Drugs, Health Technologies, Health Systems
Reimbursement Recommendation
Daratumumab (Darzalex SC)
Indication: Daratumumab in combination with bortezomib, lenalidomide, and dexamethasone for the treatment of adult patients with newly diagnosed multiple myeloma who are not candidates for autologous stem cell transplant.
Sponsor: Janssen Inc.
Final recommendation: Reimburse with conditions
Summary
What Is the Reimbursement Recommendation for Darzalex SC?
Canada’s Drug Agency (CDA-AMC) recommends that Darzalex SC (daratumumab) in combination with bortezomib, lenalidomide, and dexamethasone (D-VRd) be reimbursed by public drug plans for the treatment of adult patients with newly diagnosed multiple myeloma (NDMM) who are not suitable for autologous stem cell transplant (ASCT) or for whom ASCT is not planned as the initial treatment, if certain conditions are met.
Why Did CDA-AMC Recommend Reimbursement?
The pan-Canadian Oncology Drug Review Expert Review Committee (pERC) determined that D-VRd demonstrates acceptable clinical value versus the combination of bortezomib, lenalidomide, and dexamethasone (VRd) in patients with NDMM who are not candidates for ASCT. Evidence from a clinical trial (CEPHEUS; N = 395) demonstrated that when compared to VRd, D-VRd given for 58 months prolonged the time until disease progression or death and was associated with an improved response to treatment in patients with NDMM who are not candidates for ASCT. Evidence from indirect treatment comparisons (ITCs) showed that in these patients, time to disease progression or death and response to treatment were improved with D-VRd when compared to daratumumab in combination with lenalidomide and dexamethasone (DRd) or compared with daratumumab in combination with bortezomib, melphalan, and prednisone (DVMp). However, the magnitude of benefit is uncertain, mainly due to differences in patients’ baseline characteristics between the clinical trials included in the ITCs. Evidence from ITCs also showed that time to disease progression or death and response to treatment were similar between groups receiving D‑VRd or the combination of isatuximab with VRd (Isa-VRd).
In the CEPHEUS trial, there was a large amount of missing data for health-related quality of life (HRQoL) outcomes; therefore, the clinical value of the improvements in HRQoL associated with D-VRd cannot be determined. Additionally, Darzalex SC was considered an additive therapy to VRd, and there were higher incidences of serious adverse events (AEs), infections and infestations, and low levels of certain blood cells associated with D-VRd.
Which Patients Are Eligible for Coverage?
Darzalex SC should only be reimbursed for adult patients with NDMM who are not suitable for ASCT or do not plan to receive ASCT as the initial treatment. Patients should also have good performance status and must not have received prior treatments for multiple myeloma. They also should not have signs of meningeal involvement of multiple myeloma.
What Are the Conditions for Reimbursement?
Darzalex SC should only be reimbursed if prescribed in combination with VRd, if prescribed by clinicians with expertise in diagnosis and management of multiple myeloma, and if the cost of Darzalex SC is reduced.
Review Background
Disease background:
Multiple myeloma is a cancer of plasma cells (the white blood cells that make immunoglobulins) found in the bone marrow. It causes a range of symptoms and can substantially impair patients’ and their caregivers’ HRQoL. For patients with NDMM who are not suitable for ASCT or do not plan to receive ASCT as the initial treatment, median overall survival (OS) is 4.5 years, which is shorter than that of those who receive ASCT (median OS = 8 to 10 years).
In 2025, approximately 4,285 people in Canada had NDMM. Among them, 2,125 were not suitable for ASCT or did not plan to receive ASCT as initial treatment.
Indication and reimbursement request: Daratumumab (Darzalex SC) has been approved by Health Canada for use in combination with bortezomib, lenalidomide, and dexamethasone for the treatment of adult patients with NDMM who are not candidates for ASCT. The sponsor is seeking reimbursement for this patient population.
