Drugs, Health Technologies, Health Systems
Reimbursement Recommendation
Encorafenib (Braftovi)
Indication: In combination with cetuximab and mFOLFOX6, for the treatment of patients with mCRC with a BRAF V600E mutation, as detected by a validated test.
Sponsor: Pfizer Canada ULC
Final recommendation: Reimburse with conditions
Summary
What Is the Reimbursement Recommendation for Braftovi?
Canada’s Drug Agency (CDA-AMC) recommends that Braftovi, in combination with cetuximab and modified leucovorin (folinic acid), fluorouracil, and oxaliplatin (mFOLFOX6), be reimbursed by public drug plans for the treatment of patients with metastatic colorectal cancer (mCRC) with a BRAF V600E gene mutation, as detected by a validated test, if certain conditions are met.
Why Did CDA-AMC Recommend Reimbursement?
Evidence from 1 clinical trial showed that Braftovi, in combination with cetuximab and mFOLFOX6, results in improved progression-free and overall survival in patients with mCRC with a BRAF V600E gene mutation, compared with the trial investigator’s choice of chemotherapy, with or without bevacizumab. The pan-Canadian Oncology Drug Review Expert Review Committee determined that adding Braftovi to cetuximab plus mFOLFOX6, demonstrates acceptable clinical value compared with chemotherapy with or without bevacizumab in patients with mCRC with a BRAF V600E gene mutation, and addresses the need identified by both patients and clinicians for more effective therapy to delay disease progression and extend survival. This determination was enough for the pan-Canadian Oncology Drug Review Expert Review Committee to recommend that Braftovi be reimbursed for this indication. Given that Braftovi is expected to be an alternative to chemotherapy with or without bevacizumab, acceptable clinical value refers to added value over chemotherapy with or without bevacizumab.
Which Patients Are Eligible for Coverage?
Braftovi, in combination with cetuximab and mFOLFOX6, should only be covered for adult patients with mCRC with a confirmed BRAF V600E mutation. Patients should have good performance status and should not have active or symptomatic cancer in the brain or spinal cord. Braftovi should not be covered for patients who have received prior drug treatments for mCRC, or oxaliplatin treatment before (neoadjuvant) or after (adjuvant) surgery, if they experienced disease progression during treatment or recurrence within 6 months of completing it.
What Are the Conditions for Reimbursement?
Braftovi, in combination with cetuximab and mFOLFOX6, should only be reimbursed if the patient is under the care of a clinician who has expertise in managing mCRC and the cost of Braftovi is reduced. Treatment should be discontinued if the cancer worsens or if the patient experiences unacceptable side effects. Important budget impact considerations must be addressed for health systems to be able to adopt Braftovi.
Review Background
Disease background: Colorectal cancer (CRC) is caused by the abnormal growth of mucosal cells in the inner lining of the colon or rectum. In most cases, CRC starts as a polyp on the intestinal mucosa, which eventually develops into carcinoma.
In Canada, CRC is the fourth most commonly diagnosed cancer (estimated 25,200 cases in 2024) and the third leading cause of cancer-related mortality (estimated 9,400 deaths in 2024). Approximately 55% of patients present with metastatic CRC (mCRC), which has a poor 5-year survival rate (11% to 13%). The BRAF V600E is the most common BRAF mutation, occurring in 8% to 12.5% of mCRC cases, and it is a well-established poor prognostic factor.
In Canada, CRC is the fourth most common cancer, with an estimated 25,200 cases diagnosed in 2024, and the third leading cause of cancer-related mortality (an estimated 9,400 deaths in 2024).
CRC is the third leading cause of cancer-related mortality (an estimated 9,400 deaths in 2024). Approximately 55% of patients present with mCRC at diagnosis, which has a poor prognosis and survival rate (5-year survival rate of between 11% and 13%).
The BRAF V600E is the most common type of BRAF mutation affecting mCRC cases; it occurs in 8% to 12.5% of mCRC cases and is a well-established poor prognostic factor.
