Drugs, Health Technologies, Health Systems
Reimbursement Review
Durvalumab (Imfinzi)
Sponsor: AstraZeneca Canada Inc.
Therapeutic area: Gastric or gastroesophageal junction adenocarcinoma
Summary
What Is Gastric or Gastroesophageal Junction Cancer?
Gastric or gastroesophageal junction (GEJ) adenocarcinomas are serious cancers that start in the stomach or where the stomach meets the esophagus (the tube that connects the throat to the stomach). These cancers can grow quickly and spread to nearby lymph nodes. In the patient input received, patients identified physical symptoms like pain, fatigue, trouble eating, along with emotional strain, difficulty with daily activities, financial burdens from treatment and travel, and changes in their sense of identity and relationships as key negative impacts of gastric or GEJ cancer.
In 2024, approximately 4,000 people living in Canada were diagnosed with gastric cancer, and approximately 2,000 people died from the disease.
What Are the Treatment Goals and Current Treatment Options for Gastric or GEJ Cancer?
Treatment goals for gastric or GEJ cancer include slowing or controlling the disease, improving quality of life, and reducing side effects. Patients with gastric or GEJ cancer emphasized the need for fair and timely access to treatments that help them live longer, feel better, and manage their symptoms.
The patient group input identified the following outcomes as important: living longer, managing disease symptoms, delaying the disease from getting worse, having fewer side effects, improving quality of life, keeping treatment as short as possible, and reducing financial stress. Other important outcomes identified through clinician input included achieving a long-lasting cure, improving the cancer’s response to treatment to support curative surgery, and helping patients return to their normal daily activities.
The current treatment options for resectable (can be removed with surgery) gastric or GEJ cancer include perioperative chemotherapy with the fluorouracil, leucovorin, oxaliplatin, and docetaxel (FLOT) regimen, neoadjuvant chemoradiation followed by surgical resection and adjuvant nivolumab therapy, and doublet regimens, including fluoropyrimidine plus oxaliplatin, and fluoropyrimidine plus cisplatin.
What Is Imfinzi and Why Did Canada’s Drug Agency Conduct This Review?
Imfinzi is a drug that is administered by IV infusion. At the time this review was conducted, Health Canada was reviewing Imfinzi in combination with FLOT chemotherapy as neoadjuvant and adjuvant treatment, followed by adjuvant Imfinzi monotherapy, for the treatment of adult patients with resectable gastric or GEJ cancer.
Canada’s Drug Agency (CDA-AMC) reviewed Imfinzi in combination with FLOT to inform a recommendation to the participating public drug programs on whether it should be reimbursed for the treatment of adult patients with resectable gastric or GEJ cancer.
How Did CDA-AMC Evaluate Imfinzi Plus FLOT?
CDA-AMC reviewed the clinical evidence on the beneficial and harmful effects, as well as the economic evidence, for Imfinzi plus FLOT chemotherapy versus other treatments used in Canada for the treatment of resectable gastric or GEJ cancer. Neoadjuvant chemoradiation followed by adjuvant nivolumab therapy, perioperative FLOT chemotherapy, as well as fluoropyrimidine plus oxaliplatin and fluoropyrimidine plus cisplatin were considered relevant treatments to compare with Imfinzi plus FLOT when reviewing the clinical evidence.
CDA-AMC identified equity and ethical considerations relevant to Imfinzi plus FLOT and resectable gastric or GEJ cancer.
The review was informed by materials submitted by the sponsor, which included clinical and economic evidence.
The review was also informed by 1 patient group submission, 2 clinician group submissions, and 1 industry submission in response to our call for input, and by input from the participating public drug programs on issues that may impact their ability to implement a recommendation.
Two medical oncologists representing Ontario and British Columbia were consulted as part of the review process.
What Were the Findings?
Clinical Evidence
CDA-AMC reviewed the following clinical evidence:
1 randomized, double-blind, placebo-controlled phase III trial (the MATTERHORN trial) comparing Imfinzi plus FLOT chemotherapy with placebo plus FLOT in 948 adult patients with resectable gastric or GEJ cancer
Imfinzi plus FLOT group: received Imfinzi with FLOT chemotherapy before and after surgery, followed by Imfinzi alone
placebo plus FLOT group: received placebo with FLOT chemotherapy before and after surgery, followed by placebo alone.
The findings for the comparison of Imfinzi plus FLOT versus placebo plus FLOT were as follows:
Imfinzi plus FLOT may result in a clinically meaningful improvement in overall survival at 36 months when compared with placebo plus FLOT. The certainty of the evidence was low.
Imfinzi plus FLOT likely results in a clinically meaningful improvement in event-free survival at 36 months when compared with placebo plus FLOT. The certainty of the evidence was moderate.
Imfinzi plus FLOT may result in little to no difference in health-related quality of life at the end of treatment when compared with placebo plus FLOT. The certainty of the evidence was low.
In the overall study period, Imfinzi plus FLOT may result in an increase in the proportion of patients with serious adverse events when compared with placebo plus FLOT. The certainty of the evidence was low.
Harms were consistent with the known safety profile of chemotherapy and PD–L1 inhibitors, with no new safety signals identified.
There was no evidence to inform how Imfinzi plus FLOT compares with neoadjuvant chemoradiation followed by adjuvant nivolumab, particularly in the treatment of GEJ cancer.
Economic Evidence
Imfinzi is available as a solution for IV infusion (50 mg/mL). At the submitted price of $938.67 per 2.4 mL vial and $3,911.11 per 10 mL vial, the cost per 28-day cycle of durvalumab is expected to be $11,733 per patient, based on the Health Canada–recommended dosage. When used in combination with FLOT, the total cost of Imfinzi plus FLOT is expected to be $17,582 per cycle for the first 4 cycles and $11,733 for subsequent cycles.
Key clinical efficacy data (disease recurrence, time to death, postrecurrence survival) in the economic model were derived from the MATTERHORN trial, which compared Imfinzi plus FLOT with placebo plus FLOT. Evidence submitted by the sponsor indicates that Imfinzi plus FLOT likely improves event-free survival compared with placebo plus FLOT and may improve overall survival at 36 months in patients with resectable gastric or GEJ adenocarcinoma.
The results of the CDA-AMC base case suggest the following:
Imfinzi plus FLOT is predicted to be associated with higher costs to the health care system than FLOT alone (incremental costs = $96,818), primarily driven by increased costs associated with drug acquisition.
Imfinzi plus FLOT is predicted to be associated with a gain of 1.63 life-years compared to FLOT alone and may result in a gain of 1.44 quality-adjusted life-years (QALYs) compared to FLOT alone.
The incremental cost-effectiveness ratio (ICER) of Imfinzi plus FLOT compared to FLOT was $67,176 per QALY gained in the CDA-AMC base case. The estimated ICER was sensitive to the choice of model used for long-term time-to-disease recurrence extrapolation. An alternative analysis that utilized a different extrapolation for long-term time to recurrence increased the ICER to $81,175 per QALY gained.
CDA-AMC estimates that the budget impact of reimbursing Imfinzi for use in combination with FLOT for the treatment of resectable gastric or GEJ cancer will be approximately $113 million over the first 3 years of reimbursement compared to the amount currently spent on comparators. The expenditure on Imfinzi over this period is predicted to be $114 million (Imfinzi plus FLOT = $137 million). The actual budget impact of reimbursing Imfinzi will depend on the proportion of patients who receive postoperative treatment as well as the market uptake. The incremental budget impact of reimbursing Imfinzi is predicted to be greater than $40 million in year 2 and year 3, and the economic feasibility of adoption must be addressed.
Abbreviations
BIRC
blinded independent review committee
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
CGOEN
Canadian GI Oncology Evidence Network
CROSS
Chemoradiotherapy for Esophageal Cancer Followed by Surgery Study
DCO
data cut-off
DFS
disease-free survival
ECOG
Eastern Cooperative Oncology Group
EFS
event-free survival
EORTC
European Organisation for Research and Treatment of Cancer
FAS
full analysis set
FLOT
fluorouracil, leucovorin, oxaliplatin, and docetaxel
GEJ
gastroesophageal junction
GI DAC
Gastrointestinal Cancer Drug Advisory Committee
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HR
hazard ratio
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
IL38
item library 38
ITC
indirect treatment comparison
KM
Kaplan-Meier
MID
minimal important difference
OS
overall survival
pCR
pathological complete response
PS
performance status
QALY
quality-adjusted life-year
QLQ-C30
Quality of Life Questionnaire Core 30
QLQ-STO22
Quality of Life Questionnaire Stomach 22
RCT
randomized controlled trial
RECIST
Response Evaluation Criteria in Solid Tumours
TAP
tumour area positivity
TEAE
treatment-emergent adverse event
Background
Introduction
The objectives of this report are as follows:
Review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of durvalumab at a dose of 1,500 mg in both neoadjuvant and adjuvant periods in combination with fluorouracil, leucovorin, oxaliplatin, and docetaxel (FLOT) chemotherapy, followed by adjuvant durvalumab monotherapy, for the treatment of adult patients with resectable gastric or gastroesophageal junction (GEJ) adenocarcinoma. The focus will be placed on comparing durvalumab to relevant comparators in clinical practice in Canada, including perioperative FLOT chemotherapy, neoadjuvant chemoradiation plus adjuvant nivolumab, and chemotherapy regimens such as fluoropyrimidine plus oxaliplatin and fluoropyrimidine plus cisplatin, as well as identifying gaps in the current evidence. This focus is outlined in Table 1.
Review and critically appraise the economic information submitted by the sponsor, including a cost-effectiveness analysis and budget impact analysis. The focus of the Economic Review is aligned with the scope of the Clinical Review, unless otherwise stated. For most reviews, a Canada’s Drug Agency (CDA-AMC) base case is developed, informed by clinical expert input, the available clinical evidence, and the best interpretation of the economic evidence based on the information provided by the sponsor.
The application was submitted by the sponsor before receiving a Notice of Compliance from Health Canada. This report reflects the anticipated indication and recommended dosage for durvalumab in combination with FLOT during the initial CDA-AMC review period.
Table 1: Information on the Drug Under Review and on the CDA-AMC Review
Item | Description |
|---|---|
Information on the application submitted for review | |
Drug | Durvalumab (Imfinzi), 50 mg/mL, concentrate for IV infusion |
Sponsor | AstraZeneca Canada Inc. |
Health Canada indication | Durvalumab in combination with FLOT chemotherapy as neoadjuvant and adjuvant treatment, followed by adjuvant durvalumab monotherapy, for the treatment of adult patients with resectable gastric or gastroesophageal junction adenocarcinoma (stages II to IVa). |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review and Project Orbis (Type A) |
NOC date | January 22, 2026 |
Mechanism of action | Durvalumab is a human monoclonal antibody that acts as a potent inhibitor of human PD-L1, selectively blocking the interaction of PD-L1 with PD-1 and CD80. This promotes T-cell activity and antitumour immune responses. |
Recommended dosage | The recommended dose of durvalumab in the neoadjuvant period is 1,500 mg in combination with FLOT chemotherapy every 4 weeks for up to 2 cycles before surgery. In the adjuvant period, the recommended dose is durvalumab 1,500 mg in combination with FLOT chemotherapy every 4 weeks for up to 2 cycles, followed by durvalumab 1,500 mg as monotherapy every 4 weeks for up to 10 cycles. Patients with a body weight of 30 kg or less must receive weight-based dosing of durvalumab at 20 mg/kg every 4 weeks in combination with FLOT chemotherapy for 2 cycles before surgery and 2 cycles after surgery, followed by durvalumab 20 mg/kg every 4 weeks as monotherapy until weight increases to greater than 30 kg. |
Submission type | Initial |
Sponsor’s reimbursement request | Per proposed indication |
Submitted price | $938.67 per 2.4 mL vial (120 mg durvalumab) $3,911.11 per 10 mL vial (500 mg durvalumab) |
Information on the CDA-AMC review | |
Review type | Standard |
Clinical review focusa | Population: As defined in the Health Canada indication Subgroups: None Intervention: Per recommended dosage Comparators:
Efficacy outcomes: EFS, OS, pCR, DFS, surgery rate, R0 rate, MFS, DSS, HRQoL Harms outcomes: AEs, SAEs, WDAEs, mortality, AESIs (pneumonitis, hepatic events, diarrhea or colitis, hypothyroid or hyperthyroid events, thyroiditis, adrenal insufficiency, dermatitis or rash events, infusion-related reaction) |
AE = adverse event; AESI = adverse event of special interest; CDA-AMC = Canada’s Drug Agency; DFS = disease-free survival; DSS = disease-specific survival; EFS = event-free survival; FLOT = fluorouracil, leucovorin, oxaliplatin, and docetaxel; HRQoL = health-related quality of life; MFS = metastasis-free-survival; NOC = Notice of Compliance; OS = overall survival; pCR = pathological complete response; R0 = complete resection; SAE = serious adverse event; WDAE = withdrawal due to adverse event.
aThe Economic Review aligns with the scope of the Clinical Review, unless otherwise stated.
bAlthough several different chemotherapy regimens have been used historically, FLOT is the current standard of care for patients receiving perioperative treatment.
cCDA-AMC has previously issued a reimbursement recommendation for this drug for the same indication or a similar indication.
Submission History for the Drug Under Review
CDA-AMC has previously reviewed durvalumab for multiple indications through the Reimbursement Review process and, in each case, issued a recommendation to reimburse with clinical criteria and/or conditions, as follows:
durvalumab in combination with etoposide and platinum chemotherapy (cisplatin or carboplatin) for the first-line treatment of adult patients with extensive-stage small cell lung cancer
durvalumab in combination with etoposide and platinum chemotherapy (cisplatin or carboplatin) for the first-line treatment of adult patients with unresectable hepatocellular carcinoma requiring systemic therapy
durvalumab in combination with gemcitabine and platinum-based chemotherapy for the first-line treatment of patients with locally advanced (not amenable to surgery) or metastatic biliary tract cancer
durvalumab following curative-intent, platinum-based concurrent chemoradiation therapy for the treatment of patients with locally advanced, unresectable stage III non–small cell lung cancer.
Sources of Information
The contents of the Reimbursement Review report are informed by materials submitted by the sponsor,1 input received from interested parties (patient groups, clinician groups, and drug programs), and input from clinical experts consulted for this review.
Calls for patient group, clinician group, and industry input are issued for each Non-Sponsored Reimbursement Review. The following submissions were received: 1 patient group submission from My Gut Feeling–Stomach Cancer Foundation of Canada and 2 clinician group submissions from the Canadian GI Oncology Evidence Network (CGOEN) and the Ontario Health (Cancer Care Ontario) Gastrointestinal Cancer Drug Advisory Committee (GI DAC). Patient input from the My Gut Feeling–Stomach Cancer Foundation of Canada was gathered through an international online survey of patients and caregivers affected by gastric, esophageal, and/or gastroesophageal cancer between September 15 and 24, 2025. In total, 29 people completed the survey. Information included in the clinician input from CGOEN was based on the MATTERHORN trial and expert consensus review by gastrointestinal cancer specialists in Canada. Information in the clinician group input from GI DAC was gathered by email. The full submissions received are available on the project landing page in the consolidated input document. The drug programs provide input on each drug being reviewed through the Reimbursement Review process by identifying issues that may impact their ability to implement a recommendation.
