Drugs, Health Technologies, Health Systems
Reimbursement Review
Toripalimab (Loqtorzi)
Sponsor: Apotex Inc.
Therapeutic area: Recurrent or metastatic nasopharyngeal carcinoma
Summary
What Is Recurrent or Metastatic Nasopharyngeal Carcinoma?
Nasopharyngeal carcinoma (NPC) is a rare malignancy of the nasopharynx with distinct features; it has strong geographic and ethnic variation due to its association with Epstein-Barr virus and other risk factors. While the 5-year overall survival (OS) rate in Canada is 70% for all stages, up to 30% of patients still experience recurrence — half of these within 2 years of initial treatment.
Globally, NPC incidence is low (< 1 per 100,000 person-years), but it is much higher in endemic regions such as Southeast Asia and among certain populations in Canada, such as people of Asian descent and Inuit communities.
What Are the Treatment Goals and Current Treatment Options for Recurrent or Metastatic NPC?
Reducing tumour burden, improving symptoms, improving quality of life, delaying disease progression, and improving survival are the treatment goals in the first-line setting, as well as minimizing adverse events (AEs) and prolonging cancer control.
Progression-free survival (PFS), OS, and health-related quality of life (HRQoL) were identified as important by clinical experts consulted for this review and patient group input. Other important outcomes identified by the clinical experts were objective response rate and duration of response (DoR).
The current standard of care for NPC in the first-line setting is gemcitabine plus platinum-based chemotherapy (cisplatin or carboplatin). Tislelizumab is available through special access programs but is not routinely funded by provincial jurisdictions.
What Is Toripalimab and Why Did Canada’s Drug Agency Conduct This Review?
Toripalimab is a humanized immunoglobulin G4 kappa monoclonal antibody that binds to human PD-1 and is administered by IV infusion. At the time this review was conducted, Health Canada reviewed toripalimab in combination with cisplatin and gemcitabine for the first-line treatment of adults with metastatic or recurrent, locally advanced NPC.
Canada’s Drug Agency (CDA-AMC) reviewed toripalimab to inform a recommendation to the participating public drug programs on whether it should be reimbursed for the indication reviewed by Health Canada.
How Did CDA-AMC Evaluate Toripalimab?
CDA-AMC reviewed the clinical evidence on the beneficial and harmful effects, as well as the economic evidence, of toripalimab versus other treatments used in Canada for the first-line treatment of recurrent or metastatic NPC. Gemcitabine plus platinum-based chemotherapy (cisplatin or carboplatin) was considered a relevant treatment to compare with toripalimab in combination with cisplatin and gemcitabine when reviewing the clinical evidence.
CDA-AMC identified equity and ethical considerations relevant to toripalimab and the first-line treatment of recurrent or metastatic NPC.
The review was informed by materials submitted by the sponsor, which included clinical and economic evidence.
The review was also informed by a joint submission from 3 patient groups and 1 clinician group submission in response to the call by CDA-AMC for input, and by input from the public drug programs participating in the CDA-AMC reimbursement review process around issues that could affect their ability to implement a recommendation.
Two medical oncologists and 1 radiation oncologist were consulted as part of the review process.
What Were the Findings?
Clinical Evidence
CDA-AMC reviewed the following clinical evidence:
1 randomized, controlled, phase III trial (the JUPITER-02 study) comparing toripalimab in combination with gemcitabine and cisplatin to gemcitabine plus cisplatin in 289 patients with recurrent or metastatic NPC that was not amenable to curative treatment and was treated in the first-line care setting.
For the comparison of toripalimab plus gemcitabine and cisplatin versus gemcitabine plus cisplatin, the following points were noted:
Treatment with toripalimab demonstrated a statistically significant improvement in median PFS, resulted in a clinically important increase in the probability of having disease that is progression-free at 1 year (there was moderate certainty due to imprecision), and may result in a clinically important increase in the probability of having disease that is progression-free at 2 years (there was low certainty due to study limitations and imprecision).
Treatment with toripalimab likely results in a clinically important increase in the probability of being alive at 1 year, 2 years, and 3 years (there was moderate certainty due to imprecision).
Other outcomes (objective response rate and DoR) were supportive of PFS and OS results; however, the evidence was very uncertain about the effect of treatment with toripalimab on HRQoL as measured by the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 score and European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire 35-item Head and Neck pain and swallowing score.
The evidence was limited by an inestimable median OS rate. PFS and DoR also had some inestimable confidence intervals. Furthermore, the JUPITER-02 study was unblinded after the interim PFS analysis, which adds bias to the HRQoL results.
The JUPITER-02 study population enrolled a narrower inclusion criterion (i.e., recurrent or metastatic NPC not amenable to curative treatment) than in the Health Canada indication (i.e., metastatic or recurrent, locally advanced NPC), although clinical experts consulted for this review noted it is rare for patients with recurrent NPC to be considered for curative treatment.
The generalizability of the results was also limited by factors such as the JUPITER-02 study sites being only in NPC-endemic areas, the study including only patients of Asian descent, and most patients having nonkeratinizing NPC.
AEs were largely consistent between study arms, suggesting that the gemcitabine plus cisplatin treatment may contribute to harms; however, there were differences in immune-related AEs, suggesting that toripalimab results in an increase in these types of harms.
Economic Evidence
Loqtorzi is available as a solution for IV injection (240 mg per 6 mL). At the submitted price of $8,800.00 per vial, the cost of Loqtorzi is expected to be $8,800 per patient per 21-day cycle, based on the Health Canada–recommended dosage.1 When used in combination with cisplatin and gemcitabine, the total cost of treatment is expected to be $10,285 per patient per 21-day cycle. When considering a 28-day cost, the Loqtorzi cost is expected to be $11,733 per patient or $13,713 per patient when used in combination with cisplatin and gemcitabine.
Clinical efficacy in the economic analysis was derived from the JUPITER-02 trial, which compared Loqtorzi in combination with cisplatin and gemcitabine with chemotherapy alone.2 Evidence submitted by the sponsor indicates that Loqtorzi in combination with cisplatin and gemcitabine versus gemcitabine and cisplatin alone results in a clinically important increase in the proportion of patients with PFS at 1 year, may result in an increase in the proportion of patients with PFS at 2 years, and likely increases the proportion of patients alive at 1 year, 2 years, and 3 years among patients with metastatic or recurrent, locally advanced NPC that was not amenable to local–regional or curative treatment. However, there is uncertainty in the efficacy outcomes as the evidence was limited by high degrees of censoring, early unblinding, and generalizability concerns.
The results of the CDA-AMC base case suggest the following:
Loqtorzi plus chemotherapy is predicted to be associated with higher costs to the health care system than chemotherapy alone (incremental costs = $219,624), primarily driven by increased costs associated with drugs costs and health care resource use.
Loqtorzi plus chemotherapy is predicted to be associated with a gain of 1.56 life-years compared to chemotherapy alone and may result in a gain of 1.16 quality-adjusted life-years compared to chemotherapy alone.
The incremental cost-effectiveness ratio of Loqtorzi plus chemotherapy compared to chemotherapy alone was $189,118 per quality-adjusted life-year gained in the CDA-AMC base case. The estimated incremental cost-effectiveness ratio is uncertain due to uncertainty in the comparative efficacy data informing the model, long-term survival estimates, and the economic model structure. As a result, the economic analysis may not accurately assess the true impact of Loqtorzi plus chemotherapy on patient health and health care resources. Thus, the cost-effectiveness of Loqtorzi plus chemotherapy remains uncertain and higher price reductions may be required to achieve a given willingness-to-pay threshold.
CDA-AMC estimates that the budget impact of reimbursing Loqtorzi for use in combination with gemcitabine and cisplatin for the treatment of NPC will be approximately $52 million over the first 3 years of reimbursement compared to the amount currently spent on comparators. The expenditure on Loqtorzi over this period is predicted to be $52 million (Loqtorzi plus gemcitabine and cisplatin as a regimen = $55 million). The actual budget impact of reimbursing Loqtorzi will depend on the number of people eligible for treatment who will receive treatment, the duration of treatments, and Loqtorzi uptake.
Abbreviations
AE
adverse event
BIA
budget impact analysis
BIRC
blinded independent review committee
CCS
Canadian Cancer Society
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
DCO
data cut-off
DoR
duration of response
EBV
Epstein-Barr virus
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
EORTC QLQ-H&N35
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire 35-item Head and Neck
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HR
hazard ratio
HRQoL
health-related quality of life
IA
interim analysis
ITC
indirect treatment comparison
ITT
intention to treat
LTE
long-term extension
MID
minimal important difference
NPC
nasopharyngeal carcinoma
ORR
objective response rate
OS
overall survival
PFS
progression-free survival
PPS
per-protocol analysis set
QALY
quality-adjusted life-year
RCT
randomized controlled trial
SAE
serious adverse event
SD
standard deviation
TEAE
treatment-emergent adverse event
Background
Introduction
Context for the Review
The objectives of this report are as follows:
Review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of toripalimab 240 mg per 6 mL (40 mg per mL) sterile solution for IV infusion, in combination with cisplatin and gemcitabine, for the first-line treatment of adults with metastatic or recurrent, locally advanced nasopharyngeal carcinoma (NPC). The focus will be placed on comparing toripalimab to relevant comparators in clinical practice in Canada and identifying gaps in the current evidence; this focus is outlined in Table 1.
Review and critically appraise the economic information submitted by the sponsor, including a cost-effectiveness analysis and budget impact analysis (BIA). The focus of the economic review is aligned with the scope of the clinical review, unless otherwise stated. For most reviews, a Canada’s Drug Agency (CDA-AMC) base case is developed, informed by clinical expert input, the available clinical evidence, and the best interpretation of the economic evidence based on the information provided by the sponsor.
Table 1: Information on the Application Submitted for Review and on the CDA-AMC Review
Item | Description |
|---|---|
Information on the application submitted for review | |
Drug | Toripalimab 240 mg per 6 mL (40 mg per mL) sterile solution for IV infusion |
Sponsor | Apotex Inc. |
Health Canada indication | In combination with cisplatin and gemcitabine, for the first-line treatment of adults with metastatic or with recurrent, locally advanced NPC |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | October 17, 2025 |
Mechanism of action | Humanized IgG4 monoclonal antibody that binds to the PD-1 receptor and blocks its interaction with PD-L1 and PD-L2, releasing PD-1 pathway–mediated inhibition of the immune response, including the antitumour immune response. Upregulation of PD-1 ligands occurs in some tumours and signalling through this pathway can contribute to inhibition of active T-cell immune surveillance of tumours. |
Recommended dosage | First-line NPC: 240 mg intravenously every 3 weeks in combination with cisplatin and gemcitabine for up to 6 cycles, followed by 240 mg every 3 weeks until disease progression, unacceptable toxicity, or up to 24 months Recurrent NPC: 3 mg/kg body weight intravenously every 2 weeks. Administer until disease progression or unacceptable toxicity. |
Submission type | Initial |
Sponsor’s reimbursement request | Per indication |
Submitted price | Toripalimab: $8,800.00 per 6 mL vial |
Information on the CDA-AMC review | |
Review type | Complex |
Clinical review focusa | Population: As defined in the Health Canada indication Subgroups:
Intervention: Per recommended dosage Comparators:
Outcomes:
|
BIRC = blinded independent review committee; CDA-AMC = Canada’s Drug Agency; DoR = duration of response; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-H&N35 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire 35-item Head and Neck; IgG4 = immunoglobulin G4; NOC = Notice of Compliance; NPC = nasopharyngeal carcinoma; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours version 1.1; vs. = versus.
aThe economic review aligns with the scope of the clinical review, unless otherwise stated.
bAssessed by BIRC according to RECIST 1.1.
Submission History for the Drug Under Review
CDA-AMC has not previously reviewed toripalimab through the reimbursement review process.
Sources of Information
The contents of the Reimbursement Review report are informed by materials submitted by the sponsor, input received from interested parties (patient groups, clinician groups, and drug programs), and input from clinical experts consulted for this review.
Calls for patient group and clinician group input are issued for each reimbursement review. One joint patient group submission from 3 organizations, including the Canadian Organization for Rare Disorders, the Canadian Cancer Survivor Network, and the Canadian Cancer Society (CCS), and 1 clinician group submission from the Ontario Health (Cancer Care Ontario) Head and Neck Cancer Drug Advisory Committee were received. The CCS, the Canadian Organization for Rare Disorders, and the Canadian Cancer Survivor Network distributed the survey targeting all patients with NPC through a patient panel, a cancer connection forum, a mailing list, a newsletter, social media platforms, and so forth. Responses from 12 patients with NPC and 3 caregivers were collected between May 29, 2025, and June 13, 2025. The CCS conducted 3 interviews with certain survey respondents (patient A, patient C, and patient D). Among the respondents, 5 patients had localized NPC and 5 patients had metastatic or recurrent disease. The status of the rest of the patients was unclear. The Ontario Health (Cancer Care Ontario) Head and Neck Cancer Drug Advisory Committee gathered information via email from 3 clinicians. The full submissions received are available on the project landing page. The drug programs provide input on each drug being reviewed through the reimbursement review process by identifying issues that may impact their ability to implement a recommendation.
Input from patient and clinician groups is considered throughout the review, including in the selection of outcomes to include in the clinical review and in the interpretation of the clinical and economic evidence. Relevant patient and clinician group input is summarized in the Disease Background, Current Management, and Unmet Needs and Existing Challenges sections.
Each review team includes at least 1 clinical expert with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process. Two medical oncologists and 1 radiation oncologist with expertise in the diagnosis and management of recurrent or metastatic NPC participated as part of the review team.