Indication and reimbursement request: Encorafenib (Braftovi), in combination with cetuximab and modified leucovorin (folinic acid), fluorouracil, and oxaliplatin (mFOLFOX6), has been approved by Health Canada for the treatment of patients with mCRC with a BRAF V600E mutation, as detected by a validated test. The sponsor is seeking reimbursement for this indication.
Drug under review: Encorafenib is a BRAF inhibitor available as a 75 mg oral capsule. The product monograph recommends a daily dose of 300 mg (i.e., four 75 mg capsules).
Treatment costs: At the submitted price of $52.76 per 75 mg capsule, the per 28-day cost of encorafenib is expected to be $5,909 per patient, based on the Health Canada–recommended dosage. Encorafenib is indicated for use in combination with cetuximab and mFOLFOX6. The cost of the regimen is expected to be $18,843 per patient per 28 days.
Highlights of Input From Interested Parties
The patient group (Colorectal Cancer Resource & Action Network in collaboration with the Canadian Cancer Survivor Network) provided the following input regarding the impacts of the disease, unmet needs, and outcomes of importance to patients:
There is a significant unmet clinical need for efficacious and tolerable therapeutics for patients with BRAF-mutant mCRC, who often experience poor clinical outcomes.
Current first-line therapy for patients with BRAF-mutant mCRC typically involves aggressive multiagent chemotherapy regimens (e.g., FOLFOX [leucovorin (folinic acid), fluorouracil, and oxaliplatin], FOLFIRI [leucovorin (folinic acid), fluorouracil, and irinotecan], FOLFOXIRI [leucovorin (folinic acid), fluorouracil, oxaliplatin, and irinotecan]), with or without bevacizumab. These treatments have limited effectiveness in BRAF-mutant mCRC, are often associated with substantial toxicity, and can be difficult for patients to tolerate, resulting in significant impacts on their quality of life.
Patients and caregivers reported that it was very important that new drug therapies improve their physical condition and quality of life.
The clinician groups (Canadian Gastrointestinal Oncology Evidence Network with the Medical Advisory Board of Colorectal Cancer Canada, and Ontario Health [Cancer Care Ontario] Gastrointestinal Cancer Drug Advisory Committee) and the clinical experts consulted by Canada’s Drug Agency (CDA-AMC) noted the following regarding unmet needs arising from the disease and place in therapy for the drug under review:
Unmet needs: BRAF-mutant mCRC is an aggressive form of the disease that responds poorly to treatment, with most standard-of-care (SOC) options often proving ineffective. Compared to patients without a BRAF mutation, patients with BRAF-mutant mCRC have significantly shorter overall survival (OS), and they frequently experience earlier and more extensive cancer recurrence.
There is an urgent need for novel therapies for patients with BRAF-mutant mCRC that can improve OS, provide more durable disease control, reduce symptom burden, and prevent the development of symptoms due to the aggressive progression of these cancers.
Anticipated place in therapy: The adoption of encorafenib, in combination with cetuximab and mFOLFOX6, represents a paradigm shift, establishing a new SOC for the management of BRAF V600E–mutant mCRC. It should be considered a first-line treatment option for patients with mCRC harbouring a BRAF V600E mutation.
The participating public drug programs raised potential implementation issues related to considerations for initiation, renewal, discontinuation, and prescribing of therapy; generalizability of trial findings to broader populations; care provision issues; system and economic issues; and the potential need to update the provisional funding algorithm. These issues are addressed in a separate Supplemental Material document found on the project landing page.
Recommendation
With a vote of 16 in favour and none against, the pan-Canadian Oncology Drug Review Expert Review Committee (pERC) recommends that encorafenib in combination with cetuximab plus mFOLFOX6 be reimbursed for the treatment of patients with mCRC with a BRAF V600E mutation, as detected by a validated test, only if the conditions listed in Table 1 are met.
