this therapy, particularly as there are capacity limitations (e.g., health human resources, bed limitations) in some jurisdictions. The plans anticipate that capacity may not be able to meet demand and out-of-province or out-of-country care may be needed. There may be issues with access and the need for prolonged stays near specialized centres, especially for patients from remote areas, and financial support for travel and accommodation would be needed. The plans noted significant resource use for patient preparation, including leukapheresis, cell processing, and use of bridging and lymphodepleting chemotherapy. There is a high resource burden to obtain and maintain certification. The plans wondered whether it would be safe to administer ciltacabtagene autoleucel in an outpatient setting. Finally, patient privacy and patient cell ownership concerns were noted in cases where the CAR T-cell therapy was manufactured outside of Canada.
Several of these concerns were addressed in the sponsor’s model:
The sponsor included pomalidomide-dexamethasone (± cyclophosphamide), and carfilzomib-dexamethasone (± cyclophosphamide as a weighted basket comparator.
In addition, CADTH addressed some of these concerns as follows:
CADTH included costs associated with CAR T-cell infusion, including apheresis and bridging therapy.
CADTH was unable to address the following concerns raised from stakeholder input:
There are a lack of data available on re-treatment with ciltacabtagene autoleucel.
Economic Review
The current review is for ciltacabtagene autoleucel (Carvykti) for the treatment of adult patients with relapsed or refractory multiple myeloma (r/rMM) who have received at least 3 prior lines of therapy, including a proteasome inhibitor, an immunomodulatory drug, and an anti-CD38 antibody.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis comparing ciltacabtagene autoleucel with a mixed basket comparator (hereafter, SOC) consisting of carfilzomib-dexamethasone (33.3%), carfilzomib-dexamethasone-cyclophosphamide (6.9%), pomalidomide-dexamethasone (27.5%), and pomalidomide-dexamethasone-cyclophosphamide (32.4%), the proportions of which were based on an observational study, described in greater detail subsequently.1 The model population was based on the CARTITUDE-1 trial and consisted of patients with r/rMM who had received at least 3 lines of therapy.2 This is reflective of the proposed Health Canada indication and reimbursement request.3
Ciltacabtagene autoleucel is available as a single dose for infusion containing a suspension of CAR-positive viable T cells. The target dose of ciltacabtagene autoleucel is 0.5 × 106 to 1.0 × 106 CAR-positive viable T cells per kilogram of body weight, with a maximum dose of 1 × 108 CAR-positive viable T cells per single infusion.3 Ciltacabtagene autoleucel should be administered as a single IV infusion at a qualified health care facility.3 Patients should be monitored daily for 14 days after the ciltacabtagene autoleucel infusion and then periodically for an additional 2 weeks for symptoms of cytokine release syndrome, neurologic events, and other toxicities.3 The sponsor’s submitted price of ciltacabtagene autoleucel is $632,455 per infusion, which is assumed to be a 1-time cost.4 For SOC, the sponsor calculated a 28-day cost of approximately $12,748 when considering wastage and each regimen’s specific dosing schedule.4
The outcomes of interest were QALYs and LYs, and the analysis took the perspective of the Canadian publicly funded health care system. The time horizon was lifetime (i.e., 20 years) with a 1-week cycle length and half-cycle correction applied. Costs and outcomes were discounted at a rate of 1.5% annually.4
Model Structure
The sponsor’s model consisted of an initial, short-term decision tree followed by a partitioned survival model. The decision tree was only relevant for patients expected to receive ciltacabtagene autoleucel as, in clinical practice, patients may be selected as candidates for CAR T-cell therapy and be initiated into the pre-treatment process but may ultimately not receive the infusion due to death, AEs, or other reasons. Patients receiving ciltacabtagene autoleucel enter the partitioned survival model after a pre-infusion period of 52 days, during which time they are considered progression-free. Patients assigned to but not receiving ciltacabtagene autoleucel or those receiving SOC enter the partitioned survival model immediately, at day 0. The partitioned survival model includes 3 health states: progression-free, postprogression, and death. The proportion of patients in each state at any point in time was based on direct modelling of OS and PFS curves, which the sponsor extrapolated over the time horizon of the analysis using parametric methods. All patients enter the model in the progression-free state. The proportion of patients in the progression-free state is estimated as the area under the PFS curve while the proportion of patients in the postprogression state is estimated as the difference between the OS and PFS curves. A summary of the sponsor’s model structure is available in Figure 1 (Appendix 3).
Model Inputs
Patients’ baseline characteristics such as age, weight, and body surface area were obtained from the CARTITUDE-1 trial (n = 113). Patients were mostly male (57.5%), with a mean age of 61.7 years, mean body weight of 80.7 kg, and mean body surface area of 1.91 m2. All patients had received at least 3 prior lines of therapy and 90% had received previous ASCT.2
Efficacy data for patients receiving ciltacabtagene autoleucel were based on the modified intention-to-treat cohort of the CARTITUDE-1 trial.2 Parametric extrapolations for OS and PFS were fit to Kaplan-Meier data for these patients, using a gamma distribution in both cases.4 Patients assigned to but not receiving ciltacabtagene autoleucel were modelled directly using Kaplan-Meier data specific to patients who were not infused in CARTITUDE-1 (n = 16; 14%). No extrapolation was performed for these patients, as all had died by 6 months and extrapolation was not needed.4
Data for SOC were derived from a prospective, observational study, LocoMMotion, evaluating current US and European therapies for patients with r/rMM who have received at least 3 lines of therapy (n = 248).1 The study was designed such that clinical outcome measures and eligibility criteria were aligned with CARTITUDE-1 to generate a matched control. To conduct the ITC, individual patient data for CARTITUDE-1 (clinical cut-off: January 2022) and LocoMMotion (clinical cut-off: May 2021) were used. Adjusted comparisons were performed to balance patients in terms of prognostic factors and included refractory status, International Staging System stage, time to progression on last treatment regimen, Eastern Cooperative Oncology Group (ECOG) Performance Status, age, sex, years since MM diagnosis, extramedullary disease, average duration of prior lines of therapy, baseline hemoglobin and lactate dehydrogenase levels, creatinine clearance, and MM type.5 Inverse probability weighting was used to balance baseline characteristics using propensity scores derived from a logistic regression. The estimated propensity scores were used to derive weights for each patient to derive the average treatment effect in the treated population and were used in the extrapolations of PFS and OS data from LocoMMotion for SOC.5 For both PFS and OS for SOC, a gamma distribution was used.
In addition to the extrapolations described previously, the model considered age- and sex-adjusted probabilities of death of the general population in Canada to ensure that the probability of death predicted by the extrapolations was at least equal to that of the general population.4,6
Regarding safety outcomes, modelled AEs included those events of grade 3 or higher in severity that had occurred in at least 5% of patients in either CARTITUDE-1 or the LocoMMotion study. In addition, grade 1 and 2 events were included for cytokine release syndrome and neurotoxicity.1,2
The CARTITUDE-1 trial collected health-related quality of life data via the EQ-5D scales. These data were converted into utility indexes based on a published study.7 Based on the EQ-5D data from CARTITUDE-1, patients in the pre-infusion stage (i.e., 0 to 52 days) experienced a utility of 0.786 and patients in the progression-free state had a utility of 0.826.4 Due to the limited number of progression events observed in CARTITUDE-1, a utility value could not be calculated and was instead determined from the literature to be 0.676.8 In addition, patients experienced utility decrements due to AEs, the duration of which was based on CARTITUDE-1.2 Patients with grade 3 or higher cytokine release syndrome events experienced a complete loss of utility (i.e., utility equals 0.0) for the duration of these events.4
The economic model included costs related to drugs (acquisition, administration), follow-up care and monitoring, AE management, subsequent treatment, and terminal care. The sponsor-submitted drug cost for ciltacabtagene autoleucel was $632,455 per patient.4 This cost was reduced by 14% to account for the patients who were assigned to but did not receive ciltacabtagene autoleucel. The cost was further reduced by 4.1%, as it was determined that CAR T-cell products that are OOS (i.e., insufficient cell count) would still be administered but not reimbursed.4 Thus, the sponsor’s calculated drug acquisition cost for ciltacabtagene autoleucel was $520,516 per infusion. The sponsor’s base-case analysis assumed all patients would receive ciltacabtagene autoleucel in an inpatient setting and require a hospital stay of 7 days, costing $8,788.9 Other costs related to CAR T-cell infusion (i.e., pre-treatment costs, eligibility assessment, apheresis, bridging therapy, and lymphodepleting condition therapy) were not included in the base case but were available as a scenario analysis. Drug acquisition costs for SOC were obtained from the Ontario Drug Benefit Formulary, Ontario Exceptional Access Program, Saskatchewan Formulary, and a previous CADTH report.10-13 Drug dosages were based on the mean body surface area from CARTITUDE-1, with wastage considered for all IV and subcutaneous therapies. In addition, a treatment administration cost of $75 was applied for IV and subcutaneous SOC therapies.9 The sponsor’s model also provided an illustrative example to consider different valued-based agreements (VBAs) for ciltacabtagene autoleucel; an exploratory scenario analysis was conducted wherein rebates of 30% were applied for patients not alive at 6 and 18 months.
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (3,000 iterations for the base-case and scenario analyses). The deterministic and probabilistic results were similar. The probabilistic findings are presented subsequently.
Base-Case Results
In the sponsor’s base case, ciltacabtagene autoleucel was associated with an estimated cost of $640,970 and 3.40 QALYs over a lifetime horizon (Table 3). Compared with SOC, ciltacabtagene autoleucel was associated with an ICER of $187,779 (incremental cost: $469,538; incremental QALYs: 2.50). In the sponsor’s base case, 2.19 incremental QALYs were accrued in the progression-free state while 0.34 incremental QALYs were accrued in the postprogression state. Improvement in life expectancy (incremental LYs: 3.14) was the main driver of incremental QALY gains. CADTH notes that 47% of incremental QALYs are accrued in the first 4 years after initiation of CAR T-cell therapy; this is due to the short life expectancy associated with the current SOC (median OS = 1.1 years). In the sponsor’s base case, ciltacabtagene autoleucel had a 0% probability of being cost-effective at a WTP threshold of $50,000 per QALY. Additional results from the sponsor’s base case are available in Appendix 3.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. SOC ($/QALY) |
|---|---|---|---|---|---|
SOC | 171,431 | Reference | 0.90 | Reference | Reference |
Ciltacabtagene autoleucel | 640,970 | 469,538 | 3.40 | 2.50 | 187,779 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care.
Source: Sponsor’s pharmacoeconomic submission.4
Sensitivity and Scenario Analysis Results
The sponsor conducted several scenario analyses involving OS extrapolations, inclusion of CAR T-cell therapy–related costs, and alternate assumptions around the length of inpatient stay for CAR T-cell infusion, proportion of OOS products, and source of the matched comparator data (i.e., Flatiron database). When ||||% of products were assumed to be OOS and not reimbursed, the ICER for ciltacabtagene autoleucel versus SOC was $160,324 per QALY. When Flatiron was used as the source for comparator data, the ICER was $208,481. Other scenarios tested had minimal impact on the ICER.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
The OS benefit with ciltacabtagene autoleucel is uncertain. The sponsor modelled the survival of patients with ciltacabtagene autoleucel based on OS data from the single-arm, phase Ib and phase II CARTITUDE-1 study. However, OS was not considered a primary or key secondary end point in this trial. As noted in the CADTH Clinical Review, overall response rate (ORR) was the primary end point in this trial, and it cannot be firmly concluded to what extent the improvements in ORR observed in patients would translate into OS benefits. After a median follow-up of 27.7 months (range, 1.5 to 40.4) the median OS was still not reached. To provide an estimate of survival for the model, the sponsor extrapolated OS Kaplan-Meier data from CARTITUDE-1 using a parametric gamma distribution up to the time horizon of 20 years. The clinical feedback received by CADTH for this review indicated that the OS extrapolations were highly uncertain, given the immaturity of results. It was suggested that patients might deteriorate over time such that the hazard for mortality would increase substantially after the trial period. Clinicians noted that the gamma distribution nearly matched OS outcomes for patients who remain progression-free on first-line treatments and, therefore, was seen as a likely upper limit of potential OS for those receiving CAR T-cell therapy. Although the gamma extrapolation of OS was seen as plausible, in the absence of long-term data, alternative survival extrapolations with shorter OS, such as the Gompertz, were seen as equally plausible by the clinical experts consulted by CADTH.
Furthermore, as the CARTITUDE-1 trial was single-arm, with no comparator group, the relative treatment effects of ciltacabtagene autoleucel compared with other comparators are uncertain. Regarding the sponsor’s submitted ITC, the CADTH Clinical Review noted that this analysis was limited by differences in study design, heterogeneity, various biases, and imprecision in the results. Canadian evidence from the literature shows the median OS for patients on current fourth-line therapies tends to be between 12 and 18 months.14 In the sponsor’s analysis, median OS for current therapies is assumed to be around 13 months. However, this naive comparison of real-world evidence may not match the survival outcomes of those in the CARTITUDE-1 trial. If OS outcomes are homogenous for patients on fourth-line MM therapy, then it is likely that an OS benefit will be realized for patients with MM receiving CAR T-cell therapy compared with those receiving SOC, assuming OS outcomes match that seen in the CARTITUDE-1 trial. However, without robust data, this conclusion remains speculative.
Due to uncertainty in the long-term extrapolations of OS for ciltacabtagene autoleucel and its comparative efficacy against SOC, CADTH conducted 2 distinct reanalyses that represented 2 plausible scenarios of OS extrapolation. In CADTH reanalysis A, CADTH maintained the sponsor’s assumptions around OS (permanent and enduring impact of CAR T-cell therapy). In CADTH reanalysis B, CADTH used a Gompertz function for OS for ciltacabtagene autoleucel. As the changes to reanalysis B would result in the PFS curve intersecting the OS curve (an implausible assumption), CADTH made PFS for ciltacabtagene autoleucel a function of OS, which matched the observed PFS data based on visual assessment.
Exclusion of CAR T-cell therapy–related costs. In the sponsor’s base case, costs related to CAR T-cell infusion were excluded (i.e., eligibility assessment, apheresis, bridging therapy, and lymphodepleting conditioning therapy). Although the model included the functionality to include these costs, these were considered in a scenario analysis only. No justification was provided for the exclusion of these costs in the base case. As these costs may be substantial and specific only to patients receiving ciltacabtagene autoleucel, they should be included in an economic evaluation undertaken from a health care system perspective. Exclusion of these costs underestimates costs for patients receiving ciltacabtagene autoleucel, biasing results in favour of this product. The clinical experts consulted by CADTH reviewed and appraised the CAR T-cell therapy–related costs provided by the sponsor in a disaggregated manner and suggested they were underestimated. Specifically, the cost of apheresis ($2,633) was felt to be low, as was the duration of bridging therapy and inpatient stay (7 days). CADTH consulted the Ontario Case Costing Initiative for apheresis costs and obtained a cost of $5,426 for stem cell apheresis (code 1.LZ.58.HX).15 Data were not available for leukapheresis, specifically due to a small number of events. Clinician feedback suggested the inpatient stay would likely be closer to 10 to 16 days. CADTH updated these parameters in the reanalysis. Duration of bridging therapy was not updated, as it was expected to have minimal impact on the results. Table 11 in Appendix 4 outlines the costs used by CADTH.
In the reanalysis, CADTH included the additional CAR T-cell therapy–related costs outlined previously and updated the cost for apheresis and the inpatient stay. Given that there remains outstanding uncertainty regarding the degree of these costs, CADTH explored additional infusion-related costs using scenario analyses.
Exclusion of immunoglobulin-related costs. In the consideration of CAR T-cell therapy–related costs, the clinical experts consulted by CADTH also noted that some patients may require lifelong IV immunoglobulin (IVIG) therapy after their infusion. The feedback received suggested that 50% of patients receiving ciltacabtagene autoleucel may require 0.4 g/kg IVIG every month. CADTH sourced the cost of IVIG (i.e., Octagam) from a previous CADTH report,16 and calculated a weekly cost of $213 for IVIG based on an 80.7 kg patient (CARTITUDE-1) and 2 hours of nursing time.17 As there are limited published data on the effectiveness of IVIG for patients treated with CAR T-cell therapy, CADTH considered the cost of these products only for those patients experiencing hypogammaglobulinemia. There is biological plausibility for treating hypogammaglobulinemia with IVIG, and this practice has been recommended in the literature.18 This AE was experienced by 12.4% of patients in CARTITUDE-1.2
In reanalysis, CADTH included the cost of IVIG products for 12.4% of patients receiving ciltacabtagene autoleucel.
Uncertainty regarding the reimbursement of OOS products. In its pharmacoeconomic report, the sponsor noted that |||% of ciltacabtagene autoleucel products in CARTITUDE-1 were deemed OOS but were still administered to patients.2 As a result, the sponsor excluded drug acquisition costs for |||% of patients, under the assumption that OOS products would not be reimbursed.4 This assumption is uncertain and subject to individual jurisdiction-specific practices and policies. CADTH requested additional justification from the sponsor on the exclusion of these costs, which it was not able to provide.19 The exclusion of drug acquisition costs for these products may underestimate costs for patients receiving ciltacabtagene autoleucel, biasing results in favour of this product.
In reanalysis, CADTH assumed that OOS products would be reimbursed (i.e., drug acquisition costs would be incurred by the health care system). Exclusion of these costs was tested in a scenario analysis.
The frequency of subsequent therapy use has been underestimated. The sponsor assumed that, upon progression, 50% of patients would receive subsequent therapy consisting of 6 months of SOC. The clinical experts consulted by CADTH agreed this would be reasonable for most patients; however, for those performing well (i.e., progression-free after 1 year), it is expected that 90% of these patients would be eligible for subsequent therapy. Those patients who are still progression-free after 1 year would likely be healthier and fitter than those progressing earlier, and the vast majority would be expected to receive subsequent therapy.
In reanalysis, CADTH assumed that, of the patients progressing after 1 year on either ciltacabtagene autoleucel or SOC, 90% would receive subsequent therapy. All other assumptions regarding subsequent therapy remained unchanged.
Uncertainty regarding utility values. In deriving utility values, the sponsor used EQ-5D data from CARTITUDE-1 for the pre-infusion and progression-free state. However, due to a limited number of progression events observed during follow-up, a postprogression utility value of 0.676 was sourced from the literature.8 The use of multiple different sources for utility values is uncertain, as the populations in both studies are unlikely to be homogenous; for example, half of the patients in the Weisel et al., 2018, study received elotuzumab, which differs from CARTITUDE-1.2,8 In addition, the Weisel publication is an abstract and lacks details on baseline patient characteristics such as age, further increasing the uncertainty in comparing these populations. Lastly, the utility value of 0.676 is substantially lower than the value of 0.826 used for PFS. While it may be expected that those who progress would have a lower quality of life than during preprogression, the target population for this analysis represents patients who have already progressed on 3 prior lines of therapy. The assumption that quality of life would be substantially worse upon progression for a fourth time lacks face validity. Indeed, a study on health state utility valuation in patients with r/rMM using Canadian weights derived a postprogression utility of 0.80, which is not substantially different than the utility in preprogression and also higher than the value used for baseline (0.76).20 That study suggests that utility for patients with r/rMM who have received at least 3 lines of therapy may not decrease substantially upon progression.
In reanalysis, to mitigate the use of multiple different sources for utility values, CADTH assumed the same utility for progressed disease as in the pre-infusion period from CARTITUDE-1 (0.786).
Limitations with the model programming and transparency. The sponsor’s model lacked transparency, as it included multiple hidden rows and columns, hard coding of deterministic results requiring a macro to display, and more than 144,000 IFERROR statements. The systematic use of IFERROR statements makes thorough auditing of the sponsor’s model impractical, as it remains unclear whether the model is running inappropriately by overriding errors. In addition, CADTH discovered an error in the sponsor’s presentation of disaggregated drug costs for the probabilistic analysis, whereby undiscounted drug acquisition costs were referenced for ciltacabtagene autoleucel. Finally, the sponsor’s method of incorporating CAR T-cell therapy–related costs into the model was not transparent, as it compiled all costs into CAR T-cell therapy drug acquisition costs, further complicating validation and reanalysis.
CADTH was unable to address the limitations with model programming and transparency.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
14% of patients assigned to ciltacabtagene autoleucel underwent apheresis but did not receive the infusion and were assumed to not incur ciltacabtagene-related costs. | Not appropriate. CADTH obtained a cost of $5,426 per patient for apheresis, which was not considered by the sponsor. While this omission biases results slightly in favour of ciltacabtagene autoleucel, the impact is expected to be minimal. |
Bridging therapy was modelled according to individual drug components (i.e., dexamethasone, bortezomib, cyclophosphamide, pomalidomide) instead of complete drug regimens. | Not appropriate. The sponsor’s base-case proportions of patients on bridging therapy imply that some patients would receive dexamethasone monotherapy, which is not appropriate for disease management of MM. The clinical experts consulted by CADTH suggested that patients would more likely receive CyBorD or another SOC treatment regimen. |
CyBorD = cyclophosphamide, bortezomib, and dexamethasone; MM = multiple myeloma; SOC = standard of care.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
Given the magnitude of uncertainty surrounding the OS for ciltacabtagene autoleucel, CADTH was unable to derive a robust base-case estimate of cost-effectiveness. CADTH conducted separate reanalyses (Table 5) involving different assumptions for OS, along with applying a consistent set of changes to CAR T-cell therapy–related costs, immunoglobulin costs, OOS product reimbursement, frequency of subsequent therapy, and utility values.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. CAR T-cell therapy–related costs | Excluded |
|
2. Immunoglobulin costs | Excluded | Included (weekly cost: $213) |
3. Acquisition costs for OOS products | Excluded | Included |
4. Subsequent therapy | 50% of patients would receive subsequent therapy upon progression |
|
5. Utility values |
|
|
6. Survival assumptions |
|
|
CADTH reanalysis A | Reanalysis 1 + 2 + 3 + 4 + 5a | |
CADTH reanalysis B | Reanalysis 1 + 2 + 3 + 4 + 5 + 6 | |
CAR = chimeric antigen receptor; OOS = out of specification; OS = overall survival; PFS = progression-free survival.
aCADTH reanalysis A maintains the sponsor’s original survival assumptions, as the stepwise change in analysis 6 is not included.
The results of the 2 CADTH reanalyses (i.e., reanalysis A and B) were generally aligned: ciltacabtagene autoleucel is not cost-effective at a $50,000 WTP threshold compared with SOC. In CADTH reanalysis A (enduring impact of CAR T-cell therapy), ciltacabtagene autoleucel was associated with an ICER of $201,901 per QALY compared with SOC (incremental costs: $517,233; incremental QALYs: 2.56). In CADTH reanalysis B (waning impact of CAR T-cell therapy), ciltacabtagene autoleucel was associated with an ICER of $286,972 per QALY compared with SOC (incremental costs: $521,954; incremental QALYs: 1.82). In both reanalyses, most incremental QALYs were due to substantial improvements in LYs. Results are driven by the high drug acquisition cost and health care resource utilization associated with ciltacabtagene autoleucel. Full results are available in Appendix 4 for both reanalyses.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results (Deterministic)
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case | SOC | 171,215 | 0.90 | Reference |
Ciltacabtagene | 641,301 | 3.39 | 188,623 | |
CADTH reanalysis 1: CAR T-cell therapy costs | SOC | 171,215 | 0.90 | Reference |
Ciltacabtagene | 656,814 | 3.39 | 194,847 | |
CADTH reanalysis 2: Immunoglobulin costs | SOC | 171,215 | 0.90 | Reference |
Ciltacabtagene | 646,991 | 3.39 | 190,905 | |
CADTH reanalysis 3: OOS products | SOC | 171,215 | 0.90 | Reference |
Ciltacabtagene | 663,638 | 3.39 | 197,585 | |
CADTH reanalysis 4: Subsequent therapy | SOC | 173,156 | 0.90 | Reference |
Ciltacabtagene | 647,100 | 3.39 | 190,170 | |
CADTH reanalysis 5: Utility values | SOC | 171,215 | 0.98 | Reference |
Ciltacabtagene | 641,301 | 3.52 | 184,984 | |
CADTH reanalysis 6: Survival changes | SOC | 171,215 | 0.90 | Reference |
Ciltacabtagene | 643,938 | 2.64 | 270,667 | |
CADTH reanalysis A (reanalysis 1 to 5): Deterministic | SOC | 173,156 | 0.98 | Reference |
Ciltacabtagene | 690,639 | 3.52 | 203,635 | |
CADTH reanalysis B (reanalysis 1 to 6): Deterministic | SOC | 173,156 | 0.98 | Reference |
Ciltacabtagene | 695,306 | 2.75 | 294,812 | |
CADTH reanalysis A: Probabilistic | SOC | 173,137 | 0.98 | Reference |
Ciltacabtagene | 690,371 | 3.54 | 201,901 | |
CADTH reanalysis B: Probabilistic | SOC | 173,477 | 0.98 | Reference |
Ciltacabtagene | 695,431 | 2.80 | 286,972a |
CAR = chimeric antigen receptor; ICER = incremental cost-effectiveness ratio; OS = overall survival; QALY = quality-adjusted life-year; SOC = standard of care.
Note: CADTH reanalyses are based on publicly available prices of comparator treatments and do not reflect confidential, negotiated prices.
aWhen running probabilistically, CADTH noticed that the Gompertz survival function led to inappropriate results in some model iterations (e.g., more than half of patients still alive at the model time horizon of 20 years). This was determined to be due to the gamma shape parameter, which led to inappropriate results when it became negative. In reanalysis, CADTH prevented this parameter from sampling values of less than 0.
Scenario Analysis Results
CADTH undertook price reduction analyses based on the sponsor’s results and CADTH’s reanalyses. Results of CADTH reanalysis A suggested a price reduction of 72% would be required to achieve cost-effectiveness of ciltacabtagene autoleucel relative to SOC at a $50,000 per QALY threshold. In CADTH reanalysis B, a price reduction of 80% would be required (Table 7).
Table 7: CADTH Price Reduction Analyses
Analysis | ICERs for ciltacabtagene autoleucel vs. SOC | ||
|---|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis A | CADTH reanalysis B |
No price reduction | 187,779 | 201,901 | 286,971 |
10% | 167,283 | 180,715 | 257,248 |
20% | 146,751 | 159,527 | 227,524 |
30% | 126,218 | 138,339 | 197,801 |
40% | 105,686 | 117,152 | 168,078 |
50% | 85,153 | 95,964 | 138,355 |
60% | 64,621 | 74,777 | 108,631 |
70% | 44,088 | 53,589 | 78,908 |
80% | 23,556 | 32,401 | 49,185 |
90% | 3,023 | 11,214 | 19,461 |
100% | Dominant | Dominant | Dominant |
ICER = incremental cost-effectiveness ratio; SOC = standard of care.
CADTH undertook 2 scenario analyses on each of the CADTH reanalyses, outlined as follows:
CADTH conducted a scenario in which OOS products were assumed to not be reimbursed.
Feedback from CADTH’s clinical experts suggested that more appropriate milestones for a VBA were at 12 and 24 months. Therefore, CADTH undertook a scenario analysis in which a 30% rebate was applied for patients not alive at 12 and 24 months.
Feedback from experts noted that infusion-related costs associated with CAR T-cell therapy may have been underestimated by CADTH.
If OOS products are not reimbursed by public plans, then this slightly decreases the ICER in both the CADTH reanalyses (Table 14). Given the percentage of OOS was small (|||%), the impact of this scenario analysis was limited.
In the VBA scenarios, total costs and ICERs decreased for ciltacabtagene autoleucel. For a VBA for CADTH reanalysis A, the ICER for ciltacabtagene autoleucel was $188,237 per QALY compared with SOC. For a VBA for CADTH reanalysis B, the ICER for ciltacabtagene autoleucel was $263,839 per QALY compared with SOC.
Uncertainty remains in the analysis pertaining to CAR T-cell–related costs that are incurred for patients in addition to drug acquisition costs. The clinical expert feedback indicated that these supplementary costs would be substantial, with 1 jurisdictional estimate suggesting a cost of approximately $97,000 per patient would be required to deliver ciltacabtagene autoleucel. In the CADTH reanalyses, CAR T-cell–related costs amounted to approximately $68,000 for eligibility, apheresis, bridging and conditioning chemotherapy, and AE management. If a total cost of $97,000 was assumed instead, the price of ciltacabtagene autoleucel would need to be reduced by 78% to 86% to achieve cost-effectiveness at a $50,000 per QALY threshold.
Issues for Consideration
Drug plan feedback indicated there may be issues with access and prolonged stays required near specialized centres, especially for patients from remote areas, and financial support for travel and accommodation would be needed. CADTH surveyed the jurisdictions and found that some participating drug plans would cover travel and/or accommodation costs.
To be able to treat patients with ciltacabtagene autoleucel, specialized centres need to be trained and accredited by the sponsor. Both obtaining and maintaining this accreditation process can result in a high resource burden, including the development of various protocols and supporting yearly audits. In addition, this treatment has the added complexity of needing to coordinate patient care and product preparation with an external manufacturer. Since there are likely multiple CAR T-cell therapies being administered by specialized centres, there will be a need to managing various protocols for preparation and delivery of each product type, which can increase the overall administrative burden.