Disease Background
NPC is a rare malignancy of the nasopharynx with distinct epidemiological, etiological, and histopathological characteristics, showing strong geographic and ethnic variation due to its association with Epstein-Barr virus (EBV) and other environmental or genetic risk factors. The incidence of NPC among males is 2 to 3 times higher than that among females in most populations.3 The use of alcohol and the use of commercial tobacco products are established but less influential risk factors, and the cancer is generally characterized by a low tumour mutational burden.4 In endemic regions, NPC is more common in middle age (40 years to 60 years), with incidence often increasing at up to 50 years to 59 years; however, in nonendemic or low-incidence areas, there is sometimes a bimodal distribution: 1 peak in younger individuals (i.e., those in their late teens or early adulthood) and another peak later in life.5 First-degree relatives of patients with NPC have substantially elevated risks; there is evidence of heritability of around 60% in some studies. Studies of familial NPC have found rare pathogenic variants in known cancer predisposition genes (e.g., ERCC2, TP63, MUTYH, BRCA1) and novel genes (e.g., RAD54L, EML2).6 Diagnosis of NPC relies on histopathological confirmation via tissue biopsy, including EBV-related markers for nonkeratinizing subtypes and HPV association in keratinizing subtypes, with further diagnostic staging supported by MRI, CT, PET, and endoscopy.7-14
NPC is often diagnosed at advanced stages (stage III to stage IV) due to its deep anatomic location, vague symptoms (e.g., hearing loss, nasal congestion), and early lymph node involvement, making early detection challenging.15-18 While Canadian data report a 5-year overall survival (OS) rate of 70% for all stages, up to 30% of patients still experience recurrence, with half of these occurring within 2 years of initial treatment.19 Patients with recurrent or metastatic NPC, especially those with de novo metastases, face poor long-term outcomes, with limited curative options and a 5-year disease-specific survival rate as low as 20%.20,21
Globally, the incidence of NPC is low (< 1 per 100,000 person-years), but incidence rates are significantly higher in endemic regions such as Southeast Asia and among specific populations in Canada, including people of Asian descent and Inuit communities.3,22-24 WHO classifies NPC into 3 histologic subtypes: keratinizing squamous cell carcinoma, nonkeratinizing squamous cell carcinoma (which comprises undifferentiated and differentiated forms), and basaloid squamous cell carcinoma; the EBV-associated nonkeratinizing subtype is the most prevalent subtype, particularly in the endemic regions and in Canada.25 In Canada, more than 80% of NPC cases are nonkeratinizing, reflecting the influence of immigration patterns and EBV prevalence; however, data remain limited due to the low incidence of the disease.19,26 Despite subtype differences, treatment approaches for both keratinizing and nonkeratinizing NPC are similar, with poor prognosis in the recurrent and metastatic setting. In Canada, NPC is characterized by a national-level incidence rate of 0.5 to less than 1 per 100,000 per year, according to reports from the Global Cancer Observatory (WHO International Agency for Research on Cancer) and Statistics Canada.22,27 Approximately 300 cases to 400 cases of NPC are estimated annually in Canada, with approximately 120 cases (± 40 cases) being potentially recurrent or metastatic NPC.22
Patients experience various symptoms, which depend on the site of recurrence or metastasis. Per the patient group input, patient-reported symptoms include difficulty swallowing (16%), changes in senses (13.5%), nasal congestion (11%), nosebleeds (11%), hearing loss or ringing in ears (11%), headaches (8%), and swelling in the neck (8%). A total of 50% of respondents to the survey of the input reported moderate to severe pain and discomfort, and adverse impacts on nutritional intake likely due to difficulty with eating and drinking. Participation in work and routine activities was moderately to severely affected in 50% of patients, 70% of patients experienced moderate to severe impact on sleep, and 60% of patients experienced substantial levels of anxiety or depression.
Current Management
Treatment Goals
The clinical experts consulted for this review noted that reducing tumour burden, improving symptoms, improving quality of life, delaying disease progression, and improving survival are the main goals of treatment in the first-line setting. Clinician group input agreed that improving OS was an important treatment goal, as well as minimizing adverse events (AEs) and prolonging cancer control. Patient input on goals of treatment was consistent with the observations of the clinical experts and clinician groups but also highlighted that radiation and chemotherapy are associated with substantial side effects and that treatment options are desired that minimize AEs.
Current Treatment Options
The clinical experts consulted for this review noted that in Canada, the standard of care for first-line treatment of recurrent or metastatic NPC is gemcitabine plus platinum-based chemotherapy (carboplatin or cisplatin), typically for 6 cycles. They noted that treatment with immunotherapies (i.e., PD-L1 inhibitors) is not routinely funded across jurisdictions, although special access programs are available for tislelizumab. Tislelizumab is also under review by CDA-AMC for reimbursement in the same line of therapy but was not considered a relevant comparator.
Unmet Needs and Existing Challenges
Patients with recurrent or metastatic NPC will eventually experience disease progression, even after multiple courses of chemotherapy. As such, the intent of currently available treatments in recurrent or metastatic NPC is mainly palliative and not curative. The clinical experts consulted for this review noted that in the recurrent and metastatic setting, cytotoxic drug combinations are the current standard of care; they do not alter underlying disease mechanisms but are typically effective in relieving disease-related symptoms. However, they are also associated with poor long-term progression-free survival (PFS) and OS (e.g., at 5 years or 10 years). In addition, gemcitabine and platinum-based chemotherapy have permanent cumulative toxicities (e.g., renal toxicity, ototoxicity, neuropathy) and in patients with comorbidities or older adults may require dose reductions or modifications. In some rare instances, chemotherapy cannot be given safely due to limitations in patients’ health conditions. Clinician groups also noted that although the initial response to chemotherapy is generally favourable, treatment of recurrent or metastatic disease remains a challenge given the limited available therapies and risks of toxicity with further lines of therapy. The clinical experts further noted that treatment in later lines becomes challenging as resistance to treatment may develop.
The clinical experts consulted for this review also noted that while most treatments for NPC are usually available at most cancer treatment centres, including local community clinics, more advanced care that includes disease-specific experts and multidisciplinary care teams may only be available at large tertiary academic centres, which may be more difficult for patients in remote locations to reach. In addition, IV treatments require going to a treatment centre, which may also require travel and time off work to attend. If patients develop AEs, they may also need to be admitted to hospital for treatment.
Patients expressed satisfaction with the outcomes of treatment but found simultaneous radiation and chemotherapy — the typical treatment for locally advanced NPC — difficult due to toxicity. Patient input noted that the standard of care for NPC can cause discomfort for some and, for others, serious side effects that impact quality of life during or after treatment. Some of the physical symptoms that patients reported included difficulty swallowing, alteration in the senses, nosebleeds, hearing loss, and neck swelling. The patient group input didn’t distinguish between initial treatment for NPC or treatment for recurrent or metastatic NPC, but noted that some of the side effects from treatment included pulmonary embolism, complex neck surgery, incomplete recovery of the sense of smell, persistent leaky eye, damaged nasal passages due to radiation treatments, tinnitus, hearing loss requiring hearing aids, nerve pain, loss of appetite, weight loss, radiation burns, brain fog, and hypothyroidism secondary to the radiation treatment. Populations at higher risk of NPC include patients of Asian ancestry, Indigenous populations, and people who have emigrated from endemic regions, all of whom represent some equity-deserving groups.
Considerations for Using the Drug Under Review
Contents in this section have been informed by input from the clinical experts consulted for the purpose of this review and from clinician groups, as well as the reimbursement conditions proposed by the sponsor (refer to Table 1 of Appendix 1 in the Supplemental Material document). The implementation questions from the public drug programs and corresponding responses from the clinical experts consulted for this review are summarized in Table 2 of Appendix 1 in the Supplemental Material. The following has been summarized by the review team.
Place in Therapy
Clinical experts consulted for this review indicated that if recommended for the indication under review, toripalimab in combination with gemcitabine and carboplatin or cisplatin would become the new first-line treatment option for patients with recurrent or metastatic NPC that is not amenable to local–regional therapy because it addresses the underlying mechanism of the disease and compliments the chemotherapy. The choice of cisplatin or carboplatin would be made considering patient tolerance and organ function, among other factors. The clinical experts noted that while the mechanism of action is different than chemotherapy, toripalimab would still be considered symptomatic or palliative management, rather than curative treatment. They noted that patients should not be required to trial other treatments first.
Patient Population
The clinical experts and clinician groups consulted for this review indicated that all patients newly diagnosed with recurrent or metastatic NPC who are considered fit to receive therapy would be candidates for treatment with toripalimab plus platinum-based chemotherapy and gemcitabine; it would be the new standard first-line treatment for patients with recurrent or metastatic NPC and would be suitable for all patients. Fitness is typically assessed by clinical judgment and considers factors such as performance status, organ function, and toxicities from prior treatments. Patients would be considered even if they have minimal to no symptoms and particularly if salvage surgery, primary radiotherapy, or reirradiation are not options. They noted that salvage surgery is rarely an option in the recurrent (including local–regional recurrence) or metastatic setting, although reirradiation may be possible depending on the amount of prior exposure a patient has had or their tolerance for radiotherapy.
The clinical experts noted that potential criteria for initiating treatment with toripalimab should align with the inclusion criteria from the JUPITER-02 study (i.e., patients with NPC that is metastatic or recurrent after curative treatment and not amenable to local–regional treatment or curative treatment, and who had not been given prior systemic treatment for metastatic or recurrent disease), but also stated that patients with locally advanced NPC who are not candidates for curative treatment would be considered for toripalimab as well.
Both the experts and the clinician groups highlighted that patients would be identified based on clinical or radiographic evidence of recurrent or metastatic disease from imaging (CT, PET, and MRI), supported by histological confirmation of viable tumours. In patients with a known history of locally advanced NPC that has been histologically confirmed, clinical or radiographic diagnosis might be sufficient. The clinical experts noted that patients with recurrent or metastatic NPC generally have high responses to therapy, and no companion diagnostic test is required because PD-L1 status, genomic mutational analysis, and tumour mutational burden are generally not associated with clinical efficacy. Patients who have absolute contraindications to toripalimab, such as those with solid organ transplants (due to the increased risk of rejection), would not be eligible for treatment. Patients with EBV-keratinizing NPC were not included in the JUPITER-02 study, but the clinical experts noted that they would also be potential candidates for treatment with toripalimab.
While NPC is considered a rare disease in Canada, the clinical experts noted that the risk of developing NPC is heavily concentrated in people of Asian descent and Indigenous Peoples. These groups may also experience additional barriers to care, including language, immigration-related factors, geographical isolation, potentially reduced health literacy, and low awareness of the disease, which can impact the outcomes of treatment. Misdiagnosis is unlikely at the recurrent or metastatic stage given that patients are often seen at tertiary academic centres, but underdiagnosis and delayed diagnosis could be possible in patients who are from rural or remote communities or equity-deserving groups who may lack access to care.
Assessing the Response to Treatment
According to clinical experts consulted for this review, clinical exams occur every 3 weeks and imaging is conducted every 2 months or 3 months. In the JUPITER-02 study, patients had more frequent imaging than would be possible in clinical practice. The outcomes used to assess response are typically aligned with those employed in clinical trials, although PFS and OS are considered longer-term outcomes that aren’t typically used for clinical decision-making on a day-to-day basis. Depth of response (complete or partial), duration of response (DoR), and objective response rate (ORR) were highlighted as clinically meaningful measures. Outcomes that correspond to symptomatic control are also important, such as health-related quality of life (HRQoL) measures, although the experts noted that structured HRQoL tools are not often used in practice and symptom improvement as reported by patients during clinical visits is more often used. The experts highlighted that a response that lasts a substantial amount of time (i.e., more than 4 weeks) with no improvement or minimal improvement in symptoms or intolerable AEs would not be considered clinically meaningful.
With regard to the suggested renewal criteria from the sponsor, the experts noted that they would generally agree with a 2-year duration of therapy but if patients have stopped treatment, they might prefer to have the option to reinitiate treatment before 6 months have elapsed if a patient’s disease has progressed.
Discontinuing Treatment
According to the clinical experts consulted for this review, disease progression, a patient’s request, and intolerable toxicity would be reasons to discontinue treatment. Any decision to discontinue should also consider patient factors such as the burden of disease and response to treatment; 1 expert noted that if patients have aggressive disease that has stabilized on treatment, they should not be mandated to stop at 2 years of treatment if there are risks of disease progression or mortality. The clinical experts noted that the renewal and discontinuation criteria proposed by the sponsor would cover both situations and be easily implementable.
Prescribing Considerations
Clinical experts and the clinician groups noted that NPC is diagnosed and monitored by a medical oncologist and patients should receive treatment from physicians with expertise in head and neck cancers. They also noted that the toxicity profile of toripalimab is not expected to be any different than that of other drugs in its class. However, the experts also noted that patients who live in more rural or remote locations may have challenges accessing chemotherapy units that are closer to home, and some community oncology centres may prefer to refer patients to tertiary academic centres due to less volume-driven experience and expertise in NPC.
Additional Considerations
The clinical experts consulted for this review noted that in general, there is a lack of data on treatment with toripalimab in first-line recurrent or metastatic NPC in Canada because the JUPITER-02 study sites were located only in NPC-endemic countries, and therefore the disease profiles in Canada and other countries are not always represented (e.g., keratinizing NPC, nonkeratinizing undifferentiated NPC, basaloid squamous cell cancers). They noted that clinical research into EBV and non–EBV-associated NPC is ongoing.
Clinical Review
Methods
The review team considered studies in the sponsor’s systematic review (pivotal studies and randomized controlled trials [RCTs]), sponsor-submitted long-term extensions (LTEs), indirect treatment comparisons (ITCs), and studies addressing gaps in the evidence for inclusion. Eligible studies for the systematic review included published and unpublished pivotal studies and phase III and phase IV RCTs. Relevant patients and interventions were defined by the indication and the recommended dosage in the product monograph. Locally advanced NPC versus recurrent or metastatic NPC was considered as potentially important for informing the reimbursement recommendation. Relevant comparators were drugs and nondrug treatments used in clinical practice in Canada to treat patients described in the indication under review — there were no other restrictions placed on the comparators. LTEs of included pivotal studies and RCTs were included, regardless of whether there was a comparison group. There were no ITCs, LTE studies, or studies addressing gaps submitted by the sponsor.
The review team selected outcomes (and follow-up times) for review considering the sponsor’s Summary of Clinical Evidence,28 clinical expert input, and patient and clinician group input. Included outcomes are those considered relevant to expert committee deliberations, and they were selected in consultation with committee members. Evidence from the systematic review for the most important outcomes was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. The following outcomes were included in the GRADE assessment because they address main treatment goals and are considered outcomes important to patients as well as clinicians: PFS at 1 year and 2 years, and OS at 1 year, 2 years, and 3 years. The change from baseline to cycle 13, day 1, in the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) global health status score, the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire 35-item Head and Neck (EORTC QLQ-H&N35) pain score, and the EORTC QLQ-H&N35 swallowing score were also included as HRQoL measures. Harms selected for GRADE assessment (i.e., serious adverse events [SAEs] and immune-related AEs) were identified as being important from patient group and clinical expert input. Additional outcomes selected for inclusion in the report were DoR and ORR because they provide additional context to the results.
Methods for data extraction, risk of bias appraisal, and certainty of evidence assessment are provided in Appendix 2 in the Supplemental Material document.