Drug under review: Daratumumab is an IgG1 kappa human monoclonal antibody. It is available as a solution for subcutaneous injection. In the combination therapy (D-VRd), the dosage recommended for daratumumab in the product monograph (for a 3-week cycle dosing regimen) is 1,800 mg administrated subcutaneously — weekly during weeks 1 to 6, every 3 weeks during weeks 7 to 24, and every 4 weeks from week 25 onward until disease progression.
Treatment costs: At the submitted price of $8,028.00 per 1,800 mg vial and based on the Health Canada–recommended dosage, the 21-day cycle cost of daratumumab is expected to be $24,084 per patient in cycles 1 and 2 and $8,028 per patient in cycles 3 to 8, and the 28-day cycle cost of daratumumab is expected to be $8,028 per patient in cycles 9 and onward. Daratumumab is indicated for use in combination with VRd; the cost of the regimen is expected to be $28,210 per patient in cycles 1 and 2 (21 days each), $12,154 per patient in cycles 3 to 8 (21 days each), and $10,278 per patient in cycles 9 and beyond (28 days each).
Highlights of Input From Interested Parties
The patient group that provided input (Myeloma Canada) noted the following points regarding impacts of the disease, unmet needs, and important outcomes:
In a survey of patients with NDMM and their caregivers, respondents reported that NDMM greatly affected their HRQoL, with effects on their physical and psychological well-being and on daily activities. Multiple myeloma also placed heavy financial stress on patients and their caregivers.
Results of the survey emphasized that an ideal treatment for NDMM should be accessible to those who are not candidates for or choose not to undergo ASCT as initial therapy. It should also be effective in achieving long-term remission, preserving HRQoL and autonomy, minimizing side effects of the treatment, and ensuring continuity of care.
The clinician group (the Ontario Health [Cancer Care Ontario] Hematology Cancer Drug Advisory Committee) and the clinical experts consulted by CDA-AMC noted the following points regarding unmet needs arising from the disease and the place in therapy for the drug under review:
Although the current standard treatment (e.g., DRd) for the target patient population is highly effective, a small proportion of these patients do not initially experience disease responses, and patients eventually experience refractory disease or do not survive.
Clinical experts and the clinician group expect that D-VRd will be used as 1 of the first-line therapies for patients with NDMM who are not candidates for or choose not to undergo ASCT. Subsequently, this 4-drug combination could replace the existing 3-drug regimen (e.g., DRd) for appropriate patients.
Participating public drug programs raised potential implementation issues related to considerations for initiation, renewal, discontinuation, and prescribing of therapy; generalizability of trial populations to broader populations; care provision issues; system and economic issues; and the potential need to amend the provisional funding algorithm.
Recommendation
With a vote of 16 in favour to 0 against, pERC recommends that D-VRd be reimbursed for adult patients with NDMM who are not candidates for ASCT only if the conditions listed in Table 1 are met.
Table 1: Reimbursement Conditions and Reasons
Reimbursement condition | Reason | Implementation guidance |
|---|---|---|
Initiation | ||
1. Treatment with D-VRd should only be initiated in adult patients with previously untreated multiple myeloma for whom ASCT is not planned as initial therapy due to ineligibility or patient or clinician preference. | Evidence from the CEPHEUS trial demonstrated that treatment with D-VRd resulted in a clinically meaningful benefit in adult patients (aged 18 years or older) with symptomatic multiple myeloma, as defined by the IMWG criteria, among whom ASCT is not received as initial therapy due to their age (70 years or older), comorbid conditions, or patient preference. | In the trial, bortezomib was administered twice weekly, which differs from dosing used in most Canadian centres. Once-weekly bortezomib administration is also an option. |