Input from patient and clinician groups is considered throughout the review, including in the selection of outcomes to include in the Clinical Review and in the interpretation of the clinical and economic evidence. Relevant patient and clinician group input is summarized in the Disease Background, Current Management, and Unmet Needs and Existing Challenges sections.
Each review team includes at least 1 clinical expert with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process. Two oncologists with expertise in the diagnosis and management of gastric or GEJ adenocarcinoma participated as part of the review team, representing Ontario and British Columbia.
Disease Background
Gastric cancer is the fifth most commonly diagnosed malignancy and the fourth leading cause of cancer-related deaths worldwide.2 Adenocarcinoma is the most common type of gastric cancer, accounting for approximately 95% of all gastric cancer cases.3 Gastric or GEJ adenocarcinoma are a heterogeneous group of highly lethal malignancies of the upper gastrointestinal tract, characterized by diverse molecular subtypes and poor clinical outcomes.4,5 These cancers are defined by progressive local invasion and early spread to regional lymph nodes.5-7 Because gastric or GEJ adenocarcinoma are often asymptomatic in the early stages of disease, they often remain undetected until later stages.7 In North America, diagnosis of gastric or GEJ adenocarcinoma is commonly made at an advanced stage, leading to poor overall outcomes.5,8 At the time of diagnosis, approximately 40% of patients present with disease that has extended beyond the locoregional confines, and only about one-quarter of patients are eligible for potentially curative resection with adjuvant or neoadjuvant therapy.7-9 As tumours progress, patients may experience dysphagia, abdominal pain, dyspepsia, reflux, weight loss, bleeding, and anemia.7,10 Gastric or GEJ adenocarcinoma has a profound negative impact on health-related quality of life (HRQoL) due to physical symptoms and difficulties in eating, as well as financial difficulties related to reduced ability to work and the associated social consequences.11,12
In 2024, an estimated 4,000 Canadians were diagnosed with gastric cancer.13 Between 65% and 75% of gastric or GEJ adenocarcinoma cases occur in males, most commonly between the ages of 50 and 70 years.13-15 In 2024, gastric cancer accounted for an estimated 2,000 deaths in Canada, with mortality rates 1.6 times higher in males (1,250 deaths) than in females (760 deaths).16,17 In Canada, the overall 5-year net survival rate for gastric or GEJ adenocarcinoma across all stages is approximately 29%, although survival differs substantially by stage.18,19 For patients with stage I GC or GEJ adenocarcinoma, the 5-year survival rate exceeds 60%. Survival declines to approximately 40% to 50% for stage II disease and further decreases to 20% to 30% for stage III disease.18,19 There is some evidence suggesting that equity-deserving groups in Canada, particularly Indigenous populations, experience higher rates of late-stage diagnosis and lower survival.20
Patient group input: The patient group highlighted that gastric or GEJ adenocarcinoma has a profound impact on quality of life. Patients reported numerous physical challenges, including difficulty eating, poor appetite, reflux, weight loss, nausea, pain, and fatigue, which impacted daily functioning. Both patients and caregivers also noted significant mental health challenges. In addition, patients shared that cancer reshaped their identity, relationships, and social roles, with some withdrawing from social interactions due to visible physical changes. Patients also described a significant financial burden, citing costs such as medications, hospital parking, meals, and travel as ongoing stressors.
Current Management
Treatment Goals
Patient group input: The patient group identified improving quality of life as the top priority. Patients also emphasized the importance of reducing treatment-related side effects, minimizing financial burden, and increasing the convenience of treatment. In addition, they highlighted optimizing treatment duration and improving overall survival (OS) and progression-free survival as key goals.
Clinician input: The clinician groups (CGOEN and the Ontario Health [Cancer Care Ontario] GI DAC) identified several key treatment goals, including reducing relapse risk, prolonging recurrence-free survival and OS, improving pathological response rates to enable curative surgery, enhancing quality of life, and minimizing long-term toxicities. Clinicians also emphasized the importance of achieving durable cure by engaging both cytotoxic and immune-mediated antitumour mechanisms; improving chances of completing treatment around the time of surgery; and supporting patients’ nutrition, function, and independence.
Clinical experts consulted for this review: The clinical experts identified the key treatment goals as improving OS, preventing or delaying relapse, maintaining quality of life, maximizing the likelihood of achieving a complete surgical resection, and minimizing ling-term toxicities.
Current Treatment Options
The current treatment pathway for patients with resectable gastric or GEJ adenocarcinoma is multimodal and includes chemotherapy (neoadjuvant, adjuvant, or perioperative), with or without radiotherapy, in combination with radical surgery with curative intent and lymph node dissection to reduce the risk of recurrence and improve survival.21-24 In Canada, the standard treatment for resectable gastric or GEJ adenocarcinoma involves perioperative chemotherapy along with radical gastrectomy and lymphadenectomy. According to the clinical practice guideline, the FLOT regimen is the preferred option for patients who can tolerate triple-drug therapy.22 Prophylactic granulocyte colony-stimulating factor (G-CSF) treatment is considered for patients receiving FLOT chemotherapy.22 For patients who are unable to receive FLOT, doublet regimens combining fluoropyrimidine-platinum with cisplatin or oxaliplatin are appropriate alternatives. Additionally, anthracycline-containing regimens such as epirubicin, cisplatin, and capecitabine (ECX) or epirubicin, cisplatin, and fluorouracil (ECF) may still be considered in selected cases. For patients who have not received preoperative chemotherapy and have not undergone lymphadenectomy, adjuvant chemotherapy or chemoradiotherapy remains an option.21-24
According to the clinical experts consulted for this review, the primary goal of treatment in this setting is cure, with surgical resection remaining the cornerstone of therapy. Systemic therapy and, in select cases, radiation are incorporated to optimize cure rates. The clinical experts indicated that 2 principal curative strategies are currently employed. The first involves neoadjuvant chemoradiation, followed by surgical resection and adjuvant nivolumab for 1 year in patients with residual disease, primarily for patients with GEJ cancer. The second approach is perioperative chemotherapy with the FLOT regimen.
The clinical experts noted that, in gastric cancer, perioperative FLOT represents the predominant treatment strategy, whereas the Chemoradiotherapy for Esophageal Cancer Followed by Surgery Study (CROSS) regimen is generally reserved for esophageal adenocarcinoma and squamous cell carcinoma. The clinical experts indicated that in selected cases — particularly among patients with pure GEJ or Siewert type I tumours involving the lower esophagus — the CROSS regimen may still be considered appropriate. The clinical experts further highlighted that the use of perioperative FLOT has increased among patients with esophageal adenocarcinoma, including those with mid- to upper esophageal involvement, although such cases currently account for approximately 20% of treated patients. The clinical experts noted the evolving data on the use of FLOT in esophageal adenocarcinoma. According to the clinical experts, the addition of radiation therapy in the adjuvant or perioperative setting has not demonstrated clinical benefit in the context of contemporary D2 lymphadenectomy practices.
Key characteristics of durvalumab plus FLOT are summarized, with other treatments available for the treatment of resectable gastric or GEJ adenocarcinoma, in the Supplemental Material document (available on the project landing page), in Table 1, Appendix 1.
Unmet Needs and Existing Challenges
Patient group input: Input from the patient group underscored the need for treatments that improve quality of life, manage symptoms, minimize side effects, reduce financial burden, and ultimately lead to better survival outcomes. Patients experience serious physical symptoms that severely restrict eating, activity, and daily life. These challenges lead to depression, anxiety, social isolation, grief for families, and major financial strain from lost income and treatment-related costs.
Clinician input: Input from the clinician groups highlighted several challenges with currently available treatment options, including high relapse rates, lack of tailoring to tumour biology, toxicity, poor tolerance in frailer patients, limited curative options after recurrence, lack of immune-based strategies in the curative gastric or GEJ cancer setting, and a need for therapies that provide durable benefit. Clinicians highlighted that treatments should reduce the risk of recurrence and improve OS.
Considerations for Using the Drug Under Review
Contents within this section have been informed by input from the clinical expert(s) consulted for the purpose of this review and from clinician groups, as well as the reimbursement conditions proposed by the sponsor (refer to Table 2 in Appendix 1 of the Supplemental Material document available on the project landing page). The implementation questions from the public drug programs and corresponding responses from the clinical experts consulted for this review are summarized in the Supplemental Material document, in Table 3, Appendix 1. The following has been summarized by the review team.
Place in Therapy
Clinical experts consulted for this review: According to the clinical experts, durvalumab in combination with FLOT as neoadjuvant and adjuvant therapy, followed by adjuvant durvalumab monotherapy, introduces immunotherapy as the standard of care in the perioperative setting for the first time. This approach represents a shift toward curative intent rather than symptomatic management. The clinical experts indicated that, when added to FLOT, durvalumab appears to act synergistically with chemotherapy to enhance tumour downstaging, increase pathologic complete response (pCR) rates, and improve event-free survival (EFS), thereby facilitating surgical resection and potentially reducing micrometastatic burden. FLOT alone may remain an option in selected clinical circumstances. However, the clinical experts agreed that durvalumab in combination with FLOT is anticipated to replace FLOT as the preferred treatment approach for most patients with resectable gastric or GEJ adenocarcinoma. The clinical experts further noted that there will likely remain a role for chemoradiation followed by adjuvant nivolumab in selected patients with GEJ adenocarcinoma. However, its use is expected to decline compared with current practice.
Clinician group input: According to input from the clinician groups, durvalumab in combination with FLOT as neoadjuvant and adjuvant therapy, followed by adjuvant durvalumab monotherapy, represents the first perioperative immunotherapy approach in gastric or GEJ adenocarcinoma and complements the current perioperative strategy. Clinicians noted that this therapy is likely to become the new standard of care and can be used as first-line treatment for resectable gastric or GEJ adenocarcinoma.
Patient Population
Clinical experts consulted for this review: According to the clinical experts consulted for this review, patients most in need of intervention are those with stage II to IVa disease, specifically those with tumours classified as greater than T2 with any nodal involvement up to N3 and no distant metastases, or tumours classified as T0 to T4 with positive lymph nodes and no distant metastases. The clinical experts indicated that patients best suited for treatment with durvalumab plus FLOT are those who can tolerate FLOT chemotherapy and do not have contraindications to immunotherapy. Immunotherapy may be used cautiously in patients with autoimmune conditions, based on clinical judgment. According to the clinical experts, patients with tumours classified as T1 were not considered candidates for this intervention. The clinical experts further indicated that patients least suitable for treatment with durvalumab plus FLOT are those with tumour-related complications, such as obstruction or bleeding, that require immediate surgery; individuals who are not surgical candidates; and patients with poor performance status (PS). The clinical experts indicated that there is currently no established biomarker to identify patients most likely to respond to this treatment. They further noted that clinical benefit appears to increase with higher levels of PD-L1 expression (according to the Combined Positive Score) in the metastatic setting, consistent with emerging data on adjuvant nivolumab.
Regarding the initiation conditions proposed by the sponsor, the clinical experts indicated that they are standard and reasonable.
Clinician group input: Input from the clinician groups identified that patients best suited for this therapy are those with surgically resectable stage II to IVa gastric or GEJ adenocarcinoma who are eligible for perioperative chemotherapy and curative-intent surgery. Clinicians noted that patients with contraindications to immunotherapy, autoimmune disease, poor PS, or mismatch repair-deficient tumours require individualized risk-benefit assessment but should not be excluded from this treatment. They further indicated that no companion diagnostic testing is required for durvalumab.
Assessing the Response to Treatment
Clinical experts consulted for this review: According to the clinical experts consulted for this review, the main outcomes used to assess treatment response in clinical practice are a reduced risk of relapse and improved survival, reflecting the curative intent of therapy. The clinical experts agreed that improvement in survival is particularly important, as patients who experience relapse after receiving durvalumab may lose the opportunity for subsequent immunotherapy in the relapsed setting, depending on the timing of recurrence. The clinical experts indicated that a clinically meaningful response to treatment would be demonstrated by improvements in EFS or disease-free survival (DFS) and, ultimately, by an improvement in OS. The clinical experts further noted that an improvement in response rate would be desirable, as it may facilitate surgical resection and increase the likelihood of achieving complete resection. According to the clinical experts, treatment response should be assessed using imaging before initiating FLOT and then reassessed about 2 to 3 months later, following completion of preoperative FLOT chemotherapy and before surgery. Postoperative imaging practices vary. However, for patients receiving 10 months of immunotherapy, ongoing imaging every 3 to 4 months is typically performed to monitor for recurrence during treatment.
Clinician group input: Input from the clinician groups noted that the key outcomes used to assess treatment response include:
preoperative chemotherapy response and operability
pathologic complete response, complete resection, major pathological response, and nodal status at surgery
DFS, tolerance of ongoing therapy, and absence of recurrence postoperatively.
Clinicians noted that clinically meaningful responses include enabling curative surgery, achieving complete response, increased complete resection rates, and improved quality and quantity of life.
Discontinuing Treatment
Clinical experts consulted for this review: The clinical experts indicated that treatment with durvalumab plus FLOT should be discontinued in cases of patient preference, treatment-related toxicity, or complications that necessitate early surgery, as well as upon completion of the planned treatment course. The clinical experts further noted that discontinuation of durvalumab does not necessarily require discontinuation of FLOT, and vice versa, as the 2 components may be managed independently based on clinical circumstances.
The clinical experts agreed with the discontinuation conditions proposed by the sponsor, with the addition of patient preference as an important consideration.
Clinician group input: Input from the clinician groups indicated that treatment with durvalumab plus FLOT should be discontinued based on patient preference, disease progression before surgery, severe or unmanageable side effects (immune-mediated toxicities), disease recurrence, and postoperative complications preventing further systemic therapy.
Prescribing Considerations
Clinical experts consulted for this review: According to the clinical experts consulted for this review, durvalumab plus FLOT can be administered at any centre with the capacity and expertise to deliver both chemotherapy and immunotherapy. The clinical experts indicated that most remote sites already provide these treatments, and, thus, administration in such settings should not pose challenges. However, they emphasized that treatment decisions should be made in specialized centres with access to multidisciplinary team input, even if the actual delivery of therapy occurs in community or remote settings.
The clinical experts noted some uncertainty regarding the need for the full 1 year of treatment of durvalumab in combination with FLOT. The clinical experts further highlighted that patients who experience relapse following durvalumab plus FLOT may have limited options for subsequent immunotherapy. The clinical experts referenced findings from the SPACE-FLOT25 study, indicating that patients with nonmetastatic GEJ cancer who achieve a partial pathologic response to neoadjuvant FLOT appear to benefit from adjuvant FLOT, although it is unclear whether this applies to immunotherapy. They further noted that patients with a complete pathologic response, or those who do not respond, do not seem to benefit from adjuvant FLOT.
The clinical experts agreed with the prescribing conditions proposed by the sponsor.