Table 1: Reimbursement Conditions and Reasons
Reimbursement condition | Reason | Implementation guidance |
|---|---|---|
Initiation | ||
1. Treatment with EC + mFOLFOX6 should be reimbursed in adults (aged ≥ 18 years) with mCRC with a BRAF V600E mutation as detected by a validated test who meet the following criteria: 1.1. Have not received prior systemic therapy for mCRC. | Evidence from the BREAKWATER trial showed that treatment with EC + mFOLFOX6 resulted in clinically meaningful benefit in patients with these characteristics compared with mFOLFOX6, FOLFOXIRI, or CAPOX, with or without bevacizumab. | pERC agreed with the clinical experts that patients may be treated with EC plus alternative double chemotherapy regimens (e.g., FOLFIRI or CAPOX) at the discretion of the treating clinician. No evidence was identified to support using panitumumab in place of cetuximab in the EC + mFOLFOX6 combination. However, pERC agreed with clinical experts that this substitution may be made at the discretion of the attending clinician, given that the efficacy of the 2 drugs is expected to be comparable. According to the clinical experts consulted by CDA-AMC on this review, patients with BRAF V600E–mutated small bowel, appendiceal adenocarcinoma, or DPD deficiency could be considered for treatment with EC + mFOLFOX6. pERC noted that jurisdictions should follow DPD deficiency policies with respect to adjustments to chemotherapy regimens. pERC agreed with the clinical experts that it would be reasonable to offer EC + mFOLFOX6 as first-line treatment to patients with both a BRAF V600E mutation and locally confirmed dMMR or MSI-H who are unable to receive immune checkpoint inhibitors. This is aligned with the BREAKWATER trial, which allowed enrolment of patients with MSI-H or dMMR who could not receive immune checkpoint inhibitors due to a pre-existing medical condition, and included 1 such patient. |
2. Patients should have a good performance status. | The BREAKWATER trial included patients with an ECOG performance status of 0 to 1. | pERC agreed with the clinical experts consulted by CDA-AMC on this review that patients with an ECOG performance status of 2 may be treated at the discretion of the treating clinician. |
3. Treatment with EC + mFOLFOX6 should not be used in patients who have: 3.1. Symptomatic CNS metastases 3.2. Received prior oxaliplatin adjuvant or neoadjuvant therapy if they experienced new lesions or recurrence during or within 6 months from the end of adjuvant or neoadjuvant treatment. | The BREAKWATER trial excluded patients with such characteristics, and the CDA-AMC review did not identify any evidence regarding the efficacy and safety of EC + mFOLFOX6 in patients with symptomatic CNS metastases or with new lesions or recurrence during or within 6 months from the end of adjuvant or neoadjuvant treatment. | It would be reasonable to consider offering EC + FOLFIRI to patients who received mFOLFOX6 in the adjuvant setting and whose disease progressed within 6 months, given that these patients would be considered to have disease that is resistant to mFOLFOX6. |
Discontinuation | ||
4. Treatment with EC + mFOLFOX6 should be discontinued upon the occurrence of any of the following: 4.1. Progressive disease per RECIST 1.1 4.2. Unacceptable toxicity. | In the BREAKWATER trial, tumour response was assessed every 6 weeks for the first 18 months, and every 8 weeks thereafter, using RECIST 1.1 criteria. Treatment was discontinued due to disease progression or unacceptable toxicities. | pERC indicated that if either encorafenib or cetuximab is discontinued for toxicity, the companion drug (of the pair) should be discontinued as well, given that BRAF-mutant tumours are resistant to EGFR inhibitors alone (e.g., cetuximab or panitumumab) and encorafenib monotherapy would be insufficient treatment. pERC agreed with the clinical experts that patients who discontinue encorafenib or cetuximab for reasons other than progression (e.g., due to a lack of tolerability) may be eligible for downstream encorafenib (or cetuximab or panitumumab). However, patients whose disease progresses on encorafenib or cetuximab are not eligible for treatment with a subsequent line of therapy. |