Clinical Evidence
In this report, the following sources of evidence submitted by the sponsor are reviewed and appraised:
1 RCT included in the systematic review, the JUPITER-02 study.
One feasibility assessment for an indirect comparison was also included in the submission; however, the results of the systematic literature search conducted by the sponsor did not yield any RCTs for relevant comparators in the area of NPC. Therefore, no indirect comparison was included.
Systematic Review
Description of Studies
Study Characteristics
Characteristics of the included study are summarized in Table 2. Details pertaining to the eligibility criteria, interventions and comparators, and relevant outcome measures are provided in Appendix 3 in the Supplemental Material document.
The JUPITER-02 study was a phase III, double-blind, placebo-controlled RCT conducted in Taiwan, China, and Singapore to evaluate the efficacy and safety of toripalimab in combination with gemcitabine and cisplatin compared with placebo in combination with gemcitabine and cisplatin as first-line treatment of histologically or cytologically confirmed recurrent or metastatic NPC. The primary objective of the JUPITER-02 study was to evaluate the PFS per Response Evaluation Criteria in Solid Tumours version 1.1, with secondary objectives of evaluating OS, ORR, DoR, and HRQoL (EORTC QLQ-C30 and EORTC QLQ-H&N35). Notable exclusion criteria were patients with any malignancies other than NPC within 5 years of randomization, a history of autoimmune disease, or treatment with systemic corticosteroids equivalent to more than 10 mg per day of prednisone.
In total, 289 patients were randomized 1:1 using permuted block randomization via Interactive Web Response System and stratified on Eastern Cooperative Oncology Group Performance Status (0 or 1) and disease stage (recurrent or metastatic) to receive toripalimab (n = 146) or placebo (n = 143). Patients had to be aged between 18 years and 75 years, with a confirmed diagnosis of NPC that was either metastatic or recurrent after curative treatment, and not amenable to local–regional or curative treatment. The interval between NPC recurrence and the last dose of previous radiotherapy or chemotherapy had to be 6 months or more. After randomization, the JUPITER-02 study included a chemotherapy phase during which patients received either toripalimab plus gemcitabine and cisplatin or placebo plus gemcitabine and cisplatin for up to 6 cycles. Following the chemotherapy phase, patients without progressive disease entered the postchemotherapy maintenance phase, where they continued treatment with toripalimab or placebo as monotherapy every 3 weeks until the event of unacceptable toxicity, progressive disease, withdrawal of consent, a judgment by the investigator, or a maximum of 2 years (including the chemotherapy and postchemotherapy phases) had elapsed. Tumour evaluation scans were performed at screening, every 6 weeks for the first 12 months, and then every 9 weeks thereafter, regardless of treatment delays, until confirmed disease progression.
Table 2: Characteristics of the JUPITER-02 Study
Study name, design, and sample size | Key inclusion criteria | Key exclusion criteria | Intervention and comparator | Relevant end points |
|---|---|---|---|---|
JUPITER-02 study Placebo-controlled, multicentre, double-blind, phase III RCT Total N = 289 |
|
| Intervention arm: Gemcitabine 1,000 mg/m2 IV on day 1 and day 8 in 3-week cycles for up to 6 cycles, plus cisplatin 80 mg/m2 IV q.3.w. for up to 6 cycles, plus toripalimab 240 mg IV q.3.w. starting on day 1 Placebo arm: Placebo IV q.3.w. on day 1, plus gemcitabine 1,000 mg/m2 IV on day 1 and day 8 in 3-week cycles for up to 6 cycles, plus cisplatin 80 mg/m2 IV q.3.w. for up to 6 cycles Both arms: Treatment continued until the event of toxicity, progressive disease, withdrawal of consent, a judgment by the investigator, or a maximum of 2 years had elapsed. Patients had the opportunity to continue their treatment beyond progression per RECIST 1.1, provided they were still experiencing clinical benefit. |
|
AE = adverse event; AJCC = American Joint Committee on Cancer; BIRC = blinded independent review committee; CNS = central nervous system; CTCAE v5.0 = Common Terminology Criteria for Adverse Events Version 5.0; DoR = duration of response; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-H&N35 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire 35-item Head and Neck; NCI = National Cancer Institute; NPC = nasopharyngeal cancer; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; q.3.w. = every 3 weeks; RCT = randomized controlled trial; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours version 1.1; SAE = serious adverse event; WDAE = withdrawal due to adverse event.
aStage IVb, as defined by the Union for International Cancer Control and the AJCC Cancer Staging Manual, Eighth Edition.
bFor recurrent NPC after curative treatment (including radiotherapy and/or induction, and concurrent or adjuvant chemotherapy), the interval between recurrence and the last dose of previous radiotherapy or chemotherapy must be ≥ 6 months.
cPatients who had prior therapies for brain or leptomeningeal metastasis and were stabilized for ≥ 2 months and had discontinued systemic steroid therapy (more than 10 mg/day prednisone or equivalent) more than 4 weeks before randomization could be included.
dUnless they had been curatively treated with a negligible risk of metastasis or death (e.g., expected 5-year OS > 90%).
eIncluding, but not limited to, myasthenia gravis, myositis, autoimmune hepatitis, systemic lupus erythematosus, rheumatoid arthritis, inflammatory bowel disease, vascular thrombosis associated with antiphospholipid syndrome, Wegener granulomatosis, Sjögren syndrome, Guillain-Barré syndrome, multiple sclerosis, vasculitis, or glomerulonephritis. Patients with a history of autoimmune-related hypothyroidism on a stable dose of thyroid replacement hormone may have been eligible for this study. Patients with controlled type 1 diabetes mellitus on a stable insulin regimen were eligible for this study.
fUse of topical, ocular, intra-articular, intranasal, and inhalational corticosteroids was allowed. Patients who had received acute, low-dose, systemic immunosuppressant medications (e.g., a 1-time dose of dexamethasone for nausea) may have been enrolled in the study after discussion with and approval by the medical monitor. Patients with a history of allergic reaction to IV contrast requiring steroid pretreatment had baseline and subsequent tumour assessments performed on MRI. The use of inhaled corticosteroids for chronic obstructive pulmonary disease, mineralocorticoids (e.g., fludrocortisone) for patients with orthostatic hypotension, and low-dose supplemental corticosteroids for adrenocortical insufficiency was allowed.
gSuch as New York Heart Association cardiac disease (class II or greater), myocardial infarction within 3 months before randomization, unstable arrhythmias, or unstable angina. Patients with known coronary artery disease, congestive heart failure not meeting the aforementioned criteria, or a left ventricular ejection fraction of 50% must have been following a stable medical regimen that was optimized in the opinion of the treating physician, in consultation with a cardiologist if appropriate.
hThe original study design had only PFS controlled for multiple comparisons, and other outcomes as secondary; following an FDA request in April 2020, the study design was changed to add hierarchical testing for OS and ORR, and control for multiple comparisons of these outcomes.
Sources: Details included in the table are from the sponsor’s Summary of Clinical Evidence28 and the JUPITER-02 trial Clinical Study Report.29
Statistical Testing and Analysis Populations
A total of 280 patients (140 patients per arm) were needed to observe 200 PFS events at approximately 25 months after the first patient was randomized to detect PFS improvement with an HR of 0.67 with 80% power at an overall 2-sided significance level of 0.05. According to the sponsor, the study was not designed to be fully powered for the OS analysis. Approximately 130 deaths were expected to be observed 5 years after the first patient was randomized, which provided 46% power to detect OS improvement with an HR of 0.72 under a 2-sided alpha level of 0.05.
One interim analysis (IA) of PFS was planned when approximately 130 PFS events had been observed (approximately 18 months after the first patient was randomized), and the predefined O’Brien-Fleming stopping boundary based on the Lan-DeMets spending function was established to preserve an overall 2-sided P value of 0.05. The key secondary efficacy end points, including blinded independent review committee (BIRC)-assessed ORR and OS, were to be tested hierarchically under a 2-sided alpha level of 0.05. ORR was formally tested at the IA for PFS and reached statistical significance. Two IAs of OS were planned at the interim and final analyses of PFS for descriptive purposes, where it was expected approximately 49 deaths and 74 deaths would be observed, respectively. A type I error penalty of 10–6 (2-sided) was taken for each interim look at OS. OS was planned to be formally tested when 130 deaths had been observed in the intention-to-treat (ITT) population at a 2-sided alpha level of 0.05 minus the total alpha assigned to the IAs.
There were 3 main analysis sets for the study population:
ITT population — This included all randomized patients, and patients were analyzed according to the study arm to which they were randomized.
Per-protocol analysis set (PPS) — This included all ITT patients who did not have any major protocol violations that might have any potential impact on key efficacy or safety end points. Major protocol violations were defined and the inclusion of patients in the PPS population was finalized before study unblinding. Patients were analyzed according to the study arm to which they were randomized. The PPS population was used for some secondary and exploratory analysis as well as sensitivity analysis of the primary efficacy end point.
Safety analysis set — This included all randomized patients who received any amount of toripalimab or placebo. Patients were analyzed according to actual treatment received.
The main RCT milestones (and corresponding data cut-offs [DCOs]) included in the clinical review were as follows:
First planned IA for PFS (May 30, 2020, DCO) — This included data from the fully blinded portion of the study. After analysis, the Independent Data Monitoring Committee recommended the JUPITER-02 study be unblinded due to a statistically significant effect on PFS and no adverse effects on OS. After unblinding, patients randomized to toripalimab continued to receive it open label, but patients randomized to placebo no longer received the placebo infusion. Both groups completed the chemotherapy phase of treatment as usual, regardless of unblinding.
Additional analysis of PFS (June 8, 2021, DCO) — This included data from the prespecified final PFS analysis and the second IA of OS, and contained results from both the blinded and unblinded portions of the study.
Updated safety analysis (May 8, 2022, DCO) — This included data from the end of safety follow-up (the last dose of study treatment administered on November 18, 2021).
Final analysis of OS (November 18, 2022, DCO) — This included data from the end of OS follow-up.
Patient Disposition
Tables containing further detail on the patient disposition for the JUPITER-02 study are provided in Appendix 4 in the Supplemental Material. Briefly, in total, 408 patients were screened and 119 patients (29.2%) were excluded before randomization; the most common reason was not meeting the eligibility criteria (108 patients [26.5%]). The submission did not provide details on which inclusion or exclusion criteria were not met. As noted, 146 patients were randomized to toripalimab and 143 patients were randomized to placebo. As of the June 8, 2021, DCO, 39 patients (26.7%) in the toripalimab arm and 50 patients (35.0%) in the placebo arm discontinued the study, primarily due to death (20.5% versus 32.2%, respectively). During the chemotherapy phase, 21.9% of patients in the toripalimab arm and 17.5% of patients in the placebo arm discontinued treatment, primarily due to disease progression (5.5% versus 8.4%, respectively). During the postchemotherapy maintenance phase, 55.5% of patients in the toripalimab arm and 82.5% of patients in the placebo arm discontinued treatment, primarily due to disease progression (30.8% versus 53.5%, respectively).
As of the end of OS analysis (November 18, 2022, DCO), of the 146 patients randomized to toripalimab, 76 patients (52.1%) had completed the study; the most common reason for study discontinuation was death (57 patients [39.0%]). Of the 143 patients randomized to placebo, 57 patients (39.9%) completed the study. Of the remaining 86 patients (60.1%) who had discontinued, the most common reason was death (76 patients [53.1%]). No information was provided on study drug discontinuations at the final OS analysis.
The original study protocol was issued in March 2018. There were 6 protocol amendments up to October 2020. At the final protocol amendment, there was a change to remove crossover to toripalimab. It is unclear how many patients were enrolled and treated before this change. At the time of study closing (November 2022 DCO), 80 patients (54.8%) in the toripalimab arm and 76 patients (53.1%) in the placebo arm reported at least 1 major protocol deviation. The most common deviations were procedural deviations (e.g., missing or incorrectly performed tumour assessments at screening, laboratory tests that were not performed or not available before infusion), reported by 37.0% of patients in the toripalimab arm and 24.5% of patients in the placebo arm. Other protocol deviations were broadly balanced across treatment arms with the exception of procedural deviations, which were more commonly reported in the toripalimab arm.
Baseline Characteristics
A summary of key baseline characteristics is provided in Table 3; additional baseline characteristics are provided in Appendix 4 in the Supplemental Material. Briefly, the baseline characteristics were broadly balanced between study arms apart from cigarette and alcohol use, which were more common in the toripalimab arm. Of note, the patient population was predominantly male in each study arm (18.9% of patients were female and 81.1% of patients were male in the placebo arm; 15.1% of patients were female and 84.9% of patients were male in the toripalimab arm). The entire patient population was of Asian descent. Most patients reported undifferentiated nonkeratinizing squamous cell carcinoma (71.3% of patients in the placebo arm and 71.2% of patients in the toripalimab arm). In the toripalimab arm and the placebo arm, most patients had recurrent disease (58.2% of patients versus 60.8% of patients, respectively), which was primarily distant recurrence (45.2% of patients versus 45.5% of patients, respectively), and 41.8% of patients versus 39.2% of patients had primary metastatic disease, respectively.