2. Patients must have good performance status. | The CEPHEUS trial excluded adults with ECOG Performance Status scores > 2. Overall, 37 patients (9.4%) enrolled in the CEPHEUS trial had an ECOG Performance Status score of 2. | In clinical practice, most patients older than 80 years or with ECOG Performance Status scores > 2 would not be treated with D-VRd. However, older patients who do not have frailty may still be considered for this treatment. |
3. Patients must not have 3.1. received prior systemic therapy (except corticosteroids) or SCT for multiple myeloma 3.2. clinical signs of meningeal involvement of multiple myeloma. | Patients with NDMM exhibiting clinical signs of meningeal involvement were excluded from the CEPHEUS trial; therefore, the efficacy and safety of D‑VRd in this population is unknown. | Patients with concomitant plasma cell leukemia should be eligible for treatment with D-VRd. Patients with the following conditions would not be eligible for treatment with D‑VRd:
|
Discontinuation | ||
4. Treatment should be discontinued upon the occurrence of either of the following: 4.1. evidence of disease progression according to IMWG criteria 4.2. unacceptable toxicity. | Patients in the CEPHEUS trial discontinued treatment upon disease progression or unacceptable toxicity, consistent with clinical practice. This condition reflects the parameters for treatment discontinuation used in the CEPHEUS trial. | If prolonged treatment breaks occur, treatment with D-VRd can be resumed if disease progression had not occurred before the treatment break. If 1 of the drugs in the regimen is discontinued, treatment can continue with the other drugs in the regimen until disease progression or unacceptable toxicity occurs. |
Prescribing | ||
5. D-VRd should be prescribed by clinicians with expertise in managing patients with multiple myeloma. | To ensure that D-VRd is prescribed for appropriate patients and that adverse effects are managed in an optimized and timely manner. | — |
Pricing | ||
6. A reduction in price. | Using the CDA-AMC base-case analysis, the ICER for D-VRd was $10,623,156 per QALY gained when compared with VRd and $7,029,398 per QALY gained when compared with DRd in the indicated population. A band 4a price reduction would be required to achieve cost-effectiveness at a $50,000 per QALY gained threshold compared with VRd and a band 2a price reduction would be required to achieve cost-effectiveness at a $50,000 per QALY gained threshold compared with DRd. A band 4a price reduction would be required to achieve cost-effectiveness at a $100,000 per QALY gained threshold compared with VRd, and a band 2a price reduction would be required to achieve cost-effectiveness at a $100,000 per QALY gained threshold compared with DRd. Exact price reductions at any given willingness-to-pay threshold can be found in the CDA-AMC Main Report and Supplemental Material documents. | The CDA-AMC analysis is based on public list prices for all treatments. Further price reductions may be required if there are price arrangements (discounts) currently in place for any treatment included in the economic analysis. |
ASCT = autologous stem cell transplant; CDA-AMC = Canada’s Drug Agency; DRd = daratumumab in combination with lenalidomide and dexamethasone; D-VRd = daratumumab in combination with bortezomib, lenalidomide, and dexamethasone; ECOG = Eastern Cooperative Oncology Group; ICER = incremental cost-effectiveness ratio; IMWG = International Myeloma Working Group; NDMM = newly diagnosed multiple myeloma; QALY = quality-adjusted life-year; SCT = stem cell transplant; VRd = bortezomib, lenalidomide, and dexamethasone.
aFor statements regarding the size of the price reduction required, band 1 = 1% to 24%, band 2 = 25% to 49%, band 3 = 50% to 74%, and band 4 = 75% or greater.
Rationale for the Recommendation
Clinical Value
Based on the totality of the clinical evidence, pERC concluded that D-VRd demonstrates acceptable clinical value compared with appropriate comparators (e.g., VRd, DRd, DVMp) in patients with NDMM who are not candidates for ASCT. An acceptable clinical value refers to prolonged survival or higher rates of disease response with D-VRd versus with these comparators.
