CADTH Reimbursement Review
Lisocabtagene Maraleucel (Breyanzi)
Sponsor: Celgene Inc., a Bristol Myers Squibb Company
Therapeutic area: Relapsed or refractory large B-cell lymphoma
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Ethics Review
Stakeholder Input
Clinical Review
Abbreviations
3L+
third line or later
AE
adverse event
AESI
adverse event of special interest
allo
allogeneic
auto
autologous
axi-cel
axicabtagene ciloleucel
BCL2
B-cell lymphoma gene 2
BCL6
B-cell lymphoma gene 6
BOR
best overall response
CAR
chimeric antigen receptor
CI
confidence interval
CNS
central nervous system
CR
complete response
CrCl
creatinine clearance
CRR
complete response rate
CRS
cytokine release syndrome
CT
computed tomography
DC
dose confirmation
DE
dose expansion
DF
dose finding
DL
dose level
DL1D
dose level 1 (50 × 106 CAR-positive T cells), 2-dose regimen
DL1S
dose level 1 (50 × 106 CAR-positive T cells), single-dose regimen
DL2S
dose level 2 (100 × 106 CAR-positive T cells), single-dose regimen
DL3S
dose level 3 (150 × 106 CAR-positive T cells), single-dose regimen
DLBCL
diffuse large B-cell lymphoma
DLT
dose-limiting toxicity
DOR
duration of response
ECG
electrocardiogram
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
EQ-5D-5L
EuroQol 5-Dimensions 5-Levels questionnaire
EQ VAS
EuroQol Visual Analogue Scale
ESS
effective sample size
FL3B
follicular lymphoma grade 3B
HGL
high-grade lymphoma
HR
hazard ratio
HRQoL
health-related quality of life
HSCT
hematopoietic stem cell transplant
ICU
intensive care unit
iiNT
investigator-identified neurologic toxicity
iNHL
indolent non-Hodgkin lymphoma
IPD
individual patient data
IPI
International Prognostic Index
IRC
Independent Review Committee
ITC
indirect treatment comparison
ITT
intention to treat
LDC
lymphodepleting chemotherapy
LDH
lactate dehydrogenase
liso-cel
lisocabtagene maraleucel
LVEF
left ventricular ejection fraction
MAIC
matching-adjusted indirect comparison
MCL
mantle cell lymphoma
mCRM
modified continual reassessment method
MID
minimal important difference
MYC
myelocytomatosis oncogene
NHL
non-Hodgkin lymphoma
NOS
not otherwise specified
NR
not reached
NT
neurologic toxicity
OR
odds ratio
ORR
overall response rate
OS
overall survival
PAS
primary analysis set
PD
progressive disease
PFS
progression-free survival
PK
pharmacokinetic
PMBCL
primary mediastinal B-cell lymphoma
PP
per protocol
PR
partial response
PRO
patient-reported outcome
QoL
quality of life
R/R
relapsed or refractory
SAE
serious adverse event
SCT
stem cell transplant
SD
stable disease
SOC
system organ class
TEAE
treatment-emergent adverse event
tisa-cel
tisagenlecleucel
tFL
transformed from follicular lymphoma
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Lisocabtagene maraleucel cell suspension in patient-specific single-dose vials, 60 × 106 to 120 × 106 chimeric antigen receptor-positive viable T cells (consisting of CD4 and CD8 components at a ratio range from 0.8 to 1.2), for IV infusion |
Indicationa | For the treatment of adult patients with relapsed or refractory large B-cell lymphoma after 2 or more lines of systemic therapy, including diffuse large B-cell lymphoma not otherwise specified, primary mediastinal large B-cell lymphoma, high-grade B-cell lymphoma, and diffuse large B-cell lymphoma arising from follicular lymphoma |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | May 6, 2022 |
Sponsor | Celgene Inc., a Bristol Myers Squibb Company |
NOC = Notice of Compliance.
aNote that the CADTH Reimbursement Review was conducted before issuance of the Health Canada NOC and the scope was based on the anticipated indication.
Introduction
Lymphomas comprise a complex group of hematological malignancies with varying molecular hallmarks and prognoses. They are overall divided into non-Hodgkin lymphoma (NHL) and Hodgkin lymphoma.1 In Canada, the incidence of NHL is reported at 24.4 per 100,000 with age-standardized incidence rates of 29.3 per 100 000 and 20.2 per 100 000 among men and women, respectively.2 The median age at diagnosis for NHL is 66 years.3
Diffuse large B-cell lymphoma (DLBCL) is the most common type of NHL, comprising 30% to 40% of all cases.1 Most people are diagnosed when they are in their seventh decade of life. The DLBCL named “not otherwise specified” (NOS) is the most common type of DLBCL, representing 80% to 85% of all cases.4,5 Other subtypes of DLBCL include primary mediastinal B-cell lymphoma (PMBCL), a rare subtype of DLBCL.1,5 Patients with treatment failure after initial treatment often have a poor outcome—in particular, those with disease that is refractory to frontline or subsequent therapies—although some patients can have a durable remission and be cured after secondary therapies. Outcomes are worse in patients with chemotherapy-refractory disease, with only 7% achieving a complete response (CR) to standard treatment and overall survival (OS) of 6 months.6 People of older age (> 65 years) and those with central nervous system (CNS) involvement and comorbidities have higher possibility of adverse outcomes.7 No more than 50% of patients with relapsed or refractory (R/R) large B-cell lymphomas achieve a response to subsequent treatment after a standard second-line salvage regimen, and few are cured.8
The objective of this report is to perform a systematic review of the clinical efficacy and safety of lisocabtagene maraleucel (liso-cel) for the treatment of adult patients with R/R large B-cell lymphoma including DLBCL NOS (including DLBCL arising from indolent lymphoma), high-grade B-cell lymphoma, PMBCL, and follicular lymphoma grade 3B (FL3B) after at least 2 prior therapies. Of note, this CADTH Reimbursement Review was conducted before the issuance of the Health Canada Notice of Compliance for liso-cel and the scope was based on this anticipated indication.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input and from clinical expert(s) consulted by CADTH for the purpose of this review.
Patient Input
Input was obtained from 1 patient group. Raw patient group input is presented in the Stakeholder Input section. Overall, Lymphoma Canada, a Toronto-based, national Canadian registered charity that empowers the lymphoma community, provided an anonymous survey of patients with large B-cell lymphoma conducted online from June 21 to August 25, 2021. The survey participants (N = 331) were from Canada, US, Europe, and other countries. In this survey, patients highlighted symptoms such as fatigue and lack of energy as the most difficult part of living with lymphoma and how the treatments they receive impact on their QoL, such as hair loss, fatigue, nausea, vomiting, and fear of relapse or progression. Even though the access to the current lymphoma treatments was not a major concern, the patients surveyed were worried about not being able to get chimeric antigen receptor (CAR) T-cell therapies on time and/or high costs that would be incurred due to limited regional availability of CAR T-cell therapies. In addition, the majority of patients desired to have new treatments that improve QoL and extend remission and survival. None of the patients surveyed had direct experience with liso-cel therapy. To supplement this information, another survey was conducted from April 18 to June 15, 2018, which collected feedback from patients who underwent other CAR T-cell therapies through clinical trials. Out of 7 patients who had experiences with the CAR T-cell therapies, 5 responded to questionnaires asking about CAR T-cell therapy’s impact on QoL. These patients rated less than 3 (1 = no negative impact on my life; 5 = significant negative impact on my life) for all aspects of CAR T-cell therapy,(i.e., number of clinic visits, travel to treatment centre, CAR T-cell infusion, short-term side effects, activity level, treatment-related fatigue, lasting side effects, and leukapheresis). When asked about recommending CAR T-cell therapy to other eligible patients, 5 out of 7 patients said they would recommend, 1 said not to recommend, and 1 remained unsure. Lastly, the patients expressed that having a choice in treatment options is paramount.
Clinician Input
Input From Clinical Experts Consulted by CADTH
Clinical experts consulted by CADTH agreed that there is an unmet need for drugs that are better tolerated and with better safety profiles that can be used more frequently in the outpatient setting and that can be used in a broader population of patients with lymphoma. Suboptimal availability of commercially available CAR T-cell products in some provinces generates the need to refer patients outside of the province or country for commercial CAR T-cell therapies. Other innovative therapies (e.g., polatuzumab vedotin) may not be widely available, or are likely costly.
Although liso-cel is not the first CAR T-cell therapy on the market for R/R DLBCL in Canada, some clinical experts mentioned that it may have a better profile in terms of decreased toxicity, as suggested by the evidence from the TRANSCEND study, although others mentioned how newer therapies may benefit from prior clinical experience with similar therapies. Liso-cel would still be used as a third-line therapy (in patients who have already tried 2 lines of chemotherapy) but will have the advantage of being able to be used in a broader population.
Clinical experts suggested that patients most likely to benefit from liso-cel have similar characteristics to those included in the TRANSCEND study (e.g., Eastern Cooperative Oncology Group Performance Status [ECOG PS] of 0 or 1, low lactate dehydrogenase [LDH]), although the experts mentioned that more data on specific subgroups (e.g., ECOG PS of 2) are needed. Patients who have had an autologous stem cell transplant (auto-SCT) and then relapsed or those who are not eligible for a transplant are likely to be favoured for liso-cel administration. The clinical experts mentioned that patients who would not be suitable for treatment with liso-cel would be those not meeting established criteria (i.e., eligibility criteria from the TRANSCEND study) for CAR T-cell therapy. However, as with other CAR T-cell therapies, it remains difficult to predict at the start of treatment which patients would likely benefit from treatment with liso-cel.
Improved survival, reduction in the frequency and severity of symptoms, and cure were considered adequate measurements of response in clinical practice. Imaging may also be used as an objective means of assessing response to treatment.
The clinical experts recommended assessments of patients every 1 to 3 months. Criteria for discontinuing treatment with CAR T-cell therapy was not discussed as it is a treatment administered as a single dose (although re-treatment may be possible). Some patients may become clinically unstable during the liso-cel manufacturing process and require discontinuation (e.g., patients with ECOG PS of 4, sudden clinical deterioration, opportunistic infections, and so on).
CAR T-cell treatment is primarily performed in Canada at transplant centres. Currently, most provinces in Canada have (or will have) the necessary expertise and resources to perform the administration of liso-cel. In some areas, however, access to these centres may be challenging (e.g., in rural areas). Therefore, access to Health Canada and Foundation for the Accreditation of Cellular Therapy-accredited SCT centres in Canada is a limitation. The clinical experts expressed that outpatient therapy is feasible provided such programs have the appropriate infrastructure and accreditation.
Clinician Group Input
The collection of clinician group responses was coordinated by Lymphoma Canada. The clinician group stated that addition of liso-cel to the current third-line therapies or beyond is important for the following reasons: 1) as a curative therapy, liso-cel is expected to improve remission, (e.g., CRs and partial responses [PRs], and prolong survival, (e.g., overall and progression-free survival [PFS], of the eligible patients); 2) availability of liso-cel would prevent unnecessary delay in treatment caused by short supply of the existing CAR T-cell therapies; 3) liso-cel has demonstrated fewer frequent adverse effects [AEs], (i.e., cytokine release syndrome [CRS] and neurotoxicity [NT], compared to axicabtagene ciloleucel (axi-cel) without compromising efficacy (note: no head-to-head trial is available.); 4) liso-cel can be safely administered in an outpatient setting similarly to tisagenlecleucel (tisa-cel).
Other input was provided by the Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee. The committee indicated that liso-cel would fulfill the unmet needs of indications that are not covered by the other CAR T-cell therapies such as FL3B and secondary CNS lymphoma. Moreover, the committee identified that the limited number of CAR T-cell therapy centres available across Canada could cause access issues for patients.
Drug Program Input
The drug programs identified relevant implementation issues to be addressed through CADTH’s reimbursement review processes.
In terms of considerations for initiation of therapy, the drug program inquired if patient eligibility criteria would overlap with existing commercial CAR T-cell therapy eligibility criteria (e.g., tisa-cel and axi-cel). The clinical experts consulted by CADTH mentioned that overlap exists with axi-cel but not with tisa-cel as it does not include criteria for PMBCL.
The drug program detected that liso-cel was also evaluated in patients with DLBCL transformed from indolent lymphomas. The clinical experts considered that these patients would also need at least 2 lines of systemic therapy from the time of diagnosis of a transformation to be considered as failed treatment. Potential exceptions may include individuals with follicular lymphoma for which they already have received treatment (e.g., with rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone; gemcitabine, dexamethasone, and cisplatin, and auto-SCT) but then transforms to DLBCL/HGBL. For these cases, clinicians may want to move directly to offer CAR T-cell therapies since other options are limited. Clinical experts suggest criteria could stipulate the minimum types of therapy required in these situations.
The clinical experts believed that there were sufficient data to recommend liso-cel in patients older than 75 years, with FL3B, ECOG PS lower than 2, and with CNS involvement. More data are desirable, but all of the above have a class effect on CD19. The clinical experts mentioned that patients with comorbidities might be eligible for liso-cel use.
The drug programs also inquired about the use of liso-cel in patients who have already received a CAR T-cell therapy. The clinical experts consulted by CADTH were not aware of any evidence that supported this notion.
Clinical experts suggested that patients with CNS lymphoma (as long as their disease is controlled), should also be eligible to receive liso-cel. As mentioned in the clinical expert input and related to concerns about implementation from the drug programs, the administration of liso-cel would be done preferably in Health Canada and Foundation for the Accreditation of Cellular Therapy-accredited SCT centres (most centres are medium size, some are large). Outpatient therapy is feasible provided such programs have the infrastructure and accreditation.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
One clinical study9 is included in this report evaluating the safety and efficacy of liso-cel in patients on the third line or later (3L+) of treatment for R/R DLBCL. The TRANSCEND NHL 001 study (from now on, the TRANSCEND study) is a single-arm, open-label, phase I (seamless design) multi-centre study, conducted in the US. The population included in the study consists of patients with DLBCL NOS (de novo, transformed from FL [tFL], and transformed indolent non-Hodgkin lymphoma [iNHL]), high-grade B-cell lymphoma with myelocytomatosis oncogene (MYC) and B-cell lymphoma gene 2 (BCL2) and/or B-cell lymphoma gene 6 (BCL6) rearrangements, PMBCL, and FL3B were eligible if they were R/R to at least 2 prior lines of therapy, and had ECOG PS of 0 to 2, PET-positive disease, secondary CNS involvement, prior auto-SCT, and prior allogeneic (allo)-SCT. Patients with primary CNS involvement and allo-hematopoietic SCT (HSCT) within 90 days of leukapheresis were excluded. The seamless design allowed the study to go from dose-finding (DF) phases (groups of patients) to dose-expansion (DE) and then dose-confirmation groups. The study evaluated 3 levels of dose regimens, dose level 1 at 50 × 106 CAR-positive T cells (2-dose regimen [DL1D] and single-dose regimen [DL1S]); dose level 2 at 100 × 106 CAR-positive T cells, single-dose regimen (DL2S); and dose level 3 at 150 × 106 CAR-positive T cells, single-dose regimen (DL3S); of these, the DL2S regimen was selected for the current indication assessed in this review, for clinical use, and regulatory approval. Patients in the TRANSCEND study had a mean age of 60 years (median = 63) and were overall in relatively good health status.
After enrolment, patients went through a leukapheresis to allow for the product (liso-cel) to be manufactured (bridging therapy consisting of systemic anticancer therapy was allowed) and were required to have PET-positive disease. After product generation, patients went through lymphodepleting chemotherapy (LDC) with fludarabine plus cyclophosphamide followed by 1 or 2 doses of JCAR017 administered IV on day 1. After day 29, patients were followed on this study for safety, disease progression, and survival for 2 years after the last dose of liso-cel. Of 427 screened patients (341 in the DLBCL cohort), 344 went through leukapheresis (the intention-to-treat [ITT] set), of which 50 could not be treated with any product, 25 received nonconforming product, and 269 patients were treated with liso-cel (the DLBCL treated set) and analyzed as of the cut-off date of August 12, 2019. The main analysis was conducted on the primary analysis set (PAS) population consisting of those patients at the DL2S regimen.
Primary end points included AEs and overall response rate (ORR) as assessed by an independent review committee (IRC). Secondary end points included complete response rate (CRR) (as assessed by IRC), duration of response (DOR), PFS, and OS. The ORR was defined as the proportion of patients with a best overall response (BOR) of either CR or PR based on the Lugano 2014 criteria.10 A sequential testing procedure started with the first hypothesis test of ORR of 40% or less. The procedure proceeded to the second hypothesis test only after rejecting the null hypothesis in the first hypothesis test, and so on. Other efficacy end points were summarized. The Kaplan–Meier method was used to estimate the DOR, PFS, and OS rates at months 6, 12, 18, and 24. The manufacturing success rate using the proposed commercial manufacturing process was 90.0% and the median time from leukapheresis to JCAR017 product availability was 24.0 days (range = 17 days to 51 days).
Efficacy Results
In this specific population with 3L+ DLBCL (i.e., those with DLBCL NOS, HGL or tFL) assigned to the recommended regimen of DL2S (100 × 106 CAR-positive T cells), the ORR in the PAS (primary end point) was 74.4% (95% confidence interval [CI], 66.2 to 81.6) against a null hypothesis of ORR of 40% or less. The CR rate (key secondary end point) in the PAS was 54.1% (95% CI, 45.3 to 62.8; 1-sided P < 0.0001). Sensitivity analyses using the per-protocol (PP) set showed similar results. The leukapheresed set (ITT population) included patients treated with nonconforming product (n = 25) as well as those who received no treatment (n = 50). The primary reason for not receiving treatment was death (n = 33); most of those patients died from progressive disease (PD; n = 27). The leukapheresed set had an ORR per IRC of 60.5% (95% CI, 55.1 to 65.7), and a CR rate of 43.6% (95% CI, 38.3 to 49.0). The lower limit of each CI was equal or higher than the null hypotheses used for the PAS (40% and 20%, respectively). With a median follow-up for PFS of |||||| months, the median PFS was 4.8 months (95% CI, 4.3 to 7.3). With a median survival follow-up of 18.8 months, the median OS was 14.0 months (95% CI, 11.1 to 21.1). The estimated survival rates at 6 and 12 months were 70.2% (95% CI, 65.0 to 74.8) and 54.0% (95% CI, 48.5 to 59.2), respectively. Only 7 of 269 patients were never hospitalized. Nineteen patient (7.1%) were admitted to the intensive care unit (ICU), with a variable duration from 2 to 88 days.
Health-related quality of life (HRQoL) outcomes improved during treatment with liso-cel, although not all HRQoL domains reached statistical significance as compared to a minimal important difference (MID) and were not included in the adjustment for multiplicity.
Harms Results
The most frequently reported treatment-emergent AEs (TEAEs) were neutropenia (169 of 269 patients; 62.8%), anemia (129 of 269 patients; 48.0%), and fatigue (119 of 269 patients; 44.2%), followed by CRS (113 of 269 patients; 42.0%). CRS was also the most frequently reported serious AE (SAE; occurring in 44 of 269 patients; 16.4%), but grade 3 or higher CRS occurred in only 6 of 269 patients (2.2%). The second most frequently reported treatment-emergent SAE was encephalopathy (occurring in 14 of 269 patients; 5.2%), the most frequent symptom of investigator-identified neurologic toxicity (iiNT). All other treatment-emergent SAEs were reported in less than 5% of patients. Grade 3 or higher CRS occurred in 6 of 269 subjects (2.2%) and grade 3 or higher iiNT in 27 of 269 subjects (10.0%), while no grade 5 CRS or iiNT AEs were reported. Admission to the ICU occurred infrequently. During initial hospitalization, 19 of 269 patients (7.1%) were admitted to the ICU; the median number of ICU days was 7 days (range = 1 day to 56 days). Considering all hospitalizations through the end of the study, 33 of 269 patients (12.3%) were admitted to the ICU; the median number of ICU days in those hospitalized was 8 (range = 1 day to 56 days).
A summary of key results is presented in Table 2.
Table 2: Summary of Key Results from Pivotal and Protocol Selected Studies
Variable | DL2S | DL1S | DL1D | DL3S | Total |
|---|---|---|---|---|---|
DLBCL efficacy set | n = 169 | n = 40 | n = 6 | n = 41 | N = 256 |
Overall response rate | |||||
CR + PR, n (%) | 125 (74.0) | 27 (67.5) | 4 (66.7) | 30 (73.2) | 186 (72.7) |
95% CIa | 66.7 to 80.4 | 50.9 to 81.4 | 22.3 to 95.7 | 57.1 to 85.8 | 66.8 to 78.0 |
CR rate | |||||
CR, n (%) | 88 (52.1) | 24 (60.0) | 3 (50.0) | 21 (51.2) | 136 (53.1) |
95% CI | 44.3 to 59.8 | 43.3 to 75.1 | 11.8 to 88.2 | 35.1 to 67.1 | 46.8 to 59.4 |
Duration of response (months) | |||||
Median, 95% CI | |||||| | |||||| | |||||| | |||||| | NR, 8.6 to NR |
Min., max. | |||||| | |||||| | |||||| | |||||| | 0.0, 27.4 |
PFS events, n (%) | |||||| | |||||| | |||||| | |||||| | |||||| |
Progression | |||||| | |||||| | |||||| | |||||| | |||||| |
Death | |||||| | |||||| | |||||| | |||||| | |||||| |
Censored | |||||| | |||||| | |||||| | |||||| | |||||| |
PFS (months) | |||||
Median, 95% CI | |||||| | |||||| | |||||| | |||||| | 6.8, 3.3 to 14.1 |
Min., max. | |||||| | |||||| | |||||| | |||||| | |||||| |
OS, n (%) | |||||
Death | 82 (48.5) | 19 (47.5) | 3 (50.0) | 12 (29.3) | 116 (45.3) |
Alive | 87 (51.5) | 21 (52.5) | 3 (50.0) | 29 (70.7) | 140 (54.7) |
OS (months) | |||||
Median, 95% CI | 19.9, 11.3 to NR | NR, 6.8 to NR | NR, 1.6 to NR | NR, 10.3 to NR | 21.1, 13.3 to NR |
Min., max. | 0.2, 33.9 | 0.6, 42.0 | 1.6, 36.3 | 1.2, 14.5 | 0.2, 42.0 |
Follow-up (months) | |||||
Median, 95% CI | 17.5, 13.4 to 17.8 | 24.5, 24.1 to 34.5 | 31.6, 31.0 to 36.3 | 9.2, 8.8 to 9.7 | 17.5, 12.9 to 17.8 |
Primary analysis set | N = 133 | N = 133 | |||
ORR | |||||
CR + PR, n (%) | 99 (74.4) | NA | NA | NA | 99 (74.4) |
95% CI | 66.2 to 81.6 | NA | NA | NA | 66.2 to 81.6 |
P valueb | NA | NA | NA | NA | < 0.0001 |
CR rate, n (%) | |||||
CR | 72 (54.1) | NA | NA | NA | 72 (54.1) |
95% CI | 45.3 to 62.8 | NA | NA | NA | 45.3 to 62.8 |
P valuec | NA | NA | NA | NA | < 0.0001 |
Duration of response (months) | |||||
Median, 95% CI | 16.8, 6.0 to NR | NA | NA | NA | 16.8, 6.0 to NR |
Min., max. | |||||| | |||||| | |||||| | |||||| | |||||| |
PFS events, n (%) | |||||| | |||||| | |||||| | |||||| | |||||| |
Progression | |||||| | |||||| | |||||| | |||||| | |||||| |
Death | |||||| | |||||| | |||||| | |||||| | |||||| |
Censored | |||||| | |||||| | |||||| | |||||| | |||||| |
PFS (months) | |||||
Median, 95% CI | 9.0, 3.1 to NR | NA | NA | NA | 9.0, 3.1 to NR |
Min., max. | |||||| | NA | NA | NA | |||||| |
OS | |||||
Death, n (%) | |||||| | |||||| | |||||| | |||||| | |||||| |
Alive, n (%) | |||||| | |||||| | |||||| | |||||| | |||||| |
OS (months) | |||||
Median, 95% CI | 19.9, 10.4 to NR | NA | NA | NA | 19.9, 10.4 to NR |
Min., max. | |||||| | |||||| | |||||| | |||||| | |||||| |
Follow-up (months) | |||||
Median, 95% CI | |||||| | |||||| | |||||| | |||||| | |||||| |
AEs | |||||
Patients with any AE, n (%) | 177 (100.0) | 44 (97.8) | 6 (100.0) | 40 (97.6) | 267 (99.3) |
Most common AEs, n (%) | |||||
Neutropenia | |||||| | |||||| | |||||| | |||||| | 169 (62.8) |
Anemia | |||||| | |||||| | |||||| | |||||| | 129 (48.0) |
Fatigue | |||||| | |||||| | |||||| | |||||| | 119 (44.2) |
Patients with ≥ 1 SAEs | |||||
n (%) | 140 (79.1) | 36 (80.0) | 5 (83.3) | 32 (78.0) | 213 (79.2) |
Most common grade ≥ 3 events, n (%) | |||||
Neutropenia | |||||| | |||||| | |||||| | |||||| | 161 (59.9) |
Anemia | |||||| | |||||| | |||||| | |||||| | 101 (37.5) |
Thrombocytopenia | |||||| | |||||| | |||||| | |||||| | 72 (26.8) |
Cytokine release syndrome | |||||| | |||||| | |||||| | |||||| | 113 (42.0) |
Grade ≥ 3 infections | |||||| | |||||| | |||||| | |||||| | 33 (12.3) |
Grade ≥ 3 prolonged cytopenias | |||||| | |||||| | |||||| | |||||| | 100 (37.2) |
Hypogammaglobulinemia | |||||| | |||||| | |||||| | |||||| | 37 (13.8) |
Death (occurred any time after the first infusion of liso-cel or nonconforming product) | NA | NA | NA | NA | |||||| |
AE = adverse event; CI = confidence interval; CR = complete response; DL1D = dose level 1, 2 dose; DL1S = dose level 1, single dose; DL2S = dose level 2, single dose; DL3S = dose level 3, single dose; DLBCL = diffuse large B-cell lymphoma; HSCT = hematopoietic stem cell transplant; liso-cel = lisocabtagene maraleucel; max. = maximum; min. = minimum; NA = not applicable; NR = not reached; OS = overall survival; PFS = progression-free survival; PR = partial response; SAE = serious adverse event.
Note: Data cut-off was August 19, 2019.
aAll the CIs were 2-sided 95% exact Clopper-Pearson.
bOne-sided P value was calculated based on the null hypothesis ORR of 40% or less.
cOne-sided P value was calculated based on the null hypothesis CR of 20% or less.
Source: Clinical Study Report for the TRANSCEND Study.9
Critical Appraisal
The main limitation of the TRANSCEND study stems from the single-arm design and lack of comparator groups. In lieu of an available direct comparator, the investigators evaluated the primary end point of ORR against a null hypothesis (in the PAS population) of an ORR of 40% or less, with an alternate hypothesis of greater than 40% and an effect size of 25% (ORR = 65%). The hypothesis testing and adjustment for multiplicity were evaluated only for the PAS population, which can instill uncertainty in the effect estimates for other sets such as the leukapheresed set (ITT) and the DLBCL treated set. An open-label design may also increase uncertainty in patient-reported outcomes (PROs; i.e., HRQoL) introducing bias due to inherent subjectivity of the outcome in an unblinded assessor (patients and investigators). Furthermore, HRQoL outcomes were evaluated as secondary end points with no adjustment for multiplicity and with decreasing sample sizes at later time points of evaluation, decreasing precision due to fewer patients available to be analyzed. Any magnitude of effect that the anticancer interventions (bridging therapies) could have on the outcomes evaluated in the TRANSCEND study in patients receiving liso-cel is unknown. Sensitivity analyses based on assessing the leukapheresed set, by PP analysis, disease histology, and response determined by the investigator were overall supportive of the robustness of results. No subgroup effects were informative since the sample size was small and only in the PAS population.
Issues of generalizability of the results originate from the differences in the population included in the TRANSCEND study, which can be considered relatively young (mean age of 60.1 years in the DLBCL treated set as compared to mean age of 65 years from clinical guidelines and reviews) and with fewer baseline risks (only 4 patients in the DLBCL treated population was classified as ECOG PS = 2). This agreed with input from clinical experts consulted by CADTH, when considering the similarities between the populations from the TRANSCEND study and those likely to be encountered in clinical practice in Canada. The impact of these issues on the full implementation of the intervention, however, is uncertain. Other issues of generalizability are the low number of patients with FL3B, DLBCL transformed from indolent lymphomas other than follicular lymphoma, and patients with secondary CNS lymphoma that were included in the TRANSCEND study. These numbers make it difficult to draw conclusions on the effects of liso-cel in these populations. Furthermore, the relatively short time of follow-up for the main analysis on the PAS population (median of 11.5 months in the DLBCL treated set at the cut-off date of August 12, 2019) in the study can include some uncertainty in the effect estimates and in the generalizability of results in long-term outcomes, although further data from the June 19, 2020 and January 4, 2021 cut-off dates with median study follow-up durations of 19.1 and 19.9 months, respectively, ameliorate these issues.
Indirect Comparisons
Description of Studies
Two sponsor-submitted reports with 3 indirect treatment comparisons (ITCs) are included. The first 2 ITCs11,12 include comparisons evaluating individual patient data (IPD) evidence from a single-arm study (TRANSCEND) to be compared against aggregated data from 2 published sources evaluating tisa-cel and axi-cel, respectively . In these 2 unanchored matching-adjusted indirect comparisons (MAICs; 1 of liso-cel against tisa-cel, and the other against axi-cel), patients from these populations had R/R large B-cell lymphomas and included the lymphoma subtypes that were common among the 3 bodies of evidence, (i.e., DLBCL NOS, HGL, and transformed from follicular lymphoma). The second submitted report11 (ITC-2) includes an ITC as an unanchored MAIC comparing the same IPD from the TRANSCEND study against aggregated data from the SCHOLAR-113 study, which includes a population of patients with DLBCL treated with salvage therapies. The lymphoma subtypes included in the ITC-2 (i.e., those common among both bodies of evidence) were DLBCL, PMBCL, and tFL.
Efficacy Results
In the comparison of liso-cel versus tisa-cel, after matching and weighting 6 clinical factors, the primary analysis showed an ORR odds ratio (OR) favouring liso-cel over tisa-cel (OR = 2.77; 95% CI, 1.63 to 4.73; P < 0.001). For CRR, the OR significantly favoured liso-cel than over tisa-cel (OR = 1.92; 95% CI, 1.17 to 3.17; P = 0.010). For survival outcomes, the results of the MAICs showed longer median PFS and OS for liso-cel than for tisa-cel. For instance, the liso-cel group had a median PFS of 6.7 months (95% CI, 3.5 to not reached [NR]) as compared to tisa-cel of 2.8 months (2.3 to 4.2), and the rate of disease progression or mortality was significantly lower for liso-cel than for tisa-cel (hazard ratio [HR] = 0.66; 95% CI, 0.47 to 0.92; P = 0.013). Similarly, for OS, liso-cel had a median OS of 28.9 months (95% CI, 19.9 to NR) as compared to 11.7 (7.2 to not reached). For this comparison, the rate of mortality was significantly lower for liso-cel than for tisa-cel (HR = 0.66; 95% CI, 0.46 to 0.93; P = 0.019).
For the ITC analyzing the comparison of liso-cel versus axi-cel, the results of the MAICs showed no statistically significant difference for any of the end points (ORR, CRR, PFS, or OS).
The sponsor submitted an ITC evaluating liso-cel versus salvage chemotherapy in a MAIC, evaluating OS, CRR, and ORR. In the base-case analysis that accounted for 7 clinical factors to match and weight, the median OS for the TRANSCEND study was 21.1 months (95% CI, 12.1 to NR), with an effective sample size (ESS) of 142 (from an original N = 257); The analysis resulted in a HR of 0.47 (95% CI, 0.37 to 0.60) relative to salvage chemotherapy. Adjusted for 7 clinical factors, the CRR for liso-cel compared with salvage chemotherapy was greater with an OR of 12.89 (95% CI, 8.04 to 20.68; P < 0.001). PFS was not reported in the SCHOLAR-1 study. Unadjusted median OS was 27.3 months (95% CI, 16.8 to NR) for liso-cel (n = 257) and 6.0 months (95% CI, 5.6 to 6.8) for salvage chemotherapy (n = 603). In the base-case analysis that adjusted for 7 clinical factors, the median OS for TRANSCEND was 21.1 months (95% CI, 12.1 to NR), with an ESS of 142 (from an original N = 257); this results in a HR of 0.47 (95% CI, 0.37 to 0.60) relative to salvage chemotherapy. Adjusted for 7 clinical factors, the CRR for liso-cel was 49.2% with an ESS of 142, and when compared with salvage chemotherapy (CRR of 7.0%; n = 523) the matched and adjusted treatment effect on CRR was greater with an OR of 12.89 (95% CI, 8.04 to 20.68; P < 0.001). No data on harms were available in ITC-2.
For harms, liso-cel showed fewer AEs of special interest (AESI) such as CRS, NT, and neutropenia when compared to axi-cel or tisa-cel. Against tisa-cel, liso-cel had lower odds of CRS (OR = 0.52; 95% CI, 0.31 to 0.87) as well as for prolonged cytopenia (0.43; 95%CI, 0.26 to 0.73), but the rest of the AEs were similar overall. Relative to axi-cel, liso-cel had lower odds of CRS (0.03; 95% CI, 0.01 to 0.07), NT (0.16; 0.08 to 0.32), febrile neutropenia (0.09; 0.03 to 0.28), prolonged thrombocytopenia (0.34; 0.13 to 0.86), infections (0.19; 0.07 to 0.47), and any grade 3 or above level AE (0.04; 0.01 to 0.19). No data on harms were available for the ITC comparing liso-cel against salvage chemotherapy.
Critical Appraisal
Both ITC reports aimed at comparing IPD from a single-arm clinical trial (TRANSCEND) against aggregated data from observational studies. For the first report, 1 ITC compared liso-cel against axi-cel (ZUMA-1 study) and another ITC compared liso-cel against tisa-cel (JULIET study). The second report includes 1 ITC which compared liso-cel against salvage chemotherapy (from the SCHOLAR-1 study). All ITCs compared the interventions via an unanchored MAIC. One main limitation of unanchored MAICs is the lack of inclusion of relevant prognostic variables and effect modifiers that are not included in the weighting process. Differences in baseline characteristics of variables between the included studies suggest that other potential unmeasured confounders might be present, and that these can be unevenly distributed between groups. In both ITCs, authors attempted to obtain all possible prognostic variables/effect modifiers to be included in the weighting process of the MAIC. This effort for finding relevant clinical factors was data driven and included a literature search and clinician input. However, as mentioned by the authors, data-driven methods still have the probability of missing relevant factors, and there is no guarantee that all relevant factors were identified. Important differences in the measured variables were detected (e.g., age, International Prognostic Index [IPI] scores, ECOG PS) which can further increase the risk of bias. The ESS decreased in substantial numbers in both ITCs, which speaks of the amount of information lost due to the matching and adjustment process which also begets uncertainty and speaks of heterogeneity among original studies. There were also concerns of probable violations of the proportional hazards assumptions for time to event in end points such as OS in ITC-1. Overall, populations with R/R large B-cell lymphoma in the salvage chemotherapy had poor outcomes (e.g., OS close to a median of 6 months). Comparing the interventions used in these populations against newer CAR T-cell therapies might imply differences in baseline risks and uncertainty in the generalizability of effect estimates.
Other Relevant Evidence
An ongoing study (TRANSCEND WORLD) is included as “other relevant evidence” in this report. This is a single-arm, open-label, multi-cohort, multi-centre, phase II clinical trial to test efficacy and safety of liso-cel in adult patients with DLBCL NOS (de novo or tFL), HGL with MYC and BCL2 and/or BCL6 rearrangements with DLBCL histology and FL3B (Europe cohort 1, N = |||||| leukapheresed patients) and patients with DLBCL who are not eligible for transplant (Japan cohort 3, N = 14 leukapheresed patients). Both cohorts included |||||| leukapheresed patients, |||||| who received JCAR017 or a nonconforming product, and 37 who eventually received the JCAR017 (liso-cel) product. The median age of this cohort was also relatively young (58 years) and only 4 patients had an ECOG PS of 2.
Efficacy Results
The study met the primary efficacy end point, with an IRC-assessed ORR of ||||||||||||||||||||||||||||||| in the “efficacy-evaluable set,” thereby rejecting the null hypothesis of ORR of 40% or less (1-sided P value = 0.020). In the “liso-cel-treated set,” the ORR based on IRC assessment was ||||||||||||||||||||||||. Overall (N = 37), the Kaplan–Meier estimate median PFS was |||||||||||||||||||||||||||||||| Kaplan–Meier estimate for the median OS was |||||||||||||||||||||||||||||||||||||||||||||||||||||| and the median follow-up time was 6.39 months (95% CI, 3.09 to 9.33). Only 1 of the total 37 patients was admitted to the ICU.
Harms
The most common TEAEs were neutropenia (||||||), anemia |||||| and pyrexia |||||| The most frequently reported treatment-emergent SAEs were CRS |||||| and aphasia |||||| The deaths |||||| observed in the “enrolled set” |||||| were primarily due to progression of disease |||||| The most frequent notable harms, known to be associated with CAR T-cell therapies, were CRS |||||| prolonged cytopenias |||||| iiNT |||||| and hypogammaglobulinemia ||||||
Limitations are in line with the TRANSCEND study and include a lack of control group that makes it challenging to make conclusions about efficacy and safety. In addition, the small sample size and short follow-up period are another methodological limitation. Lastly, an open-label design may introduce a bias in interpreting results.
The study population included 1 patient with an ECOG PS score of 2 and none of the patients had CNS lymphoma at the beginning of the study. Patients may have developed secondary CNS lymphoma during the trial as noted in the study; however, there is no confirmed case. This selected population could make it difficult to generalize to patients with more severe burden of disease.
Conclusions
Evidence from a single-arm study (TRANSCEND) suggests that treatment with liso-cel is associated with benefits in outcomes deemed relevant to both patients and clinicians (OS, PFS, ORR, CRR) when compared to typical effects and evolution observed by clinical experts in patients with 3L+ R/R DLBCL not using a CAR T-cell treatment. The evidence also suggests that treatment with liso-cel may have benefits in terms of improving HRQoL and decreased health care utilization. Clinical experts considered that liso-cel safety profile was adequate and may perform better when compared to the 1 observed in clinical practice with other CAR T-cell therapies. Important limitations exist around these effect estimates due to lack of comparative evidence, risk of bias (attrition bias, no blinding), lack of adjustment for multiplicity, and imprecision in the effect estimates. Furthermore, there were concerns about the generalizability of the results due to characteristics of the populations in the TRANSCEND study that suggest a relatively stable and generally healthier population.
Evidence from sponsor-submitted ITCs using IPD from the TRANSCEND study matched and weighted in a MAIC against aggregated data from studies of 2 CAR T-cell therapies (axi-cel and tisa-cel) suggested improvements in ORR, CRR, PFS, and OS compared with tisa-cel, but not against axi-cel. Similarly, evidence from a second sponsor-submitted ITC using IPD from the TRANSCEND study against aggregated data of patients who underwent salvage therapies (SCHOLAR-1 study) suggests that liso-cel has greater improvements in efficacy and survival outcomes (OS, CRR, ORR) relative to the use of salvage chemotherapies. In all ITCs, liso-cel showed a better safety profile with fewer odds of AEs such as CRS and NT relative to axi-cel, tisa-cel, or salvage chemotherapy. The evidence from the ITCs has considerable limitations due to the observational nature of the included studies, difficulties in estimating all adequate prognostic variables, and possible residual confounding.
Overall, highly uncertain evidence from a single-arm trial and indirect comparative evidence suggest that liso-cel may be more efficacious than salvage chemotherapy and may provide clinical beneficial effects and a safety profile that are similar or better than what is expected of other CAR T-cell therapies.
Introduction
Disease Background
Lymphomas comprise a complex group of hematological malignancies with varying molecular hallmarks and prognoses. They are overall divided into NHL and Hodgkin lymphoma.1
In Canada, the incidence of NHL is reported at 24.4 per 100,000 with age-standardized incidence rates of 29.3 per 100,000 and 20.2 per 100,000 among men and women, respectively.2 It has been estimated that approximately 36,175 Canadians are living with, or are in remission from, a NHL. An estimated 8,000 new cases of lymphoma were diagnosed in Canada in 2016 and 10,400 estimated for the year 2020.2 The median age at diagnosis is 66 years for NHL; however, it can present at any age.3
There are many subtypes of NHL, including B-cell lymphomas. Diagnosis of B-cell lymphomas relies on a comprehensive examination of tumour tissue, best achieved with an excisional biopsy specimen evaluated by an expert hematopathologist. In addition to morphologic characteristics, an accurate lymphoma classification can be achieved with specialized tests, including immunohistochemistry, flow cytometry, fluorescence in situ hybridization, and molecular testing.
DLBCL is the most common type of NHL, comprising 30% to 40% of all cases.1 Most people with DLBCL are diagnosed when they are in their seventh decade of life. DLBCL is more common in men. DLBCL classified as NOS is the most common type of DLBCL, representing 80% to 85% of all cases.4,5 Other subtypes of DLBCL include PMBCL, a rare subtype of DLBCL.1,5 It occurs in the thymus or in lymph nodes in the mediastinum. It represents approximately 10% of all DLBCLs and it is more commonly seen in women in their third to fourth decades of life. DLBCL NOS and PMBCL both have a similar course and a similar treatment.1 tFL or DLBCL arising from indolent lymphoma are additional DLBCL subtypes, which are all initially slow-growing types of B-cell lymphomas that transform into DLBCL.
Patients with treatment failure after frontline rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone (see Standards of Therapy) often have a poor outcome—in particular, those with disease that is refractory to frontline or subsequent therapies—although some patients can have a durable remission and be cured after secondary therapies. Outcomes are worse in patients with chemotherapy-refractory disease, with only 7% achieving a CR to standard treatment and OS of 6 months.6 People of older age (> 65 years) and those with CNS involvement and comorbidities have higher possibility of adverse outcomes.7 No more than 50% of patients with R/R large B-cell lymphomas achieve a response to subsequent treatment after a standard second-line salvage regimen, and few are cured.8
Standards of Therapy
Treatment goals are directed at curing disease when possible, improving HRQoL with the ability for patients to return to work or daily activities, and prolong survival with the least symptoms, while minimizing adverse treatment effects.
Cyclophosphamide, doxorubicin, vincristine, and prednisone plus rituximab has been the first-line treatment of DLBCL since the early 2000s. Further treatment of DLBCL that is refractory or relapsing following first-line therapy will depend on patient status in relation to the eligibility for further intensive therapy (i.e., SCT or CAR T-cell therapies). Approximately 40% of patients will be refractory or have relapsed disease and of these, approximately 50% will be eligible for SCT.1
Patients eligible for SCT can further receive therapy with platinum-based salvage therapy (second line). Salvage therapy regimens may be gemcitabine, dexamethasone, and cisplatin, with or without rituximab, other options include rituximab plus ifosfamide-carboplatin-etoposide, rituximab plus dexamethasone, cisplatin, and cytarabine; and dexamethasone, ifosfamide, cyclophosphamide, etoposide, and procarbazine with existing variation in some regimens based on funding in specific jurisdictions across Canada. Patients with PR or CR to these regimens can enter into high-dose chemotherapy plus SCT. If despite these there is relapse and the patient is eligible for intensive therapy, then CAR T-cell therapy is an option. If the patient is not eligible for intensive therapy, then clinicians and patients can consider palliative care.
From the outset, patients who are not fit for intensive therapy or ineligible for SCT can be considered for salvage chemotherapy as second line.
Polatuzumab vedotin is an antibody-drug conjugate targeting CD79b, a component of the B-cell receptor complex, that is currently being used in combination with bendamustine and rituximab for patient’s ineligible for SCT.14
Eligible CAR-positive T-cell therapies (axi-cel, tisa-cel) are considered as third-line therapy. Some patients who are fit for intensive therapy and eligible for SCT may still be unable to undergo the transplant due to unsuccessful stem cell collection (which occurs in approximately 10% of attempts).
Patients with secondary CNS disease will follow similar pathways, but with the necessary use of CNS active regimens such as “MATRix-RICE” or high-dose methotrexate added to gemcitabine, dexamethasone, and cisplatin plus rituximab; or carboplatin, etoposide, ifosfamide, and Mesna; or dexamethasone, cytarabine, and cisplatin plus rituximab; or multiple doses of intrathecal chemotherapy.15
Palliative care usually includes gemcitabine, dexamethasone, and cisplatin, or methotrexate, etoposide, cisplatin, or prednisone, chlorambucil, etoposide, or combinations of these.
Drug
Liso-cel (also known as JCAR017) is a patient-specific cell suspension containing a target of 60 × 106 to 120 × 106 CAR-positive viable T cells (consisting of CD4 and CD8 components at a ratio range from 0.8 to 1.2) with each component supplied separately in 4 single-dose vials, for IV infusion. It has a proposed Health Canada indication for the treatment of adult patients with R/R large B-cell lymphoma after 2 or more lines of systemic therapy, including DLBCL NOS, PMBCL, high-grade B-cell lymphoma, and DLBCL arising from follicular lymphoma.
Liso-cel targets CD19, a marker expressed on B-cell precursors and malignant B cells present in DLBCL and other lymphomas. When CD19 markers are detected, T-cell activation ensues, and localized secretion of cytokines follows, leading to destruction of targeted cancer cells. Liso-cel consists of purified CD8+ and CD4+ T cells in a defined composition, that have been separately activated and transduced with a replication-incompetent lentiviral vector encoding an anti-CD19 CAR.
CADTH has not reviewed liso-cel for other indications, and the sponsor’s reimbursement request did not differ from the proposed Health Canada indication. The product was granted a Notice of Compliance by Health Canada on May 6, 2022.
In Table 3, characteristics of liso-cel and the other available CAR T-cell therapies are presented.
Table 3: Key Characteristics of Liso-Cel and Main Comparators
Criteria | Liso-cel | Axi-cel | Tisa-cel |
|---|---|---|---|
Mechanism of action | CD19-directed genetically modified autologous T-cell immunotherapy | CD19-directed genetically modified autologous T-cell immunotherapy | CD19-directed genetically modified autologous T-cell immunocellular therapy |
Indicationa | For the treatment of adult patients with R/R large B-cell lymphoma after 2 or more lines of systemic therapy, including DLBCL not otherwise specified, primary mediastinal large B-cell lymphoma, high-grade B-cell lymphoma, and DLBCL arising from follicular lymphoma | For the treatment of adult patients with R/R large B-cell lymphoma after 2 or more lines of systemic therapy, including DLBCL not otherwise specified, primary mediastinal large B-cell lymphoma, high-grade B-cell lymphoma, and DLBCL arising from follicular lymphoma | For the treatment of:
|
Route of administration | IV infusion | IV infusion | IV infusion |
Recommended dose | Patient-specific cell suspension in single-dose vials, 60 × 106 to 120 × 106 CAR-positive viable T cells (consisting of CD4 and CD8 components at a ratio range from 0.8 to 1.2), for IV infusion. A single dose of Breyanzi contains 60 × 106 to 120 × 106 CAR-positive viable T cells (consisting of CD4 and CD8 components at a ratio range from 0.8 to 1.2), with each component supplied separately in 1 to 4 single-dose vials. CD8 component Vials containing ≥ 8.0 × 106 CAR-positive viable T cells in 4.6 mL (≥ 1.6 × 106 CAR-positive viable T cells/mL). CD4 component Vials containing ≥ 8.0 × 106 CAR-positive viable T cells in 4.6 mL (≥ 1.6 1 × 106 CAR-positive viable T cells/mL). | Suspension of anti-CD19 CAR T cells in approximately 68 mL. The target dose is 2 × 106 CAR-positive viable T cells per kg body weight (range: 1 × 106 to 2.4 × 106 cells/kg), with a maximum of 2 × 108 CAR T cells for patients ≥ 100 kg. | Single-dose, one-time treatment, in a patient-specific infusion bag(s). Pediatric and young adult B-cell ALL:
Adult R/R DLBCL:
|
Serious adverse effects or safety issues | CRS, neurologic toxicities, secondary malignancies, hypogammaglobulinemia, prolonged cytopenias, infections, febrile neutropenia, tumour lysis syndrome have been observed | CRS, tumour lysis syndrome, neurologic toxicities, secondary malignancies, hypogammaglobulinemia, prolonged cytopenias, infections, febrile neutropenia | CRS, neurologic toxicities, secondary malignancies, hypogammaglobulinemia, prolonged cytopenias, infections, tumour lysis syndrome, febrile neutropenia |
Other | Must be administered in a qualified treatment centre under the supervision of health care professionals experienced in the treatment of hematological malignancies. Product must be kept frozen at ≤ –130°C until it is ready to use. | Must be administered in a qualified treatment centre under the supervision of health care professionals experienced in the treatment of hematological malignancies. Product must be kept frozen at ≤ –130°C until it is ready to use. | Must be administered in a qualified treatment centre under the supervision of health care professionals experienced in the treatment of hematological malignancies. Product must be kept frozen at ≤ –120°C until it is ready to use. |
ALL = acute lymphoblastic leukemia; axi-cel = axicabtagene ciloleucel; CAR = chimeric antigen receptor; CRS = cytokine release syndrome; DLBCL = diffuse large B-cell lymphoma; liso-cel = lisocabtagene maraleucel; R/R = relapsed or refractory; tisa-cel = tisagenlecleucel.
aThis is the Health Canada Notice of Compliance approved indication as of May 6, 2022. This CADTH Reimbursement Review was conducted before issuance of the Health Canada Notice of Compliance.
Source: Product monographs of liso-cel,16 axi-cel,17 and tisa-cel.18
Stakeholder Perspectives
Patient Group Input
Input was obtained from 1 patient group. Raw patient group input is presented in the Stakeholder Input section.
Lymphoma Canada, a Toronto-based, national Canadian registered charity that empowers the lymphoma community through education, support, advocacy, and research, provided an anonymous survey of patients with large B-cell lymphoma conducted online from June 21 to August 25, 2021. The survey participants (total = 331; DLBCL = 126, FL = 191, other LBCLs = 14) were from Canada, US, Europe, and other countries. Past survey data for subgroup of patients with DLBCL (2018 and 2020 surveys), follicular lymphoma (2017 and 2018), and those with CAR T-cell therapy experiences (April 18 to June 15, 2018) were also provided to supplement the current survey.
Respondents (n = 63) highlighted night sweat (57%), fatigue and lack of energy (54%), and aches and pains (54%) as the top symptoms of lymphoma that impact their quality of life. In addition, anxiety or worry (75%), stress related to the diagnosis (73%), and fear of progression (64%) were cited as the key psychosocial impacts. Diagnosis, symptoms, and mental health effects altogether significantly impacted patients’ daily activities (43%), ability to sleep (41%), concentration (40%), and ability to attend work or school (40%).
Of 230 respondents, 7% of patients had not yet received therapy (“watch and wait”), 50% received 1 line of therapy, and 43% received 2 or more lines of therapies at the time of survey. For patients with DLBCL receiving treatment, the most common side effects (n = 103) were hair loss (87%), fatigue (84%), and cognitive issues (68%), and the most intolerable side effects (n = 85) were fatigue (41%), nausea/vomiting (19%), and “chemo-brain” (15%). For patients with follicular lymphoma receiving treatment, the most common side effects (n = 61) were fatigue (85%), nausea or vomiting (51%), and hair loss (39%), and the most intolerable side effects (n = 49) were fatigue (37%), nausea or vomiting (10%), and pain (10%). Specific psychosocial impacts (n = 49) caused by treatments included fear of progression or relapse (67%), anxiety or worry (65%), and depression (47%). The most significant negative impacts on quality of life or daily living caused by treatments were treatment-related fatigue (57%, n = 273), late-onset or long-term side effects (41%, n = 49), and low activity level (39%, n = 176). In terms of difficulty accessing treatment options, 13% of patients (n = 44) found it very difficult to access. Living in a community without a cancer centre (35%, n = 49) was the most common reason for difficulty accessing treatment. Absence from work (62%), travelling costs (28%), and supplementary drug costs (26%) were the top financial impacts associated with accessing necessary treatments (n = 39).
The most desired outcomes from treatments included improved quality of life and performance of daily activities (93%, n = 176), longer survival (88%, n = 223), and longer disease remission (85%, n = 223). Forty-seven percent of patients (n = 297) responded that they would be willing to tolerate the short-term side effects of a new effective treatment and 47% (n = 297) said they would take the treatment recommended by their physicians even if it has potentially serious side effects.
According to the past survey data (2018), none of the patients had a direct experience with liso-cel therapy. Out of 7 patients who had experiences with other CAR T-cell therapies through clinical trials, 5 responded to questionnaire asking about CAR T-cell therapy’s impact on quality of life. These patients rated less than 3 (1 = no negative impact on my life; 5 = significant negative impact on my life) for all aspects of CAR T-cell therapy, meaning the number of clinic visits (2.8), travel to treatment centre (2.8), CAR T-cell infusion (2.6), short-term side effects (2.5), activity level (2.5), treatment-related fatigue (2.5), lasting side effects (2.0), and leukapheresis (1.8). When asked about recommending CAR T-cell therapy to other eligible patients, 5 out of 7 patients said they would recommend, 1 said they would not recommend, and 1 remained unsure.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). In addition, as part of the liso-cel review, a panel of 4 clinical experts from across Canada was convened to characterize unmet therapeutic needs, assist in identifying and communicating situations where there are gaps in the evidence that could be addressed through the collection of additional data, promote the early identification of potential implementation challenges, gain further insight into the clinical management of patients living with a condition, and explore the potential place in therapy of the drug (e.g., potential reimbursement conditions). A summary of this clinical discussion from panel and the clinical experts is presented below.
Unmet Needs
Clinical experts consulted by CADTH agreed that there is an unmet need for drugs that are better tolerated (better safety profiles), that can be used more frequently in the outpatient setting and that can be used in a broader population of patients with lymphoma (i.e., in patients with transformed from iNHL, FL3B, and CNS disease). Suboptimal availability of commercially available CAR T-cell products in some provinces generated the need to refer out of province or out of country for commercial CAR T-cell therapies.
Other therapies (e.g., polatuzumab) may not be widely available, or are costly.
Place in Therapy
According to the clinical experts consulted by CADTH, liso-cel would be used in a similar manner as the other available CAR T-cell therapies, as third-line therapy (in patients who have already tried 2 lines of chemotherapy). However, the clinical experts noted that the proposed indication for liso-cel includes a broader population than the indications for axi-cel and tisa-cel, such as those patients with iNHL (including chronic lymphocytic leukemia) and FL3B. The clinical experts noted that liso-cel would also be considered for use in patients with CNS disease. It was a consensus among clinical experts that patients who have had a previous CAR T-cell therapy would not be recommended to receive liso-cel as the evidence for this strategy is absent.
Patient Population
The clinical experts considered that patients most likely to benefit from liso-cel would be those with similar characteristics of the TRANSCEND study (e.g., ECOG PS of 0 or 1, low LDH), but the data on specific subgroups is still uncertain. Patients who have had an autologous stem-cell transplant (ASCT) and then relapsed or those who are not eligible for a transplant are likely to be favoured for liso-cel administration.
Clinicians mentioned that patients that would not be suitable for treatment with liso-cel would be those not meeting established criteria (i.e., eligibility criteria from TRANSCEND) for CAR T-cell therapy and would be excluded from therapy with liso-cel; however, the information is still uncertain to provide a definitive answer. For this same reason, is difficult to predict which patients would likely exhibit a response to treatment with liso-cel.
Assessing Response to Treatment
Clinicians considered that to determine a response to liso-cel, using commonly known parameters of efficacy and survival will suffice in clinical practice, such as survival with better HRQoL measures.
Overall, improved survival and reduction in the frequency and severity of symptoms, and cure would be good measurements of response throughout follow-up of patients.
When asked about clinically meaningful effects, the clinical experts considered that the hypotheses tested by the investigators in the TRANSCEND study with effect sizes of 25% improvement in survival and progression were deemed meaningful, but any improvement in survival or symptoms is desirable. Some clinicians prefer imaging as it is sometimes considered more objective to assess response to treatment. All these measurements are widely used by clinical experts without significant variations.
Experts preferred assessments of patients every 1 month to 3 months with varying frequency at the beginning of treatments.
Discontinuing Treatment
Discontinuation of CAR T-cell therapies would not be relevant as it is a single dose (although re-treatment is possible). However, some patients might be inherently unstable such that during the process that it may be necessary to discontinue (e.g., ECOG 4, sudden deterioration, opportunistic infections, and so on). This is when patients, after leukapheresis, are no longer able to receive liso-cel.
Prescribing Conditions
Patients and clinicians will need to be in large transplant centres in Canada. Currently, most provinces in Canada have (will have) the necessary expertise. In some areas, however, it cannot be done (e.g., a rural area). Outpatient is possible in well-resourced outpatient programs. According to the experts, Health Canada and Foundation for the Accreditation of Cellular Therapy-accredited SCT centres in Canada are needed (most are medium size, some are large). Outpatient therapy is feasible provided such programs have built the infrastructure to do so. Foundation for the Accreditation of Cellular Therapy accreditation is not uniform in Canada, but the clinical experts expect that the manufacturers may require this as a stipulation for distribution.
Additional Considerations
Experts noted that liso-cel may be associated with fewer toxicities than other CAR T-cell products (although no direct comparison were conducted), with CRS events of equal or greater severity in only 2% and NT in 10% (referring information from the TRANSCEND NHL001 study). For many patients with aggressive B-cell lymphoma, outcomes from currently available treatments are good. However, not all patients respond to currently available treatments. For those who achieve CR, the latter is not always sustained, and patients may relapse. Toxicity of treatments including intensive chemotherapy, SCT, and currently approved CAR T-cell therapies can be substantial. For transplant and even more so, CAR T-cell therapy, patients may need to travel out of province or even out of country to get treatment. Significant health care system resources are needed to safely provide these treatments.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups. Raw clinician group input can be found in the Stakeholder Input section.
Two clinician groups provided input on behalf of Lymphoma Canada and Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee. Lymphoma Canada is a national, non-for-profit organization for lymphoma and patients with chronic lymphocytic leukemia. The Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee is a committee that offers timely evidence-based clinical and health system guidance on drug-related matters.
The Lymphoma Canada clinician group stated that addition of liso-cel to the current third-line therapies or beyond is important for the following reasons: 1) as a curative therapy, liso-cel is expected to improve remission (e.g., CR and PRs) and prolong survival (e.g., overall and PFS) of the eligible patients; 2) availability of liso-cel would prevent unnecessary delay in treatment caused by short supply of the existing CAR T-cell therapies; 3) liso-cel has shown less frequent adverse effects (i.e., CRS and NT) compared to axi-cel without compromising efficacy (note: no head-to-head trial is available); 4) liso-cel can be safely administered in an outpatient setting similarly to tisa-cel.
The Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee recognized that liso-cel would fulfill the unmet needs of indications that are not covered by the other CAR T-cell therapies (e.g., FL3B and secondary CNS lymphoma). Moreover, the Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee identified that the limited number of CAR T-cell therapy centres available across Canada could cause access issues for patients.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Implementation issues | Clinical experts’ response |
|---|---|
Relevant comparators | |
The TRANSCEND NHL-001 study was a single-arm trial. Relevant comparators include axicabtagene ciloleucel, tisagenlecleucel, salvage chemotherapy (GDP, DHAP, ifosfamide, carboplatin, and etoposide, gemcitabine monotherapy, oral cyclophosphamide and etoposide) and polatuzumab plus bendamustine and rituximab. | Clinical experts agreed with the comparators stated in the protocol for this review (i.e., other CAR T-cell therapies such as axicabtagene ciloleucel and tisagenlecleucel, and drug regimens/salvage chemotherapy). |
Two other CAR T-cell products for the treatment of DLBCL (tisa-cel, axi-cel) have been assessed by CADTH and are funded in Canada. Based on the pivotal trial data and approved indication, does liso-cel expand the eligible patient population beyond that which is currently eligible for CAR T-cell therapy? | Clinical experts indicated that DLBCL transformed from iNHL (including CLL), follicular lymphoma grade 3B, and CNS disease would be additional indications for liso-cel, if funded, as these are indications or populations that were included in the TRANSCEND trial. |
Considerations for initiation of therapy | |
Can it be clarified if patients should receive reconfirmation of PET-positive disease before lymphodepleting therapy? (This is not required for the 2 currently funded CAR T-cell products in Canada). | The clinical experts consulted by CADTH indicated that negative PET results are not required before infusion as PET results are expected to be positive in most patients. |
For transformed DLBCL, do patients need to have received or failed treatment for the diagnosis of DLBCL or is biopsy-proven DLBCL sufficient? (e.g., the patient only received treatment for SLL/CLL then transformed to DLBCL). | Clinical experts noted that patients would need at least 2 lines of systemic therapy (usually considered to be effective) from the time of diagnosis of the transformed DLBCL. Potential exceptions may include individuals with follicular lymphoma for which they already have received treatment (e.g., with R-CHOP, GDP, and auto-stem cell transplant) but then transforms to DLBCL or high-grade B-cell lymphoma. For these cases, clinicians may want to move directly to offer CAR T-cell therapies since other options are limited. Clinical experts suggest criteria could stipulate the minimum types of therapy required in these situations. |
Do patient eligibility criteria overlap with existing commercial CAR T-cell therapy eligibility criteria (tisa-cel and axi-cel)? Liso-cel was also evaluated in DLBCL from indolent lymphomas and in follicular lymphoma grade 3B. | Eligibility criteria for liso-cel would overlap with axi-cel. Tisa-cel, on the other hand, does not include criteria for primary mediastinal lymphoma. |
Is liso-cel recommended (i.e., are there outcome data specifically for) in the following groups:
| The clinical experts indicated that liso-cel would be considered for use in patients who are > 75 years, have follicular lymphoma grade 3B, ECOG Performance Status < 2, and have CNS involvement. The clinical experts emphasized the need for more data, especially comparative data. TRANSCEND is the first study to include the patients with CNS involvement and prior allo-stem cell transplant. The clinical experts noted that both of these subgroups of patients represent a small proportion of the population practice making it difficult for studies to be conducted with these subgroups specifically. |
Can we confirm that patients with comorbidities are eligible? (e.g., reduced cardiac and renal function) | Yes, but patients require sufficient cardiac function to survive CRS or sepsis, and renal function to tolerate fludarabine. Currently there is variability on the approach to patients with comorbidities by Canadian centres. |
Should patients that have received other CAR T-cell therapies for DLBCL be eligible for liso-cel? | There are currently no data to support that patients that have received previous CAR T-cell therapies for DLBCL should receive liso-cel. Response to a second (different) CAR T-cell product is unknown and should be studied independently. |
Please confirm that this is a single-dose treatment, and that re-treatment is not recommended. | According to the clinical experts, there are no data to support re-treatment. |
Would patients with secondary CNS involvement be eligible? | Experts agreed that as long as disease is controlled, patients can be eligible. This population is in great need of better therapies. |
Is liso-cell sufficiently distinct from axi-cel and tisa-cel to warrant separate eligibility criteria? Consider alignment with reimbursement criteria for CAR T-cell therapy with tisa-cel and axi-cel. | Experts would treat the same as axi-cel but would add the DLBCL transformed from iNHL (including CLL), follicular lymphoma grade 3B, and CNS disease. |
Considerations for prescribing of therapy | |
The sponsor’s budget impact analysis assumes a single infusion, but the pivotal trial allowed for second infusions in refractory patients. | Re-treatment was discussed by the clinical experts as a possibility in a proportion of patients like those included in the TRANSCEND trial. |
Delivery must take place at specialized treatment centres that are FACT accredited and certified by the sponsor. A patient advisory group notes that the timelines for the sponsor’s assumptions regarding delivery locations may be unrealistic, as the roll-out of CAR T-cell therapy is dependent on provincial funding and site capacity to deliver. This may affect budget impact analysis assumptions. | Administration would be done preferably in Health Canada and FACT-accredited stem cell transplant centres. Outpatient therapy is feasible provided such programs have built the infrastructure to do so. FACT accreditation is not uniform in Canada. Sponsor companies will work with any transplant centre that has standards deemed to be at the level of FACT accreditation. All stem cell transplant centres are Health Canada–approved, and most centres are already FACT accredited. Those that are not FACT accredited may try to justify to the sponsor that they can administer CAR T-cell therapies, so implementation in these centres is still possible. One expert noted that in one centre, all companies have reached out to clinicians to state that they no longer require FACT accreditation. However, they do require a program at the FACT standards, hence would effectively imply that it is a centre that does routine apheresis for stem cells/donor lymphocyte infusion. One expert noted that, ideally, programs should meet FACT standards. FACT accreditation is not mandated by Canadian authorities, hence the variability across Canada. |
There is limited access to CAR T-cell services in Canada. While access is expanding, interprovincial travel, or out-of-country funding remains necessary in many parts of Canada. Due to geographical site limitations, patients may need to travel for treatment requiring interprovincial agreements to ensure equitable access as is needed for 2 prior CAR T-cell therapies that have been approved for DLBCL. | For pERC consideration. |
Delivery sites may have capacity and feasibility issues with being certified by more than one CAR T-cell sponsor (training, ongoing auditing, slightly different protocols) | For pERC consideration. |
Funding algorithm (oncology only) | |
Drug may change place in therapy of comparator drugs. When would liso-cel be preferred over currently funded CAR T-cell therapies? Is there sufficient clinical evidence to favour one CAR T-cell therapy over another, either generally or in any subpopulation? If this drug is the same price as tisa-cel or axi-cel, will it replace them? | Overall, it is not expected that liso-cel would be better than other CAR T-cell therapies, but it may be offered to a broader population of patients with lymphoma (i.e., transformed from iNHL, follicular lymphoma grade 3B, or CNS disease). Although there is a perception of better safety profile, experts agreed that it may be a result of clinicians having a better understanding on how to better manage CRS and immune effector cell-associated neurotoxicity syndrome, which would lead to more favourable outcomes, although the evidence is still uncertain to support any assumption. Another expert mentioned that no clear clinical evidence to favour one CAR T-cell therapy over the other for the overlapping indications. However, in practice some centres may choose to align with a limited number of manufacturers to minimize contractual and pharma specific requirements (i.e., it is possible one will be favoured for logistical reasons). |
Complex therapeutic space with multiple lines of therapy, subpopulations, or competing products Competing products: tisa-cel and axi-cel | For pERC consideration. |
Other aspects: Concerns around delivery sites processing 3 different manufacturers of CAR T cells. Additional costs incurred by non-delivering sites when sending patients out of province for treatment | For pERC consideration. |
Care provision issues | |
Like other CAR T-cell therapies, hospitalization for adverse events is not uncommon, which may include admission to an intensive care unit. Does the adverse effect profile differ significantly from currently funded CAR T-cell therapies? CRS is sometimes managed with tocilizumab. Tocilizumab is on the Canada Drug Shortages website list due to its use in COVID-19 treatment, with anticipated resolution date of December 31, 2021. Is there another treatment that can be used to manage CRS if tocilizumab is not available? Should treating centres ensure that tocilizumab is available before starting liso-cel? (Would also be an issue for other CAR T-cell therapies.) | Clinical experts mention that liso-cel may have a better safety profile, but there is still uncertainty around this issue. For now, it is important to focus on the proportion treated as an outpatient in the TRANSCEND study. The use of tocilizumab and possible shortages is a concern as the companies require 2 doses on hand for each patient. The use of siltuximab has been considered by some clinicians if there is a severe shortage. A biosimilar tocilizumab would be helpful in the future. |
System and economic issues | |
CAR T-cell therapy is an expensive therapy that requires considerable resources to deliver. As patients with DLBCL are already potentially eligible for CAR T-cell therapy in Canada, the patient advisory group is interested to know the extent to which the eligible patient population will expand (assuming no delivery constraints) if liso-cel is funded. | For pERC consideration. Refer to CADTH Economic Report. |
Accessing CAR T-cell therapy may require interprovincial travel. A program to cover travel expenses should be offered by the sponsor until widespread access across Canada is available. Due to geographical site limitations, patients may need to travel for treatment requiring interprovincial agreements to ensure equitable access as is needed for 2 prior CAR T-cell therapies that have been approved for DLBCL. | For pERC consideration. |
Tisa-cel and axi-cel are already funded in Canada for the treatment of relapsed/refractory DLBCL after 2 or more lines of therapy. Both tisa-cel and axi-cel have gone through price negotiations for the same indication. | For pERC consideration. |
Cost-effectiveness of therapy based on long-term data not available. Unknown burden and cost to staff to process cells for third product and to maintain level of training. Patient privacy and patient cell ownership concerns due to fact that CAR T cells are manufactured by US-based companies outside of Canadian jurisdiction. (This is also the case for the other CAR T-cell therapies that are publicly funded.) | For pERC consideration. |
allo = allogeneic; auto = autologous; axi-cel = axicabtagene ciloleucel; CAR = chimeric antigen receptor; CLL = chronic lymphocytic leukemia; CNS = central nervous system; CRS = cytokine release syndrome; DHAP = dexamethasone, cytarabine, and cisplatin; DLBCL = diffuse large B-cell lymphoma; ECOG = Eastern Cooperative Oncology Group; FACT = Foundation for the Accreditation of Cellular Therapy; GDP = gemcitabine, dexamethasone, and cisplatin; iNHL = indolent non-Hodgkin lymphoma; liso-cel = lisocabtagene maraleucel; pERC = CADTH pCODR Expert Review Committee; R-CHOP = rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone; SLL = small lymphocytic lymphoma; tisa-cel = tisagenlecleucel.