Table 3: Summary of Baseline Characteristics From the JUPITER-02 Study
Characteristic | JUPITER-02 study | |
|---|---|---|
Placebo (N = 143) | Toripalimab (N = 146) | |
Age (years) | ||
Mean (SD) | 49.7 (10.4) | 45.8 (11.3) |
Median (range) | 50.7 (21.3 to 71.8) | 45.6 (18.9 to 72.2) |
Sex, n (%) | ||
Female | 27 (18.9) | 22 (15.1) |
Male | 116 (81.1) | 124 (84.9) |
Race, n (%) | ||
Asian | 143 (100.0) | 146 (100.0) |
Cigarette use, n (%) | ||
Yes | 59 (41.3) | 76 (52.1) |
No | 84 (58.7) | 70 (47.9) |
Alcohol consumption, n (%) | ||
Yes | 18 (12.6) | 30 (20.5) |
No | 125 (87.4) | 116 (79.5) |
ECOG Performance Status, n (%) | ||
0 | 80 (55.9) | 83 (56.8) |
1 | 62 (43.4) | 63 (43.2) |
Disease stage, n (%)a | ||
Recurrentb | 87 (60.8) | 85 (58.2) |
Local recurrence only | 20 (14.0) | 19 (13.0) |
Distant recurrence | 65 (45.5) | 66 (45.2) |
Unknownc | 2 (1.4) | 0 (0.0) |
Primary metastatic | 56 (39.2) | 61 (41.8) |
Metastasis observed at the time of initial diagnosis, n (%) | ||
Yesd | 54 (37.8) | 59 (40.4) |
No | 89 (62.2) | 87 (59.6) |
Metastatic organs at baseline, n (%) | ||
Liver | 57 (39.9) | 61 (41.8) |
Lung | 56 (39.2) | 59 (40.4) |
Bone | 55 (38.5) | 60 (41.1) |
Other | 124 (86.7) | 123 (84.2) |
Histology type, n (%) | ||
Nonkeratinizing squamous cell carcinoma, undifferentiated | 102 (71.3) | 104 (71.2) |
Nonkeratinizing squamous cell carcinoma, differentiated | 6 (4.2) | 2 (1.4) |
Keratinizing squamous cell carcinoma | 2 (1.4) | 1 (0.7) |
NPC, unclassified | 29 (20.3) | 30 (20.5) |
Nonkeratinizing carcinoma, unclassified | 3 (2.1) | 9 (6.2) |
Other | 1 (0.7) | 0 (0.0) |
ECOG = Eastern Cooperative Oncology Group; NPC = nasopharyngeal cancer; SD = standard deviation.
aPer the case report form.
bLocal recurrence only was defined from stage I to stage IVa and distant recurrence was defined as stage IVb, based on the stage of disease at the time of informed consent.
cTwo patients were not diagnosed with NPC — 1 was diagnosed with colorectal cancer and the other with rhabdomyosarcoma.
dFour patients had nonmetastatic NPC at initial diagnosis but didn't receive any treatment until enrolment in the study. They were classified as having metastatic disease at randomization.
Sources: Details included in the table are from the sponsor’s Summary of Clinical Evidence28 and the JUPITER-02 trial Clinical Study Report.29
Treatment Exposure and Concomitant Medications
Details of patients’ treatment exposure and relative dose intensity, the use of concomitant medications, and subsequent anticancer treatments in the JUPITER-02 study are provided in Appendix 4 the Supplemental Material document. Briefly, the relative dose intensity was high (99.4%) in the toripalimab arm. On average, the number of cycles of gemcitabine and cisplatin was similar across arms (mean = approximately 5 cycles), while more cycles of toripalimab were received than placebo (mean = 19.9 cycles [SD = 12.2 cycles] versus mean = 12.7 cycles [SD = 6.8 cycles], respectively).
As of the June 8, 2021, DCO, a total of 73 patients (50.0%) in the toripalimab arm and 69 patients (48.3%) in the placebo arm had interrupted study drug treatment due to AEs. A total of 104 patients (71.2%) and 103 patients (72.0%) in the toripalimab and placebo arms, respectively, had interruptions of gemcitabine due to AEs while 63 patients (43.2%) and 49 patients (34.2%) had interruptions of cisplatin due to AEs, respectively. Dose reductions of gemcitabine occurred in 71 patients (48.2%) and 74 patients (51.7%) in the toripalimab and placebo arms, respectively, and dose reductions of cisplatin occurred in 59 patients (40.4%) and 62 patients (43.34%) in the toripalimab and placebo arms, respectively.
Concomitant medications were broadly balanced between study arms, with the most common therapy being serotonin antagonists (100% of patients in both arms), proton pump inhibitors (91.1% of patients in the toripalimab arm and 92.3% of patients in the placebo arm), and colony stimulating factors (87.0% of patients in the toripalimab arm and 90.9% of patients in the placebo arm).
As of the final OS analysis, most patients had received a subsequent anticancer therapy (74.1% of patients in the placebo arm and 56.2% of patients in the toripalimab arm). A total of 73.4% of patients in the placebo arm and 52.7% of patients in the toripalimab arm had received new systemic anticancer treatment. A total of 34.3% of patients in the placebo arm and 32.9% of patients in the toripalimab arm had received subsequent PD-1 or PD-L1 inhibitors. A numerically greater proportion of patients in the placebo arm had received cytotoxic therapy (69.2%) relative to those in the toripalimab arm (37.7%), protein kinase inhibitors (26.6% versus 19.2%, respectively), and EGFR inhibitors (13.3% versus 4.8%, respectively). A total of 16.1% of patients in the placebo arm and 12.3% of patients in the toripalimab arm had received subsequent radiotherapy.
Critical Appraisal
Internal Validity
Overall, there was a low risk of bias arising from the randomization and allocation concealment process. Randomization was stratified and undertaken with permuted block randomization via Interactive Web Response System, and the sponsor noted that study radiologists were fully blinded to treatment arm, patient demographics, site response assessments, time point, and clinical information about the patient. There were imbalances between study arms in the proportion of patients reporting cigarette use (41.3% in the placebo arm and 52.1% in the toripalimab arm), and the proportion of patients reporting alcohol use (12.6% in the placebo arm and 20.5% in the toripalimab arm) at baseline. The clinical experts noted that these factors were more impactful on a patient’s overall fitness for treatment than being prognostic factors for the outcomes from NPC treatment directly, but the reason for and overall impact of these imbalances are unclear.
Each of the radiologists forming the BIRC were also blinded to the other radiologists’ assessments, as was an independent adjudicator. PFS, ORR, and DoR were determined by the BIRC while OS, HRQoL outcomes, and safety data were investigator-assessed. There was an amendment to the protocol changing investigator-assessed outcomes to BIRC-assessed outcomes in May 2020 after the study started enrolment, and the study was unblinded after the database lock in November 2020. Therefore, changes to treatments and events of disease progression may have been ascertained by the investigator before the protocol change, and the DCOs after May 2020 (the IA for PFS) were from patients who were unblinded. While for PFS, ORR and DoR, knowledge of the treatment allocation was unlikely to impact outcome ascertainment due to the ascertainment by the BIRC after study unblinding, knowledge of the treatment arm puts the results for the HRQoL measures and the safety reporting (subjective harms) at a risk of bias after the May 2020 DCO. In addition, there is a risk of performance bias in the results due to the possibility of deviating from the intended interventions, where knowledge of the interventions may result in altered expectations of care, which could exaggerate or minimize the effects of the intervention. During the study, the proportion of patients with major protocol deviations was high (more than half of patients), though it was broadly balanced between study arms apart from procedural deviations. Procedural deviations included incorrect tumour assessments or unavailable laboratory measures and were more commonly reported in the toripalimab arm (37.0% versus 24.5% in the placebo arm). This raises the possibility of bias in the results of the toripalimab arm, which could go in either direction depending on the nature of the deviations because the potential deviations listed may have impacted tumour assessment by the BIRC. In addition, a high proportion of patients reported “other deviations,” which included SAEs not being reported in adequate time and randomization not complying with the prespecified stratification factors (17.1% in the toripalimab arm and 19.6% in the placebo arm). While balanced between study arms, they increase the overall uncertainty in the results because some of these deviations may pertain to randomization, although given that the baseline characteristics were broadly balanced, this does not seem to have fundamentally compromised the study design.
The evaluation methods for PFS, OS, ORR, and DoR were likely at a low risk of bias due to the use of a BIRC; however, there was a high degree of censoring for PFS (56.8% in the toripalimab arm and 39.2% in the placebo arm at the June 8, 2021, DCO). A considerable proportion of patients was censored in the PFS analysis due to starting a new anticancer therapy before progression (13.7% in the toripalimab arm and 21.0% in the placebo arm). This raises concern for bias due to informative censoring, which would arise if the change to a subsequent therapy is associated with a patient’s risk for the outcome (e.g., at increased risk of progression), as well as a degree of performance bias, which could bias the results in favour of toripalimab because censoring for new treatment was more prominent in the placebo arm after unblinding (at the first IA for PFS, only 8.4% of patients in the placebo arm and 8.2% of patients in the toripalimab arm were censored for starting a new anticancer therapy). The sponsor’s sensitivity analysis using this time as an event instead of censoring had similar results. Though neither analysis considers the specific PFS date, corresponding results using different assumptions improve confidence in the findings. Additional sensitivity analyses of PFS (using stratification factors on the electronic case report form, considering events after 2 or more missing assessments, and considering missing assessments due to COVID-19) also showed results similar to those of the primary analysis.
The JUPITER-02 trial included both an initial chemotherapy phase for 6 cycles and a postchemotherapy maintenance phase. At the final PFS analysis, the PFS curves only began separating after 6 months (approximately the duration of the initial chemotherapy phase). As such, there is a risk that the effect of toripalimab on PFS is overestimated and although this is mostly consistent with standards of care, it is unclear whether the benefit of toripalimab on PFS is due to maintenance treatment in the toripalimab arm, or if it is influenced by the lack of therapy in the placebo arm following the initial chemotherapy phase. In addition to this, the results for PFS were not fully estimable in the toripalimab arm; a total of 51.9% of all PFS events had occurred at the final PFS analysis (June 8, 2021, DCO); thus, how well these results predict long-term progressive disease outcomes is uncertain. Similarly, the upper bound of the CI for DoR was not estimable at the May 2020 DCO in the toripalimab arm, and OS was not estimable in either treatment arm at the end of the study (November 2022 DCO), with only 46% of total OS events having occurred. This suggests that there is uncertainty in the PFS results beyond 20 months when a large proportion of patients are censored and few remain at risk. For OS, there is uncertainty beyond 36 months due to few patients remaining at risk and high degrees of censoring toward the tail of the Kaplan-Meier curve.
Control for multiple comparisons was only preplanned for PFS; however, control for OS and ORR was added in April 2020 at the request of the US FDA. This took place before the first IA for PFS, but DoR and the EORTC QLQ-H&N35 swallowing score were not controlled for multiple comparisons and therefore there is an increased risk of type I error (i.e., erroneously rejecting the null hypothesis). DoR is also at higher risk of bias because the analysis was not conducted in a randomized population, but in a population selected based on the response outcome. In addition, the Kaplan-Meier curves for PFS and OS do not separate until several months into follow-up, suggesting the proportional hazards assumption underlying the hazard ratio (HR) is violated. Therefore, the HR may not accurately reflect the treatment effect at each point in time, although the absolute between-group differences in event probabilities used in the GRADE certainty of evidence appraisal are unaffected by this limitation.
There were relatively few losses to follow-up during the study for reasons other than death and, as previously noted, the time-to-event analyses did not appear to be impacted by informative censoring. There were low patient numbers reported at cycle 13 for all 3 HRQoL measures (n = 94 patients in the toripalimab arm and n = 60 patients in the placebo arm) and only 6 patients reporting in the placebo arm at cycle 26, compared to 60 patients in the toripalimab arm. No imputation measures were used to account for missing data when less than 50% of the questionnaire was filled out, although a prorated score was calculated for measures that were 50% filled out or more, but not completed. This high and uneven loss to follow-up across arms (39.9% of patients in the placebo arm completed the study compared to 52.1% of patients in the toripalimab arm) suggests a high risk of bias due to the open-label ascertainment of the outcomes and substantial missing data. This increases the uncertainty in the HRQoL results and makes it difficult to draw firm conclusions on the impact of treatment.
External Validity
The inclusion criteria for the JUPITER-02 study included patients with metastatic or recurrent NPC that was not amenable to local–regional treatment or curative treatment; this is narrower than the Health Canada indication of recurrent, locally advanced NPC. The clinical experts consulted for this review also noted that the study population was not entirely representative of the population they might encounter in practice; they noted that their patient population would be approximately 85% Asian people, varying from province to province, but would also include Indigenous Peoples (including Inuit) as well as people who have recently immigrated to Canada who might have delays in diagnoses due to access barriers such as language or living in more remote locations. They also noted their patient population would be slightly older, although still majority male, and with a similar mix of histologies observable (the majority being EBV-driven, nonkeratinizing, undifferentiated NPC). Despite the listed eligibility criteria for the JUPITER-02 trial, the clinical experts noted that they would also consider treatment for patients aged older than 75 years, patients with an Eastern Cooperative Oncology Group Performance Status of greater than 1, and patients with other malignancies, depending on the location and type of cancer. The results of the JUPITER-02 study therefore might not be generalizable to patients with other NPC histologies, with other malignancies or comorbidities, who are older or with less functional status, and who may be candidates for treatment in the real-world setting.
The clinical experts consulted for this review also flagged some differences in concomitant and subsequent treatments. They noted there was a high proportion of patients who received sulfonamides, which is not common in Canadian practice. In addition, they noted that gemcitabine maintenance therapy could be considered for patients instead of no treatment after the initial chemotherapy combination, which was not conducted in the trial; although there is no firm guidance, this anecdotal experience has been cited in the literature.3 Further, the clinical experts noted that carboplatin could be considered as part of the platinum backbone in combination with gemcitabine (and for toripalimab), when only cisplatin was used in the trial. They flagged a high proportion of patients proceeding from toripalimab to another PD-1 or PD-L1 inhibitor, noting that no PD-1 inhibitor treatment options would be available to them in Canada. The different treatment paths available may impact the generalizability of the harms and OS results in this patient population.
Results
The key efficacy and harms results and findings from the GRADE assessment are presented in this section. Detailed efficacy and harms results can be found in Appendix 4 in the Supplemental Material document.
Efficacy
At the time of the final OS analysis (November 18, 2022, DCO), the median follow-up duration was 30.95 months (range, 0.2 months to 48.3 months) in the placebo arm and 36.73 months (range, 1.0 months to 47.4 months) in the toripalimab arm.
Except where noted, the most recently available DCO was reported for each outcome. This corresponded to the May 30, 2020, DCO for DoR and ORR; the June 8, 2021, DCO for PFS, EORTC QLQ-C30, EORTC QLQ-H&N35 pain score, and EORTC QLQ-H&N35 swallowing score; and the November 18, 2022, DCO for OS.
Key results include the following.
PFS by BIRC: At the final PFS analysis (June 8, 2021, DCO), a total of 63 patients (43.2%) in the toripalimab arm and 87 patients (60.8%) in the placebo arm experienced an event. In the toripalimab arm, 60 patients (41.4%) had a progressive disease event and 3 patients (2.1%) had died. In the placebo arm, 86 patients (80.1%) had a progressive disease event and 1 patient (0.7%) had died. The median PFS was 21.40 months (95% confidence interval [CI], 11.73 months to not estimable) in the toripalimab arm and 8.20 months (95% CI, 7.03 months to 9.79 months) in the placebo arm. The stratified HR was 0.52 (95% CI, 0.37 to 0.73; P < 0.0001), favouring toripalimab. The probability of having disease that is progression-free at 1 year was 59.0% (95% CI, 49.7% to 67.16%) in the toripalimab arm and 32.9% (95% CI, 24.9% to 41.5%) in the placebo arm; at 2 years, the probability of having disease that is progression-free was 44.8% (95% CI, 34.4% to 54.1%) in the toripalimab arm and 25.4% (95% CI, 17.0% to 34.8%) in the placebo arm.