Clinician group input: Input from the clinician groups noted that treatment with durvalumab plus FLOT can be administered in cancer centres and outpatient oncology clinics with access to infusion services. Clinicians identified that experienced gastroenterologists and surgical oncologists are needed to manage treatment. Additionally, they noted that radiation oncologists should be involved when GEJ chemoradiation is used, and multidisciplinary team support (nutrition, rehab, supportive care) is imperative.
Additional Considerations
Both the clinical expert and clinician groups consulted for this review indicated that the MATTERHORN trial findings may be extrapolated to include patients with mid- and upper esophageal adenocarcinoma to avoid treatment uncertainty in this population. The clinical experts indicated that adenocarcinomas of the esophagus, GEJ, and stomach share similar prognosis and are increasingly treated with comparable perioperative strategies in current clinical practice. The clinical experts further noted that, although the MATTERHORN study used a flat durvalumab dose of 1,500 mg, weight-based dosing remains appropriate, consistent with other immunotherapies.
Clinical Review
Methods
The review team considered studies in the sponsor’s systematic review (pivotal studies and randomized controlled trials [RCTs]), sponsor-submitted long-term extensions, indirect treatment comparisons (ITCs), and studies addressing gaps in the evidence for inclusion. Eligible studies for the systematic review included published and unpublished pivotal studies and phase III and IV RCTs. Relevant patients and interventions were defined by the indication and the recommended dosage in the product monograph. The following subgroups were considered potentially important for informing the reimbursement recommendation: age (younger than 65 years versus 65 years or older), sex (male versus female), region (Asia versus non-Asia), clinical lymph node status (positive versus negative), PD-L1 expression status (tumour area positivity [TAP] of 1% or greater versus less than 1%), primary tumour location (gastric versus GEJ cancer), and Eastern Cooperative Oncology Group (ECOG) PS score (0 versus 1). Relevant comparators were drugs and nondrug treatments used in clinical practice in Canada to treat patients described in the indication under review. These included perioperative FLOT chemotherapy, neoadjuvant chemoradiation plus adjuvant nivolumab, fluoropyrimidine plus cisplatin, and fluoropyrimidine plus oxaliplatin.
The review team selected outcomes and follow-up times for review, considering the sponsor’s Summary of Clinical Evidence, clinical expert input, and patient and clinician group input. Included outcomes are those considered relevant to expert committee deliberations, and they were selected in consultation with committee members. Evidence from the systematic review for the most important outcomes was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach:
OS at 36 months
EFS by blinded independent review committee (BIRC) at 36 months
HRQoL: change from baseline to end of treatment (cycle 14) in European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) score
serious adverse events.
OS, EFS, HRQoL, and serious adverse events were selected, as they address the main treatment goals of the disease — prolonging life, achieving longer disease remission, controlling disease symptoms, improving and enhancing quality of life, and minimizing long-term toxicities. These outcomes were identified as important to both patients and clinicians, based on input from patient and clinician groups.
Methods for data extraction, risk of bias appraisal, and certainty-of-evidence assessment are in the Supplemental Material document, in Appendix 2.
Clinical Evidence
In this report, the following sources of evidence submitted by the sponsor are reviewed and appraised:
One pivotal study, the MATTERHORN study, was included in the systematic review.
Systematic Review
Description of Studies
Study Characteristics
Characteristics of the included study are summarized in Table 3. Details pertaining to the eligibility criteria, interventions and comparators, and relevant outcome measures are found in the Supplemental Material document, in Appendix 3. The MATTERHORN study is an ongoing, randomized, double-blind, placebo-controlled, multicentre, global phase III study evaluating the efficacy and safety of durvalumab in combination with FLOT chemotherapy in both neoadjuvant and adjuvant periods, followed by adjuvant durvalumab monotherapy, for the treatment of patients with resectable gastric or GEJ adenocarcinoma. Patients were randomized in a 1:1 ratio, using block stratified randomization via an interactive response technology or randomization and trial supply management system, to receive durvalumab plus FLOT (N = 474) or placebo plus FLOT (N = 474). Randomization was stratified by geographic region (Asia versus non-Asia), clinical lymph node status (positive versus negative), and PD-L1 expression level (TAP of 1% or greater versus less than 1%). Patients were enrolled globally across 147 study sites in 20 countries, including North America (with 6 sites in Canada), Argentina, Belgium, Brazil, Chile, Denmark, France, Germany, Hungary, Japan, the Netherlands, Peru, Poland, the Republic of Korea, the Russian Federation, Spain, Taiwan, Türkiye, the UK, and the US.
Only data from prespecified interim analyses of the MATTERHORN trial were submitted for this Reimbursement Review, with data cut-off (DCO) dates of February 1, 2023, (DCO1) for assessment of pCR, and December 20, 2024, (DCO2) for the primary analysis of EFS and OS. The submission also included the final OS results, with a DCO date of September 1, 2025. At DCO2, the median duration of follow-up in censored patients was 31.64 months (range, 0.03 months to 48.10 months) in the durvalumab plus FLOT group and 31.44 months (range, 0.03 months to 48.07 months) in the placebo plus FLOT group. At the time of final analysis, the median duration of follow-up in censored patients was 43.0 months (range, 3.4 months to 57.0 months) in the durvalumab plus FLOT group and 42.9 months (range, 0.0 months to 56.6 months) in the placebo plus FLOT group.
Table 2: Characteristics of Studies Included in the Systematic Review
Study name, design, and sample size | Key inclusion criteria | Key exclusion criteria | Intervention and comparator | Relevant end points |
|---|---|---|---|---|
MATTERHORN study Randomized, double-blind, placebo-controlled, multicentre, global phase III study N = 948a |
|
| Intervention: Durvalumab 1,500 mg on day 1 plus FLOT on days 1 and 15 every 4 weeks for 4 cycles (2 cycles neoadjuvant phase and 2 cycles adjuvant phase), followed by durvalumab 1,500 mg on day 1 every 4 weeks for 10 additional cyclesg (28 days each cycle) Comparator:
|
Harms: Incidence of AEs, SAEs, AESIs, and AEs leading to study drug dose modification or treatment discontinuation |
AE = adverse event; AESI = adverse event of special interest; BICR = blinded independent central review; DFS = disease-free survival; DSS = disease-specific survival; ECOG = Eastern Cooperative Oncology Group; EFS = event-free survival; EFS24 = event-free survival at 24 months; EFS36 = event-free survival at 36 months; EORTC = European Organisation for Research and Treatment of Cancer; FLOT = fluorouracil, leucovorin, oxaliplatin, and docetaxel; GC = gastric cancer; GEJC = gastroesophageal junction adenocarcinoma; GI = gastrointestinal; HRQoL = health-related quality of life; IL38 = item library 38; MFS = metastasis-free-survival; OS = overall survival; OS24 = overall survival at 24 months; OS36 = overall survival at 36 months; pCR = pathological complete response; PS = performance status; QLQ-C30 = Quality of Life Questionnaire Core 30; QLQ-STO22 = Quality of Life Questionnaire Stomach 22; R0 = complete resection; SAE = serious adverse event.
aOne patient was randomized twice in error under 2 different e-codes: E7820001, randomized in error receiving no study treatment, and E7820002, proceeding to receive study treatment (confirmed by site). The exclusion of E7820001 has been performed at the level of the FAS. One participant (E7606006) was randomized to the placebo plus FLOT group and included in the FAS but received both placebo and durvalumab and therefore was included in the durvalumab plus FLOT group for the purpose of the safety analysis set, which includes 475 patients in the durvalumab plus FLOT group and 469 patients in the placebo plus FLOT group.
bFor patients aged < 20 years and enrolled in Japan, a written informed consent should be obtained from the patients and their legally acceptable representatives.
cType 1 tumour is also eligible as long as the patient is intended to be treated in the same way as for Siewert Type 2 and 3 tumours: Per the judgment of the investigator, patient must be medically fit for treatment with neoadjuvant FLOT therapy before radical surgery. At screening, complete surgical resection of the primary gastric or GEJ cancer must be deemed achievable, as assessed by a multidisciplinary evaluation, which must include a board-certified GI surgeon. Patients must have had no prior anticancer therapy (e.g., chemotherapy, radiation therapy, or chemoradiation therapy) for the current malignancy. Siewert classifications are defined as follows: Siewert type 1 — adenocarcinoma of the lower esophagus with the centre located between 1 cm to 5 cm above the anatomic GEJ; Siewert type 2 — true carcinoma of the cardia at the GEJ, with the tumour centre within 1 cm above and 2 cm below the GEJ; Siewert type 3 — subcardial carcinoma with the tumour centre between 2 and 5 cm below GEJ, which infiltrates the GEJ and lower esophagus from below.
dHemoglobin of at least 9.0 g/dL; absolute neutrophil count of at least 1.5 × 109 /L; platelet count of at least 100 × 109/L; serum bilirubin less or equal to 1.5 × the upper limit of normal; alanine aminotransferase and aspartate aminotransferase less or equal to 2.5 × the upper limit of normal; measured creatinine clearance greater than 50 mL/min or calculated creatinine clearance greater than 50 mL/min as determined by Cockcroft-Gault (using actual body weight).
eIncluding, but not limited to, ongoing or active infection, symptomatic congestive heart failure, uncontrolled hypertension, unstable angina pectoris, uncontrolled cardiac arrhythmia, active interstitial lung disease, serious chronic gastrointestinal conditions associated with diarrhea, or psychiatric illness or social situations that would limit compliance with study requirements, substantially increase risk of incurring adverse events, or compromise the patient’s ability to give written informed consent.
fPatients with a past or resolved hepatitis B virus infection (defined as the presence of hepatitis B core antibody and absence of hepatitis B surface antigen) are eligible. Patients positive for hepatitis C virus antibody are eligible only if a polymerase chain reaction test is negative for hepatitis C virus RNA.
gFor patients with body weight 30 kg or less, durvalumab was administered at 20 mg per kg every 4 weeks.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence and MATTERHORN Clinical Study Report.26
Statistical Testing and Analysis Populations
The MATTERHORN study aimed to randomize approximately 900 patients to evaluate the superiority of perioperative durvalumab plus FLOT versus placebo plus FLOT in terms of EFS in patients with resectable gastric or GEJ adenocarcinoma. With an estimated 461 EFS events (51% maturity) at the final analysis, the study had approximately 85% power to detect a hazard ratio (HR) of 0.75 at a 2-sided significance level of 4.2%. This corresponded to an approximately 10-month improvement in median EFS for durvalumab plus FLOT compared with an assumed 30-month median EFS for placebo plus FLOT, based on the assumption of an exponential EFS distribution. The smallest treatment difference that would achieve statistical significance at the final analysis corresponded to an EFS HR of 0.83.
To control the overall 2-sided type I error at the 0.05 level, a fixed alpha of 0.1% (2-sided) was allocated to the analysis of pCR at DCO1, with the remaining 4.9% (2-sided) reserved for the analysis of EFS and OS at DCO2 and the final analysis. If pCR was statistically significant at DCO1, the 0.1% alpha was recycled to the EFS and OS testing hierarchy, preserving the overall 2-sided 5% type I error rate. Alpha allocation for EFS between DCO2 and the final analysis was controlled using a Lan-DeMets spending function, approximating the O’Brien-Fleming approach, with significance thresholds determined by the observed information fraction. A minimal fixed alpha spend of 0.01% was assigned to OS testing at DCO2, provided EFS was statistically significant at that time point.
At the final analysis, OS was formally tested using the Haybittle-Peto approach. The study assumed an accrual period of 24 months and 26.5 months of follow-up, with approximately 314 OS events (approximately 35% maturity) expected. Based on an assumed median OS of 50 months for placebo plus FLOT and 68 months for durvalumab plus FLOT, corresponding to a true treatment effect (HR = 0.735), the study was designed to provide approximately 77% power to detect a statistically significant difference in OS at a 2-sided significance level of 4.89%. The smallest treatment effect expected to reach statistical significance corresponded to an OS HR of 0.799.
All efficacy analyses were conducted using the full analysis set (FAS), based on treatment as randomized. DFS was analyzed in the R0 (complete) resected analysis set, which included all patients in the FAS who had a surgical resection that was defined as a complete resection. All safety analyses were conducted using the safety analysis set, which included all patients who received at least 1 dose of the study drug.
Patient Disposition
Patient disposition for the MATTERHORN study is summarized in the Supplemental Material document, in Appendix 4.
Of the 1,258 patients screened, 949 were randomized into 2 treatment groups: 474 patients to the durvalumab plus FLOT group and 474 patients to the placebo plus FLOT group. One patient was randomized twice in error under 2 different identifiers, with the initial randomization excluded from the FAS and the second used for analysis. As of the December 20, 2024, DCO, all patients in the durvalumab plus FLOT group received at least 1 dose, while 4 patients in the placebo plus FLOT group did not receive neoadjuvant treatment. During the neoadjuvant period, 16 patients (3.4%) in the durvalumab plus FLOT group and 21 (4.5%) in the placebo plus FLOT group discontinued durvalumab or placebo treatment, primarily due to adverse events (0.6% versus 1.9%, respectively) or patient decision (1.1% versus 0.4%, respectively). A total of 26 patients (5.5%) in the durvalumab plus FLOT group and 33 (7.0%) in the placebo plus FLOT group discontinued at least 1 FLOT component, primarily due to adverse events (1.7% versus 3.4%, respectively) or patient decision (1.7% versus. 0.6%, respectively). A total of 19 patients (4.0%) in the durvalumab plus FLOT group or 28 patients (5.9%) in the placebo plus FLOT group did not complete surgery. Additionally, 48 patients (10.1%) in each group underwent surgery but did not initiate adjuvant therapy.
As of the December 20, 2024, DCO, of the 716 patients who received treatment in the adjuvant period, 360 patients (98.9%) in the durvalumab plus FLOT group and 350 patients (99.4%) in the placebo plus FLOT group received adjuvant durvalumab or placebo treatment. A total of 248 patients (68.1%) in the durvalumab plus FLOT group and 245 patients (69.6%) in the placebo plus FLOT group completed all 12 cycles of adjuvant durvalumab or placebo. A total of 112 patients (30.8%) in the durvalumab plus FLOT group and 105 (29.8%) in the placebo plus FLOT group discontinued durvalumab or placebo treatment, primarily due to adverse events (7.4% versus 5.1%, respectively) or patient decision (4.4% versus 4.5%). Additionally, 124 patients (34.1%) and 101 patients (28.7%), respectively, discontinued at least 1 FLOT component, primarily due to adverse events (27.5% versus 22.7%) or investigator decision (3.3% versus 3.1%). A total of 344 patients in the durvalumab plus FLOT group and 332 patients in the placebo plus FLOT group received adjuvant durvalumab or placebo monotherapy, while 96 patients (27.9%) and 87 patients (26.2%), respectively, discontinued adjuvant durvalumab or placebo treatment, primarily due to worsening gastric or GEJ cancer (11.0% versus 16.3%), adverse events (6.1% versus 3.0%), or patient decision (3.8% versus 3.0%).