Clinical Evidence
The clinical evidence included in the review of liso-cel is presented in 3 sections. The first section, the Systematic Review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor and indirect evidence selected from the literature that met the selection criteria specified in the review. The third section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of liso-cel for the treatment of adult patients with R/R large B-cell lymphoma including DLBCL NOS (including DLBCL arising from indolent lymphoma), HGL, PMBCL, and FL3B after at least 2 prior therapies.
Methods
Studies selected for inclusion in the systematic review include pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 5. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans. Of note, the systematic review protocol presented below was established before the granting of a Notice of Compliance from Health Canada.
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Adult patients with relapsed or refractory large B-cell lymphoma including DLBCL not otherwise specified (including DLBCL arising from indolent lymphoma), HGBCL, PMBCL, and FL3B after at least 2 prior therapies. Subgroups:
|
Intervention | Lisocabtagene maraleucel, (IV, cell suspension in patient-specific single-dose vials, target dose of 100 × 106 CAR T cells) |
Comparator |
|
Outcomes | Efficacy outcomes:
Harms outcomes:
Notable harms and harms of special interest: B-cell aplasia, secondary malignancies, febrile neutropenia, cytopenia, neurologic effects (ICANS), infections, replication-competent lentivirus, development of anti-CAR antibody response, CRS, anaphylaxis. |
Study designs | Published and unpublished phase I, II, III, and IV RCTs and clinical trials. |
AE = adverse event; CAR = chimeric antigen receptor; CRR = complete response rate; CRS = cytokine release syndrome; DHAP = cytarabine, dexamethasone, cisplatin, and etoposide; DLBCL = diffuse large B-cell lymphoma; DOR = duration of response; ECOG = Eastern Cooperative Oncology Group; EFS = event-free survival; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EQ-5D-5L = EuroQol 5-Dimensions 5-Levels questionnaire; FACT-Lym = Functional Assessment of Cancer Therapy–Lymphoma; FL = Follicular lymphoma; FL3B = follicular lymphoma grade 3B; GDP = gemcitabine, dexamethasone, and cisplatin; GemOx = gemcitabine and oxaliplatin; HGBCL = high-grade B-cell lymphoma; HRQoL = health-related quality of life; HSCT = hematopoietic stem cell transplant; ICAN = immune effector cell-associated neurotoxicity syndrome; ICE = carboplatin, etoposide, ifosfamide, and Mesna; MEP = methotrexate, etoposide, cisplatin; OS = overall survival; PEP-C = prednisone, etoposide, procarbazine, cyclophosphamide; PFS = progression-free survival; PMBCL = primary mediastinal large B-cell lymphoma; RCT = randomized controlled trial; SAE = serious adverse event; TTR = time to response; WDAE = withdrawal due to adverse event.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.19
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946‒) via Ovid and Embase (1974‒) via Ovid. All Ovid searches were run simultaneously as a multi-file search. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Patient Headings), and keywords. The main search concepts were Breyanzi (liso-cel). Clinical trials registries were searched: the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register. No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Refer to Appendix 1 for the detailed search strategies.
The initial search was completed on September 2, 2021. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee on April 13, 2022. Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool for Searching Health-Related Grey Literature checklist. Included in this search were the websites of regulatory agencies (FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Refer to Appendix 1 for more information on the grey literature search strategy. These searches were supplemented by reviewing bibliographies of key papers and through contacts with appropriate experts. In addition, the sponsor of the drug was contacted for information regarding unpublished studies. Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
Two studies were identified as potentially relevant from other sources and from the literature for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 6. A list of excluded studies is presented in Appendix 4 with reasons for exclusion.
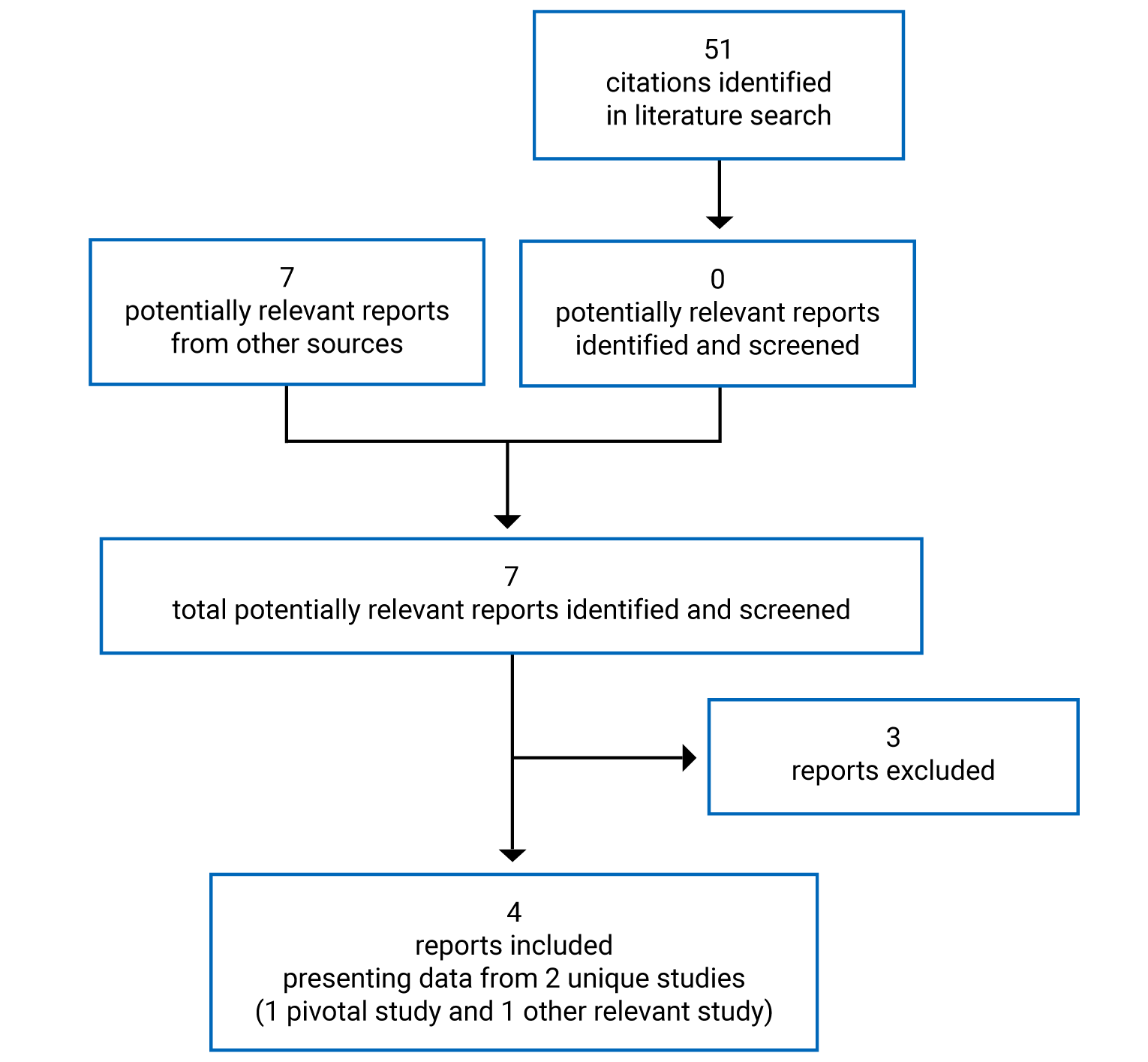
Table 6: Details of Included Study
Criteria | TRANSCEND NHL 001 |
|---|---|
Designs and populations | |
Study design | Phase I open-label, multi-centre, multi-cohort, single-arm study |
Locations | 14 cancer centres (sites) in the US |
Patient enrolment dates | First patient enrolled: January 6, 2016 Data cut-off date: August 12, 2019 The study will be considered completed when all patients in each cohort have been followed for safety, disease progression, and survival for 2 years after their last dose. |
Enrolled (N) | 344 to undergo leukapheresis |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Liso-cel IV cell suspension. Dose level 1, at day 1: 50 × 106 total CAR T cells. Dose level 1D, at day 1 and day 15: 50 × 106 total CAR T cells. Dose level 2, at day 1: 100 × 106 total CAR T cells. Dose level 3, at day 1: 150 × 106 total CAR T cells. 3 single-dose schedules were tested (dose level 1, 2, and 3). Dose level 1 was also tested as a 2-dose schedule (dose level 1D), with a second dose of liso-cel given at day 15. Lymphodepleting chemotherapy was not given before the second dose of liso-cel in the 2-dose schedule. |
Comparator(s) | No comparator arm |
Duration | |
Phase | |
Pre-treatment | Informed consent, screening, and evaluation: 28-day window Leukapheresis (liso-cel manufacturing): 28-day window |
Treatment | Lymphodepleting chemotherapy: 2 to 7 days before liso-cel infusion Liso-cel infusion in the 1 and 2-dose schedule, a first dose of liso-cel was given 2 to 7 days after LDC and a second dose was given 14 days after the first dose of liso-cel (without further LDC between the 2 doses). |
Post-treatment | Follow-up for OS, safety, and disease progression: 2 years Cut-off date for this report: August 12, 2019. Follow-up is ongoing. |
Outcomes | |
Primary end points |
|
Secondary and exploratory end points | Key secondary:
Exploratory:
|
Notes | |
Publications | |
AE = adverse event; CAR = chimeric antigen receptor; CR = complete response; DLBCL = diffuse large B-cell lymphoma; DLT = dose-limiting toxicity; DOR = duration of response; ECOG = Eastern Cooperative Oncology Group; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EQ-5D-5L = EuroQol 5-Dimensions 5-Levels questionnaire; FISH = fluorescence in situ hybridization; HRQoL = health-related quality of life; ICU = intensive care unit; LDC = lymphodepleting chemotherapy; liso-cel = lisocabtagene maraleucel; mCRM = modified continual reassessment method; NHL = non-Hodgkin lymphoma; ORR = objective response rate; OS = overall survival; PCR = polymerase chain reaction; PD = progressive disease; p[DLT] = probability of DLT; PFS = progression-free survival; PK = pharmacokinetic; PR = partial response; R/R = relapsed or refractory.
Source: Clinical Study Report for the TRANSCEND study.9
Description of Studies
The TRANSCEND study is a phase I (stated as seamless), single-arm, multi-centre, multi-cohort trial conducted in 14 cancer centres in the US. The first patient was enrolled on January 6, 2016, and last data cut-off date available was August 12, 2019. The study will be considered completed when all patients in each cohort have been followed for safety, disease progression, and survival for 2 years after their last dose. The main objective of the study was to evaluate the safety of liso-cel in adult patients with R/R B-cell NHL including DLBCL NOS (de novo and transformed from indolent lymphoma), high-grade B-cell lymphoma (HGL) with MYC and BCL2 and/or BCL6 rearrangements with DLBCL histology, PMBCL, FL3B, and mantle cell lymphoma (MCL), as well as the antitumour activity of liso-cel (measured as ORR). The key secondary objectives include assessing the rate of CR and durability of antitumour activity (measured as DOR) of liso-cel and estimate the PFS and OS an HRQoL of patients treated with liso-cel.
The study consisted of 3 main periods: pre-treatment, treatment, post-treatment. A schematic of the treatment plan is depicted in Figure 2.
Figure 2: Study Schematic of TRANSCEND NHL 001
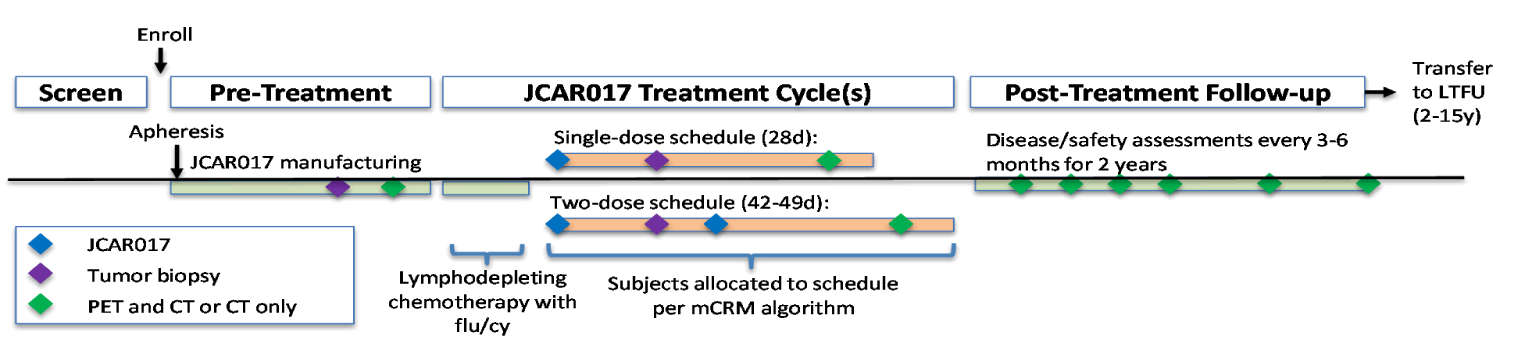
d = day; flu/cy = fludarabine/cyclophosphamide; LTFU = long-term follow-up; mCRM = modified continual reassessment method.
Source: Clinical Study Report TRANSCEND study.9
Two cohorts based on disease specifics were evaluated: the DLBCL cohort (patients with DLBCL NOS [de novo or transformed from indolent lymphoma]), HGL, PMBCL, and FL3B having received at least 2 prior therapies; and the MCL cohort, with MCL having received at least 1 prior therapy. Data from the ongoing MCL cohort are not included in this report.
The pre-treatment phase consisted of screening and enrolment of eligible patients who then underwent leukapheresis to enable the product (liso-cel) generation. In addition, disease assessments and other measures were taken. If necessary, bridging therapy, consisting of systemic anticancer therapy for disease control was allowed while the product was being manufactured (i.e., during the period between screening and LDC). In this case, patients were required to have PET-positive disease and meet relevant eligibility criteria before treatment with LDC and liso-cel.
Upon liso-cel product generation, patients entered the treatment phase of the study, which commenced with LDC and ended with the day 29 evaluation. The treatment cycle included LDC with fludarabine and cyclophosphamide followed by 1 (single-dose schedule) or 2 (2-dose schedule) doses of liso-cel administered IV on day 1. Day 1 was defined as the day of first liso-cel administration. In the single-dose schedule, liso-cel was administered 2 to 7 days after completion of LDC. In the 2-dose schedule, patients received the first dose as described above, and a second dose of liso-cel was given 14 days after the first dose of liso-cel (without further LDC between the 2 doses).
The post-treatment follow-up phase consisted, after day 29, of patients who were followed in this study for safety, disease progression, and survival for 2 years after their last dose of liso-cel, including after disease progression and/or the initiation of additional anticancer therapies.
After completion of the final efficacy and safety assessments, long-term follow-up for survival, long-term toxicity, and viral vector safety is to be continued under a separate protocol for up to 15 years post-last dose of liso-cel per FDA guidance on viral vector-based gene therapy products.
As of the data cut-off date of August 19, 2019, 6 amendments to the protocol study were filed and implemented during the conduct of the TRANSCEND study. A summary of the substantive changes made in each amendment is provided in Appendix 4.
Further data from the cut-off dates of June 19, 2020, and January 4, 2021, were also submitted by the sponsor to assess outcomes at later points and were included in this report to address key efficacy end points (ORR, CRR, DOR, PFS, and OS) and harms. However, these later cut-off dates data will be considered supplemental evidence to the main analysis (August 19, 2019) which was based on the PAS population and where the end points were tested and adjusted for multiplicity.
Populations
Inclusion and Exclusion Criteria
As described in Table 6, patients 18 years of age and older with R/R B-cell NHL of the following histologies were included. The DLBCL cohort included DLBCL and NOS, including transformed DLBCL from indolent histology [transformed iNHL]), HGL with MYC and BCL2 and/or BCL6 rearrangements with DLBCL histology, PMBCL, and FL3B. These patients must have been treated with an anthracycline and rituximab (or other CD20-targeted agent) and have R/R disease after at least 2 lines of therapy or after auto-HSCT. Exclusion criteria included CNS pathology, cardiovascular conditions, graft-versus-host disease, use of corticosteroids, low-dose chemotherapy, other cytotoxic or lymphotoxic chemotherapy, experimental agents, and use of immunosuppressive agents.
Of note, a PET-positive disease was necessary according to the Lugano Classification10 and an ECOG PS of 2. An ECOG PS status of 0, 1, or 2 was allowed initially, but it was changed after the Protocol Amendment 5 to include only an ECOG PS status of 0 or 1.
All patients included had to have adequate organ function (i.e., bone marrow, renal, liver, pulmonary, and cardiac). Patients with secondary CNS involvement were allowed, except if it was a CNS-only involvement by malignancy. Patients with other malignancies, uncontrolled systemic infections, and treatment with alemtuzumab within 6 months of leukapheresis, or treatment with fludarabine or cladribine within 3 months of leukapheresis, were not eligible to enter the study.
Baseline Characteristics
Baseline demographic information, disease characteristics, and prior medications of patients included in the TRANSCEND study (DLBCL treated set) are described in Table 7. Since the main study effects of end points were analyzed in the PAS population, the baseline characteristics for this population are presented in Table 8.
In the DLBCL treated set, the study included mostly male patients (65%) with a diagnosis of R/R DLBCL; the total population had a median age of 63 years (range = 18 to 86) and a mean age of 60.1 (standard deviation = 13.35) years, ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||; this is a relatively young population below the median age of diagnosis of 65 years of age commonly reported in epidemiology reviews and current clinical guidelines.1,21 A total of 25 patients were allowed to be treated as outpatients (13 in the DL2S group).
Based on baseline disease characteristics, most patients did not exhibit severe status and had a relatively stable health status, beyond their R/R DLBCL condition. For instance, only 4 patients (3 in the D2LS subpopulation) had an ECOG PS of 2 at baseline, 83.6% had a creatinine clearance (CrCl) pre-LDC greater than 60 mL/min, and 96% had a left ventricular ejection fraction (LVEF) greater than 50%.
DLBCL NOS was the most common histologic type among patients with DLBCL (51%), with 35% of patients having a previous SCT, and a median of 3 previous systemic treatments. Only 4 patients in the DL2S treatment group had CNS involvement, mainly due to the amendment that allowed the eligibility and inclusion of these patients in the study. Of the leukapheresed set of patients (N = 344), 214 (62.2%) received anticancer therapies before LDC (140 in the DL2S group, 61.7%), which included bridging therapies.
Table 7: Summary of Baseline Characteristics, DLBCL Treated Set
Variable | DL2S n = 177 | DL1S n = 45 | DL1D n = 6 | DL3S n = 41 | Total N = 269 |
|---|---|---|---|---|---|
Baseline Demographic | |||||
Age, mean (standard deviation) | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | 60.1 (13.35) |
Age group, n (%) | |||||
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
< 65 years | |||||||||||| | 30 (66.7) | |||||||||||| | 18 (43.9) | 157 (58.4) |
≥ 65 years | 71 (40.1) | 15 (33.3) | 3 (50.0) | 23 (56.1) | 112 (41.6) |
< 75 years | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | 242 (90.0) |
≥ 75 years | 15 (8.5) | 4 (8.9) | 0 (0.0) | 8 (19.5) | 27 (10.0) |
Sex, n (%) | |||||
Male | 117 (66.1) | 31 (68.9) | 5 (83.3) | 21 (51.2) | 174 (64.7) |
Female | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | 95 (35.3) |
Race, n (%) | |||||
American Indian or Alaska Native | 2 (1.1) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 (0.7) |
Asian | 9 (5.1) | 1 (2.2) | 0 (0.0) | 1 (2.4) | 11 (4.1) |
Black or African American | 9 (5.1) | 2 (4.4) | 0 (0.0) | 1 (2.4) | 12 (4.5) |
Multiple | 0 (0.0) | 1 (2.2) | 0 (0.0) | 0 (0.0) | 1 (0.4) |
White | 149 (84.2) | 41 (91.1) | 6 (100.0) | 36 (87.8) | 232 (86.2) |
Not reported | 8 (4.5) | 0 (0.0) | 0 (0.0) | 3 (7.3) | 11 (4.1) |
BMI (kg/m2), mean (standard deviation) | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Weight (kg), mean (standard deviation) | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
ECOG PS at screening, n (%) | |||||
0 | 65 (36.7) | 24 (53.3) | 2 (33.3) | 19 (46.3) | 110 (40.9) |
1 | 109 (61.6) | 20 (44.4) | 4 (66.7) | 22 (53.7) | 155 (57.6) |
2 | 3 (1.7) | 1 (2.2) | 0 (0.0) | 0 (0.0) | 4 (1.5) |
LVEF at screening, n (%) | |||||
≥ 40% to < 50% | 7 (4.0) | 2 (4.4) | 0 (0.0) | 4 (9.8) | 13 (4.8) |
≥ 50% | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
CrCl pre-LDC, n (%) | |||||
< 60 mL/min | 29 (16.4) | 9 (20.0) | 1 (16.7) | 12 (29.3) | 51 (19.0) |
≥ 60 mL/min | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Disease characteristics | |||||
Type of B-cell non-Hodgkin lymphoma, n (%) | |||||
DLBCL NOS | 94 (53.1) | 21 (46.7) | 2 (33.3) | 20 (48.8) | 137 (50.9) |
HGL, including DLBCL with double/triple hit | 26 (14.7) | 6 (13.3) | 1 (16.7) | 3 (7.3) | 36 (13.4) |
DLBCL transformed from indolent lymphoma | 41 (23.2) | 16 (35.6) | 3 (50.0) | 18 (43.9) | 78 (29.0) |
Follicular lymphoma | 34 (19.2) | 12 (26.7) | 1 (16.7) | 13 (31.7) | 60 (22.3) |
Marginal zone lymphoma | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | 10 (3.7) |
CLL/SLL | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | 5 (1.9) |
Other | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | 3 (1.1) |
FL3B | 2 (1.1) | 1 (2.2) | 0 (0.0) | 0 (0.0) | 3 (1.1) |
PMBCL | 14 (7.9) | 1 (2.2) | 0 (0.0) | 0 (0.0) | 15 (5.6) |
Cell of origin (for DLBCL) n (%) | |||||
GCB | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | 119 (44.2) |
Non-GCB | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | 76 (28.3) |
Unknown | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | 56 (20.8) |
Refractory or relapsed, n (%) | |||||
Refractory | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | 213 (79.2) |
Relapsed | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | 56 (20.8) |
Chemorefractory or chemosensitive, n (%)a | |||||
Chemorefractory | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Refractory due to relapse < 12 months after ASCT | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Last chemotherapy | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Chemosensitive | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
CNS involvement by lymphoma at first liso-cel infusion, n (%) | |||||
Yes | 4 (2.3) | 2 (4.4) | 0 (0.0) | 1 (2.4) | 7 (2.6) |
No | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | 262 (97.4) |
Prior treatments | |||||
Prior treatment, n (%) | |||||
Hematopoietic stem cell transplant | 61 (34.5) | 24 (53.3) | 2 (33.3) | 7 (17.1) | 94 (34.9) |
Allogeneic | 4 (2.3) | 4 (8.9) | 0 (0.0) | 1 (2.4) | 9 (3.3) |
Autologous | 61 (34.5) | 21 (46.7) | 2 (33.3) | 6 (14.6) | 90 (33.5) |
Radiotherapy | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Systemic treatment | 177 (100) | 45 (100) | 6 (100) | 41 (100) | 269 (100) |
Number of prior systemic treatments | |||||
Median | 3.0 | 3.0 | 3.5 | 2.0 | 3.0 |
Minimum, maximum | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
1 prior regimen, n (%) | 6 (3.4) | 1 (2.2) | 1 (16.7) | 1 (2.4) | 9 (3.3) |
2 prior regimens, n (%) | 80 (45.2) | 14 (31.1) | 1 (16.7) | 26 (63.4) | 121 (45.0) |
3 prior regimens, n (%) | 45 (25.4) | 12 (26.7) | 1 (16.7) | 10 (24.4) | 68 (25.3) |
4 prior regimens, n (%) | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | 43 (16.0) |
≥ 5 prior regimens, n (%) | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | 28 (10.4) |
ASCT = autologous hematopoietic stem cell transplant; BMI = body mass index; CAR = chimeric antigen receptor; CLL = chronic lymphocytic leukemia; CNS = central nervous system; CrCl = creatinine clearance; DL = dose level; DL1D = dose level 1 (50 × 106 CAR-positive T cells), 2-dose regimen; DL1S = dose level 1 (50 × 106 CAR-positive T cells), single-dose regimen; DL2S = dose level 2 (100 × 106 CAR-positive T cells), single-dose regimen; DL3S = dose level 3 (150 × 106 CAR-positive T cells), single-dose regimen; DLBCL = diffuse large B-cell lymphoma; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FL3B = follicular lymphoma grade 3B; GCB = germinal centre B-like; HGL = high-grade lymphoma; LDC = lymphodepleting chemotherapy; liso-cel = lisocabtagene maraleucel; LVEF = left ventricular ejection fraction; NOS = not otherwise specified; PMBCL = primary mediastinal B-cell lymphoma; SLL = small lymphocytic lymphoma.
aThe status was chemorefractory if a patient achieved stable disease or progressive disease to last chemotherapy-containing regimen or relapsed less than 12 months after ASCT; otherwise, the status was chemosensitive.
Source: Clinical Study Report for the TRANSCEND study.9
Table 8: Summary of Baseline Characteristics, Primary Analysis Set
Category/demographic | Total (N = 133) |
|---|---|
Baseline demographic | |
||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||| | |
||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||||||||||| |
Note: Redacted rows have been deleted.
Source: Clinical Study Report for the TRANSCEND study.9
Interventions
Leukapheresis
For each patient, leukapheresis was performed after meeting eligibility criteria to obtain a sufficient quantity of peripheral blood mononuclear cells for the production of liso-cel. If liso-cel could not be manufactured, patients could have additional leukaphereses performed. Patients were required to continue to meet eligibility requirements for additional leukaphereses, but no repeated PET or electrocardiogram was necessary.
Anticancer Therapies Between Screening and LDC
Anticancer treatment was allowed for disease control while liso-cel was being produced. Low-dose chemotherapy (e.g., vincristine, rituximab, cyclophosphamide ≤ 300 mg/m2) was allowed if completed at least 7 days before the start of LDC. If other agents were used, the washout periods noted in the exclusion criteria must had been met. Pre-treatment PET and CT (CT) assessments and other pre-treatment study procedures were to have been performed after the anticancer treatment was completed. For the purpose of this review, any anticancer therapy received during this period was considered a bridging therapy.
Lymphodepleting Chemotherapy
Eligibility criteria were confirmed before starting LDC. If patients experienced a significant worsening in clinical status compared with that during eligibility screening, they were not treated with liso-cel.
LDC was performed by administering fludarabine (30 mg/m2/day for 3 days) plus cyclophosphamide (300 mg/m2/day for 3 days) before treatment with liso-cel. Dose reductions of either or both agents were allowed at the discretion of the investigator and/or in compliance with approved labels for these products. LDC was completed between 2 and 7 days before the liso-cel administration.
Liso-cel (JCAR017) Product
To establish a recommended regimen for liso-cel, the study design included a DF group or phase, followed by DE and DC groups. The DF and DE portions of this study were designed to evaluate and refine the dose and schedule of liso-cel needed for adequate safety and antitumour activity, to be tested further in the DC group.
Liso-cel dosing started at 50 × 106 CAR T cells single dose (DL1S) and the dose could escalate or de-escalate based on a modified continual reassessment method (mCRM) algorithm that implements a Bayesian methodology to estimate the probabilities of dose-limiting toxicity and informed by the cumulative data from included patients. Clinical experience with 2 other CAR T-cell products (each using the same CAR construct, transgene, and lentiviral vector as liso-cel) informed the starting dose selection of 50 × 106 CAR-positive T cells. Then, dose escalation using the mCRM method to 2 other dose levels (100 × 106 CAR-positive T cells [DL2] and 150 × 106 CAR-positive T cells [DL3]) was performed if safety and efficacy data from the lower doses were acceptable. The enrolling of eligible patients was defined as an open enrolment assignment to the dose regimen best considered for each next patient based on the information obtained from the algorithm. Assignment on the DE group was based on the aforementioned dose-limiting toxicity (DLT) of the liso-cel product and on criteria of the probability of the product to be safe (probability of dose-limiting toxicity) and probability of being efficacious (probability of CR). Dose selection for each patient occurred after leukapheresis (and before LDC) and was dependent on the dosing groups open at the time of assignment (for example, DL1S DE group and DL2S DF group) and other factors such as gating of patients for DLT information collection. Based on cumulative data from the DF and DE phases of the study, a recommended regimen for the DLBCL cohort was selected as a DC group or portion of the flow of the study (i.e., the DL2S regimen, see Figure 3).

This figure has been redacted.
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Initially, patients could be assigned to receive either 1 or 2 doses of liso-cel per treatment cycle. In the single-dose schedule, liso-cel was given 2 to 7 days after completion of LDC. In the 2-dose schedule, liso-cel was given on day 1 (2 to 7 days after completion of LDC), and again 14 days later. The allocation to a 1-dose or 2-dose schedule was also based on the mCRM algorithm during the DF process. LDC was not given before the second dose of liso-cel in the 2-dose schedule.
Patients were premedicated with 650 mg acetaminophen orally and 25 mg to 50 mg diphenhydramine hydrochloride or equivalent antihistamine (orally or IV) 30 to 60 minutes before liso-cel administration. Liso-cel was administered as separate IV infusions that consisted of CD8+ CAR c and CD4+ CAR-positive T cells. The CD8+ drug product component was administered first, followed by the CD4+ drug product component; this order was set by the sponsor based on the concept that CD8+ cells play a greater role in tumour killing than the CD4+ cells. The product had to be administered within 2 hours of removing it from the shipping container. Monitoring of all patients was required after IV administration. Liso-cel could had been delivered in an outpatient setting at the investigator’s discretion.
Nonconforming Product
The sponsor defines a product that does not meet the specification criteria for certain non-safety attributes as a “nonconforming product.” This was identified as “any product wherein a component did not meet a release specification limit.” Nonconforming product could be administered under certain conditions (e.g., that there were not issues about safety). Patients receiving nonconforming product were analyzed separately.
Additional Cycles or Re-treatment
Re-treatment cycles with liso-cel were allowed but only under 3 pre-specified situations:
2-dose schedule: This was a protocol-defined schedule into which a patients may have been assigned at study enrolment to receive 2 doses of liso-cel approximately 14 days apart as their treatment cycle.
Re-treatment cycles: Subsequent liso-cel cycles may have been administered to a patient only if PD occurred following CR to liso-cel.
Additional cycles: Additional liso-cel cycles may have been administered to a patient only if stable disease (SD) or PR was their BOR after the initial response assessment. (Note: this option for additional cycles was removed in Amendment 6.)
“Dose” refers to infusion of liso-cel product, while the word “cycle” refers to repeating the complete LDC, liso-cel product infusion.
Outcomes
The objective of the TRANSCEND study was to evaluate the safety of liso-cel in patients with R/R large B-cell lymphomas as well as the antitumour activity based on the ORR (CR + PR). Key secondary objectives were the assessment of rate of CR and durability of antitumour activity of liso-cel (CR rate and DOR, defined as the time from first response to PD or death); to estimate the PFS and OS (PFS, OS); estimate the pharmacokinetic (PK) profile, and HRQoL and health economics (ICU and non-ICU inpatient days). Exploratory end points included antitumour activity using Bayesian methods, pharmacodynamic effects, and the effect of tumour and tumour microenvironment on liso-cel.
A list of efficacy end points identified in the CADTH review protocol that were assessed in the pivotal clinical trial included in this review is provided in Table 9. These end points are further summarized below. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 3.
Table 9: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome Measure | TRANSCEND study |
|---|---|
Overall response rate | Primarya |
Complete response | Key secondary |
Duration of response | Key secondary |
Overall survival | Key secondary |
Progression-free survival | Key secondary |
HRQoL
| Key secondary |
Hospitalization and intensive care unit utilization | Key secondary |
Harms (adverse events, serious adverse events, adverse events of special interest) | Key secondary |
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EQ-5D-5L = EuroQol 5-Dimensions 5-Levels questionnaire; FACT-Lym = Functional Assessment of Cancer Therapy–Lymphoma; HRQoL = health-related quality of life.
aOverall response rate was changed from a secondary to a primary end point in amendment 3 of the protocol and it is defined as complete response plus partial response.
bThis measurement tool was identified in the CADTH protocol for this review, but it was not assessed in the pivotal trial.
The ORR was defined as the proportion of patients with BOR of either CR or PR based on the Lugano 2014 criteria.10 The BOR is the BOR recorded from the time of the final liso-cel infusion (i.e., the first dose of the 1-dose schedule and the second dose for 2-dose schedule) until disease progression, end of study, or the start of another anticancer therapy or HSCT. Best response was assigned according to the following order: CR, PR, SD, PD, not evaluable, or not done. The ORR was included as a primary end point (IRC review based) and as determined at the end of each treatment cycle and approximately 3, 6, 9, 12, 18, and 24 months following the last dose of liso-cel. Radiographic disease assessments by PET and/or diagnostic quality CT scans (chest, neck, abdomen, and pelvis) were performed pre-treatment, after any anticancer therapy for disease control (if applicable), at the end of the treatment cycle, and approximately 3, 6, 9, 12, 18, and 24 months following the last dose of liso-cel or until disease progression or treatment with additional anticancer therapy.
The CR rate was defined as the proportion of patients with a BOR of CR by IRC assessment based on the Lugano 2014 criteria, while the DOR was defined as the interval from the first documentation of CR or PR to the earlier date of disease progression or death. The first documentation of CR or PR was defined as the latest of all dates of required measurements to establish the response. DOR was evaluated based on the IRC evaluations for patients who achieved a CR or PR based on the Lugano 2014 criteria.10
The PFS was defined as the time from the date of the first JCAR017 infusion to the earlier date of disease progression or death due to any cause. The progression date was defined as the earliest date of all assessments that led to a progression. The date of progression was provided by the IRC for PFS analysis.
OS was defined as the interval from the date of the first JCAR017 infusion to the date of death due to any reason. The OS analysis included all available survival information with long-term follow-up data. Data from surviving patients were censored at the last time that the patient was known to be alive.
HRQoL changes were assessed using the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) and the EuroQol 5-Dimensions 5-Levels (EQ-5D-5L) questionnaire. EORTC QLQ-C30 is 1 of the most commonly used PRO measures in oncology clinical trials.22 It is a multi-dimensional, cancer-specific, evaluative measure of HRQoL. It consists of 30 questions that are scored to create 5 multi-item functional scales, 3 multi-item symptom scales, 6 single-item symptom scales, and a 2-item quality of life (QoL) scale, and uses a 1-week recall period in assessing function and symptoms. Most questions have 4 response options (“not at all,” “a little,” “quite a bit,” “very much”), with scores on these items ranging from 1 to 4. For the 2 items of the global QoL scale, however, the response format is a 7-point Likert-type scale, with anchors between 1 (very poor) and 7 (excellent). All of the scales and single-item measures range in score from 0 to 100. Higher score for the functioning scales and global health status denotes a better level of functioning (i.e., a better state of the patient), while higher scores on the symptom and single-item scales indicate a higher level of symptoms (i.e., a worse state of the patient). Each raw scale score is converted to a standardized score that ranges from 0 to 100 using a linear transformation, with a higher score reflecting better function on the function scales, higher symptoms on the symptom scales, and better QoL (i.e., higher scores simply reflect higher levels of response on that scale). MIDs for improvement in the global QoL scale range from 5 to 8 in the global scale, while a decrease of –10 to –5 is used as MID for deterioration.
The EQ-5D-5L is a generic, preference-based measure of health outcomes. This instrument is applicable to a wide range of health conditions and treatments and provides a simple descriptive profile or health state and a single value for health status. The EQ-5D-5L is a self-administered instrument comprising of the EQ-5D-5L index scale and a visual analogue scale. The EuroQol Visual Analogue Scale (EQ VAS) records the respondent’s self-rated health status on a vertical graduated scale and assesses current health status, ranging from 0 to 100, with 0 representing the “worst imaginable health state” and 100 representing the “best imaginable health state.” The EQ-5D-5L index scale is scored on the UK value set scale, with a score of 0 indicating “death,” 1.00 indicating “full health,” and negative scores reflecting states perceived to be “worse than death.” No specific MID for patients with myeloma has been estimated.
The health economics and outcomes research end point was hospital resource utilization, including numbers of ICU inpatient days and non-ICU inpatient days and reasons for hospitalization.
Statistical Analysis
Since the TRANSCEND study is referred as a phase I study, 1 of the primary end points of the study was stated as the type, frequency, and severity of AEs and laboratory abnormalities and all AEs are listed and summarized in the Harms section.
The study investigators estimated that the ORR and CR rates in patients with large aggressive B-cell lymphomas who have received at least 2 prior therapies was 12% to 46% and 6% to 38%, respectively, and median PFS and OS results are also poor, less than 6 months and less than 12 months, respectively. Based on a meta-analysis data from 8 published studies23 of recommended regimens for patients with R/R aggressive large B-cell NHL, the estimated ORR was 30% (95% CI, 24 to 38) and CR is 19% (95% CI, 13 to 26). For the primary analysis in the TRANSCEND study, the efficacy end point of ORR was based on the null hypothesis of an of ORR 40% or less and an alternative hypothesis of ORR of greater than 40% with the effect size of 25% (ORR = 65%).
The analysis for ORR was conducted on the PAS based on the IRC assessments. The ORR was calculated along with the 2-sided 95% exact Clopper-Pearson CIs.
The study tested the hypothesis of a CR rate of greater than 20% against the null hypothesis of a CR rate of 20% or less, at a 1-sided 2.5% level of significance for the primary analysis of the study.
The analysis of CR rate was conducted similarly to the analysis of the primary efficacy end point.
DOR was defined as the interval from the first documentation of CR or PR to the earlier date of disease progression or death. The first documentation of CR or PR was defined as the latest of all dates of required measurements to establish the response. In the case that a patient did not have disease progression or death before the data cut-off date, DOR was censored at the date of the last adequate disease assessment on or before the earliest censoring event.
The censoring reason could have been:
ongoing
completed the study
discontinued the study
received re-treatment
received a new anticancer therapy
proceeded to HSCT
experienced an event after missing at least 2 consecutive scheduled disease assessments.
The Kaplan–Meier method was used to estimate the median DOR along with the 95% CI. The estimated percentage of patients with response duration of 6, 12, 18, and 24 months or greater was also presented with 95% CIs using the Kaplan–Meier method. Sensitivity analyses were performed (1) without censoring HSCT and (2) in alignment with the European Medicines Agency guidelines, without censoring new anticancer therapy, HSCT, and missing at least 2 consecutive scheduled disease assessments.
PFS was defined as the time from the date of the first JCAR017 infusion to the earlier date of disease progression or death due to any cause. The progression date was defined as the earliest date of all assessments that led to a progression. If a patient did not experience disease progression or death before the data cut-off date, PFS was censored at the date of the last adequate disease assessment on or before the earliest censoring event.
The censoring reasons were the same as with DOR.
The Kaplan–Meier method was used to estimate the PFS rate at months 6, 12, 18, and 24, and the median PFS along with the 95% CI.
Sensitivity analyses were performed (1) without censoring HSCT and (2) in alignment with European Medicines Agency guidelines, without censoring new anticancer therapy, HSCT, and missing at least 2 consecutive scheduled disease assessments. These sensitivity analyses were performed using the investigators’ assessment of disease response.
OS was defined as the interval from the date of the first JCAR017 infusion to the date of death due to any reason. The OS analysis included all available survival information with long-term follow-up data. Data from surviving patients were censored at the last time that the patient was known to be alive. The Kaplan–Meier method was used to estimate the OS rate at months 6, 12, 18, and 24, and the median OS along with the 95% CI.
All PRO/HRQoL analyses were performed on the PRO (EORTC QLQ-C30 or EQ-5D-5L) evaluable population. For continuous variables, descriptive statistics (n, mean, standard deviation, minimum, 25th percentile, median, 75th percentile, and maximum) for baseline, raw score at specified visits, and change from baseline were provided. Categorical variables were summarized with frequency tabulations (counts and percentages). For time-to-event analyses, the Kaplan–Meier method, including Kaplan–Meier plot were used to estimate the survival distribution with the median and its 2-sided 95% CI. Cumulative distribution frequency plots were generated for post-baseline assessment points.
The ICU inpatient days, non-ICU inpatient days, and reasons for hospitalization were assessed using descriptive statistics for patients in the JCAR017-treated analysis set . The number and percent of outpatient patients who were treated with JCAR017 cell product and who were admitted post-JCAR017 infusion were also summarized.
Sensitivity analyses of primary and secondary efficacy end points, including ORR, CR rate, ORR for chemorefractory patients, CR rate for chemorefractory patients, DOR, PFS, and OS, were performed based on the:
leukapheresed set (ITT set)
PP analysis set and/or PP DLBCL analysis set
disease histology determined by central pathology review
response determined by investigator
A patient in the leukapheresed set who did not receive cell product was considered not evaluable (i.e., a nonresponder) for the sensitivity analysis of ORR and CR rate. The analysis method was the same as previously described for the corresponding end points.
Missing data were not imputed. Further detail was not provided for how missing data were handled for specific end points. However, based on reported results, it seems likely patients with missing data were treated as non-responders with exception of the time-to-event end points where such patients were censored.
Subgroup Analysis
In the PAS and treated efficacy analysis set, efficacy subgroup analyses were performed on the following variables:
age: (1) younger than 40, 40 or older to younger than 65, and 65 years or older; (2) younger than 65 versus 65 years or older; (3) younger than 75 versus 75 years or older at the time of the first JCAR017 infusion
sex: male versus female
ethnicity: Hispanic or Latino versus not Hispanic or Latino
race: White versus other races
prior HSCT status: yes versus no
prior response status: refractory versus relapsed to last prior therapy; the status was refractory if a patient achieved less than a CR to last prior therapy, otherwise the status was relapsed
prior chemo-response status: chemorefractory versus chemosensitive to last prior chemotherapy-containing therapy; the status was chemorefractory if a patient achieved SD or PD to last chemotherapy-containing regimen or relapsed less than 12 months after auto-HSCT, otherwise the status was chemosensitive
CNS disease status: known CNS disease versus no known CNS disease at the time of the first JCAR017 infusion
cell of origin: germinal centre B-like versus non-germinal centre B-like.
Subgroup analyses and forest plots were performed for the primary efficacy end point and secondary efficacy end points, including ORR, CR rate, DOR, PFS, and OS. Some grouping of classes was considered if there were too few patients in some subgroups. Other subgroup analyses were also performed if deemed appropriate.
Power and Sample Size
As described in the statistical methods above, the study investigators estimated that the ORR and CR rates in patients who had received at least 2 prior therapies was 12% to 46% and 6% to 38%, respectively, and median PFS and OS results were also poor, at less than 6 months and less than 12 months, respectively. Based on a meta-analysis of data from 8 published studies23 of recommended regimens, the estimated ORR was 30% (95% CI, 24 to 38) and CR was 19% (95% CI, 13 to 26). For the primary analysis in the TRANSCEND study, for the efficacy end point of ORR, based on the null hypothesis of an ORR of 40% or less with the effect size of 25% (ORR = 65%), a sample size of 75 patients in the PAS will provide approximately 98% power to demonstrate statistical significance at a 1-sided significance level of 0.021 based on an exact test. For the efficacy end point of CR rate, based on the null hypothesis of a CR rate of 20% or less and an alternative hypothesis of CR rate of greater than 20% with the effect size of 20% (CR rate = 40%), 75 patients in the PAS will provide approximately 96% power to demonstrate statistical significance at a 1-sided significance level of 0.021 based on an exact test.
Across protocol amendments, the study sample size was increased as deemed appropriate by the sponsor. The number of patients allocated to each DF group depended on the Bayesian assessment of safety and efficacy. It was anticipated that at least 274 patients would be enrolled in the study. The maximum planned sample size for the DF phase was 114 patients; the planned sample size for DL1 and/or DL-1 was 60 patients across the 2 disease cohorts with a maximum of 35 patients within each disease cohort. The planned sample size for DL2 was 30 patients across the 2 disease cohorts with a maximum of 20 patients within each disease cohort. For DL3, the planned sample size was 24 patients across the 2 disease cohorts with a maximum of 12 patients within each disease cohort, and for a DC group the planned sample size was at least 100 patients to ensure at least 75 patients in the PAS. The number of patients allocated to each DF group depended on the Bayesian assessment of safety and efficacy.
Multiple Comparisons or Multiplicity
Adjustment of multiple comparisons was designed to preserve the overall type I error rate at 0.025 for both the preplanned interim and primary analysis. However, since the planned interim analysis was ultimately not conducted, the full alpha was preserved for the primary analysis. Thus, for the primary analysis, 4 hypothesis tests were performed in the following sequential order at a 1-sided significance level of 0.025:
Null hypothesis that ORR was 40% or less against alternative hypothesis that ORR was greater than 40%
Null hypothesis that CR rate was 20% or less against alternative hypothesis that CR rate was greater than 20%
Null hypothesis that ORR was 30% or less against alternative hypothesis that ORR was greater than 30% for chemorefractory patients
Null hypothesis that CR rate was 10% or less against alternative hypothesis that CR rate was greater than 10% for chemorefractory patients
Analysis Populations
Patients were enrolled into 1 of 2 disease-specific cohorts in the study, as follows:
DLBCL cohort, including patients with the following histologies: DLBCL NOS (de novo or transformed from indolent lymphoma), HGL, PMBCL, and FL3B failing at least 2 prior lines of therapy
MCL cohort, including patients with MCL failing at least 1 prior line of therapy; this cohort is not described in this CADTH report
Within the DLBCL and MCL cohorts, patients were enrolled into DF, DE, or DC groups after leukapheresis depending on the study status.
For the statistical analyses, within each cohort, patients were categorized into analysis sets. The definitions of each set and distribution during the study are represented in Figure 4.
ITT Analysis Set (Leukapheresed)
The ITT (leukapheresed) set included all patients who had signed informed consent, who met all inclusion and exclusion criteria, and who underwent leukapheresis. In the case of protocol deviations where patients underwent leukapheresis without having met all inclusion and exclusion criteria, the patients were still included in the leukapheresed set.
Liso-cel Treated Set
The liso-cel-treated analysis set included all patients who received at least 1 dose of liso-cel. In the case where a patient received multiple liso-cel doses, the first dose of liso-cel should have been the conforming product, which met specifications at the time of product release. In the Clinical Study Report, the DLBCL cohort liso-cel-treated analysis set is referred as the “DLBCL treated set.”
Safety end points were analyzed in this liso-cel-treated set.
Liso-cel-Treated Efficacy-Evaluable Set
The liso-cel-treated efficacy-evaluable analysis set is a subset of the treated set and included all patients who had PET-positive disease present before liso-cel administration based on the IRC assessment. Patients who did not have a baseline PET or CT assessment repeated after bridging therapy (when bridging therapy was indicated) and before liso-cel administration were excluded from the liso-cel-treated evaluable set. In the sponsor’s Clinical Study Report, this set is referred as the DLBCL efficacy set.
Primary Analysis Set
The PAS was a subset of the liso-cel-treated efficacy-evaluable set that focused on patients who were treated at dose level 2. This set included patients in the DF, DE, and DC groups who failed at least 2 therapies in the DLBCL cohort treated at 1 recommended regimen (determined to be DL2S). The PAS was used for the primary efficacy analysis.
This set excluded patients with an ECOG PS of 2 before LDC, prior allo-HSCT, PMBCL, FL3B, or transformation from indolent lymphoma other than follicular lymphoma; these patients were analyzed separately. Patients in the PAS must have had PET-positive disease present before liso-cel administration based on IRC assessment. Those who did not have a baseline PET or CT assessment repeated after anticancer therapy for disease control and before liso-cel administration were excluded from the PAS.
DLT-Evaluable Analysis Set
The DLT-evaluable analysis set included all patients in the DF and DE groups who received liso-cel, and who either experienced a DLT or were followed for the full DLT-evaluation period. This analysis set was used for DF purposes.
Figure 4: Sankey Diagram of the Analysis Sets Defined in the TRANSCEND Study
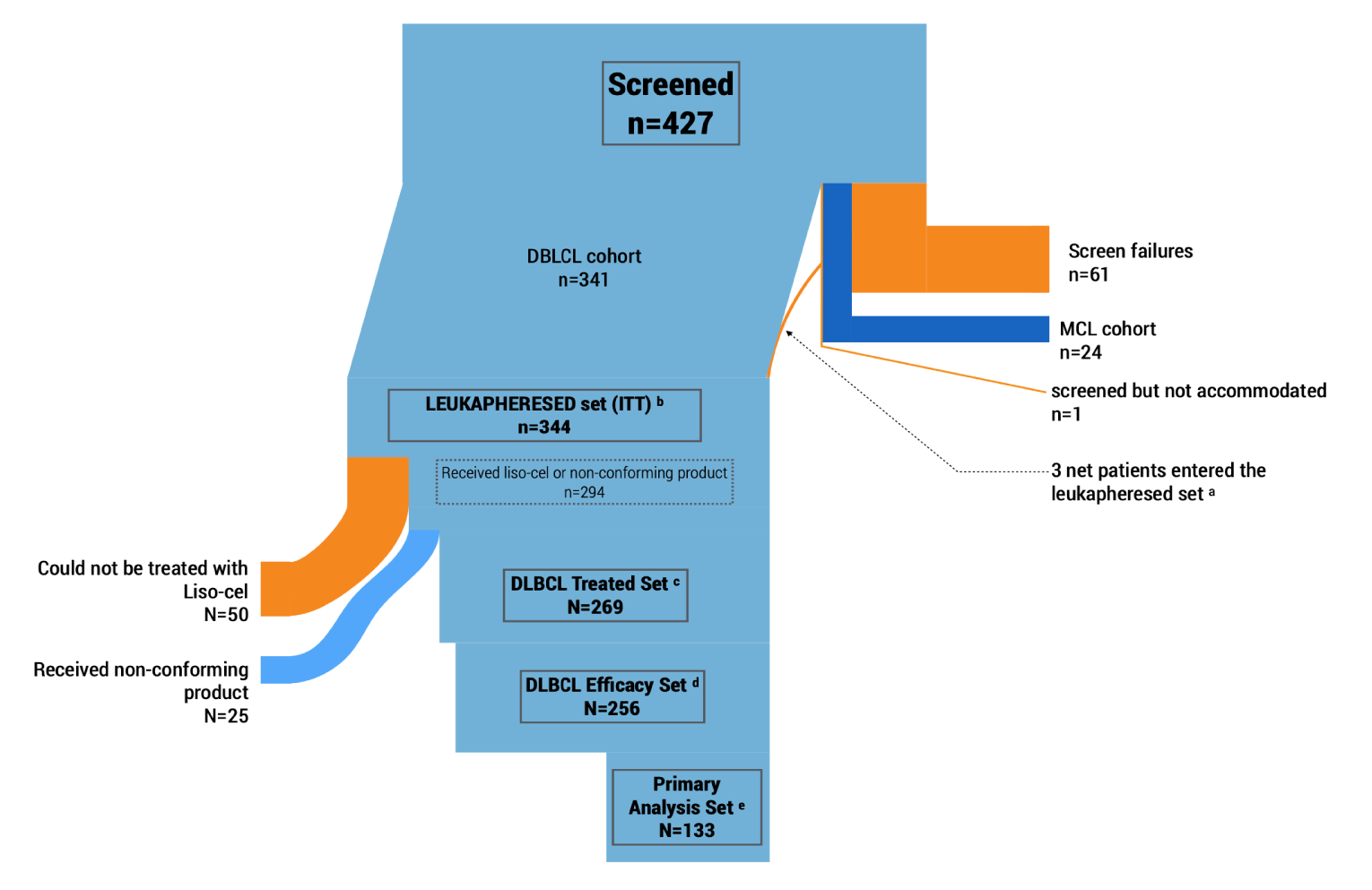
DLBCL = diffuse large B-cell lymphoma; ITT = intention to treat; liso-cel = lisocabtagene maraleucel; MCL = mantle cell lymphoma.
a Three patients were excluded because they could not be leukapheresed, plus 6 originally screen failure patients who were leukapheresed and entered the leukapheresed set.
b The leukapheresed or intention-to-treat analysis set included all patients who underwent leukapheresis. Bridging therapy could be offered between this phase and the administration of liso-cel or nonconforming product.
c Only received liso-cel, but not the nonconforming product. Harms (safety) end points were analyzed in this set.
d The DLBCL efficacy set (or liso-cel-treated efficacy-evaluable set) included all patients in the liso-cel-treated set who had confirmed PET-positive disease before liso-cel administration based on independent review committee assessment.
e A subset of the DLBCL efficacy set. This set focused on patients who were treated at dose level 2.
Source: Adapted from data from Clinical Study Report for the TRANSCEND study.9
Results
Patient Disposition
The TRANSCEND study screened a total of 427 patients, of which 61 failed the eligibility criteria as shown in Figure 5 and Table 10. The study was then divided in the MCL (n = 24) and DLBCL (n = 341) cohorts, of which the latter is the main focus of this report.
A total of 344 patients underwent leukapheresis and were considered in the enrolled (ITT) population, or leukapheresed set (a net gain of 3 patients from the screened cohort due to 6 screen failures that were leukapheresed). A majority of patients (294 [85.4%]) who were leukapheresed received an infusion with either the liso-cel or a nonconforming product.
Of the 344 patients in the DLBCL cohort who underwent leukapheresis, 25 patients received nonconforming product and were not included in the DLBCL cohort liso-cel-treated analysis set. Additionally, 50 patients in the DLBCL cohort did not receive treatment with liso-cel. The reasons, per investigator assessment, that patients did not receive treatment after leukapheresis were death (n = 33), PD (n = 27), unknown reasons (n = 3), bowel perforation (n = 1), cardiogenic shock (n = 1), and AE (n = 1; sepsis considered related to protocol-mandated procedures). Six others had disease-related complications, 3 no longer met eligibility criteria, and 2 withdrew consent. In 2 patients, the product could not be manufactured.
At the time of the data cut-off date, out of the 269 patients in the DLBCL cohort liso-cel-treated analysis set who received treatment with liso-cel, 35 had completed the study, 103 were still on study in the post-treatment follow-up portion of the study, and |||||| had discontinued. Twenty-one of the 35 patients who completed the study had consented to the long-term follow-up study to be followed for up to 15 years after liso-cel treatment. Among the |||||| patients who discontinued, the most common reason for discontinuation was death (||||||||||||)

At the cut-off date of August 12, 2019, patients were followed up for a median of 11.5 months in the total DLBCL treated set population (n = 269) and |||||| months in the DL2S subgroup (n = 177). A total of 199 patients (74.0%) had 6 months or more of follow-up, ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Table 10: Patient Disposition, TRANSCEND Study
Patient characteristics | TRANSCEND - NHL 001 |
|---|---|
Total screened (DLBCL and MCL cohorts) | 427 |
Screen failures | 61 (14.3) |
DLBCL cohort | 341 (79.8) |
Enrolled and leukapheresed | 344a |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||| |
Reason for discontinuation | |
Death | 33 (9.6) |
Adverse eventsb | 6 (1.7) |
No longer eligible | 3 (0.8) |
Not eligible for liso-cel infusion | 2 (0.6) |
Withdrew consent | 2 (0.6) |
Product could not be manufactured | 2 (0.6) |
Other | 2 (0.6) |
Received product infusionc | 294 (85.4) |
Received liso-celd | 269 (78.2) |
Discontinued after product infusion | 131 (38.0) |
Reasons for discontinuation after product infusion | |
Death | 121 (35.1) |
Withdrew consent | 7 (2) |
Lost to follow-up | 2 (0.6) |
Other | 1 (0.3) |
||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||| |
Primary analysis set, Ne | 133 |
ITT populationf | 344 |
Safety DLBCL analysis setg, N | 269 |
DLBCL = diffuse large B-cell lymphoma; ITT = intention to treat; liso-cel = lisocabtagene maraleucel; MCL = mantle cell lymphoma.
Note: Values are expressed as n (%).
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
bStated as “Disease-related complications.”
cReceived either liso-cel or nonconforming product.
dReceived only liso-cel but not the nonconforming product.
eThis is the Primary Analysis Set population in which the primary efficacy end points were analyzed.
fThis is the leukapheresed analysis set.
gAnalyzed in the liso-cel-treated analysis set.
Source: Clinical Study Report for the TRANSCEND study.9
The DF and DE portions of this study were designed to evaluate and refine the dose and schedule of liso-cel needed for adequate safety and antitumour activity, to be tested further in the DC group. Dosing started at DL1S (single dose of 50 × 106 CAR-positive T cells), then proceeded to 2 doses of 50 × 106 CAR-positive T cells given 14 days apart (DL1D), a single dose of 100 × 106 CAR-positive T cells (DL2S), and eventually a single dose of 150 × 106 CAR-positive T cells (DL3S). Dose escalation or de-escalation in this study was guided by a mCRM that implemented Bayesian methodology to estimate the probabilities of DLT and CR. With each patient’s information, the dose–toxicity and dose–response model was updated, and new probability of DLT and probability of CR were estimated.
The number and distribution of patients by dose levels are presented in Table 11.
Table 11: Analysis Populations by Dose Level, DLBCL Cohort
Analysis populations | DL2S n (%) | DL1S n (%) | DL1D n (%) | DL3S n (%) | Total N (%) |
|---|---|---|---|---|---|
Screened set | NR | NR | NR | NR | 347 |
Eligible set | NR | NR | NR | NR | 341 |
Leukapheresed set (ITT)a | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | 344 |
Liso-cel-treated analysis set (DLBCL treated set) | |||||||||||||| | 45 (71.4) | 6 (85.7) | 41 (87.2) | 269 (78.2) |
Liso-cel-treated efficacy analysis set (DLBCL efficacy set) | |||||||||||||| | 40 (63.5) | 6 (85.7) | 41 (87.2) | |||||||||||||| |
PAS (DL2S only)b | 133 (58.6) | NR | NR | NR | 133 (38.7) |
DLT-evaluable analysis setc | 48 (21.1) | 44 (69.8) | 6 (85.7) | 41 (87.2) | 139 (40.4) |
Efficacy-evaluable analysis setb | 51 (22.5) | 44 (69.8) | 6 (85.7) | 41 (87.2) | 142 (41.3) |
Per-protocol analysis set (within the PAS) | 131 (57.7) | NR | NR | NR | 131 (38.1) |
Per-protocol DLBCL analysis set (subset of DLBCL treated set) | |||||||||||||| | 42 (66.7) | 6 (85.7) | 41 (87.2) | |||||||||||||| |
PRO/QoL QLQ-C30 evaluable set | 137 (60.4) | 5 (7.9) | 0 (0.0) | 39 (83.0) | 181 (52.6) |
DE = dose expansion; DF = dose finding; DL1D = dose level 1, 2 dose; DL1S = dose level 1, single dose; DL2S = dose level 2, single dose; DL3S = dose level 3, single dose; DLBCL = diffuse large B-cell lymphoma; DLT = dose-limiting toxicity; ITT = intention to treat; liso-cel = lisocabtagene maraleucel; mCRM = modified continual reassessment method; NR = not reported; PAS = Primary Analysis Set; PRO = patient-reported outcomes; QLQ-C30 = Quality of Life Questionnaire Core 30; QoL = quality of life.
Note: The denominator is the number of patients in the leukapheresed set. Data cut-off date: August 12, 2019.
aMore patients are included in the leukapheresed set than the eligible set due to patients having enrolled in the study although they did not meet eligibility criteria. In some cases, the patients were allowed on study after discussion with the sponsor and in other cases the deviations were identified retrospectively.
bThe PAS was the population used for the primary end point analyses.
cOnly used for mCRM calculations in the DF and DE groups.
Source: Clinical Study Report for the TRANSCEND study.9
Exposure to Study Treatments
Lymphodepleting Chemotherapy
After leukapheresis, it was possible to obtain from 294 patients either the liso-cel (JCAR017) or nonconforming product, defined by the sponsor as “any product wherein a component did not meet a release specification limit.” Of these patients, 25 (9%) patients received a nonconforming product (described in the interventions section and Figure 4).
LDC was completed between 2 days to 7 days before liso-cel administration. LDC consisted of fludarabine 30 mg/m2/day for 3 days plus cyclophosphamide 300 mg/m2/day for 3 days. All 269 patients from the DLBCL treated dataset completed LDC before cycle 1 of liso-cel. The median time from last dose of LDC to JCAR017 treatment was 4 days (range = 3 days to 9 days). Of note, 4 patients received LDC but did not receive JCAR017. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Liso-cel Product
The dose regimens assigned in the TRANSCEND study were:
DL1S: 50 × 106 CAR-positive T cells (25 × 106 CD8+ CAR-positive T cells and 25 × 106 CD4+ CAR-positive T cells), single-dose regimen
DL1D: 50 × 106 CAR-positive T cells, 2-dose regimen
DL2S: 100 × 106 CAR-positive T cells (50 × 106 CD8+ CAR-positive T cells and 50 × 106 CD4+ CAR-positive T cells), single-dose regimen
DL3S: 150 × 106 CAR-positive T cells (75 × 106 CD8+ CAR-positive T cells and 75 × 106 CD4+ CAR-positive T cells), single-dose regimen
The median CD8 dose in the DLBCL treated set and within the DL2S group was ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. The median ratio of CD4 to CD8 cells was 1 in all dose groups.
Additional Cycles and Re-treatment
Under the original protocol and Amendments 1 through 5 (and as defined in the “interventions” section), patients could have received additional cycles of liso-cel if “SD” or “PR” was their BOR after the initial response assessment.
A total of 7 patients in the DLBCL treated set (3 in the DL2S and 4 in the DL1S groups) received more than 1 cycle of liso-cel (maximum, 3 cycles) after achieving SD or PR to initial treatment. Meanwhile, 16 patients received re-treatment cycles with liso-cel for PD following CR.
Manufacturing Failure
Manufacturing failure was defined as the inability to manufacture liso-cel-conforming product (as defined before). Manufacturing failure rate was defined as the number of patients for whom liso-cel could not be manufactured divided by the number of patients who had leukapheresis and manufacturing information available. Manufacturing failure occurred in 39 of 341 patients (manufacturing failure rate, 11.4%); 25 of these patients received infusion of the nonconforming product.
Nonconforming Product
As defined previously in the “Interventions” section, when pre-specified criteria were met, patients could have been treated with nonconforming product if the sponsor and the investigator agreed that the benefit/risk profile was acceptable. In the DLBCL cohort, 25 patients received nonconforming product because 1 of the drug product components (either CD8+ or CD4+) did not meet 1 of the release specification limits. The reasons products were considered to be nonconforming for patients in the DLBCL cohort were:
Received CD8+ component only (no CD4+ component administered), n = 10
Received CD4+ component only (no CD8+ component administered), n = 3
Received both components (n = 12), nonconforming due to 1 component not meeting the following specification: potency (n = 5); purity (n = 1); sterility (n = 1); passed initial release for infusion but failed final; and viability (n = 5)
In cases where the patient was treated with only 1 drug product component (CD8+ or CD4+ CAR-positive T cells), they were infused with half of the assigned dose, using the conforming component. Data from patients treated with nonconforming product were analyzed separately from those treated with liso-cel.
Outpatient Treatment
After Amendment 4 in the protocol, guidance was provided regarding outpatient treatment of patients at investigator discretion. Patients were considered to have received outpatient treatment if their first JCAR017 infusion day did not overlap with any hospitalization stays during the study. A total of 25 of 269 patients in the DLBCL treated set were treated in the outpatient setting.
Efficacy
Survival
Results are presented separately for the leukapheresed set, the DLBCL efficacy set, and the PAS below. A summary of the results for PFS and OS across all dose regimens is presented in Table 12.
Leukapheresed Set
OS in the DLBCL-leukapheresed set was defined as the interval from the date of leukapheresis to the date of death. With a median survival follow-up of 18.8 months, patients had a median OS of 14.0 months (95% CI, 11.1 to 21.1 months) in all dose levels, while the median OS in the DL2S regimen was 12.8 months (95% CI, 9.7 to 18.7). The estimated survival rate at 6 months and 12 months was 70.2% (95% CI, 65.0 to 74.8) and |||||||||||||||||||||||||||||||||||||||||||||||||||||||| respectively.
PFS in the DLBCL-leukapheresed set (ITT) analysis was defined as the time from leukapheresis to the earlier date of PD or death due to any cause. With a median PFS follow-up of 13.5 months, patients in the DLBCL-leukapheresed set had a median PFS of 4.8 months (95% CI, 4.3 to 7.3) in all regimen groups, while it was 5.3 months (95% CI, 4.3 to 8.9) in the DL2S liso-cel regimen. The estimated PFS rate at 6 months and 12 months was 46.3% (95% CI, 40.5 to 51.8) and 38.2% (95% CI, 32.5 to 43.9), respectively.
Table 12: Efficacy Outcomes, Survival
Outcome | DL2S | DL1S | DL1D | DL3S | Total |
|---|---|---|---|---|---|
Leukapheresed (ITT) analysis set | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | 6.8, 3.3 to 14.1 |
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | 116 (45.3) |
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | 140 (54.7) |
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
Median, 95% CI | 19.9, 11.3 to NR | NR, 6.8 to NR | NR, 1.6 to NR | NR, 10.3 to NR | 21.1, 13.3 to NR |
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
Follow-up (months) | |||||
Median, 95% CI | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
Primary analysis set | N = 133 | N = 133 | |||
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
PFS (months) | |||||
Median, 95% CI | 9.0, 3.1 to NR | NA | NA | NA | 9.0, 3.1 to NR |
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
Min., max. | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
OS | |||||
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
OS (months) | |||||
Median, 95% CI | 19.9, 10.4 to NR | NA | NA | NA | 19.9, 10.4 to NR |
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
Follow-up (months) | |||||
|||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
CI = confidence interval; DL1D = dose level 1, 2 dose; DL1S = dose level 1, single dose; DL2S = dose level 2, single dose; DL3S = dose level 3, single dose; DLBCL = diffuse large B-cell lymphoma; HSCT = hematopoietic stem cell transplant; ITT = intention to treat; max. = maximum; min. = minimum; NA = not applicable; NR = not reached; OS = overall survival; PFS = progression-free survival.
Note: Redacted rows have been deleted.
Source: Clinical Study Report for the TRANSCEND study.9
DLBCL Efficacy Set
The summary of OS for the DLBCL efficacy set in all regimens is shown in Table 12. With a median survival follow-up of 17.5 months, patients had a median OS of 21.1 months (95% CI, 13.3 to NR) in all regimens, and 19.9 months (95% CI, 11.3 to NR months) in the DL2S regimen group. The estimated survival rate at 6 months and 12 months was 74.7% (95% CI, 68.9 to 79.6%) and 57.9% (95% CI, 51.3 to 63.8%), respectively (Figure 6).
Patients in the DLBCL efficacy set, with a median follow-up of 12.3 months, had a median PFS of 6.8 months (95% CI, 3.3 to 14.1) in all dose regimens, while the PFS was 9.5 months (95% CI, 3.2 to NR) in the DL2S regimen group. The estimated PFS rate at 6 months and 12 months was 51.4% (95% CI, 44.6% to 57.7%) and 44.1% (95% CI, 37.3% to 50.7%), respectively (Figure 7).
Figure 6: Overall Survival by Best Overall Response, DLBCL Efficacy Set
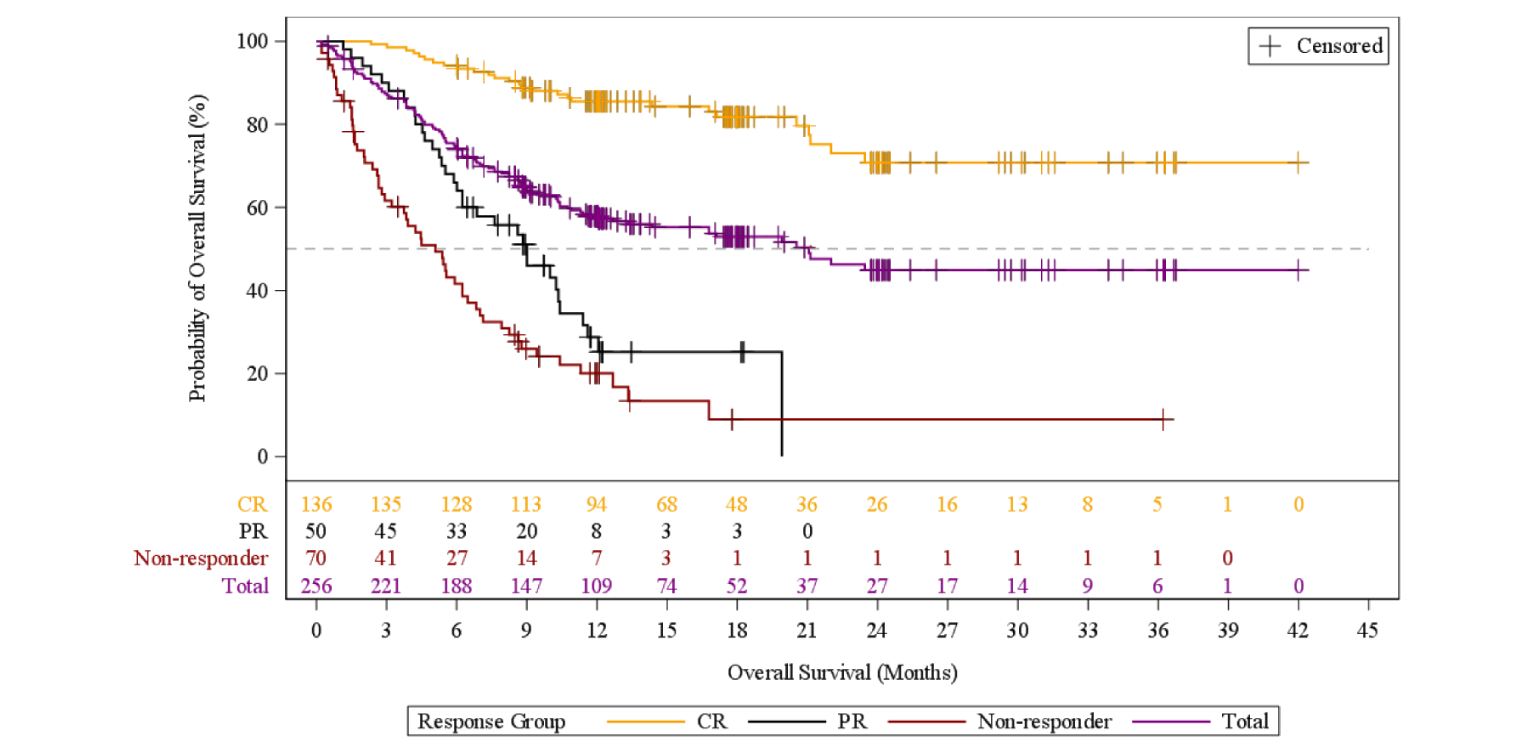
CR = complete response; DLBCL = diffuse large B-cell lymphoma; PR = partial response.