Subgroup analysis of PFS at the final PFS analysis in the subgroups of recurrent and metastatic patients was consistent with the primary analysis.
Overall survival: At the final OS analysis (November 18, 2022, DCO), 57 patients (39.0%) in the toripalimab arm and 76 patients (53.1%) in the placebo arm had died. The median OS could not be estimated in the toripalimab arm (95% CI, 38.7 months to not estimable), and was 33.7 months (95% CI, 27.0 months to not estimable) in the placebo arm. The stratified HR was 0.63 (95% CI, 0.45 to 0.89; P = 0.0083) in favour of toripalimab. The probability of being alive at 1 year was 90.9% (95% CI, 84.9% to 94.6%) in the toripalimab arm and 87.1% (95% CI, 80.4% to 91.7%) in the placebo arm; at 2 years, it was 78.0% (95% CI, 70.2% to 84.0%) in the toripalimab arm and 65.1% (95% CI, 56.5% to 72.4%) in the placebo arm; and at 3 years, it was 64.5% (95% CI, 55.9% to 71.9%) in the toripalimab arm and 49.2% (95% CI, 40.5% to 57.3%) in the placebo arm.
Subgroup analysis of OS in subgroups of interest to this review (recurrent versus metastatic) favoured the toripalimab arm for the recurrent subgroup (HR = 0.45; 95% CI, 0.28 to 0.71), with 34% of patients in the toripalimab arm (n of N = 28 of 83) and 63% of patients in the placebo arm (n of N = 51 of 82) with recurrent disease at baseline experiencing an OS event. In the subgroup of patients with metastatic disease at baseline, HR versus placebo was 1.09 (95% CI, 0.64 to 1.9), with 46.0% of patients in the toripalimab arm (n of N = 29 of 63) and 41.0% of patients in the placebo arm (n of N = 25 of 61) with metastatic disease at baseline experiencing an OS event.
ORR by BIRC: As of the June 8, 2021, DCO (final PFS analysis), 78.8% of patients and 67.1% of patients in the toripalimab arm and the placebo arm, respectively, had experienced an objective response: 39 patients (26.7%) and 19 patients (13.3%) experienced a complete response, and 76 patients (52.1%) and 77 patients (53.8%) had experienced a partial response in the toripalimab and placebo arms, respectively. The difference in ORR between study arms was 11.4% (95% CI, 1.65% to 21.23%; P = 0.0221).
DoR by BIRC: As of the June 8, 2021, DCO (final PFS analysis), in the patients who had a confirmed objective response, the median DoR was 18.0 months (95% CI, 10.51 months to not estimable) in the toripalimab arm and 6.0 months (95% CI, 5.55 months to 8.25 months) in the placebo arm. The stratified HR was 0.49 (95% CI, 0.33 to 0.72; P = 0.0014).
EORTC QLQ-C30 global health status (0 [worst] to 100 [best]): As of the June 8, 2021, DCO (final PFS analysis), the baseline score for the EORTC QLQ-C30 global health status score was █████ points (standard deviation [SD] = █████) in the toripalimab arm and █████ points (SD = █████) in the placebo arm. The change from baseline to cycle 13, day 1, was ███ points (95% CI, ███ ██ ████) in the toripalimab arm and ████ points (95% CI, ███ ██ ████) in the placebo arm (difference = ████ points [95% CI, █████ ██ ███).
EORTC QLQ-H&N35 pain score (0 [worst] to 100 [best]): As of the June 8, 2021, DCO (final PFS analysis), the baseline score for the EORTC QLQ-H&N35 pain score was ███ points (SD = ████) in the toripalimab arm and ███ points (SD = ████) in the placebo arm. The change from baseline to cycle 13, day 1, was ████ points (95% CI, ████ ██ ████) in the toripalimab arm and ████ points (████ ██ ███) in the placebo arm (difference = ████ points; 95% CI ████ ██ ███).
EORTC QLQ-H&N35 swallowing score (0 [worst] to 100 [best]): As of the June 8, 2021, DCO (final PFS analysis), the baseline score for the EORTC QLQ-H&N35 swallowing score was ████ points (SD = ████) in the toripalimab arm and ████ points (SD = ████) in the placebo arm. The change from baseline to cycle 13, day 1, was ████ points (95% CI, ████ ██ ████) in the toripalimab arm and ███ points (████ ██ ███) in the placebo arm (difference = ████ points; 95% CI, █████ ██ ████).
Harms
Harms were recorded up until 60 days after the last dose of study drug was given (November 18, 2021). Key results include the following.
Treatment-Emergent Adverse Events
All patients (100%) in both treatment arms reported treatment-emergent adverse events (TEAEs), and most patients (90.2% in the toripalimab arm and 89.7% in the placebo arm) reported TEAEs of grade 3 or higher.
The most common TEAEs in the toripalimab arm versus the placebo arm were leukopenia (91.1% versus 94.4%, respectively), anemia (89.0% versus 94.4%, respectively), neutropenia (86.3% versus 93.0%, respectively), nausea (70.5% versus 84.4%, respectively), vomiting (67.8% versus 65.7%, respectively), thrombocytopenia (64.4% versus 61.5%, respectively), decreased appetite (55.5% versus 62.9%, respectively), increased aspartate aminotransferase (39.7% versus 31.5%, respectively), constipation (39.7% versus 46.2%, respectively), and increased alanine aminotransferase (38.4% versus 39.9%, respectively).
There were numeric differences in the proportion of patients in the toripalimab arm versus the placebo arm reporting hypothyroidism (36.3% versus 17.5%, respectively), rash (34.9% versus 27.3%, respectively), pyrexia (32.2% versus 24.5%, respectively), diarrhea (30.8% versus 23.1%, respectively), hyponatremia (26.0% versus 37.1%, respectively), upper respiratory tract infection (25.3% versus 14.0%, respectively), hypochloremia (18.5% versus 25.9%, respectively), pneumonia (17.8% versus 7.0%, respectively), and pruritus (17.1% versus 7.7%, respectively).
Serious Adverse Events
A similar proportion of patients in both treatment arms reported SAEs (43.8% in the toripalimab arm versus 43.4% in the placebo arm).
The most common SAEs in the toripalimab arm versus the placebo arm were thrombocytopenia (14.4% versus 16.1%, respectively), neutropenia (10.3% versus 6.3%, respectively), pneumonia (9.6% versus 3.5%, respectively), anemia (8.9% versus 9.8%, respectively), and leukopenia (8.2% versus 9.1%, respectively).
A numerically greater proportion of patients in the toripalimab arm versus the placebo arm reported neutropenia (10.3% versus 6.3%, respectively) and pneumonia (9.6% versus 3.5%, respectively).
Withdrawals Due to Adverse Events
More patients in the toripalimab arm discontinued treatment due to AEs relative to the placebo arm (17 patients [11.6%] versus 7 patients [4.9%], respectively). The most common reasons for discontinuation in the toripalimab arm were pneumonia (3 patients [2.1%]), as well as thrombocytopenia, vomiting, pulmonary tuberculosis, electrolyte imbalance, and rash (each reported in 2 patients [1.4%]). In the placebo arm, the reasons for discontinuation were individual patient reports of anemia, cardiac failure, hypothyroidism, malignant gastrointestinal obstruction, disease progression, pulmonary tuberculosis, and cerebral infarction.
Mortality
As of the June 8, 2021, DCO, a total of 20.5% of patients in the toripalimab arm and 32.2% of patients in the placebo arm had died. The most common reason in both arms was disease progression (11.6% in the toripalimab arm and 23.1% in the placebo arm). A total of 2 patients in the toripalimab arm and 1 patient in the placebo arm died due to AEs.
As of the November 18, 2022, DCO, a total of 5 patients (3.4%) in the toripalimab arm and 3 patients (2.1%) in the placebo arm had died within 60 days of the last dose of study drug. The causes of death in the toripalimab arm were disease progression (2 patients [1.4%]) and death, intracranial hemorrhage, and epistaxis (1 patient each). The causes of death in the placebo arm were disease progression (2 patients [1.4%]) and cerebral infarction (1 patient).
Adverse Events of Special Interest
More patients in the toripalimab arm reported immune-related TEAEs relative to the placebo arm (79 patients [54.1%] versus 31 patients [21.7%]). A numerically higher proportion of patients in the toripalimab arm also reported grade 3 or higher immune-related TEAEs relative to the placebo arm (19.6% versus 1.4%).
The most common grade 3 or higher immune-related TEAEs in the toripalimab arm were rash (3.4%) and thrombocytopenia (2.1%); the remaining grade 3 or higher immune-related TEAEs were reported in 1 patient each.
Summary of Findings and Certainty of the Evidence
Literature-based minimal important difference (MID) estimates were used as the thresholds for the following outcomes: EORTC QLQ-C30 global health status, EORTC QLQ-H&N35 pain score, and EORTC QLQ-H&N35 swallowing score (MID = 5 points for improvement and MID = 7 points for deterioration based on literature for the EORTC QLQ-C30 in head and neck cancer).30 Refer to the summary of outcome measures in Appendix 3 in the Supplemental Material document. In the absence of literature-based MID estimates, thresholds suggested by the clinical experts were applied for the following outcomes: the probability of PFS at 1 year and 2 years (threshold, 8% to 10%) and the probability of being alive at 1 year, 2 years, and 3 years (threshold, 5% to 10%). In the absence of a known threshold, the certainty in the presence of a non-null effect was rated for AEs.
Table 4: Summary of Findings for Toripalimab vs. Placebo as First-Line Treatment for Patients With Recurrent or Metastatic Nasopharyngeal Carcinoma
Outcome and follow-up | Patients, N (studies) | Relative effect (95% CI) | Absolute effects (95% CI) | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
Placebo | Toripalimab | Difference | |||||
Survival outcomes | |||||||
Progression-free survival | |||||||
Proportion of patients with PFS at 1 yeara Median follow-up: 20.08 months (placebo arm) and 20.58 months (toripalimab arm) | 289 (1 RCT) | NA | 329 per 1,000 patients | 590 per 1,000 patients (497 to 672 per 1,000 patients) | 261 more per 1,000 patients (138 to 383 more per 1,000 patients) | High | Toripalimab in combination with gemcitabine and cisplatin results in a clinically important increase in the probability of PFS at 1 year when compared to gemcitabine plus cisplatin. |
Proportion of patients with PFS at 2 yearsa Median follow-up: 20.08 months (placebo arm) and 20.58 months (toripalimab arm) | 289 (1 RCT) | NA | 254 per 1,000 patients | 448 per 1,000 patients (344 to 541 per 1,000 patients) | 194 more per 1,000 patients (57 to 331 more per 1,000 patients) | Lowb,c (serious study limitations and imprecision) | Toripalimab in combination with gemcitabine and cisplatin may result in a clinically important increase in the probability of PFS at 2 years when compared to gemcitabine plus cisplatin. |
Overall survival | |||||||
Proportion of patients who are alive at 1 yeard Median follow-up: 30.95 months (placebo arm) and 36.73 months (toripalimab arm) | 289 (1 RCT) | NA | 871 per 1,000 patients | 909 per 1,000 patients (849 to 946 per 1,000 patients) | 38 more per 1,000 patients (35 fewer to 111 more per 1,000 patients) | Moderatee (serious imprecision) | Toripalimab in combination with gemcitabine and cisplatin likely results in little to no clinically important difference in the probability of being alive at 1 year when compared to gemcitabine plus cisplatin. |
Proportion of patients who are alive at 2 yearsd Median follow-up: 30.95 months (placebo arm) and 36.73 months (toripalimab arm) | 289 (1 RCT) | NA | 651 per 1,000 patients | 780 per 1,000 patients (702 to 840 per 1,000 patients) | 129 more per 1,000 patients (23 to 234 more per 1,000 patients) | Moderatef (serious imprecision) | Toripalimab in combination with gemcitabine and cisplatin likely results in a clinically meaningful increase in the probability of being alive at 2 years when compared to gemcitabine plus cisplatin. |
Proportion of patients who are alive at 3 yearsd Median follow-up: 30.95 months (placebo arm) and 36.73 months (toripalimab arm) | 289 (1 RCT) | NA | 492 per 1,000 patients | 645 per 1,000 patients (559 to 719 per 1,000 patients) | 153 more per 1,000 patients (36 to 269 more per 1,000 patients) | Moderatef (serious imprecision) | Toripalimab in combination with gemcitabine and cisplatin likely results in a clinically meaningful increase in the probability of being alive at 3 years when compared to gemcitabine plus cisplatin. |
Health-related quality of life | |||||||
EORTC QLQ-C30 Global Health Status score (100 [best] to 0 [worst]) | |||||||
Mean change from baseline to cycle 13, day 1, pointsa Median follow-up: 20.08 months (placebo arm) and 20.58 months (toripalimab arm) | 289 (1 RCT) | NA | ████ | ███ ███ ██ ████ | ████ █████ ██ ████ | Very lowg,h (serious study limitations and imprecision) | The evidence is very uncertain about the effect of toripalimab plus gemcitabine and cisplatin on the change from baseline to cycle 13, day 1, in the EORTC QLQ-C30 global health status score when compared to gemcitabine plus cisplatin. |
EORTC QLQ-H&N35 pain score (100 [best] to 0 [worst]) | |||||||
Mean change from baseline to cycle 13, day 1, pointsa Median follow-up: 20.08 months (placebo arm) and 20.58 months (toripalimab arm) | 289 (1 RCT) | NA | ████ | ████ █████ ██ █████ | ████ █████ ██ ████ | Very lowg,h (serious study limitations and imprecision) | The evidence is very uncertain about the effect of toripalimab plus gemcitabine and cisplatin on the change from baseline to cycle 13, day 1, in the EORTC QLQ-H&N35 pain score when compared to gemcitabine plus cisplatin. |
EORTC QLQ-H&N35 swallowing score (100 [best] to 0 [worst]) | |||||||
Mean change from baseline to cycle 13, day 1, pointsa Median follow-up: 20.08 months (placebo arm) and 20.58 months (toripalimab arm) | 289 (1 RCT) | NA | ███ | ████ ████ ██ █████ | ████ █████ ██ █████ | Very lowg,h (serious study limitations and imprecision) | The evidence is very uncertain about the effect of toripalimab plus gemcitabine and cisplatin on the change from baseline to cycle 13, day 1, in the EORTC QLQ-H&N35 swallowing score when compared to gemcitabine plus cisplatin. |
Harms | |||||||
Proportion of patients with ≥ 1 SAEi | 289 (1 RCT) | NR | 434 per 1,000 patients | 438 per 1,000 patients (356 to 523 per 1,000 patients) | 5 more per 1,000 patients (110 fewer to 120 more per 1,000 patients) | Lowj (serious imprecision) | Toripalimab in combination with gemcitabine and cisplatin may result in little to no difference in the proportion of patients with 1 or more SAE when compared to gemcitabine plus cisplatin. |
Proportion of patients with ≥ 1 immune-related AEi | 289 (1 RCT) | NR | 217 per 1,000 patients | 541 per 1,000 patients (457 to 624 per 1,000 patients) | 324 more per 1,000 patients (219 to 430 more per 1,000 patients) | High | Toripalimab in combination with gemcitabine and cisplatin results in an increase of the proportion of patients with 1 or more immune-mediated AE when compared to gemcitabine plus cisplatin. The clinical importance is uncertain. |
AE = adverse event; CI = confidence interval; DCO = data cut-off; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-H&N35 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire 35-item Head and Neck; HRQoL = health-related quality of life; MID = minimal important difference; NA = not applicable; NR = not reported; PFS = progression-free survival; RCT = randomized controlled trial; SAE = serious adverse event; vs. = versus.