As of the September 1, 2025, DCO, ███ ████████ ███████ in the durvalumab plus FLOT group and ███ ████████ ███████ in the placebo plus FLOT group remained on study in survival follow-up. A total of ███ ████████ ███████ in the durvalumab plus FLOT group and ███ ████████ ███████ in the placebo plus FLOT group discontinued study participation, primarily due to █████ ██████ ██████ ██████ █████████████ ███ ███████ ██████████ ██ ███████ █████ ██████ ██████.
As of the December 20, 2024, DCO, 7.0% of patients in the durvalumab plus FLOT group and 5.3% of patients in the placebo plus FLOT group experienced at least 1 important protocol deviation. The most common protocol deviations were related to the use of prohibited medications (3.2% versus 1.9%), and investigational product administration errors (2.3% versus 1.1%) in the durvalumab plus FLOT and placebo plus FLOT groups, respectively. As of the September 1, 2025, DCO ████ of patients in the durvalumab plus FLOT group and ████ of patients in the placebo plus FLOT group experienced at least 1 important protocol deviation, with overall deviations generally balanced between groups.
Baseline Characteristics
Table 3: Summary of Baseline Characteristics From Study Included in the Systematic Review
Characteristic | MATTERHORN study | |
|---|---|---|
Durvalumab plus FLOT (N = 474) | Placebo plus FLOT (N = 474) | |
Age (years) | ||
Mean (SD) | 59.9 (11.53) | 61.6 (10.14) |
Median (range) | 62.0 (26 to 84) | 63.0 (28 to 83) |
Age group (years), n (%) | ||
< 50 | 86 (18.1) | 57 (12.0) |
50 to < 65 | 205 (43.2) | 208 (43.9) |
65 to < 75 | 146 (30.8) | 166 (35.0) |
≥ 75 | 37 (7.8) | 43 (9.1) |
Sex, n (%) | ||
Female | 148 (31.2) | 118 (24.9) |
Male | 326 (68.8) | 356 (75.1) |
Race, n (%) | ||
American Indian or Alaska Native | 18 (3.8) | 20 (4.2) |
Asian | 96 (20.3) | 97 (20.5) |
Black or African American | 7 (1.5) | 3 (0.6) |
White | 321 (67.7) | 322 (67.9) |
Other | 8 (1.7) | 8 (1.7) |
Not reported | 24 (5.1) | 24 (5.1) |
Geographic region, n (%) | ||
Asia | 90 (19.0) | 90 (19.0) |
Non-Asia | 384 (81.0) | 384 (81.0) |
ECOG PS score, n (%) | ||
0 | 337 (71.1) | 366 (77.2) |
1 | 137 (28.9) | 108 (22.8) |
Clinical lymph node status (IRT)a, n (%) | ||
Positive | 329 (69.4) | 330 (69.6) |
Negative | 145 (30.6) | 144 (30.4) |
Clinical lymph node status (eCRF)b, n (%) | ||
Positive | 334 (70.5) | 333 (70.3) |
Negative | 137 (28.9) | 140 (29.5) |
Missing | 3 (0.6) | 1 (0.2) |
PD-L1 expression level (IRT)a, n (%) | ||
TAP ≥ 1% | 426 (89.9) | 427 (90.1) |
TAP < 1% | 48 (10.1) | 47 (9.9) |
PD-L1 expression level (eCRF)b, n (%) | ||
TAP ≥ 1% | 426 (89.9) | 427 (90.1) |
TAP < 1% | 48 (10.1) | 47 (9.9) |
Primary tumour location, n (%) | ||
Gastric | 324 (68.4) | 316 (66.7) |
Gastric cardia | 65 (13.7) | 69 (14.6) |
Fundus of the stomach | 13 (2.7) | 15 (3.2) |
Body of stomach | 162 (34.2) | 164 (34.6) |
Antrum pylori | 84 (17.7) | 68 (14.3) |
Gastroesophageal junction | 150 (31.6) | 158 (33.3) |
Siewert type 1 | 44 (9.3) | 55 (11.6) |
Siewert type 2 | 72 (15.2) | 68 (14.3) |
Siewert type 3 | 34 (7.2) | 35 (7.4) |
Tumour grade, n (%) | ||
Well differentiated (G1) | 49 (10.3) | 46 (9.7) |
Moderately differentiated (G2) | 144 (30.4) | 154 (32.5) |
Poorly differentiated (G3) | 212 (44.7) | 201 (42.4) |
Undifferentiated (G4) | 8 (1.7) | 4 (0.8) |
Unassessable (GX) | 60 (12.7) | 67 (14.1) |
Missing | 1 (0.2) | 2 (0.4) |
AJCC stagingc, n (%) | ||
Stage IIa | 37 (7.8) | 25 (5.3) |
Stage IIb | 109 (23.0) | 108 (22.8) |
Stage III | 287 (60.5) | 298 (62.9) |
Stage IVa | 41 (8.6) | 42 (8.9) |
Missing | 0 (0.0) | 1 (0.2) |
Microsatellite instability status, n (%) | ||
High | 25 (5.3) | 24 (5.1) |
Not high | 301 (63.5) | 310 (65.4) |
Not evaluable | 69 (14.6) | 52 (11.0) |
Missing | 79 (16.7) | 88 (18.6) |
Histology type, n (%) | ||
Intestinal | 245 (51.7) | 238 (50.2) |
Diffuse type | 130 (27.4) | 119 (25.1) |
Indeterminate type | 99 (20.9) | 117 (24.7) |
AJCC = American Joint Committee on Cancer; ECOG = Eastern Cooperative Oncology Group; eCRF = electronic case report form; FLOT = fluorouracil, leucovorin, oxaliplatin, and docetaxel; IRT = interactive response technology; PS = performance score; SD = standard deviation; TAP = tumour area positivity.
Notes: The data cut-off date was December 20, 2024.
Racial categories used in the table are as reported in the original source and may not align with Canada's Drug Agency inclusive language guidelines.
aAs recorded at randomization on the interactive response technology or randomization and trial supply management system.
bAs recorded at randomization on the electronic case report form or from external vendor data from samples collected on or before randomization.
cStages according to AJCC Cancer Staging Manual, eighth edition.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence and MATTERHORN Clinical Study Report.26
Treatment Exposure and Concomitant Medications
Details of patients’ treatment exposure, use of concomitant medications, and subsequent treatments in the MATTERHORN study are in the Supplemental Material document, in Appendix 4. As of the December 20, 2024, DCO, the median actual duration of exposure to durvalumab or placebo for the overall MATTERHORN study was 12.68 months (range, 0.3 months to 13.4 months) in the durvalumab plus FLOT group versus 12.48 months (range, 0.4 months to 13.2 months) in the placebo plus FLOT group. The median actual duration of exposure to FLOT for the overall study was 3.68 months (range, 0.3 months to 4.0 months in the durvalumab plus FLOT group, and 0.4 months to 0.4 months in the placebo plus FLOT group). During the neoadjuvant period, 461 patients (97.1%) in the durvalumab plus FLOT group and 451 patients (96.2%) in the placebo plus FLOT group completed the 2 neoadjuvant treatment cycles of durvalumab or placebo, respectively. Completion of all 12 adjuvant treatment cycles of durvalumab or placebo was achieved by 246 patients (51.8%) in the durvalumab plus FLOT group and 240 patients (51.2%) in the placebo plus FLOT group.
Following randomization, the majority of patients in the MATTERHORN study (99.6%) received at least 1 concomitant medication, including 473 patients (99.8%) in the durvalumab plus FLOT group and 471 patients (99.4%) in the placebo plus FLOT group. The most common concomitant mediations were dexamethasone (64.6% versus 68.6%), ondansetron (52.5% versus 51.5%), filgrastim (47.7% versus 51.1%), paracetamol (45.4% versus 40.7%), and omeprazole (30.2% versus. 27.4%) in the durvalumab plus FLOT and placebo plus FLOT groups, respectively.
As of the September 1, 2025, DCO, subsequent anticancer therapy was reported for █████ of patients in the durvalumab plus FLOT group and █████ in the placebo plus FLOT group. ███████ proportion of patients in the durvalumab plus FLOT group used subsequent immunotherapy ██████ compared with the placebo plus FLOT group ████████ ████ ███ ████████ █████████ █████████████ ██ ███████████ ████ █████████ █████████████
Critical Appraisal
Internal Validity
Randomization was performed using an appropriate methodology with adequate allocation concealment, and stratification factors were prespecified. A centralized interactive response system employing a permuted-block randomization scheme was used, which is generally associated with a low risk of bias. Overall, baseline patient and disease characteristics were balanced across treatment groups. Treatment completion rates for durvalumab or placebo and FLOT were comparable between groups in both phases. Surgical attempt rates were also well balanced (90.9% versus 90.3%, in the durvalumab plus FLOT and placebo plus FLOT groups, respectively). Reasons for not undergoing or not completing surgery were consistent across groups, reducing concern for differential attrition during the perioperative period. The clinical experts consulted indicated that overall patient disposition in the MATTERHORN study was consistent with expectations for a perioperative gastric or GEJ cancer population, with high completion rates of neoadjuvant therapy and surgery across groups. The clinical experts indicated discontinuation rates in the MATTERHORN study were higher in the adjuvant versus neoadjuvant phases, which they considered expected given that many patients are unable to complete postoperative FLOT due to recovery demands and treatment-related toxicity. The proportion of protocol deviations was comparable between groups and identified before the database lock. The duration of exposure to durvalumab or placebo and to FLOT chemotherapy was comparable between treatment groups across the treatment periods in the MATTERHORN study.
Based on the enrolled sample size, the study was powered to test its primary and key secondary end points: EFS, OS, and pCR. The analyses of primary and key secondary outcomes were conducted using the FAS population, which maintains randomization and minimizes the risk of bias by comparing groups with similar prognostic factors. Statistical analysis methods appear to be acceptable. In the MATTERHORN study, no information was available regarding the testing of proportionality assumptions, although such testing was planned as part of the statistical analysis plan. Two interim and the final analyses were planned a priori. A hierarchical testing strategy to sequentially test the primary and secondary outcomes was used to reduce the risk of type I error across these analyses.
At the final analysis, OS was formally tested using the Haybittle-Peto approach. Although OS reached statistical significance at the final analysis, the median OS had not been reached in either group. The OS data reflected an information fraction of approximately 37%, which exceeded the prespecified assumption of approximately 35% maturity. However, the OS data remain relatively immature and limit the precision of the estimated long-term overall survival benefit. Censoring patterns ████ ███████ ███████ ███████ ███████ with █████████████ ██████████ ██ ████████ ████████ (████% in the durvalumab plus FLOT group and ████% in the placebo plus FLOT group). ████ █ █████ ██████████ terminated follow-up before death in either treatment group (████ versus ████ in the durvalumab plus FLOT and placebo plus FLOT groups, respectively), which unlikely to introduce bias in the estimation of OS. Patients were allowed to receive posttreatment anticancer medications after discontinuing study treatment. At the time of final analysis, the subsequent treatments were not balanced between groups (█████ versus █████ in the durvalumab plus FLOT and placebo plus FLOT groups, respectively). This was expected because fewer patients progressed in the durvalumab plus FLOT group. The clinical experts consulted by CDA-AMC indicated that the use of postprogression immunotherapy in the placebo plus FLOT group was markedly lower than would be expected in clinical practice, which could bias the OS results in favour of durvalumab plus FLOT. In the durvalumab plus FLOT group, 1.1% of patients received postprogression immunotherapy alone and 4.9% received immunotherapy plus chemotherapy.
Results for the primary outcome, EFS, were based on a prespecified second interim analysis. Although interim analyses carry some risk of overestimating treatment effects, the extent of any potential overestimation in this case is uncertain.27-29 The interim analysis was conducted after 84% of the prespecified EFS events occurred (385 of 461 EFS events), nearly reaching the target for the final analysis. Additionally, the observed P value for the between-group comparison in EFS was below the interim analysis boundary, suggesting a low risk of bias from early stopping. The criteria used for disease progression and tumour response are based on radiographic images and clinical assessment, with the potential for subjective interpretation. To mitigate this potential bias, a BIRC reviewed all available radiographic tumour assessments to determine tumour response based on Response Evaluation Criteria in Solid Tumours (RECIST) Version 1.1. Censoring patterns for EFS were broadly similar between treatment groups. Only a small proportion of patients was censored due to withdrawal of consent, loss to follow-up, or other reasons, and these proportions were comparable between groups. These patterns do not suggest informative censoring and are unlikely to have introduced bias into the estimation of EFS. Results of sensitivity analyses for EFS — including those addressing potential ascertainment bias, evaluation-time bias, subsequent nonprotocol therapy censoring, and censoring rules for missed RECIST assessments — were consistent with the primary analysis. While subgroup analyses were planned a priori and generally showed consistent results with the primary analysis, they may not be powered to identify differences between subgroups. No information was available regarding the testing of proportionality assumptions, although such testing was planned as part of the statistical analysis plan. Visual inspection of the Kaplan-Meier plots for progression-free survival and OS by CDA-AMC showed no obvious violations of the proportional hazards assumption.
Biases resulting from the self-reporting nature of patient-reported outcomes were deemed to be minimal, as patients in the MATTERHORN study were blinded to their assigned intervention. However, the risk of unblinding due to adverse events in the MATTERHORN study could introduce performance and detection bias by affecting the assessment of subjective outcomes (i.e., patient-reported outcomes), as well as treatment management and monitoring intensity. HRQoL was measured using standard, validated instruments commonly employed in oncology trials (EORTC QLQ-C30 and Quality of Life Questionnaire Stomach 22 [QLQ-STO22]). No strong conclusions could be drawn about the effect of durvalumab plus FLOT compared with placebo plus FLOT on HRQoL due to a high risk of attrition bias, particularly at longer follow-up. At the end of treatment (cycle 14), 49.7% of patients in the durvalumab plus FLOT group and 48.4% in the placebo plus FLOT groups were available to complete EORTC QLQ-C30 and QLQ-STO22 plus item library 38 (IL38) assessments. The analysis method for HRQoL outcomes, conducted using the mixed model for repeated measures, relied on the likely implausible assumption that data were missing at random. No sensitivity analyses were conducted to assess robustness to different missingness mechanisms.
The results of the pCR, DFS, surgery rate, and complete resection rates were consistent with and supportive of the primary analysis. Although pCR rate was higher in the durvalumab plus FLOT group than in the placebo plus FLOT group, the clinical experts noted that pCR serves as a prognostic factor rather than a marker of therapeutic efficacy. Complete resection rates were comparable between treatment groups. The clinical experts consulted indicated that complete resection does not necessarily reflect treatment benefit because it occurs only after surgery. Additionally, complete resection and DFS analyses are limited to the complete resected analysis set (n = 662). Because this represents a subgroup of the FAS population, randomization is not maintained, and the results do not directly reflect the effect of treatment assignment.