Note: Data as of the August 12, 2019 cut-off date.
Source: Clinical Study Report for the TRANSCEND study.9
Figure 7: Progression-Free Survival Per Independent Review Committee Assessment by Best Overall Response, DLBCL Efficacy Set
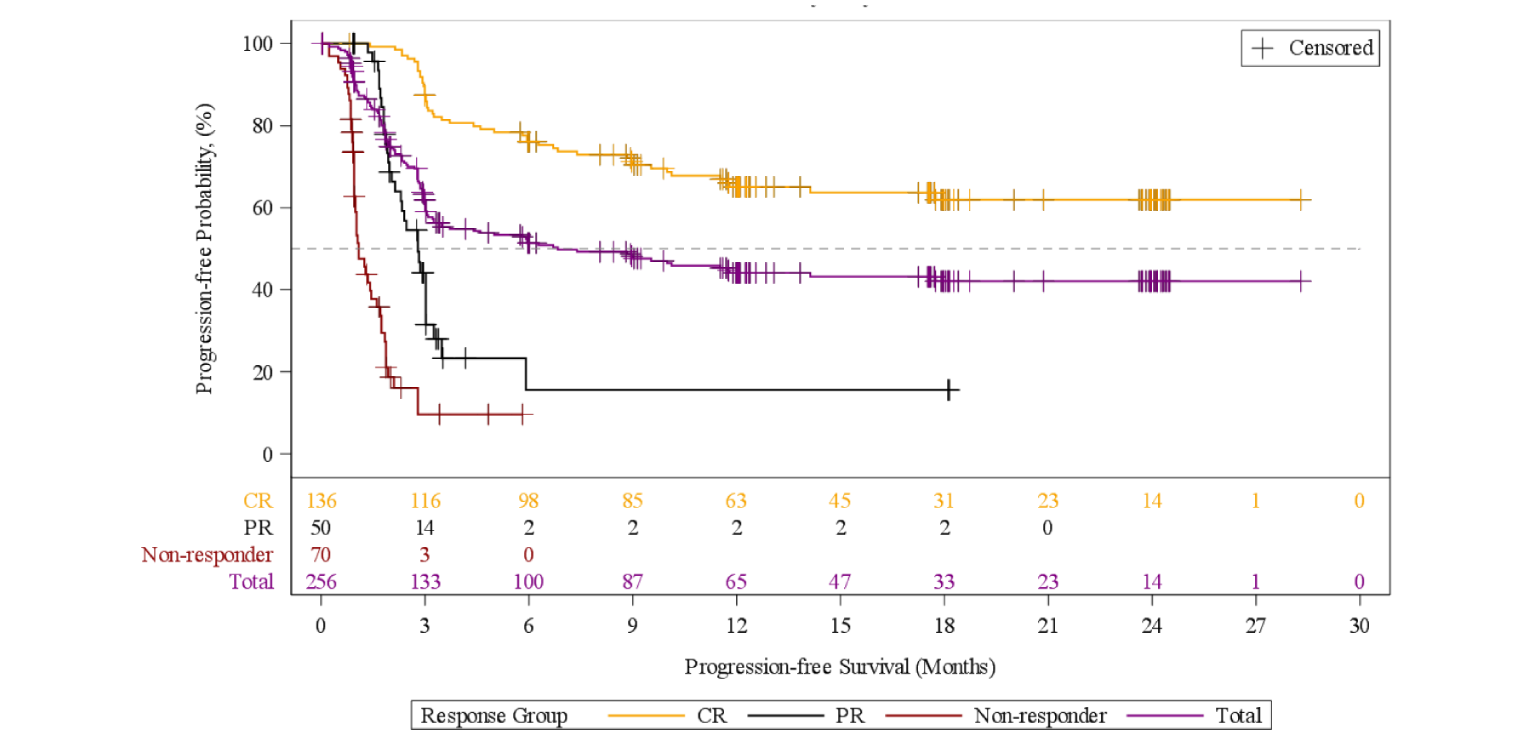
CR = complete response; DLBCL = diffuse large B-cell lymphoma; PR = partial response.
Note: Data as of the August 12, 2019 cut-off date.
Source: Clinical Study Report for the TRANSCEND Study.9
Response/Remission Rates
Results are presented separately for the leukapheresed set, the DLBCL efficacy set, and the PAS below. A summary of the results for response and remission across all dose regimens is presented in Table 13
Leukapheresed Set
The leukapheresed set (ITT) analysis was performed as a sensitivity analysis by the sponsor. The ORR was 60.5% (95% CI, 55.1 to 65.7), and the CR rate was 43.6% (95% CI, 38.3 to 49.0). In the DL2S regimen, the ORR was 60.4% (95% CI, 53.7 to 66.8), and the CR rate was 41.9% (95% CI, 35.4 to 48.6).
The DOR was based on IRC assessment for the DLBCL-leukapheresed set across assigned dose regimens. With a median follow-up of 12.4 months, the median DOR was 18.2 months (95% CI, 8.2 to NR). In total, 117 of the 208 patients who achieved a CR or PR (56.3%) were censored, and 91 of the 208 patients (43.8%) relapsed or died after initial response. Ninety of 208 patients (43.3%) were censored with ongoing response or had completed the study. Twenty-four of 208 patients (11.5%) were censored for receipt of new anticancer therapy and 3 were censored for subsequent HSCT.
Table 13: Efficacy Outcomes, Response
Variable | DL2S | DL1S | DL1D | DL3S | Total |
|---|---|---|---|---|---|
Leukapheresed (ITT) analysis set | n = 227 | n = 63 | n = 7 | n = 47 | N = 344 |
Overall response rate, n (%) | |||||
CR + PR | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | 208 (60.5) |
95% CI | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
CR rate, n (%) | |||||
CR | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | 150 (43.6) |
95% CI | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
Duration of response (months) | |||||
Median, 95% CI | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | 18.2, 8.2 to NR |
Minimum, maximum | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
DLBCL efficacy set | n = 169 | n = 40 | n = 6 | n = 41 | N = 256 |
Overall response rate, n (%) | |||||
CR + PR | 125 (74.0) | 27 (67.5) | 4 (66.7) | 30 (73.2) | 186 (72.7) |
95% CI | 66.7 to 80.4 | 50.9 to 81.4 | 22.3 to 95.7 | 57.1 to 85.8 | 66.8 to 78.0 |
CR rate, n (%) | |||||
CR | 88 (52.1) | 24 (60.0) | 3 (50.0) | 21 (51.2) | 136 (53.1) |
95% CI | 44.3 to 59.8 | 43.3 to 75.1 | 11.8 to 88.2 | 35.1 to 67.1 | 46.8 to 59.4 |
Duration of response (months) | |||||
Median, 95% CI | |||||||||||||| | NR, 3.7 to NR | NR, 0.9 to NR | |||||||||||||| | |||||||||||||| |
Minimum, maximum | 0.0, 23.5 | 0.0, 27.4 | 0.9, 23.0 | 0.0, 11.3 | 0.0, 27.4 |
Primary analysis set | n = 133 | NA | NA | NA | N = 133 |
Overall response rate, n (%) | |||||
CR + PR | 99 (74.4) | NA | NA | NA | 99 (74.4) |
95% CI | 66.2 to 81.6 | NA | NA | NA | 66.2 to 81.6 |
P valuea | NA | NA | NA | NA | < 0.0001 |
CR rate, n (%) | |||||
CR | 72 (54.1) | NA | NA | NA | 72 (54.1) |
95% CI | 45.3 to 62.8 | NA | NA | NA | 45.3 to 62.8 |
P valueb | NA | NA | NA | NA | < 0.0001 |
Duration of response (months) | |||||
Median, 95% CI | 16.8, 6.0 to NR | NA | NA | NA | 16.8, 6.0 to NR |
Minimum, maximum | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
CI = confidence interval; CR = complete response; DL1D = dose level 1, 2 dose; DL1S = dose level 1, single dose; DL2S = dose level 2, single dose; DL3S = dose level 3, single dose; DLBCL = diffuse large B-cell lymphoma; ITT = intention to treat; NA = not applicable; NR = not reached; PR = partial response.
aOne-sided P value was calculated based on the null hypothesis overall response rate of 40% or less.
bOne-sided P value was calculated based on the null hypothesis CR of 20% or less.
Source: Clinical Study Report for the TRANSCEND study.9
DLBCL Efficacy Set
The ORR (based on IRC) was 72.7% (95% CI, 66.8 to 78.0%), and the CR rate was 53.1% (95% CI, 46.8 to 59.4%). Responses, including CRs, were seen in all assigned dose regimens tested, with no evidence of a relationship between assigned dose regimen and response (overlapping CIs across all assigned dose regimens). Sensitivity analysis using the PP DLBCL analysis set (N = 259) for the ORR per IRC assessment was ||||||||||||||||||||||||||||| and the CR rate was |||||||||||||||||||||||||||||||||||||||||| Also, the concordance between IRC and investigator assessments was high (||||||||||||||||||||||||||||)
With a median follow-up of 12.0 months, the median DOR was NR (95% CI, 8.6 to NR months). After initial response, the probability of continued response at 6 months and 12 months was ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Primary Analysis Set
The primary efficacy end point of the TRANSCEND study was the ORR (per IRC) based on the PAS. A summary of response rates per IRC assessment in the PAS (by definition, assigned to DL2S) is also shown in Table 13. The ORR for patients in the PAS was 74.4% (95% CI, 66.2% to 81.6%). Based on data with a cut-off date of April 12, 2019, the study met its primary efficacy end point by rejecting the null hypothesis of an ORR of 40% or less (P < 0.0001). The CR rate for patients in the PAS was 54.1% (95% CI, 45.3% to 62.8%). Based on data with a cut-off date of April 12, 2019, the study rejected the null hypothesis of a CR of 20% or less (P < 0.0001). No additional hypothesis testing was conducted for the current data cut-off of August 12, 2019.
DOR was also based on IRC assessment for the PAS. With a median follow-up of 16.4 months, among the 99 patients achieving CR or PR, the median DOR was 16.8 months (95% CI, 6.0 to NR). After initial response, the probability of continued response at 6 months and 12 months was (||||||||||||||||||||||||||||||||||||||||||||||||||||||||), respectively. The most common reason for censoring was that the patient was still ongoing in the study (||||||||||||||||||||||||||||||||||||||||||%). Among the 72 patients in the PAS achieving CR, the median DOR was NR (95% CI, 13.3 to NR), ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||).
Intensive Care Admission and Utilization
In the total population (N = 269), 7 patients were never hospitalized. The median time for the initial hospitalization from liso-cel administration (N = 262) was 11 days (range = 2 days to 88 days). During the initial hospitalization, 19 of 269 patients (7.1%) were admitted to the ICU; the median number of ICU days was 7 days (range = 1 days to 56 days). Considering all hospitalizations through the end of the study, the median total days of hospitalization was 17 days (range = 2 days to 127 days). During this time, 33 of 269 patients (12.3%) were admitted to the ICU; the median number of ICU days was 8.0 (range = 1 days to 56 days).
In the patients who received liso-cel in the inpatient setting (N = 244), the median time from liso-cel infusion to discharge for the initial hospitalization was 11 days (range = 3 days to 88 days).
During the initial hospitalization, 18 of 244 patients (7.4%) were admitted to the ICU; the median number of ICU days was 7.5 (range = 1.0 days to 56.0 days). Considering all hospitalizations through the end of the study, the median total days of hospitalization after liso-cel infusion was 18 days (range = 3 days to 127 days). Throughout the entire study period, 32 of 244 patients (13.1%) were admitted to the ICU; the median number of ICU days was 8 (range = 1 days to 56 days).
In the patients who received liso-cel in the outpatient setting (N = 25), 18 (72.0%) were admitted to the hospital (all for AEs), a median of 5 days after liso-cel administration (range = 3 days to 22 days). The median time of first hospitalization was 6 days (range = 2 days to 23 days). During the initial hospitalization, 1 of 25 patients (4.0%) was admitted to the ICU for 3 days. Considering all hospitalizations through the end of the study, the median total days of hospitalization was 6.5 days (range = 2.0 days to 48.0 days).
HRQoL: Patient-Reported Outcomes
The PRO evaluable populations of the DLBCL cohort of the TRANSCEND study reported numerically decreased symptoms and increased PRO and QoL compared to pre-treatment baseline assessments through months 6 and 18. Specifically, patients in the PRO (EORTC QLQ-C30 and EQ-5D-5L) evaluable population of the DLBCL treated set were observed to numerically increase in HRQoL across several validated domains as early as month 1 post-liso-cel infusion. Specific results are presented in Table 14 and Table 15, and Figure 8 and Figure 9.
Table 14: Patient-Reported Outcomes: HRQoL, EORTC QLQ-C30
Variable | Global health | Physical functioning | Fatigue | Pain |
|---|---|---|---|---|
EORTC QLQ-C30a | ||||
Baseline | ||||
N | 181 | 181 | 181 | 181 |
Mean (standard deviation) | 62.3 (20.3) | 77.8 (19.2) | 38.2 (21.8) | 25.6 (25.8) |
Month 18 | ||||
N | 25 | 25 | 25 | 25 |
Mean (standard deviation) | |||||||||||||| | |||||||||||||| | |||||||||||||| | |||||||||||||| |
Change from baseline at month 18 | ||||
Mean (standard deviation) | 19.67 (25.559) | 6.93 (22.729) | –15.11 (29.897) | –8.67 (29.705) |
P valueb | < 0.001 | 0.331 | 0.021 | 0.160 |
DLBCL = diffuse large B-cell lymphoma; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; HRQoL = health-related quality of life.
aEvaluable population in DLBCL treated set. The range of EORTC QLQ-C30 scales is 0 to 100; a higher functional score indicates a more preferred health status, whereas a higher symptom score (fatigue and pain) indicates increased symptom impact. A minimal important difference of 10 points was considered significant by the sponsor and investigators.
bP values not adjusted for multiple comparisons.
Source: Clinical Study Report for the TRANSCEND study.9
Table 15: Patient-Reported Outcomes: HRQoL, EQ-5D-5L
Variable | Health utility index score |
|---|---|
Baseline | |
Na | 186 |
Mean (standard deviation) | 0.8 |||||||||| |
Month 18 | |
N | 25 |
Mean (standard deviation) | |||||||||||||| |
Change from baseline | |
Mean (standard deviation) | |||||||||||||| |
P value | |||||||||||||| |
DLBCL = diffuse large B-cell lymphoma; EQ-5D-5L = EuroQol 5-Dimensions 5-Levels questionnaire; HRQoL = health-related quality of life.
aEvaluable population in DLBCL treated set.
Source: Clinical Study Report for the TRANSCEND study.9
Figure 8: Mean Change From Baseline in Global Health Status in PRO (EORTC QLQ-C30) Evaluable Population in DLBCL Treated Set
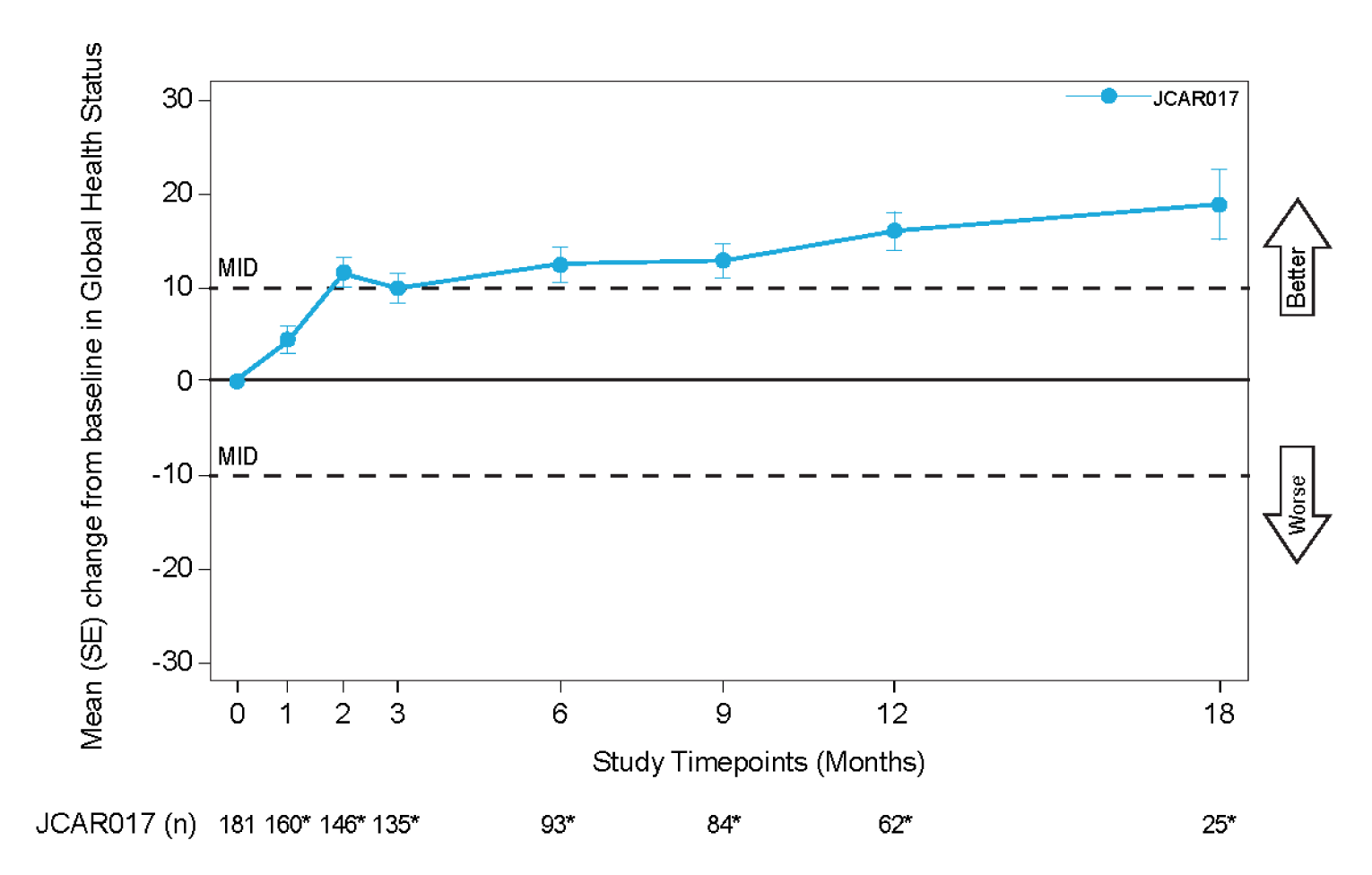
DLBCL = diffuse large B-cell lymphoma; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; MID = minimal important difference; PRO = patient-reported outcome; SE = standard error.
Note: The Wilcoxon signed rank test was used. The test was performed only if the sample size at any given assessment visit was at least 10. Month 0 represents baseline; month 1 = day 29.
*Indicates data point of a significant change from baseline with a P value of less than 0.05 based on the 2-sided unadjusted for multiple comparisons.
Source: Clinical Study Report for the TRANSCEND study.9
Figure 9: Mean Change From Baseline for EQ-5D-5L Index Scores in PRO (EQ-5D-5L) Evaluable Population in DLBCL Treated Set
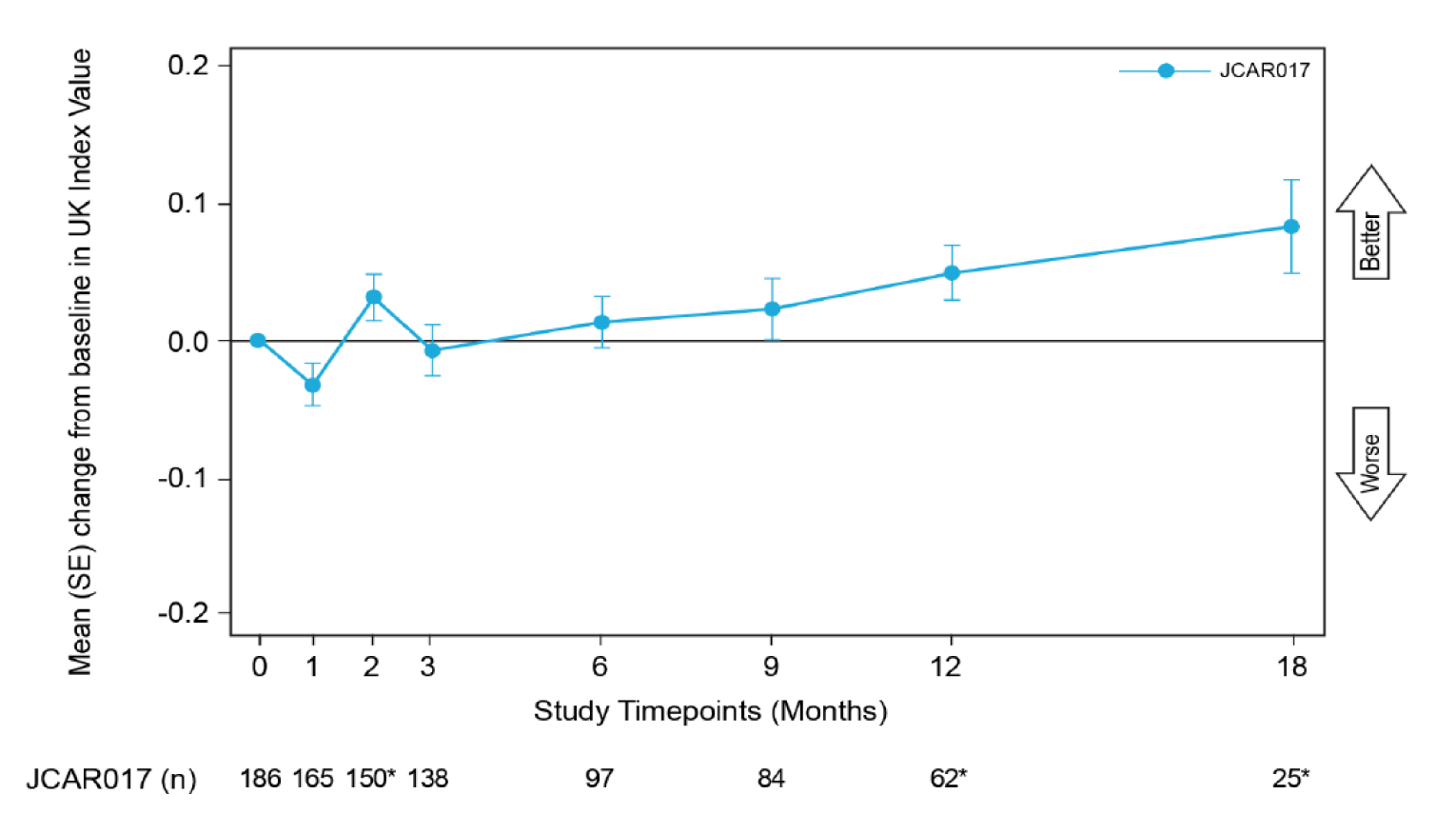
DLBCL = diffuse large B-cell lymphoma; EQ-5D-5L = EuroQol 5-Dimensions 5-Levels questionnaire; PRO = patient-reported outcome; SE = standard error.
Note: The Wilcoxon signed rank test was used. The test was performed only if the sample size at any given assessment visit was at least 10. Month 0 represents baseline; month 1 indicates day 29.
* Indicates data point of a significant change from baseline with a P value of less than 0.05 based on the 2-sided unadjusted for multiple comparisons.
Source: Clinical Study Report for the TRANSCEND study.9
At the data cut-off date (August 12, 2019), the PRO (EORTC QLQ-C30) evaluable population included 181 out of 269 patients in the DLBCL treated set. The mean change from baseline demonstrated numerical differences that ranged between 19.67 in global health status, 6.93 in physical functioning, –15.1 for fatigue, and –8.67 in pain scores through month 18. However, the number of evaluated patients also decreased to 25 by 18 months.
The evaluable population for the PRO of EQ-5D-5L included 186 out of 269 patients in the DLBCL treated set, who received liso-cel. At 18 months of follow-up, only 25 patients remained to be evaluated. At baseline, mean (standard deviation) EQ-5D-5L health utility index scores and EQ VAS scores were 0.82 (0.20) and 68.3 (19.5), respectively. By month 18, the utility index score dropped to |||||||||||||||||||||||||||| with a change from baseline ||||||||||||||||||||||||||||||||||||| (not adjusted for multiple comparisons); and ||||||||||||||||||||||||||||) in the EQ VAS.
Harms
AEs were summarized from the DLBCL treated set population (n = 269). Only those harms identified in the review protocol are reported below. See Table 16 for detailed harms data.
Table 16: Summary of Harms, DLBCL Treated Set
Harms | DL2S n = 177 | DL1S n = 45 | DL1D n = 6 | DL3S n = 41 | Total N = 269 |
|---|---|---|---|---|---|
Patients with ≥ 1 adverse event | 177 (100.0) | 44 (97.8) | 6 (100.0) | 40 (97.6) | 267 (99.3) |
Most common eventsa | |||||
Neutropenia | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 169 (62.8) |
Anemia | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 129 (48.0) |
Fatigue | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 119 (44.2) |
Cytokine release syndrome | 66 (37.3) | 18 (40.0) | 3 (50.0) | 26 (63.4) | 113 (42.0) |
Nausea | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 90 (33.5) |
Thrombocytopenia | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 84 (31.2) |
Headache | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 80 (29.7) |
Decreased appetite | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 76 (28.3) |
Diarrhea | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 71 (26.4) |
Constipation | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 62 (23.0) |
Dizziness | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 60 (22.3) |
Hypotension | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 60 (22.3) |
Cough | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 57 (21.2) |
Vomiting | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 56 (20.8) |
Hypokalemia | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 52 (19.3) |
Hypomagnesemia | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 50 (18.6) |
Pyrexia | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 45 (16.7) |
Abdominal pain | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 44 (16.4) |
Leukopenia | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 44 (16.4) |
Edema peripheral | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 42 (15.6) |
Sinus tachycardia | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 42 (15.6) |
Tremor | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 41 (15.2) |
Confusional state | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 39 (14.5) |
Hypertension | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 37 (13.8) |
Hypogammaglobulinemia | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 37 (13.8) |
Dyspnea | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 36 (13.4) |
Insomnia | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 36 (13.4) |
Back pain | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 33 (12.3) |
Chills | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 31 (11.5) |
Anxiety | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 27 (10.0) |
Hypophosphatemia | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 27 (10.0) |
Patients with ≥ 1 SAEa | 140 (79.1) | 36 (80.0) | 5 (83.3) | 32 (78.0) | 213 (79.2) |
Most common grade ≥ 3 events | |||||
Neutropenia | 106 (59.9) | 28 (62.2) | 5 (83.3) | 22 (53.7) | 161 (59.9) |
Anemia | 64 (36.2) | 20 (44.4) | 1 (16.7) | 16 (39.0) | 101 (37.5) |
Thrombocytopenia | 49 (27.7) | 13 (28.9) | 3 (50.0) | 7 (17.1) | 72 (26.8) |
Leukopenia | 26 (14.7) | 10 (22.2) | 1 (16.7) | 2 (4.9) | 39 (14.5) |
Febrile neutropenia | 13 (7.3) | 4 (8.9) | 0 (0.0) | 7 (17.1) | 24 (8.9) |
Hypophosphatemia | 10 (5.6) | 1 (2.2) | 0 (0.0) | 5 (12.2) | 16 (5.9) |
Encephalopathy | 5 (2.8) | 4 (8.9) | 1 (16.7) | 2 (4.9) | 12 (4.5) |
Hypertension | 5 (2.8) | 4 (8.9) | 0 (0.0) | 3 (7.3) | 12 (4.5) |
Deaths | N = 344 | ||||
Death occurred after leukapheresis and before lymphodepletion | NA | NA | NA | NA | 40 (11.6) |
Death occurred after lymphodepletion and before the first infusion of liso-cel or nonconforming product | NA | NA | NA | NA | 4 (1.2) |
Death occurred any time after the first infusion of liso-cel or nonconforming product | NA | NA | NA | NA | 137 (39.8) |
Notable harms | |||||
Cytokine release syndrome or neurologic toxicity | 79 (44.6) | 19 (42.2) | 3 (50.0) | 26 (63.4) | 127 (47.2) |
Cytokine release syndrome | 66 (37.3) | 18 (40.0) | 3 (50.0) | 26 (63.4) | 113 (42.0) |
Grade ≥ 3 infections | 20 (11.3) | 4 (8.9) | 0 (0.0) | 9 (22.0) | 33 (12.3) |
Grade ≥ 3 prolonged cytopenias | 73 (41.2) | 16 (35.6) | 3 (50.0) | 8 (19.5) | 100 (37.2) |
Hypogammaglobulinemia | 28 (15.8) | 3 (6.7) | 1 (16.7) | 5 (12.2) | 37 (13.8) |
DL1D = dose level 1, 2 dose; DL1S = dose level 1, single dose; DL2S = dose level 2, single dose; DL3S = dose level 3, single dose; DLBCL = diffuse large B-cell lymphoma; liso-cel = lisocabtagene maraleucel; NA = not applicable; SAE = serious adverse event.
Note: Values are represented as n (%).
aFrequency of greater than 10%.
Source: Clinical Study Report for the TRANSCEND study.9
Adverse Events
The investigators considered TEAEs to be those defined as an AE that started any time from initiation of liso-cel administration through and including 90 days following the final cycle (i.e., final infusion) of liso-cel. Any AE occurring after the initiation of another anticancer therapy or liso-cel re-treatment was not considered a liso-cel TEAE. Data from the regimen DL2S appears in the left-most column of all by-dose regimen tables, because it was the recommended regimen selected by the sponsor for evaluation in the DC group in the DLBCL cohort of the TRANSCEND study.
AEs occurred in 267 of 269 patients in all regimens and in all of the patients from the DL2S regimen. TEAEs occurred most frequently in the system organ class (SOC) of blood and lymphatic system disorders (209 of 269 patients; 77.7%). The 3 most frequently reported TEAEs (any grade) were neutropenia (169 of 269 patients; 62.8%), anemia (129 of 269 patients; 48.0%), and fatigue (119 of 269 patients; 44.2%). The fourth most commonly reported TEAE was CRS (113 of 269 patients; 42.0%). Grade 3 or higher TEAEs occurred most frequently in the SOC of blood and lymphatic system disorders (198 of 269 patients; 73.6%) and were neutropenia, anemia, and thrombocytopenia. Grade 3 or higher CRS occurred in 6 of 269 patients (2.2%), and no patient was reported to have grade 5 CRS.
From screening to leukapheresis, 94 of 347 patients (27.1%) reported AEs, including 13 of 347 patients (3.7%) with grade 3 to grade 4 AEs and 2 of 347 patients (0.6%) with SAEs. No grade 5 AEs were reported during this time period.
From leukapheresis to LDC, 192 of 344 patients (55.8%) reported AEs, including 48 of 344 patients (14.0%) with grade 3 to grade 4 AEs, 1 of 344 patients (0.3%) with a grade 5 AE of sepsis, and 20 of 344 patients (5.8%) with SAEs.
From LDC (from first day of last LDC) to first JCAR017 infusion, 272 of 298 patients (91.3%) reported AEs, including 113 of 298 patients (37.9%) with grade 3 to grade 4 AEs and 25 of 298 patients (8.4%) with SAEs. No grade 5 AEs were reported during this time period. During this time period, 225 of 298 patients (75.5%) experienced an AE related to LDC. LDC-related TEAEs occurred most frequently in the SOC of blood and lymphatic system disorders (198 of 269 patients: 73.6%). The 3 most frequent TEAEs considered related to LDC were neutropenia, occurring in 161 of 269 patients (59.9%); anemia, occurring in 113 of 269 patients (42.0%), and thrombocytopenia, occurring in 73 of 269 patients (27.1%).
A total of 10 patients were retreated at DL2S, 5 at DL1S, and 1 at DL3S. AEs were reported after re-treatment in 15 of 16 patients (93.8%), grade 3 or grade 4 AEs were reported in 13 of 16 patients (81.3%), and 1 of 16 patients (6.3%) had a grade 5 AE. AEs after re-treatment occurred most frequently in the SOC of blood and lymphatic system disorders (13 of 16 patients; 81.3%). The most frequent AEs after re-treatment were neutropenia (10 of 16 patients; 62.5%), anemia (8 of 16 patients; 50.0%), pyrexia and nausea (each in 6 of 16 patients; 37.5%), and headache and CRS (each in 5 of 16 patients; 31.3%). CRS occurred after re-treatment in 5 of 16 patients (31.3%), with 1 patient (6.3%) reporting grade 3 CRS. One patient experienced neurotoxicity (iiNT) after re-treatment.
Serious Adverse Events
In the DLBCL treated set, 122 of 269 patients (45.4%) reported treatment-emergent SAEs. SAEs were reported most frequently in the SOCs of immune system disorders (44 of 269 patients; 16.4%), nervous system disorders (41 of 269 patients; 15.2%), and infections and infestations (28 of 269 patients; 10.4%). The most frequent treatment-emergent SAEs were CRS (44 of 269 patients; 16.4%) and encephalopathy (14 of 269 patients; 5.2%). All other treatment-emergent SAEs were reported in less than 5% of patients.
Withdrawals Due to Adverse Events
Withdrawals due to AEs were not applicable as liso-cel was a single dose for most patients, and follow-up continued for patients regardless of AEs.
Mortality
Forty-four of 344 patients (12.8%) died before treatment with JCAR017 or nonconforming product. Deaths in these 44 patients were attributed to disease progression (n = 37), unknown causes (n = 3), other causes (n = 3), and sepsis (n = 1) considered related to protocol-mandated procedures.
A total of 137 deaths among the 344 patients (39.8%) were reported at any time after the first infusion of JCAR017 or nonconforming product. Deaths in these patients were attributed to disease progression (n = 116), AE (n = 12), other causes (n = 5), and unknown causes (n = 4).
Twelve patients in the DLBCL-leukapheresed set died due to AEs after treatment with JCAR017 (n = 10) or nonconforming product (n = 2).
Notable Harms
CRS was reported in 113 of 269 patients (42.0%) in the DLBCL treated set. Grade 3 or grade 4 CRS was reported in 6 of 269 patients (2.2%). No grade 5 CRS was reported. CRS was reported as an SAE in 44 of 269 patients (16.4%) in the DLBCL treated set. In the 113 patients with all-grade CRS, the median time to onset was 5 days (range = 1 days to 14 days). The events have resolved in 111 of these 113 patients. The median time to resolution of CRS in those with resolution as of the data cut-off date was 5 days (range = 1 days to 17 days). At DL3S, the incidence of all-grade CRS was more than 20% higher than at DL2S or DL1S. Treatment for CRS included tocilizumab, corticosteroids, vasopressors, supplemental oxygen, and empiric treatment with antibiotics.
In the DLBCL treated set, iiNT was reported in 80 of 269 patients (29.7%). The events resolved in 72 of these 80 patients. The median time to resolution of iiNT in those with resolution as of the data cut-off date was 11 days (range = 1 days to 86 days). Grade 3 or grade 4 iiNT was reported in 27 of 269 patients (10.0%). No grade 5 iiNT was reported. iiNT events were reported as SAEs in 39 of 269 patients (14.5%). In 45 of 269 patients (16.7%) corticosteroids and/or tocilizumab for iiNTs were used as treatment.
Other AESIs included tumour lysis syndrome which was reported in 2 of 269 patients (0.7%) in the DLBCL treated set (not reported as SAE); while 3 of 269 patients (1.1%) reported an infusion-related reaction to liso-cel. Hypogammaglobulinemia was reported in 37 of the total 269 patients (13.8%) in the DLBCL treated set, and, after the treatment-emergent period, it was reported in 12 of 247 (4.9%) of patients in the DLBCL treated set, with all events reported as grade 1 or grade 2. Treatment with IV immunoglobulin was not specified PP but rather left at investigator discretion following local guidelines. IV immunoglobulin was reported as a concomitant medication for 58 of 269 (21.5%) patients in the DLBCL treated set. In some cases, at the investigators’ discretion, IV immunoglobulin was administered for other reasons (e.g., low immunoglobulin G levels, thrombocytopenia, among others).
Updated Data
Data from 3 data cut-off dates were included in the sponsor’s submission for this review: August 19, 2019, June 19, 2020, and January 4, 2021, with median study follow-up duration of 11.5, 19.1, and 19.9 months, respectively. The 2 latest sponsor-provided updates also address efficacy and harm outcomes. However, the main analysis considered by CADTH for this review is from the August 12, 2019, cut-off date since the main hypothesis tests and adjustments for multiplicity were defined a priori and based on this date and using the PAS. Therefore, key end points from the updated cut-off dates were considered supplemental and supportive for the main analyses and are presented descriptively in Appendix 5.
Overall, the results of the new cut-off dates agree with the main analyses of the base-case data from the PAS and initial cut-off date of August 19, 2019. A total of 257 and 270 patients for the DLBCL efficacy and treated analysis sets, respectively, were included in both cut-off dates.
As of the cut-off date of January 4, 2021, in the total population of the DLBCL efficacy set, an ORR was reached in 187 (72.8%) patients (95% CI, 66.9 to 78.1), median DOR of 23.1 months (95% CI, 8.6 to NR), a median of PFS of 6.8 months (95% CI, 3.3 to 12.7), and median OS of 27.3 months (95% CI, 16.2 to 45.6). Deaths occurring at any point after the first infusion of liso-cel occurred in 40 patients (11.6%). AEs, SAEs, and deaths were observed in similar numbers at these later cut-off dates when compared to the initial cut-off date. These data are presented in Table 45 and Table 46 as well as Figure 25, Figure 26, Figure 27, and Figure 28 of Appendix 5.
Critical Appraisal
Internal Validity
The TRANSCEND study is a single-arm, open-label, phase I, seamless design study. The main limitation from the study stems from the single-arm design and lack of comparator groups giving place to risk of selection bias. In lieu of an available direct comparator, the investigators evaluated the primary end point of ORR against a null hypothesis of an ORR of 40% or less, with an alternate hypothesis of greater than 40% and effect size of 25% (ORR = 65%) based on a random effects meta-analysis of 8 studies of current recommended regimens for patients with 3L+ R/R aggressive large B-cell lymphoma. The hypothesis testing and adjustment for multiplicity was evaluated only for the PAS population; this situation can instill uncertainty in the effect estimates due to selection bias since it deviates from the ITT principle by not focusing on the population that provides most of the information as it would occur in a randomized controlled trial (i.e., the ITT population and the DLBCL treated set population) All patients in the enrolled population after screening (leukapheresed or ITT population) should be considered critical in any analysis that intends to evaluate the effect of assigning patients to an intervention (i.e., liso-cel) to evaluate the effects of all the procedures and co-interventions involved once it has been decided to start treatment; this is, including the manufacturing process, LDC, bridging therapy, and all possible consequences of these steps. An analysis based on the PAS could bias the effect estimate against a null hypothesis favouring the intervention.
An open-label design may also increase uncertainty in PROs (HRQoL) introducing bias due to inherent subjectivity of the outcome in an unblinded assessor. This bias would be less likely in more objective outcomes such as ORR, OS, or PFS. Furthermore, HRQoL outcomes were evaluated as secondary end points with no adjustment for multiplicity and with decreasing sample sizes at later time points of evaluation resulting in increasing imprecision and potential bias from missing data.
Anticancer treatments (which occurred in 62.2% of the leukapheresed patients) were considered an intervention needed for patients waiting for the manufactured product to be administered. These included bridging therapies. Any magnitude of effect that these anticancer interventions could have on the outcomes evaluated in patients who received liso-cel in the TRANSCEND study is uncertain.
Deviations from the protocol occurred in 10 of 269 (3.7%) patients in the DLBCL treated set. Sensitivity analyses were overall supportive of the robustness of results among populations. Some subgroups were pre-specified in the protocol; however, information on any subgroup effects was not possible to obtain since the sample size was small and only performed in the PAS population.
External Validity
Issues of generalizability of the results originate from the differences in the population included in the TRANSCEND study, which can be considered relatively young (mean age of 60.1 years in the DLBCL treated set). This is a relatively young population below the median age of diagnosis of 65 years of age commonly reported in epidemiology reviews and current clinical guidelines.1,21 Baseline and disease characteristics were overall similar between the DLBCL treated set and the PAS population, hence the issues of generalizability would apply to both populations for these variables.
Patients have good baseline performance status (only 4 patients in the DLBCL treated population and 1 in the PAS were classified as ECOG PS = 2) compared with patients typically seen in Canadian clinical practice. This agreed with input from clinical experts consulted by CADTH, when considering the similarities between the populations from TRANSCEND and those likely to be encountered in clinical practice in Canada. Also, some other baseline disease characteristics suggest that the included population might be healthier when compared to the Canadian clinical practice (e.g., low number of patients with ECOG PS = 2). The clinical experts consulted by CADTH noted that re-treatment cycles might be unusual in Canada; however, re-treatment in the TRANSCEND study was more common than they would expect in their clinical practice.
Other issues of generalizability are the low number of patients with FL3B, DLBCL transformed from indolent lymphomas other than follicular lymphoma, and patients with secondary CNS lymphoma that were included in the TRANSCEND study. These numbers make it difficult to draw conclusions on the effects of liso-cel in these populations.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
The objective of this section is to summarize and appraise indirect evidence comparing the relative effects and safety of liso-cel against relevant comparators in patients with R/R large B-cell lymphomas, as established in the protocol for this review. The main objective of performing ITCs is to fill a gap created by the absence of trials directly comparing available CAR T-cell therapies or comparing liso-cel to other 3L+ treatments.
A supplemental literature search was conducted by CADTH to identify further ITCs. A focused literature search for network meta-analyses dealing with large B-cell lymphoma was run in MEDLINE All (1946-) on September 2, 2021. No limits were applied. Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers made a final selection of studies included in the review, and differences were resolved through discussion. Based on this literature search conducted by CADTH, out of 22 search titles found and screened, 5 were evaluated as full texts, with no additional ITCs identified that assessed the relative effects of liso-cel against included comparisons (i.e., tisa-cel, axi-cel, or salvage therapy). One Cochrane systematic review assessed the effects of CAR T-cell therapies for people with R/R DLBCL but did not evaluate relative effects and reported results narratively.24
Description of Indirect Comparisons
Two ITC reports were provided by the sponsor and included a total of 3 ITCs in this clinical review report. The first ITC report12 comprises unanchored MAICs of liso-cel against 2 CAR T-cell therapies (i.e., tisa-cel and axi-cel), in patients with R/R large B-cell lymphomas. Data were obtained as IPD from the TRANSCEND study and as aggregated level data from the single-arm studies ZUMA-125 (axi-cel) and JULIET26 (tisa-cel).
The second ITC11 is an unanchored MAIC of the efficacy of liso-cel versus salvage chemotherapy by using IPD from the TRANSCEND NHL 001 study and aggregated level data from the SCHOLAR 1 study, respectively.
A description of the study selection criteria and methods is presented in Table 17.
Table 17: Study Selection Criteria and Methods for ITC reports
Criteria | ITC report 1 – liso-cel vs. CAR T-cell therapies | ITC report 2 – liso-cel vs. salvage chemotherapy |
|---|---|---|
Population | Patients with 3L+refractory/relapsed large B-cell lymphomas (DLBCL NOS, HGL, transformed from FL, tiNHL), secondary CNS lymphoma | Patients with 3L+refractory/relapsed large B-cell lymphomas (DLBCL NOS, HGL, transformed from FL, tiNHLs), secondary CNS lymphoma |
Intervention | Liso-cel at dose level 2: 100 × 106 CAR-positive T cells | Liso-cel at dose level 2: 100 × 106 CAR-positive T cells |
Comparators | Axi-cel as single dose of 2 × 106 CAR T cells/kg, maximum of 2 × 108 CAR T cells Tisa-cel as single infusion of 1 to 5 × 108 CAR T cells Other: Single or multi-agent chemotherapy, allo- or auto-HSCT, best supportive care, placebo | Salvage chemotherapy (no details on the type of each salvage chemotherapy) Other: Single or multi-agent chemotherapy, allo- or auto-HSCT, best supportive care, placebo |
Outcomes | ORR, CRR, PFS, and OS Harms (adverse events) Patient-reported outcomes | ORR, CRR, PFS, and OS Harms (adverse events) Patient-reported outcomes |
Study design | Phase I (IPD) and phase II single-arm trials (AD). Other: RCTs, observational studies with minimum sample size of 50 patients per study; conference abstracts. From countries: Belgium, Netherlands, Switzerland, Denmark, Finland, Norway, Sweden, Germany, France, Italy, Spain, UK, US, Japan, Australia, Canada | Phase I (IPD) and phase II single-arm trials (AD). Other: RCTs, observational studies with minimum sample size of 50 patients per study; conference abstracts. From countries: Belgium, Netherlands, Switzerland, Denmark, Finland, Norway, Sweden, Germany, France, Italy, Spain, UK, US, Japan, Australia, Canada |
Exclusion criteria | Articles published before 2003; in vitro, animal studies, commentaries, letters | Articles published before 2003; in vitro, animal studies, commentaries, letters |
Databases searched | MEDLINE, Embase, Cochrane CENTRAL, American Society of Clinical Oncology, European Society for Medical Oncology, European Hematology Association, American Society of Hematology, International Conference on Malignant Lymphoma, American Association for Cancer Research, European Organisation for Research and Treatment of Cancer, and the International Workshop on non-Hodgkin Lymphoma. Additionally, grey literature searches of clinicaltrials.gov, WHO clinical trials registry, FDA, EMA, European Union Drug Regulating Authorities Clinical Trials Database, and bibliographic handsearching of published systematic literature reviews were also conducted. | MEDLINE, Embase, Cochrane CENTRAL, American Society of Clinical Oncology, European Society for Medical Oncology, European Hematology Association, American Society of Hematology, International Conference on Malignant Lymphoma, American Association for Cancer Research, European Organisation for Research and Treatment of Cancer, and the International Workshop on non-Hodgkin Lymphoma. Additionally, grey literature searches of clinicaltrials.gov, WHO clinical trials registry, FDA, EMA, European Union Drug Regulating Authorities Clinical Trials Database, and bibliographic handsearching of published systematic literature reviews were also conducted. |
Selection and data extraction process | Title/abstract and full-text screening using an a priori set of criteria by 2 independent reviewers and conflicts resolved by consensus with a third reviewer. Data extraction by using a standardized form with 2 reviewers. | Title/abstract and full-text screening using an a priori set of criteria by 2 independent reviewers and conflicts resolved by consensus with a third reviewer. Data extraction by using a standardized form with 2 reviewers. |
Quality assessment | By using checklists recommended by National Institute for Health and Care Excellence | By using checklists recommended by National Institute for Health and Care Excellence |
3L+ = third line or later; AD = aggregated data; allo = allogeneic; auto = autologous; axi-cel = axicabtagene ciloleucel; CAR = chimeric antigen receptor; CNS = central nervous system; CRR = complete response rate; DLBCL = diffuse large B-cell lymphoma; FL = follicular lymphoma; HGL = high-grade lymphoma; HSCT = hematopoietic stem cell transplant; IPD = individual patient data; ITC = indirect treatment comparison; liso-cel = lisocabtagene maraleucel; NOS = not other specified; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; tisa-cel = tisagenlecleucel; tiNHL = transformed indolent non-Hodgkin lymphoma.
Source: Sponsor-submitted study reports; ITC112 and ITC2.11
Methods of ITC Report-1
Objectives
The objective of the ITC report-1 was to determine the comparative efficacy and safety of liso-cel relative to 2 other CAR T-cell therapies, tisa-cel and axi-cel, in patients with R/R large B-cell lymphoma on third-line therapy using MAICs for regulatory and health technology assessment purposes. An overview of the ITCs methods is presented in Table 18.
Table 18: ITC Report-1 Analysis of MAIC Methods
Criteria | ITC report-1 |
|---|---|
ITC methods | Unanchored MAICs of IPD from liso-cel (TRANSCEND) vs. AD from axi-cel (ZUMA-1) vs. AD from tisagenlecleucel (JULIET) |
Measures of effect | Generalized linear models for binary outcomes (i.e., ORR, CRR, AESI) were used to estimate odds ratios and Cox proportional hazards models for time-to-event outcomes (i.e., OS, PFS) were used to estimate HRs |
Clinical factors used for weighting | Prognostic factors were identified through a targeted literature search on, inspection of clinical factors reported in TRANSCEND, JULIET, and ZUMA-1 trials, and input from clinical experts by ranking of the factors to be included.
|
Weighting process | Method-of-moments propensity score algorithm for each comparison |
Outcomes | ORR, CRR, PFS, OS, and adverse events |
Follow-up time points | Up to 27 months |
Sensitivity analyses | Based on infused patients vs. ITT populations. Based on incorporating additional clinical factors for each outcome previously discarded in the weighting process. |
AD = aggregated data; AESI = adverse events of special interest; allo = allogeneic; axi-cel = axicabtagene ciloleucel; CNS = central nervous system; CRR = complete response rate; ECOG PS = Eastern Cooperative Oncology Group Performance Status; HSCT = hematologic stem cell transplant; IPD = individual patient data; ITC = indirect treatment comparison; ITT = intention to treat; liso-cel = lisocabtagene maraleucel; MAIC = matching-adjusted indirect comparison; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; SCT = stem cell transplant.
Source: Sponsor-submitted ITC-1 report.12
Study Selection Methods
ITC report-1 included a systematic literature search strategy to identify randomized and non-randomized studies of therapies used as 3L+ in patients with R/R LBCL, including DLBCL, FL3B, PMBCL, DLBCL transformed from iNHL, HGL, and DLBCL with CNS involvement. The search strategy included databases such as MEDLINE, Embase, Cochrane CENTRAL, and grey literature restricted to certain high-income countries and language (articles published in English, French, German, Italian, Spanish, Japanese, Danish, Finnish, Norwegian, or Swedish). The search criteria were also restricted to studies published from January 2003 to December 2019. Authors conducted, by pairs, the screening, selection, and data extraction of studies with specific inclusion or exclusion study criteria, and resolved disagreements with a third investigator. Data extraction was performed by investigators using pre-specified and piloted data extraction forms. Quality assessment of the included studies was assessed using checklists recommended by the National Institute for Health and Care Excellence.
The authors included and assessed data from 3 selected studies. For tisa-cel and axi-cel, authors used the peer-reviewed publications of the latest data cut-offs for the JULIET26 (data cut-off = December 8, 2017) and ZUMA-125 (data cut-off = August 11, 2018) trials, respectively, while using IPD from the TRANSCEND study for liso-cel. Secondary data sources for JULIET and ZUMA-1 from the same data cut-offs were assessed only when information was not available in the primary publication or when additional clarity was required.
First, the authors performed a feasibility assessment to conduct the ITC. This was an assessment of how similar, with regard to study design and patient characteristics, the pivotal studies to be included were to allow for adequate adjustment of the liso-cel IPD to the published aggregated data for the comparators tisa-cel and axi-cel. Thus, a qualitative comparison of the pivotal trials of liso-cel (TRANSCEND), tisa-cel (JULIET), and axi-cel (ZUMA-1) was conducted to assess the feasibility of ITCs in terms of study design and eligibility criteria (e.g., bridging therapy and median follow-up time), reporting of baseline characteristics, efficacy outcomes, safety outcomes, clinical definitions of baseline characteristics, and reported categorizations of clinical variables, as well as based on a quantitative assessment of the degree of imbalances between studies across baseline clinical factors.
The authors concluded that it was feasible to conduct the ITC for 4 efficacy outcomes (ORR, CRR, PFS, and OS) in comparisons of liso-cel to tisa-cel and liso-cel to axi-cel. For AESI, MAICs were feasible for grade 3 or grade 4 AEs, CRS, study-defined NT, encephalopathy, infections, hypogammaglobulinemia, and febrile neutropenia in comparisons of liso-cel to tisa-cel and liso-cel to axi-cel. MAICs of grade 3 or higher and grade 5 AEs were possible for liso-cel versus axi-cel.
The feasibility assessment was determined based on differences in study populations and design between trials that necessitated adjustment of variables to permit comparison of outcomes but were not large enough to preclude the comparison of outcomes altogether. Comparison of the study design, eligibility criteria, and baseline characteristics of the TRANSCEND, JULIET, and ZUMA-1 studies showed sufficient similarities between the studies to allow comparison, although there were still differences across trials that needed adjustment in a MAIC to reduce bias when indirectly comparing liso-cel to tisa-cel and axi-cel. Large differences in the definitions or categorizations of patient characteristics such as IPI score, disease histology, number of prior lines of therapy, and R/R to last therapy between trials were redefined within the liso-cel IPD to align more closely to those in each comparator study.
ITC Analysis Methods
The analyses in the ITCs included 2 sets of patients. The first set was composed of all patients who were enrolled and had received (were infused with) CAR T-cell therapy in the studies (i.e., the infused patients). The second set included all patients who were enrolled in the study and were leukapheresed (i.e., the leukapheresis set, also referred as the ITT).
To account for study heterogeneity, study eligibility criteria and baseline characteristics were examined. For each comparison, patients from the TRANSCEND study were removed from the IPD set if they did not satisfy the eligibility criteria and treatment protocol of the comparator trial (i.e., the ZUMA-1 or JULIET studies; refer to Table 19). Other clinical factors relevant for weighting were identified through a targeted literature search for variables that were prognostic factors in patients with 3L+ R/R large B-cell lymphoma and from inspection of clinical factors reported in the TRANSCEND, JULIET, and ZUMA-1 trials, as well as input from external clinical experts. Five clinical experts from different countries (Canada, France, Germany, the UK, and the US) supervised the identification and rank of the prognostic factors or effect modifiers relative to the outcomes of interest evaluating each efficacy outcome (4 lists of factors, 1 for each efficacy outcome), and all AEs (1 list of factors for all AEs). A final ranked list of clinical factors important for each efficacy outcome was derived using an evidence-informed ranking process that considered both the ranks informed by clinical experts and statistical approaches (i.e., random forest methodology27) to obtain data-driven rankings of the included factors. For safety outcomes, the identification and ranking methods underwent an expedited approach based on input from the clinical experts since, according to the authors, AEs would have fewer factors to consider and would be more difficult to rank.
Table 19: ITC Report-1. Patient Exclusions in Liso-cel Versus Tisagenlecleucel and Liso-cel Versus Axi-cel Comparisons
Outcome | Eligibility criteria | Liso-cel vs. tisagenlecleucel | Liso-cel vs. axi-cel |
|---|---|---|---|
Action | |||
Efficacy outcomes | Disease histology | Patients with FL3B or PMBCL were removed | Patients with FL3B were removed |
Prior allo-HSCT | Patients who had received prior allo-HSCT were removed | Patients who had received prior allo-HSCT were removed | |
ECOG PS | Patients with ECOG PS of 2 were removed | Patients with ECOG PS of 2 were removed | |
Secondary CNS involvement | Patients with secondary CNS involvement were removed | Patients with secondary CNS involvement were removed | |
Bridging therapy | No adjustment needed | Patients who received bridging therapy were removed | |
AESI | Secondary CNS involvement | Patients with secondary CNS involvement were removed | Patients with secondary CNS involvement were removed |
ECOG PS | Patients with ECOG PS of 2 were removed | Patients with ECOG PS of 2 were removed | |
Prior allo-HSCT | Patients who had received prior allo-HSCT were removed | Patients who had received prior allo-HSCT were removed | |
Bridging therapy | No adjustment needed | Patients who received bridging therapy were removed | |
AESI = adverse events of special interest; allo = allogenic; auto = autologous; axi-cel = axicabtagene ciloleucel; CNS = central nervous system; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FL3B = follicular lymphoma grade 3B; HSCT = hematologic stem cell transplant; ITC = indirect treatment comparison; liso-cel = lisocabtagene maraleucel; PMBCL = primary mediastinal large B-cell lymphoma.
Source: Sponsor-submitted ITC-1 report.12
Both the TRANSCEND and JULIET studies allowed bridging therapy for most patients. These studies provided bridging therapy as needed to patients awaiting CAR T-cell infusion. In contrast, the ZUMA-1 study did not permit bridging therapy. Due to this issue, analyses of liso-cel (from TRANSCEND) versus tisa-cel (from the JULIET study) included treated patients regardless of whether they received bridging therapy, while analyses of liso-cel (from the TRANSCEND study) versus axi-cel (from the ZUMA-1 study) involved removing patients from the TRANSCEND study who received bridging therapy. Sensitivity analyses were conducted that included patients who received bridging therapy.
After the exclusion of patients based on eligibility, the patients that remained and were included from the TRANSCEND study were weighted, using a method-of-moments propensity score algorithm for each comparison aimed at balancing clinical factors between the studies of interest. That is, after weighting patients, the means (or proportions) and standard deviations of clinical factors from the TRANSCEND study should be equal to those published in the JULIET and ZUMA-1 studies.
The final clinical factors deemed relevant to efficacy outcomes are depicted in Table 20. Of note, there were a total 24 clinical factors considered relevant to efficacy outcomes and available for analysis in the TRANSCEND study IPD data, and 17 were reported and available within the JULIET safety set/full analysis set data for comparison of OS and PFS. The 7 factors not available were:
tumour burden LDH
C-reactive protein
refractory subgroups (i.e., chemorefractory to last therapy, relapsed to prior auto-HSCT, chemosensitivity)
best response to any prior therapy
tumour burden sum of the products of diameters
extranodal disease
bulky disease.
For the CRR and ORR end points, 15 clinical factors were available within the JULIET efficacy analysis set, and 9 factors were not available, including tumour burden LDH, CRP, refractory subgroups (i.e., chemorefractory to last therapy, relapsed to prior auto-HSCT, chemosensitivity), best response to any prior therapy, tumour burden sum of the products of diameters, extranodal disease, bulky disease, age, and sex.
Of the 16 clinical factors deemed relevant to AESI, 8 were available for comparison between the TRANSCEND and JULIET studies’ safety set or full analysis set, and included secondary CNS involvement, number of prior lines of therapy, bone marrow involvement, bridging therapy, age, ECOG PS, prior allo-HSCT, and prior auto-HSCT.
The comparative efficacy of liso-cel relative to tisa-cel and axi-cel was assessed as the difference between (1) an estimate of the outcome of interest for liso-cel based on adjusted IPD from the TRANSCEND study (to align with patients in the JULIET or ZUMA-1 studies), and (2) the estimated outcome for tisa-cel or axi-cel based on published aggregated data from the JULIET or ZUMA-1 studies, respectively.
For binary end points, after exclusion of patients from the TRANSCEND study, a weighted estimate of the liso-cel outcome was derived using MAIC adjustment weights. Estimates of binary outcomes (ORR, CRR, AESI) were derived from an intercept-only logistic regression model with MAIC adjustment weights. The intercept represents a prediction of the log odds of the outcome of interest if a typical patient from the JULIET or ZUMA-1 studies had received liso-cel. Robust standard errors were estimated using the sandwich estimator via the R package “sandwich.” An estimate of the log OR for liso-cel versus tisa-cel or axi-cel was derived as the difference between the predicted log odds for liso-cel and the estimated log odds based on aggregated data from the JULIET or ZUMA-1 studies. The variance of the log OR between liso-cel versus tisa-cel or axi-cel was estimated as the sum of the variances of the log odds for liso-cel and tisa-cel or axi-cel.
Table 20: ITC Report-1. Clinical Factors and Rankings Used to Inform the Adjusting Process for Efficacy Analyses in the Comparison of Liso-cel to Tisagenlecleucel
Clinical factorb | Final rankingsa | |||
|---|---|---|---|---|
OS | PFS | CRR | ORR | |
Bridging therapy | 1 | 5 | 1 | 3 |
Disease histology | 2 | 1 | 5 | 8 |
ECOG PS | 3 | 2 | 7 | 7 |
Prior auto-HSCT | 4 | 7 | 3 | 2 |
R/R to last therapy | 5 | 4 | 2 | 6 |
Number of prior therapies | 6 | 8 | 9 | 9 |
Agec | 7 | 6 | 8 | 10 |
IPI score | 8 | 9 | 12 | 15 |
Absolute lymphocyte count | 9 | 13 | 4 | 5 |
Secondary CNS involvement | 10 | 10 | 14 | 12 |
Disease stage | 11 | 12 | 16 | 11 |
Prior allo-HSCT | 12 | 16 | 17 | 4 |
CrCl | 13 | 3 | 10 | 1 |
Sexc | 14 | 14 | 15 | 13 |
LVEF | 15 | 11 | 11 | 14 |
Cell of origin | 16 | 15 | 6 | 16 |
Double/triple hit or double expressor | 17 | 17 | 13 | 17 |
allo = allogenic; auto = autologous; CNS = central nervous system; CrCl = creatinine clearance; CRR = complete response rate; ECOG PS = Eastern Cooperative Oncology Group Performance Status; HSCT = hematologic stem cell transplant; IPI = International Prognostic Index; ITC = indirect treatment comparison; liso-cel = lisocabtagene maraleucel; LVEF = left ventricular ejection fraction; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; R/R = relapsed or refractory.
aFactors are ranked in order of importance where 1 represent the most important factor and 17 represents the least important factor.
bOnly 17 of the 24 factors available for analysis in the TRANSCEND individual patient data were available for comparison with the JULIET phase I and II safety analysis set.
cFactor was available for JULIET safety set and full analysis set, but not for JULIET efficacy analysis set.
Source: Sponsor-submitted ITC-1 report.12
For time-to-event end points (PFS and OS), weighted IPD from the TRANSCEND study were combined with pseudo-IPD (setting weights for pseudo-observations = 1) representing patients from the JULIET or ZUMA-1 studies. This dataset was then used to fit a weighted Cox proportional hazards model with a binary treatment indicator (i.e., liso-cel versus tisa-cel or axi-cel). The estimated regression coefficient for the treatment indicator was used to represent the log HR for liso-cel versus tisa-cel or axi-cel. Pseudo-IPD for PFS and OS from the JULIET or ZUMA-1 studies were generated by first digitizing the Kaplan–Meier survival curves and then using the Guyot 2012 approach to derive time-to-event data for both outcomes.28 “Log transformation” was used to estimate CIs of the median time-to-event. The authors did not adjust for multiplicity.
The following criteria were used to assess the performance and suitability of each MAIC model:
ESS: a low ESS compared to the original sample size (N) indicates large differences in patient weights due to large imbalances in patient populations before reweighting
Distribution of patient weights: extreme patient weights can indicate uncertainty in the resulting relative treatment effect
Summary statistics (e.g., means, proportions): for each clinical factor, before and after weighting were assessed to evaluate the improvement in balance between trial populations; balance was assessed using the absolute value of the standardized mean difference for each covariate and a standardized mean difference of 0.10 or greater was considered indicative of potentially important imbalances between comparisons.29
OS and PFS: the assumption of proportional hazards underlying Cox proportional hazards models was assessed by examining crossover in Kaplan–Meier curves and applying the Grambsch-Therneau statistical test for proportional hazards30
The primary analysis of the MAIC model was chosen based on achieving a balance between these criteria, while also considering the number of clinical factors included. Sensitivity analysis was chosen by incorporating the additional clinical factors for each outcome.
Results of ITC Report-1
Summary of Included Studies
The 3 studies included in the ITC were the TRANSCEND, ZUMA-1, and JULIET trials.
The TRANSCEND study is the pivotal study included in this CADTH report and has been described in the respective sections. Briefly, it is a phase I, single-arm, multi-centre, open-label trial assessing the efficacy and safety of liso-cel as a 3L+ treatment in patients with R/R large B-cell lymphoma. Primary end points were AEs and ORR as assessed by an IRC. Secondary end points included CRR (as assessed by IRC), DOR, PFS, and OS. A total of 270 patients received liso-cel, of which 257 formed the DLBCL efficacy analysis set.
The JULIET study was a phase I, single-arm, multi-centre, open-label, registrational trial of the efficacy and safety of tisa-cel in patients with R/R large B-cell lymphoma. This study did not include patients with PMBCL, transformed iNHL, and FL3B categories of lymphoma. The ECOG PS status in patients in this study was also different and set at 1 or lower. Patients were excluded if they had received allo-HSCT or had secondary CNS involvement. The primary end point was ORR and key secondary end points included DOR, OS, and safety. In total, 111 patients received an infusion and were included in the evaluation of efficacy, among which 93 patients were assessed for response rates. Median follow-up time was 14 months (range = 0.1 to 26).
Finally, the ZUMA study was a phase I/II, single-arm, multi-centre, open-label study evaluating the efficacy and safety of axi-cel in patients with refractory large B-cell lymphoma. The study included patients with the same types of lymphoma as in the TRANSCEND study (i.e., DLBCL, PMBCL, or tFL), but it did not include patients with FL3B. Patients were refractory to the most recent chemotherapy regimen or relapsed after auto-HSCT. Patients had an ECOG PS similar to those in the JULIET study (0 to 1), but lower than the TRANSCEND study. Furthermore, patients were excluded if they had secondary CNS lymphoma or prior allo-HSCT. The primary end points were safety for phase I and ORR for phase II. Key secondary end points were PFS, OS, and DOR. Of the 108 patients who received axi-cel, 101 were evaluable for efficacy in the phase II study. Median follow-up time was 27.1 months (interquartile range = 25.7 to 28.8).
A comparison of the characteristics of the included studies is presented in Table 21.
Table 21: ITC-1. Characteristics of Included Studies and Patient Characteristics
Characteristic | TRANSCEND NHL 001 (liso-cel) | JULIET (tisagenlecleucel) | ZUMA-1 (axi-cel) |
|---|---|---|---|
Design and phase | Phase I, single-arm, open-label, multi-centre (US) | Phase I, single-arm, open-label, multi-centre (US, Canada, Europe, Japan) | Phase I and II, single-arm, open-label, multi-centre (US and Israel) |
NHL subtypes | DLBCL NOS, HGL, tFL, PMBCL, tiNHL, FL3B | DLBCL NOS, HGL, tFL | DLBCL NOS, HGL, tFL, PMBCL, tiNHLa |
CAR T-cell regimen and dosage | Dose level 1, single-dose regimen: 50 × 106 CAR-positive T cells Dose level 1, 2-dose regimen: 50 × 106 CAR-positive T cells Dose level 2, single-dose regimen: 100 × 106 CAR-positive T cells Dose level 3, single-dose regimen: 150 × 106 CAR-positive T cells | Single infusion of 1 to 5 × 108 CAR-positive T cells | Single infused dose of 2 × 106 CAR-positive T cells per kg, with a maximum permitted dose of 2 × 108 CAR T cells |
Bridging therapy allowed | Yes | Yes | No |
PET-positive disease after bridging therapy | Confirmed | Not always confirmed | Not applicable |
Lymphodepleting chemotherapy | Yes, fludarabine and cyclophosphamide | Yes (omitted if WBC ≤ 1,000 cells/μL); fludarabine and cyclophosphamide. Alternatively, bendamustine | Yes, fludarabine and cyclophosphamide |
Data cut-off | June 19, 2020 | December 8, 2017 | August 11, 2018 |
Median study follow-up, months (range unless otherwise specified) | 19.1 (0.2 to 45.2) | 14 (0.1 to 26) for PFS, OS NA for ORR, CRR | 27.1 (IQR 25.7, 28.8) |
Analysis sets for efficacy (N) | DLBCL efficacy set (257) | Efficacy analysis set (93) | Phase II mITT set (101) |
Analysis sets for safety outcomes (N) | DLBCL treated set (270) | Safety/full analysis set (111) | Phase I and II safety analysis set (108) |
ECOG PS | ≤ 2 | ≤ 1 | ≤ 1 |
Prior lines of therapy | ≥ 2 | ≥ 2 | ≥ 2 |
Prior regimen required | Anthracycline and rituximab (or other CD20-targeted agents) | Included rituximab and anthracycline | Anti-CD20 monoclonal antibody unless tumour is CD20 negative, and an anthracycline containing chemotherapy regimen |
Response to prior therapies | R/R disease after at least 2 lines of therapy or after auto-HSCT | R/R disease after ≥ 2 lines of chemotherapy, including rituximab and anthracycline; patients had to have either failed auto-HSCT, or be ineligible for, or not consent to auto-HSCT | No response to first-line therapy (primary refractory disease); or no response to second or greater lines of therapy; or refractory post-auto-HSCT (disease progression or relapsed ≤ 12 months of auto-HSCT). |
Prior allo-HSCT | Allowed (not within 90 days of leukapheresis) | Not allowed | Not allowed |
Active CNS involvement | Secondary CNS involvement allowed | Not allowed | Not allowed |
allo = allogenic; auto = autologous; axi-cel = axicabtagene ciloleucel; CAR = chimeric antigen receptor; CNS = central nervous system; CRR = complete response rate; DLBCL = diffuse large B-cell lymphoma; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FL3B = follicular lymphoma grade 3B; HGL = high-grade B-cell lymphoma with rearrangements of MYC and BCL2 and/or BCL6; HSCT = hematopoietic stem cell transplant; IQR = interquartile range; ITC = indirect treatment comparison; liso-cel = lisocabtagene maraleucel; mITT = modified intention to treat; NA = not applicable; NHL = non-Hodgkin lymphoma; NOS = not otherwise specified; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; PMBCL = primary mediastinal B-cell lymphoma; R/R = relapsed or refractory; tFL = DLBCL transformed from follicular lymphoma; tiNHL = DLBCL transformed from other indolent non-Hodgkin lymphoma; WBC = white blood cell.