Selinexor has recently received a positive recommendation from CADTH in combination with bortezomib and dexamethasone for MM21 and is under consideration for negotiation with the pan-Canadian Pharmaceutical Alliance.22 The clinical experts consulted by CADTH for this review identified selinexor as a relevant comparator for transplant-ineligible patients but noted that, currently, there is no comparative evidence for ciltacabtagene autoleucel available. Therefore, the cost-effectiveness of ciltacabtagene autoleucel versus selinexor is unknown.
Overall Conclusions
The CADTH Clinical Review noted that the CARTITUDE-1 trial, although limited by its open-label design and absence of a comparator group, resulted in OS and PFS results that were considered clinically meaningful by the clinical experts consulted by CADTH. Due to a lack of a comparator treatment in the trial, comparative efficacy data were derived from the sponsor-submitted ITC. The CADTH Clinical Review highlighted numerous limitations with the ITC, including various biases and unresolved heterogeneity. Overall, the Clinical Review concluded that the ITC and other indirect evidence were not suitable to conclude a treatment effect on survival outcomes (OS or PFS), and the comparisons with external data are nonconfirmatory and can only be interpreted in an exploratory, supportive manner.
Given the magnitude of uncertainty surrounding OS for ciltacabtagene autoleucel and its comparative efficacy against SOC, CADTH was unable to derive a robust base-case estimate of cost-effectiveness. The feedback CADTH received from clinical experts noted long-term OS extrapolation was highly uncertain, as there is no long-term data on the durability of ciltacabtagene autoleucel effectiveness with regard to progression and OS in the MM population beyond the current data cut-off (approximately 3.5 years). To address this, CADTH conducted 2 reanalyses. In both reanalyses, CADTH addressed key limitations with respect to CAR T-cell therapy–related costs, immunoglobulin costs, OOS product costs, subsequent therapy uptake, and utility values. These reanalyses differed, however, in the assumptions surrounding OS. CADTH reanalysis A assumed that long-term progression and mortality rates for those who received ciltacabtagene autoleucel would remain fairly constant over time. This assumes that the OS and PFS hazard rates seen in the CARTITUDE-1 trial do not change substantially over time. CADTH reanalysis B assumed increasing progression and mortality rates over time. This could occur, for example, if the rate of relapse for patients receiving ciltacabtagene autoleucel response increases over time.
In CADTH reanalysis A (long-term OS and PFS hazard rates remain close to constant over time), the ICER for ciltacabtagene autoleucel was $201,901 per QALY compared with SOC (incremental costs, $517,233; incremental QALYs, 2.56; incremental LYs, 3.16). In CADTH reanalysis B (OS and PFS hazard rates increase over time), ciltacabtagene autoleucel was associated with an ICER of $286,972 per QALY compared with SOC (incremental costs, $521,954; incremental QALYs, 1.82; incremental LYs, 2.26). CADTH notes that both analyses assume substantial life expectancy increases for patients receiving ciltacabtagene autoleucel relative to current SOCs. In the absence of evidence from randomized controlled trials, the true comparative impact of ciltacabtagene autoleucel on OS relative to SOC is highly uncertain. The CADTH reanalyses assume that the impact of potential confounding that could drive the results seen in the CARTITUDE-1 is limited, and that these results will be replicated in the real-world setting. Both assumptions are highly uncertain. The estimates presented within the CADTH reanalyses therefore likely represent the upper limits on what incremental gains could be realized from this therapy.
A price reduction of 72% or 80% would be required for ciltacabtagene autoleucel to be cost-effective at a WTP threshold of $50,000 per QALY, depending on the long-term impact on OS. Results are driven by the high drug acquisition cost of ciltacabtagene autoleucel, as well as other supplementary costs required for CAR T-cell infusion (e.g., eligibility, apheresis, and bridging and conditioning chemotherapy). The clinical expert feedback indicated that these supplementary costs would be substantial, with 1 jurisdictional estimate suggesting a cost of approximately $97,000 per patient would be required to deliver ciltacabtagene autoleucel, a cost incurred additionally to the drug acquisition cost. If a cost of $97,000 is assumed per patient, the price of ciltacabtagene autoleucel would need to be reduced by an additional 6%. This would increase price reductions to 78% to 86% for CADTH reanalysis A and B, respectively.
References
1.Mateos M, Weisel K, De Stefano V, et al. LocoMMotion: a prospective, non-interventional, multinational study of real-life current standards of care in patients with relapsed and/or refractory multiple myeloma. Leukemia. 2022;36(5):1371-1376. PubMed
2.Janssen Research & Development. A Phase 1b-2, Open-Label Study of JNJ-68284528, a Chimeric Antigen Receptor T cell (CAR-T) Therapy Directed Against BCMA in Subjects with Relapsed or Refractory Multiple Myeloma - CARTITUDE-1 CSR. 2021.
3.Carvykti™ (ciltacabtagene autoleucel): Cell suspension in infusion bag, 0.5-1.0x106 CAR-positive viable T-cells per kg body weight with a maximum of 1x108 CAR-positive viable T-cells, for intravenous infusion [product monograph]. Toronto: Janssen Inc.; 2022.
4.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: ciltacabtagene autoleucel. Toronto: Janssen Inc. 2022 Sep 23.
5.Janssen. Adjusted comparison of ciltacabtagene autoleucel (JNJ-68284528) versus standard of care in tri-exposed multiple myeloma patients based upon data from CARTITUDE-1 and the LocoMMotion Study (MMY4001). 2022.
6.Table: 13-10-0114-01. Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island. Ottawa (ON): Statistics Canada; 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed 2022 Nov.
7.Xie F, Pullenayegum E, Gaebel K. A time trade-off-derived value set of the EQ-5D-5L for Canada. Medical care. 2016;54(1):98. PubMed
8.Weisel K, Paner A, Engelhardt M, al. e. Quality-of-life outcomes in patients with relapsed/refractory multiple myeloma treated with elotuzumab plus pomalidomide and dexamethasone: results from the phase 2 randomized eloquent-3 study. Blood. 2018;132(Supplement 1):2288-2288.
9.Canadian Institute for Health Information. Care in Canadian ICUs. 2016; https://secure.cihi.ca/estore/productSeries.htm?pc=PCC1475. Accessed 2022 Nov 9.
10.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2022: https://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2022 Nov.
11.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2022; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2022 Nov 10.
12.Saskatchewan Drug Plan: search formulary. 2022; https://formulary.drugplan.ehealthsask.ca/SearchFormulary. Accessed 2022 Nov.
13.CADTH. CADTH Reimbursement Review: Idecabtagene Vicleucel (Abecma). 2022; https://www.cadth.ca/idecabtagene-vicleucel. Accessed 2022 Nov 9.
14.Mian H, Reece D, Masih-Khan E, et al. Survival and outcomes of newly diagnosed multiple myeloma patients stratified by transplant status 2007-2018: retrospective analysis from the Canadian Myeloma Research Group database. Clinical lymphoma, myeloma & leukemia. 2022;22(8):608-617. PubMed
15.Ontario Case Costing Initiative (OCCI). Toronto (ON): Ontario Health and Long-Term Care; 2017: https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi. Accessed 2022 Nov.
16.CADTH. HyQvia CADTH Reimbursement Review. 2022; https://www.cadth.ca/sites/default/files/DRR/2022/ST0695-HyQvia-meta.pdf. Accessed 2022 Dec 7.
17.Blackhouse G, Gaebel K, Xie F, Campbell K, Assasi N. Cost-utility of intravenous immunoglobulin compared with corticosteroids for the treatment of chronic inflammatory demyelinating polyneuropathy (CIDP) in Canada. Cost Eff Resour Alloc. 2010;8:14. PubMed
18.Hill J, Giralt S, Torgerson T, Lazarus H. CAR-T– and a side order of IgG, to go? – Immunoglobulin Replacement in Patients Receiving CAR-T Cell Therapy. Blood Rev. 2019;38:100596. PubMed
19.Janssen Canada. Sponsor-provided additional information. Drug Reimbursement Review sponsor submission: ciltacabtagene autoleucel. 2022 Nov 10.
20.Delforge M, Shah N, Rodriguez-Otero P, et al. Health State Utility Valuation in Patients with Triple-Class-Exposed Relapsed and Refractory Multiple Myeloma Treated with the Bcma-Directed CAR T Cell Therapy, Idecabtagene Vicleucel (ide-cel, bb2121): Results from the Karmma Trial. Blood. 2020;136(supplement 1):14.
21.CADTH. CADTH Reimbursement Recommendation Selinexor. 2022; https://www.cadth.ca/sites/default/files/DRR/2022/PC0276%20Xpovio%20-%20Final%20CADTH%20Recommendation_KT_KAS_KT_GP-meta.pdf. Accessed 2022 Dec 13.
22.pan Canadian Pharmaceutical Alliance. Xpovio (selinexor). 2022; https://www.pcpacanada.ca/negotiation/21962. Accessed 2022 Dec 13.
23.Cancer Care Ontario. CARFDEXA Regimen. 2021; https://www.cancercareontario.ca/en/drugformulary/drugs/carfilzomib. Accessed 2022 Nov 10.
24.BC Cancer. BC Cancer Protocol Summary for Therapy of Multiple Myeloma Using Carfilzomib and Dexamethasone With or Without Cyclophosphamide. 2022; http://www.bccancer.bc.ca/chemotherapy-protocols-site/Documents/Lymphoma-Myeloma/UMYCARDEX_Protocol.pdf. Accessed 2022 Nov 10.
25.Cancer Care Ontario. DEXAPOMA Regimen. 2020; https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/46761. Accessed 2022 Nov 10.
26.Cancer Care Ontario. CYCLDEXAPOMA. 2019; https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/47786. Accessed 2022 Nov 10.
27.DeltaPA. [Ottawa (ON)]: IQVIA; 2022: https://www.iqvia.com/. Accessed 2022 Nov 10.
28.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: ciltacabtagene autoleucel. Toronto: Janssen Inc. 2022 Sep 23.
29.Brenner D, Poirier A, Woods R. Projected estimates of cancer in Canada in 2022. Canadian Medical Association Journal. 2022;194(17):E601. PubMed
30.Canadian Cancer Society. Canadian Cancer Statistics - 2021. 2021; https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2021-statistics/2021-pdf-en-final.pdf. Accessed 2022 Nov 14.
31.Fonseca R, Usmani SZ, Mehra M. Frontline treatment patterns and attrition rates by subsequent lines of therapy in patients with newly diagnosed multiple myeloma. BMC Cancer. 2020;20(1):1087. PubMed
32.Despiegel N, Touboul C, Flinois A. Health related quality of life in patients with multiple myeloma treated in routine clinical practice in France. Clinical lymphoma, myeloma & leukemia. 2019;19(1):e13-e28. PubMed
33.CADTH. Brexucabtagene autoleucel (Tecartus) Reimbursement Recommendation. 2021; https://www.cadth.ca/sites/default/files/DRR/2021/PG0219%20Tecartus%20-%20CADTH%20Final%20Rec.pdf. Accessed 2022 Dec 2.
Appendix 1: Cost Comparison Table
Note this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Patients With Relapsed or Refractory Multiple Myeloma Who Have Received at Least 3 Prior Therapies
Treatment | Strength/ concentration | Form | Price ($) | Recommended dosage (28-day cycles) | Daily cost ($) | 28-day cost ($) |
|---|---|---|---|---|---|---|
Ciltacabtagene autoleucel | 0.5 to 1.0 × 106 CAR-positive viable T cells per kg, with a maximum of 1 × 108 T cells | Cell suspension in patient-specific single infusion bag | 632,455.0000a | One-time doseb | NA | NA |
Carfilzomib + dexamethasone23 | ||||||
Carfilzomib | 10 mg 30 mg 60 mg | Powder in vial | 255.5500c 766.6590 1,533.3300 | Cycle 1: 20 mg/m2 on days 1, 2; 56 mg/m2 on days 8, 9, 15, 16 Cycles 2+: 56 mg/m2 on days 1, 2, 8, 9, 15, 16 | Cycle 1: 106.96 Cycles 2+: 474.60 | Cycle 1: 13,289 Cycles 2+: 16,867 |
Dexamethasone | 0.5 mg 4 mg | Tablet | 0.1564 0.6112 | 20 mg on days 1, 2, 8, 9, 15, 16, 22, 23 | 0.87 | 24 |
Carfilzomib + dexamethasone regimen | Cycle 1: 107.83 Cycle 2+: 475.47 | Cycle 1: 13,313 Cycle 2+: 16,891 | ||||
Carfilzomib + cyclophosphamide + dexamethasone24 | ||||||
Carfilzomib | 10 mg 30 mg 60 mg | Powder in vial | 255.5500c 766.6590 1,533.3300 | Cycle 1: 20 mg/m2 on Day 1; 70 mg/m2 on days 8 and 15 Cycle 2+: 70 mg/m2 on days 1, 8, 15 | Cycle 1: 292.06 Cycles 2+: 383.33 | Cycle 1: 8,178 Cycles 2+: 10,733 |
Cyclophosphamide | 25 mg 50 mg | Tablet | 0.3545 0.4773 | 300 mg/m2 on days 1, 8, 15 | 0.60 | 17 |
Dexamethasone | 0.5 mg 4 mg | Tablet | 0.1564 0.6112 | 40 mg on days 1, 8, 15, 22 | 0.87 | 24 |
Carfilzomib + cyclophosphamide + dexamethasone regimen | Cycle 1: 293.54 Cycles 2+: 384.81 | Cycle 1: 8,219 Cycles 2+: 10,775 | ||||
Dexamethasone + pomalidomide25 | ||||||
Dexamethasone | 0.5 mg 4 mg | Tablet | 0.1564 0.6112 | 20 to 40 mg on days 1, 8, 15, 22 | 0.44 to 0.87 | 12 to 24 |
Pomalidomide | 1 mg 2 mg 3 mg 4 mg | Capsule | 500.0000d | 4 mg on days 1 to 21 | 375.00 | 10,500 |
Dexamethasone + pomalidomide regimen | 375.44 to 375.87 | 10,512 to 10,524 | ||||
Cyclophosphamide + dexamethasone + pomalidomide26 | ||||||
Cyclophosphamide | 25 mg 50 mg | Tablet | 0.3545 0.4773 | 400 mg on days, 1, 8, 15 | 0.41 | 11 |
Dexamethasone | 0.5 mg 4 mg | Tablet | 0.1564 0.6112 | 20 to 40 mg on days 1, 8, 15, 22 | 0.44 to 0.87 | 12 to 24 |
Pomalidomide | 1 mg 2 mg 3 mg 4 mg | Capsule | 500.0000d | 4 mg on days 1 to 21 | 375.00 | 10,500 |
Cyclophosphamide + dexamethasone + pomalidomide regimen | 375.85 to 376.28 | 10,524 to 10,536 | ||||
CAR = chimeric antigen receptor.
Note: All prices are from the Ontario Drug Benefit Formulary (accessed November 2022),11 unless otherwise indicated, and do not include dispensing fees. Daily and 28-day costs are calculated based on a mean body surface area of 1.91 m2 from the CARTITUDE-1 trial.2
aSponsor-submitted price.4
bCiltacabtagene autoleucel is delivered as a 1-time dose. Daily and annual costs were not calculated.
cIQVIA DeltaPA database, accessed November 2022.27
dOntario Exceptional Access Program (EAP) formulary, accessed November 2022.10
Appendix 2: Submission Quality
Note this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | Selinexor, which was identified as a relevant comparator by clinical experts, was not included in the sponsor’s analysis. |
Model has been adequately programmed and has sufficient face validity | No | There was an error in the reporting of the disaggregated results. Some inputs were hardcoded using visual basic application, requiring a macro to present deterministic results. |
Model structure is adequate for decision problem | No | Clinical efficacy data for ciltacabtagene autoleucel were based on a single-arm phase Ib and phase II trial with immature survival data. The sponsor’s decision tree and approach to calculating ciltacabtagene infusion costs precluded CADTH from including apheresis costs for those who were not infused. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | Probabilistic sampling of the Gompertz extrapolation for OS resulted in unreasonable survival curves for ciltacabtagene autoleucel. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | CADTH was unable to derive a base case. The decision problem has not been addressed. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment. |
OS = overall survival.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note this appendix has not been copy-edited.
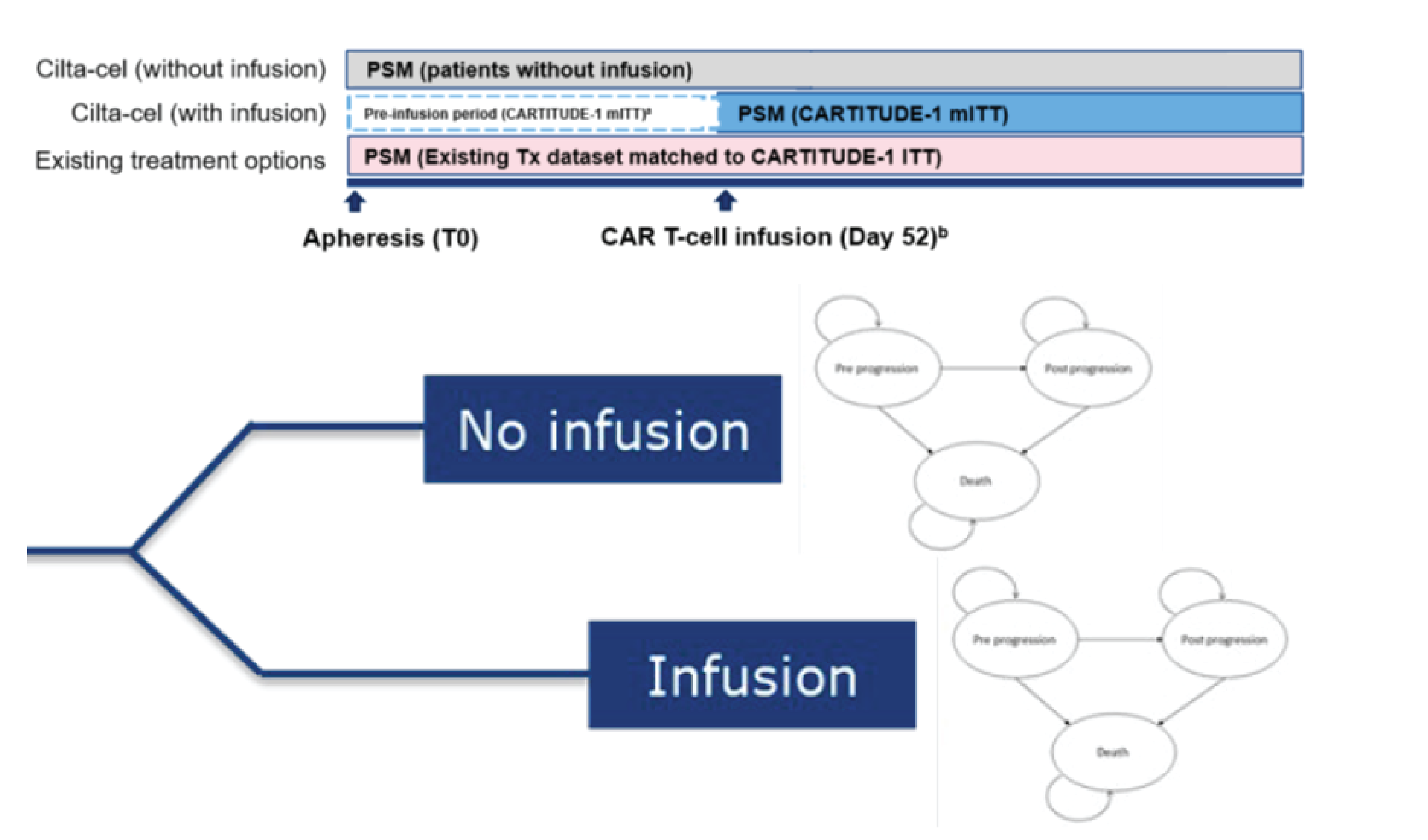
ITT = intention-to-treat; mITT = modified intention-to-treat; PSM = partitioned survival model; T0 = time zero; Tx = treatment.
Source: Sponsor’s pharmacoeconomic submission.4
Detailed Results of the Sponsor’s Base Case
Table 10: Disaggregated Results of the Sponsor’s Base Case
Parameter | Ciltacabtagene autoleucel | SOC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 4.37 | 1.23 | 3.14 |
Progression-free LYs | 3.15 | 0.50 | 2.65 |
Postprogression LYs | 1.22 | 0.73 | 0.50 |
Discounted QALYs | |||
Total | 3.40 | 0.90 | 2.50 |
Progression-free QALYs | 2.61 | 0.42 | 2.19 |
Postprogression QALYs | 0.83 | 0.49 | 0.34 |
Disutilities due to AEs | −0.04 | −0.01 | −0.03 |
Discounted costs ($) | |||
Total | 640,970 | 171,431 | 469,538 |
Cilta-cel drug acquisition and administration | 526,949a | 0 | 526,949 |
SOC drug acquisition | 0 | 83,557 | −83,557 |
Administration of SOC | 0 | 1,106 | −1,106 |
Monitoring: Preprogression | 8,259 | 1,153 | 7,106 |
Adverse events | 44,961 | 5,359 | 39,602 |
Monitoring: Postprogression | 2,825 | 1,667 | 1,158 |
Subsequent therapy | 10,144 | 27,384 | −17,240 |
Terminal care | 47,832 | 51,206 | −3,374 |
ICER ($/QALY) | 187,779 | ||
AE = adverse event; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; SOC = standard of care.
aThe sponsor’s pharmacoeconomic report and model contained an error in the calculation of disaggregated drug costs for ciltacabtagene autoleucel. CADTH has corrected the error in this table. Total costs and the ICER remain unchanged.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note this appendix has not been copy-edited.
Table 11: Disaggregated Costs Associated With CAR T-Cell Administration
Step | Components included | Cost per patient |
|---|---|---|
0. Eligibility | CAR T-cell therapy consult and testing to confirm eligibility | $3,000 |
1. Apheresis | Apheresis procedure | $5,42615 |
2. Bridging therapy | Treatment with either:
| $1,487 to $10,536 |
3. Conditioning therapy | Treatment for 3 days with:
| $2,374 |
4. One-time CAR T-cell infusion | 10 to 16 days inpatient general ward stay | $12,554 to $20,080 ($1,255/day) |
5. Short-term monitoring / follow-up (first month) | 3 visits per week with hematologist visit + bloodwork | $2,295 ($574/week) |
6. Costs associated with managing AEsa | AEs and frequency of occurrence
| $45,032 (total) |
Total CAR T-cell infusion-related costs | $72,168 to $88,743 | |
7. Long-term monitoring/follow-up (1 month onward for remainder of patient life) | Monthly costs associated with:
| $176 |
8. Intravenous immunoglobulin | 0.4 g/kg IVIG (Octagam) monthly | $106 |
Monthly CAR T-cell therapy costs postinfusion: | $282 | |
AE = adverse events; CAR = chimeric antigen receptor; CRP = C-reactive protein; CRS = cytokine release syndrome; IVIG = IV immunoglobulin.
aSome AEs may not be related exclusively to CAR T-cell therapy; however, without comparative evidence the relative difference of AEs between CAR T-cell therapy and current standards of care is uncertain. Some AEs, such as CRS, are exclusively associated with CAR T-cell therapy and would be unlikely to occur otherwise.
Figure 2: OS and PFS in CADTH Reanalysis A
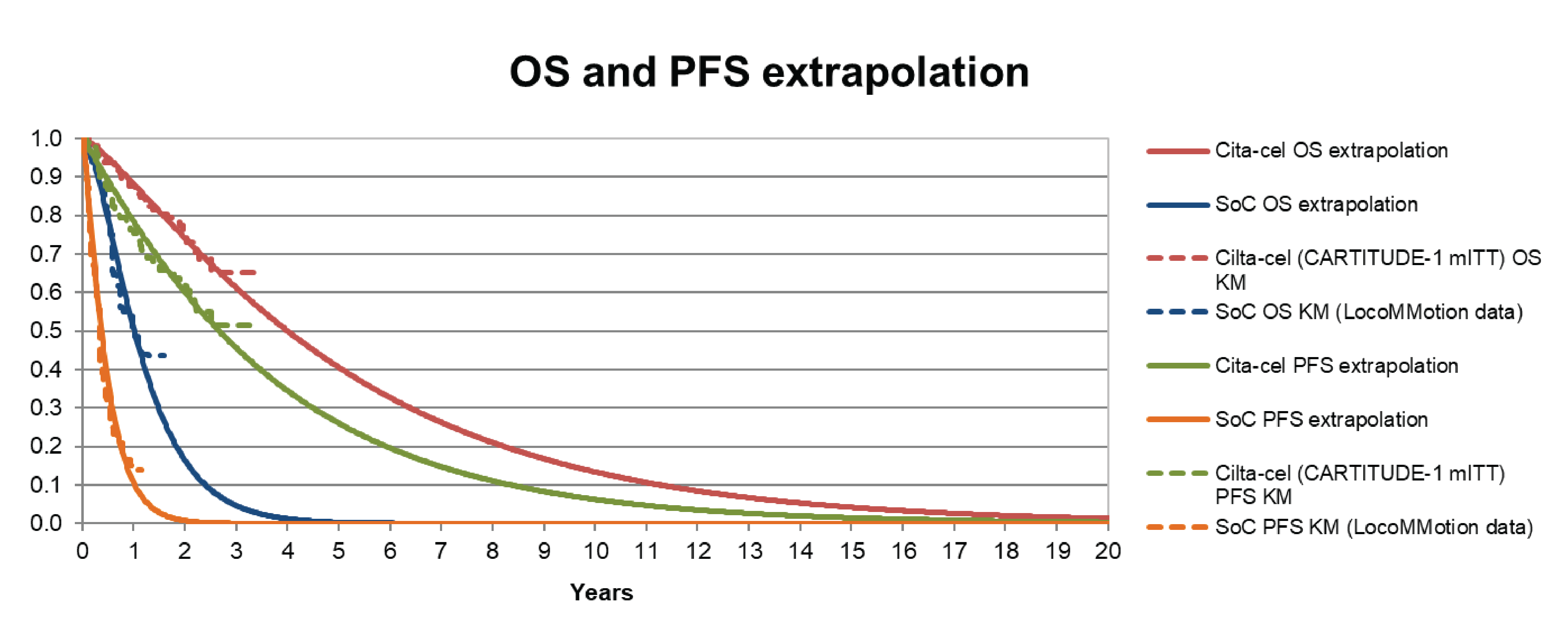
AE = adverse events; cita-cel = ciltacabtagene autoleucel; KM = Kaplan-Meier; OS = overall survival; PFS = progression-free survival; SoC = standard of care
Source: Sponsor’s pharmacoeconomic submission.4
Figure 3: OS and PFS in CADTH Reanalysis B
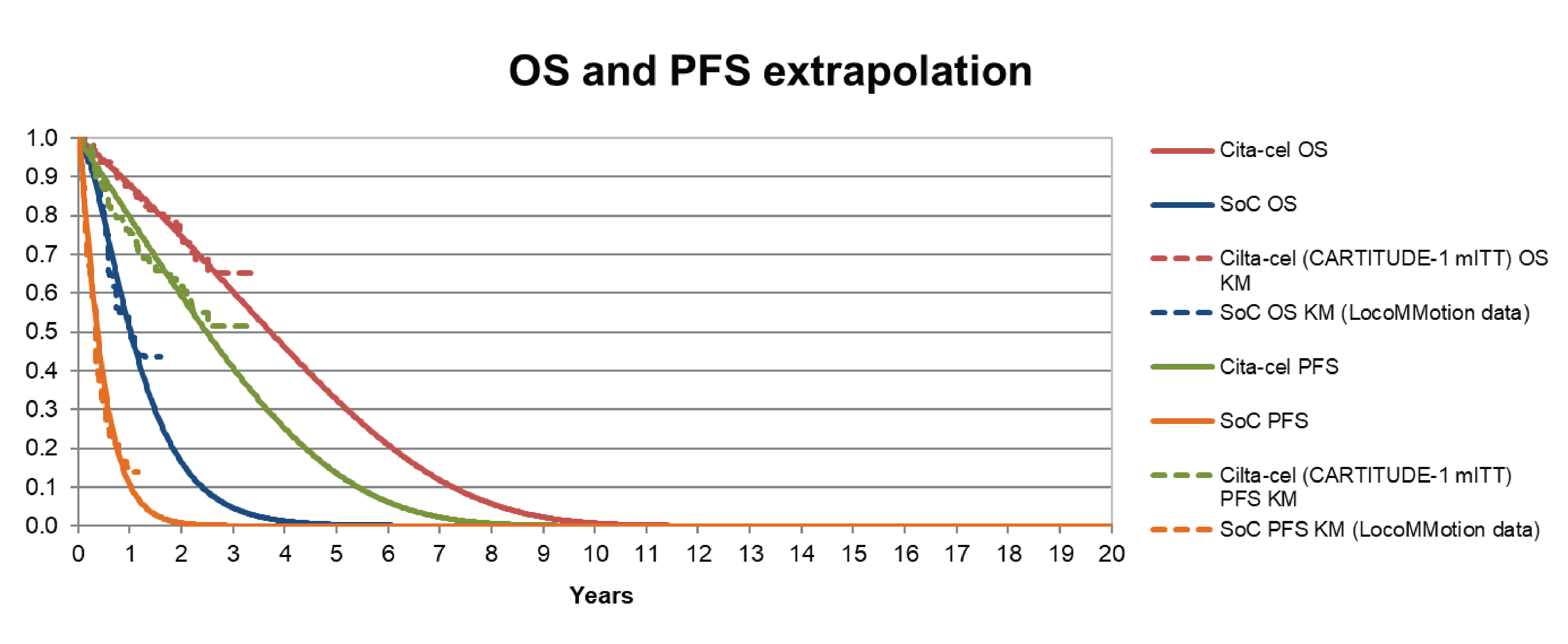
AE = adverse events; cita-cel = ciltacabtagene autoleucel; KM = Kaplan-Meier; mITT = modified intention-to-treat; OS = overall survival; PFS = progression-free survival; SoC = standard of care.