External Validity
According to the clinical experts consulted by CDA-AMC, the patient population in the MATTERHORN study generally reflects patients in clinical practice in this setting. In the MATTERHORN trial, the study population was drawn from a number of sites around the globe, including Canada. The clinical experts indicated that there are no major concerns with generalizing the findings from the trial to the clinical setting in Canada. The clinical experts considered the eligibility criteria of the MATTERHORN study broadly appropriate and reflective of clinical practice in Canada. They agreed that restricting enrolment to stage II to III disease and excluding T1 tumours in the MATTERHORN study was reasonable, as patients with T1 disease may not receive perioperative chemotherapy and would be unlikely candidates for the treatment with durvalumab plus FLOT. Requiring resectable disease at baseline was also deemed appropriate. However, the clinical experts noted that borderline resectable disease could have been included, as conversion to resectability after treatment would be clinically meaningful, although this was not evaluated in the study. Patients with active or prior autoimmune disease were excluded from the study, which clinical experts viewed as consistent with standard immunotherapy trial practice. Overall, laboratory and organ-function requirements of the study were considered appropriate by clinical experts and aligned with expectations for a population undergoing perioperative chemo-immunotherapy. In the MATTERHORN study, 67.5% of patients had gastric primary tumours and 32.5% had GEJ tumours. The clinical experts indicated that this distribution of gastric and GEJ tumours in the study was broadly consistent with real-world clinical practice. They further noted that it would be reasonable to extend eligibility for durvalumab plus FLOT to patients with esophageal adenocarcinoma, noting that adenocarcinomas of the esophagus, GEJ, and stomach share a similar prognosis and are increasingly managed with comparable perioperative treatment strategies in clinical practice.
The clinical experts agreed that FLOT chemotherapy was an appropriate comparator in the MATTERHORN study. They agreed that perioperative FLOT chemotherapy remains the standard of care in Canada for patients with resectable gastric or GEJ adenocarcinoma who have good PS. They further noted that durvalumab plus FLOT is expected to replace FLOT for most eligible patients, while FLOT alone will continue to be used in patients who cannot receive immunotherapy. The clinical experts agreed that the lack of RCT evidence comparing durvalumab plus FLOT with other reimbursed chemotherapy regimens, or with chemoradiotherapy followed by adjuvant nivolumab, is a limitation of the submitted evidence. In particular, they indicated that, for GEJ adenocarcinoma, the absence of the neoadjuvant chemoradiation (CROSS regimen) followed by adjuvant nivolumab as a comparator limits the ability to contextualize the efficacy of durvalumab plus FLOT in this population. However, with evolving evidence, there is increasing movement toward perioperative FLOT chemotherapy over chemoradiation for GEJ adenocarcinoma. Based on the information provided by the sponsor, a feasibility assessment determined that an ITC of durvalumab plus FLOT with adjuvant nivolumab following neoadjuvant chemoradiotherapy and surgery was unfeasible due to substantial clinical, methodological, and statistical heterogeneity across studies, which were deemed to preclude the assumptions necessary for a valid and reliable analysis (Appendix 6). The review team considered the sponsor’s conclusion plausible. However, no independent feasibility assessment was conducted to verify this. The comparative efficacy and safety of durvalumab plus FLOT versus relevant comparators other than FLOT remain unknown.
According to the clinical experts consulted, the demographic and disease characteristics of the MATTERHORN study population were reflective of patients with gastric or GEJ adenocarcinoma living in Canada. However, they identified several baseline characteristics that may limit generalizability. The mean age of patients was approximately 60 years, which the clinical experts considered broadly reflective of the treatment-eligible population. However, the clinical experts noted that fewer than 10% of enrolled patients were 75 years or older, indicating an underrepresentation of older adults relative to real-world practice, likely reflecting concerns about the tolerability of FLOT in this age group. In the MATTERHORN study, the proportion of females was higher in the durvalumab plus FLOT group than in the placebo plus FLOT group. The clinical experts consulted indicated that females with gastric cancer generally experience better outcomes. Therefore, this imbalance may introduce potential bias favouring durvalumab plus FLOT. The clinical experts indicated that restricting study eligibility to patients with ECOG PS score of 0 or 1 is understandable given the intensity and toxicity profile of FLOT chemotherapy. However, they noted that the predominance of patients with ECOG PS score of 0 (approximately 70%) is not reflective of real-world practice, where a substantially higher proportion of patients present with an ECOG PS score of 1 or 2. The clinical experts noted that representation of some groups, including Indigenous people and Black people, was low in the trial and that all Asian patients were categorized as a single group in the study, which they considered inappropriate given the substantial genetic and biological differences between populations, such as those from Japan or Korea and those from India. The clinical experts indicated that the proportion of patients with PD-L1 TAP of 1% or higher was unexpectedly high. However, they noted that PD-L1 testing has not been routinely performed in Canada, limiting the ability to determine the true prevalence in the treatment-eligible population. The clinical experts further noted that Combined Positive Score, rather than TAP, is used to guide immunotherapy decisions in both the metastatic and adjuvant settings in Canada. The majority of patients in the MATTERHORN study had node-positive disease. The clinical experts indicated that these patients are at the highest risk of relapse and are more likely to benefit from intensive treatment, which may amplify the observed treatment effect relative to a broader population with a lower baseline risk.
The clinical experts consulted for this review considered the end points used in the MATTERHORN study appropriate. The input from the clinical experts, patients, and clinician groups noted OS, EFS, and HRQoL as the most important outcomes for assessing treatment response. Although maintaining HRQoL is a key priority for patients, the difference in HRQoL outcomes between the groups was not formally tested in the study and was analyzed only in the HRQoL-evaluable population. Including only evaluable patients in the model can introduce selection bias, as this group may not be representative of the broader patient population. For example, these patients may represent a subgroup with different clinical profiles (e.g., older, more comorbid), and their exclusion reduces the applicability of the findings to the broader populations with gastric or GEJ cancer.
Results
The key efficacy and harms results and findings from the GRADE assessment are presented in this section. Detailed efficacy and harms results can be found in Appendix 4 in the Supplemental Material document. The EFS, HRQoL, and complete resection rate results are based on the December 20, 2024, data cut-off (DCO2), the pCR results are based on the February 1, 2023, data cut-off (DCO1), and the OS results are based on the final analysis (September 1, 2025).
Efficacy
Key results include the following:
OS: At the time of DCO2 (December 20, 2024), the median follow-up duration was 31.6 months (range, 0.03 months to 48.10 months) and 31.4 months (range, 0.03 months to 48.07 months) in the durvalumab plus FLOT and placebo plus FLOT groups, respectively. The Kaplan-Meier (KM) estimated between-group difference in the probability of being alive at 36 months was 6.7% (95% CI ███% to ████%). At the time of the final analysis (September 1, 2025), the median duration of follow-up was 43.0 months (range, 3.4 months to 57.0 months) and 42.9 months (range, 0.0 months to 56.6 months) in the durvalumab plus FLOT and placebo plus FLOT groups, respectively. There were 160 deaths (33.8%) in the durvalumab plus FLOT group and 192 deaths (40.5%) in the placebo plus FLOT group. The median OS was not reached in either group (HR = 0.78; 95% confidence interval [CI], 0.63 to 0.96; P = 0.021). The KM between-group difference in the probability of being alive at 36 months was 6.7% (95% CI ████ to ████%) in favour of durvalumab plus FLOT. Refer to Appendix 4 for OS KM curves in the FAS population.
EFS per BIRC assessment: At the time of DCO2 (December 20, 2024), a BIRC-assessed EFS event was reported in 35.2% of patients in the durvalumab plus FLOT group and 46.0% of patients in the placebo plus FLOT group. The median EFS for the durvalumab plus FLOT group was not reached, compared with a median EFS of 32.8 months (95% CI, 27.86 months to not estimable) in the placebo plus FLOT group (HR = 0.71; 95% CI, 0.58 to 0.86; P < 0.001). The KM estimated between-group difference in the probability of being alive or event-free at 36 months was 14.7% (95% CI, █████ to ██████) in favour of durvalumab plus FLOT. Refer to Appendix 4 for EFS KM curves in the FAS population. The EFS results were consistent across the prespecified sensitivity analyses. Findings in key subgroups generally aligned with those observed in the overall population, with HRs favouring durvalumab plus FLOT. However, estimates for certain subgroups were less precise, including females (HR = 0.84; 95% CI, 0.58 to 1.24), patients in Asia (HR = 0.74; 95% CI, 0.44 to 1.22), negative lymph node status (HR = 0.85; 95% CI, 0.57 to 1.27), PD-L1 expression of less than 1 (HR = 0.77; 95% CI, 0.40 to 1.46), and ECOG PS score of 1 (HR = 0.69; 95% CI, 0.46 to 1.02, with CIs touching or crossing unity.
HRQoL: At the end of treatment (cycle 14), EORTC QLQ-C30 data were available for 231 patients in the durvalumab plus FLOT group and 222 patients in the placebo plus FLOT group. The between-group difference in the mean change from baseline was 0.1 points (95% CI, –2.81 to 3.02 points) in Global Health Status or Quality of Life, –0.2 points (95% CI, –2.44 to 2.09 points) in physical functioning, 1.3 points (95% CI, –2.36 to 4.95 points) in role functioning, –0.7 points (95% CI, –4.10 to 2.74 points) in fatigue, and 2.6 points (95% CI, –1.14 to 6.39 points) in appetite loss.
At the end of treatment (cycle 14), EORTC QLQ QLQ-STO22 plus IL38 data were available for 230 patients in the durvalumab plus FLOT group and 222 patients in the placebo plus FLOT group. The between-group difference in the mean change from baseline was –0.1 points (95% CI, –2.92 to 2.71 points) in reflux, 1.5 points (95% CI, –1.57 to 4.65 points) in eating restrictions, –1.3 points (95% CI, –5.12 to 2.56 points) in anxiety, 0.5 points (95% CI, –3.18 to 4.16 points) in dry mouth, –0.6 points (95% CI, –4.02 to 2.88 points) in taste, –2.1 points (95% CI, –5.50 to 1.31 points) in hair loss, –0.3 points (95% CI, –4.59 to 3.92 points) in body image, –1.0 points (95% CI, –4.50 to 2.51 points) in difficulty swallowing, –1.3 points (95% CI, –5.62 to 2.95 points) in weight loss, –0.8 points (95% CI, –3.43 to 1.90 points) in dysphagia, and –1.0 points (95% CI, –3.77 to 1.81 points) in pain.
Complete resection: At the time of DCO2 (December 20, 2024), complete resection was achieved in 79.5% patients (95% CI, 75.62% to 83.08%) in the durvalumab plus FLOT group and 77.8% patients (95% CI, 73.84% to 81.51%) in the placebo plus FLOT group, with odds ratio of 1.11 (95% CI, 0.81 to 1.51).
pCR rate: At the time of DCO1 (February 1, 2023), the pCR rate was 19.2% (95% CI, 15.75% to 23.04%) in the durvalumab plus FLOT group compared with 7.2% (95% CI, 5.02% to 9.88%) in the placebo plus FLOT group. The between-group difference in response rate was 12.0%, with odds ratio of 3.08 (95% CI, 2.03 to 4.67).
DFS: At the time of DCO2 (December 20, 2024), a DFS event was reported in 90 patients (26.5%) in the durvalumab plus FLOT group and 119 patients (36.8%) in the placebo plus FLOT group. The median DFS was not reached in the durvalumab plus FLOT group, whereas it was 39.75 months (95% CI, 38.67 months to not estimable) in the placebo plus FLOT group (HR = 0.760; 95% CI, 0.53 to 0.93). The KM estimated between-group difference in the DFS probability at 36 months was 7.7% (95% CI, ██████ ██ ██████).
Harms
Key results include the following:
Treatment-emergent adverse events (TEAEs) were reported in 99.2% of patients (471 of 475) in the durvalumab plus FLOT group and 98.7% of patients (463 of 469) in the placebo plus FLOT group. TEAE rates were comparable between groups during neoadjuvant combination treatment (96.4% versus 95.3%), adjuvant combination treatment (96.7% versus 96.3%), and adjuvant monotherapy (79.4% versus 78.5%). TEAEs of grade 3 or 4 occurred in 71.6% of patients receiving durvalumab plus FLOT and in 71.2% of those treated with placebo plus FLOT. The most frequently reported grade 3 or 4 TEAEs in the durvalumab plus FLOT group, as compared to the placebo plus FLOT group, were neutropenia (21.3% versus 22.2%), followed by diarrhea (6.3% versus 6.0%) and decreased white blood cell count (5.3% versus 6.0%).
Serious adverse events were reported in 48.2% of patients in the durvalumab plus FLOT group and 44.1% of patients in the placebo plus FLOT group. The most common serious adverse events in the durvalumab plus FLOT group, as compared to the placebo plus FLOT group, were pneumonia (2.9% versus 3.4%), febrile neutropenia (2.1% versus 3.2%), and neutropenia (2.1% versus 0.9%). A total of 4.8% of patients in the durvalumab plus FLOT group and 4.3% in the placebo plus FLOT group died as a result of TEAEs. The most common TEAEs resulting in death were septic shock (1.1% versus 0.4%), pulmonary embolism (0.4% versus 0.2%), and abdominal sepsis (0.2% versus 0.0%) in the durvalumab plus FLOT and placebo plus FLOT groups, respectively.
The study treatment was discontinued due to adverse events in 29.9% of patients in the durvalumab plus FLOT group, compared with 22.8% in the placebo plus FLOT group. The most common adverse events leading to treatment discontinuation in the durvalumab plus FLOT versus placebo plus FLOT groups were neutropenia (2.9% versus 1.1%), infusion-related reactions (2.7% versus 1.1%), and peripheral sensory neuropathy (2.3% versus 3.4%). In the durvalumab plus FLOT group, 48 patients (10.1%) discontinued durvalumab, 121 patients (25.5%) discontinued any component of FLOT due to TEAEs, and 21 patients (4.4%) discontinued both durvalumab and FLOT. In the placebo plus FLOT group, 30 patients (6.4%) discontinued placebo, 95 patients (20.3%) discontinued any component of FLOT, and 14 patients (3.0%) discontinued both placebo and FLOT.
Hypothyroid events were reported in 8.2% of patients in the durvalumab plus FLOT group and 1.5% in the placebo plus FLOT group. Hepatic events occurred in 2.7% of patients in the durvalumab plus FLOT group versus 2.3% in the placebo plus FLOT group. A higher proportion of patients in the durvalumab plus FLOT group experienced diarrhea or colitis and dermatitis or rash events compared with the placebo plus FLOT group (2.7% versus 2.3% and 2.7% versus 1.7%, respectively). A higher proportion of patients in the durvalumab plus FLOT group experienced hypophysitis and adrenal insufficiency events compared with the placebo plus FLOT group (0.8% versus 0.0% and 1.5% versus 1.2%, respectively).
Summary of Findings and Certainty of the Evidence
A literature-based estimate of the minimal important difference (MID) was used as the threshold for the EORTC QLQ-C30 Global Health score (MID = 5 to 10 points for both improvement and deterioration) in the GRADE certainty-of-evidence assessment. Refer to the summary of outcome measures in Appendix 3 of the Supplemental Material document. In the absence of literature-based MID estimates, thresholds suggested by the clinical experts were used for EFS (threshold = 100 per 1,000 patients at 36 months) and OS (threshold = 70 per 1,000 patients at 36 months). For serious adverse events, where no empirically estimated or expert opinion-based threshold was available, the certainty was assessed based on the presence of a non-null effect.