Prescribing | ||
5. Treatment with EC + mFOLFOX6 should be prescribed by medical oncologists with expertise in managing mCRC, and cetuximab should be administered in an approved setting for oncology infusions. | This will ensure that EC + mFOLFOX6 is prescribed for patients for whom the treatment is appropriate and that adverse effects are managed in an optimal and timely manner. | — |
6. EC + mFOLFOX6 for mCRC with a BRAF V600E mutation should only be reimbursed when started in combination. | There is no evidence from the BREAKWATER trial indicating an efficacy or safety benefit in using either component of the regimen as monotherapy. | According to the clinical experts, the majority of patients will be treated with the combination; however, situations exist (e.g., patients who experience limited tolerability) in which EC without chemotherapy may be considered the preferred option. pERC noted that encorafenib plus an EGFR inhibitor may be added for a time-limited period to first-line doublet chemotherapy in patients whose disease has not progressed. In the absence of supporting evidence, pERC could not provide guidance regarding the use of EC without chemotherapy in patients with mCRC with a BRAF V600E mutation. |
Pricing | ||
7. A reduction in price | Using the CDA-AMC base-case analysis, the ICER for EC + mFOLFOX6 was $432,400 per QALY gained when compared with SOC chemotherapy in the indicated population. A band 4a price reduction would be required to achieve cost-effectiveness at a $50,000 per QALY threshold. A band 4 price reduction would be required to achieve cost-effectiveness at a $100,000 per QALY threshold. This price reduction estimate is influenced by both the cost of encorafenib and the cost of cetuximab. Price reductions for any given willingness-to-pay threshold are available in the CDA-AMC main report and Supplemental Material document. | The CDA-AMC analysis is based on public list prices for all treatments. Further price reductions may be required if there are price arrangements (discounts) currently in place for any treatment included in the economic analysis. Likewise, further price reductions may be required to address the economic feasibility of adoption. |
Feasibility of adoption | ||
8. The economic feasibility of adoption of EC + mFOLFOX6 must be addressed. | At the submitted price, the incremental budget impact of EC + mFOLFOX6 is expected to be greater than $40 million in year 2 and year 3. | The estimated budget impact is highly sensitive to assumptions about the rate of uptake, which may be higher than estimated within the CDA-AMC BIA base case. |
BIA = budget impact analysis; CAPOX = capecitabine and oxaliplatin; CDA-AMC = Canada’s Drug Agency; CNS = central nervous system; dMMR = deficient mismatch repair; DPD = dihydropyrimidine dehydrogenase; EC = encorafenib plus cetuximab; ECOG = Eastern Cooperative Oncology Group; FOLFIRI = leucovorin (folinic acid), fluorouracil, and irinotecan; FOLFOXIRI = folinic acid, fluorouracil, oxaliplatin, and irinotecan; ICER = incremental cost-effectiveness ratio; mCRC = metastatic colorectal cancer; mFOLFOX6 = modified leucovorin, fluorouracil, and oxaliplatin; MSI-H = microsatellite instability-high; pERC = pan-Canadian Oncology Drug Review Expert Review Committee; QALY = quality-adjusted life-year; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours version 1.1; SOC = standard of care.
aFor the statement regarding the size of the price reduction required, band 1 = 1% to 24%, band 2 = 25% to 49%, band 3 = 50% to 74%, and band 4 = 75% or greater.
Rationale for the Recommendation
Clinical Value
Based on the totality of the clinical evidence, pERC concluded that, in patients with a BRAF V600E mutation, encorafenib in combination with cetuximab (EC) plus mFOLFOX6 demonstrates acceptable clinical value compared with the investigator’s choice of chemotherapy with or without bevacizumab. The investigator’s choice of chemotherapy included mFOLFOX6, FOLFOXIRI, or CAPOX. Given that EC plus mFOLFOX6 is expected to be an alternative to chemotherapy with or without bevacizumab, acceptable clinical value refers to added value versus chemotherapy with or without bevacizumab.