Source: Sponsor-submitted ITC-1 report.12
Studies also differed in their enrolment process. Specifically, the ZUMA-1 study did not permit enrolment and leukapheresis unless a CAR T-cell manufacturing slot was available. In contrast, the TRANSCEND and JULIET studies enrolled patients before confirming a manufacturing slot, and therefore allowed bridging therapy as needed to patients awaiting leukapheresis. This difference is evident in the median time from leukapheresis to product availability, which varied across studies (the TRANSCEND study = 24 days [range, 17 to 51], the JULIET trial = 113 days [range, 47 to 196], and the ZUMA-1 trial = 17 days [range, 14 to 51]).
In the comparison of trials, redefinition of some of the variables was undertaken for the weighting process, as presented in Table 22 and Table 23.
Table 22: ITC-1. Main Baseline Characteristics Differences Between TRANSCEND and JULIET
Baseline characteristic | TRANSCEND NHL 001 (liso-cel) | JULIET (tisagenlecleucel) | Action taken in TRANSCEND IPD and rationale |
|---|---|---|---|
IPI score | |||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| |
ECOG PS at screening | 0; 1; 2 | 0; 1 | None |
Tumour burden | SPD (cm2) measured before lymphodepleting chemotherapy and at enrolment | Reported as tumour volume (mL) | No action was taken as variables were measured differently and not included in subsequent analyses |
Disease histology | DLBCL NOS, HGL, tFL, tiNHL, PMBCL, FL3B | DLBCL NOS, HGLa, tFL, Other | Recategorized in TRANSCEND and JULIET to improve comparability of DLBCL patients and retain TRANSCEND patients, where DLBCL NOS, HGL, and tiNHL were combined as “DLBCL.” In JULIET, DLBCL NOS and Other were combined into “DLBCL” |
Number of prior lines of therapy | Assessed number of prior systemic lines of therapy, where systemic therapy did not include HSCT, only chemotherapies | Defined as prior lines of antineoplastic therapies. Antineoplastic therapies included medications, radiotherapies, surgeries, and HSCTs | Redefined in TRANSCEND such that a line of therapy included chemotherapy, auto-HSCT, allo-HSCT, and radiotherapy to align with JULIET definition |
R/R to last therapy | Refractory: Best response to last therapy as progressive disease, stable disease, or partial response. Relapsed: Best response to last therapy as complete response | Refractory: Best response to last therapy as progressive disease, stable disease, or response unknown Relapsed: Best response to last therapy as partial response or complete response | Redefined in TRANSCEND to align with JULIET definition. Specifically, in TRANSCEND, percent refractory to last therapy was rederived to include progressive disease, stable disease, or response unknown, whereas percent relapse was rederived to include partial response and complete response |
allo = allogenic; auto = autologous; DLBCL = diffuse large B-cell lymphoma; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FL3B = follicular lymphoma grade 3B; HGL = high-grade B-cell lymphoma with rearrangements of MYC and BCL2 and/or BCL6; HSCT = hematopoietic stem cell transplant; IPD = individual patient data; IPI = International Prognostic Index; ITC = indirect treatment comparison; liso-cel = lisocabtagene maraleucel; NOS = not otherwise specified; PMBCL = primary mediastinal B-cell lymphoma; R/R = relapsed or refractory; SPD = sum of the longest perpendicular diameters; tFL = DLBCL transformed from follicular lymphoma; tiNHL = DLBCL transformed from other indolent non-Hodgkin lymphoma.
Source: Sponsor-submitted ITC-1 report.12
Table 23: ITC-1. Main Baseline Characteristics Differences Between TRANSCEND and ZUMA-1
Baseline characteristic | TRANSCEND NHL 001 (liso-cel) | ZUMA-1 (axi-cel) | Action taken in TRANSCEND IPD and rationale |
|---|---|---|---|
IPI score | |||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| |
ECOG PS at screening | 0; 1; 2 | 0; 1 | None |
Disease histology | DLBCL NOS, HGL, tFL, tiNHL, PMBCL, FL3B | DLBCL NOS HGLc; PMBCL, tFL | Recategorized TRANSCEND to align with ZUMA-1 definition for DLBCL. Specifically, DLBCL NOS, HGL, and tiNHL from TRANSCEND were grouped together in “DLBCL” for comparison to “DLBCL” category in ZUMA-1. |
Number of prior lines of therapy | Assessed number of prior systemic lines of therapy, where systemic therapy did not include HSCT, only chemotherapies | Salvage chemotherapy and auto-HSCT were considered separate regimens | Redefined in TRANSCEND such that salvage chemotherapy and auto-HSCT were considered as 2 separate lines of therapy to align with ZUMA-1 definition |
R/R to last therapy | Refractory: Best response to last therapy as progressive disease, stable disease, or partial response Relapsed: Best response to last therapy as complete response | Refractory: Best response to last therapy as progressive disease or stable disease Relapsed: best response to last therapy of partial response or complete response | Redefined in TRANSCEND to align with ZUMA-1 definition. Specifically, percent refractory to last therapy was rederived to include progressive disease and stable disease, whereas percent relapse was rederived to include partial response and complete response |
auto = autologous; axi-cel = axicabtagene ciloleucel; DLBCL = diffuse large B-cell lymphoma; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FL3B = follicular lymphoma grade 3B; HGL = high-grade B-cell lymphoma with rearrangements of MYC and BCL2 and/or BCL6; HSCT = hematopoietic stem cell transplant; IPD = individual patient data; IPI = International Prognostic Index; ITC = indirect treatment comparison; liso-cel = lisocabtagene maraleucel; NOS = not otherwise specified; PMBCL = primary mediastinal B-cell lymphoma; R/R = relapsed or refractory; tFL = DLBCL transformed from follicular lymphoma tiNHL = DLBCL transformed from other indolent non-Hodgkin lymphoma.
Source: Sponsor-submitted ITC-1 report.12
For the liso-cel versus tisa-cel comparison, primary analyses of efficacy outcomes included 2 clinical factors in the weighting process. The investigators limited inclusion to these factors to ensure sufficient ESS across all outcome comparisons. The factors included were specific to each outcome based on a ranking system informed by expert opinion. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
For the liso-cel versus axi-cel comparison, analyses of efficacy outcomes were conducted for patients who did not receive bridging therapy (i.e., patients who received bridging therapy were excluded from the TRANSCEND study). In total, 5 clinical factors were included in the weighting. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Sensitivity analyses were also performed: first, a repeat of the primary analysis but including patients who received bridging therapy in the TRANSCEND study. Second, a repeat of the primary analyses but including patients who received bridging therapy in the TRANCSEND study and weighting for additional factors (exact factors were not specified). This was conducted to assess the effect of balancing more factors after gaining ESS upon including patients who received bridging therapy.
Results
Comparison of Liso-cel Versus Tisa-cel
For each set of efficacy outcomes, comparisons of ranked clinical factors at baseline were conducted without weighting patients from the TRANSCEND study. This exercise showed that few factors were similar between liso-cel and tisa-cel. Notable differences (i.e., standardized mean differences ≥ 0.2) were observed for age, ECOG PS, secondary CNS involvement, disease histology, cell of origin, prior allo-HSCT, prior auto-HSCT, bridging therapy, number of prior lines of therapy, CrCl before LDC, and pre-leukapheresis absolute lymphocyte count. After the weighting process, some key factors remained different between the data from the TRANSCEND and JULIET studies, such as age, bridging therapy, and prior lines of therapies. A comparison of clinical factors and standardized mean differences before and after weighting based on the MAIC for the end point of OS is presented in Table 24.
Table 24: ITC-1. Comparison of Clinical Factors and SMDs Before and After MAIC for Primary Analysis of Overall Survival for Liso-cel and Tisagenlecleucel
Clinical factor | Tisagenlecleucel (JULIET) safety set/full analysis set | Liso-cel (TRANSCEND) DLBCL efficacy set N = 257 overall survival | |
|---|---|---|---|
Before MAIC (unweighted) | After MAIC (weighted) | ||
N = 111 | ||||||||||||||||||| | ESS = 180.0 | |
Age, years | |||
Mean (standard deviation) | 53.9 (12.9) | ||||||||||||||||||| | 61.3 (11.8) |
SMD | NR | ||||||||||||||||||| | 0.605 |
Sex, male, % | 61.3 | ||||||||||||||||||| | 66.5 |
SMD | NR | ||||||||||||||||||| | 0.108 |
IPI Score, per JULIET categorization, % | |||
0 to 1 | 27.9 | ||||||||||||||||||| | 28.7 |
SMD | NR | ||||||||||||||||||| | 0.020 |
2 to 5 | 72.1 | ||||||||||||||||||| | 70.9 |
Missing | 0.0 | ||||||||||||||||||| | 0.3 |
ECOG PS at screening, % | |||
0 | 55.0 | ||||||||||||||||||| | 55.0 |
SMD | NR | ||||||||||||||||||| | 0.0 |
1 | 45.0 | ||||||||||||||||||| | 45.0 |
2 | 0.0 | ||||||||||||||||||| | 0.0 |
Secondary CNS involvement at time of treatment, % | |||
No | 100 | ||||||||||||||||||| | 100 |
SMD | NR | ||||||||||||||||||| | 0.0 |
Yes | 0.0 | ||||||||||||||||||| | 0.0 |
Disease histology, per JULIET categorization, % | |||
DLBCL | 81.1 | ||||||||||||||||||| | 81.1 |
SMD | NR | ||||||||||||||||||| | 0.0 |
DLBCL tFL | 18.9 | ||||||||||||||||||| | 18.9 |
PMBCL | 0.0 | ||||||||||||||||||| | 0.0 |
FL3B | 0.0 | ||||||||||||||||||| | 0.0 |
Prior HSCT, % | |||
Allo-HSCT | 0.0 | ||||||||||||||||||| | 0.0 |
SMD | NR | ||||||||||||||||||| | 0.0 |
Auto-HSCT | 48.6 | ||||||||||||||||||| | 48.6 |
SMD | NR | ||||||||||||||||||| | 0.0 |
Bridging therapy, % | |||
No | 8.1 | ||||||||||||||||||| | 47.4 |
SMD | NR | ||||||||||||||||||| | 0.977 |
Yes | 91.9 | ||||||||||||||||||| | 52.6 |
Prior lines of therapy per JULIET definition, % | |||
1 | 4.5 | ||||||||||||||||||| | 0.6 |
SMD | NR | ||||||||||||||||||| | 0.894 |
2 | 44.1 | ||||||||||||||||||| | 16.9 |
3 | 30.6 | ||||||||||||||||||| | 28.0 |
4 to 6 | 20.7 | ||||||||||||||||||| | 46.1 |
≥ 7 | 0 | ||||||||||||||||||| | 8.4 |
allo = allogenic; auto = autologous; CNS = central nervous system; DLBCL = diffuse large B-cell lymphoma; ECOG PS = Eastern Cooperative Oncology Group performance status; ESS = effective sample size; FL3B = follicular lymphoma grade 3B; HSCT = hematologic stem cell transplant; IPI = International Prognostic Index; ITC = indirect treatment comparison; liso-cel = lisocabtagene maraleucel; MAIC = matching-adjusted indirect treatment comparison; NR = not reported; PMBCL = primary mediastinal B-cell lymphoma; SMD = standardized mean difference; tFL = transformed from follicular lymphoma.
Source: Sponsor-submitted ITC-1 report.12
In the primary analysis of the ORR that weighted for 2 factors, liso-cel had an ORR of 74.7% and an ESS of 164.0 (representing 63.8% of the 257 patients before weighting in the liso-cel DLBCL efficacy set). Based on the primary analysis, the odds of response were estimated to increase for liso-cel compared to tisa-cel (OR = 2.77; 95% CI, 1.63 to 4.73; P < 0.001). ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
In the primary analysis for CRR that weighted for 2 factors, liso-cel was associated with a CRR of 56.0%, with an ESS of 200.1 (77.8% of pre-weighting sample). The odds of response were estimated to increase for liso-cel compared to tisa-cel (OR = 1.92; 95% CI, 1.17 to 3.17; P = 0.010). ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

For the primary analysis of PFS that weighted for 2 factors, liso-cel had a median PFS of 6.7 months (95% CI, 3.5 to NR), with an ESS of 149.3 (58.0% of unweighted population). The HR for PFS estimated a decreased hazard for liso-cel compared to tisa-cel (HR = 0.66; 95% CI, 0.47 to 0.92; P = 0.013; Figure 11). ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

The HRs reported above for PFS were derived from a Cox proportional hazards model, which assumes that the relative hazard for progression for liso-cel compared with tisa-cel is constant over time. This assumption was tested by visual inspection of the Kaplan–Meier curves and the Grambsch-Therneau test on the slope of the Schoenfeld residuals. There were some concerns regarding the validity of the proportional hazard assumption, with visual inspection of the Kaplan–Meier curves suggesting the assumption was likely to be appropriate and the Grambsch-Therneau test suggesting potential violations for the naive, primary, and sensitivity analyses. Kaplan–Meier curves for PFS for the naive, primary, and sensitivity analyses are depicted in Figure 12.
Figure 12: ITC-1. Kaplan–Meier Curves of Progression-Free Survival for Liso-cel and Tisagenlecleucel in Infused Patients, Unmatched and Unadjusted (Naive) and Primary Analyses

This figure has been redacted.
Note: Updated data from the cut-off point of January 4, 2021.
Source: Sponsor-submitted ITC-1 report.12
In the primary analysis for OS that adjusted for 2 factors, liso-cel had a median OS of 28.9 months (95% CI, 19.9 to NR) with an ESS of 180.0 (70.0% of the unweighted population). For this comparison, the HR for OS estimated a decreased hazard for liso-cel compared to tisa-cel (HR = 0.66; 95% CI, 0.46 to 0.93; P = 0.019). |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

Kaplan–Meier curves liso-cel for OS are presented in Figure 14. After 44 months there was a decrease in the probability of survival and a small number of patients at risk due to loss to follow-up (through censoring or deaths) at the time of the analysis (June 19, 2020 data cut-off), as well as weighting of patients in the remaining risk set.

Simulated treatment comparisons were performed as a structural sensitivity analysis to MAIC for the efficacy outcomes of ORR, CRR, PFS, and OS. Overall, the simulated treatment comparison results were consistent to those obtained via MAIC.
In terms of safety outcomes, analyses of AESI were conducted for infused patients using the DLBCL treated set from the TRANSCEND study and safety set/full analysis set from the JULIET study. After including 1 clinical factor in the weighting process, liso-cel had an ESS of 124.7. For most end points, the odds of AESI were similar or lower for liso-cel (N = 270) than for tisa-cel (N = 111). Figure 15 shows that liso-cel had statistically significantly lower odds of grade 3 or 4 AEs, all-grade and grade 3 or higher CRS, and grade 3 or higher prolonged cytopenia by laboratory assessment. No statistically significant difference was found in the odds of all-grade and grade 3 or higher study-defined NT, all-grade and grade 3 or higher neurologic events, all-grade study-defined NT of encephalopathy (preferred term), all-grade and grade 3 or higher encephalopathy, all-grade study-defined NT of aphasia (preferred term), all-grade and grade 3 or higher aphasia, and febrile neutropenia. The odds of grade 3 or higher infections and all-grade hypogammaglobulinemia were also not statistically significantly different between treatments.


Comparison of Liso-cel Versus Axi-cel
For each efficacy outcome, comparisons of ranked clinical factors at baseline were conducted first without matching or adjusting patients from the TRANSCEND study (infused patients). Notable differences (i.e., standardized mean differences ≥ 0.2) were observed for age, disease stage, tumour burden, secondary CNS involvement, extranodal disease, disease histology, prior allo-HSCT, bridging therapy, R/R to last therapy, CrCl before LDC, and LVEF at screening. After the weighting process, key factors remained different between the data from the TRANSCEND and ZUMA-1 studies, such as prior auto-HSCT and prior line of therapy. A comparison of clinical factors and standardized mean differences before and after weighting based on the MAIC for the end point of OS is presented in Table 25.
Table 25: ITC Report-1. Comparison of Clinical Factors and SMDs Before and After MAIC for Primary Analysis of Overall Survival for Liso-cel and Axi-cel
Clinical factor | Axi-cel (ZUMA-1) phase II analysis set | Liso-cel (TRANSCEND) DLBCL efficacy set overall survival | |
|---|---|---|---|
Before MAIC (unweighted) | After MAIC (weighted) | ||
N or ESS | N = 101 | 257 | ESS = 38.3 |
Age, years | |||
Mean (standard deviation) | 56.3 (12.0) | 60.2 (13.3) | 56.3 (12.1) |
SMD | NA | 0.308 | 0.0 |
Sex, male, % | 67.3 | 65.8 | |||||||||||||||||| |
SMD | NA | |||||||||||||||||| | |||||||||||||||||| |
IPI score, per ZUMA-1 categorization, % | |||
0 to 2 | 54.5 | 58.8 | 54.5 |
SMD | NA | 0.164 | 0.0 |
4 to 4 | 45.5 | 39.7 | 45.5 |
5 | 0.0 | 0.8 | 0.0 |
Missing | 0.0 | 0.8 | 0.0 |
ECOG PS at Screening, % | |||
0 | 41.6 | 40.9 | |||||||||||||||||| |
SMD | NA | 0.178 | |||||||||||||||||| |
1 | 58.4 | 57.6 | |||||||||||||||||| |
2 | 0.0 | 1.6 | |||||||||||||||||| |
Secondary CNS involvement at time of treatment, % | |||
No | 100.0 | 97.7 | 100.0 |
SMD | NA | 0.219 | 0.0 |
Yes | 0.0 | 2.3 | 0.0 |
Disease histology, per ZUMA-1 categorization, % | |||
DLBCL | 76.2 | |||||||||||||||||| | 76.3 |
SMD | NA | |||||||||||||||||| | 0.0 |
DLBCL tFL | 15.8 | |||||||||||||||||| | 15.8 |
PMBCL | 7.9 | |||||||||||||||||| | 7.9 |
FL3B | 0.0 | |||||||||||||||||| | 0.0 |
Prior HSCT, % | |||
Allo-HSCT | 0.0 | 2.7 | 0.0 |
SMD | NA | 0.237 | 0.0 |
Auto-HSCT | 24.8 | 33.1 | 40.3 |
SMD | NA | 0.183 | 0.336 |
Bridging therapy, % | |||
No | 100.0 | 41.6 | 100 |
SMD | NA | 1.674 | 0.0 |
Yes | 0.0 | 58.4 | 0.0 |
Prior lines of therapy per ZUMA-1 definition, % | |||
1 | 3.0 | 0.8 | |||||||||||||||||| |
SMD | NA | 0.178 | |||||||||||||||||| |
2 | 27.7 | 25.3 | |||||||||||||||||| |
3+ | 69.3 | 73.9 | |||||||||||||||||| |
allo = allogenic; auto = autologous; axi-cel = axicabtagene ciloleucel; CNS = central nervous system; DLBCL = diffuse large B-cell lymphoma; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ESS = effective sample size; FL3B = follicular lymphoma grade 3B; HSCT = hematopoietic stem cell transplant; IPI = International Prognostic Index; ITC = indirect treatment comparison; liso-cel = lisocabtagene maraleucel; MAIC = matching-adjusted indirect treatment comparison; PMBCL = primary mediastinal B-cell lymphoma; SMD = standardized mean difference; tFL = DLBCL transformed from follicular lymphoma.
Source: Sponsor-submitted ITC-1 report.12
Efficacy analyses were conducted for infused patients using the DLBCL efficacy set from the TRANSCEND study and the phase II modified ITT set from the ZUMA-1 study. For each outcome, a primary analysis and 2 sensitivity analyses were conducted. The primary analysis was conducted after removing patients from the TRANSCEND study who received bridging therapy before infusion. Both sets of sensitivity analyses included patients from the TRANSCEND study who received bridging therapy before infusion. The first sensitivity analysis weighted for the same set of factors as the primary analysis. In contrast, the second sensitivity analysis leveraged the additional sample size obtained by including patients who received bridging therapy to adjust for a larger set of factors.
For the primary analysis for ORR that included 5 factors in the weighting process, the ORR for liso-cel was 80.1%, with an ESS of 42.1 (16.3% of the unweighted population). For this comparison, the odds of overall response did not show a statistically significant difference between liso-cel and axi-cel (OR = 1.40; 95% CI, 0.56 to 3.50; P = 0.473). ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Overall, the ITT population showed similar results when compared to the infused population.
In the primary analysis for CRR that included 5 factors in the weighting process, the CRR for liso-cel was 59.2%, with an ESS of 39.6. This comparison showed no statistically significant difference in the odds of response between liso-cel and axi-cel (OR = 1.21; 95% CI, 0.56 to 2.64; P = 0.627). In both sensitivity analyses there were again no statistically significant differences observed. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

In the primary analysis for PFS that included 5 factors in the weighting process, the median PFS for liso-cel increased to 6.3 months (95% CI, 3.0 to NR), with an ESS of 40.0 (15.5% of the unweighted population). The HR for PFS showed that there was no statistically significantly difference in the hazards between liso-cel and axi-cel (HR = 0.94; 95% CI, 0. 57 to 1.55; P = 0.818). In both sensitivity analyses, there were no statistically significant differences between liso-cel and axi-cel detected (Figure 18).
Figure 18: ITC-1. Forest Plot for Progression-Free Survival for Liso-cel Versus Axi-cel, Infused Patients
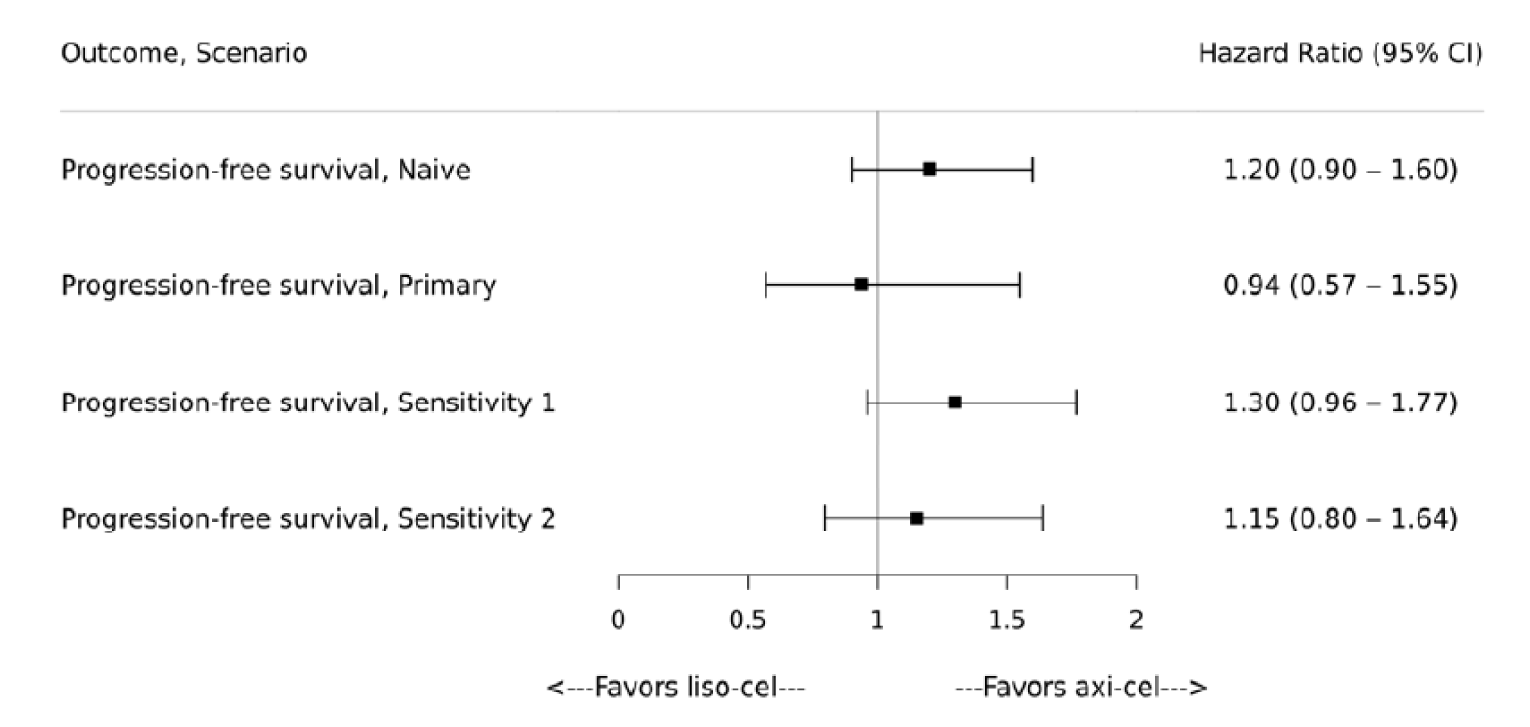
axi-cel = axicabtagene ciloleucel; ITC = indirect treatment comparison; liso-cel = lisocabtagene maraleucel; PFS = progression-free survival.
Note: For primary analysis of PFS, 5 clinical factors were used for matching and 5 factors were used for the weighting process.
Source: Sponsor-submitted ITC-1 report.12
Kaplan–Meier curves for the primary analysis are presented in Figure 19. Visual inspection of the Kaplan–Meier curve and the Grambsch-Therneau test suggested that the proportional hazards assumption was generally appropriate for these analyses. In the primary analysis for OS that included 5 factors in the weighting process, the median OS for liso-cel was 48.5 (95% CI, 11.6 to NR), with an ESS of 38.3 (14.9% of the unweighted population). The HR for OS showed that there was not a statistically significant difference in the hazards between liso-cel and axi-cel (HR = 0.78; 95% CI, 0.44 to 1.42; P = 0.421). Similarly, sensitivity analyses showed no statistically significant differences between liso-cel and axi-cel.
Figure 19: ITC-1. Comparison Kaplan–Meier Curves of Progression-Free Survival Between Liso-cel and Axi-cel for Infused Patients, Matched and Adjusted Comparison (Primary Analysis; ESS = 40.0)
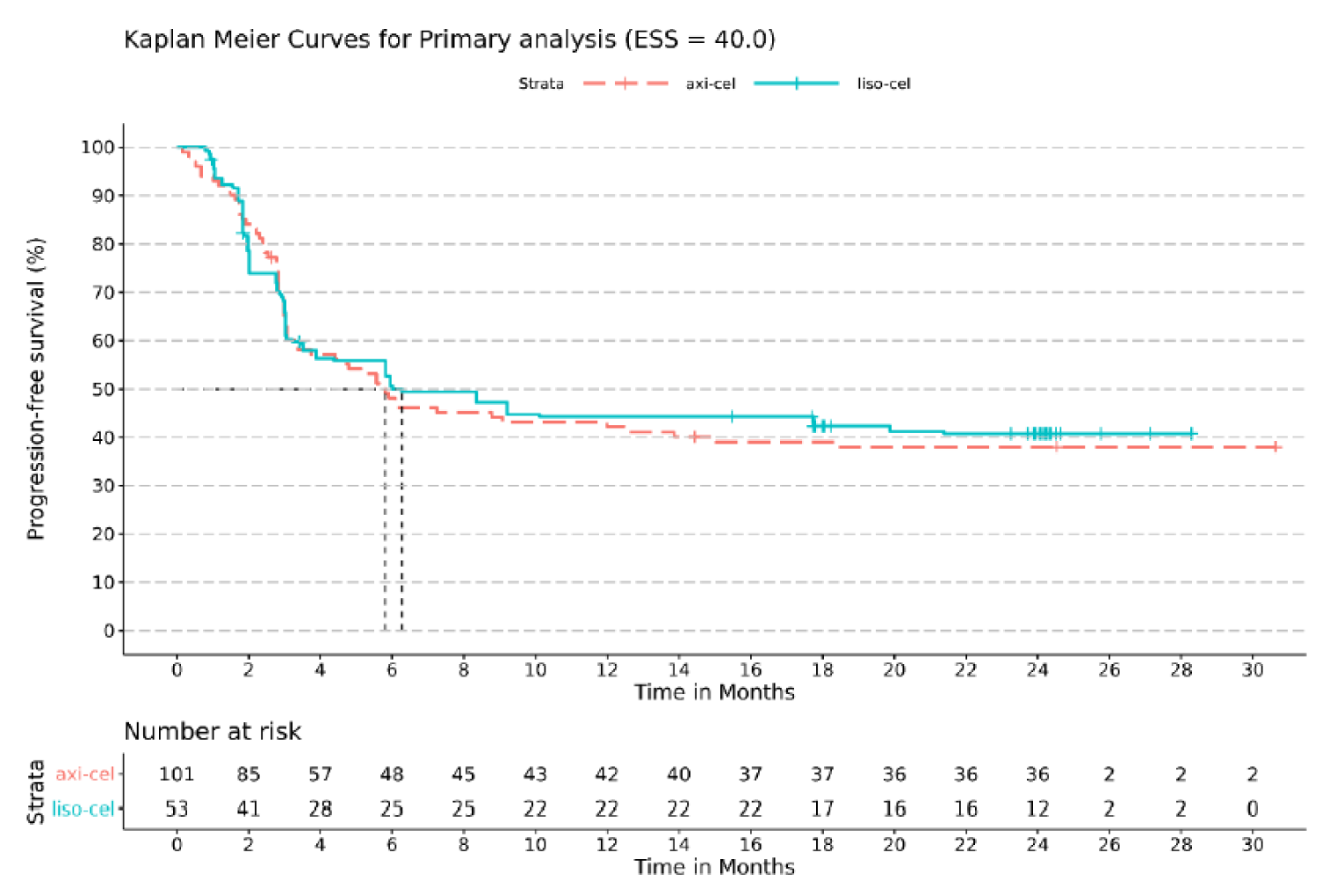
axi-cel = axicabtagene ciloleucel; ESS = effective sample size; ITC = indirect treatment comparison; liso-cel = lisocabtagene maraleucel.
Source: Sponsor-submitted ITC-1 report.12


Figure 22: ITC-1. Forest Plot for AEs (Grade ≥ 3) of Special Interest for Liso-cel Versus Axi-cel, Infused Patients
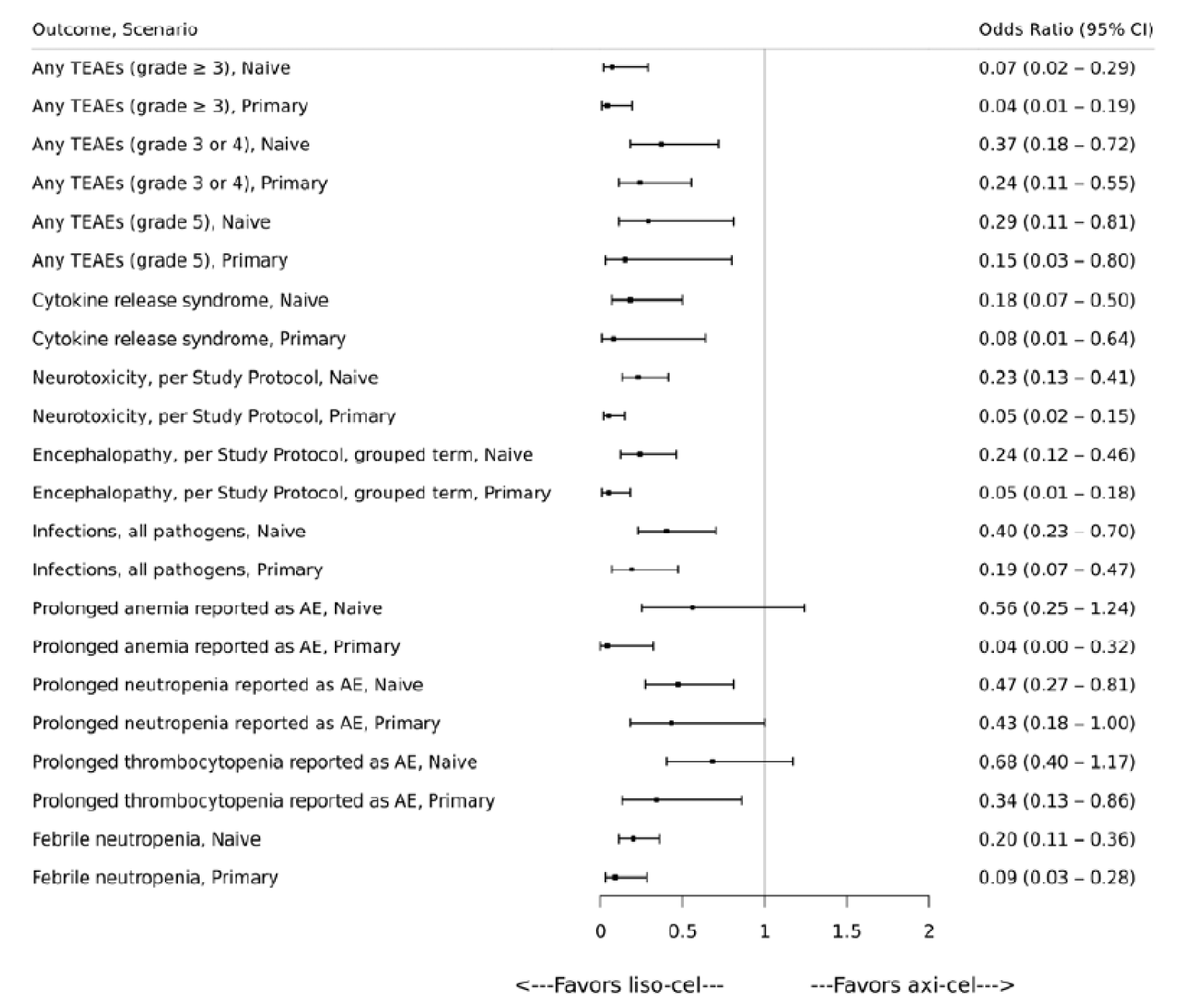
AE = adverse event; axi-cel = axicabtagene ciloleucel; CI = confidence interval; ESS = effective sample size; ITC = indirect treatment comparison; liso-cel = lisocabtagene maraleucel; TEAE = treatment-emergent adverse event.
Source: Sponsor-submitted ITC-1 report.12
Simulated treatment comparisons were performed as a structural sensitivity analysis to MAIC for the efficacy outcomes of ORR, CRR, PFS, and OS. Overall, the simulated treatment comparisons results showed no statistically significant differences between liso-cel and axi-cel for ORR, CRR, PFS, and OS, consistent with those obtained via MAIC.
In terms of safety outcomes, analyses of AESI were conducted using the DLBCL treated set from the TRANSCEND study and phase I and II safety analysis set from the ZUMA-1 study. After including 5 clinical factors in the weighting process, liso-cel had an ESS of 66.0. Overall, liso-cel had statistically significantly lower odds of AESI than axi-cel. Specifically, liso-cel was associated with a significantly lower odds of grade 3 or higher AEs, grade 3 or 4 AEs, grade 5 AEs, all-grade and grade 3 or higher CRS, all-grade and grade 3 or higher study-defined NT, all-grade and grade 3 or higher NEs, all-grade and grade 3 or higher study-defined NT of encephalopathy, all-grade and grade 3 or higher encephalopathy, all-grade study-defined NT of aphasia, all-grade aphasia, grade 3 or higher infections, all-grade hypogammaglobulinemia, grade 3 or higher prolonged anemia, neutropenia, and thrombocytopenia as AEs, and all-grade and grade 3 or higher febrile neutropenia.
Critical Appraisal of ITC Report-1
The ITC report-1 aimed at comparing IPD from a single-arm clinical trial (TRANSCEND) against aggregated data from 2 studies evaluating each tisa-cel and axi-cel in an unanchored MAIC. For the approach to be a valid comparison, the investigators would need to achieve balance on all prognostic factors and all effect modifiers between each arm of treatment by including all such factors in a weighting process to make the population similar for comparison to evaluate efficacy and safety end points. In other words, the method aims at mitigating between-study differences in baseline characteristics and variables that might modify the outcomes.
A systematic literature process is defined in a separate technical report, describing appropriate search methods that identified the JULIET and ZUMA-1 studies as key resources for the efficacy and safety evaluations. Overall, the search strategy, screening process, and quality of individual studies are described and were conducted properly.
The main limitation in any MAIC is the incompatibility of the assumption that all relevant prognostic variables and effect modifiers are detected and included in the adjustment and matching process.31 Baseline differences of variables between the 3 included studies suggest that other potential unmeasured confounders might be present, and that these can be unevenly distributed between groups—a common situation when a proper randomization is lost or not possible.
Efforts were made to obtain all possible clinical variables to be included in the weighting process of the MAIC by, for example, obtaining the prognostic variables and effect modifiers from a literature search (data driven) and by clinician input. However, as mentioned by the authors, there is no guarantee that all relevant factors will be identified, and some important variables (e.g., tumour burden, LDH) were missing in the ZUMA-1 and JULIET studies. The degree of imbalance among the 3 trials makes it impossible to weight all identified factors. Authors did not clearly state which factors were weighted for each end point which limits the ability to critically appraise the information. Even after recalculation and recategorization of the variables to align comparator arms, differences in the measured variables were detected (e.g., response criteria, bridging therapy) which can further increase the risk of bias, despite the evaluation of some of these differences through sensitivity analyses that gave similar results to the base-case analysis. The ESS went from 257.0 to 180.0 (i.e., 70.0%) in the MAIC of liso-cel versus tisa-cel and from 257.0 to 38.3 (i.e., 14.9%) in the liso-cel versus axi-cel comparisons, which speaks of the amount of information lost due to the exclusion of patients and the weighting process which also begets uncertainty due to imprecision and may limit the generalizability of the results. No sample sizes after the exclusion of patients (the matching step, as defined in the technical report) were reported, which limits the opportunity to assess the impact of the ESS in the weighting process.
There were also uncertainties due to concerns of violations of the proportional hazards assumptions for the end points of OS and PFS by visually assessing the Kaplan–Meier curves and based on the Grambsch-Therneau tests.
Overall, populations among the 3 studies are pre-treated patients with R/R large B-cell lymphoma. These patients included would be similar to the ones seen in clinical practice in the Canadian landscape and to whom the indication for liso-cel is directed. However, there are still differences in the populations, interventions, and end points evaluated in the 3 trials included in this ITC that can increase the uncertainty in the generalizability of results. For instance, the lack of bridging therapy in the ZUMA-1 trial, the unknown amount of CD8+ and CD4+ cells administered in all 3 studies (which speaks for differences in drug manufacturing and time to receive the drug after leukapheresis), the differences in the number of patients with ECOG PS of 2, the time to infusion after leukapheresis, among other factors, increase the uncertainty in the generalizability of the effect estimates from these comparisons. The end point of HRQoL was not reported in the results of these ITCs, limiting the scope of the results.
Methods of ITC Report-2
Objectives
The objective of the ITC-2 was to determine the comparative efficacy of liso-cel relative to salvage chemotherapy in the treatment of R/R large B-cell lymphomas using MAIC. This analysis used IPD from the TRANSCEND study for liso-cel and published summary-level data also called aggregated data from the SCHOLAR-1 retrospective database study for salvage chemotherapy.13
Table 26: Analysis of MAIC Methods
Method | ITC-2 |
|---|---|
ITC methods | Unanchored MAICs of IPD from liso-cel (TRANSCEND) vs. AD of salvage chemotherapy (SCHOLAR-1) |
Measures of effect | Generalized linear models for binary outcomes and Cox proportional hazards regressions for time-to-event outcomes were used to estimate odds ratios or hazard ratios from time of first infusion. |
Clinical factors used for weighting | Prognostic factors were identified through a targeted literature search, input from clinical experts by ranking of the factors to be included, data-driven prognostic associations, and assessment of prognostic factors reported in both TRANSCEND and SCHOLAR-1.
|
Weighting process | Patients from TRANSCEND were adjusted via weights derived from a method-of-moments propensity score algorithm. Method-of-moments was chosen to accommodate the availability of only summary-level data for SCHOLAR-1 to balance clinical factors between the interventions of interest. |
Outcomes | OS, CRR, ORR |
Follow-up time points | Median of 19.1 months (TRANSCEND study) |
Sensitivity analyses | Based on age (≥ 65 years) Based on OS from leukapheresis (intention-to-treat set) for TRANSCEND study. |
AD = aggregated data; auto = autologous; CRR = complete response rate; HSCT = hematologic stem cell transplant; IPD = individual patient data; IPI = International Prognostic Index; liso-cel = lisocabtagene maraleucel; ITC = indirect treatment comparison; MAIC = matching-adjusted indirect comparison; OS = overall survival; ORR = overall response rate.
Source: Sponsor-submitted ITC-2 report.11
Study Selection Methods
The ITC report-2 included a systematic literature search strategy to identify randomized and non-randomized studies of therapies used as 3L+ in patients with R/R LBCL, including DLBCL, FL3B, PMBCL, DLBCL transformed from iNHL, HGL, and DLBCL with CNS involvement. The search strategy included databases such as MEDLINE, Embase, Cochrane CENTRAL, and grey literature restricted to certain high-income countries and language (articles published in English, French, German, Italian, Spanish, Japanese, Danish, Finnish, Norwegian, or Swedish). The search criteria were also restricted to studies published from January 2003 to December 2019. Authors conducted, by pairs, the, screening, selection, and/or data extraction of studies with specific inclusion or exclusion study criteria and resolved disagreements using a third investigator. Data extraction was performed by investigators using pre-specified and piloted data extraction forms. Quality assessment of the included studies was assessed using checklists recommended by the National Institute for Health and Care Excellence.
After full-text screening and exclusion of studies based on their predefined criteria, authors included evidence from IPD from the TRANSCEND study and aggregated data from the SCHOLAR-1 study.
ITC-2 Analysis Methods
Unanchored MAICs were conducted to determine the relative efficacy of liso-cel versus salvage chemotherapy (the SCHOLAR-1 study) based on OS, CRRs, and ORR outcomes. MAICs for time-to-event outcomes were used to derive comparisons between interventions for OS, and HRs were used to summarize comparative efficacy. Furthermore, MAICs for binary outcomes were used to derive relative treatment effects for CRRs and ORRs, with ORs used to summarize comparative efficacy. All models adjusted for clinical factors identified by the investigators that were reported in both the TRANSCEND and SCHOLAR-1 studies. Analyses were conducted based on the guidance outlined in the National Institute for Health and Care Excellence Evidence Synthesis Technical Support Document Series.
IPD for liso-cel from the TRANSCEND trial were used for this analysis. The TRANSCEND trial was a phase I, single-arm, multi-centre, open-label trial that investigated the efficacy and safety of liso-cel as 3L+ treatment in patients with R/R large B-cell lymphoma. The population included from the TRANSCEND study in this ITC is the DLBCL efficacy set (n = 257).
Summary-level data for salvage chemotherapy for this analysis were derived from the SCHOLAR-1 study.13 SCHOLAR-1 was a retrospective database study including patients from 4 sources, as follows:
2 real-world databases:
follow-up of 2 phase III randomized controlled trials:
Patients with DLBCL, tFL, and PMBCL were eligible for inclusion in the SCHOLAR-1 study if they were refractory to at least 1 prior line of therapy, including an anti-CD20-targeted agent and anthracycline. Refractory status was defined as a best response of PD to any line of chemotherapy, a best response of SD to 4 or more cycles of first-line therapy, a best response of SD to 2 or more cycles of second or later-lines of therapy, or relapse 12 months or earlier after auto-HSCT. Key outcomes of interest included OS, CRR, and ORR.
In the TRANSCEND trial, patients received infusions of liso-cel at the following doses, as a single- or 2-dose regimen:
dose level 1, single-dose regimen: 50 × 106 CAR-positive T cells
dose level 1, 2-dose regimen: 50 × 106 CAR-positive T cells
dose level 2, single-dose regimen: 100 × 106 CAR-positive T cells
dose level 3, single-dose regimen: 150 × 106 CAR-positive T cells.
All patients included in the SCHOLAR-1 retrospective database study received a chemotherapy regimen, with the goal of consolidative HSCT in the LY.12 and CORAL studies34,35; no specifics on each regimen were presented.
Estimates of the comparative efficacy of liso-cel versus salvage chemotherapy were derived as the difference between (1) an estimate of the outcome of interest for patients in the SCHOLAR-1 study, had they received liso-cel, and (2) the estimated outcome based on published summary-level data from SCHOLAR-1.
Factors used for the MAIC process were selected based on a multi-faceted strategy that incorporated a targeted literature review, clinical expert opinion, data-driven prognostic associations, and assessment of prognostic factors reported in both the TRANSCEND and SCHOLAR-1 studies. In total, 37 factors were identified. Clinical experts were interviewed to validate this list of factors and to add any additional factors to be considered. Each clinical expert was then asked to rank clinical factors in order of importance for the OS, PFS, CRR, and ORR outcomes. A final ranked list of clinical factors important for efficacy and safety outcomes was derived using an evidence-informed ranking process that considered the degree of concordance of both ranks by clinical experts and statistical approaches (i.e., estimates of variable importance as derived via random forest). For efficacy outcomes there were 24 clinical factors deemed relevant and available for analysis in the TRANSCEND study IPD, and 7 were reported in the SCHOLAR-1 study and available for comparison. No information was provided for the rest of the clinical factors not included in the rankings.
||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| | ||
|---|---|---|---|
||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| | |
||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| |
||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| report.11
A weighted estimate of the outcomes was derived using MAIC adjustment weights. For binary end points (i.e., CRR, ORR), estimates were derived from an intercept only of a generalized linear model with MAIC adjustment weights. The intercept represents a prediction of the log odds of the outcome of interest if a typical patient from the SCHOLAR-1 study had received liso-cel. Robust standard errors were estimated using the sandwich estimator via the R package “sandwich.” An estimate of the log OR for liso-cel versus salvage chemotherapy was derived as the difference between the predicted log odds for liso-cel and the estimated log odds based on summary-level data from the SCHOLAR-1 study. The variance of the log OR between liso-cel versus salvage chemotherapy was estimated as the sum of the variances of the log odds for liso-cel and salvage chemotherapy.
For time-to-event end points, such as OS, weighted IPD from the TRANSCEND study were combined with pseudo-IPD (setting weights for pseudo-observations = 1) representing patients from the SCHOLAR-1 study. This dataset was then used to fit a weighted Cox proportional hazards regression with a binary treatment indicator (i.e., liso-cel versus salvage chemotherapy). The estimated regression coefficient for the treatment indicator was used to represent the log HR for liso-cel versus salvage chemotherapy. Pseudo-IPD for OS from the SCHOLAR-1 study was generated by first digitizing Kaplan–Meier survival curves and then using the Guyot 2012 approach28 to derive time-to-event data for OS.
For the ranked clinical factors, separate MAICs were conducted sequentially, adjusting for 1 additional variable at a time in order of ranked importance. After fitting each model, the performance and suitability of each MAIC model was assessed based on the following criteria:
ESS: a low ESS compared with the original sample size, N, indicates large differences in patient weights due to large imbalances in patient populations before reweighting; the ESS is interpreted as the number of independent, non-weighted individuals needed to obtain an equally precise estimate compared to that calculated from the weighted sample
distribution of patient weights: extreme patient weights can indicate uncertainty in the resulting relative treatment effect
summary statistics (e.g., means, proportions) for each clinical factor before and after weighting were assessed to evaluate the improvement in balance between trial populations; balance was assessed using the absolute value of the standardized mean difference for each covariate. A standardized mean difference of 0.10 or greater is considered indicative of potentially important imbalances between comparisons
Sensitivity analyses were conducted by iteratively removing 1 clinical factor at a time in reverse order of clinical importance, per the evidence-informed rankings. Furthermore, a sensitivity analysis was conducted for each outcome by re-running the base-case analysis after adjusting for the proportion of participants aged 65 years or older instead of the mean and standard deviation of age. An additional sensitivity analysis was conducted based on OS from leukapheresis (ITT set) for the TRANSCEND population. This comparison adjusted for 5 of the 7 characteristics used in the base case for the MAIC, as 2 factors (IPI score and disease stage) were missing for 77 of 344 patients who underwent leukapheresis.
Results of ITC Report-2
Summary of Included Studies
Study design characteristics were considered by the authors sufficiently comparable to allow for indirect comparisons between studies. Both studies were multi-centre, open-label, and single-arm. The TRANSCEND trial was conducted in the US only, whereas the SCHOLAR-1 study enrolled patients in Canada, the US, Australia, and several European countries. Baseline prognostic factors had low to moderate imbalance between studies before adjustment (Table 28).
Table 28: ITC Report-2. Characteristics of Studies Included in the MAIC
Study design characteristics | TRANSCEND (liso-cel) | SCHOLAR-1 (salvage chemotherapy) |
|---|---|---|
Design | Single arm | Retrospective database analysis |
Phase | 1 | NA |
Blinding | Open label | Open label |
Centres | Multi-centre - US | Multi-centre - Australia, Canada, US, Europe |
Inclusion criteria | ||
NHL subtypes | DLBCL NOS, HGL, tFL, Other, PMBCL, FL3B | DLBCL, PMBCL, tFL |
Age | ≥ 18 years | ≥ 18 years |
ECOG score | ≤ 2 | 0 to 4 |
Prior lines of treatment | ≥ 2 | ≥ 1 |
Prior auto-HSCT | Allowed | Allowed |
auto = autologous; DLBCL = diffuse large B-cell lymphoma; ECOG = Eastern Cooperative Oncology Group; FL3B = follicular lymphoma grade 3B; HGL = high-grade B-cell lymphoma with rearrangements of MYC and BCL2 and/or BCL6; HSCT = hematopoietic stem cell transplant; ITC = indirect treatment comparison; liso-cel = lisocabtagene maraleucel; MAIC = matching-adjusted indirect comparison; NA = not applicable; NHL = non-Hodgkin lymphoma; NOS = not otherwise specified; PMBCL = primary mediastinal B-cell lymphoma; tFL = DLBCL transformed from follicular lymphoma.
Source: Sponsor-submitted ITC-2 report.11
Overall, 7 baseline characteristics (NHL subtype, sex, age, prior auto-HSCT, R/R status to last therapy, disease stage, and IPI score) were reported in both the TRANSCEND and SCHOLAR-1 studies (out of 24 initially stated). Differences in the categorization of variables and extent of missing data were noted between studies for NHL subtype and IPI score. The definitions of these variables were aligned by reclassifying variables, collapsing variables into a narrower set of categories, or adding published patient data with missing covariate values into non-missing categories. Patients were removed from the TRANSCEND study dataset if they had missing data on any of the 7 clinical factors reported in SCHOLAR-1.
Table 29: ITC-2 Baseline Characteristics and Actions to Align for MAIC
Baseline characteristics | TRANSCEND (liso-cel) | SCHOLAR-1 (salvage chemotherapy) | Data derivation actions taken to align categories and ensure convergence of the MAIC |
|---|---|---|---|
Sample size | 257 | 636 | NA |
NHL subtype (%) | |||
DLBCL or DLBCL transformed from FL or from other NHL | 93.0 | 91.0 | DLBCL and tFL were combined into a single category |
PMBCL | 5.4 | 2.0 | NA |
FL3B | 1.6 | 0.0 | Patients in TRANSCEND were removed |
Indeterminate/missing | 0.0 | 7.0 | Categories were collapsed into DLBCL and tFL and PMBCL or indeterminate/missing |
Male sex (%) | 66.0 | 64.0 | None |
Age ≥ 65 years (%) | 42.0 | 13.8 | Used in sensitivity analysis |
Prior auto-HSCT (%) | 33.1 | 29.9 | None |
Refractory to last therapy (%) | 61.5 | 78.0 | Patients from TRANSCEND who had missing data were removed from sample |
Relapsed ≤ 12 months post-HSCT | 36.1 | 22.0 | Patients from TRANSCEND who had missing data were removed from sample |
Disease stage (%) | |||
I or II | 27.2 | 27.0 | Patients from TRANSCEND who had missing data were removed. Proportion assigned as missing in SCHOLAR-1 was redistributed to non-missing categories. |
III or IV | 72.0 | 72.0 | |
Missing | 0.8 | < 1 | |
IPI score | |||
0 to 2 (low to low-intermediate risk) | 58.8 | 49.0 | IPI score recoded to 0 to 2 and 3 to 5. Patients from TRANSCEND who had missing data were removed from the sample. Proportion assigned as missing in SCHOLAR-1 was redistributed to non-missing categories |
3 to 4 (high-intermediate to high risk) | 39.7 | 33.0 | |
5 | 0.8 | 0.0 | |
Missing | 0.8 | 18 | |
ECOG PS (%) | |||
0 to 1 | 98.5 | 73.0 | ECOG PS was not included in the matching/adjusting phase because SCHOLAR-1 included patients with a broader range of ECOG PS (0 to 4) than TRANSCEND (0 to 2). |
≥ 2 | 1.6 | 14.0 | |
Missing | 0.0 | 13.0 |
auto = autologous; DLBCL = diffuse large B-cell lymphoma; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FL = follicular lymphoma; FL3B = follicular lymphoma grade 3B; HSCT = hematopoietic stem cell transplant; IPI = International Prognostic Index; ITC = indirect treatment comparison; liso-cel = lisocabtagene maraleucel; MAIC = matching-adjusted indirect comparison; NA = not applicable; NHL = non-Hodgkin lymphoma; PMBCL = primary mediastinal B-cell lymphoma; tFL = DLBCL transformed from follicular lymphoma.
Source: Sponsor-submitted ITC-2 report.11
Standardized mean differences were used to describe imbalances between the TRANSCEND and SCHOLAR-1 studies or baseline patient characteristics. The investigators considered standardized mean differences exceeding 0.10 or 0.20 as indicative of statistically meaningful imbalances. For the TRANSCEND and SCHOLAR-1 studies, notable imbalances (i.e., standardized mean differences ≥ 0.10) were observed for age and R/R status to last therapy. The remaining variables were balanced between trials, according to the definition used by the investigators of a standardized mean difference of less than 0.10.
Efficacy Results
Efficacy outcomes included OS, CRR, and ORR. PFS was not reported in the SCHOLAR-1 study and was therefore not included in the analysis. Outcome definitions were similar for OS and PFS between the TRANSCEND and SCHOLAR-1 studies.
Of the 24 clinical factors deemed relevant to efficacy outcomes and available for analysis in the TRANSCEND study IPD, 7 were reported in the SCHOLAR-1 study and were available for comparison.
For all efficacy outcomes, comparisons of clinical factors before MAIC showed that most factors were similar (5 of 7 clinical factors with standardized mean difference < 0.1) between liso-cel (the TRANSCEND study) and salvage chemotherapy (the SCHOLAR-1 study). Notable differences were observed for age and R/R to last therapy.
Overall Survival
In the base-case analysis that adjusted for 7 clinical factors, the median OS for the TRANSCEND study was 21.1 months (95% CI, 12.1 to NR), with an ESS of 142 (55.2% of the unweighted population; Figure 23 and Table 30).

Table 30: ITC-2 Results for Overall Survival in Comparisons of Liso-cel to Salvage Chemotherapy (SCHOLAR-1)
Result | SCHOLAR-1 (salvage chemotherapy) | TRANSCEND (liso-cel) | Liso-cel vs. salvage chemotherapy |
|---|---|---|---|
Naive comparison (unweighted) | |||
N | 603 | 257 | NA |
OS, months, median (95% CI) | 6.0 (5.6 to 6.8) | 27.3 (16.8 to NR) | NA |
HR (95% CI) | NA | NA | 0.44 (0.36, 0.53) |
P value | NA | NA | < 0.001 |
Base-case comparison (weighted) | |||
EES | NA | 142 | NA |
OS, months, median (95% CI) | NA | 21.1 (12.1, NR) | NA |
HR (95% CI) | NA | NA | 0.47 (0.37, 0.60) |
P value | NA | NA | < 0.001 |
CI = confidence interval; ESS = effective sample size; HR = hazard ratio; ITC = indirect treatment comparison; liso-cel = lisocabtagene maraleucel; MAIC = matching-adjusted indirect comparison; NA = not applicable; NR = not reached; OS = overall survival.
Note: Estimates were derived from an intercept-only generalized linear model with MAIC adjustment weights. Of 24 possible clinical factors, only 7 were included in the weighting process. The median was obtained from pseudo-individual patient data based on digitized Kaplan–Meier curve.
Source: Sponsor-submitted ITC-2 report.11
Response Rates
In the base-case analysis that adjusted for 7 clinical factors, the adjusted CRR for liso-cel was 49.2% with an ESS of 142 (55.2% of the unweighted population), and the matched and adjusted treatment effect on CRR was, again, statistically significantly greater for liso-cel than for salvage chemotherapy (OR 12.89; 95% CI, 8.04 to 20.68; P < 0.001).
The base-case analysis that adjusted for 7 clinical factors showed that the adjusted ORR for liso-cel was 71.1% with an ESS of 142 (55.2% of the unweighted population), and the matched and adjusted treatment effect on ORR was, again, statistically significantly greater for liso-cel compared with salvage chemotherapy (OR 6.99; 95% CI, 4.64 to 10.54; P < 0.001).
For both ORR and CRR, adjustment for the proportion of participants aged 65 years and older — instead of the mean and standard deviation of age — generated similar relative treatment effects. Furthermore, the results of each scenario analysis were similar to the base-case analyses.
Critical Appraisal of ITC Report-2
The ITC-2 aimed at comparing IPD from a single-arm clinical trial (TRANSCEND) against aggregated data from 1 observational study (SCHOLAR-1) in an unanchored MAIC. For the approach to be a valid comparison, the investigators would need to achieve balance on all prognostic factors and all effect modifiers between each arm of treatment by including all such factors in a weighting process to make the population similar for comparison to evaluate efficacy and safety end points. The main objective was to mitigate the between-study differences in baseline characteristics and variables that might modify the outcomes.
Another limitation stems from the lack of information for other outcomes that might be considered important for patients and other stakeholders such as HRQoL and PFS. The search strategy, screening, and data extraction processes were the same as for the ITC report 1, with no serious limitations in these areas. The evidence obtained for this MAIC does, however, come with a high risk of bias due to the observational nature of the data.
The main limitation of this unanchored MAIC was the lack of comparability on many relevant prognostic variables and effect modifiers that were detected and included in the weighting process. The differences in baseline characteristics of variables between the included studies suggest that other potential unmeasured confounders might be present, and that these can be unevenly distributed between groups.
In this ITC, authors attempted to obtain all possible prognostic variables/effect modifiers to be included in the weighting process of the MAIC. The effort for finding relevant clinical factors included a literature search, a data-driven approach, and clinician input. However, as mentioned in the appraisal of the previous ITC report 1, even with these techniques there is no guarantee that all relevant factors will be identified. Of the 24 identified clinical factors, only 7 were used for the models to estimate the effects. However, no information about the factors not included in the weighting process was provided.
Important differences in the measured variables (e.g., ECOG PS, number of prior therapies) at baseline and after the weighting process speak of the possibility that not all relevant factors can be accounted for, which can further increase uncertainty in the effect estimates.
The ESS decreased in substantial numbers, going from 257 to 142.0 (55.2% of the unweighted population) in the OS end point, which indicates the amount of information lost due to the exclusion of patients and the weighting process which also begets uncertainty due to imprecision and may limit the generalizability of the results.
There were also uncertainties due to concerns of probable violations of the proportional hazards assumptions for time-to-event end points such as OS.
Overall, populations with R/R large B-cell lymphoma in the salvage chemotherapy had poor outcomes (e.g., OS close to a median of 6 months). Comparing the interventions used in these populations against newer CAR T-cell therapies might imply differences in baseline risks and uncertainty in the effect estimates. The intent of treatment for patients from the SCHOLAR population could have been different for the TRANSCEND study population, due to differences in the population per se (more treatments in the SCHOLAR study could had been considered palliative), and different baseline risks could be present.
Overall patients included in the TRANSCEND study would be in some instances similar to the ones seen in clinical practice in the Canadian landscape and to whom the indication for liso-cel is directed. Minor yet significant differences in the populations, interventions, and end points evaluated in the population included in the SCHOLAR study could increase the uncertainty in the generalizability of results, such as the aim of the salvage chemotherapy, and baseline risks.
Other Relevant Evidence
This section includes long-term extension studies and additional relevant studies that were included in the sponsor’s submission to CADTH and were considered as supplementary information to address important gaps in the evidence identified in the systematic review.
TRANSCEND WORLD Study
The sponsor submitted the TRANSCEND WORLD (JCAR017-BCM-001) study, which investigated safety and efficacy of liso-cel in patients from multiple population groups (Cohorts 1 to 6) based on different inclusion criteria. The purpose of study was to generate clinical experience in Europe and Japan, as well as to evaluate feasibility of manufacturing liso-cel product for delivery in Europe. At the time of the data cut-off date (September 13, 2019), the study only enrolled patients in Cohort 1 (Europe) and Cohort 3 (Japan). Later, the sponsor provided results from the data cut-off date of June 19, 2020, which also contain results for Cohort 1 (Europe) and Cohort 3 (Japan). Therefore, this report will focus on the efficacy and safety outcomes from Cohort 1 (Europe) and Cohort 3 (Japan).
Methods
This ongoing study is a single-arm, open-label, multi-cohort, multi-centre, phase II clinical trial to test efficacy and safety of liso-cel in adult patients with DLBCL NOS (de novo or tFL), HGL with MYC and BCL2 and/or BCL6 rearrangements with DLBCL histology and FL3B (Europe Cohort 1) and patients with DLBCL who are not eligible for transplant (Japan Cohort 3). Out of 68 patients screened, 37 (“liso-cel treated set” for baseline characteristics) or 34 (“efficacy-evaluable set” for efficacy results) patients were analyzed. The intervention was liso-cel (1 × 108 cells) with no comparator because the sponsor deemed no appropriate comparator available. The primary end point was ORR and the secondary end points included safety among others listed below in detail. The study period was approximately 24 months consisting of 3 periods:
pre-treatment period: all recruited patients were screened for eligibility; eligible patients underwent leukapheresis, liso-cel product generation, anticancer treatment (if needed) and a pre-treatment evaluation before LDC
treatment period: eligible patients received LDC (i.e., fludarabine and cyclophosphamide IV) for 3 days before liso-cel infusion, which occurred 2 days to 7 days after completion of LDC; a first response evaluation was performed approximately 28 days after liso-cel infusion
post-treatment period (2 to 24 months post-liso-cel infusion): efficacy and safety follow-up visits were conducted at approximately 2, 3, 6, 9, 12, 18, and 24 months after liso-cel infusion; after the end of study visit or at time of withdrawal, all patients were followed for survival every 3 months (± 30 days) until the last patient’s last visit and a long-term follow-up was planned for up to 15 years
Populations
Inclusion Criteria
Cohort 1 (Europe): Age 18 years or older, ECOG PS of 0 or 1, DLBCL NOS (de novo or tFL), HGL with MYC and BCL2 and/or BCL6 rearrangements with DLBCL histology (double-hit lymphoma/triple-hit lymphoma [DHL/THL]) and FL3B per WHO 2016 classification, after ≥ 2 lines of therapy, including anthracycline and rituximab (or other CD20-targeted agent). Subjects with secondary CNS lymphoma involvement could have been enrolled.
Cohort 3 (Japan): Age 18 years or older, ECOG PS of 0 to 2, transplant ineligible with DLBCL NOS (de novo or tFL), HGL with MYC and BCL2 and/or BCL6 rearrangements with DLBCL histology (DHL/THL) and FL3B per WHO 2016 classification, who failed first-line therapy including anthracycline and rituximab (or other CD20-targeted agent).
Cohort 3 (Japan) only: Transplant ineligible for high-dose chemotherapy (HDCT) and hematopoietic stem cell transplant (HSCT) due to age, ECOG PS, or comorbidity (e.g., age ≥ 70 years, ECOG PS ≥ 2, impaired pulmonary function [diffusion lung capacity ≤ 60%], impaired cardiac function [LVEF < 50%], impaired renal function [CrCl < 60 mL/min], or impaired hepatic function [aspartate aminotransferase/alanine aminotransferase < 2 upper limit of normal, bilirubin > 2 mg/dL or cirrhosis, Child-Pugh B or C]).
Exclusion Criteria
prior gene therapy
previous CD19-targeted therapy
previous history of or active hepatitis B, hepatitis C, or HIV infection
presence of acute or chronic graft-versus-host disease
active autoimmune disease requiring immunosuppressive therapy
alemtuzumab within 6 months of leukapheresis
fludarabine or cladribine within 3 months of leukapheresis
therapeutic doses of corticosteroids (> 20 mg/day prednisone or equivalent) within 7 days before leukapheresis or 72 hours before liso-cel infusion
low-dose chemotherapy (e.g., vincristine, rituximab, cyclophosphamide ≤ 300 mg/m2) within 7 days before LDC
cytotoxic chemotherapeutic agents not considered lymphotoxic within 1 week before leukapheresis; oral anticancer therapies, including lenalidomide and ibrutinib allowed if at least 3 half-lives elapsed before leukapheresis
lymphotoxic chemotherapeutic agents (e.g., cyclophosphamide > 300 mg/m2, ifosfamide, bendamustine) within 2 weeks before leukapheresis
immunosuppressive therapies within 4 weeks before leukapheresis and liso-cel infusion (e.g., calcineurin inhibitors, methotrexate, mycophenolate, rapamycin, thalidomide, anti–tumour necrosis factor, anti-IL-6[R])
allo-HSCT within 90 days before leukapheresis
uncontrolled systemic fungal, bacterial, viral, or other infection (including tuberculosis) despite appropriate antibiotics or other treatment at the time of leukapheresis or JCAR017 infusion
history of any 1 of the following cardiovascular conditions within the past 6 months: heart failure, New York Heart Association class III or IV, cardiac angioplasty or stenting, myocardial infarction, unstable angina, or other clinically significant cardiac disease
history or presence of clinically relevant CNS pathology such as epilepsy, seizure, aphasia, stroke, cerebral edema, severe brain injuries, dementia, Parkinson disease, cerebellar disease, organic brain syndrome, or psychosis.
The baseline characteristics were reported for 37 patients included in “liso-cel treated set” (Table 31). From the data from the cut-off date of September 13, 2019, the median age was 58 years (from 40 years to 73 years) and 24 (64.9%) were male. Most patients had an ECOG PS score of 0 (56.8%) or 1 (40.5%) and only 1 patient (2.7%) had a score of 2 at the beginning of study. Prior to LDC, 16 (43.2%) and 17 (45.9%) patients had ECOG PS scores of 0 and 1, respectively, and 4 (10.8%) patients had scores of 2. Of total 37 patients, 31 (83.8%) patients had DLBCL NOS, of which 9 (24.3%) had tFL, 4 (10.8%) patients had HGBL, and 2 (5.4%) patients had FL3B. With respect to previous therapies, 32 (86.5%) patients had more than 3 prior therapies and 11 (39.7%) patients had more than 5 prior therapies. In terms of response status to last prior therapy, 27 (73%) patients were refractory, and 10 (27%) patients were relapsed. Also, 13 (35.1%) patients had prior auto-HSTC. None of patient had confirmed CNS lymphoma at screening. As for bridging therapies, 31 (83.8%) of patients received either systemic or radiation therapy for disease control during the period between leukapheresis and LDC. Prior to receiving LDC, the proportion of patients with LDH of 500 U/L or greater was 10 (27.0%) of patients. Lastly, 12 (32.4%) and 7 (18.9%) patients fell into high-intermediate risk and high-risk IPI categories, respectively. As for the data cut-off date of June 19, 2020, the baseline characteristics remain largely similar to those from the earlier data cut-off date except for age (distribution), IPI (low-intermediate risk), and the number of prior systemic treatments (2 prior regimens).