Source: Sponsor’s pharmacoeconomic submission.4
Detailed Results of CADTH Reanalyses
Table 12: Disaggregated Summary of CADTH Reanalysis A (Enduring CAR T-Cell Therapy Impact)
Parameter | Ciltacabtagene autoleucel | SOC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 4.39 | 1.23 | 3.16 |
Progression-free LYs | 3.15 | 0.50 | 2.65 |
Postprogression LYs | 1.24 | 0.72 | 0.51 |
Discounted QALYs | |||
Total | 3.54 | 0.98 | 2.56 |
Progression-free QALYs | 2.61 | 0.42 | 2.19 |
Postprogression QALYs | 0.98 | 0.57 | 0.41 |
Disutilities due to AEs | −0.04 | −0.01 | −0.03 |
Discounted costs ($) | |||
Total | 690,371 | 173,137 | 517,233 |
Cilta-cel drug acquisition and administration | 564,902 | 0 | 564,902 |
SOC drug acquisition | 0 | 83,750 | −83,750 |
Administration of SOC | 0 | 1,107 | −1,107 |
Monitoring: Preprogression | 12,060 | 1,154 | 10,905 |
Adverse events | 45,005 | 5,360 | 39,645 |
Monitoring: Postprogression | 4,527 | 1,661 | 2,866 |
Subsequent therapy | 15,953 | 29,119 | −13,166 |
Terminal care | 47,923 | 50,986 | −3,064 |
ICER ($/QALY) | 201,901 | ||
AE = adverse event; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; SOC = standard of care.
Table 13: Disaggregated Summary of CADTH Reanalysis B (Waning Impact of CAR T-cell Therapy)
Parameter | Ciltacabtagene autoleucel | SOC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 3.49 | 1.23 | 2.26 |
Progression-free LYs | 2.47 | 0.50 | 1.96 |
Postprogression LYs | 1.02 | 0.72 | 0.30 |
Discounted QALYs | |||
Total | 2.80 | 0.98 | 1.82 |
Progression-free QALYs | 2.04 | 0.42 | 1.62 |
Postprogression QALYs | 0.80 | 0.57 | 0.23 |
Disutilities due to AEs | −0.04 | −0.01 | −0.03 |
Discounted costs ($) | |||
Total | 695,431 | 173,477 | 521,954 |
Cilta-cel drug acquisition and administration | 565,078 | 0 | 565,078 |
SOC drug acquisition | 0 | 83,926 | −83,926 |
Administration of SOC | 0 | 1,108 | −1,108 |
Monitoring: Preprogression | 9,567 | 1,155 | 8,411 |
Adverse events | 45,026 | 5,347 | 39,680 |
Monitoring: Postprogression | 3,743 | 1,656 | 2,087 |
Subsequent therapy | 22,936 | 29,188 | −6,252 |
Terminal care | 49,090 | 51,097 | −2,017 |
ICER ($/QALY) | 286,971 | ||
CAR = chimeric antigen receptor; AE = adverse event; cilta-cel = ciltacabtagene autoleucel; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; SOC = standard of care.
Scenario Analyses
Table 14: Scenario Analyses Conducted on the CADTH Reanalyses
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
CADTH reanalysis A: scenario 1 (OOS products) | SOC | 172,577 | 0.98 | Reference |
Ciltacabtagene | 667,840 | 3.55 | 192,640 | |
CADTH reanalysis B: scenario 1 (OOS products) | SOC | 172,529 | 0.98 | Reference |
Ciltacabtagene | 671,750 | 2.79 | 276,062 | |
CADTH reanalysis A: scenario 2 (VBA) | SOC | 173,049 | 0.98 | Reference |
Ciltacabtagene | 651,305 | 3.52 | 188,237 | |
CADTH reanalysis B: scenario 2 (VBA) | SOC | 172,917 | 0.98 | Reference |
Ciltacabtagene | 655,557 | 2.81 | 263,839 |
ICER = incremental cost-effectiveness ratio; OOS = out of specification; QALY = quality-adjusted life-year; SOC = standard of care; VBA = value-based agreement.
Appendix 5: Submitted BIA and CADTH Appraisal
Note this appendix has not been copy-edited.
Table 15: Summary of Key Take-Aways
Key take-aways of the BIA |
|---|
|
ECOG PS = Eastern Cooperative Oncology Group Performance Status.
Summary of Sponsor’s BIA
The submitted budget impact analysis (BIA) assessed the introduction of ciltacabtagene autoleucel for the treatment of r/rMM in the third-line or greater.28 The analysis was derived using an epidemiologic-based approach over a 3-year time horizon, from 2025 to 2027 with 2024 as a base year. The population was derived starting with the number of incident patients with MM followed by a series of attritions. The analysis was taken from the perspective of the public drug plans and included drug acquisition costs only.
The reference case scenario included 4 regimens: carfilzomib-dexamethasone, carfilzomib-cyclophosphamide-dexamethasone, pomalidomide-dexamethasone, and pomalidomide-cyclophosphamide-dexamethasone. The new drug scenario included the same comparators along with ciltacabtagene autoleucel. Market uptake for ciltacabtagene autoleucel was based on market research data and clinical expert opinion.28 Key inputs to the BIA are documented in Table 16.
Table 16: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Incident cases of MM in Canada | |
Proportion becoming triple-refractory | 18.0%31 |
Proportion eligible for CAR T-cell therapy | 56.8%32 |
Number of patients eligible for drug under review | 389 / 415 / 441 |
Market uptake (3 years) | |
Uptake (reference scenario) Carfilzomib-dexamethasone Carfilzomib-cyclophosphamide-dexamethasone Pomalidomide-dexamethasone Pomalidomide-cyclophosphamide-dexamethasone | 25.0% / 25.0% / 25.0% 25.0% / 25.0% / 25.0% 25.0% / 25.0% / 25.0% 25.0% / 25.0% / 25.0% |
Uptake (new drug scenario) Ciltacabtagene autoleucel Carfilzomib-dexamethasone Carfilzomib-cyclophosphamide-dexamethasone Pomalidomide-dexamethasone Pomalidomide-cyclophosphamide-dexamethasone | 5.0% / 14.0% / 20.0% 23.8% / 21.5% / 20.0% 23.8% / 21.5% / 20.0% 23.8% / 21.5% / 20.0% 23.8% / 21.5% / 20.0% |
Total cost of treatment (per patient)a | |
Ciltacabtagene autoleucel (1-time cost) Carfilzomib-dexamethasone Carfilzomib-cyclophosphamide-dexamethasone Pomalidomide-dexamethasone Pomalidomide-cyclophosphamide-dexamethasone | $632,455 $38,606 $38,695 $42,045 $42,135 |
BIA = budget impact analysis; MM = multiple myeloma; PFS = progression-free survival.
aCosts for comparators were based on a treatment duration of 3.5 months, based on the area under the PFS curve from CARTITUDE-1.2 As the model was based on incident cases only and the treatment duration is less than1 year, these represent the total costs incurred to patients in the BIA.
Summary of the Sponsor’s BIA Results
The estimated budget impact of the reimbursement of ciltacabtagene autoleucel for the treatment of third-line and greater r/rMM was expected to be $11,512,346 in year 1, $34,391,999 in year 2, and $52,213,473 in year 3, and a 3-year total of $98,117,818.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The sponsor only considered incident cases of MM. In their derivation of the population size the sponsor only considered incident cases of MM for the years 2025 to 2027. Incident cases were multiplied by the proportion of patients becoming triple-refractory from a treatment patterns study by Fonseca et al.31 This approach to deriving the population size fails to consider patients diagnosed in 2024 and earlier who may still be alive and eligible for ciltacabtagene autoleucel (i.e., a prevalent cohort). Moreover, published Canadian data suggest that the median time to fourth-line treatment is 45.8 months and 34.7 months for an ASCT and non-ASCT population, respectively.14 Therefore, incident cases of MM diagnosed in 2025 would not be expected to immediately receive fourth-line therapy, as is assumed in the sponsor’s base case. Rather, the patients eligible for fourth-line therapy would be those diagnosed a median of 3 years prior (i.e., 2022). Importantly, as the Health Canada indication for ciltacabtagene autoleucel stipulates that patients had to have failed at least 3 prior lines of therapy, patients in fifth-, sixth-, and seventh-line therapy would be eligible as well.3 Overall, the sponsor’s omission of a prevalent cohort of patients with MM miscalculates the population that would be eligible for ciltacabtagene autoleucel.
As part of the base case, CADTH derived a new estimate of the population size. Using the sponsor’s cited incidence data,29,30 adjusted for CADTH-participating drug plans only, and estimates of time to next treatment from Mian et al., 2022,14 CADTH calculated the eligible population size for the years 2024 to 2027.
CADTH calculated the number of patients who would require 4L therapy in 2023 onward (base year of the CADTH reanalysis) by looking at incident rates of MM diagnosis going back to 2017. It was assumed that 18.4% would require 4L therapy and that it would take on average 3 to 4 years to move onto 4L therapy. Finally, it was assumed all patients who move to 4L therapy will have done so by 7 years post diagnosis. Table 18 details the full calculations to derive patient numbers for each year of the CADTH budget impact reanalysis.
CADTH notes this estimate may be an underestimation as it does not account for those who initiate 5L therapy or later within the budget time horizon. The sponsor’s model is not sufficiently programmed to consider this.
The market share of ciltacabtagene autoleucel is underestimated. In the sponsor’s base case, the market uptake of ciltacabtagene autoleucel in the new drug scenario was assumed to be 5%, 14%, and 20% in years 1, 2, and 3, respectively. This was deemed to be an underestimate according to clinical experts consulted by CADTH, who stated that the vast majority of patients with third-line or greater r/rMM who are eligible for CAR T-cell therapy would likely receive this product or be initiated into the CAR T-cell therapy process. The experts noted reasons why a patient might not receive ciltacabtagene autoleucel include poor ECOG status, poor renal function, and a lack of health system capacity. However, the sponsor has already accounted for patients who are triple-refractory and eligible for CAR T-cell therapy (defined as an ECOG of 0 to 1)32 in their calculation of the population size (Table 16). Furthermore, the experts noted that individual jurisdictions and hospital systems are anticipating the introduction of CAR T-cell therapy, as several products have already received positive recommendations from CADTH in other disease areas,33 and suggested that system capacity should exceed demand by 2026 (CADTH’s base case year 3). Finally, while there may be patients with poor renal function who would not be eligible for CAR T-cell therapy, this is not expected to represent a significant proportion of the patient population. Ultimately, it was suggested by clinical experts that there would be very few eligible patients for whom ciltacabtagene autoleucel would not be considered. Therefore, the sponsor’s base case market uptake of ciltacabtagene autoleucel is considered an underestimate.
As part of the base case, CADTH increased the sponsor’s market share estimates for ciltacabtagene autoleucel to 50%, 70%, and 90% in years 1, 2, and 3, respectively. An additional scenario was conducted in which the midpoint of the sponsor’s and CADTH’s base-case market share estimates was considered (i.e., 27.5%, 42%, and 55%).
The sponsor’s time horizon is too far into the future. The sponsor’s base-case BIA considered the time from year 2025 to 2027, with 2024 as a base year. It is unclear why the sponsor modelled the time horizon of the BIA to start in 2025 but this appears to be an overestimate of the time required for drug negotiations and the potential listing given that the draft recommendation for ciltacabtagene autoleucel is scheduled for posting on March 30, 2023.
As part of the base case, CADTH rolled back the analysis by 1 year and considered the budget impact from 2024 to 2026, with 2023 as a base year. This affected the projected incidence of MM cases into the future, ultimately reducing the population size.
The proportion of patients eligible for CAR T-cell therapy may be underestimated. The sponsor assumed that only patients with an ECOG score of 0 to 1 would be eligible for CAR T-cell therapy. However, the clinical experts noted that some patients with ECOG PS 2 would likely be eligible and want to receive this therapy as well. Using the sponsor’s source, 31.8% of patients in fourth-line therapy or later would have an ECOG PS of 2.32
As part of a scenario analysis, CADTH increased the proportion eligible for CAR T-cell therapy to 88.6% (i.e., 56.8% + 31.8%).
CADTH Reanalyses of the BIA
Based on the identified limitations, CADTH’s base case included changes to the population size, the market shares of ciltacabtagene autoleucel, and the time horizon.
Table 17: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. Population size and time horizon | Base year (2024): 363 Year 1 (2025): 389 Year 2 (2026): 415 Year 3 (2027): 441 | Base year (2023): 295 Year 1 (2024): 304 Year 2 (2025): 318 Year 3 (2026): 345 |
2. Market shares of ciltacabtagene autoleucel | Year 1: 5% Year 2: 14% Year 3: 20% | Year 1: 50% Year 2: 70% Year 3: 90% |
CADTH base case | Reanalysis 1 + 2 | |
Table 18: Calculations to Derive Number of Patients Eligible for CAR T-Cell Therapy Each Year
Year of diagnosis | Number of MM diagnoses per year | Total who receive 4L therapya | Total who initiate 4L in 2023b | Total who initiate 4L in 2024 | Total who initiate 4L in 2025 | Total who initiate 4L in 2026 |
|---|---|---|---|---|---|---|
2017 | 2,900 | 534 | 76 | 0 | 0 | 0 |
2018 | 2,900 | 534 | 76 | 76 | 0 | 0 |
2019 | 2,246 | 413 | 59 | 59 | 59 | 0 |
2020 | 2,546 | 468 | 67 | 67 | 67 | 67 |
2021 | 2,845 | 524 | 75 | 75 | 75 | 75 |
2022 | 2,995 | 551 | 79 | 79 | 79 | 79 |
2023 | 3,294 | 606 | 87 | 87 | 87 | 87 |
2024 | 3,549 | 653 | NA | 93 | 93 | 93 |
2025 | 3,804 | 700 | NA | NA | 100 | 100 |
2026 | 4,058 | 747 | NA | NA | NA | 107 |
Total (patients initiating 4L therapy each year) | 519 | 536 | 559 | 607 | ||
Total (patients initiating 4L therapy each year and have an ECOG score 0 to 1).c | 295 | 304 | 318 | 345 | ||
4L = fourth line; MM = multiple myeloma; NA = not applicable.
aAssumed 18.4% of those diagnosed with MM receive 4L therapy.3
bAssumed of the 18.4% who receive 4L therapy, 14.28% receive it each year after diagnosis. Meaning that after 7 years all patients who move onto 4L therapy will have received it. This was based on a median time to 4L therapy of 3.5 years.3
cAssumed 56.8% have ECOG 0 to 1.32
The results of the CADTH stepwise reanalysis are presented in summary format in Table 19 and a more detailed breakdown is presented in Table 20. Based on the CADTH base case, the estimated budget impact of the reimbursement of ciltacabtagene autoleucel for the treatment of r/rMM in the third-line or greater is expected to be $90,059,041 in year 1, $131,673,837 in year 2, and $183,710,617 in year 3, for a 3-year total of $405,443,496.
A scenario analysis conducted on the eligibility of patients according to their ECOG status indicated that the budget impact was sensitive to assumptions about the population size, with the 3-year budget impact estimated to be $632,434,749 if patients with ECOG PS 2 are also eligible.
An additional scenario analysis was conducted that included health care costs associated with administering CAR T cells and managing AEs. To conduct this CADTH assumed $72,000 (aligning with the cost-utility analysis) of nondrug health care costs would be incurred by the health care system for all patients receiving CAR T-cell therapy. The 3-year budget impact for the health care system (including both drug- and nondrug-related costs) was found to be $439,559,841.
Table 19: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case (patients initiating 4L only) | $98,117,818 |
CADTH reanalysis 1: Population size and time horizon | $76,165,253 |
CADTH reanalysis 2: Market shares | $522,044,079 |
CADTH base case (patients initiating 4L only) | $405,443,496 |
BIA = budget impact analysis.
Table 20: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation - $) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 14,648,475 | 15,699,210 | 16,749,946 | 17,800,679 | 64,898,309 |
New drug | 14,648,475 | 27,211,556 | 51,141,944 | 70,014,152 | 163,016,127 | |
Budget impact | 0 | 11,512,346 | 34,391,999 | 52,213,473 | 98,117,818 | |
CADTH base case | Reference | 11,890,040 | 12,281,214 | 12,825,828 | 13,917,964 | 50,915,047 |
New drug | 11,890,040 | 102,340,255 | 144,499,665 | 197,628,582 | 456,358,544 | |
Budget impact | 0 | 90,059,041 | 131,673,837 | 183,710,617 | 405,443,496 | |
CADTH scenario analysis 1: ECOG PS 0 to 2 | Reference | 18,546,788 | 19,156,964 | 20,006,486 | 21,710,065 | 79,420,303 |
New drug | 18,546,788 | 159,636,385 | 225,399,127 | 308,272,753 | 711,855,053 | |
Budget impact | 0 | 140,479,420 | 205,392,640 | 286,562,689 | 632,434,749 | |
CADTH scenario analysis 2: 80% price reduction | Reference | 11,890,040 | 12,281,214 | 12,825,828 | 13,917,964 | 50,915,047 |
New drug | 11,890,040 | 25,380,536 | 31,978,132 | 40,639,153 | 109,887,862 | |
Budget impact | 0 | 13,099,322 | 19,152,303 | 26,721,188 | 58,972,814 | |
CADTH scenario analysis 3: health systems perspective (including CAR T-cell–related infusion costs) | Reference | 15,874,306 | 16,396,560 | 17,123,671 | 18,581,774 | 67,976,313 |
New drug | 15,874,306 | 114,033,687 | 159,877,301 | 217,750,858 | 507,536,154 | |
Budget impact | 0 | 97,637,126 | 142,753,630 | 199,169,084 | 439,559,841 | |
CADTH scenario analysis 4: market shares | Reference | 11,890,040 | 12,281,214 | 12,825,828 | 13,917,964 | 50,915,047 |
New drug | 11,890,040 | 61,813,687 | 91,830,131 | 126,185,564 | 291,719,423 | |
Budget impact | 0 | 49,532,473 | 79,004,302 | 112,267,600 | 240,804,375 |
BIA = budget impact analysis; CAR = chimeric antigen receptor; ECOG PS = Eastern Cooperative Oncology Group Performance Status.
Ethics Review
Abbreviations
CAR
chimeric antigen receptor
cilta-cel
ciltacabtagene autoleucel
CRS
cytokine release syndrome
ECOG
Eastern Cooperative Oncology Group
MM
multiple myeloma
r/r
relapsed or refractory
VBA
value-based agreement
Summary
CADTH reviewed patient and clinician group, clinical expert, and drug program input gathered in the course of this review as well as relevant published literature to identify and describe ethical considerations relevant to the use of ciltacabtagene autoleucel (cilta-cel) for the treatment of adult patients with multiple myeloma (MM) who have received at least 3 prior lines of therapy, including a proteasome inhibitor, an immunomodulatory drug, and an anti-CD38 antibody, and whose disease was refractory to their last treatment.
Ethical considerations arising in the context of MM highlighted impacts on patients and caregivers as well as disparities in incidence, diagnosis, treatment, and outcomes of MM, especially as they affect people who are racialized, structurally marginalized, have lower incomes, or face other barriers to health care, as well as people residing in rural areas. MM is recognized as a currently incurable condition for which treatment is burdensome for patients and their caregivers and for which there are no effective fourth-line therapies currently available.
Ethical considerations arising in the evidence used to evaluate cilta-cel indicate some limitations, including in the representativeness of the clinical trial population and the absence of long-term safety and efficacy data and comparative effectiveness data. Uncertainty about the magnitude of the clinical benefit of cilta-cel presented challenges for the pharmacoeconomic assessment and may expose payers to greater financial risks. How the proposed value-based agreement (VBA) for the reimbursement of cilta-cel is designed has implications for the distribution of the potential benefits and burdens associated with such arrangements (e.g., for patients, the public, payers, and manufacturers). As well, budget forecasting may underestimate the overall budget impact of cilta-cel if implemented fairly and as needed.
Ethical considerations arise with respect to the potential benefits and harms related to the use and delivery of cilta-cel. Several access considerations arise in the context of cilta-cel and chimeric antigen receptor (CAR) T-cell therapies in Canada, including those related to geographical access, especially as they may disproportionately impact racialized, structurally marginalized, people with lower incomes, and patients lacking caregiver support, as well as those who face other barriers to health care. Considerations related to privacy and cultural-sensitive practices also arise in the context of cell and tissue ownership, as well as considerations related to informed consent, shared decision-making, and balanced communication related to CAR T-cell therapies.
Ethical considerations for health systems include challenges associated with implementing cilta-cel and the scaling of CAR T-cell treatment centres across Canada due to the complex infrastructure and personnel requirements. There are also considerations related to fair priority-setting criteria if demand exceeds manufacturing or delivery capacity and considerations related to the opportunity costs associated with reimbursing and implementing a high-cost, resource-intensive therapy.
Objective
To identify and describe ethical considerations associated with the use of cilta-cel for the treatment of adult patients with MM who have received at least 3 prior lines of therapy, including a proteasome inhibitor, an immunomodulatory drug, and an anti-CD38 antibody, and whose disease is refractory to their last treatment, including in the context of relapsed or refractory (r/r) MM, the evidentiary basis and use of cilta-cel as a CAR T-cell therapy, and considerations related to health systems.
Research Questions
This report addresses the following research questions:
What ethical considerations arise in the context of r/rMM in adult patients, including those related to the diagnosis, treatment, and outcomes?
What ethical considerations arise related to the evidence (e.g., clinical and economic data) used to evaluate cilta-cel?
What ethical considerations arise in the use of cilta-cel as a CAR T-cell therapy for patients, their caregivers, and clinicians?
What ethical considerations for health systems are involved in the context of cilta-cel as a CAR T-cell therapy?
Methods
Overview
To identify ethical considerations relevant to the use of cilta-cel in the treatment of r/rMM, this ethics report was driven by relevant questions identified in the European Network for Health Technology Assessment (EUnetHTA) Core Model 3.0 Ethical Analysis domain1 and supplemented by relevant questions from the Equity Checklist for Health Technology Assessment (ECHTA).2 These guiding questions were organized to respond to the research questions posed. In response to each of these 4 questions, this report investigated ethical considerations in 4 domains of interest:
The people living with r/rMM and their caregivers (i.e., disparities in incidence, treatment, or outcomes; challenges related to diagnosis or clinical care; factors that might prevent patients from gaining access to therapies).
The evidence used to demonstrate the benefits, harms, and value of cilta-cel (i.e., ethical considerations in relevant clinical trials, including their representativeness; choice of outcome measures; appropriateness of analytical methods and models to all population groups; and ethical considerations related to the data or assumptions in the economic evaluation).
The use of cilta-cel as a CAR T-cell therapy, including considerations related to benefits and harms to patients, relatives, caregivers, clinicians, or society, and considerations related to access to these therapies.
The uptake of cilta-cel and CAR T-cell therapies in health systems, including considerations related to the distribution of health care resources.
These were explored through a review and synthesis of project inputs and relevant literature to highlight ethical considerations across each of the domains.
Data Collection: Review of Project Inputs and Literature
Data to inform this ethics report drew from an identification of ethical considerations (e.g., values, norms, or implications related to the harms, benefits, and implications for equity, justice, and resource allocation, and ethical considerations in the evidentiary basis) in the patient and clinician group, clinical expert, and drug program input collected throughout this review, as well as a complementary search of the published literature. Ongoing collaboration and communication with CADTH reviewers working on the clinical and economic reviews for this submission also assisted in the clarification and identification of the ethical considerations raised.
Review of Project Inputs
During this CADTH review, a single reviewer collected and considered input from 6 main sources for content related to ethical considerations relevant to addressing the research questions guiding this ethics report. In addition to published literature, this report considered the following sources:
the sponsor submission, including relevant information and external references or sources relevant to each of the research questions driving this report
clinician group input received by CADTH from the Canadian Myeloma Research Group and Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee
patient input received by CADTH from Myeloma Canada
drug program input received by CADTH
discussion with clinical experts who were practising hematologists or oncologists (n = 4) treating patients with r/rMM in Canada who were directly engaged by CADTH over the course of this Reimbursement Review, including through 2 teleconference discussions involving 2 experts, and 1 panel discussion involving 3 experts (the summary of which was reviewed by a fourth expert). During each of the 3 discussions, the clinical experts were asked targeted questions related to ethical considerations corresponding to the research questions driving this report
engagement with CADTH clinical and economic reviewers to identify domains of ethical interest arising from their respective reviews as well as relevant questions and sources to further pursue in this report.
Literature Search Methods
The literature search strategies used in this review include 2 literature search strategies that were developed for 2 previous CADTH reports and were updated for this review.3,4 As well, 1 literature search strategy was developed de novo for this review.
Details of the updated searches are as follows: a search run on November 3, 2022, to update a search originally run on December 8, 2020, with the main search concept of multiple myeloma using the databases MEDLINE through Ovid, PsycINFO through Ovid, PubMed, and the Cumulative Index to Nursing and Allied Health Literature (CINAHL) through EBSCO;4 and a search run on November 3, 2022, to update a search originally run on July 5, 2022, with the main search concept of CAR T-cell therapy using the databases MEDLINE through Ovid, Philosopher’s Index through Ovid, CINAHL through EBSCO, and Scopus.3 Due to the advancing nature of CAR T-cell technology, additional search terms were added to the original search strategy to capture articles on B-cell maturation antigen. The search for these additional terms was not restricted by date. CADTH-developed search filters were applied to both searches to limit retrieval to citations related to ethical concepts or considerations. Duplicates were removed by manual deduplication in EndNote. Retrieval was limited to the English language.
One de novo literature search was conducted by an information specialist on key resources, including MEDLINE through Ovid, Philosopher’s Index through Ovid, CINAHL through EBSCO, and Scopus. The database search was run on November 3, 2022. Duplicates were removed by manual deduplication in EndNote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was ciltacabtagene autoleucel. CADTH-developed search filters were applied to limit retrieval to citations related to ethical considerations. Retrieval was limited to the English language.
Grey literature (literature that is not commercially published) was identified by searching sources listed in the ethics section of the Grey Matters: A Practical Tool for Searching Health-Related Grey Literature checklist. The grey literature search for ethical considerations was conducted on November 7, 2022. The main search concepts were ciltacabtagene autoleucel, multiple myeloma, or CAR T-cell therapy. Search results were not limited by publication date but were limited to the English language. Google was used to search for additional internet-based materials. These searches were supplemented by reviewing bibliographies of key papers, manual searching of additional key concepts, and through contacts with experts, as appropriate.
Literature Screening and Selection
The ethics reports for 3 previous CADTH reviews of CAR T-cell therapies that identified ethical considerations in the use of idecabtagene vicleucel for adults with r/rMM4 and axicabtagene ciloleucel for adults with r/r large B-cell lymphoma3,5 served as foundational sources for this ethics report. Additional literature retrieved according to the search and selection methods detailed previously was screened in 2 stages. First, titles and abstracts of citations retrieved were screened for relevance by a single reviewer. Articles were identified and retrieved for full-text review by a single reviewer if their titles or abstracts identified ethical considerations or provided normative analysis (i.e., focusing on “what ought to be” through argumentation), or presented empirical research (i.e., focusing on “what is” through observation) of ethical considerations related to: the incidence, diagnosis, treatment, or outcomes of MM; the evidence on, use of, or implications of cilta-cel as a CAR T-cell therapy for adults with r/rMM; the implications or use of CAR T-cell therapies generally. In the second stage, full-text publications categorized as “retrieve” were reviewed by the same reviewer. Texts that included substantive information meeting the aforementioned criteria were included in the review, and reports that did not meet these criteria were excluded.
As a parallel process, grey literature and other sources drawn from relevant bibliographies, relevant key concepts, consultation with experts or other CADTH reviewers were retrieved and reviewed following the selection criteria listed previously.
Data Analysis
Data analysis included the collection, coding, and thematic analysis of data drawn from the literature and project inputs, driven by the 4 research questions guiding this report. The reviewer conducted 3 iterative cycles of coding and analysis to abstract, identify, and synthesize relevant ethical considerations from the literature and relevant project inputs.