Note: Study limitations (which refer to internal validity or risk of bias), indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aBased on the June 8, 2021, DCO.
bRated down 1 level for serious study limitations. There remained few patients (n = 11) at risk at this time point and a large proportion of patients were censored, which may impact the stability and increase the uncertainty in the estimates.
cRated down 1 level for serious imprecision. Based on a target threshold of 8% to 10% provided by the clinical experts consulted for this review, the CI includes the possibility of an effect that is not clinically meaningful.
dBased on the November 18, 2022, DCO.
eRated down 1 level for serious imprecision. Based on a target threshold of 5% provided by the clinical experts consulted for this review, the point estimate is not clinically meaningful, but the CI includes the possibility of an effect that is clinically meaningful.
fRated down 1 level for serious imprecision. Based on a target threshold of 5% provided by the clinical experts consulted for this review, the CI includes the possibility of an effect that is not clinically meaningful.
gRated down 2 levels for serious study limitations. The JUPITER-02 study was unblinded after early demonstration of statistical significance on PFS in May 2020, and knowledge of the treatment arm assignment risks biasing the results of subjective outcomes such as patient-reported HRQoL. In addition, there is a high risk of bias due to a substantial portion of missing outcome data.
hRated down 1 level for serious imprecision. Based on literature-based MIDs for head and neck cancer (5 points for improvement and −7 points for deterioration), the point estimate suggests little to no clinically important difference and the CI includes the potential for harm.
iBased on the May 8, 2022, DCO.
jRated down 2 levels for very serious imprecision. Based on a non-null target of assessment, the CI includes the possibility of no effect, the possibility of harm, and the possibility of improvement in the outcome.
Sources: Details included in the table are from the sponsor’s Summary of Clinical Evidence,28 the JUPITER-02 trial Clinical Study Report,29 the JUPITER-02 trial Clinical Study Report Addendum 1,31 the JUPITER-02 trial Clinical Study Report Addendum 3,32 and additional information provided by the sponsor.33,34
LTE Studies
The submission did not include any LTE studies.
Indirect Evidence
The submission included a feasibility assessment for an ITC that consisted of a systematic literature review and a corresponding Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram. The sponsor included pembrolizumab and nivolumab as comparators. They noted that the systematic literature review did not yield any RCTs for these comparators and therefore, an ITC was not feasible. Furthermore, the clinical experts noted that pembrolizumab and nivolumab are not funded in Canadian jurisdictions; therefore, they are not relevant comparators for toripalimab in Canada. As such, no ITC was submitted by the sponsor.
Studies Addressing Gaps in the Systematic Review Evidence
The submission did not include any studies addressing gaps in the systematic review evidence.
Discussion
This report summarizes the evidence for toripalimab combined with gemcitabine and cisplatin compared to placebo plus gemcitabine and cisplatin for the treatment of recurrent or metastatic NPC. The evidence appraised was based on 1 phase III RCT (the JUPITER-02 study) with multiple analyses, including an IA containing data reported by fully blinded patients and investigators (May 30, 2020, DCO), a final analysis for PFS that took place after study unblinding (June 8, 2021, DCO) and a final analysis for OS (November 18, 2022, DCO). The JUPITER-02 trial (N = 289) randomized patients 1:1 to either toripalimab combined with gemcitabine and cisplatin for up to 6 cycles followed by toripalimab monotherapy (n = 168) or placebo combined with gemcitabine and cisplatin for up to 6 cycles, followed by placebo (n = 163), and then followed by toripalimab maintenance or placebo.
Efficacy
The inclusion criteria for the JUPITER-02 study included patients with metastatic or recurrent NPC that was not amenable to local–regional treatment or curative treatment; this is narrower than the Health Canada indication of recurrent, locally advanced NPC. While clinical experts consulted for this review noted that it is rare for patients with recurrent or metastatic NPC to be considered candidates for surgery, patients with locally advanced NPC would not have been included in the JUPITER-02 study unless they were also recurrent. Chemotherapy is standard of care in the recurrent or metastatic disease setting and is therefore the main comparator to toripalimab in the first-line setting. There are no PD-1 or PD-L1 inhibitors indicated for the first-line treatment of recurrent or metastatic NPC in the Canadian clinical setting unless available in clinical trials or special access programs. The outcomes assessed in the JUPITER-02 trial were important and relevant to patients and clinicians, including PFS, OS, and HRQoL measures that are specific to head and neck cancers. Although patients and clinicians note that while the initial response to NPC treatment often results in symptom relief, there are few treatment options for recurrent or metastatic cases and long-term, cumulative toxicities that impact quality of life as well as resistance to treatment are a concern. Because patients will eventually experience disease progression, even after multiple courses of chemotherapy, pharmacologic treatment is considered palliative.
The etiology of NPC is multifactorial, and risk factors include use of commercial tobacco products and having had an EBV infection. The presence (or lack) of EBV is associated with specific histological subtypes of NPC. The JUPITER-02 trial was conducted in study sites located in Asia, which is considered endemic for NPC; the trial recruited a patient population that was 100% of Chinese ethnicity and most patients (approximately 70%) had nonkeratinizing NPC. In addition, there were imbalances between study arms in the proportions of patients who reported smoking and alcohol consumption, which suggested that there may remain associations between the use of alcohol, the use of commercial tobacco products, and other patient baseline characteristics that were not fully controlled for in the randomization, and the importance of this imbalance is uncertain. While clinical experts noted that most of their patients with NPC are of Asian descent (approximately 85%, varying between provinces), they noted that other patients, such as Indigenous Peoples (including Inuit), were not represented in this trial. Furthermore, they noted that while the histologies of NPC that were represented in the trial were also broadly representative of the those observed in Canadian practice, not all histopathological subtypes were included. They also flagged some differences in the concomitant treatments, which may affect harms reporting due to different side effects, as well as in subsequent treatments because a higher proportion of patients used PD-1 or PD-L1 inhibitors after toripalimab (including additional treatments with toripalimab), which would not be a treatment option in Canada. Additionally, twice as many patients in the placebo arm received cytotoxic chemotherapy as their subsequent treatment relative to patients in the toripalimab arm. Subsequent therapy may have an impact on OS and harms reporting; however, a subsequent sensitivity analysis requested by Health Canada using inverse probability of censoring weighting, which accounted for anti–PD-1 and anti–PD-L1 postprogression treatment, was consistent with the primary OS results (HR = 0.60; 95% CI, 0.42 to 0.85). Together, these limitations represent generalizability concerns, and it is unclear how directly the results of the study may apply to patients with histological subtypes other than nonkeratinizing, undifferentiated NPC, as well as in other countries with different treatment options as standard of care and beyond progression.
There were some general concerns with the conduct of the trial, which increased the uncertainty in the results, although not all concerns are sources of bias. That which may contribute to bias was the high degree of protocol violations noted in the trial, which were more commonly reported for the toripalimab arm. This may have been a result of early unblinding because the placebo arm discontinued treatment and patients were simply followed, with less concern for violations pertaining to medication administration; however, most of the protocol deviations that were more commonly reported in the toripalimab arm pertained to incorrect tumour assessments or unavailable laboratory measures. This raises the possibility of bias in the results of the toripalimab arm, which could go in either direction depending on the nature of the deviations because the potential deviations listed may affect tumour assessment by the BIRC. In addition, as of the June 8, 2021, DCO, a higher proportion of patients in the placebo arm had reported discontinuing treatment before disease progression than in the toripalimab arm. The imbalance between study arms suggests that the study unblinding may have impacted whether some patients remained on treatment; however, there were sensitivity analyses that suggested that the impact on the results may be limited.
In November 2020, the JUPITER-02 study was unblinded early at the recommendation of the Independent Data Monitoring Committee; this resulted in the discontinuation of the placebo arm and the beginning of open-label treatment with toripalimab in the toripalimab arm. Given that the duration of treatment for toripalimab was capped at 2 years, the last treatment dose was received on November 18, 2021, and the last patient visit took place on November 18, 2022 (the DCO for the final OS analysis). The early unblinding resulted in a reduced information fraction for PFS where only 43.2% of patients in the toripalimab arm experienced a PFS event. As such, the results for PFS were not fully estimated in the toripalimab arm. Furthermore, the median OS in the toripalimab arm remained inestimable at the end of the study. Subgroup analyses for recurrent and metastatic patients suggested no difference in OS for patients with primary metastatic disease; however, these subgroups were only considered exploratory and generally had smaller numbers of patients. Landmark analyses demonstrated statistically significant improvement in median PFS for toripalimab relative to placebo, and showed that toripalimab likely results in a clinically important improvement in PFS at 1 year (moderate certainty) and may result in a clinically important improvement at 2 years (low certainty) compared to placebo. Additionally, the evidence showed that toripalimab likely results in clinically important improvements in OS at 1-year, 2-year, and 3-year time points. Due to the relatively short follow-up, there remains uncertainty in the long-term benefit of toripalimab. In particular, there is uncertainty in PFS results beyond 20 months when a large proportion of patients were censored and few remain at risk. For OS, there is uncertainty beyond 36 months due to few patients remaining at risk and high degrees of censoring toward the tail of the Kaplan-Meier curve. In addition, the JUPITER-02 trial included an initial chemotherapy phase for 6 cycles followed by a maintenance phase for up to 2 years. Patients randomized to the placebo arm received maintenance placebo without chemotherapy. While there is no firm guidance on the use of gemcitabine maintenance therapy in recurrent or metastatic NPC in Canada, the clinical experts noted that the placebo arm of the JUPITER-02 study may not be reflective of clinical practice in Canada because patients may receive gemcitabine maintenance. At the final PFS analysis (June 8, 2021, DCO), PFS curves began separating after 6 months, which is approximately the duration of the initial chemotherapy phase, after which patients in the placebo arm were no longer receiving any active treatment. As such, there is a risk that the effect of toripalimab on PFS is overestimated and it is unclear whether the benefit of toripalimab on PFS is due to maintenance treatment in the toripalimab arm, or if it is influenced by the lack of therapy in the placebo arm following the initial chemotherapy phase.
HRQoL was highlighted as an outcome of importance to patients and was assessed in the JUPITER-02 study using 1 cancer-specific measure (EORTC QLQ-C30) as well as the head and neck cancer subscale of the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire. Results were very uncertain due to the risk of bias and imprecision. As such, the effect of toripalimab on HRQoL remains unknown. The change from baseline in scores did not reach the between-group MIDs available in the literature for head and neck cancers.
Harms
All patients reported TEAEs during the JUPITER-02 study; however, most individual AEs and SAEs were consistently reported between the toripalimab and placebo arms, suggesting that the harms reported by most patients were attributable to chemotherapy. However, as expected based on the mechanism of action, immune-mediated TEAEs including hypothyroidism, pyrexia, rash, upper respiratory tract infections, as well as pneumonia were more commonly reported in the toripalimab arm. In addition, a numerically higher proportion of patients in the toripalimab arm withdrew due to TEAEs relative to the placebo arm. While this suggests that toripalimab treatment does have some additional harms compared to chemotherapy alone, the overall proportion of withdrawals due to TEAEs was low during the study.
The harms reporting is subject to some limitations. Harms were not reported separately for the chemotherapy and postchemotherapy maintenance phases, which pose some challenges identifying additional long-term harms that may be attributable to toripalimab. As the duration of treatment with toripalimab was capped at 2 years, information on harms beyond the duration of the JUPITER-02 trial is not available. As of the June 8, 2021, DCO, more patients had died in the placebo arm than in the toripalimab arm, primarily driven by disease progression (23.1% versus 11.6%, respectively). Information on deaths at the final OS analysis was missing in the original submission materials; thus, the most up-to-date information on deaths was not included for appraisal. Information on causes of death within the last 60 days of study dose administration as of the final OS analysis was provided, but this represented a numerically small proportion of patients given that the most common reason for study discontinuation was death, and those causes of death are not known.
Ethics and Equity Considerations
In general, a high proportion of patients at risk for NPC are also from equity-deserving groups. In Canada, this particularly includes people of Asian descent and Indigenous populations. These people may also be more likely to face treatment access barriers related to location, language, culture, and potential low trust in the health care system, all of which may result in delays seeking care and delays in diagnosis. Given that NPC is endemic in other parts of the world such as East Asia, there is a global geographical inequity for patients who are newly immigrated to Canada from these regions who may be at increased risk of NPC but also face language barriers or have less knowledge of the health care system to seek care. Furthermore, the fact that NPC is a rare disease in Canada means that knowledge of the disease may be more concentrated in academic centres and, as a result, patients in rural or remote areas may have less access to timely care or may be unduly burdened by travel to access care. This impact can compound the burden of NPC on Indigenous populations in Canada, who also tend to live in more remote locations. These burdens can lead to subsequent financial and caregiver burdens due to transportation costs and time away from paid employment.
There are additional barriers associated with current treatments that could be partially addressed by toripalimab. The requirement for IV treatments in a cancer centre may be difficult for patients in more remote locations, a factor that would not be addressed by toripalimab, which is also an IV treatment. However, if gemcitabine is used as a maintenance therapy as has been noted in the literature, compared to this treatment, the safety profile of toripalimab may be preferable if it reduces side effects and cumulative toxicities. Toripalimab may also be suitable for patients with certain comorbidities such as solid organ transplant, or patients who are older adults, who might not be ideally suited to chemotherapy maintenance.