Table 31: Summary of Baseline Characteristics (Liso-cel-Treated Set)
Baseline demographic | Data cut-off date: September 13, 2019 Cohort 1 (Europe) N = 27 | Cohort 3 (Japan) N = 10 | Overall N = 37 | Cohort 1 (Europe) N = 36 | Data cut-off date: June 19, 2020 Cohort 3 (Japan) N = 10 | Overall N = 46 |
|---|---|---|---|---|---|---|
Age, mean (standard deviation) | 58.4 (9.13) | 60.4 (9.03) | 59.0 (9.02) | 58.8 (10.93) | 60.4 (9.03) | 59.1 (10.47) |
||||||||||||||||||||||||||| | ||||||||||||||||||||||||||| | |||||||||||||||||| | ||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||| |
≥ 40 to < 65 years | 19 (70.4) | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | 7 (70.0) | 28 (60.9) |
≥ 65 years | 8 (29.6) | 3 (30.0) | 11 (29.7) | 14 (38.9) | |||||||||||||||||| | |||||||||||||||||| |
Sex, male, n (%) | 18 (66.7) | |||||||||||||||||| | |||||||||||||||||| | 25 (69.4) | 6 (60.0) | |||||||||||||||||| |
Female | 9 (33.3) | |||||||||||||||||| | |||||||||||||||||| | 11 (30.6) | 4 (40.0) | |||||||||||||||||| |
Race | ||||||
Asian / Japanese, n (%) | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
White | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Unknown | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
BMIa (kg/m2), mean (standard deviation) | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Weight (kg), mean (standard deviation) | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
ECOG PS at screening, n (%) | ||||||
0 | 15 (55.6) | 6 (60.0) | 21 (56.8) | 19 (52.8) | 6 (60.0) | 25 (54.3) |
1 | 11 (40.7) | 4 (40.0) | 15 (40.5) | 16 (44.4) | 4 (40.0) | 20 (43.5) |
2b | 1 (3.7) | 0 (0.0) | 1 (2.7) | 1 (2.8) | 0 (0.0) | 1 (2.2) |
ECOG PS before LDC, n (%) | ||||||
0 | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
1 | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
2b | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
LDH before LDC, n (%) | ||||||
≥ 500 U/L | 8 (29.6) | 2 (20.0) | 10 (27.0) | 8 (22.2) | 2 (20.0) | 10 (21.7) |
< 500 U/L | 19 (70.4) | |||||||||||||||||| | |||||||||||||||||| | 28 (77.8) | |||||||||||||||||| | |||||||||||||||||| |
IPI, n (%) | ||||||
Low risk | 7 (25.9) | 6 (60.0) | 13 (35.1) | 8 (22.2) | 6 (60.0) | 14 (30.4) |
Low-intermediate risk | 4 (14.8) | |||||||||||||||||| | |||||||||||||||||| | 10 (27.8) | |||||||||||||||||| | |||||||||||||||||| |
High-intermediate risk | 9 (33.3) | |||||||||||||||||| | |||||||||||||||||| | 11 (30.6) | |||||||||||||||||| | |||||||||||||||||| |
High risk | 7 (25.9) | |||||||||||||||||| | |||||||||||||||||| | 7 (19.4) | |||||||||||||||||| | |||||||||||||||||| |
DLBCL NOS, n (%) | 22 (81.5) | 9 (90.0) | 31 (83.8) | 31 (86.1) | 9 (90.0) | 40 (87.0) |
Transformed FL | 6 (22.2) | 3 (30.0) | 9 (24.3) | 7 (19.4) | 3 (30.0) | 10 (21.7) |
HGBL | 4 (14.8) | 0 (0.0) | 4 (10.8) | 4 (11.1) | 0 (0.0) | 4 (8.7) |
FL grade 3B | 1 (3.7) | 1 (10.0) | 2 (5.4) | 1 (2.8) | 1 (10.0) | 2 (4.3) |
Cell of origin (for DLBCL), n (%) | ||||||
GCB | 17 (63.0) | 4 (40.0) | 21 (56.8) | 22 (61.1) | 4 (40.0) | 26 (56.5) |
ABC, non-GCB | 7 (25.9) | 5 (50.0) | 12 (32.4) | 10 (27.8) | 5 (50.0) | 15 (32.6) |
Double-hit lymphoma, n (%) | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Triple-hit lymphoma | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Refractoryc, n (%) | |||||||||||||||||| | 7 (70.0) | |||||||||||||||||| | 28 (77.8) | 7 (70.0) | 35 (76.1) |
Relapsedd | 7 (25.9) | 3 (30.0) | 10 (27.0) | 8 (22.2) | 3 (30.0) | 11 (23.9) |
Chemorefractorye, n (%) | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Chemosensitivef | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Confirmed CNS involvement of DLBCL, n (%) | 0 (0.0) | 0 (0.0)g | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Prior treatments | ||||||
Hematopoietic stem cell transplant, n (%) | 11 (40.7) | 2 (20.0) | 13 (35.1) | 12 (33.3) | 2 (20.0) | 14 (30.4) |
Allogeneic | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Autologous | 11 (40.7) | 2 (20.0) | 13 (35.1) | 12 (33.3) | 2 (20.0) | 14 (30.4) |
Radiotherapy | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Systemic treatment | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Number of prior systemic treatments, median (min., max.) | 3.0 (0, 5) | 3.0 (1, 9) | 3.0 (0, 9) | 2.0 (0, 5) | 3.0 (1, 9) | 3.0 (0, 9) |
Q1, Q3 | 2.0, 4.0 | 3.0, 4.0 | 2.0, 4.0 | 2.0, 3.5 | 3.0, 4.0 | 2.0, 4.0 |
1 prior regimen, n (%) | 0 (0.0) | |||||||||||||||||| | |||||||||||||||||| | 0 (0.0) | |||||||||||||||||| | |||||||||||||||||| |
2 prior regimens, n (%) | 10 (37.0) | |||||||||||||||||| | |||||||||||||||||| | 18 (50.0) | |||||||||||||||||| | |||||||||||||||||| |
3 prior regimens, n (%) | 9 (33.3) | |||||||||||||||||| | |||||||||||||||||| | 8 (22.2) | |||||||||||||||||| | |||||||||||||||||| |
4 prior regimens, n (%) | 5 (18.5) | |||||||||||||||||| | |||||||||||||||||| | 7 (19.4) | |||||||||||||||||| | |||||||||||||||||| |
≥ 5 prior regimens, n (%) | 2 (7.4) | |||||||||||||||||| | |||||||||||||||||| | 2 (5.6) | |||||||||||||||||| | |||||||||||||||||| |
ABC = activated B-cell; BMI = body mass index; CNS = central nervous system; DLBCL = diffuse large B-cell lymphoma; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FL = follicular lymphoma; GCB = germinal centre B-cell; HGBL = high-grade B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements with DLBCL histology; IPI = International Prognostic Index; LDC = lymphodepleting chemotherapy; LDH = lactate dehydrogenase; liso-cel = lisocabtagene maraleucel; max. = maximum; min. = minimum; NOS = not otherwise specified; Q1 = quartile 1; Q3 = quartile 3.
Note: Baseline characteristic is defined as the latest measurement on or before the date of the JCAR017 infusion.
aCalculation used for BMI is weight (kg)/(height [m] × height [m]).
bStudy began accrual with the requirement of ECOG PS 0 to 2, and protocol was later amended to only permit ECOG 0 to 1.
cRefractory disease is defined as a less than 50% decrease in lesion size or the appearance of new lesions.
dRelapsed disease reflects the (re)appearance of lesions after attainment of a partial or complete response.10
eChemorefractory is defined as not responding to chemotherapy.
fChemosensitive is defined as responding to chemotherapy.
gSubject 6011008 in Cohort 3 developed secondary CNS involvement after screening but before liso-cel infusion. A full narrative for this patient is provided in Section 14.3.3 of the Clinical Study Report.
Source: TRANSCEND WORLD (JCAR017-BCM-001) study.
Interventions
Lymphodepleting Chemotherapy
Patients were treated with fludarabine IV (30 mg/m2/day) and cyclophosphamide IV (300 mg/m2/day) for 3 days before liso-cel infusion as lymphodepleting procedure. LDC could start 5 days to 10 days before liso-cel infusion and should be finished at least 2 days before liso-cel infusion.
Liso-cel Infusion
Approximately 2 days to 7 days after completion of LDC, patients were infused with a single dose of liso-cel composed of 100 × 106 CAR-positive T cells (50 × 106 from the CD8+ component and 50 × 106 from the CD4+ component). Patients were premedicated with 500 mg to 650 mg of acetaminophen orally and 25 mg to 50 mg of diphenhydramine orally or IV (or another H1 antihistamine) 30 minutes to 60 minutes before liso-cel infusion. These supportive medications were repeated every 6 hours as needed.
Outcomes
The primary end point was ORR, defined by BOR of either CR or PR based on the Lugano criteria10 from liso-cel infusion until disease progression, end of study, the start of another anticancer therapy, or HSCT.
The secondary end points were safety, feasibility of administering liso-cel, ORR in subgroup of patients with chronic lymphocytic leukemia (Richter transformation: Cohort 6), other efficacy measures (CRR, EFS, PFS, OS, DOR), PK profile, and HRQoL measures (EORTC QLQ-C30, EQ-5D-5L, Functional Assessment of Cancer Therapy—Lymphoma).
Statistical Analysis
For binary end points, such as ORR, the frequency distribution (n, %) as point estimate with 2-sided exact 95% (Clopper-Pearson) CI were calculated. The null hypothesis was an ORR of 40% or less, which was determined based on the retrospective SCHOLAR-1 study (i.e., study hypothesis, H1: ORR > 40%). An interpolated spending function was used as efficacy boundary for this interim analysis with a significance level of 0.01. Patients with missing or unknown responses were treated as non-evaluable and were excluded from calculations of rates, CIs, and P values.
Patient Disposition
A disposition diagram is provided in the Figure 24 and Table 32. The formal interim analysis was conducted with the “liso-cel treated set” (all patients who have received liso-cel in accordance with drug product release specifications) and “efficacy-evaluable set” (all patients who received the liso-cel product in accordance with drug product release specifications and had a baseline assessment with at least 1 post-infusion assessment). The “liso-cel treated set” includes 37 patients (27 patients from Cohort 1 [Europe] and 10 patients from Cohort 3 [Japan]), whereas the “efficacy-evaluable set” includes 34 patients (24 patients from Cohort 1 [Europe] and 10 patients from Cohort 3 [Japan]).
Figure 24: Flow Diagram for Patient Disposition
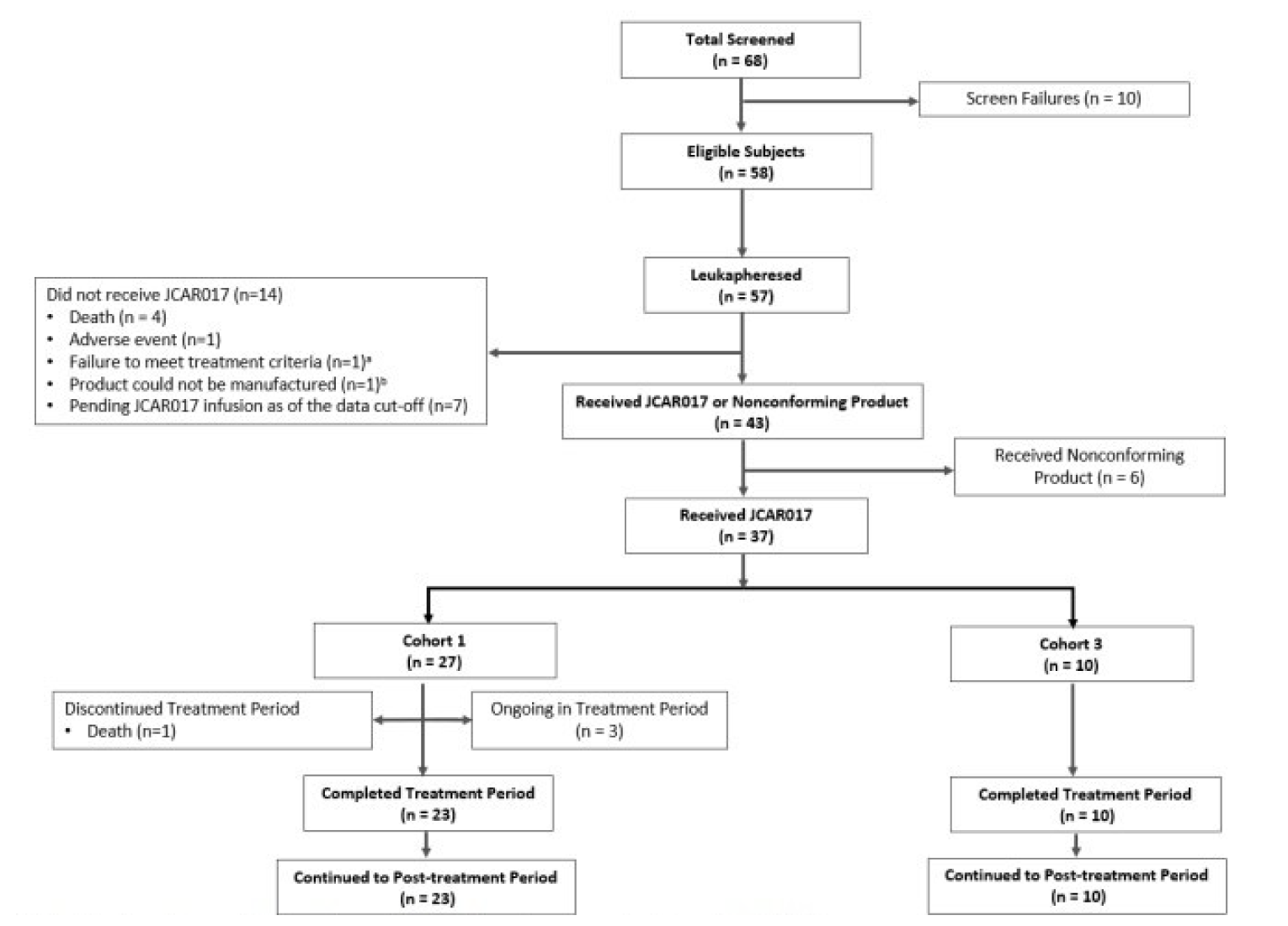
Note: Data cut-off date was September 13, 2019.
a Patient underwent leukapheresis but did not pass pre-treatment eligibility.
b Manufacturing failure: patient had no cell growth for both components.
Source: TRANSCEND WORLD (JCAR017-BCM-001) study.36
Variable | Data cut-off date: September 13, 2019 | Data cut-off date: June 19, 2020 | ||||
|---|---|---|---|---|---|---|
Cohort 1 (Europe) | Cohort 3 (Japan) | Overall | Cohort 1 (Europe) | Cohort 3 (Japan) | Overall | |
Screeneda | |||||||||||||||||| | 14 (100.0) | |||||||||||||||||| | 53 (100.0) | 16 (100.0) | 69 (100.0) |
Leukapheresed (ITT) setb | |||||||||||||||||| | 14 (100.0) | |||||||||||||||||| | 45 (84.9) | 14 (87.5) | 59 (85.5) |
Enrolled setc | |||||||||||||||||| | 14 (100.0) | |||||||||||||||||| | 44 (83.0) | 14 (87.5) | 58 (84.1) |
Liso-cel-treated setd | |||||||||||||||||| | 10 (71.4) | |||||||||||||||||| | 36 (67.9) | 10 (62.5) | 46 (66.7) |
Efficacy-evaluable sete | |||||||||||||||||| | 10 (71.4) | |||||||||||||||||| | 36 (67.9) | 10 (62.5) | 46 (66.7) |
ITT = intention to treat; liso-cel = lisocabtagene maraleucel.
Note: Values are presented as n (%).
aAll patients who signed informed consent. On the data cut-off date of September 13, 2019, there were 7 patients not assigned to a cohort; therefore, these patients will only appear in the Overall column.
bAll patients who have undergone leukapheresis.
cAll patients who signed informed consent, who passed all eligibility criteria at screening, and underwent leukapheresis.
dAll patients who received liso-cel in accordance with drug product release specifications.
eAll patients who received the liso-cel product in accordance with drug product release specifications, and who had a baseline assessment and at least 1 post-liso-cel infusion disease assessment.
Source: TRANSCEND WORLD (JCAR017-BCM-001) study.
Efficacy
The PFS is defined as time from liso-cel infusion to the first documentation of PD, or death due to any cause, whichever occurs first. Overall (N = 37), the Kaplan–Meier estimated median PFS was 3.19 months (95% CI, 2.00 to 10.15) based on FDA criteria and data from the cut-off date of September 13, 2019. The PFS data are limited due to short follow-up time (Table 33). The PFS data remain largely similar between the data from 2 cut-off dates.
As for OS, which is defined as the time from liso-cel infusion to time of death due to any cause, the Kaplan–Meier estimate for the median OS was |||||||||||||||||||||||||||||||||||||||||||||| and the median follow-up time was ||||||||||||||||||||||||||||||||||||||||||| (Table 33) based on results from the September 13, 2019 cut-off. The median OS increased to |||||||||||||||||||||||||||||||||||| with the median follow-up time of |||||||||||||||||||||||||||||||||||||||||||||||||||||| based on the data from cut-off date of June 19, 2020 (Table 33).
Based on the data from cut-off date of September 13, 2019, the study met its primary efficacy end point, with an IRC-assessed ORR of 58.8% (95% CI, 40.7 to 75.4) in the “efficacy-evaluable set,” thereby rejecting the null hypothesis of an ORR of 40% or less (1-sided P value = 0.020; Table 34). In the “liso-cel treated set,” the ORR based on IRC assessment was 54.1% (95% CI, 36.9 to 70.5). From the data from cut-off date of June 19, 2020, both datasets (i.e., “efficacy-evaluable set” and “liso-cel treated set”) met the primary end point with ORR of 63% (95% CI, 47.5 to 76.8; P value = 0.01; Table 34). A high rate of concordance (> 96%) was observed between IRC and investigator assessments of ORRs.
The DOR is defined as time from first response to progressed disease or death from any cause, whichever occurs first. Overall (N = 37), the Kaplan–Meier estimated median DOR was 9.23 months (95% CI, 2.04 to 9.23) based on FDA criteria and data from the cut-off date of September 13, 2019. The sponsor noted that the DOR data are limited due to the median on-study follow-up time of 3.38 months and 3.25 months in Cohort 1 (Europe) and Cohort 3 (Japan), respectively. The DOR results remain similar between data from either cut-off date with slightly reduced median DOR of 8.38 months (95% CI, 2.23 to not evaluable) from the data cut-off date of June 19, 2020 (Table 34).
According to the hospital resource utilization data, from a total of 37 patients, 4 patients visited the ICU with a median of 1 (range = 1 to 1) visit and 37 patients visited a standard unit with a median of 2 (range = 1 to 10) visits. The sponsor did not provide the hospitalization utilization results from data cut-off date of June 19, 2020 (Table 35).
Lastly, the analyzed results from the data cut-off date of September 13, 2019, for the subscales (fatigue, physical functioning, cognitive functioning, global health/QoL) of EORTC QLQ-C30, EQ-5D-5L (health utility index and EQ VAS scores), and Functional Assessment of Cancer Therapy — Lymphoma were reported in the Clinical Study Report. Due to small sample size (N = 37), which led to large error bars encompassing MIDs and significant drop in compliance rates after day 180 (N < 10; data not analyzable), the results cannot be definitely interpreted as stable (i.e., no improvement or deterioration), from day 1. Therefore, the detailed results are not included in this report. The sponsor did not provide the PRO results from the data cut-off date of June 19, 2020.
Table 33: Survival Analyses Based on IRC Assessment (Liso-cel-Treated Set)
Variable | Data cut-off date: September 13, 2019 | Data cut-off date: June 19, 2020 | ||||
|---|---|---|---|---|---|---|
Cohort 1 (Europe) n = 27 | Cohort 3 (Japan) n = 10 | Total N = 37 | Cohort 1 (Europe) n = 36 | Cohort 3 (Japan) n = 10 | Total N = 46 | |
Progression-free survival | ||||||
Total events, n (%) | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Progression | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Death | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Censored, n (%) | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Median, months (95% CIa) | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | 3.25 (2.79, 6.90) | 6.34 (0.62, NE) | 3.25 (2.99, 6.90) |
Q1, Q3a | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Min., max. | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Overall survival | ||||||
Death, n (%) | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | 17 (47.2) | 5 (50.0) | 22 (47.8) |
Alive, n (%) | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | 19 (52.8) | 5 (50.0) | 24 (52.2) |
Median, months (95% CIa) | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | 18.56 (5.82, NE) | 14.72 (1.71, NE) | 14.72 (6.28, NE) |
Q1, Q3a | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | 5.48, NE | 3.02, NE | 5.36, NE |
Min., max | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | 0.5, 20.5 | 1.7, 16.7 | 0.5, 20.5 |
Overall survival follow-up | ||||||
Median, months (95% CIa) | 9.07 (1.94, 11.17) | 5.88 (1.68, 7.59) | 6.93 (3.09, 9.33) | 9.53 (8.57, 14.32) | 13.72 (12.35, 16.66) | 12.35 (8.90, 14.46) |
CI = confidence interval; IRC = independent review committee; liso-cel = lisocabtagene maraleucel; max. = maximum; min. = minimum; NE = not evaluable; Q1 = quartile 1; Q3 = quartile 3.
aMedian, Q1, Q3 are estimated from Kaplan–Meier product-limit estimates.
Source: TRANSCEND WORLD (JCAR017-BCM-001) study.
Table 34: Response Analyses Based on IRC Assessment
Variable | Data cut-off date: September 13, 2019 | Data cut-off date: June 19, 2020 | ||||
|---|---|---|---|---|---|---|
Cohort 1 (Europe) n = 24 | Cohort 3 (Japan) n = 10 | Total N = 34 | Cohort 1 (Europe) n = 36 | Cohort 3 (Japan) n = 10 | Total N = 46 | |
Efficacy-evaluable set, overall response ratea | ||||||
n (%) | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | 22 (61.1) | 7 (70.0) | 29 (63.0) |
Complete responseb | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | 12 (33.3) | 5 (50.0) | 17 (37.0) |
Partial response | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | 10 (27.8) | 2 (20.0) | 12 (26.1) |
95% CIc | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | 43.5 to 76.9 | 34.8 to 93.3 | 47.5 to 76.8 |
P value for test of hypothesisd | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | 0.008 | 0.055 | 0.001 |
Liso-cel-treated set, overall response ratea | ||||||
n (%) | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | 22 (61.1) | 7 (70.0) | 29 (63.0) |
Complete responseb | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | 12 (33.3) | 5 (50.0) | 17 (37.0) |
Partial response | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | 10 (27.8) | 2 (20.0) | 12 (26.1) |
95% CIc | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | 43.5 to 76.9 | 34.8 to 93.3 | 47.5 to 76.8 |
P value for test of hypothesisd | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | 0.008 | 0.055 | 0.001 |
Liso-cel-treated set, duration of response (months) | ||||||
Median, 95% CIe | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | 3.98 (2.20 to NE) | 9.07 (2.10 to NE) | 8.38 (2.23 to NE) |
Min., max. | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | 0.03, 16.95 | 2.10, 12.06 | 0.03, 16.95 |
CI = confidence interval; IRC = independent review committee; liso-cel = lisocabtagene maraleucel; max. = maximum; min. = minimum; NE = not estimable.
Note: Overall response rate derivation does not consider the initiation of subsequent anticancer therapy. However, all responses in this table were achieved before any initiation of subsequent anticancer therapy.
aOverall response rate (for Cohorts 1 and 3) is defined as the proportion of patients who achieved an objective response of partial response or better according to Lugano criteria. Complete response rate is defined as the proportion of patients who achieved a best overall response of complete response. Patients with missing or unknown responses were treated as non-evaluable and were excluded from calculations of rates, CIs, and P values.
bComplete response rate is defined as the proportion of patients who achieved a best overall response of complete response.
cTwo-sided 95% CI based on exact Clopper-Pearson method.
dOverall response rate greater than 40% against the null hypothesis that the overall response rate is 40% or less. Significance level is 1-sided alpha = 0.025.
eMedian is calculated from Kaplan–Meier product-limit estimate.
Source: TRANSCEND WORLD (JCAR017-BCM-001) study.
Table 35: Hospital Resource Utilization (Liso-cel-Treated Set)
Variable | Data cut-off date: September 13, 2019 | Data cut-off date: June 19, 2020 | ||||
|---|---|---|---|---|---|---|
Cohort 1 (Europe) n = 27 | Cohort 3 (Japan) n = 10 | Total N = 37 | Cohort 1 (Europe) n = 36 | Cohort 3 (Japan) n = 10 | Total N = 46 | |
Total ICU inpatient stays per patient, n | 4 | 0 (0.0) | 0 (0.0) | NR | NR | NR |
Mean (standard deviation) | 1 (0.0) | NR | 1 (0.0) | NR | NR | NR |
Median | 1.0 | NR | 1.0 | NR | NR | NR |
Q1, Q3 | 1.0, 1.0 | NR | 1.0, 1.0 | NR | NR | NR |
Min., max. | 1, 1 | NR | 1, 1 | NR | NR | NR |
Total standard unit stays per patient, n | 27 | 10 | 37 | NR | NR | NR |
Mean (standard deviation) | 2.3 (2.0) | 2.4 (0.52) | 2.3 (1.72) | NR | NR | NR |
Median | 1.0 | 2.0 | 2.0 | NR | NR | NR |
Q1, Q3 | 1.0, 3.0 | 2.0, 3.0 | 1.0, 3.0 | NR | NR | NR |
Min., max. | 1, 10 | 2, 3 | 1, 10 | NR | NR | NR |
ICU = intensive care unit; liso-cel = lisocabtagene maraleucel; max. = maximum; min. = minimum; NR = not reported; Q1 = quartile 1; Q3 = quartile 3.
Source: TRANSCEND WORLD (JCAR017-BCM-001) study.
Harms
Among the 37 patients included in the safety analysis, the most common TEAEs were neutropenia (81.1%), anemia (62.2%), CRS (43.2%), and thrombocytopenia (43.2%). The most frequently reported treatment-emergent SAEs were CRS (16.2%), confusional state (8.1%), and aphasia (8.1%). The deaths (35.1%) observed in the “enrolled set” (n = 57) were primarily due to progression of disease (21.1%). The most frequent notable harms, known to be associated with CAR T-cell therapies, were CRS (43.2%), prolonged cytopenias (43.2%), iiNT (16.2%), and hypogammaglobulinemia (16.2%). The safety profile as shown by the data from the cut-off date of September 13, 2019 largely remains the same for the data from the cut-off date of June 19, 2020. In general, the frequency increased in the later cut-off data with the largest increase observed in thrombocytopenia and lymphoma progression. (Table 36)
Table 36: Summary of Harms (Liso-cel-Treated Set)
Variable | Data cut-off date: September 13, 2019 | Data cut-off date: June 19, 2020 | ||||
|---|---|---|---|---|---|---|
Cohort 1 (Europe) n = 27 | Cohort 3 (Japan) n = 10 | Overall N = 37 | Cohort 1 (Europe) n = 36 | Cohort 3 (Japan) n = 10 | Total N = 46 | |
Patients with ≥ 1 adverse event (≥ 10%) | ||||||
n (%) | 27 (100.0) | 10 (100.0) | 37 (100.0) | 36 (100.0) | 10 (100.0) | 46 (100.0) |
Neutropenia | |||||||||||||||||| | 9 (90.0) | 30 (81.1) | 32 (88.9) | 9 (90.0) | 41 (89.1) |
Anemia | 15 (55.6) | 8 (80.0) | 23 (62.2) | 18 (50.0) | 8 (80.0) | 26 (56.5) |
Pyrexia | 14 (51.9) | 1 (10.0) | 15 (40.5) | 19 (52.8) | 1 (10.0) | 20 (43.5) |
Cytokine release storm | 11 (40.7) | 5 (50.0) | 16 (43.2) | 14 (38.9) | 5 (50.0) | 19 (41.3) |
Thrombocytopenia | 7 (25.9) | 9 (90.0) | 16 (43.2) | 16 (44.4) | 9 (90.0) | 25 (54.3) |
Headache | 6 (22.2) | 0 (0.0) | 6 (16.2) | 7 (19.4) | 0 (0.0) | 7 (15.2) |
Febrile neutropenia | |||||||||||||||||| | 0 (0.0) | 4 (10.8) | 8 (22.2) | 0 (0.0) | 8 (17.4) |
Hypogammaglobulinemia | 4 (14.8) | 1 (10.0) | 5 (13.5) | 4 (11.1) | 2 (20.0) | 6 (13.0) |
Confusional state | 3 (11.1) | 1 (10.0) | 4 (10.8) | 6 (16.7) | 1 (10.0) | 7 (15.2) |
Fatigue | 0 (0.0) | 4 (40.0) | 4 (10.8) | 2 (5.6) | 4 (40.0) | 6 (13.0) |
Patients with ≥ 1 SAE (≥ 10%) | ||||||
n (%) | 11 (40.7) | 2 (20.0) | 13 (35.1) | 18 (50.0) | 2 (20.0) | 20 (43.5) |
Cytokine release syndrome | 6 (22.2) | 0 (0.0) | 6 (16.2) | 7 (19.4) | 0 (0.0) | 7 (15.2) |
Confusional state | 3 (11.1) | 0 (0.0) | 3 (8.1) | 5 (13.9) | 0 (0.0) | 5 (10.9) |
Aphasia | 3 (11.1) | 0 (0.0) | 3 (8.1) | 4 (11.1) | 0 (0.0) | 4 (8.7) |
Febrile neutropenia | 1 (3.7) | 0 (0.0) | 1 (2.7) | 4 (11.1) | 0 (0.0) | 4 (8.7) |
Tremor | 2 (7.4) | 0 (0.0) | 2 (5.4) | 4 (11.1) | 0 (0.0) | 4 (8.7) |
Patients who stopped treatment due to adverse events | ||||||
n (%) | 0 | 0 | 0 | 0 | 0 | 0 |
Deathsa | ||||||
Enrolled set, total N | 43 | 13 | 57 | 44 | 14 | 58 |
n (%) | 16 (37.2) | 4 (28.6) | 20 (35.1) | 23 (52.3) | 8 (57.1) | 31 (53.4) |
Lymphoma progression | 12 (27.9) | 0 (0.0) | 12 (21.1) | 18 (40.9) | 3 (21.4) | 21 (36.2) |
Multiple organ failure | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Neutropenia sepsis | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Progressive disease of lymphoma | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Respiratory failure | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Sepsis Candida albicans | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Unknown | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Missing | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Patients with notable harms | ||||||
Cytokine release syndrome | 11 (40.7) | 5 (50.0) | 16 (43.2) | 14 (38.9) | 5 (50.0) | 19 (41.3) |
Investigator-identified neurologic toxicity | 5 (18.5) | 1 (10.0) | 6 (16.2) | 8 (22.2) | 1 (10.0) | 9 (19.6) |
Infusion-related reaction | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Macrophage activation syndrome | 2 (7.4) | 0 (0.0) | 2 (5.4) | 2 (5.6) | 0 (0.0) | 2 (4.3) |
Tumour lysis syndrome | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Prolonged cytopeniab | 10 (37.0) | 6 (60.0) | 16 (43.2) | 15 (41.7) | 6 (60.0) | 21 (45.7) |
Infections, grade ≥ 3c | 4 (14.8) | 0 (0.0) | 4 (10.8) | 7 (19.4) | 0 (0.0) | 7 (15.2) |
Second primary malignancy | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Hypogammaglobulinemia | 5 (18.5) | 1 (10.0) | 6 (16.2) | 5 (13.9) | 2 (20.0) | 7 (15.2) |
Autoimmune disorders | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Liso-cel = lisocabtagene maraleucel; SAE = serious adverse event.
aDeaths were reported from the “Enrolled Set,” which includes all patients who signed informed consent, who passed all eligibility criteria at screening, and underwent leukapheresis.
bLaboratory-based assessments of grade 3 or higher cytopenias of neutropenia, thrombocytopenia, or anemia not resolved at day 29.
cInfections that occurred include Candida sepsis, pneumonia, cellulitis, and pulmonary mycosis.
Source: TRANSCEND WORLD (JCAR017-BCM-001) study.
Critical Appraisal
Internal Validity
Overall, a robust conclusion about the efficacy and safety of liso-cel in the population of interest cannot be made due to the lack of a control group, small sample sizes, a short follow-up period, and the open-label nature of the study (with bias favouring the treatment effects).
External Validity
The study population included 1 patient with an ECOG PS score of 2 and none of the patients had CNS lymphoma at the beginning of the study. Patients may have developed secondary CNS lymphoma during the trial as noted in the study; however, there is no confirmed case. This selected population could limit the generalizability of the study results to patients with more severe disease. Lastly, Europe and Japan may have different treatment landscape compared to Canadian practice and their population may not necessarily reflect the Canadian population.
Discussion
Summary of Available Evidence
One clinical study is included in this report evaluating the safety and efficacy of liso-cel in patients with 3L+ R/R DLBCL. The TRANSCEND study is a single-arm, open-label, phase I (seamless design) multi-centre study, conducted in the US. The population included in the study consists of patients with DLBCL NOS (de novo, tFL, and tiNHL), HGL with MYC and BCL2 and/or BCL6 rearrangements, PMBCL, and FL3B who were eligible if they were R/R to at least 2 prior lines of therapy, and had an ECOG PS score of 0 to 2, PET-positive disease, secondary CNS involvement, prior auto-HSCT, and prior allo-HSCT. Patients with primary CNS involvement and allo-HSCT within 90 days of leukapheresis were excluded. Primary end points were adverse events and ORR as assessed by an IRC. Secondary end points included CRR (as assessed by IRC), DOR, PFS, OS, HRQoL, and ICU admission. The study evaluated 3 levels of dose regimens, of which the DL2S regimen, whose dose is 100 × 106 CAR T cells, was the 1 selected for the current indication assessed in this review, for clinical use, and regulatory approval. Patients in the TRANSCEND study had a mean age of 60 years and were overall in relatively good health status (e.g., most had an ECOG PS score of 0 and 1 and good cardiac and renal function). Two updated cut-off dates (June 19, 2020, and January 4, 2021, with median study follow-up duration of 19.1 and 19.9 months, respectively) report supplementary data that are consistent with, and support, the results from the main primary analysis.
Another ongoing study is included as “other relevant evidence” in this report. This is a single-arm, open-label, multi-cohort, multi-centre, phase II clinical trial to test efficacy and safety of liso-cel in adult patients with DLBCL NOS (de novo or tFL), HGL with MYC and BCL2 and/or BCL6 rearrangements with DLBCL histology and FL3B (Europe Cohort 1) and patients with DLBCL who are not eligible for transplant (Japan Cohort 3).
Two sponsor-submitted ITCs are included. First, a comparison evaluating evidence from a single-arm study (TRANSCEND) that provides IPD was compared against 2 bodies of evidence in the form of aggregated data from 2 published sources evaluating tisa-cel and axi-cel, respectively . These formed 2 unanchored MAICs (1 of liso-cel against tisa-cel, and the other against axi-cel). Patients from these populations were R/R large B-cell lymphomas and included the lymphoma subtypes that were common among the 3 bodies of evidence (i.e., DLBCL NOS, HGL, and transformed from follicular lymphoma). The second submitted ITC is another unanchored MAIC comparing the same IPD from the TRANSCEND study against aggregated data from the SCHOLAR-1 study, which includes a population of patients with DLBCL treated with salvage therapies. The lymphoma subtypes included in the ITC-2 (i.e., those common among both bodies of evidence) were DLBCL, PMBCL, and tFL.
Interpretation of Results
Efficacy
The TRANSCEND study evaluated end points of efficacy such as ORR, CR, and DOR, as well as survival outcomes such as OS and PFS, and HRQoL and hospital utilization; all these end points were considered by the clinical experts consulted by CADTH as critical for clinical decision-making, as well as relevant in the Canadian landscape according to other stakeholders such as patient groups and the drug programs. The primary end point in the TRANSCEND study was ORR, evaluated and adjusted for multiplicity in the PAS only. Secondary end points (that were considered important for stakeholders) were also not included in the adjustment for multiplicity (including OS, PFS, DOR, HRQoL measures and hospitalization, and ICU utilization)
At a median follow-up of 18.8 months, the TRANSCEND trial met its primary end point for the ORR with a value of 74.4% (which was greater than the null hypothesis of 40%) in the PAS set. When considering the ITT population, the ORR showed lower values of 60.4% in the DL2S and 60.5% in the total population. Both numbers indicate an improvement above the expected level even if these were not set to be adjusted in the multiple testing procedures in the ITT or DLBCL treated sets.
OS reached a median of 14 months in the total leukapheresed population (12.8 months in the DL2S regimen population) with median of PFS of 4.8 months in both the total and the DL2S regimens. Both numbers were considered meaningful effects by clinical experts consulted by CADTH.
HRQoL end points are frequently brought up by patient groups and clinicians as highly valued outcomes that will impact decisions, usually by putting higher value on decreasing symptoms, improving physical functioning, and minimizing side effects from drugs. In the TRANSCEND study, treatment with liso-cel was associated with improvements in the EORTC QLQ-C30 instrument after 18 months. The EQ-5D-5L also showed improvements during follow-up. However, both of these measurements were not adjusted for multiple testing and had severe limitations due to bias from the open-label design of the study and loss of patients through the study, which introduced imprecision in the effect estimates. A small number of patients were required to use the ICU (7.4% of the total leukapheresed population) and a sizable minority (25 patients of the total leukapheresed population) was able to receive liso-cel as outpatients. This may have implications for shared decision-making between patients and their clinicians in terms of accessibility and acceptability of the intervention.
Due to lack of direct comparative evidence, information from 2 ITC reports (3 comparisons) were used, suggesting effect estimates in favour of liso-cel against tisa-cel (in ORR, CRR, PFS, and OS), and similar effects when compared to axi-cel (in ORR, CRR, PFS, and OS). For the comparison of liso-cel against salvage chemotherapies, the evidence from the ITCs suggests that liso-cel results in improvements in the OS, CRR, and ORR. For all comparisons, however, there were multiple limitations due to the observational nature of the included studies, difficulties in estimating all adequate prognostic variables, and possible residual confounding, hence the question of whether liso-cel provides an additional clinical value of efficacy is still uncertain.
Harms
Adverse events were reported in all but 2 patients receiving liso-cel and in all of the patients receiving the D2LS regimen (100 × 106 CAR T cells). Most of these events were related to neutropenia, anemia, and fatigue. These events varied by period of the study; for instance, 27% were present from screening to leukapheresis, 56% from leukapheresis to LDC, and 91% from LDC to the first infusion of liso-cel or nonconforming product. A total of 10 patients were retreated in the DL2S regimen, 5 at DL1S, and 1 at DL3S. AEs were reported after re-treatment in 15 of 16 patients (93.8%).
SAEs were present in almost half of the treated population (45%) with immune system disorder and neurologic effects being the most common SAEs. Individually, CRS was the most common SAE (16.4% of patients) followed by encephalopathy (10%). This agreed with the expectations from clinical experts who usually see these events in patients treated with CAR T-cell therapies. The clinical experts indicated that accumulating experience with CAR T-cell therapies is improving how safety issues are managed in the clinic. Most of the deaths occurring during the study (37 out of 44) were related to disease progression.
Results from ITC-1 suggested that liso-cel may have a better safety profile in terms of the CRS and prolonged cytopenias when compared to tisa-cel and a better safety profile for CRS, NT, and neutropenia when compared to axi-cel. However, some limitations include the uncertainty due to different best clinical practices in regard to toxicity management across geographical locations and different years (i.e., older trial data might not reflect current practices). According to clinical experts consulted by CADTH, management of AEs has improved over time. Nonetheless, the safety profile of liso-cel based on these numbers was considered important by the clinical experts.
Conclusions
Evidence from a single-arm study (TRANSCEND) suggests that treatment with liso-cel is associated with benefits in outcomes deemed relevant to both patients and clinicians (OS, PFS, ORR, CRR) when compared to typical effects and evolution observed by clinical experts in patients with R/R DLBCL not using a CAR T-cell treatment in the third-line setting. The evidence also suggests that treatment with liso-cel may have benefits in terms of improving HRQoL and decreased health care utilization. Clinical experts considered that the liso-cel safety profile was adequate and may perform better when compared to that observed in clinical practice with other CAR T-cell therapies. Important limitations exist around these effect estimates due to lack of comparative evidence, risk of bias (attrition bias, no blinding), lack of adjustment for multiplicity, and imprecision in the effect estimates. Furthermore, there were concerns about the generalizability of the results due to characteristics of the populations in the TRANSCEND study that suggest a relatively stable and generally healthier population.
Results from sponsor-submitted ITCs using IPD from the TRANSCEND study matched and weighted in a MAIC against aggregated data from studies of 2 CAR T-cell therapies (axi-cel and tisa-cel) suggested improvements in ORR, CRR, PFS, and OS compared with tisa-cel, but not against axi-cel. Similarly, evidence from a second sponsor-submitted ITC using IPD from the TRANSCEND study against aggregated data of patients who underwent salvage therapies (SCHOLAR-1 study) suggests that liso-cel has greater improvements in efficacy and survival outcomes (OS, CRR, ORR) relative to the use of salvage chemotherapies. In all ITCs, liso-cel showed a better safety profile with fewer odds of AEs such as CRS and NT relative to axi-cel, tisa-cel, or salvage chemotherapy. The evidence from the ITCs has considerable limitations due to the observational nature of the included studies, difficulties in estimating all adequate prognostic variables, and possible residual confounding.
Overall, highly uncertain evidence from a single-arm trial and indirect comparative evidence suggest that liso-cel may be more efficacious than salvage chemotherapy and may provide clinically beneficial effects and a safety profile that are similar or better than what is expected of other CAR T-cell therapies.
References
1.Sehn LH, Salles G. Diffuse Large B-Cell Lymphoma. N Engl J Med. 2021;384(9):842-858. PubMed
2.Brenner DR, Weir HK, Demers AA, et al. Projected estimates of cancer in Canada in 2020. CMAJ. 2020;192(9):E199-E205. PubMed
3.Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics 2019. Toronto (ON): Canadian Cancer Society; 2019: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2019-statistics/canadian-cancer-statistics-2019-en.pdf. Accessed 2021 Oct 20.
4.Vitolo U, Seymour JF, Martelli M, et al. Extranodal diffuse large B-cell lymphoma (DLBCL) and primary mediastinal B-cell lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2016;27(suppl 5):v91-v102. PubMed
5.Li S, Young KH, Medeiros LJ. Diffuse large B-cell lymphoma. Pathology. 2018;50(1):74-87. PubMed
6.Gonzalez-Barca E, Boumendil A, Blaise D, et al. Outcome in patients with diffuse large B-cell lymphoma who relapse after autologous stem cell transplantation and receive active therapy. A retrospective analysis of the Lymphoma Working Party of the European Society for Blood and Marrow Transplantation (EBMT). Bone Marrow Transplant. 2020;55(2):393-399. PubMed
7.Thanarajasingam G, Maurer MJ, Farooq U, et al. Event-free survival at 24 months captures central nervous system relapse of systemic diffuse large B-cell lymphoma in the immunochemotherapy era. Br J Haematol. 2018;183(1):149-152. PubMed
8.Abramson JS, Palomba ML, Gordon LI, et al. Lisocabtagene maraleucel for patients with relapsed or refractory large B-cell lymphomas (TRANSCEND NHL 001): a multicentre seamless design study. Lancet. 2020;396(10254):839-852. PubMed
9.Clinical Study Report: JCAR017-017001. A phase 1, multicenter, open-label study of JCAR017, CD19-targeted chimeric antigen receptor (CAR) T cells, for relapsed and refractory (R/R) b-cell non-hodgkin lymphoma (NHL) [internal sponsor's report]. Summit (NJ): Celgene Corporation; 2020 Feb 25.
10.Cheson BD, Fisher RI, Barrington SF, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J Clin Oncol. 2014;32(27):3059-3068. PubMed
11.Technical report: Indirect treatment comparison of liso-cel CAR T-cell therapy and salvage chemotherapy for the third-line or later treatment of relapsed or refractory large B-cell lymphoma: Transcend NHL 001 versus Scholar-1 [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Breyanzi (lisocabtagene maraleucel), cell suspension in patient-specific single-dose vials for intravenous infusion. Saint-Laurent (QC): Bristol Myers Squibb; 2020 Nov 16.
12.Technical report: Indirect treatment comparison of CAR T-Cell therapies for the third-line or later treatment of relapsed or refractory large B-cell lymphoma: Liso-cel versus Tisagenlecelucel and axicabtagene ciloleucel [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Breyanzi (lisocabtagene maraleucel), cell suspension in patient-specific single-dose vials for intravenous infusion. Saint-Laurent (QC): Bristol Myers Squibb; 2021 Aug 24.
13.Crump M, Neelapu SS, Farooq U, et al. Outcomes in refractory diffuse large B-cell lymphoma: results from the international SCHOLAR-1 study. Blood. 2017;130(16):1800-1808. PubMed
14.Sehn LH, Herrera AF, Flowers CR, et al. Polatuzumab Vedotin in Relapsed or Refractory Diffuse Large B-Cell Lymphoma. J Clin Oncol. 2020;38(2):155-165. PubMed
15.Ferreri AJM, Doorduijn JK, Re A, et al. MATRix-RICE therapy and autologous haematopoietic stem-cell transplantation in diffuse large B-cell lymphoma with secondary CNS involvement (MARIETTA): an international, single-arm, phase 2 trial. Lancet Haematol. 2021;8(2):e110-e121. PubMed
16.Breyanzi (lisocabtagene maraleucel): target of 100 × 106 chimeric antigen receptor (CAR)-positive viable T cells, cell suspension in patient-specific single-dose vials for intravenous infusion [product monograph]. Saint-Laurent (QC): Celgene Inc.; 2022 May 06.
17.Yescarta (axicabtagene ciloleucel): cell suspension in patient-specific single infusion bag, chimeric antigen receptor (CAR)-positive viable T cells, for intravenous infusion [product monograph]. Mississauga (ON): Gilead Sciences Canada, Inc.; 2020 Dec 22: https://pdf.hres.ca/dpd_pm/00059323.PDF. Accessed 2022 Mar 06.
18.Kymriah (tisagenlecleucel): cell suspension in infusion bag, 1.2 x 106 to 6.0 x 108 CAR-positive viable T cells, for intravenous use [product monograph]. Dorval (QC): Novartis Pharmaceuticals Canada Inc.; 2020 Dec 24: https://pdf.hres.ca/dpd_pm/00059488.PDF. Accessed 2022 Mar 06.
19.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
20.Palomba ML, Jun MP, Lymp J, et al. Postinfusion monitoring costs by site of care for patients with relapsed/refractory large B-cell lymphoma receiving third- or later-line treatment with lisocabtagene maraleucel in the TRANSCEND NHL 001 and OUTREACH trials. Leuk Lymphoma. 2021:1-8. PubMed
21.Cerhan JR, Kricker A, Paltiel O, et al. Medical history, lifestyle, family history, and occupational risk factors for diffuse large B-cell lymphoma: the InterLymph Non-Hodgkin Lymphoma Subtypes Project. J Natl Cancer Inst Monogr. 2014;2014(48):15-25. PubMed
22.Giesinger JM, Kieffer JM, Fayers PM, et al. Replication and validation of higher order models demonstrated that a summary score for the EORTC QLQ-C30 is robust. J Clin Epidemiol. 2016;69:79-88. PubMed
23.Rigacci L, Puccini B, Cortelazzo S, et al. Bendamustine with or without rituximab for the treatment of heavily pretreated non-Hodgkin's lymphoma patients: A multicenter retrospective study on behalf of the Italian Lymphoma Foundation (FIL). Ann Hematol. 2012;91(7):1013-1022. PubMed
24.Ernst M, Oeser A, Besiroglu B, et al. Chimeric antigen receptor (CAR) T-cell therapy for people with relapsed or refractory diffuse large B-cell lymphoma. Cochrane Database Syst Rev. 2021;9:CD013365. PubMed
25.Locke FL, Ghobadi A, Jacobson CA, et al. Long-term safety and activity of axicabtagene ciloleucel in refractory large B-cell lymphoma (ZUMA-1): a single-arm, multicentre, phase 1-2 trial. Lancet Oncol. 2019;20(1):31-42. PubMed
26.Schuster SJ, Bishop MR, Tam CS, et al. Tisagenlecleucel in Adult Relapsed or Refractory Diffuse Large B-Cell Lymphoma. N Engl J Med. 2019;380(1):45-56. PubMed
27.Breiman L. Random Forests. Machine Learning. 2001;45(1):5-32.
28.Guyot P, Ades AE, Ouwens MJ, Welton NJ. Enhanced secondary analysis of survival data: reconstructing the data from published Kaplan-Meier survival curves. BMC Med Res Methodol. 2012;12:9. PubMed
29.Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat Med. 2009;28(25):3083-3107. PubMed
30.Grambsch PM, Therneau TM. Proportional hazards tests and diagnostics based on weighted residuals. Biometrika. 1994;81(3):515-526.
31.Phillippo DM, Ades AE, Dias S, Palmer S, Abrams KR, Welton NJ. Methods for Population-Adjusted Indirect Comparisons in Health Technology Appraisal. Med Decis Making. 2018;38(2):200-211. PubMed
32.Ahmed MA, Chihara D, Vargas N, et al. Outcome of relapsed/refractory diffuse large B-cell lymphoma after second salvage therapy: MD Anderson Experience. Hematol Oncol. 2015;33:279-280.
33.Maurer MJ, Ghesquieres H, Jais JP, et al. Event-free survival at 24 months is a robust end point for disease-related outcome in diffuse large B-cell lymphoma treated with immunochemotherapy. J Clin Oncol. 2014;32(10):1066-1073. PubMed
34.Crump M, Kuruvilla J, Couban S, et al. Randomized comparison of gemcitabine, dexamethasone, and cisplatin versus dexamethasone, cytarabine, and cisplatin chemotherapy before autologous stem cell transplantation for relapsed and refractory aggressive lymphomas: NCIC-CTG LY.12. J Clin Oncol. 2014;32(31):3490-3496. PubMed
35.Gisselbrecht C, Glass B, Mounier N, et al. Salvage regimens with autologous transplantation for relapsed large B-cell lymphoma in the rituximab era. J Clin Oncol. 2010;28(27):4184-4190. PubMed
36.Clinical Study Report: JCAR017-BCM-001. A phase 2, single-arm, multi-cohort, multi-center trial to determine the efficacy and safety of JCAR017 in adult subjects with aggressive B-cell non-Hodgkin lymphoma (TRANSCEND WORLD) [internal sponsor's report]. Summit (NJ): Celgene Corporation; 2020 Apr 22.
37.Cocks K, King MT, Velikova G, et al. Evidence-based guidelines for interpreting change scores for the European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30. Eur J Cancer. 2012;48(11):1713-1721. PubMed
38.McClure NS, Sayah FA, Xie F, Luo N, Johnson JA. Instrument-Defined Estimates of the Minimally Important Difference for EQ-5D-5L Index Scores. Value Health. 2017;20(4):644-650. PubMed
39.EORTC Quality of Life. EORTC QLQ-C30 FAQ Categories: Scoring. https://qol.eortc.org/faq-category/scoring/. Accessed 2021 Oct 01.
40.EORTC Quality of Life Group. EORTC Quality of Life Questionnaire - Non Hodgkin Lymphoma Low Grade Module (EORTC- QLQ-NHL-LG20). Lyon (FR): eProvide; 2021: https://eprovide.mapi-trust.org/instruments/eortc-quality-of-life-questionnaire-non-hodgkin-lymphoma-low-grade-module. Accessed 2021 Oct 01.
41.EORTC Quality of Life Group. EORTC Quality of Life Questionnaire - Non Hodgkin Lymphoma High Grade Module (EORTC QLQ-NHL-HG29). Lyon (FR): ePROVIDE; 2021: https://eprovide.mapi-trust.org/instruments/eortc-quality-of-life-questionnaire-non-hodgkin-lymphoma-high-grade-module. Accessed 2021 Oct 01.
42.EORTC Quality of Life Group. EORTC Quality of Life Questionnaire - Chronic Lymphocytic Leukaemia Module (EORTC QLQ-CLL17). Lyon (FR): eProvide; 2021: https://eprovide.mapi-trust.org/instruments/eortc-quality-of-life-questionnaire-chronic-lymphocytic-leukaemia-module. Accessed 2021 Oct 01.
43.van Reenen M, Janssen B, Oppe M, Kreimeier S, Greiner W, Stolk E. EQ-5D-Y User Guide. 2020; https://euroqol.org/publications/user-guides. Accessed 2022 Mar 06.
44.Clinical Study Report: JCAR017-017001; Data cut-off: 2020-06-19. A phase 1, multicenter, open-label study of JCAR017, CD19-targeted chimeric antigen receptor (CAR) T cells, for relapsed and refractory (R/R) b-cell non-hodgkin lymphoma (NHL) [internal sponsor's report]. Summit (NJ): Celgene Corporation; 2020.
45.Clinical Study Report: JCAR017-017001; Data cut-off: 2021-01-04. A phase 1, multicenter, open-label study of JCAR017, CD19-targeted chimeric antigen receptor (CAR) T cells, for relapsed and refractory (R/R) b-cell non-hodgkin lymphoma (NHL) [internal sponsor's report]. Summit (NJ): Celgene Corporation; 2021.
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Patient headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: September 02, 2021
Alerts: Bi-weekly search updates until project completion
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits:
Publication date limit: none
Humans
Language limit: none
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a patient heading |
MeSH | Medical Patient Heading |
* | Before a word, indicates that the marked patient heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes patient headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.kw | Author keyword (Embase) |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
(breyanzi* or lisocabtagene maraleucel* or liso-cel or lisocel or "jcar 017" or jcar017 or jcar 17 or jcar17 or 7K2YOJ14X0).ti,ab,kf,ot,hw,rn,nm.
1 use medall
*lisocabtagene maraleucel/
(breyanzi* or lisocabtagene maraleucel* or liso-cel or lisocel or "jcar 017" or jcar017 or jcar 17 or jcar17).ti,ab,kw,dq.
or/3-4
5 use oemezd
6 not conference abstract.pt.
2 or 7
remove duplicates from 8
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- Studies with results | Breyanzi OR lisocabtagene maraleucel OR liso-cel OR jcar-017 OR jcar-17 OR 7K2YOJ14X0]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
[Search terms -- Breyanzi OR lisocabtagene maraleucel OR liso-cel OR jcar-017 OR jcar-17 OR 7K2YOJ14X0]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- Breyanzi OR lisocabtagene maraleucel OR liso-cel OR jcar-017 OR jcar-17 OR 7K2YOJ14X0]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- Breyanzi OR lisocabtagene maraleucel OR liso-cel OR jcar-017 OR jcar-17 OR 7K2YOJ14X0]
Grey Literature
Search dates: August 25, 2021 – August 31, 2021
Keywords: [Breyanzi OR lisocabtagene maraleucel OR liso-cel OR large B-cell lymphoma OR CAR-T]
Limits: Publication years: all years
Updated: Search updated prior to the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee (pERC)
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Internet Search
Ethics
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for Exclusion |
|---|---|
Study 017007 (TRANSCEND OUTREACH) Safety trial of JCAR017 for Relapsed and Refractory (R/R) B-cell Non-Hodgkin Lymphoma (NHL) in the Outpatient Setting (TRANSCEND OUTREACH) https://clinicaltrials.gov/ct2/show/NCT03744676 | Ongoing. Safety only. |
JCAR017-BCM-002 (PLATFORM) An Exploratory Phase 1/2 Trial To Evaluate The Safety And Efficacy Of JCAR017 Combinations In Subjects With Relapsed/Refractory B-Cell Malignancies (PLATFORM) | Ongoing. |
GC-LTFU-001 (LONG-TERM Follow-up) LONG-TERM FOLLOW-UP PROTOCOL FOR SUBJECTS TREATED WITH GENE-MODIFIED T CELLS | Ongoing. |
Appendix 3: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
EORTC QLQ-C30
EuroQol 5-Dimensions 5-Level (EQ-5D-5L)
Findings
A focused literature search was conducted to identify the psychometric properties and MID of each of the stated outcome measures.
The findings about validity, reliability, responsiveness, and MID of each outcome measure are summarized in Table 39.
Table 39: Summary of Outcome Measures and Their Measurement Properties
Outcome Measure | Type | Conclusions about Measurement Properties | MID |
|---|---|---|---|
EORTC QLQ-C30 | The EORTC QLQ-C30 is a standardized, patient self-administered questionnaire for evaluating the quality of life of patients with cancer. Consists of 5 functional scales, 3 symptom scales, 6 single-item scales, and 1 global quality of life scale. | Measurement properties of validity, reliability, and responsiveness not assessed in NHL patients. | For improvement and deterioration in patients with various types of cancers including hematological diseases37:
|
EQ-5D-5L | Generic, preference-based HRQoL instrument, consisting of an index score and VAS scale score. Higher the score represents better health-related quality of life The index score is based on 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. EQ VAS scale ranges from 0 (worst health imaginable) to 100 (best health imaginable) | Measurement properties of validity, reliability, and responsiveness not assessed in NHL patients. | Simulation-based MID – Canadian general population: 0.056 ± 0.011 (mean ± standard deviation)38 Unknown in NHL patients |
ECOG = Eastern Cooperative Oncology Group; EORTC QLQ-C30 = European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Cancer 30; EQ-5D-5L = EuroQol 5-Dimensions 5-Levels; HRQoL = health-related quality of life; MID = minimal important difference; NHL = non-Hodgkin lymphoma; PSR = performance status rating; SF-36 = Short Form-36; VAS = visual analogue scale
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-C30
Description
The EORTC QLQ-C30 is one of the most commonly used PRO measures in oncology clinical trials.22 It is a multi-dimensional, cancer-specific, evaluative measure of HRQoL. It was designed specifically for the purpose of assessing changes in participants’ HRQoL in clinical trials, in response to treatment. The core questionnaire of the EORTC QLQ-C30 consists of 30 questions that are scored to create 5 multi-item functional scales, 3 multi-item symptom scales, 6 single-item symptom scales, and a 2-item QoL scale, as outlined in Table 40. Version 3.0 of the questionnaire is the most current version and has been in use since December of 1997. It is available in 90 different languages and is intended for use in adult populations only. Notably, the global QoL scale is also known as the Global Health Status.
Table 40: Scales of EORTC QLQ-C30
Functional Scales (15 Questions) | Symptom Scales (7 Questions) | Single-Item Symptom Scales (6 Questions) | Global Quality of Life (2 Questions) |
|---|---|---|---|
Physical function (5) | Fatigue (3) | Dyspnea (1) | Global Quality of Life (2) |
Role function (2) | Pain (2) | Insomnia (1) | — |
Cognitive function (2) | Nausea and vomiting (2) | Appetite loss (1) | — |
Emotional function (4) | — | Constipation (1) | — |
Social function (2) | — | Diarrhea (1) | — |
— | — | Financial impact (1) | — |
Scoring
The EORTC QLQ-C30 uses a 1-week recall period in assessing function and symptoms. Most questions have 4 response options (“not at all,” “a little,” “quite a bit,” “very much”), with scores on these items ranging from 1 to 4. For the 2 items form the global QoL scale, however, the response format is a 7-point Likert-type scale, with anchors between 1 (very poor) and 7 (excellent).
Raw scores for each scale are computed as the average of the items that contribute to a particular scale. This scaling approach is based upon the assumption that it is appropriate to provide equal weighting to each item that comprises a scale. There is also an assumption that, for each item, the interval between response options is equal (for example, the difference in score between “not at all” and “a little” is the same as “a little” and “quite a bit,” at a value of 1 unit). All of the scales and single-item measures range in score from 0 to 100. Higher score for the functioning scales and global health status denotes a better level of functioning (i.e., a better state of the patient), while higher scores on the symptom and single-item scales indicate a higher level of symptoms (i.e., a worse state of the patient). Each raw scale score is converted to a standardized score that ranges from 0 to 100 using a linear transformation, with a higher score reflecting better function on the function scales, higher symptoms on the symptom scales, and better QoL (i.e., higher scores simply reflect higher levels of response on that scale). According to the EORTC QLQ-C30’s scoring algorithm, if there are missing items for a scale (i.e., the participant did not provide a response), the score for the scale can still be computed if there are responses for at least one-half of the items. In calculating the scale score, the missing items are simply ignored — an approach that assumes that the missing items have values equal to the average of those items for what the respondent completed.39
The EORTC QLQ-C30 has been extensively validated across countries around the world and in various conditions. However, psychometric properties of the EORTC QLQ-C30 have not been assessed in patients with lymphoma, therefore its validity, reliability, and responsiveness to change in this patient population remain unknown. Instead, there are 3 supplemental modules available to assess HRQoL in patients with low-grade non-Hodgkin lymphoma (LG-NHL), high-grade NHL (HG-NHL), and chronic lymphocytic leukemia: EORTC QLQ-NHL-LG20, EORTC QLQ-NHL-HG29, and EORTC QLQ-CLL17. The psychometric analyses of hypothesized scale structures, internal consistency, convergent and discriminate validity on these modules have been conducted in patients with various types of lymphoma.40-42
Minimal Important Difference
A study by Cocks et al.37 used a systematic review of the literature and experts’ opinion to evaluate meaningful differences and magnitude of change in the QLQ-C30 scores. In a meta-analysis of 118 relevant papers (13.6% from US and Canada, 5.1% about hematological diseases) with timescales ranging from 4 days to 5 years, authors estimated trivial, small, medium, and large size classes for meaningful change in the scales. Since medium and large changes could not be estimated for all scales due to insufficient data and response shift (i.e., psychological adaption of patients to their changing health status), small differences, as defined by subtle but nevertheless clinically meaningful changes, have been taken to represent the MIDs. (Table 41)
Table 41: Minimal Important Differences of EORTC QLQ-C30 Subscales
EORTC QLQ-C30 Scales | MID for Improvement | MID for Deterioration |
|---|---|---|
Functional Scales | ||
Physical function | 2-7 | -10 to -5 |
Role function | 6-12 | -14 to -7 |
Cognitive function | 3-7 | -7 to -1 |
Emotional function | 6-9 | -12 to -3 |
Social function | 3-8 | -11 to -6 |
Symptom Scales | ||
Fatigue | -9 to -4 | -5-10 |
Pain | -9 to -5 | 3-11 |
Nausea and vomiting | -9 to -3 | 5-11 |
Single-Item Symptom Scales | ||
Dyspnea | -9 to -2 | 5-11 |
Insomnia | -9 to -5 | 2-9 |
Appetite loss | -13 to -7 | 2-14 |
Constipation | -10 to -4 | 5-15 |
Diarrhea | -11 to -3 | 5-15 |
Financial impact | < -3 | 2-10 |
Global Quality of Life | ||
Global Quality of Life | 5-8 | -10 to -5 |
EORTC QLQ-C30 = The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; MID = minimal important difference
EuroQol 5-Dimensions 5-Levels Questionnaire
The EQ-5D-5L is a generic preference-based HRQoL instrument that has been applied to a wide range of health conditions and treatments. The EQ-5D-5L was developed by the EuroQol Group as an improvement to the EQ-5D 3 level (EQ-5D-3L), to measure small and medium health changes and reduce ceiling effects. The EQ-5D-5L consists of the EQ-5D descriptive system and EQ VAS. The descriptive system is comprised of 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension is rated on 5 levels: level 1 “no problems,” level 2 “slight problems,” level 3 “moderate problems,” level 4 “severe problems,” and level 5 “extreme problems” or “unable to perform.” A total of 3,125 unique health states are possible, with 55555 (extreme problems in all of the dimensions) representing the worst health state and 11111 (no problems in any of the dimensions) representing the best state. The corresponding scoring of EQ-5D-5L health states is based on a scoring algorithm that is derived from preference data obtained from interviews using choice-based techniques (e.g., time trade-off) and discrete choice experiment tasks. The lowest score varies depending on the scoring algorithm used. The anchors are 0 (dead) and 1 (full health), however negative values are also allowed to represent health states that a society considers worse than death. As an example, a Canadian scoring algorithm results in a score of -0.148 for health state 55555 (worst health state).43
Another component of the EQ-5D-5L, the EQ VAS, asks respondents to rate their health on a visual scale from 0 (worst health imaginable) to 100 (best health imaginable). The EQ VAS records the respondent’s self-rated health on a vertical VAS where the end points are labelled 0 and 100. The respondents are asked to mark an X on the point of the VAS that best represents their health on that day.
The EQ-5D index and VAS scores can be summarized and analyzed as continuous data. Hence, the EQ-5D produces 3 types of data for each respondent:
a profile indicating the extent of problems on each of the 5 dimensions represented by a 5-digit descriptor, such as 11121 or 21143
a population preference-weighted health index score based on the descriptive system
a self-reported assessment of health status based on the EQ VAS
The EQ-5D-5L has been extensively validated across countries around the world and in various conditions.43 However, the psychometric properties of the EQ-5D-5L have not been assessed in patients with lymphoma, therefore its validity, reliability, and responsiveness to change in this patient population remain unknown.
Minimal Important Difference
To estimate the MID values of the EQ-5D-5L for each country-specific scoring algorithm, a simulation-based approach based on instrument-defined single-level transitions has been used. The simulation-based instrument-defined generally accepted MID estimate (mean ± standard deviation) for Canada is 0.056 ± 0.011.38 However, MID in patients with lymphoma specifically has not been estimated.
Appendix 4: Amendments to the Protocol of Included Studies
Note that this appendix has not been copy-edited.
TRANSCEND NHL 001
Amendment 1
Protocol 017001 Amendment 1 was approved on 24 Sep 2015. The changes to this amendment occurred as a result of additional investigator and health authority feedback. The following changes were made in this amendment:
Corrected and completed eligibility criteria for adequate renal function
Provided additional information for continued JCAR017 treatment (additional cycles) in patients who achieve a response following JCAR017 therapy. (Note, the option for additional cycles was removed in Amendment 6)
Modified language to require consultation with Sponsor if delay in starting LDC is more than 14 days
Made local analysis of cytokines an optional evaluation
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Added details regarding number of patients enrolled in the regimen-finding portion of the study, the number of patients within each disease cohort, and the number of patients that may be added to a given dose regimen for further evaluation.
Updated the simulation report to include the hierarchical dose–response model, simulation results, and model operating characteristics by borrowing efficacy data across disease cohorts.
Amendment 2
Approved on March 14, 2016 (the first patient was enrolled on January 6, 2016). Amendment 2 was prepared primarily to allow for possible investigation of a higher dose level of JCAR017 in a second group of patients. The following changes were made:
A second group of patients may be enrolled and treated at a higher dose of JCAR017 (100 × 106 CAR-positive T cells) on the single- and 2-dose schedules if acceptable safety is observed among at least 6 patients treated with 50 × 106 CAR-positive T cells (Group A) on a single-dose schedule.
The planned maximum sample size was increased from 70 to 90 patients.
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| A separate Bayesian adaptive design simulation report for Dose Level 2 (Group B) was added.
Amendment 3
Approved on June 29, 2016. Amendment 3 of Protocol 017001 was prepared primarily to expand the number of patients allowed at each dose and to allow for a third (higher) dose level, if needed. The main following changes were made:
Allowed for a third, higher JCAR017 dose level (150 × 106 CAR-positive T cells)
Allowed for expansion groups to be opened at a dose level once that level has been shown likely to be safe and efficacious during the DF portion of the study
Made efficacy a primary end point rather than secondary
Updated the sample size of the study and other statistical methods as a result of the above changes
Specified that efficacy evaluations will be performed both by the investigator and by a central IRC
Lengthened the follow-up time on this study to 2 years before patients enroll in the long-term follow-up study, and added appropriate evaluations for this time period
Clarified that patients with PMBCL are allowed
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Added an exclusion for prior CAR T-cell or other genetically modified T-cell therapy
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Amendment 4
Approved on January 5, 2017, and was prepared primarily to allow inclusion of a DC group for the DLBCL cohort. The following changes were made in this amendment:
Defined a more homogeneous PAS for efficacy analyses.
Added provision for a DC group to further test the safety and efficacy at a recommended dose regimen already estimated to be safe and effective. Once a recommended regimen is determined, the study will continue enrolling patients at the recommended regimen for DC to reach a sample size of approximately 100 DLBCL cohort patients in the DC group to ensure at least 75 patients in the PAS. Updated analysis sets, sample size, power calculations, and timing of analyses accordingly, and specified analysis methods for the DC group.
Added a pre-specified interim analysis after approximately 50 patients in the PAS have been followed for at least 3 months or until death, disease progression, or withdrawal from study, and the primary analysis after at least 75 patients in the PAS have been treated and the last patient has been followed for at least 6 months or until death, disease progression, or withdrawal from study. A final analysis will be carried out after all patients have completed or discontinued the study due to any reason. No formal hypothesis testing will be performed at the final analysis. As a result of the changed sample size and follow-up time, increased estimated enrolment time and study duration.
Added chemorefractory subgroup and an efficacy hypothesis for this subgroup.
Changed CR and DOR from primary to secondary end points, changed assessment of CR using Bayesian methods to exploratory, and added PFS ratio as a secondary end point.
Added subgroup analyses for safety and efficacy analyses.
Clarified that all patients in the DLBCL cohort must have R/R disease after at least 2 lines of therapy or after autologous HSCT and clarified definition of DLBCL patients with regard to current WHO guidelines.
Allowed patients with CNS involvement of their lymphoma and excluded patients with CNS-only disease.
Added HRQoL and health economics and outcomes research as secondary objectives.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Amendment 5
Approved on August 14, 2017, and was prepared primarily to update the definition of the PAS, to amend the timing of the pre-specified interim analyses, to refine CRS and NT management algorithms, and to omit some assessment time points. The following changes were made:
Allowed for more than 1 DC group, and added reference to stopping rules for a DC group.