In the initial coding phase, the main ethical considerations posed and discussed in the 3 previous CADTH ethics reports were abstracted. These considerations were used to guide the questions posed to the clinical experts and the reviews of project inputs and additional literature sources. In the second coding phase, publications retrieved from the updated search as well as from project input sources were reviewed for ethical content (e.g., claims related to potential harms, benefits, equity, justice, resource allocation, and ethical issues in the evidentiary basis). Once identified, claims related to ethical content were coded using methods of qualitative description.6 In the final coding phase, major themes and subcodes were identified through repeated readings of the data6 and comparisons with the initial themes and considerations that emerged in the previous CADTH reviews. These were then summarized into thematic categories within each domain or research question. Where ethical content did not fit into the categories or domains outlined in the research questions, this was noted, as were discrepancies or conflicts between ethical considerations or values identified between project sources or within thematic categories. The data analysis was iterative, and themes identified in the literature, in project inputs, and during consultations with clinical experts were used to further refine and reinterpret the ethical considerations identified.
Data collected and analyzed from these sources were thematically organized and described according to the 4 research questions and domains driving this report. The results of this analysis and its limitations and conclusions are described subsequently.
Results
Description of Included Sources
Three previous CADTH reports on ethical considerations in the context of CAR T-cell therapies provided the foundation for both the literature search strategy and the thematic analysis of ethical considerations in this report. These 3 reports had undertaken reviews of relevant ethical considerations in the use of idecabtagene vicleucel for adults with r/rMM4 and axicabtagene ciloleucel for adults with r/r large B-cell lymphoma.3,5
The literature search identified a total of 323 results. Following title and abstract screening, 273 citations were excluded and 50 potentially relevant publications from the electronic search were retrieved for full-text review. Of the potentially relevant publications, 30 publications were excluded because they did not discuss ethical considerations of cilta-cel or MM (n = 14) or were not relevant to the Canadian context (n = 16). Twenty publications met the inclusion criteria and were included in this report. Four additional publications were retrieved by backward searching the reference lists of included publications or through a manual search.
In addition to the 3 previous CADTH reviews, a total of 24 publications were used to inform this report. Of these publications, 10 publications discussed ethical considerations in the context of access, use, or implementation of CAR T-cell therapies; 5 publications discussed disparities in MM treatment; 6 publications discussed patient and/or caregiver experiences in the context of MM; 1 publication discussed patient experiences in the context of the CARTITUDE-1 trial; and 2 publications discussed VBAs. Details regarding the characteristics of included publications are reported in Table 1.
In addition to sources from the published literature, data to inform this ethics report drew from a review of the patient group input, clinician group input, drug program input, and consultation with the clinical experts engaged by CADTH for this review. All clinical experts were active in relevant clinical roles in Canada, and all had experience as hematologists or oncologists treating patients with r/rMM. A description and summary of these sources are included in the Clinical Review report.
Key Ethical Considerations
Experiences of MM
Several ethical considerations related to experiences of MM were identified, including with respect to the treatment pathway for MM; patient and caregiver experiences of MM; and disparities in incidence, diagnosis, treatment, and outcomes of MM.
Treatment Pathway for MM
The patient and clinician group input received, and the clinical experts engaged by CADTH discussed how there is currently no curative treatment available for MM. As a result, the treatment pathway for patients diagnosed with MM extends over multiple years, during which patients will undergo successive lines of therapy to control the disease and associated symptoms, with progressively worsening outcomes, and will eventually develop refractory disease. Treatment for MM is thus considered continuous, requiring ongoing treatments, monitoring, and follow-up by clinicians; the “relentlessness of active treatment” has been described as a feature that distinguishes the treatment of MM from that of other cancers.7
The clinical experts also discussed the challenges of determining when to initiate the next line of therapy, given the need to initiate treatment neither too early nor too late (with the latter risking patients being too ill and thus no longer being sufficiently fit or eligible for treatment). They also noted that existing treatments for MM were very expensive. As noted by the clinical experts and in the clinician and patient group input, a treatment for patients with relapsed or refractory disease following 3 prior lines of therapy represents the greatest unmet need in the MM treatment landscape because there are no effective fourth-line therapies currently available.
Patient and Caregiver Experiences of MM
As described further in this section, MM negatively impacts patients’ physical, psychosocial, and mental well-being owing to the effects of the disease itself and the burdensome nature of existing treatments (both due to toxicities and the need for ongoing administration and follow-up). Relatedly, MM negatively impacts caregivers’ psychosocial and mental well-being, and has financial implications for both patients and caregivers.
As a disease, MM impacts patients’ physical well-being in various ways, including resulting in pain, fatigue, gastrointestinal issues, neuropathy, bone destruction and pain, renal failure, hypercalcemia, and low blood counts. In addition, MM — and its nature as a treatment-intensive, life-threatening, and currently incurable disease — has psychosocial impacts on patients’ and caregivers’ well-being. The patient input reported that patients’ ability to work, travel, and exercise were most significantly impacted by symptoms associated with MM. Further, both the patient group input and the published literature reported that MM has a significant impact on patients’ and caregivers’ mental health8-11 and relational well-being.7,12 Patients with MM can suffer from anxiety and depression, including due to disease-related and treatment-related burdens, social isolation, and existential fears related to their disease trajectory and uncertainty about the future.8,10
In addition to the physical and psychosocial impacts resulting from MM itself, the patient and clinician group input and clinical experts engaged by CADTH spoke to the challenges for patients, as well as their caregivers, associated with the treatment of MM as an incurable, relapsing cancer that requires continuous treatment and clinical follow-up and currently offers no treatment-free windows. They noted that existing treatments for MM are burdensome for patients in at least 2 ways. First, existing treatments are burdensome because they bear serious toxicities. For example, 1 respondent in the patient input noted that “the current treatments are so harsh they destroy all the goodness of living.”
Second, and in the absence of curative treatment, the administration of existing treatments is burdensome because it requires ongoing administration and clinical follow-up, which require routine (e.g., weekly or monthly) clinical visits and ongoing work by patients and caregivers to manage treatment.12 The clinical experts noted that this was time-consuming for patients and caregivers, and especially burdensome for patients residing in rural or remote regions and/or those who were older and had comorbid conditions that affected their ability to tolerate treatment or travel. They also emphasized that the burdensome nature of MM treatment could factor into patients’ decision-making concerning the choice of treatment or whether to pursue further treatment (e.g., forgoing treatment, or more effective treatment, to avoid the need to travel and leave one’s community or to reduce caregiver burden), which was also noted in the published literature.7,12The burdensome nature of MM treatment, including frequent hospital visits, was also reported as having negative psychosocial and mental health impacts, with patients and caregivers facing greater challenges with anxiety and depression in the days following a hospital visit.12
Treatment for MM is also financially burdensome for patients and caregivers. The patient group input reported that living with and undergoing treatment for MM has multiple financial implications, including costs related to drugs, travel, parking, and supportive care and treatment to manage side effects; lost income due to absence from work or disability; and lost job or pension income due to early retirement, considerations that were also reported in the published literature.7,10,13 Noting the various burdens associated with MM, the patient group input reported that key factors considered to be most important to any myeloma treatment included: quality of life and making side effects manageable, the effectiveness (especially achieving remission) and the accessibility and/or portability of treatment (including minimizing visits to a hospital or community treatment centre), and the accessibility of a supportive and communicative care team.
Disparities in Incidence, Diagnosis, Treatment, and Outcomes of MM
A previous CADTH review of ethical considerations in MM reported on disparities in terms of incidence, treatment, and outcomes of MM. Disparities in incidence have been reported with respect to race and ethnicity, socioeconomic status, and geography.4 Disparities in access and receipt of treatment have been reported with respect to age, race and ethnicity, socioeconomic status, geography, proximity or access to treatment centres, insurance status, and supply.4 Disparities in MM outcomes are reported with respect to age, race and ethnicity, socioeconomic status, proximity and access to treatment centres, and insurance status.4 The review noted that underlying reasons for the observed disparities across racial and ethnic groups were debated in the published literature, with some studies reporting that race-based disparities were better explained by disparities in socioeconomic status.4
Notably, most of the published literature available at the time of the previous CADTH review of MM reflected the US context. However, racial, socioeconomic, or age-based disparities in MM have been reported more recently in other jurisdictions,14,15 including in Canada.16 In Canada, the incidence of MM has been reported as being higher in smaller cities and rural areas, which were associated with increased density of agricultural facilities, while lower incidence has been reported in large metropolitan cities and high-latitude regions.17 However, the published literature concerning the distribution of MM incidence, treatment, and outcomes in Canada remains limited; analytic limitations have been attributed to gaps in the collection of age-related, sex-related, and race-related demographic data in Canadian health information databases.17,18 The absence of more fulsome demographic data collection may limit a contextualized understanding of the MM-related disparities observed in other jurisdictions within the Canadian context (or even between subnational jurisdictions).
The clinical experts consulted for this review noted that considerations related to geography and the social determinants of health could impact the distribution of MM diagnosis, treatment, and disease-related outcomes in Canada. Moreover, they suggested that greater disparities in access were likely to be observed before the diagnosis of MM (e.g., resulting from disparities in access to primary care) rather than after a patient has entered and is being actively followed in the cancer care system.19 A study from Ontario reported on geographic, age-related, and socioeconomic disparities with respect to the receipt of high-quality end-of-life care in MM; it identified that patients aged 80 years or older were less likely to receive aggressive and supportive care, patients residing in smaller-sized rural communities of fewer than 10,000 people (compared with patients in communities exceeding a population of 1.5 million) were more likely to receive aggressive care, and patients residing in neighbourhoods with the lowest income quintile were less likely to receive supportive care compared with people residing in neighbourhoods with the highest income quintile.18 The authors also noted that their analysis was limited because data on race and ethnicity were not collected in the provincial databases used.
In sum, the disease and treatment landscape for MM is characterized by a life-threatening, treatment-intensive, and currently incurable disease, which presents multiple physical, mental, psychosocial, and financial burdens for patients with r/rMM and their caregivers. Moreover, how patients with r/rMM experience the harms from MM, as well as the balance of harms and benefits associated with the diagnosis and treatment of MM, is impacted by broader factors such as geography, socioeconomic status, race and ethnicity, and age, thus highlighting considerations related to equity.
Ethics of Evidence and Evaluation of Cilta-Cel
Ethical Considerations in Clinical Trial Data
Several ethical considerations related to clinical trial data for cilta-cel — including relating to the representativeness of the clinical trial population and the quality of available evidence — were discussed by the clinical experts engaged for this review and have been reported in published literature concerning other CAR T-cell therapies.
The Representativeness of the Clinical Trial Population
The clinical evidence used to evaluate the use of cilta-cel for r/rMM is drawn from the US-based pivotal phase Ib/II trial, CARTITUDE-1, which is discussed in greater detail in the Clinical Review report. The clinical experts noted that while the trial population was broadly representative of the patient populations that they encountered in their clinical practices in Canada, there were some differences. Compared with patients with r/rMM in Canada, the patients included in the trial were generally younger (with a median age of 62 years, with the majority younger than 65 years) and healthier (with an Eastern Cooperative Oncology Group [ECOG] Performance Status score of 1 or less and with creatinine clearance ≥ 40 mL/min/1.73 m2). However, the clinical experts also noted that the expected introduction of bispecific antibodies as an alternate fourth-line therapy for r/rMM, which would be used preferentially for older patients, would likely lower the median age of patients in practice who are referred to CAR T-cell therapy, putting them closer to the age of the trial participants. Although the clinicians noted the trial population was generally healthier than the patients observed in clinical practice, they also noted that trial eligibility would have favoured patients sufficiently healthy to endure — and not have their health deteriorate significantly before — the pretreatment and manufacturing processes in advance of cilta-cel infusion. The clinical experts also noted that as CARTITUDE-1 was conducted at tertiary centres in large metropolitan areas, patients residing in rural areas or those who faced barriers in accessing care may have been inadvertently excluded from the trials, and thus may not reflect the population of patients with r/rMM in Canada. The impact that access to treatment centres has on being included in a CAR T-cell clinical trial has been reported as well.20
The underrepresentation of certain racial and ethnic minority groups in cancer clinical trials, including for MM, has previously been reported and has been argued to contribute to the limited understanding of, and thus to obfuscating, the racial and ethnic disparities reported on in the incidence, treatment, and outcomes of MM.4 Disparities in access to and inclusion within clinical trials have also been reported with respect to clinical trials for CAR T-cell therapies and other novel MM therapies (e.g., bispecific antibodies) in the US.20,21 For instance, African American and Black persons were underrepresented in CAR T-cell clinical trials for 5 CAR T-cell products across 7 indications for hematological malignant neoplasms, with the greatest degree of underrepresentation observed in patients with MM, which was noted as potentially exacerbating the existing health disparities observed in these populations.20 It has also been noted that these groups are often not reported on directly in clinical trial data (e.g., they are included in an “other” category).20 In the US, the incidence of MM in Black or African American people has been reported as being greater compared with the incidence in those who are white;4 yet, in CARTITUDE-1, 17.5% of participants were Black and 71.1% were white.
Demographically representative clinical trial data for CAR T-cell therapies may contribute to understanding whether and how therapeutic efficacy varies between subgroups, or how nontherapeutic factors affect effectiveness in the real world. For example, a subgroup analysis reported in the CARTITUDE-1 trial concerning the efficacy of cilta-cel found that the Black or African American participants enrolled in the trial tended to have a reduced overall survival rate (although it was not confirmed statistically because it was based on a univariate analysis due to the small sample size).22 The clinical experts engaged for this review were uncertain about the clinical implications of this reported finding, and noted they were unaware of evidence suggesting a different response due to genetic or biological differences between patients of different racial or ethnic backgrounds. Instead, they discussed the importance of considering the impact of socioeconomic status (e.g., through the ability to afford supplementary treatment and care) and the availability of caregiver support on outcomes following treatment with CAR T-cell therapy. For example, they discussed the critical role of caregiver support and vigilant care (e.g., monitoring for and notifying the clinical team of side effects) for safer recovery following treatment with CAR T-cell therapy. Similarly, 1 study reported that low socioeconomic status was associated with worse biological and clinical outcomes (e.g., levels of cytokines, neurotoxic kynurenine metabolites, onset of cytokine release syndrome [CRS], pain levels, and quality of sleep) in patients receiving CAR T-cell therapy for treatment of r/r CD19- or CD20-positive B-cell malignancies.23 Given the disproportionate impact of MM on certain racial and ethnic groups, and the tendency reported in the results of the subgroup analysis with Black participants in the CARTITUDE-1 trial, it is important to consider whether the results are generalizable to all races and ethnicities (e.g., Black patients), and whether additional clinical, demographic, and socioeconomic data could better inform decision-making in the Canadian context.
Availability and Quality of Clinical Evidence
An additional ethical challenge associated with the clinical trial data used to evaluate cilta-cel in this review concerns evidentiary limitations, since CARTITUDE-1 is a phase Ib and II, single-arm, open-label trial and thus presents only an understanding of the short-term safety and efficacy of cilta-cel, and no long-term or comparative data. The clinical experts noted that the risks associated with the limited evidence were partially mitigated due the growing body of evidence on CAR T-cell therapies as a class of therapies, and that patients eligible for cilta-cel were without alternative treatment options. However, they also emphasized the importance of paying special attention to treatment-related toxicities with such limited evidence.
As with previous CAR T-cell therapies, the absence of long-term evidence for the safety and efficacy of cilta-cel necessitates robust post-market surveillance to better understand the risk-benefit profile and cost-effectiveness of cilta-cel in practice.3,5,24 Moreover, post-market surveillance and the use of real-world evidence may contribute to a better understanding of how the safety and efficacy of cilta-cel in clinical practice may be impacted by nonclinical factors, and whether this has an impact on how the benefits and burdens associated with the use of this therapy are distributed fairly across diverse demographic groups within the population of patients with MM in Canada.
Ethical Considerations in Economic Models
The clinical experts and published literature raised several ethical considerations related to the economic models used to evaluate cilta-cel, including stakeholder consultation in pharmacoeconomic assessments, the uncertainty of pharmacoeconomic assessments due to the absence of long-term survival and comparative effectiveness data, the use and design of VBAs, and the budget impact analysis.
Stakeholder Consultation
The importance of including diverse stakeholders in economic modelling has been reported, given the high costs associated with CAR T-cell therapies and the opportunity costs they present in the Canadian health care system, as well as for informing how the benefit or value of drugs is understood.3,24 The sponsor noted that it consulted clinical experts to inform the pharmacoeconomic model it submitted to CADTH, but it is unclear whether a diverse range of stakeholders was included to inform the economic modelling used to support the pharmacoeconomic evaluation of cilta-cel.
Challenges to Pharmacoeconomic Assessments
The limited availability of data concerning the safety and efficacy of CAR T-cell therapies, including cilta-cel, not only presents a challenge for assessing clinical risks and benefits, but also for pharmacoeconomic assessments.24,25 In particular, the absence of long-term safety and efficacy (including survival) data as well as a lack of head-to-head comparative effectiveness data, hinders cost-effectiveness assessments.25 The collection of evidence on long-term safety, efficacy, and comparative effectiveness (e.g., through long-term follow-up studies with a greater number of participants and head-to-head studies with comparator therapies) may better support robust pharmacoeconomic assessments to inform reimbursement recommendations and decisions.25
Value-Based Agreements
Uncertainty in pharmacoeconomic assessments has ethical implications for resource allocation; this uncertainty makes it more difficult to assess opportunity costs and poses a high financial risk for payers because they may incur high costs for uncertain benefits.25 In the pharmacoeconomic evaluation submitted for this review, the sponsor suggested that VBAs could offer an opportunity to improve patient access while mitigating the uncertainty of the long-term efficacy of cilta-cel in the real world. As discussed subsequently in the section on funding models, VBAs have been proposed in published literature as a risk-sharing mechanism to possibly mitigate the risks that payers face when reimbursing high-cost therapies, including CAR T-cell therapies, based on uncertain clinical and pharmacoeconomic evidence.3,25,26 However, how a VBA is designed has ethical implications for the distribution of the potential benefits and burdens associated with such arrangements (e.g., for patients, the public, payers, and manufacturers).27 For example, how the “value” of a drug is defined, such as which surrogate outcomes are selected to evaluate efficacy, has implications for how financial risks are distributed between manufacturers and payers (e.g., with a more generous interpretation of therapeutic value placing a greater share of this risk on payers, and a more stringent interpretation of value placing a greater share of the risk on manufacturers).24,27
The clinical experts engaged for this review questioned the sponsor’s proposed VBA reimbursement cut-offs (6 and 18 months), which were provided by the sponsor as illustrative examples to demonstrate functionality, since the clinical experts expected that most patients eligible for cilta-cel would have lived past 6 months, even without receiving CAR T-cell therapy. Instead, they proposed that reimbursement assessments at 12 and 24 months would more appropriately capture the value of cilta-cel, which has been described as inducing a durable response by the sponsor, and because the average duration of progression-free survival would be approximately 9 to 12 months with the alternative treatments that are currently available beyond the third line. The clinical experts also noted a preference for using overall survival rather than progression-free survival as the outcome in a VBA because the latter is more clinically nuanced and thus more complicated to assess.
Budget Impact Analysis
In considering the budget impact analysis submitted for this review by the sponsor, the clinical experts engaged for this review questioned the sponsor’s low projected uptake of cilta-cel, as discussed in the Pharmacoeconomic Report for this review. They noted that the uptake of cilta-cel would be affected by manufacturing capacity, the capacity of health systems to deliver CAR T-cell therapy, and uptake by clinicians and patients. In the absence of capacity challenges, they anticipated that cilta-cel would be widely adopted by clinicians and patients, were it reimbursed. The greater the uptake of cilta-cel, the greater its potential impact on health care budgets and the associated financial burden it may place on Canadian health care budgets.
Ethical Considerations in the Use of Cilta-Cel
Potential Benefits in the Use and Delivery of Cilta-Cel
The patient and clinician group input and the clinical experts all noted that cilta-cel could offer an additional and novel therapeutic option for patients whose condition had failed 3 previous lines of therapy and who were largely without additional treatment options. The clinical experts also noted that cilta-cel could potentially represent a unique therapeutic opportunity — thus expanding access to treatment — for some patients who are ineligible for a stem cell transplant (e.g., patients who are still sufficiently healthy to receive CAR T-cell therapy but not healthy enough to undergo stem cell transplant because the latter is more onerous; patients who exceed age cut-offs for stem cell transplant; and patients for whom no suitable match for stem cell transplant can be found).
In addition to a novel therapeutic option, the patient and clinician group input and clinical experts noted that cilta-cel could offer practical advantages over existing therapies as a therapy requiring a single infusion and 1 that might offer patients with MM the first treatment-free period following their initial diagnosis. The clinical experts noted that a treatment offering a durable response could be less burdensome than existing treatments, especially for patients residing in rural or remote regions or with mobility issues, since the period for intensive care would be limited to a defined period, rather than requiring ongoing travel for infusions and follow-up. The potential benefit of a single treatment was echoed in the patient input, such as in several respondents’ comments: “The idea of not having to continue ongoing treatments after cart [sic] is extremely appealing” and “a one and done treatment in spite of the inherent risks is important and has merit with me.” Such hopes and benefits were echoed in the results of a qualitative study conducted with patients with r/rMM in the CARTITUDE-1 trial.11 Before treatment, patients reported seeking improvements in their MM symptoms and a return to perceived normalcy. Following treatment, patients reported finding cilta-cel easier than their prior treatments and chemotherapy, appreciating the treatment-free window and experiencing improvements in symptoms, physical functioning, and health-related quality of life (including psychological and emotional impact and activities of daily living), although most did not report changes in their relationships or social functioning.
Potential Harms in the Use and Delivery of Cilta-Cel
While CAR T-cell therapies may offer a novel therapeutic opportunity for patients with MM, they also bear the risk of severe toxicities, including CRS and other adverse events detailed in the Clinical Review report, which require serious consideration when assessing the risks and benefits of pursuing CAR T-cell therapy. The clinical experts noted that the evidence for cilta-cel suggest it has a more favourable safety profile than early CAR T-cell therapies, but that the safety of CAR T-cell therapies had also improved as clinicians have become more knowledgeable at administering treatment and identifying and responding to adverse events. This suggests that the safety of CAR T-cell therapies such as cilta-cel may in part be context-dependent, where safety and efficacy may be impacted by the level of experience of the treating team and centre as well as the availability of supportive resources.24 The collection of postmarket data and real-world evidence related to the use of novel CAR T-cell therapies, such as cilta-cel, including as new CAR T-cell treatment centres are established, could contribute to a more robust understanding of the real-world safety and efficacy of CAR T-cell therapies, and the balance of risks and benefits, in diverse clinical practice settings and communities.
The clinical experts also noted that as MM is primarily a disease of older adults, it would be important to consider patients’ fitness for treatment and frailty, such as with respect to stability of ECOG Performance Status and the increased risks of severe adverse events such as CRS, when assessing the risks and benefits of pursuing treatment with cilta-cel. Finally, the clinical experts noted the time-sensitive nature of using cilta-cel for the treatment of r/rMM; as a result, they noted that patients could be harmed by delays in access to therapy, since they had to be in sufficiently stable and good health to be eligible for cilta-cel, and to be able to withstand treatment and its potential side effects.
Equitable Access to CAR T-Cell Therapies
Besides health system–level funding and capacity concerns, which are discussed in greater detail in the subsequent section, several access issues were identified, including disparities in access to CAR T-cell therapies, the impact of geographic and financial barriers on equitable access, and the impact of referral patterns on equitable access.
Disparities in Access to CAR T-Cell Therapies
As with disparities observed in clinical trial enrolment and access to non–CAR T-cell therapies for MM, racial disparities in access to CAR T-cell therapies have been reported in the US context, with Hispanic patients — and especially Black patients —being less likely to receive CAR T-cell therapy than white patients.28,29 Geographic and socioeconomic disparities in access to CAR T-cell therapies have also been reported in the US. To date, most CAR T-cell recipients have resided in metropolitan areas with access to teaching hospitals,29 and few recipients have resided lower income neighbourhoods or in rural areas.28,29 Additionally, most CAR T-cell recipients residing outside of metropolitan areas with access to CAR T-cell centres have been from higher income groups.28 These results suggest that adequate financial resources for patients and caregivers may be important for enabling equitable access to CAR T-cell therapies by mitigating cost-related barriers that are exacerbated by geography (e.g., costs associated with travel, accommodations, and lost income for patients and caregivers who reside outside of cities with CAR T-cell treatment facilities).
Geographic and Financial Barriers to Equitable Access
The drug program input noted there might be issues related to access and prolonged stay in (or near) treatment centres, especially for patients from remote areas, and that financial support for travel and accommodation would be needed. In Canada, some financial support for travel and/or accommodation-related costs associated with CAR T-cell therapy is currently provided by jurisdictions and/or manufacturers. The drug program input noted that most, albeit not all, jurisdictions in Canada have provided some support for accommodation and/or food-related expenses for residents residing a certain distance from an infusion centre, while fewer have provided support for travel costs. In its implementation plan submitted to CADTH, the sponsor noted that it is in the process of developing a patient support program that “may also offer CAR T-cell therapy specific elements pending results of ongoing physician and patient research and subsequent internal compliance reviews, such as financial and/or accommodation support for required travel.” Previous CADTH ethics reviews of CAR T-cell therapies3 and the clinical experts engaged for this review discussed the importance of providing sufficient travel-related and accommodation-related supports for patients and caregivers to facilitate equitable access to CAR T-cell therapies. Moreover, although not yet known for cilta-cel, they noted that other, existing manufacturer-sponsored support programs for CAR T-cell therapies often included distance-related eligibility cut-offs (e.g., residing 2 hours or 200 km from the treatment centre), which could still present access challenges or leave gaps in coverage for some patients or provide insufficient support to cover all costs borne by patients and caregivers.3
The clinical experts consulted stressed that geographic disparities in access to CAR T-cell therapies may prove especially salient in the Canadian context, given Canada’s vast geography and the limited number of established and proposed CAR T-cell centres. Experts noted that disparities in access could be most pronounced for populations residing in rural and Northern communities, as well as for persons residing in provinces or territories without CAR T-cell centres. In the Canadian context, race-based disparities in access should be considered as they impact Indigenous Peoples — especially noting their disproportionately increased representation in rural and Northern communities — as well as other structurally marginalized peoples or groups underserved by health care services. Experts noted that the financial and psychosocial burdens resulting from geographic distance could impact patient decision-making regarding pursuing therapies (e.g., patients in remote or Northern communities opting for noncurative or inferior treatments to avoid leaving their communities or spending an extended time in hospital). At the same time, and as discussed previously, clinical experts also discussed how cilta-cel could perhaps offer access-related advantages over, and be less burdensome than, existing MM treatments for patients in rural and remote communities because it only required a single treatment. Ensuring equitable access to high-quality care across Canada may thus also require considering what, if anything, might be owed to patients who are eligible for but opt not to pursue effective therapeutic options, such as CAR T-cell therapy, due to geographic or other barriers.
Referral Barriers to Equitable Access
Previous CADTH ethics reviews of CAR T-cell therapies,3 the clinical experts engaged for this review, and the published literature19,24,30 have noted that referral practices can also impact access (and the distribution of access, and thus equitable access) to CAR T-cell therapies in Canada. For example, a US study reported that community oncologists who were less confident in their knowledge about CAR T-cell therapies were less likely to refer.30 Another US study reported that racial and ethnic disparities observed in the distribution of patients receiving CAR T-cell therapy occurred due to disparities in referral patterns rather than in treatment practices.19 Similarly, the clinical experts noted that to be referred for CAR T-cell therapy, patients required their physicians be aware of available therapies and eligibility criteria as well as the processes involved in making a referral to a treatment centre (which could be located in a different jurisdiction if they resided in a province or territory lacking a CAR T-cell therapy facility). Accordingly, they emphasized the importance of having clear and simplified referral practices, educating clinicians about CAR T-cell therapies and referral processes, facilitating and communication between clinicians and treatment centres, and providing systems-level supports for clinicians practising outside of large metropolitan centres where CAR T-cell centres are located (and who would otherwise be tasked with advocating for their patients to have access to CAR T-cell therapy).
The clinical experts and drug program input also noted the rapidly changing therapeutic landscape for MM, with the ongoing introduction of new therapies and changes to therapeutic regimens or sequencing, and its potential impact on access to cilta-cel. They noted that a small subset of patients with r/rMM may find themselves ineligible for referral to access cilta-cel “for no fault of their own or that of their physician” because they were not able to access 1 of the therapeutic classes outlined in the proposed Health Canada indication for this treatment due to changes in the therapeutic landscape. For example, the clinical experts and drug program input questioned whether there was a time-limited need to consider expanding access to patients who were unable to access anti-CD38 monoclonal antibodies (e.g., patients previously treated with the lenalidomide, bortezomib, and dexamethasone regimen whose disease ended up being refractory to both lenalidomide and bortezomib) to prevent them from “falling through the cracks.”