Table 4: Summary of Findings for Durvalumab Plus FLOT vs. Placebo Plus FLOT for Patients With Gastric or GEJ Cancer
Outcome and follow-up | Patients (MATTERHORN study), N | Absolute effects (95% CI) | Certainty | What happens | ||
|---|---|---|---|---|---|---|
Placebo plus FLOT | Durvalumab plus FLOT | Difference | ||||
Overall survival | ||||||
Probability of being alive at 36 months Median follow-up: 43.0 months (durvalumab plus FLOT) and 42.9 months (placebo plus FLOT) | 948 (1 RCT) | 619 per 1,000 | 686 per 1,000 (642 to 726 per 1,000) | 67 more per 1,000 (██ ███ more per 1,000) | Lowa,b (serious imprecision and risk of bias) | Durvalumab plus FLOT may result in a clinically meaningful increase in the probability of being alive at 36 months when compared with placebo plus FLOT. The clinical importance of the improvement is uncertain. |
Event-free survival | ||||||
Probability of being event-free or alive at 36 months Median follow-up: 31.6 months (durvalumab plus FLOT) and 31.4 months (placebo plus FLOT) | 948 (1 RCT) | 472 per 1,000 | 620 per 1,000 (569 to 666 per 1,000) | 147 more (██ ███ more per 1,000) | Moderatec,d (serious imprecision) | Durvalumab plus FLOT likely results in a clinically meaningful increase in the probability of being event-free or alive at 36 months when compared with placebo plus FLOT. |
Health-related quality of life | ||||||
EORTC QLQ-C30, Global Health Status and Quality of Life score: mean change from baseline at the end of treatment Median follow-up: end of treatment (14 cycles) | 453 (1 RCT) | 77.9 | 76.1 (16.98) | 0.1 (–2.81 to 3.02) | Lowe,f,g (risk of bias) | Durvalumab plus FLOT may result in little to no difference in quality of life when compared with placebo plus FLOT. |
Serious adverse events | ||||||
Serious adverse events Median follow-up: 31.6 months (durvalumab plus FLOT) and 31.4 months (placebo plus FLOT) | 944 (1 RCT) | 441 per 1,000 | 482 per 1,000 | 41 more (██ ███ per 1,000) | Lowe,h (serious imprecision) | Durvalumab plus FLOT may result in an increase in the proportion of patients with serious adverse events when compared with placebo plus FLOT. There is some uncertainty about the clinical importance of the estimates. |
CDA-AMC = Canada’s Drug Agency; CI = confidence interval; DCO = data cut-off; EFS = event-free survival; EORTC = European Organisation for Research and Treatment of Cancer; FLOT = fluorouracil, leucovorin, oxaliplatin, and docetaxel; GEJ = gastroesophageal junction; GRADE = Grading of Recommendations Assessment, Development and Evaluation; MID = minimal important difference; OS = overall survival; QLQ-C30 = Quality of Life Questionnaire Core 30; RCT = randomized controlled trial; vs. = versus.
Note: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aAn empirically derived MID was not identified for the between-group difference for this outcome. A difference of 7% between the groups was identified by the clinical expert consulted by CDA-AMC as a threshold of clinical importance for this outcome.
bRated down 1 level for serious imprecision. Based on the MID identified by clinical experts (7% between-group difference), the point estimate suggests clinically important benefit (borderline), while the lower boundary of the 95% CI suggests the possibility of no clinically important benefit. The median OS was not reached in either treatment group. OS data have reached 37% overall maturity, and statistical significance was achieved. Rated down 1 level for risk of bias. Use of subsequent anticancer treatment was not balanced across treatment groups. The use of subsequent immunotherapy (alone or in combination with chemotherapy) was markedly lower in the placebo plus FLOT group than would be expected in clinical practice, according to the consulted clinical experts. These factors may introduce bias in the estimated treatment effect.
cAn empirically derived MID was not identified for the between-group difference for this outcome. A difference of 10% between the groups was identified by the clinical expert consulted by CDA-AMC as a threshold of clinical importance for this outcome.
dRated down 1 level for serious imprecision. Based on the MID identified by clinical experts (10% between-group difference), the point estimate suggests clinically important benefit. However, the lower bound of the 95% CI crosses this threshold. It was not rated down for serious risk of bias. Although interim analyses carry some risk of overestimating treatment effects, the extent of any potential overestimation in this case is uncertain. At the time of DCO2, 84% of the prespecified EFS events (365 of 461) had occurred, nearly reaching the target for the final analysis.
eThis analysis was not part of the statistical analysis plan and was requested from the sponsor by CDA-AMC to facilitate the GRADE assessment.
fStatistical testing for this outcome was not adjusted for multiplicity. The results are considered supportive evidence.
gRated down 2 levels for serious risk of bias due to missing data, as the proportion of patients available for assessment substantively diminished over time. Additionally, the CI is wide relative to the small observed effect, leaving uncertainty about the magnitude of any true impact on quality of life.
hRated down 2 levels for serious imprecision. An empirically derived MID was not identified for the between-group difference for this outcome, and an expert-based threshold was not available. With the null specified as the threshold of importance, the point estimate suggested an increase in the proportion of patients with serious adverse events in the durvalumab plus FLOT group compared with placebo plus FLOT. However, the 95% CI around the point estimate contains the potential for a decrease as well as an increase in serious adverse events. The CI is wide, indicating substantial uncertainty around the true magnitude and direction of the effect. Differences in treatment discontinuation rates between study groups may influence the interpretation of harm outcomes as a potential risk of bias.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence and MATTERHORN Clinical Study Report.26
Long-Term Extension Studies
The submission did not include any long-term extension studies.
Indirect Evidence
The submission did not include any indirect evidence (Appendix 6).
Studies Addressing Gaps in the Systematic Review Evidence
The submission did not include any studies addressing gaps in the systematic review evidence.
Discussion
Efficacy
This report summarizes evidence from the ongoing, double-blind, phase III MATTERHORN study assessing the efficacy and safety of durvalumab in combination with FLOT as neoadjuvant and adjuvant treatment, followed by adjuvant durvalumab monotherapy, for the treatment of resectable gastric or GEJ adenocarcinoma. The clinical experts consulted for this review indicated that this combination represents an important addition to the treatment landscape in Canada. According to the clinical experts, this regimen introduces immunotherapy as the standard of care in the perioperative setting for the first time. This approach represents a shift toward curative intent rather than symptomatic management. Patient input revealed that, despite effective therapies, unmet needs persist, including profound impact on quality of life, treatment-related toxicities, and logistical challenges such as travel and costs.
The clinical experts agreed that FLOT chemotherapy was an appropriate comparator for perioperative treatment in this population. However, they noted that, for patients with GEJ adenocarcinoma, the clinically relevant standard of care is neoadjuvant chemoradiation using the CROSS regimen, followed by adjuvant nivolumab, which was not evaluated in the MATTERHORN study. The clinical experts further noted that, for patients who are unable to receive FLOT, doublet regimens combining fluoropyrimidine-platinum with cisplatin or oxaliplatin remain acceptable alternatives. Therefore, the absence of comparative evidence against these relevant treatment options represents a limitation of the submitted evidence. Based on information provided by the sponsor, an ITC was deemed unfeasible due to substantial clinical, methodological, and statistical heterogeneity across studies. The review team considered this conclusion plausible. However, no independent feasibility assessment was conducted.
In the MATTERHORN study, durvalumab was administered as a fixed dose of 1,500 mg every 4 weeks during both the neoadjuvant and adjuvant phases. According to the clinical expert consulted, this differs from typical practice in Canada, where durvalumab is generally prescribed using weight-based dosing (20 mg/kg up to a maximum of 1,500 mg), consistent with other immunotherapy protocols. The clinical experts agreed that similar treatment effects would be expected for durvalumab, whether the dosing is weight-based or flat. In the study, durvalumab was administered during both the neoadjuvant and adjuvant phases ― initially in combination with FLOT chemotherapy and subsequently as adjuvant monotherapy. The clinical experts consulted questioned the need for a full year of adjuvant durvalumab following perioperative therapy for gastric or GEJ adenocarcinoma. The clinical experts indicated that the therapeutic effect of adding immunotherapy may derive largely from the neoadjuvant phase rather than from prolonged adjuvant treatment. They further noted that adjuvant durvalumab may not be necessary for patients who achieve a complete response to neoadjuvant therapy or show no response to neoadjuvant therapy, although continuation in the adjuvant phase could still be appropriate for those with a partial response. Because the MATTERHORN study evaluated the entire treatment sequence — neoadjuvant and adjuvant durvalumab plus FLOT, followed by adjuvant durvalumab monotherapy — it is unclear how much of the observed benefit is attributable to the preoperative versus postoperative durvalumab treatment phases.
The clinical experts considered the MATTERHORN study population to be broadly reflective of practice in Canada but noted several features that may limit generalizability. According to the clinical experts, esophageal adenocarcinoma should have been included in the study because it is biologically similar to gastric and GEJ adenocarcinoma and increasingly treated with similar perioperative immunotherapy approaches in clinical practice. Thus, its exclusion creates a gap in applicability, leading to inconsistent access to treatment and limiting generalizability of the study results. The clinical experts indicated that the underrepresentation of older adults, the predominance of patients with ECOG PS score of 0, and imbalances in sex distribution and PD-L1 expression in the study may collectively overestimate the expected benefit in routine care.
Based on patient group input, most patients identified a pressing need for therapies that reduce the risk of recurrence and prolong survival. At the time of the final analysis, the median OS was not reached in either treatment group. OS data have reached 37% overall maturity and met the prespecified significance boundary. At the time of final analysis, the KM plot for OS shows that the curves overlapped during the early months of follow-up, began to separate gradually after approximately 14 to 15 months, and maintained a consistent separation thereafter. The early overlap of the curves and gradual divergence suggest a delayed treatment effect, consistent with immunotherapy. Despite achieving statistical significance, the KM curves were relatively immature, yet they still demonstrated a consistent pattern of sustained separation after approximately 15 months. Using the 7% clinical importance threshold identified by the clinical experts consulted by CDA-AMC, the OS benefit at 36 months falls into the borderline clinically meaningful range, while the lower bound of the 95% CI crosses this threshold. Patients in the MATTERHORN study received posttreatment anticancer therapy after discontinuing study treatment, which could influence OS and complicate interpretation of the OS treatment effect. These subsequent treatments were not balanced between groups. The clinical experts indicated that the use of postprogression immunotherapy was markedly lower than expected in the placebo plus FLOT group. These factors may bias the OS results in favour of durvalumab plus FLOT.
Both clinical groups and clinical experts consulted for this review considered EFS as an important end point for patients with resectable gastric or GEJ adenocarcinoma. Based on a 10% clinical importance threshold suggested by clinical experts, durvalumab plus FLOT likely results in a clinically meaningful increase in EFS at 36 months when compared with placebo plus FLOT. The median EFS for the durvalumab plus FLOT group was not reached, while the median EFS for the placebo plus FLOT group was 32.8 months. Although interim analyses carry some risk of overestimating treatment effects, the extent of any potential overestimation in this case is uncertain.27-29 The median duration of follow-up was 31.6 months in the durvalumab plus FLOT group and 31.4 months in the placebo plus FLOT group. The clinical experts consulted indicated that this duration of follow-up is sufficient to assess an EFS benefit in this setting. At the time of DCO2, 84% of the prespecified EFS events had occurred, nearly reaching the target for the final analysis (40.6% maturity). The KM curves for EFS show early overlap, with a gradual and consistent separation beginning around 8 to 9 months, which is sustained thereafter. The shape of the curves suggests a delayed immunotherapy effect, which is biologically plausible in the perioperative setting, and the separation appears durable over time.
HRQoL was highlighted as an outcome of importance to patients and was assessed in the trial using the EORTC QLQ-C30 and EORTC QLQ-STO22 plus IL38 scores. For the EORTC QLQ-C30 Global Health Status score, there is low-certainty evidence that durvalumab plus FLOT may result in little to no difference in the HRQoL compared with placebo plus FLOT at cycle 14 (end of treatment). The between-group mean difference and the corresponding CI were below the literature-established MID of 5 to 10 points. The certainty of the evidence was rated down as low, primarily due high attrition rate, lack of appropriate account of missing data (particularly with the potential of data missing not at random), reliance on evaluable data only, and imprecision. These points increase uncertainty and compromise the validity and generalizability of the results. The results for pCR, complete resection, and DFS were supportive of the OS and EFS findings.
Harms
According to the clinical experts consulted for this review, durvalumab was generally well tolerated in the MATTERHORN study, and no new safety signals were observed in either the neoadjuvant or adjuvant settings. Almost all patients in both treatment groups experienced at least 1 adverse event, which clinical experts considered expected given the intensity of perioperative FLOT chemotherapy. The clinical experts indicated that some reported adverse events are more likely attributable to underlying disease or to surgery factors rather than to durvalumab or FLOT chemotherapy. According to the clinical experts, although some toxicities, such as neutropenia, occurred more frequently with durvalumab plus FLOT than placebo plus FLOT, these differences were not clinically meaningful and remained within the expected range for this regimen. The clinical experts observed that pulmonary embolism and septic shock were reported more frequently in the durvalumab plus FLOT group, as compared with the placebo plus FLOT group, which they considered unexpected for immunotherapy (0.4% versus 0.2% and 0.2% versus 0.0%, respectively). The MATTERHORN study showed, with low certainty, that durvalumab plus FLOT may result in an increase in serious adverse events compared with placebo plus FLOT. The clinical experts indicated that treatment discontinuation in the study was expected, given the intensity and toxicity burden of FLOT chemotherapy, noting that a substantial proportion of patients discontinue perioperative chemotherapy in routine clinical practice. The clinical experts further noted the difficulty in determining whether adverse events leading to discontinuation were attributable to chemotherapy or to immunotherapy due to overlapping toxicity profiles. According to the clinical experts consulted, adverse events of special interest in the study were generally consistent with known effects of PD-L1 inhibitors. However, the clinical experts highlighted that several immune-related adverse events associated with immunotherapy, including durvalumab ― particularly adrenal insufficiency, hypophysitis, and myocarditis ― are permanent and life-altering conditions rather than transient toxicities. The clinical experts indicated that adrenal insufficiency requires lifelong hormone replacement and characterized hypophysitis as a serious and enduring diagnosis. The clinical experts further noted that other immune-mediated events, such as thyroid dysfunction, pneumonitis, and certain cases of colitis, may also persist, in contrast to reversible chemotherapy-related effects like alopecia or diarrhea. According to the clinical experts, the possibility of irreversible or long-term immune-related toxicity is important when evaluating the overall benefits and harms of durvalumab in gastric or GEJ adenocarcinoma, especially in the absence of biomarkers to identify patients most likely to benefit.