Evidence from 1 randomized, open-label, active-controlled, multicentre phase III trial (CEPHEUS; N = 395) demonstrated that treatment with D-VRd resulted in acceptable clinical value — in progression-free survival (PFS) and the minimal residual disease (MRD) negativity rate — for patients with NDMM who are not candidates for ASCT, compared with VRd. After a median follow-up time of 58.71 months, the median PFS was not reached in the D-VRd group and was 52.63 months in the VRd group. At 54 months, the Kaplan-Meier (KM) estimates of the probability of PFS were 68.1% (95% confidence interval [CI], 60.8% to 74.3%) in the D-VRd group and 49.5% (95% CI, 41.8% to 56.8%) in the VRd group, with a between-group difference of ████% (95% CI, ███% to ████%). The overall MRD negativity rate at 10-5 was 60.9% (95% CI, 53.7% to 67.8%) in the D-VRd group and 39.4% (95% CI, 32.5% to 46.6%) in the VRd group. The between-group difference in the overall MRD negativity rate at 10-5 was ████% (95% CI, ████% to ████%).
In the CEPHEUS trial, after a median follow-up time of 58.71 months, OS data were not mature; the median OS was not reached for either treatment group. The 54-month KM estimates of the OS rate were 74.2% (95% CI, 67.3% to 79.8%) in the D-VRd group and 69.6% (95% CI, 62.5% to 75.7%) in the VRd group, with a between-group difference of ███% (95% CI, ████% to ████%).
With respect to quality of life, the data from the CEPHEUS trial suggest that D-VRd may not result in any clinically important difference in patients’ HRQoL compared to VRd, and no firm conclusions could be drawn on HRQoL due to the large amount of missing data. D-VRd likely results in an increase in the incidence of serious AEs, infections and infestations, and cytopenia compared to VRd. The committee agreed with the clinical experts that the types of AEs in the trial were as expected for D-VRd.
Evidence from 3 ITC analyses suggests an improvement in PFS and the MRD negativity rate with D-VRd when compared to DRd or DVMp, although the magnitude of benefit is uncertain. This uncertainty was likely related to cross-trial heterogeneity (e.g., patients’ characteristics differed at baseline). There was no statistically significant difference in OS between D-VRd and DRd or DVMp. The ITC of the comparison of D-VRD with Isa-VRd showed no statistically significant difference between the 2 treatment regimens; the evidence is insufficient to conclude whether D-VRd or Isa-VRd is favoured for prolonging PFS or OS, or for improving the MRD negativity rate in this population.
Further information on the committee’s discussion around clinical value is provided in the Summary of Deliberation section.
Developing the Recommendation
The determination of acceptable clinical value was sufficient for pERC to recommend reimbursement of D-VRd. As part of the deliberation on whether to recommend reimbursement, the committee also considered unmet clinical need, unmet nonclinical need, and health inequity. Information on this discussion is provided in the Unmet Clinical Need and the Distinct Social and Ethical Considerations domains in the Summary of Deliberation section.
Because pERC recommended that D-VRd be reimbursed, the committee also deliberated on whether reimbursement conditions should be added to address important economic considerations, health system impacts, or social and ethical considerations, or to ensure clinical value is realized. The resulting reimbursement conditions, with accompanying reasons and implementation guidance, are stated in Table 1.
Summary of Deliberation
pERC considered all domains of value of the deliberative framework before developing its recommendation: clinical value, unmet clinical need, distinct social and ethical considerations, economic considerations, and impacts on health systems. For further information on the domains of value, refer to Expert Committee Deliberation at Canada’s Drug Agency.
The committee considered the following key discussion points, organized by the 5 domains of value.