Cell Ownership
Previous CADTH ethics reviews of CAR T-cell therapies have reported that the collection and storage of patients’ cells during the manufacture of CAR T cells may raise questions related to patient privacy and cell ownership.3,5 The drug program input also cited concerns related to privacy and cell ownership, given that cilta-cel is manufactured in the US and outside of Canadian jurisdiction. The clinical experts engaged for this review felt that patients currently receiving CAR T-cell therapy are adequately informed of patient data and privacy considerations during the consent process, and that related policies and legislation were in place. Nonetheless, it has been reported that tissue and genetic materials are valued differently by different cultural groups (e.g., Indigenous groups internationally), and that consent processes need to clearly detail cell processing and ownership, as well as how remaining cells that are produced but not infused will be handled or disposed of.31 Accordingly, consultation with diverse groups has been identified as essential to CAR T-cell research and implementation to ensure that cell handling and disposal practices, as well as educational and consent materials, are sensitive to the needs and values of diverse patients and communities.3,5,31 For example, in the Canadian context, attention should be paid to understanding Indigenous communities’ values and practices with respect to cell and tissue ownership and governance (e.g., with reference to guidance such as the First Nations Principles of OCAP [ownership, control, access, and possession]32). Moreover, as a matter of equity, it is necessary to consider how the benefits of cell ownership may accrue to different actors (e.g., patients, the public, and manufacturers), and what implications this might have for public trust in, and the legitimacy of, CAR T-cell initiatives.3,5
Considerations for Informed Consent
Previous CADTH ethics reviews of CAR T-cell therapies have noted reports of “hype” surrounding CAR T-cell therapies by media, clinicians, or patients, in which CAR T-cell therapies may be presented as curative in the absence of supporting long-term evidence and treatment-related harms or uncertainties may be underreported.3,5 As noted by the clinical experts consulted for this review, more is known about the side effects of CAR T-cell therapies — and especially the clinical management of side effects — since the introduction of the first CAR T-cell therapies. Nonetheless, CAR T-cell therapies still present a risk of harm to patients owing to treatment-related toxicities, and they offer uncertain long-term benefits owing to limited evidence. Processes should be in place to ensure that patients are apprised of the unique risks of, and uncertainties related to, cilta-cel to support robust and ongoing informed consent.3 The patient input reported that many patient respondents described a desire to speak with their treating clinician before considering whether to pursue cilta-cel as a next treatment, suggesting that despite the potential “hype” surrounding CAR T-cell therapies, patients still sought and trusted the advice of their clinicians and desired to make informed choices about their treatment. Accordingly, robust consent processes should recognize both the unique vulnerabilities of patients with r/rMM who have limited or no alternative therapeutic options as well as their autonomous decision-making capacity.3,4 Moreover, as discussed in the preceding section, consent procedures should explicitly outline information concerning cell ownership, storage, disposal, and privacy considerations.31
Given the importance of decision-making capacity to provide informed consent regarding treatment, determining how to enhance and support medical decision-making capacity also requires considering the potential for increased challenges with decision-making due to cognitive impairment and increasing age that may be observed in patients with MM.4 At the same time, it is important to recognize that patients with MM still expressed the desire to have an active role in decision-making related to their treatment, and that all efforts should be made to respect and facilitate (such as through the provision of information and help to understand information) the autonomous decision-making capacity of patients and to promote shared decision-making as a component of patient-centred care.4,13 Furthermore, studies conducted with patients with MM and their caregivers have reported the importance of having, and supporting, conversations about serious illness to improve the quality of end-of-life care for patients with MM.8,9 Furthermore, studies have reported on the importance of studying and considering patient-reported outcomes and patient experiences to better facilitate shared decision-making for MM,10,12,13 including for the use of CAR T-cell therapies.24
Health Systems Considerations
Manufacturing and Health Systems Capacity
The sponsor’s implementation plan indicates that cilta-cel will initially be rolled out in 2024 through 12 centres (3 of which are pending) in 7 provinces, and that access for patients in the remaining provinces and territories (New Brunswick, Prince Edward Island, Newfoundland and Labrador, the Northwest Territories, Nunavut, and Yukon) is expected to be managed through agreements for out-of-province treatment. Nonetheless, the concentration of CAR T-cell centres could leave gaps in access to treatment in jurisdictions without CAR T-cell facilities and for patients residing far from CAR T-cell facilities.
The delivery of CAR T-cell therapies presents at least 2 systems-level, capacity-related challenges.24 The first challenge, as described by the clinical experts and in clinician group input, concerns the capacity of manufacturers to manufacture CAR T-cell therapies, and for the timely coordination between manufacturers and CAR T-cell centres for limited manufacturing slots and a multiweek preparatory and manufacturing period (e.g., stabilizing patients’ conditions before apheresis, manufacturing and treatment, coordinating bridging therapy, apheresis, and transport of cells). While manufacturing challenges were reported with early CAR T-cell therapies,5 the sponsor for this submission has indicated that it believes there is capacity to produce cilta-cel for all patients deemed eligible for this treatment in Canada. Nonetheless, as each of the many steps within the complex sequence of manufacturing and delivery requirements for CAR T-cell therapy presents a potential opportunity for disruption or delay, it may be important to consider the development of contingency plans to ensure stable supply. The drug program input also noted the growing administrative burden for centres offering CAR T-cell therapies, which not only had to maintain resource-intensive accreditation, but also manage various protocols for preparation and delivery of a growing number of CAR T-cell therapy types.
The second challenge, which has also been reported on in past CADTH reviews of other CAR T-cell therapies,3,5 concerns the health systems capacity required to meet the therapeutic demand for CAR T-cell therapies in Canada. As noted in the clinician group input, capacity challenges arise in part due to the complex constellation of infrastructure and personnel requirements required to implement CAR T-cell therapies in clinical practice (e.g., tertiary medical centres with specialized expertise, specialized training for staff, infrastructure modifications, close interactions between experienced inpatient, intensive care unit, outpatient, and emergency personnel and facilities, and identification and planning of patients before and following treatment). In this review, health systems capacity was raised as a potential concern in the drug program and clinician group input and by clinical experts. The clinical experts noted that while capacity concerns already existed with currently implemented CAR T-cell therapies, demand for CAR T-cell therapy with MM is anticipated to exceed demand for patients with B-cell lymphomas, which could exacerbate existing capacity challenges. The clinical experts also noted that a significant increase in demand for CAR T-cell therapy could result in increased demands on clinical staff (e.g., workload associated with applying for access to CAR T-cell therapies for patients), which could prove challenging for clinical staff with limited time, and especially during an era of high rates of burnout and staffing shortages.
Although currently not proposed for cilta-cel, the clinical experts suggested that shifting to outpatient delivery of CAR T-cell therapies in the future could potentially help address capacity limitations and expand access to a greater number of patients by circumventing limitations in inpatient capacity (e.g., health human resources, hospital beds), as well as reduce implementation costs for health systems. However, they also stressed that outpatient delivery would heighten the need for patients to have access to social supports and a reliable caregiver, since the responsibility for care would be shifted largely onto patients and caregivers and away from trained health care personnel and health systems. The clinical experts noted that a shift to outpatient delivery could thus potentially exacerbate burdens and resulting inequities associated with accessing CAR T-cell therapies for patients and caregivers in lower socioeconomic strata and those residing outside of cities with CAR T-cell centres; for example, they noted that inadequate caregiver support already presented challenges to patients in accessing stem cell transplants. Similarly, it has been reported that the growing shift of delivery of care for MM from hospital to home following the introduction of novel oral drugs in Canada has required patients and caregivers to increasingly engage in active illness management,12 thus emphasizing the importance of caregiver support in implementing safe and effective care. The clinical experts cautioned that outpatient delivery would still require significant health system resources to deliver safe follow-up care for patients who may present with severe side effects or require ongoing care.
Although the clinical experts were frank about the health system capacity challenges facing the implementation of cilta-cel, they noted the potential benefits of doing so for patients and thus emphasized the need to address capacity issues. Thus, the findings in this review echo previous CADTH ethics reviews of CAR T-cell therapies, which have identified the need to also invest in the infrastructure required to implement CAR T-cell therapies.3,5
Resource Allocation in the Context of Capacity Limitations
While the clinical experts stressed the importance of addressing capacity limitations, they noted that, in the interim, capacity insufficiency necessitates developing fair priority-setting criteria to inform the prioritization of patients for access to cilta-cel. The need for priority-setting guidance was also raised in the clinician group and drug program input and has been identified in previous CADTH ethics reviews of CAR T-cell therapies.3-5
Insufficient supply and/or capacity to deliver cilta-cel were cited as raising ethical questions related to distributive justice (e.g., who should be prioritized for access to cilta-cel?) as well as procedural justice (e.g., who should decide how to allocate limited resources and capacity? What constitutes a fair allocation process?). The development of pan-Canadian priority-setting criteria and/or pan-Canadian coordination were identified as important for facilitating fair processes, equitable access to CAR T-cell therapies across the country, and reducing inefficiencies related to the duplication of efforts involved in developing priority-setting criteria. In the absence of such guidance, it was noted that individual centres or jurisdictions would likely need to develop their own criteria, but that this could result in discrepancies across the country, as some centres and jurisdictions could implement cilta-cel more easily than others. The clinical experts noted that discussions related to priority-setting criteria were under way for already established CAR T-cell therapies for other indications in Canada, and that these could potentially inform related criteria for the use of cilta-cel for the treatment of r/rMM.
The clinical experts suggested the value of developing pan-Canadian guidance that would outline at least the minimal expectations or criteria for prioritizing access to cilta-cel. The clinical experts discussed, but did not outline or agree on, a finalized list of potential priority-setting criteria, such as: first-come, first-served after meeting a basic list of eligibility criteria; most likely to benefit (e.g., based on durability of response, fitness to undergo treatment, ECOG Performance Status); least likely to benefit from alternative therapies or those ineligible for alternative therapies (e.g., stem cell transplant); and least likely to incur severe morbidity (e.g., CRS) or mortality due to treatment. However, the clinical experts agreed that criteria should be informed by biological and clinical considerations rather than, for example, the use of strict age- or other demographic-related cut-offs. Previous CADTH ethics reviews of CAR T-cell therapies have also noted the importance of considering the allocation of CAR T-cell centres in a way that explicitly considers regional, rural–urban, and sociodemographic equity.3 Accordingly, the implementation of novel CAR T-cell therapies, including cilta-cel, can be understood as necessitating the development of priority-setting criteria to inform the equitable allocation of limited resources using fair decision-making processes. The absence of such guidance risks hampering the equitable delivery of cilta-cel in Canada.
Funding Models and Opportunity Costs
Clinical experts, drug program input, and published literature have reported concerns about the Canadian health care system’s ability to sustain the financial costs associated with the reimbursement and implementation of additional CAR T-cell therapies, including cilta-cel.3,24 Moreover, as discussed earlier in the section on economic models, uncertainty about the cost-effectiveness of cilta-cel could present challenges for decision-making with respect to reimbursement and resource allocation for CAR T-cell therapies.25
A past CADTH ethics review of another CAR T-cell therapy noted that funding reforms for high-cost therapies have been suggested in the Canadian context, such as through the use of performance- or outcomes-based funding agreements to share the risks associated with funding high-cost therapies.3 Risk-sharing payment models have been used in other jurisdictions (especially in Europe), including, for example, the use of outcome-based payment agreements in Germany for CAR T-cell therapies.26 As discussed earlier in the section on economic models, the sponsor has suggested that VBAs “may be uniquely suited for CAR T-cell therapies” for facilitating patient access while mitigating the uncertainty of cilta-cel long-term efficacy in the real world. From a health system perspective, it is important to consider the clinical and data infrastructure required to implement VBAs. While VBAs could potentially mitigate some of the financial risks associated with reimbursing CAR T-cell therapies in the absence of long-term data,25-27 the clinical experts noted CAR T-cell therapies would still remain highly expensive therapies from a health system perspective — a point that was made in a previous CADTH ethics review of CAR T-cell therapies concerning the limited impact of price negotiations and the high costs associated with the delivery of CAR T-cell therapies.5
The clinical experts also discussed the opportunity costs associated with reimbursing CAR T-cell therapies, including cilta-cel, and funding the associated implementation requirements and the challenges that reimbursing such therapies might present for fixed health care budgets where not all services or therapies can be funded or reimbursed. They also noted that the implementation of resource-intensive CAR T-cell therapies, including cilta-cel, raised concerns related to the opportunity costs of allocating limited health system resources (e.g., hospital beds, intensive care unit capacity, access to clinical specialists) to the implementation of CAR T-cell therapies. As discussed earlier, the uncertainty in the pharmacoeconomic models used to evaluate cilta-cel due to the absence of long-term and comparative effectiveness data presents an additional challenge for assessing the opportunity costs of implementing cilta-cel — and thus informing the equitable and fair allocation of limited health care resources — as it hinders the ability to assess the magnitude of the benefit of cilta-cel relative to other therapies or health care services under consideration. A previous CADTH ethics review of CAR T-cell therapies noted that the funding of CAR T-cell therapies could impact the sustainability of health systems, and that fair and just funding allocation criteria, and the fair distribution of the risks and benefits of innovation, should be considered; moreover, these concerns have become even more salient as a growing number of CAR T-cell therapies, such as cilta-cel, are approved and may be reimbursed for use in Canada.3,5,24,25 Accordingly, clarity and transparency are required to justify policy decisions about expanding access to CAR T-cell therapies in the context of existing systems constraints, competing health care priorities, and the long-term sustainability of health systems.3
Limitations
This review is limited by the paucity of published literature examining ethical considerations directly related to the use of cilta-cel for the treatment of adult patients with r/rMM in Canada. Notably, demographic data (e.g., socioeconomic, racial and ethnic) for MM, as well as data concerning the postmarket and real-world use and implementation of CAR T-cell therapies (including for population subgroups), is lacking in the Canadian context. Nonetheless, the absence of directly related published ethical analyses does not mean that ethical considerations are absent in this context; many ethical considerations that arise and have been identified in the context of MM more broadly, or those related to CAR T-cell therapies in general, are also pertinent to this context. Inputs from patient and clinician groups, drug programs, and the clinical experts gathered for this Reimbursement Review supplemented the available published literature to provide a more thorough understanding of the ethical considerations related to the use of cilta-cel for the treatment of r/rMM.
It is possible that more explicit engagement with a broader range of stakeholders (such as through direct interviews with patients, caregivers, family members, health care providers, or health system decision-makers) might have revealed additional domains of analysis. Given the proposed high cost and budget impact of this therapy, is it also possible that inputs from, or consultation with, the general public might have contributed additional ethical considerations concerning the funding, priority setting, and implementation of cilta-cel within the context of the Canadian health care system and the resource limitations that it faces.
Conclusion
Cilta-cel has been proposed as a novel fourth-line therapy for adults with r/rMM. Inputs from patient and clinician groups, clinical experts, and drug programs, and relevant published literature, were reviewed to identify ethical considerations relevant to the use of cilta-cel for adults with r/rMM beyond the third line of therapy. Ethical considerations in the context of MM as a currently incurable disease that requires unrelenting treatment highlighted the burden of MM on patients and caregivers, who expressed the need for an effective treatment that improves symptoms and quality of life, has manageable side effects, and offers a treatment-free window. Furthermore, disparities in incidence, diagnosis, treatment, and outcomes for racialized, marginalized, and low socioeconomic groups were reported in the context of MM, although more data are required to inform a greater understanding of disparities within the Canadian context. With respect to the evidence used to evaluate cilta-cel, evidence from the pivotal clinical trial may not have been fully representative (e.g., across race and age) of patients living in Canada. Moreover, the lack of long-term and comparative clinical data limited the certainty of pharmacoeconomic assessments, and the proposed funding model may have overestimated the value of the therapy and underrepresented the budget impact of implementation.
The implementation of cilta-cel in clinical practice raises several access-related considerations, given limited delivery capacity and resulting geographic barriers to accessing CAR T-cell therapy; notably, barriers to access may disproportionately impact racialized, marginalized, and low socioeconomic groups as well as those lacking caregiver support. As well, the implementation of cilta-cel raises several ethical considerations for health systems, including challenges associated with scaling CAR T-cell delivery across Canada due to complex and resource-intensive infrastructure and personnel requirements. The development of fair, consistent criteria to prioritize access to cilta-cel would facilitate equitable access across Canada, especially if demand, which may be exacerbated for r/rMM in the absence of curative or other effective fourth-line therapies, exceeds supply or delivery capacity. Additionally, the high cost of implementing cilta-cel, including in the context of an increasing number of CAR T-cell therapies, presents a challenge for health care budgets and raises questions about the systems-level opportunity costs of reimbursing cilta-cel.
As with previous CAR T-cell therapies, the absence of long-term and comparative evidence for the safety and efficacy of cilta-cel necessitates robust postmarket surveillance to better understand the risk-benefit profile as well as the cost-effectiveness of cilta-cel in practice. Moreover, where possible, postmarket surveillance and the use of real-world evidence may contribute to a better understanding of how the safety and efficacy of cilta-cel in clinical practice may be impacted by nonclinical factors, and whether this has an impact on how the benefits and burdens associated with the use of this therapy are distributed fairly across diverse demographic subgroups within the population of patients with MM in Canada.
References
1.EUnetHTA Joint Action 2 Work Package 8, HTA Core Model version 3.0 2016; https://www.htacoremodel.info/BrowseModel.aspx. Accessed 2023 Feb 15.
2.Benkhalti M, Espinoza M, Cookson R, Welch V, Tugwell P, Dagenais P. Development of a checklist to guide equity considerations in health technology assessment. Int J Technol Assess Health Care. 2021;37(1). PubMed
3.CADTH. CADTH Reimbursement Review: axicabtagene ciloleucel (Yescarta) [in progress]. Ottawa: CADTH; 2022: https://www.cadth.ca/axicabtagene-ciloleucel. Accessed 2022 Dec 7.
4.CADTH Reimbursement Review: idecabtagene vicleucel (Abecma). Canadian Journal of Health Technologies. Vol 22022: https://www.cadth.ca/sites/default/files/DRR/2022/PG0240-Abecma.pdf. Accessed 2022 Dec 1.
5.Axicabtagene ciloleucel for large B-cell lymphoma: ethics and implementation report. (CADTH optimal use report vol. 9, no. 1e). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/pdf/car-t/ct0002-ipe-report.pdf. Accessed 2022 Jul 7.
6.Sandelowski M. Whatever happened to qualitative description? Research in nursing & health. 2000;23(4):334-340. PubMed
7.LeBlanc MR, LeBlanc TW, Bryant AL, Pollak KI, Bailey Jr DE, Smith SK. A Qualitative Study of the Experiences of Living With Multiple Myeloma. Oncology Nursing Forum. 2021;48(2):151-160. PubMed
8.Borregaard Myrhoj C, Novrup Clemmensen S, Sax Rogind S, Jarden M, Toudal Viftrup D. Serious illness conversations in patients with multiple myeloma and their family caregivers-A qualitative interview study. Eur J Cancer Care (Engl). 2022;31(1):e13537. PubMed
9.Cormican O, Dowling M. Providing Care to People Living with a Chronic Hematological Malignancy: A Qualitative Evidence Synthesis of Informal Carers' Experiences. Semin Oncol Nurs. 2022:151338. PubMed
10.Richter J, Sanchez L, Biran N, et al. Prevalence and Survival Impact of Self-Reported Symptom and Psychological Distress Among Patients With Multiple Myeloma. Clin Lymphoma Myeloma Leuk. 2021;21(3):e284-e289. PubMed
11.Cohen AD, Hari P, Htut M, et al. Patient Perceptions Regarding Ciltacabtagene Autoleucel Treatment: Qualitative Evidence From Interviews With Patients With Relapsed/Refractory Multiple Myeloma in the CARTITUDE-1 Study. Clinical Lymphoma, Myeloma and Leukemia.
12.Pritlove C, Jassi M, Burns B, McCurdy A. The work of managing multiple myeloma and its implications for treatment-related decision making: a qualitative study of patient and caregiver experiences. BMC Cancer. 2021;21(1):793. PubMed
13.Choon-Quinones M, Hose D, Kalo Z, et al. Patient and Caregiver Experience Decision Factors in Treatment Decision Making-Results of a Systematic Literature Review of Multiple Myeloma Decision Aids. Value Health. 2022;22:22. PubMed
14.Delon C, Brown KF, Payne NWS, Kotrotsios Y, Vernon S, Shelton J. Differences in cancer incidence by broad ethnic group in England, 2013-2017. Br J Cancer. 2022;126(12):1765-1773. PubMed
15.Xu J, Xu P, Han Q, Sun J, Chen B, Dong X. Socioeconomic status-based survival disparities and nomogram prediction for patients with multiple myeloma: Results from American and Chinese populations. Front. 2022;12:941714. PubMed
16.Mian HS, Seow H, Wildes TM, et al. Disparities in treatment patterns and outcomes among younger and older adults with newly diagnosed multiple myeloma: A population-based study. J Geriatr Oncol. 2021;12(4):508-514. PubMed
17.Tsang M, Le M, Ghazawi FM, et al. Multiple myeloma epidemiology and patient geographic distribution in Canada: A population study. Cancer. 2019;125(14):2435-2444. PubMed
18.Mohyuddin GR, Sinnarajah A, Gayowsky A, Chan KKW, Seow H, Mian H. Quality of end-of-life care in multiple myeloma: A 13-year analysis of a population-based cohort in Ontario, Canada. Br J Haematol. 2022;10:10. PubMed
19.Molina A, Muffly L. CT-095 Disparities and Incomplete Capture of Race/Ethnicity Data in Adults With Hematologic Malignancies Referred for Cellular Therapies. Clin Lymphoma Myeloma Leuk. 2022;22 Suppl 2:S433-S434.
20.Al Hadidi S, Schinke C, Thanendrarajan S, Zangari M, van Rhee F. Enrollment of Black Participants in Pivotal Clinical Trials Supporting US Food and Drug Administration Approval of Chimeric Antigen Receptor-T Cell Therapy for Hematological Malignant Neoplasms. JAMA netw. 2022;5(4):e228161.
21.Alqazaqi R, Schinke C, Thanendrarajan S, et al. Geographic and Racial Disparities in Access to Chimeric Antigen Receptor-T Cells and Bispecific Antibodies Trials for Multiple Myeloma. JAMA netw. 2022;5(8):e2228877.
22.Martin T, Usmani SZ, Berdeja JG, et al. Ciltacabtagene Autoleucel, an Anti-B-cell Maturation Antigen Chimeric Antigen Receptor T-Cell Therapy, for Relapsed/Refractory Multiple Myeloma: CARTITUDE-1 2-Year Follow-Up. J Clin Oncol. 2022:JCO2200842. PubMed
23.Knight JM, Hackett E, Szabo A, et al. Associations between socioeconomic status and bispecific LV20.19 CAR T cell therapy outcomes. Haematologica. 2022;06:06.
24.Gagelmann N, Sureda A, Montoto S, et al. Access to and affordability of CAR T-cell therapy in multiple myeloma: an EBMT position paper. Lancet Haematol. 2022;9(10):e786-e795. PubMed
25.Choi G, Shin G, Bae S. Price and Prejudice? The Value of Chimeric Antigen Receptor (CAR) T-Cell Therapy. Int J Environ Res Public Health. 2022;19(19):28. PubMed
26.Goncalves E. Value-based pricing for advanced therapy medicinal products: emerging affordability solutions. Eur J Health Econ. 2022;23(2):155-163. PubMed
27.Kannarkat JT, Good CB, Parekh N. Value-Based Pharmaceutical Contracts: Value for Whom? Value Health. 2020;23(2):154-156. PubMed
28.Ahmed N, Shahzad M, Shippey E, et al. Socioeconomic and Racial Disparity in Chimeric Antigen Receptor T Cell Therapy Access. Transplant Cell Ther. 2022;28(7):358-364. PubMed
29.Emole J, Lawal O, Lupak O, Dias A, Shune L, Yusuf K. Demographic differences among patients treated with chimeric antigen receptor T-cell therapy in the United States. Cancer Med. 2022;08:08.
30.Blue B. Socioeconomic and Racial Disparity in Chimeric antigen receptor T cell (CART)Therapy Access. Transplant Cell Ther. 2022;28(7):345-346. PubMed
31.Weinkove R, George P, Ruka M, Haira TH, Giunti G. Chimeric antigen receptor T-cells in New Zealand: challenges and opportunities. N Z Med J. 2021;134(1542):96-108. PubMed
32.First Nations Information Governance Centre. The First Nations Principles of OCAP®. https://fnigc.ca/ocap-training/. Accessed 2022 Dec 5.