Ethics and Equity Considerations
Evidence indicated that equity-deserving groups, particularly Indigenous populations, experience higher rates of late-stage diagnosis and lower survival outcomes due to longstanding barriers to timely detection and treatment.20 Consistent with these findings, the clinical experts consulted by CDA-AMC noted that Indigenous communities, people living in rural or remote areas, and individuals experiencing homelessness often face reduced access to diagnostic imaging, specialist care, and supportive services. The clinical experts emphasized that many rural communities are located far from major hospitals, resulting in limited or delayed access to specialized oncology services, including diagnostic imaging, surgical teams, and multidisciplinary cancer care. These geographic and systemic barriers may reduce the feasibility of completing complex perioperative regimens and contribute to poorer outcomes in these populations.
Patient group input further highlighted the substantial physical, psychosocial, and financial burdens experienced throughout the perioperative treatment course. Patients and caregivers described profound mental health impacts, including anxiety, emotional distress, and the psychological toll of prolonged treatment, with some patients noting that cancer reshaped their identity, roles, and relationships, occasionally leading to social withdrawal due to visible physical changes. The clinical experts indicated that perioperative therapy is difficult to tolerate and often requires extensive supportive care, including nutritional supplementation and symptom management, adding considerable caregiver burden. Caregivers frequently assume a major role, including time away from work to provide daily support. Additionally, patients face notable out-of-pocket costs ― such as nutritional supplements (e.g., Boost, which is not publicly covered), medications, parking, meals, and travel ― which contribute to financial strain. The clinical experts further noted that rural patients often lack the onsite infrastructure and support services available in urban centres, such as dietitian support, rapid-access clinics, and symptom-management programs, leading to increased reliance on family members or caregivers and further amplifying caregiver burden. According to the clinical experts consulted, durvalumab plus FLOT can be administered at any centre with capacity and resources to deliver both chemotherapy and immunotherapy, including most remote sites where these treatments are already available. However, they emphasized that treatment decisions should be made in specialized centres with multidisciplinary team input, even if the administration of therapy occurs in community or remote settings.
Conclusion
The primary goal of treatment for resectable gastric or GEJ adenocarcinoma is cure, with surgical resection remaining the cornerstone of therapy. Patients and clinicians highlighted the need for new, effective, and better-tolerated perioperative treatments for resectable gastric or GEJ adenocarcinoma that minimize side effects, prolong life, prolong disease remission, and improve quality of life. One sponsor-submitted trial was included in this review. The trial is the ongoing, phase III, multicentre, double-blind, randomized MATTERHORN study, evaluating durvalumab in combination with FLOT chemotherapy as neoadjuvant and adjuvant treatment, followed by adjuvant durvalumab monotherapy in patients with resectable gastric or GEJ adenocarcinoma. According to the clinical experts consulted for this review, the study population was broadly representative of patients seen in clinical practice in Canada. Results from the MATTERHORN study demonstrated that durvalumab plus FLOT likely improves EFS compared with placebo plus FLOT and may improve OS at 36 months. The impact of durvalumab plus FLOT on HRQoL was uncertain due to missing data and imprecision in the effect estimates. Harms were consistent with the known safety profile of chemotherapy and PD–L1 inhibitors, with no new safety signals identified in this study. Uncertainty remains regarding the relative contribution of the neoadjuvant and adjuvant durvalumab combination phases, as well as the adjuvant durvalumab monotherapy phase, to the overall treatment benefit. Although FLOT chemotherapy is considered the standard of care for perioperative treatment of resectable gastric or GEJ adenocarcinoma, the comparative benefit of durvalumab against other relevant therapies, including neoadjuvant chemoradiotherapy followed by adjuvant nivolumab for GEJ cancer, remains unknown.
Economic Review
Methods
The review team appraised the pharmacoeconomic evidence submitted by the sponsor on the cost-effectiveness and budget impact of durvalumab plus FLOT compared to FLOT alone for the treatment of adult patients with resectable gastric or GEJ adenocarcinoma.
Summary of the Submitted Economic Evaluation
The sponsor submitted a cost-utility analysis to estimate the cost-effectiveness of durvalumab plus FLOT from the perspective of a public health care payer in Canada over a lifetime horizon (39 years).30 The modelled population consisted of adult patients with resectable gastric or GEJ cancer (stages II to IVa, according to the American Joint Committee on Cancer’s AJCC Cancer Staging Manual, eighth edition ), which is aligned with the Health Canada indication and the reimbursement request and was based on the participants in the MATTERHORN trial.1,31 The sponsor’s base-case analysis included costs related to drug acquisition, administration, subsequent treatments, health care resource use, terminal care, and adverse events.30
In the sponsor’s base, durvalumab plus FLOT was associated with incremental costs of $86,881 and 2.03 incremental quality-adjusted life-years (QALYs) compared to FLOT alone. This resulted in an incremental cost-effectiveness ratio (ICER) of $42,742 per QALY gained. Of the incremental benefit compared to FLOT (2.03 incremental QALYs), approximately 92% of benefit was predicted to be accrued after the observation period of the 4-year trial. Additional information about the sponsor’s submission is summarized in the Supplemental Material document, in Appendix 10. CDA-AMC identified several key issues with the sponsor’s analysis (Table 5; full details are provided in the Supplemental Material document, in Appendix 10).
Table 5: Key Issues With the Sponsor’s Economic Submission
Issue | What evidence is there to inform this issue? | How was this issue addressed by CDA-AMC? | Did CDA-AMC explore uncertainty in a scenario analysis? |
|---|---|---|---|
Subsequent therapies are not appropriately modelled and do not reflect clinical practice in Canada. | Clinical experts consulted by CDA-AMC advised that a higher proportion of patients who experience disease progression would receive a next line of therapy than assumed in the model. Clinical experts also noted that the modelled treatment mix does not reflect current practice in Canada. | CDA-AMC addressed this issue by increasing the proportion of patients receiving subsequent therapies as a next line of therapy following disease progression to 42% in the base case. However, due to structural limitations of the model and limited data on real-world treatment patterns and durations, CDA-AMC was unable to adjust the types or distribution of subsequent therapies. | No scenario analysis was conducted. |
Long-term recurrence, postrecurrence survival, and event-free mortality are uncertain due to extrapolation assumptions. | The sponsor used parametric models fitted to the MATTERHORN trial data to extrapolate recurrence, time to first death, and postrecurrence survival over a lifetime horizon.30 Clinical experts consulted by CDA-AMC indicated that these extrapolations are likely optimistic, as real-world patients may experience earlier recurrence and limited long-term survival compared to the sponsor’s estimates. | CDA-AMC addressed this uncertainty by using transition probabilities in observed Kaplan-Meier estimates, where available, and restricting parametric modelling to extrapolated tails beyond trial follow-up, thereby reducing reliance on statistical assumptions and improving consistency across recurrence and survival transitions. | Given the lack of long-term data, CDA-AMC explored alternative extrapolation of time to first recurrence in a scenario analysis. |
Health state utility values for recurrent disease are uncertain and may be overestimated. | How the utility decrement for recurrent disease derived from the MATTERHORN trial was insufficiently documented and could not be independently appraised.30 Clinical experts advised that the resulting utility value for recurrent disease is likely too high relative to real-world experience. | CDA-AMC adopted a more conservative utility value of 0.730 for recurrent disease, while retaining the event-free health state utility used in the sponsor’s base case. This change was based on the sponsor-provided scenario and aligned with external evidence, including NICE appraisals for recurrent gastric cancer.30 | No scenario analysis was conducted. |
Relevant comparators were excluded. | The sponsor’s model compared durvalumab plus FLOT with FLOT alone and excluded other relevant comparators. However, other regimens are used in clinical practice in Canada (e.g., neoadjuvant chemoradiation with adjuvant nivolumab and doublet chemotherapy), and their exclusion limits conclusions on the relative cost-effectiveness of durvalumab plus FLOT. | CDA-AMC could not address this issue because comparative efficacy data for durvalumab plus FLOT vs. these alternative treatments were not available. | No scenario analysis was conducted. |
CDA-AMC = Canada’s Drug Agency; FLOT = fluorouracil, leucovorin, oxaliplatin, and docetaxel; NICE = National Institute for Health and Care Excellence; vs. = versus.
Note: Full details of the issues identified by CDA-AMC are provided in the Supplemental Material document, in Appendix 11.
CDA-AMC Assessment of Cost-Effectiveness
The CDA-AMC base case was derived by making changes to model parameter values and assumptions (refer to Table 15 in the Supplemental Material document), in consultation with clinical experts. Detailed information about the CDA-AMC base case is provided in the Supplemental Material document, in Appendix 11.
Impact on Health Care Costs
Durvalumab plus FLOT is predicted to be associated with additional health care costs compared to FLOT alone (incremental costs = $96,818). This increase in health care spending results from drug acquisition costs associated with durvalumab (refer to Figure 1).
Figure 1: Impact of Durvalumab Plus FLOT vs. FLOT on Health Care Costs
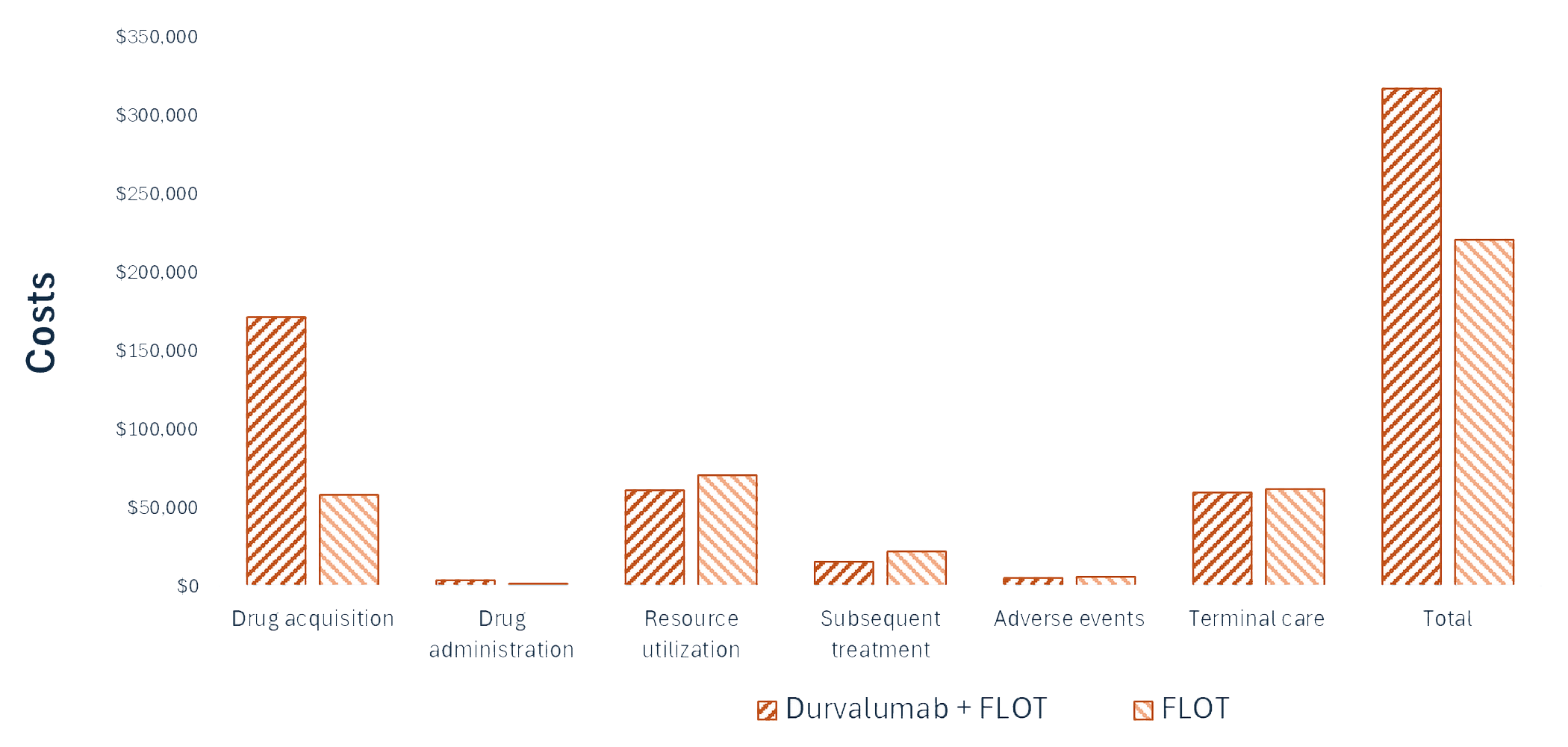
FLOT = fluorouracil, leucovorin, oxaliplatin, and docetaxel; vs. = versus.
Impact on Health
Relative to FLOT, durvalumab plus FLOT is predicted to increase OS and the amount of time a patient remains in the event-free health state by approximately 2 years. Considering the impact of treatment on both quality and length of life, durvalumab plus FLOT is predicted to result in 1.44 additional QALYs per patient compared to FLOT alone (refer to Figure 2). Approximately 89% of the predicted incremental benefit was accrued on the basis of extrapolation.
Figure 2: Impact of Durvalumab Plus FLOT vs. FLOT on Patient Health
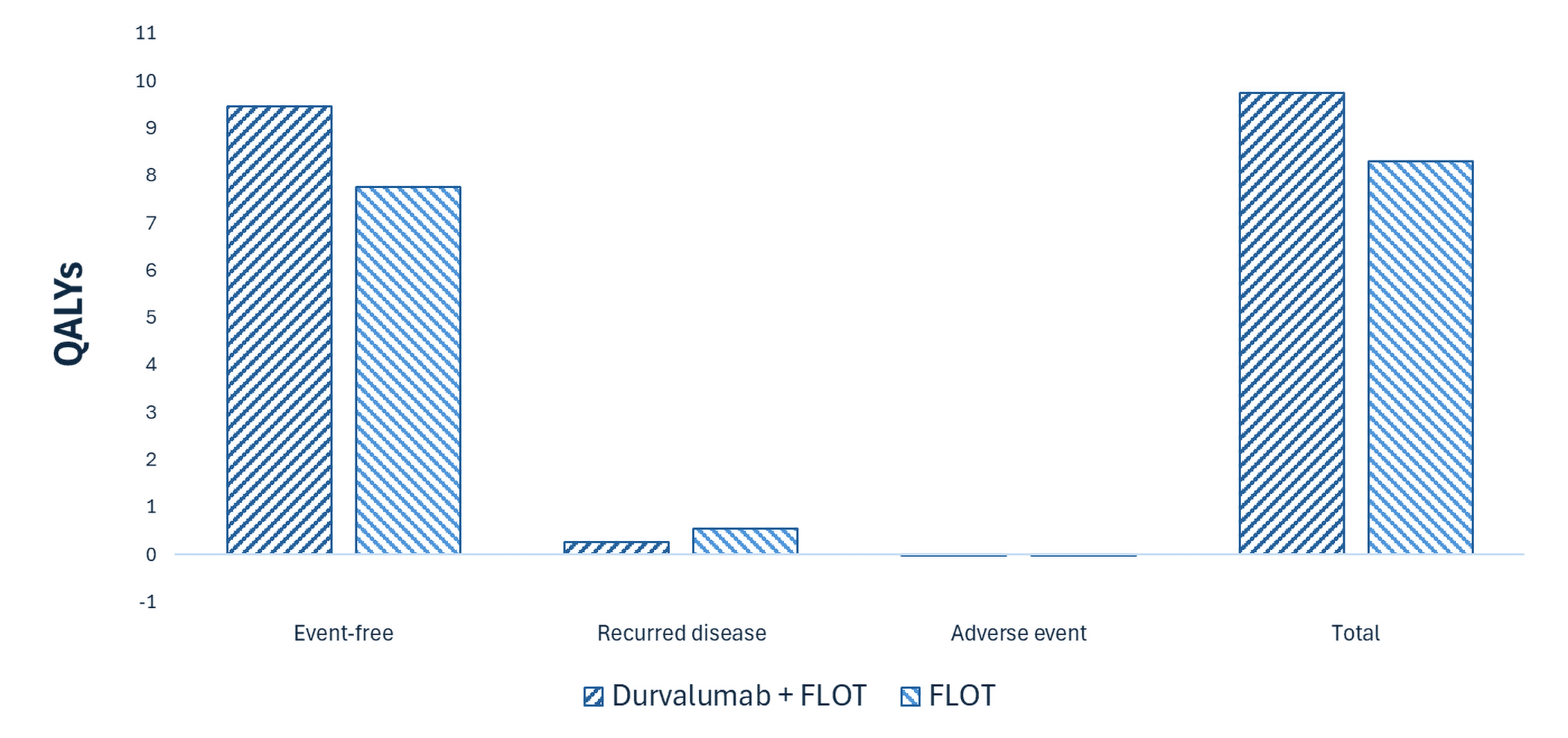
FLOT = fluorouracil, leucovorin, oxaliplatin, and docetaxel; QALY = quality-adjusted life-year; vs. = versus.