Conclusion
NPC is a rare cancer in Canada but has unique global geographic distribution and tends to disproportionately affect people of Asian descent and Indigenous Peoples (including Inuit). Recurrent or metastatic NPC is currently managed by platinum-based chemotherapy and/or radiation. Patients with recurrent or metastatic NPC will eventually experience disease progression, even after multiple courses of chemotherapy. Patients and clinicians identified a need for new treatments in the first-line setting that reduce tumour burden, delay progression, and extend survival. One phase III, placebo-controlled RCT (the JUPITER-02 study) provided evidence for the efficacy and safety of toripalimab plus gemcitabine and cisplatin as first-line treatment for 289 patients with recurrent or metastatic NPC. The population included in the reimbursement request was broader than the population included in the JUPITER-02 trial, which only included patients with recurrent or metastatic NPC not amenable to curative treatment; thus, the results of the JUPITER-02 trial cannot be generalized to locally advanced NPC.
The JUPITER-02 study demonstrated that the addition of toripalimab to standard of care for 6 cycles followed by toripalimab maintenance demonstrated a statistically significant improvement in PFS, as well as a significant improvement in OS compared to gemcitabine and cisplatin alone. Landmark analyses showed that toripalimab likely results in a clinically important improvement in PFS at 1 year (moderate certainty) and may result in a clinically important improvement at 2 years (low certainty) compared to placebo. Additionally, the evidence showed that toripalimab likely results in clinically important improvements in OS at 1-year, 2-year, and 3-year time points. However, survival estimates have added uncertainty and a risk of bias given that the JUPITER-02 trial did not include an active comparator in the maintenance phase, which may not reflect current clinical practice in Canada, as well as the fact there were differences in subsequent treatments received, though sensitivity analyses for subsequent therapy was consistent with the primary analysis. Results from the JUPITER-02 trial for HRQoL, which was an outcome important to patients, were very uncertain due to missing data and imprecision. As expected, toripalimab is associated with more immune-related AEs than chemotherapy; however, withdrawals due to AEs were low in the JUPITER-02 trial and the clinical experts consulted for this review considered the toxicity profile of toripalimab to be similar to that of other PD-1 or PD-L1 therapies.
Economic Review
Methods
The review team appraised the submitted pharmacoeconomic evidence, which included an economic evaluation comparing the cost-effectiveness of toripalimab in combination with cisplatin and gemcitabine (toripalimab plus chemotherapy) compared to chemotherapy alone for the first-line treatment of adults with metastatic or recurrent, locally advanced NPC. This is aligned with the Health Canada indication and there is an accepted deviation request to exclude pembrolizumab and nivolumab from the cost-effectiveness analysis. The review team also appraised a BIA assessing the budgetary impact of reimbursing toripalimab for the full Health Canada indication in comparison with chemotherapy, pembrolizumab plus chemotherapy, and nivolumab plus chemotherapy. The sponsor’s economic submission is summarized in Appendix 10 in the Supplemental Material.
Summary of the Submitted Economic Evaluation
The sponsor submitted a cost-utility analysis to estimate the cost-effectiveness of toripalimab in combination with cisplatin and gemcitabine from the perspective of a public health care payer in Canada over a lifetime horizon (15 years).35 The modelled population consisted of patients with metastatic or recurrent NPC, which is aligned with the Health Canada indication and was based on the participants in the JUPITER-02 trial.35 The sponsor’s base-case analysis included costs related to drug acquisition, administration, monitoring, and AEs.35
In the sponsor’s base case, toripalimab in combination with cisplatin and gemcitabine was associated with incremental costs of $219,825 and 1.30 incremental quality-adjusted life-years (QALYs) gained relative to chemotherapy alone.35 This resulted in an incremental cost-effectiveness ratio of $169,313 per QALY gained.35 Of the incremental benefit compared to chemotherapy alone (1.30 incremental QALYs gained), approximately 82% of the benefit was predicted to be accrued after the treatment duration of the JUPITER-02 trial (a median survival follow-up of 36.0 months).2,35 Additional information about the sponsor’s submission is summarized in Appendix 10 in the Supplemental Material.
CDA-AMC identified several key issues with the sponsor’s analysis (refer to Table 5; full details are provided in Appendix 11 in the Supplemental Material).
Table 5: Key Issues With the Sponsor’s Economic Submission
Issue | What evidence is there to inform this issue? | How was this issue addressed by CDA-AMC? | Did CDA-AMC explore uncertainty in a scenario analysis? |
|---|---|---|---|
The long-term comparative efficacy of toripalimab plus chemotherapy vs. chemotherapy alone is uncertain — driven by the clinical evidence combined with the modelling approach. | Evidence from the JUPITER-02 trial suggests that treatment with toripalimab plus chemotherapy may result in a clinically important increase in the proportion of patients whose disease has not progressed at 2 years and likely increases the proportion of patients alive vs. treatment with chemotherapy alone. However, the study was unblinded early and had high degrees of censoring, and the OS data were likely immature.2 Clinical expert feedback noted that long-term efficacy estimates for chemotherapy alone, chemotherapy treatment duration, and subsequent treatments used in the trial did not align with clinical expectations, and it is unclear if the OS benefit observed in the trial would be reflective of the OS benefit expected in clinical practice in Canada. PFS and OS KM data from the JUPITER-02 trial were used to program a PSM model using a piecewise approach that has structural limitations about the relationship between PFS and OS that may not accurately reflect the causal disease pathway. Altogether, the underlying data and the modelling approach resulted in postprogression benefits of chemotherapy over toripalimab, assuming no uncertainty for the trial period, and alternative curve selections resulted in improbable outcomes. | CDA-AMC selected the generalized gamma curve for chemotherapy PFS. The remaining issues could not be addressed owing to a lack of long-term data and limitations with the sponsor’s model. | Two scenario analyses were conducted where, in the first analysis, OS KM data were restricted to 40 months, and in the second analysis, parametric extrapolations for PFS and OS for the full time horizon were used for both treatment arms, removing the piecewise approach. |
Exclusion of treatment-effect waning for toripalimab is uncertain. | The sponsor assumed no treatment-effect waning.35 Clinical expert feedback indicated that it is plausible for treatment-waning to occur; however, the degree and magnitude of waning is unknown. | CDA-AMC could not address this issue owing to the structure of the sponsor’s model. | No scenario analysis was conducted. |
Cost of chemotherapy was overestimated. | Unit costs for carboplatin and cisplatin were informed by the Association québécoise des pharmaciens propriétaires medication list. Based on the generic pricing available in the IQVIA DeltaPA database, unit costs of carboplatin and cisplatin are expected to be lower.36 Additionally, the sponsor assumed a dose of 569 mg for carboplatin; however, this may underestimate the dose of carboplatin as there is variability in renal function. | CDA-AMC used the lower unit costs for carboplatin and cisplatin. Additionally, a full dose of carboplatin was assumed. | No scenario analysis was conducted. |
Utility values informed by patients with head and neck cancer are uncertain. | Clinical expert feedback noted that patients with head and neck cancer compared to patients with NPC may experience differences in quality of life. Utility values derived from patients with NPC are preferred. | CDA-AMC used utility values from the Yen et al. (2009) study. | Utility values from the NICE head and neck cancer review were explored in a scenario analysis. |
Model lacked transparency due to poor modelling practice. | The submitted model had numerous IFERROR statements that resulted in automatized overwriting errors. Additionally, the model contained some poor information presentation that made thorough auditing of the sponsor’s model impractical. | CDA-AMC could not address this issue owing to the structure of the sponsor’s model. | No scenario analysis was conducted. |
CDA-AMC = Canada’s Drug Agency; KM = Kaplan-Meier; NICE = National Institute for Health and Care Excellence; NPC = nasopharyngeal carcinoma; OS = overall survival; PFS = progression-free survival; PSM = partitioned survival model; vs. = versus.
Note: Full details of the issues identified by CDA-AMC are provided in Appendix 11 in the Supplemental Material.
CDA-AMC Assessment of Cost-Effectiveness
The CDA-AMC base case was derived by making changes to model parameter values and assumptions (refer to Appendix 11 in the Supplemental Material) in consultation with clinical experts. Detailed information about the CDA-AMC base case is provided in Appendix 11 in the Supplemental Material.
Impact on Health Care Costs
Toripalimab plus chemotherapy is predicted to be associated with additional health care costs compared to chemotherapy alone (incremental costs = $219,624). This increase in health care spending results predominantly from drug acquisition costs (incremental costs = $201,226) and nondrug health care resource use associated with toripalimab (incremental costs = $21,174) (refer to Figure 1).
Figure 1: Impact of Toripalimab Plus Chemotherapy vs. Chemotherapy Alone on Health Care Costs
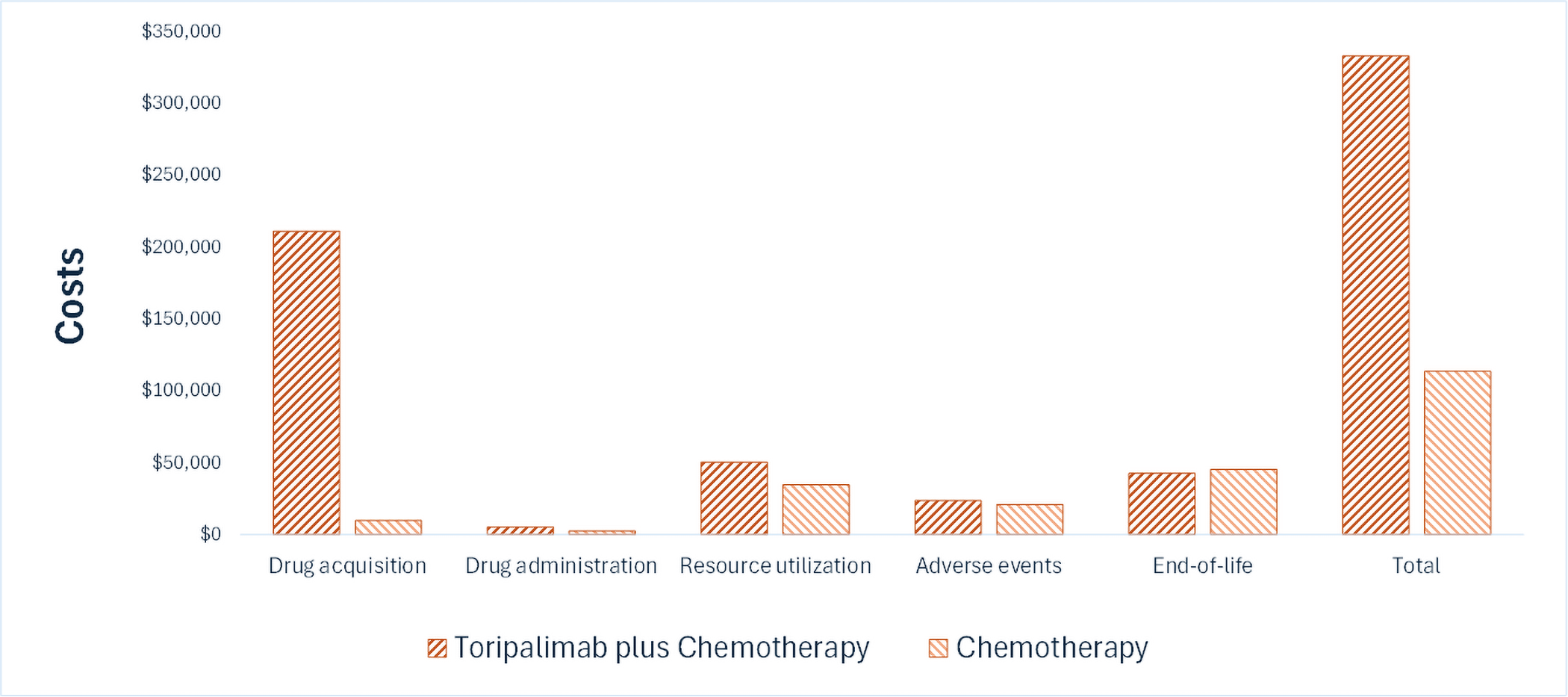
Vs. = versus.
Impact on Health
Relative to chemotherapy alone, toripalimab plus chemotherapy is predicted to increase the amount of time a patient’s disease remains in the progression-free state by approximately 1.39 years (refer to Figure 2). Considering the impact of treatment on both quality and length of life, toripalimab plus chemotherapy is predicted to result in 1.16 additional QALYs per patient compared to chemotherapy alone. Approximately 80% of the predicted incremental benefit was accrued on the basis of extrapolation.
Figure 2: Impact of Toripalimab Plus Chemotherapy vs. Chemotherapy Alone on Patient Health
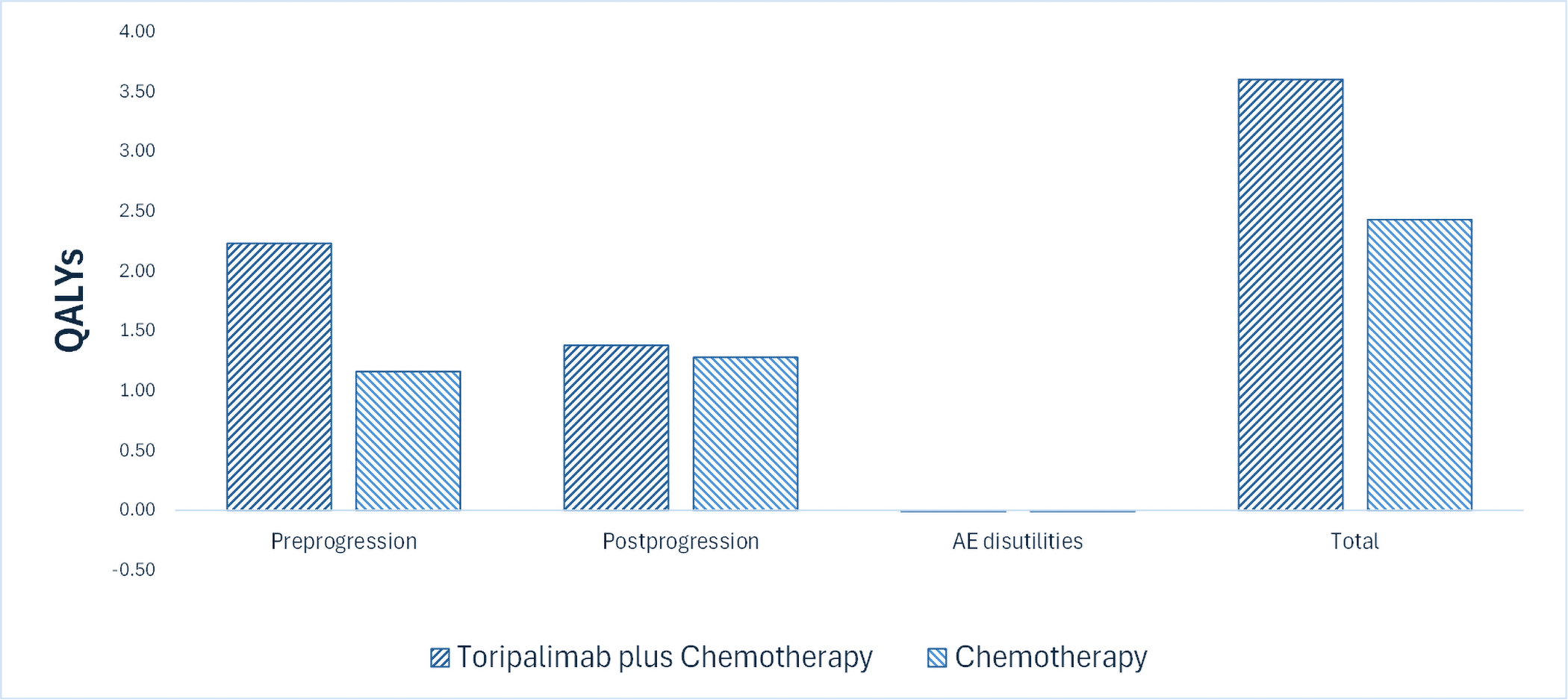
AE = adverse event; QALY = quality-adjusted life-year; vs. = versus.