Evidence from the phase III, open-label BREAKWATER trial (N = 479; study arms B and C) demonstrated that in patients with mCRC with a BRAF V600E mutation, first-line treatment with EC plus mFOLFOX6 results in added clinical benefit versus chemotherapy with or without bevacizumab. Treatment with EC plus mFOLFOX6 demonstrated statistically significant and clinically meaningful improvements in progression-free survival (PFS) and OS compared with mFOLFOX6, FOLFOXIRI, or CAPOX, with or without bevacizumab. The median PFS was 12.8 months with EC plus mFOLFOX6 versus 7.1 months with comparator chemotherapy, with or without bevacizumab (hazard ratio 0.53; 95% confidence interval [CI], 0.40 to 0.68). The 15-month between-group difference in PFS rates was ██████ ███ ███ █████ ██ █████. The median OS was 30.3 months with EC plus mFOLFOX6 versus 15.1 months with comparator chemotherapy, with or without bevacizumab (hazard ratio 0.49; 95% CI, 0.37 to 0.63). The 24-month between-group difference in OS rates was ██████ ███ ███ ████ █ ██ █████. Moderate-certainty evidence suggests that EC plus mFOLFOX6 likely results in little to no clinically important difference in the proportion of patients who experienced 1 or more serious adverse events. The impact of EC plus mFOLFOX6 on health-related quality of life (HRQoL) compared to the investigator’s choice of chemotherapy with or without bevacizumab was very uncertain due to the large amount of missing data and the open-label design of the trial. pERC considered input from clinicians and clinical experts consulted by CDA-AMC indicating that the safety profile of EC plus mFOLFOX6 observed in the BREAKWATER trial appeared consistent with the known, predictable, and generally manageable safety profiles of the individual components of the regimen.
Patients and clinicians identified the need for effective treatment options that delay disease progression, extend survival, improve quality of life, reduce adverse events, and provide additional treatment choice. pERC concluded that, compared to the comparator chemotherapy, with or without bevacizumab, EC plus mFOLFOX6 met some of the identified needs in that it delays disease progression, prolongs survival, and offers an additional treatment option.
Further information on the committee’s discussion on clinical value is provided in the Summary of Deliberation section.
Developing the Recommendation
The determination of acceptable clinical value was sufficient for pERC to recommend reimbursement of EC plus mFOLFOX6. As part of the deliberation on whether to recommend reimbursement, the committee also considered unmet clinical need, unmet nonclinical need, and health inequity. Information on this discussion is provided in the Unmet Clinical Need and Distinct Social and Ethical Considerations domains in the Summary of Deliberation section.
Because pERC recommended that EC plus mFOLFOX6 be reimbursed, the committee also deliberated whether reimbursement conditions should be added to address important economic considerations, health system impacts, or social and ethical considerations so that the clinical value of the treatment is realized. The resulting reimbursement conditions, with accompanying reasons and implementation guidance, are stated in Table 1.
Summary of Deliberation
pERC considered all the following domains of value of the deliberative framework before developing its recommendation: clinical value, unmet clinical need, distinct social and ethical considerations, economic considerations, and impacts on health systems. For further information on the domains of value, refer to Expert Committee Deliberation at Canada’s Drug Agency.
The committee considered the following key discussion points, organized by the 5 domains of value.
Clinical Value
Appropriate comparators: pERC observed that FOLFIRI, identified as a relevant comparator for the target patient population, was not evaluated in the BREAKWATER trial. The committee considered the clinical experts’ input indicating that, based on outcomes observed in clinical practice, FOLFIRI is expected to provide comparable efficacy versus other doublet chemotherapy regimens such as mFOLFOX6 and CAPOX, although differences in safety and tolerability may exist. In the absence of supporting evidence, pERC could not determine the relative efficacy and safety of EC plus mFOLFOX6 compared with FOLFIRI. However, the committee agreed with the clinical experts that the choice of chemotherapy backbone should be based on the attending clinician’s discretion, guided by patient preferences, comorbidities, and the side effects of the specific chemotherapy regimen.
Efficacy versus investigator’s choice of chemotherapy, with or without bevacizumab: Evidence from the BREAKWATER trial demonstrated that treatment with EC plus mFOLFOX6 was associated with clinically meaningful and statistically significant improvements in PFS and OS compared with the investigator’s choice of chemotherapy with or without bevacizumab. HRQoL benefit was inconclusive due to potential bias and the large amount of missing data.
Clinical importance of treatment effects: pERC considered outcomes identified as most relevant by patients and clinicians, including efficacy, tolerability, as well as improvement in physical condition and HRQoL. The committee noted that compared with mFOLFOX6, FOLFOXIRI, or CAPOX (with or without bevacizumab), treatment with EC plus mFOLFOX6 resulted in meaningful survival benefits as demonstrated by the statistically significant and clinically meaningful improvements in PFS and OS observed in the BREAKWATER trial. pERC noted that the trial identified no new safety signals beyond the known and generally manageable adverse events observed with the individual components of this regimen. However, the committee could not determine whether treatment with EC plus mFOFOX6 resulted in a meaningful improvement in patients’ quality of life due to potential bias and the substantial amount of missing data.