Amended the timing of the pre-specified interim analysis to occur when the following conditions were met: 1) at least 75 patients in the PAS have been treated at 1 recommended regimen ||||||||||||||||||||||||||||||||||||||||||||||||||||||; 2) approximately the first 50 patients treated in the DC group of the PAS have been followed for at least 3 months, or until death, disease progression, or withdrawal from the study; 3) at least the first 20 patients treated in the DC group of the PAS have been followed for at least 6 months or until death, disease progression, or withdrawal from the study.
Excluded further enrolment of patients with ECOG performance status of 2 at Screening.
Updated CRS management algorithm and guidance regarding NT based on most recent data. More specific language was added regarding actions to be taken in cases of potential CRS, especially for grade 1 and 2 events.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Updated PAS to exclude FL3B and DLBCL transformed from indolent histologies, as well as those with ECOG performance status of 2 or prior allo-HSCT.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Amendment 6
Approved on April 13, 2018, and was prepared primarily to modify the windows for the day 180 and day 270 visits and to incorporate changes previously sent to sites via administrative letter, including clinical stability measures and requirements prior to JCAR017 infusion. The following changes were made in this amendment:
Added sentence to emphasize that fludarabine doses should be adjusted in patients with renal insufficiency, in accordance with the fludarabine label
Changed the PK objective from primary to secondary
Refined CRS and NT management algorithms to be consistent with letter previously sent to sites
Appendix 5: Efficacy and Harm Outcomes From Updated Cut-off Dates
Note that this appendix has not been copy-edited.
To obtain a comprehensive view of the information related to efficacy and harm data for lisocabtagene maraleucel, updated data provided by the sponsor from 2 additional cut-off dates were added. The first cut-off date is the 2020-June-19 data and the second is the 2021-January-04 cut-off date.
Cut-Off Date 2020-June-19
The data are presented in Table 42, Figure 25, and Figure 26 and mentioned throughout the clinical review report for the main outcomes initially identified by CADTH in the protocol of this review (ORR, CRR, DOR, PFS, and OS). Harm data are also presented at this cut-off date.
Table 42: Summary of Key Results, Cut-Off Date 2020-June-19
DLBCL Efficacy Set | DL2S | DL1S | DL1D | DL3S | Total |
|---|---|---|---|---|---|
|||||||||| | |||||||||| | |||||||||| | |||||||||| | N = 257 | |
Overall response rate, n(%) | |||||
CR + PR | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 187 (72.8) |
95% CI a | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 66.9, 78.1 |
Complete response rate, n (%) | |||||
Complete Response | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 136 (52.9) |
95% CI | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 46.6, 59.2 |
Duration of response (months) | |||||
Median, 95% CI | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 20.5, 8.8-NR |
Min., max. | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 0.0, 27.4 |
PFS events, n(%) | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
Progression | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
Death | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
Censored, n (%) | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
PFS (months) | |||||
Median, 95% CI | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 6.8, 3.3-12.7 |
Min., max. | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 0.0, 28.3 |
Overall survival | |||||
Death, n (%) | 88 |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
Alive, n (%) | 82 |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
OS (Months) | |||||
Median, 95% CI | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 27.3, 16.2-45.6 |
Min., max. | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
Follow-up (months) | |||||
Median, 95% CI | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 24.1, 23.8-24.3 |
Adverse events – treated analysis set | |||||||||| | |||||||||| | |||||||||| | |||||||||| | N = 270 |
Any AE, n (%) | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 268 (99.3) |
Most common AEs, n (%) | |||||
Neutropenia | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 169 (62.6) |
Anemia | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 129 (47.8) |
Thrombocytopenia | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 85 (31.5) |
Fatigue | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 119 (44.1) |
Any serious AE, n (%) | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 122 (45.2) |
Cytokine release syndrome, n (%) | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 113 (41.9) |
Grade ≥ 3 infections | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 33 (12.2) |
Grade ≥ 3 Prolonged cytopenias | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
Hypogammaglobulinemia | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
Death – occurred any time after the first infusion of liso-cel or nonconforming product, i.e., leukapheresed set (N = 345) | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
Disease progression Adverse event Unknown Other | — | — | — | — | |||||||||| |
CI = confidence interval; DL1D = Dose Level 1, 2 Dose; DL1S = Dose Level 1, Single Dose; DL2S = Dose Level 2, Single Dose; DL3S = Dose Level 3, Single Dose; DLBCL = diffuse large B-cell lymphoma; HSCT = hematopoietic stem cell transplant; max. = maximum; min. = minimum; NA = not applicable; NR = not reached; OS = overall survival.
aAll the confidence intervals were 2-sided 95% exact Clopper-Pearson.
Data cut-off 2020-June-19.
Source: CSR TRANSCEND Study and update data cut-off 2020-06-19.9,44
Figure 25: Progression-Free Survival, DLBCL Efficacy Set, Cut-Off Date 2020-June-19
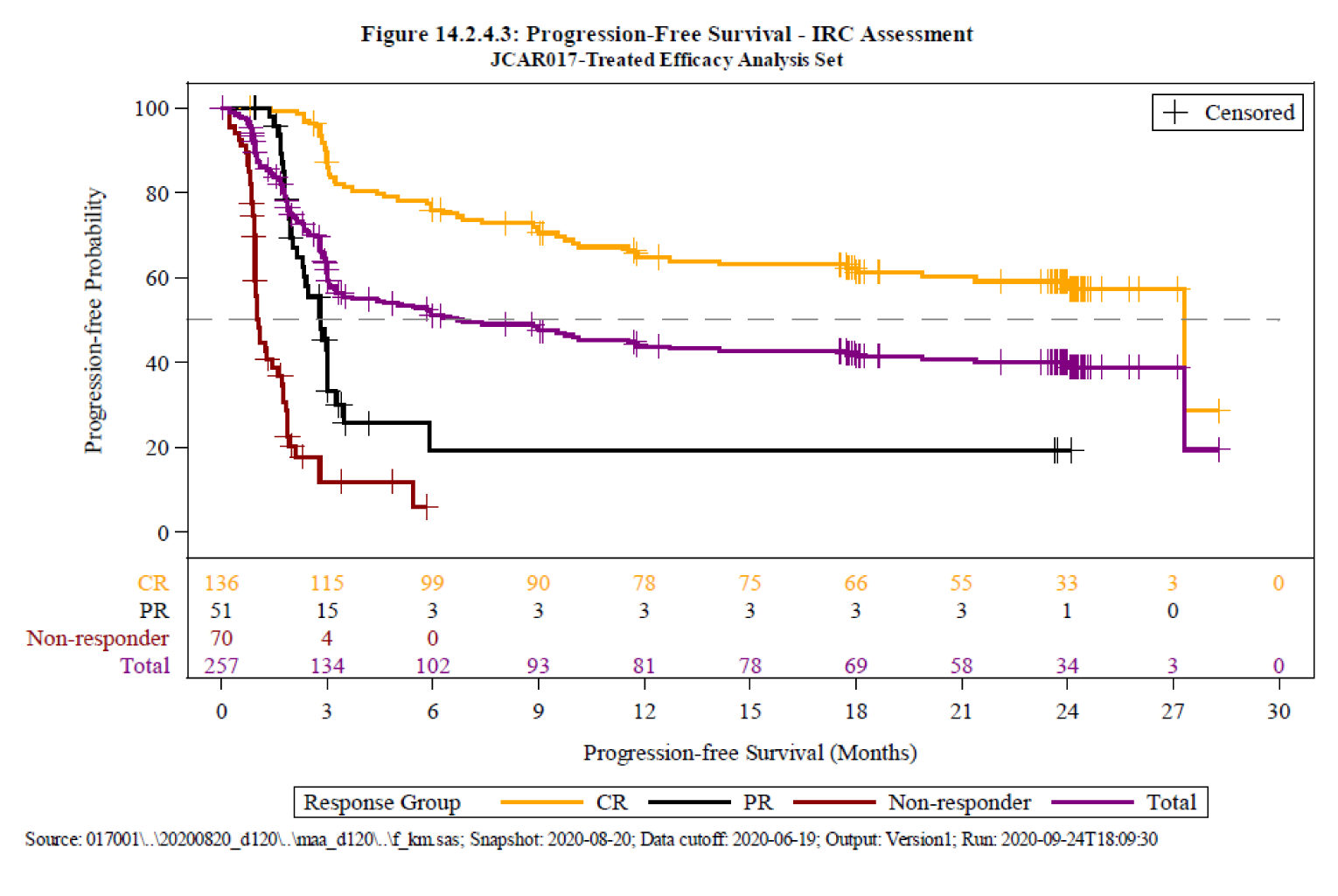
Source: CSR TRANSCEND Study and update data cut-off 2020-06-19.9,44
Figure 26: Overall Survival, DLBCL Efficacy Set, Cut-Off Date 2020-June-19
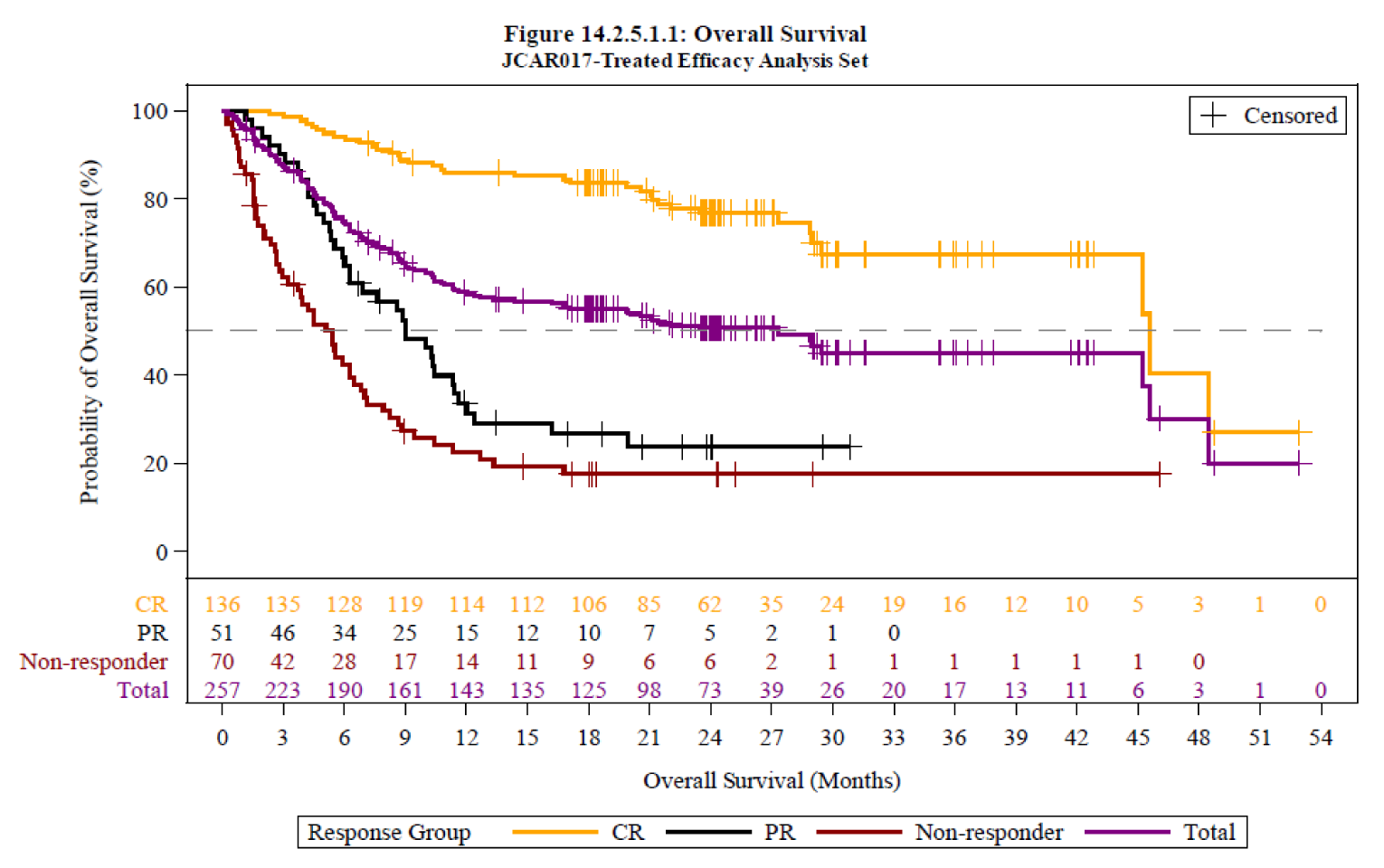
Source: CSR TRANSCEND Study and update data cut-off 2020-06-19.9,44
Cut-Off Date 2021-January-04
The data are presented in Table 43, Figure 27, and Figure 28 and mentioned throughout the clinical review report for the main outcomes initially identified by CADTH in the protocol of this review (ORR, CRR, DOR, PFS, and OS). No harms data were presented at this cut-off date.
Table 43: Summary of Key Results, Cut-Off Date 2021-January-04
DLBCL Efficacy Set | DL2S | DL1S | DL1D | DL3S | Total |
|---|---|---|---|---|---|
|||||||||| | |||||||||| | |||||||||| | |||||||||| | N = 257 | |
Overall response rate, n(%) | |||||
CR + PR | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 187 (72.8) |
95% CI a | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 66.9, 78.1 |
Complete response rate, n (%) | |||||
Complete Response | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 136 (52.9) |
95% CI | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 46.6, 59.2 |
Duration of response (months) | |||||
Median, 95% CI | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 23.1, 8.6-NR |
Min., max. | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
PFS events, n(%) | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
Progression | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
Death | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
Censored, n (%) | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
PFS (months) | |||||
Median, 95% CI | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 6.8, 3.3-12.7 |
Min., max. | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 0.0, 28.3 |
Overall survival | |||||
Death, n (%) | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
Alive, n (%) | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
OS (Months) | |||||
Median, 95% CI | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 27.3, 16.2-45.6 |
Min., max. | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
Follow-up (months) | |||||
Median, 95% CI | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 29.3, 26.2-30.4 |
Adverse events – treated analysis set | |||||||||| | |||||||||| | |||||||||| | |||||||||| | N = 270 |
Any AE, n (%) | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 268 (99.3) |
Most common AEs | |||||
Neutropenia | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 169 (62.6) |
Anemia | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 129 (47.8) |
Thrombocytopenia | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 85 (31.5) |
Fatigue | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 119 (44.1) |
Any serious AE, n (%) | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 122 (45.2) |
Cytokine release syndrome, n (%) | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 113 (41.9) |
Grade ≥ 3 infections | |||||||||| | |||||||||| | |||||||||| | |||||||||| | 33 (12.2) |
Grade ≥ 3 Prolonged cytopenias | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
Hypogammaglobulinemia | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
Death – occurred any time after the first infusion of liso-cel or nonconforming product, i.e., leukapheresed set (N = 345) | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
Disease progression Adverse event Unknown Other | — | — | — | — | |||||||||| |
CI = confidence interval; DL1D = Dose Level 1, 2 Dose; DL1S = Dose Level 1, Single Dose; DL2S = Dose Level 2, Single Dose; DL3S = Dose Level 3, Single Dose; DLBCL = diffuse large B-cell lymphoma; HSCT = hematopoietic stem cell transplant; max. = maximum; min. = minimum; NA = not applicable; NR = not reached; OS = overall survival.
aAll the confidence intervals were 2-sided 95% exact Clopper-Pearson.
Data cut-off 2020-June-19.
Source: CSR TRANSCEND Study and update data cut-off 2021-01-04.45
Figure 27: Progression-Free Survival, DLBCL Efficacy Set, Cut-Off Date 2021-January-04
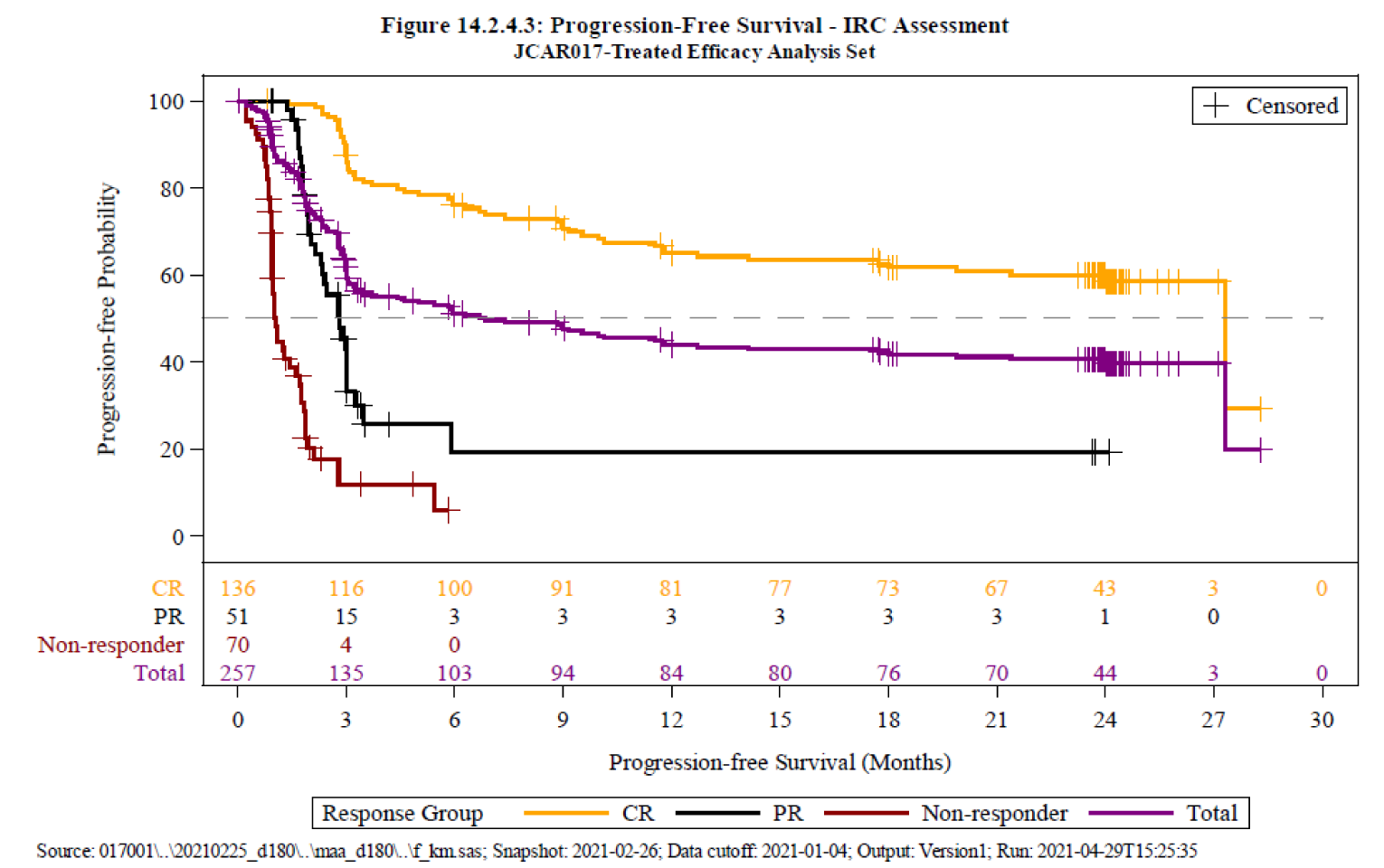
Source: CSR TRANSCEND Study and update data cut-off 2021-01-04.45
Figure 28: Overall Survival, DLBCL Efficacy Set, Cut-Off Date 2021-January-04
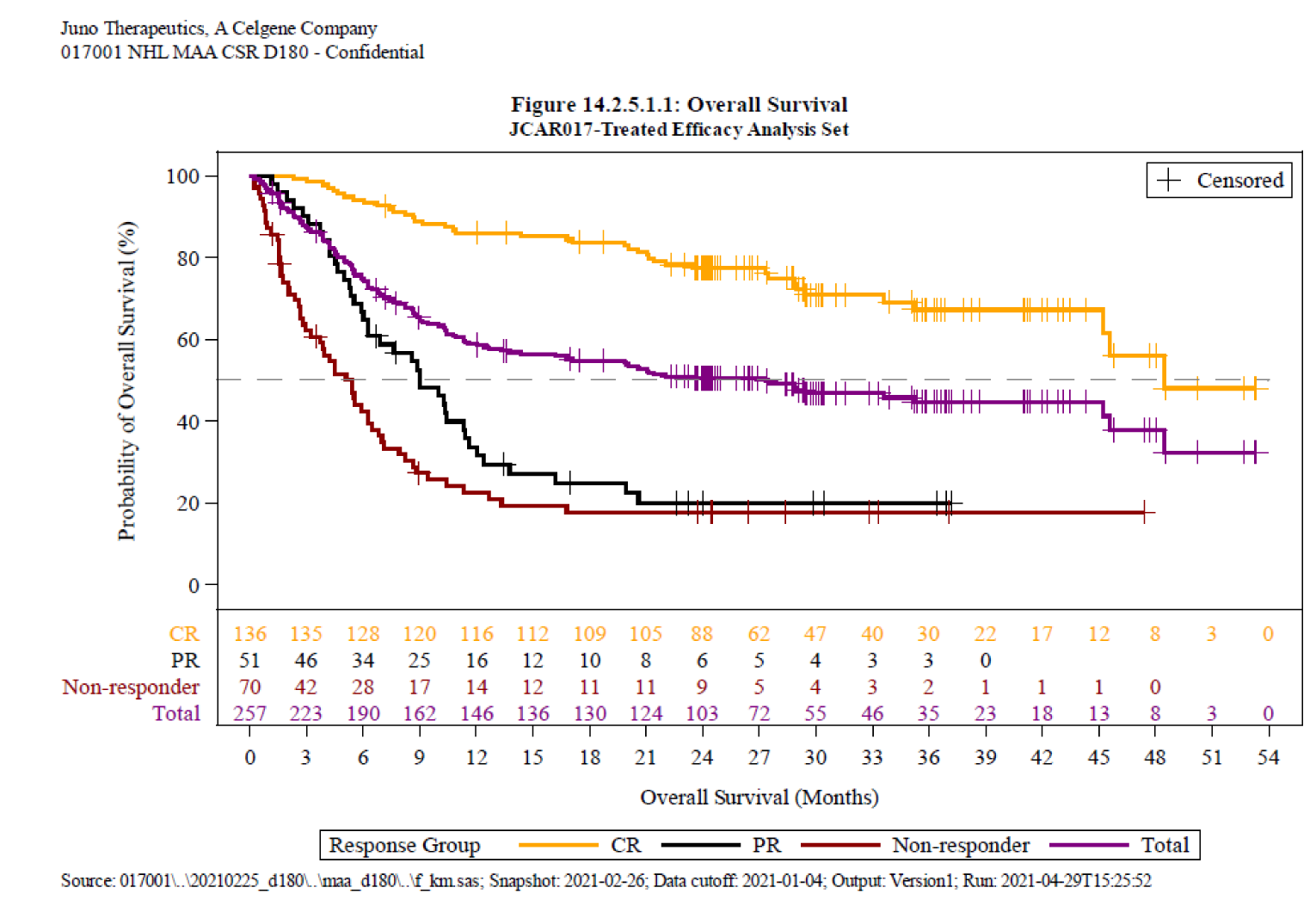
Source: CSR TRANSCEND Study and update data cut-off 2021-01-04.45
Pharmacoeconomic Review
Abbreviations
ASCT
autologous stem cell transplant
axi-cel
axicabtagene ciloleucel
CAR
chimeric antigen receptor
CRR
complete response rate
CRS
cytokine release syndrome
DHAP
cytarabine, dexamethasone, and cisplatin
DLBCL
diffuse large B-cell lymphoma
FL
follicular lymphoma
GDP
gemcitabine, dexamethasone, and cisplatin
HSCT
hematopoietic stem cell transplant
ICE
carboplatin, etoposide, and ifosfamide
ICER
incremental cost-effectiveness ratio
LBCL
large B-cell lymphoma
liso-cel
lisocabtagene maraleucel
MAIC
matching-adjusted indirect comparison
ORR
overall response rate
OS
overall survival
PFS
progression-free survival
Pola-BR
polatuzumab in combination with bendamustine and rituximab
PSM
partitioned survival model
QALY
quality-adjusted life-year
R/R
relapsed or refractory
tisa-cel
tisagenlecleucel
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Lisocabtagene maraleucel (Breyanzi), cell suspension for IV infusion |
Submitted price | Lisocabtagene maraleucel: $501,900 per administration |
Indication | Treatment of adult patients with relapsed or refractory large B-cell lymphoma after 2 or more lines of systemic therapy, including diffuse large B-cell lymphoma not otherwise specified, primary mediastinal large B-cell lymphoma, high-grade B-cell lymphoma, and diffuse large B-cell lymphoma arising from follicular lymphoma |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | May 6, 2022 |
Reimbursement request | As per indication |
Sponsor | Celgene Inc., a Bristol Myers Squibb Company |
Submission history | Previously reviewed: no |
NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Decision tree, followed by a PSM with a mixture-cure component |
Target population | Adults with R/R LBCL who failed at least 2 prior lines of treatment |
Treatment | Liso-cel |
Comparators | Axi-cel (Yescarta) Tisa-cel (Kymriah) Salvage chemotherapy; modelled as a basket of chemotherapy regimens including GDP, DHAP, ICE, gemcitabine monotherapy, and oral cyclophosphamide and etoposide |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (50 years) |
Key data source | Clinical efficacy data were derived from the TRANSCEND (liso-cel), JULIET (tisa-cel), ZUMA-1 (axi-cel), or SCHOLAR-1 (salvage chemotherapy) studies. Relative efficacy was assessed based on naive comparison and 3 pairwise unanchored MAICs. |
Submitted results | ICER = $127,679 per QALY compared with salvage chemotherapy (incremental QALYs = 3.32; incremental costs = $423,404). Tisa-cel is extendedly dominated through salvage chemotherapy and liso-cel. Axi-cel is dominated by liso-cel. |
Key limitations |
|
CADTH reanalysis results |
|
axi-cel = axicabtagene ciloleucel; CAR = chimeric antigen receptor; DHAP = cytarabine, dexamethasone, cisplatin; GDP = gemcitabine, dexamethasone, cisplatin; ICE = carboplatin, etoposide, ifosfamide; ICER = incremental cost-effectiveness ratio; LBCL = large B-cell lymphoma; liso-cel = lisocabtagene maraleucel; LY = life-year; MAIC = matching-adjusted indirect comparison; PSM = partitioned survival model; QALY = quality-adjusted life-year; R/R = relapsed or refractory; tisa-cel = tisagenlecleucel.
Conclusions
Evidence from the TRANSCEND trial suggests that liso-cel is associated with improvements in overall response rate (ORR), complete response rate (CRR), progression-free survival (PFS), overall survival (OS) and health-related quality of life when compared against historical outcomes for patients with relapsed or refractory large b-cell lymphoma (LBCL). There are important caveats with these findings given the sponsor’s single-arm study design generates bias, due to an inability to control for confounding and multiplicity, imprecision in the effect estimates, and high amount of censoring. CADTH also noted that the data were not mature at last follow-up and identified some concerns regarding the generalizability of the trial population to the Canadian setting. Due to the lack of head-to-head studies comparing liso-cel with the relevant comparators, the sponsor submitted 3 unanchored matching-adjusted indirect comparisons (MAICs) as indirect evidence of the clinical efficacy of lisocabtagene maraleucel (liso-cel) compared with axicabtagene ciloleucel (axi-cel), liso-cel with tisagenlecleucel (tisa-cel), and liso-cel with salvage chemotherapy. Although the sponsor-submitted MAICs indicated that liso-cel was associated with meaningful improvements in ORR, CRR, PFS, and OS relative to tisa-cel and salvage chemotherapy, and no differences when compared to axi-cel, due to several identified limitations with the MAICs (e.g., residual confounding, population heterogeneity, lack of precision, generalizability), no conclusions can be drawn on the comparative clinical effectiveness of liso-cel with regards to other chimeric antigen receptor (CAR) T-cell therapies. Further, the magnitude of benefit for liso-cel relative to salvage chemotherapy is considered highly uncertain.
In addition to the aforementioned limitations with the comparative effectiveness, evidence, and limitations with the clinical trial data for liso-cel, CADTH identified several major limitations with the sponsor’s economic submission to CADTH that introduced further uncertainty in the cost-effectiveness assessment of liso-cel. These limitations included: the sponsor’s use of a sequential analysis to assess the relative effectiveness of liso-cel, axi-cel, tisa-cel, and salvage chemotherapy does not align with the MAIC approach which altered the liso-cel population (and therefore baseline effects of treatment) for each comparison; the use of a model structure which incorporated pre-treatment assumptions that favoured liso-cel due to fewer patients receiving treatment and assumptions regarding fewer acquisition costs; and the assumption that a proportion of patients were “cured” immediately after receiving treatment. CADTH identified additional concerns regarding the utility values used, resource use assumptions, adverse event rates, and management practices, which appeared to benefit liso-cel relative to other comparator treatments.
As such, based on the limitations identified, the incremental cost-effectiveness ratio (ICER) for liso-cel relative to salvage chemotherapy is likely higher than the sponsor’s base case, while the assumption that liso-cel is more effective and less costly than tisa-cel and axi-cel is considered highly uncertain. No robust evidence has been provided to suggest that liso-cel is associated with improved efficacy and safety relative to other CAR T-cell therapies used to treat LBCLs. Feedback from the clinical experts consulted by CADTH indicated that liso-cel is likely similarly effective to other CAR T-cell therapies.
At the submitted price of $501,900 per administration, liso-cel has a higher publicly available acquisition cost than either tisa-cel ($450,000) or axi-cel ($485,021), and is considerably more costly over the modelled time horizon than salvage chemotherapy.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process (specifically, information that pertains to the economic submission).
Patient group input was received from Lymphoma Canada. The input was based on an anonymous online survey conducted in 2021 to capture the perspectives of patients with LBCL in Canada and the US. As no patients in the survey had experience with liso-cel, feedback on patient experience with CAR T-cell therapy was obtained from a previous survey. Additional information was derived from previous surveys about disease experience collected from patients with diffuse large B-cell lymphoma (DLBCL) and follicular lymphoma (FL). The survey collected information from 331 patients with LBCL (38% DLBCL, 58% FL, 4% other); no caregiver feedback was provided. LBCL affects quality of life; symptoms of the condition can lead to anxiety and stress and limit patients’ ability to continue their daily activities, including sleeping, concentrating, and attending work or school. Current treatments noted were chemotherapy alone or in combination with rituximab, radiation therapy, bendamustine plus rituximab, high-dose therapy, and stem cell transplant; a small proportion had received CAR T-cell therapy, while others noted a standard treatment approach is watch and wait or active surveillance. Ninety-three percent of patients had received prior treatment (50% received 1, 43% received 2 or more). Current treatments are associated with notable side effects, including fatigue, hair loss, nausea, neuropathy, neutropenia, memory loss/confusion, and pain. Patients reported that current treatments (mainly chemotherapies, chemo-immunotherapies, and radiation) can have a negative impact on quality of life, causing anxiety or depression and inability to work or attend school. The most significant impacts of current treatment on quality of life were fatigue, long-term side effects, low levels of activity, not seeing friends and family, clinic visits, and duration of treatment administration. Patients reported challenges with access to treatment due to both funding and travel required. Patients want treatments to improve quality of life and allow them to perform daily activities, improve survival, increase duration of disease remission, improve disease control symptoms, and decrease side effects.
Two registered clinician group inputs were received: from the Ontario Health Hematology Disease Site Drug Advisory Committee and a group of lymphoma experts whose input was coordinated by Lymphoma Canada. Clinicians stated the key unmet needs that liso-cel will address is the expanded patient population that other CAR T-cell therapies do not have. Clinicians indicated requirements regarding patient eligibility and access to CAR T-cell administration centres may prove a barrier for access for some patients, and suggested an additional treatment option may improve manufacturing times and result in fewer delays. Clinician group input also suggested that liso-cel may have fewer treatment-related toxicities than comparator products. Clinically meaningful benefits, such as reduced frequency and severity of symptoms, improvement or stabilization of symptoms, remission, and improvement in abilities to perform daily activities and general quality of life are treatment goals.
CADTH-participating drug plans highlighted several implementation and economic considerations for liso-cel. There were concerns the introduction of liso-cel may expand the patient population with access to CAR T-cell therapy given the difference in patient population indicated between the CAR T-cell therapies. Other concerns included: the patient support program may not fully cover interprovincial travel for patients leading to a requirement for interprovincial agreements to ensure equitable access across Canada for patients that meet the eligibility requirements; the requirement for specialized centres in which the therapy can be administered; a high human resource burden to obtain and maintain site certification; use of multiple infusions; and privacy concerns relating to patient cell ownership (due to CAR T-cell therapy being manufactured by a US-based company outside of Canadian jurisdiction).
Several of these concerns were addressed in the sponsor’s model.
The comparators included were aligned with those listed by patients, clinicians, and the CADTH-participating drug plans.
PFS and OS were used as key health states.
Adverse events were incorporated via disutilities and costs.
CADTH was unable to address the following concerns raised from stakeholder input.
Data were not available for the broader population for the comparator treatments.
While pre-treatment considerations were included in the sponsor’s model, manufacturing and administration burdens were not fully elucidated. Clinical expert feedback noted that additional experience with currently available CAR T-cell therapies has seen improvements in manufacturing and patient management since the initial trials of those treatments.
Economic Review
The current review is for liso-cel (Breyanzi) for the treatment of adult patients with relapsed/refractory (R/R) LBCL after 2 or more lines of therapies.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis comparing liso-cel with axi-cel, tisa-cel, and salvage chemotherapy. Salvage chemotherapy was defined as a basket of chemotherapy regimens including gemcitabine, dexamethasone, and cisplatin (GDP), cytarabine, dexamethasone, and cisplatin (DHAP), carboplatin, etoposide, and ifosfamide (ICE), gemcitabine monotherapy, and oral cyclophosphamide-etoposide. The sponsor indicated that salvage chemotherapy is not considered an appropriate comparator and was included for historical purposes only. Additionally, polatuzumab in combination with bendamustine and rituximab (Pola-BR) is indicated by Health Canada for the treatment of adult patients with R/R DLBCL, not otherwise specified, who are not eligible for autologous stem cell transplant (ASCT) and have received at least 1 prior therapy. The sponsor did not include Pola-BR as part of the analysis, indicating that it would not replace the use of CAR T-cell therapies in patients suitable to receive them. The reimbursement population aligns with the Health Canada-indicated population.1
Liso-cel is a CAR T-cell therapy targeting CD19, a marker expressed on B-cell precursors and malignant B-cells present in DLBCL and other lymphomas. It is available as a cell suspension for infusion containing 60 × 106 to 120 × 106 CAR T-cells, consisting of CD8 and CD4 components at a ratio range of 0.8 to 1.2, with each component supplied separately in 1 to 4 single-dose vials. The sponsor’s submitted price of liso-cel is $501,900 per infusion, not including costs associated with pre- and post-infusion management (i.e., leukapheresis, bridging therapy, conditioning chemotherapy).1 The comparators for this analysis included tisa-cel and axi-cel, other CAR T-cell therapies. The costs of tisa-cel and axi-cel were reported as $450,000 and $485,021 respectively. In addition, salvage chemotherapy was included, derived evenly from GDP, DHAP, ICE, gemcitabine monotherapy, and cyclophosphamide plus etoposide (the cost of salvage chemotherapy over the first 8 cycles is $5,265 including administration costs).1 Patients in the various CAR T-cell therapy trials were able to receive out-of-specification product or were re-treated with the same CAR T-cell product; these assumptions were incorporated into the sponsor’s economic analysis, though no additional drug cost was attributed to these patients.1
The outcomes of interest were quality-adjusted life-years (QALYs) and life-years. The analysis takes the perspective of a public health care payer. The time horizon in the base case was specified by the sponsor as a lifetime time horizon (50 years). The discount rate for costs and outcomes was 1.5% annually.1
Model Structure
The model consists of 2 components: a decision tree in the pre-treatment setting; and, in the post-treatment setting, a partitioned survival model (PSM) with a mixture-cure component with 3 different model states (pre-progression, post-progression, and death; Figure 1).1
Patients enter the model in the pre-treatment stage, which is equivalent to leukapheresis for CAR T-cell therapy and to the start of treatment for patients on salvage chemotherapy. During the pre-treatment period, patients may: die before receiving CAR T-cell therapy (in which case they move to the death health state); survive but fail to receive CAR T-cell therapy (due to adverse events from bridging therapy, CAR T-cell therapy manufacturing failure, or other reasons), in which case they are simulated to receive salvage chemotherapy instead, accruing the costs and health outcomes associated with salvage chemotherapy going forward; or, survive and receive CAR T-cell therapy as planned. Patients entering the PSM entered the model in the pre-progression health state. Patients who progress can remain in the post-progression health state or transition to the death state but never go back to the progression-free health state. All patients eventually enter the death health state. For the first 5 years, the model uses a weekly cycle; thereafter, the model shifts to an annual cycle. The total benefits accrued in the post-treatment PSM are then weighted based on the proportion of patients who make it through the pre-treatment phase and receive treatment.1
The mixture-cure component estimates the proportion of patients who are “cured” and predicts the survival of those who are “not cured.” Cured patients are defined as those who are no longer at risk of experiencing the event of interest (e.g., death-overall and/or due to disease) and are assumed to be cured from time of treatment administration (for CAR T-cell therapy or salvage chemotherapy). In the model, OS of cured patients is assumed to be the same as the age- and sex-adjusted general population mortality, accelerated by an excess mortality risk. Survival of non-cured patients is extrapolated based on parametric functions; it is assumed that non-cured patients will progress and eventually die from their disease. To estimate the OS curve, distributions assigned to the not cured proportion are combined with the cure proportion.1
Life-years and QALYs for patients who die before CAR T-cell therapy administration are accrued by the appropriate treatment arm in the model to fully capture the survival of each cohort. The costs and outcomes (e.g., death or switch to salvage chemotherapy) experienced by patients during the pre-treatment period are applied as patients enter the PSM.1
Model Inputs
The patients’ baseline characteristics, such as age, weight, and body surface area, were obtained from the “treated analysis dataset” of the TRANSCEND trial (N = 344). These patients were predominantly male (64.6%), with mean age of |||| years, mean body weight of |||| kg, and mean body surface of |||| m2.1
In the pre-treatment phase, data from the TRANSCEND (January 4, 2021 data cut-off), JULIET, and ZUMA-1 trials were used to inform the clinical information for liso-cel, tisa-cel, and axi-cel, respectively. Based on these non-comparative data, different pre-treatment assumptions were made between treatments (Table 7). In the pre-treatment period, the duration and success differed based on data from the individual trials. Per trial data, patients could receive the product out of specification, though when this occurred, acquisition costs were not incorporated. For salvage chemotherapy, no adjustment was performed as patients were assumed to immediately move into the PSM. The duration of the pre-treatment period was used to discount cost and health outcomes in the PSM.1
In the post-treatment phase, the sponsor considered 2 approaches for comparing clinical outcomes—MAICs and a naive comparison. The sponsor chose to use the unanchored pairwise MAICs in the base-case analysis, due to concerns that the naive comparison approach could introduce biases due to differences in baseline demographics and clinical characteristics which are either prognostic or treatment effect modifiers. The sponsor conducted 3 pairwise unanchored MAICs to compare liso-cel with tisa-cel, axi-cel, and salvage chemotherapy, respectively.1-5 Each MAIC produced a set of weights to be applied to the starting population of the TRANSCEND study (N = 257) to more closely reflect the patient population in each of the relevant comparator trials. In each MAIC, individual patient data from the TRANSCEND study were adjusted to match clinical factors of patients from the JULIET, ZUMA-1, and SCHOLAR-1 trials; patients who did not satisfy the sponsor’s criteria were removed from the TRANSCEND dataset (refer to CADTH Clinical Report for further information). For the purposes of economic evaluation, the MAIC weights were incorporated into the statistical analyses for extrapolating PFS and OS to derive relative treatment effect terms based on matched populations.
Health-related quality of life data were collected as part of the TRANSCEND trial and assessed using the EuroQol 5-Dimensions 5-Levels (EQ-5D-5L) questionnaire. Using the repeated-measures mixed-effect analysis method, these data were used to inform utility values for the PFS (||||) and post-progression health states (||||). The sponsor stated that the repeated-measures mixed-effect analysis accounted for baseline EQ-5D-5L questionnaires, adverse events, and progressive disease, although for the PFS health state, the values represented were considered independent of any adverse events and thus decrements associated with treatment specific adverse events are applied separately. The utility value for the pre-treatment period was assumed to be the same as for a patient with progressed disease. An age adjustment was incorporated by the sponsor. Patients who progressed and subsequently received HSCT obtained a utility value equal to that of the PFS state 6 months after surgery. Utility decrements were applied to treatments for adverse events for specific durations based on a vignette study, trial data, and sponsor assumption.1 A utility decrement was also applied to treatments requiring IV administration, exclusive of CAR T-cell therapies.1,6
The sponsor incorporated a variety of costs within the model. Costs specific to CAR T-cell therapies included in the model were drug acquisition, leukapheresis, lymphodepleting chemotherapy, bridging therapy, and administration (including infusion time and monitoring). All costs associated with CAR T-cell therapies were assumed to be 1-time costs to be incurred in the first model cycle. The administration cost of $1,326, equivalent to a 1-off inpatient stay in hospital,1,7 was assumed for all patients receiving CAR T-cell therapies and applied for a total of 11 days (per the TRANSCEND study) post-administration of CAR T-cell therapy, using cost data from the Ontario Case Costing Initiative. The sponsor incorporated re-treatment within the model to reflect the clinical evidence (Table 8), though the sponsor noted re-treatment would not be sought within the reimbursement request. Re-treatment costs were assumed to include only lymphodepleting chemotherapy and the 1-time administration cost; no additional costs associated with CAR T-cell therapy acquisition, bridging treatment, leukapheresis, or adverse events were included. The cost of salvage chemotherapy was determined from the Ontario Drug Benefit Formulary, IQVIA Delta PA database, and prior CADTH reports. Dosing information and resource used for these regimens was sourced from Cancer Care Ontario, the Ontario Ministry of Health and Long-Term Care Schedule of Benefits for Physician Services, published literature, and adaptations from other sources and disease areas.1,8-11 Costs are reported in Table 9, Table 10, and Table 12. Patients who experience progressive disease were simulated to receive a subsequent treatment. The treatment options included allogeneic and autologous HSCT, fourth line or later standard of care, which includes salvage chemotherapy and radiation therapy, or no treatment (e.g., palliative care). Patients who did not receive CAR T-cell therapy were assumed not eligible for HSCT either. Costs for autologous and allogeneic HSCT were informed by the Ontario Case Costing Initiative. Adverse event costs for grade 1 to 2 and 3 or higher cytokine release syndrome (CRS), neurotoxicity, and hypogammaglobulinemia were derived via a micro-costing approach. Post-infusion resource use was assumed to include 8 oncology consultations for a total cost of $1,256.9 Further resource use costs were associated with the various health states; for the progression-free health state, these included costs associated with active disease management such as drug costs, physician and laboratory visits, and radiological tests. In the post-progression health state, patients continue to incur costs associated with medical management of the condition.9 Patients who died in each model cycle incurred an end-of-life cost of $33,005.1,12 Indirect costs and direct non-medical costs were incorporated within the sponsor’s scenario analysis from the societal perspective.
Total cost and outcomes of each CAR T-cell treatment arm are an average of the CAR T-cell therapy and salvage chemotherapy cost and outcomes, weighted according to the proportions receiving CAR T-cell therapies and those who do not receive CAR T-cell therapy per the pre-treatment period stratification (Table 7). Patients assigned CAR T-cell therapy in the intention-to-treat population of the TRANSCEND study who did not receive the CAR T-cell infusion were assigned the costs and outcomes of the salvage chemotherapy arm.1 Based on these assumptions, approximately 70% of patients receiving tisa-cel and 90% of patients receiving axi-cel received treatment and were incurred the cost of treatment. Although approximately ||% of patients received liso-cel (per the trial data), less than 80% of patients incurred the cost of treatment in the model.
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically using 400 iterations for the base-case and scenario analyses. The sponsor reported both probabilistic and deterministic results in their analysis; results were similar. The probabilistic findings are reported below.
Base-Case Results
In the sponsor’s base-case analysis, the results indicated that treatment with liso-cel was associated with higher incremental costs than salvage chemotherapy and tisa-cel, and greater incremental QALYs than salvage chemotherapy, tisa-cel, and axi-cel. Over the 50-year (i.e., lifetime) time horizon, liso-cel had an ICER of $127,679 per QALY gained. Disaggregated results are provided in in Appendix 3 (Table 11 through Table 14). The sponsor’s cost-effectiveness acceptability curve indicated that liso-cel had a 0% probability of being cost-effective at a willingness-to-pay threshold of $50,000 per QALY. The sponsor’s analysis predicted that liso-cel was associated with a longer duration of life (i.e., “life-years;” 7.80) than salvage chemotherapy (3.81) and tisa-cel (4.81), but fewer life-years than axi-cel (7.85).1
Importantly, given the duration of the clinical trial observation period in contrast to the model time horizon (50 years), it is likely that most of the QALYs realized by patients receiving liso-cel in the model were gained outside of what was observed in the clinical trial (i.e., extrapolated period); however, the extent of this could not be examined given the sponsor’s model structure and programming.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Salvage chemotherapy | 44,630 | 3.17 | Reference |
Liso-cel | 467,972 | 6.49 | 127,679 |
ICER = incremental cost-effectiveness ratio; liso-cel = lisocabtagene maraleucel; QALY = quality-adjusted life-year.
Note: Only treatments that are on the efficiency frontier are reported in the main body. Full results can be found in Appendix 3. If a treatment is not on the frontier, it is dominated (i.e., more costly and no more effective than a comparator) or extendedly dominated (i.e., has an ICER that is greater than that of a more effective intervention on the frontier).
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor reported a series of univariate scenario analyses in their pharmacoeconomic report to assess the impact of alternate assumptions regarding the time horizon, age, health-state utilities, wastage, perspective, discount rate, parametric functions for OS and PFS for all treatment arms, excess mortality for cured versus the general population, the comparative data used to inform the model, and other efficacy, administration, and hospitalization assumptions.1
The key assumptions driving the ICER were assumptions regarding efficacy for out-of-specification treatment, alternate parametric fits for OS, alternate data sources used to inform the model, age, and time horizon. In these scenarios, liso-cel was not the optimal treatment (i.e., less effective than axi-cel, and/or the ICER relative to salvage chemotherapy increased or decreased by more than 15% from the sponsor’s submitted base-case ICER). The results of the analysis from the societal perspective were similar to the results from the health care payer perspective.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
Unknown comparative effectiveness. The TRANSCEND study was a non-comparative trial of liso-cel in adult patients with R/R B-cell non-Hodgkin lymphomas including DLBCL not otherwise specified (de novo and transformed from indolent lymphoma), high-grade B-cell lymphoma with myelocytomatosis oncogene and B-cell lymphoma gene 2 and/or 6 (BCL2 and/or BCL6) rearrangements with DLBCL histology, primary mediastinal B-cell lymphoma, FL grade 3B, and mantle cell lymphoma, as well as the antitumour activity of liso-cel. In the subgroup of interest (i.e., the indicated population), the results suggested that liso-cel was associated with an improvement in the ORR, complete response, as well as in end points of OS and PFS in patients with R/R DLBCL in the third-line setting. As the study was non-comparative, the relative effectiveness of liso-cel with axi-cel, tisa-cel, and salvage chemotherapy was obtained from MAICs.
CADTH identified several limitations with the TRANSCEND trial including concerns regarding the generalizability of the population to the Canadian setting, hypothesis testing, that adjustment for multiplicity was evaluated only for the primary analysis set population, the open label design may also introduce bias, and decreasing precision due to fewer patients available for analysis over time. These concerns suggest caution must be applied when interpreting these data.
Although the sponsor-submitted MAICs claimed that the studies were similar enough to allow indirect comparison, there are fundamental differences between the trials that were not adjusted for within the MAIC (e.g., differences between data collection from a clinical trial compared with an observational trial). Inherent study design differences existed between the TRANSCEND trial and the JULIET, ZUMA-1, and SCHOLAR-1 trials that could not be adjusted for statistically. Furthermore, the MAIC-weighting process resulted in substantially decreased sample sizes, which suggests much information is lost, speaking to uncertainty and heterogeneity concerns. These items introduce concerns with precision and generalizability.
When translating this information to the economic model, the sponsor noted that as PFS was not available for salvage chemotherapy (PFS was not reported in the SCHOLAR-1 study). As such, the relative efficacy of liso-cel compared with salvage chemotherapy observed for OS would apply to PFS. While this claim is associated with some uncertainty, it is unlikely to impact the overall clinical conclusion, though the magnitude of the difference is highly uncertain.
Furthermore, according to clinical experts consulted by CADTH, clinicians that treat this patient population have gained a better sense of the management of patients with CAR T-cell therapy over time, meaning events assessed in earlier CAR T-cell trials may be overestimated. The following observations were made by the clinical experts consulted by CADTH: 1) the adverse event rates in the earlier CAR T-cell trials are likely overestimated relative to current Canadian clinical practice (specifically CRS and neurotoxicity), 2) the differences in use of bridging therapy and IV immunoglobulin between the trials does not match current Canadian practice for the use of CAR T-cell therapy, 3) there may be differences between the manufacturing time associated with the CAR T-cell therapies, but the time to manufacture CAR T-cell products has reduced since the trials, as has been published,13,14 and 4) any results suggesting notable treatment effect differences between the CAR T-cell therapies must be viewed with caution, as these differences are not expected in clinical practice based on the currently available evidence.
The MAIC-weighted analyses were based on multiple datasets. The safety analyses were derived from 19.1-month median follow-up for the TRANSCEND study, which differed from the follow-up from the ZUMA-1 trial (27.1 months),1,15 and JULIET (28.6 months).1,16 The median follow-up for SCHOLAR-1 was not reported.1,17 Survival outcomes were derived from more recent data cuts for all comparators (for the most part) which noted similar differences in follow-up duration, although the CADTH Clinical Review Report noted limitations with the more recent data cuts as these analyses were not assessed with an a priori hypothesis testing or adjustments for multiplicity. The absolute and relative effectiveness on PFS and OS beyond the study duration is not available and was extrapolated using mathematical models. The appropriateness and quality of any extrapolation is dependent on the quantity of observed data available. As previously mentioned, closer to the data cut-off period, there was an increasingly smaller number of patients at risk of death to inform survival. With the smaller sample sizes, greater imprecision is introduced with the survival estimates at those time periods and in the extrapolation. PFS data beyond follow-up time was similarly uncertain given more than 50% of patients were censored at the median PFS follow-up duration for liso-cel.
CADTH could not adequately address the limitations associated with the comparative clinical efficacy. CADTH conducted exploratory reanalyses over a plausible range of relative effectiveness and safety scenarios.
Inappropriate modelling approach. The sponsor conducted sequential analyses comparing liso-cel with axi-cel, tisa-cel, and salvage chemotherapy, where the sponsor used data from the base liso-cel population and adjusted other populations based on the MAIC output. As the sponsor’s MAICs created different patient populations for liso-cel in their “final analysis set,” the sponsor did not take the correct approach with the incorporation of liso-cel data within the model. MAICs are pairwise analyses that use the base population from the comparator trial and adjust the population from the liso-cel trial to match characteristics of the comparator trial population. The sequential analysis does not appropriately take into account the different baseline characteristics for the patient population and different treatment efficacy for liso-cel for the specific population analyzed within each MAIC.
The sponsor also incorporated a mixture-cure component within their model. While the experts noted that there is the potential that CAR T-cells may be a curative therapy, and that there may be some encouraging early signs, there is a lack of robust long-term information to validate this assumption at this time.
CADTH could not address this limitation due to the sponsor’s model structure and information included within the sponsor’s economic model.
Differences in pre-treatment efficacy assumptions associated with uncertainty. The sponsor assumed that patient prognosis differed in the pre-treatment administration phase, based on information from the trials. The pre-treatment components included the proportion of patients who died before CAR T-cell administration, the proportion of patients who failed to receive treatment due to change in clinical profile, the proportion of patients receiving out-of-specification product, and the duration of manufacturing (Table 7). Based on these assumptions, approximately 70% of patients assigned to tisa-cel and approximately 90% of patients assigned to axi-cel were assumed to receive treatment, accrue benefits, and accrue treatment costs; however approximately ||% of patients assigned to liso-cel were assumed to receive treatment and accrue benefits, but only approximately ||% were assumed to incur treatment costs due to the proportion of patients who received out-of-specification product (out-of-specification product was assumed to be paid for by the sponsor, as opposed to the public payer). Feedback from the clinical experts consulted for this review indicated that these assumed differences in pre-treatment assumptions were considered highly uncertain. The experts noted that manufacturing of tisa-cel appears to take longer than axi-cel based on real-world evidence, and time to treatment administration may have an impact on severity of the patient’s condition. Canadian experience with manufacturing and time to administration of liso-cel has not been reported.
CADTH undertook scenario analyses that assumed the same proportion of patients were treated and paid for treatment across the CAR T-cell therapies.
Utility values associated with uncertainty. The sponsor’s utility values were derived from the trial, by taking EQ-5D-5L questionnaire data from the repeated measures mixed effect analysis and transforming it to utility weights based on Canadian tariffs. As the sponsor noted, the utility value for PFS (|||||) is higher than the general population utility for a 60-year-old Canadian (0.82).1,18 As such, the utility values are viewed with substantial uncertainty. CADTH reviewed published literature, and identified health-state utility values from published studies of R/R DLBCL19,20 in the absence of information for the broader population that could represent a reasonable proxy, and better align with the expected impact of disease relative to general population utility weights.
Uncertain generalizability. The sponsor’s trial included a broader patient population than that included in the studies of the other CAR T-cell therapies. Furthermore, the SCHOLAR-1 study (used to derive efficacy of salvage chemotherapy) was in patients with DLBCL (including primary mediastinal B-cell lymphoma and DLBCL-transformed FL). As such, data from the pivotal trial have limited generalizability to the target population eligible for reimbursement. The CADTH Clinical Review Report also noted concerns regarding the generalizability of the results to current practice, as characteristics of the populations in the TRANSCEND study suggested the patient population is relatively stable and with overall better health status than would have access to CAR T-cell therapy in the Canadian setting.
CADTH could not address this limitation.
Treatment and resource use assumptions were considered uncertain. While the proportion of patients receiving bridging therapy and IV immunoglobulin (and therefore, costs associated with these components) were assumed to differ between treatments, this does not align with current Canadian clinical practice. Additionally, the clinical experts consulted by CADTH indicated that the treatments that comprised bridging therapy did not align with Canadian practice, particularly the use of rituximab monotherapy. Furthermore, substantial cost differences were observed to treat CRS, neurotoxicities and “other adverse events” for, particularly, axi-cel relative to liso-cel. Feedback from the clinical experts consulted by CADTH indicated that the large differences in cost and resource use based on the trial numbers was unlikely to align with what is observed in clinical practice as clinicians have become more used to using CAR T-cell therapies.
CADTH undertook scenario analyses assuming equal use of bridging therapy and IV immunoglobulins across the CAR T-cell therapies, though was unable to adjust for the impact this may have on survival before or post-CAR T-cell therapy administration.
CADTH undertook scenario analyses assuming alternate weightings for treatments comprising salvage chemotherapy.
CADTH undertook scenario analyses assuming alternate adverse event rate assumptions for the CAR T-cell therapies.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
Baseline age, sex, height, and weight distribution of the TRANSCEND trial population were generalizable to the Canadian patient populations. | Uncertain, but likely reasonable. |
Leukapheresis and lymphodepleting therapy are given to all patients who are infused with CAR T-cell therapy. | Reasonable. |
Utility values in pre-treatment assumed equivalent to post-progression. | Uncertain, but given short duration of application of these values and the minimal impact on the results, CADTH did not present reanalysis of this parameter. |
Patients receiving treatment outside of product specification would not accrue the CAR T-cell therapy acquisition cost but would accrue administration and AE costs. | May not be reasonable. While this may be the intent, it is pre-requisite on an agreement between the sponsor and public payers which may not be realized. |
The sponsor did not consider Pola-BR as a comparator, bridging therapy, or subsequent treatment within the submitted economic evaluation. | Pola-BR was recently given a conditional positive recommendation by CADTH for use in adult patients with relapsed or refractory diffuse large B-cell lymphoma, not otherwise specified, who are not eligible for autologous stem cell transplant and have received at least 1 prior therapy.21 While the clinical experts consulted by CADTH considered that Pola-BR may not be a direct comparator for liso-cel, it may be considered for use as a bridging therapy. |
Subsequent treatment distributions were the same between all treatments. | Reasonable. |
AE = adverse event; CAR = chimeric antigen receptor; Pola-BR = polatuzumab in combination with bendamustine and rituximab.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
Due to the limitations with the comparative effectiveness data, CADTH could not determine a base-case estimate of the cost-effectiveness of liso-cel in the modelled population.
Exploratory Analysis Results
CADTH undertook a series of exploratory analyses to assess the impact of several parameters on the results. The reanalysis details results can be found in Table 15 and Table 16, respectively. In the 1-way exploratory analyses, the ICERs for liso-cel ranged from $115,000 per QALY (based on a naive comparison) to $150,000 per QALY (based on alternate health-state utility values). However, there is limited validity in assessing the individual steps; the revisions are more appropriate to be considered in combination. In the combined analysis, the ICER for liso-cel ranged from more than $13M per QALY (equal pre-treatment assumption, equal efficacy, alternate adverse event assumptions, and revised bridging therapy assumptions) to liso-cel not being on the cost-effectiveness frontier (dominated; i.e., more costly and same or fewer QALYs as the optimal treatment, tisa-cel), based on assumptions of equal pre-treatment outcomes, equal efficacy and safety, and revised bridging therapy assumptions.
Issues for Consideration
CRS is sometimes managed with tocilizumab. CADTH-participating drug plans noted that tocilizumab is on the Canada Drug Shortages website list due to its use in COVID-19 treatment, with an anticipated resolution date of December 31, 2021. The use of siltuximab has been considered by some clinicians if there is a severe shortage, though this treatment is currently only publicly funded via the Alberta drug formulary.22 Shortage of treatments for CRS may impact CAR T-cell therapy use due to risk of CRS with CAR T-cell therapies.
Evidence for the sequential use of CAR T-cell therapies was not provided, thus the cost-effectiveness, and budget impact of sequential use of CAR T-cell therapies is unknown.
Feedback from the clinical experts consulted by CADTH indicated that immunosuppressive treatments such as pembrolizumab or nivolumab may be considered for use post-CAR T-cell failure to augment the residual effects of CAR T-cell therapy. These treatments were not included in the sponsor’s submission, and it is unclear whether there would be differential use based on the CAR T-cell therapy received.
The evidence for the effectiveness of CAR T-cell therapy is still in its early stages and evidence is emerging about the rate of complications, the duration of treatment effect, and what comprises follow-up for patients receiving CAR T-cell therapy in Canada. Furthermore, if the therapy is curative as claimed, there would be an expectation that patients with LBCL will live a longer life, and as such, will incur additional costs to the health system. This would likely lead to an increase in the ICER for liso-cel relative to salvage chemotherapy.
Travel costs for patients (and their families) and the requirement for time spent away from work was not included in the sponsor’s base case given the perspective required for submissions to CADTH. The sponsor’s implementation plan indicated that not all provinces and territories will have a site to provide liso-cel.23 For jurisdictions that do not currently have a site to provide liso-cel, there will be a need for patients to travel out-of-province or out-of-country for treatment. Travel costs were not considered in the economic submission. Furthermore, it was noted by clinical experts that some provinces do not even have capacity to assess patients’ eligibility for CAR T-cell therapy, which would result in substantive out-of-pocket costs for patients travelling out-of-province to meet the eligibility requirements. The sponsor’s implementation plan suggests that the sponsor will coordinate travel and lodging logistics for the patient and their caregiver who arrive to receive treatment and who need to remain within proximity of the qualified treatment centre for at least 4 weeks following infusion, and provide financial support to cover travel, lodging, and food costs for the patient and their caregiver during the pre-treatment and treatment period and for at least the 4 weeks when they are required to stay within close proximity of the qualified treatment centre.23 If this support program is not operationalizable and travel expenses (e.g., travel, lodging, booking, on so on) are absorbed by the patient or public payer, this would increase the expected costs of liso-cel which would result in a higher ICER estimate, or limit access to liso-cel. Disparities in funding and treatment access may vary depending on the province or territory and the requirement for access to a tertiary care centre for delivery of liso-cel may have equity of access implications, which were not substantively considered in the economic submission.
In situations where patients need to access care outside of the jurisdiction they live in (as based on recent experience), the costs associated with out-of-province or out-of-country care may be largely underestimated. This would suggest that the cost-effectiveness of CAR T-cell therapy relative to salvage chemotherapy is underestimated.
The sponsor’s implementation plan indicated the manufacturing process took, on average || days from leukapheresis to the time liso-cel is ready to be infused back into the patient.23 Issues pertaining to the manufacturing are important to the successful delivery of CAR T-cell therapies. Moreover, manufacturing failure may occur due to inadequate number of T-cells in the apheresed product, poor selection of T-cells on day 0 of manufacturing, or irreversibly impaired T-cells (i.e., no response to stimulation in culture), microbial contamination, equipment-related cell loss, high endotoxin level, and accidents. Manufacturing failure was observed in 10% to 12% of patients enrolled in the TRANSCEND study, depending on the population analyzed. The sponsor stated that, in cases of manufacturing failure, jurisdictions will not pay for the cost of the failed product.23 However, this does not account for the costs associated with increased hospital stay while a second sample is prepared, if possible and required, nor alternate treatment if initiated, nor the impact on patient outcomes due to treatment delays or compromised doses. Manufacturing failure is likely to increase ICER because patients may require creation of an additional dose of liso-cel and/or experience disease progression that needs intensive formal and informal care. CADTH noted that manufacturing failure was higher in the TRANSCEND study than was reported in the review of axi-cel.24,25
The sponsor’s implementation plan did not indicate the capacity for production of liso-cel for Canadian patients annually.23 The sponsor did not consider potential capacity constraints within the submitted economic evaluation, not just due to challenges in the process of creating the therapy but also in terms of a site being able to provide the therapy (i.e., those considered eligible for treatment would not have adverse clinical outcomes or additional costs arising from treatment delays due to capacity issues). Given the onboarding activities required before a site being eligible to treat patients with liso-cel (e.g., training and certification) and the number of planned sites, the availability of CAR T-cell therapy may be constrained by site capacity and impact the efficacy and success of administration of liso-cel.
Axi-cel and tisa-cel were reviewed by CADTH, and both treatments were given conditional positive recommendations, with substantial price reductions by CADTH’s Health Technology Expert Review Panel committee. The rationale for the price conditions were based on CADTH reanalyses indicating that a price reduction of 83% was required to achieve an ICER of $50,000 per QALY for axi-cel, and a price reduction of 65% was required to achieve an ICER of $50,000 per QALY for tisa-cel. Further, it was noted in both recommendations that these results should be interpreted with caution given the uncertainty associated with the clinical evidence.
Although the budget impact analysis assumes public drug programs will be paying for CAR T-cell therapy, it remains unclear who would be paying for this therapy. This may vary by jurisdiction.
Overall Conclusions
Evidence from the TRANSCEND trial suggests that liso-cel is associated with improvements in ORR, CRR, PFS, OS, and health-related quality of life when compared to historical outcomes for these patients. There are important limitations with these findings given the sponsor’s single-arm study design generates bias, due to an inability to control for confounding and multiplicity, imprecision in the effect estimates, and high amount of censoring. CADTH also noted that the data were not mature at last follow-up and identified some concerns regarding the generalizability of the trial population to the Canadian setting. Due to the lack of head-to-head studies comparing liso-cel with the relevant comparators, the sponsor submitted 3 unanchored MAICs as indirect evidence of the clinical efficacy of liso-cel compared with axi-cel, liso-cel with tisa-cel, and liso-cel with salvage chemotherapy. Although the sponsor-submitted MAICs indicated that liso-cel was associated with meaningful improvements in ORR, CRR, PFS and OS relative to tisa-cel and salvage chemotherapy, and no differences when compared to axi-cel, due to several identified limitations with the MAICs (e.g., residual confounding, population heterogeneity, lack of precision, generalizability), no conclusions can be drawn on the comparative clinical effectiveness of liso-cel with regards to other CAR T-cell therapies. Further, the magnitude of benefit for liso-cel relative to salvage chemotherapy is considered highly uncertain.
In addition to the aforementioned limitations with the comparative effectiveness evidence and limitations with the clinical trial data for liso-cel, CADTH identified several major limitations with the sponsor’s economic submission to CADTH that introduced further uncertainty in the cost-effectiveness assessment of liso-cel. These limitations included: the sponsor’s use of a sequential analysis to assess the relative effectiveness of liso-cel, axi-cel, tisa-cel, and salvage chemotherapy does not align with the MAIC approach which altered the liso-cel population (and therefore baseline effects of treatment) for each comparison; the use of a model structure which incorporated pre-treatment assumptions that favoured liso-cel due to fewer patients receiving treatment and assumptions regarding fewer acquisition costs; and the assumption that a proportion of patients were “cured” immediately after receiving treatment. CADTH identified additional concerns regarding the utility values used, resource use assumptions, and adverse event rates and management practices, which appeared to benefit liso-cel relative to other comparator treatments.
As such, based on the limitations identified, the ICER for liso-cel relative to salvage chemotherapy is likely higher than the sponsor’s base case. No robust evidence has been provided to suggest that liso-cel is associated with improved efficacy and safety relative to other CAR T-cell therapies used to treat large B-cell lymphomas. Feedback from the clinical experts consulted by CADTH indicated that liso-cel is likely similarly effective to other CAR T-cell therapies. As such, the assumption that liso-cel is more effective and less costly than tisa-cel and axi-cel is considered highly uncertain.
Where there are no differences in the proportion of patients treated or adverse event costs, at the submitted price of $501,900 per administration, liso-cel has a higher publicly available acquisition cost than tisa-cel ($450,000) and axi-cel ($485,021), and is considerably more costly over the modelled time horizon than salvage chemotherapy. If, despite the limited comparative effectiveness evidence available, liso-cel is considered similarly effective and safe as other CAR T-cell therapies, then liso-cel is associated with greater costs without any additional benefits, and thus would not be considered cost-effective at the submitted price.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Breyanzi (lisocabtagene maraleucel), cell suspension in patient-specific single-dose vials for intravenous infusion. Saint-Laurent (QC): Bristol Myers Squibb; 2021 Aug 24.
2.Technical report: Indirect treatment comparison of liso-cel CAR T-cell therapy and salvage chemotherapy for the third-line or later treatment of relapsed or refractory large B-cell lymphoma: Transcend NHL 001 versus SCHOLAR-1 [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Breyanzi (lisocabtagene maraleucel), cell suspension in patient-specific single-dose vials for intravenous infusion. Saint-Laurent (QC): Bristol Myers Squibb; 2020 Nov 16.
3.Technical report: Indirect treatment comparison of CAR T-cell therapies for the third-line or later treatment of relapsed or refractory large b-cell lymphoma: Liso-cel versus tisagenlecleucel and axicabtagene ciloleucel [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Breyanzi (lisocabtagene maraleucel), cell suspension in patient-specific single-dose vials for intravenous infusion. Saint-Laurent (QC): Bristol Myers Squibb; 2021 Jan 27.
4.Technical report addendums 1 and 2: Indirect treatment comparison of CAR T-cell therapies for the third-line or later treatment of relapsed or refractory large b-cell lymphoma: JCAR017 versus tisagenlecleucel and axicabtagene ciloleucel [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Breyanzi (lisocabtagene maraleucel), cell suspension in patient-specific single-dose vials for intravenous infusion. Saint-Laurent (QC): Bristol Myers Squibb; 2021 June 4.
5.Technical report addendum 1: Indirect treatment comparison of liso-cel CAR T-cell therapy and salvage chemotherapy for the third-line or later treatment of relapsed or refractory large B-cell lymphoma: Transcend NHL 001 versus SCHOLAR-1 [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Breyanzi (lisocabtagene maraleucel), cell suspension in patient-specific single-dose vials for intravenous infusion. Saint-Laurent (QC): Bristol Myers Squibb; 2021 June 7.
6.Matza LS, Cong Z, Chung K, et al. Utilities associated with subcutaneous injections and intravenous infusions for treatment of patients with bone metastases. Patient Prefer Adherence. 2013;7:855-865. PubMed
7.Canadian Institute for Health Information (CIHI). Patient Cost Estimator. 2019; https://www.cihi.ca/en/patient-cost-estimator. Accessed 2021 Nov 29.
8.Cancer Care Ontario: funded evidence-informed regimens. 2021; https://www.cancercareontario.ca/en/drugformulary/regimens. Accessed 2021 Oct 09.
9.Schedule of Benefits and Fees for Physican Services. Toronto (ON): Ontario Ministry of Health and Ontario Ministry of Long-Term Care; 2021: https://health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master20210314.pdf. Accessed 2021 Jun 10.
10.Guideline Resource Unit, Cancer Care Alberta. Lymphoma. (Clinical practice guideline LYHE-002 V16). Edmonton (AB): Alberta Health Services (AHS); 2021: https://www.albertahealthservices.ca/assets/info/hp/cancer/if-hp-cancer-guide-lyhe002-lymphoma.pdf. Accessed 2022 Feb 28.