Appendix 1: Details of Included Studies
Table 1: Details of Included Publications
First author (year) | Publication type | Objective | Key ethical considerations | Funding source |
|---|---|---|---|---|
Ahmed (2022)28 | Database analysis | To determine patterns of racial and ethnic distribution, socioeconomic strata, insurance coverage, and travel time of CAR T-cell recipients | Universal access to CAR T-cell therapy is limited. There are disparities in access to commercial and clinical trial CAR T-cell therapy for racialized groups, especially Black and Hispanic patient populations. Majority of patients in clinical trials are white; Black patients are less likely to receive CAR T-cell therapy. Few CAR T-cell recipients are from neighbourhoods with lower incomes. | None declared |
Alqazaqi (2022)21 | Cross-sectional study | To examine whether there is equitable geographic access to CAR T-cell therapy and bispecific antibodies trials for MM in the US | Few Black patients live in a county with open CAR T-cell and bispecific antibodies trials for MM, and states with the highest proportion of Black residents had no or few trials. Geographic distribution of clinical trials may contribute to disparities in access to clinical trials for new MM therapies. | None declared |
Al Hadidi (2022)20 | Cross-sectional study | To examine the enrolment of Black participants in clinical trials that resulted in subsequent FDA approval of CAR T-cell products in hematological malignant neoplasms | Black persons were underrepresented in clinical trials that supported CAR T-cell therapies in the US. Lack of access to trials may further widen existing disparities. Need to match enrolment to disease prevalence. | None declared |
Blue (2022)30 | Commentary | To highlight similarities in social barriers to access between stem cell transplant and novel CAR T-cell therapies | CAR T-cell therapies are not universally accessible — particularly for “minority” [from original source] populations or those living outside geographic catchment areas of specialized treatment centres. Disparities in access to CAR T-cell therapies across racial and socioeconomic factors are reflective of those for stem cell transplant. Community oncologists may have limited familiarity with CAR T-cell therapies, which could result in their patients not being referred to tertiary cancer centres; education is necessary. | None Reported |
Borregaard (2022)8 | Qualitative interview study | To discuss the role of serious illness conversations with patients and their family caregivers in MM care | Need to support serious illness conversations to address anxiety and improve quality of end-of-life care. | Danish Cancer Society; Raimond and Dagmar Foundation |
CADTH (2019)5 | Ethics Review Report | To discuss the major ethical issues raised by the implementation of axicabtagene ciloleucel for adults with relapsed or refractory non-Hodgkin lymphoma | The long-term risks and benefits of CAR T-cell therapies remain unknown. There are several access challenges in the context of CAR T-cell therapies, including those related to geography, supply, and patient selection. Need to consider the context of “hype” around CAR T-cell therapies and implications for informed consent. Considerations of ownership of genetic materials in the context of CAR T-cell therapy. | Canada’s federal, provincial, and territorial governments, with the exception of Quebec |
CADTH (2022)4 | Ethics Review Report | To identify and describe ethical considerations raised in the literature associated with the use of idecabtagene vicleucel for treatment of relapsed or refractory MM who have received at least 3 prior therapies | There are disparities in the incidence, treatment, and outcomes of patients with MM. There are disparities in clinical trial inclusion for cancer therapies, including for MM. Considerations related to consent for CAR T-cell therapy in persons with MM. | Canada’s federal, provincial, and territorial governments, with the exception of Quebec |
CADTH (2022)3 | Ethics Review Report | To identify and describe ethical considerations associated with the use axicabtagene ciloleucel for the treatment of adults with relapsed or refractory large B-cell lymphoma | There are disparities in the incidence, treatment, and outcomes of patients with LBCL. Barriers to access for CAR T-cell therapies include those related to costs, geography, patient selection, and inequities that may arise during referral. Need to balance risks and benefits of CAR T-cell therapies and provide informed consent and balanced communication to patients. Resource allocation considerations call for fair prioritization processes, opportunities to expand access, and implications for health systems. | Canada’s federal, provincial, and territorial governments, with the exception of Quebec |
Choi (2022)25 | Commentary | To describe the challenges of providing a reliable cost-effectiveness analysis for CAR T-cell therapies | High costs of CAR T-cell therapies are a barrier to access. Serious adverse events are a barrier of access to CAR T-cell therapies. Limited long-term data for clinical effectiveness and safety data are barriers to access and present financial risks for payers as they make it challenging to produce accurate cost-effectiveness analyses. | National Research Foundation |
Choon-Quinones (2022)13 | Systematic literature review | To describe the range of patient and caregiver decision factors in MM | Many patients with MM, irrespective of older age on average, wish to have an active role in decision-making. Patients with MM and their caregivers consider various factors in MM-related decision-making, including related to finances, administration and transportation, beliefs and values, quality of life, social support, and caregiver burden. | International Myeloma Foundation; Bristol-Myers Squibb |
Cohen (2022)11 | Qualitative interview study | To describe the experiences of participants enrolled in the CARTITUDE-1 trial pre–cilta-cel and post–cilta-cel on living with MM, therapy expectations, and treatment experiences | At intake, participants reported seeking improvements in their MM symptoms and a return to perceived “normalcy.” Following treatment, participants reported finding cilta-cel easier than prior treatments and chemotherapy, appreciating the treatment-free window, and experiencing improvements in symptoms, physical functioning, and health-related quality of life; most reported no change in relationships and social functioning. | Janssen Research and Development, LLC; Legend Biotech US Inc. |
Cormican (2022)9 | Qualitative evidence synthesis | To describe the experiences of informal carers for a patient with a chronic hematological malignancy | Late end-of-life discussions impair informal carers’ focus on patients’ quality of life; conversations on end-of-life care can be promoted by early supportive relationships with clinicians. | Structured Population health, Policy and Health-services Research Education (SPHeRE) program |
Delon (2022)14 | Database analysis | To determine patterns of age-related and racial and ethnic distribution of cancer incidence in England | Incidence rates for most cancers were lower in racialized groups, with some exceptions, including a higher incidence of MM in Black people. | None declared |
Emole (2022)29 | Database analysis | To evaluate if demographic differences existed among adult patients who received CAR T-cell therapy and to assess predictors of CAR T-cell treatment outcomes | Not all Americans have benefited equally from CAR T-cell therapy. Recipients of CAR T-cell therapies are more likely to be white and to be residents of metropolitan areas with access to teaching hospitals. Racial disparity in receiving CAR T-cell therapy affected Black patients more disproportionately than other racialized groups. | None declared |
Gagelman (2022)24 | Consensus statement (for the European Society for Blood and Marrow Transplantation) | To identify considerations and proposed solutions related to the affordability and access of CAR T-cell therapies for patients with multiple myeloma | The high costs of CAR T-cell therapies, especially as the number of CAR T-cell therapies continues to grow, present multiple access and affordability-related challenges, including related to manufacturing and delivery capacity, and individual and societal financial toxicity. | Authors received support from Janssen, Kite/Gilead, Novartis, Bristol-Myers Squibb, and Celgene |
Gonçalves (2022)26 | Commentary | To describe the challenges of traditional value assessment and price reimbursement models in the evaluation of advanced therapy medicinal products (ATMPs), and describe current and prospective financing solutions, including value-based agreements for ATMPs | Outcome-based payment agreements have been implemented in the context of CAR T-cell therapies, including in Germany. Outcome-based agreements represent a risk-sharing mechanism aimed at allowing patient access while protecting payer affordability. | None reported |
Leblanc (2021)7 | Qualitative interview study | To describe the experiences of persons with MM with respect to diagnosis and treatment | MM and MM-related treatment impact patients’ lives in multiple ways, including through the impact of life-long treatment, social impacts and isolation, financial pressures, and impact on relationships. | Duke University School of Nursing Student Pilot Fund; LeBlanc and the Duke Palliative Care: Pilot Awards to Integrate Palliative Care into Duke Health; National Institute of Nursing Research of the National Institutes of Health |
Kannarkat (2020)27 | Commentary | To identify considerations related to the design of value-based pharmaceutical contracts | It is often unclear who benefits, and how, from value-based pharmaceutical contracts. Use of meaningful clinical outcomes, rather than short-term surrogate outcomes, for contracts can incentivize favourable clinical outcomes. | None declared |
Knight (2022)23 | Observational cohort study | To determine patterns of socioeconomic distribution in patient response to treatment with novel bispecific antibodies or CAR T-cell therapy | Patients of lower socioeconomic status had significantly elevated levels of cytokines, circulating neurotoxic kynurenine metabolites, earlier onset of CRS, greater pain, and worse quality sleep. | Authors received support from Phytecs, Inc., Formulate Biosciences, Miltenyi Biotec, Kite Pharma, Bristol-Myers Squibb, TG therapeutics, Lilly, Epizyme, Legend, Incyte, Novartis, and Umoja |
Mian (2021)16 | Database analysis | To determine patterns of age-related disparities in treatment patterns and outcomes in adults with newly diagnosed MM in Canada | Despite improvements, age-related treatment disparities exist, with rates of no treatment and early mortality among patients not treated and those started on novel drugs are higher in older adults with newly diagnosed MM. | Juravinski Cancer Centre Foundation; Institute for Clinical and Evaluative Sciences (ICES) |
Mohyuddin (2022)18 | Database analysis | To determine patterns of age-related, geographic, and socioeconomic distribution of high-quality end-of-life care for persons with MM in Ontario, Canada | There are disparities in the provision of end-of-life care, with patients aged 80 or older less likely to receive aggressive and supportive care, patients residing in smaller-size rural communities more likely to receive aggressive care, and patients residing in lower-income neighbourhoods less likely to receive supportive care. | Canadian Centre for Applied Research in Cancer Control (ARCC); Canadian Cancer Society Research Institute (CCSRI) |
Molina (2022)19 | Retrospective review of patient electronic medical records (abstract) | To determine patterns of racial and ethnic distribution in cellular therapy referral of adults with hematologic malignancies | The racial and ethnic distribution of patients treated is consistent with the distribution of patients referred, which may suggest that reported disparities occur at the level of referral. | None reported |
Pritlove (2021)12 | Qualitative interview study | To describe the experiences of patients with MM and their caregivers in treatment, treatment management, and treatment-related decision-making | The shift of delivery of care for MM from hospital to home has required increased patient and caregiver active illness management. MM impacts psychosocial and relational well-being. Patients’ treatment-related decision-making includes consideration of burden on caregivers and loved ones. | Takeda Canada, Inc. |
Richter (2021)10 | Survey study | To identify the prevalence and nature of patient-reported symptom burden and psychological distress in patients with MM | Patients with MM suffer from anxiety, depression, and psychological distress due to various illness- and treatment-related factors, including symptom, financial, and psychosocial concerns. Patient-reported outcomes can help inform therapeutic decisions. | None declared |
Tsang (2019)17 | Database analysis | To determine patterns of geographic and urban-rural distribution on the incidence of MM in Canada | There are geographic disparities in MM incidence, with lower incidence in large urban centres and high-latitude regions, and higher incidence in smaller municipalities and rural areas; the latter were associated with increased agricultural density. | Grants from the Cole Foundation, Canadian Dermatology Foundation, and Fonds de Recherche du Quebec–Santé |
Weinkove (2021)31 | Review | To outline CAR T-cell manufacturing and logistical considerations, with a focus on New Zealand’s environment for personalized cell and gene therapy | CAR T cells are manufactured in a limited number of sites; shipping of cells can pose challenges. Tissue and genetic material valued differently by different cultural groups (e.g., Māori). Details of processing and ownership must be made clear in consent processes. Consultation with diverse groups (e.g., Māori) is essential in CAR T-cell research and delivery, including development of educational material for these groups and their clinicians. | Health Research Council of New Zealand; Ministry of Business Innovations and Employment; LifeBlood Trust; Freemasons New Zealand |
Xu (2022)15 | Database analysis | To determine patterns of socioeconomic strata on the survival and clinical outcomes of MM patients in US and China | There are socioeconomic-related disparities in survival, with lower socioeconomic status significantly associated with lower overall survival and myeloma-specific survival. | Jiangsu Provincial Medical Innovation Team, the Nanjing Medical Science and Technique Development Foundation |
CAR = chimeric antigen receptor; LBCL = large B-cell lymphoma; MM = multiple myeloma.
Stakeholder Input
Patient Input
Myeloma Canada
About Myeloma Canada
Multiple myeloma, also known as myeloma, is the 2nd most common form of blood cancer. Myeloma affects a type of immune cell called the plasma cell, found in the bone marrow. Every day, 11 Canadians are diagnosed, yet despite its growing prevalence, the disease remains relatively unknown. Myeloma is a relapsing cancer which with treatment can enter periods of remission, but myeloma will always ultimately return and require further treatment. Myeloma patients also become ‘refractory’ to a treatment, meaning it can no longer control their myeloma, and they require a new regimen. Myeloma Canada has existed for over 15 years to support the growing number of Canadians diagnosed with myeloma each year, and those living longer than ever with the disease through access to new and innovative therapies. Over the years, as a part of this mission Myeloma Canada has collected data on the impact of myeloma and its treatments on patients and caregivers, by conducting surveys. The compiled data are then presented to the Pan-Canadian Oncology Drug Review. www.myeloma.ca
Information Gathering
Myeloma Canada is sharing the input received from patient and caregiver surveys regarding cilcabtagene autoleucel (ciltacel) CAR T-cell therapy. Our patient and caregiver surveys were available from August 28 to September 29, 2022, and both were shared across Canada and internationally, via email and social media. 200 complete responses to the patient survey were received, from Alberta (19), British Columbia (43), Manitoba (2), New Brunswick (3), Newfoundland and Labrador (4), Nova Scotia (4), Ontario (86), Quebec (32), Saskatchewan (5), and (2) from outside of Canada, (France and Trinidad and Tabago). To the caregiver survey, 26 complete responses were received, from Ontario (11), British Columbia (5), Quebec (5), Saskatchewan (3), Manitoba (1), and Nova Scotia (1). Survey eligibility was determined by patient and caregiver self-report of their experience with myeloma, that they have relapsed/refractory myeloma, received at least one prior line of therapy, or they care for someone who does. 71 incomplete responses wherein a respondent did not finish answering survey questions, and 21 disqualified responses wherein a respondent answers indicated they did not meet the eligibility requirements were removed from the patient and caregiver datasets. All patients and caregivers were asked similar questions regarding disease experience, then were divided into subsets, and posed different questions based on their experience with CAR-T cell therapy and/or the treatment under review. These subsets are, relapsed/refractory patients referred to as ‘R/R patients’ and relapsed/refractory caregivers, referred to as ‘R/R caregivers’, CAR T patients (who have not received cilta-cel), and finally, cilta-cel patients and caregivers.
Disease Experience
All patients were asked “How important it is for you to control various aspects of myeloma (Please rate on a scale of 1 ‘Not important,’ to 5 ‘extremely important’)”. Among the 199 patient responses ‘infections’ was the most important aspect to control and was rated ‘5-extremely important’ most frequently (136). By the weighted average of responses, patients (199) also felt mobility (4.38; SD 0.94), and kidney problems (4.31; SD 1.02) were slightly more important to control, though all options listed received an average rating of ‘4 – very important’. Patients also left comments that frequently mentioned gastrointestinal, and mental health issues were important. COVID-19 was also mentioned in patient comments.
When asked to “Rate on a scale of 1–5 (1 is ‘Not at all’, and 5 is ‘Significant impact’), how symptoms associated with myeloma impact or limit your day-to-day activities and quality of life.”; by weighted average rating, patients (198) indicated that their ability to work (3.92; SD 1.24) was most significantly impacted, followed by ability to travel (3.84; SD 1.23), and to exercise (3.65; SD 1.18). Patient comments included multiple mentions of myeloma’s significant impact on mental health. Caregivers were asked “Please rate on a scale of 1 – 5, how caring for a person with multiple myeloma impacts or limits your day-to-day activities and quality of life. 1 is ‘Not at all l’, and 5 is ‘Significant impact l’”. By weighted average rating, caregivers’ ‘ability to travel’ (4; SD 1.36) was most significantly impacted, followed by ‘ability to work’ (3.6; SD 1.37), and ‘ability to spend time with family and friends’ (3.3; SD 1.40).
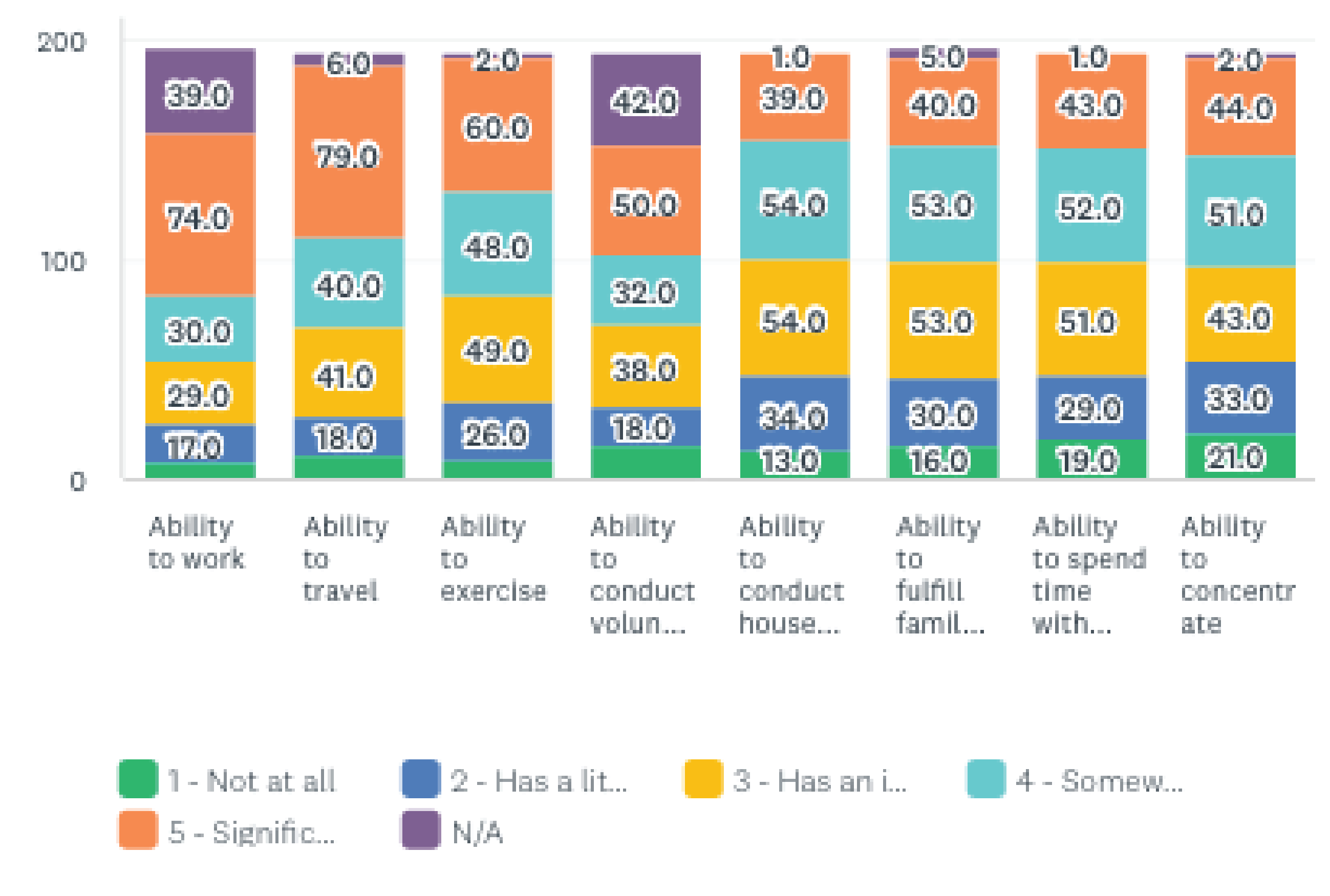
Patients and caregivers were asked, “What is the most significant financial implication of your treatment? /What are the most significant financial implications of caring for someone undergoing myeloma treatment? If there is more than one implication, please check all that apply.” Patients (198) identified: travel costs 33.8% (67), drug costs and parking costs, both receiving 28.3% (56 responses), lost income due to absence from work or disability 26.8% (53), and lost income/pension due to early retirement 20.2% (40) to be the most significant financial implications they had experienced. Patients and caregivers’ responses together rated ‘lost income/income or retirement’ as the most significant implications with 93 responses (47%).). 13 respondents selected ‘other’ and provided comments, noting the costs of supportive care treatments to manage side effects. Caregivers only (26) identified the most significant implications to be drug costs 46.2% (12), parking costs 42.3 (11), and travel costs 38.5% (10).
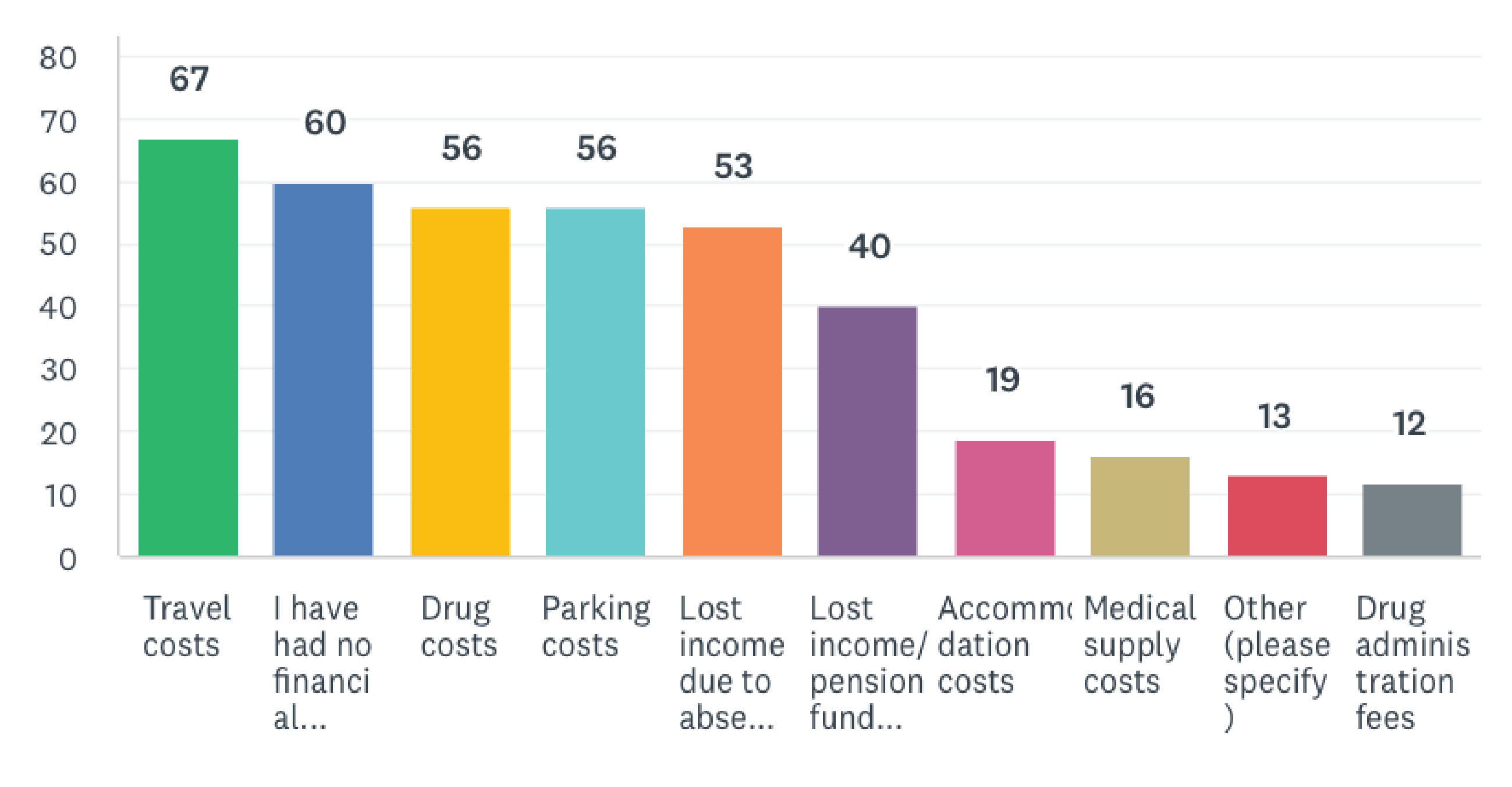
When patients (197) were asked “Do you need the support of a caregiver or family member to help you manage your myeloma or your treatment-related symptoms?”, 58% (114) responded that they required a caregiver, of which 2% (4) indicated ‘yes but I am unable to access the help I need’. Caregivers (26) were asked to identify “Are you a… A) Family caregiver B) Professional caregiver C) Friend caregiver D) Other (please specify)”. The majority of respondents (23) chose ‘A) Family caregiver’, one indicated they were a friend caregiver, and two responding caregivers selected ‘Other’ but their comments indicated they were family caregivers (an aunt, and a common-law spouse); so ultimately 96.2% (25) of respondents were family caregivers.
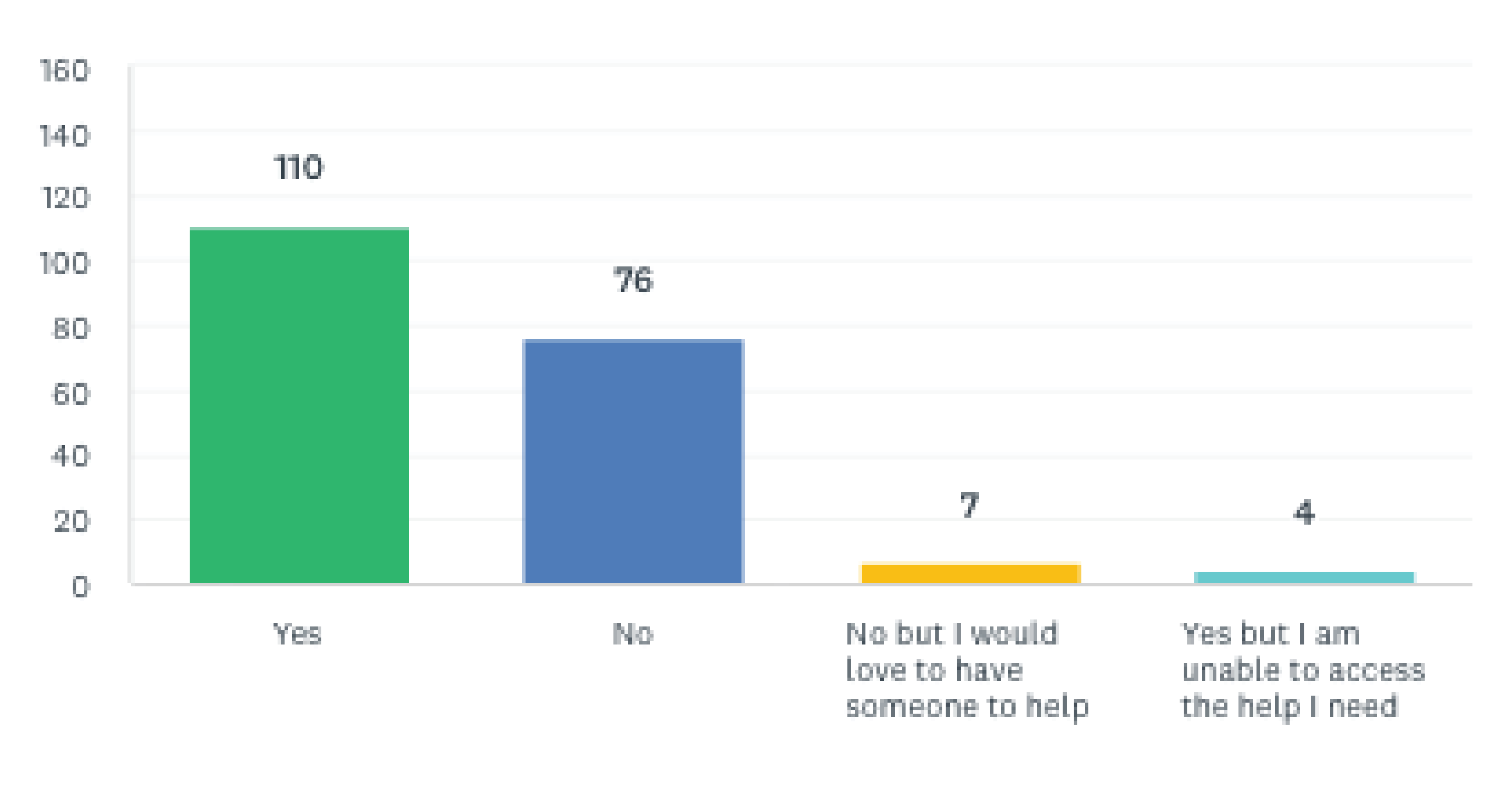
Experiences With Currently Available Treatments
When patients and caregivers were asked how often they leave home or accompany their loved ones to undergo tests or treatment, patient respondents (200)—most frequently selected ‘once a month’ 40%, then ‘once a week’ 28.7%. Caregivers (26) most often selected ‘once a week’ 34.5% (9), followed by ‘once a month’ 19.2% (5). Patients (188) were asked, “If you have received a stem cell transplant to treat your myeloma please rate the severity of side effects, you experienced due to maintenance therapy, on a scale of 1-5 where 1 is ‘no side effects’, and 5 is ‘very severe side effects’”. The greatest proportion of respondents chose ‘3- some side effects’ at 36.4% (47), followed by ‘4- significant side effects’ at 29% (37). Then patients (189) were asked what kind of impact the side effects associated with maintenance therapy had on their overall wellbeing, and quality of life? 50.4% (64) chose ‘2-some negative impact’, for a weighted average rating of 2.5. Caregivers (26) were asked “Following a stem cell transplant, patients typically are required to take certain drugs to control the growth of their myeloma, referred to as maintenance. If the person you care for received a stem cell transplant, please rate on a scale of 1 – 5, what kind of impact the side effects associated with maintenance therapy had on your duties as a caregiver? 1 is ‘significant negative impact’, and 5 is ‘significant positive impact’.” The weighted average of responses was 2.5, and the greatest proportion of caregivers to whom the question applied, 31% (8), chose ‘2-some negative impact’. All patients were asked to identify the factors they consider to be most important to (any) myeloma treatment. Respondents (173) most frequently mentioned quality of life and making side effects manageable, along with the effectiveness (especially achieving remission), accessibility/portability of treatment, and having a supportive and communicative care team accessible, to be key factors. Some responses of relevance are as follows:
The current treatments are so harsh they destroy all the goodness of living… Canadians need access to treatments that are available in many other countries. A right to choose alternative newer treatments please help make it a right for all Canadians!
First priority would be good control of my myeloma (remission) with minimal side effects and no organ/bone damage. And ideally minimal trips to the hospital or other community treatment center.
Anything that ties me to hospital prevents me from living my life as a young retiree… side effects that cause low immunities are a real obstacle to travel and the enjoyment of life.
As well, the importance of access to new treatments and funding for them was often stated: “Access to treatment from a financial perspective; quality of life”. Caregivers (22) were asked “What do you think is most important when it comes to caring for someone undergoing myeloma treatment?” The importance of providing emotional support to the person with myeloma and helping keep all disease information/medical records straight were most frequently mentioned. Comments included:
Emotional support is very important in my role as a caregiver. Other important aspects of my role are as medical secretary, medications manager and personal care support.
To understand the experience with the treatment under review or the same category of treatments, we asked patients (200) and caregivers (26) to identify if they or the person they care for received this type of treatment. 3 patients and 1 caregiver indicated “I have...”/” The person I care for has received CAR T-cell therapy, or I am/they are currently waiting to receive CAR T-cell therapy”; while 197 patients (98.8%) and 25 caregivers (96.15%) selected “I have…/The person I care for has not received CAR T-cell therapy and I/they currently have no plan to.” Patients and caregivers who indicated they had experience with CAR T-cell therapy were separated from the group and asked to identify which CAR T-cell therapy they/the person they care for received; 1 patient and 1 caregiver indicated they were treated or the person they care for was treated with ciltabtagene autoleucel (cilta-cel). Both were directed to questions about their experience with the drug under review (discussed in section 6). One patient responded they received ‘ide-cel, bb2121’, while two patients responded they had received an “Other CAR T-cell therapy than those mentioned above”. These three (non-cilta-cel) patients were posed questions about their experience accordingly and will herein be referred to as ‘CAR T patients’. The 197 patients who have not received CAR-T cell therapy but met the relapsed/refractory eligibility requirement will be referred to as R/R patients; the 25 caregivers whose patients have not received CAR-T-cell therapy but met the eligibility requirement will herein be referred to as R/R caregivers. The R/R and CAR T groups are discussed separately below.
R/R patients (197) were asked “How many prior lines of therapy have you received?” 53 patients (27%) indicated they received 3 lines of therapy, 46 patients (23.4%) responded 2 lines of therapy. 134 patients (68%) received 1-3 lines of therapy, 20.3% (40) of patients received 4 or more lines of therapy, and 12% (23) responded ‘I am unsure’.