Certainty of the evidence: pERC discussed the certainty of evidence as assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) method. For PFS at 12 and 16 months, as well as OS at 12 and 24 months, the certainty of evidence was rated as “High,” indicating that the survival benefits from treatment with EC plus mFOLFOX6 were clinically important. The certainty in the evidence regarding HRQoL at 24 and 48 weeks (as measured by the EORTC QLQ-C30 Global Health Status score) was rated as “Very low” due to risk of bias associated with patient-reported outcomes, missing data, and imprecision, as indicated by the lower bound of the 95% CI suggesting deterioration in HRQoL. Certainty of the serious adverse event evidence was rated “Moderate,” suggesting that EC plus mFOLFOX6 likely results in little to no clinically meaningful difference in the proportion of patients with at least 1 serious adverse event.
Clinical value: Based on the preceding considerations, pERC determined that in patients with mCRC with a BRAF V600E mutation, treatment with EC plus mFOLFOX6 demonstrates acceptable clinical value compared with mFOLFOX6, FOLFOXIRI, or CAPOX, with or without bevacizumab.
Unmet Clinical Need
Input on unmet clinical need: pERC acknowledged that patients and clinicians emphasized the need for effective treatment options that extend survival, improve disease control, and enhance patients’ quality of life. The committee noted clinical experts’ input indicating that, despite combining bevacizumab with chemotherapy in first-line treatment, patients with BRAF-mutant mCRC experience more aggressive disease, lower response rates, and shorter survival than patients with BRAF wild-type mCRC. Currently, patients with BRAF-mutant mCRC do not have access to targeted therapies in the first-line setting. The clinical experts consulted by CDA-AMC noted that initiating targeted treatment early is important to improve outcomes in BRAF V600E-mutant mCRC and that treatment options in the second-line and later-line settings are limited.
Severity of the disease: The BRAF V600E mutation is the most common type of BRAF mutation affecting mCRC cases; it occurs in 8% to 12.5% of mCRC cases and is a well-established poor prognostic factor. Five-year survival rates of patients with mCRC are poor (stage IV colon cancer is associated with a 5-year survival rate of 11% to 12%, and stage IV rectal cancer is associated with a 5-year survival rate of 13%).
Availability of treatment options: pERC noted the clinical experts’ input indicating that FOLFIRI and FOLFOX (with or without bevacizumab) are the most commonly used first-line chemotherapy regimens for patients with BRAF V600E-mutant mCRC in clinical practice, whereas FOLFOXIRI and CAPOX are used less frequently. For patients with mCRC harbouring a BRAF V600E mutation and microsatellite instability-low, microsatellite stable, or proficient mismatch repair, the recommended first-line treatment is a multiagent chemotherapy regimen (e.g., FOLFIRI, mFOLFOX6, FOLFOXIRI, or CAPOX) with or without bevacizumab.
pERC noted the need for a funding algorithm that covers alternative double chemotherapy regimens (e.g., FOLFIRI) as backbone with EC as first-line therapy and that offers options for patients with mCRC who have a poor prognosis and limited treatment options, such as those with liver metastases who may derive benefit from EC plus mFOLFOX6.
Distinct Social and Ethical Considerations
Ethical implications: pERC noted that patients who identified as Black or multiracial were underrepresented in the BREAKWATER trial, with only 1 patient who received SOC chemotherapy in the trial. Although the limited representation in certain groups in the trial may lead to decisional uncertainties for these groups, pERC heard from the clinical experts consulted by CDA-AMC that all patients with BRAF V600E-mutant mCRC would be eligible for treatment with EC plus mFOLFOX6 regardless of race or ethnicity. The committee discussed the fact that EC plus mFOLFOX6 should be prescribed by a medical oncologist. However, pERC agreed with the clinical experts that patients living in remote areas with limited access to medical oncologists may receive treatment at a local hospital, with follow-up visits occurring every few months at a cancer centre with expertise in managing mCRC. Patient group input highlighted the need for better, quicker, and equitable access to funded drug therapies and clinical trials in Canada.