Overall Results
The results of the CDA-AMC base case suggest an incremental cost-effectiveness ratio of $189,118 per QALY gained for toripalimab plus chemotherapy compared to chemotherapy alone (refer to Table 6). Additional details on the CDA-AMC base case are available in Appendix 11.
Table 6: Summary of CDA-AMC Economic Evaluation Results
Drug | Total costs ($) | Total LYs | Total QALYs | ICER vs. chemotherapy ($/QALY) |
|---|---|---|---|---|
Chemotherapy | 113,493 | 3.74 | 2.44 | Reference |
Toripalimab plus chemotherapy | 333,117 | 5.30 | 3.60 | 189,118 |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; vs. = versus.
Note: Publicly available list prices were used for all comparators.
Uncertainty and Sensitivity
Uncertainty was explored in a scenario analysis outlined in Table 19 of Appendix 11 in the Supplemental Material. Uncertainty around toripalimab dosing assumptions had the largest impact on the cost-effectiveness (refer to Table 19 of Appendix 11 in the Supplemental Material).
Summary of the Budget Impact
The sponsor submitted a BIA to estimate the 3-year (2026–2028) budget impact of reimbursing toripalimab in combination with cisplatin and gemcitabine for use in patients with metastatic or recurrent, locally advanced NPC. The sponsor assumed that the payer would be CDA-AMC and derived the size of the eligible population using an epidemiological approach. The price of toripalimab was aligned with the price included in the sponsor’s economic evaluation, while the prices of comparators were based on the publicly available list prices. Additional information pertaining to the sponsor’s submission is provided in Appendix 11 in the Supplemental Material.
CDA-AMC identified a number of issues with the sponsor’s estimated budget impact and made changes to model parameters and assumptions in consultation with clinical experts to derive the CDA-AMC base case (described in Appendix 12 in the Supplemental Material). CDA-AMC estimated 647 patients would be eligible for treatment with toripalimab in combination with gemcitabine and cisplatin over a 3-year period (year 1 = 211 patients; year 2 = 216 patients; year 3 = 221 patients); of these patients, 473 are expected to receive toripalimab in combination with gemcitabine and cisplatin (year 1 = 85 patients; year 2 = 183 patients; year 3 = 204 patients). The estimated incremental budget impact of reimbursing toripalimab is predicted to be approximately $52 million over the first 3 years, with an expected expenditure of $52 million on toripalimab. The actual budget impact will depend on the number of eligible people receiving treatment, the duration of treatments, and toripalimab uptake.
Conclusion
Based on the CDA-AMC base case, toripalimab plus chemotherapy would be considered cost-effective at the submitted price if the public health care system was willing to pay at least $189,118 for each additional QALY gained. If the public health care system is not willing to pay that amount, a price reduction should be considered (refer to Figure 3; full details of the impact of price reductions on cost-effectiveness are presented in Table 18 of Appendix 11 in the Supplemental Material). The estimated cost-effectiveness of toripalimab plus chemotherapy compared to chemotherapy alone is uncertain due to the uncertainty in the long-term comparative efficacy and structure of the submitted economic model.
The budget impact of reimbursing toripalimab to the public drug plans in the first 3 years is estimated to be approximately $52 million. The 3-year expenditure on toripalimab (i.e., not accounting for current expenditure on comparators) is estimated to be approximately $52 million. The estimated budget impact is uncertain mostly due to the uncertainty around the number of eligible patients who will receive treatment, the duration of treatments, and the uptake of toripalimab.

References
1.Apotex Inc. Loqtorzi (toripalimab solution for injection): Sterile solution, 240 mg/6 mL (40 mg/mL) for intravenous infusion after dilution [product monograph]. October 31, 2024.
2.Shanghai Junshi Bioscience Co., Ltd. Clinical Study Report: JS00l-015-III-NPC. A Phase 3, Randomized, Placebo Controlled, Multicenter, Double Blind Study Comparing Toripalimab Injection (JS00l) Combined With Chemotherapy Versus Placebo Combined With Chemotherapy For Recurrent Or Metastatic Nasopharyngeal Cancer [internal sponsor's report]. January 15, 2021.
3.Spreafico A, Winquist E, Ho C, et al. A Canadian Perspective on Systemic Therapy for Recurrent or Metastatic Nasopharyngeal Carcinoma. Curr Oncol. 2025;32(1):48. doi:10.3390/curroncol32010048 PubMed
4.Bruce JP, Yip K, Bratman SV, Ito E, Liu FF. Nasopharyngeal Cancer: Molecular Landscape. J Clin Oncol. 2015;33(29):3346-55. doi:10.1200/JCO.2015.60.7846 PubMed
5.American Cancer Society. Survival Rates for Nasopharyngeal Cancer [sponsor supplied reference]. Updated March 1, 2023. Accessed June 5, 2025. https://www.cancer.org/cancer/types/nasopharyngeal-cancer/detection-diagnosis-staging/survival-rates.html
6.Wang TM, He YQ, Xue WQ, et al. Whole-Exome Sequencing Study of Familial Nasopharyngeal Carcinoma and Its Implication for Identifying High-Risk Individuals. J Natl Cancer Inst. 2022;114(12):1689-1697. doi:10.1093/jnci/djac177 PubMed
7.Xu T, Tang J, Gu M, Liu L, Wei W, Yang H. Recurrent nasopharyngeal carcinoma: a clinical dilemma and challenge. Curr Oncol. 2013;20(5):e406-19. doi:10.3747/co.20.1456 PubMed
8.Lo AK, Dawson CW, Lung HL, Wong KL, Young LS. The Role of EBV-Encoded LMP1 in the NPC Tumor Microenvironment: From Function to Therapy. Front Oncol. 2021;11:640207. doi:10.3389/fonc.2021.640207 PubMed
9.Shah AB, Nagalli S. Nasopharyngeal Carcinoma [sponsor supplied reference]. StatPearls. 2025.
10.Pathology Outlines. Nasal cavity, paranasal sinuses, nasopharynx [sponsor supplied reference]. Updated December 15, 2020. Accessed June 13, 2025. https://www.pathologyoutlines.com/topic/nasalnasopharyngealgeneral.html
11.Zhao BY, Hirayama S, Goss D, Zhao Y, Faden DL. Human papillomavirus-associated nasopharyngeal carcinoma: A systematic review and meta-analysis. Oral Oncol. 2024;159:107057. doi:10.1016/j.oraloncology.2024.107057 PubMed
12.Wang WH, Lin YC, Chen WC, Chen MF, Chen CC, Lee KF. Detection of mucosal recurrent nasopharyngeal carcinomas after radiotherapy with narrow-band imaging endoscopy. Int J Radiat Oncol Biol Phys. 2012;83(4):1213-9. doi:10.1016/j.ijrobp.2011.09.034 PubMed
13.Ng SH, Chang JT, Ko SF, Wan YL, Tang LM, Chen WC. MRI in recurrent nasopharyngeal carcinoma. Neuroradiology. 1999;41(11):855-62. doi:10.1007/s002340050857 PubMed
14.Liu T, Xu W, Yan WL, Ye M, Bai YR, Huang G. FDG-PET, CT, MRI for diagnosis of local residual or recurrent nasopharyngeal carcinoma, which one is the best? A systematic review. Radiother Oncol. 2007;85(3):327-35. doi:10.1016/j.radonc.2007.11.002 PubMed
15.Cancer Care Alberta. Nasopharyngeal Cancer Treatment [sponsor supplied reference]. 2021. Accessed February 2025. https://www.albertahealthservices.ca/assets/info/hp/cancer/if-hp-cancer-guide-hn003-nasopharyngeal.pdf
16.Abdullah B, Alias A, Hassan S. Challenges in the management of nasopharyngeal carcinoma: a review. Malays J Med Sci. 2009;16(4):50-4. PubMed
17.Li AC, Xiao WW, Shen GZ, et al. Distant metastasis risk and patterns of nasopharyngeal carcinoma in the era of IMRT: long-term results and benefits of chemotherapy. Oncotarget. 2015;6(27):24511-21. doi:10.18632/oncotarget.4312 PubMed
18.Li Y, Huang Z, Zeng X, et al. Early recurrence as a pivotal event in nasopharyngeal carcinoma: identifying predictors and key molecular signals for survivors. Head Face Med. 2024;20(1):55. doi:10.1186/s13005-024-00457-7 PubMed
19.Howlett J, Hamilton S, Ye A, et al. Treatment and outcomes of nasopharyngeal carcinoma in a unique non-endemic population. Oral Oncol. 2021;114:105182. doi:10.1016/j.oraloncology.2021.105182 PubMed
20.Liu Q, Li J, Ng WT, Lee AWM. Treatment strategy for de novo metastatic nasopharyngeal carcinoma: a literature review. Chin Clin Oncol. 2023;12(4):43. doi:10.21037/cco-23-32 PubMed
21.Lee AWM, Ng WT, Chan LK, et al. The strength/weakness of the AJCC/UICC staging system (7th edition) for nasopharyngeal cancer and suggestions for future improvement. Oral Oncol. 2012;48(10):1007-1013. doi:10.1016/j.oraloncology.2012.03.022
22.World Health Organization International Agency for Research on Cancer. Cancer Today [sponsor supplied reference]. Updated August 2, 2024. Accessed February 11, 2025. https://gco.iarc.who.int/today/en/dataviz/maps-heatmap?mode=population&cancers=4&zoom=3
23.Statistics Canada. Table 13-10-0751-01: Number of prevalent cases and prevalence proportions of primary cancer, by prevalence duration, cancer type, attained age group and sex [sponsor supplied reference]. 2025. https://doi.org/10.25318/1310075101-eng
24.Young TK, Kelly JJ, Friborg J, Soininen L, Wong KO. Cancer among circumpolar populations: an emerging public health concern. Int J Circumpolar Health. 2016;75:29787. doi:10.3402/ijch.v75.29787 PubMed
25.Badoual C. Update from the 5th Edition of the World Health Organization Classification of Head and Neck Tumors: Oropharynx and Nasopharynx. Head Neck Pathol. 2022;16(1):19-30. doi:10.1007/s12105-022-01449-2
26.Peterson BR, Nelson BL. Nonkeratinizing undifferentiated nasopharyngeal carcinoma. Head Neck Pathol. 2013;7(1):73-5. doi:10.1007/s12105-012-0401-4 PubMed
27.Statistics Canada. Table 13-10-0747-01, Number of new cases and age-standardized rates of primary cancer, by cancer type and sex [sponsor supplied reference]. 2025. https://doi.org/10.25318/1310074701-eng
28.Apotex Inc. CDA-AMC Reimbursement Review Sponsor Summary of Clinical Evidence: Toripalimab for the Treatment of Recurrent/ Metastatic Nasopharyngeal Carcinoma [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Loqtorzi (toripalimab solution for injection), Sterile solution, 240 mg/6 mL (40 mg/mL) for intravenous infusion after dilution. July 15, 2025.
29.Shanghai Junshi Bioscience Co Ltd. JS001-015-III-NPC: Phase III Clinical Study Report of Toripalimab [sponsor supplied reference]. 2021. Accessed January 15, 2021.
30.Musoro JZ, Coens C, Sprangers MAG, et al. Minimally important differences for interpreting EORTC QLQ-C30 change scores over time: A synthesis across 21 clinical trials involving nine different cancer types. Eur J Cancer. 2023;188:171-182. doi:https://doi.org/10.1016/j.ejca.2023.04.027 PubMed
31.Shanghai Junshi Bioscience Co Ltd. Addendum 1 to Clinical Study Report: A Phase III, Randomized, Placebo Controlled, Multicenter, Double-Blind Study Comparing Toripalimab Injection (JS001) Combined with Chemotherapy Versus Placebo Combined with Chemotherapy for Recurrent or Metastatic Nasopharyngeal Cancer [sponsor supplied reference]. 2021.
32.Shanghai Junshi Bioscience Co Ltd. Addendum 3 to Clinical Study Report: A Phase III, Randomized, Placebo Controlled, Multicenter, Double-Blind Study Comparing Toripalimab Injection (JS001) Combined with Chemotherapy Versus Placebo Combined with Chemotherapy for Recurrent or Metastatic Nasopharyngeal Cancer [sponsor supplied reference]. 2023.
33.Apotex. Apotex Inc. response to Canada's Drug Agency request for additional information regarding toripalimab review on September 3, 2025 [internal additional sponsor's information].
34.Apotex. Apotex Inc. response to Canada's Drug Agency request for additional information regarding toripalimab review on September 10, 2025 [internal additional sponsor's information].
35.Apotex Inc. Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Loqtorzi (toripalimab solution for injection), Sterile solution, 240 mg/6 mL (40 mg/mL) for intravenous infusion after dilution. Accessed July 16, 2025.
36.IQVIA. DeltaPA. 2025. Accessed July 7, 2025. https://www.iqvia.com/
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.