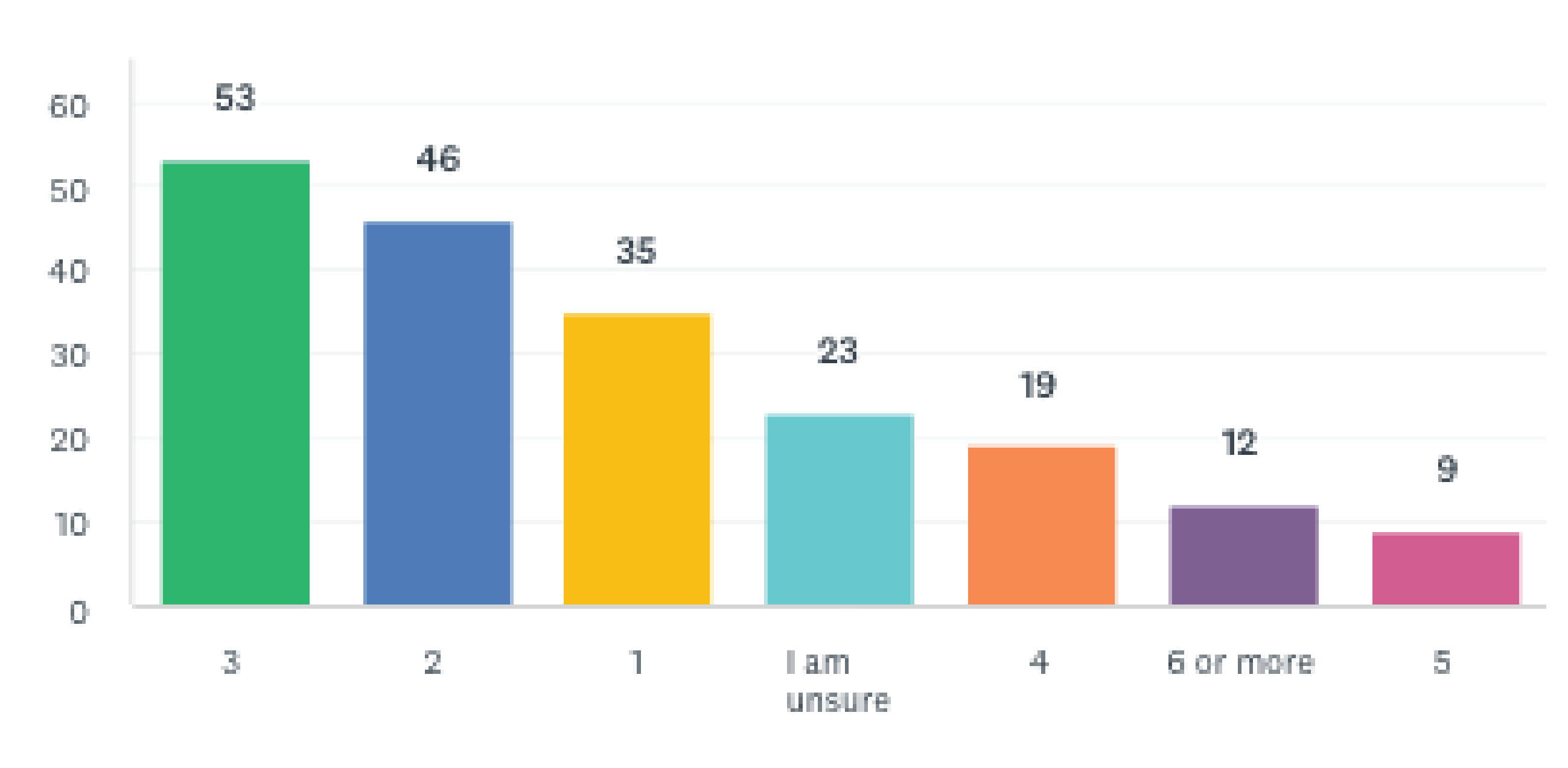
CAR T patients (patients who received a CAR-T cell therapy other than cilta-cel) (2), were asked “Please indicate how long ago you received CAR T-cell therapy?”; one responded, ‘Over two or more years ago’, and one chose ‘I don’t remember’. When asked the current status of their myeloma, one CAR T patient responded, ‘My myeloma did come back, and I am currently on a new treatment”. When asked “Based on your experience with CAR T-cell therapy, how would you rate the effectiveness of this treatment in helping to control your myeloma? 1 being ‘not effective’ and 5 ‘extremely effective’.”, one CAR T patient responded ‘5- extremely effective’. When CAR T patients were asked “Based on your experience with CAR T-cell therapy, how would you rate the effectiveness of this treatment in helping improve your quality of life? 1 being ‘not effective’ and 5 ‘extremely effective’,”, one responded ‘4-very effective’, and one responded ‘N/A’ and provided the comment “Waiting for CAR T- cell therapy. Fall of 2022.”. When asked, “Based on your experience with CAR T-cell therapy, how would you rate the overall tolerability of side effects? 1 being ‘very intolerable’ and 5 ‘Extremely tolerable’.”, the one responding CAR T patient chose ‘4-very tolerable’. CAR T patients were asked “After receiving CAR T-cell therapy, you were most likely not on a treatment for your myeloma either for a prolonged or indeterminate period. How long was this treatment interruption for you?”, one patient indicated this interruption was between ‘1-3’ months. Following which, CAR T patients were asked “How important was this treatment interruption for you?”, the one responding patient chose ‘3- somewhat important’. When asked, “Did treatment with CAR T-cell therapy improve your overall quality of life?” one CAR T patient responded ‘Yes’. When asked “Did treatment with CAR T-cell therapy meet your expectations in treating your myeloma?” the one responding patient chose ‘Yes’.
Improved Outcomes
To the question, “If you are taking a treatment or were to consider taking a treatment for your myeloma, how important is it for the treatment to improve your overall quality of life? Rate on a scale of 1 - 5, 1 is ‘Not important’ and 5 is ‘Extremely important’“, 70.3% (128) of 182 patient respondents from all groups felt it was ‘extremely important’ and 23.6% (43) answered ‘4- very important/R patients (143) and R/R caregivers (15) were asked how desirable an estimated minimum 1-2 years of extended life without needing any drugs to control their or their loved ones myeloma means to them, considering the limited options available for them or their loved one. 74.1% (106) of R/R patients and 60% (9) of caregivers responded, ‘extremely desirable’, and only two R/R patients (0 caregivers) chose ‘Not desirable’. Patient and caregiver comments noted desirability is dependent on the severity of side effects and thus quality of the extended life.
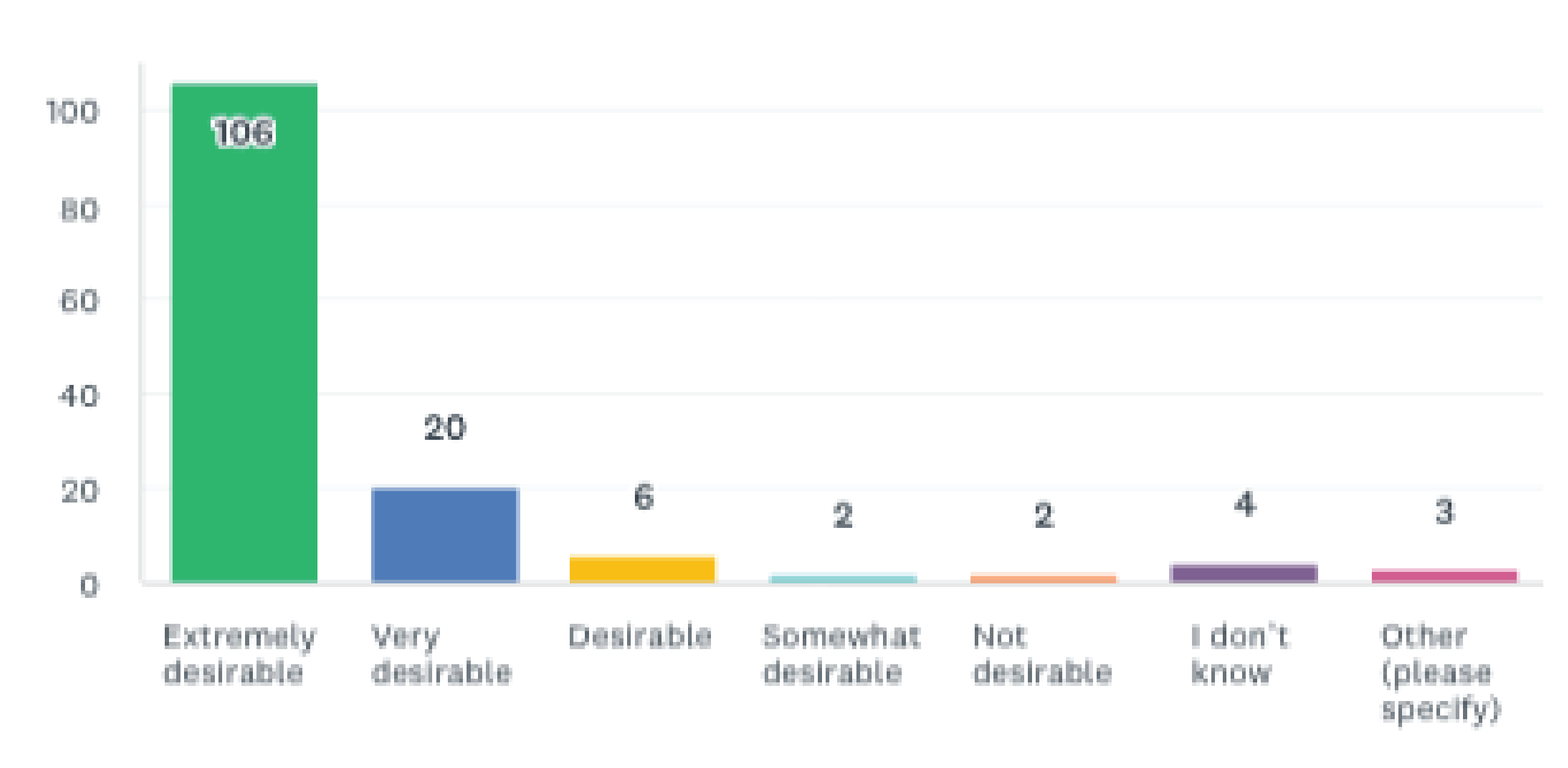
It was described to R/R patients and caregivers, that while preparing to receive CAR T-cell therapy patients must wait for their modified T-cells to be reintroduced: “In some cases, the patient’s myeloma can progress during this time (i.e., the myeloma comes back) and the patient may require an additional (bridging) therapy. If this happens the patient may no longer be eligible to proceed to the next step which is to receive their modified T-cells. In this case other treatment options are available and will be presented to the patient.”. R/R patients (145) were asked what best reflects their sentiments about this kind of situation, to which 40% (58) responded “I am concerned about my myeloma coming back but I can live with waiting for my T-cells to be reintroduced”, 30% (43) responded “I am willing to take the risk that my myeloma comes back while I wait for my T-cells to be reintroduced”, 27% (39) indicated “I am unsure… and would like to discuss this further with my hematologist /oncologist”, and only two patients were unwilling to take the risk.
R/R patients (145) and caregivers (15) were presented information about side effects: Cytokine Release Syndrome, Leukopenia, Lymphopenia, Neutropenia, Neurotoxicity. Then they were asked “Which ciltacabtagene autoleucel (cilta-cel) side effects listed below are most concerning to you/ to you as a caregiver? On a scale of 1 (most troublesome) to 5 (least troublesome), please rate each of the following side effects.” Ordered by weighted average of responses R/R patients and caregivers rated ‘Cytokine release syndrome’ as ‘Most troublesome’ (R/R patients 1.9; SD 1.2) (R/R caregivers 1.3; SD 1.01) followed by neutropenia (R/R patients 2.1; SD 1.06) (R/R caregivers 2; SD 1.13), followed by neutropenia (R/R patients 2.1; SD 1.06) (R/R caregivers 2; SD 1.13).
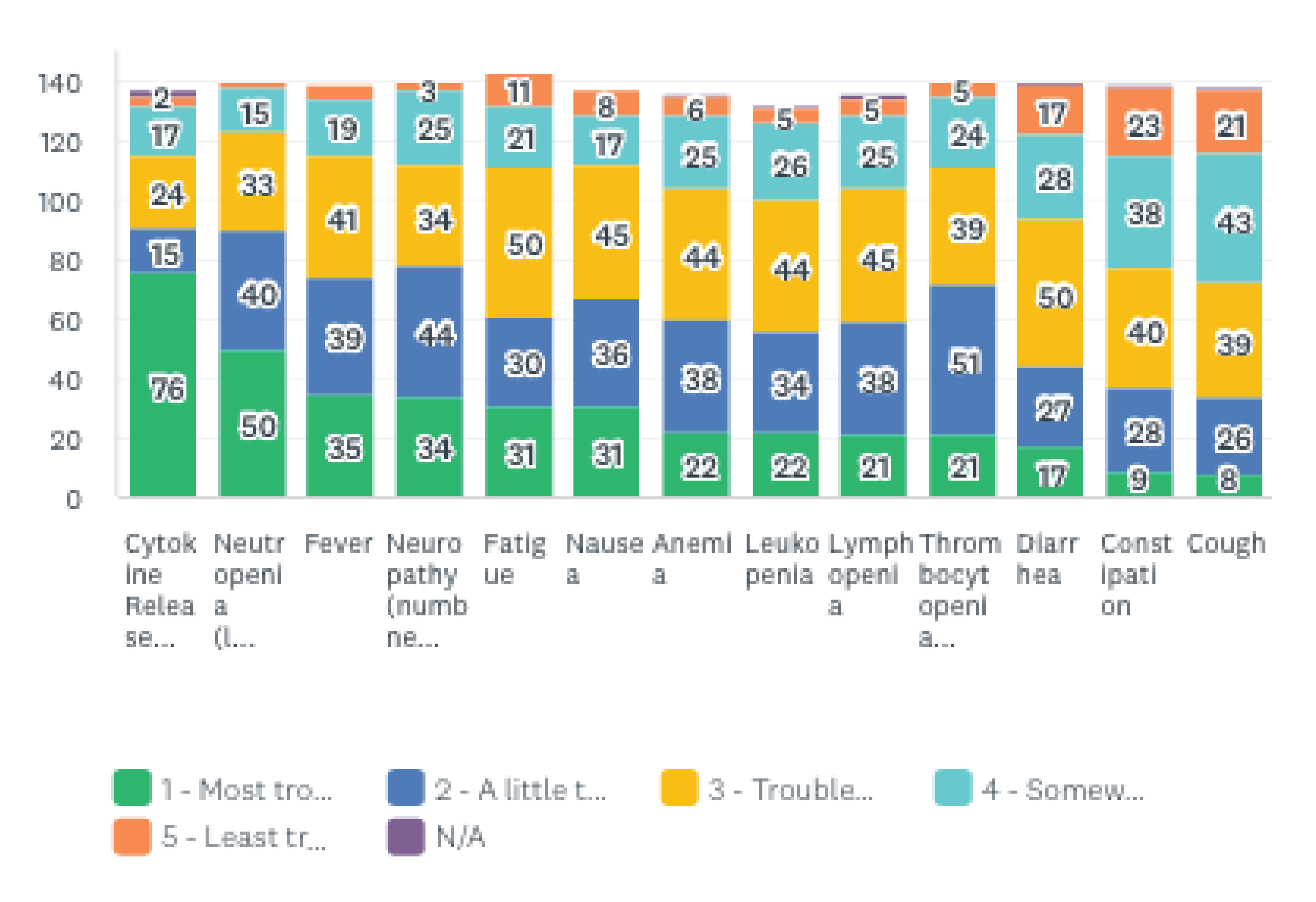
R/R caregivers (15) were asked “Do you feel that treatment with ciltacabtagene autoleucel (cilta-cel) would impact the amount of care you needed to provide? Please rate on a scale of 1-5 where 1 is ‘significantly more care’ and 5 is ‘significantly less care’.”7 (47%) chose ‘3- no change’, and 3 (20%) chose ‘4-Less care needed’. When R/R patients (145), were asked “Do you feel that treating your myeloma with cilcabtagene autoleucel (cilta-cel) could improve your health and well-being?” 57.9% (84) responded ‘Yes’, and 40% (58) chose ‘I don’t know’. Similarly, 66.2% (99) of R/R patients responded, ‘yes’ to the question “Do you feel that ciltacabtagene autoleucel (cilta-cel) to treat your myeloma could improve your long-term health outlook?”, while 32.4% (47) said ‘I don’t know”. R/R patients (144) and R/R caregivers (15 ) were asked, “If you../the person you care for were eligible to receive cilcabtagene autoleucel (cilta-cel), what do you believe the benefits would be for you, compared to the type of treatment you/they are currently receiving, or have received?” 57.3% (82) patients chose ‘All of the above”, and ‘Prolonged remission—where myeloma is not present’ at 47% (71). “Not having to take treatment because my myeloma is in remission” was chose by 50% (71), and ‘Better quality of life’ by 36.4% (52). Most comments provided by those who selected ‘Other (6)’ indicated they were unsure of the potential advantages. Caregivers most frequently chose ‘Prolonged remission where their myeloma is not present’ (8; 53.3%), and ‘All of the above’ (7; 46.7%).
Figure 7: Perceived Benefits (top) and Disadvantages (bottom) of Treatment With Cilta-cel (R/R Patients = 143)
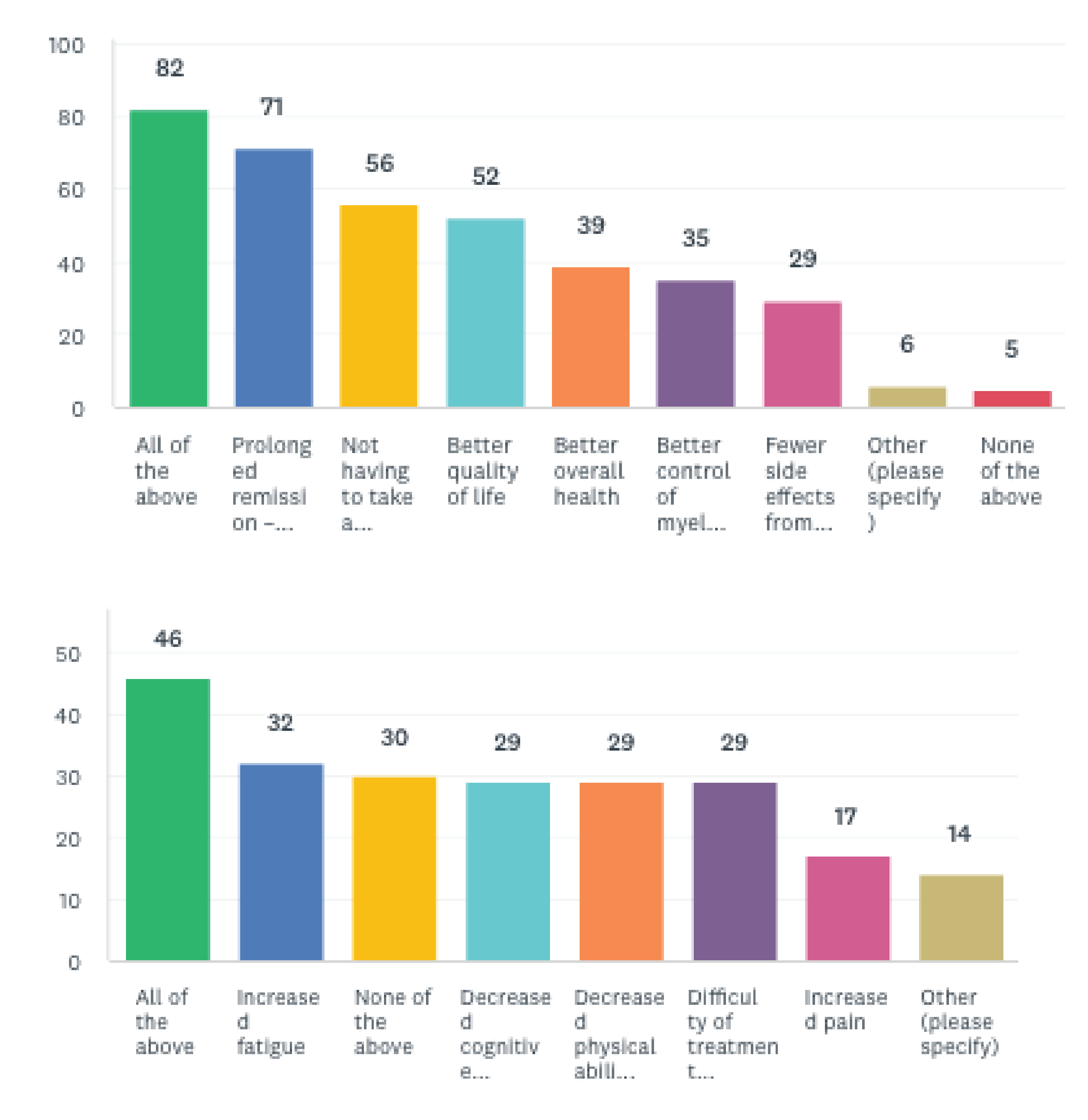
R/R patients (144) and caregivers (13) were asked ‘If you../the person you care for were eligible to receive cilcabtagene autoleucel (cilta-cel), what do you think the disadvantages would be for you, compared to the type of treatment you/they are currently receiving, or have already received)?’The responding patients most frequently chose “All of the above” 31.9% (46) followed by ‘increased fatigue’ 22.2% (32). Comments left were similarly indicative of respondents’ uncertainty surrounding what disadvantages they might experience. Caregivers most frequently chose ‘None of the above’ (8; 53.3%), followed by “Difficulty of treatment (travel, injection time, etc…)’ (5; 33.3%). To the question “With what you know today, which treatment option would you consider first as your next treatment? (Presuming your doctor has confirmed that the below treatments are an option for you). Tell us why you chose the option you did.”50% (72) of R/R patient respondents (145) indicated ‘I do not know”, while 26.2% (38) said ‘Yes’. Among the 55 patient comments many described a desire to speak with their hematologist/ oncologist before answering. Other comments expressed excitement regarding the prospect of treatment with cilta-cel/ CAR T-cell therapy in general, for example:
The idea of not having to continue ongoing treatments after cart[sic] is extremely appealing.
A one and done treatment in spite of the inherent risks is important and has merit with me.
I would rather have my T cells target cancer cells. The ‘shotgun’ effect of current chemo medications is already causing other issues with me. … I am open and excited to have the opportunity to try a Car-T therapy but will have to do more research into which type may be better for me. I really hope the gov will fund this and make it available. Though it is a high initial cost it will reduce the number of patients actively in treatment in the cancer clinics. this would reduce strain and long term costs on the medical system.
I am having trouble accessing Daratumamab due to current Bc protocols so would welcome access to Car-T
When R/R caregivers (15) were asked the same question 40% (6) of respondents chose cilta-cel, while 33.3% (5) indicated ‘I do not know’.
Figure 8: What Treatment Option Would You Consider First for Your Next Treatment? (R/R Patients = 145)
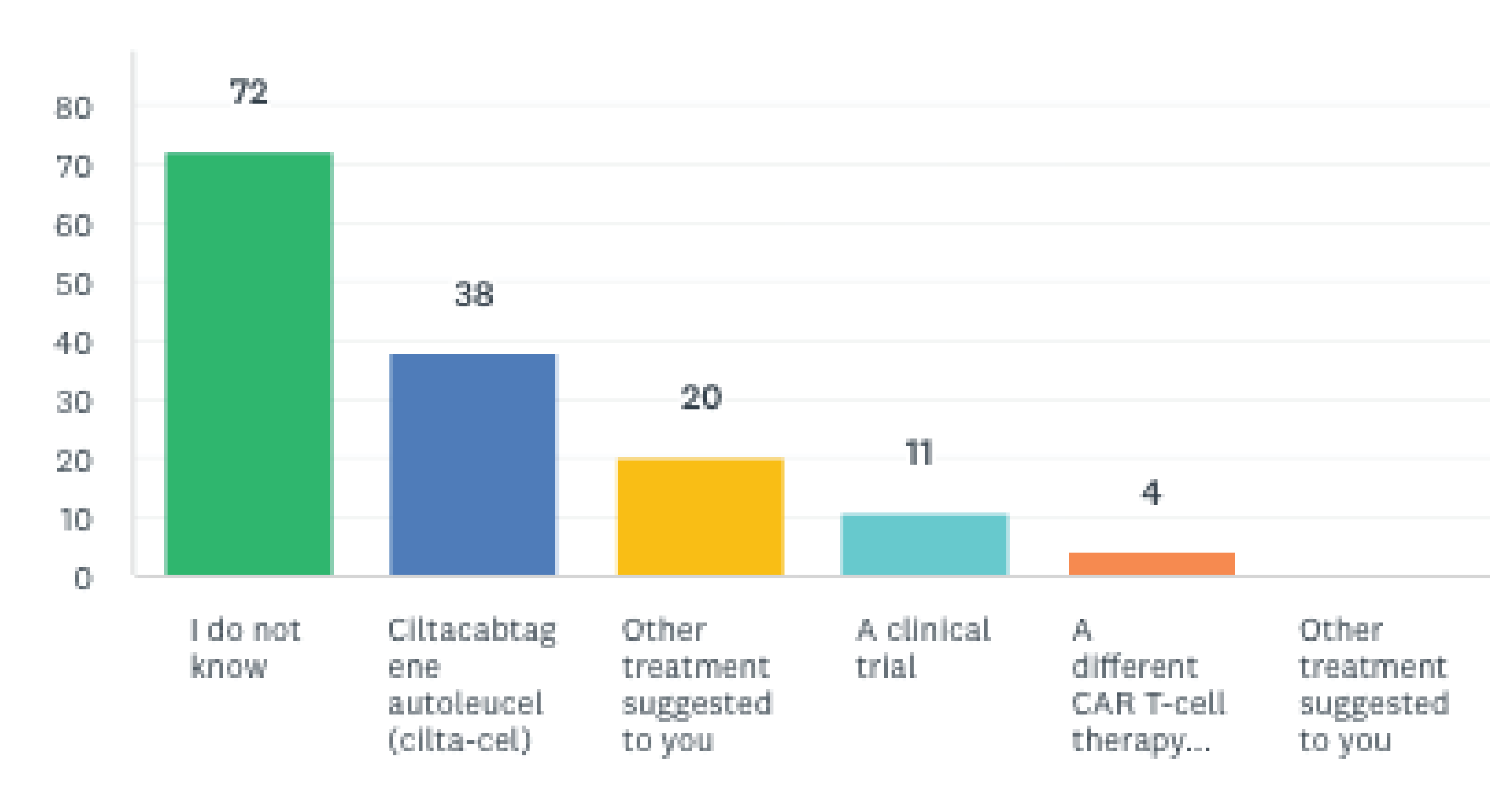
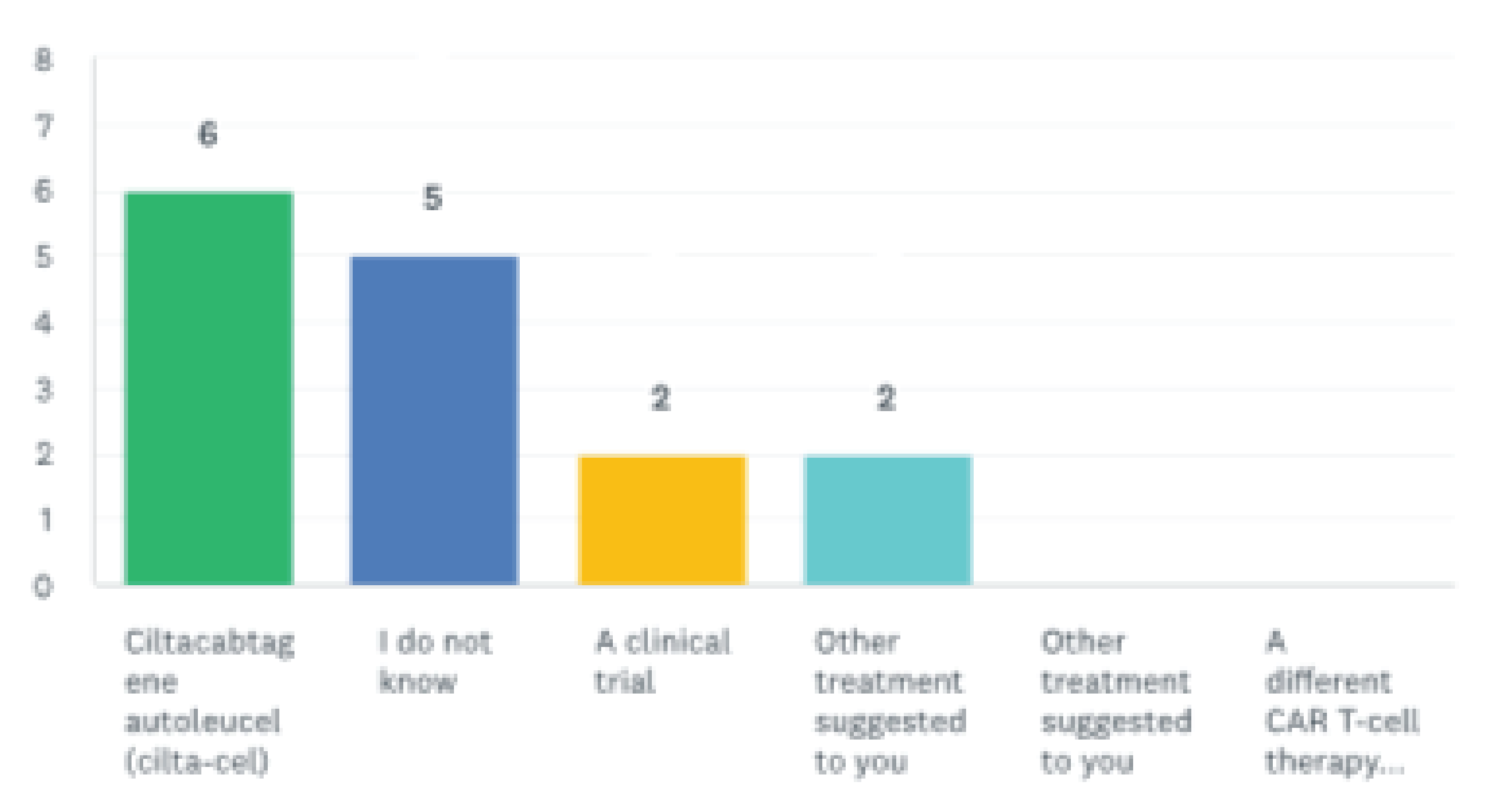
Experience With Drug Under Review
As mentioned in the Experiences With Currently Available Treatments section, among all respondents, one patient received cilta-cel and one caregiver is caring for someone who received cilta-cel. They were asked to indicate how long ago they or the person they care for received treatment with ciltacabtagene autoleucel (cilta-cel). The patient commented “I received one in 2015 and one in 2021”, while the caregiver indicated this was ‘less than three months ago”. When asked if they had relapsed since receiving treatment with cilta-cel, the patient responded, “My myeloma did come back, and I am currently under a new treatment”, while the one caregiver indicated the person, they care for is still in remission. The patient and caregiver were asked “After receiving ciltacabtagene autoleucel (cilta-cel), you/the person you care for most likely did not need to take drugs to control your/ their myeloma (not on a treatment) for a prolonged or indeterminate period. How long was this treatment interruption? The patient responded ‘4-7 months’ and the caregiver responded ‘1-3 months’. When asked “You were…/The person you care for was, most likely not on a treatment for your/their myeloma after receiving ciltacabtagene autoleucel (cilta-cel) either for a prolonged or indeterminate period of time (i.e., they did not need any drugs to control their MM). Was this treatment interruption important for you and your quality of life?”, the patient responded ‘3- somewhat important’, and the caregiver chose ‘5- extremely important’. When asked, “Based on your experience with ciltacabtagene autoleucel (cilta-cel), how would you rate the effectiveness of this treatment in helping to control your/the person your care for’s myeloma? 1 being ‘not effective’ and 5 ‘extremely effective’, the 1 patient chose ‘3-effective’ and the 1 caregiver chose ‘5-extremely effective’. When asked “Based on your experience with ciltacabtagene autoleucel (cilta-cel) how would you rate the overall side effects? 1 being ‘very intolerable’ and 5 ‘very tolerable’, the patient responded ‘4- Tolerable’. When asked “Did treatment with ciltacabtagene autoleucel (cilta-cel) impact the amount of care you needed to provide? Please rate on a scale of 1-5 where 1 is ‘significantly more care’ and 5 is ‘significantly less care’”, the one caregiver responded ‘4- less care needed’. The patient was asked, “Which of the most frequent cilta-cel side effects listed below have you experienced? Please select all that apply and rate the side effects’ severity on a scale of 1 ‘very unbearable’ to 5 ‘very bearable’.” The lowest side effect rating was ‘3-bearable’, which the patient gave to ‘Thrombocytopenia’, ‘Neutropenia’, ‘Neuropathy’, ‘Nausea’, ‘Leukopenia’, ‘Lymphopenia’, ‘Diarrhea’, ‘Constipation,’ and ‘Anemia’. The patient also rated ‘Fatigue’ as ‘4- somewhat bearable’ and ‘Fever’ as ‘5- very bearable’. Similarly, the caregiver was asked which side effects they had witnessed in the person they care for and to rate the difficulty of caring for each. The lowest rating was ‘2- difficult to care for’, which was given to the following side effects: ‘Cytokine release syndrome’, ‘Neurotoxicity’ ‘Thrombocytopenia’, ‘Neutropenia’, ‘Neuropathy’, ‘Lymphopenia’, ‘Diarrhea’, ‘Constipation,’. They also rated ‘Anemia’, ‘Nausea’, ‘Fatigue’, Fever’, ‘Chills’, ‘Cough’, ‘Constipation’, as ‘3- somewhat difficult to care for’. The patient answered ‘Yes’, when asked, “Did treatment with ciltacabtagene autoleucel (cilta-cel) improve your overall quality of life?”. When asked “Did treatment with ciltacabtagene autoleucel (cilta-cel) improve your long-term health outcomes?” the patient responded it was ‘Too soon to tell’. The one patient was asked “Did treatment with ciltacabtagene autoleucel (cilta-cel) meet your expectations in treating your myeloma?”, to which they responded ‘Yes’. Finally, the patient and caregiver were asked to share their thoughts on the treatment in an open question. The caregiver did not respond, and the patient provided the following comment:
For my 2 transplants I went in with a positive attitude and trusted my doctors. My first lasted 5 years. I’m positive that the second one will last longer. Each person is different and what happen to me doesn’t mean it will happen to someone else. Our side effects are not the same.