Economic Considerations
Health impacts of EC plus mFOLFOX6 versus relevant comparators: EC plus mFOLFOX6 is predicted to be associated with a gain of 1.04 life-years compared to SOC chemotherapy and may result in a gain of 0.85 quality-adjusted life-years (QALYs) compared to SOC chemotherapy.
Cost of EC plus mFOLFOX6 versus relevant comparators: EC plus mFOLFOX6 is predicted to be associated with higher costs to the health care system than SOC chemotherapy (incremental costs = $367,543), primarily driven by increased costs associated with drug acquisition.
Key findings of the economic evaluation: Based on the submitted evidence using the sponsor’s cost-utility analysis, the CDA-AMC base-case analysis estimated that the incremental cost-effectiveness ratio (ICER) for EC plus mFOLFOX6 in patients with mCRC with a BRAF V600E mutation was $432,400 per QALY gained when compared with SOC chemotherapy (Figure 1).
Figure 1: Estimate of the ICER Used by pERC to Inform the Price Condition
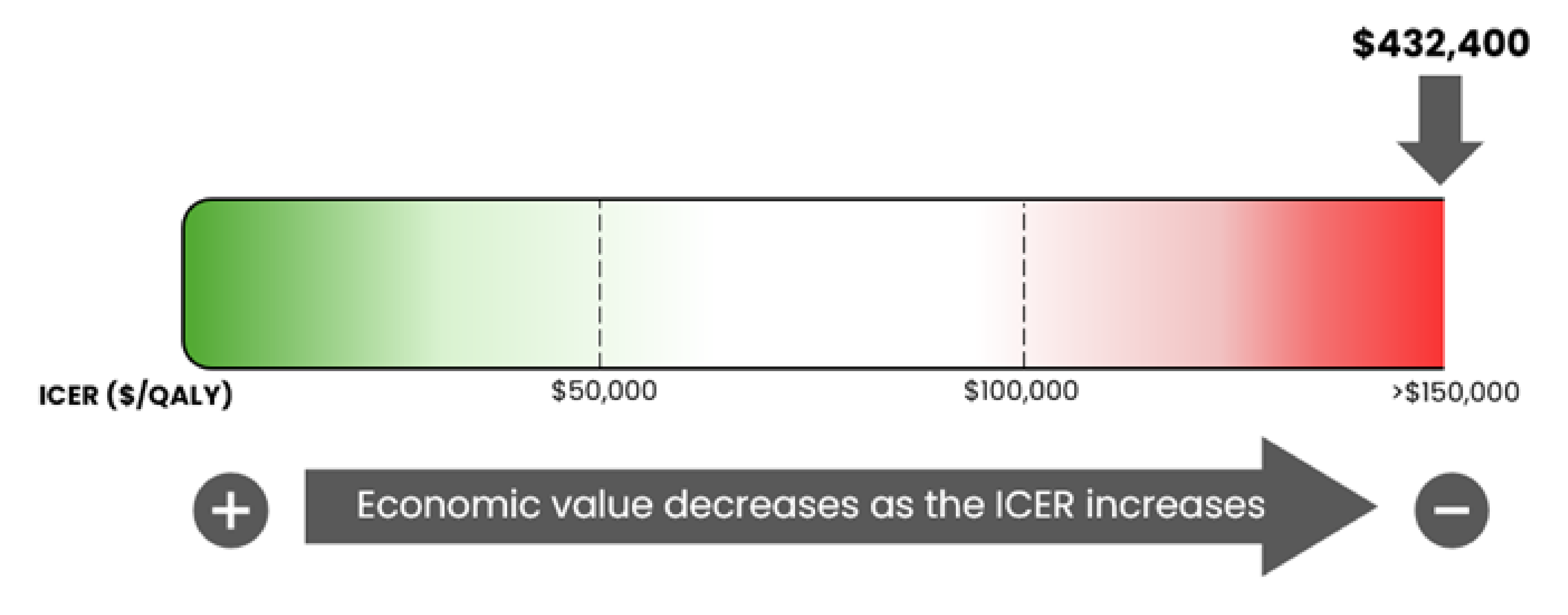
ICER = incremental cost-effectiveness ratio; pERC = pan-Canadian Oncology Drug Review Expert Review Committee; QALY = quality-adjusted life-year
Certainty of the evidence: The estimated ICER was sensitive to the distribution of subsequent treatment and was lower when the distribution was more reflective of clinical practice in Canada.