Overall Results
The results of the CDA-AMC base case suggest an ICER of $67,176 per QALY gained for durvalumab plus FLOT compared to FLOT alone (refer to Table 6). Additional details on the CDA-AMC base case are available in the Supplemental Material document, in Appendix 11.
Table 6: Summary of CDA-AMC Economic Evaluation Results
Drug | Total costs ($) | Total LYs | Total QALYs | ICER vs. FLOT ($/QALY) |
|---|---|---|---|---|
FLOT | 220,742 | 9.79 | 8.29 | Reference |
Durvalumab plus FLOT | 317,557 | 11.42 | 9.74 | 67,176 |
CDA-AMC = Canada’s Drug Agency; FLOT = fluorouracil, leucovorin, oxaliplatin, and docetaxel; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; vs. = versus.
Note: Publicly available list prices were used for all comparators.
Uncertainty and Sensitivity
Due to the lack of long-term evidence, extrapolation of both time to first recurrence and survival outcomes is subject to considerable uncertainty. Long-term time to first recurrence had the greatest impact on cost-effectiveness results. Under more conservative assumptions for long-term recurrence risk, the ICER for durvalumab plus FLOT increased to $81,175 per QALY (refer to Table 19, Appendix 11, in the Supplemental Material document).
Summary of the Budget Impact
The sponsor submitted a budget impact analysis to estimate the 3-year (2027 to 2029) budget impact of reimbursing durvalumab plus FLOT for use in the Health Canada–indicated population.32 The sponsor assumed that the payer would be CDA-AMC–participating public drug plans and derived the size of the eligible population using an epidemiologic approach.32 The price of durvalumab was aligned with the price in the sponsor’s economic evaluation, while the prices of comparators were based on the publicly available list prices.33,34 Additional information pertaining to the sponsor’s submission is provided in the Supplemental Material document, in Appendix 12. CDA-AMC identified issues with the sponsor’s estimated budget impact that could not be addressed. The sponsor estimated that 1,661 patients would be eligible for durvalumab plus FLOT over a 3-year period (year 1 = 541; year 2 = 554; year 3 = 566), of whom 1,136 would be expected to receive durvalumab plus FLOT (year 1 = ███; year 2 = ███; year 3 = ███).32 The estimated incremental budget impact of reimbursing durvalumab plus FLOT is predicted to be approximately $113 million over the first 3 years, with an expected expenditure of $114 million on durvalumab (not including the expenditure on FLOT).32 The actual budget impact will depend on the proportion of patients who receive postoperative treatment and the market uptake, both of which are uncertain.
Conclusion
Based on the CDA-AMC base case, durvalumab for use in combination with FLOT would be considered cost-effective at the submitted price if the public health care system was willing to pay at least $67,176 for each additional QALY gained. If the public health care system is not willing to pay that amount, a price reduction should be considered (Figure 3; full details of the impact of price reductions on cost-effectiveness are presented in the Supplemental Material document, in Table 18). In the absence of mature, long-term evidence, the projected treatment benefits are highly uncertain and may be overestimated. Additional price reductions may therefore be required.
The sponsor estimated that the budget impact of reimbursing durvalumab plus FLOT to the public drug plans in the first 3 years is estimated to be approximately $113 million. The 3-year expenditure on durvalumab (i.e., not accounting for current expenditure on comparators) is estimated to be $114 million. The estimated budget impact is uncertain due to the proportion of patients who receive postoperative treatment and the market uptake.
Figure 3: Summary of the CDA-AMC Economic Analysis and Price Reduction
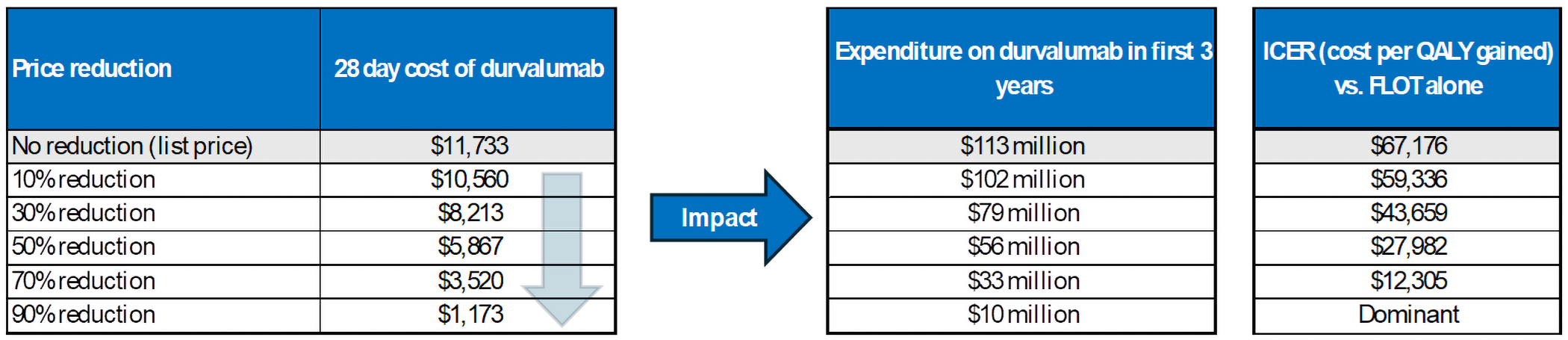
CDA-AMC = Canada’s Drug Agency; FLOT = fluorouracil, leucovorin, oxaliplatin, and docetaxel; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Note: Expenditure includes only the drug cost of durvalumab. The term dominant indicates that a drug costs less and provides more QALYs than the comparator.
References
1.AstraZeneca. A Randomized, Double-blind, Placebo-controlled, Phase III Study of Neoadjuvant-Adjuvant Durvalumab and FLOT Chemotherapy Followed by Adjuvant Durvalumab in Patients with Resectable Gastric and Gastroesophageal Junction Cancer (GC/GEJC) (MATTERHORN) - Clinical Study Protocol (CSP) [sponsor supplied reference]. 2024.
2.Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209-249. doi:10.3322/caac.21660 PubMed
3.Snow S, Gabrielson D, Lim H, Tehfe M, Brezden-Masley C. Best Practices for Managing Patients with Unresectable Metastatic Gastric and Gastroesophageal Junction Cancer in Canada. Curr Oncol. 2024;31(5):2552-2565. doi:10.3390/curroncol31050191 PubMed
4.Barbour AP, Rizk NP, Gonen M, et al. Adenocarcinoma of the gastroesophageal junction: influence of esophageal resection margin and operative approach on outcome. Ann Surg. 2007;246(1):1-8. doi:10.1097/01.sla.0000255563.65157.d2 PubMed
5.Ajani JA, D'Amico TA, Bentrem DJ, et al. Gastric Cancer, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2022;20(2):167-192. doi:10.6004/jnccn.2022.0008 PubMed
6.Smyth EC, Nilsson M, Grabsch HI, van Grieken NC, Lordick F. Gastric cancer. Lancet. 2020;396(10251):635-648. doi:10.1016/s0140-6736(20)31288-5 PubMed
7.Lordick F, Carneiro F, Cascinu S, et al. Gastric cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2022;33(10):1005-1020. doi:10.1016/j.annonc.2022.07.004 PubMed
8.Mamun TI, Younus S, Rahman MH. Gastric cancer—Epidemiology, modifiable and non-modifiable risk factors, challenges and opportunities: An updated review. Cancer Treatment and Research Communications. 2024;41:100845. doi: https://doi.org/10.1016/j.ctarc.2024.100845 PubMed
9.Purich K, Skubleny D, Ghosh S, et al. A prospective Canadian gastroesophageal cancer database: What have we learned? Can J Surg. 2023;66(4):E422. doi:10.1503/cjs.005122 PubMed
10.Ramachandran R, Grantham T, Parvataneni S, et al. Gastric Cancer: Clinical Features, Screening, Diagnosis, Treatment, and Prevention. J Community Hosp Intern Med Perspect. 2024;14(2):49-57. doi:10.55729/2000-9666.1304 PubMed
11.Kundes MF, Kement M, Yegen F, Alkan M, Kaya S, Kaptanoglu L. Effects of clinical factors on quality of life following curative gastrectomy for gastric cancer. Niger J Clin Pract. 2019;22(5):661-668. doi:10.4103/njcp.njcp_181_18 PubMed
12.Yamauchi H, Nakagawa C, Fukuda T. Social impacts of the work loss in cancer survivors. Breast Cancer. 2017;24(5):694-701. doi:10.1007/s12282-017-0759-y PubMed
13.Brenner DR, Gillis J, Demers AA, et al. Projected estimates of cancer in Canada in 2024. CMAJ. 2024;196(18):E615-e623. doi:10.1503/cmaj.240095 PubMed
14.Lou L, Wang L, Zhang Y, et al. Sex difference in incidence of gastric cancer: an international comparative study based on the Global Burden of Disease Study 2017. BMJ Open. 2020;10(1):e033323. doi:10.1136/bmjopen-2019-033323 PubMed
15.Xing Y, Hosaka H, Moki F, et al. Gender Differences in Patients with Gastric Adenocarcinoma. J Clin Med. 2024;13(9). doi:10.3390/jcm13092524 PubMed
16.Canadian Cancer Society. Canadian Cancer Statistics Advisory Committee in collaboration with the Canadian Cancer Society, Statistics Canada and the Public Health Agency of Canada. Canadian Cancer Statistics 2024. Toronto, ON: Canadian Cancer Society; 2024.
17.Canadian Cancer Society. Stomach cancer statistics.. 2024. Accessed September 25, 2025. https://cancer.ca/en/research/cancer-statistics
18.Canadian Cancer Society. Survival statistics for stomach cancer. 2019. Accessed September 25, 2024. https://cancer.ca/en/cancer-information/cancer-types/stomach/prognosis-and-survival/survival-statistics
19.Zhang H, Yang W, Tan X, et al. Long-term relative survival of patients with gastric cancer from a large-scale cohort: a period-analysis. BMC Cancer. 2024;24(1):1420. doi: 10.1186/s12885-024-13141-5 PubMed
20.Cattelan L, Ghazawi FM, Le M, et al. Geographic and Socioeconomic Disparity of Gastric Cancer Patients in Canada. Curr Oncol. 2021;28(3):2052-2064. doi:10.3390/curroncol28030190 PubMed
21.National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology. Gastric Cancer. Version 2.2025 — April 4, 2025 [sponsor supplied reference].
22.Alberta Health Services. Gastric Cancer. Clinical Practice Guideline GI-008– Version 6 [sponsor supplied reference]. Accessed February 2025. https://www.albertahealthservices.ca/assets/info/hp/cancer/if-hp-cancer-guide-gi008-gastric.pdf
23.National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Gastric Cancer, Version 3.2025 [sponsor supplied reference]. 2025. https://www.nccn.org/professionals/physician_gls/pdf/gastric.pdf
24.Lordick F, Carneiro F, Cascinu S, et al. Gastric cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2022;33(10):1005-1020. doi:10.1016/j.annonc.2022.07.004 PubMed
25.Investigators S-F. Pathological response guides adjuvant 5-fluorouracil, leucovorin, oxaliplatin, and docetaxel (FLOT) chemotherapy in surgically resected gastro-oesophageal cancer (SPACE-FLOT): international cohort study. BJS. 2025;112(4). doi:10.1093/bjs/znaf056
26.AstraZeneca. Clinical Study Report: D910GC00001. A Randomized, Double-blind, Placebo-controlled, Phase III Study of Neoadjuvant-Adjuvant Durvalumab and FLOT Chemotherapy Followed by Adjuvant Durvalumab in Patients with Resectable Gastric and Gastroesophageal Junction Cancer (GC/GEJC) (MATTERHORN) [internal sponsor's report]. May 15, 2025.
27.Bassler D, Briel M, Montori VM, et al. Stopping randomized trials early for benefit and estimation of treatment effects: systematic review and meta-regression analysis. JAMA. 2010;303(12):1180-7. doi:10.1001/jama.2010.310 PubMed
28.Briel M, Bassler D, Wang AT, Guyatt GH, Montori VM. The dangers of stopping a trial too early. J Bone Joint Surg Am. 2012;94 Suppl 1:56-60. doi: 10.2106/jbjs.K.01412 PubMed
29.Wilcox RA, Djulbegovic B, Moffitt HL, Guyatt GH, Montori VM. Randomized trials in oncology stopped early for benefit. J Clin Oncol. 2008;26(1):18-9. doi:10.1200/jco.2007.13.6259 PubMed
30.AstraZeneca Canada Inc. Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Imfinzi (durvalumab for injection), concentrate for solution for infusion, 50 mg/mL, intravenous. September 17, 2025.
31.AstraZeneca Canada Inc. Imfinzi (durvalumab for injection): concentrate for solution for infusion, 50 mg/mL, intravenous [product monograph]. June 30, 2025. Updated January 1, 1800.
32.AstraZeneca Canada Inc. Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Imfinzi (durvalumab for injection), concentrate for solution for infusion, 50 mg/mL, intravenous. September 17, 2025.
33.AstraZeneca Canada Inc. Drug Reimbursement Review sponsor submission: Imfinzi (durvalumab for injection), concentrate for solution for infusion, 50 mg/mL, intravenous [internal sponsor's package]. September 17, 2025.
34.IQVIA. DeltaPA. 2023. Accessed October 28, 2025. https://www.iqvia.com/
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@cda-amc.ca.