Clinical Value
Efficacy of D-VRd versus VRd: The phase III CEPHEUS trial (N = 395) showed that first-line treatment with D-VRd resulted in a statistically significant meaningful improvement in the primary end point of the overall MRD negativity rate at 10-5, after a median follow-up of 58.71 months: 60.9% (95% CI, 53.7% to 67.8%) in the D-VRd group and 39.4% (95% CI, 32.5% to 46.6%) in the VRd group. The between-group difference in the overall MRD negativity rate at 10-5 was ████% (95% CI, ████% to ████%). D-VRd resulted in a statistically significant and clinically meaningful improvement in PFS compared to VRd. After a median follow-up time of 58.71 months, the median PFS was not reached in the D-VRd group and was 52.63 months in the VRd group. At 54 months, the KM estimates of the probability of PFS were 68.1% (95% CI, 60.8% to 74.3%) in the D-VRd group and 49.5% (95% CI, 41.8% to 56.8%) in the VRd group, with a between-group difference of ████% (95% CI, ███% to ████%). After a median follow-up time of 58.71 months, OS data were not mature. The median OS was not reached for either treatment group. The 54-month KM estimates of the OS rate were 74.2% (95% CI, 67.3% to 79.8%) in the D-VRd group and 69.6% (95% CI, 62.5% to 75.7%) in the VRd group, with a between-group difference of ███% (95% CI, ████% to ████%). Furthermore, D-VRd may not result in any clinically important difference in patients’ HRQoL, which was assessed using the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ) Core 30 Global Health Status/Quality of Life (GHS/QoL) and EORTC QLQ Multiple Myeloma Module (MY20) scores, compared to VRd. However, pERC was unable to draw conclusions on HRQoL due to the large amount of missing data.
Safety of D-VRd versus VRd: In the CEPHEUS trial, D-VRd likely resulted in an increase in the incidence of serious AEs, infections and infestations, and cytopenia compared to VRd. The committee agreed with the clinical experts that the types of AEs in the trial were as expected for D-VRd, and these AEs would be mostly anticipated and manageable.
Certainty of the evidence: pERC discussed the certainty of evidence as assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) method. For the added PFS value, the certainty was rated as high at 54 months, indicating a clinically important improvement in PFS with the addition of daratumumab to VRd (i.e., D-VRd) in PFS at this time point. The certainty for the added value of OS was rated as moderate (rated down for imprecision) at 54 months, suggesting that D-VRd likely results in a clinically important improvement in patients’ OS; however, the clinical importance of the increase is uncertain. The imbalanced use of subsequent anti-myeloma therapies after disease progression may contribute to the uncertainty in OS benefit. The certainty of evidence for EORTC QLQ-C30 GHS/QoL and EORTC QLQ-MY20 scores was rated as low at cycle 36, suggesting that D-VRd likely results in little to no difference in HRQoL at this time point. The large amount of missing HRQoL data may explain the low certainty of evidence. The certainty of evidence for serious AEs and infection or infestation (notable harm identified by the clinical experts consulted by CDA-AMC) was rated as moderate, as the 95% CI for the difference between groups spans from a possible benefit to possible harm.
Appropriate comparators: pERC considered DRd to be an appropriate comparator. This is the current first-choice regimen for patients with NDMM who are not candidates for ASCT. VRd and DVMp remain potential alternatives but are not preferred treatment options for these patients. Isa‑VRd for patients with NDMM who are not eligible for ASCT was recently reviewed by CDA-AMC and received a positive reimbursement recommendation in June 2025.
Efficacy versus DRd, DVMp, and Isa-VRd (indirect evidence): Evidence from 3 ITCs suggested improvements in PFS and the MRD negativity rate with D-VRd when compared to DRd or DVMp, although the magnitude of benefit is uncertain. This uncertainty was likely related to cross-trial heterogeneity (e.g., patients’ characteristics differed at baseline). It is also possible that not all effect modifiers have been adjusted for in the analysis. There were no statistically significant differences in OS between D-VRd and DRd or DVMp. Additionally, ITC results suggested that evidence is insufficient to conclude whether D-VRd or Isa-VRd is favoured for prolonging PFS or OS, or for improving the MRD negativity rate, in patients with NDMM who are not candidates for ASCT.
MRD status: Although MRD status was the primary end point in the CEPHEUS trial, it has not yet been used as a standard treatment end point in routine clinical practice for this indication. However, MRD negativity is increasingly recognized as a prognostic factor and a surrogate for longer-term outcomes in patients with multiple myeloma. Recent evidence suggests that MRD negativity is associated with improved PFS and OS across disease settings, MRD assays and sensitivity thresholds, cytogenetic risk categories, and timing of assessment. In Canada, MRD testing is neither routinely available nor used to guide clinical management. More studies evaluating MRD-guided treatment de-escalation are needed, as they could reshape current decision pathways and clarify whether indefinite therapy with regimens of an anti-CD38 monoclonal antibody with lenalidomide and a steroid is warranted.