Other considerations: The price reduction necessary to make EC plus mFOLFOX6 cost-effective is also driven by the price of cetuximab. A price reduction in excess of 90%, in addition to reductions in the cost of cetuximab, would be required to achieve cost-effectiveness at a threshold of $100,000 per QALY gained. The estimated price reduction is also complicated by the fact that encorafenib and cetuximab are part of subsequent therapy for patients receiving SOC chemotherapy. Additionally, the committee noted that the uptake of EC plus mFOLFOX6 may be underestimated and the true 3-year budget impact of reimbursement is likely to be substantially higher than $175 million.
Impacts on Health Systems
Anticipated budget impact: CDA-AMC estimates that the budget impact of reimbursing Braftovi in combination with cetuximab and mFOLFOX6 for the indicated population will be approximately $175 million over the first 3 years of reimbursement compared to the amount currently spent on SOC chemotherapy, with an estimated expenditure of $70 million on Braftovi over this period. The actual budget impact of reimbursing Braftovi in combination with cetuximab and mFOLFOX6 will depend on its uptake. The incremental budget impact of reimbursing Braftovi in combination with cetuximab and mFOLFOX6 is predicted to be greater than $40 million in year 2 and year 3. pERC noted that the economic feasibility of adoption must be addressed.
Testing procedure considerations: pERC acknowledged the need to evaluate BRAF V600E status before the initiation of EC plus mFOLFOX6. pERC also noted that BRAF V600E testing is currently performed as the SOC for patients with mCRC in Canada and is not anticipated to be an implementation or access barrier.
Sources of Information Used by the Committee
To make its recommendation, the committee considered the following information (links to the full documents for the review can be found on the project webpage):
the CDA-AMC review of the clinical and pharmacoeconomic evidence submitted by the sponsor as well as relevant ethical issues related to encorafenib (refer to the main report and Supplemental Material document)
the sponsor’s comments on the draft report and the CDA-AMC responses
patients' perspectives gathered by 1 patient group, Colorectal Cancer Resource & Action Network, in collaboration with the Canadian Cancer Survivor Network (refer to the Patient and Clinician Group Input document)
input from 2 clinician groups, 1 joint submission from the Canadian Gastrointestinal Oncology Evidence Network and the Medical Advisory Board of Colorectal Cancer Canada, and 1 from Ontario Health (Cancer Care Ontario) Gastrointestinal Cancer Drug Advisory Committee (refer to the Patient and Clinician Group Input document)
input from public drug programs that participate in the reimbursement review process (refer to the Supplemental Material document)
input from 2 clinical experts with expertise in the management of CRC, consulted by CDA-AMC.
All feedback received in response to the draft recommendation is available on the CDA-AMC project webpage.
pERC Information
Members of the Committee
Dr. Catherine Moltzan (Chair), Dr. Kelvin Chan (Vice-Chair), Paul Agbulu, Dr. Phillip Blanchette, Dr. Matthew Cheung, Dr. Michael Crump, Annette Cyr, Dr. Jennifer Fishman, Dr. Jason Hart, Terry Hawrysh, Dr. Yoo-Joung Ko, Dr. Aly-Khan Lalani, Amy Peasgood, Dr. Anca Prica, Dr. Michael Raphael, Dr. Adam Raymakers, Dr. Patricia Tang, Dr. Pierre Villeneuve, and Danica Wasney.
Meeting date: January 14, 2026
Regrets: One expert committee member did not attend.
Conflicts of interest: One expert committee member did not participate due to considerations of conflict of interest.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.