11.Gisselbrecht C, Glass B, Mounier N, et al. Salvage regimens with autologous transplantation for relapsed large B-cell lymphoma in the rituximab era. J Clin Oncol. 2010;28(27):4184-4190. PubMed
12.Institut national d'excellence en santé et services sociaux. Review of axicabtagene ciloleucel for the treatment of relapsed or refractory large B-cell lymphoma. Quebec City (QC): INESSS; 2019: https://www.inesss.qc.ca/publications/repertoire-des-publications/publication/avis-sur-laxicabtagene-ciloleucel-pour-le-traitement-des-lymphomes-a-grandes-cellules-b-recidivants-ou-refractaires.html. Accessed 2021 Nov 29.
13.Pasquini MC, Hu ZH, Curran K, et al. Real-world evidence of tisagenlecleucel for pediatric acute lymphoblastic leukemia and non-Hodgkin lymphoma. Blood Adv. 2020;4(21):5414-5424. PubMed
14.Sermer D, Batlevi C, Palomba ML, et al. Outcomes in patients with DLBCL treated with commercial CAR T cells compared with alternate therapies. Blood Adv. 2020;4(19):4669-4678. PubMed
15.Locke FL, Ghobadi A, Jacobson CA, et al. Long-term safety and activity of axicabtagene ciloleucel in refractory large B-cell lymphoma (ZUMA-1): a single-arm, multicentre, phase 1-2 trial. Lancet Oncol. 2019;20(1):31-42. PubMed
16.Schuster SJ, Bishop MR, Tam CS, et al. Tisagenlecleucel in Adult Relapsed or Refractory Diffuse Large B-Cell Lymphoma. N Engl J Med. 2019;380(1):45-56. PubMed
17.Crump M, Neelapu SS, Farooq U, et al. Outcomes in refractory diffuse large B-cell lymphoma: results from the international SCHOLAR-1 study. Blood. 2017;130(16):1800-1808. PubMed
18.EQ-5D-5L Index Norms for Alberta Population. Calgary (AB): Health Quality Council of Alberta (HQCA); 2016: https://d10k7k7mywg42z.cloudfront.net/assets/57a3b0c2edb2f37e7700562a/HQCA_EQ_5D_AB_Norms_Report_Addendum_DRAFT___June_28.pdf. Accessed 2022 Feb 25.
19.Committee papers: axicabtagene ciloleucel for treating diffuse large B-cell lymphoma and primary mediastinal B-cell lymphoma after 2 or more systemic therapies [ID1115]. (NICE Single Technology Appraisal). London (UK): National Institute for Health and Care Excellence; 2018: https://www.nice.org.uk/guidance/ta559/evidence/appraisal-consultation-committee-papers-pdf-6661404973. Accessed 2021 Nov 29.
20.Wang XJ, Wang YH, Li SCT, et al. Cost-effectiveness and budget impact analyses of tisagenlecleucel in adult patients with relapsed or refractory diffuse large B-cell lymphoma from Singapore's private insurance payer's perspective. J Med Econ. 2021;24(1):637-653. PubMed
21.CADTH pCODR Expert Review Committee (pERC) final recommendation: polatuzumab vedotin (Polivy). Ottawa (ON): CADTH; 2021 Apr 21: https://www.cadth.ca/sites/default/files/pcodr/Reviews2021/10227PolatuzumabDLBCL_fnRec_EC21Apr2021_final.pdf. Accessed 2021 Oct 09.
22.DeltaPA. Ottawa (ON): IQVIA; 2021: https://www.iqvia.com/. Accessed 2022 Feb 28.
23.Drug Reimbursement Review sponsor submission: Breyanzi (lisocabtagene maraleucel), cell suspension in patient-specific single-dose vials for intravenous infusion [internal sponsor's package]. Saint-Laurent (QC): Bristol Myers Squibb; 2021 Aug 24.
24.Axicabtagene ciloleucel for large B-cell lymphoma: clinical report. (CADTH optimal use report vol. 9, no. 1c). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/pdf/car-t/ct0002-clinical-report-redacted.pdf. Accessed 2022 Feb 28.
25.Riedell PA, Bishop MR. Safety and efficacy of axicabtagene ciloleucel in refractory large B-cell lymphomas. Ther Adv Hematol. 2020;11:2040620720902899. PubMed
26.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Breyanzi (lisocabtagene maraleucel), cell suspension in patient-specific single-dose vials for intravenous infusion. Saint-Laurent (QC): Bristol Myers Squibb; 2021 Aug 24.
27.Chemotherapy protocol: lymphoma: cyclophosphamide-etoposide oral. Version 1.1. London (UK): NHS UK; 2015: https://www.uhs.nhs.uk/Media/SUHTExtranet/Services/Chemotherapy-SOPs/Lymphoma/Cyclophosphamide-Etoposide%20PO%20Ver%201.1.pdf. Accessed 2021 Oct 09.
28.Nastoupil LJ, Jain MD, Feng L, et al. Standard-of-Care Axicabtagene Ciloleucel for Relapsed or Refractory Large B-Cell Lymphoma: Results From the US Lymphoma CAR T Consortium. J Clin Oncol. 2020;38(27):3119-3128. PubMed
29.Table: 13-10-0111-01. Number and rates of new cases of primary cancer, by cancer type, age group and sex. Ottawa (ON): Statistics Canada; 2021: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011101. Accessed 2021 Sep 29.
30.Table: 17-10-0057-01. Projected population, by projection scenario, age and sex, as of July 1 (x 1,000). Ottawa (ON): Statistics Canada; 2020: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710005701. Accessed 2021 Sep 29.
31.Raut LS, Chakrabarti PP. Management of relapsed-refractory diffuse large B cell lymphoma. South Asian J Cancer. 2014;3(1):66-70. PubMed
32.Ellis K. Cost-effectiveness of Chimeric Antigen Receptor T-cell Therapy for Treating Large B-cell Lymphoma Patients in Canada. Waterloo (ON): UWSpace; 2020: https://uwspace.uwaterloo.ca/handle/10012/15515. Accessed 2021 Oct 18.
33.Crump M, Kuruvilla J, Couban S, et al. Randomized comparison of gemcitabine, dexamethasone, and cisplatin versus dexamethasone, cytarabine, and cisplatin chemotherapy before autologous stem-cell transplantation for relapsed and refractory aggressive lymphomas: NCIC-CTG LY.12. J Clin Oncol. 2014;32(31):3490-3496. PubMed
34.van Imhoff GW, McMillan A, Matasar MJ, et al. Ofatumumab Versus Rituximab Salvage Chemoimmunotherapy in Relapsed or Refractory Diffuse Large B-Cell Lymphoma: The ORCHARRD Study. J Clin Oncol. 2017;35(5):544-551. PubMed
35.Institut national d’excellence en santé et en services sociaux. Axicabtagene ciloleucel pour le traitement des lymphomes à grandes cellules B récidivants ou réfractaires. Annexes. Quebec City (QC): INESSS; 2019: https://www.inesss.qc.ca/fileadmin/doc/INESSS/Rapports/Therapies_cellulaires/INESSS_Yescarta-annexes_Cav.pdf. Accessed 2021 Oct 18.
36.Clinical Study Report: JCAR017-BCM-001. A phase 2, single-arm, multi-cohort, multi-center trial to determine the efficacy and safety of JCAR017 in adult subjects with aggressive B-cell non-Hodgkin lymphoma (TRANSCEND WORLD) [internal sponsor's report]. Summit (NJ): Celgene Corporation; 2020 Apr 22.
37.Abramson JS, Palomba ML, Gordon LI, et al. Lisocabtagene maraleucel for patients with relapsed or refractory large B-cell lymphomas (TRANSCEND NHL 001): a multicentre seamless design study. Lancet. 2020;396(10254):839-852. PubMed
38.Kymriah (tisagenlecleucel): 1.2 x 106 to 6.0 x 108 CAR-positive viable T cells, cell suspension in infusion bag for intravenous use [product monograph]. Dorval (QC): Novartis Pharmaceuticals Canada Inc.; 2020 Dec 24: https://pdf.hres.ca/dpd_pm/00059488.PDF. Accessed 2021 Nov 11.
39.Matching-adjusted indirect comparison (MAIC) of lisocabtagene maraleucel (liso-cel) vs axicabtageneciloleucel (axi-cel) and tisagenlecleucel in relapsed/refractory (R/R) large b-cell lymphoma (LBCL) - slides [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Breyanzi (lisocabtagene maraleucel), cell suspension in patient-specific single-dose vials for intravenous infusion. Saint-Laurent (QC): Bristol Myers Squibb; 2021 Aug 24.
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s). Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 5: CADTH Cost Comparison Table for R/R DLBCL
Treatment | Strength / concentration | Form | Price | Recommended dosage | Cost per cycle or 1-time use | Cost per 28 days |
|---|---|---|---|---|---|---|
CAR T-cell therapies | ||||||
Lisocabtagene maraleucel (Breyanzi) | Refer to dosage | Suspension for IV infusion | 501,900.0000a | 60 × 106 to 120 × 106 CAR-positive viable T-cells, consisting of separate CD4+CAR+ and CD8+CAR+ components | 501,900 | NA |
Axicabtagene ciloleucel (Yescarta) | Refer to dosage | Suspension for IV infusion | 485,021.0000b | Target of 2 × 106 anti-CD19 CAR T-cell/kg body weight (range: 1 × 106 to 2.4 × 106 cells/kg) to a maximum of 2 × 108 anti-CD19 CAR T-cell | 485,021 | NA |
Tisagenlecleucel (Kymriah) | Refer to dosage | Suspension for IV infusion | 450,000.0000b | 0.6 to 6.0 × 108 CAR-positive viable T-cells (non-weight based) | 450,000 | NA |
BR(Pola) | ||||||
Bendamustine (Treanda) | 25 mg vial | Powder for IV infusion | 312.5000 | 21- or 28- day cycles: 90 mg/m2 on days 1 and 2d | 4,375 | 4,375 to 5,833 |
Rituximab (biosimilars) | 100 mg vial | IV infusion | 297.0000c | 21- or 28- day cycles: 375 mg/m2 on day 1d | 2,079 | 2,079 to 2,772 |
Polatuzumab (polivy) | 140 mg vial | Lyophilized powder for solution | 14,750.0000e | Per 21-day cycle: 1.8 mg/kg on day 1d | 14,750 | 19,667 |
BR regimen Cost (21- or 28-day cycle) | 6,454 | 6,454 to 7,751 | ||||
Pola-BR regimen cost (21-day cycle) | 21,204 | 28,272 | ||||
Cyclophosphamide-Etoposide | ||||||
Cyclophosphamide (Procytox) | 25 mg 50 mg | Tablet | 0.3545c 0.4773c | 21-day cycles: 100 mg on days 1 through 5f | 4.77 | 6 |
Etoposide (Vepesid) | 50 mg | Capsule | 41.5875c | 21-day cycles: 100 mg on days 1 through 5f | 416 | 554 |
Cyclophosphamide-etoposide regimen cost per 21-day cycle | 421 | 561 | ||||
DHAP(R) | ||||||
Dexamethasone (generic) | 4 mg | Tablet | 0.3046c | 21- or 28-day cycles: 40 mg days 1 to 4dg | 12 | 12 to 16 |
Cytarabine (generic) | 500 mg 2000 mg | 100 mg/mL IV solution | 76.8500 306.5000 | 21- or 28-day cycles: 2000 mg/m2 every 12 hours on Day 2d | 1,230 | 1,230 to 1,639 |
Cisplatin (generic) | 50 mg vial 100 mg vial | 1 mg/mL IV solution | 135.0000 270.0000 | 21- or 28-day cycles: 100 mg/m2 on Day 1d | 540 | 540 to 720 |
Rituximab (biosimilars) | 100 mg vial | IV infusion | 297.0000c | 21- or 28-day cycles: 375 mg/m2 on day 1d | 2,079 | 2,079 to 2,772 |
DHAP regimen cost (21- or 28-day cycle) | 1,782 | 1,782 to 2,376 | ||||
R-DHAP regimen cost (21- or 28-day cycle) | 3,861 | 3,861 to 5,148 | ||||
GDP(R) | ||||||
Gemcitabine (generic) | 1,000 mg 2000 mg | Lyophilized powder | 270.0000 540.0000 | 21-day cycles: 1,000 mg/m2 Days 1 and 8d | 1,080 | 1,440 |
Dexamethasone (generics) | 4 mg tab | Tablet | 0.3046c | 21-day cycles: 40 mg days 1 to 4d | 12 | 16 |
Cisplatin (generic) | 50 mg vial 100 mg vial | 1 mg/mL solution for injection | 135.0000 270.0000 | 21-day cycles: 75 mg/m2 on Day 1d | 405 | 540 |
Rituximab (biosimilars) | 100 mg vial | IV infusion | 297.0000c | 21-day cycles: 375 mg/m2 on day 1d | 2,079 | 2,772 |
GDP regimen cost (21-day cycle) | 1,497 | 1,996 | ||||
R-GDP regimen cost (21-day cycle) | 3,576 | 4,768 | ||||
Gemcitabine monotherapy | ||||||
Gemcitabine (generic) | 1,000 mg 2000 mg | Lyophilized powder | 270.0000 540.0000 | 21- or 28-day cycles: 1,000 mg/m2 Days 1 and 8d | 1,080 | 1,080 to 1,440 |
Gemcitabine regimen cost (21- or 28- day cycle) | 1,080 | 1,080 to 1,440 | ||||
GemOx(R) | ||||||
Gemcitabine (generic) | 1,000 mg 2000 mg | Lyophilized powder | 270.0000 540.0000 | 14-day cycles: 1,000 mg/m2 on Day 1d | 540 | 1,080 |
Oxaliplatin (generic) | 100 mg 200 mg | Solution for injection | 72.54 145.08 | 14-day cycles: 100 mg/m2 on Day 1d | 145 | 290 |
Rituximab (biosimilars) | 100 mg vial | IV infusion | 297.0000c | 14-day cycles: 375 mg/m2 on day 1d | 2,079 | 4,158 |
GemOx regimen cost (14-day cycle) | 685 | 1,370 | ||||
R-GemOx regimen cost (14-day cycle) | 2,764 | 5,528 | ||||
ICE(R) | ||||||
Ifosfamide (Ifex) | 1,000 mg vial 3,000 mg vial | Powder for solution | 131.4900 403.4900 | 21-day cycles:1,667 mg/m2 on days 1 to 3d | 1,183 | 1,578 |
Carboplatin (generic) | 50 mg 150 mg 450 mg 600 mg | 10 mg/mL vial for injection | 70.0000 210.0000 600.0000 775.0020 | 21-day cycles: AUC 5 on day 1; maximum dose for AUC 5 is 750 mgd | Max: 1,050 | 1,400 |
Etoposide (generic) | 100 mg | 20 mg/mL injection | 75.0000 | 21-day cycles: 100 mg/m2 on days 1 to 3d | 450 | 600 |
Rituximab (biosimilars) | 100 mg vial | IV infusion | 297.0000c | 21-day cycles: 375 mg/m2 on day 1d | 2,079 | 2,772 |
ICE regimen cost (21-day cycle) | 2,683 | 3,578 | ||||
ICER regimen cost (21-day cycle) | 4,762 | 6,350 | ||||
PEP-C | ||||||
Procarbazine (Matulane) | 50 mg | Capsule | 56.7958c | 28-day cycles: 60 mg/m2 days 1 to 10d | 1,704 | 1,704 |
Etoposide (generic) | 100 mg | 20 mg/mL injection | 75.0000 | 28-day cycles: 140 mg/m2 days 2 and 3d | 450 | 450 |
Prednisone (generic) | 5 mg 50 mg | Tablet | 0.0220c 0.1735c | 28-day cycles: 60 mg/m2 days 1 to 10d | 5 | 5 |
Cyclophosphamide (Procytox) | 500 mg 1,000 mg | Powder for injection | 93.1400 168.8300 | 28-day cycles: 600 to 750 mg/m2 days 1 and 8d | 559 | 559 |
PEP-C regimen cost (28-day cycle) | 2,718 | 2,718 | ||||
R-CEOP | ||||||
Cyclophosphamide (Procytox) | 500 mg 1,000 mg | Powder for injection | 93.1400 168.8300 | 21-day cycles: 750 mg/m2 day 1d | 279 | 373 |
Etoposide (generics) | 100 mg | 20 mg/mL injection | 75.0000 | 21-day cycles: 50 mg/m2 on day 1d | 75 | 100 |
Etoposide (Vepesid) | 50 mg | Capsule | 41.5875c | 21-day cycles: 100 mg/m2 daily days 2 and 3d | 333 | 444 |
Vincristine (generic) | 1mg 2 mg 5 mg | 1 mg/mL injection | 30.6000 61.2000 153.0000 | 21-day cycles: 1.4 mg/m2 on day 1d | 92 | 122 |
Prednisone (generic) | 5 mg 50 mg | Tablet | 0.0220c 0.1735c | 21-day cycles: 100 mg Days 1 to 5d | 2 | 2 |
Rituximab (biosimilars) | 100 mg vial | IV infusion | 297.0000c | 21-day cycles: 375 mg/m2 on day 1d | 2,079 | 2,772 |
R-CEOP regimen cost (21-day cycle) | 2,860 | 3,813 | ||||
BR = bendamustine plus rituximab; CAR = chimeric antigen receptor; DHAP = dexamethasone plus cytarabine and cisplatin; GDP = gemcitabine plus dexamethasone and cisplatin; GemOx = gemcitabine plus oxaliplatin; ICE = ifosfamide plus carboplatin and etoposide; m = metre; mg: milligram; mL = millilitre; PEP-C = procarbazine plus etoposide, prednisone and cyclophosphamide; Pola-BR = polatuzumab plus bendamustine and rituximab; R-CEOP = cyclophosphamide plus etoposide, vincristine, prednisone, and rituximab; R-DHAP = dexamethasone plus cytarabine, cisplatin and rituximab; R-GDP = gemcitabine plus dexamethasone, cisplatin and rituximab; R-ICE = ifosfamide plus carboplatin, etoposide and rituximab; R-GemOx = gemcitabine plus oxaliplatin and rituximab; IV = IV.
Note: All prices are wholesale from IQVIA Delta PA (accessed October 2021), unless otherwise indicated, and do not include dispensing fees. Calculations assume a patient body weight of 75kg and a body surface area of 1.8 m2.
aSponsor’s submitted price.1
bCited as from the IQVIA TSA database.1,26
cOntario Drug Benefit Formulary or Exceptional Access Program list price (accessed October 2021).
dCancer Care Ontario Formulary: Regimens database.8
ePolivy CADTH pan-Canadian Oncology Drug Review Committee Final Recommendation.21
fNational Health Service (UK) regimen.27
gAssumed same as GDP regimen dosing.
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | Refer to CADTH appraisal. There are evidence gaps for the comparator treatments that were not addressed within the submission. |
Model has been adequately programmed and has sufficient face validity | No | Refer to CADTH appraisal. The model is overly complex and does not address the incorporation of data from multiple MAICs appropriately. |
Model structure is adequate for decision problem | No | Refer to CADTH appraisal. The sponsor includes a cure component without an easy medium to remove this function. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
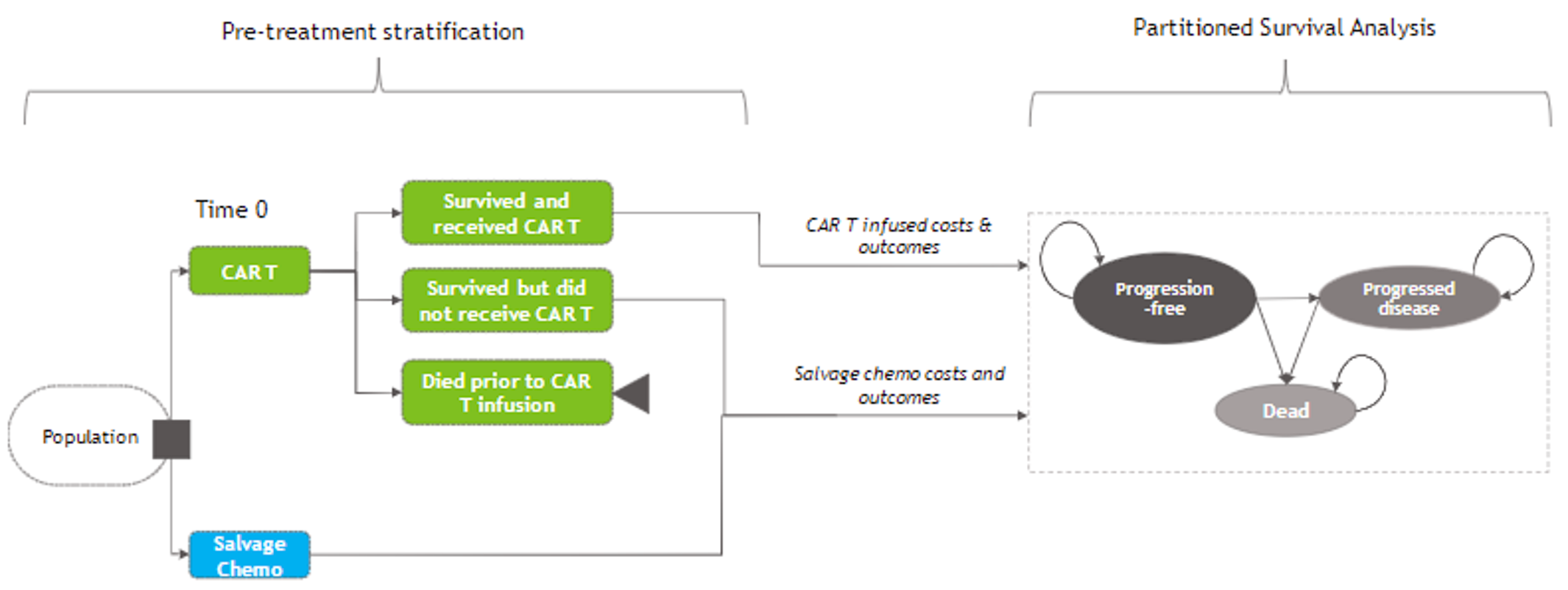
CAR t = chimeric antigen receptor T-cell; salvage chemo = salvage chemotherapy.
Source: Pharmacoeconomic submission.1
Table 7: Pre-Treatment Assumptions
Intervention | Duration of pre-treatment (days) | Patients who died pre-infusion | Patients who failed to received infusion | Patients who received treatment as planned | Patients who receive treatment off specifications |
|---|---|---|---|---|---|
Liso-cel | ||a | ||||% | ||||% | |||||% | ||||% |
Tisa-cel | 54b | 20.61% | 9.70% | 69.69% | 0.00% |
Axi-cel | 23c | 7.56% | 1.68% | 90.76% | 0.00% |
Salvage chemotherapyd | 0 | NA | N/a | 100% | NA |
axi-cel = axicabtagene ciloleucel; liso-cel = lisocabtagene maraleucel; NA = not applicable; tisa-cel = tisagenlecleucel.
aMedian time from leukapheresis to liso-cel treatment in the DLBCL leukapheresed set.
bMedian time from enrolment to infusion (range: 30 to 357 days).
cMedian duration from leukapheresis to infusion (IQR: 21 to 28 days).
dAssumptions.
Source: Sponsor’s Pharmacoeconomic Report.1
Table 8: Assumptions for CAR T-Cell Re-Treatment
Intervention | Proportion of patients re-treated with CAR T-cells | Proportion of patients receiving additional cycles of CAR T-cells | Time from first CAR T-cell infusion to re-treatment | Time from first CAR T- cell infusion to additional cycles |
|---|---|---|---|---|
Liso-cel | 6.30% | 2.59% | |||| | |||| |
Tisa-cel | 0.00%a | 0.00%a | ||||b | ||||b |
Axi-cel | 8.91% | 0.00% | ||||b | ||||b |
axi-cel = axicabtagene ciloleucel; CAR = chimeric antigen receptor; liso-cel = lisocabtagene maraleucel; tisa-cel = tisagenlecleucel.
aNo data so assumed to be 0%.
bAssumed to be the same as liso-cel.
Source: Sponsor’s Pharmacoeconomic Report.1
Table 9: Cost of Salvage Chemotherapy
Parameter Cost Item | Salvage Chemotherapy Cost per Weekly Cycle | |||
|---|---|---|---|---|
Cycle 1 | Cycle 2 | Cycle 3 | Cycle 4 | |
Drug acquisition | $1,676 | $24 | $0 | $1,571 |
Administration | $105 | $30 | $0 | $90 |
Source: Sponsor’s Pharmacoeconomic Report.1
Table 10: Annual Resource Use and Cost by Health State
Resource | Unit Cost | Progression Free | Patients in PFS for More Than 2 Years | Post-progression | |
|---|---|---|---|---|---|
CAR T-Cell | Salvage Chemotherapy | ||||
Medical oncology consultation | $157 | 8.5 | 4.0 | 2.3 | 1.7 |
Bone marrow biopsy | $1,217 | 1.0 | 1.0 | 0.0 | 0.0 |
Biochemistry | $24 | 8.5 | 4.0 | 2.3 | 1.7 |
Complete blood count | $4 | 8.5 | 4.0 | 2.3 | 1.7 |
PET/CT scan | $238 | 3.0 | 3.0 | 0.0 | 0.0 |
Total cost per year | $3,501 | $2,669 | $431 | $308 | |
CAR = chimeric antigen receptor; CT = CT; PET = PET; PFS = progression-free survival.
aIn PFS before year 2: CAR T-cell therapy frequency calculated as average of 11 visits in year 1, and 6 per year in year 2. Salvage chemotherapy frequency was calculated as an average of 4 units in year 1 and year 2.
bIn PFS for more than 2 years: CAR T-cell therapy frequency obtained as average of 4 visits in year 3, 2 visits in year 4 and 1 visit in year 5; salvage chemotherapy frequency obtained as average of 2 visits in year 3, 2 visits in year 4 and 1 visit in year 5.
cAssume one bone marrow biopsy for both CAR T-cell therapies and salvage chemotherapy.
dDerived from Lin et al. 2019, indicating that 3 PET/CT scans are recommended for CAR T-cell therapies (year 1: 3 scans, year 2: 2 to 4 scans) and salvage chemotherapy (1 after 2 to 3 cycles of chemo and 2 per year in year 1 and 2).
Source: Sponsor’s Pharmacoeconomic Report.1
Detailed Results of the Sponsor’s Base Case
Table 11: Breakdown of Clinical Outcomes in the Sponsor’s Economic Evaluation Results
Clinical benefit breakdown | Liso-cel | Tisa-cel | Axi-cel | Salvage chemotherapy |
|---|---|---|---|---|
Life-years | 7.80 | 4.81 | 7.85 | 3.81 |
Pre-treatment | 0.10 | 0.14 | 0.06 | 0.00 |
Progression free | 7.03 | 3.94 | 7.19 | 3.43 |
Post-progression | 0.66 | 0.72 | 0.60 | 0.38 |
QALYs | 6.49 | 3.96 | 6.49 | 3.17 |
Pre-treatment | 0.08 | 0.11 | 0.05 | 0.00 |
Progression free | 5.91 | 3.31 | 6.04 | 2.88 |
Post-progression | 0.51 | 0.56 | 0.46 | 0.29 |
3L+ treatment-related decrement | 0.00 | 0.00 | 0.00 | 0.00 |
Subsequent treatment-related decrement | 0.00 | 0.00 | 0.00 | 0.00 |
3L+ treatment-related AE decrement | −0.01 | −0.02 | −0.06 | 0.00 |
3L+ = third line or later; AE = adverse event; axi-cel = axicabtagene ciloleucel; HSCT = hematopoietic stem cell transplant; liso-cel = lisocabtagene maraleucel; QALY = quality-adjusted life-year; tisa-cel = tisagenlecleucel.
Source: Sponsor’s pharmacoeconomic submission.1
Table 12: Breakdown of Cost Outcomes in the Sponsor’s Economic Evaluation Results
Cost breakdown | Liso-cel | Tisa-Cel | Axi-cel | Salvage chemotherapy |
|---|---|---|---|---|
Total cost | $468,036 | $389,921 | $545,133 | $44,632 |
Pre-treatment | $4,806 | $4,728 | $3,255 | $0 |
Primary 3L+ treatment | $393,621 | $315,535 | $442,085 | $5,487 |
Subsequent treatment | $2,344 | $2,403 | $2,004 | $327 |
HSCT | $1,812 | $1,889 | $1,534 | $0 |
Treatment-related AEs | $19,338 | $21,923 | $48,965 | $4,603 |
Resource use | $17,114 | $12,875 | $18,322 | $3,140 |
End-of-life care | $29,001 | $30,568 | $28,968 | $31,076 |
AE = adverse event; axi-cel = axicabtagene ciloleucel; HSCT = hematopoietic stem cell transplant; liso-cel = lisocabtagene maraleucel; tisa-cel = tisagenlecleucel.
Source: Sponsor’s pharmacoeconomic submission.1
Table 13: Summary of the Sponsor’s Economic Evaluation Pairwise Results
Drug | Liso-cel vs. | ||
|---|---|---|---|
Tisa-cel | Axi-cel | Salvage chemotherapy | |
Incremental life-years | 2.98 | −0.06 | 3.98 |
Incremental QALYs | 2.53 | 0.002 | 3.32 |
Incremental costs | $78,114 | -$77,097 | $423,404 |
ICER (cost per life-year) | $26,176 | Less costly, less effective | $106,300 |
ICER (cost per life-year) | $30,884 | Dominant | $127,576 |
AE = adverse event; axi-cel = axicabtagene ciloleucel; HSCT = hematopoietic stem cell transplant; ICER = incremental cost-effectiveness ratio; liso-cel = lisocabtagene maraleucel; QALY = quality-adjusted life-year; tisa-cel = tisagenlecleucel.
Source: Sponsor’s pharmacoeconomic submission.1
Table 14: Summary of the Sponsor’s Economic Evaluation Sequential Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Salvage chemotherapy | 44,630 | 3.17 | Ref. |
Liso-cel | 467,972 | 6.49 | 127,679 |
Tisa-cel | 389,904 | 3.96 | Extendedly dominated through salvage chemotherapy and liso-cel |
Axi-cel | 545,067 | 6.49 | Dominated by liso-cel |
axi-cel = axicabtagene ciloleucel; ICER = incremental cost-effectiveness ratio; liso-cel = lisocabtagene maraleucel; QALY = quality-adjusted life-year; ref. = reference; tisa-cel = tisagenlecleucel.
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Not applicable.
Exploratory Analyses
CADTH undertook a series of exploratory analyses (Table 15).
Table 15: CADTH Exploratory Analyses
Exploratory analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
1. Pre-treatment: time from apheresis to infusion, proportion of patients treated, proportion of patients who died before treatment. | Based on individual trial information | Assumed all equivalent to liso-cel, with the added assumption no out-of-spec (free) product given (i.e., proportion of out-of-spec treated patients are combined with in-spec treated patients – all treated patients are costed) |
2. Clinical efficacy: PFS/OS | Based on the results for the MAICs (though liso-cel results were based on the direct trial information, unadjusted) | Based on naive comparison |
3. Clinical efficacy: PFS/OS | Based on the results for the MAICs (though liso-cel results were based on the direct trial information, unadjusted) | Assumed all equivalent to liso-cel (log-logistic distribution for both PFS and OS curves) |
4. Adverse event rates | Based on individual trial information | Alternate CRS and Neurotoxicity estimates based on Pasquini13 (tisa-cel) and Nastoupil28 (axi-cel) |
5. Adverse event rates | Based on individual trial information | Assumed all equivalent to liso-cel |
6. Health-state utility values | Trial-derived | NICE axi-cel |
7. Health-state utility values | Trial-derived | Wang et al.20 |
8. Bridging therapy | Based on individual trial information | Assumed 50% for each CAR T-cell therapy (based on clinical expert opinion) |
9. Combined analysis (1 + 3 + 4 + 8) | — | — |
10. Combined analysis (1 + 3 + 5 + 8) | — | — |
axi-cel = axicabtagene ciloleucel; CAR = chimeric antigen receptor; CRS = cytokine release syndrome; liso-cel = lisocabtagene maraleucel; MAIC = matching-adjusted indirect comparison; NICE = National Institute for Health and Care Excellence; PFS = progression-free survival; OS = overall survival; tisa-cel = tisagenlecleucel.
Table 16: Summary of the CADTH Exploratory Analysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case | Salvage chemotherapy | 44,630 | 3.17 | Ref. |
Liso-cel | 467,972 | 6.49 | 127,679 | |
CADTH Scenario analysis 1: Equal pre-treatment assumptions for CAR T-cells | Salvage chemotherapy | 44,632 | 3.17 | Ref. |
Liso-cel | 504,067 | 6.49 | 138,428 | |
CADTH Scenario analysis 2: Naive comparison | Salvage chemotherapy | 44,693 | 2.72 | Ref. |
Liso-cel | 468,018 | 6.38 | 115,771 | |
Axi-cel | 546,235 | 6.62 | 318,703 | |
CADTH Scenario analysis 3: Equal efficacy for CAR T-cells | Salvage chemotherapy | 44,691 | 2.72 | Ref. |
Liso-cel | 467,944 | 6.01 | 128,938 | |
Axi-cel | 545,609 | 6.37 | 216,256 | |
CADTH Scenario analysis 4: AEs revised with alternate sources | Salvage chemotherapy | 44,632 | 3.17 | Ref. |
Liso-cel | 468,036 | 6.49 | 127,576 | |
Axi-cel | 537,674 | 6.52 | 2,072,781 | |
CADTH Scenario analysis 5: AEs were assumed equal across CAR T-cells | Salvage chemotherapy | 44,632 | 3.17 | Ref. |
Liso-cel | 468,036 | 6.49 | 127,576 | |
Axi-cel | 517,506 | 6.54 | 979,824 | |
CADTH Scenario analysis 6: Alternate HSUVs (NICE) | Salvage chemotherapy | 44,566 | 2.89 | Ref. |
Liso-cel | 467,867 | 5.88 | 141,760 | |
Axi-cel | 543,802 | 5.89 | 6,108,577 | |
CADTH Scenario analysis 7: Alternate HSUVs (Wang et al.) | Salvage chemotherapy | 44,515 | 2.59 | Ref. |
Liso-cel | 468,154 | 5.40 | 151,117 | |
Axi-cel | 544,635 | 5.44 | 1,659,422 | |
CADTH Scenario analysis 8: Equal bridging therapy use across all CAR T-cells (50%) | Salvage chemotherapy | 44,632 | 3.17 | Ref. |
Liso-cel | 467,715 | 6.49 | 127,649 | |
CADTH Scenario analysis 9: Scenarios 1 + 3 + 4 + 8 | Salvage chemotherapy | 44,507 | 2.71 | Ref. |
Tisa-cel | 461,880 | 6.01 | 126,736 | |
Liso-cel | 503,877 | 6.01 | 13,360,090 | |
CADTH Scenario analysis 10: Scenarios 1 + 3 + 5 + 8 | Salvage chemotherapy | 44,661 | 2.72 | Ref. |
Tisa-cel | 465,896 | 6.01 | 128,000 |
AE = adverse events; axi-cel = axicabtagene ciloleucel; CAR = chimeric antigen receptor; HSUV = health-state utility value; liso-cel = lisocabtagene maraleucel; NICE = National Institute for Health and Care Excellence; tisa-cel = tisagenlecleucel.
Note: Only treatments on the cost-effectiveness frontier were included in this table – if a treatment is not on the frontier, it is dominated (i.e., more costly and no more effective than a comparator) or extendedly dominated (i.e., has an incremental cost-effectiveness ratio that is greater than that of a more effective intervention on the frontier).
Appendix 5: Submitted BIA and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 17: Summary of Key Take-Aways
Key Take-aways of the BIA |
|---|
|
Summary of Sponsor’s BIA
In the submitted budget impact analysis (BIA), the sponsor assessed the introduction of liso-cel for the treatment of adult patients with R/R LBCL who have had at least 2 prior lines of therapy. The BIA was from the perspective of a Canadian public drug payer over a 3-year time horizon using an epidemiological approach (refer to Figure 2). The sponsor included acquisition costs associated with all comparators, including wastage, markups, and dispensing fees in the base case. Data for the model were obtained from a variety of sources including Statistics Canada,29,30 the published literature,11,31-34 the INESSS report on axi-cel for DLBCL,35 and the pivotal trials of the 3 CAR T-cell products indicated for the treatment of LBCL.15,16,36,37 Key inputs to the BIA are documented in Table 18.
Key assumptions made by the sponsor include:
The results of the TRANSCEND, SCHOLAR, and ZUMA-1 trials can be directly compared and are relevant to current Canadian practice.
Liso-cel will not increase CAR T-cell capacity nor increase the number of patients receiving CAR T-cell therapy.
CAR T-cell therapy acquisition costs will come from jurisdictional drug plan budgets.
Figure 2: Sponsor’s Estimation of the Size of the Eligible Population
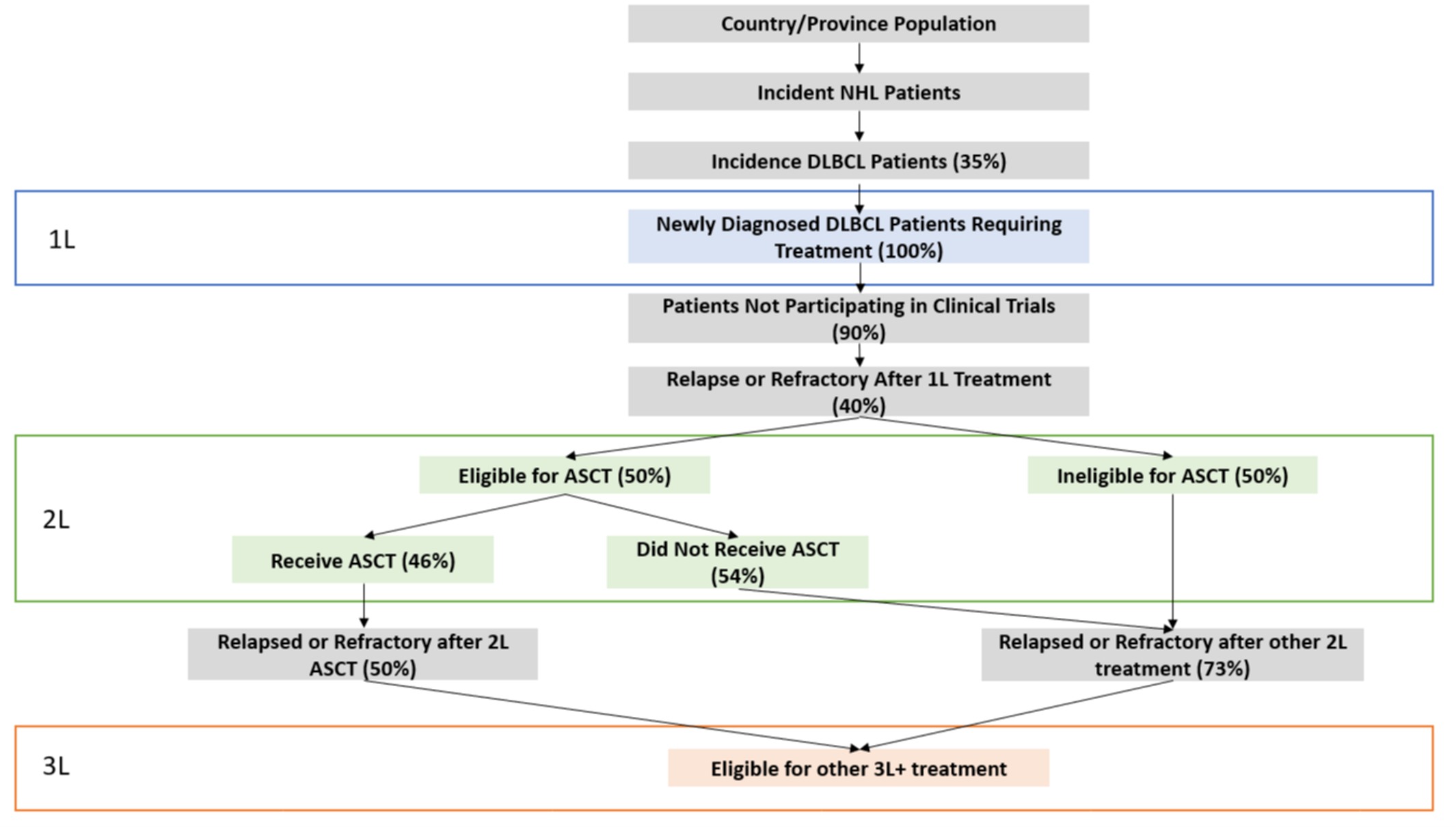
Source: Submitted Budget Impact Analysis Report, Figure 6.1.26
Table 18: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (Reported as Year 1 / Year 2 / Year 3 if appropriate) |
|---|---|
Target population | |
General population, sum of included jurisdictions in base year | 29,971,100a |
Annual incidence of diagnosed NHL per 100,000 | Varies by jurisdiction from 19.99 to 33.42b |
Percentage NHL cases that are DLBCL | 35%c |
Percentage incident DLBCL patients requiring 1L treatment | 100%d |
Percentage patients who are not participating in clinical trials | 90%e |
Percentage DLBCL patients who relapse after 1L treatment | 40%ce |
Percentage eligible for ASCT after 1L treatment | 50%ef |
Percentage eligible for ASCT who receive ASCT | 46%g |
Percentage who receive ASCT who relapse after ASCT | 50%e |
Percentage who are ineligible for ASCT or who were eligible but did not receive it who relapse after other 2L treatment | 73%e |
Number of patients eligible for drug under review | 701 / 708 / 715 |
Market uptake – reference scenario (3 years)e | |
Tisa-cel | 22.5% / 25.0% / 27.5% |
Axi-cel | 22.5% / 25.0% / 27.5% |
Salvage Chemotherapy | 55.0% / 50.0% / 45.0% |
Market uptake – new drug scenario (3 years) | |
Liso-cel | 3.0% / 10.0% / 18.0% |
Tisa-cel | 21.0% / 20.0% / 18.5% |
Axi-cel | 21.0% / 20.0% / 18.5% |
Salvage Chemotherapy | 55.0% / 50.0% / 45.0% |
Cost of treatment (per patient) | |
Liso-cel | $501,900, one time |
Bridging Chemotherapy | $635 |
Lymphodepleting Chemotherapy | $1,389 |
Tisa-cel | $450,000, one time |
Bridging Chemotherapy | $755 |
Lymphodepleting Chemotherapy | $1,132 |
Axi-cel | $485,021, one time |
Bridging Chemotherapy | $0 |
Lymphodepleting Chemotherapy | $1,474 |
Salvage Chemotherapy | $2,523 per month |
1L = first line; 2L = second line; ASCT = autologous stem cell transplant; axi-cel = axicabtagene ciloleucel; DLBCL = diffuse large B-cell lymphoma; liso-cel = lisocabtagene maraleucel; NHL = non-Hodgkin lymphoma; tisa-cel = tisagenlecleucel.
aStatistics Canada reported population projections.30
bStatistics Canada reported number and rates of new cases of primary cancer.29 plus an assumed 1% growth rate.
cRaut et al. 2014.31
dAssumption that all incident patients will receive treatment.
eINESSS report on axicabtagene ciloleucel (Yescarta) for the treatment of LBCL.35
fEllis 2020.32
gWeighted average of transplant weights across 3 DLBCL studies.11,33,34
Summary of the Sponsor’s BIA Results
Results of the sponsor’s base-case BIA suggest that the incremental expenditures associated with the reimbursement of liso-cel for the indicated population would be, when considering the drug plan perspective, $303,582 in year 1, $1,022,060 in year 2, and $1,858,105 in year 3, for a 3-year cumulative total of $3,183,747. When considering a health care system perspective, the sponsor’s base case reports a budgetary impact of $28,259 in year 1, $98,526 in year 2, and $185,179 in year 3, for a 3-year cumulative total of $311,963.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Refractory patients were not considered: The sponsor’s model considers that 40% of patients with LBCL will relapse after first-line therapy, based on Raut et al., 2014,31 who report that 30% to 40% of patients with DLBCL will relapse after initial therapy. However, this study also reports that an additional 10% of patients are refractory to first-line therapy. As the indication for liso-cel includes both R/R LBCL, refractory patients are also part of the population of interest.
CADTH reanalyses considered that 35% of patients with LBCL would relapse after first-line therapy, consistent with the 30% to 40% reported in the literature,31 and an additional 10% of patients would be refractory, for a total of 45%.
Differences in pre-treatment assumptions are associated with uncertainty. The sponsor assumed that patient prognosis differed in the pre-treatment administration phase, based on information from the trials. These components included the proportion of patients who died before CAR T-cell cell administration, the proportion of patients who failed to receive treatment due to change in clinical profile, the proportion of patients receiving out-of-specification product, the duration of manufacturing, and the proportion of patients receiving bridging therapy. Based on these assumptions, differences in the proportion of those treated, and the proportion of patients whose treatment was paid for by sponsor’s (as out-of-specification treatment was assumed to be provided for free) was assumed to differ between CAR T-cell therapies. Feedback from the clinical experts consulted for this review indicated that differences in these assumptions were considered highly uncertain, with the caveat that manufacturing of tisa-cel appears to take longer than axi-cel.
CADTH reanalyses assumed the same proportion of patients were treated across the CAR T-cell therapies, using the sponsor’s values for liso-cel, while 50% of patients receiving any CAR T-cell therapy was assumed to receive bridging therapy, and no patient received out-of-specification product. A scenario analysis was conducted where all 3 CAR T-cell products were assumed to have the proportion of out-of-specification product assumed by the sponsor for liso-cel, where such patients would not accrue CAR T-cell acquisition costs.
Individual trials may not reflect current real-world AE rates: AE rates in the economic model and BIA were derived from the sponsor’s MAIC39 and these rates differed substantially between individual trials. However, as none of the trials were comparative and clinical understanding of how to manage patients receiving CAR T-cell therapy has improved over time, AE rates in earlier trials are likely overestimated relative to current Canadian clinical practice, especially regarding CRS and neurotoxicity.
CADTH reanalyses explored the impact of adjusting CRS and neurotoxicity rates for tisa-cel and axi-cel to match those reported in 2 recent large-scale non-interventional studies, Pasquini et al., 202013 and Nastoupil et al., 2020,28 respectively. A scenario analysis was also conducted assuming all CAR T-cell-associated AEs were equal to those used by the sponsor for liso-cel.
CADTH Reanalyses of the BIA
Due to limitations in the sponsor’s economic and budget impact models, CADTH was unable to determine a base-case analysis. Instead, CADTH conducted a series of reanalyses including: increasing the number of patients who will access CAR T-cell therapy by receiving liso-cel by 20% with the introduction of liso-cel, including refractory patients in those eligible for CAR T-cell therapy, assuming all CAR T-cell therapies have pre-treatment inputs equivalent to liso-cel, and adjusting the probability of patients experiencing CRS or neurotoxicity when receiving tisa-cel and axi-cel to match newer source data. These individual reanalyses were then combined, refer to Table 19.
Table 19: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
ODB dispensing fee for oral medications | $9.93 per claim | $8.83 per claim |
Changes to derive the CADTH combined reanalysis | ||
1. Adding refractory patients | 40% of patients assumed to have relapsed LBCL | 45% of patients assumed to have relapsed or refractory LBCL |
2. Pre-treatment: time from apheresis to infusion, proportion of patients treated, proportion of patients who died before treatment. | Based on individual trial information. | All CAR T-cell therapies assumed equivalent to liso-cel, and 50% of all CAR T-cell therapy patients received bridging therapy. No patients received out-of-specification product. |
3. AEs revised with alternate source | Based on sponsor’s MAIC | Axi-cel based on Nastoupil 2020a Tisa-cel based on Pasquini 2020b |
AE = adverse event; axi-cel = axicabtagene ciloleucel; CAR = chimeric antigen receptor; CRS = cytokine release syndrome; LBCL = large B-cell lymphoma; liso-cel = lisocabtagene maraleucel; MAIC = matching-adjusted indirect comparison; ODB = Ontario Drug Benefit; tisa-cel = tisagenlecleucel.
aNastoupil et al., 2020.28
bPasquini et al., 2020.13
The results of the CADTH step-wise reanalyses are presented in summary format in Table 20 and a more detailed breakdown is presented in Table 21. When combined, these changes resulted in a 3-year budget impact of $6,878,682 when considering the drug plan perspective, or $4,366,522 when considering the health care payer perspective.
Table 20: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total (Drug plan perspective) | Three-year total (Health care perspective) |
|---|---|---|
Submitted base case | $3,183,747 | $311,963 |
Corrected submitted base case | $3,183,875 | $312,105 |
CADTH reanalysis 1 – refractory patients added | $3,581,859 | $351,118 |
CADTH reanalysis 2 – same pre-treatment for all CAR T-cell therapies | $6,067,026 | $2,856,795 |
CADTH reanalysis 3 – AEs from alternate sources | $3,229,795 | $1,331,844 |
CADTH combined reanalysis 1 through 3 | $6,878,682 | $4,366,522 |
AE = adverse event; BIA = budget impact analysis; CAR = chimeric antigen receptor.
Note: The budgetary impact of the combined analysis is less than that of reanalysis 1 as the increased number of patients resulting from reanalysis 2 brings the reference scenario closer to the maximum CAR T-cell treatment capacity, and thus fewer additional patients can be treated in the new drug scenario. For the budgetary impact of removing this constraint on maximum capacity, refer to scenario A in Table 21.
CADTH also conducted additional scenario analyses to explore areas of uncertainty, including assuming 10% more patients access CAR T-cell therapy due to the availability of liso-cel as an additional CAR T-cell product, assuming all CAR T-cell therapies are associated with AEs as those receiving liso-cel are, and assuming the 7.25% of patients receiving any CAR T-cell therapy receive out-of-specification product and thus do not accrue CAR T-cell product acquisition costs. Refer to Table 21.
Table 21: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Drug Plan Perspective | ||||||
Submitted base case | Reference | $122,990,315 | $124,220,218 | $138,898,198 | $153,857,315 | $416,975,731 |
New drug | $122,990,315 | $124,523,800 | $139,920,258 | $155,715,420 | $420,159,478 | |
Budget impact | $0 | $303,582 | $1,022,060 | $1,858,105 | $3,183,747 | |
CADTH combined reanalysis | Reference | $95,280,667 | $145,854,272 | $163,114,431 | $180,705,207 | $489,673,910 |
New drug | $95,280,667 | $146,510,180 | $165,322,654 | $184,719,758 | $496,552,592 | |
Budget impact | $0 | $655,908 | $2,208,224 | $4,014,550 | $6,878,682 | |
CADTH scenario A: 10% increase in CAR T-cell (liso-cel) use | Reference | $95,280,667 | $145,854,272 | $163,114,431 | $180,705,207 | $489,673,910 |
New drug | $95,280,667 | $153,402,944 | $177,491,409 | $197,122,422 | $528,016,776 | |
Budget impact | $0 | $7,548,672 | $14,376,978 | $16,417,215 | $38,342,866 | |
CADTH scenario B: AEs set equal to liso-cel | Reference | $144,038,920 | $145,479,310 | $162,693,640 | $180,237,708 | $488,410,658 |
New drug | $144,038,920 | $146,160,215 | $164,986,021 | $184,405,258 | $495,551,495 | |
Budget impact | $0 | $680,905 | $2,292,382 | $4,167,550 | $7,140,837 | |
CADTH scenario C: 7.25% out-of-spec product for all CAR T-cell therapies | Reference | $134,391,927 | $135,735,846 | $151,759,309 | $168,089,667 | $455,584,822 |
New drug | $134,391,927 | $136,341,571 | $153,798,583 | $171,797,067 | $461,937,222 | |
Budget impact | $0 | $605,725 | $2,039,274 | $3,707,401 | $6,352,400 | |
Health care System Perspective | ||||||
Submitted base case | Reference | $142,399,022 | $144,296,330 | $160,900,226 | $177,815,903 | $483,012,458 |
New drug | $142,399,022 | $144,324,588 | $160,998,751 | $178,001,081 | $483,324,421 | |
Budget impact | $0 | $28,259 | $98,526 | $185,179 | $311,963 | |
CADTH combined reanalysis | Reference | $110,576,369 | $167,116,246 | $186,448,583 | $206,096,690 | $559,661,519 |
New drug | $110,576,369 | $167,531,085 | $187,848,700 | $208,648,256 | $564,028,041 | |
Budget impact | $0 | $414,838 | $1,400,117 | $2,551,566 | $4,366,522 | |
CADTH scenario A: 10% increase in CAR T-cell (liso-cel) use | Reference | $110,576,369 | $167,116,246 | $186,448,583 | $206,096,690 | $559,661,519 |
New drug | $110,576,369 | $174,741,006 | $200,862,819 | $221,913,653 | $597,517,478 | |
Budget impact | $0 | $7,624,760 | $14,414,236 | $15,816,963 | $37,855,959 | |
CADTH scenario B: AEs set equal to liso-cel | Reference | $160,974,255 | $163,116,322 | $181,894,076 | $201,022,998 | $546,033,396 |
New drug | $160,974,255 | $163,802,984 | $184,209,332 | $205,238,286 | $553,250,602 | |
Budget impact | $0 | $686,662 | $2,315,256 | $4,215,288 | $7,217,206 | |
CADTH scenario E: 7.25% out-of-spec product for all CAR T-cell therapies | Reference | $155,210,043 | $157,298,663 | $175,365,792 | $193,770,553 | $526,435,009 |
New drug | $155,210,043 | $157,660,083 | $176,586,113 | $195,995,332 | $530,241,529 | |
Budget impact | $0 | $361,420 | $1,220,321 | $2,224,779 | $3,806,520 | |
AE = adverse event; BIA = budget impact analysis; CAR = chimeric antigen receptor; liso-cel = lisocabtagene maraleucel.
Ethics Review
Abbreviations
CAR
chimeric antigen receptor
DLBCL
diffuse large B-cell lymphoma
LBCL
large B-cell lymphoma
NHL
non-Hodgkin lymphoma
Summary
The literature on ethical issues related to large B-cell lymphoma (LBCL) and chimeric antigen receptor (CAR) T-cell therapies was reviewed to identify ethical considerations in the context of lisocabtagene maraleucel for the treatment of relapsed or refractory LBCL.
Ethical issues identified in the context of LBCL include disparities in incidence, treatment, and outcomes of patients with LBCL, especially as they impact patients who are racialized, marginalized, or have lower socioeconomic status; disparities in clinical trial access; and considerations relevant to clinical care for LBCL, including issues related to patient-physician relationships.
Ethical issues identified in the context of CAR T-cell therapies relate to barriers to access for CAR T-cell therapies, including those based on costs, geography, and patient selection. Resource allocation considerations identified relate to access and fair patient prioritization processes, opportunities to expand access, and implications for health systems.
Balancing the risks and benefits of novel CAR T-cell therapies highlights the importance of informed consent and balanced communication between clinicians and patients, as well as mitigating “hype” or the inflation of positive outcomes over potential harms.
Objective(s)
To identify and describe ethical considerations raised in the literature associated with the use of lisocabtagene maraleucel for the treatment of adult patients with relapsed or refractory LBCL including diffuse LBCL (DLBCL) not otherwise specified (including DLBCL arising from indolent lymphoma), high-grade B-cell lymphoma, primary mediastinal LBCL, and follicular lymphoma grade 3B after at least 2 prior therapies.
Research Question
What are the ethical considerations raised in the published literature relevant to the use of lisocabtagene maraleucel for the treatment of adult patients with relapsed or refractory LBCL, including DLBCL not otherwise specified (including DLBCL arising from indolent lymphoma), high-grade B-cell lymphoma, primary mediastinal LBCL, and follicular lymphoma grade 3B after at least 2 prior therapies?
Methods
Data Collection: Review of Empirical and Normative Ethics Literature
A review of the empirical (i.e., focused on explaining “what is” through observation) and normative (i.e., focused on explaining “what ought to be” through argumentation) literature relevant to ethical considerations in the context of the use of lisocabtagene maraleucel was conducted. This included a review of the literature relevant to ethical issues in the conditions that lisocabtagene maraleucel is aimed at treating (i.e., LBCL) and the literature relevant to ethical considerations in the use of lisocabtagene maraleucel as a CAR T-cell therapy.
Literature Search Methods
A literature search was conducted by an information specialist on key resources including MEDLINE All (1946–) via Ovid, Philosopher’s Index via Ovid, the Cumulative Index to Nursing and Allied Health Literature (CINAHL) via EBSCO, and Scopus. Duplicates were removed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were Breyanzi (lisocabtagene maraleucel), LBCL, or CAR T-cell.
CADTH-developed search filters were applied to limit retrieval to citations related to empirical and normative ethical considerations. Retrieval was not limited by study design or publication date but was limited to the English language. The initial search was completed on August 23, 2021.
Grey literature (literature that is not commercially published) was identified by searching sources listed in the ethics section of the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.1 The grey literature search for ethical considerations was conducted on August 31, 2021. The main search concepts were Breyanzi (lisocabtagene maraleucel), LBCL, or CAR T-cell. Search results were not limited by publication date but were limited to the English language. Google was used to search for additional internet-based materials. These searches were supplemented by reviewing bibliographies of key papers, as appropriate.
Literature Screening and Selection
The selection criteria for eligible publications can be found in Table 1.
Criteria | Description |
|---|---|
Population(s) | Adult patients with relapsed or refractory large B-cell lymphoma including diffuse large B-cell lymphoma not otherwise specified, high-grade B-cell lymphoma, primary mediastinal large B-cell lymphoma, and follicular lymphoma grade 3B after at least 2 prior therapies |
Intervention(s) | Lisocabtagene maraleucel or other chimeric antigen receptor T-cell therapies, or drug regimens |
Context/setting | Any health system |
Outcome(s) | Normative literature: provides normative analysis of an ethical consideration (e.g., “what ought to be” through argumentation) Empirical literature: provides empirical research directly addressing an ethical issue (e.g., “what is” through observation) |
The selection of relevant literature proceeded in 2 stages. In the first stage, the titles and abstracts of citations were screened for relevance by a single reviewer. Articles were categorized as “retrieve” or “do not retrieve” according to the selection criteria outlined in Table 1, and the following criteria:
Explicitly provides normative analysis of ethical considerations arising in the use of lisocabtagene maraleucel or CAR T-cell therapies more broadly, or of ethical considerations related to the incidence, treatment, or outcomes of adults with LBCL
Presents empirical research addressing ethical considerations arising in the use of lisocabtagene maraleucel or CAR T-cell therapies more broadly, or related to ethical considerations in the incidence, treatment, or outcomes of adults with LBCL
Explicitly identifies, but does not investigate empirically, ethical considerations arising from the use of lisocabtagene maraleucel or CAR T-cell therapies more broadly, or ethical considerations related to the incidence, treatment, and outcomes of adults with LBCL.
In the second stage, the full-text reports categorized as “retrieve” were reviewed by the same reviewer. Reports meeting the above criteria were included in the review, and reports that did not meet these criteria were excluded. Members of the CADTH review team were consulted to resolve uncertainties related to eligibility of full-text reports. As a parallel process, grey literature was reviewed, and relevant sources were retrieved and reviewed following the selection criteria listed previously
Data Extraction
One reviewer extracted basic details on publications using a data extraction form. The following publication details were recorded: first author, article title, publication objectives, characteristics of study design and methodology, date of publication, country of affiliation, funding source, and key findings identified related to ethical considerations.
Data Summary
The same reviewer conducted 2 cycles of coding to abstract, identify, and synthesize relevant ethical issues in the literature. In the initial coding phase, the publications were reviewed for ethical content, and ethically relevant claims made in the literature were noted and grouped according to theme. The Core Model 3.0 (Ethical Analysis Domain)2 questions deemed by the European Network for Health Technology Assessment (EUnetHTA) as “critically important” were used as a guide to identify and categorize ethical considerations related to the use of lisocabtagene maraleucel and ethical issues related to large B-cell lymphoma incidence, treatment, and outcomes. The Core Model was chosen because it is a wide-ranging framework; the assessment questions in the domain are intended especially for identifying ethically relevant issues and conflicts.2 This guiding framework highlights the context of a technology and focuses on the following topics: benefit–harm balance, autonomy, respect for persons, justice and equity, legislation, and ethical consequences of the health technology assessment.
Once identified, passages or claims related to ethical content were coded using methods of qualitative description.3 Initial descriptive coding of the reports focused broadly on categories concerning what ethical considerations were described. Major themes and subcodes were identified through repeated readings of the data.3 Once subcodes emerged, they were deductively applied to all reports in the set and ethical content was summarized into the thematic categories. This review focused on ethical considerations relating specifically to the use of lisocabtagene maraleucel and related ethical issues deriving from LBCL incidence, treatment, and outcomes. Other ethical considerations raised in the literature, but not related to the use of lisocabtagene maraleucel in the treatment of LBCL, were outside of the scope of the current review and are not included in the summary.
Results
Description of Included Publications
A total of 1,822 citations were identified in the search of the published literature. Following screening of titles and abstracts, 1,719 citations were excluded and 103 potentially relevant publications from the electronic search were retrieved for full-text review. In addition, 4 potentially relevant reports were retrieved from other sources, including the grey literature search. Of the potentially relevant publications, 46 publications were excluded for various reasons (e.g., they did not make any ethical claims [N = 30]; their ethical claims were not specific to the use of CAR T cells as a therapy [N = 12]; they were only available as an abstract [N = 2]; or they presented on a brief mention of an already included publication [N = 2]). Sixty-one publications met the inclusion criteria and were included in this report. Figure 1 presents the flow diagram for inclusion and exclusion of publications of the study selection process.
Details regarding the characteristics of included publications are reported in Table 2. None of the included publications reported directly on ethical considerations in the use of lisocabtagene maraleucel for the treatment of adults with relapsed or refractory LBCL. A total of 27 publications examined ethical issues related to patients with LBCL, including disparities in the incidence, treatment, and outcomes of patients with LBCL, disparities with regards to clinical trials inclusion, and patient experiences with LBCL. Thirty-four publications examined ethical considerations related to the use of CAR T-cell technologies, including patient access issues, resource allocation considerations, and considerations related to balancing risks and benefits of CAR T-cell therapies.
Key Ethics Considerations From the Literature
To examine the ethical issues relevant to the use of lisocabtagene maraleucel for the treatment of relapsed or refractory LBCL, it is relevant to examine the literatures on both LBCL and on CAR T-cell therapies. Ethical issues raised in relation to LBCL include discussions of disparities in incidence, treatment, and outcomes of LBCLs, especially as they impact marginalized and lower socioeconomic groups; disparities in clinical trial access; and considerations relevant to the organization of clinical care of LBCL, including issues related to patient-physician relationships. Ethical issues related to CAR T-cell therapies are centred around barriers to access for CAR T-cell therapies, including those based on cost, geography, and patient selection. Also relevant are considerations related to resource allocation, balancing risks and benefits, and informed consent.
Ethical Issues in LBCL
The literature on LBCL raises several ethical issues, both explicitly and implicitly, related to disparities in incidence, treatment, and outcomes for patients with LBCL, demonstrating how LBCL may affect different groups differently. Literature on LBCL clinical trials also shows how certain groups have lacked access to trials, and the implications of this for understanding and treatment of LBCL. Finally, the literature on clinical care and LBCL explores disease experience and the implications of this for informing and treating patients with LBCL.
Disparities in Incidence
Significant disparities have been noted in the incidence of LBCL and associated lymphomas, including non-Hodgkin lymphoma (NHL) and DLBCL. The incidence of these lymphomas has been more prevalent in certain racialized groups, especially Black communities in the US, who have faced a greater disease burden than White populations related to these lymphomas.4-9 It has, however, been noted that incidence rates may be decreasing among this patient group.10 Black patients with DLBCL tend to present at a younger age, with more advanced stage, and have inferior survival.8 Some reports have attributed these disparities to behaviours, exposures to environmental risks, and socioeconomic determinants.4,7,9 Disparities in incidence are also reported based on location,11,12 and authors have suggested that environmental exposures in urban areas may disproportionately affect Hispanic people and non-Hispanic Black people with regards to DLBCL incidence.11
Disparities in Treatment and Outcomes
Disparities in treatment, or access to treatment, for LBCL have also disproportionately affected many of the same groups indicated above. Studies have found that women and White patients had significantly longer survival outcomes compared to other racialized groups.7,8,13-15 As well, those with higher socioeconomic status face superior treatment and survival outcomes.5,10,12,15 These disparities persist in older patients, where racial disparities in the receipt of treatment and survival exist for older Black patients.16,17 In addition, despite recent decreases in incidence of NHL and DLBCL in Black patients in the US, outcomes have remained inferior in terms of survival.9,10,18 Living in more socioeconomically deprived areas has been associated with an emergency route to diagnosis, leading to worse treatment outcomes,19 and substantially worse survival from DLBCL,20 indicating neighbourhood-based barriers for effective access to treatment among socioeconomically disadvantaged patients. Authors have also noted disparities found in treatment and outcomes based on treatment centre type or location, with those receiving treatment at a teaching or research facility being more likely to receive chemoimmunotherapies for DLBCL5; receipt of optimal treatment being less likely for those being treated in a non-metropolitan hospital21; and those who receive treatment in a regional teaching hospital being more likely to adhere to treatment plans.22
Some hypothesized rationales for disparities in treatment and outcomes include differential access to health care, challenges with patient-physician relationships, and socioeconomic status.7,10,15 In particular, authors suggest that states of extreme poverty can make compliance with medical care for NHL and DLBCL difficult.23 Notably, these disparities in access to treatment can reflect obstacles or barriers to receiving health care services,9,17,23,24 indicating that minority populations may require more assistance and navigation of treatment for LBCL to mitigate disparities.24 Similar findings have been indicated in elderly patients with DLBCL, where improvement in outcomes depends on social and financial supports to comply with scheduled treatments.25
Disparities in Clinical Trial Access
Authors have also reported disparities in access to clinical trials for DLBCL in the US, specifically where Black patients tend to be poorly represented in these trials.4 Younger adults are also poorly represented in lymphoma clinical trials, and knowledge of age-specific outcomes, toxicities, and the development of care models are minimal for this population.26 Similarly, elderly patients, as well as patients who are people of colour, tend to be under-represented in phase III lymphoma trials in the US, meaning that trial results may not be applicable to them.27
Clinical Care and LBCL
Patients’ experiences with LBCL, falling in the domain of clinical ethics, include considerations related to how patients navigate their own illness experiences and their interactions with clinicians. Authors reports that patients with advanced B-cell lymphomas may underestimate the severity of their illness, despite having these discussions with their medical teams.28 In addition, these patients tend not to document their care preferences or participate in Advanced Care Planning.28 Learning about B-cell lymphoma has been found to be difficult for patients, and there is a need to expand the availability and accessibility of patient information.29 Similarly, experiences of living with B-cell NHL differ between patients, and educational materials aimed at these patients should reflect a diversity of lived experiences.29 Authors have also suggested that the COVID-19 pandemic has brought unique psychosocial impacts for patients with lymphoma, and highlighted the importance of screening these patients for emotional and distress conditions.30
Ethical Issues in CAR T-Cell Therapies
Alongside ethical issues described in the incidence, treatment, outcomes, and clinical care for those with LBCL, ethical issues reported in other CAR T-cell therapies are relevant to the consideration of lisocabtagene maraleucel. The literature on ethical considerations in the use of CAR T-cell therapies relates to a range of issues from barriers to access for CAR T-cell therapies, resource allocation considerations, risks and burdens of CAR T-cell therapies to patients, and implications for informed consent.
Access to CAR T-Cell Therapies
There are several barriers to access for CAR T-cell therapies for certain groups of patients. Cost considerations related to CAR T-cell therapy access are most prominent in the literature, where access to CAR T-cell therapies is restricted to those who can afford it within non-Canadian health care systems.31-36 Yet, some authors have argued that the full costs of CAR T-cell therapies may be unknown to patients, providers, or payers and have argued for full transparency around total costs of CAR T-cell therapies, including costs associated with pre- and post-infusions, treatment for severe side effects, and other clinical costs.37
Alongside monetary barriers for CAR T-cell therapies themselves, access has also been hindered by the limited capacity of hospitals and manufacturers to provide opportunities for receipt of CAR T-cell therapies. Geographical access barriers thus exist, where those who do not reside in close proximity to centres that offer CAR T-cell therapy face difficulties accessing these therapies.36 Significant costs incurred by provider organizations (hospitals and other care clinics) in delivering CAR T-cell therapies have also been shown to be barriers to access and limited treatment availabilities.31,38 The costs incurred by hospitals who deliver CAR T-cell therapy, especially where these might not be reimbursed, can limit the number of hospitals willing to undertake these procedures, thereby further limiting availability and access.39
The evaluation and selection of patients eligible for CAR T-cell therapy involves access challenges in clinical settings,40 where access barriers can be identified at the patient referral and selection time point.41 There are finite time points where patients can benefit most from the administration of CAR T-cell therapies, where they must be sick enough to be eligible (i.e., relapsed or refractory), but not sick enough to be precluded.42 The value of CAR T-cell therapies to patients can be lost with treatment delays or manufacture time.42,43
Direct patient costs and resource challenges also create access barriers for certain groups. Access to caregivers, or lack thereof, is a significant barrier for patients undergoing CAR T-cell therapies.41 Other out-of-pocket costs, including transportation and lodging at therapeutic sites, may cause additional access barriers for some patients, especially where distance to the treatment centre is significant.41,44,45 Patients with DLBCL often face long travel times to academic hospitals that administer CAR T-cell therapies, and this travel burden impacts access to care.46,47 Patients living in rural areas and those living below the poverty line tend to be disadvantaged with regard to access to CAR T-cell therapy.46
Access and Resource Allocation
The limited availability of treatment sites for CAR T-cell therapies implies important resource allocation considerations,48 and authors have argued that equity should be considered as a factor in these resource allocation considerations, and not just costs and benefits.49 Overall, authors point to a need for fair priority setting and allocation for CAR T-cell therapies,50 where patients are entitled to a fair selection process.51 Patient prioritization and selection criteria may be increasingly challenging during the COVID-19 pandemic,52,53 especially where the availability of personnel and resources may be limited and safety considerations may be enhanced.53
Suggestions for expanding access to care have included offering CAR T-cell therapies in outpatient settings to address sociodemographic and socioeconomic disparities and equity, especially related to patient travel costs.41,48 It has been suggested that manufacturers may also have a role in increasing access by shortening the production time of CAR T cells, and working to scale up more rapid manufacturing methods.41 Many, however, have argued that increased access to CAR T-cell therapies through the implementation of more availability and more therapeutic sites also needs to be balanced with safety of these treatment locations and quality control.34,36,37,39,41,44,54,55 Clinical sites thus may have a role in developing infrastructure to deliver CAR T-cell therapies at scale and diminish access inequities,56 though need to do so in a way where access benefits are balanced with an ability to minimize potential harms.