Clinical value: Based on the preceding considerations, pERC determined there was added clinical value for D-VRd versus relevant comparators in the population of patients with NDMM who are not candidates for ASCT.
Unmet Clinical Need
Input on unmet clinical need: The patient group, the clinician group, and clinical experts consulted by CDA-AMC identified the need for treatments that can alleviate symptoms, achieve long-term remission, preserve HRQoL, minimize treatment side effects, and prolong survival.
Severity of the disease: pERC discussed input from the patient group, the clinician group, and clinical experts consulted by CDA-AMC, indicating that multiple myeloma is an incurable, life-threatening, chronic disease associated with serious symptoms. It imposes a substantial burden on multiple aspects of life including physical health, emotional well-being and mental health, social interactions, work or daily activities, sleep, and pain. It follows a relapsing-remitting course despite initial treatment responses. The committee also acknowledged that the prognosis for patients with NDMM who are not candidates for ASCT tends to be poorer than that for those who receive ASCT (median overall survival < 5 years versus 8 to 10 years, respectively).
Availability of treatment options: Currently, DRd is the standard first-line treatment for adults with transplant-ineligible NDMM who are fit enough to tolerate an anti-CD38 monoclonal antibody. DRd is publicly funded in Canada. For patients who have frailty, high-risk disease, or renal insufficiency, the use of a daratumumab-containing regimen is also recommended; however, additional considerations are necessary to ensure tolerability and selection of the most appropriate combination therapy. For other daratumumab-containing regimens — DVMp and daratumumab in combination with cyclophosphamide, bortezomib, and dexamethasone (DCyBorD) — the clinical experts consulted by CDA-AMC noted that neither is commonly used as first-line treatment due to their safety profiles and generally lower efficacy compared with DRd. Furthermore, DCyBorD is only explicitly mentioned in recommendations for subpopulations of patients with high-risk disease or severe and/or rapidly progressing acute renal insufficiency related to multiple myeloma. Currently, regimens that do not contain daratumumab, such as VRd, CyBorD, and lenalidomide with dexamethasone (Rd), for patients unable to tolerate triplet regimens or living in rural settings), remain potential alternatives but are not preferred options. In addition, Isa-VRd, the most recently approved treatment option in this setting, is undergoing price negotiations and is not yet publicly funded.
Subcutaneous formulation: pERC discussed that subcutaneous formulations would offer a more convenient, accessible treatment choice for patients compared to IV formulations. pERC also noted the subcutaneous administration route required for daratumumab is a facilitator for access to quadruplet therapy, versus the IV administration required for isatuximab.
Distinct Social and Ethical Considerations
Input on unmet nonclinical need: pERC acknowledged unmet nonclinical needs of patients with NDMM who are not candidates for ASCT. The patient group highlighted challenges related to achieving greater autonomy in treatment decisions due to the financial and quality of life burdens associated with ASCT. The patient group also commented on challenges related to barriers to care, such as delayed treatments due to shortages in clinic space; inaccessibility of treatments in rural areas or in regions with physician shortages; and costs not being covered comprehensively by insurance. The committee also recognized the financial burden of treatment that this patient population experiences, including frequent clinic visits and the travel and time burdens that disproportionately affect patients and caregivers living in rural and remote areas.
Equity considerations: pERC acknowledged that the disease and treatments disproportionately affect patients and caregivers who live in rural and remote areas, who have frailty, who have low incomes, or otherwise have with limited resource. This would reduce the acceptability of D-VRd and equity of access to D-VRd. pERC also noted that multiple myeloma disproportionately affects Black individuals, who have a higher risk for this disease but have historically been underrepresented in clinical trials.
Economic Considerations
Economic considerations focus on VRd, for which direct comparative evidence exists, and DRd, which accounts for most of the use in Canadian clinical practice. The Pharmacoeconomic Review report presents results comparing D-VRd to DVMp, Isa-VRd, and Rd.