Anything Else?
R/R patients and R/R caregivers were posed questions to establish their awareness and understanding of CAR T-cell therapy. Survey responses indicate knowledge of CAR T-cell therapy is relatively widespread, as most patients and caregivers had heard of CAR T and were able to correctly define it when asked. As well numerous comments left by both patients and caregivers show that attitudes towards it as a potential treatment option, especially from those who were already aware of it, are generally favourable. It appears respondents have also heard largely good things about cilta-cel specifically, some patient comments indicated learning this was a promising treatment from their oncologist:“
…I know carT is on the horizon and is having tremendous success with many people…
I would like to have a choice for new treatments like Car-T and/or BITE as they treatments appear to have the least amount of side effects!
I think this may be the most effective treatment available.
Similarly, the prospect of CAR T-cell therapy has provided hope to Canadians living with multiple myeloma.
Je suis dans mes dernières ressources après 11 ans. Ce traitement me donne espoir tout à coup...
Overall demand for caregivers is higher than in HTA surveys previously conducted by Myeloma Canada in the recent past. The question ‘Do you need the help of a caregiver or family member to manage your myeloma or treatment-related symptoms” has been asked on all previous HTA survey the answer choices ‘no but I would love someone to help’, ‘yes’, and ‘yes but I cannot access the help I need’, are considered together as this demand, it amounts to 61.4% of responding patients (197).
Finally, patients demonstrate notable difficulty understanding their treatment experience within the language of ‘relapsed/refractory’ and ‘lines of treatment’, thus many had trouble self-determining their eligibility for the survey. When asked how many lines of therapy they had received, 12% of patients were unsure. As well, of the 21 disqualified respondents, 19 were disqualified by indicating they did not meet the eligibility requirements or did not know if they did, and two additional patients’ responses were removed from the data because, despite indicating they have ‘relapsed/refractory myeloma and had received at least one prior line of therapy’, the comments they provided to further questions described they were still on their first treatment. This September, the author conducted pre-interviews by telephone in recruitment for a focus group with the same eligibility requirements as the survey (relapsed/refractory myeloma patients who have received one or more prior line of therapy, and their caregivers). Patients and caregivers in these calls, especially those who have undergone numerous treatments, similarly had difficulty defining their disease experience in terms of ‘lines of treatment’ and the distinction between relapsed and refractory is quite unclear to patients.
Conflict of Interest Declaration — Myeloma Canada
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission?
No.
Did you receive help from outside your patient group to collect or analyze data used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 1: Financial Disclosures for Myeloma Canada
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Amgen Canada Inc. | — | — | — | X |
Abbvie | — | — | — | X |
AstraZeneca | — | — | — | X |
Binding Stie | — | — | — | X |
Cellpoint | — | X | — | — |
Sanofi | — | — | — | X |
Karyopharm | — | — | X | — |
Lonza | — | X | — | — |
Janssen | — | — | — | X |
Bristol-Myers Squibb Canada Co. | — | — | — | X |
Takeda Canada Inc. | — | — | — | X |
Merck Canada Inc. | — | — | — | X |
Pfizer Canada | — | — | — | X |
Forus Therapeutics | — | — | — | X |
Novartis | — | — | X | — |
GlaxoSmithKline Inc. | — | — | X | — |
Rapid Novor Inc. | — | X | — | — |
Roche | — | — | — | X |
Sebia | — | X | — | — |
Telo Genomics | — | X | — | — |
Apotex | — | — | X | — |
JAMP | — | — | X | — |
Clinician Input
Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee
About the Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee
OH-CCO’s Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs (PDRP) and the Systemic Treatment Program.
Information Gathering
Information was jointly discussed at a DAC meeting.
Current Treatments and Treatment Goals
In Ontario, Patients can be treated with pomalidomide-dexamethasone or carfilzomib-dexamethasone or other chemotherapy (e.g., cyclophosphamide) or SAP drugs (selinexor-dex +/- bortezomib; balantamab). Treatment goals would be prolonged life, disease progression and control disease.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Currently available treatments show low response rate and short duration of response.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
As per the clinical trial, in triple-class exposed multiple relapsed/refractory myeloma patients.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
As per the clinical trial, in triple-class exposed multiple relapsed/refractory myeloma patients. Patients best suited would be patients with an ECOG status of 0-2 and acceptable comorbidities.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
Standard myeloma response criteria. Outcomes used to determine would be improved survival, disease control, symptom improvement.
What factors should be considered when deciding to discontinue treatment with the drug under review?
This is a single treatment. Therefore, no subsequent treatments.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
The delivery will be at tertiary hospitals/transplant centres with expertise in cellular therapy.
Additional Information
Not applicable.
Conflict of Interest Declarations — Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
Yes. Ontario Health provided secretariat functions to the DAC.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Tom Kouroukis
Position: Lead, Ontario Health Cancer Care Ontario Hematology Cancer Drug Advisory Committee
Date: 22-09-2022
Table 2: COI Declaration for Ontario Health (CCO) Hematology Cancer DAC — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Canadian Myeloma Research Group
About the Canadian Myeloma Research Group
The Canadian Myeloma Research Group (CMRG) is a Canada-wide network of researchers aiming to develop better treatments for extending life of myeloma patients, enhancing the quality of life for those living with myeloma and related disorders and working to find a cure for these diseases and other plasma cell disorders. The three main purposes of CMRG consist of: 1) conducting investigator-initiated academic clinical trials to improve the outcome of myeloma patients; 2) maintenance of a national Myeloma Database, now consisting of over 8500 patients, to evaluate real-word patterns of treatment, outcomes, risk factors and areas for future research in myeloma; and 3) generation of consensus statements for myeloma management. Website: cmrg.ca
Information Gathering
CMRG holds monthly teleconferences, and participants agreed to submit a single document for feedback to CADTH which would be signed by the physicians who agreed with the information. The initial draft of the document was prepared in consultation with the CMRG Chief Medical Officer and sent to all members to obtain input. Comments and suggestions were incorporated as appropriate. The final draft was signed by physicians who agreed with all the content and their Conflict of Interest obtained as required.
Current Treatments and Treatment Goals
Regardless of the line of therapy the overall treatment goals in patients are to: 1) control the disease and its associated sequalae (bone destruction/pain, renal failure, hypercalcemia, low blood counts) by achieving an anti-myeloma response; 2) maintain control of myeloma and its manifestations for as long as possible given the current incurable nature of the disease (i.e. maximize progression free survival); 3) Improve overall survival; 4) minimize adverse effects of treatment; and 5) optimize QOL by adequately controlling the disease and minimizing toxicity with the aim to tailor the treatment approach to the individual patient.
Initial Therapy: Currently, newly diagnosed Canadian myeloma patients are still divided into those who are transplant-eligible (TE), or transplant-ineligible (TI) based on age and fitness. TE patients receive bortezomib-based induction with CyBorD (or RVD if possible) followed by high-dose melphalan + ASCT and then lenalidomide-maintenance until disease progression. TI patients receive Rd, RVd (typically “lite”) with single- agent lenalidomide also given until disease progression. More recently daratumumab-based combinations such as DRd or Dara-CYBORD/VMP have become available in the public system for TI patients, and it is expected that the majority of TI patients will be treated with DRd going forward. Support for these algorithms comes from published phase 3 trials as well as real-world CMRG analyses. These approaches have also been endorsed by CADTH in the recent Provisional Funding Algorithm.
Second-line therapy (after 1 prior regimen): Second-line therapy depends on whether or not patients have progressed on lenalidomide (currently, this includes most ASCT and TI patients). A key priority has been the inclusion of an anti-CD38 antibody, such as daratumumab (or in the future, isatuximab, when funded) as soon as feasible in the sequence of treatments. In Canada, this has resulted in the use of a daratumumab combination in the second-line setting in virtually all patients. Thus, prior to the recent funding of frontline daratumumab combinations in TI patients, the majority of patients have received daratumumab and dexamethasone combined with bortezomib (DVd) as second-line therapy. The minority of patients who did not progress on first-line therapy with a continuous lenalidomide-containing regimen have been preferentially treated with DRd. (The recent funding of DRd and Dara-CyBorD/VMP in newly diagnosed TI patients will of course mean that such patients will not receive an anti-CD38 agent at the time of first relapse except in the unlikely situation in which the antibody was stopped due to reasons other than myeloma progression or significant toxicity.)
However, there are also several other relevant novel anti-CD38 monoclonal antibody-containing regimens that have been approved by Health Canada which could be used in second-line treatment and beyond. These newer regimens appear to be more appropriate than DVd in the setting of progression on lenalidomide, which produces a median PFS of less than 1 year in lenalidomide-refractory individuals as demonstrated by CMRG data. Ideally, such patients would instead have the option to receive either 1) daratumumab or isatuximab partnered with dexamethasone and pomalidomide (P, POM) (DPd, IsaPd), as POM has typically been restricted for use only after failure of lenalidomide by the manufacturer, or 2) daratumumab or isatuximab in combination with dexamethasone and carfilzomib (DKd, IsaKd). However, none of these 4 regimens are publicly funded despite positive CADTH reviews evaluating efficacy. Thus, only those with insurance or capable of private pay can access them so that only a small minority of patients across Canada can receive these regimens (which have to be delivered outside the provincially-funded cancer clinics). This situation has fostered a growing 2-tiered health care system for patients with this cancer.
As more TI patients progress after DRd as initial therapy, second-line therapy will need to be based on combinations of either proteasome inhibitors (PIs) (bortezomib or carfilzomib) or POM -- without an anti-CD38 monoclonal antibody. Funded options include bortezomib + dex +/- cyclophosphamide (Vd or CyBorD) and carfilzomib + dex +/- cyclophosphamide (Kd or KCd). POM-based regimens such as Pd or PCd are also appropriate, although POM-based therapy typically requires exposure to both a PI and lenalidomide for provincial funding—a limitation which has often restricted access in the second-line setting. In any event, triplet regimens are generally preferable as second-line treatment in myeloma. (Of note, there is no publicly- reimbursed access to any BCMA-targeted agents.)
Third-line therapy (after 2 prior regimens): If patients have not yet received an anti-CD38 monoclonal antibody by the time of third-line treatment is needed, every effort is made to procure a combination containing such agents (as clinical trials or upcoming regimens in relapsed/refractory myeloma require patients to be “triple-exposed” or “triple-refractory” to the 3 main drug classes: a PI, an immunomodulatory derivative (IMiD) and an anti-CD38 antibody). Of note, this represents a dwindling population of patients. However, at this time, third-line therapy is based on either POM or carfilzomib with less efficacious partners. Funded options include POM + dex +/- cyclophosphamide (PCd) or carfilzomib + dex +/- cyclophosphamide (Kd or KCd). Again, triplet regimens are generally preferable. (Of note, there is no publicly- reimbursed access to any BCMA-targeted agents, as mentioned above.)
Fourth-line therapy: Options are extremely limited. A POM- or carfilzomib-based regimen such as Pd or Kd may be utilized if not used earlier in the third line. Additional treatment options include a regimen of bortezomib + steroids (Vd) but yields a short PFS and often cannot be revisited in many jurisdictions if patients are previously refractory to proteasome inhibitors. Although cyclophosphamide can be added to many regimens or even used with steroids as a doublet (CyDex or cyclo/prednisone), the cumulative lifetime exposure to cyclophosphamide is limited to 1 to 2 years for each patient due to the risks of secondary MDS/AML and bladder cancer from this alkylating agent. This risk may further restrict use of alternative alkylating agents like melphalan. As such, palliation/best supportive care and local radiotherapy is often all that can be pursued within the confines of the publicly funded system.
While antibody drug conjugates, bispecific antibodies and cellular therapy — often directed against BCMA on myeloma cells — are positioned to fill this “triple-class exposed or refractory” space none are currently available in Canada.
Clinical trials are key to improving survival of Canadian patients through early access to promising agents in this setting but clinical trial participation is markedly limited by: 1) strict eligibility criteria such as platelets over 75 x 109/L or near-normal renal function that may be challenging to meet in advanced myeloma; 2) the decision by pharma to open promising trials in only a few Canadian sites; 3) the policy of pharma to offer a time-limited trial spot for only few days so if a patient is not available immediately, the opening is removed and given to a centre in another country; 4) slow trial accrual to promising agents undergoing evaluation in a phase 1 study as DSMB reviews need to take place before a new cohort can be opened.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Myeloma remains incurable and patients eventually become refractory to all available funded agents. The highest unmet need in myeloma consists of patients with advanced disease who have received multiple lines of treatment and have already received the three major classes of drugs (“triple-class exposed or triple-class refractory”) including an IMID, PI and anti-CD38 monoclonal antibody. Outcomes in this patient population are dismal in the Canadian landscape due to the lack of access to additional novel agents including anti-BCMA therapy. This is supported by recent data from our CMRG group examining outcomes in these triple-class refractory patients. The ORR to subsequent line of treatment was approximately 40% with the median PFS from start of subsequent therapy being 4.4 months, and the median OS being 10.5 (95% CI 8.5-13.8) months (Visram A, et al. Abstract accepted for presentation at the American Society of Hematology Annual Meeting, 2022). The features associated with advanced disease progression and short duration of responses lead to a poor quality of life, advanced caregiver burden and a shortened lifespan. Thus, this situation represents one of the most important unmet needs in Canada for patients with multiple myeloma.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
The drug in question would be appropriate for “triple-class exposed or triple-class refractory” myeloma patients. Based upon the latest data, the results with this new agent, ciltacabtagene autoleucel, (i.e. cilta-cel), are expected to far exceed that of any previous standard of care regimen for this group of “triple-class exposed or refractory” patients—who currently represent a group with a great unmet need (Costa LJ, et al. Meta-analysis of ciltacabtagene autoleucel versus physician’s choice therapy for the treatment of patients with relapsed or refractory multiple myeloma (Curr Med Res Opin 2022 Oct;38(10):1759-1767). Cilta-cel addresses the myeloma in an entirely novel way thus overcoming resistance mechanisms to the more traditional approved approaches. Currently, it would be used in sequence after the other lines of therapy described in the Current Treatments and Treatment Goals section.
As there are very few options in patients with “triple-class exposed or refractory disease”, the issue of intolerance to other treatments or contraindications to other treatments is less relevant. Specifically, all other options that are currently available in this setting yield markedly inferior results.
As this drug will be used late in the current lines of myeloma treatment, i.e., after failure of multiple agents, it is not expected to impact the sequencing of agents earlier in the disease course or lead to a major change in treatment algorithms prior to patients becoming “triple-refractory”. However, given its impressive efficacy in terms of both response and durability of response, it is expected to lead to a major shift in the current treatment paradigm for those with advanced disease. Approval of, and access to, cilta-cel for myeloma patients will represent a major shift in Canada as it will for the first time provide a new cellular therapy for this disease.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
The least suitable patients would include frail patient as well as those with rapidly proliferating disease, ongoing infection, significant organ dysfunction and/or with pre-existing pancytopenia.
Patients with a good performance status, minimal or no comorbidities, low tumor burden and adequate organ function and blood counts are the most likely to have the best outcomes.
Patients with other disease-related adverse prognostic factors, such as extramedullary disease and high-risk cytogenetics, do not fare significantly worse and should be eligible for cilta-cel. Chronological older age alone per se does not seem to be an exclusion factor. From a practical point of view, patients whose disease is progressing at a rate anticipated to allow them to remain stable and relatively well during the 4–5-week time period necessary for CAR-T cell processing would be the best suited for this treatment in order to avoid death prior to cell therapy product delivery.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
Responses are based on the monoclonal protein marker in the serum and/or urine, bone marrow biopsy and in some instances imaging studies (standardized International Myeloma Working Group Criteria, IMWG). These are aligned with those used in the trials, which also included the emerging parameter of marrow minimal residual disease (MRD).
Clinically meaningful responses usually correlate with at least a partial remission by IMWG Consensus Criteria. These include improvement in symptoms (cessation of bone destruction with less pain, fractures and need for radiotherapy), improvement in energy and better ability to perform activities of daily living. In myeloma, responses are generally assessed every 1-3 months depending on clinical stability and regimen used for therapy.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Cilta-cel therapy represents a single infusion and therefore patients who meet eligibility criteria should receive the agent. Conventional factors for drug discontinuation such as progressive disease or adverse events are therefore not applicable in this context given the single infusion.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
This therapy is appropriate for a major medical facility with expertise in other cellular therapies for hematologic malignancies. There needs to be close interaction between a specialized inpatient service, an ICU familiar with immunosuppressed cancer patients, and an outpatient facility experienced in handling urgent hematologic problems. Appropriate coordination with the Emergency Department to expedite care of patients recently discharged following this treatment is also required.
The identification and planning of patients for cilta-cel therapy will require careful matching of available resources with the potential numbers of patients with relapsed myeloma. Treated patients may required an inpatient bed for about 2 weeks (or longer if complications occur) and may require readmission. They potentially require ancillary measures to treat CRS, neurotoxicity, and infections, and may need ICU support. Specialized training is required for staff, and the medical centre’s infrastructure and clinical pathways must be modified to meet the safety standards for cilta-cel treatment and subsequent follow-up. These realities are expected to limit the numbers of myeloma patients that can be treated. Effector Cell Therapy Committees/programs will likely need to establish guidelines for each institution or jurisdiction.
Conflict of Interest Declarations — Canadian Myeloma Research Group
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
No.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Donna Reece
Position: Chief Medical Officer, CMRG
Date: 11-10-2022
Table 3: COI Declaration for Canadian Myeloma Research Group — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
BMS/Celgene | — | — | X | — |
Janssen | — | — | X | — |
Amgen | — | — | X | — |
Sanofi | X | — | — | — |
GSK | X | — | — | — |
Takeda | X | — | — | — |
Declaration for Clinician 2
Name: Dr. Christopher Venner
Position: Hematologist Lymphoma and Myeloma Program, BC Cancer Vancouver Centre
Date: 11-10-2022
Table 4: COI Declaration for Canadian Myeloma Research Group — Clinician 2
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Celgene/BMS | X | — | — | — |
Takeda | X | — | — | — |
Janssen | X | — | — | — |
Amgen | X | — | — | — |
Sanofi | X | — | — | — |
GSK | X | — | — | — |
Declaration for Clinician 3
Name: Hira Mian
Position: Assistant Professor
Date: 11-10-2022
Table 5: COI Declaration for Canadian Myeloma Research Group — Clinician 3
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Takeda, Jansen, BMS, Sanofi, Amgen, GSK (advisory board fees) | — | X | — | — |
Jansen Research Funding | — | — | — | X |
Declaration for Clinician 4
Name: Dr. Kevin Song
Position: Hematologist, Vancouver General Hospital
Date: 11-10-2022
Table 6: COI Declaration for Canadian Myeloma Research Group — Clinician 4
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Bristol Myers Squibb | — | X | — | — |
Janssen | — | X | — | — |
Amgen | — | X | — | — |
Declaration for Clinician 5
Name: Dr. Sita Bhella
Position: Hematologist, Princess Margaret Cancer Centre
Date: 11-10-2022
Table 7: COI Declaration for Canadian Myeloma Research Group — Clinician 5
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Gilead | X | — | — | — |
Novartis | X | — | — | — |
Sanofi | X | — | — | — |
Amgen | X | — | — | — |
Celgene/Bristol Myers Squibb | X | — | — | — |
Declaration for Clinician 6
Name: Dr. Michael Pavic
Position: Hematologist
Date: 10-10-2022
Table 8: COI Declaration for Canadian Myeloma Research Group — Clinician 6
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 7
Name: Dr. Amaris Balitsky
Position: Malignant Hematologist, Juravinski Hospital and Cancer Centre
Date: 11-10-2022
Table 9: COI Declaration for Canadian Myeloma Research Group — Clinician 7
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
BMS | X | — | — | — |
Novartis | — | — | X | — |
Declaration for Clinician 8
Name: Dr. Rami Kotb
Position: Hematologist, Oncologist, Cancer Care Manitoba
Date: 11-10-2022
Table 10: COI Declaration for Canadian Myeloma Research Group — Clinician 8
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
BMS, Amgen, JNJ | — | X | — | — |
Takeda | X | — | — | |
Sanofi, Merck | — | — | — | X |
Karyopharm | — | — | — | X |
Declaration for Clinician 9
Name: Dr. Arleigh Mccurdy
Position: Hematologist, Oncologist
Date: 11-10-2022
Table 11: COI Declaration for Canadian Myeloma Research Group — Clinician 9
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
BMS/Celgene | X | — | — | — |
Takeda | X | — | — | — |
Amgen | X | — | — | — |
Janssen | X | — | — | — |
Sanofi | X | — | — | — |
Forus Therapeutics | X | — | — | — |
Declaration for Clinician 10
Name: Dr. Richard LeBlanc
Position: Hematologist, Oncologist at Hopital Maisonneuve-Rosemont, Montreal Associate Professor of Medicine, Universite de Montreal
Date: 11-10-2022
Table 12: COI Declaration for Canadian Myeloma Research Group — Clinician 10
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Janssen | X | — | — | — |
Declaration for Clinician 11
Name: Dr. Nicole Laferriere
Position: Hematologist / Chief of Oncology
Date: 12-10-2022
Table 13: COI Declaration for Canadian Myeloma Research Group — Clinician 11
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Astra Zeneca, AMGEN Canada, ROCHE, Abbvie, Sanofi Canada, Lundbeck, Janssen, Celgene, Teva Pharm, Novartis, KiTE, AbbVie, Incyte | X | — | — | — |
Declaration for Clinician 12
Name: Dr. Jean Roy
Position: Full professor, Université de Montréal, hematologist, Maisonneuve-Rosemont Hospital
Date: 12-10-2022
Table 14: COI Declaration for Canadian Myeloma Research Group — Clinician 12
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 13
Name: Dr. Irwindeep Sandhu
Position: MD, Associate Professor Dept of Oncology University of Alberta
Date: 12-10-2022
Table 15: COI Declaration for Canadian Myeloma Research Group — Clinician 13
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Celgene/BMS | X | — | — | — |
Janssen | X | — | — | — |
Amgen | X | — | — | — |
Takeda | X | — | — | — |
Sanofi | X | — | — | — |
Kite / Gilead | X | — | — | — |
Declaration for Clinician 14
Name: Dr. Julie Côté
Position: Hematologist/Oncologist
Date: 12-10-2022
Table 16: COI Declaration for Canadian Myeloma Research Group — Clinician 14
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
BMS | X | — | — | — |
Janssen | X | — | — | — |
Sanofi | X | — | — | — |
Declaration for Clinician 15
Name: Dr. Anthony Reiman
Position: MD/Oncologist
Date: 12-10-2022
Table 17: COI Declaration for Canadian Myeloma Research Group — Clinician 15
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 16
Name: Dr. Heather Sutherland
Position: Hematologist, Vancouver General Hospital
Date: 12-10-2022
Table 18: COI Declaration for Canadian Myeloma Research Group — Clinician 16
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Sanofi | X | — | — | — |
Amgen | X | — | — | — |
Declaration for Clinician 17
Name: Dr. Debra Bergstrom
Position: Associate Professor
Date: 13-10-2022
Table 19: COI Declaration for Canadian Myeloma Research Group — Clinician 17
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Janssen | X | — | — | — |
Declaration for Clinician 18
Name: Dr. Anca Prica
Position: Hematologist
Date: 13-10-2022
Table 20: COI Declaration for Canadian Myeloma Research Group — Clinician 18
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 19
Name: Dr. Rodger Tiedemann
Position: Consultant Hematologist, Senior Scientist, Princess Margaret Cancer Centre, UHN, Toronto
Date: 13-10-2022
Table 21: COI Declaration for Canadian Myeloma Research Group — Clinician 19
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Janssen | X | — | — | — |
Declaration for Clinician 20
Name: Christine Chen
Position: Hematologist, Princess Margaret Cancer Centre
Date: 13-10-2022
Table 22: COI Declaration for Canadian Myeloma Research Group — Clinician 20
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
BMS | X | — | — | — |
Janssen | X | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.