Resource allocation decisions also exist at a policy or systems level, where the high costs of adopting CAR T-cell therapies can impact the sustainability of health systems.34,37,44,57 The manufacture of CAR T-cell therapies is resource intensive, and this poses challenges for their introduction into health systems,58 especially where pre- and post-care may be insufficiently reimbursed.39,57 As health systems have finite resources, they must make decisions about how to fairly and justly allocate funds and distribute the risks and benefits of innovations.49 As CAR T-cell therapies become applied to more cancer subtypes, there will be a need to consider how to manage health system costs.49 Though, some have argued that costs of CAR T-cell therapies could decrease over time, thereby improving access.57
Balancing Risks and Benefits, and Informed Consent
Due to the novelty of CAR T-cell therapies, unknown safety and risks have been positioned as an ethical issue.34,51,59,60 To assess the ethical legitimacy of CAR T-cell therapy, there is a need to weigh the therapeutic risks and benefits, though there is no expert consensus on what an ethically justifiable balance of risks and benefits would be in this context.50 There is particular uncertainty in terms of the long-term harms and benefits of these therapies, where current clinical trial data do not provide clinical insights on long-term outcomes.61-63 Patients who receive CAR T-cell therapies may also experience psychosocial burdens and may require community supports.45,50
Authors have noted that CAR T-cell therapies may be considered a treatment of “last resort,”62 and that many patients who feel they lack alternative therapeutic options may be willing to undergo CAR T-cell treatments that bear risks of harm.44 For clinicians, this highlights the importance of informed consent and open communication about the risk–benefit profile of these therapies.35,44 Physicians should engage in informed discussions with patients about whether they are appropriate candidates for CAR T-cell therapies and weigh benefits and harms collectively.64
While benefits, risks, and potential side effects of CAR T-cell therapies have been discussed widely in the clinical literature, the role of the media and their portrayal of CAR T-cell risks and benefits has also been explored.37,64 This literature has shown how the media may have a role in inflating the positive outcomes of cancer immunotherapies such as CAR T-cell therapies,37 when only a few patients have access to and benefit from these therapies, and overlooking the harms.64 The media may not be the only source of overstating benefits or “hype” of CAR T-cell therapies, and it has been suggested that clinical and research communities as well as industry have also favoured benefits over risks in their discussions of CAR T-cell therapies.34,35,37,50 Balanced communication from clinicians about the benefits and risks of CAR T-cell therapies can serve to mitigate these forms of “hype.”34,37
Limitations
This review is limited by the lack of published literature examining ethical considerations directly relevant to the use of lisocabtagene maraleucel for the treatment of adult patients with LBCL. No published ethical analyses were retrieved specifically on the topic of lisocabtagene maraleucel. The absence of directly applied published ethical analyses does not indicate that ethical considerations are not present. Many of the ethical issues associated with the incidence and treatment of LBCL, including the potential for disparities, and many ethical issues associated with the use of CAR T-cell therapies, including access and resource allocation challenges, are likely of relevance to lisocabtagene maraleucel as well.
Finally, this review is limited to ethical considerations explicitly discussed in the published literature, and lacked ethical insights that might be derived from primary research, stakeholder engagement, or primary normative analysis. Some of the results and insights raised relating to clinical effectiveness, safety, and costs might be discussed more comprehensively in the clinical and pharmacoeconomic review sections, and these sections may hold implicit ethical implications.
Conclusion
Normative and empirical literatures relevant to ethical considerations in the use of lisocabtagene maraleucel for the treatment of adult patients with relapsed or refractory LBCL were reviewed. Ethical considerations raised in the context of LBCL indicate disparities in incidence, treatment, and outcomes of LBCL patients, as well as disparities in clinical trial access and challenges related to patient navigation of their illness experiences. In the context of CAR T-cell therapies, ethical issues identified relate to access barriers and disadvantages for certain patients based on treatment costs (direct and indirect), geography, and patient selection criteria. Resource allocation considerations have identified the need for fair priority setting and allocation of CAR T-cell therapies, expanding access to CAR T-cell therapies through more therapeutic sites while also balancing safety and quality considerations, and considerations for health systems adopting CAR T-cell therapies. Finally, the literature has highlighted a need to weigh therapeutic risks and benefits, and for balanced communication between physicians and patients about these risks and benefits, as well as mitigating “hype” or the overinflation of positive outcomes over potential harms.
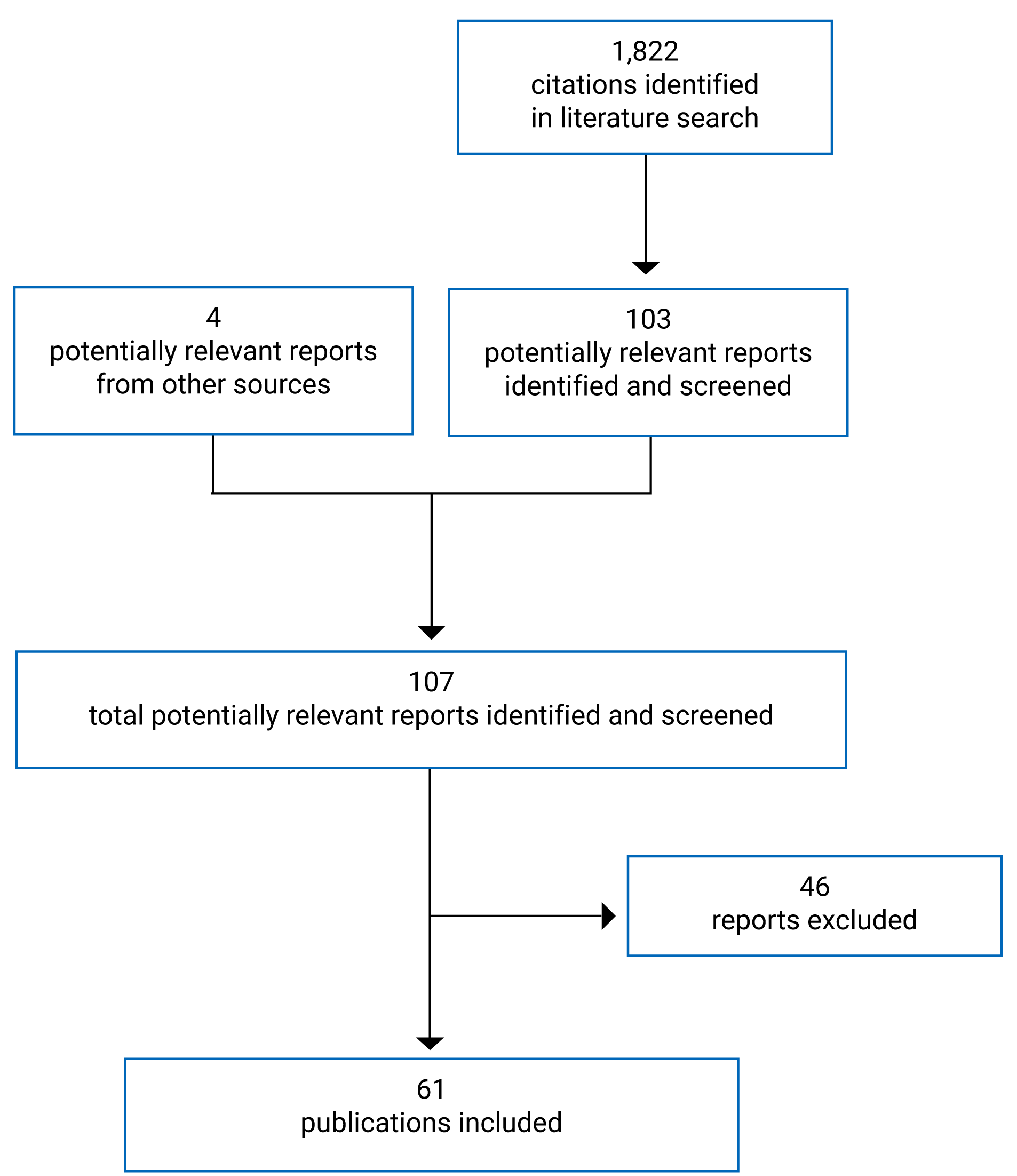
Table 2: Details of Included Publications
First author, year | Publication type | Objective | Key ethical considerations | Funding source |
|---|---|---|---|---|
Abbas, 202031 | Case study | To highlight the potential role of civil society in improving equitable and affordable access to innovative health technologies |
| None declared |
Atilla, 201834 | Review | To describe the current position of CAR T-cell therapies and compile information related to regulations and marketing of cellular therapeutic approaches worldwide |
| None declared |
Ayers, 20194 | Retrospective analysis | Examine NHL incidence rates by lymphoma subtype and racial differences in baseline characteristics and outcomes for DLBCL and follicular lymphoma in Georgia, US |
| National Cancer Institute, National Institutes of Health |
Bach, 201737 | Commentary | To discuss CAR T-cell therapies, their promise, and their associated costs |
| None declared |
Bachanova, 202052 | Review and recommendations | To review and address questions and concerns regarding cellular therapy administration in the setting of COVID-19 |
| None declared |
Blansky, 202011 | Retrospective study | To evaluate the association between urban–rural status and racial and ethnic disparities in 3 major NHL subtypes in the US |
| National Institutes of Health, National Center for Advancing Translational Science |
Buitrago, 201945 | Review | Review survivorship considerations and the physical, psychosocial, and financial effects for adults who have undergone CAR T-cell therapy |
| Bristol Myers Squibb |
CADTH, 201935 | Review and ethical analysis | To identify and analyze ethical issues and considerations for the use of axicabtagene ciloleucel |
| Canada’s federal, provincial, and territorial governments, with the exception of Quebec |
CADTH, 201950 | Review and ethical analysis | To identify and analyze ethical issues and considerations for the use of tisagenlecleucel |
| Canada’s federal, provincial, and territorial governments, with the exception of Quebec |
Carvalho, 201732 | Review | To review the current European legal framework for advanced therapy medicinal products, provide an overview of clinical applications and discusses critical challenges in the development of gene therapy medicinal products |
| PRA Health Sciences |
Crozier, 201513 | Retrospective analysis | To describe outcome disparities in different subgroups of patients with T-cell and B-cell NHL, with a focus on various ethnicities in the US |
| None declared |
De Lima Lopes, 201842 | Commentary | To discuss CAR T-cell therapies and their costs |
| None declared |
Dhakal, 201914 | Retrospective study | Examine effect of centre type and socioeconomic factors on mortality and survival of patients with DLBCL in the US |
| None declared |
El-Galaly, 202059 | Review | Describe challenges in DLBCL and opportunities for CAR T-cell therapy in international settings |
| Danish Cancer Society |
Ellis, 202138 | Qualitative study | Examine stakeholders’ attitudes to the development, administration, implementation, and logistical planning of CAR T-cell therapy in Canada |
| Biotherapeutics for Cancer Treatment Networks of Centres of Excellence |
Flowers, 20125 | Retrospective study | To examine associations between race, insurance, and treatment allocation for patients with DLBCL diagnosed in the US between 2001 and 2004 |
| Georgia Cancer Coalition; American Society of Hematology; National Cancer Institute, National Institutes of Health |
Forsberg, 201836 | Review | To summarize the journey of tisagenlecleucel from preclinical study to FDA approval and review strategies to improve the efficacy, safety, and patient access to CAR T-cell therapy |
| Stand Up To Cancer St Baldrick’s Pediatric Dream Team Translational Research Grant; National Cancer Institute/National Institutes of Health; National Science Foundation |
Gopishetty, 202027 | Retrospective study | To explore the representation of geriatric and racial minority patients in phase III cancer clinical trials |
| None declared |
Gotti, 202040 | Review | To summarize the clinical, logistic, and regulatory requirements of CAR T-cell centres |
| None declared |
Greinix, 202055 | Position statement | Develop criteria for patient selection and infrastructure of CAR T-cell centres in Austria |
| Medical University of Graz |
Griffiths, 201017 | Retrospective study | To identify patient factors associated with treatment and survival in DLBCL in the US |
| Genentech |
Guadamuz, 201916 | Retrospective cohort study | To examine racial disparities in older patients with regard to DLBCL treatment in the US |
| None declared |
Heine, 202157 | Economic review | To estimate the costs and budget impact associated with CAR T-cell therapies for current and future indications in hematological cancers from 2019 to 2029 in France, Germany, Spain, Italy, and the UK |
| European Haematology Association |
Howson, 201829 | Qualitative study | To report on the qualitative characteristics of self efficacy in the context of B-cell NHL, in the US context |
| Pharmacyclics LLC, AbbVie; Janssen Biotech; Genentech |
Hu, 202124 | Prospective study | To present the outcomes of White and minority patients with aggressive LBCL at a US-based institution with an active nurse navigation program |
| None declared |
Jacobson, 201933 | Commentary | Review CAR T-cell therapies, and their current coverage and reimbursement environment in the US |
| Pfizer |
Jecker, 201751 | Normative analysis | To develop a system for selecting individuals to participate in CAR T-cell trials and discuss principles of distributive justice and fair access |
| None declared |
Kansagra, 202041 | Commentary | To review opportunities for centres, manufacturers, payers, and policy-makers to address barriers to care with CAR T-cell therapies |
| None declared |
Kew, 202161 | Review | To provide an overview of the principles of CAR T-cell therapy, how it is delivered, who is eligible, and evidence on efficacy and safety in the UK context |
| None declared |
Kim, 201654 | Review | To address the challenges and regulatory perspectives of CAR T-cell therapies worldwide |
| Ministry of Food and Drug Safety |
Komrokji, 201118 | Retrospective study | To compare survival trends among patients with DLBCL from 1973 to 2004 in the US |
| None declared |
Lamy, 201622 | Cohort study | To investigate the association between the type of care centre in France and the relative dose intensity after adjustment for patients‘ recruitment differences |
| French National Research Agency |
The Lancet Oncology, 201862 | Commentary | To discuss CAR T-cell therapy as major clinical advance or overpromise |
| None declared |
Llaurador, 202126 | Review | To discuss current knowledge of lymphoma disease biology in adolescents and young adults, treatments and ongoing clinical trials, and review unique considerations for treatment-related toxicities in this population |
| None declared |
Lyman, 202048 | Economic evaluation | To estimate economic differences in the administration of CAR T-cell therapy by site of care and incidence of adverse events in the US context |
| Juno Therapeutics, Bristol Myers Squibb |
Madden, 201864 | Review | To discuss the history of cancer immunotherapy, recent advances, and discusses limitations and harms of immunotherapies |
| None declared |
Manz, 202039 | Commentary | To describe how payment policy affects hospital reimbursement for CAR T-cell therapy and the unintended effects and potential solutions in the US context |
| None declared |
Maschke 201744 | Commentary | To discuss challenges related to safety, access, and costs for CAR T-cell therapies |
| None declared |
Migdady, 20166 | Retrospective analysis | To compare conditional survival in common NHL subtypes of varying malignant behaviour and to identify factors that retain prognostic effect on long-term disparities in survival in the US |
| None declared |
Nieto, 202110 | Retrospective study | To analyze time trends for incidence, mortality, and prevalence of NHL in the US |
| National Institutes of Health |
Ortiz de Landazuri, 202053 | Review | How the COVID-19 pandemic has affected CAR T-cell therapy, considering production in the pharmaceutical industry vs. manufacturing in the academic/hospital environment |
| Instituto de Salud Carlos III with Fondos FEDER; Fundación Bancaria la Caixa; CELLNEX TELECOM |
Pepper, 201858 | Review | To review the implications of introducing cell and gene therapies into the health care sector in South Africa |
| South African Medical Research Council |
Phillips, 20177 | Review | Provide information about health disparities in lymphoma in the US and across the globe |
| None declared |
Pillai, 202056 | Review | Explore the challenge to delivery of cell therapies in the clinical setting in the UK |
| Manchester Clinical Research Facility, National Institute for Health Research |
Pulte, 201523 | Retrospective study | To estimate overall and cause-specific survival according to insurance status within 3 years after diagnosis of patients with NHL and DLBCL in the US |
| None declared |
Romito, 202030 | Prospective study; qualitative study | To analyze the psychosocial impact of the COVID-19 pandemic on lymphoma patients in Italy |
| None declared |
Sarker, 202125 | Retrospective study | To analyze factors associated with DLBCL in the elderly and real-world outcomes across economic disparities in India |
| None declared |
Shah, 201515 | Retrospective study | To evaluate disparities in receipt of radiotherapy and survival among patients with DLBCL on the basis of age, sex, and ethnicity in the US |
| None declared |
Shenoy, 20118 | Retrospective study | To examine differences in incidence and survival for DLBCL by race in the US |
| Georgia Cancer Coalition; American Society of Hematology |
Silbert, 201949 | Commentary | To examine whether and how to offer patients CAR T-cell therapy, and specifically to address: (1) value analysis and its application to CAR T-cell therapy; (2) factors that might complicate equitable access to these drugs; and (3) how much patients and families should be told about these therapies’ costs |
| None declared |
Smith, 202119 | Cross-sectional study | To assess the association between comorbidities and diagnostic delay among patients with DLBCL or follicular lymphoma in the UK |
| Cancer Research UK |
Snyder, 2021a47 | Geographic information system mapping study | To examine how expanding access to CAR T-cell therapy administration sites impacts patient travel distances and time in the US |
| Bristol Myers Squibb |
Snyder, 2021b46 | Study | Estimate travel-related economic burden for site of care options for patients with DLBCL in the US |
| Bristol Myers Squibb |
Snider, 201943 | Economic evaluation | Measure the social value of CAR T-cell therapy for DLBCL and quantify social value lost due to treatment delays in the US context |
| Novartis |
Tao, 201420 | Retrospective study | To consider the association between neighbourhood socioeconomic status and race/ethnicity on DLBCL mortality before and after the introduction of rituximab in California, US |
| California Department of Public Health; National Cancer Institute, National Institutes of Health |
Tiu, 20219 | Cohort study | To examine persistent racial disparities in survival among patients with DLBCL in the US context |
| None declared |
Trevino, 202028 | Cross-sectional observational study | To examine illness understanding, rates of engagement in Advance Care Planning and reasons for lack of engagement in patients with advanced B-cell lymphomas in the US context |
| Weill Cornell Medicine Lymphoma Program; National Institute on Aging; American Federation for Aging Research |
Tripathy, 201860 | Commentary | To discuss CAR T-cell therapies |
| None declared |
Williams, 202012 | Review | To define a framework for overcoming disparities for patients with hematologic malignancies and improve patient enrolment in clinical trials |
| None declared |
Wong Doo, 201921 | Population-based cohort study | To examine the factors associated with optimal DLBCL treatment and survival in the Australian context |
| Victorian Cancer Agency |
Wu, 202063 | Delphi Study | To reach a consensus with experts on the most relevant set of risks that practically occur in CAR T-cell therapy clinical trials in China |
| National Natural Science Foundation of China; Shanghai Municipal Health Commission; Shanghai Municipal Education Commission; Clinical Science and Technology Program of Shanghai Shen Kang Hospital Development Center |
CAR = chimeric antigen receptor; DLBCL = diffuse large B-cell lymphoma; LBCL = large B-cell lymphoma; NHL = non-Hodgkin lymphoma.
References
1.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2021 Aug 21.
2.EUnetHTA Joint Action 2 Work Package 8, HTA Core Model version 3.0 2016; http://www.htacoremodel.info/BrowseModel.aspx. Accessed 2020 Aug 20.
3.Sandelowski M. Whatever happened to qualitative description? Res Nurs Health. 2000;23(4):334-340. PubMed
4.Ayers AA, Lyu L, Dance K, et al. Characterizing Lymphoma Incidence and Disparities for a Cancer Center Catchment Region. Clin Lymphoma Myeloma Leuk. 2019;19(11):699-708 e695. PubMed
5.Flowers CR, Fedewa SA, Chen AY, et al. Disparities in the early adoption of chemoimmunotherapy for diffuse large B-cell lymphoma in the United States. Cancer Epidemiol Biomarkers Prev. 2012;21(9):1520-1530. PubMed
6.Migdady Y, Salhab M, Dang NH, Markham MJ, Olszewski AJ. Disparities in conditional net survival among non-Hodgkin lymphoma survivors: a population-based analysis. Leuk Lymphoma. 2016;57(3):676-684. PubMed
7.Phillips AA, Smith DA. Health Disparities and the Global Landscape of Lymphoma Care Today. Am Soc Clin Oncol Educ Book. 2017;37:526-534. PubMed
8.Shenoy PJ, Malik N, Nooka A, et al. Racial differences in the presentation and outcomes of diffuse large B-cell lymphoma in the United States. Cancer. 2011;117(11):2530-2540. PubMed
9.Tiu A, Jorge V, Moussa P, et al. Survival Disparities of Diffuse Large B-Cell Lymphoma in a Community-Based Inner-City Cancer Center. Clin Lymphoma Myeloma Leuk. 2021;21(4):205-215. PubMed
10.Nieto MJ, Li Z, Rehman H, Saif MW. Lower 24-Month Relative Survival among Black Patients with Non- Hodgkin's Lymphoma: An Analysis of the SEER Data 1997-2015. J Clin Haematol. 2021;2(1):5-13. PubMed
11.Blansky D, Mantzaris I, Rohan T, Hosgood HD, 3rd. Influence of Rurality, Race, and Ethnicity on Non-Hodgkin Lymphoma Incidence. Clin Lymphoma Myeloma Leuk. 2020;20(10):668-676 e665. PubMed
12.Williams S, Ayers AA, Hildebrandt MT, McNeill LH, Flowers CR. Strategies for Overcoming Disparities for Patients With Hematologic Malignancies and for Improving Enrollment on Clinical Trials. Oncology (Williston). 2020;34(6):216-223. PubMed
13.Crozier JA, Sher T, Yang D, et al. Persistent Disparities Among Patients With T-Cell Non-Hodgkin Lymphomas and B-Cell Diffuse Large Cell Lymphomas Over 40 Years: A SEER Database Review. Clin Lymphoma Myeloma Leuk. 2015;15(10):578-585. PubMed
14.Dhakal P, Chen B, Giri S, Vose JM, Armitage JO, Bhatt VR. Effects of center type and socioeconomic factors on early mortality and overall survival of diffuse large B-cell lymphoma. Future Oncol. 2019;15(18):2113-2124. PubMed
15.Shah BK, Bista A, Shafii B. Disparities in receipt of radiotherapy and survival by age, sex and ethnicity among patients with stage I diffuse large B-cell lymphoma. Leuk Lymphoma. 2015;56(4):983-986. PubMed
16.Guadamuz JS, Ozenberger K, Qato DM, et al. Mediation analyses of socioeconomic factors determining racial differences in the treatment of diffuse large B-cell lymphoma in a cohort of older adults. Medicine (Baltimore). 2019;98(46):e17960. PubMed
17.Griffiths R, Gleeson M, Knopf K, Danese M. Racial differences in treatment and survival in older patients with diffuse large B-cell lymphoma (DLBCL). BMC Cancer. 2010;10:625. PubMed
18.Komrokji RS, Al Ali NH, Beg MS, et al. Outcome of diffuse large B-Cell lymphoma in the United States has improved over time but racial disparities remain: review of SEER data. Clin Lymphoma Myeloma Leuk. 2011;11(3):257-260. PubMed
19.Smith MJ, Fernandez MAL, Belot A, et al. Investigating the inequalities in route to diagnosis amongst patients with diffuse large B-cell or follicular lymphoma in England. Br J Cancer. 2021;125(9):1299-1307. PubMed
20.Tao L, Foran JM, Clarke CA, Gomez SL, Keegan TH. Socioeconomic disparities in mortality after diffuse large B-cell lymphoma in the modern treatment era. Blood. 2014;123(23):3553-3562. PubMed
21.Wong Doo N, White VM, Martin K, et al. The Use of Optimal Treatment for DLBCL Is Improving in All Age Groups and Is a Key Factor in Overall Survival, but Non-Clinical Factors Influence Treatment. Cancers (Basel). 2019;11(7):02.
22.Lamy S, Bettiol C, Grosclaude P, et al. The care center influences the management of lymphoma patients in a universal health care system: an observational cohort study. BMC Health Serv Res. 2016;16(a):336.
23.Pulte D, Jansen L, Brenner H. Survival disparities by insurance type for patients aged 15-64 years with non-Hodgkin lymphoma. Oncologist. 2015;20(5):554-561. PubMed
24.Hu B, Boselli D, Pye LM, et al. Equal access to care and nurse navigation leads to equitable outcomes for minorities with aggressive large B-cell lymphoma. Cancer. 2021;127(21):3991-3997. PubMed
25.Sarker C, Radhakrishnan VS, Mandal P, et al. Outcomes of diffuse large B-cell lymphoma in elderly patients-real-world experience from a middle-income country setting. Ecancermedicalscience. 2021;15:1242. PubMed
26.Llaurador G, Giulino-Roth L. AYA Considerations for Aggressive Lymphomas. Curr Hematol Malig Rep. 2021;16(1):61-71. PubMed
27.Gopishetty S, Kota V, Guddati AK. Age and race distribution in patients in phase III oncology clinical trials. Am J Transl Res. 2020;12(9):5977-5983. PubMed
28.Trevino KM, Rutherford SC, Marte C, et al. Illness Understanding and Advance Care Planning in Patients with Advanced Lymphoma. J Palliat Med. 2020;23(6):832-837. PubMed
29.Howson A, Turell W, Roc A. Perceived self-efficacy in B-cell non-Hodgkin lymphomas: Qualitative outcomes in patient-directed education. Health Educ J. 2018;77(4):430-443.
30.Romito F, Dellino M, Loseto G, et al. Psychological Distress in Outpatients With Lymphoma During the COVID-19 Pandemic. Front Oncol. 2020;10:1270. PubMed
31.Abbas MZ. Strategic use of patent opposition safeguard to improve equitable access to innovative health technologies: A case study of CAR T-cell therapy Kymriah. Glob Public Health. 2020:1-11. PubMed
32.Carvalho M, Sepodes B, Martins AP. Regulatory and scientific advancements in gene therapy: State-of-the-art of clinical applications and of the supporting european regulatory framework. Front Med (Lausanne). 2017;4(OCT):182. PubMed
33.Jacobson C, Emmert A, Rosenthal MB. CAR T-Cell Therapy: A Microcosm for the Challenges Ahead in Medicare. JAMA. 2019;322(10):923-924. PubMed
34.Atilla E, Kilic P, Gurman G. Cellular therapies: day by day, all the way. Transfus Apher Sci. 2018;57(2):187-196. PubMed
35.Axicabtagene ciloleucel for large B-cell lymphoma: implementation and ethics project protocol. (CADTH optimal use report vol. 9, no. 1b). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/pdf/ct0002-axi-cel-for-dlbcl-implementation-and-ethics-protocol.pdf. Accessed 2022 Feb 23.
36.Forsberg MH, Das A, Saha K, Capitini CM. The potential of CAR T therapy for relapsed or refractory pediatric and young adult B-cell ALL. Ther Clin Risk Manag. 2018;14:1573-1584. PubMed
37.Bach PB, Giralt SA, Saltz LB. FDA Approval of Tisagenlecleucel: Promise and Complexities of a $475000 Cancer Drug. JAMA. 2017;318(19):1861-1862. PubMed
38.Ellis K, Grindrod K, Tully S, McFarlane T, Chan KKW, Wong WWL. Understanding the Feasibility of Implementing CAR T-Cell Therapies from a Canadian Perspective. Healthc Policy. 2021;16(3):89-105. PubMed
39.Manz CR, Porter DL, Bekelman JE. Innovation and Access at the Mercy of Payment Policy: The Future of Chimeric Antigen Receptor Therapies. J Clin Oncol. 2020;38(5):384-387. PubMed
40.Gotti M, Defrancesco I, D'Angelo M, et al. Cancer Immunotherapy Using Chimeric Antigen Receptor Expressing T-Cells: Present and Future Needs of Clinical Cancer Centers. Front Immunol. 2020;11:565236. PubMed
41.Kansagra A, Farnia S, Majhail N. Expanding Access to Chimeric Antigen Receptor T-Cell Therapies: Challenges and Opportunities. Am Soc Clin Oncol Educ Book. 2020;40:1-8. PubMed
42.de Lima Lopes G, Nahas GR. Chimeric antigen receptor T cells, a savior with a high price. Chin Clin Oncol. 2018;7(2):21. PubMed
43.Thornton Snider J, Brauer M, Kee R, et al. The potential impact of CAR T-cell treatment delays on society. Am J Manag Care. 2019;25(8):379-386. PubMed
44.Maschke KJ, Gusmano MK, Solomon MZ. Breakthrough Cancer Treatments Raise Difficult Questions. Health Aff (Millwood). 2017;36(10):1698-1700. PubMed
45.Buitrago J, Adkins S, Hawkins M, Iyamu K, Oort T. Adult Survivorship: Considerations Following CAR T-Cell Therapy. Clin J Oncol Nurs. 2019;23(2):42-48. PubMed
46.Snyder S, Albertson T, Garcia J, Gitlin M, Jun MP. Travel-Related Economic Burden of Chimeric Antigen Receptor T Cell Therapy Administration by Site of Care. Adv Ther. 2021;38(8):4541-4555. PubMed
47.Snyder S, Chung KC, Jun MP, Gitlin M. Access to Chimeric Antigen Receptor T Cell Therapy for Diffuse Large B Cell Lymphoma. Adv Ther. 2021;38(9):4659-4674. PubMed
48.Lyman GH, Nguyen A, Snyder S, Gitlin M, Chung KC. Economic Evaluation of Chimeric Antigen Receptor T-Cell Therapy by Site of Care Among Patients With Relapsed or Refractory Large B-Cell Lymphoma. JAMA Netw Open. 2020;3(4):e202072. PubMed
49.Silbert S, Yanik GA, Shuman AG. How Should We Determine the Value of CAR T-Cell Therapy? AMA J Ethics. 2019;21(10):E844-851. PubMed
50.Tisagenlecleucel for acute lymphoblastic leukemia and diffuse large B-cell lymphoma: project protocol, ethics and implementation report. (CADTH optimal use report vol. 8, no. 3b). Ottawa (ON): CADTH; 2018: https://www.cadth.ca/sites/default/files/pdf/OP0538_Tisagenlecleucel_for_B-Cell_Protocol.pdf. Accessed 2022 Feb 23.
51.Jecker NS, Wightman AG, Rosenberg AR, Diekema DS. From protection to entitlement: selecting research subjects for early phase clinical trials involving breakthrough therapies. J Med Ethics. 2017;43(6):391-400. PubMed
52.Bachanova V, Bishop MR, Dahi P, et al. Chimeric Antigen Receptor T Cell Therapy During the COVID-19 Pandemic. Biol Blood Marrow Transplant. 2020;26(7):1239-1246. PubMed
53.Ortiz de Landazuri I, Egri N, Munoz-Sanchez G, et al. Manufacturing and Management of CAR T-Cell Therapy in “COVID-19's Time”: Central Versus Point of Care Proposals. Front Immunol. 2020;11:573179. PubMed
54.Kim MG, Kim D, Suh SK, Park Z, Choi MJ, Oh YK. Current status and regulatory perspective of chimeric antigen receptor-modified T cell therapeutics. Arch Pharm Res. 2016;39(4):437-452. PubMed
55.Greinix HT, Attarbaschi A, Girschikofsky M, et al. Ensuring center quality, proper patient selection and fair access to chimeric antigen receptor T-cell therapy: position statement of the Austrian CAR-T Cell Network. Memo. 2020;13(1):27-31.
56.Pillai M, Davies MM, Thistlethwaite FC. Delivery of adoptive cell therapy in the context of the health-care system in the UK: challenges for clinical sites. Ther Adv Vaccines Immunother. 2020;8:2515135520944355. PubMed
57.Heine R, Thielen FW, Koopmanschap M, et al. Health Economic Aspects of Chimeric Antigen Receptor T-cell Therapies for Hematological Cancers: Present and Future. Hemasphere. 2021;5(2):e524. PubMed
58.Pepper MS, Alessandrini M, Pope A, Van Staden W, Green RJ. Cell and gene therapies at the forefront of innovative medical care: Implications for South Africa. S Afr Med J. 2018;109(1):20-22. PubMed
59.El-Galaly TC, Cheah CY, Kristensen D, et al. Potentials, challenges and future of chimeric antigen receptor T-cell therapy in non-Hodgkin lymphomas. Acta Oncol. 2020;59(7):766-774. PubMed
60.Tripathy D. CAR-T Cell Therapy: What We Never Dreamed Of. CURE Cancer Updates Res Educ. 2018 Special Issue;1(1):36-36.
61.Kew K. What is CAR T-cell therapy? Drug Ther Bull. 2021;59(5):73-76. PubMed
62.The Lancet O. CAR T-cell therapy: perceived need versus actual evidence. Lancet Oncol. 2018;19(10):1259. PubMed
63.Wu W, Huo Y, Ding X, Zhou Y, Gu S, Gao Y. Identification of the risks in CAR T-cell therapy clinical trials in China: a Delphi study. Ther Adv Med Oncol. 2020;12:1758835920966574. PubMed
64.Madden DL. From a Patient Advocate's Perspective: Does Cancer Immunotherapy Represent a Paradigm Shift? Curr Oncol Rep. 2018;20(1):8. PubMed
Stakeholder Input
Patient Input
Lymphoma Canada
About Lymphoma Canada
Lymphoma Canada is a national Canadian registered charity that empowers the lymphoma community through education, support, advocacy, and research. Based out of Toronto (ON), we collaborate with patients, caregivers, healthcare professionals, and other organizations and stakeholders, to promote early detection, find new and better treatments for lymphoma patients, help patients access those treatments, learn about the causes of lymphoma, and work together to find a cure. Resources are provided in both English and French. For more information about our organization, please visit us at www.lymphoma.ca
Information Gathering
Lymphoma Canada (LC) conducted an anonymous online survey for Large B-Cell Lymphoma patients between June 21, 2021 – August 25, 2021. Links to the surveys were sent via e-mail to patients registered through the LC database. The survey was also made available via social media outlets, including Twitter, Instagram and Facebook accounts, and was also sent to healthcare professionals across Canada to share with their patients. As there were no clinical trial sites in Canada, the survey was shared with lead clinicians of clinician trial sites in the United States. The survey had a combination of multiple choice, rating and open‐ended questions. Skipping logic was built into the survey so that respondents were asked questions only relevant to them. Open-ended responses to surveys that reflected the sentiment of a majority are included verbatim to provide a deeper understanding of patient perspectives. Survey data about disease experience collected from past surveys for patients with DLBCL (2018 and 2020 surveys) and FL (2017 & 2018) were included for additional support. As no patient experience with liso-cel was collected through this survey, general patient feedback on experience with CAR-T therapy from a previous survey (April 18th – June 15th, 2018) was included.
Disease Experience
There were 331 Large B-Cell Lymphoma patients that responded to the surveys, of which subtypes included diffuse large B-cell lymphoma (DLBCL) (126), Follicular lymphoma (FL) (191), and other large-b-cell lymphomas (14) including indolent lymphoma transformed to DLBCL, High-grade B-cell lymphoma, and peripheral mediastinal B-cell lymphoma (PMBCL) patients. LC had a tremendous difficulty finding patients with liso-cel treatment experience as there were no Canadian clinical trial sites, despite significant effort by LC staff, therefore general information on CAR T-cell therapy was provided. There were no caregivers that participated in this survey. Of the Large B-Cell lymphoma patients who provided their demographic information for this survey (see Table 1 to Table 3), 58% live in Canada, 57% are female, and 42% are ≥ 60 years-old.
Patients with large B-cell lymphoma shared their overall experience with their disease, with greater specifics provided on the two largest subtypes, DLBCL and FL. The top symptoms experienced by large b-cell lymphoma patients and their impact on quality of life are listed in Table 4.
Table 1: Country of Survey Respondents (331 respondents)
Respondents | CAN | USA | Europe | Other | Skipped | Total |
|---|---|---|---|---|---|---|
Patients with DLBCL | 103 | 5 | 3 | n/a | 15 | 126 |
Patients with FL3B | 87 | 52 | 24 | 4 | 24 | 191 |
Patients with other Large B-Cell Lymphomas | 3 | 1 | 1 | 0 | 9 | 14 |
Table 2: Age Range of Survey Respondents (331 respondents)
Respondents | Age Range | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
<20 | 20-39 | 40-49 | 50-59 | 60-69 | 70-79 | 80-89 | >90 | Skipped | Total | |
Patients with DLBCL | 2 | 13 | 15 | 27 | 34 | 16 | 3 | 1 | 15 | 126 |
Patients with FL3B | 0 | 10 | 32 | 55 | 54 | 30 | 2 | 0 | 18 | 191 |
Patients with other Large B-Cell Lymphomas | 0 | 2 | 1 | 2 | 0 | 0 | 0 | 0 | 9 | 14 |
Table 3: Gender of Survey Respondents (331 respondents)
Respondents | Gender | |||
|---|---|---|---|---|
Female | Male | Skipped | Total | |
Patients with DLBCL | 66 | 45 | 15 | 126 |
Patients with FL3B | 120 | 52 | 19 | 191 |
Patients with other Large B-Cell Lymphomas | 3 | 2 | 9 | 14 |
Table 4: Symptoms and Negative Impacts to QoL (63 respondents)
Symptom | Number that experienced symptom | Percentage Rating Significant Negative Impact to QoL (4-5*) |
|---|---|---|
Fatigue, lack of energy | 50 | 54% |
Enlarged lymph node(s) | 44 | 50% |
Night sweats | 37 | 57% |
Bodily Aches and pains | 35 | 54% |
Shortness of breath | 35 | 49% |
Weight loss | 33 | 27% |
Low platelet counts | 32 | 19% |
*Scale of impact rating from 1 (no impact) to 5 (significant negative impact)
These symptoms can have a large impact on quality of life. As mentioned by one patient:
“Overall tiredness so bad that I could not speak with my grandchildren” – Large B-Cell Lymphoma patient
There are a number of psychosocial impacts to patients with large b-cell lymphomas, aside from their symptoms. The majority of patients experiences anxiety/worry (75%) and stress related to their diagnosis (73%), followed by fear of progression (64%) as the top three impacts (63 respondents). Symptoms and diagnosis, as well as mental health impacts, have affected patients’ ability to continue with daily activities (43%), ability to sleep (41%), problems concentrating (40%), and ability to attend work/school (40%) (63 respondents). Some patients shared their personal experiences:
“I had to relocate to get help from my family, I left my job and my dearest ones” - Large B-Cell Lymphoma patient
“Huge shock of diagnosis at a young age of 33 years old. Quality of life impacted by potentially poor prognosis and change in life plans as we held off on having children”- Large B-Cell Lymphoma patient
“This diagnosis has impacted my ability to live the normal life I previously had. I am stressed out and I cannot plan anything for the future” – Large B-Cell Lymphoma patient
Diffuse Large B-Cell Lymphoma disease experience: Symptoms of DLBCL that most commonly affected respondents’ quality of life at diagnosis (104 respondents) were fatigue or lack of energy (69%), enlarged lymph nodes (48%), drenching night sweats (36%), unexplained weight loss (29%), loss of appetite (25%), flu-like symptoms (18%), and persistent cough (18%). 55% and 45% of patients indicated that their DLBCL had a negative impact on their ability to work or attend to family obligations, respectively. The majority of respondents (86%), had one or more symptom and mental/emotional impact negatively affect their quality of life, with the most negative impacts related to fear of recurrence (67%), anxiety/worry (38%) and problems concentrating/memory loss (38-39%) (104 respondents).
Follicular Lymphoma disease experience: Symptoms of FL that most commonly affected respondents’ quality of life at diagnosis (90 respondents) were fatigue or lack of energy (46%), enlarged lymph nodes (46%), drenching night sweats (24%), pain (23%), and shortness of breath (17%). Notably, 40/89 (45%) of respondents indicated that FL had a negative impact on their ability to work and the majority of respondents (76%; 89 respondents) reported that their quality of life was negatively affected by mental and emotional problems associated with their disease such as anxiety/worry, problems concentrating, and stress of diagnosis.
Experiences With Currently Available Treatments
Patients with large b-cell lymphomas can have different experiences with treatments as there are different treatment options funded and available for specific b-cell lymphoma subtypes. There are important concerns however that are general across all lymphoma subtypes however related to the impacts of treatment on quality of life and outcome. As expressed by one patient:
“I am afraid of how chemo will affect my quality of life as I receive more treatments” – Large B-Cell Lymphoma patient
230 respondents provided information about their experience with large b-cell lymphoma treatments. As some of these lymphomas are indolent, a standard treatment approach is watch and wait or active surveillance. A small percentage of patients (7%) had not yet received therapy at the time of their survey response, which is a standard approach for patients diagnosed with indolent lymphomas. The remainder of respondents had received at least one line of treatment; 50% of patients received one line of therapy, and 43% of patients received two or more lines of therapy. Of those that provided further detail about the number of lines of therapy received following two lines of treatment (49 respondents). The most commonly reported treatments received related to the two most commonly reported subtypes are recorded in Table 5.
Side effects of current treatments: Only 5% of patients did not experience any side-effects related to their treatments. The most common side effects respondents experienced during their FL treatments are listed in Table 6.
Table 5: Lines of Treatment per Subtype (147 respondents)
Subtype | 1st line | 2nd line or later | 3rd line+ | Total |
|---|---|---|---|---|
DLBCL | R-CHOP ± radiation (96%); EPOCH-R (3%); CEPP (1%) | HDT + SCT (9%), chemo (DHAP, R-ICE, EPOCH) (10%) | CAR-T (2%) | 101 |
FL | Bendamustine-Rituximab (33%), R-CHOP (25%), R-CVP (17%), Rituximab (14%), Radiation (4%) | Rituximab (27%), Radiation (10%), BR (9%), R-CHOP (8%) | Chemo (R-CVP, R-CHOP, BR), HDT+SCT | 147 |
Table 6: Side-effects of Current FL Therapies (276 respondents)
Side effect | % of respondents | Side effect | % of respondents |
|---|---|---|---|
Fatigue | 86% | Neuropathy | 26% |
Hair Loss | 65% | Low platelet count | 26% |
Nausea | 53% | Constipation | 25% |
Low red blood cell counts | 36% | Skin rash/itching | 24% |
Mouth sores | 35% | Infections | 24% |
Low white blood cell counts | 34% | Back/joint pain | 21% |
Confusion or memory loss | 31% | Breathing difficulties/ pneumonia | 16% |
Side effects specific to major B-cell lymphoma subtypes:
DLBCL: The most common side effects respondents experienced during their DLBCL treatments include hair loss (87%), fatigue (84%), memory problems/confusion (68%), neutropenia (65%) and nausea (59%) (103 respondents). When asked which side effects they found most difficult to tolerate, respondents most often reported fatigue (35/85; 41%), nausea/vomiting (16/85; 19%), chemo-brain (13/85; 15%), and hair loss (8/85; 9%) (85 respondents).
FL: The most common side effects respondents experienced during their FL treatments include fatigue (85%), nausea/vomiting (51%), hair loss (39%), mouth sores (30%), and neutropenia (61 respondents). Individuals noted that fatigue (18/49; 37%), nausea/vomiting (5/49; 10%), and pain (5/49; 10%) were the most difficult side effects to tolerate (49 respondents).
Impact of treatments on quality of life: When asked about the impact of various aspects of treatment on quality of life, top psychosocial impacts experienced include fear of progression/relapse (67%), anxiety/worry (65%), depression (47%), inability to attend work/school (22%), and difficulty sleeping (43%) (49 respondents). When asked about the impact of various aspects of their treatment on daily living (on a scale of 1 – 5, where 1= No impact and 5 = significant negative impact), the most significant negative impacts were treatment-related fatigue and long-term side effects of treatment. A full list can be found in Table 7.
Table 7: Impact of Treatment on Quality of Life (49-273 respondents)
Treatment aspect | Mild Impact (rating 2-3) | Significant negative impact (rating = 4-5) | Total Number of Patients |
|---|---|---|---|
Treatment-related Fatigue | 26% | 57% | 273 |
Late/Long-Term Side Effects of Treatment | 39% | 41% | 49 |
Low activity level | 37% | 39% | 176 |
Not seeing friends/family | 33% | 33% | 49 |
Immediate Side Effects of Treatment | 36% | 31% | 271 |
Number of clinic visits | 45% | 24% | 273 |
Infusion time | 45% | 24% | 271 |
Access and Financial Impacts to Treatment in Canada: Patients with B-cell lymphomas were asked about their difficulty accessing treatment options. Of those that provided information on access challenges (44 respondents), only a small percentage of patients of patients found it somewhat difficult to very difficult to access treatments (13%). For patients that could not access treatment locally, the main reason included living in a community without a cancer centre (35%) and the treatment not being available at my local cancer centre (10%) (49 respondents). As reported by one patient:
“Travel time, required ferry ride, extra hotel stays and time away from home and children” – Large B-cell lymphoma patient
As CAR-T is a treatment that is still not locally accessible for all patients in all the provinces in Canada, this remains a concern for patients as CAR-T is an effective treatment option in the relapsed/refractory setting. As expressed by patients:
“I likely need car T-cell therapy next and will need to travel to another province since BC does not currently offer it (except under clinical trial). I expect to wait longer than for my SCT previously. I am worried about this since I got serious side effect while waiting longer than necessary last time and needing ongoing chemo while I waited (including cardiac hf symptoms that could have impacted my sct eligibility)” – Large B-cell lymphoma patient
“At this point I've have full access to treatment, however, my next relapse I would like to have full access to CAR-T in my community and covered by OHIP, which at this point that I know - it isn't” – Large B-cell lymphoma patient
Top financial impacts to patients accessing treatments for their large b-cell lymphoma include an absence from work (62%), travelling costs (28%), and supplementary drug costs (26%) (39 respondents). As travel may be required for patients to access CAR-T treatment in Canada, it is important to note the financial strain that can burden a patient should CAR-T not be approved locally for the patient. As expressed by two patients:
“I worry about the cost in the future of these treatments if they aren’t covered by OHIP” – Large B-cell lymphoma patient
“It would be nice if these new drugs are covered by the government. Once you have a difficult diagnosis like this you should not have the stress of dealing with drug-related costs” – Large B-cell lymphoma patient
Improved Outcomes
Patient preferences: Respondents were asked to rate, on a scale of 1 -5 (1 = not important; 5 = extremely important), the importance of various factors regarding a new drug or therapy for large b-cell lymphomas. “Improved quality of life”, “longer survival”, and “longer remission” than current therapies were rated as the most important outcomes for large B-cell lymphoma patients related to a new therapy (Table 8).
Table 8: Treatment Preferences (45-178 respondents)
Treatment outcome or factor | Rating = 5 (Extremely important) | Number of responses |
|---|---|---|
Improve quality of life and perform daily activities | 93% | 176 |
Longer survival | 88% | 223 |
Longer disease remission | 85% | 223 |
Control disease symptoms | 73% | 45 |
Normalize blood counts | 51% | 45 |
Fewer side effects | 51% | 178 |
As reported by one patient:
“I would like therapies that avoid relapses and extend life expectancy. If they are so that I can bear side effects, even serious, until a certain extent, and during a certain length of time” – Large B-cell lymphoma patient
Choice of Treatment options: Though there CAR-T therapies are available in Canada, patients note it is very important to still have a choice in treatment. On a scale of 1 (not important) to 5 (very important), 87% of patients rated it as important to very important to have a choice of treatment options and which drug to take depending on the known side effects and expected outcomes of treatment (297 respondents). Therefore it is important for patients to have an option regarding CAR-T therapies. 32% of patients further feel there is a need for more therapy options to become available for large b-cell lymphomas. As expressed by patients:
“For myself I am most interested in options that along me to live as long as possible. Being 34 years old I want as many options available for me as possible. When diagnosed with large diffuse B cell lymphoma last year my oncologist outlined 3 steps for treatment - 1 chemo chopR, - 2 autologous sct and 3 car T cell therapy. I was shocked and disappointed there were only 3 definitive treatments to cure. My plans for the future are totally on hold as I fight this disease” – Large B-cell lymphoma patient
“I would like to have equal access across the country for the best available treatment options, that have the most prolonged treatment effects!” – Large B-cell lymphoma patient
Respondents were asked if they would be willing to tolerate the side effects of a new treatment if they were short term. 47% of respondents would be willing to tolerate potential side effects, while 12% were not; the remaining were unsure (41%) (297 respondents). Respondents were also asked if they would choose a treatment with known side effects, potentially serious, if their doctor recommended it was the best option for them. Of the 297 respondents who answered this question, 47% selected “Yes”, while only 7% selected “No”. The remaining 46% of respondents selected “I’m not sure”. As patients shared:
“Any side effect which is minimal in severity and short term, if it can help me to recover or live normally” – Large B-cell lymphoma patient
“I would be willing to tolerate any side effects of treatment if they are temporary” – Large B-cell lymphoma patient
“If my cancer returns, I’m willing to go through another round of treatment to stay alive” – Large B-cell lymphoma patient
Experience With Drug Under Review
Unfortunately, Lymphoma Canada could not locate patients with liso-cel experience to participate in this survey. However, data had been collected on DLBCL patients general experience related to their quality of life and use of CAR-T therapy for greater insight.
There were 7 DLBCL patients that provided their feedback on CAR-T therapy, all of whom accessed this treatment option through a clinical trial at the time
Quality of Life: Five respondents answered a question asking them to rate the impact of different aspects of their CAR-T therapy on a scale of 1 (no negative impact on my life) to 5 (significant negative impact on my life). None of the weighted averages for these responses was higher than 3 and only one out of the five respondents gave a rating > 3 for any aspect of CAR-T therapy, suggesting that the administration of CAR-T treatment had a reasonably benign effect on their quality-of-life. Patients shared their experience with CAR-T therapy administration and its impact on quality of life (Table 9).
Table 9: Impact of CAR-T Therapy on Patients’ Lives (5 respondents)
Aspect of CAR-T therapy | Weighted average |
|---|---|
Number of clinic visits | 2.8 |
Travel to treatment centre | 2.8 |
CAR-T cells infusion | 2.6 |
Short-term side effects of treatment | 2.5 |
Activity level | 2.5 |
Treatment-related fatigue | 2.5 |
Lasting side effects of treatment | 2.0 |
Leukapheresis | 1.8 |
One patient commented:
“For all intents and purposes, despite having reviewed and discussed all of the potential side effects with respect to the CAR-T cell therapy program, the experience was fairly uneventful. I did not experience any significant adverse effects from the treatment.” – DLBCL patient
Recommendation of CAR-T Therapy: Of the patients that responded, five patients would recommend this treatment to others with r/r DLBCL; one said no and one was unsure (7 respondents). When asked to describe the positive and negative effects of CAR-T therapy, patients mentioned:
“It was so much easier than the auto stem cell transplant.” – DLBCL patient
“After 25 days I am cancer free, so that was worth it; nothing else worked.” – DLBCL patient
“I would recommend it to any patient with relapsed DLBCL.” – DLBCL patient
Companion Diagnostic Test
CD19 CAR-T cell therapy requires expression of CD19 on the tumour cells. Hematologists and oncologists with knowledge of CAR- T therapy and experience treating DLBCL indicated that this is a routine test that can be performed on archival biopsy tissue using readily available laboratory testing and would not need to be performed on new tissue prior to the initiation of CAR-T therapy.
Anything Else?
N/A
Patient Group Conflict of Interest Declaration — Lymphoma Canada
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
No
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 10: Lymphoma Canada Financial Disclosures
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
BMS/Celgene | — | — | X | — |
I hereby certify that I have the authority to disclose all relevant information with respect to any matter involving this patient group with a company, organization, or entity that may place this patient group in a real, potential, or perceived conflict of interest situation.
Name: Kaitlyn Beyfuss-Laski
Position: Manager of Patient Programs, Research & Advocacy Patient Group: Lymphoma Canada
Date: 02-09-2021
Clinician Input
Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee
About Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee (OH-CCO Hem DAC)
OH-CCO’s Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs (PDRP) and the Systemic Treatment Program.
Information Gathering
This input was jointly discussed via email.
Current Treatments
Currently Kymriah and Yescarta are funded for DLBLC in Ontario. There is a large overlap (~90%) of the diseases between this product and the existing CAR-T products.
For the disease indications that are new to lisocabtagene maraleucel (“liso-cel”), the treatment options include potential autologous or allogeneic SCT (FL3B), palliative chemotherapy, clinical trials, or high-dose chemotherapy and autologous SCT (in select patients) or CNS radiation (secondary CNS lymphoma).
Treatment Goals
What are the most important goals that an ideal treatment would address?
Examples: Prolong life, delay disease progression, improve lung function, prevent the need for organ transplant, prevent infection or transmission of disease, reduce loss of cognition, reduce the severity of symptoms, minimize adverse effects, improve health- related quality of life, increase the ability to maintain employment, maintain independence, reduce burden on caregivers.
Prolong life, delay disease progression, reduce the severity of symptoms, minimize adverse effects, improve health-related quality of life,
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Examples: Not all patients respond to available treatments; Patients become refractory to current treatment options; No treatments are available to reverse the course of disease; No treatments are available to address key outcomes; Treatments are needed that are better tolerated; Treatment are needed to improve compliance; Formulations are needed to improve convenience
This product include additional indications to the existing CAR-T products for DLBCL. Patient eligibility based on fitness and co- morbidities may be a significant barrier.
Which patients have the greatest unmet need for an intervention such as the drug under review?
Would these patients be considered a subpopulation or niche population? Describe characteristics of this patient population. Would the drug under review address the unmet need in this patient population?
The two expanded indications would be the greatest unmet need.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Is there a mechanism of action that would complement other available treatments, and would it be added to other treatments? Is the drug under review the first treatment approved that will address the underlying disease process rather than being a symptomatic management therapy? Would the drug under review be used as a first-line treatment, in combination with other treatments, or as a later (or last) line of treatment? Is the drug under review expected to cause a shift in the current treatment paradigm?
Liso-cel may have less treatment-related toxicities. It would be an alternate treatment option to the existing CAR-T products for DLBCL and a new treatment option for the 2 expanded indications.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective. If so, please describe which treatments should be tried, in what order, and include a brief rationale.
No. It would be desirable to offer this treatment after 2 lines of therapy rather than waiting.
How would this drug affect the sequencing of therapies for the target condition?
If appropriate for this condition, please indicate which treatments would be given after the therapy has failed and specify whether this is a significant departure from the sequence employed in current practice. Would there be opportunity to treat patients with this same drug in a subsequent line of therapy? If so, according to what parameters?
Liso-cel can be used after 2 prior lines of therapy as per indication.
Which patients would be best suited for treatment with the drug under review?
Which patients are most likely to respond to treatment with the drug under review? Which patients are most in need of an intervention? Would this differ based on any disease characteristics (e.g., presence or absence of certain symptoms, stage of disease)?
Patients need to be reasonably fit, with adequate end organ functions, and reasonable performance status.
How would patients best suited for treatment with the drug under review be identified?
Examples: Clinician examination or judgement, laboratory tests (specify), diagnostic tools (specify) Is the condition challenging to diagnose in routine clinical practice? Are there any issues related to diagnosis? (e.g., tests may not be widely available, tests may be available at a cost, uncertainty in testing, unclear whether a scale is accurate or the scale may be subjective, variability in expert opinion.) Is it likely that misdiagnosis occurs in clinical practice (e.g., underdiagnosis)? Should patients who are pre-symptomatic be treated considering the mechanism of action of the drug under review?
Patients can be identified through existing networks of lymphoma treating hematologists and cellular therapy treatment centres.
Often in cases of secondary CNS lymphoma, pathology is not available as biopsy is often considered difficult or risky.
Which patients would be least suitable for treatment with the drug under review?
Patients who are frail and have exclusions for CAR-T treatment.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review? If so, how would these patients be identified?
Not applicable
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? Are the outcomes used in clinical practice aligned with the outcomes typically used in clinical trials?
Standard lymphoma response measurements
What would be considered a clinically meaningful response to treatment?
Examples: Reduction in the frequency or severity of symptoms (provide specifics regarding changes in frequency, severity, and so forth); Attainment of major motor milestones; Ability to perform activities of daily living; Improvement in symptoms; Stabilization (no deterioration) of symptom. Consider the magnitude of the response to treatment. Is this likely to vary across physicians?
Reduction in the frequency or severity of symptoms (provide specifics regarding changes in frequency, severity, and so forth)
Ability to perform activities of daily living
Improvement in symptoms
Stabilization (no deterioration) of symptoms
How often should treatment response be assessed?
Within the first 100 days and as needed thereafter.
What factors should be considered when deciding to discontinue treatment?
Examples: Disease progression (specify; e.g., loss of lower limb mobility); Certain adverse events occur (specify type, frequency, and severity); Additional treatment becomes necessary (specify)
Not applicable as it is a single treatment.
Some patients will become ineligible based on performance status and organ function during/after cell collection and manufacturing.
What settings are appropriate for treatment with the drug under review?
Examples: Community setting, hospital (outpatient clinic), specialty clinic
Cellular therapy/CAR-T centres
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review? If so, which specialties would be relevant?
NA
Additional information
Is there any additional information you feel is pertinent to this review?
Across Canada, there are a limited number of CAR-T centres available. Patient access may be an issue.
Conflict of Interest Declarations — Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee (OH-CCO Hem DAC)
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
OH-CCO provided secretariat support to the DAC in completing this input.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician that contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Tom Kouroukis
Position: Provincial Head – Complex Malignant Hematology (OH-CCO)
Date: 09-Sep-2021
Table 11: Conflict of Interest Declaration for Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee — Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Lymphoma Canada
About Lymphoma Canada
Lymphoma Canada, a national non-for-profit organization for Canadian lymphoma and CLL patients, and assisted in the coordination of the group clinician response. Lymphoma Canada was not involved in the development of this submission, nor are the clinician’s involved members of Lymphoma Canada. For more information about Lymphoma Canada, please visit www.lymphoma.ca.
The following clinicians, leading experts in lymphoma across Canada, have provided feedback on this therapeutic for the submitted indication.
Dr. Mona Shafey (lead)
Dr. Neil Berinstein
Dr. John Kuruvilla
Dr. Mahmoud Elsawy
Dr. Kevin Hay
Information Gathering
Please describe how you gathered the information included in the submission.
Clinicians provided responses to the questions in the submission based on research results, clinical experience, and understanding of patient needs and challenges.
Current Treatments
The current standard of care for patients with relapsed/refractory DLBCL failing at least two lines of therapy is anti-CD19+- directed chimeric antigen receptor (CAR) T cell therapy for all patients who are fit to receive this treatment. This is supported by both provincial and national guidelines. Currently, two commercial products, namely tisagenleucel and axicabtagene ciloleucel, are available and funded in Canada, and provided through CAR-T programs currently established in three provinces (namely Quebec, Ontario, and Alberta) and will soon be available in a fourth province (Nova Scotia). Patients outside of these provinces can access CAR-T through interprovincial agreements or out-of-country access.
CAR-T therapy is a potentially curative option for these patients who otherwise will have a dismal prognosis with an estimated median survival of 6 months. Patients who are not fit for CAR-T therapy (based on eligibility criteria, such as organ function and performance status), generally receive palliative treatments or enroll on clinical trials, with no expectation for long-term survival.
Lisocabtagene maraleucel (liso-cel) is an anti-CD19+-direct CAR-T, with similar mechanism of action as the established commercial products and offers another potential curative option for large b-cell lymphoma patients.
Treatment Goals
What are the most important goals that an ideal treatment would address?
The most important goal is long-term survival, with emphasis on overall survival and progression-free survival. This is considered curative-intent treatment, with long-term disease control in 35-45% of patients.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
The delivery of CAR-T therapy is resource-intensive and requires key interactions between all relevant parties, namely the referral centre, the treatment centre, and the manufacturing site. From a manufacturing perspective, this is not in our control, and with the uptake in CAR-T therapy across the world, the demand has exceeded the supply, and as such delays in manufacturing have been noted with both available commercial products. Having access to a third treatment would address this issue and allow patients to proceed with treatment in a timely fashion in order to maximize outcomes by avoiding delays in treatment.
The toxicity of these therapies is an ongoing concern, and despite certain interventions, these patients are at high risk for both cytokine release syndrome (CRS) and neurotoxicity (ICANS). Liso-cel has been shown to have less frequent CRS and ICANS as compared to axi-cel without compromising on efficacy. This translates into less frequent high-grade complications, less need for ICU care, and shorter hospitalizations. In fact, it is the second product (tisagenlecleucel being the other) that has been shown to be safely delivered in an outpatient setting (albeit in a specialized center). Given the nature of the current clinical environment, any decrease in hospitalization is a clear advantage.
Which patients have the greatest unmet need for an intervention such as the drug under review?
The patients being considered for this therapy are all those with relapsed/refractory DLBCL who have failed at least two lines of therapy. The patient considered for this therapy should have adequate organ function, with good performance status (ECOG 0-2) and expected to survive through the process (apheresis, manufacturing, and delivery, generally 6-8 weeks in duration).
Liso-cel would be an addition to the CAR-T therapy arsenal we have for patients with this aggressive, poor prognosis entity. For the reasons stated above in 5.1, it is an ideal agent for CAR-T therapy given its established efficacy and toxicity profile.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
The drug under review would be considered alongside the two commercially-available CAR-T products for the same population and indication, namely in the 3rd line setting or beyond. At this point in time, there is no head-to-head comparison of one CAR-T product vs. another, and none is expected in the future. Clinicians must rely on clinical trial efficacy and toxicity data, plus real world data, to decide which product to use for which patient. Currently, there is no standard or guideline established that addresses this question. In most cases, it comes down to availability and feasibility, as manufacturing availability, apheresis availability and timing, eligibility for outpatient care vs. requirement for inpatient treatment, patient co-morbidities etc. are all used to determine which product is ultimately used. At the end of the day, the aim is the give the most efficacious treatment as quickly as possible, with acceptable toxicity.
Liso-cel would be considered a stand-alone treatment, to be given once. In general, repeat CAR-T therapy with another product has not been permitted outside of a clinical trial. Patients may receive bridging therapy (e.g. steroids, radiation, chemotherapy) during the manufacturing period to hold patient disease prior to delivery of CAR-T (as is the case for the other CAR-T products).
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
In is not recommended that patients receive other therapies once they meet eligibility for CAR-T therapy. Delays in referral for CAR T therapy leads to poorer outcomes, with CAR-T treatment being less efficacious in patients with more advance disease, particularly bulky disease.
A standard DLBCL patient would receive R-CHOP (or in some cases DA-EPOCH-R) as frontline therapy. At second line, salvage chemotherapy is given (e.g R-GDP) and those that are found to be chemo-sensitive AND fit for autologous transplant proceed to ASCT. Those who fail salvage or later fail ASCT, and are physically fit to proceed with CAR-T therapy, should be referred for CAR-T therapy as soon as possible. Once the patient is deemed fit to proceed with CAR-T therapy, then the drug under review would be considered as a treatment choice. Non-transplant eligible patients with recurrent DLBCL will likely have short responses to other salvage therapies that they may be offered.
How would this drug affect the sequencing of therapies for the target condition?
Failure of CAR-T therapy is associated with a very dismal prognosis. This is also the case for patients treated with liso-cel. At this time, re-treatment has not been established as an efficacious strategy and is not considered standard. Other therapies that are generally attempted are palliative in nature, including polatuzumab-BR (not currently funded), and clinical trials (e.g. BITE antibodies). This is the general approach for all patients who fail CAR-T therapy (i.e. not specific to liso-cel).
Which patients would be best suited for treatment with the drug under review?
Patients with DLBCL who have failed two lines of therapy would be suitable for liso-cel treatment. They must meet provincial eligibility criteria for CAR-T therapy (at a minimum adequate organ function and good performance status). Patients most likely to respond to treatment are those with ECOG <2, normal LDH, low bulk disease, and low inflammatory markers prior to CAR-T therapy. The patients most in need of this intervention are the primary refractory DLBCL patients who are ineligible for transplant due to chemo-refractory disease. There does not appear to be any unique population that would benefit more from liso-cel vs. other commercial CAR-T products at this time.
How would patients best suited for treatment with the drug under review be identified?
The patients are identified by their primary treating physician. There are standard guidelines that address the approach to relapsed patients, that include CAR T therapy and when to refer. Referrals are made to the specialized CAR-T therapy programs. Diagnosis and staging are standard and widely available and even patients without symptoms should be referred given the aggressive nature of this lymphoma. For patients with a history of indolent lymphoma with biopsy-proven transformation, it is important to establish that recurrent disease is also due to transformation and not recurrence of the indolent disease, thus biopsy is required in this setting.
Which patients would be least suitable for treatment with the drug under review?
Patients with poor performance status (ECOG 3-4), unfit due to significant co-morbidities, and unexpected to survive the 6-8 weeks required for this treatment would be least suitable for this treatment. Patients with uncontrolled infections would not be acceptable candidates.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
Not at this time. There are no predictors to accurately identify which patients will exhibit response and which will not.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
Standard Lugano criteria for lymphoma is used to confirm remission status (via CT and PET scans).
What would be considered a clinically meaningful response to treatment?
Achievement of remission would be considered clinically meaningful, with complete remission (CR) associated with long-term outcomes. There are some patients with early partial remissions who later convert to complete remission (generally within 1 year of CAR-T therapy). CRs are generally associated with resolution of all lymphoma-related symptoms, improvement in functional status and quality of life indicators, and return to normal activities.
How often should treatment response be assessed?
At a minimum, remission status should be established via standard diagnostic imaging within 3 months after CAR-T infusion. Thereafter, ongoing disease response is assessed at every subsequent patient visit, generally clinically, as relapse in this setting is almost universally accompanied by patient symptoms related to lymphoma. The frequency of these assessments is variable, but generally q3 months in the first year, then q3-6 months for a few years, then yearly thereafter (as we are mandated to follow for 15 years post CAR-T).
What factors should be considered when deciding to discontinue treatment?
Treatment failure occurs with confirmation of disease progression. If there is a significant change in the patient’s status during the manufacturing period prior to infusion, this could result in treatment discontinuation. This is generally due to too rapid disease progression resulting in life-threatening organ toxicity or significant decline in performance status (e.g. ECOG 4) rendering it unsafe to proceed with CAR-T therapy from a toxicity perspective. Even patients with CNS disease that is controlled may benefit from this therapy so this is not a reason to discontinue treatment.
What settings are appropriate for treatment with the drug under review?
Liso-cel should only be administered in established CAR-T therapy programs approved to deliver this treatment.
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
Not relevant
Additional information
Liso-cel is an important addition to the CAR-T therapy landscape that will improve accessibility to this potentially life-saving therapy for patients, and should be available as a treatment option because of its relatively favourable toxicity profile and its ability to be considered for outpatient delivery or early outpatient follow-up.
Conflict of Interest Declarations — Lymphoma Canada
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
No
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician that contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Mona Shafey
Position: Clinical Associate Professor, University of Calgary
Date: 29-Aug-2021
Table 12: Conflict of Interest Declaration for Lymphoma Canada — Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Novartis | X | — | — | — |
Kite/Gilead | X | — | — | — |
BMS | X | — | — | — |
Declaration for Clinician 2
Name: Dr. Mahmoud Elsawy
Position: Assistant Professor, Dalhousie University
Date: 01-09-2021
Table 13: Conflict of Interest Declaration for Lymphoma Canada — Clinician 2
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Kite/Gilead | X | — | — | — |
Celgene/BMS | X | — | — | — |
Novartis | X | — | — | — |
Declaration for Clinician 3
Name: Dr. Neil Berinstein
Position: Medical Oncologist/Hematologist, Odette Sunnybrook cancer centre, 2075 Bayview Avenue, Toronto, Ontario, M4N3M5
Date: 30-08-2021
Table 14: Conflict of Interest Declaration for Lymphoma Canada — Clinician 3
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
n/a | — | — | — | — |
Declaration for Clinician 4
Name: Dr. Kevin Hay
Position: Hematologist, BC Cancer
Date: 02-09-2021
Table 15: Conflict of Interest Declaration for Lymphoma Canada — Clinician 4
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Celgene/BMS | — | X | — | — |
Kite/Gilead | — | X | — | — |
Novartis | X | — | — | — |
Declaration for Clinician 5
Name: Dr. John Kuruvilla
Position: Hematologist, Princess Margaret Cancer Centre
Date: 03-09-2021
Table 16: Conflict of Interest Declaration for Lymphoma Canada — Clinician 5
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Celgene/BMS | — | X | — | — |
Kite/Gilead | — | X | — | — |
Novartis | — | X | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.