Health impacts of D-VRd versus relevant comparators: D-VRd is predicted to result in no additional life-years compared to VRd or DRd. D-VRd may result in a gain of 0.10 quality-adjusted life-years (QALYs) compared to VRd and 0.04 QALYs compared to DRd.
Cost of D-VRd versus relevant comparators: D-VRd is predicted to be associated with higher costs to the health care system than VRd (incremental costs = $1,072,043) and DRd (incremental costs = $311,182). These cost increases are driven by drug acquisition costs associated with D-VRd.
Key findings of the economic evaluation: Based on the submitted evidence using the sponsor’s cost-utility analysis, the CDA-AMC base-case analysis estimated that the incremental cost-effectiveness ratios (ICERs) for D-VRd for the treatment of adult patients with newly diagnosed multiple myeloma who are not candidates for ASCT were $10,623,156 per QALY gained compared to VRd and $7,029,398 per QALY gained compared to DRd (Figure 1).
Figure 1: Estimates of the ICERs Used by pERC to Inform the Price Condition
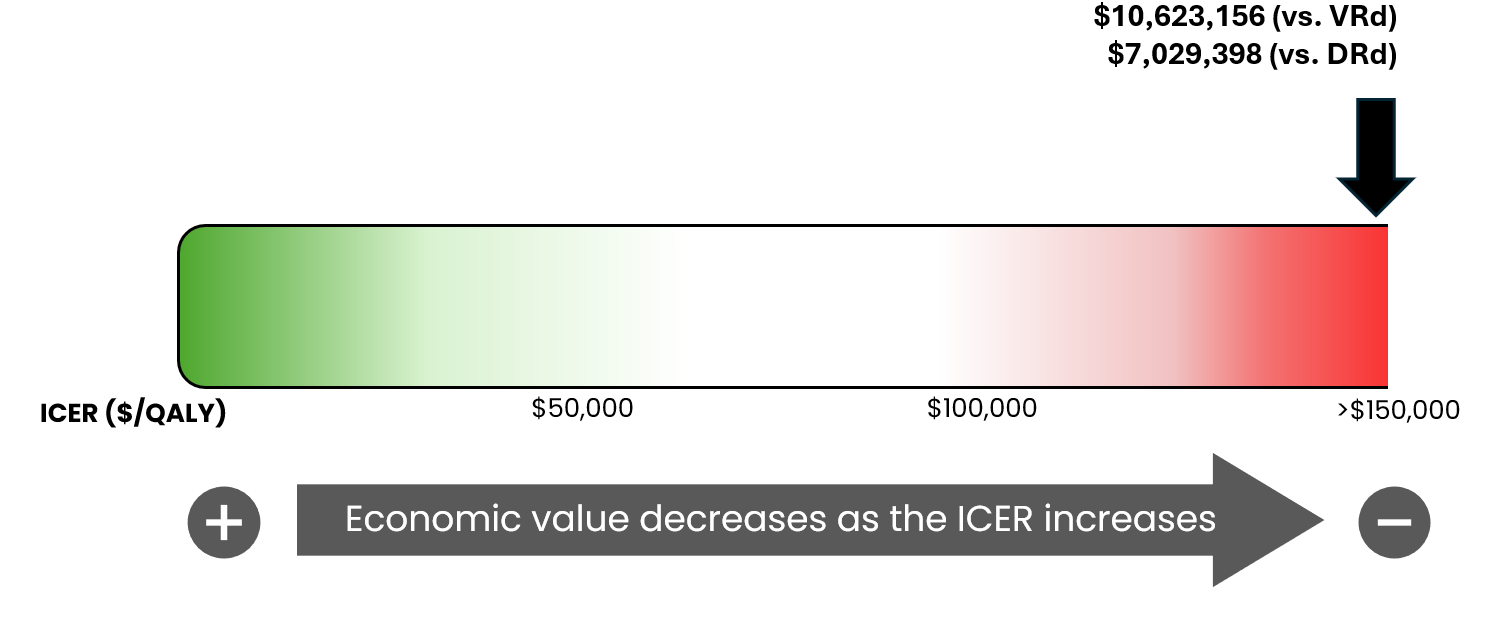
DRd = daratumumab in combination with lenalidomide and dexamethasone; ICER = incremental cost-effectiveness ratio; pERC = pan-Canadian Oncology Drug Review Expert Review Committee; QALY = quality-adjusted life-year; VRd = bortezomib, lenalidomide, and dexamethasone; vs. = versus.
Economic value considerations: pERC acknowledged that, at publicly available list prices, the CDA-AMC base-case ICERs for D-VRd versus VRd and D-VRd versus DRd are very high, reflecting substantial incremental drug acquisition costs with minimal incremental QALY gains and no predicted life-year benefit. pERC also discussed that the cost-effectiveness results are highly uncertain due to reliance on extrapolated benefits and due to sensitivity to OS assumptions and daratumumab acquisition costs, and it considered these factors when informing the price condition.
Certainty of the evidence: The estimated ICER was highly sensitive to the predicted OS benefit and the drug acquisition costs of daratumumab. Approximately 82% and 89% of the incremental benefit relative to VRd and DRd, respectively, was gained in the extrapolated period (i.e., after 5.3 years). In the absence of comparative evidence beyond this time point and uncertainty in the comparative clinical evidence, the QALYs gained remain highly uncertain and may be overestimated. Higher price reductions than those presented in this report may therefore be required to achieve cost-effectiveness at a given willingness-to-pay threshold.
Impacts on Health Systems
Anticipated budget impact: CDA-AMC estimated that 6,866 patients would be eligible for D-VRd over a 3-year period (year 1 = 2,188; year 2 = 2,287; year 3 = 2,391), of whom 1,214 are expected to receive D-VRd (year 1 = 223; year 2 = 485; year 3 = 507). The estimated incremental budgetary savings of reimbursing D-VRd are predicted to be approximately $39 million over the first 3 years relative to current spending, with an expected expenditure of $369 million on D-VRd. The actual budgetary savings of reimbursing D-VRd will depend on the market uptake of D-VRd, the negotiated prices of reimbursed comparators, and the distribution of therapies that are likely to be displaced by D-VRd. The magnitude of uncertainty in the budget impact must be addressed to ensure the feasibility of adoption given the difference between the sponsor’s estimate and the CDA-AMC estimate.
Sources of Information Used by the Committee
To make its recommendation, the committee considered the following information (links to the full documents for the review can be found on the project web page):
the CDA-AMC review of the clinical and pharmacoeconomic evidence submitted by the sponsor, as well as relevant ethical issues related to daratumumab (refer the Main Report and Supplemental Material document)
the sponsor’s comments on the draft report and the CDA-AMC responses
patients' perspectives gathered by 1 patient group, Myeloma Canada (refer to the Patient and Clinician Group Input document)
input from 1 clinician group, the Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee (refer to the Patient and Clinician Group Input document)
input from public drug programs that participate in the reimbursement review process (refer to the Supplemental Material document)
input from 2 clinical experts with expertise in the management of multiple myeloma consulted by CDA-AMC.
pERC Information
Members of the Committee
Dr. Catherine Moltzan (Chair), Dr. Kelvin Chan (Vice-Chair), Paul Agbulu, Dr. Phillip Blanchette, Dr. Matthew Cheung, Dr. Michael Crump, Annette Cyr, Dr. Jennifer Fishman, Dr. Jason Hart, Terry Hawrysh, Dr. Yoo-Joung Ko, Dr. Aly-Khan Lalani, Amy Peasgood, Dr. Anca Prica, Dr. Michael Raphael, Dr. Adam Raymakers, Dr. Patricia Tang, Dr. Pierre Villeneuve, and Danica Wasney.
Meeting date: January 14, 2026
Regrets: Two expert committee members did not attend.
Conflicts of interest: None
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.